CADTH Health Technology Review
Treatment of Adult Patients With Chronic Immune Thrombocytopenia After Failure of First-Line Therapies
PROSPERO Registration Number: CRD42021276565
Health Technology Assessment
Abbreviations
AE
adverse event
DB
double blind
HRQoL
health-related quality of life
HTA
health technology assessment
ITP
immune thrombocytopenia
ITT
intent to treat
IVIG
IV immunoglobulin
NMA
network meta-analysis
OL
open label
RCT
randomized controlled trial
SAE
serious adverse event
TPO-RA
thrombopoietin receptor agonist
Key Messages
What is the issue?
Immune thrombocytopenia (ITP) is an autoimmune disorder characterized by low platelets and an increase in bleeding risk. It has an incidence rate of 3.3 per 100,000 adults per year.
After first-line corticosteroid treatment, there is limited evidence on the best subsequent-line therapies based on evidence of low certainty. Subsequent therapies after failure of corticosteroid use include several treatments, such as rituximab, eltrombopag, romiplostim, fostamatinib, avatrombopag, and splenectomy.
The goal of treatment is to reduce bleeding and prolong life. Increases in platelet count are considered a surrogate to these treatment goals.
What did we do?
We conducted a narrative review of 15 publications (10 randomized controlled trials) found through a systematic literature search.
The review addressed the following policy questions:
What treatment(s) should be used in adult patients with ITP who have failed first-line treatments?
What is the place in therapy of splenectomy in adult patients with ITP?
What did we find?
We found that eltrombopag and romiplostim increased platelet count response and improved ITP symptoms and health-related quality of life compared to placebo.
Interpretation of the effectiveness of avatrombopag, rituximab, and fostamatinib was inconclusive due to the limited availability of evidence and varying risks of bias in the trials.
There was a lack of evidence in specific subgroups of patients and on the role of splenectomy in the sequency of subsequent-line therapies.
Further research is needed to compensate for clinical data gaps to inform an appropriate and relevant economic evaluation.
What does this mean?
CADTH suggests that jurisdictions may consider requesting that an implementation advice panel be conducted to bring together clinical experts to suggest measures (e.g., discontinuation criteria) to manage the clinical and economic uncertainty identified in this report.
Executive Summary
Background and Policy Context
Immune thrombocytopenia (ITP) is an autoimmune disorder characterized by low platelets and an increase in bleeding risk,1-4 with a reported incidence rate varying between 2 and 4 per 100,000 adults per year according to various epidemiological studies around the world.5 Severe bleeding, such as in the gastrointestinal tract or in the brain, is seen in approximately 10% of adults.6,7 First-line therapy is a short course of corticosteroids;8 alternatively, IV immunoglobulin (IVIG) and anti-D immunoglobulin may be used in patients who are unresponsive or have a contraindication to taking corticosteroids.8 Recommendations for subsequent-line therapies are based on evidence of low certainty.8 Therefore, a systematic review was undertaken at the request of public drug plans to determine the efficacy and safety of subsequent-line therapies — that is, rituximab, eltrombopag, romiplostim, fostamatinib, avatrombopag, and splenectomy — in adult patients with ITP who have failed first-line treatments.
Clinical Evidence
The research protocol was developed a priori, by engaging with patient groups, and the systematic review used robust methodology. A total of 15 publications met the final inclusion criteria, reporting findings from 10 unique trials. The study populations in the trials were considered generalizable to most ITP patients and the concomitant use of other ITP medications was allowed. A narrative synthesis was conducted due to clinical heterogeneity between studies and methodological constraints that precluded a network meta-analysis (NMA).
Findings from 4 randomized controlled trials (RCTs) showed that, compared to placebo, eltrombopag generated a long-lasting platelet count response (at least 6 weeks and up to 6 months) and improved health-related quality of life (HRQoL), in addition to reducing bleeding events and the need for rescue medication. In 3 RCTs, romiplostim increased platelet count response, improved ITP symptoms and HRQoL, and reduced the need for rescue medication compared to placebo or standard of care. Interpretation of the effectiveness of avatrombopag, rituximab, and fostamatinib was inconclusive due to the limited availability of evidence, which was 1 single trial for each intervention, with varying risks of bias.
Due to a scarcity of evidence, conclusions could not be drawn for the clinically meaningful outcomes of emergency department visits, hospitalization, and treatment-free remission.
Economic Evidence
An economic evaluation could not be conducted due to significant clinical data gaps, including the methodological limitations precluding assessment of comparative treatment efficacy in an NMA. Therefore, the comparative cost-effectiveness of treatments for ITP is unknown.
Limitations
No head-to-head study, or study with comparisons to splenectomy, was identified from the literature search. Methodological consideration prevented an NMA from being conducted. As such, direct comparisons of effectiveness between ITP treatments cannot be made. Similarly, there was insufficient evidence to inform the efficacy or sequence of subsequent-line therapies in subgroups of adult patients with ITP or the role of splenectomy in the sequency of subsequent-line therapies.
The narrative review was limited by availability of evidence. The risk of bias across the 10 studies ranged from low9-11 to high.12-15 An overall limitation of the included trials was the small sample size, which limited the level of precision and affected the certainty in the findings.
Conclusions and Implications for Decision-Making or Policy-Making
Considering that the evidence of a clinical benefit was restricted to eltrombopag or romiplostim, public drug plans may want to consider revisiting reimbursement criteria for ITP. CADTH suggests that interested jurisdictions request an implementation advice panel to suggest strategies (e.g., discontinuation criteria) to manage the clinical and economic uncertainty identified in the report.
Introduction and Rationale
Background and Rationale
ITP is an autoimmune disorder characterized by low platelets and an increase in bleeding risk due to increased platelet destruction and impaired platelet production.1-4 It was previously called “idiopathic thrombocytopenic purpura,” but is no longer considered to be an idiopathic disease.1,4 The specific cause of ITP is unknown but may be a mix of genetic and environmental factors.16 In addition, not all patients will experience bleeding symptoms such as purpura (hemorrhages in the skin and mucous membranes).16 Symptoms associated with ITP are excessive bruising, superficial bleeding that appears as reddish spots on the skin (petechiae), bleeding from the gums or nose, blood in urine or stool, and unusually heavy menstrual flow; however, ITP may present with no signs or symptoms.
Primary ITP is defined as isolated thrombocytopenia — that is, peripheral blood platelet count less than 100 × 109/L — in the absence of other causes or disorders that may be associated with thrombocytopenia.1 The disorder falls into 1 of the following 3 disease groups according to disease duration:
Newly diagnosed ITP: active disease duration of 0 to 3 months
Persistent ITP: active disease duration of 3 to 12 months, including those patients who do not reach spontaneous remission or do not maintain complete response of therapy1
Chronic ITP: ongoing, active disease lasting longer than 12 months1
Spontaneous remission may occur when there is an improved platelet count in the absence of ongoing or recent therapy, which occurs in 45% of adults at 6 months and 49% of adults at 12 months. Among those with chronic ITP, 30% of adults achieve spontaneous remission at 24 months.17
ITP has a reported incidence rate varying between 2 and 4 per 100,000 adults per year according to various epidemiological studies around the world.5 Bleeding symptoms are often present, including severe bleeding (such as in the gastrointestinal tract or the brain) in approximately 10% of adults.6,7 At least 1 comorbid condition is reported in more than 30% of patients.7
First-line therapy for newly diagnosed adult patients, according to both the American Society of Hematology 2019 Guidelines for Immune Thrombocytopenia8 and the Updated international consensus report on the investigation and management of primary immune thrombocytopenia,18 is a short course (approximately 6 weeks) of corticosteroids. For patients with ITP who are unresponsive or have a contraindication to taking corticosteroids, other first-line therapies include IVIG and anti-D immunoglobulin.8 The international standardized definition1 of a platelet response is a platelet count of 30 × 109/L or higher with at least a 2-fold increase in platelet count from baseline and an absence of bleeding, while a platelet count of 100 × 109/L or higher would typically be considered a complete response as long as there is an absence of bleeding.1
Patients who do not respond to first-line treatment within the first 3 months, or who are corticosteroid-dependent, will have a disease duration that falls within the persistent ITP category and may benefit from second-line treatment options.19 These include thrombopoietin receptor agonists (TPO-RA) romiplostim and eltrombopag, as well as rituximab.19 After 12 months of ongoing, active disease, patients are considered to have chronic disease and, in addition to second-line treatment options, become candidates for splenectomy.8 The choice of treatment will be based on patient preferences, such as whether they prefer a durable response, or if they would rather avoid long-term medication or avoid surgery.
Refractory ITP is characterized by nonresponse to splenectomy, or relapse after surgery, and either severe ITP or a high risk of bleeding that requires continued subsequent therapy.1 Treatments may include 1 of the following: TPO-RAs (i.e., eltrombopag, avatrombopag, or romiplostim), spleen tyrosine kinase inhibitor fostamatinib, or rituximab.18
There are other second-line treatment options, including azathioprine, cyclophosphamide, cyclosporine, danazol, dapsone mycophenolate mofetil, and the vinca alkaloids; however, guidelines such as that of the American Society of Hematology do not provide recommendations on these drugs due to limitations in the current evidence, mainly the small sample sizes of studies and heterogeneous patient populations.8 A brief summary of the reported efficacy of immunosuppressive drugs without American Society of Hematology guideline recommendations can be found in Table 1.
Table 1: Immunosuppressive Drugs Without Guideline Recommendations
Immunosuppressive drug | Reported efficacy | Reported safety concerns |
|---|---|---|
Azathioprine |
|
|
Cyclophosphamide |
|
|
Cyclosporine A |
|
|
Danazol |
|
|
Dapsone |
|
|
Mycophenolate mofetil |
|
|
Vinca alkaloids |
|
|
AE = adverse event; G6PD = glucose-6-phosphate dehydrogenase; PML = progressive multifocal leukoencephalopathy.
Note: All data presented are reported in Neunert et al. (2019).8 Studies had small sample sizes and heterogeneous patient populations; disease duration, disease severity, and previous treatments received may vary substantially from current clinical practice.8
Source: American Society of Hematology 2019 Guidelines for Immune Thrombocytopenia.8
It is unclear which treatments are most appropriate for adult patients with chronic ITP who have failed first-line treatments. The federal, provincial, and territorial public drug plans have requested an evaluation on the comparative evidence of available treatments for adults with ITP who have already received first-line therapies (i.e., corticosteroids, IVIG, and/or anti-D immunoglobin) and the place in therapy of splenectomy.
Summary of Patient Group Input
Lived Experience of Chronic ITP
CADTH welcomed feedback from the patient community on the proposed project entitled Treatment of Adult Patients With Chronic ITP After Failure of First-Line Therapies.” The Platelet Disorder Support Association encouraged its patient community to contribute feedback. Twenty people living with chronic ITP shared their experiences and expectations of ITP therapies, in addition to the information provided by the Platelet Disorder Support Association. Many contributors were in their 50s, 60s, and 70s, with a few contributors in their early 30s. Many had lived with ITP for more than 10 years, with a range of 12 months to 55 years. Most contributors identified that they were from Ontario or British Columbia.
Several contributors described living with the fear of serious or fatal bleeds and the exhaustion associated with low platelets. “Having ITP and living with the fear of bleeding is a very stressful and unpredictable situation. I am not able to work full-time owing to the fatigue associated with ITP. I cannot travel or participate in overly vigorous activities because of the fear of a sudden drop in platelets and bleeding.”
Patients’ Experiences of Therapies for ITP
Contributors described a wide range of experiences of therapies: corticosteroids, including prednisone and dexamethasone; IVIG; rituximab; TPO-RAs, including romiplostim and eltrombopag; immunosuppressants, including cyclosporine and azathioprine; and/or splenectomy.
Contributors described trying multiple therapies over the years. “After trying prednisone — did not respond; IVIG which did respond; then splenectomy which did not work; IVIG only lasted a few weeks; rituximab, only last a few weeks; cyclosporine which proved to be the best medication for controlling ITP for the next 11 years. Now on Revolade for the past 4 years, which has worked well.”
Temporary and/or waning effectiveness were concerns shared by contributors. “IVIG treatments which are a lifesaver but temporary.” Time spent in hospital or spent receiving IV therapy was another concern. “During the first six months, I was admitted to the hospital on 5 separate occasions with platelet readings of between 0k and 3k, accompanied by various indications (e.g., unexplained bruises, blood blisters, slight nose bleeds and bleeding gums), with an average stay of 3-5 days in each case.” “I opted for a watch and wait approach because I hated the side effects of prednisone, and the amount of school I was missing for IVIG treatments every 3-4 weeks was not sustainable.”
Many contributors described the side effects they experienced using corticosteroids. “I had terrible side effects from the steroids including manic-like episodes, weight gain, heart racing, insomnia, and eye disturbances. I have had to take bone health supplements and have regular bone scans to monitor bone loss due to long term use of steroids.” One person described being unable to work due to side effects of prednisone, while others described permanent side effects of “brain fog” and osteonecrosis, as a consequence of steroids. A few contributors described a willingness to use steroids only if platelets were extremely low, for example: “I do respond to steroids and have used prednisone but will only use them in an emergency—platelets at 10 or less—as I have a great deal of difficulty dealing with the side effects.”
One person shared their experience of 28 years of remission following removal of their spleen. When ITP returned, use of prednisone and dexamethasone raised platelets levels temporarily until an accessory spleen was found and removed, allowing the person to return to remission. Other contributors shared that splenectomy had not helped them. One person described experiencing portal vein thrombosis, resulting in 2 emergency surgeries and an intensive care unit stay; deep vein thrombosis; bowel resection; permanent daily incontinence; reduced immune system response; and a reliance on blood thinners as a consequence of splenectomy that did not offer remission, to access rituximab, which was also not effective. For this person, only prednisone has been effective.
Rationale Behind Treatment Decisions
Outside of Alberta, patients with chronic ITP must try splenectomy to be eligible for public funding of second-line drug treatments. Many contributors described how they faced an uncertain disease path, uncertain benefit of splenectomy in the short term and long term, and knowledge that the removal of their spleen was permanent, required surgery, and increased their risk of infection.
I have been highly resistant to the idea of a splenectomy for a number of reasons, including uneven record of success in treating ITP; surgical risks including long term effects of general anaesthetic; availability of alternative noninvasive medications.
Once the spleen is gone, it is gone forever.
I ended up having a splenectomy that, within a few months, indicated that it had failed. In hindsight I would not have had a splenectomy. But I felt I did not have a choice, as I could not access the more expensive treatments like Rituxan or the TPOs without having first “failed” three other lines of treatment.
Given the variability and unpredictability of the disease, some respondents described refusing splenectomy and the potential for remission, to accept the risks of bleeding and to treat only serious episodes with first-line therapy. “As there is no cure for ITP, I decided that I would rather live with what I know than a whole new batch of side effects with treatment that may or may not help bring my platelets up.”
Patients’ Expectations for ITP Treatment
A desire to see different types of therapies accessible to patients in Canada — including avatrombopag, fostamatinib, eltrombopag, romiplostim, rituximab, and oral veltuzumab — was expressed by contributors. “I understand this is a rare condition but, to me, it feels like there is really no treatment for me because what is available is so very inadequate.”
One contributor asked for public funding of TPO-RA medications. Another emphasized that health care providers should explain to patients and their families the full range of treatments available for ITP, even if not all are publicly funded. “As other new treatment advances are made, more favourable medications should constantly be re-evaluated in terms of coverage and accessibility. For now, I remain in a position where my only next treatment option is the same one offered over 100 years ago.”
Many contributors expressed a desire to avoid surgery (splenectomy) and the side effects associated with the long-term use of steroids. “It seems like an inhumane choice to force surgery to remove an organ before access to other treatments, especially when splenectomy is less often successful the older a patient is and does not have a high percentage of success in the ITP population as a whole.”
Several sought public funding of the use of indium white blood cell screening, to gauge the likelihood that splenectomy would be successful for the individual, before considering surgery.
The collection of patient perspectives highlighted the unmet need for treatment options for adult patients with chronic ITP after failure of first-line therapies.
Objectives
CADTH undertook a Health Technology Assessment (HTA) to review the effectiveness and cost-effectiveness of treatments for ITP in adults after failure of first-line treatments. A secondary objective was to determine the place of splenectomy in therapy.
Policy Questions
The following policy questions were addressed with this project:
What treatment(s) should be used in adult patients with ITP who have failed first-line treatments?
What is the place in therapy of splenectomy in adult patients with ITP?
Research Questions
The project addressed the following research questions. Details on the specific interventions and outcomes are included in Table 2.
Clinical Evaluation
What is the comparative effectiveness and safety of subsequent-line therapies in adult patients with ITP who have failed first-line treatments?
What is the comparative effectiveness and safety of splenectomy compared with second-line therapies (rituximab, fostamatinib, or TPO-RA [romiplostim, eltrombopag, avatrombopag]) in adult patients with ITP?
Economic Analysis
What is the cost-effectiveness of therapies in adult patients with ITP who have failed first-line treatments?
What is the cost-effectiveness of splenectomy compared with second-line therapies (rituximab, fostamatinib, or TPO-RA [romiplostim, eltrombopag, avatrombopag]) in adult patients with ITP?
Methods
To inform the conduct of this HTA, a preliminary informal scoping of the existing literature was conducted. A protocol was written a priori and was followed throughout the study process. The project is an HTA that includes clinical and economic reviews. Stakeholder feedback was solicited at key steps. The key elements of the project, including the population of interest, the interventions and comparators, and the main outcomes of interest, are outlined in Table 2. The protocol was registered (registration number: CRD42021276565) in PROSPERO.20 No deviations in the protocol occurred.
Opportunities for Stakeholder Feedback
The project scope was posted on the CADTH website for 10 days and feedback from the patient community was reviewed and summarized. The collection of patient perspectives enabled the research team to consider the evidence found in the literature alongside an understanding of the wider experiences of patients and family caregivers. In addition, the draft list of included studies in the review, the statistical analyses plan, and a draft of the report were also posted on the CADTH website and all stakeholders (e.g., patient community, clinician groups, industry) were given the opportunity to provide written feedback.
Clinical Review
This clinical evaluation was designed as a systematic review and an NMA to answer the first and second research questions. The systematic review and NMA of the primary studies focused on the clinical effectiveness, comparative clinical effectiveness, safety, and comparative safety of ITP medications, as well as on the clinical effectiveness, comparative clinical effectiveness, safety, and comparative safety of splenectomy in ITP. The systematic review was conducted following standard methodology and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement,21 with consideration of relevant elements of PRISMA-NMA.22 The NMA was conducted in accordance with the Professional Society for Health Economics and Outcomes Research (ISPOR) guidelines for NMAs.23
Literature Search Methods
An information specialist developed and conducted a literature search for clinical studies using a peer-reviewed search strategy according to CADTH’s PRESS Peer Review of Electronic Search Strategies checklist.24 The complete search strategy is presented in Appendix 1.
Published literature was identified by searching the following bibliographic databases: MEDLINE via Ovid, Embase via Ovid, and the Cochrane Central Register of Controlled Trials (CENTRAL) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the PICOS (Population(s), Intervention(s), Comparator(s), Outcome(s), Study Design(s)) framework and research questions. The main search concepts were rituximab, fostamatinib, TPO-RAs (romiplostim, eltrombopag, avatrombopag), or splenectomy and ITP. Clinical trials registries with results were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
CADTH-developed search filters were applied to limit retrieval to HTAs, systematic reviews, meta-analyses, or NMAs, RCTs, or controlled clinical trials. Systematic reviews were included in the literature search to inform the initial scoping of the project. Retrieval was not limited by publication date but was limited to the English or French language. Conference abstracts were excluded from the search results.
The initial search was completed on July 23, 2021. Regular alerts updated the database literature searches until July 26, 2022. The clinical trials registries search was updated before the completion of the stakeholder feedback period. Studies meeting the selection criteria of the review and identified in the alerts before the completion of the stakeholder feedback period were incorporated into the analysis of the final report. Any studies that were identified after the stakeholder feedback period are described in the discussion, with a focus on comparing the results of these new studies with the results of the analysis conducted for this report.
Grey literature (literature that is not commercially published) was identified by searching sources listed in relevant sections of Grey Matters: A Practical Tool For Searching Health-Related Grey Literature, which includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations. Google was used to search for additional internet-based materials. These searches were supplemented by screening articles identified by clinical experts and by industry following the stakeholder feedback period.
Eligibility Criteria
Studies were included if they met the eligibility criteria, including the specific population, intervention, comparators, and study designs, presented in Table 2. Drug regimens eligible for inclusion in the review were those that have been approved by Health Canada for ITP or were considered of clinical relevance based on expert advice or international clinical practice guidelines. The inclusion criteria were informed by the informal scoping review of the existing literature, patient engagement, stakeholder feedback, and consultation with the clinical experts. Studies were excluded if they did not report outcomes of interest. The language of publications was limited to English and French, with no limitation on publication date, and conference abstracts were excluded.
Criteria | Description |
|---|---|
Population | Adult patients (3 aged18 years or older) with ongoing, active ITP who have failed first-line treatments Subgroups of interest:
|
Interventions |
|
Comparators |
|
Outcomes | Clinical effectiveness:
Safety:
|
Study design | Phase III and phase IV randomized controlled trials |
ITP = immune thrombocytopenia; IVIG = IV immunoglobulin.
aRituximab dose for ITP: 375 mg/m2 IV infusion once a week for 4 weeks (4 total doses; days 1, 8, 15, and 22). There is also a lower dose that can be used for ITP: 100 mg IV infusion once a week for 4 weeks (4 total doses; days 1, 8, 15, and 22).
bIncludes biosimilars.
Population and Subgroups
The patient population included in the review consisted of adults with ongoing, active ITP who did not respond to first-line treatments. Relevant subgroups included duration of disease as persistent ITP (between 3 and 12 months) or chronic ITP (more than 12 months), and previous failure of at least 1 second-line therapy. Patients were eligible for inclusion in the studies if they were adults with a diagnosis of ITP that was either newly diagnosed, persistent, or chronic, depending on the study inclusion criteria. Platelet count was typically required to be less than 30 × 109/L. It was standard for patients to be excluded from the studies if they had significant comorbidities such as other blood disorder, history of thrombosis, cardiovascular disease, or active malignancy.
Intervention and Comparators
All currently available subsequent-line therapies for ITP were considered potentially relevant interventions and comparators, including rituximab, eltrombopag, romiplostim, fostamatinib, avatrombopag, and splenectomy. Comparators also included placebo and/or standard of care (IVIG; immunosuppressants, including azathioprine, cyclosporine, cyclophosphamide, mycophenolate mofetil, danazol, dapsone; and corticosteroids). Recognizing that rescue therapies are sometimes given in combination with these drugs, no distinction was made between monotherapy or combination therapy for any of the included treatments.
It should be noted that standard of care was included as a background treatment, or as an add-on treatment to any of the included second-line therapies because the clinical expert noted that standard of care is generally given to all patients. IVIG, immunosuppressants (azathioprine, cyclosporine, cyclophosphamide, mycophenolate mofetil, danazol, dapsone), or corticosteroids were considered as standard of care.
Outcomes Definition
In consultation with a clinical expert, outcomes were selected to assess the clinical effectiveness and safety of the interventions, including platelet count response, bleeding events, emergency department visits, hospitalization, HRQoL, symptoms (e.g., fatigue), treatment-free remission, need for rescue medication (e.g., IVIG, corticosteroids, platelet transfusions), reduction or discontinuation of corticosteroids, and mortality. Various other harms outcomes were considered important for clinical decision-making and were therefore included in the protocol. Any reasonable measurement tool or definition used by study authors for the outcomes presented, as well as any relevant follow-up time point, was considered and critically appraised when needed.
Study Designs
Published phase III and phase IV RCTs were eligible for inclusion.
Study Selection Process
Two reviewers independently screened titles and abstracts of all retrieved citations in duplicate (i.e., literature searches of academic databases, grey literature searches, and clinical trial database) against the eligibility criteria (Table 2). Exclusion by both reviewers was required for a record to be excluded at the title and abstract level. Full-text articles that were judged to be potentially relevant by at least 1 reviewer were retrieved for the second level of screening. The same 2 reviewers independently examined all full-text articles against the eligibility criteria, and consensus was required for inclusion in the review. Discrepancies between reviewers were resolved by discussion. Reasons for exclusion at the full-text level were documented. The list of final included studies was posted publicly on the CADTH website and feedback was solicited from stakeholders. Studies later identified via monthly database search alerts and semiannual grey literature search alerts meeting the selection criteria of the review were incorporated into the analysis.
Quality Assessment
Risk of bias in the individual trials was assessed using the Cochrane risk of bias 2 (RoB 2) tool at the level of the reported result.24 Risk of bias was appraised for the effect of assignment to the intervention (i.e., intent-to-treat [ITT]). Risk of bias assessments were completed by 2 reviewers independently in duplicate for each trial. The RoB 2 tool allowed for the assessment of 5 sources of bias or “domains”: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Each question within each domain was answered with a “yes,” “probably yes,” “probably no,” “no,” or “no information.” Afterward, a judgment of “low risk of bias,” “high risk of bias,” or “some concerns” was assigned for each domain, with the rationale for each decision included in the comments box field.
For each unique RCT, we assessed the risk of bias of the original primary publication, with additional details sought from supporting literature (e.g., published protocol and ClinicalTrials.gov records). Disagreements were resolved by consensus. The risk of bias of each included study and how it affects the study findings was described narratively. Other critical appraisal points were noted by reviewers, such as assessment of the generalizability of the findings.
Data Analyses and Synthesis
Data were extracted by 1 reviewer by the use of piloted and standardized data abstraction forms, and the extracted data were checked for accuracy and completeness by a second reviewer. Any disagreements were resolved by consensus. Modification to the extraction sheet was conducted after a pilot of 5 studies.
The original, primary publication for each included RCT was used for data extraction, with supplementary data obtained from companion reports and ClinicalTrials.gov records to address the research questions. In situations where multiple publications for a unique RCT were available (e.g., supplemental online appendices, companion publications of specific outcomes, or populations from the original study), the most recent data for each outcome were extracted, with preference given to published records.
The following relevant information was extracted, where available:
Study level: description of publication (e.g., first author last name, title, publication year), study characteristics (e.g., clinical trial registry identification number, trial acronym, study design, year of study conduct, sample size, study setting, country of study conduct, randomization ratio, blinding status, superiority or noninferiority design, eligibility criteria, study duration)
Patient level: number of patients, age, sex (as reported by study authors), clinical situation of the diagnosis, duration of disease
Intervention and comparator level: type, dose, total duration of treatment, dosing frequency, route of administration, and concurrent and previous relevant therapies
Outcome level: description of outcomes (e.g., method of measurement, unit of measurement, length of follow-up) and all data related to an eligible outcome domain
Type of analysis: ITT or safety population; data from figures were extracted if explicit numerical data were reported on the figure.
After the conclusion of data extraction, a feasibility assessment was conducted for addressing the posed research questions, which included evaluating sources of methodological and clinical heterogeneity between the included studies. Study design, patients’ baseline characteristics, treatment characteristics, as well as outcome definitions were compared between studies. A qualitative assessment of feasibility was determined through close collaboration between the reviewers, methodologists, and clinical experts. Because the NMA was deemed infeasible, an alternate NMA was conducted with simplified assumptions. Ultimately, it was concluded that the NMA was not informative; therefore, a narrative summary was reported. Refer to the prespecified statistical analysis plan for this report provided in Appendix 2 for further details of the planned analysis.
Results of Clinical Evaluation
Selection of Primary Studies
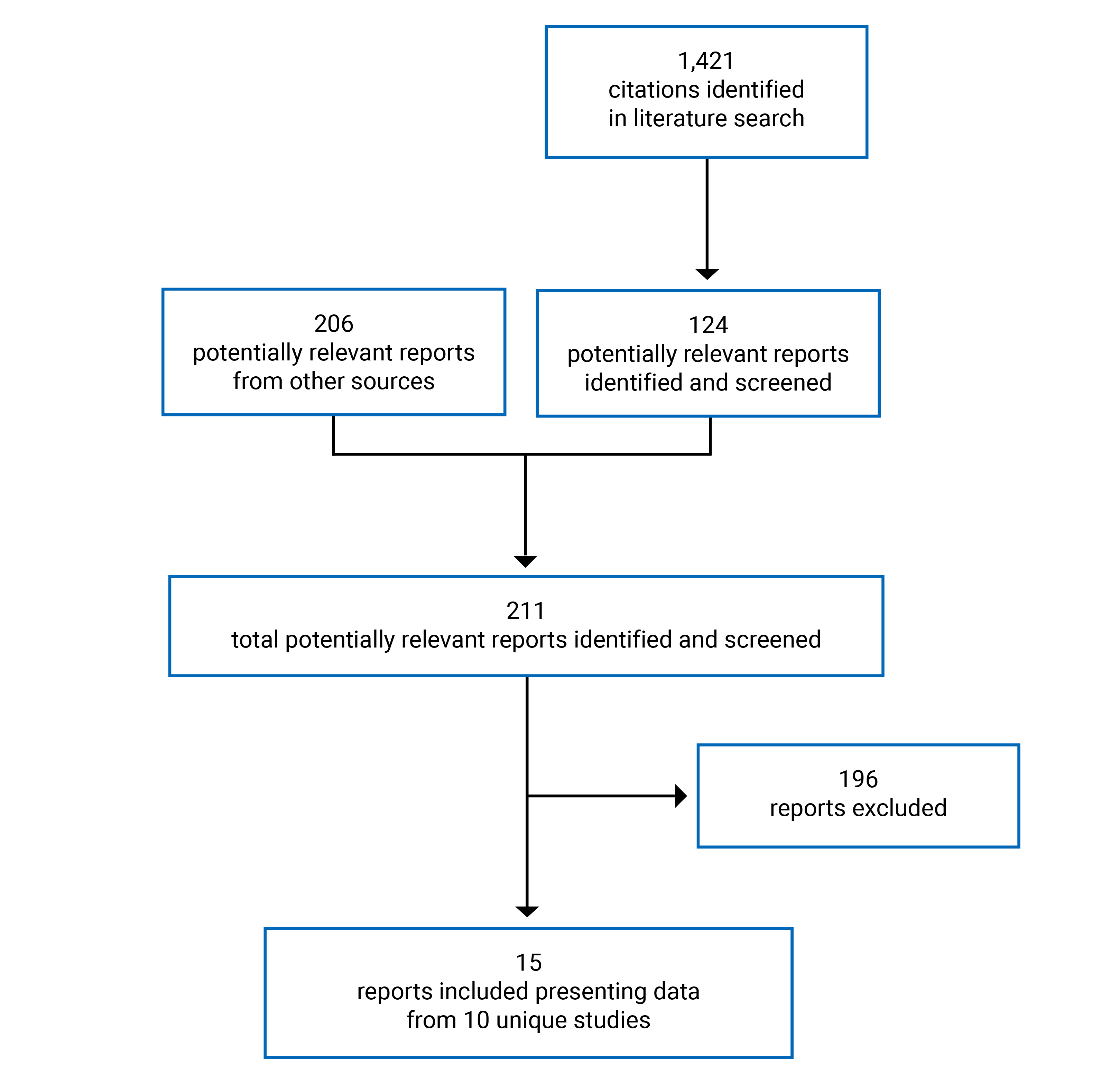
A total of 1,421 citations were identified in the literature searches. Following screening of titles and abstracts, 124 studies were identified as potentially relevant and retrieved for full-text review. A total of 206 reports were retrieved from other sources (i.e., grey literature, handsearch, and search alerts). Of these 330 potentially eligible reports, 15 reports9-15,25-32 presenting data from 10 unique studies met the inclusion criteria and were included for review. The report selection process is outlined in Figure 1. A list of included and excluded reports, with details describing the rationale for those excluded, is presented in Appendix 3 and Appendix 4, respectively.
Study and Patient Characteristics
A total of 15 publications met the inclusion criteria and were included in the systematic review, reporting results from 10 individual RCTs. Peer-reviewed publications were selected for inclusion if they met the prespecified review protocol criteria. Study characteristics are shown in Appendix 6.
Populations
One study was performed in patients who received corticosteroids without achieving a sustained response or who relapsed after discontinuation,32 and 3 studies included patients who had insufficient response or relapse to any previous therapies for ITP.9,25,27 While this was the main population of interest for the review, it limited the number of drug comparisons that could be evaluated and used to inform decision-making. Additional trials included patients who had experience with prior ITP therapies, without specifically requiring treatment failure, and these were included in the review as well.
Interventions and Comparators
Four included studies were double-blind (DB), placebo-controlled RCTs comparing eltrombopag to placebo over 6 weeks9,25,27 or 6 months10 One included study was a small DB RCT evaluating the use of avatrombopag compared with placebo over 26 weeks.12 Three included RCTs compared romiplostim to either placebo in a DB setting11,13 or standard of care in an open-lavel (OL) setting.14 Two included studies evaluated interventions other than TPO-RA: 1 DB RCT evaluated the use of rituximab compared with placebo over 4 weeks32 and 1 DB RCT compared fostamatinib to placebo over 24 weeks.15 In addition to the interventions and comparators, the concomitant use of various ITP medications was allowed in all trials. These medications included, but were not limited to, corticosteroids, azathioprine, and danazol.
Outcomes
All the studies included in the systematic review reported platelet count response as a primary or major outcome; however, the outcome measures used to assess platelet response varied substantially across the studies. The most frequently used was the proportions of patients achieving response. There were notable differences observed in thresholds and definitions for platelet count response across studies, including some that were not consistent with the international standardized definition1 of a platelet count of 30 × 109/L or higher with at least a 2-fold increase in platelet count from baseline and an absence of bleeding, while a platelet count of 100 × 109/L or higher would typically be considered a complete response, as long as there is an absence of bleeding.1 In addition, there were differences among all of the studies as to the conditions to be observed for patients to be considered responders, such as the time needed to be spent above the threshold value (ranging from at least once during the study to throughout the entire study follow-up), as well as criteria related to the use of rescue medication.
Nine studies reported bleeding as an outcome for either efficacy or harms assessment.9-12,14,15,25,27,32 Definitions of bleeding and reporting methods varied across the studies. Other frequently reported outcomes included the need for rescue medication (e.g., IVIG and corticosteroids), reduction or discontinuation of concomitant ITP medications, and various safety outcome measures. Three studies reported findings on HRQoL or ITP symptoms using various scales: the Functional Assessment of Chronic Illness Therapy (FACIT) – Fatigue subscale;10 the Functional Assessment of Cancer Therapy – Thrombocytopenia 6-item questionnaire (FACT-Th6);10 the Motivation and Energy Inventory – Short Form (MEI-SF);10 the Short Form (36) Health Survey, Version 2 (SF-36v2);10 EQ-5D;11 and the Immune Thrombocytopenic Purpura Patient Assessment Questionnaire (ITP-PAQ).11,14
No data were reported for the outcomes of treatment-free remission, emergency department visits, or hospitalization.
Eltrombopag Versus Placebo
In the 4 studies comparing eltrombopag to placebo, eltrombopag was administered at a dosage ranging from 12.5 mg to 75 mg orally once daily, with the dose to be adjusted based on platelet count response. The mean age of the patients ranged from 41 to 58 years across treatment groups at baseline. The median platelet count ranged from 9,500/µL to 21,000/µL; approximately half of the trials’ populations had a platelet count of 15,000/µL or less. The proportions of patients using concomitant ITP medication at baseline was 82% in 1 trial,25 and ranged from 42% to 55% in the other studies. All studies included a portion of patients who had a splenectomy; however, the proportions varied substantially from 1 trial to another.
Avatrombopag Versus Placebo
One study evaluated the superiority of avatrombopag administered orally once daily, with the dose to be adjusted based on platelet count response and need for concomitant ITP medications, over placebo for 26 weeks. The mean age of the patients ranged from 41 to 46 years across treatment groups at baseline. Median platelet count at baseline was not reported; however, approximately half of the patient population had a platelet count of 15,000/µL or less, while the other half had a platelet count between 15,000/µL and 30,000/µL.12 In this study, 45% of patients had concomitant ITP medication at baseline and 33% of patients had a prior splenectomy.12
Romiplostim Versus Placebo or Standard of Care
In the 3 studies comparing romiplostim to placebo or standard of care, romiplostim was administered at a dosage ranging from 1 to 3 mcg/kg subcutaneously once weekly, with the dose to be adjusted up to a maximum between 10 and 15 mcg/kg based on platelet count response. In 1 study, the mean age of the patients at baseline was 59 years in the romiplostim treatment group and 48 years in the placebo treatment group;13 in the 2 other romiplostim trials, the median age of the patients ranged from 52 to 58 years across treatment groups.11,14 In 2 of the 3 studies, baseline mean or median platelet count was less than 20,000/µL;11,13 however, 1 study included patients with a numerically higher median platelet count (33,000/µL in the romiplostim treatment arm and 27,000/µL in the placebo arm).14 The proportions of patients using concomitant ITP medication at baseline varied substantially from 1 trial to another. Two studies reported the proportions of patients who had a splenectomy, ranging from 42% to 51% across treatment groups.11,13
Table 3: High-Level Study Characteristics
Criteria | Tomiyama et al. (2012) n = 23 | Yang et al. (2017) n = 155 | Bussel et al. (2009) n = 114 | Cheng et al. (2011) n = 197 | Jurczak et al. (2018) n = 49 | Shirasugi et al. (2011) n = 34 | Kuter et al. (2008) n = 125 | Kuter et al. (2010) n = 234 | Ghanima et al. (2015) n = 150 | Bussel et al. 2018 n = 112 |
|---|---|---|---|---|---|---|---|---|---|---|
Population | Subsequent-line treatment in patients who have failed ≥ 1 prior ITP therapies | Subsequent-line treatment in patients who have experience with prior ITP therapies | second-line after corticosteroid failure | |||||||
Interventions | Eltrombopag adjusted based on platelet count | Avatrombopag adjusted based on platelet count | Romiplostim adjusted based on platelet count | Rituximab 375 mg/m2 IV weekly | Fostamatinib 100 to 150 mg orally twice daily | |||||
Comparators | Matching placebo | Standard of care | Matching placebo | |||||||
Primary outcome | Platelet count response (various outcome measures) | Treatment failure | Platelet count response | |||||||
Other key outcomes |
|
|
|
|
|
|
|
|
|
|
HRQoL = health-related quality of life; ITP = immune thrombocytopenia; IVIG = IV immunoglobulin.
Table 4: Outcomes Assessing Platelet Count Response
Intervention | Eltrombopag | Avatrombopag | Romiplostim | Rituximab | Fostamatinib | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Tomiyama et al. (2012) | Yang et al. (2017) | Bussel et al. (2009) | Cheng et al. (2011) | Jurczak et al. (2018) | Shirasugi et al. (2011) | Kuter et al. (2008) | Kuter et al. (2010) | Ghanima et al. (2015) | Bussel et al. (2018) | |
Primary platelet count response outcome | Proportion of responders | Cumulative number of weeks of platelet response | Number of weeks of platelet count response, median (IQR) | Proportion of patients with durable platelet count response rate | Incidence of treatment failure | Treatment failure | Proportion of patients with stable response | |||
60% vs. 0%; at week 6 | 58% vs. 6%; at week 6 | 59% vs. 16%; at week 6 | 79% vs. 28%; throughout 6 months | 12.0 ± 8.75 weeks vs. 0.1 ± 0.49 week | IQR 9 to 12 vs. IQR 0 to 0; median 11 weeks | 49% vs. 2%; last 8 weeks | 11% vs. 30%; 52 weeks | NS | 18% vs. 2%; 24 weeks | |
Secondary platelet count outcome | Proportion of responders | Proportion of responders | Proportions of patients with platelet count increase ≥ 20,000/µL, n | Proportions of patients with ≥ 4 weekly platelet count response | Platelet count /µL, median range | Complete response (platelet count ≥ 100,000/µL) | Overall response (platelet count ≥ 50,000/µL) | |||
33% vs. 0%; throughout 6 weeks | NR | NR | 38% vs. 7%; ≥ 75% of assessments | 66% vs. 0%; day 8 | 96% vs. 25% | 83% vs. 7%; throughout 24 weeks | 2.3 (95% CI 2.0 to 2.6); between week 2 and week 52 | 51% vs. 39%; at 78 weeks | 43% vs. 14%; 24 weeks | |
CI = confidence interval; IQR = interquartile range; NR = not reported; NS = did not meet the a priori defined threshold for statistical significance; vs. = versus.
Intervention | Eltrombopag | Avatrombopag | Romiplostim | Rituximab | Fostamatinib | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Tomiyama et al. (2012) | Yang et al. (2017) | Bussel et al. (2009) | Cheng et al. (2011) | Jurczak et al. (2018) | Shirasugi et al. (2011) | Kuter et al. (2008) | Kuter et al. (2010) | Ghanima et al. (2015) | Bussel et al. (2018) | |
Bleeding events | Proportion of patients with any bleeding symptom | Any bleeding | Any bleeding | Incidence of bleeding symptoms | Incidence of significant bleeding events (severe, life-threatening, or fatal) | Proportions of patients with bleeding events throughout trial | Any bleeding symptoms | |||
No change | 16% vs. 34% | 39% vs. 60% | 79% vs. 93% | 44% vs. 53% | 36% vs. 83%; 12 weeks | 7% vs. 12% | 52% vs. 53% | 38% vs. 50% | NR | |
Improvement in health-related quality of life | NR | NR | NR | FACT-Th questionnaire and SF-36v2 scales (physical role, vitality, and emotional role subscales; mental component summary score) | NR | NR | EQ-5D index score, EQ-5D index VAS score, the ITP-PAQ scales (symptoms, fatigue, bother, activity, psychological, fear, social quality of life, and women’s reproductive health), and the EQ-5D index score | Improvement on ITP-PAQ scales (symptoms, bother, activity, psychological, fear, overall quality of life, and social quality of life) | NR | NR |
Need for rescue medication | Proportion of patients with rescue treatment | Proportion of patients administered ITP treatment | Proportion of patients receiving rescue treatment | |||||||
NR | 9% vs. 34% | NR | 18% vs. 40% | 22% vs. 12% | 9% vs. 17% | 22% vs. 60% | 44% vs. 79% | NR | 30% vs. 45% | |
Reduction or discontinuation of concomitant ITP medication | NR | NR | NR | 59% vs. 32% | 33% vs. 0% | NR | 52% vs. 19% | NR | NR | NR |
Adverse events | 73% vs. 25% | 64% vs. 67% | 59% vs. 37% | 87% vs. 92% | 97% vs. 59% | 91% vs. 92% | 100% vs. 95% | 82% vs. 87% | NR | 83% vs. 75% |
Serious adverse events | 7% vs. 0% | 5% vs. 10% | NR | NR | 28% vs. 6% | 9% vs. 8% | 2% vs. 0% | 23% vs. 37% | NR | 13% vs. 21% |
Withdrawals due to adverse events | NR | 3% vs. 2% | 4% vs. 5% | 10% vs. 7% | 9% vs. 0% | 0% vs. 0% | 2% vs. 2% | NR | 0% vs. 0% | 10% vs. 8% |
Mortality | NR | 3% vs. 2% | 4% vs. 5% | 10% vs. 7% | 0% vs. 0% | 0% vs. 0% | 1% vs. 5% | 1% vs. 3% | 0% vs. 2% | 1% vs. 2% |
Notable harm: infection | NR | NR | NR | NR | NR | NR | NR | NR | 40% vs. 24% | NR |
FACT-Th = Functional Assessment of Cancer Therapy – Thrombocytopenia questionnaire; ITP = immune thrombocytopenia; ITP-PAQ = Immune Thrombocytopenic Purpura – Patient Assessment Questionnaire; NR = not reported; SF-36v2 = Short Form (36) Health Survey, Version 2; VAS = visual analogue scale; vs. = versus.
This section highlights a summary of studies included for each treatment comparison. Additional study characteristics are shown in Appendix 6.
Interventions Other Than TPO-RA Versus Placebo
One study (Ghanima et al.; n = 112)32 evaluated the superiority of rituximab over placebo. Rituximab was administered at a dosage of 375 mg/m2 IV every week for 4 weeks and patients were followed for a total duration of 78 weeks. The median age of the patients was 46 years at baseline. The median platelet count ranged from 16,000/µL to 21,000/µL across treatment groups.
One trial evaluated the superiority of fostamatinib administered at a dosage of 100 mg orally twice daily over placebo for 24 weeks (Bussel et al.; n = 150).15 The median age of the patients was 54 years at baseline. The mean platelet count ranged from 16,052/µL to 19,818/µL across treatment groups.
Summary of Critical Appraisal
The detailed risk of bias appraisal of all the included trials is available in Appendix 7. The key limitations — that is, those having an impact on the interpretation of the findings — are summarized in this section for each treatment comparison.
Eltrombopag Compared to Placebo
Eltrombopag was compared to placebo in 4 DB RCTs of a minimum of 6 weeks’ duration. Of these, Yang et al. (n = 155)9 and Cheng et al. (n = 197)10 were both rated as having a low risk of bias and, therefore, were considered well conducted. Bussel et al. (n = 114)27 was rated as having some concerns for overall risk of bias; the main issue with this study was that the differences in the incidence of adverse events (AEs) may have jeopardized blinding and have affected subjective outcome measurements.
Tomiyama et al. (n = 23)25 was rated as having some concerns for overall risk of bias. The small sample size of the study limits precision and affects confidence in the findings. Patients in the eltrombopag group had a higher baseline platelet count compared to placebo (mean platelet count of 21,000/µL versus 9,500/µL, and proportions of patients with platelet count of 15,000/µL or lower of 20% versus 75%, respectively). This is indicative of the failure of the randomization process, resulting in less severe ITP in patients randomized to eltrombopag, and may bias the results in favour of active treatment. Bleeding was not defined and, therefore, multiple and inconsistent definitions could have been used by assessors, again affecting precision and confidence in the findings.
Of note, 2 of the 4 trials9,25 were performed exclusively in Asia; it is possible that standard of care is different in other countries, which would affect generalizability of the results to the Canadian population.
Avatrombopag Compared to Placebo
Avatrombopag was compared to placebo in 1 DB RCT of 26 weeks’ duration. Jurczak et al. (n = 49)12 was rated as having an overall high risk of bias. The small sample size of the study limits precision and affects confidence in the findings. In addition, there were high discontinuation rates in both treatment arms, especially due to inadequate therapeutic response. Differences between groups in terms of reduction of concomitant ITP medications from baseline and AEs may have jeopardized blinding and affected subjective outcome measurements.
Romiplostim Compared to Placebo
Romiplostim was compared to placebo in 3 RCTs with substantial heterogeneity in methodology (e.g., DB versus OL setting) and follow-up duration. Of these, Kuter et al. (n = 125)11 was a DB RCT of 24 weeks’ duration rated as having a low risk of bias.
The other 2 studies were rated as having an overall high risk of bias. Shirasugi et al. (n = 34)13 was a DB RCT of 12 weeks’ duration and small sample size, limiting precision and affecting confidence in the findings. Kuter et al. (n = 234)14 was an RCT of 52 weeks’ duration with an OL design; considering that the definition of treatment failure, the primary outcome in the trial, included 1 subjective component (requirement for a change in therapy, which was based on clinical decision-making), it may be subject to bias in favour of active treatment due to the OL study design. In both studies, features suggestive of failure of the randomization process were observed, leading to imbalances between treatment groups in terms of disease severity. In Shirasugi et al.,13 a higher proportion of patients in the placebo group had concomitant ITP medication at baseline compared to romiplostim (83% versus 59%, respectively), suggesting more severe ITP in patients randomized to placebo and biasing the results in favour of active treatment. In contrast, in Kuter et al.,14 a higher proportion of patients in the romiplostim group had concomitant ITP medication at baseline compared to placebo (13% versus 6%, respectively), suggesting more severe ITP in patients in the romiplostim group, and may bias the results against active treatment. Shirasugi et al.13 was also subject to blinding issues, as differences between groups in terms of AEs were observed, hence affecting subjective outcome measurements. The trial was performed exclusively in Japan; it is possible that standard of care is different in other countries, which would affect generalizability of the results to the Canadian population.
Rituximab Compared to Placebo
Rituximab was compared to placebo in 1 DB RCT of 78 weeks’ duration. Ghanima et al. (n = 112)32 was rated as having some concerns for overall risk of bias. Not all hospital staff were blinded to treatment allocation, because it was communicated to local hospital pharmacies for infusion bag preparation; in addition, differences between groups in some AEs may also have jeopardized blinding, affecting subjective outcome measurements. The definition of treatment failure, the primary outcome in the trial, was a composite outcome that was amended during the study at a timing that was unclear to include being a candidate for splenectomy. Although this decision seemed to be based on clinical considerations, this may be perceived as an issue due to the lack of details surrounding it reported in the publication.
Fostamatinib Compared to Placebo
Fostamatinib was compared to placebo in 1 DB RCT of 24 weeks’ duration. Bussel et al. (n = 150)15 was rated as having an overall high risk of bias. Discontinuation rates were high, especially due to inadequate therapeutic response, in both fostamatinib and placebo groups. Differences between groups in some AEs may have jeopardized allocation concealment, but this would only affect the subjective outcome measurements.
Data Analysis and Synthesis
Findings of the NMA
Ten RCTs met the inclusion criteria. A network diagram is shown in Figure 2 and additional details of the feasibility assessment are reported in Appendix 5. Several issues were identified by the feasibility assessment both in terms of methodological and clinical heterogeneity of the network. As a result, the data in the network as described in the prespecified statistical analyses plan was considered infeasible for pooling and analyzing using NMA methodology. Alternative networks for analysis were also considered but had similar limitations for feasibility of conducting an NMA. For these reasons, a narrative synthesis of the evidence was conducted for the studies included in the network.
Figure 2: Network for Platelet Count Response Using the Most Encompassing Threshold (20 Thousand or More Platelets)
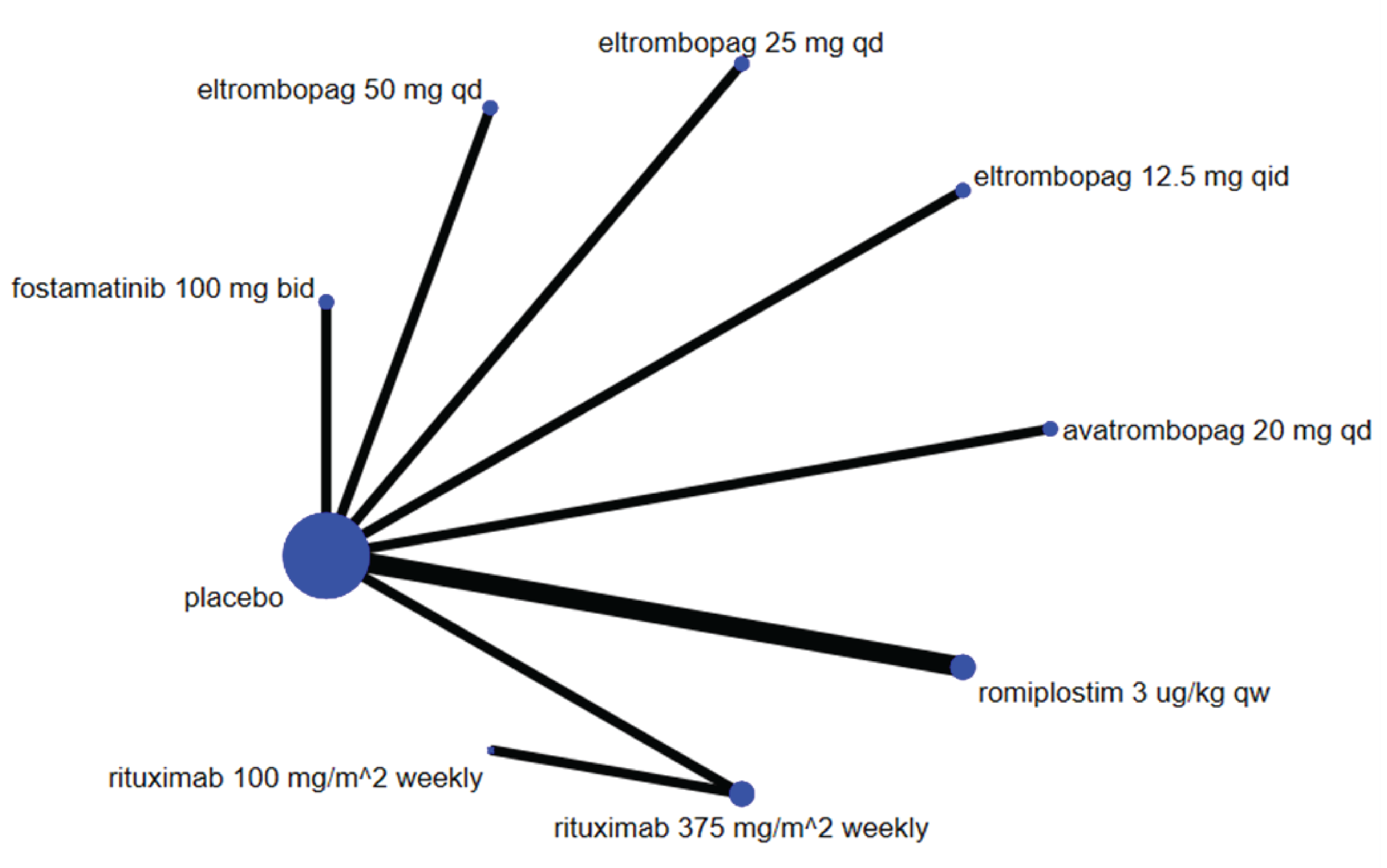
bid = twice daily; qd = once daily; qw = weekly.
Narrative Synthesis
To mitigate the lack of informative results from the NMA, a narrative synthesis was conducted. The narrative review was conducted due to heterogeneity across the publications; as such, there were several differences in the way that outcomes were defined, measured, and reported. There was no additional restriction set other than the selection criteria for inclusion in the systematic review. The outcome measures that were considered by the review team to be the most relevant to decision-making were extracted from the peer-reviewed publications. This section lays out the body of evidence, as well as the results and findings, for each treatment comparisons that were available in the 10 studies included in the systematic review — that is, a total of 5 placebo or standard of care comparisons of ITP drugs used as subsequent-line treatment in patients who have had experience with prior ITP therapies.
Results
Detailed outcome results for studies included in the narrative review are presented in Appendix 6 to Appendix 9.
Splenectomy
Among the studies identified for inclusion in the NMA, 8 studies reported the proportion of patients splenectomized at baseline. Only 1 study reported cohort-specific outcomes for splenectomized and nonsplenectomized groups.11 Four studies reported splenectomy as an outcome on its own or within a composite outcome.9,32 No studies were identified to draw conclusions on the place of splenectomy in second-line therapies.
Economic Analysis
Economic Evaluation
The intended economic evaluation was to address the following research questions:
What is the cost-effectiveness of therapies in adult patients with ITP who have failed first-line treatments?
What is the cost-effectiveness of splenectomy compared with second-line therapies (rituximab, fostamatinib, or TPO-RA [romiplostim, eltrombopag, avatrombopag]) in adult patients with ITP?
Primary Economic Analysis
Given the findings from the CADTH clinical review, conclusions regarding the comparative clinical effects of treatments could not be drawn. As such, a primary economic evaluation could not be conducted due to both evidence gaps and limitations with the existing clinical evidence. Specifically, the disease trajectory of patients with ITP across different treatments could not be modelled due to limited and heterogeneous treatment-specific response data; heterogeneity across studies in the definition of treatment response thresholds, bleeding, and other adverse outcomes; and limited information on the time-dependent risk of bleeding events across treatments. Further, both baseline characteristics for patients with ITP and the measurement of outcomes of interest on standard or care treatment within a Canadian context were lacking.
Because CADTH conducted a scoping exercise for the economic evaluation, Appendix 11 provides a review of existing published decision-analytic models in this clinical area, an in-depth discussion of the limitations of the current evidence that precludes the conduct of an economic evaluation but can help inform areas for further research, and, a proposed structure for the “ideal” decision-analytic model that would be able to address the above research questions, highlighting the potential model inputs required and data gaps that would need to be resolved.
Discussion
Summary of Evidence
The aim of this HTA was 2-fold: to determine what treatment(s) should be used in adult patients with ITP who have failed first-line treatment, and to establish the place in second-line therapy of splenectomy in adult patients with ITP. The project scope and research protocol were informed by engaging with patient groups to better understand the challenges associated with ITP and current treatments. A total of 15 publications met the final inclusion criteria, reporting findings from 10 unique trials on the use of subsequent-line ITP treatments. No study with comparisons to splenectomy could be identified from the literature search.
Patients were eligible for inclusion in the studies if they were adults with a newly diagnosed, persistent, or chronic ITP, with a platelet count of less than 30 × 109/L. Four RCTs compared eltrombopag to placebo over a minimum of 6 weeks, 1 RCT compared avatrombopag to placebo over 26 weeks, and 3 RCTs compared romiplostim to placebo or standard of care. Two RCTs evaluated interventions other than TPO-RA, including 1 comparing rituximab to placebo over 4 weeks and 1 comparing fostamatinib to placebo over 26 weeks. Trials permitted concomitant use of other ITP medications including corticosteroids, azathioprine, and danazol. The primary efficacy outcome was platelet count response; however, there were several differences across the included trials in the way that platelet count response was defined, measured, and reported.
A feasibility assessment determined that an NMA of RCTs was not feasible due to clinical heterogeneity between studies and methodological constraints. An alternate NMA with simplified assumptions based on the limitations of the network was conducted and results were not deemed informative. For these reasons, conclusions from the NMA could not be drawn. Rather, a narrative synthesis of the evidence was conducted for the included studies.
The risk of bias across the 10 studies ranged from low9-11 to high.12-15 An overall limitation of the included trials was the small sample size, which limited the level of precision and affected the certainty in the findings. The study populations were generalizable to most ITP patients, bearing in mind that there were likely differences in local background standard of care treatments across the various countries where the studies were performed. Baseline characteristics between treatment groups were balanced in most cases, with few trials having baseline imbalances that could have introduced bias.13,25 Study discontinuation rates were significant in some studies.12,15 Finally, the concomitant use of other ITP medications, likely to be a significant confounding factor, was not always reported in publications, which could affect the interpretation of the findings.
Eltrombopag
In patients with prior ITP treatment, 4 RCTs found that eltrombopag was superior to placebo at generating a long-lasting platelet count response (at least 6 weeks and up to 6 months), reducing bleeding events, and improving HRQoL. Eltrombopag was associated with a reduced need for rescue medication and concomitant ITP medications compared to placebo, including corticosteroids. Eltrombopag appeared to be well tolerated in the studies and no strong safety signal was identified.
Romiplostim
In patients who have experience with prior ITP therapies, 3 RCTs found that romiplostim induced a platelet count response compared to placebo or standard of care. Romiplostim also reduced the need for rescue medication and was associated with improvements in HRQoL compared with placebo and standard of care. Although romiplostim was generally well tolerated, there were inconsistencies in the harm profiles across studies.
Avatrombopag
In patients who have experience with prior ITP therapies, avatrombopag was assessed in a single, small, placebo-controlled study that had a high risk of bias, which contributed to a high level of uncertainty and limited the conclusions that could be drawn from this trial.
Rituximab
In patients with primary ITP who failed a short course of corticosteroid therapy, 1 RCT with a moderate risk of bias evaluated treatment failure (i.e., the absence of platelet response) in those receiving either rituximab or placebo. However, the a priori defined threshold for statistical significance for treatment failure was not met, limiting the conclusions that could be drawn from the trial.
Fostamatinib
In patients who have experience with prior ITP therapies, 1 RCT with a high risk of bias found that fostamatinib was associated with a higher proportion of patients with stable platelet response compared to placebo. However, the magnitude of the treatment response appeared low and discontinuation rates were high.
Interpretation of Clinical Results
The systematic review was undertaken at the request of public drug plans to determine the efficacy and safety of therapies in adult patients with ITP who have failed first-line treatments. In consulting with patient groups, patients with ITP expressed a desire for more accessibility to additional therapies for ITP and a desire to avoid splenectomy.
A narrative synthesis of the trials identified in the systematic review found that eltrombopag and romiplostim increased platelet count response and demonstrated an improvement in symptoms and quality of life compared to placebo. Interpretation of the effectiveness of avatrombopag, rituximab, and fostamatinib were inconclusive due to the limited availability of evidence (i.e., 1 single trial for each intervention with varying risks of bias). Due to a scarcity of evidence, conclusions could not be drawn about the outcomes of time to platelet response, time to treatment failure, emergency department visits, hospitalization, and treatment-free remission.
No head-to-head study was identified, and the trials included in the systematic review were limited to comparisons to placebo or standard of care. In addition, methodological consideration prevented an NMA from being conducted. As such, direct comparisons of effectiveness between ITP treatments cannot be made. Similarly, there was insufficient evidence to inform the efficacy or sequence of subsequent-line therapies in subgroups of adult patients with ITP or the role of splenectomy in the sequency of subsequent-line therapies.
A de novo economic model could not be conducted due to various clinical data gaps; therefore, the comparative cost-effectiveness of treatments for ITP remains unknown.
Strengths and Limitations of the Systematic Review
Strengths
The systematic review was developed using robust methodology. The research protocol was developed a priori and registered with the PROSPERO database, and a detailed scoping plan was posted publicly for stakeholder input. Input from those with lived experience was used to inform the research protocol. The literature search was comprehensive and was also publicly posted for stakeholder feedback.
Evidence collection, data extraction, and evaluation of the quality of the studies were completed by a single reviewer, with verification by a second. Conflicts in data collection were adjudicated by a third reviewer. Heterogeneity across trials was assessed and the analytical approach for the NMA was aligned with ISPOR guidelines and employed a standard methodology.
Limitations
Following an NMA feasibility analysis, it was determined that an alternate and more simplified NMA be conducted. The number of trials that contributed to the NMA was limited and results reported were highly heterogeneous. Due to the limited size of the network, it was not possible to adequately account for the level of heterogeneity, and as a result, the variation around estimated effects were extremely wide and generally not informative. Thus, we were unable to use the findings of the NMA to draw conclusions for the report. The narrative review was based on limited availability of evidence, including single trials with low sample sizes for avatrombopag, rituximab, and fostamatinib.
Interpretation of Economic Evaluation
Given that an economic model could not be conducted due to various clinical data gaps, the comparative cost-effectiveness of treatments for ITP is unknown.
Conclusions and Implications for Decision-Making or Policy-Making
Public drug plans may consider revisiting reimbursement criteria for eltrombopag and romiplostim when used in ITP. CADTH suggests that interested jurisdictions request an implementation advice panel to suggest strategies (e.g., discontinuation criteria) to manage the clinical and economic uncertainty identified in the report. Outlining what specific discontinuation criteria should be considered is beyond the scope of this report.
Patients with ITP expressed a desire to avoid surgery (splenectomy) and the side effects associated with long-term steroid use. Patients also voiced a desire to see different types of therapies accessible to patients in Canada, including avatrombopag, fostamatinib, eltrombopag, romiplostim, and rituximab.
To determine what treatment(s) should be used in adult patients with ITP who have failed first-line treatments, a systematic review of the efficacy of treatments was undertaken at the request of public drug plans. A narrative review of 15 publications, reporting findings from 10 RCTs, found that eltrombopag and romiplostim increased platelet count response and improved ITP symptoms and HRQoL compared to placebo. Interpretation of the effectiveness of avatrombopag, rituximab, and fostamatinib was inconclusive due to limited evidence (i.e., 1 single trial for each intervention, with varying risks of bias). Of note, recently, CADTH recommended that fostamatinib not be reimbursed for the treatment of thrombocytopenia in adult patients with chronic ITP who have had an insufficient response to other treatments.33 Avatrombopag for the treatment of thrombocytopenia in adult patients with chronic ITP who have had an insufficient response to a previous treatment is currently under CADTH Reimbursement Review.34
Due to the scarcity of evidence, conclusions could not be drawn about the outcomes of emergency department visits, hospitalizations, or treatment-free remission for any of the interventions. No direct treatment comparisons were identified, and methodological consideration prevented an NMA from being conducted; therefore, direct comparisons of effectiveness between ITP treatments could not be made. Similarly, there was insufficient evidence to inform the efficacy or sequence of subsequent-line therapies in specific subgroups of adult patients with ITP or the place in therapy of splenectomy. The comparative cost-effectiveness of treatments for ITP is unknown; further research is needed to compensate for clinical data gaps to inform an appropriate and relevant economic evaluation.
References
1.Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386-2393. Medline PubMed
2.Provan D, Stasi R, Newland AC, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010;115(2):168-186. Medline PubMed
3.Neunert C, Lim W, Crowther M, et al. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood. 2011;117(16):4190-4207. Medline PubMed
4.Michel M. Immune thrombocytopenia nomenclature, consensus reports, and guidelines: what are the consequences for daily practice and clinical research? Semin Hematol. 2013;50 Suppl 1:S50-54. Medline PubMed
5.Terrell DR, Beebe LA, Vesely SK, Neas BR, Segal JB, George JN. The incidence of immune thrombocytopenic purpura in children and adults: A critical review of published reports. Am J Hematol. 2010;85(3):174-180. Medline PubMed
6.Kuhne T, Berchtold W, Michaels LA, et al. Newly diagnosed immune thrombocytopenia in children and adults: a comparative prospective observational registry of the Intercontinental Cooperative Immune Thrombocytopenia Study Group. Haematologica. 2011;96(12):1831-1837. Medline PubMed
7.Schifferli A, Holbro A, Chitlur M, et al. A comparative prospective observational study of children and adults with immune thrombocytopenia: 2-year follow-up. Am J Hematol. 2018;93(6):751-759. Medline PubMed
8.Neunert C, Terrell DR, Arnold DM, et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3(23):3829-3866. Medline PubMed
9.Yang R, Li J, Jin J, et al. Multicentre, randomised phase III study of the efficacy and safety of eltrombopag in Chinese patients with chronic immune thrombocytopenia. Br J Haematol. 2017;176(1):101-110. Medline PubMed
10.Cheng G, Saleh MN, Marcher C, et al. Eltrombopag for management of chronic immune thrombocytopenia (RAISE): a 6-month, randomised, phase 3 study. Lancet. 2011;377(9763):393-402. Medline PubMed
11.Kuter DJ, Bussel JB, Lyons RM, et al. Efficacy of romiplostim in patients with chronic immune thrombocytopenic purpura: a double-blind randomised controlled trial. Lancet. 2008;371(9610):395-403. Medline PubMed
12.Jurczak W, Chojnowski K, Mayer J, et al. Phase 3 randomised study of avatrombopag, a novel thrombopoietin receptor agonist for the treatment of chronic immune thrombocytopenia. Br J Haematol. 2018;183(3):479-490. Medline PubMed
13.Shirasugi Y, Ando K, Miyazaki K, et al. Romiplostim for the treatment of chronic immune thrombocytopenia in adult Japanese patients: a double-blind, randomized Phase III clinical trial. Int J Hematol. 2011;94(1):71-80. Medline PubMed
14.Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. Medline PubMed
15.Bussel J, Arnold DM, Grossbard E, et al. Fostamatinib for the treatment of adult persistent and chronic immune thrombocytopenia: Results of two phase 3, randomized, placebo-controlled trials. Am J Hematol. 2018;93(7):921-930. Medline PubMed
16.Swinkels M, Rijkers M, Voorberg J, Vidarsson G, Leebeek FWG, Jansen AJG. Emerging Concepts in Immune Thrombocytopenia. Front Immunol. 2018;9(880). Medline
17.Despotovic JM, Grimes AB. Pediatric ITP: is it different from adult ITP? Hematology Am Soc Hematol Educ Program. 2018;2018(1):405-411. Medline PubMed
18.Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22):3780-3817. Medline PubMed
19.Nazaryan H, Liu Y, Sirotich E, Duncan J, Nazy I, Arnold D. Second-line therapy for immune thrombocytopenia: real-world experience in Canada. Can J Gen Intern Med. 2020;15(4):28-35.
20.Perras C, Sirotich E, Mbuagbaw L, et al. Treatment of adult patients with immune thrombocytopenia after failure of first-line therapies (CRD42021276565). PROSPERO: International prospective register of systematic reviews. York (GB): University of York Centre for Reviews and Dissemination; 2021: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=276565. Accessed 2022 Nov 23.
21.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Medline
22.Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777-784. Medline PubMed
23.Jansen JP, Fleurence R, Devine B, et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision-making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health. 2011;14(4):417-428. Medline PubMed
24.Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. Medline PubMed
25.Tomiyama Y, Miyakawa Y, Okamoto S, et al. A lower starting dose of eltrombopag is efficacious in Japanese patients with previously treated chronic immune thrombocytopenia. J Thromb Haemost. 2012;10(5):799-806. Medline PubMed
26.Liu X, Hou M, Li J, et al. Efficacy and safety of eltrombopag in Chinese patients with chronic immune thrombocytopenia: stage 2 results from a multicenter phase III study. Platelets. 2022;33(1):82-88. Medline PubMed
27.Bussel JB, Arnold DM, Boxer MA, et al. Long-term fostamatinib treatment of adults with immune thrombocytopenia during the phase 3 clinical trial program. Am J Hematol. 2019;94(5):546-553. Medline PubMed
28.George JN, Mathias SD, Go RS, et al. Improved quality of life for romiplostim-treated patients with chronic immune thrombocytopenic purpura: results from two randomized, placebo-controlled trials. Br J Haematol. 2009;144(3):409-415. Medline PubMed
29.Gernsheimer TB, George JN, Aledort LM, et al. Evaluation of bleeding and thrombotic events during long-term use of romiplostim in patients with chronic immune thrombocytopenia (ITP). J Thromb Haemost. 2010;8(6):1372-1382. Medline PubMed
30.Sanz MA, Aledort L, Mathias SD, Wang X, Isitt JJ. Analysis of EQ-5D scores from two phase 3 clinical trials of romiplostim in the treatment of immune thrombocytopenia (ITP). Value Health. 2011;14(1):90-96. Medline PubMed
31.Kuter DJ, Mathias SD, Rummel M, et al. Health-related quality of life in nonsplenectomized immune thrombocytopenia patients receiving romiplostim or medical standard of care. Am J Hematol. 2012;87(5):558-561. Medline PubMed
32.Ghanima W, Khelif A, Waage A, et al. Rituximab as second-line treatment for adult immune thrombocytopenia (the RITP trial): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2015;385(9978):1653-1661. Medline PubMed
33.CADTH reimbursement recommendation: fostamatinib (Tavalisse). Can J Health Technol. 2022;2(4). https://canjhealthtechnol.ca/index.php/cjht/article/view/sr0701. Accessed 2022 Nov 2.
34.CADTH. Avatrombopag. 2022: https://www.cadth.ca/avatrombopag. Accessed 2022 Nov 2.
35.Harbord RM, Egger M, Sterne JA. A modified test for small‐study effects in meta‐analyses of controlled trials with binary endpoints. Stat Med. 2006;25(20):3443-3457. Medline PubMed
36.White IR, Barrett JK, Jackson D, Higgins JPT. Consistency and inconsistency in network meta-analysis: model estimation using multivariate meta-regression. Res Synth Methods. 2012;3(2):111-125. Medline PubMed
37.Gagnier JJ, Morgenstern H, Altman DG, et al. Consensus-based recommendations for investigating clinical heterogeneity in systematic reviews. BMC Med Res Methodol. 2013;13:106-106. Medline PubMed
38.Shim S, Yoon BH, Shin IS, Bae JM. Network meta-analysis: application and practice using Stata. Epidemiol Health. 2017;39:e2017047. Medline PubMed
39.White IR. Network meta-analysis. Stata J. 2015;15(4):951-985. Medline PubMed
40.Higgins J, Jackson D, Barrett J, Lu G, Ades A, White I. Consistency and inconsistency in network meta‐analysis: concepts and models for multi‐arm studies. Res Synth Methods. 2012;3(2):98-110. Medline PubMed
41.Brignardello-Petersen R, Murad MH, Walter SD, et al. GRADE approach to rate the certainty from a network meta-analysis: avoiding spurious judgments of imprecision in sparse networks. J Clin Epidemiol. 2019;105:60-67. Medline PubMed
42.Chaimani A, Salanti G. Visualizing assumptions and results in network meta-analysis: the network graphs package. Stata J. 2015;15(4):905-950.
43.Jurczak W, Chojnowski K, Mayer J, Jamieson B, Tian W, Allen LF. Avatrombopag demonstrates superiority to placebo for the treatment of chronic immune thrombocytopenic purpura in a phase 3, multicenter, randomized, double-blind, placebo-controlled trial. Hemasphere. 2018;2(280).
44.Allen R, Bryden P, Grotzinger KM, Stapelkamp C, Woods B. Cost-Effectiveness of Eltrombopag versus Romiplostim for the Treatment of Chronic Immune Thrombocytopenia in England and Wales. Value Health. 2016;19(5):614-622. Medline PubMed
45.Lee D, Thornton P, Hirst A, Kutikova L, Deuson R, Brereton N. Cost effectiveness of romiplostim for the treatment of chronic immune thrombocytopenia in Ireland. Appl Health Econ Health Policy. 2013;11(5):457-469. Medline PubMed
46.Tremblay G, Dolph M, Roy AN, Said Q, Forsythe A. The Cost-effectiveness of Eltrombopag for the Treatment of Immune Thrombocytopenia in the United States. Clin Ther. 2020;42(5):860-872 e868. Medline PubMed
47.Xie F, Blackhouse G, Assasi N, et al. Results of a model analysis to estimate cost utility and value of information for intravenous immunoglobulin in Canadian adults with chronic immune thrombocytopenic purpura. Clin Ther. 2009;31(5):1082-1091; discussion 1066-1088. Medline PubMed
48.Neunert C, Noroozi N, Norman G, et al. Severe bleeding events in adults and children with primary immune thrombocytopenia: a systematic review. J Thromb Haemost. 2015;13(3):457-464. Medline PubMed
49.Fernando SM, Qureshi D, Talarico R, et al. Intracerebral Hemorrhage Incidence, Mortality, and Association With Oral Anticoagulation Use: A Population Study. Stroke. 2021;52(5):1673-1681. Medline PubMed
50.Norgaard M, Jensen AO, Engebjerg MC, et al. Long-term clinical outcomes of patients with primary chronic immune thrombocytopenia: a Danish population-based cohort study. Blood. 2011;117(13):3514-3520. Medline PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Cochrane Central Register of Controlled Trials (CCTR)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: July 23, 2021
Alerts: Monthly search updates until July 26, 2022
Search filters applied: Systematic reviews; meta-analyses; network meta-analyses; health technology assessments; guidelines; overview of reviews; randomized controlled trials; and controlled clinical trials.
Limits:
Humans
Language limit: English- and French-language
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.kw | Author keyword (Embase); keyword (CDSR) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
(romiplostim* or Nplate* or Romiplate* or amg531 or amg 531 or amgen megakaryopoiesis protein 531 or GN5XU2DXKV).ti,ab,kf,kw,ot,hw,nm,rn.
(eltrombopag* or Revolade* or Promacta* or Elbonix* or SB-497115 or SB497115 or SB-497-115 or SSS-20 or SSS20 or HSDB-8212 or HSDB8212 or S56D65XJ9G).ti,ab,kf,kw,ot,hw,nm,rn.
(avatrombopag* or Doptelet* or AKR 501 or AKR501 or E 5501 or E5501 or AS 1670542 or AS1670542 or YM 477 or YM477 or 3H8GSZ4SQL or GDW7M2P1IS).ti,ab,kf,kw,ot,hw,nm,rn.
(((thrombopoietin or TPO) adj2 (receptor agonist* or RA or RAs)) or TPORA or TPORAS).ti,ab,kf,kw.
Rituximab/ or (rituximab* or Rituxan* or Truximab* or MabThera* or Mab Thera* or Truxima* or blitzima* or reditux* or ritemvia* or rituxin* or rituzena* or rixathon* or riximyo* or truxella* or HSDB 7455 or HSDB7455 or IDEC-102 or IDEC102 or IDEC-C2B8 or IDECC2B8 or PF-05280586 or PF05280586 or RO-452294 or RO452294 or RG-105 or RG105 or CT-P10 or CTP10 or 4F4X42SYQ6).ti,ab,kf,kw,ot,hw,nm,rn.
(fostamatinib* or Tavalisse* or Tavlesse* or R935788 or R788 or R-788 or SQ8A3S5101 or 86EEZ49YVB or X9417132K8 or R 406 or R406 or R950091 or R 950091 or tamatinib fosdium).ti,ab,kf,kw,ot,hw,nm,rn.
Splenectomy/ or (splenectom* or (spleen* adj2 (removal or resection))).ti,ab,kf,kw.
((secondary or tertiary or failure or failed) adj3 (therap* or treatment*)).ti,ab,kf,kw.
(second-line or secondline or third-line or thirdline).ti,ab,kf,kw.
or/1-9
Purpura, thrombocytopenic/ or idiopathic thrombocytopenic purpura/
((autoimmune* or immun* or idiopathic* or purpur*) adj2 thrombocytop*).ti,ab,kf,kw.
(Werlhof disease* or morbus werlhof*).ti,ab,kf,kw.
ITP.ti,ab,kf,kw.
11 or 12 or 13 or 14
10 and 15
16 use cctr
16 use medall
*romiplostim/ or (romiplostim* or Nplate* or Romiplate* or amg531 or amg 531 or amgen megakaryopoiesis protein 531 or GN5XU2DXKV).ti,ab,kw,dq.
*eltrombopag/ or (eltrombopag* or Revolade* or Promacta* or Elbonix* or SB-497115 or SB497115 or SB-497-115 or SSS-20 or SSS20 or HSDB-8212 or HSDB8212).ti,ab,kw,dq.
*avatrombopag/ or (avatrombopag* or Doptelet* or AKR 501 or AKR501 or E 5501 or E5501 or AS 1670542 or AS1670542 or YM 477 or YM477 or 3H8GSZ4SQL or GDW7M2P1IS).ti,ab,kw,dq.
(((thrombopoietin or TPO) adj2 (receptor agonist* or RA or RAs)) or TPORA or TPORAS).ti,ab,kw,dq.
*rituximab/ or (rituximab* or Rituxan* or Truximab* or MabThera* or Mab Thera* or Truxima* or blitzima* or reditux* or ritemvia* or rituxin* or rituzena* or rixathon* or riximyo* or truxella* or HSDB 7455 or HSDB7455 or IDEC-102 or IDEC102 or IDEC-C2B8 or IDECC2B8 or PF-05280586 or PF05280586 or RO-452294 or RO452294 or RG-105 or RG105 or CT-P10 or CTP10 or 4F4X42SYQ6).ti,ab,kw,dq.
*fostamatinib/ or (fostamatinib* or Tavalisse* or Tavlesse* or R935788 or R788 or R-788 or SQ8A3S5101 or 86EEZ49YVB or X9417132K8 or R 406 or R406 or R950091 or R 950091 or tamatinib fosdium).ti,ab,kw,dq.
Splenectomy/ or (splenectom* or (spleen* adj2 (removal or resection))).ti,ab,kw,dq.
((secondary or tertiary or failure or failed) adj3 (therap* or treatment*)).ti,ab,kw,dq.
(second-line or secondline or third-line or thirdline).ti,ab,kw,dq.
or/19-27
thrombocytopenic purpura/ or idiopathic thrombocytopenic purpura/
((autoimmune* or immun* or idiopathic* or purpur*) adj2 thrombocytop*).ti,ab,kw,dq.
(Werlhof disease* or morbus werlhof*).ti,ab,kw,dq.
ITP.ti,ab,kw,dq.
or/29-32
28 and 33
34 use oemezd
(conference abstract or conference review).pt.
35 not 36
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
“Randomized Controlled Trial (topic)”/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
“Controlled Clinical Trial (topic)”/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf,kw.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf,kw.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf,kw.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf,kw.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(pragmatic study or pragmatic studies).ti,ab,hw,kf,kw.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf,kw.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(phase adj3 (III or “3”) adj3 (study or studies or trial*)).ti,hw,kf,kw.
or/38-68
(systematic review or meta-analysis).pt.
meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or “meta analysis (topic)”/ or “systematic review (topic)”/ or exp technology assessment, biomedical/ or network meta-analysis/
((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf,kw.
((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf,kw.
((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf,kw.
(data synthes* or data extraction* or data abstraction*).ti,ab,kf,kw.
76 (handsearch* or hand search*).ti,ab,kf,kw.
(mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf,kw.
(met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf,kw.
(meta regression* or metaregression*).ti,ab,kf,kw.
(meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw.
(medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw.
(cochrane or (health adj2 technology assessment) or evidence report).jw.
(comparative adj3 (efficacy or effectiveness)).ti,ab,kf,kw.
(outcomes research or relative effectiveness).ti,ab,kf,kw.
((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf,kw.
[(meta-analysis or systematic review).md.]
(multi* adj3 treatment adj3 comparison*).ti,ab,kf,kw.
(mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf,kw.
umbrella review*.ti,ab,kf,kw.
(multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kw,kf.
(multiparamet* adj2 evidence adj2 synthesis).ti,ab,kw,kf.
(multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kw,kf.
or/70-92
69 or 93
18 and 94
37 and 94
17 or 95 or 96
limit 97 to (english or french)
remove duplicates from 98
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | ITP or immune thrombocytopenia]
WHO ICTRP
International Clinical Trials Registry Platform, produced by WHO. Targeted search used to capture registered clinical trials.
[Search terms -- ITP or immune thrombocytopenia]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- ITP or immune thrombocytopenia]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- ITP or immune thrombocytopenia]
Grey Literature
Search dates: August 9 to 15, 2021, July 26, 2021.
Keywords: ITP or immune thrombocytopenia
Limits: none
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
The complete search archive of sites consulted for this report is available on request.
Appendix 2: Statistical Analysis Plan
Note that this appendix has not been copy-edited.
Objectives
The aim of this HTA to inform 2 policy questions:
What treatment(s) should be used in adult patients with immune thrombocytopenia who have failed first-line treatments?
What is the place in second-line therapy of splenectomy in adult patients with immune thrombocytopenia?
The objective is to review the available evidence on the use of therapies for ITP in adults with the objective of determining their comparative effectiveness.
The project will address the following research questions. Details on the specific interventions and outcomes are included in the selection criteria (See Protocol Table 2: Selection criteria).
What is the efficacy and safety of therapies in adult patients with immune thrombocytopenia who have failed first-line treatments?
What is the efficacy and safety of splenectomy compared with second-line therapies (rituximab, fostamatinib, or TPO-RAs [romiplostim, eltrombopag, avatrombopag]) in adult patients with immune thrombocytopenia?
Study Population
The study population are adult patients with ongoing active immune thrombocytopenia who have failed first-line treatments. Among the trials that meet the eligibility criteria (See Protocol Table 2: Selection criteria), data will be grouped according to the following patient characteristics and used for subgroup analyses.
Adult patients with chronic ITP (> 12 months)
Adult patients with persistent ITP (between 3 to 12 months)
Patients who have previously failed at least 1 second-line therapy.
For studies including more than 1 of these subpopulations, with no subgroup analysis reported, the study will be considered to belong to 1 of these subgroups if 80% of more of the enrolled patients belong to that subgroup.
Interventions and Comparators
Intervention and comparators of interest will include all drugs specified here or belonging to the overall drug category specified here:
Rituximab
Eltrombopag
Romiplostim
Fostamatinib
Avatrombopag
Corticosteroids
IVIG
Immunosuppressants (e.g., azathioprine, cyclosporine, cyclophosphamide, mycophenolate mofetil, danazol, dapsone)
Splenectomy
Placebo/ standard of care
We will include studies reporting the standard doses of the treatment approved by Health Canada and doses considered of clinical relevance based on expert guidance or international clinical practice guidelines. All data on dosages and treatment duration for each included treatment will be reported.
In cases where there are variations in the dose or dosing schedule of 1 treatment across different studies, we will seek published literature to inform on the effect of such variations. In cases where no published literature is satisfactory, the clinical expert opinion on whether these differences are substantial enough to be a treatment effect modifier, in which case they will be analyzed as separate interventions. However, if dose and dosing schedule differences do not represent a substantial treatment difference in the opinion of the clinical expert, then they will be pooled together as a single intervention. In cases of a pooled treatment with variations in the dose or dosing schedule, a subsequent sensitivity analysis will be conducted to determine the effect of the pooling.
Any follow-up period without active intervention or open-label extension phase where all patients receive the same intervention will not be eligible for analysis.
Outcomes
Clinical Effectiveness Outcomes
Platelet Count Response
The proportion of patients with complete response, response, or no response as defined by the authors. We will also consider the mean difference in platelet count.
Time to Platelet Response
Time from starting treatment to time of achievement of complete response or response.
Bleeding Events
The proportion of patients with bleeding events.
Emergency Room Visits
Number of emergency room visits for ITP-related clinical problem per patient.
Hospitalization
Number of hospitalizations for ITP-related clinical problem per patient.
Health-Related Quality of Life
The assessment of quality of life using any relevant metric will be eligible for analysis if an aggregate score is provided that represents the change from baseline to the end of treatment in the intervention groups. Domain-specific scores will not be eligible for analysis. Disease-specific measures will not be pooled with generic measures. Total scores will be converted to standardized mean differences and analyzed as a continuous outcome.
Symptoms (E.g., Fatigue)
The proportion of patients with fatigue as reported by the authors or mean difference in fatigue scores.
Treatment-Free Remission
The proportion of patients with treatment-free remission
Need for Rescue Medication:
The proportion of patients who are given rescue medication, i.e., IVIG or corticosteroids.
Reduction or Discontinuation of Corticosteroids:
The proportion of patients who reduce or discontinue their corticosteroid use.
Safety
Adverse Events
Proportion of patients reported to have any AEs.
Serious AEs
Proportion of patients reported to have any serious AEs. Serious AEs as defined by the authors of the study or when a patient dies, has a life-threatening event, is hospitalized, or experiences disability or permanent damage.
Withdrawal Due to AEs
Proportion of patients reported to have withdrawn from the study due to AEs.
Death
Proportion of patients who die during the study.
Check the Quality of Evidence
Risk of bias in the individual trials will be assessed using the Cochrane risk of bias 2 (RoB 2) tool.24 Risk of bias assessments will be completed in duplicate for each trial. The RoB 2 tool can be used to assess bias arising from the randomization process, due to deviations from intended interventions, due to missing outcome data, measurement of the outcome, and bias in selection of the reported results. For each of these domains, a judgment of high risk of bias (the study is judged to be at high risk of bias in at least 1 domain or some concerns for multiple domains), some concerns (the study is judged to raise some concerns in at least 1 domain, but not at high risk of bias for any domain) or low risk of bias (the study is judged to be at low risk of bias from all domains) can be made. An assessment will be conducted separated for each outcome, and an overall risk of bias will be reached using the signalling questions algorithm included in the tool. We do not anticipate including any crossover or cluster RCTs. If we find any crossover or cluster trials, we will only use estimates that account for the correlation between participants in cluster trials and within participants in crossover trials. For each trial, the estimate regarding the effect of randomization i.e., ITT (as opposed to the effect of adhering to the intervention i.e., per protocol) will be considered. The results of these assessments will be displayed using the robvis tool for visualizing risk of bias. Overall risk of bias will be used as the basis for sensitivity analyses in which we will drop the studies at high risk of bias and examine how this affects the results.
In addition to searching for unpublished and ongoing studies, we will investigate small-study effects using Harbord’s test for binary outcomes and Egger’s test for continuous outcomes. 35 We will also inspect the network funnel plot for asymmetry.
Construct Evidence Network
The evidence network for each outcome will be displayed graphically as a network plot. The lines will indicate direct comparisons and the thickness of the line will reflect the number of studies in each comparison. The vertices (“nodes”) will represent individual interventions. Sizes of nodes will be directly proportional to the total sample size of participants contributing data to the node across all studies involving that intervention.
Datasets
A standardized excel extraction sheet is piloted to abstract data from included studies. Modification to the extraction sheet will be conducted after a pilot of 5 studies. The data extraction will cover information pertaining to each study overall publication characteristics, study design, intervention, comparators, patients’ characteristics, outcomes definitions, outcomes results, and AEs.
The primary publication for each unique study included will be used for data extraction, except where multiple publications for a single primary study are found. Multiple publications for a unique study (e.g., substudies, reports of additional outcomes or longer follow-up) will be used if they include data relevant to our research question. The data will be entered as coming from the same study, but the related articles will be referenced as needed.
Where reported, patients’ baseline characteristics and clinical efficacy outcomes will be abstracted from the ITT population in each study while AEs will be abstracted from the per-protocol i.e., safety population. The ITT approach implies the availability of a complete dataset i.e., no missing data. If an ITT analysis is not reported in the paper, we will use the per-protocol analysis. We will conduct sensitivity analyses to determine if the analytical strategy used in the trial affects the effect estimates. Trial definitions for intention to treat, modified intention to treat, and per-protocol data will be noted and compared for consistency.
For dichotomous outcomes, we use the number of patients with the event and the total number of patients in each arm. For continuous outcomes, we will extract the mean, standard deviation, and number of participants in each arm. For time to event outcomes, we will extract the mean/median time to event, standard deviation and the number of participants per-arm (arm-based approach). If only comparative effect estimates are reported, the NMA can be conducted with generic measures of effect such as the log of the odds ratio and hazard ratio and the corresponding standard errors (contrast-based approach).36 For continuous outcomes, the standardized mean difference and its standard error can be used.
Screening, data extraction and risk of bias assessments will be conducted by 1 reviewer and verified by a second reviewer using a standardized data extraction form developed a priori, which will be piloted and modified as necessary.
The Feasibility Assessment of an NMA
Prior to commencing the NMA, a qualitative feasibility assessment will be undertaken to assess clinical and methodological heterogeneity in the available data. Trials included in the same evidence network will be compared to identify any potential heterogeneity based on differences in participants, interventions, comparisons, outcomes, or study design. If substantial heterogeneity exists in certain comparisons or subsets of studies and the data are not meaningful to pool, narrative summaries of findings will be reported, including the report on the types of trials required to fill the knowledge gap. Quantitative analyses will not be conducted where there is insufficient data.
Where potential clinical or methods-related heterogeneity is identified and the degree of heterogeneity is considered large, and if we have data on potential effect modifiers, we will use meta-regression (if there are 10 or more studies) to adjust for these sources of heterogeneity.37 If meta-regression is not possible, we will perform subgroup analyses or sensitivity analyses. Our process for assessing the feasibility of a NMA is outlined in Appendix 5. If the feasibility assessment is positive, we can continue to the next steps in this analysis plan. If feasibility assessment is negative, then we may summarize why the network is not sufficient to support a valid NMA.
Check Assumptions
Provided the NMA is deemed feasible, the identified network will be evaluated and tested for homogeneity.38 For each study in the network, the patient population, definitions of interventions, definitions of outcomes, inclusion and exclusion criteria, and designs will be described and examined for similarity across the network. Patient baseline characteristics for potential effect modifiers identified by clinical experts will be examined for homogeneity across studies.
We will observe the logical structure of the graphs i.e., whether direct evidence is similar to indirect evidence, and evaluate the fitness of the statistical models. We will also measure the confidence intervals of the difference between the direct and indirect comparisons. We will use the node-splitting method, which will allow us to assess consistency locally within each closed loop of the network. We will also run an overall (global) test for inconsistency using the Wald test. 39
We will use sensitivity analyses to determine the role of effect modifiers and meta regression to adjust for identified effect modifiers.
Statistical Models
The NMAs will be conducted under a Frequentist framework using the multivariate meta-analysis approach.39,40 Random-effects models will be used as the primary approach when feasible due to the anticipated clinical and methodological heterogeneity across studies. For sparse networks,41 fixed effects models will be considered when the available network for a given outcome is insufficient for estimating a random-effects model, i.e., the confidence intervals are inaccurate. For each NMA we will use the design-by-treatment model (global test) to assess network coherence, and the side-splitting method to assess loop specific coherence,40 computed as the difference between direct and indirect evidence. If there is large incoherence, we will use an inconsistency model to conduct the NMA.
The multivariate random-effects meta-analysis is estimated using restricted maximum likelihood that will be applied to arm-based or contrast-based data.36 The results will be presented as network plots, contribution plots, and league tables.42
If an NMA is not feasible. We will conduct a pairwise random-effects meta-analysis, comparing all available treatments to placebo or to the most common (i.e., reported in most studies) available comparison or the most relevant standard of care. If this alternative approach is also not informative a narrative synthesis will be conducted.
For binary outcomes, odds ratios and 95% confidence intervals will be reported. In cases when events are rare, the Peto odds ratio will be used. For continuous outcomes measured on the same scale, mean differences and 95% confidence intervals will be reported. For continuous outcomes measured on different scales, standardized mean differences and 95% confidence intervals will be reported. If insufficient data are found for conducting meta-analyses, narrative descriptions will be provided.
For the network or pairwise meta-analysis, we will conduct subgroup analyses comparing outcomes in trials belonging to the following subgroups:
Adult patients with chronic ITP (> 12 months)
Adult patients with persistent ITP (between 3 to 12 months)
Patients who have previously failed at least 1 second-line therapy
We will conduct additional sensitivity analysis by excluding studies with high risk of bias or studies with missing data to a relevant outcome. We will also explore the effect of outliers and influential trials by running models with and without them. All analyses will be conducted using Stata 16.0 (StataCorp, College Station, Texas, US). All comparisons will be 2 tailed using a threshold P ≤ 0.05.
Appendix 3: List of Included Studies
Note that this appendix has not been copy-edited.
Appendix 4: List of Excluded Studies During Data Extraction
Note that this appendix has not been copy-edited.
Table 7: List of Excluded Studies During Data Extraction
Author (year) NCT Number (If Available) | Reason for Exclusion |
|---|---|
Abdallah et al. (2021) | Intervention |
Zhou et al. (2015) | Intervention (rhTPO) |
Zaja et al. (2010) Hoffman-La Roche (2014) | Patient population (treatment naive) |
Cui et al. (2013) | Intervention (rhTPO) |
Gudbrandsdottir et al. (2013) | Patient population – includes treatment naive patients |
Wang et al. (2012) | Intervention (rhTPO) |
Li et al. (2011) | Patient population – includes treatment naive patients |
Jamali et al. (2009) | Regulatory approval summary - unable to identify referenced studies |
Newman et al. (2001) | Intervention |
Lang et al. (1987) | Study design |
Appendix 5: Network Meta-Analysis
Note that this appendix has not been copy-edited.
Prior to conducting an NMA, we performed a qualitative feasibility assessment to determine if the data were sufficiently similar to pool from a clinical and a methodological perspective. Clinical heterogeneity is concerned with the homogeneity in participants, interventions, comparisons, and outcomes, while methodological heterogeneity is concerned with the design and analysis.
Methodological Heterogeneity
While all the included studies were all phase III or IV two-arm parallel group randomized trials, we identified some design concerns. Three of the included studies were OL.14,15,43 The study durations ranged from 6 to 78 weeks. These differences on their own would not have precluded an NMA.
We noted some differences in how data were analyzed across some outcomes. For example, in some studies the same outcome was reported as hazard ratio and in others only figures were reported. In some instances, percentages were reported without numerators or denominators, thus precluding the estimation of variances.
Clinical Heterogeneity
Participant homogeneity was assured based on the inclusion criteria. All the studies met the inclusion criteria which included adult patents with ongoing active ITP who had failed first-line treatments.
Intervention and comparator homogeneity was ensured based on the inclusion criteria. All the included studies used either rituximab (100mg/m2/week, 375mg/m2/week), Eltrombopag (12.5mg once daily, 25mg once daily, 50mg once daily), Romiplostim (1mcg/kg qw, 3mcg/kg qw), Fostamatinib (100 mg bd) or Avatrombopag (20 mg once daily) compared to placebo or to each other. Placebo groups were uniform across studies.
There was considerable outcome heterogeneity. For example, platelet count response was defined at different thresholds (≥ 20,000, ≥ 30,000, ≥ 50,000 and ≥ 100,000 platelets/µl). Some studies reported more than 1 threshold, but even when we had multiple studies with the same threshold, the definitions were different. These differences included the number of measurements and the timing of the measurements. Three examples are shown below:
“Platelet counts ≥ 50 x 109 on at least 4 of the 6 clinic visits occurring every 2 weeks during weeks 14–24 inclusive”
“Proportion of patients with platelet counts ≥ 50 000/μL and at least twice the baseline amount”
“At least 1 platelet count ≥ 50 x 109 within first 12 weeks”
This heterogeneity was present for other outcomes such as bleeding, in which some studies used WHO-defined grades and others did not.
We attempted to pool all the studies with a threshold of ≥ 20,000 and ≥ 30,000 and found that the threshold impacted the relative effects of treatments (e.g., at higher thresholds, romiplostim was less likely to be better than placebo).
Other Issues
In addition to the concerns with heterogeneity noted above, the data were sparse i.e., we had too few comparisons per study and any attempts to create smaller more homogenous groups further aggravated the issue, leading to very wide confidence intervals. These wide confidence intervals produced results (most active treatments were not statistically significantly better than placebo) that were contradictory to the findings from the individual studies.
Further, consistency could not be estimated since there was limited direct evidence for the same comparison (almost all comparisons were treatments versus placebo) i.e., there were no closed loops.
Based on this, we concluded that the available data were not meaningful to pool and have presented narrative summaries of the findings. This decision is in line with recommended guidance for addressing feasibility in NMA and our statistical analysis plan.
Appendix 6: Summary Tables of Studies With Eltrombopag as Intervention
Note that this appendix has not been copy-edited.
Table 8: Details of Included Studies — Eltrombopag as Intervention (N = 4 Studies)
Criteria | Tomiyama et al. 2012 | Yang et al. 2017 | Bussel et al. 2009 | Cheng et al. 2011 |
|---|---|---|---|---|
Designs and Populations | ||||
Study Design | DB RCT | DB RCT | DB RCT | DB RCT |
Locations | Multicenter: Japan | Multicenter: China | Multicenter: 23 countries | Multicenter: Canada, US, UK, New-Zealand, Peru, Europe, Asia |
Randomized | n = 23 | n = 155 | n = 114 | n = 197 |
Place in Therapy | Subsequent-line treatment in patients who have failed one or more prior ITP therapies | Subsequent-line treatment in patients who have failed one or more prior ITP therapies | Subsequent-line treatment in patients who have failed one or more prior ITP therapies | Subsequent-line treatment in patients who have experience with prior ITP therapies |
Inclusion Criteria |
|
|
|
|
Exclusion Criteria |
|
|
|
|
Intervention | Eltrombopag 12.5 to 50 mg orally once daily for 6 weeks Dose depending on the platelet count response + standard of care | Eltrombopag 25 mg orally once daily for 8 weeks (start dose) Dose to be adjusted based on platelet count + standard of care | Eltrombopag 50 mg orally once daily for 6 weeks Dose up to 75 mg based on platelet count + standard of care | Eltrombopag 50 mg orally once daily for 6 months (start dose) Dose to be adjusted based on platelet count + standard of care |
Comparator(s) | DB PL orally once daily for 6 weeks + standard of care | DB PL orally once daily for 8 weeks + standard of care | DB PL orally once daily for 6 weeks + standard of care | DB PL orally once daily for 6 months + standard of care |
Concomitant Medications |
| Maintenance immunosuppressive therapy (stable dose for ≥ 1 month) | Chronic maintenance steroid or ITP therapy – including azathioprine, danazol, cyclosporine A, and mycophenolate mofetil (stable dose for ≥ 1 month) |
|
Duration | ||||
DB Phase | 6 weeks | 8 weeks (primary end point evaluated at week 6) | 6 weeks | 6 months |
OLE Phase | 6 months | 24 weeks | ¾ | ¾ |
Outcomes | ||||
Primary Outcome | Platelet count response Outcome measure: Number of responders at week 6 (defined as patients with platelet count ≥ 50 000/µL and £ 400 000/µL) | Platelet count response Outcome measure: Number of responders during week 6 (defined as patients with platelet count ≥ 50 000/µL) | Platelet count response Outcome measure: Proportion of responders after 6 weeks (defined as patients with platelet count ≥ 50 000/µL) | Platelet count response Outcome measure: Proportion of responders (platelet count between 50 000 and 400 000/µL) at each on-therapy day and 4 weeks after |
Secondary / Exploratory Outcomes |
|
|
|
|
Notes | ||||
Publications | Tomiyama et al. 201225 | Yang et al. 20179 Liu et al. 202026 | Bussel et al. 201927 | Cheng et al. 201110 |
AEs = adverse events; DB = double-blind; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue questionnaire; FACT-Th = Functional Assessment of Cancer Therapy – Thrombocytopenia questionnaire; HRQoL = health-related quality of life; ITP = immune thrombocytopenia; MEI-SF = Motivation and Energy Inventory – Short Form questionnaire; MI = myocardial infarction; NSAIDs = nonsteroidal anti-inflammatory drugs; OLE = open-label extension; PL = placebo; RCT = randomized controlled trial; SAEs = serious adverse events; SF-36v2 = Short Form – 36v2 questionnaire.
Table 9: Patient Characteristics — Eltrombopag as Intervention (N = 4 Studies)
Patient Characteristic | Tomiyama et al. 2012 | Yang et al. 2017 | Bussel et al. 2009 | Cheng et al. 2011 | ||||
|---|---|---|---|---|---|---|---|---|
Eltrombopag (N = 15) | Placebo (N = 8) | Eltrombopag (N = 104) | Placebo (N = 51) | Eltrombopag (N = 76) | Placebo (N = 38) | Eltrombopag (N = 135) | Placebo (N = 62) | |
Age, years | ||||||||
Mean (SD) | 53.7 (13.72) | 58.4 (11.72) | 44.7 (15.91) | 41.3 (12.83) | 51 (17) | 48 (16) | 46.5 (15.61) | 51.0 (14.72) |
Sex, n (%) | ||||||||
Female | 8 (53.3) | 7 (87.5) | 77 (74.0) | 40 (78.4) | 43 (57) | 27 (71) | 93 (69) | 43 (69) |
Male | 7 (46.7) | 1 (12.5) | 27 (26.0) | 11 (21.6) | 33 (43) | 11 (29) | 42 (31) | 19 (31) |
Race / Ethnicity, n (%) | ||||||||
Caucasian | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 58 (76) | 26 (68) | 101 (75) | 44 (71) |
Black | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1) | 0 | nr | |
Asian | 15 (100.0) | 8 (100.0) | 104 (100.0) | 51 (100.0) | nr | 21 (16) | 13 (21) | |
Other | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 17 (22) | 12 (32) | 13 (10) | 5 (8) |
Time since ITP diagnosis, years | ||||||||
Mean (SD) | nr | nr | nr | nr | ||||
Platelet count /µL | ||||||||
Median (IQR) | 21 000 (16 000 to 25 000) | 9 500 (7 500 to 19 000) | 14 000 (IQR nr) | 13 500 (IQR nr) | nr | 16 000 (8 000 to 22 000) | 16 000 (9 000 to 24 000) | |
Platelet count, n (%) | ||||||||
£ 15 000/µL | 3 (20.0) | 6 (75.0) | 54 (51.9) | 28 (54.9) | 38 (50) | 17 (45) | 67 (50) | 30 (49) |
> 15 000 /µL | 12 (80.0) | 2 (25.0) | 50 (48.1) | 23 (45.1) | 38 (50) | 21 (55) | 68 (50) | 32 (51) |
Concomitant ITP medication(s), n (%) | ||||||||
Yes | 12 (80) | 7 (88) | 53 (51.0) | 28 (54.9) | 32 (42) | 17 (45) | 63 (47) | 31 (50) |
Splenectomy, n (%) | ||||||||
Yes | 11 (73) | 5 (63) | 18 (17.3) | 7 (13.7) | 31 (41) | 14 (37) | 50 (37) | 21 (34) |
ITP = immune thrombocytopenia; IQR = interquartile range; nr = not reported; SD = standard deviation.
Table 10: Patient Disposition — Eltrombopag as Intervention (N = 4 Studies)
Category, n | Tomiyama et al. 2012 | Yang et al. 2017 | Bussel et al. 2009 | Cheng et al. 2011 | ||||
|---|---|---|---|---|---|---|---|---|
Eltrombopag | Placebo | Eltrombopag | Placebo | Eltrombopag | Placebo | Eltrombopag | Placebo | |
Randomized | 15 | 8 | 104 | 51 | 76 | 38 | 135 | 62 |
Completed | 14 | 8 | 100 | 49 | 52 | 30 | 112 | 55 |
Discontinued | 1 | 0 | 4 | 2 | 24 | 8 | 23 | 7 |
AEs | 1 | 0 | 2 | 1 | 3 | 2 | 13 | 4 |
Lack of efficacy | 0 | 0 | 0 | 1 | 0 | 3 | 1 | 0 |
Patient decision | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 2 |
Lost to follow- up | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 |
Protocol violation | 0 | 0 | 1 | 0 | 2 | 1 | 0 | 0 |
Platelet count > 200 000 /µL | 0 | 0 | 0 | 0 | 18 | 1 | 0 | 0 |
Other | 0 | 0 | 1 | 0 | 1 | 1 | 2 | 1 |
AE = adverse events.
Four DB RCTs evaluated eltrombopag compared to placebo.9,10,25,27 Detailed outcome results are presented in Table 8.
Outcomes Assessing Clinical Effectiveness
Platelet Count Response
The use of eltrombopag was associated with higher proportions of responders compared with placebo at week 6 in 3 trials (60% versus 0% respectively, p value not reported;25 58% versus 6% respectively, P < 0.001;9 and 59% versus 16% respectively, P < 0.001;27) as well as throughout 6 months in another trial (79% versus 28%, respectively; P < 0.0001).10 These were the primary outcome results in the studies, where response was mainly defined as a platelet count ≥ 50 000/µL, with slight variations across trials.
Other outcome measurements for platelet count response were included as secondary or exploratory outcomes with comparative data reported in 2 of these 4 studies.10,27 The use of eltrombopag was associated with a higher proportion of responders compared with placebo, that is, at any time over the 6-week period in 1 trial,27 and at ≥ 75% of the monthly assessments during the 6-month follow-up in the other trial.10
Bleeding Events
Comparative data for any bleeding events were reported in 3 studies according to the WHO bleeding scale.9,10,27 The use of eltrombopag was associated with fewer bleeding events compared with placebo in all 3 trials (OR 0.28; 95% CI 0.13 to 0.59; P < 0.001;9 39% versus 60% respectively, P = 0.029;27 79% versus 93% respectively, P < 0.00110).
Health-Related Quality of Life
HRQoL was assessed in 1 study using various scales.10 The use of eltrombopag was associated with greater improvements from baseline to week 26 compared to placebo in the FACT-Th questionnaire and in some of the SF-36v2 scales (physical role, vitality and emotional role subscales, as well as in the mental component summary score), supporting an improvement in HRQoL among patients treated with eltrombopag versus placebo. Greater improvements from baseline were also observed with eltrombopag compared with placebo in the SF-36v2 physical component summary, the MEI-FS and the FACIT-Fatigue questionnaires; however, statistical significance was not reached for these subscales. Detailed results are shown in Appendix 6. Caution is advised however when interpreting nonsignificant findings to draw conclusions regarding difference between groups in HRQoL.
Need for Rescue Medication
Two studies reported data pertaining to the use of rescue medications.9,10 In both trials, eltrombopag was associated with a smaller proportion of patients necessitating rescue treatments compared with placebo (9% versus 34% respectively, OR = 0.13 with 95% CI 0.05 to 0.37, P < 0.001;9 18% versus 40% respectively, OR = 0.33 with 95% CI 0.16 to 0.64; P = 0.00110). Rescue medications were defined similarly as either a new ITP medication, an increase in the dosage of a concomitant ITP medication, platelet transfusion, or splenectomy.9,10
Reduction or Discontinuation of Concomitant ITP Medication
Two studies assessed the reduction or discontinuation of concomitant ITP medication;9,10 however, comparative data were reported in only 1 of the 2 studies.10 Eltrombopag was associated with a reduction in the proportions of patients with reduction or discontinuation of ITP baseline treatments compared with placebo (59% versus 32%, respectively; OR = 3.10 with 95% CI 1.24 to 7.75; P = 0.02). The publication indicates that the drugs most frequently tapered or discontinued in both treatment groups were corticosteroids.
Other Prespecified Effectiveness Outcomes
No data were reported to inform on the effectiveness of eltrombopag versus placebo for the outcomes of time to platelet response, emergency department visits, hospitalization, patient-reported specific symptoms of ITP and treatment-free remission.
Outcomes Assessing Harms
Adverse Events
There was inconsistency across the 4 studies in the proportions of patients with at least 1 AE, which ranged from 25% to 92% across treatment groups. In 2 studies, a numerically higher proportion of patients in the eltrombopag group experienced AEs compared to patients in the placebo group.25,27 The proportions of patients experiencing AEs in the 2 other studies were relatively similar between treatment arms.9,10
Serious AEs
Two studies reported the proportions of patients experiencing serious adverse events (SAEs),9,25 which were less than 10% of patients per treatment arm. Only 1 trial reported the nature of the events; in this study, 1 patient receiving eltrombopag experienced a transient ischemic attack.25
Withdrawals Due to AEs
Discontinuations of study treatment due to AEs were reported in 3 trials.9,10,27 The proportions of patients who discontinued were less than 10% per treatment arm and differed between treatment arms only in 1 trial (9.6% with eltrombopag versus 6.6% with placebo).10
Mortality
Mortality was assessed as a harm outcome in the studies and therefore, is reported as such in this report. Three studies reported mortality data;9,10,27 overall, 2 patients in placebo groups died over the study period. The causes of death were undetermined or not individually reported.
Notable Harm: Infection
No data were reported to specifically inform on the comparative effectiveness of eltrombopag versus placebo for the outcome of infection, except for patient-reported AEs of some types of infections.
Table 11: Summary of Key Efficacy Outcomes — Eltrombopag as Intervention (N = 4 Studies)
Outcome | Tomiyama et al. 2012 | Yang et al. 2017 | Bussel et al. 2009 | Cheng et al. 2011 | ||||
|---|---|---|---|---|---|---|---|---|
Eltrombopag N = 15 | Placebo N = 8 | Eltrombopag N = 104 | Placebo N = 50 | Eltrombopag N = 74 | Placebo N = 38 | Eltrombopag N = 135 | Placebo N = 62 | |
Key Efficacy Outcomes | ||||||||
Primary outcome in trial | ||||||||
DB follow-up | 6 weeks | 6 weeks | 6 weeks | 6 months | ||||
Platelet count response | Proportions of responders at week 6 | Proportions of responders at week 6 | Proportions of responders after week 6 | Proportions of responders throughout 6 months | ||||
n (%) | 9 (60) | 0 (0) | 60 (58) | 3 (6) | 43 (59) | 6 (16) | 106 (79) | 17 (28) |
Between-group difference (95% CI) and p value | Absolute difference 0.6 (0.35 to 0.85) p nr | OR 26.08 (7.29 to 93.26) P < 0.001 | OR 9.61 (3.31 to 27.86) P < 0.001 | OR 8.2 (99% CI 3.59 to 18.73) P < 0.0001 | ||||
Secondary or exploratory outcomes in trial | ||||||||
Platelet count response | Proportions of responders throughout the trial | nr | Proportions of responders at any time | Proportions of responders at 3 75% of assessments | ||||
n (%) | 5 (33) | 0 (0) | nr | 51 (38) | 4 (7) | |||
Between-group difference (95% CI) and p value | nr | OR 8.79 (3.54 to 21.86) P < 0.001 | OR 10.53 (3.48 to 31.91) P < 0.0001 | |||||
Time to platelet count response | nr | nr | Median platelet count /µL on Day 15 | Median platelet count /µL - Range from Day 15 throughout treatment | ||||
Median (IQR) | nr | nr | 53 000 (IQR nr) | nr | Lowest: 53 000 (22 000 to 97 000) Highest: 73 500 (32 000 – 131 000) | Lowest: 17 500 (8 000 to 29 000) Highest: 23 000 (10 000 – 40 000) | ||
Bleeding | Proportions of patients with any bleeding symptoms | Any bleeding (WHO bleeding scale)a | Any bleeding (WHO bleeding scale)a | Any bleeding (WHO bleeding scale)a | ||||
Baseline, n (%) | 5 (33) | No change reported | 68 (65) | 36 (72) | nr | 47 (77) | 98 (73) | |
End of trial, n (%) | 2 (14) | 17 (16) | 17 (34) | 20 (39) | 18 (60) | 106 (79) | 56 (93) | |
Between-group difference (95% CI) and p value | nr | OR 0.28 (0.13 to 0.59) P < 0.001 | OR at any time 0.49 (0.26 to 0.89) P = 0.021 OR after 6 weeks 0.27 (0.09 to 0.88) P = 0.029 | OR 0.24 (0.16 to 0.38) P < 0.001 | ||||
Need for rescue medication | nr | Proportions of patients with rescue treatment | nr | Proportions of patients with rescue treatment | ||||
n (%) | 9 (9) | 17 (34) | 24 (18) | 25 (40) | ||||
Between-group difference (95% CI) and p value | OR 0.13 (0.05 to 0.37) P < 0.001 | OR 0.33 (0.16 to 0.64) P = 0.001 | ||||||
Concomitant ITP medication use | nr | nr | nr | Reduction or discontinuation of ITP baseline treatments | ||||
N patients with baseline ITP medication | N = 63 | N = 31 | ||||||
n (%) | 37 (59) | 10 (32) | ||||||
Between-group difference (95% CI) and p value | OR 3.10 (1.24 to 7.75) P = 0.02 | |||||||
HRQoL | nr | nr | nr | Improvement from baseline in HRQoL scores | ||||
Instrument | nr | nr | nr | SF-36v2 * Physical component summary | ||||
Mean change | nr | nr | nr | 1.8 | 0.3 | |||
Difference (95% CI); p value | nr | nr | nr | 1.3 (−0.2 to 2.9); P = 0.09 | ||||
Instrument | nr | nr | nr | SF-36v2 * Mental component summary | ||||
Mean change | nr | nr | nr | 1.7 | −0.6 | |||
Difference (95% CI); p value | nr | nr | nr | 2.1 (0.2 to 4.0); P = 0.03 | ||||
Instrument | nr | nr | nr | FACT-Th6 | ||||
Mean change | nr | nr | nr | 2.1 | 0.7 | |||
Difference (95% CI); p value | nr | nr | nr | 1.5 (0.5 to 2.5); P = 0.004 | ||||
Instrument | nr | nr | nr | MEI-SF | ||||
Mean change | nr | nr | nr | nr | ||||
Difference (95% CI); p value | nr | nr | nr | 3.3 (−0.6 to 7.3); P = 0.10 | ||||
Instrument | nr | nr | nr | FACIT-Fatigue | ||||
Mean change | nr | nr | nr | nr | ||||
Difference (95% CI); p value | nr | nr | nr | 1.6 (−0.2 to 3.5); P = 0.08 | ||||
DB = double-blind; CI = confidence interval; FACIT-F = Functional Assessment of Chronic Illness Therapy – Fatigue questionnaire; FACT-Th = Functional Assessment of Cancer Therapy – Thrombocytopenia questionnaire; HRQoL = health-related quality of life; IQR = interquartile range; MEI-SF = Motivation and Energy Inventory – Short Form questionnaire; nr = not reported; OR = odds ratio; SF-36v2 = Short Form – 36v2 questionnaire.
Note: There were greater improvements from baseline for patients receiving eltrombopag than for patients receiving placebo in the following SF-36v2 scales: physical role, vitality and emotional role (statistical significance reached).
aBleeding symptoms included WHO bleeding scale grades 1 to 4
Table 12: Summary of Key Harms Outcomes — Eltrombopag as Intervention (N = 4 Studies)
Outcome | Tomiyama et al. 2012 | Yang et al. 2017 | Bussel et al. 2009 | Cheng et al. 2011 | ||||
|---|---|---|---|---|---|---|---|---|
Eltrombopag | Placebo | Eltrombopag | Placebo | Eltrombopag | Placebo | Eltrombopag | Placebo | |
Key Harms Outcomes | ||||||||
Safety population | N = 15 | N = 8 | N = 104 | N = 51 | N = 76 | N = 38 | N = 135 | N = 61 |
Patients with ≥ 1 adverse events | ||||||||
n (%) | 11 (73) | 2 (25) | 66 (64) | 34 (67) | 45 (59) | 14 (37) | 118 (87) | 56 (92) |
Most common events, n (%) | Any AEs | Treatment-emergent AEs | Any AEs | Any AEs (in > 5% of patients) | ||||
Nasopharyngitis | 4 (27) | 0 (0) | nr | 5 (7) | 3 (8) | 14 (10) | 8 (13) | |
ALT increased | 3 (20) | 0 (0) | 7 (6.7) | 3 (5.9) | 2 (3) | 0 | 10 (7) | 4 (7) |
Headache | 1 (7) | 1 (13) | 3 (2.9) | 0 (0) | 6 (8) | 4 (11) | 41 (30) | 20 (33) |
AST increased | 1 (7) | 0 (0) | 6 (5.8) | 3 (5.9) | 2 (3) | 0 | 7 (5) | 2 (3) |
Blood bilirubin increased | 0 (0) | 0 (0) | 7 (6.7) | 0 (0) | nr | nr | ||
Hypokalemia | 0 (0) | 0 (0) | 4 (3.8) | 1 (2.0) | nr | nr | ||
Hemoglobin increased | nr | 3 (2.9) | 0 (0) | nr | nr | |||
Neutrophil count increased | nr | 3 (2.9) | 0 (0) | nr | nr | |||
Rash | nr | 3 (2.9) | 1 (2.0) | nr | nr | |||
Nausea | 1 (7) | 0 (0) | nr | 6 (8) | 0 (0) | 16 (12) | 4 (7) | |
Diarrhea | nr | nr | 4 (5) | 1 (3) | 17 (13) | 6 (10) | ||
Total protein increased | nr | nr | 3 (4) | 1 (3) | nr | |||
Vomiting | nr | nr | 4 (5) | 0 (0) | 10 (7) | 1 (2) | ||
Fatigue | 1 (7) | 0 (0) | nr | 3 (4) | 0 (0) | 13 (10) | 8 (13) | |
Myalgia | nr | nr | 3 (4) | 0 (0) | 8 (6) | 2 (3) | ||
Upper respiratory tract infection | nr | nr | nr | 14 (10) | 7 (11) | |||
Limb pain | nr | nr | nr | 9 (7) | 6 (10) | |||
Urinary tract infection | nr | nr | nr | 9 (7) | 4 (7) | |||
Arthralgia | 0 (0) | 0 (0) | nr | nr | 9 (7) | 3 (5) | ||
Oropharyngeal pain | nr | nr | nr | 9 (7) | 3 (5) | |||
Pharyngitis | nr | nr | nr | 8 (6) | 1 (2) | |||
Patients with ≥ 1 serious adverse events | ||||||||
n (%) | 1 (7) | 0 (0) | 5 (4.8) | 5 (9.8) | nr | nr | ||
Most common events, n (%) | ||||||||
TIA | 1 (7) | 0 (0) | nr | nr | nr | |||
Patients who stopped treatment due to adverse events | ||||||||
n (%) | nr | 3 (2.9) | 1 (2.0) | 3 (4) | 2 (5) | 13 (9.6) | 4 (6.6) | |
Events listing, n (%) | ||||||||
Abnormal renal function | n/a | 1 | nr | 0 | 0 | 0 | 1 | |
Increased ALT | n/a | 1 | nr | 0 | 0 | 4 | 0 | |
Cerebral infarction | n/a | 1 | nr | 0 | 0 | 0 | 0 | |
Abnormal hepatic function | n/a | 0 | nr | 1 | 0 | 0 | 0 | |
Hemorrhage | n/a | 0 | nr | 2 | 1 | 1 | 1 | |
Facial injury | n/a | 0 | nr | 0 | 1 | 0 | ||
Thromboembolic event | n/a | 0 | nr | 0 | 0 | 2 | 0 | |
Cataract | n/a | 0 | nr | 0 | 0 | 1 | 2 | |
Rash / urticaria | n/a | 0 | nr | 0 | 0 | 2 | 0 | |
Tachycardia | n/a | 0 | nr | 0 | 0 | 1 | 0 | |
Headache | n/a | 0 | nr | 0 | 0 | 1 | 0 | |
Cancer | n/a | 0 | nr | 0 | 0 | 1 | 0 | |
Mortality | ||||||||
n (%) | nr | 0 (0) | 1 (2.0) | 0 (0) | 0 (0) | 0 (0) | 1 (2) | |
Causes of death, n (%) | ||||||||
Undetermined | n/a | 0 | 1 | n/a | nr | |||
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate transaminase; n/a = not applicable; nr = not reported; TIA = transient ischemic attack.
Appendix 7: Summary Tables of Studies With Avatrombopag as Intervention
Note that this appendix has not been copy-edited.
Table 13: Details of Included Studies – Avatrombopag as Intervention (N = 1 Study)
Criteria | Jurczak et al. 2018 |
|---|---|
Designs and Populations | |
Study Design | DB RCT, with OLE phase |
Locations | Multicenter: Australia, New-Zealand, Singapore, South-Africa, Europe |
Randomized | n = 49 |
Place in Therapy | Subsequent-line treatment in patients who have experience with prior ITP therapies |
Inclusion Criteria |
|
Exclusion Criteria |
|
Drugs | |
Intervention | Avatrombopag 20 mg orally once daily (start dose) for 26 weeks Dose to be titrated to maintain platelet count between 50 000/µL and 150 000/µL and reduce the dose or number of concomitant ITP medications + standard of care |
Comparator(s) | DB PL orally once daily for 26 weeks + standard of care |
Concomitant Medications |
|
Duration | |
DB Phase | 26 weeks |
OLE Phase | 76 weeks |
Outcomes | |
Primary Outcome | Platelet count response Outcome measure: Cumulative number of weeks of platelet response during the 6-month treatment period (defined as platelet count ≥ 50 000/µL in the absence of rescue therapy) |
Secondary / Exploratory Outcomes |
|
Notes | |
Publications | Jurczak et al. 201812 |
AEs = adverse events; DB = double-blind; ITP = immune thrombocytopenia; OLE = open-label extension; PL = placebo; RCT = randomized controlled trial; SAEs = serious adverse events.
Table 14: Patient Characteristics — Avatrombopag as Intervention (N = 1 Study)
Patient Characteristic | Jurczak et al. 2018 | |
|---|---|---|
Avatrombopag (N = 32) | Placebo (N = 17) | |
Age, years | ||
Mean (SD) | 46.4 (14.2) | 41.2 (14.7) |
Sex, n (%) | ||
Female | 23 (71.9) | 8 (47.1) |
Male | 9 (28.1) | 9 (52.9) |
Race / Ethnicity, n (%) | ||
Caucasian | 31 (96.9) | 15 (88.2) |
Black | 0 | 1 (5.9) |
Asian | 1 (3.1) | 1 (5.9) |
Time since ITP diagnosis, years | ||
Mean (SD) | nr | |
Platelet count /µL | ||
Median (IQR) | nr | |
Platelet count, n (%) | ||
£ 15 000/µL | 18 (56.3) | 10 (58.8) |
> 15 000 /µL | 14 (43.7) | 7 (41.2) |
Concomitant ITP medication(s), n (%) | ||
Yes | 15 (46.9) | 7 (41.2) |
Splenectomy, n (%) | ||
Yes | 11 (34.4) | 5 (29.4) |
ITP = immune thrombocytopenia; IQR = interquartile range; nr = not reported; SD = standard deviation.
Table 15: Patient Disposition — Avatrombopag as Intervention (N = 1 Study)
Category, n | Jurczak et al. 2018 | |
|---|---|---|
Avatrombopag | Placebo | |
Randomized | 32 | 17 |
Completed | 22 | 1 |
Discontinued | 10 | 16 |
AEs | 3 | 0 |
Lack of efficacy | 7 | 15 |
Sponsor decision | 0 | 0 |
Withdrawal of consent | 0 | 1 |
AE = adverse events.
One DB RCT evaluated avatrombopag compared to placebo.12 Detailed outcome results are presented in Table 13.
Outcomes Assessing Clinical Effectiveness
Platelet Count Response
The use of avatrombopag was associated with a higher cumulative mean number of weeks of platelet response compared with placebo at week 26 (12.0 ± 8.75 weeks in the avatrombopag group versus 0.1 ± 0.49 week in the placebo group). The cumulative number of weeks of platelet response was the primary outcome in the trial, where response was defined as a platelet count ≥ 50 000/µL in the absence of rescue therapy. The use of avatrombopag was associated with a higher proportion of responders at day 8 compared to placebo (66% versus 0%, respectively; difference in response rate 65.63, 95% CI 49.17 to 82.08; P < 0.0001).
Bleeding Events
Comparative data for bleeding events were reported according to the WHO bleeding scale. The proportions of patients with any bleeding event were 44% with avatrombopag and 53% with placebo (p nonsignificant).
Need for Rescue Medication
The proportions of patients who received rescue medication were 22% with avatrombopag and 12% with placebo (p nonsignificant).
Reduction or Discontinuation of Concomitant ITP Medication
The proportions of patients who reduced or discontinued concomitant ITP medication were 33% with avatrombopag and 0% with placebo (difference in reduction rate of 33.33, 95% CI 9.48 to 57.19; p nonsignificant).
Other Prespecified Effectiveness Outcomes
No data were reported to inform on the comparative effectiveness of avatrombopag versus placebo for the outcomes of time to platelet response, emergency department visits, hospitalization, HRQoL, patient-reported specific symptoms of ITP and treatment-free remission.
Outcomes Assessing Harms
Adverse Events
A numerically higher proportion of patients in the avatrombopag group experienced AEs compared to patients in the placebo group (97% versus 59%, respectively).
Serious AEs
Nine patients in the avatrombopag group experienced SAEs. There was 1 SAE in the placebo group, the nature of which was not reported (28% versus 6%, respectively).
Withdrawals Due to AEs
Three patients (9%) in the avatrombopag group discontinued study treatment due to AEs; the nature of the events was not reported. There was no withdrawal due to adverse event in the placebo group.
Mortality
Mortality was assessed as a harm outcome in the study and therefore, is reported as such in this report. No patient died over the course of the study.
Notable Harm: Infection
No data were reported to specifically inform on the comparative effectiveness of avatrombopag versus placebo for the outcome of infection, except for patient-reported AEs of some types of infections.
Table 16: Summary of Key Efficacy Outcomes — Avatrombopag as Intervention (N = 1 Study)
Outcome | Jurczak et al. 2018 | |
|---|---|---|
Avatrombopag (N = 32) | Placebo (N = 17) | |
Key Efficacy Outcomes | ||
Primary outcome in trial | ||
DB follow-up | 6 months (26 weeks) Note: Mean duration of exposure was 22.8 weeks for avatrombopag patients and 8.9 weeks for placebo patients. | |
Platelet count response | Cumulative number of weeks of platelet response | |
Mean (SD) | 12.0 (8.75) | 0.1 (0.49) |
Between-group p value | P < 0.0001 | |
Secondary or exploratory outcomes in trial | ||
Platelet count response | Proportions of responders at Day 8 | |
n (%) | 21 (65.6) | 0 (0) |
Between-group difference (95% CI); p value | Difference in response rate 65.63 (49.17 to 82.08); P < 0.0001 | |
Bleeding | Any bleeding (WHO bleeding scale)a | |
n (%) | 14 (43.8) | 9 (52.9) |
Between-group p value | P = 0.5394 | |
Need for rescue medication | Proportions of patients with rescue treatment | |
n (%) | 7 (21.9) | 2 (11.8) |
Between-group p value | P = 0.4668 | |
Concomitant ITP medication use | Reduction in use of ITP baseline treatments | |
N patients with baseline ITP medication | N = 15 | N = 7 |
n (%) | 5 (33.3) | 0 (0) |
Between-group difference (95% CI); p value | Difference in reduction rate 33.33 (9.48 to 57.19); P = 0.1348 | |
DB = double-blind; CI = confidence interval; nr = not reported.
aBleeding symptoms included WHO bleeding scale grades 1 to 3
Table 17: Summary of Key Harms Outcomes — Avatrombopag as Intervention (N = 1 Study)
Outcome | Jurczak et al. 2018 | |
|---|---|---|
Avatrombopag | Placebo | |
Key Harms Outcomes | ||
Safety population | N = 32 | N = 17 |
Patients with ≥ 1 adverse events | ||
n (%) | 31 (96.9) | 10 (58.8) |
Most common events, n (%) | Treatment-emergent AEs (in > 10% of patients) | |
Headache | 12 (37.5) | 2 (11.8) |
Contusion | 10 (31.3) | 4 (23.5) |
Upper respiratory tract infection | 6 (18.8) | 1 (5.9) |
Arthralgia | 4 (12.5) | 0 (0) |
Epistaxis | 4 (12.5) | 3 (17.6) |
Fatigue | 4 (12.5) | 1 (5.9) |
Gingival bleeding | 4 (12.5) | 0 (0) |
Petechiae | 4 (12.5) | 1 (5.9) |
Diarrhea | nr | |
Nausea | nr | |
Nasopharyngitis | 3 (9.4) | 0 (0) |
Musculoskeletal pain | nr | |
Dizziness | nr | |
Insomnia | nr | |
Patients with ≥ 1 serious adverse events | ||
n (%) | 9 (28.1) | 1 (5.9) |
Headache | 2 (6.3) | 0 (0) |
Vomiting | 2 (6.3) | 0 (0) |
Platelet count decreased | 1 (3.1) | 0 (0) |
Idiopathic thrombocytopenic purpura | 0 (0) | 1 (5.9) |
Thrombocytopenia | 1 (3.1) | 0 (0) |
Food poisoning | 1 (3.1) | 0 (0) |
Mouth hemorrhage | 1 (3.1) | 0 (0) |
Nausea | 1 (3.1) | 0 (0) |
Polyserositis | 1 (3.1) | 0 (0) |
Urinary tract infection | 1 (3.1) | 0 (0) |
Cerebrovascular accident | 1 (3.1) | 0 (0) |
Uterine hemorrhage | 1 (3.1) | 0 (0) |
Epistaxis | 1 (3.1) | 0 (0) |
Petechiae | 1 (3.1) | 0 (0) |
Deep vein thrombosis | 1 (3.1) | 0 (0) |
Patients who stopped treatment due to adverse events | ||
n (%) | 3 (9.4) | 0 (0) |
Events listing, n (%) | nr | |
Mortality | ||
n (%) | 0 (0) | 0 (0) |
AE = adverse event; nr = not reported.
Appendix 8: Summary Tables of Studies With Romiplostim as Intervention
Note that this appendix has not been copy-edited.
Table 18: Details of Included Studies — Romiplostim as Intervention (N = 3 studies)
Criteria | Shirasugi et al. 2011 | Kuter et al. 2008 | Kuter et al. 2010 |
|---|---|---|---|
Designs and Populations | |||
Study Design | DB RCT | DB RCTs (parallel trials), with OLE phase | OL RCT |
Locations | Multicenter: Japan | Multicenter: US, Europe | Multicenter: North America, Europe, Australia |
Randomized | n = 34 | n = 125 in two parallel trials: n = 62 nonsplenectomized patients n = 63 splenectomized patients | n = 234 |
Place in Therapy | Subsequent-line treatment in patients who have experience with prior ITP therapies | Subsequent-line treatment in patients who have experience with prior ITP therapies | Subsequent-line treatment in patients who have experience with prior ITP therapies |
Inclusion Criteria |
|
|
|
Exclusion Criteria |
|
|
|
Drugs | |||
Intervention | Romiplostim 3 mcg/kg SC (start dose) once weekly for 12 weeks Dose to be titrated to maintain platelet count between 50 000/µL and 200 000/µL (max dose 10 mcg/kg) | Romiplostim 1 mcg/kg SC (start dose) once weekly for 24 weeks Dose to be titrated to maintain platelet count between 50 000/µL and 200 000/µL (max dose 15 mcg/kg) | Romiplostim 3 mcg/kg SC (start dose) once weekly for 52 weeks Dose to be titrated to maintain platelet count between 50 000/µL and 200 000/µL (max dose 10 mcg/kg) |
Comparator(s) | DB PL SC once weekly for 12 weeks | DB PL SC once weekly for 24 weeks | OL standard of care for 52 weeks |
Concomitant Medications | Oral corticosteroids, azathioprine, or danazol (stable dose for ≥ 4 weeks) | Oral corticosteroids, azathioprine, or danazol (stable dose and schedule) | ITP therapies including short-term rescue therapies (e.g., IV immunoglobulin) but excluding other thrombopoietin mimetics |
Duration | |||
DB Phase | 12 weeks | 24 weeks | 52 weeks |
OLE Phase | ¾ | 285 weeks | ¾ |
Outcomes | |||
Primary Outcome | Platelet count response Outcome measure: Number of weeks with weekly platelet response | Platelet count response Outcome measure: Durable platelet response, defined as ≥ 6 of the last 8 weeks of treatment with weekly platelet counts ≥ 50 000/µL and no rescue medication | Platelet count response Coprimary outcome measures:
|
Secondary / Exploratory Outcomes |
|
|
|
Notes | |||
Publications | Shirasugi et al. 201113 | Kuter et al. 200811 George et al. 200928 Gernsheimer et al. 201029 Sanz et al. 201130 | Kuter et al. 201014 Kuter et al. 201231 |
AEs = adverse events; DB = double-blind; ECOG = Eastern Cooperative Oncology Group; OL = open label; HRQoL = health-related quality of life; ITP = immune thrombocytopenia; ITP-PAQ = Immune Thrombocytopenic Purpura – Patient Assessment Questionnaire; OLE = open-label extension; PL = placebo; RCT = randomized controlled trial; SC = subcutaneously; WDAE = withdrawal from therapy due to adverse event.
Table 19: Patient Characteristics — Romiplostim as Intervention (N = 3 studies)
Patient Characteristic | Shirasugi et al. 2011 | Kuter et al. 2008 | Kuter et al. 2010 | |||
|---|---|---|---|---|---|---|
Romiplostim (N = 22) | Placebo (N = 12) | Romiplostim (N = 83) | Placebo (N = 42) | Romiplostim (N = 157) | Standard of care (N = 77) | |
Age, years | ||||||
Mean (SD) | 58.5 (12.6) | 47.6 (13.4) | nr | nr | ||
Median (range) | nr | 52 (21 to 88) | 52 (23 to 88) | 58 (18 to 90) | 57 (18 to 86) | |
Sex, n (%) | ||||||
Female | 14 (63.6) | 10 (83.3) | 54 (65) | 27 (64) | 85 (54) | 46 (60) |
Male | 8 (36.4) | 2 (16.7) | 29 (35) | 15 (36) | 72 (46) | 31 (40) |
Race / Ethnicity, n (%) | ||||||
Caucasian | 0 | 0 | 65 (78) | 37 (88) | 137 (87) | 69 (90) |
Black | 0 | 0 | 6 (7) | 3 (7) | 6 (4) | 0 |
Asian | 22 (100.0) | 22 (100.0) | nr | nr | ||
Other | 0 | 0 | 12 (14) | 2 (5) | 14 (9) | 8 (10) |
Time since ITP diagnosis, years | ||||||
Mean (SD) | 9.7 (10.4) | 7.6 (5.9) | nr | nr | ||
Median (range) | nr | nr | 2.1 (0 to 44.2) | 2.3 (0 to 33.2) | ||
Platelet count /µL | ||||||
Mean (SD) | 18 400 (8 300) | 15 800 (600) | nr | nr | ||
Median (range) | nr | 16 000 (2 000 to 29 000) | 18 000 (2 000 to 31 000) | 33 000 (1 000 to 123 000) | 27 000 (2 000 to 62 000) | |
Concomitant ITP medication(s), n (%) | ||||||
Yes | 13 (59.1) | 10 (83.3) | 23 (28) | 16 (38) | 21 (13) | 5 (6) |
Splenectomy, n (%) | ||||||
Yes | 10 (45.5) | 5 (41.7) | 42 (51) | 21 (50) | n/a | |
ITP = immune thrombocytopenia; n/a = not applicable; nr = not reported; SD = standard deviation.
Table 20: Patient Disposition — Romiplostim as Intervention (N = 3 studies)
Category, n | Shirasugi et al. 2011 | Kuter et al. 2008 | Kuter et al. 2010 | |||
|---|---|---|---|---|---|---|
Romiplostim | Placebo | Romiplostim | Placebo | Romiplostim | Standard of care | |
Randomized | 22 | 12 | 83 | 42 | 157 | 77 |
Completed | 22 | 12 | 79 | 36 | 145 | 62 |
Discontinued | 0 | 0 | 4 | 6 | 12 | 15 |
AEs | 0 | 0 | 3 | 1 | nr | |
Withdrawn consent | 0 | 0 | 1 | 2 | 5 | 4 |
Other | 0 | 0 | 0 | 3 | 7 | 11 |
AE = adverse events.
Three RCTs evaluated romiplostim compared to placebo.11,13,14 Detailed outcome results are presented in Table 18.
Outcomes Assessing Clinical Effectiveness
Platelet Count Response
The 3 romiplostim trials used different outcome measurements as primary end point for platelet count response (number of weeks in response, response rates and incidence of treatment failure), as well as different definitions and thresholds for platelet response.
In 1 12-week DB RCT, the use of romiplostim was associated with a higher number of weeks of platelet count response compared with placebo (median 11 weeks, IQR 9 to 12; versus 0, IQR 0 to 0, respectively; P < 0.0001).13 Platelet count response was defined as ≥ 50 000/µL in the publication. The use of romiplostim was also associated with a higher proportion of patients with platelet count increase ≥ 20 000/µL compared with placebo (96% versus 25%, respectively; P < 0.001).13
One 24-week DB RCT evaluated the platelet count response rate during at least 8 weeks, which was higher with romiplostim compared with placebo (49% versus 2%, respectively; P < 0.01).11 In this study, platelet count response was defined as ≥ 6 of the last 8 weeks of treatment with weekly platelet counts ≥ 50 000/µL and no rescue medication. The use of romiplostim was also associated with a higher proportion of patients with ≥ 4 weekly platelet count response at any time compared with placebo (83% versus 7%, respectively; P < 0.0001).11
The third study was a 52-week OL RCT with incidence of treatment failure (i.e., patients who did not have a platelet response) as primary outcome, which was lower in patients receiving romiplostim compared with standard of care (11% versus 30%, respectively; between-group difference of 0.31; 95% CI 0.15 to 0.61; P < 0.001).14 Treatment failure was defined in the study as a recurrent platelet count ≤ 20 000/µL despite optimal dosage, a major bleeding or withdrawal due to adverse event. The use of romiplostim was also associated with a higher median platelet count between week 2 and end of trial compared with standard of care (between-group difference of 2.3 (95% CI 2.0 to 2.6); P < 0.001).14
Bleeding Events
The 3 studies reported some data for bleeding events; however, definitions for bleeding as well as comparative data were not consistently provided. The proportions of patients with any bleeding event were 36% after 12 weeks with romiplostim versus 83% with placebo (no statistical analysis was performed) in 1 trial;13 57% with romiplostim versus 61% with placebo in the second trial (p nonsignificant);11 and 52% with romiplostim versus 53% with OL standard of care in the third trial (no statistical analysis was performed).14.
Health-Related Quality of Life
HRQoL was assessed in 2 studies using the ITP-PAQ questionnaire11,14 and in 1 study using the EQ-5D.11 The use of romiplostim was associated with greater improvements from baseline to week 24 compared to placebo in the some of the ITP-PAQ scales (symptoms, bother, activity, psychological, fear, social quality of life, and women’s reproductive health – menstrual symptoms) as well as in the ED-5D index score.11 At week 52, romiplostim was associated with greater improvements from baseline compared to OL standard of care in the following ITP-PAQ scales: symptoms, bother, activity, fear, overall quality of life, and social quality of life.14 Standard of care treatments were at the discretion of the investigators and based on local practices or therapeutic guidelines.14
Greater improvements from baseline were also observed with romiplostim compared with placebo at 24 weeks in the EQ-5D VAS score and in the ITP-PAQ fatigue and overall quality of life scales,11 as well as at 52 weeks in the ITP-PAQ fatigue scale;14 however, statistical significance was not reached.
Need for Rescue Medication
The studies11,13,14 reported some data pertaining to the use of rescue medications. All results are presented in Appendix 6. One trial performed a between-group comparison with sufficient power to show a difference between treatments. In a 24-week DB RCT, romiplostim was associated with a reduction in the proportions of patients necessitating rescue treatments compared with placebo (22% versus 60%, respectively; P < 0.0001).11 Rescue medications were defined in the trial as an increase in the dosage of a concomitant ITP medication or the use of any new drug to increase platelet count.
Reduction or Discontinuation of Concomitant ITP Medication
One study assessed the reduction or discontinuation of concomitant ITP medication.11 More patients in the romiplostim treatment group were able to discontinue a concomitant ITP medication or reduce the dose of at least 1 medication by more than 25% compared with placebo; however, no analysis between treatment groups was reported.
Other Prespecified Effectiveness Outcomes
No data were reported to inform on the comparative effectiveness of romiplostim versus placebo or standard of care for the outcomes of time to platelet response, emergency department visits, hospitalization, patient-reported specific symptoms of ITP and treatment-free remission.
Outcomes Assessing Harms
Adverse Events
AEs were reported in 2 studies.11,13 Almost all patients in these 2 trials experienced at least 1 AE. The most common AEs reported across all studies included headache, nasopharyngitis, fatigue, contusion, epistaxis, arthralgia, and petechiae.
Serious AEs
There was inconsistency across the 3 studies in the proportions of patients with SAEs. In 2 studies, the proportions of patients experiencing SAEs were similar between treatment groups and were less than 10% of patients per treatment arm.11,13 In the OL 52-week trial, the proportions of patients with SAEs were much higher, being 23% of patients under romiplostim and 37% of patients receiving standard of care.14 In this study, the most common SAEs reported included thrombocytopenia, pneumonia, peripheral edema, and pulmonary embolism.
Withdrawals Due to AEs
Discontinuations due to AEs were reported in 1 study and the proportions of patients who discontinued were similar between groups and less than 10% per treatment arm.11
Mortality
Mortality was assessed as a harms outcome in the studies and therefore, is reported as such in this report. The 3 studies reported mortality data; however, no death was observed in 1 trial.13 One patient randomized to romiplostim died in each of the 2 other trials, as well as 2 patients in the placebo or standard of care groups over each study period.11,14 The causes of death included cerebral or intracranial hemorrhage, pulmonary embolism, pneumonia, and hepatic failure.
Notable Harm: Infection
No data were reported to specifically inform on the comparative effectiveness of romiplostim versus placebo for the outcome of infection, except for patient-reported AEs of some types of infections.
Table 21: Summary of Key Efficacy Outcomes — Romiplostim as Intervention (N = 3 Studies)
Outcome | Shirasugi et al. 2011 | Kuter et al. 2008 | Kuter et al. 2010 | |||
|---|---|---|---|---|---|---|
Romiplostim N = 22 | Placebo N = 12 | Romiplostim N = 83 | Placebo N = 42 | Romiplostim N = 157 | Standard of care N = 77 | |
Key Efficacy Outcomes | ||||||
Primary outcome in trial | ||||||
DB follow-up | 12 weeks | 24 weeks | 52 weeks | |||
Platelet count response | Number of weeks of platelet count response, median (IQR) | Durable platelet count response rate during last 8 weeks, n (%) | Incidence of treatment failure | |||
Response per group | 11 (9 to 12) | 0 (0 to 0) | 41 (49) | 1 (2) | 18 (11) | 23 (30) |
Between-group difference (95% CI) and/or p value | P < 0.0001 | Splenectomized patients: 38% (23.4% to 52.8%); P = 0.0013 Nonsplenectomized patients: 56% (38.7% to 73.7%); P < 0.0001 | 0.31 (0.15 to 0.61); P < 0.001 | |||
Secondary or exploratory outcomes in trial | ||||||
Platelet count response | Proportions of patients with platelet count increase ≥ 20 000 /µL, n (%) | Proportions of patients with ≥ 4 weekly platelet count response at any time during the study, n (%) | Platelet count /µL between Week 2 and Week 52, median range | |||
Response per group | 21 (96) | 3 (25) | 69 (83.1) | 3 (7.1) | 108 000 – 176 000 | 35 000 – 52 000 |
Between-group difference (95% CI) and/or p value | P < 0.0001 | P < 0.0001 | 2.3 (2.0 to 2.6); P < 0.001 | |||
Bleeding | Incidence of bleeding symptoms | Incidence of significant bleeding events (severe, life-threatening, or fatal) | Proportions of patients with bleeding eventsa | |||
Baseline, n (%) | 14 (63.6) | 10 (83.3) | nr | nr | ||
After 4 weeks, n (%) | 7 (31.8) | 10 (83.3) | ||||
After 8 weeks, n (%) | 7 (31.8) | 12 (100.0) | ||||
After 12 weeks, n (%) | 8 (36.4) | 10 (83.3) | ||||
Throughout the trial, n (%) | 16 (72.7) | 12 (100.0) | 6 (7) | 5 (12) | 80 (52) | 40 (53) |
Need for rescue medication | Proportions of patients with rescue treatment | Proportions of patients with rescue treatment | Proportions of patients administered ITP treatment | |||
n (%) | 2 (9) | 2 (17) | 26 (21.7) | 25 (59.5) | 67 (44) | 59 (79) |
Between-group p value | P = 0.6015 | P < 0.0001 | nr | |||
Concomitant ITP medication use | nr | Concomitant ITP medication use | nr | |||
N patients with baseline ITP medication | N = 23 | N = 16 | ||||
Discontinued, n (%) | 12 (52) | 3 (19) | ||||
Reduced at least 1 drug by more than 25%, n (%) | 8 (35) | 3 (19) | ||||
HRQoL | nr | Improvement in HRQoL scores | ||||
Instrument or scale | nr | EQ-5D index score | nr | |||
N patients with data | nr | N = 76 | N = 41 | nr | ||
Mean change from baseline to end of treatment (SE) | nr | 0.05 (0.02) | −0.03 (0.02) | nr | ||
Between-group p value | nr | P = 0.015 | nr | |||
Instrument or scale | nr | EQ-5D index score VAS score | nr | |||
N patients with data | nr | N = 73 | N = 41 | nr | ||
Mean change from baseline to end of treatment (SE) | nr | 6.42 (2.08) | 0.48 (2.59) | nr | ||
Between-group p value | nr | P = 0.066 | nr | |||
Instrument or scale | nr | ITP-PAQ Symptoms Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 16.0 (1.9) | 12.5 (2.1) | |
LSM estimate (SE) | nr | 7.48 (2.08) | nr | |||
Between-group p value | nr | P = 0.0005 | P = 0.0133 | |||
Instrument or scale | nr | ITP-PAQ Fatigue Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 11.2 (3.1) | 9.5 (3.2) | |
LSM estimate (SE) | nr | 1.78 (2.83) | nr | |||
Between-group p value | nr | P = 0.53 | P = 0.3434 | |||
Instrument or scale | nr | ITP-PAQ Bother Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 16.8 (2.5) | 13.0 (2.7) | |
LSM estimate (SE) | nr | 8.94 (2.76) | nr | |||
Between-group p value | nr | P = 0.002 | P = 0.0076 | |||
Instrument or scale | nr | ITP-PAQ Activity Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 17.1 (3.5) | 8.2 (3.7) | |
LSM estimate (SE) | nr | 8.52 (3.47) | nr | |||
Between-group p value | nr | P = 0.016 | P = 0.0246 | |||
Instrument or scale | nr | ITP-PAQ Psychological Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 18.9 (2.7) | 15.7 (2.8) | |
LSM estimate (SE) | nr | 5.71 (2.77) | nr | |||
Between-group p value | nr | P = 0.042 | P = 0.0490 | |||
Instrument or scale | nr | ITP-PAQ Fear Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 13.9 (1.7) | 8.7 (1.7) | |
LSM estimate (SE) | nr | 7.13 (1.99) | nr | |||
Between-group p value | nr | P = 0.0005 | P = 0.0001 | |||
Instrument or scale | nr | ITP-PAQ Overall quality of life Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 16.1 (3.6) | 15.0 (3.7) | |
LSM estimate (SE) | nr | 4.14 (3.07) | nr | |||
Between-group p value | nr | P = 0.18 | P = 0.0246 | |||
Instrument or scale | nr | ITP-PAQ Social quality of life Scale | ||||
Mean change from baseline to end of treatment (SE) | nr | nr | nr | 9.7 (2.4) | 5.5 (2.5) | |
LSM estimate (SE) | nr | 9.66 (3.12) | nr | |||
Between-group p value | nr | P = 0.0025 | P = 0.0020 | |||
Instrument or scale | nr | ITP-PAQ Women’s reproductive health – menstrual symptoms | nr | |||
LSM estimate (SE) | nr | 24.23 (5.86) | nr | |||
Between-group p value | nr | P = 0.0001 | nr | |||
HRQoL = health-related quality of life; IQR = interquartile range; ITP = immune thrombocytopenia; ITP-PAQ = Immune Thrombocytopenic Purpura Patient Assessment Questionnaire; LSM = least square means; nr = not reported; SD = standard deviation; SE = standard error; VAS = visual analogue scale.
aIncluding grade 2 bleeding events (moderate severity)
Table 22: Summary of Key Harms Outcomes — Romiplostim as Intervention (N = 3 Studies)
Outcome | Shirasugi et al. 2011 | Kuter et al. 2008 | Kuter et al. 2010 | |||
|---|---|---|---|---|---|---|
Romiplostim | Placebo | Romiplostim | Placebo | Romiplostim | Standard of care | |
Key Harms Outcomes | ||||||
Safety population | N = 22 | N = 12 | N = 83 | N = 41 | N = 154 | N = 75 |
Patients with ≥ 1 adverse events | ||||||
n (%) | 20 (90.9) | 11 (91.7) | 83 (100) | 39 (95) | 136 (82) | 60 (87) |
Most common events, n (%) | Any AEs (in > 10% of patients) | Any AEs (in > 10% of patients) | Any AEs (in > 10% of patients) | |||
Nasopharyngitis | 9 (41) | 2 (17) | 7 (8) | 7 (17) | 36 (23) | 14 (19) |
Headache | 7 (32) | 2 (17) | 29 (35) | 13 (32) | 54 (35) | 14 (19) |
Peripheral edema | 4 (18) | 0 (0) | NR | NR | 15 (10) | 3 (4) |
Back pain | 3 (14) | 0 (0) | 11 (13) | 4 (10) | 16 (10) | 4 (5) |
Pain in extremity | 3 (14) | 0 (0) | 11 (13) | 2 (5) | 20 (13) | 6 (8) |
Malaise | 1 (5) | 2 (17) | NR | NR | NR | NR |
Contusion | 0 (0) | 2 (17) | 21 (25) | 10 (24) | 22 (14) | 13 (18) |
Fatigue | nr | 28 (33) | 12 (29) | 43 (28) | 16 (22) | |
Epistaxis | nr | 27 (32) | 10 (24) | 29 (19) | 17 (23) | |
Arthralgia | nr | 22 (26) | 8 (20) | 23 (15) | 4 (5) | |
Petechiae | nr | 14 (17) | 9 (22) | 25 (16) | 13 (18) | |
Diarrhea | nr | 14 (17) | 6 (15) | 21 (13) | 4 (5) | |
Upper respiratory tract infection | nr | 14 (17) | 5 (12) | 18 (12) | 6 (8) | |
Dizziness | nr | 14 (17) | 0 (0) | 21 (13) | 6 (8) | |
Insomnia | nr | 13 (16) | 3 (7) | 14 (9) | 9 (12) | |
Myalgia | nr | 12 (14) | 1 (2) | 17 (11) | 1 (1) | |
Nausea | nr | 11 (13) | 4 (10) | 24 (16) | 6 (8) | |
Cough | nr | 10 (12) | 7 (17) | 25 (16) | 4 (5) | |
Anxiety | nr | 9 (11) | 5 (12) | NR | NR | |
Gingival bleeding | nr | 9 (11) | 5 (12) | NR | NR | |
Abdominal pain | nr | 9 (11) | 0 (0) | NR | NR | |
Ecchymosis | nr | 6 (7) | 6 (15) | NR | NR | |
Pyrexia | nr | NR | NR | 15 (10) | 8 (11) | |
Haematoma | nr | NR | NR | 12 (8) | 9 (12) | |
Pruritus | nr | NR | NR | 16 (10) | 5 (7) | |
Urinary tract infection | nr | NR | NR | 18 (12) | 7 (10) | |
Constipation | — | — | — | 16 (10) | 6 (8) | |
Patients with ≥ 1 serious adverse events | ||||||
n (%) | 2 (9.1) | 1 (8.3) | 2 (2.4) | 0 (0) | 35 (23) | 28 (37) |
Most common events, n (%) | ||||||
Increased bone marrow reticulin | nr | 1 (1.2) | 0 (0) | nr | ||
Popliteal artery thrombosis | nr | 1 (1.2) | 0 (0) | nr | ||
Thrombocytopenia | nr | 0 (0) | 0 (0) | 5 (3) | 9 (12) | |
Pneumonia | nr | 0 (0) | 0 (0) | 4 (3) | 2 (3) | |
Edema, peripheral | nr | 0 (0) | 0 (0) | 3 (2) | 0 (0) | |
Pulmonary embolism | nr | 0 (0) | 0 (0) | 3 (2) | 0 (0) | |
Patients who stopped treatment due to adverse events | ||||||
n (%) | 0 (0) | 0 (0) | 2 (2.4) | 1 (2.4) | nr | |
Event listing, n (%) | n/a | nr | ||||
Mortality | ||||||
n (%) | 0 (0) | 0 (0) | 1 (1.2) | 2 (4.9) | 1 (0.6) | 2 (2.6) |
Causes of death, n (%) | ||||||
Cerebral hemorrhage | 0 (0) | 0 (0) | 0 (0) | 1 (2.4) | 0 (0) | 0 (0) |
Pulmonary embolism | 0 (0) | 0 (0) | 0 (0) | 1 (2.4) | 0 (0) | 0 (0) |
Intracranial hemorrhage | 0 (0) | 0 (0) | 1 (1.2) | 0 (0) | 0 (0) | 0 (0) |
Pneumonia | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1) | 0 (0) |
Hepatic failure | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.3) |
Cardiorespiratory arrest | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.3) |
AE = adverse event; n/a = not applicable; nr = not reported.
Appendix 9: Summary Tables of Studies With Interventions Other Than TPO-RA
Note that this appendix has not been copy-edited.
Table 23: Details of Included Studies — Interventions other than TPO-RA (N = 2 Studies)
Criteria | Ghanima et al. 2015 | Bussel et al. 2018 |
|---|---|---|
Designs and Populations | ||
Study Design | DB RCT | DB RCTs (parallel trials), with OLE phase |
Locations | Multicenter: Norway, Tunisia, France | Multicenter: North America, Australia, Europe |
Randomized | n = 112 | n = 150 in two parallel trials: n = 76 (FIT1) n = 74 (FIT2) |
Place in Therapy | Second-line treatment in patients with primary ITP who failed a short course of corticosteroid therapy | Subsequent-line treatment in patients who have experience with prior ITP therapies |
Inclusion Criteria |
|
|
Exclusion Criteria |
|
|
Drugs | ||
Intervention | Rituximab 375 mg/m2 IV once weekly for 4 weeks | Fostamatinib 100 mg orally twice daily for 24 weeks |
Comparator(s) | DB PL IV once weekly for 4 weeks | DB PL orally once daily for 24 weeks |
Concomitant Medications | Corticosteroids |
|
Duration | ||
DB Phase | 78 weeks | 24 weeks |
OLE Phase | ¾ | 6 months |
Outcomes | ||
Primary Outcome | Treatment failure, defined as:
| Platelet count response Outcome measure: Number of patients with stable platelet response by week 24 (defined as patients with platelet count ≥ 50 000/µL on at least 4 of the last 6 scheduled visits) |
Secondary / Exploratory Outcomes |
|
|
Notes | ||
Publications | Ghanima et al. 201532 | Bussel et al. 201815 |
DB = double-blind; ITP = immune thrombocytopenia; OLE = open-label extension; PL = placebo; RCT = randomized controlled trial; TPO-RA = thrombopoietin receptor agonists.
Table 24: Patient Characteristics — Interventions Other Than TPO-RA (N = 2 Studies)
Patient Characteristic | Ghanima et al. 2015 | Bussel et al. 2018 | ||
|---|---|---|---|---|
Rituximab (N = 55) | Placebo (N = 54) | Fostamatinib (N = 101) | Placebo (N = 49) | |
Age, years | ||||
Mean (SD) | nr | nr | ||
Median (range) | 46 (27 to 61) | 46 (28 to 60) | 54 (20 to 88) | 53 (20 to 78) |
Sex, n (%) | ||||
Female | 40 (73) | 39 (72) | 61 (60) | 30 (61) |
Male | 15 (27) | 15 (28) | 40 (40) | 19 (39) |
Race / Ethnicity, n (%) | ||||
Caucasian | nr | 94 (93) | 45 (92) | |
Black | nr | 2 (2) | 2 (4) | |
Asian | nr | 3 (3) | 2 (4) | |
Other | nr | 2 (2) | 0 | |
Time since ITP diagnosis | ||||
Mean (SD), years | nr | nr | ||
Median (range), years | nr | 8.7 (0.3 to 53) | 7.8 (0.4 to 45) | |
Median (IQR), weeks | 37 (8 to 288) | 50 (14 to 211) | nr | |
Platelet count /µL | ||||
Median (IQR) | 16 000 (6 000 to 27 000) | 21 000 (9 000 to 29 000) | nr | |
Mean (SD) | nr | nr | ||
Mean (range) | nr | 16 052 (1 000 to 51 000) | 19 818 (1 000 to 156 000) | |
Platelet count, n (%) | ||||
£ 15 000/µL | nr | 54 (53.5) | 28 (57.1) | |
> 15 000 /µL | 47 (46.5) | 21 (42.9) | ||
Concomitant ITP medication(s), n (%) | ||||
Yes | nr | nr | ||
Splenectomy, n (%) | ||||
Yes | nr | 34 (34) | 19 (39) | |
ITP = immune thrombocytopenia; IQR = interquartile range; nr = not reported; SD = standard deviation.
Table 25: Patient Disposition — Interventions Other Than TPO-RA (N = 2 Studies)
Category, n | Ghanima et al. 2015 | Bussel et al. 2018 | ||
|---|---|---|---|---|
Rituximab | Placebo | Fostamatinib | Placebo | |
Randomized | 58 | 54 | 101 | 49 |
Completed | 55 | 52 | 25 | 3 |
Discontinued | 3 | 2 | 76 | 46 |
AEs | 0 | 0 | 9 | 4 |
Lack of efficacy | 0 | 0 | 61 | 41 |
Patient decision | 0 | 1 | 2 | 1 |
Lost to follow-up | 0 | 1 | 1 | 0 |
Investigator decision | 0 | 0 | 3 | 0 |
Refused treatment | 3 | 0 | 0 | 0 |
AE = adverse events.
One DB RCT evaluated rituximab compared to placebo.32 Detailed outcome results are presented in Table 23. It should be noted that the primary outcome for this study, which was treatment failure, did not meet the a priori defined threshold for statistical significance and therefore, formal testing was halted for all secondary outcomes. As a result, any conclusion drawn from this study must consider the increased risk of type I error due to the failed primary end point.
Outcomes Assessing Clinical Effectiveness
Platelet Count Response
The proportions of patients with overall response in the trial (platelet count ≥ 30 000 /µL) were 73% with rituximab versus 67% with placebo (p nonsignificant); for complete response (platelet count ≥ 100 000 /µL), the proportions were 51% with rituximab versus 39% with placebo (p nonsignificant).
Bleeding Events
The proportions of patients with any bleeding symptoms were 38% with rituximab versus 50% with placebo (p nonsignificant).
Other Prespecified Effectiveness Outcomes
No data were reported to inform on the comparative effectiveness of rituximab versus placebo for the outcomes of time to platelet response, emergency department visits, hospitalization, HRQoL, reduction, or discontinuation of concomitant ITP medication, patient-reported specific symptoms of ITP, need for rescue medication, and treatment-free remission.
Outcomes Assessing Harms
Adverse Events
A higher proportion of patients in the rituximab group experienced AEs compared to patients in the placebo group (40% versus 24%, respectively). The most common AEs included infections, influenza, throat irritation, headache, bronchitis, and pyrexia.
Serious AEs
No data were reported to inform on the comparative effectiveness of rituximab versus placebo for the outcome of SAEs.
Withdrawals Due to AEs
No patient experienced withdrawal due to adverse event throughout the study duration.
Mortality
Mortality was assessed as a harms outcome in the studies and therefore, is reported as such in this report. One patient in the placebo group died over the study period. The cause of death was gastrointestinal bleeding.
Notable Harm: Infection
A total of 40% of patients (n = 20) in the rituximab group and 24% of patients in the placebo group (n = 13) reported an AE of infection.
One DB RCT evaluated fostamatinib compared to placebo.15 Detailed outcome results are presented in Table 23.
Outcomes Assessing Clinical Effectiveness
Platelet Count Response
The use of fostamatinib was associated with higher proportions of patients with what was labelled as stable platelet response by week 24 compared with placebo (18% versus 2%, respectively; P = 0.0003).15 This was the primary outcome in the trial and was defined as a platelet count ≥ 50 000/µL on at least 4 of the last 6 scheduled visits during weeks 14 to 24. Despite being statistically significant, the proportions of patients with platelet response appeared low in the study. It should be noted however that the median time since ITP diagnosis in the study was approximately 8 years. There was also an improvement with fostamatinib in the proportions of patients with overall response (platelet count ≥ 50 000/µL) at any time compared with placebo (43% versus 14%, respectively; P = 0.0006).
Need for Rescue Medication
Greater improvements from baseline were observed with fostamatinib compared with placebo in the proportions of patients receiving rescue medication (30% versus 45%, respectively; p nonsignificant).
Other Prespecified Effectiveness Outcomes
No data were reported to inform on the comparative effectiveness of fostamatinib versus placebo for the outcomes of time to platelet count response, bleeding, emergency department visits, hospitalization, HRQoL, patient-reported specific symptoms of ITP, reduction or discontinuation of concomitant ITP medication and treatment-free remission.
Outcomes Assessing Harms
Adverse Events
A higher proportion of patients in fostamatinib group experienced AEs compared to patients in the placebo group (83% versus 75%, respectively). The most common AEs included diarrhea, hypertension, nausea, dizziness respiratory infections, and ALT increase.
Serious AEs
A total of 13% of patients in the fostamatinib group experienced SAEs, which is numerically lower than the proportion of patients experiencing SAEs in the placebo group (21%). The most common AEs included thrombocytopenia, epistaxis, and menorrhagia.
Withdrawals Due to AEs
The proportions of patients who discontinued due to AEs were 10% in the fostamatinib group and 8% in the placebo group.
Mortality
Mortality was assessed as a harm outcome in the studies and therefore, is reported as such in this report. One patient in each group died over the study period. The causes of death were myeloma and sepsis.
Notable Harm: Infection
No data were reported to specifically inform on the comparative effectiveness of fostamatinib versus placebo for the outcome of infection, except for patient-reported AEs of some types of infections.
Table 26: Summary of Key Efficacy Outcomes — Interventions Other Than TPO-RA (N = 2 Studies)
Outcome | Ghanima et al. 2015 | Bussel et al. 2018 | ||
|---|---|---|---|---|
Rituximab N = 55 | Placebo N = 54 | Fostamatinib N = 101 | Placebo N = 49 | |
Key Efficacy Outcomes | ||||
Primary outcome in trial | ||||
DB follow-up | 4 weeks of treatment 78 weeks of follow-up | 24 weeks | ||
Platelet count response | Treatment failure | Proportions of patients with stable response | ||
n (%) | 32 (58) | 37 (68) | 18 (18) | 1 (2) |
Kaplan-Meier estimate of cumulative incidence | 46% | 52% | nr | |
Between-group difference (95% CI) and / or p value | HR 0.89 (0.55 to 1.45); P = 0.65 | P = 0.0003 | ||
Secondary or exploratory outcomes in trial | ||||
Platelet count response | Complete response at 78 weeks (platelet count ≥ 100 000/µL) | Overall response (platelet count ≥ 50 000/µL) | ||
n (%) | 28 (51) | 21 (39) | 43 (43) | 7 (14) |
Kaplan-Meier estimate of cumulative incidence | 58% | 50% | nr | |
Between-group p value | P = 0.12 | P = 0.0006 | ||
Platelet count response | Overall response at 78 weeks (platelet count ≥ 30 000/µL) | nr | ||
n (%) | 40 (73) | 36 (67) | ||
Kaplan-Meier estimate of cumulative incidence | 81% | 73% | ||
Between-group p value | P = 0.15 | |||
Bleeding | Any bleeding symptoms | nr | ||
n (%) | 21 (38) | 27 (50) | ||
Between-group p value | P = 0.08 | |||
Need for rescue medication | Probability of receiving rescue treatment | Proportions of patients receiving rescue medication | ||
n (%) | nr | 30 (30) | 22 (45) | |
Between-group p value | P = 0.09 | P = 0.07 | ||
HR = hazard ratio; ITP = immune thrombocytopenia; nr = not reported; SD = standard deviation.
Table 27: Summary of Key Harms Outcomes — Interventions Other Than TPO-RA (N = 2 Studies)
Outcome | Ghanima et al. 2015 | Bussel et al. 2018 | ||
|---|---|---|---|---|
Rituximab | Placebo | Fostamatinib | Placebo | |
Key Harms Outcomes | ||||
Safety population | N = 55 | N = 54 | N = 102 | N = 48 |
Patients with ≥ 1 adverse events | ||||
n (%) | nr | 85 (83) | 36 (75) | |
Most common events, n (%) | Any AEs (Grade 2 to 3) | Treatment-emergent AEs | ||
Infections | 20 (40) | 13 (24) | nr | |
Influenza | 8 (15) | 4 (7) | nr | |
Throat irritation | 8 (5) | 1 (2) | nr | |
Headache | 5 (9) | 2 (4) | nr | |
Bronchitis | 4 (7) | 2 (4) | nr | |
Pyrexia | 4 (7) | 2 (4) | nr | |
Upper respiratory tract infection | 3 (5) | 2 (4) | nr | |
Rash | 3 (5) | 2 (4) | 9 (9) | 1 (2) |
Diarrhea | nr | 32 (31) | 7 (15) | |
Hypertension | nr | 29 (28) | 6 (13) | |
Nausea | nr | 19 (19) | 4 (8) | |
Dizziness | nr | 11 (11) | 4 (8) | |
ALT increase | nr | 11 (11) | 0 (0) | |
Respiratory infection | nr | 11 (11) | 3 (6) | |
AST increase | nr | 9 (9) | 0 (0) | |
Fatigue | nr | 6 (6) | 1 (2) | |
Chest pain | nr | 6 (6) | 1 (2) | |
Neutropenia | nr | 6 (6) | 0 (0) | |
Patients with ≥ 1 serious adverse events | ||||
n (%) | nr | 13 (13) | 10 (21) | |
Epistaxis | nr | 1 (1) | 1 (2) | |
Thrombocytopenia | 1 (1) | 2 (4) | ||
Menorrhagia | 0 (0) | 2 (4) | ||
Patients who stopped treatment due to adverse events | ||||
n (%) | 0 (0) | 0 (0) | 10 (10) | 4 (8) |
Chest pain / syncope | n/a | 1 (1) | nr | |
Pneumonia | 1 (1) | nr | ||
Thrombocytopenia | 1 (1) | nr | ||
Mortality | ||||
n (%) | (0) | 1 (2) | 1 (1) | 1 (2) |
Gastrointestinal bleeding | 0 (0) | 1 (2) | 0 (0) | 0 (0) |
Sepsis | 0 (0) | 0 (0) | 0 (0) | 1 (2) |
Myeloma | 0 (0) | 0 (0) | 1 (1) | 0 (0) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate transaminase; n/a = not applicable; nr = not reported.
Appendix 10: Critical Appraisal
Note that this appendix has not been copy-edited.
Table 28: Critical Appraisal of Included Studies
First Author, Publication Year | Strengths and Limitations |
|---|---|
Jurczak et al. (2018) was rated as an overall high risk of bias. | There were differences in baseline characteristics between treatment arms at baseline, the proportion of females was 72% for AVA and 47% for PBO. All other baseline characteristics reported were balanced. Investigators, investigational site personnel and sponsor staff were blinded to treatment codes but not dose levels. Differences in reduction in use of concomitant ITP meds from baseline and differences in treatment-related TEAEs (63% AVA vs. 18% PBO) and other safety data may have made patients aware of the treatment received. The most frequent reason for discontinuation from the core study was lack of treatment effect (avatrombopag, N = 7; placebo, N = 15). The full analysis set included all randomized patients. The FAS was used, but there was a high discontinuation rate (> 50%). The timing of discontinuation and availability of data at later time points is unknown. High discontinuation rates due to inadequate therapeutic response: 70% (7/10) of discontinuations from AVA and 94% (15/16) of discontinuations from PBO. “cumulative number of weeks with ≥50 x 109/L during the core study in the absence of rescue therapy,” the clinical expert indicated that a threshold of 30 would be more appropriate - this would miss clinically relevant responders. Down-titration of concomitant ITP medication was implemented at the discretion of the investigator and could only be considered if the patient’s platelet count remained > 150 × 109/L. Patients with a platelet count > 150 × 109/L to ≤ 250 × 109/L could have their concomitant ITP medication down titrated by ≤ 25% of the original dose for 14 days, whereas the dose was reduced by ≤ 50% in patients with a platelet count > 250 × 109/L for 14 days. If a patient was receiving ≥ 2 concomitant ITP medications, only one medication was down titrated at a time. Decision to reduce concomitant meds was at the discretion of the investigator, which could introduce bias. |
Yang et al. (2017) was rated as low overall risk of bias. | All patients randomized into this study were assigned a unique randomization code, with randomization stratified by splenectomy status (Yes/No), use of maintenance concomitant ITP therapy at baseline (Yes/No), and baseline platelet counts (≤ 15 × 109/L or > 15 × 109/L). No information about allocation concealment, although it was likely concealed given the randomization strategy. Patients, caregivers, investigators, and outcomes assessors were blinded to treatment assignment. The analysis of the primary efficacy end point was performed for both the ITT and PP populations. 149/154 of the patients included in the ITT population completed stage I. 135 patients were included in the PP population. Proportion of patients with a platelet count ≥ 50 × 109/L after day 42 in the absence of rescue therapy. Very unlikely. The primary efficacy end point was the proportion of patients who had a platelet count ≥ 50 × 109/L after day 42 (week 6) during stage I without use of rescue treatment. Defined as either a new ITP medication, an increase in dose of concomitant ITP medication from baseline, platelet transfusion, or splenectomy. The decision to use rescue treatment is a clinical decision and therefore may vary slightly between the evaluators. The odds of bleeding and clinically significant bleeding in the eltrombopag-treated group relative to placebo, based on information at each stage I assessment, were compared using a generalized linear mixed model with a Logit canonical link function for repeated binary data, which allowed for baseline dichotomized WHO bleeding grade, use of ITP medication at baseline, splenectomy, baseline platelet count, and treatment arm as fixed effects. In addition, the patient was treated as a random effect and assumed to follow a normal distribution [~N (0, r2)]. |
Ghanima et al. (2015) was rated as some concerns for overall risk of bias. | Patients were randomized using precoded concealed envelopes, permuted block randomization with stratification by centre with a block size of 4. Patients, investigators, and reviewers were masked to allocation. Treatment allocation was communicated to local hospital pharmacies by fax. Infusion bags were concealed in opaque plastic bags that were sealed to mask the solution from the patient and health care providers. Pharmacists were not masked to treatment allocation. Treatment group imbalances (R vs. PBO): median bleeding score (2 vs. 4), treatment with corticosteroids (58% vs. 44%), Duration of ITP in weeks (newly diagnosed: 33% vs. 22%, persistent: 24% vs. 30%, chronic: 44% vs. 48%). Double-blind study. Infections were higher with rituximab (40% vs. 24%) and bleeding was higher with placebo (38% vs. 50%). Outcomes were assessed using the full analysis set (ITT). Low discontinuation rate. Platelet count ≥ 30 × 109/L (overall response) after week 4; and platelet count needed to be at least double that at baseline without administration of any platelet increasing therapy (except stable/decreasing prednisone or prednisolone) in the past 4 weeks. Efficacy outcomes were adjudicated by 2 reviewers who were masked to treatment allocation. Treatment failure was defined as a composite of splenectomy or meeting criteria for splenectomy after week 12 if splenectomy was not done, assessed in all patients who received at least one dose of study treatment. The primary end point was amended from splenectomy within 78 weeks to the rate of treatment failure, defined as a splenectomy or meeting the criteria for a splenectomy after week 12, if a splenectomy was not done because of contraindications or patients’ refusal. At which point in the study the end point was amended is unclear. |
Shirasugi et al. (2011) was rated at overall high risk of bias. | The randomization procedure was conducted centrally by Transcosmos Inc. (Tokyo, Japan) using a preprepared randomization list and communication via fax. No information about allocation concealment. Treatment group imbalances (ROM vs. PBO): female (64% vs. 83%), age (mean of 58.5 vs. 47.6), ECOG scores (0 = 77% vs. 92%, 1 = 23% vs. 8%), concomitant ITP therapy (59% vs. 83%). Double-blind study design. Frequency of AEs were much higher with romiplostim than placebo, which may have resulted in knowledge of treatment assignment. Full analysis set used. Rescue medication was defined as any medication administered for the intended purpose of raising platelet counts; permitted were IVIG, platelet transfusions, corticosteroids, and an increase in dose or frequency of a concomitant oral corticosteroid, azathioprine, and/or danazol. The decision to use rescue medication may vary between assessors. Throughout the study, rescue medication was permitted for severe bleeding or if the investigator believed that the patient was at immediate risk of bleeding. |
Kuter et al. (2010) was rated as a high overall risk of bias. | Randomized in a 2:1 ratio, stratified by geographic region. Open-label study design. In general, the treatment groups were fairly balanced. Treatment group imbalances were present for the following (ROM vs. SOC): previous treatment with IVIg (57% vs. 64%), previous treatment with rituximab (20% vs. 31%), more than 2 previous treatments (70% vs. 78%), medications for ITP at baseline (13% vs. 6%). No information about protocol deviations; but discontinuations from study were 8% vs. 19% for ROM vs. SOC and the most common reason was withdrawal of consent. Primary and secondary efficacy end points were analyzed using the ITT set. Discontinuations from study were 8% vs. 19% for ROM vs. SOC. Patients who received study treatment and discontinued from study were counted as having had both treatment failure and splenectomy. A platelet count of 20 × 109/L or lower for 4 consecutive weeks at the highest recommended dose, a major bleeding event, or requirement for a change in therapy (including splenectomy) because of an adverse event or bleeding symptoms. The outcome is based on mostly objective components, with the exception of “requirement for a change in therapy,” which is based on clinical decision-making and may be subject to bias due to open-label study design. The definition of major bleeding was not defined; however, it is unlikely that this outcome would not be assessed appropriately given the level of severity. Definition of major bleed is unclear. The definition of treatment failure was a composite outcome. Further, “Given the length of the treatment period, it was anticipated that some patients might discontinue the study early; therefore, in the primary end point analyses, a patient who had received any study treatment and had then discontinued the study was counted as having had both treatment failure and splenectomy”. |
Bussel et al. (2018) was rated as an overall high risk of bias. | Diarrhea, hypertension, nausea, and dizziness were reported more frequently in the fostamatinib treatment group, which may have allowed patients and assessors to deduce the assigned intervention. ITT analysis set. Very high discontinuation rates in both studies. High discontinuation rates due to lack of response the majority of nonresponders on fostamatinib and most patients on placebo discontinued study treatment at week 12 to enter the open-label, long-term extension study: 88% of patients in FIT1 and 79% in FIT2 on placebo vs. 55% in FIT1 and 66% in FIT2 on fostamatinib. The outcome was defined a priori but details of the analysis are unclear. Further, it is unclear why the denominator is less than the ITT set. |
Eisai Inc. (2019) was rated as some concerns for overall risk of bias. | Not enough information to assess. Only baseline characteristics available were age and sex. Study was double-blind, but SAE were only reported in the avatrombopag group. The study was terminated early due to significant enrolment challenges. |
Cheng et al. (2011) was rated as an overall low risk of bias. | Patients were randomly allocated in a 2:1 ratio to receive treatment with local standard of care plus either 50 mg eltrombopag or matching placebo. All randomizations were done with RAMOS, an automated interactive voice recognition telephone randomization and drug ordering system. Patients, investigators, and those assessing the data were masked to allocation. Well balanced groups, but higher baseline bleeding symptoms and clinically significant bleeding symptoms among the placebo group. ITT population was used. All randomized patients were included in the efficacy analysis, but 23/135 discontinued from eltrombopag; 7/62 discontinued from placebo. Response to treatment (platelet count 50,000 to 400,000 per uL) during the 6-month treatment period; a period of rescue treatment was recorded as a nonresponse. Unlikely, but decisions regarding concomitant ITP medication use may differ between clinicians/investigators. |
Tomiyama, et al. (2012) was rated as some concerns for overall risk of bias. | Patients were randomly allocated to either eltrombopag or placebo, and randomization was performed centrally. Treatment assignment was unblinded at week 7 (before entry into the open-label phase) on an individual patient basis. Treatment group imbalances by (PBO vs. E): sex % female (88% vs. 53%), median platelet count (9500 vs. 21,000), splenectomy (64% vs. 73%), platelet count < 15 000 uL (75% vs. 20%). Double-blind during the 6-week evaluation; AEs were more frequent with eltrombopag vs. placebo. Minimal information about the analyses conducted. All patients in the 6-week double-blind period were enrolled in the OLE. Assume that data were available for all patients. Patient disposition was not reported, but the results appear to include data for all patients. A responder was defined as a patient achieving a platelet count ≥ 50 × 10^9/L and ≤ 400 × 10^9/L. This was predefined as the primary end point. The primary end point for 6-week evaluation was the proportion of responders at week 6 in the eltrombopag group vs. the placebo group. The definition of bleeding was not defined. It is possible that assessors recorded incidence of bleeding differently, although it is unlikely. Bleeding was not defined; therefore multiple definitions could have been used. |
Kuter et al. (2008) was rated as an overall low risk of bias. | Patients were randomly assigned 2:1 to receive romiplostim or placebo. Random allocation sequence was generated by Amgen Inc. (Thousand Oaks, CA, US) with the blocked randomization method. Clinphone was used to randomly assign patients into the study with the interactive voice response system. Difference in the proportion of patients receiving concurrent ITP therapy (38% placebo, 28% romiplostim). Double-blind study and no major differences between AEs. Analysis was per protocol. Discontinuations were balanced between groups and limited so this was unlikely to cause attrition bias. Weekly platelet responses during 6 or more weeks of the last 8 weeks of treatment in the absence of rescue therapy. The decision of the treating physician to use recue treatment may vary, although there is no reason to expect this to differ systematically between treatment groups. |
Bussel et al. (2009) was rated with some concerns for overall risk of bias. | Patients were randomly assigned 2:1 to receive standard of care and either eltrombopag or placebo. Patients were randomly assigned by an in-house validated randomization system (RANDALL). Some treatment group imbalances to note (E vs. PBO): % women (57% vs. 71%), race, white (76% vs. 68%), baseline platelet counts = < 15,000 per uL (50% vs. 45%), at least 2 previous ITP therapies (74% vs. 68%). Differences in AEs may have lead to patients inferring treatment received. Nausea, vomiting, fatigue, and myalgia were only reported in the eltrombopag group. Bleeding was more common in the placebo group. ITT population was reported. Proportion of responders, defined as patients who had an increase in platelet counts to ≥ 50 000/μL at day 43 (i.e., 6 weeks after the start of treatment); patients who withdrew prematurely because of a platelet count greater than 200 000/μL were considered responders. |
Figure 3: Risk of Bias Assessments Per Outcome Within Each Study (Jurczak, Arnold, Yang, Ghanima, Shirasugi)
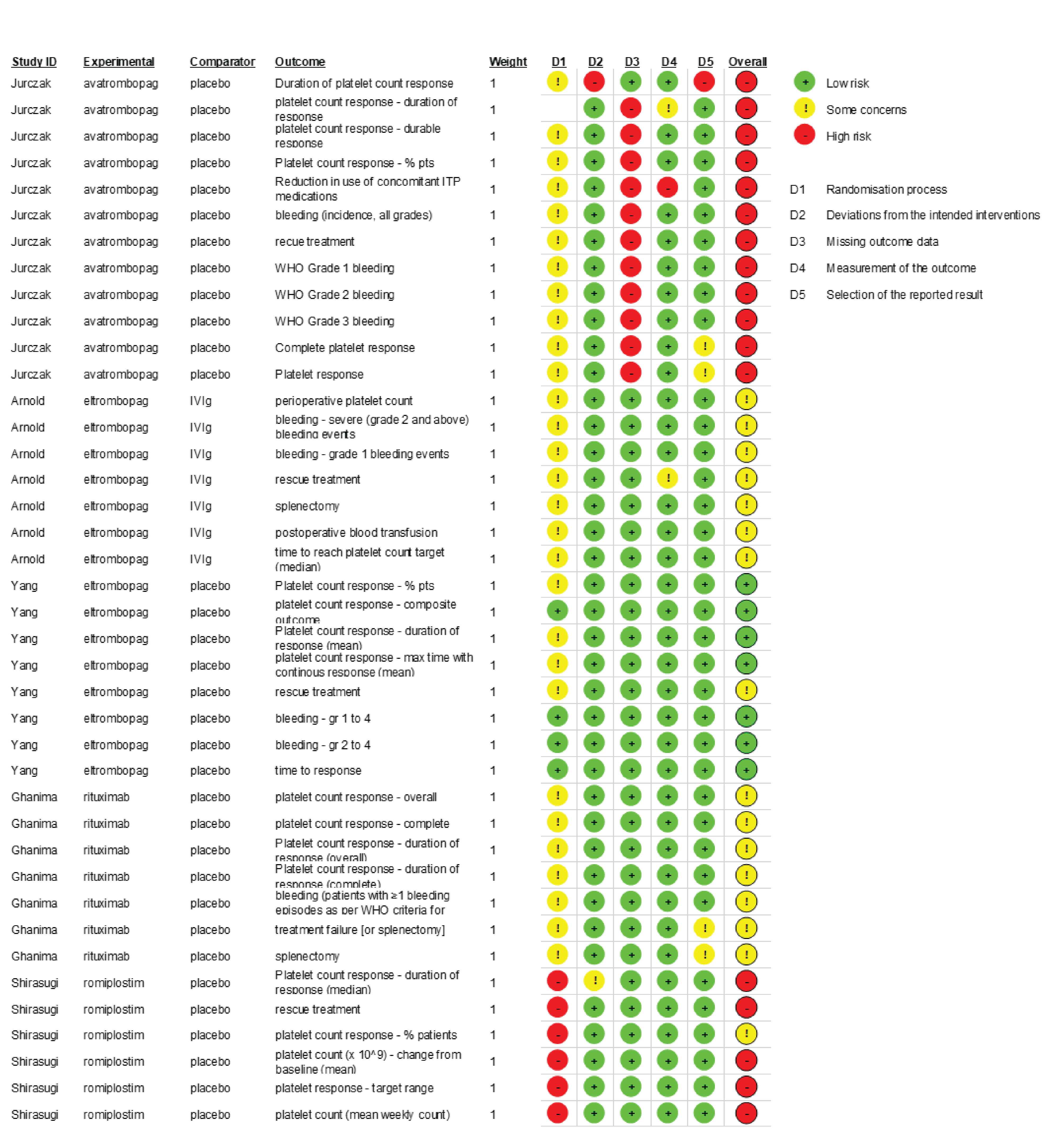
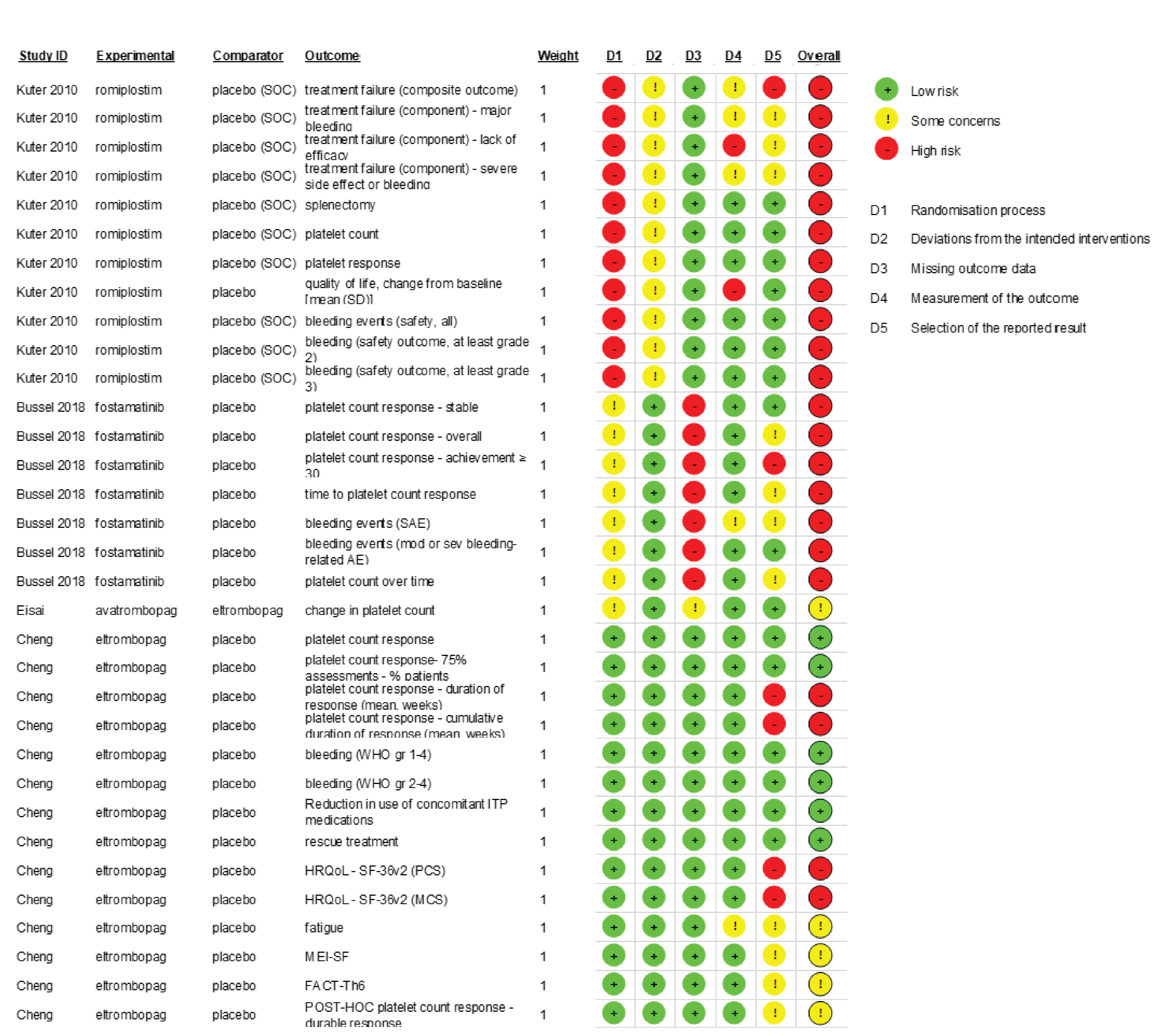
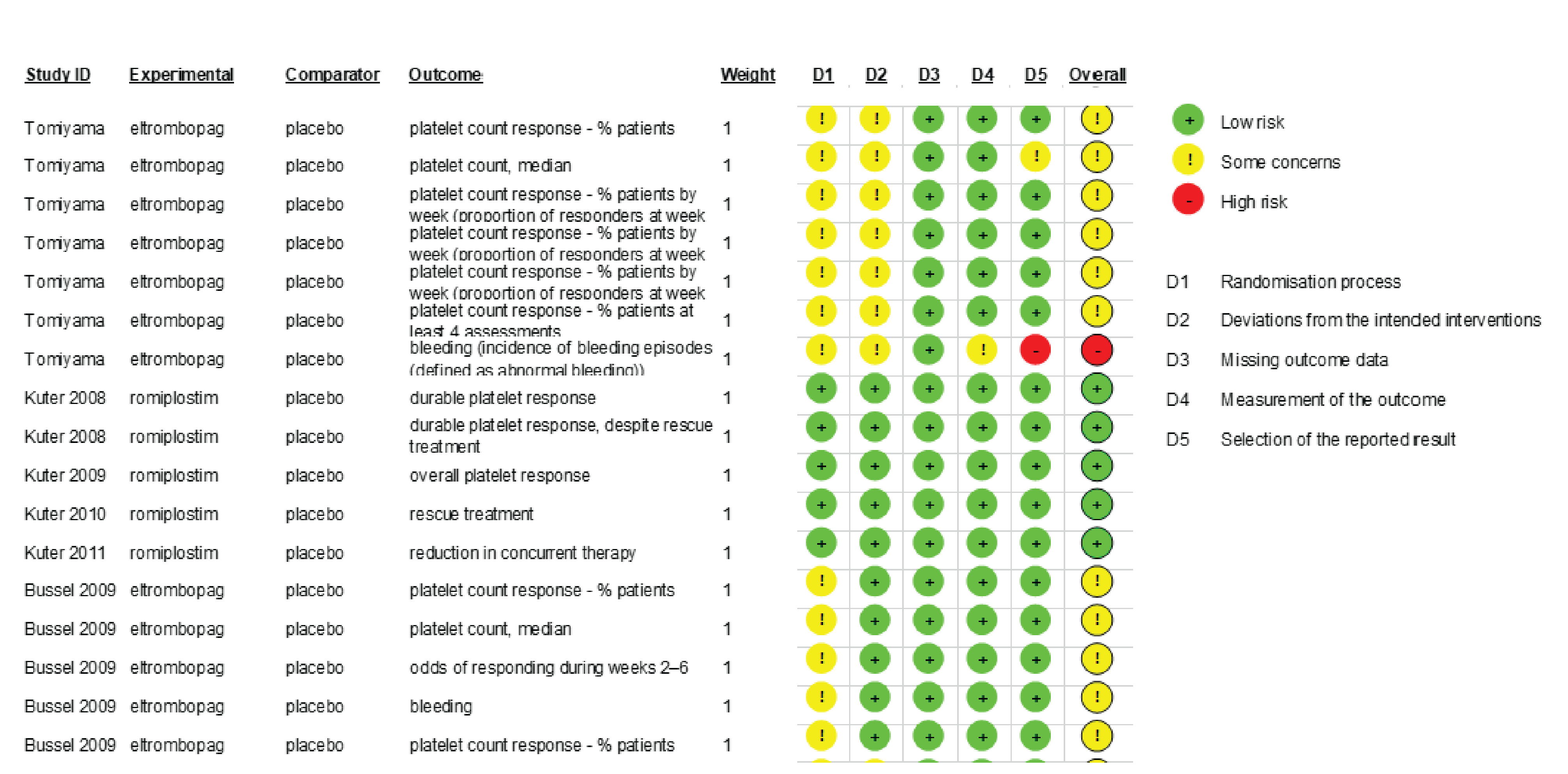
Appendix 11: Economic Evaluation
Note that this appendix has not been copy-edited.
Literature Review
As part of the development of the economic evaluation for chronic ITP, a literature review of existing decision-analytic models in chronic ITP was conducted. With the goal to determine whether any of the published economic evaluations could directly address the research questions; and, if not, whether details on the model structure could assist the development of a model. This was not a systematic review and hence likely to be nonexhaustive. Conference abstracts and manuscripts published in a different language than English were excluded.
Table 29 below summarizes the main characteristics of the identified studies. None of the identified studies were directly applicable to the economic analysis research questions. Given that the rationale for conducting this review was to further inform the development of a decision-analytic model, less emphasis was placed on the results of the analysis. Instead, the review focused on the model structure.
Table 29: Summary of ITP Decision-Analytic Models
Source | Model type | Target population | Intervention/ Comparators | Health states | Time horizon | Cycle length | Perspective |
|---|---|---|---|---|---|---|---|
Allen 201644 | Markov | UK patients with chronic ITP | Eltrombopag | 1.NR w1 to 4 2.NR w5 to 8 3.NR w9 to 12 4.NR w13 to 16 5.Responder 6.Long-term NR | Lifetime | 4 weeks | Public health care (UK) |
Lee 201345 | Markov / decision tree combination | Irish adults with chronic ITP | Romiplostim + SoC Eltrombopag + SoC SoC, including rituximab | 1.Sufficient platelets 2.Low platelets 3.Death | Lifetime | 4 weeks | Public health care (Irish) |
Tremblay 202046 | Markov | American patients with chronic ITP | Eltrombopag | 1.On treatment 2.Treatment failure/discontinuation 3.Mortality | Lifetime | 28 days | US payer perspective |
Xie 200947 | Markov | Canadian adults with chronic ITP | IVIG Prednisone | 1.Remission 2.No response 3.Refractory 4.Post splenectomy remission 5.Death | Lifetime | 1 year | Public health care (Canada) |
ITP = immune thrombocytopenia; NR = no response; SoC = standard of care.
Four studies were identified that had developed a decision-analytic model to support either a cost-effectiveness or a cost-utility analysis. All analyses were models and adopted the same national public health care perspective (except for Tremblay 2020 in which the US payer perspective was used). All studies used a cohort state-transition (Markov) model with discrete time cycles. The cycle lengths varied but all models used a lifetime time horizon. Disease progression, modelled by health states, varied across the published models but could be broadly categorized as response, nonresponse, and death.
Ideal Model Structure
As part of the scoping process, existing published models were reviewed, and clinical experts were consulted to determine the most appropriate characterization of ITP. The conceptual structure below was the outcome of the exercise, which clinical experts considered an appropriate representation of the natural history of chronic ITP. Of note, the proposed structure below was developed without taking data availability into consideration.
As the model’s target population is adults with ongoing, active ITP after failure of first-line therapy, the baseline characteristics of the target population ideally would be defined in such a way that resemble the characteristics of ITP patients diagnosed across Canadian jurisdictions. Real world administrative data would be a source to inform this set of model parameters, assuming that the population can be adequately identified through administrative data.
The base-case analysis would be conducted from the perspective of the Canadian publicly funded health care system. The model time horizon would be life-long with weekly cycle lengths. As per CADTH guideline, the discount rates for costs and utilities would be 1.5% annually. We assumed that a weekly cycle length would be a sufficient minimum duration to capture recurrent events (e.g., bleeding) or transitions between health states. A lifetime horizon would be appropriate since some of the modelled events (e.g., severe bleeding/intracranial hemorrhage) can be life altering with an increased risk of mortality.
The model would be an individual-level state-transition model, also known as a microsimulation model, with discrete time cycles. A microsimulation approach was proposed so that time dependency (e.g., differential response and bleeding events over time), the effect of past events, and individual heterogeneity is adequately considered in the model. Treatment choice after nonresponse to therapy is dependent on past treatment exposure, hence, treatment history may be considered a past event that needs to be recorded within the model. An example of individual heterogeneity relevant to consider within this decision problem, as per input from clinical experts consulted by CADTH, was the increased risk of bleeding for individuals who already experienced a bleeding episode. Hence, history of bleeding events should be taken into consideration as this would impact an individual’s risk of bleeding and have associated utility and cost impacts.
Using input from the clinical team, the model should capture the following 6 treatments: rituximab, eltrombopag, romiplostim, fostamatinib, avatrombopag, and splenectomy. It remains unclear presently whether IVIG, immunosuppressants (azathioprine, cyclosporine, cyclophosphamide, mycophenolate mofetil, danazol, dapsone) and corticosteroids constitute real world treatment alternatives.
The proposed model structure would have 4 states: nonresponse, response, and ITP-related death and death from all-cause mortality. The model diagram is presented below (Figure 6). As patients transition between states, they can experience bleeding (major and minor), experience a serious infection, switch treatment, or require rescue medication. Only some of these events are included in the model diagram for simplicity. All states lead to both ITP-related death (through bleeding or infection) and non-ITP-related death (death from other causes). These transition arrows are omitted from the model diagram for simplicity. Transitions may be modelled with time and state residence dependencies, where appropriate, to factor time dependencies, the effect of past events, and individual heterogeneity. The relationships among these events are also modelled, as noted in the transition arrows within the Figure 6.
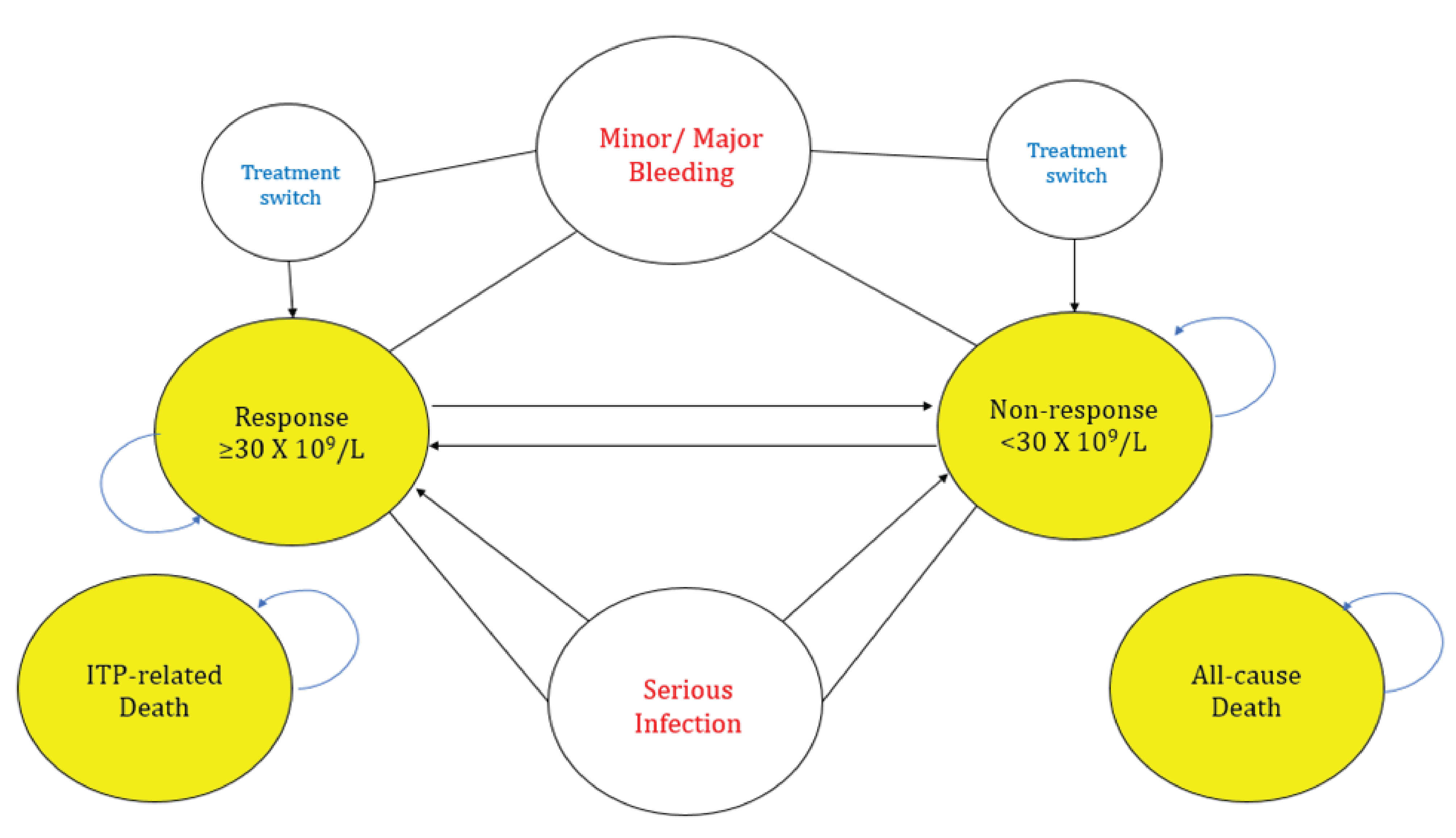
Model Inputs
The following outcomes would be needed to meaningfully inform the proposed economic model:
Clinical effectiveness outcomes would include time to platelet count response; time and treatment-dependent risk of (severe) bleeding and (severe) infections; time to treatment discontinuation; need for rescue medication (e.g., IVIG, corticosteroids, platelet transfusions), and mortality.
Severity and location of bleeding would be a function of treatment (e.g., intracranial hemorrhage vs. other bleeding) and the risk of bleeding would depend on response status.
Treatment adherence would be dependent on time and treatment history.
Safety outcomes should include AEs, serious AEs, discontinuation due to AEs, and adverse event-related death. Preference based HRQoL estimates would be required to assign utility values in occupying a given health state or experiencing an event such as severe bleeding or infection. Treatment effectiveness, AEs, treatment adherence, and costs would ideally be conditional on treatment dosage.
Table 30 and Table 31 provide a subset of the probability, utility, and cost input parameters currently available that could be used to develop a chronic ITP decision-analytic model. Of note, provided utility estimates were by platelet count and not categorized by response (where ideally a model could simulate platelet count movement).
Table 30: Model Input Parameters That Were Successfully Identified and Sourced
Input parameter | Value | Source | ||||
|---|---|---|---|---|---|---|
Proportion with ITP-related minor bleed | 1.4% [0.9%, 2.1%] | Neunert 2015 48 | ||||
Proportion with ITP-related major bleed | 9.6% [4.1%, 17.1%] | Neunert 2015 48 | ||||
Major bleed mortality (1-year) | 0.454 | Fernando 2021 49 | ||||
5-year MRR after severe bleeding | 10.6 [4.2, 26.6] | Norgaard 2011 50 | ||||
Adjusted 1-year relative risk of infection | 4.5 [3.3, 6.1] | Norgaard 2011 50 | ||||
Mortality rate ratio after infection (5-year) | 4.2 [2.4, 7.2] | Norgaard 2011 50 | ||||
Utility estimates | < 10k (n = 25) | 11 to 29k (n = 75) | 30 to 49k (n = 109) | 50 to 99k (n = 210) | 100 to 149k (n = 139) | > 150k (n = 444) |
EQ-5D Index Score | 0.75 | 0.83 | 0.82 | 0.82 | 0.79 | 0.82 |
Table 31: Treatment Costs That Were Successfully Identified and Sourced
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Course or annual cost ($) |
|---|---|---|---|---|---|---|
Fostamatinib (Tavalisse) | 100 mg 150 mg | Tablet | 80.8700 121.3050 | Initially 100 mg twice daily. After 4 weeks, increase to 150 mg twice daily if platelet count has not reached at least 50 × 109/L | 161.74 to 242.61 | 59,035 to 88,553 |
TPO-RAs | ||||||
Eltrombopag (Revolade) | 25 mg 50 mg | Tablet | 65.0000 130.0000 | Initially 50 mg once daily (25 mg in Asian patients). After 2 weeks, increase dose by 25 mg if platelet count < 50 × 109/L, up to a maximum of 75 mg daily. Reduce dose when platelet count is above 200 × 109/L | 65.00 to 195.00 | 23,725 to 71,175c |
Romiplostim (Nplate) | 250 mcg/0.5 mL 500 mcg/1 mL | Vial of lyophilized powder for solution | 1,021.7900 2,043.6000 | 1 mcg/kg SC weekly, adjusting by increments of 1 mcg/kg until platelet count ≥ 50 × 109/L. Do not exceed 10 mcg/kg | 145.97 initially, up to 437.91 | 53,279 initially, up to 159,837 |
CD20 Inhibitor (off-label) | ||||||
Rituximab (Rituxan, Truxima, Riximyo, Ruxince) | 10 mg/mL | 10 mL 50 mL Single use vials | 297.0000 1,485.0000 | 375 mg/m2 IV once per week for 4 weeks | NA | Cost per 4-week course: 8,316 |
100 mg IV once per week for 4 weeks | NA | Cost per 4-week course: 1,188 | ||||
Immunosuppressants (off-label) | ||||||
Azathioprine (generic) | 50 mg | Tablet | 0.2405 | 1 to 2 mg/kg daily, maximum 150 mg/day | 0.48 to 0.72 | 176 to 263 |
Cyclosporin A (Neoral, generic) | 10 mg 25 mg 50 mg 100 mg | Tablet | 0.6700 0.9952 1.9400 3.8815 | 5 mg/kg/day for 6 days, then 2.5 to 3 mg/kg/day | Initial: 15.53 Then: 7.76 to 9.70 | 2,881 to 3,577 |
100 mg/mL | Oral solution | 5.4030 | Initial: 21.61 Then: 10.81 to 12.97 | 4,009 to 4,785 | ||
Cyclophosphamide (Procytox) | 25 mg 50 mg | Tablet | 0.3545 0.4773 | 1 to 2 mg/kg daily for at least 16 weeksd | 0.83 to 1.43 | 304 to 523 |
200 mg 500 mg 1000 mg 2000 mg | Vial for injection 20mg/mL | 74.23 93.14 168.8300 310.6000 | 0.3 to 1 g/m2 IV every 2 to 4 weeks for one to 3 doses | NA | Per course: 167 to 932 | |
Danazol (Cyclomen) | 50 mg 100 mg 200 mg | Capsule | 1.0212 1.5156 2.4220 | 200 mg 2 to 4 times daily | 4.84 to 9.69 | 1,768 to 3,536 |
Dapsone (generic) | 100 mg | Tablet | 0.7031 | 100 mg per day | 0.70 | 257 |
Mycophenolate mofetil (generic) | 250 mg 500 mg | Capsule | 0.3712 0.7423 | 1.5 to 2 g/day for at least 12 weeks | 2.23 to 2.97 | 813 to 1,084 |
Vincristine (generic) | 1 mg/mL | Solution for injection | 30.6000 | 6 mg total at 1 to 2 mg per weekly infusion | NA | Per course: 184 |
Vinblastine (generic) | 10 mg/ 10 mL | Solution for injection | 185.6300 | 30 mg total at 10 mg per weekly infusion | NA | Per course: 557 |
IV Immunoglobulins (Human), 10% | ||||||
Gamunexb | 5g/50mL 10 g/100mL 20 g/100mL | Injectable solution | 27.2743 | 0.1 and 0.6 g/kg every 3 or 4 weeks | 7.32 to 56.49 | 2,673 to 20,619 |
IGIVnexc | 10% solution | Injectable solution | 27.2743 | 0.1 and 0.6 g/kg every 3 or 4 weeks | 7.32 to 56.49 | 2,673 to 20,619 |
Gammagard Liquidb | 1 g/10 mL 2.5 g/25 mL 5 g/50 mL 10 g/100 mL 20 g/200 mL 30 g/300mL | Solution for infusion | 26.9247 | Starting dose: 0.4 to 0.8 g/kg Thereafter: 0.2 to 0.8 g/kg | Initial: 28.92 to 74.36 Subsequent: 14.46 to 111.53 | Initial: 10,554 to 27,140 Subsequent: 5,277 to 40,710 |
Gammagard S/Dd | 5 g 10 g | Vial | 40.8342 | At least 0.1 mg/kg, monthly recommended. (Initially, patients may receive 0.2 to 0.4 g/kg) | 9.40 | 3,430 |
Octagamb,e | 5 g/50 mL 10 g/100 mL 20 g/100 mL 50 mg/mL | Solution for infusion | 24.4666 | Replacement therapy in PID: Monthly doses of at least 0.1 g/kg recommended. Replacement therapy in SIDs: 0.2 to 0.4 g/kg body weight every 3 to 4 weeks | 16.89 to 26.28 | 6,166 to 9,591 |
Panzyga | 100 mg/mL | Solution for infusion | 59.5375 | 0.2 to 0.8 g/kg, every 3 to 4 weeks | 31.97 to 164.42 | 11,669 to 60,013 |
Privigenb | 5 g/50 mL 10 g/ 100 mL 20 g/200 mL 40 g/ 400 mL | Solution for infusion and IV | 41.9715 | 0.2 to 0.8 g/kg, every 3 to 4 weeks | 22.54 to 115.91 | 8,226 to 42,307 |
Weighted IVIG cost from public sources | $47.39 per gram | http://www.cdha.nshealth.ca/nova-scotia-provincial-blood-coordinating-program-9 | ||||
Discussion
The existing published decision-analytic models informed the fundamental structure of the proposed economic model. A Markov model was considered to be a less effective approach to incorporate the complexities of the course of treatment and disease trajectories, as well as the interrelationships between treatment, AEs, and other clinical outcomes. As such, a microsimulation was felt to allow the flexibility to capture these effects and could represent the ideal modelling approach. The data collected, described in the Model inputs section of this Appendix, provide several core input parameters to this model. However, these data would not be sufficient by themselves to support the development of the model described in the model section of this Appendix.
Given the lack of data at this time, simplifications to the ideal model may be required to what could be feasible, however this should be revisited as data in this space evolves. A simplified model would have the same structure and components as the ideal model except that treatment effects would be time-independent, while bleeding and infection risks would not be treatment or time-specific (given the current lack of information). To overcome these limitations, several data points and input parameter estimates, which we could not successfully source, are required. Time-dependent treatment effects and time-dependent transition probabilities between health states need to come from a robust NMA; where the heterogeneity around the definition of treatment response, both across the studies identified in the NMA, but also in real world clinical practice complicate the comparison of the alternative identified treatment strategies in a common framework. Estimates of population baseline risk of infection, estimates of treatment-specific bleeding, and infection risks are needed, and would ideally be sourced from data reflective of the population of interest (chronic ITP patients in Canada who have failed first-line treatment). More recent and more accurate estimates of health utility associated with treatment response and bleeding or infection outcomes would also be required.
Once data that are reflective of the need of such model are generated and/or collected, we can then inform core components of the economic model, such as the risk of treatment switching or treatment-specific rates of bleeding events. If Canadian patient databases exist, this would ideally be able to be used to inform the baseline characteristics of the model population. If patient data are sufficiently granularly reported (e.g., age, splenectomy at baseline), subgroup analyses of interest, such as splenectomy status, could further be supported in the economic analysis. Another possibility that comes with these data are the ability to model treatment effectiveness more explicitly, by modelling the waning of treatment efficacy and adherence with differential waning across treatments (e.g., Rituximab vs. Fostamatinib). Thus, the effects of treatment switching on treatment effectiveness can also be more explicitly estimated and modelled.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.