CADTH Health Technology Review
Ibrutinib for Chronic Graft-Versus-Host Disease
Rapid Review
Authors: Sara D. Khangura, Aleksandra Grobelna
Abbreviations
CGvHD
chronic graft-versus-host disease
GvHD
graft-versus-host disease
Key Messages
No eligible evidence was identified comparing ibrutinib to another intervention for the management of treatment-refractory chronic graft-versus-host disease.
Currently available evidence describing second- or third-line therapies for treatment-refractory chronic graft-versus-host disease was ineligible for this review because of the use of non-comparative research methods (i.e., single-arm trials, case series, and case reports).
One randomized controlled trial is currently under way investigating the use of ibrutinib as first-line therapy for chronic graft-versus-host disease; however, no randomized controlled trials of ibrutinib for the management of treatment-refractory chronic graft-versus-host disease are currently being conducted.
The need for high-quality randomized controlled trials of ibrutinib for treatment-refractory chronic graft-versus-host disease has been highlighted repeatedly in recent literature.
Context and Policy Issues
Graft-versus-host disease (GvHD) can occur in patients who have undergone a blood or bone marrow transplant from a human donor (also known as an allogeneic hematopoietic transplant).1,2 The disease is caused by the graft when its cells initiate an immune response to, and attack, the transplant recipient’s body.3 Broad estimates indicate that between 30% and 70% of patients with allogeneic hematopoietic transplants experience GvHD.1,2,4,5
GvHD is often a serious condition that causes significant morbidity; it is a prognostic indicator of poor outcomes and is 1 of the leading causes of mortality in patients following stem cell transplant.2,4,6 A risk factor for developing GvHD is receipt of a graft from an unrelated or unmatched donor.4 Symptoms of GvHD often manifest initially as mouth sores and/or skin rash,4 and can progress to include dry mouth, gastrointestinal distress, elevated serum bilirubin, fatigue, shortness of breath and/or trouble breathing, and musculoskeletal pain and weakness.1,7,8 The severity of disease is primarily characterized clinically by the extent of organ involvement (including the skin) and the effects on lung capacity and function.8-10 Patients can experience significantly limited quality of life and negative impacts to their activities of daily life,11-13 with more severe disease associated with less favourable patient experiential outcomes.3,14
GvHD can be either acute or chronic, with the primary distinction traditionally being onset before or after 100 days following transplant3 and a longer duration of illness in patients with chronic GvHD (CGvHD).1,4,15 Although CGvHD is a distinct condition from acute GvHD, symptoms and treatments for both conditions are similar.2,3 An accurate diagnosis of either acute GvHD or CGvHD can be challenging to establish, but is important for ensuring that patients are treated optimally.8 This and other challenges in diagnosing and treating CGvHD are exacerbated by current limitations in understanding of both conditions because of insufficient data from small and/or methodologically limited studies as well as a lack of standardized thresholds and definitions.6,16 For instance, although CGvHD was originally thought to be a disease primarily of the T cells, recent research suggests that both T cells and B cells are involved,15 This finding catalyzed further studies investigating the role of treatments targeting B cells.6,16
Treatments for CGvHD target the reduction of symptoms while aiming to mitigate side effects and adverse events caused by therapy.8,17 Drug treatment for CGvHD can include localized and/or systemic interventions, with the former favoured in cases of milder disease, to avoid the toxicity and side effects that can occur with systemic therapies.1,8 Treatment can also include non-pharmaceutical interventions, including physiotherapy and stem cell and immunomodulatory therapies.2 First-line systemic therapy is often corticosteroidal; prednisone is a mainstay of early treatment.2,8 However, estimates indicate that fewer than half of patients experience a sufficiently durable response with first-line corticosteroid treatment and will require second-line (and often third-line) treatment (i.e., steroid-refractory CGvHD).1,2,6 These second- and third-line treatments may include nucleoside analogues, immunosuppressants, mechanistic target of rapamycin (mTOR) inhibitors, anti-CD20 monoclonal antibodies, and kinase inhibitors such as ruxolitinib, imatinib, and ibrutinib.2,6,8 Until recently, there have been no regulatory-approved drugs available for the second-line treatment of CGvHD.4,6,14
Ibrutinib (brand name Imbruvica) is a Bruton’s tyrosine kinase (BTK) inhibitor that received approval from Health Canada and the FDA as second-line treatment for CGvHD in 2017.4,5,7,14,18 Ibrutinib is prescribed as a once-daily tablet for patients with CGvHD which is administered until treatment is no longer required (i.e., CGvHD has resolved) or in the event that toxicity becomes intolerable.4 Ibrutinib can cause side effects including cardiovascular conditions (e.g., arrhythmias, atrial fibrillation, and heart failure), central nervous system effects (e.g., fatigue, weakness), gastrointestinal toxicity (e.g., nausea, diarrhea), hematologic conditions (e.g., thrombocytopenia and anemia), dermatologic conditions, as well as pneumonia (among others).4,9,19,20 A widely cited single-arm trial (N = 42) of ibrutinib demonstrated that more than two-thirds of patients with CGvHD had either a complete or partial response to therapy with ibrutinib.14,21 Similarly, patient-reported symptoms were significantly improved for almost half of study patients.22 Longer-term follow-up of this study has demonstrated similarly favourable findings, with more than half of responders experiencing a sustained response at a median follow-up of more than 2 years.23 However, this study was limited by its open-label, non-randomized design and small sample size.5,7
Because of the early data indicating that ibrutinib can be an effective intervention for treatment-refractory CGvHD, as well as the relatively recent Health Canada approval of its use for CGvHD, a review of the most current comparative evidence is needed to inform health care and policy decisions that will optimally benefit patients. Consequently, this report aims to synthesize and assess currently available comparative evidence describing the clinical effectiveness of ibrutinib for the treatment of patients with CGvHD who have experienced inadequate response to corticosteroids or other systemic therapies.
Research Question
What is the clinical effectiveness of ibrutinib in patients with chronic graft-versus-host disease who have inadequate response to corticosteroids or other systemic therapies?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were ibrutinib and chronic graft-versus-host disease (CGvHD). No filters were applied to limit the retrieval by study type. Conference abstracts were excluded from search results. If possible, retrieval was limited to the human population. The search was completed on April 26, 2022, and limited to English-language documents published after January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients (of all ages) with chronic graft-versus-host disease who have an inadequate response to corticosteroids or other systemic therapies |
Intervention | Ibrutinib |
Comparator | Extracorporeal photopheresis, mycophenolate mofetil, etanercept, low-dose methotrexate, infliximab, mTOR inhibitor (e.g., sirolimus, everolimus), imatinib, rituximab, pentostatin, cyclosporine, placebo |
Outcomes | Clinical effectiveness (e.g., failure-free survival, overall response rate, HRQoL, symptom severity, duration of response, overall survival, non-relapse mortality, malignancy relapse or progression, steroid dosing); safety (e.g., adverse events, severe adverse events) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies |
HrQoL = health-related quality of life; mTOR = mechanistic target of rapamycin.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017.
Summary of Evidence
Quantity of Research Available
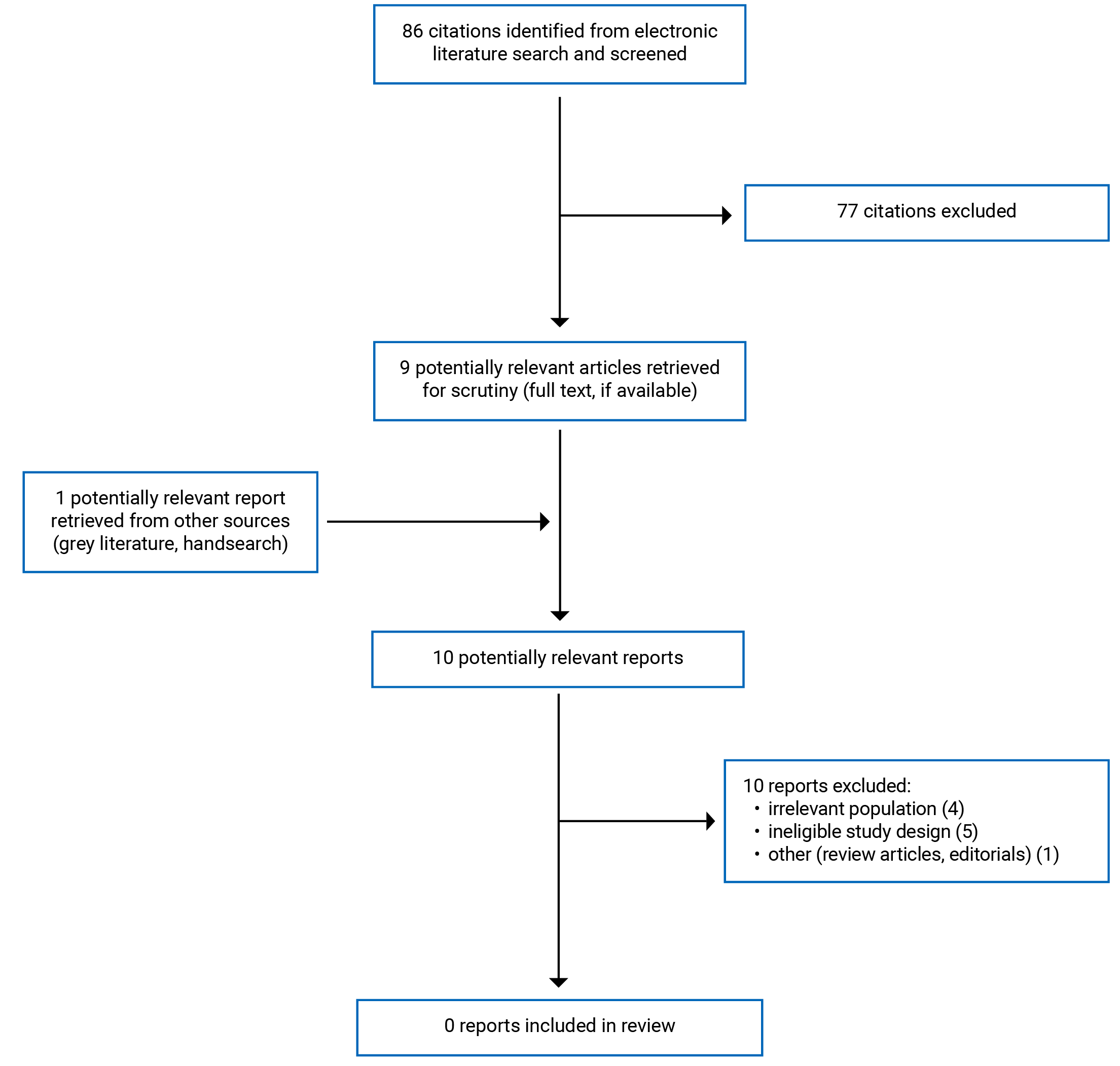
A total of 86 citations were identified in the electronic database literature search. Following screening of the titles and abstracts, 77 citations were excluded and 9 potentially relevant sources from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 10 publications were excluded for various reasons because no studies met the inclusion criteria for this report.
Additional references of potential interest are provided in Appendix 2.
Summary of Findings
Clinical Effectiveness of Ibrutinib for Chronic Graft-Versus-Host Disease
There were no eligible studies identified that described the comparative clinical effectiveness of ibrutinib for the treatment of CGvHD; thus, no summary can be provided.
Limitations
This report is limited by the lack of any eligible studies identified that answered the research question posed.
Currently available evidence describing ibrutinib for treatment-refractory CGvHD was not eligible for this review (i.e., the studies published to date use single-arm, non-randomized, non-comparative designs that cannot offer robust insight into comparative clinical effectiveness).7,15 Specifically, single-arm trials lack the comparison group(s) necessary to provide a frame of reference that can establish whether observed effect(s) were due to the intervention under study or some other factor(s).24
Comparative randomized controlled trials are needed to inform clinical and health care decisions concerning the use of ibrutinib for treatment-refractory CGvHD.13,16
Conclusions and Implications for Decision- or Policy-Making
This review did not identify any eligible studies describing the clinical effectiveness of ibrutinib for treatment-refractory CGvHD. Available research to date is limited, with most studies reporting data from single-arm trials25-27 and case reports or case series.28-30 These study designs are insufficient to provide insight into the comparative effectiveness of ibrutinib for patients with previously treated CGvHD.4
Although available studies of ibrutinib for patients with treatment-refractory CGvHD are few and of low quality, there are multiple studies describing related topics. Studies examining the effect of ibrutinib for the treatment of CGvHD in a first-line setting have been characterized as critical to understanding its optimal use for these patients.7 One randomized controlled trial is currently under way examining the effect of ibrutinib as a first-line therapy for the treatment of CGvHD31 and other single-arm trials are investigating the effects of ibrutinib as either first-line or second-line treatment as monotherapy or in parallel with other drugs (e.g., corticosteroids or rituximab).32
Other non-comparative research is focused on minimizing the side effects and adverse events caused by ibrutinib while treating various conditions (including CGvHD), such as fungal infections.33,34 One recent systematic review investigated adverse events among patients with GvHD (both acute and chronic) receiving second- and third-line treatments (following first-line corticosteroids), but no evidence describing ibrutinib was identified or included.2 However, other studies have examined the role of ibrutinib and other drug therapies on various hematological malignancies and measured the occurrence and/or severity of CGvHD as an outcome.35-38
As more evidence is generated describing the clinical effectiveness of ibrutinib as second-line therapy for CGvHD, the cost and cost-effectiveness of ibrutinib and other agents used to treat steroid-refractory CGvHD are important considerations for health systems and care providers. In 1 cost-effectiveness analysis of treatments for steroid-refractory CGvHD, ibrutinib was found to be the most costly among 11 drugs reviewed.39 The authors of this 2018 study reported that response rates across all drugs reviewed were comparable and the cost-effectiveness findings were driven mostly by the costs of the agents themselves.39 However, the analyses identified only 1 study of low quality describing ibrutinib; therefore, the extent to which robust findings describing cost-effectiveness for the drug can be generated is limited.
Further research focused on B cell–targeted therapies (including ibrutinib) remains ongoing,6 and is needed to produce higher quality data and evidence to help answer some of the many questions that remain about the optimal treatment and management of CGvHD. The current shortfall in available evidence for ibrutinib and other second- and third-line therapies for treatment-refractory CGvHD is an important limitation when considering the optimal clinical management of patients. One study described a survey of clinicians in 3 European countries and reported consistency in the approach to managing newly diagnosed CGvHD (i.e., usually corticosteroids), but found significant variability in the preferred approaches to second- and third-line treatment.40 This lack of clinical consensus is thought to be driven largely by the limited body of available and/or robust evidence informing best practice for the management of treatment-refractory CGvHD.40 This need for more (and more rigorous) evidence is a common theme in the literature describing the management of treatment-refractory CGvHD.12,39 Likewise, additional studies are needed to inform the diagnosis and prevention of CGvHD and are critical areas of future research.12,41,42
Some CADTH work to date has addressed a related research question concerning GvHD. One recent Reference List review sought evidence describing the management of GvHD with infliximab (similar to the current review); however, no eligible studies were identified.43
In conclusion, comparative evidence of high quality remains a gap in the literature that is necessary to better inform the use of ibrutinib for patients with treatment-refractory CGvHD.
References
1.Justiz Vaillant AA, Modi P, Mohammadi O. Graft versus host disease. Treasure Island (FL): StatPearls Publishing; 2022: https://www.ncbi.nlm.nih.gov/books/NBK538235/. Accessed 2022 May 25.
2.Velickovic VM, McIlwaine E, Zhang R, Spelman T. Adverse events in second- and third-ine treatments for acute and chronic graft-versus-host disease: systematic review. Ther Adv Hematol. 2020;11:1-18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7727084/pdf/10.1177_2040620720977039.pdf. Accessed 2022 May 25. PubMed
3.Zeiser R. Clinical manifestations and diagnosis of chronic graft-versus-host disease. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 May 25.
4.Raedler LA. Imbruvica (ibrutinib) first drug approved specifically for marginal-zone lymphoma and for chronic graft-versus-host disease. (American Health & Drug Benefits, volume 11). 2018: https://www.ahdbonline.com/issues/2018/april-2018-vol-11-ninth-annual-payers-guide/2545-imbruvica-ibrutinib-first-drug-approved-specifically-for-marginal-zone-lymphoma-and-for-chronic-graft-versus-host-disease. Accessed 2022 May 25.
5.Greinix HT. Chronic GVHD: progress in salvage treatment? Blood. 2017;130(21):2237-2238. PubMed
6.Rhoades R, Gaballa S. The role of B cell targeting in chronic graft-versus-host disease. Biomedicines. 2017;5(4):17. PubMed
7.Martino M, Ferreri A, Naso V, et al. The use of ibrutinib before and after allogeneic stem cell transplantation. Expert Opinion on Orphan Drugs. 2019;7(4):171-180.
8.Zeiser R. Treatment of chronic graft-versus-host disease. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 May 25.
9.Singer S, Tan SY, Dewan AK, et al. Cutaneous eruptions from ibrutinib resembling EGFR inhibitor-induced dermatologic adverse events. J Am Acad Dermatol. 2019;20:20. PubMed
10.Vaidya T, Menzer C, Ponce DM, Markova A. Inpatient management of mucocutaneous GVHD. Curr Dermatol Rep. 2019;8(4):258-278. PubMed
11.Martini DJ, Chen YB, DeFilipp Z. Recent FDA approvals in the treatment of graft-versus-host disease. Oncologist. 2022;20:20. PubMed
12.Gonzalez RM, Pidala J. Evolving therapeutic options for chronic graft-versus-host disease. Pharmacotherapy. 2020;40(8):756-772. PubMed
13.Jaglowski SM, Blazar BR. How ibrutinib, a B-cell malignancy drug, became an FDA-approved second-line therapy for steroid-resistant chronic GVHD. Blood Adv. 2018;2(15):2012-2019. PubMed
14.Janssen Inc. announces IMBRUVICA® (ibrutinib) as the first approved treatment for chronic graft-versus-host disease (cGVHD) granted by Health Canada Priority Review. 2017; https://www.newswire.ca/news-releases/janssen-inc-announces-imbruvica-ibrutinib-as-the-first-approved-treatment-for-chronic-graft-versus-host-disease-cgvhd-granted-by-health-canada-priority-review-654066423.html. Accessed 2022 May 23.
15.Saidu NEB, Bonini C, Dickinson A, et al. New approaches for the treatment of chronic graft-versus-host disease: current status and future directions. Front Immunol. 2020;11:578314. PubMed
16.Shapiro RM, Antin JH. Therapeutic options for steroid-refractory acute and chronic GVHD: an evolving landscape. Expert Rev Hematol. 2020;13(5):519-532. PubMed
17.Flowers MED. Progress in the management of chronic GVHD insights into novel therapies to treat and manage GVHD lasting longer than 12 Months. Baillieres Best Pract Res Clin Haematol. 2021;34(1):101253. PubMed
18.Ozturk C, Bozdag SC. New approaches to allogeneic haematopoietic cell transplantation. US Oncol Hematol Rev. 2021;17(1):28-35.
19.Paydas S. Management of adverse effects/toxicity of ibrutinib. Crit Rev Oncol Hematol. 2019;136:56-63. PubMed
20.Pineda-Gayoso R, Alomar M, Lee DH, Fradley MG. Cardiovascular toxicities of Bruton's tyrosine kinase inhibitors. Curr Treat Options Oncol. 2020;21(8) (no pagination).
21.Miklos D, Cutler CS, Arora M, et al. Ibrutinib for chronic graft-versus-host disease after failure of prior therapy. Blood. 2017;130(21):2243-2250. PubMed
22.King-Kallimanis BL, Wroblewski T, Kwitkowski V, et al. FDA review summary of patient-reported outcome results for ibrutinib in the treatment of chronic graft versus host disease. Qual Life Res. 2020;29(7):1903-1911. PubMed
23.Waller EK, Miklos D, Cutler C, et al. Ibrutinib for chronic graft-versus-host disease after failure of prior therapy: 1-year update of a phase 1b/2 study. Biol Blood Marrow Transplant. 2019;25(10):2002-2007. PubMed
24.Evans SR. Clinical trial structures. J Exp Stroke Transl Med. 2010;3(1):8-18. PubMed
25.Doki N, Toyosaki M, Shiratori S, et al. An open-label, single-arm, multicenter study of ibrutinib in Japanese patients with steroid-dependent/refractory chronic graft-versus-host disease. Transplant Cell Ther. 2021;27(10):867.e861-867.e869. PubMed
26.Chin KK, Kim HT, Inyang EA, et al. Ibrutinib in steroid-refractory chronic graft-versus-host disease, a single-center experience. Transplant Cell Ther. 2021;27(12):990.e991-990.e997. PubMed
27.Teusink-Cross A, Davies SM, Grimley MS, et al. Ibrutinib for the treatment of chronic graft-vs-host disease in pediatric hematopoietic stem cell transplant patients: A single-center experience. Pediatr Transplant. 2020;24(3):e13692. PubMed
28.Innocenti I, Sora F, Autore F, et al. Efficacy of ibrutinib in late relapse chronic lymphocytic leukemia after allogeneic hematopoietic stem cell transplantation. Hematol Oncol. 2021;39(2):267-269. PubMed
29.Wilkinson M, Yeung D, Limaye V. A case of inflammatory myopathy in graft vs host disease - A potential role for ibrutinib. Neuromuscul Disord. 2021;31(9):865-869. PubMed
30.Fantozzi PJ, Villa A, Antin JH, Treister N. Regression of oral proliferative leukoplakia following initiation of ibrutinib therapy in two allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2020;55(9):1844-1846. PubMed
31.National Cancer Institute (NCI). NCT04294641: Front line ibrutinib for newly diagnosed chronic graft-versus host disease. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://clinicaltrials.gov/ct2/show/record/NCT04294641. Accessed 2022 May 25.
32.Zhu S, Jung J, Victor E, Arceo J, Gokhale S, Xie P. Clinical trials of the BTK inhibitors ibrutinib and acalabrutinib in human diseases beyond B cell malignancies. Front Oncol. 2021;11:737943. PubMed
33.Rogers K. Ibrutinib and fungus: an invasive concern. Blood. 2018;131(17):1882-1884. PubMed
34.Kaloyannidis P, Ayyad A, Bahaliwah Z, et al. Ibrutinib for steroid refractory chronic graft-versus-host disease: therapeutic efficiency can be limited by increased risk of fungal infection. Bone Marrow Transplant. 2021;56(8):2034-2037. PubMed
35.Mukherjee A, Milton DR, Jabbour EJ, et al. Clinical outcome of allogeneic stem cell transplantation in patients with B-cell lymphoid malignancies following treatment with targeted small molecule inhibitors. Leuk Lymphoma. 2022;63(4):885-893. PubMed
36.Arcari A, Morello L, Vallisa D, et al. Allogeneic stem cell transplantation in patients with mantle cell lymphoma: results from the MANTLE-FIRST study on behalf of Fondazione Italiana Linfomi. Leuk Lymphoma. 2021;62(14):3474-3483. PubMed
37.Roeker LE, Dreger P, Brown JR, et al. Allogeneic stem cell transplantation for chronic lymphocytic leukemia in the era of novel agents. Blood Adv. 2020;4(16):3977-3989. PubMed
38.Dreger P, Michallet M, Bosman P, et al. Ibrutinib for bridging to allogeneic hematopoietic cell transplantation in patients with chronic lymphocytic leukemia or mantle cell lymphoma: a study by the EBMT Chronic Malignancies and Lymphoma Working Parties. Bone Marrow Transplant. 2019;54(1):44-52. PubMed
39.Yalniz FF, Murad MH, Lee SJ, et al. Steroid refractory chronic graft-versus-host disease: cost-effectiveness analysis. Biol Blood Marrow Transplant. 2018;24(9):1920-1927. PubMed
40.Wolff D, Hilgendorf I, Wagner-Drouet E, et al. Changes in immunosuppressive treatment of chronic graft-versus-host disease: comparison of 2 surveys within allogeneic hematopoietic stem cell transplant centers in Germany, Austria, and Switzerland. Biol Blood Marrow Transplant. 2019;25(7):1450-1455. PubMed
41.Zeiser R, Lee SJ. Three US Food and Drug Administration-approved therapies for chronic GVHD. Blood. 2022;139(11):1642-1645. PubMed
42.Kondo T, Ikegawa S, Fukumi T, et al. Pretransplant short-term exposure of donor graft cells to ITK selective inhibitor ameliorates acute graft-versus-host disease by inhibiting effector T cell differentiation while sparing regulatory T cells. Immunohorizons. 2021;5(6):424-437. PubMed
43.Infliximab for graft versus host disease. (CADTH reference list: summary of abstracts). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/infliximab-graft-versus-host-disease. Accessed 2022 May 25.
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Note that this appendix has not been copy-edited.
Related CADTH Report
Infliximab for graft versus host disease. (CADTH reference list: summary of abstracts). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/infliximab-graft-versus-host-disease. Accessed 2022 May 25.
Review Articles
Non-Systematic Reviews on Related Topics
Martini DJ, Chen YB, DeFilipp Z. Recent FDA approvals in the treatment of graft-versus-host disease. Oncologist. 2022;20:20. PubMed
Zhu S, Jung J, Victor E, Arceo J, Gokhale S, Xie P. Clinical trials of the BTK inhibitors ibrutinib and acalabrutinib in human diseases beyond B cell malignancies. Front Oncol. 2021;11:737943. PubMed
Martino M, Ferreri A, Naso V, et al. The use of ibrutinib before and after allogeneic stem cell transplantation. Expert Opinion on Orphan Drugs. 2019;7(4):171-180.
Systematic Review (With No Evidence Reported for Ibrutinib)
Velickovic VM, McIlwaine E, Zhang R, Spelman T. Adverse events in second- and third-ine treatments for acute and chronic graft-versus-host disease: systematic review. Ther Adv Hematol. 2020;11:1-18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7727084/pdf/10.1177_2040620720977039.pdf. Accessed 2022 May 25. PubMed
Additional References
Non-Comparative Studies (Single-Arm Trials and Case Reports/Series)
Chin KK, Kim HT, Inyang EA, et al. Ibrutinib in steroid-refractory chronic graft-versus-host disease, a single-center experience. Transplant Cell Ther. 2021;27(12):990.e991-990.e997. PubMed
Doki N, Toyosaki M, Shiratori S, et al. An open-label, single-arm, multicenter study of ibrutinib in Japanese patients with steroid-dependent/refractory chronic graft-versus-host disease. Transplant Cell Ther. 2021;27(10):867.e861-867.e869. PubMed
Innocenti I, Sora F, Autore F, et al. Efficacy of ibrutinib in late relapse chronic lymphocytic leukemia after allogeneic hematopoietic stem cell transplantation. Hematol Oncol. 2021;39(2):267-269. PubMed
Wilkinson M, Yeung D, Limaye V. A case of inflammatory myopathy in graft vs host disease - A potential role for ibrutinib. Neuromuscul Disord. 2021;31(9):865-869. PubMed
Fantozzi PJ, Villa A, Antin JH, Treister N. Regression of oral proliferative leukoplakia following initiation of ibrutinib therapy in two allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2020;55(9):1844-1846. PubMed
Teusink-Cross A, Davies SM, Grimley MS, et al. Ibrutinib for the treatment of chronic graft-vs-host disease in pediatric hematopoietic stem cell transplant patients: A single-center experience. Pediatr Transplant. 2020;24(3):e13692. PubMed
Miklos D, Cutler CS, Arora M, et al. Ibrutinib for chronic graft-versus-host disease after failure of prior therapy. Blood. 2017;130(21):2243-2250. PubMed
Cost-Effectiveness
Yalniz FF, Murad MH, Lee SJ, et al. Steroid refractory chronic graft-versus-host disease: cost-effectiveness analysis. Biol Blood Marrow Transplant. 2018;24(9):1920-1927. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca