CADTH Health Technology Review
Adalimumab for the Treatment of Adults With Non-Infectious Uveitis
Rapid Review with Expert Input
Authors: Daphne Hui, Monika Mierzwinski-Urban, Carolyn Spry
External Reviewer
This document was externally reviewed by a content expert who has granted permission to be cited.
Dr. Jean Deschênes, MD, FRCSC
Professor, Ophthalmologist-in-Chief
McGill University and McGill University Health Center
Acknowledgements
The authors would like to thank Michael Mallinson for contributing to the report by commenting on the clinical outcomes and sharing insights into and experience of non-infectious uveitis.
Abbreviations
BCVA
best-corrected visual acuity
HTA
health technology assessment
MUST
Multicenter Uveitis Steroid Treatment
NICE
National Institute for Health and Care Excellence
NHS
National Health Service
RCT
randomized controlled trial
SR
systematic review
TNF
tumour necrosis factor
WTP
willingness to pay
Key Messages
Four systematic reviews (SRs) and 1 economic evaluation were identified regarding the clinical effectiveness (including safety) and cost-effectiveness of adalimumab in adults with non-infectious uveitis.
In adults with active non-infectious uveitis (VISUAL I), adalimumab significantly lowered the risk of treatment failure and significantly improved changes in best-corrected visual acuity, anterior chamber cell grade, and vitreous haze grade. Additionally, the number and rate of adverse events and serious adverse events were greater in the adalimumab group compared to the placebo group. Clinical effectiveness and safety findings from the Japanese sub study (VISUAL I Japan) and data from a randomized controlled trial of a younger adult population (ADUR) demonstrated that adalimumab may have no treatment effect.
In adults with inactive non-infectious uveitis (VISUAL II), adalimumab significantly lowered risk of treatment failure; however, adalimumab may have no treatment effect on changes in best-corrected visual acuity, anterior chamber cell grade, and vitreous haze grade. Additionally, the number and rate of adverse events and serious adverse events were variable in the adalimumab versus placebo groups (e.g., number of adverse events was greater in the adalimumab group but the rate of adverse events was higher in the placebo groups). Clinical effectiveness and safety findings from the Japanese substudy (VISUAL II Japan) demonstrated that adalimumab may have no treatment effect.
Considering both active and inactive non-infectious uveitis (VISUAL I, VISUAL I [Japan], VISUAL II, VISUAL II [Japan], and ADUR), change in vitreous haze grade improved significantly more in the adalimumab group than the control group.
In the perspective of the health care system in the UK, adalimumab (plus systemic corticosteroid and immunosuppressant therapy) is not more cost-effective than systemic corticosteroid and immunosuppressant use alone (modelled by placebo data) in adults with active and inactive non-infectious uveitis influencing the posterior segment (i.e., back of the eye).
No evidence-based guidelines regarding the use of adalimumab for the treatment of adults with non-infectious uveitis were identified.
Context and Policy Issues
Non-infectious uveitis refers to the presence of intraocular inflammation of the uvea (i.e., middle layer of the eye) not caused by an infection that can affect individuals of any age among various etiologies.1,2 Active versus inactive uveitis refers to the activity status of the inflammation.3 The anterior segment of the uvea contains the ciliary body and iris; whereas, the posterior segment contains the choroid.3 Non-infectious uveitis may be idiopathic, caused by a reaction to a medication (but this is rare), or immune-mediated; therefore, it presents among many systemic autoimmune diseases such as juvenile idiopathic arthritis, Behçet’s disease, or ankylosing spondylitis.1,3,4 Of note, this report focuses on adults with non-infectious uveitis. As juvenile idiopathic arthritis predominantly affects pediatric patients much of the included evidence will not focus on this patient population. Up to 80% of patients with Behçet’s disease develop non-infectious uveitis. Uveitis associated with Behçet’s disease typically presents bilaterally.3
Timely treatment is critical as uveitis is the second foremost treatable cause of blindness in the Western world accounting for up to 10% of cases of loss of vision.5 The incidence of uveitis is difficult to measure due to the varying etiologies (Canadian specific prevalence and incidence was not found) but 1 of the largest studies measuring the incidence and prevalence of uveitis in the US reported the incidence to be 11.53 per 100 000 person-years.5 If left untreated, uveitis may lead to vision loss, early complications such as cystoid macular edema and vitreous haze, and late complications such as cataracts, glaucoma, and irreversible retinal damage.4
Treatment for non-infectious uveitis depends on whether it presents alongside a systemic disease (and if the disease is controlled), if the inflammation affects 1 (unilateral) or both (bilateral) eyes, and if there is anatomic localization of the uveitis.4,6 Initially, it is usually treated with corticosteroids with topical (e.g., prednisolone acetate drops) or local (e.g., intravitreal implants or injections or periocular injections) administration. For instance, posterior-, intermediate-, or panuveitis is initially treated with triamcinolone (glucocorticoid); of note, posterior non-infectious uveitis is typically not responsive to topical medication.6 Long-term use of corticosteroids is not recommended as it can result in cataracts and glaucoma.4,6 Immunosuppressive drugs can reduce corticosteroid use and associated complications.4 Systemic administration is generally used for resistant inflammation, if previously administered treatments are not tolerated, and in individuals with high risk for vision loss and/or uveitis associated with systematic disease.4 Patients with bilateral uveitis and some particular forms of uveitis (e.g., systemic inflammatory diseases such as Behçet’s disease related uveitis) are more likely to require systemic therapy.6 Systemic treatment includes corticosteroids, immunosuppressive or anti-inflammatory drugs (e.g., methotrexate, cyclosporine), and biologics.6 Biologics are used in non-infectious uveitis that does not respond to aforementioned systemic therapies.6
Adalimumab (Humira) is a biologic drug, specifically a monoclonal antibody, administered through subcutaneous injection that inhibits tumour necrosis factor-alpha (TNF-alpha).1,7 Multiple biosimilars such as Abrilada, Amgevita, Hadlima, Hulio, Hyrimoz, and Idacio (brand names) are approved for various indications in Canada including uveitis in adults.7 For individuals with non-infectious uveitis, adalimumab is generally administered in those with an incomplete response to first-line treatments and who have received at least 1 other systemic therapy.7 Adalimumab with or without concomitant immunosuppressants may increase risk of severe infections (e.g., tuberculosis) and sepsis that require hospitalization or may lead to death.7 The purpose of this rapid review is to evaluate recent evidence regarding the clinical effectiveness (including safety), cost-effectiveness, and evidence-based guidelines regarding the use of adalimumab for the treatment of adults with non-infectious uveitis. This report was carried out in series with another report that focuses on adalimumab for the treatment of pediatric populations with non-infectious uveitis.
Research Questions
What is the clinical effectiveness of adalimumab for the treatment of adults with non-infectious uveitis?
What is the cost-effectiveness of adalimumab for the treatment of adults with non-infectious uveitis?
What are the evidence-based guidelines regarding the use of adalimumab for the treatment of adults with non-infectious uveitis?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the international health technology assessment (HTA) database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were adalimumab and uveitis. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded from the search results. The search was also limited to English-language documents published between January 1, 2016 and October 19, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. SRs that met the selection criteria of this review were included regardless of the study designs of included primary studies (e.g., SRs of non-randomized studies were included). Of note, the search identified a health technology assessment published by the National Institute for Health Research in 20178 and an individual economic evaluation published in 2019.4 Both documents report the same model, similar inputs, and the same conclusions; thus, the more recent publication4 was included.
Criteria | Description |
|---|---|
Population | Adults (≥ 18 years of age) with non-infectious uveitis |
Intervention | Adalimumab, alone or in combination with background therapy (e.g., methotrexate, cyclosporin, azathioprine) |
Comparator | Q1 and Q2: Pharmacological therapy for uveitis (e.g., other biologic agents and non-biologic anti-inflammatory agents such as corticosteroids and methotrexate), and placebo Q3: Not applicable |
Outcomes | Q1: Clinical benefit (e.g., best-corrected visual acuity, disease inactivity or dormancy [quiescence], vascular lesions, uveitic macular edema, changes in uveitis-related systemic corticosteroids use) and safety (e.g., ocular complications) Q2: Cost-effectiveness (e.g., the incremental cost per health benefit or QALY gained) Q3: Recommendations regarding the use of adalimumab for uveitis |
Study designs | HTAs, SRs, RCTs, and economic evaluations |
HTA = health technology assessment; QALY = quality-adjusted life-year; RCT = randomized controlled trial.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded. For SRs and meta-analyses that had broader eligibility criteria than the current review, data were only extracted from relevant primary studies or analyses that met the eligibility criteria of the current review. For instance, data from non-comparative and/or non-randomized studies were not extracted as that does not meet the comparator and study design components of the selection criteria of this review. Literature specific to juvenile idiopathic arthritis was excluded due to its prevalence in individuals less than 18 years of age.3 Further, post-hoc analyses of randomized controlled trials (RCTs) were excluded from this rapid review as CADTH does not consider post-hoc analyses of RCTs to constitute randomized study designs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)9 for SRs and the Drummond checklist10 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Patient Engagement
Overview
CADTH involves patients, families, and patient groups to improve the quality and relevance of our assessments, ensuring that those affected by the assessments have an opportunity to contribute to them. CADTH has adopted a Framework for Patient Engagement in HTA.11 The Framework includes Standards for Patient Involvement in Individual HTAs and is used to support and guide our activities involving patients. For this rapid review CADTH engaged a patient collaborator with lived experience of uveitis.
Methods
Invitation to Participate and Consent
CADTH reached out to Arthritis Consumer Experts (ACE). ACE is national organization that provides free, science-based information and education programs to people with arthritis. A CADTH Patient Engagement Officer contacted the group by email to share the purpose and scope of the project, the purpose of engagement, and the nature of engagement activities. They also invited the group to selectively share this information with individuals who might be suited for the project and interested in sharing their experiences with CADTH. An individual interested in participating reached out to the Patient Engagement Officer, who obtained the person’s informed consent to share their lived experiences with uveitis with CADTH staff.
Engagement Activities
A patient shared his personal experiences during drafting of the report.
Patient perspectives gained through engagement processes were used to ensure relevance of outcomes of interest for the clinical assessment, to provide insights, background and context to inform the discussion section. Patient involvement enabled the research team to consider the evidence alongside an understanding of the wider experiences of Canadian patients and families.
Results
The reporting of this section followed the GRIPP2 Short Form12 reporting checklist.
Summary of Evidence
Quantity of Research Available
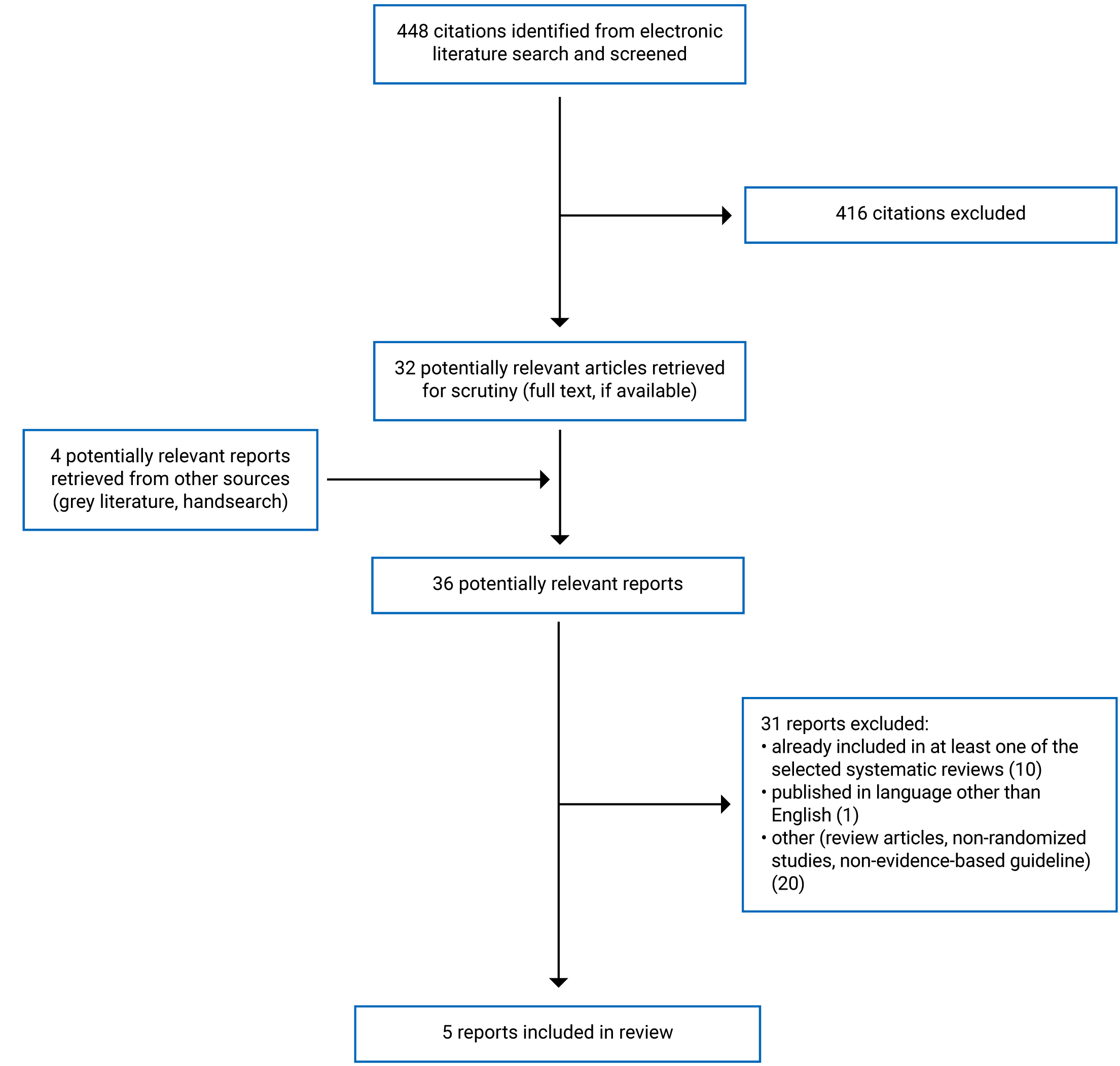
A total of 448 citations were identified in the literature search. Following screening of titles and abstracts, 416 citations were excluded and 32 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 31 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. These comprised 4 SRs and 1 economic evaluation. No evidence-based guidelines were identified. Of note, 1 SR1 and the economic evaluation4 both included data from the VISUAL I and II trials. Appendix 1 presents the PRISMA13 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One economic evaluation4 and 4 SRs1,14-16 were included in this review. Of the 4 SRs, 2 included meta-analyses.1,14 All 4 included SRs had broader inclusion criteria than this review.
Li et al. (2021) performed a meta-analysis of RCTs for efficacy outcomes (changes in best-corrected visual acuity [BCVA], anterior chamber cell grade, vitreous haze, and time to treatment failure). A total of 6 RCTs were included but data from 1 RCT were not extracted due to the focus on pediatric patients; therefore, 5 included RCTs are relevant to this review (focus on adults with non-infectious uveitis). Among the pooled analyses, all efficacy outcomes except for change in vitreous haze grade included data from pediatric and adult patients. Therefore, these meta-analyses consisted of a mixed population as it did not report findings specific to adults and is irrelevant to this review. For the outcomes of change in BCVA, time to treatment failure, and change in anterior chamber cell grade, only the results of the relevant primary studies are summarized below. Of note, Li et al. (2021) did not perform a meta-analysis for the safety outcomes; accordingly, safety outcomes of the 5 relevant RCTs (i.e., non-pooled data) are also summarized below.
Hu et al. (2020) performed a meta-analysis of prospective and retrospective studies published from January 2010 to September 2019 to evaluate the safety and effectiveness of anti-TNF-Alpha therapy for Behçet’s disease associated uveitis. The meta-analysis assessed adalimumab and infliximab; thus, it consisted of a mixed intervention as it did not report findings of adalimumab separately and is irrelevant to this review. Relevant primary studies could not be identified as the eligibility criteria regarding study design and comparators were unclear with minimal details provided. Namely, it was not possible to identify if the studies assessing adalimumab were comparative as included studies were only described as prospective or retrospective and relevant comparators were not reported.
The SR by Leal et al. (2018) assessed the safety and efficacy of intravitreal anti-TNF agents in adults with non-infectious uveitis and included literature published up to April 2017. The SR by Gόmez-Gόmez et al. (2017) assessed the safety and efficacy of immunomodulatory agents in adults with nonmalignant active non-infectious anterior uveitis. Gόmez-Gόmez et al. (2017) included literature published up to March 2016 from the Cochrane Library search and from 1961 to March 2016 from the PubMed and Embase searches.16 Both of these SRs15,16 evaluated adalimumab in adults with non-infectious uveitis with non-randomized study designs. As non-randomized studies were not eligible for this rapid review, no relevant primary studies were identified from these SRs.15,16
Among the SRs with broader inclusion criteria than this review, only the subset of relevant studies of Li et al. (2021) will be described in this report. Additional details regarding the characteristics of all included publications are provided in Appendix 2.
Study Design
The SR of RCTs by Li et al. (2021) consisted of a meta-analysis of 6 RCTs among which, 5 RCTs (VISUAL I, VISUAL I [Japan], VISUAL II, VISUAL II [Japan], and ADUR trials) are relevant to this review.1 This SR included a literature search of PubMed, Web of Science, Embase, Cochrane Library, and Clinical from inception to November 19, 2020.
One economic evaluation was included in this review. Bermejo et al. (2019) conducted a cost-effectiveness analysis using a Markov model over a lifetime time horizon with 5 health states: on treatment, post-treatment failure, blindness, remission, and death. The evaluation was performed in the perspective of the Personal Social Services and National Health Service (i.e., UK perspective). Model inputs were derived from the VISUAL I and II trials, British National Formulary, National Institute for Health and Care Excellence (NICE) documentation, National Health Service (NHS) Reference costs (2014 to 2015), and published guidelines and clinical studies. The VISUAL I and II trials were identified from the SR that informed the related clinical effectiveness review that complimented this economic evaluation as part of a National Institute for Health Research HTA (Squires et al. [2017]8 and project number 15/64/07). Most of the model outcomes were from the VISUAL I and II trials; for instance, the EuroQol- 5 Dimension (EQ-5D) scores measured in these trials were used for utility values representing health-related quality of life.
Key assumptions of the base-case analysis: placebo arm of the VISUAL I and II trials would be representative of standard practice; 10% of patients would require assistance from a nurse for adalimumab injection, all patients would be monitored for risk of adverse events every 6 weeks through outpatient visits, and patients receiving immunosuppressant therapy would also undergo 6 additional blood monitoring visits annually; patients would not become blind before treatment failure; patients would be treated with immunosuppressants and corticosteroids (modelled by the placebo arm of VISUAL I and II) following treatment failure; and probability of remission was assumed to be zero due inadequate data.
Multiple sensitivity analyses were conducted with different evidence sources and assumptions, which were not clearly and minimally reported (see the Summary of Critical Appraisal and Appendix 3 for more details). Namely, 1 sensitivity analysis estimated the cost-effectiveness using data from the Multicenter Uveitis Steroid Treatment (MUST) trial, which was conducted in a younger population (13 years of age or older). Another sensitivity analysis was based on the assumption that following 2 years of successful treatment, some patients would no longer require adalimumab (i.e., remission health state).
Country of Origin
The SR by Li et al. (2021) was conducted by authors from China.1 The economic evaluation was performed by authors from the UK using standard UK-based sources and in the perspective of the Personal Social Services and the NHS (i.e., perspective of UK services).4
Patient Population
The study population of relevant RCTs (VISUAL I, VISUAL I [Japan], VISUAL II, VISUAL II [Japan]) included in the SR by Li et al. (2021) and economic evaluation (VISUAL I and II) were similar as both consisted of adults with non-infectious intermediate-, posterior-, or panuveitis of both active and inactive forms.1,4 The SR by Li et al. (2021) and economic evaluation both included data from VISUAL I and II. The VISUAL I, VISUAL I (Japan), and ADUR trials included patients with active non-infectious uveitis and VISUAL II and VISUAL II (Japan) trials included patients with inactive non-infectious uveitis. However, the patient population of the ADUR trial included in the SR1 was slightly different as it included adults with active non-infectious anterior-, posterior-, and panuveitis (i.e., sample did not include intermediate non-infectious uveitis but included anterior non-infectious uveitis). Additionally, the ADUR trial had a younger sample (mean = 36 years) and consisted of a few etiologies not included in the VISUAL I, VISUAL I (Japan), VISUAL II, and VISUAL II (Japan) trials such as juvenile idiopathic arthritis, spondylarthritis, and granulomatosis with polyangiitis. In contrast, Behçet’s disease, sarcoidosis, Vogt-Koyanagi syndrome, and idiopathic etiologies were all reported in VISUAL I, VISUAL I (Japan), VISUAL II, and VISUAL II (Japan) trials but not the ADUR trial.
Specific to the SR,1 the mean age for the relevant trials ranged from 36.0 years (ADUR trial) to 50.9 (VISUAL I [Japan]). The percentage of patients with bilateral non-infectious uveitis ranged from 87.5% (VISUAL I [Japan]) to 96% (VISUAL II) but this was not reported for the ADUR trial. Overall, there were 515 patients across the studies relevant to the current report.
Specific to the base case of the economic evaluation,4 over 90% of the target population had bilateral non-infectious uveitis (VISUAL I: 91% and VISUAL II: 96%) and the mean age was around 43 years (VISUAL I: 42.7 and VISUAL II: 42.5). Overall, there were 452 patients included from VISUAL I (n = 223) and II (n = 229). One of the sensitivity analyses estimated the cost-effectiveness using data from the MUST trial, which consisted of patients, aged 13 and older, with active non-infectious posterior uveitis.4
Interventions and Comparators
The intervention of 4 relevant RCTs (VISUAL I, VISUAL I [Japan], VISUAL II, VISUAL II [Japan]) of the SR by Li et al. (2021) and the included economic evaluation (VISUAL I and II) consisted of subcutaneously injected adalimumab with an 80 mg loading dose followed by 40 mg doses every 2 weeks; whereas, the comparator of these aforementioned trials was placebo1,4 Patients in both the intervention and placebo groups also received a variety of immunomodulatory agents (e.g., immunosuppressants — methotrexate, mycophenolate mofetil, and ciclosporin) and an initial oral prednisone (corticosteroid) burst (i.e., short-term treatment) that was subsequently tapered.1,4 The economic evaluation reported that 32% and 47% of patients in the VISUAL I and II trials received at least 1 immunosuppressant at baseline, respectively, which was balanced across both adalimumab and placebo arms.4
All patients (both arms) in the VISUAL I and VISUAL I (Japan) trials initiated the prednisone burst at the trial start (week 0), which was tapered from 60 mg per day to 0 mg by week 15.1,4 The economic evaluation stated that all patients in the VISUAL II trial initiated the prednisone burst at week 2, which was tapered from 10 to 35 mg per day to 0 mg by week 19.4 The SR by Li et al. (2021) stated that the prednisone burst in the VISUAL II and VISUAL II (Japan) was tapered by week 15 for all patients.1 However, this reporting in the SR by Li et al. (2021) is likely an error as this does not match the source publication (Nguyen et al. [2016], NCT01124838).
The intervention of the ADUR trial (5th relevant RCT from Li et al. [2021]) consisted of 40 mg subcutaneous injections of adalimumab that were administered every 2 weeks and the SR authors reported the comparator as “blank” (p.7)1 but stated that RCTs were excluded if the control group did not constitute placebo administration. However, Li et al. (2021) noted that patients in both arms continued previous immunosuppressive treatment and received corticosteroid therapy with a dose of 1 mg/kg per body weight that was subsequently tapered following a fixed standardized protocol.1
Specific to the economic evaluation,4 1 sensitivity analysis estimated the cost-effectiveness using data from the MUST trial that compared a fluocinolone corticosteroid implant with systemic corticosteroids and immunosuppressants.
Outcomes
Clinical Effectiveness
The SR by Li et al. (2021) reported efficacy (time to treatment failure and changes in BCVA, anterior chamber cell grade, and vitreous haze grade) and safety outcomes (number and rate of adverse events and serious adverse events). Treatment failure was defined by 1 or more of the following criteria: novel active, inflammatory lesions (in reference to baseline); 2-step increase in anterior chamber cell or vitreous haze grades; worsening of BCVA by at least 15 letters as compared to the best score previously achieved in at least 1 eye using the Early Treatment Diabetic Retinopathy Study chart; “sustained non-improvement with entry grade of ≥ 3 (p.2);”1 “use of concomitant medications not allowed (p.2);”1 and intermittent or continuous interruption of study treatments (interventional or control groups) for a cumulative duration of more than 4 weeks.
Change in BCVA was reported in logarithm of the minimum angle of resolution (logMAR) units. Change in anterior chamber cell grade and change in vitreous haze grade were assessed using Standardization of Uveitis Nomenclature (SUN) criteria. A meta-analysis was only performed on the efficacy outcomes. The meta-analysis specific to change in vitreous haze grade is the only relevant pooled analysis. The rest of the efficacy and safety outcomes included in this report are based on the relevant primary studies (i.e., not pooled analyses).
Cost-Effectiveness
The included economic evaluation reported cost-effectiveness related outcomes including incremental cost-effectiveness ratio (ICERs) (expressed as cost [sterling pound] per QALY gained), incremental and total QALYs, incremental and total costs (sterling pound), and probability of cost-effectiveness at the WTP thresholds of £20 000 and £30 000. Cost data sourced from the British National Formulary were 2016 values and NHS reference costs were 2014 to 2015 values. ICERs were calculated in the base-case and sensitivity analyses.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
The 4 SRs1,14-16 were assessed to be of variable methodological quality based on the assessments using AMSTAR 2.9 Namely, the SR by Li et al. (2021)1 was considered to have satisfactory SR methodology but the other 3 SRs,14-16 which were broad and did not have identifiable relevant primary studies, were of low quality.
Specific to the Li et al. (2021) SR, which was the only SR identified to have relevant primary studies, the research question or objective and inclusion and exclusion criteria with all population, intervention, comparator, outcomes (definitions provided), and study design (RCTs only) components were clearly reported. Additionally, multiple databases were searched, and the search was conducted within 24 months before publication. The review protocol was established before conduct of the review and was registered with the International Prospective Register of Systematic Reviews (PROSPERO). Only RCTs were included, the authors justified this for the need to perform a SR with a meta-analysis without the inclusion of low-quality evidence. Despite the authors’ justification, this SR may not provide a comprehensive review of all relevant literature. Of note, the meta-analysis of the change in vitreous haze grade was the only 1 identified to be relevant to this report. Specific to that outcome, a fixed-effects model was used, and its use was justified due to low heterogeneity (i.e., I2 = 0%). Potential causes of heterogeneity were acknowledged including differences in types of non-infectious uveitis, concomitant medications, outcome measures, and age. Notably, the combination of adult and pediatric patients in the meta-analyses of all other outcomes deemed those analyses irrelevant to this report, which focuses on adults with non-infectious uveitis. The authors noted that age is associated with different systemic diagnoses (e.g., juvenile idiopathic arthritis) and anatomic localization (i.e., anterior uveitis is typically associated with juvenile idiopathic arthritis).1 Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess certainty of the evidence for all outcomes that were assessed with a meta-analysis.
The SR by Li et al. (2021) was also associated with considerable methodological limitations. The limitations included:
Risk of bias across studies was not performed, authors attributed this to the small sample size.
Interpretation of the outcome values was not described; namely, the minimal clinically important differences were not reported.
Time to treatment failure was a composite outcome consisting of some of the other evaluated outcomes (i.e., BCVA, vitreous haze grade, and anterior chamber cell grade). Composite outcomes are particularly susceptible to misleading interpretations of the overall treatment effect and treatment effect on individual components. Proper use requires the consideration of competing risks, consideration of the statistical significance and clinical importance, and assessment of effect on individual components. Of note, novel ocular inflammatory lesions was stated to be part of this composite outcome but was not an included outcome in this SR.1 Overall, the use of composite outcomes in individual clinical trials is complex given the many important considerations; therefore, pooling a composite outcome from multiple RCTs may introduce considerable heterogeneity and bias the results.
Publication bias assessments using Egger’s test and funnel plots were planned but not conducted due to the small number (6) of included studies.
Sources of funding and potential sources of conflict of interest for the included studies were not reported but it was noted that all included RCTs received support from the manufacturer of adalimumab (AbbVie).
Errors in the authors’ data extraction were identified. Namely, the SR by Li et al. (2021) stated that the prednisone burst in the VISUAL II and VISUAL II (Japan) studies was tapered by week 15.1 However, this reporting in the SR by Li et al. (2021) is likely an error as this does not match the source publication (Nguyen et al. [2016], NCT01124838).17 Overall, findings of clinical effectiveness must be interpreted with caution in light that it is only based on RCT data.
Specific to the 3 SRs14-16 without relevant primary studies identified, the research question or objective was reported, multiple databases were searched, and the search was conducted within 24 months before publication. The quality or risk of bias of included primary studies was assessed using satisfactory techniques in these SRs.14-16 Across all these studies it was reported that study selection was performed by 2 independent reviewers. In contrast, Hu et al. (2020)14 did not clearly report if data extraction and quality and risk of bias assessments were performed by 2 independent reviewers, and Gόmez-Gόmez et al. (2017)16 did not clearly report if quality and risk of bias assessments was performed by 2 independent reviewers. Unclear reporting regarding the latter increases the risk of inter-rater bias and the use of a single reviewer increases the risk of errors. Overall, these SRs14-16 had unclear reporting of the eligibility criteria, which increases the risk of selection bias. Notably, the comparator and study design components were particularly unclear, which resulted in the inability to identify relevant primary studies in the Hu et al. (2020) SR14 (which only referred to studies as prospective or retrospective) and detailed scrutiny was required to identify relevant primary studies (e.g., reviewing tables for details of characteristics of included studies) from the other SRs.15,16 Only 1 of these SRs (Leal et al. [2018])15 noted that the review protocol was established before conduct of the review and was registered with PROSPERO. This SR by Leal et al. (2018)15 also reviewed reference lists of included literature, searched trial registries, and retrieved grey literature. Alternatively, the other 2 SRs14,16 did not specify if the review protocol was established before conduct and did not search trial registries, retrieve grey literature, and/or review reference lists. The former increases the risk of reporting bias and the latter increases the risk of an inadequate, non-comprehensive SR particularly due to missing relevant, non-indexed literature.
Economic Evaluation
In the base-case analysis of the included economic evaluation4 (cost-effectiveness analysis), the research question plus the related economic importance and comparator plus the rationale for selecting the alternative intervention were clearly stated. The model structure plus health states (depicted in a diagram); input parameters with the values, sources, and references (e.g., relevant drug costs were provided in pound sterling and sourced to the British National Formulary 2016); time horizon; and discount rate for the economic model were clearly reported. Namely, the lifetime time horizon was deemed acceptable for this patient population as non-infectious uveitis tends to manifest as a chronic condition and may require long-term treatment. Model inputs were mostly derived from 2 RCTs identified from a related clinical effectiveness review (this economic evaluation4 is part of a National Institute for Health Research HTA8) that were retrieved by a systematic review in addition to other referenced publications. The specific measures/data derived were clearly reported. For instance, time to treatment failure and EQ-5D scores were extracted from the VISUAL I and II trials; whereas, data from a retrospective review of insurance claims were used to estimate the blindness rate in the base-case analysis. Overall, methods to value benefits and for the estimation of quantities and unit costs were briefly reported with reference to the related National Institute for Health Research HTA for further details. Incremental analyses were reported with relevant alternatives compared and authors reported no competing interests and reported funding sources. Major outcomes were presented in a disaggregated form by arm (e.g., limited current practice versus adalimumab plus limited current practice) but not health state.
This economic evaluation was also associated with a few considerable methodological limitations. It was clear that the perspective of this evaluation was the UK health care system; namely, the Personal Social Services and the NHS. However, services of the Personal Social Services were not reported. Placebo arms of the VISUAL I and II trials, selected as the alternative interventions, were assumed to be equivalent to current practice. However, the authors noted these data may not be entirely representative of current practice as it would likely have a greater proportion of patients treated with immunosuppressants (hence comparator referred to as “limited current practice”), which limits generalizability of the findings. Productivity changes, justification for the selected discount rate, and description of currency conversion or currency of price adjustments for inflation were not reported. Minimal details of the subjects from the MUST trial for 1 of the sensitivity analyses were provided.
Overall, the conclusion (i.e., adalimumab is not cost-effective at WTP thresholds of £20 000 to £30 000 per QALY gained in adults with active and inactive non-infectious uveitis influencing the posterior segment), should be interpreted in light that the perspective and majority of inputs were in the context of the health care system in the UK. Therefore, it may not be generalizable to Canada. Additionally, the conclusion only alludes to posterior non-infectious uveitis; however, the patient population of the base-case analysis was modelled off the VISUAL I and II trials, which included posterior-, intermediate-, or panuveitis. Thus, the applicable patient population of this cost-effectiveness conclusion is unclear.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Adalimumab for the Treatment of Individuals Adults With Non-infectious Uveitis
Results from the included evidence informing the clinical effectiveness are summarized below by outcome. Changes in BCVA, anterior chamber cell grade, and vitreous haze grade; time to treatment failure; and safety findings were extracted from relevant primary RCTs, from the broader SR by Li et al. (2021), and are reported separately for active and inactive non-infectious uveitis. CADTH did not perform any statistical comparisons for the data extracted from relevant primary RCTs. Of note, change in BCVA and time to treatment failure findings were not reported in the SR by Li et al. (2021) for the ADUR trial, it was noted that change in visual acuity was evaluated instead of BCVA and time to treatment failure was not assessed. The pooled findings for the change in vitreous haze grade was also reported as this meta-analysis met the eligibility criteria of this report.
Change in BCVA
In active non-infectious uveitis, mean differences of the change in BCVA, after treatment, were −0.07 (95% confidence interval [CI], −0.11 to −0.02) and 0.04 (95% CI, −0.22 to 0.31) in the VISUAL I and VISUAL I (Japan) trials, respectively. For the VISUAL I data, adalimumab significantly improved the change in BCVA after treatment; however, as the CI crossed 0, there may be no treatment effect for the VISUAL I (Japan) data.1 The mean difference and respective CI of the change in BCVA was not reported for the ADUR trial. For inactive non-infectious uveitis, mean differences of the change in BCVA were −0.04 (95% CI, −0.08 to 0.01) and −0.08 (95% CI, −0.20 to 0.04) for VISUAL II and VISUAL II (Japan) trials, respectively; however, as both confidence intervals crossed 0, there may be no treatment effect.1
Time to Treatment Failure
In active non-infectious uveitis, hazard ratios of time to treatment failure were 0.50 (95% CI, 0.36 to 0.70) and 1.20 (95% CI, 0.41 to 3.54) in the VISUAL I and VISUAL I (Japan) trials, respectively. For the VISUAL I data, adalimumab significantly lowered the risk of treatment failure; however, as the CI crossed 1, there may be no treatment effect for the VISUAL I (Japan) data.1 The hazard ratio and respective CI of time to treatment failure was not reported for the ADUR trial. For inactive non-infectious uveitis, hazard ratios of time to treatment failure were 0.57 (95% CI, 0.39 to 0.84) and 0.45 (95% CI, 0.20 to 1.03) in VISUAL II and VISUAL II (Japan), respectively. For the VISUAL II data, patients receiving adalimumab had a significantly lower risk of treatment failure; however, as the CI crossed 1, there may be no treatment effect for the VISUAL II (Japan) data.1
Change in Anterior Chamber Cell Grade
In active non-infectious uveitis, mean differences of the change in anterior chamber cell grade were −0.29 (95% CI, −0.51 to −0.07), 0.22 (95% CI, −0.17 to 0.61), and −0.43 (95% CI, −1.05 to 0.18) in the VISUAL I, VISUAL I (Japan), and ADUR trials, respectively. For the VISUAL I data, patients receiving adalimumab had a significant improvement in the change in anterior chamber cell grade; however, as the CIs crossed 0, there may be no treatment effect for the VISUAL I (Japan) and ADUR data.1 For inactive non-infectious uveitis, mean differences of the change in anterior chamber cell grade were −0.14 (95% CI, −0.37 to 0.08) and −0.22 (95% CI, −0.90 to 0.46) in VISUAL II and VISUAL II (Japan), respectively; however, as both CIs crossed 0, there may be no treatment effect.1
Change in Vitreous Haze Grade
The meta-analysis performed by Li et al. (2021)1 reported that the change in vitreous haze grade improved significantly more in the adalimumab group than the control group (mean difference = −0.21 [95% CI, −0.32 to −0.11]). The mean differences of change in vitreous haze grade of the included trials (VISUAL I, VISUAL I [Japan], VISUAL II, VISUAL II [Japan], and ADUR trials) were significantly different and ranged from −0.54 to −0.13 (P < 0.05). The heterogeneity of the pooled analysis was considered low as demonstrated by the Q statistic (Chi2 = 3.70, degrees of freedom = 4 [P = 0.45]) and I2 value (0%).
In active non-infectious uveitis, mean differences of change in vitreous haze grade were −0.27 (95% CI, −0.43 to −0.11), −0.41 (95% CI, −1.15 to 0.34), and −0.54 (95% CI, −1.22 to 0.14) in the VISUAL I, VISUAL I (Japan), and ADUR trials, respectively. For the VISUAL I data, patients receiving adalimumab had a significant improvement in the change in vitreous haze grade; however, as the CIs crossed 0, there may be no treatment effect for the VISUAL I (Japan) and ADUR data1 For inactive non-infectious uveitis, mean differences of the change in vitreous haze grade were −0.13 (95% CI, −0.28 to 0.01) and −0.45 (95% CI, −0.98 to 0.07) in VISUAL II and VISUAL II (Japan), respectively; however, as both CIs crossed 0, there may be no treatment effect.1
Safety
In active non-infectious uveitis, the number and rate (events per patient-years) of adverse events and serious adverse events were greater in the adalimumab group compared to the placebo group (VISUAL I, VISUAL I [Japan], and ADUR trials). Among inactive non-infectious uveitis, the number of adverse events was greater in the adalimumab group but the rate of adverse events was higher in the placebo groups. The number of serious adverse events was higher in the adalimumab group for the VISUAL II trial but the rate was slightly lower (0.138 versus 0.141 in the adalimumab versus placebo groups, respectively). The number of serious adverse events was the same in the adalimumab and placebo groups (1 and 1, respectively) for the VISUAL II (Japan) trial, but the rate was lower in the adalimumab group (0.140 versus 0.459 in the adalimumab versus placebo groups, respectively).1 Li et al. (2021) reported that the most common adverse events across all included RCTs (data of adult and pediatric populations with non-infectious uveitis) evaluating the safety of adalimumab were allergies and injection-site reactions.1
Cost-Effectiveness of Adalimumab for the Treatment of Individuals Adults With Non-infectious Uveitis
The evidence informing the cost-effectiveness is summarized separately for the base-case and sensitivity analyses.
Base-Case Analysis
Using probabilistic modelling, the estimated ICERs for adalimumab versus systemic corticosteroid and immunosuppressant therapy were £92 600 and £318 075 per QALY gained for active and inactive non-infectious uveitis, respectively.4 The authors concluded that adalimumab is not cost-effective at WTP thresholds of £20 000 to £30 000 per QALY gained in adults with active and inactive non-infectious uveitis influencing the posterior segment.4 These ICERs were estimated based on NICE standards and NHS resources (i.e., UK perspective). The incremental QALYs for active and inactive non-infectious uveitis using the probabilistic model were 0.200 and 0.119, respectively. The total QALYs for active non-infectious uveitis in adalimumab, plus systemic corticosteroid and immunosuppressant therapy, versus systemic corticosteroid and immunosuppressant use alone (comparator) was 15.421 versus 15.221, respectively. In inactive non-infectious uveitis the total QALYs were 15.668 versus 15.549 in the adalimumab versus comparator groups, respectively.
The incremental costs for active and inactive non-infectious uveitis using the probabilistic model were £18 541 and £37 784, respectively. The total costs for active non-infectious uveitis in the adalimumab versus the comparator was £67 577 versus £49 036, respectively. In inactive non-infectious uveitis the total costs were £88 014 versus £50 230 in the adalimumab versus comparator groups, respectively.
At both WTP thresholds (£20 000 and £30 000), the probabilities of cost-effectiveness for active non-infectious uveitis were 0.00 versus 1.00 for adalimumab versus placebo, respectively. At both WTP thresholds (£20 000 and £30 000), the probabilities of cost-effectiveness for inactive non-infectious uveitis were 0.00 versus 1.00 for adalimumab versus placebo, respectively.4
Sensitivity Analyses
Bermejo et al. (2019) performed the following sensitivity analyses and estimated the respective ICERs for active non-infectious uveitis. Using data from the MUST trial, the ICER was estimated to be £110 068 per QALY gained (adalimumab versus current practice); using alternative parametric survival functions of time to treatment failure, ICERs were estimated as £102 218 per QALY gained and £100 225 per QALY gained with Weibull and Gompertz distributions, respectively; following the assumption that after 2 years of successful treatment, some patients would enter the remission health state (i.e., no longer require adalimumab), ICERs were estimated as £66 176 per QALY gained and £55 161 at 0.1 and 0.2 annual remission rates, respectively.
Of note, sensitivity analyses integrating various sources for the blinding utility scores and blinding rates at different annual remission rates were also performed but details are not provided in Table 12: as the analysis was deemed unclear. Overall, this resulted in widely variable ICERs, ranging from £32 544 to £120 650 within 1 source of blindness utility scores and £48 094 to £141 099 with another source of blindness utility scores. From these findings, the authors concluded that adalimumab may be more cost-effective for patients with active non-infectious uveitis who have a greater risk of blindness; however, this is unlikely to be considered cost-effective for most patients with inactive non-infectious uveitis from a health care providers’ perspective. Please refer to the Bermejo et al. (2019) publication for the detailed findings.4
Findings for the sensitivity analyses performed on patients with inactive non-infectious uveitis were minimally reported, the authors stated, “the same sensitivity analyses were undertaken for inactive patients (except from the analysis based on the MUST trial, given that it only included active patients) and all analyses resulted in ICERs greater than £35 000 per QALY gained.” (p.1637)4 Of note, the sensitivity analysis using data from the MUST trial is based on a dataset consisting of individuals of adult and pediatric age (i.e., individuals aged 13 years or older were enrolled in the MUST trial).
Guidelines of Adalimumab for the Treatment of Individuals Adults With Non-infectious Uveitis
No evidence-based guidelines were identified regarding the use adalimumab for the treatment of individuals adults with non-infectious uveitis; therefore, no summary of guidelines can be provided.
Limitations
Overall, this report is limited in the quality and quantity of relevant evidence regarding the clinical and cost-effectiveness and evidence-based guidelines informing the use of adalimumab as treatment for adults with non-infectious uveitis. In this review, there were 4 included SRs that were all broader than the inclusion criteria of this review.1,14-16 Among these, only 1 SR1 allowed for findings to be summarized and the remaining 314-16 all had unclear eligibility criteria with a particular lack of reporting regarding eligible comparator(s) and study design(s). For instance, 1 SR14 only referred to included studies based on retrospective or prospective conduct, which did not even allow for identification of relevant primary studies. Accordingly, 314-16 of the 4 included SRs mostly contained studies that were not comparative and not randomized, which considerably limited the quantity of high-quality evidence summarized in this review. Thus, there is a need for more well-designed studies that directly assess the clinical effectiveness of adalimumab in adults with non-infectious uveitis and may inform the cost-effectiveness of adalimumab in this population. Namely, there is a particular need for more well-designed RCTs as there were 7 SRs/meta-analyses/HTAs that were excluded due to full overlap. All 7 publications included the VISUAL I and II RCTs and 2 included the ADUR RCT, which particularly highlights the small quantity of relevant evidence.
The included evidence may not be generalizable to the Canadian adult population treated with adalimumab due to the combination of various etiologies and anatomic localizations of non-infectious uveitis that are not common among adults. Namely, the ADUR trial included in the SR by Li et al. (2021),1 from which data were extracted, consisted of individuals with juvenile idiopathic arthritis and anterior-localized non-infectious uveitis. The onset of uveitis in juvenile idiopathic arthritis is typically between 2 and 8 years old, and uveitis in children tends to present with an anterior localization.1,3 Although, the ADUR trial enrolled patients aged 18 and older, the resultant sample was younger (mean age = 36 years) as the SR by Li et al. (2021) included trials with a mean age of up to 50.9 years. Therefore, inclusion of the ADUR trial limits the generalizability to the majority of Canadian adults with non-infectious uveitis as juvenile idiopathic arthritis is predominantly diagnosed under the age of 18, and the Health Canada–approved indication does not include anterior uveitis – “treatment of non-infectious uveitis (intermediate, posterior and panuveitis) in adult patients with inadequate response to corticosteroids or as corticosteroid sparing treatment in corticosteroid-dependent patients” (p. 6 to 7).18
Additionally, the included economic evaluation was not specific to Canada; therefore, the cost-effectiveness findings may not be generalizable to current clinical practice in Canada. Particularly regarding economic evaluations, perspective and model inputs should be specific to the jurisdiction of interest. The included economic evaluation was conducted in the perspective of services implemented in the UK (Personal Social Services and NHS) and many sources of model inputs were also specific to the UK (e.g., British National Formulary (2016), NICE documentation, NHS Reference costs [2014 to 2015]). Accordingly, ICERs were based on the currency of pound sterling and cost-effectiveness ICER thresholds were determined by NICE and NHS resources.4 Additionally, drug costs were based on 2016 values and some administration and monitoring and adverse event costs were based on reference costs from 2014 to 2015. The authors did not provide a description of adjustments for inflation, which also limits the generalizability to the current year.4 Thus, the interpretation of the cost-effectiveness findings in this report should be specific to the UK health care system and applicability to the current Canadian health care system is limited.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 4 SRs1,14-16 and 1 economic evaluation,4 which informed the clinical effectiveness (including safety) and cost-effectiveness of adalimumab for the treatment of adults with non-infectious uveitis, respectively. No evidence-based guidelines were identified regarding the use of adalimumab in adults with non-infectious uveitis. The SR by Li et al. (2021)1 included 5 RCTs (VISUAL I,19 VISUAL II,17 VISUAL I [Japan],20 VISUAL II [Japan],20 and ADUR21 trials) relevant to this report. Overall, the included evidence should be interpreted with caution due to methodological limitations and limited generalizability (highlighted in the Critical Appraisal and Limitations sections of this report).
The included clinical effectiveness evidence suggested that in adults with active non-infectious uveitis (VISUAL I), adalimumab significantly lowered risk of treatment failure and adalimumab significantly improved the changes in BCVA, anterior chamber cell grade, and vitreous haze grade. In adults with inactive non-infectious uveitis (VISUAL II), adalimumab significantly lowered risk of treatment failure; however, adalimumab may have no treatment effect on changes in BCVA, anterior chamber cell grade, and vitreous haze grade. Further, the Japanese VISUAL sub studies demonstrated that adalimumab may not elicit a treatment effect on risk of treatment failure and change in BCVA. Similarly, the Japanese VISUAL sub studies plus the ADUR trial (that assessed adalimumab in a younger sample with differing etiologies [e.g., included juvenile idiopathic arthritis] as compared to the VISUAL trials) demonstrated that adalimumab may not elicit a treatment effect on changes in anterior chamber cell grade and vitreous haze grade in adults with active and inactive non-infectious uveitis.1 For adults with active non-infectious uveitis, the number and rate of adverse events and serious adverse events were greater in the adalimumab group compared to the placebo group.1 Additionally, for adults with inactive non-infectious uveitis, the number and rate of adverse events and serious adverse events were variable in the adalimumab versus placebo groups.1 Pooled across active and inactive non-infectious uveitis, the change in vitreous haze grade significantly improved more in the adalimumab group than the control group.1 The clinical effectiveness and safety of adalimumab was also suggested by the other SRs from which data were not extracted; however, all 4 SRs in this report acknowledged the lack of high-quality evidence to provide certainty in the findings. Among RCTs evaluating the safety of adalimumab in adult and pediatric populations with non-infectious uveitis, allergies and injection-site reactions were the most common adverse events.1
The included cost-effectiveness analysis concluded that adalimumab is not cost-effective at WTP thresholds of £20 000 to £30 000 per QALY gained in adults with active and inactive non-infectious uveitis influencing the posterior segment.4 However, this should be interpreted in light that the economic evaluation was performed in the perspective of the UK with UK standards, resources, and cost data from 2014 to 2016 (e.g., NICE, British National Formulary, and NHS). Of note, authors did not report if adjustments for inflation were performed. Altogether, the cost-effectiveness findings may not be generalizable to Canadian jurisdictions.
CADTH was able to connect with an adult living with uveitis associated with ankylosing spondylitis. This individual noted that non-infectious uveitis may have a considerable negative impact on the quality of life particularly during the initial onset when there is a lack of knowledge of the diagnosis (i.e., individuals may mistake uveitis for dry eye or conjunctivitis especially during the first episode) in addition to the pain, irritation, discomfort, swelling, light sensitivity, blurry vision, and headache that may accompany all uveitis episodes. Additionally, it was stated that when clinicians are devising a treatment plan, they should consider the efficacy and safety of treatment(s), use of concurrent treatments, recurrence of uveitis, comorbidities, and general health of the individual. This individual’s uveitis has been controlled with prescription prednisone eye drops that are self-administered and the individual stated that they experienced no side effects from the eye drops. They had not been treated with adalimumab but noted they are aware of the higher cost of adalimumab and that adalimumab is associated with a limited ability for self-administration. The patient did not specify the frequency in which drops were administered.
Overall, there is a need for evidence-based guidelines to inform the use of adalimumab in adults with non-infectious uveitis in Canadian clinical practice and well-designed economic evaluations in the Canadian context to inform the cost-effectiveness of adalimumab in the perspective of Canadian jurisdictions. Namely, multiple biosimilars are approved in Canada with indications specific to uveitis in adult populations. As biosimilars may introduce cost-savings, there is a particular need for more evidence on individual adalimumab biosimilar drugs (i.e., not as adalimumab biosimilars collectively) as biosimilars of the same reference may perform differently. This lack of evidence is reflected in a recent CADTH report, published in February 2021, that found no evidence regarding the clinical effectiveness of switching from adalimumab (reference) to biosimilars in adults with uveitis.22 Nevertheless, the included clinical- and cost-effectiveness evidence of this rapid review may inform the use of adalimumab biosimilars in adults with non-infectious uveitis to facilitate cost-savings in some jurisdictions.
References
1.Li B, Li H, Zhang L, Zheng Y. Efficacy and safety of adalimumab in noninfectious uveitis: a systematic review and meta-analysis of randomized controlled trials. Front Pharmacol. 2021;12:673984. PubMed
2.Ming S, Xie K, He H, Li Y, Lei B. Efficacy and safety of adalimumab in the treatment of non-infectious uveitis: a meta-analysis and systematic review. Drug Des Devel Ther. 2018;12:2005-2016. PubMed
3.Rosenbaum JT. Uveitis: etiology, clinical manifestations, and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2020: www.uptodate.com. Accessed 2021 Nov 15.
4.Bermejo I, Squires H, Poku EN, et al. Adalimumab for non-infectious uveitis: is it cost-effective? Br J Ophthalmol. 2019;103(11):1633-1638. PubMed
5.Felfeli T, Christakis PG, Bakshi NK, Mandelcorn ED, Kohly RP, Derzko-Dzulynsky LA. Referral characteristics and wait times for uveitis consultation at academic tertiary care centres in Toronto. Can J Ophthalmol. 2018;53(6):639-645. PubMed
6.Rosenbaum JT. Uveitis: treatment. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Nov 15.
7.Adalimumab (including biosimilars of adalimumab): drug information. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Nov 15.
8.Squires H, Poku E, Bermejo I, et al. A systematic review and economic evaluation of adalimumab and dexamethasone for treating non-infectious intermediate uveitis, posterior uveitis or panuveitis in adults. Health Technol Assess. 2017;21(68). PubMed
9.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
10.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Nov 15.
11.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2021 Nov 8.
12.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. PubMed
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Hu Y, Huang Z, Yang S, Chen X, Su W, Liang D. Effectiveness and safety of anti-tumor necrosis factor-alpha agents treatment in behcets' disease-associated uveitis: a systematic review and meta-analysis. Front Pharmacol. 2020;11(941). PubMed
15.Leal I, Rodrigues FB, Sousa DC, et al. Efficacy and safety of intravitreal anti-tumour necrosis factor drugs in adults with non-infectious uveitis - a systematic review. Acta Ophthalmol (Oxf). 2018;96(6):e665-e675. PubMed
16.Gomez-Gomez A, Loza E, Rosario MP, et al. Efficacy and safety of immunomodulatory drugs in patients with anterior uveitis: a systematic literature review. Medicine. 2017;96(42):e8045. PubMed
17.Nguyen QD, Merrill PT, Jaffe GJ, et al. Adalimumab for prevention of uveitic flare in patients with inactive non-infectious uveitis controlled by corticosteroids (VISUAL II): a multicentre, double-masked, randomised, placebo-controlled phase 3 trial. Lancet. 2016;388(10050):1183-1192. PubMed
18.Humira (adalimumab): 40 mg in 0.8 mL sterile solution (50 mg/mL) subcutaneous injection, 10 mg in 0.1 mL sterile solution (100 mg/mL) subcutaneous injection, 20 mg in 0.2 mL sterile solution (100 mg/mL) subcutaneous injection, 40 mg in 0.4 mL sterile solution (100 mg/mL) subcutaneous injection, 80 mg in 0.8 mL sterile solution (100 mg/mL) subcutaneous injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2021 Apr 21: https://pdf.hres.ca/dpd_pm/00061690.PDF. Accessed 2021 Nov 15.
19.Jaffe GJ, Dick AD, Brezin AP, et al. Adalimumab in patients with active noninfectious uveitis. N Engl J Med. 2016;375(10):932-943. PubMed
20.Goto H, Zako M, Namba K, et al. Adalimumab in active and inactive, non-infectious uveitis: global results from the VISUAL I and VISUAL II trials. Ocul Immunol Inflamm. 2019;27(1):40-50. PubMed
21.Mackensen F, Heinz C, Jakob E, et al. Randomized controlled study to evaluate the efficacy of adalimumab in patients with different forms of refractory uveitis. Ocul Immunol Inflamm. 2018;26(7):1015-1022. PubMed
22.Switching from reference to biosimilar adalimumab for patients with various inflammatory conditions (CADTH reference list). Ottawa (ON): CADTH; 2021: https://www.cadth.ca/sites/default/files/pdf/htis/2021/RB1552%20Biosimilar%20Switching%20of%20Adalimumab%20Final.pdf. Accessed 2021 Nov 15.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included SRs and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Li et al. (2021)1 China Funding: Sichuan Provincial Department of Science and Technology, China (2019YFH0117) | SR and MA (efficacy outcomes only) of RCTs Number of included studies: 6 RCTs (combination of pediatric and adult patients) Number of relevant primary studies: 5 RCTs (VISUAL I, VISUAL I [Japan], VISUAL II, VISUAL II [Japan], ADUR) | Eligible population: patients with non-infectious uveitis of any age, ethnicity, or gender Relevant population: adults with non-infectious uveitis, n = 515 across 5 relevant RCTs Mean (SD) age in years: VISUAL I = 42.65 (14.89), VISUAL I (Japan) = 50.9 (14.72), VISUAL II = 42.56 (13.43), VISUAL II (Japan) = 46.8 (12.49), ADUR = 36 (NR) Non-infectious uveitis type:
Etiologies (not limited to):
| Intervention:
Comparator: placebo (conventional routine treatment including immunosuppressants and corticosteroids [local and systemic]), n = 257 across 5 relevant RCTs Concomitant therapy:
| Outcomes: Efficacy
Safety • AEs and SAEs (number and event/ patient-years) Follow-up: mean greater than 3 months |
Li et al. (2021)1 China Funding: Sichuan Provincial Department of Science and Technology, China (2019YFH0117) (continued) |
|
| ||
Hu et al. (2020)14 China Funding: multiple grants from 1) National Natural Science Foundation of China (U1601226, 81870649, and 81670897) and 2) Guangdong Natural Science Funds for Distinguished Young Scholar (2016A030306006) | SR and MA of prospective and retrospective studies Number of included studies: 18 (combination of adalimumab and infliximab [i.e., mixed intervention]) Number of relevant primary studiesc: could not be determined | Patients with Behçet’s disease associated uveitis receiving anti-TNF-α treatment | Eligible intervention: anti-TNF- α therapy Relevant intervention: adalimumab Comparator: conventional routine treatment (e.g., immunosuppressants, corticosteroids [local and systemic]) | Outcomes: Effectiveness
Safety
Follow-up: mean of at least 6 months |
Leal et al. (2018)15 Portugal Funding: NR | SR of non-randomized studies Number of included studies: 5 Number of relevant primary studies: 0 | Adults (> 18 years) with persistent non-infectious uveitis | Eligible intervention: intravitreal anti-TNF injections Relevant intervention: adalimumab Comparator: NR | Outcomes:
Follow-up: minimum of 4 weeks |
Gόmez-Gόmez et al. (2017)16 Spain Funding: unrestricted grant of the Spanish Society of Ocular Inflammation (SEIO) | SR of various study types (e.g., RCTs and observational studies) Number of included studies: 13 Number of relevant primary studies: 0 | Adults (≥ 18 years) with nonmalignant active non-infectious anterior uveitis | Eligible intervention: immunomodulatory drug (e.g., cyclosporine, methotrexate) or biologics (e.g., anti-TNF-α agents) Relevant intervention: adalimumab Comparator: NR | Outcomes:
• AEd Follow-up: variable periods (e.g., duration of 3 months, 20 weeks, 3 years). Eligibility criteria regarding follow-up NR. |
AC = anterior chamber; ADUR = Adalimumab in Uveitis Refractory to Conventional Therapy; AE = adverse event; BCVA = best-corrected visual acuity; CMT = central macular thickness; JIA = juvenile idiopathic arthritis; logMAR = logarithm of the minimum angle of resolution; MA = meta-analysis; NA = not applicable; NR = not reported; RCT = randomized controlled trial; SAE = serious adverse event; SR = systematic review; TNF = tumour necrosis factor; VA = visual acuity; VH = vitreous haze.
aSR by Li et al. (2021) stated that the prednisone burst in the VISUAL II and VISUAL II (Japan) was tapered by week 15.1 However, this reporting in the SR by Li et al. (2021) is likely an error as this does not match the source publication (Nguyen et al. [2016], NCT01124838).
bOnly the MA of the change in VH grade was relevant (i.e., included studies did not include a combination of pediatric and adult patients). Results of the individual studies were extracted for the other efficacy outcomes and safety outcomes.
cRelevant primary studies could not be identified as eligibility criteria regarding study design and comparators were unclear with minimal details provided. For example, relevant comparators were not reported and regarding eligible study designs, authors only stated “prospective open-label trials, uncontrolled case series reports and summaries of conferences were included to provide more evidence (p.2).”14
dGόmez-Gόmez et al. (2017) specifically states “AE” with no further details provided.
Note that this appendix has not been copy-edited.
Table 3: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysisa | Main assumptions |
|---|---|---|---|---|---|---|
Bermejo et al. (2019)4 UK Funding: National Institute of Health Research (NIHR) Health Technology Assessment (HTA) Program (Project number: 15/64/07) | Analysis: cost-effectiveness Perspective: Personal Social Services and NHS Time horizon: lifetime | Individuals with active or inactive non-infectious posterior or panuveitis, intermediate non-infectious uveitis with over 90% presenting bilaterallyb VISUAL I19: adults with active non-infectious uveitis (n = 223) Mean age: 42.7 years Bilateral non-infectious uveitis: 91% VISUAL II17: adults with inactive non-infectious uveitis (n = 229) Mean age: 42.5 years Bilateral non-infectious uveitis: 96% | Intervention: subcutaneous injection of adalimumab – 40 mg every 2 weeks Comparator: placebo (current practice including immunosuppressants [e.g., mycophenolate mofetil, ciclosporin, methotrexate] and corticosteroids) Concomitant therapies (% of patients), VISUAL I19 vs. II17:
| Markov model with 5 health states: on treatment, post-treatment failure, blindness, remission, and death. Costs and QALYs discounted at 3.5% per year. EQ-5D data modelled treatment effectiveness, which captured impact of AEs on QoL. Thus, only additional costs associated with AEs that require substantial treatment costs were included (e.g., cataract, glaucoma, elevated intraocular pressure). Multiple exploratory analyses based on different sources and assumptions were performed, only those deemed relevant and clear were included in this report. | Sources for base-case analysis: VISUAL I and II provided most of the data for the model (e.g., gender). Drug costs were from the British National Formulary (2016). Discount rate (utilities and cost) were from the NICE Reference Case. Administrating and monitoring parameters were from multiple sources (e.g., NHS Reference costs 2014 to 2015, NICE documentation, published guideline). Costs of AEs from multiple sources (e.g., NHS Reference costs 2014 to 2015, British National Formulary, VISUAL I and II RCTs, and other key clinical studies) | Current practice is assumed to be the same as the placebo arm of the VISUAL I and II RCTs, which had 32% and 47% of adults receiving at least 1 immunosuppressant at baseline, respectively. Probability of remission was assumed to be 0 in the base case due to lack of data. Following treatment failure, patients were assumed to be treated with limited current practice (immunosuppressants and corticosteroids modelled by the placebo arm in VISUAL I and II RCTs) It was assumed patients could not become blind before treatment failure. The outcome of adalimumab preventing permanent damage to the eye was assumed to prevent future blindness as VISUAL I and II did not measure occurrence of permanent blindness. |
Bermejo et al. (2019)4 UK Funding: National Institute of Health Research (NIHR) Health Technology Assessment (HTA) Program (Project number: 15/64/07 (continued) | 1 included sensitivity analysis used different parametric survival functions (vs. the log-normal distribution of the base-case) to extrapolate time to treatment failure. | Utilities of EQ-5D scores and proportion of bilateral non-infectious uveitis were from VISUAL I and II RCTs. Blindness utilities (annual blindness probability) from a UK- based retrospective review of insurance claims of patients with posterior non-infectious uveitis. 1 included sensitivity analysis estimated the ICER using MUST trial data.d | 10% of patients would require assistance from a regional nurse for adalimumab injections. All patients would be monitored for risk of AEs (and efficacy of treatments) every 6 weeks through outpatient visits. Patients receiving immunosuppressant therapy would also undergo 6 additional blood monitoring visits annually. 1 included sensitivity analysis assumed that following 2 years of successful treatment, some patients would no longer require adalimumab (remission health state) |
AE = adverse event; EQ-5D = EuroQol- 5 Dimension; MUST = Multicenter Uveitis Steroid Treatment; NA = not applicable; NHS = National Health Service; NICE = National Institute for Health and Care Excellence; NR = not reported; QALY = quality-adjusted life years; QoL = quality of life.
aFor details regarding the model input parameters for the base-case analysis see Table 2 in Bermejo et al. (2019).4
bThe modelled population is unclear as the patient population of the base-case analysis was modelled off the VISUAL I and II trials, which included posterior-, intermediate-, or panuveitis but the authors reported performing a cost-effectiveness analysis in patients with “non-infectious posterior segment uveitis.”4
cPercentage of patients taking immunosuppressant therapy was balanced across the intervention and comparator arms in the trial.
dThe MUST trial compared immunosuppressants and a fluocinolone corticosteroid implant in patients with posterior segment, active non-infectious uveitis.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of SRs and Meta-Analyses Using AMSTAR 2
Strengths | Limitations | |
|---|---|---|
Li et al. (2021)1 | ||
|
| |
Hu et al. (2020)14 | ||
|
| |
Leal et al. (2018)15 | ||
|
| |
Gόmez-Gόmez et al. (2017)16 | ||
|
| |
AC = anterior chamber; AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; BCVA = best-corrected visual acuity; GRADE = Grading of Recommendations Assessment, Development and Evaluation; MeSH = Medical Subject Headings; NA = not applicable; NR = not reported; PROSPERO = International Prospective Register of Systematic Reviews; RCT = randomized controlled trial; SR = systematic review; VH = vitreous haze.
Table 5: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist
Strengths | Limitations |
|---|---|
Bermejo et al. (2019)4 | |
Study design
| Study design
|
Data collection
| Data collection
|
Analysis and interpretation of results
| Analysis and interpretation of results
|
Other
| Other
|
HTA = health technology assessment; ICER = incremental cost-effectiveness ratio; MUST = Multicenter Uveitis Steroid Treatment; NMA = network meta-analysis; RCT = randomized controlled trial; SR = systematic review.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Change in BCVA
Details | Change in BCVA (logMAR) | ||||
|---|---|---|---|---|---|
Study | VISUAL I | VISUAL I (Japan) | VISUAL II | VISUAL II (Japan) | ADUR |
Non-infectious Uveitis Type | Active | Active | Inactive | Inactive | Active |
MD (95% CI)a | -0.07 (-0.11 to -0.02) | 0.04 (−0.22 to 0.31) | −0.04 (−0.08 to 0.01) | −0.08 (−0.20 to 0.04) | NR (NR) |
ADUR = Adalimumab in Uveitis Refractory to Conventional Therapy; BCVA = best-corrected visual acuity; CI = confidence interval; logMAR = logarithm of the minimum angle of resolution; MD = mean difference; NR = not reported.
aValues extracted from Table 2 of the source publication1
Table 7: Summary of Findings by Outcome — Time to Treatment Failure
Details | Time to Treatment Failure | ||||
|---|---|---|---|---|---|
Study | VISUAL I | VISUAL I (Japan) | VISUAL II | VISUAL II (Japan) | ADUR |
Non-infectious Uveitis Type | Active | Active | Inactive | Inactive | Active |
HR (95% CI)a | 0.50 (0.36 to 0.70) | 1.20 (0.41 to 3.54) | 0.57 (0.39 to 0.84) | 0.45 (0.20 to 1.03) | NR (NR) |
ADUR = Adalimumab in Uveitis Refractory to Conventional Therapy; CI = confidence interval; HR = hazard ratio; NR = not reported.
aValues extracted from Table 2 of the source publication1
Table 8: Summary of Findings by Outcome — Change in Anterior Chamber Cell Grade
Details | Change in Anterior Chamber Cell Grade | ||||
|---|---|---|---|---|---|
Study | VISUAL I | VISUAL I (Japan) | VISUAL II | VISUAL II (Japan) | ADUR |
Non-infectious Uveitis Type | Active | Active | Inactive | Inactive | Active |
MD (95% CI)a | −0.29 (−0.51 to −0.07) | 0.22 (−0.17 to 0.61) | −0.14 (−0.37 to 0.08) | −0.22 (−0.90 to 0.46) | −0.43 (−1.05 to 0.18) |
ADUR = Adalimumab in Uveitis Refractory to Conventional Therapy; CI = confidence interval; MD = mean difference.
aValues extracted from Table 2 of the source publication1
Table 9: Summary of Findings by Outcome — Change in Vitreous Haze Grade
Details | Change in Vitreous Haze Grade | ||||
|---|---|---|---|---|---|
Study | VISUAL I | VISUAL I (Japan) | VISUAL II | VISUAL II (Japan) | ADUR |
Non-infectious uveitis type | Active | Active | Inactive | Inactive | Active |
MD (95% CI)a | −0.27 (−0.43 to −0.11) | −0.41 (−1.15 to 0.34) | −0.13 (−0.28 to 0.01) | −0.45 (−0.98 to 0.07) | −0.54 (−1.22 to 0.14) |
SE (weight [%])b | 0.0816 (41.2) | 0.3801 (1.9) | 0.0735 (50.8) | 0.2674 (3.8) | 0.3477 (2.3) |
Pooled change in vitreous haze grade | |||||
Study | Pooled analysis of VISUAL I, VISUAL I (Japan), VISUAL II, VISUAL II (Japan), and ADUR trials | ||||
Non-infectious uveitis type | Mix of active (VISUAL I, VISUAL I [Japan], and ADUR) and inactive (VISUAL II and VISUAL II [Japan]) | ||||
Resultsb | MD = −0.21 (95% CI, −0.32 to −0.11) Heterogeneity: Chi2 = 3.70, df = 4 (P = 0.45), I2 = 0% Test for overall effect: Z = 4.10 (P < 0.0001) Range of mean differences (i.e., -0.54 to -0.13) were significantly different (P < 0.05) | ||||
ADUR = Adalimumab in Uveitis Refractory to Conventional Therapy trial; CI = confidence interval; df = degrees of freedom; MD = mean difference; SE = standard error.
aValues extracted from Table 2 of the source publication1
bValues extracted from the forest plot (Figure 6) in the source publication1
Table 10: Summary of Findings by Outcome — Safety
Details | VISUAL I | VISUAL I (Japan) | VISUAL II | VISUAL II (Japan) | ADUR | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Non-infectious uveitis type | Active | Active | Inactive | Inactive | Active | ||||||
n of intervention | ADA: 110 | Placebo: 107 | ADA: 8 | Placebo: 8 | ADA: 114 | Placebo: 111 | ADA: 16 | Placebo: 16 | ADA: 10 | Placebo: 15 | |
AEsa | |||||||||||
Number (rate [events/ patient-years]) | 657 (10.524) | 430 (9.717) | 28 (12.101) | 25 (7.962) | 831 (8.790) | 642 (9.050) | 48 (6.743) | 16 (7.344) | 54 (7.665) | 30 (5.475) | |
SAEsa | |||||||||||
Number (rate [events/ patient-years]) | 18 (0.288 ) | 6 (0.136) | 1 (0.431) | 0 (0) | 13 (0.138) | 10 (0.141) | 1 (0.140) | 1 (0.459) | 1 (0.142) | 0 (0) | |
ADA = adalimumab; AE = adverse event; SAE = serious adverse event.
aValues extracted from Table 3 of the source publication1
Table 11: Summary of Findings by Outcome — Economic Outcomes (Base-case Analysis)
Details | Base-case Analysis4 | |
|---|---|---|
Non-infectious Uveitis Type | Active | Inactive |
ICER | ||
Cost (pound sterling) per QALY gained | £92 600 and £94 262a | £318 075 |
Incremental QALYs | ||
QALY | 0.200 | 0.119 |
Incremental Costs | ||
Cost (pound sterling) | £18 541 | £37 784 |
Total QALYs | ||
Intervention, QALY | - | - |
LCP | 15.221 | 15.549 |
LCP + ADA | 15.421 | 15.668 |
Total Costs | ||
Intervention, cost (pound sterling) | - | - |
LCP | £49 036 | £50 230 |
LCP + ADA | £67 577 | £88 014 |
Probability of cost-effectiveness at WTP threshold (£20 000) | ||
Intervention, probability | - | - |
LCP | 1.00 | 1.00 |
LCP + ADA | 0.00 | 0.00 |
Probability of cost-effectiveness at WTP threshold (£30 000) | ||
Intervention, probability | - | - |
LCP | 1.00 | 1.00 |
LCP + ADA | 0.00 | 0.00 |
ADA = adalimumab; ICER = incremental cost-effectiveness ratio; LCP = limited current practice; NA = not applicable; NR = not reported; QALY = quality-adjusted life-year; vs. = versus; WTP = willingness to pay.
aICER calculated with a deterministic model.
Table 12: Summary of Findings by Outcome — Economic Outcomes (Sensitivity Analyses)a
Details | Sensitivity Analyses | |
|---|---|---|
Non-infectious Uveitis Type | Active | Inactive |
Context for Sensitivity Analysis: Data from the MUST trial | ||
ICER | Adalimumab vs. “current practice” in active non-infectious uveitis: £110 068 per QALY gained. | “The same sensitivity analyses were undertaken for inactive patients (except from the analysis based on the MUST trial, given that it only included active patients) and all analyses resulted in ICERs greater than £35 000 per QALY gained (p.1637).”4 |
Context for Sensitivity Analysis: Alternative parametric survival functions of time to treatment failure | ||
ICER | Adalimumab vs. LCP Weibull distribution £102 218 per QALY gained Gompertz distribution: £100 225 per QALY gained | “The same sensitivity analyses were undertaken for inactive patients (except from the analysis based on the MUST trial, given that it only included active patients) and all analyses resulted in ICERs greater than £35 000 per QALY gained (p.1637).”4 |
Context for Sensitivity Analysis: Assumption that following 2 years of successful treatment, some patients would no longer require adalimumab (remission health state) | ||
ICER | Adalimumab vs. LCP 0.1 annual remission rate: £66 176 per QALY gained 0.2 annual remission rate: £55 161 per QALY gained | “The same sensitivity analyses were undertaken for inactive patients (except from the analysis based on the MUST trial, given that it only included active patients) and all analyses resulted in ICERs greater than £35 000 per QALY gained (p.1637).”4 |
ICER = incremental cost-effectiveness ratio; LCP = limited current practice; MUST = Multicenter Uveitis Steroid Treatment; NA = not applicable; NR = not reported; QALY = quality-adjusted life-year; WTP = willingness to pay.
aThis table only reports the findings from sensitivity analyses deemed to be relevant and clear.
Table 13: Patient Involvement in Adalimumab for the Treatment of Adults With Non-Infectious Uveitis
Section and topic | Item | Reported on page |
|---|---|---|
Aim | The patient’s experiences of living with uveitis helped with developing the protocol and commenting on outcomes of importance to patients with uveitis. | 5 |
Methods | After giving informed consent, the patient discussed his experience via videoconference. | 5 |
Results of engagement | The researchers were made aware of the importance of several outcomes and themes. In particular, the importance of having access to an ophthalmologist and receiving care rapidly. Also, the need for health care providers to take a holistic view of patients, by considering their overall health status (including conditions that can cause uveitis), prescribed medications, frequency of flare ups, etc. When considering treatment options, patients look for something effective, safe, easy to administer, and readily available. | 13 to 14 |
Discussion and conclusions | Success of patient involvement in this report is related to several factors. The purpose and scope of the project, the purpose of engagement, and the nature of engagement activities were shared with the patient. In addition, the research team was interested in hearing the patient’s perspective first-hand, and a researcher took part in the discussion with the patient. Lastly, established processes for patient engagement were in place and compensation was offered for his involvement in the project. | 13 to 14 |
Reflections/critical perspective | The patient contributor spoke about his experiences openly and comfortably during the discussion. He shared insights around the need for a holistic approach to care and treatment. He also identified equity considerations in terms of patients needing timely access to specialized care to receive a diagnosis as well as timely access to treatment that is easy to administer and readily available. A limitation of our approach is that discussions with patients are done via teleconferencing. Patients need access to a phone or internet to collaborate with CADTH, which can exclude some voices. | 13 to 14 |
Appendix 5: References of Potential Interest
Review Articles
23.Hoy SM. Adalimumab: a review in non-infectious non-anterior uveitis. Biodrugs. 2017;31(2):135-142. PubMed
24.Knickelbein JE, Kim M, Argon E, Nussenblatt RB, Sen NH. Comparative efficacy of steroid-sparing therapies for non-infectious uveitis. Expert Rev Ophthalmol. 2017;12(4):313-319. PubMed
25.Ogbue OD, Malhotra P, Akku R, Jayaprakash TP, Khan S. Biologic therapies in sarcoidosis and uveitis: a review. Cureus. 2020;12(7):e9057. PubMed
26.Nicolela Susanna F, Pavesio C. A review of ocular adverse events of biological anti-TNF drugs. J Ophthalmic Inflamm Infect. 2020;10(1):11. PubMed
27.Rosenbaum JT, Bodaghi B, Couto C, et al. New observations and emerging ideas in diagnosis and management of non-infectious uveitis: a review. Semin Arthritis Rheum. 2019;49(3):438-445. PubMed
28.Trivedi A, Katelaris C. The use of biologic agents in the management of uveitis. Intern Med J. 2019;49(11):1352-1363. PubMed
Additional Reference – Clinical and Cost-effectiveness Review of Adalimumab Biosimilar (Amgevita) and Adalimumab (Humira)
29.Agency for Care Effectiveness. Adalimumab for treating inflammatory conditions. 2020; https://www.ace-hta.gov.sg/healthcare-professionals/ace-technology-guidances/details/adalimumab-for-treating-inflammatory-conditions. Accessed 2021 Nov 15.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca