CADTH Health Technology Review
Systemic Thrombolysis and Endovascular Therapy for Large Vessel Occlusion Acute Ischemic Stroke
Rapid Review with Expert Input
Authors: Keeley Farrell, Nicole Askin
External Reviewer
This document was externally reviewed by a content expert, who granted permission to be cited.
Grant Stotts, MD
Neurologist
Ottawa Hospital and Ottawa Hospital Research Institute
Abbreviations
EVT
endovascular therapy
mRS
modified Rankin Scale
NIHSS
National Institutes of Health Stroke Scale
RCT
randomized controlled trial
TICI
thrombolysis in cerebral infarction
Key Message
Evidence was mixed, with higher-quality evidence suggesting that there were no differences between treatment with alteplase before endovascular therapy or endovascular therapy alone in patients with large vessel occlusion acute ischemic stroke for outcomes related to safety and efficacy, and lower-quality evidence indicating a difference between the groups for certain outcomes.
Context and Policy Issues
In Canada, approximately 62,000 people with strokes and transient ischemic attacks are treated in hospitals each year.1 Stroke is a leading cause of disability in adults and the third leading cause of death in Canada.1 An acute ischemic stroke is a sudden loss of blood flow to an area of the brain due to occlusion of a blood vessel by a blood clot (thrombosis) or piece of foreign material (embolism) and the resulting loss of neurological function.2 Ischemic strokes are classified as occurring due to small vessel or large vessel occlusions.3 Small vessel strokes are due to occlusion of small (< 0.5 mm) vessels whereas large vessel occlusion strokes are due to occlusions in large (1 mm to 4 mm) vessels.3 Approximately 30% to 40% of strokes are caused by a large vessel occlusion.4
Current treatment options for large vessel occlusion acute ischemic stroke include IV thrombolysis with alteplase and/or endovascular therapy (EVT).5 Alteplase (also referred to as tissue plasminogen activator) is an enzyme that dissolves blood clots.6 In those who have had an acute ischemic stroke and receive IV alteplase, symptomatic intracranial hemorrhage and major systemic bleeding complications have been reported to occur in approximately 6% and 2% of patients, respectively.7 Due to alteplase’s narrow therapeutic window and low recanalization rate for large vessel occlusions, EVT was developed.4 EVT is a catheter-based approach that can include intraarterial thrombolysis and/or mechanical clot retrieval (thrombectomy).5
The Canadian Stroke Best Practice Recommendations for Acute Stroke Management recommend the use of IV alteplase in combination with endovascular thrombectomy in patients with large vessel occlusion acute ischemic stroke who are eligible for alteplase.1 There is uncertainty around the comparative effectiveness of IV alteplase and EVT versus EVT alone for the treatment of large vessel occlusion acute ischemic stroke.
This report is part of a series of 2 reports on the use of alteplase in acute ischemic stroke. The other report aimed to summarize the evidence regarding the safety and effectiveness of alteplase given with 3 hours, or alteplase given between 3 and 4.5 hours in adult patients with acute ischemic stroke. The aim of the current report is to summarize the evidence regarding the comparative clinical effectiveness of systemic thrombolysis with alteplase combined with EVT versus EVT alone in patients with large vessel occlusion acute ischemic stroke.
Research Question
What is the clinical effectiveness of systemic thrombolysis combined with EVT compared to EVT alone in patients with large vessel occlusion acute ischemic stroke?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Library, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were alteplase and large vessel occlusion acute ischemic stroke. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses or network meta-analyses, randomized controlled trials (RCTs), or controlled clinical trials. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2014, and February 2, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients with large vessel occlusion acute ischemic stroke |
Intervention | Endovascular therapy and systemic thrombolysis with alteplase |
Comparator | Endovascular therapy alone or with placebo |
Outcomes | Clinical effectiveness (e.g., neurological outcomes, symptom free status, disability free status) and safety (e.g., all-cause mortality, adverse events, bleeding, intracranial hemorrhage, symptomatic intracranial hemorrhage) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2014. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for systematic reviews, the “questionnaire to assess the relevance and credibility of a network meta-analysis”9 for network meta-analyses, and the Downs and Black checklist10 for randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
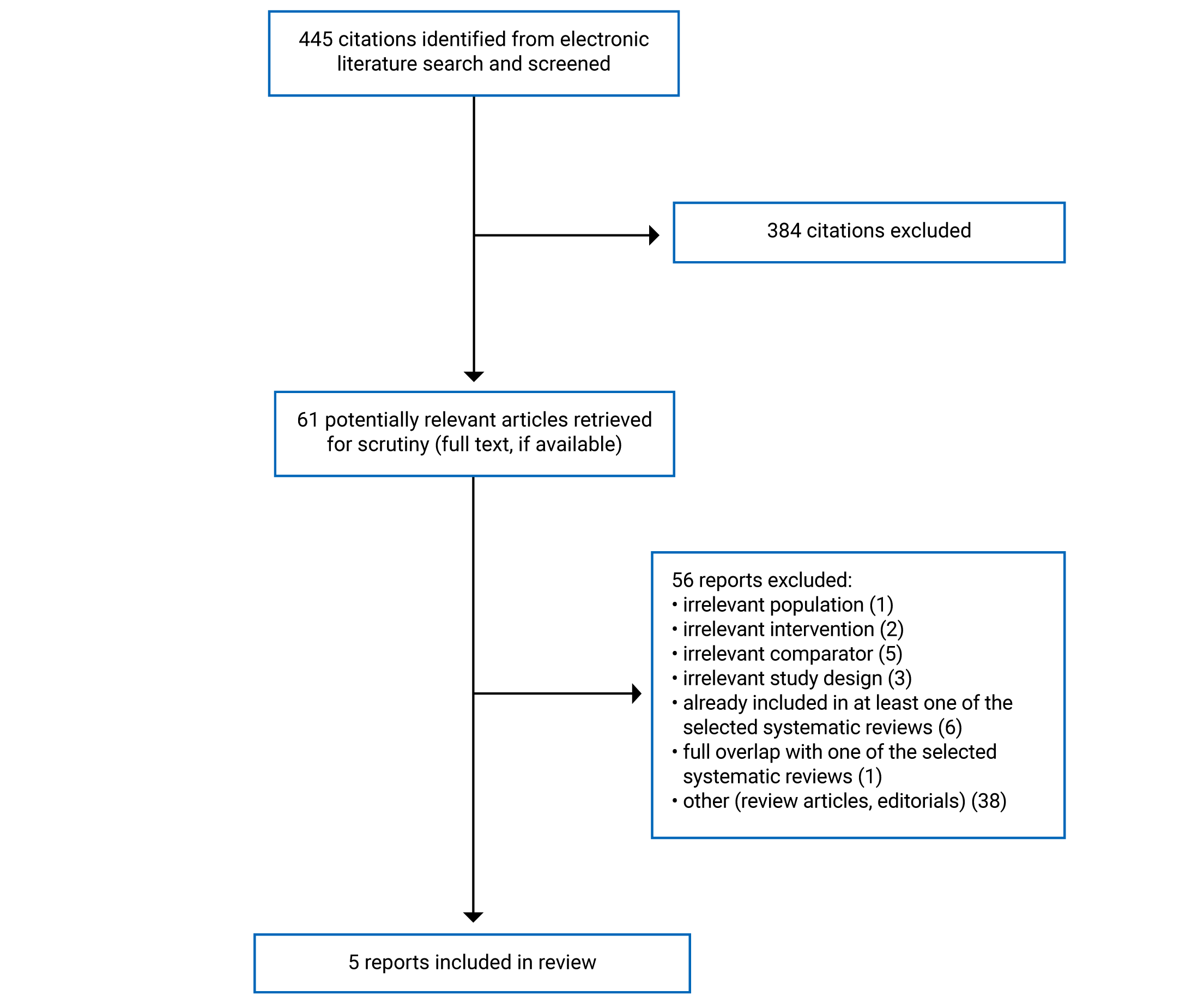
A total of 445 citations were identified in the literature search. Following screening of titles and abstracts, 384 citations were excluded and 61 potentially relevant reports from the electronic search were retrieved for full-text review. Of these potentially relevant articles, 56 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. These comprised 4 systematic reviews and 1 RCT. Appendix 1 presents the PRISMA11 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
In total, 3 systematic reviews with meta-analyses,12-14 1 systematic review with a network meta-analysis,15 and 1 RCT16 were included in this report. No relevant health technology assessments were identified.
One of the included systematic reviews15 had broader inclusion criteria than the present report. Specifically, it evaluated the clinical effectiveness of IV thrombolysis, intraarterial thrombolysis, mechanical thrombectomy, or any combination of these, and eligible thrombolytic treatments included urokinase and alteplase. Only the characteristics and results of the subset of relevant studies will be described in this report.
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
The systematic review and meta-analysis by Chen et al. (2021)12 included 3 RCTs. The search time frame was RCTs published up to and including April 16, 2021. The systematic review and network meta-analysis by Hui et al. (2020)15 included 17 RCTs (10 of which are relevant to the present report). The search was conducted from October 17, 2018, to October 19, 2018, and no restrictions were imposed based on date of publication. Only 1 of the comparisons included in the network meta-analysis was relevant to the present report (mechanical thrombectomy versus IV alteplase before mechanical thrombectomy).15 A Bayesian framework was used to perform the network meta-analysis and the relevant comparison was based on a random-effects model.15 The systematic review and meta-analysis by Kaesmacher et al. (2019)13 included 20 studies in total (10 retrospective observational studies, 6 prospective observational studies, 1 pooled analysis of 1 RCT, 1 prospective observational study, and 3 RCTs). The search time frame was from January 2007 to May 2017. The systematic review and meta-analysis by Mistry et al. (2017)14 included 13 studies in total (3 post hoc analyses of RCTs, and 10 retrospective studies). The search time frame was studies published up to and including March 21, 2017. In the RCTs included in Kaesmacher et al. (2019)13 and Mistry et al. (2017),14 patients were not randomized to receive alteplase. Patients included in these RCTs were randomized to receive alteplase and EVT or alteplase alone and in the 2 SRs13,14 the data from these studies were analyzed in patients who underwent EVT, comparing those who did and did not receive IV alteplase. Three of the included systematic reviews13-15 had overlap in their included primary studies. Thirteen primary studies were included in more than 1 systematic review. A citation matrix depicting the overlap between the included systematic reviews is provided in Appendix 5. Only primary studies that provide direct evidence relevant to this report were included in the overlap table.
The RCT was a multi-centre, open-label study.16
Country of Origin
Two of the systematic reviews were conducted by authors in China.12,15 The other systematic reviews were conducted by authors in Switzerland13 and the US.14
The RCT was conducted in the Netherlands.16
Patient Population
All the systematic reviews included adult patients with large vessel occlusion acute ischemic stroke.12-15 Two of the systematic reviews12,14 specified that the large vessel occlusions must be in the anterior circulation, and 1 review15 specified that the occlusion locations had to be identified by imaging. In the systematic review by Chen et al. (2021),12 all patients had to be eligible for IV thrombolysis within 4.5 hours of symptom onset. In the systematic review by Chen et al. (2021),12 543 patients received EVT alone and 549 patients received IV alteplase before EVT. In the systematic review by Hui et al. (2020),15 50 patients received EVT alone and 966 patients received IV alteplase before EVT. The systematic review by Kaesmacher et al. (2019)13 included 2,399 patients who received EVT alone and 2,880 patients who received IV alteplase before EVT. The systematic review by Mistry et al. (2017)14 included 1,332 patients who received EVT alone and 2,221 patients who received IV alteplase before EVT.
The RCT included 539 patients (273 in the EVT alone group, 266 in the alteplase and EVT group) with acute ischemic stroke due to an intracranial proximal occlusion of the anterior circulation who were eligible for EVT and IV alteplase within 4.5 hours of symptom onset.16 The median age of patients was 71 years and 56.6% of patients were male. A modified intention-to-treat population was analyzed that included all patients who provided consent, and patients were analyzed according to their assigned trial group.16
Interventions and Comparators
All of the included systematic reviews compared mechanical thrombectomy to IV alteplase administered before mechanical thrombectomy.12-15 The thrombectomy devices and alteplase doses used in the studies included in Chen et al. (2021)12 were not specified. In Hui et al. (2020),15 studies that used first generation thrombectomy devices were excluded and all the relevant studies used an alteplase dose of 0.9 mg per kg of body weight (maximum of 90 mg). In Kaesmacher et al. (2019),13 alteplase doses were not specified; however, most patients (≥ 80%) needed to be treated with a second generation thrombectomy device (stent retrievers or aspiration devices) for a study to be eligible. Eleven of the studies included in Mistry et al. (2017)14 used stent retrievers or aspiration devices, and 2 of the studies did not specify the device used. All the included studies in Mistry et al. (2017)14 used an alteplase dose of 0.9 mg per kg of body weight, except 1 that used a dose of 0.6 mg per kg of body weight.
In the RCT,16 patients in the EVT alone group underwent EVT performed with a stent retriever. Rescue IV alteplase at a dose of 0.9 mg per kg of body weight (maximum of 90 mg) was allowed if there was incomplete reperfusion after EVT. Patients in the control group received IV alteplase (0.9 mg per kg of body weight) administered before EVT performed with a stent retriever. In both groups, intraarterial alteplase (maximum dose of 30 mg) was permitted at the discretion of the interventionist and suction catheters could be used as a rescue approach.
Outcomes
Three of the included systematic reviews12-14 and the RCT16 assessed functional outcomes as measured by the modified Rankin Scale (mRS). The mRS measures functional outcomes on a scale ranging from 0 (no disability) to 6 (death). The 3 systematic reviews12-14 assessed 90-day functional independence, which was defined as an mRS score of less than or equal to 2. The systematic review by Chen et al. (2021)12 also assessed 90-day excellent outcome, which was defined as an mRS score of less than or equal to 1. The primary outcome in the RCT16 was median mRS score at 90 days. The primary outcome was assessed for superiority and then for noninferiority of EVT alone versus IV alteplase before EVT. The noninferiority margin was specified as 0.8 for the lower boundary of the 95% confidence interval of the common odds ratio.16 The authors state that a noninferiority boundary of 0.8 constitutes 97.5% certainty that EVT alone does not differ more than approximately 5% in the percentage of patients with an mRS score of 0 to 2 in favour of alteplase before EVT. The authors set this noninferiority margin based on research that has been published on noninferiority margins for trials of thrombectomy devices.16 Additionally, 1 of the secondary outcomes was a comparison within 3 dichotomized groups with respect to mRS scores (0 or 1, not 2 to 6; 0 to 2, not 3 to 6; 0 to 3, not 4 to 6) at 90 days.16
Two of the systematic reviews12,13 and the RCT16 assessed successful reperfusion after mechanical thrombectomy, which was defined as a thrombolysis in cerebral infarction (TICI) score of 2b, 2c, or 3. The TICI scale ranges from 0 (no reperfusion) to 3 (complete reperfusion). In the RCT,16 successful reperfusion was assessed at the last intracranial angiogram. The systematic review by Kaesmacher et al. (2019)13 also assessed complete reperfusion (TICI 3). The RCT16 also assessed recanalization on the first intracranial angiogram and after 24 hours. Recanalization was defined as a modified Arterial Occlusive Lesion score of 2 or higher. The score ranges from 0 (no recanalization) to 3 (complete recanalization).
Additional clinical outcomes assessed in the RCT16 included stroke severity, quality of life, activities of daily living, and final lesion volume. Stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS) (scores range from 0 to 42, with higher scores indicating more severe neurological deficit). Quality of life was assessed using the EQ-5D 5-Level self-report questionnaire (scores range from −0.446 to 1.00, with higher scores indicating better health status). Activities of daily living were assessed using the Barthel Index, which quantifies performance of self-care activities of daily living, with scores ranging from 0 (severe disability) to 100 (no disability). The final lesion volume was measured on MRI at 24 hours or on non-contrast CT at 5 days, 7 days, or at discharge.
All 4 systematic reviews12-15 and the RCT16 assessed mortality at 90 days. Three of the systematic reviews12-14 and the RCT16 assessed symptomatic intracranial or intracerebral hemorrhage. The systematic review by Kaesmacher et al. (2019)13 also assessed asymptomatic intracerebral hemorrhage, and the RCT16 assessed any intracerebral hemorrhage.
Additional safety end points assessed in the RCT16 included embolization to a new territory, infarction in a new territory on follow-up, femoral-artery false aneurysm, and groin hematoma.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included studies are provided in Appendix 3.
Systematic Reviews
All 4 systematic reviews12-15 had clear objectives and study eligibility criteria. The review methods were established before conducting the review in the systematic reviews by Chen et al. (2021)12 and Hui et al. (2020).15 Additionally, the protocol for the Hui et al. (2020) systematic review and network meta-analysis was registered. The other 2 systematic reviews did not include a statement that the review methods were established before conducting the review.13,14 This has the potential to introduce bias if the methods were adjusted after the review had begun. All 4 systematic reviews12-15 conducted their literature searches in multiple databases, and the search dates, any search restrictions, and key search terms used were provided. Providing details on these elements of the search strategy increases its reproducibility. None of the systematic reviews provided a list of excluded studies; however, reasons for exclusion were provided.12-15 In all the systematic reviews, study selection was performed independently by at least 2 reviewers, reducing the risk of bias in this domain. Data extraction was performed independently by at least 2 reviewers in 3 of the systematic reviews.12,14,15 In Kaesmacher et al. (2019),13 data extraction was performed by 1 reviewer and cross-checked by a second reviewer. Performing data extraction in duplicate decreases the likelihood of inconsistencies. The included primary studies were described in adequate detail in Hui et al. (2020).15 In the other 3 systematic reviews,12-14 some details of the included studies were lacking. In the systematic reviews by Chen et al. (2021)12 and Kaesmacher et al. (2019),13 alteplase dose, time frame for follow-up, and the settings of the included studies were not specified. Additionally, alteplase dose in the included studies was not specified in Chen et al. (2021).12 Limited details were provided on the populations and settings of the included studies in Mistry et al. (2017).14
The risk of bias of the included primary studies was assessed using a satisfactory technique in all 4 systematic reviews.12-15 Appropriate methods for the statistical combination of results were used in the 3 systematic reviews that included meta-analyses.12-14 In Chen et al. (2021),12 heterogeneity was assessed and the choice to use a fixed-effects or random-effects model to pool the results followed this assessment. In Kaesmacher et al. (2019),13 an inverse variance heterogeneity model was used that assumes heterogeneous studies and the presence of multiple true effect sizes. Subgroup analyses that included only data from RCTs were also performed.13 In Mistry et al. (2017),14 heterogeneity was assessed, a random-effects model was used, and subgroup analyses were conducted in data from RCTs and non-randomized studies. The included primary studies were all assessed as having a low risk of bias in the systematic review by Chen et al. (2021).12 The authors of Kaesmacher et al. (2019),13 stated that a risk of bias was noted in all the included studies, with the most common source being nonrandom allocation to treatment groups, which existed in all studies. The authors of Mistry et al. (2017)14 stated that a considerable risk of bias existed in the included studies. In the systematic reviews by Kaesmacher et al. (2019)13 and Mistry et al. (2017),14 the pooled estimates included data from non-randomized studies, and patients included in the RCTs were not randomized to receive alteplase. Therefore, many of the included patients who received mechanical thrombectomy alone were not eligible for IV alteplase, which may have led to imbalances between the treatment groups in important prognostic factors (e.g., stroke etiology, risk factors, time to treatment). The authors of the Kaesmacher et al. (2019)13 systematic review attempted to account for these differences between treatment groups by performing subgroup analyses in those who were eligible and ineligible for IV thrombolysis. The results of these 2 systematic reviews13,14 should be interpreted with caution due to the risk of bias in the included studies and the potential imbalances between the treatment groups. Publication bias was assessed in 3 of the systematic reviews.13-15 The authors of the Chen et al. (2021)12 systematic review do not state whether they performed an assessment of publication bias. Potential conflicts of interest were disclosed in all 4 systematic reviews,12-15 and 3 of the systematic reviews12,13,15 reported their funding sources. The authors of the Mistry et al. (2017)14 systematic review did not report whether they received any funding for the conduct of the review. Both the Kaesmacher et al. (2019)13 and Mistry et al. (2017)14 systematic reviews are assessed as being low quality due to the high risk of bias in the included primary studies.
Network Meta-Analysis
The systematic review by Hui et al. (2020)15 included a network meta-analysis that had several methodological strengths. Details on the strategy for the statistical analysis were specified in the protocol.17 A Bayesian framework was used to perform the network meta-analysis, the relevant comparison was based on a random-effects model, and heterogeneity was assessed. The population, intervention, comparator, and outcomes are relevant to the current report. A comprehensive search strategy was used that should have identified all relevant RCTs. The interventions of interest formed 1 connected network of RCTs. The findings of the network meta-analysis were clearly reported in graphical and tabular formats. One limitation of the network meta-analysis was that most of the included studies were open label and were assessed as having a high risk of bias. Additionally, no RCTs that directly compared the interventions of interest (mechanical thrombectomy versus IV alteplase before mechanical thrombectomy) were included; therefore, consistency between direct and indirect comparisons could not be assessed. Finally, the authors state that they could not adjust for potential effect modifiers such as NIHSS score, percentage of elderly patients, gender proportions, and specific treatment time windows. Imbalances in effect modifiers across studies can result in biased effect estimates.
Randomized Controlled Trial
The objective, patient characteristics, interventions, and main findings of the included RCT16 were clearly described. Commonly known adverse events were reported and the main outcome measures were valid and reliable. A power calculation was conducted and it was determined that 540 patients would provide 91% power to detect a true treatment effect with a 2-sided significance level of 0.05. In total, 547 patients were randomized and 539 provided consent for participation and were included in the modified intention-to-treat analysis. The analysis was based on the modified intention-to-treat population and a separate analysis was not conducted in the per-protocol population. A per-protocol analysis may be a more conservative approach when assessing noninferiority.18 There were 10 patients in each group who did not receive the treatment they were assigned. Additionally, patients in the EVT alone group were permitted to receive rescue IV alteplase if there was incomplete reperfusion after EVT. There were 19 patients (7.3%) in the EVT alone group who received rescue IV alteplase. The study used an open-label design; however, attempts were made to blind the individuals who measured outcomes to the treatment assignments. Some of the study outcomes were subjective (e.g., functional outcome, quality of life) and may have therefore been susceptible to bias due to the patients who were unblinded. Objective outcomes such as mortality are unlikely to be influenced by blinding. Patients in different intervention groups were recruited from the same population over the same time period and no patients were lost to follow-up. Patients were randomized to treatment groups using a web-based system with the use of permuted blocks stratified according to centre. The authors state that they did not keep screening logs to determine the number of patients who were eligible for enrolment; therefore, it is unclear whether the study sample is representative of the source population from which it was recruited. Adjustments to outcomes were made for age, sex, prestroke score on the mRS, duration from onset to randomization, stroke severity (NIHSS score), and collateral status. Adjusting for potential confounding factors in the analysis helps reduce the risk of bias. Although multiple secondary outcomes were assessed, the statistical analysis did not adjust for multiplicity. Adjusting for multiplicity is important in trials that assess multiple outcomes due to the potential inflation of the type I error rate. The authors reported potential conflicts of interest and the funding sources for the study, and the authors stated that the funders were not involved in trial design or planning, or in the analysis or reporting of data.
Summary of Findings
The main study findings are presented in Appendix 4.
Clinical Effectiveness of Systemic Thrombolysis and Endovascular Therapy
Evidence regarding the clinical effectiveness of systemic thrombolysis and EVT versus EVT alone for the treatment of large vessel occlusion acute ischemic stroke was available from 3 systematic reviews with meta-analyses,12-14 1 systematic review with a network meta-analysis,15 and 1 RCT.16 These findings should be considered within the context of the significant overlap between the primary studies included in 3 of the systematic reviews;13-15 therefore, the pooled estimates from these reviews contain some of the same data. A citation matrix depicting the overlap between the reviews is provided in Appendix 5.
Functional Outcome (mRS Scores)
There were no significant differences in 90-day functional independence (mRS score ≤ 2) between alteplase before EVT and EVT alone in the Chen et al. (2021)12 and Kaesmacher et al. (2019)13 meta-analyses. In the meta-analysis conducted by Mistry et al. (2017)14 there was a significant difference for 90-day functional independence in favour of alteplase before EVT versus EVT alone. However, when data from randomized and non-randomized studies were pooled separately in Mistry et al. (2017),14 there were no significant differences between the treatment groups in 90-day functional independence.
The meta-analysis by Chen et al. (2021)12 also assessed excellent outcome (mRS score ≤ 1) and there was no significant difference between alteplase before EVT and EVT alone.
In the RCT,16 there was no significant difference in the primary end point (median mRS score at 90 days) between the EVT alone and alteplase before EVT groups. These findings indicate that EVT alone was not superior or noninferior to alteplase before EVT because the lower boundary of the 95% confidence interval included 0.8. Additionally, no significant differences were found between the treatment groups for dichotomized mRS scores.
Mortality
Results from the meta-analysis by Chen et al. (2021)12 and the network meta-analysis by Hui et al. (2020)15 indicated that there were no significant differences in 90-day mortality between alteplase before EVT and EVT alone. Results from the meta-analyses by Kaesmacher et al. (2019)13 and Mistry et al. (2017)14 indicated that there were significant differences in 90-day mortality in favour of alteplase before EVT versus EVT alone. In a subgroup analysis of only those eligible for IV thrombolysis in Kaesmacher et al. (2019),13 there was no significant difference between treatment groups. In a subgroup analysis that only included data from non-randomized studies in Mistry et al. (2017),14 there was no significant difference between treatment groups.
There was no significant difference between the EVT alone and alteplase before EVT groups in regard to 90-day mortality in the RCT.16
Reperfusion and Recanalization
Results from the meta-analyses by Chen et al. (2021)12 and Kaesmacher et al. (2019)13 indicated that there were no significant differences in successful reperfusion (TICI 2b and TICI 3) between alteplase before EVT and EVT alone. Complete reperfusion (TICI 3) was also assessed in Kaesmacher et al. (2019)13 and there was no significant difference between treatment groups.
There were no significant differences between the EVT alone and alteplase before EVT groups in recanalization or successful reperfusion in the RCT.16
Hemorrhage
There was no significant difference in symptomatic intracranial hemorrhage between alteplase before EVT and EVT alone in the meta-analysis by Chen et al. (2021).12 There were no significant differences in symptomatic intracerebral hemorrhage between treatment groups in the Kaesmacher et al. (2019)13 or Mistry et al. (2017)14 meta-analyses.
The meta-analysis by Kaesmacher et al. (2019)13 indicated that there was no significant difference in asymptomatic intracerebral hemorrhage between treatment groups. However, in a subgroup analysis that only included patients eligible for IV thrombolysis, there was a significant difference in asymptomatic intracerebral hemorrhage in favour of EVT alone versus alteplase before EVT.
There were no significant differences between treatment groups in any intracerebral hemorrhage or symptomatic intracerebral hemorrhage in the RCT.16
Additional Efficacy Outcomes
The RCT16 assessed several additional efficacy outcomes. The median NIHSS score (a measure of stroke severity) was 6 in both treatment groups at 24 hours, and 4 in the EVT alone group and 3 in the alteplase before EVT group at 5 days, 7 days, or at discharge.16 The median EQ-5D 5-Level score (a measure of quality of life) was 0.8 in both treatment groups at 90 days.16 The proportion of patients with a Barthel Index score (a measure of activities of daily living) of 95 to 100 was 54.4% in the EVT alone group and 58.9% in the alteplase before EVT group at 90 days.16 The final lesion volume at follow-up imaging was 24 mL in the EVT alone group and 17 mL in the alteplase before EVT group.16
Additional Safety Outcomes
The RCT16 also assessed several additional safety outcomes. There were no significant differences between the EVT alone and alteplase before EVT groups in the proportion of patients with embolization to a new territory, infarction in a new territory on follow-up imaging, femoral-artery false aneurysm, or groin hematoma.
Limitations
The RCT by LeCouffe et al. (2021)16 and the RCTs included in the systematic review by Chen et al. (2021)12 were not conducted in Canada. The settings of the included primary studies in the other 3 systematic reviews13-15 were not specified. Therefore, it is unclear whether the findings are generalizable to patients in Canada.
In the RCT by LeCouffe et al. (2021),16 patients in the EVT alone group were permitted to receive rescue IV alteplase if reperfusion did not occur. This was not permitted in the RCTs included in the systematic review by Chen et al. (2021).12 Further, intraarterial alteplase was permitted in both groups in the RCT by LeCouffe et al. (2021),16 whereas the method used for EVT was thrombectomy alone in the RCTs included in the systematic review by Chen et al. (2021).12 Therefore, there is heterogeneity between the treatment groups in these RCTs.
In the RCTs included in 3 of the systematic reviews,13-15 patients were not randomized to receive alteplase. Additionally, 2 of the systematic reviews13,14 included non-randomized studies. Therefore, the results of these reviews are at risk of confounding and other forms of bias.
The network meta-analysis did not include studies that directly compared alteplase before EVT and EVT alone.15 Therefore, the results from the network meta-analysis presented in this report are based on an indirect comparison only.
No studies were identified that compared patients who received alteplase and EVT to those who received placebo and EVT. The RCT by LeCouffe et al. (2021)16 and the RCTs included in the systematic review by Chen et al. (2021)12 were not placebo controlled; therefore, patients were aware of their treatment group assignment. However, the use of a placebo-controlled design for these interventions presents challenges as treatment may be delayed in patients assigned to the placebo group.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 3 systematic reviews with meta-analyses,12-14 1 systematic review with a network meta-analysis,15 and 1 RCT16 on the clinical effectiveness of systemic thrombolysis and EVT versus EVT alone for the treatment of large vessel occlusion acute ischemic stroke.
Results from 1 RCT16 and 1 meta-analysis of RCTs12 in which patients were randomized to receive either alteplase before EVT or EVT alone indicated that there were no significant differences between the treatment groups in functional outcome, mortality, successful reperfusion, or symptomatic intracranial or intracerebral hemorrhage. There was no significant difference in mortality between alteplase before EVT and EVT alone in the network meta-analysis.15 Results from systematic reviews with meta-analyses that included both non-randomized studies and RCTs in which patients were not randomized to receive alteplase (Kaesmacher et al. [2019]13 and Mistry et al. [2017]14) indicated that there were significant differences in favour of alteplase before EVT versus EVT alone for certain outcomes. However, these results should be interpreted with caution due to the risk of bias in the included primary studies. There were significant differences in mortality in favour of alteplase before EVT versus EVT alone in the meta-analyses by Kaesmacher et al. (2019)13 and Mistry et al. (2017).14 In subgroup analyses that only included patients eligible for IV alteplase (Kaesmacher et al. [2019]13) and data from non-randomized studies (Mistry et al. [2017]14), there were no significant differences between the treatment groups in mortality. In Mistry et al. (2017),14 there was a significant difference in functional outcome in favour of alteplase before EVT versus EVT alone. However, when data from randomized and non-randomized studies were pooled separately, there were no significant differences between the treatment groups in functional outcome.14 There were no significant differences between the treatment groups in symptomatic intracerebral hemorrhage in either of the meta-analyses.13,14 Additionally, there were no significant differences between the treatment groups in functional outcome, successful reperfusion, or asymptomatic intracerebral hemorrhage in the meta-analysis by Kaesmacher et al. (2019).13
The limitations of the included literature (e.g., lack of blinding in the RCTs,12,16 lack of direct comparison in the network meta-analysis,15 and the inclusion of studies at high risk of bias in 2 of the meta-analyses13,14) should be considered when interpreting the findings of this report. Evidence from 1 RCT16 and 1 meta-analysis of RCTs12 suggests that there are no significant differences in functional outcome, mortality, successful reperfusion, or symptomatic intracranial or intracerebral hemorrhage between treatment with alteplase before EVT and EVT alone in patients with large vessel occlusion acute ischemic stroke treated within 4.5 hours of symptom onset. There are at least 2 additional RCTs19,20 currently underway that could help further reduce uncertainty around the clinical effectiveness of systemic thrombolysis with alteplase combined with EVT versus EVT alone for the treatment of large vessel occlusion acute ischemic stroke. Additional research that evaluates the comparative efficacy of different EVT approaches (i.e., mechanical thrombectomy, intraarterial thrombolysis, or a combined approach) could also aid decision-making around the use of EVT for patients with large vessel occlusion acute ischemic stroke.
References
1.Boulanger JM, Lindsay MP, Gubitz G, et al. Canadian Stroke Best Practice Recommendations for Acute Stroke Management: Prehospital, Emergency Department, and Acute Inpatient Stroke Care, 6th Edition, Update 2018. Int J Stroke. 2018;13(9):949-984.
2.Phipps MS, Cronin CA. Management of acute ischemic stroke. BMJ. 2020;368:l6983. PubMed
3.Smith WS. Endovascular Stroke Therapy. Neurotherapeutics. 2019;16(2):360-368. PubMed
4.Shafie M, Yu W. Recanalization Therapy for Acute Ischemic Stroke with Large Vessel Occlusion: Where We Are and What Comes Next? Transl Stroke Res. 2021;12(3):369-381. PubMed
5.Bhatia K, Bhagavan S, Bains N, et al. Current Endovascular Treatment of Acute Ischemic Stroke. Mo Med. 2020;117(5):480-489. PubMed
6.National Institute of Neurological Disorders and Stroke. Tissue plasminogen activator for acute ischemic stroke (Alteplase, Activase®). 2019; https://www.ninds.nih.gov/About-NINDS/Impact/NINDS-Contributions-Approved-Therapies/Tissue-Plasminogen-Activator-Acute. Accessed 2022 Feb 28.
7.Katsanos AH, Tsivgoulis G. Is intravenous thrombolysis still necessary in patients who undergo mechanical thrombectomy? Curr Opin Neurol. 2019;32(1):3-12. PubMed
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Chen J, Wan TF, Xu TC, Chang GC, Chen HS, Liu L. Direct Endovascular Thrombectomy or With Prior Intravenous Thrombolysis for Acute Ischemic Stroke: A Meta-Analysis. Front Neurol. 2021;12:752698. PubMed
13.Kaesmacher J, Mordasini P, Arnold M, et al. Direct mechanical thrombectomy in tPA-ineligible and -eligible patients versus the bridging approach: a meta-analysis. J Neurointerv Surg. 2019;11(1):20-27. PubMed
14.Mistry EA, Mistry AM, Nakawah MO, et al. Mechanical Thrombectomy Outcomes With and Without Intravenous Thrombolysis in Stroke Patients: A Meta-Analysis. Stroke. 2017;48(9):2450-2456. PubMed
15.Hui W, Wu C, Zhao W, et al. Efficacy and Safety of Recanalization Therapy for Acute Ischemic Stroke With Large Vessel Occlusion: A Systematic Review. Stroke. 2020;51(7):2026-2035. PubMed
16.LeCouffe NE, Kappelhof M, Treurniet KM, et al. A Randomized Trial of Intravenous Alteplase before Endovascular Treatment for Stroke. N Engl J Med. 2021;385(20):1833-1844. PubMed
17.Hui W, Wu C, Liang H, Zhao W, Ji X. Clinical efficacy and safety of intravenous thrombolysis, endovascular treatment and bridging therapy for acute ischemic stroke: protocol for a systematic review and network meta-analysis (CRD42019128604). PROSPERO: International prospective register of systematic reviews. York (GB): University of York Centre for Reviews and Dissemination; 2019: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=128604. Accessed 2022 Mar 3.
18.Wangge G, Klungel OH, Roes KC, de Boer A, Hoes AW, Knol MJ. Interpretation and inference in noninferiority randomized controlled trials in drug research. Clin Pharmacol Ther. 2010;88(3):420-423. PubMed
19.Fischer U, Kaesmacher J, P SP, et al. SWIFT DIRECT: Solitaire TM With the Intention For Thrombectomy Plus Intravenous t-PA Versus DIRECT Solitaire TM Stent-retriever Thrombectomy in Acute Anterior Circulation Stroke: Methodology of a randomized, controlled, multicentre study. Int J Stroke. 2021:17474930211048768. PubMed
20.Mitchell PJ, Yan B, Churilov L, et al. DIRECT-SAFE: A Randomized Controlled Trial of DIRECT Endovascular Clot Retrieval versus Standard Bridging Therapy. J Stroke. 2022;24(1):57-64. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix was not copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Chen et al. (2021)12 China National Nature Science Foundation of China | Study design: SR and meta-analysis Included studies: 3 RCTs | Studies of patients aged 18 years or older with acute ischemic stroke with large vessel occlusion primarily in the anterior circulation. All patients had to be eligible for IV thrombolysis within 4.5 hours of symptom onset. | Intervention: mechanical thrombectomy Comparator: IV thrombolysis using alteplase combined with mechanical thrombectomy | Outcomes: functional independence, successful reperfusion, symptomatic intracranial hemorrhage, excellent outcome, mortality Follow-up: 3 months |
Hui et al. (2020)15 China The National Key R&D Program of China, Cheung Kong Scholars Program, Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding | Study design: SR and NMA Included studies: 17 RCTs including 10 relevant to the present report | Studies of patients aged 18 years or older with large vessel occlusion acute ischemic stroke whose occlusion locations were identified by imaging. Median time from symptom onset to thrombolysis was reported individually by study and ranged from 85 to 350 minutes. | Eligible interventions: IV thrombolysis, intraarterial thrombolysis, mechanical thrombectomy or a combination of these; thrombolytic treatments included urokinase and alteplase Relevant interventions: mechanical thrombectomy, mechanical thrombectomy in combination with IV alteplase | Outcomes: all-cause mortality Follow-up: 90 days |
Kaesmacher et al. (2019)13 Switzerland The SAMW/Bangerter Foundation | Study design: SR and meta-analysis Included studies: 20 studies in total (10 retrospective studies, 6 prospective observational studies, 1 pooled analysis of 1 RCT and 1 prospective observational study, and 3 RCTs) | Studies of adult patients with acute ischemic stroke with large vessel occlusion were included. Subgroup analyses were conducted in patients eligible and ineligible for IV thrombolysis. Average time from symptom onset to groin puncture was reported individually by study and ranged from 106 to 330 minutes. | Intervention: mechanical thrombectomy Comparator: IV thrombolysis with alteplase before mechanical thrombectomy | Outcomes: functional independence, successful reperfusion, symptomatic intracerebral hemorrhage, asymptomatic intracerebral hemorrhage, mortality Follow-up: 90 days |
Mistry et al. (2017)14 US NR | Study design: SR and meta-analysis Included studies: 13 studies in total (3 post-hoc analyses of RCTs, 10 retrospective studies) | Studies of adult patients with acute ischemic stroke from a large vessel occlusion of the anterior cerebral circulation were included. Average time from symptom onset to groin puncture was reported individually by study and ranged from 130 to 300 minutes. | Intervention: IV thrombolysis with alteplase before mechanical thrombectomy Comparator: mechanical thrombectomy | Outcomes: good functional outcomes, successful recanalization, symptomatic intracerebral hemorrhage, mortality Follow-up: 90 days |
NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Randomized Controlled Trial
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
LeCouffe et al. (2021)16 The Netherlands The Collaboration for New Treatments of Acute Stroke consortium, the Brain Foundation Netherlands, the Ministry of Economic Affairs, Stryker, Medtronic, and Cerenovus | Open-label, multicentre, randomized trial | Inclusion criteria: patients aged 18 years or older with acute ischemic stroke due to an intracranial proximal occlusion of the anterior circulation that were eligible for EVT and IV alteplase within 4.5 hours of symptom onset Baseline characteristics: Overall: 539 patients with a median age of 71 years, 56.6% male EVT alone group: 273 patients with a median age of 72, 59% male, median NIHSS score of 16, medical history – 17.2% ischemic stroke, 31.5% atrial fibrillation, 14.7% diabetes, 44.3% hypertension Alteplase with EVT group: 266 patients with a median age of 69, 54.1% male, median NIHSS score of 16, medical history – 16.5% ischemic stroke, 23.7% atrial fibrillation, 18.8% diabetes, 52.5% hypertension | Intervention: EVT performed with a stent retriever Comparator: IV alteplase (0.9 mg/kg of body weight [maximum, 90 mg]) administered (10% as bolus and 90% as 1-hour infusion) before EVT performed with a stent retriever | Outcomes: functional outcome, recanalization, successful reperfusion, NIHSS score, final lesion volume, quality of life, interference with daily activities, intracranial hemorrhage, symptomatic intracerebral hemorrhage, post procedure aneurism or hematoma, embolization, infarction, mortality Follow-up: 90 days |
EVT = endovascular therapy; NIHSS = National Institutes of Health Stroke Scale.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 28 and the ISPOR Questionnaire9
Strengths | Limitations |
|---|---|
Chen et al. (2021)12 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The review methods were established before conducting the review The choice of study designs included in the review (i.e., RCTs) was explained The literature search was conducted in multiple databases and a trial registry, key search terms used were provided, and the reference lists of included articles were handsearched for additional relevant literature Study selection and data extraction were performed independently by 2 reviewers Populations of included primary studies were described in detail The risk of bias in included primary studies was assessed independently by 2 reviewers using a satisfactory technique Appropriate methods were used for the statistical combination of results Included primary studies were all assessed as having a low risk of bias Authors state that no obvious heterogeneity was observed for primary outcome The funding source for the review was reported and the authors declared that they had no conflicts of interest | List of excluded studies not provided, however reasons for exclusion were provided Some details for included primary studies were lacking such as alteplase dose, devices used for EVT, time frame for follow-up, and study settings The sources of funding for the included primary studies were not reported Assessment of heterogeneity for secondary outcomes was not described It is unclear whether authors performed an assessment of publication bias |
Hui et al. (2020)15 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The review methods were established before conducting the review and the protocol was registered The choice of study designs included in the review (i.e., RCTs) was explained The literature search was conducted in multiple databases and trial registries, full search strategy provided, no language restrictions were used, and the reference lists of included articles were handsearched for additional relevant literature | List of excluded studies not provided, however reasons for exclusion were provided Network meta-analysis Most of the included studies were open-label and were assessed as having a high risk of bias No RCTs that directly compared the interventions of interest were included The authors state that they could not adjust for factors that may impact prognosis (e.g., NIHSS score, percentage of elderly patients, gender proportions, and specific treatment time windows) |
Study selection and data extraction were performed independently by 4 reviewers Included primary studies were described in adequate detail however, the settings of included studies were not described The risk of bias in included primary studies was assessed independently by 4 reviewers using a satisfactory technique The authors state that they assessed the source of funding of the included primary studies as an additional bias item Publication bias was assessed The funding sources for the review were reported and the authors declared that they had no conflicts of interest The authors state that the funders had no role in study design, data collection, data analyses, data interpretation, or writing of the article Network meta-analysis The population, intervention, comparator, and outcomes are relevant to the current report Comprehensive search strategy that should have identified all relevant RCTs The interventions of interest formed one connected network of RCTs Statistical methods were used that preserve within-study randomization A random effects model was used, and heterogeneity was assessed The findings were clearly reported in graphical and tabular formats | |
Kaesmacher et al. (2019)13 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The choice of study designs included in the review (i.e., RCTs and non-randomized studies) was explained The literature search was conducted in multiple databases and a trial registry, full search strategy was provided, and no language restrictions were used Study selection was performed independently by 2 reviewers Data extraction was performed by 1 reviewer and cross-checked by a second reviewer Populations of included primary studies were described in adequate detail | It is unclear whether the review methods were established before conducting the review and the authors state that an analysis protocol was not published before conducting the meta-analysis List of excluded studies was not provided, however reasons for exclusion were provided Some details for included primary studies were lacking such as alteplase dose, time frame for follow-up, and study settings The sources of funding for the included primary studies were not reported Pooled estimates include data from non-randomized studies and patients in the included RCTs were not randomized to receive alteplase |
The risk of bias in included primary studies was assessed using a satisfactory technique Appropriate methods were used for the statistical combination of results Influence analysis was performed by excluding each study from the model and assessing the impact summary estimates Publication bias was assessed The funding sources for the review and potential conflicts of interest were reported | |
Mistry et al. (2017)14 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The choice of study designs included in the review (i.e., RCTs and non-randomized studies) was explained The literature search was conducted in multiple databases, key search terms used were provided, no language restrictions were used, and the reference lists of included articles were handsearched for additional relevant literature Study selection and data extraction were performed independently by 2 reviewers Interventions, comparators, outcomes, and designs of included primary studies were described in adequate detail The risk of bias in included primary studies was assessed using a satisfactory technique Appropriate methods were used for the statistical combination of results Sensitivity analysis was performed by sequential exclusion of 1 study at a time to assess the impact on summary estimates Publication bias was assessed and adjusted for Potential conflicts of interest were disclosed | It is unclear whether the review methods were established before conducting the review List of excluded studies was not provided, however reasons for exclusion were provided Limited details were provided on the populations and settings of included primary studies The sources of funding for the included primary studies were not reported Pooled estimates include data from non-randomized studies and patients in the included RCTs were not randomized to receive alteplase The authors do not state whether any funding was received for the review |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; EVT = endovascular therapy; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NIHSS = National Institutes of Health Stroke Scale; RCT = randomized controlled trial.
Table 5: Strengths and Limitations of Randomized Controlled Trial Using the Downs and Black Checklist10
Strengths | Limitations |
|---|---|
LeCouffe et al. (2021)16 | |
Objective, patient characteristics, interventions, and main findings clearly described Estimates of random variability (e.g., 95% confidence intervals) were reported Commonly known adverse events reported No patients were lost to follow-up Patients, care providers, and care setting were representative of the population and setting of interest Attempts were made to blind individuals measuring outcomes to treatment assignments The main outcome measures were valid and reliable Patients in different intervention groups were recruited from the same population over the same time period Participants were randomly allocated to intervention groups Adjustments to outcomes were made for age, sex, prestroke score on the mRS, duration from onset to randomization, stroke severity (NIHSS score), and collateral status A power calculation was conducted a priori to determine sample size The funding sources for the study and potential conflicts of interest were reported The authors state that the funders were not involved in trial design or planning, or in the analysis or reporting of data | The authors did not keep screening logs to determine the number of patients who were eligible for enrolment Study used an open-label design The statistical analysis did not adjust for multiplicity |
mRS = - modified Rankin Scale; NIHSS = National Institutes of Health Stroke Scale.
Appendix 4: Main Study Findings
Note that this appendix was not copy-edited.
Table 6: Summary of Findings by Outcome — Functional Outcome
Study citation and study design | Subgroup | OR (95% CI) | P value |
|---|---|---|---|
90-day functional independence (mRS score ≤ 2) | |||
Chen et al. (2021)12 SR and meta-analysis (3 RCTs) | NA | 1.08 (0.85 to 1.38) OR > 1 favours mechanical thrombectomy alone | 0.539 |
Kaesmacher et al. (2019)13 SR and meta-analysis | Randomized studies (3 RCTs and 1 pooled analysis of 1 RCT and 1 observational study) | 0.80 (0.58 to 1.12) OR > 1 favours mechanical thrombectomy alone | NR |
IVT-E (3 non-randomized studies) | 1.08 (0.67 to 1.76) OR > 1 favours mechanical thrombectomy alone | NR | |
IVT-IN (12 non-randomized studies, 3 RCTs) | 0.78 (0.61 to 1.01) OR > 1 favours mechanical thrombectomy alone | NR | |
Overall (IVT-E and IVT-IN) (14 non-randomized studies, 3 RCTs) | 0.82 (0.65 to 1.03) OR > 1 favours mechanical thrombectomy alone | NR | |
Mistry et al. (2017)14 SR and meta-analysis | Randomized studies (2 post-hoc analyses corresponding to 7 RCTs) | 1.28 (0.93 to 1.75) OR > 1 favours IV alteplase before mechanical thrombectomy | 0.12 |
Non-randomized studies (8 studies) | 1.31 (0.99 to 1.73) OR > 1 favours IV alteplase before mechanical thrombectomy | 0.06 | |
Overall (2 post-hoc analyses of RCTs, 8 non-randomized studies) | 1.27 (1.05 to 1.55) OR > 1 favours IV alteplase before mechanical thrombectomy | 0.02 | |
90-day excellent outcome (mRS score ≤ 1) | |||
Chen et al. (2021)12 SR and meta-analysis (3 RCTs) | NA | 1.12 (0.85 to 1.47) OR > 1 favours mechanical thrombectomy alone | 0.418 |
Note: mRS measures functional outcome on a scale ranging from 0 (no disability) to 6 (death).
CI = confidence interval; IVT-E = IV thrombolysis-eligible direct mechanical thrombectomy patients; IVT-IN, IV thrombolysis-ineligible direct mechanical thrombectomy patients; mRS = modified Rankin Scale; NA = not applicable; NR = not reported; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 7: Summary of Findings by Outcome — Mortality
Study citation and study design | Subgroup | OR | P value |
|---|---|---|---|
90-day mortality | |||
Chen et al. (2021)12 SR and meta-analysis (3 RCTs) | NA | 0.93 (95% CI = 0.68 to 1.29) OR < 1 favours mechanical thrombectomy alone | 0.673 |
Hui et al. (2020)15 SR and NMA (10 RCTs) | NA | 0.21 (95% CrI = 0.01 to 2.30) OR < 1 favours IV alteplase before mechanical thrombectomy | NR |
Kaesmacher et al. (2019)13 SR and meta-analysis | Randomized studies (3 RCTs and 1 pooled analysis of 1 RCT and 1 observational study) | 1.83 (95% CI = 1.16 to 2.91) OR < 1 favours mechanical thrombectomy alone | NR |
IVT-E (3 non-randomized studies) | 0.84 (95% CI = 0.40 to 1.75) OR < 1 favours mechanical thrombectomy alone | NR | |
IVT-IN (12 non-randomized studies, 3 RCTs) | 1.45 (95% CI = 1.22 to 1.73) OR < 1 favours mechanical thrombectomy alone | NR | |
Overall (IVT-E and IVT-IN) (14 non-randomized studies, 3 RCTs) | 1.35 (95% CI = 1.07 to 1.71) OR < 1 favours mechanical thrombectomy alone | NR | |
Mistry et al. (2017)14 SR and meta-analysis | Randomized studies (2 post-hoc analyses corresponding to 7 RCTs) | 0.56 (95% CI = 0.36 to 0.86) OR < 1 favours IV alteplase before mechanical thrombectomy | 0.007 |
Non-randomized studies (8 studies) | 0.76 (95% CI = 0.56 to 1.03) OR < 1 favours IV alteplase before mechanical thrombectomy | 0.08 | |
Overall (2 post-hoc analyses of RCTs, 8 non-randomized studies) | 0.71 (95% CI = 0.55 to 0.91) OR < 1 favours IV alteplase before mechanical thrombectomy | 0.006 | |
CI = confidence interval; CrI = credible interval; IVT-E = IV thrombolysis-eligible direct mechanical thrombectomy patients; IVT-IN, IV thrombolysis-ineligible direct mechanical thrombectomy patients; NA = not applicable; NMA = network meta-analysis; NR = not reported; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Table 8: Summary of Findings by Outcome — Reperfusion
Study citation and study design | Subgroup | OR (95% CI) | P value |
|---|---|---|---|
Successful reperfusion (TICI 2b/3) | |||
Chen et al. (2021)12 SR and meta-analysis (3 RCTs) | NA | 0.75 (0.54 to 1.05) OR > 1 favours mechanical thrombectomy alone | 0.099 |
Kaesmacher et al. (2019)13 SR and meta-analysis | Randomized studies (3 RCTs and 1 pooled analysis of 1 RCT and 1 observational study) | 1.32 (0.89 to 1.95) OR > 1 favours mechanical thrombectomy alone | NR |
IVT-E (3 non-randomized studies) | 1.67 (0.95 to 2.94) OR > 1 favours mechanical thrombectomy alone | NR | |
IVT-IN (14 non-randomized studies, 3 RCTs) | 0.86 (0.63 to 1.19) OR > 1 favours mechanical thrombectomy alone | NR | |
Overall (IVT-E and IVT-IN) (16 non-randomized studies, 3 RCTs) | 0.93 (0.68 to 1.28) OR > 1 favours mechanical thrombectomy alone | NR | |
Complete reperfusion (TICI 3) | |||
Kaesmacher et al. (2019)13 SR and meta-analysis (7 non-randomized studies, 2 RCTs) | NA | 0.98 (0.80 to 1.21) OR > 1 favours mechanical thrombectomy alone | NR |
CI = confidence interval; IVT-E = IV thrombolysis-eligible direct mechanical thrombectomy patients; IVT-IN, IV thrombolysis-ineligible direct mechanical thrombectomy patients; NA = not applicable; NR = not reported; OR = odds ratio; SR = systematic review; TICI = thrombolysis in cerebral infarction.
Table 9: Summary of Findings by Outcome — Hemorrhage
Study citation and study design | Subgroup | OR (95% CI) | P value |
|---|---|---|---|
Symptomatic intracranial hemorrhage | |||
Chen et al. (2021)12 SR and meta-analysis (3 RCTs) | NA | 0.72 (0.45 to 1.15) OR < 1 favours mechanical thrombectomy alone | 0.171 |
Symptomatic intracerebral hemorrhage | |||
Kaesmacher et al. (2019)13 SR and meta-analysis | IVT-E (3 non-randomized studies) | 0.95 (0.51 to 1.76) OR < 1 favours mechanical thrombectomy alone | NR |
IVT-IN (12 non-randomized studies, 3 RCTs) | 0.83 (0.58 to 1.19) OR < 1 favours mechanical thrombectomy alone | NR | |
Overall (IVT-E and IVT-IN) (14 non-randomized studies, 3 RCTs) | 0.86 (0.63 to 1.17) OR < 1 favours mechanical thrombectomy alone | NR | |
Mistry et al. (2017)14 SR and meta-analysis (10 non-randomized studies) | NA | 1.11 (0.69 to 1.77) OR < 1 favours IV alteplase before mechanical thrombectomy | 0.67 |
Asymptomatic intracerebral hemorrhage | |||
Kaesmacher et al. (2019)13 SR and meta-analysis | IVT-E (3 non-randomized studies) | 0.49 (0.30 to 0.81) OR < 1 favours mechanical thrombectomy alone | NR |
IVT-IN (10 non-randomized studies, 3 RCTs) | 1.07 (0.88 to 1.30) OR < 1 favours mechanical thrombectomy alone | NR | |
Overall (IVT-E and IVT-IN) (12 non-randomized studies, 3 RCTs) | 0.93 (0.72 to 1.19) OR < 1 favours mechanical thrombectomy alone | NR | |
CI = confidence interval; IVT-E = IV thrombolysis-eligible direct mechanical thrombectomy patients; IVT-IN, IV thrombolysis-ineligible direct mechanical thrombectomy patients; NA = not applicable; NR = not reported; OR = odds ratio; SR = systematic review.
Table 10: Summary of Findings of Included Randomized Controlled Trial — Efficacy
Outcome | Time point | Le Couffe et al. (2021)16 | |||
|---|---|---|---|---|---|
EVT alone (N = 273) | Alteplase before EVT (N = 266) | Measure of effect | Adjusted valuea (95% CI) | ||
Functional outcome | |||||
mRS score Median (IQR) Note: mRS measures functional outcome on a scale ranging from 0 (no disability) to 6 (death). | 90 days | 3 (2 to 5) | 2 (2 to 5) | Common OR | 0.84 (0.62 to 1.15) P value = 0.28 |
Dichotomized mRS scores No. (%) Note: mRS measures functional outcome on a scale ranging from 0 (no disability) to 6 (death). | |||||
0 or 1, not 2 to 6 | 90 days | 44 (16.1) | 41 (15.4) | OR | 1.01 (0.63 to 1.63) |
0 to 2, not 3 to 6 | 90 days | 134 (49.1) | 136 (51.1) | OR | 0.95 (0.65 to 1.39) |
0 to 3, not 4 to 6 | 90 days | 161 (59.0) | 161 (60.5) | OR | 0.99 (0.66 to 1.48) |
Stroke severity | |||||
NIHSS score Median (IQR) Note: scores range from 0 to 42 with higher scores indicating more severe neurological deficit. | 24 hours | 6 (2 to 14) | 6 (1 to 14) | Beta coefficient | 0.11 (−0.05 to 0.28) |
5 to 7 days or at discharge | 4 (1 to 13) | 3 (1 to 9) | Beta coefficient | 0.21 (0.03 to 0.38) | |
Quality of life | |||||
EQ-5D-5L score Median (IQR) Note: scores range from −0.446 to 1.00 with higher scores indicating better health status. | 90 days | 0.8 (0.7 to 0.9) | 0.8 (0.7 to 1.0) | Beta coefficient | −0.08 (−0.14 to −0.01) |
Activities of daily living | |||||
Barthel index score of 95 to 100 No./total no. (%) Note: scores range from 0 (severe disability) to 100 (no disability) | 90 days | 136/250 (54.4) | 142/241 (58.9) | OR | 0.98 (0.66 to 1.48) |
Recanalization and reperfusion | |||||
Recanalization No./total no. (%) | First intracranial angiogram | 7/250 (2.8) | 9/245 (3.7) | OR | 0.79 (0.42 to 1.47) |
24 hours | 172/220 (78.2) | 171/202 (84.7) | OR | 0.82 (0.52 to 1.28) | |
Successful reperfusion (TICI 2b/3) No./total no. (%) | Last intracranial angiogram | 192/244 (78.7) | 196/236 (83.1) | OR | 0.73 (0.47 to 1.13) |
Final lesion volume | |||||
Final lesion volume (mL) Median (IQR) | Follow-up imaging | 24 (7 to 76) | 17 (5 to 72) | Beta coefficient | 1.22 (0.92 to 1.63) |
CI = confidence interval; EQ-5D-5L = EQ-5D 5-Level; EVT = endovascular therapy; IQR = interquartile range; mRS = modified Rankin Scale; NIHSS = National Institutes of Health Stroke Scale; no. = number; OR = odds ratio; TICI = thrombolysis in cerebral infarction.
aAdjustments were made for age, sex, pre-stroke score on the mRS, duration from onset to randomization, stroke severity, and collateral status.
Table 11: Summary of Findings of Included Randomized Controlled Trial — Safety
Outcome | Le Couffe et al. (2021)16 | ||
|---|---|---|---|
EVT alone (N = 273) | Alteplase before EVT (N = 266) | ORa (95% CI) | |
Mortality at 90 days No. (%) | 56 (20.5) | 42 (15.8) | 1.39 (0.84 to 2.30) |
Any intracerebral hemorrhage No./total no. (%) | 89/248 (35.9) | 85/239 (35.6) | 0.97 (0.68 to 1.38) |
HI1 | 32/248 (12.9) | 35/239 (14.6) | 0.82 (0.50 to 1.34) |
HI2 | 23/248 (9.3) | 15/239 (6.3) | 1.27 (0.67 to 2.41) |
PH1 | 9/248 (3.6) | 14/239 (5.9) | 0.66 (0.32 to 1.39) |
PH2 | 14/248 (5.6) | 11/239 (4.6) | 1.08 (0.61 to 1.93) |
Subarachnoid hemorrhage | 28/248 (11.3) | 14/239 (5.9) | 1.65 (0.79 to 3.45) |
Symptomatic intracerebral hemorrhage No. (%) | 16 (5.9) | 14 (5.3) | 1.30 (0.60 to 2.81) |
Embolization to new territory No./total no. (%) | 13/252 (5.2) | 8/246 (3.3) | 1.31 (0.68 to 2.53) |
Infarction in new territory on follow-up CT or MRI No./total no. (%) | 38/248 (15.3) | 32/238 (13.4) | 1.05 (0.69 to 1.60) |
Small infarction | 17/248 (6.9) | 16/238 (6.7) | 0.94 (0.54 to 1.63) |
Substantial infarction | 22/248 (8.9) | 18/238 (7.6) | 0.94 (0.57 to 1.55) |
Femoral-artery false aneurysm No. (%) | 3 (1.1) | 3 (1.1) | 1.00 (0.18 to 5.36) |
Groin hematoma No. (%) | 11 (4.0) | 20 (7.5) | 0.50 (0.23 to 1.08) |
CI = confidence interval; EVT = endovascular therapy; HI1 = hemorrhagic infarction type 1; HI2 = hemorrhagic infarction type 2; IQR = interquartile range; no. = number; OR = odds ratio; PH1 = parenchymal hematoma type 1; PH2 = parenchymal hematoma type 2.
aAdjustments were made for age, sex, pre-stroke score on the mRS, duration from onset to randomization, stroke severity, and collateral status.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix was not copy-edited.
Table 12: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Hui et al. (2020)15 | Kaesmacher et al. (2019)13 | Mistry et al. (2017)14 |
|---|---|---|---|
Khoury NN, et al. J Neuroradiol. 2005;32:26-32. | Yes | No | No |
Goyal M, et al. N Engl J Med. 2015;372:1019-30. | Yes | Yes | Yesa |
Campbell BC, et al. N Engl J Med. 2015;372:1009-18. | Yes | No | Yesa |
Berkhemer OA, et al. N Engl J Med. 2015;372:11-20. | Yes | Yesb | Yesa,b |
Muir KW, et al. J Neurol Neurosurg Psychiatry. 2016;88:38-44. | Yes | No | No |
Jovin TG, et al. N Engl J Med. 2015;372:2296-306. | Yes | Yes | Yesa |
Saver JL, et al. N Engl J Med. 2015;372:2285-95. | Yes | No | Yesa |
Mocco J, et al. Stroke. 2016;47:2331-8. | Yes | No | No |
Bracard S, et al. Lancet Neurol. 2016;15:1138-47. | Yes | No | No |
Zhou H, et al. Chin J Clin Res. 2018;31:211-4. | Yes | No | No |
Broeg-Morvay A, et al. Stroke. 2016;47:1037-44. | No | Yes | Yes |
Wang H, et al. Eur J Neurol. 2017;24:935-43. | No | Yes | No |
Weber R, et al. J Neurointerv Surg. 2017;9:229-33. | No | Yes | No |
Coutinho JM, et al. JAMA Neurol. 2017;74:268-74. | No | Yes | Yes |
Abilleira S, et al. Stroke. 2017;48:375-8. | No | Yes | Yes |
Guedin P, et al. J Stroke Cerebrovasc Dis. 2015;24:952-7. | No | Yes | Yes |
Maier IL, et al. J Neurol Sci. 2017;372:300-4. | No | Yes | No |
Rai AT, et al. J Neurointerv Surg. 2018;10:17-21. | No | Yes | Yes |
Leker RR, et al. J Stroke Cerebrovasc Dis. 2015;24:1163-7. | No | Yes | Yes |
Minnerup J, et al. Stroke. 2016;47:1584-92. | No | Yes | No |
Alonso de Leciñana M, et al. J Neurointerv Surg. 2017;9:1041-6. | No | Yes | No |
Dávalos A, et al. Stroke. 2012;43:2699-705. | No | Yes | No |
Sanak D, et al. Cerbrovasc Dis. 2013;35:178. | No | Yes | No |
Kaesmacher J and Kleine JF. Clin Neuroradiol. 2018;28:81-9. | No | Yes | Yes |
Behme D, et al. J Stroke Cerebrovasc Dis. 2016;25:954-9. | No | Yes | Yes |
Nogueira RG, et al. J Neurointerv Surg. 2015;7:16-21. | No | Yes | No |
Wee CK, et al. Cerebrovasc Dis Extra. 2017;7:95-102. | No | Yes | No |
Gerschenfeld G, et al. JAMA Neurol. 2017;74:549-56. | No | No | Yes |
Mistry EA, et al. J Am Heart Assoc. 2017;6:e006167. | No | No | Yes |
Sallustio, F, et al. J Stroke Cerebrovasc Dis. 2013;22:e323-31. | No | No | Yes |
Note: Yes indicates the primary study was included within the systematic review; No indicates the primary study was not included within the systematic review
aIncluded a post-hoc analysis of Berkhemer et al. [2015], Goyal et al. [2015], Saver et al. [2015], Campbell et al. [2015], and Jovin et al. [2015] (Goyal M, et al. Lancet. 2016;387:1723-31)
bIncluded a subgroup analysis of Berkhemer et al. [2015] (Mulder MJ, et al. Int J Stroke. 2016;11:637-45)
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Endovascular thrombectomy for patients with ischemic stroke: clinical and cost-effectiveness (CADTH Rapid response report: reference list). Ottawa (ON): CADTH; 2018: https://cadth.ca/endovascular-thrombectomy-patients-ischemic-stroke-clinical-and-cost-effectiveness. Accessed 2022 Feb 28.
Endovascular therapy for ischemic stroke (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2015: https://cadth.ca/sites/default/files/pdf/htis/aug-2015/RC0687%20Endovascular%20therapy%20for%20ischemic%20stroke%20revised%20Final.pdf. Accessed 2022 Feb 28.
Review Articles
Gauberti M, Martinez de Lizarrondo S, Vivien D. Thrombolytic strategies for ischemic stroke in the thrombectomy era. J Thromb Haemost. 2021;19(7):1618-1628. PubMed
Mendelson SJ, Prabhakaran S. Diagnosis and Management of Transient Ischemic Attack and Acute Ischemic Stroke: A Review. JAMA. 2021;325(11):1088-1098. PubMed
Ferrari J, Krebs S, Sykora M. Intravenous thrombolysis and mechanical thrombectomy in patients with minor or rapidly improving neurological deficits. Curr Opin Neurol. 2019;32(1):13-18. PubMed
Sawyer RN. Intravenous Tissue Plasminogen Activator for Large Vessel Ischemic Stroke - Is There Still a Role? Neurosurg. 2019;85(suppl_1):S34-S37. PubMed
Sheen JJ, Kim YW. Paradigm Shift in Intra-Arterial Mechanical Thrombectomy for Acute Ischemic Stroke: A Review of Randomized Controlled Trials after 2015. J Korean Neurosurg Soc. 2020;63(4):427-432. PubMed
Acknowledgement: Grant Stotts, MD, Neurologist, Ottawa Hospital and Ottawa Hospital Research Institute
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.