CADTH Reimbursement Review
Macitentan and Tadalafil (Opsynvi)
Sponsor: Janssen Inc.
Therapeutic area: Pulmonary arterial hypertension
Clinical and Pharmacoeconomic Report
Abbreviations
6MWD
6-minute walking distance
6MWT
6-minute walk test
AE
adverse event
AUC
area under the curve
CDEC
CADTH Canadian Drug Expert Committee
CI
confidence interval
Cmax
peak concentration
ERA
endothelin receptor antagonist
EOT
end of treatment
FC
functional class
FDC
fixed-dose combination
FPAH
familial pulmonary arterial hypertension (or heritable pulmonary arterial hypertension)
HR
hazard ratio
HRQoL
health-related quality of life
IPAH
idiopathic pulmonary arterial hypertension
ITT
intention to treat
LOCF
last observation carried forward
ODB
Ontario Drug Benefit
PAH
pulmonary arterial hypertension
PDE5
phosphodiesterase type 5
SAE
serious adverse event
ULN
upper limit of normal
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Macitentan plus tadalafil fixed-dose combination Film-coated tablets (10 mg and 40 mg) for oral administration |
Indication | For the long-term treatment of PAH (WHO Group 1) to reduce morbidity in patients of WHO FC II or III whose PAH is either idiopathic or heritable or associated with connective tissue disease or congenital heart disease. Macitentan and tadalafil should be used in patients who are currently treated concomitantly with stable doses of macitentan 10 mg and tadalafil 40 mg (20 mg × 2) as separate tablets. |
Reimbursement request | As per indication |
Health Canada approval status | Pre-NOC |
Health Canada review pathway | Standard review |
NOC date | Target: October 14, 2021 |
Sponsor | Janssen Inc. |
FC = functional class; NOC = Notice of Compliance; PAH = pulmonary arterial hypertension.
Introduction
Pulmonary arterial hypertension (PAH) (also classified as WHO Group 1 pulmonary hypertension) is a rare, debilitating, life-limiting disease of the pulmonary vasculature characterized by vascular proliferation and remodelling of the distal pulmonary arteries. The symptoms of PAH include fatigue, weakness, chest pain, light-headedness, fainting, abdominal distension, dyspnea during exercise, swelling of the legs and ankles, and respiratory difficulties.1 Health-related quality of life (HRQoL) of these patients is often compromised.1 In early stages, patients affected by PAH are asymptomatic or they have mild nonspecific symptoms; delayed diagnosis is common.2
The estimated annual incidence of diagnosed PAH in the general population ranges from 0.9 to 10.7 cases per million persons, while the prevalence is between 6 and 26 cases per million persons.3-8 A recent study in Canada indicated a much higher rate, with estimated incidence of PAH of 4 per 100,000 persons per year and a prevalence of 29 per 100,000 persons.9 Females represent 60% to 83% of patients with PAH.10 Approximately half (43% to 50%) of diagnosed patients have idiopathic PAH (IPAH) or familial (i.e., heritable) PAH (FPAH), and half (50% to 56%) have PAH associated with another disease or drug- or toxin-induced PAH.4
There are various therapies, including drugs to relieve the symptoms of PAH. Patients with PAH are typically prescribed supportive care (i.e., oxygen, calcium channel blockers, oral anticoagulants, and diuretics) as well as drugs from the following classes of drugs approved to treated PAH: phosphodiesterase type 5 (PDE5) inhibitors (sildenafil, tadalafil), endothelin receptor antagonists (ERAs) (bosentan, ambrisentan, macitentan), soluble guanylate cyclase stimulator (riociguat), prostacyclin receptor agonists (selexipag), or prostanoids (epoprostenol, treprostinil).11 Treatment typically follows a sequential approach, starting with a single drug (often a PDE5 inhibitor or an ERA) and adding subsequent drugs as the patient’s disease progresses. The use of initial combination therapy is recommended in certain patients12 following the results of the combination therapy trial, AMBITION (ambrisentan plus tadalafil versus ambrisentan or tadalafil).13
Macitentan is an ERA and tadalafil is a PDE5 inhibitor; both have Health Canada indications for the treatment of patients with WHO Group 1 PAH and WHO functional class (FC) II or III. The product monograph for macitentan notes that it is effective when used as monotherapy or in combination with PDE5 inhibitors. Both drugs have been reviewed by CADTH and received recommendations to reimburse with conditions. Macitentan-tadalafil fixed-dose combination (FDC) is the first FDC therapy for the treatment of PAH. Macitentan-tadalafil FDC was submitted to CADTH before Notice of Compliance. The indication is for the long-term treatment of PAH (WHO Group 1) to reduce morbidity in patients of WHO FC II or III whose PAH is either idiopathic or heritable or associated with connective tissue disease or congenital heart disease. The product monograph states that macitentan-tadalafil FDC should be used in patients who are currently treated concomitantly with stable doses of macitentan 10 mg and tadalafil 40 mg (20 mg × 2) as separate tablets. The sponsor’s requested reimbursement is per the indication in patients switching from treatment with the individual components to the FDC.14
The objective of this report is to review the potential benefits and harms of macitentan-tadalafil FDC in patients with PAH (WHO Group 1) and WHO FC II or III whose PAH is either idiopathic or heritable or associated with connective tissue disease or congenital heart disease and switching from concomitant treatment with macitentan 10 mg and tadalafil 40 mg as separate tablets to the FDC. The sponsor has suggested that an unmet need exists for additional therapies that reduce pill burden and improve adherence and reduce hospitalization, while improving stability of product availability and providing cost-savings to payers.
Stakeholder Perspective
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
CADTH received no patient group submission for the review of macitentan-tadalafil FDC.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
One clinical expert with expertise in the diagnosis and management of PAH was consulted by CADTH. The clinical expert indicated that the macitentan-tadalafil FDC would mostly be prescribed to patients switching from existing dual therapy with tadalafil and macitentan. Patients would be switched to the macitentan-tadalafil FDC for convenience to reduce overall pill burden unless the individual components have not been tolerated by the patient.
Initiation of the macitentan-tadalafil FDC in newly diagnosed patients would be of interest, pending data from the A DUE study on initial therapy with the FDC. Currently, most newly diagnosed patients would be prescribed ambrisentan plus tadalafil in patients appropriate to receive this combination upfront because of the available data supporting the long-term efficacy of that specific combination from the AMBITION trial. However, this is outside of the Health Canada switch indication and reimbursement request from the sponsor.
Clinician Group Input
CADTH received no clinician group submission for the review of macitentan-tadalafil FDC.
Drug Program Input
Drug programs asked about the place in therapy for macitentan-tadalafil FDC and the potential for prescribing it to patients outside of the indication and reimbursement request. The responses to the questions are shown in Table 3. The clinical expert consulted by CADTH responded to the main question about place in therapy.
Clinical Evidence
Description of the Study
The CADTH clinical review was based on a summary of clinical evidence provided by the sponsor with the CADTH tailored review process, including bioequivalence studies and the SERAPHIN study. The SERAPHIN trial was previously evaluated as part of the CADTH review of macitentan, which received a recommendation to reimburse in 2015 with the clinical condition of a contraindication or inadequate response to sildenafil or tadalafil.15 Therefore, the combination use of macitentan and tadalafil was previously established and recommended by CADTH. The data on the macitentan 3 mg group were not presented for this submission because this dose is not aligned with the Health Canada–approved dose.
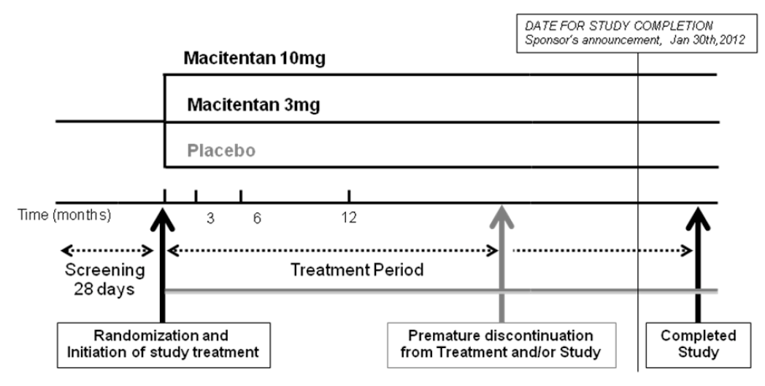
SERAPHIN was a multinational study that included 5 centres in Canada.16 A total of 742 patients were randomly assigned (1:1:1) to receive placebo (250 patients), macitentan 3 mg (250 patients), or macitentan 10 mg (242 patients) and were included in the intention-to-treat (ITT) population.16 Patients were aged 12 years or older at study entry, with a hemodynamically confirmed diagnosis of symptomatic PAH, with WHO FC II to IV. IPAH, FPAH, and PAH associated with collagen vascular disease, congenital heart disease, HIV infection, or drugs and toxins were eligible. Patients were required to have a 6-minute walking distance (6MWD) of 50 m or more at screening and randomization. Importantly, concomitant treatment with oral PDE5 inhibitors, oral or inhaled prostanoids, calcium channel blockers, or L-arginine was allowed at study entry and could be continued throughout, provided that the patient had been receiving a stable dose for at least 3 months before randomization and remained on a stable dose. Patients receiving IV or subcutaneous prostanoids were excluded. At baseline of the SERAPHIN study, 61% of patients had been treated with a PDE5 inhibitor (61.4%) and 5% with oral or inhaled prostanoids. Sildenafil was the most common PAH therapy at baseline (58%).
The primary end point was a composite outcome of the time to first morbidity event or all-cause death. Morbidity events were atrial septostomy, lung transplantation, initiation of treatment with IV or subcutaneous prostanoids, worsening of PAH atrial septostomy, lung transplantation, initiation of IV or subcutaneous prostanoids, or worsening of PAH. Secondary efficacy end points included the change from baseline to month 6 in 6MWD, the percentage of patients with an improvement in WHO FC from baseline to month 6, time to death due to PAH or hospitalization for PAH up to the end of treatment (EOT), and time to death from any cause up to EOT and up to the end of the study.
Efficacy Results
A total of 192 patients in the full population of the SERAPHIN study had a composite primary end point event over a median treatment period of 115 weeks: 116 patients (46.4%) in the placebo group and 76 patients (31.4%) in the macitentan 10 mg group. Worsening of PAH was the most frequent primary end point event (37.2% versus 24.4% for placebo and macitentan 10 mg, respectively). The hazard ratio (HR) for the time to first morbidity event or mortality was 0.55 (97.5% confidence interval [CI], 0.39 to 0.76; log-rank P < 0.001) in favour of macitentan versus placebo.
The SERAPHIN study included a mixed population of patients who received monotherapy (macitentan or placebo) or dual therapy (baseline PAH therapy plus macitentan or placebo). More than 60% of patients were in the latter group, with most patients treated with macitentan plus sildenafil; a minority of patients (approximately 1%) were treated with macitentan plus tadalafil. In the subgroup of patients receiving background PAH therapy, the HR for the composite primary end point of time to first morbidity event or mortality was 0.62 (95% CI, 0.43 to 0.89) in favour of the macitentan group. The most frequent event was clinical worsening.
Harms Results
The overall frequency of adverse events (AEs) was similar between the groups in the full population of the SERAPHIN trial (94.6% macitentan 10 mg, 96.4% placebo). Worsening of PAH was the most frequently reported AE (21.9% macitentan 10 mg, 34.9% placebo). Serious AEs (SAEs) were reported less frequently in the macitentan 10 mg group compared with the placebo group. During the study, 45% of patients in the macitentan 10 mg group and 55% of patients in the placebo group experienced SAEs. Worsening of PAH reported as “pulmonary arterial hypertension” and right ventricular failure were the most frequently reported SAEs, and both occurred at lower frequencies in the macitentan group than in the placebo group. SAEs of anemia occurred more frequently in the macitentan 10 mg group (2.5%) compared with placebo (0.4%). Withdrawals due to AEs (WDAEs) were similar between the macitentan 10 mg arm (10.7%) and placebo (12.4%). Consistent with the overall AE profile and the SAE profile, the most frequently reported AEs that led to discontinuation of study treatment across the groups were PAH (1.7% macitentan 10 mg, 4.0% placebo) and right ventricular failure (1.7% macitentan 10 mg, 2.4% placebo). The frequency of alanine aminotransferase (ALT) or aspartate aminotransferase (AST) greater than 3 times the upper limit of normal (ULN) was lower in the macitentan 10 mg group (3.4%) compared with the placebo group (4.5%). Edema occurred at similar frequency in both groups (macitentan 10 mg: 21%; placebo: 20%). More patients in the macitentan group than in the placebo group had laboratory findings of decreased hemoglobin (4.3% versus 0.4%). The SERAPHIN clinical study report did not report overall AEs, SAEs, or WDAEs by subgroup. Data provided in the macitentan-tadalafil FDC submission indicated that the AEs in the subgroup of patients on background therapy plus macitentan were similar to what is expected with the individual components and with AEs observed in the overall SERAPHIN population. The percentages of patients receiving background therapy plus macitentan or placebo who experienced an AE were 93.5% and 97.4%, respectively. Incidences of WDAEs were similar between those receiving macitentan and those receiving placebo (9.1% versus 11.8%, respectively).
The results of the SERAPHIN study are summarized in Table 2.
Table 2: Summary of Key Results From SERAPHIN Study
Outcomes | Placebo (n = 250) | Macitentan 10 mg (n = 242) |
|---|---|---|
Efficacy results | ||
Time to first morbidity event or mortality (up to EOT + 7 days) | ||
Total patients with at least 1 confirmed event, n (%) | 116 (46.4) | 76 (31.4) |
HR (97.5% CI) | — | 0.55 (0.39 to 0.76) |
P valuea | — | < 0.0001 |
First confirmed event, n (%) | ||
Worsening of PAH | 93 (37.2) | 59 (24.4) |
Death from any cause | 17 (6.8) | 16 (6.6) |
IV/SC prostanoids initiation | 6 (2.4) | 1 (0.4) |
Lung transplantation | 0 | 0 |
Time to first morbidity event or mortality (up to EOT + 7 days), subgroup of patients with background PAH therapy at baseline, n | 154 | 154 |
Total patients with at least 1 confirmed event, n (%) | 68 (44.2) | 50 (32.5) |
HR (95% CI) | — | 0.62 (0.43 to 0.89) |
Adverse events, n (%) | ||
Patients with at least 1 adverse event | 240 (96.4) | 229 (94.6) |
Patients with at least 1 adverse event, subgroup of patients with background PAH therapy at baseline | 149 of 153 (97.4) | 144 of 154 (93.5) |
Patients with at least 1 serious adverse event | 137 (55.0) | 109 (45.0) |
Patients with at least 1 adverse event, subgroup of patients with background PAH therapy at baseline | Not reported | Not reported |
Withdraw due to adverse events | 31 (12.4) | 26 (10.7) |
Patients with at least 1 adverse event, subgroup of patients with background PAH therapy at baseline | 18 of 153 (11.8) | 14 of 154 (9.1) |
Adverse events of special interest | ||
Edema | 50 (20.1) | 50 (20.7) |
Subgroup of patients with background PAH therapy at baseline | 41 of 153 (26.8) | 35 of 154 (22.7) |
Hemoglobin decrease | 12 (4.8) | 38 (15.7) |
Subgroup of patients with background PAH therapy at baseline | 10 of 153 (6.5) | 22 of 154 (14.3) |
Abnormal liver function | 36 (14.5) | 21 (8.7) |
Subgroup of patients with background PAH therapy at baseline | 5 of 153 (3.3) | 11 of 154 (7.1) |
Hypotension | 11 (4.4) | 17 (7.0) |
Subgroup of patients with background PAH therapy at baseline | 28 of 153 (18.3) | 15 of 154 (9.7) |
CI = confidence interval; EOT = end of treatment; HR = hazard ratio; PAH = pulmonary arterial hypertension; SC = subcutaneous.
Note: All end points were evaluated up to the end of the double-blind treatment period (median duration of treatment, 115 weeks), except for death from any cause up to the end of the study (median follow-up, 129 weeks).
Source: Pulido 2013.16
Bioequivalence Studies
Results from 3 bioequivalence studies17-20 were included in the sponsor’s submission to CADTH. These studies compared the FDC with treatment by 10 mg macitentan and 40 mg tadalafil as separate tablets. The studies were phase I trials conducted in healthy individuals with a crossover design. The primary objective was to demonstrate bioequivalence of the peak concentration (Cmax), the area under the curve (AUC) from time 0 to time t of the last measured concentration above the lower limit of quantification (AUC0–t), and AUC from time 0 to infinity (AUC0–inf) of macitentan-tadalafil FDC and as a free combination of macitentan and tadalafil. The secondary objectives were to evaluate the safety and tolerability of concomitant macitentan and tadalafil administered as an FDC product or as a free combination and to investigate other pharmacokinetic parameters of concomitant macitentan and tadalafil administered as an FDC product or as a free combination. Determination of bioequivalence was based upon 90% CI for the ratios of the geometric means (test/reference) for macitentan and tadalafil AUC0–inf, AUC0–t, and Cmax. The results of these studies suggested bioequivalence between FDC and treatment by 10 mg macitentan and 40 mg tadalafil as separate tablets.17-20 No patients died or reported SAEs. Most of the AEs were mild, and the proportion of individuals who had at least 1 AE was similar for the FDCs and the free combinations for both groups, varying between 70.0% and 78.7%.17-20
Other Evidence
The sponsor provided evidence from interventional studies and observational studies that had completed and were just initiating. However, all the studies were designed to investigate the effects of combination macitentan-tadalafil in treatment-naive patients; therefore, these were out of scope for the current review which is focused on patients switching from macitentan and tadalafil to the FDC.
Critical Appraisal
The evidence to support the indication and reimbursement request for macitentan-tadalafil FDC includes bioequivalence data. The SERAPHIN study was provided as supportive efficacy and safety data; it was not submitted as the primary study. The SERAPHIN trial has been previously evaluated as part of the macitentan CADTH review and received a positive recommendation in 2015,21 with the clinical condition of a contraindication or inadequate response to sildenafil or tadalafil. Therefore, the combination use of macitentan and tadalafil has been previously established and recommended by CADTH.
The overall design of the SERAPHIN study appears to be appropriate with respect to randomization and standardized assessment of the efficacy and safety outcomes. Based on the information available in the sponsor’s summary of the clinical evidence, the trial appears to be generally well-balanced in terms of baseline demographic and disease characteristics. The main analyses for the primary and secondary end points were performed by the ITT approach, which included all patients who had undergone randomization. The clinical study report stated that no imputation method was used for the primary efficacy end point because of the time-to-event design. The last observation carried forward (LOCF) approach was used to impute missing values of secondary and exploratory outcomes. More patients in the placebo group versus the macitentan group prematurely discontinued treatment (59.4% versus 44.2%) and the study (22.0% versus 16.9%), mostly due to death (17.6% versus 14.0%) and loss to follow-up (2.8% versus 0.8%). These differences may impact the validity of the secondary analyses with LOCF imputation because the method relies on data missing at random, which does not appear to have been met. Bonferroni correction was applied to ensure an overall alpha level of 0.01 for the primary outcome analysis. Overall, the handling of multiplicity in the outcome comparison is reasonably presented and acceptable due to the hierarchical testing procedure for the secondary end points.
No data were provided from a higher-level study such as a randomized controlled trial on the efficacy and safety of the FDC itself and the whole submission is based on extrapolation from existing trial data and bioequivalence data. Because only approximately 1% of patients received tadalafil plus macitentan and the study did not use a treatment switch design, the results do not directly apply to the target patient group for the submission. Nonetheless, the subgroup analyses, in combination with evidence from the CADTH therapeutic review on drugs for PAH, support the notion that combination use of macitentan and tadalafil improves outcomes for patients with WHO FC II or III PAH. Bioequivalence data suggest that the FDC is equivalent to the individual components administered separately.
The HRs reported for the time-to-event outcomes have been interpreted as a relative risk reduction, which is incorrect. The HRs represent instantaneous risk over the study time period which was lower for the treatment group.
A total of 158 centres participated in this trial, and 492 eligible patients with PAH were randomized into the 2 arms (242 to macitentan 10 mg arm and 250 placebo). Given the large number of centres involved, if there are differences in quality of care in the participating centres, the overall results may not be balanced because stratification by centre procedures were not employed in the randomization scheme. However, PAH is a rare disease, and the reason that so many countries and centres participated in this study was to ensure that the study could recruit enough patients to attempt clinically important outcome instead of just change in 6MWD like previous studies.
The total observation period was 728 days. This time period may not be realistic for some outcome measures such as lung transplantation.
The proportion of patients who discontinued from the trial was high (44.2% in the macitentan 10 mg arm and 59.4% in the placebo arm). However, most discontinuations were outcome related so it would not affect the primary end point, although secondary assessments that relied on complete case analysis would be expected to be affected by the drop-outs.
Cost Information
At the submitted price of $132.06 per tablet, macitentan-tadalafil FDC costs $48,202 per patient annually. The annual cost-savings associated with macitentan-tadalafil FDC compared with macitentan and tadalafil taken as individual products at the same dose range from $7,388 to $9,140 per patient, depending on the list price of tadalafil. The incremental savings are based on publicly available list prices and may not reflect actual prices paid by Canadian public drug plans.
The sponsor’s cost comparison assumes clinical similarity between macitentan-tadalafil FDC and macitentan and tadalafil taken as individual products. The clinical review conducted by CADTH identified several limitations with the submitted clinical evidence but concluded the FDC is similar to its components taken as individual products based on bioequivalence information. If the clinical effectiveness of macitentan-tadalafil FDC is different than that of macitentan and tadalafil taken as individual products in real-world use, the cost-effectiveness of macitentan-tadalafil FDC is unknown.
The sponsor’s submission and CADTH reanalyses focused on the sponsor’s proposed Health Canada indication and reimbursement request population, which consisted solely of patients previously treated with macitentan and tadalafil taken as individual products.
Conclusions
The SERAPHIN trial results showed that, compared with placebo, macitentan 10 mg once daily improved outcomes when administered in combination with a PDE5 inhibitor (primarily sildenafil) in patients with PAH. This study included several Canadian centres, so the results should be generalizable to Canadian patients affected by PAH. However, because only approximately 1% of patients received tadalafil plus macitentan and the study did not use a treatment switch design, the results do not directly apply to the target patient group for the submission. Nonetheless, the subgroup analyses, in combination with evidence from the CADTH therapeutic review on drugs for PAH, support that combination use of macitentan and tadalafil improves outcomes for patients with WHO FC II or III PAH. Bioequivalence data suggest that the FDC is equivalent to the individual components administered separately. A major implication of the macitentan-tadalafil FDC for the treatment of PAH is the clinical benefit of a dual treatment in patients who require this treatment approach with a reduction in pill burden. The hypothesized benefits of improved adherence and patient outcomes specific to use of the macitentan-tadalafil FDC is unclear because neither has been directly evaluated for the FDC.
At the submitted price, macitentan-tadalafil FDC costs $48,202 per patient annually and is cost-saving compared with the cost of macitentan and tadalafil taken as individual products at list prices. The appropriateness of a cost comparison to assess the cost-effectiveness of macitentan-tadalafil FDC compared with macitentan and tadalafil taken as individual products relies on the assumption of clinical similarity. If the clinical effectiveness of macitentan-tadalafil FDC is different than that of macitentan and tadalafil taken as individual products in real-world use, its cost-effectiveness is unknown.
Introduction
Disease Background
PAH is a specific type of pulmonary hypertension (classified as WHO Group 1 pulmonary hypertension) that is caused when the small arteries in the lung become thickened and narrowed. This narrowing blocks the blood flow through the lungs, which raises the blood pressure in the lungs. This increased blood pressure in the lungs causes the heart to have to work harder. As a result, the heart loses the ability to effectively pump blood throughout the body.22,23 The exact cause of PAH is unknown. It is unlike other forms of pulmonary hypertension, in which high blood pressure in the lungs is caused by underlying heart or lung disease. Researchers believe that PAH occurs when there is injury to the cells that line the blood vessels of the lung, and PAH results over time. If the cause of this change is unknown, it is referred to as IPAH. If the change is believed to be caused by a genetic mutation, it is called heritable PAH or FPAH. Approximately 15% to 20% of patients with PAH have FPAH. Since there is an inherited form of PAH, a family history of the disease may increase the risk of developing PAH. In the early stages of PAH, patients may not notice any symptoms at all. As the disease progresses, patients will start to experience symptoms common to other lung diseases, such as asthma or chronic obstructive pulmonary disease. The most common symptoms of PAH are increased shortness of breath; fatigue; edema or swelling of the feet, legs, and eventually the abdomen and neck; dizziness and fainting spells; chest pain; heart palpitations (racing or pounding); and blue lips and fingers.22,23 PAH is classified by the WHO FC, ranging from I to IV, with higher numbers indicating greater functional limitations.24-26 For example, FC I indicates no limitation on usual physical activity and no associated symptoms, while FC IV indicates an inability to perform any physical activity, who may have signs of right ventricular failure, and may have dyspnea and/or fatigue present at rest and symptoms increased by almost any physical activity.
Globally, the estimated annual incidence of diagnosed PHA in the general population ranges from 0.9 to 10.7 cases per million persons, whereas the prevalence is between 6 and 26 cases per million persons.3-8 A recent study in Canada indicated a much higher rate, with estimated incidence of 4 per 100, 000 persons per year and a prevalence of PAH of 29 per 100,000 persons.9 Females represent 60% to 83% of patients with PAH.10 Approximately half (43% to 50%) of diagnosed patients have IPAH or FPAH (i.e., heritable) and half (50% to 56%) have associated PAH or drug- or toxin-induced PAH.4
PAH is a devastating disease that is associated with a poor prognosis and causes debilitating symptoms that contribute to reduced functioning and HRQoL.27 In addition to high morbidity and mortality in the PAH population and the impact on HRQoL, patients with PAH experience high pill burden and often have several comorbid conditions, which may impact adherence to treatments.28,29
Because symptoms for patients affected by PAH are similar to other common lung diseases, it is difficult to diagnose PAH, requiring a pulmonologist or cardiologist to establish the diagnosis.22,23 The diagnosis is often established by eliminating other diseases, with assistance by the results from a number of laboratory tests, electrocardiogram, lung function tests, 6-Minute Walk Test (6MWT), echocardiogram, and right heart catheterization.22,23 PAH used to be defined as an increase in mean pulmonary artery pressure of at least 25 mm Hg (assessed by right heart catheterization), a pulmonary artery wedge pressure of 15 mm Hg or less, and pulmonary vascular resistance (PVR) greater than 3 wood units.23 Recently, a mean pulmonary artery pressure of greater than 20 mm Hg (with PVR > 3 wood units) has been recommended for the diagnosis of PAH.30
Standards of Therapy
Although there is no cure for PAH, there are medications and procedures that can slow the progression of the disease and improve the patient’s quality of life.1,22 Treatment options vary from person to person, so the patients need to work closely with the care providers to determine the best plan. Newly diagnosed patients with PAH should be referred to an accredited pulmonary hypertension care centre for evaluation and right heart catheterization. The mechanisms contributing to disease progression involve vasoconstriction, endothelial dysfunction, dysregulated smooth muscle cell growth, inflammation, and thrombosis that typically lead to overload of right ventricle and progressive right-sided heart failure.31 The therapeutic objectives of drugs for PAH are to normalize these mechanisms. Several drugs used in other indications form background supportive therapies for PAH, including diuretics, oxygen, anticoagulants, calcium channel blockers, and digoxin. Many patients with PAH initially receive supportive therapy despite limited or no evidence of effectiveness. Consequently, the majority of patients with PAH will require advanced therapy, which is directed at the disease itself. Eight drugs are approved in Canada for advanced therapy of PAH. They belong to 4 classes: PDE5 inhibitors (sildenafil, tadalafil), ERAs (bosentan, ambrisentan, and macitentan), prostacyclin receptor agonists (selexipag), soluble guanylate cyclase stimulators (riociguat), and prostanoids (epoprostenol, treprostinil).15 The approach to therapy has been to individualize the choice of initial therapy, starting with 1 of these treatments and adding on drugs from different classes as the patient’s disease progresses, moving sequentially to dual then triple therapy. Initiation of upfront dual therapy is recommended for certain patients12 following results from the AMBITION trial that reported initial combination therapy with ambrisentan plus tadalafil resulted in a statistically significantly lower risk of clinical failure events than with ambrisentan or tadalafil monotherapy.13
Although comparative assessments between sildenafil and tadalafil have not been conducted, studies evaluating a switch from sildenafil to tadalafil generally show no change in the 6MWD and other parameters.32,33 A CADTH health technology review used indirect comparison methods that showed the 2 PDE5 inhibitors are similarly effective and cost-effective.15 The review recommended the PDE5 inhibitors as first-line treatment unless a patient has a contraindication or is unable to take sildenafil or tadalafil. A recommendation for the subsequent treatment could not be determined because of a limited evidence base on sequencing of treatments. Among the ERA class, bosentan may not be considered a first choice in newly diagnosed patients given the “unfavourable long-term data as well as the hepatotoxicity and potentially and clinically relevant drug interactions.”34 This is based in part on results from the phase IV COMPASS-2 trial, which compared bosentan and sildenafil versus sildenafil monotherapy and did not achieve its primary end point of time to first morbidity or mortality event.35
Drug
Tadalafil was reviewed by CADTH in 2010 and macitentan was reviewed in 2014, and both drugs received recommendations to reimburse with conditions for patients with group 1 PAH and WHO FC II or III.15 The condition for reimbursing tadalafil was in a similar manner to the reimbursement of sildenafil, and for the cost not to exceed that of sildenafil. The conditions for the reimbursement of macitentan were if the patient had a contraindication or inadequate response to sildenafil or tadalafil, and for the price to be reduced to ensure that the drug plan cost for macitentan does not exceed the drug plan cost for bosentan. Both drugs have restricted reimbursement in some of the CADTH-participating drug plans.
Macitentan-tadalafil is a FDC of macitentan 10 mg and tadalafil 40 mg. It was submitted to CADTH before Notice of Compliance and a proposed indication for the long-term treatment of PAH (WHO Group 1) to reduce morbidity in patients of WHO FC II or III whose PAH is either idiopathic or heritable or associated with connective tissue disease or congenital heart disease. The product monograph states that the FDC of macitentan and tadalafil should be used in patients who are currently treated concomitantly with stable doses of macitentan 10 mg and tadalafil 40 mg (20 mg × 2) as separate tablets. The dosage is 1 tablet of the FDC daily. Macitentan-tadalafil FDC is the first combination therapy for the treatment of PAH. The sponsor’s request for reimbursement is per the indication in the population of patients described in the indication who are switching from macitentan and tadalafil used in combination but administered separately. The sponsor has suggested that an unmet need exists for additional therapies that reduce pill burden and improve adherence and reduce hospitalization while improving stability of product availability and providing cost-savings to payers.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
CADTH received no patient group submission for the review of macitentan-tadalafil FDC.
Clinician Input
Input From the Clinical Expert Consulted by CADTH
One clinical expert with expertise in the diagnosis and management of PAH was consulted by CADTH.
The clinical expert indicated that macitentan-tadalafil FDC would mostly be prescribed to patients switching from existing dual therapy with tadalafil and macitentan. Patients would be switched to the macitentan-tadalafil FDC for convenience to reduce overall pill burden unless the individual components have not been tolerated by the patient. There would be consideration for switching from other dual therapy combinations, such as tadalafil plus ambrisentan, sildenafil plus ambrisentan, sildenafil plus bosentan, sildenafil plus macitentan, or tadalafil plus bosentan, but this would be a much smaller proportion of patients because of concerns of clinical destabilization, patient preference, and cost.
Although trial data and clinical experience suggest that macitentan has fewer side effects leading to treatment discontinuation than ambrisentan or bosentan, it is not prescribed as much as the other ERAs in part because of issues of access; macitentan has only recently been reimbursed or is not reimbursed in some provinces. As well, tadalafil plus ambrisentan is currently the most commonly prescribed dual therapy based on the results of the AMBITION trial (for starting newly diagnosed patients on combination therapy).
Of the PDE5 inhibitors, tadalafil 40 mg daily is currently prescribed more than sildenafil because clinicians consider it to be more potent than sildenafil 20 mg 3 times daily and it is more convenient in terms of pill burden.
Initiation of the macitentan-tadalafil FDC in newly diagnosed patients would be of interest pending data from the A DUE study on initial therapy with the FDC. However, this is outside of the Health Canada switch indication and reimbursement request from the sponsor. Currently, most newly diagnosed patients who are identified as appropriate for initial dual therapy would be prescribed ambrisentan plus tadalafil because there are data supporting the long-term efficacy of that specific combination from the AMBITION trial.
Clinician Group Input
CADTH received no clinician group submission for the review of macitentan-tadalafil FDC.
Drug Program Input
Input from drug programs explored the generalizability to patients with PAH and the lack of comparators in the clinical studies. The responses to the questions are presented in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
The proposed indication submitted to Health Canada appears to contain 2 groups: initial combination therapy and switching therapy to the combination as FDC. The sponsor’s reimbursement request is for macitentan-tadalafil FDC to be funded only for patients previously treated with the individual components only (i.e., macitentan and tadalafil), and not the initiation of macitentan-tadalafil FDC in patients not previously treated with the individual components. How will clinicians use the FDC in practice? | Refer to the Clinician Input section for the answer. The sponsor clarified that the requested indication submitted to Health Canada is in the patient population switching from macitentan and tadalafil administered separately to the FDC. |
Would clinicians prescribe the FDC to pediatric patients with PAH? | The clinical expert indicated that pediatric specialists would consider prescribing the FDC to reduce the overall pill burden for children with PAH. However, there would have to be a real clinical need because this would be outside of the indications for the individual components and FDC and it would require safety data and pharmacokinetic and/or pharmacodynamic studies of these in pediatric patients. |
FDC = fixed-dose combination; PAH = pulmonary arterial hypertension.
Sponsor’s Summary of the Clinical Evidence
Note that the Sponsor’s Summary of the Clinical Evidence section has not been copy-edited.
Submitted Studies
The evidence to support the indication and reimbursement request for macitentan/tadalafil FDC includes bioequivalence data. The SERAPHIN study was provided as supportive efficacy and safety data and is not the primary study for this submission. SERAPHIN was not a pivotal study for the regulatory submission given the proposed Health Canada switch indication. The SERAPHIN trial was previously evaluated as part of the macitentan CADTH review and received a positive recommendation in 2015, with the clinical condition of a contraindication or inadequate response to sildenafil or tadalafil.21 Therefore, the combination use of macitentan and tadalafil was previously established and recommended by CADTH.
Additional information on the clinical trials, bioequivalence trials, and additional data pertaining to the combination use of macitentan and tadalafil has been provided in the file entitled “Disease and Treatment” submitted by the sponsor as an attached document. Details of the included studies are summarized in Table 4.
Table 4: Details of Included Studies
SERAPHIN (Perchenet, 2021; Pulido, 2013) | |
|---|---|
Designs & Populations | |
Study Design | Multicenter, double-blind, randomized, placebo-controlled, Phase III trial |
Locations | 158 centers in 39 countries (United States, Argentina, Australia, Austria, Belarus, Belgium, Bulgaria, Canada, Chile, China, Colombia, Croatia, France, Germany, Hong Kong, Hungary, India, Israel, Italy, Malaysia, Mexico, Netherlands, Norway, Peru, Poland, Romania, Russian Federation, Serbia, Singapore, Slovakia, South Africa, Spain, Sweden, Taiwan, Thailand, Turkey, Ukraine, United Kingdom) |
Randomized (N) | 742 patients |
Inclusion Criteria |
|
Exclusion Criteria |
|
Drugs | |
Intervention | Treatment arm 1: Macitentan 10 mg by mouth once daily Treatment arm 2: Macitentan 3 mg by mouth once daily |
Comparator(s) | Placebo by mouth once daily |
Duration | |
Phase | Phase III |
Run-in | Screening period: up to 28 days |
Double-blind | When target of 285 events confirmed (up to 4.5 years) |
Follow-up |
|
Outcomes | |
Primary Endpoint | The time from the initiation of treatment to the first morbidity or mortality event, defined as:
|
Secondary and Exploratory Endpoints | Secondary endpoints:
Exploratory endpoints:
|
Notes | |
Publications | ClinicalTrials.gov Identifier: NCT00660179 Pulido T, Adzerikho I, Channick RN, et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013 Aug 29;369(9):809-18. doi: 10.1056/NEJMoa1213917. Jansa P, Pulido T. Macitentan in Pulmonary Arterial Hypertension: A Focus on Combination Therapy in the SERAPHIN Trial. Am J Cardiovasc Drugs. 2018 Feb;18(1):1-11. doi: 10.1007/s40256-017-0260-1. Review. Mehta S, Sastry BKS, Souza R, et al. Macitentan Improves Health-Related Quality of Life for Patients With Pulmonary Arterial Hypertension: Results From the Randomized Controlled SERAPHIN Trial. Chest. 2017 Jan;151(1):106-118. doi: 10.1016/j.chest.2016.08.1473. Epub 2016 Sep 23. Erratum in: Chest. 2018 May;153(5):1287. Torbicki A, Bacchi M, Delcroix M, et al. Integrating Data From Randomized Controlled Trials and Observational Studies to Assess Survival in Rare Diseases. Circ Cardiovasc Qual Outcomes. 2019 May;12(5):e005095. doi: 10.1161/CIRCOUTCOMES.118.005095. |
Publications (continued) | Krause A, Zisowsky J, Dingemanse J. Modeling of pharmacokinetics, efficacy, and hemodynamic effects of macitentan in patients with pulmonary arterial hypertension. Pulm Pharmacol Ther. 2018 Apr;49:140-146. doi: 10.1016/j.pupt.2018.02.005. Epub 2018 Feb 28. McLaughlin VV, Hoeper MM, Channick RN, et al. Pulmonary Arterial Hypertension-Related Morbidity Is Prognostic for Mortality. J Am Coll Cardiol. 2018 Feb 20;71(7):752-763. doi: 10.1016/j.jacc.2017.12.010. Simonneau G, Channick RN, Delcroix M, et al. Incident and prevalent cohorts with pulmonary arterial hypertension: insight from SERAPHIN. Eur Respir J. 2015 Dec;46(6):1711-20. doi: 10.1183/13993003.00364-2015. Epub 2015 Oct 22. Channick RN, Delcroix M, Ghofrani HA, et al. Effect of macitentan on hospitalizations: results from the SERAPHIN trial. JACC Heart Fail. 2015 Jan;3(1):1-8. doi: 10.1016/j.jchf.2014.07.013. Epub 2014 Nov 11. Galie N, Delcroix M, Ghofrani HA, et al. Anticoagulant therapy does not influence long-term outcomes in patients with pulmonary arterial hypertension (PAH): insights from the randomised controlled SERAPHIN trial of macitentan. Euro Heart J 2014;35(10-10). Galie N, Jansa P, Pulido T, et al. SERAPHIN haemodynamic substudy: the effect of the dual endothelin receptor antagonist macitentan on haemodynamic parameters and NT-proBNP levels and their association with disease progression in patients with pulmonary arterial hypertension. European Heart Journal 2017;38:1147–1155. Sitbon O, Channick R, Delcroix M, et al. Effect of macitentan on haemodynamics in SERAPHIN, a randomised controlled trial in pulmonary arterial hypertension (PAH). European Respiratory Journal 2013;42:P4060. Souza R, Channick RN, Delcroix M, et al. Association between six-minute walk distance and long-term outcomes in patients with pulmonary arterial hypertension: Data from the randomized SERAPHIN trial. PLoS One. 2018;13(3):e0193226. doi:10.1371/journal.pone.0193226. Isaac M, Dingemanse J, Sidharta PN. Pharmacokinetics of Macitentan in Patients With Pulmonary Arterial Hypertension and Comparison With Healthy Subjects. The Journal of Clinical Pharmacology 2017;00(0):1-8. Di Scala L, Jenner B, Parodi A, Lucenti I. COMPARATIVE EFFECTIVENESS OF MACITENTAN AND AMBRISENTAN VIA INDIRECT TREATMENT COMPARISON OF THE SERAPHIN AND AMBITION TRIALS. ISPOR 2020; 23(2):S716. Souza R, Pulido T, Channick RN, et al. Long-Term Survival And Safety With Macitentan In Patients With Pulmonary Arterial Hypertension: Results From The Seraphin Study And Its Open-Label Extension. Am J Respir Crit Care Med 2017;195:A2294. Correction to Figures in: Macitentan Improves Health-Related Quality of Life for Patients With Pulmonary Arterial Hypertension: Results From the Randomized Controlled SERAPHIN Trial. Chest. 2018 May;153(5):1287. doi: 10.1016/j.chest.2018.03.030. Erratum for: Chest. 2017 Jan;151(1):106-118. PMID: 29731048. |
6MWD = 6-minute walking distance, ALT = alanine aminotransferase, AST = aspartate aminotransferase, FC = functional class, ERA = endothelin receptor antagonists, IV = intravenous, NT-proBNP = N-terminal pro-B type natriuretic peptide, PAH = pulmonary arterial hypertension, QoL = quality of life, SF-36 = 36-item Short Form survey, WHO = World Health Organization.
Source: Pulido 2013 (Pulido, 2013); Actelion Pharmaceuticals Ltd. 2012 (Perchenet, 2021)Description of Studies
The efficacy of macitentan in patients with PAH is based on the double-blind, placebo controlled, randomized controlled trial SERAPHIN (Study with Endothelin Receptor Antagonist in Pulmonary arterial Hypertension to Improve cliNical outcome), a pivotal, phase III study was designed to evaluate the efficacy and safety of macitentan 3 mg and 10 mg through the primary endpoint of time to first morbidity and all-cause mortality event, in patients with symptomatic PAH who were either treatment-naïve or receiving background PAH-specific therapy. (Perchenet, 2021; Pulido, 2013)
SERAPHIN was conducted in 158 centers in 39 countries, including five centers in Canada. A total of 742 patients were randomly assigned to receive placebo (250 patients), macitentan 3 mg (250 patients), or macitentan 10 mg (242 patients) and were included in the ITT population. (Perchenet, 2021; Pulido, 2013) Patients were randomly assigned in a 1:1:1 ratio to receive either placebo, macitentan 3 mg once daily, or macitentan 10 mg once daily. (Perchenet, 2021; Pulido, 2013) The data on macitentan 3 mg group was not presented for this submission as this dose is not aligned with the Health Canada approved dose.
Populations
Inclusion and Exclusion Criteria (Perchenet, 2021; Pulido, 2013)
Patients aged 12 years or older at study entry, with a hemodynamically confirmed diagnosis of symptomatic PAH, in WHO FC II to IV, were eligible to enroll in SERAPHIN. Idiopathic PAH, familial PAH, and PAH associated with collagen vascular disease, congenital heart disease, human immunodeficiency virus infection, or drugs and toxins, were eligible. Patients were required to have a 6MWD test ≥ 50 meters at screening and randomization. Importantly, concomitant treatment with oral phosphodiesterase-5 inhibitors, oral or inhaled prostanoids, calcium channel blockers, or l-arginine was allowed, provided that the patient had been receiving a stable dose for at least 3 months before randomization. Patients receiving IV or SC prostanoids were excluded.
Baseline Characteristics (Perchenet, 2021; Pulido, 2013)
There were no significant between-group differences at baseline (Table 5). Idiopathic PAH was the most common etiology (55.0%) followed by PAH due to collagen vascular disease (30.5%), and PAH due to congenital shunts (8.4%). At baseline, approximately 52% of patients were in WHO FC II and 46% of patients were in WHO FC III, with approximately 2% in WHO FC IV. The majority (approximately 64%) of patients were receiving at least 1 background PAH therapy at baseline.
Table 5: Summary of Baseline Characteristics (All Randomized Set)
Characteristics | Placebo (n=250) | Macitentan 10 mg (n=242) |
|---|---|---|
Female sex – no. (%) | 184 (73.9) | 194 (80.2) |
Age – year ± SD | 46.7 ± 17.03 | 45.5 ± 14.99 |
Race or ethnic group – no. (%) | ||
White | 131 (52.6) | 135 (55.8) |
Black | 8 (3.2) | 6 (2.5) |
Asian | 71 (28.5) | 65 (26.9) |
Hispanic | 37 (14.9) | 35 (14.5) |
Other | 2 (0.8) | 1 (0.4) |
Etiology of PAH – no. (%) | ||
Idiopathic | 126 (51.0) | 134 (55.6) |
Heritable | 3 (1.2) | 2 (0.8) |
Associated with connective-tissue disease | 81 (32.8) | 73 (30.3) |
Associated with congenital shunts | 26 (10.5) | 21 (8.7) |
Associated with HIV infection | 3 (1.2) | 6 (2.5) |
Associated with drug use or toxin exposure | 8 (3.2) | 5 (2.1) |
Time from diagnosis of PAH – year | 2.6 ± 3.7 | 2.6 ± 3.6 |
6MWD – m | 352 ± 110.6 | 363 ± 93.2 |
WHO functional class – no. (%) | ||
I | 0 | 1 (0.4) |
II | 129 (51.8) | 120 (49.6) |
III | 116 (46.6) | 116 (47.9) |
IV | 4 (1.6) | 5 (2.1) |
Receipt of background treatment for PAH – no. (%) | ||
No | 95 (38.2) | 88 (36.4) |
Yes | 154 (61.8) | 154 (63.6) |
PDE-5 inhibitor | 150 (60.2) | 150 (62.0) |
Oral or inhaled prostanoid | 7 (2.8) | 15 (6.2) |
For the categories of female sex, age, race or ethnic group, 6MWD, WHO functional class, and receipt of treatment for PAH, data were missing for 1 patient in the placebo group. For the categories of time from diagnosis of PAH and PAH classification, data were missing for 3 patients in the placebo group and for 1 in the group that received 10 mg of macitentan.
*Please note data is not presented for the macitentan 3 mg group as this dose is not aligned with the Health Canada approved dose.
6MWD = 6-minute walk distance; HIV = human immunodeficiency virus; PAH = pulmonary arterial hypertension; PDE-5 = phosphodiesterase-5; SD = standard deviation; WHO = World Health Organization..
Source: (Perchenet, 2021; Pulido, 2013)
Interventions (Perchenet, 2021; Pulido, 2013)
The treatments in SERAPHIN were macitentan 3 mg administered by mouth once daily, macitentan 10 mg administered by mouth once daily, and matching placebo administered by mouth once daily. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||;|||||
Concomitant treatment with oral phosphodiesterase-5 inhibitors, oral or inhaled prostanoids, calcium channel blockers, or l-arginine was allowed, provided that the patient had been receiving a stable dose for at least 3 months before randomization. Additionally, treatment with oral diuretics was allowed if it had been ongoing at a stable dose for at least 1 month before randomization. Optimization of the dose of oral diuretics was allowed during the treatment period.
Outcomes
The primary endpoint of SERAPHIN was the time from the initiation of treatment to the first morbidity or mortality event, defined as: (Perchenet, 2021; Pulido, 2013)
All-cause death;
Atrial septostomy;
Lung transplantation;
Initiation of treatment with IV or SC prostanoids;
Worsening of PAH, defined as the occurrence of all 3 of the following events:
A decrease in the 6MWD of ≥ 15% from baseline, confirmed by 2 tests on different days;
Worsening of PAH symptoms, which must have included either: an increase in WHO FC by ≥ 1 class or no change in patients who were in WHO FC IV at baseline OR the appearance or worsening of signs of right heart failure that did not respond to oral diuretic therapy;
The need for additional PAH treatment.
The primary endpoint included all-cause death, atrial septostomy, or lung transplantation as indisputable events of deterioration in PAH. (Perchenet, 2021; Pulido, 2013) The initiation of IV or SC prostanoids entails a degree of invasiveness that is in itself relevant to the patient and, thus, identifies an important event of PAH worsening. The clinical relevance of ‘Other worsening of PAH’ was strengthened by the requirement for the simultaneous occurrence of components of confirmed deterioration in exercise capacity, symptomatic worsening and need for additional PAH-specific therapy. In this context, it is notable that a pre-defined decline in 6MWD, worsening of WHO FC, and/or signs and symptoms of right heart failure all have been shown to be predictive of mortality in patients with pulmonary hypertension. (Barst, 2007; Provencher, 2006) Moreover, the decrease of at least 15% in 6MWD confirmed by repeated testing on different days constitutes a loss of physical performance, which is symptomatically meaningful to the patient and clinically indicative of definitive disease progression. (Pulido, 2013) Furthermore, for patients with a high baseline 6MWD, a decrease by 15%, would bring them into a category with a high risk for poor outcome, further reinforcing its clinical significance. (Sitbon, 2002)
Secondary efficacy endpoints included (Perchenet, 2021; Pulido, 2013):
The change from baseline to month 6 in the 6MWD.
The percentage of patients with an improvement in WHO FC from baseline to month 6.
Time to death due to PAH or hospitalization for PAH up to the end of treatment.
Time to death from any cause up to the end of treatment and up to the end of the study.
Exploratory endpoints included: (Pulido, 2013)
Change in 6MWD from baseline to all assessed time-points.
Change in modified WHO FC from baseline to all assessed time-points.
Change in Borg dyspnea index from baseline to all assessed time-points.
Achievement and/or maintenance of a 6MWD ≥ 380 m at all assessed time-points.
Change in N-terminal pro-B type natriuretic peptide (NT-proBNP) from baseline to Month 6.
Change from baseline to all visits in the Quality of Life (QoL) assessed by the 36-item Short Form Survey (SF-36) for patients ≥ 14 years of age at randomization.
Time to death due to PAH up to end of study.
Death and Hospitalization
The evaluation of death of all causes up to end of treatment and end of study and death and hospitalization due to PAH were identified as important secondary endpoints in a disease with a high risk of fatal outcome. (Perchenet, 2021; Pulido, 2013)
6MWD and Borg Dyspnea Index
The 6MWD is a non-encouraged 6-minute walk test, performed in a 30 m long flat corridor, where the patient is instructed to walk as far as possible, back and forth around 2 cones, with the permission to slow down, rest, or stop if needed. (Pulido, 2013) This endpoint has been accepted by the Food and Drug Administration (FDA) and European Medicines Agency. The evaluation of dyspnea on exertion using the Borg dyspnea index is also a recommended assessment.(Galie, 2015) Borg dyspnea index was evaluated immediately after the 6MWT to obtain a rating of dyspnea at the end of the exercise using a scale from 0 (‘Nothing at all’) to 10 (‘Very, very severe – maximal’). Moreover, it has been demonstrated that the assessment of the distance achieved in a 6MWT (< 380 m or > 380 m) correlates with survival. (Sitbon, 2002) Although a minimal important difference (MID) has not been established for these assessments, studies estimate a MID of approximately 33 m in the 6MWD test and change of 0.9 units in the Borg dyspnea index. (Khair, 2016; Mathai, 2012)
WHO FC
The WHO CF status of patients with pulmonary hypertension is 1 of the strongest predictors of survival at diagnosis and during follow up. (Barst, 2013; Nickel, 2012; Sitbon, 2002) The WHO FC ranges from I to IV, with higher numbers indicating greater functional limitations. For example, FC I indicates no limitation on usual physical activity and no associated symptoms, while FC IV indicates an inability to perform any physical activity, who may have signs of right ventricular failure, and may have dyspnea and/or fatigue present at rest and symptoms increased by almost any physical activity.(Pulido, 2013) Recent clinical guidelines identify WHO FC as a prognostic factor for estimated 1-year mortality, with patients in WHO FC I-II as low risk (< 5%), WHO FC III as intermediate risk (5-10%), and WHO FC IV as high risk (> 10%).(Galie, 2015)
NT-proBNP
NT-proBNP is a biomarker for cardiac overload and has been shown to be associated with increased mortality in PAH patients.(Bernus, 2009; Lammers, 2009; Nagaya, 2000) Recent clinical guidelines identify NT-proBNP as a prognostic factor for estimated 1-year mortality, with patients who have NT-proBNP levels < 300 ng/L as low risk (< 5%), NT-proBNP levels of 300-1400 ng/L as intermediate risk (5-10%), and NT-proBNP levels > 1400 ng/L as high risk (> 10%).(Galie, 2015)
SF-36
The SF-36 (Short-form 36 Questionnaire) is a multipurpose, short-form health questionnaire with 36 questions. It yields an 8-scale profile of the functional health and well-being scores as well as 2 psychometrically-based physical and mental health summary measures and reported health transition items. (Pulido, 2013) A higher score for individual domains indicates a better condition of the patient. The questionnaire has been widely used and validated in clinical practice and research, and has been previously used in studies with PAH patients. (Kusic-Pajic, 2007) The MID has not been established in PAH for the SF-36, however in other disease states, the generally accepted threshold is 2 to 3 norm-based points for physical component summary score and 3 points for mental component summary score. (Mehta, 2018)
Statistical Analysis
Primary Outcome(s) of the Studies
Power Calculation (Perchenet, 2021; Pulido, 2013)
It was estimated that 285 events would be needed to detect a hazard ratio for the primary endpoint with macitentan (at least 1 of the dose groups), as compared with placebo, of 0.55 over an estimated maximum study duration of 4.1 years, assuming an anticipated hazard rate of 0.43 in the placebo group, an expected 5% annual attrition rate, and an annual enrollment of 200 patients. A planned blinded re-estimation of the sample size was performed 3 months before the end of the expected recruitment phase because the overall hazard rate was lower than expected, resulting in an increase in recruitment from 525 to 699 patients.
Statistical Test or Model
The main analyses for the primary and secondary endpoints were performed in the ITT population, which included all patients who had undergone randomization. The type I error was set at 0.005 (2-sided test) for the comparison of placebo with each dose of macitentan, with the use of Bonferroni correction to ensure an overall alpha level of 0.01, and power was set at 90%. The study could also be declared ‘positive’ at a global significance level of 0.05 (statistically significant). All time-to-event endpoints were estimated with the Kaplan-Meier method and analyzed with the log-rank test. Data from patients without an event who stopped receiving blinded treatment were censored at the time of treatment discontinuation. HRs with 2-sided 97.5% CIs were calculated with the use of Cox regression models.
Data Imputation Methods (Perchenet, 2021; Pulido, 2013)
Missing data of patients for whom no post-baseline values were available after applying the above imputation rules were imputed by carrying forward the baseline value.
Subgroup Analyses (Perchenet, 2021; Pulido, 2013)
Subgroup analyses were performed for the primary endpoint with the use of interaction tests. The following subgroups were considered for the evaluation of efficacy and safety (AEs of special interest):
PAH therapy(ies) at baseline: patients not receiving versus patients receiving concomitant PAH therapy[ies] of sildenafil, tadalafil, vardenafil, iloprost, beraprost, epoprostenol and treprostinil at baseline.
Sex: male versus female.
Race: White, Asian and others (includes Black, Hispanic and any other race) PAH etiology at baseline: idiopathic, familial, HIV infection, drugs and toxins versus collagen vascular disease versus congenital shunts.
Geographical regions: North America, Western Europe/Israel, Eastern Europe/Turkey, Asia, and Latin America.
The aim of the exploratory subgroup analyses, classifying patients according to important baseline characteristics, was to explore the consistency of treatment effect across different patient subgroups. Interaction tests for heterogeneity (treated vs. placebo and between each macitentan dose group and placebo) were performed for every subgroup. No multiplicity adjustment was introduced; the subgroup analyses were descriptive in nature.
For the risk reduction evaluation endpoints, a Cox model including treatment, subgroup and treatment by subgroup as factors was run for each macitentan dose versus placebo and also for the pooled doses (at patient level) “All-treated” group versus placebo. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Secondary Outcomes of the Studies (Perchenet, 2021; Pulido, 2013)
The main analyses for the secondary endpoints were performed in the intention-to-treat population, which included all patients who had undergone randomization. The secondary endpoints were tested hierarchically within each dose group to control for multiple comparisons. Statistical significance was claimed if the following conditions were met:
The pre-defined nominal significance level (p < α/2 2-sided) has been reached for the primary endpoint for the same dose group.
The pre-defined nominal significance level (p < α/2 2-sided) has been reached for all the previous endpoints in the sequence for the same dose group.
Where for each dose group, α = 0.01 2-sided for a conclusive study and α = 0.05 2-sided for a positive study. All time-to-event endpoints were estimated with the Kaplan-Meier method and analyzed with the log-rank test. Data from patients without an event who stopped receiving blinded treatment were censored at the time of treatment discontinuation. Hazard ratios with 2-sided 97.5% CIs were calculated with the use of Cox regression models.
Analysis Populations (Perchenet, 2021; Pulido, 2013)
The main analyses for the primary and secondary endpoints were performed in the intention-to-treat population, which included all patients who had undergone randomization.
Sponsor’s Summary of the Results
For additional information on results of the SERAPHIN study and analysis of patients on background therapy specifically, a file titled “Disease and Treatment document” has been submitted by the sponsor. The data is not presented for the macitentan 3 mg group as this dose is not aligned with the Health Canada approved dose.
Patient Disposition (Perchenet, 2021; Pulido, 2013)
The proportion of patients who discontinued study treatment was 44.2% in the macitentan 10 mg group and 59.4% in the placebo group. A morbidity event followed by enrollment in the SERAPHIN OL was the most frequent reason for discontinuation of study treatment in both groups (20.7% macitentan 10 mg, 32.1% placebo). An AE led to discontinuation of study treatment in 10.7% macitentan 10 mg and 12.4% placebo. These AEs included morbidity events (without subsequent enrollment into the SERAPHIN OL study) in 3.7% of patients in the macitentan 10 mg group and 8.0% of patients in the placebo group. Other reasons included death, withdrawal from treatment (i.e., permanent discontinuation of study treatment, but with the patient’s agreement to be contacted at end of study to check vital status), withdrawal of consent, and administrative reasons (Table 6).
SERAPHIN | ||
|---|---|---|
Placebo | Macitentan 10 mg | |
Screened, N | 955 | |
Randomized, N | 250 | 242 |
Discontinued, N (%) | 148 (59.4) | 107 (44.2) |
Reason for discontinuation, N (%) | ||
Disease progression leading to OL | 80 (32.1) | 50 (20.7) |
Adverse events | 31 (12.4) | 26 (10.7) |
Lost to follow-up | 3 (1.2) | 0 |
ITT, N | 250 | 242 |
All-treated, N | 249 | 242 |
ITT = intention to treat; N = number of subjects, OL = open label.
Source: Actelion Pharmaceuticals Ltd. 2012 (Perchenet, 2021; Pulido, 2013)
Exposure to Study Treatments
The data is not presented for the macitentan 3 mg group as this dose is not aligned with the Health Canada approved dose.
Study Treatments (Perchenet, 2021; Pulido, 2013)
The median duration of exposure to study treatment was 118.4 weeks in the 10 mg group compared to 101.3 weeks in the placebo group. In the macitentan 10 mg group, 64.9% of patients had at least 2 years’ exposure to study treatment. In the placebo group, 49.8% of patients had at least 2 years’ exposure. The maximum treatment duration was 188.0 weeks in the macitentan 10 mg group and 184.9 weeks in the placebo group.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Concomitant Medication (Perchenet, 2021; Pulido, 2013)
The proportion of patients who started at least 1 medication while on study treatment was 88.0% in the macitentan 10 mg group and 84.8% in the placebo group. |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Efficacy
Please note data is not presented for the macitentan 3 mg group as this dose is not aligned with the Health Canada approved dose.
Primary Endpoint: First Morbidity or Mortality Event (Perchenet, 2021; Pulido, 2013)
A total of 287 patients had a primary endpoint event over a median treatment period of 115 weeks: 116 patients (46.4%) in the placebo group and 76 patients (31.4%) in macitentan 10 mg group. Worsening of PAH was the most frequent primary endpoint event (37.2% vs 24.4% for placebo, and macitentan 10 mg, respectively). Treatment with macitentan 10 mg resulted in a 45% risk reduction HR 0.55, 97.5% CI, 0.39 to 0.76; log rank p < 0.001) in the occurrence of morbidity or mortality events up to EOT compared to placebo (Table 7).
Table 7: Primary and Secondary Endpoints for Events Related to PAH and Death*
Endpoint | Placebo (n = 250) | Macitentan 10 mg (n = 242) | Macitentan 10 mg, vs. placebo | |
|---|---|---|---|---|
Number of patients (%) | Hazard Ratio (97.5% CI) | P Value | ||
Event related to PAH or death as the first event | ||||
All events | 116 (46.4) | 76 (31.4) | 0.55 (0.39–0.76) | < 0.001 |
Worsening of PAH | 93 (37.2) | 59 (24.4) | ||
Death from any cause† | 17 (6.8) | 16 (6.6) | ||
Prostanoid initiation | 6 (2.4) | 1 (0.4) | ||
Lung transplantation | 0 | 0 | ||
Death due to PAH or hospitalization for PAH as the first event | ||||
All events | 84 (33.6) | 50 (20.7) | 0.50 (0.34–0.75) | < 0.001 |
Hospitalization for PAH | 79 (31.6) | 45 (18.6) | ||
Death due to PAH‡ | 5 (2.0) | 5 (2.1) | ||
Death from any cause | 19 (7.6) | 14 (5.8) | 0.64 (0.29–1.42) | 0.20 |
Death due to PAH§ | 14 (5.6) | 7 (2.9) | 0.44 (0.16–1.25) | 0.07 |
Death from any cause by the end of the study ¶ | 44 (17.6) | 35 (14.5) | 0.77 (0.46–1.28) | 0.25 |
*All endpoints were evaluated up to the end of the double-blind treatment period (median duration of treatment, 115 weeks), except for death from any cause up to the end of the study (median follow-up, 129 weeks).
†Two patients in the macitentan group had an adverse event leading to the discontinuation of treatment and died thereafter. The causes of death were hematemesis and sudden cardiac death and cardiorespiratory failure. These deaths were adjudicated by the clinical event committee and, as a conservative approach, were included in the analysis of the primary endpoint.
‡Data do not include patients who were hospitalized before death.
§Data include deaths that were adjudicated by the clinical event committee to be due to PAH and that occurred during the double-blind period or deaths that occurred within 4 weeks after the end of treatment, after a confirmed worsening of PAH.
¶The analysis included patients who were eligible to receive other treatments for PAH, including open-label macitentan at a dose of 10 mg. Data on vital status were not available at the end of the study for 27 patients (3.6%) who were lost to follow-up. The results of a sensitivity analysis for death from any cause up to the end of the study, which imputed death for 30 patients (4.0%) who had missing data on vital status at the end of the study, were consistent with the results of the main analysis.
CI = confidence interval; PAH = pulmonary arterial hypertension; n = number of subjects.
Source: Pulido 2013 (Pulido, 2013)
Key Secondary Endpoints (Perchenet, 2021; Pulido, 2013)
Treatment with macitentan 10 mg resulted in a 50% relative risk reduction (HR 0.50, 97.5% CI 0.34-0.75; p < 0.001) in the occurrence of PAH related death or hospitalization for PAH, up to EOT compared to placebo (Table 4). The proportion of patients without a PAH related death or hospitalization for PAH at 3 years was 70.6% in macitentan 10 mg compared to 55.4% in placebo, corresponding to an absolute risk reduction of 15.2%.
At month 6, the 6MWD had decreased by a mean of 9.4 m in the placebo group. In contrast, the 6MWD had increased by a mean of 12.5 m in the group that received 10 mg of macitentan (treatment effect with 10 mg dose vs. placebo, 22.0 m; 97.5% CI 3.2-40.8; p = 0.008). These effects were also examined according to whether or not the patient was receiving therapy for PAH at baseline and according to the WHO FC at baseline. The WHO functional class improved from baseline to month 6 in 13% of the patients in the placebo group, as compared with 22% of those in the group that received 10 mg of macitentan (p = 0.006).
A subset of patients participated in a hemodynamic study that included right heart catheterization at baseline and month 6. Patients in the macitentan 10 mg group had significant decreases in pulmonary vascular resistance and significant increases in the cardiac index, as compared with the placebo group.
Key Exploratory Endpoints
In SERAPHIN, the change in SF-36 scores from baseline to month 6 was evaluated as an exploratory endpoint. (Pulido, 2013) At month 6, macitentan 10 mg significantly improved 7 of 8 domains in the SF-36, including those evaluating physical and mental health components, providing the first clinical evidence of a benefit of PAH therapy in the majority of the SF-36 domains. (Mehta, 2017)
Harms
Data is not presented for the macitentan 3 mg group as this dose is not aligned with the Health Canada approved dose.
Safety Evaluation Plan (Perchenet, 2021; Pulido, 2013)
The safety endpoints of the study were:
AEs up to 28 days after EOT.
SAEs up to 28 days EOT.
AEs leading to premature discontinuation of study drug.
AEs of special interest (liver disorders and abnormal liver function, decrease in hemoglobin, edema and hypotension) up to 28 days after EOT.
Marked laboratory abnormalities up to 28 days after EOT.
Echocardiogram abnormalities up to 28 days after EOT.
Change in vital signs (blood pressure and pulse rate and body weight) from baseline up to 28 days after EOT.
Occurrence of liver test abnormality, i.e., elevation of liver aminotransferases (alanine aminotransferase [ALT] and/or aspartate aminotransferase [AST] > 3 and ≤ 5 × upper limit of normal [ULN], > 5 and ≤ 8 × ULN, and > 8 × ULN, and > 3 × ULN and concomitant total bilirubin > 2 × ULN).
Occurrence of hemoglobin abnormality (≤ 8 g/dL, and > 8 and ≤ 10 g/dL) up to 28 days after EOT.
Time to first appearance of ALT or AST > 3 × ULN up to 28 days after EOT (Kaplan-Meier estimates).
Overview of Safety (Table 8) (Perchenet, 2021; Pulido, 2013)
Table 8: Most Frequent Adverse Events and Laboratory Abnormalities
Adverse events | SERAPHIN | |
|---|---|---|
Placebo (n = 249) | Macitentan 10 mg (n = 242) | |
Patients with at least 1 adverse event | ||
n (%) | 240 (96.4) | 229 (94.6) |
Most common events | ||
Worsening of pulmonary arterial hypertension‡ | 87 (34.9) | 53 (21.9) |
Upper respiratory tract infection | 33 (13.3) | 37 (15.3) |
Peripheral edema | 45 (18.1) | 44 (18.2) |
Nasopharyngitis | 26 (10.4) | 34 (14.0) |
Right ventricular failure‡ | 56 (22.5) | 32 (13.2) |
Headache | 22 (8.8) | 33 (13.6) |
Anemia | 8 (3.2) | 32 (13.2) |
Dizziness | 27 (10.8) | 26 (10.7) |
Bronchitis | 14 (5.6) | 28 (11.6) |
Dyspnea | 22 (8.8) | 18 (7.4) |
Cough | 30 (12.0) | 21 (8.7) |
Laboratory abnormality — no. of patients/total no. (%) | ||
Alanine aminotransferase or aspartate aminotransferase > 3 × ULN | 11/244 (4.5) | 8/236 (3.4) |
Alanine aminotransferase or aspartate aminotransferase > 3 × ULN and bilirubin > 2 × ULN | 4/237 (1.7) | 4/230 (1.7) |
Hemoglobin ≤ 8 g/dl | 1/237 (0.4) | 10/230 (4.3) |
Patients with at least 1 serious adverse event | ||
n (%) | 137 (55) | 109 (45) |
Withdrawals due to adverse events | ||
n (%) | 31 (12.4) | 26 (10.7) |
Adverse events of special interest | ||
Edema, n (%) | 50 (20.1) | 50 (20.7) |
Hemoglobin decrease, n (%) | 12 (4.8) | 38 (15.7) |
Liver disorders and abnormal liver function, n (%) | 36 (14.5) | 21 (8.7) |
Hypotension, n (%) | 11 (4.4) | 17 (7.0) |
*One patient randomly assigned to receive placebo did not receive the study drug and was excluded from the safety analysis.
‡The majority of these events were also reported as primary endpoint events.
n = number of patients with event; ULN = upper limit of normal.
Source: Pulido 2013,2 Actelion Pharmaceuticals Ltd. 2012. (Perchenet, 2021; Pulido, 2013).
AEs (Perchenet, 2021; Pulido, 2013)
The overall incidence of AEs was similar across the groups (94.6% macitentan 10 mg, 96.4% placebo). Worsening of PAH was the most frequently reported AE (21.9% macitentan 10 mg, 34.9% placebo). This AE could also have constituted a primary endpoint event, since all those were considered as AEs in the analysis.
SAEs (Perchenet, 2021; Pulido, 2013)
SAEs were reported less frequently in the macitentan 10 mg group compared with the placebo group. During the study, 45% of patients in the macitentan 10 mg group and 55% of patients in the placebo group experienced SAEs. Worsening of PAH reported as ‘pulmonary arterial hypertension’ and right ventricular failure were the most frequently reported SAEs, and both occurred at lower frequencies in the macitentan group than in the placebo group. SAEs of anemia occurred more frequently in the macitentan 10 mg group (2.5%) compared to placebo (0.4%).
Withdrawals Due to AEs
A total of 10.7% of patients in the macitentan 10 mg group and 12.4% of patients in the placebo group experienced at least 1 AE that resulted in the permanent discontinuation of study treatment. Consistent with the overall AE profile and the SAE profile, the most frequently reported AEs that led to discontinuation of study treatment across the 3 groups were PAH (1.7% macitentan 10 mg, 4.0% placebo) and right ventricular failure (1.7% macitentan 10 mg, 2.4% placebo).
AEs of Special Interest (Perchenet, 2021; Pulido, 2013)
AEs of special interest that have been reported with other ERAs include abnormal liver function, edema, anemia, and decrease in hemoglobin and hypotension. The incidence of ALT or AST > 3 times the ULN was lower in the macitentan 10 mg group (3.4%) compared to placebo (4.5%), consistent with its known lack of clinically relevant bile salt transport inhibition. Edema related AEs, including peripheral edema, occurred at similar frequency in both groups (macitentan 10 mg: 21%; placebo: 20%), indicating that edema does not represent a significant safety concern with macitentan therapy. The incidence of hypotension and hypotension related AEs was also similar across groups. Anemia was reported in 13.2% of patients in the macitentan 10 mg arm compared to 3.2% in the placebo arm. Decreased hemoglobin was reported more frequently in the macitentan 10 mg group (4.3%) than in the placebo group (0.4%). However, there was no difference across treatment arms in the incidence of treatment discontinuation due to hemoglobin decrease.
Subgroup Analyses of Macitentan Used in Combination With Other PAH Treatments
A subgroup analyses of the SERAPHIN trial was conducted to further establish the efficacy and safety of macitentan used in combination with other PAH treatments. In total, 154 patients randomized to macitentan 10 mg and 154 randomized to placebo were receiving background PAH therapy. Background therapy consisted primarily of a PDE-5 inhibitor (97.4%) in both macitentan and placebo groups. Among PDE-5 inhibitors used as background therapy, most patients received sildenafil.
The composite primary endpoint of time to first morbidity/mortality event was examined in the subgroup of patients receiving background PAH therapy. The risk of morbidity/mortality was reduced by 38% in patients who received macitentan and background therapy compared with those receiving background therapy alone (placebo) (HR 0.62; 95% CI 0.43–0.89; p = 0.009). These data were the first randomized controlled trial-based evidence demonstrating that combination therapy improves long-term outcomes in PAH, and data was consistent with the overall population.
Time to first PAH-related hospitalization in patients receiving macitentan and background therapy had a reduction in the risk of being hospitalized for PAH of 37.4% (HR 0.63; 95% CI 0.41–0.96) compared with patients receiving background therapy only (placebo arm). These results were consistent with the findings in the overall SERAPHIN population (macitentan 10 mg vs. placebo) (HR 0.48; 95% CI 0.34–0.70; p < 0.0001).81 These data show that macitentan reduces PAH-related hospitalizations and provide further evidence of the long-term clinical benefits of macitentan when used in combination with other PAH therapies.
In SERAPHIN, the change in SF-36 scores from baseline to month 6 was evaluated as a secondary endpoint. In the background therapy subgroup, the mean placebo-corrected change in scores from baseline to month 6 was 2.8 (1.0-4.5) in the physical component summary and was 3.1 (0.3-5.8) in the mental component summary. These results were consistent with the overall population for the physical and mental component scores.
The safety profile of macitentan as part of a combination therapy regimen was consistent with that of macitentan in the overall SERAPHIN population, suggesting that, overall, combination treatment with macitentan and a PDE-5 inhibitor does not adversely affect tolerability compared with monotherapy, predominantly with a PDE-5 inhibitor. AEs experienced by patients receiving macitentan plus background therapy were similar to those recorded for patients receiving background therapy alone. The percentages of patients receiving background therapy plus macitentan or placebo who experienced at least 1 AE were 93.5% and 97.4%, respectively. Treatment discontinuations due to AEs in patients receiving background therapy were similar between those receiving macitentan and those receiving placebo (9.1% vs. 11.8%, respectively).
Bioequivalence
Study AC-077-103 (Pivotal) (Grill, 2020; Schultz, 2018)
The pivotal bioequivalence study AC-077-103 was a single-center, open-label, single-dose, 2-period, randomized, crossover Phase I studies in healthy adult subjects. The primary objective was to demonstrate bioequivalence of Cmax, AUC from time 0 to time t of the last measured concentration above the lower limit of quantification (AUC0-t), and AUC from time 0 to infinity (AUC0-∞) of macitentan/ tadalafil FDC and as a free combination of macitentan (OPSUMIT®) and tadalafil (ADCIRCA®, EU-sourced). The secondary objectives were to evaluate the safety and tolerability of concomitant macitentan and tadalafil administered as an FDC product or as a free combination and to investigate other PK parameters of concomitant macitentan and tadalafil administered as an FDC product or as a free combination. Please refer to the Disease and Treatment document for additional information.
Subjects were randomized to 2 possible treatment sequences (A/B or B/A). Treatment A (test treatment) was a single oral dose of FDC-2 (current formulation of macitentan/tadalafil FDC). Treatment B (reference treatment) was a single oral dose of macitentan 10 mg taken together with a single oral dose of tadalafil 40 mg (given as 2 × tadalafil 20 mg tablets; EU-sourced). Bioequivalence was evaluated by comparing test treatment (Treatment A [FDC-2]) to reference treatment (Treatment B [free combination]). Determination of bioequivalence was based upon 90% CI for the ratios of the geometric means (test/reference) for macitentan and tadalafil AUC0-∞, AUC0-t, and Cmax. For acceptance of bioequivalence, the 90% CIs had to be within the range of ≥ 0.8000 and ≤ 1.2500, when rounded to 4 decimal places.
Results
A total of 38 subjects were planned and enrolled, and all subjects received study drug. Two subjects discontinued study drug as well as the study. Therefore, 36 subjects completed the study. A total of 34 out of 38 subjects were evaluable for PK.
The arithmetic mean plasma concentrations of macitentan, ACT-132577 (the major and pharmacologically active metabolite of macitentan), and tadalafil were similar following administration of FDC-2 or the free combination. The median tmax of macitentan and ACT-132577 was similar when macitentan was administered as either the FDC or free combination. Geometric mean t½ of macitentan and ACT-132577 was comparable when macitentan was administered as either the FDC or free combination. Exposure to macitentan and ACT-132577 in terms of AUC0-∞, AUC0-t and Cmax was similar following administration of FDC-2 or the free combination. For tadalafil, the tmax and t½ values were comparable when administered as FDC-2 or free combination. Exposure to tadalafil in terms of Cmax, AUC0-t, and AUC0-∞ was similar following administration of FDC-2 or the free combination (Table 9).
Table 9: Summary of Pharmacokinetic Parameters of Macitentan, Tadalafil, and ACT-132577
Parameter | Geometric means (95% CI); tmax: median (range) | |||||
|---|---|---|---|---|---|---|
Macitentan | Tadalafil | ACT-132577 | ||||
FDC-2 (n = 34) | Free combination (n = 34) | FDC-2 (n = 34) | Free combination (n = 34) | FDC-2 (n = 34) | FDC-2 (n = 34) | |
Cmax ng/mL | 174.64 (161.08, 189.35) | 164.63 (152.48, 177.74) | 538.91 (492.00, 590.29) | 597.78 (542.32, 658.91) | 162.72 (145.78, 181.62) | 162.72 (145.78, 181.62) |
AUC0-t ng h/mL | 5,809.26 (5,274.06, 6398.77) | 5,787.14 (5,270.38, 6354.57) | 17 159.15 (15 516.18, 18 976.09) | 17 091.33 (15 210.43, 19 204.81) | 18 656.33 (16 888.63, 20 609.04) | 18 656.33 (16 888.63, 20 609.04) |
AUC0-∞ ng h/mL | 5,890.08 (5,354.81, 6478.85) | 5,881.08 (5,365.79, 6445.84) | 17 268.40 (15 589.27, 19 128.39) | 17 187.34 (15 278.78, 19 334.30) | 20 373.98 (18 416.42, 22 539.63) | 20 373.98 (18 416.42, 22 539.63) |
tmax h | 9.00 (4.0–12.0) | 9.00 (4.2–24.0) | 2.00 (0.5–5.0) | 1.75 (1.0–5.0) | 48.00 (24.0–72.0) | 48.00 (24.0–72.0) |
t1/2 h | 16.146 (14.778, 17.642) | 16.106 (14.841, 17.478) | 23.319 (21.092, 25.781) | 22.592 (20.460, 24.945) | 49.405 (46.240, 52.787) | 49.405 (46.240, 52.787) |
AUC = area under the plasma concentration-time curve; AUC0-t = AUC from time 0 to time t of the last measured concentration above the lower limit of quantification; AUC0-∞ = AUC from time 0 to infinity; Cmax = maximum plasma concentration; CI = confidence interval; FDC-2 = fixed-dose combination (current formulation); N = maximum number of subjects with data; t½ = terminal half-life; tmax = time to reach maximum plasma concentration.
Source: Grill 2020 (Grill 2020), Schultz 2018 (Schultz 2018)
All 90% CIs for the geometric mean ratios (FDC-2 vs. free combination) of Cmax, AUC0-t and AUC0-∞ for both macitentan and tadalafil were within the bioequivalence limits (0.8000 to 1.2500, Table 10). Therefore, bioequivalence of FDC-2 with the free combination of macitentan and EU-sourced tadalafil was demonstrated.
Table 10: Results of Bioequivalence Determination
Parameter | Ratio of geometric means (treatment A/B; 90% CI) | ||
|---|---|---|---|
FDC-2 vs. free combination | |||
Macitentan (n = 34) | Tadalafil (n = 34) | ACT-132577 (n = 34) | |
Cmax ng/mL | 1.0608 (1.0014, 1.1238) | 0.9015 (0.8413, 0.9661) | 1.0198 (0.9819, 1.0591) |
AUC0-t ng h/mL | 1.0038 (0.9677, 1.0413) | 1.0040 (0.9584, 1.0517) | 0.9970 (0.9651, 1.0300) |
AUC0-∞ ng h/mL | 1.0015 (0.9675, 1.0367) | 1.0047 (0.9591, 1.0525) | 0.9936 (0.9619, 1.0264) |
AUC = area under the plasma concentration-time curve; AUC0-t = AUC from time 0 to time t of the last measured concentration above the lower limit of quantification; AUC0-∞ = AUC from time 0 to infinity; Cmax = maximum plasma concentration; CI = confidence interval; FDC-2 = fixed-dose combination (current formulation); N = maximum number of subjects with data.
Source: Grill 2020 (Grill 2020), Schultz 2018 (Schultz 2018)
No deaths, other SAEs, or other significant AEs occurred during the study. The proportion of subjects who had at least 1 AE was similar for the FDC and the free combination (92.1% and 88.9%, respectively). The most frequently reported AE in both treatments was headache (60.5% and 66.7%, respectively). Other frequently reported AEs included back pain, pain in extremity, nasal congestion, nausea, dizziness, myalgia, and head discomfort. All reported AEs were mild or moderate in intensity, except 1 severe intensity AE of upper respiratory tract infection reported after administration of free combination.
Study AC-077-101 (Grill, 2020; Sidharta, 2017)
Study AC-077-101 was a single-center, open-label, single-dose, 2-period, randomized, crossover Phase I studies in healthy adult subjects. The primary objective was to demonstrate bioequivalence of the Cmax, AUC0-t, and AUC0-∞ of macitentan and tadalafil FDC and as a free combination of macitentan (OPSUMIT®) and tadalafil (ADCIRCA®, US-sourced). The secondary objectives were to evaluate the safety and tolerability of concomitant macitentan and tadalafil administered as an FDC product or as a free combination and to investigate other PK parameters of concomitant macitentan and tadalafil administered as an FDC product or as a free combination. Please refer to the Disease and Treatment document for additional information.
Two FDC formulations were investigated, FDC-1 and FDC-2, each containing macitentan/tadalafil 10 mg/40 mg and with different composition of excipients. Subjects were allocated to either Group 1 (FDC-1) or Group 2 (FDC-2) and within each group subjects were randomized to 1 of the 2 possible treatment sequences, A/B or B/A. Treatment A was a single FDC (test treatment: FDC-1 or FDC-2) tablet of macitentan/tadalafil 10 mg/40 mg. Treatment B was a reference treatment of the free combination.
Results
Results are presented for the FDC-2 formulation (Group 2) which is the formulation under regulatory review. A total of 124 subjects were planned and enrolled, with 62 subjects to each group. In Group 2 (FDC-2 vs. free combination), 4 subjects discontinued study drug, therefore 58 out of 62 subjects in Group 2 were evaluable for PK.
In Group 2, the PK profiles of macitentan and ACT-132577 after administration of FDC-2 showed slight differences compared to the administration as a free combination. While tmax and t½ values were comparable to those observed after administration of the free combination, exposure to macitentan was 19% higher for Cmax and 10% higher for AUC after administration of FDC-2. These differences were less noticeable for ACT-132577, where exposure was 10% higher for Cmax and 9% higher for AUC when given as the FDC-2. The PK parameters tmax and t½ for ACT-132577 were similar for FDC-2 and the free combination. However, all 90% CIs were within the bioequivalence limits of 0.8000–1.2500, fulfilling bioequivalence criteria. The PK profile of tadalafil after administration of FDC-2 was similar to the administration as a free combination. For tadalafil, the 90% CIs for the geometric mean ratios of all 3 parameters (AUC0-∞, AUC0-t and Cmax) were within the bioequivalence limits similar to macitentan. Therefore, bioequivalence of FDC-2 with the free combination of macitentan and US-sourced tadalafil was demonstrated.
No subject died and no SAEs were reported. Three subjects prematurely discontinued treatment due to AEs: 1 subject discontinued 8 days after administration of FDC-1 due to increased blood calcium; 1 subject discontinued due to increased blood triglycerides 11 days after administration of FDC-2; and 1 subject discontinued due to pain (general soreness) on the day of administration of FDC-2. The majority of the subjects in the study had at least 1 AE. The proportion of subjects who had at least 1 AE was similar for the FDCs and the free combination for both groups and varied between 70.0 and 78.7%. Headache was the most frequently reported AE for the FDCs and the free combination, with an incidence of 45.8–67.2%. Other frequently reported AEs included back pain, pain in extremity, nausea, and dizziness.
Study 67896062PAH1006 (Armas, 2020)
To attain Health Canada approval, an additional bioequivalence study was conducted to demonstrate that the tadalafil component in the FDC was bioequivalent to Canadian-sourced tadalafil (as an individual component). The results of study 67896062PAH1006 validate the results of AC-077-101 and AC-077-103 and make it applicable to the Canadian setting. The study 67896062PAH1006 was a Phase I, single-center, open-label, single-dose, 2-period, randomized, crossover study in healthy adult participants. The goal of the study was two-fold (1) to demonstrate the bioequivalence of tadalafil administered as a FDC of macitentan/tadalafil 10 mg/40 mg (test) and co-administered as a free combination (reference) of 10 mg macitentan and 40 mg Canadian-sourced tadalafil in fasted conditions, and (2) to evaluate the effect of food on the PK parameters of macitentan/tadalafil FDC. Please refer to the Disease and Treatment document for additional information.
Bioequivalence: The primary objective was to demonstrate bioequivalence on the primary PK parameters (Cmax, AUC from time 0 to time of the last quantifiable concentration [AUC0-last], and AUC0-∞) of tadalafil administered as macitentan/tadalafil FDC and as a free combination of macitentan (OPSUMIT®) and tadalafil (ADCIRCA®, Canadian-sourced). Participants were randomly assigned to 1 of 2 treatment sequences according to a classical 2-sequence, 2-period design. In the 2 sequential treatment periods, each participant was planned to receive 2 treatments (Treatment A [FDC-2] and Treatment B [free combination]) in a random order.
Food Effect: The primary objective was to evaluate the effect of food on the primary PK parameters (Cmax, AUC0-last, and AUC0-∞) of macitentan and tadalafil administered as an FDC. Participants were randomly assigned to 1 of 2 treatment sequences according to a classical 2-sequence, 2-period design. In the 2 sequential treatment periods, each participant received 2 treatments (Treatment C [fed conditions] and Treatment D [fasted conditions]) in a random order.
Results
Bioequivalence: A total of 46 participants were included in the Bioequivalence study, of which 10 participants completed only 1 period (prematurely discontinued due to COVID-19 outbreak), 3 participants discontinued, and 33 participants completed both treatment periods with evaluable PK (Cmax, AUC0-last, and AUC0-∞) parameters (additionally for Cmax, 1 participant prematurely discontinued the study, yet reliable Cmax was calculated, therefore n = 34) for determination of bioequivalence.
The mean plasma concentration time-profiles and PK parameters of macitentan, ACT-132577, and tadalafil after a single oral dose of macitentan/tadalafil FDC were comparable to free combination of 10 mg macitentan and 40 mg Canadian-sourced tadalafil under fasting conditions.
The 90% CIs for the geometric mean ratios (FDC-2 vs. free combination) of Cmax, AUC0-last, and AUC0-∞ for tadalafil and macitentan were within the bioequivalence limits.
Food Effect: A total of 16 participants were included in the Food Effect study, out of whom 15 participants completed at least 1 treatment period (15 each for Treatment C/D) and there were 14 participants who completed both treatment periods with evaluable PK (Cmax, AUC0-last, and AUC0-∞) parameters for determination of food-effect. The mean plasma concentration time-profiles of macitentan and tadalafil after a single oral dose in fed conditions were higher compared to fasted conditions up to 24 hours and 48 hours, respectively, and at later timepoints both profiles were comparable. The 90% CI of the geometric mean ratios of macitentan fell within the 80.00% to 125.00% equivalence limits for AUC0-last and AUC0-∞, however mean Cmax was slightly higher for macitentan and higher for tadalafil and fell outside equivalence limits. This increase in Cmax of tadalafil was not clinically significant, therefore the FDC-2 formulation could be taken without regards to meals.
Overall, the AE profile observed in this study is similar to that previously reported for macitentan and tadalafil in healthy adults. There were no apparent clinically relevant differences in the safety profiles between the FDC formulation and the free combination. There was no difference in the rate or severity of the TEAEs reported between fasted or fed states. Of the 46 participants enrolled and treated in the Bioequivalence study, 45 participants experienced 1 or more TEAE. No deaths were reported in this study. Of the 16 participants enrolled and treated in the Food Effects study, 15 participants experienced 1 or more TEAEs. Most of the reported TEAEs were assessed by the investigator as mild in severity.
Other Studies and Real-World Evidence
Additional data to support the efficacy and safety of macitentan and tadalafil combination use is derived from the OPTIMA trial. However, data collected through this trial evaluates the use of initial combination therapy in newly diagnosed patients with PAH which differs from the proposed Health Canada switch indication of macitentan/tadalafil FDC.
OPTIMA (Sitbon, 2020)
OPTIMA (EudraCT 2015-002078-19) was a prospective, single-arm, open-label Phase IV study evaluating the efficacy, safety, and tolerability of initial combination therapy with macitentan and tadalafil in newly diagnosed, treatment-naïve patients with PAH. The primary endpoint was PVR at Week 16, and secondary endpoints included a decrease from baseline to Week 16 in PVR ≥ 30% and change from baseline to Week 16 in hemodynamic variables, WHO FC, 6MWD, and N-terminal pro-hormone B-type Natriuretic Peptide (NT-proBNP). A pre-specified exploratory analysis included the number of low-risk criteria at baseline and Week 16. Patients initiated therapy at a dose of macitentan 10 mg and tadalafil 20 mg daily, and after 1 week the dose of tadalafil was increased to 40 mg daily. Note that patients in this study received the individual components of macitentan and tadalafil and not the FDC formulation. Overall, 46 patients were enrolled and treated. At Week 16, mean PVR was reduced by 47% compared with baseline (geometric mean ratio 0.53; 95% CI 0.47-0.59; p2.5 L/min/m2). A ≥ 30% decrease in PVR between baseline and Week 16 occurred in 87.0% (95% CI 73.7-95.1). Change in 6MWD significantly improved by 35.8 m from baseline (95% CI 15.8-55.9, p = 0.0008), and NT-proBNP was significantly reduced by 68% from baseline (0.32 ng/L, 95% CI 0.23-0.44, p < 0.0001). Mean right atrial pressure numerically decreased by 0.28 mmHg (95% CI -1.94-1.37, p = 0.7321). The number of patients meeting at least 3 low-risk criteria increased from 11/46 (23.9%) patients at baseline to 30/44 (68.2%) at Week 16. (Sitbon, 2019) At least 1 AE was reported in 43 patients (93.5%), SAEs were reported in 13 patients (28.3%) patients, and 3 patients died. The most frequent AEs were peripheral edema, headache, diarrhea, dyspnea, anemia, and asthenia. Overall, initial combination treatment with macitentan and tadalafil was well tolerated in patients with PAH and led to significant improvements, from baseline to Week 16, in cardiopulmonary hemodynamics, functional parameters, NT-proBNP as well as patients’ risk profiles in newly diagnosed, treatment-naïve patients with PAH. Although this study evaluated initial combination treatment, it validates the use of combination therapy of macitentan and tadalafil.
OPUS and ORePHuS (Chin, 2020)
This real-world use of macitentan and tadalafil has been established in 2 large datasets: OPsumit® USers (OPUS) and OPsumit® Historical USers cohort study (OrPHeUS). OPUS is a prospective, US, multicenter, long-term, drug registry ongoing since April 2014 (NCT02126943), and OrPHeUS was a retrospective, US, multicenter medical chart review with data collected between October 2013 and March 2017 (NCT03197688). A combined analysis from the OPUS and OrPHeUS datasets was conducted using patients who received initial combination therapy of macitentan and tadalafil (in any order) ≤ 60 days apart, with baseline being defined as the date the second therapy was initiated. Key endpoints assessed include the change in 6MWD from baseline to follow-up, hospitalization rates, survival, and safety. The datasets identified 1124 patients who received combination therapy with macitentan and tadalafil, 335 (30%) of which received initial macitentan and tadalafil combination therapy. The mean baseline 6MWD, recorded in 106 patients, was 280.6 ± 131.1 m and improved from baseline in every follow-up group (Figure 8). Additionally, Kaplan-Meier (KM) estimates (95% CI) showed that 63.3% (57.0-68.9) of patients were hospitalization free at 12 months and KM survival estimates at 12 months were 89.0% (84.4-92.3).
At least 1 AE was reported in 136 (80.0%) patients and ≥ 1 hepatic AE in 35 (10.4%) patients. Discontinuation of macitentan occurred in 107 (31.9%) patients, with 56 (16.7%) patients discontinuing due to AEs. Overall, this study demonstrated that in a real-world setting 6MWD is improved from baseline to follow-up in patients who received initial combination therapy with macitentan and tadalafil. Although this data analyzes initial combination treatment macitentan with tadalafil, it further demonstrates the efficacy and safety of its use in combination.
A DUE (NCT03904693)
This is an ongoing prospective, multicenter, double-blind, randomized, active-controlled, Phase III study evaluating the efficacy and safety of macitentan tadalafil monotherapies with the corresponding FDC therapy in subjects with PAH. In total, approximately 170 subjects are planned to be randomized into study to receive either macitentan/tadalafil FDC, macitentan 10 mg, or tadalafil 40 mg given once daily. The estimated primary study completion date is December 2023. Please note this study is evaluating initial combination use of macitentan/tadalafil FDC which is different from the currently reimbursement request (for patients currently treated with macitentan 10 mg and tadalafil 40 mg as separate tablets).
CADTH’s Critical Appraisal of the Clinical Evidence
CADTH conducted a critical appraisal of the clinical evidence for the macitentan-tadalafil FDC based on the summary of the evidence provided by the sponsor.
Internal Validity
The overall design of the SERAPHIN study appears to be appropriate with respect to randomization and standardized assessment of the efficacy and safety outcomes. Based on the information available in the sponsor’s summary of the clinical evidence, the trial appeared to be generally well-balanced in terms of baseline demographic and disease characteristics.
The main analyses for the primary and secondary end points were performed by the ITT approach, which included all patients who had undergone randomization. The clinical study report stated that no imputation method was used for the primary efficacy end point because of the time-to-event design. The LOCF approach was used to impute missing values of secondary and exploratory outcomes. More patients in the placebo group versus in the macitentan group prematurely discontinued treatment (59.4% versus 44.2%) and the study (22.0% versus 16.9%), mostly due to death (17.6% versus 14.0%) and loss to follow-up (2.8% versus 0.8%). These differences may impact the validity of the secondary analyses with LOCF imputation because the method relies on data missing at random, which does not appear to have been met.
To keep the study-wise type I error to a 2-sided 0.01 “conclusive” level in the presence of multiple tests, each comparison of active dose versus placebo was tested at a nominal type I error level of 0.005 (2-sided) according to the Bonferroni approach, with testing starting from the primary end point. Overall, the handling of multiplicity in the outcome comparison is reasonably presented and acceptable due to the hierarchical testing procedure for the secondary end points.
The HRs have been interpreted as relative risk reduction, which is incorrect. The HRs represent instantaneous risk over the study time period, which was lower for the treatment group.
A total of 158 centres participated in this trial, and 492 eligible patients with PAH were randomized into the 2 arms (242 to macitentan 10 mg arm and 250 placebo). Given the large number of centres involved, if there were differences in quality of care in participating centres, the overall results may not be balanced because no stratification by centre procedures were employed in the randomization scheme. However, PAH is a rare disease and the reason that so many countries and centres participated in this study is to ensure the study could recruit enough patients to attempt clinically important outcomes instead of just change in 6MWD like previous studies. The total observation period was 728 days. This time period may not be realistic for some outcome measures such as lung transplantation. The proportion of patients who discontinued from the trial was high (44.2% in macitentan 10 mg arm and 59.4% in placebo arm). However, most of the discontinuations were outcome related so it would not affect the primary end point, although secondary assessments that relied on complete case analysis would be expected to be affected by the drop-outs. AE rates were very high in both arms, most caused by worsening PAH. No concern in the interpretation of SAEs, WDAEs, and AEs of special interest was found.
The 3 bioequivalence studies were conducted in healthy volunteers and appeared to adhere to expected methods and conduct for such studies.
External Validity
A key limitation of the evidence provided by the sponsor is that it is primarily predicated on extrapolation of data for the efficacy and safety of macitentan with background PDE5 inhibitor treatment (mainly using sildenafil, not tadalafil [approximately 1%]), based on the SERAPHIN trial, and data demonstrating bioequivalence between the FDC and the individual components. There are currently no clinical trial data for the effects of the macitentan-tadalafil FDC versus a relevant comparator on clinically important outcomes, nor is there trial data informing on the efficacy and safety of switching from the components administered together to the FDC.
The SERAPHIN study recruited patients from 158 centres in 39 countries. These centres were specialized in treating patients with PAH. Because this disease is rare and the diagnosis and treatment require specialists, patients recruited from these centres should generally be representative of the patients in clinical practice, although some exceptions are noted subsequently. The study included several Canadian centres, and the results should be generalizable to Canadian patients affected by PAH.
Patients in the SERAPHIN trial were recruited based on the Venice PH Classification. Although this was the third formal PH classification introduced in 2003, and there have been updates since then, its use in SERAPHIN should not have major impact on the external validity of the results given the Venice Classification is the 1 that introduced the terms IPAH, FPAH, and associated PAH. As such, it still has clinical relevance.
Patients enrolled in the SERAPHIN study were mostly of WHO FC II (52%) and III (46%), and only 2% were of FC IV. Therefore, more than half of patients enrolled had less advanced disease but were likely to have disease progression and poor outcomes if untreated.
Sponsor-Submitted Cost Comparison
Macitentan 10 mg and tadalafil 40 mg is a FDC product indicated for the treatment of PAH.36 The product monograph notes that macitentan-tadalafil FDC can be used in patients who are currently treated concomitantly with macitentan 10 mg and tadalafil 40 mg (20 mg × 2) as separate tablets. The sponsor submitted a cost comparison of macitentan-tadalafil FDC with a regimen of macitentan and tadalafil taken as individual products from the perspective of the Canadian public health care payer (considering drug costs and dispensing fees only). The unit price of macitentan-tadalafil FDC was obtained from the sponsor. The unit prices of macitentan and tadalafil were obtained from the Ontario Exceptional Access Program and Ontario Drug Benefit (ODB) formulary, respectively.37
At a submitted price of $132.06 per tablet, the sponsor noted that macitentan-tadalafil FDC was associated with savings of $8,373 per person annually compared with macitentan and tadalafil taken as individual products (Appendix 1, Table 12). The sponsor also estimated that macitentan-tadalafil FDC is expected to reduce dispensing fees by 50%, resulting in an additional annual savings of $106 per person per year, assuming 12 dispensing fees and a dispensing fee of $8.83 per claim.
Critical Appraisal of Cost Information
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Comparative efficacy and safety of macitentan-tadalafil FDC with macitentan and tadalafil taken as individual products is uncertain. The clinical evidence submitted by the sponsor consisted of a trial comparing macitentan to placebo, as well as bioequivalence studies comparing macitentan-tadalafil FDC with macitentan and tadalafil taken as individual products. The evidence informing the assumption of clinical equivalence of macitentan-tadalafil FDC to a regimen of its individual components taken concomitantly is bioequivalence data because there is no direct evidence to inform the relative clinical effects. As a result, there is some uncertainty associated with the assumption of clinical equivalence, which is required for a cost comparison to be considered appropriate. A cost comparison is appropriate as long as the FDC product and a regimen of its individual components taken concomitantly are considered similar.
CADTH was unable to address this limitation in reanalysis.
The relative cost-effectiveness of macitentan-tadalafil FDC to other relevant regimens for the treatment of PAH is unknown. The sponsor-submitted cost comparison focused solely on the comparison of macitentan-tadalafil FDC with its individual components. According to the clinical expert consulted by CADTH for this review, clinicians may switch patients from other combinations of ERAs and PDE5 inhibitors to macitentan-tadalafil FDC. Other potential combinations that would be relevant comparators include ambrisentan plus tadalafil, ambrisentan plus sildenafil, bosentan plus sildenafil, bosentan plus tadalafil, and macitentan plus sildenafil. The indication for macitentan-tadalafil FDC notes that it should be used in patients who are currently treated concomitantly with stable doses of macitentan 10 mg and tadalafil 40 mg (20 mg × 2). CADTH confirmed with the sponsor that the proposed Health Canada indication and reimbursement request was specific to patients previously treated with the individual products, and they were not seeking reimbursement for macitentan-tadalafil FDC in patients not previously treated with macitentan and tadalafil taken as individual products. As a result, CADTH focused the review on the population switching from the individual components and did not consider the initiation of macitentan-tadalafil FDC in patients not previously treated with macitentan and tadalafil taken as individual products. The cost-effectiveness of macitentan-tadalafil in such situations is unknown.
CADTH could not address this limitation. CADTH has included a cost table listing the costs of other ERAs and PDE5 inhibitors (Appendix 1, Table 13), and a table assessing the relative costs of various combinations of these agents (Appendix 1, Table 14) for reference.
List price of tadalafil varies across jurisdictions. The sponsor’s submitted cost comparison was based on the unit price of tadalafil (20 mg tablet) on the ODB formulary ($11.47). However, the cost of tadalafil varies across the jurisdictions where tadalafil is currently listed, ranging in price from $10.12 to $11.47.38 As such, estimated cost-savings from the reimbursement of macitentan-tadalafil FDC may vary across jurisdictions.
In a CADTH reanalysis, cost-savings associated with macitentan-tadalafil FDC were estimated based on the range of publicly available list prices for 20 mg tablets of tadalafil.
CADTH Reanalyses
The CADTH reanalysis considered the drug acquisition cost comparison of macitentan-tadalafil FDC with its individual components based on the range of publicly available list prices for tadalafil. Macitentan-tadalafil FDC remained cost-saving, with a range of cost-savings in comparison with its individual components of $7,388 to $9,140 per person per year, depending on the list price of tadalafil (Table 11).
Table 11: CADTH Drug Acquisition Cost Comparison Table for Macitentan-Tadalafil FDC
Drug and comparator | Strength | Dosage form | Price ($) | Recommended dose | Average annual drug cost ($) | Difference in annual cost ($) |
|---|---|---|---|---|---|---|
Combination product | ||||||
Macitentan-tadalafil FDC (Opsynvi) | 10 mg/40 mg | Tablet | 132.0600a | 10 mg/40 mg once daily | 48,202 | Saving vs. individual component: 7,388 to 9,140 |
Individual components | ||||||
Macitentan (Opsumit) | 10 mg | Tablet | 132.0550b | 10 mg once daily | 48,200 | NA |
Tadalafil (Adcirca and generics) | 20 mg | Tablet | 10.1228c | 40 mg once daily (2 × 20 mg) | 7,390 | |
12.5220c | 9,141 | |||||
FDC = fixed-dose combination.
Note: Annual period assumes 365 days or 30.416 days per month for all comparators.
aSponsor’s submitted price.39
bOntario Exceptional Access Program (accessed August 23, 2021).40
cSaskatchewan formulary (accessed August 23, 2021).38
CADTH also conducted a cost comparison of macitentan-tadalafil FDC to other combinations of ERAs and PDE5 inhibitors in an exploratory analysis (Appendix 1, Table 14). Incremental costs of macitentan-tadalafil FDC per patient annually ranged from cost-savings of $7,985 to increased costs of $16,790.
Issues for Consideration
Analysis based on publicly available list prices: Both the sponsor’s and CADTH’s analyses are based on publicly available list prices for all comparators. Actual costs paid by public drug plans are unknown.
A previous CADTH Canadian Drug Expert Committee (CDEC) recommendation for macitentan (Opsumit) included the condition that the price of macitentan not exceed the price of bosentan. The list price of generic bosentan is $32.09 per tablet in Ontario, for a daily cost of $64.18 which is lower than the list price of macitentan ($132.06 per tablet). Should the price of macitentan be lower than its publicly available list price, this would lower or eliminate the savings associated with the reimbursement of macitentan-tadalafil FDC at the submitted price in comparison with its individual components.
Cost-savings in dispensing fees may vary across jurisdictions: The sponsor assumed pharmacy dispensing fees will be reduced by half with macitentan-tadalafil FDC, resulting in an estimated annual cost-savings of $106 in dispensing fees. The sponsor assumes a dispensing fee of $8.83 per prescription based on ODB. However, the dispensing fees payable to pharmacies in Ontario can be as high as $13.25 in some regions. In other jurisdictions, the maximum allowable dispensing fees can range from $10.00 (in British Columbia) to $30 per prescription (in Manitoba).41 Variability in dispensing fees across jurisdictions may impact the magnitude of estimated cost-savings. In jurisdictions with higher dispensing fees, estimated cost-savings may be greater with the macitentan-tadalafil FDC product when compared with macitentan and tadalafil taken as individual components.
Discussion
Summary of Available Evidence
The evidence to support the indication submitted to Health Canada and reimbursement request for macitentan-tadalafil FDC includes bioequivalence data. The SERAPHIN study was provided as supportive efficacy and safety data and is not the primary study for this submission. Although the SERAPHIN study was not submitted as a pivotal study for the regulatory submission to Health Canada for the FDC, it was the pivotal study for the approval of macitentan.
Interpretation of Results
Efficacy
The macitentan-tadalafil FDC submission for switching patients from individually administered macitentan and tadalafil to the FDC is based on extrapolation of existing data on the established efficacy and safety of both components and bioequivalence between the FDC and components administered in combination.
The SERAPHIN study included a mixed population of patients who received monotherapy (macitentan or placebo) or dual therapy (baseline PAH therapy plus macitentan or placebo). More than 60% of patients were in the latter group, with most patients treated with macitentan plus sildenafil; a minority of patients (approximately 1%) were treated with macitentan plus tadalafil. In the subgroup of patients receiving background PAH therapy, the HR for the composite primary end point of time to first morbidity event or mortality was 0.62 (95% CI, 0.43 to 0.89) in favour of the macitentan group. The most frequent event was clinical worsening.
In its assessment of macitentan, CDEC considered the results of the SERAPHIN study and the CADTH review of drugs for the treatment of PAH.21 Given the lack of head-to-head studies of drugs for PAH, the CADTH therapeutic review conducted an indirect comparison of drugs for PAH.15 The review did not find a difference in comparative effectiveness between any of the drugs evaluated for most of the outcomes, including the outcome of clinical worsening. When the CADTH therapeutic review was conducted, the outcome of time to morbidity event or mortality had only been evaluated in the SERAPHIN study. The occurrence of clinical worsening was used as the key clinical outcome for the review. The review also found that the PDE5 inhibitors were the most cost-effective treatments to initiate treatment. CDEC recommended that sildenafil or tadalafil be the initial treatment for PAH.21 Using this information and the results from the subgroup analyses of the SERAPHIN study, CDEC recommended that macitentan be added on to initial treatment with a PDE5 inhibitor, unless the patient has a contraindication or other reason they were unable to receive these as initial treatment. Therefore, although the subgroup results by baseline therapy in the SERAPHIN study were primarily based on dual therapy with sildenafil plus macitentan, the CADTH therapeutic review and results from the SERAPHIN study support similar efficacy between the PDE5 inhibitors (i.e., interchangeable) and either could be used in combination with macitentan. CDEC also noted in support of its recommendation for macitentan that the Health Canada–approved indication states that macitentan is effective when used as monotherapy or in combination with PDE5 inhibitors. Therefore, although it would have been preferable for a randomized controlled trial of the effects of macitentan-tadalafil FDC on clinically important outcomes in the population requested for reimbursement, there is evidence to support efficacy and safety of this combination of drugs (when administered separately) for the treatment of PAH.
Additional studies were submitted to support the efficacy and safety of the macitentan-tadalafil FDC. However, the OPTIMA trial and the ongoing A DUE trial and a combined analysis from the OPUS and OrPHeUS datasets evaluated the use of initial combination therapy in newly diagnosed patients with PAH, which the sponsor noted was not the proposed switch indication or reimbursement request for macitentan-tadalafil FDC. Therefore, the results of these studies are out of scope for the current review.
The 3 bioequivalence studies suggested equivalence between the FDC and components because the 90% CIs for the geometric mean ratios of Cmax various measures of AUC were within the bioequivalence limits of 0.8000 to 1.2500. At the time of drafting this review report, macitentan-tadalafil FDC was being reviewed by Health Canada; therefore, that assessment of bioequivalence is not available. If Health Canada determines the FDC and components are bioequivalent, then this would help to support switching patients to the FDC from macitentan and tadalafil in combination but administered separately.
The sponsor’s submission highlighted the pill burden patients with PAH experience. No patient group input was submitted to CADTH for the macitentan-tadalafil FDC review. Patient group input to CADTH for the formulary review of macitentan and the therapeutic review of drugs for PAH did not specifically address pill burden. However, in addition to the PAH-specific treatments, most patients receive diuretics and blood thinners as part of their treatment, and other medications to control the many reported side effects of PAH treatment. As described previously, patients typically receive several medications as supportive care and they often have comorbidities that also require medications. Patient group input has previously emphasized that PAH is a disease that has a significant impact on the daily lives of patients and their caregivers, contributing to a reduced HRQoL. There is rationale that for patients who require combination therapy, switching from the individual drugs administered together to a FDC would decrease the total number of oral pills a patient needs to take. As the sponsor points out in their submission, this approach has been used in other indications, such as type 2 diabetes mellitus and hypertension.42,43 Improved adherence is important to ensure improved outcomes.44 Nevertheless, no evidence has been provided that directly supports improved adherence or outcomes (such as HRQoL) with the macitentan-tadalafil FDC.
Harms
There are limited data on the adverse event profile of the FDC. The frequency and nature of the AEs reported in the OPTIMA phase IV single-arm study were consistent with the known AEs for macitentan and tadalafil. The most frequent AEs were peripheral edema, headache, diarrhea, dyspnea, anemia, and asthenia. Likewise, percentages of patients in the SERAPHIN study receiving background therapy plus macitentan or placebo who experienced an AE were 93.5% and 97.4%, respectively. The frequency of treatment WDAEs in patients receiving background therapy plus macitentan were 9.1% versus 11.8% for those receiving background therapy plus placebo. In the overall SERAPHIN population, the frequency of AEs was similar between the groups in the SERAPHIN study (94.6% macitentan 10 mg, 96.4% placebo). WDAEs were similar between the macitentan 10 mg arm (10.7%) and placebo (12.4%). In the 3 bioequivalence studies submitted by the sponsor, no individual died or reported SAEs. Most of the AEs were mild and the proportion of individuals who had at least 1 AE was similar for the FDCs and the free combinations for both groups and varied between 70.0% and 78.7%. Headache was the most frequently reported AE for the FDCs and the free combinations, with an incidence of 45.8% to 67.2%. Other frequently reported AEs included back pain, pain in an extremities, nausea, and dizziness.
Other Considerations
The SERAPHIN trial has been previously evaluated as part of the macitentan CADTH review and received a recommendation to reimburse in 2015, with the clinical condition of a contraindication or inadequate response to sildenafil or tadalafil. Tadalafil was reviewed by CADTH in 2010 and also received a recommendation to reimburse with clinical conditions. Currently, macitentan is a restricted benefit in Alberta, Saskatchewan, Manitoba, Ontario, New Brunswick, Yukon, Northwest Territories, and 2 federal drug programs. Tadalafil is a restricted benefit in British Columbia, Alberta, Saskatchewan, Ontario, Yukon, and 2 federal drug programs. Both drugs are reimbursed in Quebec.
Cost
At the submitted price, macitentan-tadalafil FDC costs $48,202 per patient annually. The annual cost-savings of macitentan-tadalafil FDC compared with macitentan and tadalafil taken as individual products at the same dose range from $7,388 to $9,140 per person, depending on the list price of tadalafil. Those incremental savings are based on publicly available list prices and may not reflect actual prices paid by Canadian public drug plans.
The sponsor’s cost comparison assumes clinical similarity between macitentan-tadalafil FDC and macitentan and tadalafil taken as individual products. The clinical review conducted by CADTH identified several limitations with the submitted clinical evidence but concluded the FDC is similar to its components taken as individual products. Should the clinical effectiveness of macitentan-tadalafil FDC be different than that of macitentan and tadalafil taken as individual products in real-world use, the cost-effectiveness of macitentan-tadalafil FDC is unknown.
The sponsor’s submission and CADTH reanalyses focused on the sponsor’s proposed Health Canada indication and reimbursement request population, which consisted solely of patients previously treated with macitentan and tadalafil.
Conclusions
The results from the SERAPHIN trial showed that, compared with placebo, macitentan 10 mg once daily improved outcomes when administered in combination with a PDE5 inhibitor (primarily sildenafil) in patients with PAH. This study included several Canadian centres, so the results should be generalizable to Canadian patients affected by PAH. However, because only approximately 1% of patients received tadalafil plus macitentan and the study did not use a treatment switch design, the results do not directly apply to the target patient group for the submission. Nonetheless, the subgroup analyses, in combination with evidence from the CADTH therapeutic review on drugs for PAH, support that the combination use of macitentan and tadalafil improves outcomes for patients with WHO FC II or III PAH. Bioequivalence data suggest that the FDC is equivalent to the individual components administered separately. A major implication of the macitentan-tadalafil FDC for the treatment of PAH is the clinical benefit of a dual treatment in patients who require this treatment approach with a reduction in pill burden and therefore patient adherence and outcomes. The hypothesized benefits of improved adherence and patient outcomes specific to use of the macitentan-tadalafil FDC is unclear because neither has been directly evaluated for the FDC.
At the submitted price, macitentan-tadalafil FDC costs $48,202 per patient annually and is cost-saving compared with the cost of macitentan and tadalafil taken as individual products at list prices. The appropriateness of a cost comparison to assess the cost-effectiveness of macitentan-tadalafil FDC compared with macitentan and tadalafil taken as individual products relies on the assumption of clinical similarity. If the clinical effectiveness of macitentan-tadalafil FDC is different than that of macitentan and tadalafil taken as individual products in real-world use, its cost-effectiveness is unknown.
References
1.McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation. 2009;119(16):2250-2294. PubMed
2.Vachiéry JL, Gaine S. Challenges in the diagnosis and treatment of pulmonary arterial hypertension. Eur Respir Rev. 2012;21(126):313-320. PubMed
3.Escribano-Subias P, Blanco I, López-Meseguer M, et al. Survival in pulmonary hypertension in Spain: insights from the Spanish registry. Eur Respir J. 2012;40(3):596-603. PubMed
4.Frost AE, Badesch DB, Barst RJ, et al. The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US Contemporary Registries. Chest. 2011;139(1):128-137. PubMed
5.Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173(9):1023-1030. PubMed
6.Hurdman J, Condliffe R, Elliot CA, et al. ASPIRE registry: assessing the Spectrum of Pulmonary hypertension Identified at a REferral centre. Eur Respir J. 2012;39(4):945-955. PubMed
7.Jansa P, Jarkovsky J, Al-Hiti H, et al. Epidemiology and long-term survival of pulmonary arterial hypertension in the Czech Republic: a retrospective analysis of a nationwide registry. BMC Pulm Med. 2014;14:45. PubMed
8.Peacock AJ, Murphy NF, McMurray JJ, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J. 2007;30(1):104-109. PubMed
9.Wijeratne DT, Lajkosz K, Brogly SB, et al. Increasing incidence and prevalence of World Health Organization groups 1 to 4 pulmonary hypertension: a population-based cohort study in Ontario, Canada. Circ Cardiovasc Qual Outcomes. 2018;11(2):e003973. PubMed
10.McGoon MD, Benza RL, Escribano-Subias P, et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013;62(25 Suppl):D51-59. PubMed
11.Vaid HM, Camacho X, Granton JT, et al. The characteristics of treated pulmonary arterial hypertension patients in Ontario. Can Respir J. 2016;2016:6279250. PubMed
12.Hirani N, Brunner NW, Kapasi A, et al. Canadian Cardiovascular Society/Canadian Thoracic Society position statement on pulmonary hypertension. Can J Cardiol. 2020;36(7):977-992. PubMed
13.Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Rev Esp Cardiol (Engl Ed). 2016;69(2):177. PubMed
14.Drug Reimbursement Review sponsor submission: macitentan and tadalafil, 10 mg/40 mg film-coated tablets [internal sponsor's package]. Toronto (ON): Janssen Inc.; 2021 May 20.
15.Drugs for pulmonary arterial hypertension: comparative efficacy, safety, and cost-effectiveness - recommendations report. (CADTH therapeutic review report). Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/TR0006_PAH_Recs_Report.pdf. Accessed 2021 Aug 19.
16.Pulido T, Adzerikho I, Channick RN, et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013;369(9):809-818. PubMed
17.Clinical study report: ACT-064992 Macitentan (Protocol 67896062PAH1006). Single-center, open-label, single-dose, 2-period, randomized, crossover phase 1 study to demonstrate bioequivalence of tadalafil administered as a fixed dose combination formulation of macitentan/tadalafil (10 mg/40 mg) and as the free combination of 10 mg macitentan (Opsumit®) and 40 mg tadalafil (Adcirca®), and to assess the effect of food on the pharmacokinetics of the fixed dose formulation of macitentan/tadalafil (10 mg/40 mg) in healthy adult participants [internal sponsor's report]. Mannheim (Germany): Actelion Pharmaceuticals Ltd.; 2020 Nov 9.
18.Grill S, Bruderer S, Sidharta PN, et al. Bioequivalence of macitentan and tadalafil given as fixed-dose combination or single-component tablets in healthy subjects. Br J Clin Pharmacol. 2020;86(12):2424-2434. PubMed
19.Clinical study report: AC-077-103. Single-center, open-label, single-dose, two-period, randomized, crossover, phase 1 study to demonstrate bioequivalence between a fixed dose combination product formulation of macitentan/tadalafil (10 mg / 40 mg) and the free combination of 10 mg macitentan (Opsumit®) and 40 mg tadalafil (Adcirca®) in healthy male and female subjects [internal sponsor's report]. Mannheim (Germany): Actelion Pharmaceuticals Ltd.; 2018 Mar 21.
20.Clinical study report: AC-077-101. Single-center, open-label, single-dose, two-period, randomized, crossover, phase 1 study to demonstrate bioequivalence between two fixed dose combination product formulations of macitentan/tadalafil (10 mg / 40 mg) and the free combination of 10 mg macitentan (Opsumit®) and 40 mg tadalafil (Adcirca®) in healthy male and female subjects [internal sponsor's report]. Mannheim (Germany): Actelion Pharmaceuticals Ltd.; 2017 Nov 9.
21.CADTH Canadian Drug Expert Committee (CDEC) final recommendation: macitentan (Opsumit - Actelion Pharmaceuticals Canada Inc.). Ottawa (ON): CADTH; 2015 Jan 21: https://cadth.ca/sites/default/files/cdr/complete/cdr_complete_SR0364_Opsumit_Jan-30-15.pdf. Accessed 2021 Aug 19.
22.Galiè N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. 2009;30(20):2493-2537. PubMed
23.Hoeper MM, Bogaard HJ, Condliffe R, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D42-50. PubMed
24.Barst RJ, Chung L, Zamanian RT, Turner M, McGoon MD. Functional class improvement and 3-year survival outcomes in patients with pulmonary arterial hypertension in the REVEAL Registry. Chest. 2013;144(1):160-168. PubMed
25.Nickel N, Golpon H, Greer M, et al. The prognostic impact of follow-up assessments in patients with idiopathic pulmonary arterial hypertension. Eur Respir J. 2012;39(3):589-596. PubMed
26.Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol. 2002;40(4):780-788. PubMed
27.Howard LS, Ferrari P, Mehta S. Physicians' and patients' expectations of therapies for pulmonary arterial hypertension: where do they meet? Eur Respir Rev. 2014;23(134):458-468. PubMed
28.Badesch DB, Raskob GE, Elliott CG, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest. 2010;137(2):376-387. PubMed
29.Suárez JA, Manzaneque A, Garcia NC, Creus MT, Mir JB. DI-058 Risk of drug–drug interactions in a pulmonary arterial hypertension population. European Journal of Hospital Pharmacy. 2017;24(Suppl 1):A138-A139.
30.Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019;53(1). PubMed
31.Wilkins MR. Pulmonary hypertension: the science behind the disease spectrum. Eur Respir Rev. 2012;21(123):19-26. PubMed
32.Lichtblau M, Harzheim D, Ehlken N, et al. Safety and long-term efficacy of transition from sildenafil to tadalafil due to side effects in patients with pulmonary arterial hypertension. Lung. 2015;193(1):105-112. PubMed
33.Shlobin OA, Brown AW, Weir N, Ahmad S, Lemma M, Nathan SD. Transition of PH patients from sildenafil to tadalafil: feasibility and practical considerations. Lung. 2012;190(5):573-578. PubMed
34.Hoeper MM, Apitz C, Grünig E, et al. Targeted therapy of pulmonary arterial hypertension: Updated recommendations from the Cologne Consensus Conference 2018. Int J Cardiol. 2018;272s:37-45. PubMed
35.McLaughlin V, Channick RN, Ghofrani HA, et al. Bosentan added to sildenafil therapy in patients with pulmonary arterial hypertension. Eur Respir J. 2015;46(2):405-413. PubMed
36.Budget impact analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: macitentan and tadalafil, 10 mg/40 mg film-coated tablets. Toronto (ON): Janssen Inc.; 2021 May 20.
37.Ontario Ministry of Health Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Oct 5.
38.Saskatchewan Drug Plan: search formulary. 2021; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2021 Oct 5.
39.Zhu Q, Wu Y, Zeng J, Wang X, Zhang T, Lin X. Influence of bacterial community composition and soil factors on the fate of phenanthrene and benzo[a]pyrene in three contrasting farmland soils. Environmental Pollution. 2019;247:229-237. PubMed
40.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2021: https://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2021 Oct 5.
41.Patented Medicine Prices Review Board. Dispensing fee policies in public drug plans, 2018/19. http://www.pmprb-cepmb.gc.ca/view.asp?ccid=1308. Accessed 2021 Sep 8.
42.Lauffenburger JC, Landon JE, Fischer MA. Effect of combination therapy on adherence among US patients initiating therapy for hypertension: a cohort study. J Gen Intern Med. 2017;32(6):619-625. PubMed
43.Pan F, Chernew ME, Fendrick AM. Impact of fixed-dose combination drugs on adherence to prescription medications. J Gen Intern Med. 2008;23(5):611-614. PubMed
44.Frantz RP, Hill JW, Lickert CA, et al. Medication adherence, hospitalization, and healthcare resource utilization and costs in patients with pulmonary arterial hypertension treated with endothelin receptor antagonists or phosphodiesterase type-5 inhibitors. Pulm Circ. 2020;10(1):2045894019880086. PubMed
45.Volibris (ambrisentan): 5mg and 10mg tablets Endothelin Receptor Antagoinist [product monograph]. Mississauga (ON): GlaxoSmithKline Inc; 2021 Jul 2.
46.Sandoz Bosentan (bosentan monohydrate): 62.5 mg and 125 mg film-coated tablets Endothelin Receptor Antagonist [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2018 Nov 2.
47.Opsumit (macitentan): 10 mg film-coated tablet Endothelin Receptor Antagonist [product monograph]. Laval (QC): Actelion Pharmaceuticals Ltd.; 2015 Nov 18.
48.Revatio (sildenafil tablets, Upjohn Standard): 20 mg sildenafil (as sildenafil citrate); (sildenafil injection, Upjohn Standard): 0.8 mg/mL sildenafil (as sildenafil citrate) cGMP-Specific Phosphodiesterase Type 5 Inhibitor [product monograph]. Kirkland (QC): Upjohn Canada ULC; 2021 Feb 24.
49.Cialis (tadalafil tablets): 2.5 mg, 5 mg tablets (for once-a-day use), 10 mg, 20 mg tablets (for “on-demand” dosing) cGMP-Specific Phosphodiesterase Type 5 Inhibitor [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2020 May 28.
50.DeltaPA. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed 1800 Jan 1.
Appendix 1: Additional Economic Information
Note that this appendix has not been copy-edited.
Additional Details on the Sponsor’s Submission
Table 12: Sponsor’s Drug Acquisition Cost Comparison
Generic name (Brand name) | Strength | Dosage form | Price ($)a | Recommended dosage regimen | Annual drug cost ($) | Difference in annual costb |
|---|---|---|---|---|---|---|
Macitentan-tadalafil FDC | 10 mg/40 mg | Tablet | $132.06 | 10 mg/40 mg once daily | $48,201.90 | Saving vs. individual components: ($8,373.10) |
Comparators | ||||||
Macitentan (OPSUMIT®) | 10 mg | Tablet | $132.06 | 10 mg once daily | $48,200.08 | NA |
Tadalafil (ADCIRCA® and generics) | 20 mg | Tablet | $11.47 | 40 mg once daily (2 × 20 mg) | $8,374.93 | |
aBased on ODB pricing. Pricing for tadalafil based on the least costly interchangeable price. Prices have been rounded to the nearest 2 decimal places.
bDifference in annual cost based on addition of macitentan with tadalafil vs. Opsynvi.
Additional Details on the CADTH Reanalyses and Additional Analyses
Table 13: CADTH Cost Comparison Table for Pulmonary Arterial Hypertension
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Macitentan/ tadalafil FDC | 10 mg/40 mg | Tablet | 132.0600a | 10 mg/40 mg daily | 132.06 | 48,202 |
Endothelin receptor antagonists | ||||||
Ambrisentan (generics) | 5 mg 10 mg | Tablet | 106.3288 | 5 to 10 mg daily | 106.33 | 38,810 |
Bosentan (generics) | 62.5 mg 125 mg | Tablet | 32.0893 | 62.5 mg twice daily for 4 weeks, then, 125 mg twice daily | 64.18 | 23,425 |
Macitentan (Opsumit) | 10 mg | Tablet | 132.0550 | 10 mg daily | 132.06 | 48,200 |
Phosphodiesterase type 5 (PDE5) inhibitors | ||||||
Sildenafil (Revatio, generics) | 20 mgb | Tablet | 7.2940 | 20 mg 3 times daily | 21.88 | 7,987 |
Tadalafil (generics) | 20 mgc | Tablet | 11.4725 | 40 mg daily (2 × 20 mg) | 22.95 | 8,375 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed August 23, 2021), unless otherwise indicated, and do not include dispensing fees. Recommended dosage is based on product monographs.45-49
aSponsor’s submitted price.39
bOther strengths are available as per product monograph but price was not available for 25 mg, 50 mg, and 100 mg.48
cOther strengths are available as per product monograph but price was not available for tablets 2.5 mg, 5 mg, and 10 mg.49
Table 14: CADTH Cost Comparison of Macitentan-Tadalafil FDC Relative to Other Combinations of ERAs and PDE5 Inhibitor
ERA | PDE-5 inhibitors, annual cost of PDE _ ERAs combo and incremental annual cost relative to macitentan-tadalafil FDC ($48,202)a | |
|---|---|---|
Sildenafil 20 mg 3 times daily | Tadalafil 40 mg once daily | |
Ambrisentan 5 to 10 mg daily | $46,797 -$1,405 | $47,185 -$1,017 |
Bosentan 62.5 mg b.i.d. for 4 weeks, then 125 mg twice daily | $31,412 -$16,790 | $31,800 -$16,402 |
Macitentan 10 mg daily | $56,187 $7,985 | $56,575 $8,373 |
b.i.d = twice daily; ERAs = endothelin receptor antagonists; FDC = fixed-dose combination; PDE5 = phosphodiesterase type 5.
Note: All included costs are based on publicly available list prices and may not reflect costs paid by plans.
aCost of comparator combination minus macitentan-tadalafil FDC, with negative results indicating macitentan-tadalafil FDC is more expensive than the comparator. Annual cost of macitentan-tadalafil FDC is $48,202 per patient.
Appendix 2: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The submitted budget impact analysis (BIA) assessed the expected budgetary impact of reimbursing macitentan-tadalafil FDC for the treatment of patients with pulmonary arterial hypertension (PAH) who are currently treated concomitantly with macitentan 10 mg and tadalafil 40 mg per day taken as individual products.39 The BIA was conducted from the public drug program perspective over a 3-year time horizon. Only drug acquisition costs were considered in their base case.
A claims-based approach was taken to estimate the total market size, in terms of claims, for patients currently publicly reimbursed for the individual component medications using IQVIA Pharmastat data.50 A linear trend was assumed to estimate the forecasted number of claims of macitentan and tadalafil for the relevant time horizon. The sponsor used claims data from British Columbia for Alberta and claims data from Nova Scotia for Prince Edward Island, adjusted for population size, in the absence of relevant claims data. Additionally, the sponsor made several assumptions around the capture of other ERAs products by macitentan, the discontinuation rate with macitentan, as well as the proportion of macitentan claims expected to be in combination with tadalafil (73%) to determine the final market size. Key inputs to the BIA are documented in Table 16.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Key inputs | |
Proportion of ERAs market claimed by macitentan each year | ||39 |
Annual discontinuation rate with macitentan each year | ||||50 |
Proportion of macitentan claims made in combination with tadalafil | 73%50 |
Number of eligible claims | |||| / |||| / |||| |
Market uptake (reference scenario) | |
Macitentan and tadalafil (individual components) | 100% / 100% / 100% |
Market uptake (new drug scenario) | |
Total claims in New Drug Scenario (Year 2023, 2024, 2025) Macitentan and tadalafil (individual components) Macitentan-tadalafil FDC | |||| / |||| / |||| |||| / |||| / |||| |
Cost of treatment (per claim) | |
Macitentan-tadalafil FDC Macitentan and tadalafil (individual components) | $4,017 $4,715 ($4,017 + $698) |
ERAs = endothelin receptor antagonists; PDE5 = phosphodiesterase type 5.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s base case suggest that the incremental budget savings associated with the reimbursement of macitentan-tadalafil FDC for patients previously treated with macitentan and tadalafil taken as individual products for the long-term treatment of PAH (WHO Group 1) would be $1,670,837 in year 1, $3,210,460 in year 2, and $3,720,530 in year 3, for a 3-year cumulative budgetary savings of $8,601,826. When considering markup and dispensing fees, the estimated 3-year cumulative budget savings rose to $9,507,682.
CADTH Appraisal of the Sponsor’s BIA
Use of claims-based approach to estimate market size introduces uncertainty with the anticipated budget impact of macitentan-tadalafil FDC: The sponsor assumes that all claims for macitentan are for the indication of interest. However, according to the clinical expert consulted by CADTH for this review, there is off label use of macitentan and tadalafil for the treatment of chronic thromboembolic pulmonary hypertension. The sponsor further assumed that 73% of claims of macitentan are made in combination with tadalafil, which was based on an analysis of patient claims data in Quebec, though it is unclear if this is generalizable to the rest of the Canadian population, or to the indication of interest. Given the claims database does not provide the indication and the proportion of claims pertaining to use for other indications is unknown, using a claims-based approach to estimate market size introduces significant uncertainty. Additionally, the sponsor also acknowledges that macitentan is currently not available in most jurisdictions. Given the ongoing listing of macitentan in public formularies by additional jurisdictions, there is uncertainty introduced by estimating population size based on an unstable and growing market based on claims.
CADTH was unable to address this limitation in reanalyses. CADTH explored the impact of assuming an alternative proportion of claims of macitentan made in combination with tadalafil than the value assumed by the sponsor in scenario analyses, assuming concomitant treatment rates of 50% and 100%.
The budget impact of macitentan-tadalafil FDC in situations where comparators other than its individual components will be displaced is uncertain: The sponsor-submitted BIA focused solely on the comparison of macitentan-tadalafil FDC with its individual components, with the target population consisting of patients who were treatment experienced and receiving the individual components of macitentan and tadalafil. However, according to the clinical expert consulted by CADTH for this review, macitentan-tadalafil FDC may be used in patients on treatment with other combinations of ERAs and PDE5 inhibitors, or instead of other combinations in patients who are naïve to dual therapy for PAH. The clinical expert noted ambrisentan plus tadalafil is the most frequently prescribed combination in current clinical practice, followed by bosentan plus sildenafil; and other comparators include ambrisentan plus sildenafil and bosentan plus tadalafil. The indication for macitentan-tadalafil FDC notes that it should be used in patients who are currently treated concomitantly with stable doses of macitentan 10 mg and tadalafil 40 mg (20 mg × 2). CADTH confirmed with the sponsor that the proposed Health Canada indication and reimbursement request was specific to patients previously treated with the individual components, and they were not seeking reimbursement for macitentan-tadalafil FDC in patients not previously treated with the individual components. As a result, CADTH focused the review on the population switching from the individual components and did not consider the initiation of macitentan-tadalafil FDC in patients not previously treated with the individual components. The budget impact of macitentan-tadalafil FDC in such situations is unknown, though should macitentan-tadalafil FDC displace regimens containing bosentan or ambrisentan budgetary savings may be reduced or eliminated.
CADTH could not address this limitation.
List price of tadalafil, as well as markups and dispensing fees vary across jurisdictions. The sponsor’s BIA based the unit price per 20 mg tablet of tadalafil on the price listed in the ODB formulary ($11.4725). However, the cost of tadalafil varies across jurisdictions where tadalafil is currently listed, ranging in price from $10.1228 to $12.5220 per 20 mg tablet. The sponsor also performed a scenario analysis including a markup of 8.0% and dispensing fee of $8.83 to the cost of a claim based on Ontario. However, markups and dispensing fees vary across jurisdictions, ranging from $10.00 per claim in British Columbia to a maximum of $30 per claim in Manitoba.41 As such, estimated cost-savings from the reimbursement of macitentan-tadalafil FDC may vary across jurisdictions based on the price of tadalafil, as well as the relevant markup and dispensing fee.
In CADTH scenario analysis, the budget impact associated with macitentan-tadalafil FDC was estimated based on the lowest available list price of tadalafil ($10.1228).
Actual price of drugs paid for by public drug plans is uncertain: Both the sponsor’s and CADTH’s analyses are based on publicly available list prices for all comparators. Actual costs paid by public drug plans are unknown.
This limitation could not be addressed by CADTH. Confidential negotiated prices for the individual components of macitentan and tadalafil may lead to budgetary savings being limited or eliminated.
CADTH Reanalyses of the BIA
CADTH did not undertake a base case reanalysis. Instead, CADTH conducted several scenario analyses which included:
Assuming the lowest list price identified for 20 mg tablets of tadalafil ($10.1228)
Assuming 50% of macitentan claims are made in combination with tadalafil
Assuming 100% of macitentan claims are made in combination with tadalafil
Results are presented in Table 17. The reimbursement of macitentan-tadalafil FDC was associated with cost-savings in all scenario analyses. Savings decreased as the market size decreased, as well as when a lower price of tadalafil was considered, but not substantially.
Table 17: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $36,117,837 | $41,267,672 | $45,885,674 | $49,842,107 | $136,995,454 |
New drug | $36,117,837 | $39,596,835 | $42,675,214 | $46,121,578 | $128,393,627 | |
Budget impact | $0 | –$1,670,837 | –$3,210,460 | –$3,720,530 | –$8,601,826 | |
CADTH scenario analysis: price of tadalafil ($10.1228) | Reference | $35,095,699 | $40,184,473 | $44,741,329 | $48,636,618 | $133,562,419 |
New drug | $35,095,699 | $38,710,247 | $41,908,651 | $45,353,891 | $125,972,789 | |
Budget impact | $0 | –$1,474,226 | –$2,832,678 | –$3,282,727 | –$7,589,631 | |
CADTH scenario analysis: 50% on concomitant treatment | Reference | $32,976,019 | $37,774,894 | $42,016,942 | $45,597,423 | $125,389,259 |
New drug | $32,976,019 | $36,622,403 | $39,802,447 | $43,031,032 | $119,455,882 | |
Budget impact | $0 | –$1,152,491 | -$2,214,496 | –$2,566,390 | –$5,933,378 | |
CADTH scenario analysis: 100% on concomitant treatment | Reference | $32,976,019 | $37,774,894 | $42,016,942 | $45,597,423 | $125,389,259 |
New drug | $32,976,019 | $35,473,028 | $37,594,005 | $40,471,853 | $113,538,886 | |
Budget impact | $0 | –$2,301,867 | –$4,422,937 | –$5,125,569 | –$11,850,373 |
BIA = budget impact analysis.
Appendix 3: Sponsor’s References
Note this appendix has not been copy-edited.
Armas D. Single-center, Open-label, Single-dose, 2-period, Randomized, Crossover Phase 1 Study to Demonstrate Bioequivalence of Tadalafil Administered as a Fixed Dose Combination Formulation of Macitentan/Tadalafil (10 mg/40 mg) and as the Free Combination of 10 mg Macitentan (Opsumit®) and 40 mg Tadalafil (Adcirca®), and to Assess the Effect of Food on the Pharmacokinetics of the Fixed Dose Formulation of Macitentan/Tadalafil (10 mg/40 mg) in Healthy Adult Participants. Actelion Pharmaceuticals Ltd; Clinical Study Report 67896062PAH1006. 2020 Nov 9.
Badesch DB, Raskob GE, Elliot CG, Feldkircher K, Miller DP, McGoon MD. Pulmonary Arterial Hypertension: Baseline Characteristics From the REVEAL Registry. Chest 2010;137(2):P376-387. PubMed
Barst R, Badesch D, Fleming T, et al. Risk of Mortality after Hospitalization for Pulmonary Arterial Hypertension. AJRCCM 2007;175:A1003.
Barst RJ, Chung L, Zamanian RT, et al. Functional class improvement and 3-year survival outcomes in patients with pulmonary arterial hypertension in the REVEAL Registry. Chest 2013; 144: 160–168. PubMed
Benza RL, Lickert CA, Xie Lin, et al. Comparative effectiveness of endothelin receptor antagonists on mortality in patients with pulmonary arterial hypertension in a US Medicare population: a retrospective database analysis. Pulm Circ 2020 Oct.
Bernus A, Wagner BD, Accurso F, et al. Brain natriuretic peptide levels in managing pedriatic patients with pulmonary arterial hypertension. Chest 2009; 135(3): 745–751. PubMed
CADTH. CDEC Final Recommendation – Macitentan (Opsumit – Actelion Pharmaceuticals Canada Inc). 2015 Jan 18.
CADTH. CADTH Therapeutic Review Report. Drugs for Pulmonary Arterial Hypertension: Comparative Efficacy, Safety, and Cost-Effectiveness - Recommendations Report. March 2015 (2).
Chin KM, Channick R, McLaughlin VV, et al. Real-World Upfront Combination Therapy with Macitentan and Tadalafil in Pulmonary Arterial Hypertension (PAH): Data from the Combined OPUS and OrPHeUS Datasets. Am J Resp Crit Care Med 2020;201:A2925.
Escribano-Subias P, Blanco I, Lopez-Meseguer M, et al. Survival in pulmonary hypertension in Spain: insights from the Spanish registry. Eur Respir J 2012;40:596-603. PubMed
Frantz RP, Hill JW, Lickert CA, et al. Medication adherence, hospitalization, and healthcare resource utilization and costs in patients with pulmonary arterial hypertension treated with endothelin receptor antagonists or phosphodiesterase type-5 inhibitors. Pulm Circ 2020 Mar 18;10(1):2045894019880086. PubMed
Frost AE, Badesch DB, Barst RJ, et al. The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US Contemporary Registries. Chest 2011;139:128-37. PubMed
Galiè N, Barberà JA, Frost AE, Ghofrani HA, Hoeper MM, McLaughlin VV, Peacock AJ, Simonneau G, Vachiery JL, Grünig E, Oudiz RJ, Vonk-Noordegraaf A, White RJ, Blair C, Gillies H, Miller KL, Harris JH, Langley J, Rubin LJ; AMBITION Investigators. Initial Use of Ambrisentan plus Tadalafil in Pulmonary Arterial Hypertension. N Engl J Med. 2015;27;373(9):834-44. doi: 10.1056/NEJMoa1413687.
Galiè N, Channick RN, Frantz RP, et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur Respir J 2019 Jan 24;53(1):1801889. PubMed
Galiè N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 2009;30:2493-537. PubMed
Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J 2015; 46: 903–975. PubMed
Grady D, Weiss M, Hernandez-Sanchez J, Pepke-Zaba J. Medication and patient factors associated with adherence to pulmonary hypertension targeted therapies. Pulm Circ 2018 Jan-Mar;8(1):2045893217743616. PubMed
Grill S, Bruderer S, Sidharta PN, et al. Bioequivalence of macitentan and tadalafil given as fixed-dose combination or single-component tablets in healthy subjects. Br J Clin Pharmacol. 2020;86:2424–2434. PubMed
Guillevin L, Armstrong I, Aldrighetti R, et al. Understanding the impact of pulmonary arterial hypertension on patients' and carers' lives. European respiratory review : an official journal of the European Respiratory Society 2013;22:535-42.
Hoeper MM, Apitz C, Grunig E, et al. Targeted therapy of pulmonary arterial hypertension: Updated recommendations from the Cologne Consensus Conference 2018. Int J Cardiol 2018; 272:37-45. PubMed
Hoeper MM, Bogaard HJ, Condliffe R, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol 2013;62:D42-50. PubMed
Howard LS, Ferrari P, Mehta S. Physicians' and patients' expectations of therapies for pulmonary arterial hypertension: where do they meet? European respiratory review : an official journal of the European Respiratory Society 2014;23:458-68.
Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med 2006;173:1023-30. PubMed
Hunt SA, Baker DW, Chin MH, et al. ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1995 Guidelines for the Evaluation and Management of Heart Failure): Developed in Collaboration With the International Society for Heart and Lung Transplantation; Endorsed by the Heart Failure Society of America. Circulation 2001;104:2996-3007. PubMed
Hurdman J, Condliffe R, Elliot CA, et al. ASPIRE registry: assessing the Spectrum of Pulmonary hypertension Identified at a REferral centre. Eur Respir J 2012;39:945-55. PubMed
Jansa P, Jarkovsky J, Al-Hiti H, et al. Epidemiology and long-term survival of pulmonary arterial hypertension in the Czech Republic: a retrospective analysis of a nationwide registry. BMC pulmonary medicine 2014;14:45. PubMed
Janssen Inc. CADTH Reimbursment Review Tailored Review Submission. 2021.
Khair RM, Nwaneri C, Damico RL, Kolb T, Hassoun PM, Mathai SC. The Minimal Important Difference in Borg Dyspnea Score in Pulmonary Arterial Hypertension. AnnalsATS 2016; 13(6):842-849. PubMed
Kim JD, Lee A, Choi J, et al. Epigenetic modulation as a therapeutic approach for pulmonary arterial hypertension. Exp Mol Med 2015;47:e175. PubMed
Klinger JR, Elliott CG, Levine DJ, et al. Therapy for Pulmonary Arterial Hypertension in Adults: Update of the CHEST Guideline and Expert Panel Report. Chest 2019 Mar;155(3):565-586. PubMed
Kusic-Pajic A, Giersbergen PV, Chiossi E et al. EARLY: A randomized double-blind, placebo-controlled, multicenter study to assess the efficacy, safety and tolerability of bosentan in patients with mildly symptomatic pulmonary arterial hypertension. Actelion Pharmaceuticals Ltd; Clinical Study Report AC-052-364, 2007 May 21.
Lammers AE, Hislop AA, Haworth SG. Prognostic value of B-type natriuretic peptide in children with pulmonary hypertension. Int J Cardiol 2009;135(1):21-26. PubMed
Lichtblau M, Harzheim D, Ehlken N, et al. Safety and long-term efficacy of transition from sildenafil to tadalafil due to side effects in patients with pulmonary arterial hypertension. Lung 2015 Feb;193(1):105-12. PubMed
McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009;119:2250-94. PubMed
McLaughlin V, Channick RN, Ghofrani HA, et al. Bosentan added to sildenafil therapy in patients with pulmonary arterial hypertension. Eur Respir J 2015;46:405-13. PubMed
McLaughlin VV, Shah SJ, Souza R, Humbert M. Management of pulmonary arterial hypertension. J Am Coll Cardiol 2015;65:1976-97. PubMed
Mathai SC, Puhan MA, Lam D, Wise RA. The minimal important difference in the 6-minute walk test for patients with pulmonary arterial hypertension. Am J Respir Crit Care Med. 2012;186(5):428-433. doi:10.1164/rccm.201203-0480OC. PubMed
McGoon MD, Benza RL, Escribano-Subias P, et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol 2013;62:D51-9. PubMed
Mehta S, Sastry BKS, Souza R, et al. Macitentan Improves Health-Related Quality of Life for Patients With Pulmonary Arterial Hypertension: Results From the Randomized Controlled SERAPHIN Trial. Chest. 2017 Jan;151(1):106-118. doi: 10.1016/j.chest.2016.08.1473. Epub 2016 Sep 23. Erratum in: Chest. 2018 May;153(5):1287. PubMed
Nagaya N, Nishikimi T, Uematsu M, et al. Plasma brain natriuretic peptide as a prognostic indicator in patients with primary pulmonary hypertension. Circulation 2000; 102: 865–870. PubMed
Nierlich P, Ghanim B, Jaksch P, et al. Refinement of perioperative management in lung transplantation in patients with pulmonary hypertension: A single center experience. Journal of Heart and Lung Transplantation 2013;32:S301.
Nickel N, Golpon H, Greer M, et al. The prognostic impact of follow-up assessments in patients with idiopathic pulmonary arterial hypertension. Eur Respir J 2012; 39: 589–596. PubMed
Peacock AJ, Murphy NF, McMurray JJ, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J 2007;30:104-9. PubMed
Perchenet L, Di Scala L, Lemarie JC. PRO1 MEDICAL THERAPY FOR PULMONARY ARTERIAL HYPERTENSION (PAH): AN INDIRECT TREATMENT COMPARISON OF MACITENTAN AND BOSENTAN. Value in Health Regional Issues 2019;19:S74.
Perchenet L, Mittelholzer C, Vaclavek, et al. SERAPHIN: A Multicenter, Double-Blind, Randomized, Placebo-Controlled, Parallel-Group, Event-Driven, Phase III Study to Assess the Effects of Macitentan on Morbidity and Mortality in Patients with Symptomatic Pulmonary Arterial Hypertension. Actelion Pharmaceuticals Ltd; Clinical Study Report AC-055-302. 2021 Aug 31.
Provencher S, Sitbon O, Humbert M, et al. Long-term outcome with first-line bosentan therapy in idiopathic pulmonary arterial hypertension. Eur Heart J 2006;27:589–595. PubMed
Pulido T, Adzerikho I, Channick RN, et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013 Aug 29;369(9):809-18. doi: 10.1056/NEJMoa1213917. PubMed
Rubin LJ. Diagnosis and management of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004;126:7S-10S. PubMed
Shlobin OA, Brown AW, Weir N, Ahmad S, Lemma M, Nathan SD. Transition of PH patients from sildenafil to tadalafil: feasibility and practical considerations. Lung 2012 Oct;190(5):573-8. PubMed
Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J 2019;53:1801913. PubMed
Sitbon O, Canuet M, Picard F, et al. INITIAL TREATMENT COMBINATION WITH MACITENTAN AND TADALAFIL IN PATIENTS WITH PULMONARY ARTERIAL HYPERTENSION: RESULTS FROM THE OPTIMA STUDY. Chest 2019 Oct 1;156(4):A870-A871.
Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002;40:780–788. PubMed
Schultz A. Single-center, open-label, single-dose, two-period, randomized, crossover, Phase 1 study to demonstrate bioequivalence between a fixed dose combination product formulation of macitentan/tadalafil (10 mg / 40 mg) and the free combination of 10 mg macitentan (Opsumit®) and 40 mg tadalafil (Adcirca®) in healthy male and female subjects. Actelion Pharmaceuticals Ltd; Clinical Study Report AC-077-103. 2018 Mar 21.
Sidharta P, Antonova M, Soergel M, Dingemanse J. Single-center, open-label, single-dose, two-period, randomized, crossover, Phase 1 study to demonstrate bioequivalence between two fixed dose combination product formulations of macitentan/tadalafil (10 mg / 40 mg) and the free combination of 10 mg macitentan (Opsumit®) and 40 mg tadalafil (Adcirca®) in healthy male and female subjects. Actelion Pharmaceuticals Ltd; Clinical Study Report AC-077-101. 2017 Nov 9.
Suarez JA, Manzaneque A, Garcia NC, Creus MT, Mir JB. DI-058 Risk of drug–drug interactions in a pulmonary arterial hypertension population. Eur J Hosp Pharm 2017;24(Suppl 1):A138.
Taichman DB, Shin J, Hud L, et al. Health-related quality of life in patients with pulmonary arterial hypertension. Respir Res 2005;6:92. Janssen Inc. CONFIDENTIAL PubMed
Vachiery JL, Gaine S. Challenges in the diagnosis and treatment of pulmonary arterial hypertension. European respiratory review : an official journal of the European Respiratory Society 2012;21:313-20.
Vaid HM, Camacho X, Granton JT, Mamdani MM, Yao Z, Singh S, Juurlink DN, Gomes T. The Characteristics of Treated Pulmonary Arterial Hypertension Patients in Ontario. Can Respir J. 2016;2016:6279250. PubMed
Wijeratne DT, Lajkosz K, Brogly SB, Lougheed MD, Jiang L, Housin A, Barber D, Johnson A, Doliszny KM, Archer SL. Increasing Incidence and Prevalence of World Health Organization Groups 1 to 4 Pulmonary Hypertension: A Population-Based Cohort Study in Ontario, Canada. Circ Cardiovasc Qual Outcomes. 2018 Feb;11(2):e003973. doi: 10.1161/CIRCOUTCOMES.117.003973.; PMCID: PMC5819352.PubMed
Wilkins MR. Pulmonary hypertension: the science behind the disease spectrum. Eur Respir Rev. 2012 Mar 1;21(123):19-26 PubMed
Yorke J, Armstrong I, Campbell M, Deaton C, McGowen L, Sephton P. Self-reported adherence to pulmonary hypertension medications: Preliminary results from a longitudinal cohort study. Eur Respir J 2014; 44:1414.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.