CADTH Health Technology Review
Clinical Classification and Interventions for Post–COVID-19 Condition: A Scoping Review
Protocol Registration
Open Science Framework Registration: https://www.osf.io/xmusb
National Collaborating Centre for Methods and Tools: https://www.nccmt.ca/covid-19/covid-19-evidence-reviews/492
Scoping Review
Authors: Yi-Sheng Chao, Thyna Vu, Sarah C. McGill, Michelle Gates
Author Information
Authors
Yi-Sheng Chao, Thyna Vu, Sarah C. McGill, Michelle Gates
Contributors
Camille Santos, Sinwan Basharat, Sarah Garland, David Kaunelis, Diksha Kumar, Paula Murray, Gino De Angelis
External Reviewers
This document was externally reviewed by a content expert and methodologist, and the following individuals granted permission to be cited.
Simon Décary, PhD
Assistant Professor, University of Sherbrooke
Andrea Tricco, MSc, PhD
Scientist, Unity Health Toronto
Abbreviations
HTA
health technology assessment
ICD
International Classification of Diseases
ICU
intensive care unit
IQR
interquartile range
NICE
National Institute for Health and Care Excellence
PRISMA-ScR
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews
SARS-CoV-2
severe acute respiratory syndrome coronavirus 2
SD
standard deviation
Section | Amendment | Page in protocol | Rationale |
|---|---|---|---|
Literature Search Strategy | Searches were not supplemented by reviewing bibliographies of key papers or through contacts with experts. | 11 | Due to resource and time constraints, this was not feasible. |
Literature Search Strategy | References of included studies were not searched and no content experts were contacted. | 11 | Due to resource and time constraints, this was not feasible. |
Selection and Eligibility Criteria | More details on eligibility criteria for guidelines were added. Eligibility was expanded to include Canadian guidelines regardless of the definition used for post–COVID-19 condition. | 11 | The criteria used to include guidelines were added for improved clarity. Canadian guidelines were included regardless of definition, as they were believed to be contextually important. |
Selection and Eligibility Criteria | Additional details added regarding eligibility of studies with broad follow-up time that includes some participants followed up for < 12 weeks. | 11 | Due to these studies likely providing data of interest, they were included, and the eligibility criteria were specified. |
Selection and Eligibility Criteria | Preprints were only considered for inclusion if they were systematic reviews; preprints of other study designs were excluded. | 12 | Due to resource and time constraints, it was not feasible to include preprints of primary studies. |
Charting | Age, median, interquartile range, range, eligible age, and categories, as reported by the references, were additionally extracted. | 13 | An extraction of only mean and standard deviation age data was originally planned, but after the realization that not all publications reported this, it was decided that median, interquartile range, range, eligible age, and categories, as reported by the references, would also be extracted. |
Charting | Variables related to the PROGRESS-Plus framework (i.e., place of residence, race/ethnicity/culture/language, occupation, religion, education, socioeconomic status, social capital, and other characteristics that may be associated with disadvantage) were not extracted. | 13 | Partway through charting, it was determined that these were infeasible to extract due to resource and time constraints; thus, they were removed. |
Charting | Study authors were not contacted. | 13 | Due to resource and time constraints, no attempts were made to contact study authors for missing or unclear information. |
Key Messages
Most of the identified published research focused on characteristics or outcomes of having post–COVID-19 condition (e.g., symptoms, quality of life) or predictors for developing post–COVID-19 condition. There were fewer studies related to preventing post–COVID-19 condition or treatments. Ongoing studies, according to published protocols, will investigate interventions to prevent or treat this condition.
Notable evidence gaps included post–COVID-19 condition as it relates to people living in rural or remote areas, children and adolescents, and vaccination status. There were few economic studies, qualitative studies, and studies assessing health systems issues.
Most identified guidelines regarding the diagnosis, treatment, and management of post–COVID-19 condition, including all Canadian guidelines, provided limited guidance specific to patients meeting the WHO definition. These guidelines will need continual updates as new evidence emerges.
Abstract
Background
According to WHO, post‒COVID-19 condition is characterized by new or persisting symptoms 12 or more weeks following an initial COVID-19 infection. People with post–COVID-19 condition have been reported to experience a range of heterogenous symptoms, including fatigue, shortness of breath, muscle aches, and cognitive and mental health challenges. With the vast numbers of COVID-19 cases worldwide and estimates from the literature suggesting a substantial proportion of these individuals may develop long-term complications, there is much interest in developing a clearer understanding of this condition.
The objective of this scoping review is to characterize the current evidence landscape on post–COVID-19 condition and to identify evidence gaps. Clinical classification (e.g., symptom classification, severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2] variant quantification, and reporting of pathophysiological markers), risk factors related to developing post–COVID-19 condition, diagnostic tests, interventions to prevent or manage symptoms (e.g., drugs, rehabilitation), and evidence related to health systems for people of all ages in any context were of interest.
Methods
A scoping review of primary studies and other relevant research, including systematic reviews, guidelines, and economic evaluations was undertaken. Studies and protocols or clinical trial registrations needed to be published (commercially or as grey literature); preprints were included for systematic reviews only. Studies that followed up with participants for at least 12 weeks or 3 months after COVID-19 diagnosis or symptom onset and assessed the clinical classification, predictive variables, preventive measures, diagnostic approaches, and treatments, in any setting, were eligible for inclusion. Included references were categorized by the following concepts: risk factors and prevention, classification, diagnostic tests, treatment or management, and health system issues (e.g., increased health care services use and policy impact). Country, age, sex (proportion of male participants), and rural or remote residence were also charted to identify characteristics that stratify health opportunities and outcomes related to health equity and equity considerations.
Results
Between January 1, 2019, and December 20, 2021, 637 published articles, 247 protocols, and 8 preprints of systematic reviews were identified and included. The majority of studies came from only a few countries, particularly the US (n = 180), Italy (n = 96), and the UK (n = 81). Some countries had a moderate number of studies (36 to 66), including China, Canada, and several European countries (the Netherlands, Spain, France, and Germany). Relatively few studies (30 or fewer) were found that included participants from Africa, South America, Australia, New Zealand, and Asia. We identified 10 or more systematic reviews related to characteristics or outcomes (e.g., symptoms, quality of life) of post–COVID-19 condition, as well as risk factors. Areas with fewer systematic reviews but 50 or more primary studies included pathophysiological markers assessed at fewer than 12 weeks, as well as diagnostic tests at 12 weeks or later. Fewer than 50 primary studies for preventive or treatment interventions were identified, but a large number of protocols indicate research is in progress for these topics. Finally, several areas with few protocols and fewer than 50 primary studies were identified, including economic evaluations, qualitative studies, studies related to health system issues, and guidelines specific to 12 weeks or longer (differences between variants of SARS-CoV-2, subtypes of post–COVID-19 condition, people under 18 years old, people living in rural or remote areas, and people who have received the COVID-19 vaccine).
Conclusions
A substantial amount of research has been conducted and published on post–COVID-19 condition as of December 2021. The majority of the identified evidence has looked at symptoms, risk factors, and different diagnostic tests to assess individuals with post–COVID-19 condition. As of December 2021, there appears to be limited evidence regarding preventive interventions and interventions to treat or manage post–COVID-19 condition, but published protocols indicate research in this area is ongoing. Some areas where few published studies and protocols were found include in pediatric populations, in people living in rural or remote areas, and the impact of different variants of SARS-CoV-2.
Introduction and Rationale
COVID-19 was first identified in late 2019 and has since had an enormous impact on countries around the world. As of March 1, 2022, WHO has reported more than 433 million confirmed cases and more than 5.9 million deaths globally.1 While COVID-19 was initially considered a short-term acute disease, it has since become clear that some people do not fully recover for several weeks or months after the acute phase, or experience a recurrence of symptoms.2 Initially referred to as long COVID by patient advocates, several other names have also been suggested and used, including chronic COVID condition and post-acute sequelae of COVID-19.2,3 In addition to various terms being used, there has also been a lack of consensus definition for post–covid-19 condition: some have defined it as symptoms occurring 4 weeks after infection, diagnosis, or symptom onset, while others have suggested 12 weeks or 3 months.4
At the time of writing this report (March 2022), the Government of Canada defines post–COVID-19 condition as symptoms experienced for “weeks or months after initial recovery” and differentiates between short-term (4 to 12 weeks) and long-term (12 or more weeks) symptoms.5 This Canadian definition was published in September 2021. In December 2020, the National Institute for Health and Care Excellence (NICE) in the UK released its first iteration of a rapid guideline for managing the long-term effects of COVID-19, and suggested using acute COVID-19 for the first 4 weeks of illness, ongoing symptomatic COVID-19 for symptoms occurring between weeks 4 and 12, and post–COVID-19 syndrome for symptoms occurring after 12 weeks that cannot be explained by an alternative diagnosis.6 These terms are still used in their updated guideline from November 2021. WHO released its clinical case definition of post–COVID-19 condition in October 2021, and also defined it as symptoms occurring at least 3 months after COVID-19 infection.7 Both NICE and WHO stated that symptoms can have persisted since the acute phase, or can be new symptoms that were not present during the acute phase but developed afterwards (e.g., a person’s post–COVID-19 condition symptoms include a rash even if they did not have a rash during the acute phase).6,7 This also includes people who were asymptomatic during the acute phase. The WHO and NICE definitions also state that symptoms may fluctuate or relapse.6,7
To be consistent with the WHO definition, this report uses the term post–COVID-19 condition and defines it as symptoms or sequelae occurring at least 12 weeks or 3 months after COVID-19 infection, diagnosis, or symptom onset.6,7 We have chosen the WHO definition over the Canadian definition because the WHO definition is newer, and was built on existing empirical evidence that used robust methodology to identify the domains and variables to be included.7 Development of the definition engaged patients, clinicians, researchers, and other stakeholders from all WHO regions (n = 265) in a two-round Delphi consensus (defined as at least 70% agreement) building exercise, which was followed by a mixed iterative survey.7 We recognize that some patient advocates may prefer other terms as the term post–COVID-19 condition may be interpreted as patients have recovered or imply that there is no active disease process.8 Throughout this review, post–COVID-19 may be interpreted as occurring after the acute COVID-19 and ongoing symptomatic COVID-19 phases.
With the vast numbers of COVID-19 cases worldwide and estimates from preprint systematic reviews suggesting that approximately 43% to 53% of people infected by COVID-19 may develop post–COVID-19 condition,9,10 there is much interest in developing a clearer understanding of this condition. We identified 3 previous scoping reviews on COVID-19 sequelae, or long COVID11-13; however, none focused specifically on follow-up after at least 3 months or 12 weeks, perhaps because WHO’s definition of post–COVID-19 condition is relatively new. Thus, it is unclear where evidence exists about post–COVID-19 condition as defined as sequelae after 12 weeks, from its characteristics and symptoms, what tests are being used to assess symptoms and potential causes, which interventions have been assessed, and what guidelines are available. The rapidly evolving pandemic and rapid accumulation of new research poses challenges for policy-makers and researchers as to resource allocation and task prioritization.14 As a precursor to meaningful evidence synthesis activities (e.g., systematic reviews), we believed it important to address the aforementioned lack of clarity about the depth and breadth of rapidly emerging evidence on post–covid-19 condition. As a result, a scoping review was believed to be the most relevant methodology to characterize the evidence landscape. In addition, this would address the need to understand what evidence is available on a broader range of topics compared to previous scoping reviews, including symptoms, risk factors, pathophysiology, preventive interventions, diagnostic methods, treatment and management, and issues related to health systems.
The goal of this review was to characterize the existing evidence and to identify gaps in the evidence base and determine areas where further research is needed to help support Canadian health care decision-making needs. The findings of this scoping review, specifically the identified knowledge gaps and uncertainties, will be used to inform a larger CADTH condition-level review on post–COVID-19 condition and serve as a foundation for future rapid evidence queries. The findings will also contribute to the condition-level review’s online platform that will aim to share information, provide evidence to inform decision-making, increase awareness of ongoing initiatives, reduce duplication of effort, and support connection and collaboration. A condition-level review is an assessment of the evidence that incorporates all aspects of a condition, from prevention and detection to treatment and management.
Objective
The objective of this scoping review is to characterize the current evidence landscape on post–COVID-19 condition and to identify evidence gaps. We aim to use the findings to identify areas where it may be feasible and informative to perform future systematic reviews, which will contribute to CADTH’s larger condition-level review. Clinical classification (classifying post–COVID-19 condition at least 12 weeks or 3 months after initial infection by symptoms, pathophysiological markers, variants of SARS-CoV-2, subtypes, or other approaches); risk factors related to developing post–COVID-19 condition; diagnostic tests; interventions to prevent, treat, or manage symptoms (e.g., drugs, rehabilitation); and topics related to health systems (e.g., increased health care services use, policy impact) for people of all ages in any context were of interest.
Research Questions
The scoping review addressed the following research questions:
What is the current evidence landscape on the clinical classification, preventive measures, prognostic factors, diagnostic tests, and treatment for post–COVID-19 condition for people of any age in any setting?
What are the knowledge gaps on the clinical classification, preventive measures, prognostic factors, diagnostic tests, and treatment for post–COVID-19 condition for people of any age in any setting?
Methods
Protocol Development
To inform the preparation of the protocol for this scoping review, a CADTH Horizon Scanning report of the existing literature, including health technology assessments (HTAs) and systematic reviews was conducted.15 The protocol was written a priori based on well-established methods,16 and was externally reviewed by a content expert and methodologist. The review topic was registered at the National Collaborating Centre for Methods and Tools and posted the protocol on the Open Science Framework.
Study Design
The research questions were addressed by conducting a scoping review of primary studies and other relevant research, including systematic reviews, scoping reviews, rapid reviews, preprints, and grey literature. The methodology of the scoping review was informed by the methods outlined in the JBI Manual for Evidence Synthesis17 and reporting adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR), with relevant adaptations based on PRISMA 2020 statement.18 The final report was externally reviewed by a content expert and methodologist.19
Literature Search Strategy
The literature search was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies (PRESS) checklist.20 The complete search strategy is presented in Appendix 1 (refer to Table 9 for a guide to Ovid syntax and Table 10 for a guide to EBSCO syntax).
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒), Embase (1974), APA PsycInfo (1806‒), and the Cochrane Central Register of Controlled Trials (CENTRAL), via the Ovid platform; and CINAHL (Cumulative Index to Nursing and Allied Health Literature) via EBSCO. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy was comprised of both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was post–COVID-19 condition and synonyms. Parts of the strategy were adapted from CADTH’s COVID-19 search string.21 Detailed search strategies are provided in Appendix 1.
Retrieval was limited to documents published from January 1, 2019, onwards, and in the English or French language. As COVID-19 was first identified in late 2019, we expected that all relevant papers would have been published in or after 2019. Where possible, retrieval was limited to the human population. No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, and letters were excluded.
The following clinical trial registries were searched: the US National Institutes of Health’s ClinicalTrials.gov, WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register. Preprints (preliminary reports that have not been peer reviewed) were searched through the Europe PMC database.
Grey literature (literature that is not commercially published) was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature resource,22 and the CADTH COVID-19 Grey Literature Resources,23 which includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, systematic review repositories, patient-related groups, and professional associations. Refer to Appendix 1 for more information on the grey literature search strategy.
The initial search was completed on October 15, 2021. Regular alerts updated the database literature searches, grey literature, preprints, and clinical trial registries searches until December 20, 2021. Studies meeting the selection criteria and identified in the alerts were incorporated into the final report.
Selection and Eligibility Criteria
The study eligibility criteria for the research questions can be found in Table 2. Studies of people of all ages that investigated the clinical classification (classifying post–COVID-19 condition at least 12 weeks or 3 months after initial infection by symptoms, pathophysiological markers, variants of SARS-CoV-2, subtypes, or other approaches), prevention, diagnostic tests, or treatment of post–COVID-19 condition in any setting were included. Studies that followed up with patients at least 12 weeks (equivalent to 3 months or 84 days) after initial infection or diagnosis or symptom onset were eligible for inclusion. Studies were included even if not all eligible participants developed post–COVID-19 condition; for example, this could include studies aimed at identifying incidence or risk factors for developing post–COVID-19 condition. This also includes studies that measured immunological markers or other biomarkers after 12 weeks, as these may provide insight into methods of identifying post-COVID-19 sequelae or potential causes of sequelae (e.g., assessments of inflammatory markers after 12 weeks in people experiencing persistent symptoms, compared to people who had COVID-19 but did not experience persistent symptoms or to people who did not have COVID-19 at all). For studies where follow-up time varied between participants, with some followed up for less than 12 weeks, the following criteria were used:
If the study provided the median and interquartile range (IQR) for follow-up time, if the lower quartile was at least 12 weeks, it was included.
If the study provided the mean and standard deviation (SD) follow-up time, if the mean was at least 12 weeks, it was included.
Primary studies of any design, systematic reviews (i.e., quantitative, qualitative, or mixed-methods reviews that include a research question; a list of the sources searched and a reproducible search strategy; clear inclusion and exclusion criteria; a description of methods for study selection; information about how the data were synthesized),24 scoping reviews, economic analyses, and ethical analyses were eligible. Systematic reviews that included primary studies meeting our criteria and primary studies that did not (i.e., some studies assessed at 12 weeks or later while some assessed within 12 weeks) were included. These could be commercially published or available as grey literature, and could be available as a full-text article, conference abstract, presentation, or thesis. Evidence-based guidelines and clinical practice guidelines related to post-acute COVID-19 care were included if they provided at least 1 recommendation for patients at 12 weeks or later after initial infection or diagnosis related to diagnosis or treatment. Though none of the available Canadian guidelines used this definition, they were included as they were believed to be contextually important. Though informal literature reviews and consensus statements can sometimes include relevant data, we deemed it infeasible to sift through a large volume of editorials, letters, and commentaries; therefore these were excluded.
The review was limited to studies published in English and French due to resource and time constraints. One deviation from the original protocol is that we included preprints of systematic reviews only, rather than preprints for all study designs. This decision was made for feasibility reasons, given the large volume of eligible studies.
Table 2: Selection Criteria for Clinical Research Questions
Category | Selection criteria |
|---|---|
Population | People of all ages with post–COVID-19 condition (i.e., defined as any symptoms experienced 12 weeks or more after initial infection, diagnosis, or symptom onset) |
Concept | Clinical classification, preventive measures, diagnostic approaches, treatments, for post–COVID-19 condition |
Context | Any context or setting |
Study designs | Comparative and noncomparative study designs, economic evaluations, protocols, and clinical guidelines, including:
Exclusions:
|
Time frame | 2019 to present |
Language of publication | English or French |
aThese may be quantitative, qualitative, or mixed methods, and must include a research question, a list of the sources searched and a reproducible search strategy, clear inclusion and exclusion criteria, a description of methods for study selection, and information about how the data were synthesized. Though appraisal of the quality of the included studies is often recommended for systematic reviews, this was not considered a requirement for the purpose of the present scoping review.24
Study Selection
The systematic review management software DistillerSR (Evidence Partners, Ottawa, Canada) was used to facilitate study selection. Pilot testing was conducted for the first 50 references identified in the literature search to ensure the eligibility criteria were interpreted similarly by the reviewers. Thereafter, 2 reviewers independently screened titles and abstracts of all citations retrieved from the literature search, following a liberal-accelerated approach.25,26 That is, titles and abstracts marked as include by a single reviewer moved to full-text appraisal, while only those marked as exclude were screened by a second reviewer to confirm or reject the exclusion. A liberal-accelerated approach was also used for the full-text screening of articles included after the title and abstract screening. This may have led to the inclusion of irrelevant studies at this stage; however, all included articles were read by a second reviewer during the data validation phase, at which time disagreements about the relevance of any included study were discussed between reviewers until consensus was reached about their inclusion or exclusion from the review. The reasons for exclusion of articles at the full-text level were documented.
Protocols that were implemented with results published and included in this scoping review were considered duplicate and excluded.
Charting (Data Extraction)
A charting form was developed in DistillerSR (Evidence Partners, Ottawa, Canada) and adapted for Microsoft Excel (version 2112, Microsoft, Washington, US). Charting was performed by 1 reviewer in either DistillerSR or Microsoft Excel; DistillerSR was used for most of the literature search results, while Microsoft Excel was used for the results from clinical trial registries, preprint searches, Philosopher's Index, and grey literature, and independently checked for accuracy and completeness by a second reviewer. Before charting began, the reviewers independently tested the charting form on a sample of 10 included studies to ensure a mutual understanding and that the form adequately captured the desired information. Following piloting, the reviewers met to review discrepancies. Disagreements were resolved through discussion until consensus was reached. Relevant information was charted, including the following:
study characteristics (e.g., first author’s name, publication year, country where the study was conducted) and methodology (e.g., study design and objectives)
population (e.g., number of participants, age, sex and/or gender, methods to confirm COVID-19 infection, severity of acute illness, vaccination status)
concept (i.e., risk factors and prevention, classification, diagnostic tests, treatment or management, health systems issues; subcategories were collected within each)
context (i.e., country, setting [urban, rural, remote], site of treatment during acute illness, site of treatment during follow-up).
The full list of items extracted are available in Table 11 in Appendix 2. For reviews, data presented in the review was extracted; the included primary studies were not checked, nor were extract data from them. Data were charted for all relevant concepts and contexts for this study at any duration of follow-up. If studies included a noninfected control group, population characteristics were extracted only for participants who had COVID-19, not for noninfected controls.
Charting was an iterative process, whereby additional items were added as the research team learned about the research base and recognized new items of importance. Added items were the publication date (adding the month and day), whether a study specified it was focused on patient(s) with persistent infection, and additional age data. For age data, we originally planned to extract only mean and SD, but upon realizing not all publications reported this, we decided to also extract median, IQR, range, eligible age, and categories, as reported by the studies. We also intended to extract PROGRESS-Plus framework data (i.e., place of residence, race/ethnicity/culture/language, occupation, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination, features of relationships, and time-dependent relationships) to identify characteristics that stratify health opportunities and outcomes related to health equity and equity consideration27; however, given the volume and complexity of the literature, it was not feasible to extract and validate all of these characteristics; thus, not all of the characteristics were present in this report’s results. The same charting form was used for all study designs. In addition, guideline development methods were extracted, including databases searched, literature search methods, and funding sources. We also extracted the recommendations specific to post–COVID-19 condition.
If data were missing for any variables being extracted, they was considered as missing and not estimated or imputed. No studies were excluded due to missing data. Due to resource and time constraints, no attempts were made to contact study authors for missing or unclear information. No risk of bias assessment was conducted, as the goal of the scoping review was not to comment on the quality of the evidence. The overlap between systematic reviews was not investigated, nor was the overlap between primary studies and systematic reviews. Due to the broad topic area and limited resources, details of the interventions, comparators, and outcomes in the included studies were not validated at this stage and not reported.
Descriptive Synthesis
We presented the study characteristics and findings within summary tables, visual displays, and in the main text. The number of studies identified were summarized by publication type (published commercially or as grey literature, protocols or registered clinical trials, preprints of systematic reviews) and country or countries of participants. We presented the number of studies by month of publication. We also summarized data on participants’ age, including reported mean and median ages, whether the studies included children or adolescents (younger than 18 years old), adults (18 to 64), and/or older adults (65 or older), participants’ severity of acute illness (defined as asymptomatic, symptomatic but not hospitalized, hospitalized, and intensive care unit [ICU]), and how COVID-19 was diagnosed (e.g., laboratory test, self-report). Median values and their IQRs were reported when applicable. The number of studies for each of the 5 main concepts, as well as their subcategories, were also summarized in tables, including the number and proportion by publication type, participant age categories included (younger than 18 years, 18 to 64, and 65 or older), and participants’ acute illness severity.
Results
Quantity of Research Available
A total of 3,535 unique citations were identified in the electronic literature search. Following screening of titles and abstracts, 1,998 citations were excluded, and 1,537 potentially relevant reports were retrieved for full-text review. An additional 180 potentially relevant publications were retrieved for full-text review from the grey literature search. Of these 1,717 potentially relevant articles, 825 were excluded and 892 reports of studies were included in this scoping review (refer to the list of included studies published on the Scoping Review webpage). The study selection process is outlined in Appendix 2 using a PRISMA flow chart (Figure 4). A PRISMA-ScR checklist is included in Appendix 4 (Table 2). As there were a large number of excluded studies, it did not seem informative to present the full list. We have therefore listed a sample of the included and excluded citations for each main exclusion reason, based on their order in the literature searches, in Appendix 3.
Study Characteristics
Of the 892 included studies, 637 were published commercially or as grey literature (71.4%), 247 were protocols (including clinical trial registries; 27.7%), and 8 were preprints of systematic reviews (0.9%). The published sources included 584 primary studies (91.7%), 40 systematic reviews (including scoping reviews; 6.3%), 12 guidelines (1.9%), 1 economic evaluation (0.2%), 1 qualitative primary study (0.2%), and 2 mixed-methods primary studies (0.4%). There were no ethical analyses located. Among the protocols, 239 were for primary studies (96.8%) and 8 were for systematic reviews (3.2%).
Eligible studies, including protocols and preprints, were published between January 10, 2020, and January 31, 2022 (including publications that were available online and indexed by December 20, 2021, but were officially published later). On average, there was 1 included study that became available daily (median = 2; IQR = 1 to 3). The highest number of included studies that became available in 1 day was 22 on May 14, 2021. The number of studies published over time is presented in Figure 1.
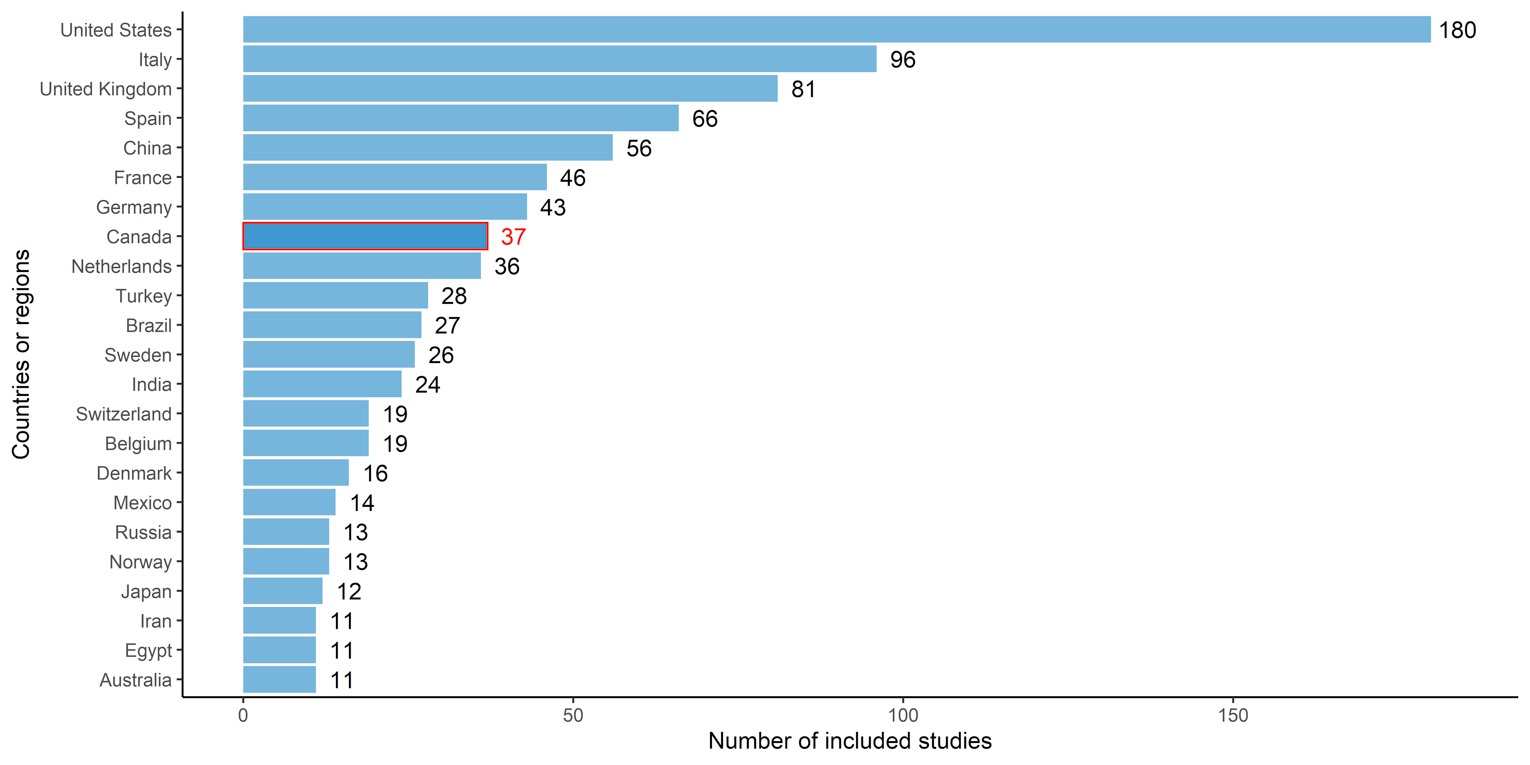
The number of sources (of any design) by country of the included participants (in countries with at least 10 included studies) is presented in Figure 2. A large proportion of studies included participants from only a few countries, particularly the US (n = 180), Italy (n = 96), and the UK (n = 81). There was lesser representation (36 to 66 studies) of participants from China, Canada, and certain European countries (primarily the Netherlands, Spain, France, and Germany). Relatively few studies (30 or fewer) included participants from areas such as Africa, South America, Australia, New Zealand, and Asia.
Additionally, lists of scoping reviews and systematic reviews are in Appendix 3 (Table 16 and Table 17, respectively).
Figure 1: Number of Included Studies by Month of Publication
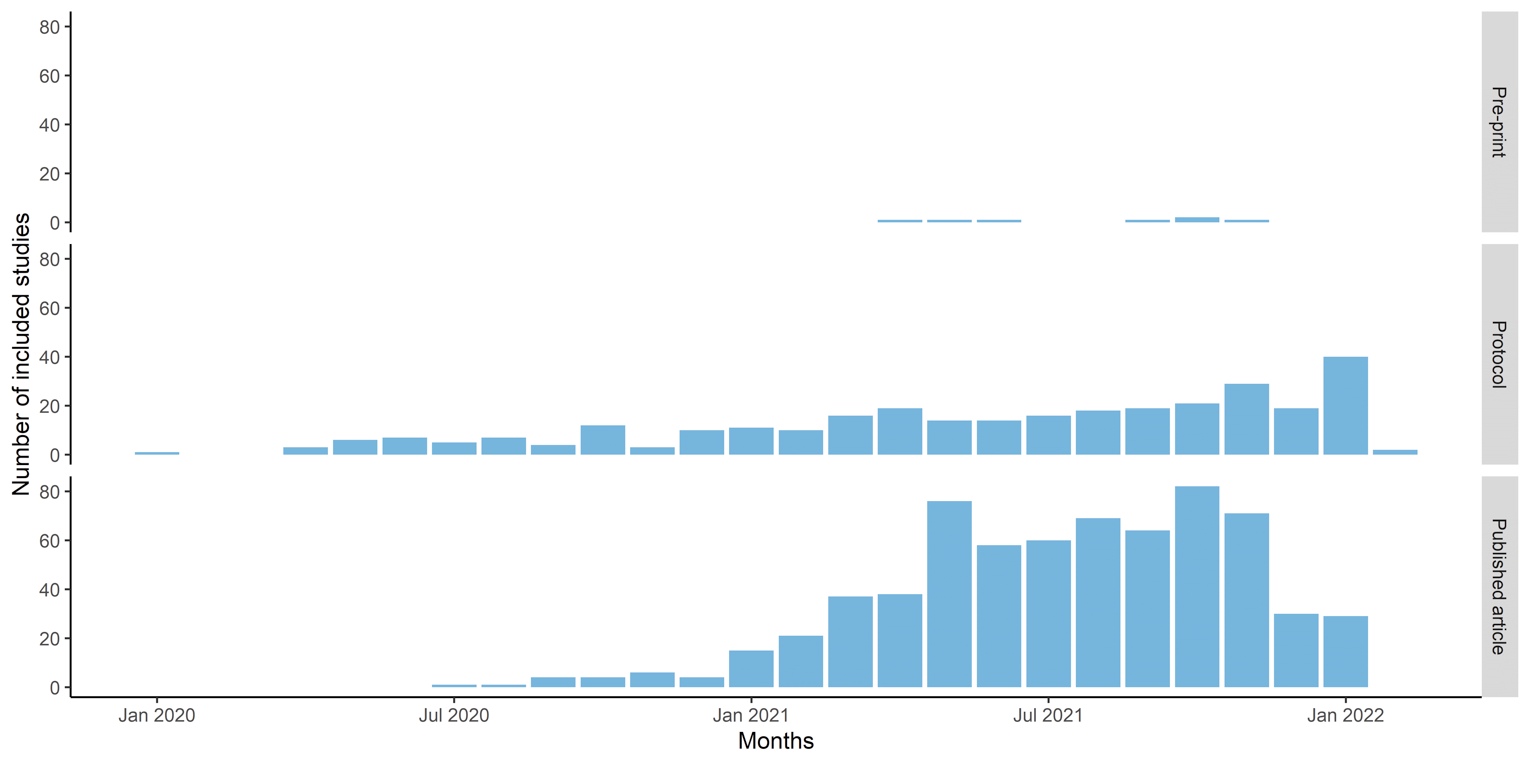
Note: Based on literature available by December 20, 2021. The first date online was extracted where available, but this was not always available, in which case the publication date was used. Some studies may have been available by December 20, 2021, but were not officially published until after; thus, some of the studies in the figure are presented as published in January.
Patient Characteristics
Demographic Characteristics
Most studies, including protocols with estimated sample sizes and systematic reviews reporting sample sizes in primary studies (n = 833; 93.4%), reported the numbers of included participants with post–COVID-19 condition. Sample sizes in guidelines were not applicable. The median sample size was 103 (range = 1 to 886,228).
The mean or median ages were reported in 503 (56.4%) studies among all sources (range = 8.5 months to 89 years). Based on reported age data in published articles and the eligible age ranges in protocols or guidelines, we determined whether studies included or planned to include children and adolescents (defined as younger than 18 years), adults (defined as 18 to 64 years), and/or older adults (defined as 65 years or older). We found that 85 (9.5%) sources included participants younger than 18 years, 720 (80.7%) included only adults between 18 and 64 years, and 473 (53.0%) included older adults who were older than 65 years. Thus, there is a notable gap in studies related to children and adolescents. The sex and/or gender distribution of the population was reported in 547 (61.3%) studies, and within these a median of 50% (IQR = 36.4% to 63.7%) of the population was male.
Data related to ethnicity and socioeconomic factors (e.g., income, education) were not widely reported in the included studies (115 [12.9%] and 54 [6.1%], respectively), which are important factors to consider when considering the potential for health inequities. Participants’ comorbidities as defined by the study authors were reported in 297 (33.3%) studies (refer to Figure 5 in Appendix 3 for the frequencies of comorbidities reported).
Few sources reported that they included individuals in rural and/or remote areas: only 11 (1.2%) and 3 (0.3%) stated they included individuals in rural and remote settings, respectively. It is possible that people living in rural or remote areas could be captured by some studies, such as those using telephone or online surveys, or online-based interventions (e.g., telerehabilitation). However, most studies did not include this information or provide subgroup analyses specific to people in rural or remote populations.
There was limited evidence identified on the role of COVID-19 vaccines. Vaccination status was not often reported in the included studies, even after COVID-19 vaccines became available in many parts of the world. Only 35 (3.9%) included references that reported data related to vaccination status, with 21 (2.4%) studies stating that participants were not vaccinated and 14 (1.6%) studies reporting that they included some participants who had received at least 1 dose of a COVID-19 vaccine. Five (0.6%) protocols have been published that plan to compare people who have been vaccinated to people who are not at risk of developing post–COVID-19 condition.
Acute Infection
The severity of acute infection (defined as asymptomatic, symptomatic but not hospitalized, hospitalized, or in ICU) was identified, though 207 (23.2%) did not report this information. Of the 685 studies where it was reported, 57 (8.3%) included participants who had been asymptomatic, 295 (43.1%) included participants who had been symptomatic but not hospitalized, 514 (75.0%) included participants who had been hospitalized, and 302 included participants (44.1%) who had been treated in the ICU. Thus, a large proportion of identified studies included people who had been hospitalized and/or treated in the ICU during the acute phase; there were comparatively fewer studies that included people who were asymptomatic in the acute phase. The frequencies of the severity of acute infection are available in Figure 6 in Appendix 3.
There were multiple methods for diagnosing or identifying COVID-19 infection used by 866 (97.1% of included sources) identified sources. Overall, there were 473 (54.6%) studies that used polymerase chain reaction tests, 122 (13.8%) that used antibody or antigen tests, 105 (11.9%) that used other or unspecified lab tests, 84 (9.5%) that used other tests (e.g., chest CT), 57 (6.5%) that confirmed using unspecified tests at the hospital or in the ICU, 53 (6.0%) that diagnosed by clinician, 11 (1.2%) that used the International Classification of Diseases (ICD) code for COVID-19, 2 (0.2%) that used the ICD code for long COVID or post–COVID-19 condition, and 9 (1.0%) that used self-report. The frequencies of these methods can be found in Figure 7 in Appendix 3.
Concepts
Main Concepts
Included studies were categorized as belonging to at least 1 main concept: risk factors and prevention, classification (e.g., classifying post–COVID-19 condition by symptoms, SARS-CoV-2 variant quantification, and reporting of pathophysiological markers), diagnostic tests, treatment or management, and health system issues (e.g., usage of health care services and pharmaceutical drugs). All concepts had additional subcategories except health system issues.
Across the 5 main categories, the most common for published studies, protocols, and preprints of systematic reviews was classification, followed by risk factors and prevention. Diagnostic tests had a high number of published studies but relatively few protocols, while treatment and management had few published studies but several protocols. We identified few sources related to few health systems issues across all publication types. The number of included sources by concept and publication status is presented in Figure 3, and a more detailed breakdown of the number of sources by various characteristics (e.g., study design, age groups) is presented in Table 3.
Figure 3: Number of Studies Included Within Each Concept, by Publication Status
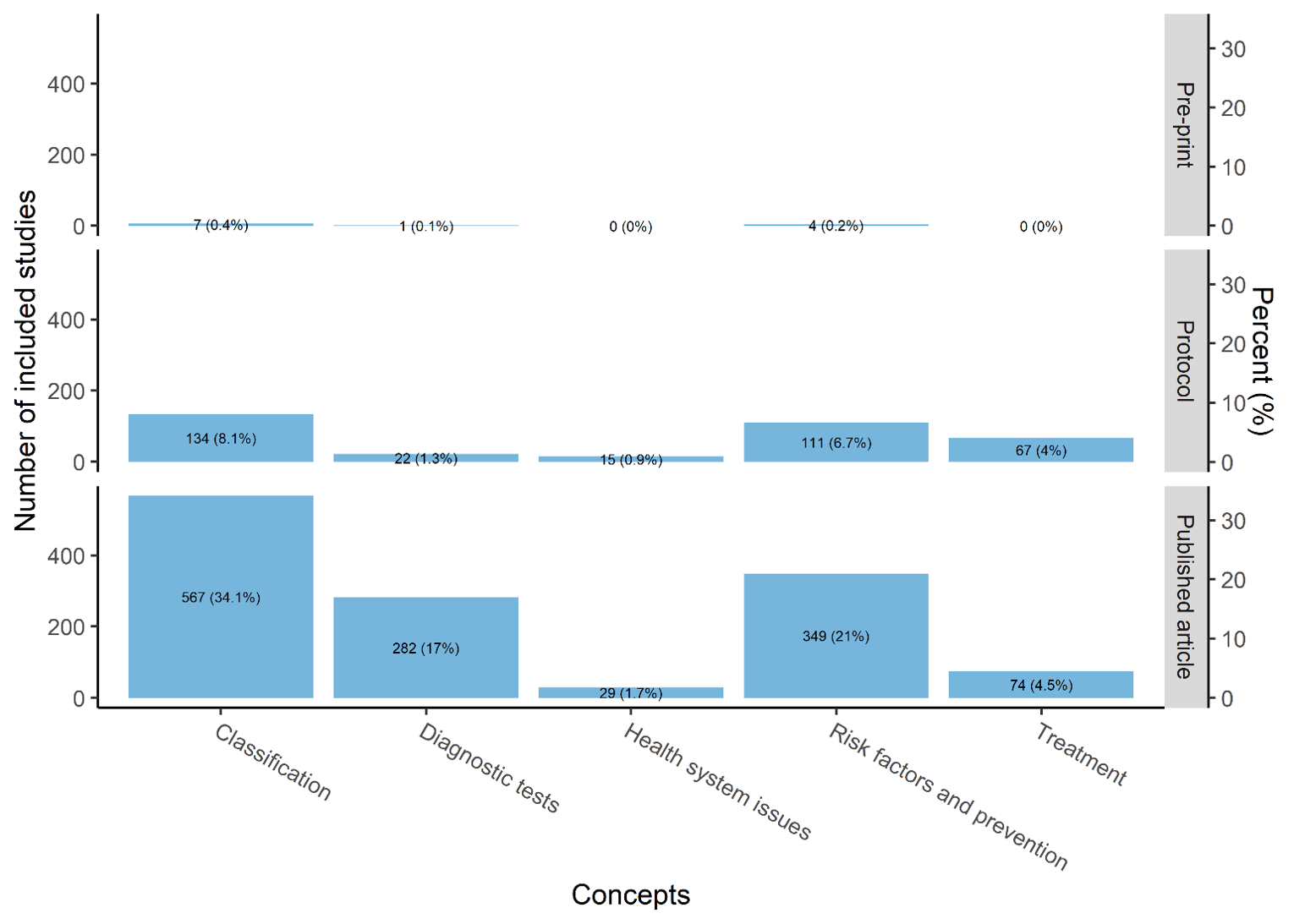
Note: Included references could be included under more than 1 main concept category.
Table 3: Characteristics of Included Studies by Concept and Publication Status
Characteristic | Treatment, n (%) | Risk factors and prevention, n (%) | Classification, n (%) | Diagnostic tests, n (%) | Health system issues, n (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Published (n = 74) | Protocol (n = 67) | Published (n = 349) | Protocol (n = 111) | Published (n = 567) | Protocol (n = 134) | Published (n = 282) | Protocol (n = 22) | Published (n = 29) | Protocol (n = 15) | |
Report type | ||||||||||
Primary study | 60 (81.1) | 65 (95.6) | 315 (90.3) | 109 (94) | 521 (92.4) | 135 (97.1) | 261 (93.2) | 21 (95.5) | 25 (89.3) | 15 (100) |
Systematic review | 4 (5.4) | 3 (4.4) | 27 (7.7) | 7 (6) | 39 (6.9) | 4 (2.9) | 10 (3.6) | 1 (4.5) | 1 (3.6) | 0 |
Scoping review | 2 (2.7) | 0 | 3 (0.9) | 0 | 3 (0.5) | 0 | 1 (0.4) | 0 | 0 | 0 |
Guideline | 11 (14.9) | 0 | 7 (2) | 0 | 6 (1.1) | 0 | 11 (3.9) | 0 | 2 (7.1) | 0 |
Economic evaluation | 0 | 0 | 1 (0.3) | 0 | 1 (0.2) | 0 | 0 | 0 | 1 (3.6) | 0 |
Study designa | ||||||||||
Interventional | 14 (18.9) | 64 (94.1) | 11 (3.2) | 69 (59.5) | 10 (1.8) | 15 (10.8) | 7 (2.5) | 8 (36.4) | 0 | 0 |
Observational | 52 (70.3) | 4 (5.9) | 332 (95.1) | 48 (41.4) | 549 (97.3) | 124 (89.2) | 264 (94.3) | 14 (63.6) | 25 (89.3) | 15 (100) |
Age categories included | ||||||||||
< 18 included | 4 (5.4) | 1 (1.5) | 33 (9.5) | 13 (11.7) | 54 (9.5) | 21 (15.7) | 20 (7.1) | 3 (13.6) | 3 (10.3) | 3 (20) |
18 to 64 included | 50 (67.6) | 61 (91) | 277 (79.4) | 103 (92.8) | 445 (78.5) | 128 (95.5) | 215 (76.2) | 19 (86.4) | 20 (69) | 15 (100) |
≥ 65 included | 18 (24.3) | 51 (76.1) | 170 (48.7) | 96 (86.5) | 238 (42) | 111 (82.8) | 102 (36.2) | 20 (90.9) | 15 (51.7) | 15 (100) |
Not reported | 12 (16.2) | 3 (4.5) | 29 (8.3) | 3 (2.7) | 43 (7.6) | 4 (3) | 29 (10.3) | 1 (4.5) | 4 (13.8) | 0 |
Severity of acute illness | ||||||||||
Asymptomatic | 4 (5.4) | 1 (1.5) | 27 (7.7) | 6 (5.2) | 39 (6.9) | 10 (7.2) | 20 (7.1) | 2 (9.1) | 2 (7.1) | 1 (6.7) |
Symptomatic, not hospitalized | 25 (33.8) | 12 (17.6) | 138 (39.5) | 28 (24.1) | 216 (38.3) | 35 (25.2) | 96 (34.3) | 6 (27.3) | 16 (57.1) | 7 (46.7) |
Hospitalized | 29 (39.2) | 16 (23.5) | 268 (76.8) | 54 (46.6) | 366 (64.9) | 71 (51.1) | 183 (65.4) | 11 (50) | 23 (82.1) | 8 (53.3) |
ICU | 16 (21.6) | 12 (17.6) | 154 (44.1) | 36 (31) | 210 (37.2) | 48 (34.5) | 94 (33.6) | 7 (31.8) | 13 (46.4) | 8 (53.3) |
Not reported | 20 (27) | 41 (60.3) | 38 (10.9) | 40 (34.5) | 92 (16.3) | 57 (41) | 41 (14.6) | 6 (27.3) | 3 (10.7) | 3 (20) |
ICU = intensive care unit; n (%) = number of references (proportions relative to all references in the same categories).
Note: Included studies could be included under more than 1 main concept category and/or study design and may have included multiple age groups and/or severity of acute illness categories.
aSystematic reviews and primary studies were classified as interventional and/or observational. Other publication types (e.g., guidelines) were not classified as either; thus, these numbers may not add up to 100%.
Classification
Studies related to classification were included in at least 1 of 5 subcategories, including:
studies that assessed characteristics or outcomes of post–COVID-19 condition (e.g., symptoms or quality of life)
pathophysiological markers that were assessed within 12 weeks (e.g., inflammation markers or lung function tests)
different variants of SARS-CoV-2 (e.g., if studies specified the variant being assessed)
subtypes of post–COVID-19 condition (e.g., studies that attempted to categorize patients with post–COVID-19 condition into different groups, based on symptoms, trajectory, and/or other factors)
other (studies that may have assessed other characteristics, such as genome sequences or follow-up studies of interventions designed for acute infection).
Overall, the largest subcategory represented under classification was characteristics for both published studies and protocols, followed by pathophysiological markers. In comparison, there were very few published studies related to different variants of the SARS-CoV-2 virus and subtypes of post–COVID-19 condition, and no protocols for either. A more detailed breakdown of the number of sources by various characteristics and publication status (published or protocols) is presented in Table 4.
Table 4: Characteristics of Included Studies Reporting on Classification, by Publication Status
Characteristic | Post–Covid-19 Characteristics, n (%) | Pathophysiological markers, n (%) | Different variants of SARS-CoV-2, n (%) | Subtypes, n (%) | Other,a n (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
Published (n = 542) | Protocol (n = 130) | Published (n = 96) | Protocol (n = 43) | Published (n = 2) | Protocol (n = 0) | Published (n = 7) | Protocol (n = 0) | Published (n = 2) | Protocol (n = 4) | |
Study design | ||||||||||
Primary study | 498 (91.9) | 126 (96.9) | 92 (95.8) | 43 (100) | 2 (100) | 0 | 7 (100) | 0 | 2 (100) | 4 (100) |
Systematic review | 39 (7.2) | 4 (3.1) | 4 (4.2) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Scoping review | 3 (0.6) | 0 | 1 (1) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Guideline | 7 (1.3) | 0 | 1 (1) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Economic evaluation | 1 (0.2) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Interventional or observationalb | ||||||||||
Interventional | 10 (1.8) | 14 (10.8) | 1 (1) | 3 (7) | 0 | 0 | 1 (14.3) | 0 | 0 | 0 |
Observational | 526 (97) | 116 (89.2) | 95 (99) | 40 (93) | 2 (100) | 0 | 6 (85.7) | 0 | 2 (100) | 4 (100) |
Age groups | ||||||||||
< 18 included | 52 (9.5) | 19 (15.2) | 8 (8.3) | 5 (11.6) | 0 | 0 | 0 | 0 | 0 | 3 (75) |
18 to 64 included | 427 (78.3) | 119 (95.2) | 74 (77.1) | 42 (97.7) | 2 (100) | 0 | 6 (85.7) | 0 | 1 (50) | 4 (100) |
≥ 65 included | 229 (42) | 105 (84) | 40 (41.7) | 36 (83.7) | 0 | 0 | 4 (57.1) | 0 | 2 (100) | 3 (75) |
Not reported | 41 (7.5) | 4 (3.2) | 10 (10.4) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Severity of acute illness | ||||||||||
Asymptomatic | 35 (6.5) | 9 (6.9) | 11 (11.5) | 2 (4.7) | 0 | 0 | 0 | 0 | 0 | 0 |
Symptomatic, not hospitalized | 211 (38.9) | 31 (23.8) | 34 (35.4) | 8 (18.6) | 1 (50) | 0 | 2 (28.6) | 0 | 0 | 3 (75) |
Hospitalized | 352 (64.9) | 66 (50.8) | 64 (66.7) | 17 (39.5) | 1 (50) | 0 | 6 (85.7) | 0 | 1 (50) | 4 (100) |
ICU | 202 (37.3) | 45 (34.6) | 35 (36.5) | 8 (18.6) | 0 | 0 | 4 (57.1) | 0 | 1 (50) | 3 (75) |
Not reported | 88 (16.2) | 53 (40.8) | 16 (16.7) | 25 (58.1) | 0 | 0 | 1 (14.3) | 0 | 0 | 0 |
ICU = intensive care unit; n (%) = number of references (proportions relative to all references in the same categories); SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Note: Included references could be included under more than 1 main concept category and/or study design and may have included multiple age groups and/or severity of acute illness categories.
aStudies that may have assessed other characteristics (e.g., genome sequences, follow-up studies of interventions designed for acute infection).
bSystematic reviews and primary studies were classified as interventional and/or observational. Other publication types (e.g., guidelines) were not classified as either; thus, these numbers may not add up to 100%.
Risk Factors and Prevention
Sources were considered as related to prevention if the intervention was provided within 12 weeks, including during the acute phase (e.g., a drug was provided during the acute phase or immediately after discharge, and the study assessed participants’ symptoms at 12 weeks or later). Studies under risk factors and prevention were included in at least 1 of the following subcategories:
risk factors (i.e., assessed any risk factors and their association with developing post–COVID-19 condition, such as age, sex, and comorbidities)
preventive drug interventions
preventive rehabilitation interventions (e.g., rehabilitation during hospital stay or immediately after discharge within 12 weeks of initial infection, may reduce the risk of developing post–COVID-19 condition)
other preventive interventions (e.g., supplements, Chinese medicine, medical devices, or surgery).
Most (n = 311; 89.1%) of the published articles in this category assessed risk factors, especially published studies. There were comparatively fewer published studies related to preventive interventions (drug: n = 34; 9.7%; rehabilitation: n = 20; 5.7%), but we identified several protocols (41 and 26 for drug and rehabilitation, respectively, or 36.9% and 24.3% of protocols in this category), indicating that these areas are currently under study and more work will be published over time. A more detailed breakdown of the number of sources by publication status (published and protocol) and various characteristics is presented in Table 5. We also identified 4 preprints of systematic reviews, all related to risk factors.
Table 5: Characteristics of Included Studies Reporting on Risk Factors and Prevention, by Publication Status
Characteristic | Drug prevention, n (%) | Preventive rehabilitation, n (%) | Risk factors, n (%) | Other, n (%) | ||||
|---|---|---|---|---|---|---|---|---|
Published (n = 34) | Protocol (n = 41) | Published (n = 20) | Protocol (n = 27) | Published (n = 311) | Protocol (n = 37) | Published (n = 9) | Protocol (n = 17) | |
Study design | ||||||||
Primary study | 33 (97.1) | 39 (95.1) | 15 (75) | 24 (88.9) | 279 (89.7) | 33 (89.2) | 7 (77.8) | 17 (100) |
Systematic review | 0 | 2 (4.9) | 1 (5) | 3 (11.1) | 27 (8.7) | 4 (10.8) | 0 | 0 |
Scoping review | 0 | 0 | 0 | 0 | 3 (1) | 0 | 0 | 0 |
Guideline | 0 | 0 | 4 (20) | 0 | 5 (1.6) | 0 | 1 (11.1) | 0 |
Economic evaluation | 1 (2.9) | 0 | 0 | 0 | 1 (0.3) | 0 | 1 (11.1) | 0 |
Interventional or observationala | ||||||||
Interventional | 2 (5.9) | 35 (85.4) | 7 (35) | 26 (96.3) | 3 (1) | 4 (10.8) | 0 | 12 (70.6) |
Observational | 31 (91.2) | 7 (17.1) | 9 (45) | 2 (7.4) | 304 (97.7) | 34 (91.9) | 7 (77.8) | 5 (29.4) |
Age groups | ||||||||
< 18 included | 1 (2.8) | 2 (5) | 0 | 2 (7.7) | 33 (10.6) | 7 (20.6) | 1 (10) | 2 (11.8) |
18 to 64 included | 29 (80.6) | 38 (95) | 15 (75) | 22 (84.6) | 244 (78.7) | 31 (91.2) | 8 (80) | 16 (94.1) |
≥ 65 included | 14 (38.9) | 34 (85) | 5 (25) | 22 (84.6) | 157 (50.6) | 27 (79.4) | 3 (30) | 15 (88.2) |
Not reported | 0 | 1 (2.5) | 5 (25) | 1 (3.8) | 27 (8.7) | 2 (5.9) | 1 (10) | 1 (5.9) |
Severity of acute illness | ||||||||
Asymptomatic | 0 | 3 (7.3) | 1 (5) | 0 | 27 (8.7) | 3 (8.1) | 0 | 1 (5.9) |
Symptomatic, not hospitalized | 9 (26.5) | 13 (31.7) | 5 (25) | 2 (7.4) | 129 (41.5) | 8 (21.6) | 2 (22.2) | 5 (29.4) |
Hospitalized | 20 (58.8) | 18 (43.9) | 14 (70) | 12 (44.4) | 249 (80.1) | 21 (56.8) | 3 (33.3) | 7 (41.2) |
ICU | 14 (41.2) | 9 (22) | 11 (55) | 12 (44.4) | 133 (42.8) | 12 (32.4) | 3 (33.3) | 7 (41.2) |
Not reported | 2 (5.9) | 12 (29.3) | 2 (10) | 8 (29.6) | 36 (11.6) | 15 (40.5) | 2 (22.2) | 7 (41.2) |
ICU = intensive care unit; n (%) = number of references (proportions relative to all references in the same categories).
Note: Included references could be included under more than 1 main concept category and/or study design and may have included multiple age groups and/or severity of acute illness categories. No qualitative or mixed-methods studies were identified.
aSystematic reviews and primary studies were classified as interventional and/or observational. Other publication types (e.g., guidelines) were not classified as either; thus, these numbers may not add up to 100%.
Diagnostic Tests
Studies were considered relevant to diagnostic tests if they conducted any kind of laboratory test, imaging test, or other kind of health assessment test (e.g., pulmonary function test) at or after 12 weeks. Thus, we categorized all sources based on whether they conducted a laboratory test, imaging test, and/or other unspecified test. Overall, there were similar numbers of published studies and protocols for imaging and laboratory tests (165 and 146 published studies, respectively, or 58.5% and 51.8% of published studies within this category; and 12 protocols for both categories, or 54.5% within this category). A more detailed breakdown of the number of sources by publication status (published or protocol) and various characteristics is presented in Table 6.
Table 6: Characteristics of Included Studies Reporting on Diagnostic Tests for Post–COVID-19 Condition, by Publication Status
Characteristic | Imaging tests, n (%) | Laboratory tests, n (%) | Other kind of health assessment test (e.g., pulmonary function test), n (%) | |||
|---|---|---|---|---|---|---|
Published (n = 165) | Protocol (n = 12) | Published (n = 146) | Protocol (n = 12) | Published (n = 85) | Protocol (n = 11) | |
Study design | ||||||
Primary study | 152 (92.1) | 12 (100) | 138 (94.5) | 12 (100) | 73 (85.9) | 10 (90.9) |
Systematic review | 7 (4.2) | 0 | 4 (2.7) | 0 | 4 (4.7) | 1 (9.1) |
Scoping review | 1 (0.6) | 0 | 0 | 0 | 0 | 0 |
Guideline | 6 (3.6) | 0 | 5 (3.4) | 0 | 8 (9.4) | 0 |
Economic evaluation | 0 | 0 | 0 | 0 | 0 | 0 |
Interventional or observationala | ||||||
Interventional | 2 (1.2) | 1 (8.3) | 5 (3.4) | 4 (33.3) | 3 (3.5) | 5 (45.5) |
Observational | 158 (95.8) | 11 (91.7) | 137 (93.8) | 8 (66.7) | 74 (87.1) | 6 (54.5) |
Age groups | ||||||
< 18 included | 11 (6.6) | 1 (8.3) | 15 (10.2) | 2 (16.7) | 5 (6) | 1 (9.1) |
18 to 64 included | 129 (77.7) | 9 (75) | 107 (72.8) | 11 (91.7) | 63 (75) | 9 (81.8) |
≥ 65 included | 51 (30.7) | 10 (83.3) | 55 (37.4) | 11 (91.7) | 32 (38.1) | 10 (90.9) |
Not reported | 14 (8.4) | 1 (8.3) | 15 (10.2) | 0 | 12 (14.3) | 1 (9.1) |
Severity of acute illness | ||||||
Asymptomatic | 4 (2.4) | 2 (16.7) | 16 (11) | 1 (8.3) | 5 (5.9) | 2 (18.2) |
Symptomatic, not hospitalized | 48 (29.1) | 3 (25) | 61 (41.8) | 4 (33.3) | 25 (29.4) | 2 (18.2) |
Hospitalized | 106 (64.2) | 7 (58.3) | 98 (67.1) | 6 (50) | 59 (69.4) | 6 (54.5) |
ICU | 60 (36.4) | 5 (41.7) | 43 (29.5) | 5 (41.7) | 35 (41.2) | 3 (27.3) |
Not reported | 17 (10.3) | 3 (25) | 21 (14.4) | 4 (33.3) | 14 (16.5) | 3 (27.3) |
ICU = intensive care unit; n (%) = number of references (proportions relative to all references in the same categories).
Note: Included references could be included under more than 1 main concept category and/or study design and may have included multiple age groups and/or severity of acute illness categories.
aSystematic reviews and primary studies were classified as interventional and/or observational. Other publication types (e.g., guidelines) were not classified as either; thus, these numbers may not add up to 100%.
Type of Treatment or Management
Any intervention provided at or after 12 weeks or 3 months was considered a treatment intervention. Treatment interventions could fall into 1 or more subcategories:
drug (any pharmaceutical intervention)
rehabilitation (i.e., any kind of exercise rehabilitation, provided in a medical setting or at home [e.g., telehealth])
care models (i.e., pathways, trajectories, frameworks, or structured clinics)28
other (e.g., supplements, Chinese medicine, medical devices, virtual reality exercise, and surgery).
References that assessed, or protocols that planned to assess, vaccines as a potential treatment for post–COVID-19 condition were considered both drug and other interventions. We identified relatively few published studies related to treatment or management interventions, but several protocols indicate that research in these areas is ongoing. However, we identified comparatively fewer published studies and protocols related to care models. A more detailed breakdown of the number of sources by publication status and various characteristics is presented in Table 7.
Table 7: Characteristics of Included Studies Reporting on Treatment or Management, by Publication Status
Characteristic | Rehabilitation, n (%) | Drug, n (%) | Care model, n (%) | Other, n (%) | ||||
|---|---|---|---|---|---|---|---|---|
Published (n = 27) | Protocol (n = 42) | Published (n = 35) | Protocol (n = 19) | Published (n = 7) | Protocol (n = 3) | Published (n = 24) | Protocol (n = 16) | |
Study design | ||||||||
Primary study | 15 (55.6) | 40 (95.2) | 33 (94.3) | 17 (89.5) | 2 (28.6) | 2 (66.7) | 20 (83.3) | 16 (100) |
Systematic review | 4 (14.8) | 2 (4.8) | 2 (5.7) | 2 (10.5) | 2 (28.6) | 1 (33.3) | 0 | 0 |
Scoping review | 2 (7.7) | 0 | 1 (2.9) | 0 | 1 (16.7) | 0 | 0 | 0 |
Guideline | 9 (33.3) | 0 | 1 (2.9) | 0 | 4 (57.1) | 0 | 4 (16.7) | 0 |
Economic evaluation | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Interventional or observationala | ||||||||
Interventional | 8 (29.6) | 40 (95.2) | 3 (8.6) | 18 (94.7) | 1 (14.3) | 1 (33.3) | 4 (16.7) | 16 (100) |
Observational | 12 (44.4) | 2 (4.8) | 33 (94.3) | 1 (5.3) | 3 (42.9) | 2 (66.7) | 16 (66.7) | 0 |
Age groups | ||||||||
< 18 included | 3 (11.5) | 1 (2.4) | 3 (8.6) | 0 | 1 (16.7) | 0 | 1 (4) | 0 |
18 to 64 included | 14 (53.8) | 38 (90.5) | 26 (74.3) | 17 (89.5) | 1 (16.7) | 2 (66.7) | 15 (60) | 13 (86.7) |
≥ 65 included | 7 (26.9) | 34 (81) | 7 (20) | 11 (57.9) | 2 (33.3) | 2 (66.7) | 6 (24) | 11 (73.3) |
Not reported | 9 (34.6) | 2 (4.8) | 1 (2.9) | 2 (10.5) | 3 (50) | 1 (33.3) | 5 (20) | 1 (6.7) |
Severity of acute illness | ||||||||
Asymptomatic | 2 (7.4) | 0 | 3 (8.6) | 1 (5.3) | 1 (14.3) | 0 | 0 | 0 |
Symptomatic, not hospitalized | 12 (44.4) | 8 (19) | 13 (37.1) | 3 (15.8) | 3 (42.9) | 0 | 7 (29.2) | 4 (25) |
Hospitalized | 11 (40.7) | 7 (16.7) | 17 (48.6) | 8 (42.1) | 3 (42.9) | 1 (33.3) | 5 (20.8) | 6 (37.5) |
ICU | 9 (33.3) | 10 (23.8) | 5 (14.3) | 0 | 2 (28.6) | 0 | 4 (16.7) | 3 (18.8) |
Not reported | 11 (40.7) | 26 (61.9) | 5 (14.3) | 11 (57.9) | 4 (57.1) | 2 (66.7) | 8 (33.3) | 7 (43.8) |
ICU = intensive care unit; n (%) = number of references (proportions relative to all references in the same categories).
Note: Included references could be included under more than 1 main concept category and/or study design and may have included multiple age groups and/or severity of acute illness categories.
aSystematic reviews and primary studies were classified as interventional and/or observational. Other publication types (e.g., guidelines) were not classified as either; thus, these numbers may not add up to 100%.
Guidelines
Among the included studies described and summarized in the previous sections, there were 12 guidelines identified. Guidelines were eligible for inclusion if they provided at least 1 recommendation specific to patients experiencing symptoms 12 or more weeks after diagnosis or symptom onset.
In Canada, guidelines from Alberta, British Columbia, Ontario, and Quebec were identified; the methods and relevant recommendations (i.e., recommendations specific to 12 weeks or later) are summarized in Table 12 and Table 13 in Appendix 2, respectively. All included guidelines define post–COVID as 4 or more weeks post-infection or diagnosis but provide limited guidance for patients experiencing symptoms after 12 weeks. Recommendations specific to people experiencing symptoms at 12 weeks or later were referral to a specialty clinic (Alberta29 and British Columbia30) and using a chest X-ray for those experiencing respiratory symptoms (Ontario31 and Quebec).32
Eight guidelines were identified from countries other than Canada and are summarized in Table 14. Most guidelines from other countries also focus on the 4 or more weeks definition, with limited diagnosis guidance for patients at 12 or more weeks post-infection or diagnosis. Four guidelines were identified that provided guidance for diagnosis as well as management for patients at 12 weeks or later.6,33-35 A summary of these guidelines’ methods and relevant recommendations are available in Table 14 and Table 15 in Appendix 2, respectively.
Evidence Gap Mapping
A summary of areas where sources were and were not identified is presented in Table 8. Thus far, much of the published literature on post–COVID-19 condition has focused on symptoms, outcomes, and risk factors, with some studies assessing for long periods of time; for example, a year after infection or hospital discharge.36-38 More than 450 studies have also assessed factors associated with a higher risk of experiencing post–COVID symptoms, and used different diagnostic tests (e.g., using biomarkers or imaging tests). We noted few systematic reviews on diagnostic tests for post–COVID-19 symptoms despite the high number of primary studies, which may be a potential area for future systematic reviews. We identified fewer than 90 published sources on treatment and management, but noted an increasing number of clinical trial registrations, indicating ongoing work to determine the effectiveness of different treatments, including pharmaceutical drugs, COVID-19 vaccines used after infection, and rehabilitation.
State of evidence map | Concepts and populations |
|---|---|
Areas where evidence was identified: several published primary studies (≥ 50) and SRs (≥ 10) |
|
Areas where there were several (≥ 50) primary studies but few SRs (< 10) |
|
Areas expecting to see evidence soon (< 50 published primary studies and/or < 10 SRs, several trial protocols, and a few SR protocols) |
|
Areas with gaps in evidence (< 50 published primary studies and < 50 protocols) | Study types:
Concepts:
Participant demographics:
|
SR = systematic reviews.
aIn total 12 guidelines were identified, but most provided limited recommendations specific to patients at 12 or more weeks and instead focused on 4 or more weeks. It is unclear if these recommendations can be applied to patients after 12 or more weeks.
bThis is based on limited studies that explicitly reported they included rural and remote or conducted a subanalysis of rural and remote. Certain study designs may include rural and remote populations (e.g., online surveys), but unless they stated that they recruited participants from rural and remote locations, they were not counted.
cThe proportion of trial protocols where severity of acute illness was not reported was relatively high for preventive and treatment and management, so it is possible that some of these trials will include participants who were asymptomatic and may have conducted subanalyses by acute illness severity. However, we identified relatively few published studies focused on this group, compared to participants who had been hospitalized.
Discussion
There were some notable evidence gaps and areas with large numbers of studies. There were limited evaluations on the economic impact of post–COVID-19 condition or the cost-effectiveness of interventions. There were also few guidelines providing recommendations for individuals living with post–COVID-19 condition according to the WHO definition (12 or more weeks after initial infection). Many of the identified guidelines provide guidance for people who still have symptoms at 4 or more weeks, and it is unclear whether these recommendations will be revised for people who are experiencing symptoms at 12 or more weeks. Early estimates suggest a lower prevalence of persistent symptoms at 12 weeks compared to 4 to 5 weeks,10,39 which may indicate that some people who have symptoms at 4 weeks will recover by 12 weeks. Currently, it is unclear if they represent a different clinical phenotype than people who have symptoms at 12 or more weeks. If this is the case, different guidance may be required at 12 or more weeks than 4 to 12 weeks. We also identified few published sources and protocols that assessed the impact of different variants of SARS-CoV-2 and different subtypes of post–COVID-19 condition (i.e., whether post–COVID-19 condition may encapsulate multiple different syndromes40,41; such as, based on different symptom trajectories).42 For example, people who had been treated in the ICU may be experiencing post-intensive care syndrome,43 which is characterized as “the worsening of the physical, mental or cognitive patient’s status after a critical illness” (p. 2),43 and may be a separate clinical phenotype from people who had milder acute illness but are also experiencing persistent symptoms.44-46
We identified few published studies and protocols for certain population groups. Relatively few studies and protocols included or plan to include children, and there may be important differences between adults and children (e.g., while many studies report shortness of breath as a common post–COVID-19 symptom, the NICE guidelines suggest that it is less common in children and older adults6). In addition, while numerous protocols for management and treatment were identified, many are not including participants under 18 years old. Thus, even if these trials indicate treatments to be effective in adults, it is not known if they can be used to treat children or adolescents with similar effects. We also did not identify many studies that included people who had been asymptomatic during the acute illness phase or focused on people living in rural and/or remote areas. This may be due in part to lack of COVID-19 testing, particularly earlier in the pandemic when access may have been restricted or otherwise difficult to access for people who were asymptomatic. It is possible the clinical phenotype of post–COVID-19 condition may differ between people who had milder acute illness (i.e., were not hospitalized) and people who had more severe acute illness and were hospitalized. Thus, the lack of published evidence and lack of planned protocols focused on people who had milder acute illness, particularly people who had been asymptomatic, is an important evidence gap. There was also a gap in studies that reported specifically on participants living in rural and/or remote areas. Many studies were conducted by major hospitals that are generally located in urban areas. While some study designs may include people living in rural and remote areas, such as surveys conducted by telephone or online,47 few studies included data on participants’ location (e.g., how many participants were living in rural or remote areas), making it unclear whether living in a rural or remote area may be associated with the severity of initial infection or influence outcomes. For example, individuals living far from a major hospital may not have received the same level of care for acute infection or may not have had access to certain treatment and management options for post–COVID-19 condition, such as a specialized clinic in the city. While telehealth-based rehabilitation has been evaluated in several primary studies,48,49 whether participants’ location may hinder accessibility and thus long-term outcomes requires further research. The lack of literature on rural and remote populations should also be considered to ensure equitable access to high-quality post–COVID care.
In Canada and many other countries, the COVID-19 vaccination coverage has reached more than 80% of adults.50 However, we did not identify many published studies that assess the impact of the COVID-19 vaccination on the development of post–COVID-19 condition. Nor many studies that reported if their participants had received the COVID-19 vaccine: thus, it is still unclear whether receiving a COVID-19 vaccine before or after developing post–COVID-19 condition will impact symptoms. We did identify some registered trials that aim to assess the impact of vaccination on post–COVID-19 condition.51-53 There are also limited studies assessing post–COVID-19 condition in breakthrough infections (i.e., for individuals who had been vaccinated, then become infected with COVID-19). This may be an important consideration with the spread of the Omicron variant, which has become dominant in Canada and many other countries, as vaccines are less effective at preventing infection from this variant, and breakthrough infections have become increasingly common.54 There was also a lack of information regarding the SARS-CoV-2 variant being assessed in studies.55,56 Determining whether different variants have different long-term effects may also be important to plan for diagnosis, treatment, or management. Finally, future guidelines or updates to existing guidelines may be needed to ensure clear and consistent recommendations for post–COVID-19 condition that incorporate the findings of emerging evidence, so that health care providers can provide adequate care.
In contrast, we identified areas with large numbers of sources. There were more systematic reviews addressing the characteristics and outcomes of post–COVID-19 condition and risk factors than other concepts. There were many recently published primary studies reporting on pathophysiological markers and diagnostic tests. These issues may be suitable for evidence synthesis or meta-analysis to provide summaries on the pandemic. While there are new SARS-CoV-2 variants emerging and new strategies are created for the long-term consequences, continued efforts in exploring these concepts in the short-term are expected.
Identified previous scoping reviews on post–COVID-19 condition were published before WHO’s release of a clinical definition for post–COVID-19 condition, and did not use the definition of 12 weeks (or 3 months) after diagnosis or symptom onset.11-13 Thus, this report has a broader scope and differs from previous scoping reviews as it focuses on studies that assessed participants at least after 12 weeks, aligning with the current NICE and WHO definitions of post–COVID-19 condition.6,7 We have also added to the evidence that pertains to a broader range of topics than previous scoping reviews, such as mapping evidence related to preventive interventions and health systems issues. Finally, we have also characterized the volume of literature by various demographic variables, allowing for a better sense of where evidence is lacking and for which groups.
Limitations
This review was limited to studies available in English or French; as this limitation was applied at the level of the search, it is not clear how many studies may have been excluded for this reason, and findings could differ slightly had other languages been included. Due to the wide breadth of topics covered and time constraints, we chose to exclude literature reviews, correspondence, editorials, and preprints of primary studies, and did not search reference lists of included studies nor contact experts to supplement the search; as a result, there is a possibility that some relevant studies were missed, but it is unlikely that this would have a large impact on the overall high-level findings. While ethical analyses were eligible for inclusion, it is possible and likely that some were missed given the specialized expertise required to identify such analyses and that these reports might be presented as narrative reviews, commentaries, or editorials, which were not eligible for this review. We also chose specific follow-up time definitions based on the reported mean with SD or median with IQR, but these are imperfect measures and had other threshold been used, there may have been differences in which studies were included and excluded. Some included sources may not have intended to assess post–COVID-19 condition; for example, a study assessed rehabilitation post-discharge to treat post-intensive care syndrome, but followed participants for at least 12 weeks after symptom onset or diagnosis. As there was no differentiation made between post-intensive care syndrome and post–COVID-19 condition, this review could include both. The overlap between systematic reviews was not investigated and certain primary studies are likely to be included in multiple systematic reviews. Resource and time constraints also prevented us from abstracting several measures, such as the definition of post–COVID-19 condition used in individual studies, details of specific interventions, and outcomes collected by the studies. Although the PROGRESS-Plus variables were charted, the text data were complex and it became infeasible to extract, validate, and organize them all in a meaningful way; thus, the data are not presented. Finally, stakeholder input on the scoping review was limited to peer review and select clinical experts. Persons with post–COVID-19 condition are an integral part of the stakeholder panel, a group of cross-jurisdictional decision-makers, clinicians, researchers, and patient representatives who are providing support for the overall direction for the larger condition-level review, but they did not provide direct input for this scoping review.
Future Updates
With the emergence of published sources of this topic monthly, an update to this scoping review will be conducted and certain aspects will transition to a living mode. A living review is one that is continually updated, incorporating relevant new evidence as it becomes available.57 Details of the exact scope of future updates are still to be determined, and future iterations will be shaped based on input from knowledge users and the patient community. This future work will provide a deeper understanding of the evidence base for post–COVID-19 condition. Additional knowledge mobilization activities to disseminate the findings of this scoping review and the larger condition-level review will also be conducted, and could include relevant educational outreach and related activities. Outreach of this project and the condition-level review will be made by CADTH’s Knowledge Mobilization and Implementation Support team to meet the needs of key stakeholders, such as patients, jurisdictional bodies, health care providers, and other users of health evidence.
Conclusions
In conclusion, as of December 2021, there has been a great deal of research conducted and published on post–COVID-19 condition. Much of the evidence identified has looked at symptoms, risk factors, and different diagnostic tests to assess individuals with post–COVID-19 condition, particularly adults and people who had been hospitalized or treated in the ICU. There is currently relatively limited research available on preventive interventions and interventions to treat or manage post–COVID-19 condition, but published protocols indicate research in this area is ongoing. Some areas where few published evidence and protocols were found include pediatric populations, people living in rural and remote areas, and the impact of different variants of SARS-CoV-2. In addition, there was a notable lack of evidence on PROGRESS-Plus variables, including few studies from low- and middle-income countries, and studies that reported factors related to disadvantage and equity (e.g., participants’ socioeconomic status, occupation, education, race, ethnicity, culture, language, and place of residence). More research in these areas may help to close some of the current evidence gaps.
References
1.World Health Organization. Weekly epidemiological update on COVID-19 - 1 March 2022. Edition 81. 2022; https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---1-march-2022. Accessed 2022 Apr 21.
2.World Health Organization. Update on the clinical long-term effects of COVID-19: the latest on the COVID-19 global situation & long-term sequelae. (Coronavirus Update 54). Geneva (Switzerland): WHO; 2021: https://www.who.int/docs/default-source/coronaviruse/risk-comms-updates/update54_clinical_long_term_effects.pdf?sfvrsn=3e63eee5_8. Accessed 2022 Apr 21.
3.Callard F, Perego E. How and why patients made Long Covid. Soc Sci Med. 2021;268:113426. PubMed
4.Greenhalgh T, Knight M, A'Court C, Buxton M, Husain L. Management of post-acute covid-19 in primary care. BMJ. 2020;370:m3026. PubMed
5.Government of Canada. Post COVID-19 condition. 2021; https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/symptoms/post-covid-19-condition.html. Accessed 2021 Dec 1.
6.National Institute for Health and Care Excellence. COVID-19 rapid guideline: managing the long-term effects of COVID-19. (NICE guideline NG188). 2020; https://www.nice.org.uk/guidance/ng188. Accessed 2022 Apr 21.
7.World Health Organization. A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021. Geneva (Switzerland): WHO; 2021: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1. Accessed 2022 Apr 21.
8.Rajan S, Khunti K, Alwan N, et al. In the wake of the pandemic: Preparing for Long COVID. European Observatory on Health Systems and Policies. 2021.
9.Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche L, Mukherjee B. Global prevalence of post-acute sequelae of COVID-19 (PASC) or long COVID: a meta-analysis and systematic review [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.11.15.21266377. Accessed 2022 Apr 21.
10.Domingo FR, Waddell L, Cheung A, et al. Prevalence of long-term effects in individuals diagnosed with COVID-19: a living systematic review [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.06.03.21258317. Accessed 2022 Apr 21.
11.Akbarialiabad H, Taghrir MH, Abdollahi A, et al. Long COVID, a comprehensive systematic scoping review. Infection. 2021;28:28. PubMed
12.Shanbehzadeh S, Tavahomi M, Zanjari N, Ebrahimi-Takamjani I, Amiri-Arimi S. Physical and mental health complications post-COVID-19: Scoping review. J Psychosom Res. 2021;147:110525. PubMed
13.Cha C, Baek G. Symptoms and management of long COVID: A scoping review. J Clin Nurs. 2021. PubMed
14.Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H. 11.1.1 Why a scoping review? In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. Adelaide (Australia): JBI; 2020: https://jbi-global-wiki.refined.site/space/MANUAL/3283910906/11.1.1+Why+a+scoping+review%3F. Accessed 2022 Mar 24.
15.Vu T, McGill SC. CADTH horizon scan: an overview of post-COVID-19 condition (Long Covid). Can J Health Technol. 2021 Sep;1(9). https://www.cadth.ca/overview-post-covid-19-condition-long-covid. Accessed 2021 Sep 28.
16.Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Adelaide (Australia): JBI; 2020: 10.46658/JBIMES-20-01. Accessed 2021 Sep 1.
17.Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H. Chapter 11: Scoping Reviews (2020 version). In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. Adelaide (Australia): JBI; 2020: https://synthesismanual.jbi.global. Accessed 2022 Apr 21.
18.Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ : British Medical Journal. 2015;349:g7647. PubMed
19.CADTH. Stakeholder feedback. 2022; https://www.cadth.ca/stakeholder-feedback. Accessed 2022 Apr 21.
20.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-46. PubMed
21.CADTH. CADTH COVID-19 search strings. 2019; https://covid.cadth.ca/literature-searching-tools/cadth-covid-19-search-strings/. Accessed 2021 Oct 15.
22.CADTH. Grey matters: a practical tool for searching health-related grey literature. 2019; https://www.cadth.ca/grey-matters. Accessed 2021 Oct 15.
23.CADTH. CADTH COVID-19 grey literature resources: a curated list of evidence-based sources for health professionals, librarians, and researchers. 2021; https://covid.cadth.ca/literature-searching-tools/cadth-covid-19-grey-literature-resources/. Accessed 2021 Oct 15.
24.Krnic Martinic M, Pieper D, Glatt A, Puljak L. Definition of a systematic review used in overviews of systematic reviews, meta-epidemiological studies and textbooks. BMC Med Res Methodol. 2019;19(1):203. PubMed
25.Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D. Evidence summaries: the evolution of a rapid review approach. Systematic Reviews. 2012;1(1):10. PubMed
26.O'Blenis P, Evidence Partners DistillerSR. One simple way to speed up your screening process. 2017; https://blog.evidencepartners.com/one-simple-way-to-speed-up-your-screening-process. Accessed 2022 Apr 21.
27.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. PubMed
28.Décary S, Dugas M, Stefan T, et al. Care models for Long COVID: a living systematic review. First update – December 2021. Toronto: SPOR Evidence Alliance, COVID-END Network; 2021: https://sporevidencealliance.ca/wp-content/uploads/2021/12/Care-Models-for-Long-COVID_Update_2021.12.04.pdf. Accessed 2022 Mar 22.
29.What is known about the optimal management for patients with post-COVID conditions or complications occurring after acute COVID-19 infection? (COVID-19 Scientific Advisory Group Rapid Evidence Report). Edmonton: Alberta Health Services; 2021: https://www.albertahealthservices.ca/assets/info/ppih/if-ppih-covid-19-sag-rapid-review-management-post-covid-conditions.pdf. Accessed 2021 Dec 1.
30.Provincial Health Services Authority. Provincial post-COVID-19 recovery care pathway. Vancouver: PHSA; 2021: http://www.phsa.ca/health-info-site/Documents/post_covid-19_Provincial_Recovery_Pathway.pdf. Accessed 2022 Apr 21.
31.Post COVID-19 condition: guidance for primary care. Assessment and management of the post-COVID-19 condition. Toronto: Ontario Health; 2021: https://www.ontariohealth.ca/sites/ontariohealth/files/2021-12/PostCovidConditionsClinicalGuidance_EN.pdf. Accessed 2022 Apr 21.
32.Post-COVID-19 conditions. Management support tool. Montreal: Institut national d'excellence en santé et en services sociaux (INESSS); 2021: https://www.inesss.qc.ca/fileadmin/doc/INESSS/COVID-19/COVID-19_INESSS_Management_support_tool_post_COVID.pdf. Accessed 2021 Dec 1.
33.COVID-19 Guidelines, version 4. Camberwell (Australia): Australian and New Zealand Intensive Care Society (ANZICS); 2021: https://www.anzics.com.au/wp-content/uploads/2021/09/ANZICS-COVID-19-Guidelines-Version-4.pdf. Accessed 2021 Dec 1.
34.Siso-Almirall A, Brito-Zeron P, Conangla Ferrin L, et al. Long Covid-19: Proposed primary care clinical guidelines for diagnosis and disease management. Int J Environ Res Public Health. 2021;18(8):20. PubMed
35.Kurtais Aytur Y, Fusun Koseoglu B, Ozyemisci Taskiran O, et al. Pulmonary rehabilitation principles in SARS-COV-2 infection (COVID-19): The revised guideline for the acute, subacute, and post-COVID-19 rehabilitation. Turk J Phys Med Rehabil. 2021;67(2):129-145. PubMed
36.Yip TCF, Wong V, Tse YK, Chan HLY, Wong GLH. Characteristics of COVID-19 patients with residual liver function abnormality: A 1-year follow-up cohort study of 1,040 patients in hong kong. Hepatology. 2021;74(SUPPL 1):311A-312A.
37.Mazza MG, Palladini M, De Lorenzo R, et al. One-year mental health outcomes in a cohort of COVID-19 survivors. J Psychiatr Res. 2022;145:118-124. PubMed
38.De Vos N, Duterme C, Ouanani Z, et al. Follow-up of novel kl-6 and routine biomarkers in covid-19 survivors 1 year post-icu. Clin Chem Lab Med. 2021;59(SUPPL 1):S95.
39.Office for National Statistics. The prevalence of long COVID symptoms and COVID-19 complications. Newport (UK): Office for National Statistics; 2020: https://www.ons.gov.uk/news/statementsandletters/theprevalenceoflongcovidsymptomsandcovid19complications. Accessed 2021 Dec 1.
40.Ursini F, Ciaffi J, Mancarella L, et al. Fibromyalgia: a new facet of the post-COVID-19 syndrome spectrum? Results from a web-based survey. RMD Open. 2021;7(3):08.
41.Mantovani E, Mariotto S, Gabbiani D, et al. Chronic fatigue syndrome: an emerging sequela in COVID-19 survivors? J Neurovirol. 2021;27(4):631-637. PubMed
42.Di Filippo L, De Lorenzo R, Cinel E, et al. Weight trajectories and abdominal adiposity in COVID-19 survivors with overweight/obesity. Int J Obes. 2021;45(9):1986-1994. PubMed
43.Ojeda A, Calvo A, Cunat T, et al. Rationale and study design of an early care, therapeutic education, and psychological intervention program for the management of post-intensive care syndrome and chronic pain after COVID-19 infection (PAIN-COVID): study protocol for a randomized controlled trial. Trials. 2021;22(1):486. PubMed
44.Bottemanne H, Gouraud C, Hulot JS, et al. Do anxiety and depression predict persistent physical symptoms after a severe COVID-19 episode? A prospective study. Frontiers in Psychiatry. 2021;12 (no pagination). PubMed
45.Behnood SA, Shafran R, Bennett SD, et al. Persistent symptoms following SARS-CoV-2 infection among children and young people: a meta-analysis of controlled and uncontrolled studies. J Infect. 2021;20:20. PubMed
46.Graham EL, Clark JR, Orban ZS, et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized Covid-19 "long haulers". Ann Clin Transl Neurol. 2021;8(5):1073-1085. PubMed
47.Vaes AW, Goertz YMJ, Van Herck M, et al. Recovery from COVID-19: a sprint or marathon? 6-month follow-up data from online long COVID-19 support group members. ERJ Open Research. 2021;7(2). PubMed
48.Turan Z, Topaloglu M, Ozyemisci Taskiran O. Is tele-rehabilitation superior to home exercise program in COVID-19 survivors following discharge from intensive care unit? - A study protocol of a randomized controlled trial. Physiother Res Int. 2021;26(4):e1920. PubMed
49.Dalbosco-Salas M, Torres-Castro R, Rojas Leyton A, et al. Effectiveness of a primary care telerehabilitation program for post-COVID-19 patients: a feasibility study. J Clin Med. 2021;10(19):27. PubMed
50.Mathieu E, Ritchie H, Ortiz-Ospina E, et al. A global database of COVID-19 vaccinations. Nat Hum Behav. 2021;5(7):947-953. PubMed
51.Southwest College of Naturopathic Medicine. NCT05104749: Homeopathic treatment of post-acute COVID-19 syndrome. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021: https://clinicaltrials.gov/show/NCT05104749. Accessed 2022 Apr 21.
52.Rodero FG, Área de Ensayos Clínicos (Spain). EUCTR2021-003331-28-ES. Randomized, double-blind, placebo-controlled clinical trial to evaluate the efficacy and safety of the COMIRNATY vaccine (COVID-19 mRNA vaccine, Pfizer-BioNTech) in people with long COVID. Geneva (Switzerland): WHO International Clinical Trials Registry Platform (ICTRP); 2021: https://trialsearch.who.int/Trial2.aspx?TrialID=EUCTR2021-003331-28-ES. Accessed 2022 Apr 21.
53.Ontanon J, Blas J, de Cabo C, et al. Influence of past infection with SARS-CoV-2 on the response to the BNT162b2 mRNA vaccine in health care workers: Kinetics and durability of the humoral immune response. EBioMedicine. 2021;73. PubMed
54.Government of Canada. COVID-19 daily epidemiology update. 2022; https://health-infobase.canada.ca/covid-19/epidemiological-summary-covid-19-cases.html. Accessed 2022 Mar 1.
55.Penetra SLS, da Silva MFB, Resende P, et al. Post-acute COVID-19 syndrome after reinfection and vaccine breakthrough by the SARS-CoV-2 Gamma variant in Brazil. Int J Infect Dis. 2022;114:58-61. PubMed
56.Guimaraes RRL, Aranda CS, Schmid LS, et al. PASC, reinfections and variants: COVID-19 in patients with inborn errors of immunity in Sao paulo-Brazil [conference abstract]. Allergy: European Journal of Allergy and Clinical Immunology. 2021;76(SUPPL 110):494.
57.The Cochrane Collaboration. Living systematic reviews. 2022; https://community.cochrane.org/review-production/production-resources/living-systematic-reviews. Accessed 2022 Apr 21.
58.Clark JM, Sanders S, Carter M, et al. Improving the translation of search strategies using the Polyglot Search Translator: a randomized controlled trial. J Med Libr Assoc. 2020;108(2):195-207.
59.Royal Australian College of General Practitioners. Caring for patients with post–COVID-19 conditions East Melbourne (Australia): RACGP; 2021: https://www.racgp.org.au/FSDEDEV/media/documents/RACGP/Coronavirus/Post-COVID-19-conditions.pdf. Accessed 2021 Dec 1.
60.van Haastregt JCM, Everink IHJ, Schols JMGA, et al. Management of post-acute COVID-19 patients in geriatric rehabilitation: EuGMS guidance. Eur Geriatr Med. 2021;13(1):291-304. PubMed
61.Managing the long-term effects of COVID-19: National guidance for identification, assessment and management. (SIGN 161). Edinburgh: Scottish Intercollegiate Guidelines Network; 2020: https://www.sign.ac.uk/media/1833/sign161-long-term-effects-of-covid19-11.pdf. Accessed 2022 Apr 21.
62.Centers for Disease Control and Prevention. Evaluating and caring for patients with Post-COVID conditions: Interim guidance. Atlanta (GA): U.S. Centers for Disease Control and Prevention; 2021: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-index.html. Accessed 2021 Dec 1.
63.So M, Kabata H, Fukunaga K, Takagi H, Kuno T. Radiological and functional lung sequelae of COVID-19: systematic review and meta-analysis [conference abstract]. Am J Respir Crit Care Med. 2021;203(9). PubMed
64.Soriano-Moreno AN, Soriano-Moreno DR, Pacheco-Barrios N, Lescano AG, Checkley W. A systematic review of the frequency of persistent constitutional and respiratory symptoms related to COVID-19: A new long COVID syndrome? [conference abstract]. Am J Respir Crit Care Med. 2021;203(9).
65.Renaud-Charest O, Lui LMW, Eskander S, et al. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J Psychiatr Res. 2021;144:129-137. PubMed
66.Anaya JM, Rojas M, Salinas ML, et al. Post-COVID syndrome. A case series and comprehensive review. Autoimmun Rev. 2021:102947. PubMed
67.Fernandez-de-Las-Penas C, Navarro-Santana M, Gomez-Mayordomo V, et al. Headache as an acute and post-COVID-19 symptom in COVID-19 survivors: A meta-analysis of the current literature. Eur J Neurol. 2021;30:30. PubMed
68.van Kessel SAM, Olde Hartman TC, Lucassen P, van Jaarsveld CHM. Post-acute and long-COVID-19 symptoms in patients with mild diseases: a systematic review. Fam Pract. 2021;16:16. PubMed
69.Malik P, Patel K, Pinto C, et al. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)-A systematic review and meta-analysis. J Med Virol. 2021;31:31.
70.Groff D, Sun A, Ssentongo AE, et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA netw. 2021;4(10):e2128568.
71.Sandler CX, Wyller VBB, Moss-Morris R, et al. Long COVID and post-infective fatigue syndrome: A review. Open Forum Infectious Diseases. 2021;8(10):ofab440. PubMed
72.Long Q, Li J, Hu X, Bai Y, Zheng Y, Gao Z. Follow-ups on persistent symptoms and pulmonary function among post-acute COVID-19 patients: a systematic review and meta-analysis. Frontiers in Medicine. 2021;8:702635. PubMed
73.Sanchez-Ramirez DC, Normand K, Zhaoyun Y, Torres-Castro R. Long-term impact of COVID-19: a systematic review of the literature and meta-analysis. Biomedicines. 2021;9(8):27. PubMed
74.Iqbal FM, Lam K, Sounderajah V, Clarke JM, Ashrafian H, Darzi A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. EClinicalMedicine. 2021;36:100899. PubMed
75.Salamanna F, Veronesi F, Martini L, Landini MP, Fini M. Post-COVID-19 syndrome: The persistent symptoms at the post-viral stage of the disease. A systematic review of the current data. Frontiers in Medicine. 2021;8:653516. PubMed
76.Fernandez-de-Las-Penas C, Palacios-Cena D, Gomez-Mayordomo V, et al. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur J Intern Med. 2021;92:55-70. PubMed
77.Michelen M, Manoharan L, Elkheir N, et al. Characterising long COVID: a living systematic review. BMJ glob. 2021;6(9):09.
78.Ahmad MS, Shaik RA, Ahmad RK, et al. "LONG COVID": an insight. Eur Rev Med Pharmacol Sci. 2021;25(17):5561-5577. PubMed
79.Schou TM, Joca S, Wegener G, Bay-Richter C. Psychiatric and neuropsychiatric sequelae of COVID-19 - A systematic review. Brain Behav Immun. 2021;97:328-348. PubMed
80.Cabrera Martimbianco AL, Pacheco RL, Bagattini ÂM, Riera R. Frequency, signs and symptoms, and criteria adopted for long COVID‐19: A systematic review. Int J Clin Pract. 2021;75(10):1-16. PubMed
81.Sun YM, Liu JY, Sun R, Zhang J, Xiao ML, Li GP. The long-term consequences of Corona Virus Disease 2019 patients receiving Chinese herbal medicine treatments in acute phase: A protocol for systematic review and meta-analysis. Medicine. 2021;100(29):e26677. PubMed
82.Ramadan MS, Bertolino L, Zampino R, Durante-Mangoni E, Monaldi Hospital Cardiovascular Infection Study G. Cardiac sequelae after coronavirus disease 2019 recovery: a systematic review. Clin Microbiol Infect. 2021;27(9):1250-1261. PubMed
83.Cares-Marambio K, Montenegro-Jimenez Y, Torres-Castro R, et al. Prevalence of potential respiratory symptoms in survivors of hospital admission after coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Chron Respir Dis. 2021;18:14799731211002240. PubMed
84.Ludvigsson JF. Case report and systematic review suggest that children may experience similar long-term effects to adults after clinical COVID-19. Acta Paediatr. 2021;110(3):914-921. PubMed
85.Vanderlind WM, Rabinovitz BB, Miao IY, et al. A systematic review of neuropsychological and psychiatric sequalae of COVID-19: implications for treatment. Curr Opin Psychiatry. 2021;34(4):420-433. PubMed
86.Kim E, Choi J, Min SY, Kim JH, Jeong A. Efficacy of traditional herbal medicine for psychological sequelae in COVID-19 survivors: A protocol for systematic review and meta-analysis. Medicine. 2021;100(20):e25609. PubMed
87.Wong TL, Weitzer DJ. Long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)-a systemic review and comparison of clinical presentation and symptomatology. Medicina. 2021;57(5):26. PubMed
88.Willi S, Luthold R, Hunt A, et al. COVID-19 sequelae in adults aged less than 50 years: A systematic review. Travel Med Infect Dis. 2021;40:101995. PubMed
89.Wang D, Li J, Zhu F, et al. Protocol for a systematic review and meta-analysis of respiratory rehabilitation following intensive care unit discharge for COVID-19 survivors. BMJ Open. 2020;10(12):e041184. PubMed
90.Jennings G, Monaghan A, Xue F, Mockler D, Romero-Ortuño R. A systematic review of persistent symptoms and residual abnormal functioning following acute COVID-19: ongoing symptomatic phase vs. post-COVID-19 syndrome [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.06.25.21259372. Accessed 2022 Apr 21.
91.Hoshijima H, Mihara T, Seki H, Hyuga S, Kuratani N, Shiga T. Incidence of long-term post-acute sequelae of SARS-CoV-2 infection related to pain and other symptoms: a living systematic review and meta-analysis [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.04.08.21255109. Accessed 2022 Apr 21.
92.Nna EO, Alao MA, Anyachukwu C, et al. Long COVID: A protocol for systematic review and meta-analysis of symptomatology and treatment approaches [non peer-reviewed preprint]. Res Sq. 2021. 10.21203/rs.3.rs-246493/v1. Accessed 2022 Apr 21.
93.De-la-Rosa-Martínez D, Delaye-Martínez MA, Bello-Chavolla OY, et al. Long-term manifestations and modifiers of prevalence estimates of the post-COVID-19 syndrome: A systematic review and meta-analysis [non-peer reviewed preprint]. medRxiv. 2021. 10.1101/2021.10.17.21265123. Accessed 2022 Apr 21.
94.Michelen M, Cheng V, Manoharan L, et al. Characterising long term Covid-19: a living systematic review [non peer-reviewed preprint]. medRxiv. 2020. 10.1101/2020.12.08.20246025. Accessed 2022 Apr 21.
95.Gyanpuri V, Dhiman N, Pathak A, Singh OP. Role of physiotherapy in long term physical and mental health of people recovered from COVID 19: a systematic review protocol [non peer-reviewed preprint]. Res Sq. 2020. 10.21203/rs.3.rs-44727/v1. Accessed 2022 Apr 21.
96.Zürcher SJ, Banzer C, Adamus C, Lehmann A, Richter D, Kerksieck P. Post-viral mental health sequelae in infected persons associated with COVID-19 and previous epidemics and pandemics: Systematic review and meta-analysis of prevalence estimates [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.06.29.21259615. Accessed 2022 Apr 21.
97.Malik J, Zaidi SMJ, Iqbal R, et al. Post-acute COVID-19 syndrome and its prolonged effects: an updated systematic review [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.05.09.21256911. Accessed 2022 Apr 21.
98.Yusuf F, Fahriani M, Mamada S, et al. Global prevalence of prolonged gastrointestinal symptoms in COVID-19 survivors and potential pathogenesis: a systematic review and meta-analysis [non peer-reviewed preprint]. F1000Res. 2021. 10.12688/f1000research.52216.1. Accessed 2022 Apr 21.
99.Fabbri L, Moss S, Khan F, et al. Post-viral parenchymal lung disease following COVID-19 and viral pneumonitis hospitalisation: a systematic review and meta-analysis [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.03.15.21253593. Accessed 2022 Apr 21.
100.Fernandez-de-Las-Penas C, Navarro-Santana M, Plaza-Manzano G, Palacios-Cena D, Arendt-Nielsen L. Time course prevalence of post-COVID pain symptoms of musculoskeletal origin in patients who had survived to severe acute respiratory syndrome coronavirus 2 infection: a systematic review and meta-analysis. Pain. 2021;23:23. PubMed
101.Rao S, Benzouak T, Gunpat S, et al. Fatigue symptoms associated with COVID-19 in convalescent or recovered COVID-19 patients; a systematic review and meta-analysis. Ann Behav Med. 2021;19:19. PubMed
102.d'Ettorre G, Gentilini Cacciola E, Santinelli L, et al. Covid-19 sequelae in working age patients: A systematic review. J Med Virol. 2021;16:16. PubMed
103.Décary S, Dugas M, Stefan T, et al. Care models for long COVID: a rapid systematic review [non peer-reviewed preprint]. medRxiv. 2021. 10.1101/2021.11.17.21266404. Accessed 2022 Apr 21.
104.Wu L, Wu Y, Xiong H, Mei B, You T. Persistence of symptoms after discharge of patients hospitalized due to COVID-19. Frontiers in Medicine. 2021;8:761314. PubMed
105.Nagarajan R, Krishnamoorthy Y, Basavarachar V, Dakshinamoorthy R. Prevalence of post-traumatic stress disorder among survivors of severe COVID-19 infections: A systematic review and meta-analysis. J Affect Disord. 2021;299:52-59. PubMed
106.Patrucco F, Zeppegno P, Baricich A, et al. Long-lasting consequences of Coronavirus disease 19 pneumonia: a systematic review. Minerva Med. 2021;03:03.
107.Razak F, Katz GM, Cheung AM, et al. Understanding the Post COVID-19 Condition (Long COVID) and the expected burden for Ontario. Science Briefs of the Ontario COVID-19 Science Advisory Table. 2021;2(44). https://covid19-sciencetable.ca/wp-content/uploads/2021/09/Understanding-the-Post-COVID-19-Condition-Long-COVID-and-the-Expected-Burden-for-Ontario_published_20210914-3.pdf. Accessed 2021 Dec 1.
108.De la Rosa-Martinez D, Delaye-Martínez MA, David Juárez-Cruz I, et al. Persistent symptoms and risk factors for post-acute COVID-19 syndrome: a systematic review and meta-analysis [protocol]. Instituto Nacional de Cancerología, Mexico. CRD42021243541. PROSPERO: International prospective register of systematic reviews. York (GB): University of York Centre for Reviews and Dissemination 2021: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021243541. Accessed 2021 Dec 1.
109.Pillay J, Rahman S, Guitard S, Wingert A, Hartling L. Risk factors and preventive interventions for post‒COVID-19 condition: systematic reviews [non-peer reviewed preprint]. Prepared by the Alberta Research Centre for Health Evidence (ARCHE), Public Health Agency of Canada (PHAC), with CADTH. medRxiv. 2021. https://www.cadth.ca/risk-factors-and-preventive-interventions-post-covid-19-condition; https://www.medrxiv.org/content/10.1101/2022.03.25.22272949v1. Accessed 2021 Dec 1.
110.ECRI. Rehabilitation for patients with postacute sequela of COVID-19. (ECRI Clinical Evidence Assessment). Plymouth Meeting (PA): ECRI; 2021: http://www.ecri.org (subscription required). Accessed 2021 Dec 1.
111.Castanares-Zapatero D, Kohn L, Dauvrin M, et al. Long COVID: pathophysiology – epidemiology and patient needs. Brussels (Belgium): Belgian Health Care Knowledge Centre; 2021: https://kce.fgov.be/sites/default/files/atoms/files/KCE_344_Long_Covid_scientific_report.pdf. Accessed 2021 Dec 1.
Appendix 1: Literature Search Methods
Note that this appendix has not been copy-edited.
Overview
Interface: Ovid and EBSCOhost
Databases:
MEDLINE All (1946-present) via Ovid
Embase (1974-present) via Ovid
APA PsycInfo (1806-present) via Ovid
Cochrane Central Register of Controlled Trials via Ovid
CINAHL (Cumulative Index to Nursing and Allied Health Literature) via EBSCO
Note: Subject headings and search fields have been customized for each database. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote.
Date of search: October 15, 2021
Alerts: Monthly search updates until December 20, 2021.
Search filters applied: No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, and letters were removed.
Limits:
Publication date limit: 2019-present
Humans
Languages: English or French
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
? | Truncation symbol for one or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE, Embase) |
.id | Author keyword (PsycInfo) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.yr | Publication year |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
psyh | Ovid database code; APA PsycInfo for the years 2019 and 2020-present. |
Ovid Multi-Database Strategy – Medline, Embase, Cochrane Central, and PsycInfo
(long COVID* or long coronavirus*).ti,ab,kf.
((chronic or post) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj2 (sequela* or syndrome* or disorder* or condition* or symptom*)).ti,ab,kf.
((post acute or postacute or post viral or postviral or post virus* or postvirus* or long duration or long last or long lasting or longstanding or long standing) adj3 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
(late sequela* adj2 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((long term or longterm) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
PASC.ti,kf.
((postcovid* or post covid* or postcoronavirus* or post coronavirus* or post SARS-COV-2 or postSARS-COV-2 or post SARS-COV2 or postSARS-COV2 or post SARSCOV-2 or post SARSCOV-2) adj3 (sequela* or syndrome* or disorder* or illness* or condition* or symptom* or prognos* or followup* or follow up*)).ti,ab,kf.
(post-covid* adj5 (care or aftercare*) adj5 (center* or centre or clinic*)).ti,ab,kf.
or/1-8 [Medline CCTR set 1 Main Long Covid Terms]
(((post acute or postacute or sub-acute or subacute or chronic) adj sequela*) or PASC).ti,ab,kf.
(long haul* or longhaul*).ti,ab,kf.
((post-intensive care or postintensive care or post-ICU) adj syndrome*).ti,ab,kf.
((persist* or long* or residual or prolonged) adj8 ((olfactory or chemosensor*) adj (disorder* or dysfunction*))).ti,ab,kf.
or/10-13 [Medline CCTR set 2 Post Acute Subtype terms to AND with COVID]
COVID-19/ or exp COVID-19 Testing/ or COVID-19 Vaccines/ or SARS-CoV-2/
(coronavirus/ or betacoronavirus/ or coronavirus infections/) and (disease outbreaks/ or epidemics/ or pandemics/)
(nCoV* or 2019nCoV or 19nCoV or COVID19* or COVID or SARS-COV-2 or SARSCOV-2 or SARS-COV2 or SARSCOV2 or SARS coronavirus 2 or Severe Acute Respiratory Syndrome Coronavirus 2 or Severe Acute Respiratory Syndrome Corona Virus 2).ti,ab,kf,nm,ot,ox,rx,px.
((new or novel or "19" or "2019" or Wuhan or Hubei or China or Chinese) adj3 (coronavirus* or corona virus* or betacoronavirus* or CoV or HCoV)).ti,ab,kf,ot.
(longCOVID* or postCOVID* or postcoronavirus* or postSARS*).ti,ab,kf,ot.
((coronavirus* or corona virus* or betacoronavirus*) adj3 (pandemic* or epidemic* or outbreak* or crisis)).ti,ab,kf,ot.
((Wuhan or Hubei) adj5 pneumonia).ti,ab,kf,ot.
or/15-21 [Medline CCTR set 3 CADTH Covid-19 filter]
(recovery adj2 (clinic or clinics or centre or center or centres or centers or program*)).ti,ab,kf.
(post* adj3 rehabilitation adj2 (clinic or clinics or centre or center or centres or centers or program*)).ti,ab,kf.
or/23-24 [Medline CCTR set 4 Post Covid Recovery Clinics]
(post adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj3 infection* adj8 (chronic* or persist* or residual or prolonged or non-recover* or nonrecover* or recover* or rehabilitat* or month or months or year or years or sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,kf.
((chronic or post) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj3 (rehabilitat* or recover* or fatigue or function*)).ti,ab,kf.
((chronic* or persist* or residual or prolonged or non-recover* or nonrecover*) adj2 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((chronic* or persist* or residual or prolonged or non-recover* or nonrecover*) adj2 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj5 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,kf.
((long-term or longterm) adj (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((post acute or postacute or post viral or postviral or post virus* or postvirus* or long duration or long last or long lasting or longstanding or long standing or late-onset or (illness adj2 duration)) adj3 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((survivor* or survived or discharg* or postdischarg* or post infect* or postinfect*) adj3 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((survivor* or survived or discharg* or postdischarg* or post infect* or postinfect*) adj3 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj5 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,kf.
or/26-33 [Medline CCTR set 5 Top Up set]
14 and 22
22 and 25
9 or 34 or 35 or 36
37 use medall
37 use cctr
(long COVID* or long coronavirus*).ti,ab,kf.
((chronic or post) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj2 (sequela* or syndrome* or disorder* or condition* or symptom*)).ti,ab,kf.
((post acute or postacute or post viral or postviral or post virus* or postvirus* or long duration or long last or long lasting or longstanding or long standing) adj3 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
(late sequela* adj2 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((long term or longterm) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
PASC.ti,kf.
((postcovid* or post covid* or postcoronavirus* or post coronavirus* or post SARS-COV-2 or postSARS-COV-2 or post SARS-COV2 or postSARS-COV2 or post SARSCOV-2 or post SARSCOV-2) adj3 (sequela* or syndrome* or disorder* or illness* or condition* or symptom* or prognos* or followup* or follow up*)).ti,ab,kf.
(post-covid* adj5 (care or aftercare*) adj5 (center* or centre or clinic*)).ti,ab,kf.
or/40-47 [Embase set 1 Main Long Covid terms]
(((post acute or postacute or sub-acute or subacute or chronic) adj sequela*) or PASC).ti,ab,kf.
(long haul* or longhaul*).ti,ab,kf.
((post-intensive care or postintensive care or post-ICU) adj syndrome*).ti,ab,kf.
((persist* or long* or residual or prolonged) adj8 ((olfactory or chemosensor*) adj (disorder* or dysfunction*))).ti,ab,kf.
or/49-52 [Embase set 2 Post Acute Subtype terms to AND with COVID]
sars-related coronavirus/
(coronavirinae/ or betacoronavirus/ or coronavirus infection/) and (epidemic/ or pandemic/)
(nCoV* or 2019nCoV or 19nCoV or COVID19* or COVID or SARS-COV-2 or SARSCOV-2 or SARS-COV2 or SARSCOV2 or SARS coronavirus 2 or Severe Acute Respiratory Syndrome Coronavirus 2 or Severe Acute Respiratory Syndrome Corona Virus 2).ti,ab,kf,hw,ot.
((new or novel or "19" or "2019" or Wuhan or Hubei or China or Chinese) adj3 (coronavirus* or corona virus* or betacoronavirus* or CoV or HCoV)).ti,ab,kf,hw,ot.
(longCOVID* or postCOVID* or postcoronavirus* or postSARS*).ti,ab,kf,hw,ot.
((coronavirus* or corona virus* or betacoronavirus*) adj3 (pandemic* or epidemic* or outbreak* or crisis)).ti,ab,kf,ot.
((Wuhan or Hubei) adj5 pneumonia).ti,ab,kf,ot.
or/54-60 [Embase set 3 CADTH Covid Filter]
(recovery adj2 (clinic or clinics or centre or center or centres or centers or program*)).ti,ab,kf.
(post* adj3 rehabilitation adj2 (clinic or clinics or centre or center or centres or centers or program*)).ti,ab,kf.
or/62-63 [Embase set 4 Post Covid Recovery Clinics to AND with Covid set 3]
(post adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj3 infection* adj8 (chronic* or persist* or residual or prolonged or non-recover* or nonrecover* or recover* or rehabilitat* or month or months or year or years or sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,kf.
((chronic or post) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj3 (rehabilitat* or recover* or fatigue or function*)).ti,ab,kf.
((chronic* or persist* or residual or prolonged or non-recover* or nonrecover*) adj2 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((chronic* or persist* or residual or prolonged or non-recover* or nonrecover*) adj2 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj5 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,kf.
((long-term or longterm) adj (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((post acute or postacute or post viral or postviral or post virus* or postvirus* or long duration or long last or long lasting or longstanding or long standing or late-onset or (illness adj2 duration)) adj3 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((survivor* or survived or discharg* or postdischarg* or post infect* or postinfect*) adj3 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,kf.
((survivor* or survived or discharg* or postdischarg* or post infect* or postinfect*) adj3 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj5 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,kf.
or/65-72 [Embase set 5 Top Up set]
53 and 61
61 and 64
48 or 73 or 74 or 75
76 use oemezd
(long COVID* or long coronavirus*).ti,ab,id.
((chronic or post) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj2 (sequela* or syndrome* or disorder* or condition* or symptom*)).ti,ab,id.
((post acute or postacute or post viral or postviral or post virus* or postvirus* or long duration or long last or long lasting or longstanding or long standing) adj3 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,id.
(late sequela* adj2 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,id.
((long term or longterm) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,id.
PASC.ti,id.
((postcovid* or post covid* or postcoronavirus* or post coronavirus* or post SARS-COV-2 or postSARS-COV-2 or post SARS-COV2 or postSARS-COV2 or post SARSCOV-2 or post SARSCOV-2) adj3 (sequela* or syndrome* or disorder* or illness* or condition* or symptom* or prognos* or followup* or follow up*)).ti,ab,id.
(post-covid* adj5 (care or aftercare*) adj5 (center* or centre or clinic*)).ti,ab,id.
or/78-85 [PsycInfo set 1 Main Long Covid terms]
(((post acute or postacute or sub-acute or subacute or chronic) adj sequela*) or PASC).ti,ab,id.
(long haul* or longhaul*).ti,ab,id.
((post-intensive care or postintensive care or post-ICU) adj syndrome*).ti,ab,id.
((persist* or long* or residual or prolonged) adj8 ((olfactory or chemosensor*) adj (disorder* or dysfunction*))).ti,ab,id.
or/87-90 [PsycInfo set 2 Post Acute Subtype terms to AND with COVID]
COVID-19/ or exp COVID-19 Testing/ or COVID-19 Vaccines/ or SARS-CoV-2/
(coronavirus/ or betacoronavirus/ or coronavirus infections/) and (disease outbreaks/ or epidemics/ or pandemics/)
(nCoV* or 2019nCoV or 19nCoV or COVID19* or COVID or SARS-COV-2 or SARSCOV-2 or SARS-COV2 or SARSCOV2 or SARS coronavirus 2 or Severe Acute Respiratory Syndrome Coronavirus 2 or Severe Acute Respiratory Syndrome Corona Virus 2).ti,ab,id,ot.
((new or novel or "19" or "2019" or Wuhan or Hubei or China or Chinese) adj3 (coronavirus* or corona virus* or betacoronavirus* or CoV or HCoV)).ti,ab,id.
(longCOVID* or postCOVID* or postcoronavirus* or postSARS*).ti,ab,id.
((coronavirus* or corona virus* or betacoronavirus*) adj3 (pandemic* or epidemic* or outbreak* or crisis)).ti,ab,id.
((Wuhan or Hubei) adj5 pneumonia).ti,ab,id.
or/92-98 [PsycInfo set 3 CADTH Covid Filter]
(recovery adj2 (clinic or clinics or centre or center or centres or centers or program*)).ti,ab,id.
(post* adj3 rehabilitation adj2 (clinic or clinics or centre or center or centres or centers or program*)).ti,ab,id.
or/100-101 [PsycInfo set 4 Post Covid Recovery Clinics to AND with Covid]
(post adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj3 infection* adj8 (chronic* or persist* or residual or prolonged or non-recover* or nonrecover* or recover* or rehabilitat* or month or months or year or years or sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,id.
((chronic or post) adj (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj3 (rehabilitat* or recover* or fatigue or function*)).ti,ab,id.
((chronic* or persist* or residual or prolonged or non-recover* or nonrecover*) adj2 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,id.
((chronic* or persist* or residual or prolonged or non-recover* or nonrecover*) adj2 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj5 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,id.
((long-term or longterm) adj (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,id.
((post acute or postacute or post viral or postviral or post virus* or postvirus* or long duration or long last or long lasting or longstanding or long standing or late-onset or (illness adj2 duration)) adj3 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,id.
((survivor* or survived or discharg* or postdischarg* or post infect* or postinfect*) adj3 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*) adj5 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2)).ti,ab,id.
((survivor* or survived or discharg* or postdischarg* or post infect* or postinfect*) adj3 (COVID* or coronavirus* or corona virus* or SARS-COV-2 or SARS-COV2 or SARSCOV-2 or nCoV* or 2019nCoV or 19nCoV or SARSCOV2) adj5 (sequela* or syndrome* or disorder* or condition* or symptom* or consequence* or outcome* or clinical outcome* or aftercare* or after-care* or issue* or complication* or following or follow-up or followup or function*)).ti,ab,id.
or/103-110 [PsycInfo set 5 Top Up set]
91 and 99
99 and 102
86 or 111 or 112 or 113
114 use psyh
exp animals/
exp animal experimentation/ or exp animal experiment/
exp models animal/
nonhuman/
exp vertebrate/ or exp vertebrates/
animal.po.
or/116-121
exp humans/
exp human experimentation/ or exp human experiment/
human.po.
or/123-125
122 not 126
(comment or newspaper article or editorial or letter or note).pt.
38 not 127
129 not 128
limit 130 to (english or french)
limit 131 to yr="2019 -Current" [Medline results with limits]
39 not 127
133 not 128
limit 134 to yr="2019 -Current" [CCTR with limits, no language limit available]
77 not 127
136 not 128
limit 137 to (english or french)
limit 138 to yr="2019 -Current" [Embase with limits]
115 not 127
140 not 128
limit 141 to (english or french)
limit 142 to yr="2019 -Current" [PsycInfo with limits]
132 or 135 or 139 or 143 [All database results with limits, combined]
remove duplicates from 144.
Syntax | Description |
|---|---|
TI | Title |
AB | Abstract |
MH | Medical Subject Heading |
PT | Publication type |
* | A truncation symbol (wildcard) to retrieve plurals or varying endings |
N# | Near operator: requires terms to be adjacent to each other within # number of words, in any order |
W# | Within operator: requires terms to be adjacent to each other within # number of words, in the order entered |
EBSCO Strategy – Cumulative Index to Nursing and Allied Health Literature (CINAHL)
The CINAHL search was translated from the Ovid Medline search with the assistance of the Polygot Search Translator.58
S1. ((TI "long COVID*" OR AB "long COVID*") OR (TI "long coronavirus*" OR AB "long coronavirus*"))
S2. (((TI chronic OR AB chronic) OR (TI post OR AB post)) W1 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)) N2 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*)))
S3. (((TI "post acute" OR AB "post acute") OR (TI postacute OR AB postacute) OR (TI "post viral" OR AB "post viral") OR (TI postviral OR AB postviral) OR (TI "post virus*" OR AB "post virus*") OR (TI postvirus* OR AB postvirus*) OR (TI "long duration" OR AB "long duration") OR (TI "long last" OR AB "long last") OR (TI "long lasting" OR AB "long lasting") OR (TI longstanding OR AB longstanding) OR (TI "long standing" OR AB "long standing")) N3 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)))
S4. ((TI "late sequela*" OR AB "late sequela*") N2 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)))
S5. (((TI "long term" OR AB "long term") OR (TI longterm OR AB longterm)) W1 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)))
S6. TI PASC
S7. (((TI postcovid* OR AB postcovid*) OR (TI "post covid*" OR AB "post covid*") OR (TI postcoronavirus* OR AB postcoronavirus*) OR (TI "post coronavirus*" OR AB "post coronavirus*") OR (TI "post SARS-COV-2" OR AB "post SARS-COV-2") OR (TI postSARS-COV-2 OR AB postSARS-COV-2) OR (TI "post SARS-COV2" OR AB "post SARS-COV2") OR (TI postSARS-COV2 OR AB postSARS-COV2) OR (TI "post SARSCOV-2" OR AB "post SARSCOV-2") OR (TI "post SARSCOV-2" OR AB "post SARSCOV-2")) N3 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI illness* OR AB illness*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI prognos* OR AB prognos*) OR (TI followup* OR AB followup*) OR (TI "follow up*" OR AB "follow up*")))
S8. ((TI post-covid* OR AB post-covid*) N5 ((TI care OR AB care) OR (TI aftercare* OR AB aftercare*)) N5 ((TI center* OR AB center*) OR (TI centre OR AB centre) OR (TI clinic* OR AB clinic*)))
S9. S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8
S10. ((((TI "post acute" OR AB "post acute") OR (TI postacute OR AB postacute) OR (TI sub-acute OR AB sub-acute) OR (TI subacute OR AB subacute) OR (TI chronic OR AB chronic)) W1 (TI sequela* OR AB sequela*)) OR (TI PASC OR AB PASC))
S11. ((TI "long haul*" OR AB "long haul*") OR (TI longhaul* OR AB longhaul*))
S12. (((TI "post-intensive care" OR AB "post-intensive care") OR (TI "postintensive care" OR AB "postintensive care") OR (TI post-ICU OR AB post-ICU)) W1 (TI syndrome* OR AB syndrome*))
S13. (((TI persist* OR AB persist*) OR (TI long* OR AB long*) OR (TI residual OR AB residual) OR (TI prolonged OR AB prolonged)) N8 (((TI olfactory OR AB olfactory) OR (TI chemosensor* OR AB chemosensor*)) W1 ((TI disorder* OR AB disorder*) OR (TI dysfunction* OR AB dysfunction*))))
S14. S10 OR S11 OR S12 OR S13
S15. (MH COVID-19) OR (MH "COVID-19 Testing"+) OR (MH "COVID-19 Vaccines") OR (MH SARS-CoV-2)
S16. ((MH coronavirus) OR (MH betacoronavirus) OR (MH "coronavirus infections")) AND ((MH "disease outbreaks") OR (MH epidemics) OR (MH pandemics))
S17. ((TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI COVID19* OR AB COVID19*) OR (TI COVID OR AB COVID) OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV2 OR AB SARSCOV2) OR (TI "SARS coronavirus 2" OR AB "SARS coronavirus 2") OR (TI "Severe Acute Respiratory Syndrome Coronavirus 2" OR AB "Severe Acute Respiratory Syndrome Coronavirus 2") OR (TI "Severe Acute Respiratory Syndrome Corona Virus 2" OR AB "Severe Acute Respiratory Syndrome Corona Virus 2"))
S18. (((TI new OR AB new) OR (TI novel OR AB novel) OR (TI 19 OR AB 19) OR (TI 2019 OR AB 2019) OR (TI Wuhan OR AB Wuhan) OR (TI Hubei OR AB Hubei) OR (TI China OR AB China) OR (TI Chinese OR AB Chinese)) N3 ((TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI betacoronavirus* OR AB betacoronavirus*) OR (TI CoV OR AB CoV) OR (TI HCoV OR AB HCoV)))
S19. ((TI longCOVID* OR AB longCOVID*) OR (TI postCOVID* OR AB postCOVID*) OR (TI postcoronavirus* OR AB postcoronavirus*) OR (TI postSARS* OR AB postSARS*))
S20. (((TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI betacoronavirus* OR AB betacoronavirus*)) N3 ((TI pandemic* OR AB pandemic*) OR (TI epidemic* OR AB epidemic*) OR (TI outbreak* OR AB outbreak*) OR (TI crisis OR AB crisis)))
S21. (((TI Wuhan OR AB Wuhan) OR (TI Hubei OR AB Hubei)) N5 (TI pneumonia OR AB pneumonia))
S22. S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21
S23. ((TI recovery OR AB recovery) N2 ((TI clinic OR AB clinic) OR (TI clinics OR AB clinics) OR (TI centre OR AB centre) OR (TI center OR AB center) OR (TI centres OR AB centres) OR (TI centers OR AB centers) OR (TI program* OR AB program*)))
S24. ((TI post* OR AB post*) N3 (TI rehabilitation OR AB rehabilitation) N2 ((TI clinic OR AB clinic) OR (TI clinics OR AB clinics) OR (TI centre OR AB centre) OR (TI center OR AB center) OR (TI centres OR AB centres) OR (TI centers OR AB centers) OR (TI program* OR AB program*)))
S25. S23 OR S24
S26. ((TI post OR AB post) W1 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)) N3 (TI infection* OR AB infection*) N8 ((TI chronic* OR AB chronic*) OR (TI persist* OR AB persist*) OR (TI residual OR AB residual) OR (TI prolonged OR AB prolonged) OR (TI non-recover* OR AB non-recover*) OR (TI nonrecover* OR AB nonrecover*) OR (TI recover* OR AB recover*) OR (TI rehabilitat* OR AB rehabilitat*) OR (TI month OR AB month) OR (TI months OR AB months) OR (TI year OR AB year) OR (TI years OR AB years) OR (TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI consequence* OR AB consequence*) OR (TI outcome* OR AB outcome*) OR (TI "clinical outcome*" OR AB "clinical outcome*") OR (TI aftercare* OR AB aftercare*) OR (TI after-care* OR AB after-care*) OR (TI issue* OR AB issue*) OR (TI complication* OR AB complication*) OR (TI following OR AB following) OR (TI follow-up OR AB follow-up) OR (TI followup OR AB followup) OR (TI function* OR AB function*)))
S27. (((TI chronic OR AB chronic) OR (TI post OR AB post)) W1 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)) N3 ((TI rehabilitat* OR AB rehabilitat*) OR (TI recover* OR AB recover*) OR (TI fatigue OR AB fatigue) OR (TI function* OR AB function*)))
S28. (((TI chronic* OR AB chronic*) OR (TI persist* OR AB persist*) OR (TI residual OR AB residual) OR (TI prolonged OR AB prolonged) OR (TI non-recover* OR AB non-recover*) OR (TI nonrecover* OR AB nonrecover*)) N2 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI consequence* OR AB consequence*) OR (TI outcome* OR AB outcome*) OR (TI "clinical outcome*" OR AB "clinical outcome*") OR (TI aftercare* OR AB aftercare*) OR (TI after-care* OR AB after-care*) OR (TI issue* OR AB issue*) OR (TI complication* OR AB complication*) OR (TI following OR AB following) OR (TI follow-up OR AB follow-up) OR (TI followup OR AB followup) OR (TI function* OR AB function*)) N5 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)))
S29. (((TI chronic* OR AB chronic*) OR (TI persist* OR AB persist*) OR (TI residual OR AB residual) OR (TI prolonged OR AB prolonged) OR (TI non-recover* OR AB non-recover*) OR (TI nonrecover* OR AB nonrecover*)) N2 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)) N5 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI consequence* OR AB consequence*) OR (TI outcome* OR AB outcome*) OR (TI "clinical outcome*" OR AB "clinical outcome*") OR (TI aftercare* OR AB aftercare*) OR (TI after-care* OR AB after-care*) OR (TI issue* OR AB issue*) OR (TI complication* OR AB complication*) OR (TI following OR AB following) OR (TI follow-up OR AB follow-up) OR (TI followup OR AB followup) OR (TI function* OR AB function*)))
S30. (((TI long-term OR AB long-term) OR (TI longterm OR AB longterm)) W1 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI consequence* OR AB consequence*) OR (TI outcome* OR AB outcome*) OR (TI "clinical outcome*" OR AB "clinical outcome*") OR (TI aftercare* OR AB aftercare*) OR (TI after-care* OR AB after-care*) OR (TI issue* OR AB issue*) OR (TI complication* OR AB complication*) OR (TI following OR AB following) OR (TI follow-up OR AB follow-up) OR (TI followup OR AB followup) OR (TI function* OR AB function*)) N5 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)))
S31. (((TI "post acute" OR AB "post acute") OR (TI postacute OR AB postacute) OR (TI "post viral" OR AB "post viral") OR (TI postviral OR AB postviral) OR (TI "post virus*" OR AB "post virus*") OR (TI postvirus* OR AB postvirus*) OR (TI "long duration" OR AB "long duration") OR (TI "long last" OR AB "long last") OR (TI "long lasting" OR AB "long lasting") OR (TI longstanding OR AB longstanding) OR (TI "long standing" OR AB "long standing") OR (TI late-onset OR AB late-onset) OR ((TI illness OR AB illness) N2 (TI duration OR AB duration))) N3 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI consequence* OR AB consequence*) OR (TI outcome* OR AB outcome*) OR (TI "clinical outcome*" OR AB "clinical outcome*") OR (TI aftercare* OR AB aftercare*) OR (TI after-care* OR AB after-care*) OR (TI issue* OR AB issue*) OR (TI complication* OR AB complication*) OR (TI following OR AB following) OR (TI follow-up OR AB follow-up) OR (TI followup OR AB followup) OR (TI function* OR AB function*)) N5 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)))
S32. (((TI survivor* OR AB survivor*) OR (TI survived OR AB survived) OR (TI discharg* OR AB discharg*) OR (TI postdischarg* OR AB postdischarg*) OR (TI "post infect*" OR AB "post infect*") OR (TI postinfect* OR AB postinfect*)) N3 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI consequence* OR AB consequence*) OR (TI outcome* OR AB outcome*) OR (TI "clinical outcome*" OR AB "clinical outcome*") OR (TI aftercare* OR AB aftercare*) OR (TI after-care* OR AB after-care*) OR (TI issue* OR AB issue*) OR (TI complication* OR AB complication*) OR (TI following OR AB following) OR (TI follow-up OR AB follow-up) OR (TI followup OR AB followup) OR (TI function* OR AB function*)) N5 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)))
S33. (((TI survivor* OR AB survivor*) OR (TI survived OR AB survived) OR (TI discharg* OR AB discharg*) OR (TI postdischarg* OR AB postdischarg*) OR (TI "post infect*" OR AB "post infect*") OR (TI postinfect* OR AB postinfect*)) N3 ((TI COVID* OR AB COVID*) OR (TI coronavirus* OR AB coronavirus*) OR (TI "corona virus*" OR AB "corona virus*") OR (TI SARS-COV-2 OR AB SARS-COV-2) OR (TI SARS-COV2 OR AB SARS-COV2) OR (TI SARSCOV-2 OR AB SARSCOV-2) OR (TI nCoV* OR AB nCoV*) OR (TI 2019nCoV OR AB 2019nCoV) OR (TI 19nCoV OR AB 19nCoV) OR (TI SARSCOV2 OR AB SARSCOV2)) N5 ((TI sequela* OR AB sequela*) OR (TI syndrome* OR AB syndrome*) OR (TI disorder* OR AB disorder*) OR (TI condition* OR AB condition*) OR (TI symptom* OR AB symptom*) OR (TI consequence* OR AB consequence*) OR (TI outcome* OR AB outcome*) OR (TI "clinical outcome*" OR AB "clinical outcome*") OR (TI aftercare* OR AB aftercare*) OR (TI after-care* OR AB after-care*) OR (TI issue* OR AB issue*) OR (TI complication* OR AB complication*) OR (TI following OR AB following) OR (TI follow-up OR AB follow-up) OR (TI followup OR AB followup) OR (TI function* OR AB function*)))
S34. S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33
S35. S14 AND S22
S36. S22 AND S25
S37. S9 OR S34 OR S35 OR S36
S38. (PT “commentary”) or (PT "editorial") or (PT "letter") or (PT "letter to the editor") or (PT "newspaper")
S39. S37 NOT S38
Search limits were: Published Date: 20190101-20221231; Exclude MEDLINE records; Language: English, French.
Clinical Trials Registries
Date of searches: October 25 to 26, 2021. Updated December 21, 2021.
ClinicalTrials.gov
Produced by the U.S. National Library of Medicine. Targeted search used to capture registered clinical trials.
Search terms – "post COVID" OR "postCOVID" OR "post COVID19" OR postCOVID19 OR "post coronavirus" OR "long COVID" OR "long COVID19" OR ("post acute" AND (COVID* OR coronavirus)) OR (sequelae AND (COVID* OR coronavirus))
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials. Duplicates removed with ClinicalTrials.gov by NCT.
Search terms – "post COVID" OR "postCOVID" OR "post COVID19" OR postCOVID19 OR "post coronavirus" OR "long COVID" OR "long COVID19" OR ("post acute" AND (COVID* OR coronavirus)) OR (sequelae AND (COVID* OR coronavirus))
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search terms – COVID, coronavirus; and reviewed results mentioning long, chronic, acute, or sequela
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search terms – "post COVID" OR "postCOVID" OR "post COVID19" OR postCOVID19 OR "post coronavirus" OR "long COVID" OR "long COVID19" OR ("post acute" AND (COVID* OR coronavirus)) OR (sequelae AND (COVID* OR coronavirus))
Other Databases
Preprints were searched via EuropePMC.org, which includes preprints from MedRxiv, bioRxiv, PsyArXiv, SSRN, and F1000 Research, among others. Preprint searches were limited to systematic reviews, meta-analyses, technology assessments, rapid reviews, scoping reviews, and other evidence reports where possible. Any preprints found in the Ovid Medline or Embase search were retained as well. Search strategies are available upon request. Date of search: October 25, 2021. Updated Dec 20, 2021.
A supplemental search of the Philosopher's Index via Ovid was conducted, with headings and keywords translated from the Ovid Medline search. Search strategies are available upon request. Date of search: October 29, 2021. Regular alerts sent with the other Ovid database alerts until December 20, 2021.
Grey Literature
Grey literature includes government information and other reports that are not published commercially and that may be inaccessible via bibliographic databases.
Search dates: October 25-29, 2021. Update of key sites on December 17-20, 2021.
Keywords: long COVID, post acute sequelae of COVID, post-COVID condition, chronic COVID condition, and synonyms.
Limits: Publication years: 2019-present
Updated: Search updated prior to the completion of stakeholder feedback period.
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
HTA Agencies
Clinical Practice Guidelines
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Large Tables and Figures
Note that this appendix has not been copy-edited.
Figure 4: Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flowchart of Selected Reports
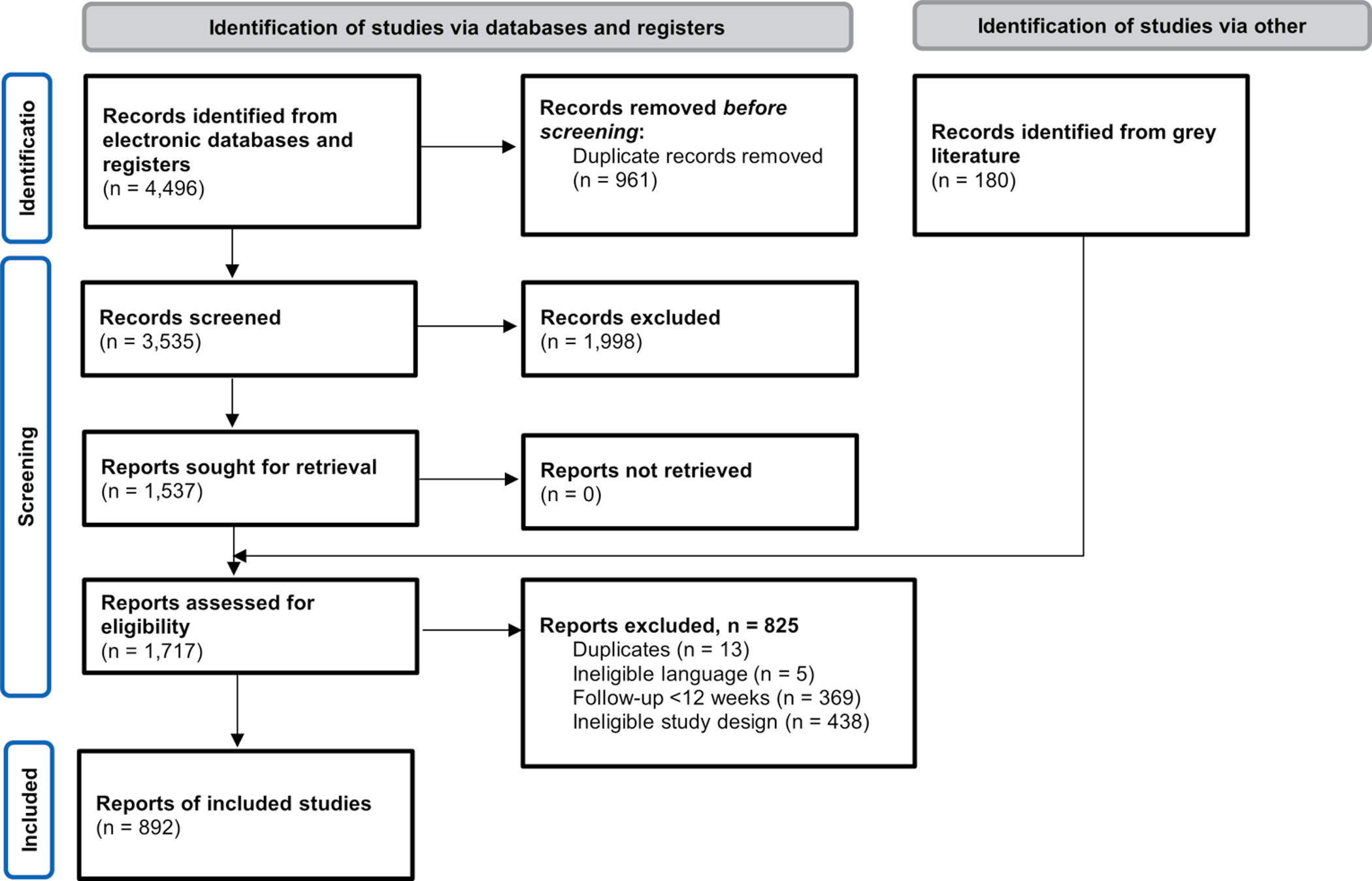
Category | Data items – Categorical (Options) | Data extracted – Open text |
|---|---|---|
Report information |
|
|
Population |
|
|
Concept a |
| Intervention/Exposure |
Context |
| NA |
COVID-19 = coronavirus disease 2019; ICD = International Classification of Diseases; ICU = intensive care unit; IQR = interquartile range; NA = not applicable; PCR = polymerase chain reaction; SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2; SD = standard deviation.
aIndicates questions where multiple categories could be selected.
bBased on date available online where available; if unavailable, date of publication was used.
c“Systematic reviews – other” was used to identify scoping reviews.
dIf at least 80% of participants must have had a COVID-19 laboratory test, defined as a PCR, antibody/antigen test, or other lab test (e.g., studies that simply stated “laboratory-confirmed”), it was considered as having a majority of laboratory-confirmed COVID-19 cases. Studies that had at least 80% of participants without a confirmed COVID-19 lab test (e.g., the methods stated patients had been diagnosed by a clinician or at the hospital, without any indication a lab test was done) were labelled as “no,” while studies that had between 20% to 80% of laboratory-confirmed COVID-19 were labelled as “mixed,” and the percentage of laboratory-confirmed participants was extracted if reported.
eInterventions were considered preventive if they occurred <12 weeks after diagnosis/discharge, including interventions provided during the acute illness phase. Interventions were considered as treatment/management if they occurred at least 12 weeks after diagnosis/discharge. If the methods were unclear regarding when the intervention occurred (e.g., if participants were eligible for the intervention if they were at least 6 weeks after diagnosis) the study was categorized as both prevention and intervention.
fPublications or protocols that assessed topics related to health ethics or equity, budget impact, and policy impact were relevant to health system issues. This included studies that assessed usage of health care services and pharmaceuticals (e.g., usage among people who had been infected with COVID-19 at least 12 weeks ago) as this was considered to potentially affect health care budget considerations.
Table 12: Methods Used by Canadian Guidelines for Post–COVID-19 Care
Method | Alberta29 | British Columbia30 | Ontario31 | Quebec32 |
|---|---|---|---|---|
Funding/sponsorship | NR | NR | NR | NR |
Did the guideline describe their methodology? | Yes | No | Yes | Yes |
Method(s) used | ||||
Systematic literature search (search strategy provided) a | No | NA | No | Yes |
Literature search, unclear if systematic | Yes | NA | No | No |
Expert feedback | No | NA | No | No |
Stakeholder feedback/consultation | No | NA | No | No |
Based on a specific guideline b | No | NA | Yes | No |
Authors’ clinical experience | No | NA | No | No |
Literature searched | ||||
CINAHL | No | NR | NR | No |
Cochrane library | No | NR | NR | Yes |
EMBASE | Yes | NR | NR | No |
Guidelines databases | No | NR | NR | Yes |
MEDLINE | Yes | NR | NR | No |
PubMed | Yes | NR | NR | Yes |
Other databases | No | NR | NR | Yes |
Other (e.g., reference list searching) | No | NR | NR | No |
End of literature search date | NR | NR | NR | June 2021 |
Publication date | July 2021 | NR | December 2021 | July 2021 |
COVID-19 = coronavirus disease 2019; NA = not applicable; NR = not reported.
aIf the methods provided a detailed search strategy and/or specified their search was systematic.
bThe guideline based their recommendations on what a previously published guideline recommends.
Table 13: Summary of Recommendations From Canadian Guidelines for Post–COVID-19 Care
Recommendation | Alberta29 | British Columbia30 | Ontario31 | Quebec32 |
|---|---|---|---|---|
Population | Children, adults a | NR | Adults | Children, adults a |
Diagnosis | ||||
Health review/follow-up at 3 months or later | NR | NR | NR | NR |
Laboratory/ imaging tests | NR | NR | NR | NR |
Chest X-ray for respiratory symptoms | NR | NR | Yes | Yes |
Management | ||||
Rehabilitation | NR | NR | NR | NR |
Referral to specialist(s) | Yes | NR | NR | NR |
Referral to post–COVID-19 clinic | Yes | Yes | NR | NR |
COVID-19 = coronavirus disease 2019; NR = not reported.
aSummarizes literature on children and adults, but unclear if guidance specific to 12+ weeks applies to children.
Table 14: Methods Used by International Guidelines for Post–COVID-19 Care
Method | Australia and New Zealand33 | Australia59 | Netherlands60 | Spain34 | Turkey35 | United Kingdom61 | United Kingdom6 | USA62 |
|---|---|---|---|---|---|---|---|---|
Funding/sponsorship | NR | NR | None | None | None | NR | NR | NR |
Did the guideline describe their methodology? | No | No | Yes | Yes | Yes | Yes | Yes | No |
Method(s) used | ||||||||
Systematic literature search a | NA | NA | No | Yes | No | Yes | Yes | NA |
Literature search, unclear if systematic | NA | NA | No | NA | Yes | NA | NA | NA |
Expert feedback | NA | NA | Yes | Yes | Yes | Yes | Yes | NA |
Stakeholder feedback/consultation | NA | NA | No | No | No | Yes | Yes | NA |
Based on a specific methodological guideline b | NA | NA | Yes | No | No | No | No | NA |
Authors’ clinical experience | NA | NA | No | Yes | No | No | No | NA |
Literature searched | ||||||||
CINAHL | NR | NR | NR | NR | Yes | Yes | Yes | NR |
Cochrane library | NR | NR | NR | NR | Yes | Yes | Yes | NR |
Embase | NR | NR | NR | NR | NR | Yes | Yes | NR |
Guidelines databases | NR | NR | NR | NR | NR | NR | NR | NR |
MEDLINE | NR | NR | NR | NR | NR | Yes | Yes | NR |
PubMed | NR | NR | NR | Yes | Yes | NR | NR | NR |
Other databases | NR | NR | NR | NR | Yes | Yes | Yes | NR |
Other sources (e.g., reference checking) | NR | NR | NR | NR | NR | Yes | Yes | NR |
End of literature search date | NR | NR | NR | January 13, 2021 | NR | October 28, 2020 | NR | NR |
Publication date | September 2021 | December 2021 | November 2021 | April 2021 | April 2021 | December 2020 | November 2021 | June 2021 |
COVID-19 = coronavirus disease 2019; NR = not reported; NA = not applicable.
aIf the methods provided a detailed search strategy and/or specified their search was systematic.
bThe guideline based their recommendations on what a previously published guideline recommends.
Table 15: Summary of Recommendations by International Guidelines for Post–COVID-19 Care
Recommendation | Australia and New Zealand33 | Australia59 | Netherlands60 | Spain34 | Turkey35 | United Kingdom61 | United Kingdom6 | USA62 |
|---|---|---|---|---|---|---|---|---|
Population | Children, adultsa treated for COVID-19 in the ICU | Children, adultsa | Older adults | NR | Adults | Children, adults, older adults | Children, adults, older adults | Children, adultsa |
Diagnosis | ||||||||
Health review/follow-up at 3+ months | Yes | NR | Yes | Yes | Yes | NR | Yes | NR |
Laboratory tests | NR | NR | NR | NR | NR | NR | NR | Yes |
Chest X-ray for respiratory symptoms | NR | Yes | NR | NR | NR | Yes | NR | NR |
Management | ||||||||
Rehabilitation | NR | NR | NR | NR | Yes | NR | NR | NR |
Referral to specialist(s) | Yes | NR | NR | Yes | NR | NR | Yes | NR |
Referral to post-COVID clinic | NR | NR | NR | NR | NR | NR | NR | NR |
COVID-19 = coronavirus disease 2019; ICU = intensive care unit; NR = not reported.
aSummarizes literature on children and adults, but unclear if guidance specific to 12+ weeks applies to children.
Appendix 3: Additional Figures and Data
Note that this appendix has not been copy-edited.
Table 16: Summary of 3 Included Scoping Reviews
First author’s surname | Year published | Countrya | Severity of acute illness | Main concepts | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Asymptomatic | Symptomatic, not hospitalized | Hospitalized | ICU | Classification | Risk factors and prevention | Diagnostic tests | Treatment and management | Health system issues | |||
Akbarialiabad11 | 2021 | Iran | NR | NR | NR | NR | Yes | Yes | Yes | Yes | NR |
Shanbehzadeh12 | 2021 | Iran | NR | Yes | Yes | NR | Yes | Yes | NR | NR | NR |
Cha13 | 2021 | South Korea | NR | Yes | Yes | NR | Yes | Yes | NR | Yes | NR |
ICU = intensive care unit; NR = not reported.
aCADTH reported the country/countries of included primary studies if it was provided in the review. If CADTH were unable to find this data, CADTH reported the country of the first author.
Table 17: Summary of Included Systematic Reviews
First author’s surname | Year published | Countrya | Severity of acute illness | Main concepts | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Asymptomatic | Symptomatic, not hospitalized | Hospitalized | ICU | Classifi-cation | Risk factors and prevention | Diagnostic tests | Treatment and management | Health system issues | |||
So63 | 2021 | Japan | NR | NR | Yes | NR | NR | NR | Yes | NR | NR |
Soriano-Moreno64 | 2021 | NR | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Renaud-Charest65 | 2021 | Canada, studies included from Italy, Austria, Spain, France, Netherlands, the US, Germany | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Anaya66 | 2021 | Colombia | NR | Yes | Yes | Yes | Yes | NR | Yes | NR | NR |
Fernandez-de-Las-Penas67 | 2021 | Spain | NR | NR | NR | NR | Yes | Yes | NR | NR | NR |
Van Kessel68 | 2021 | Netherlands | NR | Yes | NR | NR | Yes | NR | NR | NR | NR |
Malik69 | 2022 | Europe, the UK, the US, Iran, and China | NR | NR | NR | NR | Yes | NR | NR | NR | NR |
Groff70 | 2021 | US | NR | NR | NR | NR | Yes | NR | NR | NR | NR |
Sandler71 | 2021 | Australia | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Long72 | 2021 | China | NR | NR | NR | NR | Yes | Yes | NR | NR | NR |
Sanchez-Ramirez73 | 2021 | China (7), Canada (3), France (2), Norway (2), Italy (3), the US, (2), Switzerland (1), Austria (1), Iran (1), the Netherlands (1), and the UK | NR | Yes | Yes | Yes | Yes | NR | Yes | NR | NR |
Iqbal74 | 2021 | UK | NR | Yes | Yes | NR | Yes | Yes | NR | NR | NR |
Salamanna75 | 2021 | Italy | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Fernandez-de-Las-Penas76 | 2021 | Spain | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Michelen77 | 2021 | UK | NR | Yes | Yes | Yes | Yes | Yes | Yes | NR | NR |
Ahmad78 | 2021 | Saudi Arabia | NR | Yes | Yes | Yes | Yes | NR | NR | NR | NR |
Schou79 | 2021 | Asia, Europe, North America, and Oceania | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Martimbianco80 | 2021 | Brazil | NR | NR | Yes | NR | Yes | Yes | NR | NR | NR |
Sun81 | 2021 | China | NR | NR | NR | NR | Yes | Yes | Yes | NR | NR |
Ramadan82 | 2021 | Italy | NR | Yes | Yes | NR | Yes | Yes | NR | NR | NR |
Cares-Marambio83 | 2021 | Chile | NR | NR | Yes | Yes | Yes | NR | NR | NR | NR |
Ludvigsson84 | 2021 | Sweden | NR | Yes | NR | NR | Yes | NR | NR | NR | NR |
Vanderlind85 | 2021 | US | NR | NR | NR | NR | Yes | Yes | NR | NR | NR |
Kim86 | 2021 | Republic of Korea | NR | NR | NR | NR | NR | NR | NR | Yes | NR |
Wong87 | 2021 | US | NR | Yes | Yes | NR | NR | Yes | NR | NR | NR |
Willi88 | 2021 | Switzerland | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Wang89 | 2020 | China | NR | NR | NR | Yes | NR | Yes | NR | NR | NR |
Cabrera Martimbianco80 | 2021 | Brazil | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Jennings90 | 2021 | Ireland | NR | Yes | Yes | Yes | Yes | NR | Yes | NR | NR |
Hoshijima91 | 2021 | Japan | NR | NR | NR | NR | Yes | Yes | NR | NR | NR |
Nna92 | 2021 | Nigeria | NR | NR | NR | NR | Yes | Yes | NR | Yes | NR |
Michelen77 | 2021 | UK | NR | Yes | Yes | Yes | Yes | Yes | Yes | NR | NR |
De-la-Rosa-Martinez93 | 2021 | Mexico | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Domingo10 | 2021 | Canada | NR | Yes | Yes | Yes | Yes | NR | NR | NR | NR |
Michelen94 | 2021 | UK | NR | NR | NR | NR | Yes | Yes | NR | NR | NR |
Gyanpuri95 | 2020 | India | NR | NR | NR | NR | NR | Yes | NR | Yes | NR |
Zürcher96 | 2021 | Switzerland | NR | Yes | Yes | NR | Yes | NR | NR | NR | NR |
Malik97 | 2021 | Pakistan | NR | Yes | Yes | NR | Yes | NR | NR | NR | NR |
Yusuf98 | 2021 | Indonesia | NR | NR | Yes | NR | Yes | Yes | NR | NR | NR |
Fabbri99 | 2021 | UK | NR | NR | Yes | NR | Yes | Yes | Yes | NR | NR |
Fernandez-de-Las-Penas100 | 2021 | Spain | NR | Yes | Yes | Yes | Yes | NR | NR | NR | NR |
Rao101 | 2021 | Denmark, Ireland, the UK, the US, Israel, Germany, Italy, Egypt, China, Saudi Arabia, the Netherlands | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
d’Ettorre102 | 2021 | Italy | NR | NR | NR | NR | Yes | Yes | Yes | NR | NR |
Groff70 | 2021 | US | NR | Yes | Yes | NR | Yes | Yes | NR | NR | NR |
Chen9 | 2021 | China, India, Bangladesh, Iran, Russia, Italy, Norway, France, Germany, the UK, Switzerland, Spain, the UK, the US, Brazil | NR | Yes | Yes | Yes | Yes | Yes | NR | NR | NR |
Décary103 | 2021 | Canada | NR | NR | NR | NR | NR | NR | NR | Yes | NR |
Wu104 | 2021 | China | NR | NR | NR | NR | Yes | Yes | NR | NR | NR |
Nagarajan105 | 2021 | India | NR | NR | Yes | Yes | Yes | Yes | NR | NR | NR |
Patrucco106 | 2021 | Italy | NR | NR | Yes | NR | Yes | Yes | NR | NR | NR |
Behnood45 | 2021 | Australia, Faroe Islands, Germany, Italy, Latvia, the Netherlands, Russia, Spain, Sweden, Switzerland, the UK, and the US | Yes | Yes | Yes | NR | Yes | Yes | NR | NR | NR |
Razak107 | 2021 | Canada | NR | NR | NR | NR | Yes | Yes | NR | NR | Yes |
De la Rosa-Martinez108 | 2021 | Mexico | NR | NR | NR | NR | Yes | Yes | NR | NR | NR |
Pillay109 | 2021 | Canada | NR | Yes | Yes | Yes | NR | Yes | NR | NR | NR |
ECRI110 | 2021 | US | NR | Yes | Yes | Yes | Yes | Yes | NR | Yes | NR |
Castanares-Zapatero111 | 2021 | Belgium | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
ICU = intensive care unit; NR = not reported.
aCADTH reported the country/countries of included primary studies if it was provided in the review. If CADTH were unable to find this data, CADTH reported the country of the first author.
Figure 5: Number of Included References by Terms Reported for Comorbidities
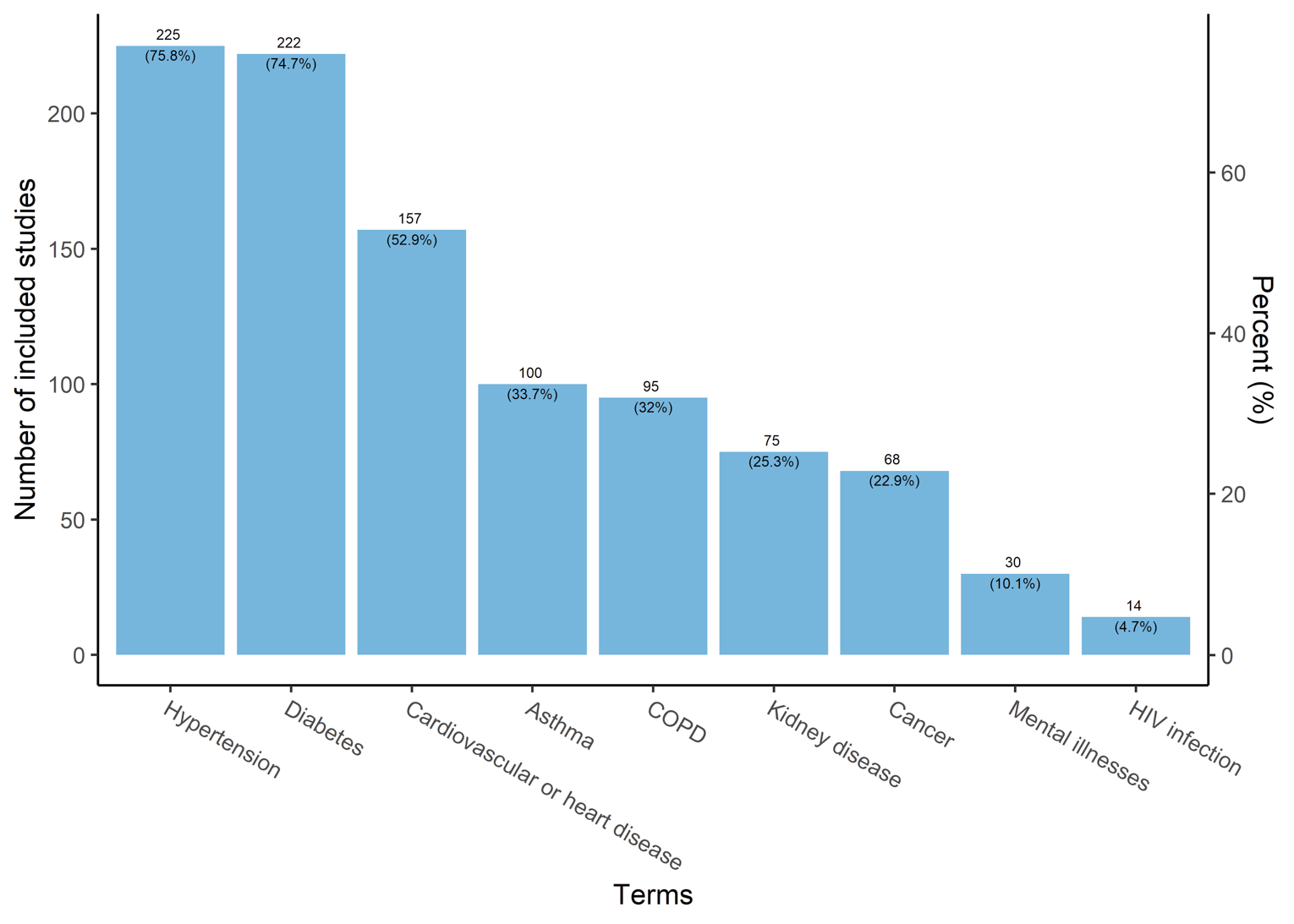
COPD = chronic obstructive pulmonary disease.
The comorbidities data were assessed in 297 (33.3%) references. The terms that were commonly investigated in 297 eligible references included hypertension (225, 75.8%), diabetes (222, 74.7%), cardiovascular or heart disease (157, 52.9%), asthma (100, 33.7%), COPD (95, 32%), kidney disease (75, 25.3%), cancer (68, 22.9%), mental health illnesses (30, 10.1%), and HIV infection or AIDS (14, 4.7%).
Figure 6: Severity of Initial COVID-19 Illness Reported in Included References
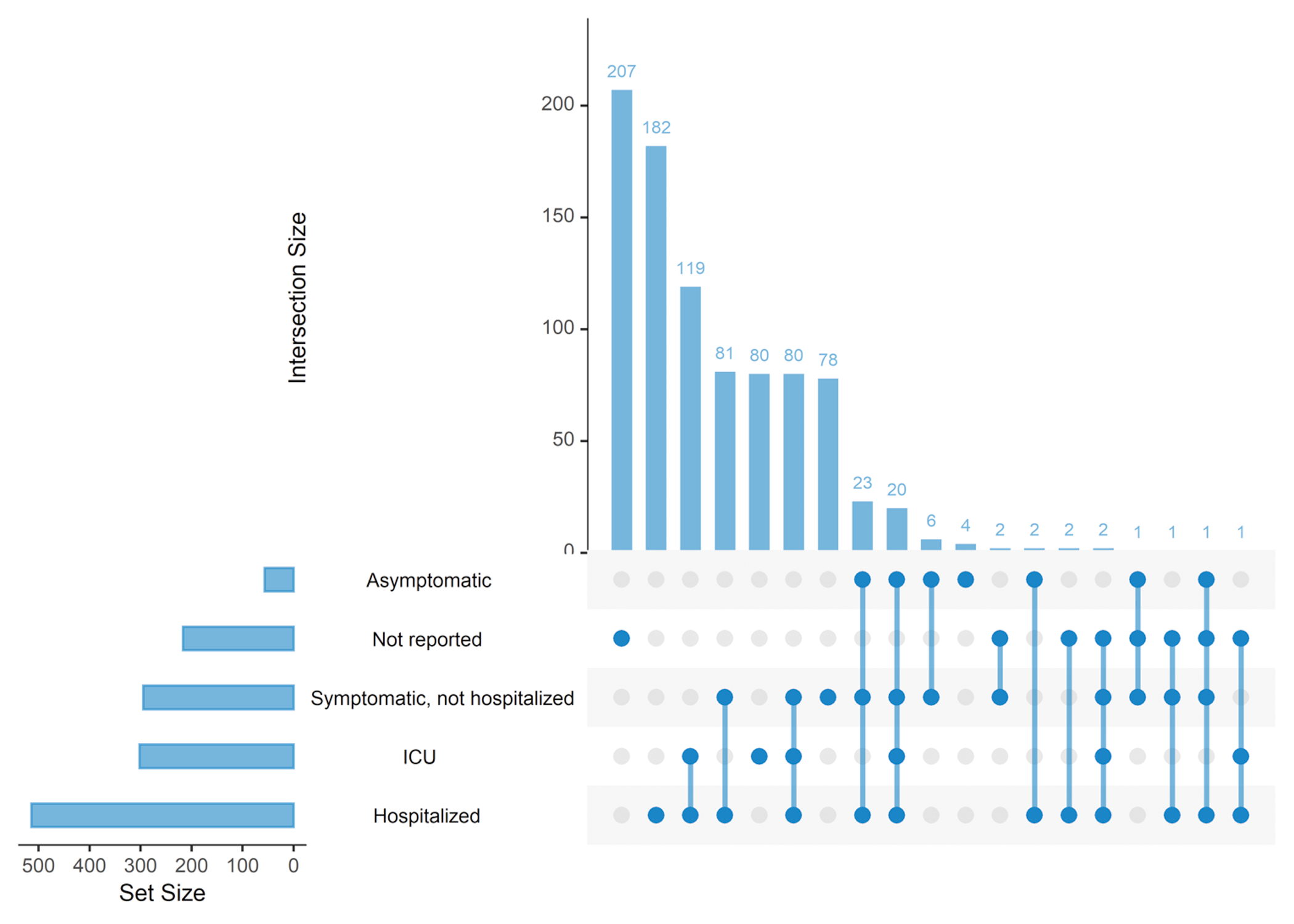
COVID-19 = coronavirus disease 2019; ICU = intensive care unit.
Note: An Upset plot is an alternative to a Venn diagram that is typically used when there are 4 or more categories. The horizontal bars represent the set sizes, or the total number of studies that are within each category. Categories are not mutually exclusive, so the sum of these sets exceeds the number of studies (e.g., a study that falls under both categories A and B would be counted in both). The vertical bars represent the intersection sizes, which are the number of studies for each unique combination of categories that was found. As these bars represent specific combinations, they are mutually exclusive groups (e.g., studies only under A, studies only under B, and studies under both A and B, are counted separately in their respective intersections). The number above the vertical bar states the number of studies in that specific combination. The dots represent which categories were included in the intersection/combination bars, with the dark blue dot representing it was included; a light grey dot indicates that category was not included.
Figure 7: Methods of Confirmation or Diagnosis of COVID-19 Reported in Eligible References
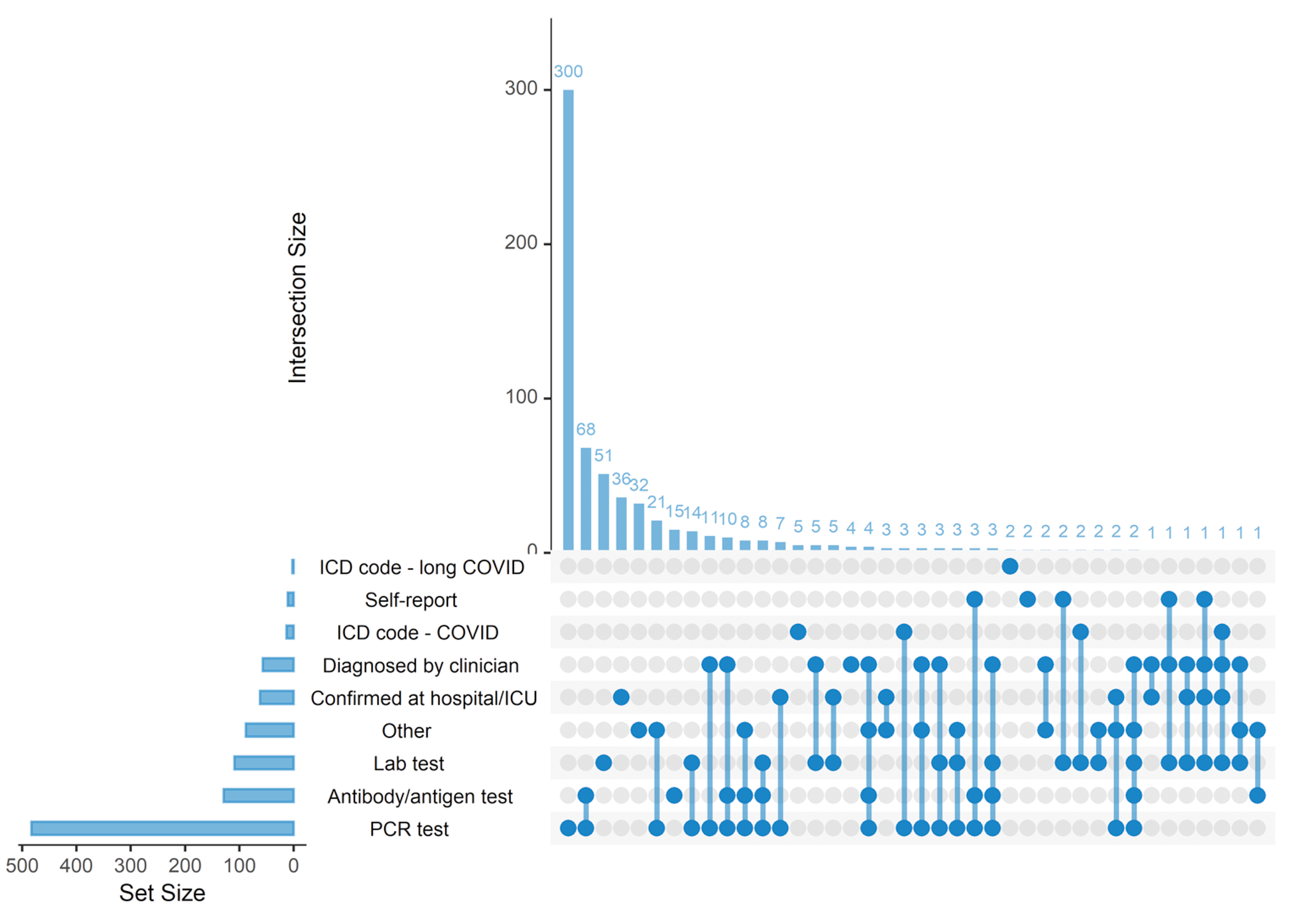
COVID = coronavirus disease; COVID-19 = coronavirus disease 2019; CT = computed tomography; ICD = International Classification of Diseases; ICU = intensive care unit; PCR = polymerase chain reaction.
Note: An Upset plot is an alternative to a Venn diagram that is typically used when there are 4 or more categories. The horizontal bars represent the set sizes, or the total number of studies that are within each category. Categories are not mutually exclusive, so the sum of these sets exceeds the number of studies (e.g., a study that falls under both categories A and B would be counted in both). The vertical bars represent the intersection sizes, which are the number of studies for each unique combination of categories that was found. As these bars represent specific combinations, they are mutually exclusive groups (e.g., studies only under A, studies only under B, and studies under both A and B, are counted separately in their respective intersections). The number above the vertical bar states the number of studies in that specific combination. The dots represent which categories were included in the intersection/combination bars, with the dark blue dot representing it was included; a light grey dot indicates that category was not included.
Sample List of Included Studies
1.Osteopathy and Physiotherapy Compared to Physiotherapy Alone on Fatigue and Functional Status in Long COVID. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT05012826. 2021.
2.Olfactory Training for Olfactory Dysfunction After Coronavirus Disease - 19 (COVID-19). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04764981. 2021.
3.Olfactory Disfunction and Co-ultraPEALut. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04853836. 2021.
4.SOLIDARITY Finland Long COVID-19. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04978259. 2021.
5.The Effect of Virtual Reality Exercises on Patients With Post-SARS-CoV-2 Syndrome. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04983394. 2021.
6.Pulmonary Rehabilitation Post-COVID-19. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT05003271. 2021.
7.Phase 2 Study of RSLV-132 in Subjects With Long COVID. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04944121. 2021.
8.Impact of Colchicine To Improve long-COVID-19 or ARDS Outcomes. WHO International Clinical Trials Registry Platform (ICTRP) http://trialsearch.who.int/?TrialID=ACTRN12621000637842. 2021.
9.tDCS for Post COVID-19 Fatigue. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04876417. 2021.
10.Coenzyme Q10 as Treatment for Long Term COVID-19. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04960215. 2021.
11.Internet-based Multidisciplinary Rehabilitation for Longterm COVID-19 Syndrome. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04961333. 2021.
12.Cardiopulmonary Rehabilitation in COVID-19 Longhaulers. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04898205. 2021.
13.Statin TReatment for COVID-19 to Optimise NeuroloGical recovERy. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04904536. 2021.
14.Inspiratory Muscle Trainer and Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) COVID-19 Persistent Symptoms. https://clinicaltrials.gov/show/NCT04919031. 2021.
15.Chinese Medicine for Patients With LCOVID-19 Symptoms. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04924881. 2021.
16.Coenzym Q10 til behandling af senfolger efter COVID-19 (QVID studiet). WHO International Clinical Trials Registry Platform (ICTRP) http://trialsearch.who.int/?TrialID=EUCTR2020-005961-16-DK. 2020.
17.The Kidney BEAM Trial. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04872933. 2021.
18.COVID-19 Pneumonia: pulmonary Physiology, Health-related Quality of Life and Benefit of a Rehabilitation Program. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04881214. 2021.
19.Safety and Efficacy of Hyperbaric Oxygen Therapy for Long COVID Syndrome. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04842448. 2021.
20.Clinical Trial of Niagen to Examine Recovery in People With Persistent Cognitive and Physical Symptoms After COVID-19 Illness (Long-COVID). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04809974. 2021.
Sample List of the Studies Excluded for Unclear Post-Infection Time
1.Diode Laser 940 nm in Management of Loss of Taste Sensation. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/show/NCT04821999. 2021.
2.Effect of Chatushashti Prahari Pippali in the management of Post COVID syndrome. WHO International Clinical Trials Registry Platform (ICTRP): http://trialsearch.who.int/?TrialID=CTRI. 2021;03(031667).
3.Powell R. 34.3 Chronic Manifestations and Prolonged Illness from Covid-19 in Children. J Am Acad Child Adolesc Psychiatry. 2021;60(10 Supplement):S51.
4.Angeli MC, Rausa F, Satta E, et al. Underestimated sleep breathing disorders in a cohort of patients admitted to post-COVID-19 follow-up program: A single center experience. J Neurol Sci. 2021;Conference: World Congress of Neurology (WCN 2021 . Rome Italy. 429 Supplement).
5.Wong J, Kudla A, Pham T, et al. Employment consequences of COVID-19 on "Long-Haul" survivors. Arch Phys Med Rehabil. 2021;102(10):e66.
6.Acanfora D, Acanfora C, Ciccone MM, et al. The cross-talk between thrombosis and inflammatory storm in acute and long-covid-19: Therapeutic targets and clinical cases. Viruses. 2021;13(10) (no pagination).
7.Blitshteyn S, Brook J, Minen M, et al. COVID-19 in patients with pre-existing neurologic disorders: Clinical course and outcomes. Neurology Conference: 73rd Annual Meeting of the American Academy of Neurology, AAN. 2021;96(15 SUPPL 1).
8.Ebel N, Kehar M, Ng V, et al. The impact of SARS-CoV2 infection in pediatric liver transplant recipients: An international observational registry study. Transplantation. 2021;105(8 SUPPL 1):157-158.
9.Marfil A, Fernandez-Garza LE, Preciado-Gonzalez O. Post COVID-19 headache: A Mexican online survey. Headache. 2021;61(SUPPL 1):33.
10.Araja D, Berkis U, Lunga A, Murovska M. PMU29 Burden of COVID-19 Consequences: an Example of Post-viral Chronic Fatigue Syndrome. Value Health. 2021;24(Supplement 1):S149-S150.
11.Cho AR, Korzan SP, Viola SR, Levine AR. Incidence of PTSD in COVID-19 survivors of critical illness and the therapeutic efficacy of steroids in the prevention of PTSD. American Journal of Respiratory and Critical Care Medicine Conference: American Thoracic Society International Conference, ATS. 2021;203(9).
12.Bandera F, Alfonzetti E, Mazzucca M, et al. Lung injury and functional capacity post-Sars-Cov-2 infection. J Am Coll Cardiol. 2021;77(18 Supplement 1):3187.
13.Patil S, Rajanikanth K. The emergence of long haul-continuing typical covid-19 symptoms long after infection. International Journal of Research in Pharmaceutical Sciences. 2020;11(Special Issue 1):1768-1772.
14.Soni SN, Nimbalkar SM. Long covid syndrome following infection with sars-cov-2- a devastating influence on health status in some affected individuals. Journal of Clinical and Diagnostic Research. 2021;15(2):LE17-LE21.
15.Jiang D. Guidelines for patient-practitioner contact and tcm management in post-covid syndromes. Journal of Chinese Medicine. 2021;2021(125):71-79.
16.Gervasoni F, LoMauro A, Ricci V, et al. Balance and visual reliance in post-COVID syndrome patients assessed with a robotic system: a multi-sensory integration deficit. Neurol Sci. 2021;06:06.
17.Horton DB, Barrett ES, Roy J, et al. Determinants and dynamics of SARS-CoV-2 infection in a diverse population: 6-month evaluation of a prospective cohort study. J Infect Dis. 2021;13:13. PubMed
18.Maniscalco M, Fuschillo S, Ambrosino P, et al. Bronchodilator response as a possible predictor of lung function improvement after pulmonary rehabilitation in post-COVID-19 patients. Arch Bronconeumol. 2021;18:18.
Sample List of the Studies Excluded for Acute or Unspecified Infection
1.A randomized, double-blind, placebo-controlled, adaptive-design study to assess the safety and efficacy of daily 200 mg fluvoxamine as add-on therapy to standard of care in moderate severity COVID-19 patients. WHO International Clinical Trials Registry Platform (ICTRP): http://trialsearch.who.int/?TrialID=EUCTR2020-002299-11; https://www.clinicaltrialsregister.eu/ctr-search/trial/2020-002299-11/HU. 2020.
2.Thornton AR. Evolution of 18F-FDG-PET/CT findings in patients following covid-19 pneumonia: An initial investigation. American Journal of Respiratory and Critical Care Medicine Conference: American Thoracic Society International Conference, ATS. 2021;203(9).
3.De Azambuja K, Agarwal S, Sehgal S. Post-acute COVID syndrome: prolonged night sweats. J Am Geriatr Soc. 2021;69(SUPPL 1):S35.
4.Weinstock LB, Brook JB, Walters AS, Goris A, Afrin LB, Molderings GJ. Mast cell activation symptoms are prevalent in Long-COVID. Int J Infect Dis. 2021;23:23. PubMed
5.Donyavi T, Bokharaei-Salim F, Baghi HB, et al. Acute and post-acute phase of COVID-19: Analyzing expression patterns of miRNA-29a-3p, 146a-3p, 155-5p, and let-7b-3p in PBMC. Int Immunopharmacol. 2021;97:107641. PubMed
6.Maniscalco M, Fuschillo S, Ambrosino P, et al. Preexisting cardiorespiratory comorbidity does not preclude the success of multidisciplinary rehabilitation in post-COVID-19 patients. Respir Med. 2021;184:106470. PubMed
7.Al Haboob AA. Miller Fischer and posterior reversible encephalopathy syndromes post COVID-19 infection. Neurosciences. 2021;26(3):295-299. PubMed
8.Raja MA, Mendoza MA, Villavicencio A, et al. COVID-19 in solid organ transplant recipients: A systematic review and meta-analysis of current literature. Transplant Rev. 2021;35(1):100588. PubMed
9.Brigham E, O'Toole J, Kim SY, et al. The Johns Hopkins Post-Acute COVID-19 Team (PACT): a multidisciplinary, collaborative, ambulatory framework supporting COVID-19 survivors. Am J Med. 2021;134(4):462-467.e461. PubMed
10.Mahmud R, Rahman MM, Rassel MA, et al. Post-COVID-19 syndrome among symptomatic COVID-19 patients: a prospective cohort study in a tertiary care center of Bangladesh. PLoS ONE. 2021;16(4):e0249644. PubMed
11.Burgess LC, Venugopalan L, Badger J, et al. Effect of neuromuscular electrical stimulation on the recovery of people with COVID-19 admitted to the intensive care unit: A narrative review. J Rehabil Med. 2021;53(3):jrm00164. PubMed
12.Agostini F, Mangone M, Ruiu P, Paolucci T, Santilli V, Bernetti A. Rehabilitation setting during and after Covid-19: an overview on recommendations. J Rehabil Med. 2021;53(1):jrm00141. PubMed
13.Grissmer J. Acupuncture for COVID Long-Haulers, Pt. 2: Case Studies. Acupuncture Today. 2021;22(9):10-22.
14.Daga M, Mawari G, Chand S, Aarthi J, Raghu R, Kumar N. Are patients with comorbidities more prone to sequalae in severe COVID-19. Indian Journal of Medical Specialities. 2021;12(3):161-164.
15.Zettersten E, Engerström L, Bell M, et al. Long-term outcome after intensive care for COVID-19: differences between men and women—a nationwide cohort study. Critical Care. 2021;25(1):1-9. PubMed
16.Brandt MP, Jäger W, Epple S, Haferkamp A, Schröder A. SARS-CoV-2 outbreak in medical employees in a large urologic department: Spread, containment and outcome. Am J Infect Control. 2021;49(6):674-677. PubMed
17.Al-Jassas HK, Al-Hakeim HK, Maes M. Intersections between pneumonia, lowered oxygen saturation percentage and immune activation mediate depression, anxiety, and chronic fatigue syndrome-like symptoms due to COVID-19: A nomothetic network approach. J Affect Disord. 2022;297:233-245. PubMed
18.Lee AS, He Z, Eggert LE, et al. The allergic asthma phenotype, associated comorbidities, and long-term symptoms in COVID-19. Allergy: European Journal of Allergy and Clinical Immunology. 2021;76(SUPPL 110):199-200.
19.Martin C, Luteijn M, Letton W, Robertson J, McDonald S. A model framework for projecting the prevalence and impact of Long-COVID in the UK. PLoS ONE. 2021;16(12):e0260843. PubMed
Appendix 4: Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist
Note that this appendix has not been copy-edited.
Table 18: Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist
Section | Item | Prisma-Scr Checklist Item | Reported on Page # |
|---|---|---|---|
Title | |||
Title | 1 | Identify the report as a scoping review. | 1 |
Abstract | |||
Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. Use the abstract reporting checklist (refer to Item 2 in PRISMA 2020). | 7-8 |
Introduction | |||
Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 9 |
Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 10 |
Methods | |||
Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. Report any protocol amendments (refer to item 24 in PRISMA 2020). | 10 |
Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 11-12 |
Information sources | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 10-11 |
Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. Include the full search strategies for all databases, registers, and websites (refer to item 7 in PRISMA 2020). | 28-42 |
Selection of sources of evidence | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. Describe if automation tools were used for study selection (refer to item 8 in PRISMA 2020). | 12 |
Data charting process | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. If outcomes were included, describe how they were defined and which results were sought (refer to item 10 in PRISMA 2020). | 13 |
Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 44-45 |
Critical appraisal of individual sources of evidence | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | NA |
Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 13 |
Results | |||
Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. Use the updated PRISMA 2020 flow diagram, which has optional boxes for review updates, as well as studies that were identified through means other than searching databases/registers and cite any studies that appeared to meet the inclusion criteria but were excluded (refer to item 16 in PRISMA 2020) | 13, 43 |
Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | Not conduced |
Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (refer to item 12). | NA |
Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | NA |
Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 14-23 |
Discussion | |||
Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 23-24 |
Limitations | 20 | Discuss the limitations of the scoping review process. | 24 |
Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 24-25 |
Funding | |||
Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. Report conflicts of interest (refer to item 26 in PRISMA 2020) 1 | Funding |
JBI = Joanna Briggs Institute; PRISMA-ScR = Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca