CADTH Reimbursement Review
Budesonide-Glycopyrronium-Formoterol Fumarate Dihydrate (Breztri Aerosphere)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Chronic obstructive pulmonary disease (COPD)
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AUC0-4
area under the curve from 0 to 4 hours post dose
BDI
Baseline Dyspnea Index
BFF
budesonide plus formoterol fumarate
BGF
budesonide plus glycopyrronium plus formoterol fumarate
BMD
bone mineral density
BUD-FOR
budesonide plus formoterol fumarate
CAT
COPD assessment test
CI
confidence interval
COPD
chronic obstructive pulmonary disease
CrI
credible interval
DIC
deviance information criterion
DPI
dry powder inhaler
E-RS
Evaluating Respiratory Symptoms in Chronic Obstructive Pulmonary Disease
EQ VAS
EuroQol Visual Analogue Scale
EQ-5D
EuroQol 5-Dimensions questionnaire
EQ-5D-5L
EuroQol 5-Dimensions 5-Levels questionnaire
EXACT-RS
Exacerbations of Chronic Pulmonary Disease Tool—Respiratory Symptoms
FEV1
forced expiratory volume in 1 second
FF-UMEC-VI
fluticasone furoate plus umeclidinium plus vilanterol
GFF
glycopyrronium plus formoterol fumarate
GOLD
Global Initiative for Obstructive Lung Disease
HR
hazard ratio
HRQoL
health-related quality of life
ICS
inhaled corticosteroid
ITT
intention to treat
LABA
long-acting beta2-agonist
LAMA
long-acting muscarinic antagonist
MCID
minimal clinically important difference
MDI
metered-dose inhaler
mMRC
Modified Medical Research Council (Dyspnea Scale)
NMA
network meta-analysis
PFT
pulmonary function test
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SGRQ
St. George’s Respiratory Questionnaire
TBH
Turbuhaler
TDI
Transition Dyspnea Index
TEAE
treatment-emergent adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Budesonide-glycopyrronium (as bromide)-formoterol fumarate dihydrate, pressurized inhalation aerosol for oral inhalation (Breztri Aerosphere) (182 mcg-8.2 mcg-5.8 mcg per metered actuation) |
Indication | Indicated for the long-term maintenance treatment to reduce exacerbations of COPD and treat airflow obstruction to relieve symptoms in patients with COPD, including chronic bronchitis and/or emphysema, who are not adequately treated by a combination of an ICS-LABA or a combination of a LAMA-LABA |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review pathway |
NOC date | July 15, 2021 |
Sponsor | AstraZeneca Canada Inc. |
COPD = chronic obstructive pulmonary disease; ICS = inhaled corticosteroid; LABA = long-acting beta-agonist; LAMA = long-acting muscarinic antagonist; NOC = Notice of Compliance.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease, often associated with chronic bronchitis and emphysema, that causes obstructed airflow from the lungs, lung hyperinflation, systemic manifestations, and increasing frequency and severity of exacerbations.1,2 COPD is a preventable and treatable disease with approximately 80% to 90% of cases being caused by smoking.1 COPD is an under-diagnosed illness; thus, prevalence statistics are likely to underestimate the number of people currently living with COPD. In Canada, COPD is the fifth-leading cause of death.1 Patients with COPD often experience negative consequences that impact their day-to-day life, including their ability to breathe, talk, sleep, work, and socialize. Overall, these patient experiences describe a physically and mentally exhausting disorder that can result in anxiety, depression, and decreased quality of life. The goals of COPD management are to reduce the frequency and severity of exacerbations, alleviate symptoms, improve exercise tolerance and daily activity, prevent and treat exacerbations and complications, improve health status, and reduce mortality.4 Management decisions are guided by disease severity (i.e., symptoms or disability and spirometry) and the frequency of acute exacerbations. Smoking cessation is the single most effective intervention to reduce the risk of developing COPD and the only intervention shown to slow the rate of lung function decline.1 Bronchodilators form the mainstay of pharmacotherapy for COPD1 and include long-acting beta-agonists (LABAs) and antimuscarinic drugs (long-acting muscarinic antagonists [LAMAs]). Antimuscarinic and beta-agonist drugs used in combination as a step-up therapy are recommended for patients with stable COPD with exacerbations despite the use of LAMA or LABA therapy.5 According to the Canadian Thoracic Society, based on consensus, a step-up to triple therapy, where a LAMA plus a LABA plus an inhaled corticosteroid (ICS) (LAMA-LABA-ICS) is used, may be considered in COPD with high symptom burden and poor health status despite the use of an inhaled LAMA plus LABA (LAMA-LABA) dual therapy.5
Breztri Aerosphere is a triple-combination therapy composed of an ICS (budesonide), a LAMA (glycopyrronium), and a LABA (formoterol fumarate dihydrate). Budesonide, the ICS component, is a well-established corticosteroid and can be administered through oral inhalation mechanisms.3,4 Glycopyrronium, the LAMA component, uses muscarinic receptors to create bronchodilatory effects on smooth muscle in the trachea and bronchi. Formoterol fumarate, the LABA component, is a well-established LABA that is often used as a monotherapy for the treatment of COPD and other indications. This fixed-dose triple therapy is administered twice daily(total dose 320 mcg budesonide plus 14.4 mcg glycopyrronium plus 9.6 mcg formoterol fumarate) through oral inhalation using a metered-dose inhalation (MDI) device, which enables delivery of an exact volume of micronized drugs at each valve actuation.5 Aerosphere offers advantages over traditional MDIs, such as consistent delivery of drugs across patient conditions, optimal particle size, and effective delivery of the particles to peripheral and central airways.6 The components of Breztri Aerosphere are available in other formulations that also have Health Canada–approved indications for the management of COPD.3,4
The objective of this review was to perform a systematic review of the beneficial and harmful effects of budesonide plus glycopyrronium plus formoterol fumarate (BGF) dihydrate inhalation aerosol (Breztri Aerosphere 182 mcg, 8.2 mcg, 5.8 mcg per metered actuation) for long-term maintenance treatment of patients with COPD, to reduce exacerbations of COPD, and to relieve symptoms, including chronic bronchitis and/or emphysema.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from a clinical expert consulted by CADTH for the purpose of this review.
Patient Input
Three patient groups, COPD Canada, the Lung Health Foundation (formerly Ontario Lung Association), and the British Columbia Lung Association, provided input for this submission. The patient groups noted that Breztri Aerosphere would be a welcome addition to provincial formularies across the country. They also expressed the belief that compliance would increase due to the ease of use of this triple therapy, and the effectiveness of the Aerosphere pressurized MDI would ensure this triple-drug combination reached the lungs without relying on a COPD patient’s ability or strength to inhale properly. However, there are continued accessibility issues throughout Canada and provincial drug coverage varies considerably between drug plans.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Input was provided by 1 clinical expert consulted by CADTH for this review. The expert noted that triple-drug combination therapy with an MDI and a spacer or holding chamber, such as an Aerochamber, would be beneficial to patients, as they are currently encouraged to use an Aerochamber for rescue medications. Having their maintenance medication administered using an MDI would also be beneficial. The expert pointed out that the pharmacological components of BGF MDI is familiar to physicians. Lastly, the clinical expert added that although small, the population that might benefit from twice-daily BGF MDI has been better identified as Canadian recommendations evolve.
Clinician Group Input
Input was provided by 3 clinicians from the COPD clinic in the Division of Respirology and Sleep Medicine at Queen’s University. The group noted that a stepwise add-on approach was used in COPD management in clinical settings. They pointed out that COPD patients who experience frequent exacerbations despite being on dual therapies would be the group that might benefit the most from BGF MDI. The clinicians added that fixed-dose triple-therapy combinations, such as BGF MDI, would likely improve the deposition of the bronchodilators and ICS in the target location, leading to better ventilated alveolar units and better outcomes for the patient.
Drug Program Input
The drug program asked about the appropriate comparators for assessing the efficacy of BGF MDI. The clinical expert noted that, although other triple-therapy combinations (fixed dose or other) would be the most appropriate comparators, dual therapies (i.e., ICS plus a LAMA [ICS-LAMA] or a LAMA plus a LABA [LAMA-LABA]) can also be considered to establish the efficacy of BGF.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
Two randomized controlled trials (RCTs), KRONOS and ETHOS, were included in the main report of the study. ETHOS was a 52-week, multi-site, double-blind, parallel-group study comparing BGF MDI with glycopyrronium plus formoterol fumarate (GFF) MDI and budesonide plus formoterol fumarate (BFF). Outcomes of the ETHOS trial included the rate of moderate or severe (primary end point) and severe COPD exacerbations, symptoms, health-related quality of life (HRQoL), pulmonary function, and safety. A total of 8,588 patients were randomized to 1 of 4 treatment groups. KRONOS was a 24-week, multi-site, double-blind parallel-group study comparing BGF MDI with GFF MDI and BFF MDI and comparing budesonide plus formoterol fumarate (BUD-FOR) inhalation powder with Symbicort Turbuhaler (TBH) inhalation powder (active control). The KRONOS trial had outcomes similar to the ETHOS trial, including rate of moderate-to-severe COPD exacerbations, symptoms, HRQoL, and safety; change in pulmonary function based on the forced expiratory volume in 1 second (FEV1) was the primary outcome. Overall, 1,902 patients were randomized among the treatment groups in the KRONOS study.
Efficacy Results
Table 2 presents a summary of key end point results from the included studies.
Exacerbations
In ETHOS, the adjusted rates of moderate or severe exacerbations per year were 1.08, 1.42, and 1.24 for the BGF MDI 320, GFF MDI, and BFF MDI arms, respectively. The rate difference between BGF MDI 320 and GFF MDI was −0.35 (95% confidence interval [CI], −0.46 to −0.23), and between BGF MDI 320 and BFF MDI it was −0.17 (95% CI, −0.27 to −0.06). In KRONOS, the adjusted annualized rates of moderate or severe exacerbations per year were numerically lower for BGF MDI 320 (0.46) compared with GFF MDI (0.95), BFF MDI (0.56), and BUD-FOR dry powder inhaler (DPI) (0.56); however, rate differences were not reported.
BGF MDI 320 was associated with significantly lower rates of moderate or severe COPD exacerbations compared with GFF MDI (rate ratio = 0.76; 95% CI, 0.69 to 0.83 at 52 weeks [ETHOS] and rate ratio = 0.48; 95% CI, 0.37 to 0.64 at 24 weeks [KRONOS]), and BFF MDI at 52 weeks (rate ratio = 0.87; 95% CI, 0.79 to 0.95 [ETHOS]). In the KRONOS trial, there was no statistically significant difference found in the rate of moderate-to-severe exacerbations between BGF MDI and BUD-FOR DPI (rate ratio = 0.83; 95% CI, 0.59 to 1.18) nor between BGF MDI and BFF MDI (rate ratio = 0.82; 95% CI, 0.58 to 1.17) at 24 weeks.
Lung Function
Lung function, measured as FEV1 area under the curve from 0 to 4 hours post dose (AUC0-4) over 24 weeks, was the primary outcome for the comparisons of BGF MDI 320 versus BFF MDI (ETHOS and KRONOS) and BGF MDI 320 versus BUD-FOR DPI (KRONOS). In ETHOS, this outcome was assessed in a pulmonary function test (PFT) substudy population. BGF MDI 320 showed statistically significant improvement in lung function compared with both BFF MDI (least squares mean = 104 mL; 95% CI, 77 to 131) and BUD-FOR DPI (least squares mean = 91 mL; 95% CI, 64 to 117). Based on a minimal clinically important difference (MCID) of 0.10 L to 0.14 L, these differences were likely clinically significant. Lung function measured as morning pre-dose trough FEV1 over 24 weeks was the primary outcome for the comparisons of BGF MDI 320 versus GFF MDI (ETHOS and KRONOS). In ETHOS, this outcome was assessed in a PFT substudy population. The change from baseline in morning pre-dose trough FEV1 at 24 weeks for BGF MDI 320 compared with GFF MDI was not clinically significant (22 mL: 95% CI, 4 to 39).
Use of Rescue Medication
In both trials, the evaluation of the average daily number of puffs of rescue medication over 24 weeks was restricted to the rescue Ventolin use population. In ETHOS, BGF MDI 320 was associated with a statistically significant reduction in the use of rescue medication compared with GFF MDI (difference = −0.51 puffs per day; 95% CI, −0.68 to −0.34) and BFF MDI (difference = −0.37 puffs per day; 95% CI, −0.54 to −0.20). No statistically significant differences were found between the groups in KRONOS.
Symptoms
The change from baseline in the Transition Dyspnea Index (TDI) focal score was used by both trials to assess improvement in dyspnea symptoms with treatment. Although both trials found that BGF MDI improved symptoms compared with GFF MDI, BFF MDI, and BUD-FOR DPI, these were not clinically significant improvements. In ETHOS, the difference in the least squares mean of the TDI focal score in BGF MDI 320 compared with GFF MDI was 0.40 units (95% CI, 0.24 to 0.55) and, compared with BFF MDI, was 0.31 units (95% CI, 0.15 to 0.46). In KRONOS, the difference in the least squares mean of the TDI focal score in BGF MDI 320 versus GFF MDI was 0.177 units (95% CI, −0.071 to 0.426), 0.237 units (95% CI, −0.068 to 0.542) compared with BFF MDI, and 0.461 units (95% CI, 0.156 to 0.766) compared with BUD-FOR DPI. Compared with other groups, there were no clinically meaningful improvements in symptoms for BGF MDI as measured using the Exacerbations of Chronic Pulmonary Disease Tool (EXACT) or the Evaluating Respiratory Symptoms in COPD (E-RS) instruments.
Health-Related Quality of Life
St. George's Respiratory Questionnaire (SGRQ) was used to measure HRQoL in both trials. Patients in all treatment groups showed clinically significant improvement in SGRQ total score before and after treatment. However, between groups, these improvements were not clinically significant (MCID = 4 units). In ETHOS, the mean difference in SGRQ total score was −1.62 units (95% CI, −2.27 to −0.97) for BGF MDI versus GFF MDI, and −1.38 (95% CI, −2.02 to −0.73) for BGF MDI 320 versus BFF MDI. These differences were statistically significant, but not clinically meaningful. In KRONOS, the mean differences were −1.22 units (95% CI, −2.30 to −0.15) and −0.45 units (95% CI, −1.78 to 0.87) for BGF MDI versus GFF MDI, and BGF MDI versus BFF MDI, respectively.
Mortality
All-cause mortality was evaluated in ETHOS (as a secondary outcome) but not in KRONOS. The risk of death (all causes) was lower during treatment with BGF MDI 320 relative to GFF MDI (hazard ratio [HR] = 0.51; 95% CI, 0.330 to 0.80), but not different relative to BFF MDI (HR = 0.72; 95% CI, 0.44 to 0.1.16) as assessed by the Cox proportional hazards model.
Harms Results
Within each trial, adverse events (AEs) were similar across treatment arms. The most common treatment-associated AEs were COPD (9.5% to 11.3% in ETHOS, 2.5% to 5.1% in KRONOS), nasopharyngitis ((9.4% to 11% in ETHOS, 7.7% to 9.4% in KRONOS), and upper respiratory tract infections (4.8% to 5.7% in ETHOS, 5.7% to 10.2% in KRONOS). Around 20% of patients in ETHOS and 9% of those in KRONOS reported 1 or more serious adverse events (SAEs). Incidence of pneumonia was 1.6% to 2.8% in ETHOS and 0 to 1.3% in KRONOS. In ETHOS, there were 112 deaths on treatment (1.3%) across all treatment groups, whereas in KRONOS there were 12 deaths (0.6%).
Approximately 6% of patients in ETHOS and 4% of patients in KRONOS withdrew due to AEs. The number of patients who withdrew was relatively similar across treatment arms. The most common reason for withdrawal was lack of efficacy, reported as COPD. Notable harms such as cardiovascular events, anticholinergic events, and corticosteroid-related events were reported in a small number of patients in each trial. The incidences were relatively similar across treatment arms. Details on these notable harms are shown in Table 2.
Table 2: Summary of Key Results From Pivotal and Protocol Selected Studies
Results | ETHOS | KRONOS | |||||
|---|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg N = 2,137 | GFF MDI 14.4 mcg-9.6 mcg N = 2,120 | BFF MDI 320 mcg- 9.6 mcg N = 2,131 | BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg N = 639 | GFF MDI 14.4 mcg- 9.6 mcg N = 625 | BFF MDI 320 mcg- 9.6 mcg N = 314 | Symbicort TBH (DPI) 400 mcg- 12 mcg N = 318 | |
Moderate-to-severe exacerbations | |||||||
n (%) | 1,026 (48.0) | 1,056 (49.8) | 1,085 (50.9) | 108 (16.9) | 157 (25.1) | 65 (20.7) | 61 (19.2) |
Adjusted rate (SE)a | 1.08 (0.04) | 1.42 (0.05) | 1.24 (0.04) | 0.46 (0.05) | 0.95 (0.09) | 0.56 (0.08) | 0.55 (0.08) |
Rate difference (95% CI) | Reference group | −0.35 (−0.46 to −0.23) | −0.17 (−0.27 to −0.06) | NR | |||
Rate ratio (95% CI) | Reference group | 0.76 (0.69 to 0.83) | 0.87 (0.79 to 0.95) | Reference group | 0.48 (0.37 to 0.64) | 0.82 (0.58 to 1.17) | 0.83 (0.59 to 1.18) |
P value | < 0.0001 | 0.0027 | < 0.0001 | 0.2792 | 0.3120 | ||
FEV1 AUC0-4 over 24 weeks | |||||||
LS mean difference (95% CI) | Reference group | 49 (31 to 66) | 99 (82 to 117) | Reference group | 16 (−6 to 38) | 104 (77 to 131) | 91 (64 to 117) |
P value | < 0.0001 | < 0.0001 | 0.1448 | < 0.0001 | < 0.0001 | ||
Morning pre-dose trough FEV1 | |||||||
LS mean difference (95% CI) | Reference group | 35 (12 to 57) | 76 (54 to 99) | Reference group | 22 (4 to 39) | 74 (52 to 95) | 59 (38 to 80) |
P value | 0.0025 | < 0.0001 | 0.0139 | < 0.0001 | < 0.0001 | ||
Use of rescue medication over 24 weeks | |||||||
Change from baseline, mean (SE) | −1.2 (0.06) | −0.7 (0.07) | −0.8 (0.06) | −1.3 (0.13) | −1.1 (0.13) | −1.1 (0.18) | −1.6 (0.17) |
Treatment group difference vs. control (95% CI) | Reference group | −0.51 (−0.68 to −0.34) | −0.37 (−0.54 to −0.20) | Reference group | −0.25 (−0.60 to 0.09) | −0.24 (−0.65 to 0.18) | 0.23 (−0.17 to 0.63) |
P value | < 0.0001 | < 0.0001 | 0.1446 | 0.2661 | 0.2667 | ||
TDI focal score over 24 weeks | |||||||
LS mean difference (95% CI) | Reference group | 0.40 (0.24 to 0.55) | 0.31 (0.15 to 0.46) | Reference group | 0.177 (−0.071 to 0.426) | 0.237 (−0.068 to 0.542) | 0.461 (0.156 to 0.766) |
P value | < 0.0001 | < 0.0001 | 0.1621 | 0.1283 | 0.0031 | ||
SGRQ total score at 24 weeks | |||||||
LS mean difference (SE, 95% CI) | Reference group | −1.62 (−2.27 to −0.97) | −1.38 (−2.02 to −0.73) | Reference group | −1.22 (−2.30 to −0.15); | −0.45 (−1.78 to 0.87) | −1.26 (−2.58 to 0.06); |
P value | — | < 0.0001 | < 0.0001 | — | 0.0259 | 0.5036 | 0.0617 |
Time to death (all-cause) | |||||||
Hazard ratio (95% CI) | Reference group | 0.51(0.33 to 0.80) | 0.72 (0.44 to 1.16) | NR | |||
P value | 0.0035 | 0.1721 | |||||
Harms, n (%) (safety population) | |||||||
AEs | 1,368 (63.8) | 1,312 (61.7) | 1,377 (64.5) | 388 (60.7) | 384(61.4) | 175 (55.7) | 183 (57.5) |
SAEs | 426 (19.9) | 433 (20.4) | 440 (20.6) | 55 (8.6) | 68 (10.9) | 21 (6.7) | 29 (9.1) |
WDAE (from study treatment) | 119 (5.6) | 146 (6.9) | 140 (6.6) | 30 (4.7) | 30 (4.8) | 11 (3.5) | 11 (3.5) |
Deaths | 20 (0.9) | 35 (1.6) | 29 (1.4) | 6 (0.9) | 3 (0.5) | 2 (0.6) | 1 (0.3) |
Notable harms | |||||||
MACE, n (%) | 31 (1.4) | 44 (2.1) | 23 (1.1) | 2 (0.3) | 3 (0.5) | 2 (0.6) | 2 (0.6) |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
||||||||||| | | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Dysphonia or aphonia | 39 (1.8) | 7 (0.3) | 31 (1.5) | 20 (3.1) | 5 (0.8) | 15(4.8) | 6 (1.9) |
Blurred vision | 2 (0.1) | 1 (< 0.1) | 4 (0.2) | 0 | 0 | 0 | 2 (0.6) |
||||||||||| | | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
||||||||||| | | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | NR | |||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Euphoric mood | NR | NR | NR | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Agitation or anxiety | 36 (1.7) | 26 (1.2) | 31 (1.5) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Insomnia | 30 (1.4) | 23 (1.1) | 11 (0.5) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
AE = adverse event; AUC0-4 = area under the curve from 0 to 4 hours post dose; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; CI = confidence interval; COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; ICS = inhaled corticosteroid; LS = least squares; MDI = metered-dose inhaler; NR = not reported; SAE = serious adverse event; SE = standard error; SGRQ = St George’s Respiratory Questionnaire; TBH = Turbuhaler; TDI = Transition Dyspnea Index; WDAE = withdrawal due to adverse event.
aAdjusted for baseline post-bronchodilator percent predicted FEV1, baseline COPD exacerbation history, log baseline blood eosinophil count, region, and ICS use at screening.
Source: ETHOS and KRONOS Clinical Study Reports.
Critical Appraisal
One of the limitations of the included study was the amount of missing data, likely due to early discontinuation. In ETHOS, in particular |||||||||||||||||||||||||||||||||||||||||||||||||| for the primary end point. The relatively high rates of treatment discontinuation (22% in ETHOS and 14% KRONOS) could have biased the results in favour of BGF MDI. The BUD-FOR TBH arm in KRONOS was open label, which could have introduced a subjective bias in patient-reported outcomes. The chances of inadvertent unblinding due to AEs were low, given the similarities in the events across the treatment groups. The degree and type of training provided for the inhaler device was not described in the trials. However, treatment adherence was high across the treatment arms in both trials, which, measured by the ratio of daily puffs taken and the expected number of daily puffs, was 93.2 and 95.2 in ETHOS and KRONOS, respectively.
There were several limitations related to generalizability. The percentage of female participants was lower than what would be expected in real-world settings. Participants’ treatment history with LAMA-LABA (14%) combinations was low compared with the Canadian COPD population. Approximately 3/4 of patients in both trials used an ICS at baseline, which was higher than in clinical settings for respirologists in Canada. This, coupled with the low threshold of baseline eosinophil levels considered for subgroup analysis, was of some concern to the clinical expert consulted by CADTH. However, the threshold and proportion of patients with a baseline eosinophil count of 150 cells/mm3 or greater in ETHOS was similar to that in trials of other triple-therapy combinations.7 Although the ideal comparator for BGF MDI would have been other triple-therapy combinations, the comparators used in the study were considered appropriate for establishing efficacy. Some outcomes that were pointed out as important by the patient groups were not considered in the trials, such as exercise tolerance and patient satisfaction, except for items within the SGRQ.
Indirect Comparisons
One network meta-analysis (NMA), submitted by the sponsor, was identified to provide indirect evidence. The NMA compared BGF MDI 320 with other open and fixed triple-therapy combinations of LAMA-LABA-ICS for the treatment of moderate-to-very-severe COPD. A systematic literature search and the study selection and quality assessments were conducted appropriately. For the NMA analysis, all LAMA-LABA combinations were grouped together into a single node to create networks and an assumption of similar efficacy was made. Analyses were conducted using a 3-level hierarchical Bayesian NMA model.
The population, intervention, comparators, and outcomes considered by the NMA were relevant. Fifteen double-blinded RCTs were included in the NMA. The baseline characteristics of the study participants and results of the included studies were not reported, making the interpretation across trials regarding potential effect modifiers and homogeneity challenging. However, an assessment of heterogeneity and planned sensitivity analyses were conducted for most of the outcomes. The results of the NMA found comparable levels of efficacy and safety between BGF MDI 320, fluticasone furoate plus umeclidinium plus vilanterol (FF-UMEC-VI) (Trelegy Ellipta) and other open triple-therapy combinations.
Other Relevant Evidence
A 52-week extension study of the KRONOS trial, the results of which were included in the appendix of the NMA, evaluated the safety of the triple BGF MDI fixed-dose combination and its effects on bone mineral density (BMD) and ocular safety in patients with moderate-to-severe COPD. Overall, 456 patients were included in the safety population and randomized to 1 of the treatment groups (BGF MDI, BFF MDI, or GFF MDI). The changes from baseline in all 3 groups were small and not clinically meaningful, and there were no new or unexpected safety findings. The main limitations of the extension safety study were the study duration and the relatively small sample size.
Conclusions
Two multinational double-blind RCTs sponsored by AstraZeneca were included in this review, ETHOS (52 weeks) and KRONOS (24 weeks), comparing the efficacy of BGF MDI 320 with that of dual therapy for patients with COPD. Overall, BGF MDI 320 reduced the rate of moderate or severe exacerbations compared with GFF MDI and BFF MDI at 52 weeks. Although numerical improvements in HRQoL and symptoms were reported, the between-group differences were not clinically significant. BGF MDI 320 improved FEV1 over 24 weeks compared with all active comparators. However, this improvement in FEV1 was not clinically significant. The average daily use of rescue medications was decreased by 1 unit after treatment with BGF MDI for 24 weeks. The between-groups difference in the use of rescue medications was inconclusive. The lack of head-to-head trials between triple-therapy combinations is an important gap in the evidence. Indirect evidence from a sponsor-submitted NMA compared BGF MDI 320 with FF-UMEC-VI (Trelegy) and other open triple-therapy combinations. BGF MDI likely showed similar or comparable efficacy and safety compared with other triple therapies, with notable limitations inherent with indirect comparison. AEs associated with BGF MDI 320 were consistent with those expected for each of the individual components.
Introduction
Disease Background
COPD is a chronic inflammatory lung disease, often associated with chronic bronchitis and emphysema, that causes obstructed airflow from the lungs, lung hyperinflation, systemic manifestations, and increasing frequency and severity of exacerbations.1,2 COPD is a preventable and treatable disease with approximately 80% to 90% of cases being caused by smoking.1 A number of factors may cause COPD and contribute to its complexity, including long-term cumulative exposure to occupational dusts and chemicals, second-hand smoke or wood smoke and other biomass fuels used for cooking; frequent lung infections as a child; or genetic reasons (alpha1-antitrypsin deficiency).2,8 This disease is associated with several comorbidities, including ischemic heart disease, osteopenia and osteoporosis, glaucoma and cataracts, cachexia and malnutrition, anemia, peripheral muscle dysfunction, cancer, and metabolic syndrome.1
COPD is an under-diagnosed illness; thus, prevalence statistics likely underestimate the number of people currently living with COPD. In 2015, the global prevalence of COPD in adults aged 40 and over was reported to be 6.4%, marking a slight decline since 2008 (7.2%).9,10 However, the prevalence, morbidity, and mortality of COPD varies across the world due to a variety of factors, including a country’s income level (high or low), air quality, and health insurance coverage.10 According to a recent Statistics Canada report, COPD is the fifth-leading cause of death in Canada and was previously ranked as the fourth-leading cause of death up until 2015.11,12 Historically, the prevalence and incidence of COPD has been higher in males compared with females; however, this has changed over the years, as the rates of smoking have increased among females.9 Moreover, new evidence suggests that women may be more susceptible to the effects of tobacco than men, possibly due to a difference in lung physiology, leading to more severe disease in women.8
Patients with COPD are often limited in their day-to-day life, including their ability to breathe, talk, sleep, work, and socialize. Overall, patients describe COPD as a physically and mentally exhausting disorder that can result in anxiety, depression, and a decrease in quality of life. In addition, COPD has a profound effect on caregivers, who cite a number of challenges, including limited time for managing their own health and well-being, feelings of depression and isolation, anxiety, stress, fatigue, feeling of unending days, and increased requirements for social support.
The goals of COPD management are to reduce the frequency and severity of exacerbations, alleviate symptoms, improve exercise tolerance and daily activity, prevent and treat exacerbations and complications, improve health status, and reduce mortality.1
Standards of Therapy
Management decisions are guided by disease severity (i.e., symptoms, disability, and spirometry) and the frequency of acute exacerbations. Smoking cessation is the single most effective intervention to reduce the risk of developing COPD and the only intervention shown to slow the rate of lung function decline; regular exercise with cardiorespiratory conditioning can improve functional status and sensation of dyspnea in COPD patients more than medications alone. Education and self-management skills are also integral to the non-pharmacological management of COPD. Pulmonary rehabilitation is recommended for all COPD patients who are symptomatic.
Bronchodilators form the mainstay of pharmacotherapy for COPD13 and include LABAs such as salmeterol, formoterol, indacaterol, and vilanterol, and LAMAs such as tiotropium, glycopyrronium, aclidinium, and umeclidinium. LAMAs and LABAs used in combination as a step-up therapy are recommended for patients with stable COPD who are still experiencing exacerbations despite the use of LAMA or LABA monotherapy.13 Combinations of a fixed-dose LABA-ICS, such as fluticasone plus salmeterol, may be considered for certain patients with COPD. ICS is not recommended as monotherapy in COPD and, should only be combined with an inhaled LABA when used.. An ICS may not be useful for mild disease; but may have more of a role in the management of patients with moderate-to-severe COPD who are experiencing 2 or more exacerbations (or 1 or more exacerbations leading to hospital admission) per year, or in those with persistent symptoms.1,8,14,15 There may also be a subpopulation of COPD patients who have concomitant asthma or airway eosinophilia where ICS use may be beneficial.8,13,16-18 Patients with persistent symptoms and poor health status who continue to experience exacerbations despite inhaled LAMA-LABA dual therapy may be recommended to step up to LAMA-LABA-ICS triple therapy.8,13 Methylxanthines (such as theophylline) and phosphodiesterase inhibitors (roflumilast) are adjunctive therapies for COPD management that have a limited place in the treatment of COPD in Canada. Oxygen therapy is used in patients with very severe COPD with persistent hypoxemia.
Drug
Breztri is a fixed-dose combination of BGF in a pressurized inhalation aerosol for oral inhalation, marketed as the Aerosphere inhaler device. BGF MDI is currently under review by Health Canada for long-term maintenance treatment to reduce exacerbations of COPD and to relieve symptoms in patients with COPD, including chronic bronchitis and/or emphysema. BGF MDI delivers budesonide 182 mcg, glycopyrronium 8.2 mcg, and formoterol fumarate dihydrate 5.8 mcg per metered actuation. Table 3 provides an overview of BGF MDI and the other currently available LAMA-LABA-ICS fixed-dose combination inhaler for COPD, FF-UMEC-VI (Trelegy Ellipta).
Table 3: Key Characteristics of LAMA-LABA-ICS Fixed-Dose Combination Inhalers
Characteristics | BGF MDI | Fluticasone furoate-umeclidinium-vilanterol (Trelegy Ellipta) |
|---|---|---|
Mechanism of action |
|
|
| COPD | COPD |
Route of administration | Oral inhalation | Oral inhalation |
Recommended dose | 182 mcg-8.2 mcg-5.8 mcg: 2 inhalations twice daily | 100 mcg-62.5 mcg-25 mcg: 1 inhalation once daily |
Serious adverse effects or safety issues |
|
|
Other | Delivery device: Aerosphere | Delivery device: Ellipta |
BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; MDI = metered-dose inhaler.
aHealth Canada–approved indication.
Source: Product monographs for Trelegy Ellipta and BGF MDI.
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups.
1. Brief Description of Patient Group(s) Supplying Input
Three patient groups, COPD Canada, the Lung Health Foundation (Ontario Lung Association), and the British Columbia Lung Association, provided input for this submission. These not-for-profit organizations help inform and support Canadians living with COPD and other lung diseases. Furthermore, these organizations act as educational resources and patient advocacy groups, providing patient education materials and services and producing quality-of-life seminars for patients and their caregivers.
COPD Canada reviews and interprets scientific literature related to emphysema and chronic bronchitis so that it can be easily interpreted by the community. The British Columbia Lung Association works closely with the Canadian Thoracic Society, Canadian Lung Association, the Lung Health Association, and other partners while providing funding to various British Columbia research initiatives pertaining to lung disease. The Lung Health Foundation invests in lung research and advocates for improved treatment and care for lung health.
Declarations of financial support for each patient group are available on the CADTH website.
2. Condition Related Information
COPD Canada collected Canadian-applicable patient input from the personal experiences of the organization’s members and from published scientific articles. Members of COPD Canada provided their experiences during group pulmonary rehabilitation sessions, lung issue support groups, and in direct one-on-one consultations. In addition, COPD Canada distributed an email survey in January 2021 for which they received 64 written responses.
The British Columbia Lung Association conducted telephone interviews with some of its members (5 patients and 5 caregivers). The interviewees were either on or caring for patients on triple therapy prescribed by a respirologist.
The Lung Health Association collected online survey responses (received in December 2020) from people living with COPD (n = 39), emphysema (n = 12), and chronic bronchitis and bronchiectasis (n = 4) as well as from 18 caregivers caring for a family member living with COPD. Additionally, 2 phone interviews were completed in January 2021 and input was received from a certified respiratory educator who reviewed disease experience and experiences with available treatments and outcomes.
COPD has a profound effect on the lives of both patients and caregivers. COPD is associated with a considerable burden of disease, affecting many things that are fundamental to everyday life, such as the ability to breathe, talk, sleep, work, and socialize. As the disease progresses and worsens, patients become less physically active and more socially isolated. Many patients with COPD are of working age, so even in the early stages of the disease, the breathlessness and fatigue caused by COPD reduces the ability of the patient to go to work or carry out their normal work activities. Some patients are forced to go into early retirement as a consequence of the progressive disease’s severity.
Even many of the day-to-day activities most take for granted are virtually impossible or extremely difficult for people with severe COPD. Changing bed sheets, bathing and dressing, shopping and carrying bags (e.g., groceries), climbing stairs, and walking and talking at the same time are all examples of such day-to-day activities.
Patients with COPD can often develop anxiety, depression, and a sense of reduced self-worth because of their inability to perform common tasks due to their lung condition. Additionally, patients with COPD often have difficulty fighting infections and ongoing exacerbations may lead to a worsening of lung function.
Caregivers face considerable challenges that commonly include limited time for managing their own health and well-being, feelings of depression and isolation, anxiety, stress, fatigue, feeling of unending days, and increased requirements for social support. In the case of grown children who become their parent’s caregivers, they are often torn between the needs of their young families and the needs of their elderly parent with COPD.
One respondent described their experience living with COPD:
It has seriously slowed activity including ruling out some of my favourites such as, hiking, walking in the woods, climbing hills, keeping up with anyone even on flat ground and I am totally unable to walk up hills. Sexual activity is very impacted. Can't do even simple jobs around the home such as mowing the grass, lifting things, or even carrying groceries and other items. The deterioration is so fast that now I could never do the renovation work I did on my house only 8 years ago.
3. Current Therapy Related Information
Typical maintenance therapy usually includes the use of tiotropium bromide (Spiriva) with fluticasone plus salmeterol (Advair), or budesonide plus formoterol (Symbicort) twice per day. Rescue medications vary from patient to patient, although salbutamol (Ventolin) is used quite extensively. These products are to control the condition, but they do not improve long-term lung function. When a patient experiences an exacerbation, prednisone and antibiotics are often prescribed. Prednisone works quickly but has very dangerous side effects. The overuse of antibiotics has become a national and international concern due to increased resistance, particularly in long-term care facilities.
The British Columbia Lung Association noted that when patients were on triple-therapy medications, symptoms subsided, and patients were able to resume or had improvements in certain activities like walking and household chores.
A respondent had the following to say about their experience with treatments they have used:
Have used Spiriva and Advair. Got thrush in my mouth a couple of times. Advair leaves too much powder behind inside my mouth and I wonder if any meds even get to my lungs. Trelegy does the same. They both seem to waste a lot of the medicine. Spiriva dispenser is much easier to use and its design seems to target the back of my mouth and throat much better.
4. Expectations About the Drug Being Reviewed
Although none of the patients with COPD who responded to the survey had direct experience with the drug under review, their input clearly identified that they want additional therapies that work to improve breathing and lung function, are easy to use, and do not just offer symptomatic or emergency relief. Because COPD is treated in a stepwise manner, where treatments are layered on as the disease progresses, additional treatment options are often needed to address continual disease progression and severity. As well, the input noted that long-term use of some of these compounds results in a perceived diminishing of the drug’s effectiveness. Thus, it would be desirable to have alternative but equivalent drugs available beyond what there is currently.
The patient groups noted that BGF MDI would be a welcome addition to provincial formularies across the country. Their input indicates they expect that adherence to treatment would increase with the ease of use of this triple therapy. They also expressed hope the Aerosphere inhaler would be easy to use and would ensure the drug is reaching the lungs without relying on a patient’s ability or strength to inhale properly to administer a dose. The British Columbia Lung Association noted that the choice of inhaler device was important and significant for COPD patients, as it has been shown that some devices do not dispense medications appropriately to large and small airways.
COPD Canada is aware of accessibility issues throughout Canada and notes that provincial drug coverage varies considerably among the plans. COPD Canada points out that most COPD patients are over 65 years of age and rely on provincial drug coverage.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in diagnosing and managing the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by a clinical specialist with expertise in the diagnosis and management of COPD.
Since the recent publications of the WISDOM, FLAME, and Trelegy studies, there has been great debate as to what the place of ICS in the management of COPD and the prevention of exacerbations should be. WISDOM and FLAME highlighted the role of dual bronchodilators in the prevention of COPD exacerbations in patients known to have had an exacerbation in the last 12 months. WISDOM provided evidence that withdrawing ICS did not lead to an increased risk of exacerbation, while FLAME showed superiority of dual bronchodilation over an ICS-LABA in preventing all exacerbations (although there was no statistically significant difference in severe exacerbations). The Global Initiative for Obstructive Lung Disease (GOLD) group published revised recommendations taking into consideration the new literature and reviewed the role of ICS in the management of COPD. To illustrate the changes proposed in GOLD, if we look at group C, a group with patients who had an exacerbation requiring hospitalization or who had more than 2 exacerbations requiring treatment with antibiotics and prednisone, dual bronchodilation is recommended and the ICS-LABA combination is an alternative treatment. Similarly, in group B, which regroups the patients with 1 exacerbation or less, there is no recommendation to use an ICS-LABA. Trelegy noted an increase in mortality rates in COPD patients with a history of exacerbations if ICS treatment was withdrawn suddenly; however, after that first month, the mortality rate stabilized between the groups of patients who were either on or off an ICS.
When reviewing AEs, especially when considering pneumonia as an AE in treating COPD patients, the risk seems less with budesonide than with other ICSs.
Something that has been missing in the treatment options for COPD is a triple-therapy combination using an MDI device. Patients are encouraged to use salbutamol as an emergency treatment using an Aerochamber, but this implies that treating teams need to teach patients how to use both their regular everyday inhaler as well as another device for emergency situations; thus, having a combination triple-therapy device in MDI format could represent an advantage.
Physicians are familiar with the individual pharmacological components of this product, as they are all available on the Canadian market, although they are in somewhat different form and delivered using different devices.
The place that a twice-daily MDI triple-therapy combination product would take is probably a small one. As the positive effects of dual-combination therapy on exacerbation rates and symptom management have been shown, and as international and Canadian recommendations have evolved, the population that would benefit from triple therapy has been better identified.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups.
A joint submission providing input from 3 clinicians from Ontario was received on the reimbursement review of BGF MDI. All 3 clinicians work at the COPD outpatient clinic in the Division of Respirology and Sleep Medicine at Queen’s University. The clinicians noted their work is at a university-based academic centre where they are involved in research, teaching, and long-term care (including rehabilitation) of patients with COPD.
Information for this input was collected through a peer-reviewed paper, recent reviews, and updates on the topic up to February 9, 2021. The clinicians also noted that they see patients with mild to end-stage COPD and are active researchers with extensive lecturing experience in clinical issues involving patients with COPD.
Unmet Needs
The clinicians noted that, as per Canadian Thoracic Society recommendations, management of COPD includes smoking cessation, anti-influenza and anti-pneumococcal vaccination, regular physical activity (or pulmonary rehabilitation in more dyspneic patients), and short-acting bronchodilators, regardless of disease severity. The clinicians also added that addressing comorbidities (e.g., chronic rhinosinusitis, gastroesophageal reflux disease, sleep disorder breathing, ischemic heart disease) is important.19
For more symptomatic patients (at least grade 1 according to the Modified Medical Research Council [mMRC] Dyspnea Scale), the clinicians noted that a stepwise add-on approach to long-acting bronchodilators is applied. The clinicians noted that patients usually start with either a LAMA or LABA followed by a LAMA and LABA combination if monotherapy is deemed insufficient for adequate control of symptoms (that are at least grade 2 according to the mMRC scale). ICSs are added to a LABA or LAMA-LABA for patients experiencing frequent exacerbations (≥ 2 moderate exacerbations that prompted a prescription for antibiotics and/or oral steroids or at least 1 severe exacerbation that required hospitalization or an emergency room visit in the last year) and the clinicians noted that some physicians use eosinophil counts to guide adding an ICS (e.g., ≥ 300 cells/mm3).20
The group of clinicians added that oral theophylline is used in some patients with advanced disease as well as low-dose opiates and anxiolytics. Additionally, they noted that macrolide prophylaxis,21 oral N-acetylcysteine, and roflumilast might be used to further decrease the frequency and severity of exacerbations. The clinicians added that action plans, usually containing a respiratory fluoroquinolone and oral steroids, are made available for patients who may be more educated on their use.22
The clinicians added that long-term oxygen therapy is considered for hypoxemic patients (either rest or exercise), whereas non-invasive positive-pressure ventilation may be helpful in hypercapnic patients.23 Furthermore, the clinicians noted that bullectomy and lung volume reduction surgeries (including endoscopic) are restricted to carefully selected patients, and eligible patients who have end-stage disease may be referred for lung transplantation. The clinicians noted that no treatment modifies the underlying disease mechanism; treatments are fundamentally focused on reducing the burden of moderate-to-severe exacerbations and dyspnea control.
The current goals of therapy for this patient population include reducing dyspnea (particularly activity-related), reducing the burden of moderate-to-severe acute exacerbations, decreasing the rate of lung function decline, and improving HRQoL. Additionally, the clinicians noted that, more recently, improving survival has been considered a potential target for treatments.24
For those patients whose needs are not being met by currently available treatments, the clinicians noted that highly variable responses are seen for dyspnea control, and there is reduced efficacy in controlling exacerbations for those who need such controls. The clinicians added there are important limitations in delivering drugs to smaller airways that need to be addressed, as well as shortcomings in the activation of DPIs due to insufficient peak inspiratory flows in patients who are hyperinflated. They also noted there is poor round-the-clock bronchodilatation in once-daily medications and there is a lack in the Canadian market of twice-daily triple therapy (which offers more consistent bronchodilation through the day and night) delivered by an MDI (which has better airway deposition). Clinicians also commented that convenience (e.g., once daily versus twice daily) is usually an issue in chronically dyspneic patients who derive sensory benefit from long-acting bronchodilators. No treatments are available to reverse the course of the disease for hypoxemic patients, apart from smoking cessation and long-term oxygen therapy.
The clinicians noted that COPD patients who experience frequent exacerbations despite being on dual therapies like LABA and ICS or LAMA and LABA and, in particular, patients who report at least moderate dyspnea in daily life (mMRC ≥ 2), are most in need of therapy.25 The clinicians added that the drug combination under review would address this unmet patient need. They added there is recent evidence that the drug combination under review may also decrease the exacerbation burden, even in patients who do not present with a recent (within the past year) exacerbation.26
Place in Therapy
The clinicians noted that BGF MDI can be used either after a trial of LABA and ICS or LAMA and LABA, or as a first-line treatment in patients with a particularly high burden of moderate-to-severe exacerbations.
In addition, the clinicians added that triple therapy in a single inhaler complements the foundations of COPD treatment. They added there is another triple therapy in the Canadian market (FF-UMEC-VI, Trelegy), but this product is administered once daily through a DPI. The clinicians expressed concerns about both drug delivery and insufficient bronchodilation over the 24 hours with FF-UMEC-VI, and that fluticasone furoate may be associated with a higher rate of bacterial pneumonia compared with budesonide.27 The clinicians noted that formoterol is a dual short- and long-acting bronchodilator with a faster onset of action compared with vilanterol, which leads to quicker relief of dyspnea.28 The clinicians noted this may result in FF-UMEC-VI being insufficient for dyspnea control in more symptomatic patients.
When asked whether it would be appropriate to recommend that patients try other treatments before initiating treatment with the drug combination under review, the clinicians noted that a standard recommendation on this is not appropriate, given the large heterogeneity of the disease. The clinician group noted that the available evidence to date clearly indicates that triple therapy (LAMA-LABA-ICS) is superior to dual therapies (LAMA and LABA and ICS and LABA) in reducing the burden of moderate-to-severe exacerbations while improving dyspnea to the same extent as LAMA and LABA.26,29 Additionally, with respect to sequencing, the clinicians note that triple therapy may be the more appropriate first choice for patients with an unordinary burden of moderate-to-severe exacerbations and who are at high risk for a negative outcome if a major exacerbation occurs. The clinicians added that the likelihood of a negative, life-threatening outcome is usually decided on a patient-by-patient basis based on the severity of functional impairment, previous history of life-threatening exacerbations (including intensive care unit [ICU] admission), and the severity of comorbidities (particularly cardiovascular disease).
Patient Population
When asked which patients would be best suited for treatment with the drug combination under review, the clinicians noted this would be COPD patients presenting with a high burden of moderate-to-severe exacerbations, as these patients are more in need of an intervention.25,30 The clinicians said they would also consider using it to treat patients without a recent (within the last year) exacerbation. In addition, the clinicians added that the presence of at least moderate dyspnea in daily life (at least grade 2 according to the mMRC scale) would strengthen the indication for use, but it should not be a requirement.
According to the clinicians, patients would be identified through the mandatory diagnosis of chronic, poorly reversible airflow limitation on spirometry. In addition, they noted that spirometry alone might underestimate the severity of functional impairment and therefore measurements of lung volumes and lung-diffusing capacity might be warranted for patients with out-of-proportion dyspnea. The clinicians also added that under-diagnosis due to the lack of PFTs is common; however, once a PFT is available, the diagnosis is usually straightforward in a patient with a high pretest likelihood of disease, i.e., smoker or ex-smoker, aged 40 or older. In addition, they added that clinical history is crucial to identify those patients experiencing frequent exacerbations and those reporting a higher dyspnea burden.24 Blood eosinophils counts were noted by the clinicians as possibly providing auxiliary information. They commented that there is not sufficient evidence to indicate that treatment with triple therapy should be considered in pre-symptomatic COPD patients.
The patients least suited for treatment with the drug combination under review would be those with a low burden of exacerbations (≤ 1 moderate exacerbation and no severe exacerbation in the preceding year).31 Patients with mild dyspnea (mMRC dyspnea grade ≤ 1) being treated with a LAMA and/or LABA and/or short-acting bronchodilators would also be least suited.
Clinical history (dyspnea burden and dyspnea in daily life) as well as, occasionally, circulating eosinophilia, may help to identify those patients who are most likely to exhibit a response to the drug combination under review. According to the clinicians, the severity of functional impairment as measured with PFTs may also influence some treatment choices.
Assessing Response to Treatment
When asked which outcomes are used to determine whether a patient is responding to treatment in clinical practice, the clinicians noted that frequency and severity of COPD exacerbations and dyspnea in daily life would be the most appropriate outcome assessed. Similarly, the clinicians noted that the absence of severe exacerbations and 1 or fewer moderate exacerbations in the year subsequent to treatment initiation would demonstrate a clinically meaningful response. This, along with improvement in at least 1 grade in mMRC dyspnea score and lower as-needed use of short-acting bronchodilators, would demonstrate a clinically meaningful response. The clinicians noted that the magnitude of the treatment effect can be assessed by any physician and response should be assessed 1 to 2 months after treatment initiation to ensure compliance and lack of side effects. Thereafter, a response assessment every 6 months would be appropriate for most patients. However, this time period may be shortened in the presence of repetitive exacerbations and the use of an action plan despite adherence to treatment.
Discontinuing Treatment
When asked about considerations for treatment discontinuation for the drug combination under review, the clinicians noted that once triple therapy is initiated in a patient for whom treatment with the drug combination is appropriate, there is conflicting evidence on whether or not it is safe to de-escalate to LABA and LAMA or LABA and ICS after exacerbation control. The clinicians noted that this situation is likely to be safely accomplished by a specialist (respirologist) on a patient-by-patient basis.32
Prescribing Conditions
Community settings such as outpatient clinics or specialty clinics were identified by the clinicians as the most appropriate treatment setting for the drug combination under review.
In addition, the clinicians noted that for most patients, a specialist is not necessary to diagnose, treat, and monitor patients who may receive the drug combination under review, provided the family physician sees the patient regularly. However, the clinicians added that a respirologist or a COPD nurse practitioner might be better at monitoring severe patients with several hospital admissions and frequent emergency room visits, and those patients who require multiple interventions such as long-term oxygen therapy, non-invasive ventilation, opiates for dyspnea control, and so forth.24
Additional Information
The clinicians noted the recent data, observed in 2 large RCTs,30,33 showing that a LAMA-LABA-ICS (including the drug combination under review) administered using a single device has a positive effect on all-cause and respiratory mortality in patients with COPD presenting with a history of moderate-to-severe exacerbations. They noted that a strong signal in relation to lower cardiovascular-related mortality, a key cause of early death in Canadians with COPD, was observed in both studies.
The clinicians added that a LAMA-LABA-ICS may be prescribed on different inhalers and there is good evidence that administration on a single inhaler is associated with decreased health care resource utilization and improved cost-effectiveness compared with multiple inhalers. The clinicians commented that the use of a single device likely improves the deposition of the bronchodilators and steroids at the same location (i.e., the better ventilated alveolar units).34
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical expert consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
What are the most appropriate comparators for BGF? | Ideally, the comparator would be other triple-therapy combinations. However, dual therapies can also be considered relevant to establish the efficacy of BGF MDI. |
BGF = budesonide-glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler.
Clinical Evidence
The clinical evidence included in the review of BGF (BGF MDI 320, Breztri Aerosphere 182 mcg per 8.2 mcg per 5.8 mcg) is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of BGF (BGF MDI 320, Breztri Aerosphere 182 mcg per 8.2 mcg per 5.8 mcg) for the long-term maintenance treatment to reduce exacerbations of COPD and to relieve symptoms in patients with COPD, including chronic bronchitis and/or emphysema.
Methods
The studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented in Table 5 was established before the granting of a Notice of Compliance from Health Canada.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Patients with COPD, including chronic bronchitis and/or emphysema who have exacerbations of COPD. Subgroups:
|
Intervention | Budesonide 182 mcg plus glycopyrronium 8.2 mcg plus formoterol fumarate dihydrate 5.8 mcg administered as 2 inhalations twice daily |
Comparator | The following comparators used in combination (as appropriate):
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; COPD = chronic obstructive pulmonary disease; HRQoL = health-related quality of life; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aThese outcomes were identified as being of particular importance to patients in the input received by CADTH from patient groups.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist (https://www.cadth.ca/resources/finding-evidence/press).35
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) through Ovid and Embase (1974‒) through Ovid. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was a combination of 3 drugs (budesonide- glycopyrrolate-formoterol). Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on February 26, 2021. Regular alerts updated the search until the meeting of the CADTH Canadian Drug Expert Committee (CDEC) on June 16, 2021.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist (https://www.cadth.ca/grey-matters).36 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contact with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 2 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 6. A list of excluded studies is presented in Appendix 2.
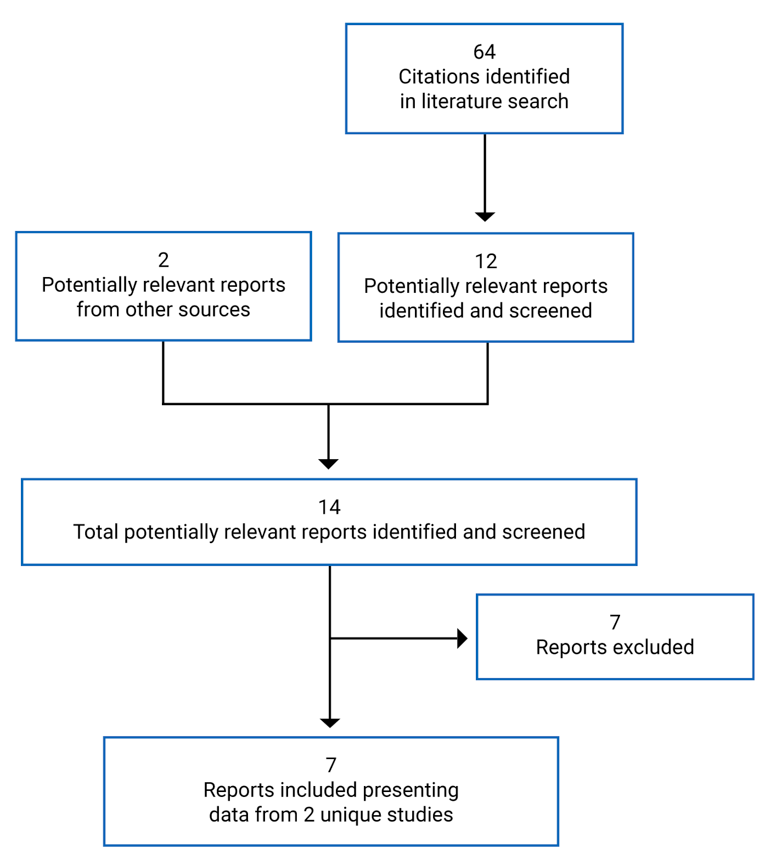
Table 6: Details of Included Studies
Detail | ETHOS | KRONOS |
|---|---|---|
Designs and populations | ||
Study design | DB parallel-group RCT | DB parallel-group RCT (with an open-label active control) |
Locations | Eastern Europe, Western Europe, Asia, North America, South America, Australia, New Zealand, South Africa | Japan, China, Canada, US |
Patient enrolment dates | June 2015 to July 2019 | August 2015 to January 2018 |
Randomized (N) | N = 8,588 (1:1:1:1)
| N = 1,902 (2:2:1:1)
|
Inclusion criteria | Male and non-pregnant female patients ≥ 40 to 80 years of age who were current or former cigarette smokers (≥ 10 pack-years at screening) diagnosed with COPD as defined by the ATS-ERS-JRS, with a score of ≥ 10 on the CAT, an FEV1 to FVC ratio of < 0.70, and an FEV1 of < 65% of the predicted normal value at visit 1; a post-bronchodilator FEV1 of ≥ 25% to < 65% of the predicted normal value at visit 2; an average of 2 FEV1 assessments conducted 60 minutes and 30 minutes pre-dose that was < 65% of the predicted normal value at visit 4; and who were on 2 or more inhaled maintenance therapies (including SABA and SAMA) for at least 6 weeks, with a documented history of exacerbations in the previous 12 months (those with a post-bronchodilator FEV1 of < 50% of predicted normal with ≥ 1 moderate or severe exacerbations, those with a post-bronchodilator FEV1 of ≥ 50% of predicted normal value with ≥ 2 moderate or ≥ 1 severe exacerbation). | Male and non-pregnant female patients ≥ 40 to 80 years of age who were current or former cigarette smokers (≥ 10 pack-years at screening) diagnosed with COPD as defined by the ATS-ERS-JRS, with a score of ≥ 10 on the CAT, an FEV1 to FVC ratio of < 0.70, and an FEV1 of < 80% of the predicted normal value at visit 1; a post-bronchodilator FEV1 to FVC ratio of < 0.70 and post-bronchodilator FEV1 of ≥ 25% to < 80% of the predicted normal value at visit 2; an average of 2 FEV1 assessments conducted 60 minutes and 30 minutes pre-dose that was < 80% of the predicted normal value at visit 4; and who were on 2 or more inhaled maintenance therapies (including SABA and SAMA) for at least 6 weeks before screening. |
Exclusion criteria | Current diagnosis of asthma, poorly controlled COPD (with recent corticosteroids or antibiotics use and hospitalization), COPD caused by alpha1-antitrypsin deficiency, other respiratory disorders, lung volume reduction within 6 months of screening, recent LRTI, long-term O2 therapy or NIPPV, cardiac diseases such as unstable ischemic heart disease, left ventricular failure, congestive heart failure, clinically significant arrhythmias, or other clinically significant diseases. | Current diagnosis of asthma, poorly controlled COPD (with recent corticosteroids or antibiotics use and hospitalization), COPD caused by alpha1-antitrypsin deficiency, other respiratory disorders, lung volume reduction within 6 months of screening, recent LRTI, long-term O2 therapy or NIPPV, other clinically significant diseases, risk factors for pneumonia, clinically significant abnormalities not believed to be due to the presence of COPD, pregnancy. |
Drugs | ||
Intervention | BGF MDI 320 mcg-14.4 mcg; 9.6 mcg, taken as 2 inhalations b.i.d. | BGF (MDI 320 mcg-14.4 mcg-9.6 mcg, taken as 2 inhalations b.i.d. |
Comparators |
|
|
Duration | ||
Phase | ||
Run-in | 4 weeks | 4 weeks |
Double-blind | 52 weeks | 24 weeks |
Follow-up | 2 weeks | 2 weeks or regional safety extension |
Outcomes | ||
Primary end point | Rate of moderate or severe COPD exacerbations |
|
Secondary and exploratory end points | Secondary:
| Secondary:
|
Exploratory:
Safety end points:
• vital sign measurements | Exploratory:
Safety:
• vital sign measurements | |
Notes | ||
Publications | ||
AE = adverse event; ATS = American Thoracic Society; AUC0-4 = area under the curve from 0 to 4 hours post dose; b.i.d. = twice daily; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; BUD = budesonide; CAT = Chronic Obstructive Pulmonary Disease Assessment Test; CI = confidence interval; CID = clinically important deterioration; COPD = chronic obstructive pulmonary disease; DB = double blind; DPI = dry powder inhaler; ECG = electrocardiogram; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; ERS = European Respiratory Society; E-RS = Evaluating Respiratory Symptoms in Chronic Obstructive Pulmonary Disease; EXACT = Exacerbations of Chronic Pulmonary Disease Tool; FEV1 = forced expiratory volume in 1 second; FOR = formoterol fumarate; FVC = forced vital capacity; GFF = glycopyrronium-formoterol fumarate; HFA = hydrofluoroalkane; JRS = Japanese Respiratory Society; LRTI = lower respiratory tract infection; LS = least squares; MCID = minimal clinically important difference; MDI = metered-dose inhaler; NIPPV = non-invasive positive-pressure ventilation; O2 = oxygen; RCT = randomized controlled trial; RS-Total = Evaluating Respiratory Symptoms in Chronic Obstructive Pulmonary Disease—Total Score; SABA = shorting-acting beta-agonist; SAMA = short-acting muscarinic antagonist; SE = standard error; SGRQ = St. George’s Respiratory Questionnaire; TBH = Turbuhaler; TDI = Transition Dyspnea Index.
aThis dose of BGF MDI was not the dosage considered for the current review. Only the characteristics and outcomes of the other 3 arms will be summarized in this report.
Source: ETHOS and KRONOS Clinical Study Reports.
Description of Studies
Two RCTs (ETHOS and KRONOS) were submitted by the sponsor and were included in the systematic review. The focus of this section is on these 2 pivotal trials. Both studies are described in Table 6.
ETHOS
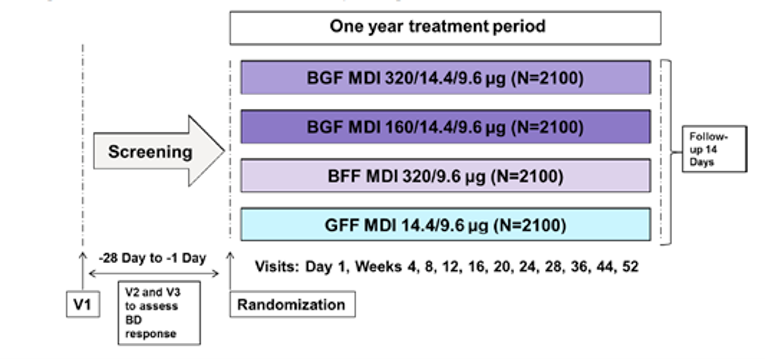
ETHOS was a multinational, 52-week, phase III, parallel-group, double-blind RCT sponsored by AstraZeneca. Patients were enrolled from Europe, Asia, North America, South America, Australia, New Zealand, and South Africa from 784 study centres (24 in Canada). This study took place from July 15, 2015 (first patient randomized) to July 26, 2019 (last patient’s last visit). Database lock was on August 9, 2019. The primary objective of ETHOS was to assess the effect of BGF MDI on the rate of moderate or severe COPD exacerbations compared with GFF MDI and BFF MDI in patients with moderate-to-severe COPD who had at least 1 exacerbation in the past year. For those patients who met the eligibility criteria, current COPD medications were reviewed and adjusted, as per the study protocol. Patients received training with an e-diary (for recording device use, symptoms, and so forth) at screening (day 1). Patients were required to demonstrate acceptable e-diary adherence during the screening period to be eligible for randomization. All patients who successfully completed the screening period of 4 weeks were randomized 1:1:1:1 to 4 treatment arms and were stratified based on exacerbation history, post-bronchodilator FEV1, blood eosinophil count, and country. Randomization was followed by a treatment period of 52 weeks that included 5 additional clinic visits and 6 telephone calls. Overall, 8,588 patients were enrolled to receive BGF MDI 320 mcg-14.4 mcg-9.6 mcg twice daily, BGF MDI 160 mcg-14.4 mcg-9.6 mcg twice daily, BFF MDI 320 mcg-9.6 mcg twice daily, or GFF MDI 14.4 mcg-9.6 mcg twice daily. Among them, BGF MDI 160 mcg-14.4 mcg-9.6 mcg is not aligned with the Health Canada review and is not considered for the current review. Figure 2 shows a visual representation of the study design for ETHOS.
KRONOS
KRONOS was a multinational, 24-week, phase III parallel-group, double-blind RCT sponsored by AstraZeneca. Patients were enrolled from the US, Canada, Japan, and China from 208 study centres (9 in Canada). The trial took place from August 20, 2015 (first patient randomized) to January 5, 2018 (last patient’s last visit). Database lock was on May 8, 2018. The primary objective of KRONOS was to assess the effect of BGF MDI and Symbicort TBH on lung function in patients with moderate-to-very-severe COPD. For those patients who met the eligibility criteria, all prohibited medications were discontinued with predetermined washout periods, and the allowed medications were adjusted as per the study protocol. Patients received training with an e-diary (for recording device use, symptoms, and so forth) at screening (day 1). All patients who successfully completed the screening period of 4 weeks were randomized in a 2:2:1:1 scheme to 4 treatment arms and were stratified based on reversibility to salbutamol (Ventolin) hydrofluoroalkane, country, and disease severity. Randomization was followed by a treatment period of 24 weeks, and each participant attended 10 study visits and a follow-up call 14 days after the last visit. Overall, 1,902 patients were randomized to receive BGF MDI 320 mcg-14.4 mcg-9.6 mcg twice daily, GFF MDI 14.4 mcg-9.6 mcg twice daily, BFF MDI 320 mcg-9.6 mcg twice daily, or BUD-FOR DPI through Symbicort TBH 400 mcg-12 mcg. Among them, the budesonide plus formoterol (Symbicort) TBH arm was designed as open label.
The KRONOS trial was designed based on local regulatory agency requirements; therefore, 3 different registration approaches were used, based on region. The approaches were based on requirements in Japan and China, the EU and Canada, and the US. The treatment comparison of interest, end points, and analysis time frames were different for each region. This review focused on the EU-Canada approach.
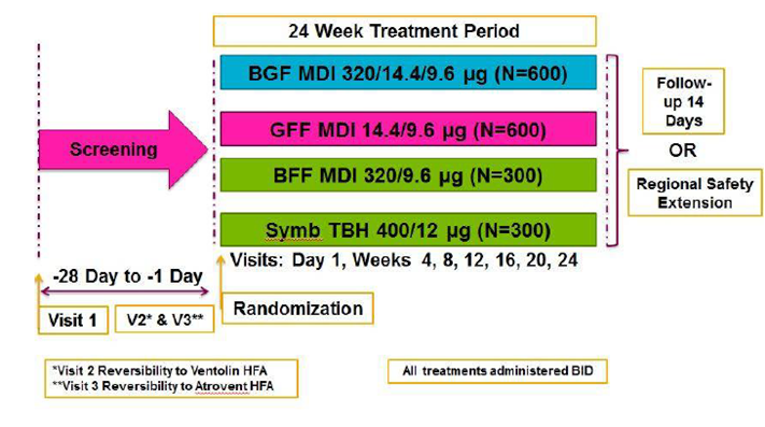
Figure 3 shows a visual representation of the study design for KRONOS.
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; BD = bronchodilator; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; V = visit.
Source: ETHOS Clinical Study Report.
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; BID = twice daily; GFF = glycopyrronium-formoterol fumarate; HFA = hydrofluoroalkane; MDI = metered-dose inhaler; Symb = Symbicort; TBH = Turbuhaler; V = visit.
Source: KRONOS Clinical Study Report.
Populations
Inclusion and Exclusion Criteria
The study population for ETHOS and KRONOS consisted of current or former smokers with COPD (diagnosed based on American Thoracic Society and European Respiratory Society definitions) who were 40 to 80 years old and were on COPD maintenance therapy with 2 or more inhaled medications for at least 6 weeks. Other inclusion criteria were an FEV1 to FVC ratio of less than 0.70 and a score of 10 or more on the COPD Assessment Test (CAT). The ETHOS trial enrolled only patients who had a documented history of at least 1 exacerbation within the previous year. On visit 1, ETHOS required the FEV1 to be less than 65% of the predicted normal value for the patient to be eligible, whereas the required FEV1 for KRONOS was less than 80% of the predicted normal. Exclusion criteria across the 2 trials were patients with: a current diagnosis of asthma, poorly controlled COPD (defined as corticosteroids or antibiotics use within the previous 6 weeks or hospitalization within the previous 3 months for KRONOS and 6 weeks for ETHOS), COPD associated with alpha1-antitrypsin deficiency, other respiratory disorders, lung volume reduction within 6 months of screening, other clinically significant diseases, or pregnancy. Patients with cardiovascular diseases such as unstable ischemic heart disease, left ventricular failure, congestive heart failure, clinically significant arrhythmias, and uncontrolled hypertension were also excluded from the trials.
Baseline Characteristics
The baseline characteristics were relatively balanced between arms for each study. The mean (standard deviation [SD]) ages of the patients were 64.7 (7.6) and 65.2 (7.7) for ETHOS and KRONOS, respectively. In ETHOS, 40.3% of patients were female compared with 28.8% female in KRONOS. In KRONOS, there was a higher proportion of Asian patients (44.9%), presumably due to the number of study centres in Japan and China. In the ETHOS trial, 60% of the patients had severe COPD and 28.5% had moderate COPD based on GOLD grade. In KRONOS, the proportion of patients with moderate and severe COPD were 49.1% and 42.9%, respectively.
Most of the patients (74.4%) in KRONOS did not have a history of COPD exacerbation within the previous 12 months, whereas more than 1-half (56.5%) of ETHOS patients had 2 or more COPD exacerbations within the year before screening. Additionally, approximately 80% of ETHOS patients and 71% of KRONOS patients were taking an ICS at baseline. Table 7 summarizes the baseline characteristics for each trial.
Table 7: Summary of Baseline Characteristics
Characteristic | ETHOS | KRONOSa | |||||
|---|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg N = 2,137 | GFF MDI 14.4 mcg-9.6 mcg N = 2,120 | BFF MDI 320 mcg-9.6 mcg N = 2,131 | BGF MDI 320 mcg- 14.4 mcg-9.6 mcg N = 639 | GFF MDI 14.4 mcg-9.6 mcg N = 625 | BFF MDI 320 mcg-9.6 mcg N = 314 | Symbicort TBH (DPI) 200 mcg-6 mcg N = 318 | |
Sex, n (%) | |||||||
Male | 1,260 (59) | 1,244 (58.7) | 1,279 (60) | 460 (72) | 430 (68.8) | 224 (71.3) | 236 (74.2) |
Female | 877 (41.0) | 876 (41.3) | 852 (40.0) | 179 (28.0) | 195 (31.2) | 90 (28.7) | 82 (25.8) |
Age, years Mean (SD) | 64.6 (7.6) | 64.8 (7.6) | 64.6 (7.6) | 64.9 (7.8) | 65.1 (7.7) | 65.2 (7.2) | 65.9 (7.7) |
Race, n (%) | |||||||
Black or African American | 78 (3.6) | 75 (3.5) | 64 (3.0) | 23 (2.6) | 38 (6.1) | 15 (4.8) | 14 (4.4) |
White | 1,819 (85.1) | 1,808 (85.3) | 1,816 (85.2) | 329 (51.5) | 301 (48.2) | 157 (50.0) | 163 (51.3) |
Native Hawaiian or Pacific Islander | 2 (0.1) | 0 | 0 | 0 | 1 (0.2) | 0 | 0 |
American Indian or Alaskan Native | 33 (1.5) | 30 (1.4) | 39 (1.8) | 1 (0.2) | 0 | 0 | 0 |
Asian | 162 (7.6) | 157 (7.4) | 166 (7.8) | 284 (44.4) | 285 (45.6) | 142 (45.2) | 141 (44.3) |
Other | 43 (2.0) | 50 (2.4) | 46 (2.2) | 2 (0.3) | 0 | 0 | 0 |
Ethnicity, n (%) | |||||||
Hispanic or Latino | 400 (18.7) | 426 (20.1) | 401 (18.8) | 16 (2.5) | 14 (2.2) | 7 (2.2) | 4 (1.3) |
Not Hispanic or Latino | 1,690 (79.1) | 1,649 (77.8) | 1,683 (79) | 623 (97.5) | 611 (97.8) | 305 (97.1) | 312 (98.1) |
Unknown | 21 (1.0) | 24 (1.1) | 25 (1.2) | 0 | 0 | 1 (0.3) | 2 (0.6) |
Not reported | 26 (1.2) | 21 (1.0) | 22 (1.0) | 0 | 0 | 1 (0.3) | 0 |
BMI | |||||||
BMI, kg/m2 Mean (SD) | 27.6 (6.2) | 27.6 (6.2) | 27.1 (6.2) | 26.1 (6.7) | 26.3 (6.4) | 26.1 (5.8) | 26.2 (6.3) |
Used ICS at screening, n (%) | |||||||
Yes | 1,706 (79.8) | 1,707 (80.5) | 1,704 (80.0) | 464 (72.6) | 447 (71.5) | 225 (71.7) | 225 (70.8) |
Smoking status, n (%) | |||||||
Current smoker | 910 (42.6) | 856 (40.4) | 864 (40.5) | 256 (40.1) | 257 (41.1) | 115 (36.6) | 122 (38.4) |
|||||||||||||||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||||||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Number of pack-years smoked mean (SD) | 47.0 (25.1) | 48.4 (26.5) | 47.1 (26.3) | 52.1 (30.0) | 49.8 (25.9) | 52.9 (29.3) | 53.5 (30.8) |
GOLD grade, n (%) | |||||||
1 (mild) | 0 | 0 | 0 | 2 (0.3) | 0 | 1 (0.3) | 0 |
2 (moderate) | 613 (28.7) | 596 (28.1) | 614 (28.8) | 310 (48.5) | 306 (49.0) | 154 (49.0) | 160 (50.3) |
3 (severe) | 1,305 (61.1) | 1,293 (61.0) | 1,283 (60.2) | 275 (43.0) | 267 (42.7) | 133 (42.4) | 138 (43.4) |
4 (very severe) | 217 (10.2) | 229 (10.8) | 233 (10.9) | 52 (8.1) | 52 (8.3) | 26 (8.3) | 20 (6.3) |
Missing | 2 (0.1) | 2 (0.1) | 1 (< 0.1) | NR | |||
Duration of COPD, years, mean (SD) | 8.4 (6.5) | 8.2 (6.1) | 8.4 (6.1) | 7.1 (6.0) | 6.5 (5.4) | 7.3 (6.2) | 6.7 (5.5) |
CAT score, mean (SD) | 19.7 (6.5) | 19.5 (6.6) | 19.5 (6.5) | 18.7 (6.4) | 18.1 (6.1) | 18.4 (6.6) | 18.0 (6.4) |
Exacerbation history | |||||||
0 | NR | 469 (73.4) | 473 (75.7) | 235 (74.8) | 234 (73.6) | ||
1 | 942 (44.1) | 909 (42.9) | 914 (42.9) | 125 (19.6) | 108 (17.3) | 61 (19.4) | 59 (18.6) |
≥ 2 | 1,195 (55.9) | 1,211 (57.1) | 1,217 (57.1) | 45 (7.0) | 44 (7.0) | 18 (5.7) | 25 (7.9) |
Baseline eosinophil count, cells/mm3, mean (SD) | 194.2 (131.4) | 194.8 (129.1) | 199.5 (140.9) | 178.6 (157.8) | 190.0 (178.9) | 178.8 (120.2) | 183.9 (137.4) |
< 150 cells/mm3, n (%) | 860 (40.2) | 847 (40.0) | 837 (39.3) | 314 (49.1) | 291 (46.6) | 151 (48.1) | 157 (49.4) |
≥ 150 cells/mm3, n (%) | 1,277 (59.8) | 1,272 (60.0) | 1,294 (60.7) | 325 (50.9) | 334 (53.4) | 163 (51.9) | 161 (50.6) |
Reversibility to Ventolin HFA, n (%) | |||||||
Change in FEV1 from pre- to post-Ventolin HFA (mL), mean (SD) | 146.3 (158.0) | 148.7 (151.1) | 142.3 (144.8) | 199.7 (144.5) | 191.7 (154.2) | 195.8 (162.1) | 212.2 (152.7) |
Reversibility to Atrovent HFA, n | |||||||
Change in FEV1 from pre- to post-Atrovent HFA (mL), mean (SD) | 144.0 (150.6) | 141.1 (144.5) | 136.6 (141.8) | 181.6 (131.5) | 180.2 (143.9) | 178.2 (147.1) | 186.9 (150.0) |
COPD-related treatment history prior to screening, n (%) | |||||||
LAMA | 23 (1.1) | 22 (1.0) | 21 (1.0) | 15 (2.3) | 8 (1.3) | 3 (1.0) | 5 (1.6) |
LABA | 15 (0.7) | 10 (0.5) | 11 (0.5) | 3 (0.5) | 3 (0.5) | 0 | 0 |
ICS | 9 (0.4) | 4 (0.2) | 7 (0.3) | 3 (0.5) | 3 (0.5) | 3 (1.0) | 2 (0.6) |
LAMA-LABA | 315 (14.7) | 286 (13.5) | 305 (14.3) | 122 (19.1) | 120 (19.2) | 66 (21.0) | 67 (21.1) |
ICS-LABA | 663 (30.9) | 660 (31.1) | 672 (31.5) | 244 (38.2) | 245 (39.2) | 102 (32.5) | 123 (38.7) |
ICS-LAMA | 14 (0.7) | 24 (1.1) | 21 (1.0) | 8 (1.3) | 7 (1.1) | 6 (1.9) | 8 (2.5) |
LAMA-LABA-ICS | 839 (39.1) | 846 (39.8) | 833 (39.0) | 177 (27.7) | 160 (25.6) | 101 (32.2) | 74 (23.3) |
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; BMI = body mass index; CAT = Chronic Obstructive Pulmonary Disease Assessment Test; COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; GOLD = Global Initiative for Chronic Obstructive Lung Disease; HFA = hydrofluoroalkane; ICS = inhaled corticosteroid; LABA = long-acting beta-agonist; LAMA = long-acting muscarinic antagonist; MDI = metered-dose inhaler; NR = not reported; SD = standard deviation; TBH = Turbuhaler.
aData from total patients in the trial.
Source: ETHOS and KRONOS Clinical Study Reports.
Interventions
In ETHOS, the study treatments were BGF 320 mcg-14.4 mcg-9.6 mcg, BFF 320 mcg-9.6 mcg, or GFF 14.4 mcg-9.6 mcg. It was administered as 2 oral inhalations twice daily using an MDI that contained 120 inhalations. Treatment duration was 52 weeks. Patients were provided with and trained to use an e-diary in which time of dosing was to be recorded along with symptoms and use of rescue medications. It was unclear whether the study patients were given training on how to use the inhaler.
In KRONOS, the study treatments were BGF 320 mcg-14.4 mcg-9.6 mcg, GFF 14.4 mcg-9.6 mcg, BFF 320 mcg-9.6 mcg, or BUD-FOR 400 mcg-12 mcg inhalation powder. In the double-blinded study arms, BGF 320 mcg-14.4 mcg-9.6 mcg, GFF 14.4 mcg-9.6 mcg, or BFF 320 mcg-9.6 mcg were administered as 2 oral inhalations twice daily using an MDI that contained 120 inhalations. In the open-label study arm, BUD-FOR inhalation powder was administered as 2 inhalations twice daily using a DPI using EU-sourced Symbicort TBH. Treatment duration was 24 weeks. Patients were provided with and trained to use an e-diary in which time of dosing was to be recorded along with symptoms and use of rescue medications.
In both trials, salbutamol (provided as Ventolin hydrofluoroalkane 90 mcg MDI) was used as rescue medication. No other COPD rescue medications were allowed. COPD medications used by the patients at screening were discontinued and a minimum washout period was observed before starting study treatments, as shown in Table 8. These medications were also not allowed to be used during the study. Medications such as systemic corticosteroids were allowed for the treatment of COPD exacerbations for a maximum of 14 days. Other prohibited medications during the study period included drugs that could prolong the QT interval, non-selective beta-blocking drugs, cardiac arrhythmic class Ia and III drugs, anticonvulsants, tricyclic antidepressants, monoclonal antibodies, mono-amine oxidase inhibitors, anti–tumour necrosis factor-alpha antibodies, and Chinese herbal therapies.
Table 8: List of Prohibited COPD Medications in ETHOS and KRONOS
Class of medication | Minimum washout period prior to starting study treatment |
|---|---|
LAMA | |
Tiotropium | 14 days |
Aclidinium | 7 days |
Glycopyrronium | 7 days |
Umeclidinium | 7 days |
SAMA | 6 hours |
LABA (inhaled) | 7 days |
Fixed combination of LABA-LAMA | 7 days |
Fixed combination of LABA-ICS | 7 days |
Fixed combination of SABA and SAMA | 6 hours |
SABA | 6 hours |
Oral beta-agonists | 2 days |
Theophylline | 7 days |
COPD = chronic obstructive pulmonary disease; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; SABA = short-acting beta2-agonist; SAMA = short-acting muscarinic antagonist.
Source: ETHOS and KRONOS Clinical Study Reports.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9. These end points are further summarized in Table 9. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | ETHOS | KRONOS |
|---|---|---|
Mortality (all causes, COPD specific) | Secondary | Not reported |
Health care resource utilization (e.g., hospitalizations, emergency room visits) | Other | Other |
Exacerbations | Primary | Secondary |
HRQoL | Secondary | Secondary |
Lung function (e.g., spirometry, expiratory capacity) | Secondary | Primary |
Symptoms (e.g., dyspnea) | Secondary | Secondary |
Use of rescue medication | Other | Secondary |
Exercise tolerance | Reported within HRQoL | Reported within HRQoL |
Patient satisfaction or adherence | Reported within HRQoL | Reported within HRQoL |
Productivity | Not reported | Not reported |
SAEs | Secondary | Secondary |
WDAEs | Secondary | Secondary |
AEs | Secondary | Secondary |
AEs of special interest (e.g., cardiovascular, pneumonia, corticosteroid AE, anticholinergic AE) | Secondary | Secondary |
AE = adverse event; COPD = chronic obstructive pulmonary disease; HRQoL = health-related quality of life; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Source: ETHOS and KRONOS Clinical Study Reports.
The primary outcome in ETHOS was the rate of moderate or severe exacerbations. COPD exacerbation was defined as a change from usual COPD symptoms that lasted for 2 or more days beyond normal variation, was acute in onset, and required a change in medication. An exacerbation was considered moderate if it required the use of systemic corticosteroids and-or antibiotics for at least 3 days. An exacerbation was considered severe if it resulted in COPD-related hospitalization for 24 hours or more or in a COPD-related death. Rate of exacerbations was considered a secondary outcome in KRONOS. Time to first moderate or severe COPD exacerbation and time to death were secondary outcomes of interest in ETHOS. In KRONOS, the rate of moderate or severe exacerbations was considered a secondary outcome.
As described previously, outcomes in KRONOS were different based on the registration requirement for that region. This review reports the outcomes per the EU-Canada approach. The primary outcome in KRONOS, lung function measured using spirometry, varied depending on the registration approach. For the EU-Canada registration approach, the primary outcome was the AUC0-4 for the FEV1 (for BGF MDI 320 versus BFF MDI, and BGF MDI 320 versus BUD-FOR DPI) and the change from baseline in the morning pre-dose trough FEV1 over 24 weeks (for BGF MDI 320 versus GFF MDI). Peak change from baseline in FEV1 within 4 hours post dosing over 24 weeks was considered a secondary outcome. In ETHOS, lung function measured as FEV1 AUC0-4 over 24 weeks was assessed as 1 of the primary outcomes in the 4-hour PFT substudy. FEV1 is the volume of air that, after a full inspiration, can be forcibly expired in 1 second. Trough FEV1 is recognized as a component of the GOLD classification of airflow limitation severity in COPD.39 The generally accepted clinically important change in FEV1 is between 0.10 L and 0.14 L.40
The change from baseline in the SGRQ total score was evaluated as a secondary outcome in ETHOS (at 52 weeks) and KRONOS (over 24 weeks). SGRQ measures health status (HRQoL), with scores ranging from 0 to 100. A higher score on the SGRQ indicates a poorer level of HRQoL and decreases in score are indicative of improvement in HRQoL. A decrease of 4 points from baseline is considered a clinically meaningful improvement.40,41 The percentage of patients who achieved this MCID were considered to be responders, which was a secondary outcome in both trials.
HRQoL was also measured using change from baseline in the EuroQol 5-Dimensions (EQ-5D) 5-Levels questionnaire (EQ-5D-5L) and was evaluated as “other” outcome in ETHOS and KRONOS. EQ-5D-5L measures the patient’s immediate situation using the EuroQol Visual Analogue Scale (EQ VAS) and 5 dimensions. The EQ VAS records the respondent’s self-rated health on a vertical VAS, where the end points are 100 (“best imaginable health state”) and 0 (“worst imaginable health state”). The MCID of the EQ VAS is estimated to be from 6.5 (anchored to the Chronic Respiratory Questionnaire [CRQ] total using receiver operating characteristic [ROC] methods) to 10.1 (distribution SD = 0.5).42
Symptoms in patients were measured using the change from baseline EXACT score in ETHOS, and the TDI focal score and E-RS score in both trials. EXACT is a valid patient-reported outcome consisting of 14 items (MCID not yet established).43 It was evaluated as a secondary outcome in ETHOS. The TDI, considered a secondary outcome in ETHOS and KRONOS, measures the change in dyspnea severity from the baseline as established by the Baseline Dyspnea Index (BDI). The TDI consists of 24 items that are graded; lower scores indicate more deterioration related to an increase in severity of dyspnea from baseline. The TDI focal score is composed of 3 different scales for functional impairment, magnitude of task, and magnitude of effort. The TDI focal score is calculated as the sum of the 3 individual scores and then divided by 2. The range of the TDI focal score is −9 to 9.0.44 A change in 1 point is considered clinically meaningful.40,45 The E-RS is an 11-item subset of the EXACT questionnaire to evaluate respiratory symptoms in COPD, with higher scores indicating greater severity.46 The E-RS was evaluated as a secondary outcome in KRONOS (over 24 weeks) and as an “other” outcome in ETHOS.
Use of rescue medications was calculated as the change from baseline in the number of average daily puffs of Ventolin hydrofluoroalkane taken by the participant. Use of rescue medications was considered as an “other” outcome in ETHOS (over 52 weeks) and was a secondary outcome in KRONOS (over 24 weeks).
Several harms outcomes were reported, including AEs, SAEs, withdrawals due to AEs, and mortality. Notable harms were reported for anticholinergic AEs, corticosteroid-associated AEs, cardiovascular effects, and pneumonia.
Lastly, health care resource utilization, such as the number of hospitalizations, ICU visits, emergency room visits, and the number of workdays missed, were measured and reported descriptively by both trials, as well.
Statistical Analysis
Summaries of the statistical analysis of the efficacy end points in ETHOS and KRONOS are presented in Table 10 and Table 11 respectively.
ETHOS
Sample size was estimated based on the primary outcome, i.e., rate of moderate-to-severe COPD exacerbations. It was assumed the average exposure would be 0.83 years, and the number of moderate or severe COPD exacerbations per year would be 1.142 in the BGF MDI 320 group, 1.344 in the GFF MDI group, and 1.344 in the BFF MDI group. A relative reduction of 15% was assumed between BGF MDI 320 and the comparator groups. With type I error controlled at a 1-sided alpha level of 0.025, enrolling 8,400 patients in a 1:1:1:1 ratio would result in a probability of demonstrating differences between the intervention and comparators of approximately 93% (96% for each comparison). A blinded sample-size reassessment was conducted before the planned interim analysis, which increased the required sample size from 8,000 to 8,400. All comparisons relevant to this review were done for superiority. The order of hypothesis testing for control of type I error is shown in Figure 4. The primary estimand of interest was the efficacy estimand, which was defined as the effect of the randomized treatments in all patients, assuming they continued the treatments for the duration of the study regardless of actual compliance. For the secondary end points, the main analysis used the efficacy estimand except for the end point time to death, which used the treatment policy estimand. The treatment policy estimand is the effect of randomized treatment over the study period, regardless of whether randomized treatment is continued.
The primary end point was analyzed using negative binomial regression, with the logarithm of time at risk as an offset term. All missed data were assumed to be missing completely at random or missing at random. The comparisons were adjusted for baseline post-bronchodilator percent predicted FEV1, log baseline blood eosinophil count, baseline COPD exacerbation history, region, and ICS use at screening. For the efficacy estimand, the time at risk was the duration of exposure to treatment, which was calculated as the days from first dose to date of treatment completion (both days inclusive), or the days from first dose to the day after premature treatment discontinuation. A sensitivity analysis for missing data was conducted using a tipping-point analysis that used a maximum delta value of 1.5 exacerbations per year. Multiple imputation techniques were used to impute the mission data, up to 10 imputations per the tipping-point analysis set. For the primary outcome, a pre-specified subgroup analysis based on several demographic categories was performed. The subgroups relevant for the current review were baseline blood eosinophil count and COPD exacerbation history.
Time to first moderate or severe COPD exacerbation and time to death were analyzed using a Cox regression model. The model for time to first moderate or severe COPD exacerbation included treatment, baseline post-bronchodilator percent predicted FEV1, log baseline blood eosinophil count, baseline COPD exacerbation history, region, and ICS use at screening. Rates of severe outcomes and the primary outcome were analyzed similarly (negative binomial regression). SGRQ total score, TDI focal score, EXACT score, E-RS score, and use of rescue medications were analyzed using a linear repeated measures analysis of covariance (ANCOVA) model. An unstructured correlation matrix was used to model additional autocorrelation within a patient. The SGRQ responder rate (percentage of patients with an improvement of ≥ 4 points) was analyzed using logistic regression with PROC GENMOD. Robustness of results to missing data was assessed using a tipping-point analysis. All covariates used in the analysis of each of the secondary outcomes are listed in Table 10.
Other end points were analyzed using log-rank tests or ANCOVA, without adjustments for multiplicity.
Figure 4: Order of Hypothesis Testing for Type I Error Control (ETHOS)
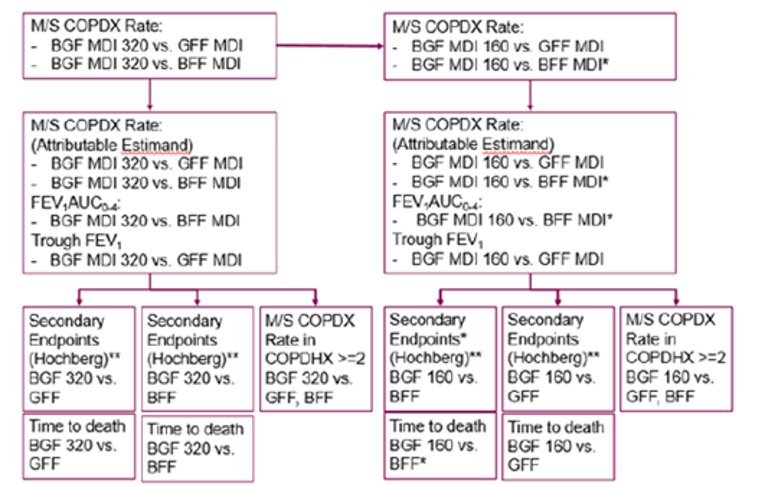
AUC0-4 = area under the curve from 0 to 4 hours post dose; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; COPDX = chronic obstructive pulmonary disease exacerbations; COPDHX = history of chronic obstructive pulmonary disease exacerbations; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; M-S = moderate or severe; vs. = versus .
*All comparisons of BGF MDI 160-14.4-9.6 mcg vs BFF MDI were for non-inferiority using the PP Estimand followed by superiority. Superiority was not required to advance to the next comparison. All other comparisons were for superiority and used the Efficacy Estimand unless otherwise stated.
**Hochberg-controlled secondary end points: Time to first moderate or severe COPD exacerbation, rescue use, rate of severe COPD exacerbation, SGRQ (ex-US), SGRQ responders (US), EXACT Total (ex-US), and TDI (ex-US).
Source: ETHOS Clinical Study Report. .
KRONOS
Sample size was estimated based on the primary outcomes. Based on these assumptions, the sample size had:
99% power to detect a difference of 75 mL between BGF MDI and BFF MDI in FEV1 AUC0-4 over 24 weeks
96% power to detect a difference of 35 mL between BGF MDI and GFF MDI in morning pre-dose trough FEV1 over 24 weeks (92% power over weeks 12 to 24)
97% power to detect a difference of 50 mL between BGF MDI and BFF MDI in morning pre-dose trough FEV1 over weeks 12 to 24
96% power to demonstrate noninferiority of BFF MDI to Symbicort TBH in morning pre-dose trough FEV1 over 24 weeks (92% power over weeks 12 to 24), based on a margin of 50 mL (1-sided alpha = 0.025); a sample size of 1,800 patients (in a 2:2:1:1 ratio) was estimated with a type I error control at a 2-sided alpha level of 0.05.
All comparisons relevant to this review were done for superiority. The type I error control approach varied based on the region and registration. For the EU-Canada approach, the order of hypothesis testing for type I error control is shown in Figure 5. The primary estimand of interest was the efficacy estimand, which is the effect of the randomized treatments in all patients, assuming they continued the treatments for the duration of the study regardless of actual compliance.
One of the primary outcomes, FEV1 AUC0-4, was analyzed using a repeated measures linear mixed model. The covariates in the analysis were baseline FEV1, percent reversibility to Ventolin hydrofluoroalkane, baseline eosinophil count, treatment, visit, treatment by visit interaction, and ICS use at screening. The other primary outcome, change from baseline in morning pre-dose trough FEV1, was also analyzed using a repeated measures linear mixed model. The covariates in the analysis were treatment, visit, treatment by visit interaction, ICS use at screening, baseline FEV1, baseline eosinophil count, and percent reversibility to Ventolin hydrofluoroalkane. Correlation within a patient was modelled using an unstructured variance-covariance matrix. Sensitivity analyses for missing data in both outcomes were conducted using tipping-point analyses. Multiple imputation techniques were used to impute the missing data under the pattern mixture model framework.
The secondary end points related to FEV1 and the primary outcomes were analyzed similarly. Peak FEV1, SGRQ total score, TDI focal score, E-RS score, and use of rescue medications were analyzed using a linear repeated measures model. The rate of moderate-to-severe exacerbations was analyzed using a negative binomial model and the SGRQ responder rate was analyzed using a logistic regression model. Other end points were analyzed using a repeated measures linear mixed model or Cox regression models, as appropriate, without adjustments for multiplicity. Other details about the analysis of each of the outcomes are listed in Table 11.
Lastly, to compare the primary and secondary continued end points (in the modified intention-to-treat [ITT] population) in each approach, a correlation analysis was conducted.
Figure 5: Order of Hypothesis Testing for Type I Error Control (KRONOS)
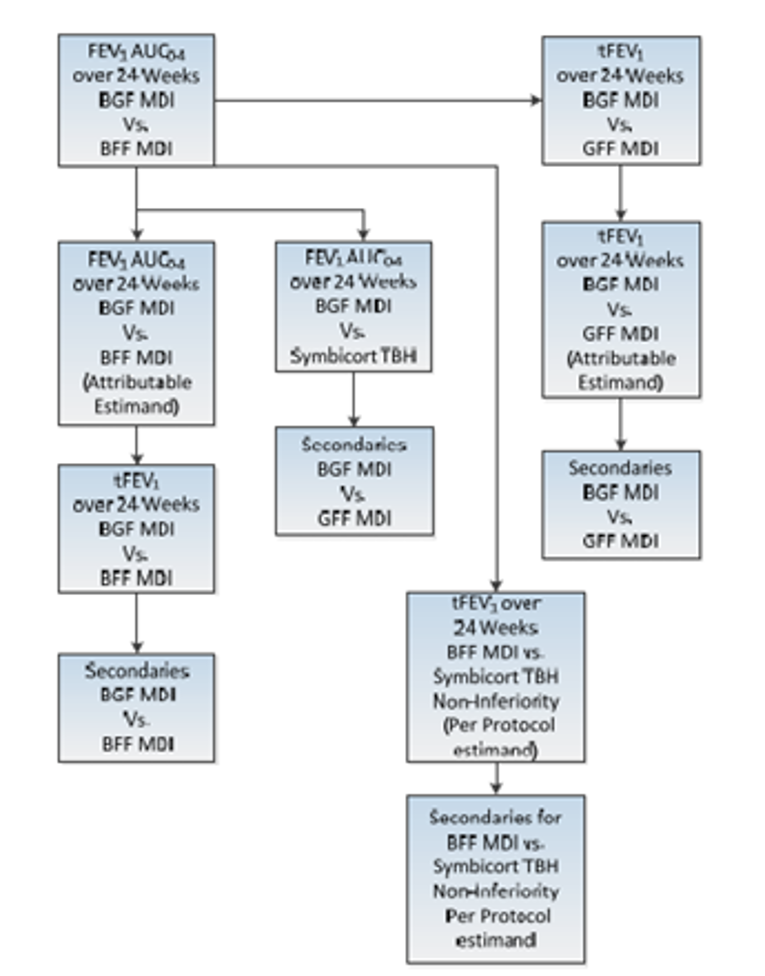
AUC0-4 = area under the curve from 0 to 4 hours post dose; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; TBH = Turbuhaler; tFEV1 = trough forced expiratory volume in 1 second; vs. = versus .
Source: KRONOS Clinical Study Report.
Table 10: Statistical Analysis of Efficacy End Points in ETHOS
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | ||
|||||||||||| | |||||||||||| | ||
|||||||||||| | |||||||||||| | ||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
ANCOVA = analysis or covariance model; COPD = chronic obstructive pulmonary disease; EXACT = Exacerbations of Chronic Pulmonary Disease Tool; FEV1 = forced expiratory volume in 1 second; HFA = hydrofluoroalkane; ICS = inhaled corticosteroid; MCID = minimal clinically important difference; MNAR = missing not at random; SGRQ = St. George’s Respiratory Questionnaire.
Source: ETHOS Clinical Study Report.
Table 11: Statistical Analysis of Efficacy End Points in KRONOS
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
ANCOVA = analysis or covariance model; AUC0-4 = area under the curve from 0 to 4 hours post dose; b.i.d. = twice daily; CID = clinically important deterioration; COPD = chronic obstructive pulmonary disease; EXACT = Exacerbations of Chronic Pulmonary Disease Tool; FEV1 = forced expiratory volume in 1 second; HFA = hydrofluoroalkane; ICS = inhaled corticosteroid; MCID = minimal clinically important difference; RM = repeated measures; SGRQ = St. George’s Respiratory Questionnaire.
Source: ETHOS and KRONOS Clinical Study Reports.
Analysis Populations
ETHOS and KRONOS included the following analysis populations:
The ITT population included all patients who were randomized to treatment and received any amount of the study drug.
The modified ITT population included all patients who were randomized with post-randomization data obtained before discontinuation from the study drug.
The per-protocol population included all patients with post-randomization data obtained before any major protocol deviation.
The safety population included all patients who were randomized to treatment and received any amount of the study drugs (similar to ITT). Patients were analyzed according to treatment received rather than randomized.
The rescue Ventolin use population included all patients in the ITT population who reported an average baseline daily use of 1 or more puffs of rescue Ventolin.
Results
Patient Disposition
Patient dispositions in ETHOS and KRONOS are summarized in Table 12. Over 8,500 patients were randomized to the 4 treatment arms in the ETHOS trial, whereas 1,902 patients underwent randomization in KRONOS. The proportion of patients who discontinued each trial was balanced between trial arms. In ETHOS, 20.6% to 25.9% of patients discontinued compared with 11.4% to 16.4% in KRONOS. This discrepancy could be due to the longer trial duration of ETHOS (52 weeks). The most common reasons for study discontinuation were AEs (5.5% to 6.9%) in ETHOS, lack of efficacy (4.8% to 8%) in ETHOS, and patient discretion (2.2% to 6.1%) in KRONOS.
Among the 16,033 and 3,047 patients screened for ETHOS and KRONOS, respectively, 7,455 (46.5%) and 1,139 (27.4%) patients were not randomized due to various reasons. The most common reason for screening failure was severity of disease in both ETHOS and KRONOS.
Disposition | ETHOS | KRONOS | |||||
|---|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg-9.6 mcg | GFF MDI 14.4 mcg-9.6 mcg | BFF MDI 320 mcg-9.6 mcg | BGF MDI 320 mcg- 14.4 mcg-9.6 mcg | GFF MDI 14.4 mcg-9.6 mcg | BFF MDI 320 mcg-9.6 mcg | Symbicort TBH 400 mcg-12 mcg | |
|||||||||||| | |||||||||||| | |||||||||||| | |||||
Randomized, N | 8,588 | 1,902 | |||||
Randomized but not treated | 1 (< 0.1) | 4 (0.2) | 5 (0.2) | 1 (0.2) | 0 | 1 (0.3) | 1 (0.3) |
Treated, n (%) | 2,156 (100) | 2,139 (99.8) | 2,146 (99.8) | 639 (99.8) | 627 (100.0) | 315 (99.7) | 318 (99.7) |
Completed study drug, n (%) | 1,711 (79.6) | 1,584 (74.1) | 1,644 (76.6) | 566 (88.6) | 524 (83.6) | 266 (84.4) | 278 (87.4) |
Discontinued study drug, n (%) | 445 (20.6) | 555 (25.9) | 502 (23.4) | 73 (11.4) | 103 (16.4) | 49 (15.6) | 40 (12.6) |
Completed study, n (%)a | 1,815 (84.2) | 1,764 (82.5) | 1,788 (83.3) | 581 (90.9) | 549 (87.6) | 279 (88.6) | 280 (88.1) |
Withdrawn from study | 342 (15.9) | 379 (17.7) | 363 (16.9) | 48 (7.5) | 74 (11.8) | 35 (11.1) | 36 (11.3) |
Reason for discontinuation, N (%) | |||||||
Adverse events | 118 (5.5) | 147 (6.9) | 138 (6.5) | 28 (4.4) | 30 (4.8) | 11 (3.5) | 11 (3.5) |
Lack of efficacy | 103 (4.8) | 171 (8.0) | 136 (6.4) | 10 (1.6) | 16 (2.6) | 6 (1.9) | 6 (1.9) |
Lost to follow-up | 25 (1.2) | 19 (0.9) | 15 (0.7) | 10 (1.6) | 2 (0.3) | 0 | 2 (0.6) |
Patient discretion | 104 (4.9) | 123 (5.8) | 130 (6.1) | 14 (2.2) | 37 (5.9) | 19 (6.1) | 15 (4.7) |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Investigator discretion | 23 (1.1) | 38 (1.8) | 28 (1.3) | 5 0.8) | 11 (1.8) | 5 (1.6) | 1 (0.3) |
Major protocol deviation | 30 (1.4) | 26 (1.2) | 28 (1.3) | 3 (0.5) | 4 (0.6) | 4 (1.3) | 4 (1.3) |
Protocol-specific discontinuation | 20 (0.9) | 9 (0.4) | 12 (0.6) | 3 (0.5) | 1 (0.2) | 3 (1.0) | 1 (0.3) |
Administrative reasons | 13 (0.6) | 11 (0.5) | 5 (0.2) | Not reported | Not reported | Not reported | Not reported |
ITT, N | 2,137 | 2,120 | 2,131 | 639 | 625 | 314 | 318 |
mITT, N | 2,137 | 2,120 | 2,131 | 639 | 625 | 314 | 318 |
PP, N | 2,086 | 2,079 | 2,088 | 608 | 587 | 298 | 295 |
Safety, N | 2,144 | 2,125 | 2,136 | 639 | 625 | 314 | 318 |
RVU | 1,430 | 1,389 | 1,429 | 293 | 270 | 141 | 157 |
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; GFF = glycopyrronium-formoterol fumarate; ITT = intention to treat; MDI = metered-dose inhaler; mITT = modified intention to treat; PP = per protocol; RVU = rescue Ventolin use; TBH = Turbuhaler.
aPatients who completed the study were defined as those who either, per the end-of-treatment electronic case report form, completed the study treatment or discontinued the study drug but continued to attend regular study visits and completed the study.
Source: ETHOS and KRONOS Clinical Study Reports.
Exposure to Study Treatments
In ETHOS, the mean duration of treatment was similar across the treatment groups, ranging from 304.2 days to 322.9 days. Overall, 78.9% of patients were exposed to the study drugs for 48 weeks or more. In KRONOS, the mean duration of treatment was similar across the treatment groups, ranging from 153.8 days to 158.5 days, with 76.5% of patients overall exposed to the study drugs for 24 weeks or more.
In both trials, treatment adherence was high and balanced across treatment groups. Compliance to treatment was measured as the number of puffs of study drug taken per day divided by the total expected number of puffs taken per day. Between trials, KRONOS had a slightly higher treatment compliance (overall mean [SD] = 95.2 [9.0]) compared with ETHOS ||||||||||||||||||||||||||||||||||||||||||, which could be due to the longer study duration of the ETHOS trial.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported subsequently. Efficacy results from the included studies are summarized in Table 13 and Table 14. See Appendix 3 for detailed efficacy data.
Mortality
The outcome mortality rates (all causes or COPD specific) were evaluated by ETHOS but not KRONOS.
Time to death (all causes) was a secondary efficacy outcome in ETHOS. The time to death was defined as the number of days from randomization to the date of death. Numerically, there were fewer deaths in the BGF MDI 320 group compared with GFF MDI and BFF MDI. The risk of death (all causes) was lower during treatment with BGF MDI 320 relative to GFF MDI (HR = 0.544; 95% CI, 0.340 to 0.870; P = 0.0111), but not different relative to BFF MDI (HR = 0.782; 95% CI, 0.472, to 1.296; P = 0.3401) as assessed by the Cox proportional hazards model.
Analysis of the final retrieved dataset (99.6% of the ITT population), which included missing week 52 vital status for 354 patients obtained after the database lock, showed similar results as the original analysis.30 The risk of death (all causes) with the supplemental vital status data (on and off treatment) was nominally lower during treatment with BGF MDI 320 relative to GFF MDI (HR = 0.51; 95% CI, 0.33 to 0.80) and was numerically lower relative to BFF MDI (HR = 0.72; 95% CI, 0.44 to 1.16). The Kaplan–Meier curve for the time of death (all causes) is shown in Figure 6.
Figure 6: Time to Death (All-cause), ETHOS
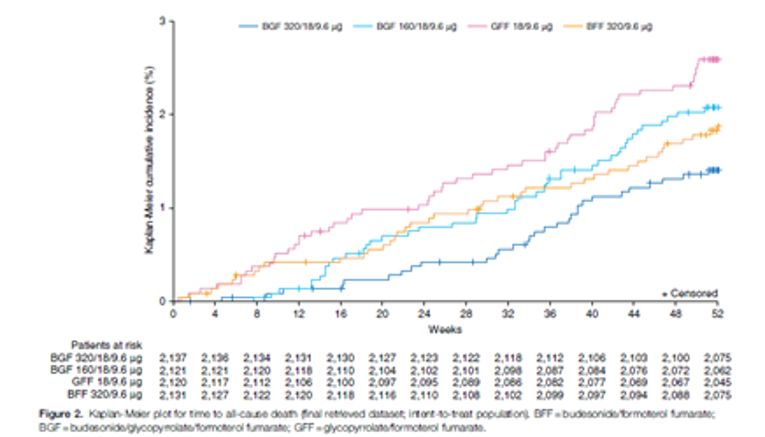
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; GFF = glycopyrronium-formoterol fumarate.
Source: Martinez et al. (2021)30. Copyright 2021 American Thoracic Society. Reprinted in accordance with Creative Licence Attribution License CC BY 4.0.30
Health Care Resource Utilization
In ETHOS and KRONOS, health care resource utilization outcomes were reported descriptively. The results were relatively balanced within trial arms. Emergency room visits ranged from |||||||||||||||||| in ETHOS and ||||||||||||||||||||||||||||. The proportion of patients who required hospitalization with time spent in ICU ranged from |||||||||||||| in ETHOS to |||||||||||| in KRONOS. Additional results for health care resource utilization outcomes are summarized in Appendix 3.
Exacerbations
In ETHOS, the rate of moderate or severe COPD exacerbations during the 52-week study was lower for BGF MDI 320 (1.02 per year) than GFF MDI (1.24 per year) and BFF MDI (1.15 per year). The rate ratio of moderate or severe exacerbations for BGF MDI 320 versus GFF MDI was 0.76 (95% CI, 0.69 to 0.83; P < 0.0001); for BGF MDI 320 versus BFF MDI, the rate ratio was 0.87 (95% CI, 0.79 to 0.95; P = 0.0027). The HRs for the time to first moderate or severe COPD exacerbation was 0.880 (95% CI, 0.807 to 0.959) for BGF MDI 320 versus GFF MDI, and 0.887 (95% CI, 0.814 to 0.966) for BGF MDI 320 versus BFF MDI (Table 13). The Kaplan-Meir curve for the time to first moderate or severe COPD exacerbation is shown in Figure 7.
The rate of severe exacerbations during the 52-week study was lower for BGF MDI 320 (0.14 per year) than for GFF MDI (0.16 per year) and BFF MDI (0.18 per year). Compared with BFF MDI, BGF MDI 320 was associated with a reduction in the rate of severe exacerbation (rate ratio = 0.80; 95% CI, 0.66 to 0.97) and an HR for the time to the first severe exacerbation of 0.805 (95% CI, 0.673 to 0.964). However, no similar statistically significant reductions were found in the BGF MDI 320 group compared with the GFF MDI group (Figure 13). The Kaplan-Meir curve for the time to first severe COPD exacerbation is shown in Figure 8.
In KRONOS, the annualized rate of moderate or severe COPD exacerbations during the 24-week study was lower for BGF MDI 320 (0.46 per year) than for GFF MDI (0.95 per year), BFF MDI (0.56 per year), and BUD-FOR DPI (0.55 per year). The rate ratio of moderate-to-severe COPD exacerbations of BGF MDI versus GFF MDI was statistically significant (rate ratio = 0.48; 95% CI, 0.37 to 0.64; P < 0.0001). . The HR for the time to first moderate or severe exacerbation also favoured BGF MDI 320 compared with GFF MDI (HR = 0.593; 95% CI |||||||||||||||||), which was statistically significant. However, the HRs were not statistically significantly different for BGF MDI 320 versus BFF MDI, or BGF MDI 320 versus BUD-FOR DPI (Table 14).
The annualized rates of severe exacerbations during the 24-week study were 0.05 per year for BGF MDI 320, 0.13 per year for GFF MDI, 0.05 per year for BFF MDI, and 0.07 per year for BUD-FOR DPI. Compared with GFF MDI, BGF MDI 320 was associated with a reduction in the rate of severe exacerbation (rate ratio = 0.36; 95% CI = 0.18 to 0.70) and in the HR for the time to first severe exacerbation (HR = 0.473; 95% CI, 0.263 to 0.850). However, no similar statistically significant reductions were found in the BGF MDI 320 group compared with the BFF MDI group or the open-label BUD-FOR DPI group (Table 14).
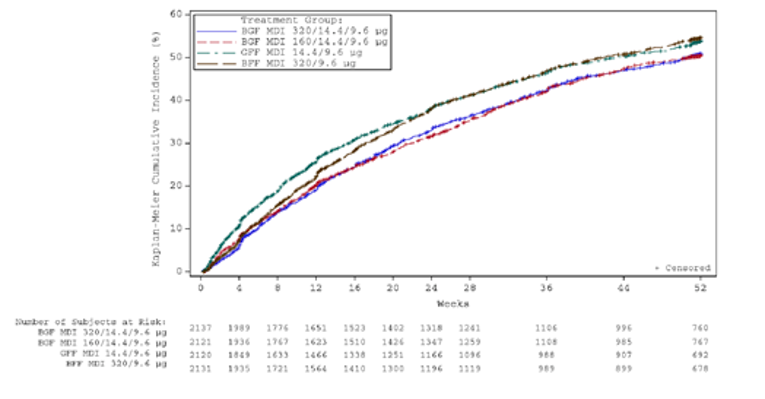
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler.
Source: ETHOS Clinical Study Report.
Figure 8: Time to First Severe COPD Exacerbation (ETHOS)

Figure 8 was removed at the request of the sponsor because it contained confidential information.
Health-Related Quality of Life
HRQoL was assessed using the change from baseline SGRQ score as a secondary outcome in ETHOS and KRONOS. HRQoL was also measured using the change from baseline in EQ-5D-5L (EQ VAS) score as an “other” outcome in both trials. The results of the EQ-5D-5L are summarized in Appendix 3.
In ETHOS, all treatment arms showed within-group improvement in SGRQ at 24 weeks from baseline. Comparing the change from baseline in SGRQ score between groups, the BGF MDI 320 arm had more improvement than the GFF MDI arm, with a mean difference of −1.62 units (95% CI, −2.27 to −0.97). Similarly, the BGF MDI 320 arm also had more improvement than the BFF MDI arm, with a mean difference of −1.38 (95% CI, −2.02 to −0.73). These differences were statistically significant (P < 0.001), but not clinically significant (MCID = 4 units). The proportion of patients achieving an improvement of at least 4 points on the SGRQ, termed as responders, was higher for BGF MDI 320 compared with GFF MDI (difference = 7.60%; 95% CI, 4.52 to 10.68) and BFF MDI (difference = 5.47%; 95% CI, 2.39 to 8.55) (Table 13).
In KRONOS, all treatment arms showed within-group improvement in SGRQ over 24 weeks from baseline. Comparing the change from baseline in SGRQ score between groups, the BGF MDI 320 arm had more improvement than the GFF MDI arm, with a mean difference of −1.22 units (95% CI, −2.30 to −0.15). This difference was statistically significant (P < 0.001), but not clinically significant (MCID = 4 units). The BGF MDI 320 arm also had more improvement than the BFF MDI arm, with a mean difference of −0.45 (95% CI, −1.78 to 0.87) as well as the BUD-FOR DPI arm, with a mean difference of −1.26 (95% CI, −2.58 to 0.06). These differences were not statistically or clinically significant. The percentage of responders was higher for BGF MDI compared with GFF MDI |||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| (Table 14).
Lung Function
In ETHOS, lung function measured as FEV1 AUC0-4 over 24 weeks was assessed as 1 of the primary outcomes in the 4-hour PFT substudy (N = 3,088) comparing BGF MDI 320 versus BFF MDI. BGF MDI 320 was associated with an improvement in the mean FEV1 AUC0-4 at week 24 compared with BFF MDI, with the mean difference being 99 units ||||||||||||||||||||||||. These improvements were statistically significant. The other primary outcome of the PFT substudy was morning pre-dose trough FEV1 for the comparison of BGF MDI 320 versus GFF MDI. The change from baseline in the morning pre-dose trough FEV1 over 24 weeks for BGF MDI 320 was significantly higher than for GFF MDI (mean difference = 35 mL: 95% CI, 12 to 57). This improvement in FEV1 was statistically significant but of uncertain clinical significance (MCID = 0.10 L to 0.14 L).40
In KRONOS, lung function measured as FEV1 AUC0-4 over 24 weeks was the primary outcome, for the comparison of BGF MDI 320 versus BFF MDI, and BGF MDI 320 versus BUD-FOR DPI (in the EU-Canada approach). Change from baseline in the morning pre-dose FEV1 over 24 weeks was the primary outcome for the comparison of BGF MDI 320 versus GFF MDI (in the EU-Canada approach). In the trial, BGF MDI 320 showed improvement in the FEV1 AUC0-4 over 24 weeks compared with BFF MDI (least squares mean = 104 mL; 95% CI, 77 to 131) and compared with BUD-FOR DPI (least squares mean = 91; 95% CI, 64 to 117) (Table 14). These improvements were statistically significant. The change from baseline in morning pre-dose trough FEV1 at 24 weeks for BGF MDI 320 compared with GFF MDI was 22 mL (95% CI, 4 to 39). This improvement in FEV1 was statistically significant but not clinically significant (MCID = 0.10 L to 0.14 L)40 (Table 14).
Symptoms
Symptoms in study participants were measured using the change from baseline in EXACT in ETHOS, and change in TDI focal score and E-RS in both trials.
In ETHOS, the difference in least squares mean for the TDI focal score showed improvement in BGF MDI 320 compared with both GFF MDI (difference = 0.40 units; 95% CI, 0.24 to 0.55) and BFF MDI (difference = 0.31 units; 95% CI, 0.15 to 0.46). The improvements were not clinically significant (MCID = 1 unit). There were statistically significant improvements in the change from baseline in the EXACT total score in BGF MDI 320 compared with GFF MDI (difference = −1.14 units; 95% CI, −1.64 to −0.65) and BFF MDI (difference = −1.04; 95% CI, −1.53 to −0.55). As for the change from baseline in E-RS score over 52 weeks, BGF MDI 320 was associated with a statistically significant improvement compared with GFF MDI |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| and BFF MDI ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||; however, these improvements were not clinically meaningful (MCID = 3.35 units) (Table 13).
In KRONOS, the difference in the least squares mean of the TDI focal score showed improvement in BGF MDI 320 compared with the open-label BUD-FOR DPI (difference = 0.46 units; 95% CI, 0.156 to 0.766). The improvement was not clinically meaningful (MCID = 1 unit). Compared with GFF MDI and with BFF MDI, BGF MDI 320 did not demonstrate a clinically or statistically significant improvement in the TDI focal score over 24 weeks (Table 13). As for the change from baseline in E-RS score over 24 weeks, BGF MDI 320 was associated with a slight improvement in scores compared with GFF MDI (difference = −0.38), BFF MDI (difference = −0.16), and the open-label BUD-FOR DPI (difference = −0.16); however, these improvements were not clinically or statistically significant (MCID = 3.35 units) (Table 14).
Use of Rescue Medication
In ETHOS and KRONOS, the evaluation of the average daily number of puffs of rescue medication over 24 weeks was restricted to the rescue Ventolin use population. In ETHOS, BGF MDI 320 was associated with a significant reduction in daily rescue medication use compared with GFF MDI (difference = −0.51 puffs per day; 95% CI, −0.68 to −0.34) and BFF MDI (difference = −0.37 puffs-day; 95% CI, −0.54 to −0.20) (Table 13).
In KRONOS, BGF MDI 320 was associated with small reductions in daily rescue medication use compared with GFF MDI (difference = −0.25 puffs-day; 95% CI, −0.60 to 0.09) and BFF MDI (difference = −0.24 puffs-day; 95% CI, −0.65 to 0.18). However, compared with BUD-FOR DPI, BGF MDI 320 was found to be associated with a slightly higher average daily use of rescue medication (difference = 0.23 puffs per day; 95% CI, −0.17 to 0.63). These differences were not statistically significant (Table 14).
Productivity
This outcome was not evaluated by any of the included trials; therefore, a summary could not be provided.
Table 13: Efficacy Outcomes for ETHOS
Outcome | Modified ITT population | ||
|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 2,137) | GFF MDI 14.4 mcg- 9.6 mcg (N = 2,120) | BFF MDI 320 mcg- 9.6 mcg (N = 2,131) | |
Rate of moderate or severe COPD exacerbations over 52 weeksa | |||
n (%) | 1,026 (48.0) | 1,056 (49.8) | 1,085 (50.9) |
Events, n | 1,852 | 2,097 | 2,018 |
Total time at risk, years | 1,820.3 | 1,687.3 | 1,752.0 |
Rate of exacerbations per year | 1.02 | 1.24 | 1.15 |
Adjusted rate (SE) | 1.08 (0.04) | 1.42 (0.05) | 1.24 (0.04) |
Rate difference (95% CI) | Reference group | −0.35 (−0.46 to −0.23) | −0.17 (−0.27 to −0.06) |
Rate ratio (95% CI) | Reference group | 0.76 (0.69 to 0.83) | 0.87 (0.79 to 0.95) |
P value | < 0.0001 | 0.0027 | |
Time to first moderate or severe COPD exacerbation over 52 weeks | |||
Time to first moderate or severe COPD exacerbation, months | 3.7 | 2.6 | 3.1 |
Hazard ratio (95% CI) | Reference group | 0.880 (0.807 to 0.959) | 0.887 (0.814 to 0.966) |
P value | 0.0035 | 0.0057 | |
Average daily use of rescue Ventolin HFA over (24 weeks) | |||
Number of patients contributing to the analysis: RVU population | 1,425 | 1,387 | 1,426 |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Change from baseline, mean (SE, 95% CI) | −1.2 (0.06, −1.3 to −1.1) | −0.7 (0.07, −0.8 to −0.5) | −0.8 (0.06, −0.9 to −0.7) |
LS mean difference (95% CI) | Reference group | −0.51 (−0.68 to −0.34) | −0.37 (−0.54 to −0.20) |
P value | < 0.0001 | < 0.0001 | |
TDI focal score (24 weeks) mITT population | |||
Number of patients contributing to the analysis | 2044 | 1983 | 2021 |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
TDI focal score at 24 weeks, mean (SE, 95% CI) | 1.3 (0.06, 1.2 to 1.4) | 0.9 (0.06, 0.8 to 1.1) | 1.0 (0.06, 0.9 to 1.1) |
LS mean difference (SE, 95% CI) | Reference group | 0.40 (0.079, 0.24 to 0.55) | 0.31 (0.078, 0.15 to 0.46) |
P value | < 0.0001 | < 0.0001 | |
Mean daily EXACT total score (52 weeks) mITT population | |||
Number of patients contributing to the analysis | 2,126 | 2,105 | 2,120 |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Change from baseline, mean (SE, 95% CI) | −1.8 (0.18, −2.2 to −1.5) | −0.7 (0.19, −1.0 to −0.3) | −0.8 (0.18, −1.1 to −0.4) |
LS mean difference (SE, 95% CI) | Reference group | −1.14 (0.252, −1.64 to −0.65) | −1.04 (0.25, −1.53 to −0.55) |
P value | < 0.0001 | < 0.0001 | |
SGRQ total score (24 weeks) mITT population | |||
Number of patients contributing to the analysis | 2,076 | 2,017 | 2,056 |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Change from baseline, mean (SE, 95% CI) | −6.5 (0.25, −7.0 to −6.0) | −4.9 (0.25, −5.4 to −4.4) | −5.1 (0.25, −5.6 to −4.6) |
LS mean difference (SE, 95% CI) | Reference group | −1.62 (0.332, −2.27 to −0.97) | −1.38 (0.330, −2.02 to −0.73) |
P value | < 0.0001 | < 0.0001 | |
Patients achieving an MCID ≥ 4 units in SGRQ total score at 24 weeks, mITT population | |||
Responders,c n (%) | 1,068 (50.4) | 893 (42.6) | 949 (44.7) |
Difference, % (95% CI) | Reference group | 7.60 (4.52 to 10.68) | 5.47 (2.39 to 8.55) |
P value | < 0.0001 | 0.0005 | |
Time to death (all causes) | |||
Deaths, n (%) | 29 (1.4) | 53 (2.5) | 38 (1.8) |
Hazard ratio (95% CI) | Reference group | 0.51(0.33 to 0.80) | 0.72 (0.44 to 1.16) |
P value | 0.0035 | 0.01721 | |
Rate of severe COPD exacerbationsa | |||
n (%) [events] | 219 (10.2) [272] | 239 (11.3) [287] | 261 (12.2) [323] |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Adjusted rate (SE)b | 0.13 (0.01) | 0.15 (0.01) | 0.16 (0.01) |
Rate difference (95% CI) | Reference group | −0.02 nv b | −0.03 nv b |
Rate ratio (95% CI) | 0.84 (0.69 to 1.03) | 0.80 (0.66 to 0.97) | |
P value | 0.0944 | 0.0221 | |
|||||||||||| | |||||||||||| |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |
BDI = Baseline Dyspnea Index; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; CI = confidence interval; COPD = chronic obstructive pulmonary disease; EXACT = Exacerbations of Chronic Pulmonary Disease Tool; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; HFA = hydrofluoroalkane; ICS = inhaled corticosteroid; ITT = intention to treat; LS = least squares; MCID = minimal clinically important difference; MDI = metered-dose inhaler; mITT = modified intention to treat; PP = per protocol; RVU = rescue Ventolin use; SE = standard error; SGRQ = St. George’s Respiratory Questionnaire; TDI = Transition Dyspnea Index.
aAdjusted for baseline post-bronchodilator percent predicted FEV1, baseline COPD exacerbation history, log baseline blood eosinophil count, region, and ICS use at screening.
bPatients achieving an MCID ≥ 4.0 units in SGRQ total score at week 24.
Source: ETHOS Clinical Study Report.
Table 14: Efficacy Outcomes for KRONOS
Outcome | Modified ITT population (over 24 weeks) (N = 1,896) | BUD-FORM DPI 400 mcg- 12 mcg (Symbicort TBH) | ||
|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 639) | GFF MDI 14.4 mcg- 9.6 mcg (N = 625) | BFF MDI 320 mcg- 9.6 mcg (N = 314) | ||
FEV1 AUC0-4 (mL) over 24 weeks | ||||
Number of patients contributing to the analysis | 501 | 485 | 245 | 248 |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
FEV1 AUC0-4 (mL) over 24 weeks, LSM (SE, 95% CI) | 305 (8.4, 288 to 321) | 288 (8.5, 272 to 305) | 201 (11.7, 178 to 224) | 214 (11.5, 192 to 237) |
LSM (95% CI) | Reference group | 16 (−6 to 38) | 104 (77 to 131) | 91 (64 to 117) |
P value | 0.1448 | < 0.0001 | < 0.0001 | |
Morning pre-dose trough FEV1 (mL) over 24 weeks | ||||
Number of patients contributing to the analysis | 622 | 601 | 300 | 301 |
Change from baseline in morning pre-dose trough FEV1 (mL) LSM (SE, 95% CI) | 147 (6.5, 134 to 159) | 125 (6.6, 112 to 137) | 73 (9.2, 55 to 91) | 88 (9.1, 70 to 105) |
LSM (95% CI) | Reference group | 22 (4 to 39) | 74 (52 to 95) | 59 (38 to 80) |
P value | 0.0139 | < 0.0001 | < 0.0001 | |
COPD exacerbations | ||||
Moderate or severe COPD exacerbations | ||||
Patients with ≥ 1 COPD exacerbation, n (%) | 108 (16.9) | 157 (25.1) | 65 (20.7) | 61 (19.2) |
Rate per year (SE) | 0.46 (0.05) | 0.95 (0.09) | 0.56 (0.08) | 0.55 (0.08) |
Rate ratio (95% CI) | Reference group | 0.48 (0.37 to 0.64) | 0.82 (0.58 to 1.17) | 0.83 (0.59 to 1.18) |
P value | < 0.0001 | 0.2792 | 0.3120 | |
Time to first moderate or severe exacerbation | ||||
Hazard ratio (95% CI) | Reference group | 0.593 |||||||||||| | 0.747 |||||||||||| | 0.853 |||||||||||| |
P value | < 0.0001 | 0.0635 | 0.3225 | |
Severe COPD exacerbation | ||||
Patients with ≥ 1 COPD exacerbation, n (%) | 17 (2.7) | 33 (5.3) | 9 (2.9) | 11 (3.5) |
Rate per year (SE) | 0.05 (0.01) | 0.13 (0.03) | 0.05 (0.02) | 0.07 (0.02) |
Rate ratio (95% CI) | Reference group | 0.36 (0.18 to 0.70) | 0.85 (0.34 to 2.13) | 0.69 (0.29 to 1.61) |
P value | 0.0026 | 0.7363 | 0.3861 | |
Time to first severe exacerbation | ||||
Hazard ratio (95% CI) | Reference group | 0.473 (0.263 to 0.850) | 0.894 (0.398 to 2.007) | 0.724 (0.339 to 1.549) |
P value | 0.0123 | 0.7856 | 0.4052 | |
TDI focal score (units) over 24 weeks | ||||
Number of patients contributing to the analysis | 614 | 587 | 296 | 291 |
BDI focal score, mean (SD) | 6.415 (2.075) | 6.496 (2.141) | 6.378 (2.223) | 6.330 (2.151) |
TDI focal score over 24 weeks, mean (SE, 95% CI) | 1.245 (0.0921, 1.064 to 1.425) | 1.067 (0.0938, 0.884 to 1.251) | 1.008 (0.1301, 0.753 to 1.263) | 0.784 (0.1298, 0.530 to 1.039) |
LSM (SE) | Reference group | 0.177 (0.1268) | 0.237 (0.1555) | 0.461 (0.1555) |
95% CI | −0.071 to 0.426 | −0.068 to 0.542 | 0.156 to 0.766 | |
P value | 0.1621 | 0.1283 | 0.0031 | |
Change from baseline in SGRQ total score (units) over 24 weeks | ||||
Number of patients contributing to the analysis | 621 | 595 | 298 | 297 |
Baseline SGRQ total score, mean (SD) | 44.1 (17.0) | 43.9 (16.4) | 43.5 (17.0) | 43.9 (17.5) |
Change from baseline, mean (SE, 95% CI) | −7.5 (0.47, −8.5 to −6.6) | −6.3 (0.47, −7.2 to −5.4) | −7.1 (0.61, −8.3 to −5.9) | −6.3 (0.62, −7.5 to −5.1) |
LSM (SE) | Reference group | −1.22 (0.549) | −0.45 (0.675) | −1.26 (0.673) |
95% CI | −2.30 to −0.15 | −1.78 to 0.87 | −2.58 to 0.06 | |
P value | 0.0259 | 0.5036 | 0.0617 | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |
|||||||||||| | |||||||||||| | |||||||||||| | ||
Change from baseline in average daily use of Ventolin HFA (puffs-day) over 24 weeks | ||||
Number of patients contributing to the analysis: RVU population | 293 | 269 | 141 | 155 |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Change from baseline, mean (SE, 95% CI) | −1.3 (0.13, −1.6 to −1.1) | −1.1 (0.13, −1.3 to −0.8) | −1.1 (0.18, −1.5 to −0.8) | −1.6 (0.17, −1.9 to −1.2) |
LSM (SE, 95% CI) | Reference group | −0.25 (0.09, 0.174 to −0.60) | −0.24 (0.18, 0.211 to −0.65) | 0.23 (0.204, −0.17 to 0.63) |
P value | 0.1446 | 0.2661 | 0.2667 | |
Peak FEV1 (mL) within 4 hours post dosing over 24 weeks | ||||
Peak change from baseline in FEV1 (mL) within 4 hours post dosing, LSM (SE, 95% CI) | 381 (8.8, ||||||||||||) | 364 (8.9, ||||||||||||) | 275 (12.2, ||||||||||) | 291 (12.0, ||||||||||) |
LSM (SE, 95% CI) | Reference group | 17 (||||, −6 to 40) | 105 (||||, 78 to 133) | 90 (||||, 62 to 118) |
P value | 0.1425 | < 0.0001 | < 0.0001 | |
Change from baseline in RS-Total score over 24 weeks | ||||
Number of patients contributing to the analysis | 638 | 621 | 313 | 313 |
Baseline RS-Total score, mean (SD) | 11.8 (5.8) | 11.2 (5.6) | 11.5 (6.0) | 11.6 (5.8) |
Change from baseline over 24 weeks, LSM (SE, 95% CI) | −1.1 (0.13, −1.4 to −0.9) | −0.7 (0.14, −1.0 to −0.5) | −1.0 (0.19, −1.3 to −0.6) | −1.0 (0.19, −1.3 to −0.6) |
LSM (SE, 95% CI) | Reference group | −0.38 (0.185, −0.74 to −0.01) | −0.16 (0.227, −0.61 to 0.28) | −0.16 (0.226, −0.60 to 0.29) |
P value | 0.0430 | 0.4790 | 0.4923 | |
AUC0-4 = area under the curve from 0 to 4 hours post dose; BDI = Baseline Dyspnea Index; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; CI = confidence interval; CID = clinically important deterioration; COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; HFA = hydrofluoroalkane; ITT = intention to treat; LS = least squares; LSM = least squares mean; MCID = minimal clinically important difference; MDI = metered-dose inhaler; mITT = modified intention to treat; RS-Total = Evaluating Respiratory Symptoms in Chronic Obstructive Pulmonary Disease–Total Score; RVU = rescue Ventolin use; SD = standard deviation; SE = standard error; SGRQ = St. George’s Respiratory Questionnaire; TBH = Turbuhaler; TDI = Transition Dyspnea Index.
Note: The noninferiority margins for BFF MDI vs. Symbicort TBH were as follows: Change from baseline morning pre-dose trough FEV1 (−50 mL), FEV1 AUC0-4 (−75 mL), TDI focal score (−0.75), peak change from baseline in FEV1 (−75 mL), SGRQ total score (3 units), RVU (0.75 puff-day), RS-Total score (−1.5), and time to CID (1.1).
Source: KRONOS Clinical Study Report.
Harms
Only those harms identified in the review protocol are reported subsequently. See Table 15 for detailed harms data.
Adverse Events
Within each trial, AEs were similar across treatment arms. In ETHOS, the proportions of patients who reported at least 1 AE at 52 weeks were 63.8% in the BGF MDI 320 arm, 61.7% in the GFF MDI arm, and 64.5% in the BFF MDI arm. The most common AEs were nasopharyngitis (9.4% to 11.3% across arms) and COPD (9.5% to 11.3%). In KRONOS at 24 weeks, AEs were reported in 60.7% of patients in the BGF MDI 320 arm, 61.4% of those in the GFF MDI arm, 55.7% of those in the BFF MDI arm, and 57.5% of those in the BUD-FOR DPI arm. The most common AEs were upper respiratory tract infections (5.7% to 10.2% across arms) and nasopharyngitis (6.6% to 9.4%). AEs that occurred in 2% or more of the population are presented in Table 15.
Serious Adverse Events
Within each trial, SAEs were similar across treatment arms. In ETHOS, the proportion of patients who reported 1 or more SAE were 19.9% in the BGF MDI 320 arm, 20.4% in the GFF MDI arm, and 20.6% in the BFF MDI arm at 52 weeks. The most common SAEs were COPD (9.4% to 11.3%) and pneumonia (1.6% to 2.8%). In KRONOS at 24 weeks, SAEs were reported in 8.6% of patients in the BGF MDI 320 arm, 10.9% of those in the GFF MDI arm, 6.7% of those in the BFF MDI arm, and 9.1% of those in the BUD-FOR DPI arm. The most common SAEs were COPD (2.5% to 5.1% across arms) and pneumonia (0 to 1.3%). Other SAEs that were reported in the trials are presented in Table 15.
Withdrawals Due to Adverse Events
Within each trial, the number of patients who stopped treatment due to AEs was relatively similar across the treatment arms. In ETHOS, 5.6% of patients in the BGF MDI 320 arm, 6.9% of patients in the GFF MDI arm, and 6.6% of patients in the BFF MDI were reported as discontinuing treatment due to AEs, most commonly due to COPD (1% to 2.1%). In KRONOS, the percentage of patients who discontinued treatment due to AEs was 4.7% in the BGF MDI arm, 4.8% in the GFF MDI arm, 3.5% in the BFF MDI arm, and 3.5% in the open-label BUD-FOR DPI arm. The most common reason for discontinuing treatment was COPD (0.3% to 1.3%). Other reasons for withdrawal from the study treatments reported in the trials are presented in Table 15.
Mortality
In ETHOS, 1.3% of the study population (n = 112) died on treatment. The most common causes of death related to cardiovascular causes (n = 33, 0.4%) and respiratory causes (n = 23, 0.3%). In KRONOS, there were 12 deaths (0.6%) reported on treatment. Among them, 3 were due to cardiovascular causes and 3 were due to respiratory causes.
Notable Harms
Cardiovascular events affected each arm similarly across trials. Among them, 1.1% to 2.1% of patients within each arm of ETHOS and 0.3% to 0.6% of patients within each arm of KRONOS reported major adverse cardiovascular events. Other notable cardiovascular AEs are presented in Table 15.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Short-term corticosteroid-related AEs were reported similarly across trials. AEs such as weight gain and insomnia were reported in less than 2% of patients in ETHOS and |||||||||||||||||||||||||||||||||||||||||. Oral candidiasis was reported by 2.3% of ETHOS patients and ||||||||||||||||||||||||||||||||. Long-term corticosteroid AEs such as osteoporosis and osteopenia were reported in a small number of patients in similar numbers across the arms of each trial. Across trials, around 2% of patients in each arm of ETHOS and |||||||||||| of patients in each arm of KRONOS reported bone fractures (overall). Other notable harms associated with corticosteroid use is presented in Table 15.
Harms | ETHOS | KRONOS | |||||
|---|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 2,144) | GFF MDI 14.4 mcg- 9.6 mcg | BFF MDI 320 mcg- 9.6 mcg | BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg | GFF MDI 14.4 mcg- 9.6 mcg | BFF MDI 320 mcg- 9.6 mcg | Symbicort TBH 400 mcg- 12 mcg | |
Patients with ≥ 1 adverse event | |||||||
n (%) | 1,368 (63.8) | 1,312 (61.7) | 1,377 (64.5) | 388 (60.7) | 384 (61.4) | 175 (55.7) | 183 (57.5) |
Number of events | 4,527 | 4,074 | 4,746 | 940 | 898 | 399 | 482 |
Most common events,a n (%) | |||||||
Nasopharyngitis | 227 (10.6) | 199 (9.4) | 234 (11.0) | 49 (7.7) | 41 (6.6) | 26 (8.3) | 30 (9.4) |
COPD | 203 (9.5) | 219 (10.3) | 242 (11.3) | 17 (2.7) | 32 (5.1) | 8 (2.5) | 13 (4.1) |
URTI | 123 (5.7) | 102 (4.8) | 115 (5.4) | 65 (10.2) | 38 (6.1) | 18 (5.7) | 22 (6.9) |
Pneumonia | 98 (4.6) | 61 (2.9) | 107 (5.0) | 12 (1.9) | 10 (1.6) | 6 (1.9) | 4 (1.3) |
Bronchitis | 66 (3.1) | 76 (3.6) | 69 (3.2) | 20 (3.1) | 15 (2.4) | 12 (3.8) | 9 (2.8) |
Back pain | 67 (3.1) | 55 (2.6) | 64 (3) | 8 (1.3) | 12 (1.9) | 4 (1.3) | 8 (2.5) |
Hypertension | 59 (2.8) | 62 (2.9) | 76 (3.6) | 13 (2.0) | 10 (1.6) | 8 (2.5) | 4 (1.3) |
Dyspnea | 54 (2.5) | 60 (2.8) | 79 (3.7) | 9 (1.4) | 9 (1.4) | 8 (2.5) | 8 (2.5) |
Headache | 57 (2.7) | 60 (2.8) | 68 (3.2) | NR | |||
Sinusitis | 56 (2.6) | 47 (2.2) | 55 (2.6) | ||||
UTI | 58 (2.7) | 60 (2.8) | 41 (1.9) | ||||
Influenza | 63 (2.9) | 42 (2) | 61 (2.9) | ||||
Cough | 58 (2.7) | 50 (2.4) | 51 (2.4) | ||||
Oral candidiasis | 65 (3.0) | 24 (1.1) | 57 (2.7) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Muscle spasm | 60 (2.8) | 19 (0.9) | 53 (2.5) | 21 (3.3) | 8 (1.3) | 17 (5.4) | 6 (1.9) |
Diarrhea | 44 (2.1) | 37 (1.7) | 38 (1.8) | NR | |||
Nausea | NR | 7 (1.1) | 3 (0.5) | 4 (1.3) | 7 (2.2) | ||
Dysphonia | 20 (3.1) | 5 (0.80) | 15 (4.8) | 6 (1.9) | |||
Patients with ≥ 1 SAE | |||||||
n (%) | 426 (19.9) | 433 (20.4) | 440 (20.6) | 55 (8.6) | 68 (10.9) | 21 (6.7) | 29 (9.1) |
Most common events,b n (%) | |||||||
COPD | 202 (9.4) | 219 (10.3) | 241 (11.3) | 17 (2.7) | 32 (5.1) | 8 (2.5) | 13 (4.1) |
Pneumonia | 61 (2.8) | 35 (1.6) | 55 (2.6) | 8 (1.3) | 6 (1.0) | 1 (0.3) | 0 |
Acute respiratory failure | 14 (0.7) | 20 (0.9) | 7 (0.3) | 4 (0.6) | 1 (0.2) | 0 | 1(0.3) |
Acute myocardial infarction | 7 (0.3) | 17 (0.8) | 7 (0.3) | 1 (0.2) | 2 (0.3) | 1 (0.3) | 5 (0.3) |
Atrial fibrillation | 9 (0.4) | 14 (0.7) | 3 (0.1) | 2 (0.3) | 0 | 0 | 0 |
Respiratory failure | 10 (0.5) | 5 (0.2) | 9 (0.4) | 4 (0.6) | 1 (0.2) | 0 | 1 (0.3) |
Pneumothorax | NR | |||||||||| | |||||||||| | |||||||||| | |||||||||| | ||
Inguinal hernia | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||
Intervertebral disc disorder | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||
Patients who stopped treatment due to adverse events | |||||||
n (%) | 119 (5.6) | 146 (6.9) | 140 (6.6) | 30 (4.7) | 30 (4.8) | 11 (3.5) | 11 (3.5) |
Most common events,b n (%) | |||||||
COPD | 22 (1.0) | 39 (1.8) | 44 (2.1) | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Dyspnea | 7 (0.3) | 9 (0.4) | 11 (0.5) | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Pneumonia | 5 (0.2) | 14 (0.7) | 4 (0.2) | |||||||||| | |||||||||| | |||||||||| | |||||||||| |
Dysphonia | NR | |||||||||| | |||||||||| | |||||||||| | |||||||||| | ||
Pulmonary mass | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||
Muscle spasms | |||||||||| | |||||||||| | |||||||||| | |||||||||| | |||
Deaths | |||||||
n (%) | 20 (0.9) | 35 (1.6) | 29 (1.4) | 6 (0.9) | 3 (0.5) | 2 (0.6) | 1 (0.3) |
Most common cause,c n (%) | |||||||
Cardiovascular cause | 4 (0.2) | 18 (0.8) | 4 (0.2) | 2 (0.3) | 1 (0.2) | 0 | 0 |
Respiratory, thoracic, and mediastinal cause | 6 (0.3) | 3 (0.1) | 9 (0.4) | 0 | 2 (0.3) | 0 | 1 (0.3) |
General disorders and administration-site conditions | 2 (< 0.1) | 8 (0.4) | 4 (0.2) | 0 | 0 | 0 | 0 |
Neoplasms benign, malignant, and unspecified (including cysts and polyps) | 1 (< 0.1) | 3 (0.1) | 5 (0.2) | 2 (0.3) | 0 | 2 (0.6) | 0 |
Infections and infestations | 2 (< 0.1) | 2 (< 0.1) | 4 (0.2) | 0 | 0 | 0 | 0 |
Nervous system disorders | 2 (< 0.1) | 1 (< 0.1) | 1 (< 0.1) | 0 | 0 | 0 | 0 |
Gastrointestinal disorders | 2 (< 0.1) | 0 | 1 (< 0.1) | 0 | 0 | 0 | 0 |
Unknown | NR | 2 (0.3) | 0 | 0 | 0 | ||
Notable harms | |||||||
MACE, n (%) | 31 (1.4) | 44 (2.1) | 23 (1.1) | 2(0.3) | 3 (0.5) | 2 (0.6) | 2 (0.6) |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Atrial fibrillation, n (%) | 18 (0.8) | 31 (1.5) | 13 (0.6) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Arrhythmia | 2 (0.1) | 2 (0.1) | 1 (< 0.1) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Dysphonia or aphonia | 39 (1.8) | 7 (0.3) | 31 (1.5) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | NR | |||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Euphoric mood | NR | |||||||||| | |||||||||| | |||||||||||| | |||||||||||| | ||
Agitation or anxiety | 36 (1.7) | 26 (1.2) | 31(1.5) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | 30 (1.4) | 23 (1.1) | 11 (0.5) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | NR | |||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; GFF = glycopyrronium-formoterol fumarate; LRTI = lower respiratory tract infection; MACE = major adverse cardiovascular event; MDI = metered-dose inhaler; NR = not reported; SAE = serious adverse event; TBH = Turbuhaler; URTI = upper respiratory tract infection; UTI = urinary tract infection.
aFrequency > 2%.
bFrequency > 0.5%.
cNumber of events (n) ≥ 2.
Source: ETHOS and KRONOS Clinical Study Reports.
Critical Appraisal
Internal Validity
ETHOS and KRONOS were randomized, double-blind, parallel-group trials. In both trials, randomization was centralized using an interactive web response system. In ETHOS, randomization was stratified by exacerbation history, post-bronchodilator FEV1, blood eosinophil count, and country. In KRONOS, randomization was stratified by reversibility to Ventolin hydrofluoroalkane, country, and disease severity. Patients in the different intervention groups were recruited over the same period of time and from the same centres. Measures were taken to ensure blinding throughout the studies. All study drugs were administered by oral inhalation devices that were provided by the sponsor as MDIs. However, in the KRONOS trial, the BUD-FOR (Symbicort TBH) arm could not be blinded, as it used the TBH inhaler. Overall, the occurrence of AEs was similar across the treatment arms in both trials. The chances of inadvertent unblinding due to AEs were low, given the similarities in the events across the treatment groups.
The baseline demographics and disease characteristics were similar between treatment arms in each trial, suggesting successful randomization. The patient disposition in both trials was described clearly.
The duration of the KRONOS trial was 24 weeks, which was a reasonable duration to evaluate the pulmonary function outcome measure (e.g., trough FEV1) and symptoms. However, for exacerbations, HRQoL, and safety outcomes, the shorter duration of the trial could have affected the results. The 52-week trial period of ETHOS was more appropriate for evaluating these outcomes, especially given the variation within the 1-year period for exacerbations.
Both trials had a 4-week screening period before randomization and the start of study treatments. There were pre-specified washout periods for the COPD medications used by the patients at screening, as well. Background medications such as rescue inhalers were standardized. However, the degree and type of training for the use of the inhalers was not described. This is particularly noteworthy for the KRONOS study, which included open-label budesonide-formoterol delivered via a different inhaler compared with the other treatment groups. Overall, treatment adherence was high and balanced across treatment arms in ETHOS and KRONOS. Despite some uncertainty as to how well patients used the inhaler devices, there did not appear to be meaningful differences between groups regarding the treatment received, other than the study treatment each patient was assigned.
The outcomes considered in the trials were validated. The primary outcomes assessed in the trials, related to trough FEV1 (KRONOS) and the annual rate of on-treatment moderate or severe exacerbations (ETHOS), are established outcomes in evaluating drug interventions for COPD. The FEV1 is used in clinical settings and recommended by GOLD to grade the severity of airflow limitation in patients with COPD. The generally accepted clinically important change in FEV1 is between 0.10 L and 0.14 L.40 The assessment of exacerbations was based on moderate exacerbations (defined as requiring treatment with oral [systemic] corticosteroids and-or antibiotics [not involving hospitalization]) and severe exacerbations (defined as requiring inpatient hospitalization); the definitions were considered acceptable by the clinical expert consulted by CADTH. In KRONOS, the primary and secondary outcomes and time points of analysis were different based on the registration approach (EU and Canada, Asia, US). The open-label study arm in KRONOS may have biased the subjective outcome results in favour of BGF MDI 320.
In ETHOS and KRONOS, all comparisons (relevant to this review) were for testing the superiority of triple therapy versus dual therapy. Appropriate statistical tests were used to analyze the study outcomes in both trials and were adequately adjusted for covariates. The primary end point in ETHOS (rate of moderate or severe COPD exacerbations) was analyzed using negative binomial regression, with the logarithm of time at risk as an offset term. Both primary outcomes in KRONOS were analyzed using a repeated measures linear mixed model. It is unknown whether the data distribution was examined for final model selection. In the presence of Poisson overdispersion, an alternative of negative binomial distribution may yield a better model fit of the count data than traditional Poisson regression. However, this needed to be tested and confirmed.
A hierarchical structure of hypothesis testing was employed for controlling type I error. The primary and secondary outcomes were analyzed, adjusting for multiplicity. Outcomes designated as “other” were analyzed without adjustments for multiplicity and should be interpreted with caution.
Approximately 22% of patients in ETHOS and 14% in KRONOS discontinued the study drug. The major reasons for early discontinuation from the trials were either AEs or lack of efficacy. In ETHOS, there were slightly more patients in the GFF and BFF arms than in the BGF arm who discontinued the trial due to lack of efficacy (8.0% or 6.4% versus 4.8%) or AEs (6.9% or 6.5% versus 5.5%). This could bias the result in favour of BGF, particularly when compared with GFF, as the percentage of patients withdrawing due to lack of efficacy was 8.0% in the GFF group compared with 4.8% in the BGF group. These percentages were relatively lower in KRONOS (lack of efficacy: 2.6% or 1.9% versus 1.6%; AEs: 4.8% or 3.5% versus 4.4%), likely because of the shorter duration of the study. The difference in efficacy is perhaps not surprising, given the stepwise treatment approach (i.e., adding medications to existing ones as the disease and symptoms progress). It has been established that stepping up to LAMA-LABA-ICS improves lung function and patient-reported outcomes and reduces exacerbations, as noted by GOLD. Most patients (> 60%) in ETHOS had severe COPD at baseline (GOLD grade 3) and had experienced 2 or more exacerbations in the previous year (> 55%). As well, one-third had been receiving an ICS-LABA and 40% had been receiving a combination LAMA-LABA-ICS at screening; only approximately 14% had been receiving dual LAMA-LABA treatment. Patients randomized to BGF MDI would have been stepping up to or staying at triple therapy, while those in the other groups mostly would have stayed on dual therapy or been stepped down to dual therapy from triple. Although testing BGF MDI against dual therapies may have been practical for establishing efficacy, it likely biased results in favour of BGF MDI, considering the baseline severity and COPD treatment history.
Generally, the robustness of the results to missing data was assessed using a tipping-point analysis under the assumption of missing not at random for the primary outcomes and most of the secondary outcomes in both trials. In ETHOS, |||||||||||||||||||||||||||||||||| missing data for the primary end point between the treatment arms. The percentage of missing data was comparable between treatment arms. In KRONOS, an attributable estimand (imputed for missing data) also showed results consistent with the efficacy estimand for the outcome change from baseline in morning pre-dose trough FEV1. As for the other primary outcome (FEV1 AUC0-4), the tipping-point analysis demonstrated that the conclusions were robust to missing data. Sensitivity analyses for missing data were not conducted for SGRQ total score, TDI focal score, EXACT score, or E-RS score in ETHOS, or for TDI focal score or E-RS score in KRONOS.
Subgroup analyses were planned a priori. Based on the randomization stratification, the subgroups relevant to this report were able to maintain randomization in ETHOS. In KRONOS, additional subgroups that were not considered during randomization stratification were analyzed. It is possible that randomization was not maintained for the baseline eosinophil subgroup or exacerbation history subgroup. Other potentially important subgroups such as prior bronchodilator therapy and baseline bronchodilator reversibility were not considered in the trials.
External Validity
The ETHOS and KRONOS trials were multi-centre multinational studies that included Canadian participation, |||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Other inclusion criteria for patient eligibility were restrictive, based on FEV1, reversibility, and past exacerbation (ETHOS). This could lower the generalizability of results to real-world settings. The clinical expert believed the demographics of patients in the included studies were generally consistent with that of the population that would be expected to use the drug, although the percentage of women was likely lower than expected (though a higher percentage were enrolled in ETHOS and KRONOS than in previous trials of COPD drugs). There was a higher proportion of Asian participants in the KRONOS trial compared with Canadian settings. The clinical expert noted that most of the patients (71% to 80%) used ICS-containing treatments at screening, which was higher than what is used in clinical settings for respirologists in Canada. As well, only 14% of patients had been receiving LAMA-LABA dual therapy at screening, which is not consistent with the current approach to treatment. Patient adherence was high for both trials which, measured by the ratio of daily puffs taken and the expected number of daily puffs, were 93.2 and 95.2 in ETHOS and KRONOS, respectively. However, it is uncertain how much of that could be translated to real-world clinical settings. The comparators and doses used in the trials were deemed by the clinical expert to be clinically relevant and appropriate; however, it was noted that comparisons with fixed-dose triple-therapy combinations would have been of interest. The concomitant medication prohibitions were found to be reasonable by the expert. The study-mandated treatment duration for exacerbations (maximum of 14 days) was also considered adequate by the expert.
For subgroup analysis, the cut-off for baseline eosinophil was 150 cells per mm3 in the studies. The clinical expert expressed concern that this was low, especially considering the majority of patients used ICS at screening.
The outcomes assessed in the included trials were appropriate and clinically important. Outcomes such as productivity, exercise tolerance, and patient satisfaction were considered important by the patient groups that provided stakeholder input for this review. Among them, exercise tolerance and patient satisfaction were included within HRQoL, as measured with the SGRQ, but were not compared separately. Productivity was not considered by any of the trials. Since the follow-up duration of ETHOS was 52 weeks, the efficacy and safety of treatments that are administered longer than that needs to be assessed, as BGF MDI 320 is indicated for long-term maintenance therapy. Lastly, the expert also noted that the percentage of patients who discontinued the study drug (22.4% in ETHOS and 14% in KRONOS) is higher than the rate of discontinuation from an inhaler device in the Canadian COPD population.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
There was limited evidence from head-to-head RCTs that compared BGF MDI 320 with other fixed-combination triple therapies in patients with COPD. The purpose of this section is to summarize and appraise the literature for the comparative efficacy and safety of BGF MDI 320 and other triple therapies for COPD through indirect comparisons or NMAs.
An NMA submitted by the sponsor was reviewed. Additionally, a focused literature search for indirect comparisons with COPD was run in MEDLINE All (1946–) on February 26, 2021. Through the search, 121 citations were identified, among which 16 potentially relevant articles were screened. After the full-text review, 1 sponsor-submitted NMA was included in this review. Sixteen NMAs were excluded due to irrelevant interventions, either because triple-therapy LAMA-LABA-ICS combinations were considered as a class, or because the specific triple therapy of BGF was not considered.
Description of NMA
One systematic review and NMA of triple combinations in moderate-to-severe COPD submitted by the sponsor was included in this review for critical appraisal. The included NMA was sponsored by the sponsor of BGF MDI (Breztri). Study selection criteria, outcomes of interest, and the methods of the NMA are described in Table 16. Of note, the NMA considered comparators such as Trimbow and Breztri 160 (BGF MDI 160), which are not available in Canada. Only the comparative results of the triple-therapy combinations relevant to the current review are summarized and presented subsequently.
Table 16: Study Selection Criteria and Methods for the Sponsor-Submitted NMA
Criteria | Sponsor-submitted NMA |
|---|---|
Population | Patients ≥ 40 years of age with moderate-to-very-severe COPD |
Intervention | Triple therapies (LAMA-LABA-ICS, both open and FDCs, including Breztri Aerosphere, Trimbow, Trelegy, and other open triple combinations) |
Comparator |
|
Outcome |
|
Study design | RCTs |
Publication characteristics | • Time frame: Inception to July 2019 • Language: English |
Exclusion criteria | • Studies involving a pediatric population • Studies including patients with mild disease • Studies involving patients with asthma and COPD overlapping (ACO) syndrome |
Databases searched | • Databases: Embase, MEDLINE, MEDLINE In-Process, and the Cochrane Central Register of Controlled Trials (CENTRAL) • Conference proceedings: American Thoracic Society, European Respiratory Society, and American College of Chest Physicians • Other sources: ClinicalTrials.gov of the US National Institutes of Health, bibliographic searching |
Selection process | Screening and selection of studies were conducted by 2 independent reviewers, with discrepancies resolved by a third independent reviewer. |
Data extraction process | Data were extracted by 2 independent reviewers using a predefined extraction grid, with results checked and reconciled by a third independent reviewer |
Quality assessment | Conducted using National Institute for Health and Care Excellence in the single technology appraisal user guide |
AE = adverse event; COPD = chronic obstructive pulmonary disease; FDC = fixed-dose combination; FEV1 = forced expiratory volume in 1 second; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; NMA = network meta-analysis; RCT = randomized controlled trial; SGRQ = St. George’s Respiratory Questionnaire; TDI = Transition Dyspnea Index.
Source: Sponsor-submitted NMA.
Methods of the Sponsor-Submitted NMA
Objectives
The objective of the included NMA was to evaluate the comparative efficacy and safety of Breztri Aerosphere and other triple-therapy combinations in the treatment of moderate-to-very-severe COPD.
Study Selection Methods
A systematic literature search was conducted to search and identify studies for inclusion in the NMA. Briefly, a systematic literature search was conducted in multiple electronic databases (MEDLINE, MEDLINE In-Process, Cochrane Central Register of Controlled Trials [CENTRAL], conference proceedings, and other sources to identify relevant studies. The searches were performed in July 2019 and updated in June 2020.
The eligible population comprised patients 40 years or older with moderate-to-severe COPD. Treatment using triple therapy (LAMA-LABA-ICS) in fixed-dose and open combinations was considered a relevant intervention. The relevant comparators of interest were triple, dual, or monotherapies of ICS, LAMA, and LABA along with placebo and best supportive care. The efficacy outcomes evaluated in the NMA were rate of exacerbations, lung function, symptom relief, use of rescue medications, HRQoL |||||||||||| ||||||||. Safety outcomes such as AEs, SAEs, pneumonia, and upper respiratory tract infection, along with withdrawals (due to any reason and due to AEs) were also analyzed.
The study selection was conducted by 2 reviewers independently with discrepancies resolved by a third reviewer. Data extraction from the included studies was conducted by 2 reviewers using a predetermined grid and was checked and reconciled by a third reviewer. The risk of bias in the included trials was assessed using the single technology appraisal guide from the National Institute for Health and Care Excellence (NICE). Quality assessment criteria included randomization, allocation concealment, blinding, baseline comparability, follow-up, selective reporting, and analysis.
NMA Analysis Methods
The NMA was conducted using a 3-level hierarchical Bayesian NMA model, which considers both treatments and classes of medications. This model assumed exchangeability between treatments within the same class. Primary base-case analyses were performed using this class-effect model. Class effects were considered for ICS-LABA and open triple therapies, in addition to including separate model nodes by individual therapy. In addition, independent treatment-effect models, in which treatments were pooled into classes defined by open triple therapies, ICS-LABAs, and LABA-LAMAs, and no differentiation was made between treatments within each class, were conducted for key outcomes relevant to economic modelling (exacerbations, use of rescue medication, |||||||| AEs, and treatment withdrawals). Multiple pairwise meta-analyses were conducted along with the NMA, following the recommended practice of the NICE decision support unit for evidence synthesis. The synthesis was conducted using WinBUGS. A total of 20,000 simulations were run for the burn-in and 180,000 simulations for inferences. Convergence was assumed if the Gelman-Rubin statistic was equal to 1 and was assessed by running 3 chains. Deviance information criterion (DIC) was used to determine the best fit, in which the model with the lowest DIC was considered to have the best fit. Markov chain Monte Carlo simulation for inference was increased to 200,000 and a thin of 30 was applied when autocorrelation was present. Models were run using non-informative priors.
A list of outcomes, the types of distribution, and output statistics is presented in Table 17. The primary outcome was exacerbations (moderate to severe and severe only). The comparative effects sizes of the NMA were reported using rate ratio (for log-normal distributions), mean difference (for continuous outcomes), odds ratio (for dichotomous outcomes), and HR (for time to event distributions) with 95% credible intervals (CrIs).
Due to the lack of a common comparator between the treatments, all LAMA-LABA combinations were grouped together to create an interlinked network under the assumption of similar efficacy for all LAMA-LABA therapies. The outcomes were analyzed at 24 and 52 weeks. All studies that reported outcome data between 20 and 28 weeks were included in the 24-weeks analysis. All studies that reported data between 48 and 56 weeks were included in the 52-weeks analysis.
Potential inconsistencies in the network were investigated with a feasibility assessment before conducting the NMA. A list of potential effect modifiers to assess clinical heterogeneity was not reported. Statistical heterogeneity in the NMA was assessed using the I2 statistic.
The base case for efficacy and safety outcomes included double-blinded studies. Some sensitivity analyses were conducted by removing outlier studies from the base-case model. For the efficacy outcomes, the planned sensitivity analyses included studies with a symptomatic population, exacerbation history, and trial duration. Other planned sensitivity analyses included analyses of open-label studies along with double-blind RCTs. Lastly, a univariate meta regression (using BMI, smoking status, COPD severity, and exacerbation history) was conducted for the rate of exacerbations (moderate and severe exacerbations as well as severe exacerbations). For safety outcomes, the planned sensitivity analyses that were performed included studies with a duration of 24 weeks and those with confirmed pneumonia cases (for the pneumonia outcome).
Table 17: Analysis Methods of the Sponsor-Submitted NMA
Methods | Sponsor-submitted NMA | |
|---|---|---|
NMA methods | Three-level hierarchical Bayesian NMA | |
Priors | Non-informative | |
Assessment of model fit | Assessed using DIC; model with the lowest DIC is generally considered the model with the best fit to the data | |
Assessment of consistency | Inconsistencies were assessed | |
Assessment of heterogeneity | Measured using the I2 statistic | |
Outcomes selected for analysis | Type of data or distribution | Output statistics |
Exacerbations Moderate to severe, severe only | Log normal | Rate ratio, 95% CrI of the estimate |
Lung function |||||||||| trough FEV1 | Continuous | Mean difference, 95% CrI of the estimate |
Symptoms TDI score, use of rescue medication | ||
Other HRQoL measures SGRQ score |||||||||| | ||
SGRQ responders | Binomial | Odds ratio, 95% CrI of the estimate |
Safety AE, SAE, pneumonia, URTI | ||
Tolerability All withdrawals, WDAE | ||
Pneumonia | Binomial | Risk difference, 95% CrI of the estimate |
|||||||||| | |||||||||| | |||||||||| |||||||||| |
Follow-up time points | 24 weeks and 52 weeks | |
Construction of nodes | All LAMA-LABA combinations combined to a single node (assumed similar efficacy for all LAMA-LABA combinations). An additional NMA was conducted for Breztri vs. other triple therapies. | |
Sensitivity analyses |
| |
Univariate meta regression | Conducted for the outcomes of moderate and severe exacerbation, and severe exacerbation. Meta regression was conducted using BMI, smoking status, COPD severity, and exacerbation history. | |
Methods for pairwise meta-analysis | Conducted | |
AE = adverse event; BMI = body mass index; COPD = chronic obstructive pulmonary disease; CrI = credible interval; DIC = deviance information criteria; ||||||||||||||||||||||||||||||||||||||||||||||||||||||||; FEV1 = forced expiratory volume in 1 second; HRQoL = health-related quality of life; ITC = indirect treatment comparison; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; NMA = network meta-analysis; SAE = serious adverse event; SGRQ = St. George’s Respiratory Questionnaire; TDI = Transition Dyspnea Index; URTI = upper respiratory tract infection; WDAE = withdrawal due to adverse event.
Source: Sponsor-submitted NMA.
Results of the NMA
The systematic review identified 15,542 publications from the original database search. After excluding irrelevant and duplicate studies, the full text of 1,589 publications was screened along with 33 publications from other sources (conferences, bibliographies, Clinical Study Reports). Nineteen trials (from 151 publications) were found to be eligible and included in the NMA. The search update did not find any additional eligible trials. Of the included studies, 7 studies were 52 weeks in duration, 5 studies were 24 weeks in duration, 1 study was 26 weeks in duration, and 6 studies were 12 weeks in duration. The FULFIL study lasted 24 weeks; however, a subgroup of patients continued in an extension study up to 52 weeks. Two of the included studies were open label (Jung, 2012 and Lee, 2016), and 17 were double-blinded RCTs.
The characteristics of the included studies, such as the inclusion criteria, number of randomized patients, baseline demographics, and clinical characteristics of patients, were not reported. The quality assessment conducted using the NICE checklist showed that all of the included studies had a low risk of bias across domains such as randomization, baseline characteristics, withdrawals, and statistical analysis. Most of the included studies (except the 2 open-label trials) had a low risk of bias in terms of blinding. All studies except 1 (Welte, 2009) had a low risk of bias in outcome selection and reporting.
The feasibility assessment conducted before the NMA showed that 2 studies (Wheeler, 2016 and Siler, 2016) were not connected in the base-case network and were therefore excluded from the NMA. Open-label studies were not included in the base-case analysis. Thus, 15 RCTs were included in the NMA.
Table 18: Summary of Results From the NMA of BGF 320 Compared With Other Triple-Therapy Treatments at 52 Weeks
Intervention | Comparator | Moderate-to-severe exacerbation | Severe exacer-bation | Trough FEV1, CFB at 52 weeks | |||||||||| | Use of rescue medication | TDI score at 52 weeks | ||||||||||| | SGRQ CFB at 52 weeks | SGRQ responders at 52 weeks | |||||||||||||| |
|---|---|---|---|---|---|---|---|---|---|---|---|
Model: Random-effects model | |||||||||||
Rate ratio (95% CrI) | Mean difference (95% CrI) | OR (95% CrI) | HR (95% CrI) | ||||||||
Studies included in the NMA, n | 14 | 13 | |||||||||
BGF MDI 320 | Trelegy | 1 (0.9 to 1.1) | 1.03 (0.84 to 1.49) | −0.01 (−0.05 to 0.03) | |||||||||| | −0.05 (−0.34 to 0.18) | 0.01 (−0.19 to 0.34) | ||||||||| | 0 (−0.93 to 0.93) | 0.99 (0.85 to 1.11) | ||||||||||| |
BGF MDI 320 | TIO 18 mcg o.d. + BDP 200 mcg b.i.d. + FOR 12 mcg b.i.d. (O) | 1 (0.86 to 1.09) | 1.01 (0.78 to 1.43) | 0.00 (−0.04 to 0.06) | |||||||||| | −0.09 (−0.48 to 0.16) | NA | ||||||| | 0.08 (−0.8 to 1.47) | 1 (0.86 to 1.17) | ||||||||||| |
BGF MDI 320 | TIO 18 mcg o.d. + BUD 320 mcg b.i.d. + FOR 9 mcg b.i.d. (O) | NA | 1.02 (0.82 to 1.58) | NA | ||||||| | NA | NA | ||||||| | NA | NA | ||||||| |
BGF MDI 320 | TIO 18 mcg o.d. + FLU 500 mcg b.i.d. + SAL 50 mcg b.i.d. (O) | 0.99 (0.83 to 1.05) | 1.00 (0.77 to 1.33) | 0.00 (−0.05 to 0.05) | ||||||| | NA | 0 (−0.36 to 0.33) | ||||||| | 0.11 (−0.74 to 1.55) | NA | ||||||| |
BGF MDI 320 | TIO 18 mcg o.d. + SAL 50 mcg b.i.d. + FLU 500 mcg b.i.d. (red) | 1 (0.86 to 1.09) | 1.01 (0.80 to 1.46) | 0.02 (−0.03 to 0.09) | ||||||| | NA | NA | ||||||| | −0.12 (−1.5 to 0.82) | NA | ||||||| |
BGF MDI 320 | TIO 18 o.d. + FLU 250 b.i.d. + SAL 50 b.i.d. (O) | 1 (0.85 to 1.09) | 1.01 (0.77 to 1.50) | NA | ||||||| | NA | NA | ||||||| | NA | NA | ||||||| |
BGF MDI 320 | UMEC 125 mcg o.d. + FLU 100 mcg o.d. + VIL 25 mcg o.d. (O) | 0.99 (0.84 to 1.08) | NA | NA | ||||||| | NA | NA | ||||||| | NA | NA | ||||||| |
BGF MDI 320 | UMEC 62.5 mcg o.d. + FLU 100 mcg o.d. + VIL 25 mcg o.d. (O) | 0.99 (0.85 to 1.07) | 1.00 (0.74 to 1.34) | NA | ||||||| | NA | NA | ||||||| | NA | NA | ||||||| |
b.i.d. = twice daily; BDP = beclomethasone; CFB = change from baseline; Crl = credible interval; ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||; FEV1 = forced expiratory volume in 1 second; FLU = fluticasone; FOR = formoterol; HR = hazard ratio; O = open triple combination; o.d. = once daily; OR = odds ratio; MDI = metered-dose inhaler; NA = not applicable; NMA = network meta-analysis; SAL = salmeterol; SGRQ = St. George’s Respiratory Questionnaire; TDI = Transition Dyspnea Index; TIO = tiotropium; UMEC = umeclidinium; VAS = visual analogue scale; VIL = vilanterol trifenatate.
Source: Sponsor-submitted NMA.
Table 19: Summary of Results From the NMA of BGF 320 Compared With Other Triple-Therapy Treatments at 24 Weeks
Intervention | Comparator | Trough FEV1, CFB at 24 weeks | TDI score at 24 weeks | ||||||||||||||||||||||||| | SGRQ CFB at 24 weeks | SGRQ responders at 24 weeks |
|---|---|---|---|---|---|---|
Model: Random-effects model | ||||||
Mean difference (95% CrI) | OR (95% CrI) | |||||
Studies included in the NMA, n | ||||||
BGF MDI 320 | Trelegy | −0.026 (−0.054 to 0.004) | 0.01 (−0.19 to 0.35) | |||||||||||||| | 0.22 (−0.39 to 1.21) | 0.98 (0.84 to 1.09) |
BGF MDI 320 | TIO 18 mcg o.d. + FLU 500 mcg b.i.d. + SAL 50 mcg b.i.d. (O) | −0.003 (−0.038 to 0.031) | 0 (−0.32 to 0.29) | ||||||||||||||| | 0.01 (−0.91 to 0.95) | N- |
BGF MDI 320 | TIO 18 o.d. + FLU 250 b.i.d. + SAL 50 b.i.d. (O) | −0.017 (−0.069 to 0.024) | NA | |||||||||||||| | NA | NA |
BGF MDI 320 | UMEC 62.5 mcg o.d. + FLU 100 mcg o.d. + VIL 25 mcg o.d. (O) | −0.003 (−0.039 to 0.031) | 0.02 (−0.2 to 0.48) | |||||||||||||| | −0.01 (−1.08 to 0.93) | 0.99 (0.8 to 1.14) |
b.i.d. = twice daily; BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; CFB = change from baseline; Crl; credible interval; ||||||||||||||||||||||||||||||||||||||||||||||||||||||; FEV1 = forced expiratory volume in 1 second; FLU = fluticasone; FOR = formoterol; HR = hazard ratio; MDI = metered-dose inhaler; NA = not applicable; NMA = network meta-analysis; O = open triple combination; o.d. = once daily; OR = odds ratio; SAL = salmeterol; SGRQ = St. George’s Respiratory Questionnaire; TDI = Transition Dyspnea Index; TIO = tiotropium; UMEC = umeclidinium; VAS = visual analogue scale; VIL = vilanterol trifenatate.
Source: Sponsor-submitted NMA.
Results
Table 18 and Table 19 present the summary of the results of the sponsor-submitted NMA for efficacy outcomes. The results of the safety outcomes are presented in Table 20.
Rate of Exacerbations
For the outcome of moderate-to-severe exacerbations without restriction on time point, 14 studies provided data for the NMA. In a random-effects model, BGF MDI showed comparable efficacy against FF-UMEC-VI (Trelegy) and other open triple-therapy combinations (Table 18). The rate ratio of BGF MDI 320 versus Trelegy was 1.0 (95% CrI, 0.9 to 1.1). The network diagram is shown in Figure 9 and a summary plot is shown in Figure 10.
A sensitivity analysis was conducted excusing studies that did not require a prior exacerbation history. Results of the sensitivity analysis and meta regression were consistent with the base-case model.
For the outcome of severe exacerbations without restriction on time point, 13 studies provided data for the NMA. BGF MDI showed comparable efficacy against FF-UMEC-VI (Trelegy) and other open triple-therapy combinations. The rate ratio of BGF MDI 320 versus FF-UMEC-VI (Trelegy) was 1.03 (95% CrI, 0.84 to 1.49). The network diagram is shown in Figure 11 and a summary plot is shown in Figure 12. A sensitivity analysis was conducted excusing studies that did not require a prior exacerbation history. Results of the sensitivity analysis and meta regression were consistent with the base-case model.
Figure 9: Network Diagram for a Composite of Moderate-to-Severe Exacerbations (n = 14; Double-Blind Studies)
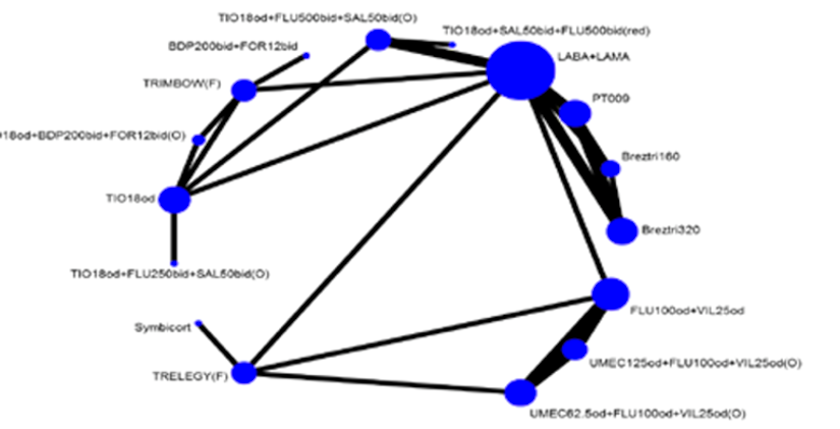
BDP = beclomethasone; bid = twice daily; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; red = reducing dose of tiotropium; SAL = salmeterol; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 10: Summary Plot of Moderate-to-Severe Exacerbations for BGF MDI 320 Versus Comparators
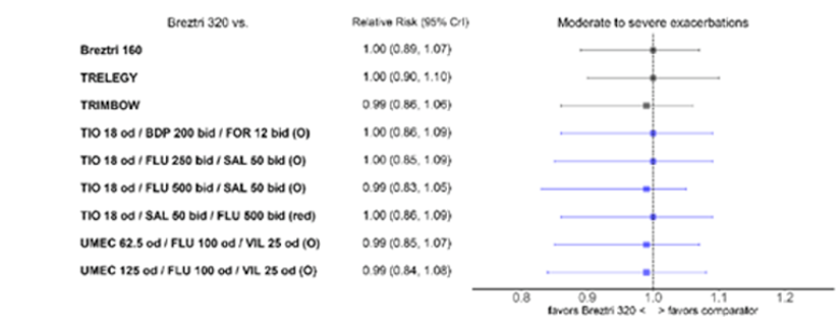
BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CrI = credible interval; FLU = fluticasone; FOR = formoterol; MDI = metered-dose inhaler; O = open triple combination; od = once daily; SAL = salmeterol; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
Figure 11: Network Diagram for a Composite of Severe Exacerbations (n = 13; Double-Blind Studies)
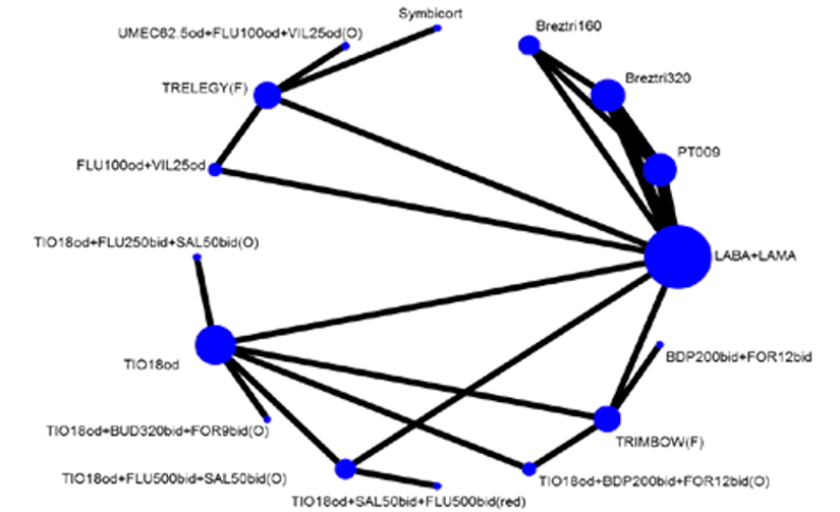
bid = twice daily; BDP = beclomethasone; BUD = budesonide; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; red = reducing dose of tiotropium; SAL = salmeterol; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 12: Summary Plot of Severe Exacerbation for BGF MDI 320 Versus Comparators
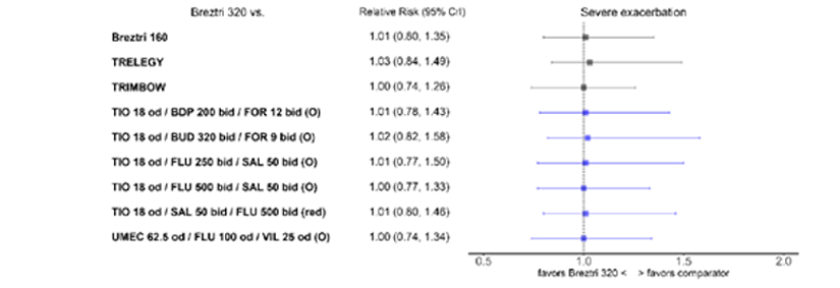
BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CrI = credible interval; FLU = fluticasone; FOR = formoterol; O = open triple combination; od = once daily; MDI = metered-dose inhaler; red = reducing dose of tiotropium; SAL = salmeterol; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
Health-Related Quality of Life
HRQoL measured using the change from baseline in SGRQ || |||||||||||||||||||| were considered outcomes of interest in the NMA.
For the NMA of change from baseline in SGRQ score at 24 weeks, 9 studies provided data to the network. Compared with FF-UMEC-VI (Trelegy) and other open triple-therapy combinations, BGF MDI showed comparable efficacy in improving HRQoL as measured using the SGRQ (Table 19). The network diagram is shown in Figure 13 and a summary plot is shown in Figure 14. For the NMA of change from baseline in SGRQ score at 52 weeks, 8 studies provided data to the network. Compared with FF-UMEC-VI (Trelegy), there was no difference in change from baseline in SGRQ score for BGF MDI at 52 weeks (mean difference = 0.0; 95% CrI, −0.93 to 0.93); the results were similar for triple-combination tiotropium 18 mcg once daily plus beclomethasone 200 mcg twice daily plus formoterol 12 mcg twice daily (Table 18). The network diagram is shown in Figure 15 and a summary plot is shown in Figure 16. A heterogeneity assessment was not performed, as the number of included studies was low. For analysis at both time points, the results of the planned sensitivity analyses were consistent with the base-case analysis.
Figure 13: Network Diagram for SGRQ CFB at 24 Weeks (n = 9; Double-Blind Studies)
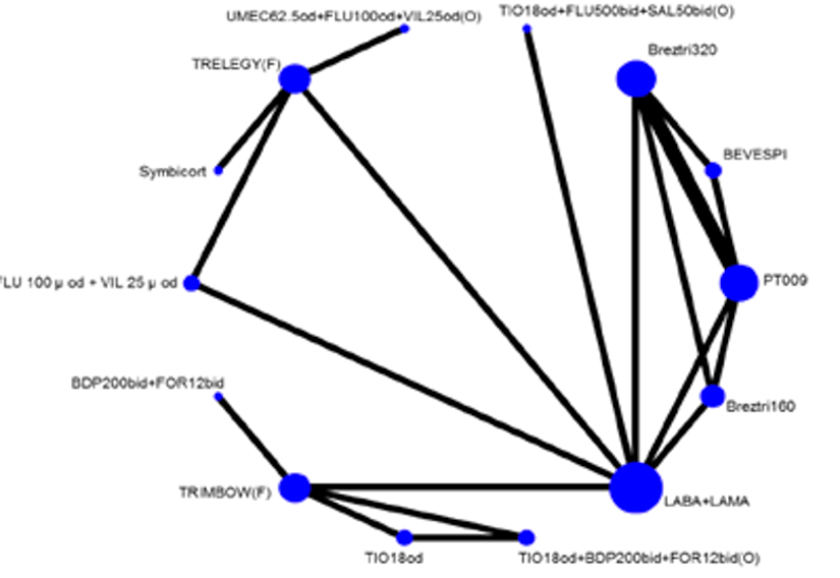
BDP = beclomethasone; bid = twice daily; CFB = change from baseline; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; red = reducing dose of tiotropium; SAL = salmeterol; SGRQ = St George’s Respiratory Questionnaire; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 14: Summary Plot of SGRQ CFB at 24 Weeks for BGF MDI 320 Versus Comparators
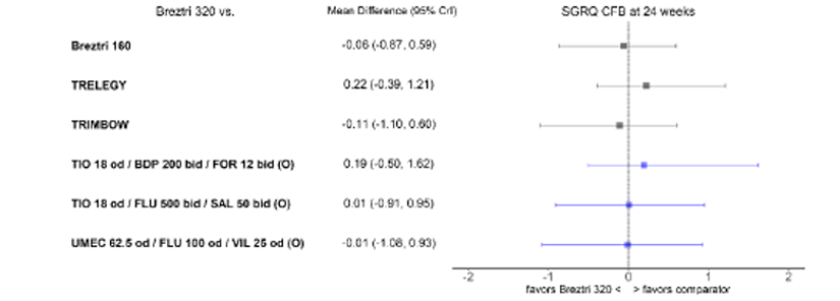
BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CFB = change from baseline; CrI = credible interval; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; MDI = metered-dose inhaler; O = open triple combination; od = once daily; SAL = salmeterol; SGRQ = St George’s Respiratory Questionnaire; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
Figure 15: Network Diagram for SGRQ CFB at 52 Weeks (n = 8; Double-Blind Studies)
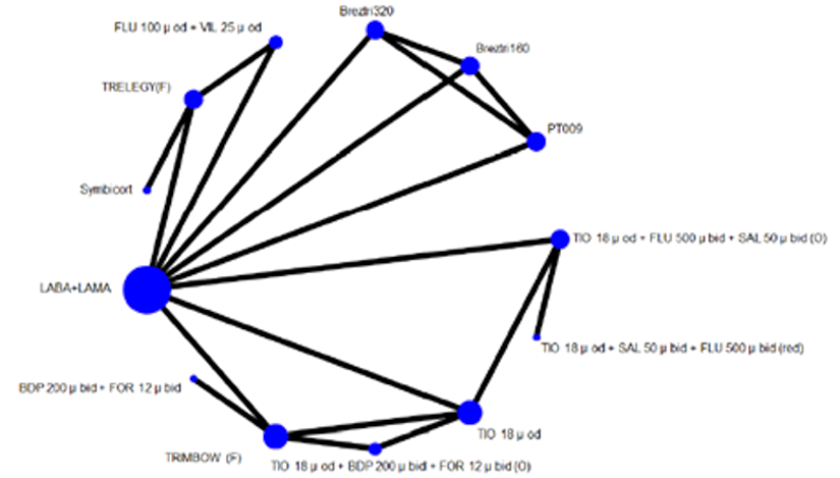
BDP = beclomethasone; bid = twice daily; CFB = change from baseline; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; red = reducing dose of tiotropium; SAL = salmeterol; SGRQ = St. George’s Respiratory Questionnaire; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 16: Summary Plot of SGRQ CFB at 52 Weeks for BGF MDI 320 Versus Comparators
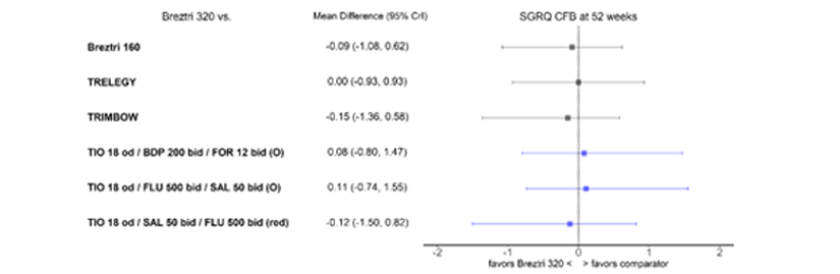
BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CFB = change from baseline; CrI = credible interval; FLU = fluticasone; FOR = formoterol; MDI = metered-dose inhaler; O = open triple combination; od = once daily; red = reducing dose of tiotropium; SAL = salmeterol; SGRQ = St. George’s Respiratory Questionnaire; TIO = tiotropium; VIL = vilanterol trifenatate; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
The data for the NMA of SGRQ responders at 24 and 52 weeks were contributed by 8 and 6 studies, respectively (network diagram not shown). The results of the analysis at 24 weeks showed that BGF MDI was associated with an improvement in the responder rate of SGRQ comparable to FF-UMEC-VI (Trelegy) and open triple-therapy combinations (Table 19). The results of the planned sensitivity analyses were consistent with the base-case analysis. At 52 weeks, compared with FF-UMEC-VI (Trelegy) and the open combination of tiotropium 18 mcg once daily plus beclomethasone 200 mcg twice daily plus formoterol 12 mcg twice daily, BGF MDI 320 showed comparable improvement in the SGRQ responder rate (Table 18).
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Lung Function
Measures of lung function such as change from baseline in the trough FEV1 (at 24 and 52 weeks) and |||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
The data for the NMA of change from baseline in trough FEV1 at 24 and 52 weeks were contributed by 10 and 8 studies, respectively. At 24 weeks, BGF MDI showed improvements in trough FEV1 comparable to FF-UMEC-VI (Trelegy) and other open triple-therapy combinations (Figure 19). The network diagram for analysis at 24 weeks is shown in Figure 17 and a summary plot is shown in Figure 18. Overall, moderate-to-low statistical heterogeneity (I2 = 0% to 45%) was observed. The results of the planned sensitivity analyses were consistent with the base-case analysis.
Figure 17: Network Diagram for Trough FEV1 CFB at 24 Weeks (n = 8; Double-Blind Studies)

BDP = beclomethasone; bid = twice daily; CFB = change from baseline; F = fixed-dose combination; FEV1 = forced expiratory volume in 1 second; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; SAL = salmeterol; SGRQ = St. George’s Respiratory Questionnaire; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 18: Summary Plot of Trough FEV1 CFB at 24 Weeks for BGF MDI 320 Versus Comparators
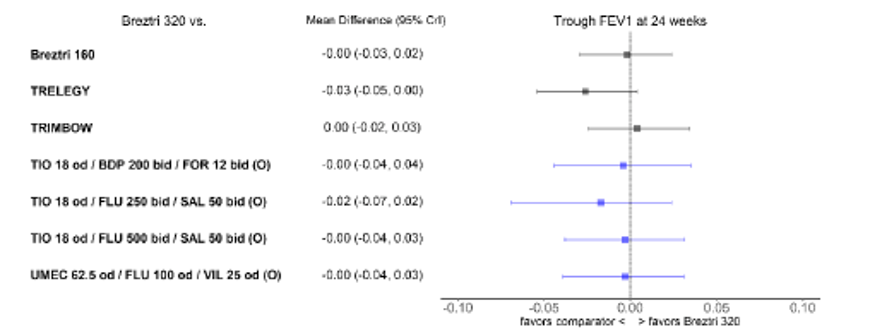
BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CFB = change from baseline; CrI = credible interval; F = fixed-dose combination; FEV1 = forced expiratory volume in 1 second; FLU = fluticasone; FOR = formoterol; MDI = metered-dose inhaler; O = open triple combination; od = once daily; SAL = salmeterol; SGRQ = St. George’s Respiratory Questionnaire; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
At 52 weeks, BGF MDI showed improvements in trough FEV1 comparable to FF-UMEC-VI (Trelegy) and other open triple-therapy combinations (Table 18). The network diagram for analysis at 52 weeks is shown in Figure 19 and a summary plot is shown in Figure 20. A heterogeneity assessment was not performed, as the number of included studies was limited. The results of the planned sensitivity analyses were consistent with the base-case analysis (Figure 18).
Figure 19: Network Diagram for Trough FEV1 CFB at 52 Weeks (n = 8; Double-Blind Studies)
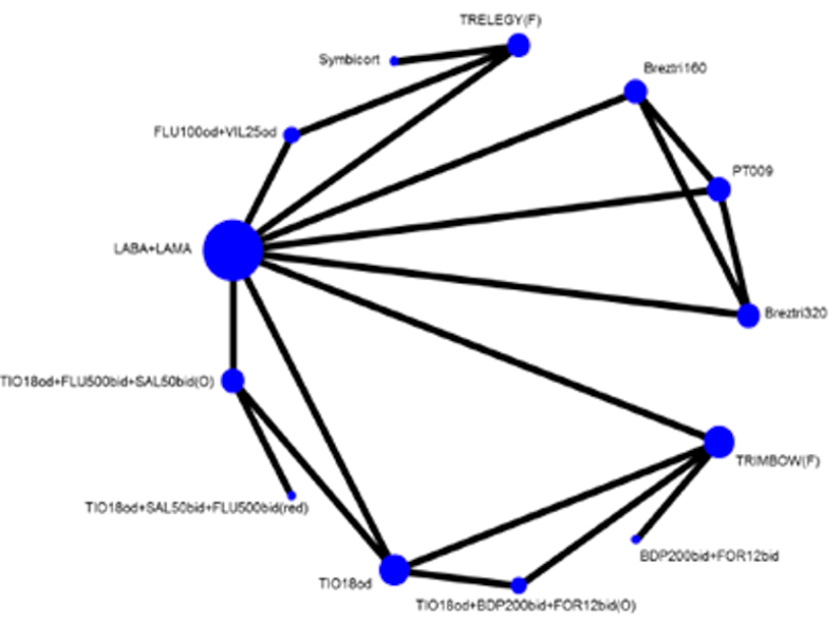
bid = twice daily; CFB = change from baseline; F = fixed-dose combination; FEV1 = forced expiratory volume in 1 second; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; red = reducing dose of tiotropium; SAL = salmeterol; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 20: Summary Plot of Trough FEV1 CFB at 52 Weeks for BGF MDI 320 Versus Comparators
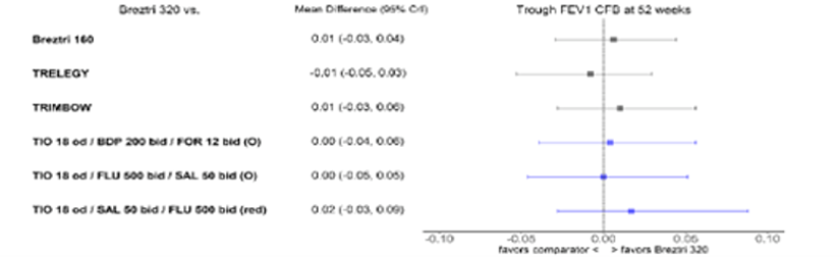
BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CFB = change from baseline; CrI = credible interval; F = fixed-dose combination; FEV1 = forced expiratory volume in 1 second; FLU = fluticasone; FOR = formoterol; MDI = metered-dose inhaler; O = open triple combination; od = once daily; red = reducing dose of tiotropium; SAL = salmeterol; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Symptoms
The burden of symptoms measured using TDI focal score at 24 and 52 weeks was considered an outcome of interest in the NMA. The data for the NMA of TDI focal score at 24 and 52 weeks were contributed by 6 and 4 studies, respectively.
At 24 weeks, BGF MDI showed improvements in TDI focal score comparable to FF-UMEC-VI (Trelegy) and other open triple-therapy combinations (Table 18). The network diagram is shown in Figure 21 and Figure 19, and a summary plot is shown in Figure 22. The results of the planned sensitivity analyses were consistent with the base-case analysis.
Figure 21: Network Diagram for TDI Focal Score at 24 Weeks (n = 6; Double-Blind Studies)
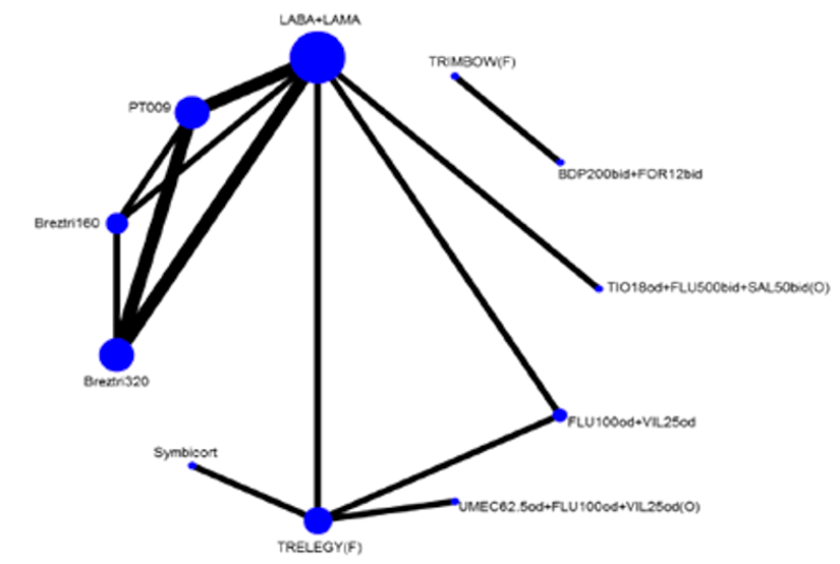
BDP = beclomethasone; bid = twice daily; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; SAL = salmeterol; TDI = Transition Dyspnea Index; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 22: Summary Plot of TDI Focal Score at 24 Weeks for BGF MDI 320 Versus Comparators
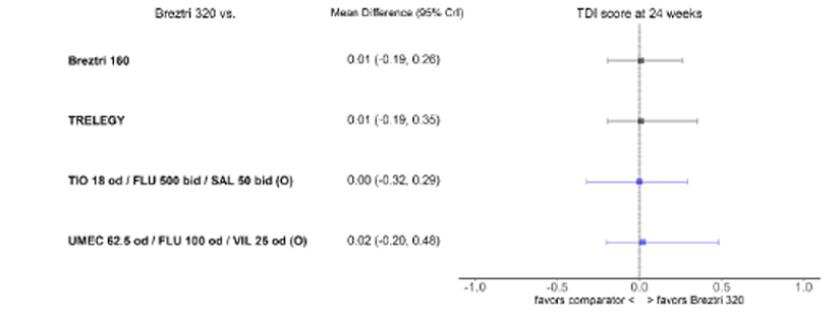
BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CrI = credible interval; FLU = fluticasone; MDI = metered-dose inhaler; O = open triple combination; od = once daily; SAL = salmeterol; TDI = Transition Dyspnea Index; TIO = tiotropium; UMEC = umeclidinium; VIL = vilanterol trifenatate; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
At 52 weeks, the TDI focal score for BGF MDI was comparable to FF-UMEC-VI (Trelegy) and tiotropium 18 mcg once daily plus fluticasone 500 mcg twice daily plus salmeterol 50 mcg twice daily (Table 18). The network diagram is shown in Figure 23 and Figure 19, and a summary plot is shown in Figure 24. As the network was sparse and the DIC did not favour a single model, a random-effects model with informative priors was chosen as the base case. A heterogeneity assessment was not performed, as the number of included studies was limited. The results of the planned sensitivity analyses were consistent with the base-case analysis.
Figure 23: Network Diagram for TDI Focal Score at 52 Weeks (n = 4; Double-Blind Studies)
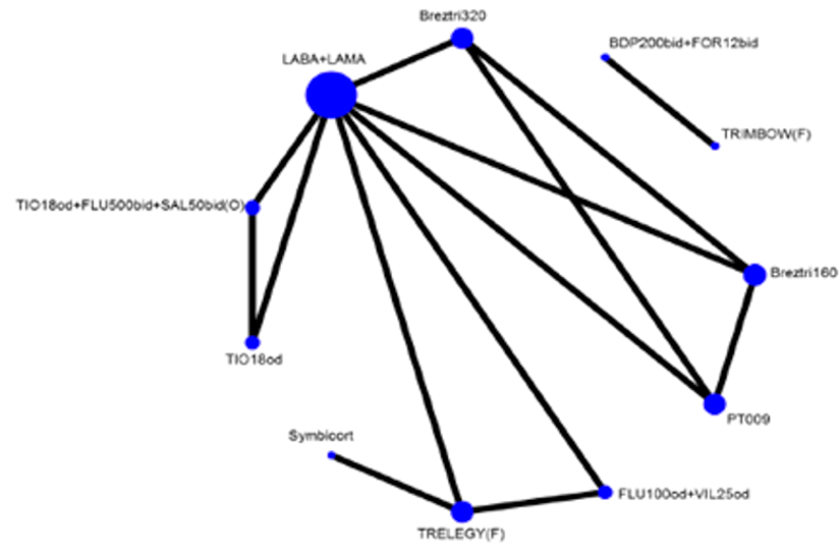
BDP = beclomethasone; bid = twice daily; CFB = change from baseline; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; SAL = salmeterol; TDI = Transition Dyspnea Index; TIO = tiotropium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 24: Summary Plot of TDI Focal Score at 52 Weeks for BGF MDI 320 Versus Comparators
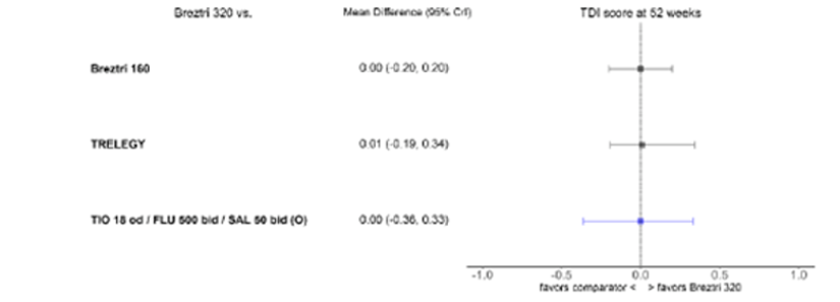
BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CrI = credible interval; FLU = fluticasone; MDI = metered-dose inhaler; O = open triple combination; od = once daily; SAL = salmeterol; TDI = Transition Dyspnea Index; TIO = tiotropium; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
Use of Rescue Medication
The mean puffs per day of rescue medication over 52 weeks was considered for an NMA, with 6 studies providing data. The results showed that BGF MDI was associated with a reduction in the use of rescue medication, which was comparable to FF-UMEC-VI (Trelegy) (mean difference = −0.05; 95% CrI, −0.34 to 0.18) and tiotropium 18 mcg once daily plus beclomethasone 200 mcg twice daily plus formoterol 12 mcg twice daily (mean difference = −0.09; 95% CrI, −0.48 to 0.16) (Table 18). The network diagram is shown in Figure 25 and Figure 19 and a summary plot is shown in Figure 26. The results of the planned sensitivity analyses were consistent with the base-case analysis.
Figure 25: Network Diagram for Use of Rescue Medication Over 52 Weeks (n = 6; Double-Blind Studies)

BDP = beclomethasone; bid = twice daily; F = fixed-dose combination; FLU = fluticasone; FOR = formoterol; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; O = open triple combination; od = once daily; TIO = tiotropium; VIL = vilanterol trifenatate.
Source: Sponsor-submitted network meta-analysis.
Figure 26: Summary Plot of Use of Rescue Medication Over 52 Weeks for BGF MDI 320 Versus Comparators
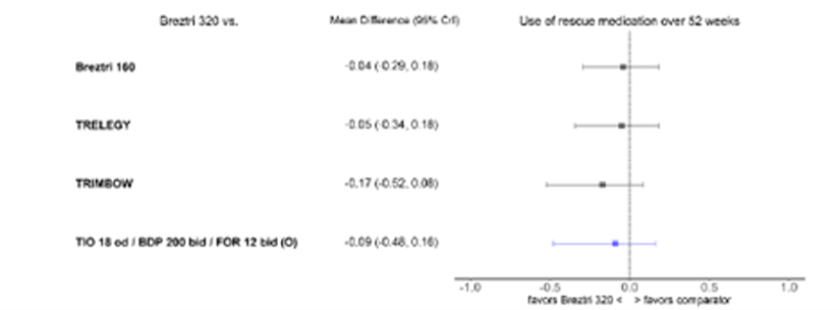
BDP = beclomethasone; BGF = budesonide-glycopyrronium-formoterol fumarate; bid = twice daily; CrI = credible interval; FOR = formoterol; MDI = metered-dose inhaler; O = open triple combination; od = once daily; TIO = tiotropium; vs. = versus .
Source: Sponsor-submitted network meta-analysis.
||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||
Figure 27: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 27 was removed at the request of the sponsor because it contained confidential information.
||||||||||||||||||||||||||||||
Figure 28: ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Figure 28 was removed at the request of the sponsor because it contained confidential information.
||||||||||||||||||||||||||||||
Table 20: Summary of Results From the NMA of Adverse Events and Withdrawals
Treatment | Any AEs at 52 weeks | Any SAEs at 52 weeks | Pneumonia at 52 weeks | URTI at 52 weeks | All withdrawals at 52 weeks | Withdrawals due to AE at 52 weeks | |
|---|---|---|---|---|---|---|---|
OR (95% CrI) | Risk difference (95% CrI) | OR (95% CrI) | |||||
Model: Random-effects model | |||||||
Studies included in the NMA, n | 8 | 8 | 8 | 3 | 8 | 8 | |
Breztri 320 | Trelegy | 1 (0.89, to 1.18) | 1 (0.88 to 1.14) | −0.001 (−0.01 to 0.01) | 1 (0.73 to 1.3) | 1.02 (0.94 to 1.26) | 1 (0.85 to 1.25) |
Breztri 320 | TIO 18 mcg o.d. + BDP 200 mcg b.i.d. + FOR 12 mcg b.i.d. (O) | 1 (0.86 to 1.2) | 1 (0.87 to 1.2) | 0.001 (−0.01 to 0.02) | NA | 1.01 (0.91 to 1.25) | 1 (0.8 to 1.31) |
Breztri 320 | TIO 18 mcg o.d. + FLU 500 mcg b.i.d. + SAL 50 mcg b.i.d. (O) | 1 (0.81 to 1.16) | 1 (0.86 to 1.17) | 0.001 (−0.01 to 0.02) | NA | 1.01 (0.91 to 1.24) | 1 (0.79 to 1.24) |
Breztri 320 | TIO 18 mcg o.d. + SAL 50 mcg b.i.d. + FLU 500 mcg b.i.d. (red) | 1 (0.81 to 1.17) | 1 (0.85 to 1.16) | 0.001 (−0.01 to 0.02) | NA | 1.01 (0.9 to 1.22) | 1 (0.82 to 1.29) |
AE = adverse event; BDP = beclomethasone; b.i.d. = twice daily; Crl = credible interval; FLU = fluticasone; FOR = formoterol; O = open triple combination; OR = odds ratio; NA = not applicable; NMA = network meta-analysis; o.d. = once daily; red = reducing dose of tiotropium; SAE = serious adverse event; SAL = salmeterol; TIO = tiotropium; URTI = upper respiratory tract infection; VIL = vilanterol trifenatate.
Source: Sponsor-submitted NMA.
Safety
The safety outcomes considered in the NMA were any AEs, any SAEs, upper respiratory tract infection, and pneumonia. The time point for analysis for all safety outcomes was 52 weeks. The overall AEs and SAEs were comparable between BGF MDI 320 and FF-UMEC-VI (Trelegy) and other triple-therapy combinations. For upper respiratory tract infections, Trelegy was the relevant comparator. Compared with Trelegy, BGF MDI showed no difference (odd ratio = 1.0; 95% CrI, 0.73 to 1.3) (Table 20). There were no differences in the occurrence of pneumonia (any grade) in BGF MDI 320 compared with FF-UMEC-VI (Trelegy) or other triple-therapy combinations. The results of the NMA of safety outcomes are presented in Table 20. The results of the planned sensitivity analyses were consistent with the base-case analysis.
Outcomes in the NMA related to tolerability were assessed as all withdrawals and withdrawals due to AEs at 52 weeks. Eight studies contributed to the NMA for each of these outcomes. The results showed that the tolerability of BGF MDI 320 is comparable to FF-UMEC-VI (Trelegy) and other triple-therapy combinations (Table 20). The results of the planned sensitivity analyses were consistent with the base-case analysis.
Critical Appraisal of NMA
The sponsor-submitted NMA was critically appraised, in part, by using recommendations from the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Task Force on Indirect Treatment Comparisons47 as a guide.
Relevance
The objectives and rationale for the NMA were clearly reported. The population, interventions, and comparators were appropriate and clear. Relevant to the current report, BGF MDI (triple therapy) was compared with other triple therapies (open and fixed dose) as well as dual and monotherapies of ICS, LAMA, and LABA. Comparisons with placebo and best supportive care were also considered. The outcomes considered in the NMA were relevant and described well. Across the included studies, the definitions of the exacerbation outcomes were similar to those used in Canadian settings, thereby increasing the generalizability of the results.
Credibility
The systematic review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, and the inclusion and exclusion criteria allowed for the identification of studies with relevant outcomes. Multiple electronic databases were searched to identify eligible RCTs. In addition, conference abstracts, trial registries, and bibliographies of systematic reviews were searched. Study selection and data extraction were conducted by 2 independent reviewers with a third reviewer employed for the resolution of discrepancies and data checking. However, the potential for publication bias was not reported and the literature search used was limited to those with an English abstract.
Quality assessments of the included RCTs were conducted using the NICE Single Technology Appraisal process. The risk of bias of the individual studies was shown. Overall, the studies were of low risk, with 2 studies having issues related to blinding (2 with unclear risk), and 1 study having a high risk associated with outcome selection (2 with unclear risk). All outcomes of interest for the NMA were not considered by all of the included studies and, therefore, not included in some of the NMAs. Additionally, a list of excluded studies (along with reason for exclusion) was not reported. As publication bias was also not assessed, it is likely the selective reporting of outcomes in the study introduced bias; however, not enough information was available to know for certain.
The baseline characteristics of the included studies were not described, except for the outcomes and follow-up time. Therefore, the number of patients in each of the included studies and their demographic and clinical characteristics were not clear. This made interpretation across trials regarding potential effect modifiers challenging. It was unclear whether all potential effect modifiers were considered, as such a list was not reported. A feasibility analysis was conducted by the reviewers for BGF MDI versus other triple-therapy combinations before conducting the NMA. Since a common comparator was lacking, all LAMA and LABA combinations were grouped together as 1 class to develop networks under the assumption of similar efficacy.
Analysis
The NMA was conducted using a 3-level hierarchical Bayesian NMA model. Convergence was assessed by running 3 chains and was assumed if the Gelman-Rubin statistic was 1. Both fixed-effect and random-effect models were generated. The goodness of fit was assessed using the DIC, and the best model was chosen based on the lowest DIC value. In the presence of autocorrelation, the Markov chain Monte Carlo simulation for inference was increased to 200,000 and a thin of 30 was applied. A class effect and independent treatment model were conducted, the base-case analysis being a class-effect model. The NMA was conducted based on relative treatment effects and no naive comparisons were made. Multiple pairwise comparisons were performed to allow indirect and direct comparisons to be synthesized. Heterogeneity in random-effect models was assessed using the I2 statistic. Consistency between direct and indirect comparisons was assessed. For 2 outcomes (moderate-to-severe exacerbation and severe exacerbation), a pre-specified univariate meta regression was conducted using BMI, smoking status, COPD severity, and exacerbation history. However, for most outcomes, meta regression was not possible due to the small number of studies reporting those outcomes.
Three different sensitivity analyses were conducted for the efficacy outcomes, as described in the earlier section (adding open-label studies to the base, symptomatic studies only, studies with a follow-up time greater than 24 weeks, and studies with a requirement of exacerbation history). Other potential effect modifiers, such as disease severity, baseline eosinophilia, and baseline reversibility of bronchodilators, were not considered.
Reporting Quality
Network diagrams and summary plots for all outcomes considered in the NMA were reported. Study results of the individual studies were not provided in the report. The results of the direct comparison and indirect comparison within the NMA were not reported separately. However, due to the lack of head-to-head trials between triple-therapy combinations, all results relevant to this review were from indirect comparisons. The results of the NMA were reported using appropriate effect estimates and measures of random variability (95% CrI). Relative treatment effects, based on certain patient characteristics such as BMI, smoking history, COPD severity, and exacerbation history were reported, as univariate meta regression, for the exacerbation outcomes. However, other potential effect modifiers, such as baseline eosinophilia and baseline reversibility to bronchodilators, were not considered.
The included NMA was funded by the sponsor of BGF MDI 320. Potential bias due to conflict of interest, and the steps taken to mitigate such bias, were not addressed.
Lastly, the authors of the sponsor-submitted NMA concluded that the efficacy and safety of BGF MDI 320 is comparable to other triple therapies for COPD. Based on the effect sizes and uncertainty levels (CrIs) of all outcomes, the relative efficacy and safety of BGF MDI 320 were found to be comparable between the treatments.
Other Relevant Evidence
Objective
The objective was to summarize the efficacy and safety results of the KRONOS extension study.38 This study was identified in the systematic review search but was not included in the main report, as the outcomes were not identified in the protocol.
Findings
Study Design
This 52-week, double-blind, randomized, parallel-group study was an extension of the phase III, 24-week, KRONOS study. The objective of the study was to assess the BMD and ocular safety of BGF MDI compared with BFF MDI and GFF MDI in patients with moderate-to-very-severe COPD. The primary end points were percentage change from baseline in lumbar spine BMD and change from baseline in the Lens Opacities Classification System version III (LOCS III) posterior subcapsular cataract score at week 52. AEs were also assessed in this study. A summary of study characteristics is presented in Table 21.
Table 21: Details of Included Study
Details | KRONOS Extension Study38 |
|---|---|
Designs and populations | |
Study design | Extension study, randomized DB |
Locations | US |
Randomized (N) | 627 |
Inclusion criteria | Inclusion and exclusion criteria of KRONOS study. Patients were 40 to 80 years of age with an established clinical history of COPD, a smoking history of ≥ 10 pack-years, a post-bronchodilator FEV1 to forced vital capacity ratio of < 0.70, and a post-bronchodilator FEV1 of < 80% that is ≥ 25% of the predicted normal value |
Exclusion criteria | Exclusion criteria specific to the 52-week study comprised severe osteoporosis, a T-score < − 2.5 at baseline or inability to achieve an acceptable BMD scan (BMD exclusion criteria), an inability to dilate pupil ≥ 6 mm, intraocular pressure ≥ 21 mm Hg (lowest of 3 readings), or an implanted artificial intraocular lens (ophthalmological exclusion criteria). |
Drugs | |
Intervention | BGF MDI 320 mcg-14.4 mcg-9.6 mcg |
Comparator(s) | GFF MDI 14.4 mcg-9.6 mcg BFF MDI 320 mcg-9.6 mcg |
Duration | |
Phase | |
Run-in | |
Double-blind | 52 weeks |
Follow-up | |
Outcomes | |
Primary end point |
|
Other end points |
Safety: AEs, AESI |
Notes | |
Publications | Kerwin et al. (2019)38 |
AE = adverse event; AESI = adverse event of special interest; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; BMD = bone mineral density; COPD = chronic obstructive pulmonary disease; DB = double blind; EXACT = Exacerbations of Chronic Pulmonary Disease Tool; EXACT-RS = Exacerbations of Chronic Pulmonary Disease Tool—Respiratory Symptoms; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; L = lumbar spine segment; LOCS III = Lens Opacities Classification System version III; MDI = metered-dose inhaler; RCT = randomized control trial; TDI = Transition Dyspnea Index.
Assessment
The primary end points of this extension study were percentage change from baseline in lumbar spine BMD and change from baseline in Lens Opacities Classification System version III posterior subcapsular cataract score at week 52. Other end points included percentage change from baseline in BMD of the total hip, change from baseline in average daily rescue salbutamol use, rate of moderate or severe exacerbations, and change from baseline in the EXACT score and E-RS total score (RS-Total). Safety was assessed using the end points, AEs, AEs of special interest, 12-lead electrocardiography, clinical laboratory testing, and vital sign measurements.
Results
Table 22: Baseline Demographics and Characteristics (Safety Population)
Characteristics | KRONOS Extension Study38 | ||
|---|---|---|---|
BGF MDI 320 mcg-18 mcg-9.6 mcg | BFF MDI 320 mcg-9.6 mcg | GFF MDI 18 mcg-9.6 mcg | |
Age, years, mean (SD) | 62.6 (7.9) | 64.0 (7.2) | 62.4 (7.8) |
Male, n (%) | 102 (52.6) | 53 (60.2) | 87 (50.0) |
Race, n (%) | |||
White | 179 (92.3) | 79 (89.8) | 156 (89.7) |
Black | 13 (6.7) | 9 (10.2) | 17 (9.8) |
Other | 2 (1.0) | 0 | 1 (0.6) |
Ethnicity, n (%) | |||
Hispanic or Latino | 9 (4.6) | 6 (6.8) | 5 (2.9) |
Not Hispanic or Latino | 185 (95.4) | 82 (93.2) | 169 (97.1) |
BMI kg/m2, mean (SD) | 29.0 (7.4) | 29.0 (5.8) | 29.0 (6.5) |
Current smoker, n (%) | 101 (52.1) | 42 (47.7) | 95 (54.6) |
Number of pack-years smoked, median (range) | 45.0 (11.2 to 256.0) | 47.3 (14.3 to 134.0) | 50.0 (10.0 to 171.0) |
COPD severity, n (%) | |||
Moderate | 95 (49.0) | 45 (51.1) | 91 (52.3) |
Severe | 86 (44.3) | 37 (42.0) | 65 (37.4) |
Very severe | 13 (6.7) | 6 (6.8) | 18 (10.3) |
COPD duration years, mean (SD) | 8.6 (6.7) | 9.6 (6.3) | 7.7 (5.3) |
Moderate or severe COPD exacerbations in the past 12 months, n (%) | |||
0 | 152 (78.4) | 67 (76.1) | 129 (74.1) |
1 | 33 (17.0) | 18 (20.5) | 34 (19.5) |
≥ 2 | 9 (4.6) | 3 (3.4) | 11 (6.3) |
Eosinophil count, cells/mm3, median, (range) | 180 (10 to 655) | 190 (15 to 505) | 185 (40 to 2,490) |
< 150 cells/mm3, n (%) | 68 (35.1) | 32 (36.4) | 54 (31.0) |
≥ 150 cells/mm3, n (%) | 126 (64.9) | 56 (63.6) | 120 (69.0) |
Use of ICS at screening, n (%) | 152 (78.4) | 73 (83.0) | 127 (73.0) |
CAT total score, mean (SD) | 21.2 (6.4) n = 192 | 22.3 (6.7) n = 86 | 20.4 (6.3) n = 172 |
EXACT total score, mean (SD) | 35.2 (10.8) n = 194 | 35.7 (10.4) n = 86 | 34.6 (10.6) n = 174 |
Rescue medication use, puffs/day 1, median (range)a | 1.9 (0.0 to 12.0) n = 194 | 2.4 (0.0 to 17.7) n = 86 | 2.0 (0.0 to 18.2) n = 174 |
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; BMI = body mass index; CAT = Chronic Obstructive Pulmonary Disease Assessment Test; COPD = chronic obstructive pulmonary disease; EXACT = Exacerbations of Chronic Pulmonary Disease Tool; GFF = glycopyrronium-formoterol fumarate; ICS = inhaled corticosteroid; MDI = metered-dose inhaler; SD = standard deviation.
aNumber of pack-years smoked = number of cigarettes smoked per day ÷ 20 × number of years smoked.
Table 23: Primary and Other BMD End Points (BMD Population)
Primary and other BMD end points | KRONOS extension study38 | ||
|---|---|---|---|
BGF MDI 320 mcg-18 mcg-9.6 mcg | BFF MDI 320 mcg-9.6 mcg | GFF MDI 18 mcg-9.6 mcg | |
Lumbar spine BMD (L2 to L4) | |||
N | 128 | 57 | 123 |
Baseline, g/cm2, mean (SD) | 1.18 (0.21) | 1.19 (0.20) | 1.16 (0.18) |
Change from baseline in primary BMD end point at week 52, % (95% CI) | −0.09 (−0.74 to 0.56) | −0.12 (−1.09 to 0.86) | 0.38 (−0.28 to 1.04) |
LS mean (95% CI) | −0.09 (−0.74 to 0.56) | −0.12 (−1.09 to 0.86) | 0.38 (−0.28 to 1.04) |
LS mean % difference between treatments (95% CI) | Reference group | 0.03 (−1.13 to 1.20) | −0.47 (−1.38 to 0.45) |
Total hip BMD | |||
N | 128 | 57 | 119 |
Baseline g/cm2, mean (SD) | 0.94 (0.15) | 0.98 (0.16) | 0.93 (0.14) |
LS mean (95% CI) | −0.87 (−1.39 to −0.34) | −1.12 (−1.90 to −0.33) | −0.32 (−0.86 to 0.23) |
LS mean % difference between treatmentsa (95% CI) | Reference group | 0.25 (−0.70 to 1.21) | −0.55 (−1.30 to 0.21) |
BFF = budesonide-formoterol fumarate; BMD = bone mineral density; BGF = budesonide-glycopyrronium-formoterol fumarate; CI = confidence interval; GFF = glycopyrronium-formoterol fumarate; L = lumbar spine segment; LS = least squares; MDI = metered-dose inhaler; SD = standard deviation.
aNot a pre-specified noninferiority comparison.
Table 24: Primary and Other Ophthalmological End Points (Ophthalmological Population)
Primary and other ophthalmological end pointsa | KRONOS extension study38 | ||
|---|---|---|---|
BGF MDI 320 mcg-18 mcg-9.6 mcg (N = 132) | BFF MDI 320 mcg-9.6 mcg (N = 54) | GFF MDI 18 mcg-9.6 mcg (N = 125) | |
LOCS III posterior subcapsular cataract score | |||
N | 218 | 98 | 184 |
Baseline, mean (SD) | 0.381 (0.880) | 0.397 (0.650) | 0.308 (0.567) |
Change from baseline at week 52, % (primary ophthalmological end point) | |||
LS mean (95% CI) | 0.153(0.079 to 0.227) | 0.022 (−0.090 to 0.135) | 0.026 (−0.055 to 0.106) |
LS mean % difference between treatments (95% CI) | Reference group | 0.130 (−0.004 to 0.265) | 0.127 (0.017 to 0.237) |
LOCS III NO score | |||
N | 220 | 98 | 187 |
Baseline, mean (SD) | 2.447 (1.082) | 2.336 (0.886) | 2.309 (1.060) |
Change from baseline to week 52 | |||
LS mean (95% CI) | 0.255 (0.170 to 0.340) | 0.186 (0.059 to 0.314) | 0.047 (−0.045 to 0.138) |
LSM % difference between treatments (95% CI) | Reference group | 0.069 (−0.084 to 0.222) | 0.208 (0.084 to 0.333) |
LOCS III NC score | |||
N | 219 | 98 | 187 |
Baseline, mean (SD) | 2.290 (1.137) | 2.287 (0.951) | 2.178 (0.858) |
Change from baseline to week 52 | |||
LS mean (95% CI) | 0.130 (0.050 to 0.209) | 0.142 (0.022 to 0.263) | 0.163 (0.077 to 0.248) |
LS mean difference between treatmentsb (95% CI) | Reference group | −0.013 (−0.157 to 0.132) | −0.033 |
LOCS III cortical cataract score | |||
N | 218 | 98 | 187 |
Baseline, mean (SD) | 0.832 (1.189) | 0.801 (0.976) | 0.727 (1.060) |
Change from baseline to week 52 | |||
LS mean (95% CI) | 0.105 (0.022 to 0.187) | 0.170 (0.047 to 0.294) | 0.067 (−0.022 to 0.155) |
LS mean difference between treatmentsb (95% CI) | Reference group | −0.065 (−0.214 to 0.083) | 0.038 (−0.083 to 0.159) |
IOP, mm Hg | |||
N | 228 | 100 | 203 |
Baseline, mean (SD) | 14.482 (2.908) | 15.490 (2.740) | 14.978 (2.971) |
Change from baseline to week 52 | |||
LS mean (95% CI) | 0.670 (0.330 to 1.010) | 0.178 (−0.339 to 0.696) | 0.680 (0.321 to 1.039) |
LS mean difference between treatmentsb (95% CI) | Reference group | 0.492 (−0.129 to 1.113) | −0.010 (−0.505 to 0.486) |
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; CI = confidence interval; GFF = glycopyrronium-formoterol fumarate; IOP = intraocular pressure; LOCS III = Lens Opacities Classification System version III; LS = least squares; MDI = metered-dose inhaler; NC = nuclear colour; NO = nuclear opalescence; SD = standard deviation.
aData presented are across eyes (irrespective of person) such that n = total number of eyes assessed.
bNot a pre-specified noninferiority comparison.
Results
Of the 627 patients who were randomized in the KRONOS study and consented to the extension study, 169 patients did not meet the extension study entry criteria. Overall, 456 patients were included in the safety population: 194 patients in the BGI MDI group, 88 patients in the BFF MDI group, and 174 patients in the GFF MDI group. Table 22 outlines the baseline demographics and characteristics of the safety population.
Efficacy Outcomes
All treatment groups had comparable and normal baseline BMD characteristics, with the mean T-scores for the lumbar spine and hip BMD equating to 0.1 and −0.6. There were small and comparable changes among treatment groups for the primary end point, percentage change from baseline at week 52 (least squares mean ranging from −0.12 to 0.38 among groups). The change in baseline at week 52 for total hip BMD was small and comparable among treatment groups (least squares mean ranging from −1.12 to −0.32 among groups).
The baseline LOCS III posterior subcapsular cataract score was slightly higher in the BFF MDI group compared with the other treatment groups. The change from baseline at week 52 for LOCS III score was small and comparable among groups (least squares mean ranging from 0.022 to 0.153).
Safety Efficacy Points
The overall incidence of treatment-emergent adverse events (TEAEs) across treatment groups was relatively similar. Rates of mild and moderate TEAEs were found to be similar across treatment groups (around 25% and 30% across groups). The rates of upper respiratory tract infections, bronchitis, and urinary tract infections were similar across treatment groups. The rate of COPD was found to be slightly higher in both the BGF (6.2%) and GFF (5.2%) treatment groups compared with the BFF treatment group (1.1%). Bone- and ocular-related TEAEs, including cataract, increased intraocular pressure, osteoarthritis, and osteoporosis, occurred minimally (0% to 3%) among the 3 treatment groups.
Table 25: Summary of TEAEs (Safety Population)
TEAEs, n (%) | KRONOS extension study38 | ||
|---|---|---|---|
BGF MDI 320 mcg-18 mcg-9.6 mcg (N = 194) | BFF MDI 320 mcg-9.6 mcg (N = 88) | GFF MDI 18 mcg-9.6 mcg (N = 174) | |
Patients with ≥ 1 TEAE | 144 (74.2) | 64 (72.7) | 133 (76.4) |
Mild | 50 (25.8) | 27 (30.7) | 46 (26.4) |
Moderate | 63 (32.5) | 29 (33.0) | 65 (37.4) |
Severe | 31 (16.0) | 8 (9.1) | 22 (12.6) |
Patients with TEAEsa | 35 (18.0) | 17 (19.3) | 29 (16.7) |
Patients with serious TEAEsb | 33 (17.0) | 7 (8.0) | 22 (12.6) |
COPDc | 12 (2.6) | 1 (1.1) | 9 (5.2) |
Pneumonia | 2 (1.0) | 0 | 4 (2.3) |
Patients with serious TEAEsa,b | 2 (1.0) | 0 | 2 (1.1) |
Patients with TEAEs leading to early discontinuation | 16 (8.2) | 6 (6.8) | 12 (6.9) |
Patients with confirmed MACEd | 3 (1.5) | 0 | 3 (1.7) |
Patients with confirmed pneumoniad | 4 (1.2) | 1 (1.1) | 6 (3.4) |
Death (all causes) | 3 (1.5) | 0 | 1 (0.6) |
TEAEs occurring in ≥ 4% of patients in any treatment arm | |||
URTI | 18 (9.3) | 6 (6.8) | 18 (10.3) |
Bronchitis | 12 (6.2) | 2 (2.3) | 8 (4.6) |
COPD | 12 (6.2) | 1 (1.1) | 9 (5.2) |
UTI | 10 (5.2) | 5 (5.7) | 6 (3.4) |
Muscle spasms | 6 (3.1) | 9 (10.2) | 5 (2.9) |
Viral URTI | 9 (4.6) | 6 (6.8) | 5 (2.9) |
Sinusitis | 11 (5.7) | 2 (2.3) | 6 (3.4) |
Hypertension | 8 (4.1) | 4 (4.5) | 6 (3.4) |
Back pain | 9 (4.6) | 1 (1.1) | 7 (4.0) |
Nasopharyngitis | 7 (3.6) | 4 (4.5) | 6 (3.4) |
Diarrhea | 5 (2.6) | 2 (2.3) | 9 (5.2) |
Dyspnea | 4 (2.1) | 5 (5.7) | 5 (2.9) |
Pneumonia | 5 (2.6) | 1 (1.1) | 8 (4.6) |
Dysphonia | 6 (3.1) | 5 (5.7) | 2 (1.1) |
Bone- and ocular-related TEAEs occurring in ≥ 1% of patients | |||
Cataract | 6 (3.1) | 2 (2.3) | 0 |
IOP increased | 2 (1.0) | 1 (1.1) | 4 (2.3) |
Osteoarthritis | 2 (1.0) | 0 | 4 (2.3) |
Osteoporosis | 2 (1.0) | 1 (1.1) | 2 (1.1) |
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; GFF = glycopyrronium-formoterol fumarate; IOP = intraocular pressure; MACE = major adverse cardiovascular event; MDI = metered-dose inhaler; TEAE = treatment-emergent adverse event; URTI = upper respiratory tract infection; UTI = urinary tract infection.
aPossibly, probably, or definitely related to treatment in the opinion of the investigator.
bTEAEs were classified as serious if, in the opinion of the investigator, they resulted in hospitalization or substantial disruption to the patient’s ability to conduct normal life functions or were life-threatening or fatal.
cClassified as a TEAE only if meeting criteria for a serious TEAE.
dConfirmed by clinical end point committee.
Limitations
The main limitations for the extension safety study relate to the length of the study and the size of the safety population. The study was 52 weeks in length, which may limit the outcomes assessed (i.e., BMD, cataracts, and so forth) and the overall results or conclusions from the study. Additionally, of the 627 patients from the KRONOS study who consented to participle in the extension study, 169 patients were not eligible to enrol due to the eligibility criteria, making the overall study population small.
Discussion
Summary of Available Evidence
This review summarizes the clinical evidence regarding the efficacy and safety of BGF MDI 320 for the long-term maintenance treatment of COPD. Two phase III double-blinded parallel-group RCTs, ETHOS and KRONOS, sponsored by AstraZeneca, met the inclusion criteria for the clinical systematic review. Both trials enrolled COPD patients over the age of 40 who had been on COPD maintenance therapy with 2 or more inhaled medications for at least 6 weeks. ETHOS enrolled patients who had moderate-to-severe disease with at least 1 documented exacerbation within the previous year. The intervention in both trials was BGF MDI 320 mcg-14.4 mcg-9.6 mcg twice daily. Relevant to this review, the comparators in ETHOS were BFF MDI 320 mcg-9.6 mcg twice daily and GFF MDI 14.4 mcg-9.6 mcg twice daily. In KRONOS, the comparators were GFF MDI 14.4 mcg-9.6 mcg twice daily, BFF MDI 320 mcg-9.6 mcg twice daily, and the open-label BUD-FOR DPI using the Symbicort TBH (400 mcg-12 mcg). The primary outcome for ETHOS was the rate of moderate and severe COPD exacerbations over 52 weeks. The primary outcomes for KRONOS were FEV1 AUC0-4 and the change from baseline in the morning pre-dose trough FEV1 over 24 weeks. Other relevant outcomes considered in the trials included HRQoL, symptoms, use of rescue medication, and safety outcomes.
The number of patients in ETHOS and KRONOS were 8,588 and 1,902, respectively, with baseline characteristics relatively balanced across the treatment arms of each trial and generally reflective of the Canadian COPD population. ETHOS enrolled a higher proportion of females than KRONOS (40.3% versus 28.8%). There was a higher proportion of Asian participants in KRONOS (44.9%) compared with ETHOS (7.7%). Most patients in the trials had moderate or severe COPD based on the GOLD criteria and most of the patients were taking either triple therapy (LAMA-LABA-ICS) or dual therapy (ICS-LABA) before the study. It is possible the results were biased in favour of BGF MDI, considering the baseline severity and prior COPD treatment. As for the external validity of the studies, the clinical expert noted that the high rate of discontinuation of the study drug (22.4% in ETHOS and 14% in KRONOS) and the rates of usage of ICS at baseline, were not reflective of the Canadian COPD population.
A sponsor-submitted NMA provided indirect evidence comparing BGF MDI 320 with other triple therapies. The NMA compared BGF MDI 320 with other open and fixed triple-therapy combinations of LAMA-LABA-ICS (including Trelegy) for the treatment of moderate-to-very-severe COPD. The baseline characteristics of the study patients and the results of the included studies were not reported, making the interpretation across trials regarding potential effect modifiers and homogeneity challenging. However, an assessment of heterogeneity and planned sensitivity analyses were conducted for most of the outcomes. General reporting quality was adequate.
Lastly, an extension study38 of KRONOS assessing the BMD and ocular safety of BGF MDI 320 was identified. In this 52-week extension, 456 patients were enrolled. The primary end points were percentage change from baseline in lumbar spine BMD and change from baseline in lens opacities. All groups (BGF MDI, BFF MDI, GFF MDI) had small and comparable changes from baseline for both the BMD end points and ocular end points. The TEAEs were small among the 3 treatment groups and no new safety concerns were identified. The relatively smaller size of the study population and the lack of safety assessment beyond 52 weeks were the major limitations of this study.
Interpretation of Results
Efficacy
One of the key outcomes of interest for this review was COPD exacerbations. From a patient perspective, exacerbations are of major concern and treatments that reduce the frequency of exacerbations, especially severe exacerbations, would likely meet some of patients’ unmet needs. Exacerbations may lead to hospitalization or the use of systemic corticosteroids or antibiotics and increase the utilization of health care resources. The 2 pivotal trials provided comparative evidence for this outcome between BGF MDI 320 and dual-therapy combinations over 24 weeks and at 52 weeks. Results from ETHOS and KRONOS showed that BGF MDI 320 was associated with significantly lower rates of moderate or severe COPD exacerbations compared with GFF MDI (rate ratio of 0.76 at 52 weeks and 0.48 at 24 weeks). BGF MDI 320 was associated with a significant decrease in the rates of moderate or severe COPD exacerbations compared with BFF MDI at 52 weeks (rate ratio of 0.87) but not at 24 weeks. One of the highest risk factors of exacerbations is a history of previous exacerbations.48,49 Results from the ETHOS subgroup analyses of patients who had 2 or more exacerbations within the previous year showed that, at 52 weeks, BGF MDI 320 significantly lowered the rates of moderate-to-severe COPD exacerbations compared with GFF MDI, but not compared with BFF MDI. A similar subgroup analysis in KRONOS showed that, over 24 weeks, these improvements were non-significant. It is possible that the subgroups were not adequately powered in KRONOS to detect a meaningful difference due to the low number of patients. Subgroup analysis in both trials showed that, in patients with a peripheral baseline eosinophil count of 150 cells per mm3 or greater, the reductions in rates were significant compared with GFF MDI but not compared with BFF MDI. Overall, the efficacy of BGF MDI 320 in lowering rates of COPD exacerbations was not significantly different compared with BFF MDI. Results from KRONOS also showed that, compared with Symbicort TBH, BGF MDI 320 was not associated with a significant reduction in the rates of moderate or severe exacerbation, likely due to the ICS component in both interventions. COPD exacerbation that resulted in hospitalization is categorized as severe. When only severe exacerbations were examined, there was a significant benefit with BGF MDI compared with BFF MDI in lowering the rates of exacerbation as well as the time to first severe exacerbation at 52 weeks. Due to a lack of direct head-to-head trials between different triple-therapy combinations, indirect evidence from an NMA was included in this review. Results from this NMA showed that BGF MDI 320 was similar to fixed-dose FF-UMEC-VI (Trelegy) and other triple-therapy combinations in reducing the rates of COPD exacerbations.
HRQoL was an outcome identified as important based on the patient input. HRQoL assessed by the SGRQ was statistically significantly improved with BGF MDI 320 compared with GFF MDI (based on results from ETHOS and KRONOS), BFF MDI (based on results from ETHOS), and Symbicort TBH (based on results from KRONOS). All treatment arms showed within-group improvement, which was clinically meaningful for the SGRQ total score (MCID = 4 units) at 24 weeks; however, none of the between-group comparisons in either study was considered clinically significant. In ETHOS, the proportion of patients who were SGRQ responders was greater in the BGF MDI 320 arm compared with GFF and BFF MDI. In KRONOS, the proportion of patients who were SGRQ responders was greater in the BGF MDI 320 arm compared with the GFF MDI arm. Overall, BGF MDI 320 was associated with an improvement in HRQoL from baseline compared with GFF MDI and BFF MDI that was not clinically meaningful. Indirect evidence from the NMA showed that BGF MDI 320 was comparable to FF-UMEC-VI (Trelegy) and other triple-therapy combinations in improving HRQoL, as measured using the SGRQ.
Another outcome of interest in the clinical review was lung function. In both trials, morning pre-dose trough FEV1 was used to assess this outcome. There was a clinically significant within-group improvement in the BGF MDI group over 24 weeks (but not for the comparators). Between groups, BGF MDI 320 showed a statistically significant increase in FEV1 over 24 weeks compared with all active comparators in both trials. However, this improvement in FEV1 was not clinically significant. Indirect evidence from the NMA showed that BGF MDI was comparable to FF-UMEC-VI (Trelegy) and other triple-therapy combinations in improving peak and trough FEV1.
Symptoms of COPD were identified as an important outcome by the patient groups. Treatment with BGF MDI 320 was associated with a within-group improvement that was clinically significant (MCID = 1 unit). Between groups, BGF MDI 320 did not clinically significantly improve TDI focal score over 24 weeks compared with GFF MDI, BFF MDI, and Symbicort TBH. A statistically significant improvement was observed between treatment groups in ETHOS, but not in KRONOS. Indirect evidence from the NMA showed that BGF MDI was comparable to FF-UMEC-VI (Trelegy) and other triple-therapy combinations in improving patient symptoms, as assessed using TDI focal score. After 24 weeks of treatment with BGF MDI 320, patients in ETHOS and KRONOS reported a decrease in the average daily use of rescue medication by more than 1 unit. Across BFF and GFF MDI, the decrease in average daily usage of rescue medications was statistically significant compared with BGF MDI 320 in ETHOS. This decrease was not statistically significant in KRONOS. Indirect evidence from the NMA showed that BGF MDI 320 was comparable to FF-UMEC-VI (Trelegy) and other triple-therapy combinations in lowering the use of rescue medication.
Other outcomes proposed by the patient groups as important, namely, exercise tolerance and patient adherence, were evaluated by the included trials and NMA within HRQoL as measured with SGRQ but were not considered separately. Productivity was not considered by any of the trials.
Harms
Within each trial, occurrences of harms outcomes were similar across treatment arms. More than 1-half of patients in each arm in both trials reported at least 1 AE. The most common AEs were COPD (indicating a lack of efficacy), nasopharyngitis, and upper respiratory tract infection. In ETHOS, at 52 weeks, SAEs were reported in around 20% of patients. In KRONOS, at 24 weeks, AEs were reported in 6.7% to 10.9% of patients in each arm. The most common SAEs were COPD (9.4% to 11.3%) and pneumonia (1.6% to 2.8%). Notable harms such as anticholinergic AEs, cardiovascular events, and corticosteroid-associated AEs were similar across treatment arms in both trials. The clinical expert consulted for the review noted that the observed AEs were aligned with the AEs observed on treatment with the components of BGF MDI 320 in clinical practice.
The KRONOS extension study, which spanned 52 weeks, found no clinically meaningful differences in BMD and ophthalmological assessments among the 3 treatment groups (BGF MDI, GFF MDI, and BFF MDI). The TEAEs were relatively low and similar across the treatment groups and did not indicate any new safety findings beyond what is expected from the components of BGF MDI.
Conclusions
Two multinational double-blind RCTs sponsored by AstraZeneca were included in this review, namely, ETHOS (52 weeks) and KRONOS (24 weeks) comparing the efficacy of BGF MDI 320 with dual therapy for patients with COPD. Overall, BGF MDI 320 reduced the rate of moderate or severe exacerbations compared with GFF MDI and BFF MDI at 52 weeks. Although numerical improvements in HRQoL and symptoms were reported, the between-group differences were not clinically significant. BGF MDI 320 improved FEV1 over 24 weeks compared with all active comparators; however, this improvement in FEV1 was not clinically significant. The average daily use of rescue medications was decreased by 1 unit after treatment with BGF MDI for 24 weeks. The between-group differences in the use of rescue medications were inconclusive. The lack of head-to-head trials comparing triple-therapy combinations is an important gap in the evidence. Indirect evidence from a sponsor-submitted NMA compared BGF MDI 320 with FF-UMEC-VI (Trelegy) and other open triple-therapy combinations. BGF MDI likely showed similar or comparable efficacy and safety compared with other triple therapies, with notable limitations that are inherent with indirect comparisons. The AEs associated with BGF MDI 320 were consistent with those expected for each of the individual components.
References
1.O'Donnell DE, Hernandez P, Kaplan A, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease - 2008 update - highlights for primary care. Can Respir J. 2008;15 Suppl A:1A-8A.
2.Lung disease A-Z. Ottawa (ON): Canadian Lung Association; 2017: https://www.lung.ca/lung-health/lung-disease/copd/. Accessed 2021 Apr 24.
3.Clinical Study Report: PT010005 (ETHOS). A Randomized, Double-Blind, Multi-Center, Parallel-Group Study to Assess the Efficacy and Safety of PT010 Relative to PT003 and PT009 on COPD Exacerbations over a 52-Week Treatment Period in Subjects With Moderate to Very Severe COPD [internal sponsor's report]. Durham (NC): AstraZeneca; 2019 Nov 08.
4.Clinical Study Report: PT010006 (KRONOS). A Randomized, Double-Blind, Parallel-Group, 24-Week, Chronic-Dosing, Multi-Center Study to Assess the Efficacy and Safety of PT010, PT003, and PT009 Compared with Symbicort® Turbuhaler® as an Active Control in Subjects with Moderate to Very Severe Chronic Obstructive Pulmonary Disease [internal sponsor's report]. Durham (NC): AstraZeneca; 2018 jun 06.
5.Lavorini F, Fontana GA, Usmani OS. New Inhaler Devices - The Good, the Bad and the Ugly. Respiration. 2014;88(1):3-15. PubMed
6.Usmani OS, Roche N, Jenkins M, Stjepanovic N, Mack P, De Backer W. Consistent Pulmonary Drug Delivery with Whole Lung Deposition Using the Aerosphere Inhaler: A Review of the Evidence. Int J Chron Obstruct Pulmon Dis. 2021;16:113-124. PubMed
7.Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671-1680. PubMed
8.Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2018 report. [place unknown]: Global Initiative for Chronic Obstructive Lung Disease; 2018.
9.Biener AI, Decker SL, Rohde F. Prevalence and Treatment of Chronic Obstructive Pulmonary Disease (COPD) in the United States. JAMA. 2019;322(7):602-602. PubMed
10.Vos T, Lim S, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. 2020;396(10258):1204-1222. PubMed
11.Canada S. Table 13-10-0801-01 Leading causes of death, total population (age standardization using 2011 population. Accessed April 14, 2021.
12.Chronic obstructive pulmonary disease under-diagnosed in Canadian adults: results from cycles 3 and 4 (2012 to 2015) of the Canadian Health Measures Survey. Health Fact Sheets. Ottawa (ON): Statistics Canada; 2017.
13.Bourbeau J, Bhutani M, Hernandez P, et al. CTS position statement: pharmacotherapy in patients with COPD — an update. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2017;1(4):222-241.
14.Sin DD, Man SF, Tu JV. Inhaled glucocorticoids in COPD: immortal time bias. Am J Respir Crit Care Med. 2003;168(1):126-127. PubMed
15.Suissa S. Effectiveness of inhaled corticosteroids in chronic obstructive pulmonary disease: immortal time bias in observational studies. Am J Respir Crit Care Med. 2003;168(1):49-53. PubMed
16.Pizzichini E, Pizzichini MM, Gibson P, et al. Sputum eosinophilia predicts benefit from prednisone in smokers with chronic obstructive bronchitis. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1511-1517. PubMed
17.Brightling CE, Monteiro W, Ward R, et al. Sputum eosinophilia and short-term response to prednisolone in chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2000;356(9240):1480-1485. PubMed
18.Leigh R, Pizzichini MM, Morris MM, Maltais F, Hargreave FE, Pizzichini E. Stable COPD: predicting benefit from high-dose inhaled corticosteroid treatment. Eur Respir J. 2006;27(5):964-971. PubMed
19.O'Donnell DE, Aaron S, Bourbeau J, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease - 2007 update. Can Respir J. 2007;14 Suppl B:5B-32B.
20.Alter P, Baker JR, Dauletbaev N, et al. Update in Chronic Obstructive Pulmonary Disease 2019. Am J Respir Crit Care Med. 2020;202(3):348-355. PubMed
21.Janjua S, Mathioudakis AG, Fortescue R, et al. Prophylactic antibiotics for adults with chronic obstructive pulmonary disease: a network meta-analysis. Cochrane Database Syst Rev. 2021;1:CD013198. PubMed
22.Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest. 2015;147(4):894-942. PubMed
23.Wilson ME, Dobler CC, Morrow AS, et al. Association of Home Noninvasive Positive Pressure Ventilation With Clinical Outcomes in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis. JAMA. 2020;323(5):455-465. PubMed
24.Reference: 2020 Global Strategy for Prevention, Diagnosis and Management of COPD. . 2020. https://goldcopd.org/gold-reports/. .
25.Rabe KF, Martinez FJ, Ferguson GT, et al. Triple Inhaled Therapy at Two Glucocorticoid Doses in Moderate-to-Very-Severe COPD. N Engl J Med. 2020;383(1):35-48. PubMed
26.Martinez FJ, Ferguson GT, Bourne E, et al. Budesonide/Glycopyrrolate/Formoterol Fumarate Metered Dose Inhaler Improves Exacerbation Outcomes in Patients with COPD without a Recent Exacerbation History: A Subgroup Analysis of KRONOS. International Journal of Copd. 2021;16:179-189. PubMed
27.Mattishent K, Thavarajah M, Blanco P, Gilbert D, Wilson AM, Loke YK. Meta-review: adverse effects of inhaled corticosteroids relevant to older patients. Drugs. 2014;74(5):539-547. PubMed
28.Maltais F, Ferguson GT, Feldman GJ, et al. A Randomized, Double-Blind, Double-Dummy Study of Glycopyrrolate/Formoterol Fumarate Metered Dose Inhaler Relative to Umeclidinium/Vilanterol Dry Powder Inhaler in COPD. Adv Ther. 2019;36(9):2434-2449. PubMed
29.Rabe KF, Martinez FJ, Ferguson GT, et al. Triple Inhaled Therapy at Two Glucocorticoid Doses in Moderate-to-Very-Severe COPD. N Engl J Med. 2020;383(1):35-48. PubMed
30.Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced All-Cause Mortality in the ETHOS Trial of Budesonide/Glycopyrrolate/Formoterol for Chronic Obstructive Pulmonary Disease. A Randomized, Double-Blind, Multicenter, Parallel-Group Study. Am J Respir Crit Care Med. 2021;203(5):553-564. PubMed
31.Mammen MJ, Lloyd DR, Kumar S, et al. Triple Therapy versus Dual or Monotherapy with Long-Acting Bronchodilators for Chronic Obstructive Pulmonary Disease. A Systematic Review and Meta-analysis. Ann Am Thorac Soc. 2020;17(10):1308-1318. PubMed
32.Magnussen H, Lucas S, Lapperre T, et al. Withdrawal of inhaled corticosteroids versus continuation of triple therapy in patients with COPD in real life: observational comparative effectiveness study. Respir Res. 2021;22(1):25. PubMed
33.Lipson DA, Crim C, Criner GJ, et al. Reduction in All-Cause Mortality with Fluticasone Furoate/Umeclidinium/Vilanterol in Patients with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2020;201(12):1508-1516. PubMed
34.Dunn LJ, Kerwin EM, DeAngelis K, Darken P, Gillen M, Dorinsky P. Pharmacokinetics of budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler formulated using co-suspension delivery technology after single and chronic dosing in patients with COPD. Pulm Pharmacol Ther. 2020;60:101873. PubMed
35.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
36.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2021 Feb 22.
37.Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, phase 3 randomised controlled trial. The Lancet Respiratory Medicine. 2018;6(10):747-758. PubMed
38.Kerwin EM, Ferguson GT, Mo M, DeAngelis K, Dorinsky P. Bone and ocular safety of budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler in COPD: a 52-week randomized study. Respir Res. 2019;20(1):167. PubMed
39.Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2021 report. Global Initiative for Chronic Obstructive Lung Disease; 2021: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf. Accessed 2021 April 23.
40.Cazzola M, MacNee W, Martinez FJ, et al. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J. 2008;31(2):416-469. PubMed
41.Jones PW FY. St. George's respiratory questionnaire manual [Internet]. Version 2.3. London (GB): St. George's University of London; 2009. https://www.sgul.ac.uk/about/our-institutes/infection-and-immunity/research-themes/research-centres/health-status/sgrq. Accessed 2021 April 23.
42.Nolan CM, Longworth L, Lord J, et al. The EQ-5D-5L health status questionnaire in COPD: validity, responsiveness and minimum important difference. Thorax. 2016;71(6):493-500. PubMed
43.Jones PW, Chen WH, Wilcox TK, Sethi S, Leidy NK. Characterizing and quantifying the symptomatic features of COPD exacerbations. Chest. 2011;139(6):1388-1394. PubMed
44.Baseline Dyspnea Index (BDI) & Transition Dyspnea Index (TDI) New York (NY): American Thoracic Society; 2014: https://www.thoracic.org/members/assemblies/assemblies/srn/questionaires/bdi-tdi.php. Accessed 2121 May 03.
45.Mahler DA, Witek TJ. The MCID of the Transition Dyspnea Index is a Total Score of One Unit. Copd. 2005;2(1):99-103. PubMed
46.Leidy NK, Murray LT. Patient-reported outcome (PRO) measures for clinical trials of COPD: the EXACT and E-RS. Copd. 2013;10(3):393-398. PubMed
47.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
48.Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128-1138. PubMed
49.Yii ACA, Loh CH, Tiew PY, et al. A clinical prediction model for hospitalized COPD exacerbations based on “treatable traits”. Int J Chron Obstruct Pulmon Dis. 2019;14:719-728. PubMed
50.EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. PubMed
51.EQ-5D User Guide, 2019. Rotterdam (NL): EuroQol Research Foundation; 2019. https://euroqol.org/publications/user-guides. Accessed 2021 Apr 24.
52.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
53.Leidy NK, Murray LT, Monz BU, et al. Measuring respiratory symptoms of COPD: performance of the EXACT- Respiratory Symptoms Tool (E-RS) in three clinical trials. Respir Res. 2014;15(1):124. PubMed
54.Leidy NK, Sexton CC, Jones PW, et al. Measuring respiratory symptoms in clinical trials of COPD: reliability and validity of a daily diary. Thorax. 2014;69(5):443-449. PubMed
55.Chronic obstructive pulmonary disease: use of the St. George's Respiratory Questionnaire as a PRO assessment tool: guidance for industry Silver Spring (MD): U.S. Food and Drug Administration; 2018: https://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm071575.pdf. Accessed 2021 Apr 24.
56.Niewoehner DE, Collins D, Erbland ML. Relation of FEV(1) to clinical outcomes during exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. Am J Respir Crit Care Med. 2000;161(4 Pt 1):1201-1205. PubMed
57.Chen CZ, Ou CY, Wang WL, et al. Using post-bronchodilator FEV1 is better than pre-bronchodilator FEV1 in evaluation of COPD severity. Copd. 2012;9(3):276-280. PubMed
58.Committee for Medicinal Products for Human Use (CHMP). Guideline on the requirements for clinical documentation for orally inhaled products (OIP) including the requirements for demonstration of therapeutic equivalence between two inhaled products for use in the treatment of asthma and chronic obstructive pulmonary disease (COPD) in adults and for use in the treatment of asthma in children and adolescents. London (GB): European Medicines Agency; 2009: https://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003504.pdf. Accessed 2021 Apr 24.
59.Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation. The St. George's Respiratory Questionnaire. Am Rev Respir Dis. 1992;145(6):1321-1327. PubMed
60.Meguro M, Barley EA, Spencer S, Jones PW. Development and Validation of an Improved, COPD-Specific Version of the St. George Respiratory Questionnaire. Chest. 2007;132(2):456-463. PubMed
61.Mahler DA, Weinberg DH, Wells CK, Feinstein AR. The measurement of dyspnea. Contents, interobserver agreement, and physiologic correlates of two new clinical indexes. Chest. 1984;85(6):751-758. PubMed
62.Witek TJ, Jr., Mahler DA. Minimal important difference of the transition dyspnoea index in a multinational clinical trial. Eur Respir J. 2003;21(2):267-272. PubMed
63.Eakin EG, Sassi-Dambron DE, Ries AL, Kaplan RM. Reliability and validity of dyspnea measures in patients with obstructive lung disease. Int J Behav Med. 1995;2(2):118-134. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–present)
Embase (1974–present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of Search: February 26, 2021
Alerts: Weekly search updates until project completion
Study Types: None applied.
Limits:
Publication date limit: None used.
Humans
Language limit: None used.
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase); |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq=# | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
Database(s): Embase 1974 to 2021 February 26, Ovid MEDLINE(R) ALL 1946 to February 26, 2021
Search Strategy:
exp budesonide/ or exp budesonide,formoterol fumarate drug combination/
(budesonide* or Q3OKS62Q6X).ti,ab,rn,nm,ot,kf.
exp glycopyrronium/
(glycopyrrolate* or glycopyrronium* or V92SO9WP2I).ti,ab,rn,nm,ot,kf.
exp formoterol fumarate/ or exp budesonide,formoterol fumarate drug combination/
(formoterol* or eformoterol* or 5ZZ84GCW8B or P3T5QA5J9N or W34SHF8J2K).ti,ab,rn,nm,ot,kf.
1 or 2
3 or 4
5 or 6
7 and 8 and 9
(breztri* or trixeo* or BGF MDI or bgfmdi or PT010).ti,ab,kf,rn,nm,ot.
10 or 11
(kronos* or ethos* or athena*).ti,ab,kf.
exp pulmonary disease, chronic obstructive/
(copd or (chronic adj2 obstructive adj2 (pulmonary or lung))).ti,ab,kf.
14 or 15
13 and 16
12 or 17
18 use medall
*budesonide/ or *budesonide plus formoterol/
budesonide*.ti,ab,kw,dq.
*glycopyrronium/ or *formoterol fumarate plus glycopyrronium bromide/
(glycopyrrolate* or glycopyrronium*).ti,ab,kw,dq.
*formoterol/ or *formoterol fumarate/ or *budesonide plus formoterol/ or *formoterol fumarate plus glycopyrronium bromide/
(formoterol* or eformoterol*).ti,ab,kw,dq.
20 or 21
22 or 23
24 or 25
26 and 27 and 28
(breztri* or trixeo* or BGF MDI or bgfmdi or PT010).ti,ab,kw,dq.
(kronos* or ethos* or athena*).ti,ab,kw.
Chronic obstructive lung disease/
(copd or (chronic adj2 obstructive adj2 (pulmonary or lung))).ti,ab,kw.
32 or 33
31 and 34
29 or 30 or 35
conference abstract.pt.
conference review.pt.
37 or 38
36 not 39
40 use oemezd
19 or 41
remove duplicates from 42
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search –(budesonide/ glycopyrrolate/ formoterol)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms -- (budesonide/ glycopyrrolate/ formoterol)]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- (budesonide/ glycopyrrolate/ formoterol)]
EU Clinical Trials
Register European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- (budesonide/ glycopyrrolate/ formoterol)]
Grey Literature
Search dates: February 22, 2021
Keywords: [(budesonide/ glycopyrrolate/ formoterol), chronic obstructive pulmonary disease]
Limits: Publication years: None used
Updated: Regulatory sections of search updated 3 weeks prior to the CDEC meeting
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool For Searching Health-Related Grey Literature (https://www.cadth.ca/grey-matters) were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
WANG, C., et al. (2020) | Irrelevant population (subgroup) |
HAN, M. K., et al. (2020) | Letter to the Editor |
DUNN, L. J., et al. (2020) | Irrelevant study design (phase I) |
CRANE, K., et al. (2020) | Review |
ICHINOSE, M., et al. (2019) | Irrelevant population (subgroup) |
ICHINOSE, M., et al. (2019) (efficacy) | Irrelevant population (subgroup) |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 28: Other Efficacy Outcomes for ETHOS
Outcomes | ETHOS | ||
|---|---|---|---|
BGF MDI 320 mcg-14.4 mcg-9.6 mcg (N = 2,137) | GFF MDI 14.4 mcg-9.6 mcg (N = 2,120) | BFF MDI 320 mcg-9.6 mcg (N = 2,131) | |
|||||||||||| | |||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |
|||||||||||| | |||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |
|||||||||||| | |||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |
|||||||||||| | |||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |
Morning pre-dose trough FEV1, 24 weeks | |||
Change from baseline (mL) over 24 weeks, LS mean (SE, 95% CI) | 111 (8.0, 95 to 127) | 76 (8.3, 60 to 93) | 35 (8.2, 19 to 51) |
LS mean difference (SE, 95% CI) | Reference group | 35 (11.5, 12 to 57) | 76 (11.4, 54 to 99) |
P value | 0.0025 | < 0.0001 | |
AUC0-4 = area under the curve from 0 to 4 hours post dose; BDI = Baseline Dyspnea Index; BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; CI = confidence interval; COPD = chronic obstructive pulmonary disease; EQ-5D-5L = EuroQol 5-Dimensions 5‑Levels questionnaire; FEV1 = forced expiratory volume in 1 second; GFF = glycopyrronium-formoterol fumarate; LS = least squares; LSM = least squares mean; MDI = metered-dose inhaler; mITT = modified intention to treat; PFT = pulmonary function test; RS = respiratory symptoms; SD = standard deviation; SE = standard error; VAS = visual analogue scale.
Source: ETHOS Clinical Study Report.
Table 29: Other Efficacy Outcomes for KRONOS
Efficacy outcomes | Modified ITT population (over 24 weeks) (N = 1,896) | BUD/FORM DPI 400-12 mcg (Symbicort TBH) | ||
|---|---|---|---|---|
BGF MDI 320 mcg-14.4 mcg-9.6 mcg (N = 639) | GFF MDI 14.4 mcg-9.6 mcg (N = 625) | BFF MDI 320 mcg-9.6 mcg (N = 314) | ||
|||||||||||| | ||||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |
BFF = budesonide-FORMOTEROL fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; CI = confidence interval; DPI = dry powder inhaler; EQ-5D-5L = EuroQol 5-Dimensions Questionnaire 5-Level; GFF = glycopyrronium-formoterol fumarate; SD = standard deviation; TBH = Turbuhaler; VAS = visual analogue scale.
Source: KRONOS Clinical Study Report.
Table 30: COPD-Related Health Care Resource Utilization Outcomes — ETHOS and KRONOS
Outcomes | ETHOS, mITT population | KRONOS, mITT population | |||||
|---|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 2,137) | GFF MDI 14.4 mcg- 9.6 mcg (N = 2,120) | BFF MDI 320 mcg- 9.6 mcg (N = 2,131) | BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 639) | GFF MDI 14.4 mcg- 9.6 mcg (N = 625) | BFF MDI 320 mcg- 9.6 mcg (N = 314) | Symbicort TBH 400-12 mcg (N = 318) | |
|||||||||||| | |||||||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; CCU = critical care unit; GFF = glycopyrronium-formoterol fumarate; ICU = intensive care unit; MDI = metered-dose inhaler; mITT = modified intention to treat; SD = standard deviation; TBH = Turbuhaler.
Source: ETHOS and KRONOS Clinical Study Report.
Table 31: Results of Subgroup Analysis of ETHOS Based on Prior Exacerbation History
Results | COPD exacerbation history: 1 | COPD exacerbation history ≥ 2 | ||||
|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg-9.6 mcg (N = 1,195) | GFF MDI 14.4 mcg-9.6 mcg (N = 1,211) | BFF MDI 320 mcg- 9.6 mcg (N = 1,217) | BGF MDI 320 mcg-14.4 mcg- 9.6 mcg (N = 1,195) | GFF MDI 14.4 mcg-9.6 mcg (N = 1,211) | BFF MDI 320 mcg-9.6 mcg (N = 1,217) | |
Rate of moderate or severe COPD exacerbations over 52 weeks a | ||||||
Patients with moderate or severe COPD exacerbations, n (%) | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Events, n | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Total time at risk, years | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Rate of exacerbations per year | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Adjusted rate (SE)b | |||||||||||| | |||||||||||| | |||||||||||| | 1.17 (0.05) | 1.60 (0.07) | 1.32 (0.06) |
Rate ratio (95% CI) | Reference group | |||||||||||| | |||||||||||| | Reference group | 0.73 (0.65 to 0.83) | 0.89 (0.79 to 1.01) |
P value | |||||||||||| | |||||||||||| | < 0.0001 | 0.0680 | ||
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; CI = confidence interval; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; mITT = modified intention to treat; SE = standard error; TBH = Turbuhaler.
Source: ETHOS Clinical Study Report.
Table 32: Results of Subgroup Analysis of ETHOS Based on Baseline Eosinophil Counts
Results | |||||||||||| | |||||||||||| | ||||
|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg-9.6 mcg (N = 860) | GFF MDI 14.4 mcg- 9.6 mcg (N = 847) | BFF MDI 320 mcg- 9.6 mcg (N = 837) | BGF MDI 320 mcg- 14.4 mcg-9.6 mcg (N = 1,195) | GFF MDI 14.4 mcg- 9.6 mcg (N = 1,211) | BFF MDI 320 mcg- 9.6 mcg (N = 1,217) | |
|||||||||||| | ||||||
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | ||
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; CI = confidence interval; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; SE = standard error; TBH = Turbuhaler.
Source: ETHOS Clinical Study Report.
Figure 29: A Forest Plot of the Rate of Moderate or Severe COPD Exacerbations by Baseline Blood Eosinophil Count Over 52 Weeks (ETHOS)
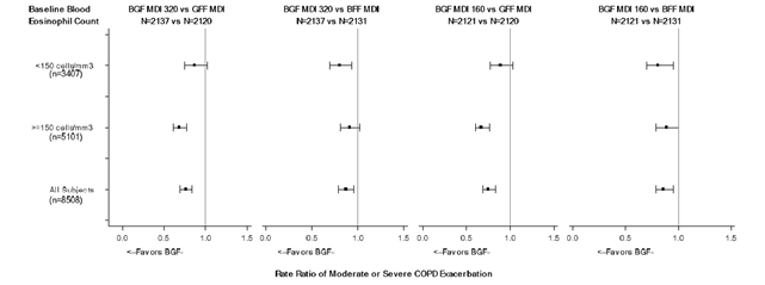
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; mITT = modified intent to treat; SE = standard error.
Source: ETHOS Clinical Study Reports.
Figure 30: A Forest Plot of the Rate of Moderate or Severe COPD Exacerbations by Prior Exacerbation History Over 52 Weeks (ETHOS)
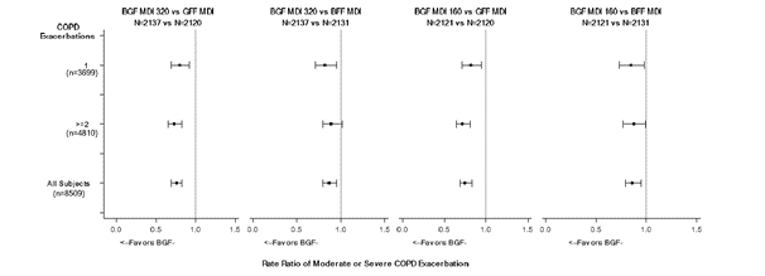
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; CI = confidence interval; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; SE = standard error.
Source: ETHOS Clinical Study Report.
Table 33: Results of Subgroup Analysis of KRONOS Based on Prior Exacerbation History
Results | COPD exacerbation history: 0 | COPD exacerbation history: 1 | COPD exacerbation history≥ 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 469) | GFF MDI 14.4 mcg- 9.6 mcg (N = 473) | BFF MDI 320 mcg- 9.6 mcg (N = 235) | Symbicort TBH 400 mcg- 12 mcg (N = 234) | BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 125) | GFF MDI 14.4 mcg- 9.6 mcg (N = 108) | BFF MDI 320 mcg- 9.6 mcg (N = 61) | Symbicort TBH 400 mcg- 12 mcg (N = 59) | BGF MDI 320 mcg- 14.4 mcg- 9.6 mcg (N = 45) | GFF MDI 14.4 mcg- 9.6 mcg (N = 44) | BFF MDI 320 mcg- 9.6 mcg (N = 18) | Symbicort TBH 400- 12 mcg (N = 25) | |
Rate of moderate or severe COPD exacerbations over 24 weeks | ||||||||||||
Patients with moderate or severe COPD exacer-bations, n (%) | 72 (15.4) | 105 (22.2) | 38 (16.2) | 37 (15.8) | 18 (14.4) | 34 (31.5) | 21 (34.4) | 18 (30.5) | 18 (40.0) | 18 (40.9) | 6 (33.3) | 6 (24.0) |
Events, n | 85 | 147 | 42 | 47 | 23 | 54 | 24 | 24 | 24 | 27 | 8 | 6 |
Total time at risk, years | 199.62 | 195.85 | 98.57 | 98.93 | 54.97 | 43.79 | 23.75 | 23.66 | 17.56 | 16.45 | 7.14 | 10.98 |
Rate of exacer-bations per year | 0.43 | 0.75 | 0.43 | 0.48 | 0.42 | 1.23 | 1.01 | 1.01 | 1.37 | 1.64 | 1.12 | 0.55 |
Adjusted rate (SE)a | 0.41 (0.05) | 0.80 (0.09) | 0.42 (0.08) | 0.47 (0.08) | 0.21 (346.66) | 0.64 (1,055.05) | 0.48 (799.96) | 0.49 (819.93) | 1.31 (0.39) | 1.81 (0.51) | 1.30 (0.59) | 0.47 (0.23) |
Rate ratio (95% CI) | Reference group | 0.52 (0.37 to 0.72) | 0.98 (0.63 to 1.54) | 0.88 (0.57 to 1.36) | Reference group | 0.33 (0.18 to 0.59) | 0.43 (0.22 to 0.87) | 0.42 (0.21 to 0.85) | Reference group | 0.72 (0.33 to 1.59) | 1.01 (0.35 to 2.88) | 2.81 (0.93 to 8.44) |
P value | 0.0001 | 0.9384 | 0.5710 | 0.0002 | 0.0193 | 0.0163 | 0.4218 | 0.9867 | 0.0660 | |||
BFF = budesonide-formoterol fumarate; BGF = budesonide-glycopyrronium-formoterol fumarate; COPD = chronic obstructive pulmonary disease; CI = confidence interval; GFF = glycopyrronium-formoterol fumarate; MDI = metered-dose inhaler; mITT = modified intention to treat; SE = standard error; TBH = Turbuhaler.
aTreatments are compared adjusting for baseline post-bronchodilator percent predicted FEV1 and baseline eosinophil count as continuous covariates and country, and inhaled corticosteroid use at screening (yes/no) as categorical covariates using negative binomial regression. Time at risk of experiencing an exacerbation is used as an offset variable in the model.
Source: KRONOS Clinical Study Report.
Table 34: Results of Subgroup Analysis of KRONOS Based on Baseline Eosinophil Counts
|||||||||||| | |||||||||||| | |||||||||||| |
|---|---|---|
|||||||||||| | |||||||||||| | |||||||||||| |
|||||||||||| | |||||||||||| | |||||||||||| |
Table 34 was removed at the request of the sponsor because it contained confidential information.
Treatments are compared adjusting for baseline post-bronchodilator percent predicted FEV1 and baseline eosinophil count as continuous covariates and baseline COPD exacerbation history (0, 1, ≥ 2), country, and ICS use at screening (yes or no) as categorical covariates using negative binomial regression. Time at risk of experiencing an exacerbation is used as an offset variable in the model.
Figure 31: Forest Plot of Moderate or Severe COPD Exacerbations by Baseline Blood Eosinophil Count Over 24 Weeks (KRONOS)

Figure 31 was removed at the request of the sponsor because it contained confidential information.
Figure 32: Forest Plot of Morning Pre-Dose Trough FEV1 (mL) (With 95% CI) by Baseline Blood Eosinophil Count Over 24 Weeks (KRONOS)

Figure 32 was removed at the request of the sponsor because it contained confidential information.
Figure 33: Forest Plot of FEV1 AUC0-4 (mL) (With 95% CI) by Baseline Blood Eosinophil Count Over 24 Weeks (KRONOS)

Figure 33 was removed at the request of the sponsor because it contained confidential information.
Appendix 4: Validity of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To summarize the validity of the following outcome measures:
EQ-5D-5L
EXACT-RS
FEV1
SGRQ
TDI
Findings
EuroQol 5-Dimensions 5-Levels Questionnaire
The EQ-5D-5L was developed by the EuroQol Group, a network of international multidisciplinary researchers devoted to the measurement of health status. It is a generic, self-reported health status assessment tool which measures the respondent’s immediate situation, in 2 parts, the EQ-5D descriptive system and the EQ VAS. The descriptive system consists of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 5 levels, ranging from 1 “no problem” to 5 “extreme problems.” Each state is reported as a 5-digit code, e.g., 23345, which is interpreted as slight problems with mobility, moderate problems with self-care and usual activities, severe problems with pain/discomfort, and extreme problems with anxiety/depression. EQ-5D health states which are defined by the descriptive system can be converted into a single utility index using a weighted formula of utilities which are specific to population and disease; the summary index can be used to calculate quality-adjusted life-years. The EQ VAS records the respondent’s self-rated health on a vertical VAS where the end points are 100 “best imaginable health state” and 0 “worst imaginable health state.” The EQ VAS scores are patient-based and not representative of the general population.50
The construct validity of the EQ-5D-5L was investigated in a cross-sectional cohort of 625 stable outpatients with COPD, of whom 616 had complete data.42 Patients were a mean 70.4 years old, with mean predicted FEV1 of 46.1%. The EQ-5D-5L, CAT, SGRQ, Clinical COPD Questionnaire (CCQ), CRQ, and Medical Research Council Dyspnea Scale (MRC) were measured and severity calculated by the ADO (age, dyspnea, airflow obstruction) index. There was moderate correlation between the EQ-5D-5L utility score and the disease-specific total scores and most subscales, with Pearson correlation coefficients with CAT of −0.528, with SGRQ total score of −0.623 (subscales −0.257 to −0.603), with CCQ total of −0.626 (subscales −0.483 to −0.674) and with CRQ total score of 0.709 (subscales 0.403 to 0.593).42 Correlation with the EQ VAS was low, with Pearson correlation coefficients with CAT of −0.428, with SGRQ total score of −0.469 (subscales −0.283 to −0.457), and with CCQ total of −0.483 (subscales −0.382 to −0.459).42
The responsiveness of the EQ-5D-5L was investigated in 400 patients undergoing pulmonary rehabilitation, of whom 324 had both baseline and 8-week measurements.42 Ceiling effects were reported, with 6% and 11% of patients reporting a maximum utility score (1.0) before and after rehabilitation, and 3% and 4% reporting a maximum EQ VAS score (100.0) before and after rehabilitation, respectively. The standardized response means were 0.39 and 0.44 for the utility scores and EQ VAS, respectively. Change in EQ-5D-5L utility index and VAS were not considered to be correlated with change in SGRQ total and symptom scores and CAT, with a Pearson correlation coefficient < 0.30. Correlation for change in EQ-5D-5L utility index and change in CRQ total score was low, 0.40 (subscales 0.25 to 0.39); correlation coefficient for change in EQ VAS and change in CRQ total score was 0.38 (subscales 0.30 to 0.32).42
EQ-5D-5L has been validated in a diverse patient population in 6 countries.51 The MCID estimates for the index score in the Canadian population have a summarized mean (SD) of 0.056 (0.011), and a summarized median of 0.056 (interquartile range 0.049 to 0.063).52 The MCID for the utility index and the EQ VAS were estimated using a variety of methods, including SD and anchor-derived estimates based on the CRQ total score and mastery and emotion subscales, in the above patient population.42 Estimates for the MCID of EQ-5D-5L utility score ranged from 0.037 (CRQ total, ROC, as anchors) to 0.109 (distribution, 0.5 SD), and those for EQ VAS from 6.5 (anchored to CRQ total, using ROC methods) to 10.1 (distribution, 0.5 SD).42
Exacerbations of Chronic Pulmonary Disease Tool—Respiratory Symptoms
The EXACT-RS score measures the effect of treatment on the severity of respiratory symptoms of COPD. It is based on the 11 respiratory symptom items of the EXACT, a 14-item daily patient diary intended to track exacerbations.53 Besides the total score, the E-RS has 3 symptom subscales: RS-Breathlessness (5 items), RS-Cough and Sputum (3 items), and RS-Chest Symptoms (3 items). Responses are according to a 5-point integer scale with descriptors that vary according to the subscale. Summation of items produces the total score and subscales. The RS-Total score ranges from 0 to 40, RS-Breathlessness ranges from 0 to 17, RS-Cough and Sputum ranges from 0 to 11, and RS-Chest Symptoms ranges from 0 to 12. In all cases, higher scores indicate more severe symptoms.
Reliability, construct validity, and responsiveness of E-RS were assessed in post-hoc analyses of 188 stable patients from a prospective study of COPD,54 and from 3 clinical trials (Mpex, AZ 1, and AZ 2) in COPD patients, with available data from 235, 749, and 597 trial patients, respectively.53 At baseline, the percentage of patients in the prospective study with mMRC dyspnea score 3 or 4 was 29.3%.54 At baseline, the percentage of trial patients with GOLD stage III or IV was 66.0%, 27.8%, and 44.3% in Mpex, AZ 1, and AZ 2, respectively.53
In the 3 trials, internal consistency for weekly measurements, measured by Cronbach alpha, was high for RS-Total, RS-Breathlessness, and RS-Chest Symptoms scales (0.90 to 0.96), and lower for cough and sputum (0.58 to 0.78).53 Reproducibility for weekly measurements, as measured by intraclass correlation coefficient [ICC], was acceptable, ranging from 0.69 to 0.74 for all scales and trials, with the exception of RS-Cough and Sputum, for the Mpex trial (0.58).53
Construct validity was assessed by correlation with measures of health status (SGRQ53,54), respiratory symptoms (breathlessness and cough and sputum scales),54 SGRQ-C,54mMRC59), airway obstruction (FEV1),53,54 and use of rescue medication.53,54 In the prospective observational study, RS-Total was highly correlated with the SGRQ total score (0.75), the correlation of the subscales of both with each other was as expected, with correlations > 0.4 for all except RS-Cough and Sputum and RS-Chest Symptoms with SGRQ Activity. Correlation of the RS and subscales with the mMRC was lower (0.33 and 0.16 to 0.38), as were correlations with rescue medication use, and percent predicted FEV1.54 In the trials, RS-Total was highly correlated with the breathlessness, cough, and sputum total score in AZ1 and AZ2 (Spearman’s rank-order correlation 0.89 in both), with correlations for individual subdomains of 0.75 to 0.92.53 RS-Total was correlated with the SGRQ total score for the Mpex trial (Spearman’s rank-order correlation 0.65), with correlations for the individual subdomains of 0.45 to 0.60.53 RS-Total score was correlated with SGRQ-C in AZ1 and AZ2 (Spearman’s rank-order correlation 0.51 to 0.54), with correlations for the individual subdomains of 0.41 to 0.52.53 Correlation of the E-RS with FEV1 was low; for the RS-Breathlessness scale, Spearman’s rank-order correlation ranged from −0.17 to −0.32. Correlation of E-RS total score and RS-Breathlessness with use of rescue medication was moderate, with Spearman’s rank-order correlation ranging from 0.42 to 0.43 in AZ1 and AZ2. The strength of correlation conformed to the authors’ pre-specified expectations, leading them to conclude that the construct was valid.
Responsiveness was assessed in the 3 trials. For patients whose health status improved from baseline to 3 months (change in SGRQ ≥ 4), E-RS total scores declined by an average −2.5 to −3.5. For those whose symptoms improved (BCSS ≥ 1), E-RS total scores declined by an average −6.53
One study of 188 patients used a distributional method (0.5 SD of the sample mean) to estimate the MCID of the RS-Total, 3.35; RS-Breathlessness,1.85; RS-Cough and Sputum, 1.15; and RS-Chest Symptoms, 1.05.54 In the 3 trials, 0.5 SD of the sample means were calculated as RS-Total, 2.97 to 3.00; RS-Breathlessness, 1.56 to 2.97; RS-Cough and Sputum, 0.78 to 1.04; and RS-Chest Symptoms, 0.96 to 1.04.53
One-Second Forced Expiratory Volume
FEV1 is the volume of air that, after a full inspiration, can be forcibly expired in 1 second. It is commonly used both in clinical practice and in clinical trials and has been correlated with treatment failure (death, intubation, readmission for COPD, or intensification of drug therapy) in hospitalized patients.55,56 In clinical practice, FEV1 is used to grade risk of death in COPD patients.57 The generally accepted clinically important change in FEV1 is between 0.10 L and 0.14 L.40 There is evidence that for patients who are undergoing COPD exacerbation, a 2-day increase of 0.10 L reduced the odds of treatment failure (odds ratio 0.80 95% CI 0.69 to 0.92).56
While both pre- and post-bronchodilator FEV1 values have been reported to be indicators of health status, risk of death, and measure of severity in COPD, the Global Initiative for Chronic Lung Disease (GOLD) criteria, indicates that post-bronchodilator values should be used.57 This is supported by evidence from a prospective study of 300 patients with COPD who were followed for at least 1.5 years and who were evaluated every 3 months until the end of the study.57 Predictors of mortality were analyzed. While FEV1, body mass index, dyspnea score, and several other factors were shown to be predictors of mortality, multivariate analyses showed that post-bronchodilator percent predicted FEV1 was a significant independent predictor of both all-cause mortality and respiratory-cause mortality; whereas the pre-bronchodilator percent predicted FEV1 was not. The all-cause mortality P = 0.008 versus 0.126; respiratory-cause mortality P = 0.016 versus 0.302). Furthermore, with respect to GOLD classifications of disease severity, the discriminative ability of the GOLD severity classification was higher using post-bronchodilator than with pre-bronchodilator percent predicted FEV1 (P = 0.009 versus 0.131).
Normalized AUC FEV1 is an average of the measurement of bronchodilatation over at least 80% of the duration of action after a single inhalation.58 No information regarding the MCID was identified.
St. George's Respiratory Questionnaire COPD (SGRQ-C)
The SGRQ is a disease-specific measure of HRQoL that was specifically developed for patients with airways obstruction.59 The COPD-specific version (SGRQ-C) was derived from it, using a Rasch analysis of the responses of a sample (n = 893) of COPD patients to identify items with the weakest measurement properties.60 The number of items was reduced from 50 to 40, corrections were made to reduce disordered responses, wording was modified, and recall period was no longer specified.60 The scoring algorithm was revised to produce scores directly comparable to the SGRQ.
The SGRQ-C questionnaire is intended for supervised self-administration. It contains 14 questions and 40 items grouped into 3 domains, Symptoms, Activity, and Impacts. Part 1 (7 items) measures the frequency of respiratory symptoms and contributes to a symptoms score. For 6 questions, patients select a response from a 3-to-5-item scale (e.g., from “not at all” to “most days”). The seventh question has a “yes/no” response. Part 2 (7 items) addresses the patient’s current state, and divides into an Activity score that measures the effect on daily physical activity, and an Impacts score that addresses psychosocial functioning.41,60 Two questions have a single response, and for the rest, patients select all the responses that apply.41Items are weighted using empirically derived weights. The SGRQ-C total score, and the 3 symptom scores are calculated by summation of the weighted items and calculation of the percentage of the maximum possible score for the total score or subscale, producing values that ranges from 0 to 100, where 0 indicates no impairment and 100 indicates worst possible health.41
Assessment of psychometric properties proceeded throughout the revision process. Correlation between the original SGRQ score and the revised SGRQ score (following removal of items and calculation of rescaling, prior to rewording and removal of recall period) was assessed using data from the original SGRQ validation study, 152 patients, mean percent predicted FEV1, 53.5%. Correlation was very high (ICC = 0.99).60
Construct validity and reliability for the revised SGRQ score were assessed using data from the original SGRQ validation study,60 against measures for respiratory function (FEV1 and FVC), physical function (6-minute walk distance), symptoms (MRC dyspnea grade, cough/phlegm, daily wheeze), global health (sickness impact profile and global health) and anxiety (Hospital Anxiety and Depression Scale [HADS]). Correlation between the revised SGRQ total score and the MRC dyspnea grade, and the SGRQ Activity subscale and MRC dyspnea grade were high (0.70 to 0.72).Moderate correlations were seen between the revised SGRQ total score and the HADS anxiety, 6-minute walk distance, and global health (absolute value 0.56 to 0.68), the SGRQ Impacts subscale with 6-minute walk test, MRC dyspnea grade, HADS anxiety, Sickness Impact Profile total, and global health were moderate (absolute value 0.59 to 0.64); and the SGRQ Activity score and the 6-minute walk distance, MRC dyspnea grade, Sickness Impact Profile total, and global health (absolute value of 0.55 to 0.72). Other correlations were low or absent.60 Reliability was assessed for this group of patients and a second described subsequently in the section on responsiveness (n = 196) as excellent, SGRQ total score 0.99 and 0.98, SGRQ Symptoms 0.96 and 0.93, SGRQ Activity 0.99 and 0.98, and SGRQ Impacts 0.98 and 0.97.60
Construct validity and reliability for the SGRQ-C score (following rewording) were assessed for a group of 63 COPD patients involved in pulmonary rehabilitation programs, 70 years old, percent predicted FEV1 of 47%.60 Moderate correlations were seen between SGRQ total score and HADS depression and global health, between SGRQ-C Activity and MRC dyspnea grade, and between SGRQ Impacts, and HADS depression. Correlation was low or not identified for the other measures. The pattern of correlation was similar between the original SGRQ and the SGRQ-C.60 Reliability for the SGRQ-C score in this group of patients was excellent for total score, Activity, and Impacts (0.91 to 0.95), and slightly lower for Symptoms (0.80).
Responsiveness of the revised SGRQ score was assessed using data from a clinical trial of salmeterol versus placebo involving 169 COPD patients, mean age 62 years and percent predicted FEV1 of 46%.60 Mean change scores were very similar between original and revised SGRQ scores. Greater improvement between baseline and 16 weeks was measured in patients receiving salmeterol , with statistically significant differences between treatment groups for SGRQ total score (mean change: salmeterol = −5.5 [SD, 13.1], placebo = −1.1 [SD, 11.6]; P = 0.04) and SGRQ Impacts (mean change: salmeterol = −6.4 [SD, 17.0], placebo = −0.1 [SD, 15.8]; P = 0.02), but not for the other 2 subscales.60
The generally accepted MCID for a change in total SGRQ from baseline is 4.0 units, and a decrease in score indicates an improvement in HRQL.40 The scoring of the SGRQ-C was adjusted to give scores equivalent to the SGRQ.60 In the manual of the SGRQ-C an MCID of 4.0 units is used for the within-group comparison, as well as the between-group comparison.41 No MCID was reported for the domain scores.
Baseline Dyspnea Index and Transition Dyspnea Index
The BDI and TDI are interviewer-administered multidimensional indices used to measure the severity of dyspnea. The BDI measures dyspnea at a single time point and the TDI measures change from baseline dyspnea as measured by the BDI.44,61 Both the BDI and TDI consist of 24 items in 3 domains: functional impairment, magnitude of task, and magnitude of effort assessed in BDI, and the changes from baseline in functional impairment, magnitude of task, and magnitude of effort in TDI. Functional impairment assesses the impact of breathlessness on the ability to carry out activities, magnitude of task determines the type of task causing breathlessness, and magnitude of effort determines the level of effort resulting in breathlessness.62 At baseline, assessed by BDI, each domain is scored from grade 0 to grade 4, where grade 0 indicates the worst affected and grade 4 indicates no effect.61 Three additional non-numeric items are available to capture reasons that a domain cannot be scored.61 The numeric domain scores are summed to produce a BDI focal score ranging from 0 to 12, with lower score indicating more severe dyspnea. Changes from baseline in dyspnea are assessed by TDI. Each domain in TDI is rated from −3 (major deterioration) to +3 (major improvement), with 1 non-numeric item available to capture further impairment for reasons other than dyspnea. The ratings for each of the 3 categories are summed to form a total TDI score ranging from −9 to +9. Lower TDI score indicates more deterioration in severity of dyspnea.
Test-retest reliability, internal consistency, and construct validity were assessed in 143 COPD patients recruited for a clinical trial, aged 40 to 86, with FEV1 0.3 to 3.53 L.63 Construct validity and responsiveness were assessed in 2 identically designed clinical trials of treatment in patients with COPD, involving 1,207 patients who were predominately male (around 75%) and had percent predicted FEV1 of 39.4% to 41.0% (depending on treatment group).63
The test-retest reliability for the BDI was 0.76 (r), and internal consistency alpha was 0.80. For both, a value greater than 0.70 is considered reasonable evidence of reliability or internal consistency.63
Construct validity for the BDI was assessed in the first study by correlation against other dyspnea measures administered to the same patients. Correlation was high for the University of California San Diego (UCSD) Shortness of Breath questionnaire (−0.70) and moderate for the American Thoracic Society Dyspnea Scale, the Oxygen Cost Diagram, and the VAS for the past week (−0.50 to −0.59).63 In the second study, construct validity for the BDI was assessed against measures of health status (SGRQ62), symptoms (dyspnea diary [DD]62), and pulmonary function (FEV1 and FVC62). Correlation between BDI and SGRQ total score was good, Pearson’s correlation coefficient −0.64, with correlation between BDI and SGRQ subscales −0.35 (SGRQ Symptom) to −0.63 (SGRQ activity). Correlation between DD score at baseline and respiratory function tests was lower, −0.34 and 0.25 to 0.31, respectively.62
Responsiveness of the TDI was assessed against changes in the SGRQ total score and subscales, DD, FEV1, and FVC, and the physician global assessment. Changes in SGRQ total score was moderately correlated with TDI (Pearson’s correlation coefficient of −0.40), with correlation between TDI and changes in SGRQ subscales −0.32 to −0.33.62 Correlation between BDI and changes in DD score, respiratory function, and Physician’s Global Evaluation (PGE) were low, −0.29 to 0.28.62 When patients are classified as responders (at least a 1-unit improvement) and non-responders, there was a statistically significant difference between groups in use of rescue medication, and a clinically meaningful difference in SGRQ (4 units).62
For the population in the clinical trials described above (75% male, moderate COPD), MCID was estimated by an anchor-based approach, relative to the PGA. A mean TDI score of one unit corresponded to clinically significant PGE changes of 1 to 2 points.62
Table 35: Summary of Outcome Measures and Their Measurement Properties
Instrument | Type | Evidence of validity | MCID | References |
|---|---|---|---|---|
EQ-5D-5L | A generic, self-reported measure of HRQL that contains the EQ-5D descriptive system and the EQ VAS. The descriptive system contains 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression; each dimension has 5 levels. A single summary index can be generated for the descriptive system. The EQ VAS score ranges from 0 to 100. | Yes | EQ-5D-5L utility score 0.037 to 0.109 EQ VAS 6.5 to 10.1. | EQ-5D-5L42 |
EXACT-RS | A patient-reported outcome scale utilizing 11 respiratory symptom items, derived from the validated 14-item EXACT scale. | Yes | 3.35a | |
FEV1 | FEV1 is the volume of air that, after a full inspiration, can be forcibly expired in 1 second. | Yes | 0.10 L to 0.14 L | FEV140 |
SGRQ-C | SGRQ-C is a disease-specific measure of HRQL that consists of 14 questions and 40 items. The questionnaire is divided into 3 dimensions: Symptoms, Activity, and Impacts of the disease. Scores for the total score and individual dimension ranges from 0 to 100, where 0 indicates no impairment and 100 indicates greatest impairment. | Yes | 4 units | |
TDI | TDI is used to measure change from baseline dyspnea as measured by the BDI and consists of 24 items measuring 3 categories: functional impairment, magnitude of task, and magnitude of effort. Items are rated in 7 grades ranging from −3 (major deterioration) to +3 (major improvement), where lower scores indicate more deterioration in the severity of dyspnea from baseline. | Yes | 1 unit |
CAT = COPD Assessment Test; EQ-5D-5L = EuroQol 5-Dimensions 5-Levels questionnaire; EQ VAS = EuroQol Visual Analogue Scale; EXACT-RS = Exacerbations of Chronic Pulmonary Disease Tool—Respiratory Symptoms; FEV1 = forced expiratory volume in 1 second; SGRQ = St. George's Respiratory Questionnaire; TDI = Transition Dyspnea Index.
aThis MCID was estimated using a distribution based method using data from a single study.59
Pharmacoeconomic Review
Abbreviations
BGF
budesonide-glycopyrronium-formoterol fumarate
COPD
chronic obstructive pulmonary disease
DPI
dry powder inhaler
FF
fluticasone furoate
ICS
inhaled corticosteroid
LABA
long-acting beta2-agonist
LAMA
long-acting muscarinic antagonist
MDI
metered-dose inhaler
ODB
Ontario Drug Benefit
UME
umeclidinium
VI
vilanterol
Executive Summary
At the submitted price of $127.00 per 120-dose inhaler, the average annual cost of treatment with the budesonide-glycopyrronium-formoterol fumarate metered-dose inhaler (BGF MDI 320, Breztri) is $1,545 per patient. Assuming equal efficacy and safety with fluticasone furoate-umeclidinium-vilanterol dry powder inhaler (FF-UME-VI DPI, Trelegy) and with available inhaled corticosteroid plus long-acting beta2-agonist (ICS-LABA) plus long-acting muscarinic antagonist (LAMA) combinations, the sponsor conducted a cost-minimization analysis over a 1-year time horizon comparing the costs of BGF MDI 320 with FF-UME-VI DPI and a weighted-average cost of available ICS-LABA plus LAMA combinations.
CADTH identified the following limitations with the sponsor’s submission:
The assumption of clinical similarity between comparators is associated with some uncertainty.
The use of a weighted-average class comparator was inappropriate.
LABA-LAMA plus ICS combinations are potentially relevant comparators in some jurisdictions.
When considering only drug costs (i.e., excluding dispensing fees and markups), and assuming similar efficacy and safety among included comparators, the annual per-patient drug-acquisition cost of BGF MDI 320 ($1,545) is $63 less expensive than FF/UME/VI DPI ($1,608) and $200 less than budesonide-formoterol plus glycopyrronium ($1,745), the combination of 2 inhalers with the same component medications as BGF MDI 320. When considering dispensing fees and markups (based on Ontario estimates), the annual cost of BGF MDI 320 ($1,776 per patient) is $237 more than that of the least expensive ICS-LABA plus LAMA combination (range: $1,580 to $2,888 per patient). The use of a single inhaler for triple therapy is associated with a reduction in dispensing fees compared with combinations of 2 inhalers, potentially saving 12 fees per year when dispensed monthly. Of note, all analyses are based on publicly available list prices and may not represent actual costs paid by plans.
Economic Review
The current review is for BGF MDI 320 (Breztri Aerosphere) for patients with chronic obstructive pulmonary disease (COPD).
Economic Information
Summary of Sponsor’s Economic Information
The sponsor submitted a cost-minimization analysis of BGF MDI 320 compared with the other available ICS-LAMA-LABA inhaler, and compared with a weighted-average cost of ICS-LABA plus LAMA (open) triple-therapy combinations approved in Canada.1 The sponsor excluded ICS plus LABA-LAMA triple-therapy combinations, as ICS therapies are not indicated for COPD except as part of combination products. The analysis population was aligned with the Health Canada indication and reimbursement request, in which BGF MDI 320 is indicated for long-term maintenance treatment to reduce exacerbations of COPD and the treatment of airflow obstruction related to COPD, including chronic bronchitis and/or emphysema, for patients who are not adequately treated by an ICS-LABA or LAMA-LABA combination.2
All triple-combination therapies were assumed to have equal efficacy and safety on the basis of the submitted network meta-analysis3 and clinical expert opinion. As such, resource use and costs, including exacerbation management, adverse event management, and rescue medication, as well as clinical benefits, were assumed to be equivalent and not included. While the sponsor’s cost-minimization analysis included health states, as the base case assumed that discontinuation and mortality were zero for all treatments over a 1-year time horizon, there were no transitions between health states. Only the drug costs associated with each triple therapy were considered. Drug-acquisition costs for other ICS-LAMA-LABA and ICS-LABA plus LAMA combination therapies were based on Ontario Drug Benefit (ODB) Formulary prices4 and included an 8% markup and an $8.83 dispensing fee per inhaler every 30 days. The cost of ICS-LABA plus LAMA therapy was based on the weighted-average cost of each class, as determined with IQVIA Pharmastat claims data (Table 4).1
When markups and dispensing fees were included, the sponsor’s results indicated that the use of BGF MDI 320 is associated with a savings of $68.37 per patient per year when compared with FF-UMEC-VI, the other available ICS-LAMA-LABA inhaler (Table 1). When compared with the weighted-average cost of ICS-LABA plus LAMA combinations, BGF MDI 320 led to a savings of $381.65 per patient per year, with $253.87 of that amount due to drug-acquisition cost savings, and $107.47 due to a reduced number of dispensing fees associated with the use of a single inhaler per 30-day supply rather than 2.
Table 1: Summary of the Sponsor’s Economic Evaluation Results
Drug | Drug costs only | Drug costs including fees and markupsa | ||
|---|---|---|---|---|
Total costs ($) | Incremental costs vs. BGF MDI 320 ($)b | Total costs ($) | Incremental costs vs. BGF MDI 320 ($)b | |
BGF MDI 320 (Breztri) | 1,546 | Reference | 1,777 | Reference |
FF-UME-VI DPI (Trelegy) | 1,610 | 63 | 1,846 | 68 |
ICS-LABA + LAMA weighted-average cost | 1,800 | 254 | 2,159 | 382 |
BGF = budesonide-glycopyrronium-formoterol fumarate; DPI = dry powder inhaler; FF-UME-VI = fluticasone furoate-umeclidinium-vilanterol; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; MDI = metered-dose inhaler.
aDispensing fees are assumed to be $8.83 per product per 30 days; the markup is 8%, consistent with that allowed by the Ontario Drug Benefit.4
bIncremental costs are BGF MDI 320 minus the comparator. Negative incremental costs indicated BGF MDI 320 is less expensive.
The sponsor also conducted scenario analyses testing alternative assumptions. Altering the distribution of ICS-LABA plus LAMA therapies to that of the Ontario BALLISTIC study reduced the cost savings associated with BGF MDI 320 from $382 per patient per year to $326, while in a scenario considering a 30-year time horizon and incorporating COPD age-adjusted mortality rates and discontinuation, BGF MDI 320 was associated with a savings of $248 when compared with FF-UME-VI DPI and a savings of $1,386 when compared with the weighted-average cost of ICS-LABA plus LAMA therapies.
CADTH Appraisal of the Sponsor’s Economic Information
CADTH identified several key limitations of the sponsor’s analysis that have notable implications on the economic analysis:
Clinical similarity to other triple-therapy combinations is associated with uncertainty: The sponsor’s analysis assumes clinical similarity between BGF MDI 320 and other ICS-LAMA-LABA and ICS-LABA plus LAMA combinations. BGF MDI 320 was not directly compared with another triple therapy in clinical trials; however, the sponsor conducted a network meta-analysis3 that compared BGF MDI 320 with FF-UME-VI DPI (Trelegy), beclomethasone dipropionate-formoterol-glycopyrronium (Trimbow; not available in Canada), and several open triple therapies (see Indirect Evidence section of the CADTH Clinical Review Report). BGF MDI 320 likely showed similar or comparable efficacy and safety compared with other triple therapies, with notable limitations inherent with indirect comparison. As such, there is some uncertainty with the assumption of clinical similarity required for a cost-minimization analysis or cost comparison.
CADTH was unable to account for this limitation in reanalysis.
Weighted-average comparator is inappropriate: Given the range of daily costs among ICS-LABA combinations in particular, the use of weighted-average costs by class (ICS-LABA plus LAMA) does not appropriately reflect the range in daily costs of ICS-LABA plus LAMA combinations. Additionally, the use of weighted-average costs implies that current market shares, as estimated by the sponsor, will remain stable over time, and thus the relative cost of BGF MDI 320 within these classes will also remain stable.
CADTH compared the daily and annual cost of BGF MDI 320 with all available ICS-LABA plus LAMA combinations individually.
Missing comparators of potential interest: While ICS inhalers are not indicated by Health Canada for use in patients with COPD, and current COPD guidelines5,6 do not endorse their use, the clinical expert consulted by CADTH indicated that with the current availability of LABA-LAMA inhalers, patients needing triple therapy who are not adequately controlled on a LABA-LAMA inhaler may be escalated to a LABA-LAMA plus ICS combination. The clinical expert further indicated that the use of an independent ICS inhaler allows for more individualization of ICS dose than the use of an ICS-LABA plus LAMA combination; thus, a separate ICS inhaler may be preferred by some clinicians or patients. For jurisdictions that reimburse ICS inhalers as a general benefit, depending on local patterns of prescribing, LABA-LAMA plus ICS combinations may be relevant economic comparators for BGF MDI 320.
CADTH compared the daily and annual cost of BGF MDI 320 with available LABA-LAMA plus ICS combinations in an exploratory analysis.
CADTH Reanalyses of the Economic Information
In addition to the sponsor’s FF-UM-VI DPI comparison, CADTH reanalyses included:
a simplification of the analysis to a cost comparison over a 1-year time horizon and assumptions of similar clinical efficacy, harms, subsequent therapies, and non-drug costs
a comparison of BGF MDI 320 with each available ICS-LABA plus LAMA combination
an exploratory analysis comparing the cost of BGF MDI 320 with available LABA-LAMA plus ICS combinations
A cost comparison of BGF MDI 320 against all available ICS-LABA plus LAMA combinations can be found in Table 2. Costs of ICS-LABA plus LAMA combinations ranged from $1,226 to $2,461 per patient per year. At $1,545 per patient per year, BGF MDI 320 is less expensive than all combinations that include budesonide-formoterol, fluticasone furoate-vilanterol, or fluticasone propionate-salmeterol MDI, but more expensive than combinations that include fluticasone propionate-salmeterol inhalation powder due to its availability in a generic formulation. Annual costs of individual components can be found in Table 5.
Of particular interest are the comparisons with FF-UME-VI DPI (Trelegy), the other available ICS-LAMA-LABA triple inhaler, and with the combination of budesonide-formoterol (Symbicort) plus glycopyrronium (Seebri), which includes the same 3 medications as BGF MDI 320, although at slightly different doses. At the submitted price, the cost of BGF MDI 320 is $63 less expensive than the annual cost of FF-UM-VI ($1,608 per patient per year) (Table 5) and $200 less than that of budesonide-formoterol plus glycopyrronium bromide ($1,745 per patient per year) (Table 2).
When dispensing fees are included, the use of single inhaler products like BGF MDI 320 or FF-UM-VI DPI is associated with 12 fewer dispensing fees per year compared with ICS-LABA plus LABA combinations, assuming inhalers are claimed monthly, or $105.96 per year when considering the ODB dispensing fee of $8.83 per product dispensed. The inclusion of markups would increase the incremental savings or costs by the allowable markup of the jurisdiction in question, e.g., 8% in the case of the ODB. Including Ontario dispensing fees and markups increases the annual cost of BGF MDI 320 to $1,776 per patient, the cost of FF-UME-VI DPI to $1,844 per patient, and the cost of the other ICS-LABA plus LAMA combinations to $1,539 to $2,888 per patient.
To be cost-neutral to the annual cost of the least expensive ICS-LABA plus LAMA combination (fluticasone propionate 250 mcg/salmeterol 50 mcg inhalation powder plus 62.5 mcg umeclidinium twice daily), the price of BGF MDI 320 would need to be reduced by 21% when markups and dispensing fees are excluded, or 14% when ODB markups and dispensing fees are considered based on dispensing at 30-day intervals.
Table 2: CADTH Cost Comparison Table of BGF MDI 320 Compared With ICS-LABA Plus LAMA Combinations
ICS-LABA annual cost and incremental annual cost relative to BGF MDI 320 ($1,545)a | LAMA | ||||
|---|---|---|---|---|---|
Aclidinium bromide (Tudorza) 400 mcg twice daily ($) | Glycopyrronium (Seebri) 50 mcg daily ($) | Tiotropium (Spiriva Respimat) 18 mcg daily ($) | Tiotropium (Spiriva) 2.5 mcg twice daily ($) | Umeclidinium (Incruse Ellipta) 62.5 mcg daily ($) | |
Budesonide/formoterol (Symbicort Turbuhaler) 400 mcg/12 mcg twice daily | 1,745 200 | 1,745 200 | 1,760 214 | 1,760 214 | 1,708 163 |
Fluticasone furoate/vilanterol (Breo Ellipta) 100 mcg/ 25 mcg daily | 1,700 155 | 1,700 155 | 1,714 169 | 1,714 169 | 1,662 177 |
Fluticasone propionate/ salmeterol (Advair Diskus, inhalation powder generic) 250 mcg/50 mcg twice daily | 1,264 −282 | 1,264 −282 | 1,278 −267 | 1,278 −267 | 1,226 −319 |
Fluticasone propionate/ salmeterol (Advair Diskus, inhalation powder generic) 500 mcg/50 mcg twice daily | 1,523 −22 | 1,523 −22 | 1,537 −8 | 1,537 −8 | 1,485 −60 |
Fluticasone propionate/salmeterol (Advair MDI) 250 mcg/50 mcg twice daily | 1,924 379 | 1,924 379 | 1,939 393 | 1,939 393 | 1,887 342 |
Fluticasone propionate/ salmeterol (Advair MDI) 500 mcg/50 mcg twice daily | 2,461 916 | 2,461 916 | 2,475 930 | 2,475 930 | 2,423 878 |
BGF = budesonide-glycopyrronium-formoterol fumarate; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; MDI = metered-dose inhaler.
All included costs are based on publicly available list prices and may not reflect costs paid by plans.
aCost of comparator combination minus BGF MDI 320, with negative results indicating BGF MDI 320 is more expensive than the comparator. Annual cost of BGF MDI 320 is $1,545 per patient.
Exploratory Analysis
While ICS inhalers are not indicated for COPD, triple-combination therapy can also be achieved by combining a LABA/LAMA inhaler with an ICS inhaler. The clinical expert consulted by CADTH viewed these combinations as relevant to Canadian practice, particularly those including ciclesonide or fluticasone furoate, despite the lack of endorsement from COPD guidelines. CADTH thus conducted a secondary analysis comparing the annual cost of BGF MDI 320 with the available LABA-LAMA plus ICS combinations (Table 3). Costs of LABA/LAMA plus ICS combinations ranged from $966 to $1,983 per patient per year. At $1,545 per patient, the annual cost of BGF MDI 320 is less than that of combinations that include high-dose ciclesonide or fluticasone propionate, but more than that of combinations that include fluticasone furoate, lower-dose ciclesonide, or lower-dose fluticasone propionate. Some combinations that include budesonide were also more expensive than BGF MDI 320, depending on which LABA-LAMA product it was combined with. The annual costs of the individual components can be found in Table 5.
As with the previous comparison, the use of a single inhaler in place of a combination of 2 inhalers would save a dispensing fee for every claim filled, e.g., $105.96 per year when considering the ODB dispensing fee of $8.83 per product dispensed and monthly claims. The inclusion of markups would increase the incremental savings or costs by the allowable markup of the jurisdiction in question (e.g., 8% in the case of the ODB).
Table 3: CADTH Cost Comparison Table of BGF MDI 320 Compared With LABA-LAMA Plus ICS Combinations
ICS Comparatorsa | LABA-LAMA | |||
|---|---|---|---|---|
Aclidinium-formoterol (Duaklir Genuair) 400 mcg/12 mcg twice daily ($) | Indacaterol-glycopyrronium (Ultibro Breezhaler) 110 mcg/50 mcg daily ($) | Tiotropium-olodaterol (Inspiolto Respimat) 5 mcg/5 mcg daily ($) | Umeclidinium-vilanterol (Anoro Ellipta) 62.5 mcg/25 mcg daily ($) | |
Budesonide (Pulmicort Turbuhaler) 400 mcg twice daily | 1,462 −83 | 1,675 130 | 1,507 −38 | 1,771 226 |
Ciclesonide (Alvesco) 200 mcg once daily | 966 −579 | 1,179 −366 | 1,011 −534 | 1,275 −270 |
Ciclesonide (Alvesco) 400 mcg twice daily | 1,675 129 | 1,887 342 | 1,719 174 | 1,983 438 |
Fluticasone furoate (Arnuity) 100 mcg daily | 1,218 −327 | 1,431 −114 | 1,263 −283 | 1,527 −19 |
Fluticasone propionate (Flovent) Diskus, 250 mcg twice daily | 1,278 −267 | 1,491 −55 | 1,322 −223 | 1,586 41 |
Fluticasone propionate (Flovent) Diskus, 500 mcg twice daily | 1,582 37 | 1,795 250 | 1,627 82 | 1,891 346 |
Fluticasone propionate (Flovent, generic) MDI, 250 mcg twice daily | 1,141 −404 | 1,354 −192 | 1,185 −360 | 1,449 −96 |
Fluticasone propionate (Flovent, generic) MDI, 500 twice daily | 1,552 6 | 1,764 219 | 1,596 51 | 1,860 315 |
BGF = budesonide-glycopyrronium-formoterol fumarate; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; MDI = metered-dose inhaler.
All included costs are based on publicly available list prices and may not reflect costs paid by plans.
aCost of comparator combination minus BGF MDI 320, with negative results indicating BGF MDI 320 is more expensive than the comparator. Annual cost of BGF MDI 320 is $1,545 per patient.
Issues for Consideration
Different formulation and schedule than other available triple-therapy inhalers: As a twice-daily MDI, BGF MDI 320 offers a different formulation than FF-UME-Vl DPI (Trelegy), a dry powder for inhalation. Patient input indicated that pressurized MDIs may assist in ensuring medication can reach the lungs without relying on the ability and strength of a patient with COPD to properly inhale. Additionally, BGF MDI 320 is used twice daily, which may be less convenient for some patients than the once-daily dose of FF-UME-VI but, according to the clinical expert consulted by CADTH and the clinician group providing input to this review, BGF MDI 320 may be more effective and perceived by patients as more effective at giving more continuous bronchodilation, particularly at night. Should these factors lead to important differences in treatment efficacy, a cost-utility analysis would be more appropriate to assess the cost-effectiveness of BGF MDI 320.
Drug plan input: The drug plan input also suggested that prescribing criteria similar to those recommended for FF-UME-VI DPI may be appropriate, and that a confidential negotiated price for FF-UME-VI DPI existed.
Conclusions
The sponsor conducted a cost-minimization analysis based on an assumption of equal efficacy and safety with FF/UME/VI DPI (Trelegy) and with available ICS-LABA plus LAMA combinations. As head-to-head studies were not conducted, this assumption was informed by a sponsor-conducted network meta-analysis and clinical expert opinion. The CADTH critical appraisal of the network meta-analysis noted that BGF MDI likely showed efficacy and safety similar or comparable to other triple therapies, though with notable limitations inherent with indirect comparison. As a result, there is some uncertainty with this assumption. Should there be differences in the efficacy and safety of BGF MDI 320 versus the comparators of interest, a cost-utility analysis would be more appropriate than a cost-minimization analysis.
When considering only drug costs (i.e., excluding dispensing fees and markups), and assuming similar efficacy and safety among included comparators, the annual per-patient drug-acquisition cost of BGF MDI 320 ($1,545) is $63 less expensive than FF-UME-VI DPI ($1,608) and $200 less than budesonide-formoterol plus glycopyrronium ($1,745), which is the combination of 2 inhalers with the same component medications as BGF MDI 320. When considering dispensing fees and markups (based on Ontario estimates), the annual cost of BGF MDI 320 ($1,776 per patient) is $237 more than that of the least expensive ICS-LABA plus LAMA combination (range: $1,580 to $2,888 per patient). The use of a single inhaler for triple therapy is associated with a reduction in dispensing fees compared with combinations of 2 inhalers, potentially saving 12 fees per year when dispensed monthly. Of note, all analyses are based on publicly available list prices and may not represent actual costs paid by plans.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Breztri Aerosphere (budesonide / glycopyrronium (as bromide) / formoterol fumarate dihydrate, pressurized inhalation aerosol for oral inhalation) 182 mcg / 8.2 mcg / 5.8 mcg per metered actuation. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Feb.
2.BREZTRI™ AEROSPHERE (budesonide / glycopyrronium (as bromide) / formoterol fumarate dihydrate, pressurized inhalation aerosol for oral inhalation), 182 mcg / 8.2 mcg / 5.8 mcg per metered actuation [DRAFT product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2020 Jul 30.
3.Systematic Review And Network Meta-Analyses Of Triple Combinations In Moderate-To-Very Severe Copd [internal sponsor's report]. In: Drug Reimbursement Review sponsor's submission: Breztri Aerosphere (budesonide / glycopyrronium (as bromide) / formoterol fumarate dihydrate, pressurized inhalation aerosol for oral inhalation) 182 mcg / 8.2 mcg / 5.8 mcg per metered actuation. Mississauga (ON): AstraZeneca Canada Inc.; 2021 Jan.
4.Ontario Ministry of H, Ontario Ministry of Long-Term C. Ontario drug benefit formulary/comparative drug index. 2020; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2021 Apr 18.
5.Bourbeau J, Bhutani M, Hernandez P, et al. Canadian Thoracic Society Clinical Practice Guideline on pharmacotherapy in patients with COPD – 2019 update of evidence. Canadian Journal of Respiratory, Critical Care, and Sleep Medicine. 2019;3(4):210-232.
6.Global Initiative for Chronic Obstructive Lung Disease. Pocket Guide to COPD Diagnosis, Management, and Prevention. A Guide for Health Care Professionals. 2021 Report. 2020: https://goldcopd.org/wp-content/uploads/2020/12/GOLD-2021-POCKET-GUIDE-v2.0-14Dec20_WMV.pdf. Accessed 2021 Apr 18.
7.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Drug name, doses and administration. City (PROV): Sponsor name; 1800.
8.PharmaStat. [Ottawa (ON)]: IQVIA; 2021: https://www.iqvia.com/. Accessed 2021 Mar 23.
Appendix 1: Additional Economic Information
Note that this appendix has not been copy-edited.
Additional Details on the Sponsor’s Submission
Table 4: Sponsor’s Daily Drug-Acquisition Costs for All Included Comparators
Drug/comparator | Strength | Doses per unit | Price ($) | Recommended dose | Average daily drug cost ($) | Assumed proportion of use within class (%) |
|---|---|---|---|---|---|---|
Closed triple therapies | ||||||
BGF MDI 320 (Breztri) | 182/10.4/5.8 mcg | 120 doses | 127.0000 | Two inhalations twice daily | 4.23 | NA |
Fluticasone furoate-umeclidinium-vilanterol (Trelegy) | 100/62.5/25 mcg | 30 doses | 132.2000 | One inhalation once daily | 4.41 | NA |
ICS-LABA Products | ||||||
Fluticasone Propionate-Salmeterol 250 (Advair Diskus-Wixela-generic) | 250/50 mcg | 60 doses | 50.7600 | One inhalation twice daily | 1.69 | |||| |
Fluticasone Propionate-Salmeterol 500 (Advair-Wixela-generic) | 500/50 mcg | 60 doses | 72.0600 | One inhalation twice daily | 2.40 | |||| |
Fluticasone Propionate-Salmeterol 125 (Advair) | 125/25 mcg | 120 doses | 105.0700 | Two inhalations twice daily | 3.50 | |||| |
Fluticasone Propionate-Salmeterol 250 (Advair) | 250/25 mcg | 120 doses | 149.1600 | Two inhalations twice daily | 4.97 | |||| |
Budesonide-formoterol (Symbicort) | 200/6 mcg | 120 doses | 90.3600 | Two inhalations twice daily | 3.01 | |||| |
Fluticasone furoate- vilanterol trifenatate (Breo Ellipta) | 100/25 mcg | 30 doses | 86.6300 | One inhalation once daily | 2.89 | |||| |
Weighted-average daily cost for ICS-LABA | 3.14 | 100 | ||||
LAMA | ||||||
Tiotropium (Spiriva Handihaler) | 18 mcg | 30 doses | 54.2600 | One inhalation once daily | 1.81 | |||| |
Tiotropium (Spiriva Respimat) | 2.5 mcg | 60 doses | 54.2600 | Two inhalations once daily | 1.81 | |||| |
Glycopyrronium (Seebri Breezhaler) | 50 mcg | 30 doses | 53.1000 | One inhalation once daily | 1.77 | |||| |
Aclidinium (Tudorza Genuair) | 400 mcg | 60 doses | 53.1000 | One inhalation twice daily | 1.77 | |||| |
Umeclidinium (Incruse Ellipta) | 62.5 mcg | 30 doses | 50.0000 | One inhalation once daily | 1.67 | |||| |
Weighted-average daily cost for LAMA | 1.79 | 100 | ||||
ICS-LABA + LAMA weighted average | 4.93 | 100 | ||||
BGF = budesonide-glycopyrrolate-formoterol fumarate; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; MDI = metered-dose inhaler; NA = not applicable.
Additional Details on the CADTH Reanalyses and Additional Analyses
CADTH Cost Comparison Table
Table 5: CADTH Cost Comparison Table for Bronchodilator Therapies for COPD
Drug/comparator | Strength | Dosage form | Price ($) | Price/ dose ($) | Recommended dose | Average daily drug cost ($) | Average annual drug cost ($) |
|---|---|---|---|---|---|---|---|
Inhaled corticosteroid/long-acting beta2-agonists/long-acting muscarinic antagonist fixed-dose combinations | |||||||
Budesonide- glycopyrronium- formoterol fumarate (Breztri Aerosphere) | 182/10.4/5.8 mcg | MDI (120 doses) | 127.0000a | 1.06 | Two inhalations twice daily | 4.23 | 1,545 |
Fluticasone furoate-umeclidinium-vilanterol (Trelegy Ellipta) | 100/62.5/25 mcg | Inhalant pwd (30 doses) | 132.2000 | 4.41 | 100/62.5/25 mcg once daily | 4.41 | 1,608 |
Long-acting beta2-agonists/long-acting muscarinic antagonist fixed-dose combinations | |||||||
Aclidinium-formoterol (Duaklir Genuair) | 400/12 mcg | Inhalant pwd (60 doses) | 60.0000 | 1.00 | 400/12 mcg twice daily | 2.00 | 730 |
Indacaterol-glycopyrronium (Ultibro Breezhaler) | 110/50 mcg | Inhalant pwd (30 capsules) | 77.4900 | 2.58 | 110/50 mcg daily | 2.58 | 1,039 |
Tiotropium-olodaterol (Inspiolto Respimat) | 2.5/2.5 mcg | Inhalation Solution (60 doses) | 63.6712 | 1.06 | 5/5 mcg once daily | 2.12 | 775 |
Umeclidinium-vilanterol (Anoro Ellipta) | 62.5/25 mcg | Inhalant pwd (30 doses) | 85.3700 | 2.85 | 62.5/25 mcg daily | 2.85 | 986 |
Inhaled corticosteroid/long-acting beta2-agonists fixed-dose combinations | |||||||
Budesonide- Formoterol (Symbicort Turbuhaler) | 100/6 mcgb 200/6 mcg | Inhalant pwd (120 doses) | 69.5400 90.3600 | 0.58 0.75 | 400/12 mcg twice daily | 3.01 | 1,099 |
Fluticasone furoate vilanterol trifenatate (Breo Ellipta) | 100/25 mcg 200/25 mcgb | Inhalant pwd (30 doses) | 86.6300 135.6900 | 2.89 | 100/25 mcg once daily | 2.89 | 1,054 |
Fluticasone propionate- Salmeterol (Advair Diskus, Wixela Inhub, generic) | 100/50 mcgb 250/50 mcg 500/50 mcg | Inhalant pwd (60 doses) | 42.4050 50.7600 72.0600 | 0.71 0.85 1.20 | 250/50 mcg or 500/50 mcg twice daily | 1.70 to 2.40 | 618 to 877 |
Fluticasone propionate- salmeterol (Advair) | 125/25 mcgb 250/25 mcgb | MDI (120 doses) | 105.0700 149.1600 | 0.88 1.24 | 250/50 or 500/50 mcg twice dailyb | 3.50 4.97 | 1,278 1,815 |
Long-acting muscarinic antagonist | |||||||
Aclidinium bromide (Tudorza Genuair) | 400 mcg | Inhalant pwd (60 doses) | 53.1000 | 0.88 | 400 mcg twice daily | 1.77 | 646 |
Glycopyrronium bromide (Seebri) | 50 mcg | Inhalant pwd (30 capsules) | 53.1000 | 1.77 | 50 mcg daily | 1.77 | 646 |
Tiotropium (Spiriva) | 18 mcg | Inhalant pwd (30 capsules) | 54,2610 | 1.81 | 18 mcg daily | 1.81 | 660 |
Tiotropium (Spiriva Respimat) | 2.5 mcg | Inhalant solution (60 doses) | 54.2607 | 0.90 | 2.5 mcg twice daily | 1.81 | 660 |
Umeclidinium (Incruse Ellipta) | 62.5 mcg | Inhalant pwd (30 doses) | 50.0000 | 1.67 | 62.5 mcg once daily | 1.67 | 608 |
Long-acting beta-agonists | |||||||
Salmeterol (SereVent) | 50 mcg | Inhalant pwd (60 doses) | 62.1300 | 1.04 | 50 mcg twice daily | 2.07 | 756 |
Formoterol (Foradil) | 12 mcgb | Inhalant pwd capsule | 0.8520c | 0.85 | 12 mcg or 24 mcg twice dailyb | 1.70 3.41 | 622 1,244 |
Indacaterol maleate (Onbrez) | 75 mcg | Inhalant pwd capsule | 1.5500 | 1.55 | 75 mcg daily | 1.55 | 566 |
Inhaled corticosteroidsb | |||||||
Budesonide (Pulmicort Turbuhaler) | 100 mcgb 200 mcgb 400 mcgb | MDI (200 doses) | 33.5900 68.7000 100.2900 | 0.1680 0.3435 0.5014 | 400 mcg twice daily | 1.00 | 366 |
Ciclesonide (Alvesco) | 100 mcgb 200 mcgb | MDI (120 doses) | 46.9200 77.6400 | 0.3910 0.6470 | 200 to 400 mcg once or twice daily | 0.65 to 2.59 | 236 to 944 |
Fluticasone furoate (Arnuity Ellipta) | 100 mcgb 200 mcgb | Inhalant pwd (30 doses) | 40.1000 80.2000 | 1.3367 2.6733 | 100 mcg once daily | 1.34 | 489 |
Fluticasone propionate (Flovent Diskus) | 250 mcgb 500 mcgb | Inhalant pwd (60 doses) | 45.0200 70.0300 | 0.7503 1.1672 | 250 or 500 mcg twice daily | 1.50 to 2.33 | 411 to 852 |
Fluticasone propionate (Flovent HFA, generic) | 125 mcgb 250 mcgb | MDI (120 doses) | 45.0200 67.5300 | 0.3752 0.7503 | 250 or 500 mcg twice daily | 1.13 to 3.00 | 5.48 to 1,095 |
COPD = chronic obstructive pulmonary disease; HFA = hydrofluoroalkane; ICS = inhaled corticosteroid; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; MDI = metered-dose inhaler; pwd = powder.
All prices are from the Ontario Drug Benefit Formulary (accessed March 2021) unless otherwise indicated and do not include dispensing fees or markups.
aSponsor’s submitted price.
bThese dose forms or strengths are not indicated for COPD. Recommended doses for ICS products in COPD are based on recommended dosing of ICS component of ICS-LABA or ICS-LAMA-LABA products, or on expert opinion where such products do not exist.
cSaskatchewan Formulary list price.
Appendix 2: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Key Takeaways of the Budget Impact Analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a claims-based budget impact analysis (BIA)7 assessing the expected budgetary impact of reimbursing BGF MDI 320 for the treatment of COPD in patients requiring escalation to triple therapy to optimally manage symptoms of dyspnea and/or activity limitation, as well as to prevent exacerbations. The BIA was from the perspective of a Canadian public drug plan payer over a 3-year time horizon and included only drug-acquisition costs in the base case. Comparators included FF-UME-VI DPI, the other available ICS-LAMA-LABA inhaler, as well as ICS-LABA plus LAMA inhaler combinations. LABA-LAMA plus ICS inhaler combinations were excluded.
The sponsor used the IQVIA Pharmastat database to estimate the number of claims of the identified comparators made between 2015 and 2020. This volume of claims was then adjusted based on IQVIA ODB RxDynamics data to reflect the proportion of claims classified as dispensed for COPD and Longitudinal Prescription Data (RxDynamics) data to reflect the proportion of ICS/LABA claims that were estimated to be used with a LAMA product (data supplied by the sponsor upon request).7 Claim volume for each ICS-LABA plus LAMA combination was estimated by multiplying the proportion of claims for each ICS-LABA product within the ICS-LABA class by the proportion of claims for each LAMA product within the LAMA class to determine the proportion of claims representing each combination overall.
Key inputs to the BIA are documented in Table 6. Other assumptions made by the sponsor include:
COPD patients do not use ICS-only inhalers as part of combination therapies as ICS-only inhalers are not indicated for COPD.
|||||% of market share captured by BGF MDI 320 would come from FF-UME-VI DPI, with the remaining |||||% coming from the ICS-LABA plus LAMA combinations in proportion to their reference scenario market shares.
The reimbursement of BGF MDI 320 will not expand the number of claims made for patients receiving triple therapy for COPD.
Table 6: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3, if appropriate) | |
|---|---|---|
Target population: Patients with COPD requiring triple therapy. | ||
Number of included claims | ||||||||||||| / ||||||||||||| / ||||||||||||| | |
Market uptake (3 years) | ||
Uptake: ICS-LAMA-LABA products (total %) BGF MDI 320 (Breztri) FF-UME-VI DPI (Trelegy) ICS-LABA + LAMA products (Total %) FP-SAL + UME (Advair/generic + Incruse) FP-SAL + GLY (Advair/generic + Seebri) FP-SAL + TIO (Advair/generic + Spiriva) FP-SAL + ACL (Advair/generic + Tudorza) FF-VIL + UME (Breo + Incruse) FF-VIL + GLY (Breo + Seebri) FF-VIL + TIO (Breo + Spiriva) FF-VIL + ACL (Breo + Tudorza) BUD-FM + UME (Symbicort + Incruse) BUD-FM + GLY (Symbicort + Seebri) BUD-FM + TIO (Symbicort + Spiriva) BUD-FM + ACL (Symbicort + Tudorza) | Reference scenario: ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| ||||||||||||||||||||||| | New-drug scenario: ||||||||||||||||||||||| |||||||||||||| |||||||||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||| |||||||||||||||||||||| |||||||||||||| |
Cost of treatment per standardized 30-day claim (Ontario costs used as example)a | ||
BGF MDI 320 (Breztri) FF-UME-VI DPI (Trelegy) FP-SAL + UME (Advair/generic + Incruse) FP-SAL + GLY (Advair/generic + Seebri) FP-SAL + TIO (Advair/generic + Spiriva) FP-SAL + ACL (Advair/generic + Tudorza) FF-VIL + UME (Breo + Incruse) FF-VIL + GLY (Breo + Seebri) FF-VIL + TIO (Breo + Spiriva) FF-VIL + ACL (Breo + Tudorza) BUD-FM + UME (Symbicort + Incruse) BUD-FM + GLY (Symbicort + Seebri) BUD-FM + TIO (Symbicort + Spiriva) BUD-FM + ACL (Symbicort + Tudorza) | $127.00 $132.20 $150.06 $153.16 $154.32 $153.16 $136.63 $139.73 $140.89 $139.73 $140.36 $143.46 $144.62 $143.46 | |
ACL = aclidinium; BUD = budesonide; BGF = budesonide-glycopyrronium-formoterol; COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; FF = fluticasone furoate; FM = formoterol; FP = fluticasone propionate; GLY = glycopyrronium; MDI – metered-dose inhaler; SAL = salmeterol; TIO = tiotropium; UME = umeclidinium.
aActual cost of treatment for each comparator in the model was based on a weighted-average cost of jurisdictional list prices and 2020 dose proportions.7,8
Summary of the Sponsor’s Budget Impact Analysis Results
Results of the sponsor’s base case suggest that reimbursement of BGF MDI 320 for patients with COPD requiring triple therapy would be associated with a budgetary savings of $1,559,158 in year 1, $4,686,782 in year 2, and $7,003,941 in year 3, for a cumulative budgetary savings of $13,249,881 over 3 years. When dispensing fees and markups are included, the budgetary savings associated with the reimbursement of BGF MDI 320 were estimated to be $2,404,418 in year 1, $7,292,754 in year 2, and $10,949,385 in year 3, for a cumulative 3-year savings of $20,646,557 (Table 7).
The sponsor also conducted sensitivity analyses increasing and decreasing the assumed market share capture of BGF MDI 320 by 25% (3-year budgetary savings of $16,562,351 and $9,937,411, respectively), and by assuming BGF MDI 320 would only displace ICS-LABA plus LAMA combinations rather than taking market share from FF-UME-VI DPI (3-year budgetary savings of $16,248,137).
CADTH Appraisal of the Sponsor’s Budget Impact Analysis
CADTH identified the following key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Relative market shares uncertain: The sponsor’s estimates of the market share of each comparator combination rely on a series of assumptions that are logical in the absence of more precise data, but which nevertheless contribute uncertainty in the results without having the ability to determine the actual values. For example, the proportion of fluticasone propionate-salmeterol (Advair, an ICS-LABA) plus UME (Incruse, a LAMA) claims is estimated by multiplying the number of claims reimbursed for fluticasone propionate-salmeterol by the estimated proportion of fluticasone propionate/salmeterol claims that were inferred by IQVIA RxDynamics data to have been filled for COPD, and then by the overall proportion of patients who IQVIA RxDynamics data inferred to have COPD and use an ICS-LABA product as well as a LAMA product, and then by the proportion of LAMA claims that were for UME.
CADTH was unable to adjust for this limitation in reanalyses. This uncertainty may impact the magnitude of savings associated with the reimbursement of BGF MDI 320 but is unlikely to eliminate them.
Missing comparators of potential interest: As noted in the economic review, triple therapy for COPD can also be achieved through the use of a LABA-LAMA plus ICS inhaler combination, although ICS products are not indicated for COPD and the proportion of claims made for ICS products which are used by COPD patients is unknown. Upon request for further information, the sponsor calculated a weighted-average 30-day cost of $129 for LAMA-LABA plus ICS combinations based on overall market share (i.e., not limited to COPD) as reported by IQVIA Pharmastat data in 2020 for ICS inhalers containing molecules and strengths that are indicated for COPD when part of ICS-LABA inhalers.8 This weighted average was more expensive than that of BGF MDI 320 ($127), although the sponsor’s method excluded ciclesonide (Alvesco) as it is not part of an ICS-LABA inhaler indicated for COPD, but was considered a comparator of interest by the expert consulted by CADTH.
CADTH was unable to adjust for this limitation in the overall BIA due to a lack of data on usage of ICS products in COPD; however, 30-day costs for all LABA/LAMA plus ICS combinations included in the economic analyses in the main report above ranged from $79 to $163. CADTH calculated the weighted-average 30-day cost8 of LABA/LAMA plus ICS to be between $126 and $132, depending upon assumptions around ciclesonide dosing. Despite this average being approximately the same as the 30-day cost of BGF MDI 320, when considering the extra dispensing fee per month required for 2-inhaler combinations, BGF MDI 320 is likely to remain cost-saving on a weighted-average per-patient basis relative to LABA-LAMA plus ICS therapies at their list prices.
Displacement of comparators is uncertain: The sponsor based their estimate of the proportion of market share that would be captured by BGF MDI 320 on internal sales forecasts and the uptake of FF-UME-VI DPI in the Canadian market. |% of BGF MDI 320 claims were assumed to have been captured from FF-UME-VI DPI with the remaining |% captured from ICS-LABA plus LAMA combinations proportional to their market share in the reference scenario. Should the actual uptake of BGF MDI 320 differ from these assumptions, the magnitude of cost savings associated with the reimbursement of BGF MDI 320 will also be altered.
CADTH was unable to adjust for this limitation in reanalysis beyond the market share scenarios already conducted by the sponsor.
Costs do not reflect confidential pricing agreements: All costs in the sponsor’s and CADTH’s base-case reanalyses are based on publicly available list prices and are unlikely to reflect true costs paid by public drug plans. Any confidential pricing agreements which are in place for comparator products would reduce or potentially eliminate the savings estimated to result from the reimbursement of BGF MDI 320 at its submitted price.
CADTH conducted price reduction analyses to find the percentage by which the list prices of the comparators would have to be reduced before BGF MDI 320 would no longer result in cost savings at its submitted price.
CADTH Reanalyses of the Budget Impact Analysis
CADTH did not undertake a base-case reanalysis. If a 21% price reduction on the submitted price of BGF MDI 320 is considered, such that its annual cost without dispensing fees or markups is cost-neutral to the lease expensive ICS-LABA plus LAMA combination, the 3-year budgetary savings associated with the reimbursement of BGF MDI 320 would be $34.8 million (Table 7).
Table 7: Detailed Breakdown of the Sponsor’s and CADTH’s BIA Scenarios
Analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 153,319,504 | 169,547,346 | 183,752,202 | 196,418,165 | 549,717,714 |
New drug | 153,319,504 | 167,988,188 | 179,065,420 | 189,414,225 | 536,467,833 | |
Budget impact | 0 | −1,559,158 | -4,686,782 | −7,003,941 | −13,249,881 | |
Sponsor scenario: markups and dispensing fees included | Reference | 184,823,346 | 203,717,143 | 220,260,812 | 235,016,654 | 658,994,609 |
New drug | 184,823,346 | 201,312,725 | 212,968,058 | 224,067,269 | 638,348,052 | |
Budget impact | 0 | −2,404,418 | −7,292,754 | −10,949,385 | −20,646,557 | |
CADTH scenario: BGF MDI 320 price reduced by 20.7% | Reference | 153,319,504 | 169,547,346 | 183,752,202 | 196,418,165 | 549,717,714 |
New drug | 153,319,504 | 165,496,912 | 171,487,272 | 177,972,500 | 514,956,685 | |
Budget impact | 0 | −4,050,434 | −12,264,930 | −18,445,665 | −34,761,029 |
BGF = budesonide-glycopyrronium-formoterol fumarate; BIA = budget impact analysis; MDI = metered-dose inhaler.
Due to the likelihood that confidential pricing agreements exist for the comparator products, CADTH calculated how much the cost of the comparators would need to be reduced to eliminate the potential savings associated with the reimbursement of BGF MDI 320 in the sponsor’s base case. An 11.4% reduction in the price of all comparators would eliminate the savings associated with the reimbursement of BGF MDI 320, while a 16.3% reduction would eliminate such savings where markups and dispensing fees are considered.
Table 8: CADTH Reanalyses of the Budget Impact Analysis Exploring Potential Comparator Price Reductions
Stepped analysis | Three-year total, drug costs only ($) | Three-year total, including dispensing fees and markups ($) |
|---|---|---|
Submitted base case | −13,249,881 | −20,646,557 |
CADTH scenario analysis: all plans pay 11.4% less for all comparators | 107,325 | −4,495,028 |
CADTH scenario analysis: all plans pay 16.3% less for all comparators | 5,848,580 | 101,154 |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.