CADTH Health Technology Review
Adalimumab for the Treatment of Pediatric Populations With Non-Infectious Uveitis
Rapid Review with Expert Input
Authors: Daphne Hui, Monika Mierzwinski-Urban, Carolyn Spry
Reviewers
External Reviewer
This document was externally reviewed by a content expert who granted permission to be cited.
Dr. Jean Deschênes, MD, FRCSC
Professor, Ophthalmologist-in-Chief
McGill University and McGill University Health Centre
Abbreviations
CAU
chronic anterior uveitis
DMARD
disease-modifying antirheumatic drugs
HUI-3
Health Utilities Index-3
JIA
juvenile idiopathic arthritis
logMAR
logarithm of the minimum angle of resolution
NICE
National Institute for Health and Care Excellence
NHS
National Health Service
RCT
randomized controlled trial
SR
systematic review
TNF
tumour necrosis factor
TNF-alpha
tumour necrosis factor-alpha
Key Messages
Two systematic reviews, 1 economic evaluation, and 2 evidence-based guidelines were identified regarding the clinical effectiveness (including safety), cost-effectiveness, and use of adalimumab in pediatric populations with non-infectious uveitis.
Pooled data of the SYCAMORE and ADJUVITE randomized controlled trials comparing adalimumab to placebo demonstrated that adalimumab significantly increased the likelihood of reducing or interrupting corticosteroid use (which is beneficial as long-term corticosteroid use can result in cataracts and glaucoma). Adalimumab significantly increased the event of a satisfactory response rate, but there was no difference in safety assessed as systemic adverse events and local adverse effects.
Specific to the ADJUVITE trial, visual acuity slightly worsened before and after treatment with adalimumab and it was unclear if adalimumab increased control of intraocular inflammation.
Specific to the SYCAMORE trial, adalimumab significantly lowered the risk of treatment failure and the rate and number of adverse events and serious adverse events were higher in the adalimumab group compared to the placebo group. For the adalimumab group, the most common adverse event type was infections and infestations and the most common serious adverse events were glaucoma, cataracts, injection site reactions, arthritis, and arthralgia.
In the perspective of the health care system in the UK, adalimumab plus methotrexate was not found to be cost-effective compared to methotrexate alone (modelled by placebo data) in uveitis associated with juvenile idiopathic arthritis.
Cost-effectiveness analyses of adalimumab at a discounted price lowered the incremental cost-effectiveness ratio, which supports the potential use of biosimilars in the future due to cost savings.
Both guidelines recommended the use of treatment that blocks proteins that cause inflammation (tumour necrosis factor-alpha inhibitors) such as adalimumab in combination with an immunosuppressive agent such as methotrexate (i.e., adalimumab plus methotrexate) in patients with uveitis associated with juvenile idiopathic arthritis who are not responsive to initial treatment (e.g., topical corticosteroids) and are at risk for severe uveitis or vision threatening complications.
The American College of Rheumatology/ Arthritis Foundation recommended the use of adalimumab and infliximab over etanercept with no preference between adalimumab and infliximab. Conversely, the guideline from multiple interdisciplinary German groups recommended that adalimumab and infliximab are the first- and second-choice tumour necrosis factor-alpha inhibiting drugs, respectively. They recommended a treatment switch to infliximab then golimumab when adalimumab is not effective or there is treatment failure with adalimumab.
Context and Policy Issues
Uveitis is the second foremost treatable cause of blindness in the Western world accounting for up to 10% of cases of loss of vision.1,2 The incidence of uveitis is difficult to measure due to the varying etiologies (Canadian specific prevalence and incidence was not found), but 1 of the largest studies measuring the incidence and prevalence of uveitis in the US reported the incidence to be 11.53 per 100 000 person-years.1,2 Non-infectious uveitis refers to the presence of intraocular inflammation of the uvea (i.e., middle layer of the eye) not caused by an infection that can present in individuals of any age among various etiologies.2 Active versus inactive uveitis refers to the activity status of the inflammation.2,3 The anterior segment of the uvea contains the ciliary body and iris, whereas the posterior segment contains the choroid.2,3 Non-infectious uveitis may be idiopathic, caused by a reaction to medication (but this is rare), or immune-mediated; therefore, it presents among many systemic autoimmune diseases such as juvenile idiopathic arthritis (JIA), Behçet disease, or ankylosing spondylitis.2-5 Of note, this report focuses on pediatric populations with non-infectious uveitis. As JIA predominantly affects pediatric patients much of the included evidence will focus on this patient population. The onset of uveitis in JIA is typically between 2 and 8 years old.3,4 Among all etiologies of uveitis in children in Europe, North America, and Israel, JIA accounts for 15 to 67%.6 Anterior uveitis is the most common (83%) anatomic localization in uveitis associated with JIA.6 Regular ophthalmology screening allows for early detection and timely treatment, which reduces the risk of visual impairment and can improve visual outcomes and prevent complications.7,8 If left untreated, uveitis may lead to vision loss, early complications such as cystoid macular edema and vitreous haze, and late complications such as cataracts, glaucoma, and irreversible retinal damage.2 Specifically in pediatric populations, uncontrolled chronic anterior uveitis may result in glaucoma in 25% to 50% and vision loss in 10 to 20% of children.8
Treatment for non-infectious uveitis depends on whether it presents alongside a systemic disease (and if the disease is controlled), if the inflammation affects 1 (unilateral) or both (bilateral) eyes, and anatomic localization of the uveitis.2,5,9 Initially, it is usually treated with corticosteroids with topical (e.g., prednisolone acetate drops) or local (e.g., intravitreal implants or injections or periocular injections) administration.2 Long-term use of corticosteroids is not recommended as it can result in cataracts and glaucoma.2,5,9 Immunosuppressive agents can reduce corticosteroid use and associated complications.2 Systemic administration is generally used for resistant inflammation, if previously administered treatments are not tolerated, and in individuals with high risk for vision loss and/ or uveitis associated with systematic disease.2,5 Systemic treatment includes corticosteroids, immunosuppressive or anti-inflammatory agents (e.g., methotrexate, cyclosporine), and biologics.2,9 Biologics are used in non-infectious uveitis that does not respond to aforementioned systemic therapies.2,9 Treatment for JIA typically begins with topical glucocorticoids. For severe or vision-threatening uveitis and/or in patients who are refractory to or dependent on corticosteroids, further systemic immunosuppressive treatment is required. Methotrexate is usually administered as the first-line systemic immunosuppressive drug. For those requiring additional treatment, immunosuppressive biologics, particularly tumour necrosis factor-alpha (TNF-alpha) inhibitors, are administered.8 Of note, TNF-alpha inhibitors are classified under the broader categorization of biologics.
Adalimumab (Humira) is a biologic agent, specifically a monoclonal antibody, administered through subcutaneous injection that is a TNF-alpha inhibitor.2,4,10 Multiple biosimilars such as Amgevita, Hadlima, Hulio, and Hyrimoz (brand names) are approved for various indications in Canada including uveitis in pediatric populations.10,11 For individuals with non-infectious uveitis, adalimumab is generally administered in those with an incomplete response to first-line treatments and who have received at least 1 other systemic therapy.2,10 Adalimumab with or without concomitant immunosuppressants may increase the risk of severe infections (e.g., tuberculosis) and sepsis that require hospitalization or may lead to death.2,10 Notably, the American College of Rheumatology/ Arthritis Foundation highlighted the need for accepted guidelines regarding the use of systemic immunosuppressive therapy in JIA-associated uveitis in North America.8 The purpose of this rapid review is to evaluate recent evidence regarding the clinical effectiveness (including safety), cost-effectiveness, and evidence-based guidelines regarding the use of adalimumab for the treatment of pediatric populations with non-infectious uveitis. This report is conducted in series with another report that focuses on adalimumab for the treatment of adults with non-infectious uveitis.2
Research Questions
What is the clinical effectiveness of adalimumab for the treatment of pediatric populations with non-infectious uveitis?
What is the cost-effectiveness of adalimumab for the treatment of pediatric populations with non-infectious uveitis?
What are the evidence-based guidelines regarding the use of adalimumab for the treatment of pediatric populations with non-infectious uveitis?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews (SRs), the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were adalimumab and uveitis. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded from the search results. The search was also limited to English language documents published between January 1, 2016 and October 19, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. SRs that met the selection criteria of this review were included regardless of the study designs of included primary studies (e.g., SRs of non-randomized studies were included).
Criteria | Description |
|---|---|
Population | Pediatric populations (< 18 years of age) with non-infectious uveitis |
Intervention | Adalimumab, alone or in combination with background therapy (e.g., methotrexate, cyclosporin, azathioprine) |
Comparator | Q1 and Q2: Pharmacological therapy for uveitis (e.g., other biologic agents and non-biologic anti-inflammatory agents such as corticosteroids and methotrexate), and placebo Q3: Not applicable |
Outcomes | Q1: Clinical benefit (e.g., best-corrected visual acuity, disease inactivity or dormancy [quiescence], vascular lesions, uveitic macular edema, changes in uveitis-related systemic corticosteroids use) and safety (e.g., ocular complications) Q2: Cost-effectiveness (e.g., the incremental cost per health benefit or QALY gained) Q3: Recommendations regarding the use of adalimumab for uveitis |
Study designs | HTAs, SRs, RCTs, and economic evaluations |
HTA = health technology assessment; Q = question; QALY = quality-adjusted life-years; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded unless the SR provided additional clinical effectiveness (including safety) data. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded. For SRs and meta-analyses that had broader eligibility criteria than the current review, data were only extracted from relevant primary studies or analyses that met the eligibility criteria of the current review. For instance, data from non-comparative and/or non-randomized studies were not extracted as that does not meet the comparator and study design components of the selection criteria of this review. Literature specific to Behçet disease was excluded due to its prevalence in individuals older than 18 years of age.3 Further, post-hoc analyses of randomized controlled trials (RCTs) were excluded from this rapid review as CADTH does not consider post-hoc analyses of RCTs to constitute randomized study designs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)12 for systematic reviews (SRs),13 the Drummond checklist14 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument15 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
A total of 448 citations were identified in the literature search. Following screening of titles and abstracts, 416 citations were excluded and 32 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 29 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. These comprised 2 SRs, 1 economic evaluation, and 2 evidence-based guidelines. Appendix 1 presents the PRISMA16 flow chart of the study selection. Of note, the 2 SRs6,17 both included data from 2 placebo controlled RCTs evaluating the use of adalimumab in JIA-associated uveitis and were both published in 2021. To provide a comprehensive summary of clinical effectiveness outcomes (including safety) both SRs were included in this report. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Two SRs with meta-analyses,6,17 1 economic evaluation,18 and 2 evidence-based guidelines7,8 were included in this review. The 2 SRs had broader inclusion criteria than this review. Li et al. (2021)6 performed a SR with meta-analyses on the safety and efficacy of anti-TNF-alpha therapies (including adalimumab) of randomized and non-randomized data. The meta-analyses of the Li et al. (2021)6 SR pooled non-randomized data; thus, the meta-analyses did not include randomized data and findings from the RCTs were reported individually. Data from the RCTs relevant to this report were summarized. Norcia et al. (2021)17 performed a SR with meta-analyses on the clinical efficacy of biologic therapy (including adalimumab) of randomized and non-randomized data. The meta-analyses in the Norcia et al. (2021)17 SR comparing adalimumab to placebo in pediatric populations with non-infectious uveitis using randomized data were deemed relevant and summarized in this report. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
SRs
Li et al. (2021)6 performed a SR with meta-analyses among which, 2 placebo controlled RCTs (SYCAMORE and ADJUVITE trials) are relevant to this review. This SR included a literature search of PubMed, Embase, the Cochrane Library, and Web of Science from inception to November 1, 2019. Norcia et al. (2021)17 performed a SR with meta-analyses, the meta-analyses pooling data from the SYCAMORE and ADJUVITE trials are relevant to this review. This SR included a literature search of SCOPUS (2004 to March 2021), PubMed (1966 to March 2021), Latin American and Caribbean Literature in Health Sciences (LILACS; 1982 to March 2021), Embase (1974 to March 2021), Web of Science (1900 to March 2021), Clinical Trials (2008 to March 2021, and Cochrane Central Register of Controlled Trials (CENTRAL; 1996 to March 2021). Searches were conducted from various start dates but all were performed up until March 2021.17
Economic Evaluation
One economic evaluation was included in this review. Hughes et al. (2019)18 conducted a cost-utility analysis using a trial-based analysis (SYCAMORE RCT) over an 18-month time horizon followed by a 10-year extrapolation performed with a Markov model. The extrapolation used data from a longitudinal cohort study of patients with idiopathic and JIA-associated uveitis of the Bristol Regional Tertiary Pediatric Uveitis clinic (Bristol cohort: 1997 to 2014). This model had 3 health states defined by survival (dead) and visual impairment (visual impairment versus no visual impairment). The evaluation was performed in the perspective of the National Health Service (NHS) (i.e., UK perspective). The base-case analysis was intended to represent the median demographics of the SYCAMORE trial (i.e., 7-year old girl).
Data sources for health utilities, unit costs, visual acuity, and long-term outcomes and surgery were reported.
Health utilities: derived from Health Utilities Index (HUI) questionnaire (health domains include vision, speech, hearing, dexterity, ambulation, pain, emotion, and cognition) responses mapped to the Mark 3 classification system, which is validated in children.18 Algorithms with preference-based scoring converted the descriptive health classifications into values for each health dimension and a multi-attribute model derived a utility score.18
Resource use: sourced from the SYCAMORE RCT. Namely, study and concomitant therapies were extracted from case report forms that were supplemented by patient diaries. Hospital and adverse event data were from patient-level costing systems or patient administration systems that were supplemented by questionnaire responses from interviews and diary entries and provided use of hospital (e.g., outpatient clinic, emergency admissions), primary care, and community care (e.g., school nurse).
Unit costs: resource use was valued at UK unit costs estimated at 2016 (time of analysis). Unit costs of treatments were from multiple NHS sources. Use of hospital services were costed to health care resource group codes from the National Tariff 2016 to 2017 or the National Schedule of Reference Costs 2015 to 2016. Primary and community care services unit costs were sourced from the Personal Social Services Research Unit 2015. Cost of surgery was assumed to be the average cost for outpatient pediatric ophthalmology procedures.
Visual acuity: measures were based on logarithm of the minimum angle of resolution (logMAR) scores in the worse eye, which was considered most clinically relevant. Namely, a score of less than 0.3 indicated no visual impairment and a score of 0.3 or more indicated a degree of visual impairment. SYCAMORE trial participants had their visual acuity measured at every visit including unscheduled visits.
Long-term outcomes and surgery: Visual acuity (logMAR scores) was measured at diagnosis and at 1, 3, 5, and 10 years of follow-up (along with the number and type of surgeries performed). The 10-year visual acuity data were utilized in the model.
Patients were initially distributed according to the proportion of time spent in each state over the preceding 18 months based on trial arm. The Bristol cohort was used to estimate the probabilities associated with transitions among health states (with or without eye surgery). The model used a cycle length of 1 year with a half-cycle correction and a standardized mortality ratio of 3.9 (95% confidence interval [CI], 0.8 to 11.3) to account for mortality. It was assumed that simulated patients were fully adherent to adalimumab and based on expert clinical opinion would continue for 3 years beyond the initial 18-month trial duration. Additionally, the progression of visual impairment after 18 months was assumed to occur at the same rate for patients receiving adalimumab or placebo.
Total costs calculated for the 18-month trial-based analysis were adjusted to apportion drug costs if administration covered the period preceding randomization or extended beyond the 18-month time horizon. QALYs were calculated as the area under each patient’s utility-time profile with the trapezium rule. QALYs and costs accruing beyond the first year were discounted at 3.5% per year. An instrumental variable regression method with QALYs and total costs as the outcome variables adjusted for age and gender was used to account for crossover effects due to early termination of the SYCAMORE RCT (i.e., recruitment of the SYCAMORE RCT was terminated early due to an interim analysis demonstrating a significantly lower risk of treatment failure in the adalimumab group). This method connected the average causal effect of compliers to the average intention-to-treat effects. For the 10-year modelled extrapolation, QALYs and costs specific to each health state were calculated with the instrumental variable regression and adjusted for time in state and treatment.
Censored data on utility and time in the visual impairment health state were imputed using predictive mean matching. Ten imputed datasets were synthesized from outcome variables (cost and exposure to adalimumab during the open-label and follow-up phases after trial treatment) and imputation models based on potential prognostic factors (e.g., age, gender, baseline visual impairment, trial arm).
Evidence-Based Guidelines
The objective of the evidence-based guideline by the American College of Rheumatology/ Arthritis Foundation was to develop recommendations for screening, monitoring, and treatment of uveitis in children with JIA.8 This guideline followed the American College of Rheumatology (ACR) guideline development process.8 Systemic comprehensive searches of multiple databases from inception to June 12, 2017 were performed to retrieve English language publications. Eligibility criteria of included evidence were not reported. Updated searches were conducted on October 13, 2017. Guideline development was performed by 5 groups:
Core Leadership Team: 4 pediatric rheumatologists involved with project supervision and coordination (e.g., drafted the clinical questions [PICO] and published guideline).
Literature Review Team: 1 experienced literature review consultant who performed the literature search and data extraction.
Expert Panel: 1 pediatric ophthalmologist and 9 pediatric rheumatologists who developed the PICO questions and decided on the scope of the guidelines.
Voting Panel: 2 pediatric ophthalmologists, 15 pediatric rheumatologists, and 2 adults with JIA who voted on the recommendations, assisted with scope development, refined PICO questions, and reviewed gathered evidence.
Parent and Patient Panel: 2 parents of children with JIA-associated uveitis and 9 adults with JIA who reviewed the gathered evidence and provided input on their values and preferences within a separate voting meeting.
When the evidence was not clear, recommendations were based on the values or preferences and experiences of the Parent and Patient Panel and the Voting Panel, respectively. The Voting Panel voted on the direction and strength of the recommendation related to each PICO question. Recommendations required a 70% level of agreement, if this level was not achieved, the Voting Panel had additional discussions, including rewording of recommendations if needed, before re-voting. For all conditional recommendations, reasons for the decision and conditions under which the alternative may be preferable was provided in writing. A subsequent round of voting was required for recommendations with additional questions. In some instances, the Voting Panel combined PICO questions into 1 recommendation for clarity. Whereas some PICO questions were dropped during the consensus meeting due to insufficient evidence to make a formal recommendation. Quality of evidence was rated for each outcome as very low, low, moderate, or high based on GRADE methodology; thus, taking into account risk of bias, inconsistency, indirectness, imprecision, and other considerations. A strong recommendation required the Voting Panel to be confident that the desirable effects of following the recommendation outweigh the undesirable effects (or vice versa); thus, the course of action would apply to all or almost all patients, and only a small proportion would not want to follow the recommendation. A conditional recommendation required the Voting Panel to believe that the desirable effects of following the recommendation would probably outweigh the undesirable effects; thus, the course of action would apply to majority of patients but some may not want to follow the recommendation. Due to patient preference and lack of strong evidence, conditional recommendations were preference-sensitive and always warranted a shared decision-making approach.
The evidence-based guideline by various interdisciplinary German groups was an update to an existing guideline, published in 2012, to include recently published literature particularly focused on biologic disease-modifying antirheumatic drugs (DMARDs).7 The guideline was developed to assist decision-making in the treatment of anterior uveitis associated with JIA by reducing variations in current practice. The methodology was based on international standards to devise high-quality guidelines highlighted in the German Association of the Scientific Medical Societies Guidance document. A literature search of MEDLINE was performed to include publications from 2 decades prior up to January 30, 2017. Eligibility criteria of included evidence were not reported but the following were considered when including evidence: clinical relevance of the outcome measures of effectiveness, applicability of the findings to the German health care system and patients, cost factors, and implementation ease in physicians’ daily routine. Guideline development was performed by representatives from professional societies involved in diagnosing and treating anterior uveitis associated with JIA and a patient group: German Ophthalmological Society, Society for Pediatric Rheumatology, Professional Association of Ophthalmologists, German Society for Rheumatology, and Parents’ Group for Children With Uveitis and their Families. This process was moderated by the Association of the Scientific Medical Societies in Germany. The initial guideline development took place on March 31, 2017 in Muenster Germany (not all members of the participating development groups were present). A nominal group process was used to collect opinions of participating individuals. Findings from the literature review were briefly presented followed by discussions to draft and fine-tune the wording of the recommendations. Consensus was required to finalize the draft recommendations and participants abstained from voting when they had relevant conflict of interest(s).
Draft guidelines were reviewed, following the Delphi process, by all development group members with modification suggestions and the individuals’ agreement or disagreement proposed. The review from the first round was summarized and sent to all members of the development group. For recommendations in which consensus was not reached, a second Delphi round was implemented. Subsequently, the guideline manuscript was externally reviewed by the German Ophthalmological Society, German Society of Rheumatology, and Society for Pediatric Rheumatology and a vote in writing followed (third Delphi round). For finalization, draft guidelines had to be approved by all participants.
The level of evidence was graded from I to III. Grade I evidence was based on at least 2 high-quality RCTs. Grade II evidence was based on a small number of RCTs, more than 1 RCT of lesser quality, nonrandomized studies (e.g., cohort or case-control studies preferably conducted by more than 1 research group or centre), and noncontrolled studies with clear observations.7 Grade III evidence was based on clinical experience or expert opinion and descriptive studies (e.g., case-control or cohort studies of poorer quality). Grade of recommendation was rated as strong (phrased as “shall”), mitigated (phrased as “should”), and open (phrased as “can”).7
Country of Origin
SRs were conducted by authors from China6 and Brazil.17 The economic evaluation was performed by authors from the UK using UK-based sources and in the perspective of the NHS (i.e., UK perspective).18 The evidence-based guideline by Angeles-Han et al. (2019) was devised by the American College of Rheumatology/Arthritis Foundation. The country where this guideline is meant to apply was not specifically stated. However, based on the participation of the American College of Rheumatology/Arthritis Foundation, it is likely the guidelines are intended for use in America and potentially North America as it was noted that there were no accepted North American guidelines for the use of systemic immunosuppressive treatments.8 The evidence-based guideline by Heiligenhaus et al. (2019) was devised by 4 clinician groups (German Ophthalmological Society, Society for Pediatric Rheumatology, Professional Association of Ophthalmologists, German Society for Rheumatology) and 1 patient/caregiver group (Parents’ Group for Children With Uveitis and their Families). Guideline development was moderated by the Association of the Scientific Medical Societies in Germany. The country where this guideline is meant to apply was not directly specified, but it is presumed to be Germany as all participating groups were German based and it was noted that the relevance to the German health care system of the included evidence was considered.7
Patient Population
The patient population of the Li et al. (2021) SR were individuals with the onset of JIA at 16 years of age or younger who were initiating anti-TNF-alpha therapy for uveitis and had an inadequate response to DMARDs (authors did not specify if this referred to non-biologic DMARDs only) and topical steroids.6 The patient population of the Norcia et al. (2021) SR were individuals under 18 years of age with non-infectious uveitis regardless of associated systemic disease.17 Both patient populations are relevant to this review. Among the 2 SRs, the patient population of the 2 relevant RCTs (SYCAMORE and ADJUVITE) included 90 patients (adalimumab group: 60 and placebo group: 30) and 31 patients (adalimumab group: 16 patients and placebo group: 15 patients), respectively.6,17 The mean age of the SYCAMORE trial in the adalimumab and placebo groups were 9.07 and 8.56 years, respectively.17 The mean age of the ADJUVITE trial in the adalimumab and placebo groups were 10.8 and 9.2 years, respectively.17 Li et al. (2021) also reported the age range for the ADJUVITE trial, which was 4.9 to 29.1 years. Both trials had a larger proportion of females.6,17
The trial-based analysis of the economic evaluation was based on the SYCAMORE trial. It was noted that the SYCAMORE trial was a double-blind placebo-controlled, multi-centre, randomized study that recruited individuals aged 2 to 18 years of age with active uveitis associated with JIA who had received stable methotrexate treatment for at least 12 weeks. It was highlighted that recruitment was terminated prematurely after an interim analysis demonstrated that adalimumab is associated with a significantly lower risk of treatment failure. In accordance with the trial protocol, participants in the adalimumab group were followed up in an open-label manner and participants in the placebo group terminated trial intervention and were followed up for 6 months.18 The 10-year extrapolation of the economic evaluation was based on the Bristol cohort study that included 91 individuals with idiopathic (42.3%) or JIA-associated (58.3%) uveitis. Mean age (standard deviation) at diagnosis was 7.9 (3.8) years with a range of 1 to 15 years. Of note, there was some overlap between the SYCAMORE RCT and Bristol cohort samples; namely, 28 of 90 trial participants were from the Bristol cohort, of which 15 were included in the longitudinal dataset of the economic evaluation.18
The target population of the evidence-based guideline by the ACR/ Arthritis Foundation were children with JIA at risk for and those with associated uveitis (chronic anterior uveitis and acute anterior uveitis). The intended users were clinicians who screen, monitor, and treat children with JIA.8 The target population of the evidence-based guideline by various interdisciplinary German groups were individuals with anterior uveitis associated with JIA.7 The intended users were not specifically stated.7
Interventions and Comparators
The interventions of interest of the Li et al. (2021) SR and Norcia et al. (2021) SR were anti-TNF-alpha therapy and biologic therapy, respectively.6,17 Adalimumab is a biologic drug and an anti-TNF-alpha therapeutic; thus, these eligible intervention criteria are broader than this report. The eligible comparators of the Li et al. (2021) SR were not reported; whereas, the comparators of the Norcia et al. (2021) SR were placebo, other drugs, or combination therapies.6,17 Among the 2 SRs, the intervention and comparator of the 2 relevant RCTs (SYCAMORE and ADJUVITE) were adalimumab plus methotrexate and placebo (methotrexate only), respectively. For the SYCAMORE trial, dosing of adalimumab was 40 mg/m2 and 20 mg/m2 for individuals at least 30 kg and less than 30 kg, respectively; dosing of the placebo was 0.8 mL; and dosing of methotrexate was 10 mg/m2 to 20 mg/m2 without exceeding 25 mg per week.6,17,18 Of note, it was not reported what “w” stands for.17 For the ADJUVITE trial, dosing of adalimumab was 40 mg/m2 and 24 mg/m2 for individuals 13 years and older and those younger than 13 years of age, respectively; dosing of the placebo was not reported; and dosing of methotrexate was 0.3 mg/kg to 0.6 mg/kg without exceeding 25 mg per week.6,17
The trial-based analysis of the economic evaluation was based on the SYCAMORE trial. The 10-year extrapolation of the economic evaluation was based on the Bristol cohort study that included patients treated with various biologics including adalimumab, abatacept, tocilizumab, etanercept, and infliximab. Namely, 47 (30%) patients received adalimumab but the dose was not reported. Of note, in the base-case analysis (18-month trial-based analysis plus 10-year extrapolation), all patients in the adalimumab group fully adhered to treatment (i.e., according to protocol) for a total of 54 months (18 months plus 3 years).18
The interventions considered in the evidence-based guideline by the ACR/ Arthritis Foundation were various treatments for uveitis associated with JIA including glucocorticoids, non-biologic DMARDs (e.g., methotrexate), and biologics (e.g., adalimumab). Non-biologic DMARDs and biologics were referred to as systemic therapy among these recommendations.8 The interventions considered in the evidence-based guideline by various interdisciplinary German groups were also various treatments for uveitis associated with JIA including anti-inflammatory therapy (e.g., corticosteroids, nonsteroidal anti-inflammatory drugs), conventional synthetic DMARDs (e.g., methotrexate), and biologic DMARDs (e.g., TNF-alpha inhibitors such as adalimumab).7 In both guidelines, recommendations pertaining to adalimumab were relevant to this report.
Outcomes
The outcomes relevant to this review reported in the SR by Li et al. (2021)6 included treatment failure, control of intraocular inflammation, visual acuity, and safety (adverse events and serious adverse events). Of note, this SR6 also reported on corticosteroid sparing but it was unclear what the reported values represented so this was not included in this report. Control of intraocular inflammation was evaluated through assessments of remission and improved activity according to the Standardization of Uveitis Nomenclature (SUN) Working Group criteria. Remission was defined as inactive disease for 3 months following discontinuation of all treatments for eye disease. Improved activity was the 2-step decrease in the level of inflammation or decreases to grade 0. Of note, other included studies of the SR by Li et al. (2021)6 followed other definitions but in this report control of intraocular inflammation was extracted from the ADJUVITE RCT, which was based on SUN criteria. Improved visual acuity was achieved with the doubling of the visual angle in at least 1 eye or eliciting 3 lines on a decimal scale. The outcomes relevant to this review reported in the SR by Norcia et al. (2021)17 included reduction or interruption of the use of corticosteroids, satisfactory response rate to treatment, and safety (local adverse events and systemic serious adverse events). Definitions of outcomes were not reported. Altogether, the clinical effectiveness outcomes summarized in this review based on the 2 SRs6,17 are categorized as change in visual acuity, change in uveitis-related corticosteroid use (i.e., reduction or interruption), control of intraocular inflammation, satisfactory response rate to treatment and treatment failure, and safety.
The primary outcome of the economic evaluation was the incremental cost per QALY gained (ICER) of adalimumab plus methotrexate versus methotrexate alone.18 Costs were in the currency of pound sterling. Accordingly, the incremental and total QALYs and costs were also reported for the base-case analysis. For the univariate sensitivity analyses, the ICERs, incremental QALYs and costs, and QALYs and costs of treatments (adalimumab plus methotrexate and methotrexate alone) were estimated. The 2-way sensitivity analyses estimated ICERs and the probabilistic sensitivity analyses estimated the probability of cost-effectiveness.18
Outcomes related to medication use in the evidence-based guideline by the American College of Rheumatology/Arthritis Foundation were categorized as critical and important. Critical outcomes included incidence and recurrence of uveitis, loss of control of uveitis including the incidence (rate or frequency — number of episodes overtime), control of uveitis at 1 month and 3 months, new ocular glucocorticoid-related complications (infection, cataracts, glaucoma/increased intraocular pressure), and new ocular complications due to inflammation. Important outcomes included side effects of systemic therapy, time to control of uveitis, and time to loss of control of uveitis.8 Outcomes for the evidence-based guideline by various interdisciplinary German groups were not reported but primary objectives of treatment were reported as sight preservation; treatment of relapses, complications, and underlying systemic diseases; prevention of complications and recurrences; and avoidance of adverse drug reactions.7
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
SRs
The 2 SRs were assessed to be of moderate methodological quality based on the assessments using AMSTAR 2.12 In both SRs, the research question/ objective was reported, multiple databases were searched, and the search was conducted within 24 months before publication. The quality or risk of bias of included primary studies was assessed using satisfactory techniques in these SRs with the ratings reported in the main publication and/or supplementary. The authors of both SRs had no conflicts of interest to disclose; however, only the SR by Li et al. (2021)6 reported funding sources. The SR by Norcia et al. (2021)17 did not report funding, which could introduce bias to the findings if the SR received financial sponsorship from parties of interest such as AbbVie, the manufacturer of adalimumab. The 2 SRs were also associated with some methodological limitations. Exclusion criteria were not specifically reported and a list of excluded studies along with the reasons for exclusion were not reported. Inclusion criteria were unclear regarding eligible study designs for both SRs. For instance, the SR by Norcia et al. (2021) noted that non-randomized controlled studies were included but this categorization is broad. In addition, the SR by Li et al. (2021) did not report the eligible comparators. Additionally, no justification was provided for the selection of eligible study designs. However, the SR by Li et al. (2021) did state that review papers, meta-analyses, editorial letters, and expert opinions were excluded to avoid duplication. Sources of funding and conflict of interest for the included studies were not reported but conflict of financial interest was noted as a main issue related to the risk of bias of included RCTs in the SR by Norcia et al. (2021). Further, it was not specified if reference lists of included studies were reviewed, grey literature were retrieved, and experts were consulted. Altogether, these limitations increase the risk of selection bias and reporting bias plus the potential for an inadequate, non-comprehensive SR, particularly as relevant literature may have been missed such as non-indexed literature that would be retrieved from grey literature.
Methodological strengths specific to the Li et al. (2021) SR included the following. Methods were established before conduct with the protocol registered with the International Prospective Register of Systematic Reviews (PROSPERO: CRD42020161749). Inclusion criteria reported the components of population, intervention, and outcomes with definitions provided. Namely, thresholds of change were reported; for instance, visual acuity control was defined as doubling of the visual angle in at least 1 eye (3 lines on a decimal scale). However, it was not reported if this threshold for visual acuity control was validated or based on clinically meaningful differences. Whereas control of intraocular inflammation was measured with SUN criteria (i.e., standardized uveitis nomenclature). Study selection was performed by 2 independent reviewers and disagreements were addressed by discussion or with a third reviewer. Data extraction used a standard form and dose of treatments, age, and length of follow-up were reported for included studies. However, age range was reported for 1 of 2 relevant studies as only pediatric populations were of interest to this report, range would be more informative and help with determining eligibility of studies. This SR was also associated with considerable methodological limitations. No explanation was provided for the restriction to English publications. Further, the findings of individual studies were not clearly reported and/or without sufficient detail; however, it was noted that a standard form was used for data extraction. Details were not reported for the data check; thus, it is possible that insufficient data were extracted if the second reviewer was checking extracted data only and was not reviewing the entire source publication. For instance, values were reported for adverse events and serious adverse events but units were not reported. It was not clear if these represented patients or number of events experiencing adverse events and serious adverse events. In addition, the change in visual acuity was reported as the change from treatment onset to a time point following treatment with adalimumab but it was not reported when the measurement was taken (i.e., time frame of the follow-up was not reported). These examples of unclear and insufficient reporting suggest that the source publications may have not been entirely reviewed by the second reviewer.6
Methodological strengths specific to the Norcia et al. (2021) SR included the following. Trial registries were searched (e.g., Cochrane Central Register of Controlled Trials); there were no restrictions regarding the language of publications; inclusion criteria reported the components of population, intervention, comparators, and outcomes; study selection, data extraction, and risk of bias assessments were performed by 2 independent reviewers with disagreements resolved through consensus and discussion with a third reviewer if required; and data extraction was performed with a standard form and resulted in the clear reporting of the characteristics of included studies (e.g., age, follow-up, and dose). Specific to the meta-analyses relevant to this report (comparisons of adalimumab to placebo based on randomized data of outcomes: reduction or interruption of the use of corticosteroids, satisfactory response rate to treatment, local AEs, and pooled systemic SAEs), strengths included appropriate methods used to assess heterogeneity (I2 statistic [considered significant when I2 > 75%] and P values from the heterogeneity chi-square test) with the results reported as risk ratios with 95% CIs and I2 values. Additionally, authors assessed the potential impact of the risk of bias in individual studies on the results of the meta-analyses but only for the outcomes presented with forest plots. This SR was also associated with specific considerable methodological limitations. Definitions of outcomes were not reported and interpretation of the outcome values were not described; namely, the minimal clinically important difference for outcomes was not reported, which limits the generalizability of the findings. Further, it was not specifically reported if GRADE ratings were performed by 2 reviewers. Specific to the meta-analyses, methods of the relevant meta-analyses were not reported. The relevant meta-analyses pooled data from 2 RCTs but methods were only reported for analyses combining data from ≥ 3 studies. Additionally, not all forest plots were provided without justification. For instance, the comparison of adalimumab to placebo on the outcomes of systemic SAEs and local AEs did not include forest plots or include assessments of the potential impact of risk of bias in individual studies on the results of the meta-analyses. Publication bias was assessed in accordance with GRADE methodology (i.e., to determine the certainty of evidence for outcomes); however, statistical evaluations or diagrams to assess publication bias such as Egger’s test or funnel plots were not performed. Nevertheless, Egger’s test or funnel plots may not have been appropriate for the meta-analyses of randomized data as data were pooled from 2 studies.17
Economic Evaluation
In the included economic evaluation (cost-utility analysis), the perspective, research question plus the related economic importance and comparator plus the rationale for selecting the alternative intervention were clearly stated. The model structure plus health states (depicted in a diagram); input parameters with the values, sources, and references (e.g., drug and resource costs were provided in pound sterling and taken from British National Formulary and NHS resources covering 2015 to 2017); time horizon; and discount rate for the economic model were reported. However, a justification for the discount rate was not provided. Namely, the time horizon of the model included an 18-month trial-based analysis and 10-year extrapolation modelled with data from a cohort study (Bristol cohort study). It may have been more appropriate to use a longer time horizon (e.g., lifetime) as the model was based on JIA patients with uveitis. These individuals would likely require chronic or longer-term treatment due to their young age and diagnosis with a systemic autoimmune disease. Nevertheless, uveitis in JIA may be chronic or acute; however, acute episodes typically do not require systemic therapy.8 Of note, the 10-year extrapolation was not justified but presumably it is because the last visual acuity measurement was evaluated at the 10-year follow-up in the Bristol cohort study. Notably, Hughes et al. (2019) explored the use of a shorter time horizon of 18 months and the ICER (£136 751 per QALY gained) was still not considered cost-effective and higher than the base-case (£129 025 per QALY gained). Methods to value benefits and estimate quantities and unit costs were reported in addition to the methods pertaining to the sensitivity analyses. Incremental analyses were reported with relevant alternatives compared and disaggregated health care resource use and costs were reported by arm and as the mean difference with 95% central range.18
This economic evaluation was also associated with considerable methodological limitations.
The datasets of the SYCAMORE RCT and Bristol cohort study may not have been comparable. Insufficient details regarding the study design, population and intervention (e.g., dosing), and results of these studies were provided, which does not allow for an assessment of how comparable the datasets were. Additionally, there were participants who were in both studies (SYCAMORE RCT and Bristol cohort study), but it is not clear if there was an impact on the results from the overlap. Nevertheless, the source publications were referenced, which allows for cross referencing.
Authors of the economic evaluation noted that the SYCAMORE RCT and Bristol cohort datasets may not be comparable regarding the treatment practice of biologic therapies. For instance, adalimumab was only prescribed to individuals with a worse health state and the frequency of biologic administration may have varied during the data collection period of 1997 to 2014 (i.e., potential for less biologic use in the earlier study periods) in the cohort study. Additionally, the Bristol centres were suggested to not be representative of the general practice across the NHS. Namely, these centres consisted of specialist care of rheumatology and ophthalmology and began administering biologic therapy to treat JIA-associated uveitis earlier than other centres in the UK. Use of aforementioned specialized care also differed between centres included in the study. Further, it was not specifically reported if only patients with JIA-associated uveitis receiving adalimumab from the Bristol cohort were included in the model. The Bristol cohort included patients with idiopathic uveitis as well. Altogether, the inclusion of the Bristol cohort data limits the internal and external validity to NHS jurisdictions and beyond (e.g., Canada).
The trial-based (SYCAMORE) analysis (18 months) was matched to the Bristol cohort study (extrapolation of 10 years) with visual acuity. However, the SYCAMORE RCT was not powered to detect differences in visual impairment and the extrapolated model did not consider severe visual impairment. Without consideration of severe visual impairment, this does not account for the substantial impact on quality of life (and employment as well as education) and high lifetime costs.
The datasets used for the economic model were not complete. Namely, the Bristol cohort study did not evaluate long-term outcome data that could have informed the progression of uveitis. Further, 28 patients (31%) of the SYCAMORE RCT had QALY data and 28% and 70% of visual acuity (VA) data in the adalimumab and placebo groups were censored, respectively.
Currency conversion or price adjustments for inflation were not provided, which limits generalizability to current Canadian health jurisdictions as the unit costs were estimated at the cost year of 2016.
A meta-analysis was not performed although data were derived from 1 RCT and 1 cohort study; thus, this may have been appropriate as combining randomized and non-randomized data could introduce considerable heterogeneity.
For the sensitivity analyses exploring the visual impairment rates, the proportion rates were referred to as high and low, but corresponding quantitative values were not reported. Overall, the assumptions for the sensitivity analyses seemed reasonable within the CADTH review team’s (of this report) level of expertise. However, the accuracy of the sensitivity analysis results were unclear, all sensitivity analysis findings summarized in this report were extracted from Table 5 of the source publication.18
Authors of the economic evaluation reported funding sources; however, multiple authors reported financial disclosures associated with AbbVie (UK), UCB (US), Eli Lilly (US), and SOBI (UK) in the form of consulting, lecturing, and drug supply. Of note, AbbVie is the manufacturer of adalimumab. For regulatory purposes, AbbVie has licensed use of the study results. The authors did specify that AbbVie had no role in funding, trial management, data analysis, or writing of the publication but was allowed to review the final draft. Nevertheless, the authors of the publication maintained complete control over the article content. Overall, this economic evaluation was conducted in the perspective of the UK health care system and many sources for input parameters (e.g., costs of drug and resources) were UK-based; thus, findings may not be generalizable to the Canadian health system.18
Evidence-Based Guidelines
Among both evidence-based guidelines,7,8 the overall objective(s) were clearly reported and the target population reported with their views and preferences considered. Both guidelines had patient representation through a parent, but it would have been more comprehensive and relevant to also have representation from a pediatric patient with non-infectious uveitis. Although, the ACR/ Arthritis Foundation guideline development group had representation from adult patients with JIA, perhaps there were ethical or legal or other concerns with having pediatric patient representatives but this was not specified. The country of relevance of users for both guidelines were not specifically stated; accordingly, they were presumed to be the US and Germany based on the countries affiliated with the development groups. Further, the target users of the interdisciplinary German groups guideline could have been more specific as the only information provided was that the guideline was intended to assist with decision-making with treatment of anterior uveitis associated with JIA. In addition, both guidelines had representatives from relevant professional groups (i.e., ophthalmology and rheumatology specialties) in the development group. However, the ACR/ Arthritis Foundation guideline was developed among panels with a substantially higher proportion of rheumatologists (e.g., expert and voting panel: 9 rheumatologists versus 1 ophthalmologist and 15 rheumatologists versus 2 ophthalmologists, respectively).8
Both guidelines performed a database literature search to retrieve evidence but the eligibility criteria were not reported. The search for the ACR/ Arthritis Foundation guideline was more comprehensive as multiple databases and registries were searched from inception. Whereas the German guideline searched 1 database with a limited search range of the previous 2 decades up to January 30, 2017. This search range may be adequate for more novel therapies such as biologics but may not capture all evidence of non-biologic DMARDs and glucocorticoids. The methods for formulating the recommendations were described but could have been clearer for the interdisciplinary German groups guideline; namely, whether the external reviewers or the development group members voted and/or reviewed the draft recommendations during the third Delphi round.7,8
Both guidelines were specific and unambiguous; considered the health benefits, side effects, and risks in formulating the recommendations (namely, the ACR/ Arthritis Foundation guideline followed GRADE methodology); and clearly presented the different treatment options. Nevertheless, both guidelines were associated with some limitations including the lack of reporting regarding facilitators and barriers, potential resource implications, monitoring and/or auditing criteria, and an updating process. Strengths of the ACR/ Arthritis Foundation guideline included key recommendations being easily identifiable, the health question(s) relevant to the guideline specifically described, and advice on how to implement the recommendation was provided. Limitations of this guideline included the strengths and limitations of the included evidence being reported for some recommendations only and only some recommendations reported additional details of the included evidence with the references provided. Specific to the interdisciplinary German groups guideline, recommendations reported additional details of the included evidence with references provided. However, limitations included key recommendations not being easily identifiable, health question(s) relevant to the guideline not specifically described, strengths and limitations of the included evidence not reported, and advice on how to implement the recommendation was not provided.
Both guidelines were published in journals with review processes. The German guideline also had an external review by the German Ophthalmological Society, German Society of Rheumatology, and the Society of Pediatric Rheumatology before finalization. For the ACR/ Arthritis Foundation guideline, financial conflict forms were submitted and it was specified that all development teams had over half of the members free of potential conflicts of interest. Additionally, the leader of the literature review team and the principal investigator were free of potential conflicts of interest. For the interdisciplinary German guideline, funding was not reported and it was stated that all participants of guideline development had no conflict of interest(s) but they were not reported.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions. 2 SRs reported on the same 2 placebo controlled RCTs; thus, pooled estimates were extracted when possible and both datasets were extracted and summarized when there were differences in values or unit measurements. CADTH did not perform any statistical comparisons for the data extracted from relevant primary RCTs.
Clinical effectiveness of adalimumab for the treatment of pediatric populations with non-infectious uveitis
Results from the included evidence informing the clinical effectiveness are summarized below by outcome.
Change in Visual Acuity
Li et al. (2021)6 reported that at the outset of the ADJUVITE trial, the median visual acuity was 0.1 logMAR (range = −0.2 to 1.3) in the adalimumab group and following treatment with adalimumab, the median visual acuity was 0.15 logMAR (range = −0.10 to 1.10). This represents a slight worsening in visual acuity through the increase in logMAR units; however, this was not statistically tested. Of note, this finding is a measure of visual acuity before and after receiving adalimumab; thus, this is single-arm (non-comparative) data and should be interpreted in light of these limitations. The change in median visual acuity for the placebo group was not reported.
Change in Uveitis-Related Corticosteroid Use
Norcia et al. (2021)17 reported that treatment with adalimumab significantly increased the likelihood of reducing or interrupting corticosteroid use compared to placebo (pooled data of the SYCAMORE and ADJUVITE RCTs), the risk ratio of the reduction or interruption of the use of corticosteroids was 2.27 (95% CI, 1.03 to 4.99; P = 0.04; I2 = 0%).17 Of note, long-term use of corticosteroids is not favourable as it is associated with side effects such as glaucoma and cataracts.5,9
Control of Intraocular Inflammation
Li et al. (2021)6 reported that there were more responders in the adalimumab group (9 of 16) compared with placebo (3 of 15) (P = 0.038), regarding control of intraocular inflammation (defined as 30% of reduction in inflammation) in the ADJUVITE RCT. The risk ratio was 2.81 (95% CI, 0.94 to 8.45) and the risk difference was 36.3% (95% CI, 2.1 to 60.6).6 Measures of risk demonstrated conflicting results: the CI crossed 1 for the relative risk, indicating a non-statistically significant difference in relative risk, which suggests there is likely no treatment effect. Alternatively, the CI of the risk difference suggested there may be a statistically significant treatment effect for intraocular inflammation control, but with a widespread (i.e., true value lying between 2.1 and 60.6).6 Overall, the effect of adalimumab on control of intraocular inflammation is unclear.
Satisfactory Response Rate to Treatment and Treatment Failure
Norcia et al. (2021)17 reported that adalimumab significantly increased the event of a satisfactory response rate compared to placebo (pooled data of the SYCAMORE and ADJUVITE RCTs). The risk ratio of the satisfactory response rate was 3.21 (95% CI, 1.65 to 6.27; P = 0.0006; I2 = 0%).17
Li et al. (2021) reported treatment failure data from the SYCAMORE RCT. The number of responders (to treatment) in the adalimumab and placebo groups were 14 of 60 and 17 of 30 patients, respectively. Adalimumab significantly lowered the risk of treatment failure with a risk ratio of 0.40 (95% CI, 0.23 to 0.72; P = 0.002).6
Safety
Li et al. (2021)6 reported safety data for the SYCAMORE trial. Regarding adverse events, there were 59 and 26 in the adalimumab and placebo groups, respectively (it was not reported if these values represented the number of patients or events).6 The rate of adverse events in the adalimumab and placebo groups were 10.60 per patient-year (95% CI, 9.77 to 11.44) and 7.12 per patient-year (95% CI, 5.89 to 8.53). For the adalimumab group, it was reported that the most common adverse event type was infections and infestations accounting for 83% (it is not clear if this proportion represents a percentage of events or patients).6 The number of patients experiencing any serious adverse event in the adalimumab and placebo groups were 13 of 60 and 2 of 30, respectively.19 The rate of serious adverse events in the adalimumab and placebo groups were 0.29 and 0.19 per patient-year, respectively (95% CIs not reported). For the adalimumab group, it was reported that the most common serious adverse events were glaucoma, cataracts, injection site reactions, arthritis, and arthralgia.6 The etiology of cataracts (i.e., related to prior corticosteroid use or due to uncontrolled inflammation) was not described. Overall, the rate and number of adverse events and serious adverse events were higher in the adalimumab group in the SYCAMORE trial.
Norcia et al. (2021)17 reported that there was no difference in safety between adalimumab and placebo (pooled data of the SYCAMORE and ADJUVITE RCTs). The risk ratios of systemic severe adverse events and local adverse effects were 2.51 (95% CI, 0.74 to 8.5; P = 0.14; I2 = 48%) and 1.15 (95% CI, 0.46 to 2.88; P = 0.76; I2 = 1%), respectively.17
Cost-Effectiveness of adalimumab for the treatment of pediatric populations with non-infectious uveitis
The evidence informing the cost-effectiveness is summarized separately for the base-case and sensitivity analyses.
Base-Case Analysis
The estimated ICER for adalimumab plus methotrexate versus methotrexate only was £129 025 per QALY gained with the estimated incremental QALYs and incremental costs reported as 0.30 and £39 316, respectively. Total QALYs for the adalimumab plus methotrexate versus methotrexate only groups were 8.60 and 8.29, respectively. Total costs for the adalimumab plus methotrexate versus methotrexate only groups were £70 719 and £31 403, respectively. Hughes et al. (2019)18 found that adalimumab plus methotrexate resulted in more QALYs but at a higher cost; further, the ICER exceeded the cost-effectiveness thresholds used by the NHS/ National Institute for Health and Care Excellence (NICE) in the UK (willingness-to-pay thresholds of £20 000 to £30 000 per QALY gained). Thus, it was concluded that adalimumab plus methotrexate is not cost-effective compared to methotrexate alone in the UK as treatment for uveitis associated with JIA. The analysis did not conduct separate analysis based on oral or subcutaneous administration of methotrexate.
Sensitivity Analyses
Among the univariate sensitivity analyses, the analyses deemed to be most relevant to this report are summarized, please refer to the source publication for the findings of all sensitivity analyses performed.18 Of note, all ICERs estimated from the univariate sensitivity analyses resulted in ICERs that were above the stated NICE thresholds of £20 000 to £30 000 per QALY gained. The following data were extracted from Table 5 in the source publication.18
Price reductions of adalimumab by 25% and 50% resulted in ICERs of £94 661 and £67 288 per QALY gained, respectively; incremental QALYs of 0.30 and 0.30, respectively; and incremental costs of £28 844 and £20 504, respectively.
Without discounting the estimated ICER was £128 886 per QALY gained and it was found that a price reduction of 84% would be required for adalimumab to be cost-effective at the £30,000 threshold. The incremental QALYs and costs were 0.32 and £40 621, respectively.
Duration of adalimumab of 18 months and 18 months plus 10 years resulted in ICERs of £133 656 and £127 646 per QALY gained, respectively; incremental QALYs of 0.11 and 0.70, respectively; and incremental costs of £14 101 and £88 858, respectively.
A shortened time horizon of 18 months increased the estimated ICER even more than the base-case analysis and different durations of adalimumab administration with a value of £136 751 per QALY gained. The incremental QALYs and costs were 0.11 and £14 374, respectively.
Reduction in the proportion of patients administered adalimumab beyond 18 months to 0.23 (reflected the observed value) resulted in an ICER of £131 511 per QALY gained. The incremental QALYs and costs were 0.15 and £19 900, respectively.
In the scenario where all participants who received placebo transited to the visual impairment state: the estimated ICER, incremental QALYs, and costs were £78 524 per QALY gained, 0.32, and £25 495, respectively. Alternatively, the scenario of all patients receiving adalimumab transitioning to the no visual impairment state and all who received placebo transition to the visual impairment state (and remain in those states): the estimated ICER, incremental QALYs, and incremental costs were £53 072 per QALY gained, 0.34, and £17 820, respectively.18
The probabilistic sensitivity analysis demonstrated that the probability of cost-effectiveness at a willingness-to-pay threshold of £30 000 per QALY was less than 1% (i.e., fewer than 1% of simulations fell below the £30 000 per QALY threshold); thus, it is very unlikely for adalimumab to be cost-effective.18 The 2-way sensitivity analyses demonstrated that the ICER was sensitive to the cost of adalimumab but not to the proportion of patients who received adalimumab and developed visual impairment or the disutility associated with visual impairment.18
Evidence-based guidelines regarding the use of adalimumab for the treatment of pediatric populations with non-infectious uveitis
American College of Rheumatology/Arthritis Foundation, 20198
Within the ACR/ Arthritis Foundation recommendations, “systemic therapy” referred to biologics and non-biologic DMARDs only (i.e., did not refer to systemic glucocorticoids). “TNFi biologics” referred to adalimumab, infliximab, and etanercept only and “monoclonal antibody TNFi” referred to adalimumab and infliximab. All recommendations in the ACR/ Arthritis Foundation guideline8 were based on very low-quality evidence. The following recommendations for DMARDs and biologics were provided: “for children and adolescents with JIA and associated active chronic anterior uveitis (CAU) who are/have
starting systemic treatment for uveitis, using subcutaneous methotrexate is conditionally recommended over oral methotrexate
starting a TNFi, starting a monoclonal antibody TNFi is conditionally recommended over etanercept
with severe active CAU and sight threatening complications, starting methotrexate and a monoclonal antibody TNFi immediately is conditionally recommended over methotrexate as monotherapy
inadequate response to one monoclonal TNFi at standard JIA dose, escalating the dose and/or frequency of the monoclonal TNFi to above-standard is conditionally recommended over switching to another monoclonal antibody TNFi (consensus was not reached regarding changes to the dose and/or frequency of treatment)
failed a first monoclonal antibody TNFi at above-standard dose and/or frequency, changing to another monoclonal antibody TNFi is conditionally recommended over a biologic in another category (p.25 to 26).”8
The following recommendations for tapering therapy for uveitis were provided:
“In children and adolescents with JIA and uveitis that is well controlled on DMARD and biologic systemic therapy only: conditionally recommend that there be at least 2 years of well-controlled disease before tapering therapy.
In children and adolescents with JIA and CAU that is controlled on systemic therapy but remain on 1–2 drops/day of prednisolone acetate 1% (or equivalent), tapering topical glucocorticoids first is strongly recommended over systemic therapy (p.26).”8
All were conditional recommendations except for the recommendation regarding tapering topical glucocorticoids over systemic therapy in those with controlled uveitis who are treated with systemic therapy and remain on 1 to 2 drops per day of prednisolone acetate 1% (or equivalent), which was a strong recommendation.8
Interdisciplinary German Groups, 20197
The evidence-based guideline by the interdisciplinary German Groups recommended that “if uveitis inactivity is not achieved by 16 weeks of methotrexate monotherapy and < 2 drops of topical corticosteroids daily, or if new, inflammation-related complications of uveitis occur, a TNF-alpha antibody therapy shall be used in combination with methotrexate (p.49).”7 Accordingly, it was recommended that adalimumab be considered in patients with anterior uveitis associated with JIA who have not responded to methotrexate. They noted that adalimumab is currently the preferred TNF-alpha inhibitor (among infliximab, golimumab, and etanercept) in the treatment of anterior uveitis associated with JIA due to the tolerability and good response rate demonstrated in RCTs. Infliximab was the second-choice TNF-alpha inhibitor due to infusion reactions but it was noted that in the event of loss of adalimumab efficacy and treatment failure, a treatment switch to infliximab or golimumab should be considered.7 The guidelines specific to adalimumab were based on level II evidence and were rated as strong.7
Limitations
Overall, this report is limited in the quality and quantity of relevant evidence regarding the clinical and cost-effectiveness and evidence-based guidelines informing the use of adalimumab as treatment in pediatric populations with non-infectious uveitis. Namely, there is a particular need for more well-designed RCTs as there were 4 SRs/meta-analyses/health technology assessments that were excluded due to full overlap. All 4 publications included the SYCAMORE and ADJUVITE RCTs. The small quantity of relevant high-quality evidence was also highlighted in the guidelines. The ACR/ Arthritis Foundation identified only 1 well-conducted RCT as evidence in children with JIA and uveitis — the SYCAMORE trial. The German evidence-based guideline identified 3 RCTs as evidence for treating anterior uveitis associated with JIA — the third being an RCT specific to etanercept. Further, the visual acuity data among the included evidence is limited. The SR by Li et al. (2021) reported that there was a slight worsening in visual acuity before and after treatment with adalimumab (0.1 logMAR versus 0.15 logMAR) from ADJUVITE trial data. This finding was non-comparative and not statistically tested. Additionally, the change in visual acuity was not reported for the placebo group, which further limits a comparison between adalimumab and placebo from the data informing this report. Further, the economic evaluation noted that the SYCAMORE trial was not powered to detect differences in visual impairment and there was no significant improvement in visual acuity of the worst-eye logMAR (i.e., worst logMAR measurement: maximum of the 2 values).18,19 As uveitis is an inflammatory condition of the eye, there is a particular need for evaluations of visual outcomes (e.g., visual acuity, best-corrected visual acuity). In addition, the economic evaluation did not perform separate analyses for orally- and subcutaneously administered methotrexate although the SYCAMORE trial allowed for both modes of administration.
The relevant RCTs of the included SRs, the economic evaluation, and evidence-based guidelines were specific to uveitis associated with JIA. Notably, there are other etiologies of non-infectious uveitis in pediatric populations; therefore, the generalizability of the findings summarized in this report may not be relevant to other pediatric populations with non-infectious uveitis. Of note, in Canada, adalimumab is specifically indicated for pediatric non-infectious uveitis: “treatment of chronic non-infectious anterior uveitis in pediatric patients from 2 years of age who have had an inadequate response to or are intolerant to conventional therapy, or in whom conventional therapy is inappropriate (p.7).”20 Additionally, adalimumab is specifically indicated for polyarticular (i.e., affecting many joints) JIA: “in combination with methotrexate, reducing signs and symptoms of moderately to severely active polyarticular JIA in patients, 2 years of age and older who have had an inadequate response to one or more DMARDs. Humira can be used as monotherapy in case of intolerance to methotrexate or when continued treatment with methotrexate is not appropriate (p.7).”20 Accordingly, recommended dosing for these indications are also different.11 Thus, interpretation of the findings of this report should be specific to adalimumab therapy for JIA-associated uveitis, which is indicated in combination with methotrexate.
Further, the included evidence were not specific to Canada; therefore, the findings of this report may not be generalizable to current clinical practice in Canada. The 2 RCTs that informed the clinical effectiveness findings were conducted in the UK (SYCAMORE) and France (ADJUVITE).6,17 The SYCAMORE trial was a multi-centre study of various sites in the UK and the ADJUVITE study was a single centre study (the Necker-Enfants Malades Hospital, Paris, France). The included economic evaluation was conducted from the perspective of the UK and model inputs were also specific to the UK (e.g., drug and resource costs were provided in pound sterling and taken from the British National Formulary and NHS resources). Accordingly, ICERs were based on the currency of pound sterling and cost-effectiveness ICER thresholds were determined by NICE. Additionally, drug and resource costs were based on 2015 to 2017 data. The authors did not provide a description of adjustments for inflation and currency conversion, which limits generalizability to the Canadian health care system in the current or recent years.18 Particularly regarding economic evaluations, perspective and model inputs should be specific to the jurisdiction of interest. Similarly, none of the included evidence-based guidelines were specific to Canada: 1 guideline7 was developed by multiple German groups with clinician and patient or caregiver representation; however, the ACR/ Arthritis Foundation guideline was potentially relevant to North America.8 Therefore, interpretation of the clinical and cost-effectiveness findings and utility of the evidence-based guidelines summarized in this report should be specific to the health care systems of the UK, France, Germany, and the US with consideration that applicability to the current Canadian health care system is limited. Specific to the evidence-based guidelines, all the recommendations in the ACR/ Arthritis Foundation guideline were based on evidence rated to be of very low quality, per GRADE methodology.8 Nevertheless, the authors of this guideline stated that the SYCAMORE study was a well-conducted RCT.8 Moreover, in the non-infectious uveitis pediatric population, consensus was not reached for recommendations regarding changes to the dose and/or frequency of treatment (in individuals with an inadequate response) before switching to another monoclonal antibody TNF inhibitor (e.g., switching from adalimumab to infliximab). However, it was noted that doses of a maximum of 20 mg per kg of infliximab every 2 weeks and adalimumab weekly have been reported among children with JIA and uveitis in observational studies.8 The recommendations specific to adalimumab in the guideline by multiple German groups were based on level II evidence, which consisted of a small number of RCTs, more than 1 RCT of lesser quality, nonrandomized studies (e.g., cohort or case-control studies preferably conducted by more than 1 research group or centre), and noncontrolled studies with clear observations.7
Conclusions and Implications for Decision- or Policy-Making
This report comprised 2 SRs with meta-analyses,17,21 1 economic evaluation,18 and 2 evidence-based guidelines,7,8 which informed the clinical effectiveness (including safety), cost-effectiveness, and use of adalimumab for the treatment of pediatric populations with non-infectious uveitis, respectively. The 2 SRs included 2 placebo controlled RCTs (SYCAMORE19 and ADJUVITE22 trials) relevant to this report. Data from the SYCAMORE trial were also used in the model of the economic evaluation.18 Overall, the included evidence should be interpreted with caution due to methodological limitations and limited generalizability (highlighted in the Critical Appraisal and Limitations sections of this report).
There was a slight worsening in visual acuity before and after treatment with adalimumab (0.1 logMAR versus 0.15 logMAR) reported in the ADJUVITE trial. However, this is non-comparative data that was not statistically tested and should be interpreted in light of these limitations.6 Pooled data of the SYCAMORE and ADJUVITE RCTs comparing adalimumab to placebo demonstrated that adalimumab significantly increased the likelihood of reducing or interrupting corticosteroid use (which is beneficial due to long-term corticosteroid use potentially resulting in glaucoma and cataracts), adalimumab significantly increased the event of a satisfactory response rate, but there was no difference in safety assessed as systemic adverse events and local adverse effects.17 Specific to the SYCAMORE trial, adalimumab significantly lowered the risk of treatment failure and the rate and number of adverse events and serious adverse events were higher in the adalimumab group compared to the placebo group. For the adalimumab group, the most common adverse event type was infections and infestations and the most common serious adverse events were glaucoma, cataracts, injection site reactions, arthritis, and arthralgia.6 Of note, it was not reported if these cataract events were due to prior corticosteroid use (and had progressed) or uncontrolled inflammation (i.e., uveitis). Specific to the ADJUVITE trial, it was unclear if adalimumab increases control of intraocular inflammation as the risk ratio and risk difference suggested contrasting conclusions (i.e., risk ratio and risk difference suggested no treatment effect and a treatment effect, respectively).6 Of note, there was a 5-year follow-up of the SYCAMORE trial from 1 of 17 participating centres.23 This study found that adalimumab did not elicit a sustained or unexplained reduction in vision from baseline (greater than 0.3 logMAR units over 2 consecutive readings during a 3-month period within the 5-year follow-up); however, drug-induced remission of uveitis did not persist after treatment with adalimumab was stopped following 1 to 2 years of therapy. Thus, it was concluded that adalimumab was well tolerated and may improve visual acuity but the optimal treatment duration of adalimumab is unclear as this 5-year follow-up data demonstrated that uveitis control did not persist throughout this period.23
The included economic evaluation concluded that the cost-effectiveness of adalimumab plus methotrexate compared to methotrexate alone could not be demonstrated in uveitis associated with JIA. The base-case analysis estimated the ICER to be £129 025 per QALY gained with incremental costs and QALYs of £39 316 and 0.30, respectively.18 At the threshold of £30 000 per QALY gained, the probability of cost-effectiveness was less than 1%. Multiple sensitivity analyses were performed and explored scenarios such as variable durations of adalimumab treatment (18 months versus 18 months plus 10 years), an 18-month time horizon, reduced prices of adalimumab by 25% and 50%, and different visual impairment rates. Nevertheless, all the sensitivity analyses estimated ICERs that were still above the NICE cost-effectiveness thresholds (£20 000 to 30 000 per QALY gained). Although the ICER decreased with a discounted price of adalimumab, a price reduction of 84% was found to be required for adalimumab to be cost-effective at the £30 000 per QALY threshold. However, these findings should be interpreted in light that the economic evaluation was performed in the perspective of the UK with UK standards, resources, and cost data (pound sterling) from 2015 to 2017 (e.g., NICE, British National Formulary, and NHS). Additionally, it was not reported if adjustments for inflation were performed. Altogether, the cost-effectiveness findings may not be generalizable to current Canadian jurisdictions. Of note, the systematic literature search performed for this report identified 4 published correspondences to the Hughes et al. (2019) economic evaluation that highlighted various limitations regarding the conduct and interpretation of the findings of the economic evaluation.24-27 A few limitations in these correspondences aligned with the limitations reported by Hughes et al. (2019); however, all critiqued the use of the Health Utilities Index-3 (HUI-3) questionnaire to inform QALYs. Lightman et al. (2019) noted that the HUI-3 reports a single measure of visual function, which is not appropriate for younger children with uveitis associated with JIA. In addition, quality of life of other stakeholders such as caregivers should have been considered (e.g., quality of life specific to the caregiver).27 Symes et al. (2019) questioned the validity of using questionnaire-based data.24 Brown et al. (2019) stated that the HUI-3 may not be sensitive to evaluating central vision, which is critical to the quality of life of a patient with an ophthalmic condition or disease.25 Pleyer et al. (2019) specified that the HUI-3 lacks elements specific to JIA and may not have detected relevant changes in quality of life.26
The ACR/ Arthritis Foundation guidelines were based on very low-quality evidence. It was conditionally (i.e., not strongly) recommended that adalimumab and infliximab be used as an initial TNF-alpha inhibitor over etanercept for active CAU in children and adolescents with JIA. However, there was no preference established between adalimumab and infliximab as the initial TNF-alpha inhibitor.8 It was noted that evidence supporting the preference for a biologic or non-biologic DMARD; combination therapies; and timing of initiation of therapies (other than adalimumab, infliximab, and methotrexate) are currently limited. Conversely, the guideline from multiple interdisciplinary German groups stated that adalimumab is the preferred TNF-alpha inhibitor in the treatment of anterior uveitis associated with JIA due to tolerability and good response rate demonstrated in published RCT data. It was noted that in the event of loss of adalimumab efficacy and treatment failure, a treatment switch to infliximab or golimumab should be considered with infliximab being the second-choice.7 Nevertheless, both guidelines suggested the use of a monoclonal antibody (TNF-alpha inhibitor: adalimumab) plus methotrexate when there is no response to initial treatment (e.g., topical corticosteroid) and risk of severe uveitis or vision threatening complications in JIA.8
CADTH was unable to connect with a pediatric patient living with non-infectious uveitis. Nevertheless, CADTH connected with an adult living with uveitis associated with ankylosing spondylitis for the companion report on non-infectious uveitis in adults.2 This individual noted that non-infectious uveitis may have a considerable negative impact on the quality of life particularly during the initial onset when there is a lack of knowledge of the diagnosis (i.e., individuals may mistake uveitis for dry eye or conjunctivitis especially during the first episode) in addition to the pain, irritation, discomfort, swelling, light sensitivity, blurry vision, and headache that may accompany all uveitis episodes. Additionally, it was stated that when clinicians are devising a treatment plan, they should consider the efficacy and safety of treatment(s), use of concurrent treatments, recurrence of uveitis, comorbidities, and general health of the individual.2
Overall, there is a need for well-designed clinical studies, economic evaluations, and evidence-based guidelines specific to Canadian health care settings to inform the clinical effectiveness, cost-effectiveness, and use of adalimumab in the perspective of Canadian jurisdictions. Namely, multiple biosimilars are approved in Canada with indications specific to uveitis in pediatric populations. Biosimilars may introduce cost-savings; thus, there is a particular need for more evidence specifically on adalimumab biosimilars as most of the current evidence is specific to adalimumab (reference). For instance, the included economic evaluation explored ICERs of adalimumab and suggested that the reduction in the ICER with a discounted price of adalimumab supports the potential use of biosimilars in the future due to cost savings.18 Further, the lack of evidence on biosimilars is reflected in a recent CADTH report, published in February 2021, that found no evidence regarding the clinical effectiveness of switching from adalimumab (reference) to biosimilars in adults with uveitis.28 Nevertheless, the included clinical- and cost-effectiveness evidence and evidence-based guidelines of this rapid review may inform the use of adalimumab biosimilars in pediatric populations with non-infectious uveitis to facilitate cost-savings in some jurisdictions.
References
1.Felfeli T, Christakis PG, Bakshi NK, Mandelcorn ED, Kohly RP, Derzko-Dzulynsky LA. Referral characteristics and wait times for uveitis consultation at academic tertiary care centres in Toronto. Can J Ophthalmol. 2018;53(6):639-645. PubMed
2.Hui D, Mierzwinski-Urban M, Spry C. CADTH health technology review: adalimumab for the treatment of adults with non-infectious uveitis. Can J Health Technol. 2022;2(1). https://www.cadth.ca/sites/default/files/pdf/htis/2022/RD0063%20Adalimumuab%20for%20Uveitis-Final.pdf. Accessed 2022 Feb 7.
3.Rosenbaum JT. Uveitis: etiology, clinical manifestations, and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Nov 15.
4.Li B, Li H, Zhang L, Zheng Y. Efficacy and safety of adalimumab in noninfectious uveitis: a systematic review and meta-analysis of randomized controlled trials. Front Pharmacol. 2021;12:673984. PubMed
5.Bermejo I, Squires H, Poku EN, et al. Adalimumab for non-infectious uveitis: is it cost-effective? Br J Ophthalmol. 2019;103(11):1633-1638. PubMed
6.Li Y, Mao X, Tang X, Mao H. Efficacy and safety of anti-TNFalpha therapy for uveitis associated with juvenile idiopathic arthritis: a systematic review and meta-analysis. Rheumatol. 2021;8(2):711-727. PubMed
7.Heiligenhaus A, Minden K, Tappeiner C, et al. Update of the evidence based, interdisciplinary guideline for anti-inflammatory treatment of uveitis associated with juvenile idiopathic arthritis. Semin Arthritis Rheum. 2019;49(1):43-55. PubMed
8.Angeles-Han ST, Ringold S, Beukelman T, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the screening, monitoring, and treatment of juvenile idiopathic arthritis-associated uveitis. Arthritis Care Res (Hoboken). 2019;71(6):703-716. PubMed
9.Rosenbaum JT. Uveitis: treatment. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Nov 15.
10.Adalimumab (including biosimilars of adalimumab): drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Nov 15.
11.Adalimumab (including biosimilars of adalimumab): pediatric drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Nov 15.
12.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
13.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
14.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Nov 15.
15.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Nov 15.
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
17.Norcia LF, Kiappe OP, Jorge EC. Biological therapy in noninfectious pediatric uveitis: a systematic review. Clin Ophthalmol. 2021;15:3765-3776. PubMed
18.Hughes DA, Culeddu G, Plumpton CO, et al. Cost-effectiveness analysis of adalimumab for the treatment of uveitis associated with juvenile idiopathic arthritis. Ophthalmology. 2019;126(3):415-424. PubMed
19.Ramanan AV, Dick AD, Jones AP, et al. Adalimumab plus methotrexate for uveitis in juvenile idiopathic arthritis. N Engl J Med. 2017;376(17):1637-1646. PubMed
20.Humira (adalimumab): 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection, 10 mg in 0.1 mL sterile solution (100 mg/mL) subcutaneous injection, 20 mg in 0.2 mL sterile solution (100 mg/mL) subcutaneous injection, 40 mg in 0.4 mL sterile solution (100 mg/mL) subcutaneous injection, 80 mg in 0.8 mL sterile solution (100 mg/mL) subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2021 Apr 21: https://pdf.hres.ca/dpd_pm/00061690.PDF. Accessed 2021 Nov 15.
21.Maccora I, Fusco E, Marrani E, Ramanan AV, Simonini G. Changing evidence over time: updated meta-analysis regarding anti-TNF efficacy in childhood chronic uveitis. Rheumatology. 2021;60(2):568-587. PubMed
22.Quartier P, Baptiste A, Despert V, et al. ADJUVITE: a double-blind, randomised, placebo-controlled trial of adalimumab in early onset, chronic, juvenile idiopathic arthritis-associated anterior uveitis. Ann Rheum Dis. 2018;77(7):1003-1011. PubMed
23.Horton S, Jones AP, Guly CM, et al. Adalimumab in juvenile idiopathic arthritis-associated uveitis: 5-year follow-up of the Bristol participants of the SYCAMORE trial. Am J Ophthalmol. 2019;207:170-174. PubMed
24.Symes RJ, Zagora SL, Younan C, McCluskey PJ. Re: Hughes et al.: Cost-effectiveness analysis of adalimumab for the treatment of uveitis associated with juvenile idiopathic arthritis (Ophthalmology. 2019;126:415-424). Ophthalmology. 2019;126(10):e77. PubMed
25.Brown GC, Brown MM. Re: Hughes et al.: Cost-effectiveness analysis of adalimumab for the treatment of uveitis associated with juvenile idiopathic arthritis (Ophthalmology. 2019;126:415-424). Ophthalmology. 2019;126(10):e76. PubMed
26.Pleyer U, Minden K, Klotsche J, Heiligenhaus A, Foeldvari I. Re: Hughes et al.: Cost-effectiveness analysis of adalimumab for the treatment of uveitis associated with juvenile idiopathic arthritis (Ophthalmology. 2019;126:415-424). Ophthalmology. 2019;126(10):e75-e76. PubMed
27.Lightman S, Niederer R, Sharma S, et al. Re: Hughes et al.: Cost-effectiveness analysis of adalimumab for the treatment of uveitis associated with juvenile idiopathic arthritis (Ophthalmology. 2019;126:415-424). Ophthalmology. 2019;126(3):e22-e24. PubMed
28.Switching from reference to biosimilar adalimumab for patients with various inflammatory conditions (CADTH reference list). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/pdf/htis/2021/RB1552%20Biosimilar%20Switching%20of%20Adalimumab%20Final.pdf. Accessed 2021 Nov 15.
Appendix 1: Selection of Included Studies
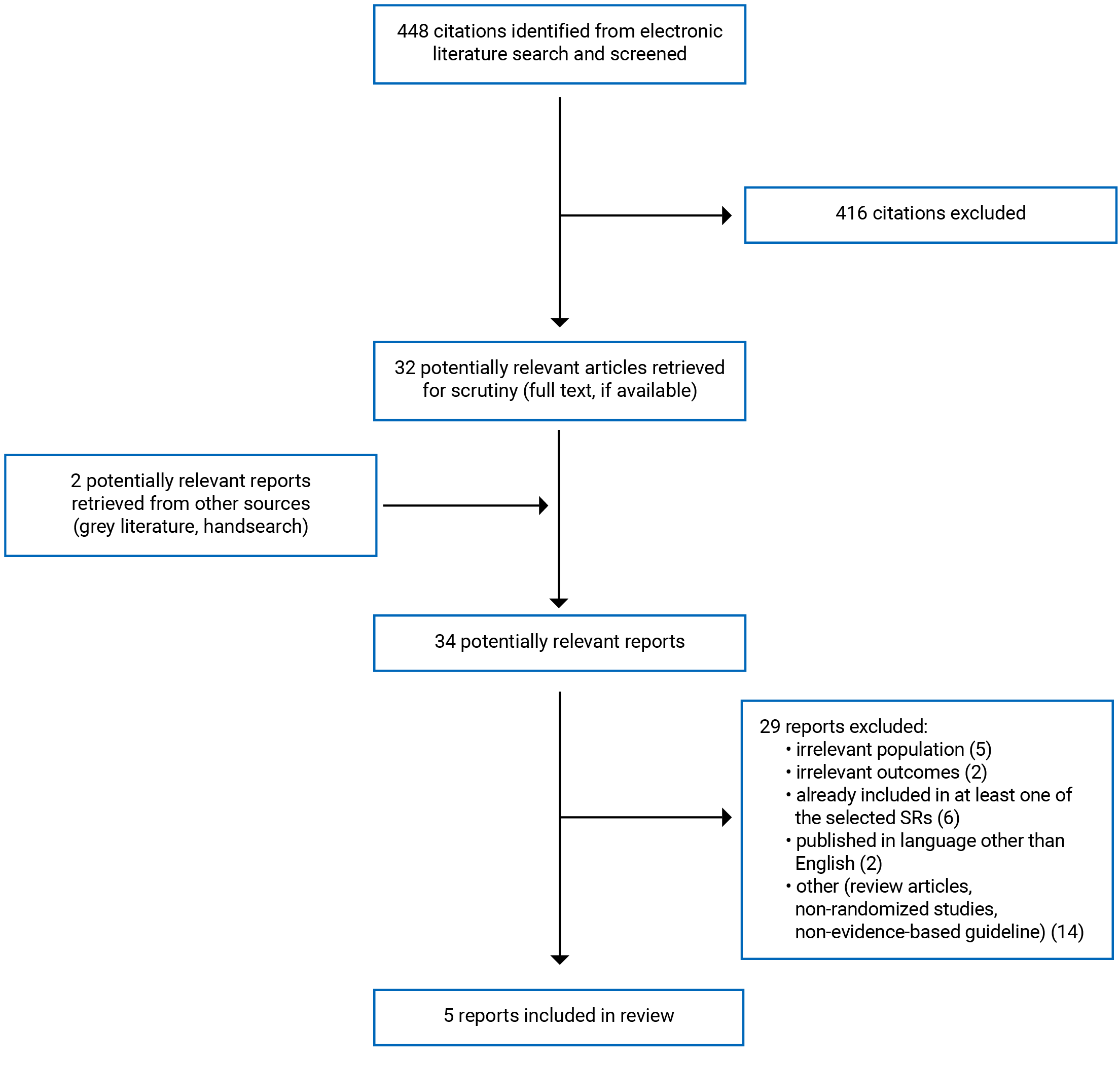
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included SRs and Meta-analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Li et al. (2021)6 China Funding: National Natural Science Foundation of China (81971547) and the Research Fund for Outstanding Youth Scholar of Chongqing Talents (CQYC201905003). | SR and MA of cohort studies, and case reports and case series (non-randomized data). Number of included studies: 21 Number of relevant primary studies: 2 placebo controlled RCTs specific to adalimumab as treatment for JIA-associated uveitis (SYCAMORE and ADJUVITE)a Objective: evaluate safety and efficacy of anti-TNF-alpha therapy for JIA-associated uveitis. | Onset of JIA at ≤ 16 years of age of individuals starting anti-TNF-alpha therapy for uveitis with an inadequate response to DMARDs and topical steroids. | Eligible intervention: anti-TNF-alpha therapy Relevant intervention: adalimumab Comparator: NR | Outcomes:
Follow-up: at least 3 months |
Norcia et al. (2021)17 Brazil Funding: NR. | SR and MA of RCTs and non-randomized controlled studies Number of included studies: 8 in the meta-analysis and 9 in the qualitative syntheses Number of relevant primary studies: 2 placebo controlled RCTs specific to adalimumab as treatment for JIA-associated uveitis (SYCAMORE and ADJUVITE)a Objective: evaluate clinical efficacy of biologic therapy for non-infectious uveitis in pediatric populations through an updated systemic search of the literature. | Individuals under 18 years of age with non-infectious uveitis regardless of related systemic disease. | Eligible intervention: biologic therapy Relevant intervention: adalimumab Comparator: placebo, other drugs, or combination therapies | Outcomes:
Follow-up:
|
AE = adverse event; BCVA = best-corrected visual acuity; CMT = central macular thickness; DMARD = disease-modifying antirheumatic drug; JIA = juvenile idiopathic arthritis; MA = meta-analysis; NA = not applicable; NR = not reported; RCT = randomized controlled trial; SAE = serious adverse event; SR = systematic review; SUN = Standardization of Uveitis Nomenclature; TNF = tumour necrosis factor; VA = visual acuity.
aBaseline characteristics of the SYCAMORE and ADJUVITE RCTs are summarized in the Summary of Study Characteristics section above.
bNot summarized in this report as the findings of this outcome in the Li et al. (2021)6 SR were unclear.
Table 3: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Hughes et al. (2019)18 UK Funding: Supported by the National Institute for Health Research Health Technology Assessment Programme (project #: 09/51/01); and Arthritis Research UK (grant #: 19612). Some authors reported financial disclosures involving manufacturers including AbbVie (UK), SOBI (UK), UCB (US), and Eli Lilly (US). | Analysis: cost-utility analysis Perspective: NHS (UK) Time horizon: 18-month trial-based analysis (SYCAMORE RCT) with a 10-year extrapolation (Bristol cohort study) | Individuals aged 2 to 18 years with persistent active uveitis associated with JIA uveitisa SYCAMORE (n = 90): age NR Bristol cohort —1997 to 2014 (n total = 91; n = 15 included in the 10 year extrapolation):
Bristol cohort study included 91 individuals with JIA-associated uveitis. | Intervention: adalimumab plus methotrexate SYCAMORE: subcutaneous adalimumab (participants < 30 kg: 20 mg and participants ≥ 30 kg: 40 mg) until treatment failure or 18 months following. Up to 25 mg of methotrexate weekly. Bristol cohort: dose NR 47 (30%) of patients received adalimumab Comparator: methotrexate only (placebo arm of SYCAMORE data) | Analysis was based on the 18-month trial period plus the 10-year modelled extrapolation. Markov model with 3 health states defined by visual impairment and survival. Patients initially distributed according to proportion of time spent in each state over the preceding 18 months based on trial arm. Bristol cohort data estimated probabilities associated with transitions among health states (with or without eye surgery). Model used a cycle length of 1 year with a half-cycle correction and a standardized mortality ratio of 3.9 (95% CI, 0.8 to 11.3). Analysis used the imputed dataset for missing data and adjusted for the crossover of participants from the placebo arm (due to early termination of SYCAMORE). | Health utilities: HUI responses mapped to the Mark 3 classification systemb Resource use: Study and concomitant therapies derived from case report forms and supplemented by patient diaries. Hospital use (or primary or community care) and AEs from patient-level costing systems or patient administration systems supplemented by interviews and diary entries. Unit costs: Resource use valued at UK unit costs estimated at 2016 (time of analysis). Unit costs of treatments were from multiple NHS sources. Use of hospital services were costed to health care resource group codes from the National Tariff 2016 to 2017 or the National | Simulated patients were considered to be fully adherent to adalimumab and based on expert clinical opinion would continue adalimumab for 3 years beyond the initial 18-month trial duration. Progression of visual impairment after 18 months would occur at the same rate for patients receiving adalimumab or placebo. Base-case analysis was intended to represent the median demographics of the SYCAMORE RCT (i.e., 7-year old girl). |
(continued) | Total costs calculated for the 18-month trial-based analysis were adjusted to apportion drug costs if administration covered the period preceding randomization or extended beyond the 18-month time horizon. QALYs calculated as the area under each utility-time profile with the trapezium rule for each patient. QALYs and costs accruing beyond the first year discounted at 3.5% per year. | Schedule of Reference Costs 2015 to 2016. Primary and community care services unit costs were sourced from the Personal Social Services Research Unit 2015. Cost of surgery was assumed to be the average cost for outpatient pediatric ophthalmology procedures. VA (logMAR): measures based on scores in the worse eye. Score of < 0.3 indicated no visual impairment. Score of ≥ 0.3 indicated a degree of visual impairment. Long-term outcomes and surgery: Bristol cohort provided the 10-year logMAR scores (VA). |
AE = adverse event; CI = confidence interval; EQ-5D = EuroQol- 5 Dimension; HUI = Health Utilities Index; JIA = juvenile idiopathic arthritis; kg = kilogram; logMAR = logarithm of the minimum angle of resolution; mg = milligram; NA = not applicable; NHS = National Health Service; NICE = National Institute for Health and Care Excellence; NR = not reported; QALY = quality-adjusted life-years; QoL = quality of life; RCT = randomized controlled trial; SD = standard deviation; VA = visual acuity; vs. = versus.
aIt was not specifically reported if only patients with JIA-associated uveitis receiving adalimumab from the Bristol cohort were included in the model. The Bristol cohort included patients with idiopathic uveitis as well.
bMark 3 classification system is validated in children.18
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
American College of Rheumatology/Arthritis Foundation, 20198 | ||||||
Intended users: clinicians who screen, monitor, and treat children with JIA in North America.a Target population: children with JIA at risk for and those with associated chronic anterior uveitis and acute anterior uveitis.b | Treatments of uveitis in JIA (e.g., glucocorticoids, non-biologic DMARDs [methotrexate], and biologics [anti-TNFAlphac]). Intervention relevant to this report: adalimumab | Outcomes related to medication use:
| Systematic, comprehensive searches of OVID MEDLINE, PubMed, Embase, and the Cochrane Library (including Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, and Health Technology Assessments) from inception through June 12, 2017. Updated searches conducted on October 13, 2017. | Recommendations rated as high, moderate, low, or very low quality (for each outcome). Evidence grading followed GRADE methodology: risk of bias, inconsistency, indirectness, and impression were considered. | Development teams: 1. Core Leadership Team: 4 pediatric rheumatologists — project supervision and coordination (e.g., drafted the clinical questions [PICO] and the published guideline) 2. Literature Review Team: experienced literature review consultant —performed the literature search and data extraction 3. Expert panel: 1 pediatric ophthalmologist and 9 pediatric rheumatologists — developed the PICO questions and decided on the scope of the guidelines | None. |
(continued) |
| Restricted to English publications. Other selection criteria NR. | 4. Voting panel: 2 pediatric ophthalmologists, 15 pediatric rheumatologists, 2 adults with JIA — voted on the recommendations, assisted with scope development, refined PICO questions, and reviewed gathered evidence 5. Parent and Patient Panel: 2 parents of children with JIA-associated uveitis and 9 adults with JIA – reviewed the gathered evidence and provided input on their values and preferences within a separate voting meeting. | |||
(continued) | When literature did not provide clear evidence, recommendations were based on values/preferences and experiences from the Parent and Patient Panel and Voting Panel (including physicians and the 2 patients present), respectively. Group consensus required for final recommendations and associated strength rating (i.e., conditional or strong). Voting panel voted on the strength and direction of the recommendation related to each PICO question. Recommendations required a 70% level of agreement, if that was not achieved during the initial vote, additional discussions and rewording of recommendations were performed before re-voting. | |||||
Interdisciplinary German Groups, 20197 | ||||||
Intended Users: individuals involved with decision-making in the treatment of anterior uveitis associated with JIA in the German health care system. Target Population: patients with anterior uveitis associated with JIA. | Treatments of anterior uveitis in JIA (e.g., anti-inflammatory treatment, DMARDs including biologics such as TNF-alpha inhibitors) Intervention relevant to this report: adalimumab This is an update to an existing guideline, published in 2012, to include recently published literature particularly focused on biologic DMARDs. | Outcomes NR but primary objectives of treatment were reported:
| Literature search of MEDLINE to include publications from 2 decades prior up to January 30, 2017. Selection criteria NR but these were considered when including evidence:
| Level of evidence:
Grade of recommendation:
| Guideline development group consisted of professional societies involved in diagnosing and treating anterior uveitis associated with JIA and a patient group: German Ophthalmological Society, Society for Pediatric Rheumatology, Professional Association of Ophthalmologists, German Society for Rheumatology, and Parents’ Group for Children With Uveitis and their Families. Consensus conference (March 31, 2017) — 69.2% of members present:
| Draft guidelines reviewed by all development group members following the Delphi process: modification suggestions and agreement or disagreement proposed. Review from 1st round was summarized and sent to all members of the development group. Recommendations in which consensus was not reached, a 2nd Delphi round was implemented. Guideline manuscript was externally reviewed by the German Ophthalmological Society, German Society of Rheumatology, and |
(continued) |
|
| Society for Pediatric Rheumatology and a vote in writing followed (3rd Delphi round). For finalization, draft guidelines had to be approved by all participants. | |||
DMARD = disease-modifying antirheumatic drug; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; JIA = juvenile idiopathic arthritis; NA = not applicable; NR = not reported; PICO = population, intervention, comparator, outcome; RCT = randomized controlled trial; TNF = tumour necrosis factor.
aThe jurisdiction of relevance is not specifically stated but the authors noted that there are no accepted guidelines in North America regarding the use of systemic immunosuppressive agents.
bRecommendations specific to children with non-systemic polyarthritis, sacroiliitis, and enthesitis related JIA were devised but reported in a separate document.
cRecommendations referring to “TNFi biologics” pertained to adalimumab, infliximab, and etanercept only. “Monoclonal antibody TNFi” referred to adalimumab and infliximab.8
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of SRs and Meta-Analyses Using AMSTAR 212
Strengths | Limitations | |
|---|---|---|
Li et al. (2021)6 | ||
Research question/ objective of the SR was reported. Protocol was registered with PROSPERO (CRD42020161749). Multiple databases were searched with the date range of search (commencement to November 1, 2019) and keywords searched reported. Literature search was conducted within 24 months before publication. Inclusion criteria reported the components of population, intervention, and outcomes with definitions provided. Namely, thresholds of change were reported. VA control defined as doubling of visual angle in at least 1 eye (3 lines on a decimal scale). Study selection performed by 2 independent reviewers and disagreements were addressed by discussion or with a third reviewer. Data extraction used a standard form. Risk of bias assessments (Cochrane tool for RCTs, Newcastle-Ottawa scale for cohort studies, and JBI checklists for case reports and case series) were performed. Ratings were reported in the main text and summary table provided in the Supplementary. Dose of treatments, age, and length of follow-up reported for included studies. Age range reported for 1 of 2 relevant studies as only pediatric populations were of interest to this report, range would be more informative to help with determining eligibility of studies. Authors of this SR had no conflicts of interest to disclose and reported funding sources. | No explanation provided for the selection of eligible study designs but it was stated that review papers, meta-analyses, editorial letters, and expert opinions were excluded to avoid duplication. It was not specified if reference lists of included studies were reviewed, grey literature were retrieved, and experts were consulted. Exclusion criteria not specifically reported. Inclusion criteria related to study design and comparators were not clearly reported. Comparators were not specifically reported. It was noted that RCTs and cohort studies were included as well as “qualified case series and case reports” but it was not specified what deemed these studies as qualified. No justification provided for restriction to English publications. A list for excluded studies along with the reasons for exclusion were not reported. Data extracted by one reviewer and checked by a second reviewer. Details on the data checking were not provided. If the reviewer only checked the extraction form and not the entire source publication, this may have resulted in incomplete or inaccurate reporting. It was not reported if the risk of bias assessments were performed by two reviewers. It was not clear if the thresholds of change for VA control were validated or clinically meaningful. Results of individual studies were not clearly reported and/or without sufficient detail. The units and/or values were unclear. For instance, values were reported for AEs and SAEs but the units were not reported. It was not clear if these values represented number of patients experiencing AEs and SAEs or the number of AEs and SAEs. Further, the change in VA was reported from treatment onset to after treatment with adalimumab but the follow-up time point was not reported. Sources of funding and potential sources of conflict of interest for included studies were not reported. | |
Norcia et al. (2021)17 | ||
Research question/ objective of the SR was clearly reported. Multiple databases (7) were searched with the search date ranges and searched MeSH terms reported. Trial registries were searched (e.g., Cochrane Central Register of Controlled Trials). Literature search was conducted within 24 months before publication. No restrictions regarding the language of publications. Inclusion criteria reported the components of population, intervention, comparators, and outcomes. Study selection, data extraction, and risk of bias assessments were performed by 2 independent reviewers. Disagreements were resolved through consensus and addressed by discussion with a third reviewer if required. Risk of bias assessments (Cochrane tool for RCTs and ROBINS-I for non-randomized controlled studies) and GRADE ratings were reported. Data extraction used a standard form. Characteristics of included studies were clearly reported (e.g., age, follow-up, and treatment dose). Appropriate methods used to assess heterogeneity (I2 statistic [considered significant when I2 > 75%] and P value from the heterogeneity chi-square test). For the meta-analyses relevant to this report, (comparisons of adalimumab to placebo based on randomized data of outcomes: reduction or interruption of the use of corticosteroids, satisfactory response rate to treatment, local AEs, and pooled systemic SAEs) results reported as risk ratios with 95% CIs and I2. Authors assessed the potential impact of risk of bias in individual studies on the results of the meta-analyses but only for the outcomes presented with forest plots (i.e., not for outcomes: systemic SAEs and local AEs). Authors of this SR reported no potential conflict of interests. | Searches conducted from varying start dates up to March 2021 for the 7 databases (e.g., SCOPUS searched from 2004); however, no justification was provided for the varying search date ranges. No explanation provided for the selection of eligible study designs. It was not specified if reference lists of included studies were reviewed, grey literature were retrieved, and experts were consulted. A list for excluded studies along with the reasons for exclusion were not reported. Exclusion criteria were not specifically stated. Eligible study designs were not clearly reported. It was noted that non-randomized controlled studies were included but this categorization is broad. Definitions of outcomes were not reported. Interpretation of the outcome values were not described; namely, the minimal clinically important difference. It was not specifically reported if GRADE ratings were performed by 2 reviewers. Methods were reported for conducting meta-analyses including data from ≥ 3 studies for which a random-effects model was performed but methods for pooled analyses of 2 studies (extracted in this report) were not reported. Not all forest plots were provided for all comparisons (e.g., systemic SAEs and local AEs were not reported with forest plots) with no justifications provided. Publication bias assessed in accordance with GRADE methodology. Statistical evaluations or diagrams to assess publication bias such as Egger’s test or funnel plots were not performed. Nevertheless, Egger’s test or funnel plots may not have been appropriate for the meta-analyses of randomized data as data were pooled from 2 studies. Sources of funding and potential sources of conflict of interest for the included studies were not reported but conflict of financial interest was noted as a main issue related to the risk of bias of included RCTs. Funding for this SR was not reported. | |
AE = adverse event; AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CI = confidence interval; GRADE = Grading of Recommendations Assessment, Development and Evaluation; JBI = Joanna Briggs Institute; kg = kilogram; MeSH = Medical Subject Headings; mg = milligram; NA = not applicable; NR = not reported; PROSPERO = International Prospective Register of Systematic Reviews; RCT = randomized controlled trial; ROBINS-I = Risk of Bias in Non-Randomized Studies of Interventions; SAE = serious adverse event; SR = systematic review; VA = visual acuity.
Table 6: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist14
Strengths | Limitations |
|---|---|
Hughes et al. (2019)18 | |
Study design Research question, economic importance of the research question, perspective, and the alternative interventions plus the rationale were clearly stated. It was clearly stated that a cost-utility analysis was performed in the perspective of the NHS. Choice of form of economic evaluation (cost-utility analysis) was justified in relation to the questions addressed. | Study design The trial-based analysis (18 months) was matched to the Bristol cohort study (extrapolation of 10 years) with VA. However, the trial was not powered to detect differences in visual impairment and the extrapolated model did not consider severe visual impairment, which would not account for the considerable impact on quality of life (and employment/education) and high lifetime costs. Authors noted that the Bristol cohort dataset may not have been comparable to the trial dataset based on treatment practice particularly regarding biologics. For instance, adalimumab was used in patients with a worse health state and adalimumab use varied during the data collection period of 1997 to 2014 (i.e., earlier in the study, biologic use may have been less). Further, the Bristol cohort dataset was highlighted to not be representative of general practice across the NHS. Use of this data limits internal and external validity. There were participants who were in both studies (SYCAMORE RCT and Bristol cohort study) but it is not clear if there was an impact on the results from the overlap. |
Data collection Sources of the model input parameters (e.g., health utilities, resource use, unit costs, visual acuity, and long-term outcomes and surgery) were clearly reported. Primary outcome for the economic evaluation was clearly stated. Methods to value benefits and for the estimation of quantities and unit costs were reported. Price data of medication and health care resources with the currency (pound sterling) and references (e.g., NHS: Prescription cost analysis [2016], National Tariff Payment System [2016/2017], and Reference costs [2015 to 2016] and British National Formulary [accessed 2017]) reported. Structure of the model was described and summarized with a diagram. Methods pertaining to the sensitivity analyses were reported. | Data collection Insufficient details regarding the designs, characteristics, participants, and results of the SYCAMORE RCT and Bristol cohort study (the effectiveness studies from which assumptions were based) were provided. Baseline characteristics of both studies should have been provided to allow one to evaluate the comparability of the SYCAMORE and Bristol cohort datasets. Authors noted the datasets may not have been comparable (please see above). Additionally, dosing of treatments (including adalimumab) was not reported for the Bristol cohort study. Although, source publications were referenced. Bristol cohort study did not evaluate long-term outcome data that could have informed the progression of uveitis. Authors highlighted the incomplete datasets for QALYs and VA. 31% of trial participants had QALY data and 28% and 70% of VA data in the ADA and placebo groups were censored, respectively. |
A meta-analysis was not performed although data were derived from 1 RCT and 1 cohort study; thus, this may have been appropriate as combining randomized and non-randomized data could introduce considerable heterogeneity. Productivity changes were not reported. Key parameters of the model were not clearly justified. Description of currency conversion or currency of price adjustments for inflation were not provided, which limits generalizability as the unit costs were estimated at the cost year of 2016. For the sensitivity analyses exploring the visual impairment rates, proportion rates were referred to as high and low but corresponding quantitative values were not reported. | |
Analysis and interpretation of results Time horizon of costs and benefits were stated. Discount rate for costs and benefits was stated (3.5% per year). Incremental analyses were reported with relevant alternatives compared. Disaggregated health care resource use and costs were reported by arm and as the mean difference with 95% central range. Health care resource costs and use were presented in a disaggregated form by intervention with the difference provided from randomization to 18 months. Answer to the study question was given. Conclusions followed from the data reported and were accompanied by appropriate caveats. | Analysis and interpretation of results Time horizon of 18 months was based on the SYCAMORE trial and the 10-year extrapolation was not justified but presumably it is because the last VA measurement was evaluated at the 10-year follow-up in the Bristol cohort study. This time horizon may not be appropriate as the population of interest was individuals with JIA-associated uveitis. These individuals would likely require chronic or longer-term treatment due to their young age and diagnosis with a systemic autoimmune disease. Therefore, a longer time horizon may be more appropriate. Justification for the selected discount rate was not reported. Accuracy of the sensitivity analysis results were unclear, all sensitivity analysis findings summarized in this report were extracted from Table 5 in the source publication.18 |
Other Authors of the publication reported funding sources. AbbVie (adalimumab manufacturer) had no role in funding, trial management, data analysis, or writing of the publication. | Other Multiple authors reported financial disclosures associated with AbbVie (UK), UCB (US), Eli Lilly (US), and SOBI (UK) in the form of consulting, lecturing, and drug supply (AbbVie is the manufacturer of adalimumab). For regulatory purposes, AbbVie has licensed use of the study results. AbbVie was allowed to review the final draft but it was noted that the authors of the publication maintained complete control over the article content. Evaluation was in the perspective of the UK health care system and many sources for input parameters were UK-based; thus, findings may not be generalizable to the Canadian health system. |
HTA = health technology assessment; ICER = incremental cost-effectiveness ratio; JIA = juvenile idiopathic arthritis; NHS = National Health Service; NMA = network meta-analysis; QALY = quality-adjusted life-years; RCT = randomized controlled trial; SR = systematic review; VA = visual acuity.
Table 7: Strengths and Limitations of Guidelines Using AGREE II15
Item | American College of Rheumatology/Arthritis Foundation, 20198 | Interdisciplinary German Groups, 20197 |
|---|---|---|
Domain 1: Scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | No |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes – but there were disproportionately more pediatric rheumatologists compared to ophthalmologists (e.g., Expert and Voting panels: 9 rheumatologists vs. 1 ophthalmologist and 15 rheumatologists vs. 2 ophthalmologists, respectively). | Yes – representation from ophthalmology and rheumatology specialties. |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes – Parent and Patient Panel consisted of 2 parents of children with JIA-associated uveitis among the guideline development group. | Yes – representation from the Parents’ Group for Children With Uveitis and their Families in the guideline development group. |
6. The target users of the guideline are clearly defined. | Yes – target users were specified (clinicians, patients, and parents) but the country the guideline is meant to be used was not specifically stated. | Partially yes – it was noted that the guideline is intended to assist decision-making with treating anterior uveitis associated with JIA. |
Domain 3: Rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes | Partially yes – 1 database was searched with a limited search range of the previous 2 decades up to January 30, 2017. No explanation was provided for this search date range. |
8. The criteria for selecting the evidence are clearly described. | NR | NR |
9. The strengths and limitations of the body of evidence are clearly described. | Yes – but for some recommendations only. | No |
10. The methods for formulating the recommendations are clearly described. | Partially yes – eligibility criteria used to select evidence should have been reported. | Partially yes – methods pertaining to the 3rd Delphi round were unclear. |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes – guideline development followed GRADE methodology. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Probably yes – for some guidelines additional details were provided with the included evidence referenced. | Yes – supporting evidence was cited. |
13. The guideline has been externally reviewed by experts before its publication. | Yes – guideline published in a peer-reviewed journal. | Yes – external review by the German Ophthalmological Society, German Society of Rheumatology, and the Society of Pediatric Rheumatology. Also, guideline published in Seminars in Arthritis and Rheumatism (journal). |
14. A procedure for updating the guideline is provided. | No | No |
Domain 4: Clarity of presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes, for relevant recommendations. Recommendations for glucocorticoid use and DMARDs plus biologics were provided. | Yes |
17. Key recommendations are easily identifiable. | Yes | No |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | No | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No |
Domain 6: Editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Probably yes – publication noted that the financial conflict forms were submitted as required. | Funding NR. |
23. Competing interests of guideline development group members have been recorded and addressed. | Probably yes. Members of the guideline development teams reported in the Supplementary Appendix. It was noted that all teams had over half of the members free of potential conflicts of interest. The leader of the literature review team and the principal investigator were free of potential conflicts of interest. | Partially yes – it was reported that all participants had no conflict of interest(s) that had the potential to influence the guideline development. Conflict of interest(s) were NR. |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; DMARD = disease-modifying antirheumatic drugs; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; JIA = juvenile idiopathic arthritis; NA = not applicable; NR = not reported; vs. = versus.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Change in VA6
Details | SYCAMORE RCTa | ADJUVITE RCTa | ||
|---|---|---|---|---|
ADA | Placebo | ADA | Placebo | |
Median logMAR (range)b | NR | NR | At study treatment onset: 0.1 (−0.2 to 1.3) After treatment with ADA: 0.15 (−0.10 to 1.10)c | NR |
ADA = adalimumab; logMAR = logarithm of the minimum angle of resolution; NR = not reported; VA = visual acuity.
aThe SYCAMORE and ADJUVITE RCTs included patients with active non-infectious uveitis.
bLi et al. (2021) did not report what the values represented. This was identified as the median and range from the source publication of the SYCAMORE trial (Ramanan et al. [2017]).19
cThis finding is a measure of visual acuity before and after receiving adalimumab; thus, this is single-arm (non-comparative) data and should be interpreted in light of these limitations.
Table 9: Summary of Findings by Outcome — Change (Reduction or Interruption) in Uveitis-Related Corticosteroid Use17
Details | SYCAMORE RCTa | ADJUVITE RCTa | Pooled analysis of SYCAMORE and ADJUVITE RCTsa | |||
|---|---|---|---|---|---|---|
ADA | Placebo | ADA | Placebo | ADA | Placebo | |
Events | 26 | 5 | 1 | 1 | 27 | 6 |
Total | 54 | 26 | 12 | 10 | 66 | 36 |
Weight | 86.1% | 13.9% | 100% | |||
RR (95% CI) | 2.50b (1.09 to 5.77) | 0.83b (0.06 to 11.70) | 2.27 (1.03 to 4.99) | |||
Heterogeneity | — | — | Chi2 = 0.61, df = 1 (P = 0.44), I2 = 0% | |||
Overall effect | — | — | Z = 2.04 (P = 0.04) | |||
Anticipated absolute effects (95% CI)c | — | — | Risk = 378 per 1.000 (172 to 832) | Risk = 167 per 1.000 (NR) | ||
ADA = adalimumab; CI = confidence interval; df = degrees of freedom; NR = not reported; RCT = randomized controlled trial; RR = risk ratio.
aThe SYCAMORE and ADJUVITE RCTs included patients with active non-infectious uveitis.
bFixed Mantel-Haenszel risk ratios.
cExtracted from Figure 11 in the source publication. Authors stated that “ the risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) (p.3773).”17
Table 10: Summary of Findings by Outcome — Control of Intraocular Inflammation6
Details | SYCAMORE RCTa | ADJUVITE RCTa | ||
|---|---|---|---|---|
ADA | Placebo | ADA | Placebo | |
n/N of responders | NR | NR | 9/16 | 3/15 |
RR (95% CI); RD (95% CI) | NR | NR | 2.81 (0.94 to 8.45); 36.3% (2.1 to 60.6) | |
P value | NR | NR | 0.038 | |
ADA = adalimumab; CI = confidence interval; NR = not reported; RCT = randomized controlled trial; RD = risk difference; RR = risk ratio.
aThe SYCAMORE and ADJUVITE RCTs included patients with active non-infectious uveitis.
Table 11: Summary of Findings by Outcome — Satisfactory Response Rate to Treatment and Treatment Failure
Outcome and details | SYCAMORE RCTa | ADJUVITE RCTa | Pooled analysis of SYCAMORE and ADJUVITE RCTsa | ||||
|---|---|---|---|---|---|---|---|
ADA | Placebo | ADA | Placebo | ADA | Placebo | ||
Satisfactory response rate to treatment17 | |||||||
Events | 34 | 5 | 9 | 3 | 43 | 8 | |
Total | 60 | 30 | 16 | 15 | 76 | 45 | |
Weight | 68.3% | 31.7% | 100% | ||||
RR (95% CI) | 3.40b (1.48 to 7.80) | 2.81b (0.94 to 8.45) | 3.21 (1.65 to 6.27) | ||||
Heterogeneity | — | — | Chi2 = 0.07, df = 1 (P = 0.79), I2 = 0% | ||||
Overall effect | — | — | Z = 3.42 (P = 0.0006) | ||||
Anticipated absolute effects (95% CI)c | — | — | Risk = 571 per 1.000 (293 to 1.000) | Risk = 178 per 1.000 (NR) | |||
Treatment failure6 | |||||||
n/N (patients) | 14/60 | 17/30 | NR | NR | NR | NR | |
RR (95% CI) | 0.40 (0.23 to 0.72) | NR | NR | NR | NR | ||
P value | 0.002 | NR | NR | NR | NR | ||
ADA = adalimumab; CI = confidence interval; df = degrees of freedom; NR = not reported; RCT = randomized controlled trial; RR = risk ratio.
aThe SYCAMORE and ADJUVITE RCTs included patients with active non-infectious uveitis.
bFixed Mantel-Haenszel risk ratios.
cExtracted from Figure 10 in the source publication. Authors stated that “ the risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) (p.3773).”17
Table 12: Summary of Findings by Outcome — Safety
Outcome and details | SYCAMORE RCTa | ADJUVITE RCTa | Pooled analysis of SYCAMORE and ADJUVITE RCTsa | |||
|---|---|---|---|---|---|---|
ADA | Placebo | ADA | Placebo | ADA | Placebo | |
AEs6 | ||||||
n (patients) | 59b | 26b | NR | NR | NR | NR |
Rate (per patient-year) (95% CI) | 10.60 (9.77 to 11.44) | 7.12 (5.89 to 8.53) | NR | NR | NR | NR |
Most common AE type | infections and infestations (83%) | NR | NR | NR | NR | NR |
Pooled Local AEs17 | ||||||
RR (95% CI) | — | — | — | — | 1.15 (0.46 to 2.88) | |
Heterogeneity (I2) | — | — | — | — | 1% | |
P value | — | — | — | — | 0.76 | |
SAEs6 | ||||||
n (patients) | 13c | 2c | NR | NR | NR | NR |
Rate (per patient-year) (95% CI) | 0.29 (NR) | 0.19 (NR) | NR | NR | NR | NR |
Most common SAE types | glaucoma, cataracts, injection site reactions, arthritis, and arthralgia | NR | NR | NR | NR | NR |
Pooled systemic SAEs17 | ||||||
RR (95% CI) | — | — | — | — | 2.51 (0.74 to 8.54) | |
Heterogeneity (I2) | — | — | — | — | 48% | |
P value | — | — | — | — | 0.14 | |
ADA = adalimumab; AE = adverse event; CI = confidence interval; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; SAE = serious adverse event.
aThe SYCAMORE and ADJUVITE RCTs included patients with active non-infectious uveitis.
bLi et al. (2021)6 did not report if these values represented the number of patients or events. This table reports AEs as the number of patients experiencing an event to correspond with the reporting of SAEs (see footnote below).
cLi et al. (2021)6 did not report if these values represented the number of patients or events. However, it was confirmed in the source publication (Ramanan et al. [2017])19 that these values represent the number of patients experiencing any SAE.
Table 13: Summary of Findings by Outcome — Economic Outcomes (Base-case Analysis)
Outcome | ADA plus methotrexate | Methotrexate | Incremental |
|---|---|---|---|
ICER (cost [£] per QALY gained) | — | — | 129 025 |
QALYs | 8.60 | 8.29 | 0.30 |
Costs (£) | 70 719 | 31 403 | 39 316 |
ADA = adalimumab; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 14: Summary of Findings by Outcome — Economic Outcomes (Sensitivity Analyses)a
Outcome | ADA plus methotrexate | Methotrexate | Incremental |
|---|---|---|---|
Duration of ADA (18 months only) | |||
ICER (cost [£] per QALY gained) | — | — | 133 656 |
QALYs | 8.40 | 8.29 | 0.11 |
Costs (£) | 45 504 | 31 403 | 14 101 |
Duration of ADA (18 months plus 10 years) | |||
ICER (cost [£] per QALY gained) | — | — | 127 646 |
QALYs | 8.99 | 8.29 | 0.70 |
Costs (£) | 120 262 | 31 403 | 88 858 |
Reduction in the proportion of patients administered ADA beyond 18 months (reduced to 0.23 [reflected the observed value]) | |||
ICER (cost [£] per QALY gained) | — | — | 131 511 |
QALYs | 8.44 | 8.29 | 0.15 |
Costs (£) | 51 304 | 31 403 | 19 900 |
Time horizon: 18 months | |||
ICER (cost [£] per QALY gained) | — | — | 136 751 |
QALYs | 1.36 | 1.25 | 0.11 |
Costs (£) | 16 336 | 1962 | 14 374 |
25% price reduction of ADA | |||
ICER (cost [£] per QALY gained) | — | — | 94 661 |
QALYs | 8.60 | 8.29 | 0.30 |
Costs (£) | 56 665 | 27 821 | 28 844 |
50% price reduction of ADA | |||
ICER (cost [£] per QALY gained) | — | — | 67 288 |
QALYs | 8.60 | 8.29 | 0.30 |
Costs (£) | 48 865 | 28 361 | 20 504 |
Discount rate (no discounting) | |||
ICER (cost [£] per QALY gained) | — | — | 128 886 What would be required for ADA to be cost-effective at the £20, 000 to 30,000 thresholds? -Price reduction of 84% −1.00 additional QALY over the 10-year time frame. Of note, the QALY gain over the trial was 0.11. |
QALYs | 9.88 | 9.57 | 0.32 |
Costs (£) | 77 634 | 36 743 | 40 621 |
Visual impairment rates: all placebo group participants transition to the visual impairment state | |||
ICER (cost [£] per QALY gained) | — | — | 78 524 |
QALYs | 8.60 | 8.27 | 0.32 |
Costs (£) | 70 719 | 45 224 | 25 495 |
Visual impairment rates: all ADA patients transition to the no visual impairment state and all placebo patients transition to the visual impairment state (and remain in those states) | |||
ICER (cost [£] per QALY gained) | — | — | 53 072 |
QALYs | 8.60 | 8.26 | 0.34 |
Costs (£) | 68 722 | 50 902 | 17 820 |
Visual impairment rates: visual impairment proportions in ADA and placebo groups are high and low, respectivelyb | |||
ICER (cost [£] per QALY gained) | — | — | 130 586 |
QALYs | 8.60 | 8.29 | 0.30 |
Costs (£) | 70 864 | 31 147 | 39 716 |
Visual impairment rates: visual impairment proportions in ADA and placebo groups are low and high, respectivelyb | |||
ICER (cost [£] per QALY gained) | — | — | 127 471 |
QALYs | 8.60 | 8.29 | 0.31 |
Costs (£) | 70 574 | 31 659 | 38 915 |
ADA = adalimumab; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aThe following data were extracted from Table 5 in the source publication.18
bProportions were only referred to as high and low, quantitative values were not given to match these categorizations.
Table 15: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidencea | Quality of evidence and strength of recommendations |
|---|---|
American College of Rheumatology/Arthritis Foundation, 20198 b,c | |
Recommendations for DMARDs and biologics | |
Recommendation 10: “In children and adolescents with JIA and actived CAU who are starting systemic treatment for uveitis, using subcutaneous methotrexate is conditionally recommended over oral methotrexate (p.25).”8 Supporting evidence/ additional details: none. | Very low quality of evidence, conditional recommendation |
Recommendation 11: “In children and adolescents with JIA with severe active CAU and sight threating complications, starting methotrexate and a monoclonal antibody TNFi immediately is conditionally recommended over methotrexate as monotherapy (p.10 and p.25).”8 Supporting evidence/ additional details: “Methotrexate and monoclonal antibody TNFi are the mainstays of systemic treatment of uveitis. Subcutaneous methotrexate was considered preferable to oral administration for uveitis, but this recommendation was conditional given the lack of strong data on differential efficacy, and that family preferences as to route of administration may differ. In children with severe active uveitis and sight-threatening complications, combining methotrexate with a monoclonal antibody TNFi at the time of initiation of systemic immunosuppressive treatment was recommended over methotrexate as monotherapy. Severe uveitis could be considered the presence of ocular structural complications due to uveitis, or complications of topical steroid therapy (30). This recommendation was conditional, based upon the lack of direct evidence from studies, risk of permanent vision loss, and anticipated differences in patient values and preferences (p.10).”8 | Very low quality of evidence, conditional recommendation |
Recommendation 12: “In children and adolescents with JIA and active CAU who are starting a TNFi, starting a monoclonal antibody TNFi is conditionally recommended over etanercept (p.11 and p.25).”8 Supporting evidence/ additional details: “Monoclonal antibody TNFi, specifically adalimumab and infliximab, were conditionally recommended over etanercept for active CAU. Although there is a paucity of direct comparisons, benefit has been shown to using monoclonal antibody TNFi. The Voting Panel was not able to make recommendations on preferred TNFi for children with active JIA to prevent uveitis onset, or for children with known CAU to prevent uveitis flares due to lack of evidence (31–35). The Voting Panel also did not make a recommendation on preference between adalimumab and infliximab for use as initial TNFi (p.11).”8 | Very low quality of evidence, conditional recommendation |
Recommendation 13: “In children and adolescents with JIA and active CAU who have an inadequate response to one monoclonal antibody TNFi at standard JIA dose, escalating the dose and/or frequency to above-standard is conditionally recommended over switching to another monoclonal antibody TNFi (p. 11 and p.25).”8 Supporting evidence/ additional details: none. | Very low quality of evidence, conditional recommendation |
Recommendation 14: “In children and adolescents with JIA and active CAU who have failed a first monoclonal antibody TNFi at above-standard dose and/or frequency, changing to another monoclonal antibody TNFi is conditionally recommended over a biologic in another category (p.11 and p.25).”8 Supporting evidence/ additional details: “These two recommendations assume that uveitis activity or severity guides therapy in the patient, irrespective of joint disease activity. The Voting Panel did not make a recommendation on preference between adalimumab and infliximab as first-line TNFi, or use of above-standard TNFi dosing at treatment initiation. For children treated with a monoclonal antibody TNFi at standard JIA dosing who have an inadequate response to therapy, the Voting Panel conditionally recommended escalating the dose and/or frequency to above-standard dosing used for arthritis prior to switching to another monoclonal antibody TNFi. Although consensus was not reached regarding a specific dose or frequency, doses as high as infliximab 20 mg/ kg every 2 weeks and adalimumab weekly have been reported in observational studies in children with JIA and uveitis (36–38). If the initial monoclonal antibody TNFi fails at an increased dose/frequency, the recommendation was to change to another monoclonal antibody TNFi prior to changing to a biologic agent in another category (p.11).”8 | Very low quality of evidence, conditional recommendation |
Recommendation 15: “In children and adolescents with JIA and active CAU who have failed methotrexate and 2 monoclonal antibody TNFi at above-standard dose and/or frequency, conditionally recommend abatacept or tocilizumab as biologic DMARD options, and mycophenolate, leflunomide or cyclosporine as alternative non-biologic options (p.11 and p.26).”8 Supporting evidence/ additional details: “The quality of evidence for subsequent treatment in children who have failed methotrexate in combination with monoclonal antibody TNFi treatment is very low. Based on current literature, recommended alternative non-biologic options are mycophenolate mofetil (39), leflunomide (40) or cyclosporine (41), and recommended alternative biologic options are abatacept (42–44) or tocilizumab (45, 46); however, evidence supporting preference for a specific non-biologic or biologic DMARD, combination therapies, and timing of initiation beyond methotrexate, adalimumab, and infliximab is currently lacking. (p.11 to 12).”8 | Very low quality of evidence, conditional recommendation |
Recommendations for tapering therapy for uveitis | |
Recommendation 18: “In children and adolescents with JIA and CAU that is controlled on systemic therapy but remain on 1–2 drops/day of prednisolone acetate 1% (or equivalent), tapering topical glucocorticoids first is strongly recommended over systemic therapy. (p.12 and p.26).”8 Supporting evidence/ additional details: There is very low quality of evidence for timing of tapering of topical glucocorticoids and systemic therapy (24, 48, 49). Some ophthalmologists feel that in selected cases, it is not possible to discontinue topical glucocorticoids altogether, despite attempts to do so, and the patients may be continued on 1 to 2 drops daily for extended periods. Despite the very low quality of evidence, the Voting Panel strongly recommended attempting to taper topical glucocorticoids before tapering systemic therapy because of the secondary complications that can occur with prolonged and frequent use of glucocorticoids (28, 29). Tapering of systemic therapy first may lead to the need for increased frequency of topical glucocorticoids for uveitis flares (p.12).”8 | Very low quality of evidence, strong recommendation |
Recommendation 19: “In children and adolescents with JIAe and uveitis that is well controlled on DMARD and biologic systemic therapy only: conditionally recommend that there be at least 2 years of well-controlled disease before tapering therapy (p.26).”8 Supporting evidence/ additional details: “The Voting Panel conditionally recommends attempted tapering of DMARD and biologic systemic therapy (DMARDs and biologics) only after uveitis has been well controlled for at least 2 years. Relapse-free survival after withdrawal of methotrexate was significantly longer in patients treated with methotrexate for more than 3 years, and who had controlled uveitis greater than 2 years before the withdrawal (49). Duration of systemic therapy may be greater than 2 years since tapering should not begin until at least 2 years of uveitis control. Decisions to taper systemic therapy should also take into consideration other JIA manifestations including arthritis activity (p.13).”8 | Very low quality of evidence, conditional recommendation |
Interdisciplinary German Groups, 20197 | |
Key statement 7: “If uveitis inactivity is not achieved by 16 weeks of methotrexate monotherapy and < 2 drops of topical corticosteroids daily, or if new, inflammation-related complications of uveitis occur, a TNFalpha anti-body therapy shall be used in combination with methotrexatef (p.49).”7 Specific to adalimumab: “Currently, preferred TNF alpha inhibitor (p.50).”7 among infliximab, golimumab, and etanercept. Infliximab was noted to be the second-choice TNFalpha inhibitor due to infusion reactions. Adalimumab was noted to be the currently preferred TNFalpha inhibitor in the treatment of anterior uveitis associated with JIA due to the tolerability and good response rate demonstrated in published RCTs. It was noted that in the event of loss of adalimumab efficacy and treatment failure, a treatment switch to infliximab or golimumab should be considered. Dosage was noted to be < 30 kg: 20 mg, ≥ 30 kg: 40 mg every 2 weeks (subcutaneous injections) “Adalimumab shall be considered for use in patients with JIAU who have not responded to treatment with methotrexate (p.50).”7 Supporting evidence/ additional details:
| Adalimumab guidelines: level II evidence, strong recommendation. Level II evidence consisted of small number of RCTs, more than 1 RCT of lesser quality, non-randomized studies (e.g., cohort or case-control studies preferably conducted by more than 1 research group or centre), and noncontrolled studies with clear observations. |
| |
CAU = chronic anterior uveitis; DMARD = disease-modifying antirheumatic drug; JIA = juvenile idiopathic arthritis; JIAU = juvenile idiopathic arthritis associated with anterior uveitis; kg = kilogram; mg = milligram; NR = not reported; NA = not applicable; RCT = randomized controlled trial; TNF = tumour necrosis factor; TNFi = tumour necrosis factor inhibitor.
aBolded wording is specific to adalimumab.
b”Systemic therapy” pertained to non-biologic DMARDs and biologics (not systemic glucocorticoids). “TNFi biologics” pertained to adalimumab, infliximab, and etanercept only. “Monoclonal antibody TNFi” pertained to adalimumab and infliximab.8
cNumbers in brackets within direct quotes refer to the cited evidence that supported the evidence-based guidelines.
dThis wording directly matches the wording in Table 3. The recommendation in the main body (p.10) does not state active CAU.8
eThis wording directly matches the wording in Table 3. The recommendation in the main body (p.10) does not specify JIA.8
fSee source publication (p.49)7 for further details regarding severity of uveitis.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Review Articles
Welzel T, Winskill C, Zhang N, Woerner A, Pfister M. Biologic disease modifying antirheumatic drugs and Janus kinase inhibitors in paediatric rheumatology - what we know and what we do not know from randomized controlled trials. Pediatr Rheumatol Online J. 2021 Mar 25;19(1):46. PubMed
Additional References
Consensus treatment plans
Angeles-Han ST, Lo MS, Henderson LA, et al. Childhood Arthritis and Rheumatology Research Alliance consensus treatment plans for juvenile idiopathic arthritis-associated and idiopathic chronic anterior uveitis. Arthritis Care Res (Hoboken). 2019;71(4):482-491. PubMed
SR with epidemiological outcomes and single-arm treatment response
Jari M, Shiari R, Salehpour O, Rahmani K. Epidemiological and advanced therapeutic approaches to treatment of uveitis in pediatric rheumatic diseases: a systematic review and meta-analysis. Orphanet J Rare Dis. 2020;15(1):41. PubMed
National Institute for Health Research (NIHR) health technology assessment (informing evidence for NIHR and NICE — UK agencies)
Ramanan AV, Dick AD, Jones AP, et al. Adalimumab in combination with methotrexate for refractory uveitis associated with juvenile idiopathic arthritis: a RCT. Health Technol Assess. 2019;23(15):1-140. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca