CADTH Reimbursement Review
Incobotulinumtoxina (Xeomin)
Sponsor: Merz Therapeutics, a business of Merz Pharma Canada Ltd.
Therapeutic area: Chronic sialorrhea associated with neurological disorders
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
ALS
amyotrophic lateral sclerosis
ANCOVA
analysis of covariance
ANOVA
analysis of variance
AP
atypical parkinsonism
BOCF
baseline observation carried forward
BoNT
botulinum neurotoxin
BoNT-A
botulinum neurotoxin type A
CI
confidence interval
CP
cerebral palsy
DBS
deep brain stimulation
DSFS
Drooling Severity and Frequency Scale
EP
extension period
EQ-5D-3L
EuroQol 5-Dimensions 3-Levels questionnaire
EQ VAS
EuroQol 5-Dimensions Visual Analogue Scale
GICS
Global Impression of Change Scale
HRQoL
health-related quality of life
LSM
least squares mean
MID
minimal important difference
MMAS
modified motor assessment scale
MMRM
mixed model for repeated measures
MP
main period
mROMP
modified Radboud oral motor inventory for Parkinson disease
MS
multiple sclerosis
PD
Parkinson disease
PPS
per-protocol set
PT
preferred term
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SE
standard error
SES-EP
safety evaluation set, extension period
SES-MP
safety evaluation set, main period
TBI
traumatic brain injury
UPDRS
unified Parkinson disease rating scale
uSFR
unstimulated salivary flow rate
VAS
visual analogue scale
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | IncobotulinumtoxinA (Xeomin), powder for solution for injection, 50 and 100 units per vial |
Indication | For the treatment of chronic sialorrhea associated with neurologic disorders in adults |
Reimbursement request | As per indication |
Health Canada approval status | Notice of Compliance |
Health Canada review pathway | Standard |
Notice of Compliance date | November 17, 2020 |
Sponsor | Merz Therapeutics, a business of Merz Pharma Canada Ltd. |
Source: CADTH review submission for incobotulinumtoxinA.1
Introduction
Sialorrhea, or drooling, can occur when there is excessive saliva production or when saliva pools in the mouth due to poor swallowing and/or neuromuscular dysfunction.2 Sialorrhea is associated with several neurologic conditions in adults, including Parkinson disease (PD), atypical parkinsonism (AP), stroke, traumatic brain injury (TBI), amyotrophic lateral sclerosis (ALS), multiple sclerosis (MS), cerebral palsy (CP), and dementias such as Alzheimer disease. Sialorrhea is linked with the severity of the underlying neurologic condition. Chronic troublesome sialorrhea can lead to speech difficulties, facial skin maceration, halitosis, infections, and, potentially, dehydration, choking, aspiration, and pneumonia; together, these have a significant negative impact on patient health-related quality of life (HRQoL) (speaking, eating, social interaction, emotional distress, and social isolation).3
The prevalence and incidence of chronic troublesome sialorrhea in adult patients with neurologic disorders in Canada is unclear, in part because of the lack of a standardized definition for the condition. According to the clinical expert consulted by CADTH for this review, patients with PD represent the largest group of patients treated for sialorrhea in Canadian clinical practice, although the incidence of sialorrhea is higher in patients with conditions that occur more rarely in the Canadian population (e.g., CP, ALS, and TBI). Diagnosis of chronic troublesome sialorrhea in adult patients with neurologic conditions is made by a neurologist or physiatrist based on clinical evaluation. Patients with mild sialorrhea may be treated with chewing gum, hard candy, mouth exercises and/or speech therapy. The need for further treatment arises when symptoms worsen and patients need to carry a cloth to wipe away saliva, experience skin breakdown, or begin to choke on their saliva. Only a subset of these patients will choose to receive pharmacological treatments, including 1% atropine drops or anticholinergics such as amitriptyline (both used off-label). However, according to the clinical expert consulted by CADTH for this review, the therapeutic effects of atropine drops are often temporary, while anticholinergics have systemic side effects and are not well tolerated by many patients.
According to the clinical expert consulted by CADTH for this review, an ideal treatment for sialorrhea would have minimal adverse effects and effectively reduce the frequency and severity of sialorrhea. The treatment goals are to reduce social isolation and prevent or ameliorate maceration of the skin around the mouth, dehydration, speech disturbances, interference with eating, and risk of aspiration. Injection of off-label botulinum neurotoxins (BoNTs) into the salivary glands has been used clinically for many years to reduce sialorrhea in patients with neurologic disorders.4-6 According to the clinical expert consulted by CADTH for this review, BoNT injections are desirable because they are focal treatments for symptomatic therapy, easy to administer (typically requiring less than 5 minutes), and have limited side effects.
IncobotulinumtoxinA is a purified botulinum neurotoxin type A (BoNT-A) that inhibits acetylcholine production and contraction of the salivary glands. It is the only BoNT and drug of any type approved by Health Canada for the treatment of chronic sialorrhea associated with neurologic disorders in adults. According to the Health Canada–recommended dose, incobotulinumtoxinA is injected at a total dosage of 100 U (30 U per side in the parotid glands and 20 U per side in the submandibular glands) every 16 weeks.7
The objective of this review was to perform a systematic review of the beneficial and harmful effects of incobotulinumtoxinA (100 U) administered by intraglandular injection for the treatment of chronic sialorrhea associated with neurologic disorders in adults.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
Input for this review was provided by 1 patient group, Parkinson Québec, which is a not-for-profit organization that supports patients with PD in Québec through advocacy, service development, research funding, revenue development, communication, and network management. Parkinson Québec distributed an online survey to traditional users of their services (individuals living with PD and their caregivers). The survey was promoted through the group’s newsletter and social networks between January 19, 2021, and March 1, 2021. Respondents had to be individuals living with PD and sialorrhea or their caregivers, at least 18 years of age, and Québec residents. Among the respondents, 138 individuals living with PD (47%) and 44 caregivers (40%) reported sialorrhea; of these, 116 individuals living with PD and 36 caregivers fully completed the survey.
Respondents were asked how sialorrhea affected their lives. Approximately 1/3 of individuals with PD reported that sialorrhea affected various aspects of their day-to-day lives, including their self-esteem, social discomfort, ability to eat or swallow, and ability to speak or communicate. Approximately 40% to 1-half of caregivers reported that sialorrhea affected their loved ones’ self-esteem, social comfort, personal relationships, ability to speak or communicate, and ability to eat or swallow. The most common methods used by individuals living with PD to manage sialorrhea were tissues or cloths to wipe drool (87%), followed by chewing gum (17%) and muscle exercises (16%). Few individuals living with PD had used medications (5%) or BoNTs (1%) to manage sialorrhea. Respondents were asked to indicate their perceptions regarding the effectiveness of methods currently used to manage sialorrhea. Overall, 61% to 63% of individuals living with PD and 40% to 47% of caregivers were satisfied with the management of their sialorrhea and felt it was being well managed. Approximately 1/3 of individuals with PD and 43% of caregivers agreed that there was a need for new treatments to manage sialorrhea. Respondents were asked to indicate their expectations for new treatments for sialorrhea. Overall, 82% of individuals with PD and 77% of caregivers desired government coverage of treatments, while 65% of individuals with PD and 71% of caregivers desired treatments with rare and mild side effects. Also desired were treatments that reduced the frequency and severity of sialorrhea, oral treatment options, and treatments with longer durations of action.
None of the survey respondents had any previous experience with incobotulinumtoxinA and only 1 respondent had received BoNT injections. No specific treatment outcomes or measures for reduced sialorrhea were identified in the patient input.
Clinician Input
Input from Clinical Experts Consulted by CADTH
One clinical specialist with expertise in the diagnosis and management of chronic troublesome sialorrhea associated with neurologic disorders in adults provided input for this review. The clinical expert stated that there is a significant unmet therapeutic need among adult patients with sialorrhea. Unlike pharmacological or surgical interventions, BoNT injections are easy to administer, have limited side effects, and are helpful for symptomatic therapy. However, they not covered by drug plans and special access must be requested through pharmacare support programs that have limited resources.
IncobotulinumtoxinA does not modify the disease process, but has several advantages compared to other options. It is already part of the current treatment paradigm but cannot be easily accessed by many patients due to funding limitations. Patients best suited for treatment with incobotulinumtoxinA would be those with significant disabling sialorrhea (e.g., those who need to use a cloth to wipe away drool and those for whom the condition is socially isolating). Patients would need to attend injection sessions every 3 to 6 months and have no major swallowing difficulties due to risk of worsening. Patients with sialorrhea that is too mild or patients with swallowing difficulties would be least suitable for treatment. Many neurologic patients have high risks of urinary retention and confusion, and anticholinergics would not be appropriate for many of these patients.
The objective measures used in trials to assess sialorrhea (e.g., radioisotope scanning, collection cups, and counting napkins) are impractical and not used in clinical practice. Response is usually assessed by taking a history. If necessary, a visual analogue scale (VAS), or tools such as the Drooling Severity and Frequency Scale (DSFS), can be used to assess response. A clinically meaningful response would be an improvement in the patient’s HRQoL as described previously. Response can be assessed subjectively at each visit as the drug is an injectable treatment. Treatment should be discontinued when it is not efficacious or when patients develop adverse events (AEs) such as swallowing problems or dental issues. IncobotulinumtoxinA should be administered in a hospital outpatient or community setting. Neurologists or physiatrists would typically be the specialists involved in the care of patients with neurologic conditions and would perform the injections.
Clinician Group Input
No clinician group input was provided for this review.
Drug Program Input
Drug programs identified several key issues related to implementation. The first is whether coverage would be restricted to the specific neurologic conditions assessed in the pivotal phase III trial of incobotulinumtoxinA. The clinical expert consulted by CADTH for this review noted that the study enrolled primarily patients with PD for feasibility reasons but that the results were most likely generalizable to patients with sialorrhea arising from other neurologic conditions who may also benefit from treatment. Second, drug programs asked which criteria would be used to assess the severity of sialorrhea necessitating treatment. The clinical expert noted that eligibility would be based on patient needs and clinician decisions; even patients with moderate but daily issues with drooling may benefit from treatment. Third, drug programs asked whether patients should try off-label systemic medications such as anticholinergics before treatment with incobotulinumtoxinA. The clinical expert stated that these medications are not often used in clinical practice, primarily due to the risks of side effects, but that disease-specific therapy would be routinely optimized in clinical practice before starting treatment with a BoNT. Fourth, drug programs asked whether a combination of incobotulinumtoxinA and anticholinergics would be excluded from coverage. The clinical expert stated that stable concomitant therapies such as anticholinergics have different mechanisms and indicated that there could be a combined benefit. Fifth, drug programs asked whether coverage would be considered for doses other than those studied in the pivotal phase III trial and the Health Canada–approved dose of 100 U. The clinical expert stated that most clinicians would use a dose close to 100 U to avoid side effects. Sixth, drug programs asked whether specific assessment scales such as the DSFS or the Global Impression of Change Scale (GICS) would be used to determine whether treatment should be continued. The clinical expert responded that questions similar to those used in these scales are routinely asked in clinical practice and that treatment decisions would be grounded in assessment of response by both the patient and clinician. Finally, drug programs had questions related to resumption of treatment following discontinuation. The clinical expert stated that treatment could be restarted and used as necessary to manage symptoms; even if treatment was discontinued due to lack of efficacy, sialorrhea may subsequently become more severe or more frequent and patients may benefit from re-treatment at a later stage. The only exceptions would occur in patients who experienced severe side effects of incobotulinumtoxinA treatment such as swallowing impairment; in these patients, treatment might not be resumed if the risk was too high as judged by the clinician.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
One phase III, double-blind, placebo-controlled, multi-centre study (SIAXI8-10) with an extension period (EP) of dose-blinded active treatment was included. The study enrolled adults aged 18 to 80 years with moderate to severe sialorrhea resulting from neurologic conditions (PD/AP, stroke, or TBI; N = 184). Chronic troublesome sialorrhea was defined as sialorrhea lasting for at least 3 months, with a DSFS sum score of 6 or greater, DSFS scores for both severity and frequency of at least 2, and a modified Radboud oral motor inventory for Parkinson disease (mROMP) Section III “Drooling,” Item A score of 3 or greater at both screening and baseline. The objective of the study was to investigate the efficacy and safety of injection of 2 doses of incobotulinumtoxinA (75 U or 100 U) into the salivary glands, compared with placebo, in reducing the unstimulated salivary flow rate (uSFR) as well as the frequency and severity of chronic troublesome sialorrhea as evaluated by patients, caregivers, and investigators using multiple rating tools (GICS, DSFS, and mROMP), drooling scores, and HRQoL evaluated using a VAS. The study comprised 4 consecutive 16-week treatment cycles. Following each incobotulinumtoxinA injection, patients were assessed over the course of each cycle through in-person visits to study sites and telephone calls. In the main period (MP) of the study (cycle 1), patients were randomized 2:2:1 to receive 75 U of incobotulinumtoxinA, 100 U of incobotulinumtoxinA, or placebo (saline) via 4 bilateral injections in the parotid and submandibular glands. For the EP, which covered cycles 2 to 4, patients who received placebo were re-randomized 1:1 to receive either 75 U or 100 U of incobotulinumtoxinA. All participants were blinded to dose level. The total duration of the study was 64 weeks. Efficacy outcomes for the 75 U incobotulinumtoxinA dose are not presented in this report because these data are not aligned with the Health Canada–approved dose (100 U).
The co-primary efficacy outcomes in SIAXI were the change in uSFR from baseline to week 4 and patient-reported GICS score at week 4 of the MP. The secondary outcomes were change in uSFR from baseline to weeks 8 and 12 and patient-reported GICS score at weeks 1, 2, 8, and 12 of the MP. Exploratory outcomes included DSFS sum and subscores, mROMP speech and drooling scores, and HRQoL assessed using the EuroQol 5-Dimensions 3-Levels questionnaire (EQ-5D-3L) during the MP and the EP.
The mean age of the study population at the MP baseline was 65.2 years (standard deviation [SD] = 11.4 years). Patients were mostly men (70.7%), White (99.5%), and predominantly had sialorrhea secondary to PD (70.7%) or stroke (19.0%). Smaller numbers of patients had AP (8.7%) or TBI (2.7%). The mean duration of sialorrhea was 32.7 months (SD = 34.5 months). Patients had moderate to severe sialorrhea based on DSFS and mROMP scores. Baseline demographic and clinical characteristics (including baseline uSFR, DSFS sum scores, DSFS severity scores, DSFS frequency scores, and mROMP drooling scores) were generally well balanced between study arms in the MP, as well as between the MP and EP. However, 13.9% of placebo-treated patients compared to 24.3% of incobotulinumtoxinA 100 U–treated patients reported receiving prior and concomitant deep brain stimulation (DBS). The clinical expert consulted by CADTH for this review stated that this imbalance was unlikely to affect the internal validity of the study, as patients were kept on the same therapy (medications and/or DBS) before and throughout the study.
Efficacy Results
In the co-primary efficacy analysis, change in uSFR from baseline and patient-reported GICS scores were assessed at week 4 post-injection using a mixed model for repeated measures (MMRM) analysis (Table 2). In exploratory efficacy analyses, DSFS and mROMP scores and HRQoL were also assessed at multiple time points post-injection, including at week 4.
At week 4 of the MP, the least squares mean (LSM) change in uSFR in the incobotulinumtoxinA 100 U arm was −0.13 g/min (standard error [SE] = 0.026; 95% confidence interval [CI], −0.18 to −0.08) compared to −0.04 g/min (SE = 0.033; 95% CI, −0.11 to 0.03) in the placebo arm. The LSM difference in uSFR between the incobotulinumtoxinA 100 U arm and the placebo arm of −0.09 g/min (SE = 0.031; 95% CI, −0.15 to −0.03) was statistically significant in favour of incobotulinumtoxinA 100 U (P = 0.004). In the EP (cycles 2, 3, and 4), similar mean changes in uSFR from study baseline to week 4 were observed for patients treated with incobotulinumtoxinA 100 U, although mean changes with reference to the baseline for each cycle were much smaller in magnitude (−0.03 to −0.06 g/min).
At week 4 of the MP, the LSM patient GICS score in the incobotulinumtoxinA 100 U arm was 1.25 (SE = 0.144; 95% CI, 0.97 to 1.53) compared to 0.67 (SE = 0.186; 95% CI, 0.30 to 1.04) in the placebo arm. The LSM difference in GICS scores between the incobotulinumtoxinA 100 U arm and the placebo arm of 0.58 (SE = 0.183; 95% CI, 0.22 to 0.94) was statistically significantly in favour of incobotulinumtoxinA 100 U (P = 0.002). In the EP (cycles 2, 3, and 4), similar mean GICS scores at week 4 were reported by patients treated with incobotulinumtoxinA 100 U to describe changes in sialorrhea since the previous injection.
At week 4 of the MP, the LSM change in DSFS sum score in the incobotulinumtoxinA 100 U arm was −1.66 (SE = 0.234; 95% CI, −2.12 to −1.20) compared to −0.50 (SE = 0.296; 95% CI, −1.08 to −0.09) in the placebo arm; the LSM difference in DSFS sum scores between the incobotulinumtoxinA 100 U arm and the placebo arm was −1.17 (SE = 0.278; 95% CI, −1.71 to −0.72). In the EP (cycles 2, 3, and 4), similar mean changes in DSFS sum scores for patients treated with incobotulinumtoxinA 100 U were observed with respect to study baseline.
At week 4 of the MP, larger mean decreases were observed in mROMP drooling scores in the incobotulinumtoxinA 100 U arm (−5.66 [SD = 6.16]) compared to the placebo arm (−1.00 [SD = 4.71]) were observed. In the EP (cycles 2, 3, and 4), similar or larger mean changes in mROMP drooling scores for patients treated with incobotulinumtoxinA 100 U were observed with respect to study baseline.
No significant changes in HRQoL measured using the EuroQol 5-Dimensions Visual Analogue Scale (EQ VAS) were observed during the MP or EP for patients treated with incobotulinumtoxinA 100 U or placebo.
Consistent differences of similar magnitudes in efficacy outcomes (uSFR, GICS, DSFS, and mROMP), but not in HRQoL, were observed between incobotulinumtoxinA 100 U and placebo-treated patients at weeks 8 and 12 of the MP. For patients treated with incobotulinumtoxinA 100 U, similar magnitudes of change from study baseline were observed during each of the additional 3 treatment cycles of the EP.
According to the clinical expert consulted by CADTH for this review, the LSM differences in GICS and DSFS scores between the incobotulinumtoxinA 100 U and placebo arms observed during the MP of the study were clinically meaningful.
Harms Results
In the MP of the SIAXI study, AEs and serious adverse events (SAEs) occurred at similar frequencies in the placebo arm (41.7% and 8.3%, respectively) and incobotulinumtoxinA 100 U arm (45.9% and 12.2%, respectively); withdrawal due to adverse events (WDAEs) were extremely rare (0% and 1.2%, respectively) and no deaths occurred. In 48-week follow-up EP, only slightly higher rates of AEs and SAEs were observed in patients treated with incobotulinumtoxinA 100 U (60.7% and 15.7%, respectively). During the EP, WDAEs occurred in 9.0% of patients treated with incobotulinumtoxinA 100 U, more than half of whom (4.5%) discontinued due to a dry mouth. Adverse events of special interest (AESIs) considered by investigators as potentially related to toxin spread occurred in 6.8% of patients in the incobotulinumtoxinA 100 U arm (but no placebo-treated patients) in the MP, as well as 13.5% of incobotulinumtoxinA 100 U–treated patients in the EP. These AESIs were generally manageable in most patients. Dysphagia occurred in 4.5% of incobotulinumtoxinA-treated patients in the EP. Dental-related AEs did not occur more frequently in patients treated with 100 U of incobotulinumtoxinA compared with placebo.
Table 2: Summary of Key Results from Pivotal and Protocol-Selected Studies
End point | SIAXI MP Placebo FAS (N = 36) | SIAXI MP IncobotulinumtoxinA 100 U FAS (N = 74) | SIAXI EP IncobotulinumtoxinA 100 U SES-EP (N = 89) |
|---|---|---|---|
uSFR (g/min) | |||
Number of patients contributing to the analysis | 36 | 73 | C2: 89 C3: 89 C4: 84 |
Baseline/cycle baseline, mean (SD) | 0.38 (0.23) | 0.40 (0.27) | C2: NRa / 0.30 (0.18)b C3: NRa / 0.30 (0.16)b C4: NRa / 0.22 (0.16)b |
Week 4, mean (SD) | 0.36 (0.19) | 0.27 (0.18) | C2: 0.24 (0.20) C3: 0.22 (0.16) C4: 0.18 (0.11) |
Change from baseline/cycle baseline, mean (SD) | −0.03 (0.21) | −0.12 (0.21) | C2: −0.14 (0.27)b / −0.06 (0.19)c C3: −0.17 (0.25)b / −0.03 (0.13)c C4: −0.20 (0.22)b / −0.05 (0.12)c |
LSM change from baseline (SE) (95% CI)c | −0.04 (0.033) (−0.11 to 0.03) | −0.13 (0.026) (−0.18 to −0.08) | — |
LSM difference vs. placebo (SE) (95% CI)c | Reference | −0.09 (0.031) (−0.15 to −0.03) | — |
P value | — | 0.004 | — |
Patient GICS | |||
Number of patients contributing to the analysis | 36 | 73 | C2: 88 C3: 84 C4: 77 |
Week 4, mean (SD)d | 0.47 (0.84) | 1.04 (1.03) | C2: 1.18 (1.16) C3: 1.13 (1.34) C4: 1.40 (1.14) |
LSM (SE) (95% CI)e | 0.67 (0.186) (0.30 to 1.04) | 1.25 (0.144) (0.97 to 1.53) | — |
LSM difference vs. placebo (SE) (95% CI)e | Reference | 0.58 (0.183) (0.22 to 0.94) | — |
P value | — | 0.002 | - |
DSFS sum score | |||
Number of patients contributing to the analysis | 36 | 73 | C2: 89 C3: 84 C4: 78 |
Baseline, mean (SD)f | 6.97 (1.06) | 6.78 (0.90) | NR |
Week 4, mean (SD)f | 6.44 (1.40) | 5.21 (1.50) | C2: 4.42 (1.91) C3: 4.14 (1.55) C4: 3.77 (1.75) |
Change from baseline, mean (SD)f | NR | NR | C2: −2.34 (1.55) C3: −2.64 (1.56) C4: −3.04 (1.71) |
LSM change from baseline (SE) (95% CI)g | −0.50 (0.296) (−1.08 to 0.09) | −1.66 (0.234) (−2.12 to −1.20) | — |
LSM difference vs. placebo (SE) (95% CI)g | Reference | −1.17 (0.278) (−1.71 to −0.62) | — |
P valueh | — | < 0.001 | — |
mROMP drooling score | |||
Number of patients contributing to the analysis | 36 | 72 | C2: 88 C3: 84 C4: 77 |
Baseline, mean (SD)i | 24.67 (6.08) | 24.76 (5.68) | NR |
Week 4, mean (SD)i | 23.67 (8.09) | 19.27 (6.69) | C2: 16.10 (7.29) C3: 15.65 (7.24) C4: 14.56 (7.55) |
Change from baseline, mean (SD)i | −1.00 (4.71) | −5.66 (6.16) | C2: −8.43 (6.48) C3: −9.07 (7.70) C4: −10.38 (7.56) |
EuroQol 5-Dimensions Visual Analogue Scale | |||
Number of patients contributing to the analysis | 35 | 73 | C2: 88 C3: 84 C4: 77 |
Baseline, mean (SD)j | 59.31 (18.00) | 58.62 (17.08) | NR |
Week 4, mean (SD)j | 56.72 (20.32) | 60.45 (17.20) | C2: 63.57 (18.55) C3: 60.40 (19.31) C4: 62.82 (17.45) |
Change from baseline, mean (SD)j | −2.20 (12.82) | 1.58 (13.29) | C2: 4.49 (18.33) C3: 0.88 (19.36) C4: 3.61 (16.69) |
Safety population | SES-MP (N = 36) | SES-MP (N = 74) | SES-EP |
Harms, n (%) | |||
AEs | 15 (41.7) | 34 (45.9) | 54 (60.7) |
SAEs | 3 (8.3) | 9 (12.2) | 14 (15.7) |
WDAE (from study treatment) | 0 | 1 (1.4) | 8 (9.0) |
Deaths | 0 | 0 | 2 (2.2) |
Notable harms, n (%) | |||
AESIs | 0 | 5 (6.8) | 12 (13.5) |
Dry mouth | 0 | 3 (4.1) | 10 (11.2) |
Dysphagia | 0 | 0 | 4 (4.5) |
Dysarthria | 0 | 1 (1.4) | 0 |
Dysphonia | 0 | 2 (2.7) | 0 |
Pneumonia aspiration | 0 | 0 | 1 (1.1) |
Dental-related AEs | 3 (8.3) | 4 (5.4) | 10 (11.2) |
AE = adverse event; C2 = cycle 2; C3 = cycle 3; C4 = cycle 4; DSFS = Drooling Severity and Frequency Score; EP = extension period; GICS = Global Impression of Change Scale; LSM = least squares mean; MMR = mixed model for repeated measures; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; NR = not reported; SAE = serious adverse event; SD = standard deviation; SE = standard error; SES = safety evaluation set; uSFR = unstimulated salivary flow rate; WDAE = withdrawal due to adverse event.
aStudy baseline.
bCycle baseline.
cLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and uSFR at baseline included as the covariate. For MMRM visit × treatment is the interaction term and visit is the repeated factor.
dGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
eLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and DSFS sum score at baseline included as the covariate. For MMRM visit*treatment is interaction term and visit is the repeated factor.
fDSFS sum scores range from 2 (best) to 9 (worst).
gLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and DSFS sum score at baseline included as the covariate. For MMRM visit × treatment is the interaction term and visit is the repeated factor.
hExploratory analysis, P value not adjusted for multiplicity.
IScores ranges from 9 (best) to 45 (worst).
jVAS ranges from 0 (worst imaginable health state) to 100 (best imaginable health state).
Source: SIAXI Clinical Study Report.8
Critical Appraisal
The SIAXI trial was rigorously designed with no major risks of bias. Some areas of potential concern that may affect interpretation of the study results should be noted. The treatment arms were imbalanced in terms of some concomitant medications and therapies, most notably DBS. The clinical expert consulted by CADTH for this review stated that this imbalance was unlikely to affect the internal validity of the study as patients were kept on the same therapy (medications and/or DBS) before and throughout the study. The study used unvalidated outcome measures and no evidence was available to support validity, reliability, and responsiveness to change; placebo effects were observed for all outcomes. For categorical outcomes measured using Likert scales, such as the GICS, the degree to which these constructs were sensitive in delineating true treatment responses from placebo effects was unclear. The study was overpowered for efficacy (based on effect sizes from a prior study of rimabotulinumtoxinB) because of the larger sample size required for safety evaluation, but still detected relatively small mean differences in efficacy outcomes between incobotulinumtoxinA 100 U and placebo. The clinical meaningfulness of differences of these magnitudes was uncertain in part because no evidence was available to suggest a minimal important difference (MID) for any of the outcome measures. Despite these caveats, consistent differences in favour of incobotulinumtoxinA were observed across all study outcomes with similar timing (weeks 4, 8, and 12 post-injection).
The characteristics of patients treated in SIAXI were generally similar to the Canadian context, although there were no study sites in Canada. However, patients were mostly White, male, and from only 2 countries (Germany and Poland), and almost all had sialorrhea secondary to either PD/AP or stroke. In addition, over the complete study (MP plus EP), patients were followed and monitored frequently for 64 weeks, and whether the study’s findings are generalizable to patients with different levels of background care or less-stringent dosing schedules is unclear. None of the efficacy outcomes used in SIAXI are used routinely in clinical practice, and their clinical relevance, importance to patients, and correlation with HRQoL was not clear.
Indirect Comparisons
No indirect evidence was identified for this review. A feasibility assessment conducted by the sponsor also concluded that no data were currently available to inform an indirect treatment comparison between incobotulinumtoxinA and other interventions, including injection of other BoNTs.
Other Relevant Evidence
One additional exploratory single-centre, double-blind, randomized controlled trial (RCT) was summarized to provide additional evidence from patients with other neurologic conditions and comparative evidence for incobotulinumtoxinA and onabotulinumtoxinA. This study was not designed as a direct head-to-head comparison of these 2 BoNTs.
Description of Studies
The study by Restivo et al.11 recruited a consecutive series of patients (aged 18 to 75 years) with PD, stroke, TBI, ALS, or CP (N = 90) with severely disabling sialorrhea. The primary goal of the study was to assess the relationship between efficacy in reducing sialorrhea and the number of glands injected; however, analyses of interest to this review included comparative efficacy assessment of incobotulinumtoxinA versus onabotulinumtoxinA and of BoNT efficacy in patients with different neurologic conditions. Patients were randomized to receive BoNT-A injections (either incobotulinumtoxinA or onabotulinumtoxinA) in different numbers of salivary glands (2, 3, or 4), resulting in a total dose received of 50 U, 75 U, or 100 U. At baseline and 2 weeks post-injection, salivary production was measured by weighing dental rolls placed in the patient’s mouth for 5 minutes. The change in salivary production from baseline was evaluated on a Likert scale (0 = no reduction, 1 = 25% reduction, 2 = 50% reduction, and 3 = 75% reduction in salivary weight).
Efficacy Results
There was a clear pattern in the dose response for both BoNT-A types, with Likert scores increasing with the number of glands injected (P < 0.001), but there was no interaction between BoNT-A type and number of glands injected. The Likert scores of patients treated with the 2 types of BoNT-A appeared to be similar, although the numerical data were not reported (P = 0.12). Subgroup analysis by etiology of sialorrhea in the overall population treated with all doses of a BoNT-A (either incobotulinumtoxinA or onabotulinumtoxinA) suggested a potential difference in treatment effect by neurologic condition (P < 0.001).
Harms Results
Harms were not formally analyzed.
Critical Appraisal
The study by Restivo et al. was described in limited detail and there was significant uncertainty regarding its internal and external validity. Because randomization was by number of glands injected rather than BoNT received, the comparative evidence from this study (incobotulinumtoxinA versus onabotulinumtoxinA) was potentially susceptible to bias and confounding. Furthermore, inability to account for imbalances in the type of BoNT administered to patients with different neurologic conditions (and vice versa) weakened analysis of either factor. Only 8 patients in the study were treated with the Health Canada–approved dose of incobotulinumtoxinA (100 U) and none of these had neurologic conditions that differed from those assessed in the SIAXI study. The study was therefore unable to address the evidence gaps relating to the efficacy of incobotulinumtoxinA in patients with neurologic conditions other than PD/AP and stroke and to comparative efficacy versus other BoNT-A injections for this indication
Conclusions
Evidence from the SIAXI study suggested that injection of incobotulinumtoxinA 100 U into the salivary glands of adult patients with neurologic disorders resulted in reduced salivary production and improvements in patients’ perceptions of frequency and severity of sialorrhea. At 4 weeks post-injection, the mean difference in change from baseline on the uSFR and patient GICS scores was statistically significant in favour of incobotulinumtoxinA versus placebo. Treatment effects in the uSFR and GICS were also observed at weeks 8 and 12 post-injection, and similar results were obtained on the investigator-rated DSFS. The clinical significance of post-treatment changes in sialorrhea between incobotulinumtoxinA- and placebo-treated patients was uncertain because the outcome measures were unvalidated, not used in clinical practice, and subjective (apart from uSFR), and therefore the magnitudes of treatment effects were of unclear relevance to patients. However, the clinical expert consulted by CADTH for this review indicated that questions similar to those asked in the GICS, DSFS, and mROMP drooling scales are part of the clinical assessment, and that the differences in GICS and DSFS between the incobotulinumtoxinA 100 U and placebo arms were clinically meaningful. Despite the uncertain clinical relevance of the magnitude of treatment differences between incobotulinumtoxinA and placebo, and despite the observation of a placebo effect for most outcomes, consistent mean changes with similar timings were observed in favour of incobotulinumtoxinA across all assessed outcomes. Numerical differences in the effects of treatment with incobotulinumtoxinA 100 U versus placebo were observed (via GICS responses) but not statistically significant at weeks 1 and 2 post-injection, clearly manifested at weeks 4, 8, and 12, and then waned by week 16, at which point a subsequent dose was administered. However, this did not translate into improvement for incobotulinumtoxinA-treated patients in terms of HRQoL measured via the EQ VAS. Injection with incobotulinumtoxinA was tolerated in most patients and side effects were generally manageable, with some infrequent but expected notable harms related to toxin spread (e.g., dry mouth and dysphagia). Key evidence gaps included a lack of comparative data on the efficacy of different BoNTs and a lack of evidence from patients with a variety of neurologic conditions
Introduction
Disease Background
Sialorrhea, or drooling, occurs when excess saliva spills over the lip margin. In healthy individuals, approximately 1 L of saliva is continuously produced by 3 pairs of major salivary glands (parotid, sublingual, and submandibular) and swallowed each day. Saliva flow is mediated by acetylcholine binding to muscarinic receptors in the salivary glands.12 Sialorrhea arises when there is excessive saliva production or when saliva pools in the oral cavity because of poor swallowing; pooling can be anterior (resulting in spilling of saliva from the open mouth), posterior (resulting in spilling into the pharynx with increased risk of aspiration and infection), or both.2 Hypersalivation can be caused by some medications or conditions (e.g., gastroesophageal reflux disease), while poor swallowing can be due to anatomic abnormalities (e.g., macroglossia, oral incompetence, or dental malocclusion), neuromuscular dysfunction (e.g., PD, stroke, TBI, or CP), and/or decreased swallowing reflexes (e.g., AP). In adults with neurologic disorders, sialorrhea is linked with the severity of the underlying neurologic condition. Sialorrhea becomes chronic and troublesome when the frequency and/or severity of drooling begins to significantly and consistently disrupt the patient’s life. For example, the patient may require frequent changes of clothes or regular use of a cloth to wipe away saliva. The adverse effects of chronic troublesome sialorrhea include speech difficulties, facial skin maceration, halitosis, infections, and potentially, dehydration, choking, aspiration, and pneumonia; together, these have a significant negative impact on HRQoL (speaking, eating, social interaction, emotional distress, and social isolation).3 Sialorrhea can also be burdensome for caregivers, who may need to regularly monitor loved ones for drooling and risk of aspiration.13
The exact prevalence and incidence of sialorrhea and of chronic troublesome sialorrhea in adult patients with neurologic disorders is unclear in Canada and elsewhere, in part because of the lack of a standardized definition for this condition. The prevalence of sialorrhea in patients with PD ranges from 32% to 74%.14 According to the clinical expert consulted by CADTH for this review, patients with PD represent the largest group treated for sialorrhea in Canadian clinical practice. However, only a relatively small subset of all patients with PD (typically those with more advanced disease) would receive pharmacological treatment for sialorrhea. While patients with PD and sialorrhea may be the most numerous, the clinical expert consulted by CADTH for this review stated that the incidence of sialorrhea is higher in patients with conditions that occur more rarely in the Canadian population, such as CP, ALS, and TBI. Based on 2010 to 2011 estimates of the prevalence of various neurologic conditions (PD, TBI, stroke, ALS, MS, AD, and other dementias) from a Canadian Community Health Survey, a National Population Health Study of Neurologic Disorders, and the Ontario Federation for Cerebral Palsy,15-18 and multiplying these by estimates of the proportions of patients experiencing severe neurologic disease19-24 and the proportions experiencing sialorrhea,14,25-27 the sponsor estimated that more than 20,000 Canadians may be living with chronic sialorrhea associated with a neurologic disorder.
Diagnosis of chronic troublesome sialorrhea in adult patients with neurologic conditions is made by a neurologist or physiatrist based on clinical evaluation.
Standards of Therapy
According to the clinical expert consulted by CADTH for this review, an ideal treatment for sialorrhea would have minimal adverse effects (an issue with anticholinergics) and effectively reduce the frequency and severity of sialorrhea. The treatment goals would be to reduce social isolation and prevent or ameliorate maceration of the skin around the mouth, dehydration, speech disturbances, interference with eating, and risk of aspiration. The most relevant indicator of response to treatment and change in sialorrhea is clinical history and/or self-reporting by patients or caregivers. Drooling scales used in clinical trials (e.g., the DSFS) are typically not used in clinical practice, while saliva collection and measurement are impractical.
According to the clinical expert consulted by CADTH for this review, mild sialorrhea can be treated with chewing gum or hard candy, oral exercises, and/or speech therapy. These methods become ineffective when a certain level of impairment is reached. There is no standardized definition of chronic or troublesome sialorrhea. According to the clinical expert consulted by CADTH for this review, treatment would be considered when patients need to carry a cloth to wipe saliva multiple times a day, when skin breakdown is observed, or when caregivers report that the patient is choking on saliva. Only a subset of patients with neurologic disorders and sialorrhea would choose to receive pharmacological treatments for sialorrhea. When symptoms worsen, patients may be treated with 1% atropine drops or anticholinergics such as amitriptyline (both off-label). However, according to the clinical expert consulted by CADTH for this review, the therapeutic effect of atropine drops is often temporary, while anticholinergics have systemic side effects and are not well tolerated in all patients, particularly those with PD who have significant comorbidities (e.g., urinary retention or confusion). Dopaminergic medications for parkinsonism have a limited impact on sialorrhea, although optimization of anti-parkinsonian medications can be effective in reducing neuromuscular dysfunction and is typically accomplished before additional interventions. Surgery (e.g., gland excision and duct ligation) or irradiation of the salivary glands can be used to control sialorrhea but these interventions are expensive, highly invasive, and, according to the clinical expert consulted by CADTH for this review, are not used in most patients.
Since the first description of sialorrhea treatment with BoNT injections into the salivary glands,28 multiple studies have evaluated the safety and efficacy of BoNT injections into the salivary glands in reducing sialorrhea among adult patients with PD or ALS.6,29-33 Most studies used doses of 55 U to 450 U of BoNT-A34-37 and 2,500 U to 4,000 U of botulinum neurotoxin type B31,32,38 injected into the salivary glands. Preliminary evidence based on non-randomized studies or studies with small sample sizes was suggestive of a clinical benefit in reducing salivary production and drooling severity.39 There is a general consensus among clinicians and specialists that BoNT-A injections are potentially efficacious in controlling drooling in patients with sialorrhea.4-6 However, due to the potential for worsening of swallowing issues, patients need to be chosen carefully. According to the clinical expert consulted by CADTH for this review, BoNT injections have several desirable characteristics: they are focal treatments for symptomatic therapy, injections are easy to administer (typically requiring less than 5 minutes for 4 injections), and they have limited side effects. The number of salivary glands injected and the dose can be customized to each patient to optimize the therapeutic effect. The clinical expert stated that the treatment effect of BoNT-A injections begins within a few days, peaks within several weeks, then wanes over several months; repeat injections 3 or 4 times a year are therefore required. Injections with BoNTs in the form of a BoNT-A (incobotulinumtoxinA [Xeomin], onabotulinumtoxinA [Botox], abobotulinumtoxinA [Dysport], or prabotulinumtoxinA [Nuceiva]) or botulinum neurotoxin type B (rimabotulinumtoxinB [Myobloc]) are also used off-label to treat sialorrhea in adults with neurologic conditions. RimabotulinumtoxinB is not currently marketed in Canada and prabotulinumtoxinA is indicated for cosmetic use only. According to the clinical expert consulted by CADTH for this review, most commonly onabotulinumtoxinA would be used off-label in Canada at present as abobotulinumtoxinA is less widely available and dosing requires an inconvenient calculation. As this treatment is not covered, it can only be provided by compassionate access through pharmaceutical companies. IncobotulinumtoxinA is the only approved treatment for sialorrhea in adults with chronic troublesome sialorrhea resulting from neurologic conditions.
Drug
IncobotulinumtoxinA is a purified BoNT-A free from complexing proteins that is produced from anaerobic fermentation of the Hall strain of Clostridium botulinum. The drug blocks transmission at the neuromuscular junction by inhibiting the release of acetylcholine from peripheral cholinergic nerve endings (Table 3). The mechanism of action involves: (1) binding to an as-yet uncharacterized site on presynaptic cholinergic axon terminals, (2) uptake within an endocytic vesicle, (3) pore formation and translocation of the light chain into the cytosol, and (4) proteolytic cleavage of SNAP 25, which is a component of the vesicle fusion machinery required for the release of acetylcholine.7 Following injection into salivary glands, muscular contraction and salivary production controlled by acetylcholine may be reduced.
IncobotulinumtoxinA is indicated for the treatment of chronic sialorrhea associated with neurologic disorders in adults.7 In this indication, the regimen recommended by Health Canada is a total dosage of 100 U (30 U per side in the parotid glands and 20 U per side in the submandibular glands) every 16 weeks. Note that the definition of units is specific to incobotulinumtoxinA and thus dosing is not interchangeable between different BoNTs. The drug received a Notice of Compliance from Health Canada for this indication on November 17, 2020. The sponsor’s reimbursement request is for the Health Canada–approved indication. The timing for repeat treatment should be determined based on the clinical needs of the individual patient, and no sooner than every 16 weeks.
Table 3: Key Characteristics of IncobotulinumtoxinA, Other BoNTs, and Anticholinergics for Treatment of Sialorrhea in Adults with Neurologic Disorders
Characteristic | IncobotulinumtoxinA | Other BoNTs (e.g., onabotulinumtoxinA) | Anticholinergics (e.g., amitriptyline) |
|---|---|---|---|
Mechanism of actiona | Blockade of transmission at the neuromuscular junction by inhibiting the release of acetylcholine from peripheral cholinergic nerve endings | Similar to incobotulinumtoxinA | Inhibition of the membrane pump mechanism responsible for the re-uptake of transmitter amines, such as norepinephrine and serotonin, thereby increasing their concentration at the synaptic clefts of the brain |
Indication(s)b | For the treatment of chronic sialorrhea associated with neurologic disorders in adults For the treatment of hypertonicity disorders of the seventh nerve, such as blepharospasm, including benign essential blepharospasm and hemifacial spasm in adults To reduce the subjective symptoms and objective signs of cervical dystonia (spasmodic torticollis) in adults For the treatment of upper limb spasticity associated with stroke in adults | Blepharospasm, strabismus, cervical dystonia, focal spasticity, primary hyperhidrosis of the axillae, chronic migraine, bladder dysfunction, cosmetic use (onabotulinumtoxinA) Cervical dystonia, focal spasticity, cosmetic use (abobotulinumtoxinA) Cosmetic use (prabotulinumtoxinA) Cervical dystonia (rimabotulinumtoxinB)c | For the drug management of depressive illness |
Route of administration | Intraglandular injection in the parotid (30 U per side) and submandibular glands (20 U per side) | As for incobotulinumtoxinA (various doses) | Oral |
Recommended dosage | 100 U no sooner than every 16 weeks | NAd | 25 to 50 mg 3 times daily |
Serious adverse effects or safety issues | Toxin spread (swallowing, speech, or respiratory problems) | As for incobotulinumtoxinA | QT-interval prolongation and other cardiac issues; confusion, cognitive impairment hallucinations, and delusions; urinary retention and constipation |
BoNT = botulinum neurotoxin; NA = not applicable.
aProposed mechanism of action based on molecular drug mechanisms; mechanism of action in humans is not fully understood.
bHealth Canada–approved indication(s).
cRimabotulinumtoxinB is not currently marketed in Canada.
dInformation on recommended dosage unavailable because these products are used off-label.
Source: Product monographs for incobotulinumtoxinA,7 onabotulinumtoxinA,40 abobotulinumtoxinA,41 prabotulinumtoxinA,42 rimabotulinumtoxinB,43 and amitriptyline.44
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on input provided by patient groups. The statistical data reported have been reproduced as is according to the submission, without modification.
About the Patient Group and Information Gathered
Input for this review was provided by 1 patient group, Parkinson Québec, which is a not-for-profit organization that supports patients with PD in Québec through advocacy, service development, research funding, revenue development, communication, and network management. Parkinson Québec serves the entire province of Québec, and its services and resources are available free of charge to the 25,000 Quebecers living with PD and their families.
Parkinson Québec distributed an online survey to traditional users of their services (individuals living with PD and their caregivers). The survey was promoted through a newsletter and social networks between January 19 and March 1, 2021. Respondents had to be individuals living with PD and sialorrhea or their caregivers, at least 18 years of age, and Québec residents. A total of 405 individuals responded, 295 of whom were living with PD and 110 of whom were caregivers. Among the respondents, 138 individuals living with PD (47%) and 44 caregivers (40%) reported sialorrhea. Results were reported only for respondents who had completed the entire survey (116 individuals living with PD and 36 caregivers). The characteristics of respondents are shown in Table 4.
Table 4: Demographic Information of Survey Respondents With Sialorrhea
Characteristics of patients with sialorrhea | Responses from individuals with PD (N = 116) | Responses from caregivers (N = 36) |
|---|---|---|
Gender, n (%) | ||
Female | 44 (37.9) | 5 (13.9) |
Male | 72 (62.1) | 31 (86.1) |
Age (years), mean (SD) | 66 (8) | 71 (9) |
Age at diagnosis (years), mean (SD) | 60 (8) | 61 (10) |
Duration of disease (years), mean (SD) | 7 (5) | 9 (8) |
Hoehn and Yahr score, mean (SD) | 1.8 (1.0) | 2.6 (1.2) |
Duration of sialorrhea, n (%) | ||
< 6 months | 28 (24.1) | 5 (13.9) |
6 months to 1 year | 34 (29.3) | 10 (27.8) |
1 to 3 years | 30 (25.9) | 11 (30.6) |
3 to 5 years | 14 (12.1) | 5 (13.9) |
> 5 years | 8 (6.9) | 4 (11.1) |
Severity of sialorrhea, n (%) | ||
Mild | 54 (46.6) | 12 (33.3) |
Moderate | 51 (44.0) | 15 (41.7) |
Severe | 7 (6.0) | 8 (22.2) |
Abundant | 2 (1.7) | 0 |
Frequency of sialorrhea, n (%) | ||
Several times a month | 11 (10%) | 4 (11.1) |
Several times a week | 43 (38%) | 14 (38.9) |
Several times a day | 55 (48%) | 12 (33.3) |
Constant | 5 (4%) | 5 (13.9) |
SD = standard deviation.
Disease Experience
Respondents were asked how sialorrhea affected their lives. Approximately 1/3 of individuals with PD reported that sialorrhea affected various aspects of their day-to-day lives, including their self-esteem, social comfort, ability to eating or swallow, and ability to speak or communicate. Approximately 40% to 50% of caregivers reported that sialorrhea affected their loved ones’ self-esteem, social comfort, personal relationships, ability to speak or communicate, and ability to eat or swallow.
Experiences with Currently Available Treatments
The most common methods used by individuals living with PD to manage sialorrhea were tissues or cloths to wipe away drool (87%), followed by chewing gum (17%) and muscle exercises (16%). Comparatively few individuals living with PD had used medications (5%) or BoNTs (1%) to manage sialorrhea.
Respondents were asked to indicate their perceptions of the effectiveness of methods currently used to manage sialorrhea. Overall, only 61% to 63% of individuals living with PD and 40% to 47% of caregivers were satisfied with the management of their sialorrhea and felt it was being managed well. Approximately 1/3 of individuals with PD and 43% of caregivers agreed that there was a need for new treatments to manage sialorrhea.
Improved Outcomes
Respondents were asked to indicate their expectations for new treatments for sialorrhea. Overall, 82% of individuals with PD and 77% of caregivers desired government coverage of treatments, while 65% of individuals with PD and 71% of caregivers desired treatments with rare and mild side effects. Many respondents also desired treatments that would reduce the frequency and severity of sialorrhea. Oral treatment options and treatments with longer durations of action were also preferred.
Experience with Drug Under Review
No respondents reported having experience with incobotulinumtoxinA.
Additional Information
Parkinson Québec’s input noted that most respondents had mild to moderate PD. The survey methodology may have recruited a biased and younger set of respondents with fewer significant sialorrhea-associated problems. However, studies of more advanced cases of PD show that severe and frequent sialorrhea can significantly affect patients’ HRQoL. New treatments to effectively manage sialorrhea in individuals with PD are therefore needed.
Clinician Input
Input from Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 1 clinical specialist with expertise in the diagnosis and management of chronic troublesome sialorrhea associated with neurologic disorders in adults.
Unmet Needs
In contrast to pharmacological or surgical interventions, BoNTs are easy to administer and have limited side effects. Because injection of BoNTs is helpful for symptomatic therapy but is not covered by drug plans, special access must be requested through pharmacare support programs, which may not be approved due to limited resources.
Place in Therapy
IncobotulinumtoxinA would not modify the disease process, but has several advantages compared to other options. This treatment is already part of the current treatment paradigm but cannot be accessed by many patients due to funding limitations. Clinicians can sometimes use extra stock on hand or a support program, but supplies are limited. In some patients it would be reasonable to use sublingual atropine before incobotulinumtoxinA; however, anticholinergics are not appropriate for use in many patients, including those at high risk of urinary retention or confusion.
Patient Population
Patients best suited for treatment with incobotulinumtoxinA would be those with significant disabling sialorrhea (e.g., those who need to use a cloth to wipe away drool and those for whom the condition is socially isolating). Patients would need to attend injection sessions every 3 to 6 months and have no major swallowing difficulties due to risk of worsening. These patients would be identified based on clinical diagnosis. Patients with sialorrhea that is too mild or patients with swallowing difficulties would be least suitable for treatment. Patients with sialorrhea resulting from diverse neurologic conditions may benefit from treatment. Patient selection by a neurologist or physiatrist is essential.
Assessing Response to Treatment
The objective measures used in trials to assess sialorrhea (e.g., radioisotope scanning, collection cups, and counting napkins) are impractical and not used in clinical practice. Response is usually assessed by taking a history. If necessary, a VAS or tools such as the DSFS can be used to assess response. A clinically meaningful response would be an improvement in the patient’s HRQoL relating to the issues described previously. Response can be assessed subjectively at each visit as this is an injectable treatment.
Discontinuing Treatment
Treatment should be discontinued when it is not efficacious or when patients develop AEs such as swallowing problems or dental issues.
Prescribing Conditions
IncobotulinumtoxinA should be administered in a hospital outpatient or community setting. Neurologists or physiatrists would typically be the specialists involved in the care of patients with neurologic conditions and would perform the injections.
Additional Considerations
The clinical expert consulted by CADTH for this review noted that pediatric patients with sialorrhea would not be covered in the indication under review but could benefit from treatment. The sponsor emphasized that incobotulinumtoxinA is indicated for treatment of chronic sialorrhea associated with neurologic disorders in adults only.
Clinician Group Input
No clinician group input was received for this review.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
The indication (neurologic disorders) is somewhat vague, and the pivotal trial did not include all adult neurologic disorders resulting in sialorrhea. Would it be reasonable to restrict coverage to the specific disorders included in the study? Would only specific neurologic disorders be eligible under the Health Canada–approved indication? Conditions like ALS, CP, MS, dementia, and AD are also associated with sialorrhea but patients with these conditions were not part of the pivotal trial. | For the purposes of the SIAXI trial, the investigators may have restricted the study population to certain diseases for simplicity. Patients with other conditions (ALS, CP, MS, dementia, and AD), including pediatric patients, can certainly have severe sialorrhea. The SIAXI trial enrolled mostly patients with PD because they are the most numerous. However, patients with other neurologic conditions also suffer from severe sialorrhea and it would be unfortunate if they were unable to access this treatment. |
Would the results of the SIAXI trial be generalizable to patients with other neurologic disorders? | Yes, the results can be generalized to patients with other neurologic conditions; the underlying pathophysiology is the same. |
In the first teleconference, the clinical expert indicated that only patients with moderate/severe sialorrhea would use this medication and only a portion would be appropriate for treatment. Presentations that would suggest initiating therapy could include: the need to carry a cloth to wipe away saliva, when choking occurs, or when skin begins to break down. What would criteria look like in terms of severity for eligibility of treatment? What severity was treated in the study? | In addition to the criteria listed, daily, bothersome sialorrhea that has a significant impact on daily functioning or is socially disabling would be eligible for treatment. |
Should patients have tried off-label medications (e.g., anticholinergics, adrenergic receptor antagonists) before being eligible for treatment with incobotulinumtoxinA? Should disease-specific therapy (such as levodopa for PD) be optimized before being eligible, and if so, how would this be addressed specifically? | In practice, many of the medications listed as comparators (anticholinergics and alpha-adrenergics) are rarely used. For example, anticholinergics pose increased risks of dementia and hallucinations and they are therefore not used unless necessary. Disease-specific therapy should be optimized. The neurologist or physiatrist would optimize these therapies; no special steps need to be taken, as these discussions would be had during patient visits. It is unlikely that incobotulinumtoxinA would be administered by a family physician. Administration of Xeomin requires mixing the drug with a saline solution and some familiarity with calculating dilutions, in addition to the injection technique. It would therefore most likely be administered by neurologists and physiatrists who have nursing support and are already injecting for other indications. |
When determining whether a patient should continue treatment, would specific reassessment scales or notes of subjective improvement be used? If so, would it use a scale or scoring system (DSFS, GICS)? Which one? | The questions in the DSFS regarding severity and frequency, or similar ones, are routinely asked in clinical practice. |
If treatment stops due to a social or other non-treatment-related issue, and the patient’s disease progresses to a level where the sialorrhea is severe, would re-initiation of treatment be considered if requested by patient/family/physician? | Physicians use it as necessary when we need to control symptoms as it is a symptomatic, not a disease-modifying treatment. |
If a patient discontinues the treatment, would you try it again after a while? | It depends on what the reason was for the treatment failure. If there was a side effect such as swallowing impairment, in most cases treatment would not be resumed. If treatment was stopped for lack of efficacy, the patient may benefit later; perhaps initially the severity of sialorrhea was insufficient to observe a treatment effect. |
The Health Canada–approved dose is 100 U (30 U per parotid gland and 20 U per submandibular gland) per treatment session with repeat session no sooner than 16 weeks. In speaking with the clinical expert, she advised there is a lot of variability among patients with dosing sometimes being above 100 U and, administration is not always per each of the 4 glands. The dosing is reflective of what was studied, but would consideration be given to doses outside of this? | A dose of 100 U is reasonable. Most physicians would not use significantly more than 100 U. Doses past 100 U could present some issues and side effects, and a dose significantly higher than that may not be beneficial. In addition, because the drug comes in 50 U and 100 U vials, and clinicians cannot order 120 U, the cost of 60 U or 100 U is the same. |
Some study participants were taking a combination of anticholinergic medication and incobotulinumtoxinA (4 patients were treated with biperiden during the main phase of the study). Would combination use with anticholinergics be excluded for coverage or would it be irrelevant to eligibility? | Stable concomitant treatments would be irrelevant. Anticholinergics could be partially effective but not effective enough to provide a clinically significant benefit. These treatments work in different ways and a combination effect could be achieved and should not be an exclusion criterion. Some patients with PD take anticholinergics for tremor control and urinary frequency (fewer than previously, as recent literature suggested a negative effect on cognition and hallucinations), but this should not be an exclusionary factor. |
Although not part of the indication, the clinical expert advised that she would not want to see certain pediatric populations excluded from accessing incobotulinumtoxinA. These may include CP patients as well as patients with developmental delays. Would incobotulinumtoxinA would be used as a first-line option in pediatric patients or upon treatment failure of off-label anticholinergic medications? This is a group that falls outside of the listed indication but for whom jurisdictions may see requests for coverage. | There is a high level of need for this drug in pediatric patients as there are many social factors such as schooling and socializing with friends. The mechanism would be the same, but dosage may require adjustment in the pediatric population. The sponsor emphasized that incobotulinumtoxinA is indicated for treatment of chronic sialorrhea associated with neurologic disorders in adults only. |
AD = Alzheimer disease; ALS = amyotrophic lateral sclerosis; CP = cerebral palsy; DSFS = Drooling Severity and Frequency Scale; GICS = global impression of change scale; MS = multiple sclerosis; PD = Parkinson disease.
Clinical Evidence
The clinical evidence included in the review of incobotulinumtoxinA is presented in 2 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. No indirect evidence met the inclusion criteria for this review. The second section includes an additional relevant study that was considered to address an important gap in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of incobotulinumtoxinA (100 U) intraglandular injection for the treatment of chronic sialorrhea associated with neurologic disorders in adults.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adults (age ≥ 18 years) with chronic sialorrhea associated with neurologic disorders Subgroups:
|
Intervention | IncobotulinumtoxinA (100 U injection in the salivary glands every 16 weeks) |
Comparator |
|
Outcomes | Efficacy:
Harms:
|
Study designs | Published and unpublished III and IV RCTs |
AE = adverse events; BoNT = botulinum neurotoxin; DSFS = Drooling Severity and Frequency Scale; GICS = Global Impression of Change Scale; HRQoL = health-related quality of life; mROMP = modified Radboud oral motor inventory for Parkinson disease; RCT = randomized controlled trial; SAE = serious adverse event; uSFR = unstimulated salivary flow rate; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies checklist.45 Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid and Embase (1974‒) via Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Xeomin (incobotulinumtoxinA) and sialorrhea. Clinical trials registries searched included the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register. For the main search, no filters were applied to limit the retrieval by study type. A supplemental search was also run using generic BoNT terms; for this search, search filters were applied to limit retrieval to RCTs or controlled clinical trials. Retrieval was not limited by publication date or by language. For the supplemental search, where possible, retrieval was limited to the human population. Conference abstracts were excluded from all search results.
Appendix 1 provides detailed search strategies. The initial search was completed on March 26, 2021. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee on July 21, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.46 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies. Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
A focused literature search for network meta-analyses dealing with sialorrhea was run in MEDLINE All (1946–) on March 25, 2021. No limits were applied to the search. No relevant network meta-analyses were identified in the search.
Findings from the Literature
One study was identified from the literature for inclusion in the systematic review (Figure 1). The included study is summarized in Table 7. A list of excluded studies is presented in Appendix 2.
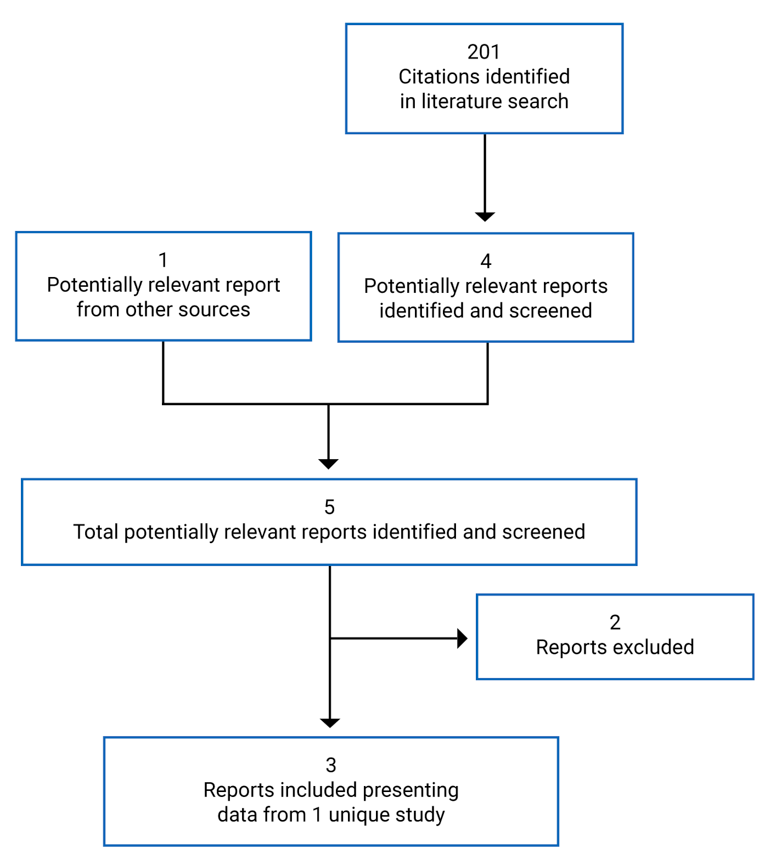
Table 7: Details of Included Studies
Detail | SIAXI | |
|---|---|---|
Designs and Populations | ||
Study design | Phase III, double-blind, placebo-controlled RCT with dose-blinded extension period | |
Locations | 33 sites in Germany and Poland | |
Patient enrolment dates | April 11, 2014, to August 26, 2015 | |
Randomized (N) | 184 | |
Inclusion criteria |
| |
Exclusion criteria |
| |
Drugs | ||
Intervention | IncobotulinumtoxinA (intraglandular injection in the parotid and submandibular glands at a concentration of 5 units/0.1 mL in physiologic saline, total dose 75 Ua or 100 U) every 16 weeks | |
Comparator | Placebo (physiologic saline) administered in the same manner as incobotulinumtoxinA | |
Screening | 4 weeks | |
Double-blind main period | 16 ± 2 weeks | |
Dose-blind extension period | 48 ± 6 weeks | |
Outcomes | ||
Co-primary end points | • Change in uSFR from baseline to week 4 • Patient GICS entry (or carer GICS entry if patient unable to answer) at week 4 | |
Secondary and exploratory end points | Secondary: • Change in uSFR from baseline to weeks 8 and 12 • Patient GICS entry (or carer GICS entry if patient unable to answer) at weeks 1, 2, 8, and 12 Exploratory (MP): • Change in DSFS subscores and sum score from baseline to weeks 4, 8, 12, and 16 • Change in uSFR from baseline to week 16 • Patient GICS entry (or carer GICS entry if patient unable to answer) at week 16 • Number of responders according to patient GICS entry at weeks 1, 2, 4, 8, 12, and 16 • Carer GICS entry at weeks 1, 2, 4, 8, 12, and 16 • Change in mROMP speech symptom and drooling score from baseline to week 4, 8, 12, and 16 • Change in EQ-5D-3L single items and EQ VAS from baseline to weeks 4, 8, 12, and 16 • Length of between-treatment interval Exploratory (EP): • Change in uSFR from baseline to all visits in the EP, and change from each injection (weeks 16, 32, and 48) to the respective assessment visits (weeks 20, 36, and 52) and to the end-of-cycle/end-of-study visits (weeks 32, 48, and 64) • Patient GICS entry (or carer GICS entry if patient was unable to answer) at all assessment visits in the EP (weeks 20, 36, and 52) and the end-of-cycle/end-of-study visits (weeks 32, 48, and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40, and 56) • Number of responders according to patient GICS entry at all assessment visits in the EP (weeks 20, 36, and 52) and the end-of-cycle/end-of-study visits (weeks 32, 48, and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40, and 56) • Change in DSFS subscores and sum score from baseline to all assessment visits in the EP • Carer GICS entry at all assessment visits in the EP (weeks 20, 36 and 52) and the end-of-cycle/end-of-study visits (weeks 32, 48, and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40, and 56) • Change in mROMP speech symptoms and drooling scores from baseline to all assessment visits in the EP • Change in EQ-5D-3L single items and EQ VAS from baseline to all assessment visits in the EP • Length of interval between consecutive injections in the EP | |
Notes | ||
Publicationsb | ||
AP = atypical parkinsonism; DSFS = Drooling Severity and Frequency Scale; EP = extension period; EQ-5D-L = EuroQol-5 Dimension-3 Level questionnaire; EQ VAS = EuroQol 5-Dimensions Visual Analogue Scale; GICS = Global Impression of Change Scale; HRQoL = health-related quality of life; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; PD = Parkinson disease; RCT = randomized controlled trial; TBI = traumatic brain injury; uSFR = unstimulated salivary flow rate.
a75 U is not a Health Canada–approved dose, and efficacy outcome data for this group are not part of this report.
bOne additional report was included (SIAXI Clinical Study Report).8
Source: SIAXI Clinical Study Report.8
Description of Studies
The SIAXI (Sialorrhea in Adults Xeomin Investigation, N = 184)8-10 trial was a prospective, double-blind, placebo-controlled, parallel-group, multi-centre, phase III RCT with an EP of dose-blinded active treatment. The study was funded by the sponsor. The objective of the study was to investigate the efficacy and safety of 2 doses of incobotulinumtoxinA (incobotulinumtoxinA, 75 U or 100 U), compared with placebo in reducing salivary flow rate as well as the frequency and severity of chronic troublesome sialorrhea in adults with various neurologic conditions. The study enrolled adults aged 18 to 80 years with chronic troublesome sialorrhea resulting from PD or AP (multiple system atrophy, corticobasal degeneration, or progressive supranuclear palsy), stroke, or TBI. A total of 216 patients were screened at 12 sites in Germany and 21 sites in Poland. Screened patients were given a screening number and members of the subset of randomized patients were given a randomization number through an interactive web response system. Initially, a target was set of at least 20% of the study population for each of the etiology subgroups (PD/AP, stroke, and TBI) but this was dropped to ensure an adequate sample size. Patients were enrolled from April 11, 2014, to August 26, 2015, and the database was closed on January 4, 2017.
Following screening, the study comprised 4 consecutive 16-week treatment cycles (Figure 2). The length of treatment cycles was based on previous observations that BoNT treatment effects occur approximately 2 weeks post-injection then wane after 8 to 12 weeks.47,48 At baseline, inclusion and exclusion criteria and randomization were re-checked. Following each incobotulinumtoxinA injection, patients were assessed over the course of the 16 ± 2–week cycle through in-person visits to study sites and telephone calls. Randomization was conducted using an unspecified method implemented in RANCODE version 3.6 and stratified by the etiology (neurologic condition) of sialorrhea. In the study’s MP, which comprised the first treatment cycle, patients were randomized 2:2:1 to receive 75 U incobotulinumtoxinA, 100 U incobotulinumtoxinA, or placebo (saline) via 4 bilateral injections in the parotid (100 U incobotulinumtoxinA dose: 30 U per side; 75 U incobotulinumtoxinA dose: 22.5 U per side) and submandibular (100 U incobotulinumtoxinA dose: 20 U per side; 75 U incobotulinumtoxinA dose: 15 U per side) glands. Eligibility for the EP was based on agreement between patient and investigator regarding continued need for treatment, continued absence of clinically relevant dysphagia (an mROMP score for Section II “Swallowing Symptoms,” Item A of no more than 2 and Item C of no more than 3), absence of AEs, absence of infection and/or inflammation at injection sites, a negative pregnancy test, and low risk of suicidality. For cycles 2 to 4 (EP), patients who received placebo were re-randomized 1:1 to receive either 75 U or 100 U of incobotulinumtoxinA. Those receiving active treatment in the MP remained in the same dose group unless dose reduction was required due to AEs. A third, dose-reduced group (56 U, corresponding to a 25% reduction from 75 U) was planned for patients in the 75 U group in the MP who experienced AEs but was not used. All participants were blinded to dose level. The fourth injection occurred 48 ± 6 weeks after the first, making for a total study duration of 64 ± 6 weeks (not including the screening period).
Efficacy outcomes for the incobotulinumtoxinA 75 U arms of both the MP and EP are not presented in this report because these data are not aligned with the Health Canada–approved dose (100 U).
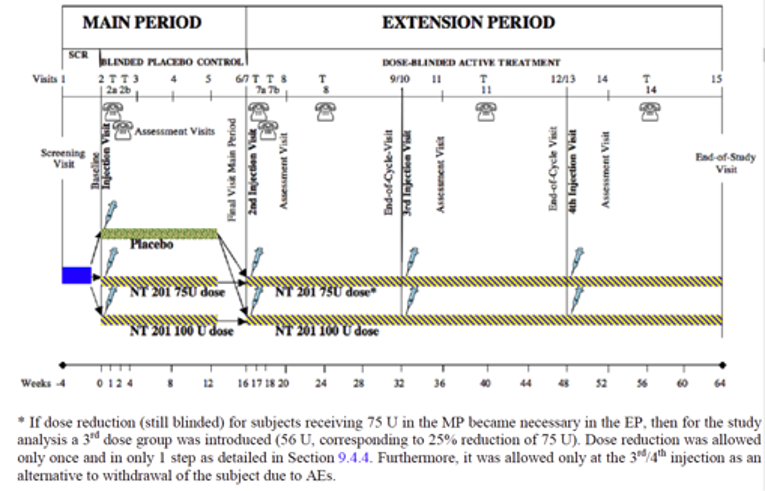
NT 201 = incobotulinumtoxinA; SCR = screening; t = telephone.
* If dose reduction for patients receiving 75 U in the MP due to AEs became necessary in the EP, then a third dose group was planned (56 U, corresponding to a 25% reduction of 75 U). Dose reduction was to be allowed only once in a single step at the third or fourth injection as an alternative to withdrawal.
Source: SIAXI Clinical Study Report.8
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria for the SIAXI study are summarized in Table 7. Patients (age 18 to 80 years inclusive) with chronic troublesome sialorrhea resulting from PD/AP, stroke, or TBI (onset ≥ 6 months before screening) were included. All diagnoses of PD were made according to the UK PD Brain Bank criteria.49 It was initially planned that 20% of patients be recruited from each etiology subgroup; however, this requirement was dropped for feasibility to achieve the necessary sample size. Chronic troublesome sialorrhea was defined as sialorrhea lasting for 3 months or longer, with a DSFS sum score of at least 6, DSFS scores for both severity and frequency of at least 2, and mROMP Section III “Drooling,” Item A score of 3 or greater at both screening and baseline. Troublesome sialorrhea had to persist after stabilization and/or optimization of medications influencing sialorrhea (e.g., anti-parkinsonian medication). Only patients with no swallowing difficulties were included (an mROMP score for Section II “Swallowing Symptoms,” Item A of no more than 2 and Item C of no more than 3 at screening and baseline). Patients with non-neurologic causes of sialorrhea, generalized neuromuscular junction disorders of muscle activity (e.g., myasthenia gravis), extremely poor dental condition or oral hygiene, history of aspiration pneumonia, previous and/or current infections or tumours of the salivary glands or injection sites, or any concurrent diseases or conditions (hematological, hepatic, renal, gastrointestinal, endocrine, pulmonary, musculoskeletal, or psychiatric) judged by investigators as potential risks were excluded. Patients unable to tolerate keeping cotton rolls in their mouths for 5 minutes (as judged by investigators), patients unable to open their mouths voluntarily, patients at significant risk of suicidality (based on investigator judgment or the electronic Columbia Suicide Severity Rating Scale50) were also excluded. Pregnant women were excluded and contraceptive use was required for women of child-bearing potential. Patients with unstable concomitant medications influencing sialorrhea (e.g., anticholinergics for parkinsonism), other concomitant medications known to cause hypersalivation (e.g., clozapine), prior or planned surgery or irradiation to treat sialorrhea, recent treatment with BoNTs (≤ 1 year for sialorrhea and ≤ 14 weeks for other indications), or known hypersensitivities to BoNTs were excluded. Detailed information on inclusion and exclusion criteria related to prior and concomitant medications and therapies is provided in the Interventions section.
Baseline Characteristics
The mean age of the study population in the MP was 65.2 years (SD = 11.4 years) (Table 8). Most patients were men (70.7%) and nearly all were White (99.5%). The most common etiology of sialorrhea was PD (70.7%) followed by stroke (19.0%), AP (8.7%), and TBI (2.7%). Among patients with PD/AP, the mean unified Parkinson disease rating scale (UPDRS)51 section III “motor examination” score was 31.2 (SD = 15.6). Among patients with stroke or TBI, the mean modified motor assessment scale (MMAS)52 score (left/right) was 38.7/39.9 (SD = 10.2/9.9). The mean duration of sialorrhea was 32.7 months (SD = 34.5 months). Baseline mean (and SD) uSFR, DSFS sum scores, DSFS severity scores, DSFS frequency scores, and mROMP drooling scores were well balanced between the placebo and the incobotulinumtoxinA 100 U arms. Baseline demographic and clinical characteristics were generally well balanced between study arms.
Most patients had at least 1 medical history finding; the most common finding, beyond the underlying neurologic condition, was DBS (placebo: 13.9%; incobotulinumtoxinA 100 U: 24.3%). Patients had a variety of concomitant diseases that occurred with similar frequency across arms; however, dysarthria (placebo: 8.3%; incobotulinumtoxinA 100 U: 20.3%), dysphonia (placebo: 2.8%; incobotulinumtoxinA 100 U: 6.8%), and dysphagia (placebo: 5.6%; incobotulinumtoxinA 100 U: 8.1%) were more common in the incobotulinumtoxinA 100 U arm compared with the placebo arm. Compared with the placebo arm, more patients in the incobotulinumtoxinA 100 U arm had a treatment history of DBS (placebo: 13.9%; incobotulinumtoxinA 100 U: 24.3%).
The demographic characteristics of the 173 patients participating in the EP were similar to those in the MP (Appendix 3). Data on severity of sialorrhea (uSFR, DSFS sum scores and subscores, and mROMP drooling scores) at the beginning of the EP are not presented in this table as these values were identical to the week 16 efficacy data for the MP. Baseline demographic and clinical characteristics were again well balanced between arms. Medical history was not evaluated separately for the EP. Concomitant diseases and medications in the EP were similar to those in the MP.
Table 8: Summary of Baseline Characteristics (SIAXI MP, FAS, and SES-MP)
Characteristic | Placebo (N = 36) | IncobotulinumtoxinA 75 U (N = 74) | IncobotulinumtoxinA 100 U (N = 74) | Total (N = 184) |
|---|---|---|---|---|
Sex, n (%) | ||||
Male | 28 (77.8) | 50 (67.6) | 52 (70.3) | 130 (70.7) |
Female | 8 (22.2) | 24 (32.4) | 22 (29.7) | 54 (29.3) |
Age, years | ||||
Mean (SD) | 63.5 (10.6) | 65.2 (11.7) | 66.0 (11.6) | 65.2 (11.4) |
Median (range) | 64.0 (23 to 80) | 67.0 (27 to 80) | 67.5 (21 to 80) | 66.5 (21 to 80) |
Age group, n (%) | ||||
18-64 years | 19 (52.8) | 30 (40.5) | 28 (37.8) | 77 (41.8) |
65-84 years | 17 (47.2) | 44 (59.5) | 46 (62.2) | 107 (58.2) |
Race, n (%) | ||||
White | 36 (100.0) | 74 (100.0) | 73 (98.6) | 183 (99.5) |
Asian | 0 | 0 | 1 (1.4) | 1 (0.5) |
Ethnicity, n (%) | ||||
Hispanic/Latino | 0 | 0 | 1 (1.4) | 1 (0.5) |
Not Hispanic/Latino | 36 (100.0) | 74 (100.0) | 73 (98.6) | 183 (99.5) |
Weight (kg) | ||||
Mean (SD) | 80.6 (16.4) | 78.4 (17.1) | 79.8 (14.0) | 79.4 (15.7) |
Median (range) | 81.4 (50 to 128) | 78.0 (37 to 127) | 79.0 (49 to 116) | 79.0 (37 to 128) |
Body mass index (kg/m2) | ||||
Mean (SD) | 28.5 (6.0) | 26.7 (5.2) | 27.7 (3.8) | 27.5 (4.9) |
Median (range) | 28.3 (19 to 41) | 26.4 (14 to 51) | 27.5 (19 to 35) | 27.5 (14 to 51) |
Medical history, n (%) | ||||
Yes | 26 (72.2) | 50 (67.6) | 58 (78.4) | 134 (72.8) |
DBS | 5 (13.9) | 8 (10.8) | 18 (24.3) | 31 (16.8) |
Diseases causing sialorrhea, n (%) | ||||
PD/AP | 29 (80.6) | 59 (79.7) | 58 (78.4) | 146 (79.3) |
PD | 26 (72.2) | 51 (68.9) | 53 (71.6) | 130 (70.7) |
AP | 3 (8.3) | 8 (10.8) | 5 (6.8) | 16 (8.7) |
MSA | 1 (2.8) | 6 (8.1) | 3 (4.1) | 10 (5.4) |
CD | 0 | 0 | 1 (1.4) | 1 (0.5) |
PSP | 2 (5.6) | 2 (2.7) | 1 (1.4) | 5 (2.7) |
Stroke | 7 (19.4) | 14 (18.9) | 14 (18.9) | 35 (19.0) |
TBI | 1 (2.8) | 2 (2.7) | 2 (2.7) | 5 (2.7) |
Concomitant diseases, n (%) | ||||
Yes | 36 (100.0) | 74 (100.0) | 74 (100.0) | 184 (100.0) |
Hypertension | 19 (52.8) | 37 (50.0) | 39 (52.7) | 95 (51.6) |
Hypercholesterolemia | 7 (19.4) | 13 (17.6) | 10 (13.5) | 30 (16.3) |
Hyperlipidemia | 4 (11.1) | 13 (17.6) | 10 (13.5) | 27 (14.7) |
Spinal osteoarthritis | 5 (13.9) | 8 (10.8) | 7 (9.5) | 20 (10.9) |
Dysarthria | 3 (8.3) | 11 (14.9) | 15 (20.3) | 29 (18.5) |
Dysphonia | 1 (2.8) | 2 (2.7) | 5 (6.8) | 8 (4.3) |
Dysphagia | 2 (5.6) | 7 (9.5) | 6 (8.1) | 15 (8.2) |
Speech disorder | 1 (2.8) | 0 | 2 (2.7) | 3 (1.6) |
Baseline uSFR, g/min | ||||
Mean (SD) | 0.38 (0.23) | 0.42 (0.28) | 0.40 (0.27) | NR |
Baseline DSFS score | ||||
Sum, mean (SD)a | 6.97 (1.06) | 6.88 (0.91) | 6.78 (0.90) | NR |
Severity, mean (SD)b | 3.72 (0.85) | 3.72 (0.73) | 3.69 (0.78) | NR |
Frequency, mean (SD)c | 3.25 (0.44) | 3.16 (0.41) | 3.09 (0.44) | NR |
Baseline mROMP score | ||||
Speechd | 19.08 (7.15) | 17.28 (6.99) | 17.20 (6.37) | NR |
Droolinge | 24.67 (6.08) | 25.84 (6.96) | 24.76 (5.68) | NR |
UPDRS section III “motor examination”f | ||||
Mean (SD) | 29.2 (12.7) | 33.1 (17.2) | 30.3 (15.1) | 31.2 (15.6) |
Median (range) | 29.0 (7 to 61) | 30.0 (7 to 80) | 29.0 (3 to 73) | 29.0 (3 to 80) |
Left MMAS scoreg | ||||
Mean (SD) | 40.4 (6.2) | 39.2 (12.0) | 37.4 (10.2) | 38.7 (10.2) |
Median (range) | 42.0 (30 to 48) | 45.0 (11 to 48) | 40.0 (15 to 48) | 41.5 (11 to 48) |
Right MMAS scoreg | ||||
Mean (SD) | 41.6 (14.0) | 39.3 (10.3) | 39.6 (7.9) | 39.9 (9.9) |
Median (range) | 47.0 (10 to 48) | 42.0 (17 to 48) | 40.5 (23 to 48) | 42.5 (10 to 48) |
Time since first diagnosis of sialorrhea at screening (months) | ||||
Mean (SD) | 37.1 (38.7) | 29.6 (28.3) | 33.7 (38.4) | 32.7 (34.5) |
Median (range) | 19.8 (5 to 157) | 15.9 (5 to 119) | 16.7 (3 to 171) | 17.4 (3 to 171) |
Edentulous, n (%) | ||||
Yes | 10 (27.8) | 20 (27.0) | 19 (25.7) | 49 (26.6) |
• Dentures | 8 (22.2) | 17 (23.0) | 15 (20.3) | 40 (21.7) |
• No dentures | 2 (5.6) | 3 (4.1) | 4 (5.4) | 9 (4.9) |
AP = atypical parkinsonism; CD = corticobasal degeneration; DBS = deep brain stimulation; DSFS = Drooling Frequency and Severity Scale; FAS = full analysis set; MMAS = modified motor assessment scale; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; MSA = multiple system atrophy; NR = not reported; PD = Parkinson disease; PSP = progressive supranuclear palsy; SD = standard deviation; SES-MP = safety evaluation set, main period; TBI = traumatic brain injury; UPDRS = unified Parkinson disease rating scale; uSFR = unstimulated salivary flow rate.
aDSFS sum scores range from 2 (best) to 9 (worst).
bSeverity: 1 = dry (never drools), 2 = mild (only lips wet), 3 = moderate (wet on lips and chin), 4 = severe (drool extends to clothes wet), 5 = profuse (hands, tray and objects wet).
cFrequency: 1 = never, 2 = occasionally (not every day), 3 = frequently (part of every day), 4 = constantly.
dScores ranges from 8 (best) to 40 (worst).
eScores ranges from 9 (best) to 45 (worst).
fMeasured by investigators based on 14 items with 27 total scores as each item may assess more than 1 part of the body. Each score was rated on a 5-point scale only in patients with PD/AP. For patients with “on-off” motor fluctuations, assessments were performed in comparable “on” states, preferably at the same day and time, at least throughout the MP. Scores range from 0 (best) to 56 or 108 (worst).
gMeasured by investigators based on 8 items, each rated on a 6-point scale only in patients with stroke or TBI. Scores range from 0 (worst) to 48 (best).
Source: SIAXI Clinical Study Report.8
Interventions
In the MP, patients were randomized 2:2:1 to receive 1 of 2 doses of incobotulinumtoxinA (75 U or 100 U) or placebo (physiologic saline) via 4 intraglandular injections administered on a single day by study personnel at the baseline visit. To maintain the double-blind study status, similarly marked vials were provided containing defined amounts of incobotulinumtoxinA that, when resuspended in 4 mL of physiologic saline, yielded solutions of 50 U/mL incobotulinumtoxinA (100 U dose group) or 37.5 U/mL incobotulinumtoxinA (75 U dose group). The placebo vials contained an excipient only (human serum albumin and sucrose). Identical volumes were injected in all patients (0.6 mL bilaterally per parotid gland and 0.4 mL bilaterally per submandibular gland). Injections were guided either by ultrasound or using anatomic landmarks; individual patients consistently received injections using 1 or the other technique. Based on input from the FDA, at least 50% of patients were targeted to receive ultrasound-guided injections, and investigators received special training for this technique. The EP involved 3 additional 16-week treatment cycles with injections administered identically as in the MP, unless dose reduction was required. If patients met the eligibility criteria for the next treatment cycle, the injection could take place at the assessment visit; otherwise, the next injection could be postponed for up to 2 weeks.
Patients treated with BoNTs for sialorrhea within the past 1 year or for other indications within 14 weeks were excluded; treatment with BoNTs (other than protocol therapy) was forbidden during the screening period and during the entire study period. Concomitant use of aminoglycoside antibiotics, curare-like agents, or other medications that could interfere with neuromuscular function was forbidden. Pharmacological treatments for sialorrhea and medications known to cause hypersalivation (e.g., clozapine) were forbidden from 4 weeks before baseline throughout the MP. Concomitant medications influencing sialorrhea (e.g., anticholinergics) were forbidden from 4 weeks before baseline throughout the MP, except for drugs taken at a stable dosage throughout this period. Changes in dosing of medications to treat PD/AP were forbidden from 4 weeks before screening throughout the MP. Salivary gland surgery or irradiation was forbidden at any time before or during the entire study period including screening. Prior (≤ 6 months) functional neurosurgery (e.g., pallidotomy, DBS) or functional neurosurgery planned during the MP was forbidden, as was any other prior (≤ 3 months) or planned (during the MP) surgery, except for minor surgery outside the head and neck region. Anticoagulants were forbidden, but Aspirin and platelet aggregation inhibitors were allowed. Use of illegal and legal drugs (except for alcohol/tobacco) for recreational purposes was forbidden. Excessive use of alcohol and/or tobacco (as judged by the investigator) was forbidden. Smoking was disallowed within 1 hour of assessments. During protocol therapy, a dry mouth could be eased by ice chips, cold water, sugar-free chewing gum, sour sugar-free sweets, sprays, gels, and mouth rinses. Patients were advised to try saliva substitutes and choose their preferred agent, but to avoid use of these agents before and during saliva collection.
Nearly all patients received concomitant medications, including dopaminergic agents for PD (placebo: 77.8%; incobotulinumtoxinA 100 U: 79.7%) during the MP (Table 9), but few received anticholinergic agents (placebo: 0%; incobotulinumtoxinA 100 U: 2.7%). Compared with the placebo arm, more patients in the incobotulinumtoxinA arm received psychoanaleptics (placebo: 19.4%; incobotulinumtoxinA 100 U: 36.5%) and fewer received diuretics (placebo: 27.8%; incobotulinumtoxinA 100 U: 14.9%), calcium channel blockers (placebo: 27.8%; incobotulinumtoxinA 100 U: 14.9%), or cardiac therapy (placebo: 19.4%; incobotulinumtoxinA 100 U: 6.8%). Compared with the placebo arm, more patients in the NT201 arm reported concomitant DBS (placebo: 13.9%; incobotulinumtoxinA 100 U: 24.3%).
Concomitant medications received during the EP were similar to those received during the MP (Appendix 3).
Table 9: Concomitant Medications and Therapies (SIAXI MP, FAS, and SES-MP)
Characteristic | Placebo (N = 36) | IncobotulinumtoxinA 75 U (N = 74) | IncobotulinumtoxinA 100 U (N = 74) | Total (N = 184) |
|---|---|---|---|---|
Concomitant non-drug therapies, n (%) | ||||
Yes | 8 (22.2) | 16 (21.6) | 27 (36.5) | 51 (27.7) |
DBS | 5 (13.9) | 8 (10.8) | 18 (24.3) | 31 (16.8) |
Concomitant medications, n (%) | ||||
Yes | 36 (100.0) | 73 (98.6) | 74 (100.0) | 183 (9.5) |
Dopaminergic agents | 28 (77.8) | 57 (77.0) | 58 (78.4) | 143 (77.2) |
Anticholinergic agents | 0 | 2 (2.7) | 2 (2.7) | 4 (2.2) |
Agents acting on the renin-angiotensin system | 16 (44.4) | 28 (37.8) | 33 (44.6) | 77 (41.8) |
Antithrombotic agents | 15 (41.7) | 30 (40.5) | 28 (37.8) | 73 (39.7) |
Lipid modifying agents | 13 (36.1) | 26 (35.1) | 20 (27.0) | 59 (32.1) |
Beta blocking agents | 11 (30.6) | 20 (27.0) | 18 (24.3) | 49 (26.6) |
Psychoanaleptics | 7 (19.4) | 16 (21.6) | 27 (36.5) | 50 (27.2) |
Diuretics | 10 (27.8) | 14 (18.9) | 11 (14.9) | 35 (19.0) |
Calcium channel blockers | 10 (27.8) | 9 (12.2) | 11 (14.9) | 30 (16.3) |
Cardiac therapy | 7 (19.4) | 3 (4.1) | 5 (6.8) | 15 (8.2) |
Antibacterials for systemic use | 4 (11.1) | 11 (14.9) | 5 (6.8) | 20 (10.9) |
Drugs for constipation | 1 (2.8) | 4 (5.4) | 12 (16.2) | 17 (9.2) |
DBS = deep brain stimulation; FAS = full analysis set; MP = main period; SES-MP = safety evaluable set, main period.
Source: SIAXI Clinical Study Report.8
Stopping criteria included withdrawal of informed consent, pregnancy, AEs for which treatment continuation constituted an unacceptably high risk (described in the Outcomes sections), and positive suicidality assessment (a “yes” response to sections 4 and 5 of the electronic Columbia Suicide Severity Rating Scale, any suicidal behaviour, or any non-suicidal self-injurious behaviour). Patients who were withdrawn due to AEs were to be followed up until the end-of-study visit or 28 days after the AE occurred, whichever was later. In addition, dose reductions of incobotulinumtoxinA due to AEs were allowed once and only once at either the third or the fourth injections in the EP; if the AE did not recur, the full dose could be given in the fourth injection for patients receiving reduced doses in the third injection. Dose reduction included planned movement of patients from the 100 U to the 75 U dose group as well as, potentially, movement to a third dose-reduced group (56 U, corresponding to a 25% reduction from 75 U). All dose reductions were based on 25% reductions in the injection volume.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 10. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4. No evidence was available to inform the validity, reliability, responsiveness to change, or MID for any of the outcome measures used in the SIAXI trial.
All primary and secondary outcomes were evaluated in the MP. In the EP, all outcomes were exploratory and were measured as in the MP. In patients with PD/AP and “on-off” motor fluctuations, all efficacy outcomes were assessed in comparable “on” states (typically 60 to 180 minutes after taking anti-parkinsonian medication).
Table 10: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | SIAXI MP | SIAXI EP | Scale |
|---|---|---|---|
Change in uSFR from baseline to week 4 | Co- primary | — | Continuous |
Patient GICS entry (or carer GICS entry if patient unable to answer) at week 4 | Co-primary | — | −3 (worst) to 3 (best) |
Change in uSFR from baseline to weeks 8 and 12 | Secondary | — | Continuous |
Patient GICS entry (or carer GICS entry if patient unable to answer) at weeks 1, 2, 8, and 12 | Secondary | — | −3 (worst) to 3 (best) |
Change in DSFS subscores and sum score from baseline to weeks 4, 8, 12, and 16 | Exploratory | — | Severity: 1 (best) to 5 (worst) Frequency: 1 (best) to 4 (worst) Sum: 2 (best) to 9 (worst) |
Change in uSFR from baseline to week 16 | Exploratory | — | Continuous |
Patient GICS entry (or carer GICS entry if patient unable to answer) at week 16 | Exploratory | — | −3 (worst) to 3 (best) |
Number of responders according to patient GICS entry at weeks 1, 2, 4, 8, 12, and 16 | Exploratory | — | Percentage |
Carer GICS entry at weeks 1, 2, 4, 8, 12, and 16 | Exploratory | — | −3 (worst) to 3 (best) |
Change in mROMP speech symptom and drooling score from baseline to week 4, 8, 12, and 16 | Exploratory | — | mROMP speech: 8 (best) to 40 (worst) mROMP drooling: 9 (best) to 45 (worst) |
Change in EQ-5D-3L single items and EQ VAS from baseline to weeks 4, 8, 12, and 16 | Exploratory | — | EQ-5D-3L single items: 1 (best) to 3 (worst) EQ VAS: 0 (worst) to 100 (best) |
Change in uSFR from baseline to all visits in the EP, and change from each injection (weeks 16, 32, and 48) to the respective assessment visits (weeks 20, 36, and 52) and to the end-of-cycle/end-of-study visits (weeks 32, 48, and 64) | — | Exploratory | Continuous |
Patient GICS entry (or carer GICS entry if patient unable to answer) at all assessment visits in the EP (weeks 20, 36, and 52) and the end-of-cycle/end-of-study visits (weeks 32, 48, and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40, and 56) | — | Exploratory | −3 (worst) to 3 (best) |
Number of responders according to patient GICS entry at all assessment visits in the EP (weeks 20, 36, and 52) and the end-of-cycle / end-of-study visits (weeks 32, 48, and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40, and 56) | — | Exploratory | Percentage |
Change in DSFS subscores and sum score from baseline to all assessment visits in the EP | — | Exploratory | Severity: 1 (best) to 5 (worst) Frequency: 1 (best) to 4 (worst) Sum: 2 (best) to 9 (worst) |
Carer GICS entry at all assessment visits in the EP (weeks 20, 36, and 52) and the end-of-cycle/end-of-study visits (weeks 32, 48, and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40, and 56) | — | Exploratory | −3 (worst) to 3 (best) |
Change in mROMP speech symptoms and drooling scores from baseline to all assessment visits in the EP | — | Exploratory | mROMP speech: 8 (best) to 40 (worst) mROMP drooling: 9 (best) to 45 (worst) |
Change in EQ-5D-3L single items and EQ VAS from baseline to all assessment visits in the EP | — | Exploratory | EQ-5D-3L single items: 1 (best) to 3 (worst) EQ VAS: 0 (worst) to 100 (best) |
DSFS = Drooling Severity and Frequency Scale; EP = extension period; EQ-5D-5L = EuroQol-5 Dimension-3 Level questionnaire; EQ VAS EuroQol -Dimensions Visual Analogue Scale; GICS = Global Impression of Change Scale; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; uSFR = unstimulated salivary flow rate.
Source: SIAXI Clinical Study Report.8
The uSFR was evaluated during onsite assessment visits at screening, baseline, and various times post-injection by direct saliva collection using the swab method. A negative change in the uSFR represents a reduction in salivary flow and therefore an improvement in sialorrhea. Four cotton rolls were placed in the patient’s mouth (1 between the cheek and gums and 1 between the tongue and gums on each side) for 5 minutes, then weighed; after 30 minutes, the procedure was repeated, and the 2 measurements were averaged. In the MP, change in uSFR was evaluated from baseline to all visits. In the EP, change in uSFR was evaluated from baseline to all visits as well as from each injection to the respective assessment visits and the end-of-cycle visit.
Scores for the GICS were evaluated by patients and by caregivers independently on a 7-point Likert scale (−3, very much worse; −2, much worse; −1, minimally worse; 0, no change; 1, minimally improved; 2, much improved; and 3, very much improved) at various times post-injection via self-reported questionnaires or phone interviews. The recall period for GICS was since before the previous injection. If patients were unable to answer, caregiver responses were used in place of the patient’s responses. The number of responders (defined as patient GICS response of at least 1, minimally improved; denominator all patients receiving injections) was calculated at all post-injection assessments. The rationale for defining responders using a threshold of a GICS score of at least 1 was not stated.
Sialorrhea and speech symptoms were evaluated by patients at screening, baseline, and at various times post-injection using the self-administered mROMP inventory containing 8 and 9 questions in the speech and drooling domains, respectively; each domain was evaluated on a 5-point Likert scale yielding total scores from 8 to 40 and 9 to 45, respectively. Changes from study baseline were evaluated.
In addition, sialorrhea severity and frequency were rated on the DSFS by study investigators at screening, baseline, and various times post-injection using 5- and 4-point Likert scales, respectively; the resulting DSFS sum score ranged from 2 to 9. The recall periods for both the mROMP and DSFS were over the previous 1 week. Changes from study baseline were evaluated.
The HRQoL was assessed by patients at baseline and at various times post-injection using the EQ-5D-3L;53 patients descriptively rated each of 5 dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) on a 3-point scale (1, no problems; 2, some problems; or 3, extreme problems) and rated their overall health using a VAS ranging from 0 (worst imaginable health state) to 100 (best imaginable health state). Changes from study baseline were evaluated.
Harms outcomes included treatment-emergent AEs, SAEs, WDAEs, and AESIs. All harms outcomes were analyzed for the MP, the full EP, and each cycle in the EP separately. AEs were defined as any untoward medical occurrence and were coded according to Medical Dictionary for Regulatory Activities version 18.1. Incidence was calculated at the system organ class and preferred term (PT) levels. Adverse events in the MP were defined as AEs with onset or worsening after the first injection up to the cycle 2 injection (the first injection of the EP), 176 weeks after the first injection, or the last study visit, whichever was later. Adverse events in the EP were defined as AEs with onset or worsening after the cycle 2 injection (the first injection of the EP) up to 16 weeks after the cycle 4 injection (the last injection of the EP) or the date of last study visit, whichever was later. Serious AEs were defined as an untoward medical occurrence that was life-threatening, requires inpatient hospitalization or prolongation of hospitalization, results in persistent or significant disability and/or incapacity, results in death, is a congenital abnormality, or consists of any other medically important condition as per the International Conference on Harmonisation's E2A guidelines.54 Adverse events of special interest (AESI) were defined as in Table 11 to capture all AE PTs potentially reflective of toxin spread. In addition, a dry mouth that was severe, serious, or irreversible was reported as an AESI. At post-injection visits, a focused physical exam was used to assess AESIs for potential toxin spread; if necessary, a full physical exam was administered.
Table 11: AESIs Potentially Indicating Toxin Spread
AESIs Potentially Indicating Toxin Spread | ||
|---|---|---|
Accommodation disorder | Eyelid ptosis | Peripheral nerve palsy |
Areflexia | Seventh nerve paralysis | Peripheral paralysis |
Aspiration | Facial paresis | Pelvic floor muscle weakness |
Botulism | Hemiparesis | Pneumonia aspiration |
Bradycardia | Hypoglossal nerve paresis | Pupillary reflex impaired |
Bulbar palsy | Hyporeflexia | Quadriparesis |
Constipation | Hypotonia | Respiratory arrest |
Cranial nerve palsies, multiple | Third nerve paresis | Respiratory depression |
Cranial nerve paralysis | Ileus paralytic | Respiratory failure |
Diaphragmatic paralysis | Fourth nerve paresis | Speech disorder |
Diplopia | Monoparesis | Trigeminal nerve paresis |
Dysarthria | Muscular weakness | Urinary retention |
Dysphagia | Paralysis | Vision blurred |
Dysphonia | Paralysis flaccid | Vocal cord paralysis |
Dyspnea | Paraparesis | Vocal cord paresis |
Extraocular muscular paresis | Paresis | |
Eyelid function disorder | Paresis cranial nerve | |
AESI = adverse event of special interest.
Note: Wording of adverse event PTs is according to the Medical Dictionary for Regulatory Activities version 15.1.
Source: SIAXI Clinical Study Report.8
Statistical Analysis
Power Calculation
The planned sample size for co-primary analysis of uSFR and GICS in SIAXI was based on a study of rimabotulinumtoxinB.47 For uSFR, the study found mean changes of −0.381 (SD = 0.34) for the rimabotulinumtoxinB 2,500 U group and −0.052 (0.33) for the placebo group 4 weeks post-injection. Assuming a dropout rate of 5% by week 4, a mean change in uSFR from baseline to week 4 of −0.362 (SD = 0.341) was calculated for the incobotulinumtoxinA 100 U group, with a corresponding change of −0.049 (SD = 0.322) for the placebo group. Based on these assumptions and a 2:2:1 randomization ratio, 46 patients in each incobotulinumtoxinA treatment arm and 23 patients in the placebo arm would provide 95% power to show a statistically significant difference between either of the incobotulinumtoxinA groups and placebo (2-sided Satterthwaite t-test, alpha = 0.05). The total sample size required was at least 115 patients.
For the GICS, the study of rimabotulinumtoxinB47 found mean changes in the Clinical Global Impression score of 2.0 (SD = 1.04)55 for the rimabotulinumtoxinB 2,500 U group and 4.1 (SD = 1.03) for the placebo group 4 weeks post-injection (smaller values reflect greater improvement). Assuming a dropout rate of 5% by week 4 and converting to GICS as (−Clinical Global Impression − change + 4), a mean GICS score at week 4 of 2.100 (SD = 1.103) was calculated for the incobotulinumtoxinA group, with a corresponding change of 1.195 (SD = 1.344) in the placebo arm. Based on these assumptions and a 2:2:1 randomization ratio, 20 patients in each incobotulinumtoxinA treatment arm and 10 patients in the placebo arm would provide 95% power to show a statistically significant difference between either of the incobotulinumtoxinA groups and placebo (2-sided Satterthwaite t-test, alpha = 0.05). The total sample size required was at least 50 patients.
Statistical Models
Two-sided hypotheses were used to test for between-treatment differences. Methods used for statistical analysis of primary and secondary outcomes are summarized in Table 12 and those used for analysis of all outcomes are shown in Appendix 3. For the co-primary outcomes (change in uSFR from baseline to week 4 in the MP and patient GICS score at week 4 in the MP), an MMRM analysis (2-sided, alpha = 0.05) comparing LSMs was used for the confirmatory analysis of differences between the incobotulinumtoxinA treatment and placebo groups. The dependent variables were change from baseline in uSFR or GICS score. The independent variables were treatment group, etiology subgroup, use of ultrasound, country, and gender as fixed factors, visit × treatment as an interaction term, and visit as a repeated factor. To adjust for baseline status, the MMRM analysis of change in uSFR included baseline uSFR as a covariate and the MMRM analysis of GICS scores included baseline DSFS as a covariate. For the co-primary outcomes, a sequence test procedure was used to control type I error when comparing the LSMs from the MMRM analysis for the 2 incobotulinumtoxinA treatment groups versus placebo at week 4. Because of the hierarchical test procedure, no additional adjustment for multiplicity was performed. First, the hypotheses of equivalence versus non-equivalence for change in uSFR and GICS score between the incobotulinumtoxinA 100 U arm and placebo were tested. Subsequently, and only if both previous equivalence hypotheses could be rejected, the hypotheses of equivalence versus non-equivalence for change in uSFR and GICS between the incobotulinumtoxinA 75 U and placebo arms were tested. The confirmatory analyses were performed in the full analysis set (FAS), and the MMRM approach accounted for missing values by assuming they were missing at random. Sensitivity analyses were performed in the same manner using the per-protocol set (PPS). Additional sensitivity analyses were performed for the FAS and PPS using the baseline observation carried forward (BOCF) approach for uSFR and imputing missing GICS entries at week 4 as “no change,” and without replacing missing data (observed cases). For the BOCF and observed cases analyses, analysis of covariance (ANCOVA) models were used without visit × treatment as an interaction term and without visit as a repeated factor. Finally, a non-parametric Wilcoxon rank sum test (FAS and PPS, using BOCF and observed cases analysis) was used as a sensitivity analysis of the change in uSFR to account for potential deviation from normality.
Secondary efficacy outcomes (change in uSFR from baseline to weeks 8 and 12 in the MP and patient GICS score at weeks 1, 2, 8, and 12 in the MP) were analyzed in the same manner as the co-primary outcomes in both the FAS and PPS. These tests were descriptive, not adjusted for multiplicity, and interpreted in an exploratory manner. Comparisons were between the incobotulinumtoxinA 100 U and placebo arms as well as the incobotulinumtoxinA 75 U and placebo arms. There was no hierarchical test procedure or strategy for multiplicity control.
Exploratory efficacy outcomes in the MP were evaluated in the FAS, except for change in uSFR at week 16 and patient GICS score at week 16, which were evaluated in both the FAS and PPS. Change in uSFR at week 16 and patient GICS score at week 16 were analyzed in the same manner as the co-primary outcomes (BOCF and observed cases). Comparison of the number of responders based on patient GICS entries across treatment groups were performed in a manner similar to that used in the primary efficacy analysis, except using logistic regression models with response to treatment as the dependent variable and treatment group, use of ultrasound, etiology subgroup, gender, and country as factors. To account for baseline status, the models included baseline DSFS score as a covariate. Odds ratios and 95% Wald CIs were calculated. Analysis was performed in the FAS without imputation of missing values and imputing missing GICS entries as nonresponders. If logistic regression models were not estimable, descriptive summary statistics were provided. For analysis of GICS responders at week 16, only summary statistics, 95% CIs, and P values from Fisher’s exact tests or chi-square tests were reported, both without imputation of missing values and imputing missing GICS entries as nonresponders. Percentages were based on all patients (BOCF) or patients with data at the respective visit (observed cases). Carer GICS scores at all time points were summarized using descriptive statistics and frequency tables. Changes in DSFS sum scores from baseline to weeks 4, 8, and 12 were analyzed as per the primary efficacy analysis. For changes in DSFS sum scores from baseline to week 16 and changes in DSFS subscores from baseline to weeks 4, 8, 12, and 16, descriptive statistics were provided. For changes in mROMP speech and drooling scores from baseline to all time points, analyses were performed of observed cases with the BOCF applied to single questions; descriptive statistics were provided. Single items from the EQ-5D-3L were analyzed using frequency tables and shift tables for changes from baseline, and the EQ VAS was analyzed using summary statistics for all visits and changes from baseline; analysis was performed without imputation of missing values. None of the exploratory analyses were controlled for multiplicity.
Exploratory efficacy outcomes in the EP were evaluated in the safety evaluation set, extension period (SES-EP) and missing data were not imputed. None of the exploratory analyses of the EP were controlled for multiplicity.
Subgroup analyses were performed as described previously for selected outcomes (uSFR, GICS, and DSFS). All subgroup analyses were exploratory and not controlled for multiplicity. Among others, the SIAXI trial pre-specified a subgroup analysis by etiology of sialorrhea (PD/AP, stroke, or TBI) that was identified as of interest in the CADTH review protocol. This subgroup was well balanced in the treatment arms. A post hoc subgroup analysis of efficacy outcomes was conducted by severity of sialorrhea (uSFR ≤ or > median uSFR at baseline), which was also identified as of interest in the CADTH review protocol but not presented in this report due to its post hoc nature. No subgroup analyses by severity of underlying neurologic condition were conducted.
Table 12: Statistical Analysis of Primary and Secondary Efficacy End Points in SIAXI
Period | Type | End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|---|---|
MP | Co-primary | Change in uSFR from baseline to week 4 | MMRM (2-sided, significance level alpha = 0.05, FAS) with comparison of LSMs |
|
|
Co-primary | Patient GICS entry (or carer GICS entry if patient unable to answer) at week 4 | MMRM (2-sided, significance level alpha = 0.05, FAS) with comparison of LSMs |
|
| |
Secondary | Change in uSFR from baseline to weeks 8 and 12 | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | |
Secondary | Patient GICS entry (or carer GICS entry if patient unable to answer) at weeks 1, 2, 8, and 12 | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) |
ANCOVA = analysis of covariance; BOCF = baseline observation carried forward; CI = confidence interval; DSFS = Drooling Severity and Frequency Scale; FAS = full analysis set; GICS = Global Impression of Change Scale; LSM = least squares mean; MMRM = mixed model for repeated measures; OC = observed cases; PPS = per-protocol set; uSFR = unstimulated salivary flow rate.
Source: SIAXI Clinical Study Report.8
Analysis Populations
The safety evaluation set, main period (SES-MP) was defined as the set of all patients who received study medication (incobotulinumtoxinA or placebo) during the MP. The FAS was defined as the subset of patients within the SES-MP for whom the primary efficacy outcome was measured (i.e., all patients who were treated and had uSFR measured at baseline; no post-baseline measurement was required for inclusion in the FAS). The PPS was defined as the subset of patients within the FAS without major protocol deviations. If patients were not treated according to the randomization list, analyses of the SES-MP and FAS were by intention to treat.
In the EP, the SES-EP was defined as the set of all patients who received study medication (incobotulinumtoxinA) at least once during the EP. Because medication was assigned for each cycle individually, treatment not according to the randomization list could occur in some but not all cycles. For efficacy outcomes over the entire EP, analysis was by intention to treat even if treatment deviated from the randomization list. For efficacy outcomes for each treatment cycle, analysis was by intention to treat. Patients receiving reduced doses were analyzed as randomized. For harms outcomes, analysis was based on treatment received.
Efficacy analyses in the MP were based on the FAS, and for sensitivity analyses, the PPS. Efficacy analyses in the EP were based on the SES-EP. In the EP, analysis was performed by combined MP/EP treatment group: placebo (MP) + incobotulinumtoxinA 100 U (EP); placebo (MP) + incobotulinumtoxinA 75 U (EP); incobotulinumtoxinA 100 U (MP) + incobotulinumtoxinA 100 U (EP); and incobotulinumtoxinA 75 U (MP) + incobotulinumtoxinA 75 U (EP). Analyses were also performed by treatment group in the EP (incobotulinumtoxinA 100 U or 75 U).
Results
Patient Disposition
A total of 216 patients were screened, of whom 184 were randomized and treated in the MP (incobotulinumtoxinA 100 U: N = 74; incobotulinumtoxinA 75 U: N = 74; placebo: N = 36) (Table 13). Among the 32 screening failures, the most common causes were violation of inclusion and/or exclusion criteria (19; 59.4%), withdrawal of consent (7; 21.9%), inability to participate in study follow-up visits (3; 9.4%), and physician decision or unknown (3; 9.4%). The most common inclusion and/or exclusion criterion violated was extremely poor oral and/or dental condition (9; 28.1%).
The SES-MP and FAS of the MP comprised all 184 patients. The PPS comprised 165 patients (89.7%) (incobotulinumtoxinA 100 U: 85.1%; incobotulinumtoxinA 75 U: 93.2%; placebo: 91.7%). Overall, 11 patients (6.0%) discontinued the study prematurely (incobotulinumtoxinA 100 U: 2.7%; incobotulinumtoxinA 75 U: 6.8%; placebo: 11.1%). The most common reason for discontinuation was withdrawal by patient (4.3%). A higher proportion of patients in the placebo arm discontinued the MP (11.1%) compared with the incobotulinumtoxinA 100 U arm (2.7%).
Table 13: Patient Disposition (SIAXI MP)
Patient disposition | Placebo | IncobotulinumtoxinA 75 U | IncobotulinumtoxinA 100 U | Total |
|---|---|---|---|---|
Screened, N | 216 | |||
Randomized, N (%) | 36 (100.0) | 74 (100.0) | 74 (100.0) | 184 (100.0) |
Treated, n (%) | 36 (100.0) | 74 (100.0) | 74 (100.0) | 184 (100.0) |
Discontinued from study, n (%) | 4 (11.1) | 5 (6.8) | 2 (2.7) | 11 (6.0) |
Reason for discontinuation, n (%)a | ||||
AEs | 1 (2.8) | 1 (1.4) | 1 (1.4) | 3 (1.6) |
Withdrawal by patient | 3 (8.3) | 4 (5.4) | 1 (1.4) | 8 (4.3) |
Physician decision | 1 (2.8) | 0 | 1 (1.4) | 2 (1.1) |
Lost to follow-up | 0 | 0 | 1 (1.4) | 1 (0.5) |
FAS, n (%) | 36 (100.0) | 74 (100.0) | 74 (100.0) | 184 (100.0) |
PPS, n (%) | 33 (91.7) | 69 (93.2) | 63 (85.1) | 165 (89.7) |
SES-MP, n (%) | 36 (100.0) | 74 (100.0) | 74 (100.0) | 184 (100.0) |
AE = adverse event; FAS = full analysis set; MP = main period; PPS = per-protocol set; SES-MP = safety evaluation set, main period.
aMultiple entries possible.
Source: SIAXI Clinical Study Report.8
A total of 173 patients completed the MP and entered the EP (incobotulinumtoxinA 100 U: N = 89; incobotulinumtoxinA 75 U: N = 84) (Table 14). These patients constituted the SES-EP. Overall, 22 patients (12.7%) discontinued the EP (14 patients [15.7%] in the incobotulinumtoxinA 100 U arm and 8 patients [9.5%] in the incobotulinumtoxinA 75 U arm). Among discontinuations during the EP, 10 (5.8%) occurred in cycle 2, 6 (3.5%) occurred during cycle 3, and 6 (3.5%) occurred during cycle 4. The most common reasons given for study discontinuation were AEs (6.9%) and withdrawal by patient (6.9%). A trend toward higher study discontinuation was evident in the incobotulinumtoxinA 100 U arm.
Table 14: Patient Disposition (SIAXI EP)
Patient disposition | IncobotulinumtoxinA 75 U | IncobotulinumtoxinA 100 U | Total incobotulinumtoxinA |
|---|---|---|---|
Completed MP and entered EP, N (%) | 84 (100.0) | 89 (100.0) | 173 (100.0) |
Treated, n (%) | 84 (100.0) | 89 (100.0) | 173 (100.0) |
Discontinued from study, n (%) | 8 (9.5) | 14 (15.7) | 22 (12.7) |
Reason for discontinuation, n (%)a | |||
Death | 3 (3.6) | 2 (2.2) | 5 (2.9) |
AEs | 4 (4.8) | 8 (9.0) | 12 (6.9) |
Lack of efficacy | 0 | 1 (1.1) | 1 (0.6) |
Withdrawal by patient | 4 (4.8) | 8 (9.0) | 12 (6.9) |
Physician decision | 0 | 2 (2.2) | 2 (1.2) |
Other | 1 (1.2) | 0 | 1 (0.6) |
SES-EP, n (%) | 84 (100.0) | 89 (100.0) | 173 (100.0) |
AE = adverse event; EP = extension period; MP = main period; SES-EP = safety evaluation set, extension period.
aMultiple entries possible.
Source: SIAXI Clinical Study Report.8
A total of 19 patients (10.3%) experienced major protocol deviations in the MP and were excluded from the PPS (Table 15). A higher number of major protocol deviations (11; 14.9%) occurred in the incobotulinumtoxinA 100 U arm compared with the placebo arm (3; 8.3%). The most common major protocol deviation was concomitant medication influencing sialorrhea (7; 3.8%). Four patients (5.4%) in the incobotulinumtoxinA 100 U arm but no patients in the placebo arm had no chronic troublesome sialorrhea as measured by the DSFS and mROMP drooling scores. All protocol deviations in the EP were classified as minor.
Table 15: Major Protocol Deviations (SIAXI MP)
Protocol deviationsa | Placebo (N = 36) | IncobotulinumtoxinA 75 U (N = 74) | IncobotulinumtoxinA 100 U (N = 74) | Total (N = 184) |
|---|---|---|---|---|
Exclusion criterion 14 (concomitant medication influencing sialorrhea), n (%) | 1 (2.8) | 2 (2.7) | 4 (5.4) | 7 (3.8) |
Inclusion criterion 5 (chronic troublesome sialorrhea measured by DSFS and mROMP drooling scales), n (%) | 0 | 0 | 4 (5.4) | 4 (2.2) |
Unallowed concomitant medication, n (%) | 0 | 1 (1.4) | 2 (2.7) | 3 (1.6) |
Exclusion criterion 15 (other concomitant medication known to cause hypersalivation), n (%) | 1 (2.8) | 0 | 1 (1.4) | 2 (1.1) |
Efficacy measurement, n (%) | 0 | 1 (1.4) | 1 (1.4) | 2 (1.1) |
GICS visit window deviation, n (%) | 1 (2.8) | 0 | 0 | 1 (0.5) |
Off-state motor fluctuation, n (%) | 0 | 1 (1.4) | 0 | 1 (0.5) |
uSFR visit window deviation, n (%) | 1 (2.8) | 0 | 0 | 1 (0.5) |
DSFS = Drooling Severity and Frequency Scale; GICS = global impression of change scale; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; uSFR = unstimulated salivary flow rate.
aMultiple entries possible.
Source: SIAXI Clinical Study Report.8
Exposure to Study Treatments
Because injections were administered by investigators at study site visits, adherence was 100% in both the MP and EP. Injection was ultrasound-guided in more than 50% of patients treated in both the MP (Table 16) and the EP (Table 17).
Therapy received was according to the randomization schedule for 100% of patients apart from discontinuations, dose reductions, or erroneous treatment. In the MP, all patients received the study drug or placebo as intended; the mean injection cycle length was 16.56 (SD = 1.19) weeks in the placebo arm, 16.13 (SD = 3.11) weeks in the incobotulinumtoxinA 75 U arm, and 16.13 (SD = 2.20) weeks in the incobotulinumtoxinA 100 U arm. In the EP, greater than 97% of patients received the intended dose of incobotulinumtoxinA; only 7 of 173 patients (4.0%) deviated from the planned randomized treatment, 5 (2.9%) because of dose reductions due to AEs and 2 (1.1%) because of missed cycles or erroneous treatment. The mean lengths of injection cycles 2, 3, and 4 were 16.18 week (SD = 1.95), 16.22 weeks (SD = 1.23), and 15.77 weeks (SD = 1.99), respectively, in the incobotulinumtoxinA 75 U arm, and 16.13 weeks (SD = 1.73), 16.21 weeks (SD = 1.29), and 16.46 weeks (SD = 1.92), respectively, in the incobotulinumtoxinA 100 U arm.
Table 16: Injection Guidance (SIAXI MP)
Injection guidance | Placebo (N = 36) | IncobotulinumtoxinA 75 U (N = 74) | IncobotulinumtoxinA 100 U (N = 74) | Total (N = 184) |
|---|---|---|---|---|
Ultrasound-guided, n (%) | 18 (50.0) | 45 (60.8) | 41 (55.4) | 104 (56.5) |
Anatomic landmark–guided, n (%) | 18 (50.0) | 29 (39.2) | 33 (44.6) | 80 (43.5) |
MP = main period.
Source: SIAXI Clinical Study Report.8
Table 17: Injection Guidance (SIAXI EP)
Injection guidance | IncobotulinumtoxinA 75 U (N = 84) | IncobotulinumtoxinA 100 U (N = 89) | Total incobotulinumtoxinA (N = 173) |
|---|---|---|---|
Second injection | N = 83 | N = 89 | N = 172 |
Ultrasound-guided, n (%) | 46 (55.4) | 51 (57.3) | 97 (56.4) |
Anatomic landmark–guided, n (%) | 37 (44.6) | 38 (42.7) | 75 (43.6) |
Third injection | N = 79 | N = 84 | N = 163 |
Ultrasound-guided, n (%) | 42 (53.2) | 47 (56.0) | 89 (54.6) |
Anatomic landmark–guided, n (%) | 37 (46.8) | 37 (44.0) | 74 (45.4) |
Fourth injection | N = 78 | N = 79 | N = 157 |
Ultrasound-guided, n (%) | 42 (53.8) | 45 (57.0) | 87 (55.4) |
Anatomic landmark–guided, n (%) | 36 (46.2) | 34 (43.0) | 70 (44.6) |
EP = extension period.
Source: SIAXI Clinical Study Report.8
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported. Appendix 3 provides detailed efficacy data.
Reduction in Salivary Production
Main Period
As part of the co-primary efficacy analysis, change in the uSFR from baseline to week 4 of the MP was analyzed in each treatment group (Table 18). The LSM change in uSFR in the incobotulinumtoxinA 100 U arm was −0.13 g/min (SE = 0.026; 95% CI, −0.18 to −0.08) compared to −0.04 g/min (SE = 0.033; 95% CI, −0.11 to 0.03) in the placebo arm. There was a statistically significant LSM difference in uSFR in favour of the incobotulinumtoxinA 100 U arm compared with the placebo arm of −0.09 g/min (SE = 0.031; 95% CI, −0.15 to −0.03) (P = 0.004).
Sensitivity analyses of change in the uSFR from baseline to week 4 of the MP in the PPS, and in the FAS and PPS using ANCOVA models and the Wilcoxon rank sum test, produced similar results (Appendix 3). A planned subgroup analysis by the etiology of sialorrhea suggested that the treatment effects of incobotulinumtoxinA 100 U on change in uSFR from baseline to week 4 occurred in both patients with PD/AP and stroke, while the number of patients with TBI was too small to reach any conclusion (Appendix 3). It was unclear from this analysis whether patients with PD/AP and stroke saw similar magnitudes of treatment effects. The subgroup analysis of change in uSFR from baseline to week 4 by baseline severity of sialorrhea was conducted post hoc and therefore was not presented in this report.
Table 18: Change in uSFR from Baseline to Week 4 (SIAXI MP, FAS, MMRM)
uSFR result | IncobotulinumtoxinA 100 U (N = 74) | Placebo (N = 36) |
|---|---|---|
Number of patients contributing to the analysis | 73 | 36 |
Baseline, mean (SD)a | 0.40 (0.27) | 0.38 (0.23) |
Week 4, mean (SD)a | 0.27 (0.18) | 0.36 (0.19) |
Change from baseline, mean (SD)a | −0.12 (0.21) | −0.03 (0.21) |
Change from baseline, LS-mean (SE) (95% CI)b | −0.13 (0.026) (−0.18 to −0.08) | −0.04 (0.033) (−0.11 to 0.03) |
LSM difference vs. placebo (SE) (95% CI) | −0.09 (0.031) (−0.15 to −0.03) | Reference |
P value | 0.004 | — |
CI = confidence interval; FAS = full analysis set; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; SD = standard deviation; SE = standard error; uSFR = unstimulated salivary flow rate.
auSFR in g/min.
bLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and uSFR at baseline included as covariate. For MMRM analysis, visit × treatment is the interaction term and visit is the repeated factor.
Source: SIAXI Clinical Study Report.8
Change in the uSFR from baseline to weeks 8 and 12 of the MP was analyzed as a secondary outcome in each treatment group (Table 19). This analysis was not controlled for multiplicity. At week 8, the LSM change in uSFR in the incobotulinumtoxinA 100 U arm was −0.13 g/min (SE = 0.026; 95% CI, −0.19 to −0.08) compared to −0.02 g/min (SE = 0.033; 95% CI, −0.08 to 0.05) in the placebo arm; the LSM difference in uSFR between the incobotulinumtoxinA 100 U arm and the placebo arm was −0.12 g/min (SE = 0.030; 95% CI, −0.18 to −0.06). At week 12, the LSM change in uSFR in the incobotulinumtoxinA 100 U arm was −0.12 g/min (SE = 0.026; 95% CI, −0.17 to −0.07) compared to −0.03 (SE = 0.033; 95% CI, −0.09 to 0.04) in the placebo arm; the LSM difference in uSFR between the incobotulinumtoxinA 100 U arm and the placebo arm was −0.09 g/min (SE = 0.031; 95% CI, −0.15 to −0.03).
Sensitivity analyses of change in the uSFR from baseline to weeks 8 and 12 of the MP in the PPS, and in the FAS and PPS using ANCOVA models and the Wilcoxon rank sum test, showed similar results, with a trend toward lower differences between the incobotulinumtoxinA 100 U and placebo groups at week 12 (data not shown in this report).
Table 19: Change in uSFR from Baseline to Weeks 8 and 12 (SIAXI MP, FAS, MMRM)
Treatment group | uSFR (g/min) change from baseline LSM (SE) (95% CI)a | uSFR (g/min) vs. placebo LSM difference (SE) (95% CI) | P valueb |
|---|---|---|---|
Change from baseline to week 8 | |||
Placebo (N = 36) | −0.02 (0.033) (−0.08 to 0.05) | Reference | — |
IncobotulinumtoxinA 100 U (N = 73) | −0.13 (0.026) (−0.19 to −0.08) | −0.12 (0.030) (−0.18 to −0.06) | < 0.001 |
Change from baseline to week 12 | |||
Placebo (N = 36) | −0.03 (0.033) (−0.09 to 0.04) | Reference | — |
IncobotulinumtoxinA 100 U (N = 73) | −0.12 (0.026) (−0.17 to −0.07) | −0.09 (0.031) (−0.15 to −0.03) | 0.004 |
CI = confidence interval; FAS = full analysis set; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; SE = standard error; uSFR = unstimulated salivary flow rate.
aLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and uSFR at baseline included as the covariate. For the MMRM analysis, visit × treatment is the interaction term and visit is the repeated factor.
bAnalysis not controlled for multiplicity.
Source: SIAXI Clinical Study Report.8
The change in the uSFR from baseline to week 16 of the MP was an exploratory outcome (Table 20). This analysis was not controlled for multiplicity. The LSM change in uSFR in the incobotulinumtoxinA 100 U arm was −0.11 g/min (SE = 0.027; 95% CI, −0.17 to −0.06) compared to −0.01 g/min (SE = 0.035; 95% CI, −0.08 to 0.05) in the placebo arm. The LSM difference in uSFR between the incobotulinumtoxinA 100 U arm and the placebo arm was −0.10 g/min (SE = 0.033; 95% CI, −0.17 to −0.04).
Table 20: Change in uSFR from Baseline to Week 16 (SIAXI MP, FAS, MMRM)
Treatment group | uSFR (g/min) change from baseline LSM (SE) (95% CI)a | uSFR (g/min) LSM difference (SE) (95% CI) vs. placebo | P valueb |
|---|---|---|---|
Placebo (N = 36) | −0.01 (0.035) (−0.08 to 0.06) | Reference | — |
IncobotulinumtoxinA 100 U (N = 73) | −0.11 (0.027) (−0.17 to −0.06) | −0.10 (0.033) (−0.17 to −0.04) | 0.002 |
CI = confidence interval; FAS = full analysis set; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; SE = standard error; uSFR = unstimulated salivary flow rate.
aLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and uSFR at baseline included as the covariate. For the MMRM analysis, visit × treatment is the interaction term and visit is the repeated factor.
bAnalysis not controlled for multiplicity.
Source: SIAXI Clinical Study Report.8
Extension Period
The change in uSFR from baseline to each visit in the EP, as well as change from the prior injection, was assessed in an exploratory fashion (Table 21). This analysis was not controlled for multiplicity. Mean decreases (improvements) in uSFR from study baseline and from the baseline for each cycle were observed at each visit in the EP for the incobotulinumtoxinA 100 U treatment arm (Table 35). The magnitude of changes in uSFR from baseline was larger than the magnitude of changes from any of the individual cycles in the EP.
Table 21: Change in uSFR from Study Baseline to All Visits in the EP, and Change From Each Injection Visit to the Respective Assessment and End-of-Cycle Visits (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) | |
|---|---|---|
n | Mean (SD)a | |
Change from study baseline to | ||
Cycle 2 baseline | 89 | −0.08 (0.21) |
Cycle 2 week 4 | 88 | −0.14 (0.27) |
Cycle 2 week 16 | 85 | −0.14 (0.24) |
Cycle 3 baseline | 84 | −0.14 (0.24) |
Cycle 3 week 4 | 84 | −0.17 (0.25) |
Cycle 3 week 16 | 81 | −0.17 (0.23) |
Cycle 4 baseline | 78 | −0.15 (0.21) |
Cycle 4 week 4 | 77 | −0.20 (0.22) |
Cycle 4 week 16 | 74 | −0.16 (0.22) |
End of study | 80 | −0.16 (0.22) |
Change from cycle 2 baseline to | ||
Cycle 2 week 4 | 88 | −0.06 (0.19) |
Cycle 2 week 16 | 85 | −0.06 (0.14) |
Change from cycle 3 baseline to | ||
Cycle 3 week 4 | 84 | −0.03 (0.13) |
Cycle 3 week 16 | 81 | −0.02 (0.14) |
Change from cycle 4 baseline to | ||
Cycle 4 week 4 | 77 | −0.05 (0.12) |
Cycle 4 week 16 | 74 | −0.01 (0.13) |
EP = extension period; OC = observed cases; SD = standard deviation; uSFR = unstimulated salivary flow rate.
auSFR measured in g/min.
Source: SIAXI Clinical Study Report.8
Mean uSFR values over the entire course of the study at all assessment visits are shown graphically in Appendix 3.
Change in Patient and Caregiver Perceived Frequency and Severity of Sialorrhea
Main Period
Patient GICS Score
As part of the co-primary efficacy analysis, patient GICS scores at week 4 of the MP was analyzed in each treatment group (Table 22). The LSM patient GICS score in the incobotulinumtoxinA 100 U arm was 1.25 (SE = 0.144; 95% CI, 0.97 to 1.53) compared to 0.67 (SE = 0.186; 95% CI, 0.30 to 1.04) in the placebo arm. The LSM difference in GICS scores was statistically significantly in favour of the incobotulinumtoxinA 100 U arm compared with the placebo arm of 0.58 (SE = 0.183; 95% CI, 0.22 to 0.94; P = 0.002).
Sensitivity analyses of patient GICS scores at week 4 of the MP in the PPS, and in the FAS and PPS using ANCOVA models, produced similar results (Appendix 3). A planned subgroup analysis by the etiology of sialorrhea suggested that the treatment effects of incobotulinumtoxinA 100 U on both co-primary efficacy outcomes occurred in both patients with PD/AP and stroke, while the number of patients with TBI was too small to reach a conclusion (Appendix 3). It was unclear from this analysis whether patients with PD/AP and stroke saw similar magnitudes of treatment effects. The subgroup analysis of patients GICS at week 4 by baseline severity of sialorrhea was conducted post hoc and therefore is not presented in this report.
Table 22: Patient GICS at Week 4 (SIAXI MP, FAS, MMRM)
GICS Result | IncobotulinumtoxinA 100 U (N = 74) | Placebo (N = 36) |
|---|---|---|
Number of patients contributing to the analysis | 73 | 36 |
Week 4, mean (SD)a | 1.04 (1.03) | 0.47 (0.84) |
LSM (SE) (95% CI)b | 1.25 (0.144) (0.97 to 1.53) | 0.67 (0.186) (0.30 to 1.04) |
LSM difference vs. placebo (SE) (95% CI) | 0.58 (0.183) (0.22 to 0.94) | Reference |
P value | 0.002 | — |
CI = confidence interval; FAS = full analysis set; GICS = Global Impression of Change Scale; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; SD = standard deviation; SE = standard error.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
bLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and Drooling Severity and Frequency Scale sum score at baseline included as the covariate. For the MMRM analysis, visit × treatment is the interaction term and visit is the repeated factor.
Source: SIAXI Clinical Study Report.8
The LSM difference in GICS scores at week 4 of the MP between the incobotulinumtoxinA 100 U and the placebo treatment groups in the primary efficacy analysis resulted from decreased numbers of patients treated with incobotulinumtoxinA 100 U responding with “no change in function” (placebo: 50.0%; incobotulinumtoxinA 100 U: 20.3%) and increased numbers of patients selecting “minimally improved function” or “much improved function” (Table 23). At week 4, the category showing the largest difference between treatment groups was a GICS score of 2, “much improved function” (placebo: 11.1%; incobotulinumtoxinA 100 U: 28.4%).
Table 23: Frequencies of Patient GICS Responses at Week 4 (SIAXI MP, FAS)
GICS Responses | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) |
|---|---|---|
Missing, n (%) | 0 | 1 (1.4) |
−3, very much worse function, n (%) | 0 | 0 |
−2, much worse function, n (%) | 1 (2.8) | 1 (1.4) |
−1, minimally worse function, n (%) | 1 (2.8) | 4 (5.4) |
0, no change in function, n (%) | 18 (50.0) | 15 (20.3) |
1, minimally improved function, n (%) | 12 (33.3) | 28 (37.8) |
2, much improved function, n (%) | 4 (11.1) | 21 (28.4) |
3, very much improved function, n (%) | 0 | 4 (5.4) |
FAS = full analysis set; GICS = Global Impression of Change Scale; MP = main period.
Source: SIAXI Clinical Study Report.8
Patient GICS scores at weeks 1, 2, 8, and 12 of the MP were analyzed as a secondary outcome in each treatment group (Table 24). This analysis was not controlled for multiplicity. At week 1, the LSM GICS score in the incobotulinumtoxinA 100 U arm was 0.96 (SE = 0.133; 95% CI, 0.70 to 1.23) compared to 0.67 (SE = 0.170; 95% CI, 0.34 to 1.00) in the placebo arm; the LSM difference in GICS score between the incobotulinumtoxinA 100 U arm and the placebo arm was 0.29 (SE = 0.158; 95% CI, −0.02 to 0.60). At week 2, the LSM GICS score in the incobotulinumtoxinA 100 U arm was 1.11 (SE = 0.139; 95% CI, 0.84 to 1.38) compared to 0.83 (SE = 0.178; 0.47 to 1.18) in the placebo arm; the LSM difference in GICS between the incobotulinumtoxinA 100 U arm and the placebo arm was 0.29 (SE = 0.171; 95% CI, −0.05 to 0.62). At week 8, the LSM GICS score in the incobotulinumtoxinA 100 U arm was 1.30 (SE = 0.148; 95% CI, 1.01 to 1.59) compared to 0.47 (SE = 0.192; 95% CI, 0.09 to 0.84) in the placebo arm; the LSM difference in GICS score between the incobotulinumtoxinA 100 U arm and the placebo arm was 0.84 (SE = 0.192; 95% CI, 0.46 to 1.21). At week 12, the LSM GICS score in the incobotulinumtoxinA 100 U arm was 1.21 (SE = 0.152; 95% CI, 0.91 to 1.51) compared to 0.56 (SE = 0.197; 95% CI, 0.17 to 0.95) in the placebo arm; the LSM difference in GICS scores between the incobotulinumtoxinA 100 U arm and the placebo arm was 0.65 (SE = 0.201; 95% CI, 0.25 to 1.04).
Sensitivity analyses of patient GICS scores at weeks 1, 2, 8, and 12 of the MP in the PPS, and in the FAS and PPS using ANCOVA models and the Wilcoxon rank sum test, showed similar results, with a trend toward smaller differences between the incobotulinumtoxinA 100 U and placebo groups at week 12 (data not shown in this report).
Table 24: Patient GICS at Weeks 1, 2, 8, and 12 (SIAXI MP, FAS, MMRM)
Treatment group | GICSa LSMs (SE) (95% CI)b | GICSb LSM difference (SE) (95% CI) vs. placebo | P valuec |
|---|---|---|---|
Week 1 | |||
Placebo (N = 36) | 0.67 (0.170) (0.34 to 1.00) | Reference | — |
IncobotulinumtoxinA 100 U (N = 74) | 0.96 (0.133) (0.70 to 1.23) | 0.29 (0.158) (−0.02 to 0.60) | 0.065 |
Week 2 | |||
Placebo (N = 36) | 0.83 (0.178) (0.47 to 1.18) | Reference | — |
IncobotulinumtoxinA 100 U (N = 74) | 1.11 (0.139) (0.84 to 1.38) | 0.29 (0.171) (−0.05 to 0.62) | 0.096 |
Week 8 | |||
Placebo (N = 36) | 0.47 (0.192) (0.09 to 0.84) | Reference | — |
IncobotulinumtoxinA 100 U (N = 74) | 1.30 (0.148) (1.01 to 1.59) | 0.84 (0.192) (0.46 to 1.21) | < 0.001 |
Week 12 | |||
Placebo (N = 36) | 0.56 (0.197) (0.17 to 0.95) | Reference | — |
IncobotulinumtoxinA 100 U (N = 74) | 1.21 (0.152) (0.91 to 1.51) | 0.65 (0.201) (0.25 to 1.04) | 0.001 |
CI = confidence interval; FAS = full analysis set; GICS = Global Impression of Change Scale; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; SE = standard error.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
bLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and Drooling Severity and Frequency Scale sum score at baseline included as the covariate. For the MMRM analysis, visit × treatment is the interaction term and visit is the repeated factor.
cAnalysis not controlled for multiplicity.
Source: SIAXI Clinical Study Report.8
The LSM differences in patient GICS at weeks 8 and 12 between the incobotulinumtoxinA 100 U and the placebo treatment groups in the secondary efficacy analysis resulted from decreased numbers of patients treated with incobotulinumtoxinA 100 U responding with “no change in function” (week 8, placebo: 61.1%; incobotulinumtoxinA 100 U: 18.9%; week 12, placebo: 50.0%; incobotulinumtoxinA 100 U: 20.3%) and increased numbers of patients selecting “minimally improved function” or “much improved function” (Table 25). At weeks 8 and 12, the category showing the largest difference between treatment groups was a GICS score of 2, “much improved function” (week 8, placebo: 8.3%; incobotulinumtoxinA 100 U: 31.1%; week 12, placebo: 11.1%; incobotulinumtoxinA 100 U: 31.1%).
Table 25: Frequencies of Patient GICS Responses at Weeks 1, 2, 8, and 12 (SIAXI MP, FAS)
GICS Responses | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) |
|---|---|---|
Week 1 | ||
Missing, n (%) | 0 | 0 |
−3, very much worse function, n (%) | 0 | 0 |
−2, much worse function, n (%) | 0 | 0 |
−1, minimally worse function, n (%) | 0 | 3 (4.1) |
0, no change in function, n (%) | 23 (63.9) | 27 (36.5) |
1, minimally improved function, n (%) | 9 (25.0) | 29 (39.2) |
2, much improved function, n (%) | 4 (11.1) | 15 (20.3) |
3, very much improved function, n (%) | 0 | 0 |
Week 2 | ||
Missing, n (%) | 1 (2.8) | 0 |
−3, very much worse function, n (%) | 0 | 0 |
−2, much worse function, n (%) | 0 | 0 |
−1, minimally worse function, n (%) | 1 (2.8) | 2 (2.7) |
0, no change in function, n (%) | 17 (47.2) | 23 (31.1) |
1, minimally improved function, n (%) | 12 (33.3) | 30 (40.5) |
2, much improved function, n (%) | 4 (11.1) | 18 (24.3) |
3, very much improved function, n (%) | 1 (2.8) | 1 (1.4) |
Week 8 | ||
Missing, n (%) | 1 (2.8) | 2 (2.7) |
−3, very much worse function, n (%) | 0 | 0 |
−2, much worse function, n (%) | 1 (2.8) | 0 |
−1, minimally worse function, n (%) | 2 (5.6) | 3 (4.1) |
0, no change in function, n (%) | 22 (61.1) | 14 (18.9) |
1, minimally improved function, n (%) | 7 (19.4) | 29 (39.2) |
2, much improved function, n (%) | 3 (8.3) | 23 (31.1) |
3, very much improved function, n (%) | 0 | 4 (4.1) |
Week 12 | ||
Missing, n (%) | 0 | 2 (2.7) |
−3, very much worse function, n (%) | 0 | 0 |
−2, much worse function, n (%) | 1 (2.8) | 2 (2.7) |
−1, minimally worse function, n (%) | 3 (8.3) | 4 (5.4) |
0, no change in function, n (%) | 18 (50.0) | 15 (20.3) |
1, minimally improved function, n (%) | 10 (27.8) | 25 (33.8) |
2, much improved function, n (%) | 4 (11.1) | 23 (31.1) |
3, very much improved function, n (%) | 0 | 3 (4.1) |
FAS = full analysis set; GICS = Global Impression of Change Scale; MP = main period.
Source: SIAXI Clinical Study Report.8
Patient GICS scores at week 16 of the MP were analyzed as an exploratory outcome (Table 26). This analysis was not controlled for multiplicity. The LSM GICS score in the incobotulinumtoxinA 100 U arm was 0.93 (SE = 0.152; 95% CI, 0.63 to 1.23) compared to 0.41 (SE = 0.199; 95% CI, 0.02 to 0.080) in the placebo arm. The LSM difference in GICS score between the incobotulinumtoxinA 100 U arm and the placebo arm was 0.52 (SE = 0.203; 95% CI, 0.12 to 0.92).
Table 26: Patient GICS at Week 16 (SIAXI MP, FAS, MMRM)
Treatment group | GICSa LSMs (SE) (95% CI)b | GICSb LSM difference (SE) (95% CI) vs. placebo | P valuec |
|---|---|---|---|
Placebo (N = 36) | 0.41 (0.199) (0.02 to 0.080) | Reference | — |
IncobotulinumtoxinA 100 U (N = 74) | 0.93 (0.152) (0.63 to 1.23) | 0.52 (0.203) (0.12 to 0.92) | 0.011 |
CI = confidence interval; FAS = full analysis set; GICS = Global Impression of Change Scale; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; SE = standard error.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
bLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and Drooling Severity and Frequency Scale sum score at baseline included as the covariate. For the MMRM analysis, visit × treatment is the interaction term and visit is the repeated factor.
cAnalysis not controlled for multiplicity.
Source: SIAXI Clinical Study Report.8
GICS Responder Rate
The proportion of responders (GICS score ≥ 1) based on patient GICS responses at all assessment visits and telephone interviews during the MP was analyzed in an exploratory fashion (Table 27). This analysis was not controlled for multiplicity. The proportion of responders ranged from 59.5% (week 1) to 76.4% (week 8) in the incobotulinumtoxinA 100 U group and from 28.6% (week 8) to 48.6% (week 2) in the placebo group. The largest differences in GICS response rates between the incobotulinumtoxinA 100 U arm and placebo arm were observed at weeks 4 (72.6% versus 44.4%), 8 (76.4% versus 28.6%), and 12 (70.8% versus 38.9%).
Table 27: Number of Responders Based on Patient GICS at Weeks 1, 2, 4, 8, 12, and 16 (SIAXI MP, FAS, OC)
Week | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | |
|---|---|---|---|
n (%) | n (%) | P valuea | |
Week 1 (TC) | 13 (36.1) | 44 (59.5) | 0.026 |
Week 2 (TC) | 17 (48.6) | 49 (66.2) | 0.095 |
Week 4 | 16 (44.4) | 53 (72.6) | 0.006 |
Week 8 | 10 (28.6) | 55 (76.4) | < 0.001 |
Week 12 | 14 (38.9) | 51 (70.8) | 0.002 |
Week 16 | 14 (40.0) | 43 (59.7) | 0.065 |
FAS = full analysis set; GICS = global impression of change scale; MP, main period; OC = observed cases; TC = telephone call.
Note: Responder was defined as a GICS entry of at least 1 (minimally improved function).
aFisher’s exact test vs. placebo. Analysis not controlled for multiplicity.
Source: SIAXI Clinical Study Report.8
Carer GICS Score
Carer GICS entries were analyzed in an exploratory fashion at all assessments and telephone interviews during the MP (Table 28). This analysis was not controlled for multiplicity. As for patient GICS entries, mean carer GICS scores were higher at all time points in the incobotulinumtoxinA 100 U arm compared to the placebo arm, notably at week 4 (1.14 [SD = 0.98] versus 0.48 [SD = 0.83]), week 8 (1.20 [SD = 0.87] versus 0.32 [SD = 0.86]), and week 12 (1.05 [SD = 1.02] versus 0.30 [SD = 0.87]).
Table 28: Carer GICS at Weeks 1, 2, 4, 8, 12 and 16 (SIAXI MP, FAS, OC)
Week | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | ||
|---|---|---|---|---|
n | Mean (SD)a | n | Mean (SD)a | |
Week 1 (TC) | 30 | 0.57 (0.82) | 59 | 0.69 (0.93) |
Week 2 (TC) | 30 | 0.67 (0.84) | 59 | 0.90 (0.90) |
Week 4 | 29 | 0.48 (0.83) | 58 | 1.14 (0.98) |
Week 8 | 28 | 0.32 (0.86) | 59 | 1.20 (0.87) |
Week 12 | 27 | 0.30 (0.87) | 60 | 1.05 (1.02) |
Week 16 | 27 | 0.41 (0.97) | 57 | 0.95 (0.99) |
FAS = full analysis set; GICS = Global Impression of Change Scale; MP = main period; OC = observed cases; SD = standard deviation; TC = telephone call.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
Source: SIAXI Clinical Study Report.8
mROMP Speech and Drooling Scores
Main Period
Changes in mROMP speech scores from baseline were analyzed in exploratory fashion at weeks 4, 8, 12, and 16 in the MP (Table 29). This analysis was not controlled for multiplicity. Similarly modest improvements in mROMP speech symptoms from baseline were observed in both the incobotulinumtoxinA 100 U group and the placebo group at all time points.
Table 29: Change in mROMP Speech Symptoms from Baseline to Weeks 4, 8, 12, and 16 (SIAXI MP, FAS, OC)
Week | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | ||
|---|---|---|---|---|
n | Mean (SD)a | N | Mean (SD)a | |
Week 4 | 36 | −0.56 (2.57) | 72 | −0.11 (2.65) |
Week 8 | 35 | −0.43 (3.62) | 72 | −0.50 (2.73) |
Week 12 | 35 | −0.34 (2.92) | 72 | −0.75 (2.96) |
Week 16 | 35 | −0.63 (3.41) | 72 | −0.29 (3.20) |
FAS = full analysis set; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; OC = observed cases; SD = standard deviation.
aScores ranges from 8 (best) to 40 (worst).
Source: SIAXI Clinical Study Report.8
Changes in mROMP drooling scores from baseline were analyzed in an exploratory fashion for each treatment group at weeks 4, 8, 12, and 16 in the MP (Table 30). This analysis was not controlled for multiplicity. The greatest differences in the mean decreases in mROMP drooling scores in the incobotulinumtoxinA 100 U arm compared to the placebo arm were observed at week 8 (−6.58 [SD = 5.90] versus −1.26 [SD = 4.91]) and week 12 (−6.40 [SD = 5.20] versus −1.77 [SD = 4.54]).
Table 30: Change in mROMP Drooling Scores from Study Baseline to Weeks 4, 8, 12, and 16 (SIAXI MP, FAS, OC)
Week | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | ||
|---|---|---|---|---|
n | Mean (SD)a | N | Mean (SD)a | |
Week 4 | 36 | −1.00 (4.71) | 72 | −5.66 (6.16) |
Week 8 | 35 | −1.26 (4.91) | 72 | −6.58 (5.90) |
Week 12 | 35 | −1.77 (4.54) | 72 | −6.40 (5.20) |
Week 16 | 35 | −1.46 (5.03) | 72 | −4.61 (5.40) |
FAS = full analysis set; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; OC = observed cases; SD = standard deviation.
aScores ranges from 9 (best) to 45 (worst).
Source: SIAXI Clinical Study Report.8
Extension Period
Patient GICS Score
Patient GICS scores at each visit in the EP were assessed in an exploratory fashion (Table 31). This analysis was not controlled for multiplicity. Positive GICS values (improvements) were observed for the incobotulinumtoxinA 100 U arm at all visits in the EP. The magnitudes of mean patient GICS responses for the EP was similar to that observed during the MP. Patient GICS tended to peak at weeks 4 and 8 of each cycle (note that GICS referred to changes compared with the previous injection).
Table 31: Patient GICS at all Assessment Visits in the EP, at the End-of-Study Visit, and at All Telephone Contacts (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) | |
|---|---|---|
n | Mean (SD)a | |
Cycle 2 week 1 (TC) | 89 | 0.98 (1.02) |
Cycle 2 week 2 (TC) | 88 | 1.28 (0.88) |
Cycle 2 week 4 | 88 | 1.18 (1.16) |
Cycle 2 week 8 (TC) | 88 | 1.27 (1.01) |
Cycle 2 week 16 | 85 | 0.62 (1.41) |
Cycle 3 week 4 | 84 | 1.13 (1.34) |
Cycle 3 week 8 (TC) | 84 | 1.23 (1.21) |
Cycle 3 week 16 | 81 | 0.86 (1.36) |
Cycle 4 week 4 | 77 | 1.40 (1.14) |
Cycle 4 week 8 (TC) | 77 | 1.40 (1.10) |
Cycle 4 week 16 | 74 | 1.36 (1.14) |
End of study | 80 | 1.31 (1.20) |
EP = extension period; GICS = global impression of change scale; OC = observed cases; SD = standard deviation; TC = telephone call.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
Source: SIAXI Clinical Study Report.8
GICS Responder Rate
The number of responders based on patient GICS entries (score ≥ 1) at each visit in the EP was assessed in an exploratory fashion (Table 32). This analysis was not controlled for multiplicity. Response rates in the incobotulinumtoxinA 100 U arm ranged from 58.4% to 80.9% throughout the EP and tended to peak at weeks 4 and 8 of each cycle (GICS referred to changes compared with the previous injection).
Table 32: Number of Responders Based on Patient GICS at all Assessment Visits in the EP, at the End-of-Study Visit, and at All Telephone Contacts (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) |
|---|---|
n (%) | |
Cycle 2 week 1 (TC) | 62 (69.7) |
Cycle 2 week 2 (TC) | 71 (79.8) |
Cycle 2 week 4 | 72 (80.9) |
Cycle 2 week 8 (TC) | 69 (77.5) |
Cycle 2 week 16 | 52 (58.4) |
Cycle 3 week 4 | 61 (72.6) |
Cycle 3 week 8 (TC) | 61 (72.6) |
Cycle 3 week 16 | 51 (60.7) |
Cycle 4 week 4 | 60 (76.9) |
Cycle 4 week 8 (TC) | 60 (76.9) |
Cycle 4 week 16 | 55 (70.5) |
End of study | 58 (65.2) |
EP = extension period; GICS = Global Impression of Change Scale; OC = observed cases; TC = telephone call.
Note: Responder was defined as a GICS entry of at least 1 (minimally improved function).
Source: SIAXI Clinical Study Report.8
Carer GICS Score
Carer GICS scores at each visit in the EP were assessed in an exploratory fashion (Table 33). This analysis was not controlled for multiplicity. Positive carer GICS values (improvements) were observed for the incobotulinumtoxinA 100 U arm for all visits in the EP. The magnitudes of carer patient GICS responses for the EP were similar to those observed during the MP. Carer GICS scores tended to peak at weeks 4 and 8 of each cycle (GICS referred to changes compared with the previous injection).
Table 33: Carer GICS at all Assessment Visits in the EP, at the End-of-Study Visit, and at All Telephone Contacts (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) | |
|---|---|---|
n | Mean (SD)a | |
Cycle 2 week 1 (TC) | 69 | 1.07 (1.02) |
Cycle 2 week 2 (TC) | 69 | 1.36 (1.01) |
Cycle 2 week 4 | 67 | 1.22 (1.28) |
Cycle 2 week 8 (TC) | 69 | 1.33 (1.02) |
Cycle 2 week 16 | 65 | 0.65 (1.35) |
Cycle 3 week 4 | 65 | 1.28 (1.22) |
Cycle 3 week 8 (TC) | 67 | 1.27 (1.29) |
Cycle 3 week 16 | 63 | 0.79 (1.43) |
Cycle 4 week 4 | 59 | 1.42 (1.12) |
Cycle 4 week 8 (TC) | 61 | 1.44 (1.04) |
Cycle 4 week 16 | 56 | 1.38 (1.09) |
End of study | 60 | 1.38 (1.09) |
EP = extension period; GICS = global impression of change scale; OC = observed cases; SD = standard deviation; TC = telephone call.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
Source: SIAXI Clinical Study Report.8
mROMP Speech and Drooling Scores
Changes in mROMP speech scores from study baseline to all assessment visits in the EP were analyzed in an exploratory fashion (Table 34). This analysis was not controlled for multiplicity. The mROMP speech scores for the incobotulinumtoxinA 100 U treatment group remained generally stable over the course of the entire EP.
Table 34: Change in mROMP Speech Symptoms From Study Baseline to All Assessment Visits (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) | |
|---|---|---|
n | Mean (SD)a | |
Change from baseline to | ||
Cycle 2 week 4 | 88 | −0.68 (3.70) |
Cycle 3 week 4 | 84 | 0.00 (3.93) |
Cycle 4 week 4 | 77 | −0.39 (4.47) |
EP = extension period; mROMP = modified Radboud oral motor inventory for Parkinson disease; OC = observed cases; SD = standard deviation.
aScores ranges from 8 (best) to 40 (worst).
Source: SIAXI Clinical Study Report.8
Changes in mROMP drooling scores from study baseline to all assessment visits in the EP were analyzed in an exploratory fashion (Table 35). This analysis was not controlled for multiplicity. Mean decreases (improvements) in mROMP drooling scores were observed at the week 4 visits for the incobotulinumtoxinA 100 U treatment arm at each injection cycle compared with baseline. Magnitudes of changes in mROMP drooling scores were similar or greater to those observed during the MP.
Table 35: Change in mROMP Drooling Scores from Study Baseline to All Assessment Visits in the EP (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) | |
|---|---|---|
n | Mean (SD)a | |
Change from baseline to | ||
Cycle 2 week 4 | 88 | −8.43 (6.48) |
Cycle 3 week 4 | 84 | −9.07 (7.70) |
Cycle 4 week 4 | 77 | −10.38 (7.56) |
EP = extension period; mROMP = modified Radboud oral motor inventory for Parkinson disease; OC = observed cases; SD = standard deviation.
aScores ranges from 9 (best) to 45 (worst).
Source: SIAXI Clinical Study Report.8
Change in Clinician-Perceived Frequency and Severity of Sialorrhea
Main Period
Changes from baseline in DSFS sum scores at weeks 4, 8, 12, and 16 were exploratory end points in the MP (Table 36). This analysis was not controlled for multiplicity. At week 4, the LSM change in DSFS sum score in the incobotulinumtoxinA 100 U arm was −1.66 (SE = 0.234; 95% CI, −2.12 to −1.20) compared to −0.50 (SE = 0.296; 95% CI, −1.08 to 0.09) in the placebo arm; the LSM difference in DSFS sum score between the incobotulinumtoxinA 100 U arm and the placebo arm was −1.17 (SE = 0.278; 95% CI, −1.71 to −0.72). At week 8, the LSM change in DSFS sum score in the incobotulinumtoxinA 100 U arm was −1.97 (SE = 0.239; 95% CI, −2.44 to −1.49) compared to −0.68 (SE = 0.305; 95% CI, −1.28 to −0.08) in the placebo arm; the LSM difference in DSFS sum score between the incobotulinumtoxinA 100 U arm and the placebo arm was −1.29 (SE = 0.291; 95% CI, −1.86 to −0.71). At week 12, the LSM change in DSFS sum score in the incobotulinumtoxinA 100 U arm was −1.62 (SE = 0.237; 95% CI, −2.09 to −1.16) compared to −1.00 (SE = 0.301; 95% CI, −1.59 to −0.40) in the placebo arm; the LSM difference in DSFS sum score between the incobotulinumtoxinA 100 U arm and the placebo arm was −0.63 (SE = 0.286; 95% CI, −1.19 to −0.06). At week 16, the LSM change in DSFS sum score in the incobotulinumtoxinA 100 U arm was −1.18 (SE = 0.232; 95% CI, −1.64 to −0.73) compared to −0.75 (SE = 0.294; 95% CI, −1.33 to −0.17) in the placebo arm; the LSM difference in DSFS sum score between the incobotulinumtoxinA 100 U arm and the placebo arm was −0.43 (SE = 0.275; 95% CI, −0.98 to 0.11).
Table 36: Change in DSFS Sum Score from Baseline to Weeks 4, 8, 12, and 16 (SIAXI MP, FAS, MMRM)
Treatment group | DSFS sum scorea Change from baseline LSM (SE) (95% CI)b | DSFS sum scoreb LSM difference (SE) (95% CI) vs. placebo | P valuec |
|---|---|---|---|
Change from baseline to week 4 | |||
Placebo (N = 36) | −0.50 (0.296) (−1.08 to 0.09) | Reference | — |
IncobotulinumtoxinA 100 U (N = 73) | −1.66 (0.234) (−2.12 to −1.20) | −1.17 (0.278) (−1.71 to −0.62) | < 0.001 |
Change from baseline to week 8 | |||
Placebo (N = 36) | −0.68 (0.305) (−1.28 to −0.08) | Reference | — |
IncobotulinumtoxinA 100 U (N = 73) | −1.97 (0.239) (−2.44 to −1.49) | −1.29 (0.291) (−1.86 to −0.71) | < 0.001 |
Change from baseline to week 12 | |||
Placebo (N = 36) | −1.00 (0.301) (−1.59 to −0.40) | Reference | — |
IncobotulinumtoxinA 100 U (N = 73) | −1.62 (0.237) (−2.09 to −1.16) | −0.63 (0.286) (−1.19 to −0.06) | 0.030 |
Change from baseline to week 16 | |||
Placebo (N = 36) | −0.75 (0.294) (−1.33 to −0.17) | Reference | — |
IncobotulinumtoxinA 100 U (N = 73) | −1.18 (0.232) (−1.64 to −0.73) | −0.43 (0.275) (−0.98 to 0.11) | 0.116 |
CI = confidence interval; DSFS = Drooling Severity and Frequency Scale; FAS = full analysis set; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; SE = standard error.
aDSFS sum scores range from 2 (best) to 9 (worst).
bLSMs are from the model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and DSFS sum score at baseline included as the covariate. For the MMRM analysis, visit × treatment is the interaction term and visit is the repeated factor.
cAnalysis not controlled for multiplicity.
Source: SIAXI Clinical Study Report.8
Changes from baseline in DSFS severity and frequency scores were exploratory end points in the MP (Table 37). This analysis was not controlled for multiplicity. Mean decreases in DSFS severity scores were of greater magnitude in the incobotulinumtoxinA 100 U arm compared with the placebo arm, particularly at week 4 (−1.06 [SD = 1.03] versus −0.37 [SD = 0.77]) and week 8 (−0.92 [SD = 1.00] versus −0.64 [SD = 0.87]). Mean decreases in DSFS frequency scores were of greater magnitude in the incobotulinumtoxinA 100 U arm compared with the placebo arm, particularly at week 4 (−0.71 [SD = 0.70] versus −0.22 [SD = 0.64]) and week 8 (−0.83 [SD = 0.73] versus −0.22 [SD = 0.64]).
Table 37: Change in DSFS Subscores from Baseline to Weeks 4, 8, 12, and 16 (SIAXI MP, FAS, OC)
Week | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | ||
|---|---|---|---|---|
n | Mean (SD) | n | Mean (SD) | |
Severitya | ||||
Week 4 | 36 | −0.31 (0.75) | 73 | −0.86 (1.05) |
Week 8 | 35 | −0.37 (0.77) | 72 | −1.06 (1.03) |
Week 12 | 36 | −0.64 (0.87) | 72 | −0.92 (1.00) |
Week 16 | 35 | −0.40 (0.91) | 72 | −0.67 (0.95) |
Frequencyb | ||||
Week 4 | 36 | −0.22 (0.64) | 73 | −0.71 (0.70) |
Week 8 | 35 | −0.34 (0.59) | 72 | −0.83 (0.73) |
Week 12 | 36 | −0.39 (0.69) | 72 | −0.63 (0.72) |
Week 16 | 35 | −0.37 (0.55) | 72 | −0.43 (0.69) |
DSFS = Drooling Severity and Frequency Scale; FAS = full analysis set; MP = main period; OC = observed cases; SD = standard deviation.
aSeverity: 1 = dry (never drools), 2 = mild (only lips wet), 3 = moderate (wet on lips and chin), 4 = severe (drool extends to clothes wet), 5 = profuse (hands, tray, and objects wet).
bFrequency: 1 = never, 2 = occasionally (not every day), 3 = frequently (part of every day), 4 = constantly.
Source: SIAXI Clinical Study Report.8
Extension Period
Changes from baseline to each visit in the EP for DSFS sum scores as well as severity and frequency scores were assessed in an exploratory fashion (Table 38). This analysis was not controlled for multiplicity. Sum scores and subscores for the DSFS and decreased (improved), from study baseline to the week 4 visit for the incobotulinumtoxinA 100 U treatment arm at each injection cycle. Magnitudes of changes in DSFS sum scores were similar or greater to those observed during the MP.
Table 38: Change in DSFS Sum Scores and Subscores from Baseline to All Assessment Visits in the EP (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) | |
|---|---|---|
n | Mean (SD) | |
Sum scorea | ||
Change from baseline to | ||
Cycle 2 week 4 | 88 | −2.34 (1.55) |
Cycle 3 week 4 | 84 | −2.64 (1.56) |
Cycle 4 week 4 | 77 | −3.04 (1.71) |
Severityb | ||
Change from baseline to | ||
Cycle 2 week 4 | 88 | −1.28 (1.05) |
Cycle 3 week 4 | 84 | −1.50 (1.12) |
Cycle 4 week 4 | 77 | −1.70 (1.08) |
Frequencyc | ||
Change from baseline to | ||
Cycle 2 week 4 | 88 | −1.06 (0.75) |
Cycle 3 week 4 | 84 | −1.14 (0.70) |
Cycle 4 week 4 | 77 | −1.34 (0.87) |
DSFS = Drooling Severity and Frequency Scale; EP = extension period; OC = observed cases; SD = standard deviation.
aDSFS sum score ranges from 2 (best) to 9 (worst).
bSeverity: 1 = dry (never drools), 2 = mild (only lips wet), 3 = moderate (wet on lips and chin), 4 = severe (drool extends to clothes wet), 5 = profuse (hands, tray, and objects wet).
cFrequency: 1 = never, 2 = occasionally (not every day), 3 = frequently (part of every day), 4 = constantly.
Source: SIAXI Clinical Study Report.8
Health-Related Quality of Life
Main Period
Changes in EQ-5D-3L single items and EQ VAS from baseline were analyzed as exploratory end points in the MP (Table 39). This analysis was not controlled for multiplicity. At baseline the mean EQ VAS score was 59.31 (SD = 18.00) in the placebo arm and 58.62 (SD = 17.08) in the incobotulinumtoxinA 100 U arm. No clear changes in the EQ VAS from baseline were observed in any treatment group, nor were differences between treatment groups evident. No clinically relevant shifts in EQ-5D-3L single items were observed (not shown in this report).
Table 39: Change in EQ VAS from Baseline to Weeks 4, 8, 12, and 16 (SIAXI MP, FAS, OC)
Week | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | ||
|---|---|---|---|---|
n | Mean (SD)a | N | Mean (SD)a | |
Week 4 | 35 | −2.20 (12.82) | 73 | 1.58 (13.29) |
Week 8 | 34 | 2.03 (15.82) | 72 | 2.72 (14.01) |
Week 12 | 35 | −4.03 (17.89) | 72 | 3.65 (15.74) |
Week 16 | 34 | 0.44 (19.12) | 72 | 1.26 (16.70) |
EQ VAS = EuroQol 5-Dimensions Visual Analogue Scale; FAS = full analysis set; MP = main period; OC = observed cases; SD = standard deviation.
aEQ VAS ranges from 0 (worst imaginable health state) to 100 (best imaginable health state).
Source: SIAXI Clinical Study Report.8
Extension Period
Changes in EQ-5D-3L single items and EQ VAS from baseline to the week 4 assessment for each cycle in the EP were analyzed in an exploratory fashion (Table 40). This analysis was not controlled for multiplicity. No major changes in the EQ VAS from baseline were observed for the incobotulinumtoxinA 100 U treatment arm, nor were clinically relevant shifts in EQ-5D-3L single items observed (not shown in this report).
Table 40: Change in EQ VAS from Study Baseline to All Assessment Visits in the EP (SIAXI EP, OC)
Assessment Visit | IncobotulinumtoxinA 100 U (N = 89) | |
|---|---|---|
n | Mean (SD)a | |
Change from baseline to | ||
Cycle 2 week 4 | 88 | 4.49 (18.33) |
Cycle 3 week 4 | 84 | 0.88 (19.36) |
Cycle 4 week 4 | 77 | 3.61 (16.69) |
EP = extension period; EQ VAS = EuroQol 5-Dimensions Visual Analogue Scale; OC = observed cases; SD = standard deviation.
aVAS ranges from 0 (worst imaginable health state) to 100 (best imaginable health state).
Source: SIAXI Clinical Study Report.8
Harms
Only those harms identified in the review protocol are reported below. Table 41 and Table 42 provide detailed harms data for the EP.
Adverse Events
In the MP, AEs occurred in 34 patients (45.9%) treated with incobotulinumtoxinA 100 U and 15 patients (41.7%) treated with placebo. Apart from AESIs and notable harms (see below), the most common AEs reported at the PT level in the incobotulinumtoxinA 100 U group were diarrhea (3 patients; 4.1%) and hypertension (3 patients; 4.1%). No AEs in the placebo group occurred in more than 1 patient.
In the EP, AEs occurred in 54 patients (60.7%) treated with incobotulinumtoxinA 100 U. Apart from AESIs and notable harms, the most common AEs reported at the PT level in the incobotulinumtoxinA 100 U group were nasopharyngitis (6 patients; 6.7%), fall (5 patients; 5.6%), PD (3 patients; 3.4%), bronchitis (3 patients; 3.4%), amylase increased (3 patients; 3.4%), and hypertension (2 patients; 2.2%).
Serious Adverse Events
Overall, SAEs occurred in 9 patients (12.2%) treated with incobotulinumtoxinA 100 U and in 3 patients (8.3%) treated with placebo. At the PT level, all SAEs occurred in single patients.
In the EP, SAEs occurred in 14 patients (15.7%) treated with incobotulinumtoxinA 100 U. At the PT level, the only SAEs occurring in more than 1 patient were PD (2 patients; 2.2%) and urethral stenosis (2 patients; 2.2%).
Withdrawals Due to Adverse Events
In the MP, AEs leading to study discontinuation occurred in 1 patient (1.4%) treated with incobotulinumtoxinA 100 U (gastrointestinal obstruction) and in no patients treated with placebo.
In the EP, AEs leading to study discontinuation occurred in 8 (9.0%) patients treated with incobotulinumtoxinA 100 U. The most AE causing discontinuation was a dry mouth (4 patients, 4.5%).
Mortality
No patients died during the MP. In the EP, 2 patients (2.2%) treated with incobotulinumtoxinA 100 U died. Both deaths occurred during the fourth treatment cycle. The causes of death were dopamine dysregulation syndrome and pulmonary embolism.
AESIs and Notable Harms
In the MP, AESIs occurred in 5 patients (6.8%) in the incobotulinumtoxinA 100 U arm and in no patients in the placebo arm. Dry mouth (3 patients; 4.1%), dysarthria (1 patient; 1.4%), and dysphonia (2 patients; 2.7%) occurred in the incobotulinumtoxinA 100 U group but not in the placebo group. Dysphagia and speech disorder did not occur in any patients. Dental-related AEs occurred in 4 patients (5.4%) in the incobotulinumtoxinA 100 U arm and 3 patients in the placebo group (8.3%; dental caries, noninfective gingivitis, and tooth fracture). Swallowing scores for the mROMP were stable from study baseline to all assessment visits in the MP for both groups (placebo and incobotulinumtoxinA 100 U).
In the EP, AESIs occurred in 12 patients (13.5%) treated with incobotulinumtoxinA 100 U. Dry mouth (10 patients; 11.2%), dysphagia (4 patients; 4.5%), and pneumonia aspiration (1 patient; 1.1%) occurred in patients treated with incobotulinumtoxinA 100 U. No patients treated with incobotulinumtoxinA 100 U experienced speech disorder, dysphonia, dysarthria, or dyspnea. Dental-related AEs occurred in 10 patients treated with incobotulinumtoxinA 100 U (tooth extraction, 4 patients, 4.5%; dental caries, dental implantation, noninfective gingivitis, gingivitis, tooth loss, and tooth repair, 1 patient each, 1.1%). Swallowing scores for the mROMP were stable from study baseline to all assessment visits in the EP.
Table 41: Summary of Harms (SIAXI MP)
Adverse events | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) |
|---|---|---|
Patients with ≥ 1 AEa | ||
n (%) | 15 (41.7) | 34 (45.9) |
Diarrhea, n (%) | 1 (2.8) | 3 (4.1) |
Hypertension, n (%) | 1 (2.8) | 3 (4.1) |
Patients with ≥ 1 SAEb | ||
n (%) | 3 (8.3) | 9 (12.2) |
Patients who stopped treatment due to AEsb | ||
n (%) | 0 | 1 (1.4) |
Deathsb | ||
n (%) | 0 | 0 |
Notable harms | ||
AESIs, n (%) | 0 | 5 (6.8) |
Gastrointestinal disorders | ||
Dry mouth, n (%) | 0 | 3 (4.1) |
Dysphagia, n (%) | 0 | 0 |
mROMP swallowing symptoms change from baseline, mean (SD) | ||
Week 4 | 0.3 (2.1) | −0.8 (2.4) |
Week 8 | −0.1 (3.1) | −0.9 (2.9) |
Week 12 | −0.1 (3.4) | −0.9 (2.6) |
Week 16 | −0.9 (2.9) | −1.2 (2.9) |
Nervous system disorders | ||
Speech disorder, n (%) | 0 | 0 |
Dysarthria, n (%) | 0 | 1 (1.4) |
Respiratory, thoracic and mediastinal disorders | ||
Dysphonia, n (%) | 0 | 2 (2.7) |
Dental-related AEs | ||
Tooth extraction, n (%) | 0 | 4 (5.4) |
Dental caries, n (%) | 1 (2.8) | 0 |
Noninfective gingivitis, n (%) | 1 (2.8) | 0 |
Tooth fracture, n (%) | 1 (2.8) | 0 |
AE = adverse event; AESI = adverse event of special interest; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; SAE = serious adverse event; SD = standard deviation.
aSpecific events with a frequency of greater than 3 patients are shown.
bSpecific events with a frequency of greater than 1 patient are shown.
Source: SIAXI Clinical Study Report.8
Table 42: Summary of Harms (SIAXI EP)
Adverse events | IncobotulinumtoxinA 100 U (N = 89) |
|---|---|
Patients with ≥ 1 AEa | |
n (%) | 54 (60.7) |
PD, n (%) | 3 (3.4) |
Urinary tract infection, n (%) | 1 (1.1) |
Upper respiratory tract infection, n (%) | 0 |
Bronchitis, n (%) | 3 (3.4) |
Fall, n (%) | 5 (5.6) |
Hypertension, n (%) | 2 (2.2) |
Nasopharyngitis, n (%) | 6 (6.7) |
Increased amylase, n (%) | 3 (3.4) |
Increased blood creatinine, n (%) | 1 (1.1) |
Increased blood urea, n (%) | 1 (1.1) |
Patients with ≥ 1 SAEb | |
n (%) | 14 (15.7) |
PD, n (%) | 2 (2.2) |
Volvulus, n (%) | 0 |
Urinary tract infection, n (%) | 0 |
Urethral stenosis, n (%) | 2 (2.2) |
Rib fracture, n (%) | 1 (1.1) |
Pneumonia aspiration, n (%) | 1 (1.1) |
Vertigo, n (%) | 1 (1.1) |
Patients who stopped treatment due to AEsb | |
n (%) | 8 (9.0) |
Dry mouth, n (%) | 4 (4.5) |
Deathsb | |
n (%) | 2 (2.2) |
Notable harms | |
AESIs, n (%) | 12 (13.5) |
Gastrointestinal disorders | |
Dry mouth, n (%) | 10 (11.2) |
Dysphagia, n (%) | 4 (4.5) |
mROMP swallowing symptoms change from baseline, mean (SD) | |
End of cycle 2 | −0.9 (3.4) |
End of cycle 3 | −0.7 (4.6) |
End of cycle 4 | −1.1 (3.8) |
Nervous system disorders | |
Speech disorder, n (%) | 0 |
Dysarthria, n (%) | 0 |
Respiratory, thoracic and mediastinal disorders, n (%) | |
Pneumonia aspiration, n (%) | 1 (1.1) |
Dyspnea, n (%) | 0 |
Dental-related AEs | |
Tooth extraction, n (%) | 4 (4.5) |
Tooth loss, n (%) | 1 (1.1) |
Tooth repair, n (%) | 1 (1.1) |
Dental implantation, n (%) | 1 (1.1) |
Dental caries, n (%) | 1 (1.1) |
Noninfective gingivitis, n (%) | 1 (1.1) |
Gingivitis, n (%) | 1 (1.1) |
Poor dental condition, n (%) | 0 |
AE = adverse event; AESI = adverse event of special interest; EP = extension period; MP = main period; mROMP = modified Radboud oral motor inventory for Parkinson disease; PD = Parkinson disease; SAE = serious adverse event; SD = standard deviation.
aSpecific events with a frequency of greater than 5 patients are shown.
bSpecific events with a frequency of greater than 1 patient are shown.
Source: SIAXI Clinical Study Report.8
Critical Appraisal
Internal Validity
SIAXI was a double-blind, placebo-controlled, multi-centre, phase III RCT with an EP of dose-blinded active treatment (N = 184). The study was rigorously designed and the risk of bias was generally low. Randomization appeared adequate in balancing the baseline characteristics of treatment arms (e.g., age, gender, neurologic condition, concomitant diseases and medications, MMAS/UPDRS, sialorrhea severity evaluated based on uSFR, DSFS, and mROMP), although the specific algorithm used was not disclosed, and allocation was concealed using computer systems. According to the clinical expert consulted by CADTH for this review, there would be no noticeable effect of incobotulinumtoxinA injection that could lead to unblinding of patients or investigators, apart from reduction in sialorrhea due to an effect of therapy. No interim analyses or unblinding of any individuals took place until after completion of the MP. Relatively few patients (placebo: 11.1%; incobotulinumtoxinA 100 U: 2.7%) discontinued the MP of the study in which co-primary and secondary outcomes were evaluated, and there were few missing data for analysis of the co-primary outcomes (uSFR change from baseline and patient GICS score at week 4). Despite the higher discontinuation rate in the placebo arm, no patients cited lack of efficacy as the reason for discontinuation. According to the clinical expert consulted by CADTH for this review, discontinuation rates of these magnitudes are to be expected in this population and would not be likely to affect the results of the study.
Randomization was generally successful in balancing treatment arms for baseline demographic and clinical characteristics. The only notable exceptions were in the use of DBS (placebo: 13.9%; incobotulinumtoxinA 100 U: 24.3%), psychoanaleptics (placebo: 19.4%; incobotulinumtoxinA 100 U: 36.5%), diuretics (placebo: 27.8%; incobotulinumtoxinA 100 U: 14.9%), calcium channel blockers (placebo: 27.8%; incobotulinumtoxinA 100 U: 14.9%), and cardiac therapy (placebo: 19.4%; incobotulinumtoxinA 100 U: 6.8%). None of these imbalances, including DBS, were judged by the clinical expert consulted by CADTH for this review as likely to affect the internal validity of the study, as patients were kept on the same therapy (medications and/or DBS) before and throughout the study. However, several unmeasured variables, which, if imbalanced, could confound the relationship between treatment administered and salivary production measured using the uSFR. For example, rates of smoking and use of saliva substitutes were not presented, nor was the volume of water consumed by patients in each group before uSFR measurements. Testing conditions for the uSFR were standardized to the extent feasible, but the measurement of small changes in salivary production could be susceptible to various forms of confounding and bias.
The statistical approach used for analysis of co-primary efficacy outcomes in SIAXI was generally appropriate. Multiplicity control was only considered for the co-primary outcome using a fixed sequence test procedure (incobotulinumtoxinA 100 U versus placebo for both uSFR and GICS at week 4, followed by incobotulinumtoxinA 75 U versus placebo for both outcomes). This hierarchical test procedure was considered adequate by Health Canada reviewers and biostatisticians.56 Data handling and imputation procedures were satisfactory, with MMRM analysis and ANCOVA (BOCF and observed cases) used for both primary and secondary analyses, as well as several exploratory analyses, in both the FAS and PPS. Although ANCOVA with BOCF were originally specified in the statistical analysis plan and later changed to an MMRM, this was done on advice from the FDA, given that an MMRM is more appropriate for outcomes with repeated measurements over time.56
However, interpretation of the co-primary efficacy outcomes was complicated by several factors and statistical issues that should be considered. First, the sample size required in the SIAXI study for safety evaluation (N = 184) was probably significantly overpowered to detect treatment effects of the magnitudes reported in a previous study of rimabotulinumtoxinB.47 The study was powered to have a 95% probability of detecting a difference in mean change in uSFR at week 4 between the incobotulinumtoxinA and placebo arms of 0.246 g/min, and a difference in mean GICS scores at week 4 of 0.955. The actual mean changes determined in the study were 0.09 g/min (uSFR) and 0.58 (GICS). Given that the sample-size calculation was based on a study of rimabotulinumtoxinB, a potential explanation is that the treatment effect of incobotulinumtoxinA was substantially smaller in the SIAXI study compared with the rimabotulinumtoxinB study. The power of the SIAXI study to detect treatment effects of the magnitudes actually reported was not stated but may have been lower than 95%. Second, the rationale for inclusion of baseline DSFS (investigator-assigned), rather than uSFR or mROMP, as a covariate in MMRM models of GICS was not explained; whether another construct may have been more appropriate to model baseline sialorrhea severity was unclear. Third, the GICS was scored on a 7-point Likert scale with only 3 levels denoting a positive change in sialorrhea (minimally improved, much improved, and very much improved) and then modelled as a continuous variable in MMRM. A similar strategy was applied to the DSFS in exploratory analyses. Few patients in any treatment group selected a GICS score of 3 (very much improved), and many placebo-treated patients selected a score of 1 (minimally improved). These patient-reported scales therefore may not have been responsive to relatively modest but clinically significant differences in function, and comparisons of LSM differences in GICS scores may not have been sensitive to such changes. Along similar lines, the definition used in SIAXI of responder (a GICS score ≥ 1) was not explained; using this definition, 30% to 90% of placebo-treated patients responded to therapy across the MP. Analysis of GICS categories suggested that the LSM difference between incobotulinumtoxinA 100 U and placebo was driven by a relatively small proportion of incobotulinumtoxinA -treated patients with large GICS values (≥ 2). According to the clinical expert consulted by CADTH for this review, moderate to marked improvement in sialorrhea (a GICS score of 2 or 3), rather than minimal improvement (a score of 1), would constitute a clinically meaningful response to treatment. Sensitivity analyses of categorical GICS data other than the proportion of responders (e.g., using logistic regression or Fisher’s exact test) were not reported. Finally, there was no strategy for multiplicity control for secondary or exploratory outcomes (following hierarchical testing of the co-primary outcomes), all of which were treated in an exploratory fashion.
Subgroup analyses by the etiology of sialorrhea were specified a priori but the study was not specifically powered to evaluate differences in treatment effect by neurologic condition. The number of patients with stroke and TBI in particular was relatively small. There was therefore uncertainty in the extent to which treatment effects were similar or different across patients with PD/AP and stroke.
As described in Appendix 4, no evidence was available to support the validity, reliability, responsiveness to change, or MID for any of the outcome measures used in the SIAXI trial. Many of these outcome measures (e.g., GICS, DSFS, mROMP, EQ VAS) capture subjective impressions of change from patients, caregivers, or clinicians. According to the clinical expert consulted by CADTH for this review, none of the outcome measures used in the study are used routinely in clinical practice, although questions similar to those asked on the GICS, DSFS, and mROMP drooling scales are part of clinical assessments. Similarly, none of these outcomes were specifically identified by patient groups as important to them. A clear placebo effect was observed for all efficacy outcomes analyzed; for patient- or investigator-rated scales such as GICS and DSFS, this may have been partially due to limited categories of choice, such that any marginal improvement gained via the placebo effect would be scored as positive. According to the clinical expert consulted by CADTH for this review, placebo effects would be expected in this population but would wane over time. However, even uSFR (an objective measure) showed consistently negative changes from baseline to all time points in the MP, suggesting a placebo effect mediated via increased salivation in placebo-treated patients, a subconscious bias in weighing saliva on the part of investigators, or a true treatment effect of saline injection into the salivary glands. Despite these caveats, the clinical expert consulted by CADTH for this review interpreted the results (particularly changes from baseline in GICS and DSFS) as clinically significant, in part based on the consistency of effect across 4 different measures (uSFR, GICS, DSFS, and mROMP). Consistency of effect was also seen across time points in the MP, with the greatest difference in treatment effect between incobotulinumtoxinA 100 U and placebo occurring at weeks 4, 8, and 12, then waning. Given the limited dynamic ranges of the scales used in the SIAXI trial (e.g., 7 points on the GICS and 9 points on the DSFS sum score), even modest differences could be clinically meaningful, according to the clinical expert consulted for this review, provided these differences resulted in a meaningful change in the patient’s lifestyle (e.g., by reducing social isolation or allowing the patient to remain in the workforce).
External Validity
The SIAXI trial was conducted at 33 sites (12 in Germany and 21 in Poland). According to the clinical expert consulted by CADTH for this review, the ages of patients in the study (mean age = 65.2 years; SD = 11.4 years) were representative of the population seen in Canadian practice. However, most patients were men (70.7%) and nearly all were White (99.5%). Baseline disease parameters and sialorrhea severity (e.g., UPDRS/MMAS, mROMP, and DSFS) were reflective of patients typically treated with incobotulinumtoxinA, according to the clinical expert consulted by CADTH for this review. Acknowledging the restrictions and limitations of the study population, the clinical expert did not think this would impede generalization of the study results to patients in other countries and regions or patients of different genders or races; based on the mechanism of action, similar treatment effects would be expected in all adult patients with neurologic conditions. The clinical expert expected that the treatment effect would be similar irrespective of underlying neurologic condition, such that the findings of the SIAXI study (whose population consisted of 79.4% PD/AP patients and 19.0% patients with stroke) would most likely be generalizable to patients with other neurologic conditions, resulting in sialorrhea such as ALS, dementia, and CP. However, the etiology of sialorrhea was moderately associated with patient GICS scores at week 4 in MMRM models (P = 0.034), and some subgroup analyses in the SIAXI trial were unable to conclusively demonstrate homogeneity of treatment effect in patients with PD/AP versus stroke. Whether the results of the SIAXI study can be generalized to patients with other types of neurologic conditions is therefore uncertain.
Adults with many neurologic conditions, particularly PD and stroke, are expected to deteriorate over time, and the clinical expert consulted by CADTH for this review stated that the treatment effect of incobotulinumtoxinA may no longer be sufficient in such patients, especially if swallowing dysfunction becomes worse. The findings of the SIAXI study therefore may not be generalizable to older patients, those with more difficulty swallowing, and patients with more severe neuromuscular dysfunction (e.g., based on UPDRS/MMAS scores). Despite an exclusion criterion for prior (within 6 months) or planned functional neurosurgery including DBS, 13.9% of patients in the placebo arm and 24.3% of patients in the incobotulinumtoxinA 100 U arm reported previous and concomitant DBS during the study. It is therefore unclear whether the results are generalizable to patient populations with higher or lower rates of DBS.
According to the clinical expert consulted by CADTH for this review, the inclusion/exclusion criteria for SIAXI would be expected to recruit a population similar to that treated with incobotulinumtoxinA in clinical practice in Canada. To be included in the SIAXI study, patients had to have DSFS sum scores of 6 or greater, DSFS scores for both severity and frequency of at least 2, and mROMP Section III “Drooling,” Item A scores of 3 or greater at both screening and baseline. As the most common cause of screening failure was poor oral and/or dental condition, the findings may also not be generalizable to these patients. The SIAXI study population was BoNT-naive (within 1 year for sialorrhea), and study results may not be generalizable to patients recently or persistently treated with BoNTs who might develop resistance and/or neutralizing antibodies.
The treatment regimen (100 U) used in the SIAXI study was aligned with the Health Canada–approved dose and, according to the clinical expert consulted by CADTH for this review, with the doses used in Canadian clinical practice. Few patients received comedications influencing sialorrhea (e.g., anticholinergics), although these are also routinely available in Canadian clinical practice. The dosing of 100 U every 16 weeks over the 4 cycles in the EP means that the safety and efficacy results may not be generalizable to patients treated with other, potentially more sporadic, dosing schedules. This is supported by the relatively smaller changes in uSFR in the EP comparing week 4 to cycle baselines compared with study baseline, or with the MP examining BoNT-naive patients.
Although SIAXI study investigators received specialized training in administration of ultrasound-guided injections, the clinical experiment consulted by CADTH for this review stated that both ultrasound-guided and anatomic landmark–guided injections can be administered successfully and are used in clinical practice. Training for use of ultrasound to guide injections, or lack thereof, would therefore be unlikely to affect the generalizability of the study findings.
Over the course of the SIAXI study (64 weeks, approximately 15 months), patients made 15 visits for assessment and consultation and were contacted in 7 telephone interviews. This may have led to a different standard of background care than the average adult patient with a neurologic condition would receive in the Canadian context. Whether and how this affects generalizability of the study findings to patients receiving less-frequent care (e.g., optimization of anti-parkinsonism medications) is unclear.
The efficacy outcomes used in the SIAXI trial (uSFR, GICS, DSFS, mROMP, and EQ-5D-3L) are not used routinely in clinical practice according to the clinical expert consulted by CADTH for this review. However, questions such as those included on the GICS and DSFS are routinely asked as part of clinical evaluations. According to the clinical expert consulted by CADTH for this review, the duration of follow-up (1 cycle, 16 weeks for the MP; 4 cycles in total, 64 weeks) was sufficient for evaluation of efficacy and safety outcomes in this population.
Indirect Evidence
No indirect evidence was identified for this review. A feasibility assessment conducted by the sponsor also concluded that no data were available to inform an indirect treatment comparison between incobotulinumtoxinA and other interventions, including injection of other BoNTs.
Other Relevant Evidence
This section includes additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review.
Studies in Other Populations
One additional RCT of BoNT-A injections (incobotulinumtoxinA and onabotulinumtoxinA) for treatment of sialorrhea in adults with neurologic conditions was summarized to provide additional evidence in patients with other neurologic conditions (ALS and CP) as well comparative evidence for these 2 BoNTs. According to the clinical expert consulted by CADTH for this review, onabotulinumtoxinA is regularly used off-label for the treatment of sialorrhea in adults with neurologic disorders. This study was not a direct head-to-head comparison of these 2 BoNTs.
Methods
Restivo et al.11 conducted an exploratory double-blind RCT to evaluate the efficacy of BoNT-A (incobotulinumtoxinA or onabotulinumtoxinA) injections into the salivary glands for treatment of adults with chronic sialorrhea resulting from neurologic disorders (PD, stroke, TBI, ALS, and CP; N = 90). The study was unrelated to the pivotal SIAXI study and was not funded by the sponsor.
The primary goal of the study was to assess the relationship between efficacy in reducing sialorrhea and number of glands injected. A consecutive series of patients were randomized to receive ultrasound-guided injections with BoNT-A in either 4, 3, or 2 salivary glands (groups A, B, and C, respectively; N = 30 per group). The primary analysis was of the number of glands injected with either of the BoNT-A types, and not the specific type. The basis for selection of incobotulinumtoxinA or onabotulinumtoxinA for injections was not stated and this analysis was post hoc. Salivary production was measured at baseline and 2 weeks post-injection by an investigator blind to treatment-group assignments (patients were also blind to group assignments). Dental rolls were weighed, placed in the patient’s mouth for 5 minutes, then weighed again. The difference in weights was calculated. The procedure was repeated 15 minutes later, and the 2 measurements were averaged. Finally, differences in salivary weight from baseline to 2 weeks post-injection were converted to a 4-point Likert scale (0: no reduction, 1: 25% reduction, 2: 50% reduction, and 3: 75% reduction in salivary weight). The specific break points for this scale were not stated.
Populations
Patients aged 18 to 75 years inclusive with PD, stroke, TBI, ALS, or CP and severely disabling sialorrhea lasting for at least 6 months were included. The diagnostic criteria for neurologic disorders and “severely disabling sialorrhea” were not stated. Patients had to have wet dental-roll weights that were at least 10-fold greater than dry roll weights to be included. Patients with other neurologic conditions or patients who could not provide informed consent due to cognitive impairment were excluded.
Among the included patients (N = 90), 59 (65.6%) were men and 31 (34.4%) were women. The mean age was 53.4 (SD = 17.6) years. Neurologic conditions included PD (30; 33.3%) stroke (21; 23.3%), CP (20; 22.2%), ALS (11; 12.2%), and TBI (8; 8.9%). Gender and age were generally well balanced across treatment arms (group A, 66.7% male, age range = 17 to 73 years; group B, 66.0% male, age range = 18 to 72 years; group C, 66.7% male, age range = 21 to 73 years). However, the etiology of sialorrhea (underlying neurologic condition) was not well balanced: the proportions of patients with PD, stroke, CP, ALS, or TBI were 53.3%, 23.3%, 13.3%, 0%, and 10.0% in group A; 36.7%, 20.0%, 26.7%, 13.3%, and 3.3% in group B; and 10.0%, 26.7%, 23.3%, 23.3%, and 16.7% in group C, respectively.
Interventions
Patients were injected percutaneously with 25 U (0.5 mL) of BoNT-A (onabotulinumtoxinA or incobotulinumtoxinA) per salivary gland (parotid and/or submandibular). Injections were ultrasound-guided using a 27G 3-quarter-inch needle. Injections were performed only once. The total dose of BoNT-A received was therefore 100 U in patients receiving injections in 4 glands, 75 U in patients receiving injections in 3 glands, and 50 U in patients receiving injections in 2 glands. In patients receiving BoNT injections in 2 or 3 glands, the remaining glands were injected with an equivalent volume of saline solution. Information on concomitant medications and therapies was not provided.
Outcomes
The singular efficacy outcome assessed in the study by Restivo et al. was the change in salivary production from baseline to 2 weeks post-injection. Change in salivary production was converted to a 4-point Likert scale as described in the Methods section, and differences between numbers of glands injected and other parameters were analyzed by 1- and 2-way analysis of variance (ANOVA). Safety outcomes were not formally analyzed.
Statistical Analysis
Differences in efficacy (based on the Likert scale) in patients receiving injections into different numbers of glands were assessed using 2-way ANOVA. Differences in efficacy based on type of toxin injected (incobotulinumtoxinA versus onabotulinumtoxinA) were assessed using 2-way ANOVA. Subgroup analyses within patients receiving injections into 3 glands (2 parotid + 1 submandibular or 1 parotid + 2 submandibular) and patients receiving injections into 2 glands (2 parotid, 2 submandibular, or 1 parotid + 1 submandibular) were conducted using 1-way ANOVA. Subgroup analysis by neurologic condition was conducted using 1-way ANOVA. For ANOVA with 3 levels, tests were adjusted for multiple comparisons using the Bonferroni correction. Analysis was in the FAS and there were no missing data.
Patient Disposition
A consecutive series of 107 patients were evaluated for inclusion in the study, 90 of whom were randomized. No information was provided on the 17 screening failures (15.9%). All 90 patients (100.0%) received study treatment were evaluated at 2 weeks post-injection and completed the study.
Exposure to Study Treatments
All patients received the planned injections. A total of 57 patients (63.3%) were injected with onabotulinumtoxinA and 33 patients (33.7%) were injected with incobotulinumtoxinA. Among the overall study population, only 8 patients (8.9%) received the Health Canada–approved dose (100 U) of incobotulinumtoxinA (6 patients with PD, 1 patient with stroke, and 1 patient with TBI).
In group A, 8 patients (26.7%) received incobotulinumtoxinA and 22 patients (73.3%) received onabotulinumtoxinA; in group B, 15 (50.0%) patients received incobotulinumtoxinA and 15 (50.0%) patients received onabotulinumtoxinA; and in group C, 10 patients (33.3%) received incobotulinumtoxinA and 20 (67.7%) patients received onabotulinumtoxinA. Within each study group, the proportions of patients receiving incobotulinumtoxinA versus onabotulinumtoxinA were not balanced by neurologic condition.
Efficacy
Overall, 82 (91.2%) patients responded to treatment (Likert score ≥ 1) and the mean dental-roll weight was 0.25 g (SD = 0.1 g) at 2 weeks post-injection compared to 0.8 g (SD = 0.08 g) at baseline.
Differences in the treatment effects of incobotulinumtoxinA and onabotulinumtoxinA were explored using ANOVA (Figure 3). There was a clear pattern of dose response for both BoNT-A types, with Likert scores increasing along with increasing number of glands injected (P < 0.001, 2-way ANOVA, for both BoNT-A types), but no interaction between BoNT-A type and number of glands injected (P = 0.069, 2-way ANOVA with Bonferroni correction).
No difference between the incobotulinumtoxinA-treated and onabotulinumtoxinA groups was observed based on a 1-way ANOVA (P = 0.12). However, no numerical data were available in the report to substantiate this conclusion.
Subgroup analysis by etiology of sialorrhea in the overall population treated with all doses of BoNT-A (either incobotulinumtoxinA or onabotulinumtoxinA) suggested a potential difference in treatment effect by neurologic condition (P < 0.001, 1-way ANOVA). Based on the Bonferroni multiple comparison, this difference was driven by paired differences between ALS patients and CP patients (P = 0.0033), PD patients (P < 0.001) and patients with stroke (P = 0.0022), with ALS patients (N = 8) showing generally poorer responses.
Figure 3: Likert Scores for Change in Salivary Production Following Injection of BoNT-A (Restivo et al.)
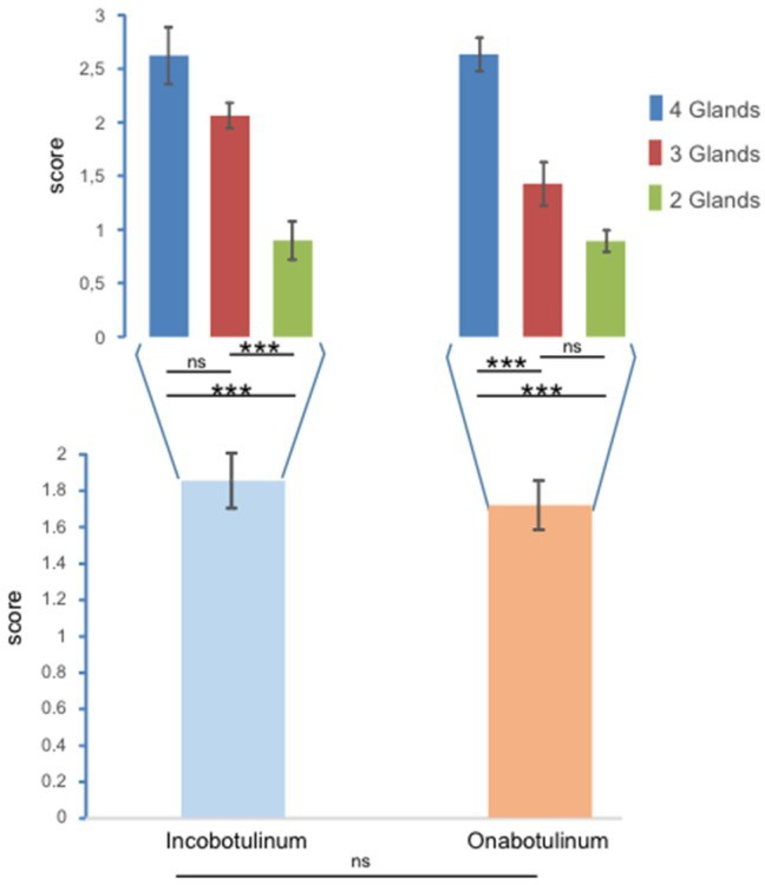
Incobotulinum = incobotulinumtoxinA (Xeomin); ns = not significant; Onabotulinum = onabotulinumtoxinA (Botox); *** = P < 0.001.
Note: Scores represent Likert transformation of response scores: 0 = no response, 1 = poor response, 2 = intermediate response, and 3 = good response. Error bars represent standard errors. Large bars (bottom) represent results for the entire study population; narrow bars (top) represent subgroup analysis for injections into 4, 3 and 2 glands.
Source: Restivo et al. (2018). Copyright 2019. This work is licensed under the Creative Commons Attribution 4.0 International (CC BY 4.0) licence. Full text available here: https://www.mdpi.com/2072-6651/10/2/55.11
Harms
Safety was not formally assessed in the study by Restivo et al. One patient (1.1%) experienced dysphagia 7 days after BoNT-A injection and 2 patients (2.2%) developed hematomas at injection sites. The specific treatments (incobotulinumtoxinA versus onabotulinumtoxinA), dose, and number of glands injected that resulted in these AEs were not stated.
Critical Appraisal
The exploratory RCT by Restivo et al. was described in limited detail, preventing CADTH from conducting a thorough critical appraisal. The evidence and any conclusions derived therefrom are therefore associated with substantial uncertainty.
Internal Validity
Limited information on the study design or statistical analysis was provided in the published study. Randomization groups were assigned by number of salivary glands injected, and the basis for treatment of some patients with incobotulinumtoxinA and others with onabotulinumtoxinA was not explained. The comparative evidence from this study for different BoNT-A types is therefore potentially susceptible to various forms of confounding and bias. Bias could not be evaluated; the randomization strategy and allocation concealment, the methods used for maintaining the DB, and reasons for screening failures were not stated. Importantly, the neurologic condition/etiology of sialorrhea was not well balanced across treatment arms. The comparative analyses of the BoNT-A drugs (incobotulinumtoxinA versus onabotulinumtoxinA) and neurologic condition (both using ANOVA) did not take into account the confounding effects of imbalances in neurologic condition (for the former) and which BoNT-A was administered (for the latter). The rationale and break points for converting salivary weight measurements into a 4-point Likert scale were not explained, and the numerical data for this outcome (mean, SD, or SE) for the comparisons between BoNT-A drug and neurologic outcomes were not provided.
External Validity
This was a study conducted at a single Italian hospital. Of the 33 patients treated with incobotulinumtoxinA, only 8 were treated with the Health Canada–approved dose of 100 U (6 patients with PD, 1 with stroke, and 1 with TBI). Limited information was provided on inclusion and/or exclusion criteria. No information was provided on patient background, including ethnicity, neurologic disease diagnosis and severity, severity of sialorrhea, concomitant therapies, and background treatments. The clinical relevance of the outcome measure (salivary production converted into a Likert scale using unclear breakpoints) was uncertain. As no control group (placebo) was assessed, the true degree of treatment effect of either BoNT-A could not be evaluated. The follow-up time (2 weeks) was relatively short and potentially insufficient to evaluate efficacy. Safety data were not collected.
In summary, the study by Restivo et al. was unable to address the evidence gaps relating to the efficacy of incobotulinumtoxinA in patients with neurologic conditions other than PD/AP and stroke and to comparative efficacy versus other BoNT-A injections for this indication. This was primarily due to the small number of patients receiving the Health Canada–approved dose of incobotulinumtoxinA (100 U), all of whom had PD, stroke, or TBI (the same groups covered included in the SIAXI study), and the design of the study, which, because it involved a non-randomized comparison of incobotulinumtoxinA with onabotulinumtoxinA, had the potential for confounding bias and limited confidence in this comparison.
Discussion
Summary of Available Evidence
One phase III, double-blind, placebo-controlled RCT (SIAXI,8-10 N = 184) was included in the CADTH systematic review. The study enrolled primarily patients with PD/AP (approximately 80%) and stroke (approximately 20%) who had moderate to severe sialorrhea (DSFS sum score ≥ 6, DSFS subscores ≥ 2, and mROMP drooling scores ≥ 3). Following injection of incobotulinumtoxinA (100 U) or placebo, patients in the MP were followed for 16 weeks. All patients in the study were subsequently treated with incobotulinumtoxinA for 3 additional cycles (the dose-blinded active treatment EP) and the same outcomes were examined. The co-primary efficacy outcomes were the mean difference in change from baseline in uSFR at week 4 and mean difference in patient-reported GICS scores at week 4 among incobotulinumtoxinA-treated patients compared with placebo-treated patients. The secondary outcomes were change in uSFR from baseline to weeks 8 and 12 and patient-reported GICS scores at weeks 1, 2, 8, and 12 of the MP. The EQ-5D-3L was used to assess HRQoL as an exploratory outcome.
The baseline characteristics of the SIAXI population were generally representative of Canadian adults requiring treatment for chronic sialorrhea. However, participants were mostly male and White, and almost all patients had sialorrhea secondary to either PD/AP or stroke. Baseline and disease characteristics were generally well balanced at baseline, there were few discontinuations, and the relatively minor degree of missing data (similar between treatment arms) was not expected to affect the results.
In addition to the SIAXI trial, 1 additional exploratory single-centre double-blind RCT was summarized to provide additional evidence from patients with other neurologic conditions and to provide comparative evidence for treatment with incobotulinumtoxinA and onabotulinumtoxinA. The study by Restivo et al.11 recruited patients with PD, stroke, TBI, ALS, and CP (N = 90) with sialorrhea. Patients were randomized to receive BoNT-A injections in 2, 3, or 4 salivary glands. Two weeks post-injection, change in salivary production was evaluated on a Likert scale. Only 33 patients were treated with incobotulinumtoxinA and only 8 patients were treated with the Health Canada–approved dose of 100 U (6 patients with PD, 1 patient with stroke, and 1 patient with TBI).
Interpretation of Results
Efficacy
According to the sponsor, there are no reports in the literature to support the validity of, or an MID for, any of the outcome measures used in the SIAXI trial (uSFR, GICS, DSFS, or mROMP). In addition, no studies were identified by CADTH to support the validity, reliability, responsiveness to change, or MID for any of the outcome measures. This is because of a lack of standard definitions and diagnostic criteria for sialorrhea, leading to wide variability in assessment tools across studies and in clinical practice.57 However, an international consensus statement on assessment of BoNTs for treatment of pediatric and adult drooling recommended 2 measures (salivary flow measurements such as uSFR and the DSFS), both of which have been used in several clinical studies.6 In an interview conducted by the sponsor, some Canadian neurologists suggested that the GICS aligns with outcomes that are meaningful to patients, and 1 neurologist suggested that a reduction of 1 on the DSFS (range = 2 to 9) would be an important difference for patients and clinicians.1
In the co-primary efficacy analysis, mean difference in uSFR change from baseline to week 4 showed a statistically significant difference in favour of incobotulinumtoxinA versus placebo using a variety of analytic approaches. Also as part of the co-primary efficacy analysis, the mean difference in patient-reported GICS scores at week 4 showed statistically significant differences in favour of incobotulinumtoxinA versus placebo using a variety of analytic approaches. Similar results and similar uncertainties were documented for secondary outcomes in the MP (uSFR at weeks 8 and 12 and GICS scores at weeks 1, 2, 8, and 12), exploratory outcomes in the MP (DSFS and mROMP), and all outcomes in the EP; none of these analyses were controlled for multiplicity. However, the clinical relevance of these differences was uncertain due to the unclear validity and MID for these outcomes. The uncertain clinical meaningfulness in changes in uSFR and patient- or investigator-perceived sialorrhea may be connected with overpowering of the SIAXI study for efficacy outcomes, allowing it to detect much smaller treatment effects than those targeted based on past investigations of BoNT injections. Despite the uncertain clinical relevance of the magnitude of treatment differences between incobotulinumtoxinA and placebo, and despite observation of a placebo effect for most outcomes, consistent mean changes, with similar timings, were observed in favour of incobotulinumtoxinA across all outcomes assessed: the effect of treatment was numerically observed (but not statistically significant) at weeks 1 and 2 post-injection, manifested at weeks 4, 8, and 12, and then waned by week 16. However, this did not translate into improvement for incobotulinumtoxinA-treated patients in terms of HRQoL measured via the EQ VAS.
The change in uSFR from cycle baseline to week 4 of each cycle was not consistent across the study. In the EP, the magnitudes of LSM differences from cycle baseline to week 4 for incobotulinumtoxinA 100 U–treated patients were much smaller than those of LSM differences from study baseline to week 4 of any of the cycles. This could imply a long-term treatment effect, with uSFR not returning to baseline even at 16 weeks post-injection. Notably, GICS scores in the EP reflected perceived improvement in sialorrhea at each cycle, and this was evaluated with reference to the previous injection, not study baseline.
Subgroup analyses in the SIAXI study did not provide substantive evidence for the presence or absence of potentially important differences in treatment effect by neurologic condition and by baseline severity of sialorrhea. A potentially relevant subgroup analysis by uSFR at baseline (≤ or > median uSFR) was conducted post hoc and therefore was not presented in this report. Neither the pre-specified subgroup analysis by neurologic condition nor the post hoc subgroup analysis by baseline uSFR provided useful evidence regarding the potentially important issue of variation in treatment effect by neurologic condition or sialorrhea severity.
According to the clinical expert consulted by CADTH for this review, the effect of sialorrhea on patient HRQoL does not correlate with neurologic disease severity. For example, in patients with moderate PD, sialorrhea may be the most troublesome issue and affect their lives in terms of social interactions. By contrast, in patients with advanced PD, sialorrhea may cause choking or skin breakdown. This suggests there may be impacts of therapy at different stages. Both identifying patients for treatment and evaluating response will often be highly dependent on circumstances. For example, a patient achieving a mild improvement in their sialorrhea who is still in the workforce might find this treatment effect sufficient to continue working and go about their daily life. It therefore may not be possible to identify a specific MID for sialorrhea that is generalizable for patients with a single neurologic condition, or even for an individual patient whose needs may change as their disease evolves. For this and other reasons, salivary production, although an objective measure, was considered by the clinical expert consulted by CADTH for this review to be less clinically relevant compared with patient- and investigator-rated scales of sialorrhea improvement.
The clinical expert stated that treatment effects following incobotulinumtoxinA injection should be marked and that clinicians are looking for at least moderate, and not minimal, improvement. Along these lines, the mean difference in GICS scores at week 4 between the incobotulinumtoxinA 100 U and placebo groups was driven by a larger proportion of patients selecting a “much improved” score of 2, (incobotulinumtoxinA 100 U: 33.8% versus placebo: 11.1%). However, the majority of patients in both the placebo and incobotulinumtoxinA 100 U groups reported a GICS score of 1 (minimal improvement) or less. A weakness of the analytic approach involving mean change and mean difference in the SIAXI study was that the mean does not describe individual patients, and potentially important variation in the proportion and degree of treatment effect was not analyzable. Many of the characteristics of an ideal treatment identified by the clinical expert consulted by CADTH for this review (minimal side effects and address social inhibition, maceration of skin, dehydration, speech disturbances, interference with eating, and risk of aspiration) were not directly addressed by the outcomes evaluated in the SIAXI study.
A limitation of the SIAXI study was unclear generalizability to patients with neurologic conditions other than PD/AP and stroke and to patients with different treatment schedules and less-regular medical care. However, the clinical expert consulted by CADTH for this review stated that, based on the mechanism of action of incobotulinumtoxinA, it would be reasonable to expect that treatment would reduce sialorrhea irrespective of neurologic condition. The exploratory double-blind RCT conducted by Restivo et al.11 was unable to extend the evidence regarding the efficacy of incobotulinumtoxinA to patients with other neurologic disorders. The CADTH review of this study was based on the limited results presented in the published study and therefore a thorough critical appraisal of internal and external validity was not possible. Only 8 patients in the study were treated with the Health Canada–approved dose of incobotulinumtoxinA (100 U) and all of these patients had sialorrhea secondary to PD or stroke, the same conditions studied in SIAXI.
Although multiple studies have evaluated injection of different BoNT preparations (in isolation) to control sialorrhea, and a variety of BoNTs are used off-label for this purpose in clinical practice, the SIAXI study provided no comparative evidence for incobotulinumtoxinA versus other BoNTs. The study by Restivo et al.11 suggested that treatment effects occurred following injection of both incobotulinumtoxinA and onabotulinumtoxinA in the salivary glands, although this issue was not the primary focus of the study. In addition, Restivo et al. was not a head-to-head comparison; the comparison of BoNT-A type was susceptible to bias and confounding, based on a partially described Likert scale of unclear clinical relevance, and not reported numerically. Whether treatment effects of the 2 BoNTs were similar therefore could not be evaluated.
Harms
The toxicity profile of incobotulinumtoxinA in the SIAXI trial was as expected, based on previous experience with salivary injection of BoNTs, including incobotulinumtoxinA, and was consistent with the product monograph. In the MP, both AEs and SAEs occurred at similar frequencies in the placebo arm (41.7% and 8.3%, respectively) and incobotulinumtoxinA 100 U arm (45.9% and 12.2%, respectively); WDAEs were extremely rare (0% and 1.2%, in the placebo and incobotulinumtoxinA 100 U groups, respectively) and no deaths occurred. In the EP, which consisted of a 48-week follow-up period, only slightly higher rates of AEs and SAEs were observed in incobotulinumtoxinA 100 U–treated patients (60.7% and 15.7%, respectively) compared to the rates of these events observed during the 16-week period of the MP. During the EP, WDAEs occurred in 9.0% of patients treated with incobotulinumtoxinA 100 U, half of whom (4.5%) discontinued due to dry mouth. Harms related to toxin spread (dry mouth, dysarthria, dysphonia, dysphagia, and pneumonia aspiration) occurred in 6.8% of patients in the incobotulinumtoxinA 100 U arm, no placebo-treated patients in the MP, and 13.5% of incobotulinumtoxinA 100 U–treated patients in the EP. These AESIs were generally manageable in most patients. Dysphagia occurred in 4.5% of incobotulinumtoxinA-treated patients in the EP, although there was no evidence of decreased mROMP swallowing scores associated with incobotulinumtoxinA treatment. Dental-related AEs did not occur more frequently in patients treated with incobotulinumtoxinA 100 U compared with those treated with placebo.
Other Considerations
Patient group input for this review indicated that no patients had experience with incobotulinumtoxinA and did not identify specific outcomes important to patients. The characteristics desired by patients were limited side effects, government coverage of treatments, treatments effective in reducing severity and frequency of drooling, and self-administered treatments. There appears to be a research gap in the assessment of drooling severity and frequency, and in connecting measurement of drooling directly with HRQoL.
The pivotal SIAXI trial did not include study sites in Canada. There are currently no reimbursed treatments for sialorrhea in adults with neurologic disorders in Canada. Although injection of several BoNTs is used off-label for this purpose, only extremely limited comparative evidence was identified to address their relative efficacy. Other evidence gaps included lack of data in patients with neurologic conditions other than PD/AP and stroke as well as lack of data regarding potential differences in treatment effects based on the severity of sialorrhea. Another research gap lies in defining the characteristics of patients who will or will not manifest treatment responses to injections with BoNTs such as incobotulinumtoxinA.
The clinical expert consulted by CADTH for this review stated that, although the SIAXI trial assessed incobotulinumtoxinA injections in adults with PD and stroke, other groups of patients would also benefit from treatment and would not be covered by the indication under review. The expectations and backgrounds of adult patients with PD may differ substantially from those of patients with CP and other childhood neurologic disorders that involve profuse sialorrhea. On a per-capita basis, these patients have higher rates of sialorrhea and it is distressing for them.
Conclusions
Evidence from the SIAXI study suggested that injection of incobotulinumtoxinA (100 U) into the salivary glands of adult patients with neurologic disorders resulted in reduced salivary production and improvements in patients’ perceptions of the frequency and severity of sialorrhea. At 4 weeks post-injection, the mean difference in change in score from baseline in the uSFR and GICS was statistically significantly in favour of incobotulinumtoxinA versus placebo. Treatment effects as measured by the uSFR and GICS were also observed at weeks 8 and 12 post-injection, and similar results were obtained on the investigator-rated DSFS. The clinical significance of post-treatment changes in sialorrhea between incobotulinumtoxinA- and placebo-treated patients was uncertain because the outcome measures were unvalidated, not used in clinical practice, and subjective apart from uSFR, and therefore the magnitudes of treatment effects were of unclear relevance to patients. However, the clinical expert consulted by CADTH for this review indicated that questions similar to those asked in the GICS, DSFS, and mROMP drooling scales are part of clinical assessments, and that the differences in GICS and DSFS between the incobotulinumtoxinA 100 U and placebo arms were clinically meaningful. Despite the uncertain clinical relevance of the magnitude of treatment differences between incobotulinumtoxinA and placebo, and despite evidence for a placebo effect in most outcomes, consistent mean changes with similar timing in favour of incobotulinumtoxinA were observed across all outcomes assessed: differences in the effects of treatment with incobotulinumtoxinA 100 U versus placebo were numerically observed (via GICS responses) but not statistically significant at weeks 1 and 2 post-injection, clearly manifested at weeks 4, 8, and 12, and then waned by week 16, at which point a subsequent dose was administered. However, this did not translate into improvement for incobotulinumtoxinA-treated patients in terms of HRQoL measured via the EQ VAS. Injection with incobotulinumtoxinA was tolerated in most patients and side effects were generally manageable, with some infrequent but expected notable harms related to toxin spread (e.g., dry mouth and dysphagia). Key evidence gaps included a lack of comparative data on the efficacy of different BoNTs and lack of evidence in patients with a variety of neurologic conditions.
References
1.Drug Reimbursement Review sponsor submission: Xeomin (incobotulinumtoxin A, clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins): powder for solution for injection, 50 and 100 units per vial [internal sponsor's package]. Burlington (ON): Merz Pharma Canada Ltd.; 2021 Mar 5.
2.Lakraj AA, Moghimi N, Jabbari B. Sialorrhea: anatomy, pathophysiology and treatment with emphasis on the role of botulinum toxins. Toxins (Basel). 2013;5(5):1010-1031. PubMed
3.Leibner J, Ramjit A, Sedig L, et al. The impact of and the factors associated with drooling in Parkinson's disease. Parkinsonism Relat Disord. 2010;16(7):475-477. PubMed
4.Miller RG, Jackson CE, Kasarskis EJ, et al. Practice parameter update: the care of the patient with amyotrophic lateral sclerosis: multidisciplinary care, symptom management, and cognitive/behavioral impairment (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2009;73(15):1227-1233. PubMed
5.Naumann M, So Y, Argoff CE, et al. Assessment: Botulinum neurotoxin in the treatment of autonomic disorders and pain (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2008;70(19 PART 1):1707-1714. PubMed
6.Reddihough D, Erasmus CE, Johnson H, McKellar GM, Jongerius PH, Cerebral Palsy Institute. Botulinum toxin assessment, intervention and aftercare for paediatric and adult drooling: international consensus statement. Eur J Neurol. 2010;17 Suppl 2:109-121. PubMed
7.Xeomin (incobotulinumtoxin A, clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins): powder for solution for injection, 50 and 100 units per vial [product monograph]. Burlington (ON): Merz Pharma Canada Ltd.; 2020 Nov 3: https://www.merzcanada.com/files/XEOMIN%20Therapeutic%20Product%20Monograph%20Nov%2017%202020.PDF. Accessed 2021 Apr 29.
8.Clinical Study Report: MRZ60201_3090_1. Prospective, randomized, double-blind, placebo-controlled, parallel-group multicenter study, with an extension period of dose-blinded active treatment, to investigate the efficacy and safety of two dose levels of NT 201 in treating chronic troublesome sialorrhea in various neurological conditions [internal sponsor's report]. Frankfurt (DE): Merz Pharmaceuticals GmbH; 2017 May 16.
9.Jost WH, Friedman A, Michel O, et al. SIAXI: Placebo-controlled, randomized, double-blind study of incobotulinumtoxinA for sialorrhea. Neurology. 2019;92(17):e1982-e1991. PubMed
10.Jost WH, Friedman A, Michel O, et al. Long-term incobotulinumtoxinA treatment for chronic sialorrhea: Efficacy and safety over 64 weeks. Parkinsonism Relat Disord. 2020;70:23-30. PubMed
11.Restivo DA, Panebianco M, Casabona A, et al. Botulinum toxin A for sialorrhoea associated with neurological disorders: evaluation of the relationship between effect of treatment and the number of glands treated. Toxins (Basel). 2018;10(2):27. PubMed
12.Prommer E. Anticholinergics in palliative medicine: an update. Am J Hosp Palliat Care. 2013;30(5):490-498. PubMed
13.Hockstein NG, Samadi DS, Gendron K, Handler SD. Sialorrhea: a management challenge. Am Fam Physician. 2004;69(11):2628-2634. PubMed
14.Kalf JG, de Swart BJ, Borm GF, Bloem BR, Munneke M. Prevalence and definition of drooling in Parkinson's disease: a systematic review. J Neurol. 2009;256(9):1391-1396. PubMed
15.Wong SL, Gilmour H, Ramage-Morin PL. Parkinson's disease: Prevalence, diagnosis and impact. Health Rep. 2014;25(11):10-14. PubMed
16.Public Health Agency of Canada. Canadian Best Practices Portal. Neurological Conditions. 2016; https://cbpp-pcpe.phac-aspc.gc.ca/chronic-diseases/neurological-conditions/. Accessed 2021 Apr 23.
17.A guide to cerebral palsy. Toronto (ON): Ontario Federation for Cerebral Palsy; 2011: https://www.ofcp.ca/pdf/Web-Guide-To-CP.pdf. Accessed 2021 Apr 23.
18.Mapping connections: an understanding of neurological conditions in Canada. The National Population Health Study of Neurological Conditions. Toronto (ON): Neurological Health Charities Canada; 2014: https://central.bac-lac.gc.ca/.item?id=HP35-45-2014-eng&op=pdf&app=Library. Accessed 2021 Apr 23.
19.GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459-480. PubMed
20.GBD 2016 Motor Neuron Disease Collaborators. Global, regional, and national burden of motor neuron diseases 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(12):1083-1097. PubMed
21.Himmelmann K, Beckung E, Hagberg G, Uvebrant P. Gross and fine motor function and accompanying impairments in cerebral palsy. Dev Med Child Neurol. 2006;48(6):417-423. PubMed
22.Krueger H, Koot J, Hall RE, O'Callaghan C, Bayley M, Corbett D. Prevalence of individuals experiencing the effects of stroke in Canada: trends and projections. Stroke. 2015;46(8):2226-2231. PubMed
23.Nguyen R, Fiest KM, McChesney J, et al. The international incidence of traumatic brain injury: a systematic review and meta-analysis. Can J Neurol Sci. 2016;43(6):774-785. PubMed
24.Yuan J, Maserejian N, Liu Y, et al. Severity distribution of Alzheimer's disease dementia and mild cognitive impairment in the Framingham Heart Study. J Alzheimers Dis. 2021;79(2):807-817. PubMed
25.Glader L, Delsing C, Hughes A, et al. Sialorrhea in cerebral palsy. Milwaukee (WI): American Academy for Cerebral Palsy and Development Medicine; 2017: https://www.aacpdm.org/publications/care-pathways/sialorrhea. Accessed 2021 Apr 23.
26.Moller E, Karlsborg M, Bardow A, Lykkeaa J, Nissen FH, Bakke M. Treatment of severe drooling with botulinum toxin in amyotrophic lateral sclerosis and Parkinson's disease: efficacy and possible mechanisms. Acta Odontol Scand. 2011;69(3):151-157. PubMed
27.Morgante F, Bavikatte G, Anwar F, Mohamed B. The burden of sialorrhoea in chronic neurological conditions: current treatment options and the role of incobotulinumtoxinA (Xeomin R). Ther Adv Neurol Disord. 2019;12:1756286419888601. PubMed
28.Jost WH. Treatment of drooling in Parkinson's disease with botulinum toxin. Mov Disord. 1999;14(6):1057. PubMed
29.Costa J, Rocha ML, Ferreira J, Evangelista T, Coelho M, de Carvalho M. Botulinum toxin type-B improves sialorrhea and quality of life in bulbaronset amyotrophic lateral sclerosis. J Neurol. 2008;255(4):545-550. PubMed
30.Intiso D, Basciani M. Botulinum toxin use in neuro-rehabilitation to treat obstetrical plexus palsy and sialorrhea following neurological diseases: A review. NeuroRehabilitation. 2012;31(2):117-129. PubMed
31.Jackson CE, Gronseth G, Rosenfeld J, et al. Randomized double-blind study of botulinum toxin type B for sialorrhea in ALS patients. Muscle Nerve. 2009;39(2):137-143. PubMed
32.Lagalla G, Millevolte M, Capecci M, Provinciali L, Ceravolo MG. Long-lasting benefits of botulinum toxin type B in Parkinson's disease-related drooling. J Neurol. 2009;256(4):563-567. PubMed
33.Lipp A, Trottenberg T, Schink T, Kupsch A, Arnold G. A randomized trial of botulinum toxin A for treatment of drooling. Neurology. 2003;61(9):1279-1281. PubMed
34.Lagalla G, Millevolte M, Capecci M, Provinciali L, Ceravolo MG. Botulinum toxin type A for drooling in Parkinson's disease: a double-blind, randomized, placebo-controlled study. Mov Disord. 2006;21(5):704-707. PubMed
35.Mancini F, Zangaglia R, Cristina S, et al. Double-blind, placebo-controlled study to evaluate the efficacy and safety of botulinum toxin type A in the treatment of drooling in parkinsonism. Mov Disord. 2003;18(6):685-688. PubMed
36.Nobrega AC, Rodrigues B, Torres AC, Enzo A, Melo A. Does botulinum toxin decrease frequency and severity of sialorrhea in Parkinson's disease? J Neurol Sci. 2007;253(1-2):85-87. PubMed
37.Porta M, Gamba M, Bertacchi G, Vaj P. Treatment of sialorrhoea with ultrasound guided botulinum toxin type A injection in patients with neurological disorders. J Neurol Neurosurg Psychiatry. 2001;70(4):538-540. PubMed
38.Ondo WG, Hunter C, Moore W. A double-blind placebo-controlled trial of botulinum toxin B for sialorrhea in Parkinson's disease. Neurology. 2004;62(1):37-40. PubMed
39.Vashishta R, Nguyen SA, White DR, Gillespie MB. Botulinum toxin for the treatment of sialorrhea: a meta-analysis. Otolaryngol Head Neck Surg. 2013;148(2):191-196. PubMed
40.Botox (onabotulinumtoxinA for injection Ph. Eur., Clostridium botulinum type A neurotoxin complex (900kD)): sterile vacuum-dried concentrate powder for solution for injection, 50, 100 and 200 Allergan units per vial [product monograph]. Markham (ON): Allergan, Inc.; 2014: https://allergan-web-cdn-prod.azureedge.net/allergancanadaspecialty/allergancanadaspecialty/media/actavis-canada-specialty/en/products/pms/botox-pm-2014-07-07_e.pdf. Accessed 2021 Apr 29.
41.Dysport therapeutic (abobotulinumtoxinA for injection Ph. Eur.): sterile lyophilized powder for solution for injection, 300 and 500 units per vial [product monograph]. Mississauga (ON): Ipsen Biopharmaceuticals Canada Inc.; 2017: https://www.cadth.ca/sites/default/files/cdr/monograph/dysport-therapeutic-product-monograph.pdf. Accessed 2021 Apr 29.
42.Nuceiva (prabotulinumtoxinA for injection): sterile vacuum-dried powder for solution for injection, 100 units per vial [product monograph]. Santa Barbara (CA): Evolus, Inc.; 2018: https://pdf.hres.ca/dpd_pm/00046932.PDF. Accessed 2021 Apr 29.
43.Myobloc (botulinum toxin type B): 5000 units/mL, sterile solution for intramuscular injection [product monograph]. San Diego (CA): Solstice NeuroSciences, LLC.; 2004: https://pdf.hres.ca/dpd_pm/00000633.PDF. Accessed 2021 Apr 29.
44.Elavil (amitriptyline hydrochloride tablets USP): 10, 25, 50 and 75 mg tablets [product monograph]. Vaughan (ON): AA PHARMA INC.; 2018: https://pdf.hres.ca/dpd_pm/00043995.PDF. Accessed 2021 Apr 29.
45.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
46.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://cadth.ca/grey-matters-practical-tool-searching-health-related-grey-literature. Accessed 2021 Mar 22.
47.Chinnapongse R, Gullo K, Nemeth P, Zhang Y, Griggs L. Safety and efficacy of botulinum toxin type B for treatment of sialorrhea in Parkinson's disease: a prospective double-blind trial. Mov Disord. 2012;27(2):219-226. PubMed
48.Solstice Neurosciences. NCT00515437: A multi-center study of MYOBLOC for the treatment of sialorrhea in Parkinson's disease patients. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2019: http://clinicaltrials.gov/ct2/show/NCT00515437. Accessed 2021 May 12.
49.Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55(3):181-184. PubMed
50.Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168(12):1266-1277. PubMed
51.Goetz CG, Tilley BC, Shaftman SR, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129-2170. PubMed
52.Loewen SC, Anderson BA. Reliability of the Modified Motor Assessment Scale and the Barthel Index. Phys Ther. 1988;68(7):1077-1081. PubMed
53.Janssen MF, Pickard AS, Golicki D, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual Life Res. 2013;22(7):1717-1727. PubMed
54.International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. ICH Harmonised Tripartite Guidelines - Clinical safety data management: definitions and standards for expedited reporting. Geneva (CH): International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH); 1994: https://database.ich.org/sites/default/files/E2A_Guideline.pdf. Accessed 2021 May 12.
55.Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont). 2007;4(7):28-37. PubMed
56.Health Canada reviewer's report: Xeomin (incobotulinumtoxinA) [internal sponsor's report]. Ottawa (ON): Therapeutics Products Directorate, Health Canada; 2020.
57.Hill F, Miller N, Walsh RA, Mockler D, McDowell R, Walsh M. Botulinum toxin for drooling in Parkinson's disease. Cochrane Database Syst Rev. 2016;10:CD012408.
58.Narayanaswami P, Geisbush T, Tarulli A, et al. Drooling in Parkinson's disease: A randomized controlled trial of incobotulinum toxin A and meta-analysis of Botulinum toxins. Parkinsonism Relat Disord. 2016;30:73-77. PubMed
59.Kalf JG, Borm GF, de Swart BJ, Bloem BR, Zwarts MJ, Munneke M. Reproducibility and validity of patient-rated assessment of speech, swallowing, and saliva control in Parkinson's disease. Arch Phys Med Rehabil. 2011;92(7):1152-1158. PubMed
60.Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53-72. PubMed
61.EuroQoL Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–present)
Embase (1974–present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: March 26, 2021
Alerts: Bi-weekly search updates until project completion
Study Types: No filters were applied to limit the main search retrieval by study type. For the search for generic terms: randomized controlled trials; controlled clinical trials.
Limits:
No publication date limits
For the search for generic terms: Humans
No language limits
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
Search Strategy
(xeomin* or xeomeen* or incobotulin* or inco A or incoA or Ainco or A inco or inco BoNT* or incoBoNT* or NT 201 or NT201 or bocouture*).ti,ab,ot,kf,hw,nm,rn.
Sialorrhea/ or Salivation/ or Saliva/ or exp Salivary Glands/
(sialorrh* or drool* or dribbl* or saliva* or hypersaliva* or hypersialorrh* or ((oral or oropharyngeal) adj1 (secret* or hypersecret*)) or polysialia or ptyalism or hyperptyalism or ptyalorrh* or sialism*).ti,ab,kf.
2 or 3
1 and 4
5 use medall
(xeomin* or xeomeen* or incobotulin* or inco A or incoA or Ainco or A inco or inco BoNT* or incoBoNT* or NT 201 or NT201 or bocouture*).ti,ab,kw,dq.
exp hypersalivation/ or salivation/ or salivation disorder/ or saliva/ or exp salivary gland/
(sialorrh* or drool* or dribbl* or saliva* or hypersaliva* or hypersialorrh* or ((oral or oropharyngeal) adj1 (secret* or hypersecret*)) or polysialia or ptyalism or hyperptyalism or ptyalorrh* or sialism*).ti,ab,kw,dq.
8 or 9
7 and 10
11 not conference abstract.pt.
12 use oemezd
6 or 13
remove duplicates from 14
Supplemental Generic Terms Search: Multi-Database Strategy
Search Strategy
Botulinum Toxins/ or Botulinum Toxins, Type A/
(Abobotulin* or AGN 191622 or AGN191622 or Allergan* or Azzalure* or Botox* or Botulax* or CNT 52120 or CNT52120 or daxibotulin* or DWP450 or DWP 450 or Dysport* or Evabotulin* or evosyal* or GSK 1358820 or GSK1358820 or HSDB 7796 or HSDB7796 or jeuveau* or Lanxoz* or letibotulin* or Mediotoxin* or Medytox* or MT 10109 or MT10109 or Nabota* or nabotulin* or Neuronox* or nuceiva* or oculinum* or onabotulin* or onaclostox* or prabotulin* or prosigne* or purtox* or QM1114 or QM 1114 or relabotulin* or reloxin* or revance* or RTT 150 or RTT150 or vistabel* or vistabex*).ti,ab,ot,kf,hw,nm,rn.
(Botulinum* or botulinium* or (botulin* adj2 (toxin* or neurotoxin*)) or BoNT-A or BoNTA or BTXA or BTX-A or toxine botulinique A or E211KPY694 or EINECS 297-253-4).ti,ab,ot,kf,hw,nm,rn.
1 or 2 or 3
Sialorrhea/ or Salivation/ or Saliva/ or exp Salivary Glands/
(sialorrh* or drool* or dribbl* or saliva* or hypersaliva* or hypersialorrh* or ((oral or oropharyngeal) adj1 (secret* or hypersecret*)) or polysialia or ptyalism or hyperptyalism or ptyalorrh* or sialism*).ti,ab,kf.
5 or 6
4 and 7
8 use medall
*botulinum toxin/ or *botulinum toxin a/
(Abobotulin* or AGN 191622 or AGN191622 or Allergan* or Azzalure* or Botox* or Botulax* or CNT 52120 or CNT52120 or daxibotulin* or DWP450 or DWP 450 or Dysport* or Evabotulin* or evosyal* or GSK 1358820 or GSK1358820 or HSDB 7796 or HSDB7796 or jeuveau* or Lanxoz* or letibotulin* or Mediotoxin* or Medytox* or MT 10109 or MT10109 or Nabota* or nabotulin* or Neuronox* or nuceiva* or oculinum* or onabotulin* or onaclostox* or prabotulin* or prosigne* or purtox* or QM1114 or QM 1114 or relabotulin* or reloxin* or revance* or RTT 150 or RTT150 or vistabel* or vistabex*).ti,ab,kw,dq.
(Botulinum* or botulinium* or (botulin* adj2 (toxin* or neurotoxin*)) or BoNT-A or BoNTA or BTXA or BTX-A or toxine botulinique A or EINECS 297-253-4).ti,ab,kw,dq.
10 or 11 or 12
exp hypersalivation/ or salivation/ or salivation disorder/ or saliva/ or exp salivary gland/
(sialorrh* or drool* or dribbl* or saliva* or hypersaliva* or hypersialorrh* or ((oral or oropharyngeal) adj1 (secret* or hypersecret*)) or polysialia or ptyalism or hyperptyalism or ptyalorrh* or sialism*).ti,ab,kw,dq.
14 or 15
13 and 16
17 not conference abstract.pt.
18 use oemezd
9 or 19
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
24.."Randomized Controlled Trial (topic)"/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
"Controlled Clinical Trial (topic)"/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf,kw.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf,kw.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf,kw.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf,kw.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf,kw.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(pragmatic study or pragmatic studies).ti,ab,hw,kf,kw.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf,kw.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf,kw.
(phase adj3 (III or "3") adj3 (study or studies or trial*)).ti,hw,kf,kw.
or/21-51
20 and 52
exp animals/
exp animal experimentation/ or exp animal experiment/
exp models animal/
nonhuman/
exp vertebrate/ or exp vertebrates/
or/54-58
exp humans/
exp human experimentation/ or exp human experiment/
or/60-61
59 not 62
53 not 63
remove duplicates from 64
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- xeomin OR incobotulinum OR incobotulinumtoxin OR incobotulinumtoxina OR NT201 OR NT 201 | sialorrhea OR sialorrhoea OR drooling OR hypersalivation OR salivation]
WHO ICTRP
International Clinical Trials Registry Platform (ICTRP), produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms – (xeomin OR incobotulinumtoxina OR incobotulinum OR incobotulinumtoxin) AND (sialorrhea OR sialorrhoea OR hypersalivation OR salivation)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- xeomin, incobotulinum, incobotulinumtoxin, incobotulinumtoxina, NT201, NT 201, botulinum]
EU Clinical Trials
Register European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- xeomin, incobotulinum, incobotulinumtoxin, incobotulinumtoxina, botulinum AND sialorrhea, botulinum AND sialorrhoea, botulinum AND hypersalivation]
Grey Literature
Search dates: March 17, 2021 – March 22, 2021
Keywords: [xeomin, incobotulinum, incobotulinumtoxin, incobotulinumtoxina, NT201, NT 201, sialorrhea, sialorrhoea, hypersalivation, salivation, drooling]
Limits: No publication limits
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reasons for exclusion |
|---|---|
| |
|
RCT = randomized controlled trial.
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 45: Summary of Baseline and End-of-Study Characteristics (SIAXI EP, SES-EP)
Characteristic | IncobotulinumtoxinA 75 U (N = 84) | IncobotulinumtoxinA 100 U (N = 89) | Total IncobotulinumtoxinA (N = 173) |
|---|---|---|---|
Sex, n (%) | |||
Male | 59 (70.2) | 65 (73.0) | 124 (71.7) |
Female | 25 (29.8) | 24 (27.0) | 49 (28.3) |
Age, years | |||
Mean (SD) | 65.0 (11.0) | 65.3 (11.8) | 65.2 (11.4) |
Median (range) | 66.0 (27, 80) | 67.0 (21, 80) | 67.0 (21, 80) |
Age group, n (%) | |||
18-64 years | 39 (46.4) | 34 (38.2) | 73 (42.2) |
65-84 years | 45 (53.6) | 55 (61.8) | 100 (57.8) |
Race, n (%) | |||
White | 84 (100.0) | 88 (98.9) | 172 (99.4) |
Asian | 0 | 1 (1.1) | 1 (0.6) |
Ethnicity, n (%) | |||
Hispanic/Latino | 0 | 1 (1.1) | 1 (0.6) |
Not Hispanic/Latino | 84 (100.0) | 88 (98.9) | 172 (99.4) |
Weight (kg) | |||
Mean (SD) | 79.8 (15.9) | 80.5 (14.8) | 80.2 (15.3) |
Median (range) | 79.5 (37, 127) | 79.9 (49, 128) | 79.9 (37, 128) |
BMI (kg/m2) | |||
Mean (SD) | 27.5 (5.0) | 28.0 (4.6) | 27.7 (4.8) |
Median (range) | 27.5 (14, 51) | 27.5 (19, 41) | 27.5 (14, 51) |
Concomitant diseases, n (%) | |||
Yes | 84 (100.0) | 89 (100.0) | 173 (100.0) |
Hypertension | 42 (50.0) | 46 (51.7) | 88 (50.9) |
Hypercholesterolemia | 15 (17.9) | 12 (13.5) | 27 (15.6) |
Hyperlipidemia | 15 (17.9) | 11 (12.4) | 26 (15.0) |
Spinal osteoarthritis | 10 (11.9) | 10 (11.2) | 20 (11.6) |
Dysarthria | 11 (13.1) | 18 (20.2) | 29 (16.8) |
Dysphonia | 2 (2.4) | 6 (6.7) | 8 (4.6) |
Dysphagia | 8 (9.5) | 6 (6.7) | 14 (8.1) |
Speech disorder | 0 | 3 (3.4) | 3 (1.7) |
Concomitant non-drug therapies, n (%) | |||
Yes | 29 (34.5) | 30 (33.7) | 59 (34.1) |
DBS | 10 (11.9) | 21 (23.6) | 31 (17.9) |
Concomitant medications, n (%) | |||
Yes | 83 (98.8) | 88 (98.9) | 171 (98.8) |
Dopaminergic agents | 64 (76.2) | 71 (79.8) | 135 (78.0) |
Anticholinergic agents | 2 (2.4) | 3 (3.4) | 5 (2.9) |
Agents acting on the renin-angiotensin system | 31 (36.9) | 39 (43.8) | 70 (40.5) |
Antithrombotic agents | 33 (39.3) | 34 (38.2) | 67 (38.7) |
Lipid modifying agents | 32 (38.1) | 25 (28.1) | 57 (32.9) |
Beta blocking agents | 23 (27.4) | 21 (23.6) | 44 (25.4) |
Psychoanaleptics | 25 (29.8) | 31 (34.8) | 66 (32.4) |
Diuretics | 18 (21.4) | 17 (19.1) | 36 (20.2) |
Calcium channel blockers | 10 (11.9) | 17 (19.1) | 27 (15.6) |
Cardiac therapy | 10 (11.9) | 8 (9.0) | 18 (10.4) |
Antibacterials for systemic use | 19 (22.6) | 10 (11.2) | 29 (16.8) |
Drugs for constipation | 4 (4.8) | 14 (15.7) | 18 (10.4) |
Diseases causing sialorrhea, n (%) | |||
PD/AP | 67 (79.8) | 71 (79.8) | 138 (79.8) |
PD | 57 (67.9) | 66 (74.2) | 123 (71.1) |
AP | 10 (11.9) | 5 (5.6) | 15 (8.7) |
MSA | 6 (7.1) | 3 (3.4) | 9 (5.2) |
CD | 0 | 1 (1.1) | 1 (0.6) |
PSP | 4 (4.8) | 1 (1.1) | 5 (2.9) |
Stroke | 16 (19.0) | 16 (18.0) | 32 (18.5) |
TBI | 2 (2.4) | 3 (3.4) | 5 (2.9) |
UPDRS section III “motor examination” a | |||
Mean (SD) | 31.4 (15.0) | 29.7 (13.4) | 30.6 (14.2) |
Median (range) | 31.0 (0, 80) | 30.5 (7, 58) | 31.0 (0, 80) |
Left MMAS score b | |||
Mean (SD) | 40.5 (11.3) | 36.4 (9.9) | 38.4 (10.6) |
Median (range) | 46.0 (11, 48) | 39.0 (9, 46) | 41.5 (9, 48) |
Right MMAS score b | |||
Mean (SD) | 37.8 (13.5) | 39.9 (8.8) | 38.9 (11.1) |
Median (range) | 43.0 (9, 48) | 42.5 (19, 48) | 42.5 (9, 48) |
Time since first diagnosis of sialorrhea at screening (months) | |||
Mean (SD) | 28.5 (29.0) | 33.2 (36.6) | 31.0 (33.1) |
Median (range) | 15.5 (5, 119) | 17.0 (3, 171) | 16.2 (3, 171) |
Edentulous, n (%) | |||
Yes | 22 (26.2) | 24 (27.0) | 46 (26.6) |
Dentures | 18 (21.4) | 19 (21.3) | 37 (21.4) |
No dentures | 4 (4.8) | 5 (5.6) | 9 (5.2) |
AP = atypical parkinsonism; BMI = body mass index; CD = corticobasal degeneration; DBS = deep brain stimulation; EP = extension period; MMAS = modified motor assessment scale; MSA = multiple system atrophy; PD = Parkinson disease; PSP = progressive supranuclear palsy; SD = standard deviation; SES-EP = safety evaluation set, extension period; TBI = traumatic brain injury; U = units; UPDRS = unified Parkinson disease rating scale.
aMeasured by investigators based on 14 items with 27 total scores since each item may assess more than one part of the body, Each score was rated on a 5-point scale only in patients with PD/AP. For patients with “On-Off” motor fluctuations, assessments were performed in comparable “On” states, preferably at the same day and time, at least throughout the MP. Scores range from 0 (best) to 56 or 108 (worst).
bMeasured by investigators based on 8 items, each rated on a 6-point scale only in patients with stroke or TBI. Scores range from 0 (worst) to 48 (best).
Source: SIAXI Clinical Study Report.8
Table 46: Concomitant Medications and Therapies (SIAXI EP, SES-EP)
Characteristic | IncobotulinumtoxinA 75 U (N = 84) | IncobotulinumtoxinA 100 U (N = 89) | Total incobotulinumtoxinA (N = 173) |
|---|---|---|---|
Concomitant non-drug therapies, n (%) | |||
Yes | 29 (34.5) | 30 (33.7) | 59 (34.1) |
DBS | 10 (11.9) | 21 (23.6) | 31 (17.9) |
Concomitant medications, n (%) | |||
Yes | 83 (98.8) | 88 (98.9) | 171 (98.8) |
Dopaminergic agents | 64 (76.2) | 71 (79.8) | 135 (78.0) |
Anticholinergic agents | 2 (2.4) | 3 (3.4) | 5 (2.9) |
Agents acting on the renin-angiotensin system | 31 (36.9) | 39 (43.8) | 70 (40.5) |
Antithrombotic agents | 33 (39.3) | 34 (38.2) | 67 (38.7) |
Lipid modifying agents | 32 (38.1) | 25 (28.1) | 57 (32.9) |
Beta blocking agents | 23 (27.4) | 21 (23.6) | 44 (25.4) |
Psychoanaleptics | 25 (29.8) | 31 (34.8) | 66 (32.4) |
Diuretics | 18 (21.4) | 17 (19.1) | 36 (20.2) |
Calcium channel blockers | 10 (11.9) | 17 (19.1) | 27 (15.6) |
Cardiac therapy | 10 (11.9) | 8 (9.0) | 18 (10.4) |
Antibacterials for systemic use | 19 (22.6) | 10 (11.2) | 29 (16.8) |
Drugs for constipation | 4 (4.8) | 14 (15.7) | 18 (10.4) |
DBS = deep brain stimulation; EP = extension period; SES-EP = safety evaluation set, extension period.
Source: SIAXI Clinical Study Report.8
Table 47: Statistical Analysis of All Efficacy End points in SIAXI
Phase | Type | End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|---|---|
MP | Co-primary | Change in uSFR from baseline to week 4 | MMRM (2-sided, significance level alpha = 0.05, FAS) with comparison of LSMs |
|
|
Co-primary | Patient GICS entry (or carer GICS entry if patient unable to answer) at week 4 | MMRM (2-sided, significance level alpha = 0.05, FAS) with comparison of LSMs |
|
| |
Secondary | Change in uSFR from baseline to weeks 8 and 12 | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | |
Secondary | Patient GICS entry (or carer GICS entry if patient unable to answer) at weeks 1, 2, 8 and 12 | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | |
Exploratory | Change in uSFR from baseline to week 16 | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS, BOCF/ANCOVA and OC/ANCOVA) | |
Exploratory | Patient GICS entry (or carer GICS entry if patient unable to answer) at week 16 | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | As per primary analysis (FAS and PPS) | |
Exploratory | Number of responders according to patient GICS entry at weeks 1, 2, 4, 8, 12 and 16 | OR and 95% Wald CIs for treatment-group comparisons were estimated using logistic regression (FAS only) If OR was not estimable, descriptive summary statistics provided. For week 16, descriptive statistics and P values from Fisher’s exact test or Χ2 test provided |
|
| |
Exploratory | Carer GICS entry at weeks 1, 2, 4, 8, 12, and 16 | Descriptive summary statistics (FAS) | NA | NR | |
Exploratory | Change in DSFS subscores and sum score from baseline to weeks 4, 8, 12 and 16 | As per primary analysis (FAS only) for change in DSFS sum score from baseline to weeks 4, 8 and 12. For change in DSFS sum score from baseline to week 16 and change in DSFS subscores from baseline to weeks 4, 8, 12 and 16, descriptive summary statistics provided | As per primary analysis (FAS only) | As per primary analysis (FAS only) | |
Exploratory | Change in mROMP speech symptom and drooling score from baseline to week 4, 8, 12 and 16 | Descriptive summary statistics (FAS) | NA | NR | |
Exploratory | Change in EQ-5D-3L single items and EQ VAS from baseline to weeks 4, 8, 12 and 16 | Frequency and shift tables, descriptive summary statistics (FAS) | NA | NR | |
EP | Exploratory | Change in uSFR from baseline to all visits in the EP, and change from each injection (weeks 16, 32 and 48) to the respective assessment visits (weeks 20, 36 and 52) and to the end-of-cycle / end-of-study visits (weeks 32, 48 and 64) | Descriptive summary statistics (SES-EP) | NA | NR |
Exploratory | Patient GICS entry (or carer GICS entry if patient unable to answer) at all assessment visits in the EP (weeks 20, 36 and 52) and the end-of-cycle / end-of-study visits (weeks 32, 48 and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40 and 56) | Frequency tables and descriptive summary statistics (SES-EP) | NA | NR | |
Exploratory | Number of responders according to patient GICS entry at all assessment visits in the EP (weeks 20, 36 and 52) and the end-of-cycle / end-of-study visits (weeks 32, 48 and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40 and 56) | Frequency tables and descriptive summary statistics (SES-EP) | NA | NR | |
Exploratory | Change in DSFS subscores and sum score from baseline to all assessment visits in the EP | Descriptive summary statistics (SES-EP) | NA | NR | |
Exploratory | Carer GICS entry at all assessment visits in the EP (weeks 20, 36 and 52) and the end-of-cycle / end-of-study visits (weeks 32, 48 and 64) as well as at all telephone contacts (weeks 17, 18, 24, 40 and 56) | Frequency tables and descriptive summary statistics (SES-EP) | NA | NR | |
Exploratory | Change in mROMP speech symptoms and drooling scores from baseline to all assessment visits in the EP | Descriptive summary statistics (SES-EP) | NA | NR | |
Exploratory | Change in EQ-5D-3L single items and EQ VAS from baseline to all assessment visits in the EP | Frequency and shift tables, descriptive summary statistics (SES-EP) | NA | NR |
ANCOVA = analysis of covariance; BOCF = baseline observation carried forward; CI = confidence interval; EP = extension phase; FAS = full analysis set; GICS = global impression of change scale; LSMs = least squares means; MMRM = mixed model repeated measures; MP = main phase; mROMP = modified Radboud oral motor inventory for Parkinson disease; NA = not applicable; NR = not reported; OC = observed cases; OR = odds ratio; PPS = per-protocol set; SES-EP = safety evaluation set, extension phase; uSFR = unstimulated salivary flow rate; VAS = visual analogue scale.
Source: SIAXI Clinical Study Report.8
Figure 4: Mean and SD uSFR Values at all Visits in the Study (SIAXI MP and EP, OC)
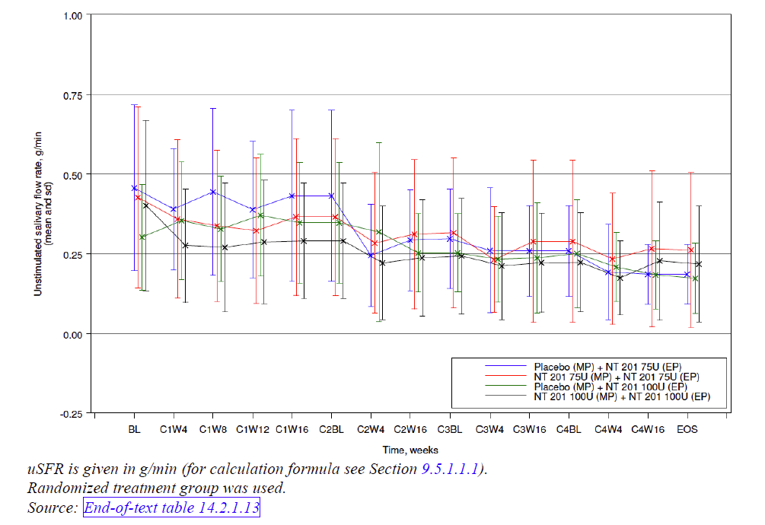
EP = extension period; MP = main period; OC = observed cases SD = standard deviation; U = units; uSFR = unstimulated salivary flow rate.
Note: uSFR measured in g/min.
Source: SIAXI Clinical Study Report.8
Sensitivity Analyses of Co-Primary Efficacy Outcomes
Table 48: Sensitivity Analyses of Change in uSFR From Baseline to Week 4 (SIAXI MP)
Statistical model (handling of missing values) | Analysis set | LSM difference IncobotulinumtoxinA 100 U versus placebo (SE) (95% CI) | Median IncobotulinumtoxinA 100 U | Median placebo | P Value |
|---|---|---|---|---|---|
MMRMa | FAS | −0.09 (0.031) (−0.15 to −0.03) | — | — | 0.004 |
ANCOVA (OC)b | FAS | −0.08 (0.031) (−0.14 to −0.02) | — | — | 0.009 |
ANCOVA (BOCF)b | FAS | −0.08 (0.030) (−0.14 to −0.02) | — | — | 0.008 |
Wilcoxon rank sum test (OC) | FAS | — | −0.08 | −0.03 | 0.010 |
Wilcoxon rank sum test (BOCF) | FAS | — | −0.08 | −0.03 | 0.012 |
MMRMa | PPS | −0.08 (0.032) (−0.14 to −0.02) | — | — | 0.014 |
ANCOVA (OC)b | PPS | −0.07 (0.032) (−0.13 to −0.01) | — | — | 0.028 |
ANCOVA (BOCF)b | PPS | −0.07 (0.032) (−0.13 to −0.01) | — | — | 0.027 |
Wilcoxon rank sum test (OC) | PPS | — | −0.08 | −0.03 | 0.010 |
Wilcoxon rank sum test (BOCF) | PPS | — | −0.08 | −0.03 | 0.010 |
ANCOVA = analysis of covariance; BOCF = baseline observation carried forward; CI = confidence interval; FAS = full analysis set; LS = least squares; MMRM = mixed model repeated measures; MP = main period; OC = observed cases; PPS = per-protocol set; SE = standard error; U = units; uSFR = unstimulated salivary flow rate.
aLSMs are from model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and uSFR at baseline included as covariate. For MMRM visit*treatment is interaction term and visit is repeated factor.
bLSMs are from model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and uSFR at baseline included as covariate.
Source: SIAXI Clinical Study Report.8
Table 49: Sensitivity Analyses of Patient GICS at Week 4 (SIAXI MP)
Statistical model (handling of missing values) | Analysis set | LSM difference incobotulinumtoxinA 100 U versus placebo (SE) (95% CI) | Median incobotulinumtoxinA 100 U | Median placebo | P Value |
|---|---|---|---|---|---|
MMRMa | FAS | 0.58 (0.183) (0.22 to 0.94) | — | — | 0.002 |
ANCOVA (OC)b | FAS | 0.59 (0.187) (0.22 to 0.96) | — | — | 0.002 |
ANCOVA (BOCF)b | FAS | 0.57 (0.187) (0.20 to 0.94) | — | — | 0.003 |
MMRMa | PPS | 0.64 (0.194) (0.25 to 1.02) | — | — | 0.001 |
ANCOVA (OC)b | PPS | 0.65 (0.197) (0.26 to 1.04) | — | — | 0.001 |
ANCOVA (BOCF)b | PPS | 0.65 (0.197) (0.26 to 1.04) | — | — | 0.001 |
ANCOVA = analysis of covariance; BOCF = baseline observation carried forward; CI = confidence interval; DSFS = Drooling Severity and Frequency Scale; FAS = full analysis set; GICS = Global Impression of Change Scale; LSM = least squares mean; MMRM = mixed model for repeated measures; MP = main period; OC = observed cases; PPS = per-protocol set; SE = standard error; U = units.
aLSMs are from model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and DSFS at baseline included as covariate. For MMRM visit*treatment is interaction term and visit is repeated factor.
bLSMs are from model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and DSFS at baseline included as covariate.
Source: SIAXI Clinical Study Report.8
Subgroup Analyses of Co-Primary Efficacy Outcomes
Table 50: Subgroup Analysis of Change in uSFR by Etiology of Sialorrhea Based on the Overall LSMs (SIAXI MP, FAS, MMRM)
Etiology of sialorrhea | n | LSM difference (SE) (95% CI)a |
|---|---|---|
PD/AP | 145 | −0.08 (0.012) (−0.10 to −0.05) |
Stroke | 32 | −0.05 (0.025) (−0.10 to −0.00) |
TBI | 5 | −0.09 (0.056) (−0.20 to 0.02) |
AP = atypical parkinsonism; CI = confidence interval; FAS = full analysis set; LSM = least squares mean; MMRM = mixed method repeated measures; MP = main period; PD = Parkinson disease; SE = standard error; uSFR = unstimulated salivary flow rate; TBI = traumatic brain injury; U = units.
auSFR measured in g/min. LSMs are from model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and uSFR at baseline included as the covariate. For MMRM visit × treatment is interaction term and visit is the repeated factor.
Source: SIAXI Clinical Study Report.8
Table 51: Subgroup Analysis of Change in uSFR by Etiology of Sialorrhea from Baseline to Week 4 (SIAXI MP, FAS, OC)
Etiology of sialorrhea | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | ||
|---|---|---|---|---|
n | Mean (SD)a | n | Mean (SD)a | |
PD/AP | 29 | −0.04 (0.23) | 58 | −0.11 (0.19) |
Stroke | 6 | 0.04 (0.12) | 13 | −0.20 (0.28) |
TBI | 1 | −0.02 (NA) | 2 | −0.12 (0.10) |
AP = atypical parkinsonism; FAS = full analysis set; MP = main period; NA = not applicable; OC = observed cases; PD = Parkinson disease; SD = standard deviation; uSFR = unstimulated salivary flow rate; TBI = traumatic brain injury; U = units.
auSFR measured in g/min.
Source: SIAXI Clinical Study Report.8
Table 52: Subgroup Analysis of Patient GICS by Etiology of Sialorrhea Based on the Overall LSMs (SIAXI MP, FAS, MMRM)
Etiology of sialorrhea | n | LSM difference (SE) (95% CI)a, b |
|---|---|---|
PD/AP | 146 | 0.58 (0.063) (0.46 to 0.71) |
Stroke | 32 | 0.78 (0.126) (0.53 to 1.03) |
TBI | 5 | 1.24 (0.285) (0.68 to 1.80) |
AP = atypical parkinsonism; CI = confidence interval; FAS = full analysis set; GICS = global impression of change scale; LSM = least squares mean; MMRM = mixed method repeated measures; MP = main period; PD = Parkinson disease; SE = standard error; TBI = traumatic brain injury; U = units.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
bLSMs are from model with treatment, country, gender, use of ultrasound and etiology included as (fixed) factors and DSFS sum score at baseline included as covariate. For MMRM visit*treatment is interaction term and visit is repeated factor
Source: SIAXI Clinical Study Report.8
Table 53: Subgroup Analysis of Patient GICS by Etiology of Sialorrhea at Week 4 (SIAXI MP, FAS, OC)
Etiology of sialorrhea | Placebo (N = 36) | IncobotulinumtoxinA 100 U (N = 74) | ||
|---|---|---|---|---|
n | Mean (SD)a | n | Mean (SD)a | |
PD/AP | 29 | 0.41 (0.82) | 58 | 0.91 (1.03) |
Stroke | 6 | 0.83 (0.98) | 13 | 1.31 (0.75) |
TBI | 1 | 0.00 | 2 | 3.00 (0.00) |
AP = atypical parkinsonism; FAS = full analysis set; GICS = Global Impression of Change Scale; MP = main period; OC = observed cases; PD = Parkinson disease; SD = standard deviation; TBI = traumatic brain injury; U = units.
aGICS: −3 = very much worse function, −2 = much worse function, −1 = minimally worse function, 0 = no change in function, 1 = minimally improved function, 2 = much improved function, 3 = very much improved function.
Source: SIAXI Clinical Study Report.8
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
Findings
No studies were identified assessing the validity, reliability, responsiveness, or MID of any of the outcome measures (Table 54) used in the pivotal SIAXI trial of incobotulinumtoxinA for chronic sialorrhea associated with neurological disorders. Each outcome measure is described in detail below.
Table 54: Summary of Outcome Measures and their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Unstimulated salivary flow rate (uSFR) | Weighing of dental rolls soaked with saliva over 5 minutes; procedure repeated after 30 minutes | • Validity: not identified • Reliability: not identified • Responsiveness: not identified | Not identified |
Global Impression of Change Scale (GICS) | Seven-point Likert scale ranging from -3 (very much worse) to +3 (very much improved); self-administered | • Validity: not identified • Reliability: not identified • Responsiveness: not identified | Not identified |
Drooling Severity and Frequency Scale (DSFS) | Five-point Likert scale for severity and 4-point Likert scale for frequency; sum score ranges from 2 to 9; investigator-rated | • Validity: not identified • Reliability: not identified • Responsiveness: not identified | Not identified |
Modified Radboud oral motor inventory for Parkinson disease (mROMP) | Inventory with a 24-item questionnaire of 5-point Likert scales; includes 8 questions to evaluate speech symptoms and 9 questions to evaluate drooling; self-administered | • Validity: not identified • Reliability: not identified • Responsiveness: not identified | Not identified |
EuroQol-5 dimension (EQ-5D-3L) | Questionnaire of the EuroQol Group with 5 items (each with 3 response options) and a VAS; self-administered | • Validity: not identified • Reliability: not identified • Responsiveness: not identified | Not identified |
MID = minimal important difference; VAS = Visual Analogue Scale.
Unstimulated Salivary Flow Rate (uSFR)
In the pivotal SIAXI trial, uSFR was measured by direct saliva collection using the swab method. Note that a negative change in the uSFR represents a reduction in salivary flow and thus an improvement in sialorrhea.
Two absorbent cotton rolls were placed directly at the orifices of the ducts of glands, one between the cheek and the gums and one between the tongue and the gums, on each side. The rolls were left in place for 5 minutes. The salivary flow rate was calculated using the following formula:
Salivary flow rate [mg/min] = Weight increase of rolls [mg] / Time of collection [min]
The procedure was repeated after 30 minutes and the average of the 2 results was calculated. The assessments were performed under the following standardized conditions:
Measurement took place at approximately the same time of day (between breakfast and lunch).
For patients with “On-Off” motor fluctuations, assessments took place in comparable “On” states, preferably at the same day and time, at least throughout the MP.
Patients were not allowed to have eaten spicy foods on the day of assessment.
Before measurement, the patient had to have fasted for 1 hour.
One hour before the measurement, the patient’s teeth were brushed by themselves or by a caregiver. Thereafter, the patient was not allowed to eat or smoke until after the measurement.
Thirty minutes before the measurement, a drink of still mineral water (maximum 200 mL) was offered to the patient. The patient was not obliged to drink this.
The patient was seated for the measurement.
Measurement was performed after the patient had swallowed their saliva and the remainder of the saliva present in the patient’s mouth had been removed using a gauze pad.
A collection cup was used to balance the scale immediately before the measurement.
The 4 cotton rolls were placed in the collection cup and their weight was measured and recorded. This was the pre-collection value (sum weight of all 4 cotton rolls).
One person was to place the 4 weighed cotton rolls in the patient’s mouth as described above and another person was to measure the collection time using a stopwatch or stop-clock. The first placement of cotton roll marked the start of the clock, and the first cotton roll was to be removed after exactly 5 minutes and placed in the collection cup, followed by the others in the same order and with the same time intervals as they were inserted. The clock was to be stopped on removal of the last cotton roll and this time was to be recorded. The collection cup (containing all 4 wet cotton rolls) was weighed, and its weight (post-collection value) was recorded. If the scale had been balanced correctly, the increase in weight represented the saliva produced during the 5-minute measurement. If the balancing of the scale was carried out incorrectly (e.g., without the cup), the scale was not balanced, or the measurement was carried out incorrectly (e.g., without the cup or without the cotton rolls), then the collection was discarded, and a fresh measurement was performed after an interval of at least 5 minutes. The same rule applied if the patient spat out a cotton roll. If the patient spat out all the cotton rolls after an interval of at least 4 minutes, these were to be weighed and the exact time of spitting out the rolls was to be recorded; in this way, the salivary flow rate could be calculated using the formula given above.8
Global Impression of Change Scale
The patient’s and caregiver’s global impression of change with respect to baseline (or for the EP, the previous injection) was recorded before the quantitative measurement of saliva production. Questions for the GICS were adapted for the indication under study.
The question of the GICS (self-administered) asked of the patient was:
Compared to how you were doing just before the last injection into your salivary gland, what is your overall impression of how you are functioning now as a result of this treatment?”
The question of the GICS (self-administered) asked of the caregiver was:
Compared to how the patient was doing just before the last injection into his/her salivary gland, what is your overall impression of how he/she is functioning now as a result of this treatment?”
The following definition was applicable for both the patient and caregiver and read: “Changes in functioning are meaningful changes you might have experienced as a result of treatment (including: changes in amount of skin irritation or need to wipe saliva, changes in difficulties eating/drinking/talking, changes in the amount or frequency of saliva getting on clothes/books/electronic devices and changes in interactions with others).”
The response options for all GICS questions (for both the patients and caregiver) were based on a common 7-point Likert scale that ranged from -3 (very much worse) to +3 (very much improved):
+3, Very much improved
+2, Much improved
+1, Minimally improved
0, No change
–1, Minimally worse
–2, Much worse
–3, Very much worse
Patients were asked to fill in the GICS independently of others, unless they needed help with reading or writing, in which case another person was to assist them (such help was to be recorded). If the patient was not able to answer this question even with assistance, then this was to be documented. In such cases the caregiver’s rating was to be used instead of the patient’s rating, which was left blank. For telephone contacts, a special version of the GICS adapted for telephone interviews was used, both for the patient and the caregiver. This version differed in that the introductory explanations, questions and options were read to the patient or caregiver and in that the interviewer had to mark the patient’s or caregiver’s responses.8
Drooling Severity and Frequency Scale
The DSFS was used to rate drooling severity (using a 5-point Likert scale from 1 [dry; never drools] to 5 [profuse; hands, tray and objects wet]) and frequency (using a 4-point Likert scale from 1 [never] to 4 [constantly]). The DSFS sum score was obtained by summation of the severity and frequency scores (range 2 to 9).
All DSFS scores were rated by investigators, possibly as part of clinical evaluation, although the specific criteria used in determining ratings were not provided. The DSFS was scored according to the following criteria:
Drooling severity
Dry (never drools)
Mild (only lips wet)
Moderate (wet on lips and chin)
Severe (drool extends to clothes wet)
Profuse (hands, tray and objects wet)
Drooling frequency
Never
Occasionally (not every day)
Frequently (part of every day)
Constantly
DSFS was evaluated for the time period “over the last week.” Instructions were provided in detail in a study-specific manual.8
Modified Radboud Oral Motor Inventory for Parkinson Disease (mROMP)
The mROMP was used for the first time in this study. The mROMP Inventory is a self-administered questionnaire designed to assess dysarthria, dysphagia, and sialorrhea in patients with PD and consists of 24 items in 3 domains: speech, swallowing and drooling. There are 8 items in the speech domain, 7 in the swallowing domain, and 9 in the drooling domain. Each item is evaluated using a 5-point Likert scale; thus, the minimum/maximum scores for the speech, swallowing and drooling domains are 8/40, 7/35, and 9/45, respectively. The mROMP was modified from the original 23-question Dutch ROMP Inventory59 to implement small changes in wording resulting from patient interviews during linguistic validation into US English. Reproducibility of the ROMP based on consecutive measurements for 60 patients with PD/AP within 24±12 days was high (overall internal consistency 0.95, intraclass correlation coefficient 0.94; domain internal consistency 0.87 to 0.94, intraclass correlation coefficients 0.83 to 0.92). Construct validity, based on blinded evaluation of 118 patients with PD/AP who had completed the ROMP by a neurologist and speech-language pathologist, was substantial to good (correlation coefficients 0.36 to 0.82). Validity of the speech and drooling domains was generally good (correlation coefficients 0.63 to 0.72 and 0.78 to 0.82, respectively). The responsiveness to change of the ROMP inventory was not assessed. No studies have directly compared the ROMP and mROMP.
The recall period for the mROMP was the last 7 days. The patient was asked to fill in the mROMP independently of others, except when they needed help with reading or writing, in which case another person was to assist them (such help was to be recorded). If the patient was not able to answer these questions even with assistance, then this was to be documented; in such cases the mROMP was left blank.8
EuroQol 5-Dimensions 3-Levels
The EQ-5D-3L is a generic preference-based HRQoL instrument that has been applied to a wide range of health conditions and treatments including inflammatory bowel disease.60,61 The first of 2 parts of the EQ-5D-3L is a descriptive system that classifies respondents (aged ≥12 years) into one of 243 distinct health states. The descriptive system consists of the following 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 3 possible levels (1, 2, or 3) representing “no problems,” “some problems,” and “extreme problems,” respectively. A scoring function can be used to assign a value (EQ-5D-3L index score) to self-reported health states from a set of population-based preference weights.60,61 The second part is a vertical, calibrated 20 cm EQ VAS that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state,” respectively. Respondents are asked to rate their own health by drawing a line from an anchor box to the point on the EQ VAS which best represents their own health on that day. Hence, the EQ-5D-3L produces 3 types of data for each respondent:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor (e.g., 11121, or 33211);
A population preference-weighted health index score based on the descriptive system; and
A self-reported current health status based on the EQ VAS that is used to assess the overall health of the respondent rather than selected dimensions of individuals’ health.
The EQ-5D-3L index score is generated by applying a multi-attribute utility function to the descriptive system. Different utility functions are available that reflect the preferences of specific populations. The lowest possible overall score (corresponding to severe problems on all 5 attributes) varies depending on the utility function that is applied to the descriptive system. Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 1.00 are assigned to the health states “dead” and “perfect health,” respectively.60,61
Patients participating in the SIAXI trial were asked to fill in the EQ-5D independently of others, except when they needed help with reading or writing, in which case another person was to assist them (such help was to be recorded). If the patients was not able to answer these questions even with assistance, then this was to be documented; in such cases the EQ-5D was left blank.8
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
BoNT-A
botulinum neurotoxin type A
EQ-5D
EuroQol 5-Dimensions questionnaire
ICER
incremental cost-effectiveness ratio
NICE
National Institute for Health and Care Excellence
PD
Parkinson disease
QALY
quality-adjusted life-year
SMR
standardized mortality ratio
SoC
standard of care
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | IncobotulinumtoxinA (Xeomin), powder for solution for injection, 50 U and 100 U per vial |
Submitted price | IncobotulinumtoxinA, 50 U: $165.00 per single-use vial IncobotulinumtoxinA, 100 U: $330.00 per single-use vial |
Indication | For the treatment of chronic sialorrhea associated with neurologic disorders in adults |
Health Canada approval status | Notice of Compliance |
Health Canada review pathway | Standard |
Notice of Compliance date | November 17, 2020 |
Reimbursement request | As per indication |
Sponsor | Merz Therapeutics, a business of Merz Pharma Canada Ltd. |
Submission history | Previously reviewed: Yes Blepharospasm: Indication: Symptomatic management in adult of blepharospasm Recommendation date: December 16, 2009 Recommendation: List in a similar manner. Cervical dystonia: Indication: Symptomatic management in adults of cervical dystonia of a predominantly rotational form (spasmodic torticollis) Recommendation date: December 16, 2009 Recommendation: List in similar manner. Spasticity, post-stroke: Indication: Symptomatic management in adults of post-stroke spasticity of the upper limb Recommendation date: December 16, 2009 Recommendation: Do not list |
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult patients with neurologic disorders who have chronic sialorrhea |
Treatment | IncobotulinumtoxinA plus SoC |
Comparators | SoC (consisting of basic non-pharmacological sialorrhea management, including physical aids such as bibs, as well as speech language pathologist and occupational therapist consultations) OnabotulinumtoxinA plus SoC |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 15 years |
Key data sources |
|
Submitted results | Based sequential analyses:
|
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; SoC = standard of care.
Conclusions
Data from the SIAXI study suggested that using incobotulinumtoxinA to manage sialorrhea in adult patients with neurologic disorders more effectively reduced mean unstimulated salivary flow rates compared with placebo after 4 weeks. Results obtained on the investigator-rated Drooling Severity and Frequency Scale (DSFS) were aligned with the primary analysis, although this was an exploratory outcome. The clinical significance of post-treatment changes in sialorrhea was uncertain because the outcome measures were unvalidated, not used in clinical practice, and of unclear importance to patients. There is no robust direct or indirect comparative evidence regarding the efficacy of incobotulinumtoxinA compared to other botulinum neurotoxin type A (BoNT-A) products, or any other treatments for sialorrhea in adults with neurologic disorders. In the sponsor’s economic analysis, BoNT-A products were assumed to have equal efficacy, which was deemed acceptable by the clinical expert for this review.
CADTH undertook reanalyses to address limitations relating to sialorrhea health-state utility values, mortality of patients with underlying neurologic conditions, discontinuation of standard of care (SoC), changing the disutility of dysphagia, and removing onabotulinumtoxinA as a comparator in the analysis. Based on CADTH reanalysis, the incremental cost-effectiveness ratio (ICER) for incobotulinumtoxinA plus SoC compared to SoC alone is $67,239 per quality-adjusted life-year (QALY). A 30% reduction in the price of incobotulinumtoxinA is required for incobotulinumtoxinA plus SoC to achieve an ICER of $50,000 per QALY compared with SoC alone. CADTH noted that changes to assumptions regarding utility values were the key driver of the results. In a scenario analysis that included onabotulinumtoxinA plus SoC in the sequential analysis, which assumed equivalent effectiveness, onabotulinumtoxinA plus SoC was more costly than incobotulinumtoxinA plus SoC.
CADTH was unable to address 2 limitations with the model conceptualization: the assumed maintenance of effectiveness without consideration of the natural history of the patient’s underlying condition(s) on the long-term effectiveness of treatments for sialorrhea (relevant comparators not included) and the lack of robust comparative data with relevant comparators. As such, the true cost-effectiveness of incobotulinumtoxinA for adults with neurologic disorders who have chronic sialorrhea is uncertain.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups and drug plans that participated in the CADTH review process. No registered clinician input was received for this review.
Patient input was received from Parkinson Québec for this review. Patient input was gathered through an online survey of 405 respondents, 295 of whom were living with Parkinson disease (PD) and 110 of whom were caregivers. Of the respondents, 47% of individuals living with PD and 40% of caregivers reported sialorrhea. In terms of the impact on daily life, it was reported that sialorrhea influenced individuals’ self-esteem, social comfort, personal relationships, ability to eat and swallow, and ability to speak and communicate. For currently available treatment options, the majority of respondents used non-pharmacological treatments to manage sialorrhea, with the most common being using a cloth to wipe drool, followed by use of chewing gum and mouth exercises. Only 5% of individuals used medications to manage sialorrhea, and 1% had experience using a botulinum toxin. No individuals surveyed had experience with incobotulinumtoxinA. Approximately 1-third of individuals living with PD and 43% of caregivers surveyed reported a need for new ways to manage sialorrhea. Expectations for new treatments included fewer or milder side effects and reduction in the frequency and severity of sialorrhea. Respondents also expressed a desire for oral treatment options and options with longer duration of action. Cost burden was an important consideration as many treatments for sialorrhea are not reimbursed by public drug plans.
Feedback from drug plans noted several concerns. These included, but were not limited to, the level of severity to initiate treatment, treatment sequencing of off-label oral medications before initiating incobotulinumtoxinA, reassessment criteria for continued coverage of incobotulinumtoxinA injections, re-initiation of treatment when treatment is stopped due to a non-treatment-related issue, dosing beyond the Health Canada–approved dose, drug administration by a specialist, use of incobotulinumtoxinA with anticholinergics, use of incobotulinumtoxinA in patients with neurologic disorders beyond those studied in the SIAXI trial or pediatric patients, and inclusion of costs of off-label medications that are listed as an open or full benefit on drug plans.
Several of these concerns were addressed in the sponsor’s model:
The clinical effectiveness of sialorrhea management in the model was based on the DSFS, which considers both the severity and frequency of sialorrhea.
Adverse events (AEs), including dysphagia and dry mouth, were incorporated in the sponsor’s model as a cost and disutility.
The sponsor’s model assumed public coverage for incobotulinumtoxinA and onabotulinumtoxinA. AbobotulinumtoxinA was not included.
Initiation of treatment in the sponsor’s model was only for those with moderate or severe sialorrhea, defined by a DSFS score of 4 or higher.
Drug administration in the pharmacoeconomic evaluation included costs for an outpatient physician consultation. Injection-training costs for specialists were not included.
CADTH was unable to address the following concerns raised from stakeholder input:
oral treatment options, such as anticholinergics, were not considered comparators to manage sialorrhea
discontinuation of incobotulinumtoxinA due to lack of clinical effect
re-initiation of treatment if a patient stops due to non-treatment-related issues
incorporating dose escalation if a patient requires dosing greater than the Health Canada–approved dose
cost-effectiveness of incobotulinumtoxinA:
in patients with prior off-label oral medications (i.e., influence of treatment sequencing)
combined with oral anticholinergic medications
in neurologic disorders beyond those specifically examined in the SIAXI trial
in a pediatric patient population.
In addition, CADTH addressed a concern that costs of off-label oral medications listed as full benefits were explored in the budget impact analysis as a scenario analysis.
Economic Review
The current review is for incobotulinumtoxinA (Xeomin) for the treatment of chronic sialorrhea in adults with neurologic disorders.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of incobotulinumtoxinA plus SoC compared with onabotulinumtoxinA plus SoC and SoC alone. SoC was assumed to consist of basic non-pharmacological sialorrhea management, including physical aids.1 The model population, which comprised adult patients with neurologic disorders who have chronic sialorrhea, was aligned with its Health Canada indication.2
IncobotulinumtoxinA is a powder for solution for either intramuscular or intraglandular injection that is available in 50 U or 100 U vials. The recommended dose for incobotulinumtoxinA is 100 U per treatment session, with repeat treatment sessions occurring no sooner than every 16 weeks.2 IncobotulinumtoxinA should be administered by physicians with suitable qualifications who are experienced in administering BoNT-A products.3 At the sponsor’s submitted price of $330.00 for a 100 U vial and $165.00 for a 50 U vial, the cost per treatment session is $330.00. Assuming patients receive 3.25 administrations per year (once every 16 weeks), the sponsor assumed that the annual cost of incobotulinumtoxinA treatment would be $1,073 if patients remained on therapy. No drug acquisition cost was modelled for SoC as this was assumed to consist of non-pharmacological interventions, and SoC was assumed to be received by all treatment groups. The cost of onabotulinumtoxinA (which does not have a Health Canada indication for sialorrhea management) reflected the publicly available price ($357.10 per 100 U vial) and dosing was assumed to be identical to that of incobotulinumtoxinA (100 U per treatment session), leading to an annual cost of $1,160.4 No wastage was assumed for incobotulinumtoxinA or onabotulinumtoxinA as the vial sizes used reflected the dose to be administered.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a 15-year time horizon from the perspective of a Canadian public health care payer. Discounting at 1.5% per annum was applied to both costs and outcomes.
Model Structure
A Markov state transition model with 5 health states with a cycle length of 16 weeks, corresponding to the reinjection interval for incobotulinumtoxinA plus SoC was submitted by the sponsor (Figure 1).1 The model consisted of 3 sialorrhea severity–based health states (mild/resolved, moderate, and severe), which were defined by the DSFS sum scores, alongside a treatment discontinuation and death health state. The DSFS is based on 2 subscales measuring drooling severity and drooling frequency that are summed to determine a sum score.1 Levels of the scales are provided in Table 11. The mild/resolved state was defined by a DSFS sum score of 2 or 3; the moderate state was defined by DSFS sum scores of 4 to 6; and the severe state was defined by DSFS sum scores of 7 to 9.1 Patients in any sialorrhea-severity health state could transition to any other sialorrhea health state, reflecting improvement or worsening of sialorrhea over time. Patients in any sialorrhea-severity health state could also transition to a treatment discontinuation health state. Patients in all health states could also transition to a death state at any model cycle.
Model Inputs
The model’s baseline population characteristics and clinical efficacy parameters were characterized according to the SIAXI study, a phase III, double-blind, randomized, placebo-controlled trial evaluating the efficacy of incobotulinumtoxinA 75 U or 100 U administered as 4 injections into the bilateral parotid and submandibular glands over 64 weeks, compared to volume-matched placebo in patients with chronic troublesome sialorrhea due to Parkinson disease or after a stroke or traumatic brain injury.5 The sponsor assumed that the SIAXI population (mean age, 65.2 years; 70.7% male)5 reflected the Canadian population. The distribution of patients across health states (55% severe, 45% moderate at baseline) was also based on baseline DSFS scores of patients in the SIAXI trial.5 SoC in the sponsor’s analysis was modelled based on the placebo arm of the SIAXI trial.
Efficacy was modelled through the DSFS sum scores, using individual patient data from the SIAXI trial to produce transition matrices. DSFS sum scores from the full analysis set for incobotulinumtoxinA were available for the 4 injection cycles; for placebo, data were limited to a single injection cycle (16 weeks). Whereas DSFS was assessed every 4 weeks in the first injection cycle, DSFS was only assessed 4 weeks after the injection in the subsequent injection cycles. As such, transitions were based on data reported at 4 weeks following each injection cycle (i.e., cycle 1 for incobotulinumtoxinA plus SoC and SoC alone were based on comparing the data observed at baseline to week 4; for cycle 2 to 4 for incobotulinumtoxinA plus SoC, transitions were calculated based on comparing data observed from weeks 4 to 20, 20 to 36, and 36 to 52). For SoC alone, only data from baseline to week 4 were available to inform the transition matrix at week 16; all patients who received placebo at baseline received an active treatment. However, data from baseline to week 52 were available for incobotulinumtoxinA plus SoC to inform the transition matrices for the first 4 treatment cycles. Beyond these time periods, the sponsor assumed that the distribution of patients observed at the end of the trial period would carry forward for the remainder of the model time horizon (i.e., sialorrhea-severity stabilizes at the end of cycles 1 and 4 for patients receiving SoC alone and incobotulinumtoxinA plus SoC, respectively, and be maintained over the 15-year time horizon). This means that, for patients receiving SoC alone, transitions between sialorrhea-severity health states only occur in cycle 1. For patients receiving incobotulinumtoxinA plus SoC, no further transitions occur after the fourth model cycle.
As there is no direct evidence regarding the relative efficacy of incobotulinumtoxinA compared to onabotulinumtoxinA, the sponsor conducted a feasibility assessment for an indirect comparison comparing the effectiveness of these treatments.1 The assessment concluded that there was insufficient evidence to conduct an indirect comparison, and that studies identified had different study designs, patient populations, and outcome ascertainment.1 As an indirect treatment comparison was not deemed feasible, the sponsor assumed equal efficacy in terms of treatment effectiveness, treatment discontinuation, and AE rates between incobotulinumtoxinA and onabotulinumtoxinA.
During all cycles, patients in all sialorrhea-severity health states could transition to the treatment discontinuation health state based on a treatment-specific, all-cause discontinuation rate. Rates of discontinuation for the first cycle for incobotulinumtoxinA plus SoC and SoC alone were based on all-cause discontinuation from the main period (baseline to week 16) of the SIAXI trial (2.7% and 11.1%, for incobotulinumtoxinA plus SoC and SoC alone, respectively).6 Discontinuation for subsequent cycles for incobotulinumtoxinA were also based on the SIAXI trial by deriving the average discontinuation rate during the extension period (week 16 and week 64; 4.7%), while the discontinuation rate for SoC alone in subsequent cycles was assumed to be the same as that observed in cycle 1.1
Mortality in the model was assumed to be equal across all health states (i.e., no excess mortality risk was associated with more severe sialorrhea).1 Mortality across all health states was assumed to be equal to that of the general Canadian population and based on age- and sex-specific rates from Canadian life tables.7
The sponsor included 2 AEs for incobotulinumtoxinA plus SoC (dry mouth and dysphagia); no AEs were associated with SoC alone. The AEs for onabotulinumtoxinA plus SoC were assumed to be equal to those of incobotulinumtoxinA plus SoC, based on clinical expert opinion.1
Health-state utility values were based on a post hoc analysis of EuroQol 5-Dimensions (EQ-5D) data from the SIAXI trial, using an Australian value set (Table 12).8 The sponsor incorporated disutilities associated with AEs sourced from the literature.9,10
Costs in the model included treatment acquisition costs for incobotulinumtoxinA and onabotulinumtoxinA; no drug acquisition cost was applied for SoC as it was assumed to consist of non-pharmacological sialorrhea management. Other costs included drug administration costs, disease management costs, and AE management costs. Drug administration costs for incobotulinumtoxinA and onabotulinumtoxinA were based on the Ontario Schedule of Benefits for Physician Services and consisted of the cost of an outpatient consultation for all patients and the cost of an ultrasound for 65% of patients, based on the proportion of patients in the SIAXI trial who had an ultrasound to guide drug administration.5,11 Disease management consisted of speech language pathology and occupational therapy consultations, with costs sourced from the Ontario Schedule of Benefits.11 Visit frequency to speech language pathologists and occupational therapists are provided in Table 13. The costs of AE management costs were applied for dry mouth and were assumed to involve at-home remedies; no AE cost was applied for dysphagia as this was assumed to be managed using existing SoC.1
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations). The deterministic and probabilistic results were similar. The probabilistic findings are presented below.
Base-Case Results
IncobotulinumtoxinA plus SoC was associated with a QALY gain of 0.51 at an additional cost of $7,287, resulting in an ICER of $14,417 per QALY gained, compared with SoC. OnabotulinumtoxinA plus SoC was dominated by (i.e., it was less effective and more expensive than) incobotulinumtoxinA plus SoC.
The sponsor reports that 0.07 of the QALY gain for incobotulinumtoxinA plus SoC occurred during the 64-week trial period and 0.33 occurred in the post-trial period; this breakdown was only reported in the deterministic analysis, in which the total QALY gain observed for incobotulinumtoxinA plus SoC was 0.41. The sponsor reports that incobotulinumtoxinA plus SoC compared to SoC alone was cost-effective at a willingness-to-pay threshold of $50,000 per QALY in 99.96% of iterations. IncobotulinumtoxinA plus SoC compared to onabotulinumtoxinA plus SoC was cost-effective in 98% of iterations.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|
SoC | 3,917 | 7.18 | Reference |
IncobotulinumtoxinA plus SoC | 11,204 | 7.68 | $14,417 |
OnabotulinumtoxinA plus SoC | 11,607 | 7.67a | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SoC = standard of care.
Note: The submitted analysis is based on the publicly available prices of the comparator treatments.
aA difference in total QALYs was observed between incobotulinumtoxinA plus SoC and onabotulinumtoxinA plus SoC in the probabilistic analysis because the relative efficacy of the comparators was included in the probabilistic analysis. The total QALYs for incobotulinumtoxinA plus SoC and onabotulinumtoxinA plus SoC are identical in the sponsor’s deterministic analysis.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters in probabilistic scenario analyses. The model was sensitive to discontinuation rates for incobotulinumtoxinA plus SoC. When the discontinuation rate for incobotulinumtoxinA plus SoC was assumed to be 20% for each cycle period, the ICER for incobotulinumtoxinA plus SoC versus SoC increased to $21,159 per QALY. When a 50% discontinuation rate was assumed, incobotulinumtoxinA plus SoC was dominated by SoC (i.e., the former was less effective and more expensive).
The model was also sensitive to the baseline distribution of patients across moderate and severe health states.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The analysis does not include all relevant comparators. The sponsor’s analysis compared incobotulinumtoxinA plus SoC with SoC alone and onabotulinumtoxinA plus SoC. In addition to onabotulinumtoxinA plus SoC, several other off-label medications for sialorrhea management are used in Canadian clinical practice, according to feedback from the clinical expert consulted for this review (per Appendix 1, and the comparator table provided by the sponsor).3 CADTH economic guidelines require all interventions currently used and potentially displaced to be identified, and those that decision-makers are currently funding or are commonly used should be included.12 While not indicated for sialorrhea, many off-label treatments are listed as a full benefit in jurisdictions, meaning that clinicians can prescribe medications for any indication, including those that are off-label.3 Additionally, CADTH economic guidelines note that comparator selection should not be limited by the availability of data.12 The sponsor rationalized excluding some oral, off-label comparators due to high AE rates that preclude their use in some neurologic disorders, such as Parkinson disease; however, these events could have been incorporated using the sponsor’s model structure.1 The exclusion of comparators that may be displaced if incobotulinumtoxinA is publicly reimbursed may favour incobotulinumtoxinA, as these comparators are associated with much lower annual costs (Appendix 1), although the comparative benefits are unknown.
CADTH was unable to address this limitation. As such, the cost-effectiveness of incobotulinumtoxinA compared to oral off-label therapies which are currently reimbursed is unknown.
The model does not reflect the natural history of sialorrhea or patients’ underlying neurologic conditions associated with sialorrhea. The sponsor’s analysis assumed that patients who discontinue treatment will revert to their baseline sialorrhea severity, which was implemented by weighting the utility for the treatment discontinuation health state by the proportion who are severe and moderate at baseline and their respective utility values. This means that 45% of patients who discontinue are moderate and are assumed to remain moderate for the entire time horizon (15 years). According to the clinical expert consulted for this review, sialorrhea is expected to worsen in severity over time, depending on the patient’s underlying condition. Therefore, it is unlikely a patient’s sialorrhea severity will remain static after discontinuing treatment for the entire time horizon.
Additionally, the sponsor’s long-term efficacy assumption for incobotulinumtoxinA plus SoC used in the sponsor’s analysis (i.e., that patients receiving incobotulinumtoxinA will remain in the same sialorrhea-severity state observed at the end of the SIAXI trial) does not reflect the progressive nature of patients’ underlying neurologic conditions. While the assumption that incobotulinumtoxinA will remain as effective as observed during the trial may be appropriate in patients whose underlying neurologic condition is not progressive, long-term efficacy for incobotulinumtoxinA is unlikely to be maintained for patients with degenerative neurologic conditions, according to the clinical expert consulted for this review. Instead, it is expected that, for neurologic conditions that worsen over time, saliva production may become more profuse and the reduction in sialorrhea achieved with incobotulinumtoxinA may not be maintained. Additionally, the clinical expert noted that, for some neurologic conditions, swallowing may become an increasingly important issue, which could contraindicate treatment with incobotulinumtoxinA. As the sponsor’s analysis assumes that both the severity of a patient’s underlying neurologic condition and their sialorrhea remain static over time, the treatment-waning effect associated with progression of underlying disease or sialorrhea was not incorporated.
CADTH was unable to incorporate the impact of the natural history of underlying disease on the model’s results. If incobotulinumtoxinA was less effective in the long-term than observed at the end of the SIAXI trial, the sponsor’s model overestimates the effectiveness of incobotulinumtoxinA, and the ICER is therefore likely underestimated.
As a scenario analysis, CADTH explored assuming that all patients who discontinue have severe sialorrhea by assigning the treatment discontinuation health-state utility associated with severe disease.
The quality of life associated with sialorrhea is uncertain. The sponsor’s base case incorporated utility values from an Australian cost-effectiveness model derived from stratifying EQ-5D data from all treatment arms of the SIAXI trial by DSFS score to determine a mean utility score associated with the DSFS-defined health states. This produced a difference between severe and mild sialorrhea of 0.19.8 The sponsor conducted additional analyses to derive health-state utilities based on the SIAXI study data. The resulting utility values, which are provided in Table 12, lead to an estimated difference in utility between severe and mild sialorrhea of 0.0543.1 The sponsor postulated that generic instruments such as the EQ-5D may be insensitive to changes in disease severity.1 As the difference between mild and severe sialorrhea was relatively small using SIAXI trial data and is therefore unlikely to reflect the difference in health-related quality of life associated with sialorrhea, the sponsor selected the Makino study utility values for its base case.1,8 The large differences between results are of concern, given the same base data source appears to have been used to inform the Makino study utility values and those tested by the sponsor.
The clinical expert consulted for this review indicated that the influence of sialorrhea on health-related quality of life is difficult to determine and patient-specific. Reducing the severity of the sialorrhea is expected to affect overall quality of life, but the magnitude of this impact may differ between patients. According to Lowin et al. (2017), progression from 1 Hoehn and Yahr Scale stage to the next most severe stage is associated with a change in utility of 0.11.13 Using the sponsor’s difference between mild and severe sialorrhea (0.19) means that the impact on quality of life of sialorrhea is similar to that of the impact of 2 Hoehn and Yahr stages (e.g., going from no signs of disease to having bilateral symptoms, or going from having balance impairment with mild to moderate disease and being physically independent to needing a wheelchair or being bedridden unless assisted).14 While the influence of sialorrhea severity is uncertain, according to the clinical expert consulted for this review, other components of the underlying condition (e.g., mobility) are expected to have a greater impact on health-related quality of life, and it is therefore unlikely that the influence of sialorrhea on quality of life will be similar to that of mobility, suggesting that the sponsor’s utility values overestimate the benefit associated with incobotulinumtoxinA. It is therefore uncertain whether the EQ-5D data from the SIAXI trial were insensitive to changes in quality of life, or whether the trial data adequately reflect the change in quality of life due to sialorrhea, and it is actually smaller than anticipated by the sponsor.
The National Institute for Health and Care Excellence (NICE) Evidence Review Group used data from the SIAXI trial, which fit latent class mixed models to individual patient data using sialorrhea-severity levels (defined by DSFS scores as explanatory variables).15 This differs from the sponsor’s approach, which used raw DSFS scores as explanatory variables, then averaged the resulting utilities according to health-state groupings. These values were more aligned with the sponsor’s own derived utility values from the SIAXI trial. CADTH used the NICE report’s values in its base case.
As the health-related quality of life associated with sialorrhea is uncertain, CADTH conducted scenario analyses using the Makino study utility values and the sponsor’s utility values derived from the SIAXI trial.
The mortality of patients’ underlying conditions was not accurately reflected in the model. The sponsor assumed that patients receiving sialorrhea treatment would have the same natural mortality as that of the general Canadian population. This meant that, for those initiating treatment at age 65, it can be expected that 71% of patients will remain alive at age 80 over the 15-year time horizon. According to the clinical expert consulted for this review, patients with severe sialorrhea are expected to have a shorter lifespan compared to that of the general population given their underlying neurologic condition. It was expected that only a small proportion of patients initiating sialorrhea treatment will remain alive at age 80. The sponsor’s model therefore overestimates the life expectancy of patients with underlying neurologic conditions. During the NICE review of incobotulinumtoxinA for sialorrhea, the sponsor provided a literature search for standardized mortality ratios (SMRs) for patients with Parkinson disease or stroke weighted by the proportion of patients in the SIAXI trial with these conditions to generate an SMR of 4.09.15 When this estimate is applied in the model, 25% of patients remain alive after 15 years, which is higher than the proportion expected by the clinical expert consulted by CADTH.
The clinical expert consulted for this review also noted the sponsor’s assumption that there is no increased mortality risk associated with severe sialorrhea was not valid, as patients could develop complications such as aspiration pneumonia. CADTH was unable to implement an increased mortality risk associated with severe sialorrhea but as this risk is likely to be small, it is not expected to significantly influence the results of the analysis.
An SMR of 4.09 was applied in the CADTH base-case reanalysis. An SMR of 10, in which approximately 3% of patients remain alive by age 80, is explored as a scenario analysis to better reflect clinical expert feedback regarding the proportion of patients likely to be alive at 80 years of age with sialorrhea and an underlying neurologic condition.
The modelling of SoC is of limited validity. The sponsor used the placebo arm of the SIAXI trial to model SoC. After the first cycle, patients receiving SoC could not transition between sialorrhea states but could “discontinue” SoC (11%) and revert to their baseline sialorrhea-severity health states. As SoC is assumed to consist of non-pharmacological interventions, such as the use of a cloth to clear drool from the face and objects, this conceptualization has limited validity as patients will not discontinue use of physical aids, nor will this influence their sialorrhea severity.
In CADTH reanalyses, discontinuation for SoC was set to 100%. Doing so assumes that all patients will remain at their baseline sialorrhea severity, thereby removing any placebo effect observed in the SIAXI trial.
CADTH explored an alternate discontinuation rate among SoC patients of 0%, which assumes any placebo effect in the model would be maintained.
The disutility for dysphagia was inappropriately extracted from its source article. The sponsor used a disutility for dysphagia of 0.004 from Stal (1998).9 The differences in mean utility for patients before and after esophageal dilation (taken as the disutility of experiencing dysphagia) using the time trade-off or standard gamble methods outlined in Stal (1998) were 0.048 and 0.094, respectively.9
In CADTH reanalyses, the disutility for dysphagia was changed to −0.048 to reflect the difference in utility values reported in the sponsor’s source article.
Lack of comparative evidence limits the usefulness of a sequential analysis. Comparison of onabotulinumtoxinA plus SoC with incobotulinumtoxin plus SoC was based on an assumption of equivalent clinical efficacy and safety. There is no robust direct or indirect comparative evidence regarding the efficacy of incobotulinumtoxinA compared to other BoNT-A products, including onabotulinumtoxinA, or any other treatments for sialorrhea in adults with neurologic disorders. As there is no robust evidence comparing incobotulinumtoxin, onabotulinumtoxinA, and SoC, a sequential analysis of cost-effectiveness results is of limited value. As comparisons with onabotulinumtoxinA are naively derived and assumption-based, pairwise comparisons between comparators for which there is some clinical evidence (i.e., incobotulinumtoxin plus SoC versus SoC) may be more appropriate.
As no direct or indirect evidence exists comparing incobotulinumtoxin plus SoC or SoC with onabotulinumtoxinA plus SoC, onabotulinumtoxinA plus SoC was removed as a comparator from the CADTH base-case reanalysis. CADTH included a scenario analysis in which incobotulinumtoxin plus SoC, onabotulinumtoxinA plus SoC, and SoC were included.
Additional limitations were identified but were not considered to be key limitations. These limitations are outlined subsequently (or in Appendix 4).
Health care resource use may not be reflective of the Canadian clinical context. Routine care for disease management in the sponsor’s base-case was assumed to consist of visits to speech language pathologists and occupational therapists, with the frequency of the visits depending on a patient’s sialorrhea severity (Table 13). According to the clinical expert consulted for this review, patients may see an occupational therapist once or twice for sialorrhea management, but not on a continual basis. Additionally, no physician visits, aside from those for injection of an active treatment, were incorporated in the model, which was deemed inappropriate by the clinical expert consulted for this review. This means that patients who discontinued active treatment had no physician visits regarding sialorrhea management. Although these assumptions are not reflective of Canadian clinical practice, CADTH explorations of alternative visit frequencies demonstrated that health care resource use is unlikely to influence analysis results and therefore health care resource use was not addressed as a key limitation in CADTH reanalyses.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation Not Noted as Limitations to the Submission
Sponsor’s key assumption | CADTH comment |
|---|---|
The efficacy, safety and treatment discontinuation of incobotulinumtoxinA plus SoC is equal to that of onabotulinumtoxinA plus SoC. | In the absence of direct or indirect evidence, the clinical expert consulted by CADTH deemed this assumption to be appropriate. |
The dose for onabotulinumtoxinA was assumed to be the same as that for incobotulinumtoxinA (i.e., 100 U per injection). | This assumption was deemed to be appropriate by the clinical expert consulted by CADTH. |
Baseline distribution of DSFS scores observed in the trial (i.e., 55% severe, 45% moderate) was reflective of the Canadian population. | This assumption was deemed to be appropriate by the clinical expert consulted by CADTH. |
SoC = standard of care.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH reanalyses addressed several limitations within the economic model, summarized in Table 5. CADTH was unable to address limitations regarding comparisons to oral off-label comparators, or incorporating natural history associated with underlying disease.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
1. Implementation of adverse event disutility | Disutility added to health-state utility values in incobotulinumtoxinA plus SoC onabotulinumtoxinA plus SoC traces, resulting in higher health-state utility values | Disutility subtracted from health-state utility values in incobotulinumtoxinA plus SoC onabotulinumtoxinA plus SoC traces |
2. Variance around comparative efficacy between incobotulinumtoxinA plus SoC onabotulinumtoxinA plus SoC | Variance applied (Cell S469 = = IF(prob = ”Deterministic”,L469,IFERROR(U469,0))) | Variance around estimates removed (S469 = 1) |
3. Inflation | 1.3% | 0% |
Changes to derive the CADTH base case | ||
1. Health-state utility values | • Mild: 0.74 • Moderate: 0.64 • Severe: 0.55 • Discontinuers: 0.59 | • Mild: 0.62 • Moderate: 0.60 • Severe: 0.58 • Discontinuers: 0.59 |
2. Standard mortality ratio | 1.0 | 4.09 |
3. Discontinuation for SoC | 11% | 100% |
4. Disutility for dysphagia | −0.0004 | −0.048 |
5. OnabotulinumtoxinA + SoC in the sequential analysis | OnabotulinumtoxinA plus SoC included as a comparator | OnabotulinumtoxinA plus SoC removed as a comparator |
CADTH base case | 1 + 2 + 3 + 4 | |
SoC = standard of care
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions, or standard errors in probabilistic analyses) that are not identified as limitations.
The results of CADTH’s stepped analysis are presented in Table 15. CADTH’s base-case reanalysis demonstrates that, compared with SoC alone, incobotulinumtoxinA plus SoC is $6,127 more expensive and yields 0.09 more QALYs, resulting in an ICER of $67,239 (Table 6). Changing the utility values resulted in the largest change to the sponsor’s base case, increasing the ICER to $64,236 (Table 15). The majority (76%) of the total costs for incobotulinumtoxinA plus SoC were treatment costs, followed by disease management costs (24%) and AE management costs (< 1%). The majority of the QALY gain compared to SoC occurs in the moderate and severe sialorrhea health states (1.35 and 1.32 more QALYs for incobotulinumtoxinA compared to SoC, respectively). The treatment discontinuation is where most QALYs were accrued for both incobotulinumtoxinA and SoC, meaning that a large proportion of the total QALYs for incobotulinumtoxinA (43%) were realized in the post-trial period.
Table 6: Summary of the CADTH Reanalysis Results
Drug | Total costs | Total QALYs | ICER vs. SoC |
|---|---|---|---|
Sponsor-corrected base case | |||
SoC | $3,917 | 7.18 | Reference |
IncobotulinumtoxinA plus SoC | $11,204 | 7.68 | $14,417 |
CADTH base case | |||
SoC | $2,606 | 5.19 | Reference |
IncobotulinumtoxinA plus SoC | $8,734 | 5.28 | $67,239 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SoC = standard of care.
Note: Reanalyses are based on publicly available prices of comparators.
Scenario Analysis Results
CADTH undertook price-reduction analyses in the sponsor’s base case and in CADTH’s base case (Table 7). These analyses demonstrated that a price reduction of 30% would be required for incobotulinumtoxinA to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for incobotulinumtoxinA plus SoC vs. SoC | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | $14,417 | $67,239 |
10% | $13,082 | $61,186 |
20% | $11,763 | $55,591 |
30% | $10,407 | $49,627 |
ICER = incremental cost-effectiveness ratio; SoC = standard of care.
To address remaining uncertainty regarding parameterization of the model, CADTH conducted several scenario analyses. Full results are presented in Table 16. The scenario analysis using the sponsor’s base-case utility values identified this as a key driver (ICER = $15,251). Additionally, assuming that patients who discontinue have a utility value equal to that of those with severe sialorrhea decreased the ICER from $67,239 per QALY to $45,660 per QALY. In the scenario where onabotulinumtoxinA plus SoC was included in a sequential analysis, based on the assumption of equivalent efficacy, onabotulinumtoxinA plus SoC was found to be more costly than incobotulinumtoxinA plus SoC. CADTH undertook analyses assuming severe or moderate sialorrhea for all patients at baseline. These scenarios appear to have a large impact on the results, although CADTH noted errors in sections of the model when this analysis was run. Additionally, although the relative risk between onabotulinumtoxinA plus SoC and incobotulinumtoxinA plus SoC was removed from the probabilistic analysis, QALYs accrued in each health-state differed between these comparators (Table 14). Removing the relative risk between these comparators should have resulted in equal QALY outcomes, which would be appropriate if the comparators were equal in terms of safety and efficacy. Differences in QALY outcomes observed despite the removal from the probabilistic analysis indicate that the outputs of the model may be of limited validity, and overall model results should be viewed with caution due to apparent errors in the model’s probabilistic analysis.
Issues for Consideration
Although incobotulinumtoxinA is indicated for the treatment of chronic sialorrhea associated with neurologic disorders in adults, according to the clinical expert consulted by CADTH, there is interest in using it as a treatment for sialorrhea in pediatric patients with neurologic conditions, such as cerebral palsy. As the SIAXI trial was in adults only, incobotulinumtoxinA use in pediatric patients has not been studied, and CADTH was unable to incorporate pediatric population in the model.
Additionally, according to the clinical expert consulted for this review, some patients using incobotulinumtoxinA for sialorrhea may require a dose of greater than 100 U to achieve an effect. However, the dose required along with the proportion of patients who may benefit from an increased dose were not available. The clinical evidence captured in the SIAXI trial did not account for this, therefore, CADTH did not address a potential increased dose for incobotulinumtoxinA in its reanalyses.
IncobotulinumtoxinA has been previously reviewed by CADTH for blepharospasm, cervical dystonia, and post-stroke spasticity at the same price as this submission’s ($330 per 100 U vial). IncobotulinumtoxinA received a listing in a similar matter for its blepharospasm and cervical dystonia indications as its submitted price was less expensive than onabotulinumtoxinA and the committee concluded that the products had similar efficacy. IncobotulinumtoxinA received a “do not list” for its spasticity post-stroke indication.
Feedback from the clinical expert consulted for this review noted that, while abobotulinumtoxinA may be used by some practitioners in Canada, it is not a relevant comparator for the management of sialorrhea due to concerns about dispersion of the medication and a higher risk of AEs; in Canada, onabotulinumtoxinA is a more commonly used BoNT-A treatment.
Overall Conclusions
Data from the SIAXI study suggested that using incobotulinumtoxinA to manage sialorrhea in adult patients with neurologic disorders more effectively reduced unstimulated salivary flow rate compared with placebo after 4 weeks. Results obtained on the investigator-rated DSFS were aligned with the primary analysis, although this was an exploratory outcome. The clinical significance of post-treatment changes in sialorrhea was uncertain because the outcome measures were unvalidated, not used in clinical practice, and of unclear importance to patients. There is no robust direct or indirect comparative evidence regarding the efficacy of incobotulinumtoxinA compared to other BoNT-A products or any other treatments for sialorrhea in adults with neurologic disorders. In the sponsor’s economic analysis, BoNT-A products were assumed to have equal efficacy, which was deemed acceptable by the clinical expert for this review.
CADTH identified several limitations with the sponsor’s model conceptualization: not including all relevant comparators; not incorporating the natural history of sialorrhea or underlying neurologic conditions; uncertain influence of sialorrhea severity on quality of life; underestimation of mortality for patients with severe neurologic conditions; the conceptualization of SoC in the model was not reflective of the Canadian context; and including onabotulinumtoxinA plus SoC in a sequential analysis in the absence of direct or indirect comparative efficacy with incobotulinumtoxinA plus SoC or SoC alone. CADTH reanalyses attempted to address some of the identified limitations with the sponsor’s analysis by using utility values from the SIAXI trial derived by NICE; increasing the SMR of death to 4.09; assuming 100% of those receiving SoC discontinue treatment (therefore remaining in their baseline sialorrhea-severity state); increasing the disutility for dysphagia; and removing onabotulinumtoxinA plus SoC as a comparator in the analysis. In the CADTH base-case reanalysis, the ICER for incobotulinumtoxinA plus SoC was $67,239 per QALY, compared with SoC alone. A price reduction of 30% would be required for incobotulinumtoxinA for incobotulinumtoxinA plus SoC to be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY compared with SoC.
The analysis was highly sensitive to sialorrhea health-state utility values. When CADTH implemented the sponsor’s base-case utility values as a scenario analysis, the ICER decreased to $15,251. The cost-effectiveness of incobotulinumtoxinA is therefore strongly driven by the difference in quality of life between having mild and severe sialorrhea. When onabotulinumtoxinA plus SoC was included in the analysis and assumed to have the same effects as incobotulinumtoxinA plus SoC, it was found to be more costly than incobotulinumtoxinA plus SoC. CADTH was unable to address several limitations with the model conceptualization: the assumed maintenance of effectiveness without consideration of the natural history of the patient’s underlying condition(s) on the long-term effectiveness of treatments for sialorrhea without inclusion of relevant comparators and the lack of robust comparative data with relevant comparators. These areas of uncertainty may bias the cost-effectiveness of incobotulinumtoxinA in either direction, although the overall direction and the magnitude of impact are unknown. Additionally, errors in the probabilistic analysis, as evidenced by the production of results that were unexpected (including conducting subgroup analyses by baseline sialorrhea severity and unequal QALY outcomes between incobotulinumtoxinA and onabotulinumtoxinA, despite removing the relative risk between products from the probabilistic analysis) means that outputs of the model may be of limited validity, and overall model results should be viewed with caution. The cost-effectiveness estimates are therefore uncertain.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Xeomin (incobotulinumtoxin A, clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins): powder for solution for injection, 50 and 100 units per vial. Burlington (ON): Merz Pharma Canada Ltd.; 2021 Mar 5.
2.Xeomin (incobotulinumtoxin A, clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins): powder for solution for injection, 50 and 100 units per vial [product monograph]. Burlington (ON): Merz Pharma Canada Ltd.; 2020 Nov 3: https://www.merzcanada.com/files/XEOMIN%20Therapeutic%20Product%20Monograph%20Nov%2017%202020.PDF. Accessed 2021 May 7.
3.Drug Reimbursement Review sponsor submission: Xeomin (incobotulinumtoxin A, clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins): powder for solution for injection, 50 and 100 units per vial [internal sponsor's package]. Burlington (ON): Merz Pharma Canada Ltd.; 2021 Mar 5.
4.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2021; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 May 7.
5.Clinical Study Report: MRZ60201_3090_1. Prospective, randomized, double-blind, placebocontrolled, parallel-group multicenter study, with an extension period of dose-blinded active treatment, to investigate the efficacy and safety of two dose levels of NT 201 in treating chronic troublesome sialorrhea in various neurological conditions [internal sponsor's report]. Frankfurt (DE): Merz Pharmaceuticals GmbH; 2017 Mar 16.
6.Jost WH, Friedman A, Michel O, et al. SIAXI: Placebo-controlled, randomized, double-blind study of incobotulinumtoxinA for sialorrhea. Neurology. 2019;92(17):e1982-e1991. PubMed
7.Government of Canada. Life Tables, Canada, provinces and territories. 2021; https://www150.statcan.gc.ca/n1/en/catalogue/84-537-X. Accessed 2021 May 7.
8.Makino K, Mahant N, Tilden D, Aghajanian L. Cost-effectiveness of incobotulinumtoxinA in the treatment of sialorrhea in patients with various neurological conditions. Neurol. 2020;9(1):117-133. PubMed
9.Stal JM, Gregor JC, Preiksaitis HG, Reynolds RP. A cost-utility analysis comparing omeprazole with ranitidine in the maintenance therapy of peptic esophageal stricture. Can J Gastroenterol. 1998;12(1):43-49. PubMed
10.Matza LS, Deger KA, Vo P, Maniyar F, Goadsby PJ. Health state utilities associated with attributes of migraine preventive treatments based on patient and general population preferences. Qual Life Res. 2019;28(9):2359-2372. PubMed
11.Schedule of benefits for physician services under the Health Insurance Act: effective April 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master20200306.pdf. Accessed 2021 May 7.
12.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/dv/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2021 May 7.
13.Lowin J, Sail K, Baj R, et al. The cost-effectiveness of levodopa/carbidopa intestinal gel compared to standard care in advanced Parkinson’s disease. J Med Econ. 2017;20(11):1207-1215. PubMed
14.European Parkinson’s Disease Association (EPDA). Rating scales. 2017; https://www.epda.eu.com/about-parkinsons/symptoms/rating-scales/. Accessed 2021 May 7.
15.Single Technology Appraisal: Clostridium botulinum neurotoxin type A for treating chronic sialorrhoea [ID1150]. Committee papers. London (GB): National Institute for Health and Care Excellence (NICE); 2019: https://www.nice.org.uk/guidance/ta605/evidence/committee-papers-pdf-6953852557. Accessed 2021 May 7.
16.Chahine L, Tarsy D. Management of nonmotor symptoms in Parkinson disease. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 May 7.
17.Saskatchewan Drug Plan: search formulary. 2021; https://formulary.drugplan.ehealthsask.ca/SearchFormulary. Accessed 2021 May 7.
18.Budget Impact Analysis [internal sponsor's report]. In: Xeomin (incobotulinumtoxin A, clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins): powder for solution for injection, 50 and 100 units per vial. Burlington (ON): Merz Pharma Canada Ltd.; 2021 March 5.
19.Public Health Agency of Canada. Canadian Best Practices Portal. Neurological conditions. 2016; https://cbpp-pcpe.phac-aspc.gc.ca/chronic-diseases/neurological-conditions/. Accessed 2021 May 7.
20.Wong SL, Gilmour H, Ramage-Morin PL. Parkinson's disease: Prevalence, diagnosis and impact. Health Rep. 2014;25(11):10-14. PubMed
21.Mapping connections: an understanding of neurological conditions in Canada. The National Population Health Study of Neurological Conditions. Toronto (ON): Neurological Health Charities Canada; 2014: https://central.bac-lac.gc.ca/.item?id=HP35-45-2014-eng&op=pdf&app=Library. Accessed 2021 May 7.
22.A guide to cerebral palsy. Toronto (ON): Ontario Federation for Cerebral Palsy; 2011: https://www.ofcp.ca/pdf/Web-Guide-To-CP.pdf. Accessed 2021 May 7.
23.GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459-480. PubMed
24.Nguyen R, Fiest KM, McChesney J, et al. The international incidence of traumatic brain injury: a systematic review and meta-analysis. Can J Neurol Sci. 2016;43(6):774-785. PubMed
25.Krueger H, Koot J, Hall RE, O'Callaghan C, Bayley M, Corbett D. Prevalence of individuals experiencing the effects of stroke in Canada: trends and projections. Stroke. 2015;46(8):2226-2231. PubMed
26.Wallin MT, Culpepper WJ, Nichols E, et al. Global, regional, and national burden of multiple sclerosis 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(3):269-285. PubMed
27.Yuan J, Maserejian N, Liu Y, et al. Severity distribution of Alzheimer’s disease dementia and mild cognitive impairment in the Framingham Heart Study [non peer-reviewed preprint]. Research Square. 2020. https://www.researchsquare.com/article/rs-34655/v1. Accessed 2021 May 7.
28.Himmelmann K, Beckung E, Hagberg G, Uvebrant P. Gross and fine motor function and accompanying impairments in cerebral palsy. Dev Med Child Neurol. 2006;48(6):417-423. PubMed
29.Kalf JG, de Swart BJ, Borm GF, Bloem BR, Munneke M. Prevalence and definition of drooling in Parkinson's disease: a systematic review. J Neurol. 2009;256(9):1391-1396. PubMed
30.Morgante F, Bavikatte G, Anwar F, Mohamed B. The burden of sialorrhoea in chronic neurological conditions: current treatment options and the role of incobotulinumtoxinA (Xeomin(R)). Ther Adv Neurol Disord. 2019;12(no pagination):1756286419888601.
31.Møller E, Karlsborg M, Bardow A, Lykkeaa J, Nissen FH, Bakke M. Treatment of severe drooling with botulinum toxin in amyotrophic lateral sclerosis and Parkinson's disease: Efficacy and possible mechanisms. Acta Odontol Scand. 2011;69(3):151-157. PubMed
32.Delsing C, Hughes A, Parr J, et al. Sialorrhea: bottom line ‘evidence-informed’ recommendations for children/youth with cerebral palsy who have sialorrhea. Milwaukee (WI): American Academy for Cerebral Palsy and Developmental Medicine; 2016: https://www.aacpdm.org/UserFiles/file/care-pathways-sialorrhea-print.pdf. Accessed 2021 May 7.
33.Sutherland G, Dinh T. Understanding the gap. A Pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: http://innovativemedicines.ca/wp-content/uploads/2017/12/20170712-understanding-the-gap.pdf. Accessed 2021 May 13.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Chronic Sialorrhea Associated With Neurological Disorders in Adults
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Average daily drug cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
IncobotulinumtoxinA (Xeomin) | 50 U 100 U | Powder for solution for injection | 165.0000a 330.0000a | 100 units every 16 weeks | 2.94 | 1,073b |
aSponsor submitted price.1
bAssumes 3.25 administrations annually.
Table 9: CADTH Cost Comparison Table for Chronic Sialorrhea Associated With Neurological Disorders in Adults (Drugs Used But Not Specifically Indicated)
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Average daily drug cost ($) | Annual cost ($) |
|---|---|---|---|---|---|---|
Botulinum toxinsa | ||||||
OnabotulintoxinA (Botox) | 50 U 100 U 200 U | Powder for solution for injection | 178.5000 357.0000 714.0000 | 100 units every 16 weeksb | 3.18 | 1,160c |
Anticholinergics | ||||||
Glycopyrrolate (Robinul, generics) | 0.2 mg / mL | Solution for oral administration | 3.9750 per mL | Initial dose: 0.5 mg once to twice dailyd Regular dose: 1 mg 3 times dailyb | Initial dose: 9.94 to 19.88 Regular dose: 59.63 | Year 1 dose: 17,589 Year 2+: 21,763 |
Trihexyphenidyl hydrochloride | 2 mg 5 mg | Tablet | 0.0376 0.0681 | 1 mg once dailye | 0.02 | 7 |
Atropine sulphate | 1% | Ophthalmic solution | 0.5490 per mL | One to 2 drops applied sublingually once or twice dailyb | 0.03 to 0.11f | 10 to 40 |
Benztropine Mesylate | 1 mg | Tablet | 0.0522 | 1 mg once dailye | 0.05 | 19 |
Amitriptyline (Elavil, generics) | 10 mg 25 mg 50 mg | Tablet | 0.0435 0.0829 0.1540 | 10 to 25 mg once dailye | 0.04 to 0.08 | 16 to 30 |
Scopolaminef (Transderm-V, generics) | 1.5 mg | Transdermal patch | 4.9300g | 1.5 mg patch every 3 dayse | 1.64 | 600 |
Note: All prices are from the Ontario Drug Benefit Formulary (accessed April 2021), unless otherwise indicated, and do not include dispensing fees.4
aAbobotulinumtoxinA (Dysport) was excluded as it was deemed not be used in Canadian clinical practice for the management of sialorrhea by the clinical expert consulted for this review. At the list price, abobotulinumtoxinA is more costly on a per unit basis than both onabotulinumtoxinA and incobotulinumtoxinA.4
bDose from Chahine16and Tarsy (2021) and confirmed to be appropriate with clinical expert.
cAssumes 3.25 administrations annually.
dInitial year dose assumes dose escalation by 0.5 mg every 4 weeks, until the regular dose is reached at 20 weeks.
eDose informed by clinical expert input.
f20 drops per mL assumed.
gSaskatchewan Formulary (accessed April 2021).
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | See CADTH Appraisal section. |
Model has been adequately programmed and has sufficient face validity | No | There is an apparent error in the probabilistic analysis yielding results that are unexpected. For example, despite removing the relative risk between IncobotulinumtoxinA + SoC and OnabotulinumtoxinA + SoC from the probabilistic analysis, QALYs between these products were not equal across health states, or across PSA iterations. Additionally, changing the baseline distribution of patients sialorrhea severity to 100% severe or moderate yields divergent deterministic and probabilistic results. |
Model structure is adequate for decision problem | No | See CADTH Appraisal section. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | When user input cells on the Model Parameters sheet are changed, the cells revert to default values during the probabilistic analysis, necessitating users to change values in multiple places in the model. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
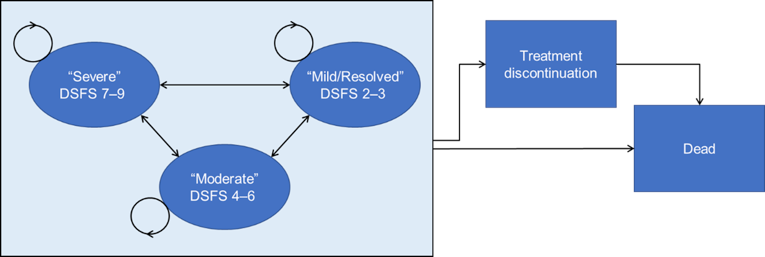
Detailed Results of the Sponsor’s Base Case
Table 11: Drooling Severity and Frequency Scale Definitions
Rank | Drooling severity | Drooling frequency |
|---|---|---|
1 | Dry: never drools | Never drools |
2 | Mild: only the lips are wet | Occasional drooling: not every day |
3 | Moderate: wet on the lips and chin | Frequent drooling: part of every day |
4 | Severe: drools to the extent that clothing becomes wet | Constant drooling |
5 | Profuse: clothing, hands, tray and objects become wet | NA – 4-point scale for frequency only |
NA = not applicable.
Source: CADTH Clinical Review Report.
Table 12: Health-State Utility Values Used in Sponsor’s Submission
Health state | SIAXI trial | ||
|---|---|---|---|
Sponsor’s base case (Makino [2019])a | Sponsor’s estimated utility valuesa | ERG estimated utility valuesb | |
Severe sialorrhea (DSFS 7-9) | 0.55 | 0.5854 | 0.5774 |
Moderate sialorrhea (DSFS 4-6) | 0.64 | 0.5974 | 0.5983 |
Mild sialorrhea (DSFS 2-3) | 0.74 | 0.6397 | 0.6227 |
Treatment discontinuation | 0.59 | 0.591 | NA |
Difference between severe and mild | 0.19 | 0.0543 | 0.0453 |
DSFS = Drooling Severity and Frequency Score, ERG = evidence review group.
aSource: Sponsor’s pharmacoeconomic submission.1
bSource : NICE Committee Papers.15
Table 13: Frequency of Consultations Used in the Sponsor’s Submission
Health state | Number of consultations per cycle | |
|---|---|---|
Occupational therapy | Speech language pathology | |
For those receiving Xeomin or Botox | ||
Severe (DSFS 7-9) | 1 | 1 |
Moderate (DSFS 4-6) | 0.5 | 0.5 |
Mild (DSFS 2-3) | 0 | 0 |
For moderate and severe sialorrhea who discontinue Xeomin or Botox | ||
Discontinuers | 0.5 | 0.5 |
DSFS = Drooling Severity and Frequency Score.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results
Treatment | Component | Value | Incremental (vs. reference) | Incremental (sequential) |
|---|---|---|---|---|
Discounted QALYs | ||||
SoC | Severe sialorrhea | 0.05 | NA | NA |
Moderate sialorrhea | 0.04 | NA | NA | |
Mild sialorrhea | 0.00 | NA | NA | |
Discontinued | 5.10 | NA | NA | |
Total | 5.19 | NA | NA | |
IncobotulinumtoxinA + SoC | Severe sialorrhea | 0.31 | 0.26 | NA |
Moderate sialorrhea | 1.39 | 1.35 | NA | |
Mild sialorrhea | 1.32 | 1.32 | NA | |
Discontinued | 2.26 | -2.84 | NA | |
Total | 5.28 | 0.09 | NA | |
OnabotulinumtoxinA + SoC | Severe sialorrhea | 0.31 | 0.26 | 0 |
Moderate sialorrhea | 1.38 | 1.33 | 0.02 | |
Mild sialorrhea | 1.31 | 1.31 | 0.01 | |
Discontinued | 2.29 | -2.81 | −0.03 | |
Total | 5.28 | 0.09 | 0 | |
Discounted costs ($) | ||||
SoC | Treatment acquisition | 0 | NA | NA |
AEs | 0 | NA | NA | |
Routine care | 2,606 | NA | NA | |
Total | 2,606 | NA | NA | |
IncobotulinumtoxinA + SoC | Treatment acquisition | 6,068 | 6,068 | NA |
AEs | 4 | 4 | NA | |
Routine care | 2,122 | -485 | NA | |
Total | 8,735 | 6,127 | NA | |
OnabotulinumtoxinA + SoC | Treatment acquisition | 6,981 | 6,981 | 373 |
AEs | 4 | 4 | 0 | |
Routine care | 2,127 | -480 | 5 | |
Total | 9,112 | 6,505 | 378 | |
ICER vs. reference ($) | Sequential ICER ($) | |||
SoC | Reference | Reference | ||
IncobotulinumtoxinA + SoC | $67,239 | $67,239 vs. SoC | ||
OnabotulinumtoxinA + SoC | $72,155 | Dominated IncobotulinumtoxinA + SoC | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; NA = not applicable; QALY = quality-adjusted life-year; SoC = standard of care; vs. = versus.
Detailed Results of CADTH Base Case
Table 15: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case | SoC | 3,917 | 7.18 | Reference |
IncobotulinumtoxinA + SoC | 11,204 | 7.68 | 14,417 | |
OnabotulinumtoxinA + SoC | 11,607 | 7.67 | Dominated | |
Sponsor’s corrected base case | SoC | 3,920 | 7.18 | Reference |
IncobotulinumtoxinA + SoC | 11,074 | 7.66 | 14,813 | |
OnabotulinumtoxinA + SoC | 11,601 | 7.66 | Dominated | |
CADTH reanalysis 1-Health-state utility values | SoC | 3,919 | 7.11 | Reference |
IncobotulinumtoxinA + SoC | 11,060 | 7.22 | 64,236 | |
OnabotulinumtoxinA + SoC | 11,629 | 7.22 | Dominated | |
CADTH reanalysis 2 – Standard mortality ratio 4.09 | SoC | 2,922 | 5.25 | Reference |
IncobotulinumtoxinA + SoC | 8,722 | 5.63 | 15,198 | |
OnabotulinumtoxinA + SoC | 9,110 | 5.63 | Dominated | |
CADTH reanalysis 3 – SoC discontinuation | SoC | 3,561 | 7.15 | Reference |
IncobotulinumtoxinA + SoC | 11,159 | 7.67 | 14,802 | |
OnabotulinumtoxinA + SoC | 11,672 | 7.66 | Dominated | |
CADTH reanalysis 4 – Dysphagia disutility | SoC | 3,855 | 7.17 | Reference |
IncobotulinumtoxinA + SoC | 9,936 | 7.57 | 15,214 | |
OnabotulinumtoxinA + SoC | 10,391 | 7.57 | Dominated | |
CADTH reanalysis 5-Removing onabotulinumtoxinA + SoC as a comparator | SoC | 3,920 | 7.18 | Reference |
IncobotulinumtoxinA + SoC | 11,074 | 7.66 | 14,813 | |
CADTH base case (1 + 2 + 3 + 4 + 5) | SoC | 2,606 | 5.19 | Ref. |
IncobotulinumtoxinA + SoC | 8,734 | 5.28 | 67,239 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SoC = standard of care.
Note: Reanalyses are based on publicly available prices of comparators.
Results of CADTH Scenario Analyses
Table 16: CADTH Common Drug Review Scenario Analyses
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
CADTH base case | SoC | 2,606 | 5.19 | Reference |
IncobotulinumtoxinA + SoC | 8,734 | 5.28 | 67,239 | |
Analysis 1 – Utility for discontinuation equal to that of severe sialorrhea | SoC | 2,606 | 5.11 | Ref. |
IncobotulinumtoxinA + SoC | 8,640 | 5.24 | 45,660 | |
Analysis 2 – Sponsor’s utility values | SoC | 2,608 | 5.23 | Reference |
IncobotulinumtoxinA + SoC | 8,729 | 5.63 | 15,251 | |
Analysis 3 – SMR of 10 | SoC | 1,697 | 3.36 | Reference |
IncobotulinumtoxinA + SoC | 6,168 | 3.42 | 70,464 | |
Analysis 4 – No discontinuation for SoC | SoC | 3,728 | 5.21 | Reference |
IncobotulinumtoxinA + SoC | 8,669 | 5.28 | 69,140 | |
Analysis 5 – Including OnabotulinumtoxinA in sequential analysis | SoC | 2,606 | 5.19 | Reference. |
IncobotulinumtoxinA + SoC | 8,734 | 5.28 | 67,239 | |
OnabotulinumtoxinA + SoC | 9,112 | 5.28 | Dominated | |
Subgroup analysis 1 – Moderate patients | SoC | 2,582 | 5.28 | Reference |
IncobotulinumtoxinA + SoC | 8,654 | 5.32 | 152,623 | |
OnabotulinumtoxinA + SoC | 9,052 | 5.32 | Dominated | |
Subgroup analysis 2 – Severe patients | SoC | 2,629 | 5.11 | Reference |
IncobotulinumtoxinA + SoC | 8,768 | 5.24 | 45,056 | |
OnabotulinumtoxinA + SoC | 9,183 | 5.24 | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years; SoC = standard of care; SMR = standard mortality ratio.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Table 17: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the budget impact of introducing incobotulinumtoxinA for the treatment of adults with chronic sialorrhea associated with neurological disorders.1 The BIA was undertaken from a publicly funded drug plan perspective considering only drug costs over a 3-year time horizon. The analytic framework, which used an epidemiology-based approach, leveraged data from multiple sources in the literature and assumptions based on clinical expert input to determine the estimated population size (Figure 2). New patients were added to the BIA via an annual population growth rate. Key inputs to the BIA are documented in Table 20.
The sponsor compared a reference scenario where incobotulinumtoxinA is not reimbursed for the treatment of adults with chronic sialorrhea associated with neurological disorders with a new drug scenario, where incobotulinumtoxin A is funded as per the Health Canada indication. Treatments available in the reference included off-label botulinum toxin products and other off-label medications (i.e., anticholinergics or adrenergic receptor antagonists). However, since these treatments are off-label comparators for sialorrhea, the sponsor assumed that these would not be covered by public drug plans in the reference or new drug scenarios; therefore, there were zero costs associated with the reference scenario. Administration fees, dispensing fees, upcharges and co-payment deductions were excluded from the sponsor’s base-case analysis.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
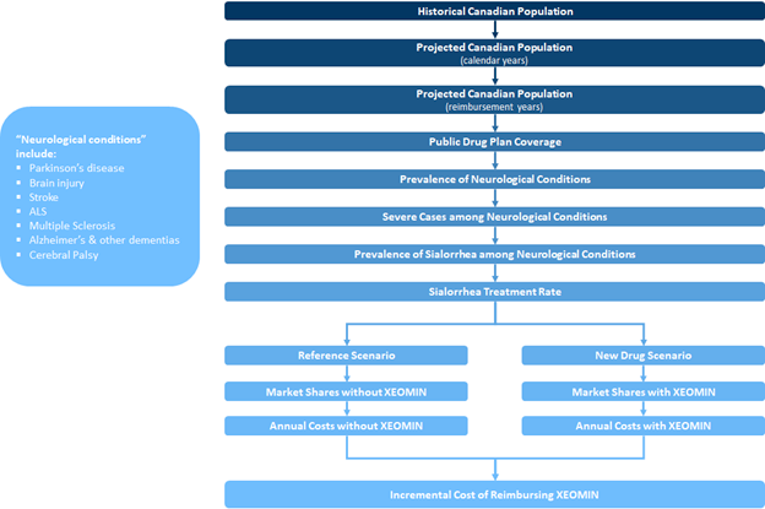
ALS = amyotrophic lateral sclerosis.
Source: Sponsor’s budget impact analysis.18
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) | ||||||
|---|---|---|---|---|---|---|---|
Target Population | |||||||
Step | PD | BI | Stroke | ALS | MS | Dementias | CP |
Prevalence (per 100,000) | 389.219 | 933.519 | 4.421 | 275.119 | 327.819 | 175.622 | |
% of cases who are severe | 45%23 | 5%24 | 25%25 | 80%- Assumption | 13%26 | 19%27 | 28%28 |
% of severe cases with sialorrhea | 56%29 | 44%30 | 58%30 | 65%31 | 20%- Assumption | 20%- Assumption | 40%32 |
% receiving pharmacological treatment | 15% | ||||||
Number of patients eligible for Incobotulinumtoxin A | 5,356 / 5,436 / 5,515 | ||||||
Market Uptake (3 years) | |||||||
Uptake (reference scenario)
| 60% / 60% / 60% 40% / 40% / 40% | ||||||
Uptake (new drug scenario)
| 18% / 28% / 43% 49% / 43% / 34% 33% / 29% / 23% | ||||||
Cost of treatment (per patient) | |||||||
Cost of treatment over one year:
| $990 $0a $0 | ||||||
ALS = amyotrophic lateral sclerosis; BI = brain injury; CP = cerebral palsy; MS = multiple sclerosis; PD = Parkinson disease.
aThe base-case analysis assumed no drug plan reimbursement of off-label botulinum toxin products (annual cost $0). The sponsor conducted 2 scenario analyses where off-label onabotulinumtoxinA was reimbursed at an annual cost of $1,071 and $1,428 (assuming 3 and 4 administrations annually at $357.004 an administration, respectively).
Table 19: Public Coverage Rates Used in Sponsor’s Budget Impact Analysis
Jurisdiction | Public coverage rate | |
|---|---|---|
Sponsor’s submission | Per cent 65+ eligible for public coverage, according to Understanding the Gap Report33 | |
British Columbia | 64.4% | 100% |
Alberta | 61.1% | 100% |
Saskatchewan | 63.4% | 100% |
Manitoba | 64.4% | 100% |
Ontario | 55.2% | 100% |
New Brunswick | 52.9% | 93.1% |
Nova Scotia | 53.2% | 100% |
Prince Edward Island | 50.0% | 100% |
Newfoundland and Labrador | 47.9% | 52.4% |
NIHB | 100.0% | 100% |
Source: Sponsor’s budget impact analysis.18
The sponsor estimated the net budget impact of introducing incobotulinumtoxin A for the treatment of adults with chronic sialorrhea associated with neurological disorders to be $954,514 in Year 1, $1,506,749 in Year 2, and $2,347,644 in Year 3 for a total budget impact over 3 years of $4,808,907.
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Underestimation of the displacement of off-label botulinum toxin products with the availability of incobotulinumtoxinA. The sponsor assumed that if incobotulinumtoxinA became publicly reimbursed, only a proportion of those currently receiving off-label botulinum toxin products, which do not have public coverage, would switch to incobotulinumtoxinA. Given that there is not coverage of off-label botulinum toxin products for sialorrhea, this means that patients who do not switch to incobotulinumtoxinA despite it being covered would be paying out of pocket for off-label botulinum toxin products, or having it covered by other third-party insurance. According to the clinical expert consulted for this review, unless patients had public coverage, it is expected that all patients would switch to the product that had public coverage. It was also noted in the patient input submission that there is a strong desire for public coverage for treatments. Though off-label botulinum toxin products are not incorporated as a cost in the analysis because they are not publicly covered, assuming a proportion of patients remain taking these off-label products decreases the number of patients using incobotulinumtoxinA in the new drug scenario, thereby underestimating the budget impact.
CADTH reanalyses assuming complete displacement of off-label botulinum toxin products (i.e., 0% market share for off-label botulinum toxin products)
Proportion of patients using pharmacological treatments underestimated in the new drug scenario. The sponsor estimates that 15% of those eligible for pharmacological treatments will use them to manage sialorrhea. According to the clinical expert consulted for this review, entry of a treatment indicated for sialorrhea means that some patients who had previously not received pharmacological treatment will now uptake treatment. The increase was expected to be modest, to a total of 20% of those eligible.
In CADTH reanalyses, it was assumed that 20% of those eligible will use pharmacological treatments to manage sialorrhea.
Costs of off-label comparators were not incorporated in the analysis. In the sponsor’s submitted base case, as there are no indicated treatments for sialorrhea, the costs associated with currently available off-label treatments were assumed to be zero as it was assumed they would not be covered on public drug plans. While not indicated for sialorrhea, many off-label treatments are listed as a full benefit in jurisdictions, meaning that clinicians can prescribe medications for any indication, including those that are off-label. Therefore, these therapies are likely covered for sialorrhea, and their costs should have been included in the analysis. However, as onabotulinumtoxinA is not listed as a full benefit in jurisdictions aside from Alberta, and because the annual costs of comparators that are full benefit is relatively low compared to incobotulinumtoxinA (up to $7, $40, $19,$30, and $600 annually for trihexyphenidyl hydrochloride, atropine sulphate, benztropine mesylate, amitriptyline and Scopolamine, respectively), the impact of excluding these comparators is not expected to be high. Also, the distribution of patients across these oral off-label comparators was not incorporated. If incobotulinumtoxinA coverage displaces reimbursement of off-label comparators, the expected budget impact of introducing incobotulinumtoxinA will be less than estimated in CADTH reanalyses.
As a scenario analysis, CADTH explored the impact of including costs for off-label comparators that are listed as a full benefit by assuming 100% of patients will take the products with the lowest and highest annual costs ($7 and $600, respectively).
The annual number of administrations of incobotulinumtoxinA in the budget impact analysis is not aligned with the sponsor’s pharmacoeconomic model. incobotulinumtoxinA is administered every 16 weeks. In the sponsor’s pharmacoeconomic model, incobotulinumtoxinA was administered 3.25 times annually; however, in their budget impact assessment, 3 annual administrations were considered.
To align with the pharmacoeconomic analysis, incobotulinumtoxinA was assumed to be administered 3.25 times annually in CADTH reanalyses.
The sponsor’s public coverage data does not account for the age of the eligible population. The sponsor sourced public coverage data from Sutherland, 2017 (see Table 19). These coverage rates appear to be for that of the general adult population, not those who are 65+. As the mean baseline age in the SIAXI trial was 65.2 years, it may be reasonable to assume that the majority of patients receiving incobotulinumtoxinA will be over 65, which, in some jurisdictions, means a higher proportion of people will be eligible for public coverage than estimated by the sponsor (see Table 19).
In CADTH reanalyses, the percent eligible for public coverage for those 65+ from Understanding the Gap (2017) was used.33 As there remains uncertainty regarding the age of all eligible patients for incobotulinumtoxinA, CADTH explored using the sponsor’s public coverage rates in a scenario analysis.
The sponsor’s epidemiological filtering approach may have underestimated the number of patients with chronic sialorrhea. The sponsor’s approach to deriving the population eligible for incobotulinumtoxinA was derived by taking the prevalence of neurological conditions, then filtering by those with severe neurological disease, then applying the proportion of those experiencing chronic sialorrhea due to their underlying condition. This approach has some uncertainty as it is unclear whether the proportion with chronic sialorrhea reported in the sponsor’s referenced articles were only those with severe disease or those with the underlying neurological condition generally. For example, the sponsor’s estimate for prevalence of chronic sialorrhea in PD (56%) was derived from a review of studies that included patients with mild and moderate PD.29 In other studies reporting prevalence of sialorrhea, the severity of the patient’s underlying conditions were not reported, so the appropriateness of the sponsor’s filtering approach could not always be assessed.
To address uncertainty regarding the sponsor’s filtering approach, CADTH removed the severe neurological disease epidemiological filter (i.e., assumed 100% of patients had severe disease) in a scenario analysis to examine the influence of chronic sialorrhea prevalence estimates used in the analysis being done in the general disease population, or just among those with severe disease, as assumed by the sponsor.
CADTH Reanalyses of the Budget Impact Analysis
CADTH revised the sponsor’s corrected base case by: assuming incobotulinumtoxinA will displace use of off-label botulinum toxin products, increasing the percentage of people using pharmacological treatments to manage sialorrhea, aligning the number of annual incobotulinumtoxinA administrations with the pharmacoeconomic analysis and using a public coverage rate for those 65 and older. Table 20 notes the assumptions used by the sponsor in comparison to those used by CADTH in its reanalysis alongside minor corrections made to the sponsor’s model.
Table 20: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Prevalence of sialorrhea in MS and Alzheimer a | 20% | 53% |
Changes to derive the CADTH base case | ||
1. IncobotulinumtoxinA uptake among off-label botulinum toxin products users | IncobotulinumtoxinA: 18% / 28% / 43% Off-label botulinum toxins: 49% / 43% / 34% Other off-label medications: 33% / 29% / 23% | IncobotulinumtoxinA: 67% / 71% / 77% Off-label botulinum toxins: 0% / 0% / 0% Other off-label medications: 33% / 29% / 23% |
2. Percent using pharmacological treatments | 15% | 20% |
3. Number of incobotulinumtoxinA administrations per year | 3 | 3.25 |
4. Public coverage rate | Sponsor’s estimates (column 2 of Table 19) | Percent 65+ eligible for public coverage (column 2 of Table 19) |
CADTH base case | Reanalysis 1 + 2 + 3 + 4 | |
MS = multiple sclerosis.
aCorrection: The proportion of MS and Alzheimer/other dementia patients with sialorrhea was estimated to be the average prevalence of sialorrhea in PD, brain injury, stroke, ALS, and CP.18 The sponsor specifies this as 53% in their submission report, but this was implemented as 20% in the model because the average calculation is referring to incorrect cells. The actual average is 53%.
Applying these changes increased the total 3-year budget impact to $31,531,777. The results of the CADTH step-wise reanalysis are presented in summary format in Table 21 and a more detailed breakdown is presented in Table 22.
Table 21: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $4,808,907 |
Corrected base case | $5,462,175 |
CADTH reanalysis 1 | $13,150,271 |
CADTH reanalysis 2 | $7,282,900 |
CADTH reanalysis 3 | $5,917,356 |
CADTH reanalysis 4 | $9,067,707 |
CADTH base case (1 + 2 + 3 + 4) | $31,531,777 |
CADTH also conducted additional scenario analyses to address remaining uncertainty:
Reduced the price of incobotulinumtoxinA to the value in which it would be cost-effective at a $50,000 per QALY threshold (30%)
Assumed incobotulinumtoxinA displaces 90% of off-label botulinum toxin products
Included an annual per patient cost ($7) for oral off-label comparator treatments
Included an annual per patient cost ($600) for oral off-label comparator treatments
Used the sponsor’s public coverage rate estimates
Assumed that the prevalence estimates for sialorrhea applied to all of those with neurological conditions, not just those whose conditions are severe
Assumed that only those with severe sialorrhea were eligible for incobotulinumtoxinA, by multiplying the population size by the proportion severe at baseline in the SIAXI trial (55%)
Assumed that only those with moderate sialorrhea were eligible for incobotulinumtoxinA, by multiplying the population size by the proportion moderate at baseline in the SIAXI trial (45%)
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is highly sensitive to the size of the eligible population (Table 22). If the prevalence of sialorrhea estimates used in the BIA are among all of those with neurological conditions, and not just among those with severe neurological conditions, the expected budget impact of introducing incobotulinumtoxinA increases more than 4-fold to $143 M over 3 years. Additionally, different population size estimates arising from alternative rates of public drug coverage and restricting eligibility by sialorrhea severity also significantly influenced the expected budget impact.
Table 22: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $954,514 | $1,506,749 | $2,347,644 | $4,808,907 | |
Budget impact | $0 | $954,514 | $1,506,749 | $2,347,644 | $4,808,907 | |
CADTH base case | Reference | $0 | $0 | $0 | $0 | $0 |
New drug | $0 | $9,674,555 | $10,405,678 | $11,451,543 | $31,531,777 | |
Budget impact | $0 | $9,674,555 | $10,405,678 | $11,451,543 | $31,531,777 | |
CADTH scenario analysis 1: 30% price reduction | Reference | $0 | $6,772,189 | $7,283,975 | $8,016,080 | $22,072,244 |
New drug | $0 | $0 | $0 | $0 | $0 | |
Budget impact | $0 | $6,772,189 | $7,283,975 | $8,016,080 | $22,072,244 | |
CADTH scenario analysis 2: 90% displacement of off-label botulinum toxin products | Reference | $0 | $8,707,100 | $9,365,110 | $10,306,389 | $28,378,599 |
New drug | $0 | $0 | $0 | $0 | $0 | |
Budget impact | $0 | $8,707,100 | $9,365,110 | $10,306,389 | $28,378,599 | |
CADTH Scenario analysis 3: $7 annual cost for off-label oral comparator | Reference | $37,133 | $9,705,656 | $10,433,418 | $11,473,869 | $31,612,943 |
New drug | $37,133 | $37,698 | $38,262 | $38,827 | $114,787 | |
Budget impact | $0 | $9,667,958 | $10,395,156 | $11,435,042 | $31,498,156 | |
CADTH Scenario analysis 4: $600 annual cost for off-label oral comparator | Reference | $3,182,855 | $12,340,334 | $12,783,416 | $13,365,161 | $38,488,911 |
New drug | $3,182,855 | $3,231,247 | $3,279,638 | $3,328,030 | $9,838,915 | |
Budget impact | $0 | $9,109,087 | $9,503,777 | $10,037,131 | $28,649,995 | |
CADTH Scenario analysis 5: sponsor public coverage rates | Reference | $0 | $5,829,141 | $6,268,466 | $6,897,228 | $18,994,836 |
New drug | $0 | $0 | $0 | $0 | $0 | |
Budget impact | $0 | $5,829,141 | $6,268,466 | $6,897,228 | $18,994,836 | |
CADTH Scenario analysis 6: Sialorrhea prevalence applies to all of those with neurological conditions | Reference | $0 | $43,933,967 | $47,254,132 | $52,003,602 | $143,191,701 |
New drug | $0 | $0 | $0 | $0 | $0 | |
Budget impact | $0 | $43,933,967 | $47,254,132 | $52,003,602 | $143,191,701 | |
CADTH Scenario analysis 7: Only severe eligible | Reference | $0 | $5,321,005 | $5,723,123 | $6,298,349 | $17,342,477 |
New drug | $0 | $0 | $0 | $0 | $0 | |
Budget impact | $0 | $5,321,005 | $5,723,123 | $6,298,349 | $17,342,477 | |
CADTH Scenario analysis 8: Only moderate eligible | Reference | $0 | $4,353,550 | $4,682,555 | $5,153,195 | $14,189,300 |
New drug | $0 | $0 | $0 | $0 | $0 | |
Budget impact | $0 | $4,353,550 | $4,682,555 | $5,153,195 | $14,189,300 |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.