CADTH Health Technology Review
Intraocular Lenses for Infants With Aphakia
PROSPERO Registration Number: CRD42021231143
Systematic Review
Authors
Clinical Effectiveness and Safety
Charlotte Wells led the systematic review; screened and selected articles; extracted, tabulated, critically appraised, and interpreted data; drafted the report; revised the report based on reviewers’ feedback; and provided final approval of the version of the report submitted for publication.
Daphne Hui supported the lead author of the review by screening and selecting studies, extracting and double-checking information, critically appraising and interpreting data, providing support in writing, reviewing the report until completion, and providing final approval of the version of the report submitted for publication.
Kwakye Peprah led the development and writing of the review protocol, participated in study selection based on the protocol-determined inclusion criteria, independently performed data extraction from assigned included studies, and checked data extracted by other reviewers for integrity and completeness.
Dr. Asim Ali contributed to the development of the review protocol and the analysis and interpretation of the study results, critically reviewed the draft report and provided feedback, and provided final approval of the version of the report submitted for publication.
Patient Engagement
Tamara Rader led family caregiver engagement activities and wrote the summary of those activities included in the report. She also reviewed the protocol and approved the Patients’ Experiences GRIPP2 Short Form Reporting Checklist table reporting family caregiver involvement in the report.
Research Information Services
Melissa Walter designed and executed the database search strategies, completed grey literature searches, maintained search alerts, prepared the search methods and appendix, and provided final approval of the version of the report submitted for publication.
David Kaunelis peer-reviewed the search strategies and approved the final version of the report submitted for publication.
Contributors
The authors would like to acknowledge Elizabeth Carson and Dr. Joanne Kim for providing project oversight and coordination and methodological support throughout the planning, conduct, and reporting of this review. They would also like to acknowledge Dr. Laura Weeks for providing project oversight and reviewing the draft protocol and draft report, Dave Marchand for his contribution to the protocol development, Dr. Brit Cooper-Jones for knowledge mobilization activities for broad public understanding of this review, and Pierre Martinelli for project management support. Finally, the authors would like to thank the 2 family members of patients with lived experience of aphakia and IOL implantation who shared their experiences with the project team members and provided their feedback on the draft protocol and draft report. Their perspectives and feedback were carefully considered by CADTH in developing this report.
Reviewers
The following individuals kindly provided comments on a draft version of the review protocol and this report.
External Reviewers
Dr. Carlos Eduardo Solarte, MD, MPH (Epi)
Assistant Professor of Ophthalmology
University of Alberta
Edmonton, Alberta
Dr. Rosanne Superstein, MD, FRCSC
Associate Professor of Ophthalmology
Université de Montréal
McGill University
Montreal, Quebec
Conflicts of Interest
There are no conflicts of interest to declare relevant to this report.
Abbreviations
BIL
bag-in-the-lens
CI
confidence interval
CL
contact lens
GRIPP2
Revised Guidance for Reporting Involvement of Patients and the Public
HRQoL
health-related quality of life
HTA
health technology assessment
IATS
Infant Aphakia Treatment Study
IOL
intraocular lens
logMAR
logarithm of the minimum angle of resolution
NRS
nonrandomized study
OTI
ocular treatment index
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PSI
parenting stress index
PVD
posterior vitreous detachment
RCT
randomized controlled trial
RoB 2
(Cochrane) Risk of Bias in Randomized Controlled Trials 2
RoBANS
Risk of Bias Assessment Tool for Non-randomized Studies
SR
systematic review
TAPS
Toddler Aphakia and Pseudophakia Study
VA
visual acuity
VAO
visual axis opacification
VO
vitreous opacity
Protocol Amendments
Section | Amendment | Page | Rationale |
|---|---|---|---|
Objectives | “Aphakia following the surgical removal of a cataract” and “aphakia” were updated to “non-congenital aphakia.” | 8 | To appropriately reflect the scope of the review, which includes all types of non-congenital aphakia, including trauma-induced aphakia, rather than limiting to cataract surgery-related aphakia. |
Research questions | A research question, as follows, was added: “What is the comparative safety of IOL implantation in infants of up to 12 months of age versus IOL implantation after 12 months of age for pediatric patients with non-congenital aphakia?” Of note, this question was added as number 4; therefore, the numbering of the research questions was updated accordingly. Where appropriate, question 4 was added throughout the protocol, and the wording around the comparison between infants and children was updated throughout the protocol (e.g., Introduction, Objectives, Methods) to reflect that clinical effectiveness, safety, and cost-effectiveness will all be in the scope of this review. | 8 | To fully assess safety outcomes of IOL implantation in all relevant age groups for this review and to complement the existing research question on comparative effectiveness in pediatric patients who received IOL implantation 12 months of age or younger vs. pediatric patients who received IOL implantation after 12 months of age and up to 12 years. |
Protocol amendments | The process for updating the project protocol on PROSPERO and the CADTH website was clarified as follows: “Updates to the PROSPERO submission (CRD42021231143) and the project protocol on the CADTH website will be made, as appropriate.” | 19 | To fully describe the process that will be used to update the project protocol, which involves not only PROSPERO as described in the original protocol, but also the CADTH website. |
IOL = intraocular lens; vs. = versus.
Key Messages
This systematic review examined intraocular lens implantation in patients aged 12 months or younger at the time of surgery compared with patients aged 12 months or younger with aphakia treated with contact lenses or glasses. It also examined intraocular lens implantation in patients aged 12 months or younger at the time of surgery (i.e., infants) compared with patients older than 12 months up to 12 years of age at the time of surgery (i.e., children).
In total, 18 studies (3 randomized controlled trials and 15 nonrandomized studies) were identified that answered the clinical questions relevant to this review. No relevant studies were identified to inform the cost-effectiveness questions.
Visual outcomes (i.e., visual acuity) did not seem to differ between patients aged 12 months or younger at the time of surgery who received intraocular lens implantation and in patients with aphakia treated with contact lenses or glasses. Parenting stress was higher in parents of infants who received intraocular lens implantation at 3 months after surgery compared with parents of infants who were treated with contact lenses; however, this difference was not maintained at 1 year after surgery.
In 1 study that examined intraocular lens implantation at different ages, age did not appear to be a significant prognostic factor in poor visual outcomes (i.e., visual acuity defined as > 0.5 logMAR).
Regarding safety, infants who underwent intraocular lens implantation experienced more frequent occurrences of complications, such as visual axis opacification, compared with infants with aphakia treated with contact lenses or glasses; therefore, more reoperations to remove the opacification were required. Many infants with aphakia who did not receive intraocular lens implantation eventually required the surgery when they got older.
There were limited statistical comparisons available for safety outcomes for intraocular lens implantation in infants at different ages. Overall, the incidence in adverse events was similar between infants and children, except for the number of additional surgeries. In the identified literature, younger patients received more additional surgeries than older patients.
The risk of bias in the included studies was high. There were many methodological concerns, including selection bias, reporting issues, statistical issues, and study designs with high risk of bias, such as retrospective cohort studies.
Family input regarding patients’ and caregivers’ experiences included reports of stress related to the use of contact lenses and stress about outcomes of the cataract removal and/or intraocular lens implantation and the effect on the child, and emphasized timely treatment to ensure optimal development of the child.
Abstract
Background: Noncongenital aphakia (i.e., a lack of a natural lens within the eye) is primarily caused by either lens removal following surgical extraction of a cataract (i.e., clouding of the natural lens) or trauma of the eye causing natural lens displacement. Cataract surgery is the leading cause of noncongenital aphakia, including aphakia in pediatric patients. This systematic review focused on noncongenital aphakia in pediatric patients, specifically in patients aged 12 months of age or younger. Treatment options for visual correction of aphakia include insertion of an intraocular lens into the eye or the use of contact lenses or glasses.
Objectives: The aims of this systematic review were to compare the clinical effectiveness and safety of intraocular lens implantation versus contact lenses or glasses in infants aged 12 months or younger and to compare the clinical effectiveness and safety of intraocular lens implantation in infants aged 12 months or younger versus intraocular lens implantation in children older than 12 months up to 12 years of age. This review also aimed to explore the cost-effectiveness data for these comparisons.
Methods: An initial comprehensive literature search of English-language articles published between January 1, 2010, and January 21, 2021, was performed by an information specialist in multiple databases, with regular search alerts conducted to update the database literature searches until the report was finalized (i.e., up to November 1, 2021). Grey literature was also searched. Two reviewers independently screened titles, abstracts, and full-text articles for relevance. Two reviewers also independently reviewed relevant articles for data extraction and performed risk of bias assessments. Study selection and risk of bias assessments were conducted with the DistillerSR software. CADTH also engaged 2 family caregivers (i.e., mothers) with lived experiences of caring for young children with aphakia to provide family perspectives.
Results: In total, 18 studies (3 randomized controlled trials and 15 nonrandomized studies) were identified that answered the clinical questions of this review. No relevant cost-effectiveness studies were identified. Regarding clinical effectiveness, there did not appear to be a benefit in visual acuity with intraocular lens implantation compared with aphakia correction with contact lenses and glasses in infants. Regarding safety, infants with intraocular lenses implanted had significantly more additional surgeries because of a greater occurrence of visual axis opacification impeding vision (i.e., clouding of the eye that can obstruct vision, thus requiring surgical removal of the opacity). However, in longer-term follow-ups, many infants who did not receive a primary intraocular lens implantation (i.e., intraocular lens implantation in the same surgery as the cataract removal) underwent additional surgery later in life to implant a lens (i.e., secondary intraocular lens implantation or intraocular lens implantation during a separate surgery from the cataract removal). The results for glaucoma were mixed. There was a trend for patients who had intraocular lens implantation at a younger age (≤ 12 months) to experience more complications as a result of the surgery than patients who had intraocular lens implantation at an older age (> 12 months and up to 12 years of age). Overall, the body of evidence was of low quality, and there were many limitations with regards to the heterogeneity of studies (i.e., studies were not similar to one another) and study designs with high risk of bias.
Conclusion: Implanting intraocular lenses in patients aged 12 months or younger does not appear to confer significant visual or safety benefits compared with implantation later in life or with aphakic correction using contact lenses or glasses.
Introduction and Rationale
Aphakia is a condition in which the eye does not have a lens — the flexible structure that enables light to focus on the retina. Congenital aphakia is rare, caused by a genetic defect, and generally associated with other eye disorders such as absence of the iris and microphthalmia (i.e., 1 or both eyes are abnormally small).1,2 However, noncongenital aphakia is primarily caused by lens removal following surgical extraction of a cataract or trauma causing lens displacement.3 Connective tissue disorders, such as Marfan syndrome, are also associated with early onset of cataracts in pediatric patients.4,5 A cataract is the clouding of the lens; cataract surgery involves the removal of the cloudy lens to manage cataract-related visual impairment.6,7 Cataract surgery is the leading cause of noncongenital aphakia, including aphakia in pediatric patients.3,8 This systematic review (SR) focuses on noncongenital aphakia in pediatric patients.
Aphakia is corrected with glasses or contact lenses (CLs), in which case the patient still has aphakia, or with an artificial, intraocular lens (IOL) implantation to replace the natural lens, in which case the patient now has pseudophakia. Glasses for aphakia require a strong prescription, which causes optical and visual field distortion, and are thick and heavy, making a well-fitting pair that stays on a young child’s face difficult to find.6,9 CLs provide better optical quality than glasses and allow for easier power adjustments required for rapidly changing eyes of pediatric patients.7 However, they can be costly, be easily lost, cause irritation and infection in the eyes, and be inconvenient and difficult to insert, remove, and keep clean.9-11 These factors may lead to poor adherence with long-term use resulting in suboptimal visual outcomes.7,9 An IOL is a tiny, artificial lens made of silicone, acrylic, or other plastic12 that is permanently fixated in the eye; therefore, it cannot produce the sensations that the patient can feel with CLs. Additionally, IOLs do not require cleaning like glasses or reusable CLs (i.e., not single-use CLs).13 The IOL may be implanted immediately after lens removal (i.e., primary implantation) or after a postponement (i.e., secondary implantation) during which aphakia is corrected using glasses or CLs.14 An IOL offers an alternative to avoid the potential for visual distortion associated with glasses and the inconvenience and risk of nonadherence associated with CLs.10 IOL implantation is meant to occur once and provide a permanent solution to aphakia; however, IOL implantation in pediatric patients poses a risk for large refractive errors because the IOL power is fixed.15 Refractive errors may arise due to the rapidly changing axial length of the growing eye (i.e., distance between the front and back of the eye), which changes power requirements over time.15 As a result, it is difficult to correctly estimate the required IOL power to achieve a minimal prescription as an adult.15
Management of childhood cataracts and associated aphakia is time-sensitive and costly because it requires care from multiple health care professionals in various specialties, community health workers, and caregivers over many years. Caregivers of patients experience considerable costs and burden associated with travel and accommodations required for clinical appointments, time off work, assistance with care for other personal obligations (e.g., childcare), and anticipated and unanticipated need for or replacement of CLs or glasses. Based on inflation-adjusted US Medicaid data that considered the mean cost of cataract surgery and all additional surgeries, examinations, and supplies, the 5-year cost of cataract surgery and optical correction in an infant with a unilateral congenital cataract was US$35,293 with IOL versus US$33,452 with CLs.16 Financial burdens are more pronounced for those with limitations to their vision coverage or those without private insurance. Additionally, complexities with treating unilateral cataracts, including amblyopia and the need to patch the eye, add complications to the management of the condition.
Glasses and CLs for aphakia have generally been used in all age populations; however, the appropriate age for IOL implantation is unclear. For instance, Vasavada and Vasavada (2017) reported a general acceptance of IOL implantation in patients aged 2 years or older.17 Alternatively, a meta-analysis (MA) by Chen et al. (2020) found that in patients younger than 2 years, those who had primary IOL implantation following cataract extraction achieved better visual outcomes than those wearing CLs and without a higher risk of complications.10 In 2019, the American Academy of Ophthalmology did not recommend IOL implantation in patients aged 6 months or younger due to a higher risk of visual axis opacities compared with patients who wear CLs.15 It is generally thought that IOL implantation in young children is associated with a high rate of postoperative complications, such as visual axis opacities, glaucoma, and inflammatory events.15,18,19 Visual axis opacification (VAO) refers to the growth of epithelial cells across the implanted lens in patients with pseudophakia or in the gap where the lens would have been in patients left with aphakia.20 VAO can lead to amblyopia and requires surgical removal when it impedes vision.21 Glaucoma in pediatric patients is typically diagnosed through a sustained increase in intraocular pressure (e.g., > 21 mm Hg) confirmed with 2 to 3 measurements plus 1 or more of the following: optic disc cupping greater than or equal to 0.3, asymmetry greater than or equal to 0.2, or progression; corneal changes; and progressive myopic shift.22 If left untreated, glaucoma can lead to irreversible vision loss.23 Therefore, determining the optimal timing for IOL implantation is favourable to maximize visual acuity (VA) outcomes, minimize complications, and balance health care resource use.
Overall, there is a need to determine if IOL implantation can be safely and effectively used to correct aphakia in infants up to 12 months of age and its cost-effectiveness, relative to conventional treatment (e.g., CLs or glasses). There is also a need to compare the clinical effectiveness, safety, and cost-effectiveness of IOL implantation between infants and children (i.e., up to 12 years of age).
Objectives
This SR aimed to evaluate the clinical effectiveness, safety, and cost-effectiveness of IOL implantation versus conventional treatment (i.e., glasses or CLs) in infants with noncongenital aphakia. This SR also aimed to assess the clinical effectiveness, safety, and cost-effectiveness of IOL implantation in infants aged 12 months or younger at the time of surgery versus children who older than 12 months up to 12 years of age at the time of surgery.
Research Questions
This SR addressed the following research questions:
What is the comparative clinical effectiveness of intraocular lens implantation versus conventional treatment in infants with noncongenital aphakia?
What is the safety of intraocular lens implantation in infants with noncongenital aphakia?
What is the comparative clinical effectiveness of intraocular lens implantation in infants of up to 12 months of age versus intraocular lens implantation after 12 months of age for pediatric patients with noncongenital aphakia?
What is the comparative safety of intraocular lens implantation in infants of up to 12 months of age versus intraocular lens implantation after 12 months of age for pediatric patients with noncongenital aphakia?
What is the cost-effectiveness of intraocular lens implantation compared with conventional treatment in infants with noncongenital aphakia?
What is the cost-effectiveness of intraocular lens implantation in infants of up to 12 months of age compared with IOL implantation after 12 months of age for pediatric patients with noncongenital aphakia?
Methods
To inform the conduct of this SR, a preliminary scoping review of the existing literature — including health technology assessments (HTAs) and SRs — was conducted. A protocol was written a priori, using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P)24 for guidance on clarity, transparency, and completeness, and was followed throughout the study process. The protocol was prospectively registered in the international repository, PROSPERO (registration number: CRD42021231143).25 Any deviations from the protocol are disclosed in this final report (Table 1) and updates were made to the PROSPERO submission accordingly.
Study Design
Research questions 1, 2, 3, and 4 were intended for the review of clinical evidence. The topic of this review did not have a broad scope, and the preliminary scoping review did not identify any high-quality SRs that comprehensively addressed these research questions. Thus, it did not appear that an overview of SRs or an update of existing SRs was an appropriate review method for this SR. Therefore, a de novo SR of all identified relevant primary studies was conducted. This approach permitted an evaluation of the various population, intervention, comparator, and outcome elements in a manner suitable to address the research questions.
For research questions 5 and 6, if relevant cost-effectiveness studies of IOL implantation for aphakia were identified through a systematic literature search, these would have been summarized and critically appraised.
Literature Search Methods
The literature search was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.26 The complete search strategy is presented in Appendix 1.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946‒) via Ovid, Embase (1974‒) via Ovid, and the Cochrane Central Register of Controlled Trials (CENTRAL) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were intraocular lenses and juvenile/congenital cataracts or aphakia. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the WHO International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was limited to English-language articles published between January 1, 2010, and January 21, 2021. When possible, retrieval was limited to the human population. Conference abstracts were excluded from the search results.
The initial search was completed on January 21, 2021. Regular alerts updated the database literature searches until the report was finalized (i.e., up to November 1, 2021). The clinical trials registries search was updated on November 2, 2021, before the completion of the stakeholder feedback period (i.e., between October 25 and November 8, 2021).
Grey literature (i.e., literature that is not commercially published) was identified by searching sources listed in relevant sections of the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist,27 which includes the websites of regulatory agencies, HTA agencies, clinical guideline repositories, SR repositories, patient-related groups, and professional associations. Google was used to search for additional internet-based materials. These searches were supplemented by reviewing bibliographies of key papers and through contacts with experts and industry, as appropriate. The grey literature search was updated on November 2, 2021, before the completion of the stakeholder feedback period (i.e., between October 25 and November 8, 2021). See Appendix 1 for more information on the grey literature search strategy.
Selection and Eligibility Criteria
Table 2 provides the study eligibility criteria for the research questions. The eligibility criteria were informed by the preliminary scoping review of the existing literature and by clinical expert input.
Criteria | Description | |
|---|---|---|
Population | Questions 1, 2, and 5
Questions 3, 4, and 6
| |
Intervention(s) | Questions 1 to 6
| |
Comparator(s) | Questions 1 and 5
Question 2
Questions 3, 4, and 6
| |
Outcomes | Questions 1 and 3: Clinical effectiveness outcomes limited to
Questions 2 and 4: Safety outcomes including but not limited to
Questions 5 and 6: Cost-effectiveness outcomes limited to
| |
Study design(s) | Included Questions 1, 3, and 4
Question 2a
Questions 5 and 6
Excluded
| |
Time frame | Studies from 2010 to presentc | |
IOL = intraocular lens; QALY = quality-adjusted life-year; vs. = versus.
aIn addition to comparative evidence vs. aphakic glasses, aphakic contact lenses, or conventional treatment as comparators, uncontrolled data for IOL was considered for inclusion to answer research question 2 if the data included a “before-and-after” comparison.
bCohort studies were defined as studies in which participants are sampled on the basis of exposure and in which outcomes are assessed in a follow-up.28 This is distinct from case series studies, in which participants are sampled on the basis of the presence of an outcome, or of both an exposure and outcome, in which absolute or relative risk cannot be calculated.28
cIOL implantation for the management of pediatric cataracts became routine practice in many countries more than 10 years ago29 and, according to clinical expert input, improvements in surgical instruments over the last decade allow for smaller surgical incisions for foldable IOLs that reduce adverse events related to cataract surgeries. Thus, studies from 2010 are likely to capture foldable IOLs and reflect current technology and instrumentation trends for cataract surgery and aphakia correction in pediatric patients.
Studies were included if they met the eligibility criteria outlined in Table 2 and were published in English. Publications in other languages were not included given the evidence suggesting that excluding non-English-language publications from evidence synthesis generally does not change conclusions.30,31 If multiple publications were identified for the same study, they were all included and cited. However, only unique data were extracted without duplication and discussed as a single study.
The population of interest was pediatric patients with noncongenital aphakia. Studies with mixed populations that included patients who did not meet the age eligibility criteria of a specific research question were considered for inclusion if they reported separate results for the eligible patients or if the eligible patients constituted 95% or more of the entire study population. The 95% threshold was chosen because it is consistent with the convention of setting the alpha at 0.05 (e.g., similar to the P = 0.05 threshold and 95% confidence interval [CI]). The decision to include or exclude a study that reported age as mean ± standard deviation would have been made by estimating the 95% predictive interval using the t-statistic or z-statistic. Studies with mixed populations that did not report on the age of the included participants in a manner that allows for the assessment of the 95% or greater rule (e.g., a range without breakdowns or a mean without a standard deviation that can be used with the t-statistic or z-statistic to determine the 95% predictive interval) would have been excluded. However, no such situation regarding the use of the 95% rule was encountered. Based on clinical expert input, it was recognized that congenital aphakia requires different treatment but that it is rare. Therefore, studies or findings were excluded if they were specifically on congenital aphakia or if they were a mix of congenital and noncongenital aphakia. Studies or findings that did not specify the type of aphakia included were eligible for inclusion.
The intervention of interest was implanted foldable IOLs. Therefore, studies or findings that focused exclusively on nonfoldable IOLs or included both foldable and nonfoldable IOLs were considered out of scope. IOL implantation for the management of pediatric cataracts became routine practice in many countries more than 10 years ago,29 and according to clinical expert input, improvements in surgical instruments over the last decade allow for smaller surgical incisions for foldable IOLs that reduce adverse events related to cataract surgeries. Therefore, on the assumption that foldable IOLs were widely implemented in many countries by 2010, studies or findings that did not report whether foldable or nonfoldable IOLs were implanted were considered for inclusion since our search was limited to 2010 onward.
Articles were excluded if they did not meet the selection criteria outlined in Table 2, if they were duplicate publications, or if they were published before 2010. If a study investigated experimental IOLs not available for usual clinical practice, it would not have been eligible for inclusion. However, no such situation occurred. Single-arm studies, eligible for 1 of the safety questions, were excluded if there was no measurement of the outcome before the cataract removal surgery (i.e., no baseline measurement) or if the specific outcome was not appropriate for a before-and-after analysis (e.g., intraocular complications).
Study Selection
Two reviewers independently selected potentially relevant citations by screening all titles and abstracts identified through the literature searches, using the eligibility criteria presented in Table 2. The study selection was conducted using the SR management software DistillerSR (Evidence Partners, Ottawa, Canada). If at least 1 reviewer considered any titles or abstracts potentially relevant during the first-level (level 1) screening, the full-text articles of the citations were retrieved for a second-level (level 2) screening to confirm their eligibility. The same 2 reviewers independently conducted the level 2 screening, examining all full-text articles for inclusion in the review. Consensus between the 2 reviewers was required for the inclusion of each article. Disagreements between the reviewers were resolved through discussion or by involving a third reviewer, if needed.
A list of studies selected for inclusion in the review was posted to the CADTH website for 10 business days to allow stakeholder review and feedback. All additional potentially relevant studies identified through stakeholder feedback were reviewed following the previously described process. In addition, publications meeting the selection criteria for the review that were identified via literature search alerts before the completion of the stakeholder feedback period for the draft report were incorporated into the analysis. Relevant studies identified after the stakeholder feedback period would have been described in the discussion, focusing on comparing their results with those obtained from the synthesis of earlier reports included in the review; however, no additional relevant studies were identified after stakeholder feedback.
The study selection process is presented in a PRISMA32 flow diagram (Appendix 2). Lists of the included and excluded studies are provided in this final report with the reasons for exclusion (Appendix 10 and Appendix 11).
Data Extraction
One reviewer performed data extraction directly into tables created in Microsoft Word, and a second reviewer independently checked the extracted data for accuracy and completeness to ensure that all relevant data from each included study were extracted. Disagreements were resolved through discussion until consensus was reached or through adjudication by a third reviewer, if necessary. The following data were extracted:
study characteristics (e.g., first author’s name, publication year, the country where the study was conducted, funding sources)
study methodology (e.g., study design and objectives, inclusion and exclusion criteria, recruitment method, setting)
population details (e.g., number of participants, age, sex, gender, unilateral or bilateral cataracts, baseline characteristics)
intervention details (e.g., information about the IOL implanted, such as the type of IOL [e.g., foldable or nonfoldable], material, the year of surgery)
comparator details (e.g., aphakic glasses, aphakic contact lenses)
outcome details (e.g., measurement method, unit of measurement, length of follow-up), results, and conclusions for the overall findings and for subgroups of interest.
For economic evaluation studies, examples of additional data that were planned for extraction included the type of analysis, time horizon, perspective, modelling approach, and main assumptions, as well as the sources of clinical, cost, and utility data used in analysis. However, no relevant economic evaluations were identified, therefore this was not performed.
Data on relevant outcomes were extracted for any duration of follow-up reported in the included studies. All unadjusted and adjusted measures of treatment effects — such as risk ratios, odds ratios, or risk differences for dichotomous outcomes and mean differences or standardized mean differences for continuous outcomes — and any results of statistical manipulations performed or statistical tests reported on those measures were reported.
Critical Appraisal of Individual Studies
Two reviewers independently conducted risk of bias assessments of the eligible studies and compared them, resolving any disagreements and reaching consensus through discussion or by involving a third reviewer, if needed. The risk of bias in randomized controlled trials (RCTs) was evaluated using the methods described in the revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2).33 The RoB 2 assessment tool is structured into 5 domains to evaluate biases arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Signalling questions in each domain helps the user make domain-level judgments about the risk of bias by answering “yes,” “probably yes,” “probably no,” “no,” and “no information.” A judgment of low risk of bias, high risk of bias, or some concerns was assigned for each domain. The overall risk of bias of each trial was rated and designated as low risk of bias, some concerns, or high risk of bias based on the domain-level determinations.33 A rationale is provided for decisions about the risk of bias for both the domain-level and overall assessments.
The risk of bias in nonrandomized studies was assessed using the Risk of Bias Assessment Tool for Non-Randomized Studies (RoBANS).34,35 RoBANS contains 8 domains that evaluate the risk of biases in a study due to the possibility of target group comparisons, target group selection, confounder, exposure measurement, blinding of assessors, outcomes assessment, incomplete outcomes data, and selective outcomes reporting.34,35 The tool was selected for its reliability, validity, and user-friendly design. A judgment of low risk of bias, high risk of bias, or unclear risk of bias was assigned for each domain using the criteria provided in the instrument.34 The overall risk of bias for each study was classified as low, some, or high based on the domain-level judgments about the risk of bias, following the RoB 2 guidance33 because RoBANS does not provide a specific approach for making study-level judgments. A rationale is provided for decisions about the risk of bias for both the domain-level and overall assessments.
For sources of bias that may differ across outcomes within a single primary study (i.e., bias due to deviations from missing outcomes data and measurement of the outcomes in RCTs; outcomes assessment and incomplete outcomes data in nonrandomized studies), the risk of bias was assessed for individual outcomes within individual studies.
In evaluating the risk of bias in the included studies, the critical appraisal tools were considered as guides and additional insight beyond the instruments’ signalling items was applied when necessary. The results of the risk of bias assessments were reported by describing each study’s strengths and limitations narratively; summary scores have not been calculated. Studies were not excluded from the review based on the results of the critical appraisal. However, the critical appraisal results and their effect on study findings were used to assess confidence in the evidence from the individual studies.
Data Analysis and Synthesis
Narrative Synthesis
Narrative syntheses were performed, summarizing relevant data in tables for each study (Appendix 3, Appendix 4, and Appendix 7) with descriptions in the main text for details and clarity. The study and patient characteristics were considered in the analysis of the clinical effectiveness and safety measures across the studies to determine the likelihood of clinical benefits or harm. The within- and between-study relationships were evaluated, and the findings about the direction and magnitude of any observed effects, trends, and deviations are summarized and discussed by research question, comparator, and outcome. If data were available, results regarding the clinical effectiveness and safety were reported separately for the comparison of IOL with aphakic glasses from CLs. Any impact of applying the 95% or greater inclusion rule for age or including studies or findings that did not specify noncongenital aphakia or foldable IOLs were examined (i.e., by summarizing the findings separately). Outcomes were reported in the measurement units used by the study authors and results were interpreted with due consideration for the differences in the instruments of assessment across the studies.
A narrative summary of the results of the critical appraisal for each included study is provided. Specifically, tables were developed to present the answers to the questions within the critical appraisal tools (Appendix 6), and a narrative description of the strengths and limitations of the included studies is provided within the main text of the report to give the reader an overview of the methodological quality of the literature. Although studies were not excluded from this review based on the critical appraisal results, the discussions and conclusions of this report emphasize the findings from higher-quality studies.
Quantitative Synthesis
The results of the included studies were examined for appropriateness for meta-analyses (i.e., if data were sufficiently homogeneous in their clinical, methodological, and statistical characteristics). Clinical, methodological, and statistical heterogeneity was assessed in consultation with clinical and methods experts, as was whether studies were sufficiently homogeneous for pooling.
MAs were considered for each outcome of interest for each research question on clinical effectiveness and safety. As the included studies were deemed too heterogeneous to combine, a quantitative pooling of results from individual studies was deemed inappropriate. Accordingly, the included studies were summarized narratively, and the reasons for not pooling are reported in Appendix 8.
Subgroup Analyses
In addition to analyzing the individual outcomes by research question for the overall population, the following subgroups were in scope:
age (e.g., studies or findings on mixed populations versus no mixed populations based on the age eligibility criteria for each research question; 0 months up to and including 6 months versus after 6 months up to and including12 months for research questions 1, 2, and 5; 0 months up to and including 6 months, after 6 months up to and including 12 months, or after 12 months up to and including 24 months versus after 24 months up to 12 years of age for research questions 3, 4, and 6)
eye involvement (e.g., bilateral versus unilateral)
time of surgery (e.g., before 2010 versus 2010 and beyond to evaluate any difference in outcomes that might be attributable to advances in surgical instruments and technology, and broader uptake in foldable IOL use compared with single-unit rigid IOLs in Canada).
Any relevant data on these subgroups of interest were extracted and described in the narrative syntheses.
Reporting of Findings
This SR was prepared in consideration of relevant reporting guidelines (i.e., PRISMA-S,36 PRISMA statement,37 PRISMA harms,38 Meta-analysis of Observational Studies in Epidemiology [MOOSE] reporting checklist,39 and Synthesis Without Meta-analysis [SWiM] guideline40) and meets the criteria outlined in A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2) checklist.41
To facilitate ease of reading and consistency in terminology, the term “IOL implantation” has been used throughout the review, in place of “pseudophakia” or “pseudophakic.” As per the inclusion criteria of this SR, eligible comparators included aphakia corrected with glasses, CLs, or both; therefore, the term “aphakia” in this report refers to aphakia with vision correction using glasses or CLs. The use of glasses or CLs was specified if possible.
Patient and Family Engagement
CADTH involves patients, families, and patient groups to improve the quality and relevance of our assessments, ensuring that the affected patients and caregivers have an opportunity to provide input into the report. CADTH has adopted a Framework for Patient Engagement in Health Technology Assessment.42 The framework includes standards for patient involvement in individual HTAs that support and guide our activities involving patients. For this SR, the value of relevance, and the belief that patients have the knowledge, perspectives, and unique experiences that contribute to essential evidence for HTA, guided our patient engagement activities. For this SR, CADTH engaged 2 family caregivers (i.e., mothers) with lived experiences of caring for young children with aphakia.
Invitation to Participate and Consent
Through conversations with Dr. Ali, the clinical expert on this report, a CADTH Patient Engagement Officer emailed interested families with an invitation to participate. The preliminary request included the purpose and scope of this SR, the purpose of engagement, and the nature of engagement activities. After corresponding with 2 family caregivers, the Patient Engagement Officer obtained both persons’ informed consent to share their lived experiences with IOL implantation for infants with aphakia with CADTH staff.
Engagement Activities
The Patient Engagement Officer and members of the project team met via teleconference with each of the 2 family caregivers and learned of their lived experiences with their child’s aphakia, and perspectives on treatments including attending regular medical appointments, wearing glasses, using contact lenses on an infant or toddler, IOL implantation, and related procedures. The family caregivers were contacted at several time points during the assessment, including:
before protocol finalization
during the drafting of the initial reviews
upon completion of the final report during the stakeholder feedback period.
Perspectives gained through the engagement process were used in several ways, including ensuring the relevance of outcomes of interest for the clinical assessment, making CADTH aware of patient-borne costs, and providing insights, background, and context to inform the discussion section. Parents or caregivers’ involvement enabled the research team to consider the evidence with an understanding of the wider real-life experiences. Participants were invited to provide feedback on the clarity of writing and comment on the relevance of the findings to Canadian patients and families.
Reporting
The reporting of the patient and family engagement activities followed the revised Guidance for Reporting Involvement of Patients and the Public (GRIPP2) Short Form reporting checklist43 and included the outcomes, discussion, and reflection items, as suggested by that guidance, to outline in the final report the process of engagement and where and how participants’ contributions were used in the assessment. The Patient Engagement Officer kept track of patient engagement activities and interactions in detailed notes and communications, which were stored on a password-protected network drive which will be permanently deleted in accordance with CADTH’s document retention policy. CADTH provided reflections and critical perspectives on the participating caregivers’ involvement with the research team in this final report.
Opportunities for Stakeholder Feedback and Unpublished Data
All stakeholders were given the opportunity to provide feedback on the draft included studies list and the draft report during 2 review periods. The draft included studies list and the draft report were each posted on the CADTH website for 10 business days. Unpublished data identified as part of the feedback process would have been included if the source of data was in the public domain; however, no unpublished data were identified through the feedback process.
Results
Quantity of Research Available
A total of 1,371 citations were identified in the literature search. Following screening of titles and abstracts, 1,162 citations were excluded, and 209 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 176 publications were excluded for various reasons, and 33 publications met the inclusion criteria and were included in this report. These comprised 3 RCTs44-61 and 15 nonrandomized studies,62-76 relevant to research questions 1, 2, 3, and 4. No economic evaluations relevant to research questions 5 and 6 were identified. There were 16 clinical publications and 1 methods publication (which was not included in the overall count)77 that reported on the same RCT — the Infant Aphakia Treatment Study (IATS).44-59
Appendix 2 presents the PRISMA32 flow diagram of the study selection process. Additional references of potential interest are provided in Appendix 12. Lists of the included and excluded studies, with reasons for exclusion, are provided in Appendix 10 and Appendix 11, respectively.
Study Characteristics
Country of Origin, Year of Publication, and Sources of Funding
The RCTs were conducted in the US44-59,77 and India.60,61 The nonrandomized studies were conducted in the US,63-65 Germany,66 Ireland,67,68 UK,69 Latvia,70 China,71 India,72-74 France,75 Brazil,62 and Korea.76
There were multiple publications for the IATS, which were published in 2020,46,50,53 2016,55,56 2015,52,59 2014,45,49,58 2013,54,57 2012,51 2011,47,48 and 2010.44 The years of publication for the remaining studies were 2021,62 2020,63,64,66,67,69,71 2019,65 2018,60 2017,61,72,75 2016,73 2014,74,76 and 2010.68
The studies were funded primarily by grants from organizations such as the National Eye Institute,44-59,77 the American Society of Cataract and Refractive Surgery Foundation,61 Mayo Clinic,63 Research to Prevent Blindness,64 National Institute for Health Research,69 Natural Science Foundation of China,71 Hyderabad Eye Research Foundation,73 Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES-DS),62 and Inje University.76
There were no funding sources for 5 studies.60,67,70,74,75 Funding sources were not reported in 4 studies.65,66,68,72
Study Design, Methods, and Settings
Three studies were RCTs.44-61,77 The 15 remaining studies were nonrandomized.62-76 Twelve NRSs were retrospective chart reviews62-68,70,72,73,75,76 and 3 were prospective cohort studies.69,71,74
All of the included studies included patients undergoing cataract removal surgery with or without IOL implantation.44-77
For the comparison of IOL implantation versus aphakia corrected by CLs or glasses, 2 RCTs44-59,77 and 7 NRSs63,65,67-69,71,74 were relevant. The IATS included patients who were 28 days of age to less than 210 days of age at the time of surgery.44-59,77 Another RCT, Vasavada et al. (2018),60 included infants up to 2 years of age. Among the NRSs, the Toddler Aphakia Pseudophakia Study (TAPS) reported by Bothun et al. (2020) included patients with the same age restrictions as the IATS (i.e., 28 days to less than 7 months).63 Other age ranges included younger than 1 year of age,67 younger than 2 years of age,69 6 months to 72 months,71 “pediatric patients” (age not specified),65 1 month to 8 months,74 and 0.5 month to 12 months.68 For the studies that included patients older than 12 months, only data on patients noted to be 12 months of age or younger at the time of surgery were extracted.
For the age comparison, 1 RCT61 and 8 NRSs62,64,66,70,72,73,75,76 were relevant. The RCT by Vasavada et al. (2017)61 included patients up to 4 years of age. The age restrictions included 5 months to 24 months,62 1 month to 72 months,64 0 years to 17 years,66 1 month to 18 years,70 2 years to 12 years,72 4 weeks to 24 months,75 less than 7 years,73 and 0.1 year to 9 years.76
Thirteen studies were single-centre studies,60-62,65-68,70-74,76 and 4 studies were multicentre studies.44-59,63,64,69,77 The setting for 1 study was not described in detail.75 The IATS was conducted at 12 clinical sites in the US,44-59,77 and the TAPS was conducted at 10 of the 12 US IATS sites.63 The IOL Under 2 study was conducted at 31 hospitals in the UK and Ireland.69 The multicentre study by Eder et al. was conducted at 2 pediatric ophthalmology practices in the US.64 All studies with known settings were conducted at research centres or hospitals44-74,76,77 (including 1 tertiary ophthalmic institute72).
There was overlap in the settings between some of the included studies. Vasavada et al. (2018),60 Vasavada et al. (2017),61 and Shah et al. (2014)74 were conducted at the same research centre in India. Additionally, Kirwan et al. (2010)68 and Murphy et al. (2020)67 were conducted at the same university hospital in Ireland. The publications from the TAPS63 and the IATS44-59,77 also shared 10 study sites in the US. However, the 2 publications by Vasavada et al.60,61 and Shah et al. (2014)74 did not include patients from the same years. The TAPS63 and IATS publications44-59,77 specifically focused on bilateral eye involvement and unilateral eye involvement, respectively; hence, there was no overlap in patient data. Although not explicitly stated, there was likely overlap between Murphy et al. (2020) and Kirwan et al. (2010) in their included patients because the years of surgery overlapped; further, it was not clear if different surgeons performed the procedures.67,68
Patient Population
Aphakia and Comorbidities
All studies included patients with aphakia due to cataract removal or lens aspiration. No aphakia was caused by a perforating wound or ulcer, lens dislocation or subluxation, or spontaneous lens absorption. One study only included patients with a cataract due to congenital rubella,74 whereas 1 study specifically excluded rubella-related cataract.71 One study only included patients with retinopathy of prematurity (ROP).72 Patients with cataracts due to trauma or general ocular traumas were excluded in 8 studies.44-61,63,67,70,71,73,77 Infants with persistent fetal vasculature were excluded in 5 studies44-60,69,71,75,77 Other ocular and chromosomal defects were excluded in 11 studies, such as microcornea,44-62,69,77 microphthalmos,62,67-69 Down syndrome,60 previous ocular surgery,44-59,63,77 and preoperative or congenital ocular hypertension or glaucoma.44-59,61-64,67,71,72,75,77 Four studies excluded “abnormalities,”69,76 “other ocular or systematic anomalies,”70 “systemic diseases,”62 and “other retinal pathologies or ocular comorbidity”72 without providing specifications or definitions of these terms.
Age at Surgery
As per the inclusion criteria, infants aged 12 months or younger at the time of surgery were eligible for inclusion for research questions 1 and 2, and infants aged 12 months or younger and children older than 12 months up to 12 years of age were eligible for research questions 3 and 4.
Two RCTs and 7 NRSs were relevant for the research questions on the treatment comparison in infants.44-60,63,65,67-69,71,74,77
One RCT and 8 NRSs were relevant for the research questions on the age comparison between infants and children.61,62,64,66,70,72,73,75,76
Seven studies44-60,63,66,69,71,75,77 reported the median age of patients in the study, and 7 studies reported the mean age of patients in the study.61,62,64,67,68,72,74
The median ages at surgery (where reported) were:
2.4 months (bilateral) and 2.2 months (unilateral)69
2.5 months63
5.7 months75
6.01 months60
21.04 months66
36 months.71
The mean ages at surgery (where reported) were:
3.46 months67
3.8 months68
3.97 months74
14.80 months and 18.26 months61
15.06 months62
18.9 months72
34.68 months.64
Neither the median nor the mean age at surgery were reported in 4 studies.65,70,73,76
Sample Sizes
Sample sizes in the studies ranged from 28 eyes72 to 1,392 eyes.65
The IATS RCT had a sample size of 114 eyes from 114 patients and did not have a high loss to follow-up over the 10 years follow-up (i.e., 3.5% attrition).44-59,77 The RCTs by Vasavada et al. (2018)60 and Vasavada et al. (2017)61 had sample sizes of 120 bilateral eyes and 61 unilateral eyes, respectively.
Sample sizes for the remaining NRSs were 28 eyes,72 37 eyes,74 46 eyes,64 61 eyes,75 90 eyes,66 93 eyes,62 131 eyes,71 135 eyes,67 137 eyes,70 144 eyes,68 172 eyes,76 178 eyes,63 378 eyes,69 814 eyes,73 and 1,392 eyes.65
Sex and Gender
The numbers of female patients and male patients were generally equal (i.e., approximately between 45% to 55% female) in most studies.44-59,62,63,69,74,76,77 Approximately one-third of patients were female in the study by Vasavada et al. (2018),60 and approximately 40% of patients were female in the studies by Vasavada et al. (2017),61 Lytvynchuk et al. (2020),66 Ezisi et al. (2017),72 and Zhang et al. (2020).71 Sex of patients was not reported in 7 studies.64,65,67,68,70,73,75
Eye Involvement
The majority of the included studies included patients with either unilateral or bilateral cataracts.61,62,64,66-70,72,74-76 One study included solely unilateral cataracts,44-59,77 and 2 studies included solely bilateral cataracts.60,63 The proportions of patients with unilateral and bilateral cataracts were not reported in 3 studies.65,71,73
Year of Surgery
The year of surgery ranged from 1984 to 2018. There were 5 studies that included patients who received surgical intervention before 2000.64,65,67,68,76 These studies did not specify the type or brand and model of IOLs implanted; therefore, despite the potential that nonfoldable IOLs were implanted in some of these patients, as per this review’s protocol, these studies were included.
Interventions and Comparators
IOLs Implanted
All included studies had an intervention of IOL implantation following cataract surgery. One study analyzed outcomes after the use of a bag-in-the-lens (BIL) technique,66 whereas the remaining studies implanted IOLs in the ciliary sulcus or capsular bag, if reported. Standard capsular bag implantation was sometimes referred to as “lens-in-the-bag” implantation. Four studies did not adequately report the location of IOL implantation.64,67,68,70 The procedures (if reported) are detailed in Appendix 4, Table 5.
Brands and models of foldable IOLs implanted included:
AcrySof SA60AT60
Hoya PC-60AD62
Aaris EC-3 PAL62
Morcher Type 89A, Type 89F or Type 89A Toric (BIL technique)66
The specific brands and models of IOLs implanted were not reported in 4 studies but were noted as “foldable lenses.”63,70,72,75 Eight studies did not specify what type of IOLs was used nor whether the IOL was foldable.64,65,67-69,71,73,76
Comparison of IOL Implantation Versus Aphakia Corrected by Glasses or Contact Lenses
The comparator was aphakia with vision correction in 10 studies.44-60,63,65,67-69,71,73,74,77 The comparator was CLs (Silsoft or rigid gas permeable) for the IATS.44-59,77 Vasavada et al. (2018) and Bothun et al. (2020) reported correction with CLs, glasses, or both CLs and glasses as the comparator.60,63 The Shah et al. (2014) study used either CLs or glasses as vision correction in patients with aphakia.74 The method of vision correction in patients with aphakia was not reported in 4 studies.65,67,68,71,73
In some publications, there were comparative data between IOL implantation and aphakia, but the reported data included a combination of patients who were younger than 1 year of age and older than 1 year of age at the time of surgery. This combination resulted in a mixed population, and therefore those data were not extracted as per the protocol.69,73
Age Group Comparison
Two studies had an objective to compare IOL implantation by age at surgery.64,66 However, there were 8 publications that did not have a primary objective to compare age groups, but included age at surgery as a subgroup, which allowed for relevant data to be extracted.61,62,69,70,72,73,75,76
Outcome Measures
Appendix 5 details the relevant outcomes extracted from each study.
Measures of Clinical Effectiveness (Research Questions 1 and 3)
Outcomes relevant to these research questions included VA67,75 and health-related quality of life (HRQoL).57
In IATS, VA was measured by 3 different methods at each follow-up. At 1 year of age, VA was measured using Teller acuity cards (molecular grating VA)44; at 5 years of age, VA was measured using Amblyopia Treatment Study HOTV (monocular optotype VA)45; and at 10 years of age, VA was measured using E-ETDRS testing protocol (monocular optotype VA).46 In the study by Vera et al. (2017),75 VA was measured using LEA pictures or matching and Snellen charts. In the study by Murphy et al. (2020), the method of measurement was not reported.67
HRQoL was measured by examining caregiver stress levels with the ocular treatment index (OTI) and the parenting stress index (PSI).57
Measures of Safety (Research Questions 2 and 4)
Outcomes relevant to the safety research questions for this SR included VAO,44-59,61-63,66-68,72-75,77 glaucoma,44-61,63,64,66-70,73-75,77 strabismus or nystagmus,44-59,62,67,76,77 additional surgeries,44-59,62-65,68,73-75,77 intraoperative complications,44-59,63,66,77 corneal changes,44-59,77 inflammatory complications,60,61,66,74,75 posterior vitreous detachment (PVD),71 and vitreous opacities (VOs).71
The method of measurement for VAO and inflammatory complications was not reported in most cases. It is likely that these outcomes were measured during a routine examination using a slit lamp, as was reported in 1 study,61 but this was not clear. PVD and VO were measured using B-scan ultrasonography.71 Strabismus and other fixation-related issues such as nystagmus were measured using the Hirschberg Test, Krimsky Test, or Alternate Prism and Cover Test in the IATS, and eye movement recordings were analyzed by an eye movement expert.54-56,58 The method of measuring strabismus was not reported in 2 studies.62,67,76
The methods of measurement and definitions of glaucoma varied across the included studies (Table 7). Methods of measuring intraocular pressure in the IATS included Goldmann applanation tonometry, Tonopen, pneumotonometry, Perkins tonometer, and rebound tonometry, depending on the patient’s age and ability to tolerate and remain still for testing (i.e., need for anesthesia).48-53 Other studies used Perkins tonometry61,62,68,73 or Goldmann applanation tonometry.68 Eight studies did not specify the method used to measure intraocular pressure.63,64,66,69,70,72,74,75
Considerations for Meta-Analysis
No MA was performed for the identified body of evidence because the identified studies were deemed too heterogeneous to facilitate appropriate pooling of data. Appendix 8 details the considerations for MA by study design, outcome, and citation.
Critical Appraisal
A summary of the risk of bias assessments for the RCTs and NRSs can be found in Table 8 and in Table 9, respectively.
Randomized Controlled Trials
The RCTs were appraised using the Cochrane RoB 2 tool.33 This tool requires that if any domain is rated at a high risk of bias, the overall risk of bias is also rated as high. Therefore, all 3 RCTs were rated as having an overall high risk of bias. However, the IATS was rated at a lower risk in most domains compared with the other RCTs.44-59,77
Randomization Process
The IATS described a randomization process in detail with minor details missing.77 There was allocation concealment and no concerns with the randomization process (i.e., baseline characteristics were similar between the 2 groups). The Vasavada et al. (2018)60 study provided few details regarding the randomization process but reported that there was allocation concealment. Conversely, the Vasavada et al. (2017)61 study lacked reporting of the details regarding allocation concealment but reported that randomization was facilitated with computer generated random numbers.
Deviations From the Intended Interventions and Blinding
There were no major concerns regarding deviations from the intended interventions for any of the RCTs, and there were no concerns regarding deviations from the protocols by the surgeons. All patients in the study by Vasavada et al. (2017)61 received IOL implantation; therefore, it was impossible for patients to not adhere to the intervention. Patients in the study by Vasavada et al. (2018) also received IOL implantation and would have also automatically adhered to the IOL intervention; however, adherence to the CLs and glasses intervention was not reported.
Adherence to the prescribed postoperative patching regimen was explored in the IATS, and it was reported that there was no difference in adherence to patching between treatment groups.78 Any differences in adherence to the treatment for CLs (e.g., not wearing CLs as prescribed) would likely reflect real-world adherence to the treatment. Patients in the IATS were not allowed to receive a secondary IOL implantation outside of extreme nonadherence, and the surgery had to be approved by a steering committee.77 Notably, by the 1-year follow-up, no patients had received a secondary IOL44; by the 5-year follow-up, 3 eyes (CL adherence failures) had received secondary IOLs.45 These deviations were minimal and consistent with the IATS prespecified protocol.77
Blinding of surgeons and participants was not possible for these surgical studies due to the nature of the procedures and the postoperative regimen. Despite this, the likelihood of bias arising from the lack of blinding was deemed to be minimal. It is unlikely that patients sought out or were successful in switching intervention groups because this would require removal of the IOL surgically or permission to implant a secondary IOL. Additionally, in the outcome evaluations, the impact of lack of blinding on bias was likely minimal for the participants undergoing the assessments, especially in the early follow-up stages, because they were infants or young children.
The IATS made a concerted effort to blind outcome assessors for VA by not informing the assessors of the clinical status of the patient and using external travelling examiners who were not involved in treatment. The 1-year follow-up required the use of Teller cards, in which an examiner looks directly at a patient’s eyes to determine eye fixation and movement; therefore, it is unclear how successful this blinding was because CLs leave a visible line on the eye. However, because the assessors were specifically trained and supervised to ensure standardization of examinations, the impact of lack of blinding on bias was likely minimal. Vasavada et al. (2017)61 also blinded assessors when examining patients for VAO; however, all patients in this study received IOL implantation and, for the purposes of this review, the attempt at blinding is not applicable.
Outcome Measurements and Missing Data
The IATS had very detailed definitions for every included outcome.44-59,77 The studies by Vasavada et al. (2017)61 and Vasavada et al. (2018)60 also had clearly defined outcomes and reported what tools were used in assessment. However, the Vasavada et al. (2018) study had a significant loss to follow-up (> 10% of patients) and did not provide reasons for this attrition rate; therefore, it is unclear if the high attrition introduced any bias into the study results.60
Statistical Analysis and Reporting
The studies by Vasavada et al. (2017)61 and Vasavada et al. (2018)60 did not have a priori statistical analysis plans; therefore, it was unclear if there were major deviations from intended analyses. Both publications took measurements from 1 eye from patients with bilateral cataracts, which was appropriate for conducting independent statistical tests. Namely, analyzing 2 eyes from the same individual would violate the assumption of independence for the tests. The IATS had a statistical analysis plan provided in the protocol with details (e.g., intention to treat) but did not appear to follow the plan for all reported results. For example, in determining the percentages of patients with a particular outcome, both the intention-to-treat number and the total number of patients with successful follow-up (i.e., per protocol) were used as a denominator.52 Despite this, the loss to follow-up in the IATS was small, especially considering the long follow-up period; therefore, this may not have affected the conclusions of the studies for most outcomes.
Some time points were not reported in the study by Vasavada et al. (2018),60 and it was unclear what the reasons were. There was also inconsistent reporting of outcomes in the Vasavada et al. (2017)61 study and the IATS.44-59,77 Namely, in different IATS publications reporting data of the same follow-up period, there were numerous reporting inconsistencies.44,48,49 This limited the interpretation of the results and reliability of the findings.
Nonrandomized Studies
The NRSs were evaluated using RoBANS.34,35 All NRSs were rated at a high62-64,66-75 or unclear overall risk of bias65,76 because methods, issues with selection bias, and selective outcomes were not reported or were not clearly reported.
Selection Bias and Confounding
Most studies were based on retrospective chart reviews, which may inherently carry selection biases. For example, in the studies by Shah et al. (2014)74 and Zhang et al. (2020),71 patients were not excluded on the basis of ocular issues such as microphthalmos (e.g., small axial length), which is often contraindicated for IOLs. Since patients in those studies were not randomized to specific cohorts, and patients with microphthalmos were unlikely to have undergone IOL implantation, the aphakic group likely had a higher percentage of patients with microphthalmos. This can introduce bias because having ocular abnormalities may increase the likelihood of poorer outcomes at follow-up, making IOL implantation appear more favourable than glasses or CLs. Accordingly, it may not be appropriate to include patients who would not likely receive the intervention in standard clinical practice because it may result in differences in baseline characteristics between comparison groups, which poses a risk or concern for selection bias.
Many studies69,71,74 specifically indicated that the decision to implant an IOL or treat aphakia with glasses or CLs was at the discretion of the surgeon as well as the parents. Other studies did not report what the decision was based on.67,68,73 It is likely that some baseline characteristics were not equal between comparative groups. In studies with mixed ages at IOL implantation, it may be likely that there were more patients in the IOL group who were closer to 12 months of age or older at the time of surgery than in the aphakia group. This may be due to the concerns surrounding the use of general anesthesia in younger patients and IOL implantation in younger patients.15,17 There was a trend for patients in the IOL groups to be older at the time of surgery than those in the aphakia groups (mean or median, if reported).67-69,71,72 Notably, patients who are diagnosed with congenital cataracts at an older age (e.g., past 6 months of age) and undergo cataract surgery and IOL implantation later in life may have worse outcomes due to a potentially more severe presentation or a delayed diagnosis (e.g., because of lack of screening).79 Therefore, patients who were older at cataract diagnosis or at the time of IOL implantation might have been different (e.g., clinically) from patients with aphakia or patients receiving surgery at an earlier age, potentially biasing results against the IOL group (compared with glasses or CLs) or later IOL implantation (in age comparisons).
No studies adequately controlled for or defined confounding factors in their analysis, except for the study by Solebo et al.69 Many studies also did not account for the differences in treatment requirements, surgeries, and potential outcome variability between patients with bilateral and unilateral cataracts. Combining these groups of patients or not reporting the laterality of cataract for included patients limits the conclusions that can be made regarding the interventions examined.
Outcome Reporting and Blinding
Overall, definitions for outcomes were poorly reported. Therefore, the risk of bias for selective reporting of outcomes potentially assessed without standardized methodologies was unclear (e.g., inflammatory complications, adverse events, strabismus). This may be of particular concern for outcome assessments prone to subjectivity. For instance, inflammatory complications that were assessed with the presence and extent of synechiae using an operating microscope (e.g., with a slit lamp attachment) were prone to subjectivity of the examiner, and inter-rater reliability was unclear, especially when the number of examiners were not reported.60,74 For outcomes that are more objective, the risk of bias for selective reporting was less of a concern. For instance, 8 studies62-64,66,69,73-75 provided a clear definition of glaucoma, although not all studies reported what method was used to determine intraocular pressure (IOP). Table 7 details the various definitions of glaucoma used in the included studies.
Eleven studies reported the results in a way that reflected the intention of the study and the methods.62,63,65,68-70,72-76 In other studies, there were unexpected additions and omissions of outcome data, and it is unclear if this was due to selective reporting, especially because no NRSs had published protocols that could be consulted for confirmation. Additionally, no studies discussed any missing data, or they excluded patients that did not reach a minimum follow-up.62,63,67,68 It was unclear if any of the patients that did not reach the minimum follow-up were missing for reasons that were associated with the intervention or the outcome, or if this differed between groups.
Similar to the RCTs, it is unlikely that it was possible to blind any of the outcome assessors to the treatment by the nature of the intervention and, in the case of retrospective studies, it is unlikely that this was done. No NRSs discussed any attempts to mask the treatment. For the objective outcomes (e.g., additional surgeries and glaucoma) this was likely not an issue. Additionally, there was likely no performance bias from the participants because the participants were young children and most of the outcomes were assessed by individuals (i.e., examiners) who were not the participants.
Statistical Analysis and Reporting
The statistical approach used may not have been appropriate in all cases in which bilateral cataracts were included in the analysis. Incorrect conclusions may have resulted from studies that treated the eye as the unit of analysis and analyzed the data using both eyes from patients with bilateral cataracts (i.e., using statistical methods that assumed independence of samples). For example, the study by Lytvynchuk et al. (2020)66 included both unilateral and bilateral cataracts in the analysis of age groups but used Fisher exact test to compare the groups, which assumed independence of samples. Koch et al. (2021) also included unilateral and bilateral cases in statistical tests that assumed independence of samples (i.e., analysis of variance [ANOVA]).62
Data Analysis and Synthesis
Appendix 7 presents the main study findings regarding outcomes with relevant information from the included studies. The tables are presented by research question and then by outcome. Details on the comparators are noted where applicable; however, most studies did not adequately report the postoperative regimen after lens removal for patients with aphakia.
The IATS had multiple follow-up time points within multiple publications; therefore, the results from those publications were summarized separately from the other studies.
Eight studies did not specify the type of IOLs used in the study (i.e., whether the IOLs were foldable or nonfoldable).64,65,67-69,71,73,76 Generally, it appears that results from these studies with unclear IOL types did not differ from the results of studies with clearly reported foldable IOLs. In this section, the studies that specified the use of foldable IOLs were identified as such. Additionally, many studies did not adequately report the laterality of the cataracts that were examined or did not disaggregate the laterality data (i.e., combined bilateral and unilateral data). These studies are noted under “unclear laterality” and “mixed laterality,” respectively.
Clinical Effectiveness of Intraocular Lens Implantation Versus Conventional Treatment in Infants With Aphakia
Visual Acuity
Three studies (1 RCT; 2 NRSs) examined VA in patients with IOL implantation or aphakia.44-46,63,67 All studies statistically examined the comparisons.44-46,63,67 Table 10 and Table 11 provide the relevant data extracted from the studies.
Unilateral Cataracts
The IATS RCT on foldable IOLs reported that at the 1-year follow-up, the median logMAR grating VA was not statistically significantly different between IOL implantation and aphakia corrected with CLs.44 At 4.5 and 10 years of follow-up, monocular optotype VA (measured using HOTV and electronic Early Treatment Diabetic Retinopathy Study, respectively) in treated eyes was also not statistically significantly different between IOLs and CLs.45,46
Bilateral Cataracts
In the NRS by Bothun et al. (2020)63 on foldable IOLs, the median VA in IOL implanted eyes and aphakic eyes treated with CLs, glasses, or both was not statistically significantly different at a maximum follow-up time of 5.8 years. When examining IOLs compared with glasses, the relationship remained numerically similar.63
Mixed Laterality
In the NRS by Murphy et al. (2020),67 treatment success was defined as a best corrected VA of 0.3 logMAR or better (i.e., ≤ 0.3 logMAR). There was a statistically significant difference in the proportion of patients achieving treatment success (77.42% versus 42.47% in the IOL implanted versus aphakia groups, respectively; P < 0.001), in favour of the IOL implanted group. However, the mean best corrected visual acuities expressed in logMAR for the IOL and aphakia groups were numerically similar (0.92 versus 0.98 in the IOL implanted versus aphakia groups, respectively; P = not reported [NR]). Therefore, it is likely that the distribution of VA scores varied between the groups; for example, there may have been more patients in the IOL group whose VA scores were just below the threshold used.
Health-Related Quality of Life
One RCT examined HRQoL in caregivers to patients with IOL implantation or aphakia.57 Table 12 provides the relevant data extracted from the study.
Unilateral Cataracts
The IATS RCT examined HRQoL in the form of caregiving stress for parents or guardians of patients with unilateral foldable IOL implantation or CLs.57
At 3 months after surgery, parenting stress was statistically significantly higher in parents of patients who had received an IOL implant compared with parents of patients who had received CLs measured by OTI and statistically significantly higher for caregivers measured by PSI (in total score as well as on the adaptability and demandingness subscales within the child domain).
At 1 year after surgery, it was reported that there were “no differences” between the groups in either the PSI or OTI although no P values were provided.57
Bilateral Cataracts or Mixed Laterality
There were no relevant results for HRQoL in bilateral cataracts or for mixed laterality.
Safety of Intraocular Lens Implantation in Infants With Aphakia
Intraoperative Complications
One RCT examined intraoperative complications in patients with IOL implantation or aphakia.44,48 Table 14 provides the relevant data extracted from the study.
Unilateral Cataracts
The IATS RCT on foldable IOLs examined intraoperative complications in patients receiving lens removal and IOL implantation compared with patients receiving lens removal and using CLs afterward.44,48 Overall, there were more intraoperative complications in the IOL group (28% versus 11% in the IOL implanted versus CL groups, respectively; P = 0.031).44 The outcomes examined included intraoperative iris prolapse, hyphema (i.e., pooling of blood inside the anterior chamber), iris damage, retained cortex (retained lens material), cloudy cornea, iris sphincterotomy, lens fragment in vitreous, and posterior capsule rupture. No individual outcomes were found to be statistically significantly different between the IOL and CL groups, except for iris prolapse, which occurred more frequently in the IOL group (21% versus 4% in the IOL implanted versus CL groups, respectively; P = 0.008).44,48
Bilateral Cataracts or Mixed Laterality
There were no relevant results for intraoperative complications in bilateral cataracts or for mixed laterality.
Visual Axis Opacification
Five studies (1 RCT; 4 NRSs) examined VAO in patients with IOL implantation or aphakia.44,45,48-50,63,67,68,74 Table 15, Table 16, Table 17, and Table 18 provide the relevant data extracted from the studies.
Unilateral Cataracts
The IATS RCT on foldable IOLs examined lens reproliferation into the visual axis that interfered significantly with vision, but it was not specified if this reproliferation was severe enough to interfere with the visual axis.44,45,48-50 The IATS also examined VAO (due to “lens reproliferation into visual axis, pupillary membrane, visually significant corectopia, retained cortex, capsular phimosis or excess deposits on IOL” [p. 6]48) in patients who were younger than 49 days (n = 25) or 49 days or older (n = 32) at the time of surgery.48 In the IATS, more events of reproliferation into the visual axis occurred in the IOL group than in the CL group (24 events44 to 27 events49 versus 1 event in the IOL implanted versus CL groups, respectively; P < 0.0001) at the 1-year follow-up.44 VAO occurred in 37 patients in the IOL group (21 [84%] in < 49 days at surgery and 16 [50%] in ≥ 49 days at surgery) and in 3 patients in the CL group (3 [12%] in < 49 days at surgery and 0 in ≥ 49 days at surgery).44
At the 5-year follow-up, lens reproliferation was numerically more common in the IOL group compared with the CL group (28 events versus 2 events), but no statistical testing results were provided.49
At the 10-year follow-up, 1 patient in the IOL group and no patients in the CL group had lens reproliferation into the visual axis. No statistical testing results were provided.50
Bilateral Cataracts
The NRS by Bothun et al. (2020)63 on foldable IOLs reported that in bilateral cataract, 32% of IOL implanted patients and 8% of patients with aphakia developed VAO (P = 0.009) within a maximum follow-up of 5.8 years.
Mixed Laterality
The NRSs by Kirwan et al. (2010) and Murphy et al. (2020) both reported that VAO occurred more frequently in the IOL implanted group than in the aphakic group (P = 0.01 and P = 0.006, respectively).67,68 Of note, these 2 studies may contain some of the same patients. In the NRS by Murphy et al., the relative risk of developing VAO was 0.5896 (95% CI, 0.3949 to 0.8803) in favour of aphakia.67 Both studies had long-term follow-ups; the longest follow-up was 26 years in Kirwan et al. (2010) and 28 years in Murphy et al. (2020).67,68
In an NRS on foldable IOLs that examined patients with rubella cataracts, 9 of 37 eyes had visual axis obscuration (VAOb) at 5 years follow-up.74 Numerically, more eyes in the IOL group (7 eyes) had VAOb than in the aphakic group (2 eyes; spectacles or CLs).74
Glaucoma and Ocular Hypertension
Five studies (1 RCT; 4 NRSs) examined glaucoma in patients with IOL implantation or aphakia.44,45,48,49,51-53,67-69,74 Table 19, Table 20, and Table 21 provide the relevant data extracted from the studies. Three studies statistically examined the comparisons,44,45,48,49,51-53,67,68 and 2 studies numerically examined the comparisons.69,74
Unilateral Cataracts
The IATS RCT on foldable IOLs reported that in the first year after surgery, there was no statistically significant difference in the incidence of glaucoma or in the incidence of glaucoma and glaucoma suspect combined between patients who received an IOL and patients who were treated with CLs (9 patients versus 5 patients).51 This continued into the 5-year45,49,52 and 10-year follow-ups.53
The NRS by Solebo et al. (2020) reported that at 5 years after surgery, there was an equal or higher incidence of glaucoma in patients with aphakia compared with patients with IOL implantation for all ages at the time of surgery except for 26.1 weeks to 52 weeks of age. However, no statistical testing results were provided.69
Bilateral Cataracts
The NRS by Solebo et al. (2020) reported that at the 5-year postsurgery follow-up, numerically there was an equal or higher incidence of glaucoma in patients with aphakia in all age groups at the time of surgery except for 8.5 weeks to 12.75 weeks of age compared with patients with IOL implantation. However, no statistical testing results were provided.69
Mixed Laterality
The NRSs by Kirwan et al. (2010) and Murphy et al. (2020) both reported that glaucoma occurred more frequently in patients with aphakia than patients with IOL implantation (P = 0.02 and P = 0.018 in the Kirwan et al. [2010] and Murphy et al. [2020] studies, respectively).67,68 Murphy et al. (2020)67 conducted a subgroup analysis of patients who had had surgery before 2.5 months of age and before 6 weeks of age. No statistically significant differences in the incidence of glaucoma between patients with IOL implantation and patients with aphakia were found in patients younger than 2.5 months of age (P = 0.188) or younger than 6 weeks of age at surgery (P = 0.067).67 A similar subgroup analysis of patients younger than 2.5 months old at time of surgery in Kirwan et al. (2010) also found no statistically significant difference in incidence of glaucoma between the 2 groups.68
In an NRS by Shah et al. (2014) on foldable IOLs that examined patients with rubella cataracts, at 5-year follow-up, numerically more eyes in the aphakic group (56.0%) had secondary glaucoma than in the IOL group (16.67%).74 However, the aphakic eyes had more ocular comorbidities, such as microphthalmos, microcornea, and preoperative glaucoma; thus, it may not have been appropriate to compare with the IOL group because it would be expected that the patients with aphakia had a higher likelihood of developing glaucoma.
Strabismus and Nystagmus
Two studies (1 RCT; 1 NRS) examined strabismus and nystagmus in patients with IOL implantation or aphakia.44,45,54-56,58,67 One study statistically examined the comparison44,45,54-56,58 and 1 study numerically examined the comparison.67 Table 22, Table 23, and Table 24 provide the relevant data extracted from the studies.
Unilateral Cataracts
The IATS RCT on foldable IOLs examined strabismus in patients at 1-year follow-up and 5-year follow-up. Within the first year, there was no statistically significant difference between patients with IOL implantation and patients with aphakia treated with CLs when examining the cumulative percentage of patients who did not have strabismus at baseline but developed strabismus by follow-up.54 Orthotropia was also not statistically significantly different between the 2 groups.44 Similarly, at 5 years, orthotropia at distance and orthophoria at distance and at near was not statistically significantly different between patients with IOL implantation and patients with aphakia treated with CLs, and the number of patients who required strabismus surgery was not statistically significantly different.45,55,56
Nystagmus was evaluated at 5-year follow-up. There was no statistically significant difference in fixation instabilities (nystagmus and saccadic oscillations) between patients with IOL implantation and patients with aphakia treated with CL.58 When divided into nystagmus and saccadic oscillations alone, there was still no statistically significant differences between the 2 groups.58
Bilateral Cataracts
There were no results for strabismus or nystagmus for bilateral cataracts alone.
Mixed Laterality
The NRS by Murphy et al. (2020) numerically compared the development of strabismus and occurrence of strabismus surgery; both were slightly higher in the IOL implantation group compared with the aphakia group (for strabismus, 67.35% versus 56.82% in the IOL implantation versus aphakia groups, respectively; for strabismus surgery, 12.24% versus 11.36% in the IOL implantation versus aphakia groups, respectively).67
Additional Surgeries
Six studies (1 RCT; 5 NRSs) examined additional surgeries in patients with IOL implantation or aphakia.44-46,48-50,65,68,74 Table 25, Table 26, Table 27, and Table 28 provide the relevant data extracted from the studies.
Unilateral Cataract
The IATS RCT on foldable IOLs examined additional surgeries in unilateral cataracts. At 1-year follow-up, significantly more patients with IOL implantation required additional surgeries compared with patients with aphakia treated with CLs (63% versus 12% in the IOL implanted versus CL groups, respectively; P < 0.0001), which was due to the significantly higher numbers of pupil-related VAO surgeries in the IOL implanted versus CL groups (60% of patients versus 7% of patients required a VAO clearing surgery in the IOL implanted versus CL groups, respectively; P < 0.0001).48 This trend was maintained at 5-year follow-up (72% versus 21%, in the IOL implanted versus aphakia groups, respectively; P < 0.001), which was also due to an increased number of VAO clearing surgeries in the IOL implantation group.45 During the post-operative years 6 to 10, more patients in the CL group had additional surgeries compared with the first 5 years.46,50 At this time, secondary IOL implantation was permitted, resulting in 21 procedures to implant a secondary IOL.46,50 However, the statistical comparison for the number of surgeries was not provided between the IOL implantation and aphakia groups during this follow-up period.
Bilateral Cataracts
There were no results regarding additional surgeries in bilateral cataracts alone.
Mixed Laterality
The NRS by Kirwan et al. (2010) reported that statistically significantly fewer patients with aphakia had surgery to remove VAO compared with patients with IOL implantation (54.5% versus 28.9% in the IOL implanted versus aphakia groups, respectively; P = 0.01).68 However, in patients younger than 2.5 months at the time of surgery, the numbers of additional VAO surgeries were comparable between the 2 groups (54.5% versus 36.1% in the IOL implanted versus aphakia groups, respectively; P = 0.15).68
In 1 NRS by Shah et al. (2014) on foldable IOLs that examined patients with rubella cataracts, at 5-year follow-up, numerically more eyes in the IOL group (41.67%) had surgery to clear the visual axis than the aphakic group (4.0%).74 This difference was not tested statistically.
Unclear Laterality
One NRS by Jackson et al. (2019) reported lens cortex reproliferation operations, which were numerically more common in the aphakic group compared with the IOL group; statistical testing results (if performed) were not provided.65
Corneal Changes
One RCT examined corneal changes in patients with IOL implantation or aphakia.59 Table 29 provides the relevant data extracted from the study.
Unilateral Cataracts
The IATS RCT on foldable IOLs examined corneal changes at 5 years of follow-up. There were statistically significant differences between the IOL and CL groups in endothelial cell density (P = 0.0012) and the coefficient of variation of cell area (P = 0.0053), favouring the CL group. The corneal thickness was also thinner among eyes with IOL implantation compared with aphakia treated with CLs.59
Bilateral Cataracts and Mixed Laterality
There were no results regarding corneal changes in bilateral cataracts or mixed laterality.
Other Safety Outcomes
Five studies (2 RCTs; 3 NRSs) examined other safety outcomes.44,49,60,62,71,73,74 Table 15, Table 16, and Table 30 provide the relevant data extracted from the studies.
Unilateral Cataracts
The IATS RCT on foldable IOLs examined a variety of safety outcomes, statistically testing the comparison between IOL implantation and CLs for corectopia and pupillary membranes.44,49 Corectopia (P = 0.004) and pupillary membranes (P < 0.0001) were statistically significantly more common in the IOL group compared with the CL group.44
Bilateral Cataracts
In the RCT by Vasavada et al. (2018) on foldable IOLs, 2 aphakic eyes and 5 IOL-implanted eyes developed posterior synechiae. These patients had received surgery before the median age of 5.7 months at the time of the surgery.60
Mixed Laterality
In an NRS by Shah et al. (2014) on foldable IOLs that examined patients with rubella cataracts, at 5-year follow-up, a numerically higher percentage of patients in the IOL group (83.3%) had posterior synechiae than in the aphakic group (48.0%).74 No statistical testing result for the difference was provided.
Unclear Laterality
A NRS by Sachdeva et al. (2016) examined uveitis in patients with IOL implantation versus patients with aphakia. Uveitis was statistically significantly more common in patients with IOL implantation (9.6% versus 0.4% in the IOL implanted versus aphakia groups, respectively; P = 0.0001) after 5 years.73
In an NRS by Zhang et al. (2020), PVD and VO were examined.71 In patients who had surgery between 6 months and 12 months of age, 2 patients in the IOL group and 1 patient in the aphakia group had PVD. Twice as many patients in the IOL group (n = 10) had VO compared with those in the aphakia group (n = 5) by 12 months of follow-up. No statistical testing result was provided for any of the comparisons.71
Clinical Effectiveness of Intraocular Lens Implantation by 12 Months of Age Versus After 12 Months of Age for Pediatric Patients with Aphakia
Visual Acuity
Two NRSs examined VA in patients of different ages at the time of surgery.62,75 Table 13 provides the relevant data extracted from the studies.
Unilateral or Bilateral Cataracts
There were no results regarding VA in unilateral or bilateral cataracts alone.
Mixed Laterality
One NRS by Vera et al. (2017) on foldable IOLs examined VA in patients receiving IOL implantation at 1 year of age or younger compared with patients receiving IOL implantation at older than 1 year of age.75 The median VA for patients younger than 6 months, between the ages of 6 months to 12 months, and between the ages of 12 months to 24 months at up to 5 years of follow-up was 0.50 logMAR, 0.85 logMAR, and 0.35 logMAR, respectively. When analyzing age as a prognostic factor for “poor visual outcome” (i.e., > 0.5 logMAR), age was not a significant predictor of the outcome. Of note, there were more patients in the younger than 6 months group (n = 33 eyes) than in the 6 months to 12 months group and the 12 months to 24 months group combined (n = 16 and 12 eyes, respectively). The authors also compared the proportion of eyes with poor VA (> 0.5 logMAR) versus eyes with good VA (≤ 0.5 logMAR) by laterality of the cataract but did not statistically test these comparisons due to lack of power.75
Another NRS by Koch et al. (2021) on foldable IOLs compared patients aged 5 months to 9 months at the time of surgery with patients aged 19 months to 24 months at the time of surgery and found no statistically significant difference between the 2 groups for corrected distance VA.62
Safety of Intraocular Lens Implantation by 12 Months of Age Versus After 12 Months of Age for Pediatric Patients With Aphakia
Intraoperative Complications
One NRS examined intraoperative complications in patients of different ages at the time of surgery.66 Table 31 provides the relevant data extracted from the study.
Unilateral and Bilateral Cataracts
There were no results regarding intraoperative complications in unilateral or bilateral cataracts alone.
Mixed Laterality
In an NRS by Lytvynchuk et al. (2020) in patients operated on with the BIL technique, there was no statistically significant difference in the proportion of eyes experiencing vitreous prolapse, iris hemorrhage, iris prolapse, iris capture, anterior capsule rupture, posterior capture rupture, or BIL IOL dislocation between patients aged 0 months up to 3 months, 3 months up to 12 months, and 12 months up to 36 months at the time of surgery.66
Visual Axis Opacification
Six studies (1 RCT; 5 NRSs) examined VAO in patients of different ages at the time of surgery.61,62,66,72,73,75 Table 32 provides the relevant data extracted from the studies.
Unilateral and Bilateral Cataracts
There were no results regarding VAO in unilateral or bilateral cataracts alone.
Mixed Laterality
In the RCT by Vasavada et al. (2017) on foldable IOLs,61 patients were not randomized by age at the time of surgery. However, in a subgroup analysis, the cumulative incidence of VAOb in patients aged 1 year or younger at the time of surgery versus patients older than 1 year up to and including 4 years of age at the time of surgery was 1 versus 0. Statistical testing results (if performed) were not provided.61
In an NRS by Lytvynchuk et al. (2020) examining BIL-implanted IOLs, there was no statistically significant difference in VAO between patients operated on at the age of 0 months up to 3 months, 3 months up to 12 months, and 12 months up to 36 months of age at the 1-year follow-up.66 In another NRS by Ezisi et al. (2017) that examined capsular bag implantation, there were 3 cases of VAO: 2 in patients aged 12 months or younger at the time of surgery and 1 in patients who were older than 12 months at the time of surgery. Statistical testing results (if performed) were not provided. There were also some discrepancies in the publication between the text and the reported tables.72
In an NRS by Vera et al. (2017) on foldable IOLs, the most common reason for VAO was lens reproliferation into the visual axis. The rate of VAO severe enough to require reintervention was 54%, 56%, and 50% in patients younger than 6 months, between 6 months and 12 months, and older than 12 months of age at IOL implantation, respectively.75 A second NRS by Koch et al. (2021) on foldable IOLs found no statistically significant difference for VAO between patients who were operated on at 5 months to 9 months of age and those at 19 months to 24 months of age. Numerically, there was a lower incidence of VAO in patients 1 year to 2 years of age compared with patients younger than 1 year of age, but no statistical testing results were provided.62
Unclear Laterality
In an NRS by Sachdeva et al. (2016), in patients younger than 1 year of age at the time of surgery compared with patients greater than 1 year of age at the time of surgery, the incidence of VAO was 7.7% versus 0.85%. Statistical testing results (if performed) were not provided.73
Glaucoma and Ocular Hypertension
Nine studies (1 RCT; 8 NRSs) examined glaucoma in patients of different ages at the time of surgery.62,64,66,69,70,72,73,75 Table 33 provides the relevant data extracted from the studies.
Unilateral Cataract
In the NRS by Solebo et al. (2020),69 unilateral cataracts were stratified by age at surgery: 0 weeks to 4.25 weeks, 4.3 weeks to 8.5 weeks, 8.5 weeks to 12.75 weeks, 12.8 weeks to 26 weeks, 26.1 weeks to 52 weeks, and 52.1 weeks up to 2 years. In the patients 12 months of age or younger at surgery, there were 3 cases of glaucoma; in patients older than 12 months of age at surgery, there were no cases of glaucoma.
Bilateral Cataracts
In the NRS by Solebo et al. (2020),69 bilateral cataracts were stratified by age at surgery: 0 weeks to 4.25 weeks, 4.3 weeks to 8.5 weeks, 8.5 weeks to 12.75 weeks, 12.8 weeks to 26 weeks, 26.1 weeks to 52 weeks, and 52.1 weeks up to 2 years. In the patients 12 months of age or younger at surgery, there were 7 cases of glaucoma; in the patients older than 12 months of age at surgery, there were no cases.
Mixed Laterality
In the RCT by Vasavada et al. (2017) on foldable IOLs,61 patients were not randomized by age at surgery. However, subgroup analyses demonstrated that 2 eyes of patients aged 1 year or younger at surgery developed glaucoma. No patients older than 1 year of age at surgery developed glaucoma.
In an NRS by Lytvynchuk et al. (2020) that examined BIL-implanted IOLs, there was no statistically significant difference in the proportion of patients who developed glaucoma between patients operated on at 0 months up to 3 months, 3 months up to 12 months, and 12 months up to 36 months of age at the 1-year follow-up.66 In another NRS by Ezisi et al. (2017), in capsular bag implantation, there was 1 case of glaucoma in patients operated on at 12 months of age or younger and no cases in patients operated on after 12 months of age. Statistical testing results (if performed) were not provided.72
The NRS by Solebo et al. (2020) reported that an independent predictor of the development of glaucoma was younger age at surgery; the adjusted odds ratio for every reduction of 1 week in age at surgery was 1.1 (95% CI, 1.1 to 1.2).69 Another NRS by Koch et al. on foldable IOLs (2021) examined glaucoma in patients who were operated on between 5 months and 24 months of age, with no cases of glaucoma occurring during an average of 70.85 months of follow-up.62
In an NRS by Vera et al. (2017) on foldable IOLs, the incidence of glaucoma in IOL-implanted eyes was 21.21% in patients younger than 6 months at surgery. There were no cases of glaucoma in patients aged 6 months to 12 months or patients aged 12 months or older. Statistical testing results (if performed) were not provided.75
The total percentage of secondary glaucoma in an NRS by Valeina et al. (2020)70 after a maximum of 10 years of follow-up was 15.5% (7 cases). Six of these cases were in patients aged 1 month to 6 months at the time of surgery. One case was in a group of patients aged 25 months to 48 months at the time of surgery.70
In an NRS by Eder et al. (2020), a study with potential follow-up to 18 years following surgery, of patients aged 0 months to 5 months, 6 months to 23 months, or 24 months to 72 months at the time of surgery, 30%, 25%, and 20% developed postoperative glaucoma, respectively. Only the right eye for bilateral cases was examined.64
No patients developed glaucoma in the NRS by Koch et al.62
Unclear Laterality
In an NRS by Sachdeva et al. (2016) on foldable IOLs that examined patients younger than 1 year of age at the time of surgery compared with patients older than 1 year of age at surgery, the incidence of glaucoma was 5.7% and 0.21%, respectively. Statistical testing results (if performed) were not provided.73
Strabismus and Nystagmus
One NRS examined strabismus in patients of different ages at the time of surgery.76 Table 34 provides the relevant data extracted from the study.
Unilateral Cataracts
The NRS by Lee and Kim (2014) compared patients with unilateral cataracts who were operated on at 1 year of age or younger with patients older than 1 year of age and found that 2 patients and 29 patients were orthotropic at follow-up, respectively (at least 2 years following surgery). The percentage of patients in either group who had strabismus was 60% and 25.6%, respectively, and this was not statistically significant (P = 0.113).76
Bilateral Cataracts
The NRS by Lee and Kim (2014) compared patients with bilateral cataracts operated on at 1 year of age or younger with patients older than 1 year of age and found that 10 patients and 43 patients were orthotropic at follow-up, respectively (at least 2 years following surgery). The percentage of patients who had strabismus in each group was 37.5% and 10.4%, respectively, and was statistically significantly different between the 2 groups (P = 0.013).76
Mixed Laterality
In the NRS by Koch et al. (2021), there was a positive correlation between age at surgery and strabismus, but this was not statistically significant.62
Additional Surgeries
Three NRSs examined additional surgeries in patients of different ages at time of surgery.62,64,73 Table 35 provides the relevant data extracted from the studies.
Unilateral and Bilateral Cataracts
There were no results regarding additional surgeries in unilateral or bilateral cataracts alone.
Mixed Laterality
Eder et al. (2020) compared the average number of surgeries in the first postoperative year in patients receiving IOLs. There was a statistically significant difference in the average number of surgeries between patients who were aged 0 months to 5 months at surgery and those aged 24 months to 72 months at surgery (1.70 versus 0.61; P = 0.005).64
The study by Sachdeva et al. (2016) on foldable IOLs reported that the patients who received IOL surgery before 1 year of age had numerically more glaucoma surgeries than patients operated on after 1 year of age.73 The NRS by Koch et al. (2021), also on foldable IOLs, found no statistically significant difference in additional surgeries between patients operated on at 5 months to 9 months of age and those at 19 months to 24 months of age.62
Inflammatory Complications
Three studies (1 RCT; 2 NRSs) examined posterior synechiae,61 peripheral synechiae,66 or postoperative inflammation.75 Table 36 provides the relevant data extracted from the studies.
Unilateral Cataract and Bilateral Cataracts
There were no results regarding inflammatory complications in unilateral or bilateral cataracts alone.
Mixed Laterality
In the RCT by Vasavada et al. (2017) on foldable IOLs,61 patients were not randomized by age at surgery but were analyzed in age subgroups of patients aged 1 year or younger versus patients after 1 year of age up to including 4 years of age (i.e., ≤ 1 year versus > 1 to ≤ 4 years).
In an NRS by Lytvynchuk et al. (2020) examining BIL-implanted IOLs, there were 1, 1, and 0 cases of peripheral synechiae in patients operated on at 0 months up to 3 months, 3 months up to 12 months, and 12 months up to 36 months of age at 1-year follow-up, respectively.66
In the NRS by Vera et al. (2017) on foldable IOLs, the incidence of postoperative inflammation (definition of inflammation not provided by the authors) in IOL-implanted eyes was 48%, 44%, and 17% in patients younger than 6 months, between 6 months and 12 months, and 12 months or older at surgery, respectively. These differences were not statistically tested.75
Other Safety Outcomes
Seven studies (1 RCT; 6 NRSs) examined other safety outcomes such at IOL centration,61 postoperative cell deposits,61 retinal detachment,62,75 endophthalmitis,75 IOL-related complications,75 intrapupillary membrane,66 iris capture,66 hyphema,66 uveitis,66,73 BIL IOL glistening,66 BIL IOL luxation,66 peripheral corneal opacification,66 IOL capture,72 corectopia,62 IOL pigments and fibrin,62 and secondary cataracts.70 Table 37 and Table 38 provide the relevant data extracted from the studies.
Unilateral and Bilateral Cataracts
There were no results regarding other safety outcomes in unilateral or bilateral cataracts alone.
Mixed Laterality
The NRS by Lytvynchuk et al. (2020) reported no statistically significant differences in intrapupillary membrane, iris capture, hyphema, uveitis, BIL IOL glistening, BIL IOL luxation, and peripheral corneal opacification in patients who received BIL surgery at 0 months up to 3 months, 3 months up to 12 months, and 12 months up to 36 months of age.66
In the NRS by Vera et al. (2017) on foldable IOLs, retinal detachment only occurred in patients operated on at age 0 months to 6 months, and endophthalmitis occurred only in patients operated on at age 6 months to 12 months.75 In patients aged 0 months to 12 months at the time of surgery, there were reported cases of IOL luxation in the vitreous (n = 3), recurrent fibrosis (n = 3), and decentering of the IOL (n = 2), whereas these were no reported cases in patients older than 12 months.75 In the NRS by Vasavada et al. (2017), no cases of decentering of the IOL occurred in any of the age groups.61 No patients with foldable IOLs had retinal detachment in the study by Koch et al.62
In an NRS by Ezisi et al. (2017), IOL capture was noted in 1 eye (7.7%) in patients aged 12 months or younger at the time of surgery; it was not noted in patients older than 12 months of age at the time of surgery.72
Secondary cataract was reported in 11, 3, 3, 9, and 19 of the eyes that were operated on in patients aged 1 month to 6 months, 7 months to 12 months, 13 months to 24 months, 25 months to 48 months, and 49 months to 84 months, respectively (i.e., 48.3% of eyes younger than 12 months at surgery and 47% of eyes older than 12 months up to 84 months at surgery) in an NRS by Valeina et al. (2020) on foldable IOLs. Statistical testing results (if performed) were not provided.70
Uveitis was reported in the NRS by Sahdeva et al. (2016), with a numerically higher proportion of patients who received surgery before 1 year of age compared with patients who received surgery after 1 year of age, but no statistical testing results were provided.
Cost-Effectiveness of Intraocular Lens Implantation Compared With Conventional Treatment in Infants With Aphakia
No relevant publications were identified regarding the cost-effectiveness of IOL implantation compared with aphakia in patients aged 12 months or younger at the time of surgery; therefore, no summary can be provided.
Cost-Effectiveness of Intraocular Lens Implantation by 12 Months of Age Compared With After 12 Months of Age for Pediatric Patients With Aphakia
No relevant publications were identified regarding the cost-effectiveness of IOL implantation in patients aged 12 months or younger at surgery compared with patients older than 12 months up to 12 years of age at the time of surgery; therefore, no summary can be provided.
Subgroup Analyses
Age
Three studies provided subgroup analyses on age for 0 months to 6 months, 6 months to 12 months, 12 months to 24 months, or 24 months to 12 years.69,70,75 Eder et al. (2020) examined patients from 0 months to 5 months, 6 months to 23 months, or 24 months to 72 months of age at time of surgery. Results for patients in different age groups are detailed above (research question 2, research question 4).
Eye Involvement
Six studies focused exclusively on unilateral or bilateral cataracts or separated results by cataract laterality.44-60,63,67,69,76,77 Results for patients with separated laterality are detailed throughout the Data Analysis and Synthesis section.
Time of Surgery
Five studies included patients with IOLs implanted before 201044-59,63,68,69,74,77 and 2 studies included patients implanted with IOLs after 2010.61,71 Ten studies included patients with surgery dates that overlapped 2010.60,64-67,70,72,73,75,76
The studies by Zhang et al. (2010)71 and Vasavada et al. (2017)61 were the only ones that exclusively included patients who had IOLs implanted from 2010 onwards. There was not enough data to examine trends in surgical outcomes before and after 2010.
Discussion
Study Limitations and Generalizability of Findings
Evidence Gaps
There were several evidentiary gaps that limited the generalizability of the conclusions of this review. For example, there were no relevant cost-effectiveness studies identified; therefore, no cost-effectiveness data were included to inform research question 5 and research question 6. Although financial burden was noted by the interviewed caregivers as a significant concern, as well as lack of equity as a major issue in receiving timely care (e.g., lack of insurance for some families or inability to access eye care in developing countries leading to delays in diagnosis and treatment), the lack of cost-effectiveness evidence limits the ability to evaluate the financial burden more broadly.
There was also no comparison of IOLs with glasses and CLs within the same study or within studies with comparable population groups; therefore, the clinical effectiveness and safety of aphakia treated with glasses alone and aphakia treated with CLs could not be separated or compared. Most studies did not specify the method of vision correction for patients with aphakia; therefore, the conclusions were also not clear regarding the comparative efficacy of IOLs versus glasses, CLs, or both.
One study (i.e., IATS RCT) reported on HRQoL by examining parenting stress57; these findings were similar to the input gathered through the Patient and Family Engagement activities. Namely, caregivers identified stress and anxiety from learning to use CLs and the outcomes and related effects on the young child from the cataract removal and/or IOL implantation (e.g., intraoperative complications and postoperative complications such as VAO). Overall, the lack of additional evidence and lack of HRQoL outcomes from the patient perspective was notable.
Definitions of Outcomes
One of the major limitations in the included evidence that limits the ability to compare conclusions between studies is the different definitions used for outcomes in the included studies. This was most common in the definitions for glaucoma. Table 7 details the different definitions of glaucoma used in the studies. Discussion with the clinical expert engaged for the review noted that there is no well-accepted or common definition for glaucoma that could be applied consistently in the pediatric population; an accepted definition would have made the conclusions more comparable across the evidence base.80 Other outcomes were not defined well (e.g., what constituted visually significant VAO or objective measurements of strabismus); therefore it was not possible to determine if the definition varied from study to study.
Heterogeneity of Studies
There was substantial heterogeneity across the included studies. Many studies included different outcomes, comparisons, and populations (e.g., rubella cataract or co-diagnoses such as microphthalmos and persistent fetal vasculature), as well as having different study designs, follow-up times, age at IOL implantation, and years with IOL implantation. There were also different proportions of patients with bilateral versus unilateral cataracts, which may have different etiologies and different responses to surgical intervention. This made it inappropriate to combine the studies for MAs and difficult to draw general conclusions regarding the effectiveness and safety of the interventions. Additionally, many studies combined unilateral and bilateral data or were not clear about the laterality of the cataracts, making it difficult to compare across these studies. Furthermore, some studies did not report if foldable IOLs were implanted, which suggests that some studies may have included patients implanted with nonfoldable IOLs. Overall, this heterogeneity did not allow for an appropriate meta-analysis of the data, which means that the included studies were narratively synthesized and, in most cases, needed to be examined in relative isolation from one another.
Quality of Evidence
The quality of the relevant evidence for this report was low. There was 1 relevant RCT that was methodologically higher in quality among certain domains but was still assessed to have an overall high risk of bias according to the Cochrane RoB 2 tool.44-59,77 The remaining studies were very low quality due to the retrospective nature of the designs and potential introduction of selection bias. Additionally, there was uncertainty in the results because, for many comparisons and outcomes, there was only 1 study that provided relevant evidence. This limited the generalizability of the conclusions for the comparisons and prevented the conduct of any meta-analysis or narrative synthesis of those outcomes.
Directions for Future Research
Future research should consist of high-quality RCTs comparing patients of different age groups and different treatments. These studies should include comparable groups at baseline (e.g., excluding patients that would only receive 1 of the treatment options under standard clinical practice) and clearly separate patients with bilateral and unilateral cataracts. Additionally, future research examining the cost-effectiveness of treatment options for patients with aphakia could assist with appropriate and equitable decision-making.
Conclusions and Implications for Decision- or Policy-Making
Overall, there were 18 relevant studies identified.44-77 Findings indicate that IOL implantation in patients aged 12 months or younger is no more effective for the outcome of VA than implantation of IOLs in patients older than 12 months and up to 12 years or treating them with glasses or CLs.44-46,62,63,67 Findings from a pivotal long-term RCT (i.e., IATS) that compared IOLs and CLs in patients younger than 1 year of age at the time of surgery were generally consistent with the limited findings from NRSs in both unilateral and bilateral cataracts. Age was not found to be a significant predictor of visual outcomes in 2 NRSs.62,75
Findings from the IATS RCT indicated that caregiver stress is an important factor in the decision to implant IOLs at an early age, but caregiving stress levels as measured by the OTI and PSI did not differ when the patient was 1 year of age.57 Interviews conducted by CADTH with 2 mothers with lived experiences suggested that stress from the financial burden of treatment (i.e., cost of CLs), stress of learning how to adequately provide visual treatment, and the stress of a child undergoing surgery (i.e., IOL implantation later in life) were major aspects of the experiences.
Safety outcomes were consistent with what is clinically expected. Patients who underwent IOL surgery at a younger age experienced more occurrences of VAO and therefore had a larger number of reoperations to remove the opacification. Other safety outcomes more common in the patients with IOL implantation compared with patients with aphakia, including corectopia, uveitis, pupillary membranes, and corneal changes. In glaucoma, there were mixed results comparing patients with IOL implantation versus patients with aphakia. This is inconsistent with previous clinical acceptance that IOLs may be protective against glaucoma for young children.52 The results for glaucoma that were compared between different age groups at the time of surgery were also mixed, but many comparisons were not statistically tested.
The evidence base was of low quality, with all studies rated to have a high or unclear risk of bias. Most commonly, the risk of selection bias was high, and the reporting for most studies was lacking, inaccurate, or inconsistent. Many studies included patients with different lateralities of the cataract (i.e., unilateral and bilateral), often combining their data into 1 outcome measure despite the different needs and outcomes for patients with different cataract lateralities. Additionally, the majority of the studies were nonrandomized,62-76 many of which were retrospective in design, which allowed the physicians and caregivers to opt for IOL implantation (or to treat aphakia with glasses or CLs) outside of a trial context. Finally, there were concerns with the choice of statistical analysis in some of the included studies. Namely, statistical tests that require an assumption of independence of samples were used on samples that may not be considered independent (i.e., bilateral cataract).
There were no relevant cost-effectiveness studies identified. This is a limitation of the evidence base and, therefore, of this review. Parents indicated that the costs associated with treatment and the lack of equity were concerns for families of children with aphakia; therefore, the lack of evidence and analysis on the cost-effectiveness of IOL implantation is notable. Other limitations include the substantial heterogeneity of the studies, which did not allow for any MAs and led to limited narrative syntheses, and the variety of definitions used for outcomes across the included studies.
Overall, the evidence is relatively consistent with clinical experience, according to clinical expert input. However, because there are many limitations to the evidence base, additional good quality RCTs and further explorations into the cost-effectiveness of treatments for aphakia in the pediatric population are needed.
References
1.National Institutes of Health Genetic and Rare Diseases Information Center (GARD). Congenital primary aphakia. 2011; https://rarediseases.info.nih.gov/diseases/9952/congenital-primary-aphakia. Accessed 2020 Sep 25.
2.Moosajee M, Sarkar H. Congenital primary aphakia. Orphanet 2020; https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=EN&Expert=83461. Accessed 2021 Jan 4.
3.Garin M. Aphakia in adults and children. Burman & Zuckerbrod Ophthalmology Associates, P.C. 2018; https://www.2020detroit.com/aphakia-in-adults-and-children/. Accessed 2020 Sep 25.
4.Esfandiari H, Ansari S, Mohammad-Rabei H, Mets MB. Management strategies of ocular abnormalities in patients with Marfan syndrome: current perspective. J Ophthalmic Vis Res. 2019;14(1):71-77. PubMed
5.Rezar-Dreindl S, Stifter E, Neumayer T, Papp A, Gschliesser A, Schmidt-Erfurth U. Visual outcome and surgical results in children with Marfan syndrome. Clin Exp Ophthalmol. 2019;47(9):1138-1145. PubMed
6.Royal National Institute of Blind People (RNIB). Congenital cataracts. 2019; https://www.rnib.org.uk/eye-health/eye-conditions/congenital-cataracts. Accessed 2020 Sep 25.
7.Wilson ME. Pediatric cataracts: overview. American Academy of Ophthalmology 2015; https://www.aao.org/disease-review/pediatric-cataracts-overview. Accessed 2020 Sep 25.
8.Christiano D. Aphakia. Healthline 2018; https://www.healthline.com/health/eye-health/aphakia. Accessed 2020 Sep 28.
9.Baradaran-Rafii A, Shirzadeh E, Eslani M, Akbari M. Optical correction of aphakia in children. J Ophthalmic Vis Res. 2014;9(1):71-82. PubMed
10.Chen J, Chen Y, Zhong Y, Li J. Comparison of visual acuity and complications between primary IOL implantation and aphakia in patients with congenital cataract younger than 2 years: a meta-analysis. J Cataract Refract Surg. 2020;46(3):465-473. PubMed
11.Giles K, Ernest M, Christelle D, et al. Aphakia correction by injection of foldable intra ocular lens in the anterior chamber. Ophthalmol Eye Dis. 2013;5:17-22. PubMed
12.Boyd K. IOL implants: lens replacement after cataracts. American Academy of Ophthalmology 2019; https://www.aao.org/eye-health/diseases/cataracts-iol-implants. Accessed 2021 Jan 3.
13.Chang DF. Intraocular lenses for cataract surgery (general info). Chang Cataract https://www.changcataract.com/cataract-information-center-los-altos/selecting-your-lens-implant/intraocular-lenses-for-cataract-surgery/. Accessed 2021 Jan 3.
14.Magli A, Forte R, Rombetto L. Long-term outcome of primary versus secondary intraocular lens implantation after simultaneous removal of bilateral congenital cataract. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):309-314. PubMed
15.Lambert SR, Aakalu VK, Hutchinson AK, et al. Intraocular lens implantation during early childhood: A report by the American Academy of Ophthalmology. Ophthalmology. 2019;126(10):1454-1461. PubMed
16.Kruger SJ, DuBois L, Becker ER, et al. Cost of intraocular lens versus contact lens treatment after unilateral congenital cataract surgery in the infant aphakia treatment study at age 5 years. Ophthalmology. 2015;122(2):288-292. PubMed
17.Vasavada AR, Vasavada V. Current status of IOL implantation in pediatric eyes: an update. Expert Rev Med Devices. 2017:1-9. PubMed
18.Koo EB, VanderVeen DK, Lambert SR. Global practice patterns in the management of infantile cataracts. Eye Contact Lens. 2018;44 Suppl 2:S292-S296. PubMed
19.Whitman MC, Vanderveen DK. Complications of pediatric cataract surgery. Semin Ophthalmol. 2014;29(5-6):414-420. PubMed
20.Khaja WA, Verma M, Shoss BL, Yen KG. Visual axis opacification in children. Ophthalmology. 2011;118(1):224-225. PubMed
21.Mohammadpour M, Shaabani A, Sahraian A, et al. Updates on managements of pediatric cataract. J Curr Ophthalmol. 2019;31(2):118-126. PubMed
22.Zhang S, Wang J, Li Y, Liu Y, He L, Xia X. The role of primary intraocular lens implantation in the risk of secondary glaucoma following congenital cataract surgery: A systematic review and meta-analysis. PLoS One. 2019;14(4):e0214684. PubMed
23.Zetterström C, Lundvall A, Kugelberg M. Cataracts in children. J Cataract Refract Surg. 2005;31(4):824-840. PubMed
24.Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647. PubMed
25.CADTH Medical Devices, Wells C, Hui D. Intraocular lenses for infants with aphakia: A systematic review of clinical effectiveness and cost-effectiveness (CRD42021231143). PROSPERO: International prospective register of systematic reviews. York (GB): University of York Centre for Reviews and Dissemination; 2021: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021231143. Accessed 2021 Aug 7.
26.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
27.Grey Matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters-practical-tool-searching-health-related-grey-literature-0. Accessed 2021 Aug 6.
28.Dekkers OM, Egger M, Altman DG, Vandenbroucke JP. Distinguishing case series from cohort studies. Ann Intern Med. 2012;156(1 Pt 1):37-40. PubMed
29.Solebo AL, Cumberland P, Rahi JS. 5-year outcomes after primary intraocular lens implantation in children aged 2 years or younger with congenital or infantile cataract: findings from the IoLunder2 prospective inception cohort study. Lancet Child Adolesc Health. 2018;2(12):863-871. PubMed
30.Morrison A, Polisena J, Husereau D, et al. The effect of English-language restriction on systematic review-based meta-analyses: a systematic review of empirical studies. Int J Technol Assess Health Care. 2012;28(2):138-144. PubMed
31.Nussbaumer-Streit B, Klerings I, Dobrescu AI, et al. Excluding non-English publications from evidence-syntheses did not change conclusions: a meta-epidemiological study. J Clin Epidemiol. 2020;118:42-54. PubMed
32.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
33.Higgins JPT SJ, Page MJ, Sterne JAC, editors. Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). London (GB): The Cochrane Collaboration; 2019: https://drive.google.com/file/d/19R9savfPdCHC8XLz2iiMvL_71lPJERWK/view. Accessed 2020 Dec 15.
34.Kim SY, Park JE, Lee YJ, et al. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J Clin Epidemiol. 2013;66(4):408-414. PubMed
35.Kim SY, Lee YJ, Seo HJ, Park JE. Revision of clinical research literature classification tool and risk of bias assessment tool. Wonju (KR): Health Insurance Review & Assessment Service; 2013: http://repository.hira.or.kr/bitstream/2019.oak/1593/2/%EC%9E%84%EC%83%81%EC%97%B0%EA%B5%AC%EB%AC%B8%ED%97%8C%20%EB%B6%84%EB%A5%98%EB%8F%84%EA%B5%AC%20%EB%B0%8F%20%EB%B9%84%EB%9A%A4%EC%9E%84%EC%9C%84%ED%97%98%20%ED%8F%89%EA%B0%80%EB%8F%84%EA%B5%AC%20%EA%B0%9C%EC%A0%95%20%EC%97%B0%EA%B5%AC.pdf. Accessed 2020 Dec 15.
36.Rethlefsen ML, Kirtley S, Waffenschmidt S, et al. PRISMA-S: an extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Systematic Reviews. 2021;10(1):39. PubMed
37.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264-269, w264.
38.Zorzela L, Loke YK, Ioannidis JP, et al. PRISMA harms checklist: improving harms reporting in systematic reviews. BMJ. 2016;352:i157. PubMed
39.Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. PubMed
40.Campbell M, McKenzie JE, Sowden A, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890. PubMed
41.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
42.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2021 Aug 16.
43.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. PubMed
44.Infant Aphakia Treatment Study Group, Lambert SR, Buckley EG, et al. A randomized clinical trial comparing contact lens with intraocular lens correction of monocular aphakia during infancy: grating acuity and adverse events at age 1 year. Arch Ophthalmol. 2010;128(7):810-818. PubMed
45.Infant Aphakia Treatment Study Group, Lambert SR, Lynn MJ, et al. Comparison of contact lens and intraocular lens correction of monocular aphakia during infancy: a randomized clinical trial of HOTV optotype acuity at age 4.5 years and clinical findings at age 5 years. JAMA Ophthalmol. 2014;132(6):676-682. PubMed
46.Lambert SR, Cotsonis G, DuBois L, et al. Long-term effect of intraocular lens vs contact lens correction on visual acuity after cataract surgery during infancy: a randomized clinical trial. JAMA Ophthalmol. 2020;138(4):365-372. PubMed
47.Morrison DG, Wilson ME, Trivedi RH, Lambert SR, Lynn MJ, Infant Aphakia Treatment Study Group. Infant Aphakia Treatment Study: effects of persistent fetal vasculature on outcome at 1 year of age. J AAPOS. 2011;15(5):427-431. PubMed
48.Plager DA, Lynn MJ, Buckley EG, Wilson ME, Lambert SR, Infant Aphakia Treatment Study Group. Complications, adverse events, and additional intraocular surgery 1 year after cataract surgery in the infant Aphakia Treatment Study. Ophthalmology. 2011;118(12):2330-2334. PubMed
49.Plager DA, Lynn MJ, Buckley EG, Wilson ME, Lambert SR, Infant Aphakia Treatment Study Group. Complications in the first 5 years following cataract surgery in infants with and without intraocular lens implantation in the Infant Aphakia Treatment Study. Am J Ophthalmol. 2014;158(5):892-898. PubMed
50.Plager DA, Bothun ED, Freedman SF, Wilson ME, Lambert SR. Complications at 10 years of follow-up in the Infant Aphakia Treatment Study. Ophthalmology. 2020;127(11):1581-1583. PubMed
51.Beck AD, Freedman SF, Lynn MJ, et al. Glaucoma-related adverse events in the Infant Aphakia Treatment Study: 1-year results. Arch Ophthalmol. 2012;130(3):300-305. PubMed
52.Freedman SF, Lynn MJ, Beck AD, et al. Glaucoma-related adverse events in the first 5 years after unilateral cataract removal in the Infant Aphakia Treatment Study. JAMA Ophthalmol. 2015;133(8):907-914. PubMed
53.Freedman SF, Beck AD, Nizam A, et al. Glaucoma-related adverse events at 10 years in the Infant Aphakia Treatment Study: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2021;139(2):165-173. PubMed
54.Bothun ED, Cleveland J, Lynn MJ, et al. One-year strabismus outcomes in the Infant Aphakia Treatment Study. Ophthalmology. 2013;120(6):1227-1231. PubMed
55.Bothun ED, Lynn MJ, Christiansen SP, et al. Sensorimotor outcomes by age 5 years after monocular cataract surgery in the Infant Aphakia Treatment Study (IATS). J AAPOS. 2016;20(1):49-53. PubMed
56.Bothun ED, Lynn MJ, Christiansen SP, et al. Strabismus surgery outcomes in the Infant Aphakia Treatment Study (IATS) at age 5 years. J AAPOS. 2016;20(6):501-505. PubMed
57.Celano M, Hartmann EE, Drews-Botsch CD, Infant Aphakia Treatment Study Group. Parenting stress in the infant aphakia treatment study. J Pediatr Psychol. 2013;38(5):484-493. PubMed
58.Felius J, Busettini C, Lynn MJ, Hartmann EE, Lambert SR, Infant Aphakia Treatment Study Group. Nystagmus and related fixation instabilities following extraction of unilateral infantile cataract in the Infant Aphakia Treatment Study (IATS). Invest Ophthalmol Vis Sci. 2014;55(8):5332-5337. PubMed
59.Morrison DG, Lynn MJ, Freedman SF, Orge FH, Lambert SR, Infant Aphakia Treatment Study Group. Corneal changes in children after unilateral cataract surgery in the Infant Aphakia Treatment Study. Ophthalmology. 2015;122(11):2186-2192. PubMed
60.Vasavada AR, Vasavada V, Shah SK, et al. Five-year postoperative outcomes of bilateral aphakia and pseudophakia in children up to 2 years of age: a randomized clinical trial. Am J Ophthalmol. 2018;193:33-44. PubMed
61.Vasavada AR, Vasavada V, Shah SK, et al. Postoperative outcomes of intraocular lens implantation in the bag versus posterior optic capture in pediatric cataract surgery. J Cataract Refract Surg. 2017;43(9):1177-1183. PubMed
62.Koch CR, Kara-Junior N, Santhiago MR, Morales M. Long-term results of in-the-bag primary intraocular lens implantation in children younger than 24 months. Arq Bras Oftalmol. 2021;84(4):316-323. PubMed
63.Bothun ED, Wilson ME, Vanderveen DK, et al. Outcomes of bilateral cataracts removed in infants 1 to 7 months of age using the Toddler Aphakia and Pseudophakia Treatment Study Registry. Ophthalmology. 2020;127(4):501-510. PubMed
64.Eder AE, Cox KF, Pegram TA, Barb SM, Hoehn ME, Kerr NC. Effect of age at primary intraocular lens implantation on refractive growth in young children. J Pediatr Ophthalmol Strabismus. 2020;57(4):264-270. PubMed
65.Jackson CM, Bickford M, Trivedi RH, Wilson ME. Unplanned returns to the operating room within three months of pediatric cataract-related intraocular surgery: indications and risk factors. J AAPOS. 2019;23(4):224 e221-224 e224.
66.Lytvynchuk LM, Thiele MV, Lorenz B. Analysis and management of intraoperative and early postoperative complications of bag-in-the-lens intraocular lens implantation in different age groups of paediatric cataract patients: report of the Giessen Paediatric Cataract Study Group. Acta Ophthalmol (Oxf). 2020;98(2):e144-e154. PubMed
67.Murphy M, Murtagh P, McAnena L, Eldouri A, Kirwan C, O'Keefe M. Secondary glaucoma and visual axis opacification in aphakic and pseudophakic patients following congenital cataract surgery: A 28-year longitudinal case series. Eur J Ophthalmol. 2020;30(6):1370-1380. PubMed
68.Kirwan C, Lanigan B, O'Keefe M. Glaucoma in aphakic and pseudophakic eyes following surgery for congenital cataract in the first year of life. Acta Ophthalmol (Oxf). 2010;88(1):53-59. PubMed
69.Solebo AL, Rahi JS, British Congenital Cataract Interest Group. Glaucoma following cataract surgery in the first 2 years of life: frequency, risk factors and outcomes from IoLunder2. Br J Ophthalmol. 2020;104(7):967-973. PubMed
70.Valeina S, Heede S, Erts R, et al. Factors influencing myopic shift in children after intraocular lens implantation. Eur J Ophthalmol. 2020;30(5):933-940. PubMed
71.Zhang F, Chang P, Zhao Y, Zhao YE. Incidence of posterior vitreous detachment after congenital cataract surgery: an ultrasound evaluation. Graefes Arch Clin Exp Ophthalmol. 2021;259(4):1045-1051. PubMed
72.Ezisi CN, Kekunnaya R, Jalali S, et al. Cataract surgery in children with retinopathy of prematurity (ROP): surgical outcomes. Br J Ophthalmol. 2017;101(8):1128-1131. PubMed
73.Sachdeva V, Katukuri S, Ali M, Kekunnaya R. Second intraocular surgery after primary pediatric cataract surgery: indications and outcomes during long-term follow-up at a tertiary eye care center. Eye. 2016;30(9):1260-1265. PubMed
74.Shah SK, Praveen MR, Vasavada AR, et al. Long-term longitudinal assessment of postoperative outcomes after congenital cataract surgery in children with congenital rubella syndrome. J Cataract Refract Surg. 2014;40(12):2091-2098. PubMed
75.Vera L, Lambert N, Sommet J, Boulkedid R, Alberti C, Bui Quoc E. Visual outcomes and complications of cataract surgery with primary implantation in infants. J Fr Ophtalmol. 2017;40(5):386-393. PubMed
76.Lee SJ, Kim WS. Factors associated with strabismus after cataract extraction and primary intraocular lens implantation in congenital cataracts. Int J Ophthalmol. 2014;7(3):522-527. PubMed
77.Infant Aphakia Treatment Study Group, Lambert SR, Buckley EG, et al. The infant aphakia treatment study: design and clinical measures at enrollment. Arch Ophthalmol. 2010;128(1):21-27. PubMed
78.Drews-Botsch CD, Hartmann EE, Celano M, Infant Aphakia Treatment Study Group. Predictors of adherence to occlusion therapy 3 months after cataract extraction in the Infant Aphakia Treatment Study. J AAPOS. 2012;16(2):150-155. PubMed
79.Sheeladevi S, Lawrenson JG, Fielder A, et al. Delay in presentation to hospital for childhood cataract surgery in India. Eye. 2018;32(12):1811-1818. PubMed
80.Beck A, Chang TCP. Glaucoma: definitions and classification. American Academy of Ophthalmology 2015; https://www.aao.org/disease-review/glaucoma-definitions-classification. Accessed 2021 Aug 15.
81.Stanford University. NCT00212134: Infant Aphakia Treatment Study (IATS) (IATS). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2005: https://clinicaltrials.gov/ct2/show/NCT00212134. Accessed 2021 Jul 8.
Appendix 1: Literature Search Methods
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases
MEDLINE All (1946-present)
Embase (1974-present)
Cochrane Central Register of Controlled Trials (CCTR)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: January 21, 2021
Alerts: Monthly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits
Publication date limit: 2010-present
Humans
Language limit: English-language
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ab | Abstract |
.kf | Author keyword heading word (MEDLINE) |
.kw | Author keyword (Embase); keyword (CDSR) |
.dv | Device trade name (Embase) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
exp aphakia/
aphaki*.ti,ab,kf,kw.
((absence or absent) adj3 lens*).ti,ab,kf,kw.
1 or 2 or 3
exp Cataract Extraction/
exp Cataract/
cataract*.ti,ab,kf,kw.
5 or 6 or 7
4 or 8
Lens Implantation, Intraocular/
exp Lenses, Intraocular/
((intraocular or intra ocular or artificial* or implant* or prosthe*) adj3 (lens or lenses)).ti,ab,kf,kw.
(pseudophaki* adj3 lens*).ti,ab,kf,kw.
(IOL or IOLs or acrysof* or enVista* or (Alcon* adj (MA60* or SA60*)) or (Artisan* adj Aphakia*)).ti,ab,kf,kw.
10 or 11 or 12 or 13 or 14
"Congenital, Hereditary, and Neonatal Diseases and Abnormalities"/ or Congenital abnormalities/ or exp Child/ or exp Infant/ or exp Pediatrics/ or Pediatricians/ or Hospitals, Pediatric/ or Child Health/
(child or children or childhood or infant* or infancy or baby or babies or newborn* or new born* or neonat* or neo nat* or preemie or preemies or months old or months of age or toddler* or paediatric* or pediatric* or girl or girls or boy or boys or kid or kids or preschool* or pre school* or schoolage* or school age* or preteen* or pre teen* or ((1 year or one year or 2 year or two year or 2 years or two years) adj2 (age or aged or old or olds)) or congenital* or juvenile*).ti,ab,kf,kw,jw.
16 or 17
9 and 15 and 18
Cataract/cn
((genetic or developmental) adj2 cataract*).ti,ab,kf,kw.
20 or 21
15 and 22
19 or 23
limit 24 to english language
25 use medall
24 use cctr
26 or 27
aphakia/
aphaki*.ti,ab,kw,dq.
((absence or absent) adj3 lens*).ti,ab,kw,dq.
29 or 30 or 31
exp cataract extraction/
exp cataract/
cataract*.ti,ab,kw,dq.
33 or 34 or 35
32 or 36
exp lens implant/
lens implantation/
((intraocular or intra ocular or artificial* or implant* or prosthe*) adj3 (lens or lenses)).ti,ab,kw,dv,dq.
(pseudophaki* adj3 lens*).ti,ab,kw,dv,dq.
(IOL or IOLs or acrysof* or enVista* or (Alcon* adj (MA60* or SA60*)) or (Artisan* adj Aphakia*)).ti,ab,kw,dv,dq.
38 or 39 or 40 or 41 or 42
newborn disease/ or congenital disorder/ or congenital malformation/ or exp Child/ or pediatric patient/ or Pediatrics/ or exp pediatric surgery/ or pediatric surgeon/ or pediatric ward/ or pediatrician/ or pediatric hospital/ or child health/ or child health care/
(child or children or childhood or infant* or infancy or baby or babies or newborn* or new born* or neonat* or neo nat* or preemie or preemies or months old or months of age or toddler* or paediatric* or pediatric* or girl or girls or boy or boys or kid or kids or preschool* or pre school* or schoolage* or school age* or preteen* or pre teen* or ((1 year or one year or 2 year or two years or 2 years or two years) adj2 (age or aged or old or olds)) or congenital* or juvenile*).ti,ab,kw,jx,dq.
44 or 45
37 and 43 and 46
exp congenital cataract/
cataract/cn
((genetic or developmental) adj2 cataract*).ti,ab,kw,dq.
48 or 49 or 50
43 and 51
47 or 52
53 not conference abstract.pt.
limit 54 to english language
55 use oemezd
28 or 56
exp animals/
exp animal experimentation/ or exp animal experiment/
exp models animal/
nonhuman/
exp vertebrate/ or exp vertebrates/
or/58-62
exp humans/
exp human experimentation/ or exp human experiment/
or/64-65
63 not 66
57 not 67
limit 68 to yr ="2010 -Current"
remove duplicates from 69
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- aphakia, intraocular lens AND (juvenile OR congenital OR pediatric OR paediatric OR infant OR children OR neonatal)]
WHO ICTRP
International Clinical Trials Registry Platform, produced by WHO. Targeted search used to capture registered clinical trials.
[Children Limit. Search terms -- intraocular lens AND cataract, intra ocular lens AND cataract, intraocular lens AND aphakia, intra ocular lens AND aphakia]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- intraocular, intra ocular, aphakia, cataract, cataracts, iols]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- aphakia, pseudophakic, intraocular AND children/juvenile/pediatric/pediatric/congenital/neonatal, “intraocular lens,” “intraocular lenses,” “intra ocular lens,” “intra ocular lenses”]
Grey Literature
Search dates: January 22, 2021 – February 4, 2021
Keywords: aphakia, “intraocular lens,” “intraocular lenses,” “intra ocular lens,” “intra ocular lenses,” pseudophakic, acrysof, alcon, envista, (juvenile OR congenital OR neonatal OR paediatric OR pediatric OR child OR children OR infant OR infants OR infancy) AND cataract*
Limits: Publication years: 2010-present
Updated: Search updated on November 2, 2021, before the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Advisories and Warnings
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
The complete search archive of sites consulted for this report is available on request.
Appendix 2: Study Selection
Note that this appendix has not been copy-edited.
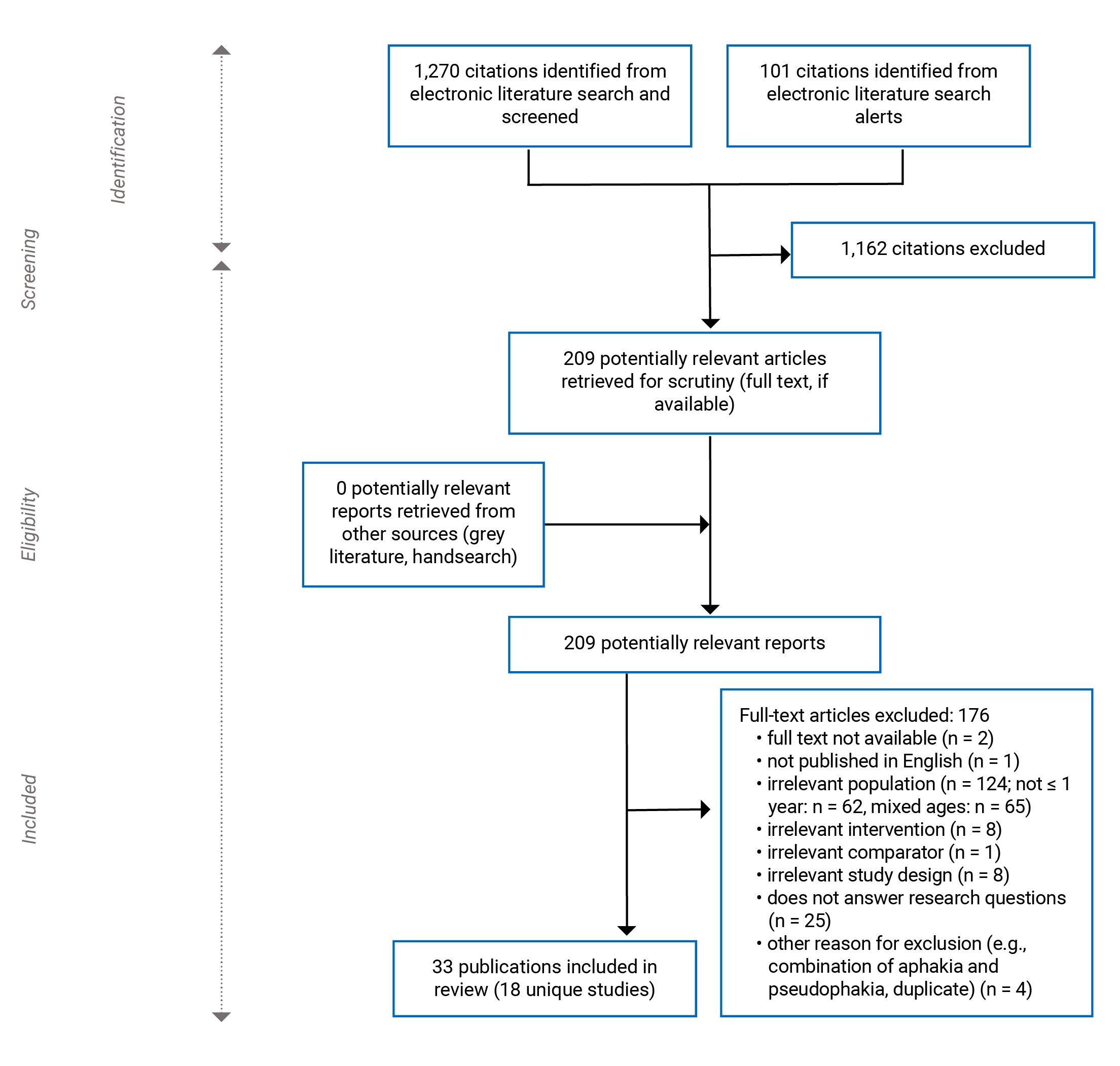
Appendix 3: Study Characteristics Table
Table 4: Study Characteristics of Included Studies
First author’s name, publication year, country, funding, and setting | Study design and objectives | Inclusion and exclusion criteria and year of IOL implantation surgery | Intervention (IOL type and implantation location) and comparator details | Outcomes assessed and measurement method, length of follow-up, and subgroups |
|---|---|---|---|---|
RCTs | ||||
Various authors as part of the IATSWGa Various publication years ranging from 2010 to 2020 US Funding: National Eye Institute NIH Departmental Core Grant and Research to Prevent Blindness, Inc. Setting: 12 sites in the US | Study design: Randomized, controlled, multicentre, superiority trial Study objectives: Compare primary IOL implantation to patients with aphakia using CL treatment after cataract surgery for patients with a unilateral congenital cataract between 1 and 6 months of age | Inclusion criteria:
Exclusion criteria:
Surgeries performed between December 2004 and January 2009 Interval between surgery on 1 eye and next: NA | N = 114 patients; 114 eyes (all unilateral cataracts) Age at surgery (total): Median: 1.8 months (Q1, Q3 1.2, 3.2 months) Intervention: IOL, n = 57
Comparator(s): Aphakia (CL), n = 57 (Silsoft or RGP CL with a 2.0 D overcorrection, or custom soft Cb)
| Clinical effectiveness outcome(s):
Safety outcome(s):
Length of follow-up:
Subgroup(s):
|
Vasavada et al. (2018)60 India Funding: None Setting: Single-centre study – Iladevi Cataract and IOL Research Centre Ahmedabad, India. A single surgeon performed all procedures. | Study design: Parallel group RCT (NCT01297153) Study objectives: Evaluate visual outcomes and complications associated with bilateral congenital cataract surgery in patients up to 2 years of age with and without primary IOL implantation | Inclusion criteria: Patients up to 2 years of age who underwent bilateral congenital cataract surgery with and without primary IOL implantation Exclusion criteria:
Surgeries performed between March 1, 2009, and February 28, 2011 Interval between surgery on 1 eye and next: Within 2 weeks of the first eye surgery | N = 60 patients; 120 eyes (aphakia n = 30 patients; IOL n = 30 patients) (All bilateral cataracts) Intervention: Primary IOL implantation with spectacles, n = 29 patients; 58 eyes
Comparator(s): Aphakia corrected with CL, glasses, or both (< 1 year: n = 25 patients; 50 eyes)
| Safety outcome(s): Posterior synechiae Length of follow-up: 5 years postoperatively Subgroup(s): Patients below and above the median age at surgery (5.7 months) |
Vasavada et al. (2017)61 India Funding: Partially supported by a research grant from the ASCRS Foundation (2013 to 2014) Setting: Single-centre study – Iladevi Cataract and IOL Research Centre Ahmedabad, India. A single surgeon performed all procedures. | Study design: Parallel group RCT Study objectives: Comparison of complications of cataract surgery with IOL implantation between, 2 techniques, in-the-bag IOL with AV vs. optic capture of IOL with no AV in patients up to 4 years of age | Inclusion criteria:
Exclusion criteria:
Surgeries performed between April 2013 and March 2014 Interval between surgery on 1 eye and next: NA (only first-operated eye was included from patients with bilateral cataracts) | N = 61 patients; 61 eyes Intervention: Primary IOL implantation (Group 1: in-the-bag IOL with limbal AV), n = 30 patients; 30 eyes
Comparator(s): Primary IOL implantation (Group 2: optic capture of the IOL with no AV), n = 31 patients and 31 eyes Comparative data: age at primary IOL implantation, i.e., ≤ 1 year vs. > 1 year to ≤ 4 years
| Safety outcome(s):
Length of follow-up: 12 months after IOL implantation Subgroup(s): Age at surgery — ≤ 1 year and > 1 year to ≤ 4 years |
NRSs | ||||
Koch et al. (2021)62 Brazil Funding: CAPES-DS Setting: Sant Joan de Déu Hospital. A single surgeon performed all procedures. | Study design: Retrospective cohort – chart review Study objectives: Evaluate safety of primary IOL implantation in patients aged 5 to 24 months | Inclusion criteria: Primary IOL implantation between ages 5 to 24 months in patients without changes observed in a fundus examination and a horizontal corneal diameter ≥ 11 mm Exclusion criteria:
Surgeries performed during period of January 1, 2006, to January 31, 2016 Interval between surgery on 1 eye and next: NR | N = 68 patients; 93 eyes Age at surgery (total): 15.06 ± 6.19 months (range 5 to 24 months) Cataract laterality (total): Unilateral: 43 patients; 43 eyes (46.2%); Bilateral: 25 patients; 50 eyes (53.8%) Intervention: IOL, n = 68 patients; 93 eyes
Comparator(s): Primary IOL implantation in children (i.e., ≥ 19 months of age) Comparison of 10 to 18 months not extracted due to combination of patients under and over 12 months of age
| Clinical effectiveness outcome(s): CDVA (< 2 years old: Teller Acuity Cards; 2 to 3.5 years old: HOTV, a LEA Symbols test, or Allen’s Picture Cards; > 3.5 years old: HOTV, a Tumbling E test, or a Snellen chart) Safety outcome(s): Postoperative complications (i.e., VAO, glaucoma [Perkins tonometer], corectopia) Length of follow-up:
Subgroup(s):
|
Bothun et al. (2020)63 2020 US Funding: Mayo Clinic, Knights Templar Setting: Various clinical centre sites in the US (10 sites). Multiple surgeons performed procedures.77 | Study design: Retrospective cohort – chart review Study objectives: Evaluate outcomes of bilateral cataract surgery in infants performed by IATS surgeons during the time of IATS recruitment | Inclusion criteria: Patients with bilateral cataracts who had surgery on at least 1 eye between 28 days and 7 months (210 days) of age from Jan. 1, 2004, to Dec. 31, 2010 (i.e., during IATS enrolment period) Exclusion criteria:
Surgeries performed during period of 2004 to 2010 Interval between surgery on 1 eye and next: Median: 4 days (range 0 to 33 days) | N = 96 patients; 178 eyes (All bilateral cataracts) Age at surgery (total): Median: 2.5 months (range 1 to 7 months) Intervention: Primary IOL implantation, n = 42 eyes
Comparator(s): Aphakia (CL, glasses, or both), n = 136 eyes
| Clinical effectiveness outcome(s): VA Safety outcome(s): Intraoperative complications, additional unplanned surgeries, AEs, glaucoma, VAO Length of follow-up: No less than 41 months Median: 4.9 years (range 4.0 to 5.8 years) Subgroup(s): No relevant subgroups |
Eder et al. (2020)64 US Funding: Partially by an unrestricted grant from Research to Prevent Blindness Setting: Two-centre study, tertiary care pediatric ophthalmology practices (Hamilton Eye Institute and St. Jude Children’s Research Hospital). Two surgeons performed all procedures. | Study design: Retrospective cohort, study – chart review Study objectives: Evaluate effect of age at primary IOL implantation on rate of refractive growth in young patients | Inclusion criteria:
Exclusion criteria:
Surgeries performed between 1999 and 2016 Interval between surgery on 1 eye and next: NA (only right eye was included from patients with bilateral cataracts) | N = 46 patients; 46 eyes Age at surgery (total): Mean: 34.68 months (range 1 to 72 months) Cataract laterality (total): Unilateral: 28 (60.87%) patients; Bilateral: 18 (39.13%) patients Intervention: Primary IOL implantation in infants (i.e., 0 to 5 months of age)
Comparator(s): Primary IOL implantation in children (i.e., 6 to 23 months and 24 to 72 months) Comparison of 6 to 23 months not extracted due to combination of patients under and over 12 months of age
| Safety outcome(s): Postoperative ocular conditions (e.g., additional surgeries, glaucoma) Length of follow-up: 35 to 226 months Subgroup(s): No relevant subgroups |
Lytvynchuk et al. (2020)66 Germany Funding: NR Setting: Single-centre study, Department of Ophthalmology, Justus-Liebig University, University Hospital Giessen and Marburg GmbH (Campus Giessen), Germany. Two surgeons performed all procedures. | Study design: Retrospective cohort study – clinical record review Study objectives: Examine and report management of intra- and early postoperative complications in pediatric patients (subgrouped by age) receiving BIL IOL | Inclusion criteria: Pediatric cataract and implantation of BIL IOL Exclusion criteria: NR Surgeries performed between January 2008 and December 2018 Interval between surgery on 1 eye and next: NR | N = 60 patients (90 eyes) Age at surgery (total): Mean: 45.25 months (range 1.05 to 200.28 months) Cataract laterality (total): Unilateral: 27 (45%) patients; Bilateral: 33 (55%) patients (3 cases of bilateral cataract, only 1 eye was operated with the BIL technique) Intervention: BIL IOL in infants (i.e., 0 to < 3 months and 3 to < 12 months of age)
Comparator(s): BIL IOL placement in children (i.e., 12 to < 36 months of age and 36 months to 17 years) 36 months to 17 years data not extracted due to inclusion of patients over 12 years of age
| Safety outcome(s): Intraoperative complications and postoperative complications (e.g., VAO, glaucoma development) Length of follow-up: Early postoperative period defined as ≤ 12 months. Follow-up > 12 months. Subgroup(s): No relevant subgroups |
Murphy et al. (2020)67 Ireland Funding: none Setting: Single-centre study (Department of Ophthalmology, Temple Street Children’s University Hospital, Dublin, Ireland). All surgeries and entirety of patients’ follow-up were performed under a single consultant surgeon. | Study design: Retrospective, longitudinal cohort – medical record reviewe Study objectives: Primary— determine incidence, characteristics, and outcomes of SG (clinical characteristics associated with increased rates of glaucoma and relation to timing of surgery). Secondary – BCVA and VAO rates | Inclusion criteria:
Exclusion criteria:
Surgeries performed between January 1, 1990, to December 31, 2017 Interval between surgery on 1 eye and next: Second eye operated on within 2 weeks of the first eye in patients with bilateral cataract | N = 93 patients; 135 eyes Statistical testing on randomly selected eye from bilateral cases (n = 93 eyes) Age at surgery (total): Mean ± SD: 3.46 ± 3.67 months (range 2 weeks to 12 months) Cataract laterality (total): Unilateral: 50 (37.04%) eyes; Bilateral: 85 (62.96%) eyes Intervention: Primary IOL implantation, n = 49 patients 1 eye each
Comparator(s): Aphakia (vision correction NR), n = 44 patients
Cataract laterality (aphakia): Unilateral: 14/50 (28%) eyes; Bilateral: 59/85 (69.41%) eyes | Clinical effectiveness outcome(s): BCVA Safety outcome(s):
Length of follow-up: Minimum of 36 months Total of 28 years (continued follow-up period from Kirwan et al. (2010)68) Total: Mean ± SD: 160.02 ± 64.42 months (range 40 to 336 months) IOL vs. Aphakia, Mean ± SD: 141.22 ± 59.88 vs. 172.86 ± 65.30 (P = 0.017) Subgroups:
|
Solebo et al. (2020)69 UK Funding: Department of Health’s NIHR BRC funding scheme Ulverscroft Vision Research Group fellowship Academy of Medical Sciences Lecturer award NIHR BRC (NIHR Clinician Scientist award) NIHR Senior Investigator Award Setting: UK and Irish hospitals (31 sites)29 | Study design: Prospective cohort (IOLunder2) Study objectives: Report glaucoma-related AEs 5 years following cataract removal with or without IOL implantation in patients of the IOLunder2 cohort | Inclusion criteria: Patients under 2 years of age with congenital or infantile cataract undergoing cataract(s) removal with or without IOL implantation Exclusion criteria:
Surgeries performed between January 1, 2009, and December 31, 2010 Interval between surgery on 1 eye and the next: NR | N = 235 patients; 378 eyes Age at surgery (total): Median (range), bilateral vs. unilateral cataract(s): 2.4 months (0.3 to 23 months) vs. 2.2 months (0.5 to 23 months) Cataract laterality (total): Unilateral: 92 (24.3%) eyes; Bilateral: 286 (75.7%) eyes Intervention: Primary IOL implantation in infants (i.e., ≤ 12 months of age)
Comparator(s): Aphakia (no relevant information on IOL vs. aphakia comparison in eligible age groups) (comparative data: age at primary IOL implantation, i.e., > 52.1 weeks to 2 years)
| Safety outcome(s): Glaucoma (measurement method NR) Length of follow-up: 5 years Subgroup(s):
|
Valeina et al. (2020)70 Latvia Funding: None Setting: Single-centre study (Clinical University Hospital – Riga, Latvia). Three different surgeons performed implantations. | Study design: Retrospective cohort – chart review Study objectives: Determine amount of myopic shift for patients ≤ 18 years old with IOLs and evaluate influencing factors. Additionally, to assess the occurrence of secondary diagnoses of glaucoma and cataract | Inclusion criteria: Patients who had congenital cataract removal and foldable IOL implantation Exclusion criteria: Traumatic, complicated, and congenital cataracts with other ocular or systemic anomalies Surgeries performed between January 1, 2006, and December 31, 2012 Interval between surgery on 1 eye and next: NR | N = 85 patients; 137 eyes Age at surgery (total): Range 1 month to 18 years Cataract laterality (total): Unilateral: 30 (22%) eyes; Bilateral: 107 (78%) eyes Intervention: Primary IOL implantation (i.e., 1 to 6 and 7 to 12 months of age)
Comparator(s): Nonef (comparative data: age at primary IOL implantation, i.e., 13 to 24, 25 to 48, 49 to 84, 85 to 216 months of age) 85 to 216 months not extracted due to inclusion of patients over 12 years of age
| Safety outcome(s):
Length of follow-up: Minimum follow-up of 6 months; maximum follow-up of 120 months Total: Mean: 47.8 months (3.9 years) Subgroup(s):
|
Zhang et al. (2020)71 China Funding: Research grants from Zhejiang Provincial Natural Science Foundation of China, National Natural Science Foundation of China, Zhejiang Provincial Key Research and Development Program, Innovation Discipline of Zhejiang Province Setting: Eye Hospital of Wenzhou Medical University, Hangzhou, China (single centre). One surgeon performed all surgeries. | Study design: Prospective cohort Study objectives: Examine changes to the vitreous body (i.e., PVD development) after congenital cataract surgery and its association with phakic status | Inclusion criteria: Patients with congenital cataract who underwent cataract surgery Exclusion criteria:
Surgeries performed during June 1, 2015, and September 1, 2018 Interval between surgery on 1 eye and next: NR | N = 131 eyes Cataract laterality: NR (only right eyes of bilateral cataract patients included) Intervention: IOL, n = 57 eyes
Comparator(s): Aphakia (vision correction NR), n = 74 eyes
| Safety outcome(s):
Length of follow-up: 12 months (1, 3, 6, 9, and 12-month follow-up) Subgroups(s):
|
Jackson et al. (2019)65 US Funding: NR Setting: Single-centre study – Storm Eye Institute. A single surgeon performed all procedures. | Study design: Retrospective cohort – medical record review Study objectives: Identify reasons and associated risk factors for unplanned returns to the operating room within 90 days of initial cataract-related intraocular surgery in pediatric patients | Inclusion criteria: Cataract extraction, with or without IOL implant, or secondary IOL implantation Exclusion criteria: Reoperations anticipated preoperatively or related to a pre-existing condition (e.g., patient with Lowes syndrome requiring subsequent glaucoma surgery) Surgeries performed between 1991 to 2018 Interval between surgery on 1 eye and next: NR | N = 989 patients; 1392 eyes Underwent cataract-related surgery at age < 1 year: n = 467 eyes Age at surgery and cataract laterality NR Intervention: Primary or secondary IOL implantation, n = 183 eyes
Comparator(s): Aphakia (vision correction NR), n = 284 eyes | Safety outcome(s): Indication and timing of unplanned reoperation within 90 days of initial surgery Length of follow-up: 90 days Subgroups: No relevant subgroups |
Ezisi et al. (2017)72 2017 India Funding: NR Setting: Single tertiary care ophthalmic institute | Study design: Retrospective cohort study – medical record review Study objectives: Examine cataract surgery outcomes (intraoperative, surgical, and visual) for patients with ROP | Inclusion criteria:
Exclusion criteria:
Surgeries performed January 2001 to December 2014 Interval between surgery on 1 eye and next: NR | N = 22 patients; 28 eyes Age at surgery (total): Mean ± SD: 18.9 ± 31.3 months (range 2 to 144 months) Cataract laterality (total): Unilateral: 16 (72.7%) patients; Bilateral: 6 (27.3%) patients Intervention: IOL implantation, n = 16 patients; 19 eyes IOL implanted in patients with a corneal diameter ≥ 10.5 mm or based on surgeon’s discretion and presence of other intraoperative complications
Comparator(s): Nonef (comparative data: aphakia and age at IOL implantation [i.e., ≤ 12 months vs. > 12 months]) Aphakia (glasses or CLs and amblyopia therapy): n = 6 patients; 9 eyes
| Safety outcome(s): AEs (e.g., VAO, IOL capture) and glaucoma Length of follow-up: Median: 12 months (range 1 to 132 months, IQR: 7 to 36 months) Subgroups: Age at surgery (≤ 12 months vs. > 12 months of age) |
Vera et al. (2017)75 France Funding: None Setting: Unclear | Study design: Retrospective cohort – medical record review Study objectives: Assess visual outcomes and postoperative complications of cataract surgery with primary IOL implantation in infants. Determine possible predictive factors related to poor visual outcome | Inclusion criteria:
Exclusion criteria:
Surgeries performed between January 2009 and December 2011 Interval between surgery on 1 eye and next: NR | N = 43 patients; 61 eyes Age at surgery (total): Median: 5.7 months (range 4 weeks to 24 months) Cataract laterality (total): Unilateral: 25 (58.00%) patients; Bilateral: 18 (42.00%) patients Intervention: Primary IOL implantation in infants (i.e., 0 to < 6 and 6 to 12 months)
Comparator(s): Nonef (comparative data: age at IOL implantation presented as subgroups, i.e., > 12 to 24 months of age) | Clinical effectiveness outcome(s): VA (LEA pictures, or matching and Snellen charts)
Safety outcome(s):
Subgroup(s): Age at surgery:
Bilateral and unilateral cataract Length of follow-up: 1 to 5 years. Median: 47.0 months (range 14 to 60 months) |
Sachdeva et al. (2016)73 India Funding: Hyderabad Eye Research Foundation (HERF) Setting: Nimmagada Prasad Children’s Eye Care Centre (single-centre study) | Study design: Retrospective cohort –medical record review Study objectives: Examine complications following lens aspiration with and without IOL implantation in patients < 7 years of age | Inclusion criteria: Patients who had lens aspiration with or without primary IOL implantation Exclusion criteria:
Surgeries between January 2006 and December 2014 Interval between surgery on 1 eye and next: 1 to 4 weeks | N = 814 eyes Age at surgery and cataract laterality NR Intervention: Primary posterior chamber IOL, n = 570 eyes
Comparator(s): Aphakia (vision correction NR), n = 244 eyes Comparative data: age at IOL implantation, i.e., < 1 year vs. > 1 year to 7 yearsf | Safety outcome(s):
Length of follow-up: 5 years Subgroup(s): Age at primary surgery – < 1 year and > 1 year to 7 yearsg |
Lee et al. (2014)76 Korea Funding: Inje University Setting: Maryknoll hospital | Study design: Retrospective cohort study – medical record review Study objectives: Examining strabismus in patients between 1.5 months and 9 years who had cataract removal and primary IOL implantation | Inclusion criteria:
Exclusion criteria:
Surgeries performed between January 1993 and August 2011 Interval between surgery on 1 eye and next: NR | N = 108 patients (172 eyes) Age at surgery (total): Range 0.1 to 9 years Cataract laterality (total): Unilateral: 44 (25.6%) eyes; Bilateral: 128 (74.4%) eyes Intervention: Primary IOL implantation
Comparator(s): Nonef (comparative data: age at IOL implantation, i.e., ≤ 1 year vs. > 1 year) | Safety outcome(s): Post-operative strabismus (method NR) Length of follow-up: At least 2 years (range of mean follow-up: 4.1 to 4.9 years) Subgroup(s): Age at surgery — ≤ 1 year and > 1 year |
Shah et al. (2014)74 India Funding: None Setting: Single-centre study – Iladevi Cataract and IOL Research Centre, Ahmedabad, India. A single surgeon performed all procedures. | Study design: Prospective cohort Study objectives: Assess intraoperative and long-term longitudinal postoperative outcomes of cataract surgery in pediatric patients with congenital rubella syndrome | Inclusion criteria: Pediatric patients with pediatrician and laboratory confirmed rubella cataract who underwent cataract surgery with or without IOL implantation. Exclusion criteria: Patients who tested negative for anti-rubella virus immunoglobulin M antibodies Surgeries performed between 2004 and 2007 Interval between surgery on 1 eye and next: NR | N = 21 patients; 37 eyes Age at surgery (total): Mean ± SD: 3.97 ± 2.1 months (range 1 to 8 months), median: 4.0 months Cataract laterality (total): Unilateral: 5 (13.51%) eyes; Bilateral: 32 (86.49%) eyes Intervention: Primary IOL implantation, n = 12 eyes
Comparator(s): Aphakia, n = 25 eyes (Spectacles or CLs, all eyes with microphthalmia were left aphakic) | Safety outcome(s):
Length of follow-up: Up to 5 years postoperatively. Additional follow-up visits were tailored to the patients' needs. Subgroup(s): No relevant subgroups |
Kirwan et al. (2010)68 Ireland Funding: NR Setting: Single-centre study. All surgeries were performed at 1 unit at Children’s University Hospital (Dublin, Ireland) | Study design: Retrospective cohort – chart review Study objectives: Examine glaucoma development in IOL implanted and aphakic eyes with following cataract surgery | Inclusion criteria: Congenital cataracts removed before 1 year of age Exclusion criteria:
Surgeries performed between 1984 and 2007 Interval between surgery on 1 eye and next: NR | N = 100 patients; 144 eyes Cataract laterality (total): Unilateral: 56 (50.9%) patients; Bilateral: 44 (40%) patients One eye selected randomly for analysis in bilateral cataract Intervention: Primary IOL implantation, n = 55 patients; 67 eyes
Comparator(s): Aphakia (vision correction NR), n = 45 patients; 77 eyes
| Safety outcome(s):
Length of follow-up: Minimum of 4 months—majority of patients continuing regular follow-up sessions at time of publication. Longer follow-up is reported in Murphy et al. (2020)67 IOL vs. Aphakia, Mean ± SD (range): 56.3 ± 43.5 months (5 to 174 months) vs. 113.4 ± 68.9 months (12 to 254 months), P < 0.001 Subgroup(s): Patients aged ≤ 2.5 months of age at cataract surgery Age at surgery, IOL vs. Aphakia: Mean ± SD: 1.5 ± 0.6 vs. 1.4 ± 0.6 months (range 0.5 to 2.5 months for both groups), P = 0.79 |
ACCC = anterior continuous curvilinear capsulorhexis; AE = adverse event; ASCRS = American Society of Cataract and Refractive Surgery; AV = anterior vitrectomy; BCVA = best corrected visual acuity; BIL = bag-in-the-lens; CAPES-DS = Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil; CL = contact lens; CDVA = corrected distance visual acuity; E-ETDRS = electronic Early Treatment Diabetic Retinopathy Study; EC = endothelial cell; GmbH = Gesellschaft mit beschränkter Haftung; HERF = Hyderabad Eye Research Foundation; IATS = Infant Aphakia Treatment Study; IATSWG = Infant Aphakia Treatment Study writing group; IO = intraocular; IOL = intraocular lens; IOP = intraocular pressure; IQR = interquartile range; NA = not applicable; NIH = National Institutes of Health; NIHR BRC = National Institute for Health Research Biomedical Research Centre; NR = not reported; NRS = nonrandomized study; OTI = Ocular Treatment Index; PCCC = posterior continuous curvilinear capsulorhexis; PFV = persistent fetal vasculature; PSI = Parenting Stress Index; PVD = posterior vitreous detachment; Q = quartile; QR = quartile range; RCT = randomized controlled trial; ROP = retinopathy of prematurity; SC = secondary cataract; SD = standard deviation; SG = secondary glaucoma; SR = systematic review; VA = visual acuity; VAO = visual axis opacification; VAOb = visual axis obscuration; VO = vitreous opacity; vs. = versus.
aIATS writing group was led by Dr. Scott Lambert.44
b“In cases where a Silsoft CL could not be worn successfully, a RGP CL was substituted and vice versa. A patient was deemed to have failed CL wear if the fitted lens was worn for fewer than 4 hours a day on average over a period of 8 consecutive weeks” (p. 4).77
cAEs included glaucoma, glaucoma suspect, pupillary membrane, lens reproliferation into the visual axis, strabismus, corectopia, vitreous hemorrhage, retinal hemorrhage, hyphema, retained cortex, retinal detachment, endophthalmitis, phthisis bulbi, keratitis, corneal abrasion, corneal opacity, corneal edema lasting > 30 days, capsular phimosis, and wound leak/dehiscence.
sIOL implantation is not routinely performed in the study institution in children aged < 5 months.
eThe authors labelled this study as a “cross-sectional single-centre prospective case series,” however, the study appears to be a retrospective chart review.67
fComparator is noted as “none” when the study did not have a comparator specified in its original methods (i.e., it was designed as a single-arm study) but was eligible for inclusion due to subgroup analyses or additional data that fit inclusion criteria.
gThe authors do not specify in which group patients exactly 1 year of age would fall.
Note that this appendix has not been copy-edited.
Appendix 4: Procedures Performed and Medications Administered
Table 5: Surgical Procedures and Medications
Study citation | Reported surgical procedures | Preoperative medications/agentsa | Intraoperative medications/agentsa | Postoperative medications/agentsa | Postoperative visual rehabilitation (non-medication) |
|---|---|---|---|---|---|
RCTs | |||||
Infant Aphakia Treatment Study (Various Authors, various years)44-59,77 | Procedures: Anterior capsulotomy: all patients Central posterior capsulectomy: all patients AV: all patients | NR | Intraoperative medications/agents: Subconjunctival injections of antibiotics and steroids after the limbal incisions were closed for infants randomized to the CL group 1 drop of 0.5% or 1% atropine Antibiotic/steroid ointment at the end of surgery for all eyes | Postoperative medications/agents: Prednisolone acetate 1% - administered topically at least 4 times a day for 1 month but never exceeding 6 months Topical antibiotic instilled 3 to 4 times a day for 1 week Atropine 0.5% or 1% instilled twice daily for 2 to 4 weeks | Postoperative visual rehabilitation (non-medication): All operated eyes were patched following the administration of atropine drop and antibiotic/steroid ointment at the end of surgery |
Vasavada et al. (2018)60 | Limbal approach in all surgeries ACCC: all surgeries PCCC: all surgeries AV: all surgeries Optic capture: only in IOL patients | For pupil dilation: 1% cyclopentolate eye drops 10% phenylephrine, administered at 1-hour intervals starting 3 hours before surgery | Antibiotics: Injected vancomycin (1%; 0.1 mL) | Prednisolone acetate 1% eye drops (6 times a day for 2 weeks and then gradually tapered over 3 months) Atropine (1%) eye drops (once at bedtime for 4 weeks) Moxifloxacin 0.05% eye drops (Vigamox; 3 times a day for 4 weeks) No oral steroids Systemic or subconjunctival steroids allowed – dosage and frequency of topical steroid administration based on the surgeon’s clinical judgment | Both IOL and patients with aphakia: Patching (at least 6 hours) Prescribed if there is squint or unilateral deterioration of vision Temporary spectacles were prescribed (before suture removal) and a final prescription were prescribed (after suture removal) with complete correction for distance |
Vasavada et al. (2017)61 | ACCC: all patients PCCC: all patients AV:
Optic capture: group 2 (n = 31 eyes) In the presence of vitreous disturbance, an AV was performed irrespective of the group allocation | NR | Sodium hyaluronate 2.3% (Healon5) injected into the anterior chamber Triamcinolone acetonide (Aurocort) 0.1 mL (intracameral injection) | Moxifloxacin 0.5% eyedrops Prednisolone acetate 1.0% eyedrops tapered over 3 months Atropine sulphate 1.0% eyedrops for 2 weeks | NR |
NRSs | |||||
Koch et al. (2021)62 | Procedures: Anterior capsulorhexis: all patients Posterior central capsulotomy: all patients AV: all patients | NR | Intraoperative medications/agents: At end of surgery: Inferior subconjunctival injection of steroids (methylprednisolone) Anterior chamber injected antibiotic (cefuroxime 1mg/0.1ml) | Postoperative medications/agents: Topical antibiotic and steroid drop combination applied every 4 hours for a week then tapered down over 4 weeks Cycloplegic eye drop (twice daily for 2 weeks) Oral steroid (7 days) | Postoperative visual rehabilitation (non-medication): Glasses or CLs (15 days after surgery) Amblyopia and ocular alignment treatment as needed |
Bothun et al. (2020)63 | 98% of implanted eyes: Primary PC AV
No other additional surgical procedures | NR | NR | NR | NR |
Eder et al. (2020)64 | NR | NR | NR | NR | NR |
Lytvynchuk et al. (2020)66 | Original bag-in the-lens surgical technique as described by Tassignon et al. (2002) Patients < 12 months of age underwent peripheral superior iridectomy Flexible iris retractors Were used in patients with small pupil or posterior synechia ACCC: all surgeries Separation of anterior vitreous surface from posterior capsule PCCC: all surgeries | NR | Anterior and posterior capsules were approached to each other with sodium hyaluronate 1.2% Intracameral injection of Adrenalin (1:1,000) and Xylocaine 2% (0.1 mL) Miochol 2 to 5 mg Cefuroxime 0.025 mg | Eye drops of antibiotics, dexamethasone and nonsteroidal anti-inflammatory agents | Prescription of glasses or CLs (in all patients, attempted within the first weeks post-surgery) and occlusion therapy as needed |
Murphy et al. (2020)67 | ACCC: NR PC:
AV, n (%)*:
Optic capture: NR | NR | NR | Standard regimen of tapering topical steroid and antibiotics administered to all patients Subconjunctival dexamethasone and intracameral cefuroxime administered to majority of patients | Patching (IOL patients)
Mean ± SD: 61.57 ± 28.29 Patching (patients with aphakia)
Mean ± SD: 43.67 ± 44.07 |
Solebo et al. (2020)69 | 91.5% of eyes underwent:
| NR | 91.5% of eyes received local corticosteroids (intraocular, subconjunctival, subtenon or orbital floor injection) | 40.0% of eyes received intensive topical steroids regimens (drops administered at least every 2 hours during the day for first week) | CL ± glasses or glasses only Occlusion/ penalization therapy |
Valeina et al. (2020)70 | NR | NR | NR | NR | Glasses were prescribed within 2 weeks. Amblyopia treatment was ongoing |
Zhang et al. (2020)71 | Patients > 2 years:
Patients < 2 years:
| NR | NR | NR | NR |
Jackson et al. (2019)65 | All surgeries: Initial incisions: NR ACCC: NR Optic capture: NR Cataract extraction without IOL implantation (aphakia): Central posterior capsulectomy performed with a vitrector handpiece AV Cataract extraction with IOL implantation: Limbal or a pars plana posterior capsulectomy Posterior vitrectomy Posterior capsulectomy was performed in patients < 8 years of age and in all eyes with posterior polar or capsular cataract. Some eyes of patients > 8 years of age had a manual PCCC without an AV | NR | Some eyes received intracameral triamcinolone, n = NR | NR | NR |
Ezisi et al. (2017)72 | Primary PC AV | NR | NR | NR | Glasses or contact lenses and, when needed, amblyopia therapy |
Vera et al. (2017)75 | ACCC: all surgeries PCCC: all surgeries AV: all surgeries Optic capture: NR | NR | At the end of all surgical procedures: dexamethasone 4 mg (subconjunctival injection) | Systemic steroids 0.7 mg/kg per day for 3 days Antibiotics and topical steroids tapered over 2 months | Glasses Prescribed at 1-week follow-up Patching |
Sachdeva et al. (2016)73 | With or without primary PC With or without AV | NR | NR | NR | NR in methods. Results noted that patients with dense amblyopia wore spectacles and underwent patching |
Lee et al. (2014)76 | 131/172 had PCCC 107/131 had optic capture of IOL 24/131 eyes had in-the-bag IOL implantation following AV using a vitreous cutter In patients without PCCC (41 eyes), 16 had scleral fixation performed due to lens decentration | NR | NR | NR | NR |
Shah et al. (2014)74 | ACCC: performed manually in all surgeries PCCC: performed manually in all surgeries AV: limbal approach in all surgeries Optic capture: NR Reported surgical procedures performed in some eyes: Pars plicata lensectomy performed in 2 eyes with microcornea and coexisting microphthalmos in which the pupil could not be dilated In eyes without microphthalmos capsular bag was inflated with a high viscosity ophthalmic viscosurgical device. | NR | Pupil was constricted with an intracameral injection Anterior chamber reformed with a balanced salt solution then injected with 0.1 mL of moxifloxacin 1.0% | Prednisolone acetate 1.0% eyedrops tapered over 12 weeks Moxifloxacin 0.5% eyedrops for 4 weeks Diclofenac sodium 0.1% 3 times a day for 4 weeks Timolol maleate 0.25% eyedrops 2 times a day for 2 weeks Cyclopentolate 1.0% eyedrops once a day for 2 weeks and then on alternate days for 15 days Oral steroids with a dose of 0.8 mg/kg of body weight in tapering doses for 2 weeks | Spectacles or CLs were prescribed for all patients |
Kirwan et al. (2010)68 | NR | NR | NR | NR | NR |
ACCC = anterior continuous curvilinear capsulorhexis; CL = contact lens; IOL = intraocular lens; NRS = nonrandomized study; NR = not reported; PC = posterior capsulotomy; PCCC = posterior continuous curvilinear capsulorhexis; RCT = randomized controlled trial; SD = standard deviation.
aExtracted data for pre-, post-, and intraoperative medications do not include the use of anesthesia during surgery or during pre- or post-operative examinations.
Note that this appendix has not been copy-edited.
Appendix 5: Outcomes by Publication
Table 6: Relevant Outcomes by Included Study
Study citation | Clinical effectiveness | Safety | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
VA | HRQoL | VAO | Glaucoma/ ocular hypertension | Strabismus/ Nystagmus | Additional surgeries | IO complications | Corneal changes/ ECD | INF complications | PVD | VO | |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | No | No | |
Vasavada et al. (2018)60 | No | No | No | Yes | No | No | No | No | Yes | No | No |
Vasavada et al. (2017)61 | No | No | Yes | Yes | No | No | No | No | Yes | No | No |
Koch et al. (2021)62 | Yes | No | Yes | Yes | Yes | Yes | Yes | No | No | No | No |
Bothun et al. (2020)63 | No | No | Yes | Yes | No | Yes | Yes | No | No | No | No |
Eder et al. (2020)64 | No | No | No | Yes | No | Yes | No | No | No | No | No |
Lytvynchuk et al. (2020)66 | No | No | Yes | Yes | No | No | Yes | No | Yes | No | No |
Murphy et al. (2020)67 | Yes | No | Yes | Yes | Yes | No | No | No | No | No | No |
Solebo et al. (2020)69 | No | No | No | Yes | No | No | No | No | No | No | No |
Valeina et al. (2020)70 | No | No | No | Yes | No | No | No | No | No | No | No |
Zhang et al. (2020)71 | No | No | No | No | No | No | No | No | No | Yes | Yes |
Jackson et al. (2019)65 | No | No | No | No | No | Yes | No | No | No | No | No |
Ezisi et al. (2017)72 | No | No | Yes | No | No | No | No | No | No | No | No |
Vera et al. (2017)75 | Yes | No | Yes | Yes | No | Yes | No | No | Yes | No | No |
Sachdeva et al. (2016)73 | No | No | Yes | Yes | No | Yes | No | No | No | No | No |
Lee et al. (2014)76 | No | No | No | No | Yes | No | No | No | No | No | No |
Shah et al. (2014)74 | No | No | Yes | Yes | No | Yes | No | No | Yes | No | No |
Kirwan et al. (2010)68 | No | No | Yes | Yes | No | Yes | No | No | No | No | No |
ECD = endothelial cell density; HRQoL = health-related quality of life; IATS = Infant Aphakia Treatment Study; INF = inflammatory; IO = intraoperative; PVD = posterior vitreous detachment; VA = visual acuity; VAO = visual axis opacification; VAOb = visual axis obscuration; VO = vitreous opacity.
Note that this appendix has not been copy-edited.
Table 7: Definitions of Glaucoma in Included Studies
Study citation | Definition of glaucoma |
|---|---|
RCTs | |
IOP > 21 mm Hg with “1) corneal enlargement; 2) asymmetrical progressive myopic shift coupled with enlargement of the corneal diameter and/or axial length; 3) increased optic nerve cupping defined as an increase of ≥ 0.2 in the cup-to-disc ratio, or 4) the use of a surgical procedure for IOP control” (p. 4)44 | |
Vasavada et al. (2018)60 | “Diagnosis required IOP >21 mm Hg, combined with at least 1 of the following:
|
Vasavada et al. (2017)61 | “Diagnosis required IOP >21 mmHg more than once with at least 1 [of the following]:
|
NRSs | |
Koch et al. (2021)62 | Based on IOP > 21 mm Hg using Perkins tonometer and fundoscopy (cup-to-disc ratio changes) |
Bothun et al. (2020)63 | Same at IATS definition, but not enforced “It was assumed that the enrolling clinicians for the TAPS used those same definitions in their diagnoses, which were gleaned from record review and were reported by the investigators based on these records.” (p. 502) |
Eder et al. (2020)64 | “Glaucoma was determined based on whether a diagnosis code with corresponding elevated IOP appeared in the chart” (p. 265) |
Lytvynchuk et al. (2020)66 | “Postoperative intraocular pressure was measured with two different methods depending on the compliance of the patients and whether the patient was awake or under general anesthesia. … postoperative intraocular hypertension was defined as IOP ≥ 12 mmHg measured with applanation tonometry Perkins Tonometer Mk2 … in general anesthesia or as IOP ≥ 20 mmHg with iCarePRO … in awake state. Secondary postoperative glaucoma on eyes operated with bag-in-the-lens technique was defined …as increase of IOP ≥ 22 mmHg measured at the beginning of the induction of general anesthesia [with Tonopen] … and presence of one or more following complications: buphthalmus [sic], enlarged cornea, corneal oedema, glaucomatous appearance of the optic disc, a myopic shift or an increase of axial length more than predicted based on individual growth curves” (p. e146) |
Murphy et al. (2020)67 | NR |
Solebo et al. (2020)69 | “Defined by the 2001 British Infantile and Childhood Glaucoma (‘BIG eye’) study group taxonomy
|
Valeina et al. (2020)70 | NR |
Ezisi et al. (2017)72 | NR |
Vera et al. (2017)75 |
|
Sachdeva et al. (2016)73 | “Glaucoma was defined as increase in the IOP (< 22 mm Hga), with the presence of increased optic nerve cupping and/or myopic refractive shift” (p.1261) |
Shah et al. (2014)74 |
|
Kirwan et al. (2010)68 | NR |
IATS = Infant Aphakia Treatment Study; IOP = intraocular pressure; mm Hg = millimetres of mercury; NRS = nonrandomized study; NR = not reported; p. = page; RCT = randomized controlled trial; TAPS = Toddler Aphakia and Pseudophakia Study.
aThe study69 reports the definition with a “less than” symbol. It is unclear if this is a typo.
Appendix 6: Critical Appraisal Tables
Table 8: Critical Appraisal of RCTs
Study citation | Bias arising from the randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcome | Bias in selection of the reported result | Overall risk of bias judgment |
|---|---|---|---|---|---|---|
Low | Effect of assignment to intervention: Low | VA 1 year (molecular grating): Low 5 years (HOTV): Low 10 years (E-ETDRS): Low Intraoperative complications: Low AEs 1 year: Low 5 years: Low 10 years: Low Glaucoma 1 year: Low 5 years: Low 10 years: Low Additional surgery 1 year: Low 5 years: Low 10 years: Low Parenting stress 3 months: Low 1 year: Low Strabismus 1 year: Low 5 years: Low Nystagmus 5 years: Low Corneal changes 5 years: SC | VA 1 year (molecular grating): Low 5 years (HOTV): Low 10 years (E-ETDRS): Low Intraoperative complications: SC AEs 1 year: SC 5 years: SC 10 years: SC Glaucoma 1 year: Low 5 years: Low 10 years: Low Additional surgery 1 year: SC 5 years: SC 10 years: SC Parenting stress 3 months: High 1 year: High Strabismus 1 year: Low 5 years: Low Nystagmus 5 years: Low Corneal changes 5 years: Low | High | High | |
Vasavada et al. (2018)60 | Low | Effect of adhering to intervention: Low | Inflammatory complications: High | Inflammatory complications: SC | High | High |
Vasavada et al. (2017)61 | Low | Effect of adhering to intervention: Low | Glaucoma: Low VAOb: Low Inflammatory complications: Low IOL centration: Low Cell deposits: Low | Glaucoma: Low VAOb: Low Inflammatory complications: Low IOL centration: Low Cell deposits: Low | High | High |
AE = adverse event; E-ETDRS = Electronic Early Treatment for Diabetic Retinopathy Study; IATS = Infant Aphakia Treatment Study; RCT = randomized controlled trial; SC = some concerns; VA = visual acuity; VAOb = visual axis obscuration.
Note that this appendix has not been copy-edited.
Table 9: Critical Appraisal of NRSs
Study citation | Risk of bias | ||||||||
|---|---|---|---|---|---|---|---|---|---|
The possibility of the target group comparisonsa | Target group selectionb | Confoundersc | Exposure measurementd | Blinding of assessorse | Outcome assessmentf | Incomplete outcome datag | Selective outcome reportingh | Overall risk of bias judgment | |
Koch et al. (2021)62 | UC | Low | VA: High VAO: High Glaucoma: High Strabismus: High IC: High Corectopia: High All other outcomes: High | Low | VA: UC VAO: UC Glaucoma: UC All other outcomes: Strabismus: UC IC: Low Corectopia: UC All other outcomes: UC | VA: Low VAO: Low Glaucoma: Low All other outcomes: Strabismus: Low IC: Low Corectopia: Low All other outcomes: UC | VA: UC VAO: UC Glaucoma: UC All other outcomes: Strabismus: UC IC: UC Corectopia: UC All other outcomes: UC | Low | High |
Bothun et al. (2020)63 | UC | UC | VA: High VAO: High | Low | VA: UC VAO: UC | VA: UC VAO: UC | VA: UC VAO: UC | Low | High |
Eder et al. (2020)64 | UC | UC | Glaucoma: High AS: High | Low | Glaucoma: UC AS: Low | Glaucoma: Low AS: Low | Glaucoma: UC AS: UC | High | High |
Lytvynchuk et al. (2020)66 | UC | UC | Intraoperative complications: High VAO: High Glaucoma: High IC: High IOL dislocation and Iris capture: High All other outcomes: High | Low | Intraoperative complications: Low VAO: UC Glaucoma: UC IC: UC IOL dislocation and Iris capture: UC All other outcomes: UC | Intraoperative complications: UC VAO: UC Glaucoma: Low IC: UC IOL dislocation and Iris capture: Low All other outcomes: UC | Intraoperative complications: UC VAO: UC Glaucoma: UC IC: UC IOL dislocation and Iris capture: UC All other outcomes: UC | High | High |
Murphy et al. (2020)67 | UC | UC | VA: High VAO: High Glaucoma: High Strabismus: High | Low | VA: UC VAO: UC Glaucoma: UC Strabismus: UC | VA: UC VAO: UC Glaucoma: UC Strabismus: UC | VA: UC VAO: UC Glaucoma: UC Strabismus: UC | High | High |
Solebo et al. (2020)69 | High | High | Glaucoma: Low | Low | Glaucoma: UC | Glaucoma: Low | Glaucoma: UC | Low | High |
Valeina et al. (2020)70 | Low | UC | Glaucoma: UC Secondary cataract: UC | Low | Glaucoma: UC Secondary cataract: UC | Glaucoma: UC Secondary cataract: UC | Glaucoma: UC Secondary cataract: UC | High | High |
Zhang et al. (2020)71 | High | High | PVD: High VO: High | Low | PVD: UC VO: UC | PVD: Low VO: Low | PVD: UC VO: UC | UC | High |
Jackson et al. (2019)65 | UC | UC | AS: UC | Low | AS: Low | AS: Low | AS: UC | UC | Unclear |
Ezisi et al. (2017)72 | Low | UC | VAO: High Glaucoma: High IOL capture: High | Low | VAO: UC Glaucoma: UC IOL capture: UC | VAO: UC Glaucoma: UC IOL capture: UC | VAO: High Glaucoma: High IOL capture: High | High | High |
Vera et al. (2017)75 | Low | High | VA: High Glaucoma: High VAO: High IC: High Endophthalmitis: High Retinal Detachment: High IOL-related complications: High | Low | VA: UC Glaucoma: UC VAO: UC IC: UC Endophthalmitis: UC Retinal Detachment: UC IOL-related complications: UC | VA: UC Glaucoma: UC VAO: UC IC: UC Endophthalmitis: UC Retinal Detachment: UC IOL-related complications: UC | VA: UC Glaucoma: UC VAO: UC IC: UC Endophthalmitis: UC Retinal Detachment: UC IOL-related complications: UC | Low | High |
Sachdeva et al. (2016)73 | UC | UC | VAO: High Glaucoma: High AS: High Uveitis: High | Low | VAO: UC Glaucoma: UC AS: Low Uveitis: UC | VAO: UC Glaucoma: UC AS: Low Uveitis: UC | VAO: UC Glaucoma: UC AS: UC Uveitis: UC | High | High |
Lee et al. (2014)76 | Low | Low | Strabismus: UC Nystagmus: UC | Low | Strabismus: UC Nystagmus: UC | Strabismus: UC Nystagmus: UC | Strabismus: UC Nystagmus: UC | Low | Unclear |
Shah et al. (2014)74 | High | Low | VAO: High Glaucoma: High AS: High IC: High Post-operative cell deposits: High | Low | VAO: UC Glaucoma: UC AS: UC IC: UC Post-operative cell deposits: UC | VAO: UC Glaucoma: Low AS: Low IC: UC Post-operative cell deposits: UC | VAO: UC Glaucoma: UC AS: UC IC: UC Post-operative cell deposits: UC: | Low | High |
Kirwan et al. (2010)68 | UC | UC | VAO: High Glaucoma: High AS: High | Low | VAO: UC Glaucoma: UC AS: UC | VAO: UC Glaucoma: Low AS: Low | VAO: UC Glaucoma: UC AS: UC | Low | High |
AS = additional surgery; IC = inflammatory complications; IOL = intraocular lens; NRS = nonrandomized study; PVD = posterior vitreous detachment; UC = unclear; VA = visual acuity; VAO = visual axis opacification; VO = vitreous opacity.
aRisk of selection bias due to selection of inappropriate comparison target group
bRisk of selection bias due to inappropriate intervention or inappropriate selection of patient group
cRisk of selection bias due to inappropriate confounder confirmation and consideration
dRisk of performance bias due to inappropriate intervention
eRisk of confirmation bias due to inappropriate blinding of assessors
fRisk of confirmation bias due to inappropriate outcome assessment methods
gRisk of attrition bias due to inappropriate handling of incomplete data
hRisk of reporting bias due to selective outcome reporting
Appendix 7: Results Tables
Note that this appendix has not been copy-edited.
Clinical Effectiveness
Table 10: Comparative Clinical Effectiveness of IOL Implantation Versus CLs — VA Results of IATS RCT by Follow-Up Time for Unilateral Cataracts
Detail | 1 year44 | 4.5 years45 | 10 years46 | |||
|---|---|---|---|---|---|---|
IOL (foldable) | CL | IOL (foldable) | CL | IOL (foldable) | CL | |
N of total sample | 57 eyes from 57 patients | 57 eyes from 57 patients | 55 eyes from 55 patients | 57 eyes from 57 patients | 55 eyes from 55 patients | 55 eyes from 55 patients |
Age at follow-up (years), mean | NR | 4.5 (range = 4.5 to 4.9) | 10.6 ± 0.3 in both groups | |||
Monocular MVA (treated eye) | ||||||
MVA, median (IQR) | 0.97 logMAR (0.80 to 1.10) | 0.80 logMAR (0.66 to 0.97) | 0.90 logMAR and 20/159 SE (0.40 to 1.73) | 0.90 logMAR and 20/159 SE (0.30 to 1.60) | 0.89 logMAR and 20/159 SE (0.38 to 1.38) | 0.86 logMAR and 20/145 SE (0.30 to 1.46) |
Between-group difference | 0.17a P = 0.19 | NR P = 0.54 | NR (99% CI, –0.54 to 0.47) P = 0.82b | |||
Patients categorized based on monocular VA (treated eye) | ||||||
N | — | — | — | — | 55 eyes from 55 patients | 57 eyes from 57 patients |
VA range (SE), n (%) | ||||||
20/20 to < 20/40 | — | — | — | — | 6 (11) | 13 (23) |
20/40 to < 20/80 | — | — | — | — | 14 (25) | 9 (16) |
20/80 to < 20/200 | — | — | — | — | 8 (15) | 7 (12) |
20/200 or worse | — | — | — | — | 27 (49) | 28 (49) |
Patients categorized based on monocular VA ranges (treated eye) | ||||||
VA range, n (%) | ||||||
0.30 logMAR; 20/40 SE or better | — | — | 12 (22) | 15 (27) | — | — |
1.00 logMAR; 20/200 SE or worse | — | — | 25 (44) | 25 (44) | — | — |
Additional details of analysis | Patients with > 1.00 logMAR, IOL vs. CL: P = 0.97 | |||||
CI = confidence interval; CL = contact lens; E-ETDRS = Electronic Early Treatment Diabetic Retinopathy Study; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; IQR = interquartile range; ITT = intention to treat; logMAR = logarithm of the minimum angle of resolution; NA = not applicable; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; SE = Snellen equivalent; VA = visual acuity; vs. = versus.
aLarger than the interval between Teller cards (0.15 logMAR) and smaller than the difference the study was designed to detect (0.20 logMAR).
bP value was reported as 0.44 in the caption of Figure 2 in the Lambert et al. (2020) publication. It is unclear which P value is correct.
Table 11: Comparative Clinical Effectiveness of IOL Implantation Versus Aphakia — VA Results of NRSs
Details | Bothun et al. (2020)63,a Follow-up: Up to 5.8 years | Murphy et al. (2020)67,b Follow-up: Up to 28 years | ||
|---|---|---|---|---|
IOL (foldable) 42 eyes from 22 patients | Aphakia (CL, glasses, or both) 136 eyes from 74 patients | IOL (NR if foldable) 62 eyes | Aphakia (NR if glasses and/or CL) 73 eyes | |
Median VA (logMAR) | 0.35 | 0.35 | — | |
P value | 0.42 | |||
Median VA (logMAR) | 0.35 | 0.35 (glasses only) | — | |
Treatment success achieved,c n (%) | — | 48 eyes (77.42%) | 31 eyes (42.47%) | |
P value | < 0.001 | |||
BCVA, n of analysis | — | 49 eyes from 49 patientsd | 44 eyes from 44 patientsd | |
Mean ± SD | 0.92 ± 0.47 | 0.98 ± 0.58 | ||
BCVA = best corrected visual acuity; CL = contact lens; IOL = intraocular lens; logMAR = logarithm of the minimum angle of resolution; NR = not reported; NRS = nonrandomized study; SD = standard deviation; VA = visual acuity; vs. = versus.
aThe Bothun et al. (2020)63 study included all bilateral cataracts.
bIn the Murphy et al. (2020)67 there were 50 (37%) eyes with unilateral cataracts and 85 (63%) eyes with bilateral cataracts.
cFinal BCVA of 0.3 logMAR or lower.
dA sample selected for subgroup analyses (i.e., 1 eye each from 1 patient, randomly selected from bilateral cataracts).
Table 12: Comparative Clinical Effectiveness of IOL Implantation Versus CLs — HRQoL (Caregiver Stress) Results of IATS RCT for Unilateral Cataracts
Details | IOL (foldable) Follow-up: 3 months57 | CL Follow-up: 3 months57 | IOL (foldable) Follow-up: 12 months57 | CL Follow-up: 12 months57 |
|---|---|---|---|---|
PSI (total score) | ||||
n of Analysis | 53 caregivers | 55 caregivers | — | |
Mean ± SD | 213.1 ± 36.8 | 197.4 ± 35.7 | ||
Additional Details of Analysis | Between-group difference = NR; P = 0.027 Cohen d = 0.42a; P = 0.006 | |||
OTI (total score) | ||||
Mean ± SD | 90.8 ± 13.1 | 82.6 ± 15.7 | — | |
Additional Details of Analysis | Between-group difference = NR; P = 0.003 Cohen d = 0.56a (higher stress in IOL group); P = 0.000 | |||
PSI (total score) (from caregivers with data at both the 3-month and 12-month follow-up) | ||||
n of Analysis | 38 caregivers | 43 caregivers | — | |
Mean ± SD | 208.0 ± 34.1 | 200.4 ± 37.8 | ||
Additional Details of Analysis | Between-group difference = NR; P = NR | |||
OTI (total score) (from caregivers with data at both the 3-month and 12-month follow-up) | ||||
n of Analysis | 37 caregivers | 43 caregivers | — | |
Mean ± SD | 91.0 ± 12.5 | 82.9 ± 15.7 | ||
Additional Details of Analysis | Between-group difference = NR; P = NR | |||
PSI subscales at 3 months follow-up57 | ||||
n of Analysis | IOL n = 53 caregivers; CL n = 55 caregivers | — | ||
Results | “…both Child Domain and Parent Domain scores were higher for caregivers of children in the IOL group than for caregivers of children in the CL group, but only the Child Domain test yielded a statistically significant result.” (p. 490) | |||
Additional Details of Analysis | Child domain sub scores of the PSI:
Score = NR and P = NS for other domains (i.e., Distractibility/Hyperactivity, Reinforces Parent, Mood, and Acceptability) | |||
PSI (total score) (from caregivers with data at both the 3-month and 12-month follow-up)b | ||||
n of Analysis | — | 38 caregiversc | 43 caregiversc | |
Mean ± SD | 208.3 ± 30.8 | 202.6 ± 34.4 | ||
P value | Between-group difference = NR; P = NR | |||
OTI (total score) (from caregivers with data at both the 3-month and 12-month follow-up)b | ||||
Mean ± SD | — | 93.6 ± 14.9 | 91.8 ± 19.1 | |
P value | Between-group difference = NR; P = NR | |||
Effect of time for PSI scores | ||||
Results (3 vs. 12 months) | — | Between-group difference = NR; P = NSd | ||
Effect of time for OTI scores | ||||
Results (3 vs. 12 months) | — | “The effect of time was only statistically significant for the OTI… with stress scores increasing over the two assessment points.” (p. 490) | ||
Between-group difference = NR; P < 0.01 | ||||
CL = contact lens; HRQoL = health-related quality of life; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; NA = not applicable; NR = not reported; NS = not significant; OTI = ocular treatment index; PSI = parenting stress index; SD = standard deviation; VA = visual acuity; vs. = versus.
aControlled for caregiver age at surgery.
bEffect sizes (Cohen d) and group differences in PSI and OTI total scores, as well as other statistics (e.g., F, df, and P value), were NR. No differences between groups (OTI or PSI) at post-VA assessment were reported (P = NR).
c9 and 6 patients were not included in the 12-month follow-up in the IOL and CL groups, respectively. In the IOL group, 8 were lost to follow-up for parenting stress, and 1 was evaluated outside the assessment window. In the CL group, 5 were lost to follow-up for parenting stress, and 1 was evaluated outside the assessment window.
d“There were no significant treatments by time interactions for any of the stress measures, suggesting that stress scores did not change differentially for participants assigned to IOL versus CL” (p. 490).
Table 13: Comparative Clinical Effectiveness of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — VA Results of NRSs for Foldable IOLs
Outcomes and age at surgery | Vera et al. (2017)75,a Follow-up: Up to 5 years | Koch et al. (2021)62,b Follow-up: Up to 14.4 years |
|---|---|---|
N | 61 eyes from 43 patients (mixed age) | 93 eyes from 68 patients (mixed age) 56 eyes (≤ 9 months and ≥ 19 months) |
Median VA, logMAR | ||
< 6 months | 0.50 | — |
6 to 12 months | 0.85 | |
≥ 12 months | 0.35 | |
Mean CDVA, logMAR ± SD (range) | ||
≤ 9 months | — | 0.44 ± 0.29 (0.1 to 1.1) |
≥ 19 months | 0.37 ± 0.37 (0.00 to 1.3) | |
P value | P = 0.085c | |
Eyes with poor VA vs. eyes with good VA, n (%)d | ||
< 6 months | 10/33 (30%) vs. 23/33 (70%) | — |
6 to 12 months | 10/16 (62.5%) vs. 6/16 (37.5%) | |
≥ 12 months | 4/12 (33.3%) vs. 8/12 (66.7%) | |
Age at surgery as a prognostic factor associated with poor visual outcome (Univariate analysis), OR (95% CI)d | ||
< 6 months | 0.84 (0.13 to 5.32) | — |
6 to 12 months | 3.28 (0.42 to 25.47) | |
≥ 12 months (reference group) | 1 (NR) | |
Difference between groups (P value) | P = 0.23 | |
Unilateral cataract, eyes with poor VA vs. eyes with good VA, n (%)d,e | ||
< 6 months | 7/12 (58%) vs. 5/12 (42%) | — |
6 to 12 months | 6/8 (75%) vs. 2/8 (25%) | |
≥ 12 months | 4/5 (80%) vs. 1/5 (20%) | |
Bilateral cataract, eyes with poor VA vs. eyes with good VA, n (%)d,e | ||
< 6 months | 3/21 (14%) vs. 18/21 (86%) | — |
6 to 12 months | 4/8 (50%) vs. 4/8 (50%) | |
≥ 12 months | 3/7 (43%) vs. 4/7 (57%) |
CI = confidence interval; logMAR = logarithm of the minimum angle of resolution; NR = not reported; NRS = nonrandomized study; OR = odds ratio; VA = visual acuity; vs. = versus.
aIn the Vera et al. (2017)75 study there were 25 (58%) patients with unilateral cataracts and 18 (42%) patients with bilateral cataracts.
bIn the Koch et al. (2021)62 study there were 43 eyes (46.2%) with unilateral cataracts and 50 eyes (53.8%) with bilateral cataracts.
cThis statistical comparison includes a third comparator group – 10 to 18 months of age. Comparison was done via ANOVA and found no statistically significant differences in the means of all 3 groups.
dEyes with poor VA were defined as eyes with > 0.5 logMAR, and eyes with good VA were defined as eyes with ≤ 0.5 logMAR on examination.
eStatistical comparisons of subgroups’ laterality were not performed due to lack of power.
Safety
Table 14: Safety of IOL Implantation — Results for Intraoperative Complications From IATS RCT for Unilateral Cataracts44,48,a
Outcomes | IOL (foldable) 57 eyes from 57 patients | CL 57 eyes from 57 patients |
|---|---|---|
Intraoperative complications (1 or more complications),44,48,b n (%) | 16 (28%)b | 6 (11%) |
P value | 0.031 | |
Intraoperative iris prolapse, n (%) | 12 (21%) | 2 (4%) |
P value | 0.008 | |
Hyphema, n (%) | 2 (4%) | 3 (5%) |
P value | NS | |
Iris damage, n (%) | 3 (5%) | 1 (2%) |
P value | NS | |
Retained cortex, n (%) | 1 (2%) | 1 (2%) |
P value | NS | |
Cloudy cornea, n (%) | 1 (2%) | 1 (2%) |
P value | NS | |
Iris sphincterotomy, n (%) | 1 (2%) | 0 (0%) |
P value | NS | |
Lens fragment in vitreous, n (%) | 1 (2%) | 0 (0%) |
P value | NS | |
Posterior capsule rupture, n (%) | 1 (2%) | 0 (0%) |
P value | NS | |
Intraoperative complications based on age at surgery, 48 n (%) | ||
< 49 days (n = 25 eyes from 25 patients) | 10 (40%) | 4 (16%) |
≥ 49 days (n = 32 eyes from 32 patients) | 6 (19%) | 2 (6%) |
P value | < 49 days vs. ≥ 49 days: 0.14 | < 49 days vs. ≥ 49 days: 0.39 |
Intraoperative complications (1 or more during the initial cataract surgery)47,c,d based on PFV Status, n of N (%) | ||
PFV (n = 18 eyes from 18 patients) | 2 of 7 (29%) | 1 of 11 (9%) |
no PFV (n = 65 eyes from 65 patients) | 10 of 34 (29%) | 5 of 31 (16%) |
Difference in proportions (95% CI); P value | No PFV vs. PFV: NR (–36% to 38%); 0.99 | No PFV vs. PFV: NR (–14% to 28%); 0.99 |
CI = confidence interval; CL = contact lens; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; NR = not reported; NS = not significant; PFV = persistent fetal vasculature; RCT = randomized controlled trial; vs. = versus.
aNo statistically significant difference in other intraoperative complications by 1 year of age was reported. P = NR for between-group comparisons.
bThis result is reported as n = 16 (21%) in Plager et al. (2011)48 and n = 16 (28%) in The Infant Aphakia Treatment Study Group (2010).44 It is believed that 21% is a typing error.
cIncluding iris prolapse, hyphema, iris damage, retained cortex, cornea cloudy, iris sphincterotomy, lens fragment in vitreous, and unintentional posterior capsule rupture.
dDifference in proportions between treatment groups was not reported.
Table 15: Safety of IOL Implantation — Results for AEs and Complications From IATS RCT at Various Follow-Up Timepoints for Unilateral Cataractsa
Outcomes and follow-up timepoint | IOL (foldable) | CL | P value | ||
|---|---|---|---|---|---|
Patients | Events | Patients | Events | ||
Total number of AEs48, n | |||||
1 Year | — | — | 22 | — | |
5 Yearsb | — | — | — | — | — |
10 Years | — | — | — | — | |
Patients with ≥ 1 AE, n (%)44, n (%) | |||||
1 Year | 88 | 14 (25%)48 (15 [26%] [22 events] in Plager et al. 201449) | < 0.0001 | ||
5 Yearsb | 46 (81%) | 108 | 32 (56%) patients (54 events) | 0.008 | |
10 Years | — | — | — | — | |
Annual rate of AEs based on number of AEs per year49 | |||||
1 Year | 1.6 | 0.4 | < 0.0001 | ||
5 Yearsb | — | — | — | ||
10 Years | — | — | — | ||
Lens reproliferation in visual axis, n (%) | |||||
1 Year | 24 (42%) (23 in Plager et al. [2014]49) | 24 (27 in Plager et al. [2014]49) | 1 (2%) | 1 | < 0.0001 |
5 Yearsb | 23 (40%) | 28 | 2 (4%) | 2 | — |
10 Years | 1 | — | 0 | 0 | — |
Retinal detachment, n (%) | |||||
1 Year | 0 | 0 | 2 (4%) | 2 | — |
5 Yearsb | 0 | 0 | 2 (4%) | 2 | — |
10 Years | 1 | — | 0 | 0 | — |
Retinal hemorrhage, n (%) | |||||
1 Year | 2 (4%) | 3 | 2 (4%) | 2 | — |
5 Yearsb | 3 (5%) | 3 | 2 (4%) | 2 | — |
10 Years | — | — | — | — | — |
Pupillary membranes, n (%) | |||||
1 Year | 17 (30%) (16 in Plager et al. [2014]49) | 0 | 0 | < 0.0001 | |
5 Yearsb | 16 (28%) | 25 | 2 (4%) | 2 | — |
10 Years | — | — | — | — | — |
Corectopia, n (%) | |||||
1 Year | 11 (19%) (13 in Plager et al. [2014],49 16 in clinical trial database81) | 11 (15 in Plager et al. [2014],49 16 in clinical trial database81) | 1 (2%) | 1 | P = 0.004 |
5 Yearsb | 16 (28%) | 19 | 1 (2%) | 1 | — |
10 Years | 5c | — | 0 | 0 | — |
CL related AEs (corneal abrasions, corneal ulcers, and episodes of keratitis), n (%) | |||||
1 Year | 0 | 0 | Abrasion: 1 (2%) Keratitis: 1 (2%) | NR | — |
5 Yearsb | NA | — | 10 (18%) | 18 | NA |
10 Years | Abrasion: 0 | 0 | Abrasion: 1 | — | — |
Retained cortex, n (%) | |||||
1 Year | 3 (5%) | 4 | 2 (4%) | 2 | — |
5 Yearsb | 3 (5%) | 4 | 2 (4%) | 2 | — |
10 Years | — | — | — | — | — |
Endophthalmitis, n (%) | |||||
1 Year | 0 | 0 | 1 (2%) | 1 | — |
5 Yearsb | 0 | 0 | 1 (2%) | 1 | — |
10 Years | — | — | — | — | — |
Phthisis bulbi, n (%) | |||||
1 Year | 0 | 0 | 1 (2%) | 1 | — |
5 Yearsb | 0 | 0 | 1 (2%) | 1 | — |
10 Years | — | — | — | — | — |
Corneal edema > 30 days, n (%) | |||||
1 Year | 1 (2%) | 1 | 0 | 0 | — |
5 Yearsb | 1 (2%) | 1 | 0 | 0 | — |
10 Years | — | — | — | — | — |
Wound leak / dehiscence, n (%) | |||||
1 Year | 1 (2%) | 1 | 0 | 0 | — |
5 Yearsb | 1 (2%) | 1 | 0 | 0 | — |
10 Years | — | — | — | — | — |
Corneal opacity due to tight contact lens, n (%) | |||||
1 Year | 0 | 0 | 1 (2%) | NR | — |
5 Yearsb | — | — | — | — | — |
10 Years | — | — | — | — | — |
Vitreous hemorrhage, n (%) | |||||
1 Year | 4 (7%) | 4 | 2 (4%) | 2 | — |
5 Yearsb | 5 (9%) | 5 | 2 (4%) | 2 | — |
10 Years | — | — | — | — | — |
Hyphema, n (%) | |||||
1 Year | 3 (5%) | 3 | 1 (2%) | 1 | — |
5 Yearsb | 4 (7%) | 5 | 1 (2%) | 1 | — |
10 Years | — | — | — | — | — |
Capsular phimosis, n (%) | |||||
1 Year | 0 | 0 | 1 (2%) | NR | — |
5 Yearsb | — | — | — | — | — |
10 Years | — | — | — | — | — |
IOL capture, n (%) | |||||
1 Year | — | — | — | — | — |
5 Yearsb | 1 (2%) | 1 | NA | NA | NA |
10 Years | — | — | — | — | — |
AE = adverse events; CL = contact lenses; IOL = intraocular lens; NA = not applicable; NR = not reported.
aNumber of eyes at 1 year follow-up were 57 and 57 in the IOL and CL group, respectively.44,48 Number of eyes at 5-year follow-up were 56 and 57 eyes in the IOL and CL group, respectively.5,45,49,55,56 Number of eyes in the 10 years follow-up were 55 and 55 in the IOL and CL group, respectively.46,50
bInformation in the publication at 1-year follow-up, the clinical trial database listing, and the information in the publication at 5-year follow-up appear to differ for some outcomes. Differences are noted where applicable.
cNone visually significant or requiring intervention.
Table 16: Safety of IOL Implantation — Results for AEs and Complications From IATS RCT in Postoperative Years 2 to 549
Outcomes | IOL n = 56 eyes from 56 patients | CL n = 57 eyes from 57 patients | P value | ||
|---|---|---|---|---|---|
Patients | Events | Patients | Events | ||
At least 1 AE, n (%) | 14 (25%) | 21 | 24 (42%) | 33 | 0.073 |
Lens reproliferation, n | 1 | 1 | 1 | 1 | — |
Pupillary membranes, n | 3 | 5 | 2 | 2 | — |
Corectopia, n | 4 | 4 | 0 | 0 | — |
Retained cortex, n | 0 | 0 b | 0 | 0 | — |
Retinal detachment, n | 0 | 0 b | 0 | 0 | — |
Endophthalmitis, n | 0 | 0 b | 0 | 0 | — |
Phthisis bulbi, n49 | 0 | 0 | 0 | 0 | — |
CL related AEs (corneal abrasions, corneal ulcers, and episodes of keratitis), n49 | NA | — | 7 | 14 | — |
Corneal edema > 30 days, n | 0 | 0 | 0 | 0 | — |
Wound leak/dehiscence, postoperative years 2 to 5, n | 0 | 0 | 0 | 0 | — |
Vitreous hemorrhage, n | 1 | 1 | 0 | 0 | — |
Retinal hemorrhage, n | 0 | 0 | 0 | 0 | — |
Hyphema, n | 1 | 2 | 0 | 0 | — |
IOL capture, n | 1 | 1 | — | — | — |
AE = adverse events; CL = contact lenses; IOL = intraocular lens.
Table 17: Safety of IOL Implantation — Results for AEs and Complications From IATS RCT in Patients of Different Ages at Time of Surgery
Outcomes | Age at surgery | P value | |
|---|---|---|---|
< 49 days (n = 25 eyes from 25 patients) | ≥ 49 days (n = 32 eyes from 32 patients)48 | ||
Any AE, n (%) | 23 (92%) vs. 21 (66%) | 7 (28%) vs. 7 (22%) | IOL < 49 days vs. ≥ 49 days: 0.026 CL < 49 days vs. ≥ 49 days: 0.76 |
Visual axis opacity, n (%) | 21 (84%) vs. 16 (50%) | 3 (12%) vs. 0 (0%) | IOL < 49 days vs. ≥ 49 days: 0.011 CL < 49 days vs. ≥ 49 days: 0.079 |
AE = adverse event; CL = contact lens; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; PFV = persistent fetal vasculature; RCT = randomized controlled trial; vs. = versus.
Table 18: Safety of IOL Implantation — VAO Results of NRSs
Details | Shah et al. (2014)74,a Follow-up: Up to 5 years | Bothun et al. (2020)63,b Follow-up: Up to 5.8 years | Kirwan et al. (2010)68,c Follow-up: Up to 26 years | Murphy et al. (2020)67,d Follow-up: Up to 28 years | ||||
|---|---|---|---|---|---|---|---|---|
IOL (foldable): 12 eyes | Aphakia (Spectacles or CLs): 25 eyes | IOL (foldable): 42 eyes from 22 patients | Aphakia (CL, glasses, or both): 136 eyes from 74 patients | IOL (NR if foldable): 67 eyes from 55 patients | Aphakia (NR if glasses and/or CL): 77 eyes from 45 patients | IOL (NR if foldable): 62 eyes | Aphakia (NR if glasses and/or CL): | |
n of Analysis | 12 eyes | 25 eyes | 22 eyes | 74 eyes | NR | NR | 49 eyes from 49 patientse | 44 eyes from 44 patientse |
VAO | ||||||||
n (%) | 7 | 2 | 7 (32%) | 6 (8%) | NR | NR | 34 (69.39%) | 18 (40.91%) |
Additional details of analysis | P = NR “incidence of … VAO was greater in pseudophakic eyes” (p. 2096)74 | P = 0.009 | P = 0.01 “The incidence of VAO was significantly higher in the pseudophakic group” (p. 55)68 | P = 0.006 RR of developing VAO = 0.5896 (95% CI, 0.3949 to 0.8803, in favour of aphakia) | ||||
Eyes with clear visual axis that persisted to end of follow-up | ||||||||
n (%) | 5 (41.67%) | 23 (92.00%) | — | — | — | |||
P value | NR | — | — | — | ||||
CI = confidence interval; IOL = intraocular lens; NA = not applicable; NR = not reported; NRS = nonrandomized study; RR = relative risk; VAO = visual axis opacification; VAOb = visual axis obscuration; vs. = versus.
aIn the Shah et al. (2014)74 study there were 5 (13.51%) eyes with unilateral cataracts and 32 (86.49%) eyes with bilateral cataracts.
bThe Bothun et al. (2020)63 study included all bilateral cataracts.
cIn the Kirwan et al. (2010)68 study there were 56 (50.9%) patient with unilateral cataracts and 44 (40%) patients with bilateral cataracts.
dIn the Murphy et al. (2020)67 there were 50 (37.04%) eyes with unilateral cataracts and 85 (62.96%) eyes with bilateral cataracts.
eA sample selected for subgroup analyses (i.e., 1 eye each from 1 patient, randomly selected from bilateral cataracts).
Table 19: Safety of IOL Implantation — Results for Glaucoma and Glaucoma Suspect From IATS RCT for Unilateral Cataracts
Details | Follow-up time | |||||
|---|---|---|---|---|---|---|
10 years53 | ||||||
IOL (foldable) | CL | IOL (foldable) | CL | IOL (foldable) | CL | |
n of Analysis | 57 eyes from 57 patients | 57 eyes from 57 patients | 56 eyes from 56 patientsa | 57 eyes from 57 patients | 55 eyes from 55 patients | 55 eyes from 55 patients |
Glaucoma | ||||||
n (%) | 7 (12%) patients; 95% CI, 5% to 24%51 | 3 (5%) patients; 95% CI, 1% to 15%51 | 11 (19%) eyes | 9 (16%) eyes | 12 (22%) eyes | 13 (25%) eyes |
Additional Details of Analysis | Difference in proportions: NR (95% CI, –3% to 17%) P = 0.32 | Difference in proportions: NR P = 0.81 | HR = 1.0 (95% CI, 0.5 to 2.3); P = NR | |||
Glaucoma suspect | ||||||
n (%) | 2 (4%) patients51 | 5 (9%) eyes | 11 (19%) eyes | 8 (15%) eyes | 13 (25%) eyes | |
P value | NR | NR | NR | |||
Combined glaucoma and suspected glaucoma | ||||||
n (%) | 9 (16%; 95% CI, 7% to 24%) patients | 5 (9%; 95% CI, 3% to 19%) patients | 16 (28%) eyes | 20 (35%) eyes | 20 (35%) eyes (20 [36%] in Plager et al.)50 | 26 (46%) eyes (26 [47%] in Plager et al.)50 |
Additional Details of Analysis | Difference in proportions: NR (95% CI, –5% to 19%) P = 0.39 | P = 0.55b | HR = 1.4 (95% CI, 0.8 to 2.5)c; P = 0.3350 | |||
Risk of glaucoma after cataract removal (Kaplan-Meier Analysis52,53) | ||||||
HR (95% CI) | — | 0.8 (0.3 to 2.0) | 1.0 (0.5 to 2.3) | |||
P value | 0.6252 | 0.9453 | ||||
Risk of glaucoma suspect diagnosis after cataract removal (Kaplan-Meier Analysis52,53) | ||||||
HR (95% CI) | — | 1.3 (0.6 to 2.5) | 1.3 (0.7 to 2.4) | |||
P value | 0.5852 | 0.3653 | ||||
CI = confidence interval; CL = contact lens; HR = hazard ratio; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; NR = not reported; SD = standard deviation; RCT = randomized controlled trial.
a1 patient was lost to follow-up at age 18 months.
b3 patients in each group progressed from glaucoma suspect to glaucoma.45
c4 eyes (1 IOL; 3 CL) progressed from glaucoma suspect to glaucoma between year 5 and year 10. 1 eye (CL) progressed from no glaucoma (normal) to glaucoma.50
Table 20: Safety of IOL Implantation — Glaucoma and Ocular Hypertension Results of NRSs
Details | Shah et al. (2014)74,a Follow-up: 5 years | Kirwan et al. (2010)68,b Follow-up: Up to 26 years | Murphy et al. (2020)67,c Follow-up: Up to 28 years | ||||
|---|---|---|---|---|---|---|---|
IOL (foldable) | Aphakia (spectacles or CLs) | IOL (NR if foldable) | Aphakia (NR if glasses and/or CL) | IOL (NR if foldable) | Aphakia (NR if glasses and/or CL) | ||
Secondary glaucoma | |||||||
n of Analysis | 12 eyes | 25 eyes | 55 eyes | 45 eyes | 49 eyesd | 44 eyesd | |
Eyes, n (%) | 2 (16.67%) | 14 (56.00%) | 7 (12.7%) | 15 (33.3%) | 10 (20.41%) | 19 (43.18%) | |
P value | NR | 0.02 | 0.018 | ||||
Glaucoma incidence | |||||||
Eyes, n (%) | — | 7 (12.7%) | 15 (33.3%) | 10 (20.41%) | 19 (43.18%) | ||
P value | — | 0.02 | 0.018 | ||||
Time to glaucoma diagnosis | |||||||
N of Total Sample | — | 67 eyes from 55 patients | 77 eyes from 45 patients | 62 eyes | 73 eyes | ||
Time (years), n | — | ||||||
0 to 1 | — | 5 | 7 | 5 | 7 | ||
1 to 2 | — | 1 | 3 | 2 | 3 | ||
2 to 3 | — | 1 | 3 | 1 | 3 | ||
3 to 4 | — | 0 | 0 | 0 | 1 | ||
4 to 5 | — | 0 | 0 | 2 | 1 | ||
5 to 6 | — | 0 | 2 | 0 | 2 | ||
6 to 7 | — | 0 | 3 | 0 | 4 | ||
7 to 8 | — | 0 | 1 | 0 | 1 | ||
8 to 9 | — | NR | NR | 1 | 0 | ||
9 to 10 | — | NR | NR | 0 | 2 | ||
10 to 11 | — | NR | NR | 0 | 0 | ||
11 to 12 | — | NR | NR | 0 | 2 | ||
12 to 13 | — | NR | NR | 0 | 1 | ||
13 to 14 | — | 0 | 1 | 1 | 1 | ||
14 to 15 | — | NR | NR | 0 | 0 | ||
15 to 16 | — | NR | NR | 0 | 0 | ||
16 to 17 | — | 0 | 3 | 0 | 3 | ||
17 to 18 | — | 0 | 1 | 0 | 1 | ||
Range | — | 3 to 26 months | 3 to 206 months | — | — | ||
Mean ± SD | — | 9 ± 9 months | 65 ± 70 months | 3.14 ± 4.2 | 6.56 ± 5.7 | ||
P value (mean comparison) | — | NR | 0.038 | ||||
Glaucoma incidence, patients age at surgery ≤ 2.5 months | |||||||
N of analysis | — | 33 | 36 | — | |||
n (%) | — | 7 (21.2%) | 15 (41.7%) | — | |||
P value | — | 0.08 | — | ||||
Glaucoma rate comparisons, patients age < 2.5 months at surgery | |||||||
N of analysis | — | — | NR | NR | |||
n (%) | — | — | NR | NR | |||
P value | — | — | 0.188 | ||||
Glaucoma rate comparisons at age < 6 weeks at surgery between IOL and aphakia groups | |||||||
N of analysis | — | — | NR | NR | |||
n (%) | — | — | NR | NR | |||
P value | — | — | 0.067 | ||||
Glaucoma incidence – All eyes (i.e., both eyes from bilateral cases included) | |||||||
N of analysis | — | — | 62 eyes | 73 eyes | |||
n (%) | — | — | 12 (19.4%) | 33 (45.2%) | |||
Glaucoma development between aphakic and IOL implanted groups compared to multiple risk factors | |||||||
RR (95% CI) | — | — | 2.1159 (1.1062 to 4.0473) | ||||
P value | — | — | 0.0235 | ||||
CI = confidence interval; IOL = intraocular lens; NA = not applicable; NR = not reported; NRS = nonrandomized study; RR = relative risk; SD = standard deviation; SG; secondary glaucoma; vs. = versus.
aIn the Shah et al. (2014)74 study there were 5 (13.51%) eyes with unilateral cataracts and 32 (86.49%) eyes with bilateral cataracts.
bIn the Kirwan et al. (2010)68 study there were 56 (50.9%) patients with unilateral cataracts and 44 (40%) patients with bilateral cataracts.
cIn the Murphy et al. (2020)67 study there were 50 (37.04%) eyes with unilateral cataracts and 85 (62.96%) eyes with bilateral cataracts.
dA sample selected for the subgroup analyses (i.e., 1 eye each from 1 patient, randomly selected from bilateral cataracts).
Table 21: Safety of IOL Implantation — Glaucoma and Ocular Hypertension Results of NRS Subgroup Analyses for Laterality and Multiple Risk Factors
Details | Solebo et al. (2020)69,a Follow-up: 5 years | Murphy et al. (2020)67,b Follow-up: Up to 28 years | ||||||
|---|---|---|---|---|---|---|---|---|
Unilateral IOL (NR if foldable) | Aphakia (NR if glasses and/or CL) | Bilateral IOL (NR if foldable) | Bilateral aphakia (NR if glasses and/or CL) | Unilateral IOL (NR if foldable)c | Unilateral aphakia (NR if glasses and/or CL)c | Bilateral IOL (NR if foldable)c | Bilateral aphakia (NR if glasses and/or CL)c | |
N | 47 eyes | 45 eyes | 116 eyes | 170 eyes | 36 eyes from 36 patients | 14 eyes from 14 patients | 13 eyes from 13 patients | 30 eyes from 30 patients |
n of analysis | 31 eyes | 42 eyes | 84 eyes | 160 eyes | 36 eyes from 36 patients | 14 eyes from 14 patients | 13 eyes from 13 patients | 30 eyes from 30 patients |
Number of patients with glaucoma | ||||||||
n (%) | — | 9 (25%) | 5 (35.7%) | 1 (7.7%) | 14 (46.7%) | |||
RR (95% CI) | — | 0.7125 (0.3657 to 1.3881) | 1.175 (0.5400 to 2.5595) | 0.2198 (0.0327 to 1.4792) | 1.96 (1.0926 to 3.5159) | |||
P value | NR | 0.3192 | 0.6836 | 0.1193 | 0.0240 | |||
Age at surgery, n of N (%); 95% CI) | ||||||||
0 to 4.25 weeks | 0 of 2 (0%; 0 to 66%) | 1 of 3 (33.3%; 6 to 79%) | 0 of 0 (0%; NA) | 2 of 5 (40%; 12 to 77%) | — | — | — | — |
4.3 to 8.5 weeks | 2 of 12 (16.7%; 5 to 45%) | 4 of 24 (16.7%; 7 to 37%) | 4 of 27 (14.8%; 6 to 32%) | 15 of 77 (19.5%; 12 to 30%) | — | — | — | — |
8.5 to 12.75 weeks | 0 of 3 (0%; 0 to 56%) | 3 of 8 (37.5%; 14 to 69%) | 2 of 8 (25%; 7 to 59%) | 7 of 34 (20.6%; 10 to 37%) | — | — | — | — |
12.8 to 26 weeks | 0 of 1 (0%; 0 to 79%) | 0 of 6 (0%; 0 to 39%) | 1 of 27 (3.7%; 1 to 18%) | 5 of 32 (15.6%; 7 to 32%) | — | — | — | — |
26.1 to 52 weeks | 1 of 13 (7.7%; 1 to 3) | 0 of 1 (0%; 0 to 79%) | 0 of 22 (0%; 0 to 15%) | 0 of 12 (0%; 0 to 24%) | — | — | — | — |
CI = confidence interval; IOL = intraocular lens; NA = not applicable; NR = not reported; NRS = nonrandomized study; RR = relative risk; SD = standard deviation; SG; secondary glaucoma; vs. = versus.
aIn the Solebo et al. (2020)69 study there were 92 (24.3%) eyes with unilateral cataracts and 286 (75.7%) eyes with bilateral cataracts.
bIn the Murphy et al. (2020)67 study there were 50 (37.04%) eyes with unilateral cataracts and 85 (62.96%) eyes with bilateral cataracts.c A sample selected for the subgroup analyses (i.e., 1 eye each from 1 patient, randomly selected from bilateral cataracts).
cA sample selected for the subgroup analyses (i.e., 1 eye each from 1 patient, randomly selected from bilateral cataracts).
Table 22: Safety of IOL Implantation — Results for Strabismus From IATS RCT at 1-Year Follow-Up for Unilateral Cataracts
Details | IOL (foldable) | CL |
|---|---|---|
N of Total Sample | 57 eyes from 57 patients | 57 eyes from 57 patients |
Cumulative percentage of patients developing strabismus within the first year after cataract surgery54 | ||
n of analysis | 57 eyes from 57 patients | 57 eyes from 57 patients |
n (%) | 38 (66.7%) patients | 42 (74.5%) patients |
Additional details of analysis | Cumulative percentage (combined groups): 70.4% Difference in proportion: NR P = 0.59 | |
Cumulative percentage of patients developing strabismus within the first year after cataract surgery (patients without strabismus at baseline)54 | ||
n of analysis (combined groups) | 86 eyes from 86 patients | |
n (%) | 45 (57.8%) patients | 41 (64.6%) patients |
Additional details of analysis | Cumulative percentage (combined groups): 60.7% Difference in proportion: NR P = 0.97 | |
Prevalence of strabismus at the 1-year follow-up (Total [patients with 12-month ocular alignment data]), n (%)54 | ||
n of analysis | 52 eyes from 52 patients | 53 eyes from 53 patients |
Results, n (%) | ||
Esotropia | 12 (23.1%) | 25 (47.2%) |
Exotropia: | 10 (19.2%) | 6 (11.3%) |
Hypertropia: | 1 (1.9%) | — |
Total | 23 (44.2%) | 31 (58.5%) |
Additional details of analysis | Among the patients with an IOL and with 1 or more AE, 30/48 (63%) had strabismus. 22/38 (58%) had strabismus in the IOL patients without an AE (P = 0.82) Proportion of patients with strabismus, IOL vs. CL: P = 0.14 | |
AE = adverse event; CL = contact lens; IATS = Infant Aphakia Treatment Study; IATSG = Infant Aphakia Treatment Study group; IOL = intraocular lens; NA = not applicable; RCT = randomized controlled trial; vs. = versus.
Table 23: Safety of IOL Implantation — Results for Strabismus, Nystagmus, and Sensorimotor Outcomes From IATS RCT for Unilateral Cataracts
Details | Follow-up time | ||||
|---|---|---|---|---|---|
1 year54 | |||||
IOL (foldable) | CL | IOL (foldable) | CL | ||
Orthotropia44 | |||||
n (%) of patients | NR (58%) | NR (38%) | — | — | |
P value | 0.051 | — | — | ||
Orthotropic at distance (patients with no strabismus surgery)45,55 | |||||
n | — | — | 56 eyes from 56 patientsa | 57 eyes from 57 patients | |
n of N (%) | — | — | 13 of 56 (23%)55 | 8 of 56 (14%)55 | |
P value | — | — | 0.3355 | ||
Orthophoric at near (patients with no strabismus surgery)45 | |||||
n | — | — | 56 eyes from 56 patientsa | 57 eyes from 57 patients | |
n of N (%) | — | — | 11of 56 (20%) | 11 of 57 (19%) | |
P value | — | — | 0.99 | ||
Orthophoric at distance (patients with no strabismus surgery)45 | |||||
n | — | — | 56 eyes from 56 patientsa | 57 eyes from 57 patients | |
n of N (%) | — | — | 14 of 56 (25%)45 | 8of 57 (14%)45 | |
P value | — | — | 0.1645 | ||
Strabismus surgery | |||||
n | — | — | 56 eyes from 56 patientsa | 57 eyes from 57 patients | |
n (%) | — | — | |||
P value | — | — | 0.70 (P = 0.57 in IATSG 2014)45 | ||
Nystagmus | |||||
n | — | — | 41 eyes from 41 patients | 39 eyes from 39 patients | |
n (%) | — | — | 16 (39%) | 14 (36%) | |
P value | — | — | 0.82 | ||
Saccadic oscillations | |||||
n of analysis | — | — | 40 eyes from 40 patients | 40 eyes from 40 patients | |
n (%) | — | — | 10/40 (25%) | 15/40 (38%) | |
P value | — | — | 0.33 | ||
AE = adverse event; CL = contact lens; IATS = Infant Aphakia Treatment Study; IATSG = Infant Aphakia Treatment Study group; IOL = intraocular lens; NA = not applicable; RCT = randomized controlled trial; vs. = versus.
a1 patient was lost to follow-up at age 18 months.
Table 24: Safety of IOL Implantation — Strabismus Results for Murphy et al. (2020)67
Details | IOL (NR if foldable): 62 eyes | Aphakia (NR if glasses and/or CL): 73 eyes |
|---|---|---|
Follow-up period | Up to 28 years | |
Laterality of cataracts, n (%) | Unilateral: 50 (37.04%) eyes; Bilateral: 85 (62.96%) eyes | |
Strabismus | ||
n of eyes in Analysis | 49 | 44 |
n (%) of eyes | 33 (67.35%) | 25 (56.82%) |
Strabismus surgery | ||
n (%) of eyes | 6 (12.24%) | 5 (11.36%) |
CL = contact lens; IOL = intraocular lens; NR = not reported; NRS = nonrandomized study.
Table 25: Safety of IOL Implantation — Results for Additional Surgeries From IATS RCT for Unilateral Cataractsa
Outcomes and follow-up timepoints | IOL (foldable) | CL | P value |
|---|---|---|---|
Number of additional surgeries between surgery and follow-up time, n of patients | |||
1 Year | 52 procedures (36 patients) (36 patients [49 procedures] in Plager et al. 201148) | 13 procedures (7 patients) (7 patients [10 procedures] Plager et al. 201148) | NR |
5 Yearsb | 66 | 17 | NR |
10 Years | 71 | 38 | NR |
Occurrence of at least 1 additional intraocular surgery (including secondary IOL placement), n (%) of patients | |||
1 Year | 36 (63%) | 7 (12%) | < 0.0001 |
5 Yearsb | 41 (72%) | 12 (21%) | < 0.001 |
10 Years | — | — | — |
At least 1 additional surgery (not including secondary IOL placement)49, n (%) of patients | |||
1 Year | 41 (72%) | 9 (16%) | < 0.0001 |
5 Yearsb | — | — | — |
10 Years | — | — | — |
Clearing visual axis opacities, n (%) of patients | |||
1 Year | 34 (60%) | 6 (11%) | NR |
5 Yearsb | 39 (68%) | 8 (14%) | NR |
10 Years | — | — | — |
Clearing pupil-related visual axis opacities, n (%) of patients | |||
1 Year | 34 (60%) | 4 (7%) | < 0.0001 |
5 Yearsb | NR | NR | NR |
10 Years | — | — | — |
Glaucoma surgery, n (%) of patients | |||
1 Year | 4 (7%) | 1 (2%) | NR |
5 Yearsb | 5 (9%) | 2 (4%) | NR |
10 Years | — | — | — |
Secondary IOL placement, n (%) of patients | |||
1 Year | NA | NR | NA |
5 Yearsb | NA | NR | NA |
10 Years | NR | NR | NR |
Repair retinal detachment, n (%) of patients | |||
1 Year | 0 (0%) | 2 (4%) | NR |
5 Yearsb | 0 (0%) | 2 (4%) | NR |
10 Years | — | — | — |
Repair wound dehiscence, n (%) of patients | |||
1 Year | 1 (2%) | 0 (0%) | NR |
5 Yearsb | 1 (2%) | 0 (0%) | NR |
10 Years | — | — | — |
IOL exchange, n (%) of patients | |||
1 Year | 1 (2%) | NA | NA |
5 Yearsb | 3 (5%) | NA | NA |
10 Years | — | — | — |
Iridectomy or iridotomy, n (%) of patients | |||
1 Year | 1 (2%) | 1 (2%) | NR |
5 Yearsb | 1 (2%) | 1 (2%) | NR |
10 Years | — | — | — |
Scleral patch graft, n (%) of patients | |||
1 Year | 1 (2%) | 0 (0%) | NR |
5 Yearsb | — | — | — |
10 Years | — | — | — |
Lysis of vitreous wick, n (%) of patients | |||
1 Year | — | — | — |
5 Yearsb | 1 (2%) | 0 (0%) | NR |
10 Years | — | — | — |
Laser treatment of lattice degeneration by 1 year of age, n (%) of patients | |||
1 Year | 0 (0%) | 1 (2%) | NR |
5 Yearsb | — | — | — |
10 Years | — | — | — |
aNumber of eyes at 1 year follow-up were 57 and 57 in the IOL and CL group, respectively.44,48 Number of eyes at 5-year follow-up were 56 and 57 eyes in the IOL and CL group, respectively.5,45,49,55,56 Number of eyes in the 10 years follow-up were 55 and 55 in the IOL and CL group, respectively.46,50
b1 patient was lost to follow-up at age 18 months.
Table 26: Safety of IOL Implantation — Results for Additional Surgeries From IATS RCT for Unilateral Cataracts
Outcomes | Postoperative years 2 to 549 | |||||
|---|---|---|---|---|---|---|
IOL n = 56 eyes from 56 patients | CL n = 57 eyes from 57 patients | P value | IOL n = 55 eyes from 55 patients | CL n = 55 eyes from 55 patients | P value | |
Number of additional surgeries, n | 8 | 4 | NR | 6 | 25 | NR |
Clearing visual axis opacities, n | 8 | 3 | NR | 0 | 0 | NR |
Glaucoma surgery, n | 2 | 1 | NR | 1 | 4 | NRc |
Secondary IOL placement, n | NA | 3 (5%)45 | NA | NA | 21 procedures | NA |
Repair retinal detachment, n | 0 | 0 | NA | 1 | 0 | NR |
Repair wound dehiscence, n | NR | NR | NR | 0 | 0 | NR |
IOL exchange, n | 2 | NA | NA | 4 | NA | NA |
Iridectomy or iridotomy, n | 0 | 0 | NA | 0 | 0 | NR |
Lysis of vitreous wick, n | 0 | 0 | NA | 0 | 0 | NR |
CI = confidence interval; CL = contact lens; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; ITT = intention to treat; NA = not applicable; PFV = persistent fetal vasculature; RCT = randomized controlled trial; vs. = versus.
Table 27: Safety of IOL Implantation — Additional Surgeries and Reoperations Results of NRSs
Details | Jackson et al. (2019)65,a Follow-up: 3 months | Shah et al. (2014)74,b Follow-up: 5 years | Kirwan et al. (2010)68,c Follow-up: Up to 26 years | |||
|---|---|---|---|---|---|---|
IOL (NR if foldable): 183 eyes (mixed age) | Aphakia (NR if glasses and/or CL): 284 eyes (mixed age) | IOL (foldable): 12 eyes | Aphakia (Spectacles or CLs): 25 eyes | IOL (NR if foldable): 67 eyes from 55 patients | Aphakia (NR if glasses and/or CL): 77 eyes from 45 patients | |
Endophthalmitis reoperation | ||||||
n (%) | 0 (0%) | 0 (0%) | — | — | ||
Lens cortex reproliferation reoperations | ||||||
n (%) | 4 (2.2%) eyes | 8 (2.8%) eyes | — | — | ||
Additional Details of Analysis | P = NR A total of 25 cases (52.1% of total [n = 48]) of early and unanticipated reoperations occurred in IOL implanted and patients with aphakia that underwent cataract-related surgery at age < 1 year | |||||
Surgery to clear visual axis | ||||||
n of N (%) | — | 5 of 12 (41.67%) eyes | 1 of 25 (4.00%) eyes | — | ||
Additional Details of Analysis | P = NR Median follow-up = 17.6 months | |||||
Procedures to remove VAO (YAG laser capsulotomy or AV) | ||||||
Mean ± SD (range) | — | — | 2.0 ± 1.4 (1 to 7) | 1.2 ± 0.4 (1 to 2) | ||
AV = anterior vitrectomy; IOL = intraocular lens; NA = not applicable; NR = not reported; NRS = nonrandomized study; SD = standard deviation; VAO = visual axis opacification; vs. = versus; YAG = yttrium aluminum garnet.
aIn the Jackson et al. (2019)65 study, the number and proportion of eyes or patients with unilateral and bilateral cataracts were not reported.
bIn the Shah et al. (2014)74 study there were 5 (13.51%) eyes with unilateral cataracts and 32 (86.49%) eyes with bilateral cataracts.
cIn the Kirwan et al. (2010)68 study there were 56 (50.9%) patients with unilateral cataracts and 44 (40%) patients with bilateral cataracts.
Table 28: Safety of IOL Implantation — VAO Removal in Patients Aged 1 Year or Younger and 2.5 Months or Younger at Time of Cataract Surgery of Kirwan et al. (2010)68 NRSa
Details | ≤ 1 year of age at cataract surgery | ≤ 2.5 months of age at cataract surgery | ||
|---|---|---|---|---|
IOL (NR if foldable): | Aphakia (NR if glasses and/or CL): | IOL (NR if foldable): | Aphakia (NR if glasses and/or CL): | |
n of N (%) eyes | 30 of 55 (54.5%) | 13 of 45 (28.9%) | 18 of 33 (54.5%) | 13 of 36 (36.1%) |
P value | 0.01 | 0.15 | ||
AV = anterior vitrectomy; IOL = intraocular lens; NA = not applicable; NR = not reported; NRS = nonrandomized study; SD = standard deviation; VAO = visual axis opacification; vs. = versus; YAG = yttrium aluminum garnet.
aOne eye selected randomly for the analysis of bilateral cataracts. The Kirwan et al. (2010)68 study had a follow-up period of up to 26 years. In the Kirwan et al. (2010)68 study there were 56 (50.9%) patients with unilateral cataracts and 44 (40%) patients with bilateral cataracts.
Table 29: Safety of IOL Implantation — Results for Corneal Changes From IATS RCT for Unilateral Cataracts at 5-year Follow-up59,a
Details | IOL (foldable): 53 eyes from 53 patientsb | CL: 52 eyes from 52 patientsb |
|---|---|---|
EC density | ||
n of analysis | 45 eyes | 43 eyes |
Mean ± SD | 3,470 ± 601 cells/mm2 | 3,893 ± 582 cells/mm2 |
Difference between means (95% CI) | 423 (173 to 674) | |
P value | 0.0012 | |
CV of cell area | ||
n of Analysis | 45 eyes | 43 eyes |
Mean ± SD | 25 ± 4 | 27 ± 4 |
Difference between means (95% CI) | 2 (0.7 to 4) | |
P value | 0.0053 | |
% Hexagonal cells | ||
n of Analysis | 44 eyes | 43 eyes |
Mean ± SD | 74 ± 7% | 72 ± 7% |
Difference between means (95% CI) | –3 (−6 to 0.1) | |
P value | 0.056 | |
Corneal thickness | ||
n of Analysis | 49 eyes | 48 eyes |
Mean ± SD (μm) | 605 ± 49 | 638 ± 53 |
Difference between means (95% CI) | 33 (12 to 54) | |
P value | 0.0020c | |
Corneal thickness with additional surgery vs. without additional surgery | ||
n of Analysis | NR | |
Mean (μm) | 614 vs. 571 | 638 vs. 638 |
P value | 0.096 | |
CI = confidence interval; CL = contact lens; CV = coefficient of variation; EC = endothelial cell; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; SD = standard deviation; RCT = randomized controlled trial; vs. = versus.
aMean age at follow-up = 5.0 years (SD 0.1 years; range 4.7 to 5.4 years). Mean length of follow-up = 4.8 years (SD 0.1 years; range 4.4 to 5.3 years).
bEight patients, who were examined at age 5, did not have any specular microscopy or corneal thickness measurements (3 and 5 were in the IOL and CL group, respectively). Of the 113 patients available for the 5-year follow-up, 80 (71%) had digitizable specular microscopy images of both eyes, 8 (7%) had images of only the treated eye, 8 (7%) had images of only the fellow eye, and 17 (15%) had no images of either eye. Of the 17 patients without images for either eye, 8 and 9 were in the IOL and CL group, respectively.
cOf patients with specular microscopy or corneal thickness data, 10 of 52 (19%) CL patients and 39 of 53 (74%) IOL patients had additional surgery. The effects of additional surgery included “lower cell density, greater CV of cell area, lower percent hexagonal cells, and greater corneal thickness in both groups” (p. 5).
Table 30: Safety of IOL Implantation — Other Safety Outcomes Results of RCTs and NRSs
Details | Zhang et al. (2020)71 – NRSa Follow-up: 12 months | Shah et al. (2014)74 – NRSb Follow-up: 5 years | Vasavada et al. (2018)60 – RCTc Follow-up: 5 years | Sachdeva et al. (2016)73 – NRSd Follow-up: 5 years | ||||
|---|---|---|---|---|---|---|---|---|
IOL (NR if foldable) | Aphakia (NR if glasses and/or CL) | IOL (foldable) | Aphakia (spectacles or CLs) | IOL (foldable) | Aphakia (CL, glasses, or both) | IOL (NR if foldable) | Aphakia (NR if glasses and/or CL) | |
N of Total Sample | 57 eyes (mixed age) | 74 eyes | 12 eyes | 25 eyes | 58 eyes from 29 patients (mixed age) | 50 eyes from 25 patients (mixed age) | 570 eyes (mixed age) | 244 eyes (mixed age) |
PVD (B-scan) in patients between 6 and 12 months of age at cataract surgery, n | ||||||||
n of Analysis | 15 eyes | 14 eyes | — | — | — | |||
n | 2 patients (1 patient at 1-month; 1 at 1 year follow-up) Another 2 patients had normal scans, NR for others) | 1 patient (at 1-year follow-up) | ||||||
VO (B-scan) incidence in patients between 6 and 12 months of age at cataract surgery, n (%) (events) | ||||||||
Age at surgery, n (%) | ||||||||
1 month | 2 (14.3%) | 0 (0%) | — | — | — | |||
3 months | 6 (42.9%), | 1 (6.7%) | ||||||
6 months | 8 (57.1%) | 3 (20.0%) | ||||||
9 months | 10 (71.4%) | 3 (20.0%) | ||||||
12 months | 10 (71.4%) | 5 (33.3%) | ||||||
Posterior synechiae (rubella congenital cataract patients) | ||||||||
n (%) | — | 10 (83.33) | 12 (48.00%) | — | — | |||
Posterior synechiae (of first-operated eye) in patients ≤ 5.7 months of age at cataract surgery | ||||||||
n (%, eyes) | — | — | 5 of 8 (62.5%) | 2 | — | |||
Uveitis | ||||||||
n of analysis | — | — | — | 104 eyes | 204 eyes | |||
n of N (%) (eyes) | 10 of 104 (9.6%) | 1 of 204 (0.4%) | ||||||
P value | 0.0001 | |||||||
IOL = intraocular lens; NA = not applicable; NR = not reported; NRS = nonrandomized study; PVD = posterior vitreous detachment; RCT = randomized controlled trial; VO = vitreous opacity; vs. = versus.
aIn the Zhang et al. (2020)71 study, the number and proportion of eyes or patients with unilateral and bilateral cataracts were not reported but only right eyes of bilateral cataract patients included.
bIn the Shah et al. (2014)74 study there were 5 (13.51%) eyes with unilateral cataracts and 32 (86.49%) eyes with bilateral cataracts.
cThe Vasavada et al. (2018)60 study included all bilateral cataracts.
dIn the Sachdeva et al. (2016)73 study, the number and proportion of eyes or patients with unilateral and bilateral cataracts were not reported.
Table 31: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — Intraoperative Complications up to 1 Year Follow-up of a NRS that Used the BIL Surgical Technique66,a
Outcome | Age at surgery (months) | P value | ||
|---|---|---|---|---|
0 to < 3 n = 10 | 3 to < 12 n = 21 | 12 to < 36 n = 19 | ||
Vitreous prolapse, n (%) | 2 (20%) | 6 (28.6%) | 9 (47.4%) | NS |
Iris hemorrhage, n (%) | 0 (0%) | 1 (4.8%) | 0 (0%) | NS |
Iris prolapse, n (%) | 0 (0%) | 2 (9.5%) | 0 (0%) | NS |
Iris capture, n (%) | 0 (0%) | 0 (0%) | 1 (5.3%) | NS |
Anterior capsule rupture, n (%) | 0 (0%) | 6 (28.6%) | 3 (15.8%) | NS |
Posterior capsule rupture, n (%) | 0 (0%) | 0 (0%) | 2 (10.5%) | NS |
BIL IOL dislocation after implantation, n (%) | 0 (0%) | 0 (0%) | 0 (0%) | NS |
Mo = month; NRS = nonrandomized study; NS = not significant; vs. = versus.
aIn the Lytvynchuk et al. (2020)66 there were a total of 90 eyes from 60 patients. There were 27 (45%) patients with unilateral cataracts and 33 (55%) patients with bilateral cataracts
Table 32: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — VAO Results of RCTs and NRSs
Details | Vasavada et al. (2017)61 – RCTa Follow-up: 1 year | Lytvynchuk et al. (2020)66 – NRSb Follow-up: Up to 1 year | Sachdeva et al. (2016)73 – NRSc Follow-up: 5 years | Vera et al. (2017)75 – NRSd Follow-up: Up to 5 years | Ezisi et al. 201772 – NRSe Follow-up: Up to 11 years | Koch et al. (2021)62 – NRSf Follow-up: Up to 14.4 years | |
|---|---|---|---|---|---|---|---|
Intervention | IOL (foldable) – Group 1: IOL with AV; Group 2: optic capture of IOL with no AV) | IOL (BIL; foldable) | IOL (NR if foldable) | IOL (foldable) | IOL (foldable) | IOL (foldable) | |
N of total sample | 61 eyes from 61 patients (mixed age) Group 1: n = 30 eyes / Group 2: 26 eyesg | 90 eyes from 60 patients (mixed age) | 570 eyes (mixed age) | 61 eyes from 43 patients (mixed age) | 19 eyes from 16 patients (mixed age) | 93 eyes from 68 patients (mixed age) | |
Age at surgery comparison | ≤ 1 year vs. > 1 to ≤ 4 years | 0 to < 3 months vs. 3 to < 12 months vs. 12 to < 36 months | < 1 year vs. > 1 year | < 6 months vs. 6 to 12 months vs. > 12 months | ≤ 12 months vs. < 12 months | ≤ 9 months vs. ≥ 19 to 24 months | < 1 year vs. ≥ 1 year to 2 years |
n of Analysis | NR | 10 eyes vs. 21 eyes vs. 19 eyes | 104 eyes vs. 466 eyes | NR | 13 eyes vs. 6 eyes | 22 eyes vs. 34 eyes | 93 eyes from 68 patients |
Cumulative incidence of postoperative VAOb | |||||||
Age at surgery and group number (6- and 12-month follow-up),h n | |||||||
Age ≤ 1 year, Group 1 | 1 | — | — | — | — | — | |
Age ≤ 1 year, Group 2 | 13 | — | — | — | — | — | |
Age > 1 to ≤ 4 years, Group 1 | 0 | — | — | — | — | — | |
Age > 1 to ≤ 4 years, Group 2 | 16 | — | — | — | — | — | |
VAO | |||||||
Age at surgery, n (%) | |||||||
0 to < 3 months | — | 2 (20%) eyes | — | — | — | — | — |
3 to < 12 months | — | 1 (4.8%) eye | — | — | — | — | — |
P value (all comparisons) | — | NS | — | — | — | — | — |
Age at surgery | |||||||
< 1 year | — | — | 8 (7.7%) eyes | — | — | — | — |
> 1 year | — | — | 4 (0.85%) eyes | — | — | — | — |
Age at surgery | |||||||
≤ 12 months | — | — | — | — | 2 of 13 eyes | — | — |
> 12 months | — | — | — | — | 1 of 6 eyes | — | — |
Age at surgery | |||||||
≤ 9 months | — | — | — | — | — | 5 eyesi | — |
≥ 19 to 24 months: | — | — | — | — | 2 eyes | — | |
P value | — | — | — | — | 0.109j | — | |
Age at surgery | |||||||
< 1 year | — | — | — | — | — | — | 8 eyes (8.6%) (7 eyes in Table of study)62 |
≥ 1 year to 2 years | — | — | — | — | — | — | 5 eyes (5.4%) (6 eyes in Table of study)62 |
Lens proliferation into the visual axis < 6 months vs. 6 to 12 months vs. > 12 months | |||||||
Age at surgery | |||||||
< 6 months | — | — | — | 54% | — | — | |
6 to 12 months | 56% | ||||||
> 12 months | 50% | ||||||
Post-operative corneal opacification | |||||||
Age at surgery, n (%) | |||||||
0 to < 3 months | — | 2 (20%) | — | — | — | — | |
3 to < 12 months | 0 | ||||||
12 to < 36 months | 0 | ||||||
P Value (all comparisons) | NS | ||||||
AV = anterior vitrectomy; IOL = intraocular lens; IQR = interquartile range; NA = not applicable; NRS = nonrandomized study; NS = not significant; RCT = randomized controlled trial; VAO = visual axis opacification; VAOb = visual axis obscuration; vs. = versus.
aIn the Vasavada et al. (2017)61 study there were 37 eyes with unilateral cataracts and 24 eyes with bilateral cataracts. Only the first-operated eye was included from patients with bilateral cataracts.
bIn the Lytvynchuk et al. (2020)66 there were 27 (45%) patients with unilateral cataracts and 33 (55%) patients with bilateral cataracts. Of 3 cases of bilateral cataract, only 1 eye was operated with the bag-in-the-lens technique.
CIn the Sachdeva et al. (2016)73 study, the number and proportion of eyes or patients with unilateral and bilateral cataracts were not reported.
dIn the Vera et al. (2017)75 study there were 25 (58.00%) patients with unilateral cataracts and 18 (42.00%) patients with bilateral cataracts.
eIn the Ezisi et al. 201772 study there were 16 (72.7%) patients with unilateral cataracts and 6 (27.3%) patients with bilateral cataracts.
fIn the Koch et al. (2021)62 study there were 43 eyes (46.2%) with unilateral cataracts and 50 eyes (53.8%) with bilateral cataracts.
gIn Group 2, optic capture could not be achieved in 5 of 31 eyes randomized to that group.
hResults for 6- and 12-month follow-up were identical.
Table 33: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — Glaucoma Results of RCTs and NRSs
Details | Vasavada et al. (2017)61 – RCTa Follow-up: 1 year | Lytvynchuk et al. (2020)66 – NRSb Follow-up: Up to 1 year | Sachdeva et al. (2016)73 – NRSc Follow-up: 5 years | Solebo et al. (2020)69 – NRSd Follow-up: Up to 5 years | Vera et al. (2017)75 – NRSe Follow-up: Up to 5 years | Valeina et al. (2020)70 – NRSf Follow-up: Up to 10 years | Ezisi et al. 201772 – NRSg Follow-up: Up to 11 years | Eder et al. (2020)64 – NRSh Follow-up: Up to 18 years | Koch et al. (2021)62 – NRSi Follow-up: Up to 14.4 years |
|---|---|---|---|---|---|---|---|---|---|
Intervention | IOL (foldable) – Group 1: IOL with AV; Group 2: optic capture of IOL with no AV): 61 eyes from 61 patients (mixed age) Group 1: 30 eyes Group 2: 26 eyesj | IOL (BIL; foldable): 90 eyes from 60 patients (mixed age) | IOL (NR if foldable): 570 eyes (mixed age) | IOL (NR if foldable): 378 eyes from 235 patients (mixed age and intervention) 163 IOL implanted eyes | IOL (foldable): 61 eyes from 43 patients (mixed age) | IOL (foldable): 137 eyes from 85 patients (mixed age) | IOL (foldable): 19 eyes (mixed age) | IOL (NR if foldable): 46 eyes from 46 patients (mixed age) | IOL (foldable): 93 eyes from 68 patients (mixed age) |
Age at Surgery Comparison | ≤ 1 year vs. > 1 to ≤ 4 years | 0 to < 3 months vs. 3 to < 12 months vs. 12 to < 36 months | < 1 vs. > 1 year | 0 to 4.25 weeks vs. 4.3 to 8.5 weeks vs. 8.5 to 12.75 weeks vs. 12.8 to 26 weeks vs. 26.1 to 52 weeks vs. > 52.1 weeks to 2 years | < 6 vs. 6 to 12 vs. ≥ 12 months | 13 to 24 months vs. 25 to 48 months vs. 49 to 84 months vs. 85 to 216 months | ≤ 12 months vs. < 12 months | 0 to 5 months vs. 6 to 23 months vs. 24 to 72 months | ≤ 9 months vs. ≥ 19 to 24 months |
Number of Patients or Proportion of Patients with Glaucoma or Intraocular Hypertension | |||||||||
n | NR | 10 eyes vs. 21 eyes vs. 19 eyes | 104 eyes vs. 466 eyes | Bilateral: 0 vs. 27 vs. 8 vs. 27 vs. 22 vs. 5 Unilateral: 2 vs. 12 vs. 3 vs. 1 vs. 13 vs. 15 | — | — | — | 10 vs. 8 vs. 28 | 22 eyes vs. 34 eyes |
n (%) | 2 eyes | Glaucoma: 1 (10%) vs. 1 (4.8%) vs. 0 (0%) Hypertension: 2 (20%) vs. 1 (4.8%) vs. 2 (10.5%) | 6 (5.7%) eyes vs. 3 (0.21%) eyes | — | 3 (30%) vs. 2 (25%) vs. 4 (20%) | 0 vs. 0 | |||
Laterality, n (%, 95% CI) | |||||||||
Unilateral | — | 0 (0%, 0 to 66%) vs. 2 (16.7%, 5 to 45%) vs. 0 (0%, 0 to 56%) vs. 0 (0%, 0 to 79%) vs. 1 (7.7%, 1 to 33%) vs. 0 (0%, 0 to 20%) | — | — | — | — | |||
Bilateral | 0 (%) vs. 4 (14.8%, 6 to 32%) vs. 2 (25%, 7 to 59%) vs. 1 (3.7%, 1 to 18%) vs. 0 (0%, 0 to 15%) vs. 0 (0%, 0 to 43%) | ||||||||
P value | NS for both | NR | — | NA | |||||
Glaucoma Incidence | |||||||||
n of analysis | — | — | — | — | 33 vs. 12 | — | — | — | — |
n (%) | 7 (21.21%) eyes vs. 0 eyes vs. 0 eyes | ||||||||
Secondary Glaucoma | |||||||||
n of analysis | — | — | — | — | — | 19 eyes from 12 patients, vs. 10 eyes from 6 patients vs. 12 eyes from 7 patients vs. 27 eyes from 20 patients vs. 27 eyes from 17 patients | 13 eyes vs. 6 eyes | — | — |
n | 6 vs. 0 vs. 0 vs. 1 vs. 0 | 1 eye vs. 0 eyes | |||||||
P value | None | None | |||||||
CI = confidence interval; IOL = intraocular lens; NA = not applicable; NRS = nonrandomized study; NS = not significant; OR = odds ratio; RCT = randomized controlled trial; SG = secondary glaucoma; vs. = versus.
aIn the Vasavada et al. (2017)61 study there were 37 eyes with unilateral cataracts and 24 eyes with bilateral cataracts. Only the first-operated eye was included from patients with bilateral cataracts.
bIn the Lytvynchuk et al. (2020)66 there were 27 (45%) patients with unilateral cataracts and 33 (55%) patients with bilateral cataracts. Of 3 cases of bilateral cataract, only 1 eye was operated with the bag-in-the-lens technique.
cIn the Sachdeva et al. (2016)73 study, the number and proportion of eyes or patients with unilateral and bilateral cataracts were not reported.
dIn the Solebo et al. (2020)69 study there were 92 (24.3%) eyes with unilateral cataracts and 286 (75.7%) eyes with bilateral cataracts.
eIn the Vera et al. (2017)75 study there were 25 (58.00%) patients with unilateral cataracts and 18 (42.00%) patients with bilateral cataracts.
fIn the Valeina et al. (2020)70 there were 30 (22%) eyes with unilateral cataracts and 107 (78%) eyes with bilateral cataracts.
gIn the Ezisi et al. 201772 study there were 16 (72.7%) patients with unilateral cataracts and 6 (27.3%) patients with bilateral cataracts.
hIn the Eder et al. (2020)64 study there were 28 (60.87%) patients with unilateral cataracts and 18 (39.13%) patients with bilateral cataracts.
iIn the Koch et al. (2021)62 study there were 43 eyes (46.2%) with unilateral cataracts and 50 eyes (53.8%) with bilateral cataracts.
jIn Group 2, optic capture could not be achieved in 5 of 31 eyes randomized to that group.
Table 34: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — Strabismus and Nystagmus Results of NRSs
Details | Lee et al. (2014)76,a Follow-up: At least 2 years | Koch et al. (2021)62,b Follow-up: Up to 14.4 years | ||
|---|---|---|---|---|
Intervention | IOL (NR if foldable): 172 eyes from 108 patients | IOL (foldable): 93 eyes from 68 patients (mixed age) | ||
n of analysis | ≤ 1 year of age (16 bilateral patients; 5 unilateral patients) | > 1 year of age (48 bilateral patients; 39 unilateral patients) | ≤ 9 months: 22 eyes | ≥ 19 to 24 months: 34 eyes |
Strabismus | ||||
n (%) | — | — | 9 (40.9%) | 16 (47.1%) |
Correlation | — | — | Positive correlation between age at surgery and strabismus R = 0.015, P = 0.886 | |
Laterality, n (%) | ||||
Bilateral | 6 (37.5%) | 5 (10.4%) | — | — |
Unilateral | 3 (60%) | 10 (25.6%) | — | — |
P Value | Bilateral: 0.013 Unilateral: 0.113 | — | ||
Patients who were orthotropic at follow-up | ||||
n | Bilateral: 10 Unilateral: 2 | Bilateral: 43 Unilateral: 29 | — | |
P value | NR | — | ||
IOL = intraocular lens; NRS = nonrandomized study; vs. = versus.
aIn the Lee et al. (2014)76 study there were 44 (25.6%) eyes with unilateral cataracts and 128 (74.4%) eyes with bilateral cataracts.
bIn the Koch et al. (2021)62 study there were 43 eyes (46.2%) with unilateral cataracts and 50 eyes (53.8%) with bilateral cataracts.
Table 35: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — Additional Surgeries Results of NRSs
Outcome | Eder et al. (2020)64,a Follow-up: < 1 year | Sachdeva et al. (2016)73,b Follow-up: Up to 5 years | Koch et al. (2021)62,c Follow-up: Up to 14.4 years |
|---|---|---|---|
Average number of surgeries in first postoperative year based on age at surgery, n | |||
0 to 5 months (10 patients in analysis) | 1.70 | — | — |
6 to 23 months (8 patients in analysis) | 1.50 | — | — |
24 to 72 months (28 patients in analysis) | 0.61 | — | — |
P value | 0 to 5 months vs. 24 to 72 months: 0.005 0 to 5 months vs. 6 to 23 months: 0.76 6 to 23 months vs. 24 to 72 months: 0.003 | — | — |
Glaucoma surgery, n (%) | |||
< 1 year of age (104 eyes in analysis) | — | 2 (1.9%) | — |
> 1 year of age (466 eyes in analysis) | — | 0 (0%) | — |
Additional surgeries (excluding strabismus surgery), n (%) | |||
≤ 9 months (22 eyes in analysis) | — | — | 6 (27.3%) |
≥ 19 to 24 months (34 eyes in analysis) | — | — | 3 (8.8%) |
P value | — | — | 0.323d |
IOL = intraocular lens; NA = not applicable; NRS = nonrandomized study; vs. = versus.
aIn the Eder et al. (2020)64 study there were 28 (60.87%) patients with unilateral cataracts and 18 (39.13%) patients with bilateral cataracts. It was not reported if the IOL implanted was foldable. 46 eyes from 46 patients were implanted with IOLs (mixed age [i.e., combination of patients aged 12 months or younger and older than 12 months]).
bIn the Sachdeva et al. (2016)73 study, the number and proportion of eyes or patients with unilateral and bilateral cataracts were not reported. Foldable IOLs were implanted in 570 eyes (mixed age [i.e., combination of patients aged 12 months or younger and older than 12 months]).
cIn the Koch et al. (2021)62 study there were 43 eyes (46.2%) with unilateral cataracts and 50 eyes (53.8%) with bilateral cataracts. Foldable IOLs were implanted in 93 eyes from 68 patients (mixed age [i.e., combination of patients aged 12 months or younger and older than 12 months]).
dThis statistical comparison includes a third comparator group – 10 to 18 months of age. Comparison was done via ANOVA and found no statistically significant differences in the means of all 3 groups.
Table 36: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — Inflammatory Complications Results of RCTs and NRSs
Details | Vasavada et al. (2017)61 – RCTa Follow-up: 1 year | Lytvynchuk et al. (2020)66 – NRSb Follow-up: Up to 1 year | Vera et al. (2017)75 – NRSc Follow-up: Up to 5 years | |||||
|---|---|---|---|---|---|---|---|---|
≤ 1 year | > 1 to ≤ 4 years | 0 to < 3 months | 3 to < 12 months | 12 to < 36 months | < 6 months | 6 to 12 months | > 12 months | |
Intervention | IOL (foldable) – Group 1: IOL with AV; group 2: optic capture of IOL with no AV): 61 eyes from 61 patients (mixed age) | IOL (BIL; foldable): 90 eyes from 60 patients (mixed age) | IOL (foldable): 61 eyes from 43 patients (mixed age) | |||||
Incidence of postoperative posterior synechiae | ||||||||
Follow-up period, n (%), group 1: n = 30 eyes vs. group 2: 26 eyesd | ||||||||
1 month | 1 (7.1%) vs. 2 (16.7%) | 2 (12.5%) vs. 0 (0%) | — | — | — | — | — | — |
3 months | 1 (7.1%) vs. 2 (16.7%) | 2 (12.5%) vs. 0 (0%) | — | — | — | — | — | — |
6 months | 1 (7.1%) vs. 2 (16.7%) | 2 (12.5%) vs. 0 (0%) | — | — | — | — | — | — |
12 months | 1 (7.1%) vs. 2 (16.7%) | 2 (12.5%) vs. 0 (0%) | — | — | — | — | — | — |
Anterior peripheral synechia | ||||||||
n of eyes in analysis | — | — | 10 | 21 | 19 | — | — | — |
n (%) | — | — | 1 (10%) | 1 (4.8%) | 0 (0%) | — | — | — |
Incidence of postoperative inflammation | ||||||||
n of eyes in analysis | — | — | — | — | — | 33 | 16 | 12 |
% | — | — | — | — | — | 48% | 44% | 17% |
AV = anterior vitrectomy; BIL = bag-in-the-lens; IOL = intraocular lens; NRS = nonrandomized study; RCT = randomized controlled trial; vs. = versus.
aIn the Vasavada et al. (2017)61 study there were 37 eyes with unilateral cataracts and 24 eyes with bilateral cataracts. Only the first-operated eye was included from patients with bilateral cataracts.
bIn the Lytvynchuk et al. (2020)66 there were 27 (45%) patients with unilateral cataracts and 33 (55%) patients with bilateral cataracts. Of 3 cases of bilateral cataract, only 1 eye was operated with the BIL technique.
cIn the Vera et al. (2017)75 study there were 25 (58.00%) patients with unilateral cataracts and 18 (42.00%) patients with bilateral cataracts.
dIn Group 2, optic capture could not be achieved in 5 of 31 eyes randomized to that group.
Table 37: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — Other Safety Outcomes Results of RCTs and NRSs
Details | Vasavada et al. (2017)61 – RCTa Follow-up: 1 year | Sachdeva et al. (2016)73 – NRSb Follow-up: 5 years | Vera et al. (2017)75 – NRSc Follow-up: Up to 5 years | Valeina et al. (2020)70 – NRSd Follow-up: Up to 10 years | Ezisi et al. (2017)72 – NRSe Follow-up: Up to 11 years | Koch et al. (2021)62 – NRSf Follow-up: Up to 14.4 years | |
|---|---|---|---|---|---|---|---|
Intervention | IOL (foldable) – Group 1: IOL w/ AV / group 2: optic capture of IOL w/ no AV): 61 eyes from 61 patients (mixed age) Group 1: n = 30 eyes / Group 2: 26 eyesg | IOL (NR if foldable): 570 eyes (mixed age) | IOL (foldable)c: 61 eyes from 43 patients (mixed age) | IOL (foldable): 137 eyes from 85 patients (mixed age) | IOL (foldable): 19 eyes (mixed age) | IOL (foldable): 93 eyes from 68 patients (mixed age) | |
Age at Surgery Comparison | ≤ 1 year vs. > 1 to ≤ 4 years | < 1 year vs. > 1 year | < 6 months vs. 6 to 12 months vs. > 12 months | 13 to 24 months vs. 25 to 48 months vs. 49 to 84 months vs. 85 to 216 months | ≤ 12 months vs. < 12 months | ≤ 9 months vs. ≥ 19 to 24 months | |
Decentering of the IOL | |||||||
n of Analysis | 61 eyes from 61 patients | — | 33 eyes vs. 16 eyes | — | — | — | |
Results | All eyes (including those implanted < 12 months) maintained a clinically well-centred IOL throughout follow-up | — | 2 cases | — | — | — | |
Uveitis | |||||||
n of analysis | — | 104 eyes vs. 466 eyes | — | — | — | — | |
n (%) | — | < 1 year: 10 (9.6) eyes > 1 year: 12 (2.5) eyes | — | — | — | — | |
P value | — | P = NR | — | — | — | — | |
Incidence of postoperative cell deposits | |||||||
n of Analysis | NR | — | — | — | — | — | |
Follow-up period, n (%), group 1 vs. group 2, ≤ 1 year | |||||||
1 month | 6 (42.8%) vs. 6 (50%) | — | — | — | — | — | |
3 months | 6 (42.8%) vs. 5 (41.7%) | — | — | — | — | — | |
6 months | 3 (21.4%) vs. 3 (25.0%) | — | — | — | — | — | |
12 months | 1 (7.1%) vs. 1 (8.3%) | — | — | — | — | — | |
Follow-up period, n (%), group 1 vs. group 2, age > 1 to ≤ 4 years | |||||||
1 month | 9 (56.3%) vs. 6 (42.9%) | — | — | — | — | — | |
3 months | 9 (56.3%) vs. 7 (50.0%) | — | — | — | — | — | |
6 months | 9 (56.3%) vs. 7 (50.0%) | — | — | — | — | — | |
12 months | 6 (37.5%) vs. 3 (21.4%) | — | — | — | — | — | |
Endophthalmitis | |||||||
n of Analysis | — | — | NR | — | — | — | |
Results | — | — | Endophthalmitis was a postoperative outcome that only developed in patients who were infants at IOL implantation – namely, it developed only in patients operated at age 6 to 12 months at IOL implantation | — | — | — | |
IOL capture | |||||||
n of eyes in Analysis | — | — | — | — | 13 vs. 6 | — | |
Age at surgery, n of eyes | |||||||
≤ 12 months of age | — | — | — | — | 1 | — | |
> 12 months of age | — | — | — | — | 0 | — | |
IOL luxation (in the vitreous) | |||||||
n of Analysis | — | — | 33 eyes vs. 16 eyes | — | — | — | |
n | — | — | 3 patients Ciliary sulcus, n = 1 Capsular bag, n = 2 | — | — | — | |
SC | |||||||
n of Analysis | — | — | — | 19 eyes from 12 patients, vs. 10 eyes from 6 patients vs. 12 eyes from 7 patients vs. 27 eyes from 20 patients vs. 27 eyes from 17 patients | — | — | |
n | — | — | — | 1 to 6 months: 11 7 to 12 months: 3 13 to 24 months: 3 25 to 48 months: 9 49 to 84 months: 19 | — | — | |
Recurrent fibrosis (surrounding IOL) | |||||||
n of Analysis | — | — | 33 eyes vs. 16 eyes | — | — | — | |
n | — | — | 3 cases | — | — | — | |
Retinal detachment | |||||||
n of Analysis | — | — | 33 eyes vs. 16 eyes | — | — | 22 eyes vs. 34 eyes | |
n | — | — | Retinal detachment only developed in patients operated at age 0 to 6 months at IOL implantation | — | — | 0 vs. 0 | |
P value | — | — | NR | — | — | NA | |
Corectopia | |||||||
Age at Surgery Comparison | ≤ 1 year vs. > 1 to ≤ 4 years | < 1 year vs. > 1 year | < 6 months vs. 6 to 12 months vs. > 12 months | 13 to 24 months vs. 25 to 48 months vs. 49 to 84 months vs. 85 to 216 months | ≤ 12 months vs. < 12 months | ≤ 9 months vs. ≥ 19 to 24 months | < 1 year vs. ≥ 1 year to 2 years |
n of Analysis | — | — | — | — | — | 22 eyes vs. 34 eyes | 93 eyes from 68 patients |
n (%) | — | — | — | — | — | 1 (4.5%) vs. 1 (2.9%) | < 1 year: 2 eyes ≥ 1 year to 2 years: 3 eyes |
P value | — | — | — | — | — | P = NR | P = NR |
Pigments in IOL | |||||||
n of Analysis | — | — | — | — | — | 22 eyes vs. 34 eyes | 93 eyes from 68 patients |
n (%) | — | — | — | — | — | 0 vs. 0 | < 1 year: 0 ≥ 1 year to 2 years: 2 eyes |
P value | — | — | — | — | — | NA | NR |
Fibrin formation | |||||||
n of Analysis | — | — | — | — | — | 22 eyes vs. 34 eyes | 93 eyes from 68 patients |
n (%) | — | — | — | — | — | 0 vs. 0 | < 1 year: 0 ≥ 1 year to 2 years: 1 eye |
P value | — | — | — | — | — | NA | NR |
IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; NA = not applicable; NRS = nonrandomized study; NS = not significant; RCT = randomized controlled trial; SC = secondary cataract; VA = visual acuity; vs. = versus.
aIn the Vasavada et al. (2017)61 study there were 37 eyes with unilateral cataracts and 24 eyes with bilateral cataracts. Only first-operated eye was included from patients with bilateral cataracts.
bIn the Sachdeva et al. (2016)73 study, the number and proportion of eyes or patients with unilateral and bilateral cataracts were not reported.
cIn the Vera et al. (2017)75 study there were 25 (58.00%) patients with unilateral cataracts and 18 (42.00%) patients with bilateral cataracts.
dIn the Valeina et al. (2020)70 there were 30 (22%) eyes with unilateral cataracts and 107 (78%) eyes with bilateral cataracts.
eIn the Ezisi et al. 201772 study there were 16 (72.7%) patients with unilateral cataracts and 6 (27.3%) patients with bilateral cataracts.
fIn the Koch et al. (2021)62 study there were 43 eyes (46.2%) with unilateral cataracts and 50 eyes (53.8%) with bilateral cataracts.
gIn Group 2, optic capture could not be achieved in 5 of 31 eyes randomized to that group.
Table 38: Comparative Safety of IOL Implantation in Patients Aged 12 Months or Younger Versus Older Than 12 Months — Other Safety Outcomes Results for Bag-In-Lens Surgery Technique at 1-Year Follow-up 1 Year for Foldable IOLs66,a
Outcome, n (%) | Age at surgery (months) | P value | ||
|---|---|---|---|---|
0 to < 3 n = 10 | 3 to < 12 n = 21 | 12 to < 36 n = 19 | ||
Uveitis | 0 (0) | 3 (14.3) | 2 (10.5) | NS |
Intrapupillary membrane | 1 (10) | 0 (0) | 0 (0) | NS |
BIO IOL luxation | 1 (10) | 2 (9.5) | 0 (0) | NS |
BIL IOL glistening | 0 (0) | 0 (0) | 0 (0) | NS |
Hyphema | 0 (0) | 0 (0) | 2 (10.5) | NS |
Iris capture | 0 (0) | 1 (4.7) | 1 (5.3) | NS |
PCO | 2 (20) | 0 (0) | 0 (0) | NS |
BIL = bag-in-the-lens; IATS = Infant Aphakia Treatment Study; IOL = intraocular lens; NA = not applicable; NRS = nonrandomized study; NS = not significant; PCO = peripheral corneal opacification; RCT = randomized controlled trial; SC = secondary cataract; VA = visual acuity; vs. = versus.
aIn the Lytvynchuk et al. (2020)66 there were a total of 90 eyes from 60 patients. There were 27 (45%) patients with unilateral cataracts and 33 (55%) patients with bilateral cataracts.
Appendix 8: Considerations for Meta-Analysis
Note that this appendix has not been copy-edited.
Table 39: Considerations for Meta-Analysis
Comparison | Outcomes | Relevant studies | Meta-analysis appropriate? - Reason |
|---|---|---|---|
Prospective nonrandomized studies | |||
IOL vs. aphakia | Glaucoma | Shah et al. (2014)74 | No – different populations (i.e., rubella cataract and non-rubella cataract) |
Solebo et al. (2020)69 | |||
Retrospective nonrandomized studies | |||
IOL vs. aphakia | VA | Bothun et al. (2020)63 | No – different follow-up times |
Murphy et al. (2020)67 | |||
VAO | Bothun et al. (2020)63 | No – different follow-up times | |
Kirwan et al. (2010)68 | |||
Murphy et al. (2020)67 | |||
Glaucoma | Kirwan et al. (2010)68 | No – different follow-up times and potentially same patients in both studies | |
Murphy et al. (2020)67 | |||
Additional surgeries | Jackson et al. (2019)65 | No – different follow-up times | |
Kirwan et al. (2010)68 | |||
Age at surgery comparison | VAO | Koch et al. (2021)62 | No – different follow-up times for Lytvynchuk et al. (2020)66 and Ezisi et al. (2017)72 vs. Vera et al. (2017)75 and Sachdeva et al. (2016)73 Lytvynchuk et al. (2020)66 and Ezisi et al. (2017)72 used different surgical techniques Vera et al. (2017)75 and Sachdeva et al. (2016)73 included different age ranges for the > 12 months group Koch et al. (2021)62 has different follow-up times than the other studies |
Lytvynchuk et al. (2020)66 | |||
Ezisi et al. (2017)72 | |||
Vera et al. (2017)75 | |||
Sachdeva et al. (2016)73 | |||
Glaucoma | Koch et al. (2021)62 | No – different follow-up times for Lytvynchuk et al. (2020),66 Ezisi et al. (2017),72 Valeina et al. (2020),70 Eder et al. (2020), and Koch et al. (2021)62,64 Vera et al. (2017)75 and Sachdeva et al. (2016)73 included different age ranges for the > 12 months group | |
Lytvynchuk et al. (2020)66 | |||
Ezisi et al. (2017)72 | |||
Valeina et al. (2020)70 | |||
Eder et al. (2020)64 | |||
Sachdeva et al. (2016)73 | |||
Vera et al. (2017)75 | |||
Inflammatory complications | Lytvynchuk et al. (2020)66 | No – different follow-up times | |
Vera et al. (2017)75 | |||
Additional surgeries | Koch et al. (2021)62 | No – different follow-up times | |
Eder et al. (2020)64 | |||
Sachdeva et al. (2016)73 | |||
Uveitis | Lytvynchuk et al. (2020)66 | No – different surgical techniques (i.e., BIL and lens in bag) | |
Sachdeva et al. (2016)73 | |||
BIL = bag-in-the-lens; IOL = intraocular lens; VA = visual acuity; VAO = visual axis opacification.
All other comparisons and outcomes not displayed in table were deemed inappropriate for MA because there was a single study that represented both the study design and relevant outcome, therefore there was no available data to meta-analyze.
Appendix 9: Patients’ Experiences — GRIPP2 Short Form Reporting Checklist
Note that this appendix has not been copy-edited.
Table 40: GRIPP2 Short Form Reporting Checklist
Section and topic | Item | Reported on page |
|---|---|---|
Aim | The caregiver contributors were involved in developing the protocol and commenting on outcomes important to children with aphakia and their families. | 18 |
Methods | Facilitated by the Patient Engagement Officer, the mothers discussed with the research team / primary report authors, their families’ experiences via video teleconference and follow-up email communication. | 18 |
Results of engagement | The researchers were made aware of the importance of several outcomes and goals of treatment for aphakia. In particular, visual acuity, preserving and protecting the children’s vision was noted as the main goal of treatment. Promptness of treatment was also important to families so the children would have the best chance for normal development. For example, speech delay can sometimes go hand in hand with vision issues, so families were motivated to use contact lenses, glasses, or surgery to support their child’s vision as they grew from infants to preschool age. The mothers commented on family-borne costs, and equity issues for those who live far from an urban centre or do not have extended health benefits. Sharing these concerns allowed the research team to consider the evidence in the context of the wider experiences of families when preparing the assessment. | 35 to 36 |
Discussion and conclusions | Success of patient involvement in this report is related to several factors. First the mothers were briefed on the objectives of the project and supported in their role as contributors. The research team was receptive to this involvement and used it in their approach to the clinical evidence appraisal and synthesis. Established processes are in place, and each mother was offered compensation for her time to participate in the project. The mothers reported patient concerns, family-borne costs, and burdens, for example regular and unexpected replacement for contact lenses or glasses, time off work, childcare, accommodation/hotel stay, and travel. | 18,35 to 36 |
Reflections/critical perspective | The time frame of a CADTH systematic review project may make it difficult for patients to participate fully, on terms that work for them (e.g., daytime teleconferences). One mother was able to participate on a vacation day. The mothers we spoke to were recommended by their ophthalmologist, (a clinical expert on the project), and were motivated to be involved because of the positive relationship with him. Ethical and equity issues are sometimes revealed in the telling of patients’ experiences. Timely access to care is an important concern, and the financial costs of contact lenses and glasses raised as an important consideration for people without private insurance coverage or with limits on vision coverage. Time away from work, and childcare costs for other children during travel for regular appointments was also discussed in this context. Although not within the scope of this project, both mothers discussed the stress of learning to use contact lenses with a baby, and the need for support during this learning phase. For 1 family, a difficult aspect of the process was the experience of a 4-year-old undergoing surgery. Being old enough to be aware of the surgery but too young to understand and fully co-operate with procedure requirements was an unexpected, significantly difficult part of the experience. People need access to telephone or internet, and to be available to attend a scheduled conversation during the weekday to collaborate with CADTH, possibly excluding some voices. | 35 to 36 |
GRIPP2 = Revised Guidance for Reporting Involvement of Patients and the Public
Appendix 10: List of Included Publications
Note that this appendix has not been copy-edited.
1.Koch CR, Kara-Junior N, Santhiago MR, Morales M. Long-term results of in-the-bag primary intraocular lens implantation in children younger than 24 months. Arq Bras Oftalmol. 2021;84(4):316-323. PubMed
2.Murphy M, Murtagh P, McAnena L, Eldouri A, Kirwan C, O'Keefe M. Secondary glaucoma and visual axis opacification in aphakic and pseudophakic patients following congenital cataract surgery: A 28-year longitudinal case series. Eur J Ophthalmol. Nov 2020;30(6):1370-1380. PubMed
3.Solebo AL, Rahi JS, British Congenital Cataract Interest Group. Glaucoma following cataract surgery in the first 2 years of life: frequency, risk factors and outcomes from IoLunder2. Br J Ophthalmol. 07 2020;104(7):967-973.
4.Plager DA, Bothun ED, Freedman SF, Wilson ME, Lambert SR. Complications at 10 years of follow-up in the Infant Aphakia Treatment Study. Ophthalmology. November 2020;127(11):1581-1583. PubMed
5.Lambert SR, Cotsonis G, DuBois L, et al. Long-term effect of intraocular lens vs contact lens correction on visual acuity after cataract surgery during infancy: a randomized clinical trial. JAMA Ophthalmol. 04 01 2020;138(4):365-372.
6.Valeina S, Heede S, Erts R, et al. Factors influencing myopic shift in children after intraocular lens implantation. Eur J Ophthalmol. Sep 2020;30(5):933-940. PubMed
7.Jackson CM, Bickford M, Trivedi RH, Wilson ME. Unplanned returns to the operating room within three months of pediatric cataract-related intraocular surgery: indications and risk factors. J AAPOS. 08 2019;23(4):224.e1-224.e4.
8.Bothun ED, Wilson ME, Vanderveen DK, et al. Outcomes of bilateral cataracts removed in infants 1 to 7 months of age using the Toddler Aphakia and Pseudophakia Treatment Study Registry. Ophthalmology. 04 2020;127(4):501-510.
9.Vasavada AR, Vasavada V, Shah SK, et al. Postoperative outcomes of intraocular lens implantation in the bag versus posterior optic capture in pediatric cataract surgery. J Cataract Refract Surg. 09 2017;43(9):1177-1183.
10.Vasavada AR, Vasavada V, Shah SK, et al. Five-year postoperative outcomes of bilateral aphakia and pseudophakia in children up to 2 years of age: a randomized clinical trial. Am J Ophthalmol. 09 2018;193:33-44.
11.Bothun, E D, Lynn, M J, Christiansen, S P, et al. Strabismus surgery outcomes in the Infant Aphakia Treatment Study (IATS) at age 5 years. J AAPOS. 12 2016;20(6):501-505.
12.Vera L, Lambert N, Sommet J, Boulkedid R, Alberti C, Bui Quoc E. Visual outcomes and complications of cataract surgery with primary implantation in infants. Journal Francais d Opthalmologie. May 2017;40(5):386-393. PubMed
13.Ezisi CN, Kekunnaya R, Jalali S, et al. Cataract surgery in children with retinopathy of prematurity (ROP): surgical outcomes. Br J Ophthalmol. 08 2017;101(8):1128-1131.
14.Sachdeva V, Katukuri S, Ali M, Kekunnaya R. Second intraocular surgery after primary pediatric cataract surgery: indications and outcomes during long-term follow-up at a tertiary eye care center. Eye. Sep 2016;30(9):1260-5. PubMed
15.Bothun ED, Lynn MJ, Christiansen SP, et al. Sensorimotor outcomes by age 5 years after monocular cataract surgery in the Infant Aphakia Treatment Study (IATS). J AAPOS. Feb 2016;20(1):49-53. PubMed
16.Morrison DG, Lynn MJ, Freedman SF, Orge FH, Lambert SR, Infant Aphakia Treatment Study Group. Corneal changes in children after unilateral cataract surgery in the Infant Aphakia Treatment Study. Ophthalmology. Nov 2015;122(11):2186-92. PubMed
17.Freedman SF, Lynn MJ, Beck AD, et al. Glaucoma-related adverse events in the first 5 years after unilateral cataract removal in the Infant Aphakia Treatment Study. JAMA Ophthalmol. Aug 2015;133(8):907-14. PubMed
18.Shah SK, Praveen MR, Vasavada AR, et al. Long-term longitudinal assessment of postoperative outcomes after congenital cataract surgery in children with congenital rubella syndrome. J Cataract Refract Surg. Dec 2014;40(12):2091-8. PubMed
19.Plager DA, Lynn MJ, Buckley EG, Wilson ME, Lambert SR, Infant Aphakia Treatment Study Group. Complications in the first 5 years following cataract surgery in infants with and without intraocular lens implantation in the Infant Aphakia Treatment Study. Am J Ophthalmol. Nov 2014;158(5):892-8. PubMed
20.Lambert SR, Lynn MJ, Hartmann EE, et al. Comparison of contact lens and intraocular lens correction of monocular aphakia during infancy: A randomized clinical trial of HOTV optotype acuity at age 4.5 years and clinical findings at age 5 years. JAMA Ophthalmol. June 2014;132(6):676-682. PubMed
21.Felius J, Busettini C, Lynn MJ, Hartmann EE, Lambert SR, Infant Aphakia Treatment Study Group. Nystagmus and related fixation instabilities following extraction of unilateral infantile cataract in the Infant Aphakia Treatment Study (IATS). Invest Ophthalmol Vis Sci. Aug 05 2014;55(8):5332-7. PubMed
22.Lee SJ, Kim WS. Factors associated with strabismus after cataract extraction and primary intraocular lens implantation in congenital cataracts. Int J Ophthalmol. 2014;7(3):522-7. PubMed
23.Celano M, Hartmann EE, Drews-Botsch CD, Infant Aphakia Treatment Study Group. Parenting stress in the infant aphakia treatment study. J Pediatr Psychol. Jun 2013;38(5):484-93. PubMed
24.Bothun ED, Cleveland J, Lynn M J, et al. One-year strabismus outcomes in the Infant Aphakia Treatment Study. Ophthalmology. Jun 2013;120(6):1227-31. PubMed
25.Beck AD, Freedman SF, Lynn MJ, et al. Glaucoma-related adverse events in the Infant Aphakia Treatment Study: 1-year results. Arch Ophthalmol. Mar 2012;130(3):300-5. PubMed
26.Morrison DG, Wilson ME, Trivedi RH, Lambert SR, Lynn MJ, Infant Aphakia Treatment Study Group. Infant Aphakia Treatment Study: effects of persistent fetal vasculature on outcome at 1 year of age. J AAPOS. Oct 2011;15(5):427-31. PubMed
27.Plager DA, Lynn MJ, Buckley EG, Wilson ME, Lambert SR, Infant Aphakia Treatment Study Group. Complications, adverse events, and additional intraocular surgery 1 year after cataract surgery in the infant Aphakia Treatment Study. Ophthalmology. Dec 2011;118(12):2330-4. PubMed
28.Infant Aphakia Treatment Study Group, Lambert SR, Buckley EG, et al. A randomized clinical trial comparing contact lens with intraocular lens correction of monocular aphakia during infancy: grating acuity and adverse events at age 1 year. Arch Ophthalmol. Jul 2010;128(7):810-8. PubMed
29.Kirwan C, Lanigan B, O'Keefe M. Glaucoma in aphakic and pseudophakic eyes following surgery for congenital cataract in the first year of life. Acta Opthalmologica. Feb 2010;88(1):53-9. PubMed
30.Freedman SF, Beck AD, Nizam A, et al. Glaucoma-related adverse events at 10 years in the Infant Aphakia Treatment Study: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. Dec 17 2020;17:17. PubMed
31.Zhang F, Chang P, Zhao Y, Zhao YE. Incidence of posterior vitreous detachment after congenital cataract surgery: an ultrasound evaluation. Graefes Arch Clin Exp Ophthalmol. Nov 12 2020;12:12. PubMed
32.Eder AE, Cox KF, Pegram TA, Barb SM, Hoehn ME, Kerr NC. Effect of age at primary intraocular lens implantation on refractive growth in young children. J Pediatr Ophthalmol Strabismus. Jul 01 2020;57(4):264-270. PubMed
33.Lytvynchuk LM, Thiele MV, Lornz B. Analysis and management of intraoperative and early postoperative complications of bag-in-the-lens intraocular lens implantation in different age groups of paediatric cataract patients: report of the Giessen Paediatric Cataract Study Group. Acta Opthalmologica. Mar 2020;98(2):e144-e154. PubMed
Appendix 11: List of Excluded Studies
Note that this appendix has not been copy-edited.
Table 41: List of Excluded Studies
Citation | Reason for exclusion |
|---|---|
Vasavada, A.R., Vasavada, V., Shah, S.K., et al. Five-Year Postoperative Outcomes of Bilateral Aphakia and Pseudophakia in Children up to 2 Years of Age: a Randomized Clinical Trial. Am J Ophthalmol 2019; 199(): 263-264. | Irrelevant population |
Abdelmassih, Y., Beaujeux, P., Dureau, P., Edelson, C., Caputo, G. Incidence and Risk Factors of Glaucoma Following Pediatric Cataract Surgery with Primary Implantation. Am J Ophthalmol Sep 17 2020; 17(): 17. | Irrelevant study design |
Adhikari, S., Shrestha, U. D. Pediatric cataract surgery with hydrophilic acrylic intraocular lens implantation in Nepalese children. Clin Ophthalmol 2018; 12(): 7-11. | Irrelevant population |
Agarkar, S., Gokhale, V. V., Raman, R., Bhende, M., Swaminathan, G., Jain, M. Incidence, Risk Factors, and Outcomes of Retinal Detachment after Pediatric Cataract Surgery. Ophthalmology 01 2018; 125(1): 36-42. | Irrelevant population |
Al-Otaibi, A. G., Al Hammad, F. Childhood penetrating eye trauma visits to the emergency room. Causes and outcomes. Saudi Med J April 2012; 33(4): 449-451. | Irrelevant population |
Allam, G., Ellakkany, R., Ellayeh, A., Mohsen, T., Abouelkheir, H. E., Gaafar, W. Outcome of pediatric cataract surgery with intraocular injection of triamcinolone acetonide: Randomized controlled trial. Eur J Ophthalmol Nov 2018; 28(6): 633-638. | Irrelevant population |
Ashok Kumar, D., Agarwal, A., Sivangnanam, S., Chandrasekar, R., Agarwal, A. Implantation of glued intraocular lenses in eyes with microcornea. J Cataract Refract Surg Feb 2015; 41(2): 327-33. | Irrelevant population |
Balakrishnan, D., Mukundaprasad, V., Jalali, S., Pappuru, R. R. A Comparative Study on Surgical Outcomes of Glued Intraocular Lens and Sutured Scleral Fixated Intraocular Lens Implantation. Semin Ophthalmol 2018; 33(4): 576-580. | Irrelevant population |
Balekudaru, S., Agarkar, S., Guha, S., Mayee, R. C., Viswanathan, N., Pandey, A., Singh, M., Lingam, V., George, R. Prospective analysis of the predictors of glaucoma following surgery for congenital and infantile cataract. Eye 05 2019; 33(5): 796-803. | Irrelevant population |
Bar-Sela, S. M., Har-Noy, N. B., Spierer, A. Secondary membrane formation after cataract surgery with primary intraocular lens implantation in children. Int Ophthalmol Aug 2014; 34(4): 767-72. | Irrelevant population |
Beheshtnejad A, Hashemian H, Kakaie S, Mahdavi A, Naderan M. Outcomes of the infantile cataract surgery: case series with a 5-year follow-up. Int Ophthalmol. 2021 Oct 11. | Irrelevant population |
Besek NK, Nacaroglu SA, Er MO, et al. The Effect of Secondary Intraocular Lens Implantation Time on Visual Prognosis in Aphakia Cases After Open Globe Injury. Korean J Ophthalmol. 2021;35(5):368-375. | Irrelevant population |
Bhusal, S., Ram, J., Sukhija, J., Pandav, S. S., Kaushik, S. Comparison of the outcome of implantation of hydrophobic acrylic versus silicone intraocular lenses in pediatric cataract: prospective randomized study. Can J Ophthalmol Oct 2010; 45(5): 531-6. | Irrelevant population |
Bolletta E, Coassin M, Iannetta D, et al. Cataract surgery with intraocular lens implantation in juvenile idiopathic arthritis-associated uveitis: Outcomes in the era of biological therapy. J Clin Med 2021; 10(11). | Irrelevant population |
Borisovsky, G., Silberberg, G., Wygnanski-Jaffe, T., Spierer, A. Results of congenital cataract surgery with and without intraocular lens implantation in infants and children. Graefes Arch Clin Exp Ophthalmol Sep 2013; 251(9): 2205-11. | Irrelevant population |
Bothun, E. D., Wilson, M. E., Traboulsi, E. I., Diehl, N. N., Plager, D. A., Vanderveen, D. K., Freedman, S. F., Yen, K. G., Weil, N. C., Loh, A. R., Morrison, D., Anderson, J. S., Lambert, S. R., Toddler Aphakia and Pseudophakia Study Group. Outcomes of Unilateral Cataracts in Infants and Toddlers 7 to 24 Months of Age: Toddler Aphakia and Pseudophakia Study (TAPS). Ophthalmology 08 2019; 126(8): 1189-1195. | Other Reason for Exclusion |
Bothun, E. D., Wilson, M. E., Yen, K. G., Anderson, J. S., Weil, N. C., Loh, A. R., Morrison, D., Freedman, S. F., Plager, D. A., Vanderveen, D. K., Traboulsi, E. I., Hodge, D. O., Lambert, S. R., Toddler Aphakia and Pseudophakia Study. Outcomes of Bilateral Cataract Surgery in Infants 7 to 24 Months of Age Using the Toddler Aphakia and Pseudophakia Treatment Study Registry. Ophthalmology Jul 15 2020; 15(): 15. | Irrelevant population |
Brandner, M., Thaler-Saliba, S., Plainer, S., Vidic, B., El-Shabrawi, Y., Ardjomand, N. Retropupillary Fixation of Iris-Claw Intraocular Lens for Aphakic Eyes in Children. PLoS ONE 2015; 10(6): e0126614. | Irrelevant population |
Burcu, A., Yalniz-Akkaya, Z., Abay, I., Acar, M. A., Ornek, F. Scleral-fixated posterior chamber intraocular lens implantation in pediatric and adult patients. Semin Ophthalmol Jan 2014; 29(1): 39-44. | Irrelevant population |
Buzzonetti L, Petroni S, De Sanctis CM, et al. Comparative analysis of visual outcomes of multifocal and monofocal intraocular lenses in congenital cataract surgery. J Cataract Refract Surg. 2021; 26. | Irrelevant study design |
Byrd, J. M., Young, M. P., Liu, W., Zhang, Y., Tate, D. B., Crandall, A. S., Owen, L. A. Long-term outcomes for pediatric patients having transscleral fixation of the capsular bag with intraocular lens for ectopia lentis. J Cataract Refract Surg May 2018; 44(5): 603-609. | Irrelevant population |
Cai, L., Han, X., Jiang, Y., Qiu, X., Qian, D., Lu, Y., Yang, J. Three-year outcomes of Cionni-modified capsular tension ring implantation in children under eight years old with ectopia lentis. Am J Ophthalmol. 2020; 27. | Irrelevant population |
Carrigan, A. K., DuBois, L. G., Becker, E. R., Lambert, S. R., Infant Aphakia Treatment Study Group. Cost of intraocular lens versus contact lens treatment after unilateral congenital cataract surgery: retrospective analysis at age 1 year. Ophthalmology Jan 2013; 120(1): 14-9. | Irrelevant study design |
Celano, M., Cotsonis, G. A., Hartmann, E. E., Drews-Botsch, C., Infant Aphakia Treatment Study Group. Behaviors of children with unilateral vision impairment in the Infant Aphakia Treatment Study. J AAPOS 08 2016; 20(4): 320-5. | Does not answer research questions |
Celano, M., Hartmann, E. E., DuBois, L. G., Drews-Botsch, C., Infant Aphakia Treatment Study Group. Motor skills of children with unilateral visual impairment in the Infant Aphakia Treatment Study. Dev Med Child Neurol Feb 2016; 58(2): 154-9. | Does not answer research questions |
Chew, F. L. M., Qurut, S. E., Hassan, I., Theng, L. S., Ramasamy, S., Rahmat, J. Paediatric cataract surgery in hospital Kuala Lumpur - A 5-year review of visual outcomes Med J Malaysia February 2019; 74(1): 15-24. | Irrelevant population |
Cleary, C., Lanigan, B., O'Keeffe, M. Artisan iris-claw lenses for the correction of aphakia in children following lensectomy for ectopia lentis. Br J Ophthalmol Mar 2012; 96(3): 419-21. | Irrelevant population |
Crockett, C., Camero, K. A., Kong, L., Yen, K. G. Visual outcomes of patients presenting with bilateral infantile cataracts and nystagmus. Can J Ophthalmol Apr 2017; 52(2): 203-206. | Irrelevant population |
Cromelin, C. H., Drews-Botsch, C., Russell, B., Lambert, S. R., Infant Aphakia Treatment Study Group. Association of Contact Lens Adherence With Visual Outcome in the Infant Aphakia Treatment Study: A Secondary Analysis of a Randomized Clinical Trial. JAMA Ophthalmol 03 01 2018; 136(3): 279-285. | Does not answer research questions |
CTRI. A clinical trial to study the comparison of hydrophilic intraocular lens and silicone lens in children undergoing cataract surgery 2010; 091(000195). | Full text not available |
Daien, V., Le Pape, A., Heve, D., Villain, M., Bremond Gignac, D., Collaborators of the, Epidemiology, Safety, Program Incidence and Characteristics of Congenital Cataract Surgery in France from 2010-2012: The EPISAFE Program. Ophthalmic Res 2017; 58(2): 114-116. | Irrelevant study design |
David, R., Davelman, J., Mechoulam, H., Cohen, E., Karshai, I., Anteby, I. Strabismus developing after unilateral and bilateral cataract surgery in children. Eye Sep 2016; 30(9): 1210-4. | Irrelevant population |
Demirkilinc Biler, E., Bozbiyik, D. I., Uretmen, O., Kose, S. Strabismus in infants following congenital cataract surgery. Graefes Arch Clin Exp Ophthalmol Oct 2015; 253(10): 1801-7. | Does not answer research questions |
Dixit, N. V., Shah, S. K., Vasavada, V., Vasavada, V. A., Praveen, M. R., Vasavada, A. R., Trivedi, R. H. Outcomes of cataract surgery and intraocular lens implantation with and without intracameral triamcinolone in pediatric eyes. J Cataract Refract Surg Sep 2010; 36(9): 1494-8. | Irrelevant population |
Eibenberger, K., Kiss, B., Schmidt-Erfurth, U., Stifter, E. Clinical characteristics and treatment of secondary glaucoma, glaucoma suspects and ocular hypertension after congenital cataract surgery. Eur J Ophthalmol. 2021. | Irrelevant population |
Eibenberger, K., Stifter, E., Pusch, F., Schmidt-Erfurth, U. Simultaneous Bilateral Pediatric and Juvenile Cataract Surgery Under General Anesthesia: Outcomes and Safety. Am J Ophthalmol 06 2020; 214: 63-71. | Irrelevant population |
El Gendy, H. A., Khalil, H. E., Haroun, H. E., El Deeb, M. W. Endoscopic-Assisted Scleral Fixated IOL in the Management of Secondary Aphakia in Children. J Ophthalmol 2016; 2016: 8501842. | Irrelevant population |
Elkin, Z. P., Piluek, W. J., Fredrick, D. R. Revisiting secondary capsulotomy for posterior capsule management in pediatric cataract surgery. J AAPOS 12 2016; 20(6): 506-510. | Irrelevant population |
Fan, F., Luo, Y., Liu, X., Lu, Y., Zheng, T. Risk factors for postoperative complications in lensectomy-vitrectomy with or without intraocular lens placement in ectopia lentis associated with Marfan syndrome. Br J Ophthalmol Oct 2014; 98(10): 1338-42. | Irrelevant population |
Faramarzi, A., Feizi, S., Maghsoodlou, A. Factors influencing intraocular pressure, corneal thickness and corneal biomechanics after congenital cataract surgery. Br J Ophthalmol 11 2017; 101(11): 1493-1499. | Irrelevant population |
Faramarzi, A., Javadi, M. A., Jabbarpoor Bonyadi, M. H., Yaseri, M. Changes in central corneal thickness after congenital cataract surgery. J Cataract Refract Surg Dec 2010; 36(12): 2041-7. | Irrelevant population |
G, I. Gawdat, M, M. Youssef, N, M. Bahgat, D, M. Elfayoumi, As Eddin, M. Incidence and Risk Factors of Early-onset Glaucoma following Pediatric Cataract Surgery in Egyptian Children: One-year Study. J Curr Glaucoma Pract Sep-Dec 2017; 11(3): 80-85. | Irrelevant population |
Gochnauer, A. C., Trivedi, R. H., Hill, E. G., Wilson, M. E. Interocular axial length difference as a predictor of postoperative visual acuity after unilateral pediatric cataract extraction with primary IOL implantation. J AAPOS Feb 2010; 14(1): 20-4. | Irrelevant population |
Gonnermann, J., Klamann, M. K., Maier, A. K., Rjasanow, J., Joussen, A. M., Bertelmann, E., Rieck, P. W., Torun, N. Visual outcome and complications after posterior iris-claw aphakic intraocular lens implantation. J Cataract Refract Surg Dec 2012; 38(12): 2139-43. | Irrelevant population |
Grzybowski, A., Kanclerz, P., Beiko, G. H. H. IOLs glistenings and quality of vision. Graefes Arch Clin Exp Ophthalmol 12 2019; 257(12): 2795-2796. | Irrelevant population |
Guindolet, D., Dureau, P., Terrada, C., Edelson, C., Barjol, A., Caputo, G., LeHoang, P., Bodaghi, B. Cataract Surgery with Primary Lens Implantation in Children with Chronic Uveitis. Ocul Immunol Inflamm 2018; 26(2): 298-304. | Irrelevant population |
Gupta, A., Kekunnaya, R., Ramappa, M., Vaddavalli, P. K. Safety profile of primary intraocular lens implantation in children below 2 years of age. Br J Ophthalmol Apr 2011; 95(4): 477-80. | Irrelevant intervention |
Hartmann, E. E., Stout, A. U., Lynn, M. J., Yen, K. G., Kruger, S. J., Lambert, S. R., Infant Aphakia Treatment Study Group, Infant Aphakia Treatment Study Group. Stereopsis results at 4.5 years of age in the infant aphakia treatment study. Am J Ophthalmol Jan 2015; 159(1): 64-70.e1-2. | Does not answer research questions |
Hildebrand, G. D., Tassignon, M. J., Vasavada, A. R., Nischal, K. K., Nystrom, A. Intraocular lens implantation in children with cataract. The Lancet Child & Adolescent Health 07 2019; 3(7): e6-e7. | Irrelevant population |
Hoehn, M. E., Irshad, F., Kerr, N. C., Wilson, M. W. Outcomes after cataract extraction in young children with radiation-induced cataracts and retinoblastoma. J AAPOS Jun 2010; 14(3): 232-4. | Irrelevant population |
Hoevenaars, N. E., Polling, J. R., Wolfs, R. C. Prediction error and myopic shift after intraocular lens implantation in paediatric cataract patients. Br J Ophthalmol Aug 2011; 95(8): 1082-5. | Does not answer research questions |
Hsu, H. Y., Edelstein, S. L., Lind, J. T. Surgical management of non-traumatic pediatric ectopia lentis: A case series and review of the literature. Saudi J Ophthalmol Jul 2012; 26(3): 315-21. | Irrelevant population |
Huang, Y., Xie, L. Short-term outcomes of dry pars plana posterior capsulotomy and anterior vitrectomy in paediatric cataract surgery using 25-gauge instruments. Br J Ophthalmol Aug 2010; 94(8): 1024-7. | Irrelevant population |
Hwang, S., Lim, D. H., Lee, S., Choi, D. D., Chung, E. S., Chung, T. Y. Temporary Piggyback Intraocular Lens Implantation Versus Single Intraocular Lens Implantation in Congenital Cataracts: Long-Term Clinical Outcomes. Invest Ophthalmol Vis Sci 04 01 2018; 59(5): 1822-1827. | Irrelevant population |
Infant Aphakia Treatment Study Group, Lambert, S. R., Buckley, E. G., Drews-Botsch, C., DuBois, L., Hartmann, E., Lynn, M. J., Plager, D. A., Wilson, M. E. The infant aphakia treatment study: design and clinical measures at enrollment. Arch Ophthalmol Jan 2010; 128(1): 21-7. | Does not answer research questions |
Infant Aphakia Treatment Study Group, Lambert, S. R., Lynn, M. J., Hartmann, E. E., DuBois, L., Drews-Botsch, C., Freedman, S. F., Plager, D. A., Buckley, E. G., Wilson, M. E. Comparison of contact lens and intraocular lens correction of monocular aphakia during infancy: a randomized clinical trial of HOTV optotype acuity at age 4.5 years and clinical findings at age 5 years. JAMA Ophthalmol Jun 2014; 132(6): 676-82. | Other Reason for Exclusion |
Jasman, A. A., Shaharuddin, B., Noor, R. A., Ismail, S., Ghani, Z. A., Embong, Z. Prediction error and accuracy of intraocular lens power calculation in pediatric patient comparing SRK II and Pediatric IOL Calculator. BMC Ophthalmol Aug 25 2010; 10: 20. | Irrelevant population |
Jinagal, J., Gupta, G., Agarwal, A., Aggarwal, K., Akella, M., Gupta, V., Suri, D., Gupta, A., Singh, S., Ram, J. Safety and efficacy of dexamethasone implant along with phacoemulsification and intraocular lens implantation in children with juvenile idiopathic arthritis associated uveitis. Indian J Ophthalmol Jan 2019; 67(1): 69-74. | Irrelevant population |
Jinagal, J., Gupta, P. C., Ram, J., Sharma, M., Singh, S. R., Yangzes, S., Sukhija, J., Singh, R. Outcomes of cataract surgery in children with persistent hyperplastic primary vitreous. Eur J Ophthalmol Mar 2018; 28(2): 193-197. | Irrelevant population |
Joshaghani, M., Soleimani, M., Foroutan, A., Yaseri, M. Visual Outcomes and Complications of Piggyback Intraocular Lens Implantation Compared to Aphakia for Infantile Cataract. Middle East Afr J Ophthalmol Oct-Dec 2015; 22(4): 495-501. | Irrelevant intervention |
Kamath, S. J., John, T. A., Jayanthi, K. Clinical profile of congenital and developmental cataract in a tertiary care centre of southern India. J Clin Diagn Res 01 Sep 2018; 12(9): NC01-NC04. | Irrelevant population |
Khan, A. O., Al-Dahmash, S. Lack of glaucoma following infantile cataract surgery with primary posterior chamber intraocular lens implantation. Ophthalmic Surgery, Lasers & Imaging Jul-Aug 2010; 41(4): 459-62. | Irrelevant study design |
Khokhar, S., Sharma, R., Patil, B., Sinha, G., Nayak, B., Kinkhabwala, R. A. A safe technique for in-the-bag intraocular lens implantation in pediatric cataract surgery. Eur J Ophthalmol Jan-Feb 2015; 25(1): 57-9. | Irrelevant population |
Khurana, S., Gupta, P. C., Vaiphei, K., Singh, R., Ram, J. A clinicopathological study of persistent fetal vasculature. Indian J Ophthalmol 06 2019; 67(6): 785-787. | Irrelevant population |
Khurana, S., Ram, J., Singh, R., Gupta, P. C., Gupta, R., Yangzes, S., Sukhija, J., Dogra, M. R. Surgical outcomes of cataract surgery in anterior and combined persistent fetal vasculature using a novel surgical technique: a single center, prospective study. Graefes Arch Clin Exp Ophthalmol Jan 2021; 259(1): 213-221. | Irrelevant population |
Kim, J. A., Lee, S. Y., Park, K. H., Yu, Y. S., Jeoung, J. W. Incidence and Risk Factors for Glaucoma Development After Bilateral Congenital Cataract Surgery in Microphthalmic Eyes. Am J Ophthalmol December 2019; 208: 265-272. | Irrelevant population |
Kleinmann, G., Zaugg, B., Apple, D. J., Bleik, J. Pediatric cataract surgery with hydrophilic acrylic intraocular lens. J AAPOS Aug 2013; 17(4): 367-70. | Irrelevant population |
Koch, C. R., Kara-Junior, N., Santhiago, M. R., Morales, M. Comparison of different surgical approaches for pediatric cataracts: complications and rates of additional surgery during long-term follow-up. Clinics (Sao Paulo) 2019; 74: e966. | Irrelevant population |
Koch, C. R., Kara-Junior, N., Serra, A., Morales, M. Long-term results of secondary intraocular lens implantation in children under 30 months of age. Eye 12 2018; 32(12): 1858-1863. | Irrelevant population |
Koch, C. R., Santhiago, M. R., Jorge, P. A., Sena, P., Kara-Junior, N. Posterior Capsule Opacification after Cataract Surgery in Children Over Five Years of Age with Square-edge Hydrophobic vs. Hydrophilic Acrylic Intraocular Lenses: A Prospective Randomized Study. Clinics (Sao Paulo) 2020; 75: e1604. | Irrelevant population |
Kraus, C. L., Trivedi, R. H., Wilson, M. E. Intraocular lens exchange for high myopia in pseudophakic children. Eye Sep 2016; 30(9): 1199-203. | Irrelevant study design |
Kruger, S. J., DuBois, L., Becker, E. R., Morrison, D., Wilson, L., Wilson, M. E., Jr., Lambert, S. R., Infant Aphakia Treatment Study Group. Cost of intraocular lens versus contact lens treatment after unilateral congenital cataract surgery in the infant aphakia treatment study at age 5 years. Ophthalmology Feb 2015; 122(2): 288-92. | Irrelevant study design |
Kruger, T. L., Monson, B. S., Baker, J. D. The role and efficacy of secondary intraocular lenses in the treatment of monocular infantile cataracts. J Pediatr Ophthalmol Strabismus Nov-Dec 2014; 51(6): 370-4. | Irrelevant population |
Kumar, D. A., Agarwal, A., Packiyalakshmi, S., Jacob, S., Agarwal, A. Complications and visual outcomes after glued foldable intraocular lens implantation in eyes with inadequate capsules. J Cataract Refract Surg Aug 2013; 39(8): 1211-8. | Irrelevant population |
Lambert, S. R., Bothun, E. D., Plager, D. A. Five-Year Postoperative Outcomes of Bilateral Aphakia and Pseudophakia in Children up to 2 Years of Age: A Randomized Clinical Trial. Am J Ophthalmol March 2019; 199: 263-264. | Irrelevant population |
Lambert, S. R., Cotsonis, G., DuBois, L., Wilson, M. E., Plager, D. A., Buckley, E. G., McClatchey, S. K., Infant Aphakia Treatment Study Group. Comparison of the rate of refractive growth in aphakic eyes versus pseudophakic eyes in the Infant Aphakia Treatment Study. J Cataract Refract Surg 12 2016; 42(12): 1768-1773. | Does not answer research questions |
Lambert, S. R., Lynn, M. J., DuBois, L. G., Cotsonis, G. A., Hartmann, E. E., Wilson, M. E., Infant Aphakia Treatment Study Groups. Axial elongation following cataract surgery during the first year of life in the infant Aphakia Treatment Study. Invest Ophthalmol Vis Sci Nov 07 2012; 53(12): 7539-45. | Does not answer research questions |
Lambert, S. R., Plager, D. A., Buckley, E. G., Wilson, M. E., DuBois, L., Drews-Botsch, C. D., Hartmann, E. E., Lynn, M. J., Infant Aphakia Treatment Study Group. The Infant Aphakia Treatment Study: further on intra- and postoperative complications in the intraocular lens group. J AAPOS Apr 2015; 19(2): 101-3. | Irrelevant study design |
Lambert, S. R., Purohit, A., Superak, H. M., Lynn, M. J., Beck, A. D. Long-term risk of glaucoma after congenital cataract surgery. Am J Ophthalmol Aug 2013; 156(2): 355-361.e2. | Irrelevant study design |
Li, Q., Fu, T., Li, Z. E., Bi, H. S., Wang, X. R., Dong, M., Xin, T. Optical correction of aphakia following unilateral infantile cataract removal. Acta Opthalmologica Dec 2014; 92(8): e657-62. | Irrelevant population |
Lin, H., Chen, W., Luo, L., Zhang, X., Chen, J., Lin, Z., Qu, B., Zhan, J., Zheng, D., Zhong, X., Tian, Z., Liu, Y., Study Group of, Ccpmoh Ocular hypertension after pediatric cataract surgery: baseline characteristics and first-year report. PLoS ONE 2013; 8(7): e69867. | Other Reason for Exclusion |
Little, B. Cataract surgical problem. J Cataract Refract Surg May 2013; 39(5): 810-811. | Irrelevant population |
Long, T., Xu, Y., Wu, X., Zhao, J., Li, Y., Xie, L. Intraocular pressure in pediatric eyes. Ophthalmology January 2013; 120(1): 212-212.e3. | Irrelevant population |
Louison, S., Blanc, J., Pallot, C., Alassane, S., Praudel, A., Bron, A. M., Creuzot-Garcher, C. Visual outcomes and complications of congenital cataract surgery. Journal Francais d Opthalmologie Apr 2019; 42(4): 368-374. | Irrelevant population |
Lu, Y., Ji, Y. H., Luo, Y., Jiang, Y. X., Wang, M., Chen, X. Visual results and complications of primary intraocular lens implantation in infants aged 6-12 months. Graefes Arch Clin Exp Ophthalmol May 2010; 248(5): 681-6. | Irrelevant study design |
Ma, F., Ren, M., Wang, L., Wang, Q., Guo, J. Visual outcomes of dense pediatric cataract surgery in eastern China. PLoS ONE 2017; 12(7): e0180166. | Irrelevant population |
Magli, A., Carelli, R., Forte, R., Chiariello Vecchio, E., Esposito, F., Torre, A. Congenital and Developmental Cataracts: Focus on Strabismus Outcomes at Long-Term Follow-Up. Semin Ophthalmol 2017; 32(3): 358-362. | Irrelevant intervention |
Magli, A., Forte, R., Carelli, R., Magli, G., Esposito, F., Torre, A. Long-Term Follow-Up after Surgery for Congenital and Developmental Cataracts. Semin Ophthalmol 2016; 31(3): 261-5. | Irrelevant intervention |
Magli, A., Forte, R., Carelli, R., Rombetto, L., Magli, G. Long-Term Outcomes of Primary Intraocular Lens Implantation for Unilateral Congenital Cataract. Semin Ophthalmol 2016; 31(6): 548-53. | Irrelevant intervention |
Magli, A., Forte, R., Rombetto, L. Long-term outcome of primary versus secondary intraocular lens implantation after simultaneous removal of bilateral congenital cataract. Graefes Arch Clin Exp Ophthalmol Jan 2013; 251(1): 309-14. | Irrelevant intervention |
Mataftsi, A., Dabbagh, A., Moore, W., Nischal, K. K. Evaluation of whether intracameral dexamethasone predisposes to glaucoma after pediatric cataract surgery. J Cataract Refract Surg Oct 2012; 38(10): 1719-23. | Other Reason for Exclusion |
Matalia, J., Anaspure, H., Shetty, B. K., Matalia, H. Intraoperative usefulness and postoperative results of the endoilluminator for performing primary posterior capsulectomy and anterior vitrectomy during pediatric cataract surgery. Eye Aug 2014; 28(8): 1008-13. | Irrelevant population |
Matsuo, T. Intraocular lens implantation in unilateral congenital cataract with minimal levels of persistent fetal vasculature in the first 18 months of life. Springerplus 2014; 3: 361. | Irrelevant population |
Mboni, C., Gogate, P. M., Phiri, A., Seneadza, A., Ramson, P., Manolakos-Tsehisi, H., Musonda, L., Benjamin, L., Overland, L. Outcomes of Pediatric Cataract Surgery in the Copperbelt Province of Zambia. J Pediatr Ophthalmol Strabismus Sep 01 2016; 53(5): 311-7. | Irrelevant population |
Mediero, S., Peralta Calvo, J., Pastora Salvador, N., Abelairas Gomez, J. Elevated intraocular pressure in paediatric cataract surgery in a reference centre. Arch Soc Esp Oftalmol Aug 2019; 94(8): 377-383. | Irrelevant population |
Meier, P., Sterker, I., Tegetmeyer, H., Wiedemann, P. 23-gauge-lentectomy for the treatment of congenital cataract. [German, English] Ophthalmologe March 2010; 107(3): 241-245. | Not published in English |
Mireskandari, K. Safety profile of primary intraocular lens implantation in children below 2 years of age. Evidence-Based Ophthalmology October 2011; 12(4): e9-e10. | Irrelevant study design |
Mndeme, F. G., Mmbaga, B. T., Msina, M., Mwende, J., Vaitha, S. J., Kim, M. J., Macleod, D., Burton, M. J., Gilbert, C. E., Bowman, R. Presentation, surgery and 1-year outcomes of childhood cataract surgery in Tanzania. Br J Ophthalmol 01 Mar 2021; 105(3): 334-340. | Irrelevant population |
Mohan, A., Kumar, A., Sen, P., Shah, C., Jain, E., Sen, A. Outcome of Surgical Membranectomy With a Vitrector via Limbal Approach for Posterior Capsular Opacity in Children. J Pediatr Ophthalmol Strabismus Jan 01 2020; 57(1): 33-38. | Irrelevant population |
Morral, M., Guell, J. L., El Husseiny, M. A., Elies, D., Gris, O., Manero, F. Paired-eye comparison of corneal endothelial cell counts after unilateral iris-claw phakic intraocular lens implantation Presented in part at the ASCRS Symposium on Cataract, IOL and Refractive Surgery, San Diego, California, US, April 2015. J Cataract Refract Surg 01 Jan 2016; 42(1): 117-126. | Irrelevant population |
NCT01297153. Aphakia Versus Pseudophakia in Children Under 2 Years Undergoing Bilateral Congenital Cataract Surgery https://clinicaltrials.gov/show/NCT01297153 2011. | Irrelevant population |
Neel, S. T. A cost-minimization analysis comparing immediate sequential cataract surgery and delayed sequential cataract surgery from the payer, patient, and societal perspectives in the United States. JAMA Ophthalmol Nov 2014; 132(11): 1282-8. | Irrelevant population |
Negalur, M., Sachdeva, V., Neriyanuri, S., Ali, M. H., Kekunnaya, R. Long-term outcomes following primary intraocular lens implantation in infants younger than 6 months. Indian J Ophthalmol 08 2018; 66(8): 1088-1093. | Irrelevant study design |
Ness, P. J., Jackson, C. M., Offerle, T. L., Briggs, T. M., Trivedi, R. H., Wolf, B., Wilson, M. E. Changes in intraocular pressure control in the first year after secondary intraocular lens implantation in children. Eye Oct 09 2020; 09: 09. | Irrelevant population |
Ngoy, J. K., Stahnke, T., Dinkulu, S., Makwanga, E., Moanda, A., Ngweme, G., Mukwanseke, E., Kundt, G., Thiesen, F., Hopkins, A., Guthoff, R. F. Bilateral paediatric cataract surgery-outcomes of 298 children from kinshasa, the democratic republic of the Congo. Afr Health Sci December 2020; 20(4): 1817-1827. | Irrelevant population |
Nuzzi, R., Baratozzi, V., Polito, M. S., Tridico, F. Efficacy and safety of an intracameral combination of two mydriatics and an anesthetic for phacoemulsification in complicated patients. Open Ophthalmology Journal 2018; 12(1): 322-329. | Irrelevant population |
Olsen, T. W., Pribila, J. T. Pars plana vitrectomy with endoscope-guided sutured posterior chamber intraocular lens implantation in children and adults. Am J Ophthalmol Feb 2011; 151(2): 287-96.e2. | Irrelevant population |
Ozbilen, K. T., Altinkurt, E. Impact of the possible prognostic factors for visual outcomes of traumatic cataract surgery. Int Ophthalmol 01 Nov 2020; 40(11): 3163-3173. | Irrelevant population |
Palsson, S., Nystrom, A., Sjodell, L., Jakobsson, G., Byhr, E., Andersson Gronlund, M., Zetterberg, M. Combined phacoemulsification, primary intraocular lens implantation, and pars plana vitrectomy in children with uveitis. Ocul Immunol Inflamm Apr 2015; 23(2): 144-51. | Irrelevant population |
Praveen, M. R., Shah, S. K., Vasavada, A. R., Vasavada, V. A., Asnani, P. K., Anwar, I., Trivedi, R. H. Incidence, management, and postoperative outcomes in pediatric eyes with coexisting posterior capsule plaque and cataract. J Cataract Refract Surg Dec 2010; 36(12): 2094-9. | Irrelevant population |
Praveen, M. R., Shah, S. K., Vasavada, V. A., Dixit, N. V., Vasavada, A. R., Garg, V. S., Trivedi, R. H. Triamcinolone-assisted vitrectomy in pediatric cataract surgery: intraoperative effectiveness and postoperative outcome. J AAPOS Aug 2010; 14(4): 340-4. | Irrelevant population |
Ram, J., Gupta, N., Sukhija, J. S., Chaudhary, M., Verma, N., Kumar, S., Severia, S. Outcome of cataract surgery with primary intraocular lens implantation in children. Br J Ophthalmol Aug 2011; 95(8): 1086-90. | Irrelevant population |
Ram, J., Jain, V. K., Agarwal, A., Kumar, J. Hydrophobic acrylic versus polymethyl methacrylate intraocular lens implantation following cataract surgery in the first year of life. Graefes Arch Clin Exp Ophthalmol Sep 2014; 252(9): 1443-9. | Irrelevant comparator |
Resende, G. M., Lupinacci, A. P. C., Arieta, C. E. L., Costa, V. P. Central corneal thickness and intraocular pressure in children undergoing congenital cataract surgery: A prospective, longitudinal study. Br J Ophthalmol September 2012; 96(9): 1190-1194. | Irrelevant population |
Rong, X., Ji, Y., Fang, Y., Jiang, Y., Lu, Y. Long-Term Visual Outcomes of Secondary Intraocular Lens Implantation in Children with Congenital Cataracts. PLoS ONE 2015; 10(7): e0134864. | Irrelevant population |
Rumelt, S., Rehany, U. The influence of surgery and intraocular lens implantation timing on visual outcome in traumatic cataract. Graefes Arch Clin Exp Ophthalmol Sep 2010; 248(9): 1293-7. | Irrelevant population |
Sachdeva, V., Reddy, P., Fernandes, M., Shah, S., Kekunnaya, R. Refractive outcomes with secondary intraocular lens implantation in children. J AAPOS Aug 2010; 14(4): 377-8. | Irrelevant population |
Sahay, P., Goel, S., Maharana, P. K. Five-Year Postoperative Outcomes of Bilateral Aphakia and Pseudophakia in Children up to 2 Years of Age: A Randomized Clinical Trial. Am J Ophthalmol March 2019; 199: 264. | Irrelevant population |
Sahin, A., Caca, I., Cingu, A. K., Turkcu, F. M., Yuksel, H., Sahin, M., Cinar, Y., Ari, S. Secondary glaucoma after pediatric cataract surgery. Int J Ophthalmol 2013; 6(2): 216-20. | Irrelevant population |
Samarawickrama, C., Li, Y. C., Kanapathipillai, N., Grigg, J. R. Changing refractive outcomes with increasing astigmatism at longer-term follow-up for infant cataract surgery. Eye Sep 2016; 30(9): 1195-8. | Irrelevant study design |
Scott Lowery, R., Nick, T. G., Shelton, J. B., Warner, D., Green, T. Long-term visual acuity and initial postoperative refractive error in pediatric pseudophakia. Can J Ophthalmol April 2011; 46(2): 143-147. | Irrelevant population |
Sen, P., Attiku, Y., Bhende, P., Rishi, E., Ratra, D., Sreelakshmi, K. Outcome of sutured scleral fixated intraocular lens in Marfan syndrome in pediatric eyes. Int Ophthalmol Jun 2020; 40(6): 1531-1538. | Irrelevant population |
Sen, P., Kshetrapal, M., Shah, C., Mohan, A., Jain, E., Sen, A. Posterior capsule opacification rate after phacoemulsification in pediatric cataract: Hydrophilic versus hydrophobic intraocular lenses. J Cataract Refract Surg 10 2019; 45(10): 1380-1385. | Irrelevant population |
Sen, P., Shah, C., Sen, A., Jain, E., Mohan, A. Primary versus secondary intraocular lens implantation in traumatic cataract after open-globe injury in pediatric patients. J Cataract Refract Surg Dec 2018; 44(12): 1446-1453. | Irrelevant population |
Sen, P., Sreelakshmi, K., Bhende, P., Gopal, L., Rishi, P., Rishi, E., Susvar, P., Attiku, Y. Outcome of Sutured Scleral-Fixated Intraocular Lens in Blunt and Penetrating Trauma in Children. Ophthalmic Surg Lasers Imaging Retina 10 01 2018; 49(10): 757-764. | Irrelevant population |
Shenoy, B. H., Mittal, V., Gupta, A., Sachdeva, V., Kekunnaya, R. Complications and visual outcomes after secondary intraocular lens implantation in children. Am J Ophthalmol Apr 2015; 159(4): 720-6. | Irrelevant population |
Shuaib, A. M., El Sayed, Y., Kamal, A., El Sanabary, Z., Elhilali, H. Transscleral sutureless intraocular lens versus retropupillary iris-claw lens fixation for paediatric aphakia without capsular support: a randomized study. Acta Opthalmologica Sep 2019; 97(6): e850-e859. | Irrelevant population |
Sijssens, K. M., Los, L. I., Rothova, A., Schellekens, P. A., van de Does, P., Stilma, J. S., de Boer, H. J. Long-term ocular complications in aphakic versus pseudophakic eyes of children with juvenile idiopathic arthritis-associated uveitis. Br J Ophthalmol Sep 2010; 94(9): 1145-9. | Irrelevant population |
Sillen H, Van Looveren J, Plaeke P, Van Os L, Tassignon MJ. Real-time intraoperative OCT imaging of the vitreolenticular interface during pediatric cataract surgery. J Cataract Refract Surg. 2021; 9: 1153-1160. | Irrelevant population |
Solebo, A. L., Cumberland, P., Rahi, J. S., British Isles Congenital Cataract Interest Group. 5-year outcomes after primary intraocular lens implantation in children aged 2 years or younger with congenital or infantile cataract: findings from the IoLunder2 prospective inception cohort study. The Lancet Child Adolescent Health 12 2018; 2(12): 863-871. | Irrelevant population |
Solebo, A. L., Hammond, C. J., Rahi, J. S. Improving outcomes in congenital cataract. Nature 04 Apr 2018; 556(7699): E1-E2. | Irrelevant population |
Solebo, A. L., Rahi, J. S., British Congenital Cataract Interest Group. Visual Axis Opacity after Intraocular Lens Implantation in Children in the First 2 Years of Life: Findings from the IoLunder2 Cohort Study. Ophthalmology 09 2020; 127(9): 1220-1226. | Irrelevant population |
Solebo, A. L., Russell-Eggitt, I., Cumberland, P. M., Rahi, J. S., British Isles Congenital Cataract Interest Group. Risks and outcomes associated with primary intraocular lens implantation in children under 2 years of age: the IoLunder2 cohort study. Br J Ophthalmol Nov 2015; 99(11): 1471-6. | Irrelevant population |
Solebo, A. L., Russell-Eggitt, I., Cumberland, P., Rahi, J. S. Congenital cataract associated with persistent fetal vasculature: findings from IoLunder2. Eye Sep 2016; 30(9): 1204-9. | Irrelevant population |
Spiess, K., Calvo, J. P. Clinical characteristics and treatment of secondary glaucoma after pediatric congenital cataract surgery in a tertiary referral hospital in spain. J Pediatr Ophthalmol Strabismus October 2020; 57(5): 292-300. | Irrelevant population |
Struck, M. C. Long-term results of pediatric cataract surgery and primary intraocular lens implantation from 7-22 months of life. JAMA Ophthalmol Oct 2015; 133(10): 1180-3. | Irrelevant population |
Sukhija, J., Kaur, S. Central corneal thickness and intraocular pressure changes after congenital cataract surgery with intraocular lens implantation in children younger than 2 years. J Cataract Refract Surg 05 2017; 43(5): 662-666. | Irrelevant population |
Sukhija, J., Kaur, S., Ram, J. Outcome of primary intraocular lens implantation in infants: Complications and rates of additional surgery. J Cataract Refract Surg 07 2016; 42(7): 1060-5. | Irrelevant study design |
Sukhija, J., Kaur, S., Ram, J. Outcome of a New Acrylic Intraocular Lens Implantation in Pediatric Cataract. J Pediatr Ophthalmol Strabismus Nov-Dec 2015; 52(6): 371-6. | Irrelevant population |
Sukhija, J., Kaur, S., Ram, J., Yangzes, S., Madan, S., Jinagal, J. Outcome of various Hydrophobic Acrylic Intraocular Lens Implantations in Children with Congenital Cataract. Eur J Ophthalmol Nov 08 2017; 27(6): 711-715. | Irrelevant population |
Sukhija, J., Ram, J., Gupta, N., Sawhney, A., Kaur, S. Long-term results after primary intraocular lens implantation in children operated less than 2 years of age for congenital cataract. Indian J Ophthalmol Dec 2014; 62(12): 1132-5. | Irrelevant population |
Sukhija, J., Ram, J., Kaur, S. Complications in the first 5 years following cataract surgery in infants with and without intraocular lens implantation in the infant aphakia treatment study. Am J Ophthalmol Dec 2014; 158(6): 1360-1. | Irrelevant study design |
Tachibana K, Maeda N, Abe K, Kusaka S. Efficacy of Toric Intraocular Lens and Prevention of Axis Misalignment by Optic Capture in Pediatric Cataract Surgery. J Cataract Refract Surg. 2021; 18. | Irrelevant population |
Tadros, D., Trivedi, R. H., Wilson, M. E. Primary versus secondary IOL implantation following removal of infantile unilateral congenital cataract: outcomes after at least 5 years. J AAPOS Feb 2016; 20(1): 25-9. | Irrelevant intervention |
Tadros, D., Trivedi, R. H., Wilson, M. E., Davidson, J. D. Ocular axial growth in pseudophakic eyes of patients operated for monocular infantile cataract: a comparison of operated and fellow eyes measured at surgery and 5 or more years later. J AAPOS 06 2016; 20(3): 210-3. | Does not answer research questions |
Tassignon, M. J., Gobin, L., Mathysen, D., Van Looveren, J., De Groot, V. Clinical outcomes of cataract surgery after bag-in-the-lens intraocular lens implantation following ISO standard 11979 to 7:2006. J Cataract Refract Surg Dec 2011; 37(12): 2120-9. | Irrelevant population |
Tataru, C. I., Tataru, C. P., Costache, A., Boruga, O., Zemba, M., Ciuluvica, R. C., Sima, G. Congenital cataract - clinical and morphological aspects. Rom J Morphol Embryol 2020; 61(1): 105-112. | Irrelevant population |
Tornquist, A. L., Olsson, M., Martin, L., Winiarski, J., Fahnehjelm, K. T. Visual field results and optic disc morphology in patients treated with allogeneic stem-cell transplantation in childhood. Acta Opthalmologica Feb 2011; 89(1): 62-9. | Irrelevant population |
Traboulsi, E. I., Drews-Botsch, C. D., Christiansen, S. P., Stout, A. U., Hartmann, E. E., Lambert, S. R. Rate of ocular trauma in children operated on for unilateral cataract in infancy-data from the Infant Aphakia Treatment Study. J AAPOS October 2020; 24(5): 301-303. | Irrelevant study design |
Trivedi, R. H., Boden, J. H., Mickler, C., Wilson, M. E. Intraocular pressure elevation during early postoperative period after secondary intraocular lens implantation in children and adolescents. J Cataract Refract Surg Sep 2012; 38(9): 1633-6. | Irrelevant population |
Trivedi, R. H., Wilson, M. E., Vasavada, A. R., Shah, S. K., Vasavada, V., Vasavada, V. A. Visual axis opacification after cataract surgery and hydrophobic acrylic intraocular lens implantation in the first year of life. J Cataract Refract Surg Jan 2011; 37(1): 83-7. | Irrelevant study design |
Tsai, T. H., Tsai, C. Y., Huang, J. Y., Hu, F. R. Outcomes of pediatric cataract surgery with triamcinolone-assisted vitrectomy. Journal of the Formosan Medical Association Dec 2017; 116(12): 940-945. | Irrelevant population |
Urban, B., Bakunowicz-Lazarczyk, A. Aphakic glaucoma after congenital cataract surgery with and without intraocular lens implantation. Klin Oczna 2010; 112(4-6): 105-7. | Full text not available |
Van Looveren, J., Ni Dhubhghaill, S., Godts, D., Bakker, E., De Veuster, I., Mathysen, D. G., Tassignon, M. J. Pediatric bag-in-the-lens intraocular lens implantation: long-term follow-up. J Cataract Refract Surg Aug 2015; 41(8): 1685-92. | Irrelevant study design |
VanderVeen, D. K., Drews-Botsch, C. D., Nizam, A., Bothun, E. D., Wilson, L. B., Wilson, M. E., Lambert, S. R. Outcomes of Secondary Intraocular Lens Implantation in the Infant Aphakia Treatment Study. J Cataract Refract Surg 2020. | Irrelevant population |
VanderVeen, D. K., Drews-Botsch, C. D., Nizam, A., Bothun, E. D., Wilson, L. B., Wilson, M. E., Lambert, S. R., Infant Aphakia Treatment Study. Outcomes of Secondary Intraocular Lens Implantation in the Infant Aphakia Treatment Study. J Cataract Refract Surg Sep 07 2020; 07: 07. | Irrelevant population |
Vasavada, A. R., Vasavada, S. A., Bobrova, N., Praveen, M. R., Shah, S. K., Vasavada, V. A., Pardo, A. Jv, Raj, S. M., Trivedi, R. H. Outcomes of pediatric cataract surgery in anterior persistent fetal vasculature. J Cataract Refract Surg May 2012; 38(5): 849-57. | Irrelevant population |
Ventura, M. C., Ventura, B. V., Ventura, C. V., Ventura, L. O., Arantes, T. E., Nose, W. Outcomes of congenital cataract surgery: intraoperative intracameral triamcinolone injection versus postoperative oral prednisolone. J Cataract Refract Surg Apr 2014; 40(4): 601-8. | Irrelevant population |
Wall, P. B., Lee, J. A., Lynn, M. J., Lambert, S. R., Traboulsi, E. I., Infant Aphakia Treatment Study Group. The effects of surgical factors on postoperative astigmatism in patients enrolled in the Infant Aphakia Treatment Study (IATS). J AAPOS Oct 2014; 18(5): 441-5. | Does not answer research questions |
Wang, J., Chen, J., Chen, W., Wang, Q., Zhao, L., Wang, R., Liu, Z., Chen, H., Cao, Q., Tan, X., Lin, Z., Li, X., Li, J., Lai, W., Zhu, Y., Chen, C., Zheng, D., Wu, M., Han, Y., Chen, W., Liu, Y., Lin, H. Incidence of and Risk Factors for Suspected Glaucoma and Glaucoma After Congenital and Infantile Cataract Surgery: A Longitudinal Study in China. J Glaucoma 01 2020; 29(1): 46-52. | Irrelevant population |
Warren, N., Trivedi, R. H., Wilson, M. E. Persistent Fetal Vasculature With Elongated Ciliary Processes in Children. Am J Ophthalmol 02 2019; 198: 25-29. | Irrelevant population |
Weakley, D. R., Jr., Lynn, M. J., Dubois, L., Cotsonis, G., Wilson, M. E., Buckley, E. G., Plager, D. A., Lambert, S. R., Infant Aphakia Treatment Study Group. Myopic Shift 5 Years after Intraocular Lens Implantation in the Infant Aphakia Treatment Study. Ophthalmology 06 2017; 124(6): 822-827. | Does not answer research questions |
Weakley, D., Cotsonis, G., Wilson, M. E., Plager, D. A., Buckley, E. G., Lambert, S. R., Infant Aphakia Treatment Study Group. Anisometropia at Age 5 Years After Unilateral Intraocular Lens Implantation During Infancy in the Infant Aphakia Treatment Study. Am J Ophthalmol Aug 2017; 180: 1-7. | Does not answer research questions |
Wilson, M. E., Jr., Hafez, G. A., Trivedi, R. H. Secondary in-the-bag intraocular lens implantation in children who have been aphakic since early infancy. J AAPOS Apr 2011; 15(2): 162-6. | Irrelevant population |
Wilson, M. E., Trivedi, R. H. Safety of piggyback intraocular lenses (polypseudophakia) in children: long-term outcomes of a 15-year, single-surgeon study. J AAPOS 08 2020; 24(4): 230.e1-230.e4. | Irrelevant intervention |
Wilson, M. E., Trivedi, R. H., Weakley, D. R., Jr., Cotsonis, G. A., Lambert, S. R., Infant Aphakia Treatment Study Group. Globe Axial Length Growth at Age 10.5 Years in the Infant Aphakia Treatment Study. Am J Ophthalmol 08 2020; 216(): 147-155. | Does not answer research questions |
Wood, K. S., Tadros, D., Trivedi, R. H., Wilson, M. E. Secondary intraocular lens implantation following infantile cataract surgery: intraoperative indications, postoperative outcomes. Eye Sep 2016; 30(9): 1182-6. | Irrelevant population |
Writing Committee for the Pediatric Eye Disease Investigator Group, Repka, M. X., Dean, T. W., Kraker, R. T., Bothun, E. D., Morrison, D. G., Lambert, S. R., Stahl, E. D., Wallace, D. K. Visual Acuity and Ophthalmic Outcomes in the Year After Cataract Surgery Among Children Younger Than 13 Years. JAMA Ophthalmol 07 01 2019; 137(7): 817-824. | Irrelevant population |
Yagev, R., Khatib, N., Barrett, C., Lior, Y., Lifshitz, T., Tsumi, E. Intraocular lens implantation as an isolated risk factor for secondary glaucoma in pediatric patients. Can J Ophthalmol 10 2019; 54(5): 621-625. | Irrelevant population |
Yang, Y., Yao, T. T., Zhou, Y. L., Wang, Y. X., Wang, Z. Y. A modified intrascleral intraocular lens fixation technique with fewer anterior segment manipulations: 27-gauge needle-guided procedure with built-in 8 to 0 absorbable sutures. BMC Ophthalmol Nov 21 2019; 19(1): 234. | Irrelevant population |
Yangzes, S., Kaur, S., Gupta, P. C., Sharma, M., Jinagal, J., Singh, J., Ram, J. Intraocular lens implantation in children with unilateral congenital cataract in the first 4 years of life. Eur J Ophthalmol May 2019; 29(3): 304-308. | Irrelevant population |
Yangzes, S., Seth, N. G., Singh, R., Gupta, P. C., Jinagal, J., Pandav, S. S., Gupta, V., Gupta, A., Ram, J. Long-term outcomes of cataract surgery in children with uveitis. Indian J Ophthalmol Apr 2019; 67(4): 490-495. | Irrelevant population |
Yeh, A. G., Kong, L., Yen, K. G. Long-term Outcomes of Primary Intraocular Lens Implantation in Patients Aged 7 to 24 Months. J Pediatr Ophthalmol Strabismus May 01 2017; 54(3): 149-155. | Irrelevant study design |
Zhang, H., Xie, L., Wu, X., Tian, J. Long-term results of pediatric cataract surgery after delayed diagnosis. J AAPOS Feb 2012; 16(1): 65-9. | Irrelevant population |
Zhang, K., Liu, X., Jiang, J., Li, W., Wang, S., Liu, L., Zhou, X., Wang, L. Prediction of postoperative complications of pediatric cataract patients using data mining. J Transl Med 01 03 2019; 17(1): 2. | Irrelevant population |
Zhao, Y. E., Gong, X. H., Zhu, X. N., Li, H. M., Tu, M. J., Coursey, T. G., Pflugfelder, S. C., Gu, F., Chen, D. Long-term outcomes of ciliary sulcus versus capsular bag fixation of intraocular lenses in children: An ultrasound biomicroscopy study. PLoS ONE 2017; 12(3): e0172979. | Irrelevant population |
Appendix 12: Additional References of Potential Interest
Note that this appendix has not been copy-edited.
TAPS
Bothun ED, Wilson ME, Yen KG, et al. Outcomes of Bilateral Cataract Surgery in Infants 7 to 24 Months of Age Using the Toddler Aphakia and Pseudophakia Treatment Study Registry. Ophthalmology. 2020;15:15. PubMed
Bothun ED, Wilson ME, Traboulsi EI, et al. Outcomes of Unilateral Cataracts in Infants and Toddlers 7 to 24 Months of Age: Toddler Aphakia and Pseudophakia Study (TAPS). Ophthalmology. 2019;126(8):1189-1195. PubMed
IOL Implantation in Children Younger Than 2 Years of Age (“IOLunder2” study)
Solebo LA, Rahi JS, Group BICCI. IOLunder2: Outcomes Following Surgery With And Without Primary Intraocular Lens Implantation In Children under 2years Old. Invest Ophthalmol Vis Sci. 2012;53(14):6769-6769.
Cost Studies
Kruger SJ, DuBois L, Becker ER, et al. Cost of intraocular lens versus contact lens treatment after unilateral congenital cataract surgery in the infant aphakia treatment study at age 5 years. Ophthalmology. 2015;122(2):288-292. PubMed
Carrigan AK, DuBois LG, Becker ER, Lambert SR, Infant Aphakia Treatment Study G. Cost of intraocular lens versus contact lens treatment after unilateral congenital cataract surgery: retrospective analysis at age 1 year. Ophthalmology. 2013;120(1):14-19. PubMed
Other Studies
Chen J, Chen Y, Zhong Y, Li J. Comparison of visual acuity and complications between primary IOL implantation and aphakia in patients with congenital cataract younger than 2 years: a meta-analysis. J Cataract Refract Surg. 2020;46(3):465-473. PubMed
Cao K, Wang J, Zhang J, et al. Efficacy and safety of vitrectomy for congenital cataract surgery: a systematic review and meta-analysis based on randomized and controlled trials. Acta Ophthalmol (Oxf). 2019;97(3):233-239. PubMed
Lambert SR, Aakalu VK, Hutchinson AK, et al. Intraocular Lens Implantation during Early Childhood: A Report by the American Academy of Ophthalmology. Ophthalmology. 2019;126(10):1454-1461. PubMed
Mohammadpour M, Shaabani A, Sahraian A, et al. Updates on managements of pediatric cataract. Journal of Current Ophthalmology. 2019;31(2):118-126. PubMed
Zhang S, Wang J, Li Y, Liu Y, He L, Xia X. The role of primary intraocular lens implantation in the risk of secondary glaucoma following congenital cataract surgery: A systematic review and meta-analysis. PLoS ONE [Electronic Resource]. 2019;14(4):e0214684. PubMed
Mataftsi A, Haidich AB, Kokkali S, et al. Postoperative glaucoma following infantile cataract surgery: an individual patient data meta-analysis. JAMA Ophthalmology. 2014;132(9):1059-1067. PubMed
Hug D. Intraocular lens use in challenging pediatric cases. Curr Opin Ophthalmol. 2010;21(5):345-349. PubMed
Ledoux DM, Trivedi RH, Wilson ME, Jr., Payne JF. Pediatric cataract extraction with intraocular lens implantation: visual acuity outcome when measured at age four years and older. J AAPOS. 2007;11(3):218-224. PubMed
Trivedi R, Wilson M, Bartholomew L, Lal G, Peterseim M. Opacification of the visual axis after cataract surgery and single acrylic intraocular lens implantation in the first year of life. J AAPOS. 2004;8:156-164. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca