CADTH Health Technology Review
Phosphodiesterase Type 5 Inhibitors for the Treatment of Secondary Raynaud Phenomenon and Digital Ulcers
Rapid Review with Expert Input
Authors: Kendra Brett, Tamara Rader, Sarah C. McGill
Reviewers
External Reviewers
This document was externally reviewed by content experts, and the following individuals granted permission to be cited.
Dr. Jacob Karsh, MDCM, FRCPC
Professor of Medicine
The Ottawa Hospital
Acknowledgements
The authors would like to thank Maureen Sauvé, Co-Chair of the Scleroderma Patient-centered Intervention Network (SPIN) Patient Advisory Board for contributing to the report by commenting on the clinical outcomes, and sharing perspectives from the patient community
Abbreviations
BHPR
British Health Professionals in Rheumatology
BSR
British Society for Rheumatology
CCB
calcium channel blocker
EULAR
European League Against Rheumatism
NMA
network meta-analysis
PDE5
phosphodiesterase type 5
RCT
randomized controlled trial
RP
Raynaud phenomenon
SPIN
Scleroderma Patient-centered Intervention Network
SR
systematic review
SSRI
selective serotonin reuptake inhibitors
Key Messages
As a first-line therapy for the treatment of secondary Raynaud phenomenon (RP), phosphodiesterase type 5 (PDE5) inhibitors are more effective than a placebo at reducing the frequency, severity, and the duration of RP attacks. PDE5 inhibitors were less effective than calcium channel blockers or selective serotonin reuptake inhibitors at reducing the severity of RP attacks. Patients treated with PDE5 inhibitors were more likely to experience an adverse event and to discontinue treatment compared with those treated with a placebo.
As a first-line therapy for the treatment of secondary digital ulcers, treatment with PDE5 inhibitors was less effective at preventing new digital ulcers than treatment with an endothelin receptor antagonist, but there was no difference in the time to healing or the size of the primary digital ulcer (findings based on 1 non-randomized study).
There is a lack of evidence on the clinical effectiveness of PDE5 inhibitors as second-line therapy (i.e., after failed treatment with calcium channel blockers) for treating secondary RP and/or digital ulcers.
There is a lack of evidence on the cost-effectiveness of PDE5 inhibitors for treating secondary RP and/or digital ulcers.
Two guidelines were identified that provide recommendations for treating RP secondary to systemic sclerosis. Two guidelines recommend calcium channel blockers as first-line therapy based on high-quality evidence; 1 guideline recommends angiotensin II receptor antagonists as first-line therapy, but this is based on weak evidence. The guidelines also include recommendations that PDE5 inhibitors, selective serotonin reuptake inhibitors, alpha blockers, and statin therapy be considered for treating RP secondary to systemic sclerosis. For severe cases of RP secondary to systemic sclerosis, IV iloprost is recommended.
Three guidelines were identified that provide recommendations for treating digital ulcers secondary to systemic sclerosis. Three guidelines recommend treatment with PDE5 inhibitors. The guidelines also recommend considering treatment with endothelin receptor antagonists, IV iloprost, and calcium channel blockers. For severe digital ulcers secondary to systemic sclerosis, treatment with IV iloprost or a PDE5 inhibitor is recommended.
A patient with lived experience with secondary RP and digital ulcers was involved in this report, and they identified outcomes that are important to patients with secondary RP and/or digital ulcers. These outcomes included pain, digit loss, fatigue, mental health, and function. None of the studies or guidelines in this report included direct measures of these patient-identified outcomes.
Context and Policy Issues
Raynaud phenomenon (RP) is a condition in which there is an exaggerated vasoconstrictive response to cold exposure or emotional stress which manifests as a rapid onset of cold digits (fingers or toes) and a sharp colour change in the digits (to white or blue) due to restricted blood flow to the digits.1 There are 2 forms of RP: primary and secondary. In primary RP, the exaggerated vasoconstriction is not associated with a specific disease or known cause, and it is often associated with less severe symptoms.1,2 Primary RP can often be managed with non-pharmacological measures, such as patient education and self-management (e.g., avoiding cold exposure, limiting emotional stress), and pharmacological therapy may be used for those who do not respond to non-pharmacological measures.2,3 Secondary RP refers to situations in which the RP occurs in association with an underlying disease.1,2 Diseases associated with secondary RP include, but are not limited to, systemic sclerosis (or scleroderma), systemic lupus erythematosus, and mixed connective tissue disease1,2; more than 95% of patients with systemic sclerosis experience secondary RP. Secondary RP is often associated with severe tissue ischemia resulting in pain and ulceration of the skin (e.g., digital ulcers).1,2 In critical cases, this can result in gangrene and the loss of digits,2 and usually requires pharmacological management. Due to the severity of symptoms associated with secondary RP (notably the associated digital ulcers) and the need for pharmacological therapy to prevent tissue injury, this report will focus on secondary RP and/or digital ulcers secondary to another medical condition.
The main objective for treatment of secondary RP and/or digital ulcers is to prevent tissue and/or digit loss and to improve quality of life.3 The first-line of pharmacotherapy in patients with secondary RP and/or digital ulcers are long-acting calcium channel blockers (CCBs), such as amlodipine or nifedipine.3 Other potential treatments for secondary RP include angiotensin II receptor blockers, selective serotonin reuptake inhibitors (SSRIs), phosphodiesterase type 5 (PDE5) inhibitors, IV prostaglandins (e.g., IV iloprost), and endothelin receptor antagonists (e.g., bosentan), but the choice of treatment may depend on the severity of the disease and potential contraindications for use.3,4
PDE5 inhibitors are vasodilators that are used to treat erectile disfunction and pulmonary arterial hypertension, and include sildenafil (brand name Viagra),5 tadalafil (brand name Cialis),6 and vardenafil (brand name Staxyn).7 In Canada, the use of PDE5 inhibitors for the treatment of secondary RP and/or digital ulcers is an off-label use5-7 and requires that physicians make a request through Health Canada’s Special Access Programme to authorize the use of these drugs.8 In patients experiencing severe acute ischemia, any delays in this authorization process have the potential for serious consequences (e.g., threat of digit loss). Establishing eligibility criteria for the use of PDE5 inhibitors in treating secondary RP and/or digital ulcers could help ensure that access to these drugs is consistent and timely.
The purpose of this report is to summarize the evidence regarding the clinical effectiveness and cost-effectiveness of PDE5 inhibitors for the treatment of secondary RP and/or digital ulcers secondary to another medical condition. Evidence-based guidelines with recommendations regarding pharmacological therapy for patients with secondary RP and/or digital ulcers secondary to another medical condition will also be reviewed.
Research Questions
What is the clinical effectiveness of phosphodiesterase type 5 (PDE5) inhibitors as first-line therapy in individuals with secondary Raynaud phenomenon (RP) and/or digital ulcers secondary to another medical condition?
What is the clinical effectiveness of PDE5 inhibitors as second-line therapy in individuals with secondary RP and/or digital ulcers secondary to another medical condition?
What is the cost-effectiveness of PDE5 inhibitors in patients with secondary RP and/or digital ulcers secondary to another medical condition?
What are the evidence-based guidelines regarding pharmacological therapy for patients with secondary RP and/or digital ulcers secondary to another medical condition?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase through Ovid, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were phosphodiesterase type 5 inhibitors and Raynaud phenomenon or digital ulcers. No filters were applied to limit the retrieval by study type. For question 4, a broader search was conducted with the search concepts of Raynaud phenomenon or digital ulcers, and CADTH-developed search filters were applied to limit retrieval to guidelines. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded from both searches. When possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2011, and May 4, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals with secondary RP and/or digital ulcers secondary to another medical condition |
Intervention | Q1: PDE5 inhibitors (i.e., sildenafil, tadalafil, and vardenafil) as first-line therapy used alone or in combination with CCBs Q2: PDE5 inhibitors as second-line therapy following treatment with CCBs (i.e., after failure of treatment with CCBs) used alone or in combination with CCBs Q3: PDE5 inhibitors as first- or second-line therapy used alone or in combination with CCBs Q4: Any pharmacotherapy (e.g., PDE5 inhibitors, CCBs, prostaglandins) |
Comparator | Q1 to Q3: Any alternative pharmacological therapy for the treatment of RP or digital ulcers (e.g., CCBs, prostaglandins, endothelin receptor antagonists, alternative PDE5 inhibitor) used alone or in combination with each other. Placebo No treatment Q4: Not applicable |
Outcomes | Q1 and Q2. Clinical benefits (e.g., degree of ischemia, degree of tissue loss, time to healing, ulcer or lesion healing, pain, health-related quality of life, function, RP or digital ulcer interference with activities of daily living, change in use of concurrent therapies) and harms (e.g., headaches, dizziness, gastrointestinal symptoms) Q3. Cost-effectiveness (e.g., cost per quality-adjusted life-years, incremental cost-effectiveness ratios, cost per patient adverse event avoided) Q4. Recommendations regarding best practices (e.g., which medications in which situations; contraindications for use) |
Study designs | Health technology assessment reports, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines. |
CCB = calcium channel blocker; PDE5 = phosphodiesterase type 5; Q = question; RP = Raynaud phenomenon.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2011. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded. Non-comparative (i.e., single-arm) before-after studies were excluded (listed in Appendix 5).
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)9 for SRs, the “Questionnaire to assess the relevance and credibility of a network meta-analysis”10 for network meta-analyses (NMAs), the Downs and Black checklist11 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument12 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Patient Engagement
CADTH has adopted the CADTH Framework for Patient Engagement in Health Technology Assessment,13 which includes standards for patient involvement in individual health technology assessments and is used to support and guide CADTH activities involving patients. For this report, CADTH engaged a patient contributor with lived experience of RP and digital ulcers secondary to scleroderma.
Invitation to Participate and Consent
CADTH reached out to the Patient Advisory Board of the Scleroderma Patient-centred Intervention Network (SPIN). SPIN is an organization of researchers, health care providers, and people living with scleroderma from around the world. A CADTH Patient Engagement Officer contacted the group by email to explore their interest in becoming involved. The preliminary request included the purpose and scope of this project, the purpose of engagement, and the nature of engagement activities. The Patient Engagement Officer obtained the person’s informed consent to share their lived experiences with RP and/or digital ulcers secondary to scleroderma with CADTH staff.
Engagement Activities
A member of the Patient Advisory Board of SPIN shared her personal experiences during drafting of the report. She was able to provide community perspectives from her past experience supporting and involving other scleroderma patients. Patient perspectives gained through engagement processes were used to ensure relevance of outcomes of interest for the clinical assessment and to provide insights, background, and context to inform the discussion section.
Patient involvement was guided by the Guidance for Reporting Involvement of Patients and the Public (version 2) Short Form reporting checklist14 (Appendix 4, Table 8).
Summary of Evidence
Quantity of Research Available
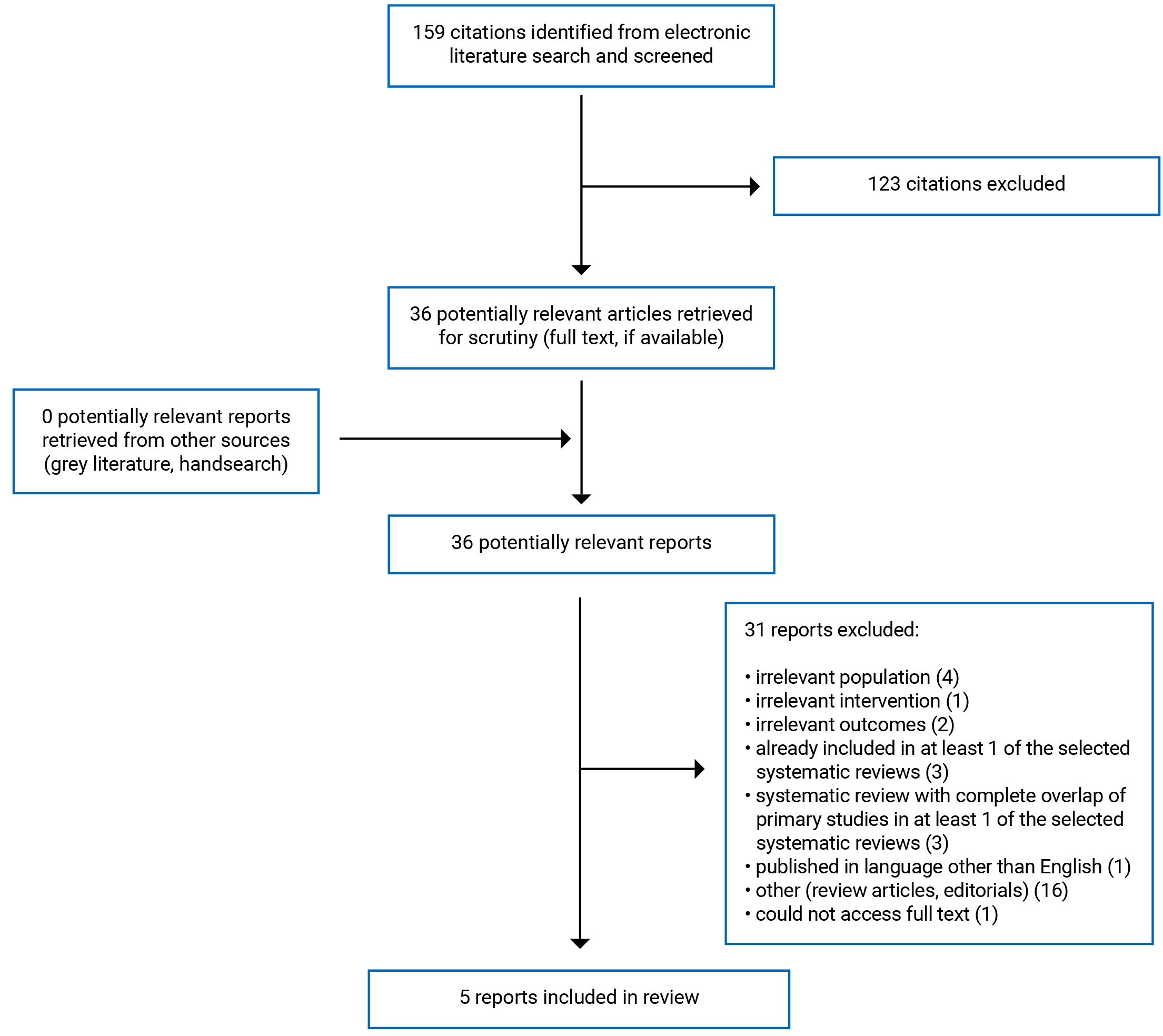
A total of 159 citations were identified in the literature search. Following screening of titles and abstracts, 123 citations were excluded and 36 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 31 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. These comprised 1 SR, 1 non-randomized study, and 3 evidence-based guidelines. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)15 flow chart of study selection is presented in Appendix 1.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One SR with an NMA,16 1 cohort study,17 and 3 evidence-based guidelines18-20 were identified and included in this report. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
One SR16 with an NMA was published in 2019. This SR16 searched the literature from the journal’s inception to January 31, 2017, and double-blind randomized controlled trials (RCTs) were eligible for inclusion. A total of 58 RCTs were identified in the SR and included in the NMA, of which 12 trials (from 11 RCTs) included PDE5 inhibitors and were directly relevant to this report. The NMA used a Bayesian approach using Markov chain Monte Carlo simulation with non-informative prior distribution to fit a normal likelihood model for continuous outcomes and a Poisson model with a logarithmic link function for safety outcomes. Due to observed heterogeneity across RCTs in the network, results were produced from random-effects models for each outcome. In addition to the NMA, this study included direct pairwise meta-analysis comparisons between all of the interventions and placebo and between interventions if relevant RCTs were available.16
One prospective, observational cohort study by Chang et al.17 was published in 2021. This non-randomized study was conducted at 13 medical centres between 2015 and 2017, and patients were followed for 24 weeks.
Three relevant guidelines18-20 were identified. One guideline19 was developed by the Japanese Dermatological Society and was published in 2020. This guideline searched the literature for evidence and included all types of evidence from the literature as well as expert opinion.19 The methods used to develop the recommendations were not reported, but the quality of the evidence was graded from I (highest) to VI (lowest), and the recommendations were rated as either 1 (strong recommendation) or 2 (weak recommendation) and from A (strong evidence) to D (weak evidence).19
One guideline from 2017 was developed by the European League Against Rheumatism (EULAR)20 and used a systematic approach to search for and select evidence for inclusion; there were no restrictions on the type of evidence included. Recommendations were developed from evidence summaries, and recommendations were discussed and refined by the development group until a consensus was reached. The quality of the evidence informing the recommendations was assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) system; evidence grades ranged from 1A (highest) to 4 (lowest).20 The strength of the recommendation ranged from A (highest) to D (lowest).20
One guideline published in 2016 was a joint publication by the British Society for Rheumatology (BSR) and the British Health Professionals in Rheumatology (BHPR).18 The BSR and BHPR guideline18 was based on a literature search to identify available evidence, and discussions of this evidence were used to develop the recommendations. The recommendations were voted on by the guideline development group; if there was agreement of 75% or higher, it was considered a consensus. The level of evidence and strength of the recommendations were graded, but the full details of the grading systems were not reported; the level of the evidence ranged from I (highest) to IV (lowest), and the recommendations were graded from A (highest) to D (lowest).18
Country of Origin
The SR with NMA16 was led by authors in France. The observational cohort study was led by authors and conducted in South Korea.17 The guideline from the Japanese Dermatological Association19 is meant to apply to Japan, the EULAR guideline20 is meant to apply to Europe, and the BSR and BHPR guideline18 is meant to apply to the UK.
Patient Population
The SR with NMA16 included RCTs with people who had secondary RP; if an RCT included people with primary and secondary RP, it was included if at least 50% of the people had secondary RP. The overall study population included in the NMA comprised 3,867 individuals of whom 91.5% had secondary RP. There were 556 individuals in the RCTs that included PDE5 inhibitors, of whom 96% had secondary RP. The conditions to which the RP was secondary were not reported in this SR with an NMA.16
The observational cohort study17 included individuals with systemic sclerosis and at least 1 active digital ulcer. There were 63 participants included in this study (60 relevant to this report); the average age was 50 years, the population was 78% female, 100% of the participants had RP, and close to half the patients in both groups had more than 1 digital ulcer.17
The target population of the Japanese Dermatological Association guideline19 is people with skin ulcers associated with connective tissue diseases; the population relevant to this report is people with skin ulcers secondary to systemic sclerosis (skin ulcers was defined in the guideline as “digital ulcers”). The target population of the EULAR guideline20 and the BSR and BHPR guideline18 is people with systemic sclerosis, and the populations relevant to this report include RP secondary to systemic sclerosis and digital ulcers secondary to systemic sclerosis. The intended users of all 3 guidelines18-20 are medical professionals; the Japanese Dermatological Association guideline19 also specifies patients as intended users of that guideline.
Interventions and Comparators
The SR with NMA16 included any pharmacological therapies for RP that were compared with any alternative pharmacological therapy for RP or a placebo. Interventions were grouped by drug class (e.g., PDE5 inhibitors, CCBs, endothelin receptor antagonists). Twelve trials included a PDE5 inhibitor (i.e., sildenafil [n = 5], tadalafil [n = 4], vardenafil [n = 1], udenafil [n = 1], and PF-00489791 [unnamed PDE5 inhibitor; n = 1]); 1 trial compared a PDE5 inhibitor (i.e., udenafil 100 mg/day; not approved for use in Canada) to a CCB (10 mg/day) and the rest compared the PDE5 inhibitor with a placebo. The dosage for the PDE5 inhibitors ranged across and within types of PDE5 inhibitors (i.e., tadalafil 10 mg/day to 40 mg/day; sildenafil 100 mg/day to 200 mg/day; vardenafil 20 mg/day; PF-00489791 4 mg/day; udenafil 100 mg/day).
In the observational cohort study by Chang et al. (2021),17 the choice of medication was determined by the physicians treating the patients (based on drugs available in Korea at the time). Of the 11 patients treated with PDE5 inhibitors, 9 received sildenafil, 1 received tadalafil, and 1 received udenafil (not approved for use in Canada).17 The relevant comparator in the observational cohort was bosentan, an endothelin receptor antagonist, which was used to treat 49 patients. The dose and duration of each treatment was not reported, although it was indicated that they followed standard recommendations.17 Nearly one-third of the patients in each group were also receiving a CCB.
Neither the SR with NMA nor the observational study16,17 reported whether the PDE5 inhibitors were first-line therapy or second-line therapy (i.e., after failure of treatment with CCBs); therefore, for the purpose of this report, all included evidence on PDE5 inhibitors was assumed to be first-line therapy.
The interventions considered by the Japanese Dermatological Association guideline19 were all therapies for skin ulcers associated with connective tissue disease. The EULAR guideline20 considered pharmacological therapies such as CCBs, prostanoids, endothelin receptor antagonists, and PDE5 inhibitors. The BSR and BHPR guideline18 considered all therapies in the management of systemic sclerosis.
Outcomes
The SR with NMA16 reported on 5 outcomes, and included the frequency of daily RP attacks; mean duration of each RP attack (in minutes); mean severity of RP attacks assessed using Raynaud’s Condition Score (i.e., level of difficulty experienced due to RP each day) or any other scale reported in the RCTs and converted to a 10-point scale to assess the standard mean difference; tolerability (i.e., proportion of patients with severe adverse event or who dropped out due to adverse events); and acceptability (i.e., all-cause discontinuation of the drug).
Most of the outcomes in the observation study were focused on digital ulcer healing, such as time to healing of the primary digital ulcer, change in the number of digital ulcers, and the size of the primary ulcer.17 The primary ulcer was selected by the treating physician, and was defined as the most painful, the largest, or the deepest digital ulcer. Once an ulcer was completely covered in skin it was considered healed.17 Adverse events were also reported in the observational study.17
None of the guidelines18-20 reported the outcomes that were considered in the supporting literature reviews.
Summary of Critical Appraisal
The critical appraisal of the included studies is summarized in this section, and additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Systematic Reviews
The SR with NMA16 had well-described eligibility criteria for the review and the protocol was published a priori, thus reducing the risk of reporting bias. A comprehensive search strategy was used (e.g., searched multiple databases, trial registries, no language restrictions), reducing the likelihood that relevant literature was missed. Only double-blind RCTs were eligible for inclusion in this SR, but the authors did not provide a justification for excluding RCTs that were not double blind, nor did they include a full list of excluded studies. The study selection diagram showed that 6 RCTs were excluded for not being double blind; it is unclear whether these missing RCTs may have affected the findings of this SR. An adequate tool was used to assess the risk of bias, and the authors did consider the quality of the evidence when discussing the findings. A brief description of the included studies was provided (e.g., sample size, country, study design, length of follow-up); however, some details were lacking, such as a complete description of the population (e.g., RP was secondary to which conditions) or the full details of the treatment regimens (e.g., length or frequency of treatment), thus limiting the ability to assess the heterogeneity of the studies. The source of funding for the RCTs included in this SR were not reported, but the authors did assess whether the studies were supported by pharmaceutical companies as part of the risk of bias assessment. This SR with NMA received no funding; however, some authors declared conflicts of interest, including funding from pharmaceutical companies. It was not reported how these potential conflicts were managed, and it is unclear whether the reporting of the findings is biased due to these potential conflicts.
The NMA conducted as part of the SR16 used an appropriate statistical model; a Bayesian approach using Markov chain Monte Carlo simulations with non-informative prior distributions was used, and the authors reported 95% credible intervals with the effect estimates. Efficacy outcomes were modelled using a normal likelihood, and safety outcomes were modelled using a Poisson likelihood with a logarithmic link function. The authors reported both the direct pairwise meta-analysis comparisons and the indirect comparisons from the NMA, and consistency was demonstrated across comparisons. To account for variation in patient characteristics and study design of the primary studies, the authors used random-effects models and reported on the between-study variance and statistical heterogeneity for each outcome. Baseline summary characteristics were reported by drug class, but due to limited information reported on the individual primary studies in the SR, the ability to assess the possible impact of the heterogeneity across the primary studies on the results of the NMA is limited. To account for heterogeneity across the studies in the NMA, the authors conducted pre-planned sensitivity analyses and meta-regressions. Three sensitivity analyses were conducted to assess the possible influence of studies with high risk of bias, studies that included both primary and secondary RP, and the method of measuring the severity of RP attacks on the effectiveness outcomes; no substantial changes to the findings were observed in these sensitivity analyses for the PDE5 inhibitors versus placebo comparison. Meta-regression was conducted to assess the potential influence of predefined variables of interest, which identified that 1 of the variables (i.e., older age) was correlated with the outcome severity. The authors conducted further Bayesian NMA that adjusted for this potential effect modifier, and some of the results of this adjusted NMA differed from the results of the primary NMA, which suggests some uncertainty in the findings. However, because age was not reported for the primary studies (and only summarized by drug class), the degree to which older age may directly influence the findings of the PDE5 inhibitor studies is unclear.
Non-Randomized Studies
The prospective observational cohort study by Chang et al. (2021)17 was generally well-reported. The objective, the main outcomes, and the eligibility criteria were well-described, simple outcome data were provided for the primary outcome (i.e., time to healing), and the distribution of potential confounders was reported for each group and in the overall study population. In this observational study, the choice of pharmacological intervention to treat the digital ulcers was at the discretion of the treating physician (based on drugs available in Korea at the time of the study), which increases the risk of selection bias in terms of which patients were enrolled in the study as well as which patients received each treatment. The majority (78%) of the patients in this study received an endothelin receptor antagonist (i.e., bosentan) and 17% of patients received a PDE5 inhibitor, which suggests that selection of the intervention may have been biased. The dose and duration of the different treatments were not reported, but the authors reported that standard recommendations were followed for each drug. The original target sample size was 200 participants, but enrolment was stopped at 71 participants due to slow recruitment. It is unclear whether a statistical power calculation was done, thus it is unclear whether the study is adequately powered to detect significant differences in the outcomes. There were 9 participants excluded from the analysis, but no details were reported about these participants (including which intervention they received), and it is unclear whether the findings would have been affected by the patients that were lost to follow-up. It was not reported whether the participants were blinded to the intervention, but it is unlikely that the patients knowing the intervention would have influenced the outcomes (e.g., time to healing). It was not reported whether the individuals assessing the outcomes were blinded to the intervention, which increases the potential for measurement bias due to the awareness of the intervention. Some of the outcome measures were accurate (i.e., time to primary ulcer healing, number of new ulcers); however, 1 outcome (size of the primary ulcer) may not provide clinically meaningful results, and an alternative measure, such as “change in size of the primary ulcer” may have provided more valuable information. One author disclosed receiving funding from pharmaceutical companies, but it was not reported how this potential conflict was managed with regards to conducting the study or reporting the results. The source of funding was reported, and the authors declared that the funder did not influence the design, data collection, analysis, or publication of the study.17
Guidelines
All 3 guidelines18-20 included a clear description of the scope of the guideline, the population to whom the guideline was meant to apply, and the target users of the guideline. Two guidelines19,20 described the specific health questions covered by the guideline, but the research questions that were used to develop the recommendations for the BSR and BHPR guideline18 were not reported. The guideline development group for the EULAR guideline20 included individuals from all relevant professional groups, including 2 patient partners, although it was not reported how the patients were involved with the development of the recommendations. The Japanese Dermatological Association guideline19 described the area of expertise of the members of the guideline development group, and the names and institutions of the guideline authors were reported in the BSR and BHPR guideline18, although it was unclear whether both guidelines included all relevant professional groups; and neither reported including the views of the target population.
The EULAR guideline20 used systematic methods to search for and select evidence, and the process for formulating the recommendations was clear with an explicit link between the evidence and the recommendations. For the other 2 guidelines, it is unclear whether systematic methods were used because they did not report the full details of their searches nor did they report the eligibility criteria for the evidence,18,19 thus it is unknown if all relevant information was considered when developing the guidelines. The Japanese Dermatological Association guideline19 did not include the methods used to formulate the recommendations, thus it is unclear how the evidence was translated into recommendations and whether consensus was reached among the members of the guideline development group. Within each of the guidelines, the level of evidence and the strength of the recommendations were reported, and 2 of the guidelines19,20 included summaries of the evidence that supported the recommendations, but there was not a summary of the supporting evidence in the BSR and BHPR guideline.18. However, none of the guidelines included evidence tables with detailed descriptions of the strengths and limitations of the body of evidence, thus it is not possible to determine whether the health benefits, side effects, and risks were considered when formulating the recommendations. It was not reported in the EULAR guideline20 or the BSR and BHPR guideline18 whether the guideline was externally reviewed. The Japanese Dermatological Association guideline19 was reviewed by other members of the Japanese Dermatological Association but it was unclear whether other external experts also reviewed the guideline. The lack of external review of the guidelines should be considered when assessing the certainty of the recommendations. The recommendations are easy to identify in 2 guidelines18,20 but more difficult to identify in the Japanese Dermatological Association guideline.19 In all 3 guidelines, the recommendations would benefit from additional details (e.g., recommended dosage, timing of treatment). No funding from public, commercial, or not-for-profit agencies was received for the development of 1 guideline18 It is unclear whether the views of the funding body could have influenced 2 guidelines19,20; conflicts of interest, including funding from pharmaceutical companies, were declared by members of the guideline development group in 2 guidelines18,20 but it was not reported how these potential conflicts were managed.
Summary of Findings
Relevant findings are summarized in this section, and a detailed summary of findings and authors conclusions are presented in Appendix 4.
Clinical Effectiveness of PDE5 Inhibitors as First-Line Therapy
One SR with NMA16 and 1 observational cohort17 were identified regarding the clinical effectiveness of PDE5 inhibitors as first-line therapy in individuals with secondary RP and/or digital ulcers secondary to another medical condition.
Frequency of RP Attacks
In patients with secondary RP, indirect comparisons in the SR with NMA16 found that PDE5 inhibitors were favoured compared with placebo and soluble guanylate cyclase stimulators in reducing the frequency of daily RP attacks, and that no therapy was favoured when comparing PDE5 inhibitors with any other drug classes included in the NMA (e.g., CCBs, IV prostacyclin analogues). A direct pairwise comparison in this SR found that PDE5 inhibitors significantly reduced the frequency of daily RP attacks compared to the placebo, which was consistent with the finding from the NMA.16
Severity of RP Attacks
For patients with secondary RP, indirect comparisons in the SR with NMA16 found that PDE5 inhibitors were favoured compared with placebo and soluble guanylate cyclase stimulators in reducing the severity of RP attacks, and that CCBs and SSRIs were favoured over PDE5 inhibitors in reducing the severity of RP attacks. Indirect comparisons did not favour any therapy for the severity of RP attack when comparing PDE5 inhibitors with any other drug class (e.g., endothelin receptor antagonists, IV prostacyclin analogues) included in the NMA. A direct pairwise comparison of PDE5 inhibitors versus placebo in the SR16 on the severity of RP attacks was consistent with the finding in the NMA in terms of magnitude and direction of the effect.
Duration of RP Attacks
Indirect comparisons from the SR with NMA16 found that PDE5 inhibitors were favoured compared with placebo in reducing the duration of each RP attack for patients with secondary RP, and that no therapy was favoured when comparing PDE5 inhibitors to the other drug classes included in the NMA (e.g., CCBs, IV prostacyclin analogues). Direct pairwise comparisons in this SR found that PDE5 inhibitors significantly reduced the duration of RP attacks compared with a placebo, and that the duration of RP attacks was comparable between PDE5 inhibitors and CCBs, which was consistent with the findings from the NMA.16
Healing of Primary Digital Ulcer
For patients with digital ulcers secondary to systemic sclerosis, findings from 1 observational cohort study found no difference in the time to healing of the primary digital ulcer between those treated with PDE5 inhibitors and those treated with bosentan (an endothelin receptor antagonist).17 This study also found no difference in the absolute size of the primary ulcer at 24 weeks between those treated with PDE5 inhibitors and those treated with bosentan.17
Occurrence of New Digital Ulcers
The findings from 1 observational cohort study found that the occurrence of new digital ulcers was statistically significantly lower in patients with digital ulcers secondary to systemic sclerosis treated with bosentan (an endothelin receptor antagonist) compared with those treated with PDE5 inhibitors.
Acceptability
For patients with secondary RP, indirect comparisons in the SR with NMA16 found that PDE5 inhibitors were less favoured compared with placebo, IV prostacyclin analogues, antioxidants, and topical nitric oxide in terms of acceptability (i.e., all-cause discontinuation of the drug), and that no therapy was favoured when comparing PDE5 inhibitors with the other drug classes included in the NMA (e.g., CCBs, endothelin receptor antagonists). Direct pairwise comparisons in this SR found that PDE5 inhibitors had statistically significantly lower acceptability compared with the placebo, and that the acceptability was comparable between PDE5 inhibitors and CCBs; these findings are consistent with the findings from the NMA.16
Tolerability
Indirect comparisons in the SR with NMA16 found that PDE5 inhibitors were less favoured compared with placebo in terms of tolerability (i.e., proportion of patients with a severe adverse event or who dropped out due to adverse events) in patients with secondary RP, and that no therapy was favoured when comparing PDE5 inhibitors to the other drug classes included in the NMA (e.g., CCBs, endothelin receptor antagonists). Consistent findings were observed in direct pairwise comparisons in the SR; PDE5 inhibitors had statistically significantly lower tolerability compared with the placebo, and that tolerability was similar between PDE5 inhibitors and CCBs.16
Adverse Events
For patients with digital ulcers secondary to systemic sclerosis, findings from 1 observational cohort study reported a similar proportion of patients who experienced an adverse event in those treated with PDE5 inhibitors (27.3%) and bosentan (an endothelin receptor antagonist; 36.7%), but no statistical test was reported.17 Patients treated with bosentan experienced liver function abnormalities (8%), headache (6%), fatigue (2%), facial flushing (12%), edema (10%), and anemia (4%). Patients treated with PDE5 inhibitors experienced restrictive heart failure (9%), facial flushing (9%), edema (9%), and palpitations (9%). The authors of this study did not report the severity of these adverse events but indicated that all adverse events were “temporary and reversible.”17
Clinical Effectiveness of PDE5 Inhibitors as Second-Line Therapy
No relevant evidence regarding the clinical effectiveness of PDE5 inhibitors as second-line therapy (i.e., after failure of treatment with CCBs) for the treatment secondary RP and/or digital ulcers secondary to another medical condition was identified, therefore no summary can be provided.
Cost-Effectiveness of PDE5 Inhibitors
No relevant evidence regarding the cost-effectiveness of PDE5 inhibitors for secondary RP or digital ulcers was identified, therefore no summary can be provided.
Guidelines
Three evidence-based guidelines18-20 included recommendations regarding pharmacological therapy for patients with secondary RP and/or digital ulcers secondary to another medical condition.
RP Secondary to Systematic Sclerosis
CCBs
Due to the increased effectiveness of CCBs when compared with placebo and the good safety profile for CCBs, the EULAR guideline20 recommends that CCBs (e.g., oral nifedipine) should be considered as first-line therapy for RP secondary to systemic sclerosis; this is a strong recommendation based on high-quality evidence. The BSR and BHPR guideline18 also recommends CCBs as a first-line treatment of RP secondary to systemic sclerosis; this is a strong recommendation that was reported to be based on high-quality evidence; however, no supporting evidence was reported in the guideline.
Angiotensin II Receptor Antagonists
Another BSR and BHPR guideline18 recommendation is that angiotensin II receptor antagonists be a first-line treatment of RP secondary to systemic sclerosis. This is a weak recommendation that was reported to be based on moderate-quality evidence; however, no supporting evidence was reported in the guideline.
Intravenous Iloprost
For severe cases of RP secondary to systemic sclerosis, the EULAR guideline20 recommends that treatment with IV iloprost should be considered; this is a strong recommendation based on high-quality evidence. The BSR and BHPR guideline18 also recommends that IV iloprost be considered in cases of severe or refractory RP secondary to systemic sclerosis; this is a moderate-strength recommendation based on high-quality evidence. For non-severe secondary RP, the EULAR guideline20 recommends that IV iloprost, due to its cost and feasibility, be considered for treatment when oral therapies (e.g., CCBs, PDE5 inhibitors) have failed; this suggestion was based on expert opinion (i.e., no supporting evidence).
PDE5 Inhibitors
For patients with RP secondary to systemic sclerosis who do not respond to treatment with CCBs, the EULAR guideline20 recommends that PDE5 inhibitors be considered as treatment; this is a strong recommendation from high-quality evidence. As part of their list of treatment recommendations for RP secondary to systemic sclerosis, the BSR and BHPR guideline18 reported that PDE5 inhibitors are being used more frequently for systemic sclerosis–related RP, but recommendations were not made for or against their use. The strength of statement was weak, and it was reported to be based on weak evidence; however, no supporting evidence was reported in the guideline.18
Other Treatments
The EULAR guideline20 includes a weak recommendation from low-quality evidence that SSRIs might be considered for the treatment of RP attacks secondary to systemic sclerosis. The BSR and BHPR guideline18 also includes a weak recommendation that was reported to be based on evidence of very low quality for other treatments that may be considered for RP secondary to systemic sclerosis include SSRIs, alpha blockers, and statin therapy; however, no supporting evidence was reported in the guideline.
Digital Ulcers Secondary to Systemic Sclerosis
PDE5 Inhibitors
The Japanese Dermatological Association guideline19 suggests that PDE5 inhibitors could be a treatment option for skin ulcers secondary to systemic sclerosis; this is a weak recommendation, and the level of evidence varies by PDE5 inhibitor (i.e., weak evidence for sildenafil, very weak evidence for tadalafil and vardenafil). The EULAR guideline20 also recommends that PDE5 inhibitors be considered in the treatment of digital ulcers secondary to systemic sclerosis; this was a strong recommendation based on high-quality evidence. In patients with digital ulcers secondary to systemic sclerosis, the BSR and BHPR guideline18 recommends that sildenafil (a PDE5 inhibitor) be used before considering an IV prostanoid or an endothelin receptor antagonist. This is a strong recommendation that was reported to be based on high-quality evidence; however, no supporting evidence was reported in the guideline. In patients with systemic sclerosis and refractory or recurrent digital ulcers, the BSR and BHPR guideline18 also includes a moderate-strength recommendation to consider treatment with a PDE5 inhibitor in conjunction with an endothelin receptor antagonist that was reported to be based on moderate-quality evidence; however, the guideline did not report supporting evidence.
Intravenous Iloprost
The EULAR guideline20 recommends that IV iloprost (a prostanoid) be considered in the treatment of digital ulcers secondary to systemic sclerosis; this is a strong recommendation from high-quality evidence. For patients with severe active digital ulcers secondary to systemic sclerosis, the BSR and BHPR guideline18 recommends treatment with an IV prostanoid. This was a moderate-strength recommendation reported to be based on moderate-quality evidence; however, no supporting evidence was cited in the guideline. This guideline also recommends considering IV prostanoid with a concomitant endothelin receptor antagonist for the treatment of patients with systemic sclerosis and refractory or recurrent digital ulcers; this was a moderate-strength recommendation based on moderate-quality evidence.
Endothelin Receptor Antagonist
The EULAR guideline20 recommends that bosentan (an endothelin receptor antagonist) be considered for patients with digital ulcers secondary to systemic sclerosis (despite use of CCBs, PDE5 inhibitors, or iloprost therapy), especially those with multiple digital ulcers; this is a strong recommendation from high-quality evidence.
CCBs
The Japanese Dermatological Association guideline19 reported that they did not identify any evidence evaluating the effectiveness of CCBs for treating digital ulcers secondary to systemic sclerosis. However, given the effectiveness in treating RP secondary to systemic sclerosis, it was proposed that CCBs may be a treatment option for skin ulcers secondary to systemic sclerosis; this is a weak recommendation based on very weak evidence.
Limitations
The evidence in this report is associated with several limitations, including several evidence gaps. First, this report did not identify any evidence regarding the clinical effectiveness of PDE5 inhibitors as second-line therapy or any evidence regarding the cost-effectiveness of PDE5 inhibitors in individuals with secondary RP and/or digital ulcers secondary to another medical condition. Therefore, no conclusions can be formed on these research questions.
Second, this report is limited in terms of the population. Limited clinical evidence specific to people with secondary digital ulcers was identified and included in this report, with findings contributed by 1 observational cohort study of 60 people with secondary digital ulcers.17 The SR with NMA16 included studies with patients with secondary RP but did not report whether the patients also experienced digital ulcers. However, the 3 guidelines included in this report18-20 do include treatment recommendations for patients with digital ulcers secondary to systemic sclerosis. Furthermore, the primary condition of the populations of interest in the cohort study17 and the guidelines18-20 was systemic sclerosis (i.e., RP or digital ulcers secondary to systemic sclerosis), whereas the SR with NMA16 did not report the primary condition for the populations in the included RCTs (i.e., whether RP is secondary to systemic sclerosis or to other conditions). Therefore, it is unknown whether the findings in this report are generalizable to other primary conditions (e.g., RP or digital ulcers secondary to systemic lupus), and clinical judgment is required if this evidence will be applied to individuals with medical conditions not covered in this report.
Third, the evidence in the report is limited in terms of which outcomes were reported. The outcomes in the SR with NMA16 focused on RP attacks, and the outcomes in the observational study17 focused on digital ulcer healing. After speaking with an individual with lived experience with digital ulcers secondary to scleroderma, the outcomes that were identified as important to patients included pain, digit loss, fatigue, function, mental health, interference with activities of daily living, the use of pain medication, and the cost of treatment (e.g., medications, bandages). Neither study16,17 nor any of the guidelines18-20 included in this report considered direct measures of these patient-identified outcomes, and it is unknown whether PDE5 inhibitors influence these key outcomes. The SR with NMA16 measured severity of the RP attacks, which could be assessed using the Raynaud’s Condition Score (which assesses the level of difficulty experienced due to RP) or other measures of severity (e.g., visual analogue scales), but the precise definition for this outcome was not provided and it is unclear whether it is a valid measure of the impact of RP on function.
Fourth, the evidence in this report was limited in terms of which PDE5 inhibitors and which comparators were investigated. Of the studies included in this report, 2 studies compared PDE5 inhibitors to an active treatment comparator; in the cohort study, bosentan (an endothelin receptor antagonist) was used,17 and in 1 of the RCTs within the SR and NMA the comparator was CCBs.16 The other studies included in this report compared PDE5 inhibitors to a placebo. There are 3 PDE5 inhibitors approved for use in Canada (i.e., sildenafil,5 tadalafil,6 and vardenafil7), and in both the SR with NMA16 and the observational study,17 some of the patients were treated with udenafil, which is not approved in Canada. In addition, in the observational study,17 no patients were treated with vardenafil, thus no evidence on that specific PDE5 inhibitor for people with secondary digital ulcers is included in this report.
Fifth, this report is limited by the heterogeneity of the evidence. In the SR with NMA,16 eligible RCTs could include people with primary RP if at least 50% of the population had secondary RP. Although 96% of the population from the studies with PDE5 inhibitors had secondary RP, the proportion of patients with secondary RP in the overall NMA ranged across drug classes from 51% to 100%. Thus, the indirect comparisons generated from the NMA include evidence from studies with a high proportion of patients with primary RP (i.e., up to 49%), which may not be applicable to this report. There was also some heterogeneity in the interventions used in the studies in this report. Eligible interventions for this report included PDE5 inhibitors alone or in combination with CCBs; in the observational cohort,17 close to one-third of participants were also taking CCB with their PDE5 inhibitor, but the data were not reported separately. In the SR with NMA,16 eligible RCTs included PDE5 inhibitors given alone or as an add-on therapy, but the concurrent treatments were not reported in the SR nor were the findings reported separately. Thus, the findings in this report combine results from PDE5 inhibitors given alone or in combination with another therapy. The SR with NMA16 was also associated with heterogeneity in the patient population, intervention, and length of follow-up, and some of this heterogeneity may explain the observed uncertainty with some of the findings of the NMA. For instance, the evidence in the SR with NMA was grouped by drug class, thus the evidence for PDE5 inhibitors combined 5 different PDE5 inhibitors, including 2 that are not approved in Canada, and it is unknown whether effectiveness varies by PDE5 inhibitor. In addition, in the NMA model adjusted for older age, the PDE5 inhibitors were no longer favoured compared with the placebo for RP attack severity. However, insufficient information was reported to fully assess the influence of age on the results of the NMA.
Finally, none of the studies on PDE5 inhibitors were conducted in Canada, some of the studies included PDE5 inhibitors that are not approved in Canada (i.e., udenafil), and none of the guidelines are meant to apply to Canada. Thus, it is unclear if the findings of this report are generalizable to Canadian clinical practice because there may be differences between countries in the availability of PDE5 inhibitors or other treatments for secondary RP and digital ulcers. For instance, although sildenafil, tadalafil, and vardenafil are available in Canada, access to these drugs for the treatment of secondary RP and/or digital ulcers currently requires a request through the Health Canada Special Access Programme.8
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 SR with NMA16 and 1 observational cohort17 with clinical evidence regarding the use of PDE5 inhibitors as first-line therapy in individuals with secondary RP and/or digital ulcers, and 3 evidence-based guidelines18-20 with recommendations regarding pharmacological therapies for secondary RP and/or digital ulcers secondary to another medical condition. No relevant evidence was identified regarding the clinical effectiveness of PDE5 inhibitors as second-line therapy or the cost-effectiveness of PDE5 inhibitors in individuals with secondary RP and/or digital ulcers secondary to another medical condition.
Regarding the clinical effectiveness of PDE5 inhibitors for the treatment of secondary RP, the findings in this report are based on 1 SR with NMA that includes 58 RCTs, of which 12 trials include direct comparisons to PDE5 inhibitors.16 The findings from the NMA suggest that PDE5 inhibitors are more effective than placebo at reducing the frequency of daily RP attacks, the severity of RP attacks, and the duration of each RP attack.16 When compared with other classes of drugs in the NMA, PDE5 inhibitors were more effective at reducing the frequency of daily RP attacks and the severity of RP attacks compared with soluble guanylate cyclase stimulators, and less effective at reducing the severity of RP attacks compared with CCBs or SSRIs.16 In the NMA, PDE5 inhibitors were also found to be less tolerable compared with placebo, and less favoured in terms of acceptability when compared with placebo, IV prostacyclin analogues, antioxidants, or topical nitric oxide.16 However, many of the credible intervals for the effect estimates in this NMA were wide, which suggests that there is limited information for these comparisons and the findings should be interpreted with caution. None of the other comparisons in the NMA between PDE5 inhibitors and the other drug classes favoured a particular therapy in terms of the frequency, severity, or duration of RP attacks, or the acceptability or tolerability of the therapies.16
Regarding the clinical effectiveness of PDE5 inhibitors for the treatment of secondary digital ulcers, limited evidence from 1 observational cohort study17 suggests that there is no difference in the time to healing or the absolute size of the primary digital ulcer in patients treated with PDE5 inhibitors compared with those treated with an endothelin receptor antagonist; however, the occurrence of new digital ulcers was lower in patients treated with an endothelin receptor antagonist.17 A similar proportion of patients in both groups experienced an adverse event, but no statistical tests were reported with these findings. There are concerns that this study was based on a limited number of patients (PDE5 inhibitors: n = 11; endothelin receptor antagonists: n = 49) and that the selection of participants for the trial may have been biased, thus the findings should be interpreted with caution.
For the treatment of RP secondary to systemic sclerosis, there are strong recommendations based on high-quality evidence that CCBs should be used as first-line therapy,18,20 and a weak recommendation that angiotensin II receptor antagonists should be used as a first-line treatment of RP secondary to systemic sclerosis.18 For severe or refractory cases of RP secondary to systemic sclerosis, IV iloprost is recommended based on high-quality evidence.18,20 For non-severe secondary RP, 1 guideline suggests that due to the reported high-cost and feasibility of administering IV iloprost that it only be considered after treatment with oral therapies has failed; however, this was based on expert opinion.20 There is also a strong recommendation that PDE5 inhibitors should be considered as a treatment of RP secondary to systemic sclerosis in those who do not respond to treatment with CCBs.20 The guidelines also include weak recommendations that SSRIs,18,20 alpha blockers,18 and statin therapy18 be considered in the treatment of RP secondary to systemic sclerosis.
Regarding the treatment of digital ulcers secondary to systemic sclerosis, none of the guidelines specified which pharmacotherapy should be considered as first-line therapy. There is a strong recommendation that sildenafil, a PDE5 inhibitor, should be used before considering treatment with an IV prostanoid (e.g., iloprost) or an endothelin receptor agonist (e.g., bosentan),18 as well as weak19 and strong20 recommendations that PDE5 inhibitors should be considered for the treatment of digital ulcers secondary to systemic sclerosis. Given its effectiveness at reducing the number of new digital ulcers, a strong recommendation was made that bosentan (an endothelin receptor antagonist) be considered in the treatment of digital ulcers secondary to systemic sclerosis, despite the use of concurrent treatments (e.g., CCBs, PDE5 inhibitors).20 For refractory or recurrent digital ulcers, there is a moderate-strength recommendation to consider treatment with a PDE5 inhibitor or IV iloprost and an endothelin receptor antagonist.18 Intravenous iloprost is also recommended for patients with severe active digital ulcers18 and for the treatment of digital ulcers secondary to systemic sclerosis.20 A weak recommendation was made that CCBs may be considered a treatment option for skin ulcers secondary to systemic sclerosis; however, this recommendation was based on evidence in a different population (i.e., secondary RP, not secondary digital ulcers).19
Overall, for secondary RP, the findings suggest that PDE5 inhibitors are less effective at reducing the severity of RP attacks compared with CCBs or SSRIs, and more effective at reducing the frequency of daily RP attacks, the severity of RP attacks, and the duration of each RP attack compared with placebo.16 Similarly, the guidelines recommend that CCBs be considered as first-line therapy for RP secondary to systemic sclerosis,18,20 but that other treatment options be considered for RP secondary to systemic sclerosis, including PDE5 inhibitors,18,20 SSRIs,18,20 and IV iloprost (for severe or refractory cases).18,20 For secondary digital ulcers, when PDE5 inhibitors were compared with endothelin receptor antagonists, no difference was observed in the time to healing or the absolute size of the primary digital ulcer; however, the occurrence of new digital ulcers was lower in patients treated with an endothelin receptor antagonist.17 None of the guidelines specified a preferred first-line treatment for digital ulcers secondary to systemic sclerosis, but there are recommendations for PDE5 inhibitors,18-20 endothelin receptor antagonists,18,20 and IV iloprost,18 with the choice of treatment depending of the severity of the digital ulcers or the use of concurrent treatments.
The findings highlighted in this report are based on 1 SR with an NMA,16 1 observational cohort,17 and 3 evidence-based guidelines18-20 that are associated with methodological limitations and a moderate degree of uncertainty. These limitations and the notable gaps in the body of evidence should be considered when interpreting the findings from this report.
Future research should explore the clinical effectiveness of PDE5 inhibitors for the treatment of secondary RP or secondary digital ulcers regarding outcomes identified as important to patients, such as pain, digit loss, and the interference with activities of daily living. In addition, future research on the cost-effectiveness of PDE5 inhibitors for the treatment of secondary RP or digital ulcers should consider the direct and indirect costs of the treatment (e.g., PDE5 inhibitors, pain medication, hospitalization), patient-borne costs (e.g., bandages, time away from work), and the cost per quality-adjusted life-years.
References
1.Wigley FM. Clinical manifestations and diagnosis of Raynaud phenomenon. In: Axford JS, Ramirez Curtis M, eds. UpToDate. Waltham (MA): UpToDate; 2019: http://www.uptodate.com. Accessed 2021 May 31.
2.Hinze AM, Wigley FM. Pharmacotherapy Options in the Management of Raynaud's Phenomenon. Current Treatment Options in Rheumatology. 2018;4(3):235-254. PubMed
3.Wigley FM. Treatment of Raynaud phenomenon: initial management. In: Axford JS, Ramirez Curtis M, eds. UpToDate. Waltham (MA): UpToDate; 2021: http://www.uptodate.com/. Accessed 2021 May 31.
4.Wigley FM. Treatment of Raynaud phenomenon: refractory or progressive ischemia. In: Axford JS, Ramirez Curtis M, eds. UpToDate. Waltham (MA): UpToDate; 2019: http://www.uptodate.com/. Accessed 2021 May 31.
5.Sildenafil: drug information. Lexicomp. Waltham (MA): UpToDate; 2021: http://www.uptodate.com/. Accessed 2021 May 31.
6.Tadalafil: drug information. UpToDate. Waltham (MA): UpToDate; 2021: http://www.uptodate.com/. Accessed 2021 May 31.
7.Vardenafil: drug information. UpToDate. Waltham (MA): UpToDate; 2021: http://www.uptodate.com/. Accessed 2021 May 31.
8.Health Canada's special access programs: request a drug. Ottawa: Health Canada; 2020: https://www.canada.ca/en/health-canada/services/drugs-health-products/special-access/drugs.html. Accessed 2021 May 18.
9.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
10.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
12.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 May 31.
13.CADTH framework for patient engagement in health technology assessment. Ottawa: CADTH; 2019: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2021 May 31.
14.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engagem. 2017;3:13. PubMed
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Khouri C, Lepelley M, Bailly S, et al. Comparative efficacy and safety of treatments for secondary Raynaud's phenomenon: a systematic review and network meta-analysis of randomised trials. The Lancet Rheumatology. 2019;1(4):e237-e246.
17.Chang SH, Jun JB, Lee YJ, et al. A clinical comparison of an endothelin receptor antagonist and phosphodiesterase-5 inhibitors for treating digital ulcers of systemic sclerosis. Rheumatology. 2021;12:12. PubMed
18.Denton CP, Hughes M, Gak N, et al. BSR and BHPR guideline for the treatment of systemic sclerosis. Rheumatology. 2016;55(10):1906-1910. PubMed
19.Fujimoto M, Asai J, Asano Y, et al. Wound, pressure ulcer and burn guidelines - 4: Guidelines for the management of connective tissue disease/vasculitis-associated skin ulcers. J Dermatol. 2020;47(10):1071-1109. PubMed
20.Kowal-Bielecka O, Fransen J, Avouac J, et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann Rheum Dis. 2017;76(8):1327-1339. PubMed
21.van der Heijde D, Aletaha D, Carmona L, et al. 2014 Update of the EULAR standardised operating procedures for EULAR-endorsed recommendations. Ann Rheum Dis. 2015;74(1):8-13. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review and Network Meta-Analysis
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Khouri et al. (2019)16 France Not funded. | Study design: SR with NMA; also includes pairwise meta-analyses. Double-blind RCTs, with a parallel or cross over design were eligible for inclusion in the SR. Included studies: 58 RCTs identified in the SR and included in the NMA Studies that include PDE5 inhibitors: 12 trials (from 11 RCTs) relevant to this report | Includes: people with secondary RP. Trials that included both primary and secondary RP were eligible if at least 50% of people had secondary RP. Overall population in NMA: N = 3,867 Secondary RP = 91.5% % Female: 81.8 Population from PDE5 inhibitor trials: N = 556 Secondary RP = 96% % Female = 86 Mean age (SD) = 47.8 (11.7) Frequency of daily RP attacks, mean (SD) = 3.01 (2.16) Severity of RP attacks, mean (SD) = 3.92 (2.50) Duration of RP attacks in minutes, mean (SD) = 15.94 (17.42) | Eligible interventions: pharmacological therapies for RP Relevant interventions: PDE5 inhibitors [tadalafil, sildenafil, vardenafil, udenafil, and PF-00489791 (unnamed PDE5 inhibitor)] Comparators: any alternative pharmacological therapy for RP, placebo | Outcomes: frequency of daily RP attacks, severity of RP attacks, duration of each RP attack, tolerability, acceptability. Follow-up (in PDE5 inhibitor RCTs): ranged from 4 to 12 weeks |
NMA = network meta-analysis; PDE5 = phosphodiesterase type 5; RCT = randomized controlled trial; RP = Raynaud phenomenon; SD = standard deviation; SR = systematic review; vs. = versus .
Table 3: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Chang et al. (2021)17 South Korea Funding: Handok, Inc. (Seoul, Republic of Korea). | Prospective, observational cohort study Conducted at 13 medical centres between January 2015 to November 2017 | Adults (18 or older), with systemic sclerosis and at least 1 active digital ulcer that is secondary to the systemic sclerosis Excluded: pregnant people, or those planning to become pregnant PDE5i, n = 11 ERA, n = 49 Age, mean years (SD) PDE5i = 50.9 (10.7) ERA = 50.1 (11.5) % Female: PDE5i = 81.8% ERA = 77.6% RP, n (%) PDE5i = 11 (100) ERA = 49 (100) With ≥ digital ulcers, n (%) PDE5i = 5 (45.5) ERA = 25 (51.0) Diffuse cutaneous systemic sclerosis, n (%) PDE5i = 7 (63.6) ERA = 28 (41.7) | Choice of medication was determined by the attending physicians. Reported that dose and duration of each drug regimen followed standard recommendations, but dosage not reported in main report (and supplemental material was not accessible at the time of writing this report) Intervention: PDE5i [sildenafil (n = 9), tadalafil (n = 1), or udenafil (n = 1)] Comparator: ERA (bosentan) Some patients also received CCBs PDE5i, n = 3 (27.7%) ERA, n = 14 (28.5%) | Outcomes:
Follow-up: 24 weeks |
CCB = calcium channel blocker; ERA = endothelin receptor antagonist; PDE5i = phosphodiesterase type 5 inhibitors; RCT = randomized controlled trial; RP = Raynaud phenomenon.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendation development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Japanese Dermatological Association (2020)19 | ||||||
Intended users: medical experts and patients Target population: people with skin ulcers associated with connective tissue diseases (e.g., SSc, SLE, RA) or vasculitis | Therapies for connective tissue disease/vasculitis-associated skin ulcers | Not reported | Multiple databases were searched for evidence. References obtained through manual searching were also included. | Quality of evidence was based on the type of studies available, and classified as follows. No other details provided. Evidence level: I = 1 or more SR II = 1 or more RCT III = non-randomized comparative trials IVa = cohort studies IVb = case-control or cross-sectional studies V = case reports or case series VI = expert opinion | Did not report methods for developing recommendations. There are 3 options for the interventions: 1. Recommended 2. Proposed as an option 3. No recommendation can be made Recommendations can be: 1 = strong recommendation 2 = weak recommendation Strength of the evidence summarized as: A = strong evidence B = moderate evidence C = weak evidence D = very weak evidence | Prior to publication the guideline was presented at annual meetings of the Japanese Dermatological Association to solicit feedback and make revisions. |
EULAR (2017)20 | ||||||
Intended Users: clinicians involved in treating patients with systemic sclerosis Target Population: people with systemic sclerosis | Calcium channel blockers, prostanoids, endothelin receptor antagonists, PDE5 inhibitors | Not reported | This is an update to the 2009 EULAR guidelines. A list clinical questions were solicited from the clinical experts, and 3 round online Delphi survey was used narrow down which questions would be prioritized and addressed. Systematic literature search was used to find and select evidence. A summary of the evidence was prepared for each clinical question. | For the clinical benefits, only studies with the highest level of available for each intervention were retained for data extraction and critical appraisal. For adverse events, meta-analyses, RCTs, and non-randomized controlled trials were always considered. Quality assessments of each included study was conducted using the Jadad scale, which considers whether the study was randomized, described as double blind, and a description of the withdrawals from the study. | Evidence from individual studies was combined to develop the recommendations in accordance with GRADE. Draft recommendations were prepared from evidence summaries, reviewed by the panel, and discussed at a face-to-face consensus meeting. The nominal group technique was used to discuss and reformulate the recommendations until a consensus was reached among all participants. For research questions for which appropriate evidence in the literature was not identified, comments from the expert committee are provided | Not reported. |
“Categories of evidence: 1A = from meta-analysis of RCTs 1B = from at least 1 RCT 2A = from at least 1 controlled study without randomization 2B = from at least 1 type of quasi-experimental study 3 = from descriptive studies, such as comparative studies, correlation studies or case-control studies 4 = from expert committee reports or opinions and/or clinical experience of respected authorities” (p. 10)21 | “Strength of the recommendations: A = Category I evidence B = Category II evidence or extrapolated recommendations from category I evidence C = Category III evidence or extrapolated recommendation from category I or II evidence D = Category IV evidence or extrapolated recommendation from category II or III evidence” (p. 10)21 | |||||
BSR/BHPR (2016)18 | ||||||
Intended Users: Health care professionals including rheumatologists, dermatologists, general physicians, nurses, trainees, and specialists treating complications of systemic sclerosis Target Population: people with systemic sclerosis | Therapies for the management of systemic sclerosis | Not reported | Literature reviews were conducted for each topic. 2 databases were searched, and reference lists of included studies were also reviewed. | The level of the evidence was graded, but full details not reported. I = at least 1 meta-analysis, SR, or RCT of evidence level Ia = not defined Ib = not defined IIa = not defined IIb = not defined III = evidence from non-analytical studies IV = expert opinion | Discussions to develop the guideline were informed by the literature reviews. Section leads for each topic lead the development of those recommendations. Members voted on each recommendation, and a minimum agreement of 75% was considered as consensus. Recommendations were graded based on the level of evidence and strength of recommendations. Full details of the grading system were not provided. Grades ranged from A (evidence from level I) to D (i.e., evidence level III or IV) | Not reported. |
BHPR = British Health Professionals in Rheumatology; BSR = The British Society for Rheumatology; EULAR = European League Against Rheumatism; GRADE = Grading of Recommendations Assessment, Development and Evaluation; PDE5 = phosphodiesterase type 5; RA = rheumatoid arthritis; RCT = randomized controlled trial; SLE = systemic lupus erythematosus; SSc = systemic sclerosis; SR = systematic review.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 29 and the ISPOR Questionnaire10
Strengths | Limitations |
|---|---|
Khouri et al. (2019)16 | |
Well-described eligibility criteria for the SR (i.e., population, intervention, comparator, outcomes) The methods for the review were established before conducting the review (PROSPERO CRD42017057518) Comprehensive search was conducted, including searching multiple databases, clinical trial registries, and speaking to leaders in the field. They reported their search date limits, and provided the search terms, and had no language restrictions. Two authors independently performed the study selection and conducted the risk of bias assessments The Cochrane risk of bias tool was used to assess the quality of the RCTs across 6 domains or bias, and reported for each trial. Reported whether each trial was supported by pharmaceutical companies (but not the source of funding) Authors reported investigating publication (small study) bias, and if publication bias was detected the authors downgraded the evidence in the NMA The study population, outcomes, and comparators used in the NMA were relevant to the current report The quality of the evidence for each drug vs. the place in the NMA was assessed and reported using GRADE Random-effects models were used due to variability in patient characteristics and study design Direct and indirect comparisons are reported No naïve comparisons were made Between-study variance and heterogeneity was reported per outcome Pre-planned sensitivity analyses and meta-regression were conducted | Only double-blind RCTs were eligible for inclusion but no explanation was provided for excluding RCTs that were not double-blinded, and 6 RCTs were excluded for this reason (impact is unclear) Did not report a list of excluded studies Did not report how many authors were involved in data extraction Description of the included studies lacked details regarding the population (e.g., RP secondary to what conditions, frequency of RP attacks), and the length of the treatment Pairwise meta-analyses were conducted to compare each drug to the placebo, but they did not report whether fixed or random-effects analyses were conducted Meta-analyses include all studies regardless of risk of bias Potential conflicts of interest were reported by the authors (e.g., funding from pharmaceutical companies), and it was not reported how these potential conflicts were managed Substantial variation in the length of follow-up in the primary studies in the NMA, ranging from 1.4 weeks to > 2 years Minimal information is reported for the primary studies limiting the assessment of the heterogeneity across studies within the model |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NMA = network meta-analysis; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; RP = Raynaud phenomenon; SR = systematic review.
Table 6: Strengths and Limitations of the Clinical Study Using the Downs and Black Checklist11
Strengths | Limitations |
|---|---|
Chang et al. (2021)17 | |
Study objective, main outcomes, and eligibility criteria were clearly described Simple outcome data were reported for primary outcome (i.e., time to healing) Distribution of potential confounders was reported (e.g., age, sex, number of digital ulcers, size of primary ulcer) Actual P values (P value) were reported Participants recruited from 13 medical centres, and participants in all groups recruited over the same time period Appropriate statistical tests were used Compliance with the interventions was comparable between groups Source of funding was reported, and the article includes a statement that the funding agency did not influence the study design or manuscript preparation | Choice of medication was decided by the physicians (risk of selection bias) based on list of available medications Dose and duration of treatment was not reported for each treatment Outcome ‘size of primary ulcer’ may not be useful, and reporting on ‘change in size of the primary ulcer’ may have provided more valuable information Enrolment was stopped at 71 people, before reaching target sample size (i.e., 200) due to slow recruitment 8 participants were excluded from the analysis (lost to follow-up, withdrew consent, or incomplete data), but did not report any details of these patients Did not report whether participants or individuals assessing the outcomes or conducting the statistical analysis were blinded to the intervention One author declared receiving funding from pharmaceutical companies |
Table 7: Strengths and Limitations of Guidelines Using AGREE II12
Item | Japanese Dermatological Association (2020)19 | EULAR (2017)20 | BSR/BHPR (2016)18 |
|---|---|---|---|
Domain 1: Scope and Purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | No |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Partially | Yes | No |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No | Partially | No |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes |
Domain 3: Rigour of Development | |||
7. Systematic methods were used to search for evidence. | No | Yes | Unclear |
8. The criteria for selecting the evidence are clearly described. | No | Partially | No |
9. The strengths and limitations of the body of evidence are clearly described. | No | No | No |
10. The methods for formulating the recommendations are clearly described. | No | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | No | Partially | No |
12. There is an explicit link between the recommendations and the supporting evidence. | Partially | Yes | No |
13. The guideline has been externally reviewed by experts before its publication. | Unclear | No | No |
14. A procedure for updating the guideline is provided. | Yes | No | Yes |
Domain 4: Clarity of Presentation | |||
15. The recommendations are specific and unambiguous. | Partially | Partially | Partially |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Partially | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | No | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No | No |
20. The potential resource implications of applying the recommendations have been considered. | No | No | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No |
Domain 6: Editorial Independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Unclear | Unclear |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; BHPR = British Health Professionals in Rheumatology; BSR = The British Society for Rheumatology; EULAR = European League Against Rheumatism.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Summary of Findings Included Systematic Review and Network Meta-Analysis
Khouri et al. (2019)16
Main Study Findings
Mean difference (MD) or standard mean difference (SMD) were reported for efficacy outcomes; negative values indicate an improvement relative to the comparator.
Incidence rate ratio (IRR) was reported for safety outcomes; values greater than 1 indicate an increased risk relative to the comparator.
Direct comparisons from the pairwise meta-analyses:
PDE5i versus placebo
Frequency of RP attacks (daily), MD: –0.31, 95% confidence interval (CI), –0.57 to –0.04
12 trials, I2 = 0%
Severity of RP attacks, SMD: –0.30, 95% CI, –0.62 to 0.01
12 trials, I2 = 0%
Duration of RP attacks, MD: –3.05, 95% CI, –5.79 to –0.31
11 trials, I2 = 0%
Acceptability, IRR: 2.64, 95% CI, 1.40 to 4.99
8 trials, I2 = 0%
Tolerability, IRR: 3.20, 95% CI, 1.45 to 7.09
6 trials, I2 = 15%
PDE5i versus CCB (1 trial)
Duration of RP attacks, MD: –0.91, 95% CI, –6.25 to 4.43
Acceptability, IRR: 2.00, 95% CI, 0.37 to 10.92
Tolerability, IRR: 4.29, 95% CI, 0.48 to 38.34
Indirect comparisons from NMA of 58 studies:
Frequency of RP attacks (daily), MD
Comparisons were made between: PDE5 inhibitors, placebo, CCBs, SSRIs, antioxidants, IV prostacyclin analogues (PGI2), topical nitric oxide, alpha antagonists, phosphodiesterase type 3 (PDE3) inhibitors, thromboxane synthase inhibitors (TSIs), oral prostacyclin receptor (IP) agonists, soluble guanylate cyclase stimulators (sGCs)
Random-effects model, Tau2 = 0.035, I2 = 16.8%
Relevant comparisons where 1 treatment was favoured compared to another at reducing frequency of RP attacks:
PDE5i versus Placebo: –0.36, 95% credible interval (CrI), –0.69 to –0.04 (moderate quality of evidence)
PDE5i versus sGCs: –2.18, 95% CrI, –3.88 to –0.47
Severity of RP attacks (scale 0 to 10), SMD
Comparisons were made between PDE5 inhibitors, placebo, CCBs, Oral IP agonists, IV PGI2, endothelin receptor antagonists (ERAs), Antioxidants, Topical nitric oxide, Alpha antagonists, anti-interleukin 6, botulinum toxin A, SSRI, PDE3 inhibitors, TSI, sGCs, angiotensin-converting enzyme (ACE) inhibitor (ACEi) and an angiotensin receptor blocker (ARB)
Random-effects model, Tau2 = 0, I2 = 0%
Relevant comparisons where 1 treatment was favoured compared to another in improving severity of RP attacks:
PDE5i versus Placebo: –0.34, 95% CrI, –0.66 to –0.03 (moderate quality of evidence)
PDE5i versus sGCs: –1.98, 95% CrI, –3.86 to –0.12
CCB versus PDE5i: –0.5, 95% CrI, –1.00 to –0.01
SSRI versus PDE5i: –1.20, 95% CrI, –2.38 to –0.03
Duration of each RP attack, MD
Comparisons were made between: PDE5 inhibitors, placebo, CCBs, Alpha antagonists, Oral IP agonists, IV PGI2, Antioxidants, TSI
Random-effects model, Tau2 = 0, I2 = 0%
Relevant comparisons where 1 treatment was favoured compared to another in improving duration of RP attacks:
PDE5i versus Placebo: –3.42, 95% CrI, –6.63 to –0.29 (low quality of evidence)
Acceptability, IRR
Comparisons were made between PDE5 inhibitors, Oral IP agonists, PDE3 inhibitors, CCBs, ACEi/ARB, Alpha antagonists, ERA, placebo, anti-interleukin 6, IV PGI2, SSRI, Antioxidants, TSI, Topical nitric oxide
Random-effects model, Tau2 = 0.077, I2 = 25.2%
Relevant comparisons where 1 treatment was less favoured compared to another for acceptability:
PDE5i versus Placebo: 2.61, 95% CrI, 1.48 to 4.81
PDE5i versus IV PGI2: 3.35, 95% CrI, 1.43 to 8.25
PDE5i versus antioxidants: 4.01, 95% CrI, 1.11 to 15.33
PDE5i versus Topical nitric oxide: 7.17, 95% CrI, 1.40 to 41.26
Tolerability, IRR
Comparisons were made between PDE5 inhibitors, CCBs, Oral IP agonists, IV PGI2, PDE3 inhibitors, Alpha antagonists, ACEi/ARB, sGCs, placebo, Topical nitric oxide, SSRI, anti-interleukin 6, ERA, TSI, Antioxidants
Random-effects model, Tau2 = 0.23, I2 = 41.0%
Relevant comparisons where 1 treatment was less favoured compared to than another for tolerability:
PDE5i versus Placebo: 3.32, 95% CrI, 1.49 to 7.61
Author’s Conclusion
“Direct and indirect evidence was consistent for all outcomes.” (p. e241)
“PDE5 inhibitors were the only class statistically more effective than placebo for all three efficacy outcomes” (p. e24)
“PDE5i had lower acceptability (IRR 2·61 [95% CrI 1·48–4·78]) and tolerability (3·30 [1·49–7·55]) than did placebo” (p. e242)
Summary of Findings of Included Primary Clinical Study
Chang et al. (2021)17
Main Study Findings
Time to healing of primary ulcer, mean, days (standard deviation [SD])
PDE5 inhibitor (PDE5i) = 81.3 (46.7)
ERA = 91.3 (49.6)
ERA versus PDE5i, hazard ratio (HR) = 0.75, 95% CI, 0.35 to 1.64, P = 0.47, unadjusted model
ERA versus PDE5i, HR = 0.80, 95% CI, 0.36 to 1.78, P = 0.59, model adjusted for age, sex, CCB use, number of digital ulcers, and area of primary ulcer
Size of primary ulcer, mm2, mean (SD)
Baseline: ERA = 21.5 (20.5) versus PDE5i = 24.2 (26.1), P = 0.40
Week 24: ERA = 4.3 (7.4) versus PDE5i = 1.2 (2.0), P = 0.13
Occurrence of new digital ulcers
ERA versus PDE5i, HR = 0.39, 95% CI, 0.16 to 0.93, P = 0.03, unadjusted model
ERA versus PDE5i, HR = 0.32, 95% CI, 0.13 to 0.81, P = 0.02, model adjusted for age, sex, CCB use, number of digital ulcers, and area of primary ulcer
Adverse events:
Patients with an adverse event, n (%)
PDE5i = 3 (27.3)
ERA = 18 (36.7)
Reported in the ERA group:
Liver function abnormalities = 4 (8%)
Headache = 3 (6%)
Fatigue = 1 (2%)
Facial flushing = 6 (12%)
Edema = 5 (10%)
Anemia = 2 (4%)
Reported in the PDE5i group:
Restrictive heart failure = 1 (9%)
Facial flushing = 1 (9%)
Edema = 1 (9%)
Palpitations = 1 (9%)
Author’s Conclusion
“CU healing was comparable between PDE5is and ERAs, but several points support a benefit of sildenafil over bosentan for digital ulcer healing. First, its effects were similar to those in the ERA group even though the dose of sildenafil was lower than in previous studies. Second, although not statistically significant, the CU was larger in the PDE5i group than in the ERA group at baseline but smaller at all subsequent time points.” (p. 5)
“In conclusion, the time to heal cardinal ulcers and the change in cardinal size were comparable between the ERA and PDE5i groups. New digital ulcer occurrence was significantly lower in patients treated with an ERA than in those treated with a PDE5i.” (p. 5)
“Overall, all adverse events were temporary and reversible.” (p. 4)
Summary of Recommendations in Included Guidelines
Japanese Dermatological Association (2020)19
Recommendations and Supporting Evidence
Recommendation 1: “No report has directly evaluated the usefulness of calcium blockers for treating SSc [systemic sclerosis]-associated skin ulcers, but they are useful for treating Raynaud’s phenomenon and can be expected to effectively treat ulcers caused by circulatory impairments. Therefore, they are proposed as an option for treating SSc-associated skin ulcers.” (p. 1082)
No evidence was identified on the effectiveness of calcium channel blocker for treating ulcers secondary to SSC, and expert opinions were used to develop the recommendation.
Supporting evidence from a RCT, and a systematic review with meta-analysis demonstrated that calcium channel blockers were more effective than a placebo at reducing the frequency, duration, and severity of RP secondary to SSc.
Recommendation 2: “Because phosphodiesterase-5 inhibitors are expected to be useful for treating SSc-associated skin ulcers, the administration of sildenafil (2C), tadalafil (2D) or vardenafil (2D) is proposed as an option. However, careful evaluation of indications is necessary for their administration.” (p. 1085)
Evidence on the usefulness of sildenafil SSc-associated skin ulcers was identified in 1 case series and 2 case reports, and demonstrated an improvement in digital ulcers. For RP secondary to SSc, evidence from 2 RCTs showed that sildenafil was associated with decreased RP symptoms.
In an RCT of people with SSc, tadalafil was associated with improvements in RP score, frequency and duration. No evidence on tadalafil for SSc skin ulcers was identified, and expert opinion was used.
One RCT of vardenafil in people with RP secondary to SSc, vardenafil was associated with significant improvements in RP symptoms.
No evidence on vardenafil for SSc skin ulcers was identified, and expert opinion was used.
Quality of Evidence and Strength of Recommendations
Recommendation 1: Evidence level VI, strength of recommendation 2D
Recommendation 2:
For sildenafil: Evidence level V, strength of recommendation 2C
For tadalafil: Evidence level VI, strength of recommendation 2D
For vardenafil: Evidence level VI, strength of recommendation 2D
EULAR (2017)20
Recommendations and Supporting Evidence
Recommendation 1: “Dihydropyridine-type calcium antagonists, usually oral nifedipine, should be considered as first-line therapy for SSc-RP. PDE5 inhibitors should also be considered in treatment of SSc-RP” (p. 1328)
One meta-analysis of 8 RCTs on the effectiveness of CCBs, indicated that when compared to placebo, the CCBs significantly reduced the frequency and severity of RP attacks in people with SSc. Common side effects include hypotension, dizziness, and headaches, but none of the studies in the meta-analysis directly examined side effects of CCBs.
A meta-analysis of 6 RCTs found that PDE5 inhibitors had a significant but moderate effect on the frequency and severity of RP attacks in people with SSc when compared to placebo. Common side effects reported in the meta-analysis included chest pain, vasomotor restrictions, dyspepsia, and myalgia.
Recommendation 2: “Intravenous iloprost should be considered for severe SSc-RP” (p. 1330)
One meta-analysis of 5 RCTs found that when compared to placebo, IV iloprost (a prostanoid) significantly reduced the frequency of ischemic attacks, and improved the severity of RP score in people with SSc. Oral iloprost was found to be less effective than IV iloprost.
When compared to a CCB, evidence from 2 RCTs demonstrated that iloprost performed slightly better than the CCB at improving symptoms of RP secondary to SSc.
Recommendation 3: “Experts recommend that intravenous iloprost should be used for treatment of SSc-RP attacks after oral therapy” (p. 1330)
Due to the costs and feasibility of IV iloprost, the experts recommended that IV prostanoids are considered when oral therapies (e.g., CCBs, PDE5 inhibitors) have failed.
Recommendation 4: “Fluoxetine might be considered in treatment of SSc-RP attacks” (p. 1330)
Evidence from 1 study of 27 people with RP secondary to SSc found that fluoxetine (an SSRI) was superior to nifedipine (a CCB) in reducing the severity of RP symptoms, but the finding was not statistically significant.
Recommendation 5: “Intravenous iloprost should be considered in the treatment of DUs [digital ulcers] in patients with SSc” (p. 1330)
Evidence from 2 RCTs found that when compared to placebo, IV iloprost significantly reduced the number of DUs and significantly improved DU healing in people with SSc. Evidence from a meta-analysis that included studies with oral and IV prostanoids, showed a trend toward beneficial effects over place in healing of DUs, with the greatest effect seen with IV iloprost. Prostanoids were not found to prevent new DUs in the meta-analysis.
Recommendation 6: “PDE5 inhibitors should be considered in the treatment of DUs in patients with SSc” (p. 1331)
A meta-analysis of 3 RCTs, found that PDE5 inhibitors significantly improved DUs (i.e., number of patients with healing DUs, and number of patients with improved DU) in patients with SSc compared to placebo. These findings were supported by an independent RCTs that found significant improvements in DU healing in patients with SSc treated with a PDE5 inhibitor compared to a placebo.
Recommendation 7: “Bosentan should be considered for reduction of the number of new DUs in SSc, especially in patients with multiple DUs despite the use of calcium channel blockers, PDE-5 inhibitors or iloprost therapy” (p. 1331)
Two RCTs assessed by the guideline group to be high-quality, found that when compared to placebo, bosentan (an endothelin receptor antagonist), significantly reduced the number of new DUs in patients with SSc and a history of or at least 1 active DU. Neither trial found a difference between bosentan and the placebo in healing active SSc-related DUs.
Quality of Evidence and Strength of Recommendations
Recommendation 1: A
Recommendation 2: A
Recommendation 3: expert opinion
Recommendation 4: C
Recommendation 5: A
Recommendation 6: A
Recommendation 7: A
BSR/BHPR (2016)18
Recommendations and Supporting Evidence
Recommendation 1: For RP in SSc “First-line treatments are CCBs (Ia, A) and angiotensin II receptor antagonists (Ib, C).” (p. 1907)
Recommendation 2: For RP in SSc “Other treatments that may be considered are: selective serotonin reuptake inhibitors, a-blockers and statin therapy (III, C). (p. 1907)
Recommendation 3: For RP in SSc “PDE5 inhibitors are being used increasingly for SSc-related RP (IIa, C).” (p. 1907)
Recommendation 4: For RP in SSc “Intravenous prostanoid (e.g., iloprost; Ia, B) and digital (palmar) sympathectomy (with or without botulinum toxin injection) should be considered in severe and/or refractory cases (III, D).” (p. 1907)
Recommendation 5: For DUs in SSc “Sildenafil should now be used before considering intravenous prostanoids and bosentan, in line with the current National Health Service (NHS) England Clinical Commissioning policy (I, A).” (p. 1908)
Recommendation 6: For DUs in SSc “In severe active digital ulceration, patients should receive intravenous prostanoid (Ia, B).” (p. 1908)
Recommendation 7: For DUs in SSc “In patients with recurrent, refractory DUs, a PDE5 inhibitor (IIa, B) or intravenous prostanoid (Ia, B) and an endothelin receptor antagonist (including bosentan; Ia, B) should be considered.” (p. 1908)
No supporting evidence was reported in the guideline for any of the recommendations.
Quality of Evidence and Strength of Recommendations
Recommendation 1: CCBs: Evidence level Ia, strength of recommendation A
Angiotensin II receptor antagonists: Evidence level Ib, strength of recommendation C
Recommendation 2: Evidence level III, strength of recommendation C
Recommendation 3: Evidence level IIa, strength of recommendation C
Recommendation 4: IV prostanoid: Evidence level Ia, strength of recommendation B
Digital sympathectomy: Evidence level III, strength of recommendation D
Recommendation 5: Evidence level I, strength of recommendation A
Recommendation 6: Evidence level Ia, strength of recommendation B
Recommendation 7: PDE5 inhibitor: Evidence level IIa, strength of recommendation B
IV prostanoid: Evidence level Ia, strength of recommendation B
Endothelin receptor antagonist: Evidence level Ia, strength of recommendation B
Table 8: Patient Involvement in PDE5 Inhibitors to Treat Patients With Secondary RP and/or Digital Ulcers
Section and topic | Item | Reported on page |
|---|---|---|
Aim | The patient contributor was involved in developing the protocol and commenting on outcomes important to patients and families with experience of Raynaud's RP and/or digital ulcers secondary to scleroderma. | 5 |
Methods | After giving informed consent, the patient contributor discussed her experiences, and perspectives on the outcomes via teleconference and follow-up email communication. | 6 |
Results of engagement | The researchers were made aware of the importance of several outcomes and themes. In particular, the relevance of the research question for patients and she explained connections between the quality-of-life outcomes (i.e., the connection between pain, disrupted sleep, and fatigue) were confirmed. She explained why some of the more technical outcomes (such as degree of ischemia) were important to people and their treatment goals, and daily activities. She commented on patient-borne costs, and equity issues in the community. | 3, 32 |
Discussion and conclusions | Success of patient involvement in this report is related to several factors. First, the patient contributor was briefed on the objectives of the project and supported in her role. The research team was receptive to this involvement and used it in their approach to the clinical evidence. Established processes are in place, and compensation was offered for her time to participate in the project. | 32 |
Reflections/critical perspective | The patient contributor was highly engaged in the conversation with researchers. She reported patient concerns, family-borne costs, and burdens, for example, that the lack of access to PDE5 inhibitors in the treatment of severe Raynaud's and digital ulcers means that the next course of treatment requires hospitalization or outpatient IV infusion clinics. Ethical and equity issues are sometimes revealed in the telling of patient experiences. Timely access to care an important concern, and the financial costs of medication, creams, and bandages was raised as an important consideration for people without private insurance coverage. One limitation of our approach is that people need reliable access to phone and internet to contribute to CADTH, which may exclude some voices. | 13, 15 |
PDE5 = phosphodiesterase type 5, RP = Raynaud phenomenon.
Appendix 5: References of Potential Interest
Review Articles
22.Fernandez-Codina A, Canas-Ruano E, Pope JE. Management of Raynaud's phenomenon in systemic sclerosis-a practical approach. Journal of Scleroderma and Related Disorders. 2019.
Additional References
Non-Comparative, Before-After Study
23.Kumar U, Sankalp G, Sreenivas V, Kaur S, Misra D. Prospective, open-label, uncontrolled pilot study to study safety and efficacy of sildenafil in systemic sclerosis-related pulmonary artery hypertension and cutaneous vascular complications. Rheumatol Int. 2013;33(4):1047-1052. PubMed
Guidance Documents, Methodology Not Reported
24.Hughes M, Herrick AL. Assessment and management of Raynaud's phenomenon. Prescriber. 2017;28(7):11-16.
25.NHS England. Clinical Commissioning Policy: Sildenafil and Bosentan for the Treatment of Digital Ulceration in Systemic Sclerosis. (NHS England: A13/P/b). 2015; https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2015/10/a13pb-sildenafil-bosentan-oct15.pdf Accessed 2021 May 6.
26.Hughes M, Ong VH, Anderson ME, et al. Consensus best practice pathway of the UK Scleroderma Study Group: digital vasculopathy in systemic sclerosis. Rheumatology. 2015;54(11):2015-2024. PubMed
27.National Institute for Health and Care Excellence. Digital ulcers: sildenafil. (NICE Evidence summary ESUOM42). 2015; https://www.nice.org.uk/advice/esuom42/resources/digital-ulcers-sildenafil-54116459119149253 Accessed 2021 May 6.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca