CADTH Reimbursement Review
Galcanezumab (Emgality)
Sponsor: Eli Lilly Canada Inc.
Therapeutic area: Prevention of migraine
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
ADA
antidrug antibodies
AE
adverse event
ALT
alanine aminotransferase
ANCOVA
analysis of covariance
ANOVA
analysis of variance
AST
aspartate aminotransferase
CGRP
calcitonin gene-related peptide receptor
CI
confidence interval
CM
chronic migraine
CrI
credible interval
EF
emotional function
EM
episodic migraine
ePRO
electronic patient-reported outcomes
EQ-5D-5L
EQ-5D 5-Levels
EQ VAS
EQ visual analogue scale
GAD-7
Generalized Anxiety Disorder 7-item
HCRU
health care resource utilization
HIT-6
6-item Headache Impact Test
HRQoL
health-related quality of life
ICER
Institute for Clinical and Economic Review
ICHD-3
International Classification of Headache Disorders, third edition
IHS
International Headache Society
ITC
indirect treatment comparison
ITT
intention-to-treat
LOCF
last observation carried forward
LS
least squares
MedDRA
Medical Dictionary for Regulatory Activities
MHD
migraine headache day
MIBS-4
4-item Migraine Interictal Burden Scale
MID
minimal important difference
MIDAS
Migraine Disability Assessment
MMRM
mixed model for repeated measures
MSQ v2.1
Migraine-Specific Quality of Life Questionnaire version 2.1
NMA
network meta-analysis
OR
odds ratio
PGI-S
Patient Global Impression of Severity
PHQ-9
Patient Health Questionnaire-9
RCT
randomized controlled trial
RD
risk difference
RF-P
role function – preventive
RF-R
role function – restrictive
RR
relative risk
SAE
serious adverse event
SD
standard deviation
SE
standard error
ULN
upper limit of normal
WPAI
Work Productivity and Activity Impairment
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Galcanezumab (Emgality), 120 mg/mL solution for subcutaneous injection |
Indication | For the prevention of migraine in adults who have at least 4 migraine days per month |
Reimbursement request | For the prevention of migraine in adults who have at least 4 migraine days per month and have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 30, 2019 |
Sponsor | Eli Lilly Canada Inc. |
NOC = Notice of Compliance.
Introduction
Migraine is a neurologic disease characterized by recurrent episodes of pulsating headache pain of at least moderate severity.1 The type of migraine can be refined based on the frequency of monthly migraine headache days (MHDs) and monthly headache days.1 The International Classification of Headache Disorders, third edition (ICHD-3), describes chronic migraine (CM) as a headache (tension-type-like or migraine-like) occurring on 15 or more days per month for more than 3 months with the features of migraine headaches on at least 8 days per month.2 In episodic migraine (EM), individuals experience headaches on 14 or fewer days per month for more than 3 months with the features of migraine headaches on at least 4 days per month.2 In Canada (2010 to 2011), 9.6% of the population over 18 years of age experienced migraine attacks, with more females (13.8%) than males (5.3%) having had migraine.3
Comprehensive migraine therapy includes management of lifestyle factors and triggers, acute and preventive (or prophylactic) medications, and migraine self-management strategies.4,5 The goals of migraine treatments are to relieve pain, restore function, improve health-related quality of life (HRQoL), reduce headache frequency, and prevent the progression of EM to CM.6 Preventive medications include a variant of the botulinum toxin (onabotulinumtoxinA; for CM only), inhibitors of the calcitonin gene-related peptide receptor (CGRP), beta-blockers, calcium-channel blockers, tricyclic antidepressants, serotonin-norepinephrine reuptake inhibitors, angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, anticonvulsants, and pizotifen. Only topiramate, onabotulinumtoxinA, and the CGRP inhibitors have been approved by Health Canada for the prevention of migraine, and of these, onabotulinumtoxinA is indicated only for the prevention of CM. Migraine prophylaxis is an important part of the overall approach for a proportion of individuals with migraine.4 Of patients with migraine who have received preventive medications, 87% have an inadequate response to 2 or more preventive therapies.7
Galcanezumab is a humanized immunoglobin G4 monoclonal antibody that binds to CGRP and prevents its biologic activity.8 Galcanezumab is administered by subcutaneous injection. Galcanezumab received a Health Canada Notice of Compliance on July 30, 2019, with an indication for the prevention of migraine in adults who have at least 4 migraine days per month. The recommended dose is a loading dose of 240 mg (administered as 2 consecutive subcutaneous injections of 120 mg) followed by once-monthly doses of 120 mg (1 injection). Galcanezumab has not been previously reviewed by CADTH.
The objective of this report is to perform a systematic review of the beneficial and harmful effects of galcanezumab (120 mg/mL solution in a 1 mL single-use, pre-filled syringe or pen) for the prevention of migraine in adults who have at least 4 MHDs per month and have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
CADTH received a joint submission from Migraine Canada and Migraine Québec.
Migraine Canada and Migraine Québec identified the following as key impacts on the lives of those living with migraine and their families: inability to work resulting in financial stress and reliance on a spouse or family members to compensate, childcare and needing additional help, restricted social activities and difficulties with relationships, and lack of understanding from others. Patients described how their spouse and/or family often must bear the burden of household and financial responsibilities, how families miss out on spending time together, difficulties with starting new relationships and stress on existing relationships, and the lack of support available for caregivers.
Patients indicated that it is important to control the frequency and severity of migraine as well as reduce or eliminate the need for acute medications (i.e., triptans and opioids). Patients indicated that they wanted a preventive medication that allowed them to be more productive at work and home. They also felt it was important that a new medication would allow them to fully participate in daily life, work, improve family and social relationships, and reduce exhaustion and side effects. In general, survey respondents felt that nearly any degree of relief would be a successful outcome for a preventive therapy. When asked about methods of administration, 73% of participants stated they would prefer a monthly injection to a daily pill.
Clinician Input
Input From Clinical Experts Consulted by CADTH
According to the clinical expert consulted by CADTH, the most important goal of treatment is a reduction in the frequency of headache. In the clinical expert’s experience, a trial of 2 to 3 oral preventive medications is often required before a patient experiences a benefit. The older preventive medications have important side effects that often limit their use and affect adherence to treatment.
If the cost of the patient’s prescription drugs is reimbursed, the patient will typically be offered 2 or 3 oral preventive medications before receiving either onabotulinumtoxinA (if they have CM) or an anti-CGRP monoclonal antibody.
Patients with a diagnosis of migraine with or without aura, more than 4 headache days per month, failure on 2 or more daily preventers used at an appropriate dose for an appropriate period of time, and no contraindication of the use of an anti-CGRP monoclonal antibody would be suitable for galcanezumab. In the clinical expert’s opinion, patients with frequent EM without medication overuse could be most likely to respond to an anti-CGRP monoclonal antibody and patients with CM may realize the greatest benefit. The clinical expert added that patients least suitable for treatment with galcanezumab would include those contemplating pregnancy, and some physicians may be reluctant to prescribe it (or any anti-CGRP monoclonal antibody) to patients with known active peripheral vascular, cardiovascular, or cerebrovascular disease. In addition, use of this family of medications in patients with Raynaud phenomenon who were taking triptans may be associated with digital ischemia leading to digit amputation, and caution is therefore needed in that area.
Reduction in frequency and/or severity of headaches, reduced use of abortive medications, improved function, and quality of life are important measures of treatment response. The clinical expert reported that the goal is to reduce the frequency of headache, ideally to fewer than 4 headache days per month. A 50% or greater reduction in headache frequency is also considered successful. A reduction in the severity of the headaches, as measured by the Migraine Disability Assessment (MIDAS) or 6-item Headache Impact Test (HIT-6), even if the frequency of headaches remains unaltered, would also be considered successful, according to the clinical expert. The clinical expert reported that patients should be assessed for response to galcanezumab treatment at 2 to 3 weeks after their third injection, and those who have not shown improvement at that time should be assessed 2 to 3 weeks after their sixth injection. If there is no improvement after 6 injections, treatment would be discontinued. The clinical expert indicated that development of intolerable side effects, comorbidities that preclude the patient being on treatment (e.g., stroke or heart attack), or pregnancy would also lead to discontinuation of treatment.
The clinical expert noted that galcanezumab could be prescribed by headache specialists, general neurologists, family doctors on the advice of a neurologist, and family doctors experienced with the use of the medication in other patients. The clinical expert cautioned against requiring patients to be supervised by a headache specialist, as few such specialists practise in Canada.
Clinician Group Input
No input from clinician groups was received for this review.
Drug Program Input
The drug programs noted that 2 other CGRP inhibitors (erenumab and fremanezumab) received recommendations to reimburse with conditions under the CADTH review process and were undergoing pan-Canadian Pharmaceutical Alliance negotiations at the time of this review. The drug programs pointed out that galcanezumab has the same Health Canada indication as both fremanezumab and erenumab, although the reimbursement requests from the sponsors for the 3 medications differ.
The drug programs noted that the reimbursement request for galcanezumab specifies patients who have tried at least 2 prophylactic migraine medications, and indicated that it would be helpful to jurisdictions for this to be defined further (e.g., at least 2 prophylactic medications of different classes and clarification of the optimal dose and duration of the trials). The clinical expert consulted by CADTH indicated that, for an adequate trial, patients are ideally within the therapeutic range for at least 8 weeks before deciding whether treatment has failed. Furthermore, although the reimbursement request specifies failure on at least 2 prophylactic drugs, the drug plans indicated it would be helpful to clarify if there is a maximum number of prophylactic drugs that would be accepted before consideration of coverage. In the clinical expert’s experience, only a small proportion of patients have tried 4 or more preventive medications, and they did not think that a maximum number of prophylactic agents would be necessary.
The drug programs added that it would be helpful to outline whether failure on or intolerance to another CGRP inhibitor would exclude patients from coverage of galcanezumab. The clinical expert reported that no data currently indicate whether failure on or intolerance to 1 or more CGRP inhibitor would exclude patients from trying a treatment with another CGRP inhibitor such as galcanezumab. In addition, the clinical expert noted that the CGRP inhibitors have different properties and can work through different mechanisms (i.e., bind to the CGRP ligand versus the receptor).
The drug programs noted that there is potential in some jurisdictions for galcanezumab to be used in combination with onabotulinumtoxinA. The clinical expert noted that anti-CGRP monoclonal antibodies work to inhibit CGRP activity on nerves different from those affected by onabotulinumtoxinA. The clinical expert therefore suggested there may be reason to consider using both medications at the same time in some patients.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
Four phase III, multi-national, double-blind, randomized, placebo-controlled trials were identified and included in the systematic review: EVOLVE-1,9 EVOLVE-2,10 REGAIN,11 and CONQUER.12 In all trials, galcanezumab and matching-administration placebo were supplied as an injectable solution in 1 mL pre-filled manual syringes designed to deliver 120 mg of galcanezumab each. The injections were administered by study-site personnel once monthly at dosing visits. The primary outcome in all trials was the overall mean change from baseline in the number of monthly MHDs during double-blind treatment.
The EVOLVE-1 (N = 862) and EVOLVE-2 (N = 922) trials were identically designed studies of patients with EM. In both studies, patients were randomized in a 2:1:1 ratio to placebo, galcanezumab 120 mg (loading dose of 240 mg), or galcanezumab 240 mg. The double-blind treatment phase of the studies was 6 months in duration. The EVOLVE-1 and EVOLVE-2 trials excluded patients who had previously failed at least 3 classes of migraine-preventive treatments. Key secondary outcomes controlled for multiplicity included the Migraine-Specific Quality of Life Questionnaire version 2.1 (MSQ v2.1) role function – restrictive (RF-R) domain and monthly MHDs with acute headache pain medication intake.
The REGAIN trial (N = 1,117) was conducted in patients with CM. Patients were randomized in a 2:1:1 ratio to placebo, galcanezumab 120 mg (loading dose of 240 mg), or galcanezumab 240 mg. The study had a 3-month-long double-blind treatment phase. The REGAIN trial excluded patients who had previously failed at least 3 classes of migraine-preventive treatments. Key secondary outcomes that controlled for multiplicity included the MSQ v2.1 RF-R domain and monthly MHDs with acute headache pain medication intake.
The CONQUER trial (N = 463) was conducted in patients with EM or CM who had a documented history of 2 to 4 migraine-preventive medication category failures due to inadequate efficacy or tolerability in the past 10 years. Patients were randomized in a 1:1 ratio to placebo or galcanezumab 120 mg (loading dose of 240 mg). The study had a 3-month double-blind treatment phase. The key secondary outcome of interest to the systematic review was the MSQ v2.1 RF-R domain.
This review only reports the results for the galcanezumab 120 mg treatment arms because it is the Health Canada–approved dose. Results for the galcanezumab 240 mg treatment arms are not reported.
In all trials, most patients were female and White, and the mean age of patients was between 39 and 46 years. Most patients (> 60%) in the EVOLVE and REGAIN studies and all patients in the CONQUER study had received prior preventive treatment. Mean baseline MIDAS total scores of 33.2 and 33.0, which reflect severe disability, were reported in EVOLVE-1 and EVOLVE-2, respectively.12 In the REGAIN trial, 29.5% of patients had failed 2 or more such treatments due to lack of efficacy in the past 5 years, and the mean baseline MIDAS total score was 67.2, which reflects very severe disability.12 Overall, 15.5% of patients in the REGAIN trial had concurrent prophylaxis use with topiramate or propranolol. In the CONQUER trial, most patients had 2 (58.2%) or 3 (30.1%) prior medication category failures and the mean baseline total MIDAS score was 50.93, which reflects very severe disability.12 During the baseline period, the mean number of monthly MHDs was 9.1 in both the EVOLVE-1 and EVOLVE-2 studies. In the REGAIN trial’s baseline period, patients had a monthly average of 21.4 headache days, of which an average of 19.4 were MHDs. During the baseline period in the CONQUER trial, patients had a monthly average of 15.0 headache days, of which an average of 13.2 were MHDs.
Efficacy Results
Key efficacy results from the double-blind treatment periods of the EVOLVE-1, EVOLVE-2, REGAIN, and CONQUER trials are summarized in Table 2 and Table 3.
Migraine-Specific Quality of Life Questionnaire Version 2.1
The mean change from baseline in the MSQ RF-R domain score was a key secondary outcome in the trials and controlled for multiplicity. In the EVOLVE-1 trial, the mean change from baseline in the MSQ RF-R domain score during months 4 to 6 of double-blind treatment was 7.74 points greater in the galcanezumab 120 mg group compared with placebo (95% confidence interval [CI], 5.20 to 10.28; P < 0.001). Similarly, in the EVOLVE-2 trial, the mean change from baseline in the MSQ RF-R domain score during months 4 to 6 was 8.82 points greater in the galcanezumab 120 mg group compared with placebo (95% CI, 6.33 to 11.31; P < 0.001). In the REGAIN trial, the least squares (LS) mean change from baseline was 5.06 points greater in the galcanezumab 120 mg arm compared with the placebo arm (95% CI, 2.12 to 7.99); however, the difference could not be tested for statistical significance based on the predefined multiple-testing procedure. In the CONQUER trial, the mean change from baseline in the MSQ v2.1 RF-R domain score at month 3 was 12.53 points greater in the galcanezumab group compared with placebo (95% CI, 9.19 to 15.87; P < 0.0001).
Migraine Headache Days With Symptoms
The overall change from baseline in number of monthly MHDs with symptoms (nausea and/or vomiting, photophobia and phonophobia, aura, and prodromal symptoms other than aura) during the double-blind treatment phase was an exploratory outcome in all pivotal trials. These outcomes were not controlled for multiplicity within the trials’ multiple-testing procedures. Results are summarized in Table 2. The LS mean change differences in the galcanezumab 120 mg arm versus the placebo arm indicated that galcanezumab treatment was associated with a numerically greater reduction in the number of monthly MHDs with all types of symptoms in all trials.
Migraine Disability Assessment
Change in MIDAS total score was a secondary outcome in all pivotal trials. This outcome was not controlled for multiplicity within the trials’ multiple-testing procedures. In the EVOLVE-1 trial, the mean change from baseline to the end of the double-blind treatment phase (month 6) in the galcanezumab 120 mg arm was −6.29 points (95% CI, −9.45 to −3.13), indicating a numerically greater reduction compared with placebo. In the EVOLVE-2 trial, the mean change from baseline to the end of the double-blind treatment phase (month 6) in the galcanezumab 120 mg arm was −9.15 points (95% CI, −12.61 to −5.69), indicating a numerically greater reduction compared with placebo. In the REGAIN trial, the mean change from baseline to the last observation carried forward (LOCF) end point for the galcanezumab 120 mg arm was −8.74 points (95% CI, −16.39 to −1.08), indicating a numerically greater reduction compared with placebo. In the CONQUER trial, the mean change in the galcanezumab 120 mg arm from baseline to the LOCF end point was −17.8 points (95% CI, −25.6 to −10.0), indicating a numerically greater reduction compared with placebo.
Number of Monthly Migraine Headache Days
The overall change from baseline in the number of monthly MHDs during the double-blind treatment phase was the primary outcome in each of the pivotal trials. The reduction in the overall LS mean change from baseline in the number of monthly MHDs during the double-blind treatment phase for galcanezumab 120 mg was statistically significantly greater compared to placebo in all studies.
In the EVOLVE-1 trial, the overall mean change from baseline in the number of monthly MHDs in the galcanezumab 120 mg arm during the double-blind treatment phase was −1.92 days (95% CI, −2.48 to −1.37; P < 0.001), indicating a greater reduction compared to placebo. In the EVOLVE-2 trial, the overall mean change in the galcanezumab 120 mg arm was −2.02 days (95% CI, −2.55 to −1.48; P < 0.001), indicating a greater reduction compared to placebo. In the REGAIN trial, the overall mean change in the galcanezumab 120 mg arm was −2.09 days (95% CI, −2.92 to −1.26; P < 0.001), indicating a greater reduction compared with placebo. In the CONQUER trial, the overall mean change in the galcanezumab arm was −3.12 days (95% CI, −3.92 to −2.32; P < 0.0001), indicating a greater reduction compared to placebo.
Number of Monthly Headache Days
The overall change from baseline in number of monthly headache days was a secondary outcome in the 4 pivotal trials. This outcome was not included in the trials’ multiple-testing procedures and therefore was not adjusted for multiplicity. In the EVOLVE-1 trial, the mean change difference in the galcanezumab 120 mg arm was −1.66 days (95% CI, −2.25 to −1.07), a numerically greater reduction compared to placebo. In the EVOLVE 2 trial, the mean change difference for the galcanezumab 120 mg arm was −2.00 days (95% CI, −2.58 to −1.42), a numerically greater reduction compared with placebo. In the REGAIN trial, the LS mean change difference in the galcanezumab 120 mg arm was −1.84 days (95% CI, −2.65 to −1.02) compared to placebo. In the CONQUER trial, the mean change difference in the galcanezumab 120 mg arm compared to placebo was a numerically greater −3.13 days (95% CI, −3.96 to −2.29).
Acute Headache Pain Medication Intake
In the EVOLVE-1, EVOLVE-2, and REGAIN trials, the overall change from baseline in monthly MHDs with acute medication use during the double-blind treatment phase was a key secondary outcome and was included in the trials’ multiple-testing procedures. In the EVOLVE-1 trial, the mean change difference from placebo in the galcanezumab 120 mg arm was a numerically greater −1.81 days (95% CI, −2.28 to −1.33; P < 0.001). In the EVOLVE-2 trial, the mean change difference from placebo in the galcanezumab 120 mg arm was a numerically greater −1.82 days (95% CI, −2.29 to −1.36; P < 0.001). In the REGAIN trial, the mean change difference in the galcanezumab 120 mg arm was −2.51 days (95% CI, −3.27 to −1.76), a numerically greater reduction compared to placebo. The difference between the galcanezumab 120 mg and placebo arms could not be tested for statistical significance based on the REGAIN trial’s predefined multiple-testing procedure. In the CONQUER trial, the overall change from baseline in MHDs with acute medication use during the double-blind treatment phase was a secondary outcome. This outcome was not included in the trial’s multiple-testing procedure, and therefore is not adjusted for multiplicity. The mean change difference in the galcanezumab 120 mg arm was −3.40 days (95% CI, −4.14 to −2.65), a numerically greater reduction compared to placebo.
Time to First Loss of Response in the Post-Treatment Phase
Time to the first loss of 50% response in patients who were 50% responders (defined as a reduction of 50% or more from baseline in monthly MHDs) in the last month of double-blind treatment and who entered the post-treatment phase was assessed in the EVOLVE-1, EVOLVE-2, and REGAIN trials. In EVOLVE-1 and EVOLVE-2, approximately half of the patients in all treatment groups had first loss of 50% response by 4 months after the end of the double-blind treatment phase.13 In the REGAIN study, the percentage of patients with first loss of 50% response at month 1 of the post-treatment phase was 24.3%.13 By month 4 of the post-treatment phase, 48.2% patients had first loss of 50% response.
Time to Initiation of Migraine-Prevention Treatment in the Post-Treatment Phase
Time to initiation of migraine-preventive medication during the post-treatment phase was assessed in EVOLVE-1, EVOLVE-2, and REGAIN. In the EVOLVE-1 study, in which 12 patients (< 2%) initiated treatment with a migraine-prevention medication, no significant differences between placebo and galcanezumab-treated patients were observed in the time of initiation.13 In the EVOLVE-2 study, 3.2% of patients in the placebo arm initiated treatment with a migraine-preventive medication, compared with 1.4% patients in the galcanezumab 120 mg arm.13 There were no significant differences between placebo and galcanezumab-treated patients with regard to the time of initiation. In the REGAIN study, |||| of patients who entered the post-treatment follow-up phase started a migraine-preventive medication during the post-treatment period.13
Health Care Resource Utilization
Health care resource utilization (HCRU) was a secondary outcome in the REGAIN and CONQUER trials. These outcomes were not adjusted for multiplicity. The number of HCRU events was recorded in the baseline period (the 6 months before randomization) and the 3-month double-blind treatment periods. Because low rates of HCRU events were observed and because of the different time periods assessed at baseline and post-baseline, rates for the migraine-related events were standardized per 100 patient-years. Migraine-related HCRU per 100 patient-years is summarized in Table 2.
Work Productivity and Activity Impairment Questionnaire
The Work Productivity and Activity Impairment (WPAI) questionnaire was assessed in the CONQUER trial. The LS mean changes for activity impairment were −20.71% (standard error [SE] = 1.95%) and −8.64% (SE = 1.92%) in the galcanezumab and placebo arms, respectively. For presenteeism, the LS mean changes were −12.50% (SE = 2.37%) and −2.56% (SE = 2.32%) in the galcanezumab and placebo arms, respectively. For overall work impairment, the LS mean changes were −14.31% (SE = 2.51%) and −3.46% (2.41%) in the galcanezumab and placebo arms, respectively. For absenteeism, the LS mean changes were −4.22% (1.29%) and −2.90% (SE = 1.24%) in the galcanezumab and placebo arms, respectively.
Harms Results
Harms results from the double-blind treatment periods of the EVOLVE-1, EVOLVE-2, REGAIN, and CONQUER trials are summarized in Table 2 and Table 3.
Adverse Events
During the double-blind treatment period, most patients in the EVOLVE-1 and EVOLVE-2 trials experienced at least 1 treatment-emergent adverse event (AE), with a numerically smaller proportion of patients experiencing at least 1 AE in the placebo arm compared to the galcanezumab 120 mg arm (60% versus 66%, respectively, in EVOLVE-1; 62% versus 65%, respectively, in EVOLVE-2). The most frequently reported AEs in the EVOLVE-1 trial were injection site pain and nasopharyngitis. The most frequently reported AEs in the EVOLVE-2 trial were injection site pain and upper respiratory tract infections.
During the double-blind treatment period of the REGAIN trial, 50% of patients in the placebo arm and 58% of patients in the galcanezumab 120 mg arm experienced at least 1 treatment-emergent AE. The most frequently reported AEs were injection site pain and nasopharyngitis.
During the double-blind treatment period of the CONQUER trial, 53% of patients in the placebo arm and 51% of patients in galcanezumab 120 mg arm experienced at least 1 treatment-emergent AE. The most frequently reported AEs were nasopharyngitis and influenza.
Serious Adverse Events
Fewer than 3% of patients experienced a serious adverse event (SAE) in the studies.
Withdrawals Due to Adverse Events
As with SAEs, a small percentage of patients (< 4%) discontinued double-blind treatment due to AEs.
Mortality
No patients died during the trials.
Notable Harms
Anaphylaxis and hypersensitivity reactions: No patients in the trials experienced an anaphylactic reaction. In the EVOLVE trials, 2% to 4% of patients in the placebo arms and 4% to 6% of patients in the galcanezumab 120 mg arms experienced a hypersensitivity event. One patient in the placebo arm experienced angioedema in each of the EVOLVE trials. In the REGAIN trial, 2% and 4% of patients experienced a hypersensitivity event in the placebo and galcanezumab 120 mg arms, respectively, during the double-blind treatment phase. Three patients in the placebo arm and 2 patients in the galcanezumab 120 mg arm experienced angioedema during double-blind treatment. In the CONQUER trial, 3% of patients in the placebo arm and 3% in the galcanezumab 120 mg arm experienced a hypersensitivity event during the double-blind treatment phase. One patient in the placebo arm and 0 patients in the galcanezumab 120 mg arm experienced angioedema during double-blind treatment.
Injection site reactions: Injection site reactions during double-blind treatment were reported in a numerically greater proportion of patients in the EVOLVE-1 study compared to the other trials. In the EVOLVE-1 trial, injection site reactions were reported by 20% of patients in the placebo arm and 28% of patients in the galcanezumab 120 mg arm. In the other trials, injection site reactions were reported by 9% to 10% and 7% to 18% of patients in the placebo and galcanezumab 120 mg arms, respectively.
Antibody formation: During the double-blind treatment periods of the EVOLVE-1, EVOLVE-2, and REGAIN studies, up to 9.4% of patients treated with galcanezumab 120 mg and up to 1.7% of patients treated with placebo were positive for treatment-emergent antidrug antibodies (ADAs). The formation of ADAs was not assessed proactively in the CONQUER study and is therefore not reported.
Vascular events: In the EVOLVE trials, approximately 2% and 3% of patients in the placebo and galcanezumab 120 mg arms, respectively, experienced a vascular disorder. In the REGAIN trial, 1.79% and 1.10% of patients in the placebo and galcanezumab 120 mg arms, respectively, experienced a vascular disorder during the double-blind treatment phase. The most frequently reported vascular disorders in EVOLVE-1, EVOLVE-2, and REGAIN were hypertension and hot flushes. In the CONQUER trial, 2.61% and 0.43% of patients in the placebo and galcanezumab 120 mg arms, respectively, experienced a vascular disorder during the double-blind treatment phase. Hypertension was the only vascular disorder experienced by more than 1 patient (1.30% in the placebo arm, 0.43% in the galcanezumab arm).
Table 2: Summary of Key Results from Pivotal and Protocol-Selected Studies — EVOLVE-1 and EVOLVE-2, Double-Blind Treatment phase
Results | EVOLVE-1 | EVOLVE-2 | ||
|---|---|---|---|---|
Placebo N = 433 | GMB 120 mg N = 213 | Placebo N = 461 | GMB 120 mg N = 231 | |
Key efficacy results – modified ITT population | ||||
MSQ v2.1 RF-R domain mean change from baseline (average of months 4 to 6)a,b | ||||
Nc | 377 | 189 | 396 | 213 |
LS mean change (95% CI) | 24.69 (22.59 to 26.79) | 32.43 (29.87 to 35.00) | 19.65 (17.85 to 21.45) | 28.47 (26.22 to 30.73) |
LS mean change difference vs. placebo (95% CI) | NA | 7.74 (5.20 to 10.28) | NA | 8.82 (6.33 to 11.31) |
P value | NA | < 0.001d | NA | < 0.001d |
Overall change from baseline in number of monthly MHDs with symptomsa | ||||
nd | 425 | 210 | 450 | 226 |
Nausea and/or vomiting | NA | NA | NA | NA |
LS mean change from baseline | −1.17 (−1.48 to −0.86) | −1.91 (−2.29 to −1.54) | −0.87 (−1.14 to −0.61) | −2.02 (−2.35 to −1.69) |
LS mean change difference vs. placebo (95% CI) | NA | −0.74 (−1.10 to −0.39) | NA | −1.14 (−1.50 to −0.79) |
P valuef | NA | < 0.001 | NA | < 0.001 |
Photophobia and phonophobia | NA | NA | NA | NA |
LS mean change from baseline | −2.10 (−2.55 to −1.66) | −3.50 (−4.03 to −2.96) | −1.47 (−1.84 to −1.10) | −3.22 (−3.69 to −2.76) |
LS mean change difference vs. placebo (95% CI) | NA | −1.39 (−1.90 to −0.89) | NA | −1.76 (−2.25 to −1.27) |
P valuef | NA | < 0.001 | NA | < 0.001 |
Aura | NA | NA | NA | NA |
LS mean change from baseline | −0.96 (−1.19 to −0.72) | −1.39 (−1.67 to −1.11) | −0.97 (−1.21 to −0.73) | −1.45 (−1.75 to −1.15) |
LS mean change difference vs. placebo (95% CI) | NA | −0.43 (−0.70 to −0.16) | NA | −0.48 (−0.81 to −0.16) |
P valuef | NA | 0.002 | NA | 0.004 |
Prodromal symptoms other than aura | NA | NA | NA | NA |
LS mean change from baseline (95% CI) | −1.23 (−1.51 to −0.95) | −1.83 (−2.18 to −1.49) | −1.01 (−1.28 to −0.75) | −1.84 (−2.17 to −1.51) |
LS mean change difference vs. placebo (95% CI) | NA | −0.61 (−0.93 to −0.28) | NA | −0.83 (−1.18 to −0.47) |
P valuef | NA | < 0.001 | NA | < 0.001 |
MIDAS total score mean change from baseline to month 6a | ||||
nd | 345 | 177 | 374 | 202 |
LS mean change from baseline (95% CI) | −14.87 (−17.55 to −12.19) | −21.16 (−24.39 to −17.93) | −12.02 (−14.51 to −9.53) | −21.17 (−24.27 to −18.07) |
LS mean change difference vs. placebo (95% CI) | NA | −6.29 (−9.45 to −3.13) | NA | −9.15 (−12.61 to −5.69) |
P valuef | NA | < 0.001 | NA | < 0.001 |
Overall average change from baseline in monthly MHDs (primary outcome)a,b | ||||
Ne | 425 | 210 | 450 | 226 |
LS mean change (95% CI) | −2.81 (−3.28 to −2.34) | −4.73 (−5.31 to −4.16) | −2.28 (−2.67 to −1.88) | −4.29 (−4.79 to −3.80) |
LS mean change difference vs. placebo (95% CI) | NA | −1.92 (−2.48 to −1.37) | NA | −2.02 (−2.55 to −1.48) |
P value | NA | < 0.001d | NA | < 0.001d |
Overall average change from baseline in monthly headache days | ||||
ne | 425 | 210 | 450 | 226 |
LS mean change (95% CI) | −3.03 (−3.54 to −2.51 | −4.69 (−5.31 to −4.07) | −2.30 (−2.73 to −1.87) | −4.31 (−4.85 to −3.76) |
LS mean change difference vs. placebo (95% CI) | NA | −1.66 (−2.25 to −1.07) | NA | −2.00 (−2.58 to −1.42) |
P valuef | NA | < 0.001 | NA | < 0.001 |
Overall average change from baseline in monthly MHDs with acute headache pain medication intakea,b | ||||
ne | 425 | 210 | 450 | 226 |
LS mean change (95% CI) | −2.15 (−2.56 to −1.74) | −3.96 (−4.46 to −3.46) | −1.85 (−2.20 to −1.50) | −3.67 (−4.11 to −3.23) |
LS mean change difference vs. placebo (95% CI) | NA | −1.81 (−2.28 to −1.33) | NA | −1.82 (−2.29 to −1.36) |
P value | NA | < 0.001d | NA | < 0.001d |
Harms – safety population | EVOLVE-1 Placebo N = 432 | EVOLVE-1 GMB 120 mg N = 206 | EVOLVE-2 Placebo N = 461 | EVOLVE-2 GMB 120 mg N = 226 |
AEs, n (%) | 261 (60.42) | 135 (65.53) | 287 (62.26) | 147 (65.04) |
SAEs, n (%) | 5 (1.16) | 6 (2.91) | 5 (1.08) | 5 (2.21) |
WDAE from study treatment, n (%) | 10 (2.31) | 7 (3.40) | 8 (1.74) | 5 (2.21) |
Deaths, n (%) | 0 | 0 | 0 | 0 |
Notable harms | ||||
Anaphylactic reaction, n (%) | 0 | 0 | 0 | 0 |
Hypersensitivity events, n (%) | 9 (2.08) | 9 (4.37) | 20 (4.34) | 13 (5.75) |
Angioedema, n (%) | 1 (0.23) | 0 | 1 (0.22) | 0 |
Injection site reactions, n (%) | 87 (20.14) | 57 (27.67) | 45 (9.76) | 40 (17.70) |
ADA-positive, n (%) | 7 (1.66) | 7 (3.47) | 2 (0.45) | 19 (8.56) |
Vascular disorders, n (%) | 7 (1.62) | 6 (2.91) | 9 (1.95) | 7 (3.10) |
ADA = antidrug antibody; AE = adverse event; ANCOVA = analysis of covariance; CI = confidence interval; CM = chronic migraine; EM = episodic migraine; GMB = galcanezumab; HCRU = health care resource utilization; ITT = intention-to-treat; LS = least squares; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MMRM = mixed model for repeated measures; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; NA = not applicable; NR = not reported; RF-R = role function – restrictive; SAE = serious adverse event; SE = standard error; vs. = versus; WDAE = withdrawal due to adverse event; WPAI = Work Productivity and Activity Impairment.
aAn MMRM was used for analysis. In the EVOLVE-1 and EVOLVE-2 trials, the MMRM included the fixed, categorical effects of treatment, geographical region, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction. In the REGAIN trial, the MMRM included the fixed, categorical effects of treatment, country, month, baseline medication overuse (yes vs. no), concurrent prophylaxis (yes vs. no), and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction. Estimates were obtained using an unstructured covariance structure. The Kenward-Roger approximation was used to estimate denominator degrees of freedom.
bOutcome included in trial’s multiple-testing procedure.
cNumber of patients in the analysis population with non-missing baseline value and non-missing value at month 3.
dResults are statistically significant after adjustment for multiplicity.
eNumber of patients in the analysis population with non-missing baseline value and at least one non-missing post-baseline value.
fP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: EVOLVE-1 Clinical Study Report9 and EVOLVE-2 Clinical Study Report.10
Table 3: Summary of Key Results from Pivotal and Protocol-Selected Studies — REGAIN and CONQUER, Double-Blind Treatment phase
Results | REGAIN | CONQUER | ||
|---|---|---|---|---|
Placebo N = 558 | GMB 120 mg N = 278 | Placebo N = 230 | GMB 120 mg N = 232 | |
Key efficacy results – modified ITT population | ||||
MSQ v2.1 RF-R domain mean change from baseline at month 3a,b | ||||
Nc | 494 | 252 | 222 | 223 |
LS mean change (95% CI) | 16.76 (14.44 to 19.07) | 21.81 (19.04 to 24.59) | 10.68 (8.04 to 13.32) | 23.21 (20.55 to 25.87) |
LS mean change difference vs. placebo (95% CI) | NA | 5.06 (2.12 to 7.99) | NA | 12.53 (9.19 to 15.87) |
P value | NA | < 0.001d,e | NA | < 0.0001e,f |
Overall change from baseline in number of monthly MHDs with symptomsa | ||||
ng | 538 | 273 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Nausea and/or vomiting | NA | NA | NA | NA |
LS mean change from baseline | −1.92 (−2.45 to −1.39) | −3.13 (−3.77 to −2.48) | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | −1.21 (−1.82 to −0.59) | NA | |||||||||||||||||||||| |
P valueh | NA | < 0.001 | NA | |||||||||||||||||||||| |
Photophobia and phonophobia | NA | NA | NA | NA |
LS mean change from baseline | −2.25 (−2.95 to −1.55) | −3.81 (−4.65 to −2.97) | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | −1.56 (−2.37 to −0.75) | NA | |||||||||||||||||||||| |
P valueh | NA | < 0.001 | NA | |||||||||||||||||||||| |
Aura | NA | NA | NA | NA |
LS mean change from baseline | −1.42 (−1.90 to −0.95) | −1.40 (−1.97 to −0.82) | |||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | 0.03 (−0.53 to 0.58) | NA | |||||||||||||||||||||| |
P valueh | NA | 0.922 | NA | |||||||||||||||||||||| |
Prodromal symptoms other than aura | NA | NA | NA | NA |
LS mean change from baseline | −1.15 (−1.69 to −0.60) | −1.81 (−2.47 to −1.15) | |||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | −0.66 (−1.29 to −0.02) | NA | |||||||||||||||||||||| |
P valueh | NA | 0.042 | NA | |||||||||||||||||||||| |
MIDAS total score mean change from baseline to last observation carried forward end point | ||||
Ng | 504 | 254 | 225 | 228 |
LS mean change from baseline (95% CI) | −11.53 (−18.17 to −4.89) | −20.27 (−28.27 to −12.28) | −3.30 (NR) | −21.10 (NR) |
LS mean change difference vs. placebo (95% CI) | NA | −8.74 (−16.39 to −1.08) | NA | −17.8 (−25.6 to −10.0) |
P valuef | NA | 0.025 | NA | < 0.0001 |
Overall average change from baseline in monthly MHDs (primary outcome)a,b | ||||
Ng | 538 | 273 | 228 | 230 |
LS mean change (95% CI) | −2.74 (−3.45 to −2.03) | −4.83 (−5.69 to −3.97) | −1.02 (−1.65 to −0.39) | −4.14 (−4.77 to −3.51) |
LS mean change difference vs. placebo (95% CI) | NA | −2.09 (−2.92 to −1.26) | NA | −3.12 (−3.92 to −2.32) |
P value | NA | < 0.001f | NA | < 0.0001f |
Overall average change from baseline in monthly headache days | ||||
ng | 538 | 273 | 228 | 230 |
LS mean change (95% CI) | −3.01 (−3.70 to −2.31) | −4.84 (−5.69 to −4.00) | −1.05 (−1.76 to −0.35) | −4.18 (−4.87 to −3.49) |
LS mean change difference vs. placebo (95% CI) | NA | −1.84 (−2.65 to −1.02) | NA | −3.13 (−3.96 to −2.29) |
P valueh | NA | < 0.001 | NA | < 0.0001 |
Overall average change from baseline in MHDs with acute headache pain medication intakea,b | ||||
ng | 538 | 273 | 228 | 230 |
LS mean change (95% CI) | −2.23 (−2.88 to −1.58) | −4.74 (−5.53 to −3.96) | −0.80 (−1.41 to −0.18) | −4.19 (−4.82 to −3.57) |
LS mean change difference vs. placebo (95% CI) | NA | −2.51 (−3.27 to −1.76) | NA | −3.40 (−4.14 to −2.65) |
P value | NA | < 0.001h | NA | < 0.0001f |
HCRUs related to migraine – mean number of events per 100 patient-years | ||||
Ne | 533 | 269 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Health care professional visits | NA | NA | NA | NA |
Baseline events | 110.69 | 102.60 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Treatment events | 44.64 | 29.04 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Mean change from baseline | NR | NR | |||||||||||||||||||||| | |||||||||||||||||||||| |
Emergency room visits | NA | NA | NA | NA |
Baseline events | 21.01 | 18.59 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Treatment events | 13.86 | 13.76 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Mean change from baseline | NR | NR | |||||||||||||||||||||| | |||||||||||||||||||||| |
Admissions to hospital | NA | NA | NA | NA |
Baseline events | 1.50 | 1.49 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Treatment events | 0 | 0 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Mean change from baseline | NR | NR | |||||||||||||||||||||| | |||||||||||||||||||||| |
Overnight hospital stays | NA | NA | NA | NA |
Baseline events | 4.88 | 2.97 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Treatment events | 0 | 0 | |||||||||||||||||||||| | |||||||||||||||||||||| |
Mean change from baseline | NR | NR | |||||||||||||||||||||| | |||||||||||||||||||||| |
WPAI mean change from baseline to last observation carried forward end point | ||||
Percent of activity impairment due to health | Not assessed | Not assessed | NA | NA |
Ng | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change (SE) | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
P valueh | Not assessed | Not assessed | NA | |||||||||||||||||||||| |
Percent of impairment while working due to health (presenteeism) | Not assessed | Not assessed | NA | NA |
Ne | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change (SE) | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
P valueh | Not assessed | Not assessed | NA | |||||||||||||||||||||| |
Percent of overall work impairment due to health | Not assessed | Not assessed | NA | NA |
Ne | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change (SE) | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
P valueh | Not assessed | Not assessed | NA | |||||||||||||||||||||| |
Percent of work time missed due to health (absenteeism) | Not assessed | Not assessed | NA | NA |
Ng | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change (SE) | Not assessed | Not assessed | |||||||||||||||||||||| | |||||||||||||||||||||| |
P valueh | Not assessed | Not assessed | NA | |||||||||||||||||||||| |
Harms – safety population | ||||
AEs, n (%) | 279 (50.00) | 159 (58.24) | 122 (53.04) | 119 (51.29) |
SAEs, n (%) | 4 (0.72) | 1 (0.37) | 2 (0.87) | 2 (0.86) |
WDAE from study treatment, n (%) | 6 (1.08) | 1 (0.37) | 0 | 1 (0.43) |
Deaths, n (%) | 0 | 0 | 0 | 0 |
Notable harms – safety population | ||||
Anaphylactic reaction, n (%) | 0 | 0 | 0 | 0 |
Hypersensitivity events, n (%) | 11 (1.97) | 12 (4.40) | 8 (3.48) | 7 (3.02) |
Angioedema, n (%) | 3 (0.54) | 2 (0.73) | 1 (0.43) | 0 |
Injection site reactions, n (%) | 51 (9.14) | 31 (11.36) | 23 (10.00) | 16 (6.90) |
ADA-positive, n (%) | 8 (1.50) | 7 (2.65) | NR | NR |
Vascular disorders, n (%) | 10 (1.79) | 3 (1.10) | 6 (2.61) | 1 (0.43) |
ADA = antidrug antibody; AE = adverse event; ANCOVA = analysis of covariance; CI = confidence interval; CM = chronic migraine; EM = episodic migraine; GMB = galcanezumab; HCRU = health care resource utilization; ITT = intention-to-treat; LS = least squares; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MMRM = mixed model for repeated measures; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; NA = not applicable; NR = not reported; RF-R = role function – restrictive; SAE = serious adverse event; SE = standard error; vs. = versus; WDAE = withdrawal due to adverse event; WPAI = Work Productivity and Activity Impairment.
aAn MMRM was used for analysis. In the REGAIN trial, the MMRM included the fixed, categorical effects of treatment, country, month, baseline medication overuse (yes vs. no), concurrent prophylaxis (yes vs. no), and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction. In the CONQUER trial, the MMRM included the fixed, categorical effects of treatment, baseline migraine frequency category (low-frequency EM, high-frequency EM, and CM), pooled country, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline value-by-month interaction. Estimates were obtained using an unstructured covariance structure. The Kenward-Roger approximation was used to estimate denominator degrees of freedom.
bOutcome included in trial’s multiple-testing procedure.
cNumber of patients in the analysis population with non-missing baseline value and non-missing value at month 3.
dP value is descriptive only because outcome could not be tested for statistical significance based on the predefined multiple-testing procedure due to a failed test for a previous end point in the testing sequence (Figure 21 and Figure 22 in Appendix 3).
eANCOVA used for analysis. In the REGAIN trial, the ANCOVA model contained the main effects of treatment, baseline medication overuse, concurrent prophylaxis use, and country, and included an appropriate baseline value as a covariate. In the CONQUER trial, the ANCOVA model contained the main effects of treatment, baseline migraine frequency category, pooled country, and appropriate baseline value.
fResults are statistically significant after adjustment for multiplicity.
gNumber of patients in the analysis population with non-missing baseline value and at least one non-missing post-baseline value.
hP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: REGAIN Clinical Study Report11 and CONQUER Clinical Study Report.12
Critical Appraisal
The pivotal trials were designed to assess the superiority of galcanezumab over placebo. The trials were double-blind and the blinding methods used were appropriate. Although the efficacy analyses used what appeared to be a modified intention-to-treat (ITT) population, which included randomized patients who received at least 1 dose of the study drug, the numerical differences between the randomized (ITT) population and the analyzed population were generally small and unlikely to be a major source of bias for most outcomes. The analyzable sample sizes for the MSQ v2.1 and MIDAS were notably smaller than the randomized sample sizes in each study except CONQUER. There was no discernable difference between treatment groups in any study regarding disproportionate missing patients, but characteristics of the patients who were not included in the analyzable set were not reported and it could not be determined what impact this reduced sample size had on the results for these outcome measures. The safety population included data from all randomized patients who received at least 1 dose of the investigational drug, with analyses conducted based on modal treatment. A numerically greater proportion of patients discontinued from double-blind treatment in the EVOLVE-1 and EVOLVE-2 trials compared to the other trials. Furthermore, the clinical expert consulted by CADTH indicated that the discontinuation rates in the EVOLVE trials were higher than is typically seen in their clinical practice, and higher than expected with anti-CGRP monoclonal antibodies. The most frequent reason for discontinuing double-blind treatment was withdrawal by the patient. Other reasons for discontinuation included lost to follow-up, lack of efficacy, and AEs. Patient compliance with the electronic patient-reported outcomes (ePRO) diary, which was used to collect data for migraine and headache-related end points, was high during the double-blind treatment period across trials. Multiple testing procedures were used in all the trials to control type I error for the primary and key secondary outcomes. Each of the trials met their primary objective for the galcanezumab 120 mg arm, which statistically significantly reduced the overall mean number of monthly MHDs during double-blind treatment. The EVOLVE-1, EVOLVE-2, and CONQUER trials also met all of their key secondary objectives. In the galcanezumab 120 mg arm in the REGAIN trial, only 1 key secondary objective (50% response rate), which was not included in the CADTH systematic review protocol, was statistically significant after multiplicity adjustment. in the REGAIN trial, monthly MHDs with acute medication use and MSQ v2.1 RF-R could not be tested for statistical significance within the pre-specified multiple-testing procedure; thus, these results cannot be interpreted to draw conclusions for this end point.
All trials were placebo-controlled. No direct comparative effect between galcanezumab and other available migraine-preventive treatments (e.g., other CGRP medications) was studied. Patients randomized to the galcanezumab 120 mg arm in the studies received a loading dose of 240 mg, which aligns with the Health Canada–approved dose. The clinical expert consulted by CADTH indicated that the numbers of monthly MHDs and headache days at baseline in the REGAIN and CONQUER trials were lower than would be expected for patients with CM typically treated in regular clinical practice, although it was acknowledged that the patients enrolled in the CM populations of the trials met the criteria for CM (i.e., headaches occurring on 15 or more days per month and MHDs on 8 or more days per month). The CONQUER trial was conducted in a treatment-resistant migraine-patient population (i.e., history of failures to 2 to 4 prior migraine-preventive medication categories due to inadequate efficacy or safety and tolerability), including patients with either EM or CM. This most closely aligns with the patient population specified in the reimbursement request. In contrast, the EVOLVE-1, EVOLVE-2, and REGAIN trials excluded patients who failed to have an efficacy response to at least 3 classes of migraine-preventive treatment, and most patients enrolled in these trials had not previously failed 2 or more prior migraine-preventive treatments. All the pivotal trials excluded patients who had been previously treated with a CGRP inhibitor. In the REGAIN trial, patients could be on 1 stable dose of prophylactic therapy (topiramate or propranolol only). This aligns with regular practice in Canada, according to the clinical expert consulted by CADTH, who indicated that galcanezumab could be used concurrently with other migraine-preventive medications.
Indirect Comparisons
Description of Studies
Two indirect treatment comparison (ITCs) were included. One is the sponsor-submitted ITC,14 which compared galcanezumab (120 mg and 240 mg) with erenumab (70 mg and 140 mg) in the prophylaxis of EM and CM in patients with a history of prior preventive treatment failures. The other identified by CADTH literature search was a network meta-analysis (NMA) by the Institute of Clinical and Economic Reviews (ICER),15 which compared galcanezumab with other migraine therapies in the treatment of patients with EM.
Efficacy Results
The sponsor-submitted ITC14 reported there was insufficient evidence to show a difference between galcanezumab and erenumab for all reported efficacy outcomes in patients with EM or CM who failed at least 2 or at least 3 preventive medications.
The ICER meta-analysis found that patients with EM in the galcanezumab 120 mg group experienced fewer days of acute medication use per month compared with the erenumab 70 mg group. No treatments were favoured when comparing galcanezumab with fremanezumab in all assessed outcomes. Patients in the galcanezumab 120 mg group experienced fewer monthly migraine days when compared with topiramate (200 mg/day and 50 mg/day) and placebo. In terms of 50% response (i.e., 50% reduction in MHDs), the results favoured galcanezumab 120 mg over placebo, with a higher proportion of patients on galcanezumab 120 mg achieving a 50% response.
Harms Results
No data on harms (AEs, SAEs, notable AEs) were reported in either of the ITCs.
Critical Appraisal
For the sponsor-submitted ITC, the main limitations were poor reporting of methods (i.e., details of the literature search, the process of study selection and data extraction, and the risk of bias assessment of individual studies were not clearly described), as well as clinical heterogeneity in the included studies (e.g., the definition of treatment response varied across the included studies). For the ICER meta-analysis, the key limitations were the population was not specifically aligned with the population indicated in the reimbursement request to CADTH, a relatively small number of trials were included for each outcome, clinical heterogeneity (e.g., the definition of the response varied), and the NMA was limited to patients with EM (i.e., no NMA evidence for patients with CM). In addition, outcomes important to patients, such as headache-related disability (as measured by HIT-6, migraine-related disability scores as measured by the MIDAS, work productivity, loss of workdays WPAI), adherence, and HCRU (hospitalizations), were not assessed in either ITC. Due to methodological limitations and clinical heterogeneities across the included studies in both ITCs, the findings from both ITCs do not clearly indicate whether galcanezumab is inferior, similar, or superior to the comparators of interest for this review.
The clinical expert CADTH consulted for this review indicated that, while there is a lack of direct clinical trial evidence, reliable and robust indirect comparison evidence, and clinical experience to compare galcanezumab with other CGRPs (e.g., erenumab or fremanezumab), the mechanism of the different CGRPs suggests it is reasonable to expect similar efficacy and safety among CGRPs approved by Health Canada. It should be noted that, clinically, not all patients respond to any individual CGRP drug, and different CGRP drugs may work for different patients. Galcanezumab may therefore provide an option for patients who do not respond to other CGRP inhibitors.
Other Relevant Evidence
Description of Studies
One long-term study (CGAJ16) was summarized to provide additional evidence regarding the safety of galcanezumab 120 mg (with a 240 mg loading dose) for patients with EM or CM. The CGAJ study was a multi-centre, phase III, randomized, open-label study. The trial consisted of a screening period, 12 months of open-label treatment with galcanezumab, and 4 months of follow-up. In total, 270 patients with migraine were enrolled and randomized in a 1:1 ratio to either galcanezumab 120 mg (with a 240 mg loading dose) or 240 mg in CGAJ. Because galcanezumab 240 mg is outside of the Health Canada–recommended dose, this summary of the CGAJ study focuses on the results of the 120 mg dose. Patients who received galcanezumab 120 mg had a single initial loading dose of galcanezumab 240 mg (2 injections of galcanezumab 120 mg) then 120 mg for the remainder of the 12-month treatment period. The study drug was administered subcutaneously using a pre-filled syringe (80.9%) or an autoinjector (19.1%), when the latter was available. Study-site personnel administered the first dose while patients and/or caregivers were trained to administer all subsequent doses. The primary outcome was long-term safety and tolerability for 12 months of treatment, which included assessments of the number of AEs, SAEs, and discontinuation rates. Secondary outcomes included long-term efficacy and HRQoL measured by change in MIDAS score, MSQ v2.1 score, and HCRU and employment status.
For patients who received galcanezumab 120 mg, the mean age was 40.2 years (standard deviation [SD] = 11.68), and most patients were female (81.5%) and White (76.3%). This group had a mean baseline MIDAS score of 45.8 (SD = 42.06), which reflects severe disability. In terms of medication history, 60% of patients had tried at least 1 prior preventive treatment, with 43% and 20% having failed at least 1 and 2 prior treatments, respectively.
Efficacy Results
In the galcanezumab 120 mg arm, the overall LS mean change from baseline was −5.61 (95% CI, −6.27 to −4.95) for MHDs and −2.17 (95% CI, −2.76 to −1.58) for headache days. The overall mean change from baseline in use of acute migraine or headache treatment was −5.09 days per month (95% CI, −5.83 to −4.35). The overall LS mean change from baseline was −33.58 (95% CI, −37.73 to −29.42) for the MIDAS total score and 28.27 (95% CI, 25.98 to 30.56) for the MSQ v2.1 total score. In months 7 to 12, the numbers of patients who had at least 1 health care visit or emergency room visit related to migraine were 12 and 3, respectively, compared with 52 and 11 patients at baseline, respectively.
Harms Results
Most patients (82.2%) experienced at least 1 treatment-emergent AE during the treatment phase of the CGAJ trial. The most frequently reported AEs were nasopharyngitis (17.8%), injection site pain (17.1%), injection site reaction (11.6%), sinusitis (10.9%), and back pain (9.3%). Three patients reported having a single SAE in the form of each of the following: lumbar radiculopathy, migraine, and osteoarthritis. In total, 6 patients (4.7%) discontinued the study due to an AE and no deaths were reported.
Notable harms included anaphylactic reaction (6.2%), hypersensitivity reaction (14.7%), injection site reaction (11.6%), and vascular disorder (4.7%). The presence of ADAs was detected in 8 (6.3%) patients at baseline and 16 (12.5%) patients during the treatment phase. A patient was considered ADA-positive when a post-baseline titre was 4 times greater than the baseline value or a post-baseline titre was greater than 1:20 if the baseline ADA tests were negative. Neutralizing antibodies were present for all ADA-positive patients at both baseline and during treatment (n = 8 and n = 16, respectively).
Critical Appraisal
The CGAJ trial did not have a control group. Additionally, the open-label design may have influenced the perception of improvement by patients and clinicians, which could affect the reporting of harms and efficacy measures. All information on migraine frequency and acute medication use was collected retrospectively by direct questioning from study personnel during visits. This form of data collection could affect the accuracy of harms and efficacy reporting, although it is unknown if this would be in favour of or against the study treatment. Limitations in the study design make it challenging to interpret the results and form conclusions with certainty. The CGAJ trial sample size was small. Patients were predominantly female and White, which the clinical expert consulted by CADTH confirmed means they were similar to patients treated in Canadian clinics. The clinical expert consulted by CADTH suggested that, ideally, patients are tried on a medication within the therapeutic range for at least 8 weeks before deciding whether the treatment had failed. The time on treatment (maximum 12 months) was therefore acceptable.
Conclusions
The EVOLVE-1 and EVOLVE-2 trials provide direct evidence regarding the efficacy and safety of galcanezumab relative to placebo for adult patients with EM. The REGAIN trial provides direct evidence regarding the efficacy and safety of galcanezumab relative to placebo for adult patients with CM. The CONQUER trial provides direct evidence regarding the efficacy and safety of galcanezumab relative to placebo in adult patients with EM or CM who have previously failed 2 to 4 classes of migraine-preventive treatments. Compared to placebo, patients who were treated with galcanezumab 120 mg showed benefits in the form of a reduction in monthly MHDs during double-blind treatment periods in all trials (6 months in the EVOLVE-1 and EVOLVE-2 trials; 3 months in the REGAIN and CONQUER trials). In addition, reductions in monthly MHDs with acute medication use and improvement in the MSQ v2.1 RF-R domain were observed in the EVOLVE-1, EVOLVE-2, and CONQUER trials. The effect of galcanezumab on MHDs with symptoms, headache days, other patient-reported outcomes, and HCRU and employment status remains uncertain due to a lack of control for multiplicity. Many study patients reported treatment-emergent AEs. The most frequently reported AEs across the trials were injection site pain and nasopharyngitis. Galcanezumab was related to a numerically higher frequency of becoming ADA-positive in the 3 trials that assessed immunogenicity. Few patients discontinued double-blind treatment due to AEs and few patients experienced SAEs. No patients died. The pivotal trials did not provide direct evidence regarding the relative efficacy and safety of galcanezumab versus other migraine-preventive medications in adults with EM or CM.
The results of the CGAJ trial, a randomized, open-label, long-term safety study of galcanezumab 120 mg and 240 mg, supported the safety of galcanezumab 120 mg. The results also supported the beneficial effect of galcanezumab in terms of monthly MHDs, headache days, use of acute medication, and HRQoL. However, limitations of this study, such as a small sample size and lack of a control group, contribute uncertainty to the results.
Neither the sponsor-submitted ITC nor the ICER meta-analysis provided sufficient evidence to conclude that galcanezumab differed in efficacy compared to other CGRPs in terms of response rate, change from baseline of monthly MHDs, change from baseline of monthly MHDs with acute medication use, discontinuation from all causes, and discontinuation from AEs in patients with CM and/or EM. Due to several limitations of both ITCs (i.e., methodological issues and clinical heterogeneity), no definitive conclusion can be drawn on the clinical efficacy and safety galcanezumab 120 mg compared with erenumab or fremanezumab in the treatment of patients with migraine (EM or CM) who failed at least 2 preventive treatments.
Introduction
Disease Background
Migraine is a neurologic disease characterized by recurrent episodes of pulsating headache pain of at least moderate severity.1 Migraine episodes may last from 4 to 74 hours and can be accompanied by symptoms such as photophobia, phonophobia, nausea, and vomiting.5 The type of migraine can be refined by the frequency of monthly MHDs and monthly headache days.1 The ICHD-3 describes CM as a headache (tension-type-like or migraine-like) occurring on 15 or more days per month for more than 3 months with the features of migraine headaches on at least 8 days per month.2 In EM, individuals experience headaches on 14 or fewer days per month for more than 3 months with the features of migraine headaches on at least 4 days per month.2 A diagnosis of migraine is made using a history, physical examination, and neurologic examination.5
In Canada (2010 to 2011), 9.6% of the population over 18 years of age experienced migraine attacks, with more females (13.8%) than males (5.3%) having had migraine.3 In a longitudinal web-based panel study of migraine in the US (N = 16,789), 91.2% of patients had EM and 8.8% had CM.17 An estimated 2.5% of patients with EM transition to having CM.18
Among those who had migraine in Canada (aged ≥ 15 years, 2011), 38.2% reported that migraine at least moderately affected their life and 25.5% reported that the pain prevented them from activities.19 In a cross-sectional, web-based observational survey of patients with migraine (N = 8,726), nearly half of all respondents reported moderate or severe disability, with more headache days per month associated with more severe disability.20 Among the respondents, 5.7% had CM and 94.3% had EM.20 Patients with CM reported longer, more painful headaches, and more comorbidities than those with EM.20 Additionally, patients with CM reported worse headache-related disability compared with those with EM, as measured by the MIDAS, which is a validated tool that measures disability in patients with migraine.20 Migraine attacks are often disabling. Headache disorders are among the 3 highest causes of years lived with disability worldwide (1990 to 2017), with migraine accounting for 47,245.4 years lost to disability (thousands) in 2017.21
Migraine attacks are associated with missed activities at work, school, and/or at home.19 Additionally, prevalence is highest during peak productive years (i.e., around 30 to 64 years of age),5 which maximizes the impact on the sufferer, family, and society.19,22-24 Migraine reduces productivity, leading to missed work days and substantial economic costs. Loss of productivity accounts for up to 70% of total migraine-related annual costs.25 In Canada, 34% of individuals with migraine reported limitations in job opportunities due to migraine in 2011; 36% of those currently employed reported missing at least 1 day of work in the past 3 months due to migraine; and 18% who had previously been employed reported that, due to migraine, they had changed their work activities (hours, type of work, or stopped work) for 3 months or longer.19
Standards of Therapy
Comprehensive migraine therapy includes management of lifestyle factors and triggers, acute and preventive (or prophylactic) medications, and migraine self-management strategies.4,5 The goals of migraine treatments are to relieve pain, restore function, improve HRQoL, reduce headache frequency, and prevent the progression of EM to CM.6 The Canadian Headache Society has guidelines for the acute treatment of migraine and for preventing attacks.5
Preventive medications include a variant of the botulinum toxin (onabotulinumtoxinA; for CM only), inhibitors of CGRP (e.g., galcanezumab, fremanezumab, erenumab), beta-blockers (e.g., propranolol, metoprolol), calcium-channel blockers (e.g., flunarizine, verapamil), tricyclic antidepressants (e.g., amitriptyline, nortriptyline), serotonin-norepinephrine reuptake inhibitors (e.g., venlafaxine), anticonvulsants (e.g., topiramate, gabapentin, or divalproex), angiotensin-converting enzyme inhibitors and angiotensin receptor blockers (e.g., candesartan), and a serotonin antagonist (pizotifen). Only topiramate, onabotulinumtoxinA, and CGRP inhibitors have been approved by Health Canada for the prevention of migraine, and onabotulinumtoxinA is only indicated for the prevention of CM. Migraine prophylaxis is an important part of the overall approach for a proportion of individuals with migraine.4 Of patients with migraine who have received preventive medications, 87% with migraine have an inadequate response to 2 or more preventive therapies.7
Drug
Galcanezumab is a humanized immunoglobin G4 monoclonal antibody that binds to CGRP and prevents its biologic activity.8 Galcanezumab does not bind to the CGRP receptor. Galcanezumab is administered by subcutaneous injection. The recommended protocol is a loading dose of 240 mg (administered as 2 consecutive subcutaneous injections of 120 mg) followed by once-monthly, single-injection doses of 120 mg. Galcanezumab received a Health Canada Notice of Compliance on July 30, 2019, with an indication for the prevention of migraine in adults who have at least 4 migraine days per month. Galcanezumab also is indicated for the reduction in the frequency of attacks throughout a cluster period in adults with episodic cluster headache with prior cluster headache periods lasting at least 6 weeks and who have had an inadequate response to, tolerated poorly, or had contraindications to conventional preventive therapies established by Canadian practice guidelines. Galcanezumab has not been previously reviewed by CADTH.
The sponsor requested reimbursement of galcanezumab for the prevention of migraine in adults who have at least 4 MHDs per month and have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications, which differs from the Health Canada indication.26
Table 4: Key Characteristics of Galcanezumab, Fremanezumab, Erenumab, OnabotulinumtoxinA, Beta-Blockers, Anticonvulsants, TCAs and SNRIs, CCBs, ACE Inhibitors and ARBs, and Pizotifen
Drug name | Mechanism of action | Indicationa | Route of administration | Recommended dosage | Serious adverse effects of safety issues | Other |
|---|---|---|---|---|---|---|
Galcanezumab | Binds to CGRP ligand | The prevention of migraine in adults who have at least 4 migraine days per month | Subcutaneous injection | 240 mg loading dose followed by 120 mg monthly | Hypersensitivity reactions | NA |
Fremanezumab | Binds to CGRP ligand | For prevention of migraine in patients who have at least 4 migraine days monthly | Subcutaneous injection | 675 mg quarterly, 675 mg followed by 225 mg monthly (patients with CM), or 225 mg monthly (patients with EM) | Hypersensitivity reactions | NA |
Erenumab | Binds to CGRP receptor | For prevention of migraine in patients who have at least 4 migraine days monthly | Subcutaneous injection | 70 mg or 140 mg once monthly | Hypersensitivity reactions | NA |
OnabotulinumtoxinA | Inhibits presynaptic release of CGRP, and other neurotransmitters | For prophylaxis of headaches in adults with chronic migraine (≥ 15 days/month with headache lasting ≥ 4 hours/day) | Intramuscular injection | 5 units to 31 different sites, across 7 different head-and-neck muscle areas | Spread of toxin beyond injection site (e.g., breathing difficulties) | NA |
Beta-blockers | Beta1-receptor antagonists | Migraine prophylaxis: propranolol, timolol Others: none for migraine Various cardiovascular indications | Oral | Varies by drug | Rebound syndrome Bronchospasm | Drugs: propranolol, timolol, nadolol, metoprolol |
Anticonvulsants | Multiple mechanisms of action | Topiramate: migraine prophylaxis Topiramate/others: epilepsy | Oral | Varies by drug | Valproic acid: hepatotoxicity | Drugs: topiramate, gabapentin, valproic acid |
TCAs and SNRIs | Inhibits reuptake of serotonin, norepinephrine | None for migraine Depression Anxiety | Oral | Varies by drug | Hypertension Serotonin syndrome Conditions that may be exacerbated by anticholinergic effects (TCA mainly) | Drugs: amitriptyline, nortriptyline, venlafaxine |
CCBs | Blocks L-type calcium channels | Flunarizine: migraine prophylaxis Others: none for migraine Various cardiovascular indications | Oral | Varies by drug | Heart block | Drugs: flunarizine, verapamil |
ACE inhibitors and ARBs | Inhibits effects of angiotensin II | None for migraine Hypertension Heart failure | Oral | Varies by drug | Angioedema | Drugs: lisinopril, candesartan |
Pizotifen | Blocks 5HT-2 receptors, histamine (H1) receptors | Prevention of migraine: recommended for those with ≥ 3 attacks monthly and fail to respond to symptomatic treatment and have reduced quality of life | Oral | 1 mg/day to 6 mg/day, up to 3 mg in a single dose | Conditions that may be exacerbated by anticholinergic effects | NA |
5HT-2 = serotonin-2; ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; CCB = calcium-channel blocker; CGRP = calcitonin gene-related peptide; CM = chronic migraine; EM = episodic migraine; NA = not applicable; SNRI = serotonin-norepinephrine reuptake inhibitor; TCA = tricyclic antidepressant.
aHealth Canada–approved indication.
Source: Galcanezumab product monograph,8 CADTH Clinical Review of fremanezumab.27
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
About the Patient Group(s) and Information Gathered
CADTH received a joint submission from Migraine Canada and Migraine Québec for the review of galcanezumab (Emgality). Migraine Canada and Migraine Québec are not-for-profit patient organizations that provide support and education to patients, caregivers, and health care professionals, and raise awareness about the impact of migraine. The groups are advocates for optimal care for those living with migraine and support improved quality of life and research toward a cure.
The information for the patient-group submission was collected through 2 online surveys conducted in 2018 and 2021. The 2018 survey was promoted through Migraine Canada’s Facebook community, Twitter platform, and in migraine clinics across Canada. In total, 597 respondents participated, the majority of whom were between 26 and 54 years old. The survey results indicated that 26% of participants had low-frequency (1 to 6 days per month) EM, 32% had high-frequency (7 to 14 days per month) EM, and 42% had CM (15 or greater days per month). The 2021 survey captured input from 115 participants and was specific to CGRP medications and galcanezumab. In this group, 97% were female, nearly 90% had been diagnosed with migraine, and 73% had experienced at least 15 migraine attacks each month. Both surveys were designed and analyzed by Migraine Canada. Direct input from 2 Canadian patients, a 37-year-old male and a 25-year-old female, was also included in the submission.
Disease Experience
Based on the survey responses, Migraine Canada and Migraine Québec identified the following key impacts on the lives of those living with migraine and their families: inability to work resulting in financial stress and relying on a spouse or family members to compensate, childcare and needing additional help, restricted social activities and difficulties with relationships, and lack of understanding from others.
The patient groups emphasized that many patients take time away from work due to active attacks (ictal state) but then try to compensate by doing more to catch up during the time between attacks (interictal state), which does not allow for rest and recovery. They added that lost productivity should include both missed working days and “presenteeism,” when patients attend work despite having migraine symptoms. When asked to rate how migraine affected their daily lives in the past 3 months, 1% of respondents indicated having no limitations, 24% avoided triggers and missed personal activities but not work, 45% missed at least 1 day of full-time work or household work, 5% were working part-time, and 25% reported being disabled or not working.
Migraine also affected patients’ family members and relationships, with 48% indicating it had a minor impact, 40% noting a major impact, and 9% attributing their lack family or intimate relationships primarily to migraine. The remaining 3% responded that migraine had no impact on their relationships. Patients described how their spouse and/or family often must bear the burden of household and financial responsibilities, how families miss out on spending time together, difficulties with starting new relationships and stress on existing relationships, and the lack of support available for caregivers.
Quality of life is severely affected during interictal states as patients often live in fear of their next attack, avoiding potential triggers, which limits their activities and social interactions, and may be continually managing medication side effects. This last impact is unacceptable to patients aiming to be active and contributing members at work, home, and in their communities. Mental health is also greatly affected by migraine and 80% of respondents stated that they have anxiety or depression.
According to the patient submission, 27% of respondents had been to the emergency department at least 4 times since the start of their condition. Patients noted that living with migraine stressful, and they also felt stigmatized and blamed for wasting health care resources and health care providers’ time when making trips for urgent care.
The following quotes are representative of patient and caregiver experiences of living with migraine:
“It is invisible. It is stigmatised. It isolates and diminishes you. Constant pain symptoms from migraine wear on the body and soul. You are trapped unable to escape or explain. Unable to live your life or enjoy simple moments.”
“Physically and emotionally exhausting! The stress of going to work (nurse) and suddenly having to leave my patients and coworkers is upsetting. The unpredictability of migraine is stressful. The loss of freedom and independence is stressful. This mostly invisible chronic pain is stressful, almost overwhelmingly so.”
“My migraines are the main reason my husband and I do not have children. My husband currently has to work full-time outside the house to support us since I am not working.”
“Chronic migraine has turned my wife's life upside down. She suffers with bouts of depression, anxiety, and even suicidal thoughts. I can't even begin to be imagine the pain she suffers on an almost daily basis.”
Experiences With Currently Available Treatments
Patients reported having experience with triptans, amitriptyline, venlafaxine, topiramate, Emtec, ibuprofen, almotriptan, ketorolac tromethamine, onabotulinumtoxinA, lidocaine, and galcanezumab, along with broader categories of medications, such as tricyclic antidepressants, beta-blockers, calcium-channel blockers, anti-epileptics, CGRP inhibitors, and nonspecific compounds such as cannabidiol oil, magnesium, and riboflavin. Many still struggle to find an effective treatment or access to 1. One patient shared, “I have daily migraine and can barely work. Amitriptyline is not working anymore which is why I am currently looking into injection types of treatment recommended by my neurologist but a lot so [sic] them are not covered by my insurance or pharmacare.”
When specifically discussing CGRP medications, patients noted the advantages of the medications’ convenience and effectiveness with minimal side effects. Unfortunately, costs and access were identified as major limitations: “They are a godsend to those who have had migraine relief with them. The costs makes [sic] them unavailable to many unless they have a private insurance plan. Side effects for some migraineurs make it impossible to take them even if they provide relief” and “Advantages are getting migraines under control with only one dose a month. Feel better in-between migraines. Only disadvantage is access to them and cost.”
The survey responses indicated that 22% had experience with 1 or 2 preventive medications, 22% had tried 3 or 4 drugs, 45% had used at least 5 medications, and the remaining 11% had not tried any. Of those who had tried oral preventive medications, 68% of respondents had experienced side effects leading to discontinuation, 25% reported having tolerable side effects, and 7% stated having no side effects. The most frequently reported side effects included somnolence, dizziness, weight gain, cognitive problems, gastrointestinal issues, and mood problems. One patient reported that, although triptans and opioids were the most effective at controlling pain, a number of side effects followed. With triptans, they experienced burning or tingling of the extremities, muscle weakness, medication overuse that made it less effective or led to medication overuse headaches, frequent urination and urine leakage, extreme irritability, and not wanting to be around other people. The patient also stated that opioids caused drowsiness that prevented them from being able to drive or work.
Not only do patients have to deal with treatment options that inadequately control migraine, but they are also faced with limited access to care. For instance, 27% of patients reported being on wait lists for neurologists or specialists that are more than a year long, and 54% of patients were dissatisfied with the care they have received.
Because there is no cure for migraine, patients are told that a 50% improvement in frequency and intensity is acceptable. Despite this, 74% of respondents did not indicate that they had experienced an improvement of at least a 50%, whereas only 6% indicated that a drug they have tried provided a 75% improvement.
Improved Outcomes
In general, survey respondents reported that nearly any degree of relief would be a successful outcome for a preventive therapy. More specifically, patients indicated that they would prefer a preventive medication that allows them to be more productive at work and home. They also raised concerns over the frequency of administration, potential side effects, affordability, accessibility, and impact on quality of life.
According to 1 patient, the most important aspects of migraine requiring control are the frequency and severity of migraine attacks, as well as reducing or eliminating the need for triptans and opioids. The patient added that it was important that a new medication would allow them to fully participate in daily life, work, improve family and social relationships, and reduce exhaustion and side effects. Another patient had similar interests and added that having more energy on migraine-free days, reducing nausea, and being able to maintain a healthy weight would be important to them.
When asked about methods of administration, 73% of participants preferred a monthly injection to a daily pill. One respondent replied that, “If I had access to a preventive that I could take only once monthly, I would be thrilled.”
Experience With the Drug Under Review
Among the participants in the 2021 survey, 36 had experience with galcanezumab. In general, patients appeared to be pleased with the drug and reported that it effectively reduced migraine severity and frequency, that it was convenient, and that acute medications offered a better response when taken. Despite the benefits, 1 patient stated that “the possibility of having to stop treatment due to cost is very stressful.” Although most responses indicated that patients had minimal to no side effects, dizziness, vertigo, vomiting, constipation, and temporary injection site pain were noted in the patient submission.
The following quotes have been selected to illustrate how galcanezumab has impacted patients’ lives:
“Emgality has been my miracle drug after trialing every other treatment available. While I still have daily headaches, it has helped reduce the severity.”
“This past year on Emgality has been life changing. I am functioning well at work, my sick time has drastically improved. My mood is upbeat, I look forward to life so much more without constantly feeling like I can’t do the things I enjoy. I feel more reliable and pleasant to be around.”
“Benefits were awesome, my migraines severity went down. I went from daily migraine/headache to 9-10 Free Days!! Severity I rank from 0-5 I went from average of 3-5s to 1-3 with only a few 4 or 5. The BIG disadvantage was vertigo. The last month I took Emgality I lost 15 pounds due to vertigo...vomiting and unable to eat.”
“Some increased dizziness in the first week and a lit bit of constipation but very well tolerated.”
Patients also reported that the benefits of treatment with galcanezumab extended to those around them as it allowed them to spend more time with their family and friends and participate in activities together:
“Greatly improved by quality of life which in turn has made my families lives happier.” [sic]
“My husband and my son are elated at the difference because I am able to be more present in our family and participate in activities that were impossible before my first Emgality shot. The symptoms get better with each subsequent injection as well.”
The 2 patients who provided direct input to the patient groups for this submission had experience with galcanezumab. One, a 37-year-old male, gained access through a prescription from a neurologist and with help from Eli Lilly patient support coverage. Treatment over the past year reportedly reduced migraine frequency from daily to only a couple of attacks per month without any reduction in effectiveness and allowed him to “reduce his effective dose of triptan to one half or one quarter” of his previous dose “to get rid of the migraine which has resulted in less side effects from the triptan.” Similar to the other experiences described, administration was convenient and side effects were minimal. It was noted that the possibility of not being able to access or afford treatment in the future has caused him to have severe anxiety.
The other patient, a 25-year-old female, accessed galcanezumab through the patient support program. Although she reported that she does not like needles, she found the drug to be convenient and easy to self-administer. For the first 6 to 7 months, there was minor irritation at the injection site but she has not experienced it since. After the first administration of galcanezumab, there was an improvement within a few days and, “Since the first month, after injection I would … have 3 weeks with only a couple migraines and by 4th week I’d start to experience an increase in migraine frequency and a few days after injection, migraine’s free up and don’t see same frequency. This pattern has held for 8 months.” She reported that “being able to increase dosage would maybe be helpful in reducing frequency.” Overall, the effects have been positive, and she shared that:
Emgality has given me back my life. I can take care of myself. I can cook. I can go out and socialize with friends. I feel like I actually have a life versus being bedridden and stuck at home.” and “My mental health is better now because she is not in pain all the time, I have more energy, less fatigue. I have a better perspective on life, and am more hopeful about the future.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of migraine.
Unmet Needs
According to the clinical expert consulted by CADTH, the most important goal of treatment is to reduce the frequency of headaches. In the clinical expert’s experience, patients have an approximately 20% chance of responding well to the first preventive medication tried. As a result, a trial of 2 to 3 preventive medications is often required before a patient experiences benefit. The clinical expert noted that often the medications have not been given in the correct dose or for a sufficient period of time to make a valid judgment as to whether they were effective or not. Ideally, patients are within the therapeutic range for at least 8 weeks before deciding whether a treatment has failed. In the clinical expert’s experience, approximately 10% to 20% of patients have not tried any preventive medications when referred to their headache clinic, 40% have tried 1 to 2 medications, and most others have tried 2 to 3 medications. Only a small proportion of Canadian patients with migraine have tried 4 or more medications, in the clinical expert’s experience.
There are limitations with the older oral medications used to prevent migraine. The clinical expert reported that many patients cannot take beta-blockers or calcium-channel blockers because these medications cause hypotension. Weight gain is a problem with gabapentin, amitriptyline, divalproex, sodium valproate, and nortriptyline. Somnolence and dry mouth limit the use of amitriptyline for many patients. Cognitive slowing and word-finding difficulty often limit topiramate use. In addition, the clinical expert reported that adherence is an issue with oral preventive medications that are taken daily, even when the patient is receiving a benefit. Furthermore, cost is a barrier for patients who might benefit from anti-CGRP monoclonal antibodies and onabotulinumtoxinA.
Place in Therapy
The clinical expert consulted by CADTH indicated that 1 of the first lines of treatment for EM and CM is to identify and eliminate or reduce factors that trigger headaches. In addition, cognitive behavioural therapy and mindfulness can be help patients manage their migraine headaches.
For headaches that occur more than 4 times per month, the clinical expert reported that a variety of preventive medications are used. Prescription medications to prevent headaches include beta-blockers (e.g., propranolol, nadolol, metoprolol, atenolol), calcium-channel blockers (e.g., verapamil, flunarizine), angiotensin-converting enzyme inhibitors (e.g., lisinopril), angiotensin receptor blockers (e.g., candesartan), tricyclic antidepressants (e.g., amitriptyline and nortriptyline), serotonin-norepinephrine reuptake inhibitors (e.g., venlafaxine), anticonvulsants (e.g., topiramate, gabapentin, and divaloproex or sodium valproate), and anti-CGRP monoclonal antibodies (e.g., erenumab, fremanezumab, galcanezumab, and eptinezumab). For CM (headaches occurring 15 days per month, with 8 meeting the criteria for migraine), onabotulinumtoxinA injections may be used.
Before the advent of anti-CGRP monoclonal antibodies, patients often tried 4 to 6 daily preventers. If they had coverage, they would try 2 before receiving either onabotulinumtoxinA (if they have CM) or an anti-CGRP monoclonal antibody. The clinical expert noted that anti-CGRP monoclonal antibodies such as galcanezumab would be a first-line treatment in practice, but, for reasons of cost-effectiveness and funding status, these are typically used in patients who first fail on 2 or more oral preventive medications.
The clinical expert consulted by CADTH indicated that galcanezumab could be used concurrently with other migraine-preventive medications if the patient had a partial response from a daily preventer. In such cases, the clinician would keep the patient on the medication if they were not having side effects and add an anti-CGRP monoclonal antibody. The clinical expert noted that anti-CGRP monoclonal antibodies inhibit CGRP activity on nerves that are different from those affected by onabotulinumtoxinA. The clinical expert indicated that there may be mechanistic reasons to consider using both medications at the same time in some patients.
Patient Population
According to the clinical expert, patients with frequent EM without medication overuse would be the most likely to respond to an anti-CGRP monoclonal antibody. Patients with severe and/or CM may realize the greatest benefit from galcanezumab. However, the clinical expert noted that many patients with severe migraine are disabled or do not have good drug coverage, and therefore do not currently have access to anti-CGRP monoclonal antibodies. The clinical expert reported that there are no disease characteristics that signal who is more likely to respond to treatment with galcanezumab.
The clinical expert reported that suitability for galcanezumab treatment is determined based on patient history. Those with a diagnosis of migraine with or without aura, more than 4 headache days per month, and failure on 2 or more daily preventers used at an appropriate dose for an appropriate period of time, and no contraindication to the use of an anti-CGRP monoclonal antibody would be suitable for galcanezumab. No tests are necessary to determine suitability for treatment. The clinical expert noted that misdiagnosis of migraine in clinical practice would be unlikely.
Patients least suitable for treatment include women contemplating pregnancy. In addition, it would be unlikely for patients with a needle phobia to be able to inject themselves, although the clinical expert noted that autoinjectors can make self-injection easier. The clinical expert indicated there would be hesitancy to prescribe an anti-CGRP monoclonal antibody to patients with known active peripheral vascular, cardiovascular, or cerebrovascular disease. The clinical expert reported that colleagues in the US prescribe anti-CGRP monoclonal antibodies to patients after a year of stability following a cardiovascular event or onset of morbidity. In addition, use of this family of medications in patients with Raynaud phenomenon who were taking triptans has been associated with digital ischemia leading to digit amputation, and the clinical expert indicated that caution is needed in these patients.
Assessing Response to Treatment
When assessing response to treatment, the clinical expert indicated that it is common practice to ask the patient for their impression (i.e., Do they like the medication and do they want to stay on it?).
Reduction in frequency and/or severity of headaches is important, which can be assessed using headache diaries. The clinical expert reported that the goal of treatment is to reduce the frequency of headache, ideally to fewer than 4 headache days per month. A 50% or greater reduction in headache frequency is also considered a successful response. The clinical expert noted that medications may only reduce the severity of headaches as measured by MIDAS or HIT-6 scores, but not the frequency, which is also considered a successful response. Reduced use of abortive medications (e.g., triptans) may also be indicative of improvement. The clinical expert reported that a change within 2 days of acute medication use is clinically significant.
In addition, the clinical expert reported that improvement in function is important. Improvement in the MIDAS and HIT-6 scores are reflective of improvement in the patient’s life. A reduction of 6 points on the HIT-6 for EM and 5 points for CM were considered significant improvements by the clinical expert. A reduction in the MIDAS score by 50% or by 5 points was considered significant.
The clinical expert reported that patients should be assessed for response to galcanezumab treatment 2 to 3 weeks after their third injection, and those who have not shown improvement at that time should be assessed 2 to 3 weeks after their sixth injection. If there is no improvement after 6 injections, then treatment would be discontinued, according to the clinical expert.
Discontinuing Treatment
The clinical expert consulted by CADTH indicated that the following would lead to discontinuation of treatment: intolerable side effects, development of comorbidities that preclude the patient being on treatment (e.g., stroke or heart attack), pregnancy, and failure to respond after 6 injections.
Prescribing Conditions
The clinical expert indicated that all physicians and nurse practitioners can make a diagnosis of EM and CM. Galcanezumab would be prescribed by headache specialists, general neurologists, family doctors, or nurse practitioners on the advice of a neurologist, and family doctors or nurse practitioners who have experience with the use of the medication in other patients. The clinical expert cautioned against requiring patients to be supervised by a headache specialist because there are too few such specialists in Canada, and this could prevent patients from accessing treatment. The clinical expert added that it is within the scope of practice for a general neurologist, nurse practitioner, or family physician to supervise management after a recommendation for use is made. Patients would self-administer the medication at home.
Clinician Group Input
No input from clinician groups was received for this review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CADTH are summarized in Table 5.
The drug programs noted that 2 other CGRP inhibitors (erenumab and fremanezumab) recently received positive reimbursement recommendations under the CADTH review process and were the subjects of pan-Canadian Pharmaceutical Alliance negotiations at the time of this review. The drug programs noted that galcanezumab has the same Health Canada indication as both fremanezumab and erenumab, although the reimbursement requests for the 3 medications differ. The drug programs noted that the reimbursement request for galcanezumab is for patients who have tried at least 2 prophylactic migraine medications, and that it would be helpful to jurisdictions for this to be defined further. In addition, the drug programs indicated that it would be helpful to outline whether failure on or intolerance to another CGRP inhibitor would exclude patients from coverage of galcanezumab.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
The reimbursement request specifies patients who have tried at least 2 prophylactic migraine medications. It would be helpful to jurisdictions for this to be defined further; for example, at least 2 prophylactic medications of different classes, and clarification of the optimal dose/duration of the trials. | The clinical expert indicated that, for an adequate trial, patients are ideally within in the therapeutic range for at least 8 weeks before deciding whether a treatment has failed. |
Outline whether failure or intolerance to 1 or more CGRP inhibitor would exclude patients from coverage of galcanezumab. | The clinical expert reported that, currently, no data are available to indicate whether failure on or intolerance to 1 or more CGRP inhibitor would exclude patients from trying treatment with another CGRP inhibitor, such as galcanezumab. In the clinical expert’s opinion, patients who experience failure on or intolerance to another CGRP inhibitor should not be excluded from galcanezumab because the different anti-CGRP monoclonal antibodies have different side-effect profiles in clinical practice. In addition, the clinical expert noted that the CGRP inhibitors have different properties and can work through different mechanisms (i.e., galcanezumab and fremanezumab bind to the CGRP ligand whereas erenumab binds to the CGRP receptor). |
The pivotal studies (EVOLVE-1, EVOLVE-2, and REGAIN) excluded patients who had failed to respond to 3 or more classes of adequately dosed migraine-preventive treatments. CONQUER excluded patients who had failed more than 4 migraine-preventive medications categories. Although the reimbursement request specifies failure on at least 2 prophylactic agents, it would be helpful to clarify if there is a maximum number of prophylactic agents that would be accepted before consideration of coverage. | In the clinical expert’s experience, approximately 10% to 20% of patients have not tried any preventive medications when referred to their clinic, 40% have tried 1 or 2 medications (but this could be an inadequate trial), and most others have tried 2 or 3 medications. In the clinical expert’s experience, only a small proportion of patients have tried 4 or more preventive medications, and a maximum number of prophylactic agents would not be necessary. |
The drug programs noted that there is potential in some jurisdictions for galcanezumab to be used in combination with onabotulinumtoxinA. Can the Committee please comment on combination use? | The clinical expert noted that anti-CGRP monoclonal antibodies work to inhibit CGRP activity on nerves that are different from those affected by onabotulinumtoxinA, and there may be reason to consider using both medications at the same time in some patients. |
CGRP = calcitonin gene-related peptide.
Clinical Evidence
The clinical evidence included in the review of galcanezumab is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes a sponsor-submitted safety study.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of galcanezumab (120 mg/mL solution in a 1 mL single-use pre-filled syringe or pen) for the prevention of migraine in adults who have at least 4 migraine days per month and have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults who have at least 4 migraine days per month and have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications. Subgroups:
|
Intervention | Galcanezumab (240 mg loading dose then 120 mg once per month, subcutaneous injection) |
Comparator | Pharmacologic interventions:
Placebo |
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality, notable harms, and harms of special interest (e.g., anaphylaxis and hypersensitivity reactions, injection site reactions, antibody formation, vascular events) |
Study designs | Published and unpublished phase III and IV randomized controlled trials |
AE = adverse event; CGRP = calcitonin gene-related peptide; HIT-6 = 6-item Headache Impact Test; HRQoL = health-related quality of life; MIDAS = Migraine Disability Assessment; MPFID = migraine physical function impact diary; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies checklist.28
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Emgality (galcanezumab). Clinical trials registries included the US National Institutes of Health’s clinicaltrials.gov, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies.
The initial search was completed on June 29, 2021. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on October 27, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.29 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for NMAs dealing with migraine was run in MEDLINE All (1946–) on June 29, 2021. No limits were applied to the search.
Findings From the Literature
A total of 24 reports presenting data from 4 unique studies from the literature were identified for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
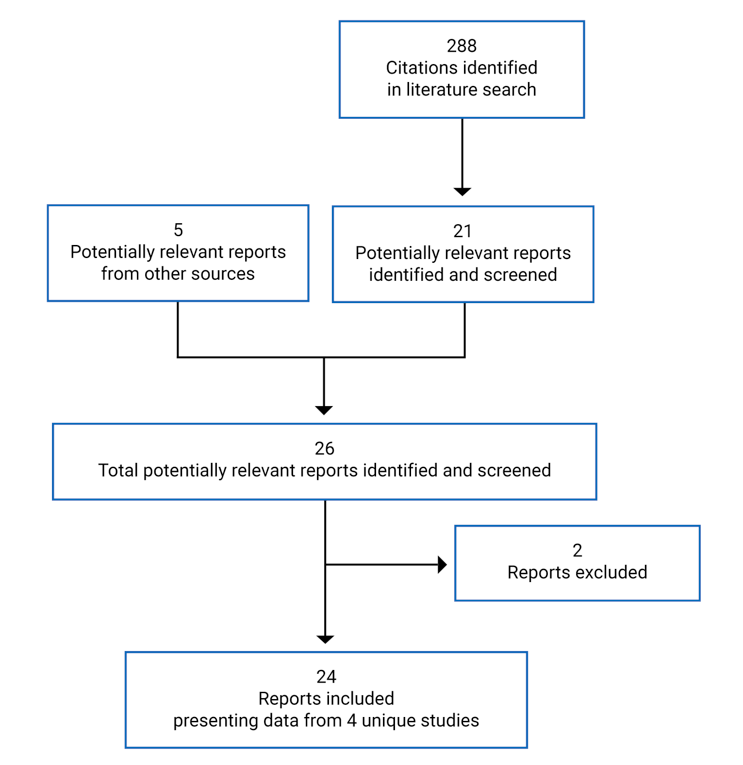
Table 7: Details of Included Studies
Detail | EVOLVE-1 | EVOLVE-2 | REGAIN | CONQUER |
|---|---|---|---|---|
Designs and populations | ||||
Study design | Phase III DB RCT, placebo-controlled, parallel group | Phase III DB RCT, placebo-controlled, parallel group | Phase III DB RCT, placebo-controlled, parallel group | Phase IIIb DB RCT, placebo-controlled, parallel group |
Locations | 90 sites in the US and Canada | 109 study sites in 11 countries in North America (excluding Canada), Europe, South America, and Asia | 116 study sites in 12 countries in North America (including Canada), Europe, South America, and Asia | 64 sites in 12 countries in North America (including Canada), Europe, and Asia |
Study period | January 11, 2016, to March 22, 2017 | January 29, 2016, to March 29, 2017 | January 12, 2016, to March 16, 2017 | September 10, 2018, to June 19, 2019 |
Randomized (N) | N = 862
| N = 922
| N = 1,117
| N = 463
|
Inclusion criteria |
|
|
|
|
Inclusion criteria (continued) |
|
|
|
|
Exclusion criteria |
|
|
|
|
Exclusion criteria (continued) |
|
|
|
|
Drugs | ||||
Intervention | Galcanezumab 120 mg once per month (240 mg loading dose at first injection) Galcanezumab 240 mg once per month | Galcanezumab 120 mg once per month (240 mg loading dose at first injection) Galcanezumab 240 mg once per month | Galcanezumab 120 mg once per month (240 mg loading dose at first injection) Galcanezumab 240 mg once per month | Galcanezumab 120 mg once per month (240 mg loading dose at first injection) |
Comparator(s) | Placebo | Placebo | Placebo | Placebo |
Duration | ||||
Screening phase | 3 to 45 days | 3 to 45 days | 3 to 45 days | 3 to 30 days |
Prospective baseline phase | 30 to 40 days | 30 to 40 days | 30 to 40 days | 30 to 40 days |
DB treatment phase | 6 months | 6 months | 3 months | 3 months |
OL treatment phase | NA | NA | 9 months (optional) | 3 months (optional) |
Post-treatment follow-up phase | 4 months | 4 months | 4 months | NA |
Outcomes | ||||
Primary end point | Overall mean change from baseline in the number of monthly MHDs during the DB treatment phase | Overall mean change from baseline in the number of monthly MHDs during the DB treatment phase | Overall mean change from baseline in the number of monthly MHDs during the DB treatment phase | Overall mean change from baseline in number of monthly MHDs during the DB treatment phase in the total population (EM or CM) |
Secondary and exploratory end points | Secondary:
| Secondary:
| Secondary:
| Secondary:
|
Secondary and exploratory end points (continued) |
|
|
|
|
Secondary and exploratory end points (continued) |
Exploratory:
| Exploratory:
|
Tertiary:
|
Tertiary:
|
Publications | ||||
Individual trial results | Stauffer et al. (2018)30 | Skljarevski et al. (2018)31 | Detke et al. (2018)32 Ruff et al. (2019)33 Ford et al. (2021)34 | Kuruppu et al. (2021)35 Mulleners et al. (2020)36 Schwedt et al. (2021)37 |
Pooled results for EVOLVE-1 and EVOLVE-2 | Detke et al. (2020)38 Ford et al. (2019)39 Rosen et al. (2018)40 Ruff et al. (2020)41 Silberstein et al. (2019)42 Stauffer et al. (2019)43 | NA | NA | |
Pooled results for EVOLVE-1, EVOLVE-2, and REGAIN | Ailani et al. (2020)44 Ailani et al. (2020)45 Ament et al. (2021)46 Dodick et al. (2021)47 Förderreuther et al. (2018)48 Pozo-Rosich et al. (2021)49 Stauffer et al. (2020)50 | NA | ||
ADA = antidrug antibody; BMI = body mass index; CGRP = calcitonin gene-related peptide; CM = chronic migraine; CV = cardiovascular; DB = double-blind; EF = emotional function; EM = episodic migraine; EQ-5D-5L = EQ-5D 5-Levels questionnaire; GAD-7 = Generalized Anxiety Disorder 7-item; HCRU = health care resource utilization; ICHD = International Classification of Headache Disorders, third edition; IHS = International Headache Society; MHD = migraine headache day; MI = myocardial infarction; MIBS-4 = 4-item Migraine Interictal Burden Scale; MIDAS = Migraine Disability Assessment; MOH = medication overuse headache; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; NA = not applicable; OL = open-label; PGI-I = Patient Global Impression of Improvement; PGI-S = Patient Global Impression of Severity; PHQ-9 = Patient Health Questionnaire-9; RCT = randomized controlled trial; RF = role function; RF-P = role function – preventive; RF-R = role function – restrictive; WPAI = Work Productivity and Activity Impairment.
Note: Five additional reports were included (EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 REGAIN Clinical Study Report,11 CONQUER Clinical Study Report,12 and the Health Canada Reviewer’s Report51).
atypes of prior preventives included propranolol or metoprolol; topiramate, valproate or divalproex; amitriptyline; flunarizine; candesartan; botulinum toxin A or B (if taken for chronic migraine); medications locally approved for prevention of migraine.
bOther types of headache included persistent daily headache, cluster headache or migraine subtypes, including hemiplegic (sporadic or familial) migraine, ophthalmoplegic migraine, and migraine with brainstem aura (basilar-type migraine).
cElectrocardiogram abnormalities indicating acute CV events and/or serious CV risk; or MI, unstable angina, percutaneous coronary intervention, or coronary artery bypass graft within 6 months; or planned CV surgery or percutaneous coronary angioplasty. In the EVOLVE-1, EVOLVE-2, and REGAIN trials, this also included lifetime history of stroke.
dSafety outcomes included treatment-emergent adverse events, serious adverse events, discontinuation rates, vital signs and weight, electrocardiograms, and laboratory measures.
Source: EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 REGAIN Clinical Study Report,11 and CONQUER Clinical Study Report.12
Description of Studies
Four phase III, multi-national, double-blind, randomized, placebo-controlled trials were included in the systematic review: EVOLVE-1,9 EVOLVE-2,10 REGAIN,11 and CONQUER.12 In all studies, patients were randomized using an interactive web response system.
EVOLVE-1 and EVOLVE-2
The EVOLVE-1 and EVOLVE-2 trials were identically designed studies conducted in patients with EM.9,10 The primary objective of the EVOLVE-1 and EVOLVE-2 studies was to test the hypothesis that at least 1 dose of galcanezumab (120 or 240 mg) is superior to placebo in the prevention of migraine headaches in patients with EM. The EVOLVE-1 trial had 90 sites in the US and Canada. The EVOLVE-2 trial had 109 study sites in 11 countries in Europe, South America, Asia, and the US. In both studies, patients were randomized in a 2:1:1 ratio to placebo, galcanezumab 120 mg (loading dose of 240 mg), or galcanezumab 240 mg. In the EVOLVE-1 trial, randomization was stratified by geographic region (eastern half of the US, western half of the US, Puerto Rico, and Canada) and migraine frequency at baseline (< 8 versus ≥ 8 MHDs per month). In the EVOLVE-2 trial, randomization was stratified by country and migraine frequency at baseline (< 8 versus ≥ 8 MHDs per month). The EVOLVE-1 trial randomized 862 patients: 433 to placebo, 213 to galcanezumab 120 mg, and 212 to galcanezumab 240 mg. The EVOLVE-2 trial randomized 922 patients: 461 to placebo, 231 to galcanezumab 120 mg, and 223 to galcanezumab 240 mg. Efficacy and harms data will not be presented for the galcanezumab 240 mg arm because this dose is not aligned with the Health Canada–approved dose.
The study design of the EVOLVE-1 and EVOLVE-2 trials is summarized in Figure 2. The studies comprised 4 study periods: screening; a prospective 30- to 40-day baseline phase to determine patient eligibility; a 6-month double-blind treatment phase; and a 4-month post-treatment follow-up phase. During the prospective baseline period, patients logged in daily to the ePRO system to answer questions about the occurrence of headaches, headache duration, headache features, severity of headaches, and use of headache medication. The purpose of the prospective baseline period was to confirm that the patient had between 4 and 14 MHDs and at least 2 migraine attacks during the 30- to 40-day period, and to establish baseline data for the comparison of end points during the treatment phase.
The data cut-off date for the main reports on the EVOLVE-1 trial was March 22, 2017, which was the last patient-visit date of the double-blind phase. The database was locked for analysis on April 28, 2017. The data cut-off date for the reports on the EVOLVE-2 trial was March 29, 2017, which was the last patient-visit date of the double-blind phase. The database was locked for analysis on May 5, 2017. According to the Clinical Study Reports, a data lock date after the data cut-off date was chosen because additional time was needed to resolve and close all data queries, process laboratory samples, and complete sign-off by investigators. These analyses are considered the final analyses of the primary and key efficacy end points during the double-blind treatment phase. In addition, Clinical Study Report addenda reporting data from the post-treatment phases were provided by the sponsor following CADTH’s request for additional information. The EVOLVE-1 Clinical Study Report Addendum was dated December 18, 2017, and the last patient completed the study on July 19, 2017. The EVOLVE-2 Clinical Study Report Addendum was dated December 18, 2017, and the last patient completed the study on August 4, 2017.
Figure 2: EVOLVE-1 and EVOLVE-2 Study Design
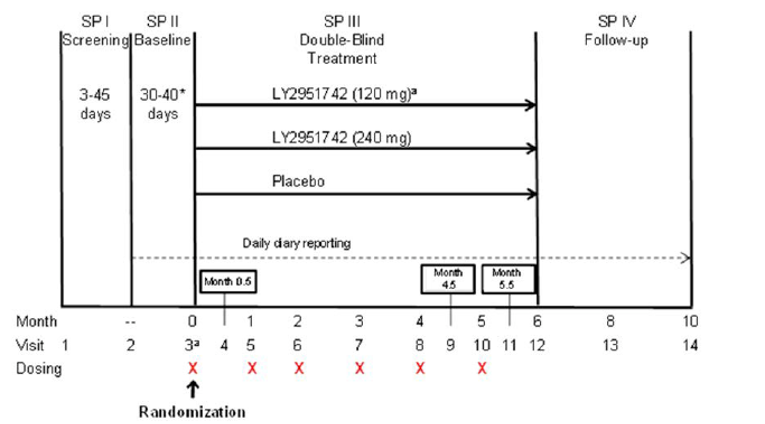
LY2951742 = galcanezumab; SP = study period.
* Eligibility period was a minimum of 30 days and a maximum of 40 days in length. Investigators may have had up to 5 additional days (beyond the 40 days) if needed to schedule a patient’s visit 3 appointment.
a Patients randomized to the 120 mg dose received a loading dose of 240 mg at the first injection only (visit 3).
Source: EVOLVE-1 Clinical Study Report9 and EVOLVE-2 Clinical Study Report.10
REGAIN
The REGAIN trial was conducted in patients with CM.11 The primary objective was to test the hypothesis that at least 1 dose of galcanezumab (120 or 240 mg) is superior to placebo in the prevention of migraine headaches in patients with CM. Patients were enrolled from 116 study sites in 12 countries in North America (including Canada), Europe, South America, and Asia. A total of 1,117 patients were randomized in a 2:1:1 ratio to placebo (N = 558), galcanezumab 120 mg (loading dose of 240 mg; N = 278), or galcanezumab 240 mg (N = 277). Randomization was stratified by country, acute headache medication overuse (yes versus no), and use of concurrent migraine prophylactic medication (yes versus no). Efficacy and harms data will not be presented for the galcanezumab 240 mg arm because this dose is not aligned with the Health Canada–approved dose.
The study design of the REGAIN trial is summarized in Figure 3. The study comprised 5 study periods: screening; a prospective 30- to 40-day baseline phase to determine patient eligibility; a 3-month double-blind treatment phase; an optional 9-month open-label extension phase; and a 4-month post-treatment follow-up phase. During the prospective baseline period, patients logged in daily to an ePRO system to answer questions about the occurrence of headaches, headache duration, headache features, severity of headaches, and use of headache medication. This prospective baseline period was to confirm that the patient had at least 15 headache days during the 30- to 40-day period, 8 of which must have had the features of a migraine headache, as well as to establish baseline data for comparison of end points during the double-blind treatment phase.
The data cut-off date for the reports on the REGAIN trial was March 16, 2017, which was the last patient-visit date of the double-blind phase. The database was locked for analysis on May 5, 2017. According to the Clinical Study Report, the data lock date was after the data cut-off date to allow for additional time needed to resolve and close all data queries, process laboratory samples, and complete sign-off by investigators. This analysis is considered the final analysis of the primary and key efficacy end points during the double-blind treatment phase. In addition, a Clinical Study Report Addendum that contained the final results of the open-label treatment and post-treatment phases was provided by the sponsor following CADTH’s request for additional information. This addendum was dated February 5, 2019, and the last patient completed the study on May 1, 2018.
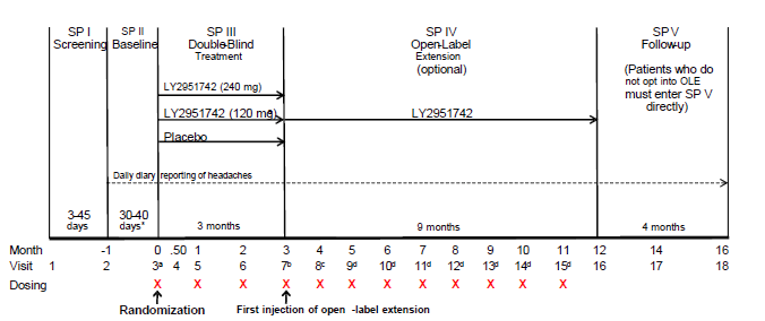
LY2951742 = galcanezumab; OLE = open-label extension; SP = study period.
* Eligibility period determined between a minimum of 30 days and maximum of 40 days. Investigators may have had up to 5 additional days (beyond the 40 days) if needed to schedule a patient’s visit 3 appointment.
a Patients randomized to the 120 mg dose received a loading dose of 240 mg at the first injection only (visit 3).
b At visit 7, all patients who entered the open-label extension received galcanezumab at a dose of 240 mg.
c At visit 8, all patients received galcanezumab at a dose of 120 mg.
d Starting at visit 9, dosing was flexible (galcanezumab 120 or 240 mg) at the discretion of the investigator.
Source: REGAIN Clinical Study Report.11
CONQUER
The CONQUER trial was conducted in patients with EM or CM who had 2 to 4 migraine-preventive medication category failures due to inadequate efficacy or tolerability in the previous 10 years.12 The primary objective of the CONQUER trial was to test the hypothesis that galcanezumab is superior to placebo in the prevention of migraine in patients with treatment-resistant migraine. Patients were enrolled from 64 sites in 12 countries in North America (including Canada), Europe, and Asia. A total of 463 patients were randomized in a 1:1 ratio to placebo (N = 230) or galcanezumab 120 mg (loading dose of 240 mg; N = 232). One patient who was a screening failure was inadvertently randomized and immediately discontinued. Randomization was stratified by country and migraine frequency from the prospective baseline period (low-frequency episodic versus high-frequency episodic versus chronic). The sponsor stopped enrolment of patients with CM when the number of patients exceeded approximately 40% of the planned sample size, which was planned per-protocol.
The study design of the CONQUER trial is summarized in Figure 4. The study comprised 4 study periods: screening, a 30- to 40-day prospective baseline period, a 3-month double-blind treatment phase, and an optional 3-month open-label treatment phase. During the prospective baseline period, patients logged in daily to an ePRO system to answer questions about the occurrence of headaches, headache duration, headache features, severity of headache, and use of headache medication. This prospective baseline period was to confirm that the patient had at least 4 MHDs and at least 1 headache-free day per 30-day period, and to establish baseline data for comparison of end points during the double-blind treatment phase.
The data cut-off date for the reports on the CONQUER trial was June 19, 2019. The reporting database was validated and locked for analysis on July 22, 2019. The reason the data lock date was after the data cut-off date was not reported in the Clinical Study Report. This analysis is considered the final analysis of the primary and key efficacy end points, as well as all other efficacy and safety analyses of the double-blind treatment phase of the CONQUER trial. In addition, a Clinical Study Report Addendum containing the final results of the open-label treatment phase was provided by the sponsor following CADTH’s request for additional information. This addendum was dated December 18, 2019, and the last patient completed the study on September 19, 2019.
Figure 4: CONQUER Study Design
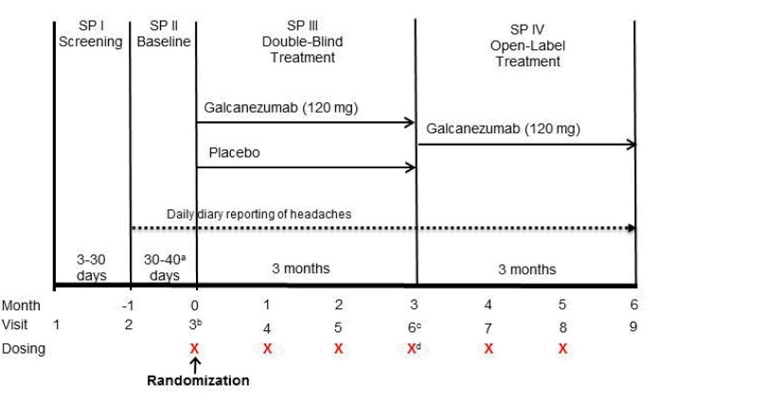
SP = study period.
a Eligibility period was a minimum of 30 days and maximum of 40 days in length, with up to 5 additional days to schedule randomization visit, if necessary.
b Patients randomized to galcanezumab 120 mg received a loading dose of 240 mg at the first injection only (visit 3).
c Patients randomized to placebo who entered the open-label treatment phase received a loading dose of galcanezumab 240 mg at the first injection only of study period IV.
d First injection of the open-label treatment phase occurred at visit 6 once all study procedures for the double-blind phase were completed.
Source: CONQUER Clinical Study Report.12
Populations
Inclusion and Exclusion Criteria
The EVOLVE-1 and EVOLVE-2 trials included adult patients (18 to 65 years of age) with a diagnosis of EM as defined by IHS ICHD-3 beta guidelines (1.1 or 1.2), with a history of migraine headaches for at least 1 year before screening, migraine onset before age 50, and a monthly frequency of 4 to 14 MHDs. The EVOLVE-1 and EVOLVE-2 trials excluded patients who had previously failed to have an efficacy response to 3 or more classes of migraine-preventive treatments, and those who were currently receiving medication or other treatments for the prevention of migraine headaches.
The REGAIN trial included adult patients (18 to 65 years of age) with a diagnosis of CM as defined by IHS ICHD-3 beta guidelines (1.3), with a history of migraine headaches for at least 1 year before screening, and migraine onset before age 50. Patients who had been on a stable dose of either topiramate or propranolol for at least 2 months before beginning the prospective baseline period could continue to take that preventive medication throughout the trial. Patients who had previously failed to have an efficacy response to 3 or more classes of migraine-preventive treatments were excluded.
The CONQUER trial included adult patients (18 to 75 years of age) with a diagnosis of EM or CM; a history of migraine headaches for at least 1 year before screening with onset before age 50; a history of at least 4 MHDs with at least 1 headache-free day per month on average within the past 3 months; and documentation of 2 to 4 migraine-preventive medication category failures in the past 10 years. Specifically, patients were required to have documentation of previous failure of 2 to 4 migraine-preventive medication categories from the following list due to inadequate efficacy (maximum tolerated dose for at least 2 months) and/or safety or tolerability reasons: propranolol or metoprolol, topiramate, valproate or divalproex, amitriptyline, flunarizine, candesartan, botulinum toxin A or B (if it was documented that botulinum toxin was taken for CM), and medication locally approved for prevention of migraine. The CONQUER trial excluded patients who had previously failed more than 4 migraine-preventive medication categories in the past 10 years from the list in the inclusion criteria due to inadequate efficacy. Patients currently receiving medication or other treatments for the prevention of migraine headaches were also excluded.
All 4 pivotal trials excluded patients with prior exposure to a CGRP antibody.
Baseline Characteristics
Demographic and baseline characteristics of patients enrolled in the EVOLVE studies, REGAIN study, and CONQUER study are summarized in Table 8, Table 9, and Table 10, respectively. In all trials, most patients were female and White, and the mean number of comorbidities other than migraine was 3 to 4.
In the EVOLVE studies, the mean age of patients was between 39 and 42 years and most patients (> 60%) had received prior preventive treatment. The mean baseline MIDAS total scores were 33.2 and 33.0, which reflect severe disability, in the EVOLVE-1 and EVOLVE-2 studies, respectively. In the EVOLVE studies, approximately 60% to 68% of patients had used at least 1 prior preventive therapy. The most frequently reported prior medications were topiramate, ibuprofen, Thomapyrin N, sumatriptan, paracetamol, propranolol, and amitriptyline. In the REGAIN trial, the mean age of patients was 41.0 years. Most patients (77.8%) in the REGAIN study reported using a prior migraine-preventive treatment, with 29.5% having failed 2 or more such treatments in the past 5 years due to lack of efficacy. In the REGAIN trial, the most frequently used medications were topiramate, amitriptyline, propranolol, ibuprofen, botulinum toxin type A, sumatriptan, paracetamol, Thomapyrin N, valproate sodium, amitriptyline hydrochloride, and nortriptyline. The mean baseline MIDAS total score in the REGAIN trial was 67.2, which reflects very severe disability. Overall, 15.5% of patients in the REGAIN trial had concurrent prophylaxis use with topiramate or propranolol. In the CONQUER trial, the mean age of patients was 45.8 years. Most patients had 2 (58.2%) or 3 (30.1%) prior medication category failures and the mean baseline total MIDAS score was 50.93, which reflects very severe disability. In the CONQUER trial, the most common medication categories failed in past 10 years were topiramate, amitriptyline, propranolol or metoprolol, valproate or divalproex, botulinum toxin A or B, candesartan, and flunarizine.
For all studies, the baseline for efficacy outcomes was derived from headache information collected using the ePRO system during the prospective baseline period. During the baseline period, the mean number of monthly MHDs was 9.1 in both the EVOLVE-1 and EVOLVE-2 studies. In the REGAIN trial, patients had an average of 21.4 headache days per month in the baseline period, of which an average of 19.4 were MHDs. During the baseline period in the CONQUER trial, patients had an average of 15.0 headache days per month, of which an average of 13.2 were MHDs.
Aside from some small demographic differences, baseline characteristics were generally similar between groups within studies.
Table 8: Summary of Baseline Characteristics — EVOLVE-1 and EVOLVE-2, Modified ITT Population
Characteristic | EVOLVE-1 | EVOLVE-2 | ||||
|---|---|---|---|---|---|---|
Placebo (N = 433) | GMB 120 mg (N = 213) | GMB 240 mg (N = 212) | Placebo (N = 461) | GMB 120 mg (N = 231) | GMB 240 mg (N = 233) | |
Demographics | ||||||
Age, years, mean (SD) | 41.33 (11.40) | 40.93 (11.87) | 39.07 (11.52) | 42.33 (11.30) | 40.91 (11.15) | 41.91 (10.77) |
Sex, n (%) | ||||||
Male | 71 (16.40) | 32 (15.02) | 37 (17.45) | 68 (14.75) | 34 (14.72) | 32 (14.35) |
Female | 362 (83.60) | 181 (84.98) | 175 (82.55) | 393 (85.25) | 197 (85.28) | 191 (85.65) |
Race | ||||||
American Indian or Alaska Native | 0 | 0 | 3 (1.42) | 20 (4.34) | 8 (3.46) | 13 (5.83) |
Asian | 13 (3.00) | 7 (3.29) | 4 (1.89) | 50 (10.85) | 28 (12.12) | 24 (10.76) |
Black or African-American | 42 (9.70) | 29 (13.62) | 23 (10.85) | 36 (7.81) | 11 (4.76) | 16 (7.17) |
Native Hawaiian or other Pacific Islander | 1 (0.23) | 0 | 2 (0.94) | 0 | 0 | 2 (0.90) |
White | 356 (82.22) | 169 (79.34) | 165 (77.83) | 325 (70.50) | 166 (71.86) | 152 (68.16) |
Multiple | 21 (4.85) | 8 (3.76) | 15 (7.08) | 30 (6.51) | 18 (7.79) | 16 (7.17) |
Body mass index, kg/m2, mean (SD) | 28.60 (5.52) | 27.77 (5.34) | 28.60 (5.68) | 26.71 (5.35) | 26.83 (5.27) | 27.15 (5.48) |
Disease characteristics | ||||||
Duration of migraine illness, years, mean (SD) | 19.89 (12.30) | 21.12 (12.97) | 19.30 (11.88) | 21.15 (12.75) | 19.93 (11.73) | 20.01 (12.12) |
Number of comorbidities, mean (SD) | 4.81 (3.57) | 4.67 (3.79) | 4.44 (3.63) | 3.66 (3.08) | 3.64 (3.41) | 3.26 (2.75) |
MHDs per month, mean (SD) | 9.08 (2.97) | 9.21 (3.05) | 9.14 (2.91) | 9.19 (2.99) | 9.07 (2.87) | 9.06 (2.92) |
Migraine attacks per month, mean (SD) | 5.79 (1.72) | 5.61 (1.70) | 5.74 (1.81) | 5.67 (1.82) | 5.54 (1.76) | 5.66 (1.80) |
MHD category ≥ 8, n (%) | 285 (65.82) | 140 (65.73) | 139 (65.57) | 307 (66.59) | 154 (66.67) | 151 (67.71) |
Mean severity of migraine headaches per month, mean (SD) | 2.09 (0.36) | 2.07 (0.37) | 2.09 (0.39) | 2.08 (0.38) | 2.08 (0.37) | 2.11 (0.38) |
MHD with acute medication use per month, mean (SD) | 7.38 (3.48) | 7.42 (3.68) | 7.34 (3.30) | 7.62 (3.40) | 7.47 (3.34) | 7.47 (3.25) |
MIDAS total score at baseline, mean (SD) | 31.84 (27.31) | 32.93 (28.18) | 36.09 (27.76) | 34.25 (31.03) | 30.87 (27.90) | 32.75 (28.84) |
MSQ v2.1 RF-R score at baseline, mean (SD) | 52.92 (15.41) | 51.39 (16.20) | 48.76 (16.82) | 51.35 (15.73) | 52.47 (14.76) | 51.71 (16.31) |
Medication use | ||||||
≥ 1 prior preventive treatment, n (%) | 257 (59.35) | 133 (62.44) | 125 (58.96) | 298 (64.64) | 157 (67.97) | 144 (64.57) |
Most frequently used medications,a n (%) | ||||||
Topiramate | 60 (13.86) | 37 (17.37) | 30 (14.15) | 103 (22.34) | 66 (28.57) | 41 (18.39) |
Ibuprofen | 78 (18.01) | 31 (14.55) | 30 (14.15) | 68 (14.75) | 29 (12.55) | 22 (9.87) |
Thomapyrin N | 64 (14.78) | 26 (12.21) | 30 (14.15) | 30 (6.51) | 15 (6.49) | 18 (8.07) |
Sumatriptan | 39 (9.01) | 22 (10.33) | 18 (8.49) | 48 (10.41) | 21 (9.09) | 23 (10.31) |
Paracetamol | 41 (9.47) | 16 (7.51) | 22 (10.38) | 38 (8.24) | 31 (13.42) | 13 (5.83) |
Propranolol | 15 (3.46) | 13 (6.10) | 12 (5.66) | 30 (6.51) | 19 (8.23) | 16 (7.17) |
Amitriptyline | 10 (2.31) | 10 (4.69) | 14 (6.60) | 21 (4.56) | 11 (4.76) | 13 (5.83) |
GMB = galcanezumab; ITT = intention-to-treat; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; RF-R = role function – restrictive; SD = standard deviation.
aFrequency of at least 5% in either EVOLVE-1 or EVOLVE-2.
Source: EVOLVE-1 Clinical Study Report9 and EVOLVE-2 Clinical Study Report.10
Table 9: Summary of Baseline Characteristics — REGAIN, Modified ITT Population
Characteristic | REGAIN | ||
|---|---|---|---|
Placebo (N = 558) | GMB 120 mg (N = 278) | GMB 240 mg (N = 277) | |
Demographics | |||
Age, years, mean (SD) | 41.63 (12.08) | 39.66 (11.88) | 41.05 (12.40) |
Sex, n (%) | |||
Male | 75 (13.44) | 41 (14.75) | 51 (18.41) |
Female | 483 (86.56) | 237 (85.25) | 226 (81.59) |
Race | |||
American Indian or Alaska Native | 4 (0.72) | 2 (0.72) | 0 |
Asian | 26 (4.66) | 13 (4.68) | 14 (5.07) |
Black or African-American | 39 (6.99) | 16 (5.76) | 17 (6.16) |
Native Hawaiian or other Pacific Islander | 1 (0.18) | 0 | 0 |
White | 432 (77.42) | 223 (80.22) | 224 (81.16) |
Multiple | 56 (10.04) | 24 (8.63) | 21 (7.61) |
Body mass index, kg/m2, mean (SD) | 26.87 (5.55) | 26.40 (5.49) | 26.67 (5.24) |
Disease characteristics | |||
Duration of migraine illness, years, mean (SD) | 21.94 (12.85) | 20.37 (12.74) | 20.06 (12.72) |
Number of comorbidities, mean (SD) | 4.39 (3.70) | 4.08 (3.33) | 4.21 (3.19) |
Number of monthly MHDs, mean (SD) | 19.55 (4.59) | 19.36 (4.27) | 19.17 (4.60) |
Number of monthly headache days, mean (SD) | 21.54 (4.10) | 21.24 (3.97) | 21.44 (4.10) |
Migraine attacks per month, mean (SD) | 6.23 (2.03) | 6.48 (1.95) | 6.30 (2.08) |
Mean severity of migraine headaches per month, mean (SD) | 2.15 (0.36) | 2.16 (0.36) | 2.16 (0.37) |
MHD with acute medication use per month, mean (SD) | 15.51 (6.57) | 15.12 (6.25) | 14.49 (6.25) |
Baseline headache medication overuse, n (%) | 353 (63.38) | 178 (64.26) | 177 (64.13) |
Baseline MIDAS total score, mean (SD) | 68.66 (57.36) | 62.46 (49.48) | 69.17 (64.08) |
Baseline MSQ RF-R score, mean (SD) | 38.37 (17.18) | 39.29 (17.30) | 38.93 (17.31) |
Medication use | |||
Prior treatment with migraine prophylactic medication, n (%) | 435 (77.96) | 211 (75.90) | 220 (79.42) |
Previously never failed prophylactic treatment | 59 (10.57) | 25 (8.99) | 31 (11.19) |
Failed ≥ 1 medication class | 274 (49.10) | 130 (46.76) | 145 (52.35) |
Failed ≥ 2 medication classes | 163 (29.21) | 68 (24.46) | 97 (35.02) |
Most frequently used medications,a n (%) | |||
Topiramate | 200 (35.84) | 79 (28.42) | 107 (38.63) |
Amitriptyline | 83 (14.87) | 38 (13.67) | 45 (16.25) |
Propranolol | 79 (14.16) | 38 (13.67) | 45 (16.25) |
Ibuprofen | 74 (13.26) | 45 (16.19) | 37 (13.36) |
Botulinum toxin type A | 74 (13.26) | 26 (9.35) | 43 (15.52) |
Sumatriptan | 54 (9.68) | 29 (10.43) | 32 (11.55) |
Paracetamol | 43 (7.71) | 23 (8.27) | 20 (7.22) |
Thomapyrin N | 44 (7.89) | 20 (7.19) | 16 (5.78) |
Valproate sodium | 32 (5.73) | 13 (4.68) | 20 (7.22) |
Amitriptyline hydrochloride | 35 (6.27) | 13 (4.68) | 18 (6.50) |
Nortriptyline | 29 (5.20) | 10 (3.60) | 17 (6.14) |
Concurrent prophylaxis use, n (%) | 82 (14.70) | 37 (13.31) | 43 (15.52) |
Propranolol | 23 (4.12) | 11 (3.96) | 14 (5.05) |
Topiramate | 59 (10.57) | 26 (9.35) | 30 (10.83) |
GMB = galcanezumab; ITT = intention-to-treat; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; RF-R = Role Function-Restrictive; SD = standard deviation.
aFrequency of at least 5%.
Source: REGAIN Clinical Study Report11 and Ruff et al. (2019).33
Table 10: Summary of Baseline Characteristics — CONQUER Trial, Modified ITT Population
Characteristic | CONQUER | |
|---|---|---|
Placebo (N = 230) | GMB 120 mg (N = 232) | |
Demographics | ||
Age, years, mean (SD) | 45.67 (12.33) | 45.87 (11.34) |
Sex, n (%) | ||
Male | 28 (12.17) | 37 (15.95) |
Female | 202 (87.83) | 195 (84.05) |
Race | ||
American Indian or Alaska Native | 1 (0.45) | 0 |
Asian | 35 (15.70) | 37 (16.52) |
Black or African-American | 2 (0.90) | 3 (1.34) |
Native Hawaiian or other Pacific Islander | 0 | 1 (0.45) |
White | 182 (79.13) | 183 (78.88) |
Multiple | 3 (1.35) | 0 |
Body mass index, kg/m2, mean (SD) | 25.58 (5.54) | 25.95 (5.51) |
Disease characteristics | ||
Duration of migraine illness, years, mean (SD) | 23.76 (13.86) | 22.73 (13.24) |
Number of comorbidities, mean (SD) | 4.19 (3.71) | 4.15 (3.65) |
Number of monthly headache days, mean (SD) | 14.75 (5.91) | 15.26 (6.38) |
Number of monthly MHDs, mean (SD) | 13.01 (5.73) | 13.44 (6.08) |
Migraine attacks per month, mean (SD) | 5.98 (1.83) | 5.75 (2.07) |
Baseline migraine frequency category, n (%) | ||
Episodic | 132 (57.39) | 137 (59.05) |
Low-frequency episodic a | 36 (15.65) | 35 (15.09) |
High -frequency episodic b | 96 (41.74) | 102 (43.97) |
Chronic | 98 (42.61) | 95 (40.95) |
Number of days with acute headache medication use per month, mean (SD) | 12.38 (5.97) | 12.28 (6.02) |
Baseline headache medication overuse, n (%) | 99 (43.04) | 108 (46.55) |
MIDAS total score at baseline, mean (SD) | 50.96 (45.50) | 50.90 (45.96) |
MSQ RF-R score at baseline, mean (SD) | 43.95 (18.49) | 45.81 (16.00) |
PHQ-9, Major depression, n (%) | 36 (15.65) | 30 (12.93) |
GAD-7, Anxiety disorder, n (%) | 36 (15.65) | 32 (13.79) |
Medication use | ||
Prior treatment with migraine prophylactic medication | 230 (100) | 232 (100) |
Qualifying medication category failures in past 10 years, n (%) | ||
2 | 139 (60.43) | 130 (56.03) |
3 | 68 (29.57) | 71 (30.60) |
4 | 19 (8.26) | 27 (11.64) |
Number of failed individual preventive meds past 10 years, mean (SD) | 3.31 (1.65) | 3.34 (1.57) |
Lifetime total number of failed individual preventive meds, mean (SD) | 3.47 (1.72) | 3.48 (1.70) |
Most common medication categories failed in past 10 years, n (%) | ||
Topiramate | 169 (73.48) | 163 (70.26) |
Amitriptyline | 111 (48.26) | 110 (47.41) |
Propranolol or metoprolol | 101 (43.91) | 108 (46.55) |
Valproate or divalproex | 63 (27.39) | 66 (28.45) |
Botulinum toxin A or B | 36 (15.65) | 41 (17.67) |
Candesartan | 26 (11.30) | 22 (9.48) |
Flunarizine | 23 (10.00) | 35 (15.09) |
GAD-7 = Generalized Anxiety Disorder 7-item; GMB = galcanezumab; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; PHQ-9 = Patient Health Questionnaire-9; RF-R = role function – restrictive; SD = standard deviation.
aLow-frequency episodic migraine defined as 4 to fewer than 8 migraine headache days per month.
bHigh-frequency episodic migraine defined as 8 to fewer than 15 MHDs per 30-day period, and with fewer than 15 headache days per 30-day period.
Source: CONQUER Clinical Study Report.12
Interventions
Administration of Study Drug
Double-Blind Treatment phase
Each of the EVOLVE-1, EVOLVE-2, and REGAIN trials had 3 study arms: placebo, galcanezumab 120 mg (with a loading dose of 240 mg), and galcanezumab 240 mg. The CONQUER trial had 2 study arms: placebo and galcanezumab 120 mg (with a loading dose of 240 mg).
In all trials, the galcanezumab or matching-administration placebo injections were administered by study-site personnel once monthly at dosing visits.12,50 Galcanezumab and matching-administration placebo were supplied as an injectable solution in 1 mL, single-dose, pre-filled, disposable manual syringes. Each syringe of galcanezumab was designed to deliver galcanezumab 120 mg. The syringes (and their contents) containing either galcanezumab or placebo were visibly indistinguishable from each other. Subcutaneous injection sites included the abdomen, thigh, upper arm, or buttocks.
In the EVOLVE-1, EVOLVE-2, and REGAIN trials, all treatment groups received 2 injections of the study drug at each dosing visit to maintain the blind (2 placebo injections, 2 galcanezumab 120 mg injections, or 1 placebo injection and 1 galcanezumab 120 mg injection). In the CONQUER study, patients in both treatment groups received 2 injections (2 placebo injections or 2 galcanezumab 120 mg injections) at the loading-dose visits during the double-blind and open-label phases to maintain the blind and 1 injection at subsequent visits.
Open-Label phase
The EVOLVE-1 and EVOLVE-2 studies did not include an open-label treatment phase.
In the REGAIN trial, doses administered were galcanezumab 240 mg at the first visit in the open-label phase (visit 7), galcanezumab 120 mg at the next visit (visit 8), and either 120 or 240 mg, thereafter, at the discretion of the investigator. Dosing and dose changes could only occur at the regular once-monthly visits.
At the first visit in the open-label treatment phase (visit 6) in the CONQUER trial, patients in the galcanezumab 120 mg arm received 120 mg galcanezumab (1 injection of 120 mg plus 1 injection of placebo to maintain the blind) and patients in the placebo arm received a loading dose of 240 mg (2 injections of 120 mg). At the subsequent dosing visits in the open-label phase, all patients received 120 mg galcanezumab (1 injection).
Treatment Duration
In the EVOLVE studies, the double-blind treatment period was 6 months (6 administrations). In the REGAIN study, the double-blind treatment period was 3 months (3 administrations) and the optional open-label treatment phase was 9 months (9 administrations). In the CONQUER trial, the double-blind treatment phase was 3 months (3 administrations) and the optional open-label treatment phase was 3 months (3 administrations).
Concomitant Medications
In all trials, acute (abortive) medications were allowed and recorded in the patient ePRO diaries.9-12 These included acetaminophen (paracetamol), nonsteroidal anti-inflammatories, triptans, ergotamine and derivatives, isometheptene mucate, dichloralphenazone and acetaminophen combination (Midrin), or combinations thereof.
In the EVOLVE-1, EVOLVE-2, and REGAIN studies, the use of concomitant medication for acute treatment of migraine was subject to some limitations, such as a restriction on the use of opioid- and barbiturate-containing medications for no more than 3 days per month, and a single dose of injectable steroids was allowed only once during the study, in an emergency setting. For patients who completed the double-blind treatment phase of the study, treatments used for the prevention of migraine were allowed 1 month after the patient entered the post-treatment phase, if clinically warranted due to a worsening of symptoms.
In the REGAIN trial, treatments used for the prevention of migraine were generally not allowed during the double-blind and open-label treatment phases. However, the study allowed approximately 1-third of enrolled patients to continue migraine prophylactic treatment with either topiramate or propranolol if the patient had been on a stable dose for at least 2 months before the prospective baseline period and if dosing was expected to remain stable throughout the double-blind treatment phase.
In the CONQUER trial, the concomitant use of acute medications to treat migraine was allowed, with some limitations, such as restricting the use of opioid- and barbiturate-containing medications to no more than 4 days per month, and a single dose of injectable steroids was allowed only once during the study, in an emergency setting. Treatments used for the prevention of migraine, including nutraceuticals and nonpharmacological interventions, were not allowed at any time during the prospective baseline, double-blind treatment, and open-label treatment phases of the study. Patients were to wash out all migraine-preventive treatments at least 5 days before beginning the prospective baseline period (visit 2). Botulinum toxin A or B in the head or neck area for therapeutic use was not allowed within 3 months before visit 2. Nerve blocks or use of therapeutic devices, such as transcranial magnetic stimulation, in the head or neck area or for migraine prevention, were not allowed within 30 days before visit 2.
In all studies, concomitant medications used for the acute treatment of migraine were recorded by the patient in the ePRO diary and all other concomitant medications taken during the study were recorded via electronic case report forms.
Discontinuation Criteria
In all studies, patients were to be discontinued from the study if the investigator or patient decided the patient should be withdrawn.
In EVOLVE-1, EVOLVE-2, and REGAIN, discontinuation of the study drug for abnormal liver tests was required when a patient met 1 of the following conditions and the event was at least possibly related to the study drug: alanine aminotransferase (ALT) or aspartate aminotransferase (AST) levels were 8 times the upper limit of normal (ULN); ALT or AST levels were greater than 5 times the ULN for more than 2 weeks; ALT or AST levels were greater than 3 times ULN and total bilirubin levels were greater than 2 times the ULN or prothrombin time was greater than 1.5 times the ULN; ALT or AST was greater than 3 times the ULN, with the appearance of fatigue, nausea, vomiting, right upper-quadrant pain or tenderness, fever, rash, and/or eosinophilia (> 5%); alkaline phosphatase levels were greater than 3 times the ULN; and alkaline phosphatase levels were greater than 2.5 times the ULN and total bilirubin was greater than twice the ULN; alkaline phosphatase was greater than 2.5 times the ULN, with the appearance of fatigue, nausea, vomiting, right-quadrant pain or tenderness, fever, rash, and/or eosinophilia (> 5%). Discontinuation of study treatment was also required in the following cases, if the event was at least possibly related to the study drug: serious allergic reaction to the study drug, serious injection site reaction, serious event of suicidality or depression, and serious cerebrovascular event.
In the CONQUER trial, discontinuation of the study drug for abnormal liver tests was to be considered by the investigator, in consultation with the sponsor. Patients must have been discontinued from the study drug if the patient requested to discontinue, in the event of pregnancy, or if the investigator decided the patient should be withdrawn.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 11. These end points are summarized in the following section. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 11: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome Measure | EVOLVE-1 | EVOLVE-2 | REGAIN | CONQUER |
|---|---|---|---|---|
MSQ v2.1 | Secondarya | Secondarya | Secondarya | Secondarya |
EQ-5D-5L | Not assessed | Not assessed | Not assessed | Secondary |
HIT-6 | Not assessed | Not assessed | Not assessed | Not assessed |
MHDs with symptoms (nausea, vomiting, photophobia, phonophobia, aura, and prodromal symptoms) | Exploratory | Exploratory | Exploratory | Exploratory |
MIDAS | Secondary | Secondary | Secondary | Secondary |
MIBS-4 | Not assessed | Not assessed | Not assessed | Secondary |
PHQ-9 | Not assessed | Not assessed | Not assessed | Exploratory |
GAD-7 | Not assessed | Not assessed | Not assessed | Exploratory |
Number of monthly MHDs | Primarya | Primarya | Primarya | Primarya |
Number of monthly headache days | Secondary | Secondary | Secondary | Secondary |
Acute headache pain medication intake | Secondarya | Secondarya | Secondarya | Secondary |
Time to first loss of response | Secondary | Secondary | Secondary | Not assessed |
Time to initiation of a migraine-prevention medication | Secondary | Secondary | Secondary | Not assessed |
HCRU and employment status | Not assessed | Not assessed | Secondary | Secondary |
WPAI | Not assessed | Not assessed | Not assessed | Secondary |
Harms | Secondary | Secondary | Secondary | Secondary |
EQ-5D-5L = EQ-5D 5-Levels questionnaire; GAD-7 = Generalized Anxiety Disorder 7-item; HCRU = health care resource utilization; HIT-6 = 6-item Headache Impact Test; MHD = migraine headache day; MIBS-4 = 4-item Migraine Interictal Burden Scale; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; PHQ-9 = Patient Health Questionnaire-9; WPAI = Work Productivity and Activity Impairment.
aControlled for multiplicity within the trial’s multiple-testing procedure.
Source: EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 REGAIN Clinical Study Report,11 and CONQUER Clinical Study Report.12
Efficacy Outcomes
Assessments of migraine and headache-related end points (i.e., MHDs with symptoms, number of monthly MHDs, number of monthly headache days, and acute headache pain medication intake) were based on headache information captured in ePRO diaries. Patients were asked to use a daily ePRO diary to record headache information (e.g., characteristics, duration, and severity) and whether any acute headache medication was taken. The system also was used to collect information about migraine-associated symptoms (e.g., photophobia, phonophobia, nausea, and/or vomiting). Based on patient responses in the daily ePRO diaries, days were defined as no headache, headache, non-migraine headache, ICHD-3 migraine headache, and MHDs (primary measure) using an automated algorithm according to the definitions in Table 12. Each month was defined as a 30-day period with migraine or headache measures normalized to a 30-day period from the actual visit intervals.
Table 12: Migraine and Headache End-Point Definitions
Diagnosis | Definition/Criteria |
|---|---|
Migraine headache | EVOLVE-1, EVOLVE-2, and CONQUER: A headache, with or without aura, of ≥ 30 minutes duration, with both of the following required features (A and B): A. At least 2 of the following headache characteristics:
AND B. During headache at least 1 of the following:
REGAIN: A headache, with or without aura, of ≥ 30 minutes duration with both of the following required features (A and B): A. At least 2 of the following headache characteristics:
AND B. During headache at least 1 of the following:
OR C. The headache was believed by the patient to be migraine at onset and was relieved by a triptan or ergot derivative. (Definitions adapted from the standard IHS ICHD-3 definition) |
Probable migraine headache | EVOLVE-1, EVOLVE-2, and CONQUER: A headache of ≥ 30 minutes duration, with or without aura, but missing 1 of the migraine features in the IHS ICHD-3 definition (i.e., it met either at least 2 of the A criteria and 0 of the B criteria, or 1 of the A criteria and at least 1 of the B criteria) REGAIN: A headache of ≥ 30 minutes, but missing 1 of the migraine features in the IHS ICHD-3 beta definition (i.e., it met either at least 2 of the A criteria and 0 of the B criteria, or one 1 of the A criteria and at least 1 of the B criteria); it must not have met criterion C |
Migraine headache day (primary objective) | A calendar day on which a migraine headache or probable migraine headache occurred |
Non-migraine headache | All headaches of at least 30 minutes duration not fulfilling the definition of migraine or probable migraine |
Headache day | A calendar day on which any type of headache occurred (including migraine, probable migraine, and non-migraine headache) |
ICHD-3 = International Classification of Headache Disorders, third edition; IHS = International Headache Society.
Source: EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 REGAIN Clinical Study Report,11 and CONQUER Clinical Study Report.12
In the EVOLVE-1, EVOLVE-2, and REGAIN trials, time to first loss of response among patients who met the 50% response criteria at the end of their treatment interval and time to initiation of treatment with a migraine-prevention medication were assessed in the post-treatment follow-up periods. A 50% response was defined as a reduction of least 50% from baseline in MHDs during the month. Time to first loss of 50% response was analyzed among patients who met the 50% response criterion during the last month of treatment and also entered the post-treatment phase. Patients who discontinued or completed the study without loss of 50% response were censored in the time-to-event analysis of first loss of response.
A detailed discussion of the MSQ v2.1, MIDAS, HRCU employment status, EQ-5D 5-Levels questionnaire (EQ-5D-5L), WPAI questionnaire, Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder 7-item (GAD-7) scale is provided in Appendix 4.
The MSQ v2.1 is a self-administered questionnaire that addresses the physical and emotional impact of migraine on functioning with a 4-week recall period.9-12 It is a 14-item instrument covering 3 domains: RF-R (impact on performance of normal activities), role function – preventive (RF-P; complete functional impairment), and emotional function (EF; feelings related to disabling migraine). Responses are captured using a 6-point Likert scale, ranging from “none of the time” to “all of the time.” The total raw score is the sum of responses for each domain, which is converted to a 0-to-100 scale. Higher scores indicate a better health status, and an increase in score reflects improvement in HRQoL. A literature by CADTH identified the following minimal important differences (MIDs): 3.2 to 5.0 for RF-R, 4.6 to 7.9 for RF-P, and 7.5 to 10.6 for EF in patients with EM, and 10.9 for RF-R, 8.3 for RF-P, and 12.2 for EF in patients with CM.52,53
The MIDAS is a 5-item instrument that measures headache-related disability over a 3-month period.54 The instrument evaluates the number of days missed or with reduced productivity at work or school, at home, and in social settings. Total scores are translated to a 4-point grading system: grade 1 (scores from 0 to 5) is for minimal or infrequent disability; grade 2 (scores from 6 to 10) is for mild or infrequent disability; grade 3 (scores from 11 to 20) is for moderate disability; and grade 4 (scores of 21 or greater) is for severe disability.12 Grade 4 can be further divided into 2 subcategories: grade 4-A (scores 21 to 40) is for severe disability and grade 4-B (scores 41 to 270) is for very severe disability. A higher value is indicative of more disability; a decrease in grade indicates a decrease in disability. CADTH identified an MID of 3.7 points in the literature.55 The clinical expert consulted by CADTH indicated a 5-point or 50% change in total MIDAS score would be considered clinically significant.
The EQ-5D-5L is a patient-reported, generic, HRQoL instrument that that assesses current health status.56-58 The recall period is “today” and the instrument consists of 2 parts: a health utility index and the EQ Visual Analogue Scale (EQ VAS). The health utility component consists of 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and patients respond to each dimension using 5 levels (1 indicates no problems, 5 indicates extreme problems or unable to perform). Results from the EQ-5D-5L descriptive system can be converted into a single index score using a scoring algorithm taking the local patient and population preferences into account. The index score therefore provides a country-specific value, which is a major feature of the instrument. The health state index score provides a single value on a scale from less than 0 to 1; negative values are for states worse than dead, 0 is a health state equivalent to death, and 1 is a health state equivalent to perfect health. For the EQ VAS, patients rate their perceived health state from 0 (the worst health imaginable) to 100 (the best health imaginable). A Canadian-specific estimate of a MID in the general population is 0.056.59 No MID was identified in populations with migraine.
The 4-item Migraine Interictal Burden Scale (MIBS-4) is a self-reported questionnaire that assesses the burden of illness related to migraine during the time in between attacks (interictal state) with a 4-week recall period.12 The 4 items address disruption at work and school, diminished family and social life, difficulty planning, and emotional difficulty. Responses range from 0 (don’t know/not applicable or never) to 3 (much or most/all of the time). The individual item scores are summed, producing a total score ranging from 0 to 12. A higher score indicates a greater interictal burden. No MID was identified in populations with migraine.
The PHQ-9 is a self-reported questionnaire used for screening patients for depression and measuring the severity of depressive symptoms over the past 2 weeks.12,60 The instrument consists of 9 items corresponding to criteria for diagnosing major depressive disorder from the Diagnostic and Statistical Manual for Mental Disorders, fourth edition. Patients score each item on a 4-point scale for how frequent symptoms occurred during a 2-week recall period (0 = not at all, 1 = several days, 2 = more than half the days, 3 = nearly every day). The total score ranges from 0 to 27, with a higher score indicating greater severity of depressive symptoms (0 to 4 = none to minimal depression, 5 to 9 = mild depression, 10 to 14 = moderate depression, 15 to 19 = moderately severe depression, and 20 to 27 = severe depression).61 No MID was identified in patients with migraine.
The GAD-7 is a patient-administered questionnaire used to screen for and measure the severity of anxiety symptoms within a 2-week recall period.12 The questionnaire consists of 7 items, including feelings of nervousness, uncontrollable worrying, excessive, worrying, trouble relaxing, restlessness, irritability, and fearfulness. Patients answer based on a 4-point rating scale (0 = not at all, 1 = several days, 2 = more than half the days, and 3 = nearly every day). Total scores range from 0 to 21, with a higher score indicating greater anxiety (0 to 4 = minimal anxiety, 5 to 9 = mild, 10 to 14 = moderate, and 15 to 21 = severe). No specific MID was identified in patients with migraine.
Data on HCRU and employment status were collected by study-site personnel in the REGAIN and CONQUER trials. Patients were asked 3 questions about the number of hospital emergency visits, overnight stays at the hospital, and other visits with a health care professional aside from study-related visits that occurred (all-cause and migraine-specific) since the patient’s last study visit. At baseline, the same questions were asked with a recall period of 6 months. A higher number (i.e., events or visits) indicates greater utilization of health care resources. Employment status information was also collected while documenting patient responses about the number of health care events (all-cause and migraine-specific) since the patient’s last study visit. No literature was found that assessed HCRU or employment status for validity, reliability, or responsiveness in patients with migraine. No MID was identified in populations with migraine.
The WPAI is a patient-reported instrument that measures the impact on work productivity and regular activities attributable to a specific health problem.62 The instrument consists of 6 items and measures impairments on both paid and unpaid work within a 7-day recall period. Four scores are calculated for absenteeism, presenteeism, work productivity loss, and activity impairment. No MID was identified in patients with migraine. The scores are reported as impairment percentages, with a higher number indicating greater impairment or lower productivity. No literature was found that assessed the WPAI for validity, reliability, or responsiveness in patients with migraine.
Harms Outcomes
In all studies, AEs related to injection sites were defined using terms from the Medical Dictionary for Regulatory Activities (MedDRA) high-level term of “injection site reactions.”
Potential treatment-emergent hypersensitivity events (immediate and non-immediate) were identified from a review of preferred terms generated from the standardized MedDRA query for anaphylactic reaction, angioedema, and hypersensitivity. Query results were narrowed by using preferred terms that are highly likely to represent the condition of interest and are reported in the CADTH systematic review.
Adverse events related to injection sites were defined using the MedDRA high-level term of “injection site reactions.”
In the EVOLVE-1, EVOLVE-2, and REGAIN studies, data on the incidence of treatment-emergent ADA were prospectively collected and reported. Treatment-emergent ADA-positive was defined as a negative baseline and a positive post-baseline ADA result with a titre of 20 or greater, or a positive baseline and a positive post-baseline result with a titre increase of at least 4-fold (e.g., baseline titre of 10 increasing to 40 or greater following baseline). A list of patients who were treatment-emergent ADA-positive at any time during the study was created and included neutralizing ADA status. Immunogenicity was not proactively evaluated in the CONQUER trial.
Vascular events included treatment-emergent AEs categorized in the MedDRA system order class of vascular disorders.
Statistical Analysis
The statistical analysis of efficacy end points conducted in the 4 trials included in the systematic review is summarized in Table 13.
All Pivotal Trials
In all trials, analyses were conducted primarily using 2 analysis populations: an ITT population and a safety population. Efficacy analyses were conducted on the ITT population. Safety analyses were conducted on the safety population.
Treatment effects were evaluated based on an overall 1-sided significance level of 0.025 (equivalent to a 2-sided 0.05 significance level) for all efficacy and safety analyses. The 95% CIs for the difference in LS means between treatment groups were presented.
Change from baseline of continuous variables with repeated measures was analyzed using a mixed model for repeated measures (MMRM) analysis.
For other continuous variables, the change from baseline to the LOCF end point was analyzed using an analysis of variance (ANOVA) or analysis of covariance (ANCOVA) model. Unless otherwise specified, when an ANOVA or ANCOVA model was used to analyze a continuous efficacy variable, type III sum of squares for the LS means was used for statistical comparisons.
For categorical efficacy variables without repeated measures, comparisons between treatment groups were performed using logistic regressions.
Comparisons between galcanezumab and placebo refer to comparisons of each galcanezumab treatment group with placebo.
Approaches to Handling Missing Data
To handle missing data, 2 statistical approaches were applied. Repeated measures analyses were used where the model parameters were simultaneously estimated using restricted-likelihood estimation incorporating all observed data.; estimates have been shown to be unbiased when the missing data are missing at random. For ANOVA and ANCOVA analyses, the LOCF was used.
In the EVOLVE-1, EVOLVE-2, and REGAIN trials, sensitivity analyses were conducted to assess the robustness of the primary analysis conclusions to deviations from missing at random assumption. The approach for these analyses was to vary the assumptions of missing data for the primary analysis in a systematic way. The method was to predict the missing outcomes, then add values (Δ120, Δ240, and ΔP) to the predictions in the galcanezumab 120 mg, galcanezumab 240 mg, and placebo treatment groups, respectively, regardless of the reason the data were missing.
The primary outcome measure (i.e., the number of monthly MHDs) was summarized from the daily ePRO data for each patient (including daily data from the baseline period before randomization and 6 months of daily data during the treatment phase). The daily data were aggregated, and the number of MHDs was provided for each of the monthly visit or dose intervals. In calculating the number of MHDs for each monthly interval, the number of MHDs was normalized to a 30-day period by multiplying the number of MHDs by 30 and dividing by the total number of non-missing diary days in the monthly interval. This approach to missing ePRO diary data assumed that the rate of migraine headache per day was the same for days with missing and non-missing ePRO diary days. The same approach was applied to secondary and exploratory efficacy measures that were derived from ePRO data. If the compliance rate for a monthly interval was no more than 50%, then all end points to be derived from the ePRO diary data for that 1-month period were considered missing.
Primary Outcome
The primary outcome (i.e., the number of monthly MHDs) was summarized from the daily ePRO data for each patient. The primary analysis evaluated the efficacy of galcanezumab compared with placebo on the overall mean change from baseline in the number of monthly MHDs during the double-blind treatment phase. The primary analysis was performed using a MMRM analysis. The overall mean change in monthly MHDs was estimated as the main effect of treatment (each galcanezumab dose group and placebo) from the MMRM analysis during the double-blind treatment phase. This provided the average treatment effect across the duration of the double-blind treatment phase. The repeated measures analysis included data from all treatment groups. The type I error rate for the study was controlled at a 2-sided 0.05 level (equivalent to a 1-sided 0.025 level).
EVOLVE-1 and EVOLVE-2
Statistical analysis was performed as previously described.
The MMRM for efficacy analyses included the fixed, categorical effects of treatment, geographical region, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction. The baseline value and baseline-by-month interaction were included to account for the differential influence over time that the baseline value has on the post-baseline values. The MMRM for the safety analyses included the fixed, categorical effects of treatment, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction.
When an ANOVA model was used to analyze a continuous efficacy variable at an LOCF end point, the model contained the main effects of treatment and region. The ANCOVA model used to analyze a continuous efficacy variable contained the same main effects as the ANOVA model, but included an appropriate baseline value as a covariate. When an ANOVA or ANCOVA model was used to analyze a continuous safety variable, the term for region was excluded from the model.
For categorical variables without repeated measures, comparisons between treatment groups were performed using Fisher’s exact test.
With the exception of efficacy analyses on MHDs or categorical analysis of response rates derived from MHDs where the continuous value of baseline MHDs was used as covariate, all other efficacy analyses included a baseline monthly MHD category (< 8 versus ≥ 8) as a covariate in the model.
Multiple Testing Procedure
Control of the familywise type I error rate for the primary and key secondary end points was achieved through an overall superchain procedure (Kordzakhia and Dmitrienko [2013]), a multiple-testing method that employs alpha recycling techniques. As part of this procedure in the EVOLVE-1 and EVOLVE-2 studies, a Dunnett test (Dunnett [1955]) was used for the primary hypotheses (galcanezumab 120 mg versus placebo, galcanezumab 240 mg versus placebo). Tests for key secondary hypotheses were conducted following rejection of at least 1 of the 2 primary null hypotheses. Specifically, the Hochberg procedure (Hochberg [1988]) was used for a 50% and 75% response rate in MHDs at the corresponding dose(s). Following rejection of the previous secondary null hypotheses, the Bonferroni-Holm procedure (Holm [1979]) was used for change in the use of acute (abortive) migraine treatment and change in functioning for the MSQ v2.1. Following rejection of these secondary null hypotheses, the remaining hypotheses of 100% response rate and Patient Global Impression of Severity (PGI-S) were tested sequentially. Alpha could be recycled between doses following testing of all secondary null hypotheses for either dose.
The multiple-testing procedure is depicted in Figure 5. Propagation weights are denoted along the edges between boxes, which represent hypothesis tests for families of hypotheses. According to this testing procedure, the parallel branches (dose sequences) are initially tested simultaneously, and the available alpha is then recycled between the branches to retest end-point families containing non-rejected null hypotheses.
Multiple testing procedure results for the EVOLVE-1 and EVOLVE-2 studies are presented in Appendix 3 (Figure 19 and Figure 20, respectively).
There were no adjustments for multiplicity for analyses of other end points.
Figure 5: Multiple Testing Procedure in the EVOLVE-1 and EVOLVE-2 Trials
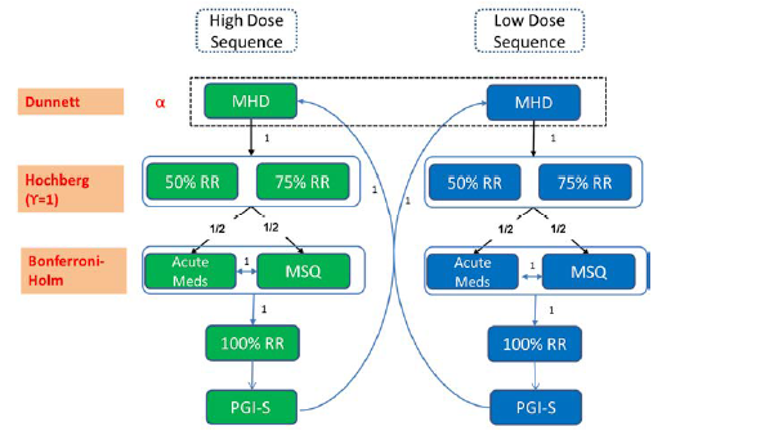
acute meds = migraine headache days with use of acute (abortive) treatment; MHD = number of monthly migraine headache days (mean change from baseline); MSQ = Migraine-Specific Quality of Life Questionnaire version 2.1 role function – restrictive domain; PGI-S = Patient Global Impression of Severity; RR = response rate in monthly migraine headache days (mean change from baseline).
Source: EVOLVE-1 Clinical Study Report9 and EVOLVE-2 Clinical Study Report.10
Primary Outcome Analysis
The primary outcome analysis was performed as previously described for all pivotal trials. The following subgroup analyses were planned for the primary outcome measure: sex, race, ethnicity, baseline monthly MHD category (< 8 or ≥ 8), baseline treatment-resistant status (previously failed 2 or more prophylactic treatments: yes or no), and having aura or not (during the baseline period). The subgroup analyses were conducted using the same MMRM applied to the primary efficacy analysis, with terms of subgroup, subgroup-by-treatment, subgroup-by-month, and subgroup-by-treatment-by-month interactions added as additional covariates. A post hoc subgroup analysis also performed for patients who failed 3 or more prophylactic treatments.
Sensitivity Analyses for the Primary Outcome: Sensitivity analyses for missing-data assumptions were planned to be performed in the EVOLVE-1 and EVOLVE-2 studies. Delta adjustments as suggested in Permutt (2016) were conducted for change from baseline in MHDs. These analyses were performed to assess the potential impact of missing-data assumptions by examining the primary conclusions under a set of plausible, worst-case scenarios around the distribution of missing outcome data. Missing outcome values were imputed to be worse than expected based on the observed values (at the extreme, even markedly worse than the baseline values) with no treatment benefit at all seen in missing outcomes data. In total, 9 delta sets were used.
In both the EVOLVE-1 and EVOLVE-2 studies, a sensitivity analysis for the raw number of MHDs (i.e., the total number of MHDs for each interval without normalization to a 30-day period) was conducted with a repeated measures negative binomial regression analysis to assess the validity of the primary MMRM results with respect to deviations from normality assumption.
In addition, a sensitivity analysis was conducted in both EVOLVE studies to assess the validity of the primary results if a minor change was made to the definition of migraine headache. This minor change was to add an additional condition that, for any diary day, even if the patient did not meet the migraine headache definition as defined by criteria A and B (Table 12) but was taking a triptan or ergot derivative (“criterion C”), this diary day for this patient was still considered an MHD. The rationale was to replicate the use of a similar criterion that is part of the ICHD-3 criteria for a diagnosis of CM. This analysis was implemented by repeating the primary analysis using the number of monthly MHDs derived based on the modified definition of migraine headache.
A post hoc sensitivity analysis was conducted to assess the impact of inadvertently enrolled patients (i.e., identified as having an important protocol deviation of inclusion or exclusion criteria not being met) on the primary efficacy analysis in the EVOLVE-1 and EVOLVE-2 studies.
In the EVOLVE-1 study, an additional post hoc sensitivity analysis was conducted to assess the impact of excluding the patients from a site that was closed due to Good Clinical Practice compliance issues.
Secondary and Exploratory End point Analyses
For the continuous efficacy measures, the change from baseline to each post-baseline period was estimated for each treatment from repeated measures analyses as described for analysis of the primary outcome, with the addition of baseline monthly MHD category (< 8 versus ≥ 8) as a covariate. For the continuous secondary efficacy measures for which the objective was to assess overall mean change during the 6-month double-blind treatment phase, the end point for comparing galcanezumab with placebo was estimated as the main effect of treatment from the MMRM analysis across months 1 to 6 (inclusive of month 6). In addition to the repeated measures analyses, the mean change from baseline to the average monthly measures or LOCF end point during the 6-month treatment phase was estimated for the continuous efficacy measures using ANCOVA models with covariate adjustments as previously described.
The mean change from baseline to each post-baseline visit for MSQ v.2.1 total and domain scores averaged across months 4 to 6 (inclusive of month 6) was evaluated using an MMRM. The mean change from baseline to each post-baseline visit for MIDAS total and item scores was also evaluated using an MMRM.
For time-to-event analyses, a stratified log-rank test was used.
Determination of Sample Size
Each study planned to enrol approximately 825 patients. Eligible patients were to be randomized in a 2:1:1 ratio to placebo (approximately 413 patients), galcanezumab 120 mg (target of 206 patients), or galcanezumab 240 mg (target of 206 patients). With the assumption of a 26% discontinuation rate and an effect size of 0.33 in the last month of the 6-month treatment phase, it was estimated that this sample would provide approximately 95% power that at least 1 dose of galcanezumab would separate from placebo at a 1-sided 0.025 significance level based on simulations using a Dunnett test. Assumptions were based on data from 2 double-blind, placebo-controlled, phase II studies, adjusted to reflect the longer treatment duration and greater variability expected in a larger phase III study.
REGAIN
Statistical analysis was performed as previously described. In addition to the primary efficacy analyses conducted on the ITT population, some analyses were conducted using the open-label treatment population, which included all patients who entered the open-label treatment phase as indicated by receiving any injections starting from visit 7.
The MMRM for efficacy analyses included the fixed, categorical effects of treatment, country, month, baseline medication overuse (yes versus no), concurrent prophylaxis (yes versus no), and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction. The baseline value and baseline-by-month interaction were included to account for the differential influence over time that the baseline value has on the post-baseline values. The MMRM for the safety analyses included the fixed, categorical effects of treatment, month, baseline medication overuse, concurrent prophylaxis, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction.
When an ANOVA model was used to analyze a continuous efficacy variable, the model contained the main effects of treatment, baseline medication overuse, concurrent prophylaxis use, and country. The ANCOVA model used to analyze a continuous efficacy variable contained the same main effects as the ANOVA model, but included an appropriate baseline value as a covariate. When an ANOVA or ANCOVA model was used to analyze a continuous safety variable, the term for country was excluded from the model.
For categorical variables without repeated measures, comparisons between treatment groups were performed using a Cochran-Mantel-Haenszel or Fisher exact test. Unless otherwise stated, the former test was controlled for baseline medication overuse (yes versus no) and concurrent prophylaxis use (yes versus no). Unless specified otherwise, the Fisher exact test was used for comparisons of baseline measures.
When a logistic regression was used to analyze a binary variable, the model included the main effect of treatment, baseline medication overuse, concurrent prophylaxis use, and country, and an appropriate baseline value as a covariate. The country could have been excluded from the model in the event of non-convergence.
Multiple Testing Procedure
Control of the familywise type I error rate for the primary and key secondary end points was achieved through an overall superchain procedure (Kordzakhia and Dmitrienko [2013]), a multiple-testing method that employs alpha recycling techniques. As part of this procedure in the present study, a Dunnett test was used for the primary hypotheses (galcanezumab 120 mg versus placebo, galcanezumab 240 mg versus placebo). Tests for key secondary hypotheses were to be conducted following rejection of at least 1 of the 2 primary null hypotheses. Specifically, following rejection of at least 1 primary null hypothesis, the Hochberg procedure (Hochberg [1988]) was to be used for the 50% and 75% response rate in MHDs at the corresponding dose(s). Following rejection of the previous secondary null hypotheses, the Bonferroni-Holm procedure (Holm [1979]) was to be used for change in the use of acute (abortive) migraine treatment and change in functioning for the MSQ v2.1. Following rejection of these secondary null hypotheses, the remaining hypotheses of PGI-S and 100% response rate were to be tested sequentially. Alpha could be recycled between doses following testing of all secondary null hypotheses for either dose. This multiple-testing procedure is depicted in Figure 6. Propagation weights are denoted along the edges between boxes, which represent tests for families of hypotheses. According to this testing procedure, the parallel branches (dose sequences) are initially tested simultaneously, and then the available alpha is recycled between the branches to retest end-point families containing non-rejected null hypotheses.
Multiple testing procedure results for the REGAIN trial are presented in Appendix 3 (Figure 21 and Figure 22).
There were no adjustments for multiplicity for analyses of other end points.
Figure 6: Multiple Testing Procedure in the REGAIN Trial
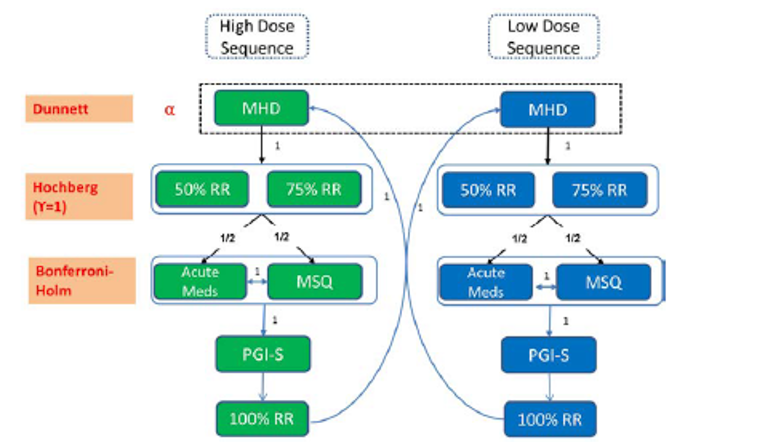
acute meds = migraine headache day with the use of acute (abortive) treatment; MHD = the number of monthly migraine headache days (mean change from baseline); MSQ = Migraine-Specific Quality of Life Questionnaire version 2.1 role function – restrictive domain; PGI-S = Patient Global Impression of Severity; RR = response rate in monthly migraine headache days (mean change from baseline).
Source: REGAIN Clinical Study Report.11
Primary Outcome Analysis
The primary outcome analysis was performed as previously described for all pivotal trials. The following subgroup analyses were planned for the primary outcome measure: sex, race, ethnicity, region, treatment-resistant status (i.e., failed at least 2 prophylactic treatments [yes versus no]), having an aura or not (during the baseline period), baseline medication overuse, and concurrent prophylaxis use. The subgroup-by-treatment interaction was tested at a 2-sided 0.10 significance level. Treatment-group differences were evaluated within each category of the subgroup variable. For all the subgroup variables, the subgroup analysis for change from baseline to each monthly interval in the number of MHDs was conducted with the same MMRM in terms of subgroup, subgroup-by-treatment, subgroup-by-month, and subgroup-by-treatment-by-month interactions added as additional covariates. In this analysis, the P values for the subgroup-by-treatment, subgroup-by-month, and subgroup-by-treatment-by-month interactions at the last monthly interval of the 3-month treatment (month 3) were reported. For subgroup analysis with both the MMRM and ANCOVA method, the LS mean and LS mean change estimate as well as the treatment comparisons within each subgroup were analyzed using the data within that specific subgroup only. The MMRM and ANCOVA models were the same as the primary analysis. A post hoc exploratory subgroup analysis was also performed for patients who failed at least 3 prophylactic treatments (yes versus no).
Sensitivity Analyses for the Primary Outcome: Two sensitivity analyses were planned in the REGAIN trial. Sensitivity analyses with delta adjustments as suggested in Permutt (2016) were conducted for change from baseline in MHDs to assess the potential impact of missing data assumptions by examining the primary conclusions under a set of plausible, worst-case scenarios around the distribution of missing outcome data. In addition, a sensitivity analysis for the raw number of MHDs (i.e., the total number of MHDs for each interval without normalization to a 30-day period) was conducted with a repeated measures negative binomial regression analysis to assess the validity of the primary MMRM results with respect to deviations from normality assumption.
Two post hoc sensitivity analyses were also conducted. One sensitivity analysis assessed the impact of inadvertently enrolled patients (i.e., identified as having an important protocol deviation of inclusion or exclusion criteria not being met) on the primary efficacy analysis. Another sensitivity analysis was conducted to assess the impact of the interactive web response system stratification error on the primary efficacy analysis.
Secondary and Exploratory End point Analyses
For the continuous efficacy measures, the change from baseline to each post-baseline period was estimated for each treatment from repeated measures analyses as described for analysis of the primary outcome. For the continuous secondary efficacy measures in which the objective was to assess overall mean change during the 3-month double-blind treatment phase, the end point for comparing galcanezumab with placebo was estimated as the main effect of treatment from the MMRM analysis assessing the average treatment effect across months 1, 2, and 3. In addition to the repeated measures analyses, the mean change from baseline to the average monthly measures or LOCF end point during the 3-month double-blind treatment phase was estimated for the continuous efficacy measures using ANCOVA models with covariate adjustments.
The mean change from baseline to each post-baseline visit for MSQ v2.1 total and domain scores was evaluated using an MMRM. The change from baseline to month 3 on the MIDAS total and item scores was evaluated using the ANCOVA model.
For time-to-event analysis (including time to first loss of 50% response and time to start of preventive treatment), a stratified log-rank test was used with the baseline monthly MHD category (< 8 versus ≥ 8) and region as covariates.
For the HCRU, numbers of the following health-related visits were enumerated and analyzed: hospital emergency room visits, overnight hospital stays, other visits with health care professional, hospital emergency room visits related to migraine headache, overnight hospital stays related to migraine headache, and other visits with health care professionals related to migraine headache. The HCRU rate during the 3-month double-blind phase was compared with the baseline 3-month rate. The baseline 3-month rate was derived from the baseline HCRU measurement, which assessed the previous 6 months. The 6-month baseline rate was then divided by 2 to establish a time frame comparable to the 3-month double-blind treatment phase. These measures were analyzed with a repeated measures negative binomial regression analysis. The model included country, month, baseline medication overuse, concurrent prophylaxis use, and treatment-by-month interaction, as well as the continuous fixed covariates of baseline and baseline-by-month interaction, and log (number of actual number of days within every 3 months divided by 90) as the offset in the model. In case of non-convergence, country and/or baseline-by-month interaction may not have been included in the model. Due to the low rates of HCRU, summary statistics were also provided. Employment status at each visit was summarized separately for each treatment group.
For the outcome of overall change in MHDs with acute migraine medication use from baseline, a post hoc exploratory subgroup analysis was performed for the number of failed prophylactic treatments (≥ 2 versus ≥ 3). For the outcome of overall change in the MSQ v2.1 RF-R domain score from baseline to month 3, a post hoc exploratory subgroup analysis was performed for the number of failed prophylactic treatments (≥ 2 versus ≥ 3).
Determination of Sample Size
A sample size re-estimation procedure was originally planned for the study due to uncertainty in the effect size of galcanezumab in CM. The final sample size could have been between the minimum (825 patients) and maximum (1,140 patients) sample sizes, as informed by the results of the planned interim sample size re-estimation computation:
Based on the assumption of an effect size of 0.33 and a dropout rate of approximately 15%, an initial minimum sample size of 825 was expected to provide more than 90% power that at least 1 dose of galcanezumab would separate from placebo at a 2-sided significance level of 0.05 based on simulations using a Dunnett test (Dunnett 1955).
The maximum sample size of 1,140 was based on the assumption of a 15% discontinuation rate and an effect size of 0.30 in the last month of the 3-month treatment phase; it was estimated that this sample size would provide approximately 95% power that at least 1 dose of galcanezumab would separate from placebo at a 1-sided 0.025 significance level.
To preserve blinding, full details of the sample size and power calculations were omitted from the protocol and were provided to the ethics review board in a separate document. Sites therefore remained blinded to the potential maximum as well as final sample size throughout the trial.
However, the planned sample size re-estimation was not conducted because the rapid rate of enrolment made this adaptive feature of the trial impossible. At the time that interim sample size re-estimation results would have been available, the study would have already surpassed the number of patients needed for screening to enrol the predefined maximum sample size. Therefore, the sample size target was set to the originally planned maximum of approximately 1,140 patients, and the sample size adaptive feature of the trial was removed. The decision to enrol approximately 1,140 patients made the sample size for this study comparable to those of the sponsor’s other global CM studies, according to publicly available records. The final sample size fell slightly short of the 1,140 target due to the variability of screening fail rates that can occur when using a prospective baseline period.
CONQUER
Statistical analysis was performed as described in the preceding section.
The MMRM included the fixed, categorical effects of treatment, baseline migraine frequency category (low-frequency EM, high-frequency EM, and CM), pooled country, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline value-by-month interaction. Baseline value and baseline-by-month interaction were included to account for the differential influence over time that the baseline value has on the post-baseline values.
The ANOVA model for continuous efficacy and health outcome variables contained the main effects of treatment, baseline migraine frequency category, and pooled country. The ANCOVA model for continuous efficacy and health outcome variables contained the main effects of treatment, baseline migraine frequency category, pooled country, and appropriate baseline value.
For categorical efficacy variables without repeated measures, the logistic model included the main effect of treatment, baseline migraine frequency category, and appropriate baseline value as a covariate.
For some health outcome variables without repeated measures during the double-blind treatment phase, the change from baseline score was analyzed using nonparametric tests as the scores of the categories or number of events in the HCRU do not usually satisfy normal assumptions. The Kruskal-Wallis test (Kruskal and Wallis [1952]) was used for treatment comparison and Wilcoxon signed rank test (Wilcoxon [1945]) was used to compare the change from baseline within each treatment group.
Control for Multiplicity
To provide control of the type I error, the key secondary analyses were to be tested using a gated approach at a 2-sided alpha level of 0.05. If the null hypothesis was rejected for the primary end point, key secondary end points were to be sequentially tested following the gatekeeping hierarchy shown in Figure 7. Following the primary objective, the sequential procedure for key secondary objectives began with the comparison between treatment groups in the number of MHDs based on the ITT episodic subpopulation. If the null hypothesis was rejected for that comparison, then the comparison of the 50% response rate between treatment groups was to be tested in the ITT population. If that null hypothesis was rejected, then the next comparison in the sequence was to be tested (50% response rate in the ITT episodic subpopulation), following this same pattern until all hypotheses were tested or until the null hypothesis was accepted for an end point, at which point any further testing stopped for the key secondary objectives.
Multiple testing procedure results for the CONQUER trial are presented in Appendix 3 (Figure 23).
No adjustments were made for multiplicity for analyses of the other secondary or exploratory end points.
Figure 7: Multiple Testing Procedure in the CONQUER Trial
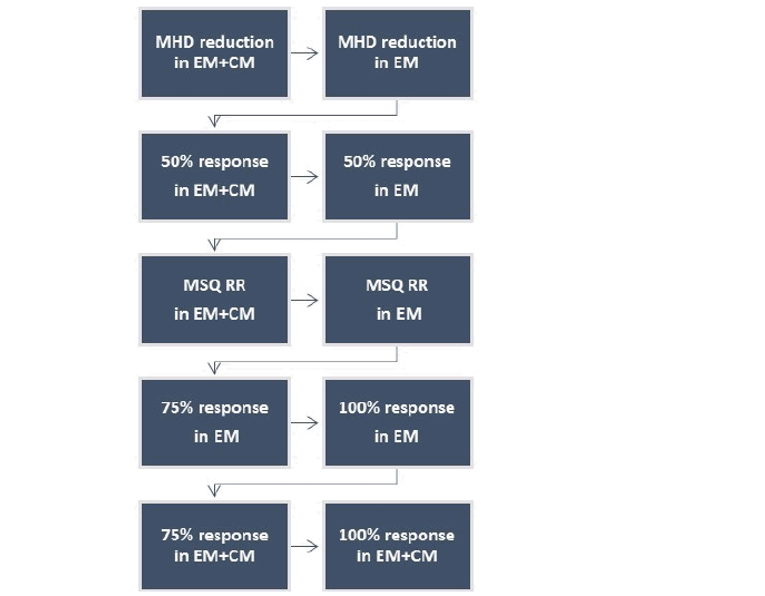
CM = chronic migraine; EM = episodic migraine; MHD = the number of monthly migraine headache days; MSQ RR = Migraine-Specific Quality of Life Questionnaire version 2.1 role function – restrictive domain; response = response rate.
Note: All testing was conducted at a 2-sided alpha of 0.05.
Source: CONQUER Clinical Study Report.12
Primary Outcome Analysis
Subgroup analyses were planned for the primary outcome measure for the ITT patients in the double-blind treatment phase. Subgroup variables for the primary efficacy measure included sex, race, age, region, baseline migraine frequency category, and number of failed preventive migraine medication categories in the past 10 years. The subgroup-by-treatment interaction was tested at a 2-sided 0.10 significance level. Treatment-group differences were evaluated within each category of the subgroup variable. The subgroup analyses were conducted with the same MMRM.
Sensitivity Analyses for the Primary Outcome: Multiple sensitivity analyses were planned in the CONQUER trial. Sensitivity analyses with delta adjustment as suggested in Permutt (2016) were conducted for change from baseline in the number of monthly MHDs. These analyses were performed to assess the potential impact of missing-data assumptions by examining the primary conclusions under a set of plausible, worst-case scenarios around the distribution of missing outcome data. A sensitivity analysis for the raw number of MHDs (i.e., the total number of MHDs for each interval without normalization to a 30-day period) was conducted with a repeated measures negative binomial regression analysis to assess the validity of the primary MMRM results with respect to deviations from normality assumption. A third sensitivity analysis was conducted after removing outliers. In this analysis, the Studentized residuals from the primary analysis model were examined and patients with outlier residuals were identified as those who had an absolute value of a Studentized residual greater than or equal to 2 at any month of the double-blind treatment phase.
Last, a per-protocol analysis of the primary efficacy end point was conducted post hoc. The per-protocol population included all ITT patients who did not have any important protocol deviations during the baseline and double-blind treatment phases.
Secondary and Exploratory End-Point Analyses
The MSQ v2.1, MIDAS, MIBS-4, WPAI, EQ-5D-5L, PHQ-9, and GAD-7 were evaluated using MMRM when there were repeated measures. When there was a single post-baseline measure, they were evaluated using an ANCOVA model.
As HCRU data are count data with excess zeros for migraine patients, they were summarized as the number of events per 100 patient-years. A Wilcoxon signed rank test was performed for comparisons within treatment group and a Kruskal-Wallis test was used for comparisons between treatment groups.
Subgroup analyses were planned for patients with 3 or more prior preventive medication category failures. These subgroup analyses were performed in the ITT population for the following outcome measures: MSQ v2.1 RF-R and MHDs with acute medication use.
Determination of Sample Size
The study planned to enrol approximately 420 patients. With the assumption of a 10% discontinuation rate and an effect size of 0.39, it was estimated that this sample size would provide approximately 96% power that galcanezumab will separate from placebo at a 2-sided significance level of 0.05 for the ITT population.13 The study was also powered for the subpopulation of patients with EM. The study aimed to enrol approximately 250 patients with EM as determined during the prospective baseline period. With the assumption of a 10% discontinuation rate and an effect size of 0.46, it was estimated that this would provide approximately 93% power that galcanezumab will separate from placebo at a 2-sided significance level of 0.05 for the EM subpopulation.
Table 13: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
EVOLVE-1 and EVOLVE-2 | |||
MSQ v2.1 | MMRM |
| None |
MHDs with symptoms | MMRM |
| None |
MIDAS | MMRM |
| None |
Monthly MHDs | MMRM |
|
|
Monthly headache days | MMRM |
| None |
Acute headache pain medication intake | MMRM |
| None |
Time to first loss of response | Stratified log-rank test | Baseline monthly MHD category (< 8 vs. ≥ 8) and region as covariates | None |
Time to initiation of a migraine-prevention medication | Stratified log-rank test | Baseline monthly MHD category (< 8 vs. ≥ 8) and region as covariates | None |
REGAIN | |||
MSQ v2.1 | MMRM |
| None |
MHDs with symptoms | MMRM |
| None |
MIDAS | ANCOVA |
| None |
Monthly MHDs | MMRM |
|
|
Monthly headache days | MMRM |
| None |
Acute headache pain medication intake | MMRM |
| None |
HCRU | MMRM |
| None |
Employment status | Descriptive summary | NA | NA |
Time to first loss of response | Stratified log-rank test | Not reported | None |
Time to initiation of a migraine-prevention medication | Stratified log-rank test | Not reported | None |
CONQUER | |||
MSQ v2.1 | MMRM |
| None |
EQ-5D-5L | ANCOVA |
| None |
MHDs with symptoms | MMRM |
| None |
MIDAS | ANCOVA |
| None |
MIBS-4 | MMRM |
| None |
PHQ-9 | ANCOVA |
| None |
GAD-7 | ANCOVA |
| None |
Monthly MHDs | MMRM |
|
|
Monthly headache days | MMRM |
| None |
Acute headache pain medication intake | MMRM |
| None |
HCRU | Wilcoxon signed rank test for within treatment-group comparison Kruskal-Wallis test for between treatment-group comparisons | None | None |
Employment Status | Descriptive summary | NA | NA |
WPAI | ANCOVA |
| None |
ANCOVA = analysis of covariance; EQ-5D-5L = EQ-5D 5-Levels questionnaire; GAD-7 = Generalized Anxiety Disorder 7-item; GCP = Good Clinical Practice; HCRU = health care resource utilization; IWRS = interactive web response system; MHD = migraine headache day; MIBS-4 = 4-item Migraine Interictal Burden Scale; MIDAS = Migraine Disability Assessment; MMRM = mixed model for repeated measures; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; NA = not applicable; PHQ-9 = Patient Health Questionnaire-9; vs. = versus; WPAI = Work Productivity and Activity Impairment Questionnaire.
Source: EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 REGAIN Clinical Study Report,11 CONQUER Clinical Study Report,12 Stauffer et al. (2019),43 and sponsor’s response to CADTH’s request for additional information.13
Analysis Populations
In all trials, efficacy analyses were performed on a modified ITT population. The modified ITT population included all randomized patients who received at least 1 dose of the study drug. For efficacy analyses, patients were analyzed according to the treatment to which they were randomized. In the CONQUER trial, efficacy analyses were also performed on the modified ITT episodic subpopulation (randomized patients diagnosed with EM) and modified ITT chronic subpopulation (randomized patients diagnosed with CM).
In all trials, the safety population included data from all randomized patients who received at least 1 dose of the study drug. Analyses in the safety population were conducted based on modal treatment the patient received during the double-blind treatment phase. Modal treatment was used to account for situations in which the patient accidentally received a treatment other than the treatment assigned, or cases in which a patient was randomized to the galcanezumab 120 mg group but discontinued after administration of the loading dose such that their exposure was predominantly to the 240 mg loading dose.
The EVOLVE-1, EVOLVE-2, and REGAIN trials also had a post-treatment population, which was used for analyses of the post-treatment phase only (excluding the double-blind treatment phase). This population included all patients who entered the post-treatment phase, as indicated by entering any post-treatment visit. Efficacy analyses using this population were conducted according to the ITT principle, whereas safety analyses were conducted based on modal treatment the patient received during double-blind treatment.
Results
Patient Disposition
Patient disposition in the EVOLVE-1 and EVOLVE-2 trials is summarized in Table 14. In the EVOLVE-1 trial, 1,671 patients were screened, and 862 patients were randomized: 433 to placebo, 213 to galcanezumab 120 mg, and 212 to galcanezumab 240 mg, with 4 excluded from the study’s ITT population because they did not receive at least 1 dose of study drug. The most common reason for screen failure was patients not meeting criteria for study enrolment based on migraine headache information collected in the ePRO diary during the prospective baseline phase. A total of 155 patients (18.1%) discontinued from the double-blind treatment phase. The most frequent reason for discontinuing from double-blind treatment was withdrawal by patient, which occurred in a similar percentage of patients across treatment groups. Overall, 67.1% of patients entered the post-treatment phase of the study as of the data cut-off date of March 22, 2017, for the final efficacy analyses for the double-blind treatment phase.
In the EVOLVE-2 trial, 1,696 patients were screened, and 922 patients were randomized: 461 to placebo, 231 to galcanezumab 120 mg, and 223 to galcanezumab 240 mg, with 7 excluded from the study’s ITT population because they did not receive at least 1 dose of study drug. The most common reason for screen failure was patients not meeting criteria for study enrolment based on migraine headache information collected in the ePRO diary during the prospective baseline phase. A total of 129 patients (14.1%) discontinued from the double-blind treatment phase. The most frequent reason for discontinuing from double-blind treatment was withdrawal by patient, which occurred in 8.5% of the placebo arm, 4.8% of the galcanezumab 120 mg arm, and 6.3% of the galcanezumab 240 mg arm. Overall, 68.5% of patients entered the post-treatment phase of the study as of the data cut-off date of March 29, 2017, for the final efficacy analyses for the double-blind treatment phase.
Patient disposition in the REGAIN trial is summarized in Table 15. A total of 1,903 patients were screened, and 1,117 patients were randomized: 558 to placebo, 278 to galcanezumab 120 mg, and 277 to galcanezumab 240 mg, with 4 excluded from the study’s ITT population because they did not receive at least 1 dose of study drug. Overall, 93.2% of patients completed the double-blind treatment phase, with 91.0% completing the placebo arm, 94.6% the galcanezumab 120 mg arm, and 96.0% the galcanezumab 240 mg arm. The most frequent reason for discontinuing from the double-blind treatment phase was withdrawal by patient (3.4% placebo, 1.4% galcanezumab 120 mg, and 2.5% galcanezumab 240 mg). Of the patients who completed the double-blind treatment phase, 98.5% entered the optional open-label treatment phase as of the data cut-off date of March 16, 2017, for the final efficacy analyses for the double-blind treatment phase.
Patient disposition in the CONQUER trial is summarized in Table 16. A total of 610 patients were screened, and 463 patients were randomized: 230 to placebo and 232 to galcanezumab 120 mg. One patient who was a screen failure was inadvertently randomized and immediately discontinued. A total of 462 randomized patients received at least 1 dose of study drug and were included in the ITT population. Overall, 97.6% of patients completed the double-blind treatment phase. The most frequent reason for discontinuing from the double-blind treatment phase was protocol deviation (1.7% galcanezumab and 0.4% placebo). Of the patients who completed the double-blind treatment phase, 99.6% entered the optional open-label treatment phase as of the data cut-off date of June 19, 2019, for the final efficacy analyses for the double-blind treatment phase.
Table 14: Patient Disposition — EVOLVE-1 and EVOLVE-2 Trials
Disposition | EVOLVE-1 | EVOLVE-2 | ||||
|---|---|---|---|---|---|---|
Placebo | GMB 120 mg | GMB 240 mg | Placebo | GMB 120 mg | GMB 240 mg | |
Screened, N | 1,671 | 1,696 | ||||
Randomized, N | 433 | 213 | 212 | 461 | 231 | 223 |
Discontinued from DB treatment phase, n (%) | 82 (18.94) | 36 (16.90) | 37 (17.45) | 74 (16.05) | 28 (12.12) | 27 (12.11) |
Adverse events | 10 (2.31) | 9 (4.23) | 7 (3.30) | 8 (1.74) | 5 (2.16) | 9 (4.04) |
Lack of efficacy | 10 (2.31) | 1 (0.47) | 2 (0.94) | 6 (1.30) | 1 (0.43) | 1 (0.45) |
Lost to follow-up | 18 (4.16) | 9 (4.23) | 5 (2.36) | 10 (2.17) | 7 (3.03) | 0 |
Physician decision | 7 (1.62) | 3 (1.41) | 2 (0.94) | 4 (0.87) | 0 | 2 (0.90) |
Pregnancy | 2 (0.46) | 1 (0.47) | 3 (1.42) | 1 (0.22) | 2 (0.87) | 0 |
Protocol deviation | 2 (0.46) | 2 (0.94) | 2 (0.94) | 5 (1.08) | 2 (0.87) | 1 (0.45) |
Terminated by sponsor | 0 | 0 | 0 | 1 (0.22) | 0 | 0 |
Withdrawal by patient | 33 (7.62) | 11 (5.16) | 16 (7.55) | 39 (8.46) | 11 (4.76) | 14 (6.28) |
Completed DB treatment phase, n (%) | 351 (81.06) | 177 (83.10) | 175 (82.55) | 387 (83.95) | 203 (87.88) | 195 (87.44) |
Entered post-treatment phase, n (%) | 282 (65.13) | 145 (68.08) | 140 (66.04) | 292 (63.34) | 156 (67.53) | 155 (69.51) |
Modified ITT, N | 433 | 213 | 212 | 461 | 231 | 223 |
Safety, N | 432 | 206 | 220 | 461 | 226 | 228 |
DB = double-blind; GMB = galcanezumab; ITT = intention-to-treat.
Note: As of the data cut-off dates for the final efficacy analyses for the double-blind treatment phase (EVOLVE-1: March 22, 2017; EVOLVE-1: March 29, 2017).
Source: EVOLVE-1 Clinical Study Report9 and EVOLVE-2 Clinical Study Report.10
Table 15: Patient Disposition — REGAIN Trial
Disposition | REGAIN | ||
|---|---|---|---|
Placebo | GMB 120 mg | GMB 240 mg | |
Screened, N | 1,903 | ||
Randomized, N | 558 | 278 | 277 |
Discontinued from DB treatment phase, n (%) | 49 (8.78) | 15 (5.40) | 11 (3.97) |
Adverse events | 6 (1.08) | 3 (1.08) | 2 (0.72) |
Lack of efficacy | 4 (0.72) | 0 | 0 |
Lost to follow-up | 10 (1.79) | 4 (1.44) | 1 (0.36) |
Physician decision | 2 (0.36) | 1 (0.36) | 1 (0.36) |
Pregnancy | 2 (0.36) | 2 (0.72) | 0 |
Protocol deviation | 6 (1.08) | 1 (0.36) | 0 |
Withdrawal by patient | 19 (3.41) | 4 (1.44) | 7 (2.53) |
Completed DB treatment phase, n (%) | 508 (91.04) | 263 (94.60) | 266 (96.03) |
Entered OL phase, n (%) | 501 (89.78) | 259 (93.17) | 261 (94.22) |
Discontinued from OL phase, n (%) | 55 (10.98) | 35 (13.51) | 35 (13.41) |
Adverse events | 15 (2.99) | 6 (2.32) | 10 (3.83) |
Lack of efficacy | 10 (2.00) | 7 (2.70) | 9 (3.45) |
Lost to follow-up | 8 (1.60) | 3 (1.16) | 4 (1.53) |
Pregnancy | 1 (0.20) | 2 (0.77) | 1 (0.38) |
Protocol Deviation | 3 (0.60) | 4 (1.54) | 1 (0.38) |
Withdrawal by patient | 18 (3.59) | 13 (5.02) | 10 (3.83) |
Modified ITT, N | 558 | 278 | 277 |
Safety, N a | 558 | 273 | 282 |
DB = double-blind; GMB = galcanezumab; ITT = intention-to-treat; OL = open-label.
Note: As of the data cut-off date of March 16, 2017, for the final efficacy analyses for the double-blind treatment phase.
aThe safety population is based on modal treatment the patient received during the double-blind treatment phase.
Source: REGAIN Clinical Study Report.11
Table 16: Patient Disposition — CONQUER Trial
Disposition | CONQUER | |
|---|---|---|
Placebo | GMB 120 mg | |
Screened, N | 610 | |
Randomized, N | 230 | 232 |
Discontinued DB treatment phase, n (%) | 4 (1.74) | 7 (3.02) |
Patient decision | 2 (0.87) | 1 (0.43) |
Protocol deviation | 1 (0.43) | 4 (1.72) |
Lack of efficacy | 1 (0.43) | 1 (0.43) |
Adverse event | 0 | 1 (0.43) |
Completed DB treatment phase, n (%) | 226 (98.3) | 225 (97.0) |
Entered OL phase, n (%) | 225 (97.8) | 224 (96.6) |
Discontinued from OL phase, n (%) | 10 (4.44) | 5 (2.23) |
Patient decision | 3 (1.33) | 0 |
Protocol deviation | 2 (0.89) | 0 |
Lack of efficacy | 3 (1.33) | 2 (0.89) |
Adverse event | 1 (0.44) | 2 (0.89) |
Lost to follow-up | 1 (0.44) | 0 |
Physician decision | 0 | 1 (0.45) |
Modified ITT, N | 230 | 232 |
Safety, N | 230 | 232 |
DB = double-blind; GMB = galcanezumab; ITT = intention-to-treat; OL = open-label.
Note: As of the data cut-off date of June 19, 2019, for the final efficacy analyses for the double-blind treatment phase.
Source: CONQUER Clinical Study Report.12
Exposure to Study Treatments
Exposure to study treatments during the double-blind treatment phases of the 4 pivotal trials is summarized in Table 17.
Most patients in the EVOLVE-1 and EVOLVE-2 trials, which included a 6-month double-blind treatment phase, received 6 doses of the study drug (> 82% in all treatment arms). Most patients in the REGAIN and CONQUER trials, which had a 3-month double-blind treatment phase, received 3 doses of the study drug (> 92% in both arms of the REGAIN trial, > 97% in both arms of the CONQUER trial).
As of the data cut-off for the REGAIN trial’s Clinical Study Report Addendum,13 the mean duration of exposure to the study drug in the open-label treatment phase (which does not include exposure in the double-blind treatment phase) was 239.5 days. Approximately 80.9% of patients (N = 827) received all 9 doses of open-label galcanezumab. A total of 1,013 patients (99.3%) received the loading dose of 240 mg galcanezumab at visit 7 (first injection of open-label treatment phase) as per protocol. Seven patients received only 1 injection at visit 7, and 2 patients did not receive any injection at visit 7. All patients (100%) who continued to visit 8 received 1 injection (120 mg galcanezumab) at visit 8, as per protocol. Most patients received 2 injections (240 mg) at the flexibly dosed visits, ranging from 64.3% of patients (at visit 9) to 75.0% (at visit 14).
As of the data cut-off for the CONQUER trial’s Clinical Study Report Addendum,13 the mean duration of exposure to galcanezumab in the galcanezumab-treated population was 130.1 days. The most common number of galcanezumab doses received was either 3 or 6 doses (47.5% and 47.7%, respectively).
Table 17: Exposure to Study Treatments — Double-Blind Treatment phase, Safety Population
Exposure | EVOLVE-1 | EVOLVE-2 | REGAIN | CONQUER | ||||
|---|---|---|---|---|---|---|---|---|
Placebo N = 432 | GMB 120 mg N = 206 | Placebo N = 461 | GMB 120 mg N = 226 | Placebo N = 557 | GMB 120 mg N = 273 | Placebo N = 230 | GMB 120 mg N = 232 | |
Mean duration of exposure (SD), days | 162.53 (36.89) | 168.47 (30.68) | 164.56 (40.69) | 171.92 (23.79) | 86.82 (14.89) | 88.66 (8.27) | 88.61 (8.09) | 87.10 (9.95) |
Doses received, n (%) | ||||||||
1 | 12 (2.78) | 0 | 24 (5.21) | 0 | 27 (4.84) | 0 | 1 (0.43) | 4 (1.72) |
2 | 24 (5.56) | 10 (4.85) | 17 (3.69) | 7 (3.10) | 15 (2.69) | 9 (3.30) | 2 (0.87) | 2 (0.86) |
3 | 14 (3.24) | 4 (1.94) | 16 (3.47) | 4 (1.77) | 516 (92.47) | 264 (96.70) | 227 (98.70) | 226 (97.41) |
4 | 13 (3.01) | 7 (3.40) | 7 (1.52) | 5 (2.21) | NA | NA | NA | NA |
5 | 11 (2.55) | 6 (2.91) | 5 (1.08) | 7 (3.10) | NA | NA | NA | NA |
6 | 357 (82.64) | 179 (86.89) | 392 (85.03) | 203 (89.82) | NA | NA | NA | NA |
GMB = galcanezumab; NA = not applicable; SD = standard deviation.
Source: EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 REGAIN Clinical Study Report,11 and CONQUER Clinical Study Report.12
Adherence With the ePRO Diary
In the EVOLVE-1 and EVOLVE-2 trials, a majority of patients (> 80%) completed at least 80% of their daily diary entries at each month during the double-blind treatment phase. In the EVOLVE-1 trial, mean compliance with the ePRO diary averaged over the 6-month treatment phase was similar across treatment groups (89.8% for placebo, 91.9% for galcanezumab 120 mg, and 90.8% for galcanezumab 240 mg). In the EVOLVE-2 trial, mean compliance with the ePRO diary averaged over the 6-month treatment phase was similar across treatment groups (91.3% for placebo, 90.9% for galcanezumab 120 mg, and 92.7% for galcanezumab 240 mg).
In the REGAIN trial, most patients (> 85%) completed at least 80% of their daily diary entries at each month during the double-blind treatment phase. Mean compliance with the ePRO diary averaged over the 3-month double-blind treatment phase was 91.0% for the placebo group and 91.8% for the galcanezumab 120 mg group.
In the CONQUER trial, > 93% of patients completed at least 80% of their daily ePRO diary entries during each month of the double-blind treatment phase. Mean compliance with the ePRO diary averaged over the 3-month double-blind treatment phase was approximately 96% in both treatment groups.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported. Efficacy data are not presented for the galcanezumab 240 mg arm of the EVOLVE-1, EVOLVE-2, and REGAIN trials because this dose is not aligned with the Health Canada–approved dose.
Results for the key efficacy outcomes for the EVOLVE-1 and EVOLVE-2 trial are summarized in Table 18. Results for the key efficacy outcomes for the REGAIN trial are summarized in Table 20. Results for the key efficacy outcomes for the CONQUER trial are summarized in Table 23.
Health-Related Quality of Life
Migraine-Specific Quality of Life Questionnaire Version 2.1
In the EVOLVE-1 and EVOLVE-2 trials, the mean change from baseline in the MSQ v2.1 RF-R domain score during months 4 to 6 (the final 3 months of double-blind treatment) was a key secondary outcome and controlled for multiplicity. In the EVOLVE-1 trial, the mean change from baseline in the MSQ RF-R during months 4 to 6 was 7.74 points greater in the galcanezumab 120 mg group compared with placebo (95% CI, 5.20 to 10.28; P < 0.001). Similarly, in the EVOLVE-2 trial, the mean change from baseline in the MSQ RF-R during months 4 to 6 was 8.82 points greater in the galcanezumab 120 mg group compared with placebo (95% CI, 6.33 to 11.31; P < 0.001).
In the REGAIN trial, the mean change from baseline in the MSQ RF-R at month 3 was a key secondary outcome and controlled for multiplicity. The mean numerical change from baseline in the MSQ RF-R at month 3 was 5.06 points greater in the galcanezumab 120 mg arm compared to placebo (95% CI, 2.12 to 7.99). The galcanezumab 120 mg arm could not be tested for statistical significance based on the predefined multiple-testing procedure because of a previously failed end point in the testing sequence (75% response rate; Figure 21 and Figure 22 in Appendix 3). Results of a post hoc exploratory subgroup analysis for the number of failed prophylactic treatments (≥ 2 versus ≥ 3) are summarized in Table 22. The results of this analysis were consistent with the analysis of overall change in the MSQ RF-R from baseline to month 3 in the ITT population.
In the CONQUER trial, the mean change from baseline in the MSQ RF-R at month 3 in the ITT population was a key secondary outcome and controlled for multiplicity. The mean change from baseline in MSQ RF-R at month 3 was 12.53 points greater in the galcanezumab group compared with placebo (95% CI, 9.19 to 15.87; P < 0.0001). The results of a planned subgroup analysis in patients with 3 or more prior preventive-medication category failures are summarized in Table 25, and are consistent with the ITT population.
EQ-5D 5-Levels Questionnaire
The EQ-5D-5L was not assessed in the EVOLVE-1, EVOLVE-2, and REGAIN trials. In the CONQUER trial, the LS mean change from baseline to the LOCF end point in EQ VAS scores was 3.38 (95% CI, not reported; SE = 1.31). The outcome was a secondary end point, but was not controlled for multiplicity.
Headache Symptoms
Migraine Headache Days with Symptoms
The overall change from baseline in number of monthly MHDs with symptoms during the double-blind treatment phase was an exploratory outcome in all pivotal trials. These outcomes were not controlled for multiplicity within the trials’ multiple-testing procedures.
In the EVOLVE-1 trial, the mean change difference from baseline in the galcanezumab 120 mg arm compared to placebo was −0.74 days (95% CI, −1.10 to −0.39) for nausea and/or vomiting, −1.39 days (95% CI, −1.90 to −0.89) for photophobia and phonophobia, −0.43 days (95% CI, −0.70 to −0.16) for aura, and −0.61 days (95% CI, −0.93 to −0.28) for prodromal symptoms other than aura.
In the EVOLVE-2 trial, the mean change difference from baseline in the galcanezumab 120 mg arm compared to placebo was −1.14 days (95% CI, −1.50 to −0.79) for nausea and/or vomiting, −1.76 days (95% CI, −2.25 to −1.27) for photophobia and phonophobia, −0.48 days (95% CI, −0.81 to −0.16) for aura, and −0.83 days (95% CI, −1.18 to −0.47) for prodromal symptoms other than aura.
In the REGAIN trial, the mean change difference from baseline in the galcanezumab 120 mg arm compared placebo was −1.21 days (95% CI, −1.82 to −0.59) for nausea and/or vomiting, −1.56 days (95% CI, −2.37 to −0.75) for photophobia and phonophobia, 0.03 days (95% CI, −0.53 to 0.58) for aura, and −0.66 (95% CI, −1.29 to −0.02) days for prodromal symptoms other than aura.
In the CONQUER trial, the mean change difference from baseline in the galcanezumab 120 mg arm compared to placebo was |||||||||||||||||||||||||||||||||||| for nausea and/or vomiting, |||||||||||||||||||||||||||||||||||||||| for photophobia and phonophobia, ||||||||||||||||||||||||||||||| for aura, and ||||||||||||||||||||||||||| for prodromal symptoms other than aura.
Other Patient-Reported Outcomes
Migraine Disability Assessment
Change in the MIDAS total score from baseline was a secondary outcome in all pivotal trials. This outcome was not controlled for multiplicity within the trials’ multiple-testing procedures.
In the EVOLVE-1 trial, the mean change from baseline to the end of double-blind treatment (month 6) was −6.29 points (95% CI, −9.45 to −3.13), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to the placebo arm.
In the EVOLVE-2 trial, the mean change from baseline to the end of double-blind treatment (month 6) was −9.15 points (95% CI, −12.61 to −5.69), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to the placebo arm.
In the REGAIN trial, the mean change from baseline to LOCF end point was −8.74 points (95% CI, −16.39 to −1.08), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to the placebo arm. The mean change from baseline to the end of double-blind treatment (month 3) was −8.74 (95% CI, −16.39 to −1.08), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to the placebo arm.
In the CONQUER trial, the mean change from baseline to LOCF end point was −17.8 points (95% CI, −25.6 to −10.0), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to the placebo arm.
4-item Migraine Interictal Burden Scale
The MIBS-4 was not assessed in the EVOLVE-1, EVOLVE-2, and REGAIN trials.
In the CONQUER trial, change in the MIBS-4 total score was assessed as a secondary outcome. The outcome was not included in the CONQUER trial’s multiple-testing procedure and therefore not controlled for multiplicity. The mean change in MIBS-4 total score from baseline during the double-blind treatment period was −1.06 points (95% CI, −1.58 to −0.54), indicating a numerically greater reduction in the galcanezumab arm compared to the placebo arm.
Patient Health Questionnaire-9
The PHQ-9 was not assessed in the EVOLVE-1, EVOLVE-2, and REGAIN trials.
In the CONQUER trial, the PHQ-9 was an exploratory outcome. The outcome was not included in the CONQUER trial’s multiple-testing procedure. The mean change in PHQ-9 total score from baseline to LOCF end point in the double-blind treatment period was −2.12 (SE = 0.32) in the galcanezumab arm compared to −1.13 (SE = 0.31) in the placebo arm.
Generalized Anxiety Disorder 7-Item
The GAD-7 was not assessed in the EVOLVE-1, EVOLVE-2, and REGAIN trials.
In the CONQUER trial, the GAD-7 was an exploratory outcome. The outcome was not included in the CONQUER trial’s multiple-testing procedure. The mean change from baseline to LOCF end point for the GAD-7 total score was |||||||||||||||||| in the galcanezumab arm and |||||||||||||||||| in the placebo arm.
Headache or Migraine Frequency
Number of Monthly Migraine Headache Days
The overall change from baseline in the number of monthly MHDs during the double-blind treatment phase was the primary outcome and included in the multiple-testing procedure in each of the pivotal trials. Galcanezumab 120 mg was associated with a statistically significant greater reduction in the overall LS mean change from baseline in the number of monthly MHDs during the double-blind treatment phase compared to placebo in all 4 trials.
EVOLVE-1 and EVOLVE-2: In the EVOLVE-1 trial, the overall mean change from baseline in the number of monthly MHDs during the double-blind treatment phase was −1.92 days (95% CI, −2.48 to −1.37; P < 0.001), indicating a greater reduction in the galcanezumab 120 mg arm compared to placebo. Results of all sensitivity analyses were consistent with the primary efficacy analysis.
In the EVOLVE-2 trial, the overall mean change from baseline in the number of monthly MHDs during the double-blind treatment phase was −2.02 days (95% CI, −2.55 to −1.48; P < 0.001), indicating a greater reduction in the galcanezumab 120 mg arm compared to placebo. Results of all sensitivity analyses were consistent with the primary efficacy analysis.
Results of the subgroup analyses conducted for overall change in monthly MHDs in the EVOLVE-1 and EVOLVE-2 are summarized in Table 19. The results of these subgroup analyses (baseline number of monthly MHDs [< 8 versus ≥ 8], failed 2 or more prophylactic treatments [yes versus no], baseline headache medication overuse [yes versus no]) were consistent with the results of the primary analysis. The subgroup analyses were not included in the multiple-testing procedure. The analysis of the subgroup of patients who failed 3 or more prophylactic treatments was a post hoc exploratory analysis.
REGAIN: In the REGAIN trial, the overall mean change from baseline in the number of monthly MHDs during the double-blind treatment phase was −2.09 days (95% CI, −2.92 to −1.26; P < 0.001), indicating a greater reduction in the galcanezumab 120 mg arm compared to placebo. Results of all sensitivity analyses were consistent with the primary efficacy analysis.
Results of the subgroup analyses conducted for overall change in monthly MHDs in the REGAIN trial are summarized in Table 21. The results of these subgroup analyses (failed 2 or more prophylactic treatments [yes versus no], failed 3 or more prophylactic treatments [yes versus no], baseline headache medication overuse [yes versus no]) were consistent with the results of the primary analysis. The subgroup analyses were not included in the multiple-testing procedure. The subgroup analyses of those who failed 2 or more prophylactic treatments (yes versus no) and baseline headache medication overuse (yes versus no) were specified a priori. The analysis of the subgroups that failed 3 or more prophylactic treatments (yes versus no) was a post hoc exploratory analysis.
CONQUER: In the CONQUER trial, the overall mean change from baseline in the number of monthly MHDs in the ITT population during the double-blind treatment phase was −3.12 days (95% CI, −3.92 to −2.32; P < 0.0001), indicating a greater reduction in the galcanezumab arm compared to placebo. Results of all sensitivity analyses were consistent with the primary efficacy analysis.
Planned subgroup analyses were conducted for baseline migraine frequency category and number of prior preventive medication category failures. Results, which are summarized in Table 24 and Table 25, were consistent with the primary analysis.
Number of Monthly Headache Days
The overall change from baseline in number of monthly headache days was a secondary outcome in the 4 pivotal trials. This outcome was not included in the trials’ multiple-testing procedures and was not adjusted for multiplicity.
In the EVOLVE-1 trial, the overall mean change from baseline in the number of monthly headache days during the double-blind treatment phase was −1.66 days (95% CI, −2.25 to −1.07), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to placebo.
In the EVOLVE 2 trial, the overall mean change from baseline in the number of monthly headache days during the double-blind treatment phase was −2.00 days (95% CI, −2.58 to −1.42), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to placebo.
In the REGAIN trial, the overall mean change from baseline in the number of monthly headache days during the double-blind treatment phase was −1.84 days (95% CI, −2.65 to −1.02), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to placebo.
In the CONQUER trial, the overall mean change from baseline in the number of monthly headache days in the ITT population during the double-blind treatment phase was −3.13 days (95% CI, −3.96 to −2.29), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to placebo.
Acute Headache Pain Medication Intake
In the EVOLVE-1, EVOLVE-2, and REGAIN trials, the overall change from baseline in monthly MHDs with acute medication use during the double-blind treatment phase was a key secondary outcome and included in the trials’ multiple-testing procedures.
In the EVOLVE-1 trial, the overall mean change was −1.81 days (95% CI, −2.28 to −1.33; P < 0.001), indicating a greater reduction in the galcanezumab 120 mg arm versus the placebo arm.
In the EVOLVE-2 trial, the overall mean change was −1.82 days (95% CI, −2.29 to −1.36; P < 0.001), indicating a greater reduction in the galcanezumab 120 mg arm compared to the placebo arm.
In the REGAIN trial, the overall mean change was −2.51 days (95% CI, −3.27 to −1.76), indicating a numerically greater reduction in the galcanezumab 120 mg arm compared to the placebo arm. The difference between the galcanezumab 120 mg and placebo arms could not be tested for statistical significance based on the predefined multiple-testing procedure because of a previously failed end point in the testing sequence (75% response rate; Figure 21 and Figure 22 in Appendix 3). Results of a post hoc exploratory subgroup analysis for the number of failed prophylactic treatments (≥ 2 versus ≥ 3) are summarized in Table 22. The results of this analysis were consistent with the analysis of overall change in MHDs with acute migraine medication use from baseline in the ITT population.
In the CONQUER trial, the overall change from baseline in MHDs with acute medication use during the double-blind treatment phase was a secondary outcome. The outcome was not included in the trial’s multiple-testing procedure, and therefore is not adjusted for multiplicity. The overall mean change from baseline in the number of monthly days with acute headache medication intake during the double-blind treatment phase was −3.40 days (95% CI, −4.14 to −2.65), indicating a numerically greater reduction in the galcanezumab arm compared to the placebo arm. The results of a planned subgroup analysis in patients with 3 or more prior preventive-medication category failures are summarized in Table 25, and are consistent with the results observed in the ITT population.
Duration of Effect and Re-Treatment Intervals
Time to First Loss of Response in the Post-Treatment phase
In the EVOLVE-1 and EVOLVE-2 trials, time to first loss of response among patients who met the 50% response rate criteria during their last month of double-blind treatment was a secondary outcome. This outcome was not controlled for multiplicity. Time to the first loss of 50% response in patients who were 50% responders at the last month of double-blind treatment and who entered the post-treatment phase in the EVOLVE-1 trial is shown in Figure 8. In the EVOLVE-1 study, approximately half of the patients in all treatment groups had first loss of 50% response by 4 months after the end of the double-blind treatment phase.13
Time to the first loss of 50% response in patients who were 50% responders at the last month of double-blind treatment and who entered the post-treatment phase in the EVOLVE-2 trial is shown in Figure 9. In the EVOLVE-2 study, approximately half of the patients in all treatment groups had first loss of 50% response by 4 months after the end of the double-blind treatment phase.13
In the REGAIN trial, time to first loss of response among patients who met the 50% response rate criteria during their last month of treatment (double-blind or open-label phase) was a secondary outcome. This outcome was not controlled for multiplicity. Time to the first loss of 50% response in patients who were 50% responders at the last month of double-blind treatment and who entered the post-treatment phase in the REGAIN trial is shown in Figure 10. In the REGAIN study, the percentage of patients with first loss of 50% response at month 1 of the post-treatment phase was 24.3%.13 By month 4 of the post-treatment phase, 48.2% patients had first loss of 50% response.
The CONQUER study design did not include a post-treatment follow-up phase; thus, time to first loss of response after stopping treatment was not assessed.
Figure 8: Time to First Loss of 50% Response After Double-Blind Treatment — EVOLVE-1 Trial, Patients Who Were 50% Responders at the Last Month of Double-Blind Treatment and Who Entered the Post-Treatment phase
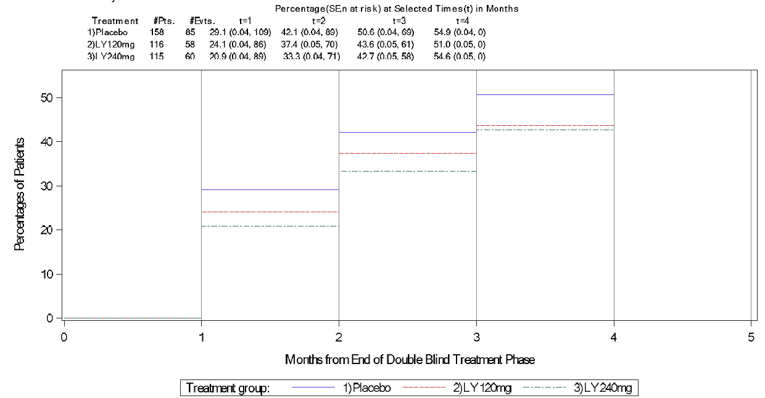
Evts = events; LY = galcanezumab; Pts = patients; SE = standard error; t = times.
Note: This analysis only includes patients who were 50% responders at the last month of double-blind treatment and who entered the post-treatment phase. Patients who were sustained 50% responders during the entire post-treatment follow-up phase are censored.
Source: EVOLVE-1 Clinical Study Report Addendum.13
Figure 9: Time to First Loss of 50% Response After Double-Blind Treatment — EVOLVE-2 Trial, Patients Who Were 50% Responders at the Last Month of Double-Blind Treatment and Who Entered the Post-Treatment phase
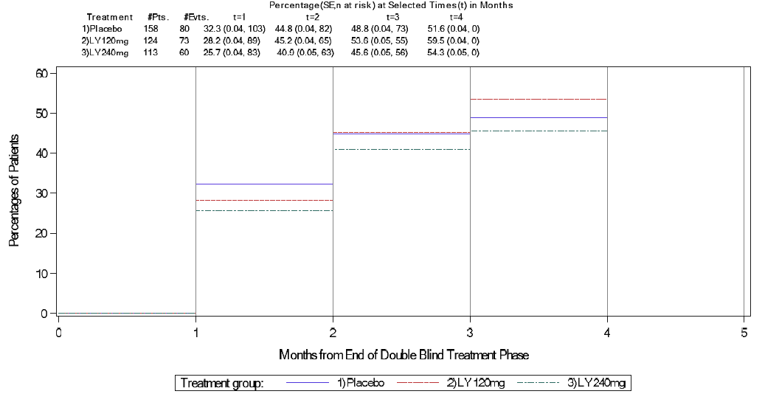
Evts = events; LY = galcanezumab; Pts = patients; SE = standard error; t = times.
Note: This analysis only includes patients who were 50% responders at the last month of double-blind treatment and who entered the post-treatment phase. Patients who are sustained 50% responders during the entire post-treatment follow-up phase are censored.
Source: EVOLVE-2 Clinical Study Report Addendum.13
Figure 10: Time to First Loss of 50% Response After Galcanezumab Treatment — REGAIN, Patients Who Were 50% Responders in the Last Month of Treatment Before Entering the Post-Treatment phase
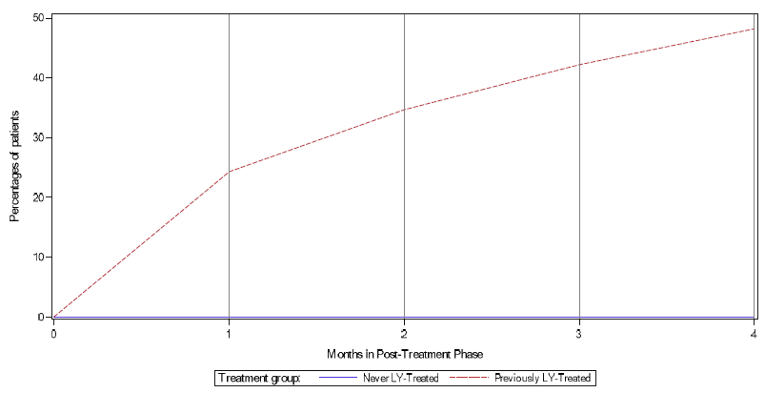
LY = galcanezumab.
Note: This analysis only includes patients who are 50% responders in the last month of treatment before entering the post-treatment phase. Patients who maintained 50% response during the entire post-treatment phase were censored at the end of the post-treatment phase.
Source: REGAIN Clinical Study Report Addendum.13
Time to Initiation of a Migraine-Prevention Treatment in Post-Treatment phase
Time to initiation of treatment with a migraine-prevention medication in the post-treatment follow-up phase was a secondary outcome in the EVOLVE-1, EVOLVE-2, and REGAIN trials. The outcome was not controlled for multiplicity.
Time to initiation of migraine-preventive medication during the post-treatment phase of the EVOLVE-1 trial is shown in Figure 11. In the EVOLVE-1 study, 12 patients (< 2%) initiated treatment with a migraine-prevention medication.13
Time to initiation of migraine-preventive medication during the post-treatment phase of the EVOLVE-2 trial is shown in Figure 12. In the EVOLVE-2 study, 3.2% of patients in the placebo arm initiated treatment with a migraine-prevention medication compared with 1.4% patients in the galcanezumab 120 mg arm.13
Time to initiation of migraine-preventive medication during the post-treatment phase of the REGAIN trial is shown in Figure 13. In the REGAIN study, 5.7% of patients who entered the post-treatment follow-up phase started a migraine-preventive medication during the post-treatment period.13
The CONQUER study design did not include a post-treatment follow-up phase; thus, time to initiation of a migraine-prevention treatment in after stopping galcanezumab treatment was not assessed.
Figure 11: Time to Initiation of Preventive Treatment After Double-Blind Treatment — EVOLVE-1, Patients Who Entered Post-Treatment Follow-Up
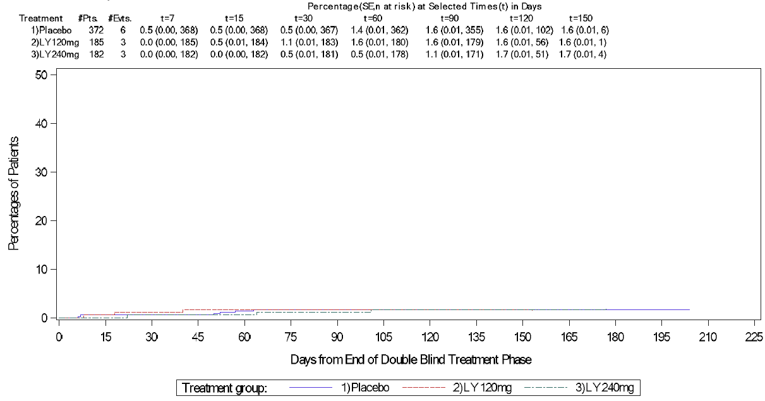
Evts = events; LY = galcanezumab; Pts = patients; SE = standard error; t = times.
Note: This analysis only includes patients who entered the post-treatment phase. Patients who never started preventive treatment are censored.
Source: EVOLVE-1 Clinical Study Report Addendum.13
Figure 12: Time to Initiation of Preventive Treatment After Double-Blind Treatment — EVOLVE-2, Patients Who Entered Post-Treatment Follow-Up
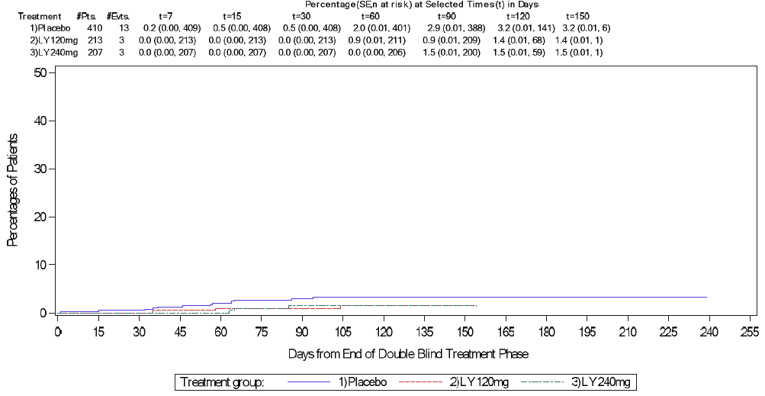
Evts = events; LY = galcanezumab; Pts = patients; SE = standard error; t = times.
Note: This analysis only includes patients who entered the post-treatment phase. Patients who never started preventive treatment are censored.
Source: EVOLVE-2 Clinical Study Report Addendum.13
Figure 13: Time to Initiation of Preventive Treatment After Galcanezumab Treatment — REGAIN, Patients Who Entered Post-Treatment Follow-up
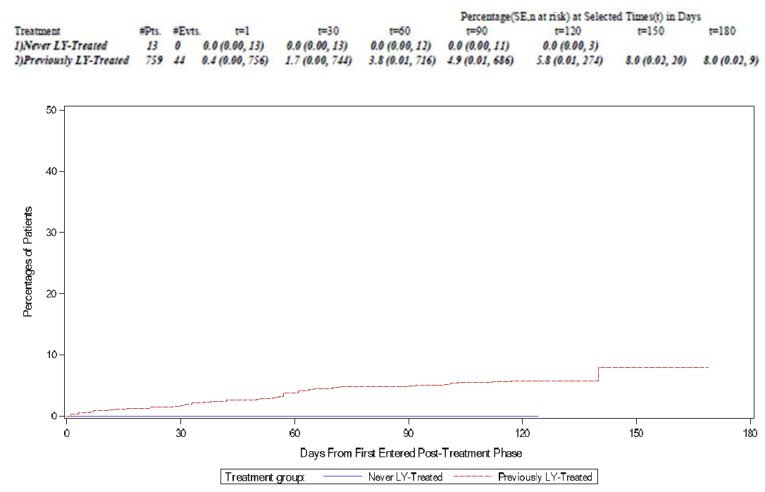
Evts = events; LY = galcanezumab; Pts = patients; SE = standard error; t = times.
Note: This analysis only includes patients who entered the post-treatment phase. Patients who never started preventive treatment are censored.
Source: REGAIN Clinical Study Report Addendum.13
Health Care Resource Utilization and Employment Status
The EVOLVE-1 and EVOLVE-2 trials did not assess HCRU and employment status; both were secondary outcomes in the REGAIN and CONQUER trials. The outcomes were not controlled for multiplicity.
In the REGAIN trial, the percentages of patients with health care professional visits related to migraine in the baseline period (6-month period before randomization) were 20.4% in the galcanezumab 120 mg arm and 18.3% in the placebo arm. Emergency room visits related to migraine were reported for 6.6% of patients in the galcanezumab 120 mg arm and 4.9% of patients in the placebo arm. Two patients (0.73%) in the galcanezumab arm and 4 patients (0.72%) in the placebo arm had an overnight hospital admission related to migraine during the baseline period. In the 3-month double-blind treatment period, the percentages of patients with health care professional visits related to migraine were 6.0% in the placebo group and 3.7% in the galcanezumab 120 mg group. Emergency room visits related to migraine were reported for 2.4% of placebo patients and 1.8% of galcanezumab 120 mg patients during the double-blind treatment phase. No patients had an overnight hospital admission related to migraine during the double-blind treatment period.
In the CONQUER trial, the percentages of patients with health care professional visits related to migraine during the 3-month double-blind treatment phase were |||| in the galcanezumab group and |||| in the placebo group. In the baseline period (i.e., | months before randomization), the percentages of patients with health care professional visits related to migraine were |||| in the placebo group and |||| in the galcanezumab group. Few patients had emergency room visits related to migraine (|||||||||||||||||||||||| |||| ||||||) or hospitalizations related to migraine (|||||||||||||||||||||||||||||||) during the double-blind treatment phase, and | |||||| had an overnight hospital admission related to migraine.
Because of the low rates of HCRU events and because of the different time periods assessed at baseline (a period of 6 months before randomization) and post-baseline in both the REGAIN and ||||||||||||||||||, rates for the migraine-related events were standardized per 100 patient-years. Migraine-related HCRU per 100 patient-years is summarized in Table 20 for the REGAIN trial and Table 23 for the CONQUER trial.
Patients’ employment status at month 0 and month 3 of the double-blind treatment phase is summarized in Table 20 for the REGAIN trial and Table 23 for the CONQUER trial.
Work Productivity and Activity Impairment Questionnaire
The WPAI questionnaire was not assessed in the EVOLVE-1, EVOLVE-2, and REGAIN trials.
In the CONQUER trial, change from baseline in the WPAI was a secondary outcome. The outcome was not controlled for multiplicity. The LS mean change from baseline to the LOCF end point and SE was reported for percent of activity impairment due to health, percent of impairment while working due to health (presenteeism), percent of overall work impairment due to health, and percent of work time missed due to health (absenteeism). The 95% CIs were not reported. The LS mean change for activity impairment was −20.71% (SE = 1.95%) and −8.64% (SE = 1.92%) in the galcanezumab and placebo arms, respectively. For presenteeism, the LS mean change (SE) was −12.50% (SE = 2.37%) and −2.56% (SE = 2.32%) in the galcanezumab and placebo arms, respectively. For overall work impairment, the LS mean change was −14.31% (SE = 2.51%) and −3.46% (SE = 2.41%) in the galcanezumab and placebo arms, respectively. For absenteeism, the LS mean change was −4.22% (SE = 1.29%) and −2.90% (SE = 1.24%) in the galcanezumab and placebo arms, respectively.
Table 18: Key Efficacy Findings — EVOLVE-1 and EVOLVE-2, Modified ITT Population, Double-Blind Treatment phase
Outcomes | EVOLVE-1 | EVOLVE-2 | ||
|---|---|---|---|---|
Placebo N = 433 | GMB 120 mg N = 213 | Placebo N = 461 | GMB 120 mg N = 231 | |
MSQ v2.1 mean change from baseline (average of months 4 to 6; secondary) – MMRM,a DB treatment phase | N = 377 | N = 189 | N = 396 | N = 213 |
MSQ v2.1 total score | ||||
LS mean change (95% CI) | 21.51 (19.50 to 23.52) | 28.85 (26.41 to 31.30) | 16.58 (14.90 to 18.26) | 25.03 (22.92 to 27.15) |
LS mean change difference vs. placebo (95% CI) | NA | 7.34 (4.91 to 9.77) | NA | 8.45 (6.13 to 10.78) |
P valueb | NA | < 0.001 | NA | < 0.001 |
MSQ v2.1 role function – restrictivec | ||||
LS mean change (95% CI) | 24.69 (22.59 to 26.79) | 32.43 (29.87 to 35.00) | 19.65 (17.85 to 21.45) | 28.47 (26.22 to 30.73) |
LS mean change difference vs. placebo (95% CI) | NA | 7.74 (5.20 to 10.28) | NA | 8.82 (6.33 to 11.31) |
P valueb | NA | < 0.001d | NA | < 0.001d |
MSQ v2.1 role function – preventive | ||||
LS mean change (95% CI) | 17.13 (15.30 to 18.97) | 22.69 (20.44 to 24.94) | 12.25 (10.64 to 13.86) | 20.09 (18.06 to 22.11) |
LS mean change difference vs. placebo (95% CI) | NA | 5.56 (3.31 to 7.80) | NA | 7.83 (5.61 to 10.06) |
P valueb | NA | < 0.001 | NA | < 0.001 |
MSQ v2.1 emotional function | ||||
LS mean change (95% CI) | 20.73 (18.26 to 23.21) | 29.03 (26.01 to 32.04) | 15.60 (13.64 to 17.57) | 24.10 (21.63 to 26.57) |
LS mean change difference vs. placebo (95% CI) | NA | 8.29 (5.30 to 11.28) | NA | 8.50 (5.78 to 11.22) |
P valueb | NA | < 0.001 | NA | < 0.001 |
Overall change from baseline in number of monthly MHDs with symptoms (exploratory) – MMRM,a DB treatment phase | N = 425 | N = 210 | N = 450 | N = 226 |
Nausea and/or vomiting | ||||
LS mean change from baseline | −1.17 (−1.48 to −0.86) | −1.91 (−2.29 to −1.54) | −0.87 (−1.14 to −0.61) | −2.02 (−2.35 to −1.69) |
LS mean change difference vs. placebo (95% CI) | NA | −0.74 (−1.10 to −0.39) | NA | −1.14 (−1.50 to −0.79) |
P valueb | NA | < 0.001 | NA | < 0.001 |
Photophobia and phonophobia | ||||
LS mean change from baseline | −2.10 (−2.55 to −1.66) | −3.50 (−4.03 to −2.96) | −1.47 (−1.84 to −1.10) | −3.22 (−3.69 to −2.76) |
LS mean change difference vs. placebo (95% CI) | NA | −1.39 (−1.90 to −0.89) | NA | −1.76 (−2.25 to −1.27) |
P valueb | NA | < 0.001 | NA | < 0.001 |
Aura | ||||
LS mean change from baseline | −0.96 (−1.19 to −0.72) | −1.39 (−1.67 to −1.11) | −0.97 (−1.21 to −0.73) | −1.45 (−1.75 to −1.15) |
LS mean change difference vs. placebo (95% CI) | NA | −0.43 (−0.70 to −0.16) | NA | −0.48 (−0.81 to −0.16) |
P valueb | NA | 0.002 | NA | 0.004 |
Prodromal symptoms other than aura | ||||
LS mean change from baseline | −1.23 (−1.51 to −0.95) | −1.83 (−2.18 to −1.49) | −1.01 (−1.28 to −0.75) | −1.84 (−2.17 to −1.51) |
LS mean change difference vs. placebo (95% CI) | NA | −0.61 (−0.93 to −0.28) | NA | −0.83 (−1.18 to −0.47) |
P valueb | NA | < 0.001 | NA | < 0.001 |
MIDAS total score mean change from baseline to month 6 (secondary) – MMRM,a DB treatment phase | N = 345 | N = 177 | N = 374 | N = 202 |
LS mean change from baseline (95% CI) | −14.87 (−17.55 to −12.19) | −21.16 (−24.39 to −17.93) | −12.02 (−14.51 to −9.53) | −21.17 (−24.27 to −18.07) |
LS mean change difference vs. placebo (95% CI) | NA | −6.29 (−9.45 to −3.13) | NA | −9.15 (−12.61 to −5.69) |
P valueb | NA | < 0.001 | NA | < 0.001 |
Headache or migraine frequency | NA | NA | NA | NA |
Overall change from baseline in monthly MHDs (primary)c – MMRM,a DB treatment phase | N = 425 | N = 210 | N = 450 | N = 226 |
LS mean change (95% CI) | −2.81 (−3.28 to −2.34) | −4.73 (−5.31 to −4.16) | −2.28 (−2.67 to −1.88) | −4.29 (−4.79 to −3.80) |
LS mean change difference vs. placebo (95% CI) | NA | −1.92 (−2.48 to −1.37) | NA | −2.02 (−2.55 to −1.48) |
P value | NA | < 0.001d | NA | < 0.001d |
Overall change from baseline in number of monthly headache days (secondary) – MMRM,a DB treatment phase | N = 425 | N = 210 | N = 450 | N = 226 |
LS mean change (95% CI) | −3.03 (−3.54 to −2.51 | −4.69 (−5.31 to −4.07) | −2.30 (−2.73 to −1.87) | −4.31 (−4.85 to −3.76) |
LS mean change difference vs. placebo (95% CI) | NA | −1.66 (−2.25 to −1.07) | NA | −2.00 (−2.58 to −1.42) |
P valueb | NA | < 0.001 | NA | < 0.001 |
Average change from baseline in number of monthly MHDs with acute headache medication use (secondary)c – MMRM,a DB treatment phase | N = 425 | N = 210 | N = 450 | N = 226 |
LS mean change (95% CI) | −2.15 (−2.56 to −1.74) | −3.96 (−4.46 to −3.46) | −1.85 (−2.20 to −1.50) | −3.67 (−4.11 to −3.23) |
LS mean change difference vs. placebo (95% CI) | NA | −1.81 (−2.28 to −1.33) | NA | −1.82 (−2.29 to −1.36) |
P value | NA | < 0.001d | NA | < 0.001d |
Duration of effect and re-treatment intervals | NA | NA | NA | NA |
Time to initiation of a migraine-prevention medication – post-treatment follow-up phase | N = 372 | N = 185 | N = 410 | N = 213 |
Patients initiating migraine preventives, n (%) | 6 (1.6) | 3 (1.6) | 13 (3.2) | 3 (1.4) |
CI = confidence interval; DB = double-blind; GMB = galcanezumab; ITT = intention-to-treat; LS = least squares; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MMRM = mixed model for repeated measures; MSQ = Migraine-Specific Quality of Life Questionnaire version 2.1; NA = not applicable; vs. = versus.
aThe MMRM included the fixed, categorical effects of treatment, geographical region, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction. Estimates were obtained using unstructured covariance structure. The Kenward-Roger approximation was used to estimate denominator degrees of freedom.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
cOutcome included in the trial’s multiple-testing procedure.
dResults are statistically significant after adjustment for multiplicity.
Source EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 and Stauffer et al. (2019).43
Table 19: EVOLVE-1 and EVOLVE-2 Trials — Subgroup Analyses of Primary End Point, Modified ITT Population
Subgroup | Categories | Treatment group | n | LS mean change from baseline (95% CI) | LS mean change difference vs. placebo (95% CI) | P valuea |
|---|---|---|---|---|---|---|
Overall change in number of monthly MHDs – double-blind treatment phase, MMRM analysisb | ||||||
EVOLVE-1 | ||||||
Baseline number of monthly MHDs (a priori) | < 8 | Placebo | 145 | −1.35 (−2.01 to −0.68) | NA | NA |
GMB 120 mg | 73 | −2.94 (−3.73 to −2.15) | −1.59 (−2.29 to −0.89) | < 0.001 | ||
≥ 8 | Placebo | 280 | −3.59 (−4.22 to −2.97) | NA | NA | |
GMB 120 mg | 137 | −5.70 (−6.46 to −4.94) | −2.10 (−2.86 to −1.34) | < 0.001 | ||
Failed ≥ 2 prophylactic treatments (a priori) | Yes | Placebo | 22 | 0.47 (−2.10 to 3.05) | NA | NA |
GMB 120 mg | 10 | −0.65 (−4.01 to 2.71) | −1.12 (−4.49 to 2.25) | 0.505 | ||
No | Placebo | 403 | −2.97 (−3.45 to −2.48) | NA | NA | |
GMB 120 mg | 200 | −4.95 (−5.53 to −4.37) | −1.99 (−2.54 to −1.43) | < 0.001 | ||
EVOLVE-2 | ||||||
Baseline number of monthly MHDs (a priori) | < 8 | Placebo | 150 | −0.54 (−1.11 to 0.03) | NA | NA |
GMB 120 mg | 77 | −2.62 (−3.32 to −1.91) | −2.07 (−2.83 to −1.32) | < 0.001 | ||
≥ 8 | Placebo | 300 | −3.17 (−3.70 to −2.63) | NA | NA | |
GMB 120 mg | 149 | −5.15 (−5.83 to −4.48) | −1.99 (−2.70 to −1.27) | < 0.001 | ||
Failed ≥ 2 prophylactic treatments (a priori) | Yes | Placebo | 63 | −1.96 (−3.18 to −0.74) | NA | NA |
GMB 120 mg | 33 | −5.16 (−6.58 to −3.74) | −3.20 (−4.75 to −1.64) | < 0.001 | ||
No | Placebo | 387 | −2.35 (−2.81 to −1.90) | NA | NA | |
GMB 120 mg | 193 | −4.25 (−4.80 to −3.69) | −1.89 (−2.46 to −1.32) | < 0.001 | ||
EVOLVE-1 and EVOLVE-2 pooled | ||||||
Baseline headache medication overuse (post hoc) | Yes | Placebo | 169 | −2.7 (−3.7 to −1.7) | NA | NA |
GMB 120 mg | 74 | −6.3 (−7.5 to −5.1) | −3.6 (−4.7 to −2.4) | < 0.001 | ||
No | Placebo | 706 | −2.5 (−2.8 to −2.2) | NA | NA | |
GMB 120 mg | 362 | −4.1 (−4.5 to −3.7) | −1.6 (−2.0 to −1.2) | < 0.001 | ||
CI = confidence interval; GMB = galcanezumab; ITT = intention-to-treat; LS = least squares; MHD = migraine headache day; MMRM = mixed model for repeated measures; NA = not applicable.
aP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
bThe MMRM included the fixed, categorical effects of treatment, geographical region, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction.
Source: EVOLVE-1 Clinical Study Report,9 EVOLVE-2 Clinical Study Report,10 and Dodick et al. (2021).47
Table 20: Key Efficacy Findings — REGAIN, Modified ITT Population, Double-Blind Treatment phase
Outcomes | REGAIN | |
|---|---|---|
Placebo N = 558 | GMB 120 mg N = 278 | |
MSQ v2.1 mean CFB at month 3 (secondary) – MMRMa | N = 494 | N = 252 |
MSQ total score | ||
LS mean change (95% CI) | 14.55 (12.18 to 16.92) | 20.51 (17.59 to 23.44) |
LS mean change difference vs. placebo (95% CI) | NA | 5.96 (2.99 to 8.93) |
P valueb | NA | < 0.001 |
MSQ v2.1 role function – restrictivec | ||
LS mean change (95% CI) | 16.76 (14.44 to 19.07) | 21.81 (19.04 to 24.59) |
LS mean change difference vs. placebo (95% CI) | NA | 5.06 (2.12 to 7.99) |
P valueb | NA | < 0.001d |
MSQ v2.1 role function – preventive | ||
LS mean change (95% CI) | 10.98 (8.73 to 13.22) | 17.98 (15.20 to 20.76) |
LS mean change difference vs. placebo (95% CI) | NA | 7.00 (4.17 to 9.83) |
P valueb | NA | < 0.001 |
MSQ v2.1 emotional function | ||
LS mean change (95% CI) | 14.07 (11.04 to 17.10) | 21.03 (17.29 to 24.78) |
LS mean change difference vs. placebo (95% CI) | NA | 6.96 (3.16 to 10.76) |
P valueb | NA | < 0.001 |
Overall CFB in number of monthly MHDs with symptoms (exploratory) – MMRMa | N = 538 | N = 273 |
Nausea and/or vomiting | ||
LS mean change from baseline | −1.92 (−2.45 to −1.39) | −3.13 (−3.77 to −2.48) |
LS mean change difference vs. placebo (95% CI) | NA | −1.21 (−1.82 to −0.59) |
P valueb | NA | < 0.001 |
Photophobia and phonophobia | ||
LS mean change from baseline | −2.25 (−2.95 to −1.55) | −3.81 (−4.65 to −2.97) |
LS mean change difference vs. placebo (95% CI) | NA | −1.56 (−2.37 to −0.75) |
P valueb | NA | < 0.001 |
Aura | ||
LS mean change from baseline | −1.42 (−1.90 to −0.95) | −1.40 (−1.97 to −0.82) |
LS mean change difference vs. placebo (95% CI) | NA | 0.03 (−0.53 to 0.58) |
P valueb | NA | 0.922 |
Prodromal symptoms other than aura | ||
LS mean change from baseline | −1.15 (−1.69 to −0.60) | −1.81 (−2.47 to −1.15) |
LS mean change difference vs. placebo (95% CI) | NA | −0.66 (−1.29 to −0.02) |
P valueb | NA | 0.042 |
MIDAS total score (secondary) – ANCOVAe | N = 504 | N = 254 |
MIDAS total score mean change from baseline to LOCF end point | ||
LS mean change from baseline (95% CI) | −11.53 (−18.17 to −4.89) | −20.27 (−28.27 to −12.28) |
LS mean change difference vs. placebo (95% CI) | NA | −8.74 (−16.39 to −1.08) |
P valueb | NA | 0.025 |
MIDAS total score mean change from baseline to month 3 | ||
LS mean change from baseline (SE) | −11.53 (3.38) | −20.27 (4.07) |
LS mean change difference vs. placebo (95% CI) | NA | −8.74 (−16.39 to −1.08) |
P valueb | NA | 0.025 |
Headache or migraine frequency | ||
Overall change from baseline in monthly MHDs (primary)c – MMRM,a DB treatment phase | N = 538 | N = 273 |
LS mean change (95% CI) | −2.74 (−3.45 to −2.03) | −4.83 (−5.69 to −3.97) |
LS mean change difference vs. placebo (95% CI) | NA | −2.09 (−2.92 to −1.26) |
P value | NA | < 0.001f |
Overall CFB in number of monthly headache days (secondary) – MMRM,a DB treatment phase | N = 538 | N = 273 |
LS mean change (95% CI) | −3.01 (−3.70 to −2.31) | −4.84 (−5.69 to −4.00) |
LS mean change difference vs. placebo (95% CI) | NA | −1.84 (−2.65 to −1.02) |
P valued | NA | < 0.001 |
Average CFB in number of monthly MHDs with acute headache medication use (secondary)c – MMRMa | N = 538 | N = 273 |
LS mean change (95% CI) | −2.23 (−2.88 to −1.58) | −4.74 (−5.53 to −3.96) |
LS mean change difference vs. placebo (95% CI) | NA | −2.51 (−3.27 to −1.76) |
P value | NA | < 0.001d |
HCRU related to migraine in patient-years (secondary) | N = 533 | N = 269 |
Health care professional visits | ||
Baseline events per 100 patient-years | 110.69 | 102.60 |
Treatment events per 100 patient-years | 44.64 | 29.04 |
Emergency room visits | ||
Baseline events per 100 patient-years | 21.01 | 18.59 |
Treatment events per 100 patient-years | 13.86 | 13.76 |
Admissions to hospital | ||
Baseline events per 100 patient-years | 1.50 | 1.49 |
Treatment events per 100 patient-years | 0 | 0 |
Overnight hospital stays | NA | NA |
Baseline events per 100 patient-years | 4.88 | 2.97 |
Treatment events per 100 patient-years | 0 | 0 |
Employment status (secondary) | ||
Employment status at month 0 | N = 532 | N = 269 |
Working for pay, n (%) | 338 (63.53) | 182 (67.66) |
Student, n (%) | 30 (5.64) | 9 (3.35) |
Keeping house, n (%) | 42 (7.89) | 30 (11.15) |
Volunteer work, n (%) | 5 (0.94) | 3 (1.12) |
Unemployed, unrelated to study disease disability, n (%) | 37 (6.95) | 20 (7.43) |
Unemployed, due to study disease disability, n (%) | 17 (3.20) | 6 (2.23) |
Retired, n (%) | 30 (5.64) | 8 (2.97) |
Self-employed, n (%) | 33 (6.20) | 11 (4.09) |
Employment status at month 3 | N = 506 | N = 256 |
Working for pay, n (%) | 328 (61.65) | 182 (67.66) |
Student, n (%) | 27 (5.08) | 8 (2.97) |
Keeping house, n (%) | 42 (7.89) | 25 (9.29) |
Volunteer work, n (%) | 4 (0.75) | 2 (0.74) |
Unemployed, unrelated to study disease disability, n (%) | 29 (5.45) | 14 (5.20) |
Unemployed, due to study disease disability, n (%) | 12 (2.26) | 5 (1.86) |
Retired, n (%) | 34 (6.39) | 7 (2.60) |
Self-employed, n (%) | 30 (5.64) | 13 (4.83) |
ANCOVA = analysis of covariance; CFB = change from baseline; CI = confidence interval; GMB = galcanezumab; HCRU = health care resource utilization; ITT = intention-to-treat; LOCF = last observation carried forward; LS = least squares; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MMRM = mixed model for repeated measures; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; NA = not applicable; OL = open-label; vs. = versus.
aThe MMRM included the fixed, categorical effects of treatment, country, month, baseline medication overuse (yes vs. no), concurrent prophylaxis (yes vs. no), and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction. Estimates were obtained using unstructured covariance structure. The Kenward-Roger approximation was used to estimate denominator degrees of freedom.
bP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
cOutcome included in the trial’s multiple-testing procedure.
dP value is descriptive only because outcome could not be tested for statistical significance based on the predefined multiple-testing procedure due to a failed test for a previous end point in the testing sequence (Figure 21 and Figure 22 in Appendix 3).
eThe ANCOVA model contained the main effects of treatment, baseline medication overuse, concurrent prophylaxis use, and country, and included an appropriate baseline value as a covariate.
fResults are statistically significant after adjustment for multiplicity.
Source: REGAIN Clinical Study Report.11
Table 21: REGAIN Trial — Subgroup Analyses of Primary End Point, Modified ITT Population
Subgroup | Categories | Treatment group | n | LS mean change from baseline (95% CI) | LS mean change difference vs. placebo (95% CI) | P valuea |
|---|---|---|---|---|---|---|
Overall change in number of monthly MHDs (primary) – double-blind treatment phase, MMRMb | ||||||
Failed ≥ 2 prophylactic treatments (a priori) | Yes | Placebo | 161 | −1.44 (−2.66 to −0.22) | −4.48 (−5.93 to −3.02) | < 0.001 |
GMB 120 mg | 66 | −5.91 (−7.46 to −4.36) | ||||
No | Placebo | 377 | −3.69 (−4.53 to −2.85) | −1.13 (−2.10 to −0.15) | 0.023 | |
GMB 120 mg | 207 | −4.82 (−5.77 to −3.87) | ||||
Failed ≥ 3 prophylactic treatments (post hoc exploratory) | Yes | Placebo | NR | −0.39 (NR) | NA | NA |
GMB 120 mg | NR | −5.64 (NR) | NR | < 0.001 | ||
No | Placebo | NR | NR | NA | NA | |
GMB 120 mg | NR | NR | NR | NR | ||
Baseline medication overuse (a priori) | Yes | Placebo | 344 | −2.25 (−3.12 to −1.37) | −2.53 (−3.57 to −1.50) | < 0.001 |
GMB 120 mg | 177 | −4.78 (−5.82 to −3.74) | ||||
No | Placebo | 193 | −3.49 (−4.51 to −2.47) | −1.44 (−2.80 to −0.09) | 0.037 | |
GMB 120 mg | 95 | −4.93 (−6.20 to −3.67) | ||||
CI = confidence interval; GMB = galcanezumab; ITT = intention-to-treat; LS = least squares; MHD = migraine head day; NA = not applicable; NR = not reported.
aP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
bThe MMRM included the fixed, categorical effects of treatment, country, month, baseline medication overuse (yes vs. no), concurrent prophylaxis (yes vs. no), and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction.
Source: REGAIN Clinical Study Report11 and Ruff et al. (2019).33
Table 22: REGAIN Trial — Post Hoc Exploratory Subgroup Analyses of Secondary End Points, Modified ITT Population
Subgroup | Categories | Treatment group | n | Overall LS mean change from baseline (SE) | LS mean change difference vs. placebo (SE) | P valuea |
|---|---|---|---|---|---|---|
Overall change in MHDs with acute migraine medication use from baseline – MMRMb | ||||||
Number of failed prophylactic treatments | ≥ 2 | Placebo | 174 | −1.35 (0.53) | NA | NA |
GMB 120 mg | 72 | −5.81 (0.69) | −4.46 (0.69) | < 0.001 | ||
≥ 3 | Placebo | NR | −0.78 (0.75) | NA | NA | |
GMB 120 mg | NR | −6.01 (0.96) | NR | < 0.001 | ||
Change in MSQ v2.1 role function – restrictive domain score from baseline at month 3 – MMRMb | ||||||
Number of failed prophylactic treatments | ≥ 2 | Placebo | 174 | 10.67 (2.12) | NA | NA |
GMB 120 mg | 72 | 19.13 (2.87) | 8.45 (2.99) | < 0.01 | ||
≥ 3 | Placebo | NR | 10.34 (2.74) | NA | NA | |
GMB 120 mg | NR | 20.34 (3.82) | NR | < 0.05 | ||
GMB = galcanezumab; ITT = intention-to-treat; LS = least squares; MHD = migraine headache days; MSQ v2,1 = Migraine-Specific Quality of Life Questionnaire version 2.1; SE = standard error.
aP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
bThe MMRM included the fixed, categorical effects of treatment, country, month, baseline medication overuse (yes vs. no), concurrent prophylaxis (yes vs. no), and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline-by-month interaction.
Source: Ruff et al. (2019).33
Table 23: Key Efficacy Findings — CONQUER Trial, Modified ITT Population, Double-Blind Treatment phase
Outcomes | CONQUER | |
|---|---|---|
Placebo (N = 230) | GMB 120 mg (N = 232) | |
MSQ v2.1 mean change from baseline at month 3 (secondary) – MMRMa | N = 222b | N = 223b |
MSQ v2.1 total score | ||
LS mean change (95% CI) | 10.08 (7.64 to 12.53) | 21.67 (19.21 to 24.14) |
LS mean change difference vs. placebo (95% CI) | NA | 11.59 (8.50 to 14.68) |
P valuec | NA | < 0.0001 |
MSQ v2.1 role function – restrictived | ||
LS mean change (95% CI) | 10.68 (8.04 to 13.32) | 23.21 (20.55 to 25.87) |
LS mean change difference vs. placebo (95% CI) | NA | 12.53 (9.19 to 15.87) |
P value | NA | < 0.0001e |
MSQ v2.1 role function – preventive | ||
LS mean change (95% CI) | 7.68 (5.34 to 10.02) | 17.53 (15.18 to 19.88) |
LS mean change difference vs. placebo (95% CI) | NA | 9.85 (6.91 to 12.79) |
P valuec | NA | < 0.0001 |
MSQ v2.1 emotional function | ||
LS mean change (95% CI) | 12.02 (8.88 to 15.16) | 24.02 (20.86 to 27.19) |
LS mean change difference vs. placebo (95% CI) | NA | 12.00 (8.01 to 16.00) |
P valuec | NA | < 0.0001 |
EQ-5D-5L (secondary) – ANCOVAc | N = 225f | N = 227f |
Change from baseline to LOCF end point in EQ-5D-5L VAS score, LS mean change (SE)g | −0.09 (1.29) | 3.38 (1.31) |
P valuec | NA | 0.0277 |
Overall change from baseline in number of monthly MHDs with symptoms (exploratory) – MMRMa | N = 228f | N = 230f |
Nausea and/or vomiting | ||
LS mean change from baseline | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | |||||||||||||||||||||| |
P valuec | NA | |||||||| |
Photophobia and phonophobia | ||
LS mean change from baseline | |||||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | |||||||||||||||||||||| |
P valuec | NA | |||||||| |
Aura | ||
LS mean change from baseline | |||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | |||||||||||||||||||||| |
P valuec | NA | |||||| |
Prodromal symptoms other than aura | ||
LS mean change from baseline | |||||||||||||||||||| | |||||||||||||||||||||| |
LS mean change difference vs. placebo (95% CI) | NA | |||||||||||||||||||||| |
P valuec | NA | |||||||| |
Other patient-reported outcomes | ||
MIDAS total score mean change from baseline to LOCF (secondary) – ANCOVAh | N = 225f | N = 228f |
LS mean change from baseline (SE)g | −3.30 (3.30) | −21.10 (3.32) |
LS mean change difference vs. placebo (95% CI) | NA | −17.8 (−25.6 to −10.0) |
P valuec | NA | < 0.0001 |
MIBS-4 total score mean change from baseline to month 3 (secondary) – MMRMa | N = 222b | N = 223b |
LS mean change (95% CI) | −0.78 (−1.18 to −0.37) | −1.83 (−2.24 to −1.42) |
LS mean change difference vs. placebo (95% CI) | NA | −1.06 (−1.58 to −0.54) |
P valuec | NA | < 0.0001 |
PHQ-9 total score mean change from baseline to LOCF end point (exploratory) – ANCOVAh | N = 225f | N = 228f |
LS mean change (SE)g | −1.13 (0.31) | −2.12 (0.32) |
P valuee | NA | 0.0091 |
GAD-7 total score mean change from baseline to LOCF end point (exploratory) – ANCOVAh | N = 225f | N = 228f |
LS mean change (SE)g | −0.40 (0.23) | −0.91 (0.24) |
P valuec | NA | 0.0693 |
Headache or migraine frequency | ||
Overall change from baseline in number of monthly MHDs (primary)d – MMRMa | N = 228f | N = 230f |
LS mean change (95% CI) | −1.02 (−1.65 to −0.39) | −4.14 (−4.77 to −3.51) |
LS mean change difference vs. placebo (95% CI) | NA | −3.12 (−3.92 to −2.32) |
P value | NA | < 0.0001e |
Overall change from baseline in number of monthly headache days (secondary) – MMRMa | N = 228d | N = 230f |
LS mean change (95% CI) | −1.05 (−1.76 to −0.35) | −4.18 (−4.87 to −3.49) |
LS mean change difference vs. placebo (95% CI) | NA | −3.13 (−3.96 to −2.29) |
P valuec | NA | < 0.0001 |
Average change from baseline in number of monthly MHDs with acute headache medication use (secondary) – MMRMa | N = 228f | N = 230f |
LS mean change (95% CI) | −0.80 (−1.41 to −0.18) | −4.19 (−4.82 to −3.57) |
LS mean change difference vs. placebo (95% CI) | NA | −3.40 (−4.14 to −2.65) |
P valuec | NA | < 0.0001 |
HCRU related to migraine (secondary) – events per 100 patient-years | N = 229f | N = 228f |
Health care professional | ||
Baseline events | |||||||||||| | |||||||||||| |
Treatment events | |||||||||||| | |||||||||||| |
Mean change from baseline | |||||||||||| | |||||||||||| |
P valuec,i | NA | |||||||||||| |
Emergency room visits | ||
Baseline events | |||||||||||| | |||||||||||| |
Treatment events | |||||||||||| | |||||||||||| |
Mean change from baseline | |||||||||||| | |||||||||||| |
P valuec,i | NA | |||||||||||| |
Admissions to hospital | ||
Baseline events | |||||||||||| | |||||||||||| |
Treatment events | |||||||||||| | |||||||||||| |
Mean change from baseline | |||||||||||| | |||||||||||| |
P valuec,i | NA | |||||| |
Overnight hospital stays | ||
Baseline events | |||||||||||| | |||||||||||| |
Treatment events | |||||||||||| | |||||||||||| |
Mean change from baseline | |||||||||||| | |||||||||||| |
P valuec,i | NA | |||||| |
Employment status (secondary) | ||
Employment status at month 0 | N = 229 | N = 228 |
Working for pay, n (%) | |||||||||||| | |||||||||||| |
Student, n (%) | |||||| | |||||| |
Keeping house, n (%) | |||||||| | |||||||| |
Volunteer work, n (%) | |||||||||||| | |||||| |
Unemployed, unrelated to study disease disability, n (%) | |||||||| | |||||| |
Unemployed, due to study disease disability, n (%) | |||||| | |||||| |
Retired, n (%) | |||||||| | |||||||| |
Self-employed, n (%) | |||||||| | |||||||| |
Employment status at month 3 | |||||||| | |||||||| |
Working for pay, n (%) | |||||||||||| | |||||||||||| |
Student, n (%) | |||||| | |||||| |
Keeping house, n (%) | |||||||| | |||||||| |
Volunteer work, n (%) | |||||||||||| | |||||| |
Unemployed, unrelated to study disease disability, n (%) | |||||||| | |||||| |
Unemployed, due to study disease disability, n (%) | |||||| | |||||| |
Retired, n (%) | |||||||| | |||||||| |
Self-employed, n (%) | |||||| | |||||||| |
WPAI mean change from baseline to LOCF end point (secondary) – ANCOVAh | ||
Percent of activity impairment due to health | N = 225f | N = 227f |
LS mean change (SE)g | −8.64 (1.92) | −20.71 (1.95) |
P valuec,h | NA | < 0.0001 |
Percent of impairment while working due to health (presenteeism) | N = 141f | N = 147f |
LS mean change (SE)g | −2.56 (2.32) | −12.50 (2.37) |
P valuec,h | NA | 0.0004 |
Percent of overall work impairment due to health | N = 145f | N = 148f |
LS mean change (SE)g | −3.46 (2.41) | −14.31 (2.51) |
P valuec,h | NA | 0.0003 |
Percent of work time missed due to health (absenteeism) | N = 145f | N = 148f |
LS mean change (SE)f | −2.90 (1.24) | −4.224 (1.29) |
P valuec,h | NA | 0.3880 |
ANCOVA = analysis of covariance; CI = confidence interval; CM = chronic migraine; EM = episodic migraine; EQ-5D-5L = EQ-5D 5-Levels questionnaire; GAD-7 = Generalized Anxiety Disorder 7-item; GMB = galcanezumab; HCRU = health care resource utilization; LOCF = last observation carried forward; LS = least squares; MIBS-4 = 4-item Migraine Interictal Burden Scale; MIDAS = Migraine Disability Assessment; MHD = migraine headache day; MMRM = mixed model for repeated measures; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; NA = not applicable; PHQ-9 = Patient Health Questionnaire-9; SE = standard error; VAS = Visual Analogue Scale; vs. = versus; WPAI = Work Productivity and Activity Impairment.
aThe MMRM included the fixed, categorical effects of treatment, baseline migraine frequency category (low-frequency EM, high-frequency EM, and CM), pooled country, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline value-by-month interaction. Estimates were obtained using unstructured covariance structure. The Kenward-Roger approximation was used to estimate denominator degrees of freedom.
bNumber of patients in the analysis population with non-missing baseline value and non-missing value at month 3.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
dOutcome included in the trial’s multiple-testing procedure.
eResults are statistically significant after adjustment for multiplicity.
fNumber of patients in the analysis population with non-missing baseline value and at least 1 non-missing post-baseline value.
gThe SE was reported because the 95% CI was not reported.
hBetween-treatment group comparison P value using an ANCOVA model for end point measures. The ANCOVA model contained the main effects of treatment, baseline migraine frequency category, pooled country, and appropriate baseline value.
iBetween-treatment group P value from a Kruskal-Wallis test.
Source: CONQUER Clinical Study Report12 and Mulleners et al. (2020).36
Table 24: CONQUER Trial — Subgroup Analyses of Primary End Point, Modified ITT Population (A Priori)
Subgroup | Categories | Treatment group | n | LS mean change from baseline (95% CI) | LS mean change difference vs. placebo (95% CI) | Subgroup-by-treatment interaction P valuea |
|---|---|---|---|---|---|---|
Overall change in number of monthly MHDs (primary) – Double-blind treatment phase, MMRMb | ||||||
Baseline migraine frequency category | Low-frequency episodic | Placebo | 36 | 1.07 (−0.59 to 2.74) | −3.26 (−5.17 to −1.35) | 0.4033 |
GMB 120 mg | 35 | −2.19 (−3.92 to −0.45) | ||||
High-frequency episodic | Placebo | 96 | −0.78 (−1.57 to 0.01) | −2.31 (−3.26 to −1.36) | ||
GMB 120 mg | 102 | −3.09 (−3.87 to −2.30) | ||||
Chronic | Placebo | 96 | −2.21 (−3.47 to −0.95) | −3.70 (−5.23 to −2.16) | ||
GMB 120 mg | 93 | −5.91 (−7.19 to −4.63) | ||||
Number of preventive medication category failures | 2 | Placebo | 139 | −1.16 (−1.92 to −0.40) | −1.98 (−2.91 to −1.04) | 0.0040 |
GMB 120 mg | 129 | −3.14 (−3.95 to −2.32) | ||||
3 | Placebo | 68 | −1.28 (−2.82 to 0.25) | −4.10 (−5.80 to −2.40) | ||
GMB 120 mg | 70 | −5.38 (−6.88 to −3.88) | ||||
4 | Placebo | 18 | 0.98 (−2.17 to 4.13) | −6.14 (−9.51 to −2.77) | ||
GMB 120 mg | 27 | −5.16 (−7.45 to −2.88) | ||||
CI = confidence interval; CM = chronic migraine; EM = episodic migraine; GMB = galcanezumab; ITT = intention-to-treat; LS = least squares; MHD = migraine headache day; MMRM = mixed model for repeated measures; vs. = versus.
aP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
bThe MMRM included the fixed, categorical effects of treatment, baseline migraine frequency category (low-frequency EM, high-frequency EM, and CM), pooled country, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline value-by-month interaction.
Source: CONQUER Clinical Study Report.12
Table 25: CONQUER Trial — Subgroup Analyses in Patients with 3 or More Prior Preventive-Medication Category Failures (A Priori)
Outcome | Treatment | n | LS mean change from baseline (95% CI) | LS mean change difference vs. placebo (95% CI) | P valuea |
|---|---|---|---|---|---|
Change in number of monthly MHDs – overall, MMRMb | Placebo | 86 | −1.03 (−2.42 to 0.35) | −4.46 (−5.88 to −3.03) | < 0.0001 |
GMB 120 mg | 98 | −5.49 (−6.77 to −4.20) | |||
MSQ v2.1 role function –restrictive – month, MMRMb | Placebo | 84 | 12.03 (6.52 to 17.55) | 15.30 (9.45 to 21.16) | < 0.0001 |
GMB 120 mg | 94 | 27.34 (21.95 to 32.72) | |||
Number of monthly MHDs with acute headache medication use – overall, MMRMb | Placebo | 86 | −0.69 (−2.10 to 0.72) | −4.63 (−6.00 to −3.27) | < 0.0001 |
GMB 120 mg | 98 | −5.32 (−6.69 to −3.95) |
CI = confidence interval; GMB = galcanezumab; LS = least squares; MHD = migraine headache day; MSQ = Migraine-Specific Quality of Life Questionnaire version 2.1; vs. = versus.
aP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
bThe MMRM included the fixed, categorical effects of treatment, baseline migraine frequency category (low-frequency EM, high-frequency EM, and CM), pooled country, month, and treatment-by-month interaction, as well as the continuous, fixed covariates of baseline value and baseline value-by-month interaction.
Source: CONQUER Clinical Study Report.12
Harms
Only those harms identified in the review protocol are reported as follows. Table 26 provides detailed harms data for the EVOLVE-1 and EVOLVE-2 trials, Table 27 provides detailed harms data for the REGAIN trial, and Table 28 provides detailed harms data for the CONQUER trial.
Adverse Events
In the EVOLVE-1 and EVOLVE-2 studies, most patients experienced at least 1 treatment-emergent AE, with a numerically smaller proportion of patients experiencing 1 or more AEs in the placebo arm compared to the galcanezumab 120 mg arm (60.42% versus 65.53%, respectively, in EVOLVE-1; 62.26% versus 65.04%, respectively, in EVOLVE-2). The most frequently reported AEs in EVOLVE-1 were injection site pain (17.36% and 16.02% in the placebo and galcanezumab 120 mg arms, respectively) and nasopharyngitis (17.36% and 16.02% in the placebo and galcanezumab 120 mg arms, respectively). The most frequently reported AEs in EVOLVE-2 were injection site pain (8.46% and 9.29% in the placebo and galcanezumab 120 mg arms, respectively) and upper respiratory tract infection (3.47% and 5.75% in the placebo and galcanezumab 120 mg arms, respectively).
During the double-blind treatment period of the REGAIN trial, 50.00% of patients in the placebo arm and 58.24% of patients in the galcanezumab 120 mg arm experienced at least 1 treatment-emergent AE. The most frequently reported AEs were injection site pain (4.30% and 6.23% in the placebo and galcanezumab 120 mg arms, respectively) and nasopharyngitis (4.66% and 6.23% in the placebo and galcanezumab 120 mg arms, respectively). During the open-label phase, 70.35% of patients experienced at least 1 treatment-emergent AE. The most frequently reported AEs in the open-label phase were nasopharyngitis (9.59%), upper respiratory tract infection (6.16%), and injection site reaction (5.87%).
During the double-blind treatment period of the CONQUER trial, 53.04% of patients in the placebo arm and 51.29% of patients in galcanezumab 120 mg arm experienced at least 1 treatment-emergent AE. The most frequently reported AEs were nasopharyngitis (9.13% and 6.90% in the placebo and galcanezumab 120 mg arms, respectively) and influenza (3.04% and 4.74% in the placebo and galcanezumab 120 mg arms, respectively). During the open-label phase, 54.92% of patients experienced at least 1 treatment-emergent AE. The most frequently reported AEs in the open-label phase were nasopharyngitis (4.2%), injection site pain (3.6%), and injection site erythema (2.7%).
Serious Adverse Events
During the EVOLVE-1 trial, 5 patients (1.16%) in the placebo arm and 6 patients (2.91%) in the galcanezumab 120 mg arm reported 1 or more SAEs. Two patients in the placebo group had an SAE of cholelithiasis. No other individual SAE was reported more than once. During the EVOLVE-2 trial, 5 patients (1.08%) in the placebo arm and 5 patients (2.21%) in the galcanezumab 120 mg arm reported 1 or more SAEs. No individual SAE was reported by more than 1 patient.
In the REGAIN trial, 4 patients (0.72%) in the placebo arm and 1 patient (0.37%) in the galcanezumab 120 mg arm reported 1 or more SAEs during the double-blind treatment phase. No individual SAE was reported by more than 1 patient. During the optional open-label phase, 33 patients (3.2%) reported SAEs (18 in the placebo, 6 in the galcanezumab 120 mg, and 9 in the galcanezumab 240 mg arms). Events reported by more than 1 patient in the open-label phase were seizure (N = 2), migraine (N = 2), appendicitis (N = 2), and urinary tract infection (N = 2).
In the CONQUER trial, 2 patients (0.87%) in the placebo arm and 2 patients (0.86%) in the galcanezumab 120 mg arm reported 1 or more SAEs during the double-blind treatment phase. During the optional open-label phase, 11 patients (2.41%) reported SAEs as of the data cut-off date. No individual SAE was reported by more than 1 patient in either treatment period.
Withdrawals Due to Adverse Events
During the EVOLVE-1 trial, 10 patients (2.31%) in the placebo arm and 7 patients (3.40%) in the galcanezumab 120 mg arm discontinued due to AEs. Migraine was the only AE that led to discontinuation in more than 1 patient (1 each in the placebo and galcanezumab 120 mg arms). In the EVOLVE-2 trial, 8 patients (1.74%) in the placebo arm and 5 patients (2.21%) in the galcanezumab 120 mg arm discontinued due to AEs. No individual AE led to discontinuation in more than 1 patient in the placebo and galcanezumab 120 mg arms.
In the REGAIN trial, 6 patients (1.08%) in the placebo arm and 1 patient (0.37%) in the galcanezumab 120 mg arm discontinued due to AEs during the double-blind treatment phase. Adverse events leading to discontinuation from the placebo group were migraine (N = 2), headache (N = 1), abdominal pain (N = 1), alopecia (N = 1), and myocardial infarction (N = 1). The AE leading to discontinuation from the galcanezumab 120 mg group was increased weight. In the open-label phase, 46 patients (4.5%) discontinued due to AEs. The most frequently reported AEs leading to discontinuation from the open-label treatment phase were urticaria (0.68%), rash (N = 2), and back pain, dyspnea, headache, hepatic enzyme increased, and rash (0.20% each).
In the CONQUER trial, 0 patients in the placebo arm and 1 patient (0.43%) in the galcanezumab arm discontinued due to an AE (rash generalized) during the double-blind treatment phase. During the open-label phase, 3 patients (0.65%) discontinued due to an AE (1 patient from the placebo arm and 2 patients from the galcanezumab arm) as of the data cut-off date for the main efficacy analysis (June 19, 2019). The AEs leading to discontinuation in the open-label phase included induration of the labia, attention-deficit/hyperactivity disorder, and rash. As of the end of the study, a total of 6 galcanezumab-treated patients (1.3%) discontinued the study due to an AE during galcanezumab treatment.
Mortality
No patients died during any phase of the EVOLVE-1, EVOLVE-2, REGAIN, and CONQUER trials.
Notable Harms
Anaphylaxis and Hypersensitivity Reactions
No patients in the EVOLVE-1, EVOLVE-2, REGAIN, and CONQUER trials experienced an anaphylactic reaction.
In the EVOLVE-1 trial, 2.08% of patients in the placebo arm and 4.37% of patients in the galcanezumab 120 mg arm experienced a hypersensitivity event. In the EVOLVE-2 trial, 4.34% of patients in the placebo arm and 5.75% of patients in the galcanezumab 120 mg arm experienced a hypersensitivity event. One patient in the placebo arm experienced angioedema in each of the EVOLVE trials.
In the REGAIN trial, 1.97% and 4.40% of patients experienced a hypersensitivity event in the placebo and galcanezumab 120 mg arms, respectively, during the double-blind treatment phase. Three patients (0.54%) in the placebo arm and 2 patients (0.73%) in the galcanezumab 120 mg arm experienced angioedema during double-blind treatment. During the open-label phase, 79 patients (7.73%) experienced a hypersensitivity event and 18 (1.76%) experienced angioedema as of the data cut-off date.
In the CONQUER trial, 3.48% and 3.02% of patients experienced a hypersensitivity event in the placebo and galcanezumab 120 mg arms, respectively, during the double-blind treatment phase. One patient (0.43%) in the placebo arm and 0 patients in the galcanezumab 120 mg arm experienced angioedema during double-blind treatment. During the open-label phase, 16 patients (3.50%) experienced a hypersensitivity event and 2 (0.44%) experienced angioedema.
Injection Site Reactions
Injection site reactions during double-blind treatment were reported in a numerically greater proportion of patients in the EVOLVE-1 study compared to the other trials.
In the EVOLVE-1 trial, injection site reactions were reported by 20.14% of patients in the placebo arm and 27.67% of patients in the galcanezumab 120 mg arm. In the EVOLVE-2 trial, injection site reactions were reported by 9.76% and 17.70% of patients in the placebo and galcanezumab 120 mg arms, respectively.
During double-blind treatment in the REGAIN trial, injection site reactions were reported by 9.14% and 11.36% of patients in the placebo and galcanezumab 120 mg arms, respectively. During open-label treatment period, 13.80% of patients experienced an injection site reaction.
During double-blind treatment in the CONQUER trial, 10.00% and 6.90% of patients in the placebo and galcanezumab 120 mg arms, respectively, reported injection site reactions. During all galcanezumab-treated time, including the double-blind and open-label treatment period, 10.94% of patients experienced an injection site reaction as of the data cut-off date.
Antibody Formation
During the double-blind treatment periods of the EVOLVE-1, EVOLVE-2, and REGAIN studies, up to 9.4% of patients treated with galcanezumab 120 mg and up to 1.7% of patients treated with placebo were treatment-emergent ADA-positive. The formation of ADAs was not assessed proactively in the CONQUER study and therefore is not reported.
In the EVOLVE-1 safety population, the percentages of patients who were treatment-emergent ADA-positive during the double-blind treatment phase were 1.66% in the placebo group and 3.47% in the galcanezumab 120 mg group. In the EVOLVE-2 safety population. Of these patients, all but 1 placebo-treated patient had neutralizing ADAs present. In the EVOLVE-2 trial, the percentages of patients in the safety population who were treatment-emergent ADA-positive during the double-blind treatment phase were 0.45% in the placebo group and 8.56% in the galcanezumab 120 mg group. Of these patients, all but 1 placebo-treated patient had neutralizing ADAs present.
During the double-blind treatment phase in the REGAIN trial, the percentages of patients in the safety population who were treatment-emergent ADA-positive were 1.5% in the placebo group and 2.7% in the galcanezumab 120 mg group. Of these patients, 0.6% in the placebo arm and 2.3% in the 120 mg arm had neutralizing ADAs present. During all galcanezumab-treated time for all patients, including the open-label extension phase (ongoing at the time of the data cut-off date of March 16, 2017), 6.35% were treatment-emergent ADA-positive. Of these patients, 5.12% had neutralizing ADAs present.
Vascular Events
In the EVOLVE-1 trial, 1.62% and 2.91% of patients in the placebo and galcanezumab 120 mg arms, respectively, experienced a vascular disorder. In the EVOLVE-2 trial, 1.95% and 3.10% of patients in the placebo and galcanezumab 120 mg arms, respectively, experienced a vascular disorder. The most frequently reported vascular disorders in the EVOLVE studies were hypertension and hot flushes.
In the REGAIN trial, 1.79% and 1.10% of patients in the placebo and galcanezumab 120 mg arms, respectively, experienced a vascular disorder during the double-blind treatment phase. The most frequently reported vascular disorders in the EVOLVE studies were hypertension and hot flushes. Vascular disorder events experienced in the open-label phase were not reported.
In the CONQUER trial, 2.61% and 0.43% of patients in the placebo and galcanezumab 120 mg arms, respectively, experienced a vascular disorder during double-blind treatment. Hypertension was the only vascular disorder experienced by more than 1 patient (N = 3 [1.30%] in the placebo arm; N = 1 [0.43%] in the galcanezumab arm). During the open-label phase, 7 patients (1.53%) reported vascular disorder AEs. The most frequently reported vascular disorders were flushing and hypertension (N = 2 [0.44%] each).
Table 26: Summary of Harms — EVOLVE-1 and EVOLVE-2, Safety Populations, Double-Blind Treatment phase
Harms | EVOLVE-1 | EVOLVE-2 | ||
|---|---|---|---|---|
Placebo N = 432 | GMB 120 mg N = 206 | Placebo N = 461 | GMB 120 mg N = 226 | |
Patients with ≥ 1 adverse event | ||||
n (%) | 261 (60.42) | 135 (65.53) | 287 (62.26) | 147 (65.04) |
Most common events,a n (%) | ||||
Injection site pain | 75 (17.36) | 33 (16.02) | 39 (8.46) | 21 (9.29) |
Nasopharyngitis | 27 (6.25) | 16 (7.77) | 41 (8.89) | 19 (8.41) |
Urinary tract infection | 15 (3.47) | 8 (3.88) | 11 (2.39) | 5 (2.21) |
Injection site erythema | 11 (2.55) | 10 (4.85) | 4 (0.87) | 6 (2.65) |
Injection site pruritus | 1 (0.23) | 9 (4.37) | 0 | 6 (2.65) |
Injection site reaction | 4 (0.93) | 7 (3.40) | 0 | 7 (3.10) |
Sinusitis | 13 (3.01) | 10 (4.85) | 13 (2.82) | 6 (2.65) |
Nausea | 15 (3.47) | 5 (2.43) | 15 (3.25) | 4 (1.77) |
Back pain | 6 (1.39) | 5 (2.43) | 20 (4.34) | 2 (0.88) |
Dizziness | 11 (2.55) | 6 (2.91) | 10 (2.17) | 8 (3.54) |
Influenza | 5 (1.16) | 5 (2.43) | 14 (3.04) | 3 (1.33) |
Upper respiratory tract infection | 31 (7.18) | 9 (4.37) | 16 (3.47) | 13 (5.75) |
Fatigue | 12 (2.78) | 5 (2.43) | 12 (2.60) | 6 (2.65) |
Diarrhea | 10 (2.31) | 4 (1.94) | 11 (2.39) | 7 (3.10) |
Rash | 7 (1.62) | 1 (0.49) | 7 (1.52) | 5 (2.21) |
Neck pain | 4 (0.93) | 3 (1.46) | 9 (1.95) | 5 (2.21) |
Viral infection | 3 (0.69) | 2 (0.97) | 5 (1.08) | 6 (2.65) |
Injection site swelling | 1 (0.23) | 3 (1.46) | 0 | 5 (2.21) |
Anxiety | 3 (0.69) | 3 (1.46) | 6 (1.30) | 5 (2.21) |
Patients with ≥ 1 SAE | ||||
n (%) | 5 (1.16) | 6 (2.91) | 5 (1.08) | 5 (2.21) |
Patients who discontinued treatment due to adverse events | ||||
n (%) | 10 (2.31) | 7 (3.40) | 8 (1.74) | 5 (2.21) |
Deaths | ||||
n (%) | 0 | 0 | 0 | 0 |
Notable harms | ||||
Anaphylactic reaction, n (%) | 0 | 0 | 0 | 0 |
Hypersensitivity events, n (%) | 9 (2.08) | 9 (4.37) | 20 (4.34) | 13 (5.75) |
Angioedema, n (%) | 1 (0.23) | 0 | 1 (0.22) | 0 |
Injection site reactions, n (%) | 87 (20.14) | 57 (27.67) | 45 (9.76) | 40 (17.70) |
ADA-positive, n (%) | 7 (1.66) | 7 (3.47) | 2 (0.45) | 19 (8.56) |
Neutralizing ADAs present | 6 (1.42) | 7 (3.47) | 1 (0.23) | 19 (8.56) |
Vascular disorders, n (%) | 7 (1.62) | 6 (2.91) | 9 (1.95) | 7 (3.10) |
Hot flushes | 2 (0.46) | 2 (0.97) | 7 (1.52) | 4 (1.77) |
Hypertension | 4 (0.93) | 2 (0.97) | 0 | 2 (0.88) |
Flushing | 0 | 1 (0.49) | 0 | 0 |
Aneurysm | 0 | 1 (0.49) | 0 | 0 |
Hematoma | 0 | 0 | 1 (0.22) | 1 (0.44) |
Deep vein thrombosis | 1 (0.23) | 0 | 0 | 0 |
Diastolic hypotension | 0 | 0 | 1 (0.22) | 0 |
ADA = antidrug antibody; GMB = galcanezumab; NA = not applicable; SAE = serious adverse event.
aFrequency of 2% or greater in either treatment arm of trial.
Source: EVOLVE-1 Clinical Study Report9 and EVOLVE-2 Clinical Study Report.10
Table 27: Summary of Harms — REGAIN, Safety Population, Double-Blind and Open-Label Treatment phases
Harms | REGAIN | |
|---|---|---|
Placebo N = 558 | GMB 120 mg N = 273 | |
Double-blind treatment phase | ||
Patients with ≥ 1 adverse event | ||
n (%) | 279 (50.00) | 159 (58.24) |
Most common events,a n (%) | ||
Injection site pain | 24 (4.30) | 17 (6.23) |
Nasopharyngitis | 26 (4.66) | 17 (6.23) |
Injection site reaction | 10 (1.79) | 8 (2.93) |
Upper respiratory tract infection | 13 (2.33) | 9 (3.30) |
Fatigue | 10 (1.79) | 6 (2.20) |
Back pain | 14 (2.51) | 9 (3.30) |
Abdominal pain | 9 (1.61) | 6 (2.20) |
Urinary tract infection | 7 (1.25) | 6 (2.20) |
Nausea | 23 (4.12) | 9 (3.30) |
Dizziness | 20 (3.58) | 6 (2.20) |
Neck pain | 8 (1.43) | 7 (2.56) |
Influenza | 15 (2.69) | 0 |
Patients with ≥ 1 SAE | ||
n (%) | 4 (0.72) | 1 (0.37) |
Patients who discontinued DB treatment due to adverse events | ||
n (%) | 6 (1.08) | 1 (0.37) |
Deaths | ||
n (%) | 0 | 0 |
Notable harms | ||
Anaphylactic reaction, n (%) | 0 | 0 |
Hypersensitivity events, n (%) | 11 (1.97) | 12 (4.40) |
Angioedema, n (%) | 3 (0.54) | 2 (0.73) |
Injection site reactions, n (%) | 51 (9.14) | 31 (11.36) |
ADA-positive,b n (%) | 8 (1.50) | 7 (2.65) |
Neutralizing ADAs present | 3 (0.56) | 6 (2.27) |
Vascular disorders, n (%) | 10 (1.79) | 3 (1.10) |
Hypertension | 4 (0.72) | 2 (0.73) |
Hot flush | 2 (0.36) | 1 (0.37) |
Orthostatic hypotension | 1 (0.18) | 0 |
Diastolic hypertension | 1 (0.18) | 0 |
Hypotension | 1 (0.18) | 0 |
Vascular pain | 1 (0.18) | 0 |
Open-label treatment phasec | ||
GMB-treatedd (N = 1,022) | ||
Patients with ≥ 1 adverse event | ||
n (%) | 719 (70.35) | |
Most common events,e n (%) | ||
Nasopharyngitis | 98 (9.59) | |
Upper respiratory tract infection | 63 (6.16) | |
Injection site reaction | 60 (5.87) | |
Urinary tract infection | 44 (4.31) | |
Influenza | 43 (4.21) | |
Back pain | 39 (3.82) | |
Sinusitis | 32 (3.13) | |
Bronchitis | 31 (3.03) | |
Patients with ≥ 1 SAE | ||
n (%) | 33 (3.23) | |
Patients who discontinued open-label treatment due to adverse events | ||
n (%) | 46 (4.50) | |
Deaths | ||
n (%) | 0 | |
Notable harms | ||
Anaphylactic reaction, n (%) | 0 | |
Hypersensitivity events, n (%) | 79 (7.73) | |
Angioedema, n (%) | 18 (1.76) | |
Injection site reactions, n (%) | 141 (13.80) | |
ADA-positive, n (%)f | 62 (6.35) | |
Neutralizing ADAs presentf | 50 (5.12) | |
Vascular disorders, n (%) | NR | |
ADA = antidrug antibody; GMB = galcanezumab; NR = not reported; SAE = serious adverse event.
aFrequency of 2% or greater.
bIncluded patients who were ADA-positive at any time during galcanezumab treatment (i.e., double-blind and/or open-label treatment phases). Patients who became ADA-positive during the open-label phase only were not reported.
cOpen-label treatment phase data cut-off was May 1, 2018 (date last patient completed the study).
dGalcanezumab dosing during the open-label extension (ongoing) comprised monthly injections at 9 office visits. The doses administered during this phase were 240 mg at visit 7, 120 mg at visit 8, and either 120 mg or 240 mg per month, thereafter, at the discretion of the investigator. Dosing and dose changes could only occur at regular once-monthly visits.
eFrequency of 3% or greater.
fDuring all galcanezumab-treated time for all patients, including the open-label extension phase (ongoing at the time of the data cut-off date of March 16, 2017).
Source: REGAIN Clinical Study Report11 and REGAIN Clinical Study Report Addendum.13
Table 28: Summary of Harms — CONQUER, Safety Population, Double-Blind and Open-Label Treatment phases
Harms | CONQUER | |
|---|---|---|
Placebo (N = 230) | GMB (N = 232) | |
Double-blind treatment phase | ||
Patients with ≥ 1 adverse event | ||
n (%) | 122 (53.04) | 119 (51.29) |
Most common events,a n (%) | ||
Nasopharyngitis | 21 (9.13) | 16 (6.90) |
Influenza | 7 (3.04) | 11 (4.74) |
Injection site erythema | 6 (2.61) | 8 (3.45) |
Constipation | 5 (2.17) | 5 (2.16) |
Injection site pain | 13 (5.65) | 5 (2.16) |
Upper respiratory tract infection | 5 (2.17) | 5 (2.16) |
Back pain | 6 (2.61) | 4 (1.72) |
Nausea | 5 (2.17) | 4 (1.72) |
Sinusitis | 5 (2.17) | 4 (1.72) |
Patients with ≥ 1 SAE | ||
n (%) | 2 (0.87) | 2 (0.86) |
Patients who discontinued treatment due to adverse events | ||
n (%) | 0 | 1 (0.43) |
Deaths | ||
n (%) | 0 | 0 |
Notable harms | ||
Anaphylactic reaction, n (%) | 0 | 0 |
Hypersensitivity, n (%) | 8 (3.48) | 7 (3.02) |
Angioedema, n (%) | 1 (0.43) | 0 |
Injection site reactions, n (%) | 23 (10.00) | 16 (6.90) |
ADA formation, n (%) | NR | NR |
Vascular disorders, n (%) | 6 (2.61) | 1 (0.43) |
Hypertension | 3 (1.30) | 1 (0.43) |
Behcet syndrome | 1 (0.43) | 0 |
Flushing | 1 (0.43) | 0 |
Hot flushes | 1 (0.43) | 0 |
Open-label treatment phaseb | ||
GMB Treated (N = 457) | ||
Patients with ≥ 1 adverse event | ||
n (%) | 193 (42.98) | |
Most common events,a n (%) | ||
Nasopharyngitis | 19 (4.23) | |
Injection site pain | 16 (3.56) | |
Injection site erythema | 12 (2.67) | |
Patients with ≥ 1 SAE | ||
n (%)c | 11 (2.41) | |
Patients who discontinued treatment due to adverse events | ||
n (%)c | 6 (1.3) | |
Deaths | ||
n (%) | 0 | |
Notable harmsc | ||
Anaphylactic reaction, n (%) | 0 | |
Hypersensitivity, n (%) | 16 (3.50) | |
Angioedema, n (%) | 2 (0.44) | |
Injection site reactions, n (%) | 50 (10.94) | |
ADA-positive, n (%) | NR | |
Vascular disorders, n (%) | 7 (1.53) | |
Flushing | 2 (0.44) | |
Hypertension | 2 (0.44) | |
Diastolic hypertension | 1 (0.22) | |
Hot flush | 1 (0.22) | |
Varicose vein | 1 (0.22) | |
ADA = antidrug antibody; GMB = galcanezumab; NR = not reported; SAE = serious adverse event.
aFrequency of 2% or greater.
bOpen-label treatment phase data cut-off was September 19, 2019 (date last patient completed the study).
cEvents reported during galcanezumab-treated time (i.e., double-blind and open-label treatment periods). Number of events reported during the completed open-label phase only was not reported.
Source: CONQUER Clinical Study Report12 and CONQUER Clinical Study Report Addendum.13
Critical Appraisal
Internal Validity
The pivotal trials were designed to assess the superiority of galcanezumab over placebo. The overall designs of the pivotal trials were justified and considered appropriate to investigate the trials’ primary and secondary objectives. The initial screening and prospective baseline periods were appropriate to accurately identify patients who had the required number of monthly MHDs, headache days, and headache-free days as well as establish a baseline for efficacy end points. The randomization procedures used were appropriate and the enrolled sample sizes were adequate. Within each of the trials, baseline demographic and disease characteristics were generally balanced. The trials were double-blind to minimize bias and the blinding methods used were appropriate. However, it is possible that accidental unblinding may have occurred due to the profile of AEs observed with galcanezumab (e.g., hypersensitivity reactions).
Multiple testing procedures were used in all the trials to control type I error for the primary and key secondary outcomes. In the EVOLVE-1, EVOLVE-2, and REGAIN trials, this included overall change in monthly MHDs, monthly MHDs with acute medication use, and MSQ v2.1 RF-R domain scores. In the CONQUER trial, this included the overall change in monthly MHDs and MSQ v2.1 RF-R. However, in the REGAIN trial, monthly MHDs with acute medication use and MSQ v2. RF-R could not be tested for statistical significance within the pre-specified multiple-testing procedure; thus, conclusions for this end point cannot be drawn from these results.
Each of the trials met their primary objective for the galcanezumab 120 mg arm of a statistically significantly reduced overall mean number of monthly MHDs during double-blind treatment. The EVOLVE-1, EVOLVE-2, and CONQUER trials also met all of their key secondary objectives. In the galcanezumab 120 mg arm in the REGAIN trial, only 1 key secondary objective (50% response rate) was statistically significant after multiplicity adjustment.
The validity and reliability of the MSQ v2.1, MIDAS, MIBS-4, PHQ-9, and GAD-7 were considered adequate. CADTH identified MIDs in the literature for the MSQ v2.1 and MIDAS scores of patients with migraine. No MID was identified in patients with migraine for the EQ-5D-5L, MIBS-4, PHQ-9, GAD-7, HCRU and employment status, and WPAI. Statistical inference on these outcomes is limited because they were not included in the multiple-testing procedure.
The REGAIN and CONQUER trials included an optional open-label extension phase (9 months and 3 months, respectively), which helped monitor the long-term effects of the drug, particularly safety. The vast majority of patients (> 98%) entered the open-label extension phase of these trials. The observation of long-term efficacy could have been compromised due to the unblinding, which would more likely bias patient reporting of headache or migraine or related subjective outcome measures, such as the MIDAS and MSQ. However, the primary analyses of efficacy end points were conducted using data from the double-blind treatment phases.
A numerically greater proportion of patients discontinued from the double-blind treatment phase of the EVOLVE-1 and EVOLVE-2 trials compared to the REGAIN and CONQUER trials. Furthermore, the clinical expert consulted by CADTH indicated that the discontinuation rates in the EVOLVE trials were higher than seen in their clinical practice, and higher than expected with anti-CGRP monoclonal antibodies. The most frequent reason for discontinuing from the double-blind treatment phase in the EVOLVE-1, EVOLVE-2, and REGAIN trials was withdrawal by patient. Other reasons for discontinuation included lost to follow-up, lack of efficacy, and AEs. The numerical differences in discontinuation between groups did not appear to be important and, despite the relatively large percentage in the EVOLVE studies, the methods for imputing missing data were generally appropriate.
A modified ITT population was used for efficacy analyses, which included all randomized patients who received at least 1 dose of the study drug. The safety population included data from all randomized patients who received at least 1 dose of the investigational product. Analyses were conducted based on modal treatment the patient received during the double-blind treatment phase.
Migraine and headache-related end points (MHDs with symptoms, number of monthly MHDs, number of monthly headache days, and acute headache pain medication intake) were derived from headache information captured via an ePRO diary, which patients were asked to complete daily. Compliance with the ePRO diary was generally high across studies. However, compliance was numerically lower in the EVOLVE-1 and EVOLVE-2 studies compared to the REGAIN and CONQUER studies. Missing data were still likely a concern, particularly when the amount of missing data differed between the 2 comparison arms. The approach taken by the sponsor for missing data for the primary end point was to normalize them to a 30-day period by multiplying by 30 and dividing by the number of non-missing diary days in the monthly interval. The approach taken by the sponsor for the primary and secondary end point assumes that the rate of migraine headaches was the same for days with missing and non-missing ePRO diary days. If patients had completed less than 50% of the required entries in a month, all end points measured through the ePRO would be considered missing for that month. This approach to missing ePRO diary data assumed that the rate of MHDs was the same for days with missing and non-missing ePRO diary days. The impact of this missing-data approach was assessed through sensitivity analyses, which were generally consistent with the primary results. In addition, the primary analytic approach (MMRM) accounts for missing data under a missing-at-random assumption. For other end points, repeated measures analyses were used or ANOVA or ANCOVA using change from baseline to the LOCF end point where data were missing. The LOCF approach was used for the analysis of the following outcomes: MIDAS total score in the REGAIN and CONQUER trials; and PHQ-9, GAD-7, and WPAI in the CONQUER trial. The Clinical Study Reports did not clearly describe how and when the LOCF approach was implemented. The LOCF method may inaccurately represent how patients would respond during the rest of the study had they continued on the medication, and it is unknown how this affects the study results and their interpretation.
The analyzable sample sizes for the MSQ and MIDAS were notably smaller than the randomized sample sizes in each study, with the exception of the CONQUER study. There was no discernable difference between treatment groups in each study regarding disproportionately missing patients, but characteristics of the patients who were not included in the analyzable set were not reported and it could not be determined what impact this reduced sample size had on the results for these outcome measures.
Subgroup analyses were conducted on the primary end point in each of the trials. Most the subgroup analyses were specified a priori: baseline number of monthly MHDs and failures on 2 or more prophylactic treatments and in the EVOLVE-1 and EVOLVE-2 studies; failures on 2 or more prophylactic treatments and baseline headache medication overuse in the REGAIN trial; and baseline migraine frequency category and number of preventive-medication category failures in the CONQUER trial. The following subgroup analyses were conducted post hoc and therefore considered exploratory: baseline headache medication overuse in the EVOLVE-1 and EVOLVE-2 trials and patients who failed at least 3 prophylactic treatments in the EVOLVE-1, EVOLVE-2, and REGAIN studies. The subgroup analyses were not adjusted for multiplicity and therefore are considered exploratory, and results can only be considered supportive evidence.
There were some differences in design between of the REGAIN trial and those of the other pivotal trials. The REGAIN trial used a different definition of MHD than the definition used in the other pivotal trials to align with IHS guidelines for trials of migraine-preventive medications in adults with CM, which included an additional criterion that, for any diary day, even if the patient did not meet the migraine headache definition as defined by criteria A and B (Table 12) but was taking a triptan or ergot derivative (“criterion C”), this diary day for this patient was still considered an MHD. It is unknown how this difference in definitions could bias results. In addition, patients enrolled in the REGAIN trial could be on 1 stable dose of prophylactic therapy (topiramate or propranolol only). The other pivotal trials did not allow patients to take a concurrent preventive medication. In the REGAIN trial, up to 1-third of the patients were allowed to take concomitant therapy with these agents per the study protocol; however, the number of patients using these therapies remained low. The number of patients using prophylactics during the trial was roughly equal in the 3 arms, and use of these concurrent therapies is unlikely to confound the results.
External Validity
Patients randomized to the galcanezumab 120 mg arm in the studies all received a loading dose of 240 mg, which aligns with the Health Canada–approved dose. Dosing in the open-label extension phase of the CONQUER trial also aligned with the Health Canada–approved dose. However, the dose of galcanezumab received by most patients during the open-label phase of the REGAIN trial did not align with the Health Canada–approved dose. The sponsor followed guidelines from IHS and the American Academy of Neurology.
The inclusion criteria of the trials adequately captured the CM and EM populations in Canada, according to the clinical expert consulted by CADTH. The EVOLVE-1, REGAIN, and CONQUER trials included study sites in Canada. The average number of monthly MHDs and headache days at baseline was lower than the clinical expert would expect to observe in the general Canadian migraine population, particularly in the REGAIN and CONQUER trials, which included patients diagnosed with CM, although the patients met the diagnostic criteria for EM or CM as appropriate in the pivotal trials. The trials excluded patients with common comorbidities such as depression and a higher risk of cardiovascular events, limiting full extrapolation of the data to the full population. However, the clinical expert indicated that this is common in migraine trials and unlikely to affect the generalizability of results. The majority of study patients in all trials were female and White, which the clinical expert indicated reflects the Canadian migraine population. On average, baseline measures indicated that the patient population in this study had been long-time sufferers of migraine, which aligns with the type of patients the clinical expert usually sees in their practice.
Patients indicated that they preferred a medication that reduces the frequency and severity of migraine and reduces or eliminates the need for acute medications (e.g., triptans and opioids). This aligns with the outcomes of monthly MHDs, monthly MHDs with acute medication use, and monthly headache days. Patients indicated that they preferred a preventive medication that allows them to be more productive at work and home and full participate in daily life, which aligns with the MIDAS, MSQ v2.1, and WPAI. The HIT-6 was not assessed in the trials, although it is a commonly used outcome measure in migraine trials.
The CONQUER trial was conducted in a treatment-resistant migraine-patient population, including patients with either EM or CM. Treatment-resistance was defined in this study as having a history of failure on 2 to 4 prior migraine-preventive medication categories due to inadequate efficacy or safety and tolerability. This trial population most closely aligns with the patient population specified in the reimbursement request. In contrast, EVOLVE-1, EVOLVE-2, and REGAIN excluded patients who failed to have an efficacy response to 3 or more classes of migraine-preventive treatment, and the majority of patients enrolled in these trials had not previously failed 2 or more prior migraine-preventive treatments. This may limit generalizability of the overall trial results to the patient population under review (i.e., patients who have experienced an inadequate response, intolerance, or are contraindicated for at least 1 prophylactic migraine medications). However, subgroup analyses in patients who failed at least 2 or at least 3 prior preventive medications were generally consistent with the primary analyses. All pivotal trials excluded patients who had been previously treated with a CGRP inhibitor. It is unclear whether results of the trials are generalizable to patients who had previously failed another CGRP inhibitor.
Patients in all the trials were able to continue the use of acute headache medications, which aligns with headache guidelines that allow preventive migraine therapy in combination with acute treatment. In the REGAIN trial, patients could be on 1 stable dose of prophylactic therapy (topiramate or propranolol only). This aligns with regular practice in Canada, according to the clinical expert consulted by CADTH, who indicated that galcanezumab could be used concurrently with other migraine-preventive medications. The clinical expert indicated that, if patients have had a partial response from a daily preventer, it would be appropriate to keep them on that medication if they were not having side effects and add an anti-CGRP monoclonal antibody.
In all the trials, the injections were administered by study personnel via manual syringes during dosing visits. According to the clinical expert consulted by CADTH, patients would inject themselves in regular clinical practice. The clinical expert noted that, currently, autoinjectors are commonly used to self-administer galcanezumab and other CGRP inhibitors. The clinical expert reported that the method of injection (i.e., manual syringe versus autoinjector) and training provided to the person administering the injection can affect whether a patient experiences an injection site reaction. As a result, safety data on injection site reactions from the pivotal trials may not be generalizable to regular use in the real-world setting.
All trials were placebo-controlled. No direct comparative effect was studied between galcanezumab versus other available migraine-preventive treatments (e.g., other CGRP medications).
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The sponsor submitted an ITC due to a lack of direct evidence comparing galcanezumab to other treatments for migraine in adults.14 CADTH also conducted a literature search and identified a single NMA of galcanezumab versus other migraine therapies that was conducted and published by the ICER.15 This section summarizes and critically appraises the sponsor-submitted ITC and NMA conducted by ICER.
Description of Indirect Comparisons
The sponsor-submitted ITC14 was based on a systematic review of drugs for CM or EM in which eligible studies were further analyzed with the Bucher method (Bucher et al. [1997]).63 The systematic literature reviews were conducted in October 2019 to identify all phase II and III randomized controlled trials (RCTs) of galcanezumab (120 mg and 240 mg) and erenumab (70 mg and 140 mg) in the prophylaxis of EM and CM in patients with a history of prior preventive-treatment failures. The population, intervention, comparator, outcomes, and study design of the sponsor-submitted ITC are presented in Table 29. An initial search was conducted in December 2017 (searched databases were not clearly described in the sponsor’s ITC report) followed by 3 updated searches of the same databases and conferences in October 2018, August 2019, and October 2019. Starting from the second update (August 2019), a search was performed in 3 health technology assessment repositories to identify relevant data in difficult-to-treat patient populations. Overall, 45 publications covering 16 individual RCTs were identified based on the wider pre-specified selection criteria. Out of these 16 trials, 4 were conducted specifically in an EM population, 6 in a CM population; and 3 in a mixed EM and CM population (for which results were not reported separately by migraine type), while in 2 trials the type of migraine was unspecified and in 1 the data were reported separately for EM and CM.
Based on a feasibility assessment, a full network Bayesian analysis was not feasible, and a series of pairwise Bucher ITCs comparing galcanezumab with erenumab were performed instead.14
Table 29: Study Selection Criteria and Methods for Indirect Treatment Comparisons
PICOS | Sponsor-submitted ITC | ICER NMAa |
|---|---|---|
Population | Adults (≥ 18 years old) (males and females) with migraine
| Adults (≥ 18 years old) with episodic or chronic migraine and eligible for preventive migraine therapy
|
Intervention | Galcanezumab 120 mg (with a loading dose of 240 mg) | Galcanezumab (120 mg, 240 mg) |
Comparatorc | Erenumab |
|
Outcome |
|
|
Study design | Phase II to IV randomized controlled trials (crossover up to time of crossover) |
|
Publication characteristics | English-language only | English language |
Exclusion criteria | NR |
|
Databases searched | An initial database searched in 2017 and the first update (August 2018) was not reported; starting from the second update (August 2019) a search was performed in 3 health technology assessment repositories |
|
Selection process | NR | Two independent reviewers with discrepancy solved through a consensus meeting |
Data extraction process | NR | Single reviewer with a second reviewer confirming accuracy |
Quality assessment | NR | US Preventive Services Task Force criteria |
HIT-6 = 6-item Headache Impact Test; ICER = Institute of Clinical and Economic Reviews; ITC = indirect treatment comparison; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; NMA = network meta-analysis; NR = not reported; OLE = open-label extension; PICOS = population, intervention, comparator, outcomes, and study design; RCT = randomized controlled trial; SAE = serious adverse event.
aOnly ICER ITC information relevant to this review was presented.
bNo ITC analysis for galcanezumab was performed in chronic migraine population.
cThe full list of comparators treatments considered were detailed in the systematic literature review; for the purpose of this ITC analysis, the focus was on erenumab (70 mg and 140 mg) only.
dErenumab (70 mg and 140 mg) and fremanezumab were reported as interventions in the ICER ITC. For the purpose of this review, erenumab (70 mg and 140 mg) and fremanezumab were classified as comparators.
eOnabotulinumtoxinA was not used for episodic migraine.15
Methods of Sponsor-Submitted Indirect Treatment Comparison
Objectives
In the absence of head-to-head studies of galcanezumab compared with erenumab, an ITC was conducted to understand the relative efficacy and safety of galcanezumab 120 mg (with a 240 mg loading dose) compared to erenumab 70 mg and 140 mg in EM and CM patients with a history of prior preventive treatment failures.
Study Selection Methods
The sponsor-submitted ITC included only studies that provided information on whether patients had had an inadequate response to at least 2 or at least 3 prior preventive migraine treatments. In addition, these studies needed to present their results separately for either CM or EM. Only erenumab was included as comparator for this ITC. However, whether study selection and data extraction were conducted by 2 reviewers independently was not clearly described. Whether the methodological quality of included studies was assessed was also not clearly described.
Indirect Treatment Comparison Analysis Methods
The sponsor-submitted ITC was conducted using the Bucher method,63 which is a frequentist approach to evidence synthesis. The following populations were of interest for the ITC conducted for EM and CM: difficult-to-treat patient population 2, defined as failure on at least 2 prior preventive treatments for all-cause reasons; and difficult-to-treat patient population 3, a population defined as failure on at least 3 prior preventive treatments for all-cause reasons. The intervention of galcanezumab 120 mg (with a loading dose of 240 mg) was compared to erenumab 70 mg and 140 mg doses. The outcomes included response rates (≥ 50%, ≥ 75%, and ≥ 100% reduction in MHDs) and monthly migraine days with acute migraine-specific medication use, as well as discontinuation for all causes and discontinuation due to AEs. Continuous outcomes were assessed in terms of weighted mean difference. Binary outcomes were assessed in terms of odds ratio (OR), relative risk (RR), and risk difference (RD); however, the focus of the ITC was interpretation of the OR results as these were the most commonly reported outcomes for binary end points. Because the number of events was small for some end points and even 0 (in the case of AEs), the conclusions drawn through OR, RR, and RD may differ. For binary outcomes for OR or RR, the treatment effect of the indirect comparison of active treatments A and B via common comparator baseline treatment C was estimated as the difference of the treatment effects of the direct comparisons on the log scale. If more than 1 study was available, the corresponding treatment effect and variance considered in the Bucher method was a pooled estimator obtained through meta-analysis using a binary outcome from the Mantel-Haenszel method. Pooling of continuous outcome was conducted by assigning inverse variance weights to the individual studies. The inverse variance refers to the relative effect of each individual study, which was considered in the pooling.14 The random effects were calculated using the DerSimonian-Laird method as the estimator for tau for both a continuous and binary outcome.14
The heterogeneity across included studies on each comparison was assessed through the inconsistency parameter (I2) statistic and the P value of the Q statistic. In the absence of heterogeneity, the results of fixed effects and random effects models were expected to be identical. The ITC analyses were performed using the Cheetah-tool (Indirect Comparison on Results from 2 Meta-Analyses version 1.1), a Lilly-developed program based on R package Meta. Treatment effects were estimated, following the approach proposed by Bucher et al. (1997).63
The base-case analyses used the estimates of the primary analyses as displayed in the publicly available information for each study. Three sensitivity analysis were relevant to the ITC. One sensitivity analysis was performed as per the base case, except that continuous estimates from EVOLVE-1 and EVOLVE-2, REGAIN and CONQUER were multiplied by 28 and divided by 30 to assess the impact of defining a month differently across study programs (28 versus 30 days); 1 sensitivity analysis used all data points at a specific time point (i.e., at month 3 and at month 6; as opposed to across a few months) to assess the impact of the different analyses choices across studies; and the third sensitivity analysis was done as per the base case, but excluding subgroup data. In other words, this sensitivity analyses considered only evidence from CONQUER (I5Q-MCCGAW) for galcanezumab or LIBERTY for erenumab.
The author of the ITC indicated that responder rates (50%, 75%, or 100%, also known as a 50%, 75%, and 100% reduction in MHD) were analyzed differently in the galcanezumab and erenumab development plans and they were therefore reported differently. In the galcanezumab studies, the responder outcomes correspond to the average of the monthly responder rates calculated across the double-blind study duration and was therefore a continuous measure. Hence, tTo allow for an indirect comparison to the erenumab studies, the number of responders in the galcanezumab studies were recalculated from the average of the response rates and the number of patients contributing to the analyses. In the erenumab studies, the responder outcomes are binary and calculated at month 3 (for LIBERTY and the chronic phase II study) or across a period of time (month 4 to month 6 for STRIVE).
The base-case analyses used the estimates of the primary analyses as displayed in the primary manuscripts of each study. The erenumab trials calculated monthly estimates based on 28 days, whereas galcanezumab studies considered a month based on 30 days. The author indicated that, overall, these estimates were comparable from 1 study to another but estimates for all studies are not always publicly available.
Results of the Sponsor-Submitted ITC
Summary of Included Studies
Galcanezumab was investigated in 4 studies (EVOLVE-1,64 EVOLVE-2,64 REGAIN,65 and CONQUER66). REGAIN65 was performed in a population with CM. The included study results were based on a subgroup analysis of REGAIN (Ruff et al. [2019a]67). CONQUER66 was an RCT investigating galcanezumab in EM and CM with a history of failure on 2 to 4 migraine-preventive medication categories (Mulleners et al., [2019]68). EVOLVE-1 and EVOLVE-2 were conducted in patients with EM (reported in conference abstracts: Zhang et al. [2018]69; results were published later in Ruff et al. [2019b]70). Erenumab was investigated in 3 trials, 2 of which were performed in an EM population (STRIVE, subgroup data NCT02456740)71 and LIBERTY (a specific trial in EM patients unsuccessfully treated with prior preventive migraine treatments, NCT03096834)72 and 1 in a CM population (subgroup, NCT02066415, AMG 334, Ashina [2018]73). The efficacy results of these trials were reported in a pooled analysis. However, the individual study data from EVOLVE-1 and EVOLVE-2 included in the ITC were based on internal documentation.64 The source documents on which the ITC was based are presented in Table 30.
Table 30: Source Documents Considered in the Sponsor’s Indirect Treatment Comparison
Study drugs | Study name and acronym | ITC alias | Full reference |
|---|---|---|---|
Galcanezumab | Evaluation of Galcanezumab in the Prevention of Episodic Migraine – the EVOLVE-1 Study (Evolve-1)64 | CGAG64 | Eli Lilly and Company (2018a). Galcanezumab Clinical Health Technology Assessment Toolkit. Assessment of Clinical Efficacy and Safety for Galcanezumab – Pooled Studies.64 |
Evaluation of Galcanezumab in the Prevention of Episodic Migraine – the EVOLVE-2 Study (Evolve-2)64 | CGAH64 | Eli Lilly and Company (2018a). Galcanezumab Clinical Health Technology Assessment Toolkit. Assessment of Clinical Efficacy and Safety for Galcanezumab – Pooled Studies.64 | |
A Study of Galcanezumab (LY2951742) in Adults With Treatment-Resistant Migraine (CONQUER)66 | CGAW66 | Eli Lilly and Company (2019c). CGAW Clinical Study Report. A randomized, double-blind, placebo-controlled study of galcanezumab in adults with treatment-resistant migraine – the CONQUER study: final results from the double-blind treatment phase and interim results from the open-label treatment phase. Sep 27, 2019.66 | |
Evaluation of Galcanezumab in the Prevention of Chronic Migraine (REGAIN)65 | CGAI65 | Eli Lilly and Company (2018b). I5Q-MC-CGAI Clinical Health Technology Assessment Toolkit Clinical Section of Health Technology Toolkit for REGAIN: Assessment of Clinical Efficacy and Safety for Galcanezumab (LY2951742). A phase 3, Randomized, Double-Blind, Placebo-Controlled Study of LY2951742 in Patients with Chronic Migraine – the REGAIN Study.65 | |
Erenumab | A Study Evaluating the Effectiveness of AMG 334 Injection in Preventing Migraines in Adults Having Failed Other Therapies (Liberty)72 | Reuter (2018)72 | Reuter U., Goadsby PJ., Lanteri-Minet M., Wen S., Hours-Zesiger P., Ferrari MD., Klatt J. (2018). Efficacy and tolerability of erenumab in patients with episodic migraine in whom 2 to-four previous preventive treatments were unsuccessful: a randomized, double-blind, placebo-controlled, phase 3b study. Lancet. pii: S0140 to 6736(18)32534 to 0. doi:10.1016/S0140-6736(18)32534-0. [Epub ahead of print]72 |
Erenumab (continued) | Study to Evaluate the Efficacy and Safety of Erenumab (AMG334) in Migraine Prevention (Strive)67,71 | Goadsby (2019)71 | Goadsby P., Paemeleire K., Broessner G., Brandes J., Klatt J., Zhang F., Picard H., Lenz R., Mikol D (2019). Efficacy and safety of erenumab (AMG334) in episodic migraine patients with prior preventive treatment failure: A subgroup analysis of a randomized, double-blind, placebo-controlled study. Cephalalgia, 39(7):817 to 826. doi:10.1177/0333102419835459. Epub 2019 Apr 1371 |
Ruff (2019a)67 | Ruff D, Ford J, Tockhorn-Heidenreich A, Sexson M, Govindan S, Pearlman E, Wang SJ, Khan A, Aurora SK (2019a). Efficacy of galcanezumab in patients with chronic migraine and a history of preventive treatment failure. Cephalalgia, May 19:333102419847957. doi: 10.1177/0333102419847957. [Epub ahead of print]67 | ||
A Study to Evaluate the Efficacy and Safety of Erenumab (AMG 334) in Chronic Migraine Prevention73 | Ashina (2018)73 | Ashina M., Tepper S., Brandes J., Reuter U., Boudreau G., Dolezil D., Mikol D. (2018). Efficacy and safety of erenumab (AMG334) in chronic migraine patients with prior preventive treatment failure: A subgroup analysis of a randomized, double-blind, placebo-controlled study. Cephalalgia, 38(10), 1611 to 1621. doi:10.1177/033310241878834773 |
ITC = indirect treatment comparison.
Source: Sponsor-submitted ITC.14
The baseline characteristics of the included studies used in the ITCs are presented in Table 31, Table 32, Table 33, and Table 34. No baseline data were available for the difficult-to-treat EM population from LIBERTY.
Table 31: Baseline Characteristics for Difficult-to-Treat Population 2 — Episodic Migraine
Trials | Intervention/ comparators | Patient number | Age, years mean (SD) | Female number, (%) | Number of monthly migraine headache days, mean (SD) | Monthly migraine days with acute medication, mean (SD) |
|---|---|---|---|---|---|---|
Galcanezumab | ||||||
EVOLVE-1 (CGAG)64 | Galcanezumab 120 mg | | | |||||||||| | |||||||||| | |||| | | |
Placebo | | | |||||||||| | |||||||| | |||| | | | |
EVOLVE-2 (CGAH)64 | Galcanezumab 120 mg | | | |||||||||| | |||||||| | |||| | | |
Placebo | | | |||||||| | |||||||| | |||| | | | |
CONQUER (CGAW)66 | Galcanezumab 120 mg | 137 | 45.9 (11.2) | 112 (81.2) | 9.5 (3.0) | 8.5 (3.1) |
Placebo | 132 | 46.3 (11.8) | 117 (88.6) | 9.2 (2.7) | 8.1 (2.9) | |
Erenumab | ||||||
STRIVE (Goadsby, 2019)71 | Erenumab 70 mg | 49 | 42.5 (10.6) | 47 (95.9) | 8.9 (2.0) | NA |
Erenumab 140 mg | 58 | 42.5 (9.8) | 53 (91.4) | 8.7 (2.5) | NA | |
Placebo | 54 | 46.4 (11.2) | 44 (81.5) | 8.1 (2.5) | NA | |
LIBERTY (Reuter, 2018)72 | Erenumab 140 mg | 121 | 44.6 (10.5) | 97 (80.0) | 9.2 (2.6) | 4.8 (2.9) |
Placebo | 125 | 44.2 (10.6) | 103 (82.0) | 9.3 (2.7) | 4.4 (2.8) | |
NA = not available; SD = standard deviation.
Source: Sponsor-submitted indirect treatment comparsion.14
Table 32: Baseline Characteristics for Difficult-to-Treat Population 2 — Chronic Migraine
Trials | Intervention/ comparators | Patient number | Age, years mean (SD) | Female number, (%) | Number of monthly migraine headache days, mean (SD) | Monthly migraine days with acute medication, mean (SD) |
|---|---|---|---|---|---|---|
Galcanezumab | ||||||
REGAIN (CGAI)65 | Galcanezumab 120 mg | 74 | 42.8 (11.3) | 68 (91.9) | 20.0 (4.3) | 16.6 (5.6) |
Placebo | 177 | 43.9 (11.8) | 157 (88.7) | 19.6 (4.7) | 15.8 (6.0) | |
CONQUER (CGAW)66 | Galcanezumab 120 mg | 95 | 45.8 (11.6) | 83 (87.4) | 19.2 (4.7) | 15.0 (6.3) |
Placebo | 98 | 44.8 (13.1) | 85 (86.7) | 18.1 (4.7) | 15.2 (5.9) | |
Erenumab | ||||||
AMG 334 (Ashina [2018])73 | Erenumab 70 mg | 93 | 42.9 (11.2) | 84 (90.3) | 18.0 (4.4) | 10.5 (7.2) |
Erenumab 140 mg | 92 | 44.2 (10.6) | 82 (89.1) | 18.8 (4.4) | 12.4 (6.2) | |
Placebo | 142 | 42.9 (11.5) | 111 (78.2) | 18.3 (4.5) | 11.4 (7.4) | |
NA = not available; SD = standard deviation.
Source: Sponsor-submitted indirect treatment comparsion.14
Table 33: Baseline Characteristics for Difficult-to-Treat Population 3 — Episodic Migraine
Trials | Intervention/ comparators | Patient number | Age, years mean (SD) | Female number, (%) | Number of monthly migraine headache days, mean (SD) | Monthly migraine days with acute medication, mean (SD) |
|---|---|---|---|---|---|---|
Galcanezumab | ||||||
CONQUER (CGAW)66 | Galcanezumab 120 mg | 56 | 44.7 (10.7) | 43 (76.8) | 10.2 (2.6) | 9.5 (2.7) |
Placebo | 44 | 47.7 (12.3) | 40 (90.9) | 9.5 (2.7) | 8.1 (2.9) | |
Erenumab | ||||||
LIBERTY (Reuter [2018])72 | Erenumab 140 mg | 76 | NA | NA | NA | NA |
Placebo | 72 | NA | NA | NA | NA | |
NA = not available; SD = standard deviation.
Source: Sponsor-submitted indirect treatment comparsion.14
Table 34: Baseline Characteristics for Difficult-to-Treat Population 3 — Chronic Migraine
Trials | Intervention/ comparators | Patient number | Age, years mean (SD) | Female number, (%) | Number of monthly migraine headache days, mean (SD) | Monthly migraine days with acute medication, mean (SD) |
|---|---|---|---|---|---|---|
Galcanezumab | ||||||
REGAIN (CGAI)65 | Galcanezumab 120 mg | | | |||||||| | |||| | |||||| | | |
Placebo | | | |||||||| | |||| | |||||| | | | |
CONQUER (CGAW)66 | Galcanezumab 120 mg | 43 | 46.3 (10.7) | 35 (81.4) | 18.8 (4.6) | 15.3 (6.2) |
Placebo | 43 | 44.7 (14.1) | 37 (86.1) | 18.8 (4.9) | 15.7 (5.9) | |
Erenumab | ||||||
AMG 334 (Ashina [2018])73 | Erenumab 70 mg | 69 | 42.8 (11.5) | 62 (89.9) | 18.9 (4.4) | 11.0 (7.6) |
Erenumab 140 mg | 65 | 44.1 (11.3) | 59 (90.8) | 19.0 (4.7) | 12.5 (6.1) | |
Placebo | 98 | 42.4 (11.5) | 72 (73.5) | 18.6 (4.3) | 12.0 (7.1) | |
NA = not available; SD = standard deviation.
Source: Sponsor-submitted indirect treatment comparison.14
Results
A summary of the key results of each outcome of the sponsor-submitted ITC are presented Table 35 and Table 36.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| to erenumab in all reported outcomes (response rate, change from baseline of monthly MHD, change from baseline of monthly MHD with acute medication use, discontinuation from all-cause, and discontinuation from adverse events in patients with EM or CM who failed at least 2 or at least 3 preventive medications).
Table 35: Base-Case Analysis ITC Results in Patients Who Failed 2 or More Medications (DTT-2, Random Effect)
Outcomes | Episodic migraine | Chronic migraine | ||
|---|---|---|---|---|
Galcanezumab vs. erenumab 70 mg | Galcanezumab vs. erenumab 140 mg | Galcanezumab vs. erenumab 70 mg | Galcanezumab vs. erenumab 140 mg | |
≥ 50% reduction in migraine headache days | ||||
Odds ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
≥ 75% reduction in migraine headache days | ||||
Odds ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
100% reduction in migraine headache days | ||||
Odds ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
CFB in monthly migraine headache days | ||||
Mean difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
CFB in monthly migraine headache days with acute medication use | ||||
Mean difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
Discontinuation due to all-cause | ||||
Odds ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
Discontinuation due to AE | ||||
Odds ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
AE = adverse event; CFB = change from baseline; CI = confidence interval; DTT-2 = difficult-to-treat population 2; ITC = indirect treatment comparison; NA = not available; vs. = versus.
Note: Odds ratio for a response reduction greater than 1 favours galcanezumab; an odds ratio smaller than 1 favours galcanezumab for discontinuation; a negative mean difference in change from baseline favours galcanezumab.
Source: Sponsor-submitted ITC.14
Table 36: Base-Case Analysis ITC Results in Patients Who Failed 3 or More Medications (DTT-3, Random Effect)
Outcomes | Episodic migraine | Chronic migraine | ||
|---|---|---|---|---|
Galcanezumab vs. erenumab 70 mg | Galcanezumab vs. erenumab 140 mg | Galcanezumab vs. erenumab 70 mg | Galcanezumab vs. erenumab 140 mg | |
≥ 50% reduction in migraine headache days | ||||
Odds ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
≥ 75% reduction in migraine headache days | ||||
Odds ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk ratio (95% CI) | | | | | | | | | | | | | | | | | | | | |
Risk difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
CFB in monthly migraine headache days | ||||
Mean Difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
CFB in monthly migraine headache days with acute medication use | ||||
Mean difference (95% CI) | | | | | | | | | | | | | | | | | | | | |
CFB = change from baseline; CI = confidence interval; DTT-3 = difficult-to-treat population 3; ITC = indirect treatment comparison; NA = not assessed; vs. = versus.
Source: Sponsor-submitted indirect treatment comparison.14
The results from fixed-effect model analysis were largely consistent with that of random effect model analysis (data not reported in this summary).14
Sensitivity Analyses
Results of all 3 relevant sensitivity analyses were largely consistent with the base case in all reported outcomes (data not reported in this summary).14
Critical Appraisal of the Sponsor-Submitted Indirect Treatment Comparison
The sponsor-submitted ITC compared galcanezumab 120 mg (with a loading dose of 240 mg) to erenumab 70 mg and 140 mg. The ITC analysis was based on migraine type and the number of previous treatments for which patients were deemed to have responded inadequately. Clinically relevant outcomes, such as response rate, change from baseline of monthly MHDs, change from baseline in monthly MHDs with acute medication, and discontinuation due to all-cause reasons or AEs, were reported. Based on the feasibility assessment, the sponsor-submitted ITC was conducted using the Bucher method. In addition to the base-case analysis, several pre-planned sensitivity analyses were conducted to assess the robust of the ITC results. However, several key limitations of the ITC are evident.
Although the ITC was based on a systematic review of the literature to identify all relevant trials from 3 health technology assessment repositories and conferences, the detail of the initial databases searched were not described in the ITC report. Whether the selection of relevant studies and data extraction were conducted by 2 reviewers independently was not described. The potential risk of bias of the included studies (methodological limitations) was not assessed and not reported. The quality of the study design was therefore not considered in the ITC analysis. In addition, details of the key baseline disease characteristics of the included studies were not provided. Due to the lack of this information, the robustness of the systematic review process remains uncertain.
Some discrepancies in study-level data (such as the number of patients included for analysis for a specific outcome) were evident between what was presented in the ITC analysis and what was presented in the pivotal studies in the main report. The discrepancy may be due to the data sources being based on different publications. The data presented in the ITCs were based mainly on conference abstracts and internal documents (the internal documents were not provided in the ITC report). In this case, CADTH was unable to audit the data and to check the accuracy of the data used in the ITCs.
Several clinical heterogeneities across the included studies were identified. For example, the duration of trials for galcanezumab varied at either 3 months or 6 months. And the trial duration for erenumab was 3 months. Consequently, the responder was determined based on variable treatment duration (3 months versus 6 months). Furthermore, the length of a month in the monthly MHDs was defined differently in different studies (28 days in the REGAIN and CONQUER trials versus 30 days in the other trials), which had a potential impact on the ITC results. However, the results of the several sensitivity analyses in which the previously described factors were adjusted were largely consistent with that reported in the base-case analysis.
In addition, patient important outcomes such as headache-related disability, as measured by HIT-6, migraine-related disability scores as measured by the MIDAS, work productivity, loss of work days (WPAI), adherence, and HCRU (hospitalizations) were not assessed.
In summary, the sponsor-submitted ITC reported a broadly similar clinical efficacy and safety profile when comparing galcanezumab with erenumab. However, due to various limitations (i.e., methodological limitations and clinical heterogeneity), any interpretation of these findings should consider these limitations.
Methods of the Institute for Clinical and Economic Review Network Meta-Analysis
Objectives
The ICER 2018 NMA15 aimed to assess the comparative clinical effectiveness of CGRP inhibitors for patients with CM or EM.
Study Selection Methods
Similarly, the ICER NMA was based on a systematic review of CGRP inhibitors for treatment of patients with CM or EM.15 The population, intervention, comparison, outcome and study design for systematic review are presented in Table 28. Several bibliographic databases were searched. Two reviewers screened abstracts and full-text articles independently. Published RCTs of any sample size were included. Non-randomized comparative studies were selected if they had at least 100 patients and crossover studies were eligible if data were reported before the crossover period. The population of interest for this systematic review was adult patients (≥ 18 years of age) with migraine who experienced at least 4 headache days per month and were eligible for preventive therapy. Studies of patients with other types of headache conditions, such as tension-type, cluster, or secondary headaches were excluded. The primary intervention was CGRP inhibitors, which included prophylactic-treatment subcutaneous injections of galcanezumab, erenumab, and fremanezumab at any dose or frequency. For both EM and CM populations, other included preventive therapies were topiramate, propranolol, and amitriptyline. For CM patients, onabotulinumtoxinA was also included.
Key outcomes were change from baseline in monthly migraine days, change from baseline in using acute medication per month, 50% or greater reduction in migraine days, and all-cause discontinuations.
One reviewer extracted data on patient population, sample size, duration of follow-up, funding source, study design, intervention, outcome assessment (definition, timing, and method of assessment), and results. A second reviewer independently verified the extracted data.
Quality assessment of included studies was based on the US Preventive Services Task Force.74
Network Meta-Analysis Methods
An NMA was conducted if data were available from at least 3 similar studies, with respect to characteristics such as population, intervention, outcome, and time point.
The NMA followed a Bayesian framework with random effects on the treatment parameters, and between-study variance was assumed to be constant across treatment comparisons. Continuous outcomes were analyzed with a normal likelihood and identity link, while binary outcomes were analyzed with a binomial likelihood and logit link. The treatment effects were presented as mean differences with 95% credible intervals (CrIs) for continuous outcomes and ORs with 95% CIs for binary outcomes. Non-informative prior distributions were used for all model parameters. The first 50,000 iterations were discarded as a “burn-in” and base inferences were made on an additional 50,000 iterations using 3 chains, with chain convergence assessed visually with trace plots. If studies reported multiple time points, the NMAs included the latest time point data. Separate NMAs were conducted at monthly time points (e.g., 4 weeks, 8 weeks, 12 weeks, and 26 weeks) where data were available. A subgroup of patients who had failed at least 1 prior preventive treatment was also analyzed.
Results of Institute for Clinical and Economic Review Indirect Treatment Comparison
Summary of Included Studies
Although the ICER 2018 ITC aimed to assess the comparative clinical effectiveness of CGRP inhibitors for patients with CM or EM, the ICER comparison of galcanezumab with other treatments was only limited to patients with EM. No ITC on galcanezumab was performed for a CM population. In this summary, only relevant results of NMA analysis comparing galcanezumab with other migraine therapies are presented.
For patients with EM, 9 trials were included for the assessment of clinical benefit of CGRP inhibitors (4 trials for galcanezumab: Dodick [2014],75 Skljarevski [2018],76 EVOLVE-1,30 and EVOLVE-231; 3 trials for erenumab: Sun [2016],77 STRIVE,78 and ARISE]79; and 2 trials for fremanezumab: Bigal [2015]80 and HALO-EM,81). All of these trials were industry-funded, multi-centred, and conducted predominately in North America and Europe. All trials were double-blinded and included a 4-week baseline period followed by a 12-week randomized, placebo-controlled treatment phase. At baseline, the average age was 40 years, patients had been diagnosed with migraine for approximately 20 years, and the average number of migraine days per month was 8 to 9, with the exception of patients in Bigal (2015)80 (a fremanezumab trial), who experienced a higher frequency at baseline with approximately 12 migraine days per month. Across the trials, the number of days using any acute medication was approximately 7 to 10.
Of the trials assessing comparator-of-interest preventive therapies (i.e., amitriptyline, propranolol, or topiramate) in the EM population, 17 compared active therapy versus placebo (4 RCTs of amitriptyline,82-85 4 RCTs86-89 and 1 crossover of propranolol,90 and 8 RCTs of topiramate91-98) and 7 head-to-head studies were conducted (3 RCTs of topiramate versus propranolol,99-101 1 RCT of topiramate versus amitriptyline,102 1 RCT of propranolol versus amitriptyline,103 1 RCT of topiramate versus amitriptyline versus topiramate plus amitriptyline,104 and 1 RCT of propranolol versus amitriptyline versus propranolol plus amitriptyline105). Most trials were industry-funded. Ten of the trials were single-centred, 10 other trials were multi-centred, and the status of 4 was unclear. Where reported, the trials were conducted in the US and Europe, except for 4 trials conducted in Turkey and 1 in Singapore. Baseline phases were typically 4 weeks, followed by randomized phases of 4 weeks to 26 weeks. At baseline, the average number of migraine days ranged from 5 to 12 days per month. The percentage of patients who experienced prior failure on at least 1 preventive treatment was not reported in any of the oral preventive therapy trials.
Of RCTs conducted in patients with EM, an overall rating of “good,” “fair,” or “poor” was given to each study. The CGRP inhibitor studies were rated to be of good quality.30,31,75-81 The amitriptyline studies were rated as poor (Couch [1979]83), fair (Couch [2011],82 and Lampl [2009]85), and good (Gonçalves [2016]84). The propranolol studies were rated as good (Diener [1996]86), fair (Pradalier [1989]88), and poor (Jafarpour [2016],87 Sargent [1985],89 and Weber [1972]90). The topiramate studies were rated as good (Silberstein [2006]96), fair (Lipton [2011],93 Brandes [2004],91 Silberstein [2004],97 Mei [2004],95 and Storey [2001]98), and poor (Gode [2010]92 and Lo [2010]94). The head-to-head trials studies were rated as fair (Diener [2004],100 Dogan [2015],101 and Keskinbora [2008]104), and poor (Ashtari [2008],99 Dodick [2009],102 Duman [2015],103 and Mathew [1981]105).
An NMA was conducted if data were available from at least 3 similar studies.
Results
Results for EM patients
Fourteen trials of change from baseline in monthly migraine days were included in the NMA. Two trials compared topiramate with either amitriptyline or propranolol, and 12 of the trials compared an active therapy to placebo only (Figure 14). Across the trials, patients receiving placebo experienced an average reduction from baseline of 1.1 to 5.3 migraine days per month.
Eighteen trials reported on the proportion of patients who experienced a reduction of migraine frequency or migraine days by at least 50%. The trials assessed response between 12 and 26 weeks of treatment. Across the trials, 10% to 62% of patients on placebo were responders as defined by a reduction in migraine days of at least 50% (Figure 15).
Twelve of the 14 trials reported on the change in the number of days using acute medications per month during follow-up. Across the trials, patients on placebo experienced an average reduction from baseline of 0.6 to 3.8 days using acute medications (Figure 16).
Monthly Migraine Days: The network diagram for the ITC analysis on monthly migraine days is presented in Figure 14. Table 37 present results from the NMA for the change from baseline in monthly migraine days in patients with EM. Galcanezumab (120 mg and 240 mg) was compared with fremanezumab 225 mg monthly and fremanezumab 675 mg quarterly, erenumab 140 mg, erenumab 70 mg, propranolol 160 mg per day, topiramate 200 mg per day, topiramate 100 mg per day, topiramate 50 mg per day, amitriptyline 25 mg per day to 100 mg per day, and placebo. Galcanezumab (both 240 mg and 120 mg) was favoured only when compared with topiramate 200 mg per day, topiramate 50 mg per day, and placebo (Table 37). The mean differences between galcanezumab 240 mg and topiramate 200 mg per day, topiramate 50 mg per day, and placebo were −0.89 (95% CrI, −1.69 to −0.03), −1.67 (95% CrI, −2.66 to −0.65), and −1.84 (95% CrI, −2.48 to −1.22), respectively. The mean differences between galcanezumab 120 mg and topiramate 200 mg per day, topiramate 50 mg per day, and placebo were −0.84 (95% CrI, −1.63 to −0.01), −1.62 (95% CrI, −2.60 to −0.62) and −1.80 (95% CrI, −2.40 to −1.20), respectively.
Figure 14: Network of Studies Assessing Monthly Migraine Days in Episodic Migraine Patients
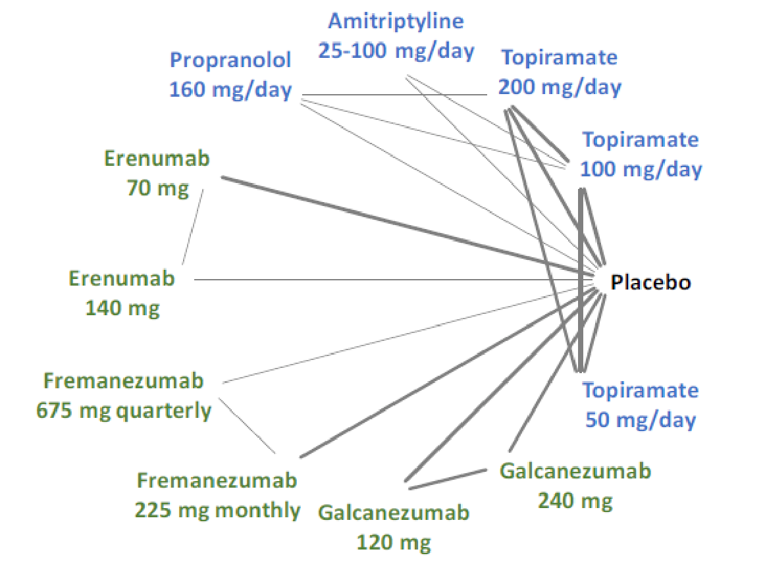
Note: Calcitonin gene-related peptide receptor inhibitors are depicted in green, existing oral preventive therapies in blue, and placebo in black. The thickness of the connecting lines is related to the number of trials available for each pair of treatments.
Source: Institute for Clinical and Economic Review network meta-analysis.15
Table 37: Network Meta-Analysis Results for Change from Baseline in Monthly Migraine Days in Episodic Migraine Patients
Comparison | Mean difference (95% CrI) |
|---|---|
Galcanezumab 240 mg vs. fremanezumab 225 mg, monthly | −0.25 (−1.28 to 0.83) |
Galcanezumab 120 mg vs. fremanezumab 225 mg, monthly | −0.20 (−1.20 to 0.85) |
Galcanezumab 240 mg vs. fremanezumab 675 mg, quarterly | −0.56 (−1.81 to 0.50) |
Galcanezumab 120 mg vs. fremanezumab 675 mg, quarterly | −0.61 (−1.73 to 0.52) |
Erenumab 140 mg vs. galcanezumab 240 mg | −0.10 (−1.07 to 0.87) |
Erenumab 140 mg vs. galcanezumab 120 mg | −0.15 (−1.09 to 0.82) |
Galcanezumab 240 mg vs. erenumab 70 mg | −0.54 (−1.36 to 0.25) |
Galcanezumab 120 mg vs. erenumab 70 mg | −0.50 (−1.29 to 0.27) |
Galcanezumab 240 mg vs. propranolol 160 mg per day | −0.64 (−1.65 to 0.38) |
Galcanezumab 120 mg vs. propranolol 160 mg per day | −0.60 (−1.57 to 0.40) |
Galcanezumab 240 mg vs. topiramate 200 mg per day | −0.89 (−1.69 to −0.03) |
Galcanezumab 120 mg vs. topiramate 200 mg per day | −0.84 (−1.63 to −0.01) |
Galcanezumab 240 mg vs. topiramate 100 mg per day | −0.68 (−1.44 to 0.12) |
Galcanezumab 120 mg vs. topiramate 100 mg per day | −0.64 (−1.38 to 0.14) |
Galcanezumab 240 mg vs. topiramate 50 mg per day | −1.67 (−2.66 to −0.65) |
Galcanezumab 120 mg vs. topiramate 50 mg per day | −1.62 (−2.60 to −0.62) |
Galcanezumab 240 mg vs. amitriptyline 25 mg per day to 100 mg per day | −0.77 (−2.09 to 0.56) |
Galcanezumab 120 mg vs. amitriptyline 25 mg per day to 100 mg per day | −0.73 (−2.02 to 0.58) |
Galcanezumab 240 mg vs. placebo | −1.84 (−2.48 to −1.22) |
Galcanezumab 120 mg vs. placebo | −1.80 (−2.40 to −1.20) |
CrI = credible interval; vs. = versus.
Note: Results displayed in bold indicate comparisons that favour galcanezumab.
Source: Institute for Clinical and Economic Review network meta-analysis.15
Proportion of Patients With 50% Response (Responder: 50% Reduction in Migraine Frequency or Migraine Headache Days): The ITC analysis network diagram for 50% responders in patients with EM is presented in Figure 15. Table 38 presents results from the NMA for the 50% response in patients with EM. In this analysis, galcanezumab (240 mg and 120 mg) was only favoured when compared with placebo.
Figure 15: Network of Studies Assessing 50% Response in Episodic Migraine Patients
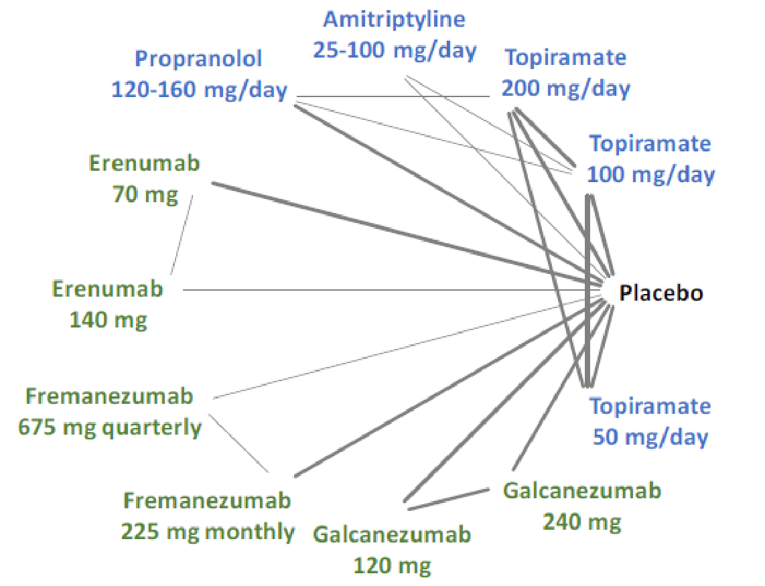
Note: Calcitonin gene-related peptide receptor inhibitors inhibitors are depicted in green, existing oral preventive therapies in blue, and placebo in black. The thickness of the connecting lines is related to the number of trials available for each pair of treatments.
Source: Institute for Clinical and Economic Review network meta-analysis.15
Table 38: Network Meta-Analysis Results for 50% Response in Episodic Migraine Patients
Comparison | Odds ratio (95% CrI) |
|---|---|
Galcanezumab 240 mg vs. fremanezumab 225 mg, monthly | 1.29 (0.79 to 2.05) |
Galcanezumab 120 mg vs. fremanezumab 225 mg, monthly | 1.21 (0.73 to 1.95) |
Galcanezumab 240 mg vs. fremanezumab 675 mg, quarterly | 1.48 (0.86 to 2.47) |
Galcanezumab 120 mg vs. fremanezumab 675 mg, quarterly | 1.39 (0.80 to 2.35) |
Galcanezumab 240 mg vs. erenumab 140 mg | 1.17 (0.70 to 1.89) |
Galcanezumab 120 mg vs. erenumab 140 mg | 1.09 (0.65 to 1.81) |
Galcanezumab 240 mg vs. erenumab 70 mg | 1.33 (0.88 to 1.99) |
Galcanezumab 120 mg vs. erenumab 70 mg | 1.25 (0.82 to 1.90) |
Propranolol 120 mg per day to 160 mg per day vs. galcanezumab 240 mg | 1.07 (0.64 to 1.78) |
Propranolol 120 mg per day to 160 mg per day vs. galcanezumab 120 mg | 1.14 (0.67 to 1.92) |
Galcanezumab 240 mg vs. topiramate 200 mg per day | 1.09 (0.72 to 1.65) |
Galcanezumab 120 mg vs. topiramate 200 mg per day | 1.02 (0.66 to 1.57) |
Topiramate 100 mg/day vs. galcanezumab 240 mg | 1.06 (0.73 to 1.62) |
Topiramate 100 mg/day vs. galcanezumab 120 mg | 1.14 (0.76 to 1.74) |
Galcanezumab 240 mg vs. topiramate 50 mg per day | 1.59 (0.97 to 2.57) |
Galcanezumab 120 mg vs. topiramate 50 mg per day | 1.49 (0.90 to 2.43) |
Galcanezumab 240 mg vs. amitriptyline 25 mg per day to 100 mg per day | 1.29 (0.71 to 2.23) |
Galcanezumab 120 mg vs. amitriptyline 25 mg per day 100 mg per day | 1.21 (0.66 to 2.12) |
Galcanezumab 240 mg vs. placebo | 2.52 (1.87 to 3.35) |
Galcanezumab 120 mg vs. placebo | 2.36 (1.72 to 3.21) |
CrI = credible interval; vs. = versus.
Note: Results displayed in bold indicate comparisons that favour galcanezumab.
Source: Institute for Clinical and Economic Review network meta-analysis.15
The ITC analysis network diagram for the change from baseline in acute medication use per month in patients with EM is presented in Figure 16. Table 39 present results from the NMA for the change from baseline in acute medication use per month in patients with EM. In this analysis, patients in galcanezumab 120 mg group experienced fewer days of acute medication use per month compared with the erenumab 70 mg group, with a between-group mean difference of change from baseline of −0.94 (95% CrI, −1.69 to −0.10). Galcanezumab (both 240 mg and 120 mg) was favoured, with patients having fewer days of acute medication use per month compared with topiramate 200 mg per day and topiramate 50 mg per day. The mean difference of change from baseline between galcanezumab 240 mg and topiramate 200 mg per day was −0.99 (95% CrI, −1.79 to −0.12), the mean difference of change from baseline between galcanezumab 120 mg and topiramate 200 mg per day was −1.08 (95% CrI, −1.89 to −0.22), the mean difference of change from baseline between galcanezumab 240 mg and topiramate 50 mg per day was −1.27 (95% CrI, −2.33 to −0.16), and the mean difference of change from baseline between galcanezumab 120 mg and topiramate 50 mg per day was −1.37 (95% CrI, −2.43 to −0.26). Galcanezumab 120 mg was favoured, with patients having fewer days of acute medication use per month compared with topiramate 100 mg per day. The mean difference of change from baseline between galcanezumab 120 mg and topiramate 100 mg per day was −0.85 (95% CrI, −1.64 to −0.04). In addition, galcanezumab (both 240 mg and 120 mg) was favoured, with patients having fewer days of acute medication use per month compared with placebo. The mean difference of change from baseline between galcanezumab 240 mg and placebo was −1.71 (95% CrI, −2.33 to −1.07) and the mean difference of change from baseline between galcanezumab 120 mg and placebo was −1.80 (95% CrI, −2.44 to −1.17).
Figure 16: Network of Studies Assessing Days of Acute Medication Use per Month in Episodic Migraine Patients
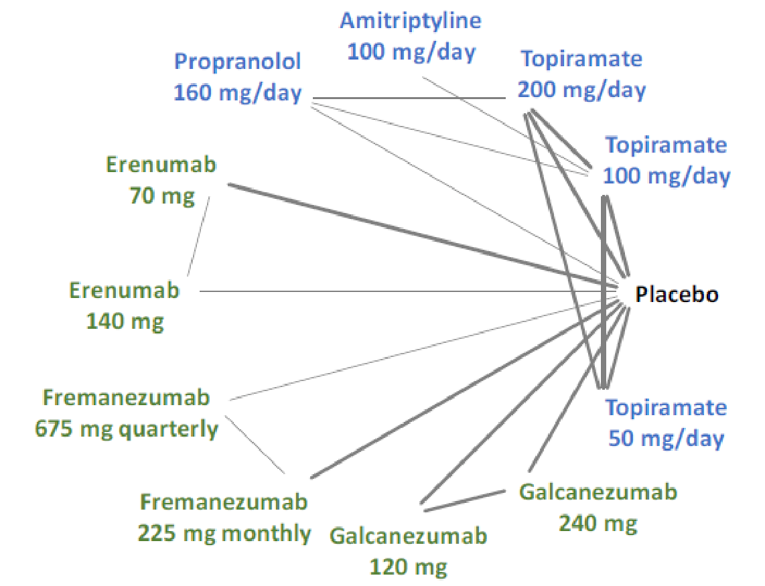
Note: Calcitonin gene-related peptide receptor inhibitors are depicted in green, existing oral preventive therapies in blue, and placebo in black. The thickness of the connecting lines is related to the number of trials available for each pair of treatments.
Source: Institute for Clinical and Economic Review network meta-analysis.15
Table 39: Network Meta-Analysis Results for Change from Baseline in Days of Acute Medication Use per Month in Episodic Migraine Patients
Comparison | Mean difference (95% CrI) |
|---|---|
Galcanezumab 240 mg vs. fremanezumab 225 mg, monthly | −0.60 (−1.58 to 0.43) |
Galcanezumab 120 mg vs. fremanezumab 225 mg, monthly | 0.49 (−1.48 to 0.53) |
Galcanezumab 240 mg vs. fremanezumab 675 mg, quarterly | −0.69 (−1.76 to 0.41) |
Galcanezumab 120 mg vs. fremanezumab 675 mg, quarterly | −0.59 (−1.66 to 0.50) |
Galcanezumab 240 vs. erenumab 140 mg | −0.07 (−1.02 to 0.91) |
Galcanezumab 120 vs. erenumab 140 mg | −0.17 (−1.12 to 0.81) |
Galcanezumab 240 mg vs. erenumab 70 mg | −0.84 (−1.58 to 0.00) |
Galcanezumab 120 mg vs. erenumab 70 mg | −0.94 (−1.69 to −0.10) |
Galcanezumab 240 mg vs. propranolol 160 mg per day | −0.62 (−1.59 to 0.38) |
Galcanezumab 120 mg vs. propranolol 160 mg per day | −0.72 (−1.69 to 0.28) |
Galcanezumab 240 mg vs. topiramate 200 mg per day | −0.99 (−1.79 to −0.12) |
Galcanezumab 120 mg vs. topiramate 200 mg per day | −1.08 (−1.89 to −0.22) |
Galcanezumab 240 mg vs. topiramate 100 mg per day | −0.76 (−1.54 to 0.07) |
Galcanezumab 120 mg vs. topiramate 100 mg per day | −0.85 (−1.64 to −0.04) |
Galcanezumab 240 mg vs. topiramate 50 mg per day | −1.27 (−2.33 to −0.16) |
Galcanezumab 120 mg vs. topiramate 50 mg per day | −1.37 (−2.43 to −0.26) |
Galcanezumab 240 mg vs. amitriptyline 100 mg per day | −0.55 (−1.91 to 0.84) |
Galcanezumab 120 mg vs. amitriptyline 100 mg per day | −0.65 (−2.02 to 0.73) |
Galcanezumab 240 mg vs. placebo | −1.71 (−2.33 to −1.07) |
Galcanezumab 120 mg vs. placebo | −1.80 (−2.44 to −1.17) |
CrI = credible interval; vs. = versus.
Note: Results displayed in bold indicate comparisons that favour galcanezumab.
Source: Institute for Clinical and Economic Review network meta-analysis.15
The ITC analysis network diagram for proportion of patients with all-cause discontinuations in patients with EM is presented in Figure 17. Table 40 present results from the NMA for all-cause discontinuations in patients with EM. In this analysis, no treatments were favoured when comparing galcanezumab (240 mg and 120 mg) with other CGRPs and other existing preventive therapies.
Figure 17: Network of Studies Assessing All-Cause Discontinuations in Episodic Migraine Patients
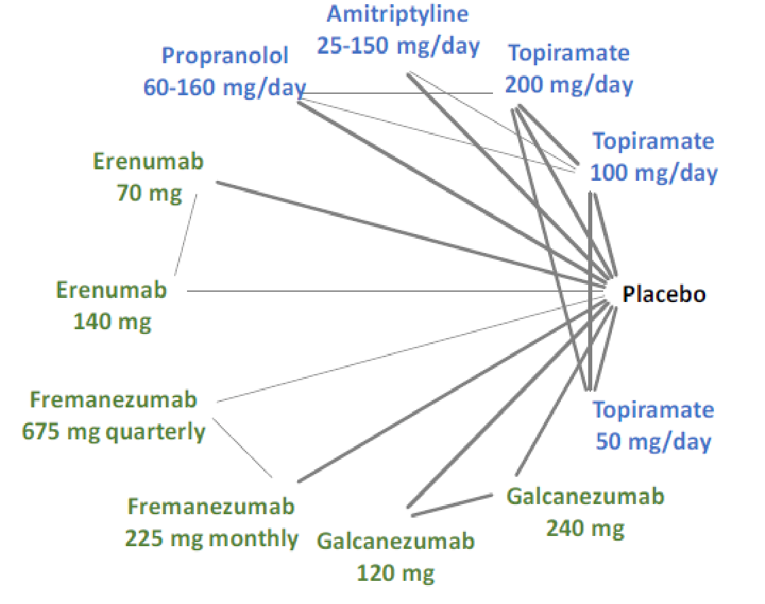
Note: Calcitonin gene-related peptide receptor inhibitors are depicted in green, existing oral preventive therapies in blue, and placebo in black. The thickness of the connecting lines is related to the number of trials available for each pair of treatments.
Source: Institute for Clinical and Economic Review network meta-analysis.15
Table 40: Network Meta-analysis Results for All-Cause Discontinuations in Episodic Migraine Patients
Comparison | Odds ratio (95% CrI) |
|---|---|
Galcanezumab 240 mg vs. fremanezumab 225 mg, monthly | 0.61 (0.24 to 1.47) |
Galcanezumab 120 mg vs. fremanezumab 225 mg, monthly | 0.64 (0.26 to 1.50) |
Galcanezumab 240 mg vs. fremanezumab 675 mg, quarterly | 0.77 (0.28 to 2.13) |
Galcanezumab 120 mg vs. fremanezumab 675 mg, quarterly | 0.80 (0.30 to 2.18) |
Erenumab 140 mg vs. galcanezumab 240 mg | 0.74 (0.26 to 1.97) |
Erenumab 140 mg vs. galcanezumab 120 mg | 0.71(0.26 to 1.83) |
Erenumab 70 mg vs. galcanezumab 240 mg | 0.83 (0.32 to 1.94) |
Erenumab 70 mg vs. galcanezumab 120 mg | 0.80 (0.32 to 1.81) |
Galcanezumab 240 mg vs. propranolol 60 mg per day to 160 mg per day | 0.91 (0.41 to 1.86) |
Galcanezumab 120 mg vs. propranolol 60 mg per day to 160 mg per day | 0.95 (0.45 to 1.87) |
Galcanezumab 240 mg vs. topiramate 200 mg per day | 0.50 (0.25 to 1.00) |
Galcanezumab 120 mg vs. topiramate 200 mg per day | 0.52 (0.27 to 1.01) |
Galcanezumab 240 mg vs. topiramate 100 mg per day | 0.86 (0.44 to 1.66) |
Galcanezumab 120 mg vs. topiramate 100 mg per day | 0.90 (0.48 to 1.67) |
Galcanezumab 240 mg vs. topiramate 50 mg per day | 0.76 (0.37 to 1.73) |
Galcanezumab 120 mg vs. topiramate 50 mg per day | 0.79 (0.40 to 1.76) |
Galcanezumab 240 mg vs. amitriptyline 25 mg per day to 100 mg per day | 0.81 (0.38 to 1.61) |
Galcanezumab 120 mg vs. amitriptyline 25 mg per day to 100 mg per day | 0.84 (0.42 to 1.63) |
Galcanezumab 240 mg vs. placebo | 0.84 (0.48 to 1.50) |
Galcanezumab 120 mg vs. placebo | 0.88 (0.53 to 1.50) |
CrI = credible interval; vs = vs..
Source: Institute for Clinical and Economic Review network meta-analysis.15
No NMA was conducted for quality of life (e.g., MIDAS or MSQ v2.1) or the HIT-6.
Critical Appraisal of Institute for Clinical and Economic Review Indirect Treatment Comparison
The NMAs were based on a systematic review of the literature to identify all relevant published trials from multiple databases, with the focus of the review on CGRP inhibitors as the intervention. A comprehensive set of safety and efficacy outcomes was evaluated, and included quality-of-life scales such as MIDAS, MSQ v2.1, and HIT-6. However, the data available for quality of life were insufficient for an NMA, and follow-up on all outcomes was limited from 12 to 26 weeks. For this review, the key limitations of the ICER comparison was the population not specifically aligned with the Health Canada–approved indicated population of adult patients who have at least 4 migraine days per month and have experienced an inadequate response, intolerance, or are contraindicated for at least 2 prophylactic migraine medications. The ITC analysis comparing galcanezumab with other CGRPs or other existing preventive therapies was limited to the EM population. There was no ITC analysis comparing galcanezumab with other CGRPs or other existing preventive therapies in CM population.
Several sources of heterogeneity included networks that reduced the overall applicability to target patient population. These sources included variations in the outcome measures related to the definition of responders, variations in the number of inadequate previous treatments, variations in the disease duration, and variations in the dosing of onabotulinumtoxinA in contrast to the Health Canada–approved indication.
The ICER report did not present the direct and indirect estimates separately when available, and the consistency of the direct and indirect estimates is therefore unclear. However, the report did indicate that, for networks that had loops, the assumption of consistency among indirect and direct estimates was examined empirically using a node-splitting approach, and that no evidence of inconsistency was observed.
The report did not provide a discussion about whether the transitivity assumption was met in the networks of trials. This is relevant considering the sources of heterogeneity. There were also differences among the trials in the exclusion of previous treatment failures, whether ongoing preventive therapy was allowed, and the percentage of patients with medication-overuse headaches (trials either excluded these patients or prevalence ranged from 41% to 68%). Although these factors may be important effect modifiers, they were not examined in analyses.
The NMA considered the time point in a meta-regression and conducted a subgroup analysis for patients who had prior failure on at least 1 other preventive treatment. No subgroup ITC data were provided in the ICER report, and no other sources of potential heterogeneity, such as number of previous treatment failures, use of concomitant migraine-preventive therapy, compliance with headache diary, onabotulinumtoxinA dose, or methodological quality of the study design, were considered.
The majority of the results showing comparative values that include the null in the credible interval should not be interpreted as evidence of similarity or equal effect. The small size of the networks and the fact that 1 study informed the direct evidence between 2 nodes did not provide a statistically robust analysis with sufficient power to determine similarity.
Overall, the comparative efficacy of galcanezumab and other CGRP inhibitors remains uncertain due to the previously discussed methodological limitations.
Summary
Two ITCs were summarized in this review. The sponsor-submitted ITC was conducted using the Bucher method to compare the clinical efficacy and safety of galcanezumab and erenumab in the treatment of adult patients with EM or CM who failed at least 2 preventive treatments. The sponsor-submitted ITC reported results for clinical efficacy and a safety profile comparing galcanezumab with erenumab in terms of responder rate, reduction of the monthly migraine headache days and reduction of the monthly MHDs with acute medication use, discontinuation due to all causes and discontinuation due to AEs. However, no evidence was found to support a difference in outcome for any of these end points. The ICER meta-analysis was conducted using a Bayesian framework. It compared galcanezumab with other CGRPs (erenumab and fremanezumab) and other preventive therapies (topiramate, propranolol, and amitriptyline) in the treatment of patients with EM. The ICER meta-analysis found that patients in the galcanezumab 120 mg group experienced fewer days in acute medication use per month compared with the erenumab 70 mg group. No treatment was favoured when comparing galcanezumab with fremanezumab in all assessed outcomes. Patients in the galcanezumab 120 mg group experienced fewer monthly migraine days when compared with topiramate (200 mg per day and 50 mg per day) and placebo. In terms of 50% response (reduction in MHDs), results favoured galcanezumab 120 mg over placebo, with a higher portion of patients achieving a 50% response.
Due to the multiple limitations of both ITCs (i.e., methodological issues, clinical heterogeneity, and the relatively small number of studies included for each ITC analysis for each outcome), no definitive conclusion can be drawn on the clinical efficacy and safety of galcanezumab 120 mg compared with erenumab or fremanezumab in the treatment patients with migraine (episodic or chronic) who failed at least 2 or at least 3 preventive treatments.
The clinical expert CADTH consulted for this review indicated that, while there is a lack of direct clinical trial evidence, reliable and robust indirect comparison evidence, and clinical experience to compare galcanezumab with other CGRPs (e.g., erenumab or fremanezumab), the mechanism of the different CGRPs suggests it is reasonable to expect similar efficacy and safety among CGRPs approved by Health Canada. From a clinical perspective, although not all patients may respond to any single CGRP drug, different CGRP drugs may work for different patients. Galcanezumab may therefore provide an option for patients who do not respond to other CGRP inhibitors.
Other Relevant Evidence
This section includes a long-term study included in the sponsor’s submission to CADTH that was considered to address important gaps in the evidence included in the systematic review.
Long-Term Extension Studies
One long-term study (CGAJ) has been summarized to provide additional evidence regarding the safety of galcanezumab 120 mg (with a 240 mg loading dose) for patients with EM or CM. Data for this summary were presented in the Clinical Study Report dated September 13, 2017, with a data cut-off date of May 12, 2017.16
Methods
The CGAJ study was a multi-centre, phase III, randomized, open-label study conducted at 28 study sites in 5 countries (Canada, Belgium, France, Hungary, and the US).106 The trial consisted of a screening period, 12 months of open-label treatment with galcanezumab, and 4 months of follow-up (Figure 18). In total, 270 patients with migraine were enrolled and randomized 1:1 to either galcanezumab 120 mg (with a 240 mg loading dose) or 240 mg. Because galcanezumab 240 mg is outside of the Health Canada–recommended dose, this summary of the CGAJ focuses on the results of the 120 mg dose. The primary outcome was long-term safety and tolerability for 12 months of treatment, and included assessments of the number of AEs, SAEs, and discontinuation rates. Secondary outcomes included long-term efficacy and HRQoL.
Figure 18: Flow Diagram for the CGAJ Study
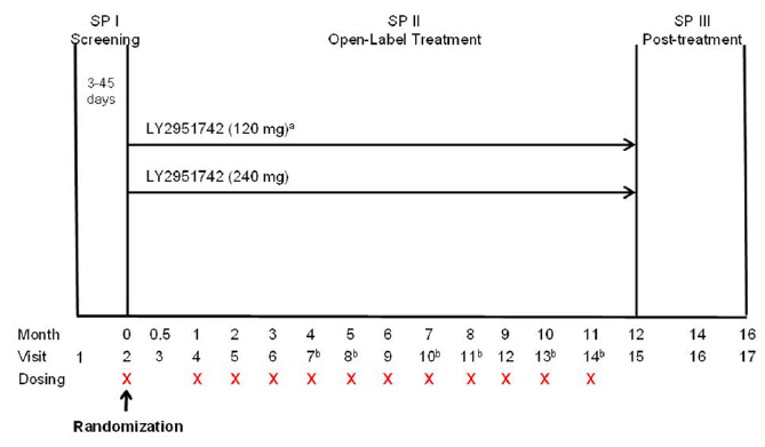
LY2951742 = galcanezumab; SP = study period.
a Patients randomized to the 120 mg dose received a loading dose of 240 mg at the first injection only (visit 2).
b Telephone visit.
Source: Clinical Study Report for CGAJ.16
Populations
Patients were eligible to participate in CGAJ if they met the following inclusion criteria:
male or female, aged 18 to 65 years (inclusive)
diagnosed with migraine, defined by IHS ICHD-3 beta guidelines
a history of migraine headaches at least 1 year before screening and had migraine onset before age 50
a mean of at least 4 MHDs per month for the 3 months before screening
at least 1 headache-free day per month for the 3 months before screening.
Patients were not eligible to participate in CGAJ if they met any of the following exclusion criteria:
previously treated with galcanezumab or another CGRP antibody
received a therapeutic antibody within the past 12 months or would need to during the study
received migraine-prevention treatment within 30 days of randomization or botulinum toxin A or B (head or neck area) within 4 months of randomization
failed at least 3 classes of migraine-preventive treatments with level A or B efficacy (according to Table 1 of the American Academy of Neurology’s Evidence-based Guidelines Update: Pharmacologic Treatment for Episodic Migraine Prevention in Adults or botulinum toxin A or B)
a history any of the following: persistent daily headache, cluster headache, migraine subtypes defined by IHS ICHD-3 beta; headache other than migraine; head or neck injury within 6 months or associated with changes in quality or frequency of headaches; abnormal electrocardiogram or other cardiovascular disease within 6 months of screening; substance abuse
a body mass index of at least 40 kg/m2
liver function tests outside the normal range
active or medical history of psychiatric disease
used opioid- and barbiturate-containing medications more than 3 times per month for pain.
Patient baseline characteristics are summarized in Table 41. For patients who received galcanezumab 120 mg, the mean age was 40.2 years (SD = 11.68), most patients were female (81.5%) and White (76.3%), and the mean body mass index was 26.6 kg/m2 (SD = 5.35). Patients had experienced migraine for a mean duration of 20.2 years (SD = 12.4), they had a mean of 9.7 MHDs per month (SD = 5.8), and more patients had EM compared to CM (80.7% versus 19.3%). This group had a mean baseline MIDAS score of 45.8 (SD = 42.06), which corresponds to the grade 4-B or very severe category,12 and a mean MSQ v2.1 score of 53.9 (SD = 20.34).
In terms of medication history, 60% of patients had tried at least 1 prior preventive treatment, with 43% and 20% having failed at least 1 and 2 prior treatments, respectively. The 3 most frequently used medications included topiramate (36.3%), propranolol (13.3%), and botulinum toxin type A (9.63%).
Table 41: Baseline Characteristics of CGAJ — ITT population
Characteristics | Galcanezumab 120 mg (N = 135) |
|---|---|
Demographics | |
Age (years), mean (SD) | 40.21 (11.68) |
Female, n (%) | 110 (81.48) |
Body mass index (kg/m2), mean (SD) | 26.55 (5.35) |
Race, n (%) | |
White | 103 (76.30) |
Black | 6 (4.44) |
Asian | 2 (1.48) |
Native Hawaiian or other Pacific Islander | 1 (0.74) |
Multiple | 23 (17.04) |
Disease characteristics | |
Duration of migraine illness, years, mean (SD) | 20.18 (12.36) |
Number of non-migraine comorbidities, mean (SD) | 4.29 (3.15) |
MHDs per month, mean (SD) | 9.72 (5.82) |
Baseline migraine frequency category, n (%) | |
EM | 109 (80.74) |
CM | 26 (19.26) |
MHD with acute medication use per month, mean (SD) | 9.84 (6.58) |
MIDAS total score at baseline, mean (SD) | 45.77 (42.06) |
MSQ v2.1 total score at baseline, mean (SD) | 53.85 (20.34) |
Medication use | |
≥ 1 prior preventive treatment, n (%) | 81 (60.00) |
Failed ≥ 1 | 58 (42.96) |
Failed ≥ 2 | 27 (20.00) |
Most frequently used medications,a n (%) | |
Topiramate | 49 (36.30) |
Propranolol | 18 (13.33) |
Botulinum toxin type A | 13 (9.63) |
Amitriptyline | 11 (8.15) |
Amitriptyline hydrochloride | 10 (7.41) |
Propranolol hydrochloride | 10 (7.41) |
Atenolol | 8 (5.93) |
Valproic acid | 8 (5.93) |
Flunarizine dihydrochloride | 7 (5.19) |
Oxetorone fumarate | 7 (5.19) |
Riboflavin | 6 (4.44) |
Lisinopril | 5 (3.70) |
CM = chronic migraine; EM = episodic migraine; ITT = intent-to-treat; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; SD = standard deviation.
aFrequency of 5% or greater in CGAJ.
Source: Clinical Study Report for CGAJ.16
Interventions
Patients who received galcanezumab 120 mg had a single initial loading dose of galcanezumab 240 mg (2 injections of galcanezumab 120 mg) then 120 mg per month for the remainder of the 12-month treatment period. The study drug was administered subcutaneously via pre-filled syringes (80.9%) or autoinjectors (19.1%), when the latter were available. Study-site personnel administered the first dose, while patients and/or caregivers were trained to administer all subsequent doses.
Acute migraine medication was permitted throughout the treatment phase, but opioids and barbiturate-containing medications were only allowed 3 times in a month. Single-dose corticosteroid injections were allowed twice throughout the trial, but oral corticosteroids were not allowed.
During the 4-month post-treatment follow-up phase, patients discontinued galcanezumab and continued to track their headache information. If warranted by worsening symptoms, 1 month after the final visit during the treatment phase (month 15 for those who completed the entire treatment phase), patients could take preventive migraine medication at the discretion of the investigator.
Outcomes
The primary outcome of long-term safety and tolerability of galcanezumab for 12 months of treatment is summarized in this report by number of AEs, SAEs, discontinuation rates, and deaths. Secondary outcomes included long-term efficacy measured by change in MHDs, reduction in medication use, and HRQoL as measured by change in MIDAS score, MSQ v2.1 score, and HCRU and employment status.
Statistical Analysis
The study planned to enrol approximately 250 patients to ensure that at least 100 patients would be treated with galcanezumab for at least 1 year.
The ITT population included all patients who were randomized to receive at least 1 dose of galcanezumab and was used for efficacy analyses, which were performed based on the treatment group to which they were randomized. The safety population included all patients who were randomized to receive at least 1 dose of galcanezumab and was used for safety analyses, which were performed based on the modal treatment received. Modal treatment accounted for instances in which the patient received a different dose than originally assigned or when a patient was assigned to the 120 mg group, received the 240 mg loading dose, then discontinued, causing their predominant dose to be 240 mg (n = 6).
Descriptive statistics were presented for safety and efficacy outcomes. A 2-sided significance level of 0.05 was used to assess safety and efficacy outcomes with 95% CIs for the difference in LS means between treatment groups. Continuous variables with repeated measures were analyzed based on change from baseline using a MMRM analysis that includes longitudinal observations at each post-baseline visit. Other continuous variables were analyzed based on change from baseline to LOCF end point using an ANOVA or ANCOVA. Categorical variables were compared between treatment groups using Fisher’s exact test.
Where data were missing, repeated measures analyses were used (model parameters were estimated using restricted-likelihood estimation incorporating all observed data) or ANOVA or ANCOVA methods were used by applying the change from baseline to LOCF end point. There was no adjustment for multiplicity.
Patient Disposition
Patient disposition is summarized in Table 42. Of the 341 individuals screened, 71 failed screening and 270 were randomized to either galcanezumab 120 mg (N = 135) or 240 mg (N = 135). Overall, 71.9% of patients in the galcanezumab 120 mg group completed the open-label treatment phase and 28.2% discontinued. The reasons for discontinuation from the galcanezumab 120 mg group included lack of efficacy (9.6%), patient decision (7.4%), AEs (5.2%), lost to follow-up (5.2%), and physician decision (0.7%).
Table 42: Patient Disposition of CGAJ Study
Patient disposition | Galcanezumab 120 mg | Galcanezumab 240 mg |
|---|---|---|
Screened | 341 | |
Randomized, N | 135 | 135 |
Completed open-label phase, n (%) | 97 (71.9) | 113 (83.7) |
Discontinued open-label phase, n (%) | 38 (28.2) | 22 (16.3) |
Lack of efficacy | 13 (9.6) | 5 (3.7) |
Withdrawal by patient | 10 (7.4) | 7 (5.2) |
Adverse event | 7 (5.2) | 6 (4.4) |
Lost to follow-up | 7 (5.2) | 4 (3.0) |
Physician decision | 1 (0.7) | 0 |
ITT population, n (%) | 135 (100) | 135 (100) |
Safety population,a n (%) | 129 (95.6) | 141 (104.4) |
ITT = intention-to-treat.
aSafety population based on modal treatment that was received. Six patients randomized to the 120 mg group received only the loading dose of 240 mg before discontinuing treatment causing them to be counted toward to 240 mg group for safety analyses.
Source: Clinical Study Report for CGAJ.16
Exposure to Study Treatments
The mean duration of exposure to galcanezumab 120 mg was 318.48 (SD = 76.71) days; median duration of exposure to galcanezumab 120 mg was 351 (minimum = 66; maximum = 421) days. By the data cut-off date, 95 patients (73.64%) in the safety population had received 12 doses during the study.
Treatment adherence was calculated for each patient as the number of completed dose visits during which the patient received the assigned number of doses divided by the total number of dose visits (completed and skipped) before the last dose visit or discontinuation. The mean overall adherence for galcanezumab 120 mg was 95.8% (SD = 9.94).
Efficacy
Efficacy results are summarized in Table 43. The overall LS mean change from baseline was −5.61 (95% CI, −6.27 to −4.95) for MHDs and −2.17 (95% CI, −2.76 to −1.58) for headache days. The overall raw rate (average of raw rates for each month) was 0.674 for 50% responders for MHDs and 0.257 for 100% responders for MHDs. The overall mean change from baseline in use of acute migraine or headache treatment was −5.09 (95% CI, −5.83 to −4.35) days per month. Measurements of HRQoL using the MIDAS and MSQ v2.1 showed improvements from baseline (lower MIDAS and higher MSQ v2.1 scores). The overall LS mean change from baseline was −33.58 (95% CI, −37.73 to −29.42) for the MIDAS total score and 28.27 (95% CI, 25.98 to 30.56) for the MSQ v 2.1 total score. In months 7 to 12, the numbers of patients who had at least 1 health care visit or emergency room visit related to migraine were 12 and 3, respectively compared to 52 and 11 patients, respectively, at baseline.
Table 43: Efficacy Outcomes of CGAJ Study — ITT Population
Outcomes | Galcanezumab 120 mg (N = 135) |
|---|---|
Migraine headache days, change from baseline | |
Month 12 (n = 95), LSM (SE; 95% CI) | −6.35 (0.43; −7.20 to −5.49) |
Overall (n = 132), LSM (SE; 95% CI) | −5.61 (0.34; −6.27 to −4.95) |
Headache days, change from baseline | |
Month 12 (n = 95), LSM (SE; 95% CI) | −1.59 (0.45; −2.47 to −0.71) |
Overall (n = 132), LSM (SE; 95% CI) | −2.17 (0.30; −2.76 to −1.58) |
50% responders for MHDs | |
Month 12, n/N (raw rate) | 72/95 (0.758) |
Model estimated ratea (SE; 95% CI) | 0.726 (0.043; 0.633 to 0.803) |
Overall,b n (raw rate) | 132 (0.674) |
Model estimated ratea (SE; 95% CI) | 0.656 (0.032; 0.591 to 0.715) |
100% responders for MHDs | |
Month 12, n/N (raw rate) | 29/95 (0.305) |
Model estimated ratea (SE; 95% CI) | 0.258 (0.046; 0.178 to 0.359) |
Overall,b n (raw rate) | 132 (0.257) |
Model estimated ratea (SE; 95% CI) | 0.214 (0.026; 0.167 to 0.271) |
Use of acute migraine or headache treatment, change from baseline | |
Month 12 (n = 95), LSM (SE; 95% CI) | −5.30 (0.51; −6.31 to −4.28) |
Overall (n = 132), LSM (SE; 95% CI) | −5.09 (0.38; −5.83 to −4.35) |
MIDAS total score, change from baseline | |
Month 12 (n = 90), LSM (SE; 95% CI) | −38.60 (2.23; −42.99 to −34.21) |
Overall (n = 124), LSM (SE; 95% CI) | −33.58 (2.11; −37.73 to −29.42) |
MSQ v2.1 total score, change from baseline | |
Month 12 (n = 90), LSM (SE; 95% CI) | 30.52 (1.47; 27.63 to 33.41) |
Overall (n = 130), LSM (SE; 95% CI) | 28.27 (1.16; 25.98 to 30.56) |
MSQ v2.1 RF-R score, change from baseline | |
Month 12 (n = 90), LSM (SE; 95% CI) | 34.18 (1.58; 31.07 to 37.28) |
Overall (n = 130), LSM (SE; 95% CI) | 31.55 (1.20; 29.19 to 33.91) |
MSQ v2.1 RF-P score, change from baseline | |
Month 12 (n = 90), LSM (SE; 95% CI) | 23.50 (1.39; 20.76 to 26.23) |
Overall (n = 130), LSM (SE; 95% CI) | 22.08 (1.11; 19.88 to 24.27) |
MSQ v2.1 EF score, change from baseline | |
Month 12 (n = 90), LSM (SE; 95% CI) | 31.50 (1.67; 28.21 to 34.79) |
Overall (n = 130), LSM (SE; 95% CI) | 28.92 (1.35; 26.26 to 31.58) |
HCRU – related to migraine | |
Baseline (n = 132), mean (SE) | 0.89 (0.15) |
Patients with ≥ 1 visit, n (%) | 52 (39.39) |
Months 7 to 12 (n = 113), mean (SE) | 0.33 (0.16) |
Patients with ≥ 1 visit, n (%) | 12 (10.62) |
HCRU – emergency room visits related to migraine | |
Baseline (n = 135), mean (SE) | 0.10 (0.03) |
Patients with ≥ 1 visit, n (%) | 11 (8.15) |
Months 7 to 12 (n = 113), mean (SE) | 0.03 (0.02) |
Patients with ≥ 1 visit, n (%) | 3 (2.65) |
CI = confidence interval; EF = emotional function; HCRU = health care resource utilization; ITT = intention-to-treat; LSM = least squares mean; MHD = migraine headache day; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; RF-P = role function – preventive; RF-R = role function – restrictive; SE = standard error.
aEstimates based on the mixed model for repeated measures were obtained using unstructured covariance structure. The Kenward-Roger approximation was used to estimate denominator degrees of freedom.
bRaw rate for overall is the average of raw rate from each month.
Source: Clinical Study Report for CGAJ.16
Harms
Safety results are summarized in Table 44. Most patients (82.2%) experienced at least 1 treatment-emergent AE during the treatment phase of the CGAJ trial. The most frequently reported AEs were nasopharyngitis (17.8%), injection site pain (17.1%), injection site reaction (11.6%), sinusitis (10.9%), and back pain (9.3%). Three patients reported an SAE, with a single occurrence of each of the following: lumbar radiculopathy, migraine, and osteoarthritis. Six patients (4.7%) discontinued the study due to an AE and no deaths were reported.
Notable harms included anaphylactic reaction (6.2%), hypersensitivity reaction (14.7%), injection site reaction (11.6%), and vascular disorder (4.7%). Antidrug antibodies were detected in 8 patients (6.3%) at baseline and 16 patients (12.5%) during the treatment phase. A patient was considered ADA-positive if a post-baseline titre was 4 times greater than the baseline value or a post-baseline titre was greater than 1:20 with a negative baseline ADA result. Neutralizing antibodies were present for all ADA-positive patients at both baseline and during treatment (n = 8 and n = 16, respectively).
Table 44: Safety Outcomes of CGAJ Study — Safety Population
Outcome | Galcanezumab 120 mg (N = 129) |
|---|---|
Patients with ≥ 1 AE,a n (%) | 106 (82.17) |
AE, n (%) | |
Nasopharyngitis | 23 (17.83) |
Injection site pain | 22 (17.05) |
Injection site reaction | 15 (11.63) |
Sinusitis | 14 (10.85) |
Back pain | 12 (9.30) |
Nausea | 10 (7.75) |
Injection site erythema | 9 (6.98) |
Upper respiratory tract infection | 9 (6.98) |
Arthralgia | 8 (6.20) |
Influenza | 8 (6.20) |
Myalgia | 8 (6.20) |
Increased weight | 7 (5.43) |
Patients with ≥ 1 SAE, n (%) | 3 (2.33) |
SAE, n (%) | |
Lumbar radiculopathy | 1 (0.78) |
Migraine | 1 (0.78) |
Osteoarthritis | 1 (0.78) |
Discontinuation due to AE, n (%) | 6 (4.65) |
Deaths, n (%) | 0 (0) |
Notable harms | |
Anaphylactic reaction | 8 (6.20) |
Hypersensitivity reaction | 19 (14.73) |
Injection site reaction | 15 (11.63) |
ADA formation | |
At baseline | 8 (6.25) |
During open-label phase | 16 (12.50) |
Vascular disorder | 6 (4.65) |
ADA = antidrug antibody; AE = adverse event; SAE = serious adverse event.
aFrequency of 5% or greater.
Source: Clinical Study Report for CGAJ.16
Critical Appraisal
Internal Validity
The CGAJ trial did not have a control group, and the galcanezumab 240 mg comparator group is not of interest for the comparison in this review, which makes it difficult to account for natural changes in migraine that may occur over time, the effects of confounders, or potential placebo response. Additionally, the open-label design may have influenced the perception of improvement by patients and clinicians which could impact the reporting of harms and efficacy measures. The reasons for the 71 screening failures were not further discussed in the report. It is worth noting that patients were not recruited from any pivotal studies and did not have any previous experience with galcanezumab or other CGRP treatments. There was also no control for multiplicity described in the report. Where data were missing, repeated measures analyses or ANOVA or ANCOVA methods using change from baseline to the LOCF end point were applied. The LOCF method may inaccurately represent how patients would respond during the rest of the study had they continued on the medication, and it is unknown how this affects the study results and their interpretation. The study focused largely on patient-reported outcome measures and, rather than having patients enter data into a daily electronic diary, all information on migraine frequency and acute medication use was collected retrospectively by direct questioning from study personnel during visits. This form of data collection could affect the accuracy of harms and efficacy reporting, although it is unknown if this would be in favour of or against the study treatment. Mean adherence during the study period was high (95.8%) for monthly galcanezumab 120 mg. Discontinuations were somewhat high (28.2%) during the open-label phase, with the most common reasons being lack of efficacy (9.6%) and patient withdrawal (7.4%). The limitations with the study design make it challenging to interpret the results and form conclusions with certainty.
External Validity
The CGAJ trial sample size was small, consisting of 135 patients who received galcanezumab 120 mg. Patients were predominantly female and White, which the clinical expert consulted by CADTH confirmed was similar to patients treated in Canadian clinics. Most patients were diagnosed with EM (80.7%) and the small proportion of patients with CM limits the information available and generalizability to others with CM. The exclusion criteria (a body mass index greater than 40 kg/m2, non-migraine headaches, or serious cardiovascular disease) also limits how the results of this study may be applied to the general population. The clinical expert consulted by CADTH suggested that patients are ideally tried on a medication within the therapeutic range for at least 8 weeks before deciding whether the treatment failed, and the time on treatment (maximum 12 months) was therefore acceptable. The clinical expert also noted that some patients in clinics would receive other acute migraine medications concurrently, which was permitted in this study, although use of opioids and barbiturate-containing medications and corticosteroids were restricted. With regards to harms outcomes, injection site pain, injection site reaction, and injection site erythema were reported by 17.0%, 11.6%, and 7.0% of patients, respectively. The clinical expert suggested that harms related to injected medications (i.e., galcanezumab) could be associated with insufficient training of drug administration or use of an autoinjector rather than a syringe. In the CGAJ trial, patients (and/or caregivers) were trained to administer the injection during the first dose visit and were expected to complete all subsequent 11 injections on their own. Furthermore, patients were transitioned from a pre-filled syringe to an autoinjector as the latter became available, unless they were close to their last visit. Input from patient groups submitted to CADTH for this review indicated that 73% of survey participants would prefer a monthly injection to a daily oral medication, and the clinical expert indicated there may be benefits in terms of adherence with injectable treatments. Last, the clinical expert noted that the MSQ v2.1 is not commonly used in clinical practice, but the MIDAS is used among clinicians. Although the HIT-6 is commonly used by clinicians, it was not used in this study. These limitations are important considerations when attempting to generalize the study results to a broader Canadian population with migraine.
Discussion
Summary of Available Evidence
Four double-blind, placebo-controlled, phase III RCTs (EVOLVE-1, EVOLVE-2, REGAIN, and CONQUER) were identified and included in the systematic review. The EVOLVE-1 (N = 862) and EVOLVE-2 (N = 922) studies were identically designed, and the primary objective of each was to test the hypothesis that at least 1 dose of galcanezumab (120 mg or 240 mg) is superior to placebo in the prevention of migraine headache in patients with EM. The REGAIN trial (N = 1,117) was designed to test the same hypothesis in patients with CM. In these trials, patients were randomized in a 2:1:1 ratio to receive placebo, galcanezumab 120 mg (with a loading dose of 240 mg), or galcanezumab 240 mg. Because galcanezumab 240 mg does not align with the Health Canada–recommended dose, the systematic review focused on the galcanezumab 120 mg versus placebo arms. The primary objective of the CONQUER trial (N = 463) was to test the hypothesis that galcanezumab is superior to placebo in the prevention of migraine in patients with EM or CM and 2 to 4 migraine-preventive medication category failures in the past 10 years. Patients were randomized 1:1 to receive placebo or galcanezumab 120 mg. The primary outcome in all trials was the overall mean change from baseline in the number of monthly MHDs during double-blind treatment. Secondary efficacy outcomes included HRQoL as measured by the MSQ v2.1, MIDAS, other patient-reported outcomes, monthly MHDs with acute headache pain medication intake, time to first loss of response post-treatment, time to initiation of a migraine-prevention medication post-treatment, HCRU and employment status, and the WPAI. Monthly MHDs with symptoms were assessed as exploratory outcomes.
In all trials, most patients were female and White. In the EVOLVE studies, the mean age of patients was between 39 and 42 years, most patients (> 60%) had received prior preventive treatment, and had an average of 9.1 MHDs per month. In the REGAIN trial, the mean age was 41.0 years and patients had an average of 19.4 MHDs per month. Most patients (77.8%) reported using prior migraine-preventive treatment, with 29.5% having failed at least 2 treatments due to lack of efficacy in the past 5 years. In the CONQUER trial, the mean age of patients was 45.8 years and patients had an average of 13.2 MHDs per month. Most patients had 2 or 3 prior medication category failures (58.2% or 30.1%, respectively). Aside from some small demographic differences, baseline characteristics were generally similar between groups within studies.
Key critical appraisal issues included the administration of the injections containing galcanezumab or placebo by study personnel at dosing visits using a manual syringe in all pivotal trials. According to the clinical expert consulted by CADTH, galcanezumab would be self-administered by patients (and/or caregivers) at home in regular practice, and autoinjectors are commonly used. Harms results (e.g., injection site reactions) may not be generalizable to these different methods of injection administration. Multiple testing procedures were used to control type I error for the primary and key secondary outcomes. Other secondary and exploratory outcomes were not adjusted for multiplicity. Subgroup analyses were also not adjusted for multiplicity. In addition, although the HIT-6 is a commonly used outcome measure among clinicians to assess treatment response, it was not included in the pivotal trials.
Two ITCs were summarized and critically appraised. One of the ITCs was provided by the sponsor and the other was an NMA conducted by the ICER. The sponsor-submitted ITC compared galcanezumab with erenumab in the prophylaxis of EM and CM in patients with a history of prior preventive-treatment failures. The ICER analysis compared galcanezumab to other migraine therapies in the treatment of patients with EM. For the sponsor-submitted ITC, the main limitations were methodological issues and clinical heterogeneity. For the ICER analysis, the key limitations were the failure to align the population with that indicated in the reimbursement request, the relatively small number of trials included in NMA for each outcome, clinical heterogeneity, and the inclusion of only patients with EM. In addition, important patient-reported outcomes were not assessed in either of the ITCs.
In addition, a long-term study (CGAJ) was summarized and critically appraised as other relevant evidence. The CGAJ study (N = 270) was a multi-centre, phase III, open-label study that randomized patients in a 1:1 ratio to either galcanezumab 120 mg (with a 240 mg loading dose) or 240 mg. The treatment period was 12 months. Patients (and/or caregivers) were trained to administer the injection during the first dose visit and then administer subsequent injections on their own. Patients were transitioned from a pre-filled manual syringe to an autoinjector as the latter became available. The primary outcome was long-term safety and tolerability. Secondary outcomes included efficacy and HRQoL as measured using the MIDAS and MSQ, HCRU, and employment status. Information on migraine frequency and acute medication use was collected retrospectively by direct questioning from study personnel during visits. This form of data collection could affect the accuracy of data, although the direction of bias is unknown.
Interpretation of Results
Efficacy
The reimbursement request under review is for the prevention of migraine in adults who have at least 4 migraine days per month and have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications. This includes patients with EM and those with CM. The EVOLVE-1 and EVOLVE-2 trials included patients with EM only, the REGAIN trial included patients with CM only, and the CONQUER trial included both patients with EM and CM. The EVOLVE-1, EVOLVE-2, and REGAIN trials excluded patients who failed to have an efficacy response to at least 3 classes of migraine-preventive treatment, and the majority of patients enrolled in these trials had not previously failed at least 2 prior migraine-preventive treatments. This may limit generalizability of the trial results to the intended patient population. The CONQUER trial was conducted in patients with a history of failures on 2 to 4 prior migraine-preventive medication categories due to inadequate efficacy or safety and tolerability in the past 10 years, including patients with either EM or CM. The patient population in the CONQUER trial most closely aligns with the patient population specified in the reimbursement request.
The patient groups that provided input for this review indicated that patients would prefer a medication that reduces the frequency and severity of migraine. The patient groups indicated that nearly any degree of relief would be a successful outcome for a preventive therapy. Similarly, the clinical expert consulted by CADTH indicated that reduction in frequency and/or severity of headaches (which is commonly assessed using headache diaries) is important. This aligns with the outcomes of monthly MHDs and monthly headache days assessed in the pivotal trials.
The primary outcome of all the pivotal trials was the overall change from baseline in number of monthly MHDs during the double-blind treatment period. Galcanezumab (120 mg per month with a 240 mg loading dose) elicited a statistically significant reduction in the overall mean number of monthly MHDs of approximately 2 to 3 days from baseline during double-blind treatment compared to placebo in the 4 pivotal trials. The clinical expert consulted by CADTH noted that this magnitude of reduction may be clinically significant for some patients, and the patient groups emphasized that nearly any reduction in MHDs would be meaningful. Results of all subgroup analyses of the primary end point favoured galcanezumab 120 mg over placebo, and were consistent with the primary analysis in the modified ITT populations.
The overall change from baseline in number of monthly headache days was a secondary outcome in all the pivotal trials. This outcome was not controlled for multiplicity and results must therefore be consider the possibility of type I error. Results were consistent with the primary end-point analysis and suggested a benefit from galcanezumab 120 mg treatment compared to placebo. The clinical expert noted that the magnitude of reduction in headache days observed in the trials may be clinically significant for some patients. The clinical expert reported that the goal of treatment is to reduce the frequency of headaches, ideally to fewer than 4 headache days per month. The patient groups indicated that nearly any reduction in headache days would be meaningful.
In addition to a reduction in MHDs and headache days, the patient groups indicated that they wanted a medication that reduces or eliminates the need for acute medications (e.g., triptans and opioids), which aligns with the outcome of monthly MHDs with acute medication use. The patient advocacy groups reported that patients felt that nearly any degree of relief would be a successful outcome for a preventive therapy. Similarly, the clinical expert indicated that reduced reliance on abortive medications (e.g., triptans) may also be indicative of improvement. The clinical expert added that a change within 2 days of acute medication use is clinically significant. For the outcome of average change from baseline in the number of monthly days with acute headache medication use during double-blind treatment in the EVOLVE-1, EVOLVE-2, and CONQUER trials, the LS mean change difference versus placebo was statistically significant in favour of galcanezumab 120 mg. Monthly MHDs with acute medication use (galcanezumab 120 mg versus placebo) could not be tested for statistical significance within the pre-specified multiple-testing procedure in the REGAIN trial.
Furthermore, the patient groups indicated that they wanted a preventive medication that would allow them to be more productive at work and home and fully participate in daily life, which aligns with the MSQ v2.1, MIDAS, and WPAI outcome measures.
Change from baseline in the MSQ v2.1 RF-R domain score was a key secondary end point included in the multiple-testing procedures of the pivotal trials. In the EVOLVE-1 and EVOLVE-2 trials, the LS mean change from baseline during the last 3 months of double-blind treatment was statistically significantly greater in the galcanezumab 120 mg group compared with placebo, and the mean changes observed were greater than the MID for the EM population. In the REGAIN trial, the LS mean change from baseline at month 3 was numerically greater in the galcanezumab 120 mg arm compared to the placebo arm, and the change was greater than the MID for the CM population. However, the difference between the galcanezumab 120 mg arm versus the placebo arm could not be tested for statistical significance based on the REGAIN trial’s predefined multiple-testing procedure. In the CONQUER trial, the mean change from baseline at month 3 was statistically significantly greater in the galcanezumab group compared with placebo, and the change was greater than the MIDs identified for the EM and CM populations. However, the clinical expert consulted by CADTH indicated the MSQ v2.1 is not commonly used to assess treatment response in regular practice, and it is therefore difficult to determine whether these results are clinically significant.
The MIDAS total score was a secondary outcome in all the pivotal trials. The outcome was not included in the trials’ multiple-testing procedures and results must therefore be considered with regards to type I error. Results of these analyses were generally consistent with the primary and key secondary outcomes in suggesting a potential benefit from galcanezumab compared to placebo. CADTH identified an MID of 3.7 points in the literature, and the clinical expert consulted by CADTH indicated that a 5-point or 50% change in total MIDAS score would be clinically significant. In the EVOLVE-1 and EVOLVE-2 trials, the mean change from baseline to end of double-blind treatment phase (month 6) and difference from placebo were numerically greater than both the MID identified in the literature and the clinical expert’s threshold for clinical significance. The mean change from baseline to the LOCF end point and difference from placebo in the REGAIN and CONQUER trials were also numerically greater than the MID identified in the literature and the clinical expert’s threshold for clinical significance. However, due to the lack of adjustment for multiplicity, the MIDAS total score analyses can only be considered supportive evidence.
The WPAI was assessed only in the CONQUER trial. Results for this outcome were consistent with the primary and key secondary analysis results in suggesting a benefit (i.e., decreased impairment) from galcanezumab treatment compared to placebo. The CONQUER trial also assessed EQ-5D-5L and MIBS-4 scores as secondary outcomes, and PHQ-9 and GAD-7 scores as exploratory outcomes. Results of these analyses were generally consistent with the primary and key secondary outcomes in suggesting a potential benefit from galcanezumab treatment compared to placebo (e.g., improved perception of health status per the EQ VAS, decreased burden related to headache in the time between attacks, and reduction in the severity of depression symptoms). There was no difference between the galcanezumab and placebo arms with respect to anxiety symptoms based on the GAD-7 total score. It is important to note that these additional patient-reported outcome measures were not included in the trial’s multiple-testing procedure; thus, results must be considered with the potential for type I error.
The EVOLVE-1, EVOLVE-2, and REGAIN trials assessed time to first loss of 50% response and time to initiation of a preventive migraine medication in the post-treatment phases. In the 3 trials, approximately half of the patients in all treatment groups had first loss of 50% response by 4 months after the end of treatment. Small numbers of patients in the 3 trials started a migraine-prevention treatment in the post-treatment phase, limiting interpretation of the results for this outcome. As the CONQUER trial did not include a post-treatment follow-up phase, time to first loss of 50% response and time to initiation of a preventive migraine medication in the post-treatment phases were not assessed. Based on the data available, CADTH cannot make conclusions about the effect of galcanezumab 120 mg compared to placebo on the time to first loss of response and time to initiation of another preventive treatment.
The degree of HCRU was assessed in the REGAIN and CONQUER trials. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| and lack of control for multiplicity for these outcomes, no conclusions can be drawn regarding the effect of galcanezumab 120 mg on HCRU compared to placebo. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Based on the data available, it is unknown whether treatment with galcanezumab 120 mg has an effect on patient employment status compared to placebo.
Both the sponsor-submitted ITC and the ICER analysis reported that there is insufficient evidence to conclude that galcanezumab was different from other CGRP inhibitors or other migraine therapies in terms of response rate, change from baseline of monthly MHDs, change from baseline of monthly MHDs with acute medication use, discontinuation from all causes, and discontinuation from AEs in patients with EM or CM. Due to the methodological issues and clinical heterogeneity of both ITCs, interpretation of the results should consider these limitations.
The CGAJ long-term study provided data on 12 months of open-label treatment with galcanezumab 120 mg. Secondary outcomes in this study included change in MHDs, reduction in medication use, MIDAS score, MSQ v2.1 score, HCRU, and employment status. Results for the secondary outcomes were generally consistent with the pivotal trials and suggested that, after 12 months of treatment, patients experienced reductions in monthly MHDs, headache days, and use of acute medication. Results for the HRQoL data were also consistent with the changes observed in the pivotal trial, suggesting that patients may experience an improvement in HRQoL and reduction in disability with galcanezumab treatment. However, due to the lack of a control group, no conclusions can be drawn about the efficacy of galcanezumab 120 mg for 12 months from these data.
Harms
The EVOLVE-1 and EVOLVE-2 trials provided harms data from 6 months of double-blind treatment, the REGAIN trial provided harms data for 3 months of double-blind treatment followed by an optional 9-month open-label extension, and the CONQUER trial provided harms data for 3 months of double-blind treatment followed by an optional 3-month open-label extension. Approximately 50% to 65% of patients in the pivotal trials experienced at least 1 treatment-emergent AE during double-blind treatment across the placebo and galcanezumab 120 mg treatment arms. In the EVOLVE-1, EVOLVE-2, and REGAIN trials, a numerically smaller proportion of patients experienced AEs in the placebo arm compared to the galcanezumab 120 mg arm; in the CONQUER trial, a numerically smaller proportion of patients experienced AEs in the galcanezumab 120 mg arm compared to the placebo arm. The most frequently reported AEs across the pivotal trials were injection site pain and nasopharyngitis. Small percentages of patients (< 4%) discontinued double-blind treatment due to AEs, small percentages of patients (< 4%) experienced SAEs, and no patients died during any phases of the pivotal trials.
Regarding notable harms, the Health Canada product monograph for galcanezumab contains warnings and precautions for serious hypersensitivity reactions, including anaphylaxis, angioedema, and urticaria. The product monograph also notes that no safety data are available for patients with cardiovascular diseases and vascular disorders. No patients in any of the pivotal trials experienced an anaphylactic reaction. Hypersensitivity events and angioedema were reported in small percentages of patients (< 6%) in each study. Vascular disorder events were experienced by a small percentage of patients (< 4%) in each study. The most frequently reported vascular disorders were hypertension, flushing, and hot flushes. During the double-blind treatment periods of the EVOLVE-1, EVOLVE-2, and REGAIN studies, up to 9.4% of patients treated with galcanezumab 120 mg and up to 1.7% of patients treated with placebo were treatment-emergent ADA-positive. Most of these patients had neutralizing ADAs present. The formation of ADAs was not assessed proactively in the CONQUER study. In the EVOLVE-1 trial, a numerically greater percentage of patients experienced injection site reactions compared to the 3 other pivotal trials. The clinical expert consulted by CADTH noted that the percentage of patients who experienced injection site reactions in the EVOLVE-1 trial was higher than expected. The reason for the numerically higher percentage of injection site reactions in the EVOLVE-1 trial is unknown because study-site personnel administered injections using a manual syringe in all trials.
The CGAJ study provided data on the safety and tolerability of galcanezumab 120 mg for 12 months of open-label treatment. During longer-term treatment in this study, the proportion of patients who experienced at least 1 treatment-emergent AE was greater than 80%, which was numerically greater than the percentages of patients who experienced AEs in the pivotal trials. The most frequently reported AEs were nasopharyngitis, injection site pain, injection site reaction, sinusitis, and back pain, which was similar to the AEs most frequently reported in the pivotal trials. In the CCAJ safety study, the study drug was administered subcutaneously via a pre-filled syringe (81%) or autoinjector (19%), when available. Study-site personnel administered the first dose, while patients and/or caregivers were trained to administer all subsequent doses. In the galcanezumab 120 mg arm of the CGAJ study, the proportion of patients who experienced injection site reactions was similar to what was observed in the EVOLVE-2, REGAIN, and CONQUER trials.
No data on harms were reported in either of the ITCs.
Conclusions
Four phase III, placebo-controlled, randomized trials (EVOLVE-1, EVOLVE-2, REGAIN, and CONQUER) with double-blind treatment periods were included in the systematic review. The EVOLVE-1 and EVOLVE-2 trials provide direct evidence regarding the efficacy and safety of galcanezumab relative to placebo for adult patients with EM; the REGAIN trial provides direct evidence regarding the efficacy and safety of galcanezumab relative to placebo for adult patients with CM. The CONQUER trial provides direct evidence regarding the efficacy and safety of galcanezumab (120 mg per month with a 240 mg loading dose) relative to placebo in adult patients with EM or CM who have previously failed 2 to 4 classes of migraine-preventive treatments. Compared to placebo, patients who were treated with galcanezumab 120 mg showed benefits in the reduction of monthly MHDs during double-blind treatment periods (6 months in the EVOLVE-1 and EVOLVE-2 trials and 3 months in the REGAIN and CONQUER trials) in all trials. In addition, reductions in monthly MHDs with acute medication use and improvement in the MSQ v2.1 RF-R domain were observed in the EVOLVE-1, EVOLVE-2, and CONQUER trials. The effect of galcanezumab on MHDs with symptoms, headache days, other patient-reported outcomes, HCRU, and employment status remains uncertain due to a lack of control for multiplicity. Many study patients reported treatment-emergent AEs. The most frequently reported AEs across trials were injection site pain and nasopharyngitis. Galcanezumab was related to a numerically higher frequency of becoming ADA-positive in the 3 trials that assessed immunogenicity. Few patients discontinued double-blind treatment due to AEs and few patients experienced SAEs. No patients died. The pivotal trials did not provide direct evidence on the relative efficacy and safety of galcanezumab versus other migraine-preventive medications in adults with EM or CM.
The CGAJ study was a randomized, open-label, long-term safety trial of galcanezumab 120 mg and 240 mg. The results supported the safety of galcanezumab 120 mg. The results also supported the beneficial effect of galcanezumab on monthly MHDs, headache days, use of acute medication, and HRQoL. However, limitations of this study, such as a small sample size and lack of a control group, contribute uncertainty to the results.
Results from the sponsor-submitted ITC and the ICER NMA both provided insufficient evidence to conclude that galcanezumab differed in efficacy compared to other CGRPs in terms of response rate, change from baseline of monthly MHDs, change from baseline of monthly MHDs with acute medication use, discontinuation from all causes, and discontinuation from AEs in patients with CM and/or EM. Due to several limitations of both ITCs (i.e., methodological issues and clinical heterogeneity), no definitive conclusion can be drawn on the comparative clinical efficacy and safety comparing galcanezumab 120 mg with erenumab or with fremanezumab in the treatment of patients with EM or CM who failed at least 2 preventive treatments.
References
1.Bigal ME, Lipton RB, Stewart WF. The epidemiology and impact of migraine. Curr Neurol Neurosci Rep. 2004;4(2):98-104. PubMed
2.Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211.
3.Cooke LJ, Becker WJ. Migraine prevalence, treatment and impact: the canadian women and migraine study. Can J Neurol Sci. 2010;37(5):580-587. PubMed
4.American Headache Society. The American Headache Society Position Statement On Integrating New Migraine Treatments Into Clinical Practice. Headache. 2019;59(1):1-18. PubMed
5.Becker WJ, Findlay T, Moga C, Scott NA, Harstall C, Taenzer P. Guideline for primary care management of headache in adults. Can Fam Physician. 2015;61(8):670-679. PubMed
6.Lipton RB, Silberstein SD. Episodic and chronic migraine headache: breaking down barriers to optimal treatment and prevention. Headache. 2015;55 Suppl 2:103-122; quiz 123-106. PubMed
7.Martelletti P, Schwedt TJ, Lanteri-Minet M, et al. My Migraine Voice survey: a global study of disease burden among individuals with migraine for whom preventive treatments have failed. J Headache Pain. 2018;19(1):115. PubMed
8.Emgality (galcanezumab): 100 mg/mL, 120 mg/mL solution for subcutaneous injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc; 2020 Sep 17.
9.Clinical Study Report: I5Q-MC-CGAG. A phase 3, randomized, double-blind, placebo-controlled study of LY2951742 in patients with episodic migraine – the EVOLVE-1 study: results from the double-blind treatment phase [internal sponsor's report]. Eli Lilly and Company; 2017.
10.Clinical Study Report: I5Q-MC-CGAH. A phase 3, randomized, double-blind, placebo-controlled study of LY2951742 in patients with episodic migraine – the EVOLVE-2 study: results from the double-blind treatment phase [internal sponsor's report]. Eli Lilly and Company; 2017.
11.Clinical Study Report: I5Q-MC-CGAI. A phase 3, randomized, double-blind, placebo-controlled study of LY2951742 in patients with chronic migraine – the REGAIN Study: final results from the double-blind treatment phase and interim results from the open-label treatment phase [internal sponsor's report]. Eli Lilly and Company; 2017.
12.Clinical Study Report: I5Q-MC-CGAW. A randomized, double-blind, placebo-controlled study of galcanezumab in adults with treatment-resistant migraine – the CONQUER study: final results from the double-blind treatment phase and interim results from the open-label treatment phase [internal sponsor's report]. Eli Lilly and Company; 2019.
13.Eli Lilly Canada Inc. response to July 26, 2019 DRR request for additional information regarding Emgality DRR review [internal additional sponsor's information]. City (PROV): Sponsor name; 1800.
14.Indirect comparison of galcanezumab compared to erenumab in patients with a history of prior migraine preventive treatment failures [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Emgality (galcanezumab), 120 mg/mL solution for subcutaneous injection Toronto (ON): Eli Lilly Canada Inc; 2020.
15.Calcitonin gene-related peptide (CGRP) inhibitors as preventive treatments for patients with episodic or chronic migraine: effectiveness and value. Boston (MA): Institute for Clinical and Economic review; 2018: https://icer-review.org/wp-content/uploads/2017/11/ICER_Migraine_Final_Evidence_Report_070318.pdf. Accessed 2020 Dec 7.
16.Clinical Study Report: I5Q-MC-CGAJ. A phase 3, long-term, open-label safety study of LY2951742 in patients with migraine: results from the open-label treatment phase [internal sponsor's report]. Eli Lilly and Company; 2017.
17.Dodick DW, Loder EW, Manack Adams A, et al. Assessing Barriers to Chronic Migraine Consultation, Diagnosis, and Treatment: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study. Headache. 2016;56(5):821-834. PubMed
18.Evans RW. A rational approach to the management of chronic migraine. Headache. 2013;53(1):168-176. PubMed
19.Ramage-Morin PL, Gilmour H. Prevalence of migraine in the Canadian household population. Health Rep. 2014;25(6):10-16. PubMed
20.Blumenfeld AM, Bloudek LM, Becker WJ, et al. Patterns of use and reasons for discontinuation of prophylactic medications for episodic migraine and chronic migraine: results from the second international burden of migraine study (IBMS-II). Headache. 2013;53(4):644-655. PubMed
21.James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392(10159):1789-1858. PubMed
22.Blumenfeld AM, Varon SF, Wilcox TK, et al. Disability, HRQoL and resource use among chronic and episodic migraineurs: results from the International Burden of Migraine Study (IBMS). Cephalalgia. 2011;31(3):301-315. PubMed
23.Buse DC, Manack AN, Fanning KM, et al. Chronic migraine prevalence, disability, and sociodemographic factors: results from the American Migraine Prevalence and Prevention Study. Headache. 2012;52(10):1456-1470. PubMed
24.Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):343-349. PubMed
25.Lanteri-Minet M. Economic burden and costs of chronic migraine. Curr Pain Headache Rep. 2014;18(1):385. PubMed
26.Drug Reimbursement Review sponsor submission: Emgality (galcanezumab), 120 mg/mL solution for subcutaneous injection [internal sponsor's package]. Toronto (ON): Eli Lilly Canada Inc; 2021 Jun 3.
27.CADTH Clinical Review Report: fremanezumab. https://cadth.ca/fremanezumab. Accessed August 13, 2021.
28.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
29.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/resources/finding-evidence/grey-matters. Accessed 2021 Jun 17.
30.Stauffer VL, Dodick DW, Zhang Q, Carter JN, Ailani J, Conley RR. Evaluation of Galcanezumab for the Prevention of Episodic Migraine: The EVOLVE-1 Randomized Clinical Trial. JAMA Neurology. 2018;75(9):1080-1088. PubMed
31.Skljarevski V, Matharu M, Millen BA, Ossipov MH, Kim BK, Yang JY. Efficacy and safety of galcanezumab for the prevention of episodic migraine: Results of the EVOLVE-2 Phase 3 randomized controlled clinical trial. Cephalalgia. 2018;38(8):1442-1454. PubMed
32.Detke HC, Goadsby PJ, Wang S, Friedman DI, Selzler KJ, Aurora SK. Galcanezumab in chronic migraine: The randomized, double-blind, placebo-controlled REGAIN study. Neurology. 2018;91(24):e2211-e2221. PubMed
33.Ruff DD, Ford JH, Tockhorn-Heidenreich A, et al. Efficacy of galcanezumab in patients with chronic migraine and a history of preventive treatment failure. Cephalalgia. 2019;39(8):931-944. PubMed
34.Ford J, Tassorelli C, Leroux E, et al. Changes in patient functioning and disability: results from a phase 3, double-blind, randomized, placebo-controlled clinical trial evaluating galcanezumab for chronic migraine prevention (REGAIN). Qual Life Res. 2021;30(1):105-115. PubMed
35.Kuruppu DK, Tobin J, Dong Y, Aurora SK, Yunes-Medina L, Green AL. Efficacy of galcanezumab in patients with migraine who did not benefit from commonly prescribed preventive treatments. BMC Neurol. 2021;21(1):175. PubMed
36.Mulleners WM, Kim BK, Lainez MJA, et al. Safety and efficacy of galcanezumab in patients for whom previous migraine preventive medication from two to four categories had failed (CONQUER): a multicentre, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. 2020;19(10):814-825. PubMed
37.Schwedt TJ, Kuruppu DK, Dong Y, Standley K, Yunes-Medina L, Pearlman E. Early onset of effect following galcanezumab treatment in patients with previous preventive medication failures. J Headache Pain. 2021;22(1):15. PubMed
38.Detke HC, Millen BA, Zhang Q, et al. Rapid Onset of Effect of Galcanezumab for the Prevention of Episodic Migraine: Analysis of the EVOLVE Studies. Headache. 2020;60(2):348-359. PubMed
39.Ford JH, Ayer DW, Zhang Q, et al. Two randomized migraine studies of galcanezumab: Effects on patient functioning and disability. Neurology. 2019;93(5):e508-e517. PubMed
40.Rosen N, Pearlman E, Ruff D, Day K, Jim Nagy A. 100% Response Rate to Galcanezumab in Patients With Episodic Migraine: A Post Hoc Analysis of the Results From Phase 3, Randomized, Double-Blind, Placebo-Controlled EVOLVE-1 and EVOLVE-2 Studies. Headache. 2018;58(9):1347-1357. PubMed
41.Ruff DD, Ford JH, Tockhorn-Heidenreich A, et al. Efficacy of galcanezumab in patients with episodic migraine and a history of preventive treatment failure: results from two global randomized clinical trials. Eur J Neurol. 2020;27(4):609-618. PubMed
42.Silberstein SD, Stauffer VL, Day KA, Lipsius S, Wilson MC. Galcanezumab in episodic migraine: subgroup analyses of efficacy by high versus low frequency of migraine headaches in phase 3 studies (EVOLVE-1 & EVOLVE-2). J Headache Pain. 2019;20(1):75. PubMed
43.Stauffer VL, Wang S, Voulgaropoulos M, Skljarevski V, Kovacik A, Aurora SK. Effect of Galcanezumab Following Treatment Cessation in Patients With Migraine: Results From 2 Randomized Phase 3 Trials. Headache. 2019;59(6):834-847. PubMed
44.Ailani J, Andrews JS, Rettiganti M, Nicholson RA. Impact of galcanezumab on total pain burden: findings from phase 3 randomized, double-blind, placebo-controlled studies in patients with episodic or chronic migraine (EVOLVE-1, EVOLVE-2, and REGAIN trials). J Headache Pain. 2020;21(1):123. PubMed
45.Ailani J, Pearlman E, Zhang Q, Nagy AJ, Schuh K, Aurora SK. Positive response to galcanezumab following treatment failure to onabotulinumtoxinA in patients with migraine: post hoc analyses of three randomized double-blind studies. Eur J Neurol. 2020;27(3):542-549. PubMed
46.Ament M, Day K, Stauffer VL, et al. Effect of galcanezumab on severity and symptoms of migraine in phase 3 trials in patients with episodic or chronic migraine. J Headache Pain. 2021;22(1):6. PubMed
47.Dodick DW, Doty EG, Aurora SK, et al. Medication overuse in a subgroup analysis of phase 3 placebo-controlled studies of galcanezumab in the prevention of episodic and chronic migraine. Cephalalgia. 2021;41(3):340-352. PubMed
48.Forderreuther S, Zhang Q, Stauffer VL, Aurora SK, Lainez MJA. Preventive effects of galcanezumab in adult patients with episodic or chronic migraine are persistent: data from the phase 3, randomized, double-blind, placebo-controlled EVOLVE-1, EVOLVE-2, and REGAIN studies. J Headache Pain. 2018;19(1):121. PubMed
49.Pozo-Rosich P, Samaan KH, Schwedt TJ, Nicholson RA, Rettiganti M, Pearlman EM. Galcanezumab Provides Consistent Efficacy Throughout the Dosing Interval Among Patients with Episodic and Chronic Migraine: A Post Hoc Analysis. Adv Ther. 2021;38(6):3154-3165. PubMed
50.Stauffer VL, Wang S, Bonner J, et al. Evaluation of injection-site-related adverse events with galcanezumab: a post hoc analysis of phase 3 studies in participants with migraine. BMC Neurol. 2020;20(1):194. PubMed
51.Health Canada reviewer's report: Emgality (galcanezumab) [internal sponsor's report]. Toronto (ON): Eli Lilly Canada Inc; 2019 Jul 3.
52.Dodick DW, Silberstein S, Saper J, et al. The impact of topiramate on health-related quality of life indicators in chronic migraine. Headache. 2007;47(10):1398-1408. PubMed
53.Cole JC, Lin P, Rupnow MF. Minimal important differences in the Migraine-Specific Quality of Life Questionnaire (MSQ) version. Cephalalgia. 2009;29(11):1180-1187. PubMed
54.Bigal ME, Rapoport AM, Lipton RB, Tepper SJ, Sheftell FD. Assessment of Migraine Disability Using the Migraine Disability Assessment (MIDAS) questionnaire: a comparison of chronic migraine with episodic migraine. Headache. 2003;43(4):336-342. PubMed
55.Lipton RB DP, Sapra S, Buse DC, Fanning KM, Reed ML. How much change in headache-related disability is clinically meaningful? Estimating minimally important difference (MID) or change in MIDAS using data from the AMPP study [abstract PF52]. . Headache. 2017;57:165–166.
56.EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
57.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
58.M van Reenen BJ. EQ-5D-5L user guide: basic information on how to use the EQ-5D-5L instrument. 2015; https://euroqol.org/wp-content/uploads/2016/09/EQ-5D-5L_UserGuide_2015.pdf.
59.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
60.Williams KG, Sanderson M, Jette N, Patten SB. Validity of the Patient Health Questionnaire-9 in neurologic populations. Neurol Clin Pract. 2020;10(3):190-198. PubMed
61.Patient Health Questionnaire (PHQ-9). Victoria (BC): gov.bc.ca: https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc-guidelines/depression_patient_health_questionnaire.pdf. Accessed 2019 Feb 14.
62.Alberta HQCo. 2014 Alberta population norms for EQ-5D-5L 2014; https://d10k7k7mywg42z.cloudfront.net/assets/542f01f2edb2f37083002e54/2014_EQ_5D_5L_report_FINALFINAL.pdf.
63.Bucher HC, Guytt GH, Griffith LE, Walter SD. (1997). The results of direct and indirect treatment comparisons in metaanalysis of randomized controlled trials. J Clin Epi, 60(6):683-91.
64.Eli Lilly and Company (2018a). Galcanezumab Clinical Health Technology Assessment Toolkit. Assessment of Clinical Efficacy and Safety for Galcanezumab—Pooled Studies. Internal doc.
65.Eli Lilly and Company (2018b). I5Q-MC-CGAI Clinical Health Technology Assessment Toolkit Clinical Section of Health Technology Toolkit for REGAIN: Assessment of Clinical Efficacy and Safety for Galcanezumab (LY2951742). A Phase 3, Randomized, Double-Blind, Placebo-Controlled Study of LY2951742 in Patients with Chronic Migraine – the REGAIN Study.
66.Eili Lilly and Company (2019c). CGAW Clinical study report. A randomized, double-blind, placebo-controlled study ofgalcanezumab in adults with treatment-resistant migraine –the CONQUER study: final results from the double-blindtreatment phase and interim results from the open-labeltreatment phase. 27 Sep 2019.
67.Ruff D, Ford J, Tockhorn-Heidenreich A, Sexson M, Govindan S, Pearlman E, Wang SJ, Khan A, Aurora SK (2019a). Efficacy of galcanezumab in patients with chronic migraine and a history of preventive treatment failure. Cephalalgia, May 19:333102419847957. doi: 10.1177/0333102419847957. [Epub ahead of print], doi:10.1177/0333102419847957.
68.Mulleners WM, Kim B, Láinez, MJ., Lanteri-Minet M, Aurora SK, Nichols RM, Wang S, Tockhorn-Heidenreich A, Detke HC. (2019). IHC-OR-042. A Randomized, Placebo-Controlled Study of Galcanezumab in Patients with Treatment-Resistant Migraine: Double-Blind Results from the CONQUER Study. IHC 2019 Late Breaking Abstracts. Cephalalgia, 39(1S):366.
69.Zhang Q, Ruff DD, Pearlman EM, Govindan S, Aurora S. Efficacy of galcanezumab in patients who failed to respond to preventives previously: Results from EVOLVE-1, EVOLVE-2 and REGAIN studies. Cephalalgia 2018;38(Suppl 1):51 [MTIS2018-069].
70.Ruff D, Ford JH, Tockhorn-Heidenreich A, Stauffer VL, Govindan S, Aurora SK, Terwindt GM, Goadsby P. (2019b). Efficacy of Galcanezumab in Patients With Episodic Migraine and a History of Preventive Treatment Failure: Results From Two Global Randomized Clinical Trials. Eur J Neurol, DOI: 10.1111/ene.14114. PubMed
71.Goadsby P., Paemeleire K., Broessner G., Brandes J., Klatt J., Zhang F., Picard H., Lenz R., Mikol D (2019). Efficacy and safety of erenumab (AMG334) in episodic migraine patients with prior preventive treatment failure: A subgroup analysis of a randomized, double-blind, placebo-controlled study. Cephalalgia, 39(7):817-826. doi: 10.1177/0333102419835459. Epub 2019 Apr 13 https://www.ncbi.nlm.nih.gov/pubmed/30982348. PubMed
72.Reuter U., Goadsby PJ., Lanteri-Minet M., Wen S., Hours-Zesiger P., Ferrari MD., Klatt J. (2018). Efficacy and tolerability of erenumab in patients with episodic migraine in whom twoto-four previous preventive treatments were unsuccessful: a randomised, double-blind, placebo-controlled, phase 3b study. Lancet. pii: S0140-6736(18)32534-0. doi: 10.1016/S0140-6736(18)32534-0. [Epub ahead of print] https://www.ncbi.nlm.nih.gov/pubmed/30360965.
73.Ashina M, Tepper S, Brandes J, Reuter U, Boudreau G, Dolezil D, Cheng S, Zhang F, Lenz R, Klatt J, Mikol D. (2018). Efficacy and safety of erenumab (AMG334) in chronic migraine patients with prior preventive treatment failure: A subgroup analysis of a randomized, double-blind, placebo-controlled study. Cephalalgia,38(10):1611-1621. doi:10.1177/0333102418788347. PubMed
74.Agency for Healthcare Research and Quality. U.S. Preventive Services Task Force Procedure Manual. 2008.
75.Dodick DW, Goadsby PJ, Spierings EL, Scherer JC, Sweeney SP, Grayzel DS. Safety and efficacy of LY2951742, a monoclonal antibody to calcitonin gene-related peptide, for the prevention of migraine: a phase 2, randomised, double-blind, placebo-controlled study. Lancet Neurol. 2014;13(9):885-892. PubMed
76.Skljarevski V, Oakes TM, Zhang Q, et al. Effect of different doses of galcanezumab vs placebo for episodic migraine prevention: a randomized clinical trial. JAMA Neurol. 2018;75(2):187-193. PubMed
77.Sun H, Dodick DW, Silberstein S, et al. Safety and efficacy of AMG 334 for prevention of episodic migraine: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol. 2016;15(4):382-390. PubMed
78.Goadsby PJ, Reuter U, Hallstrom Y, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017;377(22):2123-2132. PubMed
79.Dodick DW, Ashina M, Brandes JL, et al. ARISE: a phase 3 randomized trial of erenumab for episodic migraine. Cephalalgia. 2018;38(6):1026-1037. PubMed
80.Bigal ME, Dodick DW, Rapoport AM, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of high-frequency episodic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Neurol. 2015;14(11):1081-1090. PubMed
81.Dodick DW, Silberstein SD, Bigal ME, et al. Effect of fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. JAMA. 2018;319(19):1999-2008. PubMed
82.Couch JR. Amitriptyline in the prophylactic treatment of migraine and chronic daily headache. Headache. 2011;51(1):33-51. PubMed
83.Couch JR, Hassanein RS. Amitriptyline in migraine prophylaxis. Arch Neurol. 1979;36(11):695-699. PubMed
84.Goncalves AL, Martini Ferreira A, Ribeiro RT, Zukerman E, Cipolla-Neto J, Peres MF. Randomised clinical trial comparing melatonin 3 mg, amitriptyline 25 mg and placebo for migraine prevention. J Neurol Neurosurg Psychiatry. 2016;87(10):1127-1132. PubMed
85.Lampl C, Huber G, Adl J, et al. Two different doses of amitriptyline ER in the prophylaxis of migraine: long-term results and predictive factors. Eur J Neurol. 2009;16(8):943-948. PubMed
86.Diener HC, Foh M, Iaccarino C, et al. Cyclandelate in the prophylaxis of migraine: a randomized, parallel, double-blind study in comparison with placebo and propranolol. The Study group. Cephalalgia. 1996;16(6):441-447. PubMed
87.Jafarpour M, Yousefi G, Hamedi A, Shariat A, Salehi A, Heydari M. Effect of a traditional syrup from Citrus medica L. fruit juice on migraine headache: a randomized double blind placebo controlled clinical trial. J Ethnopharmacol. 2016;179:170-176. PubMed
88.Pradalier A, Serratrice G, Collard M, et al. Long-acting propranolol in migraine prophylaxis: results of a double-blind, placebo-controlled study. Cephalalgia. 1989;9(4):247-253. PubMed
89.Sargent J, Solbach P, Damasio H, et al. A comparison of naproxen sodium to propranolol hydrochloride and a placebo control for the prophylaxis of migraine headache. Headache. 1985;25(6):320-324. PubMed
90.Weber RB, Reinmuth OM. The treatment of migraine with propranolol. Neurology. 1972;22(4):366-369. PubMed
91.Brandes JL, Saper JR, Diamond M, et al. Topiramate for migraine prevention: a randomized controlled trial. JAMA. 2004;291(8):965-973. PubMed
92.Gode S, Celebisoy N, Kirazli T, et al. Clinical assessment of topiramate therapy in patients with migrainous vertigo. Headache. 2010;50(1):77-84. PubMed
93.Lipton RB, Silberstein S, Dodick D, et al. Topiramate intervention to prevent transformation of episodic migraine: the topiramate INTREPID study. Cephalalgia. 2011;31(1):18-30. PubMed
94.Lo YL, Lum SY, Fook-Chong S, Siow HC. A pilot study of topiramate dosages for migraine prophylaxis in an Asian population. J Headache Pain. 2010;11(2):175-178. PubMed
95.Mei D, Capuano A, Vollono C, et al. Topiramate in migraine prophylaxis: a randomised double-blind versus placebo study. Neurol Sci. 2004;25(5):245-250. PubMed
96.Silberstein SD, Hulihan J, Karim MR, et al. Efficacy and tolerability of topiramate 200 mg/d in the prevention of migraine with/without aura in adults: a randomized, placebo-controlled, double-blind, 12-week pilot study. Clin Ther. 2006;28(7):1002-1011. PubMed
97.Silberstein SD, Neto W, Schmitt J, Jacobs D. Topiramate in migraine prevention: results of a large controlled trial. Arch Neurol. 2004;61(4):490-495. PubMed
98.Storey JR, Calder CS, Hart DE, Potter DL. Topiramate in migraine prevention: a double-blind, placebo-controlled study. Headache. 2001;41(10):968-975. PubMed
99.Ashtari F, Shaygannejad V, Akbari M. A double-blind, randomized trial of low-dose topiramate vs propranolol in migraine prophylaxis. Acta Neurol Scand. 2008;118(5):301-305. PubMed
100.Diener HC, Tfelt-Hansen P, Dahlof C, et al. Topiramate in migraine prophylaxis--results from a placebo-controlled trial with propranolol as an active control. J Neurol. 2004;251(8):943-950. PubMed
101.Dogan A, Orscelik O, Kocyigit M, et al. The effect of prophylactic migraine treatment on arterial stiffness. Blood Press. 2015;24(4):222-229. PubMed
102.Dodick DW, Freitag F, Banks J, et al. Topiramate versus amitriptyline in migraine prevention: a 26-week, multicenter, randomized, double-blind, double-dummy, parallel-group noninferiority trial in adult migraineurs. Clin Ther. 2009;31(3):542-559. PubMed
103.Duman T, Dede OH, Uluduz D, Seydaoglu G, Okuyucu E, Melek I. Sleep changes during prophylactic treatment of migraine. Ann Indian Acad Neurol. 2015;18(3):298-302. PubMed
104.Keskinbora K, Aydinli I. A double-blind randomized controlled trial of topiramate and amitriptyline either alone or in combination for the prevention of migraine. Clin Neurol Neurosurg. 2008;110(10):979-984. PubMed
105.Mathew NT. Prophylaxis of migraine and mixed headache. A randomized controlled study. Headache. 1981;21(3):105-109. PubMed
106.Camporeale A, Kudrow D, Sides R, et al. A phase 3, long-term, open-label safety study of Galcanezumab in patients with migraine. BMC Neurol. 2018;18(1):188. PubMed
107.Jhingran P, Osterhaus JT, Miller DW, Lee JT, Kirchdoerfer L. Development and validation of the Migraine-Specific Quality of Life Questionnaire. Headache. 1998;38(4):295-302. PubMed
108.Bagley CL, Rendas-Baum R, Maglinte GA, et al. Validating Migraine-Specific Quality of Life Questionnaire v2.1 in episodic and chronic migraine. Headache. 2012;52(3):409-421. PubMed
109.Schober P, Boer C, Schwarte LA. Correlation coefficients: appropriate use and interpretation. Anesth Analg. 2018;126(5):1763-1768. PubMed
110.Rendas-Baum R, Bloudek LM, Maglinte GA, Varon SF. The psychometric properties of the Migraine-Specific Quality of Life Questionnaire version 2.1 (MSQ) in chronic migraine patients. Qual Life Res. 2013;22(5):1123-1133. PubMed
111.Speck RM, Yu R, Ford JH, Ayer DW, Bhandari R, Wyrwich KW. Psychometric validation and meaningful within-patient change of the Migraine-Specific Quality of Life questionnaire version 2.1 electronic patient-reported outcome in patients with episodic and chronic migraine. Headache. 2021;61(3):511-526. PubMed
112.Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology. 2001;56(6 Suppl 1):S20-28. PubMed
113.Stewart WF, Lipton RB, Kolodner K, Liberman J, Sawyer J. Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia. 1999;19(2):107-114; discussion 174. PubMed
114.Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain. 2000;88(1):41-52. PubMed
115.Sauro KM, Rose MS, Becker WJ, et al. HIT-6 and MIDAS as measures of headache disability in a headache referral population. Headache. 2010;50(3):383-395. PubMed
116.Yang M, Rendas-Baum R, Varon SF, Kosinski M. Validation of the Headache Impact Test (HIT-6 TM) across episodic and chronic migraine. Cephalalgia. 2011;31(3):357-367. PubMed
117.Silberstein SD, Lee L, Gandhi K, Fitzgerald T, Bell J, Cohen JM. Health care Resource Utilization and Migraine Disability Along the Migraine Continuum Among Patients Treated for Migraine. Headache. 2018;58(10):1579-1592. PubMed
118.Buse D, Bigal M, Rupnow M, et al. The Migraine Interictal Burden Scale (MIBS): results of a population-based validation study (abstract). Headache. 2007;47(5):778.
119.Buse DC, Rupnow MF, Lipton RB. Assessing and managing all aspects of migraine: migraine attacks, migraine-related functional impairment, common comorbidities, and quality of life. Mayo Clin Proc. 2009;84(5):422-435. PubMed
120.Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353-365. PubMed
121.Seo JG, Park SP. Validation of the Patient Health Questionnaire-9 (PHQ-9) and PHQ-2 in patients with migraine. J Headache Pain. 2015;16:65. PubMed
122.Blumenfeld AM, Tepper SJ, Robbins LD, et al. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J Neurol Neurosurg Psychiatry. 2019;90(3):353-360. PubMed
123.McMillan D, Gilbody S, Richards D. Defining successful treatment outcome in depression using the PHQ-9: a comparison of methods. J Affect Disord. 2010;127(1-3):122-129. PubMed
124.Seo JG, Park SP. Validation of the Generalized Anxiety Disorder-7 (GAD-7) and GAD-2 in patients with migraine. J Headache Pain. 2015;16:97. PubMed
125.Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097. PubMed
126.Robinson E, Titov N, Andrews G, McIntyre K, Schwencke G, Solley K. Internet treatment for generalized anxiety disorder: a randomized controlled trial comparing clinician vs. technician assistance. PLoS One. 2010;5(6):e10942. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–present)
Embase (1974–present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: June 29, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
No date or language limits were used
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(galcanezumab* or Emgality* or ly 2951742 or ly2951742 or 55KHL3P693).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*galcanezumab/
(galcanezumab* or Emgality* or ly 2951742 or ly2951742).ti,ab,kw,dq..
3 or 4
5 use oemezd
6 not (conference review or conference abstract).pt.
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | Emgality OR galcanezumab]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- Emgality OR galcanezumab]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- Emgality OR galcanezumab]
Grey Literature
Search dates: June 17, 2021-June 26, 2021
Keywords: Emgality, galcanezumab, migraine
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Blumenfeld AM, Frishberg BM, Schim JD, et al. Real-World Evidence for Control of Chronic Migraine Patients Receiving CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA: A Retrospective Chart Review. Pain Ther. 2021 Apr 21;21:21. | Study design |
Skljarevski V, Oakes TM, Zhang Q, et al. Effect of Different Doses of Galcanezumab vs Placebo for Episodic Migraine Prevention: A Randomized Clinical Trial. JAMA Neurology. 2018 02 01;75(2):187-193. | Study design |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 19: EVOLVE-1 Trial Results From Multiple Testing Procedure — ITT Population, Double-Blind Treatment Phase
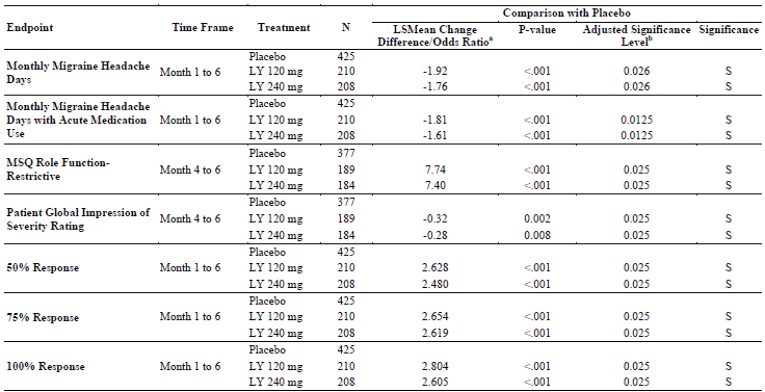
ITT = intention-to-treat; LSMean = Least Squares Mean; LY = LY2951742/galcanezumab; MSQ = Migraine-Specific Quality of Life Questionnaire; N = number of intent-to-treat patients who had non-missing baseline and at least one post-baseline value; S = significant.
a Odds ratio is provided for response measures. For the other measures, LSMean change difference is provided.
b If P value is less than or equal to the adjusted significance level, then the results are statistically significant after adjustment for multiplicity.
Source: EVOLVE-1 Clinical Study Report9
Figure 20: EVOLVE-2 Trial Results From Multiple Testing Procedure — ITT Population, Double-Blind Treatment Phase
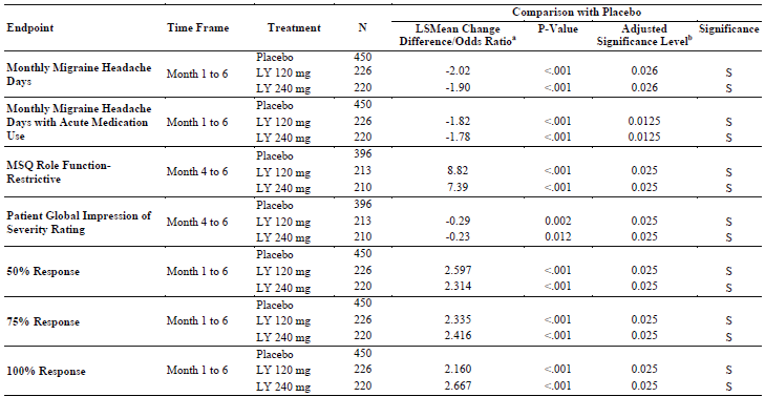
ITT = intention-to-treat; LSMean = Least Squares Mean; LY = LY2951742/galcanezumab; MSQ = Migraine-Specific Quality of Life Questionnaire; N = number of intent-to-treat patients who had non-missing baseline and at least one post-baseline value; S = significant.
a Odds ratio is provided for response measures. For the other measures, LSMean change difference is provided.
b If P value is less than or equal to the adjusted significance level, then the results are statistically significant after adjustment for multiplicity.
Source: EVOLVE-2 Clinical Study Report.10
Figure 21: REGAIN Trial Results From Multiple Testing Procedure — Overview
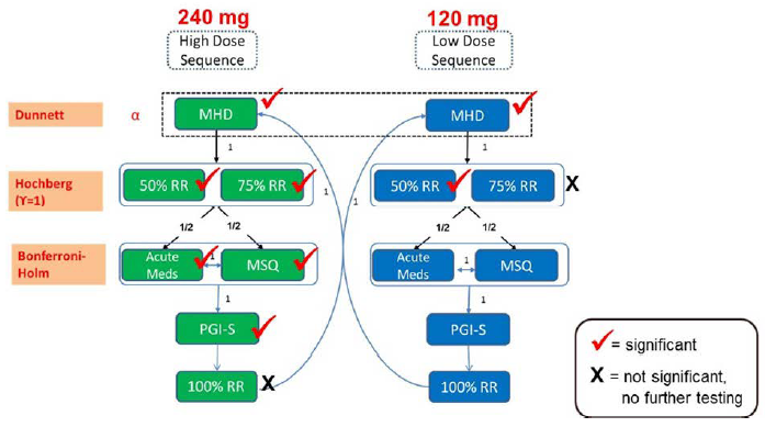
Acute Meds = MHD with the use of acute (abortive) treatment; MHD = the number of monthly migraine headache days (mean change from baseline); MSQ = Migraine-Specific Quality of Life Questionnaire Role Function-Restrictive domain; PGI-S = Patient Global Impression of Severity; RR = response rate.
Source: REGAIN Clinical Study Report.11
Figure 22: REGAIN Trial Results From Multiple Testing Procedure — ITT Population, Double-Blind Treatment Phase
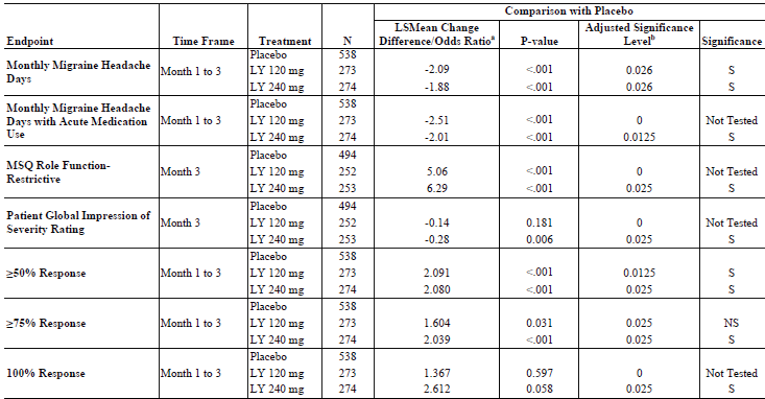
ITT = intention-to-treat; LSMean = Least Squares Mean; LY = LY2951742/galcanezumab; MSQ = Migraine-Specific Quality of Life Questionnaire; N = number of intent-to-treat patients who had non-missing baseline and at least one post-baseline value; NS = not significant; S = significant.
a Odds ratio is provided for response measures. For the other measures, LSMean change difference is provided.
b If P value is less than or equal to the adjusted significance level, then the results are statistically significant after adjustment for multiplicity.
Source: REGAIN Clinical Study Report.11
Figure 23: CONQUER Trial Results From Multiple Testing Procedure — ITT Population and ITT Episodic Subpopulation, Double-Blind Treatment Phase
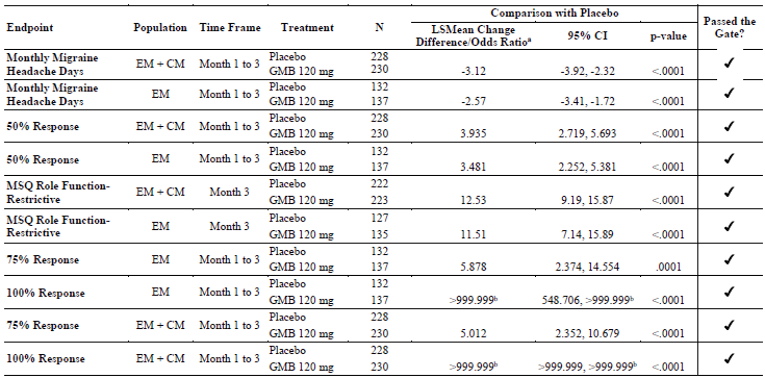
ITT = intent-to-treat; CI = confidence interval; CM = chronic migraine; EM = episodic migraine; GMB = LY2951742/galcanezumab; LSMean = Least Squares Mean; MSQ = Migraine-Specific Quality of Life Questionnaire; N = number of patients in the analysis population who had non-missing baseline and at least one post-baseline value, with the exception of MSQ, for which N = number of patients in the analysis population with non-missing baseline value and non-missing value for month 3.
a Odds ratio is provided for response measures. For the other measures, LSMean change difference is provided.
b Due to no patients meeting the responder definition in the placebo group at month 1 and low patient counts at months 2 and 3 in the placebo group, the odds ratio and corresponding 95% CI is large and reported as >999.999.
Source: CONQUER Clinical Study Report.12
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
Migraine-Specific Quality of Life Questionnaire version 2.1 (MSQ v2.1)
Migraine Disability Assessment (MIDAS)
Health care resource utilization (HCRU) and employment status
4-item Migraine Interictal Burden Scale (MIBS-4)
EQ-5D 5-Levels (EQ-5D-5L)
Work Productivity and Activity Impairment questionnaire (WPAI)
Patient Health Questionnaire-9 (PHQ-9)
Generalized Anxiety Disorder 7-Item (GAD-7).
Findings
Table 47: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
MSQ v2.1 | A 14-item instrument covering 3 domains allowing patients to rate the impact that migraine had on their physical and emotional functioning using a 6-point scale. Raw scores are rescaled from 0 to 100 and an increase in score indicates an improvement in HRQoL. | Validity: Construct, convergent, and discriminant validity were adequate when compared to other headache-related and HRQoL instruments in patients with migraine. Reliability: Internal consistency and test-retest reliability were adequate in patients with migraine. Responsiveness: Responsiveness was adequate in patients with migraine. | Patients with EM: RR = 3.2 to 5.0 RP = 4.6 to 7.9 EF = 7.5 to 10.6 Patients with CM: RR = 10.9 RP = 8.3 EF = 12.2 |
MIDAS | A 5-item instrument evaluating the number of days missed or with reduced productivity at work/school, at home, and in social settings. Total scores are translated to a 4-point grading system and a decrease in grade indicates a decrease in disability. | Validity: Concurrent validity was adequate when compared to other headache-related assessments in patients with migraine. Reliability: Internal consistency and test-retest reliability were adequate in patients with migraine. Responsiveness: No evidence found for patients with migraine. | 3.7 points for a population of patients with migraine. |
HCRU and employment status | Study personnel collected information of HCRU (emergency visits, overnight hospital stays, and other health care visits) and employment status. | Validity: No evidence found for patients with migraine. Reliability: No evidence found for patients with migraine. Responsiveness: No evidence found for patients with migraine. | Not identified in populations with migraine. |
MIBS-4 | A 4-item instrument that assesses the burden of migraine during the interictal state on a 4-point scale. Total scores range from 0 to 12 and a decrease in score indicates decrease in burden. | Validity: Moderate correlation with other migraine and headache instruments indicating some validity in patients with migraine. Reliability: No evidence found for patients with migraine. Responsiveness: No evidence found for patients with migraine. | Not identified in populations with migraine. |
EQ-5D-5L and VAS | A patient-reported, generic, QoL instrument that has been applied to a wide range of health conditions and treatments. An increase in score indicates an increase in QoL. | Validity: Adequate in diverse patient populations. No evidence found for patients with migraine. Reliability: No evidence found for patients with migraine. Responsiveness: No evidence found for patients with migraine. | Not identified in populations with migraine. |
WPAI | A 6-item questionnaire measuring impairments on work productivity and daily activities due to generic or specific health problems using an 11-point scale. A decrease in score indicates an improvement in productivity and decrease in impairment. | Validity: Adequate in general, employed populations. No evidence found for patients with migraine. Reliability: No evidence found for patients with migraine. Responsiveness: No evidence found for patients with migraine. | Not identified in populations with migraine. |
PHQ-9 | A 9-item questionnaire used to screen patients for depression based on a 4-point scale. Total scores range from 0 to 27 and a decrease in score indicates a decrease in depression severity. | Validity: Construct validity was adequate when compared to other headache-related and HRQoL instruments in patients with migraine. Reliability: Internal consistency and reliability were adequate in patients with migraine. Responsiveness: Not identified in populations with migraine. | Meaningful change: for patients with CM, a reduction of ≥1 severity category which is consistent with an improvement of ≥5 points on the scale for patients with baseline values >8. No specific MID identified. |
GAD-7 | A 7-item questionnaire used to screen patients for anxiety based on a 4-point scale. Total scores range from 0 to 21 and a decrease in score indicates a decrease in anxiety severity. | Validity: Construct validity was adequate when compared to other headache-related and HRQoL instruments in patients with migraine. Reliability: Internal consistency and reliability were adequate in patients with migraine. Responsiveness: Not identified in populations with migraine. | Meaningful change: for patients with CM, a reduction of ≥1 severity category which is consistent with a change from ≥10 points to < 10 points on the scale or a reduction ≥50% of a patient’s baseline score. No specific MID identified. |
CM = chronic migraine; EF = emotional function; EM = episodic migraine; EQ-5D-5L = EQ-5D 5-levels; GAD-7 Generalized Anxiety Disorder 7-item; HCRU = health care resource utilization and employment status; HRQoL = health-related quality of life; MIBS-4 = migraine interictal burden scale; MID = minimal important difference; MIDAS = Migraine Disability Assessment; MSQ v2.1 = Migraine-Specific Quality of Life Questionnaire version 2.1; PHQ-9 = Patient Health Questionnaire-9; QoL = quality of life; RP = role function – preventive; RR = role function – restrictive VAS = visual analogue scale; WPAI = Work Productivity and Activity Impairment.
Migraine-Specific Quality of Life Questionnaire Version 2.1
The MSQ v2.1 is a self-reported, disease-specific instrument which assesses the physical and emotional impact of migraine on functioning.9-12 MSQ version 2.1 (v2.1) was revised from the earlier MSQ version 1.0 (developed and validated by Jhingran et al.) with items that have been reworded for clarification and shortened for easier administration.107 MSQ v2.1 was used in the studies in this review.
The 14 items of the MSQ v2.1 assess HRQoL across 3 domains: role function – restrictive (RR, 7 items assessing how migraine limits daily social and work-related activities), role function – preventive (RP, 4 items assessing how migraine prevents these activities), and EF, 3 items assessing the emotions associated with migraine).108 Participants respond based on a 4-week recall period and using a 6-point Likert-type scale where 1 = none of the time, 2 = a little bit of the time, 3 = some of the time, 4 = a good bit of the time, 5 = most of the time, and 6 = all of the time. Raw dimension scores are computed as a sum of item responses and are rescaled to a 0 to 100-point scale, producing an overall score for each domain. A higher score indicates better HRQoL.
A study by Bagley et al. provided evidence of the validity and reliability of MSQ v2.1 in patients with EM and CM.108 The study was a web-based, cross-sectional survey conducted in 8,726 patients with EM (< 15 headache days per month [HDPM]) or CM (15 HDPM) from 9 countries. Construct validity was assessed using Pearson’s correlation coefficients (r) of the MSQ scores and other HRQoL instruments. Based on the overall study population (both CM and EM), correlations were moderate to strong between the MSQ and (HIT-6 (r = –0.60 to –0.71), weak to moderate for the MSQ and Patient Health Questionnaire-4 (PHQ-4) (r = –0.31 to –0.42), and weak for the MSQ and MIDAS (r = –0.38 to –0.39) and the MSQ and HDPM (r = –0.17 to –0.24).108,109 Overall, this provided some support for convergent and discriminant validity of the MSQ. Similar results were also obtained for the CM and EM groups alone.108 Known-groups validity was also demonstrated using the same HRQoL measures, as a statistically significant difference was observed for the mean MSQ scores across migraine frequency groups. Reliability and internal consistency were measured with Cronbach alpha for the study population for RR, RP, and EF (0.96, 0.90, and 0.87, respectively), and was acceptable based on a threshold of 0.70. Internal consistency was also adequate for either of the EM and CM populations with Cronbach alpha measures ≥0.86 for each of the MSQ domains.
Rendas-Baum et al. provided further validation of MSQ v2.1 in patients with CM undergoing prophylactic treatment.110 Data were pooled from 2 clinical trials of onabotulinumtoxinA, PREEMPT-1 and PREEMPT-2, and included 1,376 patients. MSQ and HIT-6 scores were moderately to strongly correlated109, Pearson values ranged from r = –0.59 (EF) to r = –0.75 (RR) at baseline and r = –0.74 (EF and RP) and r = –0.86 (RR) at 24 weeks demonstrating adequate validity.110 Internal consistency at baseline was acceptable with Cronbach alpha of 0.80 for all 3 domains, varying between 0.80 (EF) and 0.93 (RR). At 24 weeks, Cronbach alpha remained acceptable and ranged from 0.90 to 0.97 across the 3 domains and the 2 studies. MSQ change scores showed large and moderate effect sizes for patients who experienced ≥50% improvement and improvement between 30% and 50%, respectively, indicating acceptable responsiveness.
Speck et al. assessed the psychometric properties of the electronic MSQ v2.1 using data from EVOLVE-1, EVOLVE-2, and REGAIN which were studies of adult patients with EM and CM.111 For validity, they found moderate correlations between each of the 3 domains when compared to the MIDAS and PGI-S. Correlations ranged from 0.46 to 0.57 for the RR, from 0.35 to 0.57 for the RP, and from 0.38 to 0.51 for the EF domains and there were stronger correlations with the MIDAS than the PGI-S. Internal consistency and test-retest reliability were adequate for all 3 domains of the MSQ v2.1 (Cronbach alpha ranged from 0.83 to 0.93 and intraclass correlation coefficient ranged from 0.77 to 0.92). Responsiveness was demonstrated where patients who showed a ≥1 level improvement on the MIDAS, PGI-S, or Patient Global Impression of Improvement and/or at least 50% fewer HDPM during the first 3 months of treatments also had a significant improvement in all 3 MSQ domains compared to those who did not demonstrate improvements. Correlations across the MSQ domains (RR, RP, and EF) compared to HDPM were also stronger for patients with CM versus those with EM (–0.60, –0.48, and –0.47 versus –0.47, –0.35, and –0.35), respectively. Lastly, the investigators observed no significant floor or ceiling effects from the data in any of the studies.
Dodick et al. estimated MIDs based on a multi-centre, double-blind, randomized trial of 328 adults with CM who received either topiramate or placebo for 16 weeks.52 The mean age was 38.2 years (range = 18, 74) and 85% of the study population was female. An anchor-based approach was used to estimate the MIDs based on within-group differences with the subject global impression of change (SGIC) serving as the anchor. The MID was estimated as the change in MSQ domain score that corresponded to a unit improvement on the SGIC (i.e., the beta coefficient of the regression equation of MSQ domain with SGIC was the MID). MIDs (95% confidence interval [CI]) for the RR, RP, and EF were 10.9 (9.4, 12.4), 8.3 (6.7, 9.9), and 12.2 (10.2, 14.3), respectively.
Cole et al. also calculated group-level and individual-level MIDs for the 3 domains.53 The analyses were performed on pooled data from 2 clinical trials of topiramate for migraine prophylaxis (N = 916) and the QualityMetric National Headache Survey (N = 1,016). The trials were randomized, double-blind, and placebo-controlled from Canada and the US. Patients were 12 to 65 years of age and experienced 3 to 12 migraine attacks per month (but not more than 15 HDPM during the 28-day baseline period). Patients were randomized to placebo or topiramate 50, 100, or 200 mg/day and continued treatment for 18 weeks. The QualityMetric database included adults (18 to 65 years) residing in the contiguous 48 states of the US and experienced a headache at least once in the past 4 weeks prior to the phone interview. No study intervention was administered to the survey participants. Using a distribution-based method with Cohen d effect sizes from the pooled topiramate trial data, group-level MIDs were estimated to be 3.2, 4.6, and 7.5 for RR, RP, and EF, respectively.
Cole et al. also calculated individual-level MIDs with anchor-based versus distribution methods.53 Anchors included average monthly migraine rate (30%, 40%, or 50% reduction), migraine status (yes/no), MIDAS, more or less headaches compared to 3 months ago (yes/no), bothered by headaches more now compared with 3 months age (yes/no), and impact of migraine on life (i.e., everyday physical activities, feeling frustrated or irritable, limitations in daily activities, and overall quality of life). The individual-level MIDs suggested by Cole et al. from anchor-based techniques (Table 48) were between 4.9 and 5.0 for RR, 5.0 and 7.9 for RP, and 8.0 and 10.6 for EF and were generally smaller than those reported by Dodick et al.52 It is important to note that the MIDs proposed by Dodick et al.52 were based on patients with CM, whereas the datasets used by Cole et al.53 included patients with a maximum of 15 HDPM (i.e., patients would be below the threshold for classification of CM).
Using a distribution-based method, the MIDs were calculated from one-half the SD of each MSQ domain from the pooled topiramate trial dataset and the QualityMetric dataset separately.53 In a second distribution-based technique, the MIDs were calculated from the standard error of the mean (SEM) of the MSQ domains in the pooled clinical trial dataset. The MIDs ranged from 4.8 to 8.6 (RR), 7.9 to 9.9 (RP), and 10.6 to 12.4 (EF). The anchor-based MIDs were similar to the distribution-based MIDs using the SEM, however, were less than the distribution-based MIDs using one-half of the SD (Table 48).
Table 48: Individual-Level MIDs for MSQ in Patients With Fewer Than 15 HDPMs
MSQ Domain | Anchor-Based MIDa | Distribution-Based (½ SD) MIDb | Distribution-Based (SEM) MID |
|---|---|---|---|
Role function – restrictive (RR) | 4.9; 5.0 | 8.3; 8.6 | 4.8 |
Role function – preventive (RP) | 5.0; 7.9 | 9.9; 8.5 | 7.9 |
Emotional function (EF) | 8.0; 10.6 | 12.4; 11.5 | 10.6 |
EM = episodic migraine; HDPM = headache days per month; MID = minimal important difference; MSQ = Migraine-Specific Quality of Life Questionnaire; SD = standard deviation; SEM = standard error of mean.
a Estimates based on logistic and better-same-worse analysis.
b Estimates based on multiple databases (pooled topiramate trial dataset and QualityMetric dataset).
Source: Cole et al.53
Migraine Disability Assessment
The MIDAS is a self-reported, 5-item questionnaire that evaluates headache-related disability.54 Each item corresponds to the number of days missed or with reduced productivity in 3 domains: work or school; housework or chores; and family, social, or leisure activities. Answers are based on a 3-month recall interval which allows the questions to capture information on patients’ long-term experience with headaches.112 An overall score (ranging from 0 to 270) for the questionnaire is calculated by summing the number of lost days recorded across the 5 items.9-12 Two additional questions are not included in the scoring that ask about the frequency of headaches and intensity of headache pain.112 These are used to provide clinicians with additional information for managing treatment decisions. The overall score translates to a 4-point grading scale: grade 1 (scores from 0 to 5) = minimal or infrequent disability; grade 2 (scores from 6 to 10) = mild or infrequent disability; grade 3 (scores from 11 to 20) = moderate disability; grade 4 (scores 21 or greater) = severe disability. Grade 4 can be further divided into 2 subcategories: grade 4-A (scores 21 to 40) = severe and grade 4-B (scores 41 to 270) = very severe.12
The MIDAS has been validated in terms of internal consistency and test-retest reliability in studies by Stewart et al. Concurrent validity of MIDAS was assessed by comparing the MIDAS score and a 90-day headache diary, both of which were completed by 144 patients with physician-confirmed migraine diagnosis.112-114 The individual items and overall MIDAS score showed a moderate to strong correlation109 between the questionnaire and daily headache dairy (Pearson’s r = 0.50 to 0.77, Spearman’s ρ = 0.53 to 0.76) demonstrating concurrent validity.112,114
Two studies by Stewart et al. collected data using phone interviews and a clinically-validated, computer-assisted telephone interview that asked respondents about their headaches, which was used to define cases of migraine in combination with International Headache Society criteria.112,113 A total of 124 respondents with migraine and 100 non-migraine headache controls completed the MIDAS twice.113 Spearman’s and Pearson’s correlations were used to assess test-retest reliability between responses to the first and second questionnaires, and internal consistency for the overall score was evaluated using Cronbach alpha. There was substantial agreement based on a Pearson’s correlation, ranging from 0.60 to 0.75 for each question, and Spearman’s correlation, ranging from 0.67 to 0.84, demonstrating adequate test-retest reliability. The MIDAS also demonstrated acceptable internal consistency (Cronbach alpha = 0.83). Similar methods were used to evaluate reliability in the second study by Stewart et al.112 Questionnaires were collected from 197 patients living with migraine (97 from the US and 100 from the UK), which were completed a median of 21.5 days apart. Each MIDAS question score was moderately to strongly correlation based on Pearson’s correlation coefficient (r = 0.52 to 0.82) and moderately to substantially correlated according to Spearman’s correlation coefficient (ρ = 0.46 to 0.71), demonstrating variable test-retest reliability. Furthermore, the overall MIDAS score demonstrated acceptable test-retest reliability with high Pearson’s (r = 0.80 to 0.83) and Spearman’s correlations (ρ = 0.77 to 0.78).
The MIDAS is considered reliable and valid in those experiencing headaches and migraine; however, the proportion of patients with CM versus EM in these studies is unknown. No literature was found that assessed the MIDAS responsiveness in patients with migraine.
A MID was estimated based on data from 2,442 patients who reported at least 4 HDPM and had participated in the 2005 and 2006 American Migraine Prevalence and Prevention Study.55 Using anchor-based methods, Lipton et al. found that a 25% increase in HDPM (N = 54) corresponded to a 1.6 (SD = 30.9) point increase in mean MIDAS score while a 25% decrease in HDPM (N = 82) corresponded to a 5.0 (SD = 16.5) point decrease in mean MIDAS score. A weighted average was calculated and resulted in an estimated MID of 3.7 points.
Migraine Disability Assessment and 6-Item Headache Impact Test
The HIT-6 is a 6-item, self-reported questionnaire that assesses the impact of headache on patient quality of life.115 The items cover topics such as pain, social function, cognitive function, and psychological distress. Patients are asked to quantify their responses using: never, rarely, sometimes, very often, and always which correspond to values of 6, 8, 10, 11, and 13, respectively. A total score is the sum of the 6 items and translates to 4 levels of severity: little or no impact, some impact, substantial impact, and very severe impact. The HIT-6 has previously demonstrated acceptable validity, internal consistency (Cronbach alpha = 0.90), and test-retest reliability (Cronbach alpha = 0.78).
Sauro et al. used data from the Canadian Headache Outpatient Registry and Database (CHORD) to compare MIDAS and HIT-6 scores for 798 patients.115 Those who were part of the CHORD were new patients at 1 of 5 affiliated neurology clinics in Canada and most were diagnosed with migraine. The Spearman rank correlation coefficient (r) was 0.52 for the MIDAS and HIT-6 showing moderate correlation between the instruments. This correlation (r = 0.56) was also demonstrated with data from adults who recently reported headaches and participated in the National Survey of Headache Impact study and the HIT-6 Validation study.116 The investigators found that the HIT-6 was more likely to categorize patients in a higher (more severe) category than the MIDAS: 79% had very severe impact on the HIT-6 whereas 57% had severe disability on the MIDAS.115 Headache intensity also showed a stronger correlation with the HIT-6 (r = 0.46) compare to the MIDAS (r = 0.26). The recall period for the HIT-6 is typically 4 weeks versus 3 months for the MIDAS. It was also noted that the HIT-6 questions may be more subjective in nature with patients responding qualitatively (e.g., never or always). Alternatively, the MIDAS has patients quantify the number of days of lost or 50% reduced productivity, though there is still some subjectivity in patients’ opinions. Furthermore, it was suggested that the content of the HIT-6 is more emotional in nature compared to the MIDAS with the former asking how patients felt during the recall period. The MIDAS may be more easily interpreted since the score refers to the number of days that a patient recalled having lost productivity, but this could depend on employment or school status since work/school and home are considered separate domains. Responses to the HIT-6 range from never to always which may be subjective and non-linear in nature. Based on the differences, the investigators suggested that the 2 instruments are not interchangeable, but complementary.
Health Care Resource Utilization and Employment Status
Health care resource utilization information was collected by study personnel in the REGAIN and CONQUER studies.11,12 Three questions asked about the number of hospital emergency visits, overnight stays at the hospital, and other visits with a health care professional aside from study-related visits that occurred (all-cause and migraine-specific) since the patient’s last study visit. At baseline, the same questions were asked with a recall period of 6 months. A higher number (i.e., events or visits) indicates greater utilization of health care resources. Employment status information was also collected due to the association and potential confounding with health outcomes measures.
Data from a cross-sectional survey from the US National Health and Wellness Survey panel and other ailment panels were collected and used in an analysis of HCRU by Silberstein et al.117 Altogether, 1,347 respondents were included who were adults with a self-reported migraine diagnosis or had migraine symptoms in the previous 3 months and had taken acute and/or preventive migraine medication in the previous year. Patients were categorized by the frequency of their self-reported number of headaches into low-frequency EM (LFEM, < 4 headache days per month), moderate-frequency episodic migraine (MFEM, 4 to 9 days), high-frequency EM (HFEM, 10 to 14 days), and CM (≥15 days). Based on bivariate analyses, the number of migraine-related emergency room and health care practitioner visits were statistically significantly lower for the LFEM group compared to the 3 other groups of patients. There was no notable difference in the number of hospitalizations among the severities of migraine. From multivariable analyses, statistically significant differences were calculated between the LFEM versus MFEM and CM groups for both health care practitioner visits and hospitalizations as well as between the LFEM versus MFEM groups for emergency visits. Furthermore, total costs were significantly higher for both MFEM and CM groups compared to LFEM patients. It is worth noting this was an American study, migraine diagnosis was patient-reported, it is unknown if patients accurately represent the broader migraine population, and costs data were extrapolated from the 2013 Medical Expenditure Panel Survey.
A multi-national, cross-sectional survey of adults with migraine was conducted in 2009 assessing disability, HRQoL, and resource use.22 In total, 8,726 individuals reported on the frequency of resources used (e.g., visits to hospital, emergency, primary care provider, and specialist) during the previous 3 months. Of the 8,726 respondents, 499 (5.7%) reported having CM while 8,227 (94.2%) had EM (< 15 headache days per month). Overall, those with CM, compared to EM, showed greater HCRU. After adjusting for covariates such as age, gender, country, education, and comorbidities, the odds ratios ranged from 2.32 (95% confidence interval [CI] = 2.15 to 2.51) for primary care provider visits to 3.23 (95% CI = 2.78 to 3.75) for neurologist/headache specialist visits.
No literature was found that assessed HCRU or employment status for validity, reliability, or responsiveness in patients with migraine.
No MID was identified in populations with migraine.
4-Item Migraine Interictal Burden Scale
The MIBS-4 is a self-reported, 4-item questionnaire that assesses the burden of illness related to migraine during the time in between attacks (interictal state).12 Its 4 items address interruptions with work or school, diminished family and social life, difficulty making plans, and emotional distress. Responses range from 0 = don’t know/not applicable or never, 1 = rarely, 2 = some of the time, and 3 = much or most/all of the time. The individual item scores are summed for a total score ranging from 0 to 12 where a higher score indicates a greater interictal burden. Total scores can be categorized as follows: 0 = no burden, 1 to 2 = mild, 3 to 4 = moderate, and ≥5 = severe. Questions are answered based on a 4-week recall period.
Buse et al. administered 30 candidate items of the MIBS-4 as a mailed survey to 2,500 previously identified patients with migraine.118 Patients were also mailed a validated diagnostic screener such as the MIDAS, MSQ, PHQ, HIT-6, and lost productive time work and health questionnaire.119 Of the 1,734 surveys returned, 1,391 met the International Classification of Headache Disorders-2 (ICHD-2) criteria for migraine. Categorical confirmatory factor analysis yielded the 4 domains of the MIBS-4 described previously.118
The MIBS-4 showed moderate correlation with the MIDAS, MSQ, HIT-6, assessments of psychological disorders, and measures of workplace productivity indicating some validity.119 In a regression model, the total MIBS-4 score predicted MIDAS disability with R2 = 0.15, suggesting that ictal and interictal burden are correlated, but distinct.118 No literature was found that assessed MIBS-4 reliability or responsiveness in patients with migraine.
No MID was identified in populations with migraine.
EQ-5D 5-Levels Questionnaire
The EQ-5D-5L is a generic, self-reported instrument that is applicable to a wide range of health conditions and treatments.56-58 To improve sensitivity and reduce ceiling effects, the EQ-5D-3L was updated to have 5 levels in 2005, resulting in the EQ-5D-5L, which was used in the studies of this review. Questions were answered based on how the patient felt that day.12
The EQ-5D-5L consists of a descriptive system and the EQ VAS.58 The descriptive system comprises 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Patients respond to each dimension using 5 levels where 1 = no problems, 2 = slight problems, 3 = moderate problems, 4 = severe problems, and 5 = extreme problems or unable to perform. Respondents are asked to choose the level that reflects their health state. In terms of measurement properties, these are ordinal data; they do not have interval properties and therefore, are not used to produce an individual dimension score. Results from the EQ-5D-5L descriptive system can be converted into a single, country-specific index score using a scoring algorithm taking the local patient and population preferences into account.62 A score of 0 represents the health state dead and 1.0 reflects perfect health. Negative scores are also possible for health states that society, not the patient, considers to be worse than dead.
The EQ VAS records the respondent’s self-rated health on a vertical VAS where the end points are labelled 0 (the worst health imaginable) and 100 (the best health imaginable). The respondents are asked to mark an X on the scale that best represents their health on that day.58,62
The EQ-5D-5L has been validated in terms of feasibility, convergent validity, discriminatory power, and ceiling effects in a diverse patient population from 6 countries with chronic conditions.58 No literature was found that assessed the EQ-5D-5L for validity, reliability, or responsiveness in patients with migraine.
A Canadian-specific estimate of a MID for the EQ-5D-5L was generated by simulating the effects of single level transitions in each dimension.59 The results yielded MIDs with a summarized mean of 0.056 (SD = 0.011), and a summarized median of 0.056 (interquartile range = 0.049, 0.063). No MID was identified in populations with migraine.
Work Productivity and Activity Impairment Questionnaire
The WPAI questionnaire is a self-reported instrument that measures impairments on work productivity and daily activities due to generic health (WPAI-GH) or specific health problems (WPAI-SHP).62 The 2 versions were created using the same template and respondents answer based on general health status or a specific health problem, disease, or condition. The instrument consists of 6 items and measures impairments on both paid and unpaid work with a 7-day recall period. A patient’s employment status is determined first after which they answer 3 questions related to: work hours missed due to health issues, work hours missed for other reasons, and hours worked. There are 2 final questions asking how health issues have impacted productivity at work and activities outside of work rated on an 11-point scale from 0 = no impairment to 10 = complete impairment. Four scores are calculated for absenteeism, presenteeism, work productivity loss, and activity impairment and reported as impairment percentages where a higher number indicates greater impairment and/or lower productivity.12
The instrument has been validated in a sample of 106 employed individuals who had some symptom or health problem in the 7 days prior to completing the questionnaire.120 Respondents completed a baseline, self-administered questionnaire then were randomly assigned to either complete a second self-administered version or an interviewer-administered version via telephone call at least 4 hours later. The WPAI was also compared to 3 items from the SF-36 (role function physical, role function emotional, and pain). Overall, the highest correlations were observed among work productivity and non-work activities with the SF-36 as well as with the interviewer-administered questionnaires compared to self-administered formats. For reproducibility, there were no statistically significant changes from the first assessment to the second and all were done the same day.
No literature was found that assessed the WPAI for validity, reliability, or responsiveness in patients with migraine.
No MID was identified in patients with migraine.
Patient Health Questionnaire-9
The PHQ-9 is a self-reported questionnaire used for screening rather than diagnosing patients and consists of 9 items corresponding to criteria for diagnosing major depressive disorder from the Diagnostic and Statistical Manual for Mental Disorders, fourth edition.12,60 The 9 items include anhedonia; depressed mood; trouble sleeping; feeling tired; change in appetite; guilt, self-blame, or worthlessness; trouble concentrating; feeling slowed down or restless; and thoughts of being better off dead or hurting oneself.12 Patients score each item for how frequent symptoms occurred with a 2-week recall period where 0 = not at all, 1 = several days, 2 = more than half the days, and 3 = nearly every day.12,60 The total score ranges from 0 to 27 where 0 to 4 = none/minimal depression, 5 to 9 = mild depression, 10 to 14 = moderate depression, 15 to 19 = moderately severe depression, and 20 to 27 = severe depression.61
Validity and reliability of the PHQ-9 in patients with migraine was assessed by Seo et al.121 Consecutive patients (N = 132) visiting a hospital headache clinic in Korea were recruited. Patients aged 16 to 70 years were diagnosed with migraine based on the International Classification of Headache Disorders-3. In addition to the validated Korean PHQ-9, other HRQoL instruments were administered including the Mini International Neuropsychiatric Interview-Plus Version 5.0.0 (MINI), Beck Depression Inventory-II (BDI-II), MIDAS, HIT-6, and MSQOL. Of the 132 patients, 73 (55%) had CM. The PHQ-9 score correlated strongly with BDI-II (Spearman’s ρ = 0.754), HIT-6 (0.519), and MSQ (–0.538), and moderately with the MIDAS (0.377), demonstrating acceptable construct validity. Using receiver operating characteristic analyses, at a cut-off score of 7, relative to the MINI, the sensitivity of the PHQ-9 was 79.5%, specificity 81.7%, positive predictive value 64.6%, and negative predictive value 90.5%. Cronbach alpha for the PHQ-9 was 0.894 suggesting acceptable internal consistency and reliability. No literature was found that assessed the PHQ-9 for responsiveness in patients with migraine.
A study by Blumenfeld et al. investigated the use of onabotulinumtoxinA for the treatment of migraine in 716 patients with CM and how the medication affected depression and anxiety.122 The researchers considered a clinically relevant change on the PHQ-9 to be a reduction of at least 1 severity category which they noted as being consistent with an improvement of at least 5 points on the scale for patients with baseline values greater than 8.123 No MID was identified in patients with migraine.
Generalized Anxiety Disorder 7-Item
The GAD-7 is a patient-administered questionnaire used to screen for and measure the severity of anxiety symptoms with a 2-week recall period.12 The questionnaire consists of 7 items including feelings of nervousness, uncontrollable worrying, excessive, worrying, trouble relaxing, restlessness, irritability, and fearfulness. Patients answer based on a 4-point rating scale where 0 = not at all, 1 = several days, 2 = more than half the days, and 3 = nearly every day. Total scores range from 0 to 21 where a score of 0 to 4 = minimal anxiety, 5 to 9 = mild, 10 to 14 = moderate, and 15 to 21 = severe.
The GAD-7 has previously been validated in primary care settings and in 2015, Seo and Park conducted a study validating the instrument in 146 patients with migraine visiting an outpatient headache clinic in South Korea.124 Patients were aged 16 to 65 years old and were either newly diagnosed or were not already preventive medications in the past month. The Korean translation of the GAD-7 was validated and used for this study. To assess validity, the Korean version of the GAD-7 was compared to validated Korean translations of the Beck Anxiety Inventory, MIDAS, HIT-6, and MSQ. Spearman correlations (ρ) varied by instrument and all values were statistically significant (P < 0.001): Beck Anxiety Inventory rho = 0.756, MIDAS rho = 0.231, HIT-6 rho = 0.403, and MSQ rho = −0.378. In the original validating study of the GAD-7 for patients in primary care settings, at a cut-off score of 9, the instrument had a sensitivity of 89% and specificity of 82% for detecting generalized anxiety disorder when compared to structured psychiatric interviews.125 Similar results have been reported in studies of patients and the general population of other countries. In the Seo and Park study, at a cut-off score of >5, sensitivity was 78.1%, specificity 74.6%, positive predictive value 46.3%, and negative predictive value 92.4%.124 The researchers recommend that the instrument still be validated in different study settings and disease groups. The GAD-7 showed acceptable internal consistency and reliability (Cronbach alpha of 0.915) and individual items were associated with the total instrument score. No literature was found that assessed the GAD-7 for responsiveness in patients with migraine.
A study by Blumenfeld et al.122 investigated the use of onabotulinumtoxinA for the treatment of migraine in 716 patients with CM and how the medication affected depression and anxiety. The researchers considered a clinically relevant change on the GAD-7 to be a reduction of at least 1 severity category which they noted as being consistent with a change from ≥10 points on the scale to < 10 points or a reduction ≥50% of a patient’s baseline score.126 No specific MID was identified in patients with migraine.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BSC
best supportive care
CGRP
calcitonin gene-regulated peptide
CM
chronic migraine
EM
episodic migraine
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
MHD
migraine headache day
MSQ
Migraine-Specific Quality of Life Questionnaire
OnaA
onabotulinumtoxinA
QALY
quality-adjusted life-year
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Galcanezumab (Emgality), solution for subcutaneous injection |
Submitted price | Galcanezumab, 120 mg/mL: $623.00 per single-dose pre-filled pen or syringe |
Indication | For the prevention of migraine in adults who have at least 4 migraine days per month |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 30, 2019 |
Reimbursement request | For the prevention of migraine in adults who have at least 4 migraine days per month and have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications |
Sponsor | Eli Lilly Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis |
Target populations | Adults who have at least 4 migraine days per month and who have a history of at least 2 prior preventive treatment failures due to a lack of efficacy or tolerability, or both, in 2 populations:
|
Treatment | Galcanezumab. 240 mg (administered as 2 consecutive injections of 120 mg), followed by once-monthly doses of 120 mg. |
Comparator | BSC, consisting of acute medication for migraine as permitted in the CONQUER trial, including triptans, nonsteroidal anti-inflammatory drugs, and acetaminophen or acetaminophen combinations, with some restrictions on opioids and barbiturates |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs |
Time horizon | 20 years |
Key data source | CONQUER trial |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results | In CADTH reanalyses, the time horizon was reduced to 5 years, treatment-independent health-state utilities were applied, hospital costs were removed, and MHD reductions were not stratified by response
|
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; MHD = migraine headache days; QALY = quality-adjusted life-year.
Conclusions
Based on the CADTH clinical review, galcanezumab may reduce the frequency of migraine, reduce the frequency of migraine headache days (MHDs) with acute medication use, and improve quality of life as measured by the Migraine-Specific Quality of Life Questionnaire (MSQ) among patients with episodic migraine (EM) or chronic migraine (CM) compared to placebo. The effect of galcanezumab on MHDs with symptoms, headache days, and other patient-reported outcomes remains uncertain due to a lack of control for multiplicity.
CADTH undertook reanalyses to address limitations in the sponsor’s submission, including reducing the time horizon to 5 years, applying treatment-independent utilities, removing costs related to hospitalization for migraine treatment, and considering the sponsor’s combined-criteria analysis when incorporating the reduction in MHDs associated with treatment. In CADTH’s base-case reanalysis, galcanezumab was more costly and more effective than best supportive care (BSC) of no preventive therapy in patients with EM or CM who had experience with 2 or more prior preventive therapies. For patients with EM who have used 2 or more prior preventives, the incremental cost-effectiveness ratio (ICER) for galcanezumab compared to BSC was $273,560 per quality-adjusted life-year (QALY) gained, while for patients with CM and experience with 2 or more prior preventives, the ICER for galcanezumab compared to BSC was $109,325. Price reductions of 78% to 49% would be required for galcanezumab to be considered optimal compared to BSC at a willingness-to-pay threshold of $50,000 per QALY for EM and CM patients, respectively. Interpretation of these results should allow for the fact that migraine severity was not independently considered within the model. The cost-effectiveness of galcanezumab in patients who have experience with fewer than 2 prior preventive therapies for migraine is unknown.
The clinical effectiveness of galcanezumab relative to other currently reimbursed migraine-preventive therapies is uncertain due to a lack of direct comparative evidence and limitations within the sponsor’s indirect treatment comparison (ITC). Results of both the sponsor’s ITC and an ITC conducted by the Institute for Clinical and Economic Review suggest that the clinical efficacy and tolerability of galcanezumab is similar to that of erenumab or fremanezumab, although no definitive conclusion could be drawn on comparative clinical efficacy and safety specifically in patients with EM or CM who failed at least 2 preventive treatments. At the submitted price, the annual cost of galcanezumab is greater than that of erenumab and fremanezumab, and galcanezumab is more costly than onabotulinumtoxinA (OnaA) and oral therapies for the prevention of migraine in adults. The submitted evidence does not justify a price premium for galcanezumab over other, currently reimbursed comparator treatments.
Stakeholder Input Relevant to the Economic Review
This section is a summary of feedback received from the patient groups and drug plans that participated in the CADTH review process.
One joint patient input submission from Migraine Canada and Migraine Québec was received by CADTH for the review of galcanezumab for the treatment of migraine. Patient input was collected through 2 online surveys. The first survey, which was conducted in 2018, recruited 597 respondents, 32% of whom had 7 to 14 MHDs per month, while 42% had 15 or more MHDs per month. The second survey, conducted in 2021, captured input from 115 participants and was specific to calcitonin gene-regulated peptide (CGRP) medications, including galcanezumab. Two patients also provided direct input to the submission. The Summary of Patient Input section of the CADTH clinical report provides more details.
In terms of symptoms, patients with migraine report severe, throbbing, recurring pain; nausea; vomiting; dizziness; vertigo; loss of balance; extreme sensitivity to sound, light, touch, and smell; visual disturbances; loss of vision, speech, sensation, or muscle strength; and tingling or numbness in the extremities or face. Migraine can also be associated with slowed thinking, lack of focus, and difficulty reading and speaking, all of which affect an individual’s ability to perform work tasks and socialize. In total, 80% of respondents noted that their migraine headaches have led to anxiety or depression. Patients also reported living in fear of the next attack, dreading potential triggers, and having difficulty planning future events, which limits their personal and professional activities. Of the respondents, 27% reported having been to the emergency department at least 4 times since the start of their disease, with some reporting feeling stigmatized and blamed for wasting health care resources and the time of health care providers. In addition, 27% of patients reported having to wait over a year to see a neurologist or headache specialist, and 54% of patients reported being dissatisfied or very dissatisfied with the care they received from their physicians.
When asked about oral preventive treatments, 11% of the respondents to the 2018 survey had not tried any, 22% had tried 1 or 2 preventives, 22% had tried 3 or 4, and 45% had tried at least 5. In terms of adverse events (AEs), 7% of patients reported not having any side effects, 25% stated that what they experienced was tolerable, and 68% had discontinued a medication because of AEs. The most commonly reported side effects from using preventive medications were somnolence (76%), dizziness (58%), weight gain (54%), cognitive difficulties (53%), gastrointestinal upset (45%), and mood difficulties (44%). Patients valued a preventive medication that would allow them to be more productive at work and more sociable with their family, provide any degree of relief, have fewer side effects, and be affordable. A monthly injection was preferred over a daily pill by 73% of participants.
Of the 115 respondents to the 2021 survey, 36 had experience with galcanezumab. Patients generally felt that galcanezumab reduced migraine severity and frequency and was convenient, and that acute medications offered a better response when required. Most respondents had minimal to no side effects, but dizziness, vertigo, vomiting, constipation, and temporary injection site pain were noted.
The drug plans noted the lack of head-to-head trials comparing galcanezumab to other anti-CGRPs (erenumab and fremanezumab) that are currently undergoing pan-Canadian Pharmaceutical Alliance negotiations to determine their reimbursement status for the prevention of migraine.
Several of these aspects were addressed in the sponsor’s model:
The clinical effectiveness of preventive migraine therapies was based on the number of monthly migraine days, with higher frequency associated with lower health-related quality of life and higher health care costs.
Loss of productivity was considered in scenario analyses.
The lack of comparators relevant to current treatment patterns in Canada, such as oral preventive therapies, was not directly addressed in the sponsor’s model and could not be addressed by CADTH due to structural or data limitations.
Economic Review
The current review is for galcanezumab (Emgality) for adults who have at least 4 MHDs and who have who have a history of at least 2 prior preventive treatment failures due to a lack of efficacy or tolerability, or both.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Galcanezumab is indicated for the prevention of migraine in adults who have at least 4 migraine days per month,1 while the sponsor’s reimbursement request is for the prevention of migraine in adults who have at least 4 migraine days per month and who have experienced an inadequate response, intolerance, or contraindication to at least 2 prophylactic migraine medications.2 Galcanezumab is administered by subcutaneous injection, and the initial dose for the prevention of migraine is 240 mg followed by 120 mg monthly. The sponsor has submitted galcanezumab at a price of $623.00 per 120 mg single-dose, pre-filled pen or syringe, leading to an annual cost of therapy of $8,099 per patient in the first year, and $7,476 per patient thereafter.3
The sponsor submitted a cost-utility analysis to assess the cost-effectiveness of prophylactic galcanezumab compared to BSC among patients with EM, defined as at least 4 MHDs and fewer than 15 headache days per month, or with CM, defined as having at least 15 headache days per month, at least 8 of which are MHDs, with a history of treatment failure to at least 2 prior preventive treatments due to a lack of efficacy, tolerability, or both. Best supportive care was represented by the placebo group of the CONQUER trial,4 in which patients did not receive a preventive therapy but, like the galcanezumab group, were allowed to take acute medication to treat migraine attacks, including triptans, nonsteroidal anti-inflammatory drugs, and acetaminophen or acetaminophen combinations, with some restrictions on opioids and barbiturates. A scenario analysis was conducted including erenumab as a comparator.
The sponsor adopted a 20-year time horizon, with the analysis conducted from the perspective of a publicly funded health care payer. Future costs and benefits were discounted at a rate of 1.5% per year, and the model cycle length was 30 days.
Model Structure
The sponsor submitted a semi-Markov model with 4 health states: on treatment, off treatment due to nonresponse, off treatment due to AEs, and death (Figure 1, Appendix 3). Patients entered the model as they initiated galcanezumab or no preventive therapy (BSC) and were assessed for response after 3 months. Response was defined as those who met a 50% or greater reduction in MHDs from baseline for EM patients, or a 30% or greater reduction from baseline for CM patients — this definition matches the outcome reported in the CONQUER trial.4 Patients who responded to galcanezumab were assumed to maintain their responder change in MHDs until an AE was experienced, while those who discontinued galcanezumab due to nonresponse or AEs reverted to their baseline MHDs over time. Patients who initially experienced a response while treated with BSC were assumed to return to their baseline monthly MHDs over 12 months.
Model Inputs
Data from the CONQUER trial, a randomized, multi-centre, double-blind, placebo-controlled, phase III clinical trial, were used to inform the demographic characteristics of patients with 2 or more prior failures to preventive migraine therapies.4 Patients could be enrolled in the CONQUER trial if they were 18 to 75 years of age, had a diagnosis of EM or CM, and had a history of at least 4 MHDs and at least 1 headache-free day per month on average over the previous 3 months. Participants also had to have a documented treatment failure to 2 to 4 categories of migraine-preventive therapies in the past 10 years due to inadequate effect after at least 2 months at the maximum tolerated dose, safety or tolerability issues, or both.
The primary efficacy measure in the model was the mean change from baseline in the number of MHDs per 30-day period as reported at month 3 in the CONQUER trial for galcanezumab and BSC in the base case,4 and from a sponsor-conducted ITC for the scenario analysis comparing galcanezumab to erenumab.5 Mean change from baseline in number of MHDs was stratified by responder status as defined in the sponsor’s base case, while a combined-criterion option averaging the change from baseline in all patients within each treatment group was considered in scenario analyses.
Mortality was based on Statistics Canada estimates of age- and gender-matched mortality rates6 and weighted by the proportion of male and female patients in the CONQUER trial.4 Death could occur from any health state, and neither the number of MHDs nor the treatment received altered the rates.
Health-state utility values were determined by the number of MHDs, from 0 to 30, experienced by the patient per 30-day cycle. Utility values were derived from MSQ estimates from the CONQUER trial,4 which were mapped to the EuroQol 5-Dimensions 3-Levels questionnaire.7 Utilities were further divided by treatment group, with modifiers distinguishing utility values among patients on treatment with galcanezumab, those on treatment with BSC, and those off treatment.
Adverse events were not explicitly modelled due to the small number of patients experiencing serious AEs, their transient nature, and the limited impact they would have on resource use, and to avoid double counting their impact on patient health utility, as discontinuation due to AEs was included in the model.3
Costs included drug acquisition costs for galcanezumab at the submitted price,3 with erenumab included in scenario analyses at IQVIA-reported wholesale prices,8 along with triptans used as acute migraine treatment at Ontario Drug Benefit list prices.9 Additionally, the model included health care resource use costs for physician visits, emergency room visits, hospitalizations, and neurologist consultations as reported by the Ontario Schedule of Benefits for Physician Services10 and the Ontario Case Costing Initiative.11 Resource use varied by a patient’s number of MHDs per cycle. All costs were reported in 2021 Canadian dollars.3
Summary of Sponsor’s Economic Evaluation Results
The sponsor-submitted probabilistic analyses aligned with the reimbursement request (adults with at least 4 MHDs and 2 previous failures of preventive therapy) for patients with EM or CM. The sponsor’s analyses were based on 1,000 iterations. More detailed results from the sponsor’s deterministic economic evaluation are presented in Appendix 3.
Base-Case Results
The sponsor’s base-case results for both patients with EM and those with CM are presented in Table 3. For patients with EM, galcanezumab was associated with 0.706 additional QALYs and an additional cost of $27,524, for an ICER of $39,010 per QALY gained, where 99.7% of iterations were cost-effective at a willingness-to-pay threshold of $50,000 per QALY. Among patients with CM, galcanezumab was associated with 1.573 additional QALYs and an additional cost of $26,101 when compared to BSC, resulting in an ICER of $16,594 per QALY gained, with 100% of iterations deemed cost-effective at a willingness-to-pay threshold of $50,000 per QALY. Deterministic results were similar, with disaggregated results available only for the deterministic analyses (Table 11).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($ per QALY) |
|---|---|---|---|---|---|
Episodic migraine population | |||||
BSC | 50,045 | Reference | 10.411 | Reference | Reference |
Galcanezumab | 77,568 | 27,524 | 11.116 | 0.706 | 39,010 |
Chronic migraine population | |||||
BSC | 99,976 | Reference | 8.217 | Reference | Reference |
Galcanezumab | 126,077 | 26,101 | 9.790 | 1.573 | 16,594 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Adapted from the sponsor’s pharmacoeconomic submission, tables 31 and 32.3
Sensitivity and Scenario Analysis Results
The sponsor conducted a series of scenario analyses, varying the assumed discount rate, time horizon, response definition, treatment-waning assumption, and MHD distribution; removing hospitalizations from the model; incorporating all-cause discontinuation; and presenting a societal perspective. Most of these scenarios had only minimal impact on results, although the ICER increased when the time horizon was shortened to 5 or 10 years, as well as when hospitalizations were removed or the discontinuation rate increased. Taking a societal perspective lowered the ICER.
Additionally, the sponsor conducted a scenario comparing galcanezumab to erenumab 70 mg or 140 mg monthly in both EM and CM patients. For EM patients, treatment with galcanezumab was considered to be both less effective and less costly than erenumab for the 70 mg (incremental cost: −$9,665, incremental QALYs: −0.166) and 140 mg (incremental cost: −$12,930, incremental QALYs: −0.319) erenumab doses, respectively. For patients with CM, galcanezumab was associated with an ICER of $14,587 when compared to the 70 mg erenumab dose, but was dominated by (more costly and less effective than) the 140 mg dose. Both results were driven by low incremental costs and QALYs.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
Full Health Canada–indicated population not modelled: While the sponsor’s reimbursement request and economic model3 are for the prevention of migraine in adult patients with 4 or more MHDs per month who have failed with at least 2 previous preventive therapies, Health Canada did not limit the approved indication to patients with previous preventive-therapy failures.1 As such, the modelled population explores the cost-effectiveness of galcanezumab in only a subset of the indicated population in Canada. The sponsor’s model was not sufficiently flexible to report the cost-effectiveness of galcanezumab in the full population, and the cost-effectiveness of galcanezumab in patients who have not failed at least 2 previous preventive therapies is therefore unknown.
CADTH was unable to address this limitation within the model. The cost-effectiveness of galcanezumab in patients who have used fewer than 2 prior preventive therapies is unknown.
Not all relevant comparators considered in the base case: In the base case, the sponsor compared galcanezumab to BSC, which consisted of acute migraine treatment only. According to the clinical expert consulted by CADTH, this is not consistent with current clinical practice in Canada, where patients whose disease could be managed with preventive therapy are not limited to acute treatment alone in the absence of galcanezumab. Ideally, the cost-effectiveness of galcanezumab compared to oral migraine-prevention therapies currently reimbursed for the prevention of migraine in adults would be assessed.
While the sponsor did include erenumab as a comparator in scenario analyses, erenumab is not currently funded by public health care payers in Canada. No head-to-head evidence was available comparing galcanezumab to active preventive therapies. The results of a sponsor-conducted ITC5 were used to estimate the relative improvements in MHDs per month and the discontinuation rates associated with galcanezumab compared to 70 mg or 140 mg erenumab monthly. As noted in the CADTH clinical review, the interpretation of the sponsor’s ITC findings is limited by heterogeneity in the included studies and methodological issues. A network meta-analysis conducted by the Institute for Clinical and Economic Review12 found the differences between galcanezumab and other anti-CGRP therapies in important clinical outcomes, including mean difference in change from baseline MHDs, discontinuation rates, and proportion of episodic patients achieving a 50% reduction in MHDs, were not statistically significant.
CADTH was unable to address this limitation within the model. The cost-effectiveness of galcanezumab compared to oral preventive therapies, OnaA, or fremanezumab is unknown. The cost-effectiveness of galcanezumab compared to 70 mg or 140 mg erenumab is highly uncertain.
Stratification of MHD reduction by response status: The sponsor’s model stratified patient reduction in monthly MHDs by response status, defined as achieving a 50% reduction in MHDs for EM patients and a 30% reduction for CM patients as reported in the CONQUER trial. However, placebo response from the CONQUER trial is unlikely to be generalizable to patients in clinical practice who would neither receive a placebo nor experience potential improvements in care associated with enrolment in a clinical trial. A high degree of uncertainty surrounding the large reduction in MHDs is therefore associated with responders to BSC in the model. While the sponsor attempted to mitigate this effect by limiting the duration of response to 1 year for patients responding to BSC, it is unclear how much patients responding to galcanezumab may be similarly affected and therefore not sustain the initial mean reduction in MHDs for the duration of treatment. Additionally, the sponsor’s combined-criterion option included all patients within each treatment group, and therefore had more power than responder and nonresponder subgroup mean changes.
CADTH considered the sponsor’s combined-criterion option in its base case. A scenario analysis using the responder criterion was also conducted to explore the impact of this uncertainty on the ICER.
Model structure does not adequately reflect the management of migraine in clinical practice: The health states used by the sponsor to assess the cost-effectiveness of galcanezumab classify patients on treatment with galcanezumab, on treatment with BSC, or off treatment, with effectiveness defined as the reduction in MHDs per 30 days. Patients who are off treatment (e.g., discontinue galcanezumab or stop responding to BSC) were assumed to receive BSC (acute migraine treatment) only, with no additional preventive therapy. According to the clinical expert consulted by CADTH for this review, patients who discontinue galcanezumab would continue to receive preventive migraine treatment in the form of another anti-CGRP, OnaA (depending on prior treatment experience and jurisdiction of residence), or oral treatment (e.g., propranolol, amitriptyline, or topiramate). The sponsor’s assumption that patients would receive no additional preventive treatment for the remaining time horizon (up to 20 years) was not supported by data.
CADTH was unable to address these limitations associated with the model structure. The direction and magnitude of the impact on the cost-effectiveness results for galcanezumab are unknown. CADTH reduced the time horizon to 5 years in its base case to align with previous reviews for this indication. Scenario analyses considering 10- and 20-year time horizons were conducted.
Uncertainty in the long term treatment efficacy of galcanezumab: In the sponsor’s model, patients who responded to galcanezumab after 12 weeks of treatment were assumed to maintain their improved frequency of MHDs for the remainder of their time on treatment, up to the analysis time horizon. In contrast, modelled patients who responded to 3 months of BSC were assumed to revert to their baseline MHD frequency over the course of a year, despite continuing on BSC therapy. Patients with EM who either did not respond to galcanezumab and discontinued or who discontinued due to experiencing an AE, experienced post-discontinuation waning of their MHD frequency based on a quadratic function fitted to washout data from the EVOLVE-2 trial to predict the amount of time required to return to baseline. Effect-waning for CM patients who discontinued galcanezumab was based on data reported during the washout period following the open-label extension of the REGAIN trial. Additionally, according to the clinical expert consulted by CADTH, response to anti-CGRP therapies appears to be durable over the short-term (i.e., between 6 and 24 months); however, patients may not continue on successful preventive therapy as initiated indefinitely, but instead may have their preventive treatment removed or reduced to test whether improvement in MHDs, severity, and response to triptans can be maintained without it.
CADTH explored the impact of higher discontinuation rates in scenario analyses. Uncertainty remains in the maintenance of treatment effect in patients who continue on therapy.
Uncertainty in direct health care resource use: The sponsor’s analysis incorporated health care resource use taken from a 2006 survey of 7,437 migraine patients in the US reported in an economic evaluation by Lipton.13 Lipton estimated the “use per migraine day” by dividing the mean patient-reported medical resource use over 12 months by the reported annual number of headache days. In its model, the sponsor multiplied the “use per migraine day” by the number of migraine days per 30-day cycle to estimate the resource use per cycle, which was assumed to be equivalent between CM and EM patients. The 2006 survey had a 54% response rate and was based on a 12-month recall period. The relationship between data sources and the calculation of resource use per migraine day was not described transparently.
The clinical expert consulted by CADTH indicated that the management of migraine differs between Canada and the US. Canadian patients are rarely admitted to hospital for the treatment of migraine. As such, costs related to hospitalization for migraine were removed from the CADTH base case.
Inappropriate methods used to reflect health-state utilities and disease severity: The sponsor considered different sets of health utilities based on the number of monthly MHDs by treatment group. The application of these utilities in the pharmacoeconomic model included a treatment-effect variable differentiating patients who were off treatment (at baseline and those who had discontinued), receiving galcanezumab, or receiving BSC. The utility estimates were based on a mapping exercise of MSQ data from the CONQUER trial to the EuroQol 5-Dimensions 5-Levels questionnaire. The use of treatment-specific utilities is inappropriate as differences in clinical effects and costs should be reflected in the model health states. Defining health states based on MHD frequency fails to capture migraine severity, which is likely to affect patient quality of life and clinical management of EM and CM. While a statistically significant improvement in MSQ scores was found between galcanezumab and placebo in the CONQUER trial,4 it is unclear to what extent this difference was related to MHD reduction versus other factors such as severity. The sponsor’s use of treatment-specific utilities was an attempt to account for these other factors; however, this method does not adequately differentiate the mechanism by which patients experience quality-of-life differences, and there is meaningful uncertainty around the extent to which such differences are explained by MHD frequency versus severity of migraine or other factors.
CADTH assumed equal pooled utility estimates for all treatment groups in the base case. Treatment-specific utility estimates were explored in a scenario analysis.
Key assumptions made by the sponsor and listed in Table 4 have been appraised by CADTH.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
No migraine-related mortality was assumed. | Appropriate. According to the experts consulted by CADTH in this and previous reviews, migraine patients are not at higher risk of death compared with the general population. |
No administration costs were applied for galcanezumab or triptans, or to erenumab in scenario analysis. | Appropriate. Anti-CGRPs and triptans were assumed to be self-administered by the patient and would not incur additional costs. |
Acute medication use was based on overall data from the CONQUER trial. | Uncertain. The use of triptans in the CONQUER trial may not be representative of acute medication use in Canadian practice. Clinical expert feedback indicated that patients with chronic migraine have difficulty distinguishing the after effects of 1 migraine headache from the onset of another, and may therefore be less likely to use triptans compared with patients with episodic migraines. Acute migraine treatment resource use in the model therefore may not be reflective of Canadian clinical practice. |
Migraine frequency does not change except due to treatment effect. | Uncertain. The model does not consider changes in the frequency of migraine that are unrelated to treatment (i.e., no patients naturally improve or decline). According to the clinical expert consulted by CADTH, some patients may show a natural improvement or worsening in the frequency of migraines over time, regardless of treatment, as they transition between EM and CM. The effect of this assumption on the model results is unknown but is not expected to meaningfully affect the ICER as this phenomenon would not be biased in favour of or against any particular treatment. |
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH reanalyses addressed key limitations of the submitted model (Table 5). CADTH was unable to address the full indicated population (i.e., patients who have experienced fewer than 2 prior preventive therapies) and the lack of active preventive therapy as part of BSC.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | None | None |
Changes to derive the CADTH base case | ||
1. Time horizon | 20 years | 5 years |
2. Health state–specific utilities | Utilities varied by MHDs and treatment assignment | Utilities varied by MHDs, set to pooled treatment values per MHD |
3. Hospitalization costs | 0.0039 uses per MHD (at $3,306 per use) | 0 uses per MHD |
4. MHD distribution stratification | MHD distribution stratified by treatment group and response status | MHD distribution stratified by treatment group |
CADTH base case | — | Reanalyses 1 through 4 |
MHD = migraine headache day.
CADTH’s stepped reanalyses and base-case results are presented in Table 6. Disaggregated results and sensitivity analyses results are presented in Appendix 4.
Among patients with EM who have used 2 or more prior preventive migraine therapies, galcanezumab was associated with $14,563 in additional costs and 0.053 additional QALYs compared to BSC over a 5-year time horizon, leading to an ICER of $273,560 per QALY gained.
Among patients with CM who have used 2 or more prior preventive migraine therapies, galcanezumab was associated with $18,247 in additional costs and 0.167 additional QALYs compared to BSC over a 5-year time horizon, leading to an ICER of $109,325 per QALY gained.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Episodic migraine population (≥ 2 previous therapies) | ||||
Sponsor’s base case | BSC | 50,045 | 10.411 | Reference |
Galcanezumab | 77,568 | 11.116 | 39,010 | |
CADTH reanalysis 1: Time horizon | BSC | 13,956 | 2.983 | Reference |
Galcanezumab | 26,101 | 3.246 | 46,250 | |
CADTH reanalysis 2: Equal utilities pooled | BSC | 50,162 | 11.393 | Reference |
Galcanezumab | 77,537 | 11.715 | 85,021 | |
CADTH reanalysis 3: Hospitalization removed | BSC | 25,535 | 10.410 | Reference |
Galcanezumab | 57,519 | 11.115 | 45,361 | |
CADTH reanalysis 4: MHD stratification | BSC | 50,395 | 10.404 | Reference |
Galcanezumab | 82,836 | 10.941 | 60,392 | |
CADTH base cases 1 to 4 | BSC | 7,191 | 3.235 | Reference |
Galcanezumab | 21,754 | 3.288 | 273,560 | |
Chronic migraine population (≥ 2 previous therapies) | ||||
Sponsor’s base case | BSC | 99,976 | 8.217 | Reference |
Galcanezumab | 126,077 | 9.790 | 16,594 | |
CADTH reanalysis 1: Time horizon | BSC | 27,892 | 2.367 | Reference |
Galcanezumab | 40,100 | 2.936 | 21,452 | |
CADTH reanalysis 2: Equal utilities pooled | BSC | 99,897 | 9.679 | Reference |
Galcanezumab | 126,146 | 10.517 | 31,310 | |
CADTH reanalysis 3: Hospitalization removed | BSC | 50,255 | 8.211 | Reference |
Galcanezumab | 88,598 | 9.789 | 24,292 | |
CADTH reanalysis 4: MHD stratification | BSC | 100,522 | 8.200 | Reference |
Galcanezumab | 136,927 | 9.424 | 29,734 | |
CADTH base cases 1 to 4 | BSC | 14,248 | 2.748 | Reference |
Galcanezumab | 32,495 | 2.748 | 109,325 | |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
Scenario analyses were conducted using the CADTH base case to investigate the impact of including hospitalization resource use, extending the time horizon, comparing galcanezumab to erenumab, considering a societal perspective, and considering all-cause discontinuation. Results of these scenario analyses are presented in Appendix 4. The scenario analyses with the greatest impact on the ICER for EM patients were those regarding choice of comparator, the responder analysis, and treatment-specific utilities. For CM patients, the discontinuation rate, responder analysis, and treatment-specific utilities had the greatest impact on the ICER.
Price-reduction analyses were conducted for each patient subpopulation for galcanezumab versus BSC for both the sponsor and CADTH base cases. Among patients with EM and experience with at least 2 prior preventive therapies, a 78% price reduction would be required for galcanezumab to be cost-effective at a willingness-to-pay threshold of $50,000 per QALY, while for CM patients with at least 2 prior preventive therapies, a 49% price reduction would be required.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for galcanezumab vs. best supportive care ($ per QALY) | |
|---|---|---|
Episodic migraine | ||
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 39,010 | 273,560 |
10% | 33,621 | 246,850 |
20% | 28,402 | 218,514 |
30% | 23,084 | 187,334 |
40% | 17,882 | 158,767 |
50% | 12,774 | 130,555 |
60% | 7,560 | 100,955 |
70% | 2,341 | 72,144 |
80% | Dominant | 43,482 |
Chronic migraine | ||
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 16,594 | 110,266 |
10% | 13,399 | 97,909 |
20% | 10,292 | 85,520 |
30% | 7,110 | 73,422 |
40% | 3,904 | 60,531 |
50% | 659 | 48,442 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Issues for Consideration
Availability of anti-CGRP comparators: Two additional anti-CGRPs (erenumab and fremanezumab) have been approved by Health Canada for the prevention of migraines in adults with at least 4 MHDs, although neither is currently reimbursed on public formularies.14,15 Both have been reviewed by the CADTH Canadian Drug Expert Committee. Erenumab (Aimovig) received a reimbursement recommendation for the prevention of CM in adults who have had an inadequate response, intolerance, or contraindication to 2 or 3 oral prophylactic migraine medications, on condition of a price reduction.16 Fremanezumab (Ajovy) received a reimbursement recommendation for the prevention of EM or CM in adults who have an inadequate response, intolerance, or contraindication to at least 2 oral prophylactic migraine medications, also on condition of a price reduction.17 An additional anti-CGRP, eptinezumab (Vyepti), has been approved by Health Canada but has not yet been reviewed by CADTH or marketed.18
OnaA is reimbursed for the prevention of migraine in select jurisdictions: CADTH recommended that OnaA be reimbursed for the prophylaxis of headaches in adults with CM who have had an inadequate response, intolerance, or contraindication to at least 3 oral prophylactic migraine medications.19 OnaA may therefore be an additional comparator of interest for some patients in jurisdictions reimbursing it for the prevention of migraine.
Comparison to the erenumab and fremanezumab pharmacoeconomic reviews: CADTH has previously reviewed erenumab and fremanezumab for migraine prophylaxis. In the current review, CADTH implemented several changes to the sponsor’s submission to increase consistency between the 3 reviews (e.g., adopting a similar time horizon). The estimates of the ICER for these 3 submissions may not be directly comparable, due to differences in model structure, clinical effectiveness parameters, health-state utility values, and cost inputs.
Overall Conclusions
Based on the CADTH clinical review, galcanezumab may reduce the frequency of migraine, reduce the frequency of MHDs with acute medication use, and improve quality of life as measured by the MSQ among patients with EM or CM compared to placebo. The effect of galcanezumab on MHDs with symptoms, headache days, and other patient-reported outcomes remains uncertain due to a lack of control for multiplicity. The trials did not provide direct evidence on the relative efficacy and safety of galcanezumab versus other migraine-preventive medications.
CADTH undertook reanalyses to address limitations in the sponsor’s submission, reducing the time horizon to 5 years, applying treatment-independent utilities, removing costs related to hospitalization for migraine treatment, and considering the sponsor’s combined-criteria analysis in incorporating the reduction in MHDs associated with treatment. In CADTH’s base-case reanalysis, galcanezumab was more costly and more effective than BSC in patients with EM or CM who had experience with 2 or more prior preventive therapies. For patients with EM who have used 2 or more prior preventives, the ICER for galcanezumab compared to BSC was $273,560 per QALY, while for CM patients with 2 or more prior preventives, the ICER for galcanezumab compared to BSC was $109,325 per QALY. Price reductions of 78% and 49% are required to reduce the ICERs of galcanezumab to $50,000 per QALY, for patients with EM and CM, respectively.
The cost-effectiveness of galcanezumab in patients who have experience with fewer than 2 prior preventive therapies for migraine is unknown. The cost-effectiveness of galcanezumab compared to oral prevention therapies, OnaA, and fremanezumab is also unknown, and highly uncertain compared to erenumab.
Results of both the sponsor’s and the Institute for Clinical and Economic Review’s ITCs suggest that galcanezumab is generally similar to other CGRPs in terms of efficacy and discontinuation rates. At the submitted price, the annual cost of galcanezumab is more than that of erenumab and fremanezumab, and it is also more costly than OnaA and oral therapies for the prevention of migraine in adults. The submitted evidence does not justify a price premium for galcanezumab over other currently reimbursed comparator treatments.
References
1.Emgality (galcanezumab): 100 mg/mL, 120 mg/mL solution for subcutaneous injection [product monograph]. Toronto (ON): Eli Lilly Canada Inc; 2020 Sep 17.
2.Drug Reimbursement Review sponsor submission: Emgality (galcanezumab), 120 mg/mL solution for subcutaneous injection [internal sponsor's package]. Toronto (ON): Eli Lilly Canada Inc; 2021 Jun 3.
3.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Emgality (galcanezumab), 120 mg/mL solution for subcutaneous injection [internal sponsor's package]. Toronto (ON): Eli Lilly Canada Inc; 2021 Jun 3.
4.Mulleners WM, Kim BK, Lainez MJA, et al. Safety and efficacy of galcanezumab in patients for whom previous migraine preventative medication from two to four categories had failed (CONQUER): a multicentre, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. 2020;19(10):814-825. PubMed
5.Indirect comparison of galcanezumab compared to erenumab in patients with a history of prior migraine preventative treatment failures [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Emgality (galcanezumab), 120 mg/mL solution for subcutaneous injection Toronto (ON): Eli Lilly Canada Inc; 2020.
6.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2020: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 1800 Jan 1.
7.Gillard PJ, Devine B, Varon SF, Liu L, Sullivan SD. Mapping from disease-specific measures to health-state utility values in individuals with migraine. Value Health. 2012;15(3):485-494. PubMed
8.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 June 17.
9.Ontario Ministry of H, Ontario Ministry of Long-Term C. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 June 17.
10.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 1800 Jan 1.
11.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 1800 Jan 1.
12.ICER. Calcitonin Gene-Related Peptide (CGRP) Inhibitors as Preventative Treatments for Patients with Episodic or Chronic Migraine: Effectiveness and Value. 2018.
13.Lipton RB, Brennan A, Palmer S, et al. Estimating the clinical effectiveness and value-based price range of erenumab for the prevention of migraine in patients with prior treatment failures: a US societal perspective. J Med Econ. 2018;21(7):666-675. PubMed
14.Ajovy (fremanezumab): solution for subcutaneous injection 225 mg in 1.5 mL (150 mg/mL) [product monograph]. Montreal (QC): Teva Canada Innovation; 2020 Apr 9.
15.Aimovig (erenumab injection), Solution for Subcutaneous Injection, 70 mg in 1.0 mL (70 mg/mL) 140 mg in 1.0 mL (140 mg/mL) [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2020 Apr 22. Accessed Nov 18 2020.
16.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: Aimovig. Ottawa (ON): CADTH; 2020: https://cadth.ca/sites/default/files/cdr/complete/SR0578%20Aimovig%20-%20CDEC%20Final%20Recommendation%20July%2024%2C%202020%20%28redacted%29_For%20Posting.pdf. Accessed 2021 Jul 28.
17.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: Ajovy. Ottawa (ON): CADTH; 2021: https://cadth.ca/sites/default/files/cdr/complete/SR0641%20Ajovy%20-%20CDEC%20Final%20Recommendation%20April%201%2C%202021_For%20Posting.pdf. Accessed 2021 Jul 28.
18.Vyepti (eptinezumab): Solution for intravenous infusion, 100 mg/mL, [product monograph]. Saint-Laurent (QC): Lundbeck Canada Inc.; 2021 Jan 11: https://pdf.hres.ca/dpd_pm/00059556.PDF.
19.CADTH Canadian Drug Expert Committee Recommendation (Botox). 2019: https://www.cadth.ca/onabotulinumtoxina-23. Accessed November 23, 2020.
20.Alberta Interactive Drug Benefit List. Edmonton (AB): Government of Alberta; 2021: https://idbl.ab.bluecross.ca/idbl/load.do. Accessed 2021 Aug 14.
21.Pringsheim T, Davenport W, Mackie G, et al. Canadian Headache Society guideline for migraine prophylaxis. Can J Neurol Sci. 2012;39(2 Suppl 2):S1-59. PubMed
22.Osman NW, Irene., Lagman-Bartolome, Ana Marissa., Headache in adults. In: Compendium of therapeutic choices. Ottawa (ON): Canadian Pharmacists Association; 2021: https://www.pharmacists.ca. Accessed 2021 Aug 16.
23.Saskatchewan Drug Plan: search formulary. 2021; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2021 June 17.
24.Camporeale A, Kudrow D, Sides R, et al. A phase 3, long-term, open-label safety study of Galcanezumab in patients with migraine. BMC Neurol. 2018;18(1):188. PubMed
25.Canadian Institute for Health Information. Prescribed Drug Spending In Canada, 2020: A Focus on Public Drug Programs. Ottawa, ON: CIHI; 2020: https://www.cihi.ca/sites/default/files/document/prescribed-drug-spending-in-canada-2020-report-en.pdf.
26.Table: 17-10-0005-01. Population estimates on July 1st, by age and sex, Canada. Ottawa (ON): Statistics Canada; 2020: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2021-07-20.
27.O'Brien B, Goeree R, Streiner D. Prevalence of migraine headache in Canada: a population-based survey. Int J Epidemiol. 1994;23(5):1020-1026. PubMed
28.Stewart WF, Wood C, Reed ML, Roy J, Lipton RB, Group AA. Cumulative lifetime migraine incidence in women and men. Cephalalgia. 2008;28(11):1170-1178. PubMed
29.Vo P, Fang J, Bilitou A, Laflamme AK, Gupta S. Patients' perspective on the burden of migraine in Europe: a cross-sectional analysis of survey data in France, Germany, Italy, Spain, and the United Kingdom. J Headache Pain. 2018;19(1):82. PubMed
30.Stokes M, Becker WJ, Lipton RB, et al. Cost of health care among patients with chronic and episodic migraine in Canada and the USA: results from the International Burden of Migraine Study (IBMS). Headache. 2011;51(7):1058-1077. PubMed
31.Scher AI, Buse DC, Fanning KM, et al. Comorbid pain and migraine chronicity: The Chronic Migraine Epidemiology and Outcomes Study. Neurology. 2017;89(5):461-468. PubMed
32.Wachholtz A, Bhowmick A, Herbert LB, Marcus D. More is not Always Better: An Epidemiological Assessment of Migraine Frequency and the Impact on Relationships. J Pain Manag Med. 2017;3(2). PubMed
33.Lipton RB, Serrano D, Holland S, Fanning KM, Reed ML, Buse DC. Barriers to the diagnosis and treatment of migraine: effects of sex, income, and headache features. Headache. 2013;53(1):81-92. PubMed
34.Sutherland GD, T. Understanding the Gap: A Pan-Canadian Analysis of Prescription Drug Insurance Coverage. The Conference Board of Canada,; 2017: https://www.conferenceboard.ca/temp/758ed58f-2652-4178-9596-52557e8c3793/9326_Understanding-the-Gap__RPT.pdf?bcs-agent-scanner=079fbd59-37ed-dd44-9cdb-85b3ca35a1c0.
35.Indigenous Services Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2018 to 2019. 2020: https://www.sac-isc.gc.ca/eng/1584392581890/1584393350542. Accessed 2021 08 16.
36.CADTH Common Drug Review Pharmacoeconomic Review Report: Aimovig (Novartis). Ottawa (ON): CADTH; 20200: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/sr0578-aimovig-pharmacoeconomic-review-report.pdf. Accessed 2021 09 01.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in Table 8 have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Prophylaxis of Migraine
Drug/ comparator | Strength | Dosage form | Price ($) | Recommended dosage | Average daily drug cost ($) | Average annual drug cost ($) |
|---|---|---|---|---|---|---|
Galcanezumab (Emgality) | 120 mg/mL | 1 mL pre-filled syringe or pen | 623.0000a | 240 mg initial loading dose, then 120 mg once monthly | Maintenance: 20.47 | First year: 8,099 Subsequent years: 7,476 |
Comparators indicated for prophylaxis of migraine | ||||||
Erenumab (Aimovig) | 70 mg/mL 140 mg/mL | Autoinjector | 532.0000b | 70 mg or 140 mg subcutaneously monthly | 17.48 | 6,384 |
Flunarizine (generics) | 5 mg | Cap | 0.7348 | 10 mg daily | 1.47 | 537 |
Fremanezumab (Ajovy) | 225 mg / 1.5 mL | Pre-filled syringe | 585.0000a | 225 mg once a month or 675 mg every 3 months | 19.22 | 7,020 |
OnabotulinumtoxinA (Botox)d | 50 units 100 units 200 units | Injection vial | 178.5000 357.0000 714.0000 | 155 units to 195 units every 12 weeks | 8.50 | 3,105 |
Pizotyline/Pizotifen (Sandomigran) | 0.5 mg 1 mg | Tab | 0.3972 0.8716 | 1.0 to 6 mg daily | 0.79 to 4.77 | 290 to 1,741 |
Topiramate (generics) | 25 mg 100 mg 200 mg | Tab | 0.2433 0.4583 0.6748 | 100 mg per daye | 0.46 | 167 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed June 2021)9 unless otherwise indicated and do not include dispensing fees. All recommended doses sourced from respective product monographs. An average year is assumed to be comprised of 365.25 days. Excess medication in vials is assumed wasted where applicable.
aSponsor’s submitted price.3
bIQVIA Delta PA wholesale price, accessed June 2021.8
cCADTH Reimbursement Recommendation for fremanezumab (Ajovy), sponsor’s submitted price.17
dIndicated for use in chronic migraine only, 15 or more days per month with headaches lasting 4 hours a day or longer. At the time of this review, onabotulinumtoxinA is only reimbursed for the prevention of migraines in select jurisdictions (e.g., Alberta).20
eDaily and annual drug costs assume post-titration maintenance dose.
Table 9: CADTH Cost Comparison Table for Prophylaxis of Migraine (Off-Label Medications)
Drug/comparator | Strength | Dosage form | Price ($) | Recommended dosage | Average daily drug cost ($) | Average annual drug cost ($) |
|---|---|---|---|---|---|---|
Anti-Epileptics | ||||||
Divalproex sodiuma,b (generics) | 125 mg 250 mg 500 mg | Ent Tab | 0.1539 0.2767 0.5537 | 500 mg to 1,500 mg per daya,b | 0.55 to 1.66 | 202 to 607 |
Valproic acida,b (generics) | 250 mg | Cap | 0.2905 | 500 mg to 1,500 mg per daya,b | 0.58 to 1.74 | 212 to 637 |
50 mg/mL | Oral sol | 0.0398 | 0.40 to 1.19 | 145 to 436 | ||
500 mg | Ent Cap | 0.6356 | 0.64 to 1.91 | 232 to 696 | ||
Gabapentina (generics) | 100 mg 300 mg 400 mg | Cap | 0.0416 0.1012 0.1206 | 1,200 mg to 1,800 mg per day in 3 dosesa | 0.36 to 0.61 | 132 to 222 |
Anti-depressants | ||||||
Amitriptylinea,b (generics) | 10 mg 25 mg 50 mg | Tab | 0.0435 0.0829 0.1540 | 20 mg to 150 mg per daya,b | 0.09 to 0.46 | 32 to 169 |
Doxepinb (generic) | 10 mg 25 mg 50 mg 75 mg 100 mg | Cap | 0.3423 0.4201 0.7793 1.1131c 1.5152c | 25 mg to 100 mg per dayb | 0.42 to 1.46 | 153 to 534 |
Nortriptylinea,b (generic) | 10 mg 25 mg | Cap | 0.2570 0.5193 | 20 mg to 150 mg per daya,b | 0.51 to 3.12 | 188 to 1,138 |
Venlafaxinea,b (generics) | 37.5 mg 75 mg 150 mg | ER Cap | 0.0913 0.1825 0.1927 | 150 mg per daya,b | 0.19 | 70 |
Antihypertensives | ||||||
Atenolol (generics) | 50 mg 100 mg | Tab | 0.1107 0.1821 | 100 to 150 mg per dayb | 0.18 to 0.0.29 | 67 to 107 |
Metoprolol (generics) | 50 mg 100 mg | Tab | 0.0624 0.1361 | 100 mg to 200 mg per daya,b | 0.12 to 0.25 | 46 to 91 |
100 mg 200 mg | SR Tab | 0.1415 0.2568 | 0.14 to 0.26 | 52 to 94 | ||
Nadolol (generics) | 40 mg 80 mg 160 mg | Tab | 0.2375 0.3410 1.2046 | 80 mg to 160 mg per daya,b | 0.34 to 0.68 | 125 to 249 |
Propranolol (generics) | 10 mg 20 mg 40 mg 80 mg | Tab | 0.0689 0.1107 0.1225 0.2034 | 80 mg to 160 mg per day in 2 dosesa,b | 0.24 to 0.41 | 89 to 149 |
Verapamil (generics) | 80 mg 120 mg | Tab | 0.2735 0.4250 | 240 mg to 320 mg per daya,b | 0.82 to 1.12 | 300 to 410 |
120 mg 180 mg 240 mg | SR Tab | 0.5078c 0.5204 0.5075 | 0.51d | 185 | ||
Candesartan (generics) | 4 mg 8 mg 16 mg 32 mg | Tab | 0.1700 0.2281 0.2281 0.2281 | Up to 16 mg per daya,b | 0.17 to 0.23 | 62 to 83 |
Lisinopril (generics) | 5 mg 10 mg 20 mg | Tab | 0.1347 0.1619 0.1945 | 20 mg per daya | 0.19 | 71 |
Anti-Manic/Mood-Stabilizer | ||||||
Lithium carbonate (generics) | 150 mg 300 mg 600 mg | Cap | 0.0667 0.0657 0.1988d | 300 mg 3 times dailyb | 0.20 | 72 |
Lithium carbonate (Lithmax) | 300 mg | SR Tab | 0.2660d | 0.80 | 291 | |
SR = sustained release.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed June 2021)9 unless otherwise indicated and do not include dispensing fees. An average year is assumed to be comprised of 365.25 days.
aSource: 2012 Canadian Headache Society Guideline for Migraine Prophylaxis.21
bSource: CPhA Therapeutic Choices: Medications for Migraine Prophylaxis (Accessed October 2020).22
cSaskatchewan Formulary list price (accessed June 2021).23
dAssumes 240 mg, as 320 mg is not a possible dose with SR tablets.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The full population of the indication was not modelled, and the comparator of best supportive care (no preventive therapy) was not representative of current practice in Canada |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | No | Cost-effectiveness relative to relevant comparators (e.g., oral preventive therapies) could not be determined |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Note: This table has not been copy-edited.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
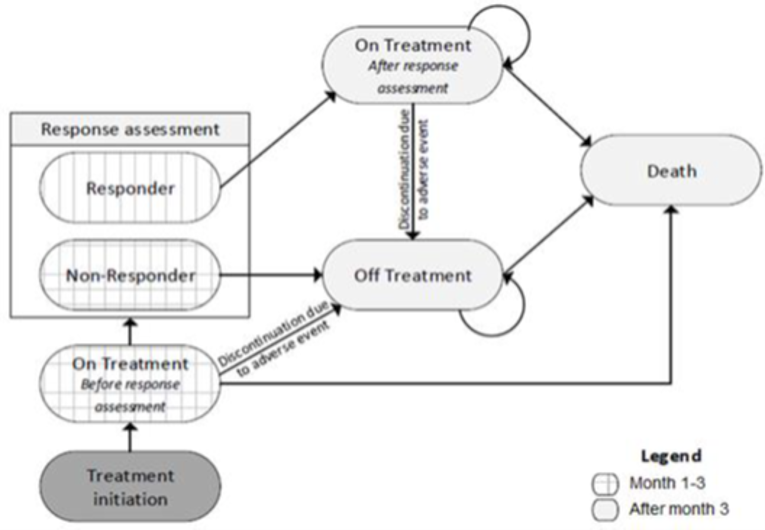
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of Sponsor’s Deterministic Economic Evaluation Results
Parameter | Galcanezumab | BSC | Incremental |
|---|---|---|---|
Episodic migraine | |||
Discounted QALYs | |||
Total | 11.117 | 10.411 | 0.705 |
On treatment | 3.619 | 0.240 | 3.379 |
AE discontinuation | 1.542 | 1.798 | −0.256 |
Nonresponse | 5.956 | 8.374 | −2.418 |
Discounted costs ($) | |||
Total | 77,537 | 50,162 | 27,375 |
Drug costs | 36,742 | 0 | 36,742 |
Administration costs | 0 | 0 | 0 |
Resource costs | 32,411 | 39,862 | −7,451 |
Acute medication costs | 8,384 | 10,300 | −1,916 |
ICER ($ per QALY) | 38,817 | ||
Chronic migraine | |||
Discounted QALYs | |||
Total | 9.788 | 8.215 | 1.572 |
On treatment | 4.653 | 0.247 | 4.406 |
AE discontinuation | 1.766 | 2.205 | −0.439 |
Nonresponse | 3.369 | 5.764 | −2.395 |
Discounted costs ($) | |||
Total | 126,073 | 99,844 | 26,229 |
Drug costs | 50,274 | 0 | 50,274 |
Administration costs | 0 | 0 | 0 |
Resource costs | 60,649 | 79,943 | −19,294 |
Acute medication costs | 15,151 | 19,901 | −4,750 |
ICER ($ per QALY) | 16,680 | ||
AE = adverse event; BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH Base-Case Deterministic Economic Evaluation Results
Parameter | Galcanezumab | BSC | Incremental |
|---|---|---|---|
Episodic migraine | |||
Discounted QALYs | |||
Total | 3.300 | 3.247 | 0.053 |
On treatment | 1.363 | 0.245 | 1.118 |
AE discontinuation | 0.146 | 0.487 | −0.341 |
Nonresponse | 1.791 | 2.515 | −0.724 |
Discounted costs | |||
Total | 21,889 | 7,195 | 14,694 |
Drug costs | 15,480 | 0 | 15,480 |
Administration costs | 0 | 0 | 0 |
Resource costs | 3,812 | 4,280 | 469 |
Acute medication costs | 2,597 | 2,914 | 317 |
ICER ($ per QALY) | 275,212 | ||
Chronic migraine | |||
Discounted QALYs | |||
Total | 2.921 | 2.756 | 0.165 |
On treatment | 1.646 | 0.250 | 1.396 |
AE discontinuation | 0.185 | 0.640 | −0.454 |
Nonresponse | 1.090 | 1.866 | −0.776 |
Discounted costs ($) | |||
Total | 32,451 | 14,245 | 18,207 |
Drug costs | 20,591 | 0 | 20,591 |
Administration costs | 0 | 0 | 0 |
Resource costs | 7,151 | 8,601 | 1,450 |
Acute medication costs | 4,709 | 5,643 | 935 |
ICER ($ per QALY) | 110,266 | ||
AE = adverse event; BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analyses
Table 13: CADTH Scenario Analyses
Parameter | CADTH base case | CADTH scenario |
|---|---|---|
Scenario analyses | ||
1. Health care resource utilization | Costs related to hospitalization for the treatment of migraine were excluded | Costs related to hospitalization for the treatment of migraine were included |
2. Time horizon of analysis | 5 years | 10 years |
3. Time horizon of analysis | 20 years | |
4. Comparators | Galcanezumab was compared to BSC | Galcanezumab was compared to erenumab 70 mg |
5. Comparators | Galcanezumab was compared to erenumab 140 mg | |
6. Perspective | Health care payer perspective | Societal perspective (i.e., productivity costs were incorporated) |
7. Treatment discontinuation | Long-term discontinuation was based on discontinuations due to AEs from the CGAJ extension study24 | Long-term discontinuation was based on all-cause discontinuation from the CGAJ extension study24 |
8. Utilities | All utilities are based on pooled treatment groups per MHD | Galcanezumab patients who have not discontinued are assigned galcanezumab-specific utilities; all patients receiving BSC, including those assigned to BSC and those who have discontinued galcanezumab, are assigned BSC-specific utilities per MHD |
9. Responder analysis | The mean reduction in monthly MHDs for all patients in each treatment group was assumed for the duration of treatment | The mean reduction in monthly MHDs in each treatment group was stratified by responder status and assumed for the duration of treatment |
AE = adverse event; BSC = best supportive care; MHD = migraine headache day.
Table 14: Summary of Scenario Analysis Around the CADTH Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALYs) |
|---|---|---|---|---|
Episodic migraine population (≥ 2 previous therapies) | ||||
Sponsor’s base case – deterministic | BSC | 50,161 | 10.411 | Reference |
Galcanezumab | 77,537 | 11.117 | 38,817 | |
CADTH base case | BSC | 7,195 | 3.247 | Reference |
Galcanezumab | 21,889 | 3.300 | 275,212 | |
Scenario 1: Hospitalizations included | BSC | 14,195 | 3.247 | Reference |
Galcanezumab | 28.122 | 3.300 | 260,852 | |
Scenario 2: Time horizon of 10 years | BSC | 13,899 | 6.221 | Reference |
Galcanezumab | 37,680 | 6.317 | 246,202 | |
Scenario 3: Time horizon of 20 years | BSC | 25,542 | 11.385 | Reference |
Galcanezumab | 60,107 | 11.533 | 233,766 | |
Scenario 4: Comparator of erenumab 70 mg | Erenumab 70 mg | 21,839 | 3.281 | Reference |
Galcanezumab | 22,771 | 3.305 | 38,714 | |
Scenario 5: Comparator of erenumab 140 mg | Erenumab 140 mg | 22,436 | 3.302 | Reference |
Galcanezumab | 22,771 | 3.305 | 119,185 | |
Scenario 6: Societal perspective | BSC | 21,466 | 3.247 | Reference |
Galcanezumab | 34,949 | 3.300 | 252,537 | |
Scenario 7: All-cause discontinuation | BSC | 7,195 | 3.247 | Reference |
Galcanezumab | 17,611 | 3.290 | 240,568 | |
Scenario 8: Utilities | BSC | 7,195 | 3.110 | Reference |
Galcanezumab | 21,889 | 3.266 | 94,257 | |
Scenario 9: Responder analysis | BSC | 7,077 | 3.255 | Reference |
Galcanezumab | 20,871 | 3.369 | 120,517 | |
Chronic migraine population (≥ 2 previous therapies) | ||||
Sponsor’s base case – deterministic | BSC | 99,844 | 8.215 | Reference |
Galcanezumab | 126,073 | 9.788 | 16,680 | |
CADTH base case – deterministic | BSC | 14,245 | 2.756 | Reference |
Galcanezumab | 32,451 | 2.921 | 110,266 | |
Scenario 1: Hospitalizations included | BSC | 28,312 | 2.756 | Reference |
Galcanezumab | 44.147 | 2.921 | 95,905 | |
Scenario 2: Time horizon of 10 years | BSC | 27,448 | 5.279 | Reference |
Galcanezumab | 57,163 | 5.587 | 96,759 | |
Scenario 3: Time horizon of 20 years | BSC | 50,429 | 9.672 | Reference |
Galcanezumab | 93,829 | 10.148 | 91,160 | |
Scenario 4: Comparator of erenumab 70 mg | Erenumab 70 mg | 15,252 | 2.797 | Reference |
Galcanezumab | 32,070 | 2.947 | 111,575 | |
Scenario 5: Comparator of erenumab 140 mg | Erenumab 140 mg | 14,994 | 2.814 | Reference |
Galcanezumab | 32,070 | 2.947 | 127,851 | |
Scenario 6: Societal perspective | BSC | 42,997 | 2.756 | Reference |
Galcanezumab | 57,049 | 2.921 | 85,103 | |
Scenario 7: All-cause discontinuation | BSC | 14,245 | 2.756 | Reference |
Galcanezumab | 26,159 | 2.929 | 68,611 | |
Scenario 8: Utilities | BSC | 14,245 | 2.631 | Reference |
Galcanezumab | 32,451 | 2.932 | 60,456 | |
Scenario 9: Responder analysis | BSC | 14,049 | 2.769 | Reference |
Galcanezumab | 30,408 | 3.071 | 55,975 | |
ICER = incremental cost-effectiveness ratio; QALY – quality-adjusted life-year.
Note: Deterministic analysis results are presented for all scenarios.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted base-case budget impact analysis (BIA), the sponsor assessed the introduction of galcanezumab for the treatment of EM or CM, compared to oral preventive migraine therapies, in adult patients with at least 4 MHDs per month, and who have failed at least 2 prior lines of preventive therapy. Additional analyses were conducted which assumed that fremanezumab and erenumab, or OnaA would also be reimbursed. The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2023 to 2025) using an epidemiological approach. The sponsor included drug acquisition costs, including wastage for OnaA when appropriate, while dispensing fees and markups were not included in the base case. Data for the model were obtained from various sources including the Canadian Institute for Health Information, Statistics Canada, the published literature, ODB Formulary list prices, and the sponsor’s internal data.
Key inputs to the BIA are documented in Table 16.
Key assumptions included:
Patients are equally likely to be diagnosed as migraine sufferers regardless of the number of MHDs per month they experience.
Patients are equally likely to receive a preventive therapy regardless of the number of MHDs per month they experience.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
Estimated active plan beneficiary population (year 1) Proportion of general population (male/female) Annual growth rate | 12,239,965a 49.7% / 50.3%b 1.3%b |
Migraine population | |
Prevalence of migraine (male/female) Incidence of migraine (male/female) Diagnosed population Prevention-treated population | 7.8% / 24.9%c 0.6% / 1.8%d 49.0%ce ||%f |
Headache days per month | |
< 4 4 to 14 ≥ 15 | 21.0%g 70.0%g 9.0%g |
Preventive treatment history | |
Prior experience with 1+ preventive (episodic/chronic) Prior experience with 2+ preventives (episodic/chronic) Prior experience with 3+ preventives (episodic/chronic) Prior experience with 4+ preventives (episodic/chronic) | 28.8% / 48.2% 11.5% / 26.6% 6.8% / 13.0% 3.2% / 6.8% |
Number of patients eligible for drug under review | 44,078 / 45,197 / 46,345 |
Market uptake (reference scenario, 3 years)h | |
Anti-depressants Anti-epileptics Beta blockers Calcium channel blockers Serotonin antagonist | 19.9% 46.3% 26.0% 6.8% 1.0% |
Market uptake (new drug scenario, 3 years)h | |
Galcanezumab Anti-depressants Anti-epileptics Beta blockers Calcium channel blockers Serotonin antagonist | |||||||||||||||||||||||| |||||||||||||||||||||||||| |||||||||||||||||||||||||| |||||||||||||||||||||||||| |||||||||||||||||||||| |||||||||||||||||||||||||| |
Cost of treatment (per patient) over 1 yearh | |
Galcanezumab Anti-depressants Anti-epileptics Beta blockers Calcium channel blockers Serotonin antagonist | $8,099 when initiated, $7,476 thereafter $500.12 $337.70 $146.99 $521.46 $1,908.80 |
aCanadian Institute for Health Information, 2020.25
bStatistics Canada, 2020,26 other genders not reported.
cObrien, 1994.27 Other genders not reported.
dStewart, 2008.28 Other genders not reported.
eVo 2018.29
fReported as Eli Lilly, data on file.
gReported as derived from Stokes (2011),30 Scher (2017),31 and Wachholtz (2017).32
hMarket shares and annual costs of oral preventive therapies have been combined into class categories by CADTH for brevity.
Source: Sponsor’s submitted budget impact model and analysis.
Summary of the Sponsor’s Budget Impact Analysis Results
Results of the sponsor’s base case suggested that the reimbursement of galcanezumab for adults with EM or CM who had failed at least 2 previous preventive therapies, in the absence of other anti-CGRPs, was associated with an incremental cost of $20,498,546, $26,377,884, and $33,668,936 in Years 1, 2, and 3, respectively, for a total of $80,545,365 over the 3-year period.
When the sponsor considered scenarios around the number of previous failures to other therapies, the 3-year total incremental cost ranged from $609,257,360 when no previous therapies were required before galcanezumab eligibility, to $21,994,962 when at least 4 previous preventive therapies were required. When the reimbursement of erenumab and fremanezumab were assumed, the 3-year incremental cost associated with also reimbursing galcanezumab fell to $2,706,731. When the reimbursement of OnaA was included, the 3-year incremental cost was $79,818,466.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Proportion of patients receiving a preventive treatment may be underestimated: Of patients with prevalent or incident migraine, the sponsor’s analysis assumed that 49% would be diagnosed,27,29 while |% of those diagnosed would receive a preventive therapy (|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||), or |% in total. However, a study by Lipton in 2013 found that of 775 survey participants with episodic migraines, 45.5% had consulted a health care professional in the previous year, 86.7% received a diagnosis of migraine, and 66.7% were receiving treatment, or 26.2% in total.33
CADTH increased the proportion of people with migraines who receive treatment to 26.3%.
Eligible Canadian population overestimated: When calculating the number of active beneficiaries covered by public drug plans, the sponsor considered the population within each jurisdiction that was over and under age 65, as reported by Statistics Canada. However, galcanezumab is indicated for the treatment of adult patients only, and thus only the population aged 18 to 64 years and those 65 years and older are of interest. Additionally, Statistics Canada data includes all persons living within the geographical borders of each province or territory. The sponsor added the population of NIHB beneficiaries to the populations of the included provincial jurisdictions reported by Statistics Canada, thus double counting most NIHB beneficiaries. As the sponsor’s source25 for the proportion of the population eligible for public reimbursement did not differentiate children from adults under 65 years of age, CADTH used data from the Conference Board of Canada.34
CADTH reduced the number of patients considered eligible for preventive migraine therapy to include only adults, removed eligible NIHB beneficiaries living within each provincial border from eligibility for reimbursement by the provincial drug plan, and included all public-plan eligible beneficiaries for patients aged 65 and above, and enrolled beneficiaries for those aged 18 to 64.
Other anti-CGRPs are likely to be reimbursed before reimbursement of galcanezumab: The sponsor’s base case assumes a reference scenario where only oral migraine-preventive therapies are reimbursed, which is currently the case in most jurisdictions in Canada (onabotulinumtoxinA is reimbursed in only a few jurisdictions). However, both erenumab and fremanezumab have received positive reimbursement recommendations from CDEC,16,17 and both are currently undergoing negotiation through the pan-Canadian Pharmaceutical Alliance. As such, CADTH also considered the budget impact of reimbursing galcanezumab when erenumab and fremanezumab are assumed to also be reimbursed to be relevant. The sponsor included a scenario analysis incorporating erenumab and fremanezumab market share, however this analysis did not consider that CDEC recommended erenumab be reimbursed only for CM patients, while fremanezumab was recommended for both EM and CM patients.
A CADTH scenario reanalysis included erenumab and fremanezumab as reimbursed comparators, while the consideration of only oral preventive therapies was presented as a scenario analysis. CADTH reduced the market share of erenumab relative to fremanezumab and galcanezumab compared to the sponsor’s estimates.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s submitted analysis by increasing the proportion of patients with migraines who receive prophylactic treatment, decreasing the eligible population (by limiting it to adults, removing double-counted NIHB beneficiaries, and updated the proportions of people reimbursed by public plans), and assuming erenumab and fremanezumab will also be publicly reimbursed (Table 17).
Table 17: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | None | None |
Changes to derive the CADTH base case | ||
1. Proportion of people with migraine receiving treatment |
|
|
2. Eligible Canadian Population |
|
|
CADTH base case | Reanalysis 1 + 2 | |
CGRP = calcitonin gene-regulated peptide; NIHB = Non-Insured Health Benefits.
aNIHB Annual Report.35 Eligible NIHB beneficiaries reported as being within the Atlantic Canada region were removed from eligibility for reimbursement by New Brunswick, Nova Scotia, Prince Edward Island, and Newfoundland and Labrador proportionally to the overall population of each province.
bCIHI (2019).25
cConference Board of Canada, 2017. 25 to 64 age group used as a proxy for the 18-to-64 age group.34
The results of the CADTH stepwise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19. Applying these changes resulted in a 3-year budget impact of $80,077,151.
Table 18: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $80,545,365 |
CADTH reanalysis 1: proportion receiving treatment | $100,819,262 |
CADTH reanalysis 2: eligible Canadian population | $63,974,317 |
CADTH base case (1 + 2) | $80,077,151 |
CADTH also conducted additional scenario analyses (Table 19) including limiting reimbursement to patients with chronic migraine, assuming other CGRPs are reimbursed with fremanezumab assumed to have more market share than erenumab as only fremanezumab was recommended for reimbursement for patients with EM, assuming other CGRPs are reimbursed at the price reductions recommended in previous CADTH reviews,17,36 and assuming price reductions for galcanezumab of 49% and 78% as established in the review of the sponsor’s economic evaluation above.
Table 19: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $15,342,520 | $15,342,520 | $15,732,161 | $16,131,697 | $47,206,378 |
New drug | $15,342,520 | $35,841,066 | $42,110,044 | $49,800,633 | $127,751,743 | |
Budget impact | — | $20,498,546 | $26,377,884 | $33,668,936 | $80,545,365 | |
CADTH base case | Reference | $15,253,333 | $15,253,333 | $15,640,709 | $16,037,923 | $46,931,965 |
New drug | $15,253,333 | $35,632,720 | $41,865,257 | $49,511,139 | $127,009,116 | |
Budget impact | — | $20,379,387 | $26,224,548 | $33,473,217 | $80,077,151 | |
Scenario A: Only chronic patients eligible | Reference | $3,496,407 | $7,325,862 | $8,925,625 | $10,588,485 | $26,839,972 |
New drug | $3,496,407 | $7,410,058 | $9,092,099 | $10,894,864 | $27,397,021 | |
Budget impact | — | $84,196 | $166,474 | $306,378 | $557,048 | |
Scenario B: Other CGRPs reimbursed | Reference | $15,253,333 | $31,959,608 | $38,938,693 | $46,193,041 | $117,091,342 |
New drug | $15,253,333 | $32,326,919 | $39,664,948 | $47,529,639 | $119,521,506 | |
Budget impact | — | $367,311 | $726,255 | $1,336,598 | $2,430,164 | |
Scenario C: Other CGRPs reimbursed with price reductions of 49% for erenumab and 71% for fremanezumab | Reference | $15,253,333 | $21,294,751 | $23,023,357 | $24,938,456 | $69,256,564 |
New drug | $15,253,333 | $22,728,548 | $26,999,399 | $32,309,358 | $82,037,304 | |
Budget impact | — | $1,433,797 | $3,976,042 | $7,370,902 | $12,780,741 | |
CADTH scenario analysis C: 49% price reduction | Reference | $15,253,333 | $15,253,333 | $15,640,709 | $16,037,923 | $46,931,965 |
New drug | $15,253,333 | $25,198,373 | $28,402,112 | $32,323,405 | $85,923,890 | |
Budget impact | — | $9,945,039 | $12,761,404 | $16,285,482 | $38,991,925 | |
CADTH scenario analysis D: 78% price reduction | Reference | $15,253,333 | $15,253,333 | $15,640,709 | $16,037,923 | 46,931,965 |
New drug | $15,253,333 | $19,022,942 | $20,434,129 | $22,151,072 | $61,608,144 | |
Budget impact | — | $3,769,609 | $4,793,420 | $6,113,150 | $14,676,179 |
CGRP = calcitonin gene-regulated peptide.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.