CADTH Reimbursement Review
Bimekizumab (Bimzelx)
Sponsor: UCB Canada Inc.
Therapeutic area: Psoriasis, moderate to severe plaque
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
BSA
body surface area
CI
confidence interval
CMH
Cochran-Mantel-Haenszel
DLQI
Dermatology Life Quality Index
EQ-5D-3L
EuroQol 5-Dimensions 3-Levels questionnaire
EQ-5D
EuroQol 5-Dimensions questionnaire
HRQoL
health-related quality of life
IGA
Investigator’s Global Assessment
IL
interleukin
ITC
indirect treatment comparison
MID
minimal important difference
NMA
network meta-analysis
OR
odds ratio
PASI
Psoriasis Area and Severity Index
PY
person year
RCT
randomized controlled trial
SC
subcutaneous
SD
standard deviation
SF-36
Short Form (36) Health Survey
TNF
tumour necrosis factor
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Bimekizumab (Bimzelx), 160 mg/mL solution for subcutaneous injection |
Indication | For the treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | February 14, 2022 |
Sponsor | UCB Canada Inc. |
NOC = Notice of Compliance.
Introduction
Plaque psoriasis is a chronic inflammatory skin disease characterized by erythematous inflammatory plaques that may be itchy or painful and are usually covered by silver, flaking scales.1 In addition to the overt dermatological symptoms, plaque psoriasis is often associated with psychosocial symptoms and may affect various aspects of social functioning, including interpersonal relationships and performance at school or work. Treatments include topical therapy, phototherapy, non-biologic systemic drugs (e.g., methotrexate, cyclosporine), and biologic therapies (e.g., interleukin [IL]-17, IL-23, IL-12/23 inhibitors and tumour necrosis factor [TNF] alpha inhibitors). An estimated 1 million Canadians are living with psoriasis, 90% of whom have plaque psoriasis.2
Bimekizumab is a humanized monoclonal antibody that belongs to the IL-17 drug class.3 Bimekizumab is approved by Health Canada for the treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy. It is available as a 160 mg/1 mL pre-filled syringe or autoinjector. The recommended dose is 320 mg, administered as 2 160 mg subcutaneous (SC) injections every 4 weeks for the first 16 weeks, followed by 320 mg SC every 8 weeks thereafter.3 The product monograph states that, at the prescriber’s discretion, discontinuation of treatment may be considered in patients who have shown no improvement after 16 weeks of treatment. The product monograph also states that, for patients with a body weight of 120 kg or more who do not achieve a complete skin response, a dosage of 320 mg every 4 weeks after week 16 may be considered.3
The objective of this report is to perform a systematic review of the beneficial and harmful effects of bimekizumab 160 mg/mL solution for SC injection for the treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical expert(s) consulted by CADTH for the purpose of this review.
Patient Input
Two responses to CADTH’s call for patient input for the bimekizumab submission were received: a submission from the Psoriasis Society of Canada and a co-operative submission from the Canadian Association of Psoriasis Patients (CAPP) and the Canadian Psoriasis Network (CPN). The information used to inform the submissions was from phone calls from psoriasis patients as well as from a survey that was hosted on the CAPP and CPN websites and sent to clinics conducting bimekizumab trials to share with patients. A total of 95 survey responses were received, in addition to a telephone interview with a bimekizumab trial participant.
The patients described psoriasis as a chronic inflammatory condition that can present potentially debilitating challenges. Most patients reported living with psoriatic arthritis and about half of all survey respondents described their psoriasis as moderate or severe. Common symptoms, experienced by more than 2-thirds of patients, included flaking, itching, and redness, and more than half of patients experienced pain. Most patients reported that their psoriasis symptoms affected their social life, self-esteem, mental health, intimate life, sleep, and work. Many patients reported feeling that their symptoms are not effectively controlled with existing therapies. Most patients indicated that an improvement in their quality of life or a reduction in symptoms would be an important treatment outcome, in addition to the desire for a faster response to treatment, clear skin, or a cure. Moreover, a new treatment should have reduced adverse effects, be affordable, assist with persistent symptoms, and be easier to take.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
According to the clinical expert consulted for this review, none of the available treatments for plaque psoriasis provide a cure, and there remains an unmet need for highly effective and safe treatments that are accessible and easy to use. The clinical expert stated that the ideal treatment would produce a sustained Psoriasis Area and Severity Index (PASI) 100 response (a 100% improvement in PASI score) in all patients, with a low risk of adverse events; would minimize or eliminate the negative impact of psoriasis on health-related quality of life (HRQoL); and would benefit 1 or more of the comorbidities, particularly psoriatic arthritis.
In the clinical expert’s opinion, bimekizumab is unlikely to cause a shift in the treatment paradigm for moderate to severe plaque psoriasis, as it is anticipated that prior treatment with methotrexate or cyclosporine will be required for reimbursement. As the fourth IL-17 inhibitor approved for plaque psoriasis in Canada, bimekizumab is an additional efficacious drug in the treatment armamentarium, thus increasing the likelihood that the patient will find a drug that works well and is tolerated.
The expert stated that bimekizumab is appropriate for adult patients with moderate to severe plaque psoriasis who are suitable candidates for systemic therapy. Most payors would limit use to patients with a minimum PASI score of 12 and 10% or more of body surface area (BSA) affected. Patients least suitable for treatment with bimekizumab would be those with active Crohn disease or those who had failed 1 or more prior trials of an IL-17 inhibitor, according to the clinical expert.
In clinical practice, response to therapy is assessed based on the PASI score, with a PASI 75 response at 16 weeks considered a clinically meaningful improvement by the clinical expert. However, clinicians expect that patients will achieve a higher threshold of improvement with newer biologic drugs. According to the clinical expert consulted, discontinuation of bimekizumab would be warranted in patients who failed to reach or maintain PASI 75 response, in those with inadequate control of comorbid psoriatic arthritis, in those who developed a high-risk malignancy or significant infection, and in those undergoing elective surgery.
Clinician Group Input
No input was received from clinician groups.
Drug Program Input
The drug programs enquired about the place in therapy of bimekizumab and whether it may cause a shift in the treatment algorithm for plaque psoriasis. The clinical expert did not anticipate that bimekizumab would affect the treatment algorithm and stated that the initiation, renewal, and discontinuation criteria for bimekizumab should be aligned with other biologic drugs used for the treatment of patients with moderate to severe plaque psoriasis.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
The systematic review included 4 multi-centre, double-blind randomized controlled trials (RCTs) that evaluated the safety and efficacy of bimekizumab in patients with moderate to severe plaque psoriasis who were candidates for systemic therapy or phototherapy (studies PS0009, PS0008, PS0015, and PS0013). The studies randomized 435 to 743 patients to receive bimekizumab compared with placebo, ustekinumab, adalimumab, or secukinumab, for 48 to 56 weeks. The dosage of bimekizumab was either 320 mg SC every 4 weeks or 320 mg every 4 weeks for the first 16 weeks and then every 8 weeks thereafter. Study PS0013 used a randomized withdrawal design, and bimekizumab-treated patients who achieved a 90% improvement in their PASI score (PASI 90) at week 16 were randomized to either switch to placebo or to continue receiving bimekizumab every 4 weeks or bimekizumab every 8 weeks.
In studies PS0009, PS0008, and PS0013, the co-primary outcomes were the proportion of patients who achieved a PASI 90 response, and an Investigator’s Global Assessment (IGA) score of “clear” or “almost clear” (i.e., 0 or 1) with at least a 2-point change from baseline, at week 16. The IGA is a 5-point composite physician assessment of the overall severity of the patient’s psoriatic lesions at a given time point. The primary outcome in study PS0015 was the proportion of patients who achieved a PASI 100 response at week 16. PASI grades the extent and severity of psoriatic lesions and combines an assessment of the BSA affected with the severity of desquamation, erythema, and plaque induration or infiltration. It is scored from 0 to 72, with higher scores representing more severe disease. A PASI response is the percentage improvement in PASI score. IGA 0/1, PASI 90, or PASI 100 response thresholds are generally accepted as representing clinically relevant improvements.
The mean age of the patients enrolled ranged from 43.5 years (standard deviation [SD] 13.1) to 49.7 years (SD 13.6) across treatment groups in the 4 trials. Most patients were male (64% to 73%) and White (74% to 94%), with psoriasis that was rated as moderate in severity based on their IGA score (59% to 72%). Most patients (69% to 83%) had received prior systemic therapy, which included prior biologic therapy for 31% to 44% of patients and prior IL-17 therapy for 11% to 24% of patients.
Efficacy Results
Initial Treatment Period
In Study PS0009, 85.0% of patients in the bimekizumab group achieved PASI 90 response at 16 weeks, compared with 49.7% for ustekinumab and 4.8% for placebo groups (Table 2). The between-group differences favoured bimekizumab versus ustekinumab (odds ratio [OR] 6.06; 95% confidence interval [CI], 3.87 to 9.47; P < 0.001) and versus placebo (OR 99.87; 95% CI, 34.02 to 293.18; P < 0.001), demonstrating that bimekizumab was superior to ustekinumab and placebo for the PASI 90 response at week 16. The results for the co-primary outcome of IGA 0/1 response at week 16 showed similar findings. At 16 weeks, 84.1%, 53.4%, and 4.8% of the bimekizumab, ustekinumab, and placebo groups, respectively, achieved an IGA score of 0 or 1 (OR 4.81 bimekizumab versus ustekinumab; 95% CI, 3.10 to 7.47; P < 0.001).
The proportion of patients who achieved PASI 90 response at 16 weeks in Study PS0008 was 86.2% and 47.2% for bimekizumab and adalimumab groups, respectively, and the OR favoured bimekizumab versus adalimumab (OR 7.46; 95% CI, 4.71 to 11.82; P < 0.001). Bimekizumab demonstrated superiority to adalimumab for the IGA 0 or 1 response at week 16 (85.3% versus 57.2%; OR 4.32; 95% CI, 2.79 to 6.77; P < 0.001).
Table 2: Summary of Key Efficacy Results From Pivotal and Protocol Selected Studies
Study / treatment group | Total, N | PASI 90 response at week 16a | IGA 0/1 response at week 16a | ||||
|---|---|---|---|---|---|---|---|
n (%) | BKZ vs. placebo OR (95% CI), P value | BKZ vs. active control OR (95% CI), P value | n (%) | BKZ vs. placebo OR (95% CI), P value | BKZ vs. active control OR (95% CI), P value | ||
PS0009 (RS) | |||||||
Placebo | 83 | 4 (4.8) | Reference | NA | 4 (4.8) | Reference | NA |
BKZ q.4.w. | 321 | 273 (85.0) | 99.87 (34.02 to 293.18), P < 0.001 | 6.06 (3.87 to 9.47), P < 0.001 | 270 (84.1) | 118.76 (36.70 to 384.31), P < 0.001 | 4.81 (3.10 to 7.47), P < 0.001 |
USTE | 163 | 81 (49.7) | NA | Reference | 87 (53.4) | NA | Reference |
PS0008 (RS) | |||||||
BKZ (pooled)b | 319 | 275 (86.2) | NA | 7.46 (4.71 to 11.82), P < 0.001 | 272 (85.3) | NA | 4.34 (2.79 to 6.77), P < 0.001 |
ADA | 159 | 75 (47.2) | NA | Reference | 91 (57.2) | NA | Reference |
PS0015 (RS) | |||||||
BKZ q.4.w. | 373 | 319 (85.5) | NA | 2.14 (1.46 to 3.14), P < 0.001c | 319 (85.5) | NA | 1.64 (1.11 to 2.41), P = 0.012c |
SECU | 370 | 275 (74.3) | NA | Reference | 291 (78.6) | NA | Reference |
PS0013 (RS) | |||||||
Placebo | 86 | 1 (1.2) | Reference | NA | 1 (1.2) | Reference | NA |
BKZ q.4.w. | 349 | 317 (90.8) | 496.32 (82.80 to 2,975.09), P < 0.001 | NA | 323 (92.6) | 657.3 (105.8 to 4,083.3), P < 0.001 | NA |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval; IGA = Investigator’s Global Assessment; NA = not applicable; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RS = randomized set; SECU = secukinumab; USTE = ustekinumab.
aStratified Cochran-Mantel-Haenszel test, stratified by region and prior biologic drug exposure (nonresponder imputation).
bPatients randomized to BKZ q.4.w., and to BKZ q.4.w. for 16 weeks then q.8.w. thereafter were pooled for the analysis of 16-week outcomes.
cNot adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
The withdrawal study, PS0013, reported that 90.8% of patients in the bimekizumab group achieved PASI 90 response at week 16 compared with 1.2% of patients in the placebo group, with an OR of 496.32 (95% CI, 82.8 to 2,975.09; P < 0.001). The results were similar for the co-primary outcome IGA 0/1 response (92.6% versus 1.2% bimekizumab versus placebo; OR 657.3; 95% CI, 105.8 to 4,083.3; P < 0.001).
In Study PS0015, 61.7% and 48.9% of patients in the bimekizumab and secukinumab groups, respectively, achieved PASI 100 response at week 16 (primary outcome). On the relative scale, the differences favoured bimekizumab versus secukinumab (OR 1.72; 95% CI, 1.27 to 2.31; P < 0.001), demonstrating that bimekizumab was superior to secukinumab. At 16 weeks, 85.5% and 74.3% achieved PASI 90 response, and 85.5 and 78.6% achieved IGA 0/1 response in the bimekizumab and secukinumab groups, respectively. Between-group differences favoured bimekizumab versus secukinumab, but these outcomes were not controlled for type I error rate and should be interpreted as supportive evidence of the overall effect of bimekizumab.
In studies PS0009, PS0008, and PS0013, the proportion of patients who achieved PASI 100 response at 16 weeks (secondary outcome) ranged from 58.6% to 68.2% in the bimekizumab groups, compared with 23.9% for adalimumab, 20.9% for ustekinumab, and 0% to 1.2% for placebo groups. The between-group differences favoured bimekizumab versus adalimumab and placebo, and all comparisons were statistically significant (P < 0.001). The comparison in PS0009 also favoured bimekizumab versus ustekinumab. This analysis was not part of the statistical testing hierarchy to control the type I error rate; thus, these data should be interpretive as supportive evidence only.
For all studies, the sensitivity analyses for the primary or co-primary outcomes showed findings that were supportive of the primary analyses. Descriptive data for PASI 90 or PASI 100 response and IGA 0/1 response at week 16 were generally consistent between subgroups, based on prior biologic therapy (yes/no), prior systemic therapy (yes/no), and baseline PASI score (< 20 versus ≥ 20). Limited post hoc data were available for patients with body weight of 120 kg or more.
HRQoL was reported based on the Dermatology Life Quality Index (DLQI), a 10-item dermatology-specific questionnaire that covers 6 domains and is scored from 0 to 30, with lower scores indicating better HRQoL. The proportion of patients with a DLQI score of 0 or 1 at 16 weeks |||||||||||||| in the bimekizumab groups than placebo groups in PS0009 |||||||||||||||||||||||||||| and in Study PS0013 |||||||||||||||||||||||||||||||||||||||||| achieved a DLQI score of 0 or 1 in the bimekizumab than the ustekinumab group in PS0009 |||||||||||||||||||||||||||| and for bimekizumab versus adalimumab in PS0008 ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. HRQoL outcomes were not controlled for type I error rate; thus, these data should be interpreted as supportive evidence only.
Maintenance Treatment Period
In Study PS0009, 81.9% of patients in the bimekizumab group and 55.8% in the ustekinumab group achieved PASI 90 response at week 52, with an OR of 3.80 (95% CI, 2.44 to 5.90; P < 0.001) favouring bimekizumab. IGA 0/1 response was reported for 78.2% and 60.7% in the bimekizumab and ustekinumab groups, respectively (OR 2.41; 95% CI, 1.57 to 3.70; P < 0.001).
In Study PS0015, the PASI 100 response at week 48 was 73.5%, 66.0%, and 48.3% in the bimekizumab every 4 weeks, bimekizumab every 4 weeks for 16 weeks then every 8 weeks, and secukinumab groups, respectively. The between-group differences favoured bimekizumab versus secukinumab for both the every 4 weeks maintenance dosage (OR 3.24; 95% CI, 2.10 to 5.00; P < 0.001) and the every 8 weeks maintenance dosage (OR 2.12; 95% CI, 1.48 to 3.04; P < 0.001). This analysis excluded 4% of patients who withdrew during the first 16 weeks and was based on patients in the bimekizumab group who were re-randomized at 16 weeks to every 4 or 8 weeks maintenance dosage regimens (maintenance set N = 716). For the analysis based on all randomized patients, the 48-week PASI 100 results were comparable (67.0% versus 46.2% for bimekizumab versus secukinumab, respectively; OR 2.46; 95% CI, 1.81 to 3.34; P < 0.001).
Descriptive data were reported at week 56 for Study PS0008. Among patients who remained on bimekizumab every 4 weeks throughout the study, 84.8% and 82.3% achieved PASI 90 and IGA 0/1 response at week 56. For patients who received bimekizumab every 4 weeks for 16 weeks, then every 8 weeks thereafter, 82.6% and 83.2% achieved PASI 90 and IGA 0/1 response at week 56.
Withdrawal Treatment Period
In Study PS0013, patients in the bimekizumab group who achieved PASI 90 response at week 16 were re-randomized to switch to placebo or to continue bimekizumab every 4 weeks or 8 weeks. At week 56, 88.8% of patients who continued on bimekizumab reported PASI 90 response, compared with 16.2% of patients who switched to placebo (OR 47.41; 95% CI, 22.09 to 101.75; P < 0.001).
Harms Results
The frequency of adverse events was generally similar between groups in Study PS0009 (initial treatment period [first 16 weeks]: 47% to 56%; total study period: 80% to 82%), Study PS0008 (70% to 77%), and Study PS0015 (81% to 86%) (Table 3). In Study PS0013, more patients who received bimekizumab reported adverse events than the placebo group during the initial treatment period (61% versus 41%), but the frequency was comparable during the withdrawal period (69% to 77%). Across the studies, infections were the most commonly reported adverse events, specifically fungal infections, of which oral candidiasis was the most commonly reported event. Across studies, the bimekizumab groups reported a higher frequency of fungal infections than the comparators. In the first 16 to 24 weeks of PS0009, PS0008, and PS0013, 12% to 16% of patients in the bimekizumab groups reported a fungal infection, compared with 0% to 2% of those who received placebo, ustekinumab, or adalimumab. In the total study period, 18% to 29% of patients who received bimekizumab experienced a fungal infection, versus 3% and 10% who received ustekinumab or secukinumab, respectively. No systemic fungal infections were reported, and the frequency of serious infections was generally low (0% to 3%).
The frequency of adverse events was generally similar between bimekizumab groups that received maintenance doses every 4 weeks compared with every 8 weeks. However, in PS0013, the frequency of fungal infections was higher among patients who continued on bimekizumab every 4 weeks (21%) than every 8 weeks (14%) or those switched from bimekizumab to placebo (7%).
Serious adverse events were reported by 3% to 6% of patients who received bimekizumab, 8% of patients who received ustekinumab, and 6% who received secukinumab during the total study period of PS0008, PS0009, and PS0015, and in 3% to 5% of patients who received bimekizumab or placebo during the withdrawal period of PS0013. Seven patients died during the 4 studies, including 3 patients (0% to 0.5%) in the bimekizumab groups, and 1 patient in each of the ustekinumab, adalimumab, secukinumab, and placebo groups (0% to 1.2%).
The number of patients who discontinued the study due to adverse events was generally low across trials, and similar between treatment groups within studies, during the overall treatment period (3% to 5%) or withdrawal period (0% to 3%).
Table 3: Summary of Key Safety Results From Pivotal and Protocol Selected Studies
Study / treatment group | Total, N | AE n (%) | SAE n (%) | WDAE n (%) | Fungal infections n (%) |
|---|---|---|---|---|---|
Initial treatment period | |||||
PS0009 (16 weeks, SS) | |||||
Placebo | 83 | 39 (47) | 2 (2) | 6 (7) | 0 |
BKZ q.4.w. | 321 | 181 (56) | 5 (2) | 6 (2) | 45 (14) |
USTE | 163 | 83 (51) | 5 (3) | 3 (2) | 1 (0.6) |
PS0008 (24 weeks, SS) | |||||
BKZ (pooled) | 319 | 228 (71) | 5 (2) | 9 (3) | 50 (16) |
ADA | 159 | 111 (70) | 5 (3) | 5 (3) | 1 (1) |
PS0013 (16 weeks, SS) | |||||
Placebo | 86 | 35 (41) | 2 (2) | 0 | 2 (2) |
BKZ q.4.w. | 349 | 213 (61) | 6 (2) | 3 (1) | 40 (12) |
Withdrawal period | |||||
PS0013 (week 16 to 56, responder set) | |||||
BKZ q.4.w./placebo | 105 | 72 (69) | 4 (4) | 3 (3) | 7 (7) |
BKZ q.4.w./q.8.w. | 100 | 77 (77) | 3 (3) | 2 (2) | 14 (14) |
BKZ q.4.w. | 106 | 78 (74) | 5 (5) | 0 | 22 (21) |
Total study period | |||||
PS0009 (52 weeks, AMS) | |||||
BKZ q.4.w.a | 395 | 323 (82) | 24 (6) | 21 (5) | 92 (23) |
USTE | 163 | 130 (80) | 13 (8) | 7 (4) | 4 (3) |
PS0008 (56 weeks, BKZ set) | |||||
BKZ q.4.w./q.8.w. | 154 | 119 (77) | 8 (5) | 5 (3) | 27 (18) |
BKZ q.4.w.b | 468 | 343 (73) | 16 (3) | 14 (3) | 97 (21) |
PS0015 (48 weeks, SS) | |||||
BKZ q.4.w. | 373 | 321 (86) | 22 (6) | 13 (4) | 108 (29) |
SECU | 370 | 301 (81) | 21 (6) | 10 (3) | 35 (10) |
ADA = adalimumab; AE = adverse event; AMS = active medication set; BKZ = bimekizumab; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SAE = serious adverse event; SECU = secukinumab; SS = safety set; USTE = ustekinumab; WDAE = withdrawal due to adverse event.
aIncludes patients randomized to BKZ and those switched from placebo to BKZ after the first 16 weeks.
bBKZ q.4.w. group includes all events that occurred during BKZ q.4.w. treatment for all 3 randomized treatment groups.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Critical Appraisal
The risk of bias related to randomization and treatment allocation concealment was rated as low for all studies, and, in general, the patient characteristics appeared to be balanced between groups at baseline. However, in studies PS0009 and PS0008, some differences were observed in the median duration of disease and the proportion of patients with PASI score 20 and higher. However, the clinical expert consulted for this review did not anticipate that the differences noted would bias the results. The trials were double blind and took steps to maintain blinding of patients and investigators. However, nonidentical pre-filled syringes were used to administer the study drugs, which may have resulted in some patients being aware of treatment assignment. It is unclear whether unblinding may have introduced any bias into the results. The statistical analyses were based on a stratified Cochran-Mantel-Haenszel (CMH) test for the intention-to-treat population, with missing data imputed as nonresponders. While the PASI 90, PASI 100, or IGA 0/1 response outcome measures are generally accepted as representing clinically important improvement in psoriasis severity, the primary outcomes for this chronic condition were measured at 16 weeks. The longer-term outcome data were limited by the lack of control group (PS0008), were affected by failure to maintain randomization (maintenance set in PS0015), were restricted to patients with a demonstrated response to treatment (PS0013), or did not use a Health Canada–recommended dosage regimen (i.e., every 4 weeks maintenance dosage for patients with weight < 120 kg) (PS0009, PS0015, PS0013). In addition, there were important limitations to HRQoL data (such as lack of control of type I error, unknown extent of missing data, incomplete reporting of between-group differences), which limit the interpretation of these results.
The safety data available for bimekizumab were limited by the sample size and study duration of the trials, which may have been insufficient to detect infrequent adverse events or those that take a longer time to develop.
With respect to external validity, the characteristics of the patients enrolled in the trials were considered representative of patients in Canada with moderate to severe plaque psoriasis in Canada who may be treated with biologic drugs, according to the clinical expert consulted for this review. The trials, however, excluded patients with a history of nonresponse to IL-17 inhibitors or nonresponse to more than 1 biologic drug other than an IL-17 inhibitor. Thus, the treatment effects of bimekizumab in these patients in unknown. Moreover, concomitant use of topical therapies, phototherapy or non-biologic systemic drugs was prohibited during the trials, as was the titration of biologic drug dosages or dosing frequency to effect, which is common in clinical practice. Thus, the prescribing patterns of biologic controls or co-interventions used during the trial may not reflect clinical practice.
Indirect Comparisons
Description of Studies
The sponsor submitted an indirect treatment comparison (ITC) that evaluated the efficacy of bimekizumab in the treatment of moderate to severe chronic plaque psoriasis compared with other biologic and non-biologic systemic treatments. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Results
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Critical Appraisal
Several sources of heterogeneity were noted across the trials, including the proportion of patients with comorbid psoriatic arthritis, prior exposure to biologics or other non-biologic therapies, region, duration of disease, study years, timing of the outcome assessment, and placebo response rate. Due to this heterogeneity, the ITC was conducted ||||||||||||||||||||||||||||||||||||||||||; however, it is uncertain whether this approach is adequate to control for differences in patient characteristics that may bias results. The ITC did not assess other outcomes of interest to this review and was limited ||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Comparative indirect evidence is lacking on ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Other Relevant Evidence
Description of Studies
The aim of the ongoing extension study, PS0014, was to examine the longer-term efficacy and safety of bimekizumab in patients who had completed 1 of the 3 pivotal studies — PS0008, PS0009, or PS0013. Interim data up to 48 weeks of the extension study were available at the time this report was written. All patients received open-label bimekizumab 320 mg SC every 4 weeks or every 8 weeks. A total of 1,286 patients were enrolled, of which 3.5% had discontinued before week 24 of the extension study. Most patients (64%) were continuing in the study and had not completed the 48-week follow-up at the time of the interim analysis of PS0014.
Efficacy Results
The proportion of patients who achieved PASI or IGA response at week 24 in Study PS0014 was similar among those who received bimekizumab every 4 weeks and every 8 weeks. At 24 weeks, 89.2% and 90.1% of patients had achieved a PASI 90 response and 87.5% and 88.3% of patients had an IGA 0/1 response, among those who received bimekizumab every 4 weeks or every 8 weeks, respectively (nonresponder imputation). PASI 100 response was reported by 72.7% and 74.9% of patients who had received bimekizumab every 4 weeks or every 8 weeks, respectively. The proportion of patients who reported a DLQI score of 0 or 1 at 24 weeks was 82.5% and 81.2% among those who received bimekizumab every 4 weeks or every 8 weeks, respectively.
Harms Results
No new safety signals were reported, based on the 48-week interim safety data in PS0014. Adverse events were reported by 59% to 71% of patients, of which infections and infestations were common (41% to 53%). Fungal infections were reported in 229 patients (18%), including Candida infections in 174 patients (14%). Serious adverse events were reported in 66 patients (5.1%), as well as 8 serious infections (0.6%) and 3 deaths.
Critical Appraisal
Limitations of the extension study include selection bias, lack of a control group, and lack of blinding. Reporting of harms and subjective measures (such as those included in the PASI score) may be biased by knowledge of treatment received. Since only descriptive statistics were published in this interim report, and since there were no comparator groups, the interpretation of the results is limited. Moreover, there is potential for selection bias, as patients who discontinued the parent RCTs due to adverse events, lack of efficacy, or other reasons were excluded. The lack of systematic follow-up after discontinuation of bimekizumab in the extension study could have missed important information regarding the long-term adverse effects of the treatment. In addition, not all patients received a maintenance dosage regimen that was consistent with Health Canada recommendations.
Conclusions
Bimekizumab showed statistically and clinically important improvement in psoriasis disease severity versus placebo, adalimumab, ustekinumab, and secukinumab, measured as PASI 90, IGA response, or PASI 100 response at week 16, among patients with moderate to severe plaque psoriasis who were candidates for phototherapy or systemic therapy. The 1-year data suggest that PASI response may be maintained in the majority of patients who continue bimekizumab therapy, with between-group differences that favour bimekizumab versus secukinumab or ustekinumab.
Short-term data suggest that patients who receive bimekizumab may be more likely to show improvements in HRQoL (measured using the DLQI) than those who receive placebo, adalimumab, and ustekinumab, but not secukinumab. However, HRQoL outcomes were outside the statistical testing procedure and should be interpreted as supportive evidence in view of the inflated risk of type I error.
The indirect evidence suggests that bimekizumab |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Several sources of heterogeneity were identified across the trials included in the ITC, and it is uncertain whether the methods used to control for potential bias were adequate, or whether the between-group differences for some comparisons were clinically important.
Infections were among the most commonly reported adverse events, and fungal infections were reported more frequently among patients who received bimekizumab than among those receiving the comparators. The incidence of serious adverse events or withdrawals due to adverse events was low among patients who received bimekizumab, and no new safety signals were identified in the interim extension study data. However, the RCTs were not designed or powered to detect rare adverse events or those with a longer lag time, and longer-term comparative safety data are lacking.
Introduction
Disease Background
Plaque psoriasis is a chronic inflammatory skin disease characterized by erythematous inflammatory plaques that may be itchy or painful and are usually covered by silver, flaking scales.1 It is a complex immune-mediated disorder, in which dysregulation of components of the innate and adaptive immune systems, keratinocyte function, and vascular structure contribute to the manifestations of the disease.8
In addition to the overt dermatological symptoms, plaque psoriasis is often associated with psychosocial symptoms, including poor self-esteem, and may affect various aspects of social functioning, including interpersonal relationships and performance at school or work. These negative impacts on social and work life were described by most patients who provided input for this CADTH Common Drug Review. Psoriasis is associated with several comorbid conditions, including depressive symptoms, conditions associated with an increased risk of cardiovascular disease (such as type 2 diabetes, metabolic syndrome, and obesity), and psoriatic arthritis.1,9
The severity of psoriasis may be classified as mild, moderate, or severe, based on the extent of BSA affected, with 10% or more of BSA affected generally considered more severe disease.10 However, for patients with involvement of the hands, feet, scalp, face, or genital area, or those experiencing significant physical discomfort or emotional impacts from the disease, psoriasis may also be considered severe, regardless of BSA affected.10 For most patients with moderate to severe plaque psoriasis, the disease cannot be adequately controlled with topical treatments or phototherapy alone.10
There are multiple forms of psoriasis, including plaque, guttate, inverse, pustular, and erythrodermic psoriasis, but plaque psoriasis is the most common form and represents approximately 90% of cases.2 It is estimated that up to 1 million Canadians are living with a type of psoriasis.2 In Ontario, the estimated the age- and sex-standardized cumulative prevalence of psoriasis in 2015 was 2.32%.11 Up to 1-third of patients with psoriasis have moderate to severe disease.12-15
Standards of Therapy
Plaque psoriasis requires lifelong treatment. Measures of treatment success include clearance (absence of signs of disease), control (satisfactory response to therapy as defined by the patient and/or physician), and remission (suppression of signs and symptoms over time). Clearance and symptom control have been identified as treatment outcomes that are important to patients, and treatment decisions depend largely on the patient’s perception of their disease.
In patients with mild psoriasis, topical treatments (such as corticosteroids, vitamin D3 analogues, retinoids, anthralin, and tars) may be sufficient to control the disease; however, for those with moderate to severe psoriasis, systemic therapies are often required.16,17 Traditional systemic drugs include cyclosporine and methotrexate, but long-term use may be limited by toxicity.17 In Canada, there are several biologic drugs approved for the treatment of psoriasis (Table 4). The first biologic drugs licensed to treat plaque psoriasis were TNF alpha inhibitors. While effective and associated with rapid disease control, TNF alpha inhibitors are associated with a number of safety concerns, including serious infections (e.g., sepsis, reactivated tuberculosis, viral infections), autoimmune conditions (e.g., lupus and demyelinating disorders), and malignancies such as lymphoma.16,17 Other available biologic drugs include the IL-23 inhibitors risankizumab, guselkumab, and tildrakizumab; the IL-12/23 inhibitor ustekinumab; and IL-17 inhibitors secukinumab, ixekizumab, and brodalumab. These drugs have been associated with serious infections; potential activation of inflammatory bowel disease, in the case of IL-17 inhibitors; and suicidal ideation, in the case of brodalumab. According to the clinical expert consulted for this review, IL-17 and IL-23 inhibitors are now chosen more frequently by Canadian dermatologists over TNF alpha inhibitors as the first biologic for the treatment of plaque psoriasis.
Drug
Bimekizumab is a humanized monoclonal antibody that binds to the IL-17A, IL-17F, and IL-17AF cytokines and inhibits their interaction with the IL-17RA/IL-17RC receptor complex.3 Bimekizumab is approved by Health Canada for the treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy. It is available as a 160 mg/1 mL pre-filled syringe or autoinjector. The recommended dose is 320 mg, administered as 2 160 mg SC injections (pre-filled single use syringe or autoinjector) every 4 weeks for the first 16 weeks, followed by 320 mg SC every 8 weeks thereafter.3 The product monograph states that, at the prescriber’s discretion, discontinuation of treatment may be considered in patients who have shown no improvement after 16 weeks of treatment. The product monograph also states that, for patients with a body weight of 120 kg or more who did not achieve a complete skin response, a dosage of 320 mg every 4 weeks after week 16 may be considered.3
Bimekizumab underwent a standard review by Health Canada. The drug has not previously been reviewed by CADTH. The sponsor is requesting reimbursement as per the anticipated indication.18
Table 4: Key Characteristics of Drugs for Psoriasis
Biologic drug | Indicationa | Recommended dose | Serious adverse effects / safety issues |
|---|---|---|---|
IL-17 inhibitors | |||
Bimekizumab (Bimzelx) | Treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy | 320 mg SC every 4 weeks for the first 16 weeks, then 320 mg SC every 8 weeks thereafter Note: For patients with a body weight ≥ 120 kg who did not achieve a complete skin response, a dose of 320 mg every 4 weeks after week 16 may be considered | Infections, including candidiasis and other fungal infections Use with caution in patients with inflammatory bowel disease |
Brodalumab (Siliq) | Treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy | 210 mg SC at weeks 0, 1, and 2, followed by 210 mg SC every 2 weeks | Suicidal ideation and behaviour Crohn disease Infection |
Secukinumab (Cosentyx) | Treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy Treatment of severe plaque psoriasis in pediatric patients 12 to under 18 years of age who are candidates for systemic therapy or phototherapy and have a body weight ≥ 50 kg | Adults: 300 mg SC at weeks 0, 1, 2, 3, and 4, followed by monthly maintenance administration Pediatric patients > 12 years and ≥ 50 kg: 150 mg (may be increased to 300 mg) at weeks 0, 1, 2, 3, and 4, followed by monthly maintenance administration | Infection Inflammatory bowel disease Serious hypersensitivity reactions |
Ixekizumab (Taltz) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy Treatment of pediatric patients from 6 to less than 18 years of age with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | Adults: 160 mg SC at week 0, followed by 80 mg SC at weeks 2, 4, 6, 8, 10, and 12, then 80 mg SC every 4 weeks Pediatric patients ≥ 6 years: > 50 kg: 160 mg at week 0, then 80 mg every 4 weeks 25 kg to 50 kg: 80 mg at week 0, then 40 mg every 4 weeks < 25 kg: 40 mg at week 0, then 20 mg every 4 weeks | Infection Serious hypersensitivity reactions Inflammatory bowel disease |
IL-23 inhibitors | |||
Tildrakizumab (Ilumya) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | 100 mg administered by SC injection at weeks 0 and 4, and every 12 weeks thereafter | Infection |
Risankizumab (Skyrizi) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | 150 mg administered by SC injection at weeks 0 and 4, and every 12 weeks thereafter | Infection Hypersensitivity reactions |
Guselkumab (Tremfya) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy | 100 mg administered SC at weeks 0 and 4, followed by maintenance administration every 8 weeks thereafter | Infection Hypersensitivity reactions |
IL-12/23 inhibitors | |||
Ustekinumab (Stelara) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for phototherapy or systemic therapy Treatment of chronic moderate to severe plaque psoriasis in adolescent patients from 12 to 17 years of age, whose psoriasis is inadequately controlled by, or who are intolerant to, other systemic therapies or phototherapies | 45 mg SC at weeks 0 and 4, then every 12 weeks thereafter. Alternatively, 90 mg SC may be used in patients with a body weight > 100 kg. For patients who respond inadequately to administration every 12 weeks, consideration may be given to treating as often as every 8 weeks Dose of 0.75 mg/kg is recommended in pediatric patients weighing < 60 kg | Infection Malignancy Serious hypersensitivity reactions |
TNF inhibitors | |||
Adalimumab (Humira, Hadlima, Hulio, Amgevita, Hyrimoz, Idacio) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy; for patients with chronic moderate plaque psoriasis, adalimumab should be used after phototherapy has been shown to be ineffective or inappropriate | Initial dose of 80 mg SC followed by 40 mg SC every other week starting 1 week after the initial dose Continued therapy beyond 16 weeks should be carefully reconsidered in a patient not responding within this time period | Malignancies Infection Congestive heart failure Hematologic events Hypersensitivity reactions Autoimmunity and immunosuppression Neurologic events |
Certolizumab pegol (Cimzia) | Treatment of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy | 400 mg SC every 2 weeks A dose of 400 mg SC initially (week 0) and at weeks 2 and 4 followed by 200 mg every 2 weeks may be considered | Malignancies Infection Heart failure Hematologic events Hypersensitivity reactions Autoimmunity and immunosuppression Neurologic events |
Etanercept (Enbrel, Erelzi, Brenzys) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy Treatment of pediatric patients ages 4 to 17 years with chronic severe psoriasis who are candidates for systemic therapy or phototherapy | Adults: Starting dose of 50 mg SC given twice weekly (administered 3 or 4 days apart) for 3 months, followed by a reduction to a maintenance dosage of 50 mg SC per week. A maintenance dosage of 50 mg SC given twice weekly has also been shown to be efficacious Pediatric patients: 0.8 mg/kg per week (up to a maximum of 50 mg per week) | Infections Malignancies Neurologic events Hematologic events Congestive heart failure Autoimmunity |
Infliximab (Remicade, Inflectra, Renflexis, Avsola) | Treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy; for patients with chronic moderate plaque psoriasis, infliximab should be used after phototherapy has been shown to be ineffective or inappropriate | 5 mg/kg IV followed by additional 5 mg/kg IV doses at 2 and 6 weeks after the first infusion, then every 8 weeks thereafter. If a patient does not show an adequate response at week 14, no additional treatment with infliximab should be given | Infection Malignancies Cardiovascular events Hematologic abnormalities Hepatic abnormalities Hypersensitivity reactions Autoimmunity and immunogenicity Neurologic events |
IL = interleukin; IV = IV; SC = subcutaneous.
aHealth Canada indication.
Source: Product monographs.3,19-39
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
Two responses to CADTH’s call for patient input for the bimekizumab submission were received: a submission from the Psoriasis Society of Canada and a co-operative submission from the Canadian Association of Psoriasis Patients (CAPP) and the Canadian Psoriasis Network (CPN). The information used to inform the submissions was from phone calls from psoriasis patients as well as from a survey hosted on the CAPP and CPN websites and sent to clinics conducting bimekizumab trials to share with patients. A total of 95 survey responses were received, in addition to a telephone interview with a bimekizumab trial participant.
The patients described psoriasis as a chronic inflammatory condition that can present potentially debilitating challenges. Most patients reported living with psoriatic arthritis, and about half of all survey respondents described their psoriasis as moderate or severe. Common symptoms experienced by more than 2-thirds of patients included flaking, itching, and redness, and more than half of patients experienced pain. Most patients reported that their psoriasis symptoms affected their social life, self-esteem, mental health, intimate life, sleep, and work. Many patients reported feeling that their symptoms are not effectively controlled with existing therapies. Most patients indicated that an improvement in their quality of life or a reduction in symptoms would be an important treatment outcome, in addition to the desire for a faster response to treatment, clear skin, or a cure. Moreover, a new treatment should have reduced adverse effects, be affordable, assist with persistent symptoms, and be easier to take.
Clinician Input
Input from the Clinical Expert Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of plaque psoriasis.
Unmet Needs
According to the clinical expert consulted for this review, none of the available treatments for plaque psoriasis provide a cure, and there remains an unmet need. The ideal treatment would produce a sustained PASI 100 response in all patients, with a low risk of adverse effects; would minimize or eliminate the negative impact of psoriasis on HRQoL; and would benefit 1 or more of the comorbidities, particularly psoriatic arthritis. Ideally, the medication would produce remission without the need for continuous long-term administration or could be administered intermittently, as required, when the patient reaches a predetermined PASI score after interruption of therapy. In addition, the treatment would be easily accessed by the patient and convenient to administer.
Place in Therapy
In the clinical expert’s opinion, bimekizumab is unlikely to cause a shift in the treatment paradigm for moderate to severe plaque psoriasis, as it is anticipated that prior treatment with methotrexate or cyclosporine will be required for reimbursement.
Bimekizumab is the fourth IL-17 inhibitor approved for the treatment of plaque psoriasis in Canada. As such, it does not have a completely unique mechanism of action compared to currently available drugs. It is the first drug in this class to inhibit both IL-17A and IL-17F.
At present, it is impossible to predict with certainty whether a patient will respond adequately to any of the available biologic drugs. In addition, not all drugs are suitable for all patients (e.g., Crohn disease is a contraindication to the IL-17 inhibitors, severe depression with suicidal ideation is a contraindication to brodalumab, and cardiac failure and multiple sclerosis are contraindications to TNF alpha inhibitors). The expert stated that bimekizumab will be an additional efficacious drug in the treatment armamentarium and will increase the likelihood that the patient will find a drug that works well and is well tolerated.
The expert indicated that dermatologists will likely favour IL-17 inhibitors, including bimekizumab, as the first biologic drugs of choice due to their high efficacy, along with IL-23 inhibitors. Bimekizumab (for patients less than 120 kg body weight) has the advantage of a longer maintenance dosage frequency (every 8 weeks), compared to ixekizumab and secukinumab (every 4 weeks), and brodalumab (every 2 weeks).
In regard to gaps in the evidence, the expert noted that the potential for intermittent therapy with bimekizumab, and its efficacy in psoriatic arthritis, are currently unknown.
The expert anticipated that it will be uncommon for dermatologists to combine bimekizumab with methotrexate or apremilast.
In general, if there are no contraindications (or reimbursement issues, in the case of apremilast) the expert recommended trials of methotrexate, cyclosporine, acitretin (in palmoplantar plaque psoriasis), and possibly apremilast before initiating bimekizumab. Trials of non-biologic drugs are required for public reimbursement for biologic drugs and for most third-party carriers, and many patients respond well without significant toxicity. As stewards of a publicly funded health care system, dermatologists are encouraged to offer these lower-cost alternatives before offering the biologic drugs.
Patient Population
According to the clinical expert, bimekizumab is appropriate for adult patients with moderate to severe plaque psoriasis who are suitable candidates for systemic therapy. Most payors would limit use to patients with a minimum PASI score of 12 and psoriasis affecting 10% or more of BSA.
The expert anticipates that most patients with moderate to severe plaque psoriasis are likely to show an improvement with bimekizumab. However, for patients with psoriatic arthritis, additional evidence is required, including data on the relative efficacy of the IL-23 inhibitors versus the IL-17 inhibitors for psoriatic arthritis. Currently, it is impossible to identify which patients are most likely to respond to bimekizumab. In general, patients who have failed multiple previous biologic therapies may be less likely to respond to subsequent therapies than patients who are biologic-naive. The expert foresees that patients who have experienced primary or secondary failure with 1 IL-17 inhibitor may be successfully treated with another member of the IL-17 class. However, additional evidence is required.
The expert expects there will be a small portion of patients who remain clear of psoriasis for a significant time after bimekizumab is discontinued. A review of treatment interruption data will be required so that start-stop therapy options can be explored.
Patients least suitable for treatment with bimekizumab would be those with active Crohn disease or those who had failed 1 or more prior trials of an IL-17 inhibitor, according to the clinical expert.
The diagnosis of psoriasis is made clinically and is not a challenging diagnosis for dermatologists, so misdiagnosis is unlikely. Basic laboratory testing before starting bimekizumab, as with all other biologic drugs, would include HIV serology, viral hepatitis screening, and screening for latent tuberculosis.
Assessing Response to Treatment
According to the clinical expert, response to therapy is assessed based on the PASI score (as a requirement for reimbursement); in some practices, the DLQI instrument may also be used. A PASI 75 response at 16 weeks would be considered a clinically meaningful response to treatment. However, clinicians expect that patients will achieve a higher threshold of improvement with newer biologic drugs.
The expert stated that patients who have achieved a PASI 90 or PASI 100 response at 16 weeks will be offered follow-up in 1 year but may be seen earlier if response wanes or the patient is concerned about a possible adverse event. If the patient has barely achieved a PASI 75 response at 16 weeks, a follow-up appointment would be booked in approximately 12 to 16 weeks to determine whether there has been additional improvement.
Discontinuing Treatment
According to the clinical expert, the following would be reasons to discontinue treatment:
Failure to reach PASI 75 improvement at 16 weeks
Failure to maintain PASI 75 response during the maintenance phase; in Canada, patients would typically receive a dosage increase and addition of topical therapy to see whether response can be recaptured
Failure of the drug to control psoriatic arthritis in patients with concomitant arthritis
Development of a high-risk malignancy, particularly if the patient’s oncologist is advising immunotherapy
Elective surgery (orthopedic, gastrointestinal, genitourinary) and development of significant infections; in most cases, these result in temporary discontinuation followed by resumption of the drug.
Prescribing Conditions
Bimekizumab may be administered by the patient at home after appropriate training but could also be administered at a community infusion clinic or at the prescribing dermatologist’s office.
A dermatologist will be required to diagnose, treat, and monitor patients on bimekizumab. Patients may be co-managed by dermatology and rheumatology if they also have psoriatic arthritis.
Clinician Group Input
No input was received from clinician groups.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Implementation issues | Advice from CADTH |
|---|---|
Relevant comparators | |
Given the available evidence, do you think that bimekizumab will affect the treatment algorithm for biologic drugs? | The clinical expert consulted did not anticipate that bimekizumab would cause shifts in the treatment algorithm for patients with plaque psoriasis. Bimekizumab offers patients another treatment option among the other interleukin inhibitors approved for use in Canada. |
Considerations for initiation of therapy | |
Jurisdictions have some differences in prior therapies required for eligibility for biologic drugs for psoriasis. In your opinion, which therapies should patients try first before they become eligible for bimekizumab? | According to the expert consulted, patients with no contraindications to therapy should receive a trial of methotrexate and cyclosporine before switching to a biologic drug, including bimekizumab. |
Do you think that the initiation criteria for bimekizumab should align with that of other biologic drugs? | The initiation criteria for bimekizumab should be consistent with other biologic drugs. |
Considerations for continuation or renewal of therapy | |
Most jurisdictions use PASI and DLQI for other biologic drugs for plaque psoriasis. Do you think it is appropriate to align the renewal criteria for bimekizumab with that for other biologic drugs for plaque psoriasis? | The renewal criteria for bimekizumab should be consistent with the criteria for other biologic drugs. |
Considerations for discontinuation of therapy | |
Treatment with biologic drugs for plaque psoriasis would be discontinued if a response has not been demonstrated after 12 to 16 weeks. Should the discontinuation criteria for bimekizumab align with that of other biologic drugs for plaque psoriasis? | The discontinuation criteria for bimekizumab should be consistent with those for other biologic drugs. |
Considerations for prescribing of therapy | |
Is it appropriate to use bimekizumab in combination with other systemic or biologic treatments? | The expert indicated that bimekizumab may be used in combination with non-biologic systemic therapies but not with other biologic treatments. |
Clinical Evidence
The clinical evidence included in the review of bimekizumab is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of bimekizumab 160 mg/mL solution for SC injection for the treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults ≥ 18 years with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy Subgroups:
|
Intervention | Bimekizumab 320 mg subcutaneous injection every 4 weeks for the first 16 weeks, then every 8 weeks thereafter (Note: For some patients with a body weight ≥ 120 kg, 320 mg every 4 weeks after week 16 may be considered) |
Comparator | The following drugs when used as monotherapy or in combination with non-biologic systemic drugs: Biologic drugs targeting interleukins: brodalumab, guselkumab, ixekizumab, risankizumab, secukinumab, tildrakizumab, ustekinumab Biologic drugs targeting TNF alpha: adalimumab, certolizumab pegol, etanercept, infliximab |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; BSA = body surface area; DLQI = Dermatology Life Quality Index; EQ-5D = EuroQol 5-Dimensions questionnaire; HRQoL = health-related quality of life; PASI = Psoriasis Area and Severity Index; RCT = randomized controlled trial; SAE = serious adverse event; SF-36 = Short Form (36) Health Survey; TNF = tumour necrosis factor; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.40
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was bimekizumab. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on September 8, 2021. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on January 26, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.41 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings from the Literature
A total of 4 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
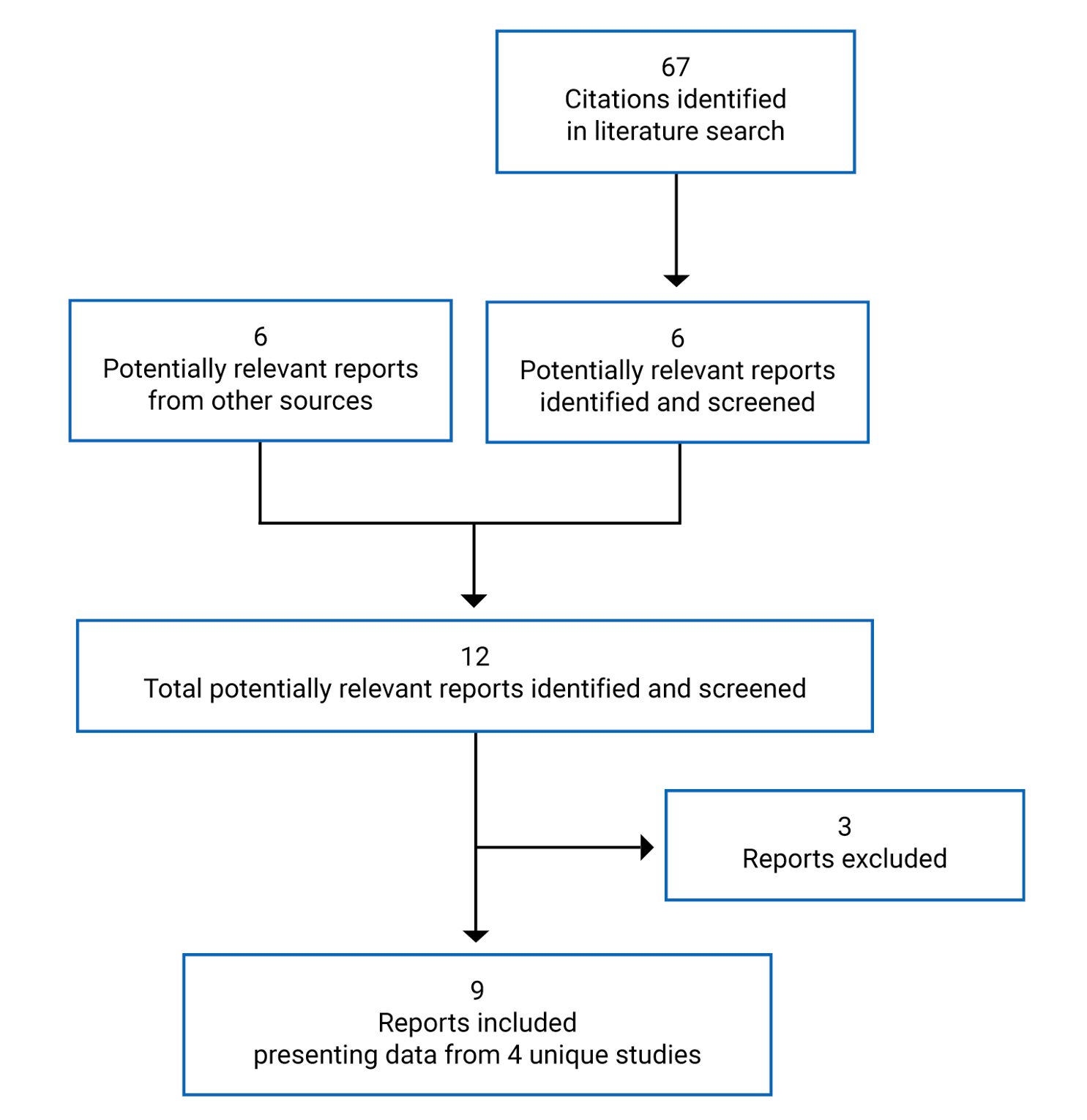
Table 7: Details of Included Studies
Item | PS0009 (BE VIVID) | PS0008 (BE SURE) | PS0015 (BE RADIANT) | PS0013 (BE READY) |
|---|---|---|---|---|
Designs and populations | ||||
Study design | DB RCT (pivotal) | DB RCT (pivotal) | DB RCT | DB RCT, withdrawal design (pivotal) |
Locations | Canada, US, Europe, Australia, (105 sites) | Canada, US, Europe, Asia, Australia (77 sites) | Canada, US, Europe, Australia (77 sites) | Canada, Europe, US, Korea, Australia (77 sites) |
Patient enrolment dates | December 6, 2017, to December 13, 2019 | January 26, 2018, to February 26, 2020 | June 13, 2018, to June 29, 2020 | February 5, 2018, to January 7, 2020 |
Randomized (N) | 567 | 478 | 743 | 435 |
Inclusion criteria | Adults 18 years or older, chronic plaque psoriasis for at least 6 months, PASI ≥ 12, ≥ 10% of BSA affected, IGA score of ≥ 3 on a 5-point scale, candidate for systemic psoriasis therapy and/or phototherapy, suitable for treatment with each study’s active control drug (i.e., ustekinumab, adalimumab, or secukinumab) | |||
Exclusion criteria |
| |||
Drugs | ||||
Intervention | Bimekizumab, 320 mg SC every 4 weeks for 52 weeksa | Bimekizumab 320 mg SC every 4 weeks for 56 weeksa Bimekizumab 320 mg SC every 4 weeks for 16 weeks, then every 8 weeks for weeks 16 to 56 | Bimekizumab 320 mg SC every 4 weeks for 16 weeks, then re-randomization to 320 mg bimekizumab every 4a or 8 weeks up to week 48 | Bimekizumab 320 mg SC every 4 weeks for 16 weeks Patients in the bimekizumab group who achieved PASI 90 response at week 16 were re-randomized to bimekizumab 320 mg every 4 weeks,a every 8 weeks, or placebob |
Comparator(s) | Ustekinumab, 45 mg or 90 mg (weight-based dosing) SC at weeks 0 and 4, and then every 12 weeks Placebo injection SC every 4 weeks for first 16 weeks, then bimekizumab 320 mg SC every 4 weeks | Adalimumab 80 mg SC at week 0, 40 mg at week 1, then every 2 weeks thereafter until week 24, when patients were switched to bimekizumab 320 mg SC every 4 weeks until week 56 | Secukinumab 300 mg SC at weeks 0, 1, 2, 3, and 4, then every 4 weeks up to week 48 | Placebo injection SC every 4 weeks for 16 weeks Patients who achieved PASI 90 response at week 16 continued on placebo; nonresponders were eligible for escape therapyb |
Duration | ||||
Phase | ||||
Screening | 2 to 5 weeks | 2 to 5 weeks | 2 to 5 weeks | 2 to 5 weeks |
Initial treatment | 16 weeks | 16 weeks | 16 weeks | 16 weeks |
Maintenance / withdrawal treatment | 36 weeks | 40 weeks | 32 weeks | 40 weeks |
Safety follow-up | 20 weeks | 20 weeks | 20 weeks | 20 weeks |
Outcomes | ||||
Primary end point | Co-primary: • Proportion of patients with a 90% or more improvement from baseline (PASI 90) at week 16 • Proportion of patients with an IGA response (score of 0 or 1) with at least a 2-category improvement from baseline at week 16 | Co-primary: • Proportion of patients with a 90% or more improvement from baseline (PASI 90) at week 16 • Proportion of patients with an IGA response (score of 0 or 1) with at least a 2-category improvement from baseline at week 16 | Primary: • Proportion of patients with a 100% improvement from baseline (PASI 100) at week 16 | Co-primary: • Proportion of patients with a 90% or more improvement from baseline (PASI 90) at week 16 • Proportion of patients with an IGA response (score of 0 or 1) with at least a 2-category improvement from baseline at week 16 |
Secondary and exploratory end points | Secondary:
Other
| Secondary:
Other
| Secondary:
Other
| Secondary:
Other
|
Notes | ||||
Publications | Reich et al. (2021)42 | Warren et al. (2021)43 | Reich et al. (2021)44 | Gordon et al. (2021)45 |
ACR = American College of Rheumatology; BCG = bacillus Calmette-Guerin; BSA = body surface area; DB = double-blind; DLQI = Dermatology Life Quality Index; EQ-5D-3L = EuroQol 5-Dimensions 3-Levels questionnaire; HAQ-DI = Health Assessment Questionnaire–Disability Index; IGA = Investigator’s Global Assessment; IL = interleukin; IV = IV; MI = myocardial infarction; mNAPSI = modified Nail Psoriasis Severity Index; PACE = Psoriatic Arthritis Screening and Evaluation; PASI = Psoriasis Area and Severity Index; P-SIM = Psoriasis Symptoms and Impacts Measure; RCT = randomized controlled trial; SC = subcutaneous; SF-36 = Short Form (36) Health Survey; VAS = visual analogue scale; WPAI-SHP = Work Productivity and Activity Impairment Questionnaire–Specific Health Problem.
Note: One additional report was included (European Public Assessment Report for Bimzelx12).
aBimekizumab 320 mg every 4 weeks after week 16 was not consistent with the Health Canada–recommended dosage unless the patient weighed more than 120 kg.
bEscape treatment was offered to patients who did not respond (i.e., achieve PASI 90 response) to study drug by week 16, and those who relapsed (i.e., did not achieve PASI 75 response) at week 20 or later.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Description of Studies
Four multi-centre, double-blind RCTs met the inclusion criteria for the systematic review (studies PS0009, PS0008, PS0015, and PS0013). Study schematics for the 4 trials are shown in Figure 2 to Figure 5.
The objective of Study PS0009 (BE VIVID) was to the compare the efficacy and safety of bimekizumab versus placebo or ustekinumab in the treatment of patients with moderate to severe chronic plaque psoriasis. The study randomized 567 patients (4:2:1) to bimekizumab every 4 weeks, ustekinumab (weight-based dosing), or placebo. After 16 weeks, patients in the placebo group were switched to receive bimekizumab every 4 weeks up to week 52.
The 56-week Study PS0008 (BE SURE) was designed to evaluate the efficacy and safety of bimekizumab versus adalimumab in patients with moderate to severe plaque psoriasis. Patients were randomized 1:1:1 to bimekizumab every 4 weeks, bimekizumab every 4 weeks for 16 weeks, then every 8 weeks, or adalimumab (with crossover to bimekizumab at 24 weeks) (N = 478).
The aim of Study PS0015 (BE RADIANT) was to evaluate the efficacy and safety of bimekizumab versus secukinumab in patients with moderate to severe plaque psoriasis. A total of 743 patients were randomized (1:1) to bimekizumab every 4 weeks or secukinumab for the first 16 weeks, after which, patients in the bimekizumab group were re-randomized (1:2) to receive maintenance therapy with bimekizumab every 4 weeks or every 8 weeks up to week 48. Patients in the secukinumab group continued to receive that drug until the end of the study at week 48.
Study PS0013 (BE READY) used a randomized withdrawal design to examine the efficacy and safety of bimekizumab versus placebo at 16 weeks, and the effects of treatment withdrawal on the efficacy and safety of bimekizumab over 56 weeks. A total of 435 patients were randomized (4:1) to bimekizumab every 4 weeks or placebo for the first 16 weeks. At 16 weeks, patients in the bimekizumab group who achieved PASI 90 response were re-randomized to bimekizumab every 4 weeks, bimekizumab every 8 weeks, or placebo (1:1:1). Patients in the placebo group with a PASI 90 response at week 16 remained on placebo, and patients in both groups who were nonresponders at week 16, or who relapsed at week 20 or later, received escape therapy with bimekizumab every 4 weeks for 12 weeks.
The trials were conducted between December 2017 and June 2020, and all included sites from Canada, US, Europe, and Australia. Two studies also included sites from Asia (PS0008, PS0013). The number of Canadian patients enrolled was 61 (11%), 77 (16%), 89 (21%), and 88 (12%) in studies PS0009, PS0008, PS0013, and PS0015, respectively. In all 4 studies, randomization was stratified by region and prior biologic drug exposure (yes/no), with patients allocated to treatments using an interactive response technology. Of note, the dosage frequency of some bimekizumab groups during the maintenance period of the trials was not consistent with the Canadian product monograph, which recommends every 8 weeks for most patients.
Patients who completed the PS009, PS0008, or PS0013 trials were eligible to enter the open-label extension study, PS0014 (BE BRIGHT) and receive bimekizumab 320 mg every 4 or 8 weeks. Patients who received escape therapy in PS0013 were also allowed to enter extension Study PS0014 if they achieved at least a PASI 50 response to rescue therapy. Patients who completed the double-blind period of PS0015 were eligible to enter a 96-week open-label extension period and continued to receive bimekizumab 320 mg every 4 or 8 weeks.
Figure 2: Study Schematic Diagram for PS0009
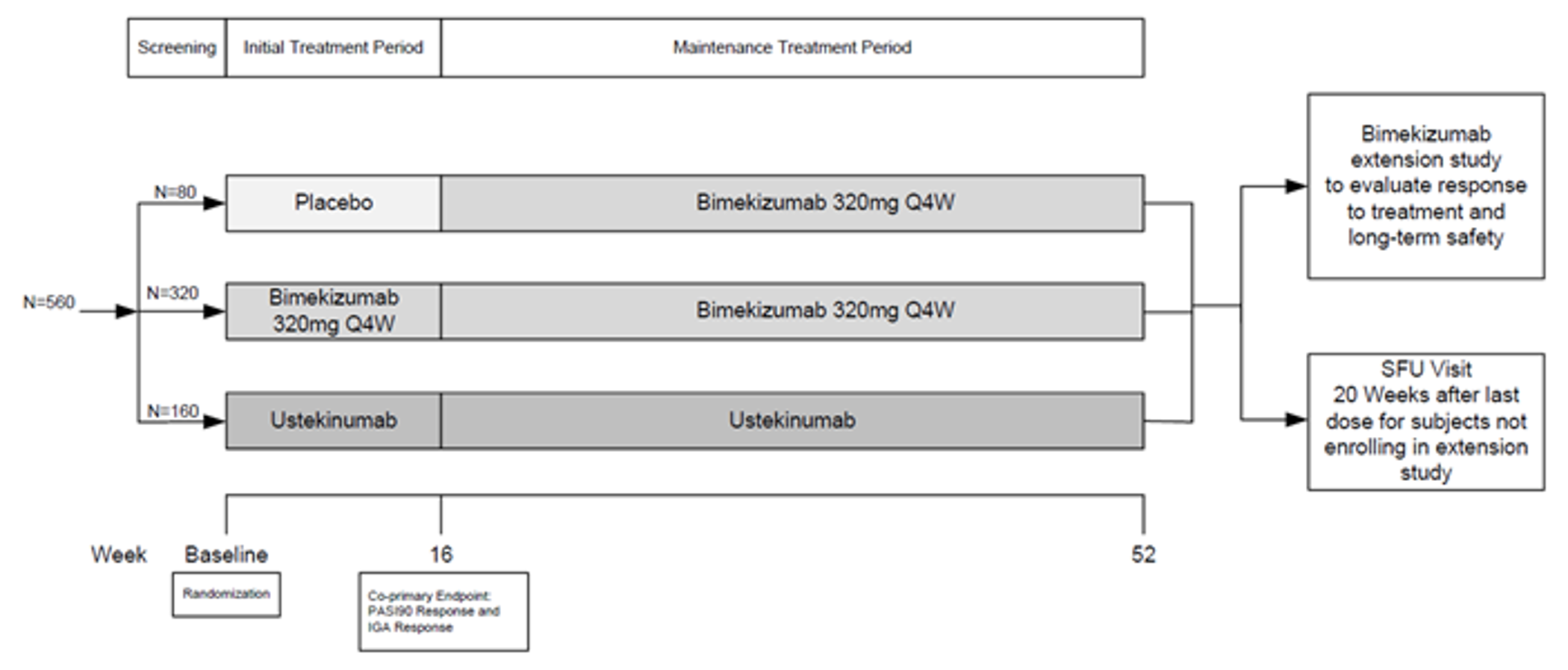
IGA = Investigator’s Global Assessment; PASI = Psoriasis Area and Severity Index; Q4W = every 4 weeks; SFU = safety follow-up.
Source: Clinical Study Report for PS000.4
Figure 3: Study Schematic Diagram for PS0008
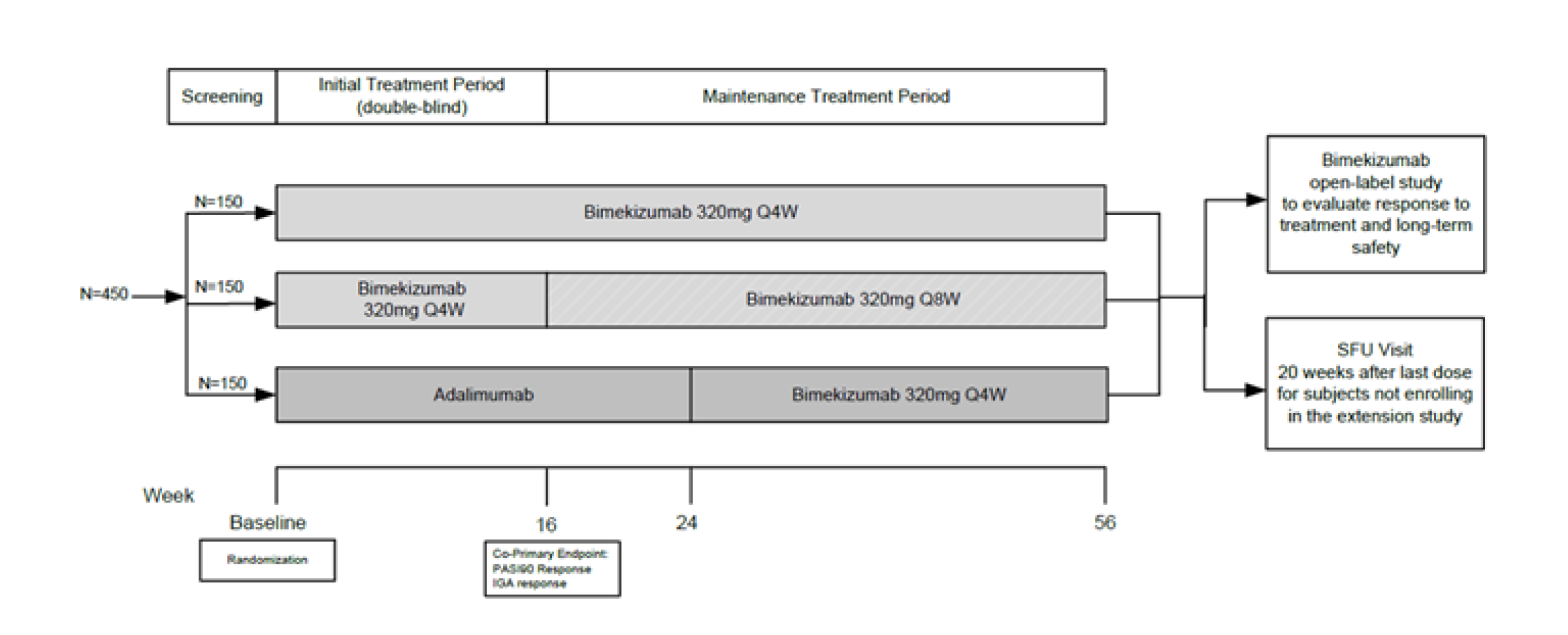
IGA = Investigator's Global Assessment; PASI = Psoriasis Area and Severity Index; Q4W = every 4 weeks; Q8W = every 8 weeks; SFU = safety follow-up.
Source: Clinical Study Report for PS0008,5
Figure 4: Study Schematic Diagram for PS0015
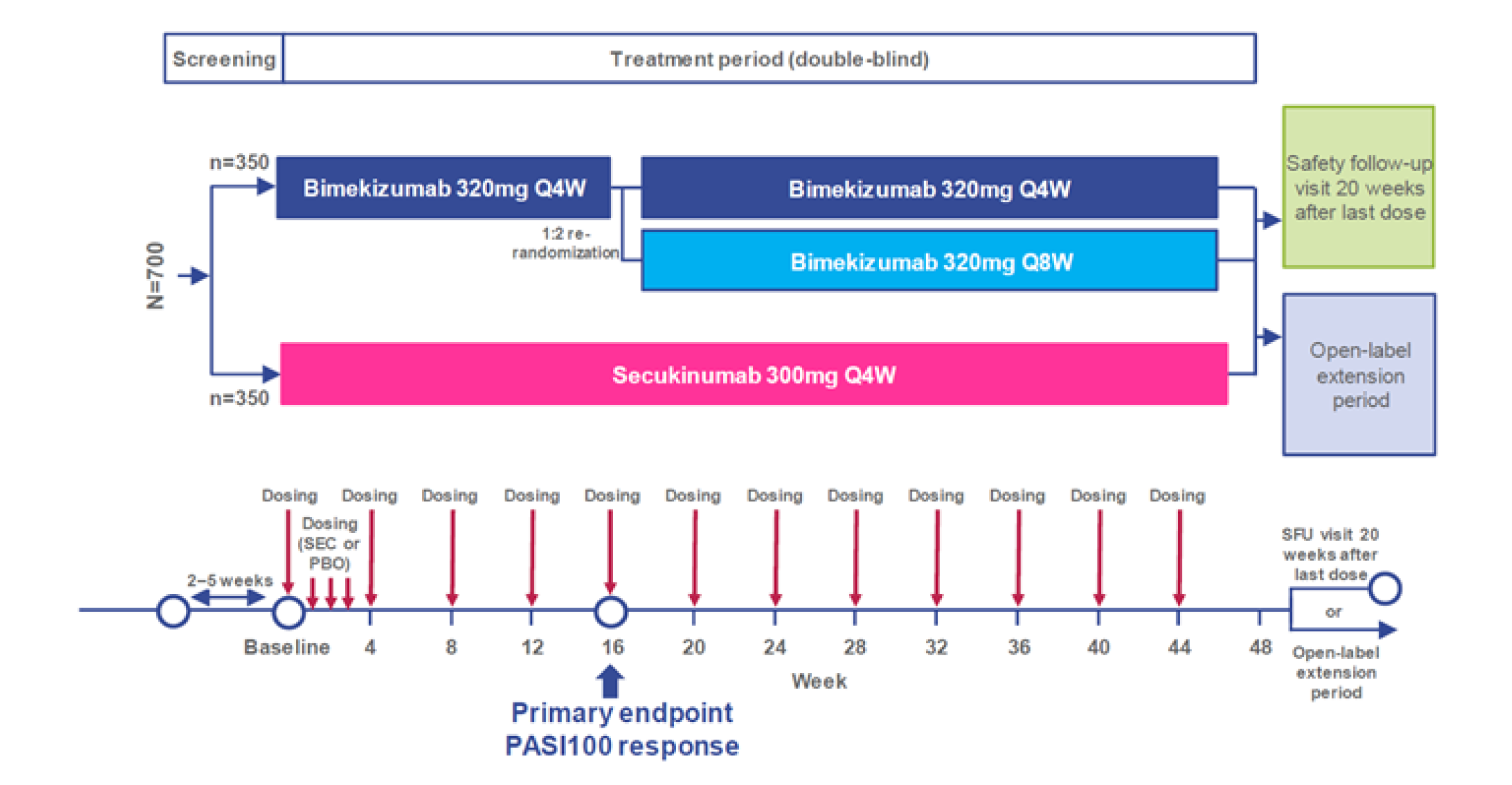
PASI = Psoriasis Area and Severity Index; PBO = placebo; Q4W = every 4 weeks; Q8W = every 8 weeks SEC = secukinumab; SFU = safety follow-up.
Source: Clinical Study Report for PS0015.6
Figure 5: Study Schematic Diagram for PS0013
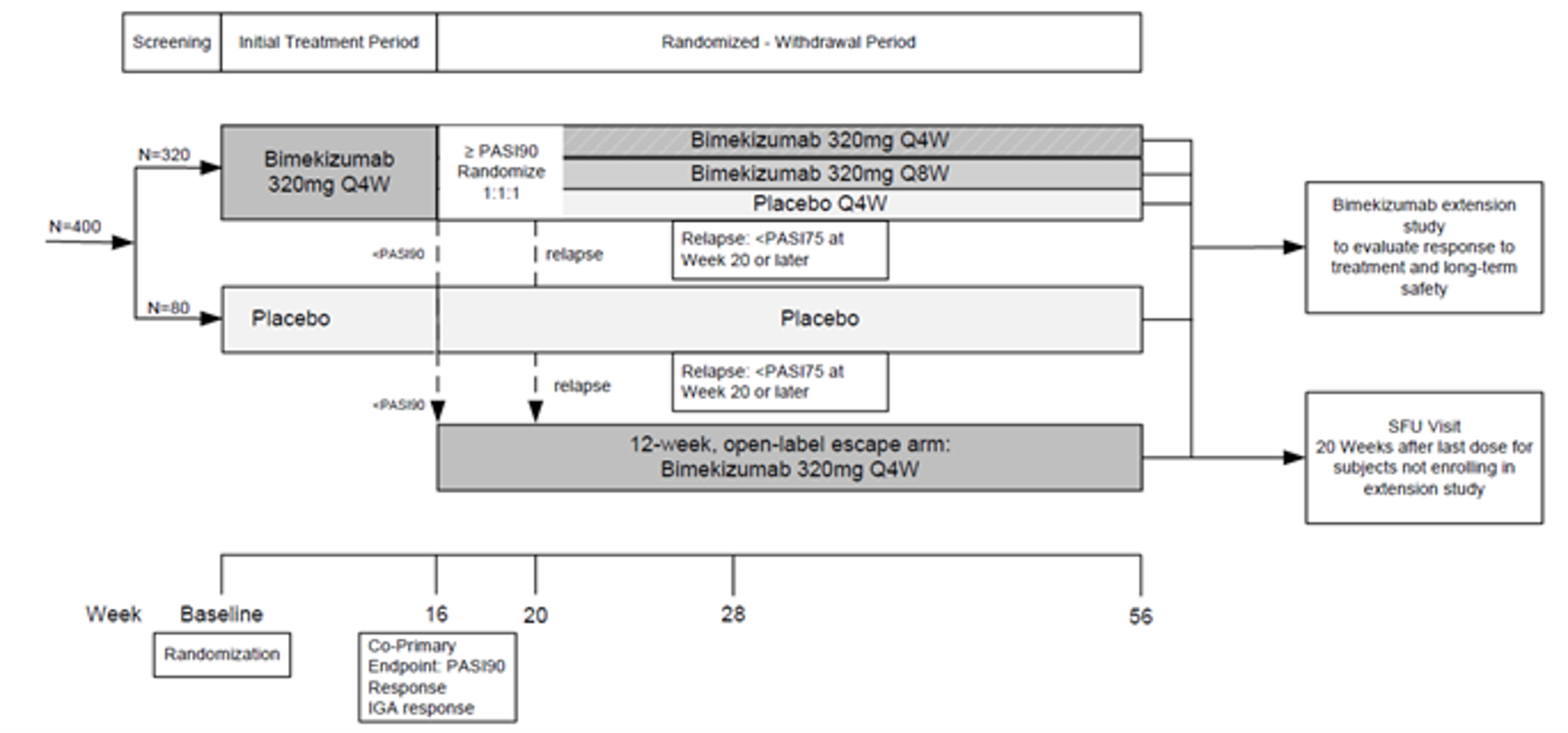
IGA = Investigator's Global Assessment; PASI = Psoriasis Area and Severity Index; Q4W = every 4 weeks; Q8W = every 8 weeks; SFU = safety follow-up.
Populations
Inclusion and Exclusion Criteria
All 4 trials used essentially the same inclusion and exclusion criteria. They enrolled adults who had had moderate or severe plaque psoriasis for at least 6 months, who had a baseline PASI score of at least 12 points, and who had at least 10% of their BSA affected. All patients had an IGA score of at least 3 points on a 5-point scale (i.e., moderate severity psoriasis) and were candidates for systemic treatment or phototherapy.
Key exclusion criteria were patients who had experienced primary failure (no response within 12 weeks) to an IL-17 biologic drug or to more than 1 biologic response modifier other than an IL-17; who had a recent infection or history of serious, opportunistic, recurrent, or chronic infection; and who had active suicidal ideation, moderate to severe depression, or history of lymphoproliferative disease or malignancy. Patients with inflammatory conditions other than psoriatic arthritis were also excluded. Those with Crohn disease or ulcerative colitis were allowed if they had no active symptomatic disease.
Baseline Characteristics
The mean age of the patients enrolled ranged from 43.5 years (SD 13.1) to 49.7 years (SD 13.6) across treatment groups in the 4 trials (Table 8, Table 9, and Table 10). Most patients were male (64% to 73%) and White (74% to 94%), with psoriasis that was rated at moderate severity based on their IGA score (59% to 72%). The proportion of patients with a PASI score greater than 20 at baseline ranged from 34% to 47% across treatment groups in all 4 studies. Most patients (69% to 83%) had received prior systemic therapy, which included prior biologic therapy for 31% to 44% of patients, and prior IL-17 therapy for 11% to 24% of patients.
The baseline characteristics were generally similar between trials except in a few instances, such as Study PS0009, that enrolled more Asian patients (22%) than other studies (2% to 7%), and fewer patients had received an IL-17 biologic drug in Study PS0015 (12%) than in other trials (approximately 22%). A few imbalances were noted between groups in studies PS0009 and PS0008, including the median duration of disease, the proportion of patients with PASI score of 20 or higher, and the mean age in PS0009. Other baseline patient characteristics appeared to be generally well balanced between groups within trials.
Table 8: Summary of Baseline Characteristics for Study PS0009 and PS0008
Characteristic | PS0009 (RS) | PS0008 (SS) | ||||
|---|---|---|---|---|---|---|
PBO/BKZ q.4.w. N = 83 | BKZ q.4.w. N = 321 | USTE N = 163 | BKZ q.4.w./q.8.w. N = 161 | BKZ q.4.w. N = 158 | ADA/BKZ q.4.w. N = 159 | |
Age, years, mean (SD) | 49.7 (13.6) | 45.2 (14.0) | 46.0 (13.6) | 44.0 (13.5) | 45.3 (13.2) | 45.5 (14.3) |
Male, n (%) | 60 (72.3) | 229 (71.3) | 117 (71.8) | 112 (69.6) | 102 (64.6) | 114 (71.7) |
Weight, kg, mean (SD) | 89.1 (26.4) | 88.7 (23.1) | 87.2 (21.1) | 93.2 (24.4) | 89.6 (21.4) | 90.5 (22.1) |
Weight > 100 kg, n (%) | 23 (27.7) | 95 (29.6) | 41 (25.2) | 53 (32.9) | 45 (28.5) | 45 (28.3) |
BMI, kg/m2, mean (SD) | 30.0 (7.6) | 29.6 (7.0) | 29.4 (6.4) | 31.0 (7.7) | 30.2 (6.9) | 30.2 (7.0) |
Race, n (%) | ||||||
White | 63 (75.9) | 237 (73.8) | 120 (73.6) | 140 (87.0) | 140 (88.6) | 141 (88.7) |
Asian | 20 (24.1) | 71 (22.1) | 36 (22.1) | 13 (8.1) | 10 (6.3) | 11 (6.9) |
Black | 0 | 9 (2.8) | 3 (1.8) | 2 (1.2) | 2 (1.3) | 2 (1.3) |
Other | 0 | 4 (1.2) | 4 (2.5) | 6 (3.7) | 6 (3.8) | 5 (3.1) |
PASI score, mean (SD) | 20.1 (6.8) | 22.0 (8.6) | 21.3 (8.3) | 19.9 (6.1) | 20.5 (6.9) | 19.1 (5.9) |
PASI score ≥ 20, n (%) | 29 (34.9) | 151 (47.0) | 60 (36.8) | 66 (41.0) | 64 (40.5) | 51 (32.1) |
IGA score, n (%) | ||||||
2 (mild) | 1 (1.2) | 1 (0.3) | 1 (0.6) | 0 | 0 | 0 |
3 (moderate) | 54 (65.1) | 201 (62.6) | 96 (58.9) | 111 (68.9) | 102 (64.6) | 114 (71.7) |
4 (severe) | 28 (33.7) | 119 (37.1) | 66 (40.5) | 50 (31.1) | 56 (35.4) | 45 (28.3) |
% BSA, mean (SD) | 27.0 (16.3) | 29.0 (17.1) | 27.3 (16.7) | 25.2 (12.4) | 26.5 (15.9) | 25.0 (14.4) |
DLQI total score, mean (SD) | 10.0 (6.8) | 9.9 (6.3) | 11.0 (6.9) | 10.8 (6.2) | 11.1 (6.5) | 10.5 (7.4) |
Duration of disease, years, median (range) | 17.5 (1.2 to 59.0) | 13.7 (0.6 to 57.7) | 15.6 (0.5 to 56.5) | 15.6 (0.6 to 53.5) | 19.5 (0.5 to 56.7) | 14.3 (0.6 to 56.6) |
Prior psoriasis therapy, n (%) | ||||||
Any systemic therapy | 64 (77.1) | 267 (83.2) | 132 (81.0) | 116 (72.0) | 112 (70.9) | 110 (69.2) |
Biologic therapy | 33 (39.8) | 125 (38.9) | 63 (38.7) | 50 (31.1) | 50 (31.6) | 53 (33.3) |
Anti-TNF therapy | 16 (19.3) | 51 (15.9) | 24 (14.7) | 10 (6.2) | 14 (8.9) | 14 (8.8) |
Anti-IL-17 therapy | 18 (21.7) | 76 (23.7) | 38 (23.3) | 37 (23.0) | 33 (20.9) | 35 (22.0) |
Systemic phototherapy or chemopho-totherapy | 38 (45.8) | 141 (43.9) | 73 (44.8) | 52 (32.3) | 59 (37.3) | 62 (39.0) |
ADA = adalimumab; BKZ = bimekizumab; BMI = body mass index; BSA = body surface area; DLQI = Dermatology Life Quality Index; IGA = Investigator's Global Assessment; IL = interleukin; PASI = Psoriasis Area and Severity Index; PBO = placebo; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RS = randomized set; SD = standard deviation; SS = safety set; TNF = tumour necrosis factor; USTE = ustekinumab.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Table 9: Summary of Baseline Characteristics for Study PS0015 and PS0013
Characteristic | PS0015 (RS) | PS013 (RS) | ||
|---|---|---|---|---|
BKZ N = 373 | SECU N = 370 | Placebo N = 86 | BKZ q.4.w. N = 349 | |
Age, years, mean (SD) | 45.9 (14.2) | 44.0 (14.7) | 43.5 (13.1) | 44.5 (12.9) |
Male, n (%) | 251 (67.3) | 235 (63.5) | 58 (67.4) | 255 (73.1) |
Weight, kg, mean (SD) | 90.1 (21.3) | 88.8 (20.0) | 91.7 (22.2) | 88.7 (20.6) |
Weight > 100 kg, n (%) | 109 (29.2) | 87 (23.5) | 28 (32.6) | 88 (25.2) |
BMI, kg/m2, mean (SD) | 30.0 (6.6) | 29.8 (6.0) | 30.4 (7.0) | 29.4 (6.2) |
Race, n (%) | ||||
White | 347 (93.0) | 348 (94.1) | 79 (91.9) | 324 (92.8) |
Asian | 10 (2.7) | 9 (2.4) | 5 (5.8) | 13 (3.7) |
Black | 6 (1.6) | 4 (1.1) | 0 | 6 (1.7) |
Other | 10 (2.7) | 9 (2.4) | 2 (2.3) | 6 (1.7) |
PASI score, mean (SD) | 20.2 (7.5) | 19.7 (6.7) | 20.1 (7.6) | 20.4 (7.6) |
PASI score ≥ 20, n (%) | 140 (37.5) | 135 (36.5) | 29 (33.7) | 132 (37.8) |
IGA score, n (%) | ||||
2 (mild) | 2 (0.5) | 0 | 0 | 0 |
3 (moderate) | 240 (64.3) | 268 (72.4) | 62 (72.1) | 242 (69.3) |
4 (severe) | 131 (35.1) | 102 (27.6) | 24 (27.9) | 107 (30.7) |
% BSA, mean (SD) | 24.8 (15.5) | 23.8 (14.3) | 24.4 (16.0) | 24.6 (15.2) |
DLQI total score, mean (SD) | 10.8 (6.6) | 11.3 (7.2) | 11.3 (6.9) | 10.4 (6.3) |
Duration of disease, years, median (range) | 16.2 (0.5 to 68.8) | 14.8 (0.6 to 65.9) | 16.4 (1.2 to 59.6) | 17.3 (0.7 to 67.5) |
Prior psoriasis therapy, n (%) | ||||
Any systemic therapy | 267 (71.6) | 272 (73.5) | 71 (82.6) | 276 (79.1) |
Biologic therapy | 125 (33.5) | 119 (32.2) | 37 (43.0) | 155 (44.4) |
Anti-TNF therapy | 71 (19.0) | 69 (18.6) | 12 (14.0) | 62 (17.8) |
Anti-IL-17 therapy | 39 (10.5) | 50 (13.5) | 18 (20.9) | 85 (24.4) |
Systemic phototherapy or chemophototherapy | 133 (35.7) | 140 (37.8) | 28 (32.6) | 129 (37.0) |
BKZ = bimekizumab; BMI = body mass index; BSA = body surface area; DLQI = Dermatology Life Quality Index; IGA = Investigator's Global Assessment; IL = interleukin; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RS = randomized set; SD = standard deviation; SECU = secukinumab; TNF = tumour necrosis factor.
Source: Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Interventions
Table 10 provides a summary of the study treatments administered during the initial treatment period (first 16 weeks) and the maintenance or withdrawal period (week 16 up to week 56) of the included studies.
In Study PS0009, patients were randomized to receive placebo, bimekizumab 320 mg SC every 4 weeks, or ustekinumab 45 mg or 90 mg SC at week 0, week 4, and every 12 weeks up to week 52. Weight-based dosing of ustekinumab was used, with patients weighing 100 kg or less receiving 45 mg dose and those more than 100 kg receiving the 90 mg dose. After the 16-week initial treatment period, patients in the placebo group were switched to bimekizumab 320 mg SC every 4 weeks until the end of the trial.
In Study PS0008, patients were randomized to receive bimekizumab 320 mg SC every 4 weeks; bimekizumab 320 mg SC every 4 weeks for 16 weeks, then every 8 weeks; or adalimumab 80 mg SC at week 0, 40 mg at week 1, and 40 mg every 2 weeks until week 24, after which they were switched to bimekizumab 320 mg every 4 weeks until week 56.
In Study PS0015, patients were randomized to bimekizumab 320 mg SC every 4 weeks or secukinumab 300 mg SC at weeks 0, 1, 2, 3, 4, and every 4 weeks up to week 16 (initial treatment period). At 16 weeks, patients in the bimekizumab group were re-randomized to 1 of 2 maintenance dosages: bimekizumab 320 mg every 4 weeks or bimekizumab 320 mg every 8 weeks. Patients in the secukinumab group continued to receive 300 mg every 4 weeks up until week 48. Of note, the re-randomization of the bimekizumab-treated patients at week 16 was implemented after enrolment had started based on Protocol Amendment 1 (October 17, 2018) and was applied only to patients enrolled after the protocol amendment. Patients randomized to bimekizumab before implementation of Protocol Amendment 1 continued to receive every 4 week dosage up until the 48-week study visit.
Study PS0013 randomized patients to receive bimekizumab 320 mg SC every 4 weeks or placebo for the first 16 weeks. At 16 weeks, patients in the bimekizumab group who achieved PASI 90 response were re-randomized to bimekizumab 320 mg every 4 weeks, bimekizumab 320 mg every 8 weeks, or placebo during the 40-week withdrawal period. Patients in the placebo group who achieved a PASI 90 response continued on placebo. At 16 weeks, any patients who had not achieved PASI 90 response entered the escape arm and received open-label bimekizumab 320 mg SC every 4 weeks for 12 weeks. In addition, patients who relapsed at 20 weeks or later were also enrolled in the escape arm and received open-label bimekizumab.
Table 10: Summary of Initial and Maintenance Period Treatments
Study | Initial treatment (week 0 to 16) | Maintenance treatment (week 16 to end of studya) |
|---|---|---|
PS0009 | BKZ q.4.w. | BKZ q.4.w. |
Ustekinumab | Ustekinumab | |
Placebo | BKZ q.4.w. | |
PS0008 | BKZ q.4.w. | BKZ q.4.w. |
BKZ q.4.w. | BKZ q.8.w. | |
Adalimumab | Adalimumab / BKZ q.4.w. (switch at 24 weeks) | |
PS00015 | BKZ q.4.w. | BKZ q.4.w.b |
BKZ q.8.w.b | ||
Secukinumab | Secukinumab | |
PS0013 (withdrawal design) | BKZ q.4.w. | Responder: BKZ q.4.w.c |
Responder: BKZ q.8.w.c | ||
Responder: Placeboc | ||
Nonresponder: open-label BKZ q.4.w. (escape treatment) | ||
Placebo | Responder: Placebo | |
Nonresponder: open-label BKZ q.4.w. (escape treatment) |
Note: Grey shading indicates maintenance dosing that is consistent with Health Canada recommendations.
BKZ = bimekizumab; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks.
aEnd of study was 52 weeks for PS0009, 56 weeks for PS0008, 48 weeks for PS0015, and 56 weeks for PS0013.
bBimekizumab group re-randomized at week 16.
cPatients in the bimekizumab group who achieved a PASI 90 response at week 16 were re-randomized at week 16. Nonresponders at week 16 or those who relapsed at week 20 or later were enrolled in the escape arm of the trial and received open-label bimekizumab every 4 weeks for 12 weeks.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
All the sponsor’s personnel, study investigators, and patients were blinded to the randomized treatment group. The study drug was administered by unblinded study staff who were not otherwise involved in the conduct of the trial. All patients received 1 or 2 SC injections of active study drug and/or placebo at each study visit so that the number and timing of injections were the same for all treatment groups within each study. In all studies, bimekizumab was supplied as a 1 mL pre-filled syringe containing 160 mg/mL solution for SC injection. Pre-filled syringes with placebo contained 1 mL of 0.9% sodium chloride. The active control drugs were commercially available and were supplied as a pre-filled syringes containing 45 mg/0.5 mL ustekinumab in Study PS0009, adalimumab 40 mg/0.8 mL or 40 mg/0.4 mL in Study PS0008, or 150 mg/1 mL secukinumab for Study PS0015. The study drug was administered into the lateral abdominal wall, upper outer thigh, or upper arm in a manner that the syringe could not be seen by the patient (i.e., the patient wore eye coverings or was instructed to turn away during injection).46
Concomitant use of topical moisturizers, over-the-counter shampoos for scalp psoriasis, and mild or low-potency topical steroids were allowed in all studies. The use of mild analgesics were allowed for treatment of arthritis pain, as were nonsteroidal anti-inflammatory drugs, if the dosages were stable before screening. Other treatments for psoriatic arthritis were not allowed. The following medications were prohibited during the trial and were required to be stopped before randomization (with a specific washout period): other topical treatments for psoriasis (2 weeks); systemic non-biologic treatments for psoriasis (e.g., immunosuppressants, systemic steroids, phototherapy) (1 month); anti-TNF biologic drugs (1 to 3 months); anti-IL-17 biologic drugs (3 months); and other biologic or systemic therapies (2 weeks to 12 months, depending on the drug).
Studies PS009, PS0008, and PS0015 had stopping rules for patients who did not respond to the randomized study drug. Patients who had a persistent IGA score of 3 or higher for at least 4 weeks despite continuous treatment with the study drug for a minimum of 12 weeks were considered nonresponders and were withdrawn from the study at 24 weeks (Study PS0009), week 28 (PS0015), or week 36 (PS0008), or any subsequent time points when these criteria were met. Other protocol-defined permanent or temporary stopping criteria that applied to all studies included active tuberculosis or untreated latent tuberculosis, newly diagnosed inflammatory bowel disease or disease flare, active suicidal ideation or behaviour, severe major depression, serious adverse events, and pregnancy. Patients were prohibited from receiving live or live-attenuated vaccines during the studies.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 11. These end points are further summarized below. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 11: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | PS0009 | PS0008 | PS0015 | PS0013 |
|---|---|---|---|---|
Initial treatment period | ||||
Week 16: PASI 90 | Co-primary | Co-primary | Secondary | Co-primary |
Week 16: IGA 0 or 1a | Co-primary | Co-primary | Secondary | Co-primary |
Week 16: PASI 100 | Secondary | Secondary | Primary | Secondary |
Week 4: PASI 75 | Secondary | Secondary | Secondary | Secondary |
Week 12: PASI 90; IGA 0 or 1a | Secondary | NA | NA | NA |
Week 16: Scalp IGA 0 or 1a | Secondary | Other | Other | Secondary |
Week 16: Palmoplantar IGA 0 or 1a | Other | Other | Other | Other |
Maintenance or withdrawal treatment period | ||||
Week 24: PASI 100; PASI 90; IGA 0 or 1a | NA | Secondary | NA | NA |
Week 48: PASI 100 | NA | NA | Secondary | NA |
Week 52: PASI 90; IGA 0 or 1 responsea | Secondary | NA | NA | NA |
Week 56: PASI 90; IGA 0 or 1 responsea | NA | Secondary | NA | NA |
Week 56: PASI 90 among week 16 PASI 90 responders | NA | NA | NA | Secondary |
Week: 56: Relapse | NA | NA | NA | Other |
Multiple time points | ||||
DLQI (change from baseline, proportion with DLQI score of 0 or 1, proportion of patients with at least a 4-point [MID] decrease from baseline) | Other | Other | Other | Other |
EQ-5D VAS (change from baseline) | Other | Other | Other | Secondary |
SF-36 MCS, PCS, individual domains (change from baseline) | Other | Other | NA | Other |
DLQI = Dermatology Life Quality Index; EQ-5D VAS = EuroQol 5-Dimensions visual analogue scale; IGA = Investigator's Global Assessment; MCS = mental component score; MID = minimal important difference; NA = not applicable; PASI = Psoriasis Area and Severity Index; PCS = physical component score; SF-36 = Short Form (36) Health Survey.
aWith at least a 2-category improvement in IGA score from baseline.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Psoriasis Area and Severity Index (PASI)
The PASI is widely used in psoriasis trials to grade the extent and severity of psoriatic lesions. It combines an assessment of the BSA affected in 4 anatomic regions (head, trunk, arms, and legs) and the severity of desquamation, erythema, and plaque induration or infiltration (thickness) in each region. Scores range from 0 to 72 points. In general, a PASI score more than 10 represents more severe disease.47 The percent improvement in PASI score is calculated as the baseline PASI score minus post-baseline PASI score, divided by baseline PASI score, multiplied by 100. Patients with a 75%, 90%, or 100% improvement are categorized as achieving a PASI 75, PASI 90, or PASI 100 response. PASI scores have shown weak to moderate correlation with DLQI scores and good inter-rater and moderate intra-rater reliability.48,49 Responsiveness may be weak, especially when the BSA affected is less than 10%.50,51
In all trials, investigators had documented training on how to perform PASI and IGA assessments, and the same investigator assessed efficacy outcomes for a given patient at all study visits. PASI 90 or PASI 100 response was the primary or co-primary outcome in all 4 studies, and these responses are generally accepted as representing clinically relevant improvements (see Appendix 4). In Study PS0013, relapse was defined as not achieving a PASI 75 response at week 20 or later during the withdrawal period (i.e., among patients who had achieved PASI 90 response at week 16).
Investigator’s Global Assessment (IGA)
The IGA is a composite score of physician assessment of the overall severity of the patient’s psoriatic lesions. The static version of the IGA, which is a measurement of the disease severity at a given time point, was used in all included studies. The investigator assessed the overall severity of psoriasis based on 5-point scale, as described in Table 12. Higher scores indicate a more severe condition.
In 3 studies, the co-primary outcome of IGA response was defined as a IGA score of “clear” or “almost clear” (i.e., 0 or 1), with at least a 2-category improvement from baseline, which is generally accepted as a clinically meaningful score. The same definition was used for separate analyses in the subgroup of patients with scalp or palmoplantar psoriasis who had a baseline IGA score of at least 2 for these areas. The IGA has shown moderate correlation with DLQI, and strong correlation with PASI scores.52,53 The IGA has shown acceptable test-retest reliability,52 but no information on responsiveness was found.
Table 12: Description of Investigator’s Global Assessment Outcome Measure
Score | Short descriptor | Detailed descriptor |
|---|---|---|
0 | Clear | No signs of psoriasis; post-inflammatory hyperpigmentation may be present |
1 | Almost clear | No thickening; normal to pink coloration; no to minimal focal scaling |
2 | Mild | Just detectable to mild thickening; pink to light red coloration; predominantly fine scaling |
3 | Moderate | Clearly distinguishable to moderate thickening; dull to bright red; moderate scaling |
4 | Severe | Severe thickening with hard edges; bright to deep dark red coloration; severe/coarse scaling covering almost all or all lesions |
Source: Clinical Study Report for PS0009.4
Health-Related Quality of Life
The DLQI is a dermatology-specific questionnaire that has been used to assess the impact of the disease on a patient’s HRQoL. It is a 10-item questionnaire that covers 6 domains: symptoms and feeling, daily activities, leisure, work and school, personal relationships, and bother with psoriasis treatment, each assessed over the past week. Each item is scored on a 4-point Likert scale: 0 (not at all affected/not relevant), 1 (a little affected), 2 (a lot affected), and 3 (very much affected). The overall DLQI score is a numeric score between 0 to 30, with lower scores indicating better quality of life.54,55 The final numeric score translates to the effect of the patient’s disease on their quality of life, where 0 to 1 = no effect, 2 to 5 = small effect, 6 to 10 = moderate effect, 11 to 20 = very large effect, and 21 to 30 = extremely large effect.56 The DLQI has shown strong correlation with the EuroQol 5-Dimensions questionnaire (EQ-5D) index score and the bodily pain and social functioning domains of the Short Form 36 Health Survey (SF-36).55 It may, however, lack conceptual validity for the psychological impact of psoriasis. There is evidence of responsiveness and test-retest reliability.54,55 Estimates of the minimal important difference (MID) range from 2.2 to 6.9.55,57 The sponsor defined a 4-point improvement in the DLQI as the MID.
The EuroQol 5-Dimensions 3-Levels questionnaire (EQ-5D-3L) questionnaire is a generic, preference-based, HRQoL measure.58 It includes 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is divided into 3 levels representing “no problems,” “some problems,” and “extreme problems” (1, 2, and 3, respectively). The 5 questions are scored and together contribute to the EQ-5D index (utility) score between 0 and 1, where 0 represents death, and 1 represents perfect health. Different utility functions are available that reflect the preferences of specific populations (e.g., US, UK). The EQ-5D also includes a visual analogue scale (VAS) of the patient’s self-rated health status on a vertical 20 cm scale that ranges from 0 (worst imaginable health status) to 100 (best imaginable health status). Estimates of the MID for the VAS range from 3.8 to 10.3 in patients with psoriasis.55
The SF-36 version 2 is a 36-item, general health status instrument that consists of 8 health domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health.59,60 The SF-36 also provides 2 component summaries, the physical component summary and the mental component summary, derived from aggregating the 8 domains according to a scoring algorithm. All domain and component scores are based on a scale of 0 to 100, with higher scores indicating higher health status. Scores are standardized with a mean of 50 and SD of 10 points in the general US population. The sponsor defined a change of 2 points in the SF-36 physical component score and 3 points in the SF-36 mental component score as the MID, which was consistent with the literature, but are not specific to patients with psoriasis.61
Harms
For the included studies, an adverse event was any untoward medical occurrence that may or may not have a causal relationship with treatment. Serious adverse events included death, any event that was life-threatening or that resulted in significant disability or incapacity, a congenital anomaly, or an important medical event that may have jeopardized the patient, required medical or surgical intervention, or hospitalization. Confirmed active tuberculosis was also reported as a serious adverse event.
The trials pre-specified several adverse events of interest and conducted special monitoring, additional data collection activities and enhanced signal detection activities for the following events: infections (serious, opportunistic, fungal, and tuberculosis), neutropenia, hypersensitivity, suicidal ideation and behaviour, depression, major cardiovascular events, liver function test changes/enzyme elevations, malignancies, and inflammatory bowel diseases. Suicidal ideation and behaviour was assessed using the self-reported electronic Columbia Suicide Severity Rating Scale questionnaire.
Statistical Analysis
Studies PS0019 and PS0013 were designed to test the superiority of bimekizumab versus placebo for the co-primary outcomes of PASI 90 and IGA 0/1 response at week 16. Study PS0008 tested the noninferiority, and then superiority, of bimekizumab versus adalimumab for the co-primary outcomes of PASI 90 and IGA 0/1 response at week 16. Both co-primary outcomes in PS0009, PS0008, and PS0013 had to show a P value of less than 0.05 for noninferiority or superiority to be demonstrated. The primary outcome in PS0015 was PASI 100 response at week 16 for bimekizumab versus secukinumab, which was tested first for noninferiority, then superiority.
The primary and other binomial outcomes in all trials were analyzed using a stratified CMH test, with prior biologic drug exposure and region as stratification factors. Patients with missing data due to early study withdrawal or who had stopped the study drug were imputed as nonresponders. For the primary and secondary outcomes, superiority versus placebo or active control was based on the CMH test P value for general association, with the OR and 95% CI reported based on the Wald test. The assessment of noninferiority of bimekizumab versus ustekinumab, adalimumab, or secukinumab in studies PS0009, PS0008, and PS0015 was established if the lower 97.5% CI for the stratified Mantel-Haenszel absolute risk difference was greater than –10%. The sponsor stated the 10% noninferiority margin was selected because it was considered to be a clinically relevant difference that could influence the choice of treatments. No citations were provided to support the noninferiority margin selected. Of note, the 16-week outcomes comparing bimekizumab to adalimumab in Study PS0008 were analyzed based on the pooled bimekizumab groups, as both groups had received the same bimekizumab dose during the first 16 weeks of the study. Table 13 describes the statistical methods used in the trials and the planned sensitivity analyses.
Table 13: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
PS0009 | |||
PASI 90 response at week 16; IGA response 0 or 1 (with at least a 2 category improvement from baseline) at week 16 Other binary outcomesa | Stratified Cochran-Mantel-Haenszel test (RS) [nonresponder imputation for missing data]b |
|
|
Change from baseline in SF-36 MCS and PCS | ANCOVA (RS) [MI (MCMC/monotone regression) for missing data] |
| NR |
Change from baseline in EQ-5D VAS | Descriptive statistics [MI (MCMC/monotone regression) for missing data] | NA | NA |
PS0008 | |||
PASI 90 response at week 16; IGA response 0 or 1 (with at least a 2 category improvement from baseline) at week 16 Other binary outcomesc | Stratified Cochran-Mantel-Haenszel test (RS) [nonresponder imputation for missing data] b 16-week efficacy outcomes based on the pooled bimekizumab groups vs. adalimumab |
|
|
Change from baseline in SF-36 MCS and PCS | ANCOVA (RS) [MI (MCMC/monotone regression) for missing data] |
| NR |
Change from baseline in EQ-5D VAS | Descriptive statistics [MI (MCMC/monotone regression) for missing data] | NA | NA |
PS0015 | |||
PASI 100 response at week 16 Other binary outcomesd | Stratified Cochran-Mantel-Haenszel test (RS) [nonresponder imputation for missing data] |
|
|
PASI 100 response at week 48 |
|
|
|
Change from baseline in EQ-5D VAS | Descriptive statistics [MI (MCMC/monotone regression) for missing data] | NA | NA |
PS0013 | |||
PASI 90 response at week 16; IGA response 0 or 1 (with at least a 2 category improvement from baseline) at week 16 Other binary outcomes at week 4 to 16d | Stratified Cochran-Mantel-Haenszel test (RS) [nonresponder imputation for missing data]b |
|
|
PASI 90 response at week 56 |
|
|
|
Change from baseline in SF-36 MCS and PCS | ANCOVA (RS) [MI (MCMC/monotone regression) for missing data] |
| NR |
Change from baseline in EQ-5D VAS | Descriptive statistics [MI (MCMC/monotone regression) for missing data] | NA | NA |
ANCOVA = analysis of covariance; EQ-5D VAS = EuroQol 5-Dimensions visual analogue scale; FAS = full analysis set; IGA = Investigator's Global Assessment; LOCF = last observation carried forward; MCMC = Markov Chain Monte Carlo; MCS = mental component score; MI = multiple imputation; NA = not applicable; NR = not reported; NRI = non-responder imputation; PASI = Psoriasis Area and Severity Index; PCS = physical component score; PP = per-protocol; RS = randomized set; SF-36 = Short Form (36) Health Survey.
aPS0009: Sensitivity analyses were performed only for secondary outcomes or those included in the statistical testing hierarchy and were limited to analyses that used multiple imputation for missing data or observed case data.
bLogit methods were used when the CMH test was not possible due to very low response rates.
cPS0008: Sensitivity analyses were performed for secondary outcomes only and were limited to analyses that used multiple imputation for missing data or observed case data. PASI 90 and IGA response at 56 weeks were reported as descriptive statistics only.
dPS0015 and PS0013: Sensitivity analyses were performed for secondary outcomes only and were limited to analyses that used multiple imputation for missing data or observed case data.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
In Study PS0015, the proportion of patients who achieved PASI 100 response at week 48 was analyzed based on 2 populations: first, patients initially randomized to either bimekizumab or secukinumab (regardless of re-randomization of bimekizumab-treated patients at week 16); and, second, patients re-randomized at week 16 to bimekizumab every 4 weeks or every 8 weeks (maintenance set) compared to secukinumab. The COVID-19 pandemic disrupted participation in Study PS0015 for 143 patients (19%) during the last few weeks of the maintenance treatment period, which resulted in some missing data, remote (telephone or video) assessment of outcomes, or out-of-window treatment assessments. Additional sensitivity and subgroup analyses were conducted to determine any the impact of the pandemic on the findings.
For all studies, the pre-planned subgroup analyses of interest to this review included patients with scalp or palmoplantar psoriasis at baseline, prior biologic drug exposure (yes/no), prior systemic therapy (yes/no), and baseline disease severity (PASI < 20, PASI ≥ 20). Of these subgroups, randomization was stratified by prior biologic drug exposure only. Efficacy results by subgroups were reported descriptively, with the exception of scalp IGA at 16 weeks in studies PS0009 and PS0013, which were part of the fixed-sequence statistical testing procedure. No pre-planned subgroup analyses were reported based on prior biologic drug class or by body weight less than 120 kg or 120 kg or more. However, the sponsor provided post hoc pooled data by body weight.
The change from baseline in the EQ-5D VAS was reported descriptively, and no between-group comparisons were reported. The change from baseline in SF-36 mental and physical component scores were analyzed using an analysis of covariance (ANCOVA) model that included covariates for treatment, region, prior biologic drug exposure, and the baseline values. Multiple imputation methods were used to impute missing data (Table 13). The proportion of patients who achieved a DLQI score of 0 or 1 was analyzed using a stratified CMH test, with prior biologic drug exposure and regions as stratification factors. Other analyses of DLQI data have not been summarized in this report.
All studies used a fixed-sequence testing procedure to control the family-wise type I error rate. Superiority was tested based on a 2-sided alpha of 0.05, and noninferiority was tested based on a 1-sided alpha of 0.025 and a 10% noninferiority margin. In studies PS0009, PS0008, and PS0013, both of the co-primary end points had to show statistical significance for the alpha to be passed to the next comparison and for the statistical testing to proceed. Details of the testing procedure and order of testing are presented in Table 14. For any outcomes or subgroup analyses outside of these lists, there was no control of the type I error rate.
Study PS0009 was powered for superiority of bimekizumab versus placebo and ustekinumab for the co-primary outcomes of PASI 90 and IGA 0/1 response at 16 weeks. The planned sample size of 560 patients was based on a 4:2:1 randomization to the bimekizumab, ustekinumab, and placebo groups, respectively, and assumed a 16-week PASI 90 response rate of 75%, 58%, and 2%, and IGA 0/1 response rate of 85%, 68%, and 5%. Response rates were based on data from the bimekizumab phase II study PS001062 and the CLEAR study63 for ustekinumab. The estimated power was greater than 99% for superiority versus placebo for both outcomes, and 95% and 98% for superiority versus ustekinumab for PASI 90 and IGA 0/1, based on 2-sided significance level of 0.05. The study had greater than 99% power for noninferiority of both outcomes, based on a 1-sided significance of 0.025 and a 10% noninferiority margin.
The planned sample size in Study PS0008 was 150 patients per treatment group, assuming PASI 90 and IGA 0/1 response rates of 75% and 85% in the bimekizumab groups and 50% and 68% in the adalimumab group (based on Study PS0010 and VOYAGE-1 and VOYAGE-2 trials).62,64,65 The trial had 97% or higher power to detect a significant difference between the bimekizumab groups and the adalimumab group for each of the co-primary outcomes at 16 weeks (2-sided significance level of 0.05 for superiority). The projected power was greater than 99% for each outcome to test for noninferiority based on a 1-sided significance level of 0.025 and 10% noninferiority margin.
The estimated sample size for Study PS0015 was 700 patients, based on which the study had 98% power to detect the superiority of bimekizumab versus secukinumab for the PASI 100 response at 16 weeks. These estimates assumed a PASI 100 response rate of 60% and 44% for bimekizumab and secukinumab, respectively (based on Study PS001062 and CLEAR63). The study had greater than 99% power for the noninferiority comparison, based on a 10% noninferiority margin.
Study PS0013 had greater than 99% power to detect superiority versus placebo for the co-primary outcomes at 16 weeks. The estimated sample size of 400 patients (randomized 4:1 to bimekizumab and placebo) was based on the same PASI 90 and IGA0/1 response rates as in Study PS0009. No power estimates were provided for outcomes tested during the withdrawal period.
Table 14: Sequence of Statistical Testing
Outcome | Time point (week) | Testing strategy |
|---|---|---|
PS0009 | ||
PASI 90 and IGA response 0 or 1 | 16 | Superiority vs. placebo |
PASI 100 response | 16 | Superiority vs. placebo |
IGA response 0 | 16 | Superiority vs. placebo |
PASI 90 response | 16 | Noninferiority vs. ustekinumab |
IGA response 0 or 1 | 16 | Noninferiority vs. ustekinumab |
PASI 90 response | 16 | Superiority vs. ustekinumab |
IGA response 0 or 1 | 16 | Superiority vs. ustekinumab |
PASI 90 response | 12 | Superiority vs. ustekinumab |
IGA response 0 or 1 | 12 | Superiority vs. ustekinumab |
PASI 75 response | 4 | Superiority vs. placebo |
PASI 75 response | 4 | Superiority vs. ustekinumab |
PSD pain response | 16 | Superiority vs. placebo |
PSD itch response | 16 | Superiority vs. placebo |
PSD scaling response | 16 | Superiority vs. placebo |
Scalp IGA response 0 or 1 | 16 | Superiority vs. placebo |
PASI 90 response | 52 | Superiority vs. ustekinumab |
IGA response 0 or 1 | 52 | Superiority vs. ustekinumab |
PS0008 | ||
PASI 90 and IGA response 0 or 1 | 16 | Noninferiority adalimumab vs. bimekizumab groups combined |
PASI 90 and IGA response 0 or 1 | 16 | Superiority adalimumab vs. bimekizumab groups combined |
PASI 100 response | 16 | Superiority adalimumab vs. bimekizumab groups combined |
PASI 75 response | 4 | Superiority adalimumab vs. bimekizumab groups combined |
PASI 100 response | 24 | Superiority adalimumab vs. bimekizumab groups combined |
PASI 90 response | 24 | Superiority adalimumab vs. bimekizumab groups combined |
IGA response 0 or 1 | 24 | Superiority adalimumab vs. bimekizumab groups combined |
PASI 100 response | 24 | Superiority adalimumab vs. bimekizumab q.4.w. group only |
PASI 90 response | 24 | Superiority adalimumab vs. bimekizumab q.4.w. group only |
IGA response 0 or 1 | 24 | Superiority adalimumab vs. bimekizumab q.4.w. group only |
PS0015 | ||
PASI 100 response | 16 | Noninferiority vs. secukinumab (RS) |
PASI 100 response | 16 | Superiority vs. secukinumab (RS) |
PASI 75 response | 4 | Superiority vs. secukinumab (RS) |
PASI 100 response | 48 | Superiority vs. secukinumab (RS) |
PASI 100 response | 48 | Bimekizumab q.4.w. superiority vs. secukinumab (MS) |
PASI 100 response | 48 | Bimekizumab q.8.w. superiority vs. secukinumab (MS) |
PS0013 | ||
PASI 90 and IGA response 0 or 1 | 16 | Superiority vs. placebo |
PASI 100 response | 16 | Superiority vs. placebo |
IGA response 0 | 16 | Superiority vs. placebo |
PASI 75 response | 4 | Superiority vs. placebo |
PSD pain response | 16 | Superiority vs. placebo |
PSD itch response | 16 | Superiority vs. placebo |
PSD scaling response | 16 | Superiority vs. placebo |
Scalp IGA response 0 or 1 | 16 | Superiority vs. placebo |
PASI 90 response | 56 | Superiority of pooled bimekizumab q.4.w. and q.8.w. groups vs. placebo (among week 16 PASI 90 responders) |
IGA = Investigator's Global Assessment; MS = maintenance set; PASI = Psoriasis Area and Severity Index; PSD = patient symptom diary; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RS = randomized set.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Analysis Populations
In studies PS0009, PS0008, and PS0015, efficacy analyses were based on the randomized set, which included all patients randomized. The maintenance set included all randomized patients who received at least 1 dose of study drug during the maintenance period of these trials.
The efficacy analysis populations in study PS0013 included the randomized set (all patients randomized) and the week 16 responder set (all patients who achieved a PASI 90 response at week 16 and received at least 1 dose of study drug in the withdrawal period). The escape study set included patients who were either nonresponders at week 16 (i.e., did not achieve PASI 90) or who experienced a relapse during the withdrawal period, and had received at least 1 dose of bimekizumab as escape therapy.
In all trials, the safety set included all patients randomized who received at least 1 dose of study drug. Study PS0009 also reported safety data for the active medication set, which included all patients who received at least 1 dose of bimekizumab or ustekinumab. The bimekizumab set in Study PS0008 included all patients who received at least 1 dose of bimekizumab.
Results
Patient Disposition
The number of patients screened ranged from 576 to 1,005, of which 73% to 78% were randomized to 1 of the included studies (Table 15, Table 16, Table 17). The main reason for screening failure was that patients did not meet study eligibility criteria.
During the initial treatment period (first 16 weeks), the proportion of patients who discontinued the study drug ranged from 5% to 11% in the placebo groups, 3% to 5% in the bimekizumab groups, and 4% to 6% in the active control groups. The proportion of discontinuations was generally similar between groups within studies, with the exception of Study PS0009, in which the frequency of study drug discontinuation was higher for placebo (11%) than ustekinumab or bimekizumab (4% and 5%, respectively).
During the maintenance treatment period, the proportion of patients who stopped the study drug ranged from 3% to 11% and was generally similar between groups within trials.
Table 15: Patient Disposition for Study PS0009 and PS0008
Patient disposition | PS0009 | PS0008 | ||||
|---|---|---|---|---|---|---|
Initial treatment perioda | PBO | BKZ q.4.w. | USTE | BKZ q.4.w./q.8.w. | BKZ q.4.w. | ADA |
Screened, N | 735 | 614 | ||||
Randomized, N (%) | 567 (77)b | 478 (78)c | ||||
83 | 321 | 163 | 161 | 158 | 159 | |
Discontinued study drug, N (%) | 9 (11) | 15 (5) | 6 (4) | 7 (4) | 5 (3) | 9 (6) |
Reason for discontinuation, N (%) | ||||||
Adverse events | 6 (7) | 6 (2) | 3 (2) | 2 (1) | 2 (1) | 4 (3) |
Lack of efficacy | 2 (2) | 1 (0.3) | 0 | 0 | 0 | 1 (1) |
Protocol violation | 0 | 0 | 2 (1) | 0 | 0 | 2 (1) |
Lost to follow-up | 0 | 3 (1) | 0 | 0 | 2 (1) | 1 (1) |
Consent withdrawn | 1 (1) | 2 (1) | 1 (2) | 4 (3) | 1 (1) | 1 (1) |
Other | 0 | 3 (1) | 0 | 1 (1) | 0 | 0 |
RS, N (%) | 83 (100) | 321 (100) | 163 (100) | 161 (100) | 158 (100) | 159 (100) |
MS, N (%) | 74 (89) | 306 (95) | 157 (96) | 154 (96) | 153 (97) | 149 (94) |
Safety, N (%) | 83 (100) | 321 (100) | 163 (100) | 161 (100) | 158 (100) | 159 (100) |
Maintenance treatment periodd | PBO/BKZ | BKZ q.4.w. | USTE | BKZ q.4.w./q.8.w. | BKZ q.4.w. | ADA/BKZ |
Started maintenance treatment, N (% of randomized) | 74 (89) | 306 (95) | 157 (96) | 149 (93) | 152 (96) | 149 (94) |
Discontinued study drug, N (%) | 5 (7) | 23 (8) | 16 (10) | 11 (7) | 10 (7) | 17 (11) |
Reason for discontinuation, N (%) | ||||||
Adverse events | 3 (4) | 12 (4) | 4 (3) | 6 (4) | 5 (3) | 6 (4) |
Lack of efficacy | 0 | 1 (0.3) | 4 (3) | 1 (1) | 1 (1) | 1 (1) |
Protocol violation | 1 (1) | 1 (0.3) | 0 | 0 | 0 | 0 |
Lost to follow-up | 0 | 4 (1) | 3 (2) | 0 | 2 (1) | 6 (4) |
Consent withdrawn | 1 (1) | 4 (1) | 4 (3) | 4 (3) | 1 (1) | 4 (3) |
Other | 0 | 1 (0.3) | 1 (1) | 0 | 1 (1) | 0 |
ADA = adalimumab; BKZ = bimekizumab; MS = maintenance set; PBO = placebo; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RS = randomized set; USTE = ustekinumab.
aFirst 16 weeks.
bStudy PS009 reasons for screen failure were as follows: study ineligibility (n = 151, 21%), consent withdrawn (n = 8, 1%), or other (n = 9, 1%)
cStudy PS008 reasons for screen failure were as follows: study ineligibility (n = 123, 20%), consent withdrawn (n = 11, 2%), or other (n = 2, 0.3%)
dWeek 16 to week 52 for Study PS0009; week 16 to week 56 for Study PS0008.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008.5
Table 16: Patient Disposition for Study PS0015
Patient disposition | PS00015 | ||
|---|---|---|---|
Initial treatment perioda | BKZ q.4.w. | SECU | |
Screened, N | 1,005 | ||
Randomized, N (%) | 743 (73)b | ||
373 | 370 | ||
Discontinued study drug, N (%) | 11 (3) | 16 (4) | |
Reason for discontinuation, N (%) | |||
Adverse events | 8 (2) | 6 (2) | |
Lost to follow-up | 0 | 3 (1) | |
Consent withdrawn | 3 (1) | 4 (1) | |
Other | 0 | 3 (1) | |
RS, N (%) | 373 (100) | 370 (100) | |
MS, N (%) | 362 (97) | 354 (96) | |
Safety, N (%) | 373 (100) | 370 (100) | |
Maintenance treatment periodc | BKZ q.4.w./q.8.w. | BKZ q.4.w. | SECU |
Started maintenance treatment, N (% of randomized) | 215 (58) | 147 (39) | 354 (96) |
Discontinued study drug, N (%) | 10 (5) | 9 (6) | 29 (8) |
Reason for discontinuation, N (%) | |||
Adverse events | 2 (1) | 3 (2) | 4 (1) |
Lack of efficacy | 0 | 1 (1) | 4 (1) |
Lost to follow-up | 1 (1) | 2 (1) | 8 (2) |
Consent withdrawn | 7 (3) | 3 (2) | 12 (3) |
Other | 0 | 0 | 1 (0.3) |
BKZ = bimekizumab; MS = maintenance set; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RS = randomized set; SECU = secukinumab.
aFirst 16 weeks.
bStudy PS015 reasons for screen failure were as follows: study ineligibility (n = 247, 25%) or other (n = 15, 2%)
cWeek 16 to week 48.
Source: Clinical Study Report for PS0015.6
Table 17: Patient Disposition for Study PS0013
Patient disposition | PS0013 | |||
|---|---|---|---|---|
Initial treatment perioda | PBO | BKZ q.4.w. | ||
Screened, N | 576 | |||
Randomized, N (%) | 435 (76)b | |||
86 | 349 | |||
Discontinued study drug, N (%) | 4 (5) | 9 (3) | ||
Reason for discontinuation, N (%) | ||||
Adverse events | 0 | 5 (1) | ||
Lack of efficacy | 2 (2) | 1 (0.3) | ||
Lost to follow-up | 1 (1) | 3 (1) | ||
Consent withdrawn | 1 (1) | 0 | ||
Received escape treatment, N (%) | 81 (94) | 23 (7) | ||
RS, N (%) | 86 (100) | 349 (100) | ||
Safety, N (%) | 86 (100) | 349 (100) | ||
Week 16 responder set, N (%) | 1 (1) | 311 (89) | ||
Withdrawal treatment periodc | PBO/ PBO | BKZ q.4.w./PBO | BKZ q.4.w./q.8.w. | BKZ q.4.w. |
Started maintenance treatment, N (% of randomized) | 1 (1) | 105 (30) | 100 (29) | 106 (30) |
Discontinued study drug, N (%) | 0 | 5 (5) | 3 (3) | 5 (5) |
Reason for discontinuation, N (%) | ||||
Adverse events | NA | 3 (3) | 2 (2) | 0 |
Lost to follow-up | NA | 2 (2) | 1 (1) | 2 (2) |
Consent withdrawn | NA | 0 | 0 | 3 (3) |
Received escape treatment, N (%) | NA | 67 (64) | 4 (4) | 7 (7) |
BKZ = bimekizumab; NA = not applicable; PBO = placebo; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RS = randomized set.
aFirst 16 weeks.
bStudy PS013 reasons for screen failure were as follows: study ineligibility (n = 129, 22%), consent withdrawn (n = 7, 1%), or other (n = 5, 1%)
cWeek 16 to week 56.
Source: Clinical Study Report for PS0013.7
Exposure to Study Treatments
During the initial treatment period, the mean duration of study drug exposure was similar between groups and ranged from 106.6 days (SD 19.5) to 110.4 days (SD 8.5) across the studies. The mean study drug exposure for the total treatment period was 321.3 days (SD 76.4) and 337.6 days (SD 74.6) for bimekizumab and ustekinumab groups in study PS0009, and 321.2 days (SD 53.4) and 315.6 days (SD 63.9) for bimekizumab and secukinumab groups in Study PS0015 (Table 18). For the patients who received bimekizumab every 4 weeks or every 8 weeks in Study PS0008, the mean treatment duration during the maintenance period was 270.9 days (SD 34.9) and 265.0 days (SD 50.3), respectively. For the total study period of PS0008, the mean total treatment duration was 230.5 days (SD 119.3) for all patients who received bimekizumab every 4 hours at any point during the trial (including those who were switched from adalimumab to bimekizumab).
For the withdrawal period of Study PS0013, patients who were switched from bimekizumab to placebo had a shorter treatment duration (192.1 days; SD 74.4) than patients who continued on bimekizumab every 4 weeks (260.0 days; SD 57.9) or every 8 weeks (268.7 days; SD 39.8) (Table 19).
Table 18: Treatment Exposure in Studies PS0009, PS0008, and PS0015
Study, treatment group | Initial treatment period (SS) | Total treatment period (SS) | ||
|---|---|---|---|---|
N | Treatment duration (days), mean (SD) | N | Treatment duration, days, mean (SD) | |
PS0009 | ||||
Placebo | 83 | 106.6 (19.5) | NA | NA |
BKZ q.4.w. | 321 | 110.4 (8.5) | 395 | 321.3 (76.4) |
USTE | 163 | 108.2 (16.5) | 163 | 337.6 (74.6) |
PS0008 | ||||
BKZ q.4.w./q.8.w. | 161 | 109.6 (11.9) | 154 | 265.0 (50.3) |
BKZ q.4.w. | 158 | 109.4 (13.1) | 468a | 230.5 (119.3) |
ADA/BKZb | 159 | 109.7 (16.2) | NR | NR |
PS0015 | ||||
BKZ q.4.w. + q.4.w./q.8.w. | 373 | 110.3 (9.5) | 373 | 321.2 (53.4) |
SECU | 370 | 109.7 (11.8) | 370 | 315.6 (63.9) |
ADA = adalimumab; BKZ = bimekizumab; NA = not applicable; NR = not reported; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SD = standard deviation; SECU = secukinumab; SS = safety set; USTE = ustekinumab.
aIncludes bimekizumab q.4.w. study drug taken in all 3 treatment groups.
bPatients in the adalimumab group were switched to bimekizumab after 24 weeks. The mean treatment exposure at 24 weeks was 163.1 days (SD 22.7) for the bimekizumab groups and 162.2 days (SD 28.8) for the adalimumab group.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015.6
Table 19: Treatment Exposure in Study PS0013
Treatment period, treatment group | N | Treatment duration (days), mean (SD) |
|---|---|---|
Initial treatment period (SS) | ||
Placebo | 86 | 107.4 (17.4) |
BKZ q.4.w. | 349 | 110.4 (8.3) |
Withdrawal period (responder set) | ||
BKZ q.4.w./Placebo | 105 | 192.1 (74.4) |
BKZ q.4.w./q.8.w. | 100 | 268.7 (39.8) |
BKZ q.4.w. | 106 | 260.0 (57.9) |
BKZ = bimekizumab; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SD = standard deviation; SS = safety set.
Source: Clinical Study Report for PS0013.7
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. See Appendix 3 for detailed efficacy data.
Skin Clearance or Psoriasis Score
Initial Treatment Period
The key 16-week outcomes for all trials are shown in Table 20 to Table 22. PASI 90 and IGA 0/1 response were co-primary outcomes in studies PS0009, PS0008, and PS0013, and PASI 100 response was the primary outcome in Study PS0015. Patients with missing data were imputed as nonresponders.
In Study PS0009, 85.0% of patients in the bimekizumab group achieved PASI 90 response at 16 weeks compared with 49.7% for ustekinumab and 4.8% for placebo (Table 20). Bimekizumab every 4 weeks demonstrated noninferiority to ustekinumab as the lower limit of the 95% CI for the absolute risk difference exceeded the –10% noninferiority margin (absolute risk difference 35.2%, 95% CI, 27.0% to 43.4%). On a relative scale, bimekizumab was superior to ustekinumab (OR 6.06; 95% CI, 3.87 to 9.47; P < 0.001) and to placebo (OR 99.87; 95% CI, 34.02 to 293.18; P < 0.001). The results for the co-primary outcome of IGA 0/1 response at week 16 showed similar findings (Table 21). At 16 weeks, 84.1%, 53.4%, and 4.8% in the bimekizumab, ustekinumab, and placebo groups, respectively, achieved an IGA score of 0 or 1 (OR 4.81 bimekizumab versus ustekinumab; 95% CI, 3.10 to 7.47; P < 0.001).
Table 20: PASI 90 Response at Week 16 (Randomized Set)
Study / treatment group | Total, N | PASI 90 response at week 16 | BKZ vs. placeboa | BKZ vs. active controla | ||
|---|---|---|---|---|---|---|
n (%) | OR (95% CI), P value | RD (95% CI) | OR (95% CI), P value | RD (95% CI) | ||
PS0009 | ||||||
Placebo | 83 | 4 (4.8) | Reference | Reference | NA | NA |
BKZ q.4.w. | 321 | 273 (85.0) | 99.87 (34.02 to 293.18), P < 0.001 | 79.9 (74.0 to 85.9) | 6.06 (3.87 to 9.47), P < 0.001 | 35.2 (27.0 to 43.4)b |
USTE | 163 | 81 (49.7) | NA | NA | Reference | Reference |
PS0008 | ||||||
BKZ (pooled)c | 319 | 275 (86.2) | NA | NA | 7.46 (4.71 to 11.82), P < 0.001 | 39.3 (30.9 to 47.7)b |
ADA | 159 | 75 (47.2) | NA | NA | Reference | Reference |
PS0015 | ||||||
BKZ q.4.w. | 373 | 319 (85.5) | NA | NA | 2.14 (1.46 to 3.14), P < 0.001d | NR |
SECU | 370 | 275 (74.3) | NA | NA | Reference | Reference |
PS0013 | ||||||
Placebo | 86 | 1 (1.2) | Reference | NR | NA | NA |
BKZ q.4.w. | 349 | 317 (90.8) | 496.32 (82.80 to 2,975.09), P < 0.001 | NR | NA | NA |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval; NA = not applicable; NR = not reported; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RD = risk difference; SECU = secukinumab; USTE = ustekinumab.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
bBimekizumab demonstrated noninferiority to ustekinumab and adalimumab as the lower limit of the 95% CI for the absolute risk difference in the 16-week PASI 90 response exceeded the –10% noninferiority margin.
cPatients randomized to BKZ q.4.w., and to BKZ q.4.w. for 16 weeks, then q.8.w. thereafter, were pooled for the analysis of 16-week outcomes.
dNot adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Table 21: IGA Response (0 or 1) at Week 16 (Randomized Set)
Study / treatment group | Total, N | IGA response (0 or 1) at week 16 | BKZ vs. placeboa | BKZ vs. active controla | ||
|---|---|---|---|---|---|---|
n (%) | OR (95% CI), P value | RD (95% CI) | OR (95% CI), P value | RD (95% CI) | ||
PS0009 | ||||||
Placebo | 83 | 4 (4.8) | Reference | Reference | NA | NA |
BKZ q.4.w. | 321 | 270 (84.1) | 118.76 (36.70 to 384.31), P < 0.001 | 78.9 (72.9 to 84.8) | 4.81 (3.10 to 7.47), P < 0.001 | 30.4 (22.2 to 38.7)b |
USTE | 163 | 87 (53.4) | NA | NA | Reference | Reference |
PS0008 | ||||||
BKZ (pooled)c | 319 | 272 (85.3) | NA | NA | 4.34 (2.79 to 6.77), P < 0.001 | 28.2 (19.7 to 36.7)b |
ADA | 159 | 91 (57.2) | NA | NA | Reference | Reference |
PS0015 | ||||||
BKZ q.4.w. | 373 | 319 (85.5) | NA | NA | 1.64 (1.11 to 2.41), P = 0.012d | NR |
SECU | 370 | 291 (78.6) | NA | NA | Reference | NR |
PS0013 | ||||||
Placebo | 86 | 1 (1.2) | Reference | NR | NA | NA |
BKZ q.4.w. | 349 | 323 (92.6) | 657.3 (105.8 to 4,083.3), P < 0.001 | NR | NA | NA |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval; IGA = Investigator’s Global Assessment; NA = not applicable; NR = not reported; OR = odds ratio; q.4.w. = every 4 weeks; RD = risk difference; SECU = secukinumab; USTE = ustekinumab.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
bBimekizumab demonstrated noninferiority to ustekinumab and adalimumab as the lower limit of the 95% CI for the absolute risk difference in the 16-week IGA 0/1 response exceeded the –10% noninferiority margin.
cPatients randomized to BKZ q.4.w. and to BKZ q.4.w. for 16 weeks, then q.8.w. thereafter, were pooled for the analysis of 16-week outcomes.
dNot adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
The 16-week co-primary outcomes of study PS0008 were analyzed based on the pooled bimekizumab groups, as all patients received bimekizumab every 4 weeks for the initial 16 weeks, as per the statistical analysis plan. The proportion of patients who achieved PASI 90 response at 16 weeks was 86.2% and 47.2% for bimekizumab and adalimumab groups, respectively, and noninferiority was demonstrated (absolute risk difference 39.3%; 95% CI, 30.9% to 47.7%). The OR favoured bimekizumab versus adalimumab, which was statistically significant (OR 7.46; 95% CI, 4.71 to 11.82; P < 0.001). Bimekizumab also demonstrated superiority to adalimumab for the IGA 0 or 1 response at week 16 (85.3% versus 57.2%; OR 4.32; 95% CI, 2.79 to 6.77; P < 0.001).
The withdrawal study, PS0013, reported that 90.8% of patients in the bimekizumab group achieved PASI 90 response at week 16 compared with 1.2% of patients in the placebo group, with an OR of 496.32 (95% CI, 82.8 to 2,975.09; P < 0.001). The results were similar for the co-primary outcome IGA 0/1 response (92.6% versus 1.2%; OR 657.3 for bimekizumab versus placebo; 95% CI, 105.8 to 4,083.3; P < 0.001).
In Study PS0015, 61.7% and 48.9% of patients in the bimekizumab and secukinumab groups, respectively, achieved PASI 100 response at week 16 (primary outcome). The study demonstrated noninferiority of bimekizumab, as the lower limit of the 95% CI for the absolute risk difference exceeded the –10% noninferiority margin (absolute risk difference 12.7%; 95% CI, 5.8% to 19.6%). On the relative scale, the differences favoured bimekizumab versus secukinumab, demonstrating superiority (OR 1.72; 95% CI, 1.27 to 2.31; P < 0.001). At 16 weeks, 85.5% and 74.3% achieved PASI 90 response, and 85.5 and 78.6% achieved IGA 0/1 response in the bimekizumab and secukinumab groups, respectively. Between-group differences favoured bimekizumab versus secukinumab, but these outcomes were not controlled for type I error rate and should be interpreted as evidence supportive of the overall effect of bimekizumab.
In studies PS0009, PS0008, and PS0013, the proportion of patients who achieved PASI 100 response at 16 weeks (secondary outcome) ranged from 58.6% to 68.2% in the bimekizumab groups, compared with 23.9% for adalimumab, 20.9% for ustekinumab, and 0% to 1.2% for placebo groups (Table 22) The between-group differences favoured bimekizumab versus adalimumab and placebo, and all comparisons were statistically significant (P < 0.001). The comparison between bimekizumab and ustekinumab in PS0009 also favoured bimekizumab but was not part of the statistical testing hierarchy to control the type I error rate. Thus, these data should be interpretive as supportive evidence only.
Table 22: PASI 100 Response at Week 16 (Randomized Set)
Study / treatment group | Total, N | PASI 100 response at week 16 | BKZ vs. placeboa | BKZ vs. active controla | |
|---|---|---|---|---|---|
n (%) | OR (95% CI), P value | OR (95% CI), P value | RD (95% CI) | ||
PS0009 | |||||
Placebo | 83 | 0 | Reference | NA | NA |
BKZ q.4.w. | 321 | 188 (58.6) | 25.59 (9.06 to 72.25), P < 0.001 | 5.68 (3.62 to 8.91), P < 0.001b | NR |
USTE | 163 | 34 (20.9) | NA | Reference | NR |
PS0008 | |||||
BKZ (pooled)c | 319 | 194 (60.8) | NA | 4.97 (3.23 to 7.66), P < 0.001 | NR |
ADA | 159 | 38 (23.9) | NA | Reference | NR |
PS0015 | |||||
BKZ q.4.w. | 373 | 230 (61.7) | NA | 1.72 (1.27 to 2.31), P < 0.001 | 12.7 (5.8 to 19.6) |
SECU | 370 | 181 (48.9) | NA | Reference | Reference |
PS0013 | |||||
Placebo | 86 | 1 (1.2) | Reference | NA | NA |
BKZ q.4.w. | 349 | 238 (68.2) | 220.0 (28.8 to 1,683.6), P < 0.001 | NA | NA |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval; NA = not applicable; NR = not reported; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RD = risk difference; SECU = secukinumab; USTE = ustekinumab.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation). Logit method used if CMH test not possible due to low response rates.
bNot adjusted for multiple testing (i.e., the type I error rate has not been controlled).
cPatients randomized to BKZ q.4.w. and to BKZ q.4.w. for 16 weeks, then q.8.w. thereafter, were pooled for the analysis of 16-week outcomes.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
For all studies, the sensitivity analyses for the primary or co-primary outcomes showed findings that were supportive of the primary analyses. The results of the per-protocol set were aligned with the randomized set (intention-to-treat population) and demonstrated noninferiority of bimekizumab versus active controls in studies PS0009, PS0008, and PS0015. Additional analyses of PASI 100 PASI 90, and IGA 0/1 response at week 24 in PS0008 (before adalimumab patients switching to bimekizumab), were comparable to results at week 16 (Appendix 3, Table 37). Across the trials, the proportion of patients who achieved PASI 75 response at week 4 ranged from 71.0% to 76.9% in the bimekizumab groups, 15.3% for ustekinumab, 31.4% for adalimumab, 47.3% in secukinumab, and 1.2% to 2.4% for placebo groups (Appendix 3, Table 38). All comparisons favoured bimekizumab versus active controls or placebo, with P values less than 0.001.
Subgroup data of interest to this review are presented in Appendix 3, Table 39 to Table 43. Descriptive data for PASI 90 or PASI 100 response and IGA 0/1 response at week 16 were generally consistent between subgroups, based on prior biologic therapy (yes/no), prior systemic therapy (yes/no), and baseline PASI score less than 20 versus 20 or higher. No data were available for subgroups based on treatment history according to biologic drug class. The European Public Assessment Report described post hoc subgroup data for patients weighing 120 kg or more that was pooled from studies PS0009, PS0008, and PS0015 (N = 88).12 Patients weighing 120 kg or more who received maintenance dosing of bimekizumab every 4 weeks (N = 51) showed greater improvement in PASI 100 response from week 16 (39.2%) to week 48 (68.6%), compared with patients who received bimekizumab every 8 weeks (week 16: 45.9%; week 48: 51.4%; N = 37).12 Additional sponsor-submitted post hoc subgroup data according to body weight less than 120 kg or 120 kg or more are presented in Appendix 3, Table 44.66
The IGA response for patients with psoriasis of the scalp and palmoplantar regions is described in Appendix 3, Table 39. Across the trials, 84% to 92% of patients in bimekizumab groups achieved an IGA score of 0 or 1 of the scalp at week 16, with at least a 2-point decrease from baseline. The proportion of patients with an IGA 0/1 response of the scalp was 71% for ustekinumab, 67% for adalimumab, 87% for secukinumab, and 7% to 15% for placebo groups. In studies PS0009 and PS0013, the comparison between bimekizumab and placebo for scalp IGA response showed OR point estimates of 37.70 and 158.0, respectively, and P values less than 0.0001, favouring bimekizumab. The between-group difference in scalp IGA response favoured bimekizumab versus ustekinumab and adalimumab in studies PS0009 and PS0008, but these comparisons were not part of the statistical testing hierarchy and should be viewed as supportive evidence. No difference was detected between bimekizumab and secukinumab in terms of scalp IGA 0/1 response at week 16 in Study PS0015.
Across the studies, the proportion who achieved IGA 0/1 response at week 16 for the palmoplantar region was 81% to 94% for bimekizumab groups, 83% for ustekinumab, 71% for adalimumab, 89% for secukinumab, and 24% to 32% for placebo. No between-group comparisons were reported.
Maintenance Treatment Period
In Study PS0009, 81.9% of patients in the bimekizumab group and 55.8% in the ustekinumab group achieved PASI 90 response at week 52, with an OR of 3.80 (95% CI, 2.44 to 5.90; P < 0.001) favouring bimekizumab. IGA 0/1 response was reported for 78.2% and 60.7% in the bimekizumab and ustekinumab groups, respectively (OR 2.41; 95% CI, 1.57 to 3.70; P < 0.001) (Table 23).
Descriptive data were reported at week 56 for Study PS0008 (Table 23). Among patients who remained on bimekizumab every 4 weeks throughout the study, 84.8% and 82.3% achieved PASI 90 and IGA 0/1 response, respectively, at week 56. For patients who received bimekizumab every 4 weeks for 16 weeks, then every 8 weeks thereafter, 82.6% and 83.2% achieved PASI 90 and IGA 0/1 response at week 56, respectively.
Table 23: PASI 90 and IGA Response at Week 52 or 56 for Study PS0009 and PS0008 (Randomized Set)
Study / treatment group | Total, N | PASI 90 response at week 52 or week 56a | IGA response (0 or 1) at week 52 or week 56a | ||
|---|---|---|---|---|---|
n (%) | OR (95% CI), P value | N (%) | OR (95% CI), P value | ||
PS0009 – Week 52 | |||||
BKZ q.4.w. | 321 | 263 (81.9) | 3.80 (2.44 to 5.90), P < 0.001 | 251 (78.2) | 2.41 (1.57 to 3.70), P < 0.001 |
USTE | 163 | 91 (55.8) | Reference | 99 (60.7) | Reference |
PS0008 – Week 56 | |||||
BKZ q.4.w./q.8.w. | 161 | 133 (82.6) | NR | 134 (83.2) | NR |
BKZ q.4.w. | 158 | 134 (84.8) | NR | 130 (82.3) | NR |
ADA/BKZ | 159 | NR | NR | NR | NR |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval; IGA = Investigator’s Global Assessment; NR = not reported; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; USTE = ustekinumab.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008.5
In Study PS0015, PASI 100 response at week 48 was reported by 67.0% of patients initially randomized to bimekizumab 320 mg every 4 weeks, and 46.2% of patients randomized to secukinumab (randomized set N = 743) (Table 24). Based on the randomized set, the between-group difference favoured bimekizumab over secukinumab (OR 2.46; 95% CI, 1.71 to 3.34; P < 0.001). At 16 weeks, patients in the bimekizumab group were re-randomized to 2 maintenance dosages: bimekizumab 320 mg every 4 weeks, or bimekizumab 320 mg every 8 weeks. The 48-week results were reported based on the maintenance set, which included all patients who received at least 1 dose of study drug during the maintenance period (N = 716, 96.4%), according to the 16-week randomized treatment groups. The PASI 100 response at week 48 was 73.5%, 66.0%, and 48.3% in the bimekizumab every 4 weeks, bimekizumab every 4 weeks/every 8 weeks, and secukinumab groups, respectively. The between-group differences favoured bimekizumab versus secukinumab for both the every 4 week maintenance dosage (OR 3.24; 95% CI, 2.10 to 5.00; P < 0.001) and the every 8 week maintenance dosage (OR 2.12; 95% CI, 1.48 to 3.04; P < 0.001).
Table 24: PASI 100 Response at Week 48 for Study PS0015 (Randomized Set and Maintenance Set)
Treatment group | Total, N | PASI 100 response at week 48a | |
|---|---|---|---|
n (%) | OR (95% CI), P value | ||
Randomized set | |||
BKZ q.4.w. | 373 | 250 (67.0) | 2.46 (1.81 to 3.34), P < 0.001 |
SECU | 370 | 171 (46.2) | Reference |
Maintenance setb | |||
BKZ q.4.w./q.8.w. | 215 | 142 (66.0) | 2.12 (1.48 to 3.04), P < 0.001 |
BKZ q.4.w. | 147 | 108 (73.5) | 3.24 (2.10 to 5.00), P < 0.001 |
SECU | 354 | 171 (48.3) | Reference |
BKZ = bimekizumab; CI = confidence interval; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SECU = secukinumab.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
bThe maintenance set included 95.7% of patients initially randomized to secukinumab and 97.1% of patients initially randomized to bimekizumab.
Source: Clinical Study Report for PS0015.6
Withdrawal Treatment Period
In Study PS0013, patients in the bimekizumab group who achieved PASI 90 response at week 16 were re-randomized to switch to placebo or to continue bimekizumab every 4 weeks or 8 weeks. At week 56, 88.8% of patients in the pooled bimekizumab group reported PASI 90 response, compared with 16.2% of patients who switched to placebo (OR 47.41; 95% CI, 22.09 to 101.75; P < 0.001) (Table 25).
Table 25: PASI 90 Response at Week 56 Among Week 16 Responders in Study PS0013 (Responder Set)
Treatment group | Total, N | PASI 90 response at week 56a | |
|---|---|---|---|
n (%) | OR (95% CI), P value | ||
Week 16 responder setb | |||
BKZ q.4.w./placebo | 105 | 17 (16.2) | Reference |
BKZ q.4.w. + q.4.w./q.8.w. (pooled) | 206 | 183 (88.8) | 47.41 (22.09 to 101.75), P < 0.001 |
BKZ = bimekizumab; CI = confidence interval; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
bResponder set included patients who received bimekizumab q.4.w. in the initial treatment period and who achieved a PASI 90 response at week 16 and were re-randomized to bimekizumab q.4.w., bimekizumab q.8.w., or placebo. Data from the 2 bimekizumab groups were pooled for this analysis according to the statistical analysis plan. The responder set included 89.1% of patients initially randomized to bimekizumab.
Source: Clinical Study Report for PS0013.7
Relapse
Patients considered responders at week 16 in PS0013 were followed to assess the proportion who relapsed (i.e., did not achieved PASI 75 response at week 20 or later). At week 56, 77 of 105 patients (73%) who were switched from bimekizumab to placebo had relapsed, compared with 9 of 100 (9%) of patients who received maintenance dosages of bimekizumab every 8 weeks, and 12 of 106 patients (11%) who received bimekizumab every 4 weeks (no between-group statistical testing was reported).
Health-Related Quality of Life
HRQoL measures were defined as “other” outcomes by the sponsor and were not part of the planned statistical testing hierarchy in any of the studies.
Data from the proportion of patients who achieved a DLQI score of 0 or 1 at 16 weeks are summarized in Table 26. A DLQI score of 0 or 1 was considered clinically relevant and has been characterized as the condition having no impact on HRQoL.56 The proportion of patients with a DLQI score of 0 or 1 at 16 weeks |||||||||||||| in the bimekizumab groups than placebo groups in PS0009 |||||||||||||||||||||||||||| and in study PS0013 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| a DLQI score of 0 or 1 in the bimekizumab than the ustekinumab group in PS0009 ||||||||||||||||||||||||||||||||| and for bimekizumab versus adalimumab in PS0008 ||||||||||||||||||||||||||||||||||||||||||||||||||||| However, these differences should be interpreted as supportive evidence due to the inflated family-wise risk of type I error. |||||||||||||||||||||||||||| between bimekizumab and secukinumab in PS0015 ||||||||||||||||||||||||||||||||||||||||||
Table 26: Proportion of Patients With DLQI Score 0 or 1 at Week 16 (RS)
Study / treatment group | Total, N | Proportion with DLQI score 0 or 1a | |
|---|---|---|---|
n (%) | P value | ||
PS0009 | |||
Placebo | 83 | |||||||||||||| | |||||||||||||| |
BKZ q.4.w. | 321 | |||||||||||||| | |||||||||||||| |
USTE | 163 | |||||||||||||| | |||||||||||||| |
PS0008 | |||
BKZ (pooled) | 319 | |||||||||||||| | |||||||||||||| |
ADA | 159 | |||||||||||||| | |||||||||||||| |
PS0015 | |||
BKZ 320 mg q.4.w. | 373 | |||||||||||||| | |||||||||||||| |
SECU | 370 | |||||||||||||| | |||||||||||||| |
PS0013 | |||
Placebo | 86 | |||||||||||||| | |||||||||||||| |
BKZ q.4.w. | 349 | |||||||||||||| | |||||||||||||| |
ADA = adalimumab; BKZ = bimekizumab; DLQI = Dermatology Life Quality Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SECU = secukinumab; USTE = ustekinumab.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Harms
Only those harms identified in the review protocol are reported below. See Table 27 to Table 30 for detailed harms data.
Adverse Events
In Study PS0009, 47%, 56%, and 51% of patients experienced an adverse event in the placebo, bimekizumab, and ustekinumab groups, respectively, during the initial treatment period, and 82% and 80% of patients had an adverse event in the bimekizumab and ustekinumab groups during the total study period (Table 27).
The frequency of events was similar between bimekizumab and adalimumab groups during the first 24 weeks of PS0008 (70% to 72%, respectively) and for the 2 bimekizumab maintenance dosage groups during the total study period (73% and 77%, respectively) (Table 28). Study PS0015 also reported a comparable frequency of adverse events in the bimekizumab (86%) and secukinumab groups (81%) during the total study period, as well as between bimekizumab every 4 weeks and bimekizumab every 8 week dosage groups (81% and 75%, respectively) during the maintenance period (Table 29).
In Study PS0013, 41% of patients in the placebo group and 61% in the bimekizumab group reported an adverse event in the initial treatment period. During the withdrawal period, 69% of patients who were switched from bimekizumab to placebo reported an adverse event, compared with 77% and 74% of patients who remained on bimekizumab (Table 30).
Across the studies, nasopharyngitis, oral candidiasis, and upper respiratory tract infections were the most commonly reported adverse events.
Table 27: Summary of Harms in Study PS0009
Adverse event | Initial treatment period (16 weeks, SS) | Total study period (52 weeks, AMS) | |||
|---|---|---|---|---|---|
Placebo N = 83 | BKZ q.4.w. N = 321 | USTE N = 163 | Total BKZ q.4.w.a N = 395 | USTE N = 163 | |
Total time at risk, PYs | 25.4 | 99.3 | 50.1 | 359.2 | 157.6 |
Patients with ≥ 1 adverse event | |||||
n (%) [IR per 100 PYs] | 39 (47) [238] | 181 (56) [287] | 83 (51) [248] | 323 (82) [221] | 130 (80) [189] |
Most common events,b n (%) | |||||
Nasopharyngitis | 7 (8) | 30 (9) | 14 (9) | 86 (22) | 36 (22) |
Oral candidiasis | 0 | 28 (9) | 0 | 60 (15) | 1 (1) |
Urinary tract infection | 5 (6) | 6 (2) | 2 (1) | 12 (3) | 7 (4) |
Upper respiratory tract infection | 9 (11) | 46 (14) | 22 (14) | 36 (9) | 18 (11) |
Psoriasis | 5 (6) | 3 (1) | 2 (1) | 9 (2) | 2 (1) |
Back pain | 2 (2) | 3 (1) | 4 (3) | 10 (3) | 9 (6) |
Headache | 0 | 11 (3) | 7 (4) | 16 (4) | 10 (6) |
Hypertension | 1 (1) | 7 (2) | 5 (3) | 14 (4) | 10 (6) |
Patients with ≥ 1 SAE | |||||
n (%) | 2 (2) | 5 (2) | 5 (3) | 24 (6) | 13 (8) |
Most common events,c n (%) | |||||
Myocardial infarction | 0 | 1 (0.3) | 0 | 2 (0.5) | 0 |
Patients who discontinued study due to adverse events | |||||
n (%) | 6 (7) | 6 (2) | 3 (2) | 21 (5) | 7 (4) |
Most common events,c n (%) | |||||
Psoriasis | 2 (2) | 0 | 0 | 3 (0.8) | 0 |
Oral candidiasis | 0 | 1 (0.3) | 0 | 3 (0.8) | 0 |
Deaths | |||||
n (%) | 1 (1.2) | 1 (0.3) | 1 (0.6) | 2 (0.5) | 1 (0.6) |
Description of events | Esophageal carcinoma | NA | Heart injury and cardiac arrest | Cardiac arrest (1), unknown cause (1) | NA |
Notable harms | |||||
Notable events, n (%) [IR per 100 PYs] | |||||
Infections and infestations (SOC) | 18 (22) [83] | 111 (35) [137] | 34 (21) [75] | 246 (62) [116] | 83 (51) [74] |
Serious infections | 0 | 0 | 2 (1) | 5 (1) | 4 (3) |
Opportunistic infections | 0 | 5 (2) | 0 | 10 (3) | 0 |
Fungal infections | 0 | 45 (14) | 1 (0.6) | 92 (23) | 4 (3) |
Major adverse cardiovascular events | 0 | 1 (0.3) | 0 | 5 (1.3) | 0 |
Malignancy | 1 (1) | 0 | 0 | 1 (0.3) | 1 (0.6) |
Inflammatory bowel disease | 0 | 1 (0.3) | 0 | 1 (0.3) | 0 |
Hepatic events | 1 (1) | 4 (1) | 0 | 10 (3) | 4 (3) |
Hypersensitivity reactions | 0 | 16 (5) | 10 (6) | 47 (12) | 15 (9) |
Anxiety symptoms | 0 | 1 (0.3) | 0 | 1 (0.3) | 0 |
Depressive disorders | 0 | 2 (0.6) | 1 (0.6) | 2 (0.5) | 2 (1.2) |
Suicidal ideation and behaviour | 0 | 0 | 0 | 1 (0.3) | 1 (0.6) |
Injection-site reactions | 1 (1) | 9 (3) | 2 (1) | 11 (3) | 3 (2) |
AMS = active medication set; BKZ = bimekizumab; IR = incidence rate; NA = not applicable; PY = patient-year; q.4.w. = every 4 weeks; SAE = serious adverse event; SOC = system organ class; SS = safety set; USTE = ustekinumab.
Note: IR reported as the number of patients with treatment-emergent adverse event per 100 PYs follow-up.
aIncludes patients randomized to BKZ and those switched from placebo to BKZ after the first 16 weeks.
bFrequency > 5%.
cReported in 2 or more patients per treatment group.
Source: Clinical Study Report for PS0009.4
Table 28: Summary of Harms in Study PS0008
Adverse event | First 24 weeks (SS) | Total study period (56 weeks. BKZ set)a | |||
|---|---|---|---|---|---|
BKZ q.4.w./q.8.w. N = 161 | BKZ q.4.w. N = 158 | ADA N = 159 | BKZ q.4.w./q.8.w. N = 154 | BKZ q.4.w. N = 468 | |
Total time at risk, PYs | 73.2 | 72.2 | 72.4 | 116.0 | 306.0 |
Patients with ≥ 1 adverse event | |||||
n (%) [IR per 100 PYs] | 116 (72) [310] | 112 (71) [301] | 111(70) [298] | 119 (77) [231] | 343 (73) [262] |
Most common events,b n (%) | |||||
Nasopharyngitis | 27 (17) | 32 (20) | 38 (24) | 28 (18) | 79 (17) |
Oral candidiasis | 19 (12) | 15 (10) | 0 | 17 (11) | 66 (14) |
Upper respiratory tract infection | 12 (8) | 7 (4) | 15 (9) | 13 (8) | 30 (64) |
Pharyngitis | 5 (3) | 4 (3) | 1 (1) | 11 (7) | 13 (3) |
Diarrhea | 5 (3) | 8 (5) | 4 (3) | 5 (3) | 14 (3) |
Hypertension | 9 (6) | 6 (4) | 13 (8) | 4 (3) | 19 (4) |
Patients with ≥ 1 SAE | |||||
n (%) | 1 (1) | 4 (3) | 5 (3) | 8 (5) | 16 (3) |
Patients who discontinued study due to adverse events | |||||
n (%) | 6 (4) | 3 (2) | 5 (3) | 5 (3) | 14 (3) |
Most common events,c n (%) | |||||
Hepatic enzyme increased | 2 (1) | 0 | 1 (1) | 2 (1) | 1 (1) |
Deaths | |||||
n (%) | 0 | 0 | 1 (0.6) | 0 | 0 |
Description of event | NA | NA | Squamous cell carcinoma | NA | NA |
Notable harms | |||||
Notable events, n (%) [IR per 100 PYs] | |||||
Infections and infestations (SOC) | 91 (57) [180] | 79 (50) [155] | 78 (49) [151] | 94 (61) [141] | 261 (56) [145] |
Serious infections | 1 (1) | 0 | 1 (1) | 2 (1) | 6 (1) |
Opportunistic infections | 3 (2) | 1 (1) | 0 | 0 | 7 (2) |
Fungal infections | 26 (16) | 24 (15) | 1 (1) | 27 (18) | 97 (21) |
Major adverse cardiovascular events | 0 | 0 | 0 | 0 | 0 |
Malignancy | 4 (3) | 0 | 1 (1) | 3 (2) | 4 (1) |
Inflammatory bowel disease | 0 | 0 | 0 | 0 | 0 |
Hepatic events | 4 (3) | 3 (2) | 11 (7) | 5 (3) | 13 (3) |
Hypersensitivity reactions | 7 (4) | 9 (6) | 5 (3) | 9 (6) | 35 (8) |
Anxiety symptoms | 0 | 0 | 1 (1) | 1 (0.6) | 2 (0.4) |
Depressive disorders | NR | NR | NR | 0 | 1 (0.2) |
Suicidal ideation and behaviour | 0 | 0 | 0 | 0 | 0 |
Injection-site reactions | 4 (3) | 5 (3) | 4 (3) | 5 (3) | 10 (2) |
ADA = adalimumab; IR = incidence rate; BKZ = bimekizumab; NA = not applicable; PY = patient-year; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SAE = serious adverse event; SOC = system organ class; SS = safety set.
Note: IR reported as the number of patients with treatment-emergent adverse event per 100 PYs follow-up.
aBKZ q.4.w. group includes all events that occurred during BKZ q.4.w. treatment for all 3 randomized treatment groups.
bFrequency > 5%.
cReported in 2 or more patients per treatment group.
Source: Clinical Study Report for PS0008.5
Table 29: Summary of Harms in Study PS0015
Adverse event | Maintenance treatment period (week 16 to 48, MS) | Total study period (48 weeks, SS) | ||
|---|---|---|---|---|
BKZ q.4.w. N = 147 | BKZ q.4.w./q.8.w. N = 215 | BKZ total N = 373 | SECU N = 370 | |
Total time at risk, PYs | 91.1 | 132.7 | 340.4 | 333.3 |
Patients with ≥ 1 adverse event | ||||
n (%) [IR per 100 PYs] | 119 (81) [280] | 162 (75) [251] | 321 (86) [282] | 301 (81) [230] |
Most common events,a n (%) | ||||
Nasopharyngitis | 20 (14) | 33 (15) | 88 (24) | 102 (28) |
Oral candidiasis | 19 (13) | 36 (17) | 72 (19) | 11 (3) |
Upper respiratory tract infection | 8 (5) | 21 (10) | 42 (11) | 36 (10) |
Urinary tract infection | 11 (8) | 10 (5) | 25 (7) | 22 (6) |
Patients with ≥ 1 SAE | ||||
n (%) | 4 (3) | 9 (4) | 22 (6) | 21 (6) |
Most common events,b n (%) | ||||
Atrial fibrillation | 0 | 1 (0.5) | 1 (0.3) | 2 (0.5) |
Appendicitis | 0 | 2 (0.9) | 2 (0.5) | 0 |
Road traffic accident | 0 | 1 (0.5) | 2 (0.5) | 0 |
Patients who discontinued study due to adverse events | ||||
n (%) | 3 (2) | 1 (0.5) | 13 (4) | 10 (3) |
Deaths | ||||
n (%) | 0 | 1 (0.5) | 1 (0.3) | 1 (0.3) |
Description of events | NA | NA | Road traffic accident (non-suicidal) | Asphyxia and aspiration |
Notable harms | ||||
Notable events, n (%) [IR per 100 PYs] | ||||
Infections and infestations (SOC) | 85 (58) [142] | 119 (55) [138] | 253 (68) [140] | 217 (59) [104] |
Serious infections | NR | NR | 8 (2) | 8 (2) |
Opportunistic infections | NR | NR | 4 (1) | 1 (0.3) |
Fungal infections | NR | NR | 108 (29) | 35 (10) |
Major adverse cardiovascular events | NR | NR | 0 | 2 (0.5) |
Malignancy | NR | NR | 5 (1) | 3 (1) |
Inflammatory bowel disease | NR | NR | 1 (0.3) | 1 (0.3) |
Hepatic events | NR | NR | 22 (6) | 21 (6) |
Hypersensitivity reactions | NR | NR | 45 (12) | 35 (10) |
Anxiety symptoms | NR | NR | 3 (1) | 4 (1) |
Depressive disorders | NR | NR | 4 (1) | 2 (0.5) |
Suicidal ideation and behaviour | NR | NR | 1 (0.3) | 0 |
Injection-site reactions | NR | NR | 14 (4) | 7 (2) |
BKZ = bimekizumab; IR = incidence rate; MS = maintenance set; NR = not reported; PY = patient-year; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SAE = serious adverse event; SECU = secukinumab; SOC = system organ class; SS = safety set.
Note: IR reported as the number of patients with treatment-emergent adverse event per 100 PYs follow-up.
aFrequency > 5%.
bReported in 2 or more patients per treatment group.
Source: Clinical Study Report for Clinical Study Report for PS0015.6
Table 30: Summary of Harms in Study PS0013
Adverse event | Initial treatment period (First 16 weeks, SS) | Withdrawal period (Week 16 to 56, responder set) | |||
|---|---|---|---|---|---|
Placebo N = 86 | BKZ q.4.w. N = 349 | BKZ q.4.w./placebo N = 105 | BKZ q.4.w./q.8.w. N = 100 | BKZ q.4.w. N = 106 | |
Total time at risk, PYs | 26.2 | 108.4 | 57.2 | 75.1 | 77.9 |
Patients with ≥ 1 adverse event | |||||
n (%) [IR per 100 PYs] | 35 (41) [177] | 213 (61) [324] | 72 (69) [242] | 77 (77) [225] | 78 (74) [209] |
Most common events,a n (%) | |||||
Nasopharyngitis | 4 (5) | 23 (7) | 20 (19) | 23 (23) | 11 (10) |
Oral candidiasis | 0 | 21 (6) | 6 (6) | 9 (9) | 12 (11) |
Upper respiratory tract infection | 7 (8) | 14 (4) | 5 (5) | 8 (8) | 12 (11) |
Arthralgia | 3 (4) | 4 (1) | 1 (1) | 5 (5) | 3 (3) |
Patients with ≥ 1 SAE | |||||
n (%) | 2 (2) | 6 (2) | 4 (4) | 3 (3) | 5 (5) |
Most common events,b n (%) | |||||
Diarrhea | NR | NR | 0 | 2 (2) | 0 |
Patients who discontinued study due to adverse events | |||||
n (%) | 0 | 3 (1) | 3 (3) | 2 (2) | 0 |
Deaths | |||||
n (%) | 0 | 0 | 0 | 0 | 0 |
Notable harms | |||||
Notable events, n (%) [IR per 100 PYs] | |||||
Infections and infestations (SOC) | 20 (23) [86] | 130 (37) [146] | 46 (44) [118] | 56 (56) [124] | 53 (50) [104] |
Serious infections | 0 | 2 (0.6) | 0 | 0 | 1 (0.9) |
Opportunistic infections | 0 | 5 (1) | 0 | 1 (1) | 2 (2) |
Fungal infections | 2 (2) | 40 (12) | 7 (7) | 14 (14) | 22 (21) |
Major adverse cardiovascular events | 0 | 0 | 0 | 1 (1) | 0 |
Malignancy | 0 | 1 (0.3) | 1 (1) | 0 | 0 |
Inflammatory bowel disease | 0 | 0 | 0 | 0 | 0 |
Hepatic events | 1 (1) | 10 (3) | 0 | 3 (3) | 8 (8) |
Hypersensitivity reactions | 1 (1) | 12 (3) | 3 (3) | 2 (2) | 3 (3) |
Anxiety symptoms | 0 | 3 (0) | 0 | 1 (1) | 0 |
Depressive disorders | NR | NR | 0 | 1 (1) | 0 |
Suicidal ideation and behaviour | 0 | 0 | 0 | 0 | 0 |
Injection-site reactions | 1 (1) | 10 (3) | 0 | 0 | 2 (2) |
BKZ = bimekizumab; IR = incidence rate; NR = not reported; PY = patient-year; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SAE = serious adverse event; SOC = system organ class; SS = safety set; USTE = ustekinumab.
Note: IR reported as the number of patients with treatment-emergent adverse event per 100 PYs follow-up.
aFrequency > 5%.
bReported in 2 or more patients.
Source: Clinical Study Report for PS0013.7
Serious Adverse Events
The frequency of serious adverse events was similar between groups during the initial treatment period and ranged from 1% to 3% across the placebo, bimekizumab, and active control groups. During the withdrawal period of Study PS0013, 3% to 5% of patients who switched from bimekizumab to placebo or who remained on bimekizumab experienced a serious adverse event. For the total study period, serious adverse events were reported by 3% to 6% of patients who received bimekizumab, 8% of patients who received ustekinumab, and 6% who received secukinumab across studies PS0008, PS0009, and PS0015. Specific serious adverse events reported in 2 or more patients in the bimekizumab groups included myocardial infarction, appendicitis, road traffic accident, and diarrhea.
Withdrawals Due to Adverse Events
During the initial treatment period of PS0009, 2% of patients in the bimekizumab and ustekinumab groups discontinued the study due to adverse events, compared with 7% in the placebo group. The frequency of discontinuations was similar for bimekizumab groups (2% and 4%) and adalimumab (3%) during the initial treatment period of PS0008. In Study PS0013, no patients in the placebo group and 1% in the bimekizumab group discontinued due to adverse events during the first 16 weeks, and none to 3% discontinued during the withdrawal period.
The number of patients who discontinued the study due to adverse events during the overall treatment period was generally low across trials and similar between treatment groups within studies PS0009 (bimekizumab 5%, ustekinumab 4%), PS0008 (bimekizumab 3%), and PS0015 (bimekizumab 4%, secukinumab 3%). Specific events that led to discontinuation in 2 or more patients in the bimekizumab groups were psoriasis, oral candidiasis, and increased hepatic enzyme levels.
Mortality
Seven patients died during the 4 studies, including 3 patients (0% to 0.5%) in the bimekizumab groups and 1 patient in each of the ustekinumab, adalimumab, secukinumab, and placebo groups (0% to 1.2%). The cause of death in the bimekizumab-treatment patients was cardiac arrest (PS0009), unknown cause (PS0009), and road traffic accident (PS0015). The cause of death in other groups was esophageal carcinoma (placebo), heart injury and cardiac arrest (ustekinumab), squamous cell carcinoma (adalimumab), and asphyxia and aspiration (secukinumab).
Notable Harms
Infections were a commonly reported adverse event in all studies. No cases of active tuberculosis, systemic fungal infections, or systemic opportunistic infections were reported in any of the trials.
In Study PS0009, the incidence rate of infections was higher in the bimekizumab versus placebo group (137 versus 83 patients with a treatment-emergent adverse event per 100 person-years [PYs]) during the initial treatment period, and higher versus ustekinumab in the overall study period (116 versus 74 patients per 100 PYs). However, the frequency of serious or opportunistic infections was generally low and ranged from 0% to 3% across the treatment groups. More patients in the bimekizumab group reported fungal infections compared with placebo (14% versus 0%; first 16 weeks) and compared with ustekinumab (23% versus 3%; 52 weeks). Oral candidiasis infections were the most common fungal infection reported in the overall study period (bimekizumab 15% versus ustekinumab 1%). Six patients in the bimekizumab group withdrew from the study due to fungal infections, including 1 patient with a serious esophageal candidiasis infection.
The incidence rate of infections ranged from 155 to 180 patients per 100 PYs in the bimekizumab groups compared with 151 patients per 100 PYs in the adalimumab group during the first 24 weeks of PS0008. More patients who received bimekizumab experienced a fungal infection compared with adalimumab (16% versus 1%), of which oral candidiasis was the most commonly reported fungal infection (11% versus 0%). No fungal infections led to study discontinuation. One patient in the bimekizumab and 1 in the adalimumab group experienced a serious infection during the first 24 weeks, and 8 patients who received bimekizumab had a serious infection in the overall study period. The incidence of infections in the overall study period was similar among patients who received bimekizumab every 4 weeks versus every 8 weeks (141 to 145 patients per 100 PYs).
In the total study period of PS0015, the incidence of infections was 140 patients per 100 PYs in the bimekizumab group compared with 104 patients per 100 PYs in the secukinumab group. Fungal infections were reported in 29% versus 10% of patients in the bimekizumab versus secukinumab groups, respectively, including 19% versus 3% of patients reporting oral candidiasis. The frequency of serious infections was 2% per group and of opportunistic infections was 1% or less per group. A skin candidiasis infection led to study discontinuation for 1 patient in the bimekizumab group. During the maintenance period, the incidence of infections was similar in the bimekizumab every 4 weeks and the every 8 weeks dosage groups (138 to 142 patients per 100 PYs).
In the first 16 weeks of study PS0013, the incidence of infections was higher in the bimekizumab group (146 patients per 100 PYs) than in the placebo group (86 patients per 100 PYs). Fungal infections were reported in 12% and 2% of patients, including oral candidiasis in 6% versus 0% of patients in the bimekizumab and placebo groups, respectively. Two patients reported serious infections, and 5 had opportunistic infections in the bimekizumab group, compared with no cases in the placebo group during the initial treatment period. During the maintenance period, the overall frequency of infections was similar between groups, but fungal infections were higher among patients who continued on bimekizumab every 4 weeks (21%) or every 8 weeks (14%) than among those switched from bimekizumab to placebo (7%). No fungal infections led to discontinuation.
Across the trials, the frequency of major adverse cardiovascular events, malignancy, inflammatory bowel disease, psychological adverse events, and injection-site reactions were low and generally similar between groups (0% to 4%).
The proportion of patients who experienced hepatic adverse events ranged from 1% to 3% across groups in PS0009, 3% to 7% in PS0008, 6% per group in PA0015, and 0% to 8% across groups in PS0013.
In the first 16 to 24 weeks, the frequency of hypersensitivity reactions was generally low (bimekizumab 3% to 6%, ustekinumab 6%, adalimumab 3%, placebo ≤ 1%) across the studies. For the total study period, 12% and 9% reported hypersensitivity reactions in the bimekizumab and ustekinumab groups in PS0009, 12% and 10% in the bimekizumab and secukinumab groups of PS0015, and 6% to 8% in the bimekizumab groups of PS0008.
Critical Appraisal
Internal Validity
All 4 clinical trials were conducted using similar study and statistical methods. Patients were allocated to treatments using interactive response technology with randomization stratified by region and history of biologic drug exposure. The baseline patient characteristics were generally well balanced between groups within trials, but in studies PS0009 and PS0008 some differences were observed in the median duration of disease and the proportion of patients with PASI score of 20 or more. However, the clinical expert consulted for this review did not anticipate that the differences noted would bias the results. The drug discontinuation rate was generally low, with 3% to 6% of patients stopping the active study drug in the first 16 weeks (11% in the placebo group in PS0009), and 3% to 11% stopping the study drug in the maintenance phase of the trial (week 16 up to week 56).
All trials were described as double blind, with patients and study personnel involved in patient care or outcome assessment blinded to treatment. Study personnel who prepared and administered the study drugs were not blinded. Patients received a combination of active and placebo pre-filled syringes to ensure that each treatment group received the same number and timing of injections to match the bimekizumab dosage regimens to the active controls or placebo. There were, however, differences in the drug volume administered (0.4 mL to 1 mL) and the appearance of the pre-filled syringes (commercial and non-commercial products). The sponsor indicated that the study drug was administered so that the product could not be seen by the patients (i.e., patients were instructed to turn away at the time of injection or wore eye coverings). This method of blinding could have resulted in patients being aware of their treatment assignment. However, it is uncertain if this introduced any bias into the results.
Statistical analyses for binary outcomes were conducted based on a stratified CMH test, based on stratification factors used during randomization. The between-group comparisons for tests of superiority were reported as OR, however the risk difference may have been more informative clinically. Any patient with missing data was imputed as a nonresponder, which is thought to be a conservative assumption, and most efficacy analyses were based on the intention-to-treat population. Sensitivity analyses were conducted using alternate imputation methods for missing data and other statistical models, and all showed findings similar to the primary analyses. All studies used a fixed-sequence statistical hierarchy to control the family-wise type I error rate for the co-primary and key secondary outcomes.
The primary outcomes were PASI 90 or PASI 100 response and IGA 0/1 response, which are commonly used in clinical trials and generally accepted as representing a clinically important improvement in psoriasis severity. These measures, however, may not correlate with HRQoL or psychological stress caused by the disease. The patient groups who provided input for this submission reported that their psoriasis had negative effects on the patients’ social life, mental health, intimate life, sleep, and work, yet these impacts were not the focus of the trials. Although HRQoL was measured in the trials, these outcomes were outside the statistical testing hierarchy and were not controlled for type I error, which limits the ability to draw conclusions from these data. Moreover, reporting of the results was incomplete, as the absolute or relative between-group differences were not reported, and, for the EQ-5D and SF-36, the extent of missing data was unknown, further limiting the interpretation of these data.
The primary outcomes were measured at 16 weeks in all studies, which provided data on early treatment effects. However, psoriasis is a chronic condition and may require lifelong therapy. The trials reported response data for longer-term outcomes (week 48 to 56), but these data had some limitations. In Study PS0008, there was no longer-term control group, and only descriptive data were available for the 2 bimekizumab maintenance dosage groups at week 56. Although 52-week comparative data were reported for bimekizumab versus ustekinumab in PS0009, the maintenance dosage of bimekizumab (every 4 weeks) was not consistent with Health Canada–recommended dose for most patients (i.e., those with body weight under 120 kg). For study PS0015, patients in the bimekizumab group were re-randomized at week 16 to every 4 or every 8 weeks maintenance regimens. The dose-specific analyses of the 48-week outcomes excluded 4.3% of patients in the secukinumab group and 2.9% in the bimekizumab group who withdrew from the study during the first 16 weeks; thus, randomization was not maintained for all treatment groups. This study did report 48-week PASI 100 response for the intention-to-treat population, but these data were based on the pooled bimekizumab maintenance dosage groups and ignored the change in dose that occurred at week 16. Study PS0013 used a withdrawal design and examined the longer-term response in patients who achieved PASI 90 response at week 16. This adaptive design provides information on the proportion of patients who can maintain response over time (versus those who discontinue therapy) in an enriched patient population.
Subgroup analyses were reported descriptively, with no pre-planned between-group differences tested, with the exception of IGA response for patients with psoriasis of the scalp. Only the analysis based on prior biologic drug exposure had randomization balanced between subgroups. Limited information was available for subgroups based on body weight of 120 kg and more, for which Health Canada, and the European Medicines Agency recommended more frequent maintenance dosage.3,12 No subgroup data were available based on prior IL-17 inhibitor exposure.
In 3 studies, noninferiority was tested based on a 10% noninferiority margin. However, no evidence was provided to support this threshold. Although this is a limitation of the testing of noninferiority, the lower limit of the 95% CI for the risk difference was positive (i.e., excluded the null) and favoured bimekizumab versus active controls.
The safety data available for bimekizumab was limited by the sample size and study duration of the trials, which may have been insufficient to detect infrequent adverse events or those that take a longer time to develop.
External Validity
All trials used similar inclusion and exclusion criteria and enrolled predominantly middle-aged, overweight, White men with a mean PASI of approximately 20 and a rate of previous systemic therapy between 69% and 83%. All studies included study sites in Canada, and 11% to 21% of patients were Canadian. Limited information was available on the 25% of patients who were screened but were not randomized; thus, it is impossible to assess whether the characteristics of these patients were different from those enrolled. Although the clinical expert consulted for this review considered that the patients enrolled would represent patients with moderate to severe psoriasis who may be treated with bimekizumab in Canada, the clinical expert noted that 2 important patient groups were excluded. Specifically, excluding patients with a history of nonresponse to IL-17 inhibitors, or those with nonresponse to more than 1 biologic other than IL-17 inhibitors, may limit the generalizability of the studies. The expert also noted that the trials excluded patients with other types of psoriasis (e.g., erythrodermic, and localized or generalized pustular psoriasis), but dermatologists may use bimekizumab off-label in these patients despite the evidence gap.
The clinical expert stated that the choice of comparators was appropriate, as adalimumab, ustekinumab, and secukinumab are commonly prescribed biologic drugs for psoriasis in Canada. The expert did note that the comparative efficacy of adalimumab and ustekinumab is lower than some other biologic drugs in the IL-17 or IL-23 drug class and that, in clinical practice, adalimumab and ustekinumab are sometimes used in combination with methotrexate to improve treatment response. The concomitant use of topical corticosteroids, phototherapy, or non-biologic systemic drugs were prohibited in all trials. Moreover, the expert indicated that off-label dosage regimens (i.e., increase in the dose or frequency of administration) for biologic drugs such as adalimumab and ustekinumab may be used in patients showing less-than-optimal response. In addition, the expert stated that biologic drugs may be used intermittently in patients who respond well to treatment, with longer intervals between doses than is recommended in the product monographs. Thus, the treatment patterns in the trials may not reflect current practice, which could affect the generalizability of the findings to the real world.
The primary outcomes measured were relevant to patients, but the impacts of treatment on HRQoL were not assessed as key secondary outcomes, thus limiting their interpretation. The RCTs were limited to 56 weeks in duration, which may be considered relatively short for this chronic condition. Moreover, the longer-term data in PS0009 did not reflect the recommended maintenance dosage in Canada and, in PS0015, was not based on the intention-to-treat population. The withdrawal period results of Study PS0013 were based on an enriched population who had responded to bimekizumab. As a result, the 56-week response rate may be inflated relative to an unselected patient population.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The aim of this section was to appraise the indirect evidence used to inform the pharmacoeconomic model and to identify indirect comparisons that fill gaps in the evidence from the systematic review. Although direct evidence is available on the efficacy and safety of bimekizumab versus 3 other biologic response modifiers, comparative efficacy studies versus other biologic drugs of interest were not identified in the systematic literature search.
A focused literature search for ITCs dealing with bimekizumab or plaque psoriasis was run in MEDLINE All (1946–) on September 8, 2021. No limits were applied. The results were reviewed by 1 researcher to select any indirect comparisons that met the patient, intervention, comparator, and outcome criteria listed in the review protocol (Table 6).
Three potentially relevant ITCs were identified in the literature. However, these reports only included data from the phase II study of bimekizumab and thus are missing key evidence to inform the indirect comparison.67-69 Thus, these 3 reports have not been summarized. This section will appraise the sponsor-submitted ITC.18
Description of Indirect Comparison(s)
The sponsor submitted an ITC that evaluated the efficacy of bimekizumab in patients with moderate to severe plaque psoriasis.
Methods of Sponsor-Submitted ITC
Objectives
The objective of the systematic literature review and network meta-analysis (NMA) was to evaluate the efficacy of bimekizumab in the treatment of moderate to severe chronic plaque psoriasis compared with other biologic and non-biologic treatments.
The methods and results for the sponsor-submitted ITC were redacted at the sponsor’s request.
Critical Appraisal of Sponsor-Submitted ITC
The selection of studies to inform the ITC was based on a systematic review of the literature that was performed using standard methods. The authors conducted a search of multiple databases and a limited grey literature search, and used a 2-stage duplicate selection process. The inclusion and exclusion criteria used for screening studies were clear, and the study selection flow chart was reported, but a list of excluded studies was not provided. The scope of the review was comprehensive and included all the biologic drugs approved for use for psoriasis in Canada. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Most of the included studies were rated as having a low risk of bias, and no studies were excluded based on study quality.
The ITC’s authors conducted a feasibility assessment of the patient and trial characteristics to determine whether the trials were sufficiently similar to conduct the NMA. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Multiple methods were used in an attempt to control for this |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Adjusting for the variation in placebo response rates across trials has been endorsed by the National Institute for Health and Care Excellence and others, as the placebo rate and the relative effect versus placebo may be related.70,71 This method assumes that study and patient characteristics that are effect modifiers of the relative treatment effect are also prognostic factors of the outcome with placebo.72,73 ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Prior exposure to biologic drugs has been identified as an important effect modifier for psoriasis, and others have limited networks to more homogeneous subgroups to reduce heterogeneity.74 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Of these, the clinical expert consulted for this review identified disease duration, prior phototherapy or systemic therapy, and prior biologic therapy as the most important potential effect modifiers.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| As a result, it is unclear whether the differences detected for some comparisons were clinically important. Although the ITC states that inconsistency and statistical heterogeneity were examined, no data were reported on these analyses.
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||The analysis was also limited to evaluation of treatment effects for ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Summary
The sponsor submitted an ITC that evaluated the efficacy of bimekizumab in the treatment of moderate to severe chronic plaque psoriasis compared with other biologic and non-biologic treatments. The NMA was based on a systematic review of the literature and data from |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Due to this heterogeneity, the ITC used ||||||||||||||||||||||||||||. However, it is uncertain whether this approach is adequate to control for differences in patient characteristics that may bias results. The ITC did not assess other outcomes of interest to this review and was limited to ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
The open-label extension study PS0014 provides longer-term safety and efficacy data that supplements the evidence from the RCTs in the systematic review.
Long-Term Extension Study
The ongoing, long-term extension study, PS0014 (BE BRIGHT),75 examined the longer-term efficacy and safety data for patients who had completed any of the 3 pivotal studies: PS0008,5 PS0009,4 or PS0013.7 Interim efficacy and safety data for up to the first 48 weeks of the extension study were available in the interim clinical study report (data cut-off June 2020; estimated completion date January 2023),75 and a summary of the data is provided below.
Methods
Patients with moderate to severe plaque psoriasis who had completed study PS0008, PS0009, or PS0013 were eligible to enrol in PS001475: an optional, long-term, open-label extension study to evaluate the efficacy and safety of bimekizumab for up to 144 weeks of treatment. In PS0014, the dosage of bimekizumab (320 mg every 4 weeks or every 8 weeks) was based on patients’ treatment regimens in the pivotal trial as well their PASI response upon entering the extension study. Relevant efficacy outcomes assessed included PASI 90 and PASI 100 response rates, as well as DLQI and IGA 0/1 responses, measurements for which were collected every 4 weeks. Safety assessments consisted of reporting all adverse events, including treatment-emergent adverse events, serious adverse events, as well as adverse events of special interest.
Populations
A total of 1,286 patients were enrolled in the extension study after completing a pivotal trial, of which 903 initially received bimekizumab every 4 weeks and 383 received bimekizumab every 8 weeks. The overall mean age for all participants PS0014 was 45.5 (SD 13.4) years. A majority of all participants were male (71.8%) and White (85.2%). A total of 59.8% had a PASI score less than 20 at baseline, and 79.1% had received prior systemic therapy. In PS0014, at baseline, the mean percentage of BSA affected was 26.4% (SD 15.7%), the mean PASI score was 20.67 (SD 7.46), and all but 2 participants had an IGA score of 3 or more. Overall, the characteristics of patients enrolled in PS0014 were generally consistent with the baseline characteristics of the patients randomized in the pivotal trials. Table 31 has a summary of baseline characteristics of patients enrolled in PS0014.
Table 31: Summary of Baseline Characteristics for Study PS0014 Extension Study (Safety Set Population)
Characteristic | BKZ 320 mg q.4.w. N = 903 | BKZ 320 mg q.8.w. N = 383 |
|---|---|---|
Age, years, mean (SD) | 45.5 (13.2) | 45.2 (13.8) |
Male, n (%) | 658 (72.9) | 265 (69.2) |
Weight, kg, mean (SD) | 90.55 (21.55) | 87.57 (21.11) |
Weight > 100 kg, n (%) | 276 (30.6) | 95 (24.8) |
BMI, kg/m2, mean (SD) | 30.08 (6.63) | 29.24 (6.29) |
Race, n (%) | ||
White | 753 (83.4) | 343 (89.6) |
Asian | 115 (12.7) | 31 (8.1) |
Black | 16 (1.8) | 1 (0.3) |
Other | 19 (2.1) | 8 (2.1) |
PASI score, mean (SD) | 20.64 (7.49) | 20.74 (7.37) |
PASI score ≥ 20, n (%) | 361 (40.0) | 155 (40.5) |
IGA score, n (%) | ||
2 (mild) | 2 (0.2) | 0 |
3 (moderate) | 584 (64.7) | 266 (69.5) |
4 (severe) | 317 (35.1) | 117 (30.5) |
% BSA, mean (SD) | 26.7 (16.4) | 25.7 (14.0) |
DLQI total score, mean (SD) | 10.4 (6.6) | 10.8 (6.3) |
Duration of disease, years, median (range) | 15.7 (0.5 to 59.6) | 16.6 (0.6 to 67.5) |
Prior psoriasis therapy, n (%) | ||
Any systemic therapy | 713 (79.0) | 304 (79.4) |
Biologic therapy | 359 (39.8) | 150 (39.2) |
Anti-TNF therapy | 132 (14.6) | 50 (13.1) |
Systemic phototherapy or chemophototherapy | 362 (40.1) | 161 (42.0) |
BKZ = bimekizumab; BMI = body mass index; BSA = body surface area; DLQI = Dermatology Life Quality Index; IGA = Investigator's Global Assessment; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; SD = standard deviation; TNF = tumour necrosis factor.
Note: Patient characteristics were collected at the baseline of the pivotal studies (PS0009, PS0008, and PS0013).
Source: Clinical Study Report for PS0014.75
Interventions
Allocation to a treatment regimen of either bimekizumab 320 mg every 4 weeks or every 8 weeks was based on patients’ treatment received in the pivotal trial and their PASI score. Patients who received ustekinumab and achieved PASI 90 at the end of the pivotal study were randomized 1:1 to the bimekizumab 320 mg every 4 weeks or every 8 weeks group, while patients who received bimekizumab 320 mg every 4 weeks and achieved PASI 90 at the end of the pivotal study were randomized 4:1 to the bimekizumab 320 mg every 4 weeks or every 8 weeks group. Patients who received ustekinumab, bimekizumab 320 mg every 4 weeks, or bimekizumab 320 mg every 8 weeks and did not achieve PASI 90 response at the end of their pivotal trial were allocated to the bimekizumab 320 mg every 4 weeks group. Figure 6 has a detailed schematic of treatment allocation. Cohort B refers to an additional open-label cohort included as a country-specific amendment in Japan and is not presented in this report.
In PS0014, at week 24, if PASI 90 was achieved among patients receiving bimekizumab 320 mg every 4 weeks, the investigator, at their own discretion, could change the patients’ dosing interval to 320 mg every 8 weeks. If PASI 90 was achieved at week 48, by patients receiving bimekizumab every 4 weeks, the dosage interval was changed by default to every 8 weeks until week 144, unless the investigator decided otherwise, based on medical judgment. During weeks 48 to 144, patients had the option to self-inject bimekizumab at home.
Figure 6: Study Schematic Diagram for PS0014 Extension Study
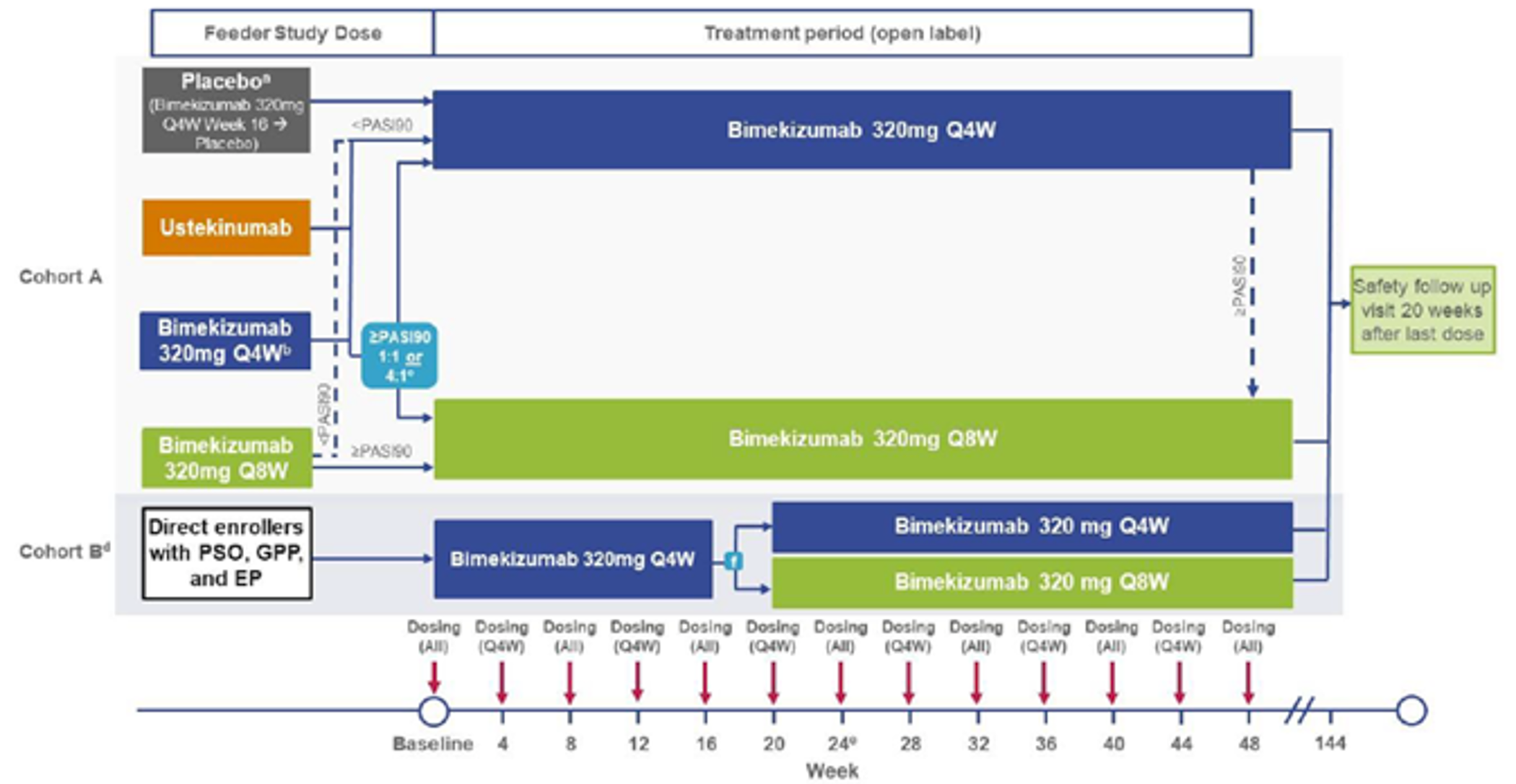
EP = erythrodermic psoriasis; GPP = generalized pustular psoriasis; PASI = Psoriasis Area and Severity Index; PSO = psoriasis; Q4W = every 4 weeks; Q8W = every 8 weeks.
Source: Clinical Study Report for PS0014.75
Outcomes
The efficacy outcomes PASI 90, PASI 100, IGA 0/1, and DLQI 0/1 presented in this section correspond to the currently available pooled data at the 24-week time point for patients enrolled in PS0014. The safety outcomes (treatment-emergent adverse events, serious adverse events, and adverse events of special interest) correspond to pooled harms data through to week 48 for patients enrolled in PS0014.
Statistical Analysis
Efficacy analyses were performed on the full analysis set unless otherwise specified, which included enrolled patients who received at least 1 dose of the study medication and had a valid efficacy measurement for PASI at baseline of a pivotal trial and at baseline of PS0014. For patients in the PS0014 extension study who did not reach, or discontinued before, week 48, only the efficacy data during the participant’s time at risk was considered in the analysis. For the key efficacy variables, including PASI 90, PASI 100, IGA 0/1, and DLQI 0/1, summary tables were provided according to treatment received. Since a majority of patients did not finish extension week 48 at the time of this interim analysis, efficacy data for the first 24 weeks of the extension study are presented. Patients with missing efficacy at week 24 were imputed as nonresponders.
Safety analyses were conducted on the PS0014 treatment group using the safety set (SS), which includes all randomized patients who received at least 1 dose of the assigned study treatment in PS0014. Any adverse event that emerged on or after the extension week 48 dose was not considered a treatment-emergent adverse event. Note that patients could be included in more than 1 treatment group if they switched from bimekizumab 320 mg every 4 weeks to every 8 weeks at week 24.
Patient Disposition
Patient disposition is summarized in Table 32. Of the 1,480 patients randomized into the 3 pivotal trials, 1,286 (87%) enrolled in PS0014. In PS0014, at extension week 24, there were 131 patients in the bimekizumab 320 mg every 4 weeks group who achieved PASI 90 and were switched to bimekizumab every 8 weeks at the investigator’s discretion. Overall, 1,245 patients (96.8%) completed extension week 24; the completion rate was high in the every 4 weeks group (96.7%) and the every 8 weeks group (96.6%). The most frequently reported reason for discontinuation through extension week 24 was an adverse event; this was the case in both the every 4 weeks group (1.4%) and the every 8 weeks group (1.3%). The majority (64.4%) of the patients in PS0014 had not yet completed extension week 48 but remained in the study at the time of the interim report. The most frequently reported primary reason for discontinuation between extension weeks 24 and 48 was consent withdrawn (0.9%) for patients who remained on bimekizumab every 4 weeks, or an adverse event for patients switched from bimekizumab every 4 to every 8 weeks (1.5%), and for those who received bimekizumab every 8 weeks throughout (1.0%). In PS0014, at week 28 onwards, patients on continuous treatment of bimekizumab every 4 weeks or every 8 weeks for at least 12 weeks with a persistent IGA score of 3 or higher over at least a 4-week period were defined as nonresponders.
Table 32: Patient Disposition in PS0014 Extension Study Through Week 48 (Safety Set Population)
Patient disposition | BKZ 320 mg q.4.w./q.4.w. N = 772 | BKZ 320 mg q.4.w./q.8.w.a N = 131 | BKZ 320 mg q.8.w./q.8.w. N = 383 |
|---|---|---|---|
Enrolled | 903 | 383 | |
Discontinued through week 24, n (%) | 30 (3.3) | 15 (3.9) | |
Adverse event | 13 (1.4) | 5 (1.3) | |
Lack of efficacy | 2 (0.2) | 1 (0.3) | |
Protocol violation | 3 (0.3) | 1 (0.3) | |
Lost to follow-up | 6 (0.7) | 3 (0.8) | |
Consent withdrawn | 4 (0.4) | 5 (1.3) | |
Other | 2 (0.2) | 0 | |
Discontinued after week 24 through week 48, n (%) | 15 (1.9) | 3 (2.3) | 5 (1.3) |
Adverse event | 1 (0.1) | 2 (1.5) | 4 (1.0) |
Lack of efficacy | 3 (0.4) | 1 (0.8) | 0 |
Protocol violation | 1 (0.1) | 0 | 0 |
Lost to follow-up | 2 (0.3) | 0 | 0 |
Consent withdrawn | 7 (0.9) | 0 | 1 (0.3) |
Other | 1 (0.1) | 0 | 0 |
BKZ = bimekizumab; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks.
aStudy participants who switched from BKZ q.4.w. to q.8.w. at week 24 were summarized in the q.4.w./q.8.w. group.
Source: Clinical Study Report for PS0014.75
Exposure to Study Treatments
In PS0014, through to week 48, the median duration of treatment exposure was 281.0 days (range 1 to 354 days) for the bimekizumab 320 mg every 4 weeks group and 253.0 days (range 1 to 344 days) for the bimekizumab every 8 weeks group. The total time at risk was 668.0 patient-years for those on bimekizumab 320 mg every 4 weeks and 328.4 patient-years for patients on bimekizumab 320 mg every 8 weeks.
Efficacy
Response rates over time by PS0014 treatment for PASI 90, PASI 100, IGA 0/1, and DLQI 0/1 were provided up to week 24 with nonresponder imputation results, as shown in Table 33. At week 24, 89.2% and 72.7% of patients in the bimekizumab 320 mg every 4 weeks, and 90.1% and 74.9% of patients in the bimekizumab 320 mg every 8 weeks group reported PASI 90 and PASI 100 responses, respectively. Furthermore, IGA 0/1 responses at week 24 were reported among 87.5% and 88.3% of patients for each of the bimekizumab 320 mg every 4 and every 8 weeks groups. High levels of DLQI total score of 0 or 1 were sustained through week 24 for both the every 4 and every 8 weeks groups at 82.5% and 81.2%, respectively. Overall, the treatment response observed up to week 24 was similar among patients who received bimekizumab 320 mg every 4 weeks and every 8 weeks.
Table 33: PASI 90, PASI 100, IGA 0/1, and DLQI 0/1 Response in PS0014 Extension Study Through Week 24 (Full Analysis Set)
Outcome, time point | BKZ 320 mg q.4.w.a N = 902 | BKZ 320 mg q.8.w. N = 383 |
|---|---|---|
PASI 90,b n (%) | ||
Baseline | 776 (86.0) | 380 (99.2) |
Week 4 | 807 (89.5) | 370 (96.6) |
Week 12 | 823 (91.2) | 350 (91.4) |
Week 24 | 805 (89.2) | 345 (90.1) |
PASI 100,c n (%) | ||
Baseline | 602 (66.7) | 313 (81.7) |
Week 4 | 630 (69.8) | 304 (79.4) |
Week 12 | 666 (73.8) | 293 (76.5) |
Week 24 | 656 (72.7) | 287 (74.9) |
IGA 0/1,d n (%) | ||
Baseline | 789 (87.5) | 371 (96.9) |
Week 4 | 797 (88.4) | 360 (94.0) |
Week 12 | 804 (89.1) | 347 (90.6) |
Week 24 | 789 (87.5) | 338 (88.3) |
DLQI 0/1, n (%) | ||
Baseline | 732 (81.2) | 351 (91.6) |
Week 24 | 744 (82.5) | 311 (81.2) |
BKZ = bimekizumab; DLQI = Dermatology Life Quality Index; IGA = Investigator’s Global Assessment; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks.
aStudy patients who started with BKZ 320 mg q.4.w. and who achieved PASI 90 at week 24 could be switched to BKZ 320 mg q.8.w.
bPASI 90 was defined as an improvement (reduction) of at least 90% in the PASI score compared with the baseline measurement in the pivotal trials.
cPASI 100 was defined as an improvement (reduction) of 100% in the PASI score compared with the baseline measurement in the pivotal trials.
dIGA 0/1 response was defined as IGA score of “clear” (0) or “almost clear” (1), with at least a 2-category improvement from the pivotal trial baseline at visit time point. Only patients with an IGA of 2 or greater at the pivotal trial baseline were included.
Source: Clinical Study Report for PS0014.5
Harms
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The summary of treatment-emergent adverse events at the interim analysis are presented in Table 34. The exposure-adjusted incidence rate for treatment-emergent adverse events were |||||||||||||||||||||||||||||||||||||||||| for the bimekizumab every 4 weeks group and every 8 weeks group, respectively. Treatment-emergent adverse events were reported among ||||||||||| of patients in the bimekizumab every 4 weeks group and |||||||||||||| in the bimekizumab every 8 weeks group for infections and infestations. Frequent adverse events reported by at least 5% of patients in 1 or more of the treatment groups were ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The most reported drug-related treatment-emergent adverse event was ||||||||||||||||||||||||||||, which was reported among ||||||||| of patients in the bimekizumab every 4 weeks group and |||||||| of patients in the bimekizumab every 8 weeks group.
|||||||||||||||||||||||||||| had treatment-emergent adverse events leading to death during the study, including ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 34: Summary of Treatment-Emergent Adverse Events in PS0014 Extension Study (Safety Set)
Adverse event | BKZ 320 mg q.4.w.a N = 903 | BKZ 320 mg q.8.w. N = 383 |
|---|---|---|
Total time at risk, PYs | |||||||||||||| | |||||||||||||| |
Any TEAEs, n (%) | |||||||||||||| | |||||||||||||| |
Infections and infestations | |||||||||||||| | |||||||||||||| |
Fungal infections | |||||||||||||| | |||||||||||||| |
Serious TEAEs | |||||||||||||| | |||||||||||||| |
Study participant discontinuations due to TEAEs | |||||||||||||| | |||||||||||||| |
Drug-related TEAEs | |||||||||||||| | |||||||||||||| |
Severe TEAEs | |||||||||||||| | |||||||||||||| |
All deaths (AEs leading to death) | |||||||||||||| | |||||||||||||| |
BKZ = bimekizumab; PY = patient-year; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; TEAE = treatment-emergent adverse event.
aStudy patients who switched from q.4.w. to q.8.w. at week 24 appear in both columns.
Source: Clinical Study Report for PS0014.5
Critical Appraisal
Limitations of the pooled results of the extension study include the absence of an active comparator or placebo group. As with most extension studies, an additional limitation is the open-label study design; unblinding of the study drugs in the extension phase can bias the reporting of end points, particularly any subjective measures included in the PASI score and adverse events. As only descriptive statistics were published in this interim report, and there are no comparator groups, the interpretation of the results is limited. Since completion of a pivotal trial was an eligibility criterion for the extension study, patients who discontinued those trials due to adverse events or death were excluded. This could result in a population of patients that were more tolerant of bimekizumab, which can lead to a response bias, since those not responding to treatment are less likely to continue. Having patients more tolerant of bimekizumab can also lead to biased estimates related to adverse events, potentially resulting in fewer adverse events being reported. The lack of systematic follow-up after discontinuation of bimekizumab in the extension study could have missed important information regarding the long-term effects of the treatment. In addition, not all patients received a maintenance dosing regimen that was consistent with Health Canada recommendations.
Discussion
Summary of Available Evidence
The systematic review included 4 multi-centre, double-blind RCTs that evaluated the safety and efficacy of bimekizumab in patients with moderate to severe plaque psoriasis who were candidates for systemic therapy or phototherapy (studies PS0009, PS0008, PS0015, and PS0013). Three trials used a parallel design, and the fourth (PS0013) was a randomized withdrawal study. The studies randomized 435 to 743 patients to receive bimekizumab compared with placebo, ustekinumab, adalimumab, or secukinumab for up to 48, 52, or 56 weeks. The dose of bimekizumab was either 320 mg SC every 4 weeks or 320 mg every 4 weeks for the first 16 weeks and then every 8 weeks thereafter. In study PS0013, bimekizumab-treated patients who achieved a PASI 90 response at week 16 were randomized to switch to placebo or to continue bimekizumab every 4 weeks or every 8 weeks. In 3 trials, the co-primary outcomes were the proportion of patients who achieved a PASI 90 response and the proportion who achieved an IGA score of 0 or 1 (with at least a 2-point change from baseline) at week 16. The primary outcome in Study PS0015 was the proportion of patients who achieved a PASI 100 response at week 16.
The mean age of the patients enrolled ranged from 43.5 years (SD 13.1) to 49.7 years (SD 13.6) across treatment groups in the 4 trials. Most patients were male (64% to 73%) and White (74% to 94%), with psoriasis that was rated as moderate in severity based on their IGA score (59% to 72%). Most patients (69% to 83%) had received prior systemic therapy, which included prior biologic therapy for 31% to 44% of patients and prior IL-17 therapy for 11% to 24% of patients.
Additional data that informed the submission included the ITC submitted by the sponsor and interim results from the open-label extension study PS0014. The ITC evaluated the PASI response at week 10 to 16 for bimekizumab versus other biologic and non-biologic systemic therapies. Study PS0014 provided longer-term efficacy and safety data for the 1,286 patients enrolled.
Interpretation of Results
Efficacy
Across all 4 RCTs, bimekizumab met the primary outcomes and demonstrated superiority to placebo, ustekinumab, adalimumab, and secukinumab in terms of PASI 90 and IGA 0/1 response or PASI 100 response at week 16. The absolute risk difference for bimekizumab versus ustekinumab or adalimumab for the proportion of patients with PASI 90 response at week 16 was 35% and 39%, respectively, and for the proportion with IGA 0/1 response at week 16 was 30% and 28%, respectively. For the comparison between bimekizumab and secukinumab, the absolute risk difference for PASI 100 response at week 16 was 13%. The secondary outcome of PASI 75 response at week 4 was also supportive of a benefit with bimekizumab versus placebo or active comparators. The PASI 75, PASI 90, PASI 100, or IGA 0/1 response outcome measures are generally accepted as representing clinically important improvements in psoriasis severity. The clinical expert consulted for this review considered the between-group differences clinically relevant. Although the expert stated that adalimumab and ustekinumab are commonly prescribed in Canada and were relevant comparators, the expert did note that the relative efficacy of these drugs is lower than some other IL-17 or IL-23 biologics available in Canada. Moreover, adalimumab and ustekinumab are sometimes used in combination with methotrexate, or at an increased dose (off-label) to improve the treatment response. In all studies, dose increases and concomitant use of topicals or non-biologic systemic drugs were prohibited. Thus, the treatment patterns in the trials may not reflect current practice, which could affect the generalizability of the findings to the real world.
In the longer term, the PASI and IGA response rates appear to be maintained up to 56 weeks in the RCTs, favouring bimekizumab versus ustekinumab in PS0009 and versus secukinumab in PS0015. Although none of the studies were designed to test for differences between the 2 maintenance dosages of bimekizumab, the efficacy of the 2 regimens appears to be similar. The Health Canada–recommended maintenance dosage of bimekizumab is 320 mg every 8 weeks for most patients, with more frequent dosing suggested for patients who weigh at least 120 kg and who do not achieve a complete response at 16 weeks.3 The available data for patients who weigh at least 120 kg, however, were limited. Interpretation of longer-term results should consider the lack of a control group in PS0008, failure to maintain randomization for the maintenance set analysis of PS0015, and use of a non-approved bimekizumab maintenance dosage in PS0009.
The 56-week outcomes in the randomized withdrawal study (PS0013) were restricted to patients with a demonstrated response to treatment at week 16 and thus represent an enriched population. This study showed that patients who remained on bimekizumab were more likely to show a PASI 90 response at week 56 than patients switched to placebo. The enrichment design may affect the external validity of the findings, and the 56-week response rate observed with bimekizumab may be inflated relative to an unselected patient population.
The interim efficacy results for the first 24 weeks in the extension study, PS0014, showed PASI and IGA response rates that were generally comparable to those observed at the end of the pivotal trials. These results suggest that treatment effects with bimekizumab may be maintained for up to 1.5 years among patients who had shown early tolerance and response to treatment. Although the efficacy data for the extension study were reported using nonresponder imputation for missing data, the potential for selection and reporting bias and the lack of a control group should be considered when interpreting these findings.
Patient input received by CADTH for this review indicates that psoriasis can have a substantial impact on HRQoL and may affect patients’ personal relationships, mental health, and work. Data on HRQoL were measured in the studies using the DLQI, EQ-5D, and SF-36. However, these data had several limitations. Reporting of the results was incomplete, as the absolute or relative between-group differences were not reported, and the extent of missing data was unknown for some analyses. Moreover, these outcomes were outside the statistical testing hierarchy and were not controlled for type I error. The available data on DLQI suggest that bimekizumab may be associated with short-term benefits in HRQoL versus placebo, adalimumab, or ustekinumab, but not secukinumab. However, these data should be interpreted as supportive evidence due to the lack of control of multiplicity and the risk of inflated type I error rate.
To supplement the direct comparative evidence for bimekizumab, and to inform the pharmacoeconomic model, the sponsor submitted an ITC that evaluated the efficacy of bimekizumab in the treatment of moderate to severe chronic plaque psoriasis compared with other biologic and non-biologic treatments. The NMA was based on a systematic review of the literature, and data from 86 RCTs were used to inform the random-effects, Bayesian multinomial, placebo-adjusted model. The NMA results favoured bimekizumab versus all other biologics approved in Canada in terms of PASI 90 and PASI 100 response at weeks 10 to 16, with a 95% credible interval that excluded the null. Several sources of heterogeneity were noted across trials, including comorbid psoriatic arthritis, prior exposure to biologics or other non-biologic therapies, region, duration of disease, study years, timing of the outcome assessment, and placebo response rate. Due to this heterogeneity, the ITC used a placebo-adjusted model. However, it is uncertain whether this approach is adequate to control for differences in patient characteristics that may bias results. Moreover, the base-case results were reported as probit differences, which can be difficult to interpret clinically. Thus, it is unclear whether some of the between-group differences reported were clinically important. The ITC did not assess other outcomes of interest to this review and was limited to PASI response during the induction period. Thus, data are lacking on comparative safety and impacts on HRQoL.
Harms
The frequency of adverse events was generally similar between groups within the RCTs, with the exception of study PS0013, in which more patients who received bimekizumab reported adverse events than the placebo group during the initial treatment period (61% versus 41%). Across the studies, infections were the most commonly reported adverse events, specifically fungal infections. The bimekizumab groups reported a higher frequency of fungal infections than comparators in all trials. This included secukinumab, another IL-17 inhibitor, with 29% versus 10% of patients in the bimekizumab and secukinumab groups, respectively, reporting fungal infections in study PS0015. Oral candidiasis was the most commonly reported fungal infection, and no patients experienced a systemic fungal infection, although some fungal infections led to discontinuation. Overall, the frequency of serious infections was low (0% to 3%) and generally similar between groups within studies.
The frequency of adverse events was generally similar between bimekizumab groups that received maintenance doses every 4 weeks, compared with every 8 weeks, except for fungal infections in PS0013, in which the data suggest that the frequency may be higher among patients who received bimekizumab every 4 weeks than every 8 weeks.
Serious adverse events were reported by 3% to 6% of patients who received bimekizumab, and 6% to 8% of patients who received secukinumab or ustekinumab, during the total study period of PS0008, PS0009, and PS0015. Seven patients died during the 4 studies, including 3 patients in the bimekizumab groups, and 1 patient in each of the ustekinumab, adalimumab, secukinumab, and placebo groups.
The number of patients who discontinued the study due to adverse events was generally low across trials and similar between treatment groups within studies during the overall treatment period (3% to 5%) or withdrawal period (0% to 3%) of the RCTs.
Of the adverse events of interest listed in this review’s protocol, no specific safety signals were observed with bimekizumab, as the frequency of these adverse events were generally low and similar between groups. However, the sample size and duration of the pivotal trials was likely insufficient to detect infrequent adverse events or those that take a longer time to develop.
No new safety signals were detected based on the 48-week interim results from the extension study PS0014. Infections, specifically fungal infections, were commonly reported among those who received open-label bimekizumab every 4 or 8 weeks. The indirect comparison ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Conclusions
Bimekizumab showed statistically and clinically important improvement in psoriasis disease severity versus placebo, adalimumab, ustekinumab, and secukinumab, measured as PASI 90, IGA response, or PASI 100 response at week 16, among patients with moderate to severe plaque psoriasis who were candidates for phototherapy or systemic therapy. The 1-year data suggest that PASI response may be maintained in the majority of patients who continue bimekizumab therapy, with between-group differences that favour bimekizumab versus secukinumab or ustekinumab.
Short-term data suggest that patients who receive bimekizumab may be more likely to show improvements in HRQoL (measured using the DLQI) than those who receive placebo, adalimumab, and ustekinumab, but not secukinumab. However, HRQoL outcomes were outside the statistical testing procedure and should be interpreted as supportive evidence in view of the inflated risk of type I error.
The indirect evidence suggests that bimekizumab |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Several sources of heterogeneity were identified across the trials included in the ITC, and it is uncertain whether the methods used to control for potential bias were adequate, or whether the between-group differences for some comparisons were clinically important.
Infections were among the most commonly reported adverse events, and fungal infections were reported more frequently among patients who received bimekizumab than comparators. The incidence of serious adverse events or withdrawals due to adverse events was low among patients who received bimekizumab, and no new safety signals were identified in the interim extension study data. However, the RCTs were not designed or powered to detect rare adverse events or those with a longer lag time, and longer-term comparative safety data are lacking.
References
1.Feldman S. Psoriasis: epidemiology, clinical manifestations, and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2019: www.updodate.com. Accessed 2021 Oct 29.
2.Canadian Dermatology Association. Psoriasis. 2021: https://dermatology.ca/public-patients/skin/psoriasis/. Accessed 2021 Oct 29.
3.Bimzelx (bimekizumab): 160 mg/mL solution subcutaneous injection [product monograph]. Oakville (ON): UCB Canada Inc; 2022 Feb 14.
4.Clinical Study Report: PS0009 (BE VIVID). A phase 3, multicenter, randomized, double-blind, placebo-and active comparator-controlled, parallel-group study to evaluate the efficacy and safety of bimekizumab in adult subjects with moderate to severe chronic plaque psoriasis [internal sponsor's report]. Brussels (BE): UCB Biopharma SRL; 2020 Aug 27.
5.Clinical Study Report: PS0008 (BE SURE). A phase 3, multicenter, randomized, double-blind study with an active-controlled initial treatment period followed by a dose-blind maintenance treatment period to evaluate the efficacy and safety of bimekizumab in adult subjects with moderate to severe chronic plaque psoriasis [internal sponsor's report]. Brussels (BE): UCB Biopharma SRL; 2020 Sep 28.
6.Clinical Study Report: PS0015 (BE RADIANT) (interim). A phase 3, multicenter, double-blind, placebo-controlled study to evaluate the efficacy and safety of bimekizumab in adult subjects with moderate to severe chronic plaque psoriasis [internal sponsor's report]. Brussels (BE): UCB Biopharma SRL; 2020 Oct 21.
7.Clinical Study Report: PS0013 (BE READY). A phase 3, multicenter, double-blind, placebo-controlled study with initial treatment period followed by a randomized-withdrawal period to evaluate the efficacy and safety of bimekizumab in adult subjects with moderate to severe chronic plaque psoriasis [internal sponsor's report]. Brussels (BE): UCB Biopharma SRL; 2020 Sep 28.
8.Baluvelt A, Ehst BD. Pathophysiology of plaque psoriasis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2019: www.uptodate.com. Accessed 2021 Oct 29.
9.Dowlatshahi EA, Wakkee M, Arends LR, Nijsten T. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: a systematic review and meta-analysis. J Invest Dermatol. 2014;134(6):1542-1551. PubMed
10.Menter A, Strober B, Kaplan D, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2019;80(4):1029-1072. PubMed
11.Eder L, Widdifield J, Rosen CF, et al. Trends in the prevalence and incidence of psoriasis and psoriatic arthritis in Ontario, Canada: a population-based study. Arthritis Care Res (Hoboken). 2019;71(8):1084-1091. PubMed
12.Committee for Medicinal Products for Human Use. Assessment report: Bimzelx (bimekizumab). (European public assessment report). Amsterdam (NL): European Medicines Agency; 2021 Jun 24: https://www.ema.europa.eu/en/documents/assessment-report/bimzelx-epar-public-assessment-report_en.pdf. Accessed 2021 Sept 21.
13.Levy AR, Davie AM, Brazier NC, et al. Economic burden of moderate to severe plaque psoriasis in Canada. Int J Dermatol. 2012;51(12):1432-1440. PubMed
14.Mrowietz U, Barker J, Boehncke WH, et al. Clinical use of dimethyl fumarate in moderate-to-severe plaque-type psoriasis: a European expert consensus. J Eur Acad Dermatol Venereol. 2018;32 (Suppl 3):3-14. PubMed
15.Petrella RJ GV, Luciani L, Barbeau M. Characteristics of chronic plaque psoriasis in Canada: a retrospective database study. Value Health. 2014;17(3):PA284.
16.Canadian Psoriasis Guidelines Addendum Committee. 2016 addendum to the Canadian guidelines for the management of plaque psoriasis 2009. J Cutan Med Surg. 2016;20(5):375-431. PubMed
17.Canadian Psoriasis Guidelines Committee. Canadian guidelines for the management of plaque psoriasis. Ottawa (ON): Canadian Dermatology Association; 2009.
18.Drug Reimbursement Review sponsor submission: Bimzelx (bimekizumab), 160 mg/mL subcutaneous injection [internal sponsor's package]. Oakville (ON): UCB Canada Inc; 2021 Aug 17.
19.Cosentyx (secukinumab): 150 mg/mL solution for injection, powder for solution for injection [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2021 May 26: https://pdf.hres.ca/dpd_pm/00061115.PDF. Accessed 2021 Oct 15.
20.Hadlima (adalimumab): 40 mg in 0.8 mL sterile solution (50 mg/mL), pre-filled syringe for subcutaneous injection [product monograph]. Kirkland (QC): Organon Canada Inc; 2021 Aug 19: https://pdf.hres.ca/dpd_pm/00062608.PDF. Accessed 2021 Oct 15.
21.Humira (adalimumab): 40 mg in 0.8 mL sterile solution (50 mg/mL), 10 mg in 0.1 mL sterile solution (100 mg/mL), 20 mg in 0.2 mL sterile solution (100 mg/mL), 40 mg in 0.4 mL sterile solution (100 mg/mL), 80 mg in 0.8 mL sterile solution (100 mg/mL), subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2021 Apr 21: https://pdf.hres.ca/dpd_pm/00061690.PDF. Accessed 2021 Oct 15.
22.Ilumya (tildrakizumab): 100 mg / 1 mL solution (100 mg/mL) for subcutaneous injection [product monograph]. Burlington (ON): C.R.I.; 2021 May 19: https://pdf.hres.ca/dpd_pm/00060995.PDF. Accessed 2021 Oct 15.
23.Inflectra (infliximab): 100 mg/vial, powder for solution, lyophilized, intravenous infusion [product monograph]. Kirkland (QC): Pfizer Canada Inc; 2020 Jul 6: https://pdf.hres.ca/dpd_pm/00057004.PDF. Accessed 2021 Oct 15.
24.Remicade (infliximab): 100 mg/vial powder for solution, sterile, lyophilized [product monograph]. Toronto (ON): Janssen Inc; 2021 Apr 1: https://pdf.hres.ca/dpd_pm/00060595.PDF. Accessed 2021 Oct 15.
25.Renflexis (Infliximab): 100 mg /vial powder for solution, sterile, lyophilized [product monograph]. Kirkland (QC): Merck Canada Inc.; 2020 Feb 25: https://pdf.hres.ca/dpd_pm/00055165.PDF. Accessed 2021 Oct 15.
26.Siliq (brodalumab): 140 mg/mL solution for subcutaneous injection [product monograph]. Laval (QC): Bausch Health, Canada Inc; 2019 Jun 7: https://pdf.hres.ca/dpd_pm/00051682.PDF. Accessed 2021 Oct 15.
27.Skyrizi (risankizumab): 75 mg in 0.83 mL sterile solution (90 mg/mL), 150 mg in 1 mL sterile solution (150 mg/mL), subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2021 Aug 19: https://pdf.hres.ca/dpd_pm/00062581.PDF. Accessed 2021 Oct 15.
28.Stelera (ustekinumab): 45 mg//0.5 mL, 90 mg/1/0 mL solution for subcutaneous injection; 130 mg/26 mL (5 mg/mL) solution for intravenous infusion [product monograph]. Toronto (ON): Janssen Inc; 2021 Sep 9: https://pdf.hres.ca/dpd_pm/00062938.PDF. Accessed 2021 Oct 15.
29.Taltz (ixekizumab): 80 mg/1.0 mL solution for injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2021 Mar 29: https://pdf.hres.ca/dpd_pm/00060574.PDF. Accessed 2021 Oct 15.
30.Tremfya (guselkumab): 100 mg/1 mL solution for injection, pre-filled syringe; Tremfya One-Press (guselkumab): 100 mg/1 mL solution for injection, patient-controlled injector [product monograph]. Toronto (ON): Janssen Inc; 2021 Sep 17: https://pdf.hres.ca/dpd_pm/00063006.PDF. Accessed 2021 Oct 15.
31.Enbrel (etanercept): 50 mg/mL solution in a prefilled syringe, 25 mg/vial lyophilized powder in a vial for reconstitution, subcutaneous injection [product monograph]. Mississauga (ON): Amgen Canada Inc.; 2021 Mar 19: https://pdf.hres.ca/dpd_pm/00060454.PDF. Accessed 2021 Oct 15.
32.Erelzi (etanercept): 50 mg/mL solution for injection in a prefilled syringe, 50 mg/mL solution for injection in a prefilled autoinjector [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2020 Jun 9: https://pdf.hres.ca/dpd_pm/00056848.PDF. Accessed 2021 Oct 15.
33.Brenzys (etanercept): 50 mg/mL solution for injection in a pre-filled syringe; 50 mg/mL solution for injection in a pre-filled auto-injector [product monograph]. Incheon (KR): Samsung Bioepis; 2020 Aug 19: https://pdf.hres.ca/dpd_pm/00058001.PDF. Accessed 2021 Oct 15.
34.Avsola (infliximab): 100 mg/vial powder for solution, sterile, lyophilized [product monograph]. Mississauga (ON): Amgen Canada Inc; 2020 Mar 12: https://pdf.hres.ca/dpd_pm/00055391.PDF. Accessed 2021 Oct 15.
35.Amgevita (adalimumab): 20 mg in 0.4 mL sterile solution (50 mg/mL), prefilled syringe for subcutaneous injection; 40 mg in 0.8 mL sterile solution (50 mg/mL), prefilled syringe for subcutaneous injection; 40 mg in 0.8 mL sterile solution (50 mg/mL), prefilled SureClick autoinjector for subcutaneous injection [product monograph]. Mississauga (ON): Amgen Canada Inc; 2021 Jul 9: https://pdf.hres.ca/dpd_pm/00062110.PDF. Accessed 2021 Oct 15.
36.Hulio (adalimumab): 20 mg in 0.4 mL sterile solution (50 mg/mL) subcutaneous injection; 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection [product monograph]. Etobicoke (ON): BGP Pharma ULC; 2020 Nov 24: https://pdf.hres.ca/dpd_pm/00059384.PDF. Accessed 2021 Oct 15.
37.Hyrimoz (adalimumab): 20 mg in 0.4 mL sterile solution (50 mg/mL) subcutaneous injection in a pre-filled syringe, 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection in a pre-filled syringe, 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection in a pre-filled autoinjector [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2021 Sep 10: https://pdf.hres.ca/dpd_pm/00062896.PDF. Accessed 2021 Oct 15.
38.Idacio (adalimumab): 40 mg / 0.8 mL (50 mg/mL) sterile solution, subcutaneous injection [product monograph]. Toronto (ON): Fresenius Kabi Canada Ltd; 2020 Oct 30: https://pdf.hres.ca/dpd_pm/00058541.PDF. Accessed 2021 Oct 15.
39.Cimzia (certolizumab pegol): 200 mg/mL solution for injection [product monograph]. Oakville (ON): UCB Canada Inc; 2019 Nov 13: https://pdf.hres.ca/dpd_pm/00053920.PDF. Accessed 2021 Oct 19.
40.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
41.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Sep 8.
42.Reich K, Papp KA, Blauvelt A, et al. Bimekizumab versus ustekinumab for the treatment of moderate to severe plaque psoriasis (BE VIVID): efficacy and safety from a 52-week, multicentre, double-blind, active comparator and placebo controlled phase 3 trial. Lancet. 2021;397(10273):487-498. PubMed
43.Warren RB, Blauvelt A, Bagel J, et al. Bimekizumab versus adalimumab in plaque psoriasis. N Engl J Med. 2021;385(2):130-141. PubMed
44.Reich K, Warren RB, Lebwohl M, et al. Bimekizumab versus secukinumab in plaque psoriasis. N Engl J Med. 2021;385(2):142-152. PubMed
45.Gordon KB, Foley P, Krueger JG, et al. Bimekizumab efficacy and safety in moderate to severe plaque psoriasis (BE READY): a multicentre, double-blind, placebo-controlled, randomised withdrawal phase 3 trial. Lancet. 2021;397(10273):475-486. PubMed
46.UCB Canada Inc. response to October 13, 2021 DRR request for additional information regarding Bimzelx (bimekizumab) DRR review: clarification on clinical trial methods [internal additional sponsor's information]. Oakville (ON): UCB Canada Inc; 2021 Oct 27.
47.Mrowietz U, Kragballe K, Reich K, et al. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Arch Dermatol Res. 2011;303(1):1-10. PubMed
48.Bozek A, Reich A. The reliability of three psoriasis assessment tools: psoriasis area and severity index, body surface area and physician global assessment. Adv Clin Exp Med. 2017;26(5):851-856. PubMed
49.Simpson MJ, Chow C, Morgenstern H, Luger TA, Ellis CN. Comparison of three methods for measuring psoriasis severity in clinical studies (Part 2 of 2): use of quality of life to assess construct validity of the Lattice System Physician's Global Assessment, Psoriasis Area and Severity Index and Static Physician's Global Assessment. J Eur Acad Dermatol Venereol. 2015;29(7):1415-1420. PubMed
50.Puzenat E, Bronsard V, Prey S, et al. What are the best outcome measures for assessing plaque psoriasis severity? A systematic review of the literature. J Eur Acad Dermatol Venereol. 2010;24 (Suppl 2):10-16. PubMed
51.Spuls PI, Lecluse LL, Poulsen ML, Bos JD, Stern RS, Nijsten T. How good are clinical severity and outcome measures for psoriasis?: quantitative evaluation in a systematic review. J Invest Dermatol. 2010;130(4):933-943. PubMed
52.Callis Duffin K, Bushmakin AG, Cappelleri JC, Mallbris L, Mamolo C. A multi-item Physician Global Assessment scale to assess psoriasis disease severity: validation based on four phase III tofacitinib studies. BMC Dermatol. 2019;19(1):8. PubMed
53.Cappelleri JC, Bushmakin AG, Harness J, Mamolo C. Psychometric validation of the physician global assessment scale for assessing severity of psoriasis disease activity. Qual Life Res. 2013;22(9):2489-2499. PubMed
54.Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210-216. PubMed
55.Shikiar R, Willian MK, Okun MM, Thompson CS, Revicki DA. The validity and responsiveness of three quality of life measures in the assessment of psoriasis patients: results of a phase II study. Health Qual Life Outcomes. 2006;4:71. PubMed
56.Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY. Translating the science of quality of life into practice: what do dermatology life quality index scores mean? J Invest Dermatol. 2005;125(4):659-664. PubMed
57.Melilli L, Shikiar R, Thompson C. Minimal clinically important difference in Dermatology Life Quality Index in moderate to severe plaque psoriasis patients treated with adalimumab. J Am Acad Dermatol. 2006;54:AB221.
58.EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
59.Frendl DM, Ware JE, Jr. Patient-reported functional health and well-being outcomes with drug therapy: a systematic review of randomized trials using the SF-36 health survey. Med Care. 2014;52(5):439-445. PubMed
60.Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-483. PubMed
61.Maruish ME. Determining important differences in scores. User's manual for the SF-36v2 health survey. 3rd ed. Lincoln (RI): Quality Metric Incorporated; 2011:169-177.
62.Papp KA, Merola JF, Gottlieb AB, et al. Dual neutralization of both interleukin 17A and interleukin 17F with bimekizumab in patients with psoriasis: results from BE ABLE 1, a 12-week randomized, double-blinded, placebo-controlled phase 2b trial. J Am Acad Dermatol. 2018;79(2):277-286.e210. PubMed
63.Thaçi D, Blauvelt A, Reich K, et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate to severe plaque psoriasis: CLEAR, a randomized controlled trial. J Am Acad Dermatol. 2015;73(3):400-409. PubMed
64.Blauvelt A, Papp KA, Griffiths CE, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol. 2017;76(3):405-417. PubMed
65.Reich K, Armstrong AW, Foley P, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76(3):418-431. PubMed
66.UCB Canada Inc. response to October 13, 2021 DRR request for additional information regarding Bimzelx (bimekizumab) DRR review: subgroup data on weight > or < 120 kg [internal additional sponsor's information]. Oakville (ON): UCB Canada Inc; 2021 Nov 4.
67.Sbidian E, Chaimani A, Afach S, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2020;1:CD011535. PubMed
68.Sbidian E, Chaimani A, Garcia-Doval I, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2021;4:CD011535. PubMed
69.Xu S, Gao X, Deng J, Yang J, Pan F. Comparative efficacy and safety of biologics in moderate to severe plaque psoriasis: a multiple-treatments meta-analysis. J. 2021;19(1):47-56.
70.Wade R, Grosso A, South E, et al. Brodalumab for the treatment of moderate-to-severe plaque psoriasis: an evidence review group evaluation of a NICE single technology appraisal. Pharmacoeconomics. 2019;37(2):131-139. PubMed
71.Cameron C, Hutton B, Druchok C, et al. Importance of assessing and adjusting for cross-study heterogeneity in network meta-analysis: a case study of psoriasis. J. 2018;7(11):1037-1051.
72.Jansen JP, Schmid CH, Salanti G. Directed acyclic graphs can help understand bias in indirect and mixed treatment comparisons. J Clin Epidemiol. 2012;65(7):798-807. PubMed
73.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
74.Wade R, Sharif-Hurst S, Dias S. Patient characteristics as effect modifiers for psoriasis biologic treatment response: an assessment using network meta-analysis subgroups. Syst. 2020;9(1):132. PubMed
75.Clinical Study Report: PS0014 (BE BRIGHT) (interim). A multicenter, randomized, open-label study to assess the long-term safety, tolerability, and efficacy of bimekizumab in adult subjects with moderate to severe chronic plaque psoriasis [internal sponsor's report]. Brussels (BE): UCB Biopharma SRL; 2020 Dec 7.
76.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
77.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
78.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
79.Berth-Jones J, Grotzinger K, Rainville C, et al. A Study examining inter- and intrarater reliability of three scales for measuring severity of psoriasis: Psoriasis Area and Severity Index, Physician's Global Assessment and Lattice System Physician's Global Assessment. Br J Dermatol. 2006;155(4):707-713. PubMed
80.Langley RG, Feldman SR, Nyirady J, van de Kerkhof P, Papavassilis C. The 5-point Investigator’s Global Assessment (IGA) Scale: a modified tool for evaluating plaque psoriasis severity in clinical trials. J Dermatolog Treat. 2015;26(1):23-31. PubMed
81.Robinson A, Kardos M, Kimball AB. Physician Global Assessment (PGA) and Psoriasis Area and Severity Index (PASI): why do both? A systematic analysis of randomized controlled trials of biologic agents for moderate to severe plaque psoriasis. J Am Acad Dermatol. 2012;66(3):369-375. PubMed
82.Ali FM, Salek MS, Finlay AY, Piguet V. Validation of the electronic PASI application: establishing measurement equivalence. J Am Acad Dermatol. 2019;81(6):1439-1441. PubMed
83.Feldman SR, Menter A, Koo JY. Improved health-related quality of life following a randomized controlled trial of alefacept treatment in patients with chronic plaque psoriasis. Br J Dermatol. 2004;150(2):317-326. PubMed
84.Ashcroft DM, Wan Po AL, Williams HC, Griffiths CE. Clinical measures of disease severity and outcome in psoriasis: a critical appraisal of their quality. Br J Dermatol. 1999;141(2):185-191. PubMed
85.Feldman SR, Krueger GG. Psoriasis assessment tools in clinical trials. Ann Rheum Dis. 2005;64 (Suppl 2):ii65-68. PubMed
86.Weisman S, Pollack CR, Gottschalk RW. Psoriasis disease severity measures: comparing efficacy of treatments for severe psoriasis. J Dermatolog Treat. 2003;14(3):158-165. PubMed
87.Carlin CS, Feldman SR, Krueger JG, Menter A, Krueger GG. A 50% reduction in the Psoriasis Area and Severity Index (PASI 50) is a clinically significant endpoint in the assessment of psoriasis. J Am Acad Dermatol. 2004;50(6):859-866. PubMed
88.Belinchón Romero I, Dauden E, Ferrándiz Foraster C, et al. PASI 100 response rates in moderate to severe psoriasis: a systematic literature review and analysis of clinical practice guidelines. J Dermatolog Treat. 2021:1-9. PubMed
89.Langley RG, Ellis CN. Evaluating psoriasis with Psoriasis Area and Severity Index, Psoriasis Global Assessment, and Lattice System Physician's Global Assessment. J Am Acad Dermatol. 2004;51(4):563-569. PubMed
90.Mattei PL, Corey KC, Kimball AB. Psoriasis Area Severity Index (PASI) and the Dermatology Life Quality Index (DLQI): the correlation between disease severity and psychological burden in patients treated with biological therapies. J Eur Acad Dermatol Venereol. 2014;28(3):333-337. PubMed
91.Basra MKA, Salek MS, Camilleri L, Sturkey R, Finlay AY. Determining the minimal clinically important difference and responsiveness of the Dermatology Life Quality Index (DLQI): further data. Dermatology. 2015;230(1):27-33. PubMed
92.Gourraud PA, Le Gall C, Puzenat E, Aubin F, Ortonne JP, Paul CF. Why statistics matter: limited inter-rater agreement prevents using the psoriasis area and severity index as a unique determinant of therapeutic decision in psoriasis. J Invest Dermatol. 2012;139(9):2171-2175. PubMed
93.Feldman SR, Fleischer ABJ, Reboussin DM, et al. The self-administered psoriasis area and severity index is valid and reliable. J Invest Dermatol. 1996;106(1):183186. PubMed
94.Perez-Chada LM, Salame NF, Ford AR, et al. Investigator and patient global assessment measures for psoriasis clinical trials: a systematic review on measurement properties from the International Dermatology Outcome Measures (IDEOM) initiative. Am J Clin Dermatol. 2020;21(3):323-338. PubMed
95.Lewis V, Finlay AY. 10 years experience of the Dermatology Life Quality Index (DLQI). J Investig Dermatol Symp Proc. 2004;9(2):169-180. PubMed
96.Shikiar R, Bresnahan BW, Stone SP, Thompson C, Koo J, Revicki DA. Validity and reliability of patient reported outcomes used in psoriasis: results from two randomized clinical trials. Health Qual Life Outcomes. 2003;1:53. PubMed
97.Mazzotti E, Picardi A, Sampogna F, Sera F, Pasquini P, Abeni D. Sensitivity of the Dermatology Life Quality Index to clinical change in patients with psoriasis. Br J Dermatol. 2003;149(2):318-322. PubMed
98.Basra MK, Fenech R, Gatt RM, Salek MS, Finlay AY. The Dermatology Life Quality Index 1994-2007: a comprehensive review of validation data and clinical results. Br J Dermatol. 2008;159(5):997-1035. PubMed
99.Both H, Essink-Bot ML, Busschbach J, Nijsten T. Critical review of generic and dermatology-specific health-related quality of life instruments. J Invest Dermatol. 2007;127(12):2726-2739. PubMed
100.Norlin JM, Steen Carlsson K, Persson U, Schmitt-Egenolf M. Analysis of three outcome measures in moderate to severe psoriasis: a registry-based study of 2450 patients. Br J Dermatol. 2012;166(4):797-802. PubMed
101.Sinnott PL, Joyce VR, Barnett PG. Guidebook: preference measurement in economic analysis. Menlo Park (CA): Health Economics Research Center; 2007: https://www.herc.research.va.gov/files/BOOK_419.pdf. Accessed 2021 Sep 30.
102.McDowell I. Measuring health: a guide to rating scales and questionnaires. New York (NY): Oxford University Press; 2006.
103.Mease PJ, Menter MA. Quality-of-life issues in psoriasis and psoriatic arthritis: outcome measures and therapies from a dermatological perspective. J Am Acad Dermatol. 2006;54(4):685-704. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: September 8, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Search Strategies:
(bimekizumab* or Bimzelx* or ucb-4940 or ucb4940 or cdp-4940 or cdp4940 or WHO 9870 or WHO9870 or 09495UIM6V).ti,ab,kf,ot,hw,nm,rn.
1 use medall
*bimekizumab/ or (bimekizumab* or Bimzelx* or ucb-4940 or ucb4940 or cdp 4940 or cdp4940 or WHO 9870 or WHO9870).ti,ab,kw,dq.
3 use oemezd
4 not (conference review or conference abstract).pt.
2 or 5
remove duplicates from 6
Clinical Trials Registries
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms – bimekizumab; plaque psoriasis]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – bimekizumab; plaque psoriasis]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms – bimekizumab; plaque psoriasis]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms – bimekizumab; plaque psoriasis]
Grey Literature
Search dates: September 2-8, 2021
Keywords: bimekizumab; plaque psoriasis
Limits: Publication years: none
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Open Access Journals.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Clinical Study Report: PS0014 (BE BRIGHT) (interim). A phase 3, open-label extension study to evaluate the efficacy and safety of bimekizumab in adult subjects with moderate to severe chronic plaque psoriasis [internal sponsor's report]. Brussels (BE): UCB Biopharma SRL; 2020 Dec 7. | Study Design |
Papp KA, Merola JF, Gottlieb AB, et al. Dual neutralization of both interleukin 17A and interleukin 17F with bimekizumab in patients with psoriasis: results from BE ABLE 1, a 12-week randomized, double-blinded, placebo-controlled phase 2b trial. J Am Acad Dermatol. 2018;79(2):277-286.e210. | Study Design |
Blauvelt A, Papp KA, Merola JF, et al. Bimekizumab for patients with moderate to severe plaque psoriasis: 60-week results from BE ABLE 2, a randomized, double-blinded, placebo-controlled, phase 2b extension study. J Am Acad Dermatol. 2020;83(5):1367-1374. | Study Design |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 37: PASI 90, PASI 100 and IGA Response at Week 24 in Study PS0008 (RS)
Treatment group | Total N | PASI 90 response a | PASI 100 response a | IGA 0 or 1 responsea | |||
|---|---|---|---|---|---|---|---|
n (%) | OR (95% CI), P value | n (%) | OR (95% CI), P value | n (%) | OR (95% CI), P value | ||
Bimekizumab versus adalimumab at week 24 | |||||||
BKZ q.4.w./q.8.w. | 161 | 137 (85.1) | 5.28 (3.08 to 9.05), P < 0.001b | 106 (65.8) | 4.69 (2.90 to 7.57), P < 0.001b | 140 (87.0) | 4.78 (2.74 to 8.35), P < 0.001b |
BKZ q.4.w. | 158 | 136 (86.1) | 6.23 (3.52 to 11.05), P < 0.001 | 107 (67.7) | 5.25 (3.21 to 8.59), P < 0.001 | 136 (86.1) | 4.72 (2.68 to 8.32), P < 0.001 |
ADA | 159 | 82 (51.6) | reference | 47 (29.6) | reference | 92 (57.9) | reference |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval; IGA = Investigator's Global Assessment; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RS = randomized set.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
bNot adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for PS0008.5
Table 38: PASI 75 Response at Week 4 (RS)
Study / treatment group | Total N | PASI 75 response at week 4 | BKZ versus placeboa | BKZ versus active controla | ||
|---|---|---|---|---|---|---|
n (%) | OR (95% CI), P value | P value | OR (95% CI), P value | P value | ||
PS0009 | ||||||
Placebo | 83 | 2 (2.4) | reference | reference | NA | NA |
BKZ q.4.w. | 321 | 247 (76.9) | 123.02 (29.39 to 514.86) | <0.001 | 18.20 (11.00 to 30.12) | <0.001 |
USTE | 163 | 25 (15.3) | NA | NA | reference | reference |
PS0008 | ||||||
BKZ q.4.w. (pooled) b | 319 | 244 (76.5) | NA | NA | 7.10 (4.64 to 10.88) | P < 0.001 |
ADA | 159 | 50 (31.4) | NA | NA | reference | reference |
PS0015 | ||||||
BKZ q.4.w. | 373 | 265 (71.0) | NA | NA | 2.81 (2.06 to 3.82) | <0.001 |
SECU | 370 | 175 (47.3) | NA | NA | reference | reference |
PS0013 | ||||||
Placebo | 86 | 1 (1.2) | 316.64 (39.42 to 2,543.25) | <0.001 | NA | NA |
BKZ q.4.w. | 349 | 265 (75.9) | reference | reference | NA | NA |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval NA = not applicable; NR = not reported; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RS = randomized set; SECU = secukinumab; USTE = ustekinumab.
aStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
bPatients randomized to BKZ q.4.w., and to BKZ q.4.w. for 16 weeks then q.8.w. thereafter were pooled for the analysis of 4-week outcomes.
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Table 39: Scalp and Palmoplantar IGA Response at Week 16 (RS)
Study / treatment group | Scalp IGA responsea | Palmoplantar IGA responsea | ||||
|---|---|---|---|---|---|---|
Total N | Week 16 n (%) | OR (95% CI), P valueb | Total N | Week 16 n (%) | P valueb | |
PS0009 | ||||||
Placebo | 72 | 11 (15) | reference | 29 | 7 (24) | reference |
BKZ q.4.w. | 285 | 240 (84) | 37.70 (16.92 to 83.99), P < 0.001 vs placebo 2.41 (1.47 to 3.94), P < 0.001 vs USTEc | 105 | 85 (81) | P < 0.001 vs placeboc P = 0.97 vs USTE |
USTE | 146 | 103 (71) | reference | 47 | 39 (83) | reference |
PS0008 | ||||||
BKZ q.4.w./q.8.w. | 154 | 131 (85) | BKZ total P <0.001c | 44 | 37 (84) | BKZ total P = 0.07 |
BKZ q.4.w. | 142 | 125 (88) | 46 | 38 (83) | ||
ADA | 138 | 93 (67) | reference | 34 | 24 (71) | reference |
PS0015 | ||||||
BKZ q.4.w. | 331 | 294 (89) | P = 0.45 | 92 | 79 (86) | P = 0.57 |
SECU | 331 | 288 (87) | reference | 89 | 79 (89) | reference |
PS0013 | ||||||
Placebo | 74 | 5 (7) | reference | 31 | 10 (32) | reference |
BKZ q.4.w. | 310 | 286 (92) | 158.00 (49.26 to 506.75), P < 0.001 | 97 | 91 (94) | P <0.001 c |
ADA = adalimumab; BKZ = bimekizumab; CI = confidence interval; IGA = Investigator's Global Assessment; NA = not applicable; NR = not reported; OR = odds ratio; q.4.w. = every 4 weeks; RD = risk difference; RS = randomized set; SECU = secukinumab; USTE = ustekinumab.
aData reported for the subgroup of patients who had scalp or palmoplantar psoriasis at baseline and a baseline scalp or palmoplantar IGA score of at least 2 (nonresponder imputation for patients with missing data).
bStratified CMH test, stratified by region and prior biologic drug exposure (nonresponder imputation).
cNot adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Table 40: Subgroup Analyses for Study PS0009 (RS)
Subgroup | Treatment group | Total N (% total) | PASI 90 response at week 16a, n (%) | IGA response at week 16a, n (%) |
|---|---|---|---|---|
Prior biologic therapy | ||||
Prior biologic therapy - Yes | Placebo | 33 (40) | 0 | 0 |
BKZ q.4.w. | 125 (39) | 106 (85) | 102 (82) | |
USTE | 63 (39) | 27 (43) | 31 (49) | |
Prior biologic therapy - No | Placebo | 50 (60) | 4 (8) | 4 (8) |
BKZ q.4.w. | 196 (61) | 167 (85) | 168 (86) | |
USTE | 100 (61) | 54 (54) | 56 (56) | |
Prior systemic therapy | ||||
Prior systemic therapy - Yes | Placebo | 64 (77) | 2 (3) | 1 (2) |
BKZ q.4.w. | 267 (83) | 228 (85) | 224 (84) | |
USTE | 132 (81) | 65 (49) | 68 (52) | |
Prior systemic therapy - No | Placebo | 19 (23) | 2 (11) | 3 (16) |
BKZ q.4.w. | 54 (17) | 45 (83) | 46 (85) | |
USTE | 31 (19) | 16 (52) | 19 (61) | |
Baseline PASI score | ||||
PASI score <20 | Placebo | 54 (65) | 3 (6) | 4 (7) |
BKZ q.4.w. | 170 (53) | 135 (79) | 138 (81) | |
USTE | 102 (63) | 47 (46) | 53 (52) | |
PASI score ≥20 | Placebo | 29 (35) | 1 (3) | 0 |
BKZ q.4.w. | 151 (47) | 138 (91) | 132 (87) | |
USTE | 60 (37) | 34 (57) | 33 (55) | |
BKZ = bimekizumab; IGA = Investigator's Global Assessment; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RS = randomized set; USTE = ustekinumab.
aNonresponder imputation for patients with missing data.
Source: Clinical Study Report for PS0009.4
Table 41: Subgroup Analyses for Study PS0008 (RS)
Subgroup | Treatment group | Total N (% total) | PASI 90 response at week 16a, n (%) | IGA response at week 16a, n (%) |
|---|---|---|---|---|
Prior biologic therapy | ||||
Prior biologic therapy - Yes | BKZ q.4.w./q.8.w. | 50 (31) | 43 (86) | 40 (80) |
BKZ q.4.w. | 50 (32) | 47 (94) | 47 (94) | |
ADA | 53 (33) | 25 (47) | 31 (59) | |
Prior biologic therapy - No | BKZ q.4.w./q.8.w. | 111 (69) | 94 (85) | 94 (85) |
BKZ q.4.w. | 108 (68) | 91 (84) | 91 (84) | |
ADA | 106 (67) | 50 (47) | 60 (57) | |
Prior systemic therapy | ||||
Prior systemic therapy - Yes | BKZ q.4.w./q.8.w. | 116 (72) | 100 (86) | 97 (84) |
BKZ q.4.w. | 112 (71) | 101 (90) | 100 (89) | |
ADA | 110 (69) | 58 (53) | 68 (62) | |
Prior systemic therapy - No | BKZ q.4.w./q.8.w. | 45 (28) | 37 (82) | 37 (82) |
BKZ q.4.w. | 46 (29) | 37 (80) | 38 (83) | |
ADA | 49 (31) | 17 (35) | 23 (47) | |
Baseline PASI score | ||||
PASI score <20 | BKZ q.4.w./q.8.w. | 95 (59) | 79 (83) | 80 (84) |
BKZ q.4.w. | 94 (59) | 76 (81) | 77 (82) | |
ADA | 108 (68) | 50 (46.3) | 68 (63) | |
PASI score ≥20 | BKZ q.4.w./q.8.w. | 66 (41) | 58 (88) | 54 (82) |
BKZ q.4.w. | 64 (41) | 62 (97) | 61 (95) | |
ADA | 51 (32) | 25 (49) | 23 (45) | |
ADA = adalimumab; BKZ = bimekizumab; IGA = Investigator's Global Assessment; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks; RS = randomized set.
aNonresponder imputation for patients with missing data.
Source: Clinical Study Report for PS0008.5,
Table 42: Subgroup Analyses for Study PS0015 (RS)
Subgroup | Treatment group | PASI 100 response at week 16a | |
|---|---|---|---|
Total N (% total) | n (%) | ||
Prior biologic therapy | |||
Prior biologic therapy - Yes | BKZ q.4.w. | 125 (34) | 75 (60) |
SECU | 119 (32) | 56 (47) | |
Prior biologic therapy - No | BKZ q.4.w. | 248 (66) | 155 (63) |
SECU | 251 (68) | 125 (50) | |
Prior systemic therapy | |||
Prior systemic therapy - Yes | BKZ q.4.w. | 267 (72) | 163 (61) |
SECU | 272 (74) | 134 (49) | |
Prior systemic therapy - No | BKZ q.4.w. | 106 (28) | 67 (63) |
SECU | 98 (26) | 47 (48) | |
Baseline PASI score | |||
PASI <20 | BKZ q.4.w. | 233 (62) | 152 (65) |
SECU | 235 (64) | 116 (49) | |
PASI ≥20 | BKZ q.4.w. | 140 (38) | 78 (56) |
SECU | 135 (36) | 65 (48) | |
BKZ = bimekizumab; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RS = randomized set; SECU = secukinumab.
aNonresponder imputation for patients with missing data.
Source: Clinical Study Report for PS0015,6
Table 43: Subgroup Analyses for Study PS0013 (RS)
Subgroup | Treatment group | Total N | PASI 90 response at week 16a, n (%) | IGA response at week 16 a, n (%) |
|---|---|---|---|---|
Prior biologic therapy | ||||
Prior biologic therapy - Yes | Placebo | 37 (43) | 0 | 0 |
BKZ q.4.w. | 155 (44) | 142 (92) | 144 (93) | |
Prior biologic therapy - No | Placebo | 49 (57) | 1 (2) | 1 (2) |
BKZ q.4.w. | 194 (56) | 175 (90) | 179 (92) | |
Prior systemic therapy | ||||
Prior systemic therapy - Yes | Placebo | 71 (83) | 0 | 0 |
BKZ q.4.w. | 276 (79) | 251 (91) | 255 (92) | |
Prior systemic therapy - No | Placebo | 15 (17) | 1 (7) | 1 (7) |
BKZ q.4.w. | 73 (21) | 66 (90) | 68 (93) | |
Baseline PASI score | ||||
PASI <20 | Placebo | 57 (66) | 1 (2) | 1 (2) |
BKZ q.4.w. | 217 (62) | 191 (88) | 199 (92) | |
PASI≥20 | Placebo | 29 (34) | 0 | 0 |
BKZ q.4.w. | 132 (38) | 126 (96) | 124 (94) | |
BKZ = bimekizumab; CI = confidence interval; IGA = Investigator's Global Assessment; NA = not applicable; NR = not reported; OR = odds ratio; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; RS = randomized set; SECU = secukinumab; USTE = ustekinumab.
aNonresponder imputation for patients with missing data.
Source: Clinical Study Report for PS0013.7
Table 44: Pooled PS0008, PS0009, and PS0015 Data for Post Hoc Subgroups Based on Body Weight
Outcomes | Weight < 120 kg | Weight ≥120 kg | ||
|---|---|---|---|---|
BKZ q.4.w./q.8.w. N = 332 | BKZ q.4.w. N = 555 | BKZ q.4.w./q.8.w. N = 37 | BKZ q.4.w. N = 51 | |
PASI 90 Week 16 | 90.4% | 88.6% | 83.8% | 84.3% |
PASI 90 Week 48 | 86.7% | 87.4% | 83.8% | 76.5% |
IGA 0/1 Week 16 | 89.5% | 88.1% | 78.4% | 86.3% |
IGA 0/1 Week 48 | 87.3% | 85.6% | 83.8% | 80.4% |
PASI 100 Week 16 | 68.4% | 62.5% | 45.9% | 39.2% |
PASI 100 Week 48 | 69.9% | 72.1% | 51.4% | 68.6% |
BKZ = bimekizumab; IGA = Investigator's Global Assessment; PASI = Psoriasis Area and Severity Index; q.4.w. = every 4 weeks; q.8.w. = every 8 weeks.
Source: Additional data supplied by Sponsor.66
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the outcome measures summarized in Table 45, and review their measurement properties including validity, reliability, responsiveness to change, and MID.
Of the 5 outcome measures, the PASI and IGA are described in greater detail as these were co-primary or secondary end points, respectively, in the 4 pivotal trials under review. Validation of the generic tools EQ-5D-3L and SF-36 in patients with psoriasis was included.
Table 45: Outcome Measures Included in Each Study
Outcome measure | PS0008 | PS0009 | PS0013 | PS0015 |
|---|---|---|---|---|
PASI 75/90/100 | Primary: PASI 90 at week 16 Secondary: PASI 75 at week 4, PASI 90 at week 24, and PASI 100 at weeks 16 and 24 | Primary: PASI 90 at week 16 Secondary: PASI 75 at week 4, PASI 90 at weeks 12 and 52, and PASI 100 at week 16 | Primary: PASI 90 at week 16 Secondary: PASI 75 at week 4 and PASI 100 at week 16 | Primary: PASI 100 at week 16 Secondary: PASI 75 at week 4, PASI 90 at week 16, and PASI 100 at week 48 |
IGA 0/1 | Primary | Primary | Primary | Secondary |
DLQI | Other | Other | Other | Other |
EQ-5D-3L | Other | Other | Other | Other |
SF-36 | Other | Other | Other | NA |
EQ-5D-3L = EuroQol 5-Dimensions 3-Levels questionnaire; DLQI = Dermatology Life Quality Index; NA= Not Applicable; PASI = Psoriasis Area and Severity Index; IGA = Physician’s Global Assessment; SF-36 = Short Form (36) Health Survey;
Source: Clinical Study Report for PS0009,4 Clinical Study Report for PS0008,5 Clinical Study Report for PS0015,6 Clinical Study Report for PS0013.7
Findings
The validity, reliability, and responsiveness of each outcome measure were summarized and evaluated. Interpretation of the reliability and validity metrics were based on the following criteria:
Inter-rater reliability, kappa statistics (level of agreement)76:
< 0 = poor agreement
0.00–0.21 = slight agreement
0.21–0.40 = fair agreement
0.41–0.60 = moderate agreement
0.61–0.8 = substantial
0.81–1.00 = almost perfect agreement
Internal consistency (Cronbach alpha) and test-retest reliability: ≥ 0.7 is considered acceptable77
Validity; i.e., between-scale comparison (correlation coefficient, r)78:
≤ 0.3 = weak
0.3 to ≤ 0.5 = moderate
> 0.5 = strong
Table 46: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MIDa |
|---|---|---|---|
PASI 75/90/100 | Disease-specific composite severity index based on an average score of erythema, scaling, and thickness of the lesions, weighted by the area of involvement. PASI scores range from 0 to 72, with higher scores indicating greater severity. | Validity: Construct validity was demonstrated through correlation of the PASI and DLQI scores (0.36 ≤ r ≤ 0.54).49 Correlation between the LS-IGA and IGA (Spearman’s rank correlation 0.92 and 0.73).79 Reliability: PASI was shown to have good inter-rater reliability (ICC > 0.75). The coefficient of variation for the PASI score was 36.9, indicating moderate inter-rater reliability.48 Responsiveness: Responsiveness was found to be low when the affected BSA is < 10%.50,51 | A 75% reduction in the PASI score (i.e., PASI 75), is used as a benchmark in clinical trials in psoriasis |
Static IGA | Five-point scale used to measure the severity of disease at a single point in time (static IGA). IGA scores range from 0 (clear) to 4 (severe). | Validity: Relatively high correlation with both the PASI and PtGA (Pearson correlation coefficient >0.5),52,53 moderate correlation with DLQI,11 and a low correlation with the OCI,53 supporting convergent and divergent validity. Reliability: Acceptable test-retest reliability (ICC 0.8).52 High internal consistency reliability in IGA scores, Cronbach coefficient alpha > 0.80 at week 2 and onwards53 and ≥ 0.90 in 4 examined trials.52 Responsiveness: Not assessed to date | A score of 0 or 1 is generally accepted that a clinically meaningful.80 Some trials define efficacy as a 2-point reduction in the total score.81 Clinically important difference estimates included point changes of about half of a PGA category; 0.52 and 0.55 points in 2 studies, respectively.52,53 |
DLQI | 10-item dermatology-specific quality of life questionnaire to assess limitations related to the impact of skin disease. The response options range from 0 (not affected at all) to 3 (very much affected). DLQI scores range from 0 to 30, with lower scores indicating better quality of life. | Validity: Correlated with the bodily pain (r = 0.61) and social functioning domains (r = 0.68) of the SF-36, and the EQ-5D index score (r = 0.71).55 Reliability: The test–retest reliability correlation coefficients were high for both the overall score (Spearman rank correlation 0.99) and for individual questions (0.95 to 0.98).54 Responsiveness: Equal responsiveness to the PASI and IGA scores with correlation coefficients of r = 0.69 and r = 0.7155 | The MID estimates ranged from 2.2 to 6.9 using 3 anchor-based methods.55 A study in patients with psoriasis treated with adalimumab reported an MID of 3.2.57 In a review of RCTs in psoriasis, the MID was reported to be a score change of 5.82 |
EQ-5D-3L | Generic, preference-based, health-related quality of life measure consisting of 6 descriptive questions comprising 5 dimensions and a VAS which records the subject’s self-rated health. | The evidence for the validity of EQ-5D-3L in the psoriasis population is limited. The EQ-5D-3L was found to be highly correlated with the DLQI, though not as responsive to change in patient status.55 EQ-5D-3L showed similar responsiveness as the SF-36 version 1.55 | Estimates derived using distributional and anchor-based approaches.55 Estimates ranged from 0.09 to 0.20 for the index score and 3.82 to 10.34 for the VAS among psoriasis patients.55 |
SF-36 version 2 | 36-item general health status instrument. It consists of 8 domains. A physical component score (PCS) and a mental component score (MCS) can be computed. | In a systematic review examining both version 1 and 2 of the SF-36, the instrument was observed to be responsive (when compared with primary clinical measures) in patients with psoriasis.59,55 | 55A review examining both version 1 and 2 of the SF-36 indicated PCS or MCS improvement of at least 3 points.59 |
EQ-5D-3L = European Quality of Life 5-Dimensions 3-Levels questionnaire; DLQI = Dermatology Life Quality Index; HRQoL = Health-related quality of life; IGA = Investigator’s Global Assessment; LS-IGA = Lattice System Physician’s Global Assessment; MID = minimal important difference; OCI = Ocular Comfort Index; PASI = Psoriasis Area and Severity Index; PtGA = Patient Global Assessment; SF-36 = Short Form (36) Health Survey; VAS = visual analogue scale.
aMIDs were identified for continuous outcomes only. For outcomes measured by responder analysis (i.e., PASI and IGA), a clinically meaningful score was reported.
Psoriasis Area and Severity Index (PASI)
The PASI is the most used instrument for the assessment of psoriasis severity.83,84 It is a single estimate of disease severity based on lesion characteristics weighted by area of body involvement. Psoriatic lesion characteristics are assessed separately for erythema, induration, and scaling in the 4 major body areas: head, upper extremities, trunk, and lower extremities. Severity of each item is graded on a scale of 0 to 4 (0 = clear, 1 = mild, 2 = slight, 3 = moderate, 4 = severe), which is then summed by body region and weighted by the percentage of BSA involvement converted on a scale of 0 to 6 (0 = no involvement, 1 = 1–9%, 2 = 10–29%, 3 = 30–49%, 4 = 50–69%, 5 = 70–89%, 6 = 90–100%). The individual body region scores are then multiplied by weighting factors representing their respective proportion of the total BSA (0.1 for head, 0.2 for upper extremities, 0.3 for trunk and 0.4 for lower extremities), as in the following formula85:
The generated PASI score is a numeric score ranging from 0 to 72, with a score greater than 10 representing more severe disease.47 In clinical trials, PASI is often reported as an overall mean percentage improvement with treatment, and is used most commonly for responder analyses.86 A 75% reduction in the PASI score, i.e., PASI 75, is used as a benchmark in clinical trials in psoriasis.87 While the PASI 75 is still used for legacy drugs, the treatment goal in clinical practice for newer treatment should be the achievement of PASI 90, according to the clinical expert consulted for this review. A recent systematic review noted that achieving a PASI 100 indicates total clearing of the skin and is commonly used in clinical trials, although more real-world evidence is required to determine its role in daily practice.88
Validity
Simpson et al. (2015)49 studied data from a phase III clinical trial (N = 445) to validate 3 systems of physician-scoring psoriasis severity, which included the PASI, static IGA, and Lattice System IGA (LS-IGA) measures. Construct validity of PASI was assessed by evaluating the correlation between the PASI score and the DLQI score, a skin-related HRQoL measure in grading psoriasis severity. The PASI correlated moderately with both the DLQI overall score as well as a single item of DLQI related to psoriasis symptoms (0.36 ≤ r ≤ 0.54), demonstrating that psoriasis severity is correlated with the DLQI score. The same study also investigated the content validity of the 3 measures by assessing the relative impact of the individual components of the measures on HRQoL using multiple linear regression analysis; BSA was most consistently associated with DLQI scores, followed by plaque induration and erythema. The scaling score was found to be minimally and inconsistently associated with DLQI scores which may be in part due to the static measurement of scaling which does not encompass the flaking of the skin over time which can be very distressing to patients.49 The authors therefore concluded that weighing erythema, induration and scaling equally would not accurately capture the varying degrees to which these factors affect the patient’s rating of quality of life. Lastly, the construct and content validity of the PASI were found to be stronger during active treatment compared to pre-therapy.49
Another study of 10 trained dermatologists evaluating 9 adult patients with plaque type psoriasis assessed the correlations of PASI with other commonly used instruments in psoriasis, including the BSA and the IGA.48 The authors reported a strong correlation with both measures (Pearson correlation coefficient > 0.78 and > 0.61, respectively).48 Similarly, Berth-Jones et al. (14 trained dermatologists, 16 patients with chronic plaque psoriasis) reported a strong correlation between PASI and the LS-IGA (Spearman’s rank correlation, r = 0.92), and a moderate correlation with the IGA (r = 0.73).79 Berth-Jones et al. also found that the PASI and IGA were in good agreement for the clearance state (kappa = 0.64) but poor agreement for the severe state (kappa = 0.18).79
Reliability
The reliability of the PASI measure has been assessed in several studies.48,79,89 Bożek et al. reported the interclass correlations (ICCs) for all components of the PASI to be > 0.75, indicating very good intra-rater reliability, except for scaling (0.72). The highest ICC was observed for the area score (0.97). The coefficients of variation (CV) for the PASI was 36.9 overall, indicating moderate inter-rater reliability. The highest variability was observed for the head and neck (CV = 117.8) and the lowest variability was for the area score (CV = 26.8).48 Langley et al. (17 physicians, 25 patients with psoriasis) reported similar results, with higher variability observed in the PASI scores derived by inexperienced physicians compared with experienced investigators (σ = 3.2 vs. 1.2).89 Berth-Jones et al. found excellent intra-rater and inter-rater reliability for the PASI score (ICCs > 0.81).79 The systematic review by Puzenat et al. (4 studies, N = 281) reported good internal consistency, limited intra-rater variation, and moderate inter-rater variation for the PASI.50
Responsiveness
The PASI score was found to have a moderate sensitivity to change.50 In a review by Spuls et al. (2010)51 the authors commented on the responsiveness of PASI being weak when less than 10% of the BSA is affected given that the PASI score would be entirely dependent on the plaque severity scores, and therefore may underestimate the general degree of improvement.
Clinical Relevance
A systematic review by Mattei et al. (2013)90 including 13 RCTs evaluating biologics in psoriasis, reported that a ≥ 75% reduction in the PASI score translates to clinically-significant HRQoL improvement in patients assessed using the DLQI. This is based on the several studies that have demonstrated that a reduction in PASI scores can predict a reduction in DLQI scores, particularly when the patients were achieving a PASI 75 or higher (PASI 75 versus PASI 50 to 75 versus mean difference of 3.24). According to the approximate mean MID for the DLQI of 3.2, this difference suggests a meaningful clinical benefit in HRQoL.90,91 The clinical expert consulted for this review indicated that PASI 90 or even PASI 100 is increasingly being used in clinical settings for newer biologics.
Limitations
The PASI can be difficult to interpret because it is not a linear index.81 For example, a small increase in the BSA affected from 9% to 10%, results in a doubling of the PASI score (with all other parameters constant). Moreover, the PASI lacks sensitivity at its lower end of the scale, where most patient scores fall into, leaving the higher end of the scale redundant, and decreasing the usefulness of the full range of scores (0 to 72).50,84,92 Erythema, induration, and scaling are equally-weighted within each of the 4 body regions, therefore, a reduction in one item with a concomitant increase in another item could be recorded with the same PASI score. Similarly, a drastic (and maybe temporary) change in one subscore can change the overall score.86
The PASI has been criticized for not correlating the clinical extent of the disease with HRQoL and the psychological stress caused by psoriasis. Improvements in the PASI score are not linearly related to severity or improvements in disease state, and therefore some severe diseases may be scored low.51,79 For example, a PASI score as low as 3 on the palms and soles may represent psoriasis that disables a patient from work and other life activities. The score also lacks sensitivity to body sites such as the nails, feet, face, genitalia, and symptoms such as pruritus, or other disease-related comorbidities.50,81 As a result, the sensitivity of the PASI is highly dependent on the initial baseline score, and patients with low initial scores may not achieve a PASI 75, but still have a clinically meaningful response to treatment.89 While a highly effective treatment should overcome this lack of sensitivity, it is for these reasons why the PASI score should be accompanied by patient-reported HRQoL measures.89 PASI scores can also vary substantially between experienced and inexperienced physicians, raising concerns for inter-rater reliability. Despite these limitations, the PASI score remains the most extensively validated, and most complete score which is highly producible. It has also been shown to correlate strongly with its counterpart, the self-administered PASI50,93
Investigator’s Global Assessment (IGA)
The IGA, also known as the Physician Global Assessment (PGA) is a simple measurement of the clinical signs of psoriasis, frequently used as a co-primary end point with the PASI score in psoriasis clinical trials.85 Various IGAs have been used in psoriasis with different descriptions and scores, with the most common IGA versions using 5- to 6-point scales.85,89 The 5-point scale is reported to have a more strict criteria for the score of 1 (“almost clear”) than the 6-point scale score of 1 (“minimal”).80 There are 2 types of IGAs, a static form which measures the physician’s measurement of the disease at a given time point, and a dynamic form in which the physician evaluates the level of improvement or deterioration from a baseline.81,85 The static form of the IGA is preferred as it does not rely on the investigator’s recall of the patient’s disease severity observed at baseline or a previous visit. In the 4 studies under review, a 5-point, static version of the IGA was used, as shown in Table 47, where a higher score indicates a more severe condition.4-7
Table 47: Investigator’s Global Assessment Scoring
Score | Short Descriptor | Detailed Descriptor |
|---|---|---|
0 | Clear | No signs of psoriasis; post-inflammatory hyperpigmentation may have been present |
1 | Almost Clear | No thickening; normal to pink coloration; no to minimal focal scaling |
2 | Mild | Just detectable to mild thickening; pink to light red coloration; predominately fine scaling |
3 | Moderate | Clearly distinguishable to moderate thickening; dull to bright red; moderate scaling |
4 | Severe | Severe thickening with hard edges; bright to deep dark red coloration; severe/coarse scaling covering almost all or all lesions |
Source: Clinical Study Report PS00137
Validity
The most recent study assessing the validity of the IGA evaluated data from 4 Phase III clinical studies of tofacitinib in patients with psoriasis (N = 3,641).52 Construct validity was assessed using a known-group approach, measuring the relationship between IGA and PASI through a repeated measures model. A positive relationship between the IGA and PASI scores was observed which was stable and replicable across the 4 studies, indicating that the IGA could discriminate between different degrees of disease severity.52
Convergent validity was assessed in the aforementioned study by comparing the IGA with 3 additional outcome measures: the PASI, patient global assessment, and DLQI.52 Pearson correlation coefficients between IGA and the 3 scales ranged from 0.4 to 0.79 at primary assessment time points in the 4 clinical studies. Results showed a strong correlation between the IGA and the PASI (r = 0.77 to 0.79) even though the IGA does not consider the amount of BSA affected by psoriasis. A moderately strong correlation was found between the IGA and DLQI (0.44 to 0.57). None of the correlations were very large (> 0.8, indicating that the IGA considers some different information than the PASI and DLQI. Baseline correlations were smaller likely due to the limited range of responses from relatively homogeneous subjects. An earlier study by Cappelleri et al. (2013)53 conducted a psychometric validation of the IGA using data from a phase II study of tofacitinib among 197 patients. Results found a relatively high correlation between the IGA and patient global assessment as well as the IGA and PASI with correlation coefficient values > 0.5, except for at baseline. The study also examined correlations between the IGA and the Ocular Comfort Index and the Pain/Discomfort Assessment with all correlation coefficient values < 0.2, indicating relatively high divergent validity. These findings were consistent with several other studies examining the 6-point IGA.48,79,89
Reliability
A recent systematic review noted that the 5-point IGA appears to be based on a formative model where a change in the severity of the disease does not necessarily mean a change in all 3 components of erythema, induration, and scaling, and therefore an assessment of internal consistency would not be applicable.94 However, Callis Duffin et al. (2019)52 assessed the internal consistency reliability, demonstrating that the scoring items (erythema, induration, and scaling) were highly consistent with each other (Cronbach coefficient alpha ≥ 0.90) at the primary assessment points in all 4 trials. The internal consistency reliability was less convincing (Cronbach coefficient alpha 0.50 to 0.63) for the values observed at baseline, likely a result of the specific inclusion criteria of the trials.52 This study also evaluated the consistency of IGA measurements between screening and baseline visits, when no change in terms of disease severity was expected. The ICC values for the pooled data were 0.70, suggesting an acceptable test-retest reliability over a stable period.
Cappellleri et al. (2013)53 also examined the test-retest reliability of IGA scores at baseline and week 2 among patients with little to no change in their PASI scores, resulting in a high ICC of 0.80. The study also examined internal consistency reliability of the IGA, with Cronbach coefficient alpha > 0.80 at all time points from week 2 onwards, indicating high correlations after baseline. Langley et al. (2013)89 conducted an analysis of variance (ANVOA) to examine the variability in the IGA and PASI. The intra-rater variation in the 6-point IGA was lower than the PASI with standard deviations of 0.2 and 2.5, respectively.89 The systematic review by Puzenat et al. also reported low intra-observer variability but moderate inter-observer variability for the IGA.50
Responsiveness
No evidence regarding the responsiveness of the IGA was identified from the literature at this time.
Clinical Relevance
It is generally accepted that a clinically meaningful score in the IGA is a score of 0 (“clear”) or 1 (“almost clear” or “minimal”).80 Furthermore, some trials define efficacy as a 2-point reduction in the total IGA score.81 Both Cappellleri et al. (2013)53 and Callis Duffin et al. (2019)52 assessed the clinically important difference for the IGA. Both studies used the patient global assessment score as a continuous anchor and determined a clinically important difference score of 0.52 (95% CI, 0.42 to 0.56) and 0.55 (95% CI, 0.546 to 0.563) in each study, respectively. It should be noted that the clinically important difference does not necessarily imply a minimum clinically important difference and although it is not possible to measure less than 1 category difference for an individual on the IGA scale, the clinically important difference was deemed appropriate to determine a group difference.53
Limitations
The IGA is more subjective than the PASI in that there is no attempt to quantify the individual elements of plaque morphology or BSA involvement.83,86 This could lead to potentially misleading scores when there is clearance of BSA involvement, but the remaining lesions appear the same.81 Despite this, it is possible that physicians consider the extent of the psoriasis when grading each item, as one study found that the sum of the area scores from the PASI were more correlated with IGA than were the sum scores for each item.89 The IGA has been shown to be reliable based on test–retest data and internal consistency, however inter-rater reliability can be poor due to variability, especially among untrained observers.86 Furthermore, given that the IGA has many different scales and scoring variations, comparisons between studies is made very difficult.86 Within a study, however, the IGA correlated well with the PASI and HRQoL measures.51 Furthermore, a systematic review by Robinson et al. included 30 RCTs of biologic drugs in psoriasis from 2001 to 2010 and found that the IGA (0, 1) correlated very closely with the PASI 75 (correlation coefficient 0.9157), suggesting potential redundancy in measuring both scores as primary end points.81
Dermatology Life Quality Index (DLQI)
The DLQI is a widely used dermatology-specific health-related HRQoL instrument which assesses limitations related to the impact of skin disease.54 It is a 10-item questionnaire that covers 6 domains: symptoms and feeling, daily activities, leisure, work and school, personal relationships, and bother with psoriasis treatment. Each item is scored on a 4-point Likert scale: 0, (not at all affected/not relevant), 1 (a little affected), 2 (a lot affected), and 3 (very much affected). The overall DLQI score is a numeric score between 0 to 30, with lower scores indicating better quality of life. At least 80% of the questions must be answered for a score to be reported54,55 The final numeric score translates to the effect of the patient’s disease on their quality of life where 0 to 1 = no effect, 2 to 5 = small effect, 6 to 10 = moderate effect, 11 to 20 = very large effect and 21 to 30 = extremely large effect.56 The DLQI can be completed within a few minutes, making it a very time-efficient scoring system for use in clinical settings.95
Validity
The DLQI was developed in 1994, and since has been validated in many studies.54,55,95-98 Construct validity of the DLQI was based on the correlation of the instrument with either generic, dermatologic, or disease-specific instruments in more than 37 separate studies.98 Shikiar et al. (2003)96 reported a good correlation (Correlation coefficient, r, > 0.61) with 3 different itch measures in a study combining results from trials in moderate to severe plaque psoriasis (N = 1,095). A later study by Shikiar et al. (2006)55 demonstrated excellent correlation between the DLQI and generic HRQoL instruments in a population of 147 with moderate to severe plaque psoriasis randomized to adalimumab versus placebo; the DLQI correlated the greatest with the bodily pain (r = 0.61) and social functioning domains (r = 0.68) of the 36-item Short Form Health Survey (SF-36), as well as the overall EuroQol 5-Dimensions 3-Levels questionnaire (EQ-5D-3L) index score (r = 0.71).
Reliability
In the original validation study by Finlay and Khan, the reliability of the DLQI was assessed with 53 patients with a variety of skin diseases by completing the questionnaire twice, 7 to 10 days apart.54 The test‒retest reliability correlation coefficients were obtained using the Spearman rank correlation test, which were high for both the overall score (0.99) and individual questions (0.95 to 0.98).54 The good test‒retest reliability of the DLQI was also confirmed in a systematic review by Basra et al., with eight of 12 international studies reporting correlation coefficients greater than 0.56, up to 0.99.98 The same review reported good internal consistency reliability of the DLQI which is based on 22 international studies with Crohnbach alpha coefficients ranging from 0.75 to 0.92.98
Responsiveness
Responsiveness to change in the clinical status of a patient was measured by comparing DLQI data with PASI and IGA scores.55 The correlations between the DLQI and the 2 disease severity scores were r = 0.69 and r = 0.71, respectively. The DLQI demonstrated equal responsiveness to the PASI and IGA scores with correlation coefficients of r = 0.69 and r = 0.71, which was not achieved by the general tools, the EQ-5D -3L(r = 0.44) and SF-36 (r = 0.44).55 In a second study assessing responsiveness, Shikiar et al. contrasted change in DLQI scores in patients who were defined as clinical responders (achievement of PASI 75 response by week 12) with those characterized as nonresponders (< PASI 50); DLQI scores in responders improved by 12.17 points, compared with 1.77 points in the nonresponders subgroup (effect size 0.40).55 Additional studies demonstrating the responsiveness of the DLQI were also identified in the systematic review by Basra et al.97,98
MID
Shikiar et al. (2006)55 estimated the MID of the DLQI in patients with psoriasis (N = 147) using 3 anchor-based methods; MID-1 was based on scores from near-responders (PASI improvement of 25 to 49%), MID-2 was based on partial responders (PASI improvement 50 to 74%), and MID-3 corresponded to the difference between nonresponders and minimal responders for the IGA score. The authors also estimated the MID using standard error of measurement and one-half SD of baseline scores. Estimates ranged from 2.33 to 6.95.55 It should be noted that these approaches lack patient-based anchors, and therefore do not necessarily identify the minimal difference that a patient would consider important. Another study in patients with psoriasis (N = 147) treated with adalimumab reported an MID of 3.2.57 In the most recent systematic review of RCTs in psoriasis, the DLQI MID was reported to be a score change of 5.82
Limitations
The DLQI was the first dermatology-specific tool to evaluate skin-related HRQoL, and was originally developed for use in routine practice.54 While the tool focuses on the patient’s daily functioning, it has been criticized for not fully capturing emotional and mental states.99 Therefore, the DLQI may lack conceptual validity in the psychological consequences of living with psoriasis.
EuroQol 5-Dimensions 3-Levels Questionnaire (EQ-5D-3L)
The EQ-5D-3L questionnaire is a generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS.58 The descriptive questions comprise of 5 dimensions, mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is divided into 3 levels (1, 2, 3) representing “no problems,” “some problems,” “extreme problems,” respectively. Respondents are asked to choose one level that reflects their own health state for each of the 5 dimensions. The 5 questions are scored and together contribute to the EQ-5D index (utility) score between 0 and 1, where 0 represents death, and 1 represents perfect health. The EQ-5D also includes a VAS of the patient’s self-rated health status on a vertical 20 cm scale that ranges from 0 (worst imaginable health status) to 100 (best imaginable health status). Different utility functions are available that reflect the preferences of specific populations (e.g., US, UK).
The evidence for the validity of EQ-5D-3L in the psoriasis population is limited. A Swedish observational cohort study found good correlation of EQ-5D-3L with other outcome measures DLQI and PASI.100 However, EQ-5D was not as responsive to change in patients’ clinical status as the DLQI and the study authors recommend the use of EQ-5D in complement with DLQI and PASI.100 An additional study found the EQ-5D-3L to be highly correlated with the DLQI, though not as responsive to change in patient status.55 EQ-5D showed similar responsiveness as the SF-36.55 Estimates of the MID for EQ-5D-3L VAS and index score were derived using 5 methods including 3 anchor-based (PASI and IGA anchors) and 2 distributional approaches (standard error of measurement and one-half SD of baseline scores) as described previously for the DLQI.55 The estimated MIDs in the psoriasis population for the VAS ranged from 3.82 to 10.34 and the MIDS for the index score ranged from 0.09 to 0.22.55 This estimated MID range compared to the general MID range of 0.033 to 0.074, suggests that a larger difference in EQ-5D-3L index score is necessary for patients with psoriasis to regard the change as clinically beneficial.101
Short Form (36) Health Survey
The SF-36 is a 36-item, general health status instrument that has been used extensively in clinical trials in many disease areas.59,60 The SF-36 consists of 8 health domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. For each of the 8 domains, a subscale score can be calculated. The SF-36 also provides 2 component summaries, the physical component summaries (PCS) and the mental component summary (MCS), derived from aggregating the 8 domains according to a scoring algorithm. All scores are based on a scale of 0 to 100, with higher scores indicating higher HRQoL. The scores can also be standardized to the general US population, where an average score is 50, with a SD of 10 (t score). Version 2 of the SF-36 was made available to researchers in 199661 and was developed to address the shortcomings of the version 1 of the survey; including changing response options for role function scales from dichotomous to 5-point scale responses and altering the wording of certain items to make them easier to understand.102
A systematic review by Frendl and Ware (2014)59 examined SF-36 concordance and its MID across many different indications in 185 studies (using either version 1 or version 2 of the SF-36) evaluating drug therapy effectiveness. The SF-36 was observed to be responsive (when compared with primary clinical measures) in patients with psoriasis in these studies. In addition, of the 10 psoriasis studies identified, PCS or MCS improvement of at least 3 points versus placebo was observed in 70% of these studies.59,103
Based on anchor data, the developer of both versions of the SF-36 proposed the following minimal mean group differences for the individual domain scores: physical functioning (3), role physical (3), bodily pain (3), general health (2), vitality (2), social functioning (3), role emotional (4), and mental health (3).61 It should be noted that these MID values were determined as appropriate for groups with mean t score ranges of 30 to 40. For higher t score ranges, MID values may be higher. Furthermore, as these MID values were based on clinical and other non–patient-reported outcomes, they do not necessarily identify the smallest difference that patients would consider important.
Conclusions
The evaluation of severity of disease in psoriasis is largely dependent on ratings of physical signs and symptoms. The PASI is the most commonly used summary score both in clinical trials and clinical practice of psoriasis, while the IGA is used mostly in clinical trials. Given its relative objectivity, the PASI score remains the most widely used end point, and as such all other investigator-derived (IGA) and patient-reported outcome measures (DLQI, EQ-5D-3L, SF-36) used in psoriasis have been validated against the PASI score. The IGA score is criticized for being more subjective than the PASI score and for lacking a BSA involvement component. As the DLQI may not fully capture emotional and mental states, this instrument can be supported by the EQ-5D-3L and the SF-36v2 which include mental health measures.
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
EQ-5D
EuroQol 5-Dimensions questionnaire
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
IL
interleukin
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
PASI
Psoriasis Area and Severity Index
QALY
quality-adjusted life-year
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Bimekizumab (Bimzelx), solution for subcutaneous injection |
Submitted price | Bimekizumab, 160 mg per 1 mL pre-filled syringe or autoinjector, $1,625.00 |
Indication | Proposed: For the treatment of moderate to severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | February 14, 2022 |
Reimbursement request | As per indication |
Sponsor | UCB Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy, which aligns with the reimbursement request |
Treatment | Bimekizumab |
Comparators | Adalimumab, brodalumab, certolizumab pegol, etanercept, guselkumab, infliximab, ixekizumab, risankizumab, secukinumab, tildrakizumab, ustekinumab |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 10 years |
Key data source | A network meta-analysis of 84 clinical trials was used to compare the ability of bimekizumab to achieve PASI 75 (or greater) at 16 weeks compared to the other biologic drugs. This network included 4 phase III and IIIb clinical trials for bimekizumab: PS0009, PS0008, PS0015, and PS0013. |
Submitted results | The 3 treatments on the efficiency frontier were adalimumab, brodalumab, and bimekizumab. The ICER of bimekizumab vs. brodalumab was $1,805,071 per QALY (including costs: $33,594; including QALYs: 0.019). |
Key limitations |
|
|
|
ICER = incremental cost-effectiveness ratio; LY = life-year; NICE = National Institute for Health and Care Excellence; PASI = psoriasis area severity index; QALY = quality-adjusted life-year.
Conclusions
The CADTH clinical review concluded that bimekizumab showed a statistically and clinically important improvement in psoriasis disease severity (as measured by Psoriasis Area and Severity Index [PASI] and Investigator’s Global Assessment) versus placebo, adalimumab, ustekinumab, and secukinumab in the evaluated studies (PS0009, PS0008, PS0015, and PS0013) after 16 weeks in patients with moderate to severe plaque psoriasis who were candidates for phototherapy or systemic therapy. The 1-year data from these clinical trials suggest that PASI response may be maintained in the majority of patients who continue bimekizumab therapy; the incremental differences that favoured bimekizumab versus secukinumab or ustekinumab were also maintained. However, these longer-term outcome data were limited by the lack of control group and failure to maintain randomization. The data were restricted to patients with a demonstrated response to treatment or those who did not use a Health Canada–recommended dosage regimen. In addition, there were important limitations in health-related quality of life (HRQoL) data, which limit the interpretation of these results. The safety data available for bimekizumab were limited by the sample size and study duration of the trials, which may have been insufficient to detect infrequent adverse events or those that take a longer time to develop.
As there were important comparators not assessed in the clinical trials, the sponsor submitted indirect evidence, which suggests that ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. However, several sources of heterogeneity were identified across the trials included in the indirect comparison, and it is uncertain whether the methods used to control for potential bias were adequate, or whether the between-group differences for some comparisons were clinically important.
CADTH identified several limitations with the sponsor’s pharmacoeconomic model, including the clinical evidence used to inform the model, utility estimates, discontinuation rate, lack of treatment waning, and adverse events. As part of the base case, CADTH used alternative utility values derived from the National Institute for Health and Care Excellence (NICE) submission for ixekizumab. Based on the CADTH base case, bimekizumab was associated with incremental costs of $33,526 and quality-adjusted life-years (QALYs) of 0.0135, resulting in an incremental cost-effectiveness ratio (ICER) of $2,475,397 per QALY compared to brodalumab. The probability of cost-effectiveness of bimekizumab at a $50,000 per QALY willingness-to-pay (WTP) threshold was 0%, and a price reduction of 41% would be required to achieve cost-effectiveness at this threshold.
Scenario analyses were performed regarding treatment discontinuation rate and PASI response threshold. The scenario involving differential discontinuation rates resulted in an ICER for bimekizumab of $2,617,920 per QALY compared to brodalumab. The scenario that assumed a PASI90 response threshold resulted in an ICER of $2,393,618 per QALY for bimekizumab compared to brodalumab. These analyses had little impact on the overall ICER, which is predicated upon small incremental QALYs and a high drug acquisition cost.
CADTH acknowledges that both the clinical trial data and indirect evidence have limitations, which leads to some uncertainty with the clinical findings. Furthermore, the lack of transparency in the sponsor’s overly complex model contributes additional uncertainty to the results of the economic analysis. As an exploratory analysis, CADTH assumed the same efficacy for all comparators based on the efficacy of the weighted bucket. In this analysis, a price reduction of 49.5% would be required to ensure cost parity with the cheapest comparator, adalimumab.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
As part of the call for patient input CADTH received 2 submissions, a joint patient input submission from the Canadian Psoriasis Network and the Canadian Association for Psoriasis Patients and another submission from the Psoriasis Society of Canada. All are national, non-profit organizations dedicated to helping patients with psoriasis. The Canadian Psoriasis Network and the Canadian Association for Psoriasis Patients conducted an online survey and received 95 responses from Canadians. The Psoriasis Society of Canada distributes newsletters to its members across Canada and received phone calls from psoriasis patients. Patients reported being treated with phototherapy, topical corticosteroids, biologic drugs, methotrexate, and vitamin D. Approximately half of patients surveyed reported that skin irritation and itching — side effects of current treatments — were difficult to tolerate. For patients, the most important outcomes from a new therapy were symptom improvement, improvement in quality of life, reduced side effects, affordability, and easier administration. Thirteen patients had experience with bimekizumab, likely obtained through clinical trials. Eleven patients reported that bimekizumab was better at managing their psoriasis symptoms than other therapies and that it improved their mental well-being and quality of life, and 9 stated that side effects were more tolerable than therapies they had previously tried.
No clinician input was received for this review.
Drug plans providing feedback for this review enquired how the introduction of bimekizumab would affect current treatment algorithms for biologic drugs for this disease. The plans noted that bimekizumab could be self-administered and that it was the only interleukin (IL)-17 inhibitor with a maintenance dosage frequency of every 8 weeks. Last, the plans noted that most biologic drugs for plaque psoriasis have confidential, negotiated prices and that biosimilars are also used for this disease.
Several of these concerns were addressed in the sponsor’s model:
The sponsor used the prices for biosimilars in its analysis, where applicable.
In addition, CADTH addressed some of these concerns as follows:
CADTH included the prices for biosimilars in the cost comparison table (Table 8), where applicable.
CADTH was unable to address the following concerns raised from stakeholder input:
Adverse events such as itchy skin and irritation were not included in the sponsor’s model.
CADTH was not able to use the confidential, negotiated prices for comparators.
Economic Review
The current review is for bimekizumab (Bimzelx) for adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of bimekizumab compared with other biologic comparators. The modelled population consisted of adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy, which aligns with both the Health Canada indication and the reimbursement request.1
Bimekizumab is available as a pre-filled syringe or autoinjector, each containing 1 mL of 160 mg of bimekizumab. The recommended dose of bimekizumab is 320 mg (given as 2 subcutaneous injections of 160 mg each) every 4 weeks for the first 16 weeks and every 8 weeks thereafter. For patients with a body weight of 120 kg or more who do not achieve a complete skin response, 320 mg every 4 weeks after week 16 may be considered.1 Bimekizumab is given subcutaneously and may be self-administered by patients after they are trained in the proper technique. The cost for bimekizumab is $1,625 per 160 mg bimekizumab as a pre-filled syringe or autoinjector. The cost for bimekizumab is $30,631 in year 1 and $22,921 in subsequent years (i.e., maintenance cost). In the base case, the sponsor assumed that 8.5% of patients had a body weight of 120 kg or more and would receive the drug every 4 weeks.
The comparators for this analysis include the biologic drugs adalimumab, brodalumab, certolizumab pegol, etanercept, guselkumab, infliximab, ixekizumab, risankizumab, secukinumab, tildrakizumab, and ustekinumab. The recommended dosage regimens for each drug were derived from the respective product monographs and are summarized in Table 8. The annual maintenance costs for the comparators ranged from $12,253 for adalimumab to $34,555 for certolizumab pegol, based on the recommended dosages. The sponsor assumed that all patients would receive up to 5 lines of therapy. Subsequent lines of therapy were represented by a weighted bucket of all relevant treatments, with costs and efficacy (based on the network meta-analysis [NMA]) weighted according to the year 3 market shares from the budget impact analysis (BIA). This weighted bucket comparator was used for each line of subsequent therapy for lines 2 through 5. Annual maintenance costs for this weighted bucket were $19,232.
Wastage was not relevant for most of the treatments in this analysis, including bimekizumab, as the recommended dose is based on pre-filled syringes or autoinjectors. Only 1 product, infliximab, had weight-based dosing, for which the sponsor assumed there would not be any wastage.
Outcomes of the model included QALYs and life-years over a time horizon of 10 years. The base-case analysis was conducted from the perspective of the Canadian public health care system, with discounting (1.5% per annum) applied to both costs and outcomes. The cycle length was 2 weeks.
Model Structure
The sponsor submitted a Markov model with health states generally based on PASI scores. Patients entered the model and received their initial treatment for 16 weeks, after which they were assessed for treatment response according to their PASI score. Those achieving treatment response at 16 weeks (defined as PASI ≥ 75) continued on maintenance with that treatment until discontinuation for any cause or death. Those not achieving treatment response at 16 weeks (PASI < 75) were moved to the next line of therapy, which was a weighted bucket comparator, described previously. The assignment of patients to PASI states at 16 weeks was determined by the NMA. The sponsor’s model structure is shown in Appendix 3 (Figure 1).
Model Inputs
The target population for this analysis includes adult patients with moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. Mean baseline demographic characteristics used in the model were based on pooled patient data from PS0008 (BE SURE), BE VIVID (PS0009), BE READY (PS0013), and BE RADIANT (PS0015). The mean age and weight of the population was 45.1 years and 89.6 kg, and 30.9% of the population were women.
After an initial treatment period of 16 weeks, patients were assigned to health states based on their PASI score: PASI < 50, 50 ≤ PASI < 75, 75 ≤ PASI < 90, 90 ≤ PASI < 100, and PASI100.
Assignment to these health states was determined through a sponsor-commissioned systematic literature review and NMA.2 Using a random-effects model, the sponsor’s analysis calculated the probability of achieving each PASI score for each comparator. These data were converted into proportions of patients achieving each PASI score at 16 weeks (Table 12).
Beyond the 16-week initial period, the model assumed that all patients remained in the same health state, although it included a constant annual discontinuation rate of 15% for all treatments. Patients that discontinued moved to the next line of treatment. Subsequent lines of therapy were represented by a weighted bucket of all relevant treatments, with costs and efficacy (based on the NMA) weighted according to the year 3 market shares from the BIA (Table 21). Patients who reached the fifth line of treatment remained there until death or for the rest of the time horizon. All-cause mortality was included in the model based on age- and gender-specific data from Canadian life tables.3 The risk of death was not affected by a patient’s psoriasis.
The dosage used in the model was consistent with the product monograph and as described previously for bimekizumab: 320 mg every 4 weeks for the first 16 weeks and every 8 weeks thereafter, or every 4 weeks thereafter for patients with a body weight of 120 kg or more.1 From pooled data from PS0009, PS0008, PS0013, and PS0015, the model estimated that 8.5% of patients had a body weight of 120 kg or more, and these patients were assumed to receive the drug every 4 weeks in the base case. The dosage used for other comparators was consistent with their product monographs and is described in the CADTH cost comparison (Table 8).
Health state utilities were calculated for the various PASI scores based on pooled bimekizumab and certolizumab pegol EuroQol 5-Dimensions questionnaire (EQ-5D) data from patients in the CIMPASI-2 (PS0002), CIMPACT (PS0003), CIMPASI-1 (PS0005), PS0009, PS0008, PS0013, and PS0015 trials, and were converted to utility scores using UK tariffs (Table 11).4 It was assumed that, when a patient discontinued a treatment and moved to the initial period of the next treatment in the sequence, they were assigned utilities for baseline PASI. The only adverse event included in the model was oral candidiasis, and the sponsor assumed that this did not significantly affect a patient’s quality of life and, therefore, it did not have an associated disutility.
The annual maintenance drug acquisition costs for the biologic drugs used in the model ranged from $12,253 for adalimumab to $34,555 for certolizumab pegol. Costs for most of the biologic drugs were derived from the Ontario Drug Benefit formulary5 and Ontario Exceptional Access Program,6 while the costs for guselkumab and tildrakizumab were derived from the respective CADTH reports.7,8 The cost for the weighted bucket comparator for subsequent line therapy was calculated as the sum of the products of the maintenance costs for each comparator multiplied by their market shares, resulting in a maintenance cost of $19,232. Monitoring costs were included and consisted of dermatologist visits, chest X-rays, tuberculosis tests, and liver function tests. The monitoring costs for patients receiving subcutaneous therapy were calculated to be $96 initially and $0 during the maintenance period. Costs for disease management were also applied and consisted of inpatient and emergency department visits for sepsis. The unit cost per day for an inpatient stay was $1,455 based on the Canadian Institute for Health Information patient cost estimator9 and the Ontario Schedule of Benefits10; an emergency department cost of $585.79 was derived from the Alberta Interactive Health Database Application.11 Oral candidiasis was assumed to be treated with a 14-day course of fluconazole, costing $34.34 per treatment.5
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in this section.
Base-Case Results
The results of the sponsor’s analysis demonstrated that 3 drugs remained on the cost-effectiveness frontier: adalimumab, brodalumab, and bimekizumab (Table 3). All other products were dominated or subject to extended dominance (Table 14).
Compared to brodalumab, bimekizumab was associated with incremental costs of $33,594 and QALYs of 0.0186, resulting in an ICER of $1,805,071 per QALY. The probability of cost-effectiveness of bimekizumab at a $50,000 per QALY WTP threshold was 0%. Additional results from the sponsor’s submitted economic evaluation base case are available in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Adalimumab | 163,823 | 8.345 | Reference |
Brodalumab | 177,325 | 8.382 | 371,500 |
Bimekizumab | 210,919 | 8.401 | 1,805,071 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The submitted analyses are based on the publicly available prices of comparators and may not reflect confidential, negotiated prices. Only treatments on the cost-effectiveness frontier are reported in this table.
Source: Sponsor’s pharmacoeconomic submission.4
Sensitivity and Scenario Analysis Results
The sponsor conducted a number of sensitivity and scenario analyses involving the time horizon, adverse events, patient weight, and market shares for the weighted bucket comparator. All scenarios tested showed that comparators that were dominated or extendedly dominated in the base case remained so, such that the main comparison between bimekizumab and brodalumab remained relevant. The scenario that had the largest influence on the ICER was shortening the time horizon to 1 year, resulting in an ICER of $2,532,411 per QALY for bimekizumab compared to brodalumab. When 0% of patients were assumed to weigh 120 kg or more (i.e., no dosage every 4 weeks), the resulting ICER was $1,443,480 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Uncertainty with respect to the clinical and indirect evidence: The sponsor submitted an NMA that ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. According to the CADTH clinical review, there was heterogeneity among included trials regarding the proportion of patients with prior exposure to biologic drugs or phototherapy, study region, time since diagnosis, timing of assessment, and the year the study was conducted, which may have biased the results of the NMA.
Of particular significance is the assumption that ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, which was done according to previous CADTH reviews.12,13 |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||; this introduces uncertainty into the analysis.
In addition, there were important limitations in the HRQoL data (such as lack of control of type I error, unknown extent of missing data, incomplete reporting of between-group differences), which limit the interpretation of these results. The safety data available for bimekizumab were limited by the sample size and study duration of the trials, which may have been insufficient to detect infrequent adverse events or those that take a longer time to develop.
As part of a scenario analysis, CADTH assumed the same efficacy for all comparators based on the NMA, namely, that of the weighted bucket comparator.
Utility values did not meet face validity: The utility values used by the sponsor were overestimated, suggesting higher quality of life for patients with plaque psoriasis than for the general population. In its base case, the sponsor used pooled bimekizumab and certolizumab pegol EQ-5D data from various trials, and converted these data to utility scores ranging from 0.7879 for baseline PASI to 0.9304 for PASI100 using UK tariffs.14 These values do not meet face validity, as the maximum observed EQ-5D Canadian utility value in the general population ranges from 0.863 to 0.885.15,16 Furthermore, Canadian tariffs have been previously published and are more appropriate for use in a Canadian setting.17 In consultation with the clinical expert, CADTH determined that the values from the NICE appraisal of ixekizumab most accurately reflected Canadian utility values for plaque psoriasis.18
In addition, the clinical expert consulted by CADTH highlighted the heterogeneous nature of plaque psoriasis disease presentation at baseline. The expert stated that a patient with a baseline PASI score of 12 would be much better off than a patient with a baseline PASI score of 30, for example, and that an associated PASI50 response would look different in these 2 patients. Thus, the sponsor’s use of health state utility values based on different PASI responses does not appear to address the heterogeneous nature of the disease. The clinical expert noted that improvements to quality of life should consider a patient’s baseline PASI state. CADTH was unable to address this feedback in its reanalysis.
As part of the base case, CADTH used the health state utility values from the NICE appraisal of ixekizumab, using the sponsor-provided option to do so.18
Model was cumbersome and lacked transparency: CADTH noted that the sponsor’s submission was overly complex, making simple validation checks very difficult. For example, there was duplication of key parameters across multiple sheets, making it unclear which parameter needed to be edited to implement a change. Likewise, the sponsor’s submitted model also included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately as a result of overwriting errors. The lack of transparency and of a detailed user guide for the sponsor’s macros further complicated the validation process. Finally, the Markov trace included by the sponsor was unwieldy and overly complex. A transparent Markov trace is crucial for validation, as it allows CADTH to ensure that inputs into the model are being correctly programmed to generate results. Without a transparent Markov trace, CADTH could not fully validate the model.
CADTH was unable to address these deficiencies in the model structure and noted that results from the analysis could not be fully validated.
Uncertainty in treatment discontinuation rate: The sponsor assumed a constant annual discontinuation rate of 15% for all biologic drugs, which did not align with clinical expert opinion. The clinical expert stated that, for new generation IL-17 (secukinumab, ixekizumab, brodalumab, and bimekizumab) and IL-23 inhibitors (guselkumab, risankizumab, tildrakizumab), a lower rate of discontinuation (10%) may be more appropriate. This is mainly due to the expected increase in efficacy of newer products and is supported by a retrospective cohort study, which found low rates of discontinuation due to ineffectiveness.19 This parameter assumption is associated with uncertainty, given the findings of the clinical review.
As part of a scenario analysis, CADTH used a constant annual discontinuation rate of 10% for bimekizumab, secukinumab, ixekizumab, brodalumab, guselkumab, risankizumab, and tildrakizumab, while discontinuation rates remained at 15% for other comparators.
Treatment waning was not considered: In the sponsor’s base case, it was assumed that patients would achieve different PASI scores based on treatment received, according to the proportions derived from the NMA. Patients were assumed to remain in this PASI state until discontinuation for any reason, at which point they would transition to the next line of therapy. This methodology does not allow for consideration of treatment waning, which can occur, according to the clinical expert. The expert noted that, while PASI75 or PASI90 may be considered a relevant threshold by which to assess response, patients may not actually switch therapy until their score drops below PASI 50. Thus, patients could experience treatment waning in which their condition progresses and quality of life decreases, while still remaining on the same therapy, a factor not accounted for in the sponsor’s discontinuation assumptions. It is uncertain what effect this has on the cost-effectiveness results.
Due to limitations in the model structure, CADTH was unable to address treatment waning in its reanalysis.
Uncertainty concerning the appropriate threshold for treatment response: In the sponsor’s base case, patients were assumed to respond to and maintain their current therapy provided they had achieved a response of PASI75 at 16 weeks. The clinical expert noted that, especially for newer biologic drugs entering the market, a PASI90 score would be a more appropriate measure of treatment response. This factor was also noted in the CADTH reviews of tildrakizumab and risankizumab.8,13
As part of a scenario analysis, CADTH considered a PASI90 threshold for treatment response, using the sponsor-provided option to do so.
The sponsor did not consider all relevant adverse events: Relevant adverse events, such as other infections and/or systemic lupus erythematosus, were not included in the sponsor’s pharmacoeconomic analysis and are expected to entail costs and decreases in quality of life. The CADTH clinical review noted higher rates of fungal infections in patients treated with bimekizumab compared to other biologic drugs, which include candidiasis and other such infections. Taken together, this oversight likely biases the results in favour of bimekizumab, as the reduction in quality of life associated with these higher rates of adverse events was not considered.
CADTH was unable to address all relevant adverse events in its reanalysis.
Additionally, the sponsor made the following key assumptions, which CADTH has appraised (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
A 10-year time horizon was considered. | Reasonable. Given the continually evolving field of plaque psoriasis treatments, a shorter time horizon is appropriate as new biologic drugs will likely be added to the treatment paradigm in the future. |
All-cause mortality was included in the model, with no additional risk of mortality associated with moderate to severe plaque psoriasis. | Appropriate. Plaque psoriasis is not expected to influence survival. |
Patients can receive up to 5 lines of therapy with a weighted bucket comparator including all biologic drugs. | Uncertain. While the expert noted that patients could technically receive every biologic if all failed, this is unlikely to make up a significant number of patients or to meaningfully affect the results. |
Efficacy of the weighted bucket comparator based on the sum of the products of BIA year 3 market shares for Ontario and the NMA efficacy. | Uncertain. There was heterogeneity in the NMA regarding the proportion of patients who had previously received biologic drugs. The same NMA and data were used to determine the efficacy of initial treatment with all the biologic drugs and subsequent treatment with the weighted comparator. |
BIA = budget impact analysis; NMA = network meta-analysis.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making 1 change to health state utility values, in consultation with clinical experts. This change is summarized in Table 5.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Utility values | Pooled bimekizumab and certolizumab:
| NICE ixekizumab appraisal:
|
CADTH base case | — | Reanalysis 1 |
PASI = psoriasis area severity index.
The results of the CADTH reanalysis were similar to the sponsor’s, in that the same 3 drugs remained on the cost-effectiveness frontier: adalimumab, brodalumab, and bimekizumab (Table 6). All other products were dominated or subject to extended dominance.
Compared to brodalumab, bimekizumab was associated with incremental costs of $33,526 and QALYs of 0.0135, resulting in an ICER of $2,475,397 per QALY. The probability of cost-effectiveness of bimekizumab at a $50,000 per QALY WTP threshold was 0%. A detailed breakdown of the disaggregate results in available in Appendix 4.
Table 6: Summary of the CADTH Reanalysis Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Adalimumab | 165,100 | 7.173 | Reference |
Brodalumab | 178,413 | 7.200 | 492,461 |
Bimekizumab | 211,939 | 7.214 | 2,475,397 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
CADTH undertook price reduction analysis based on the sponsor’s and CADTH’s base case. Based on the CADTH base case, a price reduction of 41% would be necessary to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for bimekizumab vs. reference product | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 1,805,071 (vs. brodalumab) | 2,475,397 (vs. brodalumab) |
10% | 1,203,540 (vs. brodalumab) | 1,651,581 (vs. brodalumab) |
20% | 599,339 (vs. brodalumab) | 828,051 (vs. brodalumab) |
30% | 243,804 (vs. adalimumab) | 344,068 (vs. adalimumab) |
40% | 39,409 (vs. adalimumab) | 73,981 (vs. adalimumab) |
41% | 18,969 (vs. adalimumab) | 46,972 (vs. adalimumab) |
ICER = incremental cost-effectiveness ratio; vs. = versus.
CADTH undertook a series of exploratory analyses to determine the impact of alternative assumptions on the cost-effectiveness of bimekizumab, which are outlined as follows:
An analysis used a constant annual discontinuation rate of 10% for bimekizumab, secukinumab, ixekizumab, brodalumab, guselkumab, risankizumab, and tildrakizumab and maintained a rate of 15% for other comparators.
An analysis considered a PASI90 threshold for treatment response.
An analysis assumed the same efficacy based on the NMA for all comparators, namely, that of the weighted bucket comparator.
An analysis assumed a greater proportion of patients may require more frequent dosage of bimekizumab in the maintenance phase.
The results of these analyses are presented in Appendix 4, Table 19. The scenario involving differential discontinuation rates resulted in an ICER for bimekizumab of $2,617,920 per QALY compared to brodalumab. The scenario assuming a PASI90 response threshold resulted in an ICER of $2,393,618 per QALY for bimekizumab compared to brodalumab. The scenario assuming a greater proportion of patients require more frequent dosage of bimekizumab resulted in an ICER of $3,111,076 per QALY for bimekizumab compared to brodalumab.
Issues for Consideration
There is evidence that many patients experience delays from symptom onset to treatment for their plaque psoriasis.20 Moreover, as psoriasis is a disease that can flare up, patients can go for long periods in relative remission before re-treatment. The impact of these factors on cost-effectiveness is unknown.
For some patients with a body weight of 120 kg or more, a dosage of 320 mg every 4 weeks after week 16 may be considered, effectively doubling the cost of bimekizumab. Limited post hoc data were available in the clinical submission for patients with body weight of 120 kg or more. Furthermore, the NMA considered only the induction period (first 16 weeks) and did not incorporate weight-based dosing. Therefore, while costs for bimekizumab are expected to increase with increasing proportions of patients with body weight of 120 kg or more, the clinical efficacy and impact on cost-effectiveness are unknown.
Bimekizumab may be self-administered and is the only IL-17 inhibitor with maintenance dosage frequency of every 8 weeks. This ease of administration was noted as an important outcome for patients in the patient input.
For patients with a body weight of 120 kg or more who did not achieve a complete skin response, a dose of 320 mg every 4 weeks after week 16 may be considered for bimekizumab. As there is some uncertainty in the estimate of patients with a body weight of 120 kg or more, there is also uncertainty in the ICER and price reduction required, but higher proportions of patients receiving the drug every 4 weeks will result in a higher ICER and thus require greater price reductions.
The final product monograph states that “at the prescriber’s discretion, discontinuation of treatment may be considered in patients who have shown no improvement after 16 weeks of treatment.” If treatment is continued in patients who do not achieve a PASI75 response, the impact on cost-effectiveness is uncertain, as the total costs will increase, but the impact on incremental benefit is not known.
Overall Conclusions
The CADTH clinical review concluded that bimekizumab showed a statistically and clinically important improvement in psoriasis disease severity (as measured by PASI and Investigator’s Global Assessment) versus placebo, adalimumab, ustekinumab, and secukinumab in the evaluated studies (PS0009, PS0008, PS0015, and PS0013) after 16 weeks in patients with moderate to severe plaque psoriasis who were candidates for phototherapy or systemic therapy. The 1-year data from these clinical trials suggest that PASI response may be maintained in the majority of patients who continue bimekizumab therapy; the incremental differences that favoured bimekizumab versus secukinumab or ustekinumab were also maintained. However, these longer-term outcome data were limited by the lack of control group and failure to maintain randomization. The data were restricted to patients with a demonstrated response to treatment or those who did not use a Health Canada–recommended dosage regimen. In addition, there were important limitations in HRQoL data, which limit the interpretation of these results. The safety data available for bimekizumab were limited by the sample size and study duration of the trials, which may have been insufficient to detect infrequent adverse events or those that take a longer time to develop.
As there were important comparators not assessed in the clinical trials, the sponsor submitted indirect evidence suggests that ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. However, several sources of heterogeneity were identified across the trials included in the indirect comparison, and it is uncertain whether the methods used to control for potential bias were adequate, or whether the between-group differences for some comparisons were clinically important.
CADTH identified several limitations with the sponsor’s pharmacoeconomic model, including the clinical evidence used to inform the model, utility estimates, discontinuation rate, lack of treatment waning, and adverse events. As part of the base case, CADTH used alternative utility values from the NICE submission for ixekizumab. Based on the CADTH base case, bimekizumab was associated with incremental costs of $33,526 and QALYs of 0.0135, resulting in an ICER of $2,475,397 per QALY compared to brodalumab. The probability of cost-effectiveness of bimekizumab at a $50,000 per QALY WTP threshold was 0%, and a price reduction of 41% would be required to achieve cost-effectiveness at this threshold.
Scenario analyses were performed regarding treatment discontinuation rate and PASI response threshold. The scenario involving differential discontinuation rates resulted in an ICER for bimekizumab of $2,617,920 per QALY compared to brodalumab. The scenario that assumed a PASI90 response threshold resulted in an ICER of $2,393,618 per QALY for bimekizumab compared to brodalumab. These analyses had little impact on the overall ICER, which is predicated upon small incremental QALYs and a high drug acquisition cost.
CADTH acknowledges that both the clinical trial data and indirect evidence have limitations, which leads to some uncertainty with the clinical findings. Furthermore, the lack of transparency in the sponsor’s overly complex model contributes additional uncertainty to the results of the economic analysis. As an exploratory analysis, CADTH assumed the same efficacy for all comparators based on the efficacy of the weighted bucket. In this analysis, a price reduction of 49.5% would be required to ensure cost parity with the cheapest comparator, adalimumab.
References
1.Bimzelx (bimekizumab): 160 mg/mL solution subcutaneous injection [DRAFT] [product monograph]. Oakville (ON): UCB Canada Inc; 1800.
2.Systematic literature review and network meta-analysis of treatments for moderate-to-severe plaque psoriasis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Bimzelx (bimekizumab), 160 mg/mL subcutaneous injection. Oakville (ON): UCB Canada Inc; 2021 Aug 17.
3.Statistics Canada. Life expectancy and other elements of the complete life table, three-year estimates, Canada, all provinces except Prince Edward IslandLife tables, Canada, provinces and territories [Table: 13-10-0114-01]. 2020; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2021 Oct 27.
4.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Bimzelx (bimekizumab), 160 mg/mL subcutaneous injection. Oakville (ON): UCB Canada Inc; 2021 Aug 17.
5.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Sept 22.
6.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Sept 22.
7.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: guselkumab (Tremfya) - (Janssen Inc.). Ottawa (ON): CADTH; 2018 Feb 21: https://www.cadth.ca/sites/default/files/cdr/complete/SR0530_Tremfya_complete_Feb-23-18.pdf. Accessed 2021 Oct 27.
8.CADTH pharmacoeconomic review report: tildrakizumab (Ilumya) - (Sun Pharma Global FZE). Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0624-ilumya-pharmacoeconomic-review-report.pdf. Accessed 2021 Oct 27.
9.Patient cost estimator. 2021; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2021 Oct 27.
10.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2021: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2021 Oct 27.
11.Alberta Health Interactive Health Data Application. Health costing: hospital ambulatory care case costs - CACS - 2018 version. 2018; http://www.ahw.gov.ab.ca/IHDA_Retrieval/selectSubCategoryParameters.do. Accessed 2021 Oct 27.
12.CADTH pharmacoeconomic review report: guselkumab (Tremfya) - (Janssen Inc.). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0530_Tremfya_PE_Report.pdf. Accessed 2021 Oct 27.
13.CADTH pharmacoeconomic review report: risankizumab (Skyrizi) - (AbbVie). Ottawa (ON): CADTH; 2019: https://cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0583-skyrizi-pharmacoeconomic-review-report.pdf. Accessed 2021 Oct 27.
14.Drug Reimbursement Review sponsor submission: Bimzelx (bimekizumab), 160 mg/mL subcutaneous injection [internal sponsor's package]. Oakville (ON): UCB Canada Inc; 2021 Aug 17.
15.Bansback N, Tsuchiya A, Brazier J, Anis A. Canadian valuation of EQ-5D health states: preliminary value set and considerations for future valuation studies. PLoS One. 2012;7(2):e31115. PubMed
16.Guertin J, Feeny D, Tarride J. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;12(190):E155-161. PubMed
17.Xie F, Pullenayegum E, Gaebel K, Bansback N, Stirling B, Ohinmaa A. A time trade-off-derived value set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
18.Ixekizumab for treating moderate to severe plaque psoriasis. (Technology appraisal guidance TA442). London (GB): National Institute for Health and Care Excellence; 2017: https://www.nice.org.uk/guidance/ta442/resources/ixekizumab-for-treating-moderate-to-severe-plaque-psoriasis-pdf-82604781265093. Accessed 2021 Oct 27.
19.Torres T, Puig L, Vender R, Lynde C, al e. Drug survival of IL-12/23, IL-17 and IL-23 inhibitors for psoriasis treatment: a retrospective multi-country, multicentric cohort study. Am J Clin Dermatol. 2021;22(4):567-579. PubMed
20.Maza A, Richard M, Aubin F, et al. Significant delay in the introduction of systemic treatment of moderate to severe psoriasis: a prospective multicentre observational study in outpatients from hospital dermatology departments in France. Br J Dermatol. 2012;167(3):643-648. PubMed
21.Cimzia (certolizumab pegol): 200 mg/mL solution for injection [product monograph]. Oakville (ON): UCB Canada Inc; 2019 Nov 13: https://pdf.hres.ca/dpd_pm/00053920.PDF. Accessed 2021 Sep 22.
22.Cosentyx (secukinumab): 150 mg/mL powder for solution for injection [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc; 2021 May 26: https://pdf.hres.ca/dpd_pm/00061115.PDF. Accessed 2021 Sep 22.
23.Erelzi (etanercept): 50 mg/mL solution for injection in a prefilled syringe, 50 mg/mL solution for injection in a prefilled autoinjector [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2020 Jun 9: https://pdf.hres.ca/dpd_pm/00056848.PDF. Accessed 2021 Sep 22.
24.Hyrimoz (adalimumab): 20 mg in 0.4 mL sterile solution (50 mg/mL) subcutaneous injection in pre-filled syringe, 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection in a pre-filled syringe, 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection in a pre-filled autoinjector [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2021 Sep 10: https://pdf.hres.ca/dpd_pm/00062896.PDF. Accessed 2021 Sep 22.
25.Ilumya (tildrakizumab): 100 mg in 1 mL sterile solution (100 mg/mL) for subcutaneous injection [product monograph]. Burlington (ON): C.R.I; 2021 May 19: https://pdf.hres.ca/dpd_pm/00060995.PDF. Accessed 2021 Sep 22.
26.Renflexis (infliximab): 100 mg/vial powder for solution, sterile, lyophilized [product monograph]. Kirkland (QC): Merck Canada Inc; 2020 Feb 25: https://pdf.hres.ca/dpd_pm/00055165.PDF. Accessed 2021 Sep 22.
27.Siliq (brodalumab): 140 mg/mL solution for subcutaneous injection [product monograph]. Laval (QC): Bausch Health, Canada Inc; 2019 Jun 7: https://pdf.hres.ca/dpd_pm/00051682.PDF. Accessed 2021 Sep 22.
28.Skyrizi (risankizumab): 150 mg in 1 mL sterile solution (150 mg/mL), 75 mg in 0.83 mL sterile solution (90 mg/mL), subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2021 Aug 19: https://pdf.hres.ca/dpd_pm/00062581.PDF. Accessed 2021 Sep 22.
29.Stelara (ustekinumab): 45 mg/0.5 mL, 90 mg/1.0 mL solution for subcutaneous injection; Stelara I.V. (ustekinumab): 130 mg/26 mL (5 mg/mL) solution for intravenous infusion [product monograph]. Toronto (ON): Janssen Inc; 2021 Sep 9: https://pdf.hres.ca/dpd_pm/00062938.PDF. Accessed 2021 Sep 22.
30.Taltz (ixekizumab): 80 mg / 1.0 mL solution for injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc; 2021 Mar 29: https://pdf.hres.ca/dpd_pm/00060574.PDF. Accessed 2021 Oct 27.
31.Tremfya (guselkumab): 100 mg/1 mL solution for injection pre-filled syringe, Tremfya One-Press (guselkumab): 100 mg/1 mL solution for injection patient-controlled injector [product monograph]. Toronto (ON): Janssen Inc; 2020 Sep 4: https://pdf.hres.ca/dpd_pm/00057930.PDF. Accessed 2021 Sep 22.
32.DeltaPA. Ottawa (ON): IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 Oct 27.
33.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Bimzelx (bimekizumab), 160 mg/mL subcutaneous injection. Oakville (ON): UCB Canada Inc.; 2021 August 17.
34.Papp K, Gulliver W, Lynde C, Poulin Y, Ashkenas J. Canadian guidelines fro the management of plaque psoriasis: overview. J Cutan Med Surg. 2011;15(4):210-219. PubMed
35.CADTH final reimbursement recommendation: tildrakizumab (Ilumya). Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/cdr/complete/SR0624%20Ilumya%20-%20CDEC%20Final%20Recommendation%20June%2023%2C%202021_for%20posting%20(1).pdf. Accessed 2021 Oct 27.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Moderate to Severe Plaque Psoriasis
Treatment | Strength / concentration | Form | Price | Recommended dosagea | Annual cost |
|---|---|---|---|---|---|
Bimekizumab (Bimzelx) | 160 mg/mL | 1 mL Pre-filled syringe or autoinjector | $1,625.0000b | 320 mg at weeks 0, 4, 8, 12, 16 followed by 320 mg every 8 weeks (or every 4 weeks for those ≥120 kg) | First year: $29,250 Subsequent years: $22,750 For ≥120 kg First year: $45,500 Subsequent years: $42,250 |
Adalimumab (Hyrimoz - biosimilar) | 50 mg/mL | 0.4 mL 0.8 mL Pre-filled syringe | $235.6350 $471.2700 | 80 mg at week 0 followed by 40 mg every 2 weeks starting one week after initial dose | First year: $13,196 Subsequent years: $12,253 |
Brodalumab (Siliq) | 140 mg/mL | 1.5 mL Pre-filled syringe | $645.0000 | 210 mg at weeks 0, 1, 2 followed by 210 mg every 2 weeks | First year: $18,060 Subsequent years: $16,770 |
Certolizumab pegol (Cimzia) | 200 mg/mL | 1 mL Pre-filled syringe | $664.5100c | 400 mg at weeks 0, 2, 4 followed by 200 mg or 400 mg every 2 weeks | First year: $19,935 to $35,884 Subsequent years: $17,277 to $34,555 |
Etanercept (Erelzi - biosimilar) | 50 mg/mL | 0.5 mL 1 mL Pre-filled syringe or autoinjector | $120.5000 $241.0000 | 50 mg twice per week for 12 weeks followed by 50 mg per week | First year: $15,906 Subsequent years: $12,532 |
Guselkumab (Tremfya) | 100 mg/mL | 1 mL Pre-filled syringe or autoinjector | $3,059.7400d | 100 mg at weeks 0 and 4 followed by 100 mg every 8 weeks | First year: $24,478 Subsequent years: $18,358 |
Infliximab (Renflexis - biosimilar) | 0.4 mg/mL | 100 mg Powder for IV injection | $493.0000 | 5 mg/kg at weeks 0, 2, 6 followed by 5 mg/kg every 8 weeks | First year: $19,720 Subsequent years: $17,255 |
Ixekizumab (Taltz) | 80 mg | 1 mL Pre-filled syringe | $1,670.4400 | 160 mg at week 0 followed by 80 mg at weeks 2, 4, 6, 8, 10, 12 followed by 80 mg every 4 weeks | First year: $30,068 Subsequent years: $21,716 |
Risankizumab (Skyrizi) | 90 mg/mL | 0.83 mL Pre-filled syringe | $2,467.5000 | 150 mg at weeks 0, 4 followed by 150 mg every 12 weeks | First year: $29,610 Subsequent years: $19,740 |
Secukinumab (Cosentyx) | 150 mg/mL | 1 mL Pre-filled syringe | $840.0000 | 300 mg at weeks 0, 1, 2, 3, 4 followed by 300 mg every 4 weeks | First year: $28,560 Subsequent years: $21,840 |
Tildrakizumab (Ilumya) | 100 mg/mL | 1 mL Pre-filled syringe | $4,935.0000e | 100 mg at weeks 0, 4 followed by 100 mg every 12 weeks | First year: $29,610 Subsequent years: $19,740 |
Ustekinumab (Stelara) | 90 mg/mL | 0.5 mL 1 mL Pre-filled syringe | $4,593.1400 | 45 mg to 90 mg at weeks 0, 4, followed by 45 mg to 90 mg every 12 weeks | First year: $27,559 Subsequent years: $18,373 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed September 2021),5 unless otherwise indicated, and do not include dispensing fees. For weight-based dosing a weight of 89.6 kg was assumed based on pooled data from bimekizumab trials.4
aRecommended dosages are from the respective product monographs.21-31
bSponsor submitted price.4
cOntario Exceptional Access Program formulary (accessed September 2021).6
dIQVIA DeltaPA database (accessed September 2021).32
ePrice taken from CADTH review of tildrakizumab (Ilumya).8
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | The model was unwieldy and computationally complex, making for slow validation and run times. The model relied heavily on VBA, making it difficult to validate. The Markov trace was massive and overly complex on account of it being converted from VBA code after creation of the original model. The model contained numerous “IFERROR” statements. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | There was a slight discrepancy between the deterministic results provided in the sponsor’s model and the results observed when running the model provided deterministically. This suggests a parameter was changed after finalization of the model but before the CADTH submission. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The technical report was lacking in detail, especially pertaining to how the NMA results were incorporated into the model. Some slight discrepancies between the results reported in the manuscript and those found in the model. The sponsor indicated that the differences were due to sampling variation between the NMA report and CODA file included within the model. |
CODA = Co-Design Architecture; NMA = network meta-analysis; VBA = visual basic application.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
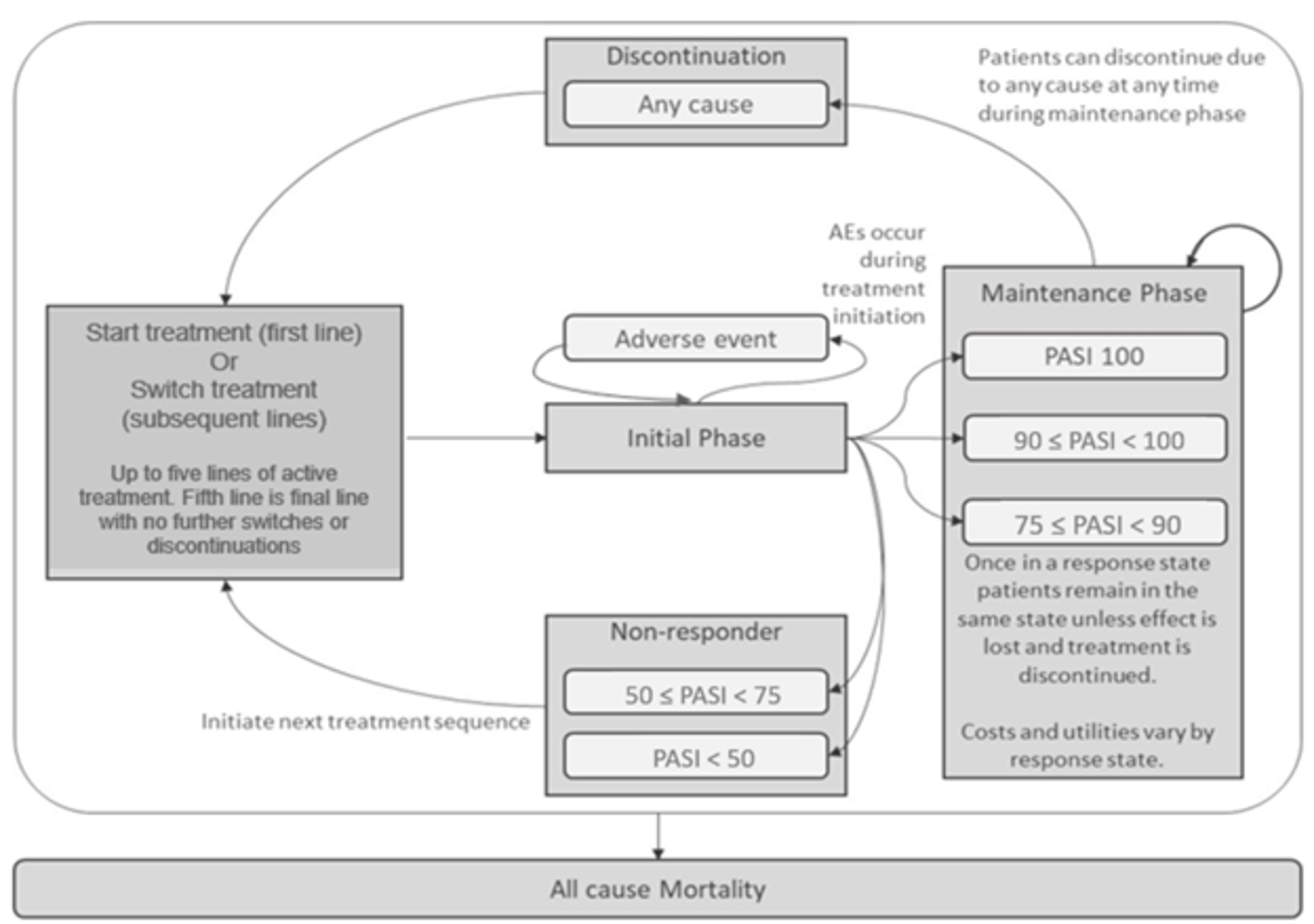
AE = adverse event; PASI = psoriasis area sensitivity index.
Source: Sponsor’s pharmacoeconomic report.4
Detailed Results of the Sponsor’s Base Case
|||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||| |
|---|---|
|||||||||||||||||||||||||||||| | |||||||||| |
|||||||||||||||||||||||||||||| | |||||||||| |
||||||||||||||||||||||||||||||||||
Note that this table has been redacted.
Source: Sponsor’s pharmacoeconomic report.4
Table 11: Health State Utilities Used in the Model
Health state | Utility value |
|---|---|
Baseline PASI | 0.7879 |
PASI <50 | 0.7905 |
50 ≤ PASI < 75 | 0.8743 |
75 ≤ PASI < 90 | 0.8934 |
90 ≤ PASI < 100 | 0.9170 |
PASI100 | 0.9304 |
PASI = psoriasis area severity index.
Source: Sponsor’s pharmacoeconomic report.4
Table 12: Disaggregated Costs in the Sponsor’s Base Case
Treatment | Drug acquisition | Monitoring | Health state | Adverse events | Total |
|---|---|---|---|---|---|
Bimekizumab | $209,920.88 | $456.25 | $538.37 | $3.01 | $210,918.51 |
Adalimumab | $162,746.71 | $475.29 | $600.61 | $0.48 | $163,823.09 |
Brodalumab | $176,309.62 | $461.17 | $553.54 | $0.43 | $177,324.77 |
Certolizumab pegol 200 mg | $181,871.00 | $474.18 | $597.13 | $0.47 | $182,942.78 |
Certolizumab pegol 400 mg | $246,575.17 | $469.08 | $580.46 | $0.46 | $247,625.17 |
Etanercept | $177,333.84 | $502.15 | $689.57 | $0.56 | $178,526.11 |
Guselkumab | $192,936.88 | $461.18 | $554.42 | $0.43 | $193,952.92 |
Infliximab | $170,278.43 | $964.68 | $574.28 | $0.45 | $171,817.84 |
Ixekizumab | $204,765.95 | $459.52 | $547.98 | $0.43 | $205,773.87 |
Risankizumab | $202,767.24 | $458.35 | $545.02 | $0.43 | $203,771.02 |
Secukinumab 300 mg | $196,271.49 | $463.50 | $562.40 | $0.44 | $197,297.84 |
Tildrakizumab | $199,997.75 | $480.85 | $619.22 | $0.49 | $201,098.31 |
Ustekinumab 45 mg | $195,031.00 | $474.52 | $597.76 | $0.47 | $196,103.76 |
Ustekinumab 90 mg | $195,014.97 | $474.42 | $598.23 | $0.48 | $196,088.09 |
Source: Sponsor’s pharmacoeconomic report.4
Table 13: Disaggregated QALYs Gained in the Sponsor’s Base Case
Treatment | Initial phasea | PASI < 50 | 50 ≤ PASI < 75 | 75 ≤ PASI < 90 | 90 ≤ PASI < 100 | PASI 100 | Total |
|---|---|---|---|---|---|---|---|
Bimekizumab | 0.643 | 0.031 | 0.038 | 1.262 | 2.424 | 4.004 | 8.401 |
Adalimumab | 0.699 | 0.043 | 0.053 | 2.145 | 2.788 | 2.618 | 8.346 |
Brodalumab | 0.657 | 0.034 | 0.041 | 1.578 | 2.587 | 3.486 | 8.383 |
Certolizumab pegol 200 mg | 0.696 | 0.043 | 0.052 | 2.327 | 2.762 | 2.460 | 8.340 |
Certolizumab pegol 400 mg | 0.681 | 0.039 | 0.048 | 2.239 | 2.848 | 2.490 | 8.346 |
Etanercept 50 mg | 0.777 | 0.062 | 0.076 | 2.416 | 2.502 | 2.488 | 8.321 |
Guselkumab | 0.658 | 0.034 | 0.042 | 1.768 | 2.855 | 3.015 | 8.371 |
Infliximab | 0.676 | 0.038 | 0.047 | 2.079 | 2.767 | 2.749 | 8.355 |
Ixekizumab | 0.652 | 0.033 | 0.040 | 1.706 | 2.738 | 3.207 | 8.377 |
Risankizumab | 0.650 | 0.032 | 0.039 | 1.632 | 2.559 | 3.471 | 8.383 |
Secukinumab 300 mg | 0.665 | 0.036 | 0.044 | 1.841 | 2.741 | 3.042 | 8.368 |
Tildrakizumab | 0.715 | 0.047 | 0.058 | 2.245 | 2.720 | 2.553 | 8.339 |
Ustekinumab 45 mg | 0.696 | 0.043 | 0.053 | 2.197 | 2.751 | 2.606 | 8.345 |
Ustekinumab 90 mg | 0.697 | 0.043 | 0.053 | 2.299 | 2.697 | 2.554 | 8.342 |
QALY = quality-adjusted life-year; PASI = psoriatic area severity index.
aThe initial phase was considered to be the first 16 weeks of treatment with each line of therapy, and QALYs gained in this run-in period were summed across all lines of therapy. Similarly, for all other categories, the QALYs gained in each PASI state were the sum of QALYs gained in those states in each line of therapy.
Table 14: Probabilistic Cost-Effectiveness Sequential Analysis From Sponsor’s Base Case
Treatment | Cost | QALYs | Incremental Cost | Incremental QALYs | ICER |
|---|---|---|---|---|---|
Adalimumab | $163,823 | 8.345 | Ref. | Ref. | Ref. |
Infliximab | $171,818 | 8.355 | — | — | Extendedly dominated |
Brodalumab | $177,325 | 8.382 | $13,502 | 0.036 | $371,500 |
Etanercept | $178,526 | 8.321 | — | — | Dominated |
Certolizumab pegol 200 mg | $182,943 | 8.340 | — | — | Dominated |
Guselkumab | $193,953 | 8.371 | — | — | Dominated |
Ustekinumab 90 mg | $196,088 | 8.342 | — | — | Dominated |
Ustekinumab 45 mg | $196,104 | 8.345 | — | — | Dominated |
Secukinumab 300 mg | $197,298 | 8.368 | — | — | Dominated |
Tildrakizumab | $201,098 | 8.339 | — | — | Dominated |
Risankizumab | $203,771 | 8.383 | — | — | Extendedly dominated |
Ixekizumab | $205,774 | 8.377 | — | — | Dominated |
Bimekizumab | $210,919 | 8.401 | $33,594 | 0.019 | $1,805,071 |
Certolizumab pegol 400 mg | $247,625 | 8.346 | — | — | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 15: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | Adalimumab | 163,823 | 8.345 | Ref. |
Brodalumab | 177,325 | 8.382 | 371,500 | |
Bimekizumab | 210,919 | 8.401 | 1,805,071 | |
CADTH reanalysis 1 and base case | Adalimumab | 165,100 | 7.173 | Ref. |
Brodalumab | 178,413 | 7.200 | 492,461 | |
Bimekizumab | 211,939 | 7.214 | 2,475,397 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Table 16: Disaggregated Costs in the CADTH Reanalysis
Treatment | Drug acquisition | Monitoring | Health state | Adverse events | Total |
|---|---|---|---|---|---|
Bimekizumab | $210,940.65 | $456.87 | $538.50 | $3.01 | $211,939.03 |
Adalimumab | $164,024.15 | $475.32 | $599.92 | $0.48 | $165,099.87 |
Brodalumab | $177,398.58 | $461.08 | $552.78 | $0.43 | $178,412.87 |
Certolizumab pegol 200 mg | $183,141.22 | $474.28 | $596.63 | $0.48 | $184,212.60 |
Certolizumab pegol 400 mg | $247,789.66 | $469.44 | $579.81 | $0.46 | $248,839.37 |
Etanercept | $178,941.97 | $502.24 | $688.83 | $0.56 | $180,133.60 |
Guselkumab | $194,045.50 | $461.33 | $553.72 | $0.44 | $195,060.99 |
Infliximab | $171,428.67 | $965.33 | $573.38 | $0.45 | $172,967.83 |
Ixekizumab | $205,857.38 | $459.32 | $546.74 | $0.43 | $206,863.87 |
Risankizumab | $203,822.61 | $458.68 | $544.84 | $0.43 | $204,826.56 |
Secukinumab 300 mg | $197,415.66 | $464.16 | $562.25 | $0.44 | $198,442.52 |
Tildrakizumab | $201,334.69 | $481.19 | $619.02 | $0.50 | $202,435.40 |
Ustekinumab 45 mg | $196,298.34 | $474.26 | $596.38 | $0.48 | $197,369.45 |
Ustekinumab 90 mg | $196,284.71 | $475.09 | $598.74 | $0.48 | $197,359.02 |
Table 17: Disaggregated QALYs Gained in the CADTH Reanalysis
Treatment | Initial phasea | PASI < 50 | 50 ≤ PASI < 75 | 75 ≤ PASI < 90 | 90 ≤ PASI < 100 | PASI 100 | Total |
|---|---|---|---|---|---|---|---|
Bimekizumab | 0.529 | 0.026 | 0.032 | 1.098 | 2.092 | 3.436 | 7.214 |
Adalimumab | 0.574 | 0.036 | 0.046 | 1.867 | 2.401 | 2.250 | 7.173 |
Brodalumab | 0.539 | 0.028 | 0.035 | 1.373 | 2.229 | 2.996 | 7.200 |
Certolizumab pegol 200 mg | 0.571 | 0.036 | 0.045 | 2.027 | 2.374 | 2.116 | 7.169 |
Certolizumab pegol 400 mg | 0.559 | 0.033 | 0.041 | 1.948 | 2.450 | 2.143 | 7.174 |
Etanercept 50 mg | 0.638 | 0.051 | 0.065 | 2.102 | 2.154 | 2.139 | 7.150 |
Guselkumab | 0.540 | 0.028 | 0.036 | 1.540 | 2.459 | 2.590 | 7.193 |
Infliximab | 0.554 | 0.032 | 0.040 | 1.808 | 2.383 | 2.365 | 7.182 |
Ixekizumab | 0.535 | 0.027 | 0.034 | 1.483 | 2.361 | 2.757 | 7.198 |
Risankizumab | 0.534 | 0.027 | 0.034 | 1.420 | 2.207 | 2.981 | 7.202 |
Secukinumab 300 mg | 0.546 | 0.030 | 0.037 | 1.601 | 2.361 | 2.614 | 7.190 |
Tildrakizumab | 0.588 | 0.039 | 0.050 | 1.951 | 2.345 | 2.194 | 7.168 |
Ustekinumab 45 mg | 0.571 | 0.036 | 0.045 | 1.911 | 2.371 | 2.240 | 7.173 |
Ustekinumab 90 mg | 0.573 | 0.036 | 0.045 | 2.004 | 2.322 | 2.190 | 7.170 |
aThe initial phase was considered to be the first 16 weeks of treatment with each line of therapy, and QALYs gained in this run-in period were summed across all lines of therapy. Similarly, for all other categories, the QALYs gained in each PASI state were the sum of QALYs gained in those states in each line of therapy.
Table 18: Probabilistic Cost-Effectiveness Sequential Analysis From the CADTH Reanalysis
Treatment | Cost | QALYs | Incremental Cost | Incremental QALYs | ICER |
|---|---|---|---|---|---|
Adalimumab | $165,100 | 7.173 | Ref. | Ref. | Ref. |
Infliximab | $172,968 | 7.182 | — | — | Extendedly dominated |
Brodalumab | $178,413 | 7.200 | $13,313 | 0.027 | $492,461 |
Etanercept | $180,134 | 7.150 | — | — | Dominated |
Certolizumab pegol 200 mg | $184,213 | 7.169 | — | — | Dominated |
Guselkumab | $195,061 | 7.193 | — | — | Dominated |
Ustekinumab 90 mg | $197,359 | 7.170 | — | — | Dominated |
Ustekinumab 45 mg | $197,369 | 7.173 | — | — | Dominated |
Secukinumab 300 mg | $198,443 | 7.190 | — | — | Dominated |
Tildrakizumab | $202,435 | 7.168 | — | — | Dominated |
Risankizumab | $204,827 | 7.202 | — | — | Extendedly dominated |
Ixekizumab | $206,864 | 7.198 | — | — | Dominated |
Bimekizumab | $211,939 | 7.214 | $33,526 | 0.014 | $2,475,397 |
Certolizumab pegol 400 mg | $248,839 | 7.174 | — | — | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Scenario Analyses
Table 19: Summary of Scenario Analyses Conducted on CADTH Base Case
Scenario analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CADTH base case | Adalimumab | 165,100 | 7.173 | Ref. |
Brodalumab | 178,413 | 7.200 | 492,461 | |
Bimekizumab | 211,939 | 7.214 | 2,475,397 | |
1. Differential discontinuation rates | Adalimumab | 165,105 | 7.180 | Ref. |
Brodalumab | 174,435 | 7.225 | 205,191 | |
Bimekizumab | 213,853 | 7.240 | 2,617,920 | |
2. PASI90 considered as response threshold | Adalimumab | 175,428 | 7.164 | Ref. |
Brodalumab | 181,848 | 7.191 | 240,325 | |
Bimekizumab | 211,877 | 7.203 | 2,393,618 | |
3. Same efficacy for all comparatorsa | Adalimumab | 161,578 | 7.191 | Ref. |
Brodalumab | 179,732 | 7.191 | Dominated | |
Bimekizumab | 210,341b | 7.191 | Dominated | |
4. 15% of bimekizumab patients assumed to require Q4W dosing | Adalimumab | 165,765 | 7.178 | Ref. |
Brodalumab | 179,037 | 7.206 | 471,977 | |
Bimekizumab | 218,454c | 7.219 | 3,111,076 |
ICER = incremental cost-effectiveness ratio; PASI = psoriasis area severity index; QALY = quality-adjusted life-year; Ref. = reference.
aDeterministic analysis undertaken, given the underlying efficacy assumption.
bIn this scenario assuming equal efficacy, bimekizumab would require a 49.5% price reduction to ensure cost parity with adalimumab.
cIn this scenario assuming 15% require bimekizumab Q4W dosing, bimekizumab would require a 43.7% price reduction to achieve cost-effectiveness at a $50,000 per QALY threshold.
Note: Other treatments were included in these analyses, but were dominated (i.e., more costly and less effective).
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 20: Summary of Key Takeaways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The submitted BIA assessed the introduction of bimekizumab for the treatment of adult patients with moderate to severe plaque psoriasis (plaque psoriasis) who are candidates for systemic therapy or phototherapy. The analysis was taken from the perspective of the Canadian public drug plans using a claims-based approach, with only drug acquisition costs included. A 3-year time horizon was used, from 2023 to 2025, with 2022 as a base year. Prescription claims data were obtained from the IQVIA Pharmastat database from January 1, 2018, to December 31, 2020, and were used to estimate the market sizes for each of the comparators. Claims data from the IQVIA RxDynamics database were used to determine the proportion of Pharmastat claims that were related to plaque psoriasis. The number of plaque psoriasis drug units was converted to number of patients based on the number of drug units received per year.
The reference case scenario included all biologic comparators used in the pharmacoeconomic analysis, namely, adalimumab, brodalumab, certolizumab pegol, etanercept, guselkumab, infliximab, ixekizumab, risankizumab, secukinumab, tildrakizumab, and ustekinumab. The new drug scenario included bimekizumab along with these other comparators. Bimekizumab was assumed to capture market share from all comparators equally, as an equal proportion of their current market share in the reference scenario. Of note, the drugs certolizumab pegol, guselkumab, and tildrakizumab were not assumed to possess any market share in either the new or reference scenario on account of their novelty and not being reimbursed by any of the drug programs. Key inputs to the BIA are documented in Table 21.
Table 21: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review in Canada | |||||||||| / |||||||||| / |||||||||| |
Market Uptake (3 years) | |
Uptake in Ontario (new drug scenario) | |
Bimekizumab | ||||||||||% / ||||||||||% / ||||||||||% |
Adalimumab | ||||||||||% / ||||||||||% / ||||||||||% |
Brodalumab | ||||||||||% / ||||||||||% / ||||||||||% |
Certolizumab pegol | ||||||||||% / ||||||||||% / ||||||||||% |
Etanercept (Enbrel) | ||||||||||% / ||||||||||% / ||||||||||% |
Etanercept (biosimilars) | ||||||||||% / ||||||||||% / ||||||||||% |
Guselkumab | ||||||||||% / ||||||||||% / ||||||||||% |
Infliximab (Remicade) | ||||||||||% / ||||||||||% / ||||||||||% |
Infliximab (biosimilars) | ||||||||||% / ||||||||||% / ||||||||||% |
Ixekizumab | ||||||||||% / ||||||||||% / ||||||||||% |
Risankizumab | ||||||||||% / ||||||||||% / ||||||||||% |
Secukinumab | ||||||||||% / ||||||||||% / ||||||||||% |
Tildrakizumab | ||||||||||% / ||||||||||% / ||||||||||% |
Ustekinumab | ||||||||||% / ||||||||||% / ||||||||||% |
Cost of treatment (per patient) | |
Cost of annual treatment in first year in Ontario | |
Bimekizumab | $29,250 |
Adalimumab | $13,196 |
Brodalumab | $18,060 |
Certolizumab pegol 200 mg | $19,935 |
Certolizumab pegol 400 mg | $35,884 |
Etanercept (Enbrel) | $26,795 |
Etanercept (biosimilars) | $15,906 |
Guselkumab | $24,478 |
Infliximab (Remicade) | $17,666 |
Infliximab (biosimilars) | $17,666 |
Ixekizumab | $30,068 |
Risankizumab | $29,610 |
Secukinumab | $26,880 |
Tildrakizumab | $29,610 |
Ustekinumab | $27,559 |
Cost of annual treatment in maintenance year in Ontario | |
Bimekizumab | $21,125 |
Adalimumab | $12,253 |
Brodalumab | $16,770 |
Certolizumab pegol 200 mg | $17,277 |
Certolizumab pegol 400 mg | $34,554 |
Etanercept (Enbrel) | $21,111 |
Etanercept (biosimilars) | $12,532 |
Guselkumab | $19,888 |
Infliximab (Remicade) | $14,354 |
Infliximab (biosimilars) | $14,354 |
Ixekizumab | $21,715 |
Risankizumab | $21,385 |
Secukinumab | $20,160 |
Tildrakizumab | $21,385 |
Ustekinumab | $19,903 |
Note: Costs and market shares vary by jurisdiction. Ontario presented here as an example.
Source: Sponsor’s budget impact report.33
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding bimekizumab for the treatment of adult patients with moderate to severe plaque psoriasis was $2,908,857 in year 1, $6,718,044 in year 2, and $9,729,169 in year 3, for a 3-year total of $19,356,070.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Uncertainty with the use of a claims-based approach to estimate market size: The sponsor estimated the market size for plaque psoriasis using IQVIA Pharmastat claims data for the included biologic drugs from 2018 to 2020. To determine how many of the claims were for plaque psoriasis specifically, the sponsor used IQVIA RxDynamics data from the Ontario Drug Benefit (ODB), which categorized drugs by indication. The proportion of claims for plaque psoriasis from RxDynamics was multiplied by the number of units in IQVIA Pharmastat. While this approach is more thorough than one in which Pharmastat data alone are used, the derivation of market size using claims data is still associated with uncertainty. CADTH attempted to corroborate the sponsor’s IQVIA Pharmastat data through their own access and found the sponsor’s methods of including Pharmastat units to be inconsistent. For some drugs in some jurisdictions, the sponsor included both public and private claims, while for others only private or only public claims were considered relevant. No information was provided in the technical reports describing this methodology. In addition, no information or source was provided for the RxDynamics database from which the claims by indication data were derived. Furthermore, it is unclear whether the claims by indication data for Ontario would be generalizable to the other jurisdictions, as is assumed in the sponsor’s base case. Finally, there was no correlation between the number of plaque psoriasis patients estimated by the ODB RxDynamics data and the number of plaque psoriasis patients in Ontario calculated using the sponsor’s approach. If the sponsor’s methodology were valid, it is expected that these numbers would be similar.
CADTH was unable to address this uncertainty in reanalysis due to the modelling approach and lack of transparency in the technical guidance.
Underestimation of population size: The use of a claims-based approach appears to have underestimated the population size when considering the epidemiology of plaque psoriasis. The sponsor’s approach led to an estimate of ||||||||||, ||||||||||, and |||||||||| patients in each of years 1, 2, and 3 of the BIA. However, the sponsor’s own budget impact report estimated that approximately 160,000 to 260,000 Canadians are currently living with moderate to severe plaque psoriasis based on a prevalence estimate of 1.7%.33,34 The clinical expert suggested the prevalence was even higher, and estimated that approximately 315,000 Canadian (including children) are currently living with plaque psoriasis. This large discrepancy between the epidemiology and claims-based estimates introduces uncertainty into the calculation of the budget impact. CADTH emphasizes that the population size is correlated with the incremental budget impact, and that if the population size is underestimated the budget impact is expected to be as well.
As part of a scenario analysis, CADTH doubled the population size.
Uncertainty with comparator displacement: There was uncertainty around the sponsor’s assumptions about the comparators displaced by bimekizumab. The sponsor assumed that the market shares for all comparators would decrease by the same proportion as bimekizumab would be expected to uptake; thus, the displacement was the same from all comparators. It is uncertain whether this assumption is valid and would reflect clinical practice. Furthermore, the sponsor assumed that tildrakizumab would not capture any market share over the 3-year time horizon of the BIA, despite it receiving a positive recommendation from CADTH in 2021.35 The clinical expert stated that tildrakizumab may achieve some market penetrance by year 3 of the analysis.
CADTH was unable to address this in reanalysis due to the way in which the claims-based market shares were programmed.
CADTH Reanalyses of the BIA
CADTH did not undertake reanalyses of the sponsor’s BIA due, in part, to the sponsor’s methodology and lack of transparency. Without conducting a full de novo budget impact analysis using an epidemiological approach, CADTH was unable to address the limitations of the claims-based BIA. A scenario analysis was conducted to explore the uncertainty surrounding the population size.
Table 22: Detailed Breakdown of the CADTH Scenario Analyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $270,233,704 | $302,170,029 | $334,206,702 | $366,717,319 | $1,003,094,051 |
New drug | $270,233,704 | $305,078,886 | $340,924,746 | $376,446,488 | $1,022,450,121 | |
Budget impact | $0 | $2,908,857 | $6,718,044 | $9,729,169 | $19,356,070 | |
CADTH scenario analysis 1: population size doubled | Reference | $540,467,408 | $604,340,058 | $668,414,404 | $733,434,639 | $2,006,188,101 |
New drug | $540,467,408 | $610,157,773 | $681,849,492 | $752,892,977 | $2,044,900,241 | |
Budget impact | $0 | $5,817,714 | $13,436,087 | $19,458,338 | $38,712,140 | |
CADTH scenario analysis 2: 15% of bimekizumab patients assumed to require Q4W dosing | Reference | $270,233,704 | $302,170,029 | $334,206,702 | $366,717,319 | $1,003,094,051 |
New drug | $270,233,704 | $305,749,402 | $342,505,143 | $378,771,950 | $1,027,026,495 | |
Budget impact | $0 | $3,579,373 | $8,298,441 | $12,054,631 | $23,932,444 | |
CADTH scenario analysis 3: 41% price reduction from pharmaco-economic analysis | Reference | $270,233,704 | $302,170,029 | $334,206,702 | $366,717,319 | $1,003,094,051 |
New drug | $270,233,704 | $299,550,115 | $327,893,492 | $357,271,765 | $984,715,372 | |
Budget impact | $0 | -$2,619,914 | -$6,313,210 | -$9,445,554 | -$18,378,679 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Psoriasis Society of Canada
About the Psoriasis Society of Canada
Describe the purpose of your organization. Include a link to your website.
The Psoriasis Society of Canada is a National organization and has members across Canada including Quebec. The Psoriasis Society of Canada (PSC) is a non-profit organization and is registered with Revenue Canada. Website: psoriasissociety.org.
Information Gathering
CADTH is interested in hearing from a wide range of patients and caregivers in this patient input submission. Describe how you gathered the perspectives: for example, by interviews, focus groups, or survey; personal experience; or a combination of these. Where possible, include when the data were gathered; if data were gathered in Canada or elsewhere; demographics of the respondents; and how many patients, caregivers, and individuals with experience with the drug in review contributed insights. We will use this background to better understand the context of the perspectives shared.
The Psoriasis Society receives phone calls from psoriasis patients who share their experiences of living with psoriasis. The PSC sends a newsletter to members across Canada with the latest information on psoriasis and treatments.
Disease Experience
CADTH involves clinical experts in every review to explain disease progression and treatment goals. Here we are interested in understanding the illness from a patient’s perspective. Describe how the disease impacts patients’ and caregivers’ day-to-day life and quality of life. Are there any aspects of the illness that are more important to control than others?
Members have reported they have been discriminated at their workplace, hairdressers refuse to touch their hair because of psoriasis on the scalp. Members report stress and depressive symptoms. Patients are more interested effective drugs so they can have clearing of their skin.
Experiences With Currently Available Treatments
CADTH examines the clinical benefit and cost-effectiveness of new drugs compared with currently available treatments. We can use this information to evaluate how well the drug under review might address gaps if current therapies fall short for patients and caregivers.
Describe how well patients and caregivers are managing their illnesses with currently available treatments (please specify treatments). Consider benefits seen, and side effects experienced and their management. Also consider any difficulties accessing treatment (cost, travel to clinic, time off work) and receiving treatment (swallowing pills, infusion lines).
When members are on biological treatments and they stop being effective, they begin looking for a new biological treatment. It is important to have easy access to new treatments so patients are able to continue effectively manage their psoriasis. Patients are always looking for new innovative treatments to provide better results versus the currently available treatments.
Improved Outcomes
CADTH is interested in patients’ views on what outcomes we should consider when evaluating new therapies. What improvements would patients and caregivers like to see in a new treatment that is not achieved in currently available treatments? How might daily life and quality of life for patients, caregivers, and families be different if the new treatment provided those desired improvements? What trade-offs do patients, families, and caregivers consider when choosing therapy?
Patients are looking for complete skin clearance(PASI 100) and faster response. They want better treatment versus actual available treatment now.
Experience With Drug Under Review
CADTH will carefully review the relevant scientific literature and clinical studies. We would like to hear from patients about their individual experiences with the new drug. This can help reviewers better understand how the drug under review meets the needs and preferences of patients, caregivers, and families.
How did patients have access to the drug under review (for example, clinical trials, private insurance)? Compared to any previous therapies patients have used, what were the benefits experienced? What were the disadvantages? How did the benefits and disadvantages impact the lives of patients, caregivers, and families? Consider side effects and if they were tolerated or how they were managed. Was the drug easier to use than previous therapies? If so, how? Are there subgroups of patients within this disease state for whom this drug is particularly helpful? In what ways? If applicable, please provide the sequencing of therapies that patients would have used prior to and after in relation to the new drug under review. Please also include a summary statement of the key values that are important to patients and caregivers with respect to the drug under review.
The PSC has no comment on the drug under review as we do not have any testimony from members on this new treatment.
Companion Diagnostic Test
If the drug in review has a companion diagnostic, please comment. Companion diagnostics are laboratory tests that provide information essential for the safe and effective use of particular therapeutic drugs. They work by detecting specific biomarkers that predict more favourable responses to certain drugs. In practice, companion diagnostics can identify patients who are likely to benefit or experience harms from particular therapies, or monitor clinical responses to optimally guide treatment adjustments.
What are patient and caregiver experiences with the biomarker testing (companion diagnostic) associated with regarding the drug under review?
Consider:
Access to testing: for example, proximity to testing facility, availability of appointment.
Testing: for example, how was the test done? Did testing delay the treatment from beginning? Were there any adverse effects associated with testing?
Cost of testing: Who paid for testing? If the cost was out of pocket, what was the impact of having to pay? Were there travel costs involved?
How patients and caregivers feel about testing: for example, understanding why the test happened, coping with anxiety while waiting for the test result, uncertainty about making a decision given the test result.
N/A
Anything Else?
Is there anything else specifically related to this drug review that CADTH reviewers or the expert committee should know?
Psoriasis Society Canada is pleased to see that clinical trials have taken place at Canadian hospital clinics.
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. Thi Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Conflict of Interest Declaration for the Psoriasis Society of Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
UCB | — | X | — | — |
novartis | — | X | — | — |
Sun pharma | — | X | — | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Position: President, Psoriasis Society of Canada
Date: September 1, 2021
Canadian Psoriasis Network (CPN) and Canadian Association of Psoriasis Patients (CAPP)
About the Canadian Psoriasis Network (CPN) and the Canadian Association of Psoriasis Patients (CAPP)
The Canadian Psoriasis Network (CPN) is working in collaboration with the Canadian Association of Psoriasis Patients (CAPP) for the completion of this submission. CPN is a national, not-for-profit organization dedicated to improving the quality of life of people in Canada who live with psoriasis and psoriatic arthritis. We do this by providing current information on research and treatment options and by working with others to build awareness and advocacy about the complexity of these conditions. CAPP is a national, not-for-profit organization formed to better serve the needs of psoriasis patients across the country. CAPP is a partner organization of CSPA and strives to improve the quality of life for all Canadian psoriasis patients. CAPP’s mission is to be a resource and advocate for psoriatic patients and their families to improve patient care and quality of life.
Information Gathering
Data Gathering
Information for this submission was obtained primarily through a survey hosted on both CPN and CAPP’s websites from July 19, 2021-August 29, 2021 in English and French. CPN and CAPP also sent the survey to clinics in Canada that conducted bimekizumab trials and asked that they share it with patients. We received 95 survey responses from all provinces. There were no responses from participants in the Northwest Territories, the Yukon or Nunavut. In addition to the written survey, we conducted one telephone interview with an individual who had taken bimekizumab through a clinical trial.
Regional Data
The majority of survey responses were from Ontario (53%, n=49) followed by Quebec (18%, n=17) and British Columbia (11%, n=10). We received one response from Saskatchewan, one from New Brunswick, and one from Nova Scotia. The remaining responses came from Alberta (5%, n=5), Newfoundland and Labrador (3%, n=3) and Prince Edward Island (2%, n=2).
Survey Demographics
The vast majority of participants (95%, n=90) identified as living with psoriasis. Another 5% (n=5) identified as a caregiver and/or family member of someone who lives with psoriasis. One caregiver/family member participant indicated that the patient in their life takes bimekizumab for their psoriasis and 12 (18%) participants who identified as patients stated that they take bimekizumab for their psoriasis.
One-third of survey participants (34%, n=21) stated that they are between the ages of 55-65; 30%, (n=18) indicated that they are over 65; 18% (n=11) stated that they are between 45-54; 11% (n=7) are between the ages of 25-34; and the remainder (3%, n=2) are 18-24.
The majority of participants (66%, n=40) indicated that they are female and 34% (n=21) stated that they are male.
Most participants (61%, n=30%) live with psoriatic arthritis and 29% (n=14) live with another type of arthritis. Some participants indicated living with comorbidities, including anxiety (33%, n=16), diabetes (27%, n=13), depression (22%, n=11), heart disease or stroke (12%, n=6), another inflammatory condition (12%, n=6), another skin condition (12%, n=6), cancer (6%, n=3), kidney disease (6%, n=3) and lung disease (4%, n=2). In the open-ended text option for this question, a few participants mentioned living with cardiovascular conditions, such as hypertension and metabolic conditions, including high cholesterol.
Disease Severity
Nearly half (46%, n=36) of participants described their psoriasis severity as “mild” (less than 3% of body surface area, or BSA); 40% (n=31) of participants described their severity as “moderate” (between 3-10% of BSA); and 14% (n=11) described their severity as “severe” (greater than 10% of BSA).
Disease Experience
Patient survey participants provided insights into how psoriasis affects their lives including living with the following symptoms outlined in Table 2.
Table 2: Symptoms That Patient Survey Participants Experience That Affect Their Ability to Participate in Day-To-Day Life and/or Quality of Life
Symptom | Total (%) | Total (n) |
|---|---|---|
Flaking | 89.6 | 69 |
Itch | 85.7 | 66 |
Redness | 85.7 | 66 |
Flares | 75.3% | 58 |
Pain/burning | 59.7% | 46 |
In open-ended responses, survey participants reported other symptoms, including pain, inflammation and joint stiffness related to psoriatic arthritis, peeling skin on feet, swelling, and hair loss. The majority of survey participants indicated that their symptoms have an impact on multiple aspects of their lives including social life (70%, n=53), self-esteem (69%, n=52), mental health (65%, n=49), intimate life (63%, n=47), sleep (61%, n=46), work (54%, n=41), exercise (52%, n=39), family life (40%, n=30), and finances (38%, n=28).
When asked to share any additional information about challenges participants face living with psoriasis that are important to them, we were told:
“I basically hide from life. I never married, had children, had the career I wanted because I had such low self-esteem. It’s truly devastating and now that this current trial drug has completely cleared my psoriasis do I fully appreciate how much of life I’ve been robbed of up until now.”
“Past twenty years have been extremely difficult. Psoriasis and my psoriatic arthritis worsen with stress. The topical cream [and] steroid[s] are not very effective. The other stronger options are either too expensive or have side effects.”
“As a lady I had to look for alternatives to shaving my legs as the razor would cause lots of bleeding. Psoriasis on the scalp causes dandruff and sometimes this would be really bad and embarrassing. When my skin was flaking I would get up in the morning and the sheets would be covered in skin which is embarrassing when staying at someone else’s house.”
“I had psoriasis almost all my life and in the last two years I have psoriatic arthritis. I live in [a major city] and I didn’t have a rheumatologist in the last two years. I will have a rheumatologist in three months that will retire soon. I’m worst in the last year and don’t have the support I need.”
“I live approximately 30 min away from phototherapy. It is difficult to get in also as you have to pay for parking. I would be interested in biologics or being able to purchase my own phototherapy machine with the right coverage offered.”
“Not getting the right treatment. Would like to see a dermatologist but no referral yet. I don’t have a regular doctor which doesn’t help.”
“After 60 years nothing has changed. No cure.”
“Fatigue [and] lack of motivation.”
Two survey participants who identify as caregivers/family members provided insights into how supporting someone with psoriasis impacts their life. Specifically, they identified impacts on their social life and on their intimate life. They also described providing emotional support to the person with psoriasis and arranging for transportation or driving the individual to appointments. One caregiver/family member (from Quebec) indicated that the person with psoriasis pays for their psoriasis treatment out of pocket and the other (from PEI) stated that the person has private insurance. Both participants indicated that the patient has had financial hardships for paying for medications and has had to stop taking their medications as a result. Other caregiver/family member participants provided insights into how psoriasis symptoms impact aspects of the patient’s life including school, social life, intimate life and mental health.
Experiences With Currently Available Treatments
Survey participants were asked to identify the treatments that they have used for psoriasis and to rate how effective they were at treating symptoms. Specifically, participants told us what they had found to be effective: 40% (n=25) rated phototherapy as effective; 38% (n=27) participants rated topical corticosteroids (e.g., betamethasone, mometasone, etc.) as effective; 37% (n=23) rated biologics as effective; 29% (n=20) rated topical combination treatments as effective; 29% (n=19) rated methotrexate as effective; and 18% (n=12) rated topical vitamin D derivatives as effective. Table 3 provides a full breakdown of responses.
Table 3: Patient Survey Participant Rating of Effectiveness of Psoriasis Treatments They Have Used
Treatment | Very effective (%, n) | Effective (%, n) | Ineffective (%, n) | Very ineffective (%, n) | N/A (%, n) |
|---|---|---|---|---|---|
Topical corticosteroids (e.g., betamethasone, mometasone, etc.); n=70 | 7.1% (5) | 31.4% (22) | 45.7% (32) | 11.4% (8) | 4.3% (3) |
Topical vitamin D derivatives (e.g., Dovonex, Silkis, etc.); (n=67) | 3.0% (2) | 14.9% (10) | 41.8% (28) | 13.4% (9) | 27% (18) |
Topical combination treatment (e.g., Dovobet, Enstilar, etc.; n=69 | 5.8% (4) | 23.2% (16) | 31.9% (22) | 8.7% (6) | 30.4% (21) |
Topical retinoids; n=62 | 0 (0) | 6.5% (4) | 19.4% (12) | 3.2% (2) | 80.0% (53) |
Apremilast; n=59 | 3.4% (2) | 1.7% (1) | 5.1% (3) | 0 (0) | 90.0% (53) |
Cyclosporine; n=60 | 0 (0) | 1.7% (1) | 10.0% (6) | 3.3% (2) | 85.0% (51) |
Methotrexate; n=64 | 9.4% (6) | 20.3% (13) | 15.6% (10) | 9.4% (6) | 45.3% (29) |
Oral retinoids; n=59 | 0 (0) | 0 (0) | 8.5% (5) | 5.1% (3) | 86.4% (51) |
Oral steroids; n=19 | 1.7% (1) | 10.0% (6) | 6.7% (4) | 3.3% (2) | 78.3% (47) |
Biologics n=62 | 17.7% (11) | 19.4% (12) | 1.6% (1) | 1.6% (1) | 59.7% (37) |
Phototherapy; n=63 | 4.8% (3) | 34.9% (22) | 15.9% (10) | 4.7% (3) | 39.7% (25) |
Medical cannabis; n=60 | 0 (0) | 6.7% (4) | 10.0% (6) | 1.7% (1) | 81.7 (49) |
Overall, the majority of participants (including those who are on a clinical trial for bimekizumab) (70%, n=47) indicated that their current treatment allows them to resume daily activities (e.g., work, household tasks, caring for children) but 7% (n=5) disagreed this was the case for them.
When asked if participants experience any side effects of treatments that are difficult to tolerate or manage, the most common responses were noted in Table 4.
Table 4: Side Effects of Treatment that are Difficult to Tolerate or Manage for Patient Survey Participants
Side effect | Respondents who found it difficult to tolerate (%, n) |
|---|---|
Skin irritation or redness | (51%, n=35) |
Skin itching | (46%, n=32) |
Muscle soreness or joint stiffness | (43%, n=30) |
Skin thinning | (42%, n=29) |
Changes in skin pigmentation (i.e., affected skin turns lighter or darker) | (42%, n=29) |
Unexplained fatigue | (41%, n=28) |
Dry skin, eyes, or lips | (36%, n=25) |
Headache | (28%, n=19) |
Hair loss | (26%, n=18) |
Development of rash/acne | (23%, n=16) |
Pain | (23%, n=16) |
Nearly one-third (31%, n=23) of participants stated that they take medications or over-the-counter products to help them manage the side effects noted in Table 4, including moisturizers, pain medication (e.g., acetaminophen, ibuprofen, codeine), and vitamins (e.g., vitamin D, folic acid).
Affordability of Treatment
Survey participants were also asked to respond to a series of statements regarding their current treatments. In terms of affordability, 41% (n=27) indicated that they do not think their current treatment is affordable. In addition, about one third of participants (34%, n=22) disagreed with the statement “I can afford my medication.”
Participants indicated paying for their medications in various ways. Most participants (48%, n=32) have private insurance either through their employer, union or professional association, or through their partner/spouse. Nearly one-third (29%, n=19) are covered through a public drug program. Other ways that people accessed their treatments included: participating in a clinical trial (23%, n=15); paying for medications out of pocket (12%, n=8); and receiving medication from the manufacturer through a Patient Support Program or compassionate access (12%, n=8).
Comments from participants regarding drug plans included the following:
“Have insurance but most of time [it does] not cover [my medication].”
“My private drug [plan] gives me nothing but grief and basically ruins any chance I have to go on a biologic.”
When asked if they had ever experienced financial hardship with paying for treatments, 52% (n=35) of participants said yes. Of those that did experience financial hardships, some said they managed (18%, n=12), while others stopped taking their medications (15%, n=10), took less than prescribed (10%, n=7), and/or did not fill their prescription at the pharmacy (9%, n=6).
Accessibility
In terms of being prescribed the treatment they need, 71% (n=47) agreed that their prescriber can prescribe the preferred/appropriate treatment for their circumstances, however only 54% (n=35) indicated that they are receiving their preferred choice of treatment. The dissonance between these responses were not explored in the current survey, however it is important to recognize that survey participants expressed some level of dissatisfaction with being able to access the treatment that they would prefer.
The vast majority (88%, n=59) agreed that instructions for using the treatment are easy to follow and 68% (n=44) agreed that their current dosing schedule is convenient.
Participant Satisfaction With Treatments
Notably, less than half (41%, n=28) of participants either disagreed or were neutral with regards to the statement “Overall, my needs are met with the treatment I receive” indicating that there is room for improvement. Section 5 – Improved Outcomes – may provide some insights into participants’ perspectives in this regard. Moreover, 14% (n=9) do not feel that the travel to and from medical appointments is manageable.
Improved Outcomes
When asked what survey participants’ expectations for a new medication are, given their experience with existing treatments for psoriasis, 68% (n=41) indicated “improves my symptoms” as the top response.
Other responses included “better quality of life (e.g., return to work, able to socialize more, mental wellbeing, fewer doctor visits)” (63%, n=38); reduced side effects (50%, n=30); affordable (50%, n=30); help with persistent symptom(s) (47%, n=28); and easier to take (e.g., improved dosing schedule) (42%, n=25).
When asked, “What is the biggest improvement that you would like to see in psoriasis treatment?” participants shared a range of responses including the following:
“Clear skin and pain free.”
“Life changing biologic drugs made more easily accessible to psoriasis sufferers without private insurance. The cost is prohibitive and to access it through i.e. Ontario Trillium requires a lot of effort and commitment from the dermatologist to get approved for their patient use. I shouldn’t feel like there are haves and have nots in Canadian health care but I had to get on a trial to get this outstanding drug, yet a family member working for the government with excellent health care has been on a biological drug for years with far less severe psoriasis than my own. I believe this trial drug is superior to any other biological drug when I compare my complete and quick improvement to what others have shared on other biological drugs. I am so very thankful to have been on this trial for bimekizumab, it changed my life.”
“Length of remission extended.”
“No redness and colour discolouration [sic].”
“Would like to find a medication that doesn’t make me sick, works, and is safe to take for the long term.”
“Reduction of plaques.”
“The itching to be gone, and the flakes to be gone.”
“No more inflammation and flaking.”
“It works and I’m clear for longer periods with minimum side effects.”
“I want to walk or sleep without too much pain.”
“More information on how best to treat my inverse psoriasis, particularly my genital area.”
“Reduced costs, fewer side effects.”
The majority of the 51 participants who responded to this question provided some form of “a cure” and/or “clear skin” as responses. Drug coverage and affordability were also common responses from participants. A few participants commented on the benefits of different treatment modalities (e.g., “Oral would be great. I am on scheduled injections which is a bit harder to apply…”)
Experience With Drug Under Review
Summary of Participants
As mentioned above, one caregiver/family member survey participant indicated that the patient in their life takes bimekizumab for their psoriasis and 12 (18%) participants identifying as patients stated that they take bimekizumab for their psoriasis. In addition, one telephone interview was conducted with a patient who has accessed bimekizumab through a clinical trial. His perspectives are provided in summary form as an example of one person’s experience.
Though we do not have specific information about how survey participants accessed bimekizumab, given its status in Canada at the time of the survey and our outreach efforts to clinical trial sites, as well as some of the open-ended comments in the survey, it is likely that all respondents accessed the drug under review by participating in a clinical trial.
Of the survey participants who indicated that they have taken bimekizumab, the following number also report having tried the other treatments: topical corticosteroids (99%, n=11), topical vitamin D derivatives (80%, n=8), topical combination treatments (90%, n=9), topical retinoids (33%, n=3), cyclosporine (11%, n=1), methotrexate (55%, n=5), oral retinoids (33%, n=3), biologics 66%, n=6), phototherapy (54%, n=6), and medical cannabis (33%, n=3).
The Impact of Bimekizumab on Participants / Patients
When asked to share their positive and negative experiences with bimekizumab, survey participants shared the following:
“To start, I have no side effects. Within two months of starting the trial my skin is clear and has remained that way. My skin is completely clear and I didn’t realize how much my psoriasis affected me mentally until it was gone. I was part of a clinical trial so the drug cost to me was zero.”
“I am in a clinical trial and when I am done, I will not be able to afford the cost. I have great, almost clear results.”
“This trial drug has completely cleared my moderate to severe psoriasis and changed every aspect of my life to the better in ways I couldn’t have even imagined. The thought that the drug trial will come to an end and my psoriasis will return is devastating. When approved, I fear this drug will be unattainable to me as I do not have insurance and rely on Ontario Trillium for my prescriptions. The side effects are negligible – nasal drip, periodically have small rashes in body folds that are easily treated and cleared. I was significantly clear within a short amount of time of starting this drug and have been COMPLETELY CLEAR for close to 3 years taking it every 2 months after the initial few months. I also have normal nails for the first time in my life.”
“I have been totally clear since starting the trial 3 years ago. The self injections are simple. I had a minor rash side effect at the start that cleared within a couple of months as my body adjusted…”
“My skin was clear very early on in the clinical trials. No negative side effects whatsoever.”
“My psoriasis cleared up.”
“I don’t know about the costs as I was part of a clinical study, but this medication literally changed my life for the better. I’m not trying to sound melodramatic, but I was applying topical medications for 2 hrs daily just to keep a semblance of control over my outbreaks. I have been completely symptom free from the first week I took my first injection, and have remained so ever since. My old life centered around controlling my psoriasis. I cannot say enough positive things…”
“My overall quality of life has improved. I don’t feel any side effects yet but the known risks are for sure always at the back of my mind which sometimes makes me worry.”
Survey participants were asked to rank how effectively bimekizumab manages their psoriasis symptoms: pain/burning (90%, n=9); itch (100%, n=11); flaking (90%, n=10); redness (100%, n=10); flares (100%, n=9).
Table 5 describes survey participant responses when asked to rate the following statements related to their experience with using bimekizumab compared to other treatments.
Table 5: Experiences With Bimekizumab Statement Rating
Statement | Strongly agree/agree | Neutral | N/A |
|---|---|---|---|
Bimekizumab is easier to use than other therapies | 64%, n=7 | 36%, n=4 | — |
Bimekizumab is better at managing my psoriasis symptoms than other therapies | 100%, n=11 | — | — |
Bimekizumab’s side effects are more tolerable than other therapies | 82%, n=9 | 9%, n=1 | 9%, n=1 |
Bimekizumab’s instructions are easier to follow than other therapies | 81%, n=9 | 18%, n=2 | — |
I expect that bimekizumab will improve my long-term health and well-being | 91%, n=10 | 9%, n=1 | — |
Bimekizumab improved my quality of life (i.e., return to work, ability to socialize more, mental well-being) | 100%, n=11 | — | — |
Bimekizumab helped me return to my day-to-day activities | 82%, n=9 | 9%, n=1 | 9%, n=1 |
Bimekizumab reduced my flares | 100%, n=10 | — | — |
Overall, my needs are better met with bimekizumab | 100%, n=11 | — | — |
When asked to describe what impact (if any) bimekizumab had on their quality of life and day-to-day activities, examples of survey participant responses include:
“I didn’t realize how much having psoriasis bothered me until my skin was clear. I didn’t have to think about trying to control my itching when we were out.”
“My self awareness and self esteem are a lot better.”
“I no longer need to hide and I can live my life to the fullest. I am in a long term relationship for the first time, I have started a new career and I no longer hide my body with long sleeves and pants. I just go out now without worrying about camouflaging anything or heavy makeup to conceal what I could.”
“The last three years have been my best years for managing and controlling my psoriasis. I have had psoriasis for over 40 years. I am no longer itching, in pain or fatigued. I am also no longer embarrassed to wear shorts, go swimming, change for sports in dressing rooms.”
“Improved my quality of life in every conceivable aspect.”
“It cleared up my psoriasis.”
“This medication has completely eliminated my plaques. For the first time in over 40 years, I was able to wear shorts and t-shirts, go swimming in a bathing suit, and not have to constantly worry about my psoriasis. It really has been a godsend.”
“Being able to live life normally. The smallest things like standing up from your bed without seeing flakes of your skin.”
All patients reported positive outcomes of bimekizumab treatment, with a few participants noting side effects including dry skin, eyes, or lips (50%, n=3), development of new rash/acne (50%, n=3), or muscle soreness or joint stiffness (33%, n=2). These participants commented that with additional treatment, the side effects went away and/or could be well managed. For instance, one participant who indicated that they experienced a rash/acne stated that “the rash did not last very long, less than a month.”
Summary of Interview With Bimekizumab Clinical Trial Patient
The interviewee shared that he started to experience psoriasis in his early 40s (about 25 years ago) with a little bit of itching on his scalp and left hip. At first, he thought it was “just dry skin”, but it was itchy and “never seemed to go away”. Eventually he also started to have issues with his lungs and with arthritis. He saw a pulmonary specialist and was diagnosed with sarcoidosis – but, he reflected, “back then people didn’t know that psoriasis was more than skin deep”. As a result, he had to have angioplasty surgery due to a blocked artery in the heart and it was at the cardio clinic that he was first informed that psoriasis is an inflammatory condition that can impact other organs.
Just before turning 50 in 2003, he had to see an orthopedic surgeon because his knees were terribly swollen – he was told that it was psoriatic arthritis and that there was “nothing you can do about it.” Eventually he was referred to a rheumatologist and was “finally able to get some relief”. They had to drain his knee and he was prescribed Celebrex.
Though he had seen dermatologists for his psoriasis, it was not until he saw his current specialist that he said he received appropriate care and treatment for his symptoms. Previously, he reflected that he was “lucky to get five minutes with dermatologists…they would only prescribe topicals” which in his experience were not effective at treating his symptoms. He further reflected that previous dermatologists wanted to prescribe methotrexate but he said no, “that’s an awful drug”. He considered phototherapy but it was “a terrible location” which was far from his home and where there was no parking.
He indicated that he had heard about the clinical trial from someone in his community. He met with the dermatologist conducting the clinical trial who reassured him about finding appropriate treatment options. The interviewee shared that he was relieved and finally felt heard.
Regarding his experience with the clinical trial, he described having an injection once every 4 weeks right at first, and then every 8 weeks. He said that after his first injection, the plaques on the back of his hands were gone the next day. Within a week, his skin was clear. He said that he knew from the beginning he was on the treatment arm of the trial because the results were so fast. He shared that in three months, he found renewed growth in his fingernails and within six months, his toes were cleared. He also shared that his arthritis pain has since been manageable, and he believes the treatment is impacting this – he described that the swelling in his knees has been minimal and that he only occasionally has to take a Tylenol for his pain. He shared that some redness and skin discoloration lasted about a year.
Prior to the clinical trial, the interviewee said that if he went to someone’s home, he’d ask them to put a cover on furniture. He described having psoriasis all over his body – “back, rear end, back of legs, elbows, everywhere” – and that as his skin was drying after a shower, it felt like his skin was on fire; touch or sunshine would also feel like burning on his skin. He described waking up several times during the night because he’d be itching – “If you scratched, you’d bleed. “It was just awful”.
He said, “I can understand why some people could take their own lives.”
Since he has been on the clinical trial, the interviewee says that he cannot remember what it was like to live that way. He made an analogy to smoking – he doesn’t remember what it was like to smoke but he did at a time and similarly, he can’t even remember what it was like having psoriasis.
Values That Are Important to Patients
In terms of values that are important to patients and caregivers with respect to the drug under review, a few themes stood out to us based on survey responses from people with experience of bimekizumab. Specifically, finding care and treatment that works for the individual, achieving clear skin, safety of treatment, treatment that works over the long term, increased self-esteem and social engagement, and generally living life freely – in a way that is not consumed by symptoms and by vigilance related to one’s disease.
Companion Diagnostic Test
N/A
Anything Else?
Psoriasis is a chronic and potentially debilitating condition that poses many challenges, including high prevalence, chronicity, disfiguration, disability, and associated comorbidities. Psoriasis is linked to anxiety, depression, and social isolation, and can interfere with relationships, productivity, family life and work life. The physical, psychological, social, and economic impact of psoriasis can significantly burden patients and their families. Access to effective care and appropriate treatment is needed but management of psoriasis can be complex partly due to varied patient response to treatments, differences in social determinants of health, lifestyle considerations, and other factors that affect one’s condition. Moreover, due to the chronicity of this disease, patients are concerned about recurrence and resistance to earlier therapies.
Psoriasis is more than a skin condition. It is an inflammatory disease that can impact several organ systems. It is estimated that up to 30 percent of people with psoriasis develop psoriatic arthritis. People with psoriatic disease also are at greater risk of developing cardiovascular disease, depression and anxiety, diabetes, and cancer.
For more information about the challenges of living with psoriasis, please see the following resources:
CAPP’s report Pso Serious 2018: A Report on Access to Care and Treatment for Psoriasis Patients in Canada
CPN and CAPP’s joint report, Journey to Stability
CPN and CAPP’s joint infographic on Impact of COVID-19 on the Psoriasis and Psoriatic Community in Canada – Highlights from a National Survey
CPN’s fact sheet for health care providers on Women and Psoriasis: Findings from a Survey of Women-identified People with Psoriatic Disease
Patients are looking for a treatment that will control all of their symptoms but ultimately, they want and value a cure for psoriasis.
Conflict of Interest Declaration for the Canadian Psoriasis Network (CPN) and the Canadian Association of Psoriasis Patients (CAPP)
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
We received help with developing the survey and outreach to clinical trial sites by two medical student volunteers.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
N/A
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 6: Conflict of Interest Declaration for the Canadian Psoriasis Network
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AbbVie Canada | — | — | — | X |
Amgen Canada | — | — | X | — |
BMS | — | — | X | — |
Bausch Health Canada | — | X | — | |
Boehringer Ingelheim Canada | — | — | X | — |
Boehringer Ingelheim International | X | — | — | — |
Eli Lilly Canada | — | X | — | — |
Janssen Canada | — | — | X | — |
LEO Pharma Canada | — | — | X | — |
Novartis Canada | — | — | X | — |
Pfizer | — | — | X | — |
UCB Canada | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Position: Executive Director, Canadian Psoriasis Network
Date: Sept 13, 2021
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 7: Conflict of Interest Declaration for the Canadian Association of Psoriasis Patients
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
AbbVie Canada | — | — | X | — |
Amgen Canada | — | — | X | — |
Bausch Health Canada | — | — | X | — |
Boehringer Ingelheim International | — | — | X | — |
Eli Lilly Canada | — | — | X | — |
Janssen Canada | — | — | X | — |
LEO Pharma Canada | — | — | X | — |
Novartis Canada | — | — | X | — |
Novartis Global | — | X | — | — |
UCB Canada | — | — | X | — |
I hereby certify that I have the authority to disclose all relevant information with respect to any matter involving this patient group with a company, organization, or entity that may place this patient group in a real, potential, or perceived conflict of interest situation.
Position: Executive Director, Canadian Association of Psoriasis Patients
Date: Sept 13, 2021
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.