Drugs, Health Technologies, Health Systems
Health Technology Review
Health System Readiness for Disease-Modifying Therapies for Alzheimer Disease
Key Messages
What Is the Issue?
Alzheimer disease (AD) is a chronic neurologic degenerative disease and 1 of the most common causes of dementia. It affected an estimated 368,200 people in Canada in 2020.1
Mild cognitive impairment (MCI) is a clinical condition involving memory loss that can progress to dementia and is often due to underlying AD. It was estimated to affect around 917,000 people in Canada aged 60 and older in 2020.1,2
Disease-modifying therapies (DMTs) are being developed that target underlying pathologic processes of AD to slow disease progression, unlike contemporary treatments that focus on managing symptoms. A prominent target of these therapies is amyloid-beta, a protein known to contribute to amyloid plaques. Many of the anti–amyloid-beta DMTs are intended for people with early-stage AD, which includes MCI and mild dementia due to AD.
At least 7 countries have approved a therapy from this treatment class, and, at the time of writing, 2 therapies are undergoing regulatory review by Health Canada and reimbursement review by Canada's Drug Agency (CDA-AMC).
DMTs demand more frequent health care visits and higher use of medical imaging for safe treatment and monitoring. This would greatly impact current care pathways for early-stage AD, necessitating an examination of health system readiness in Canada.
What Did CDA-AMC Do?
CDA-AMC sought to examine health system readiness in Canada and care pathways for early-stage patients with AD in preparation for the potential use of these anti–amyloid-beta DMTs in Canada.
CDA-AMC reviewed publicly available data and literature about health systems and AD treatment pathways for improving dementia care to prepare for the possible introduction of DMTs in health systems in Canada.
What Did CDA-AMC Find?
CDA-AMC found that, if DMTs were approved by Health Canada and provincial and territorial drug plans, a new model of care for AD in Canada would be necessary. The new care pathway would require:
earlier screening and diagnosis, at the MCI or mild dementia stages of AD
guidance for optimal use of diagnostic imaging and biomarker-based tests, as well as an increase in equitable access to PET-CT units for amyloid PET exams or cerebrospinal fluid (CSF) testing to assess treatment eligibility
increased capacity to administer IV infusions
guidance for optimal use of MRI to avoid overuse and increase equitable access to MRI to monitor individuals through treatment
a combination of reliable and validated methods and tools for evaluating cognitive decline in diverse populations, including Indigenous Peoples and racialized groups, presenting with cognitive symptoms or undergoing treatment
clear criteria for discontinuing treatment.
CDA-AMC found that assessment and diagnosis of early-stage AD and timely access to DMTs could be delayed due to:
a lack of education and awareness of symptoms of early-stage AD among the general public and care providers, as well as cultural barriers, including a fear of stigma or cultural perceptions of the condition3
staffing shortages in care providers capable of assessing and treating dementia and other supporting staff, including primary care providers (PCPs), dementia specialists, nurses, imaging staff, and social care providers
limited capacity of medical imaging (e.g., PET-CT and MRI) and laboratory services (i.e., CSF analysis) to confirm early-stage AD and treatment eligibility and to monitor drug response and disease progression.
A variety of new technologies are in development, including new AD biomarker testing methods, that may alleviate some capacity concerns in dementia detection, treatment eligibility screening, treatment administration, and patient monitoring.
Alternative DMTs that target other AD pathologic processes are also in development.
What Does This Mean?
There may be challenges in providing equitable and timely access to DMTs for AD, given the geographic distribution of the population (especially in rural and remote locations), cultural barriers, and lack of awareness of the condition in the population in Canada.
Not all individuals with mild dementia due to early-stage AD or MCI who are eligible for treatment may have timely access to screening and diagnosis, which could prevent them from receiving DMTs.
Additionally, an increased number of individuals — some of whom may not be eligible for DMTs — may be motivated to seek screening, leading to higher demand and potential delays in the screening process.
Health system decision-makers may want to consider system-wide adaptations to enhance screening and care for individuals with suspected early-stage AD, given the projected rise in AD prevalence, which is expected to exceed 1.1 million people by 2050.1 This may include:
adding more health and social care staff
providing enhanced training to effectively assess and diagnose early-stage AD
improving access to diagnostic imaging to screen and monitor patients using anti–amyloid-beta DMTs.
Abbreviations
AD
Alzheimer disease
AI
artificial intelligence
ARIA
amyloid-related imaging abnormalities
CADRO
Common Alzheimer’s Disease Research Ontology
CCCDTD
Canadian Consensus Conference on the Diagnosis and Treatment of Dementia
CSF
cerebrospinal fluid
DMT
disease-modifying therapy
GFAP
glial fibrillary acidic protein
LP
lumbar puncture
mAb
monoclonal antibody
MCI
mild cognitive impairment
MINT
multispecialty interprofessional team
NfL
neurofilament light chain
NICE
UK National Institute for Health and Care Excellence
p-tau
phosphorylated tau
PCP
primary care provider
Background
New DMTs using monoclonal antibodies (mAbs) may provide new treatment options for people with MCI and mild dementia due to early-stage AD. Unlike existing treatments that focus on managing the symptoms of AD or MCI, DMTs are intended to slow disease progression.4
Currently, no DMTs are approved for use in Canada for any type of dementia, but, if DMTs are approved by Health Canada, a surge in demand is possible. Resource implications are anticipated, as DMTs would place new requirements on the health care system for their optimal use.4,5
Objective
This report examines the readiness of health care systems in Canada for the potential introduction of anti–amyloid-beta mAb DMTs. While there are several new AD therapies on the horizon, this report focuses on mAb DMTs targeting amyloid-beta in patients with early-stage AD, including MCI or mild dementia due to AD. In some countries, these therapies have received regulatory approval and positive recommendations for reimbursement and are being implemented in the health care system.
This report also explores emerging technologies that could enhance health systems’ efficiency in implementing anti–amyloid-beta mAb DMTs for AD and provides an estimate of the number of patients with incident early-stage AD who could receive treatment with anti–amyloid-beta mAb DMTs.
Approach
Information specialists conducted a tailored literature search, balancing comprehensiveness and relevance, across various sources, including a focused internet search conducted on March 8 and 9, 2024, as well as regular search updates. Content experts were consulted for input and peer review. This document delineates the current patient pathway for AD and outlines 4 domains of a potential future AD treatment pathway for novel anti–amyloid-beta mAb DMTs: assessment and diagnosis of early-stage AD, treatment eligibility assessment, treatment administration, and patient monitoring.
What Is the Context?
Alzheimer Disease and Mild Cognitive Impairment
Dementia is a condition characterized by symptoms such as memory loss and difficulties with attention, language, and problem solving resulting from specific disruptions to brain function, reducing a person’s ability to perform everyday activities.1
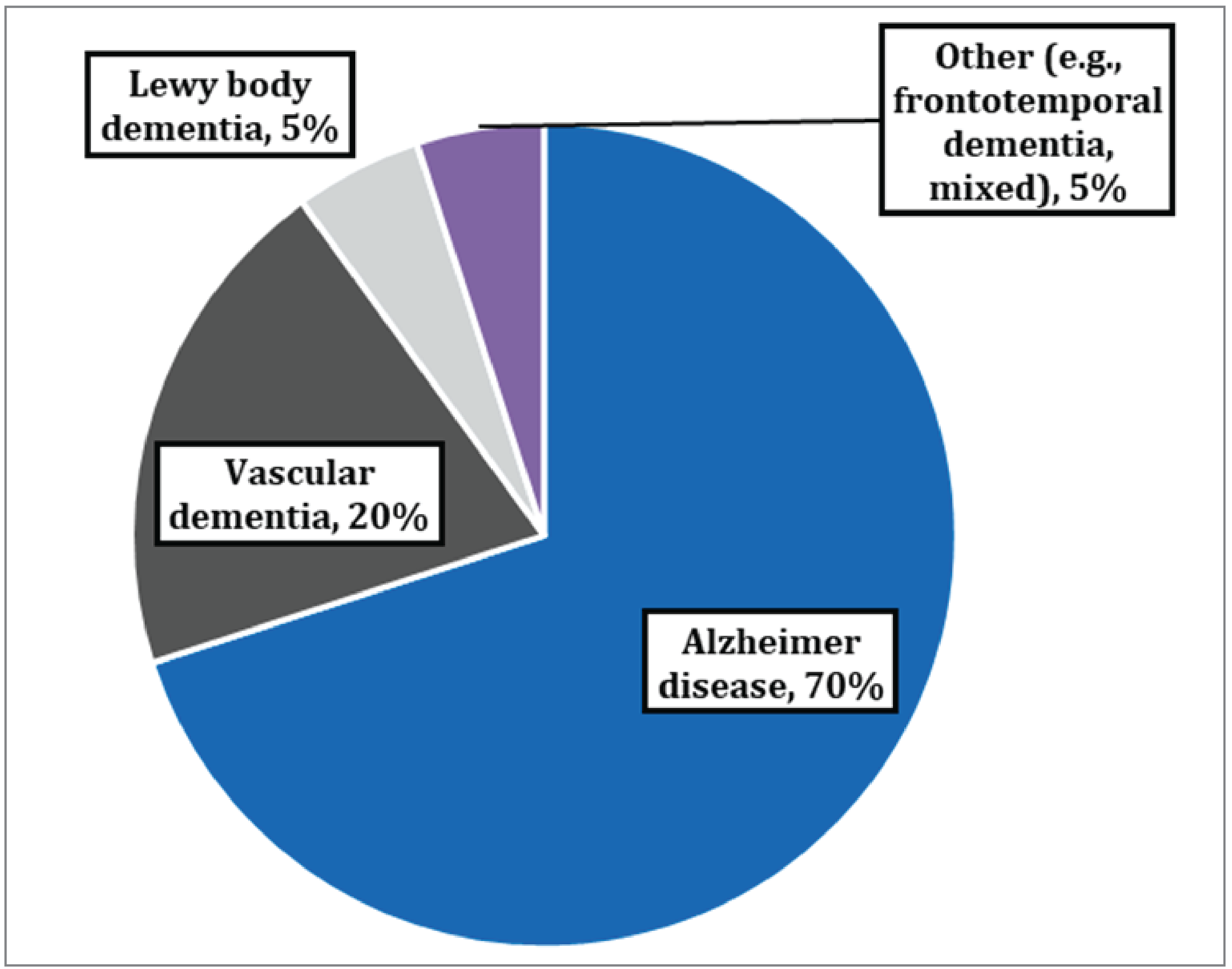
AD is a chronic neurologic degenerative disease that results in a progressive loss of cognition, function, and social capabilities.6,7 AD can cause changes to brain structures years before any symptoms develop and is 1 of the most common causes of dementia, contributing to 60% to 70% of dementia cases (Figure 1) and often affecting people aged older than 65.1,4,5
MCI is a neurocognitive disorder that is characterized by mild symptoms such as memory impairment but that does not functionally affect everyday activities.7,9 MCI frequently goes undetected until symptoms become more severe.10
MCI is often described as an intermediate stage of cognitive impairment between the changes in cognition associated with aging and the onset of dementia. Around 10% to 15% of MCI diagnoses progress to dementia caused by underlying AD annually.2,9 Not all MCI diagnoses result from AD pathology, as MCI can be caused by a variety of conditions.7,9 Early-stage AD includes both MCI due to AD and mild dementia due to AD.1,2,11
Figure 1: Proportions of Common Causes of Dementia8
AD in the Context of Canada
In Canada in 2020, there were an estimated 368,200 people living with AD, with that total expected to rise to more than 1.1 million people by 2050.1
Applying US estimates of MCI prevalence to the population in Canada, approximately 917,000 individuals aged 60 and older in Canada would have been affected by MCI in 2020.2,12
In 2020, the total annual economic burden of dementia in Canada was estimated at $40.1 billion, an average of $67,200 per person with dementia, and this cost is projected to rise to approximately $65.2 billion by 2030.13 According to the Alzheimer Society of Canada and the Public Health Agency of Canada, the total health care system costs and out-of-pocket costs of caring for people with dementia are 5.5 times greater than for those without dementia.14 The latter stages of AD involve the largest health care costs due to loss of independence, necessitating more attentive and intensive care, typically provided in long-term care or assisted-living residences.15,16
AD diagnosis currently relies on clinical presentation and family history, complemented by clinical assessment of cognition and functional impairment. Neuroimaging and AD biomarker testing are recommended only when initial evaluations are inconclusive in identifying the underlying cause of cognitive impairment.17 Routine screening of asymptomatic older adults with cognitive testing or diagnostic imaging is not recommended by the 5th Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (CCCDTD) guidelines,17 although there is some disagreement on this recommendation.17,18
Current AD treatment focuses on primary care, where available, and involves psychosocial interventions and pharmacological therapies (e.g., cholinesterase inhibitors and memantine). These approaches are not intended to slow disease progression and instead are intended to manage symptoms and late-stage disease.17,19 Currently, MCI is treated with preventive lifestyle measures, such as regular physical exercise, mentally stimulating activities, and improved nutrition. These lifestyle adjustments may reduce the risk of progression to dementia, but there are no recommended pharmaceutical treatments for MCI.17,20
Recent Developments in DMTs Using Monoclonal Antibodies for AD
The development of several novel mAb DMTs is predicated on recent advances in the understanding of AD biomarkers, which are indicators of pathological change of the disease.4 These therapies are designed to target protein accumulation associated with these biomarkers, thereby aiming to slow disease progression.21,22
One such target of these mAb DMTs is amyloid-beta, a protein believed to contribute to the formation of amyloid plaques in the brain, a signature biological milestone of AD that can lead to brain cell death. The amyloid hypothesis posits that removal of amyloid-beta can slow plaque formation and AD progression, prompting the development of anti–amyloid-beta mAb DMTs.23
Six anti–amyloid-beta mAb DMTs have advanced to or completed phase III clinical trials: aducanumab, donanemab, gantenerumab, lecanemab, remternetug, and solanezumab. Eligibility for these treatments requires early diagnosis of MCI or dementia due to AD.24 While 2 of these therapies have received FDA approval, others are still under evaluation in clinical trials, with additional treatments in active development.21,25,26 For the anti–amyloid-beta mAb DMTs that have been approved in the US and other countries, at least 3 MRI neuroimaging exams were required to monitor for adverse events during early phases of treatment, to allow treatment regimens to be tailored accordingly.27-30 However, if adverse events occur, additional MRI exams would be needed until symptoms resolve.27-30
A reported limitation of this approach to anti–amyloid-beta mAb DMT development is that cognitively healthy individuals will sometimes have abnormal biomarker results. Abnormal biomarker levels do not necessarily indicate that patients will develop AD in the future, meaning that some individuals may receive treatment that is not needed.31,32 There is also some uncertainty as to whether clearing amyloid-beta accumulations actually improves memory and cognition.32,33
If regulatory bodies and provincial and territorial formularies approve the use and reimbursement of these novel anti–amyloid-beta mAb DMTs, the current paradigm for treatment and management of AD in Canada may need to change. Potential gaps in the current system would need to be addressed so that:5,20,32,33
individuals with cognitive symptoms receive timely and equitable access to dementia specialists for an early cognitive assessment of AD and to imaging specialists for neuroimaging
there is increased capacity and equitable access to amyloid PET scans or lumbar puncture (LP) procedures to determine levels of abnormal amyloid-beta required to assess treatment eligibility and there are standardized optimal-use guidelines for amyloid PET and LP procedures
staffing capacity, particularly of dementia specialists, matches expected demand for services
there is timely access to MRI scans for screening that follows standardized optimal-use guidelines and for monitoring adverse events during treatment and health care systems are equipped to manage effectively and address any adverse events that may arise.
Health System Readiness
The Patient Pathway
Currently, the diagnostic and treatment pathway for people with early-stage AD, which includes MCI and mild dementia due to AD, typically begins with the presentation of symptoms. However, a significant portion of the general public remains unaware of the symptoms of early-stage AD.34,35
Patients and their caregivers initially seek care from social care services or from a PCP who can recognize, assess, and diagnose AD, possibly collaborating with a dementia specialist if their expertise is required. Upon confirmation of early-stage AD, current treatments primarily focus on managing symptoms.
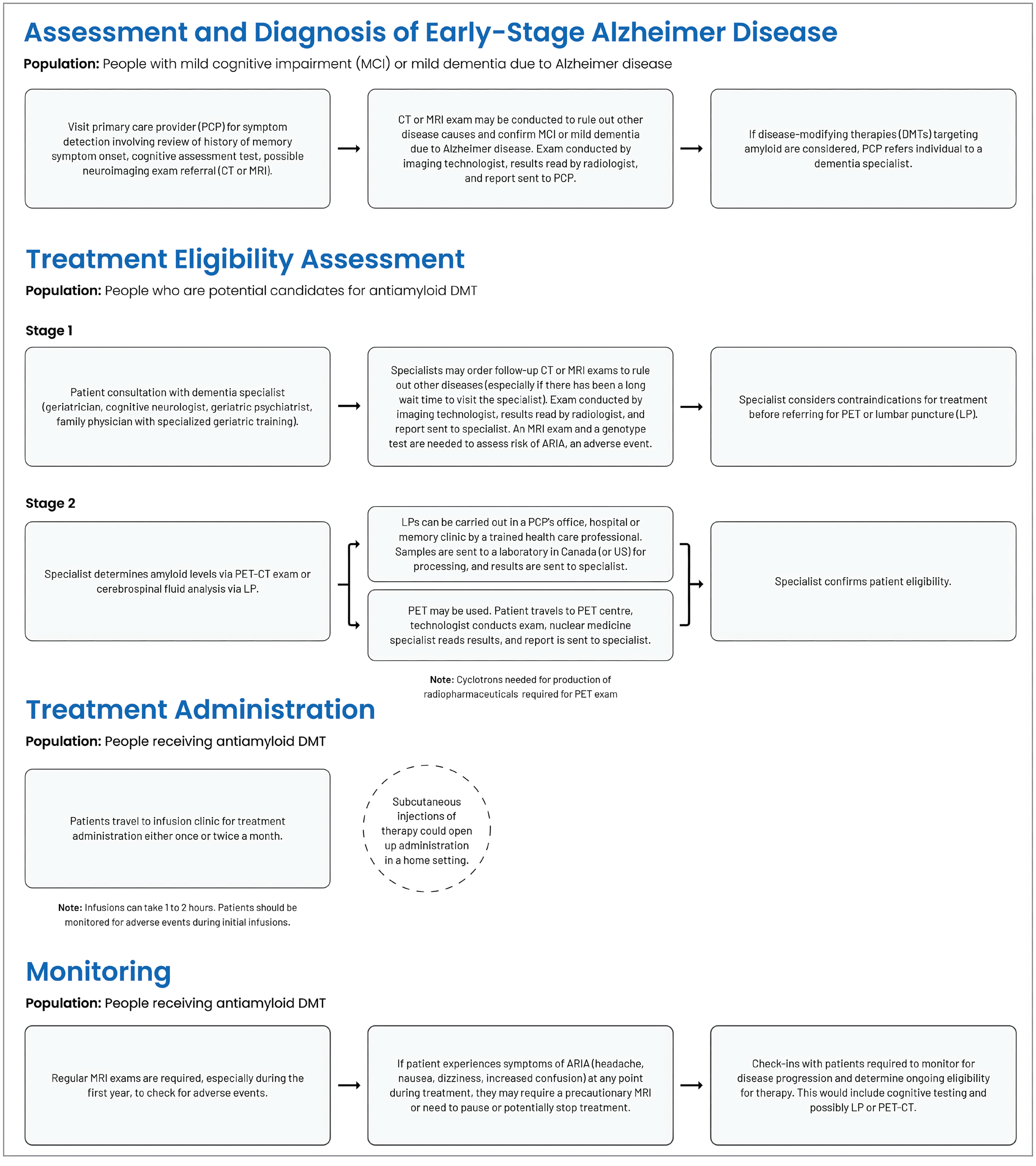
It is anticipated that a new model of care and clinical pathway for early-stage AD and additional public education and outreach campaigns may be needed for the successful implementation of anti–amyloid-beta mAb DMTs, if they are approved in Canada. The potential disease treatment pathway for anti–amyloid-beta mAb DMTs could encompass 4 clinical domains (Figure 2): assessment and diagnosis of early-stage AD, treatment eligibility assessment, treatment administration of anti–amyloid-beta mAb DMTs, and patient monitoring.
Assessment and Diagnosis of Early-Stage AD
The assessment and diagnosis domain of the clinical pathway may include identifying individuals at risk of AD who are experiencing cognitive symptoms in social care services or primary care settings and administering cognitive assessments through trained care providers. The expertise of dementia specialists and medical imaging professionals to confirm suspected diagnosis of early-stage AD via cognitive assessments and neuroimaging (i.e., MRI or CT exams) may also be required.
Treatment Eligibility Assessment
The treatment eligibility assessment domain of the clinical pathway may involve assessing whether people with early-stage AD are eligible to receive anti–amyloid-beta mAb DMTs. In countries where these therapies have been approved, assessment of individuals includes LP or amyloid PET scans to determine amyloid-beta positivity. Additionally, individuals are evaluated for susceptibility to adverse events, such as brain hemorrhages, using MRI and genotyping.
Treatment Administration of Anti–Amyloid-Beta mAb DMTs
The treatment administration domain of the clinical pathway would involve travel to and from an outpatient clinic. Individuals are administered anti–amyloid-beta mAb infusions at these clinics every 2 or 4 weeks.
Patient Monitoring
The treatment monitoring phase of the clinical pathway would be concurrent with treatment administration and involves regular MRI monitoring for adverse events, supervised by a specialist. The frequency of MRI monitoring may increase if symptoms of adverse events develop.
In addition, disease progression could also be monitored with cognitive tests and repeat amyloid PET and LP exams, to determine whether patients are still eligible for the therapy.
Assessment and Diagnosis of Early-Stage AD
Identifying MCI and AD and Seeking Help
Currently, clinical diagnosis of early-stage AD, encompassing MCI and mild dementia due to AD, involves a comprehensive evaluation by a trained primary health care professional, such as a family doctor or primary care nurse. This assessment requires a careful corroborated history of the onset of symptoms and progression from both the patient and caregiver, using pen-and-paper psychometric screening tools, in addition to neurologic exams.17,36,37 Novel anti–amyloid-beta mAb DMTs were designed for people with early-stage AD, underscoring the importance of diagnosing MCI or AD at an early stage to optimize treatment effectiveness.26
Current guidance from the CCCDTD does not recommend routine cognitive testing to screen older adults who are asymptomatic.17 However, these guidelines were published before the advent of anti–amyloid-beta mAb DMTs, and it is unclear how these recommendations would change in this new context. Up to 60% of dementia cases worldwide remain undetected, suggesting that many individuals with early-stage disease may be unaware of or are overlooking symptoms associated with early-stage AD.34,35 Public education and advocacy campaigns as well as additional support resources may create better public awareness and understanding of early-stage AD, its symptoms, and how it can be managed.38
With the potential introduction of new therapies offering the promise of slowing disease progression, more individuals may be motivated to seek screening, including those who may not necessarily be eligible.39 A recent survey from Alzheimer’s Disease International has reported that more than 90% of carers and the general public would be more likely to seek a diagnosis if DMTs were available.40 Jurisdictions in Canada may not be fully prepared for an increase in screening demand, given the challenges in accessing both primary and specialist care, as well as gaps in physician training for diagnosing early-stage AD. This highlights a significant gap in readiness to diagnose individuals at an early enough stage, should anti–amyloid-beta mAb DMTs be approved.7
Implementation considerations for identifying early-stage AD include the following:
There is a lack of awareness among the general population regarding symptoms of early-stage AD. Symptoms such as forgetting names and places, as well as disorientation, are often conflated with “normal” aspects of aging rather than being seen as symptoms that warrant further investigation.41 The survey from Alzheimer’s Disease International found that 80% of the general public and 65% of health and care providers believe that dementia is a normal part of aging.40
Caregivers, whether paid or unpaid, often play a pivotal role in recognizing symptoms and supporting individuals with early-stage AD.42-44 A 2011 survey of caregivers in Canada reported that up to half of their family members waited a year or more before seeking help for their symptoms, which included frequent memory loss, disorientation of time and location, or personality changes.45
The stigma associated with MCI or AD diagnosis has been reported to cause hesitancy among individuals with new-onset symptoms to speak about the condition and seek help from social care services or a PCP. A 2017 Alzheimer Society survey found that 1 in 5 Canadians would avoid seeking help for as long as possible if they thought they had dementia.46,47 A different survey conducted by Alzheimer’s Disease International found that approximately 24% of people with dementia concealed their diagnosis due to the stigma associated with the disease.40
Accessing Primary Care
The diagnostic pathway for early-stage AD begins when individuals or their caregivers recognize symptoms and seek medical attention. Current guidance in Canada suggests the pathway to diagnosis should begin at the primary care level.17
Implementation considerations for diagnosing early-stage AD and accessing primary care and treatment include the following:
Limited primary care: As of 2023, an estimated 5.4 million people (17%) living in Canada lack stable access to a PCP, who serve as the initial point of contact for beginning the diagnosis of early-stage AD.17,48,49 These individuals and their caregivers are often forced to seek care from family doctors or general practitioners at walk-in clinics or emergency departments, or they may go without treatment altogether. An absence of an established relationship with a PCP is associated with decreased likelihood of the care provider noticing symptoms of early-stage AD.50,51
Geographic disparities: People living in rural or remote areas, constituting around 18% of Canada’s population, and who tend to be older, encounter challenges in accessing primary care. These regions are served by only 8% of practising PCPs.52,53 Furthermore, people living in rural or remote areas often rely on caregivers for transportation to health care services, further complicating access to timely care.54
Barriers to care for Indigenous Peoples: Indigenous communities in rural and remote areas encounter unique challenges, such as difficulties in recruiting and retaining health care professionals. Additionally, there is a lack of consistent access to PCPs for at least half of First Nations people living off-reserve, as well as Métis and Inuit populations in remote communities.55,56 Furthermore, although research indicates that Indigenous Peoples may have higher rates of dementia, it is important to note that structural barriers, a lack of trust in colonial institutions, and fears of experiencing racism or discrimination in the health care system may contribute to reluctance in seeking care as well as to underdiagnosis or misdiagnosis in this population.3
Health care system navigation: Many jurisdictions in Canada do not have a comprehensive system of care navigators or case managers who could assist prospective patients with dementia in finding the care they need, which often spans multiple health care services and programs. There is also inequitable access to individual care navigators, which may affect certain groups more than others, including people living in rural communities, as well as newcomers to Canada who may lack familiarity with navigating the health care systems in Canada.42,57,58 As a result, these patients and their caregivers are often left to navigate a fragmented health care system on their own.59
Lack of equitable access to care: Racialized groups and some newcomers to Canada may encounter obstacles in accessing culturally appropriate care or locating primary care services.60-62 In addition, people from racialized communities may have different cultural views and stigma about dementia, making it challenging for individuals from these communities to seek help or accept a dementia diagnosis.3 There is a wide variation in dementia rates among different racialized groups, which may necessitate further study to understand these differences and to ensure that health care systems provide equitable treatment for these groups.3,63 These groups may require caregivers, often family members and friends, to assist in navigating the health care system while providing translation between patients and health care providers.3
Patient and caregiver advocacy: Individuals with symptoms, along with their caregivers, have reported a need to advocate for access to services to determine an early-stage AD diagnosis and subsequent treatment. This advocacy stems from reported challenges; some PCPs may struggle to recognize symptoms of early-stage AD. As well, there are instances of PCPs being perceived as dismissive of patient concerns regarding these symptoms.41,64-67 This can result in patients and their caregivers coordinating different appointments to obtain an accurate diagnosis, while keeping multiple care providers informed, requiring both time and effort.65,68,69 However, this can deepen inequities in access to care, as only those who are persistent and have the necessary resources may be able to navigate the system effectively and receive timely care, which could include anti–amyloid-beta mAb DMTs.
Additional training for physicians: There are a variety of different methods for diagnosing early-stage AD, including a large range of cognitive assessment tools (e.g., Montreal Cognitive Assessment [MoCA], the General Practitioner Assessment of Cognition [GPCOG], the Canadian Indigenous Cognitive Assessment [CICA], and the Mini–Mental State Examination [MMSE]). The accuracy of a diagnosis depends on the PCP’s knowledge of MCI and dementia and their proficiency in administering and interpreting results of cognitive assessment tools for diagnosing these conditions.17,70 In addition, it was reported in an Alzheimer’s Disease International survey that 65% of health care professionals believed that dementia was a normal part of aging.40 The survey also highlighted a phenomenon known as “therapeutic nihilism,” in which some providers refrain from making diagnoses because they believe there are no effective treatments for dementia. Increasing training on the symptoms, causes, and available treatments for dementia could help health care providers better identify and diagnose symptoms.
Difficulty in identifying early-stage AD: Clinical trials for anti–amyloid-beta mAb DMTs used a research framework based on biological definitions of early-stage AD, which were not intended for real-world clinical practice to diagnose people with early-stage AD.17 This can make it challenging to determine how many patients can be identified with early-stage AD in routine primary care practice.17 Studies of PCPs in Canada indicate variability in awareness of guideline details and the overall purpose and use of these tests.64,66 According to the 2019 Commonwealth Fund Survey of Family Physicians, 40% of doctors in Canada felt adequately prepared to care for individuals with dementia.71
Equitable cognitive assessments: The cognitive assessment tools used for diagnosing early-stage AD can be administered by any trained professional, such as family physicians and nurses. However, these tools were originally designed for Western populations and may have cultural biases that can result in poor test accuracy in ethnically diverse populations.72-74
In Canada, there are numerous Indigenous Peoples and racialized groups who may have different cultural perspectives and understandings of early-stage AD.75-77 Culturally sensitive cognitive assessment methods, screening tools, and care may provide more reliable results and help prevent inequities in diagnosis in these populations.78,79
Accessing Specialist Care and Receiving a Diagnosis
After seeking help in a primary care setting, individuals with symptoms of early-stage AD typically receive a final diagnosis from their PCP, without referral to a specialist, unless the cause of symptoms remains unclear or neuroimaging is required.17,41 However, if anti–amyloid-beta mAb DMTs are being considered as a treatment option for these individuals, confirmation of the diagnosis and evaluation of treatment eligibility would likely require the involvement of a dementia specialist. To facilitate shared decision-making, the benefits and risks of treatment should also be discussed between the patient and their caregiver, on the 1 hand, and a dementia specialist, on the other. The specialist would oversee the coordination of care and administration of treatment to ensure appropriate management.17,41
Accessing dementia specialists in Canada presents several challenges:
Geographic disparities: Specialized clinics are often located in urban settings, posing challenges for individuals living in rural or remote areas to equitably access specialist care, diagnostic imaging, and support services.7,80,81 This disparity necessitates additional costs for travel and time away from home and work to receive treatment.82,83 Programs such as the multispecialty interprofessional team (MINT) memory clinics and Saskatchewan’s Rural and Remote Memory Clinic demonstrate efforts to enhance care accessibility in rural and remote areas, aiming to mitigate geographic barriers.84-87
Wait times: Referral times for specialist care can be lengthy, with estimated average wait times of 28 months from diagnosis to specialist assessment. Symptoms will continue to progress while patients await care, potentially closing the window of patient eligibility for anti–amyloid-beta mAb DMTs.7 The development of a standardized approach to assessing potential patients — including checklists of cognitive tests and assessments, to be completed by PCPs before specialist referral — could reduce delays in early diagnosis.88
Limited human resources: Long referral times stem, at least in part, from a shortage of dementia specialists with training and experience in diagnosing early-stage AD (i.e., geriatricians, cognitive neurologists, family physicians with specialized geriatric training, and geriatric psychiatrists). As well, there are challenges with timely access to diagnostic equipment (e.g., PET-CT and MRI machines) to diagnose patients due to high demand and limited capacity.88-91 These factors collectively contribute to delays in diagnosis and access to specialized care for individuals seeking evaluation and treatment for cognitive symptoms.
Lack of multidisciplinary care coordination: Multidisciplinary teams that incorporate PCPs, AD specialists, nurses, social workers, and other health care providers, with specialized training and cross-collaboration among staff, may allow for quicker detection and coordinated care of early-stage AD by focusing specifically on patients with cognitive symptoms. The Family Medicine Groups in Quebec and MINT memory clinics across Canada are examples of multidisciplinary teams that allow for the administration of cognitive tests and focused care.4,84,92-94
Imaging capacity: The method for AD diagnosis recommended in the current CCCDTD guidelines depends on ruling out alternative causes of symptoms.17,19 Family physicians or specialists may order MRI or CT scans to exclude other causes of dementia unrelated to AD. If underlying pathological processes remain unclear, PET-CT or single-photon emission CT exams may also be ordered. However, accessing medical imaging often entails substantial wait times due to general high demand for these services, potentially delaying diagnosis.95-97
Future Diagnostic Technologies
A variety of new and emerging technologies have been developed or are currently in development to improve the identification of early-stage AD. The adoption of digital cognitive tests, ocular biomarkers, and artificial intelligence (AI) has the potential to enhance health system efficiencies by replacing pen-and-paper psychometric screening methods. While these technologies are showing promise in research settings, their widespread clinical adoption depends on further validation, regulatory approvals, and integration into health care systems.
Digitization of Cognitive Tests
The digitization of cognitive screening tools has the potential to transform patient screening by enabling broader access, integrating real-time data, tracking cognitive trends, and reducing clinician workload.36,98 A shift toward digital platforms has the potential to improve early diagnosis and monitoring, facilitating more effective management of early-stage AD.
Developments in the digital administration of cognitive screening tools include:
adapting traditional psychometric screening tools to computer platforms, including remotely administered tablet- and smartphone-based cognitive assessments, which may expedite in-clinic or remote administration, automate scoring, and allow data integration36
the introduction of new digital cognitive screening tests aimed to mitigate the effects of language, cultural, racial, and ethnic biases in cognitive assessment36,99
wearable devices that track sleep and activity patterns continuously, facilitating detection of presymptomatic functional decline without having to rely on participant self-report.100
While these digital platforms have the potential to enhance early diagnosis and monitoring, particularly in early-stage AD, traditional cognitive testing may still play an important role, especially for patients and care providers who may not have access to, or be comfortable operating, digital devices. Ensuring equitable access to cognitive assessments will likely require a balance between digital innovations and traditional approaches.
Ocular Biomarkers and Retinal Imaging Technologies
In recent years, some AD research has focused on potential biomarkers correlated with AD development that occur biologically in the eye or are related to functionality of the eye. AI use in conjunction with ocular biomarkers of AD, including tears, corneal nerves, retina, visual function, and eye movement tracking, may be able to detect early-stage AD. This technology may improve the accuracy of identifying AD and could become a screening tool to detect AD before symptoms develop.101
Recent developments to advance ocular diagnostics in MCI and AD include the following:
A machine-learning model uses retinal imaging technologies to differentiate between normal cognition and MCI. By analyzing specific features in the images along with demographic and quantitative data, the model aims to provide a noninvasive approach for the early detection of MCI. Researchers plan to further validate and potentially enhance the model’s clinical utility by collecting images from a larger and more diverse cohort of representative individuals.102
An eye-tracking technology uses a tablet-based camera to analyze eye movement parameters. Health Canada has approved an application for use in clinics or remotely through self-testing in patients with multiple sclerosis.103 The manufacturer is currently conducting trials to evaluate this technology for tracking progression and cognitive changes in patients with AD.104
Despite these advances, barriers to implementing ocular diagnostics may persist. These include a lack of consensus on clinical integration strategies and limited understanding of the relationship between retinal changes and AD, underscoring the need for further research.105 Additionally, challenges such as the need for specialized training for eye care professionals and variations in optometrists' scope of practice across provinces would need to be addressed.
AI Detection and Machine Learning
AI and machine-learning models, especially those that optimize MRI scans, have the potential to improve diagnostic processes. These technologies have the capability to analyze neuroimaging data with greater precision, detecting subtle brain changes that indicate AD and standardizing pattern identification for radiologists, potentially reducing the need for specialized training. This capability could lead to earlier and more accurate AD diagnoses, distinguishing it from other neurologic conditions.106-110 However, an important consideration, discussed later in this report, is the need to address implementation challenges associated with MRI access.
Additionally, other key considerations and challenges include the following:
Biases in predictive models: Identifying and mitigating potential biases in predictive machine-learning models is important to ensure they maintain accuracy across diverse populations, including multicultural groups.107
Privacy safeguards: Implementing appropriate safeguards to protect patient data privacy is essential when using AI and machine learning in clinical settings.111
Further research: Continued research is necessary to develop reliable and clinically applicable AI and machine-learning models for diagnosing and monitoring AD.111
These advances underscore the potential of AI to support AD diagnosis and care and highlight the importance of addressing ethical, technical, and practical challenges to maximize their benefits in health care settings.111
Recent developments in AI detection and machine learning include the following:
The FDA has granted De Novo approval of a clinical test that uses AI and standard MRI to predict progression from MCI to AD in individuals within 5 years.109
Other novel AI models that use machine-learning techniques are also being developed to analyze neuroimaging data to detect subtle brain changes, assess disease risk, and differentiate AD from other conditions.106,108,110
Treatment Eligibility Assessment
Once diagnosed with early-stage AD, which includes MCI and mild dementia due to AD, individuals would undergo assessment for treatment options, including anti–amyloid-beta mAb DMTs, if approved by Health Canada. In countries where these therapies are approved, regulatory authorities typically require patients to have abnormal levels of amyloid-beta pathology to be eligible for treatment.28,29 For example, 21% to 40% of people with MCI do not display enough amyloid-beta biomarker load to confirm a diagnosis of AD.112,113 These amyloid-beta levels are currently determined by an amyloid PET exam or an analysis of CSF obtained via LP.114 The required amyloid-beta levels for eligibility may vary among different anti–amyloid-beta mAb DMTs, and clinicians would need training to discern the nuances among these therapies.115
The CCCDTD does not currently recommend amyloid PET exams or LPs as a regular part of the diagnosis pathway for early-stage AD unless there is diagnostic uncertainty. However, the CCCDTD recommendations were made in 2020, before the introduction of anti–amyloid-beta mAb DMTs as a potential AD treatment.17 Integrating these forms of testing may involve considerations of appropriate use, equitable access, and additional training for PCPs and dementia and neuroimaging specialists in the health care systems in Canada.
In addition to determining biomarker levels, regulatory authorities in countries that have approved anti–amyloid-beta mAb DMTs have also required an MRI scan within 12 months before treatment initiation and suggested APOE genotyping to evaluate patients’ predisposition to adverse events.114 After patients complete treatment eligibility testing, dementia specialists would have to review the results and determine the treatment plan.4
CSF Analysis and LPs
CSF collection via LP is considered a convenient and cost-effective method to determine amyloid-beta levels compared to amyloid PET exams, primarily due to its lower resource requirements.116 The procedure requires basic equipment, consisting of a LP kit, which includes a needle and collection tube, making it more accessible for individuals living in rural or remote areas.117 In some provinces, both PCPs and nurses can perform LPs, although additional training would likely be required.118-121
Most often, LPs are performed in the hospital setting by neurologists.118 While these procedures could be conducted in outpatient settings, which could improve access in the health care system, this would necessitate appropriate training to ensure the procedure is conducted safely.117,122 An additional advantage of LP, compared to amyloid PET, is that CSF assays can examine multiple different biomarkers concurrently.117 However, the CCCDTD does not recommend CSF testing and LPs as part of the routine diagnosis pathway unless there is diagnostic uncertainty in people under the age of 65.17
Implementing CSF analysis via LPs may present several challenges, and these include the following:
LP safety: Common patient complaints following LP include headaches and back pain, which are generally mild and manageable. Approximately 0.7% of patients experience serious adverse events that require hospitalization, such as cerebral or spinal hemorrhaging; cerebral thrombosis, hematomas, or herniation; or infection.117,123,124 Additionally, in approximately 10% of cases, LPs do not draw sufficient CSF fluid, necessitating subsequent amyloid PET imaging to determine biomarker load.125 Amyloid PET exams may also be used after LPs if CSF results do not match clinical diagnosis.126
PCP acceptance: Some PCPs have expressed that they feel unprepared or would require training to perform LPs to reduce the risk of adverse events.64,117 Others have expressed that the procedure is invasive for their patients and there is difficulty in coordinating with specialists to perform LPs.127 This hesitancy may push PCPs and people with early-stage AD toward seeking this procedure in hospitals or specialized memory clinics. While the performance of LPs in these settings may be perceived as safer, it could strain resources and increase demand at these facilities. While amyloid PET exams are an alternative option, they are less available.64,117
Patient comfort and acceptance: While research has shown that LPs are well tolerated and are generally safe for older people, patient acceptance of the procedure, particularly among those who are frail or have symptoms of confusion, can present a barrier to its widespread implementation.117 Some people, particularly in certain racialized communities, may feel hesitant about undergoing LP due to concerns about the procedure’s invasiveness.126,128 Effective communication and comprehensive shared decision-making with health care providers regarding the safety, effectiveness, and other aspects of the procedure are crucial to increasing patient and caregiver comfort and acceptance.129,130
Laboratory capacity: Currently, Canada has at least 3 laboratories capable of processing CSF samples, with an expected turnaround time ranging from 5 to 28 days. Alternatively, samples can be sent to the US for processing.4,131-133 However, these CSF samples require specific storage conditions, which raises the risk of spoilage during transition to the laboratories.134,135 Furthermore, there is a lack of clarity on the number of laboratories that have the capability to process CSF samples beyond these 3 laboratories. With projected annual dementia prevalence rates expected to increase by 51% by 2030 compared to 2020, this projected demand could overwhelm the capacity of laboratories in Canada to process these tests. In scenarios such as equipment failures or when demand exceeds capacity, the necessity to send excess CSF samples to the US for processing could lead to extended wait times for pathological confirmation. Moreover, this process introduces additional complexities regarding the privacy of patient data.4,136 An expansion of the current CSF processing infrastructure, as well as inclusion of newer automated platforms, could increase the capacity to deliver timely results and system resilience.137
Reimbursement pathways: Reimbursement for LPs currently varies across provincial and territorial health care systems in Canada.4,117 For instance, some jurisdictions do not reimburse LPs related to AD, whereas others require a special approval for reimbursement, creating inequitable access to this procedure.4,138 Studies have indicated that LPs can be financially burdensome for PCPs, as reimbursement may not adequately cover the time and resources required to perform the procedure. This financial aspect, especially when considering large workloads, may serve as a disincentive for PCPs to offer LPs, potentially impacting patient access to timely diagnostic assessments for AD.125
Amyloid PET Imaging
PET-CT is an advanced, hybrid, diagnostic imaging modality that combines PET and CT imaging in a single unit. This modality uses radiopharmaceuticals to attach to AD biomarkers, such as amyloid-beta plaques in the brain, allowing medical imaging specialists to determine the biomarker load of patients in a noninvasive manner. PET-CT can be used in cases where LP is contraindicated.7,139-141 However, PET-CT exposes people to ionizing radiation and requires specialized equipment and staff.142,143
Amyloid PET imaging is not part of the routine AD diagnosis pathway in Canada and is not recommended for use in those who show no clinical symptoms. Amyloid PET imaging is primarily used in an AD research setting, although it can be used clinically under special authorization, and is usually ordered by a dementia expert, as indicated by the CCCDTD.17 PET-CT does not currently allow for concomitant tracking of multiple biomarkers, unlike CSF analysis.118
Implementing amyloid PET imaging presents several challenges. These include:
Capacity: There are 60 PET-CT machines in Canada, located in 9 provinces and all in urban centres.144 There are no PET-CT machines in the territories. Expanding PET-CT capacity is complex; it can take up to 5 years to introduce new PET-CT units due to regulatory and licensing requirements, as well as the need to develop or modify facilities to support PET-CT units with proper radiation shielding.142 The distribution of PET-CT units raises concerns about equitable access for individuals residing outside urban areas. People who do not live close to a PET-CT would need to travel to urban settings or out of their province or territory for imaging, incurring additional cost and logistical challenges.
Radiopharmaceutical availability: Radiopharmaceuticals, a necessity for PET-CT imaging, are in short supply due to a limited number of cyclotrons that generate these reagents.7 Some radiopharmaceuticals have a very short active half-life; if a cyclotron is farther away, more reagents would need to be purchased in order for a usable amount to remain active by the time the reagents arrive at the imaging unit.142 Additionally, if a cyclotron experiences downtime, this could lead to rebooking or cancelling appointments, disrupting the continuity of service.145 Addressing these challenges requires strategies to enhance cyclotron infrastructure and supply chain logistics. This might involve increasing the number of cyclotrons, improving distribution networks, and implementing contingency plans to minimize disruptions in radiopharmaceutical supply.
Regulatory approvals: Currently, 1 radiopharmaceutical is approved in Canada for amyloid imaging. Others are used in the research setting but are unavailable for clinical use in Canada.145,146
Competing priorities: Existing PET-CT units are primarily allocated for oncology exams in Canada and frequently operate at full capacity.144 The prioritization of oncology exams can significantly extend the waiting times for non-oncology exams, including those that would be needed for AD. A 2021 survey of PET-CT clinicians reported that average wait times for non-oncology exams were more than 1 year.147 This extended wait period underscores the challenges faced by individuals requiring PET-CT scans for diagnoses other than cancer.
Limited human resources: There is a shortage of trained staff capable of operating PET-CT units and specialists capable of interpreting the images.144,148,149 Staffing shortages may be increasing and have been noted to contribute to long wait times to access PET-CT imaging.147,150
Amyloid-Related Imaging Abnormalities, MRI, and APOE Genotyping
In addition to testing for biomarker levels, regulatory authorities and appropriate-use guidelines also require prospective patients to undergo an MRI examination and APOE genotyping for their susceptibility to amyloid-related imaging abnormalities (ARIA), an adverse event related to anti–amyloid-beta mAb DMTs.28,114
In countries that have already approved anti–amyloid-beta mAb DMTs, regulatory authorities require an MRI scan within the 12 months before treatment initiation. This precaution ensures potential patients can begin treatment safely.28,29 This scan identifies patients with microhemorrhages in the brain, which puts them at higher risk of ARIA.114,151 ARIA can be categorized as 2 different subtypes, which can co-occur: ARIA-E (presenting as edema and effusion) or ARIA-H (presenting as microhemorrhages). An MRI exam and reporting of the intensity of symptoms is used to grade the severity of ARIA.152
If an MRI examination was conducted within the 12-month period to assess early-stage AD symptoms and included sequences to evaluate the risk of ARIA, a second MRI scan may not be necessary as a baseline before initiating treatment with anti–amyloid-beta mAb DMTs. This is because the initial MRI would have already captured the necessary imaging sequences to determine ARIA risk. However, if a CT exam was used to confirm diagnosis of AD, an MRI would still be required because the CT scan would not have sufficient resolution to identify ARIA.114
Implementing MRI may present several challenges, and these include the following:
Capacity: There are 432 MRI units in Canada, in all provinces and 1 territory, with approximately 80% located in urban facilities. This geographic concentration forces patients living in rural and remote areas, especially in the territories, to travel for these scans, incurring additional costs.153 Limited capacity places strain on wait times, with the national median wait time for an MRI exam in 2023 reaching up to 3 months, although this varies by jurisdiction.96 Increasing MRI capacity would take time because MRI exams must be carried out in dedicated rooms with sufficient radiofrequency shielding to prevent electromagnetic interference, and a supply chain must be in place to support the advanced cooling systems needed to operate the units.154
Limited human resources: According to a survey by the Canadian Association of Medical Radiation Technologists, there is a shortage of staff trained to operate MRI units, with 11% of positions for MRI technologists being vacant as of 2021. This staffing gap contributes to longer wait times for imaging.148,149,155 This highlights the importance of appropriate use of diagnostic imaging to reduce unnecessary exams and optimize the use of limited MRI capacity.156
Education and training: Radiologists may need additional training in MRI acquisition protocols that are optimized to detect and monitor brain structures susceptible to ARIA.4,157 For example, measuring for ARIA-H on baseline MRI exams can be difficult due to its similarities to other brain microbleeds.151 Standardized MRI protocols and clear criteria for how ARIA could affect treatment plans should be included as part of this training.152
Along with the MRI examination before treatment initiation, regulatory authorities and appropriate-use guidelines have recommended that patients undergo genetic testing to determine whether they are carriers of APOE4 alleles.28,114 It has been found that people carrying APOE4 alleles are especially at risk for ARIA events. APOE genotyping can allow better-informed discussions of the risk of anti–amyloid-beta mAb DMTs and ensure better patient monitoring.114
Currently, AD genotyping is offered only for patients who have young-onset familial AD; it involves a detailed review of family history by a genetic counsellor or physician and does not include APOE genotyping.158 Genetic testing is conducted at research laboratories in Canada or commercial laboratories in the US.158 While commercial genetic testing is available at clinical laboratories in Canada, it may not be covered by public health plans.158,159 If anti–amyloid-beta mAb DMTs were approved in Canada, ensuring equitable access to APOE genotyping would be important for ensuring the safety of patients receiving this class of treatment. Such genotyping tests could be undertaken at community laboratories in the future, mitigating the need to travel to hospitals for patients and caregivers.160-162
Figure 3: Mechanisms of Action of Drugs in Phase III Clinical Trials for AD, Classified Using the CADRO Approach
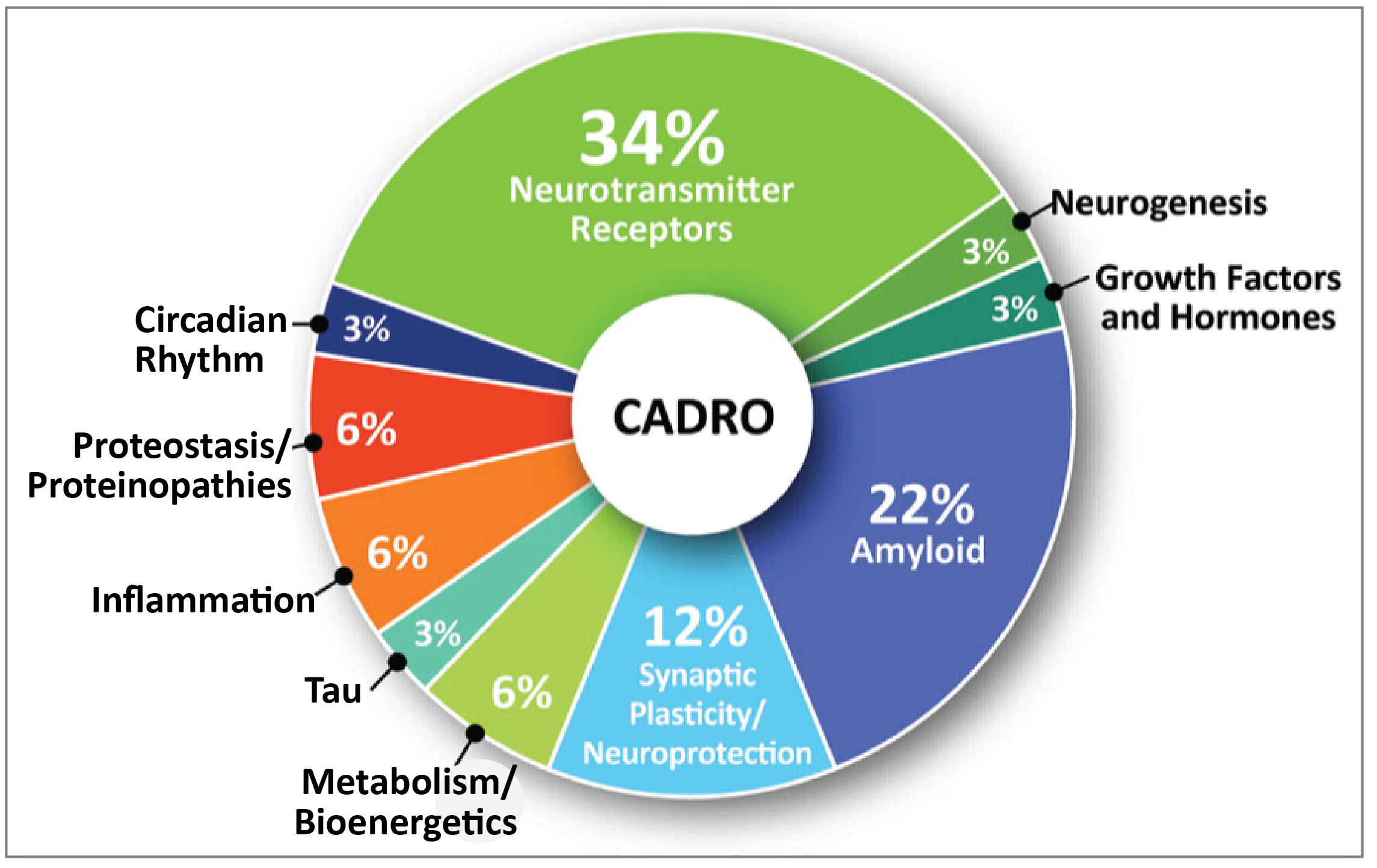
Source: Cummings J, Zhou Y, Lee G, Zhong K, Fonseca J, Cheng F. Alzheimer’s disease drug development pipeline: 2024. Alzheimer’s Dement (N Y). 2024;10(2):e12465. Available from: https://www.pubmed.ncbi.nlm.nih.gov/38659717/. Reprinted in accordance with Creative Commons Attribution 4.0 International License (CC BY 4.0): https:// creativecommons.org/licenses/by/4.0/50.24
Future Biomarker Detection Technologies
As of January 1, 2024, 164 clinical trials evaluating 127 drugs for AD were registered on clinicaltrials.gov, an international voluntary database of clinical research studies from 200 countries, with DMTs constituting 76% of drugs for AD in the database. These drugs are designed to target nearly all disease processes mentioned in the Common Alzheimer’s Disease Research Ontology (CADRO) approach, a method of classifying AD processes into key categories reflecting different aspects of AD pathology and progression.24 Figure 3 illustrates the mechanisms of action of drugs in phase III clinical trials for AD, classified according to the CADRO approach. The increased use of biomarkers, refined target identification, and enhanced methodologies in clinical trials could improve the success rate of AD drug development.24 Ongoing research has identified several promising AD-related biomarkers.
Table 1 presents the emerging fluid biomarkers linked to the drugs in Figure 3, categorized by their clinical development stage: FDA breakthrough-device designation, research-only use, and emerging biomarkers needing further clinical validation. This is not an exhaustive list, as drugs and biomarkers in development are evolving rapidly.
Table 1: Emerging Fluid Biomarkers Linked to the Drugs in Phase III Clinical Trials for AD
CADRO category of drugs in phase III clinical trials24 | Fluid biomarkers163 | Stage of clinical development |
|---|---|---|
Amyloid | CSF and plasma amyloid-beta | FDA breakthrough-device designation164 |
Tau | CSF and plasma p-tau | FDA breakthrough-device designation164 |
Growth factors and hormones | BDNF | Emerging biomarker requiring further clinical validation165 |
HSD1, trial-specific hormones | Research use only166 | |
Proteostasis or proteinopathies | Proteomics | Research use only166 |
Inflammation | GFAP | |
YKL-40, sTREM2, MCP-1 | Emerging biomarker requiring further clinical validation167-169 | |
Synaptic plasticity or neuroprotection | Neurogranin, synaptotagmin, and SNAP-25 | Emerging biomarker requiring further clinical validation163,170 |
Metabolism or bioenergetics | Metabolomics | Emerging biomarker requiring further clinical validation163,171 |
Neurotransmitter receptors | None identified | — |
Neurogenesis | None identified | — |
Circadian rhythm | None identified | — |
AD = Alzheimer disease; BDNF = brain-derived neurotrophic factor; CADRO = Common Alzheimer’s Disease Research Ontology; CSF = cerebrospinal fluid; GFAP = glial fibrillary acidic protein; HSD1 = hydroxysteroid dehydrogenase type 1; MCP-1 = monocyte chemoattractant protein-1; p-tau = phosphorylated tau; SNAP-25 = synaptosomal-associated protein 25; sTREM2 = soluble triggering receptor expressed on myeloid cells 2; YKL-40 = chitinase-3-like protein 1.
Blood-Based Biomarkers
Blood-based biomarkers, collected through a blood draw, offer a promising alternative to CSF analysis via LPs or amyloid PET exams, potentially reducing reliance on invasive and resource-intensive methods.172,173 Such biomarkers are intended to complement comprehensive clinical assessments rather than serve as standalone diagnostic tools. While the clinical applications of these biomarkers may introduce some challenges, including scalability, accuracy, robustness, and standardization, they may be less resource-intensive than current options.164,172,174 Notable biomarkers nearing clinical implementation include plasma amyloid-beta42/40 ratio, various tau and phosphorylated tau (p-tau) isoforms, plasma neurofilament light chain (NfL), and glial fibrillary acidic protein (GFAP).164,172 There are potential benefits and challenges associated with these biomarkers (Appendix 1).
Composite Panels
Several manufacturers are also exploring the use of panels that combine multiple biomarkers to improve diagnostic accuracy, such as:164,166
C2N’s PrecivityAD (amyloid-beta42/40, APOE, age)
Roche’s Amyloid Plasma Panel (p-tau181 + APOE4)
Labcorp’s ATN Profile (amyloid-beta42/40, p-tau181, NfL)
Fujirebio’s AD-BBB testing (amyloid-beta42/40, p-tau181, p-tau217)
C2N’s PrecivityAD2 (amyloid-beta42/40, p-tau 217, np-tau217)
Quanterix’s ALZpath (p-tau181, p-tau217, p-tau231, YKL-40, GFAP)
Luminex (21-protein panel)
Alamar (p-tau217 and large multiplex assays)
Meso Scale (p-tau181, p-tau217, p-tau231).
Fingerprick Blood Sample and Remote Collection
A fingerprick blood test for measuring NfL, GFAP, p-tau181, and p-tau217 has been developed. In a study involving patients at a memory clinic, both vein and fingerprick blood samples were transferred onto dried blood spot cards and transported without temperature control to a laboratory for interpretation. Upon arrival, biomarkers were successfully detected in both sample types.175 In the vein blood spots, levels of GFAP, NfL, p-tau217, and p-tau181 closely matched those found in standard blood tests. Similarly, the fingerprick blood samples showed results that closely matched standard blood tests for these biomarkers, indicating the potential of fingerprick blood sampling and remote collection as alternatives to traditional blood draws.175 This approach could improve access for patients in remote and underserved communities across Canada, where limited capacity and the absence of standard laboratory facilities make traditional blood draws challenging.
Further Development of Blood-based Biomarkers
Research into plasma protein changes that precede the onset of dementia has identified potential blood-based biomarkers in the immune, lipid, metabolic signalling, and hemostasis pathways. These findings may allow for earlier preclinical AD detection.176,177 RNA sequencing analysis of blood samples has also identified biomarkers for early diagnosis of AD.178
Considerations for Clinical Use
There are some considerations for the clinical use of biomarkers for AD that may support their successful integration into the management of AD. These include the following:
Standardization: Widespread implementation of AD blood biomarkers in clinical settings may require not only analytical standardization, but also compatibility with laboratory analyzers used in smaller, nonspecialized hospitals, along with standardized sample-collection, processing, and storage procedures.172 Variations in sample processing — such as time of collection, fasting status, temperature, time from collection to centrifugation, and centrifugation parameters — can introduce measurement variations, reducing clinical reliability and complicating result comparisons across laboratories.179 With numerous tests under development, harmonizing efforts across laboratories, such as establishing references and quality-control programs, as well as promoting interlaboratory collaboration (for sharing best practices and troubleshooting challenges) would be important for ensuring consistent and reliable assay results.164,179
Implementation: Integration of blood-based biomarkers into routine clinical practice may require clear guidelines for use and interpretation.174 If standardizations and guidelines are sufficiently clear, blood biomarker tests could be implemented at community laboratories, expanding access for patients, especially those in rural or remote areas.164
Treatment Administration of Anti–Amyloid-Beta mAb DMTs
The main method of treatment administration for anti–amyloid-beta mAb DMTs is infusions at regular intervals, ranging from biweekly to monthly.114,180 These infusions can take between 1 and 2 hours to complete. Individuals are often required to remain at the treatment administration centre immediately after the initial infusions to monitor for any adverse reactions.4,114 Over time, infusions could be administered at home if the therapies prove to be sufficiently safe and patients respond without adverse reactions.181 Administration for anti–amyloid-beta mAb DMTs may also be possible via subcutaneous injections in the future, which could also be administered in the home setting. However, mAbs have limited bioavailability beyond the injection site, and a large volume injection may be difficult to administer.182,183
Infusion Clinics
In Canada, there is increased reliance on private infusion clinics, funded by pharmaceutical companies, to provide early access to new therapies, before public drug plan approval.184-187 Of the outpatient infusion clinics identified in Canada, 573 (52.2%) are owned by private entities and are funded by patient support programs from pharmaceutical companies, or private insurance; or required out-of-pocket patient payments to cover services.187 It is unclear whether these clinics have capacity or are authorized to administer anti–amyloid-beta mAb DMTs, as they are not required to publicly identify their available capacity or the clinical indications and therapies they support.188 A coordinated system for collecting and maintaining information on publicly and privately funded infusion clinics would allow for assessment of the regional availability and capacity to administer anti–amyloid-beta mAb DMTs.
There may be several considerations for the successful implementation of treatment administration. These include the following:
Geographic disparities: Individuals living in rural and remote areas would need to travel to infusion clinics for each treatment administration, presenting a potential challenge for equitable access to treatment.188 This would incur substantial costs and effort for patients and their caregivers and may make coordinating care between the clinics and PCPs more challenging.82,83
Capacity: Public infusion clinics may not have the capacity to administer a new therapy to a new and large patient population.185,189 A 2018 survey of medical oncologists reported wait times of up to 3 weeks to initiate treatments in public infusion clinics.190,191 Capacity would be limited by the availability of health care professionals, such as nurses and pharmacists, to administer these therapies.4 Some reports have raised the concern of nurses and other staff moving to work in private infusion clinics, which could further impact capacity in publicly funded infusion sites.192-194
Education and training: Reports indicate that infusion-related adverse events occur in 8% to 25% of patients, with the most common symptoms being fever, headache, nausea, or vomiting.114 Clinic staff would need training to recognize and treat these reactions. Patients may need to stay at infusion clinics longer to monitor for early adverse events.4,114 Staff may also require additional training to interact with cognitively impaired patients.180
Continuity of care: Patient care may be difficult to coordinate when patients are treated by both nurses and on-call physicians at private infusion clinics and by specialists and PCPs in publicly funded health systems. There may also be concerns that private infusion clinics may lack connections to trained medical staff to monitor ARIA-related reactions.195,196
Regulatory compliance: The oversight and regulation of private infusion clinics in Canada can be challenging due to ambiguity regarding which jurisdiction — federal or provincial — holds primary responsibility. This uncertainty particularly pertains to areas such as licensing, inspections, data protection, public safety, and patient advocacy, complicating effective regulation and oversight.185
Data privacy: Data privacy concerns of individuals treated at private infusion clinics are an emerging area of concern. It has been noted in other areas of for-profit health care in Canada that patient data may be collected and used to market products and services.197,198 Patient consent for data collection and transparency around data storage and use could help to address these concerns.
Future Administration Technologies
New and emerging technologies may play a role in enhancing the operational capacity of infusion clinics, and some of these technologies have already been adopted in other care settings. Integrating smart IV pump technology and remote IV monitoring in infusion clinics, for example, may help to streamline drug-administration processes and workflows and reduce medication errors.
Developments in treatment administration include the following:
Smart pumps are advanced, programmable infusion devices with built-in drug libraries to set dosage limits and alerts. They have been reported to improve the accuracy of drug delivery and reduce medication errors.199,200
Bidirectional IV smart-pump interoperability enables real-time, two-way communication between the pump and the centralized hospital software, automating programming and documentation. Implementation considerations include a need to integrate diverse technologies, establish reliable wireless networks, and maintain detailed drug libraries.201,202
Remote monitoring of multiple infusion metres using a device that combines software applications with infusion technology could reduce workload and increase operational capacity.203
Patient Monitoring
When patients begin anti–amyloid-beta mAb DMT, they require monitoring over the course of the treatment, by both caregivers and clinicians, to ensure safe drug administration and to watch for serious adverse effects.4 Monitoring can lead to dose adjustments, temporary pauses, or discontinuation in therapy, and may require regular MRIs and routine cognition tests administered by a health care provider.4
MRI Monitoring
The most common adverse effect of anti–amyloid-beta mAb DMTs is ARIA. Studies have found that most cases of ARIA are transient and asymptomatic, but ARIA can on occasion lead to serious adverse events such as swelling in the brain (ARIA-E) or hemorrhagic brain bleeds (ARIA-H).157,204 If an individual experiences ARIA, treatment is suspended until symptoms resolve or treatment is discontinued permanently.157
In countries that have approved anti–amyloid-beta mAb DMTs, regulatory authorities require patients receiving treatment to undergo routine MRI scans at set infusion intervals to monitor for ARIA.27-30 In addition to these routine scans, if patients exhibit symptoms of ARIA (noticed by the patient, caregivers, or clinicians), a precautionary MRI scan could be clinically indicated based on the severity and intensity of the symptoms, as determined by their care provider. If ARIA is confirmed, repeated scans would be required until the ARIA symptoms have resolved.27-30 Symptoms of ARIA are broad and can include headaches, nausea, dizziness, or increased confusion.205
A recent meta-analysis of anti–amyloid-beta mAb DMTs found that approximately 6.5% to 7.8% of trial patients developed ARIA, although the incidence of ARIA has been found to be as high as 30%, depending on the specific therapy.206 While 80% of these cases are asymptomatic and transient, typically occurring early in treatment with reduced incidence after the first year of treatment, ARIA can still occur at any time, and recurrences are possible.157,206 In rare cases with severe symptoms, hospitalization may be necessary, and there is a risk of death.206
There may be several considerations for the successful implementation of MRI monitoring. These include the following:
Capacity: There are 432 MRI units in Canada, with 87.5% of units concentrated in Ontario, Quebec, British Columbia, and Alberta.153 Almost 80% of MRI units are in urban facilities, limiting equitable access for those living in rural and remote areas. Travel costs to receive routine MRI monitoring exams would also represent an additional burden of care for patients and their families, if they live far from imaging sites.82,83,153
Limited human resources: Based on data from the Canadian Medical Imaging Inventory 2022–2023 national survey, the number of full-time medical imaging staff has not kept pace with the growing volume of exams.149 Medical imaging staff shortages can lead to longer wait times or service disruptions, with vacancies increasing five-fold from 2019 to 2021, potentially affecting capacity to monitor patients as well as increasing exhaustion among staff.4,149,155,207 Efforts to streamline credentialing and licensing processes, recruit foreign-trained medical imaging staff, invest in and adopt information technologies and AI to eliminate repetitive tasks, cross-train staff for interoperability, and support existing staff may help to retain and increase available staff capacity.155
Education and training: Radiologists may need training to apply appropriate MRI acquisition protocols for ARIA screening as well as training to detect ARIA in MRI images and ensure that baseline and monitoring MRI scans are comparable.4,157
Wait times: In 2023, median wait times for an MRI exam peaked at more than 3 months, although this was dependent on the urgency of the exam.96 The additional volume of MRI exams for scheduled monitoring or unscheduled precautionary scans, would, in the absence of changes to streamline or address appropriate use of diagnostic imaging, almost certainly increase current MRI wait times.4
Patient safety: It has been observed that patients with AD and APOE4 alleles receiving anti–amyloid-beta mAb DMTs are more susceptible to ARIA.4,208 APOE4 alleles are most common in people with European or African ancestry.209,210 APOE4 testing is not currently routine in Canada, as APOE4 mutations indicate susceptibility to AD rather than confirm development of the disease.158,211 However, given the susceptibility of patients with AD and APOE4 to ARIA, regulatory agencies and appropriate-use guidelines recommend that APOE4 testing is warranted to better assess patient risk of developing ARIA and identify those who may require closer and more frequent MRI monitoring.4,28-30,114,212 Such APOE4 tests could be combined with other blood-based AD biomarker tests.164,166
Continuation of Treatment
It is unclear how long patients should continue to use anti–amyloid-beta mAb DMTs, as clinical trials have been conducted over a relatively short period. Additionally, clinical trials included patients with early-stage disease, which was assessed by experts using cognitive tests, and it remains unclear what benefits are gained by continued treatment when AD progresses beyond the early stage.21,213 This may necessitate routine check-ins with a care provider to monitor disease progression.21
There are several considerations related to monitoring for disease progression. These include the following:
Recurrent cognitive assessments: Assessment of cognitive decline during anti–amyloid-beta mAb DMT use would require routine administration of cognitive tests. Given that many people in Canada do not have access to a PCP, routine monitoring of cognitive decline may be difficult.48 Additionally, clinical trials used tests such as the Clinical Dementia Rating Scale Sum of Boxes (CDR-SB) and the Alzheimer’s Disease Assessment Scale–Cognitive Subscale (ADAS-cog) to measure cognitive decline, which are not recommended by CCCDTD for use in clinical practice, as most clinicians are not familiar with these tests.17,21 Therefore, optimal use of anti–amyloid-beta mAb DMTs would require training PCPs or other care providers on the use of cognitive tests or the development of an alternative validated test that can sufficiently measure cognitive decline in patients using anti–amyloid-beta mAb DMTs.
Repeat treatment eligibility assessments: According to clinician engagement by the National Institute for Health and Care Excellence (NICE), the UK health technology assessment agency, patients may also need repeated amyloid PET exams or LPs to confirm ongoing eligibility for treatment, which could contribute to longer wait times for PET-CT scans and increase radiation exposure. Additionally, CSF analysis following LPs could place added strain on laboratory processing networks.21
Emerging blood-based biomarkers: New blood-based biomarkers may play an important role in determining the cessation of treatment.
Future Monitoring Technologies
Advances in MRI technology could ease current capacity constraints in imaging centres and provide a lower-cost and more accessible alternative to conventional MRI. Some current and emerging MRI technologies include the following:
Modular MRI systems are designed to be smaller and more portable than traditional MRI machines, enabling them to be used in a variety of settings, including smaller clinics and remote areas. This capability has the potential to enhance equitable access to MRI.214 However, their smaller size, lower magnetic field strength, and portability might limit the scope of imaging capabilities, as currently the CCCDTD recommends full-size MRI units with sufficient field strength (1.5 or 3.0 Tesla) for neuroimaging.17 Investigations are under way to determine whether these portable units with low magnetic field strength have sufficient resolution to reliably detect ARIA.215
Remote MRI operation, like virtual cockpits, could provide support to facilities that have MRI machines but lack specialized MRI operators. A key consideration is the need for robust and secure communication networks to ensure data privacy and prevent interruptions during remote operations.216,217 It should be noted that technologists would still be required to ensure safety protocols are followed and patients receive care and support.
Integrating telemedicine with MRI services may streamline workflows by allowing remote prescan and postscan consultations, as well as potentially supporting specialists from different jurisdictions to assist in MRI interpretations if local expertise is unavailable. Challenges for integration of telemedicine with MRI services include ensuring the safety and privacy of patient data, addressing billing issues for specialists, and resolving cross-jurisdictional licensing (5 jurisdictions permit teleradiology services from outside their borders).95,218
Blood-based biomarkers have also shown promise for monitoring treatment effectiveness, particularly in anti–amyloid-beta mAb DMT trials. The use of biomarkers such as amyloid-beta42/40, p-tau 217, and p-tau181 have been correlated with reductions in use of amyloid PET across various trials, suggesting the potential of these biomarkers for dynamic monitoring and in determining treatment cessation. However, further research is needed to establish the relationship between biomarker changes and clinical outcomes, particularly at the individual level, to support personalized treatment decisions and to better demonstrate treatment effectiveness.219
Estimation of Treatable Population With Incident Early-Stage AD and Medical Imaging Demand
CDA-AMC estimated the size of the treatable population (those eligible for treatment with anti–amyloid-beta mAb DMTs) with incident cases of early-stage AD in 2020 and the associated demand on medical imaging. In addition, the treatable population and medical imaging demand were projected over a 5-year period from 2020 to 2025. Data availability limited calculations and estimation to this period. Incident cases were used instead of prevalent cases to estimate the number of patients for capacity planning. This approach assumes that prevalent cases of AD would be too advanced to benefit from anti–amyloid-beta mAb DMTs, although this may not accurately reflect all prevalent cases in a real-world setting. The methodology used was adapted from a NICE report that examined potential issues and challenges in evaluating DMTs.21,220
Treatable Population Estimation
A funnel approach was used to estimate a treatable population with incident cases of early-stage AD by narrowing down a starting population of people aged 65 years or older in Canada in stages, as follows (Figure 4):
those who develop dementia of any kind
those who present to health care services
those who are assessed and diagnosed to have early-stage AD
those who have sufficient amyloid-beta to be eligible for treatment with anti–amyloid-beta mAb DMTs.
A literature scan was undertaken to find incidence rates and proportions for each calculation stage. Details on specific methodology and calculations at each stage are provided in Appendix 2.
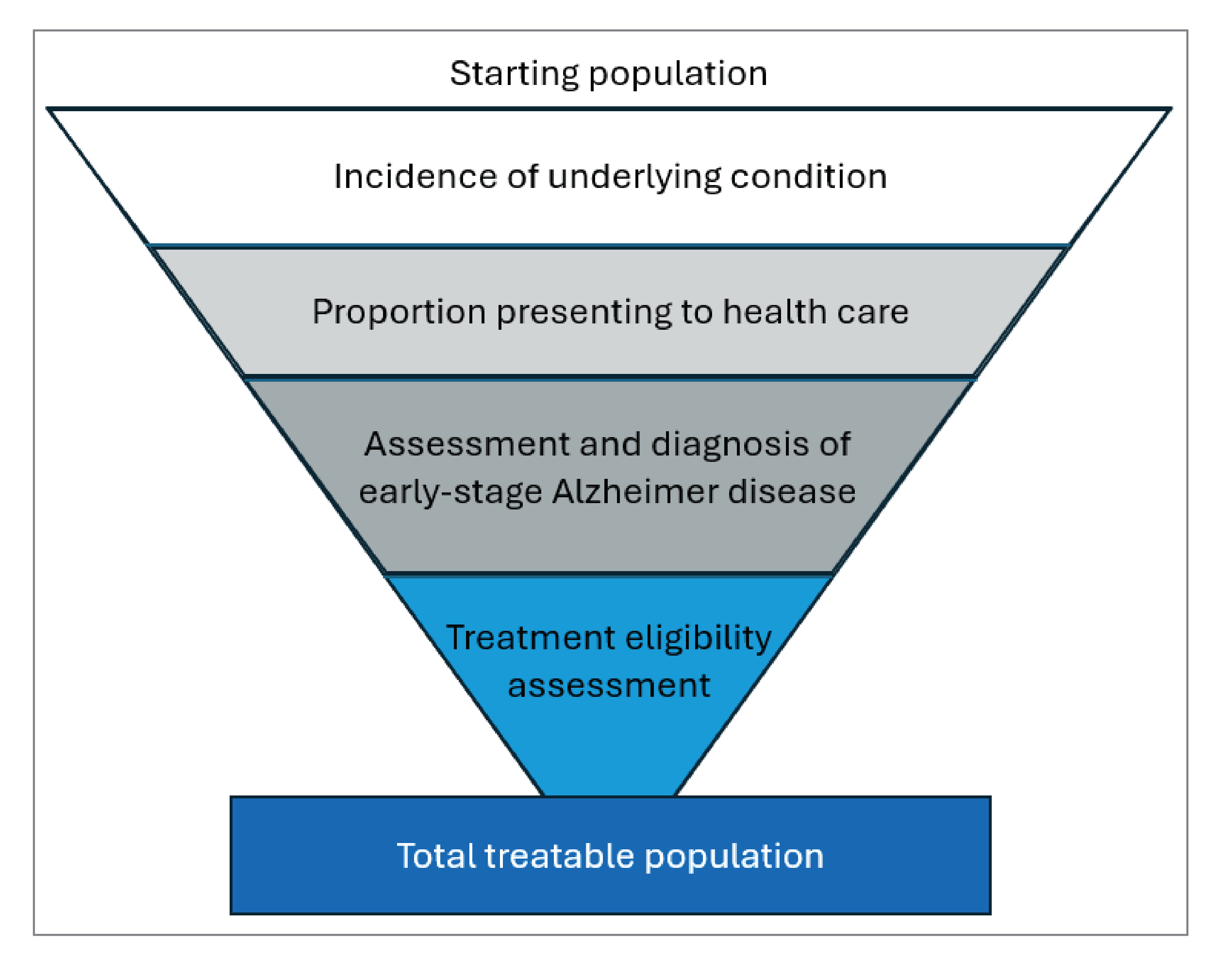
In 2020, the total estimated incident treatable population in Canada was 22,652 people, representing 0.3% of people aged 65 years or older in Canada (6,809,521; Table 2). This number reflects only 1 year of newly diagnosed cases and provides a conservative estimate of the potential treatable population if anti–amyloid-beta mAb DMTs were available in Canada. It does not account for patients with existing early-stage AD who might also seek treatment, potentially increasing the total treatable population. Additionally, not everyone with sufficient amyloid-beta to qualify for the DMTs may choose to pursue treatment due to comorbidities, frailties, or concerns about potential serious adverse effects, for example.
Table 2: Combined Estimated Incident Treatable Population With Early-Stage AD in Canada for Anti–Amyloid-Beta mAb DMTs in 2020
Stage | Mild cognitive impairment | Mild dementia due to AD | Total incident treatable population | |||
|---|---|---|---|---|---|---|
N | % of starting population | N | % of starting population | N | % of starting population | |
People 65 years or older in Canada | 6,809,521 | — | 6,809,521 | — | 6,809,521 | — |
Incidence of underlying condition | 347,286 | 5.1 | 86,000 | 1.3 | 433,286 | 6.4 |
Proportion presenting to health care | 46,189 | 0.7 | 32,938 | 0.5 | 79,127 | 1.2 |
Assessment and diagnosis of early-stage AD | 25,404 | 0.4 | 11,621 | 0.2 | 37,025 | 0.5 |
Treatment eligibility assessment | 14,506 | 0.2 | 8,146 | 0.1 | 22,652 | 0.3 |
AD = Alzheimer disease; DMT = disease-modifying therapy; mAb = monoclonal antibody.
A 2023 report examining current health system capacity found that less than 2% of potential patients would be able to access the health care resources required to be treated with anti–amyloid-beta mAb DMTs, with eligibility assessment creating the largest capacity gap to treat patients.5 This further reinforces the need to modify the current patient pathway to treat AD should anti–amyloid-beta mAb DMTs be approved, as well as to prepare for the adoption of emerging technologies such as blood-based biomarkers.
The estimate used here limited the treatable population to those 65 years of age or older. In clinical trials of DMTs, the average age of trial participants skewed older, exceeding 70 years of age. However, if anti–amyloid-beta mAb DMT were approved in Canada, it is likely that those under the age of 65 with symptoms would also seek assessment and treatment, increasing the treatable population beyond what was estimated. Additionally, this report relies on publicly available information from a literature scan, including studies from a variety of countries, which may affect its accuracy in reflecting the context of Canada. Much of the literature was published before the introduction of DMTs, so the values underpinning the calculation stages may change as new data and studies examining how patient behaviour is affected by DMTs are made available.
Estimation of Medical Imaging Demand
Using the estimated incident treatable population with early-stage AD, the number of PET-CT and MRI exams required for anti–amyloid-beta mAb DMTs was calculated and matched to the domains of the patient pathway for AD. This is a novel extension to the work done in the NICE report.21,220 Details on specific methodology and assumptions are listed in Appendix 2.
In 2020, an estimated 7,475 PET-CT exams and 70,900 MRI exams would be required to support the 22,652 patients with incident early-stage AD eligible for anti–amyloid-beta mAb DMTs for 1 year (Table 3). This represents 6% and 3% of the 2019 to 2020 exam volumes for PET-CT and MRI, respectively, adding an additional volume to medical imaging capacity, which would be expected to further contribute to long wait times.144,153 As previously mentioned, eligibility assessment, including PET-CT exams, was 1 of the largest identified capacity gaps in the current health care system, leading to a reduced access to anti–amyloid-beta mAb DMTs for the treatable population.5
Table 3: Estimated PET-CT and MRI Exams Required Based on Estimated Incident Treatable Population in Canada With Early-Stage AD for Anti–Amyloid-Beta mAb DMTs in 2020
Domain | PET-CT exams | MRI exams |
|---|---|---|
Treatment eligibility assessment | 7,475 | 22,652 |
Treatment administration of anti-amyloid-beta mAb DMTs | NA | NA |
Patient monitoring | NA | 48,248 |
Total | 7,475 | 70,900 |
AD = Alzheimer disease; DMT = disease-modifying therapy; mAb = monoclonal antibody; NA = not available.
These exam volumes also represent a conservative estimate of potential exams, as it was assumed only patients contraindicated for LPs (33%) would receive PET-CT exams, whereas patient preference may lead to more PET-CT exams than projected.221 In addition, it may be necessary to conduct recurrent PET-CT exams each year to confirm continued eligibility for anti–amyloid-beta mAb DMTs. The estimated MRI exam volumes include a baseline exam and 2 scheduled monitoring exams for all patients and the associated exams needed for the 6.5% of patients who experience ARIA. However, the estimated MRI exam volumes did not take into account the need for precautionary MRI exams when symptoms of adverse events appear that do not progress to full cases of ARIA, which could significantly inflate the exam volume. Additionally, if people with existing early-stage AD were to seek treatment, the subsequent exam volume would increase as well.
Estimating Future Demand
The 5 years from 2020 to 2025 were examined by combining the estimation of the treatable incident population with the estimated medical imaging demand to aid in potential capacity planning. Details on specific methodology and assumptions are provided in Appendix 2.
Over the 5-year period, an initial jump in the number of patients, from 22,625 patients to 71, 249, was seen in the first 3 years as anti–amyloid-beta mAb DMTs were introduced. The health system may not be able to handle a large influx of patients and medical imaging exams within a relatively short period of time. With patients remaining on treatment for 2 years before being taken off, a steadier increase of patients was projected, increasing by approximately 4,000 annually.
Table 4: Estimated Incident Treatable Population With Early-Stage AD in Canada for Anti–Amyloid-Beta mAb DMTs From 2020 to 2025 and Estimated Demand on Medical Imaging
Year | Total annual number of patients eligible for treatment | Annual number of incident cases | Annual PET-CT exams | Annual MRI exams |
|---|---|---|---|---|
2020 | 22,625 | 22,625 | 7,475 | 70,900 |
2021 | 46,357 | 23,732 | 15,307 | 75,752 |
2022 | 71,249 | 24,892 | 23,521 | 79,456 |
2023 | 74,733 | 26,109 | 24,662 | 83,339 |
2024 | 78,387 | 27,386 | 25,868 | 87,415 |
2025 | 82,220 | 28,725 | 27,133 | 91,689 |
AD = Alzheimer disease; DMT = disease-modifying therapy; mAb = monoclonal antibody.
This projection assumes a constant demand for anti–amyloid-beta mAb DMTs, which may not reflect reality, as demand could grow as the treatment becomes more established. In addition, the projection assumes the treatment period lasts 2 years based on clinical trial parameters, but it remains unclear how long patients would remain on anti–amyloid-beta mAb DMTs, as open-label extension studies are ongoing.222,223 Additionally, a constant increase in the incidence rate was assumed over the 5-year period, which may not reflect the potential future demand, as more patients with symptoms may seek assessment if anti–amyloid-beta mAb DMTs become more established as a treatment option. Finally, health care providers may be cautious concerning adverse events and limit patient eligibility, or the health system may limit where treatments will be offered during the early phases of anti–amyloid-beta mAb DMTs implementation, lowering the number of patients who will be treated. For instance, 6 months after regulatory approval, it has been reported that only 2,000 to 3,000 people in the US have received treatment with anti–amyloid-beta mAb DMT because treatment was mainly being provided at large neurology centres.224
Future Considerations for Anti–Amyloid-Beta mAb DMTs
With numerous potential treatments for AD in development, the current care pathway may not provide the range of health care resources required for optimal patient support. If these therapies are approved, substantial changes to existing patient care pathways may be necessary to ensure equitable access to them. This may include:
enhancing care by implementing interdisciplinary teams to better support and manage patients presenting with cognitive symptoms as well as coordinating care while patients receive anti–amyloid-beta mAb DMTs
increasing health system capacity to treat patients with AD, including dementia specialists, AD care providers, lab capacity, and infusion sites to meet the needs of a growing aging population
increasing medical imaging capacity, with consideration for staffing levels and the number and location of MRI and PET-CT units, as well as supporting medical imaging staff with education and training
improving equitable access to primary and social services for underserved groups — such as racialized communities and Indigenous populations — which requires expanding culturally appropriate care, addressing structural barriers, implementing equitable cognitive-assessment tools, and educating and training health care providers to better support these communities to ensure they receive the care and support they need
increasing outreach and awareness of cognitive decline symptoms among PCPs, patients, and the general public, especially in racialized groups that may be less aware of AD
establishing criteria for accessing limited medical imaging resources without disrupting access for current patients (i.e., oncology patients receiving PET-CT exams)
conducting postmarket drug evaluations to assess long-term safety and effectiveness of anti–amyloid-beta mAb DMTs, including their impact on AD progression and potential side effects over time
ensuring appropriate follow-up and monitoring, potentially with a patient registry, to determine when patients should discontinue treatment.
The landscape of anti–amyloid-beta mAb DMTs implementation is already evolving, with the development of blood-based AD biomarker testing. As well, the adoption of portable or remote operating MRI units may play a role in alleviating some equity and travel concerns for patients living in rural or remote areas in the future. These developments may greatly increase access to anti–amyloid-beta mAb DMTs, and care needs to be taken to ensure that these advances can be deployed in a timely and equitable manner. This includes:
developing a standardized threshold for determining AD using blood-based biomarker tests as well as accrediting labs throughout the country to ensure timely analysis of biomarker tests
combining newly developed technologies and key alterations in how patients with AD receive care to improve patient care and health system readiness and resilience to treat patients with anti–amyloid-beta mAb DMTs if they are approved in Canada.
Limitations
The aim of this report is to provide a high-level overview of considerations for health care systems in relation to the potential market entry of anti–amyloid-beta mAb DMTs. Some of the challenges may differ in magnitude across different provinces and territories. Additionally, this report specifically focused on anti–amyloid-beta mAb DMTs, as they are the most developed treatment option, they have been approved in some countries, and they share many considerations for potential effects on the treatment pathway and the health care system. Other DMTs for AD that target alternative pathologic processes or use different administration methods (e.g., oral intake) are still in earlier stages of development and may involve additional considerations not covered here. However, these other DMTs for AD may have considerations that overlap with some of the proposed changes to the current treatment pathway for potential uptake of anti–amyloid-beta mAb DMTs.
This report is also limited by information that is publicly accessible via a literature search. Access to provincial and territorial health systems data could provide key information about demographic aspects and the clinical profile of people with early-stage AD, current processes of care, and outcomes of the disease, which would assist in projections and planning to optimize care.
Conclusions
CDA-AMC has highlighted some key considerations in relation to the readiness of health care systems if emerging DMTs were adopted in Canada.
The regulatory approval and public reimbursement of DMTs for AD in Canada would require a new pathway of care to ensure equitable and timely access to these novel therapies.
Implementing the changes to the clinical pathway for the use of anti–amyloid-beta mAb DMTs will require considerations for adaptations across the continuum of care, including health and social human resources planning and additional clinical training, increased capacity for diagnostic imaging, laboratory networks, and IV infusion. Careful consideration of processes and systems would be needed to promote best clinical practice and appropriate use of finite health care resources.
Across different provincial and territorial health care systems, challenges will vary, necessitating open communication and multidisciplinary collaboration between health system partners to facilitate the optimal delivery of patient care. It would take time to design, plan, and operationalize models of care for novel DMTs, and careful consideration would need to be given to emerging technologies that may support their delivery. New blood-based biomarkers, for example, could largely obviate the need for LP via CSF and PET-CT to assess amyloid positivity. An ongoing awareness of emerging health technologies in relation to screening, diagnosis, treatment, monitoring, and assessment of their benefits and limitations would be important to support optimal care and health system sustainability.
This report highlights that certain groups of people in Canada may face challenges in accessing the technologies, services, and clinicians needed to diagnose the presence and severity of the disease, determine eligibility for treatment, administer therapies, and provide ongoing monitoring. Rural and remote populations, newcomers to Canada, Indigenous Peoples, and other groups may experience barriers in accessing and navigating the health care systems, challenging the principle of health equity.
Pan-Canadian alignment among the provinces and territories, as well as input from patients and caregivers, is required to promote a standardized, patient-centred approach to screening, diagnosing, treating, and monitoring patients. Such an approach may help achieve long-term success in expanding capacity and ensuring the delivery of optimal and sustainable care.
References
1.Navigating the path forward for dementia in Canada: the Landmark study: Report 1. Toronto (ON): Alzheimer Society of Canada; 2022: https://alzheimer.ca/sites/default/files/documents/Landmark-Study-Report-1-Path_Alzheimer-Society-Canada_0.pdf. Accessed 2024 Apr 25.
2.Petersen RC, Lopez O, Armstrong MJ, et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2018;90(3):126-135. PubMed
3.The Many Faces of Dementia in Canada: the Landmark Study: Report 2. Toronto (ON): Alzheimer Society of Canada; 2024: https://alzheimer.ca/sites/default/files/documents/ASC_The%20Many%20Faces%20of%20Dementia%20In%20Canada_Landmark%20Study_Vol2.pdf. Accessed 2024 Aug 5.
4.Frank A, Ismail Z, Wilson M, et al. Health System Change for Alzheimer's Disease-Modifying Therapies in Canada: Beginning the Discussion. Can J Neurol Sci. 2023:1-9. PubMed
5.Black SE, Budd N, Nygaard HB, et al. A Model Predicting Healthcare Capacity Gaps For Alzheimer's Disease-Modifying Treatment in Canada. Can J Neurol Sci. 2023:1-8. PubMed
6.National Institute on Aging. Alzheimer's Disease Fact Sheet. 2021; https://www.nia.nih.gov/health/alzheimers-and-dementia/alzheimers-disease-fact-sheet. Accessed 2024 Apr 29.
7.Liu J, Hlavka JP, Coulter DT, Baxi SM, Mattke S, Gidengil CA. Assessing the Preparedness of the Canadian Health Care System Infrastructure for an Alzheimer's Treatment. Santa Monica (CA): RAND Corporation; 2017: https://www.rand.org/pubs/research_reports/RR2744.html. Accessed 2024 Apr 29.
8.Duong S, Patel T, Chang F. Dementia: What pharmacists need to know. Can Pharm J (Ott). 2017;150(2):118-129. PubMed
9.Petersen RC, Caracciolo B, Brayne C, Gauthier S, Jelic V, Fratiglioni L. Mild cognitive impairment: a concept in evolution. J Intern Med. 2014;275(3):214-228. PubMed
10.Fitzpatrick-Lewis D, Warren R, Ali M, Sherifali D, Raina P. Treatment for mild cognitive impairment: a systematic review and meta-analysis. CMAJ Open. 2015;3(4):E419-E427. https://www.cmajopen.ca/content/3/4/E419. Accessed 2024 Apr 30. PubMed
11.Morris JC, Storandt M, Miller JP, et al. Mild cognitive impairment represents early-stage Alzheimer disease. Arch Neurol. 2001;58(3):397-405. PubMed
12.Statistics Canada. Table 17-10-0005-01: Population estimates on July 1, by age and gender. 2024; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2024 Apr 29.
13.Dementia in Canada: Economic Burden 2020 to 2050. Toronto (ON): Canadian Centre for Economic Analysis; 2023: https://www.cancea.ca/wp-content/uploads/2023/07/CANCEA-Economic-Impact-of-Dementia-in-Canada-2023-01-08.pdf. Accessed 2024 Oct 31.
14.Canadian Institute for Health Information (CIHI). How dementia impacts Canadians. Dementia in Canada [2018?]; https://www.cihi.ca/en/dementia-in-canada/how-dementia-impacts-canadians. Accessed 2024 May 02.
15.Herrmann N, Tam DY, Balshaw R, et al. The relation between disease severity and cost of caring for patients with Alzheimer disease in Canada. Can J Psychiatry. 2010;55(12):768-775. PubMed
16.Progression - Late Stage. The Progression of Alzheimer's Disease. Toronto (ON): Alzheimer Society of Canada; 2022: https://alzheimer.ca/sites/default/files/documents/Progression-Late-Stage-Alzheimer-Society.pdf. Accessed 2024 Apr 30.
17.Ismail Z, Black SE, Camicioli R, et al. Recommendations of the 5th Canadian Consensus Conference on the diagnosis and treatment of dementia. Alzheimers Dement. 2020;16(8):1182-1195. PubMed
18.Bergman H, Borson S, Jessen F, et al. Dementia and comorbidities in primary care: a scoping review. BMC Prim Care. 2023;24(1):277. PubMed
19.Gauthier S, Patterson C, Chertkow H, et al. Recommendations of the 4th Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (CCCDTD4). Can Geriatr J. 2012;15(4):120-126. PubMed
20.Watt JA, Isaranuwatchai W, Grossman L, Straus SE. Disease-modifying drugs for Alzheimer disease: implications for people in Canada. CMAJ. 2023;195(42):E1446-E1448. https://www.cmaj.ca/content/cmaj/195/42/E1446.full.pdf. Accessed 2024 Apr 30. PubMed
21.Potential issues and challenges in evaluation of disease-modifying dementia treatments. HTA Innovation Laboratory Report. London (UK): National Institute for Health and Care Excellence (NICE); 2023: https://www.nice.org.uk/Media/Default/About/what-we-do/HTA%20Lab/HTA-lab-dmdt.pdf. Accessed 2024 Apr 29.
22.Cummings J, Fox N. Defining Disease Modifying Therapy for Alzheimer's Disease. J Prev Alzheimers Dis. 2017;4(2):109-115. PubMed
23.Selkoe DJ, Hardy J. The amyloid hypothesis of Alzheimer's disease at 25 years. EMBO Mol Med. 2016;8(6):595-608. PubMed
24.Cummings J, Zhou Y, Lee G, Zhong K, Fonseca J, Cheng F. Alzheimer's disease drug development pipeline: 2024. Alzheimers Dement (N Y). 2024;10(2):e12465. PubMed
25.Cummings J, Ritter A, Zhong K. Clinical Trials for Disease-Modifying Therapies in Alzheimer's Disease: A Primer, Lessons Learned, and a Blueprint for the Future. J Alzheimers Dis. 2018;64(s1):S3-S22. PubMed
26.Cummings J, Zhou Y, Lee G, Zhong K, Fonseca J, Cheng F. Alzheimer's disease drug development pipeline: 2023. Alzheimers Dement (N Y). 2023;9(2):e12385. PubMed
27.Biogen Inc. Prescribing information: Aduhelm (aducanumab-avwa) injection, for intravenous use. Silver Spring (MD): U.S. Food and Drug Administration; 2021: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/761178s003lbl.pdf. Accessed 2024 May 23.
28.Eisai Inc. Prescribing information: Leqembi (lecanemab-irmb) injection, for intravenous use. Silver Springs (MD): U.S. Food and Drug Administration; 2023: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761269s000lbl.pdf. Accessed 2024 May 23.
29.Report on the Deliberation Results: Leqembi for Intravenous Infusion 200 mg. Tokyo (JP): Pharmaceuticals and Medical Devices Agency, Pharmaceutical Evaluation Division, Pharmaceutical Safety and Environmental Health Bureau; 2023: https://www.pmda.go.jp/files/000267068.pdf. Accessed 2024 May 23.
30.Eli Lilly and Company. Prescribing information: Kisunla (donanemab-azbt) injection, for intravenous use. Silver Spring (MD): U.S. Food and Drug Administration; 2024: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/761248s000lbl.pdf. Accessed 2024 Aug 19.
31.Sturchio A, Dwivedi AK, Young CB, et al. High cerebrospinal amyloid-β 42 is associated with normal cognition in individuals with brain amyloidosis. eClinicalMedicine. 2021;38. PubMed
32.Morris GP, Clark IA, Vissel B. Questions concerning the role of amyloid-beta in the definition, aetiology and diagnosis of Alzheimer's disease. Acta Neuropathol. 2018;136(5):663-689. PubMed
33.Brucki SMD, Cesar-Freitas KG, Spera RR, Borges CR, Smid J. Are we ready to use anti-amyloid therapy in Alzheimer's disease? Arq Neuropsiquiatr. 2022;80(5 Suppl 1):15-23. PubMed
34.Lang L, Clifford A, Wei L, et al. Prevalence and determinants of undetected dementia in the community: a systematic literature review and a meta-analysis. BMJ Open. 2017;7(2):e011146. PubMed
35.Sternberg SA, Wolfson C, Baumgarten M. Undetected dementia in community-dwelling older people: the Canadian Study of Health and Aging. J Am Geriatr Soc. 2000;48(11):1430-1434. PubMed
36.Öhman F, Hassenstab J, Berron D, Schöll M, Papp KV. Current advances in digital cognitive assessment for preclinical Alzheimer's disease. Alzheimers Dement (Amst). 2021;13(1):e12217. PubMed
37.Chun CT, Seward K, Patterson A, Melton A, MacDonald-Wicks L. Evaluation of Available Cognitive Tools Used to Measure Mild Cognitive Decline: A Scoping Review. Nutrients. 2021;13(11). PubMed
38.Cahill S, Pierce M, Werner P, Darley A, Bobersky A. A systematic review of the public's knowledge and understanding of Alzheimer's disease and dementia. Alzheimer Dis Assoc Disord. 2015;29(3):255-275. PubMed
39.Laurell AAS, Venkataraman AV, Schmidt T, et al. Estimating demand for potential disease-modifying therapies for Alzheimer's disease in the UK. Br J Psychiatry. 2024;224(6):198-204. PubMed
40.World Alzheimer Report 2024: Global changes in attitudes to dementia. London (UK): Alzheimer’s Disease International; 2024: https://www.alzint.org/u/World-Alzheimer-Report-2024.pdf. Accessed 2024 Oct 31.
41.Aminzadeh F, Molnar FJ, Dalziel WB, Ayotte D. A review of barriers and enablers to diagnosis and management of persons with dementia in primary care. Can Geriatr J. 2012;15(3):85-94. PubMed
42.CADTH Horizon Scan: Dementia Concerns and Considerations: A CADTH Panel of People with Lived Experience. Can J Health Technol. 2022;2(4). https://www.cadth.ca/sites/default/files/hta-he/HC0022-Dementia-Panel.pdf. Accessed 2024 May 02.
43.Canadian Institute for Health Information (CIHI). Unpaid caregiver challenges and supports. Dementia in Canada 2018; https://www.cihi.ca/en/dementia-in-canada/unpaid-caregiver-challenges-and-supports. Accessed 2024 Oct 28.
44.Black SE, Gauthier S, Dalziel W, et al. Canadian Alzheimer's disease caregiver survey: baby-boomer caregivers and burden of care. Int J Geriatr Psychiatry. 2010;25(8):807-813. PubMed
45.The Canadian Press. Canadians dismiss early signs of dementia. CBC. 2012 Jan 4. https://www.cbc.ca/news/health/canadians-dismiss-early-signs-of-dementia-1.1187103. Accessed 2024 May 02.
46.Foin G. Expérience des personnes qui vivent avec un trouble neurocognitif au Québec [Experience of people who live with a neurocognitive disorder in Quebec]. Quebec (QC): Institut national d’excellence en santé et en services sociaux (INESSS); 2024: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Usage_optimal/INESSS_Alzheimer_TNC_EC_VF.pdf. Accessed 2024 May 02.
47.2017 Awareness Survey Executive Summary. Toronto (ON): Alzheimer Society of Canada; 2017: https://ilivewithdementia.ca/wp-content/uploads/2019/12/2017_AWARENESS-SURVEY_EXECUTIVE_SUMMARY.pdf. Accessed 2024 Oct 31.
48.Duong D, Vogel L. National survey highlights worsening primary care access. CMAJ. 2023;195(16):E592-E593. PubMed
49.Canadian Institute for Health Information (CIHI). Better access to primary care key to improving health of Canadians. Taking the pulse: Measuring shared priorities for Canadian health care, 2024 2024; https://www.cihi.ca/en/taking-the-pulse-measuring-shared-priorities-for-canadian-health-care-2024/better-access-to-primary-care-key-to-improving-health-of-canadians. Accessed 2024 Nov 7.
50.Pimlott NJ, Persaud M, Drummond N, et al. Family physicians and dementia in Canada: Part 2. Understanding the challenges of dementia care. Can Fam Physician. 2009;55(5):508-509 e501-507.
51.Risdon C. Analysis: The impact of not having a family doctor: Patients are worse off, and so is the health system. McMaster University Brighter World 2023 Oct 19; https://brighterworld.mcmaster.ca/articles/analysis-the-impact-of-not-having-a-family-doctor-patients-are-worse-off-and-so-is-the-health-system/. Accessed 2024 May 02.
52.Bacsu J, Novik N, Johnson S, et al. Addressing the needs of rural and remote people in a national dementia strategy for Canada. Can J Public Health. 2019;110(6):752-755. PubMed
53.Wilson CR, Rourke J, Oandasan IF, Bosco C. Progress made on access to rural health care in Canada. Can Fam Physician. 2020;66(1):31-36.
54.Roberts JR, Windle G, Story A, et al. Dementia in rural settings: a scoping review exploring the personal experiences of people with dementia and their carers. Ageing and Society. 2023:1-30.
55.Access to health services as a social determinant of First Nations, Inuit and Métis health. Prince George (BC): National Collaborating Centre for Indigenous Health; 2019: https://www.nccih.ca/docs/determinants/FS-AccessHealthServicesSDOH-2019-EN.pdf. Accessed 2024 May 28.
56.Yangzom K, Masoud H, Hahmann T. Primary health care access among First Nations people living off reserve, Métis and Inuit, 2017 to 2020. Ottawa (ON): Statistics Canada, Centre for Indigenous Statistics and Partnerships; 2023: https://www150.statcan.gc.ca/n1/pub/41-20-0002/412000022023005-eng.htm. Accessed 2024 May 28.
57.Anthonisen G, Luke A, MacNeill L, MacNeill AL, Goudreau A, Doucet S. Patient navigation programs for people with dementia, their caregivers, and members of the care team: a scoping review. JBI Evid Synth. 2023;21(2):281-325. PubMed
58.Tang KL, Kelly J, Sharma N, Ghali WA. Patient navigation programs in Alberta, Canada: an environmental scan. CMAJ Open. 2021;9(3):E841-E847. PubMed
59.Hinton L, Tran D, Peak K, Meyer OL, Quinones AR. Mapping racial and ethnic healthcare disparities for persons living with dementia: A scoping review. Alzheimers Dement. 2024;20(4):3000-3020. PubMed
60.Gauthier S, Rosa-Neto P, Morais JA, Webster C. World Alzheimer Report 2021: Journey through the diagnosis of dementia. London (UK): Alzheimer's Disease International; 2021: https://www.alzint.org/u/World-Alzheimer-Report-2021.pdf. Accessed 2024 May 01.
61.Miedema B, Hamilton R, Easley J. Climbing the walls: Structural barriers to accessing primary care for refugee newcomers in Canada. Can Fam Physician. 2008;54(3):335-336, 338-339. PubMed
62.Ravichandiran N, Mathews M, Ryan BL. Utilization of healthcare by immigrants in Canada: a cross-sectional analysis of the Canadian Community Health Survey. BMC Prim Care. 2022;23(1):69. PubMed
63.Mayeda ER, Glymour MM, Quesenberry CP, Whitmer RA. Inequalities in dementia incidence between six racial and ethnic groups over 14 years. Alzheimers Dement. 2016;12(3):216-224. PubMed
64.Pimlott NJ, Persaud M, Drummond N, et al. Family physicians and dementia in Canada: Part 1. Clinical practice guidelines: awareness, attitudes, and opinions. Can Fam Physician. 2009;55(5):506-507 e501-505.
65.Bradford A, Kunik ME, Schulz P, Williams SP, Singh H. Missed and delayed diagnosis of dementia in primary care: prevalence and contributing factors. Alzheimer Dis Assoc Disord. 2009;23(4):306-314. PubMed
66.Liss JL, Seleri Assuncao S, Cummings J, et al. Practical recommendations for timely, accurate diagnosis of symptomatic Alzheimer's disease (MCI and dementia) in primary care: a review and synthesis. J Intern Med. 2021;290(2):310-334. PubMed
67.Bacsu J, Mateen FJ, Johnson S, Viger MD, Hackett P. Improving Dementia Care Among Family Physicians: From Stigma to Evidence-Informed Knowledge. Can Geriatr J. 2020;23(4):340-343. PubMed
68.Kokorelias KM, Markoulakis R, Hitzig SL. Considering a Need for Dementia-Specific, Family-Centered Patient Navigation in Canada. J Appl Gerontol. 2023;42(1):19-27. PubMed
69.Boise L, Morgan DL, Kaye J, Camicioli R. Delays in the diagnosis of dementia: Perspectives of family caregivers. American Journal of Alzheimer's Disease. 1999;14(1):20-26.
70.Walker JD, O'Connell ME, Pitawanakwat K, et al. Canadian Indigenous Cognitive Assessment (CICA): Inter-rater reliability and criterion validity in Anishinaabe communities on Manitoulin Island, Canada. Alzheimers Dement (Amst). 2021;13(1):e12213. PubMed
71.How Canada Compares: Results From the Commonwealth Fund's 2019 International Health Policy Survey of Primary Care Physicians - Accessible Report. Ottawa (ON): Canadian Institute for Health Information (CIHI); 2020: https://www.cihi.ca/sites/default/files/document/cmwf-2019-accessible-report-en-web.pdf. Accessed 2024 Jun 10.
72.Ng KP, Chiew HJ, Lim L, Rosa-Neto P, Kandiah N, Gauthier S. The influence of language and culture on cognitive assessment tools in the diagnosis of early cognitive impairment and dementia. Expert Rev Neurother. 2018;18(11):859-869. PubMed
73.Chithiramohan T, Santhosh S, Threlfall G, et al. Culture-Fair Cognitive Screening Tools for Assessment of Cognitive Impairment: A Systematic Review. J Alzheimers Dis Rep. 2024;8(1):289-306. PubMed
74.O'Driscoll C, Shaikh M. Cross-Cultural Applicability of the Montreal Cognitive Assessment (MoCA): A Systematic Review. J Alzheimers Dis. 2017;58(3):789-801. PubMed
75.Halseth R. Alzheimer's Disease and Related Dementias in Indigenous Populations: Knowledge, Needs, and Gaps. Chronic and Infectious Diseases. Prince George (BC): National Collaborating Centre for Indigenous Health; 2022: https://www.nccih.ca/Publications/Lists/Publications/Attachments/10385/Alzheimers-Disease-and-Related%20Dementias-in-Indigenous-Populations_Web_2022-08-11.pdf. Accessed 2024 Oct 28.
76.McCleary L, Persaud M, Hum S, et al. Pathways to dementia diagnosis among South Asian Canadians. Dementia (London). 2013;12(6):769-789. PubMed
77.Iroanyah N, Savundranayagam MY, Mundadan RG, Sivananthan S. Equity, diversity, and inclusion in dementia diagnosis: a Canadian perspective. World Alzheimer Report 2021: Journey through the diagnosis of dementia London (UK): Alzheimer's Disease International; 2021: https://www.alzint.org/u/World-Alzheimer-Report-2021.pdf. Accessed 2024 Oct 28.
78.Jacklin K, Pitawanakwat K, Blind M, et al. Developing the Canadian Indigenous Cognitive Assessment for Use With Indigenous Older Anishinaabe Adults in Ontario, Canada. Innov Aging. 2020;4(4):igaa038. PubMed
79.Gove D, Nielsen TR, Smits C, et al. The challenges of achieving timely diagnosis and culturally appropriate care of people with dementia from minority ethnic groups in Europe. Int J Geriatr Psychiatry. 2021;36(12):1823-1828. PubMed
80.Constantinescu A, Li H, Yu J, Hoggard C, Holroyd-Leduc J. Exploring Rural Family Physicians' Challenges in Providing Dementia Care: A Qualitative Study. Can J Aging. 2018;37(4):390-399. PubMed
81.Canadian Institute for Health Information (CIHI). Family doctor preparedness. Dementia in Canada [2018?]; https://www.cihi.ca/en/dementia-in-canada/spotlight-on-dementia-issues/family-doctor-preparedness. Accessed 2024 May 02.
82.Kornelsen J, Khowaja AR, Av-Gay G, et al. The rural tax: comprehensive out-of-pocket costs associated with patient travel in British Columbia. BMC Health Serv Res. 2021;21(1):854. PubMed
83.Mathews M, West R, Buehler S. How important are out-of-pocket costs to rural patients' cancer care decisions? Can J Rural Med. 2009;14(2):54-60. PubMed
84.Lee L, Molnar F, Hillier LM, Patel T, Slonim K. Multispecialty Interprofessional Team Memory Clinics: Enhancing Collaborative Practice and Health Care Providers' Experience of Dementia Care. Can J Aging. 2022;41(1):96-109. PubMed
85.Elbeddini A, Tayefehchamani Y, Yilmaz Z, Villegas JJ, Zhang EY. Evaluation of a community-based memory clinic in collaboration with local hospitals to support patients with memory decline. J Taibah Univ Med Sci. 2022;17(2):220-234. PubMed
86.ARTIC. Memory Clinics expanded to underserviced areas in Ontario. New ARTIC project helps patients living with dementia receive care, closer to home. Toronto (ON): Health Quality Ontario; 2017 Jan 23: https://www.hqontario.ca/portals/0/Documents/qi/artic/artic-pcmc-media-release-2016-en.pdf. Accessed 2024 May 29.
87.Morgan DG, Crossley M, Kirk A, et al. Improving access to dementia care: development and evaluation of a rural and remote memory clinic. Aging Ment Health. 2009;13(1):17-30. PubMed
88.CADTH Horizon Scan: Understanding the Portrait of Dementia Care in Canada: A CADTH Panel of Experts. Can J Health Technol. 2022;2(8). https://www.cadth.ca/sites/default/files/hs-eh/EH0110-Dementia-Clinician-Panel-v2.0-Final.pdf. Accessed 2024 May 02.
89.Kirby S, Weston LE, Barton JJ, Buske L, Chauhan TS. Report of the Canadian Neurological Society Manpower Survey 2012. Can J Neurol Sci. 2016;43(2):227-237. PubMed
90.Glauser W. Lack of interest in geriatrics among medical trainees a concern as population ages. CMAJ. 2019;191(20):E570-E571. PubMed
91.Basu M, Cooper T, Kay K, et al. Updated Inventory and Projected Requirements for Specialist Physicians in Geriatrics. Can Geriatr J. 2021;24(3):200-208. PubMed
92.Vedel I, Sourial N, Arsenault-Lapierre G, Godard-Sebillotte C, Bergman H. Impact of the Quebec Alzheimer Plan on the detection and management of Alzheimer disease and other neurocognitive disorders in primary health care: a retrospective study. CMAJ Open. 2019;7(2):E391-E398. PubMed
93.Lee L, Hillier LM, Harvey D. Integrating community services into primary care: improving the quality of dementia care. Neurodegener Dis Manag. 2014;4(1):11-21. PubMed
94.Lee L, Hillier LM, Heckman G, et al. Primary Care-Based Memory Clinics: Expanding Capacity for Dementia Care. Can J Aging. 2014;33(3):307-319. PubMed
95.CADTH Health Technology Review: Canadian Medical Imaging Inventory 2022-2023: Provincial and Territorial Overview. Can J Health Technol. 2024;4(8):1-81. https://www.cda-amc.ca/sites/default/files/hta-he/HC0024_Overview.pdf. Accessed 2024 May 1.
96.Moir M, Barua B, Wannamaker H. Waiting your turn: Wait times for health care in Canada, 2023 Report. Vancouver (BC): Fraser Institute; 2023: https://www.fraserinstitute.org/studies/waiting-your-turn-wait-times-for-health-care-in-canada-2023. Accessed 2024 May 13.
97.Addressing the Medical Imaging Dilemma in Canada: Restoring Timely Access for Patients Post-Pandemic. Ottawa (ON): Canadian Association of Radiologists; 2022: https://car.ca/wp-content/uploads/2022/02/CAR-PreBudgetSubmission-2022-e-web-FINAL_edited_Feb.pdf. Accessed 2024 May 2.
98.Staffaroni AM, Tsoy E, Taylor J, Boxer AL, Possin KL. Digital Cognitive Assessments for Dementia: Digital assessments may enhance the efficiency of evaluations in neurology and other clinics. Pract Neurol (Fort Wash Pa). 2020;2020:24-45. PubMed
99.Jannati A, Toro-Serey C, Gomes-Osman J, et al. Digital Clock and Recall is superior to the Mini-Mental State Examination for the detection of mild cognitive impairment and mild dementia. Alzheimers Res Ther. 2024;16(1):2. PubMed
100.Britton GB, Huang LK, Villarreal AE, et al. Digital phenotyping: An equal opportunity approach to reducing disparities in Alzheimer's disease and related dementia research. Alzheimers Dement (Amst). 2023;15(4):e12495. PubMed
101.Chaitanuwong P, Singhanetr P, Chainakul M, Arjkongharn N, Ruamviboonsuk P, Grzybowski A. Potential Ocular Biomarkers for Early Detection of Alzheimer's Disease and Their Roles in Artificial Intelligence Studies. Neurol Ther. 2023;12(5):1517-1532. PubMed
102.Wisely CE, Richardson A, Henao R, et al. A Convolutional Neural Network Using Multimodal Retinal Imaging for Differentiation of Mild Cognitive Impairment from Normal Cognition. Ophthalmol Sci. 2024;4(1):100355. PubMed
103.Biospace. Health Canada grants approval of the Eye-Tracking Neurological Assessment for Multiple Sclerosis (ETNA-MS) for use in tracking disease progression in people living with MS. 2024 Mar 25; https://www.biospace.com/article/releases/health-canada-grants-approval-of-the-eye-tracking-neurological-assessment-for-multiple-sclerosis-etna-and-8482-ms-for-use-in-tracking-disease-progression-in-people-living-with-ms/. Accessed 2024 May 6.
104.Innodem Neurosciences. Development and Validation of a Novel Functional Eye-Tracking Software Application for Alzheimer's Disease. 2024; https://innodemneurosciences.com/blogs/clinical-trials/development-and-validation-of-a-novel-functional-eye-tracking-software-application-for-alzheimers-disease. Accessed 2024 May 6.
105.García-Bermúdez MY, Vohra R, Freude K, et al. Potential Retinal Biomarkers in Alzheimer's Disease. Int J Mol Sci. 2023;24(21). PubMed
106.Businesswire. AIRAmed Receives FDA 510(k) Clearance for Its AIRAscore Brain Volumetry Software: Novel Technology Aids Physicians in Early Detection of Alzheimer’s and Other Dementias. 2023 Sep 19; https://www.businesswire.com/news/home/20230919787530/en/AIRAmed-Receives-FDA-510-k-Clearance-for-Its-AIRAscore-Brain-Volumetry-Software. Accessed 2024 May 6.
107.Yuan C, Linn KA, Hubbard RA. Algorithmic Fairness of Machine Learning Models for Alzheimer Disease Progression. JAMA Netw Open. 2023;6(11):e2342203. PubMed
108.Yin C, Imms P, Cheng M, et al. Anatomically interpretable deep learning of brain age captures domain-specific cognitive impairment. Proc Natl Acad Sci U S A. 2023;120(2):e2214634120. PubMed
109.PR Newswire. Darmiyan Receives FDA Approval for BrainSee, the First Prognostic Test for Predicting Likelihood of Progression to Alzheimer's Dementia. 2024; https://www.prnewswire.com/news-releases/darmiyan-receives-fda-approval-for-brainsee-the-first-prognostic-test-for-predicting-likelihood-of-progression-to-alzheimers-dementia-302033616.html. Accessed 2024 May 6.
110.Zou H, Xiao L, Zeng D, Luo S. Multivariate functional mixed model with MRI data: An application to Alzheimer's disease. Stat Med. 2023;42(10):1492-1511. PubMed
111.Bucholc M, James C, Khleifat AA, et al. Artificial intelligence for dementia research methods optimization. Alzheimers Dement. 2023;19(12):5934-5951. PubMed
112.Papaliagkas V, Kalinderi K, Vareltzis P, Moraitou D, Papamitsou T, Chatzidimitriou M. CSF Biomarkers in the Early Diagnosis of Mild Cognitive Impairment and Alzheimer's Disease. Int J Mol Sci. 2023;24(10):8976. PubMed
113.Kim JP, Kim J, Jang H, et al. Predicting amyloid positivity in patients with mild cognitive impairment using a radiomics approach. Sci Rep. 2021;11(1):6954. PubMed
114.Cummings J, Apostolova L, Rabinovici GD, et al. Lecanemab: Appropriate Use Recommendations. J Prev Alzheimers Dis. 2023;10(3):362-377. PubMed
115.Schiffman C, Bittner T, Giacobino C, et al. Determining the amyloid PET and CSF inclusion criteria for the SKYLINE secondary prevention study with gantenerumab. Alzheimers Dement. 2022;18(S6):e062376.
116.Lee SA, Sposato LA, Hachinski V, Cipriano LE. Cost-effectiveness of cerebrospinal biomarkers for the diagnosis of Alzheimer's disease. Alzheimers Res Ther. 2017;9(1):18. PubMed
117.Hampel H, Shaw LM, Aisen P, et al. State-of-the-art of lumbar puncture and its place in the journey of patients with Alzheimer's disease. Alzheimers Dement. 2022;18(1):159-177. PubMed
118.Stiffel M, Bergeron D, Mourabit Amari K, et al. Use of Alzheimer's Disease Cerebrospinal Fluid Biomarkers in A Tertiary Care Memory Clinic. Can J Neurol Sci. 2022;49(2):203-209. PubMed
119.Wetmore SJ, Rivet C, Tepper J, Tatemichi S, Donoff M, Rainsberry P. Definining core procedure skills for Canadian family medicine training. Can Fam Physician. 2005;51(10):1365. PubMed
120.Yeo CT, Davison C, Ungi T, Holden M, Fichtinger G, McGraw R. Examination of Learning Trajectories for Simulated Lumbar Puncture Training Using Hand Motion Analysis. Acad Emerg Med. 2015;22(10):1187-1195. PubMed
121.Gouvernement du Québec. Services offered by specialized nurse practitioners. 2024; https://www.quebec.ca/en/health/health-system-and-services/service-organization/specialized-nurse-practitioners/services-offered-specialized-nurse-practitioners. Accessed 2024 May 30.
122.Sweeney M, Al-Diwani A, Hadden R. Improving the safety and efficiency of outpatient lumbar puncture service. BMJ Qual Improv Rep. 2016;5(1). PubMed
123.Duits FH, Martinez-Lage P, Paquet C, et al. Performance and complications of lumbar puncture in memory clinics: Results of the multicenter lumbar puncture feasibility study. Alzheimers Dement. 2016;12(2):154-163. PubMed
124.Mayo Clinic. Lumbar puncture (spinal tap). 2024; https://www.mayoclinic.org/tests-procedures/lumbar-puncture/about/pac-20394631. Accessed 2024 Jun 18.
125.Bonomi S, Gupta MR, Schindler SE. Inadequate reimbursement for lumbar puncture is a potential barrier to accessing new Alzheimer's disease treatments. Alzheimers Dement. 2023;19(12):5849-5851. PubMed
126.Bouwman FH, Frisoni GB, Johnson SC, et al. Clinical application of CSF biomarkers for Alzheimer's disease: From rationale to ratios. Alzheimers Dement (Amst). 2022;14(1):e12314. PubMed
127.Menendez-Gonzalez M. Routine lumbar puncture for the early diagnosis of Alzheimer's disease. Is it safe? Front Aging Neurosci. 2014;6:65. PubMed
128.Moulder KL, Besser LM, Beekly D, Blennow K, Kukull W, Morris JC. Factors Influencing Successful Lumbar Puncture in Alzheimer Research. Alzheimer Dis Assoc Disord. 2017;31(4):287-294. PubMed
129.Vitali P. How to reassure people in need of a lumbar puncture. World Alzheimer Report 2021. Chapter 11 Spinal fluid. London (UK): Alzheimer's Disease International; 2021: https://www.alzint.org/u/World-Alzheimer-Report-2021-Chapter-11.pdf. Accessed 2024 May 8.
130.Babapour Mofrad R, Fruijtier AD, Visser LNC, et al. Lumbar puncture patient video increases knowledge and reduces uncertainty: An RCT. Alzheimers Dement (N Y). 2021;7(1):e12127. PubMed
131.Providence Health Care. Neurodegenerative Profile, CSF. [date unknown]; https://www.providencelaboratory.org/test-catalog/628. Accessed 2024 May 10.
132.Western University Schulich School of Medicine & Dentistry, Pathology and Labratory Medicine. Under the Microscope: PaLM Quarterly Newsletter Issue No. 4. London (ON): Pathology and Labratory Medicine; 2023: https://www.schulich.uwo.ca/pathol/about_us/utm_newsletter/Under%20the%20Microscope%20December%202023.pdf. Accessed 2024 Oct 28.
133.BC Neuroimmunology Laboratory Inc. Test Directory. Vancouver (BC): BC Neuroimmunology; 2024: https://bcneuro.ca/wp-content/uploads/2024/10/BCNI-Test-Directory_Rev2.1.pdf. Accessed 2024 Oct 28.
134.Hansson O, Batrla R, Brix B, et al. The Alzheimer's Association international guidelines for handling of cerebrospinal fluid for routine clinical measurements of amyloid beta and tau. Alzheimers Dement. 2021;17(9):1575-1582. PubMed
135.Ferrer R, Zhu N, Arranz J, et al. Importance of cerebrospinal fluid storage conditions for the Alzheimer's disease diagnostics on an automated platform. Clin Chem Lab Med. 2022;60(7):1058-1063. PubMed
136.Teitlebaum C, Collins A. Canadian Privacy Legislation and the Cross-Border Transfer of Personal Information Part One: Personal Health Information. Toronto (ON): Aird & Berlis LLP; [2008]: https://www.airdberlis.com/docs/default-source/articles/article—cross-border-transfer-of-personal-health-information.pdf?sfvrsn=2. Accessed 2024 May 30.
137.Willemse EAJ, Tijms BM, van Berckel BNM, et al. Comparing CSF amyloid-beta biomarker ratios for two automated immunoassays, Elecsys and Lumipulse, with amyloid PET status. Alzheimers Dement (Amst). 2021;13(1):e12182. PubMed
138.Help for Today, Hope for Tomorrow: Pre-Budget Submission 2024. Toronto (ON): Alzheimer Society of Ontario; 2024: https://alzheimer.ca/on/sites/on/files/documents/2024%20Budget%20Submission_EN.pdf. Accessed 2024 May 14.
139.Filippi L, Chiaravalloti A, Bagni O, Schillaci O. 18F-labeled radiopharmaceuticals for the molecular neuroimaging of amyloid plaques in Alzheimer's disease. Am J Nucl Med Mol Imaging. 2018;8(4):268-281. PubMed
140.Cummings J, Osse AML, Cammann D, Powell J, Chen J. Anti-Amyloid Monoclonal Antibodies for the Treatment of Alzheimer's Disease. Biodrugs. 2023. PubMed
141.Garibotto V, Albert NL, Barthel H, et al. The approval of a disease-modifying treatment for Alzheimer's disease: impact and consequences for the nuclear medicine community. Eur J Nucl Med Mol Imaging. 2021;48(10):3033-3036. PubMed
142.The Implementation Considerations of PET-CT. (Canadian Medical Imaging Inventory Service Report). Ottawa (ON): CDA-AMC; 2022: https://www.cadth.ca/sites/default/files/attachments/2022-01/implementation_considerations_of_PET-CT.pdf. Accessed 2024 May 14.
143.Verfaillie G, Franck C, De Crop A, Beels L, D'Asseler Y, Bacher K. A systematic review and meta-analysis on the radiation dose of computed tomography in hybrid nuclear medicine imaging. EJNMMI Phys. 2023;10(1):32. PubMed
144.CADTH Health Technology Review: Canadian Medical Imaging Inventory 2022-2023: PET-CT and PET-MRI. Can J Health Technol. 2024;4(8):1-72. https://www.cda-amc.ca/sites/default/files/hta-he/HC0024-04-CMII4-PET-Hybrid.pdf. Accessed 2024 May 1.
145.The Role of PET-CT in Drugs Targeting Amyloid-Beta in Alzheimer Disease: Part 2. (Canadian Medical Imaging Inventory Service Report). Ottawa (ON): CDA-AMC; 2022: https://www.cadth.ca/sites/default/files/attachments/2022-01/role_of_PET-CT_in_drugs_targeting_amyloid_beta_in_alzheimer_disease_part_2FINAL.pdf. Accessed 2024 May 13.
146.Health Canada. Product Information: NeuraCeq (Florbetaben (18F)): 3 µg/mL Solution for Intravenous Administration. 2024; https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=94968. Accessed 2024 May 14.
147.The future of PET-CT in Canada. (Canadian Medical Imaging Inventory Service Report). Ottawa (ON): CDA-AMC; 2021: https://www.cda-amc.ca/sites/default/files/attachments/2021-10/cmii_service_future_of_PET_CT.pdf. Accessed 2024 May 13.
148.Cao DJ, Hurrell C, Patlas MN. Current Status of Burnout in Canadian Radiology. Can Assoc Radiol J. 2023;74(1):37-43. PubMed
149.CADTH Health Technology Review: Canadian Medical Imaging Inventory 2022–2023: The Medical Imaging Team. Can J Health Technol. 2024;4(8). https://www.cda-amc.ca/sites/default/files/hta-he/HC0024-08-Medical-Imaging-Team.pdf. Accessed 2024 May 1.
150.Gerwing M. New PET scanner sits idle at Winnipeg hospital without staff to operate it. CTV News. 2023 Apr 6. https://winnipeg.ctvnews.ca/new-pet-scanner-sits-idle-at-winnipeg-hospital-without-staff-to-operate-it-1.6346224. Accessed 2024 May 30.
151.Hampel H, Elhage A, Cho M, Apostolova LG, Nicoll JAR, Atri A. Amyloid-related imaging abnormalities (ARIA): radiological, biological and clinical characteristics. Brain. 2023;146(11):4414-4424. PubMed
152.Roytman M, Mashriqi F, Al-Tawil K, et al. Amyloid-Related Imaging Abnormalities: An Update. AJR Am J Roentgenol. 2023;220(4):562-574. PubMed
153.CADTH Health Technology Review: Canadian Medical Imaging Inventory 2022–2023: MRI. Can J Health Technol. 2024;4(8). https://www.cda-amc.ca/sites/default/files/hta-he/HC0024-006-CMII4-MRI.pdf. Accessed 2024 May 1.
154.Deoni SCL, Medeiros P, Deoni AT, et al. Development of a mobile low-field MRI scanner. Sci Rep. 2022;12(1):5690. PubMed
155.Improving Access to Lifesaving Imaging Care for Canadians. Ottawa (ON): Canadian Association of Radiologists; 2022: https://car.ca/wp-content/uploads/2022/11/CAR_Multistakeholder_Brief_FINAL_2022_Nov.pdf. Accessed 2024 Jul 31.
156.Canadian Institute for Health Information (CIHI). Unnecessary Care in Canada. Ottawa (ON): CIHI; 2017: https://secure.cihi.ca/free_products/choosing-wisely-baseline-report-en-web.pdf. Accessed 2024 Jun 19.
157.Barakos J, Purcell D, Suhy J, et al. Detection and Management of Amyloid-Related Imaging Abnormalities in Patients with Alzheimer's Disease Treated with Anti-Amyloid Beta Therapy. J Prev Alzheimers Dis. 2022;9(2):211-220. PubMed
158.Understanding Genetics and Alzheimer's Disease. Toronto (ON): Alzheimer Society of Canada; 2018: https://alzheimer.ca/ab/sites/ab/files/documents/research_understanding-genetics-and-alzheimers-disease.pdf. Accessed 2024 May 24.
159.Maruf AA, Fan M, Arnold PD, Muller DJ, Aitchison KJ, Bousman CA. Pharmacogenetic Testing Options Relevant to Psychiatry in Canada: Options de tests pharmacogenetiques pertinents en psychiatrie au Canada. Can J Psychiatry. 2020;65(8):521-530. PubMed
160.Zhong L, Xie YZ, Cao TT, et al. A rapid and cost-effective method for genotyping apolipoprotein E gene polymorphism. Mol Neurodegener. 2016;11(2):2. PubMed
161.LifeLabs Genetics. Did You Know: Dementia and Hereditary Testing. 2019; https://www.lifelabsgenetics.com/2019/01/30/dementia-and-hereditary-testing/. Accessed 2024 Oct 29.
162.Dynacare. APOE-ALZHEIMER'S RISK (National). [date unknown]; https://www.dynacare.ca/specialpages/secondarynav/find-a-test/nat/apoe-alzheimer-s%C2%A0risk.aspx?sr=NAT&st=. Accessed 2024 Oct 29.
163.Cummings J, Kinney J. Biomarkers for Alzheimer's Disease: Context of Use, Qualification, and Roadmap for Clinical Implementation. Medicina (Kaunas). 2022;58(7). PubMed
164.Hampel H, Hu Y, Cummings J, et al. Blood-based biomarkers for Alzheimer's disease: Current state and future use in a transformed global healthcare landscape. Neuron. 2023;111(18):2781-2799. PubMed
165.Gliwińska A, Czubilińska-Łada J, Więckiewicz G, et al. The Role of Brain-Derived Neurotrophic Factor (BDNF) in Diagnosis and Treatment of Epilepsy, Depression, Schizophrenia, Anorexia Nervosa and Alzheimer’s Disease as Highly Drug-Resistant Diseases: A Narrative Review. Brain Sci. 2023;13(2):163. PubMed
166.Pleen J, Camerucci E, Al-Sabbagh M, Cunningham K. Blood-Based Biomarkers in Alzheimer Disease: Clinical Implementation and Limitations. Pract Neurol. 2024;23:27-29,35.
167.Pelkmans W, Shekari M, Brugulat-Serrat A, et al. Astrocyte biomarkers GFAP and YKL-40 mediate early Alzheimer's disease progression. Alzheimers Dement. 2024;20(1):483-493. PubMed
168.Morenas-Rodríguez E, Li Y, Nuscher B, et al. Soluble TREM2 in CSF and its association with other biomarkers and cognition in autosomal-dominant Alzheimer's disease: a longitudinal observational study. Lancet Neurol. 2022;21(4):329-341. PubMed
169.Wang T, Yao Y, Han C, et al. MCP-1 levels in astrocyte-derived exosomes are changed in preclinical stage of Alzheimer's disease. Front Neurol. 2023;14:1119298. PubMed
170.Agnello L, Lo Sasso B, Vidali M, et al. Neurogranin as a Reliable Biomarker for Synaptic Dysfunction in Alzheimer's Disease. Diagnostics (Basel). 2021;11(12). PubMed
171.Oka T, Matsuzawa Y, Tsuneyoshi M, et al. Multiomics analysis to explore blood metabolite biomarkers in an Alzheimer's Disease Neuroimaging Initiative cohort. Sci Rep. 2024;14(1):6797. PubMed
172.Hansson O, Blennow K, Zetterberg H, Dage J. Blood biomarkers for Alzheimer's disease in clinical practice and trials. Nat Aging. 2023;3(5):506-519. PubMed
173.Ashton NJ, Brum WS, Di Molfetta G, et al. Diagnostic Accuracy of a Plasma Phosphorylated Tau 217 Immunoassay for Alzheimer Disease Pathology. JAMA Neurol. 2024;81(3):255-263. PubMed
174.Dark HE, Duggan MR, Walker KA. Plasma biomarkers for Alzheimer's and related dementias: A review and outlook for clinical neuropsychology. Arch Clin Neuropsychol. 2024;39(3):313-324. PubMed
175.Alzheimer’s Association Media Line. From the Alzheimer’s Association International Conference 2023: Simple finger prick test exemplifies advances in Alzheimer’s disease blood tests. Chicago (IL): Alzheimer’s Association; 2023: https://aaic.alz.org/downloads2023/Blood-Tests-AAIC-2023.pdf. Accessed 2024 May 15.
176.Tin A, Sullivan KJ, Walker KA, et al. Proteomic Analysis Identifies Circulating Proteins Associated With Plasma Amyloid-β and Incident Dementia. Biol Psychiatry Glob Open Sci. 2023;3(3):490-499. PubMed
177.Walker KA, Chen J, Zhang J, et al. Large-scale plasma proteomic analysis identifies proteins and pathways associated with dementia risk. Nat Aging. 2021;1(5):473-489. PubMed
178.Shigemizu D, Mori T, Akiyama S, et al. Identification of potential blood biomarkers for early diagnosis of Alzheimer's disease through RNA sequencing analysis. Alzheimers Res Ther. 2020;12(1):87. PubMed
179.Zeng X, Chen Y, Sehrawat A, et al. Alzheimer blood biomarkers: practical guidelines for study design, sample collection, processing, biobanking, measurement and result reporting. Mol Neurodegener. 2024;19(1):40. PubMed
180.Cummings J, Aisen P, Apostolova LG, Atri A, Salloway S, Weiner M. Aducanumab: Appropriate Use Recommendations. J Prev Alzheimers Dis. 2021;8(4):398-410. PubMed
181.Belder CRS, Schott JM, Fox NC. Preparing for disease-modifying therapies in Alzheimer's disease. Lancet Neurol. 2023;22(9):782-783. PubMed
182.Rosa-Neto P, Gauthier S. World Alzheimer Report 2022: Life after diagnosis: Navigating treatment, care and support. London (UK): Alzheimer's Disease International; 2022: https://www.alzint.org/u/World-Alzheimer-Report-2022.pdf. Accessed 2024 May 21.
183.Varkhede N, Forrest ML. Understanding the Monoclonal Antibody Disposition after Subcutaneous Administration using a Minimal Physiologically based Pharmacokinetic Model. J Pharm Pharm Sci. 2018;21(1s):130s-148s. PubMed
184.Market Intelligence Report: Biologic Response Modifier Agents, 2015. Ottawa (ON): Patented Medicine Prices Review Board; 2016: https://www.pmprb-cepmb.gc.ca/view.asp?ccid=1286&lang=en. Accessed 2024 May 17.
185.Grant K. Oversight gap at private infusion clinics poses health risk, Ontario documents say. The Globe and Mail. 2018 Nov 11. https://www.theglobeandmail.com/canada/article-oversight-gap-at-private-infusion-clinics-poses-health-risk-ontario/. Accessed 2024 May 17.
186.Mattke S, Wang M, Ullrich A. Implications of Alzheimer's Treatment for Organization and Payment of Medical Practices in Canada. Los Angeles (CA): USC Dornsife Center for Economic and Social Research; 2021: https://cesr.usc.edu/sites/default/files/Implications_of_Alzheimers_Treatment_for_Organization_and_Payment_of_Medical%20_Practices_in_Canada.pdf. Accessed 2024 May 17.
187.Grundy Q, Hart D, Elkhalifa S, et al. Mapping the landscape of infusion care for people prescribed intravenous medicines in Canada [forthcoming].
188.CADTH Health Technology Review: Health System Readiness Report: The Availability of Privately Funded IV Infusion Clinics in Canada. Can J Health Technol. 2022;2(6). https://canjhealthtechnol.ca/index.php/cjht/article/view/372. Accessed 2024 May 20.
189.Schultz TJ, Thomas A, Georgiou P, et al. Developing a Model of Care for Home Infusions of Natalizumab for People With Multiple Sclerosis. J Infus Nurs. 2019;42(6):289-296. PubMed
190.Batist G, Ghedira S, Khan A, et al. Pcn252 Time-to-Treatment Initiation (Tti) in Community Infusion Clinics: Decreasing Wait Times for Canadian Oncology Patients. Value Health. 2020;23:S67.
191.Sekhon T, Tejani A. Ironing out the problem of outpatient infusion wait times: look for process improvements first [preprint]. Authorea. 2024. https://www.authorea.com/doi/full/10.22541/au.170670506.63555340/v1. Accessed 2024 May 21.
192.Baumann A, Crea-Arsenio M. The Crisis in the Nursing Labour Market: Canadian Policy Perspectives. Healthcare (Basel). 2023;11(13):1954. PubMed
193.Canada's nursing shortage at a glance: A media reference guide. Ottawa (ON): Canadian Federation of Nurses Unions; 2022: https://nursesunions.ca/wp-content/uploads/2022/07/nurses_shortage_media_ref_guide_comp.pdf. Accessed 2024 May 21.
194.Jones AM, Favaro A. Why some worry about the rise of private agency health-care staffing firms in Canada. CTV News 2023 Oct 15; https://www.ctvnews.ca/health/why-some-worry-about-the-rise-of-private-agency-health-care-staffing-firms-in-canada-1.6600637. Accessed 2024 May 31.
195.Goodwin JS. Continuity of Care Matters in All Health Care Settings. JAMA Netw Open. 2021;4(3):e213842. PubMed
196.Amjad H, Carmichael D, Austin AM, Chang C, Bynum JPW. Continuity of Care and Healthcare Utilization in Older Adults with Dementia in Fee-for-Service Medicare. JAMA Intern Med. 2017;176(9):1371-1378. PubMed
197.Spithoff S, McPhail B, Vesely L, Rowe RK, Mogic L, Grundy Q. How the commercial virtual care industry gathers, uses and values patient data: a Canadian qualitative study. BMJ Open. 2024;14(2):e074019. PubMed
198.Spithoff S, Grundy Q. Commercializing Personal Health Information: A Critical Qualitative Content Analysis of Documents Describing Proprietary Primary Care Databases in Canada. Int J Health Policy Manag. 2023;12:6938. PubMed
199.Alamer F, Alanazi AT. The Impact of Smart Pump Technology in the Healthcare System: A Scope Review. Cureus. 2023;15(3):e36007. PubMed
200.Sproul A, Newman H. Get Smart, Canada: Exploring Smart Pump Implementation, Management, and Compliance with Standards through a Nationwide Survey. Can J Hosp Pharm. 2023;76(3):185-195. PubMed
201.Giuliano KK, Mahuren RS, Balyeat J. Data-based program management of system-wide IV smart pump integration. Am J Health Syst Pharm. 2024;81(1):e30-e36. PubMed
202.Mackenzie Health. Mackenzie Health launches first-of-its-kind technology in Canada designed to help reduce IV pump programming medication errors. 2024; https://www.mackenziehealth.ca/about-us/news/~368-Mackenzie-Health-launches-first-of-its-kind-technology-in-Canada-designed-to-help-reduce-IV-pump-programming-medication-errors. Accessed 2024 May 21.
203.Puolitaival A, Savola M, Tuomainen P, Asseburg C, Lundström T, Soini E. Advantages in Management and Remote Monitoring of Intravenous Therapy: Exploratory Survey and Economic Evaluation of Gravity-Based Infusions in Finland. Adv Ther. 2022;39(5):2096-2108. PubMed
204.Sperling RA, Jack CR, Jr., Black SE, et al. Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: recommendations from the Alzheimer's Association Research Roundtable Workgroup. Alzheimers Dement. 2011;7(4):367-385. PubMed
205.Withington CG, Turner RS. Amyloid-Related Imaging Abnormalities With Anti-amyloid Antibodies for the Treatment of Dementia Due to Alzheimer's Disease. Front Neurol. 2022;13:862369. PubMed
206.Jeong SY, Suh CH, Shim WH, Lim JS, Lee JH, Kim SJ. Incidence of Amyloid-Related Imaging Abnormalities in Patients With Alzheimer Disease Treated With Anti-beta-Amyloid Immunotherapy: A Meta-analysis. Neurology. 2022;99(19):e2092-e2101. PubMed
207.CADTH Health Technology Review: Wait List Strategies for CT and MRI Scans. Can J Health Technol. 2023;3(1). https://www.cadth.ca/sites/default/files/attachments/2023-01/CM0002-HC0052-Wait-List%20Strategies-for-CT-and-MRI-Scans.pdf. Accessed 2024 May 27.
208.Doran SJ, Sawyer RP. Risk factors in developing amyloid related imaging abnormalities (ARIA) and clinical implications. Front Neurosci. 2024;18:1326784. PubMed
209.Wang YY, Ge YJ, Tan CC, Cao XP, Tan L, Xu W. The Proportion of APOE4 Carriers Among Non-Demented Individuals: A Pooled Analysis of 389,000 Community-Dwellers. J Alzheimers Dis. 2021;81(3):1331-1339. PubMed
210.Barnes LL, Bennett DA. Dementia: Cognitive resilience in APOE*epsilon4 carriers-is race important? Nat Rev Neurol. 2015;11(4):190-191. PubMed
211.Alzheimer Society of Canada. Genetic testing and Alzheimer's disease. [2024]; https://alzheimer.ca/en/about-dementia/what-alzheimers-disease/genetic-testing-alzheimers-disease. Accessed 2024 May 24.
212.Leqembi 100mg/ml concentrate for solution for infusion. Public Assessment Report. National Procedure. London (UK): Medicines & Healthcare products Regulatory Agency; 2024: https://mhraproducts4853.blob.core.windows.net/docs/6ed2db79b7202feb5a8edbecfa5c35bb434381e6. Accessed 2024 Oct 30.
213.Liu KY, Villain N, Ayton S, et al. Key questions for the evaluation of anti-amyloid immunotherapies for Alzheimer's disease. Brain Commun. 2023;5(3):fcad175. PubMed
214.Ontario’s first modular MRI department opens at Brockville. Canadian Healthcare Technology. 2023 Sep 20. https://www.canhealth.com/2023/09/20/ontarios-first-modular-mri-department-opens-at-brockville/. Accessed 2024 May 28.
215.Hyperfine. Leading Institutions Enroll First Alzheimer's Patients Receiving Amyloid-Targeting Therapy in CARE PMR Study. 2024; https://hyperfine.io/about/news/press-release-leading-institutions-enroll-first-alzheimers-patients-receiving-amyloid-targeting-therapy-in-care-pmr-study. Accessed 2024 May 30.
216.Hudson D, Sahibbil JP. Remote scanning support in magnetic resonance imaging: Friend or foe? Radiography (Lond). 2022;28(3):739-745. PubMed
217.MacLean T. A first look inside. A new, relocatable MRI funded by the QEII Foundation will be helping more patients receive their critical scan. QEII Health Sciences Centre Foundation 2024; https://qe2foundation.ca/our-impact/news/first-look-inside-new-relocatable-mri-funded-qeii-foundation-will-be-helping-more. Accessed 2024 Aug 12.
218.Ahmed A. The Case for a Pan-Canadian Teleradiology Network. Policy Magazine. 2023 Dec 6. https://www.policymagazine.ca/the-case-for-a-pan-canadian-teleradiology-network/. Accessed 2024 May 28.
219.Hampel H, Gao P, Cummings J, et al. The foundation and architecture of precision medicine in neurology and psychiatry. Trends Neurosci. 2023;46(3):176-198. PubMed
220.Wailoo A. Appendix D: Estimates of the size of the English eligible population in for amyloid targeting therapies in Alzheimer’s Disease. In: National Institute for Health and Care Excellence (NICE), ed. Potential issues and challenges in evaluation of disease-modifying dementia treatments: HTA Innovation Laboratory Report. Sheffield (UK): School of Health and Related Research (ScHARR), University of Sheffield; 2023: https://www.nice.org.uk/Media/Default/About/what-we-do/HTA%20Lab/Appendix-D.pdf. Accessed 2024 Jul 12.
221.Verger A, Yakushev I, Albert NL, et al. FDA approval of lecanemab: the real start of widespread amyloid PET use? - the EANM Neuroimaging Committee perspective. Eur J Nucl Med Mol Imaging. 2023;50(6):1553-1555. PubMed
222.van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in Early Alzheimer's Disease. N Engl J Med. 2023;388(1):9-21. PubMed
223.Sims JR, Zimmer JA, Evans CD, et al. Donanemab in Early Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial. JAMA. 2023;330(6):512-527. PubMed
224.AlzForum. Rising Leqembi Prescriptions Are Straining Clinic Capacity. 2024; https://www.alzforum.org/news/research-news/rising-leqembi-prescriptions-are-straining-clinic-capacity. Accessed 2024 Oct 31.
225.Mila-Aloma M, Ashton NJ, Shekari M, et al. Plasma p-tau231 and p-tau217 as state markers of amyloid-beta pathology in preclinical Alzheimer's disease. Nat Med. 2022;28(9):1797-1801. PubMed
226.Roberts R, Knopman DS. Classification and epidemiology of MCI. Clin Geriatr Med. 2013;29(4):753-772. PubMed
227.Manly JJ, Tang MX, Schupf N, Stern Y, Vonsattel JP, Mayeux R. Frequency and course of mild cognitive impairment in a multiethnic community. Ann Neurol. 2008;63(4):494-506. PubMed
228.Anstey KJ, Cherbuin N, Eramudugolla R, et al. Characterizing mild cognitive disorders in the young-old over 8 years: prevalence, estimated incidence, stability of diagnosis, and impact on IADLs. Alzheimers Dement. 2013;9(6):640-648. PubMed
229.Glynn K, O'Callaghan M, Hannigan O, et al. Clinical utility of mild cognitive impairment subtypes and number of impaired cognitive domains at predicting progression to dementia: A 20-year retrospective study. Int J Geriatr Psychiatry. 2021;36(1):31-37. PubMed
230.Petersen RC, Aisen P, Boeve BF, et al. Mild cognitive impairment due to Alzheimer disease in the community. Ann Neurol. 2013;74(2):199-208. PubMed
231.Ravaglia G, Forti P, Montesi F, et al. Mild cognitive impairment: epidemiology and dementia risk in an elderly Italian population. J Am Geriatr Soc. 2008;56(1):51-58. PubMed
232.Solfrizzi V, Panza F, Colacicco AM, et al. Vascular risk factors, incidence of MCI, and rates of progression to dementia. Neurology. 2004;63(10):1882-1891. PubMed
233.Knopman DS, Gottesman RF, Sharrett AR, et al. Mild Cognitive Impairment and Dementia Prevalence: The Atherosclerosis Risk in Communities Neurocognitive Study (ARIC-NCS). Alzheimers Dement (Amst). 2016;2:1-11. PubMed
234.Lee SH, Lee JH, Byun MS, et al. Comparison of Amyloid Positivity Rate and Accumulation Pattern between Amnestic and Non-Amnestic Type Mild Cognitive Impairment. Psychiatry Investig. 2020;17(6):603-607. PubMed
235.Kim JY, Lim JH, Jeong YJ, Kang DY, Park KW. The Effect of Clinical Characteristics and Subtypes on Amyloid Positivity in Patients with Amnestic Mild Cognitive Impairment. Dement Neurocogn Disord. 2019;18(4):130-137. PubMed
236.Public Health Agency of Canada. Dementia: Overview. 2024; https://www.canada.ca/en/public-health/services/diseases/dementia.html. Accessed 2024 Aug 5.
237.Alzheimer's Association. 2020 Alzheimer's disease facts and figures. Alzheimers Dement. 2020;16(3):391-460.
238.Yuan J, Maserejian N, Liu Y, et al. Severity Distribution of Alzheimer's Disease Dementia and Mild Cognitive Impairment in the Framingham Heart Study. J Alzheimers Dis. 2021;79(2):807-817. PubMed
239.Rabinovici GD, Gatsonis C, Apgar C, et al. Association of Amyloid Positron Emission Tomography With Subsequent Change in Clinical Management Among Medicare Beneficiaries With Mild Cognitive Impairment or Dementia. JAMA. 2019;321(13):1286-1294. PubMed
240.Public Health Agency of Canada. Canadian Chronic Disease Surveillance System (CCDSS). 2024; https://health-infobase.canada.ca/ccdss/data-tool/Index?G=00&V=16&M=4&Y=2021. Accessed 2024 Aug 16.
241.Jonsson L, Wimo A, Handels R, et al. The affordability of lecanemab, an amyloid-targeting therapy for Alzheimer's disease: an EADC-EC viewpoint. Lancet Reg Health Eur. 2023;29:100657. PubMed
242.Jansen WJ, Janssen O, Tijms BM, et al. Prevalence Estimates of Amyloid Abnormality Across the Alzheimer Disease Clinical Spectrum. JAMA Neurol. 2022;79(3):228-243. PubMed
Appendix 1: Additional Information on Blood-Based Biomarkers for AD
Please note that this appendix has not been copy-edited.
Examples of some of the strengths and weaknesses of emerging biomarkers:
Plasma Amyloid-Beta
While CSF amyloid-beta42/amyloid-beta40 ratios are associated with amyloid plaques in the brain, plasma amyloid-beta42/amyloid-beta40 testing encounters challenges related to accurate blood sampling and variability in diagnostic utility. Studies have shown that integrating genotyping and age into plasma amyloid-beta42/amyloid-beta40 testing may enhance its performance.164,166,172
Plasma p-tau
Studies have suggested that plasma phospho-tau (p-tau) isoforms, including p-tau181, p-tau217, and p-tau231, elevate early in the AD disease process and increase with disease progression.164,172 While some comparative studies have reported that p-tau217 may be a better diagnostic biomarker for symptomatic AD, p-tau181 is easier to measure due to higher levels in plasma.166,172,173
Some studies have shown that plasma p-tau231, when combined with plasma amyloid-beta42/amyloid-beta40, age, sex, and APOE4 status, may detect amyloid-beta pathology earlier in younger individuals who have yet to develop cognitive impairment.225
Plasma GFAP
Plasma GFAP concentrations increase following central nervous system injury and have been associated with early amyloid-beta pathology in some studies, potentially predicting cognitive decline and conversion to AD in cognitively unimpaired individuals and those with MCI.164
Additionally, significant reductions in plasma GFAP levels have been observed following the removal of amyloid-beta plaques through anti–amyloid-beta AD immunotherapy, suggesting that plasma GFAP may potentially be useful in monitoring treatment response.172
Plasma NfL
Studies suggest that serum NfL is a sensitive, nonspecific biomarker for neuronal damage across conditions such as dementia, brain injury, cardiovascular diseases, and multiple sclerosis.164
NfL offers limited utility for specific detection of AD pathology, but it may hold prognostic value in predicting future cognitive decline in patients with MCI or dementia.172
Appendix 2: Methodology for Estimation of Treatable Population With Incident Early-Stage AD
Please note that this appendix has not been copy-edited.
Treatable Patient Population Estimation
To facilitate the adaptation of the NICE model to the context of Canada, a literature scan was undertaken to find incidence rates and proportions for each calculation stage, from individuals aged older than 65 through to those receiving treatment. Where updated studies could not be found, the same studies in the NICE report were used for their equivalent calculation stage. These estimates could increase if those who have prevalent AD and those under the age of 65 with cognitive symptoms sought treatment.
To accommodate ranges of incidence and proportions, upper and lower estimates were calculated for each stage of the patient pathway using the NICE approach for MCI and mild dementia due to AD (Tables A1 and A2, respectively). The midrange results were presented in the Treatable Patient Population Estimation section with methodology detailed in this section for MCI and mild dementia due to AD.
Mild Cognitive Impairment
For calculating stage I (incidence of underlying condition), an annual MCI incidence of 5.1% was applied to the 2020 starting population of Canadians aged 65 years or older. This value comes from a table in Roberts et al. that reported a variety of incidence rates among different age cohorts.226 The listed 5.1% annual MCI incidence rate was from Manly et al. from a racially diverse cohort of people aged 65 years or older in the US.227 Calculating MCI incidence is a novel addition to the methodology used in the NICE report which only examined prevalence of MCI.21
For calculating stage II (proportion presenting to health care), Anstey et al. reported that 13.3% of those with MCI presented to health care.228 Anstey et al. was used in the NICE report and is a study following a cohort of Australian participants who were assessed every 4 years for MCI.
For calculating stage III (assessment and diagnosis of early-stage AD), Glynn et al. reports 55% of MCI cases are amnestic.229 Amnestic MCI is a subtype of MCI that progresses to AD and is likely caused by underlying AD etiology. Glynn et al. is a 20-year retrospective study of MCI patients at a memory clinic.229
For calculating stage 4 (treatment eligibility assessment), Petersen et al. reports 57.1% of MCI cases show amyloid positivity.230 Petersen et al. examined a cohort of amnestic MCI patients from the Mayo Clinic Study on Aging and examined AD biomarkers, including amyloid positivity.230
Mild Dementia Due to AD
For calculating stage I (incidence of underlying condition), this statistic comes from the Government of Canada’s web page on dementia and had the same parameters (statistic was for those aged 65 years or older in 2020 to 2021 with dementia of any kind).236
For calculating stage II (proportion presenting to health care), Lang et al. reported that 38.3% of those with dementia presented to health care.34 Lang et al. was used in the NICE report and is a systematic review and meta-analysis examining the prevalence of undetected dementia in communities.34
For calculating stage III (assessment and diagnosis of early-stage AD), a two-step process was done. First, it was assumed that 70% of dementia cases were due to underlying AD etiology from the 2020 Alzheimer’s Association fact sheet.237 Second, Yuan et al. found that 50.4% of Alzheimer patients had mild dementia due to AD.238 Yuan et al. was a study examining the distribution of Alzheimer severity among participants of the Framingham Heart Study.238
For calculating stage 4 (treatment eligibility assessment), Rabinovici et al. reports 70.1% of mild dementia cases due to AD show amyloid positivity.239
Table 5: Upper and Lower Ranges of Estimates for Treatable Population in Canada With Incident MCI From 2020 to 2021
Stage | Upper Estimate | % of starting population | Source | Midrange Estimate | % of starting population | Source | Lower Estimate | % of starting population | Source |
|---|---|---|---|---|---|---|---|---|---|
2020 | |||||||||
People 65 years or older in Canada | 6,809,521 | — | StatsCan 65+ (2020)12 | 6,809,521 | — | StatsCan 65+ (2020)12 | 6,809,521 | — | StatsCan 65+ (2020)12 |
Incidence of underlying condition | 522,971 | 7.7% | Ravaglia et al. (76.8/1000 person-years)231 from Roberts et al.226 | 347,286 | 5.1% | Manly et al. (5.1% annual incidence)227 from Roberts et al.226 | 146,405 | 2.2% | Solfrizzi et al. (21.5/1000 person- years)232 from Roberts et al.226 |
Proportion presenting to health care | 69,555 | 1.0% | 13.3% from Anstey et al.228 | 46,189 | 0.7% | 13.3% from Anstey et al.228 | 19,472 | 0.3% | 13.3% from Anstey et al.228 |
Assessment and diagnosis of early-stage Alzheimer disease | 52,166 | 0.8% | 75% from Knopmann et al.233 | 25,404 | 0.4% | 55% from Glynn et al.229 | 10,710 | 0.2% | 55% from Glynn et al.229 |
Treatment eligibility assessment | 33,751 | 0.5% | 64.7% from Lee et al.234 | 14,506 | 0.2% | 57.1% from Petersen et al.230 | 4,391 | 0.1% | 41% from Kim et al.235 |
2021 | |||||||||
People 65 years or older in Canada | 7,045,990 | StatsCan 65+ (2021)12 | 7,045,990 | StatsCan 65+ (2021)12 | 7,045,990 | StatsCan 65+ (2021)12 | |||
Incidence of underlying condition | 541,132 | 7.7% | Ravaglia et al. (76.8/1000 person-years)231 from Roberts et al.226 | 359,345 | 5.1% | Manly et al. (5.1% annual incidence)227 from Roberts et al.226 | 151,489 | 2.2 | Solfrizzi et al. (21.5/1000 person- years)232 from Roberts et al.226 |
Proportion presenting to health care | 71,971 | 1.0% | 13.3% from Anstey et al.228 | 47,793 | 0.7% | 13.3% from Anstey et al.228 | 20,148 | 0.3 | 13.3% from Anstey et al.228 |
Assessment and diagnosis of early-stage Alzheimer disease | 53,978 | 0.8% | 75% from Knopmann et al.233 | 26,286 | 0.4% | 55% from Glynn et al.229 | 11,081 | 0.2 | 55% from Glynn et al.229 |
Treatment eligibility assessment | 34,924 | 0.5% | 64.7% from Lee et al.234 | 15,009 | 0.2% | 57.1% from Petersen et al.230 | 4,543 | 0.1 | 41% from Kim et al.235 |
Table 6: Upper and Lower Ranges of Estimates for Treatable Population in Canada With Incident Mild Dementia Due to AD From 2020 to 2021
Stage | Upper Estimate | % of starting population | Source | Midrange Estimate | % of starting population | Source | Lower Estimate | % of starting population | Source |
|---|---|---|---|---|---|---|---|---|---|
2020 | |||||||||
People 65 years or older in Canada | 6,809,521 | — | StatsCan 65+ (2020)12 | 6,809,521 | — | StatsCan 65+ (2020)12 | 6,809,521 | — | StatsCan 65+ (2020)12 |
Incidence of underlying condition | 124,000 | 1.8% | Alzheimer Society of Canada Landmark Report (likely includes those under 65)1 | 86,000 | 1.3% | Government of Canada ‘Dementia: Overview’236 | 82,872 | 1.2% | Crude incidence rate of dementia (1,217/100K) from CCDSS for 2020 to 2021240 |
Proportion presenting to health care | 55,800 | 0.8% | 45% from Lang et al.34 | 32,938 | 0.5% | 38.3% from Lang et al.34 | 20,718 | 0.3% | 25% from World Alzheimer Report 202160 |
Assessment and diagnosis of early-stage Alzheimer disease | 25,891 | 0.4% | (80% from 2020 Alzheimer’s Association fact sheet)237 x (58% from Jonsson et al.)241 | 11,621 | 0.2% | (70% from 2020 Alzheimer’s Association fact sheet)237 x (50.4% from Yuan et al.)238 | 5,967 | 0.1% | (60% from 2020 Alzheimer’s Association fact sheet)237 x (48% from Jonsson et al.)241 |
Treatment eligibility assessment | 22,007 | 0.3% | 85% from Jansen et al.242 | 8,146 | 0.1% | 70.1% from Rabinovici et al.239 | 4,183 | 0.06% | 70.1% from Rabinovici et al.239 |
2021 | |||||||||
People 65 years or older in Canada | 7,045,990 | StatsCan 65+ (2021)12 | 7,045,990 | StatsCan 65+ (2021)12 | 7,045,990 | StatsCan 65+ (2021)12 | |||
Incidence of underlying condition | 92,725 | 1.3% | Crude incidence rate of dementia (1,316/100K) from CCDSS for 2021 to 2022240 | 92,091 | 1.3% | Crude incidence rate of dementia (1,307/100K) from CCDSS for 2021 to 2022240 | 91,527 | 1.3% | Crude incidence rate of dementia (1,299/100K) from CCDSS for 2021 to 2022240 |
Proportion presenting to health care | 41,726 | 0.6% | 45% from Lang et al.34 | 35,271 | 0.5% | 38.3% from Lang et al.34 | 22,882 | 0.3% | 25% from World Alzheimer Report 202160 |
Assessment and diagnosis of early-stage Alzheimer disease | 19,361 | 0.3% | (80% from 2020 Alzheimer’s Association fact sheet)237 x (58% from Jonsson et al.)241 | 12,444 | 0.2% | (70% from 2020 Alzheimer’s Association fact sheet)237 x (50.4% from Yuan et al.)238 | 6,590 | 0.1% | (60% from 2020 Alzheimer’s Association fact sheet)237 x (48% from Jonsson et al.)241 |
Treatment eligibility assessment | 16,457 | 0.2% | 85% from Jansen et al.242 | 8,723 | 0.1% | 70.1% from Rabinovici et al.239 | 4,620 | 0.07% | 70.1% from Rabinovici et al.239 |
Estimation of Medical Imaging Demand
After estimating the incident treatable population eligible to receive anti–amyloid-beta mAb DMTs for early-stage AD, estimates of the number of PET-CT and MRI exams were calculated and matched to the domains of the patient pathway for AD. This is a new extension to the work done in the NICE report. It should be noted that while CT exams may be used to rule out other causes of dementia in patients, it is insufficient for determining treatment eligibility, so it was excluded from the estimation.
For PET-CT exams, Verger et al. reported that up to 33% of patients are not able to receive LP to determine amyloid positivity and will need a PET-CT exam.221 This was applied to the estimated incident population eligible for treatment (22,652) to get 7,475 potential PET-CT exams. Verger et al. is a position paper put forward by the European Association of Nuclear Medicine Neuroimaging Committee which cites a study noting that up to one-third of patients may require amyloid PET over LP to determine amyloid positivity.221
For MRI exams, a baseline MRI exam is required during treatment eligibility assessment to ensure that patients’ brain structures are not at high risk of adverse events, leading to 22,652 baseline scans. This has been a requirement in countries that have approved anti–amyloid-beta mAb DMTs.28,29 In addition, at least 2 MRI exams are taken within the first year of treatment to monitor for the development of adverse events, leading to an additional 45,304 scans, for a total of 67,956 exams if no adverse events occur. In some countries that have approved the use of anti–amyloid-beta mAb DMTs, this can be up to 3 MRI exams, potentially adding another 22,652 exams.28,29
However, if an adverse event were to occur, MRI monitoring exams would increase to once every 2 to 4 months. Jeong et al. reports an adverse event incidence rate of 6.5%, with the majority of cases resolving within 4 months.206 Assuming an incidence rate of 6.5% and that cases resolve within 4 months with a monitoring rate of 1 MRI scan every 2 months, this leads to an additional 2,944 MRI exams. This leads to an estimated 70,900 MRI exams.
Estimating Future Demand
After estimating the incident treatable population eligible to receive anti–amyloid-beta mAb DMTs for early-stage AD, and the number of PET-CT and MRI exams to support treatment, a 5-year projection was estimated. This is a new extension to the work done in the NICE report to assist in capacity planning.
Several key assumptions underpin the 5-year projection. Subsequent changes to these assumptions would affect the numbers. The assumptions used to create the initial treatable incident population estimate and medical imaging demand estimate were carried forward into the calculations made for the projection.
The percent increase in incidence rate between 2020 to 2021 was calculated and applied to each subsequent year. This assumes a constant incidence rate increase which may not necessarily be accurate as more people with cognitive symptoms could seek health care if there was a treatment available for them. Additionally, it was assumed that patients would receive anti–amyloid-beta mAb DMTs for 2 years before AD progression removed them from treatment eligibility. It remains unclear how long patients will be able to remain on anti–amyloid-beta mAb DMTs.21,213 Furthermore, it was assumed that patients would undergo annual treatment eligibility assessments to ensure they are still able to receive treatment.21 This means that those who received PET-CT exams previously would receive another for each year of treatment. It was also assumed that those who experienced an ARIA event within the first year of treatment will require an additional MRI exam 1 year after treatment initiation.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.