CADTH Health Technology Review
Abiraterone Acetate for Metastatic Castration-Sensitive Prostate Cancer
Rapid Review with Expert Input
Authors: Amanda Shane, Melissa Walter
External Reviewer
This document was externally reviewed by a content expert who has granted permission to be cited.
Christian Kollmannsberger, MD FRCPC
Clinical Professor
BC Cancer Vancouver Centre, University of British Columbia
Abbreviations
AAP
abiraterone acetate plus prednisone or prednisolone
ADT
androgen deprivation therapy
AE
adverse event
APA
apalutamide
DOC
docetaxel
ECOG
Eastern Cooperative Oncology Group
ENZ
enzalutamide
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
MA
meta-analysis
mCRPC
metastatic castration-resistant prostate cancer
mCSPC
metastatic castration-sensitive prostate cancer
NMA
network meta-analysis
PSA
prostate-specific antigen
QALY
quality-adjusted life-year
RCT
randomized controlled trial
SR
systematic review
Key Messages
The use of abiraterone acetate for the treatment of metastatic castration-sensitive prostate cancer is clinically effective.
Compared with standard of care, abiraterone acetate was associated with increased overall survival, increased prostate cancer–specific survival, increased progression-free survival, and improved quality of life.
Patients treated with abiraterone acetate were at higher risk for grade III to grade V adverse events (severe, life-threatening, or fatal) and were more likely to discontinue treatment compared with standard of care.
The incremental cost-effectiveness ratios for both brand and generic abiraterone acetate were estimated to be higher than common willingness-to-pay thresholds.
Context and Policy Issues
Prostate cancer is the most commonly diagnosed cancer among men in Canada, with 1 in 9 males expected to be diagnosed in their lifetime.1 Prostate cancer accounts for approximately 20% of new cancer diagnoses2 and is responsible for 9.5% of cancer-related deaths among men.1 The 10-year relative survival for localized prostate cancer is nearly 100% but this decreases to less than 20% if distant metastasis occurs.3
Androgen deprivation therapy (ADT) is a hormone therapy that has been the standard of care for metastatic prostate cancer since the 1940s.4 The goal of ADT is to lower the level of androgens produced by the testes, either through surgery (surgical castration) or medication (medical castration).5,6 Metastatic prostate cancer that is responsive to hormone therapy is termed metastatic castration-sensitive prostate cancer (mCSPC). Initially, ADT is often effective in slowing the growth of prostate cancer cells, but within 18 to 24 months, the clinical benefits of ADT slow and patients progress to metastatic castration-resistant prostate cancer (mCRPC).
Within the past 5 years, new systemic therapies have been approved for use in the treatment of mCSPC.4 One such treatment is abiraterone acetate. Abiraterone acetate is an agent that inhibits cytochrome P17 enzyme, resulting in decreased testosterone production.7 The aim of this treatment is to delay the progression from mCSPC to mCRPC. With the advance of new treatment options, institutional coverage decisions are required.
This report aims to summarize the clinical effectiveness and cost-effectiveness of abiraterone acetate for the treatment of mCSPC.
Research Questions
What is the clinical effectiveness of abiraterone acetate combined with ADT for mCSPC?
What is the cost-effectiveness of abiraterone acetate combined with ADT for mCSPC?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were abiraterone acetate and castration-sensitive prostate cancer. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded. The search was also limited to English-language documents published between January 1, 2016, and March 8, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients with newly diagnosed metastatic castration-sensitive prostate cancer |
Intervention | Abiraterone acetate with dexamethasone or with prednisone in combination with androgen deprivation therapy |
Comparator | Placebo plus androgen deprivation therapy, other androgen receptor–targeted agents (i.e., apalutamide, darolutamide, enzalutamide) with androgen deprivation therapy, docetaxel plus androgen deprivation therapy |
Outcomes | Q1: Clinical effectiveness (e.g., progression-free survival [e.g., radiographic progression-free survival, prostate-specific antigen progression-free survival, clinical progression-free survival], overall survival, response rate, quality of life, time to prostate-specific antigen progression); adverse events; discontinuation Q2: Cost-effectiveness (e.g., quality-adjusted life-years, incremental cost-effectiveness ratio) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, economic evaluations |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published prior to 2016. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs, unless they included different outcomes, were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Due to the volume of literature and lack of generalizability to the Canadian decision-making context, economic evaluations conducted outside of Canada were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for SRs, the ISPOR (International Society for Pharmacoeconomics and Outcomes Research) Questionnaire to Assess the Relevance and Credibility of a Network Meta-Analysis9 for network meta-analyses (NMAs), the Downs and Black checklist10 for randomized and non-randomized studies, and the Drummond checklist11 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
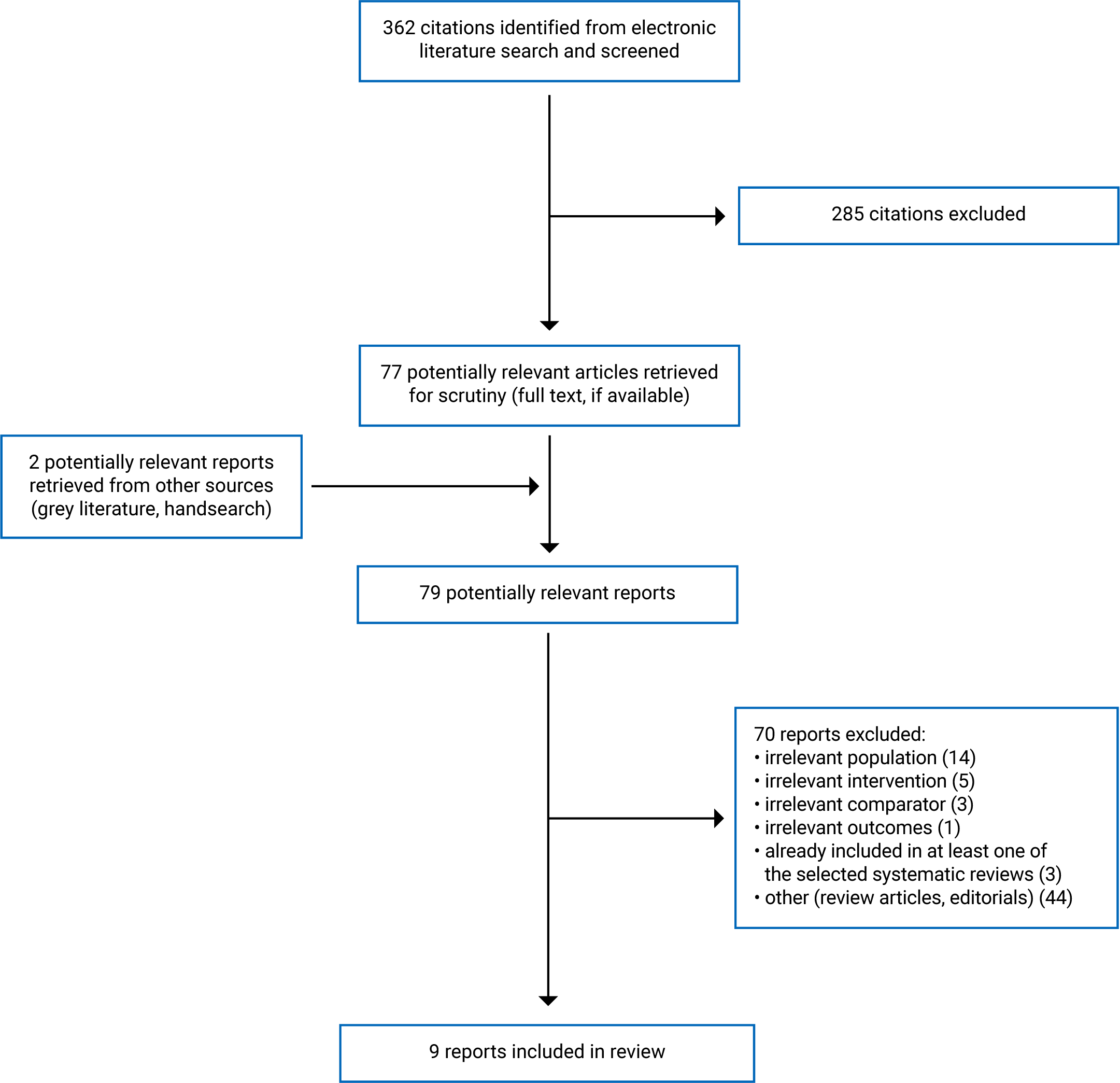
A total of 362 citations were identified in the literature search. Following screening of titles and abstracts, 285 citations were excluded and 77 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 70 publications were excluded for various reasons, and 9 publications met the inclusion criteria and were included in this report. These comprised 5 SRs, 3 publications related to 1 randomized controlled trial (RCT), and 1 economic evaluation. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)12 flowchart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Three13-15 of the 5 SRs had broader inclusion criteria than the present review. Specifically, these 3 SRs included studies with both mCSPC and either non-mCSPC14,15 or mCRPC.13 Only the characteristics and results of the subset of relevant studies will be described in this report.
Study Design
Of these 5 SRs, 3 were published in 2020,13,16,17 1 in 2019,14 and 1 in 2018.15 The literature searches ranged from database inception to May 15, 2020. All the SRs included only RCTs as study design. Two SRs contained NMAs15,17 and 3 contained meta-analyses (MAs).13,14,16 One was a Cochrane review.16 There was overlap of included primary studies across the SRs. The extent of this overlap is summarized in Appendix 5. There have been 2 RCTs conducted that meet the selection criteria for this report: LATITUDE and STAMPEDE. Results from 1 or both of these trials have been included in each of the 5 SRs.
Three primary clinical studies18-20 related to 1 RCT were included. Two studies were exploratory subgroup analyses of patients enrolled in the LATITUDE trial in Japan: 1 based on the interim results which was published in 201819 and 1 based on the final results which was published in 2020.18 The third study was a subgroup analysis of patient-reported outcomes from the LATITUDE trial which was published in 2018.20 Although the data in these reports were captured in the full, final results of the LATITUDE trial, they provided additional information about time points or specific sub-populations that may be of interest, but were not meant to replace or supersede the findings from the full study which was captured in the SRs.
The economic evaluation21 was a cost-effectiveness analysis published in 2020. It had a lifetime horizon and was from the health care payer perspective. Clinical data were obtained from the literature, cost data were obtained from the Canadian Institute of Health Information and the literature, and utility data were obtained from Tufts-New England Medical Center Cost-Effectiveness Analysis Registry. The evaluation was based on a microsimulation Markov model with a simulation of 100,000 patients. The main assumptions were that therapy was completed without interruption or adjustments unless the patient experienced an adverse event (AE), progression, or death; patients that did not complete at least 3 months of their treatment plan had no survival benefit; patients who received docetaxel first received abiraterone acetate as second-line treatment (and vice versa); third-line treatment was cabazitaxel; and there were no long-term treatment-related complications after the primary treatment phase.
Country of Origin
The primary author for 3 of the SRs were from China.13,15,17 One SR was authored by an investigator in the US16 and 1 from France.14 Two primary studies were authored by investigators in Japan18,19 and 1 by an investigator in Canada.20 However, Chi et al. (2018)20 was an international collaboration with the remaining authors from the UK, Spain, Italy, Germany, Japan, China, South Korea, Brazil, the US, Belgium, and France.
The primary author for the economic evaluation21 was from Canada.
Patient Population
All SRs included patients with mCSPC. One study17 limited study inclusion to those with patients18 years and older, another limited to patients older than 70 years,14 and 3 studies had no age restrictions.13,15-17 The number of mCSPC patients included in each SR ranged from 499 to 11,494.
The 3 primary studies18-20 presented analyses of the LATITUDE trial, so the inclusion and exclusion criteria for that trial applied to patients with newly diagnosed mCSPC, who were at least 18 years of age, and had an Eastern Cooperative Oncology Group (ECOG) score of less than or equal to 2. Patients with high-risk disease were included if they had at least 2 of the following: a Gleason score higher than 7, more than 2 bone lesions, or measurable visceral metastasis. A total of 1,119 patients were randomized 1:1 to the intervention or placebo groups. The median age of the LATITUDE participants was 68 years (range = 38 years to 89 years) in the treatment group and 67 years (range = 33 years to 92 years) in the control group. Two primary studies18,19 were subgroup analyses of patients enrolled in Japan in the LATITUDE trial (n = 70 participants). Chi et al. (2018)20 included all LATITUDE trial participants.
The base case of the economic evaluation21 was a 65-year-old patient with newly diagnosed mCSPC and a candidate for either intervention (docetaxel or abiraterone acetate). The modelled patients were a cohort with ECOG status of 0 to 2 and radiographic evidence of metastasis.
Interventions and Comparators
The intervention of interest was abiraterone acetate combined with either prednisone or prednisolone (AAP) plus ADT (AAP + ADT). The comparator for the 3 SRs with an MA was ADT alone16 or ADT plus placebo.13,14 The comparators for the SRs with an NMA were docetaxel plus ADT (DOC + ADT) and ADT alone,15 and enzalutamide plus ADT (ENZ + ADT), apalutamide plus ADT (APA + ADT), and DOC + ADT.17
Outcomes
All SRs13-17 and the 2 LATITUDE subgroup analyses of patients enrolled in Japan18,19 reported overall survival as a primary outcome. It was defined as the time from randomization to death from any cause. Four SRs13,14,16,17 reported progression-free survival (PFS) (time to disease progression). Time to chemotherapy was reported in 1 SR17 and the 2 publications focused on patients enrolled in Japan.18,19 Time to prostate-specific antigen (PSA) progression was reported in 1 SR,13 and 1 publication focused on patients enrolled in Japan.18 The second publication that focused on the Japanese subgroup included radiographic PFS.19 The Cochrane review16 reported 3 additional outcomes not included in other studies: time to death due to prostate cancer (planned after 50% of events occurred, measured at median follow-up time of 30.4 months), quality of life (measured via the Functional Assessment of Cancer Therapy-Prostate [FACT-P], measured at 12 months), and discontinuation of treatment due to AEs (measured at a median follow-up time of 30 months). PSA response rate was reported by Tan et al. (2020).13 It was defined as a decrease in PSA level of 50% or more from baseline. Failure-free survival was reported by Sun et al. (2018)15 and was defined as the time from randomization to PSA progression, onset of metastases, or death from any cause. Subsequent prostate cancer therapy was reported by Suzuki et al. (2020).18 It was defined as the time from randomization to the start of any subsequent prostate cancer therapy. Secondary PFS was reported by Sun et al. (2018).15 It was defined as the time from randomization to second disease progression or death.
Several AE outcomes were reported across the studies. Grade III to V AEs (grouped), defined as severe to life-threatening according to the Common Toxicity Criteria, were reported by Sathianathen et al. (2020).16 Time to symptomatic skeletal events and time to pain progression were reported in 3 studies.15,17,19
The publication by Chi et al. (2018)20 focused on patient-reported outcomes and health-related quality of life (HRQoL) from the LATITUDE trial.22 Data were collected via several standardized questionnaires (the Pain Inventory-Short Form, Brief Fatigue Inventory, FACT-P scale, and the EuroQol 5-Dimensions, 5-Levels [EQ-5D-5L] questionnaire). The patient-reported outcomes included fatigue intensity and fatigue interference; average pain progression, pain interference progression, and pain intensity; and time to HRQoL deterioration.
Summary of Critical Appraisal
Systematic Reviews
Several strengths were shared across all included SRs13-17: the research question and inclusion criteria had PICO (population, intervention, comparator, and outcome) components, the methods were established a priori, the characteristics of included studies were provided, and appropriate meta-analysis methods were used. Appropriate risk of bias (RoB) methods were used in all studies, but only Sathianathen et al. (2020)16 and Tan et al. (2020)13 discussed the impact of the RoB assessment on the results. Landre et al. (2019)14 did not assess RoB. All SRs conducted comprehensive literature reviews. All provided the search strategy except Landre et al. (2019).14 Duplicate study selection and extraction were conducted in most SRs.13,15,16 Author conflicts of interest were reported, with none declared in all SRs except Sathianathen et al. 2020 (did not declare). Finally, Tan et al. (2020),13 Wang et al. (2020),17 and Landre et al. (2019)14 discussed the impact of heterogeneity on the results.
Limitations of the systematic review methodology existed in all included studies. None provided justification for restriction to RCT study design. All but Sathianathen et al. (2020)16 failed to provide an excluded studies list with rationale for exclusion, or the sources of funding for each included study.13-15,17 Three SRs either did not include a funnel plot,13 included one but did not discuss it,14 or was unable to assess publication bias due to an insufficient number of included studies.16 The extent and impact of RoB on the study funding was not discussed by Wang et al. (2020),17 Landre et al. (2019),14 or Sun et al. (2018).15 The presence and impact of heterogeneity was not discussed in 2 SRs.15,16
An NMA was conducted in 2 SRs.15,17 In both cases, the population was relevant, there were no missing interventions or outcomes, and the study contexts were applicable. Attempts were made to identify all relevant RCTs, poor quality trials were not included, there was no selective reporting of outcomes, and measures of uncertainty were included for all pairwise comparisons. Wang et al. (2020)17 had additional strengths, mostly regarding the NMA methods: all included trials formed a connected network, there were no naive comparisons, and a rationale was provided for the use of fixed- or random-effects models (both were used depending on the specific deviance information criterion for each outcome). Ranking of interventions was provided.
Wang et al. (2020)17 had few limitations: results from direct comparisons were not reported, the number of studies was not included in the results tables or figures, individual study results were not presented, and the patient impacts were not discussed. In contrast, Sun et al. (2018)15 had more limitations. There was no information about the NMA methods (i.e., it is unknown whether a fixed- or random-effects model[s] was used, whether the trials formed a connected network, or whether statistical methods were used to preserve study randomization [no naive comparisons]). Note that naive comparisons are considered a fatal methodological flaw as per the ISPOR questionnaire, which means that “findings can be misleading and that the decision-maker should use caution in applying the findings to inform decisions (p.159).”9 In addition, heterogeneity was not explored, direct and indirect comparisons were not presented, and there was no ranking of interventions. Similar to Wang et al. (2020),17 the number of studies was not included in the results tables or figures and patient impacts were not discussed.
Primary Clinical Studies
The strengths and limitations of the primary clinical studies18-20 were similar given they were subgroup analyses of the LATITUDE RCT. The objectives, interventions, and outcomes were clearly described. The outcome measures were valid and reliable. The patient characteristics were included. Study subjects were randomized to the intervention group, and both participants and clinicians were blinded to the treatment received. The statistical tests were described and appropriate, and the main study findings were clear. Estimates of the random variability in the data were provided, and actual probability values were reported. The compliance with the intervention was reliable. The treatment was representative of the treatment that most mCSPC patients would receive, and the patients were representative of the source population.
Potential confounders and their impact on the analyses were not explicitly discussed in any clinical study. However, all 3 studies were publications of the LATITUDE trial in which stratification by key confounders (age and severity of illness) occurred before randomization and there was equal distribution of these variables between intervention and control groups. Therefore, the impact of this is likely minimal. There was no discussion of sample size or power in the studies on the Japanese subgroup (n = 35 intervention; n = 35 control).18,19 Given the small sample size, and lack of statistically significant difference for the primary outcome of overall survival, it is possible that there was insufficient power to detect differences across groups. Similarly, Chi et al. (2018)20 reported that LATITUDE was powered for the primary end point of overall survival, but not the patient-reported outcomes. Approximately 10% of the data were missing in Chi et al. (2018)20 and the reasons were unknown. However, the authors conducted sensitivity analyses to determine what impact this would have on the results and concluded that it did not have a large impact.
Economic Evaluation
The research question, rationale for the selection of the intervention, the outcomes of interest, and the economic importance were clearly stated in the economic evaluation.21 Details of the study design, including the viewpoint of the analysis, the time horizon, the source of effectiveness estimates, the analytic method, and model details, were provided. Incremental and sensitivity analyses were conducted. The discussion flowed from the results, the assumptions were reasonable, limitations were provided, and the authors clearly answered the research question. Some limitations did exist: The method to value the benefit was not stated, selection of the discount rate was not justified, and there was no mention of price adjustments for inflation.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions. For some outcomes, there was some overlap in the primary studies that were included in the SRs; therefore, the pooled estimates from separate reviews contain some of the same data. Any overlap is described in the following section. A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Clinical Effectiveness of Abiraterone Acetate for Metastatic Castration-Sensitive Prostate Cancer
Overall Survival
Direct Comparisons
The 3 SRs that reported overall survival in the general patient population13,15,16 found that AAP + ADT was favourably associated with overall survival compared with ADT plus placebo. There was overlap in the primary studies included in these SRs. The MAs were based on results from 2 RCTs. The 3 SRs included the STAMPEDE results23; however, Sathianathen et al. (2020)16 and Sun et al. (2018)15 included the interim LATITUDE results22 while Tan et al. (2020)13 included the final LATITUDE results.24
Indirect Comparisons
There was no difference in overall survival between those receiving AAP + ADT compared with APA + ADT,17 DOC + ADT,15,17 or ENZ + ADT.17 There was overlap in the primary studies included in these NMAs. Both included interim LATITUDE results22 and STAMPEDE.23
Patients Enrolled in LATITUDE in Japan
Among patients enrolled in the LATITUDE trial in Japan, there was no difference in overall survival at the first interim analyses19 and the final analyses18 between those treated with AAP + ADT compared with those who received ADT plus placebo. The sample size for this subgroup was small (intervention: n = 35; control: n = 35), and there was no discussion by the authors regarding adequate power to detect differences between groups with small numbers of participants.
Patients 70 Years and Older
There were inconsistent findings between the 2 studies that presented overall survival for participants aged 70 years or older15 and younger than 70 years14 despite both only using the interim results from LATITUDE and including the same number of participants (n = 499) to inform this outcome. In addition, there was no difference in overall survival between those treated with AAP + ADT compared with DOC + ADT.15
Patients Younger Than 70 Years
Among patients younger than 70 years of age, AAP + ADT was favourably associated with overall survival compared with ADT plus placebo.15 There was no difference in overall survival between those treated with AAP + ADT compared with DOC + ADT.15
Disease Volume
Two SRs16,17 examined the overall survival by disease volume. Wang et al. (2020)17 included an NMA of 8 RCTs by disease volume. Among patients with high-volume disease, AAP + ADT was favourably associated with overall survival compared to ADT plus placebo. There was no difference in overall survival between those receiving AAP + ADT compared with DOC + ADT, APA + ADT, or ENZ + ADT. Among patients with low-volume disease, there was no difference in overall survival between those receiving AAP + ADT compared with ADT alone, or DOC + ADT, APA + ADT, or ENZ + ADT.
The SR by Sathianathen et al. (2020)17 pooled results from 2 RCTs22,23 and determined that AAP + ADT reduced the probability of death from any cause compared with ADT alone among patients with low-volume metastases (hazard ratio [HR] = 0.68; 95% confidence interval [CI], 0.50 to 0.91) and high-volume metastases (HR = 0.61; 95% CI, 0.53 to 0.71)
Gleason Score of Less Than 8
Two SRs15,17 with an NMA examined the effect of treatment with AAP + ADT on overall survival by Gleason score. There was no difference in overall survival among patients with a Gleason score of less than 8 between AAP + ADT and any other treatment regimen.
Sun et al. (2018)15 presented a direct comparison based on data from the LATITUDE RCT22 only. There was no difference in overall survival among patients with a Gleason score of less than 8 who received AAP + ADT compared with ADT plus placebo.15,17 However, because the number of study participants with a Gleason score of less than 8 at baseline was small in this trial (n = 13 and n = 11 in intervention and control groups, respectively), power may have been insufficient to detect true differences.
From the indirect comparisons from the NMAs, there was no difference in overall survival between AAP + ADT compared with ADT plus placebo,15,17 DOC + ADT,15,17 APA + ADT,17 or ENZ + ADT.17 There was overlap among included primary studies in these NMAs: both included RCTs, 422,23,25,26 of which were included in both SRs; therefore, the pooled estimates both contain the data from these 4 RCTs.
Gleason Score of 8 or Higher
There were inconsistent findings between the 2 SRs that presented overall survival for patients with a Gleason score of 8 or higher. Through indirect comparison (direct comparisons were not presented), Wang et al. (2020)17 concluded there was no difference in overall survival between those receiving AAP + ADT compared with APA + ADT, DOC + ADT, ENZ + ADT, or ADT plus placebo. Sun et al. (2018)15 also found no difference in overall survival between AAP + ADT versus DOC + ADT but did find a favourable association in the direct evidence among those receiving AAP + ADT compared with ADT alone. There was overlap among the included primary studies in these NMAs: both included RCTs, 422,23,25,26 of which were included in both SRs; therefore, the pooled estimates both contain the data from these 4 RCTs.
ECOG Score of Zero or 1 or Higher
An SR with an NMA by Sun et al. (2018)15 found that in both ECOG subgroups (score of 0 and ≥ 1), overall survival was favourably associated with AAP + ADT compared with ADT plus placebo. There was no difference in overall survival between those treated with AAP + ADT compared with DOC + ADT.
Visceral Metastasis
A meta-analysis of 2 RCTs22,25 in 1 SR15 found no difference in overall survival between those receiving AAP + ADT and DOC + ADT for patients with visceral metastasis.
Time to Death Due to Prostate Cancer
Based on a meta-analysis of 2 RCTs22,23 from 1 SR,16 AAP + ADT reduced the time to death due to prostate cancer compared with ADT plus placebo. Among patients with low-volume metastases, there was no difference in time to death due to prostate cancer between patients receiving AAP + ADT compared with those receiving ADT alone (HR = 0.67; 95% CI, 0.44 to 1.01). Among patients with high-volume metastases, treatment with AAP + ADT reduced the probability of death due to prostate cancer compared with ADT alone (HR = 0.57; 95% CI, 0.49 to 0.67). However, the authors note that there was uncertainty around the impact of AAP + ADT on the time to death due to prostate cancer by disease volume because “there were insufficient data to conduct all the intended subgroup analyses… (p. 16).”16
Progression-Free Survival
Direct Comparisons
In the general patient population, AAP + ADT was favourably associated with PFS compared with ADT plus placebo.16,27 There was overlap in the primary studies included in these SRs. Both included the interim LATITUDE results,22 but Sathianathen et al. (2020)16 also included STAMPEDE.23 This association was consistent across patient subgroups reported in the 3 included RCTs: patients older than 70 years14 and patients enrolled in Japan.18,19
One SR13 reported direct evidence from 1 RCT28 in which AAP + ADT was favourably associated with PSA progression compared with ADT plus placebo.
One SR16 conducted a subgroup analysis by disease volume. Evidence from 2 RCTs22,23 found that AAP + ADT reduced the time to disease progression compared with ADT alone among patients with low-volume metastases (HR = 0.46; 95%CI, 0.33 to 0.63) and high-volume disease (HR = 0.46; 95% CI, 0.31 to 0.69).
Indirect Comparisons
Time to PSA Progression
One SR17 included an NMA with 9 RCTs that found AAP + ADT was favourably associated with PSA-PFS compared with DOC + ADT. There was no difference in PSA-PFS between AAP + ADT versus ENZ + ADT or APA + ADT. The authors of this SR did not specify which 9 RCTs (of the 10 total included) were part of the NMA for this outcome.
Secondary Progression-Free Survival
Among patients enrolled in Japan, secondary PFS was favourably associated with AAP + ADT compared with ADT plus placebo.18
Failure-Free Survival
One SR15 examined the impact of AAP + ADT on failure-free survival across several subgroups. Evidence for these comparisons came from 1 or 2 RCTs,22,23 depending on the subgroup. In the general patient population and in patients with an ECOG score of zero and those with a Gleason score of 8 or higher, AAP + ADT was favourably associated with failure-free survival compared with both ADT plus placebo and DOC + ADT. Among patients with an ECOG score of 1 or higher, AAP + ADT was favourably associated with failure-free survival compared with ADT plus placebo.
For those with a Gleason score of less than 8, there was no difference in failure-free survival between those receiving AAP + ADT compared with both ADT plus placebo and DOC + ADT. For those with an ECOG score of 1 or higher, there was no difference in failure-free survival between AAP + ADT and DOC + ADT.
PSA Response Rate in Patients Enrolled in Japan
Evidence from 1 subgroup analysis24 of Japanese patients summarized by Suzuki et al. (2020)18 found that AAP + ADT was favourably associated with time to deterioration compared with ADT plus placebo.
Deterioration
Evidence from 1 RCT22 summarized by Chi et al. (2018)20 found that AAP + ADT was favourably associated with time to deterioration compared with ADT plus placebo.
Time to Chemotherapy
The NMA from Wang et al. (2020)17 used data from 2 RCTs24,29 and found that AAP + ADT was favourably associated with time to chemotherapy compared with ADT plus placebo. There was no difference between those receiving AAP + ADT and those receiving APA + ADT.
Adverse Events
Grade III to V Adverse Events
Based on evidence from 1 RCT22 in 1 SR,16 the risk of grade III to V AEs, and the risk of discontinuation of treatment due to AEs, was higher among patients receiving AAP + ADT compared to those receiving ADT plus placebo. Among patients receiving AAP plus ADT, 69% experienced grade III to V AEs),22 compared with 51% in the ADT plus placebo group. In both groups, most AEs were grade III (e.g., hypertension, hypokalemia, hyperglycemia) (n = 344 of 411 in the AAP + ADT group; n = 267 of 309 in the ADT plus placebo group). The study authors24 considered most AEs to be medically manageable. For both outcomes, this was considered moderate quality evidence; the level of evidence was downgraded due to concerns related to attrition bias.
Symptomatic Skeletal Events
One SR17 included an NMA that included 4 treatment modalities in the indirect comparisons of symptomatic skeletal events. There was no difference in time to symptomatic skeletal events between patients receiving AAP + ADT and ADT + APA, ADT + ENZ, or ADT monotherapy. The authors did not specify which RCTs were included in this indirect comparison.
Pain Progression
One SR17 included an NMA that included 4 treatment modalities in the indirect comparisons of time to pain progression: ADT + APA, ADT + AAP, ADT + ENZ, and ADT monotherapy. They found that AAP + ADT was favourably associated with time to pain progression compared with ADT plus placebo, but there was no difference in pain progression between AAP + ADT compared with ADT + APA or ADT + ENZ. The authors did not specify which RCTs were included in this indirect comparison.
Evidence from a subgroup analysis of Japanese patients from 1 RCT24 suggested there was no difference in time to pain progression between those treated with AAP + ADT compared with those treated with ADT plus placebo.18
Chi et al. (2018)20 summarized additional pain-related outcomes from 1 RCT.22 Patients receiving AAP + ADT had a longer median time to worst pain intensity progression and lower median time to pain interference progression compared with those who received ADT plus placebo. There was no difference in the time to average pain progression between AAP + ADT compared with ADT plus placebo. However, this RCT was not powered for these patient-related outcomes so it is possible that the sample size was too small to detect a true difference between groups.
Fatigue
Evidence from 1 RCT22 summarized by Chi et al. (2018)20 found that AAP + ADT was favourably associated with both worst fatigue intensity and fatigue interference progression compared with ADT plus placebo.
Quality of Life
Based on evidence from 1 RCT22 in 1 SR,16 AAP + ADT was favourably associated with quality of life compared with ADT plus placebo.16 This was considered moderate quality evidence; the level of evidence was downgraded due to concerns related to attrition bias. There was no difference in quality of life between patients treated with AAP + ADT compared with ADT alone who had low-volume metastases (mean difference [MD] = –2.03; 95% CI, –11.0 to 6.9) or high-volume metastases (MD = 3.68; 95% CI, 0.73 to 6.63)
Cost-Effectiveness of Abiraterone Acetate for Metastatic Castration-Sensitive Prostate Cancer
Incremental Cost-Effectiveness Ratio
The average cost of treatment for mCSPC with initial abiraterone acetate was estimated to be $188,815.07 compared with $64,501.75 for initial docetaxel. Hird et al. (2020)21 estimated an incremental cost-effectiveness ratio (ICER) of $276,251.82 per QALY gained, which is outside traditionally accepted willingness-to-pay thresholds. With the recent approval of a generic abiraterone product, the authors produced a modified ICER using pharmacy costing data for the generic product. The result was $149,022.09 per QALY gained. The authors concluded that to reduce the willingness-to-pay threshold even further to $100,000, the monthly cost of abiraterone acetate must be less than $1,750.
Limitations
Although a large body of evidence exists related to the clinical effectiveness of abiraterone acetate for the treatment of mCSPC, the direct evidence for effectiveness comes from 2 RCTs: the LATITUDE trial22 and the STAMPEDE trial.23 The LATITUDE trial was characterized as a double-blind, placebo-controlled trial. The STAMPEDE trial23 was an open-label trial; therefore, opportunities exist for the introduction of detection bias, particularly for subjective outcomes such as quality of life. Also, the STAMPEDE trial included both non-mCRPC and mCRPC patients. Although subgroup analyses specific to mCSPC were provided, baseline characteristics were not.16 Therefore, it is not possible to assess degree of similarity in baseline characteristics across both RCTs. A degree of clinical heterogeneity did exist between the 2 trials; for example, most participants in the LATITUDE trial22 had undergone previous prostate cancer treatment (93.4%) compared with 6.1% in the STAMPEDE trial23 and the LATITUDE trial22 required the presence of at least 2 high-risk prognostic factors, whereas the STAMPEDE trial23 did not. However, taking these methodological factors into consideration, the Cochrane review16 assessed the evidence from these 2 trials, upon which most of the evidence in this report is based, to be of moderate or high certainty. Further, given these trials are multi-national (including Canadian recruitment sites and investigators), the results are likely generalizable to the Canadian context.
Adverse event outcomes were reported in 5 studies,15-17,19,20 but only 1 reported grade III to V AEs.16 Although treatment with AAP + ADT was associated with increased risk of severe, life-threatening, or fatal AEs (grade III to V), these data were presented in aggregate form; the frequency by specific AE type (e.g., frequency of hypertension, hypokalemia) was not reported. This makes it difficult to weigh clinical benefits of treatment against the risk of severe AE during decision-making.
Although additional cost-effectiveness analyses were identified, the evidence for cost-effectiveness of abiraterone acetate for the treatment of mCSPC was limited to studies conducted in Canada, which are most relevant and generalizable to the Canadian context. The included economic evaluation by Hird et al. (2020)21 was of high quality. However, consideration of additional evidence and perspective may add a level of certainty to the cost-effectiveness assessment. Further, this study compared AAP plus ADT with DOC +ADT, but not to ADT alone. Because patients may not receive docetaxel for a variety of reasons, additional cost-effectiveness evidence with ADT alone as a comparator may be beneficial for decision-making. An additional 5 economic evaluations were identified that met the selection criteria for this report, but these were not summarized. Citations for these studies are found in Appendix 6.
No research gaps were identified in this report.
Conclusions and Implications for Decision- or Policy-Making
Five SRs13-17 and 3 subgroup analyses reporting results from 1 RCT18-20 were included to address the clinical effectiveness of abiraterone acetate for the treatment of mCSPC. One economic evaluation21 was included to address the cost-effectiveness of abiraterone acetate for the treatment of mCSPC. The findings from these publications are largely based on 2 trials22,23 with moderate- to high-certainty evidence for key clinical outcomes16 and generalizable to the Canadian mCSPC patient population and economic context.
Compared to ADT monotherapy, AAP + ADT was associated with improved overall survival, prostate cancer–specific survival, PFS, and improved quality of life. Although AAP + ADT did have a favourable association with AEs, such as time to pain progression and deterioration compared with ADT monotherapy, patients treated with AAP + ADT were at increased risk of grade III to V AEs (severe, life-threatening, or fatal) and the risk of treatment discontinuation due to these AEs was higher. Hird et al. (2020)21 estimated a cost of $276,251.82 per QALY gained which is higher than traditionally accepted willingness-to-pay thresholds. Despite the recent introduction of a generic product to the Canadian market, the updated ICER was calculated to be $149,022.09 per QALY gained.
Future funding decisions for abiraterone acetate in Canada will have to weigh the benefits of a clinically effective treatment against both the evidence regarding AEs and the budgetary implications of a high-cost treatment.
References
1.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics 2019. Toronto (ON): Canadian Cancer Society; 2019: https://www.cancer.ca/~/media/cancer.ca/CW/cancer%20information/cancer%20101/Canadian%20cancer%20statistics/Canadian-Cancer-Statistics-2019-EN.pdf?la=en&la=en. Accessed 2021 Apr 7.
2.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-e205. PubMed
3.Siegel DA, O'Neil ME, Richards TB, Dowling NF, Weir HK. Prostate cancer incidence and survival, by stage and race/ethnicity - United States, 2001-2017. MMWR Morb Mortal Wkly Rep. 2020;69(41):1473-1480. PubMed
4.Swami U, McFarland TR, Nussenzveig R, Agarwal N. Advanced prostate cancer: treatment advances and future directions. Trends Cancer. 2020;6(8):702-715. PubMed
5.American Cancer Society. Hormone therapy for prostate cancer. 2020; https://www.cancer.org/cancer/prostate-cancer/treating/hormone-therapy.html. Accessed 2021 Apr 7.
6.Montanari M, Rossetti S, Cavaliere C, et al. Epithelial-mesenchymal transition in prostate cancer: an overview. Oncotarget. 2017;8(21):35376-35389. PubMed
7.Rehman Y, Rosenberg JE. Abiraterone acetate: oral androgen biosynthesis inhibitor for treatment of castration-resistant prostate cancer. Drug Des Devel Ther. 2012;6:13-18. PubMed
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Apr 7.
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Tan G, Xuan Z, Li Z, et al. The efficacy and safety of abiraterone acetate in patients with high-risk prostate cancer: a meta-analysis based on six randomized control trials. Transl Androl Urol. 2020;9(4):1691-1699. PubMed
14.Landre T, Guetz GD, Chouahnia K, Fossey-Diaz V, Taleb C, Culine S. Is there a benefit of addition docetaxel, abiraterone, celecoxib, or zoledronic acid in initial treatments for patients older than 70 years with hormone-sensitive advanced prostate cancer? A meta-analysis. Clin Genitourin Cancer. 2019;17(4):e806-e813. PubMed
15.Sun G, Zhang X, Chen J, et al. What kind of patients with castration-naive prostate cancer can benefit from upfront docetaxel and abiraterone: A systematic review and a network meta-analysis. Urol Oncol. 2018;36(12):505-517. PubMed
16.Sathianathen NJ, Oestreich MC, Brown SJ, et al. Abiraterone acetate in combination with androgen deprivation therapy compared to androgen deprivation therapy only for metastatic hormone-sensitive prostate cancer. Cochrane Database Syst Rev. 2020;12:CD013245. PubMed
17.Wang Y, Gui H, Wang J, et al. Comparative efficacy of combined radiotherapy, systemic therapy, and androgen deprivation therapy for metastatic hormone-sensitive prostate cancer: a network meta-analysis and systematic review. Front Oncol. 2020;10:567616. PubMed
18.Suzuki H, Shin T, Fukasawa S, et al. Efficacy and safety of abiraterone acetate plus prednisone in Japanese patients with newly diagnosed, metastatic hormone-naive prostate cancer: final subgroup analysis of LATITUDE, a randomized, double-blind, placebo-controlled, phase 3 study. Jpn J Clin Oncol. 2020;50(7):810-820. PubMed
19.Fukasawa S, Suzuki H, Kawaguchi K, et al. Efficacy and safety of abiraterone acetate plus prednisone in Japanese patients with newly diagnosed, metastatic hormone-naive prostate cancer: a subgroup analysis of LATITUDE, a randomized, double-blind, placebo-controlled, Phase 3 study. Jpn J Clin Oncol. 2018;48(11):1012-1021. PubMed
20.Chi KN, Protheroe A, Rodriguez-Antolin A, et al. Patient-reported outcomes following abiraterone acetate plus prednisone added to androgen deprivation therapy in patients with newly diagnosed metastatic castration-naive prostate cancer (LATITUDE): an international, randomised phase 3 trial. Lancet Oncol. 2018;19(2):194-206. PubMed
21.Hird AE, Magee DE, Cheung DC, Matta R, Kulkarni GS, Nam RK. Abiraterone vs. docetaxel for metastatic hormone-sensitive prostate cancer: A microsimulation model. Can Urol Assoc J. 2020;14(9):E418-E427. PubMed
22.Fizazi K, Tran N, Fein L, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352-360. PubMed
23.James ND, Spears MR, Sydes MR. Abiraterone in metastatic prostate cancer. N Engl J Med. 2017;377(17):1696-1697. PubMed
24.Fizazi K, Tran N, Fein L, et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019;20(5):686-700. PubMed
25.Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373(8):737-746. PubMed
26.Gravis G, Boher JM, Joly F, et al. Androgen deprivation therapy (ADT) plus docetaxel versus ADT alone in metastatic non castrate prostate cancer: impact of metastatic burden and long-term survival analysis of the randomized phase 3 GETUG-AFU15 trial. Eur Urol. 2016;70(2):256-262. PubMed
27.Tan PS, Aguiar P, Jr., Haaland B, Lopes G. Addition of abiraterone, docetaxel, bisphosphonate, celecoxib or combinations to androgen-deprivation therapy (ADT) for metastatic hormone-sensitive prostate cancer (mHSPC): a network meta-analysis. Prostate Cancer Prostatic Dis. 2018;21(4):516-523. PubMed
28.Feyerabend S, Saad F, Perualila NJ, et al. Adjusting overall survival estimates for treatment switching in metastatic, castration-sensitive prostate cancer: results from the LATITUDE study. Target Oncol. 2019;14(6):681-688. PubMed
29.Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381(1):13-24. PubMed
30.Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: a randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974-2986. PubMed
31.Boevé LMS, Hulshof M, Vis AN, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial: data from the HORRAD trial. Eur Urol. 2019;75(3):410-418. PubMed
32.Clarke NW, Ali A, Ingleby FC, et al. Addition of docetaxel to hormonal therapy in low- and high-burden metastatic hormone sensitive prostate cancer: long-term survival results from the STAMPEDE trial. Ann Oncol. 2019;30(12):1992-2003. PubMed
33.Davis ID, Martin AJ, Stockler MR, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121-131. PubMed
34.James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016;387(10024):1163-1177. PubMed
35.Fizazi K, Faivre L, Lesaunier F, et al. Androgen deprivation therapy plus docetaxel and estramustine versus androgen deprivation therapy alone for high-risk localised prostate cancer (GETUG 12): a phase 3 randomised controlled trial. Lancet Oncol. 2015;16(7):787-794. PubMed
36.Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018;392(10162):2353-2366. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Sathianathen et al. (2020)16 Country: US Funding source: University of Minnesota | This Cochrane review with meta-analysis included 2 RCTs: LATITUDE final results24 and STAMPEDE.23 | Men with metastatic prostate cancer (with or without local therapy) Men with prior adjuvant or neoadjuvant ADT were included if metastasis occurred > 12 months after stopping hormone therapy Men receiving concurrent osteoprotective therapy were included Men who received chemotherapy without known metastases or those who received any chemotherapy agent for prostate cancer were excluded | Intervention: Abiraterone acetate and prednisone in combination with ADT Comparator: ADT alone | Primary outcomes: Time to death due to any cause; quality of life Secondary outcomes: Grades III to V AEs; time to death due to prostate cancer; time to disease progression; discontinued treatment due to AEs Follow-up: LATITUDE: 5 years STAMPEDE: Until death of all randomized participants Quality of life: Measured at 12 months Grades III to V AEs; time to disease progression; and discontinued treatment due to AEs: measured at medium follow-up of 30 months Time to death due to prostate cancer: measured at median follow-up of 30.4 months |
Tan et al. (2020)13 Country: China Funding source: High-level Hospital Construction Research Project of Maoming People’s Hospital, Guangdong Medical Science and Technology Fund and Maoming Science and Technology Project | This systematic review with meta-analysis included 3 RCTs relevant to this report: LATITUDE interim22 and final24 results and STAMPEDE.23 | Patients diagnosed with mCSPC | Intervention: Abiraterone acetate and prednisone in combination with ADT Comparator: ADT plus placebo | Outcomes: Overall survival; progression-free survival; time to PSA progression; PSA response rate (≥ 50% decline in PSA level from baseline) Follow-up: NR |
Wang et al. (2020)17 Country: China Funding source: National Natural Science Foundation of China and the Cuiying Scientific and Technological Innovation program of Lanzhou University Second Hospital | This systematic review with network meta-analysis included 10 RCTs with 11,194 participants. | Patients ≥ 18 years of age with mHSPC. Patients with localized or castration-resistant prostate cancer were excluded | Interventions:
| Outcomes: Overall survival, PSA progression-free survival; time to symptomatic skeletal events; time to pain progression; and time to chemotherapy. Follow-up: NR |
Landre et al. (2019)14 Country: France Funding source: NR | This systematic review and meta-analysis included 8 RCTs, 1 of which was relevant to this report: LATITUDE interim results.22 | Patients > 70 years of age with advanced HSPC 6 of 8a RCTs included both metastatic and non-metastatic HSPC patients. The authors did not stratify the results by metastatic status. Therefore, only the crude results from the LATITUDE trial22 are reported here (all participants had mHSPC) | Intervention: Abiraterone acetate and prednisone in combination with ADT Comparator: ADT plus placebo | Outcomes: Overall survival; progression-free survival Follow-up: NR |
Sun et al. (2018)15 Country: China Funding source: National Natural Science Foundation of China, the Science and Technology Support Program of Scihuan Province, and 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University | This systematic review with network meta-analysis included 6 RCTs with 6,480 patients. Among these, 1,577 patients (24%) received abiraterone and 3,535 (55%) received ADT alone. | Patients with non-mHSPC (n = 2,018, 31%) or mHSPC (n = 4,462; 69%). Median age: 62 to 68 years | Intervention: Abiraterone acetate plus ADT; docetaxel plus ADT Comparator: ADT alone | Outcomes: Overall survival; failure-free survival With subgroup analysis by age (< 70 vs. ≥ 70 years); Gleason score (< 8 vs. ≥ 8); and ECOG PS (0 vs. ≥ 1) Follow-up: Median 28.9 months to 9.2 years |
ADT = androgen deprivation therapy; AE = adverse event; CSPC = castration-sensitive prostate cancer; ECOG PS = Eastern Cooperative Oncology Group performance status; mHSPC = metastatic hormone-sensitive prostate cancer; NR = not reported; PSA = prostate-specific antigen; RCT = randomized controlled trial; vs. = versus.
aThe other RCTs investigated docetaxel vs. ADT and not relevant to this report.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Suzuki et al. (2020)18 Country: Japan Funding source: Janssen Research & Development and Janssen Pharmaceutical K.K. | This study is a subgroup analysis of the LATITUDE trial’s final analysis (clinical cut-off date of August 15, 2018) LATITUDE RCT: Phase III double-blind (investigators and patients were blind to the randomization), active control trial Recruitment occurred across 235 clinical sites in 34 countries (including Canada) | This subgroup analysis consists of 70 participants enrolled in Japan (n = 35 each in the treatment and placebo groups), which represents 5.8% of the total number of LATITUDE trial participants. The authors reported that baseline characteristics of the Japanese subgroup were similar to the general trial population. LATITUDE population inclusion/exclusion criteria: Inclusion: Patients with newly diagnosed high-risk mCSPC:
Patients with high-risk disease were included if they had at least 2/3 high-risk prognostic factors (Gleason score > 7, presence of > 2 bone lesions, or measurable visceral metastasis) | Intervention: Abiraterone acetate and prednisone in combination with ADT Comparator: ADT plus placebo | Primary outcome: Overall survival Secondary outcomes: Time to pain progression (via BPI-SF); time to PSA progression; time to next skeletal-related event; time to initiation of chemotherapy; and time to the next therapy for prostate cancer Exploratory end point: Secondary progression-free survival (time from randomization to second disease progression or death) Safety outcomes: Incidence of AEs Follow-up: Median follow-up = 56.6 months (range = 2.5 to 64.2 months) |
Suzuki et al. (2020)18 Country: Japan Funding source: Janssen Research & Development and Janssen Pharmaceutical K.K. | This study is a subgroup analysis of the LATITUDE trial’s final analysis (clinical cut-off date of August 15, 2018) LATITUDE RCT: Phase III double-blind (investigators and patients were blind to the randomization), active control trial Recruitment occurred across 235 clinical sites in 34 countries (including Canada) | Exclusion: Patients with:
Number of trial participants: 1,119 patients were randomized 1:1 (597 to intervention and 602 to comparator) Median age: 68 years (range = 38 to 89 years) in the treatment group and 67 years (range = 33 to 92 years) in the control group | Intervention: Abiraterone acetate and prednisone in combination with ADT Comparator: ADT plus placebo | |
Fukasawa et al. (2018)19 Country: Japan Funding source: Janssen Research & Development and Janssen Pharmaceutical K.K. | LATITUDE RCT (see Suzuki et al. [2020]18 above for details about the LATITUDE trial methodology) This study is a subgroup analysis of the LATITUDE trial’s first interim analysis (clinical cut-off date of October 31, 2016) | See Suzuki et al. (2020)18 for details about the LATITUDE trial methodology This subgroup analysis consists of 70 Japanese participants (n = 35 each in the treatment and placebo groups), which represents 5.8% of the total number of LATITUDE trial participants. The authors reported that the baseline characteristics of the Japanese subgroup were similar to the general trial population except for higher baseline PSA in the treatment vs. control group, and “slight differences” in Gleason scores and disease locations between the Japanese subgroup and general trial population. | See Suzuki et al. (2020)18 for details about the LATITUDE trial methodology | Primary outcomes: Overall survival; radiographic progression-free survival Secondary outcomes: Time to pain progression (via BPI-SF); time to PSA progression; time to next skeletal-related event; time to initiation of chemotherapy; and time to the next therapy for prostate cancer Safety outcomes: Incidence of AEs Follow-up: Median follow-up = 35.0 months |
Chi et al. (2018)20 Country: Canada* Funding source: Janssen Research & Development (study); Janssen Global Services (editorial support) | This is an interim analysis of the LATITUDE trial, focused on patient-reported outcomes. LATITUDE RCT (see information presented from Suzuki et al. [2020]18 for details about the LATITUDE trial methodology) | See information presented from Suzuki et al. (2020)18 for details about the LATITUDE trial methodology | See information presented from Suzuki et al. (2020)18 for details about the LATITUDE trial methodology | Outcomes: Patient-reported outcomes of time to average pain progression; time to worst pain intensity progression; time to pain interference progression; time to worst fatigue intensity progression; time to fatigue interference progression; time to deterioration of FACT-P total score; and EQ-VAS and EQ-5D-5L health utility scores over time Follow-up: Median follow-up for all patients at the interim cut-off date was 30.4 months |
ADT = androgen deprivation therapy; AE = adverse event; BPI-SF = Brief Pain Inventory-Short Form; ECOG = Eastern Cooperative Oncology; FACT-P = Functional Assessment of Cancer Therapy-Prostate; mCSPC = metastatic castration-sensitive prostate cancer; PSA = prostate-specific antigen; RCT = randomized controlled trial.
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
Hird et al. (2020)21 Country: Canada Funding source: Ajmera Family Chair in Urologic Oncology | Type of analysis: Cost-effectiveness analysis Horizon: Lifetime Perspective: Health care payer | Population: Men with newly diagnosed mCSPC Base case: 65-year-old patient with mCSPC | Intervention and comparator: Long-term ADT with initial docetaxel (6 cycles, 1 every 3 weeks) of 75 mg/m2 vs. long-term ADT with initial abiraterone acetate and prednisone | Modelling approach: Microsimulation model with Markov cycle length of 3 months (accounts for follow-up interval in clinical practice). The base case was a 65-year-old patient with newly diagnosed mCSPC and candidate for either intervention. The modelled patients were a cohort with ECOG status of 0 to 2 and radiographic evidence of metastasis. ICER would be calculated if abiraterone acetate demonstrated superiority over docetaxel. The model conducted a simulation of 100,000 patients. Primary outcome: QALY Secondary outcomes: Overall survival; rates of use of second- and third-line therapy; and rates of AEs | Source of clinical data: From the literature and adjusted for cycle length. RCT data were preferred. The weighted average was used to combine estimates across multiple data points. Source of cost data: From the literature and CIHI PCE Source of utility data: Tufts-New England Medical Center Cost-Effectiveness Analysis Registry | It was assumed that:
|
ADT = androgen deprivation therapy; AE = adverse event; CIHI PCE = Canadian Institute for Health Information Patient Cost Estimator; ECOG = Eastern Cooperative Oncology Group; ICER = incremental cost-effectiveness ratio; mCSPC = metastatic castration-sensitive prostate cancer; QALY = quality-adjusted life-years; vs. = versus.
Appendix 3: Critical Appraisal of Included Publications
Table 5: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 2 and the ISPOR Questionnaire
Strengths | Limitations |
Sathianathen et al. (2020)16 | |
|
|
Tan et al. (2020)13 | |
|
|
Wang et al. (2020)17 | |
SR Strengths
NMA Strengths
| SR Limitations
NMA Limitations
|
Landre et al. (2019)14 | |
|
|
Sun et al. (2018)15 | |
SR Strengths
NMA Strengths
| SR Limitations
NMA Limitations
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NMA = network meta-analysis; PICO = population, intervention, comparator, and outcome; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist
Strengths | Limitations |
Suzuki et al. (2020)18 | |
|
|
Chi et al. (2018)20 | |
|
|
Fukasawa et al. (2018)19 | |
|
|
Table 7: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist
Strengths | Limitations |
Hird et al. (2020)21 | |
|
|
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings of Included Systematic Reviews and Network Meta-Analyses
Sathianathen et al. (2020)16
Main Study Findings
Evidence from the meta-analysis of the LATITUDE and STAMPEDE trials
Time to death from any cause
AAP + ADT reduced the probability of death from any cause compared with ADT alone (HR = 0.64; 95% CI, 0.56 to 0.73) (high-certainty evidence)
Subgroup: Volume of metastases
AAP + ADT reduced the probability of death from any cause compared with ADT alone among patients with low-volume metastases (HR = 0.68; 95%CI, 0.50 to 0.91) and high-volume disease (HR = 0.61; 95% CI, 0.53 to 0.71)
Time to death due to prostate cancer
AAP + ADT reduced the probability of death from prostate cancer compared with ADT alone (HR = 0.58; 95% CI, 0.50 to 0.68) (moderate-certainty evidence)
Subgroup: Volume of metastases
Among patients with low-volume metastases, there was no difference in time to death due to prostate cancer between patients receiving abiraterone acetate plus ADT compared with those receiving ADT alone (HR = 0.67; 95% CI, 0.44 to 1.01). Among patients with high-volume metastases, treatment with AAP + ADT reduced the probability of death due to prostate cancer compared with ADT alone (HR = 0.57; 95% CI, 0.49 to 0.67)
Time to disease progression
AAP + ADT reduced the probability of disease progression compared with ADT alone (HR = 0.35; 95% CI, 0.26 to 0.49) (moderate-certainty evidence)
Subgroup: Volume of metastases
AAP + ADT prolonged the time to disease progression compared with ADT alone among patients with low-volume metastases (HR = 0.46; 95% CI, 0.33 to 0.63) and high-volume disease (HR = 0.46; 95% CI, 0.31 to 0.69)
Evidence from the LATITUDE trial
Quality of life
Quality of life among men on AAP + ADT was higher than men on ADT alone (MD = 2.9 points; 0.11 to 5.69 higher) (moderate-certainty evidence)
Subgroup: volume of metastases
There was no difference in quality of life between patients treated with AAP + ADT compared to ADT alone who had low-volume metastases (MD, -2.03; 95% CI, -11.0 to 6.9) or high-volume metastases (MD = 3.68; 95% CI, 0.73 to 6.63)
Grades III to V AEs
The risk of AE among men on AAP + ADT was higher relative to men on ADT alone (relative risk [RR] = 1.34; 95% CI, 1.22 to 1.47) (high-certainty evidence)
Discontinuation of treatment due to AEs
The risk of discontinuation of treatment due to AEs was higher among men on AAP + ADT relative to men on ADT alone (RR = 1.50; 95% CI, 1.17 to 1.92) (moderate-certainty evidence)
Author’s Conclusion
“Compared to androgen deprivation therapy (ADT) alone, the addition of abiraterone acetate to ADT for metastatic hormone-sensitive prostate cancer probably improves overall and progression-free survival. The addition of abiraterone acetate to ADT appears to result in a large reduction in the risk of progression. It also probably reduces the probability of prostate cancer-specific death… (p.16).”16
“Abiraterone acetate in addition to ADT probably results in a small likely not clinically meaningful improvement in quality of life at 12 months compare to ADT alone… assuming a minimally clinically important difference of 6-10 (p. 15).”16
“We had concerns regarding attrition bias for the quality of life outcome, because only 70% of the men in the LATITUDE study completed the questionnaire at 12 months; therefore, this may not reliably reflect the true treatment effect for this population (p.16).”16
“This corresponds to 162 more (95% CI 105 to 224) grades III to V adverse event events per 1,000 men treated with abiraterone acetate and ADT compared to ADT alone, at a median follow-up of 30 months (p. 15).”16
“This corresponds to 51 more men (95% CI 17 to 93) discontinuing treatment because of adverse events per 1,000 men treated with abiraterone acetate and ADT compared to ADT alone, at a median follow-up of 30 months (p. 16).”16
Tan et al. (2020)13
Main Study Findings
Evidence from the meta-analysis of LATITUDE final results24 and the STAMPEDE trial23
• Overall survival
AAP + ADT reduced the probability of death from any cause compared with ADT alone (HR = 0.64; 95% CI, 0.56 to 0.73)
Evidence from LATITUDE final results24
Time to PSA progression
AAP + ADT improved the time to PSA progression compared with ADT alone (HR = 0.31; 95% CI, 0.27 to 0.36)
Evidence from LATITUDE interim results22
Progression-free survival
AAP + ADT was associated with improved PFS compared with ADT alone (HR = 0.47; 95% CI, 0.40 to 0.56)
PSA response rate
AAP + ADT was associated with improved PSA response rate compared with ADT alone (RR = 1.37; 95% CI, 1.02 to 1.84)
Author’s Conclusion
“All included RCTs confirmed that abiraterone acetate achieved a significant and different degree of clinical benefits in OS, the time to PSA progression, PFS (according to radiographic evidence), and PSA response rate in high-risk prostate cancer patients… (p. 1697).”13
Wang et al. (2020)17
Main Study Findings
Direct comparisons: Not reported
Indirect comparisons
Overall survival
AAP + ADT was associated with increased overall survival compared with ADT alone (HR = 0.64; 95% CI, 0.56 to 0.73)
There was no difference in overall survival between patients receiving AAP + ADT compared with those receiving 1 of the following:
ADT plus apalutamide (HR = 0.95; 95% CI, 0.70 to 1.30)
ADT plus docetaxel (HR = 1.20; 95% CI, 1.0 to 1.5)
ADT plus enzalutamide (HR = 0.82; 95% CI, 0.57 to 1.2)
AAP + ADT had the highest likelihood of being ranked second (55.7%) compared with the other treatment combinations
PSA progression-free survival
AAP + ADT was associated with improved PSA-PFS compared to ADT alone (HR = 0.30; 95% CI, 0.26 to 0.35)
ADT plus docetaxel was associated with reduced PSA-PFS compared to AAP + ADT (HR = 2.2; 95% CI, 1.7 to 2.9)
There was no difference in PSA-PFS between patients receiving AAP + ADT compared to those receiving:
Enzalutamide plus ADT (HR = 1.1; 95% CI, 0.84 to 1.5)
Apalutamide plus ADT (HR = 1.2; 95% CI, 0.9 to 1.5)
AAP + ADT had the highest likelihood of being ranked second (67.2%) behind apalutamide compared with the other treatment combinations
Time to symptomatic skeletal events
There was no difference in time to symptomatic skeletal events between patients receiving AAP + ADT compared with those receiving any of the following:
ADT (HR = 0.76; 95% CI, 0.32 to 1.8)
Apalutamide plus ADT (HR = 0.94; 95% CI, 0.27 to 3.3)
Enzalutamide plus ADT (HR = 0.68; 95% CI, 0.19 to 2.4)
AAP + ADT had the highest likelihood of being ranked second (40.5%) behind enzalutamide compared with the other treatment combinations
Time to pain progression
AAP + ADT was associated with improved time to pain progression compared with ADT alone (HR = 0.72; 95% CI, 0.61 to 0.86)
There was no difference in time to pain progression between patients receiving AAP + ADT compared with those receiving:
Apalutamide plus ADT (HR = 0.88; 95% CI, 0.65 to 1.2)
Enzalutamide plus ADT (HR = 1.3; 95% CI, 1.0 to 1.6)
AAP + ADT had the highest likelihood of being ranked first (79.9%) compared with the other treatment combinations
Time to chemotherapy
AAP + ADT was associated with improved time to chemotherapy compared to ADT alone (HR = 0.51; 95% CI, 0.41 to 0.63)
There was no difference in time to chemotherapy between those receiving AAP + ADT compared to those receiving apalutamide plus ADT (HR = 1.3; 95% CI, 0.85 to 2.0)
AAP + ADT had the highest likelihood of being ranked second (89.3%) behind apalutamide compared with the other treatment combinations
Subgroup analysis of disease volume
Overall survival: high-volume subgroup
Among patients with high-volume disease, there was improved overall survival for those receiving AAP + ADT compared with those receiving ADT alone (HR = 0.62; 95% CI, 0.50 to 0.74)
There was no difference in overall survival between patients receiving AAP + ADT compared to those receiving any of the following:
Docetaxel plus ADT (HR = 1.2; 95% CI, 0.93 to 1.5)
Apalutamide plus ADT (HR = 0.91; 95% CI, 0.64 to 1.3)
Enzalutamide plus ADT (HR = 1.0; 0.65 to 1.7)
AAP + ADT had the highest likelihood of being ranked first (62.3%) compared with the other treatment combinations
Overall survival: low-volume subgroup
There was no difference in overall survival between patients receiving AAP + ADT compared with those receiving:
ADT alone (HR = 0.72; 95% CI, 0.47 to 1.1)
Apalutamide plus ADT (HR = 1.1; 95% CI, 0.49 to 2.4)
Enzalutamide plus ADT (HR = 0.53; 95% CI, 0.25 to 1.1)
Docetaxel plus ADT (HR = 1.1; 95% CI, 0.69 to 1.8)
AAP + ADT had the highest likelihood of being ranked fourth (24.0%) compared with the other treatment combinations
Overall survival: Gleason score less than 8
There was no difference in overall survival between those receiving AAP + ADT and those receiving:
ADT alone (HR = 0.44; 95% CI, 0.15 to 1.3)
Apalutamide plus (HR = 0.78; 95% CI, 0.23 to 2.6)
Docetaxel plus ADT (HR = 1.6; 95% CI, 0.54 to 4.8)
Enzalutamide plus ADT (HR = 1.4; 95% CI; 0.38 to 4.8)
AAP + ADT had the highest likelihood of being ranked first (56.0%) compared with the other treatment combinations
Overall survival: Gleason score of 8 or higher
There was no difference in overall survival between those receiving AAP + ADT and those receiving:
ADT alone (HR = 0.67; 95% CI, 0.35 to 1.3).
Apalutamide plus (HR = 0.92; 95% CI, 0.35 to 2.4)
Docetaxel plus ADT (HR = 1.2; 95% CI, 0.54 to 2.5)
Enzalutamide plus ADT (HR = 1.0; 95% CI; 0.4 to 2.6)
AAP + ADT had the highest likelihood of being ranked first (33.0%) compared with the other treatment combinations
Author’s Conclusion
The authors did not discuss abiraterone acetate results specifically.
“The present study analyzed 10 high-quality, large-scale clinical trials involving 11,194 patients. All of the combined treatment regimens improved OS compared to ADT monotherapy, with ADT + ENZ ranking highest (although this result lacked statistical significance) (p. 9).”17
Landre et al. (2019)14
Main Study Findings
Patients aged 70 years or older
Overall survival
Abiraterone acetate with ADT and prednisone was associated with increased overall survival compared with ADT plus placebo (HR = 0.53; 95% CI, 0.38 to 0.75)
Progression-free survival
Abiraterone acetate with ADT and prednisone was associated with increased PFS compared with ADT plus placebo (HR = 0.55; 95% CI, 0.38 to 0.80)
Author’s Conclusion
The authors did not discuss the crude results from the LATITUDE trial alone.
“One of the limitations is the lack of power of the studies (the number of older patients included too small to show a real difference) as well as the fact of not knowing the cause of the deaths of the patients (p. e810).”14
Sun et al. (2018)15
Main Study Findings
Direct comparisons
Overall survival
All ages: AAP + ADT compared with ADT alone was associated with improved overall survival (HR = 0.63, 95% CI, 0.55 to 0.72)
Patients younger than 70 years: AAP + ADT compared with ADT alone was associated with improved overall survival (HR = 0.62; 95% CI, 0.45 to 0.85)
Patients 70 years or older: There was no difference in overall survival between patients receiving AAP + ADT and ADT alone (HR = 0.82; 95% CI, 0.53 to 1.27)
Patients with ECOG of zero: AAP + ADT compared with ADT alone was associated with improved overall survival (HR = 0.64, 95% CI, 0.48 to 0.85)
Patients with ECOG of 1 or higher: AAP + ADT compared with ADT alone was associated with improved overall survival (HR = 0.61, 95% CI, 0.46 to 0.81)
Patients with Gleason score less than 8: There was no difference in overall survival between patients receiving AAP + ADT and ADT alone (HR = 0.62; 95% CI, 0.18 to 2.14)
Patients with Gleason score of 8 or higher: AAP + ADT compared with ADT alone was associated with improved overall survival (HR = 0.63; 95% CI, 0.51 to 0.78)
Failure-free survival
AAP + ADT compared to ADT alone was associated with improved failure-free survival (FFS) (HR = 0.39, 95% CI, 0.35 to 0.44)
Patients with ECOG of zero: AAP + ADT compared with ADT alone was associated with improved FFS (HR = 0.40, 95% CI, 0.32 to 0.50)
Patients with ECOG of 1 or higher: AAP + ADT compared with ADT alone was associated with improved FFS (HR = 0.37; 95% CI, 0.17 to 0.81)
Patients with Gleason score less than 8: There was no difference in FFS among patients receiving AAP + ADT and ADT alone (HR = 0.47; 95% CI, 0.15 to 1.47)
Patients with Gleason score of 8 or higher: AAP + ADT compared with ADT alone was associated with improved FFS (HR = 47; 95% CI, 0.40 to 0.55)
Indirect comparisons
Overall survival
There was no difference in overall survival between patients receiving docetaxel plus ADT and those receiving abiraterone acetate (HR = 1.19; 95% CI, 0.98 to 1.44)
By subgroup
There was no difference in overall survival between docetaxel plus ADT and abiraterone acetate and ADT across all subgroups:
Patients younger than 70 years (HR = 1.26, 95% CI, 0.83 to 1.91)
Patients 70 years or older (HR = 0.76, 95% CI, 0.34 to 1.67)
Patients with ECOG of zero (HR = 1.25, 95% CI, 0.87 to 1.79)
Patients with ECOG of 1 or higher (HR = 0.72; 95% CI, 0.41 to 1.26)
Patients with Gleason score less than 8 (HR = 0.95; 95% CI, 0.26 to 3.46)
Patients with Gleason score of 8 or higher (HR = 1.29; 95% CI, 0.69 to 2.40)
Patients with visceral metastases (HR = 1.00; 95% CI, 0.42 to 2.37)
Failure-free survival
Docetaxel plus ADT was associated with decreased FFS compared with AAP + ADT (HR = 1.59; 95% CI, 1.36 to 1.86)
By subgroup
Docetaxel plus ADT was associated with decreased FFS compared with AAP + ADT for the following subgroups:
Patients with ECOG of zero (HR = 1.85; 95% CI, 1.33 to 2.57)
Patients with Gleason score of 8 or higher (HR = 1.72; 95% CI, 1.23 to 2.42)
There was no difference in overall survival between docetaxel plus ADT and abiraterone acetate and ADT for the following subgroups:
Patients with ECOG of 1 or higher (HR = 1.57; 95% CI, 0.69 to 3.57)
Patients with Gleason score less than 8 (HR = 1.28; 95% CI, 0.38 to 4.26)
Author’s Conclusion
“M1 patients [mCNPC] with younger age (< 70 years), more favorable ECOG PS (0-1), lower Gleason score (GS < 8), or visceral metastases have clear survival advantage with combination therapies. Among M1 patients < 70 years old, ECOG 0-1 or GS ≥ 8, although insufficient evidence supports better OS, early Abi administration was associated with longer FFS than Doc. The number of serious AEs ( ≥ 3) was comparable between the 2 treatment groups (p. 512).”15
“In the current meta-analysis, unlike younger men, elderly patients (≥ 70 years) did not realize improvement in OS with combination therapy (p. 513).”15
Summary of Findings of Included Primary Clinical Studies
Suzuki et al. (2020)18
Main Study Findings
Primary outcome
Overall survival
There was no difference in overall survival between Japanese participants who received abiraterone acetate with ADT and prednisone compared with those who received ADT plus placebo (HR = 0.61; 95% CI, 0.27 to 1.42; P = 0.2502). The point estimate was consistent with that of the overall population, final analysis (HR = 0.66; 95% CI, 0.56 to 0.78; P < 0.0001).
Secondary outcomes
Time to PSA progression, chemotherapy initiation, and subsequent prostate cancer therapy
Participants who received abiraterone acetate with ADT and prednisone had improved time to PSA progression (HR = 0.19; 95% CI, 0.10 to 0.38), chemotherapy initiation (HR = 0.46; 95% CI, 0.21 to 0.98), and subsequent prostate cancer therapy (HR = 0.31; 95% CI, 0.17 to 0.57) compared with participants receiving ADT and placebo.
Time to pain progression and skeletal-related initiation
There was no difference between participants treatment and control groups in the time to pain progression (HR = 0.68; 95% CI, 0.35 to 1.33) or skeletal-related initiation (HR = 1.65; 95% CI, 0.66 to 4.11)
Exploratory outcome
Secondary PFS
Participants who received abiraterone acetate with ADT and prednisone had improved secondary PFS compared with those on ADT and placebo (HR = 0.32; 95% CI, 0.17 to 0.62)
Safety outcomes
The frequency distributions of AEs across the treatment and control groups were reported and compared to the overall population. Statistical analysis was not completed.
Author’s Conclusion
“In the current Japanese subgroup analysis of LATITUDE, addition of AAP to ADT improved OS (co-primary endpoint) in comparison with the addition of placebo to ADT, which corroborates with the significant treatment benefit reported earlier in the IA [interim analysis] of Japanese subgroup (p. 816).”18 Note: this conclusion does not appear to be supported by the main study findings.
“The overall incidence of AEs was similar between the AAP group and the placebo groups in the Japanese subgroup (both 34/35 [97.1%]) as well as in the overall population (AAP group: 569/597 [95.3%], placebo group: 561/602 [93.2%]) (p. 815).”18
“Most of the results for secondary endpoints, including time to pain progression, PSA progression, initiation of chemotherapy and subsequent PC therapy in the Japanese subgroup showed consistency with the results in the overall population, supporting the addition of AAP to ADT (p. 816).”18 Note: this conclusion does not appear to be supported by the main study findings (time to pain progression and skeletal-related initiation were not significantly different between treatment and control groups.
“In this final analysis of the Japanese subgroup, the treatment effect of AAP, in terms of the primary endpoint (OS), most of secondary endpoints and the exploratory endpoint of secondary PFS were consistent with those of the overall population (p. 816).”18
Chi et al. (2018)20
Main Study Findings
Time to worst pain intensity progression: Patients receiving AAP + ADT had a longer median time to worst pain intensity progression compared with ADT (HR = 0.63; 95% CI, 0.52 to 0.77; P < 0.0001)
Time to pain interference progression: Patients receiving AAP + ADT had lower median time to pain interference progression (did not reach the predefined cut-off of the first increase by 0.5SD of baseline scores from baseline in items 9A to G from the BPI-SF) compared with ADT plus (HR = 0.67; 95% CI, 0.56 to 0.80; P < 0.0001)
Time to average pain progression: There was no significant difference in time to average pain progression between treatment groups (neither group reached the predefined cut-off of 30% or greater average pain compared with baseline via items 3 to 6 in the BPI-SF) (HR = 0.90; 95% CI, 0.69 to 1.16; P = 0.41)
Time to worst fatigue intensity: Patients receiving AAP + ADT had longer time to worst pain fatigue compared with ADT (although neither group reached the predefined cut-off of increase of 2 points or more from baseline from item 3 of the BFI) (HR = 0.65; 95% CI, 0.53 to 0.81; P = 0.001)
Time to fatigue interference progression: Patients receiving AAP + ADT had longer time to fatigue interference progression compared with ADT, although neither group reached the predefined cut-off of 1.25 points or more from baseline (HR = 0.59; 95% CI, 0.47 to 0.75; P < 0.0001)
Time to HRQoL deterioration (FACT-P): The time to deterioration was longer among patients receiving AAP + ADT, compared with those receiving ADT (HR = 0.85; 95% CI, 0.74 to 0.99; P = 0.032)
Author’s Conclusion
“ADT plus abiraterone acetate and prednisone consistently improves pain and fatigue symptoms, and overall HRQoL, when compared with those for ADT plus placebo (p. 202).”20
“Patients treated with ADT plus abiraterone acetate and prednisone showed significantly longer median time to worst pain intensity progression, worst fatigue intensity progression, and functional deterioration status as assessed by the FACT-P total score or the prostate cancer-specific subscale than those for patients treated with ADT plus placebo, and maintained or improved HRQoL (p.202).”20
“Treatment with ADT plus abiraterone acetate and prednisone led to longer median time to deterioration of physical wellbeing; however, median time to deterioration of functional, emotional, and social and family wellbeing did not differ significantly between treatment groups. These results might have been anticipated since wellbeing domains are qualitative and affected by multiple aspects of life and are therefore less likely to be dependent on disease and treatment factors (p.202).”20
“EQ-5D-5L data indicated better general health status scores (assessed by the EQ-VAS) and health utility scores in patients in the ADT plus abiraterone acetate and prednisone group than in patients in the ADT plus placebos group (p. 201).”20
Fukasawa et al. (2018)19
Main Study Findings
Primary outcomes
Overall survival
There was no significant difference in the rate of overall survival between Japanese patients receiving abiraterone acetate with ADT and prednisone compared with those receiving ADT and placebo (HR = 0.64; 95% CI, 0.15 to 2.66). The HR point estimate was comparable to that of the overall study population (HR = 0.62; 95% CI, 0.51 to 0.76), but had a higher level of uncertainty.
Radiographic progression-free survival
A total of 6 patients in the treatment group and 23 patients in the control group had evidence of radiographic PFS at time of analysis. There was a reduced risk of radiographic PFS among the Japanese patients receiving abiraterone acetate with ADT and prednisone compared with those receiving ADT and placebo (HR = 0.22; 95% CI, 0.09 to 0.56). This was consistent with the overall population (HR = 0.47; 95% CI, 0.39 to 0.55).
Secondary outcomes
Treatment with AAP + ADT and prednisone was associated with reduced time to PSA progression (HR = 0.19; 95% CI, 0.09 to 0.38) and improved time to subsequent prostate cancer therapy (HR = 0.28; 95% CI, 0.14 to 0.56)
There was no difference between the treatment and control groups with respect to time to pain progression (HR = 0.68; 95% CI, 0.35 to 1.33), time to next skeletal-related event (HR = 2.41; 95% CI, 0.82 to 7.06), or time to chemotherapy (HR = 0.43; 95% CI, 0.18 to 1.02)
Safety outcomes
The frequency distributions of AEs across the treatment and control groups were reported and compared to the overall population. Statistical analysis was not completed.
Author’s Conclusion
“…the addition of AAP to ADT improved coprimary outcomes, OS and rPFS, compared with ADT alone in Japanese men with newly diagnosed mHNPC (p. 1018).”19 Note: it doesn’t appear the conclusion about overall survival is supported by the main study findings.
“The combination of AAP plus ADT versus placebo plus ADT also prolonged time to PSA progression, along with most of the secondary endpoints (p. 1018).”19 Note: only time to PSA progression and time to subsequent prostate cancer therapy were associated with statistically significant benefit among the treatment group.
“There were no notable safety concerns identified in Japanese patients (p. 1018).”19
Summary of Findings of Included Economic Evaluation
Hird et al. (2020)21
Main Study Findings
Model costs (per patient-month)
ADT: $371
Abiraterone acetate
$3,975.69 (range: $2,370.09 to $3,975.69) (based on cost of generic abiraterone)
Emergency department visits: 129 events per 5,143 person-months
Hospitalizations: 108 events per 5,143 person-months
AE needing in-patient care: $7,099 (range: $5,574 to $7,099)
Surveillance: $3,975.69 (range: $2,370.09 to $3,975.69)
Docetaxel
$1,300.35
Emergency department visits: 703 events per 11,436 person-months
Hospitalizations: 490 events per 11,496 person-months
Chemotherapy admission for neoplasm: $7,099 (range: $6,343 to $7,099)
Chemotherapy AE needing outpatient care: $2,056 (range: $1,848 to $2,056)
Surveillance: $526.35
Third-line therapy
$9,166.35
AE on third-line: $7,099 (range: $5,679 to $7,099)
Surveillance: $155.35
Palliation
$3,671
Preferred treatment pathway
The abiraterone acetate + ADT pathway was preferred over the docetaxel + ADT pathway (overall survival of 3.36 QALYs versus 2.91 QALYs)
Median overall survival 51 months with initial abiraterone acetate compared with 48 months with initial docetaxel
Survival begins to favour abiraterone acetate at the 40-month mark
Adverse events
Proportion of patients experiencing AE was 17.6% with initial abiraterone acetate compared with 22.3% with initial docetaxel.
Treatment-related death occurred in 0.5% of patients with docetaxel and 1.0% in those with abiraterone acetate
Cost
Average cost of treatment was $188,815.07 among those with initial abiraterone acetate compared with $64,501.75 with initial docetaxel
ICER = $276,251.82 per QALY gained with initial therapy with abiraterone acetate
Cost (generic brand of abiraterone acetate)
$2,370.09 per month (pharmacy costing data)
Treatment cost of $124,094.10 per patient
Updated ICER = $149,022.09 per QALY gained
From sensitivity analysis, for willingness-to-pay threshold to be less than $100,000, monthly cost of abiraterone acetate must be less than $1,750
Author’s Conclusion
“Initial AA resulted in a gain of 0.45 QALYs compared to DC (3.36 vs. 2.91 QALYs). Median crude OS was 51 months with AA and 48 months with DC. Graphically, 5-year OS with both therapies was similar…although survival for simulated patients in the initial AA group appeared to separate from the DC group around the 40-month mark in favor of AA (p. e423).”21
“Incremental cost-effectiveness of AA over DC was $276 251.82 per QALY gained. Sensitivity analysis estimating the ICER with the reduced cost of AA in Canada was $149 022.09 per QALY gained (p. e423).”21
Appendix 5: Overlap Between Included Systematic Reviews
Table 11: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation RCT name | Sathianathen et al. (2020)16 | Tan et al. (2020)13 | Wang et al. (2020)17 | Landre et al. (2019)14 | Sun et al. (2018)15 |
Armstrong et al. (2019)30 ARCHES | No | No | Yes | No | No |
Boeve et al. (2019)31 HORRAD | No | No | Yes | No | No |
Chi et al. (2019)29 TITAN | No | No | Yes | No | No |
Clarke et al. (2019)32 STAMPEDE – arm C | No | No | Yes | No | No |
Davis et al. (2019)33 ENZAMET | No | No | Yes | No | No |
Fizazi et al. (2019)24 LATITUDE final | Yes | Yes | Yes | No | No |
James et al. (2017)23 STAMPEDE | Yes | Yes | Yes | No | Yes |
Fizazi et al. (2017)22 LATITUDE interim | Yes | Yes | Yes | Yes | Yes |
James et al. (2016)34 STAMPEDE – arm G | No | No | No | No | Yes |
Gravis et al. (2016)26 GETUG-AFU-15 | No | No | Yes | No | Yes |
Fizazi et al. (2015)35 GETUG-12 | No | No | No | No | Yes |
Parker et al. (2018)36 STAMPEDE – arm H | No | No | Yes | No | No |
Sweeney et al. (2015)25 CHAARTED | No | No | Yes | No | Yes |
Appendix 6: References of Potential Interest
Additional References
Economic Evaluations
These economic evaluations met the selection criteria in Table 1 but were excluded from this report due to volume of evidence and lack of generalizability to the Canadian decision-making context.
1.Chiang CL, So TH, Lam TC, Choi HCW. Cost-effectiveness analysis of abiraterone acetate versus docetaxel in the management of metastatic castration-sensitive prostate cancer: Hong Kong's perspective. Prostate Cancer Prostatic Dis. 2020 03;23(1):108-115.
2.Aguiar PN, Jr., Tan PS, Simko S, et al. Cost-effectiveness analysis of abiraterone, docetaxel or placebo plus androgen deprivation therapy for hormone-sensitive advanced prostate cancer. Einstein. 2019 Mar 07;17(2):eGS4414.PubMed
3.Hu X, Qu S, Yao X, Li C, Liu Y, Wang J. Abiraterone acetate and docetaxel with androgen deprivation therapy in high-volume metastatic hormone-sensitive prostate cancer in China: an indirect treatment comparison and cost analysis. Cost Eff Resour Alloc. 2019;17:27 PubMed
4.Ramamurthy C, Handorf EA, Correa AF, Beck JR, Geynisman DM. Cost-effectiveness of abiraterone versus docetaxel in the treatment of metastatic hormone naive prostate cancer. Urol Oncol. 2019 10;37(10):688-695.
5.Sathianathen NJ, Alarid-Escudero F, Kuntz KM, et al. A cost-effectiveness analysis of systemic therapy for metastatic hormone-sensitive prostate cancer. Eur Urol Oncol. 2019 11;2(6):649-655.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca