CADTH Reimbursement Review
Colchicine (Myinfla)
Sponsor: Pendopharm, a division of Pharmascience Inc.
Therapeutic area: Atherothrombotic events in coronary artery disease
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
ACE
angiotensin-converting enzyme
ACS
acute coronary syndrome
CI
confidence interval
CYP3A4
cytochrome P450 enzyme 3A4
HR
hazard ratio
IQR
interquartile range
ITT
intention-to-treat
RCT
randomized controlled trial
SD
standard deviation
STEMI
ST-elevation myocardial infarction
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Colchicine (Myinfla), 0.5 mg extended-release oral tablet |
Indication | For the reduction of atherothrombotic events in adult patients with existing coronary artery disease, in addition to standard therapies, including low-density lipoprotein cholesterol (LDL-C)–lowering and antithrombotic drug treatment |
Reimbursement request | As per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Priority review |
NOC date | August 23, 2021 |
Sponsor | Pendopharm, a division of Pharmascience Inc. |
NOC = Notice of Compliance.
Introduction
Coronary artery disease is a leading cause of premature mortality and disability in Canada.1 An estimated 2.4 million Canadian adults have been diagnosed with coronary artery disease, including 578,000 adults (2.1%) with a history of a myocardial infarction.1 The estimated annual incidence of coronary artery disease in Canada is 6.1 per 1,000 (158,700 adults) with 63,200 Canadian adults experiencing a first myocardial infarction (2.3 per 1,000). Canadian adults with coronary artery disease are 3 times more likely, and those who survived a myocardial infarction are 4 times more likely, to die prematurely compared with those without the condition.1
The management of myocardial infarction in patients with acute coronary disease includes revascularization procedures, as well as pharmacotherapy and lifestyle modification to prevent recurrent events. Standard pharmacological therapy consists of antiplatelet drugs, high-intensity cholesterol-lowing drugs, beta-blockers, and renin-angiotensin-aldosterone system inhibitors, plus other medications to manage recognized risk factors.
Colchicine is currently available in Canada as a 0.6 mg tablet for the treatment of gout, pericarditis, and familial Mediterranean fever. Colchicine 0.5 mg extended-release oral tablets are approved by Health Canada for the reduction of atherothrombotic events in adult patients with existing coronary artery disease, in addition to standard therapies, including low-density lipoprotein cholesterol–lowering and antithrombotic drug treatments.2 The recommended dosage is 0.5 mg once daily. The sponsor has requested reimbursement as per the indication.3
The objective of this report was to perform a systematic review of the beneficial and harmful effects of colchicine 0.5 mg oral tablets for the reduction of atherothrombotic events in adults with existing coronary artery disease, in addition to standard therapies.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
No patient group input was received for this submission.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Despite widespread implementation of guideline-recommended therapies, many patients with coronary artery disease and acute coronary syndrome (ACS) continue to experience subsequent cardiovascular events (death, myocardial infarction, stroke, and hospitalization for revascularization procedures). According to the clinical experts consulted for this review, colchicine would be used long-term for the secondary prevention of ischemic cardiac events and is best suited for those with coronary artery disease who have experienced a myocardial infarction. Colchicine would be used as add-on therapy and would not replace any of the standard guideline-recommended secondary prevention drugs. Colchicine should be avoided in patients who are using certain drugs metabolized by the cytochrome P450 enzyme 3A4 (CYP34A) or P-glycoprotein pathways due to the increased risk of colchicine toxicity, or in patients with other contraindications to therapy. The development of adverse effects may lead to discontinuation of colchicine, according to the experts consulted, and the use of colchicine for secondary prevention may not be an option for patients who have experienced intolerable adverse effects with colchicine in the past.
Clinician Group Input
No clinician group input was received for this submission.
Drug Program Input
The drug programs requested input on the patients most likely to be prescribed colchicine, the longer-term safety and tolerance of colchicine, and the potential for off-label use of colchicine at a 0.6 mg dosage as a secondary prevention therapy. In response, the clinical experts indicated that colchicine will be used primarily in patients with a history of myocardial infarction, including some patients who were excluded from the clinical trials (e.g., due to a low ejection fraction or prior bypass surgery). A large number of patients are potentially eligible for treatment with colchicine, as the drug can be initiated irrespective of how much time has elapsed since a prior myocardial ischemic event. Colchicine is associated with gastrointestinal adverse effects, and a portion of patients will discontinue therapy due to intolerance. Based on previous experience with colchicine, the frequency of discontinuation due to adverse effects is expected to be similar to that of other secondary prevention drugs.
Mechanistically, colchicine may be beneficial as primary prevention therapy; however, direct evidence is lacking as no clinical trials have been conducted in this population. The experts state that some clinicians have prescribed colchicine 0.6 mg tablets for secondary prevention therapy, and it is possible that off-label use may continue after the 0.5 mg dosage form is available in Canada. There is some uncertainty surrounding the longer-term safety of colchicine in patients with coronary artery disease, and additional data are required.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
Four trials met the inclusion criteria for the systematic review, including 3 double-blind placebo-controlled studies (COLCOT, COPS, and LoDoCo2) and 1 open-label, observer-blinded trial (LoDoCo). The trials enrolled adults with an acute myocardial infarction (COLCOT), ACS (COPS), or stable coronary artery disease (LoDoCo2 and LoDoCo), with sample sizes ranging from 532 to 5,522 patients. Patients received colchicine 0.5 mg daily versus placebo or no treatment as add-on therapy to standard secondary prevention therapies. In the LoDoCo2 study, all patients received open-label colchicine during a 1-month run-in period, and those who were tolerant of and adherent to therapy were randomized. The primary outcome in all trials was the time to first occurrence of a composite outcome that included several major cardiovascular events. The duration of the median follow-up ranged from 1 to 3 years.
The mean age of patients enrolled ranged from 59.7 years (standard deviation [SD] = 10.2) to 67 years (SD = 9.2), and 78% to 89% of patients per treatment group were male. Approximately half (50% to 52%) of the patients enrolled had a history of hypertension, 18% to 33% had diabetes, and 4% to 37% were smokers. In the LoDoCo2 and LoDoCo studies, 84% and 24% of patients, respectively, had a history of ACS. In the COLCOT study, patients were enrolled a mean of 13.5 days following their myocardial infarction, and in the COPS study, patients were enrolled during their hospital admission for ACS.
Efficacy Results
The COLCOT study reported similar numbers of deaths in the colchicine (43 patients, 1.8%) and placebo groups (44 patients, 1.8%) over a median follow-up period of 22.6 months (hazard ratio [HR] = 0.98; 95% confidence interval [CI], 0.64 to 1.49, P = 0.93) (total N = 4,745). For the primary composite outcome, 131 patients (5.5%) in the colchicine group and 170 patients (7.1%) in the placebo group experienced an adjudicated event of cardiovascular death, resuscitated cardiac arrest, acute myocardial infarction, stroke, or urgent revascularization. The unadjusted HR for the time to first occurrence of the primary composite end point was 0.77 (95% CI, 0.61 to 0.96; P = 0.02) for colchicine versus placebo (Table 1).
In the 1-year COPS study, 8 patients (2.0%) who received colchicine died, compared with 1 patient in the placebo group (0.3%) (HR = 8.20, 95% CI, 1.03 to 65.61, P = 0.047, not adjusted for type I error rate). In this trial, 24 patients (6.1%) in the colchicine group and 38 patients (9.5%) in the placebo group experienced a primary adjudicated end point of either death, ACS, ischemia-driven urgent revascularization, or noncardioembolic ischemic stroke by 12 months (P = 0.09 in a log-rank test). The estimated HR for the time to first adjudicated primary end point was 0.65 (95% CI, 0.38 to 1.09; total N = 795).
The LoDoCo2 study reported 73 (2.6%) deaths in the colchicine group and 60 (2.2%) deaths in the placebo group after a median follow-up of 28.6 months (HR = 1.21; 95% CI, 0.86 to 1.71; total N = 5,522). The primary composite outcome was time to first occurrence of an adjudicated cardiovascular death, nonprocedural myocardial infarction, ischemic stroke, or ischemia-driven revascularization. In the colchicine group, 187 patients (6.8%) experienced an adjudicated primary end point compared with 264 patients (9.6%) in the placebo group, with a cause-specific HR of 0.69 (95% CI, 0.57 to 0.83; P < 0.001).
Four patients (1.4%) died in the colchicine group and 10 patients (4.0%) died in the control group of the LoDoCo study, which had a median follow-up duration of 36 months (total N = 532). Fifteen patients (5.3%) in the colchicine group and 40 patients (16.0%) in the control group experienced an adjudicated primary end point event of ACS, fatal or nonfatal out-of-hospital cardiac arrest, or noncardioembolic stroke (unadjusted HR = 0.33; 95% CI, 0.18 to 0.59; P < 0.001) (Table 1).
In the LoDoCo2 and LoDoCo studies, the treatment effects for the primary composite end point in the subgroup of patients with a history of ACS were similar to those in the overall population.
Across all 4 trials, the time-to-event analyses of the individual components of the primary composite end point showed point estimates for the HR that favoured colchicine versus control; however, the 95% CI, did not exclude the null for all outcomes. Of the major cardiovascular events included in the composite end points, myocardial infarction and revascularization procedures were the most frequently reported, with resuscitated cardiac arrest, stroke, and death reported less frequently. Only the LoDoCo2 study used a hierarchical testing procedure to control the type I error rate for secondary outcomes, which included the time to ischemia-driven revascularization (HR = 0.75, 95% CI, 0.60 to 0.94; P = 0.01), myocardial infarction (HR = 0.70, 95% CI, 0.53 to 0.93; P = 0.01), ischemic stroke (HR = 0.66, 95% CI, 0.35 to 1.25; P = 0.20) and cardiovascular death (HR = 0.80; 95% CI, 0.44 to 1.44; P value not reported as statistical testing was stopped). The experts consulted for this review noted that not all composite end points were of equal importance. A significant reduction in revascularization, while important from a health care resource use perspective, may be of lesser relevance to patients compared with death, potentially disabling stroke, or myocardial infarction. These differences in the clinical importance of the end points should be considered when interpreting the results of the composite outcomes.
Harms Results
The collection and reporting of harms data were incomplete for all studies. No studies collected data on the overall frequency of adverse events and only the COLCOT study reported the number of patients with at least 1 serious adverse event (16% in the colchicine group and 17% in the placebo group).
The overall frequency of gastrointestinal adverse effects was 17% per treatment group in the COLCOT study and 21% to 23% in the COPS study. Gastrointestinal adverse effects were the reason for treatment discontinuation for 4% of colchicine-treated patients in the COLCOT study, 9% in the COPS study, and 14% in the LoDoCo study. During the run-in period of the LoDoCo2 study, 9% of patients withdrew due to intolerance, and another 3% of patients per group stopped treatment during the double-blind phase.
Generally, the frequency of neoplasms and serious infections appeared to be numerically similar between groups in the COLCOT and LoDoCo2 studies. Myalgia was reported in 21.2% of patients in the colchicine group compared with 18.5% of patients in the placebo group, based on data from a subgroup of the LoDoCo2 study.
Table 2: Summary of Key Results From Pivotal and Protocol-Selected Studies [Redacted]
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|---|---|---|---|
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Note: Table 2 has been redacted.
Source: Clinical Study Report for the COLCOT study,4 Tong et al. (2020),5 Nidorf et al. (2020),6 and Nidorf et al. (2013).7
Critical Appraisal
No major sources of bias were identified for the pivotal COLCOT and LoDoCo2 studies. Potential limitations include unclear allocation concealment in the LoDoCo2 study, and a lack of control of multiplicity in the COLCOT study.
Several limitations were identified for the 2 other trials. This included the sample sizes (532 and 795) and lack of statistical power (COPS), as well as poor reporting of methods to maintain blinding of all participants in the double-blind COPS study or outcome assessors in the open-label, assessor-blinded LoDoCo study. In the COPS study, follow-up was incomplete for many patients (number not reported) at the time of the pre-planned primary analysis. The randomization process was potentially biased in the LoDoCo study, and some imbalances in patient characteristics were noted at baseline, making it unclear if all prognostic and effect modifiers were balanced between groups. Due to the open-label design, the LoDoCo study may also be subject to performance bias, outcome ascertainment bias, and reporting bias.
In addition, the trials were designed and powered to detect differences in the primary composite outcome, not the individual outcomes of the composite, or in mortality. None of the trials collected data on health-related quality of life, and limited hospitalization data were reported in the COPS study.
The safety data available were limited by the sample size and study duration of the key trials, which may have been insufficient to detect infrequent adverse events or those that require a longer time to develop. Moreover, the collection and reporting of adverse event data were incomplete. Although colchicine has been available in Canada for decades, some uncertainty remains regarding its comparative longer-term safety in patients with CAD.
With regard to external validity, the LoDoCo2 study enrolled an enriched population that was tolerant of and adherent to colchicine, which may overestimate the treatment effects in an unselected patient population. The pivotal trials excluded patients with more severe heart failure, valvular heart disease, or prior coronary bypass graft, as well as those with renal or hepatic impairment. As a result, the findings may not be generalizable to these patients. Although the enrolled patients may not reflect the gender, racial, or ethnic diversity of the Canadian population, the experts had no major concerns with the generalizability of the study populations.
Indirect Comparisons
No relevant indirect comparisons were identified.
Other Relevant Evidence
No other studies were identified that addressed gaps in the evidence included in the systematic review.
Conclusions
Colchicine, when used as add-on therapy to standard secondary prevention drugs, was associated with statistically significant and clinically important differences relative to placebo on the composite outcome of time to first occurrence of cardiovascular death, stroke, myocardial infarction, and urgent ischemia-driven revascularization in patients with a recent myocardial infarction, as well as those with stable coronary artery disease who had experienced a prior ACS event. Colchicine also showed statistically and clinically significant differences versus placebo in the time to myocardial infarction and the time to ischemia-driven revascularization in patients with stable coronary artery disease and a history of ACS. No conclusions about the impact of colchicine on the individual components of the primary composite end point in patients with a recent myocardial infarction can be drawn, as the COLCOT study was not designed to test for differences in these events.
No conclusions can be drawn on the impact of colchicine on health-related quality of life or hospitalization due to the lack of data, or on mortality because the trials were not designed or powered to test for differences between groups for this outcome. Gastrointestinal effects, which were common adverse events reported in the trials, may lead to treatment discontinuation in a subset of patients. The comparative evidence on safety was limited by the incomplete collection and reporting of adverse events, the sample size, and duration of the trials.
Introduction
Disease Background
Coronary artery disease is a leading cause of premature mortality and disability in Canada.1 An estimated 2.4 million Canadian adults have been diagnosed with coronary artery disease, including 578,000 adults (2.1%) with a history of a myocardial infarction.1 The estimated annual incidence of coronary artery disease in Canada is 6.1 per 1,000 (158,700 adults) with 63,200 Canadian adults experiencing a first myocardial infarction (2.3 per 1,000). Canadian adults with coronary artery disease are 3 times more likely, and those who survived a myocardial infarction are 3 times more likely, to die prematurely, compared with those without the condition.1
Standards of Therapy
The most important treatment goals following ACS include the prevention of future coronary events and of heart failure, eliminating or at least minimizing symptom recurrence (e.g., angina), and improving quality of life (mentally as well as physically).
The management of myocardial infarction in patients with acute coronary disease includes revascularization procedures, such as percutaneous coronary intervention and coronary artery bypass grafts, as well as pharmacotherapy and lifestyle modification to prevent recurrent events. Antiplatelet therapy typically includes Aspirin plus clopidogrel or ticagrelor, but may also include combination therapy with anticoagulants (e.g., rivaroxaban). Lipid-lowering therapy includes statins, which may be used alone or in combination with a different drug class (e.g., ezetimibe, alirocumab, evolocumab, or icosapent ethyl). Beta-blockers are routinely prescribed in patients with cardiac impairment following an acute coronary event. However, the clinical experts consulted indicated that the benefit in patients with preserved left ventricular ejection fraction (> 50%) has recently been questioned and that clinical trials are under way to examine the role of beta-blockers as uniform treatment for secondary prevention of a subsequent acute coronary event. Angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers may also be initiated for secondary prevention and blood pressure control. Other drugs may be indicated in select subpopulations (e.g., sodium-glucose cotransporter-2 inhibitors in patients with diabetes or heart failure). Lifestyle modification consists of maintaining a healthy diet and optimal body weight, smoking cessation, stress and alcohol reduction, and regular anaerobic exercise, which may include participation in a cardiac rehabilitation program.8
Drug
Colchicine is available in Canada as a 0.6 mg oral tablet and is indicated for the treatment of gout and familial Mediterranean fever.9 Colchicine 0.5 mg extended-release oral tablets are approved by Health Canada for the reduction of atherothrombotic events in adult patients with existing coronary artery disease, in addition to standard therapies, including low-density lipoprotein cholesterol–lowering and antithrombotic drug treatment.2 The recommended dosage is 0.5 mg once daily. The sponsor has requested reimbursement as per the indication.3
Colchicine is professed to have anti-inflammatory properties, although its mechanism of action for the secondary prevention of cardiovascular events is not fully understood.2 Colchicine is known to disrupt cytoskeletal functions through the inhibition of beta-tubulin polymerization into microtubules, which prevents the activation, degranulation, and migration of neutrophils.2 A number of other potential anti-inflammatory activities of colchicine have been proposed.2
Colchicine has not previously been reviewed by CADTH.
Table 3: Key Characteristics of Colchicine
Key characteristics | Colchicine |
|---|---|
Mechanism of action | Professed anti-inflammatory; mechanism of action not completely understood |
Indicationa | For the reduction of atherothrombotic events in adult patients with existing coronary artery disease, in addition to standard therapies, including LDL-C–lowering and antithrombotic drug treatment |
Route of administration | Oral |
Recommended dosage | 0.5 mg once daily |
Serious adverse effects or safety issues |
|
CYP3A4 = cytochrome P450 enzyme 3A4; LDL-C = low-density lipoprotein cholesterol.
aHealth Canada–approved indication.
Source: Product monograph.2
Stakeholder Perspectives
Patient Group Input
No patient group input was received for this submission.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of coronary artery disease.
Unmet Needs
Despite implementing guideline-recommended, goal-directed therapies, many patients with coronary artery disease and ACS experience subsequent cardiovascular events (death, myocardial infarction, stroke, and hospitalization for revascularization procedures). Adverse effects can limit use, or at least optimal dosing, of secondary prevention therapies in ischemic heart disease (e.g., bleeding and gastric erosion with Aspirin, myalgias with statins, lethargy and impotence with beta-blockers, and symptomatic hypotension with ACE inhibitors). There is also a need for simpler regimens, specifically fewer tablets taken fewer times each day.
Place in Therapy
The clinical experts indicated that colchicine would be used long-term as add-on therapy for the secondary prevention of ischemic cardiac events. Colchicine would not replace any of the standard guideline-recommended drugs and the dose of other concomitant drugs would not be decreased after adding colchicine.
Although inflammation is thought to play a pivotal role in the development of coronary artery obstructions that lead to acute ischemic events, none of the current secondary prevention therapies primarily address inflammation. Aspirin and statins do have some anti-inflammatory properties; however, colchicine is the first approved secondary prevention therapy that is hypothesized to act through an anti-inflammatory pathway.
Patient Population
The clinical experts expressed that the patients best suited for colchicine therapy are those with coronary artery disease who have experienced a myocardial infarction. The experts were not able to identify any specific subgroups of patients who were most likely to benefit from colchicine therapy and should therefore be primarily targeted for its use.
No specific tests are required to identify eligible patients for colchicine. In Canada most patients are admitted to hospital for the management of myocardial infarction, and colchicine could be initiated in hospital or during post-discharge care.
The experts indicated that patients who had received colchicine previously and experienced adverse effects, such as gastrointestinal symptoms, may or may not be willing to restart the drug to determine if it might be better tolerated. Colchicine should be avoided in patients who are using certain drugs metabolized via CYP3A4 or P-glycoprotein pathways, or with other contraindications to therapy.
Assessing Response to Treatment
The experts indicated that avoidance or delaying myocardial infarction or stroke and the need for expensive and resource-intensive procedures, such as coronary revascularization (percutaneous coronary intervention or surgery with coronary artery bypass graft), and death, would be indicative of response to treatment.
Discontinuing Treatment
According to the experts consulted, the primary reason for discontinuing colchicine would be intolerable adverse effects, or development of a condition that was listed as an exclusion criteria in the clinical trials. The recurrence of an ischemic event would not be viewed as treatment failure, but a reflection of the patient’s ongoing risk of coronary ischemia.
Prescribing Conditions
Colchicine could be initiated in hospital following a myocardial infarction or as part of outpatient care. The experts stated that a specialist is not required to prescribe colchicine. Potential drug-drug interactions may be monitored by a pharmacist, with treatments modified as needed, as part of routine care.
Clinician Group Input
No clinician group input was received for this submission.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert responses |
|---|---|
The inclusion criteria for the trials varied, and some studies excluded those with severe heart failure or severe valvular disease. In which patients will this drug be initiated? | Colchicine may be initiated in patients with a low ejection fraction or those who have undergone a coronary bypass, even though these patients were excluded from some studies. |
Will use be limited to patients with a previous myocardial infarction, or expand to include all adults with coronary artery disease? | The obvious time to start colchicine would be in hospital, at the time of presentation with and survival of an acute coronary event. However, it may also be prescribed later for patients who have a remote history of myocardial infarction. There is potentially a large number of patients who would be eligible for treatment with colchicine, regardless of how much time had elapsed since their index myocardial ischemic event. |
Gastrointestinal adverse effects can be common with colchicine. If treatment is stopped due to adverse effects or other reasons, can or should treatment be resumed? According to what time frame? | Patients who had previously experienced gastrointestinal adverse effects with colchicine may be willing to restart the drug to determine if it may be better tolerated. For patients who require short-term treatment with a drug that may interact with colchicine (e.g., an antifungal), it may be reasonable to hold the colchicine and then restart once the course of therapy is complete. |
How will gastrointestinal and other adverse effects be managed in clinical practice? | As is known from its role in treating pericarditis, colchicine is associated with gastrointestinal upset (specifically diarrhea) in about 10% of patients. While some patients will persist with treatment and find that the gastrointestinal symptoms attenuate and even resolve with time, others will stop treatment altogether. The proportion of patients who stop therapy due to adverse effects is on par with that of many of other treatments used for secondary prevention of coronary events. |
Will the colchicine 0.6 mg tablet, which is readily available on the Canadian market, be prescribed for secondary coronary prevention in place of the Myinfla 0.5 mg tablet? | The experts indicated that some clinicians are prescribing colchicine 0.6 mg daily for secondary prevention as the 0.5 mg dosage form is currently not available. The extent of this use is not known. |
Are there any clinical concerns with a 0.6 mg vs. 0.5 mg daily dose? | The relative risk of harm for 0.5 mg vs. 0.6 mg is not known. |
If patients are already prescribed colchicine for another condition (e.g., gout) could patients be advised to take 0.6 mg daily? | It is possible that patients prescribe colchicine for gout or other conditions may be instructed to take 0.6 mg daily for secondary prevention, rather than using the 0.5 mg dosage form once available. |
The trials primarily included White males who were approximately 65 years of age. Are the findings from the clinical trials generalizable to the Canadian population with coronary artery disease? | The experts did not have any major concerns with the external validity of the trials. Although the gender, racial, and ethnic diversity of the Canadian population may not be fully reflected in those enrolled, it is reasonable to extrapolate the studies’ findings to the Canadian population with coronary artery disease. |
Is there potential for the drug to be used in patients at high risk of myocardial infarction or other cardiac events but who do not have evidence of coronary artery disease? | Mechanistically, colchicine may be beneficial as primary prevention therapy; however, direct evidence is lacking as no clinical trials have been conducted in this population. The cost-effectiveness of primary prevention could be low because the absolute risk reduction and the number needed to treat may be substantially higher for primary vs. secondary prevention. |
Are additional studies required to demonstrate the longer-term safety of colchicine when used for secondary prevention? | Additional data are required as there is some uncertainty regarding the longer-term safety of colchicine, particularly in subsets of patients who may have a higher risk of adverse events (e.g., the elderly or those with renal or hepatic impairment). In some clinical trials, a potential signal for increased all-cause mortality with colchicine relative to placebo was observed in patients with CAD. |
Clinical Evidence
The clinical evidence included in the review of colchicine is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of colchicine 0.5 mg oral tablets for the reduction of atherothrombotic events in adult patients with existing coronary artery disease, in addition to standard therapies.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria in Table 5. Outcomes included in the CADTH review protocol reflect those considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients with coronary artery disease Subgroups
|
Intervention | Colchicine 0.5 mg tablet per day as add-on to standard treatments for secondary prevention of atherothrombotic events (e.g., antiplatelet therapy, lipid-lowering therapy, beta-blockers, ACE inhibitors, or angiotensin receptor blockers) |
Comparator | Standard treatments for secondary prevention of atherothrombotic events, such as antiplatelet therapy, lipid-lowering therapy, beta-blockers, ACE inhibitors, or angiotensin receptor blockers (with or without placebo) |
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality, gastrointestinal adverse effects, blood dyscrasias, neuromuscular toxicity and rhabdomyolysis, infections, malignancy |
Study designs | Published and unpublished phase III and IV randomized controlled trials |
ACE = angiotensin-converting enzyme; AE = adverse event; CV = cardiovascular; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aThe sponsor initially requested reimbursement for the prevention of cardiovascular events in patients who have had a myocardial infarction, but in September 2021, this was changed to include adult patients with existing coronary artery disease (i.e., the Health Canada–approved population).
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies checklist.10
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Myinfla (colchicine) and coronary artery disease. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
Search filters developed by CADTH were applied to limit retrieval to randomized controlled trials (RCTs) or controlled clinical trials. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Appendix 1 provides detailed search strategies.
The initial search was completed on June 25, 2021. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on October 27, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature resource.11 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Appendix 1 provides more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
Four studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6 and Table 7. A list of excluded studies is presented in Appendix 2.
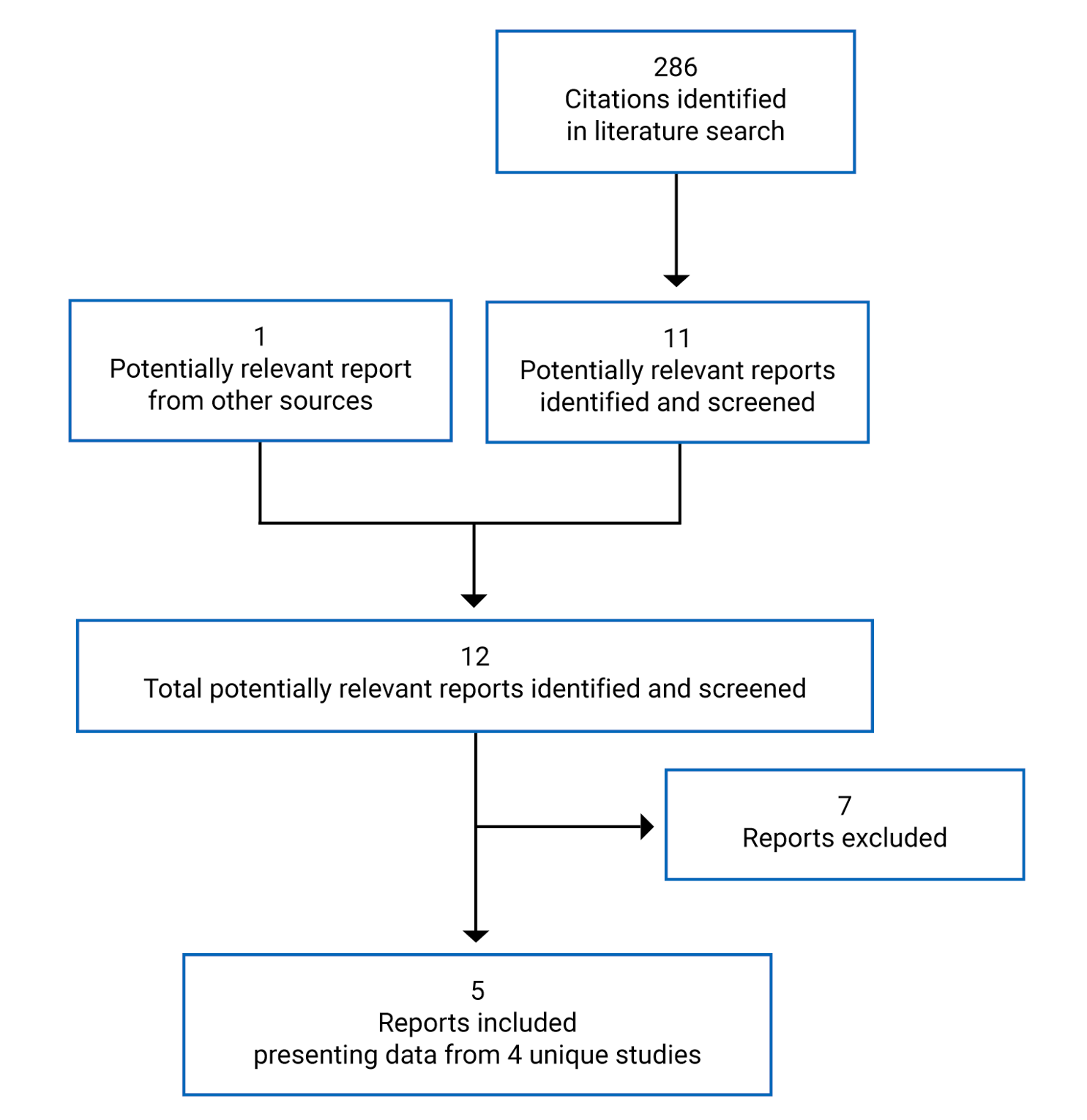
Table 6: Details of Included Studies in Patients With Acute Coronary Syndrome
Details | COLCOT | COPS |
|---|---|---|
Designs and populations | ||
Study design | Double-blind RCT (pivotal) | Double-blind RCT |
Locations | Canada, South America, Europe, Middle East, North Africa (total 167 sites) | Australia (17 hospitals) |
Patient enrolment dates | December 2015 to August 2018 Database lock: August 2019 | December 2015 and September 2018 Database lock: NR |
Randomized (N) | 4,745 | 795 |
Inclusion criteria | Adults who experienced MI in past 30 days
| Patients 18 to 85 years of age who presented to hospital with ACS (symptoms of acute myocardial ischemia with elevated troponin or ECG changes)
|
Exclusion criteria |
|
|
Drugs | ||
Intervention | Colchicine 0.5 mg once daily plus standard care | Colchicine 0.5 mg twice daily for 1 month, then 0.5 mg once daily for 11 months in addition to standard care |
Comparator(s) | Placebo plus standard care | Placebo plus standard care |
Duration | ||
Phase | ||
Run-in | NA | NA |
Double-blind | Event-driven (minimum of 301 adjudicated primary events) | At least 12 months |
Follow-up | 30 days | 7 days |
Outcomes | ||
Primary end point | Time to first event of CV death, resuscitated cardiac arrest, acute MI, stroke, or urgent hospitalization for angina requiring coronary revascularization | Time to first event of death from any cause, ACS (STEMI or non-STEMI, and/or unstable angina), ischemia-driven urgent revascularization, noncardioembolic ischemic stroke |
Secondary and exploratory end points | Secondary:
Exploratory:
Harms: SAE, gastrointestinal AE, drug-related AE, clinically significant laboratory abnormalities | Secondary:
Other: Time to CV death (post hoc) Harms: Treatment-related AE |
Notes | ||
Publications | Tardif et al. (2019)12 | Tong et al. (2020)5 |
ACS = acute coronary syndrome; AE = adverse event; ALT = alanine transaminase; CABG = coronary artery bypass graft; CAD = coronary artery disease; CPK = creatine phosphokinase; CV = cardiovascular; CYP3A4 = cytochrome P450 enzyme 3A4; ECG = electrocardiogram; eGFR = estimated glomerular filtration rate; HF = heart failure; LVEF = left ventricular ejection fraction; MI = myocardial infarction; NA = not applicable; NR = not reported; NYHA = New York Heart Association; PCI = percutaneous coronary intervention; RAAS = renin-angiotensin-aldosterone system; RCT = randomized controlled trial; SAE = serious adverse event; STEMI = ST-elevation myocardial infarction; ULN = upper limit of normal.
Source: Clinical Study Report for COLCOT,4 Tardif et al. (2019),12 and Tong et al. (2020).5
Table 7: Details of Included Studies in Patients With Coronary Artery Disease
Detail | LoDoCo2 | LoDoCo |
|---|---|---|
Designs and populations | ||
Study design | Double-blind RCT (pivotal) | RCT, open-label (observer-blinded) |
Locations | Australia (13 centres), Netherlands (30 centres) | Australia (1 outpatient cardiology clinic) |
Patient enrolment dates | Enrolment: August 2014 to December 2018 Trial end date: December 2019 | Enrolment: August 2008 and May 2010 Trial end date: May 2012 |
Randomized (N) | 5,522 | 532 |
Inclusion criteria | Adults aged 35 to 82 years with CAD on invasive angiography or CT angiography, or a coronary artery calcium score ≥ 400 Agatston units on a coronary artery calcium scan
| Adults aged 35 to 85 years with angiographically proven CAD
|
Exclusion criteria |
| NR |
Drugs | ||
Intervention | Colchicine 0.5 mg once daily plus standard care | Colchicine 0.5 mg once daily plus standard care |
Comparator(s) | Placebo plus standard care | Standard care |
Duration | ||
Phase | ||
Run-in | 1 month (open-label)a | NA |
Treatment | Event-driven (minimum of 331 adjudicated primary outcome events or 1 year follow-up) | At least 2 years |
Follow-up | NR | NR |
Outcomes | ||
Primary end point | Time to first event of CV death, MI, ischemic stroke, or ischemia-driven coronary revascularization | Time to first event of ACS, fatal or nonfatal out-of-hospital cardiac arrest, or noncardioembolic ischemic stroke |
Secondary and exploratory end points | Secondary:
Additional:
Harms: Select treatment-related adverse events | Secondary:
Harms: Withdrawal due to adverse events, deaths |
Notes | ||
Publications | Nidorf et al. (2020)6 | Nidorf et al. (2013)7 |
ACS = acute coronary syndrome; CABG = coronary artery bypass graft; CAD = coronary artery disease; CV = cardiovascular; eGFR = estimated glomerular filtration rate; MI = myocardial infarction; NA = not applicable; NR = not reported; NYHA = New York Heart Association; RCT = randomized controlled trial.
aAll patients received open-label colchicine 0.5 mg once daily. Patients who were in stable condition and were tolerant of and adherent to colchicine therapy were eligible to enter the double-blind randomized period.
Description of Studies
Four investigator-led RCTs4-7 met the inclusion criteria for this review, 2 of which were considered pivotal trials.4,6
The objective of the COLCOT trial was to determine if long-term treatment with colchicine reduced the rate of cardiovascular events in patients after myocardial infarction. This double-blind RCT enrolled 4,745 patients within 30 days of a myocardial infarction who were randomized to colchicine 0.5 mg once daily or placebo (1:1) as add-on therapy to standard treatments. Randomization was conducted using an automated interactive web response system, stratified by site, based on a computer-generated permutated block randomization schedule. The event-driven trial was to continue until 301 adjudicated primary outcome events had occurred (cardiovascular death, resuscitated cardiac arrest, acute myocardial infarction, stroke, or urgent hospitalization for angina requiring coronary revascularization). This multi-national trial included 35 sites in Canada.
The aim of the COPS study was to assess the efficacy of colchicine versus placebo, in addition to standard secondary prevention therapies, on cardiovascular events in patients presenting with ACS. The double-blind RCT enrolled 795 patients who were randomized (1:1) to colchicine 0.5 mg daily or placebo using an interactive web response system. The computer-generated permuted block randomization schedule was stratified by pre-existing history of myocardial infarction, diabetes, and study site. The study was conducted at 17 hospitals in Australia.
The objective of the LoDoCo2 trial was to determine if colchicine prevents cardiovascular events in patients with chronic coronary disease. This event-driven RCT included a 1-month open-label run-in period during which all patients received colchicine 0.5 mg daily. Patients who were in stable condition, tolerated and adhered to colchicine, and agreed to continue the study were eligible to enter the double-blind randomized period. Patients were randomized (1:1) to either colchicine 0.5 mg once daily or placebo, as add-on therapy to standard secondary prevention medications (N = 5,522). The computer-generated randomized algorithm was stratified by country. The multi-centre study was conducted in Australia and The Netherlands.
The LoDoCo study used a prospective randomized, open-label, and blinded end point design. Its objective was to determine if colchicine reduces the risk of cardiovascular events in patients with stable coronary artery disease. Patients were randomized 1:1 to either colchicine 0.5 mg once daily or no treatment, as add-on therapy to standard secondary prevention therapies (N = 532). Randomization employed a computer-generated sequence managed by a research assistant who was not involved in the management of study patients, and a central database was used to conceal allocation. Investigators and patients were advised of treatment assignment after randomization and all patients were followed for at least 2 years. The single-centre study was conducted in Australia.
A clinical study report was available for 1 study,4 and the 3 other studies were available as published reports only.5-7 None of the trials were industry-funded.
Populations
Inclusion and Exclusion Criteria
Two trials (LoDoCo2 and LoDoCo) enrolled adults with documented coronary artery disease that was stable for the past 6 months, and 2 trials (COLCOT, COPS) enrolled patients following an ACS event. For the COLCOT study, adults who had experienced an acute myocardial infarction in the previous 30 days were eligible. In the COPS study, patients who presented to hospital with ST-elevation myocardial infarction (STEMI), non-STEMI, and/or unstable angina were eligible to enter the trial.
The COLCOT study excluded patients with severe heart failure, a left ventricular ejection fraction of less than 35%, stroke within past 3 months, type 2 myocardial infarction, a prior coronary artery bypass graft in the past 3 years, progressive neuromuscular disease, inflammatory bowel disease or chronic diarrhea, elevated serum creatinine, or severe hepatic disease. The LoDoCo2 study also excluded patients with severe heart failure, moderate or severe valvular heart disease, moderate to severe renal impairment, peripheral neuritis, myositis, or myosensitivity to statins. Other inclusion and exclusion criteria are listed in Table 6 and Table 7.
Baseline Characteristics
For the 2 trials that enrolled patients with ACS (COLCOT and COPS), the mean age per group ranged from 59.7 years (SD = 10.2) to 60.6 years (SD = 10.7), and 78% to 82% of the participants were male. The majority of patients in the COLCOT study were White (57%): race was not reported in the COPS study. Patients were enrolled a mean of 13.5 days following their myocardial infarction in the COLCOT study, or during their hospital admission for ACS in the COPS study. In both trials, most patients (88% to 93%) underwent percutaneous coronary interventions for their ACS event, and approximately half had a history of hypertension (50% to 52%) or dyslipidemia (44% to 46% per treatment group). Other cardiovascular risk factors included diabetes (19% to 21%), and smoking (30% to 37% per treatment group). The baseline characteristics were generally balanced between groups, except for a family history of ischemic heart disease in the COPS study (45% in the colchicine group; 36% in the placebo group). Additional information on baseline characteristics for the COLCOT and COPS studies is listed in Table 8 and Figure 2, respectively.
The mean age of patients enrolled in the LoDoCo2 study was 66 years (SD = 8.6) and 85% were male. Overall, 84% of patients had a prior ACS event, which had occurred more than 24 months before enrolment for 58% of patients. Half the patients had a history of hypertension, 18% were receiving treatment for diabetes, and 12% were current smokers. Overall, 34% were from Australia and 66% were from The Netherlands. No information was provided on the race of the patients enrolled. The baseline characteristics appeared to be balanced between groups. Additional details are provided in Figure 3.
LoDoCo study enrolled predominately male (89%) patients with mean ages of 67 years (SD = 9.2) and 66 years (SD = 9.6) in the control and colchicine groups, respectively. (Figure 4). The study reported that 24% and 23% had a prior ACS event, 28% and 33% of patients had a history of diabetes, and 6% and 4% were smokers in the control and colchicine groups, respectively. Fewer patients in the control group than the colchicine group had undergone a percutaneous angioplasty (55% versus 60%) or CABG procedure (16% versus 22%), respectively.
The patients enrolled in the ACS studies were younger and a higher proportion were smokers compared with those enrolled in the stable coronary artery disease trials.
Table 8: Summary of Baseline Characteristics — COLCOT Study (MI Population, ITT Population)
Characteristic | Colchicine N = 2,366 | Placebo N = 2,379 |
|---|---|---|
Mean age (SD), years | 60.6 (10.7) | 60.5 (10.6) |
Male, n (%) | 1,894 (80) | 1,942 (82) |
Ethnic origin, n (%) | ||
White | 1,350 (57) | 1,329 (56) |
Hispanic or Latino | 377 (16) | 381 (16) |
North African or Middle Eastern | 70 (3) | 73 (3) |
Asian | 26 (1) | 27 (1) |
Black | 3 (< 1) | 8 (< 1) |
Other | 24 (1) | 26 (1) |
Not reported | 516 (22) | 535 (22) |
Body mass index, kg/m2, mean (SD) | 28.2 (4.8) | 28.4 (4.7) |
Index MI to randomization, mean days (SD) | 13.4 (10.2) | 13.5 (10.1) |
PCI for index MI, N (%) | 2,192 (93) | 2,216 (93) |
Smoker, n (%) | ||
Non-smoker | 787 (33) | 797 (34) |
Previous smoker | 871 (37) | 872 (37) |
Smoker | 708 (30) | 708 (30) |
Medical history, n (%) | ||
Diabetes | 462 (20) | 497 (21) |
Hypertension | 1,185 (50) | 1,236 (52) |
Dyslipidemia | 1,029 (44) | 1,105 (46) |
Prior MI | 370 (16) | 397 (17) |
Prior PCI | 392 (17) | 406 (17) |
Prior CABG | 69 (3) | 81 (3) |
Stroke or TIA | 55 (2) | 67 (3) |
Heart failure | 48 (2) | 42 (2) |
Atrial fibrillation | 110 (5) | 100 (4) |
CABG = coronary artery bypass graft; ITT = intention-to-treat; MI = myocardial infarction; PCI = percutaneous coronary intervention; SD = standard deviation; TIA = transient ischemic attack.
Source: Clinical Study Report for the COLCOT trial.4
Figure 2: Summary of Baseline Characteristics — COPS Study (Intention-to-Treat Population) [Redacted]

Source: Tong et al. (2020).5
See Table 1 in Tong DC, Quinn S, Nasis A, et al. Colchicine in Patients With Acute Coronary Syndrome: The Australian COPS Randomized Clinical Trial. Circulation. 2020;142(20):1890 to 1900. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.120.050771
Figure 3: Summary of Baseline Characteristics — LoDoCo2 Study (Intention-to-Treat Population)
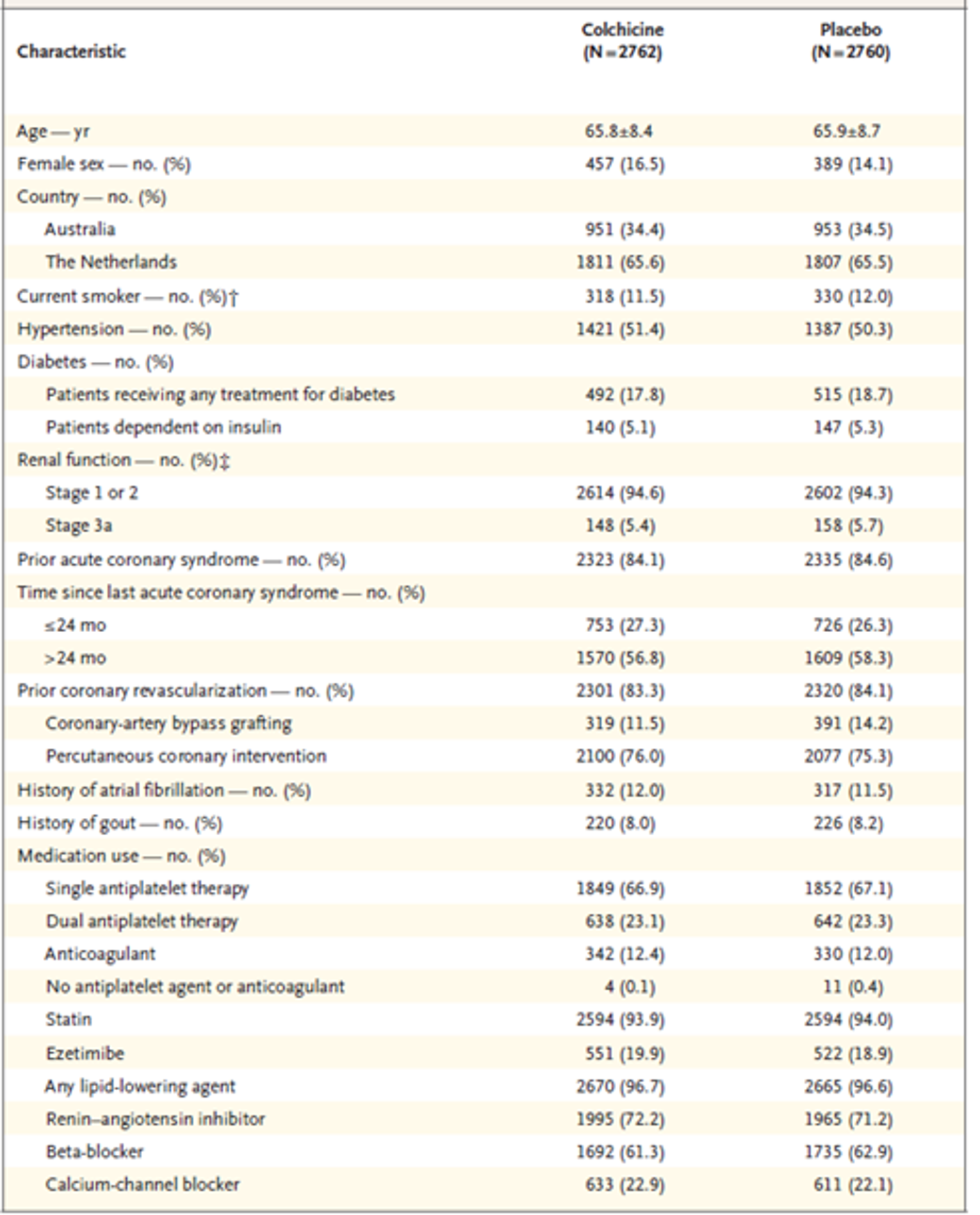
* Plus-minus values are means ± standard deviation.
† Information on smoking was missing for 21 patients.
‡ Stage 1 refers to an estimated glomerular filtration rate of at least 90 mL/min/1.73 m2 of body surface are (normal to high), stage 2 to a rate of 60 to 89 mL/min/1.73 m2 (mildly decreased), and stage 3a to a rate of 45 to 59 mL/min/1.73 m2 (mildly to moderately decreased). Stages are based on the Kidney Improving Global Outcomes Clinical Practice Guidelines for Acute Kidney Injury.
Source: Nidorf et al. (2020)6 from N Engl J Med, Nidorf SM, Fiolet ATL, Mosterd A, et al., Colchicine in Patients with Chronic Coronary Disease., volume 383, Page No. 1838 to 1847. Copyright 2020 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Figure 4: Summary of Baseline Characteristics — LoDoCo Study (Intention-to-Treat Population)
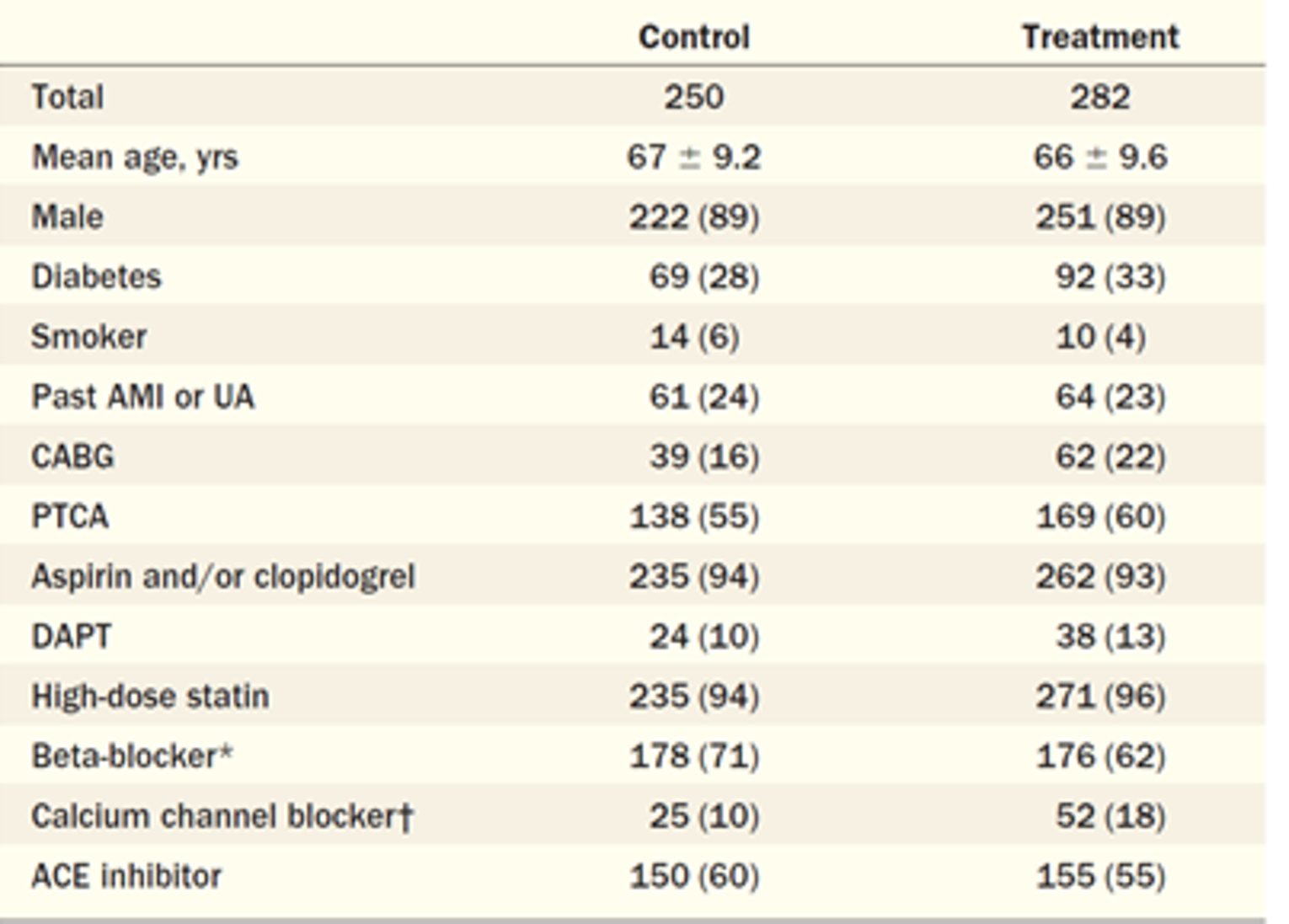
ACE = angiotensin-converting enzyme; AMI = acute myocardial infarction: CABG = coronary artery bypass graft; DAPT = dual antiplatelet therapy (Aspirin and clopidogrel); PRCA = percutaneous coronary angioplasty; UA = unstable angina.
Note: Values of mean ± standard deviation or n (%).
* P is less than 0.05.
† P is less than 0.01 for the comparison of the distribution between treatment and control.
Source: Nidorf et al. (2013).7 Reprinted from J Am Coll Cardiol, Vol 61, Nidorf SM, Eikelboom JW, Budgeon CA, Thompson PL, Low-dose colchicine for secondary prevention of cardiovascular disease, Pages No. 404 to 410, Copyright 2013, with permission from Elsevier.
Interventions
Patients enrolled in the COLCOT study were randomized 1:1 to received colchicine 0.5 mg tablets once daily or matching placebo. All patients received standard medical care for control of dyslipidemia, hypertension, angina, and diabetes at the discretion of the investigators. A summary of concomitant medications during the COLCOT study is provided in Table 9. The vast majority of patients in both groups were receiving an antithrombotic drug (99.8%), lipid-modifying therapy (99%), beta-blockers (89%), and renin-angiotensin-aldosterone system drugs (86%). Overall, 21% of patients were receiving medications to manage diabetes.
Prior to randomization, any patients receiving colchicine for other conditions were required to stop therapy, and no washout period was required. Due to potential drug interactions with P-glycoprotein and hepatic CYP3A4 substrates, which may increase the likelihood of colchicine toxicity, use of erythromycin and clarithromycin was prohibited during the study. Chronic use of systemic corticosteroids and consumption of more than 750 mL of grapefruit juice was also prohibited. Investigators were to monitor for drug interactions with statins and other lipid-lowering drugs, digoxin, and cyclosporine. Administration of other medications was allowed, provided the patients were stabilized before enrolment.
Table 9: Summary of Concomitant Medications — COLCOT Study (MI Population, ITT Population)
Drug Class | Colchicine N = 2,366 | Placebo N = 2,379 |
|---|---|---|
RAAS drugs, n (%) | 2,042 (86.3) | 2,062 (86.7) |
Beta-blocker, n (%) | 2,116 (89.4) | 2,101 (88.3) |
Antithrombotic drug, n (%) | 2,362 (99.8) | 2,375 (99.8) |
Calcium-channel blocker, n (%) | 454 (19.2) | 461 (19.4) |
Diuretics, n (%) | 477 (20.2) | 500 (21.0) |
Drugs for acid related disorders, n (%) | 1,662 (70.2) | 1,702 (71.5) |
Lipid-modifying drugs, n (%) | 2,346 (99.2) | 2,366 (99.5) |
Drugs used in diabetes, n (%) | 486 (20.5) | 516 (21.7) |
ITT = intention-to-treat; RAAS = renin-angiotensin-aldosterone system.
Source: Clinical Study Report for the COLCOT trial.4
In the COPS study, patients were randomized to receive either placebo or colchicine 0.5 mg twice daily for 1 month then 0.5 mg daily for 11 months, as add-on therapy to standard secondary prevention pharmacotherapy. Within the first month of therapy the dosage of the study drug could be reduced from twice daily to once daily if patients developed severe gastrointestinal symptoms. Most patients (97% to 99%) were receiving Aspirin or other antiplatelet drugs and statins, and 81% to 88% were administered a beta-blocker and/or an ACE inhibitor or angiotensin receptor blocker. Fifteen percent of patients were treated with an oral hypoglycemic drug and 5% to 7% were on insulin (Figure 2).
All patients enrolled in the LoDoCo2 study received open-label colchicine 0.5 mg daily during the run-in period and those who were in stable condition, tolerated and adhered to colchicine, and agreed to continue in the study were eligible to enter the double-blind randomized period. Randomized patients received either colchicine 0.5 mg once daily or matching placebo, as add-on therapy to standard secondary prevention medications. Concomitant treatments received included lipid-lowering therapy (97%), single antiplatelet (67%) or dual antiplatelet therapy (23%), anticoagulants (12%), beta-blockers (62%), renin-angiotensin inhibitors (72%) and calcium-channel blockers (22%) (Figure 3). Overall, 18% of patients were receiving treatment for diabetes, including 5% who required insulin.
In the LoDoCo study, patients randomized to colchicine received a prescription for 0.5 mg once daily, which was supplied through their usual pharmacy. Patients could request reimbursement for colchicine drug costs. Those assigned to the control group received no additional treatment. Both groups continued to receive standard secondary prevention therapies, including Aspirin or clopidogrel (94% and 93% in the control and colchicine groups, respectively), dual antiplatelet therapy (10% and 13%), high-dose statins (94% and 96%), beta-blockers (71% and 62%), calcium-channel blockers (10% and 18%), and ACE inhibitors (60% and 55%) (Figure 4).
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 10. These end points are further summarized in the following section, with study definitions listed in Table 11.
Table 10: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | COLCOT (MI) | COPS (ACS) | LoDoCo2 (CAD) | LoDoCo (CAD) |
|---|---|---|---|---|
Primary | Time to first event of:
| Time to first event of:
| Time to first event of:
| Time to first event of:
|
Secondary | Time to all-cause mortality Time to event for each component of primary outcome Time to CV death, resuscitated cardiac arrest, acute MI, or stroke Recurrent primary CV events | Time to event for each component of primary outcome Time to hospitalization for chest pain | Time to CV death, nonprocedural MI, ischemic stroke Time to MI or ischemia-driven coronary revascularization Time to CV death or nonprocedural MI Time to ischemia-driven coronary revascularization Time to nonprocedural MI Time to ischemic stroke Time to death from any cause Time to CV death | Time to each component of primary outcome Time to acute MI (unrelated to stent) Time to unstable angina (unrelated to stent) |
Exploratory | Time to coronary vascularization | Time to CV death (post hoc) | Time to sudden cardiac death, nonfatal out-of-hospital cardiac arrest, ACS (MI or UA irrespective of revascularization), or atherosclerotic ischemic stroke Time to all MI | NR |
ACS = acute coronary syndrome; CV = cardiovascular; MI = myocardial infarction; NR = not reported; STEMI = ST-elevated myocardial infarction; UA = unstable angina.
Source: Clinical Study Report for COLCOT trial,4 Tong et al. (2020),5 Nidorf et al.(2020),6 and Nidorf et al. (2013).7
COLCOT
In the COLCOT study the primary outcome was the time to first occurrence of cardiovascular death, resuscitated cardiac arrest, acute myocardial infarction, stroke, or urgent hospitalization for angina requiring coronary revascularization. Other secondary and exploratory outcomes of interest to this review are listed in Table 10. For the time-to-event analyses of mortality or cardiovascular death, patients who completed the study and were event-free were censored at the study end date, and those who withdrew or were lost to follow-up were censored on the date of last contact or the date of assessment of vital status, whichever was the latest. For the analysis of cardiovascular death, patients who died from a noncardiovascular cause were censored at the time of death. The study’s authors stated that “for all other endpoints, including the primary endpoint, the same censoring rules applied, but the survival status was not used as no formal assessment of endpoints was done at the assessment of survival status.” Potential end points were adjudicated by an independent clinical-event committee that included cardiologists and neurologists who were blinded to the treatment allocation. Follow-up visits or telephone assessments were completed 1 month, 3 months, and 6 months after randomization, and every 3 months thereafter.
COPS
In the COPS study, the primary outcome was the time to first event of death from any cause, ACS (STEMI or non-STEMI, and/or unstable angina), ischemia-driven urgent revascularization, or noncardioembolic ischemic stroke. Other secondary outcomes of interest included the time to each component of the primary composite outcome and hospitalization for chest pain, as well as the time to cardiovascular death (which was analyzed post hoc). No details were provided on censoring rules or how the time to event was calculated. Cardiovascular events were adjudicated by an independent, blinded clinical-event committee that included 2 cardiologists. The harms data included any adverse event that occurred during treatment or within 7 days of the last dose of study drug.
Patients were followed by a blinded research team member at 1 month, 6 months, and 12 months after randomization using structured telephone interviews and reviews of primary and secondary care records. All patients were followed for at least 12 months, including those who had stopped treatment early.
LoDoCo2
The primary end point for the LoDoCo2 study was the time to first event of cardiovascular death, nonprocedural myocardial infarction, ischemic stroke, or ischemia-driven revascularization. Secondary and exploratory end points are listed in Table 10. All end points were adjudicated by a blinded clinical-event committee (no details were available).
Patients were evaluated before the run-in period, at randomization and at 6-month intervals at in-person visits (if possible), otherwise via telephone. Clinical follow-up was continued until the end of the study, including for patients who discontinued the study drug early. The end-of-trial date for individual patients was the day of death, the day of the scheduled close-out visit (for patients who had stopped treatment early), or the last day of study-drug ingestion (for patients who were on treatment at the global end-of-trial date). The time to event was the difference between each patient’s end-of-trial date and the day of randomization plus 1.
The list of end points, including the primary outcome, was modified several times, with final changes made in January 2020 before the data were unblinded.
LoDoCo
The primary end point for the LoDoCo study was the time to first event of ACS, fatal or nonfatal out-of-hospital cardiac arrest, or noncardioembolic ischemic stroke. Secondary outcomes were individual components of the primary outcome and the components of ACS unrelated to stent disease. In this open-label trial, all outcomes were assessed by an experienced adjudicator who was blinded to treatment allocation. (No further details were available.)
Treatment outcomes and adherence to therapy data were collected at routine care visits and at any unplanned hospitalizations. The pre-planned study duration was 2 years for all patients, and all living patients were contacted by telephone for a final follow-up after the study closure date (May 2012). Patients were censored at the date of death, or at the study end date for those who were still alive and had not experienced an end point event. The time to event was calculated by subtracting the date of randomization from the date of an event or censoring date. Patients who stopped colchicine were followed during the trial and included in the analysis.
Table 11: Key Outcomes Definitions in the Included Studies [Redacted]
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|---|---|---|---|
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Note: Table 11 has been redacted.
Source: Clinical Study Report for COLCOT trial,4 Tong et al. (2020),5 Nidorf et al.(2020),6 and Nidorf et al. (2013).7
Statistical Analysis
COLCOT
The primary outcome of the COLCOT study (time to first occurrence of cardiovascular death, resuscitated cardiac arrest, acute myocardial infarction, stroke, or urgent hospitalization for angina requiring coronary revascularization) was analyzed using an unadjusted Cox proportional hazards model and log-rank test for the intention-to-treat (ITT) population. A single interim analysis for futility was planned and conducted once 50% of the primary outcome events had been adjudicated. The stopping rules for futility were pre-planned and, based on the interim analysis in July 2018, the study continued as planned. To control the type I error rate and account for the interim analysis, the statistical significance for the final analysis of the primary outcome was set to 0.049. The study’s authors stated that efficacy event and censoring dates were complete for all patients, eliminating the need to impute missing end point data. It is unclear if any tests were run to assess if the proportionality assumption was met.
Pre-planned sensitivity analyses were run for the primary outcome based on the per-protocol population and a multivariate Cox proportional hazards model adjusted for baseline (Table 12).
Baseline variables that showed association (P < 0.20) in a univariate model were added in a stepwise manner, and the final adjusted model included covariates for age, history of diabetes, history of prior coronary revascularization, or history of heart failure. Other post hoc sensitivity analyses were also reported.
All other secondary or exploratory time-to-event analyses were analyzed using an unadjusted Cox proportional hazards model and log-rank test. Recurrent primary end point events were analyzed using 3 methods: a negative binomial regression model (number of events as outcome and follow-up time as offset) reporting the marginal rate ratio; an Andersen and Gill model with a robust variance estimator (to account for dependency of within-patient events based on a gap-time approach considering the time since a previous event); and a Wei, Lin, and Weissfeld marginal model. The 95% CI, and P values for all secondary and exploratory outcomes were not adjusted for multiple comparisons and the sponsor stated that inferences drawn from these analyses may not be reproducible.
The event-driven COLCOT study had 80% power to detect a 27% risk reduction (HR = 0.724) on the primary composite outcome for colchicine versus placebo, based on a planned enrolment of 4,500 patients and with 301 patients experiencing an adjudicated primary outcome event (2-sided alpha 0.05). The estimates assumed an 8% nonadherence rate in the colchicine group, a 7% event rate after 24 months in the placebo group, an 18-month recruitment period, and a 1% yearly withdrawal rate over a 24-month minimum follow-up time frame.
COPS
The primary outcome of time to first event of death from any cause, ACS (STEMI or non-STEMI, and/or unstable angina), ischemia-driven urgent revascularization, or noncardioembolic ischemic stroke was analyzed using a log-rank test. Sensitivity analyses were run using Cox proportional hazards models that considered multiple correlated events within individuals, adjusted for potential confounders, and accounted for competing risks, as well as an on-treatment analysis (see Table 12).
The proportional hazards assumption was checked for all Cox models (using the STATA estat phtest command). Patients who stopped treatment early were followed and included in the ITT analysis. The methods to analyze the secondary outcomes were not explicitly stated. No procedures were implemented to control the type I error rate.
Sample-size calculations were based on previously published data and assumed 7.2% and 3.5% annual event rates for the control and colchicine groups, respectively. With a sample size of 1,009 patients and 10% attrition, the study would have 80% power to detect this difference using a log-rank test (2-sided alpha 0.05). The authors anticipated 49 primary end point events would occur, with an estimated HR of 0.47.
The trial was stopped early due to slower than expected recruitment. The decision to stop the study was made by the trial steering committee before the trial outcomes were known. The primary analysis was planned after 365 days of follow-up, but due to the large number of patients with incomplete follow-up data at this time point (N not provided) and several late events, the study’s authors stated that a secondary analysis was conducted 400 days after follow-up. Blinding was maintained until the secondary analysis.
LoDoCo2
The cause-specific HR and 95% CI for the primary outcome (time to first occurrence of cardiovascular death, nonprocedural myocardial infarction, ischemic stroke, or ischemia-driven revascularization) was estimated using a Cox proportional hazards model (stratified by country) The null hypothesis was tested using a 2-sided log-rank test. The analysis was based on the ITT principle and included all adjudicated end point events from randomization to the end-of-trial date for all randomized patients. Sensitivity analyses are described in Table 12.
The study was planned to stop when 331 adjudicated primary events had occurred, and all patients had at least 1 year of follow-up. The end-of-trial date for 1 patient who was lost to follow-up was set to the last trial visit. No patients withdrew consent for collecting follow-up data.
The event-driven trial had greater than 90% power to detect an HR of 0.7 for the primary composite outcome, based on 331 primary events (2-sided alpha 0.05). Sample-size calculations assumed an annual primary event rate of 2.6% in the placebo group and that 10% of patients would show early intolerance during the run-in period. The planned enrolment was 6,053 patients, of whom an estimated 5,447 would complete the run-in phase and be randomized. A minimum of 1-year follow-up for all patients was planned. Effect-size data from the LoDoCo study7 were used to inform the sample-size calculations.
The secondary and exploratory time-to-event outcomes were analyzed using the same model as the primary composite outcome. A hierarchical testing procedure was implemented to control the type I error rate for the secondary outcomes, which were tested in the order presented in Table 10. For testing to proceed, the previous outcome in the hierarchy had to show statistical significance (P < 0.05). No formal hypothesis testing was planned for the exploratory outcomes.
All time-to-event analyses were reviewed to determine if the proportional hazards assumptions were met. The plot of the log of the cumulative hazard between treatments was assessed visually and by adding a treatment by log-transformed time interaction to the Cox model. Nidorf et al.13 reported no violations to the proportionality assumption. A pre-planned subgroup analysis of patients with and without a history of ACS was conducted.
The study protocol underwent several changes. Initially, only Australian centres were involved, and enrolment began in August 2014. In October 2016, 30 centres in The Netherlands began recruiting patients. With the addition of The Netherlands, the primary end point, other end points, and sample-size calculations were changed. Other edits included implementing a hierarchical testing procedure for the secondary outcomes to control for multiple testing.
LoDoCo
The primary outcome of time to first event of ACS, fatal or nonfatal out-of-hospital cardiac arrest, or noncardioembolic ischemic stroke was analyzed using an unadjusted Cox proportional hazards model for the ITT population (including those who stopped colchicine early). Sensitivity analyses were run based on the on-treatment population (i.e., patients who were adherent and tolerant to colchicine), as well as an adjusted Cox model (Table 12). Secondary time-to-event outcomes were analyzed using the same methods. There was no control of type I error rate for the secondary outcomes. The authors stated that final outcomes were known for all patients, and no patients were lost to follow-up.
Subgroup data were reported for patients with a history of ACS. It is unclear if this analysis was pre-planned.
The protocol allowed for new patients to be randomized to replace those who stopped colchicine due to adverse effects in the first month. The LoDoCo study had a planned sample size of 250 patients in the control group and 250 in the treatment group who were tolerant to colchicine for at least 4 weeks after randomization. Assuming a 2-year accrual period, a 2-year follow-up period, and an event rate for the primary composite outcome of 8% in the control population, the study was estimated to have greater than 80% power to detect an HR of 0.50 or less (2-sided alpha 0.05). The control event rate was based on data from Bhatt et al. (2010).14
Table 12: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
COLCOT (myocardial infarction) | |||
Time to event (primary composite outcome) | Cox proportional hazards model; log-rank test (ITT population) | None |
|
|
|
|
|
|
|
|
|
COPS (acute coronary syndrome) | |||
Time to first event of death, ACS (STEMI or non-STEMI/UA), ischemia-driven urgent revascularization, or noncardioembolic ischemic stroke | Log-rank test (ITT population) | None |
|
LoDoCo2 (coronary artery disease) | |||
Time to first event of CV death, nonprocedural MI, ischemic stroke, or ischemia-driven revascularization | Cause-specific Cox proportional hazards model; log-rank test (ITT population) | Stratified by country |
|
|
|
|
|
LoDoCo (coronary artery disease) | |||
Time to first event of ACS, fatal or nonfatal out-of-hospital cardiac arrest, or noncardioembolic ischemic stroke | Cox proportional hazards model (ITT population) | None |
|
Secondary time to event outcomes | Cox proportional hazards model (ITT population) | None | NA |
ACE = angiotensin-converting enzyme; CABG = coronary artery bypass graph; ITT = intention-to-treat; NA = not applicable; NR = not reported; UA = unstable angina.
Source: Clinical Study Report for COLCOT trial,4 Tong et al. (2020),5 Nidorf et al.(2020),6 and Nidorf et al. (2013).7
Analysis Populations
The ITT population of the COLCOT study included all randomized patients, analyzed according to the assigned treatment, regardless of patient adherence to the planned treatment. The safety population included all ITT patients who used at least 1 dose of the study drug, analyzed according to the randomized treatment.
In the COPS, LoDoCo2, and LoDoCo studies, the ITT population included all randomized patients, irrespective of ingestion of the study drug. No description of the safety population was available for these trials.
Results
Patient Disposition
Patient disposition flow diagrams for all trials are shown in Appendix 3 (Figure 7 to Figure 10).
The COLCOT study randomized 4,745 patients to either placebo or colchicine. No information was available on the number of patients screened for study entry. Of those randomized, a similar percentage of patients in the colchicine and placebo groups never received the study drug (1.5% and 1.3%), discontinued the study drug early (18.1% and 18.5%) and discontinued from the study (5.9% and 6.2%), respectively. The most common reasons for study discontinuation were death, lost to follow-up, or patients who discontinued the study drug and visits but whose vital status was obtained at the end of the trial. At the end of the study the vital status was unknown for 23 patients (Table 13).
A total of 2,167 patients were screened for inclusion in the COPS study: 295 patients (14%) declined to participate and 1,077 patients (50%) did not meet eligibility criteria, leaving 795 (37%) to be randomized. More patients who were randomized to the colchicine group discontinued the study drug compared with the placebo group (15.4% versus 8.3%, respectively). Three patients per group never received the study drug (0.8%), and 2.8% and 4.8% discontinued the study in the colchicine and placebo groups, respectively (Table 13). Withdrawal of consent and death were the most common reasons for study discontinuation.
Table 13: Disposition of Patients With Acute Coronary Syndrome [Redacted]
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|---|---|---|---|
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Note: Table 13 has been redacted.
Source: Clinical Study Report for COLCOT trial4 and Tong et al. (2020).5
In the LoDoCo2 study, the number of patients screened was not reported. A total of 6,528 patients entered the run-in period and received open-label colchicine, of whom 1,006 patients (15%) did not undergo randomizations due to intolerance (9%), patient choice (5%), or other reasons (1%) (Table 14). Of the 5,522 patients who were randomized, 10.5% in each group permanently stopped the study drug, most commonly due to study withdrawal (4.5% per group) or adverse events (3.4% per group). Overall, 1.6% and 1.2% of patients in the colchicine and placebo groups, respectively, had their data censored early, primarily due to death from noncardiovascular causes. One patient in the placebo group was lost to follow-up.
The LoDoCo study screened 901 patients, of whom 532 (59%) were randomized. No patients in either group were lost to follow-up. The study’s authors reported that 24.5% of patients in the colchicine group stopped treatment, either due to adverse effects (16.3%), intercurrent illness (3.9%), or patient choice (1.8%). Seven patients randomized to colchicine never received the study drug (2.5%) (Table 14).
Table 14: Disposition of Patients With Coronary Artery Disease [Redacted]
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|---|---|---|---|
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Note: Table 14 has been redacted.
Exposure to Study Treatments
In the COLCOT study, the median follow-up duration was 22.6 months (range not reported). The median treatment duration was 19.6 months (range 0.03 to 41.3) in the colchicine group and 19.5 months (range 0.03 to 41.4) for the placebo group. Among patients who discontinued the study drug early, the median treatment duration was 7.1 months (interquartile range [IQR] = 1.9 to 14.6) and 6.1 months (IQR = 1.6 to 14.4) in the colchicine and placebo groups, respectively. Adherence to treatment was high (98%) in both groups among patients who did not permanently stop the study drug.
In the COPS study, 3 patients in each group (0.8%) did not receive the study drug. No other information was available on treatment exposure during the trial. Tong et al.5 reported that all patients were followed for at least 1 year (median of 371 days).
For the LoDoCo2 study, the median duration of follow-up was 28.1 months (IQR = 20.3 to 43.5) for patients in the placebo group and 29.0 months (IQR = 20.7 to 45.7) for those in the colchicine group. Treatment exposure per group was not reported.
In the LoDoCo study the median follow-up was 36 months (range = 24 to 44 months). No information was provided on the extent of colchicine exposure.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. Appendix 3 provides detailed efficacy data.
Mortality
Table 15 provides a summary of deaths from any cause in the 4 included studies. The cause of death is discussed in further detail in the Harms section.
The COLCOT study reported similar numbers of deaths in the colchicine (43 patients, 1.8%) and placebo groups (44 patients, 1.8%) over a median follow-up period of 22.6 months (HR = 0.98; 95% CI, 0.64 to 1.49). Of these events, 20 (0.8%) were cardiovascular-related deaths in the colchicine group, compared with 24 (1.0%) in the placebo group (HR = 0.84; 95% CI, 0.46 to 1.52). Noncardiovascular deaths were reported in 23 patients (5.6%) in the colchicine group and 20 patients (3.8%) in the placebo group (HR not reported). Two patients per group with an undetermined cause of death were counted as cardiovascular deaths. One additional death occurred in the colchicine group in a patient who had withdrawn consent and whose death was obtained during a review of medical records at the end of the trial. The vital status was missing for 23 patients at the end of the study (placebo: 10 [0.4%)], colchicine: 13 patients [0.5%]).
In the COPS study, 8 patients who received colchicine (2.0%) died, compared with 1 patient in the placebo group (0.3%) (HR = 8.20; 95% CI, 1.03 to 65.61; P = 0.047, not adjusted for type I error rate). Over the 1-year follow-up period 3 deaths in the colchicine group and 1 death in the placebo group were cardiovascular-related. Eight patients (2.0%) in the colchicine group and 3 patients (0.8%) in the placebo group were lost to follow-up, and their vital status was unknown.
The LoDoCo2 study reported 73 deaths (2.6%) in the colchicine group and 60 (2.2%) deaths in the placebo group after a median follow-up of 28.6 months (HR = 1.21; 95% CI, 0.86 to 1.71). Cardiovascular-related deaths were reported in 20 (0.7%) and 25 (0.9%) of patients in the colchicine and placebo groups, respectively (HR = 0.80; 95% CI, 0.44 to 1.44). Noncardiovascular-related deaths were reported in 53 (1.9%) and 35 (1.3%) of patients in the colchicine and placebo groups, respectively (HR = 1.51; 95% CI, 0.99 to 2.31). The vital status of 1 patient in the placebo group who was lost to follow-up was unknown.
A total of 4 patients (1.4%) died in the colchicine group and 10 patients (4.0%) died in the control group of the LoDoCo study, which had a median follow-up duration of 36 months. In the control group, all deaths were either cardiovascular-related or presumed to have cardiovascular causes, whereas in the colchicine group, all deaths were from noncardiac causes. No patients were lost to follow-up in either treatment group.
Table 15: All-Cause Mortality (Intention-to-Treat Population) [Redacted]
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|---|---|---|---|
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
|||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| | |||||||||||||||||| |
Note: Table 15 has been redacted.
Source: Clinical Study Report for COLCOT study,4 Tong et al. (2020),5 Nidorf et al. (2020),6 and Nidorf et al. (2013).7
Cardiovascular Events
In the COLCOT study, 131 patients (5.5%) in the colchicine group and 170 patients (7.1%) in the placebo group experienced an adjudicated primary cardiovascular event of cardiovascular death, resuscitated cardiac arrest, acute myocardial infarction, stroke, or urgent revascularization. The unadjusted HR was 0.77 (95% CI, 0.61 to 0.96; P = 0.02) for colchicine versus placebo (Table 16). A Kaplan–Meier plot of the primary adjudicated cardiovascular events in the COLCOT study is shown in Appendix 3, Figure 11.
In the COLCOT study, concordance between suspected cardiovascular events and adjudicated events was lowest for stroke (26 of 31 events, 84%), and ranged from 90% for urgent hospitalization for angina requiring revascularization to 100% for death and resuscitated cardiac arrest. In general, the sensitivity analyses for the primary composite outcome showed consistent results with the unadjusted Cox model used in the primary analysis.
Of the primary composite events, myocardial infarction was reported most frequently (3.8% versus 4.1%) followed by urgent hospitalization for angina requiring coronary revascularization (1.1% versus 2.1% in the colchicine and placebo groups, respectively) (Table 16). When each component of the composite was analyzed separately, only the time to stroke or time to urgent revascularization reported 95% CIs that excluded the null. Because these analyses were not controlled for type I error, the time to stroke (HR = 0.26; 95% CI, 0.10 to 0.70; P = 0.01) and the time to urgent revascularization (HR = 0.50; 95% CI, 0.31 to 0.81; P = 0.005) should be considered as supportive evidence for the effect of colchicine in the overall population. The secondary outcome of time to first event of cardiovascular death, resuscitated cardiac arrest, acute myocardial infarction, or stroke reported an HR of 0.85 (95% CI, 0.66 to 1.10; P = 0.22). When the time to event for all coronary revascularization procedures was analyzed, the HR was 0.81 (95% CI, 0.64 to 1.02; P = 0.067).
In the analysis of first and recurrent primary cardiovascular events, a total of 154 events were reporting in the colchicine group compared with 223 events in the placebo group, with a rate ratio of 0.66 (95% CI, 0.51 to 0.86) (Table 16). As the type I error rate was not controlled for the secondary outcomes in the COLCOT trial, this data should be interpreted as supportive evidence for the effect of colchicine in the overall population.
Table 16: Efficacy Outcomes — COLCOT Study (Intention-to-Treat Population)
Outcome | COLCOT (MI) | |||
|---|---|---|---|---|
Colchicine N = 2,366 | Placebo N = 2,379 | Treatment effect | P value | |
Primary composite outcome and its componentsa | n (%) | n (%) | HR (95% CI) | P value |
Time to first primary composite end point b | 131 (5.5) | 170 (7.1) | 0.77 (0.61 to 0.96) | 0.02 |
CV death | 20 (0.8) | 24 (1.0) | 0.84 (0.46 to 1.52) | 0.56c |
Resuscitated cardiac arrest | 5 (0.2) | 6 (0.3) | 0.83 (0.25 to 2.73) | 0.76c |
Acute MI | 89 (3.8) | 98 (4.1) | 0.91 (0.68 to 1.21) | 0.52c |
Stroke | 5 (0.2) | 19 (0.8) | 0.26 (0.10 to 0.70) | 0.01c |
Urgent hospitalization for angina requiring coronary revascularization | 25 (1.1) | 50 (2.1) | 0.50 (0.31 to 0.81) | 0.005c |
Secondary or exploratory time-to-event outcomesa | n (%) | n (%) | HR (95% CI) | P value |
Time to first event of CV death, resuscitated cardiac arrest, acute MI, or stroke | 111 (4.7) | 130 (5.5) | 0.85 (0.66 to 1.10) | 0.22c |
Time to all coronary revascularization procedures | 132 (5.6) | 164 (6.9) | 0.81 (0.64 to 1.02) | 0.067c |
Recurrent CV eventsd | n events (PYs) | n events (PYs) | Rate ratio (95% CI) | P value |
Total number of primary end point events (first and recurrent) | 154 (4,412.4) | 223 (4,421.7) | 0.66 (0.51 to 0.86) | 0.002c |
CI = confidence interval; CV = cardiovascular; HR = hazard ratio; MI = myocardial infarction; PY = patient-year.
aCox proportional hazard model (unadjusted); log-rank test; intention-to-treat population.
bTime to first occurrence of CV death, resuscitated cardiac arrest, acute MI, stroke, urgent hospitalization for angina requiring coronary revascularization. Median follow-up duration was 22.6 months. P value required to infer statistical significance was 0.049.
cP value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
dNegative binomial model.
Source: Clinical Study Report for COLCOT trial.4
In the COPS study, 24 patients in the colchicine group (6.1%) and 38 patients (9.5%) in the placebo group experienced a primary end point of either death, ACS (STEMI or non-STEMI and/or unstable angina), ischemia-driven urgent revascularization, or noncardioembolic ischemic stroke by 12 months (log-rank test P = 0.09). The estimated HR for the time to first adjudicated primary end point was 0.65 (95% CI, 0.38 to 1.09) for colchicine versus placebo. In the colchicine and placebo groups, respectively, 2.0% and 0.3% died, 2.8% and 5.0% experienced an ACS event, 0.5% and 1.3% experienced a stroke, and 0.8% and 3.0% required urgent revascularization over 12 months (Appendix 3, Figure 12). The findings were comparable across the sensitivity analyses, as well as the post hoc analysis conducted after 400 days of follow-up, which reported that 24 patients (6.1%) versus 41 patients (10.3%) in the colchicine and placebo groups, respectively, experienced a primary composite outcomes (HR = 0.60; 95% CI, 0.36 to 1.01; log-rank test P = 0.047, not adjusted for type I error rate).
In the LoDoCo2 study, the primary composite outcome was time to first occurrence of cardiovascular death, nonprocedural myocardial infarction, ischemic stroke, or ischemia-driven revascularization. The status of the primary end point was known for all but 1 patient (median follow-up of 28.6 months; IQR = 20.5 to 44.4). In the colchicine group, 187 patients (6.8%) experienced a primary end point compared with 264 patients (9.6%) in the placebo group, with a cause-specific HR of 0.69 (95% CI, 0.57 to 0.83; P < 0.001) (Figure 5).
Nidorf et al. (2020)6 analyzed different combinations of the primary cardiovascular events as secondary outcomes, which were part of the hierarchical statistical testing procedure (Figure 5). All 3 composite analyses showed differences that favoured colchicine versus placebo, with an HR and 95% CI that were consistent with the primary end point. Also included in the statistical hierarchy were the individual components of the primary composite end point. Of these, the time to ischemia-driven coronary revascularization (1.8% versus 2.4%; HR = 0.75; 95% CI, 0.60 to 0.94; P = 0.01) and time to myocardial infarction (1.1% versus 1.5%; HR = 0.70; 95% CI, 0.53 to 0.93, P = 0.01) showed statistical differences favouring colchicine versus placebo. Statistical testing was stopped after the analysis of the time to ischemic stroke resulted in a 95% CI that included the null (0.2% versus 0.3% for colchicine versus placebo (HR = 0.66; 95% CI, 0.35 to 1.25; P = 0.20).
Figure 5: Efficacy Outcomes — LoDoCo2 Study (CAD Population, ITT analysis)
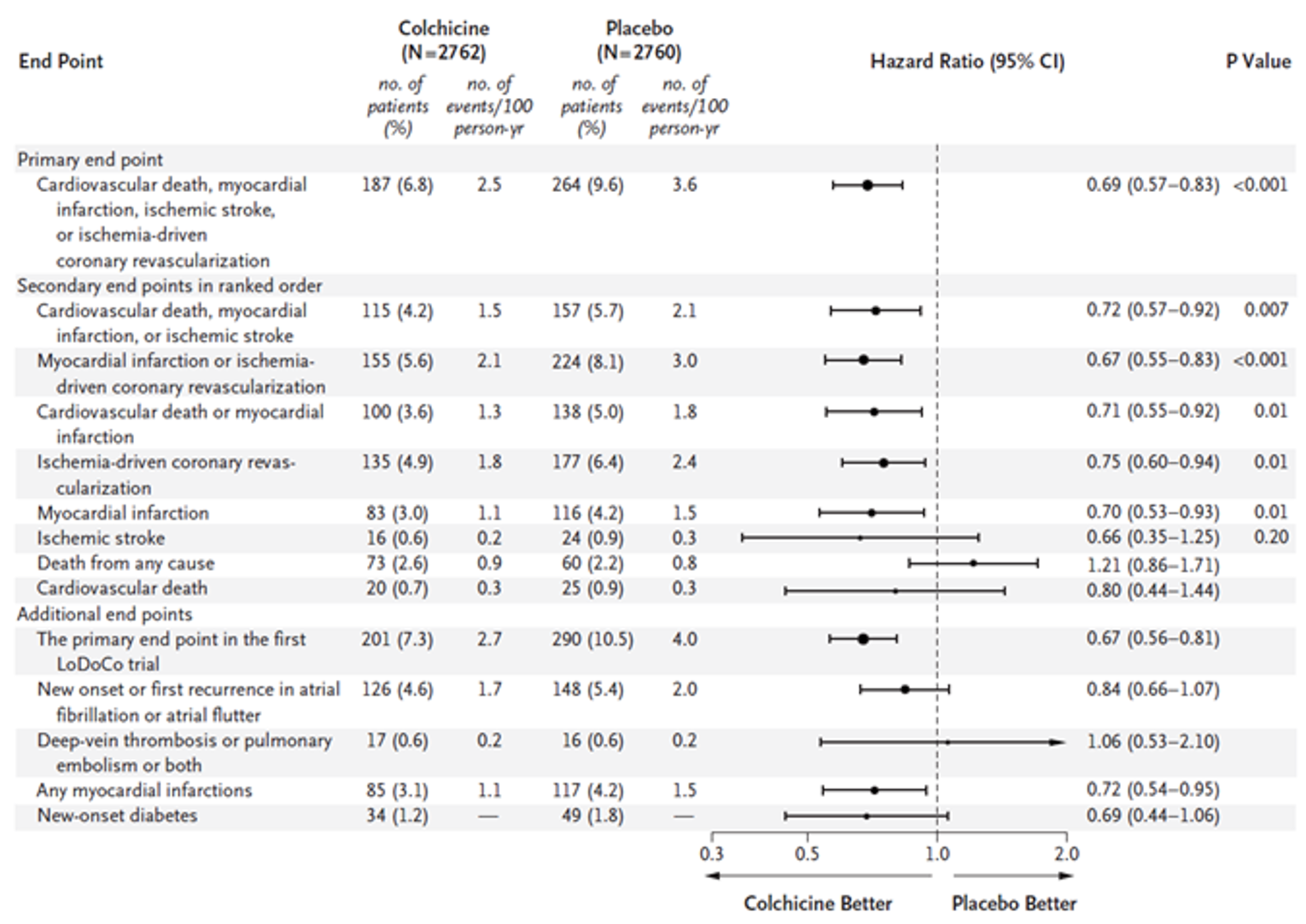
CAD = coronary artery disease; CI = confidence interval; ITT = intention-to-treat, no = number; yr = year.
Note: The cause-specific hazard ratios were estimated from a Cox proportional hazards regression analysis with death from noncardiovascular causes or death from any cause as a competing risk event. Myocardial infarction refers to spontaneous (nonprocedural) myocardial infarction. The primary end point in the first low-dose colchicine (LoDoCo) trial was a composite of sudden cardiac death, nonfatal out-of-hospital cardiac arrest, acute coronary syndrome (myocardial infarction or unstable angina irrespective of revascularization), or atherosclerotic ischemic stroke. Any myocardial infarctions refers to either spontaneous or procedural myocardial infarctions. The ratio for new-onset diabetes is presented as a cumulative incidence ratio because time-to-event data were not collected. The size of the data points is inversely proportional to the precision (the standard error of the log of the hazard ratios or cumulative incidence ratio) of the estimates, with larger data points representing more precise estimates. The testing hierarchy for statistical significance was broken at the end point of ischemic stroke.
Source: Nidorf et al. (2020)6 from N Engl J Med, Nidorf SM, Fiolet ATL, Mosterd A, et al., Colchicine in Patients with Chronic Coronary Disease., volume 383, Page No. 1838 to 1847. Copyright 2020 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
In the LoDoCo study, 15 patients (5.3%) in the colchicine group and 40 patients (16.0%) in the control group experienced a primary end point event of ACS, out-of-hospital cardiac arrest, or noncardioembolic stroke (HR = 0.33; 95% CI, 0.18 to 0.59; P < 0.001) (Appendix 3, Figure 13). The between-group differences were driven primarily by a reduction in ACS events for the colchicine versus the control group (4.6% versus 13.6%; HR = 0.33; 95% CI, 0.18 to 0.63; not adjusted for type I error rate).
Subgroup Data for Patients With Prior ACS
The subgroup of patients with a history of ACS included 4,658 patients in the LoDoCo2 study and reported an HR for the primary composite outcome of 0.67 (95% CI, 0.54 to 0.82). For patients with no history of ACS (N = 864) the HR was 0.81 (95% CI, 0.52 to 1.27).
For the LoDoCo study, patients with a history of acute myocardial infarction or unstable angina (N = 125) reported an HR of 0.29 (95% CI, 0.08 to 1.07) for the primary composite outcome, and those with no prior acute myocardial infarction or unstable angina (N = 407) had an HR of 0.33 (95% CI, 0.17 to 0.65).
Neither study stratified randomization by history of ACS, and it is unknown if the baseline characteristics were balanced between groups within the subgroups. The trials did not report the P value for the treatment-by-subgroup interaction term.
Hospitalization
No hospitalization data were reported in the COLCOT, LoDoCo2, and LoDoCo studies.
The COPS study reported data for the time to hospitalization for chest pain, defined as readmission to a medical ward with chest pain and a change in medical therapy, but without dynamic or new electrocardiogram changes or a rise in cardiac biomarkers. At 1 year, 7 patients in the colchicine group (1.8%) and 11 patients in the placebo group (2.8%) were hospitalized for chest pain (HR = 0.34; 95% CI, 0.04 to 3.31; P = 0.36) (Appendix 3, Figure 12).
Health-Related Quality of Life
None of the included studies reported data on the impact of colchicine on health-related quality of life.
Harms
Only those harms identified in the review protocol are reported below. Table 17 and Figure 6 provide detailed harms data.
Adverse Events
None of the studies reported the overall frequency of adverse events.
Serious Adverse Events
Serious adverse events were reported by 383 patients (16.4%) and 404 patients (17.2%) in the colchicine and placebo groups, respectively, in the COLCOT study. The most common serious adverse events were cardiac disorders, infections and infestations, gastrointestinal disorders, and neoplasms (Table 17).
The overall frequency of serious adverse events was not reported for the LoDoCo2, LoDoCo, or COPS study.
Withdrawals Due to Adverse Events
The COLCOT study did not report the overall number of patients who stopped treatment due to adverse events. Serious adverse events and treatment-related adverse events were the reasons for withdrawal for 1.2% and 5.7%, respectively, of the patients enrolled in the study (with a similar frequency per treatment group). In the colchicine group, 4.4% (102 patients) stopped treatment due to gastrointestinal adverse events compared with 3.8% (89 patients) in the placebo group (Table 17).
In the COPS study, 9% of patients in the colchicine group and 4% in the placebo group stopped treatment due to gastrointestinal intolerance. The overall frequency of withdrawals due to adverse events was not reported.
LoDoCo2 study reported that 3.4% of patients in each group stopped taking the study drug due to adverse events. No further details were provided.
In the LoDoCo study, 32 patients (11%) stopped colchicine therapy within the first 30 days due to gastrointestinal adverse events. Another 14 patients (5%) stopped colchicine at a later time point due to intestinal upset (7 patients, 2.5%), myalgia (2 patients, 0.9%), and 1 patient each due to myositis, rash, alopecia, itch, or peripheral neuritis.
Mortality
In the COLCOT study, 44 patients (1.9%) died in each treatment group (Table 17). For the colchicine group, the most common causes for death were general disorders of system organ class (11 patients, 0.5%), cardiac disorders (10 patients, 0.4%), neoplasms (8 patients, 0.3%) and infections or infestations (4 patients, 0.2%). The cause of death was not reported for the placebo group.
Eight patients (2.0%) in the colchicine group and 1 patient (0.3%) in the placebo group died during the COPS study. In the colchicine group, 3 deaths were cardiovascular-related (cardiac arrest, sudden death, or stroke), and 5 were noncardiovascular-related (2 cases of pneumonia, 2 of sepsis, and 1 of metastatic cancer with hemolytic anemia). One death in the placebo group was due to STEMI.
In the LoDoCo2 study, there were 53 noncardiovascular deaths in the colchicine group and 35 in the placebo group (1.9% versus 1.3%, respectively). The most common causes were cancer (26 and 22 patients in the colchicine and placebo groups, respectively), respiratory failure (9 and 4 patients) and infection (4 patients per group). Other causes reported in at least 2 patients were multi-organ failure, dementia, or accidental death.
In the LoDoCo study, 4 patients in the colchicine group died, all from noncardiovascular causes (no details reported). In the control group, 10 patients died, including 5 from presumed cardiac causes, 2 from cardiac arrest, 2 from cardiogenic shock following acute myocardial infarction, and 1 following bypass surgery.
Notable Harms
The frequency of gastrointestinal disorders was similar in the colchicine and placebo groups (17.0% versus 17.1%, respectively) in the COLCOT study. Other notable harms that were specified in the systematic review protocol (i.e., malignancy, anemia, leukopenia, neutropenia, thrombocytopenia) generally showed a similar frequency between groups (Table 17). A single serious adverse event of myopathy was reported in a patient who had received colchicine (for 8 days) in combination with high-dose statin treatment. The event occurred 3 months after stopping colchicine.
In the COPS study, gastrointestinal adverse events were reported by 23% of patients in the colchicine group and 21% in the placebo group. No patients in either group experienced myelosuppression. Myalgia was reported by 8 patients in the placebo group (2%) and 0 patients in the colchicine group, during the 1-year treatment period.
In the LoDoCo2 study, the diagnosis of cancer, hospitalization for infection or gastrointestinal reasons, and neutropenia were reported at similar frequencies in the colchicine and placebo groups (Figure 6). Myalgia was reported in 21.2% of patients in the colchicine group and 18.5% of those in the placebo group (data collected for patients in The Netherlands only).
No data were available from the LoDoCo study.
Table 17: Summary of Harms for the COLCOT Study (Safety Population)
Adverse eventa | Colchicine N = 2,330 | Placebo N = 2,346 |
|---|---|---|
Patients with ≥ 1 serious adverse event | ||
n (%) | 383 (16.4) | 404 (17.2) |
Most common events by SOC, n (%) | ||
Cardiac disorders | 140 (6.0) | 154 (6.6) |
Infections and infestations | 51 (2.2) | 38 (1.6) |
Pneumonia | 21 (0.9) | 9 (0.4) |
Urinary tract infection | 6 (0.3) | 1 (0.0) |
Neoplasms benign, malignant, and unspecified | 47 (2.0) | 45 (1.9) |
Gastrointestinal disorders | 46 (2.0) | 36 (1.5) |
Gastrointestinal hemorrhage | 8 (0.3) | 4 (0.2) |
Patients who stopped treatment due to adverse events | ||
n (%) | NR | NR |
Reason for treatment discontinuation, n (%) | ||
Treatment-related adverse event | 133 (5.7) | 132 (5.6) |
Serious adverse event | 27 (1.2) | 27 (1.2) |
Gastrointestinal events | 102 (4.4) | 89 (3.8) |
Deaths | ||
n (%) | 44 (1.9) | 44 (1.9) |
Most common causes of death by system organ class, n (%) | ||
General disorders and administration site conditions | 11 (0.5) | NR |
Cardiac disorders | 10 (0.4) | NR |
Neoplasms benign, malignant, and unspecified | 8 (0.3) | NR |
Infections and infestations | 4 (0.2) | NR |
Notable harms | ||
Gastrointestinal disorders by system organ class, n (%) | 396 (17.0) | 401 (17.1) |
Diarrhea | 225 (9.7) | 208 (8.9) |
Nausea | 43 (1.8) | 24 (1.0) |
Dyspepsia | 31 (1.3) | 32 (1.4) |
Abdominal pain | 28 (1.2) | 29 (1.2) |
Abdominal pain upper | 23 (1.0) | 23 (1.0) |
Constipation | 23 (1.0) | 22 (0.9) |
Malignancy | 43 (1.8) | 46 (2.0) |
Infections | NR | NR |
Serious adverse event: myalgia | 1 (0.0) | 2 (0.1) |
Serious adverse event: rhabdomyolysis | 1 (0.0) | 0 |
Anemia | 14 (0.6) | 10 (0.4) |
Leukopenia | 2 (0.1) | 3 (0.1) |
Neutropenia | 0 | 1 (0.0) |
Thrombocytopenia | 3 (0.1) | 7 (0.3) |
NR = not reported.
aMedian duration of study treatment was 19.6 months and follow-up was 22.6 months.
Source: Clinical Study Report for the COLCOT trial.4
Figure 6: Summary of Harms for LoDoCo2 Study (Intention-to-Treat Population)
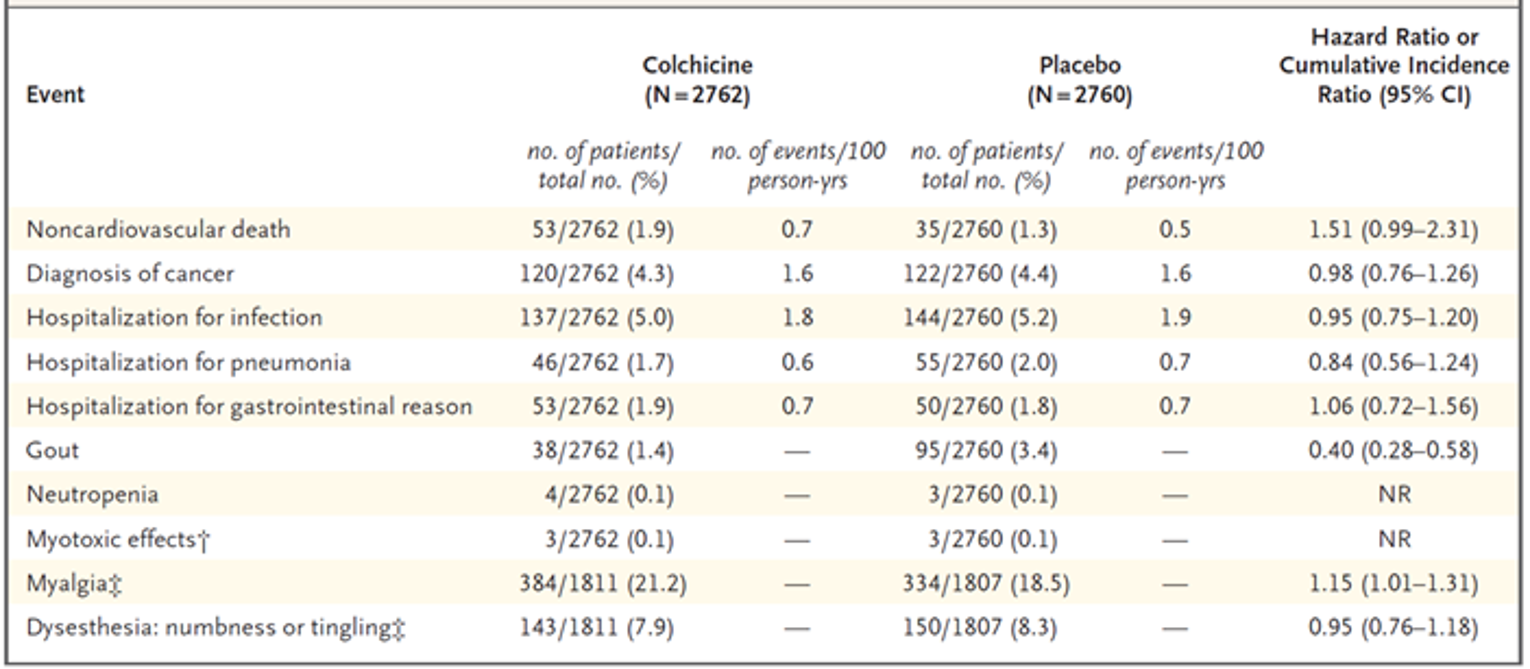
CI = confidence interval; yrs = years; NR = not reported.
* Hazard ratios are reported for noncardiovascular deaths, diagnoses of cancer, hospitalizations for infection, hospitalizations for pneumonia, and hospitalizations for gastrointestinal reasons; cumulative incidence ratios are reported for gout, myalgia, and dysesthesia because time-to-event data were not collected for these end points. Cumulative incidence ratios are not reported or neutropenia and myotoxic effects because of the low numbers of events.
† Rhabdomyolysis occurred in 1 patient in the colchicine group who had a full recovery.
‡ Data were collected for The Netherlands cohort only. Reporting of these adverse events was requested by the Medicines Evaluation Board in The Netherlands when the trial was expanded to include patients from that country.
Source: Nidorf et al. (2020)6 from N Engl J Med, Nidorf SM, Fiolet ATL, Mosterd A, et al., Colchicine in Patients with Chronic Coronary Disease. Volume 383, Page No. 1838 to 1847. Copyright © 2020 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Critical Appraisal
Internal Validity
COLCOT
Overall, the risk of bias for the COLCOT study was rated as low by the CADTH reviewer. The study used a computer-generated permuted block randomization schedule, stratified by site, and an interactive automated web response system to randomize patients and conceal allocation. A matched placebo was used to maintain blinding, and all potential cardiovascular end points were adjudicated by an independent blinded clinical-event committee that included cardiologists and neurologists.
The patient characteristics and use of secondary prevention medications appeared to be similar between groups at baseline, and efficacy analyses were run based on the ITT population, which included patients who were nonadherent to the study drug. The percentage of patients who discontinued the study was generally low and comparable between groups (5.9% in the colchicine group and 6.2% in the placebo group). This included 1.6% and 2.1% of patients in the colchicine and placebo groups, respectively, who were lost to follow-up, and 1.7% and 1.6%, respectively, who stopped study visits but whose survival status was known. Vital status data were missing for 23 patients (colchicine 13 patients, placebo 10 patients), which could potentially affect the findings of the all-cause mortality analysis.
The primary outcome was analyzed using a log-rank test and unadjusted Cox proportional hazards model. This analysis did not take into consideration competing risks and assumes that patients who continue to be followed have the same risk of future events as those who were censored or have dropped out, which may not be valid. Also, it is unclear if the authors assessed whether the proportional hazards assumption was met. One interim analysis was pre-planned in the protocol and the P value for the primary outcome was adjusted to control the type I error rate. Several secondary outcomes were pre-specified in the protocol; however, no statistical procedures were implemented to control the type I error rate. The individual components of the primary composite outcome and the analysis of recurrent cardiovascular events that reported a P value less than 0.05 should therefore be interpreted as supportive evidence only.
COPS
The risk of bias related to randomization and allocation concealment was assessed to be low for the COPS study, which used a stratified block randomization and a web response system to allocate patients to treatment groups. Few details were provided on how blinding was maintained, and the authors did not explicitly state that the placebo was identical in appearance to the active tablets; however, packing and distribution of the study drug were conducted by an independent pharmaceutical packaging company. The baseline characteristics of the enrolled patients appear to be balanced between groups. Patient follow-up was conducted by phone, creating the potential for reporting bias. However, primary physicians were also contacted, and hospital records examined, which may reduce the risk of bias. All cardiovascular events were adjudicated by an independent and blinded clinical-event committee that included 2 cardiologists.
The study was stopped early due to low enrolment, and the trial was likely underpowered as it only achieved 79% of the planned enrolment. Tong et al. (2020)5 stated that “very few” patients had complete data for the primary analysis (at 12 months), and it is unclear how missing data were handled. There was no information on censoring rules or how times to events were calculated. Because of the low completion rate at 1 year, the authors conducted a post hoc analysis at 400 days, which showed results that were similar to those of the primary analysis. The null hypothesis was tested based on a log-rank test, and the HR results reported are based on a sensitivity analysis that accounted for clustering of events within patients. The analysis of time to CV death was conducted post hoc, after unblinding.
There was excess mortality in the colchicine group; however, because the sample size was small and the follow-up duration was short (1 year), this may be a chance finding. Tong et al. stated the mortality data should be viewed with caution as the number of patients lost to follow-up (8 colchicine and 3 placebo patients) was similar to the number of deaths analyzed (8 colchicine and 1 placebo patient).
LoDoCo2
No major sources of bias were identified in the LoDoCo2 study. Patients were randomized using a computer-generated randomization algorithm that was stratified by country; however, the authors did not specify the methods used to conceal allocation. The study was double-blinded, with patients receiving either colchicine or a matched placebo. All patients received open-label colchicine during the run-in period, and some patients who had experienced adverse effects with colchicine may have inferred treatment allocation when switched to placebo. This is likely a minor source of unblinding, as any patients with significant intolerance to colchicine were withdrawn before randomization. All end points were adjudicated by a blinded clinical-event committee (no details were provided on its composition). The baseline characteristics of patients appeared to be balanced between groups and only 1 patient was lost to follow-up.
The statistical analysis was based on the cause-specific HR, which takes into consideration competing risks in the time-to-event analyses. Moreover, the study was based on the ITT population and included data from patients who stopped treatment early. LoDoCo2 was the only trial to control for the type I error rate for secondary outcomes, which included the individual components of the primary composite outcome.
Of note, the protocol for the LoDoCo2 trial underwent numerous changes: study sites from the Netherlands were added, the primary and secondary outcomes were altered, and the statistical analysis plan was changed. The authors stated that all changes were complete before the database was unlocked and the data were unblinded; thus, the risk of bias may be considered low.
LoDoCo
The risk of bias related to randomization and allocation concealment was unclear in the LoDoCo trial. A research assistant who was not involved in patient care conducted the randomization using a computer-generated sequence; however, no information was provided on how the process was conducted. The protocol allowed the research assistant to assign patients to the colchicine group to replace those with early intolerance, which is why the colchicine group was 32 patients larger than the no-treatment group. Although the study’s authors state that this process did not bias the randomization, the 2 groups were handled differently and replacement of patients was nonrandom, leaving the potential for bias. Little information was reported on the baseline characteristics of the patients, but these data showed some imbalances between groups, which may be related to the sample size as well as potential flaws in the randomization.
The study was open-label, and both patients and investigators were aware of treatment allocation. Patients in the colchicine group were given a prescription for colchicine, and the control group received no treatment. Because treatment allocation was known, there was the potential for bias in performance, outcome ascertainment, and reporting. Outcomes were adjudicated by a blinded reviewer, but no details were provided on how blinding was maintained. There may be some gaps in the outcome data as the study had no scheduled follow-up visits, but relied instead on routine clinic visits, unplanned hospitalization, and the final telephone contact at the end of the study to collect study data.
The efficacy analyses were based on the ITT population, and those patients who stopped treatment early were included. The authors stated that all patients were followed for at least 24 months, with no patients lost to follow-up. The Cox proportional hazards model did not take into consideration competing risks (e.g., noncardiovascular deaths) and no sensitivity analyses were run to test the potential impact of these events.
All Included Studies
The primary outcome in all trials was based on a composite of major cardiovascular events, which varied across trials. According to the clinical experts consulted, the trials used standard definitions of these cardiovascular events, and any differences in outcome definitions between the 2 pivotal trials were considered minor. Events were adjudicated by a blinded clinician (in LoDoCo) or clinical-event committee (in COLCOT, LoDoCo2, and COPS), which would be expected to improve the objectivity of outcome assessments. Although CADTH did not receive any input from patient groups as to which outcomes were most important to patients, the experts agreed that the outcomes included in the composite end points were clinically relevant. It should be noted that not all components were of equal importance, with revascularization rated as the least important by the experts, and cardiovascular mortality the most important. Because the trials were designed and powered to test for differences in the composite end point, not the individual components or all-cause mortality, these data should be interpreted with caution and consider that the type I error rate had not been controlled in 3 of the 4 studies.
None of the trials reported data on health-related quality of life, and limited data were available on hospitalizations.
The reporting of safety data was poor in all trials and not all potentially relevant adverse events were collected or reported. In the LoDoCo study, only data on withdrawals due to adverse events were reported for the colchicine group, and reporting may be biased by knowledge of treatment allocation. Moreover, the safety data were limited by the sample size and study duration of the trials, which may have been insufficient to detect infrequent adverse events or those with a longer lag time.
External Validity
The patients enrolled in the colchicine studies were an average of 60 to 65 years of age and predominantly male (> 80%). The race of the participants was not reported for 3 studies but, based on the countries where these trials were conducted (Australia and The Netherlands, which are predominantly White), and the demographic data reported in the COLCOT study, it is unlikely that the trials reflect the racial and ethnic diversity of the Canadian population. The 2 pivotal trials did not report any data on the patients excluded during study screening, and 41% to 63% of patients in the other 2 trials were excluded during this phase. In addition, the pivotal trials excluded patients with more severe heart failure, valvular heart disease, or prior coronary bypass graft, as well as those with renal or hepatic impairment. As a result, the findings may not be generalizable to these patients. Overall, the clinical experts identified no major issues that may affect the external validity of the trials, and the baseline characteristics of the patients enrolled appeared to be similar to those of the Canadian population with coronary artery disease. The exception was the proportion of smokers, which was higher in the COLCOT and COPS studies than in Canada. According to the clinical experts, the proportion of patients receiving antiplatelet and lipid-lowering drugs, beta-blockers, and renin-angiotensin inhibitors was high and generally similar to the Canadian situation, which suggests the patients were well managed in terms of secondary prevention therapies.
Of note, the LoDoCo2 study enrolled an enriched population of patients who were tolerant and adherent to colchicine treatment. During the run-in period 15% of patients were excluded, and the observed treatment effects may overestimate the effects observed in an unselected population.
The LoDoCo study ended in 2012 and, although not explicitly stated, it appears to be a single-centre study, which may limit its generalizability to Canadian patients. Other issues include the use of twice-daily dosing of colchicine in the first month of the COPS study, which was not consistent with the Health Canada–approved dose.
Indirect Evidence
No indirect treatment comparisons were submitted by the sponsor. CADTH conducted a literature search to identify any indirect comparisons that met the population, intervention, comparator, and outcome criteria listed in the systematic review protocol (Table 5). A focused literature search for indirect comparisons dealing with coronary artery disease was run in MEDLINE All (1946–) on June 25, 2021. No limits were applied to the search. A single researcher screened the results, and no relevant indirect comparisons were identified.
Other Relevant Evidence
No long-term extension studies or other studies were included in the sponsor’s submission to CADTH to address important gaps in the evidence included in the systematic review.
Discussion
Summary of Available Evidence
Four RCTs met the inclusion criteria for the systematic review, including 3 double-blind placebo-controlled studies (COLCOT, COPS, LoDoCo2) and 1 open-label, observer-blinded trial (LoDoCo). The trials enrolled adults with acute myocardial infarction (COLCOT), ACS (COPS), or stable coronary artery disease (LoDoCo2 and LoDoCo), and had sample sizes that ranged from 532 to 5,522 patients. Patients received colchicine 0.5 mg daily versus placebo or no treatment as add-on therapy to standard secondary prevention therapies. In the LoDoCo2 study, all patients received colchicine during a 1-month run-in period and those who were tolerant of and adherent to therapy were randomized. The primary outcome in all trials was based on the time to first occurrence of a composite outcome that included several major cardiovascular events. Although the end points included in the primary composite end point varied across trials, the clinical experts consulted stated that the trials used standard definitions, and any differences in outcome definitions between the 2 pivotal trials were considered minor. The median follow-up duration ranged from 1 to 3 years.
The mean age of enrolled patients ranged from 59.7 years (SD = 10.2) to 67 years (SD = 9.2), and 78% to 89% of patients per treatment group were male. Approximately half of the patients enrolled had a history of hypertension (50% to 52%), 18% to 33% had diabetes, and 4% to 37% were smokers. In the LoDoCo2 and LoDoCo studies, 84% and 24% of patients, respectively, had a history of ACS.
No indirect treatment comparisons or other relevant studies were identified for inclusion in this review.
Interpretation of Results
Efficacy
Two pivotal trials that enrolled patients with myocardial infarction (COLCOT) or stable coronary artery disease (LoDoCo2, 84% with a history of ACS), showed statistically and clinically important differences in the time to first occurrence of adjudicated major cardiovascular events favouring colchicine as add-on therapy relative to placebo. In both studies, myocardial infarction and revascularization procedures were the most frequently reported of the primary events, with resuscitated cardiac arrest, stroke, and cardiovascular deaths reported less frequently. The direction of the treatment effects for the individual components of the primary composite outcomes favoured colchicine versus placebo in both trials, but with a 95% CI that did not consistently exclude the null. In the LoDoCo2 study, the between-group differences were statistically significant for the time to myocardial infarction, or ischemia-driven revascularization, but not for the time to stroke or CV death. In the COLCOT study, the between-groups differences were greatest for the time to urgent revascularization or stroke, but there was no control of the type I error rate for secondary outcomes, and these analyses with P values less than 0.05 should be interpreted as supportive evidence only. The analysis of recurrent events, which showed fewer total primary cardiovascular events occurred in the colchicine group compared with the placebo group (rate ratio = 0.66; 95% CI, 0.51 to 0.86), must also be interpreted as supportive evidence due to the lack of control of the type I error rate. It should be noted that these studies were not powered to detect differences between groups in the individual outcomes included in the composite, and, although the trends consistently favoured colchicine, it is unclear if all end points are affected equally by treatment. Also, the experts consulted by CADTH indicated that not all composite end points are of equal importance to patients. A significant reduction in revascularization, while important from a health care resource use perspective, may be considered of lesser relevance to patients than death, potentially disabling stroke, or myocardial infarction. These differences in clinical importance of the end points should be considered when interpreting the results of the composite outcomes.
Two other non-pivotal trials, COPS and LoDoCo, were included in the sponsor’s submission for colchicine. The COPS study, which enrolled patients who were hospitalized for ACS, showed no statistically significant difference between colchicine and placebo for the primary cardiovascular outcome. This trial had several limitations, including a limited sample size and lack of statistical power, as randomization was stopped early before the planned sample size was accrued. The authors state that the trial was stopped early due to slow recruitment. Other limitations include poor reporting of methods to maintain blinding, possible reporting bias from patient-reported outcome data collected by telephone, and post hoc analysis of cardiovascular mortality. In addition, follow-up was incomplete for the primary analysis that was planned for 365 days after randomization, with the authors stating that they had complete data on “very few” patients at that time point.
The LoDoCo study reported a statistically significant and clinically important difference favouring colchicine plus standard of care versus standard of care in the time to the composite end point of ACS, out-of-hospital cardiac arrest, or noncardioembolic ischemic stroke. All components of the composite showed point estimates that favoured colchicine but there were relatively few strokes or cardiac arrest events compared to ACS events. Although this was an open-label study, the outcome assessor was blinded to treatment allocation. However, the study did not describe the methods used to ensure blinding of clinical data that was collected from routine health care visits, unplanned hospitalizations, and telephone contact with the patients. Considering the sample size (N = 532), potential bias in the randomization process, and baseline differences in the proportion of patients with diabetes, prior revascularization procedures, and some secondary prevention drug therapies, it is unclear if all prognostic factors and effect modifiers were balanced between the groups.
All-cause mortality was a secondary efficacy outcome in 3 studies; however, only in the LoDoCo2 trial was this outcome included in a hierarchical statistical analysis procedure to control the type I error rate. The percentage of deaths was similar in both treatment groups in the COLCOT study (1.8%), but in the LodoCo2 trial, 2.6% versus 2.2% of patients in the colchicine and placebo groups, respectively, died. (HR = 1.21; 95% CI, 0.86 to 1.71), and in the COPS study 2.0% versus 0.3% of colchicine versus placebo-treated patients died (HR = 8.20; 95% CI, 1.03 to 65.61). In all trials the frequency of noncardiovascular deaths was numerically higher in the colchicine groups than in the placebo groups. Although these data suggest possible excess noncardiovascular mortality with colchicine, it should be noted that none of the trials were designed or powered to test for differences between groups in mortality, and the implication of this potential signal is therefore unclear.
None of the trials reported data on health-related quality of life, and limited data were available from the COPS study on hospitalization for chest pain. Trial duration ranged from 1 to 3 years, with pivotal trials reporting a median follow-up duration of 22.6 and 28.6 months. The experts indicated that a longer follow-up would have been preferable for this chronic and progressive condition.
With regard to external validity, LoDoCo2 enrolled an enriched population tolerant of and adherent to colchicine, and this may overestimate the treatment effects in an unselected patient population. According to the clinical experts, the proportion of patients receiving antiplatelet and lipid-lowering drugs, beta-blockers, and renin-angiotensin inhibitors was high, suggesting the patients were well managed in terms of secondary prevention therapies. Although the enrolled patients may not reflect the gender, racial, or ethnic diversity of the Canadian population, the experts had no major concerns with the generalizability of the study populations.
Harms
Overall, reporting of harms data was poor in all studies. No trial collected data on the overall frequency of adverse events, and only 1 study reported data on the number of patients who experienced at least 1 serious adverse event (16% to 17% per group). All trials were selective in collecting and reporting harms data, in most cases focusing on events that were deemed to be treatment-related.
The overall frequency of gastrointestinal adverse effects was 17% per treatment group in the COLCOT study and 21% to 23% of patients in the COPS study. Gastrointestinal adverse effects were the reason for treatment discontinuation for 4% of colchicine-treated patients in the COLCOT study, 9% in the COPS study, and 14% in the LoDoCo study. During the run-in period of the LoDoCo2 study, where all patients received colchicine, 9% withdrew due to intolerance and another 3% of patients per group stopped treatment during the double-blind phase.
Limited data were available on the adverse events of interest listed in this review’s protocol. Generally, the frequency of neoplasms and serious infections appeared to be similar between groups in the COLCOT and LoDoCo2 studies. Myalgia data were collected for a subset of patients in the LoDoCo2 study (The Netherlands only) and were reported in 21.2% of patients in the colchicine group compared with 18.5% of patients in the placebo group.
Colchicine has a narrow therapeutic window and can be fatal in overdoses.2 It is known to interact with several other drugs, and patients with impaired renal or hepatic dysfunction may be at increased risk of toxicity.2 The safety data available in patients with coronary artery disease was limited by the sample size and study duration of the key trials, which may have been insufficient to detect infrequent adverse events or those that take a longer time to develop. Moreover, the collection and reporting of adverse event data were incomplete. Although colchicine is an established drug that has been available in Canada for decades, uncertainty remains on its comparative longer-term safety in patients with coronary artery disease.
Conclusions
Colchicine, when used as add-on therapy to standard secondary prevention drugs, was associated with statistically significant and clinically important differences relative to placebo on the composite outcome of time to first occurrence of cardiovascular death, stroke, myocardial infarction, and urgent ischemia-driven revascularization in patients with a recent myocardial infarction, as well as those with stable coronary artery disease who had experienced a prior ACS event. Colchicine also showed statistically and clinically significant differences versus placebo in the time to myocardial infarction and the time to ischemia-driven revascularization in patients with stable coronary artery disease and a history of ACS. No conclusions about the impact of colchicine on the individual components of the primary composite end point in patients with a recent myocardial infarction can be drawn, as the COLCOT study was not designed to test for differences in these events.
No conclusions can be drawn on the impact of colchicine on health-related quality of life or hospitalization due to the lack of data, or on mortality because the trials were not designed or powered to test for differences between groups for this outcome. Gastrointestinal effects, which were common adverse events reported in the trials, may lead to treatment discontinuation in a subset of patients. The comparative evidence on safety was limited by the incomplete collection and reporting of adverse events, the sample size, and duration of the trials.
References
1.Heart disease in Canada: Highlights from the Canadian Chronic Disease Surveillance System. 2017: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/heart-disease-fact-sheet/heart-disease-factsheet-eng.pdf. Accessed 2020 Jul 23.
2.Myinfla (colchicine): 0.5 mg film-coated tablets [product monograph]. Montreal (QC): Pendopharm, Division of Pharmascience Inc; 2021 Aug 20.
3.Drug Reimbursement Review sponsor submission: Myinfla (colchcine), 0.5 mg film-coated tablets [internal sponsor's package]. Montreal (QC): Pendopharm, a division of Pharmascience Inc; 2021 Jun 10.
4.Clinical Study Report: MHIPS-003. Colchicine Cardiovascular Outcomes Trials (COLCOT) [internal sponsor's report]. Montreal (QC): Montreal Heart Institute; 2020 Sep 9.
5.Tong DC, Quinn S, Nasis A, et al. Colchicine in Patients With Acute Coronary Syndrome: The Australian COPS Randomized Clinical Trial. Circulation. 2020;142(20):1890-1900. PubMed
6.Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med. 2020;383(19):1838-1847. PubMed
7.Nidorf SM, Eikelboom JW, Budgeon CA, Thompson PL. Low-dose colchicine for secondary prevention of cardiovascular disease. J Am Coll Cardiol. 2013;61(4):404-410. PubMed
8.Hennekens CH, Lopez-Sendon J. Overview of the prevention of cardiovascular disease events in those with established disease (secondary prevention) or at very high risk. Waltham (MA): UpToDate; 2021.
9.pms-Colchicine [product monograph]. Montreal (QC): Pharmascience Inc.; 2016 Jul 5: https://pdf.hres.ca/dpd_pm/00035611.PDF. Accessed 2021 Jun 29.
10.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
11.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Jun 15.
12.Tardif JC, Kouz S, Waters DD, et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N Engl J Med. 2019;381(26):2497-2505. PubMed
13.Nidorf SM, Fiolet ATL, Eikelboom JW, et al. The effect of low-dose colchicine in patients with stable coronary artery disease: The LoDoCo2 trial rationale, design, and baseline characteristics. Am Heart J. 2019;218:46-56. PubMed
14.Bhatt DL, Eagle KA, Ohman EM, et al. Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA. 2010;304(12):1350-1357. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: June 25, 2021
Alerts: Bi-weekly search updates until project completion
Search filters applied: randomized controlled trials; controlled clinical trials
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase); keyword (CDSR) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq=# | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
# Searches
exp Colchicine/
(colchi* or Myinfla* or Colchysat or colcin* or colcrys or colctab or colsaloid or condylon or goutnil or kolkicin or mitigare or gloperba or colgout or colrefuz or goutichine or kolkisin or tolchicine or "mpc 004" or mpc004 or nsc 757 or nsc757 or SML2Y3J35T).ti,ab,kf,ot,hw,rn,nm.
1 or 2
Acute Coronary Syndrome/
Myocardial Ischemia/
exp Coronary Disease/
exp Myocardial Infarction/
Plaque, Atherosclerotic/
exp Arteriosclerosis/
exp Angina Pectoris/
((coronary or isch?em* or heart) adj2 (disease* or syndrome*)).ti,ab,kf.
(atherosclerosis or atherothrombotic or atherosclerotic or atherothrombosis or arteriosclerotic or arteriosclerosis).ti,ab,kf.
(heart or myocardi* or cardiovascular or cardio-vascular or coronary or angina or cardiac or atrial).ti,kf.
or/4-13
3 and 14
15 use medall
*Colchicine/
*colchicine derivative/
(colchi* or Myinfla* or Colchysat or colcin* or colcrys or colctab or colsaloid or condylon or goutnil or kolkicin or mitigare or gloperba or colgout or colrefuz or goutichine or kolkisin or tolchicine or "mpc 004" or mpc004 or nsc 757 or nsc757).ti,ab,kw,dq.
or/17-19
exp coronary artery disease/
exp heart infarction/
exp angina pectoris/
ischemic heart disease/
((coronary or isch?em* or heart) adj2 (disease* or syndrome*)).ti,ab,kw,dq.
(atherosclerosis or atherothrombotic or atherosclerotic or atherothrombosis or arteriosclerotic or arteriosclerosis).ti,ab,kw,dq.
(heart or myocardi* or cardiovascular or cardio-vascular or coronary or angina or cardiac or atrial).ti,kw.
or/21-27
20 and 28
29 use oemezd
30 not (conference abstract or conference review).pt.
16 or 31
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
"Randomized Controlled Trial (topic)"/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
"Controlled Clinical Trial (topic)"/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf,kw.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf,kw.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf,kw.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf,kw.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(pragmatic study or pragmatic studies).ti,ab,hw,kf,kw.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf,kw.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(phase adj3 (III or "3") adj3 (study or studies or trial*)).ti,hw,kf,kw.
or/33-63
32 and 64
remove duplicates from 65
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- (Myinfla OR colchicine) AND (coronary OR heart OR myocardial OR cardiovascular OR angina OR cardiac OR atrial OR atherosclerosis OR atherothrombotic OR atherosclerotic OR atherothrombosis OR arteriosclerotic OR arteriosclerosis OR ischemic OR ischemia OR ischaemic OR ischaemia)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- (Myinfla OR colchicine) AND (coronary OR heart OR myocardial OR cardiovascular OR angina OR cardiac OR atrial OR atherosclerosis OR atherothrombotic OR atherosclerotic OR atherothrombosis OR arteriosclerotic OR arteriosclerosis OR ischemic OR ischemia OR ischaemic OR ischaemia)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- (Myinfla OR colchicine) AND (coronary OR heart OR myocardial OR cardiovascular OR angina OR cardiac OR atrial OR atherosclerosis OR atherothrombotic OR atherosclerotic OR atherothrombosis OR arteriosclerotic OR arteriosclerosis OR ischemic OR ischemia OR ischaemic OR ischaemia)]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- (Myinfla OR colchicine) AND (coronary OR heart OR myocardial OR cardiovascular OR angina OR cardiac OR atrial OR atherosclerosis OR atherothrombotic OR atherosclerotic OR atherothrombosis OR arteriosclerotic OR arteriosclerosis OR ischemic OR ischemia OR ischaemic OR ischaemia)]
Grey Literature
Search dates: June 14 to June 21, 2021
Keywords: Myinfla OR colchicine
Limits: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
Reference | Reason for exclusion |
|---|---|
Deftereos S, Giannopoulos G, Angelidis C, et al. Anti-Inflammatory Treatment With Colchicine in Acute Myocardial Infarction: A Pilot Study. Circulation. 2015;132(15):1395-1403. Deftereos S, Giannopoulos G, Raisakis K, et al. Colchicine treatment for the prevention of bare-metal stent restenosis in diabetic patients. J Am Coll Cardiol. 2013;61(16):1679-1685. O'Keefe JH, Jr., McCallister BD, Bateman TM, Kuhnlein DL, Ligon RW, Hartzler GO. Ineffectiveness of colchicine for the prevention of restenosis after coronary angioplasty. J Am Coll Cardiol. 1992;19(7):1597-1600. | Intervention |
Hennessy T, Soh L, Bowman M, et al. The Low Dose Colchicine after Myocardial Infarction (LoDoCo-MI) study: A pilot randomized placebo controlled trial of colchicine following acute myocardial infarction. Am Heart J. 2019;215:62-69. | Outcomes |
Deftereos S, Giannopoulos G, Panagopoulou V, et al. Anti-inflammatory treatment with colchicine in stable chronic heart failure: a prospective, randomized study. JACC Heart Fail. 2014;2(2):131-137. | Population, intervention |
Bouabdallaoui N, Tardif JC, Waters DD, et al. Time-to-treatment initiation of colchicine and cardiovascular outcomes after myocardial infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT). Eur Heart J. 2020;41(42):4092-4099. | Population |
Nidorf SM, Fiolet ATL, Eikelboom JW, et al. The effect of low-dose colchicine in patients with stable coronary artery disease: The LoDoCo2 trial rationale, design, and baseline characteristics. Am Heart J. 2019;218:46-56. | Study design |
Note: This table has not been copy-edited
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
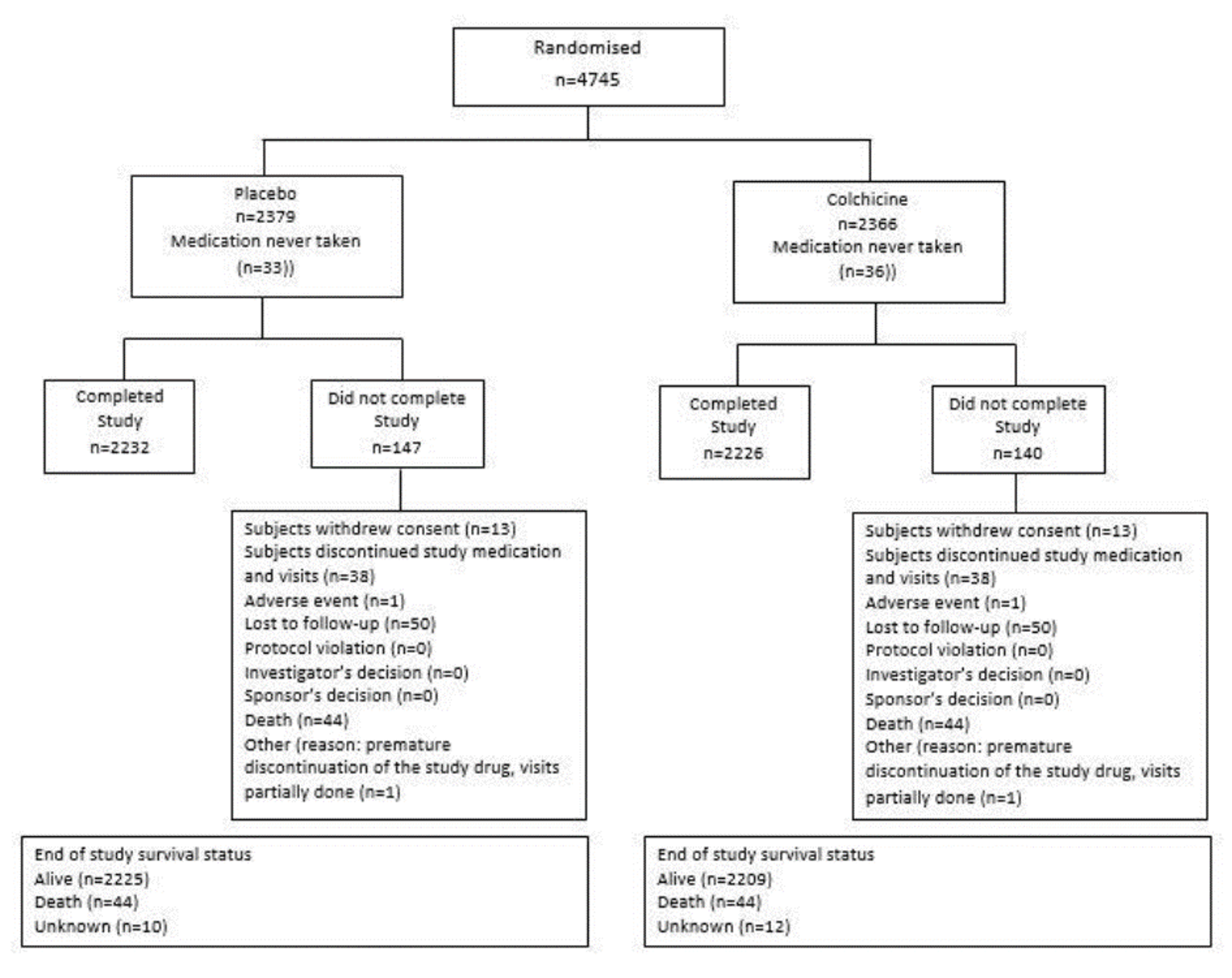
Figure 8: Disposition Flowchart for the COPS Study [Redacted]

Source: Tong et al. (2020).5
See Figure 1 in Tong DC, Quinn S, Nasis A, et al. Colchicine in Patients With Acute Coronary Syndrome: The Australian COPS Randomized Clinical Trial. Circulation. 2020;142(20):1890-1900. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.120.050771
Figure 9: Disposition Flowchart for the LoDoCo2 Study
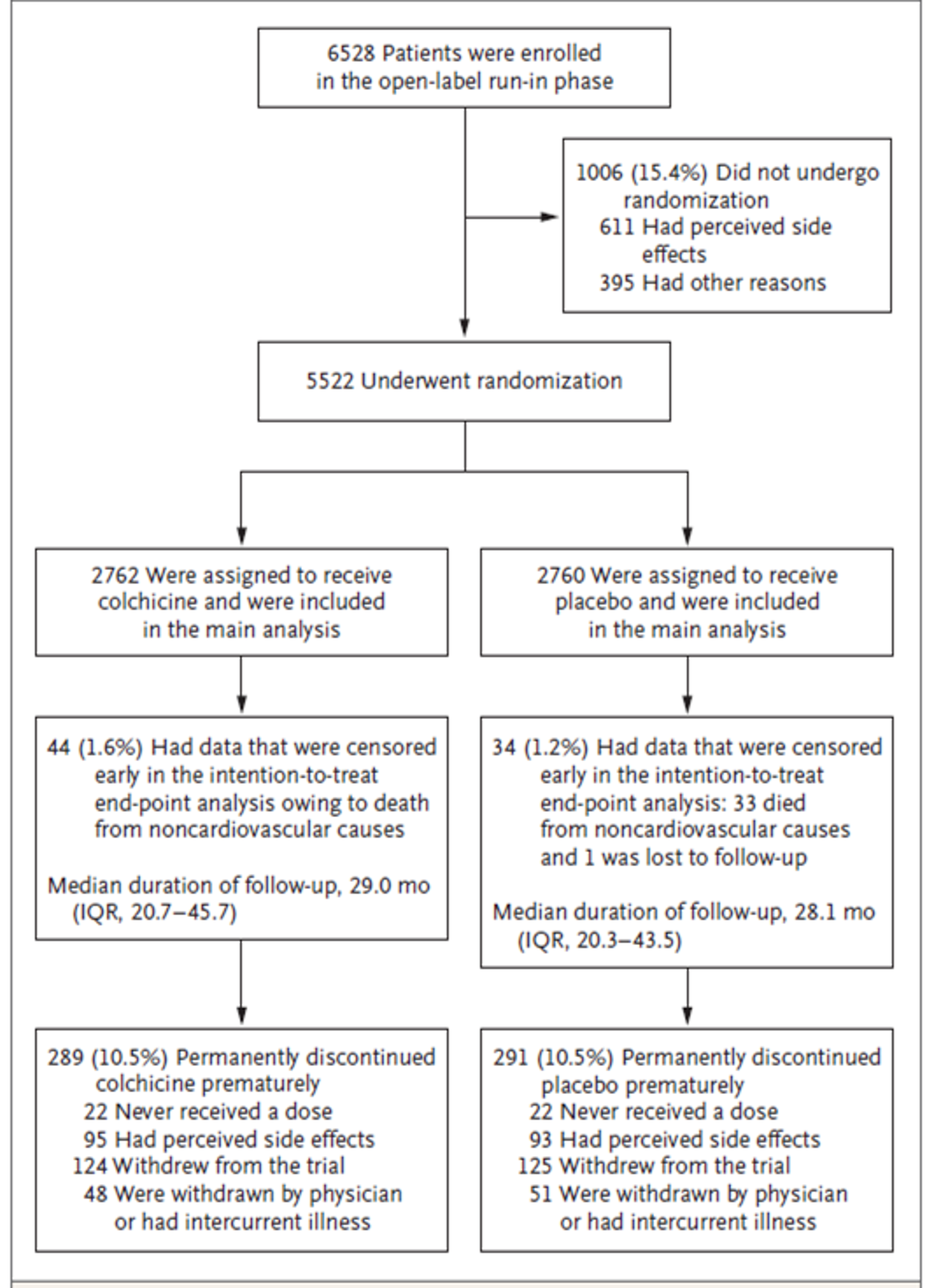
Source: Nidorf et al.(2020)6 from N Engl J Med, Nidorf SM, Fiolet ATL, Mosterd A, et al., Colchicine in Patients with Chronic Coronary Disease., Volume 383, Page No. 1838-1847. Copyright © 2020 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Figure 10: Disposition Flowchart for the LoDoCo Study
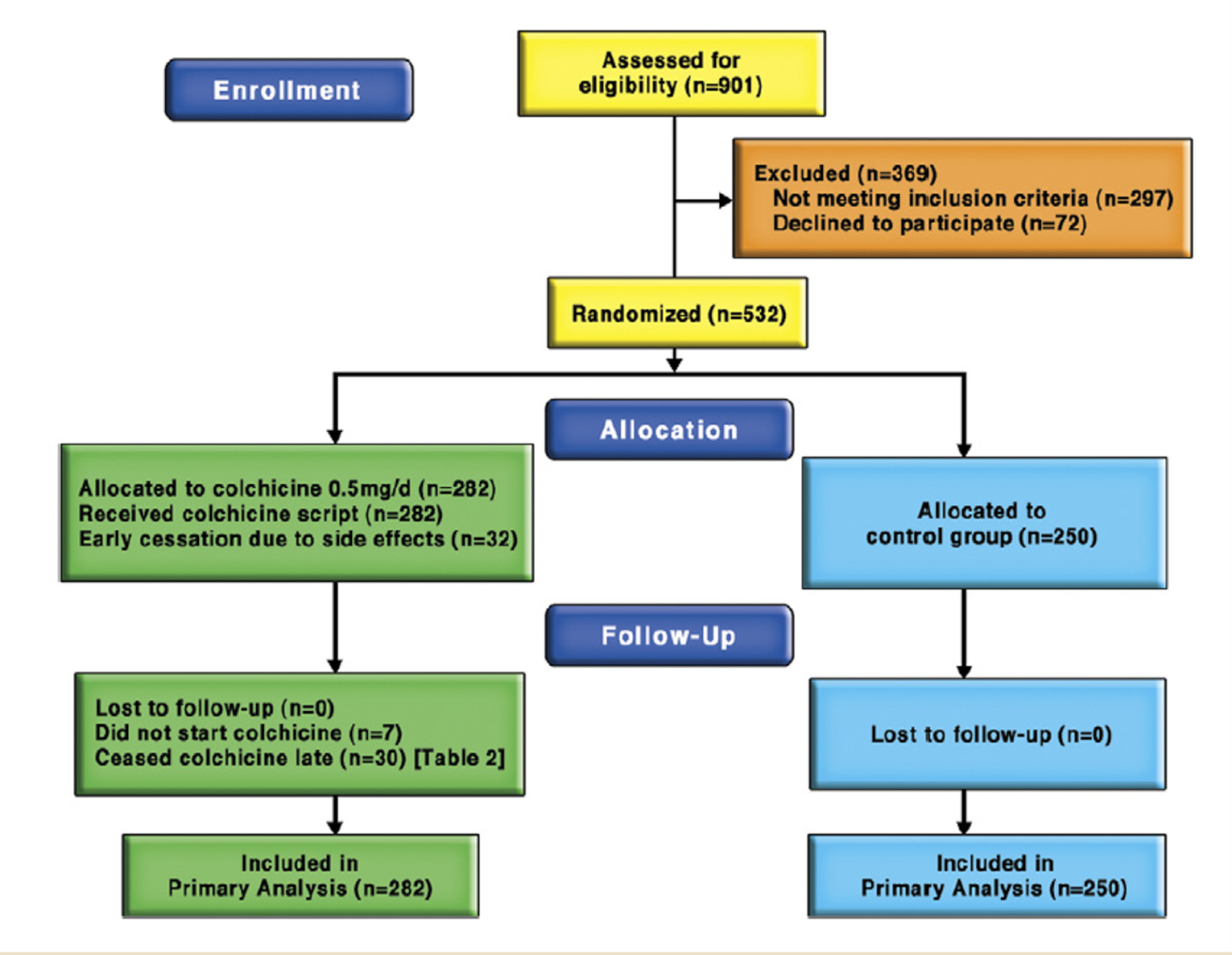
Source: Nidorf et al. (2013).7 Reprinted from J Am Coll Cardiol, Vol 61, Nidorf SM, Eikelboom JW, Budgeon CA, Thompson PL, Low-dose colchicine for secondary prevention of cardiovascular disease, Pages No. 404-410, Copyright 2013, with permission from Elsevier.
Figure 11: Kaplan-Meier Curve for the Primary Outcome — COLCOT Study (MI Population, ITT Analysis)
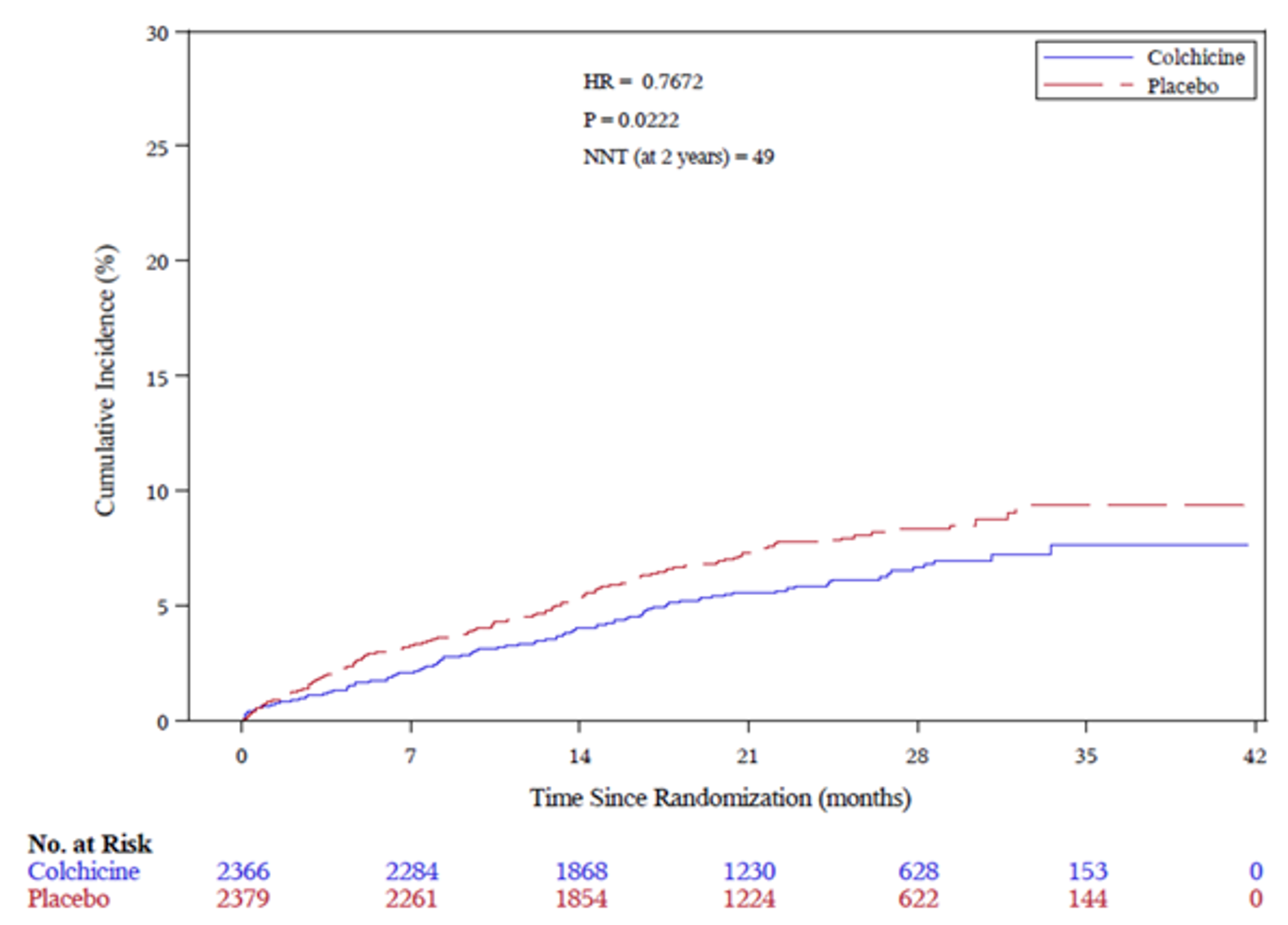
HR = hazard ratio; ITT = intention-to-treat; MI = myocardial infarction; NNT = number needed to treat.
Source: Clinical Study Report for COLCOT trial.4
Figure 12: Efficacy Outcomes — COPS Study (ACS Population, ITT Analysis) [Redacted]

Source: Tong et al. (2020).5
See Table 2 in Tong DC, Quinn S, Nasis A, et al. Colchicine in Patients With Acute Coronary Syndrome: The Australian COPS Randomized Clinical Trial. Circulation. 2020;142(20):1890-1900. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.120.050771
Figure 13: Efficacy Outcomes — LoDoCo Study (CAD Population, ITT Analysis)
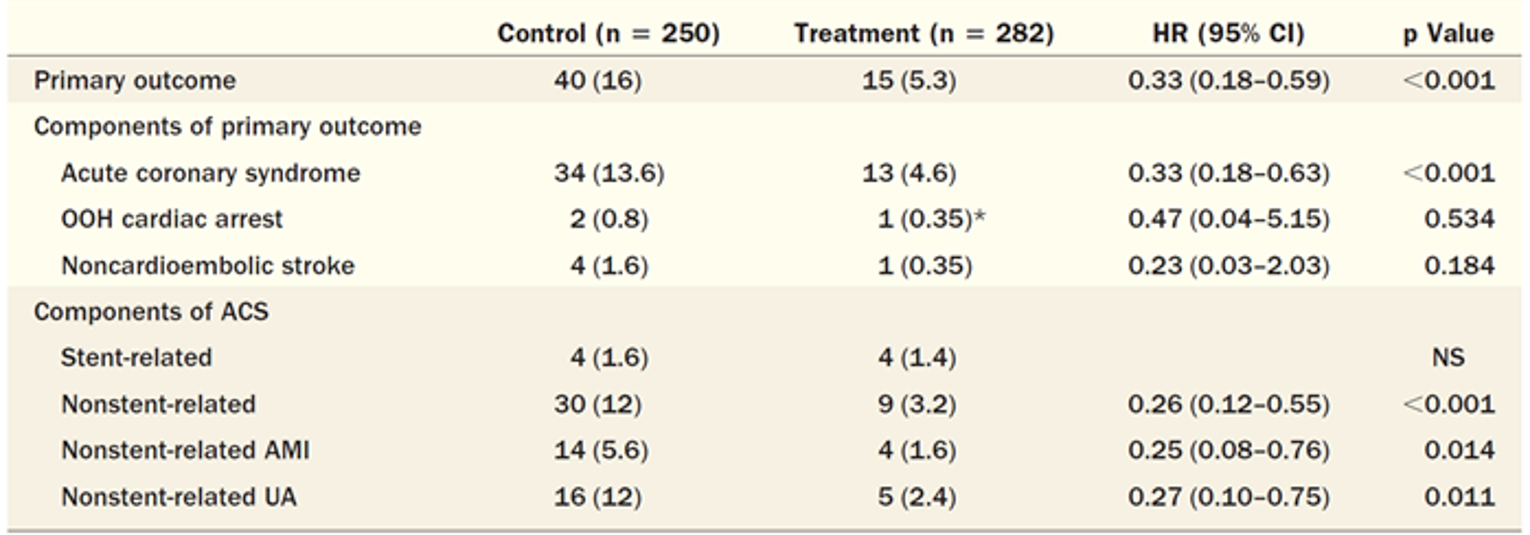
ACS = acute coronary syndrome; AMI = acute myocardial infarction; CAD = coronary artery disease; CI = confidence interval; HR = hazard ratio; ITT = intention-to-treat; UA = unstable angina.
Note: Values are n (%). The primary composite outcome was the time to first event of ACS, fatal or nonfatal out-of-hospital cardiac arrest, or noncardioembolic ischemic stroke. There was no control of type I error rate for the secondary outcomes.
* Nonfatal.
Source: Nidorf et al. (2013).7 Reprinted from J Am Coll Cardiol, Vol 61, Nidorf SM, Eikelboom JW, Budgeon CA, Thompson PL, Low-dose colchicine for secondary prevention of cardiovascular disease, Pages No. 404-410, Copyright 2013, with permission from Elsevier.
Pharmacoeconomic Review
Abbreviations
ASA
acetylsalicylic acid
BIA
budget impact analysis
CAD
coronary artery disease
CI
confidence interval
CV
cardiovascular
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
MI
myocardial infarction
QALY
quality-adjusted life-year
SOC
standard of care
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Colchicine (Myinfla), oral tablets |
Submitted price | Colchicine, 0.5 mg tablet: $0.50 |
Indication | For the reduction of atherothrombotic events in adult patients with existing coronary artery disease, in addition to standard therapies, including low-density lipoprotein cholesterol–lowering and antithrombotic drug treatment |
Health Canada approval status | Under review (pre-NOC) |
Health Canada review pathway | Priority review |
NOC date | August 23, 2021 |
Reimbursement request | As per indication |
Sponsor | Pendopharm, a division of Pharmascience Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients with existing CAD |
Treatment | Colchicine plus SOCa |
Comparator | SOCa |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs, life-years |
Time horizon | Lifetime (44 years) |
Key data sources | LoDoCo2 trial, COLCOT trial |
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
CAD = coronary artery disease; CV = cardiovascular; ICER = incremental cost-effectiveness ratio; MI = myocardial infarction; QALY = quality-adjusted life-year; SOC = standard of care.
aThe composition of SOC was not defined by the sponsor.
Conclusions
Evidence from the LoDoCo2 and COLCOT trials suggests that colchicine as an add-on to standard secondary prevention drugs is associated with a statistically significant difference in the time to first occurrence of a composite cardiovascular (CV) end point (i.e., CV death, stroke, myocardial infarction [MI], and ischemia-driven revascularization) relative to placebo plus standard of care (SOC), in patients with stable coronary artery disease (CAD), as well as those with CAD and a recent MI. In both pivotal trials used to inform the economic evaluation (i.e., LoDoCo2 and COLCOT), the time-to-event analyses of the individual CV events that made up the primary composite outcome produced point estimates that favoured colchicine over placebo. However, the benefit of colchicine was not statistically significant for all outcomes within the composite outcome in both trials. For example, while the risk of MI was significantly reduced in the LoDoCo2 trial (hazard ratio [HR] = 0.70; 95% confidence interval [CI], 0.53 to 0.93) among patients with stable CAD, there was no statistical difference in the risk of cardiovascular death (HR = 0.808; 95% CI, 0.44 to 1.44). Similarly, there was no difference in cardiovascular death between colchicine and placebo in the COLCOT study among patients with CAD and a recent MI (HR = 0.84; 95% CI, 0.46 to 1.52) and there was no significant difference in all-cause death between colchicine and placebo in either the LoDoCo2 or COLCOT trial. Without evidence from longer-term trials, any predicted survival benefit with the use of colchicine is highly uncertain. The long-term effects of colchicine relative to SOC and their impact on quality of life are also highly uncertain due to a lack of data.
Reanalyses undertaken by CADTH of the cost-effectiveness of colchicine plus SOC involved 2 patient subgroups that met the Health Canada indication of patients with stable CAD (informed by data from the LoDoCo2 trial) and patients with CAD and a recent MI (informed by data from the COLCOT trial). In the stable CAD subgroup, CADTH reanalyses adopted a shorter time horizon, treatment-specific distribution of CV events, and alternative assumptions about colchicine adherence. Changes in the reanalyses of the subgroup of patients with patients with CAD and a recent MI included assuming an annual cost of SOC and using an alternative baseline health-state utility value for patients with CAD and MI.
For the stable CAD subgroup, the CADTH base case resulted in an incremental cost-effectiveness ratio (ICER) of $100 per quality-adjusted life-year (QALY) gained for colchicine plus SOC compared to SOC alone. There was a 63% probability of colchicine plus SOC being considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY. Based on the mean ICER, no price reduction would be required; however, given the wide uncertainty around the probabilistic ICER, a price reduction may still be necessary. In a subgroup of patients with CAD and a recent MI, the ICER for colchicine plus SOC was $64,922 per QALY compared with SOC, with a 47% probability of colchicine plus SOC being cost-effective at a willingness-to-pay threshold of $50,000 per QALY. A 15% price reduction of colchicine would be needed for colchicine plus SOC to be considered cost-effective at a threshold of $50,000 per QALY in this subgroup. However, given the wide uncertainty around the probabilistic ICER, further price reductions may still be necessary for colchicine to be a cost-effective treatment in patients with CAD and a recent MI. In both patients with CAD and in patients with CAD and a recent MI, colchicine plus SOC was more costly and less effective (fewer QALYs) compared to SOC alone in 30% to 31% of simulations.
CADTH was unable to address the assumption that the comparative efficacy between colchicine and placebo observed in the pivotal trials would be consistent over the entire time horizon, which is unlikely. CADTH was also unable to address the assumption that patients are at risk of only 1 nonfatal CV event during their lifetime, which clinical experts consulted by CADTH for this review deemed inappropriate for both patients with stable CAD and patients with CAD and a recent MI. Given that CADTH was unable to address these limitations, the costs and health outcomes associated with the use of colchicine in both subgroups are uncertain. The impacts of these limitations are unknown, and as a result, the ICERs and price reductions estimated in this report are subject to a high degree of uncertainty.
Results for 2 subgroups (stable CAD and CAD plus MI), which are assumed to constitute the Health Canada indication (i.e., patients with CAD), were entirely driven by the LoDoCo2 and COLCOT trials. Due to the inclusion and exclusion criteria of these trials, the cost-effectiveness of colchicine in some additional subgroups of patients with CAD is unknown. For example, patients with unstable angina or severe heart failure would have been excluded from the LoDoCo2 trial, as only clinically stable patients (i.e., those with no cardiovascular-related hospital admission in the prior 6 months) were enrolled. As such, the cost-effectiveness estimates do not include all patients who would be eligible for colchicine under the full Health Canada indication.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
No patient or registered clinician input was received for this review.
Drug plan input received for this review included questions about the management of adverse events, particularly gastrointestinal adverse events (e.g., how these should be managed and whether colchicine should be discontinued as part of adverse event management). Drug plans were also interested in whether treatment should resume and under what time frame, should discontinuation occur. Questions about the generalizability of the patient populations included in the trial were posed, and the input noted that the studies’ patient populations were mostly male, White, and approximately 65 years old. Finally, given that there is already a 0.6 mg tablet of colchicine available, drug plans questioned whether clinicians may advise patients to take 0.6 mg daily instead of the 0.5 mg tablet given the expected difference in price.
Several of these concerns were addressed in the sponsor’s model:
The sponsor included quality-of-life decrements associated with some adverse events (i.e., diarrhea, abdominal pain, hospitalization for infection and pneumonia, diagnosis of cancer, gout, myalgia, and dysesthesia). Costs related to these adverse events, with the exception of diarrhea and abdominal pain, were included.
The following concerns raised in stakeholder input could not be addressed:
CADTH could not incorporate treatment discontinuation and/or interruption due to the structure of the sponsor’s model.
CADTH was unable to address questions related to the generalizability of the LoDoCo2 and COLCOT trials to Canadian patients.
Economic Review
The current review is for colchicine (Myinfla) for patients with CAD.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
Colchicine is indicated for the reduction of atherothrombotic events in patients with existing CAD, in addition to standard therapies, including low-density lipoprotein cholesterol–lowering and antithrombotic drug treatment. The sponsor submitted a cost-utility analysis of colchicine as an add-on to current SOC compared to SOC alone in patients with stable CAD,1 which represents a portion of the Health Canada–indicated population. The cost-effectiveness of colchicine in patients with CAD and a recent MI was explored in scenario analyses. The modelled population for the sponsor’s base case (patients with stable CAD) was based on the LoDoCo2 trial, which randomized patients with CAD that had been stable for at least 6 months to either colchicine (0.5 mg daily) or placebo in addition to standard secondary prevention medications, with a median follow-up period of 29.0 months for patients receiving colchicine. The modelled population for the subgroup of patients with CAD and a recent MI (CAD plus MI) was based on the COLCOT trial, which randomized patients within 30 days of an MI to receive colchicine (0.5 mg daily) or placebo in addition to standard treatments (median follow-up: 22.6 months).
Colchicine is available as 0.5 mg tablets in bottles of 100 tablets. The recommended dosage of colchicine is 0.5 mg once daily.2 The submitted price of colchicine is $0.5000 per 0.5 mg tablet (annual per patient cost: $182.50).1 A definition of SOC was not provided by the sponsor, and no costs for SOC were included in the model.
The clinical outcomes of interest were life-years and QALYs. The economic analysis was undertaken from a Canadian publicly funded health care system perspective over a lifetime time horizon (stable CAD subgroup: 44 years; CAD plus MI subgroup: 49 years). Costs and health outcomes were discounted at an annual rate of 1.5%.
Model Structure
The sponsor submitted a Markov model with 5 health states: CV-event-free, nonfatal CV event, post-nonfatal CV event, death from fatal CV causes, and death from other causes (Appendix 3, Figure 3).3 Patients entered the model in the CV event–free state and were at risk of a nonfatal CV event (MI, stroke, resuscitated cardiac arrest, or coronary revascularization), CV death, or death from other causes. Patients who experienced a nonfatal CV event moved to the post-nonfatal CV event state, where they were at risk of death from non-CV causes and at increased risk of death from CV causes. Patients could experience only 1 nonfatal CV event during the model time horizon. Additionally, patients were at risk of death due to CV death or death from non-CV causes in any health state.
Model Inputs
The modelled patient characteristics for the sponsor’s base case were based on the LoDoCo2 trial (mean age: 66 years; 85% male); this population represents patients with stable CAD.4 The sponsor’s scenario analyses, which involved patients with CAD and a recent MI, was based on patient characteristics from the COLCOT trial (mean age: 61 years; 80.8% male).
For the subgroup of patients with stable CAD, the incidence of CV events (a composite outcome including CV death, spontaneous MI, ischemic stroke, and ischemia-driven coronary revascularization) was based on digitized Kaplan–Meier curves from the LoDoCo2 trial.4 The sponsor assumed proportional hazards for the risk of CV events between the patients who received colchicine or placebo, and a constant HR over time (colchicine plus SOC versus SOC: HR = 0.6964; 95% CI, 0.5774 to 0.8399). The efficacy of colchicine was modelled by applying the HR for colchicine plus SOC from LoDoCo2 to the survival function for SOC. The sponsor selected a log-normal distribution for extrapolation of the trial data over the time horizon based on statistical fit (i.e., an Akaike information criterion or Bayesian information criterion), visual inspection, and clinical plausibility. The distribution of individual CV events among patients who experienced the composite outcome was based on pooled data from the colchicine and placebo arms in LoDoCo2 (i.e., the proportion of patients who experienced each CV event within the composite outcome was assumed to be equivalent for colchicine plus SOC and SOC alone) and constant over time. A proportion of patients in the LoDoCo2 trial experienced multiple CV events during follow-up. However, the sponsor included only the worst event in the calculation of the HR (i.e., death was considered the worst event followed by nonfatal MI, nonfatal stroke, and ischemia-driven coronary revascularization).3
For the subgroup of patients with CAD and a recent MI, a similar approach was adopted, with the incidence of CV events based on the COLCOT trial,5 which used a composite outcome for CV events comprising death from CV causes, MI, stroke, resuscitated cardiac arrest, and urgent hospitalization for angina leading to revascularization. The HR for CV events was based on digitized Kaplan–Meier curves from the COLCOT trial (colchicine plus SOC versus SOC: HR = 0.77; 95% CI, 0.61 to 0.96), which was applied to a survival function for SOC to estimate the efficacy of colchicine plus SOC. The sponsor selected a log-normal distribution for the long-term extrapolation of treatment efficacy based on statistical fit, visual inspection, and clinical plausibility. The distribution of CV events within the composite outcome was based on pooled data across colchicine and placebo groups in the COLCOT trial and was assumed to be constant over time.
All-cause mortality in the model was based on Statistics Canada life tables.3 To account for the increased risk of death following nonfatal CV events, the sponsor applied “mortality multipliers” to estimate the risk of death following an MI, stroke, or coronary revascularization,6,7 adjusted for a reduced risk of death over time.8 Adverse events included in the model were based on the pooled incidence rates (i.e., the total number of events in both trials divided by the total of number of patients in both trials) of the LoDoCo2 and COLCOT trials for events that occurred in at least 2% of patients in either arm of the trials. The sponsor noted that pneumonia was included in the model because it was reported in > 2% of patients in the LoDoCo2 trial and the difference between the 2 arms of the COLCOT trial was statistically significant. Infection and pneumonia were considered acute events, while the other adverse events were considered chronic (i.e., considered to recur throughout the patient’s lifetime). Disutilities from the published literature were used to account for reduced quality of life due to adverse events.
Health-related quality-of-life data were not collected in the LoDoCo2 or COLCOT trials. To inform the model, the sponsor obtained health-state utility values from the published literature. The baseline health-state utility value for patients in the CV event–free state for both the stable CAD and CAD plus MI subgroups was assumed to be 0.778.9 Patients with a nonfatal MI were assumed to have an acute utility value of 0.651 and a post-acute utility of 0.685; patients having a nonfatal stroke were assumed to have an acute utility value of 0.512 and a post-acute utility of 0.641.10,11 Patients with a coronary revascularization were assumed to return to a baseline utility of 0.778 after the acute period (acute utility: 0.629).3
Costs considered in the model included those related to treatment acquisition, management of CV events, follow-up, and adverse events. The sole drug cost in the model was for colchicine, with no cost assumed for SOC. No administration costs were included. Adherence to colchicine was assumed to be 65%, based on adherence to statins.3 Costs for managing a nonfatal MI and nonfatal stroke were obtained from Goeree et al. (2009),12 while costs associated with a fatal MI and fatal stroke were obtained from Anis et al. (2006).13 Costs for ischemia-driven coronary revascularization were obtained from Samuel et al. (2020),5 which assumed 73% of patients received a percutaneous coronary intervention and 27% received coronary artery bypass graft surgery.14 The subgroup analysis for patients with CAD plus MI included additional costs for resuscitated cardiac arrest, as it was included in the composite outcome of CV events for this population. Follow-up costs included medical visits with a cardiologist or general practitioner and laboratory tests. Adverse event costs included 1-time costs for hospitalizations (infection, pneumonia) and annual costs for chronic conditions (cancer, gout, myalgia, and dysesthesia). No costs were included for diarrhea or abdominal pain.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically using 5,000 iterations. The deterministic and probabilistic results were similar, and the probabilistic findings are presented in Table 3 and Table 4. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3. The submitted analyses were based on publicly available prices of comparator treatments.
Among patients with stable CAD, colchicine plus SOC was dominant over SOC alone, in that it was associated with lower costs (incremental: −$2,165) and higher QALYs (incremental: 0.51) compared with SOC over a lifetime horizon (Table 3). In the sponsor’s base case, colchicine plus SOC had an 100% probability of being the most cost-effective strategy at a willingness-to-pay threshold of $50,000 per QALY.
Results were driven by the costs associated with the treatment of nonfatal MIs and the accrual of QALYs among patients who remained free of CV events. The majority (96%) of the QALYs across all health states were accrued during the extrapolated period.
Table 3: Summary of Sponsor’s Economic Evaluation — Stable Coronary Artery Disease
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($ per QALY) |
|---|---|---|---|---|---|
SOC | 31,672 | Reference | 11.45 | Reference | Reference |
Colchicine + SOC | 29,507 | −2,165 | 11.96 | 0.51 | Dominanta |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
aDominant indicates that a treatment is less costly and more effective (more QALYs) than the reference.
Source: Sponsor’s pharmacoeconomic submission.3
Among patients with CAD and a recent MI, colchicine plus SOC was dominant over SOC alone, in that colchicine plus SOC was associated with lower costs (incremental: −$662) and higher QALYs (incremental: 0.52) compared to SOC over a lifetime horizon (Table 4). In the sponsor’s analysis, colchicine plus SOC had an 100% probability of being the most cost-effective strategy at a willingness-to-pay threshold of $50,000 per QALY in patients with CAD and MI.
Table 4: Summary of Sponsor’s Economic Evaluation — Coronary Artery Disease and a Recent Myocardial Infarction
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($ per QALY) |
|---|---|---|---|---|---|
SOC | 33 482 | Reference | 13.68 | Reference | Reference |
Colchicine + SOC | 32,820 | −662 | 14.19 | 0.52 | Dominanta |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
aDominant indicates that a treatment is less costly and more effective (more QALYs) than the reference.
Source: Sponsor’s pharmacoeconomic submission.3
Sensitivity and Scenario Analysis Results
The sponsor provided several scenario and sensitivity analyses for the stable CAD subgroup that assumed the clinical benefits of colchicine stopped at the end of the trial period, full treatment adherence, and no increase in the risk of death after a CV event. The analyses also adopted alternate discounting rates (0% and 3%) and time horizons (5 years and 10 years) and considered a societal perspective. Most scenarios had no meaningful effect on the ICER, with the exceptions of assuming that the clinical benefits of colchicine ceased at the end of the trial duration and adopting a time horizon of 5 years. In the sponsor’s analysis, colchicine plus SOC was no longer dominant when a 5-year analysis horizon was adopted (ICER: $1,292 per QALY versus SOC) and when the benefits of colchicine were assumed to stop after the trial duration (ICER: $2,247 per QALY versus SOC).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
Costs related to SOC were not included in the model: In both the stable CAD and CAD plus MI subgroups, the sponsor assumed that the costs of SOC would be equal in both treatment arms because colchicine is intended to be added to SOC. Although the clinical experts consulted by CADTH for this review agreed that there is likely to be no change in SOC regimens with the addition of colchicine, the exclusion of costs related to SOC is inappropriate given that the model predicts a gain in life-years with colchicine plus SOC compared to SOC alone. As such, patients who receive colchicine are expected to incur the cost of SOC for a longer duration than those who receive SOC alone. The exclusion of SOC costs from the model underestimates the total drug costs associated with the use of colchicine, biasing the ICER in favour of colchicine.
The composition of SOC was not specified by the sponsor. Based on clinical expert input, CADTH assumed that SOC in the stable CAD subgroup would include acetylsalicylic acid (ASA). For the CAD plus MI subgroup, CADTH assumed that SOC would comprise a basket of ASA, beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and statins, based on clinical expert input. In CADTH reanalyses, no cost was added for ASA due to the inconsistent reimbursement of ASA across jurisdictions and no cost was added for SOC in the stable CAD subgroup. For the CAD plus MI subgroup, an annual drug cost for SOC of $246 per patient was added. The cost of SOC may be underestimated because costs related to the use of P2Y12 inhibitors have not been included, given the limited duration of P2Y12 inhibitor use after an event (6 to 12 months for most patients). However, the exclusion of such costs is not expected to have a major impact on the ICER.
The sponsor’s model lacks face validity: In the sponsor’s model, patients who experienced a nonfatal CV event were assumed to transition to a “post-nonfatal CV event” state, in which they were at risk of CV death or all-cause death but were not at risk of further CV events. The model therefore assumes that patients are at risk of only 1 nonfatal CV event over the model time horizon. Clinical experts consulted by CADTH for this review indicated that this assumption lacks face validity, as multiple CV events are common in this patient population, which may lead to cumulative myocardial injury and heart failure. The impact of multiple CV events on quality of life and costs was not captured in the sponsor’s model. In addition, treatment discontinuation was not accounted for in the sponsor’s model, such that patients were assumed to remain on colchicine for the duration of the analysis. As noted in the CADTH clinical review, approximately 10% and 18% of patients discontinued colchicine treatment in the LoDoCo2 and COLCOT trials, respectively. In both trials, some discontinuations were due to gastrointestinal adverse events.
CADTH was unable to address limitations related to the risk of subsequent nonfatal CV events or treatment discontinuation due to the structure of the sponsor’s model.
The long-term relative effectiveness of colchicine plus SOC compared to SOC is highly uncertain: In the sponsor’s analysis of the stable CAD subgroup, the clinical effectiveness of colchicine plus SOC and SOC alone was based on data from the LoDoCo2 trial (median follow-up: 28.6 months) and extrapolated over a 44-year time horizon (lifetime). The sponsor assumed that the relative treatment effects observed during the trial (i.e., an HR of 0.69 for colchicine plus SOC compared to SOC alone) would remain constant over the entire time horizon (in a proportional hazards assumption). The sponsor justified this assumption using the results of statistical analyses (i.e., log-log survival plots and Schoenfeld residuals plots) using data from digitized Kaplan–Meier curves for the composite outcome of CV events from the published LoDoCo2 trial data. While the proportional hazards assumption may hold for the trial duration, it is unlikely to hold in the long-term in most cases,15 and statistical testing confirms only that the assumption holds during the trial period, not for the extrapolated period. The sponsor made similar assumptions for the extrapolation of outcome data from the COLCOT trial (median follow-up: 22.6 months) to a lifetime (49-year) time horizon in CAD plus MI subgroup analyses.
The assumption of proportional hazards was based on analysis of composite outcome data (including CV death, MI, ischemic stroke, and ischemia-driven coronary revascularization for the LoDoCo2 trial). The clinical experts consulted by CADTH for this review noted that the proportion of patients experiencing each type of event is likely to vary over time as the underlying characteristics of the patients at risk change. For example, the proportion of patients experiencing CV death in the modelled cohort is likely to increase as patients age, and the accumulation of events in some patients may lead to more severe events. The clinical experts further noted that the sponsor’s predicted proportion of patients who remain event-free during the extrapolation period (based on a log-normal distribution of CV events) is likely overestimated. Given that the majority of the incremental QALYs gained with colchicine plus SOC (96%) in both the stable CAD and CAD plus MI subgroups accrued during the extrapolation period, incorrectly assuming proportional hazards over the entire time horizon of the model may substantially overestimate the incremental QALYs gained by patients receiving colchicine and bias the ICER in favour of colchicine.
CADTH reviewers further noted that the sponsor’s model predicts a survival advantage with colchicine plus SOC compared to SOC alone among both patients with stable CAD and among patients with CAD plus MI, which has not been shown in clinical trials. As noted in the CADTH clinical review, the risk of death was not statistically different among patients who received colchicine or placebo in the LoDoCo2 trial (HR = 1.21; 95% CI, 0.86 to 1.71) or in the COLCOT trial (HR = 0.98; 95% CI, 0.64 to 1.49). The sponsor provided no longer-term trials to support the model findings, and as such, the predicted survival benefit with colchicine is highly uncertain.
The assumptions required for the extrapolation of short-term clinical trial data over a lifetime horizon were inappropriate in the sponsor’s model. Clinical experts were unable to identify a more appropriate distribution for the extrapolation of long-term CV outcomes due to the impact of patient characteristics on clinical outcomes. In CADTH reanalyses, a 20-year horizon was adopted to lessen the impact of such assumptions, and alternative time horizons were explored in scenario analyses.
Limitations with the use of a composite outcome: In the stable CAD subgroup, the efficacy of colchicine plus SOC in reducing CV events was based on published data from the LoDoCo2 trial for the composite outcome of CV death, nonfatal MI, nonfatal stroke, and ischemia-driven coronary revascularizations. As noted by the sponsor, a proportion of patients in the LoDoCo2 trial experienced more than 1 nonfatal CV event during the follow-up period.3 However, due to a lack of individual patient data, the sponsor included “only the worst event,” with the rank order being death, nonfatal MI, nonfatal stroke, and ischemia-driven coronary revascularization. The use of composite outcomes assumes equal importance for each of the individual components of the composite and may not appropriately capture the relative importance of each of these events to patients. According to the clinical experts consulted for this review, CV deaths, MI, and stroke are the most clinically important outcomes in practice. As indicated in the sponsor’s submission, approximately 38.5% of patients in the colchicine arm and 40.53% of patients in the placebo arm of LoDoCo2 underwent coronary revascularization; this outcome was considered by the clinical experts to be the least clinically relevant outcome among those included in the composite.
The sponsor additionally assumed that the proportion of individual CV events within the composite outcome would be equivalent between the colchicine plus SOC and SOC-alone arms, based on the pooling of events across the colchicine and placebo arms in the LoDoCo2 trial, despite the availability of treatment-specific event rates. The sponsor assumed that, of the CV events experienced by patients, 9.98% would be CV death, 42.79% would be nonfatal MI, 7.54% would be nonfatal stroke, and 39.69% would be coronary revascularization in both the colchicine plus SOC and SOC-alone groups. These values differ from the treatment-specific values provided by the sponsor for CV deaths and nonfatal stroke. Notably, the proportion of CV deaths is higher for the colchicine plus SOC group (10.7% of CV events) than the SOC-alone group (9.47%). Pooling the percentage of events across treatment arms obscures potential differences between treatments and may underestimate costs associated with the treatment of events, potentially biasing the results in favour of colchicine.
Similar assumptions were made in the sponsor’s analysis of the efficacy of colchicine among patients with CAD plus MI, based on the composite outcome of CV events from the COLCOT trial. The composite outcome in this trial included CV death, nonfatal MI, nonfatal stroke, angina requiring coronary revascularization, and resuscitated cardiac arrest, which may be of varying degrees of importance to patients. Additionally, despite differences in the distribution of individual events within the composite outcome, the sponsor assumed that the distribution of individual events would be equivalent between patients who experienced a CV event in the colchicine plus SOC arm or the SOC arm, based on pooled data from both treatment groups. This pooling obscures differences in the distribution of events between treatments, including the proportion of CV events that are nonfatal MIs (colchicine plus SOC: 64.89% of CV events; SOC: 52.35% of CV events).
In its reanalyses, CADTH applied the sponsor-provided treatment-specific distributions of individual events within the composite outcome of CV events, based on the LoDoCo2 trial for the patients with stable CAD and the COLCOT trial for patients with CAD plus MI. CADTH was unable to address limitations associated with the use of a composite outcome with components of varying severity.
The generalizability of the LoDoCo2 trial data to Canadian patients with CAD is uncertain: As noted in the CADTH clinical review, the LoDoCo2 trial was conducted in Australia and the Netherlands, with no study sites in Canada. Subgroup data showed potentially different effects of colchicine compared with placebo at Australian study centres (HR = 0.51; 95% CI, 0.39 to 0.67) compared with study centres in The Netherlands (HR = 0.92; 95% CI, 0.71 to 1.20). Given that there may be regional differences in treatment effects, it is possible that the effectiveness of colchicine in Canadian patents with stable CAD may differ from that observed in the LoDoCo2 trial.
In the LoDoCo2 study, patients received open-label colchicine (0.5 mg daily) during the run-in period. At the end of the run-in, those in stable condition who tolerated and adhered to colchicine and agreed to continue in the study were eligible to enter the double-blind randomized period. During the run-in period, 9% of patients withdrew due to intolerance. The use of an enriched population (i.e., patients who can tolerate and adhere to treatment) is likely to overestimate the effects of colchicine in clinical practice.
CADTH was unable to address the potential for differential treatment effects among Canadian patients with stable CAD due to a lack of data. Due to regional variation in treatment efficacy and a lack of Canadian study sites, the relevance of the pooled HR from the LoDoCo2 trial to the Canadian context is uncertain. CADTH explored the impact of regional variation in treatment efficacy observed in the LoDoCo2 trial in scenario analyses.
The cost of colchicine was underestimated: In the calculation of drug costs, the sponsor assumed a treatment adherence of 65% for colchicine, based on claims data for statins.3 The assumption that adherence to colchicine would be the same as that for statins was not justified by the sponsor. In the sponsor’s model, adherence was assumed to affect only treatment costs and did not consider the impact of lower adherence on treatment effectiveness. However, for oral treatments, Canadian pharmacies are likely to dispense the full quantity of medication for each prescription, and any unused treatment by the patient is unlikely to be recuperated. The cost of medication to the drug plan is therefore independent of patient adherence, and adopting a lower adherence rate inappropriately reduces the cost of colchicine in the model, biasing the results in its favour.
In CADTH reanalyses, the yearly drug cost of colchicine was based on the sponsor’s submitted price of colchicine without adjustment for adherence.
The impact of colchicine on quality of life is uncertain: There are several sources of uncertainty related to the impact of colchicine on quality of life. First, the impact of treatment with colchicine on quality of life was not assessed in the LoDoCo2 or COLCOT trials. To inform the economic model, the sponsor undertook a “targeted literature search to identify utility values for stable CAD patients (no CV event) and for patients experiencing selected CV events.”3 No details about this search were provided. The sponsor adopted utility values from multiple sources,10,11,16 and they were derived by various methods. CADTH economic guidelines recommended that utility values be derived from a consistent source,17 as the use of utilities from different patient populations, time points, and methods may introduce inconsistencies in the data informing the model. Second, although the sponsor’s model included utility values for acute health states (nonfatal MI, nonfatal stroke, resuscitated cardiac arrest, and coronary revascularization), patients were assumed to be at risk of only 1 nonfatal CV event during the model time horizon. Given that clinical experts consulted by CADTH indicated that CV events may become more frequent over the course of a disease, the utilities calculated by the model may not adequately reflect the impact of colchicine on quality of life. Third, the sponsor’s assumption that the distribution of individual CV events would be equal between colchicine plus SOC and SOC alone was not supported by clinical trial data. This assumption of an equivalent distribution of CV events, which were each associated with different utility values, further obscures the relationship between colchicine and quality of life. Fourth, for the CAD plus MI subgroup, the sponsor adopted a baseline utility value based on the utility of patients with existing CAD (0.778), which was higher than the utility value used for patients in the post-nonfatal MI state (0.685).
In CADTH reanalyses of the CAD plus MI subgroup, the baseline utility of patients with CAD and MI was assumed to be 0.685. CADTH was unable to address the additional limitations due to a lack of alternative health-state utility values.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients enrolled in the LoDoCo2 trial were assumed to be representative of the Health Canada–indicated population (i.e., patients with existing CAD who require preventive treatment for the reduction of atherothrombotic events). | The LoDoCo2 trial enrolled patients with clinically stable CAD (i.e., no cardiovascular-related hospital admission in the prior 6 months). As such, the LoDoCo2 trial does not reflect the full Health Canada–indicated population, as those with unstable disease (e.g., those with a recent MI, unstable angina, severe heart failure) are not considered. The sponsor provided scenario analyses for patients with CAD and MI, based on data from the COLCOT trial. As the COLCOT trial enrolled patients with an MI within the previous 30 days, the cost-effectiveness analyses for this scenario are specific to patients with a recent MI (i.e., those who experienced an MI in the past 30 days). A proportion of patients eligible for colchicine under the Health Canada–approved indication are not captured in the sponsor’s pharmacoeconomic analyses (i.e., those with unstable angina or severe heart failure) and the cost-effectiveness of colchicine in these populations is unknown. |
The cost of managing a myocardial infarction was assumed to be $12,775 in the first year and $3,379 in subsequent years.12 | Uncertain. CADTH identified alternative estimates of the costs of managing myocardial infarction in the first year ($21,732) and subsequent years ($925).a CADTH explored the impact of adopting alternative costs in scenario analyses. |
The sponsor assumed that patients who experience a CV event (MI, stroke, or coronary revascularization) are at higher risk of death compared to the general Canadian population. The sponsor applied relative risks of 3.70, 2.50, and 3.00 to the background probability of death from Statistics Canada life tables to account for the increased risk of death after an MI, stroke, or coronary revascularization, respectively. The sponsor applied a relative risk of 0.5 to these values to account for reduced CV event rate over time. | Uncertain. The relative risk estimates adopted by the sponsor were obtained from the literature from a variety of sources6-8 and may not fully align with the Canadian population or the population of interest for this review. |
For parameters with no available measure of variation, the sponsor assumed 10% variability in the base case to inform parameter uncertainty in input parameters. | Not appropriate. Generic ranges for variability do not reflect the full range of clinically plausible values. |
Costs related to the management of management of diarrhea and abdominal pain were not included. | Uncertain. Diarrhea and abdominal pain management may be associated with health care costs (e.g., visits to a health care provider) which were not accounted for in the sponsor’s model. Drug costs associated with these adverse events are likely borne out-of-pocket by patients. As noted in the CADTH clinical report, gastrointestinal effects were a common adverse event reported in the LoDoCo2 and COLCOT trials. |
aCosts reported in Tran (2018)18 in 2016 Canadian dollars were inflated to 2021 values using the Canadian Consumer Price Index.
CADTH Reanalyses of the Economic Evaluation
Several limitations in the sponsor’s submission could not be adequately addressed (i.e., the lack of consideration for multiple CV events, varying severity of events with the composite outcome “CV events,” generalizability of LoDoCo2 trial data to Canadian patients, and uncertainty regarding the impact of colchicine on health-related quality of life). CADTH undertook reanalyses in 2 patient subgroups (those with stable CAD and patients with CAD and a recent MI); however, these reanalyses do not capture a proportion of patients who would be eligible for colchicine under the full Health Canada–approved indication (e.g., those with unstable angina and those with severe heart failure) due to a lack of data.
CADTH undertook reanalyses that addressed limitations within the model, summarized in Table 6, for patients with stable CAD and patients with CAD and a recent MI for both subgroups. CADTH reanalyses were derived by making changes in model parameter values and assumptions in consultation with clinical experts.
Table 6: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case (stable CAD) | ||
Disutility calculation | Incorrect reference cell included in the formula for applying AE disutilities | Corrected reference cell in formula |
Corrections to sponsor’s subgroup analysis (CAD and a recent MI) | ||
Incorrect formula to calculate disutilities for chronic AEs, SOC costs, and parametric distributions | Incorrect reference cell in formula for calculating chronic AE disutilities; the cost of SOC was counted twice due to a programming error; errors within the probabilistic analysis due to issues with the Dirichlet distributions for the “individual component distribution” of CV events | Corrected reference cell in formula for AE disutilities; double counting of SOC costs was removed and the individual component distribution of CV events was assumed to be fixed |
Changes to derive the CADTH base case (stable CAD) | ||
1. Analysis time horizon | Lifetime (44 years) | 20 years |
2. Distribution of individual CV events among patients who experienced the composite outcome of “CV events” | Distribution of events assumed to be equivalent across treatments: CV death: 9.98% Nonfatal MI: 42.79% Nonfatal stroke: 7.54% Coronary revascularization: 39.69% | Treatment-specific distribution of events: Colchicine plus SOC: CV death: 10.70% Nonfatal MI: 42.78% Nonfatal stroke: 8.02% Coronary revascularization: 38.50% SOC: CV death: 9.47% Nonfatal MI: 42.80% Nonfatal stroke: 7.20% Coronary revascularization: 40.53% |
3. Colchicine treatment adherence | 65% | 100% |
CADTH base case (stable CAD subgroup) | 1 + 2 + 3 | |
Changes to derive the CADTH base case (CAD and a recent MI) | ||
1. SOC costs | $0 | $246 per patient per year, based on a basket of acetylsalicylic acid, beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and statins |
2. Analysis time horizon | Lifetime (49 years) | 20 years |
3. Distribution of individual CV events among patients who experience the composite outcome of “CV events” | Distribution of events assumed to be equivalent across treatments: CV death: 10.96% Nonfatal MI: 57.81% Nonfatal stroke: 6.98% Resuscitated cardiac arrest: 1.00% Coronary revascularization: 23.26% | Treatment-specific distribution of events: Colchicine plus SOC: CV death: 12.98% Nonfatal MI: 64.89% Nonfatal stroke: 3.82% Resuscitated cardiac arrest: 0.46% Coronary revascularization: 17.56% SOC: CV death: 9.41% Nonfatal MI: 52.35% Nonfatal stroke: 9.41% Resuscitated cardiac arrest: 1.18% Coronary revascularization: 27.65% |
4. Colchicine treatment adherence | 65% | 100% |
5. Health-state utility values | Baseline (existing CVD): 0.778 Acute health states Nonfatal MI: 0.651 Nonfatal stroke: 0.512 Resuscitated cardiac arrest: 0.677 Coronary revascularization: 0.629 Post-acute health states: Nonfatal MI: 0.685 Nonfatal stroke: 0.641 Resuscitated cardiac arrest: 0.778 Coronary revascularization: 0.778 | Baseline (CAD and post-nonfatal MI)a: 0.685 Acute health states Nonfatal MI: 0.651 Nonfatal stroke: 0.512 Resuscitated cardiac arrest: 0.677 Coronary revascularization: 0.629 Post-acute health states: Nonfatal MI: 0.685 Nonfatal stroke: 0.641 Resuscitated cardiac arrest: 0.685b Coronary revascularization: 0.685b |
CADTH base case (CAD and a recent MI subgroup) | Reanalyses 1 + 2 + 3 + 4 + 5 | |
AE = adverse event; CAD = coronary artery disease; CV = cardiovascular; CVD = cardiovascular disease; MI = myocardial infarction; SOC = standard of care.
aIn CADTH reanalysis of the CAD plus MI subgroup, the baseline utility was assumed to be that supplied by the sponsor for patients with CAD and post-nonfatal MI (0.685).
bConsistent with the assumption made in the sponsor’s base case, the utility value for patients with resuscitated cardiac arrest and coronary revascularization was assumed to be equal to the baseline utility.
Base-Case Results
CADTH undertook a stepped analysis, incorporating each change proposed in Table 6 to the sponsor’s base case for patients with stable CAD (Table 7) and for patients with CAD and a recent MI (CAD plus MI). The disaggregated results for both subgroups are presented in Appendix 4, Table 16 and Table 20, respectively.
Among stable CAD patients, colchicine plus SOC was associated with higher costs (incremental: $14) and greater QALYs gained (incremental: 0.14) over a 20-year horizon (Table 7). The ICER for colchicine plus SOC versus SOC alone was $100 per QALY. There is a 63% probability that colchicine plus SOC is cost-effective compared to SOC at a willingness-to-pay threshold of $50,000 per QALY. The impact of this uncertainty is shown in Figure 1, with colchicine plus SOC proving to be both less effective (fewer QALYs) and more costly than SOC alone in approximately 30% of simulations. The incremental number of QALYs with colchicine plus SOC during the trial period was 0.005, indicating that the majority of the incremental benefits (97%) accrued in the post-trial period, which were derived from extrapolated trial findings rather than observed benefit.
Table 7: Summary of CADTH Base Case — Stable Coronary Artery Disease
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($ per QALY) |
|---|---|---|---|---|---|
SOC | 24,435 | Ref | 10.03 | Reference | Reference |
Colchicine + SOC | 24,449 | 14 | 10.18 | 0.14 | 100 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Figure 1: Cost-Effectiveness Plane for the CADTH Base Case — Patients with Stable Coronary Artery Disease
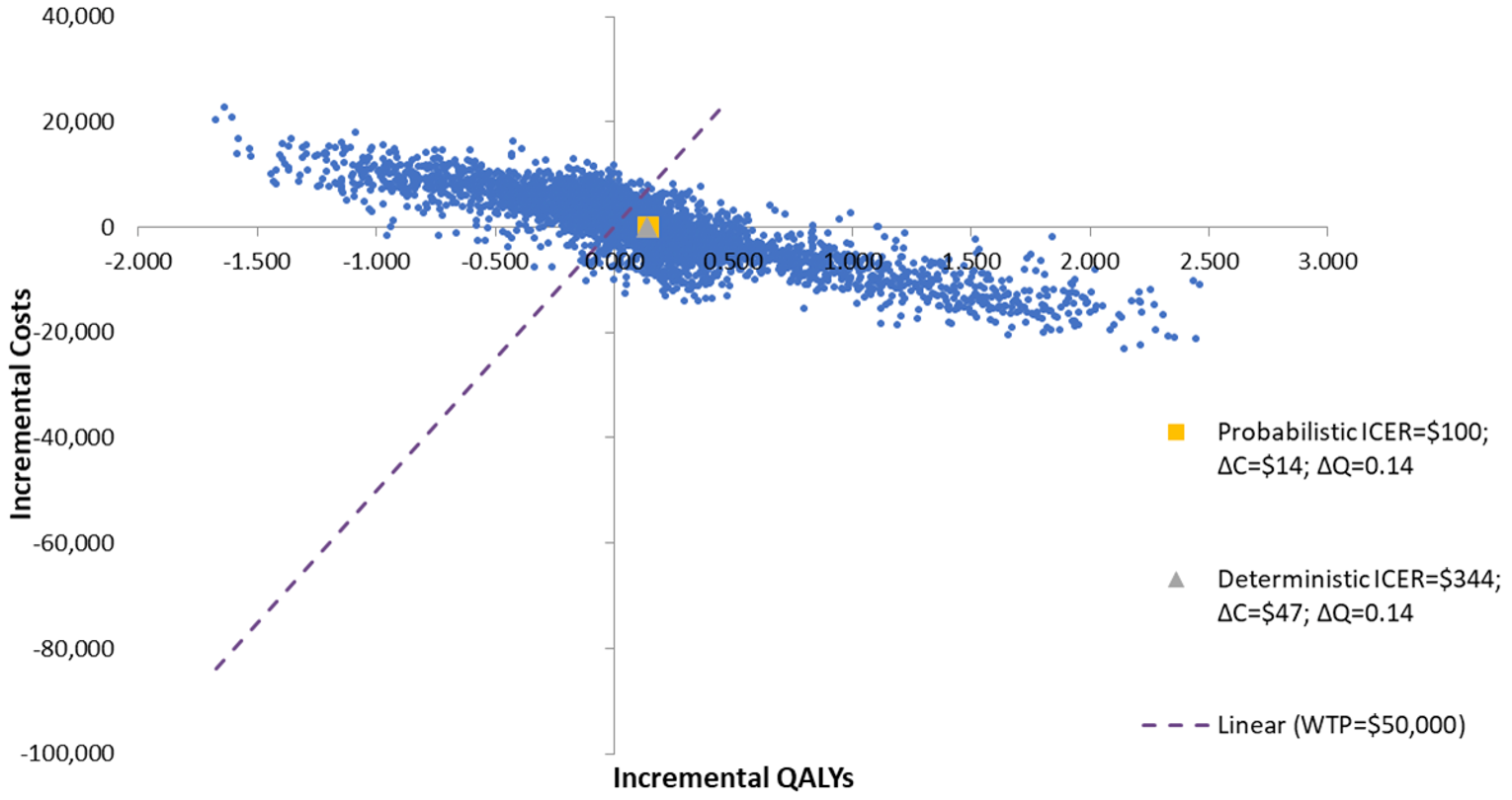
ΔC = incremental cost; ΔQ = incremental quality-adjusted life-years; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; WTP = willingness to pay.
Among patients with CAD and a recent MI, colchicine plus SOC had higher costs (incremental: $1,389) and marginal gains in QALYs (0.02), resulting in an ICER of $64,922 per QALY over a 20-year horizon among patients with CAD and MI (Table 8). There is a 47% probability that colchicine plus SOC is cost-effective compared to SOC at a willingness-to-pay threshold of $50,000 per QALY. The impact of this uncertainty is shown in Figure 2, where colchicine plus SOC was both less effective (fewer QALYs) and more costly than SOC alone in approximately 31% of simulations. The number of incremental QALYs gained with colchicine plus SOC during the trial period was 0.002, indicating that the majority of the incremental benefits (88%) were accrued in the post-trial period, which were derived from extrapolated trial findings rather than observed benefit.
Table 8: Summary of CADTH Base Case — Coronary Artery Disease and a Recent Myocardial Infarction
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. SOC ($ per QALY) |
|---|---|---|---|---|---|
SOC | 27,956 | Reference | 9.83 | Reference | Reference |
Colchicine + SOC | 29,256 | 1,301 | 9.85 | 0.02 | 64,922 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care; vs. = versus.
Figure 2: Cost-Effectiveness Plane for CADTH Base Case — Patients With Coronary Artery Disease and a Recent Myocardial Infarction
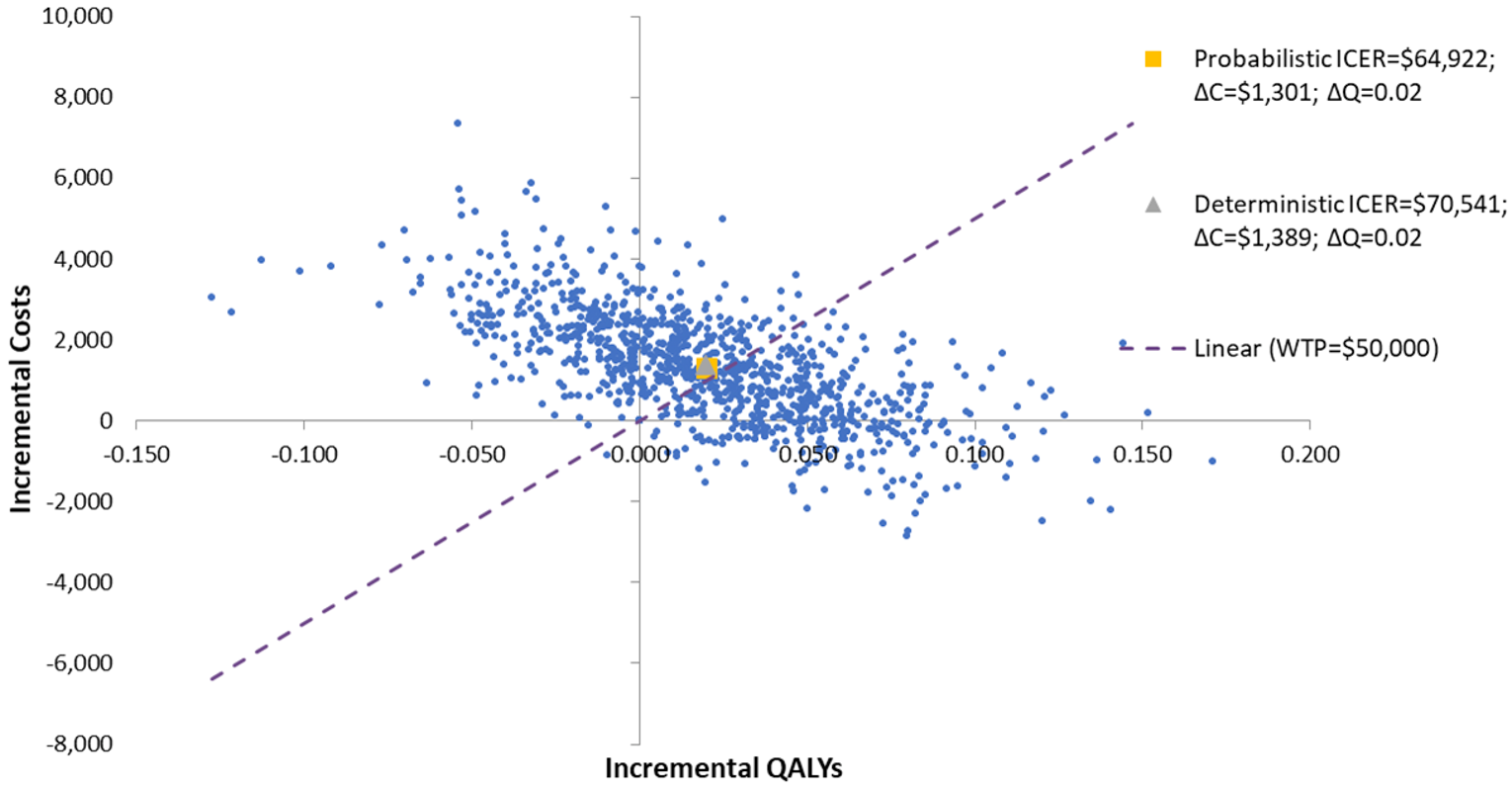
ΔC = incremental cost; ΔQ = incremental quality-adjusted life-years; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; WTP = willingness to pay.
Scenario Analysis Results
Several scenario and sensitivity analyses were conducted on the CADTH base case. These scenario analyses explored the impact of adopting alternative analysis time horizons (lifetime = 10 years), region-specific HRs (LoDoCo2 trial only), and alternative estimates for the cost of managing MI.
The results of the CADTH reanalyses for the CAD and CAD plus MI subgroups were highly sensitive to the model time horizon. Among patients with CAD, the ICER changed most notably when a lifetime horizon was adopted (colchicine plus SOC was dominant over SOC) or when the HR for CV events was based on data from LoDoCo2 study centres in the Netherlands (ICER: $117,377 for colchicine plus SOC versus SOC alone). Among patients with CAD plus MI, the ICER changed most notably when a lifetime horizon was adopted (ICER: $32,935 versus SOC) or when a 10-year horizon was adopted (ICER: $134,390 versus SOC). Analyses involving a lifetime horizon are limited by assumptions related to the long-term relative effectiveness of colchicine and SOC, as noted in the CADTH appraisal of the sponsor’s economic evaluation.
Price-Reduction Analyses
For patients with stable CAD, no price reduction for colchicine was needed when compared with SOC, given that the mean ICER for colchicine plus SOC versus SOC alone was $100 per QALY gained among patients with CAD. However, given the wide uncertainty around the probabilistic ICER (e.g., 63% probability of being cost-effective at a threshold of $50,000 per QALY), a price reduction may still be necessary.
For patients with CAD plus MI, a 15% price reduction for colchicine would be required for colchicine plus SOC to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY compared to SOC alone (Table 9). However, given the wide uncertainty around the probabilistic ICER, further price reductions may still be necessary.
Table 9: CADTH Price-Reduction Analyses — Coronary Artery Disease and a Recent Myocardial Infarction
Price reduction | Deterministic ICERs for colchicine plus SOC vs. SOC ($) | |
|---|---|---|
Sponsor analysis | CADTH reanalysisa | |
No price reduction | Colchicine dominant | 70,541 |
10% | NA | 56,661 |
15% | NA | 49,721 |
ICER = incremental cost-effectiveness ratio; SOC = standard of care; vs. = versus.
aBased on deterministic analyses.
Issues for Consideration
The sponsor indicated in its submission that it expects colchicine to be initiated in hospital and be part of patient discharge protocols. The extent to which colchicine may be initiated in hospital was not explored in CADTH’s analysis; however, coordination between hospital and community drug programs should be considered in the event that this type of prescribing should occur.
In the LoDoCo2 trial, 16% of patients did not have a previous acute CV event documented. Consequently, there is limited evidence on the use of colchicine for primary prevention of atherothrombotic events in patients with existing CAD, and the cost-effectiveness of colchicine in this setting is unknown.
No discontinuation criteria are listed in the Health Canada product monograph for colchicine. According to the clinical experts consulted by CADTH for this review, colchicine is expected to be used indefinitely.
Overall Conclusions
Evidence from the LoDoCo2 and COLCOT trials suggests that colchicine as an add-on to standard secondary prevention drugs is associated with a statistically significant difference in the time to first occurrence of a composite CV end point (i.e., CV death, stroke, MI, ischemia-driven revascularization) relative to placebo plus SOC, in patients with stable CAD, as well as those with CAD and a recent MI. In both pivotal trials used to inform the economic evaluation (LoDoCo2 and COLCOT), the time-to-event analyses of the individual CV events that made up the primary composite outcome produced point estimates that favoured colchicine over placebo. However, the benefit of colchicine was not statistically significant for all outcomes within the composite outcome in both trials. For example, while the risk of MI was significantly reduced in the LoDoCo2 trial (HR = 0.70; 95% CI, 0.53 to 0.93), there was no statistical difference in the risk of CV death (HR = 0.808; 95% CI, 0.44 to1.44). Similarly, there was no difference in CV deaths between colchicine and placebo in the COLCOT study among patients with CAD and a recent MI (HR = 0.84, 95% CI, 0.46 to 1.52) and there was no significant difference in all-cause deaths between colchicine and placebo in the LoDoCo2 or COLCOT trials. Without evidence from longer-term trials, any predicted survival benefit with the use of colchicine is therefore highly uncertain. The long-term effects of colchicine relative to SOC and its impact on quality of life are also highly uncertain due to a lack of data.
CADTH undertook reanalyses of the cost-effectiveness of colchicine plus SOC in 2 patient subgroups that would be eligible for colchicine under the Health Canada indication: patients with stable CAD (informed by data from the LoDoCo2 trial) and patients with CAD and a recent MI (informed by data from the COLCOT trial). In the stable CAD subgroup, CADTH reanalyses adopted a shorter time horizon, treatment-specific distribution of CV events, and alternative assumptions about colchicine adherence. Additional changes in the reanalyses of the CAD plus MI subgroup included assuming an annual cost of SOC and using an alternative baseline health-state utility value for patients with CAD plus MI.
Among patients with stable CAD, the CADTH base case resulted in an ICER of $100 per QALY gained for colchicine plus SOC compared to SOC alone. There was a 63% probability of colchicine plus SOC being cost-effective at a willingness-to-pay threshold of $50,000 per QALY, and in 30% of simulations colchicine plus SOC was more costly and less effective (fewer QALYs) compared to SOC alone. Based on the mean ICER, no price reduction would be required; however, given the wide uncertainty around the probabilistic ICER, a price reduction may still be necessary. Among patients with CAD and a recent MI, the ICER for colchicine plus SOC was $64,922 per QALY compared with SOC, with an 47% probability of colchicine plus SOC being cost-effective at a willingness-to-pay threshold of $50,000 per QALY. Colchicine plus SOC was more costly and less effective compared to SOC alone in 31% of simulations. A 15% price reduction of colchicine would be needed for colchicine plus SOC to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY in this subgroup. However, given the wide uncertainty around the probabilistic ICER, further price reductions may still be necessary for colchicine to be a cost-effective treatment in patients with CAD and a recent MI.
In its reanalyses, CADTH was unable to address the assumption that the efficacy of colchicine compared with placebo observed in the pivotal trials would be consistent over the entire time horizon, which is unlikely. CADTH was also unable to address the assumption that patients are at risk of only 1 nonfatal CV event during their lifetime, which clinical experts consulted by CADTH for this review deemed inappropriate, both for patients with stable CAD and for those with CAD and a recent MI. Given that CADTH was unable to address these limitations, the costs and health outcomes associated with the use of colchicine in both subgroups are uncertain. The impact of these limitations are unknown, and as a result, the ICERs and price reductions estimated in this report are subject to a high degree of uncertainty.
Results for these subgroups (stable CAD and CAD plus MI), which are assumed to constitute the Health Canada indication (i.e., patients with CAD), were entirely driven by the LoDoCo2 and COLCOT trials. Due to the inclusion and exclusion criteria of the pivotal trials used to inform the economic evaluation (LoDoCo2 and COLCOT), some patients eligible for colchicine under the Health Canada indication would not have been adequately captured in the cost-effectiveness analyses. For example, patients with unstable angina or severe (i.e., New York Heart Association class III or IV) heart failure would have been excluded from the LoDoCo2 trial, as only clinically stable patients (i.e., those with no cardiovascular-related hospital admission in the prior 6 months) were enrolled. As such, the cost-effectiveness estimates do not include all patients who would be eligible for colchicine under the full Health Canada indication.
References
1.Drug Reimbursement Review sponsor submission: Myinfla (colchcine), 0.5 mg film-coated tablets [internal sponsor's package]. Montreal (QC): Pendopharm, a division of Pharmascience Inc; 2021 Jun 10.
2.Myinfla (colchicine): 0.5 mg film-coated tablets [draft product monograph] Montreal (QC): Pendopharm, Division of Pharmascience Inc; 2020 Sep.
3.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Myinfla (colchcine), 0.5 mg film-coated tablets. Montreal (QC): Pendopharm, a division of Pharmascience Inc; 2021 Jun 10.
4.Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med. 2020;383(19):1838-1847. PubMed
5.Samuel M, Tardif JC, Khairy P, et al. Cost-Effectiveness of Low-Dose Colchicine after Myocardial Infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT). Eur Heart J Qual Care Clin Outcomes. 2020;14:14. PubMed
6.Hankey GJ, Jamrozik K, Broadhurst RJ, et al. Five-Year Survival After First-Ever Stroke and Related Prognostic Factors in the Perth Community Stroke Study. Stroke. 2000;31(9):2080-2086. PubMed
7.Lampe FC, Whincup PH, Wannamethee SG, Shaper AG, Walker M, Ebrahim S. The natural history of prevalent ischaemic heart disease in middle-aged men. Eur Heart J. 2000;21(13):1052-1062. PubMed
8.Rawshani A, Rawshani A, Franzén S, et al. Mortality and Cardiovascular Disease in Type 1 and Type 2 Diabetes. N Engl J Med. 2017;376(15):1407-1418. PubMed
9.Sullivan PW, Lawrence WF, Ghushchyan V. A National Catalog of Preference-Based Scores for Chronic Conditions in the United States. Med Care. 2005;43(7):736-749. PubMed
10.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
11.Sullivan PW, Ghushchyan V. Preference-Based EQ-5D index scores for chronic conditions in the United States. Med Decis Making. 2006;26(4):410-420. PubMed
12.Goeree R, Lim ME, Hopkins R, et al. Prevalence, Total and Excess Costs of Diabetes and Related Complications in Ontario, Canada. Canadian Journal of Diabetes. 2009;33(1):35-45.
13.Anis AH, Sun H, Singh S, Woolcott J, Nosyk B, Brisson M. A cost-utility analysis of losartan versus atenolol in the treatment of hypertension with left ventricular hypertrophy. Pharmacoeconomics. 2006;24(4):387-400. PubMed
14.Tu JV, Ko DT, Guo H, et al. Determinants of variations in coronary revascularization practices. Can Med Assoc J. 2012;184(2):179-186. PubMed
15.Guyot P, Ades AE, Beasley M, Lueza B, Pignon JP, Welton NJ. Extrapolation of Survival Curves from Cancer Trials Using External Information. Med Decis Making. 2017;37(4):353-366. PubMed
16.Melsop KA, Boothroyd DB, Hlatky MA. Quality of life and time trade-off utility measures in patients with coronary artery disease. Am Heart J. 2003;145(1):36-41. PubMed
17.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2021 Aug 23.
18.Tran DT, Welsh RC, Ohinmaa A, Thanh NX, Kaul P. Resource Use and Burden of Hospitalization, Outpatient, Physician, and Drug Costs in Short- and Long-term Care After Acute Myocardial Infarction. Can J Cardiol. 2018;34(10):1298-1306. PubMed
19.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Myinfla (colchcine), 0.5 mg film-coated tablets. Montreal (QC): Pendopharm, a division of Pharmascience Inc; 2021 Jun 10.
20.Clopidogral. Clopidogrel Tablets USP 75 mg Clopidogrel, as clopidogrel bisulfate [product monograph]. Brampton (ON): Sanis Health Inc.; 2017: https://pdf.hres.ca/dpd_pm/00042760.PDF. Accessed 2021 Sep 20.
21.Effient®prasugrel (as prasugrel hydrochloride) tablets 10 mg [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2014: https://pi.lilly.com/ca/effient-ca-pm.pdf. Accessed 2021 Sep 20.
22.Brilinta ticagrelor tablets 60 and 90 mg [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2020: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/brilinta-product-monograph-en.pdf. Accessed 2021 Sep 20.
23.Ontario Ministry of H, Ontario Ministry of Long-Term C. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021.
24.Government BC. BC PharmaCare formulary search. 2021; https://pharmacareformularysearch.gov.bc.ca.
25.Saskatchewan Drug Plan: search formulary. 2021; https://formulary.drugplan.ehealthsask.ca/SearchFormulary.
26.Wein T, Lindsay MP, Cote R, Foley N, Berlingieri J, et al. Canadian stroke best practice recommendations: Secondary prevention of stroke, sixth edition practice guidelines, update 2017. Int J Stroke. 2018;13(4):420-443. https://journals.sagepub.com/doi/pdf/10.1177/1747493017743062. Accessed 2021 Sep 20.
27.Captopril Captopril Tablets USP 12.5, 25, 50 and 100 mg [product monograph]. Laval (QC): Pro Doc Ltée 2008: https://pdf.hres.ca/dpd_pm/00005498.PDF. Accessed 2021 Sep 20.
28.APO-Perindopril Perindopril erbumine tablets Apotex Standard 2 mg, 4 mg and 8 mg [product monograph]. Weston (ON): Apotex Inc.; 2018: https://pdf.hres.ca/dpd_pm/00044113.PDF. Accessed 2021 Sep 20.
29.Sandoz Ramipril Ramipril Tablets 1.25 mg, 2.5 mg, 5.0 mg and 10.0 mg [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2015: https://www.sandoz.ca/sites/www.sandoz.ca/files/Ramipril_Tab_PM_English_20151214.pdf. Accessed 2021 Sep 20.
30.pms-TRANDOLAPRIL Trandolapril 0.5 mg, 1 mg, 2 mg and 4 mg Capsules [product monograph]. Montréal (QC): Pharmascience Inc.; 2018: https://pdf.hres.ca/dpd_pm/00045421.PDF. Accessed 2021 Sep 20.
31.Atacand® candesartan cilexetil tablets 4 mg, 8 mg, 16 mg and 32 mg [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2016: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/atacand-product-monograph-en.pdf. Accessed 2021 Sep 20.
32.Cozaar® losartan potassium tablets 25, 50 and 100 mg [product monograph]. Kirkland (QC): Merck Canada Inc.; 2018: https://www.merck.ca/static/pdf/COZAAR-PM_E.pdf. Accessed 2021 Sep 20.
33.Diovan® (valsartan) 40 mg, 80 mg, 160 mg and 320 mg tablets [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc.; 2015: https://www.ask.novartispharma.ca/download.htm?res=diovan_scrip_e.pdf&resTitleId=725. Accessed 2021 Sep 20.
34.Olmetec® Olmesartan Medoxomil 5 mg*, 20 mg, and 40 mg Tablets [product monograph]. Kirkland (QC): Merck Canada Inc.; 2020 https://www.merck.ca/static/pdf/OLMETEC-PM_E.pdf. Accessed 2021 Sep 20.
35.Micardis® Telmisartan Tablets 40 mg and 80 mg [product monograph]. Burlington (ON): Boehringer Ingelheim (Canada) Ltd.; 2013: https://www.boehringer-ingelheim.ca/sites/ca/files/documents/micardispmen.pdf. Accessed 2021 Sep 20.
36.Jamp-Carvedilol Carvedilol Tablets, House Standard 3.125, 6.25, 12.5 and 25 mg. Boucherville (QC): JAMP Pharma Corporation; 2017: https://pdf.hres.ca/dpd_pm/00038626.PDF. Accessed 2021 Sep 20.
37.Sandoz Bisoprolol Bisoprolol fumarate tablets, USP 5 mg, 10 mg [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2009: https://www.sandoz.ca/sites/www.sandoz.ca/files/Bisoprolol_TAB_Monograph.pdf. Accessed 2021 Sep 20.
38.Teva-Atenolol (Atenolol Tablets, 25mg, 50mg, & 100mg) [product monograph]. Toronto (ON): Teva Canada Limited; 2010: https://pdf.hres.ca/dpd_pm/00018948.PDF. Accessed 2021 Sep 20.
39.TEVA-METOPROLOL (Metoprolol tartrate) 25 mg, 50 mg and 100 mg Tablets [product monograph]. Toronto (ON): Teva Canada Limited; 2018: https://pdf.hres.ca/dpd_pm/00043862.PDF. Accessed 2021 Sep 20.
40.Lipitor® (atorvastatin calcium tablets) 10 mg, 20 mg, 40 mg and 80 mg atorvastatin [product monograph]. Kirkland (QC): Upjohn Canada ULC 2020: https://www.pfizer.ca/sites/default/files/202012/Lipitor_PM_E_241951_2020.12.10.pdf. Accessed 2021 Sep 20.
41.Sandoz pravastatin tablets (Pravastatin Tablets BP) Pravastatin sodium 10 mg, 20 mg and 40 mg. Boucherville (QC): Sandoz Canada Inc.; 2017: https://www.sandoz.ca/sites/www.sandoz.ca/files/Pravastatin%20Tablets%20Product%20Monograph.pdf. Accessed 2021 Sep 20.
42.CRESTOR® rosuvastatin calcium Tablets, 5, 10, 20 and 40 mg [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2020: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/crestor-product-monograph-en.pdf. Accessed 2021 Sep 20.
43.Zocor® simvastatin tablets 10, 20 and 40 mg [product monograph]. Kirkland (QC): Merck Canada Inc.; 2019: https://www.merck.ca/static/pdf/ZOCOR-PM_E.pdf. Accessed 2021 Sep 20.
44.Government of Canada. Canadian Chronic Disease Surveillance System (CCDSS). 2020; https://health-infobase.canada.ca/ccdss/data-tool/ Accessed 2021 Sep 20.
45.Samuel M, Tardif JC, Bouabdallaoui N, Khairy P, Dubé MP, et al. Colchicine for Secondary Prevention of Cardiovascular Disease: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Can J Cardiol. 2021;37(5):776-785. PubMed
46.Sutherland G, Dinh T. Understanding the Gap. A Pan-Canadian Analysis of Prescription Drug Insurance Coverage. Ottawa: The Conference Board of Canada; 2017: http://innovativemedicines.ca/wp-content/uploads/2017/12/20170712-understanding-the-gap.pdf. Accessed 2021 Aug 23.
47.Canadian Institute for Health Information. National Prescription Drug Utilization Information System - Plan Information Document Ottawa: Canadian Institute for Health Information; 2020: https://secure.cihi.ca/free_products/npduis-plan-information-2020-en.pdf. Accessed 2021 Aug 21.
48.First Nations and Inuit Health Branch. Non-Insured Health Benefits Program Annual Report 2018-2019. . Ottawa: Indigenous Services Canada; 2020: https://www.sac-isc.gc.ca/DAM/DAM-ISC-SAC/DAM-HLTH/STAGING/texte-text/nihb-Annual_Report_2018-19_1589921777815_eng.pdf. Accessed 2021 Sep 20.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in Table 10 have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 10: CADTH Cost Comparison Table for Secondary Prevention of Atherothrombotic Events in Patients With Coronary Artery Disease
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Colchicine (Myinfla) | 0.5 mg | Tablet | 0.5000a | 0.5 mg once daily | 0.50 | 183 |
aSponsor’s submitted price.19
Table 11: CADTH Cost Comparison Table for Secondary Prevention of Atherothrombotic Events in Patients With Coronary Artery Disease
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Nonsteroidal anti-inflammatory drug | ||||||
Acetylsalicylic acid (generic) | 81 mg | Tablet | 0.0262b | 75 mg to 162 mg once dailye | 0.03 to 0.05 | 10 to 19 |
P2Y12 inhibitorsa | ||||||
Clopidogrel | 75 mg | Tablets | 0.2631c | Loading dose: 300 mg Maintenance dose: 75 mg once daily | First year: 0.27 Second year+: 0.26 | First year: 97 Second year+: 96 |
Prasugrelb (generic) | 10 mg | Tablets | 1.6680 | Loading dose: 60 mg Maintenance dose: 10 mg once daily | First year: 1.70 Second year+: 1.67 | First year: 619 Second year+: 609 |
Ticagrelor (Brilinta) | 60 mg 90 mg | Tablets | 1.5840 | Loading dose: 180 mg Maintenance dose: 90 mg twice daily | First year: 3.18 Second year+: 3.17 | First year: 1,159 Second year+: 1,156 |
Note: Dosage based on product monographs20-22 for the secondary prevention of cardiovascular events. Prices are from Ontario Drug Benefit Formulary (August 2021) unless otherwise indicated.23
aTypically taken for 6-12 months. Recommended dosage for P2Y12 inhibitors is based on the product monograph dosages for acute coronary syndrome.
bBritish Columbia Formulary(August 2021).24
cSaskatchewan Drug Benefit (August 2021).25
dDosage based on Canadian stroke best practice recommendations for the secondary prevention of stroke (2017).26
Table 12: CADTH Cost-Comparison Table for Secondary Prevention of Atherothrombotic Events in Patients With Coronary Artery Disease and Myocardial Infarction
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost | Annual cost |
|---|---|---|---|---|---|---|
Nonsteroidal anti-inflammatory drug | ||||||
Acetylsalicylic acid (generic) | 81 mg | Tablet | 0.0262a | 75 mg to 162 mg once dailye | 0.03 to 0.05 | 10 to 19 |
P2Y12 inhibitorsb | ||||||
Clopidogrel | 75 mg | Tablets | 0.2631c | 75 mg once daily | 0.26 | 96 |
Prasugrela (generics) | 10 mg | Tablets | 1.6680 | Loading dose: 60 mg Maintenance dose: 10 mg once daily | First year: 1.70 Second year+: 1.67 | First year: 619 Second year+: 609 |
Ticagrelor (Brilinta) | 60 mg 90 mg | Tablets | 1.5840 | Loading dose: 180 mg Maintenance dose: 90 mg twice daily | First year: 3.18 Second year+: 3.17 | First year: 1,159 Second year+: 1,156 |
Angiotensin-converting enzyme inhibitors | ||||||
Captopril | 6.25 mg 12.5 mg 25 mg 50 mg 100 mg | Tablet | 0.1237c 0.2120 0.3000 0.5590 1.0395 | 25 mg to 100 mg twice daily 25 mg to 100 mg 3 times daily | 0.60 to 2.08 0.90 to 3.12 | 219 to 759 329 to 1,138 |
Perindopril | 2 mg 4 mg 8 mg | Tablet | 0.1632 0.2042 0.2831 | 2 mg to 8 mg once daily | 0.16 to 0.28 | 60 to 103 |
Ramipril | 1.25 mg 2.5 mg 5 mg 10 mg | Capsule | 0.0708 0.0817 0.0817 0.1034 | 2.5 mg to 10 mg once dailye | 0.08 to 0.10 | 26 to 38 |
Trandolapril | 0.5 mg 1 mg 2 mg 4 mg | Capsule | 0.0698c 0.1762 0.2025 0.2498 | 1 mg to 2 mg once dailye | 0.18 to 0.20 | 64 to 74 |
Angiotensin II receptor blockers | ||||||
Candesartan | 4 mg 8 mg 16 mg 32 mg | Tablet | 0.1700 0.2281 0.2281 0.2281 | 8 to 32 mg once daily | 0.23 | 83 |
Losartan | 25 mg 50 mg 100 mg | Tablet | 0.3147 | 50 mg to 100 mg once daily | 0.31 | 115 |
Valsartan (generics) | 40 mg 80 mg 160 mg 320 mg | Tablet | 0.2211c 0.2159 0.2159 0.2098 | 40 mg to 160 mg twice daily | 0.43 to 0.44 | 158 to 161 |
Olmesartan (generics) | 20 mg 40 mg | Tablet | 0.3019 | 20 mg to 40 mg once dailye | 0.30 | 110 |
Telmisartan (generics) | 40 mg 80 mg | Tablet | 0.2161 | 80 mg once daily | 0.22 | 79 |
Beta-blockers | ||||||
Carvedilol (generics) | 3.125 mg 6.25 mg 12.5 mg 25 mg | Tablet | 0.2431 | 3.125 mg to 25 mg twice daily | 0.49 | 177 |
Bisoprolol (generics) | 5 mg 10 mg | Tablet | 0.0715 0.1044 | 5 mg to 20 mg once dailye | 0.07 to 0.21 | 26 to 76 |
Atenolol (generics) | 50 mg 100 mg | Tablet | 0.1107 0.1821 | 50 mg to 100 mg once dailye | 0.11 to 0.18 | 40 to 66 |
Metoprolol (generics) | 25 mg 50 mg 100 mg | Tablet | 0.0643c 0.0624 0.1361 | 100 mg to 200 mg once daily | 0.14 to 0.27 | 50 to 99 |
Metoprolol (generics) | 100 mg 200 mg | Sustained Release Tablet | 0.1415 0.2568 | 100 mg to 200 mg once daily | 0.14 to 0.26 | 52 to 94 |
HMG-CoA reductase inhibitors (statins) | ||||||
Atorvastatin calcium (generics) | 10 mg 20 mg 40 mg 80 mg | Tablet | 0.1743 0.2179 0.2342 0.2342 | 10 to 80 mg once daily | 0.17 to 0.23 | 64 to 85 |
Pravastatin sodium (generics) | 10 mg 20 mg 40 mg | Tablet | 0.2916 0.3440 0.4143 | 20 to 80 mg once dailyf | 0.34 to 0.83 | 126 to 302 |
Rosuvastatin calcium | 5 mg 10 mg 20 mg 40 mg | Tablet | 0.1284 0.1354 0.1692 0.1990 | 20 mg once daily | 0.17 | 62 |
Simvastatin (generics) | 5 mg 10 mg 20 mg 40 mg 80 mg | Tablet | 0.1023 0.2023 0.2501 0.2501 0.2501 | 40 mg once daily | 0.25 | 91 |
Note: Dosage based on product monograph20-22,27-43 for the secondary prevention of cardiovascular events. Prices are from Ontario Drug Benefit Formulary (August 2021) unless otherwise indicated.23
aBritish Columbia Formulary (August 2021).24
bTypically taken for 6-12 months. Recommended dosage for P2Y12 inhibitors is based on the product monograph dosages for acute coronary syndrome.
cSaskatchewan Drug Benefit (August 2021).25
dDosage based on Canadian stroke best practice recommendations on secondary prevention of stroke (2017).26
eBased on the recommended dosage for hypertension identified from the respective treatment’s product monograph.37,38
fBased on the recommended dosage for hypertension and coronary heart disease from the product monograph.41
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor provided analyses that encompassed patients with stable CAD (informed by the LoDoCo2 trial) and patients with CAD and a recent MI (informed by the COLCOT trial). Based on the inclusion/exclusion criteria of these trials, some groups of patients eligible for colchicine under the Health Canada approved indication would have been excluded (e.g., those with unstable angina and severe heart failure). |
Model has been adequately programmed and has sufficient face validity | No | CADTH identified programming errors in the application of AE event disutilities and drug costs in the sponsor’s model; these were corrected in CADTH’s base case. Programming errors were also identified in the treatment-specific individual component distribution (Dirichlet) adopted by the sponsor for the composite outcome (CV events) in the CAD plus MI subgroup. For this subgroup, the percentage of each individual CV event within the composite was assumed to be fixed in CADTH reanalyses. |
Model structure is adequate for decision problem | No | Structural limitations of the model including not allowing for subsequent nonfatal CV events after an initial event and the potential for recurrent events to lead to a more progressed disease state. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
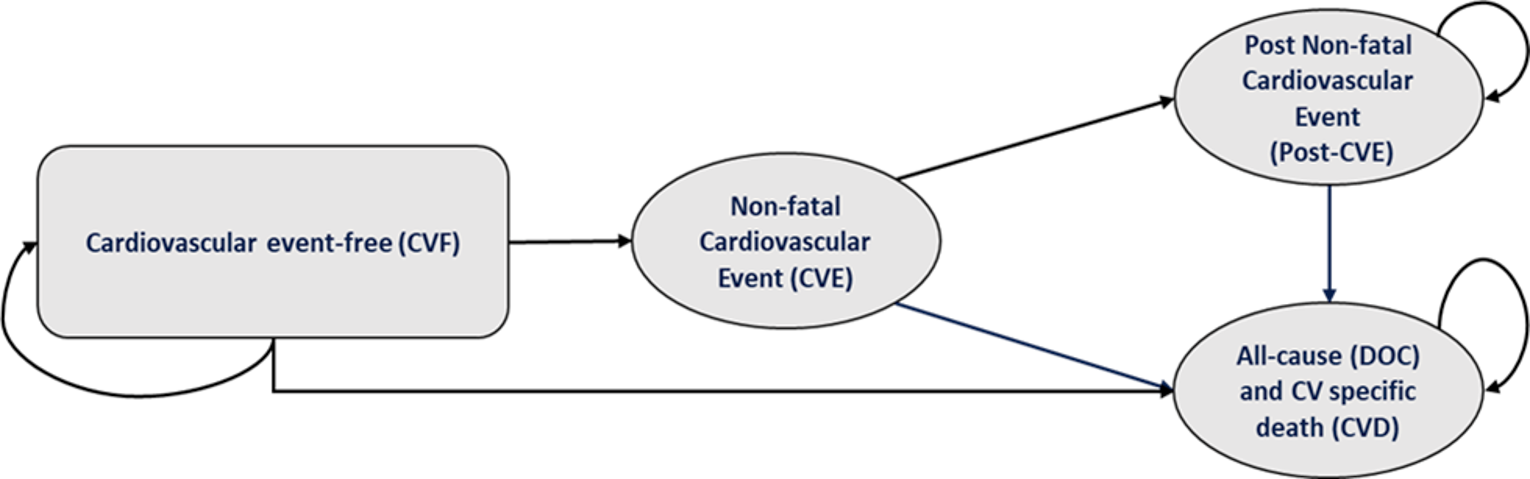
Detailed Results of the Sponsor’s Base Case
Table 14: Disaggregated Summary of the Sponsor’s Base Casea
Parameter | Colchicine plus SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 15.65 | 15.40 | 0.25 |
By health state | |||
Cardiovascular event–free | 13.51 | 12.45 | 1.05 |
Acute event states | 0.21 | 0.27 | -0.06 |
Nonfatal MI | 0.10 | 0.13 | -0.03 |
Nonfatal stroke | 0.02 | 0.02 | -0.01 |
Coronary revascularization | 0.09 | 0.12 | -0.03 |
Post–acute event states | 1.93 | 2.67 | -0.74 |
Post–nonfatal MI | 0.87 | 1.20 | -0.33 |
Post–nonfatal stroke | 0.17 | 0.24 | -0.06 |
Post–resuscitated cardiac arrest | 0.00 | 0.00 | 0.00 |
Post–coronary revascularization | 0.89 | 1.23 | -0.34 |
Discounted QALYs | |||
Total | 11.96 | 11.45 | 0.51 |
By health state | |||
Cardiovascular event–free | 10.51 | 9.69 | 0.82 |
Acute event states | |||
Nonfatal MI | 0.06 | 0.09 | -0.02 |
Nonfatal stroke | 0.01 | 0.01 | 0.00 |
Coronary revascularization | 0.06 | 0.08 | -0.02 |
Post–acute event states | |||
Post–nonfatal MI | 0.60 | 0.82 | -0.22 |
Post–nonfatal stroke | 0.11 | 0.15 | -0.04 |
Post–coronary revascularization | 0.70 | 0.96 | -0.26 |
Disutility associated with treatment-related AE | -0.08 | -0.35 | 0.27 |
By time period | |||
Utility generated within trial period | 1.49 | 1.47 | 0.03 |
Utility generated after trial period | 10.47 | 9.98 | 0.49 |
Discounted costs ($) | |||
Total | 29,507 | 31,672 | -2,165 |
Drug acquisition cost | 1,855 | 0 | 1,855 |
Total cardiovascular disease cost | 12,419 | 17,001 | -4,582 |
CV death | 4,952 | 6,777 | -1,825 |
Death from other causes | 0 | 0 | 0 |
Cardiovascular event-free | 0 | 0 | 0 |
Acute event states | |||
Nonfatal MI | 1,229 | 1,671 | -442 |
Nonfatal stroke | 395 | 536 | -141 |
Coronary revascularization | 1,207 | 1,640 | -433 |
Post-acute event states | |||
Post-nonfatal MI | 2,947 | 4,056 | -1,110 |
Post–nonfatal stroke | 861 | 1,183 | -322 |
Post–coronary revascularization | 828 | 1,138 | -310 |
Follow-up cost | 2,235 | 1,745 | 490 |
Adverse event costs | 12,997 | 12,926 | 71 |
ICER ($ per QALY) | Colchicine dominant | ||
CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY= life-year; MI = myocardial infarction; QALY = quality-adjusted life-year; SOC = standard of care.
Reference: Sponsor’s pharmacoeconomic submission.3
aThe sponsor’s base-case analysis was informed by data from the LoDoCo2 trial, which enrolled patients whose coronary artery disease had been stable for at least 6 months. Scenario analyses were provided by the sponsor for patients with CAD and a recent MI, informed by the COLCOT trial.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of the CADTH Base Case: Stable Coronary Artery Disease
Table 15: Summary of the Stepped Analysis of the CADTH Reanalysis Results — Stable Coronary Artery Disease
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 31,672 | 11.45 | Reference |
Colchicine + SOC | 29,507 | 11.96 | Dominant | |
Sponsor’s corrected base case | SOC | 31,885 | 11.43 | Reference |
Colchicine + SOC | 29,644 | 11.68 | Dominant | |
CADTH reanalysis 1: Analysis time horizon | SOC | 24,846 | 10.16 | Reference |
Colchicine + SOC | 23,710 | 10.32 | Dominant | |
CADTH reanalysis 2: Distribution of CV events | SOC | 31,374 | 11.44 | Reference |
Colchicine + SOC | 29,929 | 11.66 | Dominant | |
CADTH reanalysis 3: Treatment adherence | SOC | 31,739 | 11.42 | Reference |
Colchicine + SOC | 30,552 | 11.67 | Dominant | |
CADTH base case (1+2+3) | SOC | 24,435 | 10.03 | Reference |
Colchicine + SOC | 24,449 | 10.18 | 100 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
aDominant indicates that a treatment is less costly and more effective (higher QALYs) than the reference.
Table 16: Disaggregated Summary of CADTH’s Base-Case Reanalyses — Stable Coronary Artery Disease
Parameter | Colchicine + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 13.60 | 13.48 | 0.12 |
By health state | |||
Cardiovascular event–free | 11.88 | 11.07 | 0.81 |
Acute event states | |||
Nonfatal MI | 0.09 | 0.12 | -0.04 |
Nonfatal stroke | 0.02 | 0.02 | 0 |
Coronary revascularization | 0.08 | 0.11 | -0.03 |
Post–acute event states | |||
Post–nonfatal MI | 0.70 | 1.00 | -0.30 |
Post–nonfatal stroke | 0.15 | 0.18 | -0.03 |
Post–coronary revascularization | 0.68 | 0.97 | -0.29 |
Discounted QALYs | |||
Total | 10.18 | 10.03 | 0.14 |
By health state | |||
Cardiovascular event–free | 9.25 | 8.62 | 0.63 |
Acute-event states | |||
Nonfatal MI | 0.06 | 0.08 | -0.02 |
Nonfatal stroke | 0.01 | 0.01 | 0 |
Coronary revascularization | 0.05 | 0.07 | -0.02 |
Post–acute event states | |||
Post–nonfatal MI | 0.48 | 0.68 | -0.20 |
Post–nonfatal stroke | 0.10 | 0.12 | -0.02 |
Post–coronary revascularization | 0.53 | 0.76 | -0.23 |
Disutility associated with treatment-related AE | |||
By time period | |||
Utility generated within trial period | 1.47 | 1.47 | 0.0048 |
Utility generated after trial period | 8.70 | 8.56 | 0.14 |
Discounted costs ($) | |||
Total | 24,449 | 24,435 | 14 |
Drug acquisition cost | 2,484 | 0 | 2,484 |
Total cardiovascular disease cost | 8,591 | 11,535 | -2,944 |
CV death | 2,202 | 2,761 | -558 |
Death from other causes | 0 | 0 | 0 |
Cardiovascular event–free | 0 | 0 | 0 |
Total acute-event state | |||
Nonfatal MI | 1,130 | 1,158 | -455 |
Nonfatal stroke | 419 | 496 | -76 |
Coronary revascularization | 1,097 | 1,546 | -449 |
Total post–acute event state | |||
Post–nonfatal MI | 2,359 | 3,360 | -1,001 |
Post-nonfatal stroke | 743 | 887 | -143 |
Post–coronary revascularization | 641 | 901 | -261 |
Follow-up eost | 2,010 | 1,556 | 455 |
Adverse-event costs | 11,364 | 11,344 | 19 |
ICER ($ per QALY) | 100 | ||
CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY = life-year; MI = myocardial infarction; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analyses: Stable Coronary Artery Disease
Table 17: CADTH Scenario Analyses — Stable Coronary Artery Disease
Scenario | CADTH base case | CADTH scenario |
|---|---|---|
Scenario analyses | ||
1. Analysis time horizon | 20 years | Lifetime (44 years) |
2. Analysis time horizon | As above | 10 years |
3. Clinical effectiveness (CV events) | HR 0.69 for colchicine plus SOC vs. SOC, based on overall data reported for the LoDoCo2 trial. | HR 0.51 for colchicine plus SOC vs. SOC, based on CV event data from patients (N = 1,904) enrolled at Australian study centres in the LoDoCo2 trial. |
4. Clinical effectiveness (CV events) | As above | HR 0.92 for colchicine plus SOC vs. SOC, based on CV event data from patients (N = 3,618) enrolled at study centres in The Netherlands in the LoDoCo2 trial. |
5. Cost of managing myocardial infarction | Based on costs reported in Goeree et al. 200912: First year: $12,775 Subsequent years: $3,379 | Based on costs reported in Tran 201818: First year: $21,732a Subsequent year: $925a |
CI = confidence interval; CV = cardiovascular; HR = hazard ratio; SOC = standard of care; vs = versus.
aCosts reported in Tran (2018)18 (2016 Canadian Dollars) were inflated to 2021 Canadian Dollars by use of the Canadian Consumer Price Index.
Table 18: CADTH Scenario Analyses Results — Stable Coronary Artery Disease
Drug | Total Costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|
CADTH Base case | |||
SOC | 24,435 | 10.03 | Ref. |
Colchicine + SOC | 24,449 | 10.18 | 100 |
Scenario 1: Lifetime horizon (44 years) | |||
SOC | 31,374 | 11.44 | Ref. |
Colchicine + SOC | 30,925 | 11.66 | Dominant |
Scenario 2: 10-year horizon | |||
SOC | 14,287 | 6.39 | Ref. |
Colchicine + SOC | 14,622 | 6.44 | 7,018 |
Scenario 3: Effectiveness estimates based on Australian study centre data (LoDoCo2 trial) | |||
SOC | 24,695 | 10.18 | Ref. |
Colchicine + SOC | 22,826 | 10.41 | Dominant |
Scenario 4: Effectiveness estimates based on Netherlands study centre data (LoDoCo2 trial) | |||
SOC | 24,695 | 10.18 | Ref. |
Colchicine + SOC | 27,029 | 10.20 | 117,377 |
Scenario 5: Cost of managing myocardial infarction | |||
SOC | 23,356 | 10.18 | Ref. |
Colchicine + SOC | 23,787 | 10.31 | 3,163 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Detailed Results of the CADTH Base Case: Coronary Artery Disease and a Recent Myocardial Infarction
Table 19: Summary of the Stepped Analysis of the CADTH Reanalysis Results — Coronary Artery Disease and a Recent Myocardial Infarction
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 33,482 | 13.68 | Ref. |
Colchicine + SOC | 32,820 | 14.19 | Dominant | |
Sponsor’s corrected base case | SOC | 33,659 | 13.71 | Ref. |
Colchicine + SOC | 32,975 | 13.91 | Dominant | |
CADTH reanalysis 1: SOC costs | SOC | 36,603 | 13.71 | Ref. |
Colchicine + SOC | 35,949 | 13.91 | 11,366 | |
CADTH reanalysis 2: Analysis time horizon | SOC | 24,638 | 11.13 | Ref. |
Colchicine + SOC | 24,615 | 11.23 | Dominant | |
CADTH reanalysis 3: Distribution of CV events | SOC | 32,936 | 13.76 | Ref. |
Colchicine + SOC | 33,712 | 13.85 | 8,574 | |
CADTH reanalysis 4: Treatment adherence | SOC | 33,659 | 13.71 | Ref |
Colchicine + SOC | 34,163 | 13.91 | 2,576 | |
CADTH reanalysis 5: Health-state utility values | SOC | 33,659 | 12.18 | Ref. |
Colchicine + SOC | 32,975 | 12.32 | Dominant | |
CADTH base case: 1 + 2 + 3 + 4 + 5 | SOC | 27,956 | 9.83 | Ref. |
Colchicine + SOC | 29,256 | 9.85 | 64,922 |
CV = cardiovascular events; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference; SOC = standard of care
Table 20: Disaggregated Summary of CADTH’s Base-Case Reanalyses — Coronary Artery Disease and a Recent Myocardial Infarction
Parameter | Colchicine + SOC | SOC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 14.86 | 14.86 | 0 |
By health state | |||
Cardiovascular event–free | 13.29 | 12.77 | 0.52 |
Acute-event states | |||
Nonfatal MI | 0.11 | 0.11 | 0 |
Nonfatal stroke | 0.01 | 0.02 | -0.1 |
Coronary revascularization | 0.03 | 0.06 | -0.03 |
Resuscitated cardiac arrest | 0 | 0 | 0 |
Post–acute event states | |||
Post–nonfatal MI | 1.05 | 1.08 | -0.3 |
Post–nonfatal stroke | 0.07 | 0.21 | -0.14 |
Post–coronary revascularization | 0.29 | 0.59 | -0.30 |
Post–resuscitated cardiac arrest | 0.01 | 0.02 | -0.01 |
Discounted QALYs | |||
Total | 9.85 | 9.83 | 0.02 |
By health state | |||
Cardiovascular event–free | 9.11 | 8.75 | 0.36 |
Acute-event states | |||
Nonfatal MI | 0.07 | 0.07 | 0 |
Nonfatal stroke | 0 | 0.01 | -0.01 |
Coronary revascularization | 0.02 | 0.04 | -0.02 |
Resuscitated cardiac arrest | 0 | 0 | 0 |
Post–acute event states | |||
Post–nonfatal MI | 0.72 | 0.74 | -0.02 |
Post–nonfatal stroke | 0.04 | 0.13 | -0.09 |
Post–coronary revascularization | 0.20 | 0.40 | -0.20 |
Post–resuscitated cardiac arrest | 0.01 | 0.02 | -0.01 |
Disutility associated with treatment-related AE | -0.33 | -0.33 | 0 |
By time period | |||
Utility generated within trial period | 1.30 | 1.30 | 0.002 |
Utility generated after trial period | 8.55 | 8.53 | 0.02 |
Discounted costs ($) | |||
Total | 29,256 | 27,956 | 1,301 |
Drug acquisition cost | 6,355 | 3,648 | 2,707 |
Total cardiovascular disease cost | 8,416 | 10,072 | -1,656 |
CV death | 2,296 | 2,116 | 180 |
Death from other causes | 0 | 0 | 0 |
Cardiovascular event–free | 0 | 0 | 0 |
Total acute-event state | |||
Nonfatal MI | 1,398 | 1,425 | -27 |
Nonfatal stroke | 158 | 492 | -334 |
Coronary revascularization | 404 | 802 | -399 |
Resuscitated cardiac arrest | 13 | 25 | -12 |
Total post–acute event state | |||
Post–nonfatal MI | 3,542 | 3,632 | -89 |
Post–nonfatal stroke | 326 | 1,023 | -696 |
Post-coronary revascularization | 273 | 547 | -274 |
Post–resuscitated cardiac arrest | 6 | 11 | -5 |
Follow-up cost | 2,159 | 1,749 | 409 |
Adverse-event costs | 12,326 | 12,486 | -160 |
ICER ($ per QALY) | 64,922 | ||
CV = cardiovascular; ICER = incremental cost-effectiveness ratio; LY= life-year; MI = myocardial infarction; QALY = quality-adjusted life-year; SOC = standard of care.
Scenario Analyses: Coronary Artery Disease and a Recent Myocardial Infarction
Table 21: CADTH Scenario Analyses — Coronary Artery Disease and a Recent Myocardial Infarction
Scenario | CADTH base case | CADTH scenario |
|---|---|---|
Scenario analyses | ||
1. Analysis time horizon | 20 years | Lifetime (49 years) |
2. Analysis time horizon | As above | 10 years |
3. Cost of managing myocardial infarction | Based on costs reported in Goeree et al. (2009)12: First year: $12,775 Subsequent years: $3,379 | Based on costs reported in Tran (2018)18: First year: $21,732a Subsequent year: $925a |
aCosts reported in Tran (2018)18 in 2016 Canadian Dollars were inflated to 2021 values using the Canadian Consumer Price Index.
Table 22: CADTH Scenario Analyses Results — Coronary Artery Disease and a Recent Myocardial Infarction
Drug | Total Costs ($) | Total QALYs | ICER ($/QALY)a |
|---|---|---|---|
CADTH Base Case | |||
SOC | 28,094 | 9.90 | Reference |
Colchicine + SOC | 29,483 | 9.92 | 70,541 |
Scenario 1: Lifetime horizon (49 years) | |||
SOC | 37,481 | 12.22 | Reference |
Colchicine + SOC | 39,453 | 12.28 | 32,935 |
Scenario 2: 10-year horizon | |||
SOC | 15,984 | 5.84 | Reference |
Colchicine + SOC | 16,915 | 5.84 | 134,390 |
Scenario 3: Cost of managing myocardial infarction | |||
SOC | 26,451 | 9.90 | Reference |
Colchicine + SOC | 27,884 | 9.92 | 72,824 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
aBased on deterministic analyses.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 23: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA)19 assessed the expected budgetary impact of reimbursing colchicine for patients with existing CAD, in line with the Health Canada–indicated population. The BIA was conducted from the perspective of the Canadian public drug plans, over a 3-year time horizon and included drug acquisition costs, markup, and dispensing fees. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec), as well as the Non-Insured Health Benefits Program. Key inputs to the BIA are documented in Table 24.
The analytic framework, which used an epidemiological-based approach, leveraged data from Statistics Canada and published literature to estimate the number of patients eligible for colchicine. The sponsor assumed that CAD is synonymous with ischemic heart disease and adopted the age-standardized prevalence and incidence of ischemic heart disease in Canada to estimate the population size over the time horizon (2022-2024).44 The sponsor determined trends in annual mortality and incidence rates based on 16 years of historical data (2000-2016) retrieved from the Canadian Chronic Disease Surveillance System and the Government of Canada.44 The sponsor assumed an average annual population growth rate of 1.55%. In the baseline year (2021), the sponsor adopted an annual CAD incidence of 0.51%, CAD prevalence of 7.86%, and mortality of 1.56%. The sponsor assumed the annual CAD incidence and mortality rate decrease by 4.16% and 1.71%, respectively.44 The sponsor divided the CAD population into 2 age categories, where 56.8% of all CAD patients were under the age of 65 years and 43.2% were above the age of 65 years.45 Then, a provincial weighted average of 30.4% for CAD patients aged <65 years and 97.0% for CAD patients aged ≥65 years was used to estimate the population size covered by the public drug plans.46
The cost of colchicine was based on the sponsors submitted daily price ($0.50 per 0.5 mg tablet), assumed treatment adherence of 65%, and a dosing regimen in line with the product monograph, resulting in an average annual cost of $152.19 The sponsor’s submission considered a reference scenario in which patients received SOC and a new-drug scenario in which colchicine was reimbursed as an add-on therapy to the current SOC. SOC was not defined by the sponsor, and no costs for SOC were included in the model. The sponsor assumed colchicine would capture 20.0% and 8.0% of the total market share by year 3 for incident and prevalent population, respectively.
Table 24: Summary of Key Model Parameters — Health Canada–Indicated Population
Parameter | Sponsor’s estimate |
|---|---|
Target population | |
Annual prevalence | 7.86%44 |
Annual incidence | 0.51%44 |
Annual mortality | 1.56%44 |
Growth in annual incidence | −4.16% |
Growth in annual mortality | −1.71% |
< 65 years | 30.40%a |
≥ 65 years | 97.00%a |
Number of patients eligible for drug under review (Year 1 / Year 2 / Year 3) | 1,192,923 / 1,242,295 / 1,290,339 |
Market Uptake (Year 1 / Year 2 / Year 3) | |
Uptake (reference scenario) Colchicine Incident population Prevalent population | 0.0% / 0.0% / 0.0% 0.0% / 0.0% / 0.0% |
Uptake (new drug scenario) Colchicine Incident population Prevalent population | 8.0% / 12.0% / 20.0% 2.0% / 4.0% / 8.0% |
Cost of treatment (per patient) | |
Annual cost of treatment ($) SOC Colchicine | $0 $152b |
aProvincial weighted average.
bAssuming 65% adherence, and includes markups, dispensing fees, and copayments.
Source: Sponsor’s BIA submission,19 unless otherwise indicated.
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor estimated the net budget impact of introducing colchicine for the Health Canada–indicated population (patients with CAD) to be $3,532,544 in year 1, $6,934,344 in year 2, and $13,954,907 in year 3, for an overall 3-year budget impact of $24,421,794 to the public drug plans.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of patients eligible for public drug plan coverage of colchicine is underestimated: The sponsor estimated the proportion of patients eligible for public drug plan coverage based on the number of patients enrolled in public plans for each jurisdiction.46 However, it is more appropriate to use the proportion of patients eligible, rather than enrolled, as the market size will be determined by all patients eligible for public coverage; therefore the BIA should consider all patients eligible regardless of whether they are presently enrolled.
In the CADTH reanalysis, the proportion of patients eligible for public drug plan coverage in each jurisdiction46 was used to determine the market size for colchicine.
The cost of colchicine was underestimated: In the calculation of drug costs, the sponsor assumed a treatment adherence of 65% for colchicine, based on claims data for statins. The assumption that adherence to colchicine would be the same as that for statins was not justified by the sponsor. The LoDoCo2 study enrolled an enriched population that was tolerant and adherent to colchicine, while in the COLCOT study, adherence to treatment was high (98%) in both groups among patients who did not permanently stop the study drug. Adopting a lower adherence rate thus inappropriately reduces the cost of colchicine in the model.
In the CADTH reanalysis, the annual drug cost of colchicine was based on the sponsor’s submitted price of colchicine without adjustment for adherence. CADTH explored the impact of assuming lower adherence in a scenario analysis.
There is uncertainty in the market share and uptake of colchicine in patients with CAD and MI: In the sponsor’s base case, the market share of colchicine was assumed to be equal across all patients with CAD, without differentiation between those with stable CAD or after an acute event (e.g., MI). Clinical experts consulted for this review indicated that the market share of colchicine in incident patients is likely to be higher among patients with CAD and a recent MI compared to patients with stable MI. The sponsor also indicated that prescriptions for colchicine in incident patients would be initiated in a hospital setting and assumed that hospital-initiated products have slow uptake rates. Within the hospital setting, treatment algorithms are often used to guide clinician prescribing patterns, and given the expected algorithmically driven prescription of colchicine, the clinical experts predicted an initial jump in the market share of colchicine for patients with CAD and MI, instead of a gradual increase.
CADTH was unable to address this limitation owing to the structure of the sponsor’s model.
The cost of prolonged survival on colchicine is not captured in the estimated budget impact: As colchicine is an add-on treatment, the sponsor assumed no cost for SOC. Similarly, the sponsor assumed no difference in survival with the addition of colchicine. This is in contrast to the sponsor’s submitted economic evaluation, which predicted a survival advantage of colchicine plus SOC compared to SOC alone among patients with stable CAD and among those with CAD and a recent MI. Should colchicine be associated with increased survival, additional drug costs associated with SOC will be incurred by patients taking colchicine. As such, it is possible that the estimated budget impact of reimbursing colchicine may be underestimated. CADTH notes, however, that the increased survival predicted by the sponsor’s economic model is not supported by clinical trial data and is highly uncertain. CADTH was unable to explore the extent to which the budget impact may be underestimated by this limitation.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s base case by changing the proportion of patients eligible for public drug plan coverage and assuming higher adherence for colchicine.
Table 25: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Percentage of patients covered by public drug plans | Determined by the jurisdiction-specific percentage of patients enrolled | Determined by the jurisdiction-specific percentage of patients eligible for enrolment in public drug plans46 |
2. Colchicine treatment adherence | 65% | 100% |
CADTH base case | CADTH reanalysis 1 + 2 | |
The results of the CADTH stepwise reanalysis are presented in summary format in Table 26 and a more detailed breakdown is presented in Table 27.
In the CADTH reanalysis, the 3-year budget impact of reimbursing colchicine for patients with CAD is $52,926,508 (Year 1: $7,650,184; Year 2: $15,021,976; Year 3: $30,254,348).
Table 26: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total | |
|---|---|---|
Drug costs only ($) | Dispensing fees, markups and copayment included ($) | |
Submitted BIA | $21,127,120 | $24,921,794 |
CADTH base case | ||
CADTH reanalysis 1 – drug plan coverage | $30,199,549 | $34,402,230 |
CADTH reanalysis 2 – colchicine adherence | $32,503,262 | $37,571,991 |
CADTH base case | $46,460,845 | $52,926,508 |
CADTH also conducted an additional scenario analysis to address remaining uncertainty, using the CADTH base case. Results are provided in Table 27.
1. Assuming a lower adherence rate to colchicine (90%)
Table 27: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1a | Year 2a | Year 3a | Three-year totala |
|---|---|---|---|---|---|---|
Sponsor submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $3,532,544 | $6,934,344 | $13,954,907 | $24,421,794 | |
Budget impact | $0 | $3,532,544 | $6,934,344 | $13,954,907 | $24,421,794 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $7,650,184 | $15,021,976 | $30,254,348 | $52,926,508 | |
Budget impact | $0 | $7,650,184 | $15,021,976 | $30,254,348 | $52,926,508 | |
CADTH scenario analysis 1: 90% adherence to colchicine | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $6,885,166 | $13,519,779 | $27,228,913 | $47,633,857 | |
Budget impact | $0 | $6,885,166 | $13,519,779 | $27,228,913 | $47,633,857 |
aIncludes dispensing fees, markups, and copayments.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.