CADTH Health Technology Review
Yttrium-90 Microspheres for Intermediate- or Advanced-Stage Hepatocellular Carcinoma
Rapid Review with Expert Input
Authors: Calvin Young, Anusree Subramonian, Charlene Argáez
External Reviewer
This document was externally reviewed by a content expert who granted permission to be cited.
Dr. Kelly Burak, MD, FRCPC, MSc (Epid)
Professor
Departments of Medicine and Oncology
Cumming School of Medicine
University of Calgary
Abbreviations
90Y
yttrium-90
BCLC
Barcelona Clinic Liver Cancer
CI
confidence interval
CrI
credibility interval
cTACE
conventional transarterial chemoembolization
DEB-TACE
drug-eluting bead transarterial chemoembolization
EQ-5D
EuroQol-5 Dimensions
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ICUR
incremental cost-utility ratio
IQR
interquartile range
ITT
intention-to-treat
LYG
life-years gained
mRECIST
modified Response Evaluation Criteria in Solid Tumours
NICE
National Institute for Health and Care Excellence
NR
not reported
OR
odds ratio
QALY
quality-adjusted life-year
RCT
randomized controlled trial
RR
relative risk
SIRT
selective internal radiation therapy
TACE
transarterial chemoembolization
TARE
transarterial radioembolization
Key Messages
Transarterial radioembolization using yttrium-90 (90Y) microspheres is a therapeutic option for patients with intermediate- or advanced-stage hepatocellular carcinoma, including those with recurrent or inoperable hepatocellular carcinoma.
Overall, the evidence suggests that patients treated with 90Y-based transarterial radioembolization may experience no difference in overall survival, progression-free survival, and tumour response when compared to patients who received transarterial chemoembolization therapies or systemic treatment with sorafenib or lenvatinib.
Patients treated with transarterial radioembolization generally experienced similar rates of adverse events compared to those treated with transarterial chemoembolization, although there were some instances where treatment with transarterial radioembolization led to increased or decreased risks of specific adverse events. The comparative safety of transarterial radioembolization versus systemic treatment with sorafenib was unclear as the included studies did not statistically compare the risks of experiencing adverse events.
Evidence regarding the cost-effectiveness of 90Y microspheres for treating hepatocellular carcinoma is conflicting. Three economic evaluations suggest treatment with transarterial radioembolization is likely to be cost-effective or dominant — less costly and more effective — compared to transarterial chemoembolization or systemic therapies, while a single economic study suggested treatment with sorafenib or lenvatinib is most likely to be cost-effective or dominant compared to transarterial radioembolization.
Context and Policy Issues
Primary liver cancer has the sixth-highest incidence of all cancers and is the fourth-largest cause of cancer-related mortality worldwide.1 Estimates for 2020 suggested that 3,100 Canadians would be diagnosed with primary liver cancer and that 1,450 Canadians would die from it.2 In particular, data from the Long Form Census in Canada suggest that members of First Nations have disproportionately high rates of primary liver cancer, emphasizing the importance of attention to this condition in Canadian settings.3 While the prevalence and cancer-related mortality of primary liver cancer are higher in males (accounting for 10.2% of all cancer-related deaths in males worldwide), primary liver cancer is still a significant cause of disease burden in females (5.6% of all cancer-related deaths in females worldwide).1 The most common type of primary liver cancer is hepatocellular carcinoma, which accounts for approximately 80% to 85% of primary liver cancers.4,5 Risk factors for the development of hepatocellular carcinoma include chronic alcohol consumption, viral hepatitis (e.g., hepatitis B, hepatitis C), cirrhosis of any etiology, and non-alcoholic fatty liver disease.4,6
Treatment options for hepatocellular carcinoma consist of surgical (e.g., resection and liver transplantation) and non-surgical techniques, including locoregional therapies (e.g., percutaneous ethanol injection, radiofrequency or microwave ablation, transarterial chemoembolization [TACE] or transarterial radioembolization [TARE]) and systemic therapies (e.g., sorafenib, lenvatinib, and atezolizumab-bevacizumab).7 The selection of appropriate treatment is typically informed by tumour stage, liver function, and patient performance status, all of which are important factors that may influence treatment outcomes,8,9 and selection is best done by a multi-disciplinary team.10 Surgical resection is the treatment of choice for patients with single nodules, no underlying cirrhosis, and good liver function.10 While patients who undergo surgical resection have a reasonably good prognosis (a 5-year survival rate of approximately 70%),10 a majority of patients with hepatocellular carcinoma are diagnosed with advanced disease when patients become symptomatic and have some degree of liver impairment. In many of these cases, surgical resection may no longer be appropriate.4 As a form of radiation therapy for patients with advanced or inoperable hepatocellular carcinoma, TARE (also known as selective internal radiation therapy [SIRT]) has been used to downstage patients before surgery or to bridge patients to liver transplantation. As part of this procedure microspheres loaded with a radioactive isotope, most commonly yttirium-90 (90Y), are delivered into the hepatic artery via a catheter inserted into the femoral artery.11 The therapy delivers a high dose of targeted radiation directly to the cancer cells, while also blocking the supply of blood to the tumour.11 Conventional transarterial chemoembolization (cTACE) is administered using a procedure similar to TARE; however, instead of radiation the patient is given regional chemotherapy (usually doxorubicin or cisplatin) before an embolic agent. TACE can also be performed using drug-eluting beads that combine the chemotherapeutic agent with the embolic agent (i.e., drug-eluting bead transarterial chemoembolization [DEB-TACE]).12
The objective of this report is to evaluate the evidence regarding the clinical effectiveness and cost-effectiveness of TARE using 90Y microspheres to support decisions involving the use of this therapy to treat patients with intermediate- or advanced-stage hepatocellular carcinoma. This report complements previous CADTH evaluations of the evidence regarding the use of 90Y microspheres for the treatment of other cancers, including uveal melanoma liver metastases,13 liver metastases from colorectal cancer,14 and primary or secondary liver cancer.15
Research Questions
What is the clinical effectiveness of 90Y microspheres for TARE of intermediate- or advanced-stage hepatocellular carcinoma?
What is the cost-effectiveness of 90Y microspheres for TARE of intermediate- or advanced-stage hepatocellular carcinoma?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist using key resources, including MEDLINE, the Cochrane Library, University of York Centre for Reviews and Dissemination databases, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were yttrium microspheres and hepatocellular carcinoma. No search filters were applied to limit retrieval to study type. Comments, newspaper articles, editorials, letters, and conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and December 21, 2020.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Patients with intermediate- or advanced-stage hepatocellular carcinoma |
Intervention | TARE (also known as selective internal radiation therapy) using resin or glass microspheres loaded with radioactive yttrium-90 (i.e., Y-90, 90Y, TheraSpheres, SIR-Spheres) |
Comparator | TACE; sorafenib; lenvatinib; atezolizumab-bevacizumab (alone or in combination) |
Outcomes | Q1: Clinical effectiveness (e.g., PFS, OS, objective response, quality of life, adverse events, treatment discontinuation) Q2: Cost-effectiveness (e.g., quality-adjusted life-years gained, incremental cost-effectiveness ratios) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, and economic evaluations |
90Y = yttrium-90; OS = overall survival; PFS = progression-free survival; TACE = transarterial chemoembolization; TARE = transarterial radioembolization.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2016. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 216 for systematic reviews, the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) “Indirect Treatment Comparison/Network Meta-Analysis Study Questionnaire to Assess Relevance and Credibility to Inform Health Care Decision Making”17 for the network meta-analysis, the Downs and Black checklist18 for a non-randomized study, and the Drummond checklist19 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
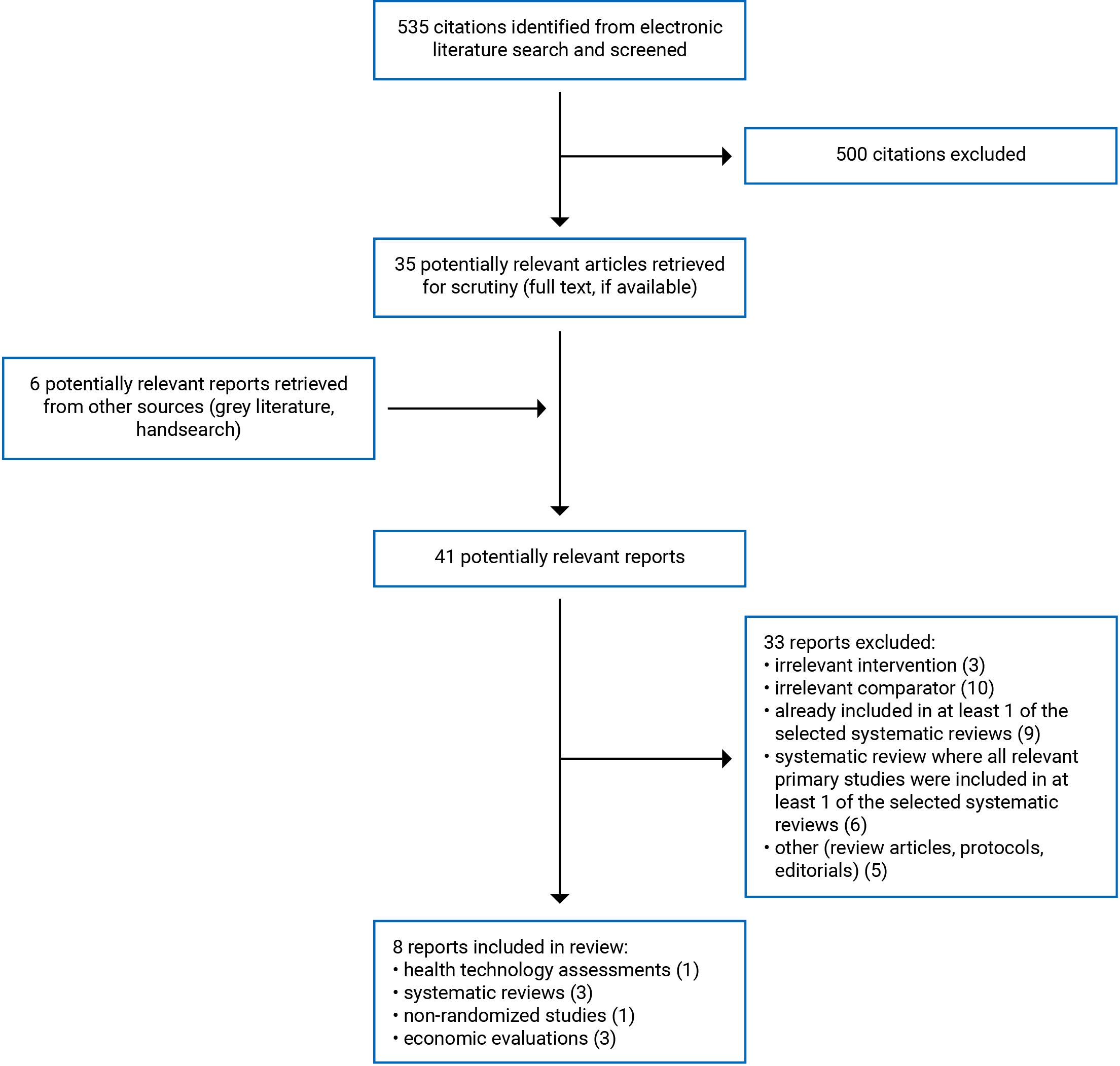
A total of 535 citations were identified in the literature search. Following screening of titles and abstracts, 500 citations were excluded and 35 potentially relevant reports from the electronic search were retrieved for full-text review. Six potentially relevant publications were identified from the grey literature for full-text review. Of these 41 potentially relevant articles, 33 publications were excluded for various reasons, and 8 publications that met the inclusion criteria were included in this report. These comprised 1 health technology assessment (which included a systematic review with network meta-analyses and an economic evaluation),20 3 systematic reviews with meta-analyses,21-23 1 non-randomized study,24 and 3 economic evaluations.25-27 Appendix 1 presents the Prevention and Recovery Information System for Monitoring and Analysis (PRISMA)28 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
One relevant health technology assessment (which included a systematic review with network meta-analyses and an economic evaluation),20 3 systematic reviews with meta-analyses,21-23 1 non-randomized study,24 and 3 economic evaluations25-27 were included in this review. No relevant randomized controlled trials (RCTs) in addition to those already included in at least 1 of the selected systematic reviews were identified. Detailed study characteristics are available in Appendix 2, Table 2, Table 3, and Table 4.
The health technology assessment20 and 1 systematic review with meta-analyses21 had objectives and inclusion criteria that were wider in scope than the current report. Specifically, Walton et al. (2020)20 assessed any form of TARE, rather than just 90Y-based therapies (e.g., holmium-166 microspheres). This health technology assessment also examined a wider range of relevant comparators beyond those considered relevant to the current report (e.g., best supportive care was considered eligible in the health technology assessment). In addition to comparing TARE with alternative therapies, the review by Yang et al. (2020)21 included primary studies that compared cTACE versus DEB-TACE. Only the characteristics and results of the subset of relevant studies will be described in this report.
Study Design
The systematic review and network meta-analysis of clinical effectiveness conducted as part of the health technology assessment by Walton et al. (2020)20 primarily included RCTs. When there was insufficient RCT evidence to address the decision problem, non-randomized comparative studies and non-comparative studies were considered for inclusion. Literature searches were conducted up to May 8, 2019, and did not impose any restrictions on date of publication. A total of 27 studies were included in the systematic review (7 RCTs, 7 prospective comparative studies, 12 retrospective comparative studies, and 1 non-comparative study; 17 studies reported in 21 publications were relevant to the current report).20 As part of their network meta-analysis, the authors created 3 different networks for 3 different patient populations: 1) adults with unresectable hepatocellular carcinoma who were eligible for transplant, 2) adults with unresectable hepatocellular carcinoma who were eligible for conventional transarterial therapies, and 3) adults with unresectable hepatocellular carcinoma who were ineligible for conventional transarterial therapies. After considering the evidence that could be used in each of these networks, networks 1 and 2 were deemed unsuitable for decision-making and were not conducted, while network 3 was deemed appropriate and was analyzed. Five primary studies, including 3 RCTs and 2 retrospective comparative studies, were included in the network meta-analysis, which was conducted using a Bayesian evidence synthesis approach. Fixed-effect models were used as they provided a better fit to the data than a random-effects model according to the deviance information criterion and residual deviance statistics due to the small number of studies and the influence of the former on between-study heterogeneity when compared to random-effects models. The authors of the Yang et al. (2020) systematic review and meta-analysis21 included RCTs and retrospective or prospective cohort studies published up to July 2019. A total of 28 primary studies were included in the systematic review21 (8 RCTs, 3 prospective cohort studies, and 17 retrospective cohort studies; 12 primary studies were relevant to the current report). The systematic review with meta-analyses by Yang and Si (2018)22 included RCTs, observational studies, and other clinical studies published between January 2009 and July 2017. The 11 studies (2 RCTs and 9 observational studies) included in the systematic review were all relevant to the current report. The authors of the Lobo et al. (2016) systematic review with meta-analyses23 included any comparative studies (i.e., RCTs and non-randomized studies) published between January 2005 and February 2016. The review included 5 observational studies (all relevant to the current report). In total, the systematic reviews20-23 included 28 unique clinical studies relevant to the current report. The relevant primary study overlap between these systematic reviews is summarized in Appendix 5, Table 11. Twelve of the 28 primary studies were included in more than 1 systematic review; only 1 study was included in all 4 systematic reviews.20-23
The non-randomized study24 was a single-centre, retrospective cohort study. Data were collected between 2010 and 2015.
Four economic evaluations20,25-27 (including an independent economic analysis20 conducted as part of the health technology assessment) were identified regarding the cost-effectiveness of 90Y microspheres for the treatment of hepatocellular carcinoma. All 4 studies were model-based cost-utility analyses. The analysis by Manas et al. (2020)25 employed a cohort-based Markov model that had a cycle length of 4 weeks and used a 20-year time horizon from the perspective of the UK National Health Service. Effectiveness inputs and utility values were derived from National Liver Offering Scheme data, key clinical trials, and assumptions informed by clinical experts. Cost inputs were derived from the National Institute for Health and Care Excellence (NICE) formulary and National Schedule of Reference Costs for 2018 to 2019.29 Muszbek and colleagues26 designed a lifetime partitioned survival analysis model from the perspective of the UK National Health Service. The model incorporated 4 health states: progression-free, post-progression, received curative therapy, and dead. Effectiveness inputs and utility values for the interventions were extrapolated from the key clinical trials or from studies retrieved in a targeted literature review. Resource uses were from registries and clinical surveys. The economic evaluation by Walter et al. (2020)20 used a decision-tree model that fed into a post-treatment Markov model with 3 states: progression-free survival, post-progression, and dead. The model was from the perspective of the UK National Health Service and Personal Social Services and used a 10-year time horizon. Treatment-effectiveness parameters were extrapolated from key clinical trials and the network meta-analysis conducted as part of the health technology assessment while costing information was obtained from manufacturers’ submissions and the National Schedule of Reference Costs for 2017 to 2018.30 The fourth economic evaluation by Rognoni et al. (2017)27 was a cohort-based multistate Markov model that had cycle lengths of 1 month. The 5 possible health states in the model were post-transplantation, stable disease, disease progression, death from the cancer, and death from other causes. The model used a lifetime horizon and was from the Italian health care service perspective. Model transition probabilities were derived from prospectively collected real-world data from patients receiving care at 3 centres in Italy, while health utility values were retrieved from studies identified in a literature search or from the Cost-Effectiveness Analysis Registry. Resource consumptions and costs were from the Regional Health Care Service price list and the diagnosis-related group-reimbursement rates in Italy.
Country of Origin
The included health technology assessment was conducted by a group in the UK.20 The 3 systematic reviews with meta-analyses were by authors in China21,22 and the US.23
The non-randomized study was conducted in the US.24
The economic evaluations were conducted by authors based in Italy27 and the UK.25,26
Patient Population
The systematic review conducted as part of the health technology assessment20 was specific to patients with unresectable early-stage hepatocellular carcinoma (Barcelona Clinic Liver Cancer [BCLC] stage A), intermediate-stage hepatocellular carcinoma (BCLC stage B), or advanced-stage hepatocellular carcinoma (BCLC stage C). Studies on participants with secondary liver metastases or other types of liver cancers (e.g., cholangiocarcinoma) were not eligible for inclusion in the synthesis. The 3 remaining systematic reviews21-23 included studies of patients with hepatocellular carcinoma without any specific restrictions while acknowledging that treatment with locoregional therapies, such as TARE, are generally appropriate when the cancer is unresectable. The review by Yang et al. (2020)21 specifically stated that studies of patients with multiple malignancies were excluded.
The non-randomized study by Padia et al. (2017)24 included data from 178 patients (between the ages of 36 and 86 years; median age was 61 years) who were treated at a single centre in the US for hepatocellular carcinoma. The proportion of male participants within the study population was 77.5%. The study authors did not place any restrictions on the cause of cirrhosis (which affects a large proportion of people with hepatocellular carcinoma),31 treatment history (e.g., prior liver transplantation, surgical resection, or ablation), or stage of disease, but patients had to have received the intervention of interest to treat a region equivalent to a single hepatic Couinaud segment.
All 4 economic evaluations20,25-27 modelled patients with unresectable hepatocellular carcinoma. The analysis by Manas et al. (2020)25 stated that their hypothetical cohort included patients ≥ 65 years of age who were eligible for transarterial embolization therapies. The cohort was assumed to be 75% male. The study by Muszbek et al. (2020)26 included patients with unresectable intermediate (BCLC stage B) or advanced (BCLC stage C) hepatocellular carcinoma who did not have extrahepatic disease, had a low tumour burden (≤ 25%), and who had preserved liver function. The analysis by Walton et al. (2020)20 modelled patients with (BCLC stage B) or advanced (BCLC stage C) hepatocellular carcinoma who did not have extrahepatic disease and for whom any conventional transarterial embolization therapies (e.g., TACE) were inappropriate. The fourth economic evaluation included patients with intermediate or advanced hepatocellular carcinoma and excluded those with metastatic disease or early or terminal hepatocellular carcinoma.
Interventions and Comparators
Consistent with the inclusion criteria for the current report, the health technology assessment20 and the 3 systematic reviews21-23 included primary studies that examined the effectiveness of TARE using resin or glass microspheres loaded with 90Y (i.e., TheraSphere or SIR-Spheres). The non-randomized study24 included patients who were given TARE using 90Y glass microspheres (i.e., TheraSphere). The 4 economic evaluations modelled the cost-effectiveness of TARE with TheraSphere25 or SIR-Spheres,26 any form of radioembolization (i.e., TheraSphere, SIR-Spheres, and QuiremSpheres),20 or an unspecified form of TARE.27
As for comparators, the systematic review conducted as part of the health technology assessment20 listed alternative SIRTs, conventional transarterial therapies (e.g., TACE), established clinical management without TARE (e.g., sorafenib, lenvatinib, and regorafenib), or best supportive care as eligible. Comparators considered within the network meta-analysis were lenvatinib and sorafenib. The 3 remaining systematic reviews21-23 included studies that compared TARE to TACE (with doxorubicin, mitomycin, adriamycin, and/or cisplatin), although the review by Yang and Si (2018)22 only considered cTACE as eligible (i.e., studies on DEB-TACE were excluded). The non-randomized study24 included a control group of participants who received TACE, using either drug-eluting embolics (i.e., 100 μm to 300 μm doxorubicin drug-eluting embolic mixed with 50 mg of doxorubicin) or an oil-based chemoembolic agent (i.e., 50 mg of doxorubicin mixed with 10 mL of ethiodized oil to create a 1:1 emulsion for infusion). The 4 economic evaluations modelled a variety of comparator interventions: Manas et al. (2020)25 considered transarterial embolization, cTACE, and DEB-TACE; Muszbek et al. (2020)26 used sorafenib; Walton et al. (2020)20 considered established clinical management using sorafenib or lenvatinib; and Rognoni et al. (2017)27 considered sorafenib with a target dosage of 800 mg/day.
For the purposes of this report, the terms cTACE and DEB-TACE were used to subclassify TACE procedures when details on the specific technique were reported in the included studies. When it was unclear if conventional or drug-eluting techniques were used, the procedure was referred to as TACE.
Outcomes
Literature assessing outcomes relating to clinical effectiveness reported on overall survival, progression-free survival, measures of tumour response, quality of life, and adverse events or complications. Four systematic reviews,20-23 including 1 network meta-analysis,20 and 1 non-randomized study24 evaluated outcomes related to overall survival. These outcomes included median overall survival (reported in weeks or months)20,24 or the proportion of patients who were still alive at various follow-up periods (e.g., 1 year, 2 years, 3 years, or 4 years).20-24 Progression-free survival was evaluated in 2 systematic reviews20,21 and was reported as the median time to progression20 or as the proportion of patients who were still experiencing progression-free survival at specific follow-up points (e.g., 1 year).20,21 Measures of tumour response were assessed in all 4 systematic reviews20-23 and in the non-randomized study.24 This was reported as the proportion of patients who experienced tumour response at follow-up according to various criteria. Criteria for tumour response considered in the identified literature included the modified Response Evaluation Criteria in Solid Tumours (mRECIST) criteria,22,24 World Health Organization (WHO) criteria,20,22 and European Association for the Study of the Liver criteria.20 Quality-of-life measures were reported in 5 primary studies included in 1 systematic review.20 The tools used to measure quality of life in these primary studies were unclear in the systematic review; however, some appeared to use the EuroQol-5 Dimensions (EQ-5D) index, the Functional Assessment of Cancer Therapy – Hepatobiliary tool, or the Trial Outcome Index. Adverse events were captured in all 4 systematic reviews20-23 and in the non-randomized study.24 Adverse events reported in these studies included nausea or vomiting, pain, fatigue, liver failure, gastrointestinal bleeding, infection or fever, diarrhea, and various biochemical toxicities (e.g., increases in aspartate aminotransferase, alanine aminotransferase, or total bilirubin). Between-group comparisons were typically made by evaluating the proportion of patients who experienced specific adverse events across the treatment groups.
As for the 4 economic evaluations,20,25-27 model outputs included treatment costs (reported in pounds or euros), life-years gained (LYG), quality-adjusted life-years (QALYs), incremental cost-effectiveness ratios (ICERs), and net monetary benefits. In some cases, the analyses also included cost-effectiveness acceptability curves that showed the probability of each treatment being cost-effective over a range of willingness-to-pay thresholds.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3, Table 5, Table 6, and Table 7.
Systematic Reviews
The 4 systematic reviews (1 with a network meta-analysis20 and 3 with meta-analyses21-23) were considered to be of high methodological quality based on the assessments using A MeaSurement Tool to Assess systematic Reviews 2.16 The reviews had clearly defined objectives and primary study eligibility criteria, included electronic searches in multiple databases, and provided a description of key search terms, dates of searches, and any search restrictions, increasing the reproducibility of the literature searches. In addition, the authors of all reviews20-23 described the included studies in adequate detail, assessed the risk of bias of included primary studies using appropriate techniques, used appropriate methods for the statistical combination of results, assessed heterogeneity using a variety of methods (e.g., Cochrane Q statistics and the I2 test) when suitable, and stated their potential conflicts of interest. The review methods for 1 systematic review20 were prospectively registered in a published protocol (with the International Prospective Register of Systematic Reviews), decreasing the risk for selective reporting. The methods used for article selection, data extraction, and quality assessment were well-documented and conducted in duplicate or triplicate (with the exception of quality assessment in the review by Yang and Si (2018)22 and article selection and quality assessment in the review by Lobo and colleagues,23 where it was unclear if these were conducted by a single author or in duplicate), decreasing the likelihood of inconsistency in these processes. While the authors of 3 systematic reviews20,22,23 considered the risk of bias in individual primary studies when interpreting and discussing the results of the reviews, Yang et al. (2020)21 provided limited discussion on risk of bias when formulating conclusions. Publication bias was assessed by the authors of 3 included systematic reviews21-23 using various methods (e.g., Begg’s and Egger’s tests, funnel plots, and examination of trial registries) and in all cases no indicators of publication bias were identified. Within 3 systematic reviews,21-23 the literature search strategies did not include grey literature, increasing the risk of missing relevant, non-indexed studies. Additionally, none of the systematic reviews20-23 included a list of excluded studies; however, reasons for excluding articles after full-text review were described. Finally, while the authors of 2 systematic reviews20,21 disclosed their sources of funding (which were considered unlikely to have influenced the findings of the reviews), it was unclear if financial support for the reviews was received by Yang and Si (2018)22 and Lobo et al. (2016).23
Network Meta-Analyses
This report included 1 network meta-analysis20 that was appraised using criteria from the ISPOR Indirect Treatment Comparison/Network Meta-Analysis Study Questionnaire to Assess Relevance and Credibility to Inform Health Care Decision Making report,17 The network meta-analysis was estimated using a Bayesian framework with normal identity link models. The network meta-analysis20 exhibited several methodological strengths: the literature search strategy used to identify studies informing the networks was comprehensive and should have identified all relevant RCTs, the populations, interventions, comparators, and outcomes were relevant to the current report (although the network meta-analysis did not compare TARE versus TACE or atezolizumab-bevacizumab), the main outcome measures (i.e., overall survival) were valid and accepted in clinical and research settings and were reported using effect sizes and 95% credibility intervals (CrIs), 4) lower-quality studies were excluded from the networks to reduce the risk of bias, 5) within-study randomization was preserved in the networks, 6) characteristics of primary studies used to generate the network were described, 7) sensitivity analyses were conducted to explore uncertainty, and 8) the conclusions of the analyses were fair and balanced. One notable limitation of the network meta-analysis was that the network relied on data from non-randomized studies to connect the interventions of interest. While this was a result of a paucity of published clinical literature investigating these interventions (and not the fault of the review authors), and the observational data were only included in scenario analyses, this limitation increased the risk of confounding and other sources of bias in the results of the network meta-analyses. In addition, there was clinical heterogeneity within the studies forming the network. Specifically, there was variation in the median age, sex, proportion of patients with portal vein thrombosis or portal venous invasion, and distribution of BCLC classification of participants from included primary studies. In addition, other potential effect modifiers, including tumour size, number of tumours, and cirrhosis etiology, were not reported. The imbalances in effect modifiers across studies may have resulted in biased treatment estimates. Finally, the authors did not provide a suitable rationale for reporting fixed-effects models over random-effects models despite notable heterogeneity between the included primary studies.
Non-Randomized Studies
The included retrospective cohort study24 had clearly described objectives, interventions, main outcomes, and patient eligibility criteria. Relevant baseline patient characteristics, such as age, sex, cirrhosis etiology, disease stage, prior treatment, number of tumours, and tumour characteristics, were presented and tested for statistically significant differences between cohorts. Additional methodological strengths were that study subjects in the intervention and control groups were recruited over the same period of time (between 2010 and 2015), compliance with the assigned treatment was reliable, outcome measures were valid, adverse events that may have been a consequence of the intervention were recorded, findings of the study were well-reported, and authors declared their potential conflicts of interest (1 author was a paid consultant for BTG International, a supplier of the intervention examined in the study). Finally, the study participants, care providers, and health care settings appeared to be representative of the population and care settings of interest, increasing the external validity of the study.
As for methodological limitations, participants were not allocated to treatment groups at random and there were significant between-group differences with respect to baseline characteristics, many of which are likely to affect the outcomes of interest (e.g., age, Eastern Cooperative Oncology Group performance status, Child-Pugh class, albumin, number of tumours, tumour size, infiltrative tumours, and the presence of portal vein thrombosis). While the propensity-score model used in the analyses adjusted for some of these imbalances, these limitations increased the risk of confounding and selection bias. Study authors did not perform a power calculation before conducting analyses, and therefore the study may not have been powered to detect statistically significant between-group differences for all reported outcomes. The sources of funding for the study were not disclosed. In addition, the generalizability of the findings from the non-randomized study to Canadian settings is unclear, given that it was conducted at a single centre in the US.
Economic Evaluations
In all 4 included economic evaluations,20,25-27 the research questions, objectives, economic importance of the research questions, time horizons, treatment strategies being compared, rationale for choosing alternative interventions, and viewpoint or perspective of the analysis were clearly stated. The selected time horizons, which were 10 years,20 20 years,25 and lifetime,26,27 were appropriate given the nature of hepatocellular carcinoma and the interventions under investigation. Additionally, the choices of the form of economic evaluations were justified and the model structures were clearly explained using figures. These methodological strengths increase confidence in the reporting methods used by the authors.
The sources of effectiveness estimates, including those used to derive model transition probabilities and health utility values, were provided and described in sufficient detail to assess their relevance in addressing the research questions. Similarly, the sources of cost data (e.g., cost estimates for TARE procedures) were appropriately referenced in all 4 economic evaluations. While this is a result of the limited number of RCTs that have examined the interventions of interest, it should be noted that many effectiveness inputs were derived from single clinical trials rather than a synthesis or meta-analysis of estimates from multiple sources; any sources of bias that may have influenced the findings of these trials would therefore translate into uncertainty in the findings of the economic models. In some cases, advice from clinical experts or extrapolation of data from clinical trials was necessary to inform the economic models, particularly when deciding on model transition probabilities; however, the parameters that were estimated from expert clinical advice and the techniques used for extrapolation appeared to be reasonable. While a majority of model assumptions made in the economic evaluations20,25-27 were rational, the study by Manas et al. (2020)25 assumed that there was no hepatocellular carcinoma recurrence after successful liver transplantation, which is not reflective of rates observed in Canadian settings.32 The approach to sensitivity analyses and the choice of variables for sensitivity analyses were justified in all economic evaluations.20,25-27 In the case of 3 economic evaluations20,26,27 the currency in which costs were expressed and the methods applied to adjust for inflation were clearly stated; however, the study by Manas et al. (2020)25 did not report the year to which costs were inflated. In all 4 studies20,25-27 an appropriate discount rate (i.e., 3.5% per year) was applied to costs and outcomes, incremental analyses were reported, and conclusions made by the authors were justified and accompanied by appropriate caveats.
There were some concerns relating to the generalizability of these economic evaluations to the Canadian setting. Because these economic models were constructed using effectiveness and cost inputs from the UK20,25,26 or Italy27, any differences between Canadian health care costs and the costs in these European countries would affect the cost-effectiveness findings. A final limitation to consider is that 2 of these economic evaluations25,26 were funded directly by companies involved in the production or distribution of TARE interventions.
Summary of Findings
The overall findings of the included studies are highlighted in the following sections. Detailed summaries of the main findings and authors’ conclusions are available in Appendix 4.
Clinical Effectiveness of 90Y Microspheres
Evidence regarding the clinical effectiveness of 90Y microspheres for TARE of intermediate- or advanced-stage hepatocellular carcinoma was available from 4 systematic reviews20-23 (1 with a network meta-analysis)20 and 1 non-randomized study.24 The findings from these studies are summarized within and across studies by outcome and comparator. These results should be interpreted while considering the significant overlap in the primary studies that were included in the systematic reviews; the pooled estimates from separate reviews therefore contain some of the same data. A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Overall Survival
TARE Versus Sorafenib
Direct comparisons in primary studies: Two primary studies included in the Walton et al. (2020)20 systematic review reported on overall survival in those treated with TARE versus those treated with sorafenib. In both studies, there were no statistically significant differences in the median overall survival or 1-year survival rates between the treatment groups. This was the result for both intention-to-treat (ITT) and per-protocol analyses.
Direct comparisons in the network meta-analysis: The network meta-analysis conducted by Walton et al. (2020)20 suggested there were no significant differences between treatment with SIR-Spheres and sorafenib in adults with unresectable hepatocellular carcinoma who were Child-Pugh class A and ineligible for conventional transarterial therapy (as they had advanced-stage disease, portal vein thrombosis, or previously failed with conventional transarterial therapy) with respect to overall survival.
TARE Versus Lenvatinib
Direct comparisons in primary studies: No studies that directly compared TARE versus lenvatinib were included in the identified literature.
Indirect comparisons in the network meta-analysis: The network meta-analysis conducted by Walton et al. (2020)20 suggested that there were no significant differences in terms of overall survival between these 2 treatments in adults with unresectable hepatocellular carcinoma who were Child-Pugh class A and ineligible for conventional transarterial therapy.
TARE Versus TACE
The Walton et al. (2020)20 systematic review included 4 primary studies that reported on the comparative effectiveness of TARE versus cTACE or DEB-TACE with respect to overall survival, including median overall survival and survival rates at 1 year, 2 years, and 3 years; however, the statistical significance of these finding was not reported in the review. The authors of the Yang et al. (2020)21 systematic review conducted several meta-analyses to compare overall survival for patients treated with TARE and cTACE or DEB-TACE. Compared to patients treated with cTACE, patients treated with TARE had improved 2-year and 3-year survival. No differences were observed at 1 year. When compared to patients treated with DEB-TACE, those treated with TARE had decreased survival after 2 years, but there were no significant differences in survival between the 2 treatments at 1 year. Meta-analyses conducted as part of the Yang and Si (2018)22 review indicated that there were no significant differences between treatment with TARE and cTACE with respect to 1-year and 2-year overall survival. The authors of the Lobo et al. (2016)23 systematic review concluded that there were no significant differences between treatment with TARE and cTACE with respect to survival at 1 year, 3 years, and 4 years, but did note that 2-year overall survival favoured patients treated with TARE.
The non-randomized study by Padia et al. (2017)24 reported overall survival rates following treatment with TARE and TACE (cTACE and DEB-TACE results were not reported separately). Within their study population, there were no statistically significant differences between the 2 study cohorts with respect to overall survival after propensity-score adjustment techniques were applied. Additionally, the authors reported on a composite outcome that included death or overall progression. Patients who were treated with TACE experienced significantly higher rates of death or overall progression, regardless of whether orthotopic liver transplantation was considered a competing risk or not, compared with those who were treated with TARE.
Progression-Free Survival and Tumour Progression
TARE Versus Sorafenib
Two primary studies included in the Walton et al. (2020)20 systematic review reported on measures of progression-free survival, including the proportion of patients who experienced progression and the median progression-free survival, in patients treated with TARE or sorafenib. Neither primary study detected statistically significant differences between treatment with TARE and treatment with sorafenib.
TARE Versus TACE
The authors of the Walton et al. (2020)20 systematic review identified 5 primary studies that assessed median progression-free survival in patient groups who were treated with TARE or TACE; however, the results were inconsistent across studies and the statistical significance of these findings was not reported in the systematic review. A meta-analysis conducted as part of the Yang et al. (2020)21 review suggested that there were no significant differences in terms of progression-free survival at 1 year between TARE and DEB-TACE.
Patients included in the non-randomized study by Padia et al. (2017)24 who received treatment with TARE were significantly less likely to experience index tumour progression than those who were treated with TACE.
Tumour Response
TARE Versus Sorafenib
The systematic review by Walton et al. (2020)20 summarized 2 primary studies that compared TARE versus sorafenib and reported on findings related to tumour response. For both primary studies, complete or partial response rates were reported but the between-group statistical significance of these rates was not calculated.
TARE Versus TACE
The Walton et al. (2020)20 review summarized information related to tumour response from 4 primary studies; however, measures used to assess response rates varied across studies and none of these findings included between-group statistical comparisons. The systematic review by Yang et al. (2020)21 estimated the effectiveness of TARE versus cTACE using objective response (defined as complete response plus a partial response) and disease control rate (objective response plus stable disease), according to an unspecified criteria for response. While there were no statistically significant between-group differences with respect to objective response, patients treated with TARE had significantly greater disease control rates compared to those treated with cTACE. The authors of the review by Yang and Si (2018)22 conducted meta-analyses to determine the effect of TARE on tumour response in studies using WHO or mRECIST criteria for response. Compared to patients treated with cTACE, patients treated with TARE had statistically significant improvements in tumour response in studies that used mRECIST criteria. There were no statistically significant differences between the treatments in studies that used WHO criteria for response or in the analysis of all studies, regardless of response criteria. The review by Lobo et al. (2016)23 included meta-analyses for radiological response, partial response, disease progression, and stable disease within 3 months of treatment. For all 4 of these outcomes, there were no statistically significant differences between patients treated with TARE and those treated with TACE.
The non-randomized study by Padia et al. (2017)24 reported on the proportion of participants who experienced complete response, partial response, stable disease, and progressive disease. Compared to those who received TACE, patients treated with TARE had statistically significantly improved per-tumour and per-patient complete response rates (using mRECIST criteria).
Quality of Life
TARE Versus Sorafenib
Two primary studies summarized within the Walton et al. (2020)20 systematic review reported on measures of quality of life in patients treated with TARE or sorafenib. In 1 of these studies, those who were treated with TARE had statistically significant improvements in the global health status subscore. Conversely, there were no statistically significant differences in mean EQ-5D scores between patients treated with TARE and those treated with sorafenib in the second primary study.
TARE Versus TACE
Three primary studies from the Walton et al. (2020)20 systematic review that compared treatment with TARE versus TACE (conventional or drug-eluting bead) reported on measures of quality of life. The between-group differences were not statistically significant in 2 of these primary studies, while the authors of the third primary study noted that those who were treated with TARE had significantly better quality of life with respect to social well-being, functional well-being, and embolotherapy-specific score.
Adverse Events
TARE Versus Sorafenib
Rates of adverse events from 2 studies summarized in Walton et al. (2020)20 that compared treatment with TARE versus sorafenib were available; however, the statistical significance of these findings was not reported. In the 2 primary studies, the proportion of patients who experienced at least 1 adverse event at unspecified lengths of follow-up were 60% and 77% in the TARE groups versus 77% and 94% in the sorafenib groups.
TARE Versus TACE
Rates of adverse events from 1 study summarized in Walton et al. (2020)20 that compared treatment with TARE versus TACE were available (i.e., 92.3% for those who received TARE versus 66.7% for those that received TACE at an unspecified length of follow-up); however, the statistical significance of these findings was not reported. The Yang et al. (2020)21 review included meta-analyses to estimate the odds ratio of experiencing adverse events in those treated with TARE versus those treated with cTACE or those treated with DEB-TACE. There were no statistically significant differences observed between TARE and either cTACE or DEB-TACE across all reported adverse events (i.e., nausea or vomiting, pain, fatigue, liver failure, infection or fever, and gastrointestinal bleeding). Similarly, the review by Yang and Si (2018)22 evaluated the relative risk of experiencing serious adverse events between those treated with TARE and those treated with cTACE. The results of the meta-analysis suggested that there were no statistically significant differences. Lobo et al. (2016)23 conducted a meta-analysis for each adverse event of interest. Contrary to the other studies, their findings indicated patients who received TARE were at increased risk of post-procedural fatigue and at decreased risk of pain compared to those who received cTACE. There were no statistically significant differences in the risk of nausea and vomiting, fever, post-treatment morbidity, or other complications (e.g., diarrhea, anorexia, headache, chest pain, confusion, gastric ulceration, bleeding from puncture site, rash, varicella zoster infection, and hepatic abscess; fixed-effects model).
The non-randomized study by Padia et al. (2017)24 reported on the incidence of adverse events within the study population. Monitored adverse events included fatigue, pain, post-embolization syndrome, leukopenia, increased aspartate aminotransferase, increased alanine aminotransferase, increased total bilirubin, hypoalbuminemia, and any biochemical toxicity. There were no statistically significant differences between patients who received TARE and those who received TACE for any of these outcomes, with the exception of pain, where the TARE group had a higher relative risk.
Cost-Effectiveness of 90Y Microspheres
Evidence regarding the cost-effectiveness of 90Y microspheres in TARE for intermediate- or advanced-stage hepatocellular carcinoma was available from 4 economic evaluations20,25-27 (1 of which was conducted as part of a health technology assessment20).
Incremental Cost-Effectiveness Ratios
TARE Versus Sorafenib
The cost-effectiveness of 90Y-based TARE versus sorafenib was modelled in 3 economic evaluations.20,26,27 One analysis26 suggested TARE was dominant compared to sorafenib; 1 analysis27 suggested TARE was cost-effective compared to sorafenib; and 1 analysis18 suggested TARE was not cost-effective compared to sorafenib.
The study by Muszbek et al. (2020)26 estimated treatment with TARE cost less and produced more QALYs compared to treatment with sorafenib; therefore, TARE was considered dominant. TARE was dominant across a range of scenario analyses, including those that tested different time horizons, discount rates, methods for extrapolating effectiveness inputs from clinical trial data, and health-state utility values. When downstaging was not allowed or when significant discounts were applied to the cost of sorafenib, TARE was no longer dominant but was considered cost-effective. The authors of the analysis by Rognoni et al. (2017)27 stratified their results by patients with intermediate- or advanced-stage disease. In those with intermediate-stage disease, TARE was estimated to have increased costs but generated more QALYs, resulting in a cost-effective ICER of €3,302 per QALY. For those with advanced-stage disease, TARE lowered costs and produced higher QALYs, resulting in TARE being dominant. Treatment with TARE was considered cost-effective or dominant across a wide range of scenario analyses that tested the robustness of the findings while varying model inputs such as time horizon, mean number of TARE procedures per patient, patient age, and the cost of sorafenib. At a cost-effectiveness threshold of £30,000 per QALY, TARE had 99.2% and 98.2% probabilities of being cost-effective versus sorafenib in patients with intermediate and advanced-stage hepatocellular carcinoma, respectively.
The economic evaluation by Walton et al. (2020)20 considered 2 different 90Y-based TARE interventions (i.e., TheraSphere and SIR-Spheres) separately within their analyses. In the deterministic base-case model, TheraSphere and SIR-Spheres were less costly but had reduced QALYs compared to sorafenib. Compared with TheraSphere (the more cost-effective of the 2 90Y-based interventions as they were assumed to produce similar QALYs although the cost of TheraSphere was lower), sorafenib had an ICER of £28,728 per QALY. Similarly, the probabilistic base-case model estimated TheraSphere and SIR-Spheres would be less costly but result in decreased QALYs compared to sorafenib; however, this model did not directly calculate the comparative cost-effectiveness of these interventions as lenvatinib was considered the most cost-effective intervention.
While these 3 analyses20,26,27 were on similar patient populations, there was some variation in the clinical inputs that informed the economic models. Two analyses20,26 primarily relied on the SARAH trial33 as a source of effectiveness inputs; however, Muszbek et al. (2020)26 used data from the ITT analysis while Walton et al. (2020)20 determined that data from the per-protocol analysis was more appropriate. Because the Rognoni et al. (2017)27 study was conducted before the completion of the SARAH trial,33 it was informed instead by real-world data that were prospectively collected from patients who received TARE or sorafenib in Italy. These differences, along with differences in the costs associated with treatments, may explain the inconsistent conclusions made by study authors.
TARE Versus Lenvatinib
Two economic evaluations estimated the cost-effectiveness of TARE versus lenvatinib. One study20 suggested that TARE was not cost-effective or was dominated by lenvatinib, while the second study26 suggested that TARE was the cost-effective intervention. The variations in clinical inputs for the 2 models (described for the TARE-versus-sorafenib comparison) may have contributed to these conflicting results.
The Walton et al. (2020)20 economic evaluation included a deterministic base-case model and a probabilistic base-case model. In the deterministic base-case model, lenvatinib was more costly but produced more QALYs compared with TheraSphere, resulting in a cost-effective ICER of £2,911 per QALY. Compared to SIR-Spheres, treatment with lenvatinib was estimated to produce more QALYs and was associated with lower costs and was therefore dominant. Lenvatinib was dominant to TARE (TheraSphere and SIR-Spheres) in the probabilistic base-case model, producing more QALYs at a lower cost. The authors concluded that lenvatinib had the highest likelihood of being cost-effective versus either TARE or sorafenib across any willingness to pay up to £100,000 per QALY.
While not considered in their base-case analysis, the authors of the Muszbek et al. (2020)26 economic evaluation conducted a scenario analysis to estimate the cost-effectiveness of 90Y-based TARE compared to lenvatinib. This analysis suggested that lenvatinib had an ICER of £58,298 per QALY versus TARE and was therefore not cost-effective at a willingness-to-pay threshold of £20,000 per QALY; however, the authors noted that these findings should be treated with caution due to high levels of uncertainty in the model.
TARE Versus TACE
The study by Manas et al. (2020)25 examined the cost-effectiveness of TARE (with TheraSphere) versus cTACE and DEB-TACE in patients (≥ 65 years of age) with unresectable hepatocellular carcinoma. While treatment with TARE was associated with higher absolute costs, it generated more QALYs and was considered cost-effective with ICERs of £17,279 per QALY versus cTACE and £23,020 per QALY versus DEB-TACE. At a willingness-to-pay threshold of £20,000, the probabilities of TARE being cost-effective were 76.8% and 15.9% versus conventional or DEB-TACE, respectively. Using a £30,000 willingness-to-pay threshold, these probabilities increased to approximately 93% and 88.6% for cTACE or DEB-TACE, respectively.
Limitations
Based on the information presented in the systematic reviews20-23 and in the non-randomized study,24 none of the included primary clinical studies were conducted in Canada. Additionally, none of the economic evaluations25-27 were conducted from the perspective of a Canadian health care payer. The cost-effectiveness of these interventions is expected to be influenced by local processes used to administer these procedures (e.g., if patients are admitted to hospital to receive treatment or if they are treated as an outpatient). Therefore, both the clinical and economic findings summarized in this report have unclear generalizability to Canadian settings.
Although the 4 included systematic reviews20-23 were considered to be of high methodological quality, the primary studies summarized in these reviews were of variable quality. The RCTs included in the Walton et al. (2020)20 systematic review were judged as being at low to high risk of bias by the authors of the review, while the retrospective comparative studies were judged as being at unclear to high risk of bias. Of the 12 relevant primary studies included in the Yang et al. (2020)21 systematic review, 3 were considered to be of high quality by the review authors (i.e., Jadad score ≥ 4 points for RCTs, ≥ 8 points on the modified Newcastle-Ottawa scale for non-randomized studies). The authors of the Yang et al. (2018)22 systematic review judged their 2 included RCTs to have a moderate and a low risk of bias, while all 9 included observational studies were considered to be of high quality, according to the Newcastle-Ottawa scale. Finally, the 5 studies included in the Lobo et al. (2016)23 systematic review had STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) scores of between 27 and 32, with a mean score of 29.6.
Tumour progression and tumour response are influenced by the frequency of follow-up imaging. While the interval between follow-up imaging visits is expected to have been consistent across treatment groups in primary clinical studies (e.g., Padia and colleagues24 conducted follow-up imaging visits 1 month after treatment and every 3 months thereafter), different primary studies assessed these outcomes at different time intervals. Therefore, between-study comparisons of these outcomes should be interpreted with caution.
When information on the gender or sex of patients was available, the identified literature20-27 included a disproportionately high number of men. While this is likely attributable to the higher prevalence of hepatocellular carcinoma in men,34 the effectiveness of 90Y-based TARE in women may be different than the treatment-effect estimates summarized in the literature.
No evidence regarding the clinical effectiveness or cost-effectiveness of 90Y-based TARE versus treatment with a combination of atezolizumab and bevacizumab was identified, and no conclusions can be drawn regarding the comparative effectiveness of these treatments. The combination of atezolizumab and bevacizumab has recently emerged as a promising treatment option that is associated with greater overall survival and progression-free survival compared with sorafenib for patients with advanced hepatocellular carcinoma.35 Additional information regarding the clinical effectiveness of 90Y-based TARE compared with newer treatment options may influence conclusions regarding its place in therapy.
Conclusions and Implications for Decision- or Policy-Making
This review comprised 1 health technology assessment (which included a systematic review with network meta-analyses and an economic evaluation),20 3 systematic reviews with meta-analyses,21-23 1 non-randomized study,24 and 3 economic evaluations25-27 regarding 90Y microspheres for TARE of intermediate- or advanced-stage hepatocellular carcinoma.
Based on the evidence summarized within this report, TARE performed using 90Y microspheres appears to result in no differences in overall survival, progression-free survival, and tumour response when compared to sorafenib or TACE. However, differences between treatment with TARE and comparator interventions were statistically significant in some instances. For example, treatment with TARE may lead to improved 2-year and 3-year overall survival rates versus cTACE21,23 and decreased 2-year overall survival rates versus DEB-TACE.21 Additionally, treatment with TARE may be associated with improvements in tumour response using mRECIST criteria compared to cTACE.22 As for the comparative safety of TARE, evidence from 4 systematic reviews20-23 and 1 non-randomized study24 suggested that in general the rates of adverse events, such as fatigue, nausea, vomiting, fever, or liver failure, were not statistically significantly different between participants who were treated with TARE and those who received comparator interventions; however, treatment with TARE led to increased or decreased risk for specific adverse events in some instances.
Four economic evaluations20,25-27 assessed the cost-effectiveness of TARE performed using 90Y microspheres versus comparator interventions for the treatment of hepatocellular carcinoma. Compared with TACE, 1 study25 suggested that TARE was likely to be cost-effective at a willingness-to-pay threshold of £30,000. The authors of the analyses20,26,27 that compared TARE with systemic therapies (i.e., sorafenib or lenvatinib) made mixed conclusions. One analysis26 suggested that TARE was dominant versus sorafenib, 1 analysis27 suggested TARE was dominant or cost-effective versus sorafenib or lenvatinib (depending on the patient population), and the third analysis20 suggested treatment with sorafenib or lenvatinib was dominant or cost-effective versus TARE. While these 3 analyses20,26,27 used similar model structures and patient populations, the cost inputs and interpretations of the findings from key clinical trials varied, which may have contributed to the divergent conclusions made by study authors.
The limitations of the included literature20-27 (e.g., the lack of evidence comparing TARE with atezolizumab-bevacizumab, variable quality of primary studies included in identified systematic reviews,20-23 uncertainty in the economic models, and paucity of literature from Canadian settings) should be considered when interpreting the findings of this report. Evidence regarding the use of 90Y microspheres for the treatment of hepatocellular carcinoma is evolving rapidly. For example, NICE is in the process of conducting a Multiple Technology Appraisal on SIRTs for treating hepatocellular carcinoma36 that is expected to be completed in the near future. In addition, Cancer Care Ontario is in the process of updating guidelines regarding the non-surgical management of advanced hepatocellular carcinoma.37 Findings from the NICE appraisal and the Cancer Care Ontario guidelines, as well as additional data from new clinical trials and other evidence syntheses, may help better define the role of 90Y microspheres in the care pathway.
References
1.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. PubMed
2.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. Can Med Assoc J. 2020;192(9):E199-E205. PubMed
3.Mazereeuw MV, Withrow DR, Diane Nishri E, Tjepkema M, Marrett LD. Cancer incidence among First Nations adults in Canada: follow-up of the 1991 Census Mortality Cohort (1992-2009). Can J Public Health. 2018;109(5-6):700-709. PubMed
4.Balogh J, Victor D, 3rd, Asham EH, et al. Hepatocellular carcinoma: a review. J Hepatocell Carcinoma. 2016;3:41-53. PubMed
5.Gelband H, Jha P, Sankaranarayanan R, Horton S. Cancer: disease control priorities Vol 3. Third ed. Washington, D.C.: The International Bank for Reconstruction and Development/The World Bank; 2015.
6.Janevska D, Chaloska-Ivanova V, Janevski V. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;3(4):732-736. PubMed
7.EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56(4):908-943. PubMed
8.Moctezuma-Velazquez C, Montano-Loza AJ, Meza-Junco J, et al. Selective internal radiation therapy for hepatocellular carcinoma across the Barcelona Clinic Liver Cancer stages. Dig Dis Sci. 2020. PubMed
9.Kim DY, Han KH. Transarterial chemoembolization versus transarterial radioembolization in hepatocellular carcinoma: optimization of selecting treatment modality. Hepatol Int. 2016;10(6):883-892. PubMed
10.Raza A, Sood GK. Hepatocellular carcinoma review: current treatment, and evidence-based medicine. World J Gastroenterol. 2014;20(15):4115-4127. PubMed
11.Tong AKT, Kao YH, Too CW, Chin KFW, Ng DCE, Chow PKH. Yttrium-90 hepatic radioembolization: clinical review and current techniques in interventional radiology and personalized dosimetry. Br J Radiol. 2016;89(1062):20150943-20150943. PubMed
12.Facciorusso A. Drug-eluting beads transarterial chemoembolization for hepatocellular carcinoma: Current state of the art. World J Gastroenterol. 2018;24(2):161-169. PubMed
13.Radioembolization with yttrium-90 microspheres for the management of uveal melanoma liver metastases: a review of clinical effectiveness and cost-effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pdf/htis/2018/RC1008%20Yttrium-90%20microspheres%20Final.pdf. Accessed 2021 Jan 5.
14.Clinical and cost effectiveness of yttrium-90 microspheres for liver metastases from colorectal cancer (Health Technology Inquiry Service). Ottawa (ON): CADTH; 2007: https://www.cadth.ca/sites/default/files/pdf/htis/Yttrium-90%20Microspheres%20for%20Liver%20Metastases%20from%20Colorectal%20Cancer.pdf. Accessed 2021 Jan 05.
15.Yttrium-90 microsphere radioembolization for the treatment of primary or secondary liver cancer: clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/htis/feb-2016/RB0963%20Yttrium-90%20Radioembolization%20Final.pdf. Accessed 2021 Jan 05.
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
18.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
19.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Jan 5.
20.Walton M, Wade R, Claxton L, et al. Selective internal radiation therapies for unresectable early-, intermediate- or advanced-stage hepatocellular carcinoma: systematic review, network meta-analysis and economic evaluation. Health Technol Assess. 2020;24(48):1-264. PubMed
21.Yang B, Liang J, Qu Z, Yang F, Liao Z, Gou H. Transarterial strategies for the treatment of unresectable hepatocellular carcinoma: A systematic review. PLoS One. 2020;15(2):e0227475. PubMed
22.Yang Y, Si T. Yttrium-90 transarterial radioembolization versus conventional transarterial chemoembolization for patients with hepatocellular carcinoma: a systematic review and meta-analysis. Cancer Biol Med. 2018;15(3):299-310. PubMed
23.Lobo L, Yakoub D, Picado O, et al. Unresectable hepatocellular carcinoma: radioembolization versus chemoembolization: a systematic review and meta-analysis. Cardiovasc Intervent Radiol. 2016;39(11):1580-1588. PubMed
24.Padia SA, Johnson GE, Horton KJ, et al. Segmental yttrium-90 radioembolization versus segmental chemoembolization for localized hepatocellular carcinoma: results of a single-center, retrospective, propensity score-matched study. J Vasc Interv Radiol. 2017;28(6):777-785.e771. PubMed
25.Manas D, Bell JK, Mealing S, et al. The cost-effectiveness of TheraSphere in patients with hepatocellular carcinoma who are eligible for transarterial embolization. Eur J Surg Oncol. 2020;14:14. PubMed
26.Muszbek N, Remak E, Evans R, et al. Cost-utility analysis of selective internal radiation therapy with Y-90 resin microspheres in hepatocellular carcinoma. Fut Oncol. 2020;23:23. PubMed
27.Rognoni C, Ciani O, Sommariva S, Tarricone R. Real-world data for the evaluation of transarterial radioembolization versus sorafenib in hepatocellular carcinoma: a cost-effectiveness analysis. Value Health. 2017;20(3):336-344. PubMed
28.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
29.National Health Service (NHS). National schedule of reference costs 2018–2019. National cost collection for the NHS 2019; https://www.england.nhs.uk/national-cost-collection/#ncc1819, 2021 Jan 28.
30.NHS Improvement. Reference costs 2017/18: highlights, analysis and introduction to the data. 2018; https://improvement.nhs.uk/documents/1972/1_-_Reference_costs_201718.pdf. Accessed 2021 Jan 28.
31.Tarao K, Nozaki A, Ikeda T, et al. Real impact of liver cirrhosis on the development of hepatocellular carcinoma in various liver diseases-meta-analytic assessment. Cancer Med. 2019;8(3):1054-1065. PubMed
32.Brahmania M, Marquez V, Kneteman NM, et al. Canadian liver transplant allocation for hepatocellular carcinoma. J Hepatol. 2019;71(5):1058-1060. PubMed
33.Vilgrain V, Pereira H, Assenat E, et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol. 2017;18(12):1624-1636. PubMed
34.Wu EM, Wong LL, Hernandez BY, et al. Gender differences in hepatocellular cancer: disparities in nonalcoholic fatty liver disease/steatohepatitis and liver transplantation. Hepatoma res. 2018;4:66. PubMed
35.Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894-1905. PubMed
36.National Institute for Health and Care Excellence. Selective internal radiation therapies for treating hepatocellular carcinoma [ID1276]. (In development [GID-TA10381]) 2020; https://www.nice.org.uk/guidance/indevelopment/gid-ta10381. Accessed 2021 Jan 28.
37.Meyers B, Knox J, Cosby R, et al. Non-surgical management of advanced hepatocellular carcinoma. Guideline 2-24: being updated. Toronto (ON): Cancer Care Ontario; 2019: https://www.cancercareontario.ca/sites/ccocancercare/files/guidelines/full/pebc2-24f.pdf. Accessed 2021 Jan 28.
38.Chow PKH, Gandhi M, Tan SB, et al. SIRveNIB: selective internal radiation therapy versus sorafenib in Asia-Pacific patients with hepatocellular carcinoma. J Clin Oncol. 2018;36(19):1913-1921. PubMed
39.Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163-1173. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Health Technology Assessment, Systematic Reviews, and Network Meta-Analyses
Author, country, funding source | Objectives, study designs, and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Health technology assessment | ||||
Walton et al. (2020)20 UK Funding source: NIHR Health Technology Assessment program | Objective: To evaluate the clinical and cost-effectiveness of SIRTs for the treatment of patients with unresectable hepatocellular carcinoma Study design: Systematic review, NMA, and economic analysis; the systematic review and NMAs included RCTs; when there was insufficient RCT evidence to address the decision problem, non-randomized comparative studies and non-comparative studies were considered for inclusion; characteristics of the economic evaluation are described in Table 4 Number of included studies: A total of 27 studies were included in the systematic review (17 studies reported in 21 publications were relevant to the current report); the network meta-analysis included 5 of these primary studies (3 RCTs and 2 retrospective comparative studies) Quality-assessment tool: RCTs were assessed using the Cochrane risk-of-bias tool; quality-assessment tools for other study designs were developed using relevant criteria (e.g., those outlined in the CRD’s guidance on undertaking systematic reviews) | Studies of people with early-stage hepatocellular carcinoma in whom curative treatment is contraindicated (BCLC stage A) and studies of people with intermediate-stage (BCLC stage B) or advanced-stage (BCLC stage C) hepatocellular carcinoma were included Three NMA models were produced to estimate relative efficacy in 3 subpopulations: 1) adults with unresectable hepatocellular carcinoma who are potentially eligible for transplant, 2) adults with unresectable hepatocellular carcinoma who are eligible for conventional transarterial therapies; and 3) adults with unresectable hepatocellular carcinoma who are ineligible for conventional transarterial therapies Excluded: Studies of people with secondary liver metastases or other types of liver cancer | Intervention: SIRTs, including TheraSphere, SIR-Spheres, and QuiremSpheres; only primary studies that examined 90Y-based SIRTs were considered relevant to the current report (i.e., studies on QuiremSpheres were not considered relevant) Comparators: Alternative SIRT interventions, conventional transarterial therapies (e.g., TACE), established clinical management without SIRT (e.g., sorafenib, lenvatinib, and regorafenib), or best supportive care Only primary studies that used TACE, sorafenib, lenvatinib, atezolizumab, or bevacizumab as comparators were relevant to the current report | Clinical outcomes:
Length of follow-up: Varied by individual study and was NR |
Systematic reviews | ||||
Yang et al. (2020)21 China Funding source: The Department of Science and Technology of Sichuan Province of China | Objective: To systematically analyze the comparative effectiveness of TARE, DEB-TACE, and cTACE for the treatment of unresectable hepatocellular carcinoma with respect to overall survival, tumour response rate, and complications Study design: Systematic review and meta-analysis of RCTs and retrospective or prospective cohort studies Number of included studies: A total of 28 studies were included in the systematic review (12 studies were relevant to the current report) Quality-assessment tool: RCTs were assessed using the Jadad score (studies with a score ≥ 4 were considered high-quality); non-randomized studies were assessed using the modified Newcastle-Ottawa scale (studies with ≥ 8 points were considered high-quality) | Studies of people with hepatocellular carcinoma confirmed by typical imaging scans or pathology were included Excluded: Studies of people with multiple malignancies | The review included primary studies that directly compared various transarterial strategies for the treatment of unresectable hepatocellular carcinoma (i.e., TARE vs. cTACE, TARE vs. DEB-TACE, and cTACE vs. DEB-TACE); only primary studies that included a group of patients that received TARE were considered relevant to the current report | Clinical outcomes:
Length of follow-up: |
Yang and Si (2018)22 China Funding source: NR | Objective: To evaluate the effectiveness and safety of 90Y TARE vs. cTACE for the treatment of hepatocellular carcinoma (particularly those with intermediate or advanced-stage disease) Study design: Systematic review and meta-analysis of RCTs, observational studies, and other clinical studies Number of included studies: A total of 11 studies were included in the systematic review (all were relevant to the current report) Quality-assessment tool: RCTs were assessed using the Cochrane Collaboration tool of RevMan; observational studies were assessed using the modified Newcastle-Ottawa scale | Studies of people who were diagnosed with hepatocellular carcinoma were included | Intervention: 90Y TARE Comparator: cTACE (i.e., studies on DEB-TACE were not eligible) | Clinical outcomes:
Length of follow-up: Varied by individual study and was NR. Overall survival was calculated for 1 year and 2 years |
Lobo et al. (2016)23 US Funding source: NR | Objective: To systematically evaluate the comparative effectiveness of TARE vs. TACE for the treatment of unresectable hepatocellular carcinoma Study design: Systematic review and meta-analysis of any comparative studies (i.e., RCTs and non-randomized studies) Number of included studies: A total of 5 studies were included in the systematic review (all were relevant to the current report) Quality-assessment tool: The included studies were assessed using the 22-item STROBE checklist | Studies of people with unresectable hepatocellular carcinoma were included | Intervention: 90Y TARE using a glass matrix (e.g., TheraSphere) or resin microspheres (e.g., SIR-Spheres) Comparator: TACE (e.g., doxorubicin, mitomycin, adriamycin, and cisplatin) | Clinical outcomes:
Length of follow-up: |
90Y = yttrium-90; BCLC = Barcelona Clinic Liver Cancer; CRD = Centre for Reviews and Dissemination; cTACE = conventional transarterial chemoembolization; DEB-TACE = drug-eluting bead transarterial chemoembolization; NIHR = National Institute for Health Research; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial; SIRT = selective internal radiation therapy; STROBE = STrengthening the Reporting of OBservational studies in Epidemiology; TACE = transarterial chemoembolization; TARE = transarterial radioembolization; vs. = versus.
Table 3: Characteristics of Included Non-Randomized Study
Study citation, country, funding source | Objective and study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Padia et al. (2017)24 US Funding source: NR | Objective: To compare segmental TARE with segmental TACE for the treatment of localized, unresectable hepatocellular carcinoma deemed inappropriate for ablation Study design: Single-centre, retrospective cohort study | Inclusion criteria: Those who received radioembolization or chemoembolization to treat a region equivalent to a single hepatic Couinaud segment between 2010 and 2015 at the study centre were included in the analysis; patients were eligible regardless of their treatment history (e.g., prior liver transplantation, surgical resection, or ablation) Excluded: Patients who received treatment to larger areas of the liber (e.g., lobar chemoembolization) Number of participants: 178 (101 in the TARE group; 77 in the TACE group) Median age, years (range): 62 (36 to 83) in the TARE group; 60 (41 to 82) in the TACE group Sex: 82.2% male in the TARE group; 71.4% male in the TACE group Cirrhosis etiology:
Child-Pugh class:
BCLC stage:
Prior liver treatment:
Number of tumours:
| Intervention: TARE using 90Y glass microspheres (TheraSphere) Comparator: DEB-TACE (using doxorubicin drug-eluting beads) or cTACE (using doxorubicin microspheres) In both treatment groups, repeat segmental TARE or TACE was considered if a partial response or stable disease was seen on follow-up imaging | Clinical outcomes:
Length of follow-up: Follow-up visits occurred at 1-month post-treatment and every 3 months thereafter; median follow-up after treatment was 322 days (IQR = 193 to 561 days) for the TARE group and 585 days (IQR = 317 to 952 days) for the TACE group |
90Y = yttrium-90; BCLC = Barcelona Clinic Liver Cancer; cTACE = conventional transarterial chemoembolization; DEB-TACE = drug-eluting bead transarterial chemoembolization; HBV = hepatitis B virus; HCV = hepatitis C virus; IQR = interquartile range; NR = not reported; TACE = transarterial chemoembolization; TARE = transarterial radioembolization.
Table 4: Characteristics of Included Economic Evaluations
Study citation country, funding source | Type of analysis, time horizon, | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
Manas et al. (2020)25 UK Funding source: A consultancy agreement between York Health Economics Consortium and Boston Scientific | Analysis: Cost-utility analysis Time horizon: 20 years Perspective: UK National Health Service | A hypothetical cohort of patients (≥ 65 years of age) with hepatocellular carcinoma who were unresectable at presentation and were eligible for transarterial embolization, cTACE or DEB-TACE; the cohort was 75% male | Intervention: TARE with TheraSphere Comparators: transarterial embolization, cTACE, and DEB-TACE | A cohort-based Markov model with a cycle length of 4 weeks. The 8 health states included: watch and wait, resection, pharmacological management, pre-transplant, post-transplant, no hepatocellular carcinoma post-transplant, no hepatocellular carcinoma (other), and dead | Effectiveness inputs and utility values were derived from National Liver Offering Scheme data, clinical trials, and assumptions informed by clinical experts; cost inputs were taken from publicly available sources, including the NICE formulary and National Schedule of Reference Costs 2018–201929 |
|
Muszbek et al. (2020)26 UK Funding source: Sirtex Medical Ltd. (a manufacturer of SIR-Spheres) | Analysis: Cost-utility analysis Time horizon: a lifetime horizon (scenario analyses considered a 5-year horizon) Perspective: UK National Health Service | Patients with unresectable intermediate (BCLC stage B) or advanced (BCLC stage C) hepatocellular carcinoma for whom any transarterial embolization therapies (e.g., TACE or transcatheter arterial embolization) were inappropriate, who did not have extrahepatic disease, had a low tumour burden (≤ 25%), and who had preserved liver function (ALBI grade 1) | Intervention: SIRT with SIR-Spheres (90Y resin microspheres) Comparator: Sorafenib | A lifetime partitioned survival analysis model that incorporated 4 health states: progression-free, post-progression, received curative therapy, and dead | Effectiveness inputs and utility values for SIRT and sorafenib were extrapolated from the SARAH trial,33 effectiveness inputs for treatments with curative intent were selected from a targeted literature review, and resource uses were from registries and clinical surveys; utility values were EQ-5D scores mapped from EORTC QLQ-C30 within the SARAH trial33 |
|
Walton et al. (2020)20 UK Funding source: The NIHR Health Technology Assessment program | Analysis: Cost-utility analysis conducted as part of an HTA Time horizon: 10 years Perspective: UK National Health Service and Personal Social Services | Patients with unresectable intermediate (BCLC stage B) or advanced (BCLC stage C) hepatocellular carcinoma and without extrahepatic disease for whom any conventional transarterial embolization therapies (e.g., TACE) were inappropriate | Intervention: SIRTs, including TheraSphere, SIR-Spheres, and QuiremSpheres Comparator: Established clinical management without SIRT using sorafenib or lenvatinib | A decision tree representing the outcome of the work-up procedure transitioning into a 3-state (i.e., progression-free survival, post-progression, and dead) partitioned survival model | Treatment-effectiveness parameters and other inputs calculated from the SARAH,33 SIRveNIB38 and REFLECT trials39 were used; additional effectiveness inputs were drawn from the NMA conducted as part of the HTA; costs of SIRTs and health-state costs were obtained from manufacture’s submissions and the National Schedule of Reference Costs 2017–201830 | The model incorporated several assumptions due to limited availability of clinical literature in some instances:
|
Rognoni et al. (2017)27 Italy Funding source: ASBM Srl through an unrestricted grant to CERGAS, Bocconi University | Analysis: Cost-utility analysis Time horizon: a lifetime horizon (scenario analyses considered the following time horizons: 1 year, 2 years, 4 years, 6 years, 8 years, 10 years, 15 years, 20 years) Perspective: Italian health care service | Patients with intermediate or advanced hepatocellular carcinoma at 3 oncology centres in Italy; patients with metastatic disease or early or terminal hepatocellular carcinoma were excluded | Intervention: TARE Comparator: Sorafenib (target dosage; 800 mg/day) | A cohort-based multistate Markov model that had a cycle length of 1 month. The model consisted of 5 possible health states (i.e., post-transplantation, stable disease, disease progression, death from the disease, and death from other causes) | Transition probabilities were obtained from prospectively collected real-world data from patients receiving care at 3 centres in Italy; health utility values were retrieved from studies identified in a literature search or came from the Cost-Effectiveness Analysis Registry; health care resource consumptions and costs were from the Regional Health Care Service price list and the from diagnosis-related group-reimbursement rates |
|
90Y = yttrium-90; ALBI = albumin-bilirubin; BCLC = Barcelona Clinic Liver Cancer; cTACE = conventional transarterial chemoembolization; DEB-TACE = drug-eluting bead transarterial chemoembolization; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer quality of life questionnaire; EQ-5D = EuroQol 5-Dimensions; HTA = health technology assessment; NICE = National Institute for Health and Care Excellence; NMA = network metanalysis; SIRT = selective internal radiation therapy; TACE = transarterial chemoembolization; TARE = transarterial radioembolization.
Appendix 3: Critical Appraisal of Included Publications
Table 5: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 216 and the ISPOR Questionnaire17
Strengths | Limitations |
Walton et al. (2020)20 | |
Network meta-analyses
|
Network meta-analyses
|
Yang et al. (2020)21 | |
|
|
Yang and Si (2018)22 | |
|
|
Lobo et al. (2016)23 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; BCLC = Barcelona Clinic Liver Cancer; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NIHR = National Institute of Health Research; NHS = National Health Service; RCT = randomized controlled trial.; WHO = World Health Organization.
Table 6: Strengths and Limitations of Non-Randomized Study Using the Downs and Black Checklist18
Strengths | Limitations |
Padia et al. (2017)24 | |
|
|
ECOG = Eastern Cooperative Oncology Group; TACE = transarterial chemoembolization; TARE = transarterial radioembolization; vs. = versus.
Table 7: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist19
Strengths | Limitations |
Manas et al. (2020)25 | |
Study design
Data collection
Analysis and interpretation of results
Miscellaneous Review authors stated their potential conflicts of interest (4 authors worked for York Health Economics Consortium, a consultancy company that was commissioned by Boston Scientific to produce this work; 1 author was paid to attend advisory panel meetings for Roche, BMS, Eisae, Celgene, Beigene, Opsen and Boston Scientific, and to be a speaker for Eisae, Ipsen, Mylan, and PrimeOncology; 1 author had attended conferences for Bayer, BMS, and Roche; 1 author had advisory roles for Boston Scientific, Sirtex, and Roche, and had been paid to be a speaker for Boston Scientific, Sirtex, and Terumo; 1 author had received travel costs and a honorarium to chair a TheraSphere advisory board) |
|
Muszbek et al. (2020)26 | |
Study design
Data collection
Analysis and interpretation of results
Miscellaneous Study authors stated their potential conflicts of interest (2 authors were partners/employees of Visible Analytics Ltd., which conducted this survey and received consultancy fees and expenses from Sirtex Medical Ltd.; 3 authors were employees of Sirtex Medical Ltd.; 1 author had received consulting fees from Sirtex Medical Ltd., but has not received honorariums for this manuscript) |
|
Walton et al. (2020)20 | |
Study design
Data collection
Analysis and interpretation of results
Miscellaneous
|
|
Rognoni et al. (2017)27 | |
Study design
Data collection
Analysis and interpretation of results
Miscellaneous Source of funding was disclosed (ASBM Srl through an unrestricted grant to CERGAS, Bocconi University) and was unlikely to have had an effect on the findings of the study |
|
NIHR = National Institute for Health Research.
Appendix 4: Main Study Findings and Authors’ Conclusions
Summary of Findings Including Systematic Reviews and Network Meta-Analyses
Walton et al. (2020)20
Main Study Findings
Systematic review with network meta-analyses that evaluated the clinical effectiveness of SIRTs for the treatment of patients with unresectable hepatocellular.
Relevant primary studies: The systematic review included 27 studies that compared various SIRTs to alternative SIRTS, conventional transarterial therapies (e.g., TACE), established clinical management without a SIRT (e.g., sorafenib, lenvatinib, and regorafenib), or best supportive care; however, only primary studies that compared 90Y-based therapies versus TACE, sorafenib, lenvatinib, atezolizumab, or bevacizumab were relevant to the current report (17 studies reported in 21 publications). Relevant results are therefore summarized individually by primary study, and treatment-effect estimates from interventions of interest were extracted from the network meta-analyses.
Summary of Relevant Findings From the Systematic Review
TARE versus sorafenib
Overall survival
Chow 2018 (SIRveNIB trial)
Median overall survival
TARE (N = 182; 95% confidence interval [CI]): 8.8 months (7.5 months to 10.8 months)
Sorafenib (N = 178; 95% CI): 10.0 months (8.6 months to 13.8 months)
ITT population hazard ratio (HR) (95% CI): 1.12 (0.9 to 1.4)
P value: 0.36
Per-protocol population HR (95% CI): 0.86 (0.7 to 1.1)
P value: 0.27
Vilgrain 2017 (SARAH trial)
1-year overall survival rate
TARE (N = 237; 95% CI): 39.5% (33.3% to 45.9%)
Sorafenib (N = 222; 95% CI): 42.1% (35.6% to 48.7%)
ITT population HR (95% CI): 1.15 (0.94 to 1.41)
P value: 0.18
Per-protocol population HR (95% CI): 0.99 (0.79 to 1.24)
P value: not reported (NR)
Progression-free survival
Chow 2018 (SIRveNIB trial)
Median progression-free survival
TARE (N = 182; 95% CI): 5.8 months (3.7 months to 6.3 months)
Sorafenib (N = 178; 95% CI): 5.1 months (3.9 months to 5.6 months)
ITT population HR (95% CI): 0.89 (0.7 to 1.1)
P value: 0.31
Vilgrain 2017 (SARAH trial)
Proportion of patients who experienced progression
TARE (N = 237; 95% CI): 92% (NR)
Sorafenib (N = 222; 95% CI): 92% (NR)
ITT population HR (95% CI): 1.03 (0.85 to 1.25)
P value: 0.76
Response
Chow 2018 (SIRveNIB trial)
Complete or partial response rates
TARE (N = 182; 95% CI): 16.5% (NR)
Sorafenib (N = 178; 95% CI): 1.7% (NR)
P value: NR
Vilgrain 2017 (SARAH trial)
Complete or partial response rates
TARE (N = 237; 95% CI): 19% (NR)
Sorafenib (N = 222; 95% CI): 12% (NR)
P value: NR
Quality of life
Chow 2018 (SIRveNIB trial): EQ-5D mean scores
“There were no statistically significant differences in the EQ-5D index between the SIR-Spheres and sorafenib groups throughout the study in either the ITT or the treated populations (p. 199).”20
Vilgrain 2017 (SARAH trial): Global health status subscores
“The global health status subscore was significantly better in the selective internal radiation therapy group than in the sorafenib group (group effect P = 0.0048; time effect P < 0.0001) and the between-group difference tended to increase with time (group*time interaction p = 0.0447) for both the ITT and per-protocol populations (p. 197).”20
Adverse events
Chow 2018 (SIRveNIB trial)
Proportion of patients who experienced at least 1 adverse event
TARE (N = 182; 95% CI): 60% (NR)
Sorafenib (N = 178; 95% CI): 84.6% (NR)
P value: NR
Vilgrain 2017 (SARAH trial)
Proportion of patients who experienced at least 1 adverse event
TARE (N = 237; 95% CI): 77% (NR)
Sorafenib (N = 222; 95% CI): 94% (NR)
P value: NR
TARE versus TACE (cTACE or DEB-TACE)
Overall survival
Hickey 2016
Median overall survival in those with BCLC stage A and Child-Pugh class A
TARE (N = NR; 95% CI): 21.4 months (9.8 months to 33.1 months)
TACE (N = NR; 95% CI): not evaluable (most patients still alive)
P value: NR
Median overall survival in those with BCLC stage A and Child-Pugh class B
TARE (N = NR; 95% CI): 27.6 months (11.6 months to 43.6 months)
TACE (N = NR; 95% CI): not evaluable (most patients still alive)
P value: NR
Median overall survival in those with BCLC stage B and Child-Pugh class A
TARE (N = NR; 95% CI): 18.3 months (12.3 months to 24.3 months)
TACE (N = NR; 95% CI): 19.2 months (16.0 months to 22.4 months)
P value: NR
Median overall survival in those with BCLC stage B and Child-Pugh class B
TARE (N = NR; 95% CI): 12.2 months (8.1 months to 16.3 months)
TACE (N = NR; 95% CI): 17.4 months (8.8 months to 26.0 months)
P value: NR
Median overall survival in those with BCLC stage C and Child-Pugh class A
TARE (N = NR; 95% CI): 9.5 months (7.0 months to 11.9 months)
TACE (N = NR; 95% CI): 8.6 months (5.1 months to 12.0 months)
P value: NR
Median overall survival in those with BCLC stage C and Child-Pugh class B
TARE (N = NR; 95% CI): 5.6 months (4.1 months to 7.1 months)
TACE (N = NR; 95% CI): 3.5 months (2.6 months to 4.4 months)
P value: NR
Salem 2016 (PREMIERE trial)
Median overall survival
TARE (N = 24; 95% CI): 18.6 months (7.4 months to 32.5 months)
TACE (N = 21; 95% CI): 17.7 months (8.3 months to NR)
P value: NR
El Fouly 2015
Median overall survival
TARE (N = 44; 95% CI): 16.4 months (7.9 months to 25.3 months)
TACE (N = 42; 95% CI): 18.0 months (12.1 months to 25.5 months)
P value: NR
1-year overall survival rate
TARE (N = 44; 95% CI): 59% (NR)
TACE (N = 42; 95% CI): 64% (NR)
P value: NR
2-year overall survival rate
TARE (N = 44; 95% CI): 40% (NR)
TACE (N = 42; 95% CI): 36% (NR)
P value: NR
3-year overall survival rate
TARE (N = 44; 95% CI): 31% (NR)
TACE (N = 42; 95% CI): 11% (NR)
P value: NR
Pitton 2015
Median overall survival
TARE (N = 12; interquartile range [IQR]: 592 days (192 days to NR)
DEB-TACE (N = 12; IQR): 788 days (178 days to 950 days)
P value: NR
Progression-free survival
Salem 2016 (PREMIERE trial)
Median time to progression
TARE (N = 24): not reached (> 26 months)
TACE (N = 21): 6.8 months
P value: NR
El Fouly 2015
Median time to progression
TARE (N = 44; 95% CI): 13.3 months (3.4 months to 23.1 months)
TACE (N = 42; 95% CI): 6.8 months (3.9 months to 8.8 months)
P value: NR
Kolligs 2015 (SIRTACE trial)
Median progression-free survival
TARE (N = 13; 95% CI): 3.6 months (2.3 months to 6.2 months)
TACE (N = 15; 95% CI): 3.7 months (1.6 months to 11.0 months)
P value: NR
Pitton 2015
Median progression-free survival
TARE (N = 12; IQR): 180 days (120 days to 414 days)
DEB-TACE (N = 12; IQR): 216 days (88 days to 355 days)
P value: NR
Memon 2013
Median time to progression
TARE (N = 42): 13.3 months (range: 9.3 months to 25.0 months)
TACE (N = 54): 8.4 months (range: 7.3 months to 10.6 months)
P value: NR
Response
Kirchner 2019
Complete or partial response rates
TARE (N = 21; 95% CI): 0% (NR)
cTACE or DEB-TACE (N = 46; 95% CI): 2.3% (NR)
P value: NR
Salem 2016 (PREMIERE trial)
Proportion of patients who achieved European Association for the Study of the Liver response
TARE (N = 24; 95% CI): 87% (NR)
TACE (N = 21; 95% CI): 74% (NR)
P value: NR
Proportion of patients who achieved WHO response
TARE (N = 24; 95% CI): 52% (NR)
TACE (N = 21; 95% CI): 63% (NR)
P value: NR
El Fouly 2015
Complete response rates
TARE (N = 44; 95% CI): 7% (NR)
TACE (N = 42; 95% CI): 5% (NR)
P value: NR
Partial response rates
TARE (N = 44; 95% CI): 68% (NR)
TACE (N = 42; 95% CI): 45% (NR)
P value: NR
Kolligs 2015 (SIRTACE trial)
Complete or partial response rates
TARE (N = 13; 95% CI): 30.8% (NR)
TACE (N = 15; 95% CI): 13.3% (NR)
P value: NR
Quality of life
Kirchner 2019
Health status and quality of life
“After treatment, the mean absolute decrease in global health status/quality of life was higher in the TACE group (−10.5%) than in the selective internal radiation therapy group (−4.8%), which was not statistically significant (p = 0.396) (p. 206).”20
Kolligs 2015 (SIRTACE trial)
Health-related quality of life
“Health-related quality of life data were analysed for 18 patients (8 SIRT and 10 TACE). Higher scores reflect higher functioning and fewer symptoms. At baseline, median scores were lower for patients receiving SIRT than for patients receiving TACE, particularly for subscales of physical functioning (82.0 vs. 96.0; p = 0.04) by Kruskal–Wallis test. This manifested in the lower scores with SIRT throughout the first 12 weeks after treatment, although the differences between the treatment groups by week 12 were not statistically significant for either FACT-Hep total or its subscales (p. 200).”20
Salem 2013
Health-related quality of life
“Despite more advanced disease at baseline (regression analysis incorporating BCLC stage), selective internal radiation therapy patients showed significantly better quality of life relative to TACE in social well-being (p = 0.019), functional well-being (p = 0.031) and embolotherapy-specific score (p = 0.018). Strong trends favouring selective internal radiation therapy were noted in overall quality of life (p = 0.055), the Trial Outcome Index (p = 0.05) and FACT-Hep (p = 0.071) (p. 209).”20
Adverse events
Kolligs 2015 (SIRTACE trial)
Proportion of patients who experienced at least 1 adverse event
TARE (N = 13; 95% CI): 92.3% (NR)
TACE (N = 15; 95% CI): 66.7% (NR)
P value: NR
Note: Several additional primary studies were identified and included in the systematic review. Detailed study characteristics were extracted, and a quality assessment was conducted by the review authors. However, detailed study findings were not extracted in cases where the primary studies were judged to be of low quality (i.e., the findings were at high risk of bias). Instead, the review authors focused on the results from higher-quality studies that examined the same intervention or comparator pairs.
Summary of Relevant Findings from the Network Meta-Analyses
Network meta-analysis #1: Adults with unresectable hepatocellular carcinoma who are eligible for transplant
Evidence from 2 RCTs was identified regarding this population and could have been used to construct a network; however, in consultation with clinical experts the authors decided that due to study quality and issues with generalizability this network would be unsuitable to inform decision-making and was therefore not analyzed
Network meta-analysis #2: Adults with unresectable hepatocellular carcinoma who are eligible for conventional transarterial therapies
Evidence from 7 studies (6 RCTs and 1 retrospective comparative study) was identified regarding this population and could have been used to construct a network; however, in consultation with clinical experts the authors decided that, due to study quality and the small number of studies on which the model would rely to form the network, the results would be unsuitable to inform decision-making and were therefore not analyzed
Network meta-analysis #3: Adults with unresectable hepatocellular carcinoma who are Child-Pugh class A and ineligible for conventional transarterial therapy (includes data from 3 RCTs)
Overall survival in the per-protocol population
SIR-Spheres versus sorafenib
Fixed-effects HR (95% CrI): 0.94 (0.77 to 1.14)
Random-effects HR (95% CrI): 0.94 (0.68 to 1.26)
SIR-Spheres versus lenvatinib
Fixed-effects HR (95% CrI): 0.91 (0.63 to 1.26)
Random-effects HR (95% CrI): 0.92 (0.52 to 1.51)
“There were no meaningful differences in overall survival in the per-protocol population between any of the three treatments and all treatments appear to have a similar effect (p. 45).”20
Overall survival in the ITT population
SIR-Spheres versus sorafenib
Fixed-effects HR (95% CrI): 1.13 (0.96 to 1.32)
Random-effects HR (95% CrI): 1.13 (0.86 to 1.47)
SIR-Spheres versus lenvatinib
Fixed-effects HR (95% CrI): 1.09 (0.77 to 1.48)
Random-effects HR (95% CrI): 1.10 (0.66 to 1.74)
“SIR-Spheres appears to increase mortality when compared with sorafenib and lenvatinib. However, the CrIs indicate that these results are uncertain (p. 46).”20
Author’s Conclusion
“The existing evidence cannot provide decision-makers with clear guidance on the comparative effectiveness of treatments in early- and intermediate-stage hepatocellular carcinoma. All of the identified studies were rated as being at a high risk of bias and included highly heterogeneous populations, limiting the conclusions that can be drawn from these results. The results of individual studies varied considerably, with some showing that conventional transarterial therapy was superior to selective internal radiation therapy and vice versa. However, the available evidence suggests that selective internal radiation therapy may be beneficial in this population, with moderate improvements in progression-free survival and transplantation rates (p. 131).”20
Yang et al. (2020)21
Main Study Findings
Systematic review with meta-analyses that examined the comparative effectiveness of TARE, DEB-TACE, and cTACE for the treatment of unresectable hepatocellular carcinoma.
Relevant primary studies: The systematic review included 28 studies that compared TARE, DEB-TACE, and cTACE to each other. Of these, 12 studies compared TARE versus DEB-TACE or TARE versus cTACE and were considered relevant to the current report. Findings related to the DEB-TACE versus cTACE comparison were not extracted.
Summary of Relevant Findings from the Systematic Review
TARE versus cTACE (8 primary studies)
Overall survival
1-year overall survival (8 primary studies)
relative risk (RR) (95% CI): 0.91 (0.79 to 1.05)
P value: 0.215
2-year overall survival (7 primary studies)
RR (95% CI): 0.87 (0.80 to 0.95)
P value: 0.003 (favours TARE)
3-year overall survival (5 primary studies)
RR (95% CI): 0.90 (0.85 to 0.96)
P value: 0.001 (favours TARE)
Tumour response
Objective response (unclear number of primary studies)
odds ratio (OR) (95% CI): 0.77 (0.57 to 1.03)
P value: 0.082
Disease control rate (unclear number of primary studies)
OR (95% CI): 1.89 (1.07 to 3.35)
P value: 0.029 (favours TARE)
Adverse events
Nausea or vomiting (unclear number of primary studies)
OR (95% CI): 0.35 (0.07 to 1.73)
P value: 0.199
Pain (unclear number of primary studies)
OR (95% CI): 0.14 (0.01 to 2.51)
P value: 0.183
Fatigue (unclear number of primary studies)
OR (95% CI): 1.63 (0.25 to 10.59)
P value: 0.61
Liver failure (unclear number of primary studies)
OR (95% CI): 1.09 (0.47 to 2.49)
P value: 0.845
Gastrointestinal bleeding (unclear number of primary studies)
OR (95% CI): 1.12 (0.29 to 4.83)
P value: 0.875
TARE versus DEB-TACE (4 primary studies)
Overall survival
1-year overall survival (4 primary studies)
RR (95% CI): 0.83 (0.68 to 1.02)
P value: 0.081
2-year overall survival (3 primary studies)
RR (95% CI): 0.40 (0.19 to 0.84)
P value: 0.016 (favours DEB-TACE)
Progression-free survival
Progression-free survival at 1 year (unclear number of primary studies)
RR (95% CI): 1.00 (0.80 to 1.25)
P value: 1.000
Adverse events
Nausea or vomiting (unclear number of primary studies)
OR (95% CI): 1.03 (0.42 to 2.50)
P value: 0.949
Pain (unclear number of primary studies)
OR (95% CI): 2.12 (0.30 to 15.03)
P value: 0.452
Infection or fever (unclear number of primary studies)
OR (95% CI): 2.08 (0.11 to 38.4)
P value: 0.623
Liver failure (unclear number of primary studies)
OR (95% CI): 0.69 (0.18 to 2.61)
P value: 0.584
Gastrointestinal bleeding (unclear number of primary studies)
OR (95% CI): 0.60 (0.09 to 3.99)
P value: 0.595
Author’s Conclusion
“The current meta-analysis suggests that both DEB-TACE and TARE are superior to conventional TACE in terms of overall survival and complications. DEB-TACE has significantly better overall survival rates for patients with hepatocellular carcinoma than TARE. Further multicenter, well-designed randomized trials are needed, especially to compare DEB-TACE with TARE (p. 15).”21
Yang and Si. (2018)22
Main Study Findings
Systematic review with meta-analyses that evaluated the effectiveness and safety of 90Y TARE versus cTACE for the treatment of hepatocellular carcinoma (particularly those with intermediate- or advanced-stage disease).
Relevant primary studies: All 11 primary studies included in the systematic review were relevant to the current report.
Summary of Relevant Findings from the Systematic Review
TARE versus cTACE (11 primary studies)
Overall survival
1-year overall survival (fixed-effects model) (10 primary studies)
OR (95% CI): 0.939 (0.705 to 1.251)
P value: 0.66
2-year overall survival (random-effects model) (9 primary studies)
OR (95% CI): 0.641 (0.382 to 1.075)
P value: 0.092
Tumour response
Tumour response in studies that used WHO criteria (random-effects model) (4 primary studies)
OR (95% CI): 1.065 (0.500 to 2.268)
P value: 0.870
Tumour response in studies that used mRECIST criteria (random-effects model) (5 primary studies)
OR (95% CI): 0.584 (0.349 to 0.976)
P value: 0.040 (favours TARE)
Tumour response in all studies regardless of response criteria (random-effects model) (9 primary studies)
OR (95% CI): 0.781 (0.454 to 1.343)
P value: 0.371
Adverse events
Serious adverse events (random-effects model) (7 primary studies)
RR (95% CI): 1.477 (0.864 to 2.526)
P value: 0.154
Author’s Conclusion
“Although additional studies are urgently needed to establish clinical trials and RCTs, our findings generally support the application of TARE (90Y) for patients with hepatocellular carcinoma (especially intermediate or advanced stages) as a therapy that might be superior to conventional TACE, in 2-year overall survival rates and objective response rates, according mRECIST criteria (p. 308–309).”22
Lobo et al. (2016)23
Main Study Findings
Systematic review with meta-analyses that compared the effectiveness of 90Y TARE versus cTACE for the treatment of unresectable hepatocellular carcinoma.
Relevant primary studies: All 5 primary studies included in the systematic review were relevant to the current report.
Summary of Relevant Findings from the Systematic Review
TARE versus cTACE (5 primary studies)
Overall survival
1-year overall survival (fixed-effects model) (5 primary studies)
RR (95% CI): 0.93 (0.81 to 1.08)
P value: 0.33
2-year overall survival (fixed-effects model) (5 primary studies)
RR (95% CI): 1.36 (1.05 to 1.76)
P value: 0.02 (favour TARE)
3-year overall survival (fixed-effects model) (5 primary studies)
RR (95% CI): 1.27 (0.88 to 1.84)
P value: 0.02
4-year overall survival (fixed-effects model) (5 primary studies)
RR (95% CI): 1.64 (0.80 to 3.34)
P value: 0.17
1-year overall survival (random-effects model) (5 primary studies)
RR (95% CI): 0.94 (0.82 to 1.08)
P value: NR
2-year overall survival (random-effects model) (5 primary studies)
RR (95% CI): 1.25 (0.83 to 1.89)
P value: NR
3-year overall survival (random-effects model) (5 primary studies)
RR (95% CI): 1.26 (0.87 to 1.82)
P value: NR
4-year overall survival (random-effects model) (5 primary studies)
RR (95% CI): 1.48 (0.40 to 5.47)
P value: NR
Tumour response
Radiological response within 3 months of treatment (fixed-effects model) (3 primary studies)
RR (95% CI): 2.35 (0.76 to 7.28)
P value: 0.14
Partial response within 3 months of treatment (fixed-effects model) (3 primary studies)
RR (95% CI): 0.85 (0.55 to 1.31)
P value: 0.45
Disease progression within 3 months of treatment (fixed-effects model) (3 primary studies)
RR (95% CI): 1.07 (0.58 to 1.97)
P value: 0.84
Stable disease within 3 months of treatment (fixed-effects model) (3 primary studies)
RR (95% CI): 0.96 (0.38 to 2.42)
P value: 0.92
Adverse events
Pain (fixed-effects model) (3 primary studies)
RR (95% CI): 0.51 (0.36 to 0.72)
P value: < 0.01 (favours TARE)
Post-procedural fatigue (fixed-effects model) (3 primary studies)
RR (95% CI): 1.60 (1.25 to 2.06)
P value: NR
Nausea and vomiting (fixed-effects model) (4 primary studies)
RR (95% CI): 0.83 (0.60 to 1.22)
P value: 0.35
Fever (fixed-effects model) (3 primary studies)
RR (95% CI): 0.94 (0.46 to 1.90)
P value: NR
Other complications (e.g., diarrhea, anorexia, headache, chest pain, confusion, gastric ulceration, bleeding from puncture site, rash, varicella zoster infection, and hepatic abscess; fixed-effects model) (5 primary studies)
RR (95% CI): 1.09 (0.67 to 1.76)
P value: 0.74
Post-treatment morbidity (fixed-effects model) (4 primary studies)
RR (95% CI): 0.85 (0.69 to 1.05)
P value: 0.41
More than 3 complications (fixed-effects model) (4 primary studies)
RR (95% CI): 0.83 (0.49 to 1.39)
P value: 0.47
Pain (random-effects model) (3 primary studies)
RR (95% CI): 0.55 (0.33 to 0.92)
P value: NR
Post-procedural fatigue (random-effects model) (3 primary studies)
RR (95% CI): 1.68 (1.08 to 2.62)
P value: < 0.01 (favours TACE)
Nausea and vomiting (random-effects model) (4 primary studies)
RR (95% CI): 0.84 (0.60 to 1.23)
P value: NR
Fever (random-effects model) (3 primary studies)
RR (95% CI): 1.16 (0.07 to 18.61)
P value: 0.92
Other complications (e.g., diarrhea, anorexia, headache, chest pain, confusion, gastric ulceration, bleeding from puncture site, rash, varicella zoster infection, and hepatic abscess; random-effects model) (5 primary studies)
RR (95% CI): 1.14 (0.70 to 1.86)
P value: NR
Post-treatment morbidity (random-effects model) (4 primary studies)
RR (95% CI): 0.84 (0.5 to 1.26)
P value: 0.41
More than 3 complications (random-effects model) (4 primary studies)
RR (95% CI): 0.83 (0.49 to 1.38)
P value: NR
Author’s Conclusion
“In conclusion, based on current available data, TARE is comparable to TACE with similar complication profile and survival rates. Larger prospective randomized trials, focusing on patient-reported outcomes and cost–benefit analysis, are required to consolidate these results. An important outcome to examine would be time to progression especially as we see wait times for liver transplant increasing. As results are reported, the role of TARE in hepatocellular carcinoma treatment algorithm will likely get to be redefined (p. 1585).”23
Summary of Findings of Included Non-Randomized Study
Padia et al. (2017)24
Main Study Findings
The single-centre, retrospective cohort study included 178 patients who received TARE (N = 101) or TACE (N = 77) to treat hepatocellular carcinoma. Participants in the TACE group received either cTACE or DEB-TACE; results were not reported separately by TACE technique.
Summary of Findings
Tumour response
Per-tumour response rates (index tumour) using mRECIST
Proportion of tumours with complete response
TARE: 92.4%
TACE: 73.8%
Adjusted response rate difference (95% CI): −23.0% (−36.2% to −9.8%)
Proportion of tumours with partial response
TARE: 5.3%
TACE: 18.4%
Adjusted response rate difference (95% CI): 17.1% (6.8% to 27.3%)
Proportion of tumours with stable disease
TARE: 1.5%
TACE: 4.9%
Adjusted response rate difference (95% CI): 1.9% (−2.0% to 5.9%)
Proportion of tumours with progressive disease
TARE: 0.8%
TACE: 2.9%
Adjusted response rate difference (95% CI): 4.0% (−1.8% to 9.8%)
P value (test for trend for the 4 response categories): 0.001
Per-patient response rates (overall) using mRECIST
Proportion of tumours with complete response
TARE: 84.0%
TACE: 58.4%
Adjusted response rate difference (95% CI): −28.9% (−43.1% to −14.7%)
Proportion of tumours with partial response
TARE: 11.0%
TACE: 26.0%
Adjusted response rate difference (95% CI): 17.2% (4.8% to 29.5%)
Proportion of tumours with stable disease
TARE: 2.0%
TACE: 7.8%
Adjusted response rate difference (95% CI): 3.8% (−2.7% to 10.3%)
Proportion of tumours with progressive disease
TARE: 3.0%
TACE: 7.8%
Adjusted response rate difference (95% CI): 8.0% (−1.1% to 17.1%)
P value (test for trend for the 4 response categories): < 0.001
Overall survival, progression-free survival, and index tumour progression
Overall survival
Death (ignoring orthotopic liver transplantation)
Adjusted HR (95% CI): 1.39 (0.69 to 2.78)
P value: 0.35
Death (censored by orthotopic liver transplantation)
Adjusted HR (95% CI): 1.83 (0.97 to 3.48)
P value: 0.064
Death (orthotopic liver transplantation is a competing risk)
Adjusted HR (95% CI): 1.52 (0.78 to 2.97)
P value: 0.22
Overall survival or overall progression
Death or overall progression (ignoring orthotopic liver transplantation)
Adjusted HR (95% CI): 2.00 (1.30 to 3.08)
P value: 0.002 (i.e., those on TACE had a higher event rate)
Death or overall progression (censored by orthotopic liver transplantation)
Adjusted HR (95% CI): 3.17 (1.95 to 5.15)
P value: < 0.001 (i.e., those on TACE had a higher event rate)
Death or overall progression (orthotopic liver transplantation is a competing risk)
Adjusted HR (95% CI): 2.13 (1.39 to 3.30)
P value: 0.001 (i.e., those on TACE had a higher event rate)
Index tumour progression
Index tumour progression (censored by orthotopic liver transplantation)
Adjusted HR (95% CI): 8.24 (3.96 to 17.12)
P value: < 0.001 (i.e., those on TACE had a higher event rate)
Index tumour progression (orthotopic liver transplantation and death are competing risks)
Adjusted HR (95% CI): 7.11 (3.35 to 15.07)
P value: < 0.001 (i.e., those on TACE had a higher event rate)
Toxicity from first treatment of each tumour
Clinical toxicity
Proportion of patients who experienced fatigue
TARE: 38.6%
TACE: 26.5%
Adjusted RR (95% CI): 0.70 (0.39 to 1.24)
P value: 0.22
Proportion of patients who experienced pain
TARE: 7.6%
TACE: 1.0%
Adjusted RR (95% CI): 0.10 (0.01 to 0.82)
P value: 0.032 (i.e., TARE had higher toxicity)
Proportion of patients who experienced postembolization syndrome
TARE: 2.3%
TACE: 8.8%
Adjusted RR (95% CI): 3.42 (0.85 to 13.73)
P value: 0.082
Biochemical toxicity
Proportion of patients who experienced leukopenia
TARE: 4.6%
TACE: 5.0%
Adjusted RR (95% CI): 0.47 (0.08 to 2.58)
P value: 0.38
Proportion of patients who experienced increased aspartate aminotransferase
TARE: 3.1%
TACE: 8.0%
Adjusted RR (95% CI): 3.46 (0.67 to 17.85)
P value: 0.14
Proportion of patients who experienced increased alanine aminotransferase
TARE: 1.5%
TACE: 3.0%
Adjusted RR (95% CI): 1.63 (0.17 to 15.39)
P value: 0.67
Proportion of patients who experienced increased total bilirubin
TARE: 3.1%
TACE: 9.0%
Adjusted RR (95% CI): 3.12 (0.73 to 13.26)
P value: 0.12
Proportion of patients who experienced hypoalbuminemia
TARE: 2.3%
TACE: 3.0%
Adjusted RR (95% CI): 0.60 (0.09 to 3.83)
P value: 0.59
Proportion of patients who experienced any biochemical toxicity
TARE: 9.9%
TACE: 20.0%
Adjusted RR (95% CI): 1.12 (0.41 to 3.03)
P value: 0.83
Note: Differences were adjusted using inverse probability of treatment weights from a propensity-score model to adjust for imbalances of patient-specific and tumour-specific factors between the 2 treatment groups (e.g., age, Eastern Cooperative Oncology Group performance status, Child-Pugh class, number of tumours, longest tumour length, presence of an infiltrative tumour, and presence of portal vein thrombosis).
Author’s Conclusion
“In conclusion, this study demonstrates that radioembolization showed equivalent toxicities, superior tumour response rates, lower local tumor recurrence rates, and superior progression-free survival compared with chemoembolization. Although prospective, randomized studies are needed to confirm these findings, segmental radioembolization has the potential to achieve durable local control with an acceptable toxicity profile (p. 785).”24
Summary of Findings of Included Economic Evaluations
Manas et al. (2020)25
Main Study Findings
Cost-utility analysis that examined the cost-effectiveness of TARE (with TheraSphere) versus transarterial embolization, cTACE, and DEB-TACE in patients (≥ 65 years of age) with unresectable hepatocellular carcinoma. Findings related to transarterial embolization as a comparator were not extracted as this was not relevant to the current report.
Summary of Findings
Base-case results
Treatment costs
TARE: £49,583
TACE: £37,038
DEB-TACE: £33,206
QALYs
TARE: 2.24
TACE: 1.57
DEB-TACE: 1.57
Undiscounted LYG
TARE: 3.72
TACE: 2.52
DEB-TACE: 2.52
Discounted LYG
TARE: 3.05
TACE: 2.14
DEB-TACE: 2.14
ICER per QALY gained (TARE versus comparator)
TACE: £17,279
DEB-TACE: £23,020
ICER per discounted LYG (TARE versus comparator)
TACE: £12,808
DEB-TACE: £17,059
Probabilistic results
Treatment costs
TARE (95% CrI): £48,572 (£44,263 to £52,925)
TACE (95% CrI): £37,139 (£33,178 to £41,503)
DEB-TACE (95% CrI): £33,312 (£29,878 to £37,274)
QALYs
TARE (95% CrI): 2.23 (1.96 to 2.50)
TACE (95% CrI): 1.57 (1.34 to 1.83)
DEB-TACE (95% CrI): 1.57 (1.34 to 1.82)
Undiscounted LYG
TARE (95% CrI): 3.72 (3.22 to 4.23)
TACE (95% CrI): 2.53 (2.11 to 2.99)
DEB-TACE (95% CrI): 2.15 (1.84 to 2.50)
Discounted LYG
TARE (95% CrI): 3.04 (2.67 to 3.41)
TACE (95% CrI): 2.15 (1.83 to 2.50)
DEB-TACE (95% CrI): 2.15 (1.83 to 2.49)
ICER per QALY gained (TARE versus comparator)
TACE (95% CrI): £17,417 (£13,394 to £25,312)
DEB-TACE (95% CrI): £23,205 (£18,690 to £34,949)
ICER per discounted LYG (TARE versus comparator)
TACE (95% CrI): £12,871 (£9,919 to £18,706)
DEB-TACE (95% CrI): £17,143 (£13,785 to £25,972)
Probabilities of cost-effectiveness
Probability of TARE being cost-effective at a willingness-to-pay threshold of £20,000
TACE: 76.8%
DEB-TACE: 15.9%
Probability of TARE being cost-effective at a willingness-to-pay threshold of £30,000
TACE: approximately 93%
DEB-TACE: 88.6%
Author’s Conclusion
“TheraSphere is likely to be cost-effective against transarterial embolization, [TACE] and DEB-TACE for patients who may be downstaged to curative treatments. TheraSphere produces a QALY gain superior to TAE, TACE and DEB-TACE (p. 6).”25
Muszbek et al. (2020)26
Main Study Findings
Cost-utility analysis that examined the cost-effectiveness of TARE (with SIR-Spheres) versus sorafenib in UK patients with unresectable hepatocellular carcinoma who were ineligible for treatment with TACE.
Summary of Findings
Base-case results
Total costs
TARE: £29,530
Sorafenib: £30,957
Total life-years
TARE: 2.637
Sorafenib: 1.890
Total QALYs
TARE: 1.982
Sorafenib: 1.381
ICER (£ per QALY)
TARE: Dominant (i.e., treatment results in more QALYs and less costs)
Sorafenib: –
Incremental net benefit with £20,000 willingness-to-pay threshold
TARE: £13,443
Sorafenib: –
“Results were robust in the sensitivity analyses [page number not specified].”26
Scenario analysis (time horizon 5 years)
ICER TARE versus sorafenib (£ per QALY)
Dominant (−7,934)
Incremental net benefit with £20,000 willingness-to-pay threshold
£9,343
Scenario analysis (discount cost and benefits 0%)
ICER TARE versus sorafenib (£ per QALY)
Dominant (−1,368)
Incremental net benefit with £20,000 willingness-to-pay threshold
£15,350
Scenario analysis (discount cost and benefits 5%)
ICER TARE versus sorafenib (£ per QALY)
Dominant (−2,807)
Incremental net benefit with £20,000 willingness-to-pay threshold
£12,782
Scenario analysis (using the ITT population)
ICER sorafenib versus TARE (£ per QALY)
58,298
Incremental net benefit with £20,000 willingness-to-pay threshold
4,003
Scenario analysis (not allowing downstaging)
ICER sorafenib versus TARE (£ per QALY)
2,848
Incremental net benefit with £20,000 willingness-to-pay threshold
10,660
Scenario analysis (comparison to lenvatinib using network meta-analyses of the SARAH and REFLECT trials)
ICER lenvatinib versus TARE (£ per QALY)
58,298
Incremental net benefit with £20,000 willingness-to-pay threshold
4,003
Additional sensitivity analyses are available in the publication.26
Author’s Conclusion
“In a selected population, selective internal radiation therapy with SIR-Spheres 90Y resin microspheres has the potential to be a dominant and in an unselected population a cost-effective alternative to sorafenib in patients with unresectable hepatocellular carcinoma ineligible for TACE. The estimated population average costs and outcomes are likely similar for selective internal radiation therapy and sorafenib in all populations. Additionally, sorafenib is associated with significant adverse effects including diarrhea, fatigue and hand and foot skin reaction compared with selective internal radiation therapy, and there is evidence that treatment with SIRT is associated with a higher likelihood of subsequent treatments with curative intent. Thus, the individual patients should have the option to receive selective internal radiation therapy treatment based on their eligibility and their preferences regarding adverse effects, quality of life and potential outcomes [page number not specified].”26
Walton et al. (2020)20
Main Study Findings
Cost-utility analysis (conducted as part of a health technology assessment) that examined the cost-effectiveness of TARE therapies (i.e., TheraSphere, SIR-Spheres, and QuiremSpheres) versus sorafenib or lenvatinib in patients with unresectable intermediate (BCLC stage B) or advanced (BCLC stage C) hepatocellular carcinoma and without extrahepatic disease for whom any conventional transarterial embolization therapies (e.g., TACE) were inappropriate. Findings related to QuiremSphere were not summarized as this intervention uses holmium-166.
Summary of Findings
Deterministic base-case results
Costs
TheraSphere: £29,888
Lenvatinib: £30,005
SIR-Spheres: £30,107
Sorafenib: £32,082
Life-years
TheraSphere: 1.110
Lenvatinib: 1.183
SIR-Spheres: 1.110
Sorafenib: 1.243
QALYs
TheraSphere: 0.764
Lenvatinib: 0.805
SIR-Spheres: 0.764
Sorafenib: 0.841
Incremental costs (versus TheraSphere)
Lenvatinib: £117
SIR-Spheres: £218
Sorafenib: £2,194
Incremental QALYs (versus TheraSphere)
Lenvatinib: 0.04
SIR-Spheres: 0.000
Sorafenib: 0.076
ICER (versus TheraSphere)
Lenvatinib: £2,911
SIR-Spheres: More costly
Sorafenib: £28,728
Incremental net monetary benefit (versus TheraSphere)
Lenvatinib: £1,090
SIR-Spheres: −£218
Sorafenib: £97
ICER (fully incremental)
Lenvatinib: £2,911
SIR-Spheres: Extendedly dominated
Sorafenib: £57,488
Probabilistic base-case results
Costs
Lenvatinib: £29,658
TheraSphere: £30,014
SIR-Spheres: £30,196
Sorafenib: £32,444
Life-years
Lenvatinib: 1.202
TheraSphere: 1.111
SIR-Spheres: 1.111
Sorafenib: 1.244
QALYs
Lenvatinib: 0.825
TheraSphere: 0.765
SIR-Spheres: 0.765
Sorafenib: 0.841
Incremental costs (versus lenvatinib)
TheraSphere: £356
SIR-Spheres: £583
Sorafenib: £2,786
Incremental QALYs (versus lenvatinib)
TheraSphere: −0.060
SIR-Spheres: −0.060
Sorafenib: 0.016
ICER (versus lenvatinib)
TheraSphere: Dominated
SIR-Spheres: Dominated
Sorafenib: £174,320
Incremental net monetary benefit (versus lenvatinib)
TheraSphere: −£2,154
SIR-Spheres: £2,323
Sorafenib: £2,306
ICER (fully incremental)
TheraSphere: Dominated
SIR-Spheres: Dominated
Sorafenib: £174,320
Probabilities of cost-effectiveness
“Lenvatinib has the highest likelihood of being cost-effective across any willingness-to-pay threshold of <£100,000 (p. 112).”20
“The results of the Assessment Group’s base-case analysis are robust to a wide range of assumptions, reflecting the completeness and quality of the included studies, and the substantial differences seen in costs and QALYs between the SIRTs and current UK practice (including confidential Patient Access Schemes). The Assessment Group’s analyses predicted lenvatinib to rank first in terms of net monetary benefit in all scenarios (excluding scenario 4), whereas sorafenib was a cost-effective alternative, producing more QALYs at a higher cost (p. 123).”20
Author’s Conclusion
“Based on the Assessment Group’s probabilistic base-case analysis at list price, none of the three selective internal radiation therapies is expected to be cost-effective at any willingness to pass threshold, being more costly and less effective than lenvatinib. When the modelled population was limited to only those with a low tumour burden and preserved liver function, the ICERs for TheraSphere and SIR-Spheres were £17,165 and £18,783 per QALY gained versus the most cost-effective systemic therapy. The most optimistic ICERs were generated in the scenario presented for the low tumour burden and preserved liver function in which downstaging to curative therapy was permitted. In this scenario, the ICERs for TheraSphere and SIR-Spheres decreased to £1440 and £2339, respectively. However, there was no scenario in which SIRT was predicted to be cost-effective at a WTP threshold of £30,000 when confidential Patient Access Scheme discounts were included (p. 122).”20
Rognoni et al. (2017)27
Main Study Findings
Cost-utility analysis that evaluated the cost-effectiveness of TARE versus sorafenib for the treatment of patients with intermediate or advanced hepatocellular carcinoma.
Summary of Findings
Base-case results in patients with intermediate-stage disease
Costs
TARE: €31,071
Sorafenib: €29,289
LYG
TARE: 2.531
Sorafenib: 1.575
QALYs
TARE: 1.178
Sorafenib: 0.638
ICER (versus sorafenib)
TARE: €1,865 per life-year
incremental cost-utility ratio (ICUR) (versus sorafenib)
TARE: €3,302 per QALY
Base-case results in patients with advanced-stage disease
Costs
TARE: €21,961
Sorafenib: €30,750
LYG
TARE: 1.445
Sorafenib: 1.306
QALYs
TARE: 0.639
Sorafenib: 0.568
ICER (versus sorafenib)
TARE: Dominant
ICUR (versus sorafenib)
TARE: Dominant
Sensitivity analysis (time horizon 1 year)
ICUR (versus sorafenib)
TARE (intermediate stage): Dominant
TARE (advanced stage): Sorafenib versus TARE €322,488
Sensitivity analysis (time horizon 2 years)
ICUR (versus sorafenib)
TARE (intermediate stage): Dominant
TARE (advanced stage): Sorafenib versus TARE €238,642
Sensitivity analysis (time horizon 4 years)
ICUR (versus sorafenib)
TARE (intermediate stage): Dominant
TARE (advanced stage): Sorafenib versus TARE €313,606
Sensitivity analysis (time horizon 6 years)
ICUR (versus sorafenib)
TARE (intermediate stage): Dominant
TARE (advanced stage): Sorafenib versus TARE €840,495
Sensitivity analysis (time horizon 8 years)
ICUR (versus sorafenib)
TARE (intermediate stage): Dominant
TARE (advanced stage): Dominant
Sensitivity analysis (time horizon 10 years)
ICUR (versus sorafenib)
TARE (intermediate stage): €1,067
TARE (advanced stage): Dominant
Sensitivity analysis (time horizon 15 years)
ICUR (versus sorafenib)
TARE (intermediate stage): €2,649
TARE (advanced stage): Dominant
Sensitivity analysis (time horizon 10 years)
ICUR (versus sorafenib)
TARE (intermediate stage): €3,116
TARE (advanced stage): Dominant
Sensitivity analysis (mean number of TARE per patient = 1)
ICUR (versus sorafenib)
TARE (intermediate stage): €744
TARE (advanced stage): Dominant
Sensitivity analysis (mean number of TARE per patient = 3)
ICUR (versus sorafenib)
TARE (intermediate stage): €51,915
TARE (advanced stage): €260,020
Sensitivity analysis (patient age = 60)
ICUR (versus sorafenib)
TARE (intermediate stage): €4,315
TARE (advanced stage): Dominant
Sensitivity analysis (patient age = 80)
ICUR (versus sorafenib)
TARE (intermediate stage): Dominant
TARE (advanced stage): Dominant
Sensitivity analysis (discount rate = 0%)
ICUR (versus sorafenib)
TARE (intermediate stage): €4,956
TARE (advanced stage): Dominant
Sensitivity analysis (discount rate = 10%)
ICUR (versus sorafenib)
TARE (intermediate stage): €151
TARE (advanced stage): Dominant
Additional sensitivity analyses are available in the publication.27
“Sensitivity and scenario analyses showed the robustness of the baseline results: only variations in the time horizon and in the number of TARE treatments per patient could lead to an ICUR of more than €50,000/QALY gained. The number of TARE treatments per patient, however, is unlikely to be greater than 1.5. Furthermore, probabilistic sensitivity analyses confirmed the results, with most of the simulations (almost all for intermediate stages) lying below the commonly accepted ICUR threshold representing value for money (p. 342).”27
Probabilities of cost-effectiveness
“Dotted lines represent a theoretical cost-effectiveness threshold of €50,000/QALY; 99.8% and 98% of points lie below this line for intermediate and advanced stages, respectively. A theoretical cost-effectiveness threshold of £30,000/QALY(€38,500) shows similar results: 99.2% and 98.2% for intermediate and advanced stages, respectively (p. 342).”27
Author’s Conclusion
“TARE seems to be a valid treatment option for patients in intermediate and advanced hepatocellular carcinoma stages. The trial results from forthcoming RCTs comparing TARE with sorafenib will increase the clinical evidence qualitatively to confirm or reject the validity of this preliminary evaluation. In the meantime, decision-makers can make use of these results to issue preliminary coverage recommendations, for approval in defined target patient populations, or using conditional approval methods (p. 342).”27
Appendix 5: Overlap Between Included Systematic Reviews
Table 8: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Walton et al. (2020)20 | Yang et al. (2020)21 | Yang and Si (2018)22 | Lobo et al. (2016)23 |
Kirchner T, et al. Abdom Radiol 2019 44:1554-1561. | X | — | — | — |
Chow PKH, et al. J Clin Oncol 2018 36:1913-1921. | X | — | — | — |
Bouattour M, et al. Ann Oncol 2017 28(Suppl. 3):iii150-153. | X | — | — | — |
Gabr A, et al. J Vasc Interv Radiol 2017 28:1272-1273. | X | — | — | — |
McDevitt JL, et al. J Vasc Interv Radiol 2017 28:1371-1377. | — | X | — | — |
Vilgrain V, et al. Eur Lancet Oncol 2017 18(12):1624-1636 | X | — | — | — |
Akinwande O, et al. Anticancer Res 2016 36:239-246. | X | X | — | — |
Akinwande O, et al. J Vasc Interv Radiol 2016 27:S248. | X | — | — | — |
Cho YY, et al. PLOS ONE 2016 11:e0154986. | X | — | — | — |
de la Torre MA, et al. Liver Int 2016 36:1206-1212. | X | — | — | — |
Gordon A, et al. J Vasc Interv Radiol 2016 27:S61-62. | X | — | — | — |
Hickey R, et al. J Vasc Interv Radiol 2016 27:795-802. | X | — | — | — |
Salem R, et al. Gastroenterology 2016 151:1155-1163.e2. | X | X | X | — |
Soydal C, et al. Nucl Med Commun 2016 37:646-649 | X | X | X | — |
Akinwande O, et al. Surg Oncol 2015 24:270-275. | — | — | — | X |
El Fouly A, et al. Liver Int 2015 35:627-635. | X | X | X | — |
Gramenzi A, et al. Liver Int 2015 35:1036-1047 | X | — | — | — |
Kolligs FT, et al. Liver Int 2015 35:1715-1721. | X | X | X | — |
Pitton MB, et al. Cardiovasc Intervent Radiol 2015 38:352-360 | X | X | — | — |
She WH, et al. Hepatobiliary Surg Nutr 2014 3:185-193. | — | — | X | — |
Memon K, et al. J Vasc Interv Radiol 2013 24:1189-1197.e2. | X | — | — | — |
Moreno-Luna LE, et al. Cardiovasc Intervent Radiol 2013 36:714-723. | X | X | X | X |
Lance C, et al. J Vasc Interv Radiol 2011 22(12):1697-1705. | — | X | X | X |
Salem R, et al. Clin Gastroenterol Hepatol 2013 11:1358-1365.e1. | X | — | — | — |
Salem R, et al. Gastroenterology 2011 140:497-507.e2 | X | — | X | X |
Carr BI, et al. Cancer. 2010 116(5):1305-1314 | — | X | X | — |
Kooby DA, et al. J Vasc Interv Radiol 2010 21:224-230. | — | X | X | X |
Lewandowski RJ, et al. Am J Transplant 2009 9:1920-1928. | — | X | X | — |
[ X ]= the primary study was included in the systematic review; [ – ] = the primary study was not included in the systematic review.
Note: Several publications report on the same study: Bouattour et al. (2017) and Vilgrain et al. (2017); Gabr et al. (2017), Gordon et al. (2016), Salem et al. (2016); and both Akinwande et al. (2016) publications.
Appendix 6: References of Potential Interest
Previous CADTH Reports
1. Clinical report: atezolizumab (tecentriq) in combination with bevacizumab, for the first-line treatment of adult patients with unresectable or metastatic hepatocellular carcinoma who require systemic therapy. (CADTH pCODR final clinical guidance report). Ottawa (ON) CADTH: 2020 Nov 17. https://www.cadth.ca/sites/default/files/pcodr/Reviews2020/10217AtezolizumabBevacizumabHCC_fnCGR_REDACT_PostEC17Nov2020_final.pdf. Accessed 2021 Jan 6.
Review Articles
2. Saini A, Wallace A, Alzubaidi S, et al. History and Evolution of Yttrium-90 Radioembolization for Hepatocellular Carcinoma. J Clin Med. 2019 Jan 07;8(1):07. PubMed
3. Titano JJ, Kim E, Patel RS. Yttrium-90 complications: prevention and management. Tech Vasc Interv Radiol. 2019 Jun;22(2):87-92. PubMed
4. Hsieh TC, Wu YC, Sun SS, Yen KY, Kao CH. Treating hepatocellular carcinoma with 90Y-bearing microspheres: a review. Biomedicine. 2016 Nov;6(4):19. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca