CADTH Health Technology Review
Aprepitant for the Prevention of Post-Operative Nausea and Vomiting in Refractory or High-Risk Patients
Rapid Review
Authors: Kylie Tingley, Melissa Severn
Abbreviations
NK1
neurokinin-1
NMA
network meta-analysis
PONV
post-operative nausea and vomiting
RCT
randomized controlled trial
SR
systematic review
Key Messages
No studies were found that evaluated the clinical effectiveness of aprepitant for the prevention of post-operative nausea and vomiting in patients with a history of post-operative nausea and vomiting refractory to conventional antiemetic prophylaxis that met the criteria for this review.
In patients with the potential for life-threatening post-operative medical complications due to emesis, limited evidence of variable quality was identified for the clinical effectiveness of aprepitant. The studies varied by population, the combination of interventions and comparators and the outcomes measured, and the findings were mixed.
No studies were found that evaluated the cost-effectiveness of aprepitant for the prevention of post-operative nausea and vomiting in patients with a history of post-operative nausea and vomiting refractory to conventional antiemetic prophylaxis that met the criteria for this review.
No studies were found that evaluated the cost-effectiveness of aprepitant for the prevention of post-operative nausea and vomiting in patients with the potential for life-threatening post-operative medical complications due to emesis that met the criteria for this review.
No evidence-based guidelines were found regarding the use of aprepitant for the prevention of post-operative nausea and vomiting in patients with a history of post-operative nausea and vomiting refractory to conventional antiemetic prophylaxis that met the criteria for this review.
No evidence-based guidelines were found regarding the use of aprepitant for the prevention of post-operative nausea and vomiting in patients with the potential for life-threatening post-operative medical complications due to emesis that met the criteria for this review.
Context and Policy Issues
Post-operative nausea and vomiting (PONV) is one of the most common complications that arise during recovery from anesthesia.1 In a study looking at patient perspectives on important clinical anesthesia outcomes to avoid, nausea and vomiting were reported as high priority for most patients,2 making PONV an important patient-centered outcome. Not only is PONV distressing for patients, but it is also associated with longer hospital stays in the post-anesthesia care unit, can result in unanticipated hospital re-admission, and increases the health resource utilization and costs.3
Management of PONV is multi-dimensional and includes risk assessment, multimodal risk reduction, prophylactic measures, and prompt rescue therapy when needed.4 The combination of ondansetron and dexamethasone is a commonly used PONV prophylactic combination therapy; however, in recent years evidence has emerged that supports the use of novel medications.3,4 Aprepitant is an orally administered neurokinin-1 (NK1) receptor antagonist.5 It is typically used in the management and treatment of chemotherapy-induced nausea and vomiting. In a recent meta-analysis, Weibel and colleagues reported that that single NK1 receptor antagonists, like aprepitant, had a similar effect to most combination therapies on preventing post-operative vomiting among patients who underwent general anesthesia.6 The use of aprepitant in Canada is generally restricted for patients undergoing chemotherapy;7 however, given the potential benefits of aprepitant there is interest in potentially expanding the use of aprepitant to prevent PONV in 2 subpopulations (i.e., patients with refractory PONV and patients at high risk for life-threatening medical complications due to emesis).
The objective of this report is to summarize the evidence regarding the clinical and cost-effectiveness of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis or who are at risk of potential for life-threatening post-operative medical complications due to emesis. In addition, this report will also summarize the available evidence-based guidance for the use of aprepitant in these 2 subpopulations.
Research Questions
What is the clinical effectiveness of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis?
What is the clinical effectiveness of aprepitant for the prevention of PONV in patients with the potential for life-threatening post-operative medical complications due to emesis?
What is the cost-effectiveness of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis?
What is the cost-effectiveness of aprepitant for the prevention of PONV in patients with the potential for life-threatening post-operative medical complications due to emesis?
What are the evidence-based guidelines regarding the use of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis?
What are the evidence-based guidelines regarding the use of aprepitant for the prevention of PONV in patients with the potential for life-threatening post-operative medical complications due to emesis?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were aprepitant and post-operative nausea and vomiting. No filters were applied to limit the retrieval by study type. The search was completed on April 14, 2022, and limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1, Q3, and Q5: Patients undergoing surgery who have a history of PONV refractory to conventional antiemetic prophylaxis Q2, Q4, and Q6: Patients undergoing surgery who have the potential for life-threatening post-operative medical complications due to emesis (e.g., jaw wiring; neurosurgery; upper gastrointestinal surgery; ear, nose, and throat surgery, etc.) |
Intervention | Aprepitant alone or in combination with conventional antiemetic drugs (e.g., dexamethasone, 5-HT3 antagonists [e.g., ondansetron, granisetron, etc.], haloperidol, etc.) |
Comparator | Q1 to Q4: Conventional dual or triple antiemetic prophylaxis (e.g., dexamethasone, 5-HT3 antagonists [e.g., ondansetron, granisetron, etc.], haloperidol, etc.) Q5 and Q6: Not applicable |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., incidence of vomiting, severity of nausea, number of rescue antiemetics, time to first emetic episode, time to discharge, prevention of medical sequela, safety, etc.) Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios, etc.) Q5 and Q6: Recommendations regarding the use of aprepitant for the prevention of PONV |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
5-HT3 = 5-hydroxytryptamine; PONV = post-operative nausea and vomiting.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for SRs, the “Questionnaire to assess the relevance and credibility of a network meta-analysis”9 for network meta-analyses (NMA), and the Downs and Black checklist10 for randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
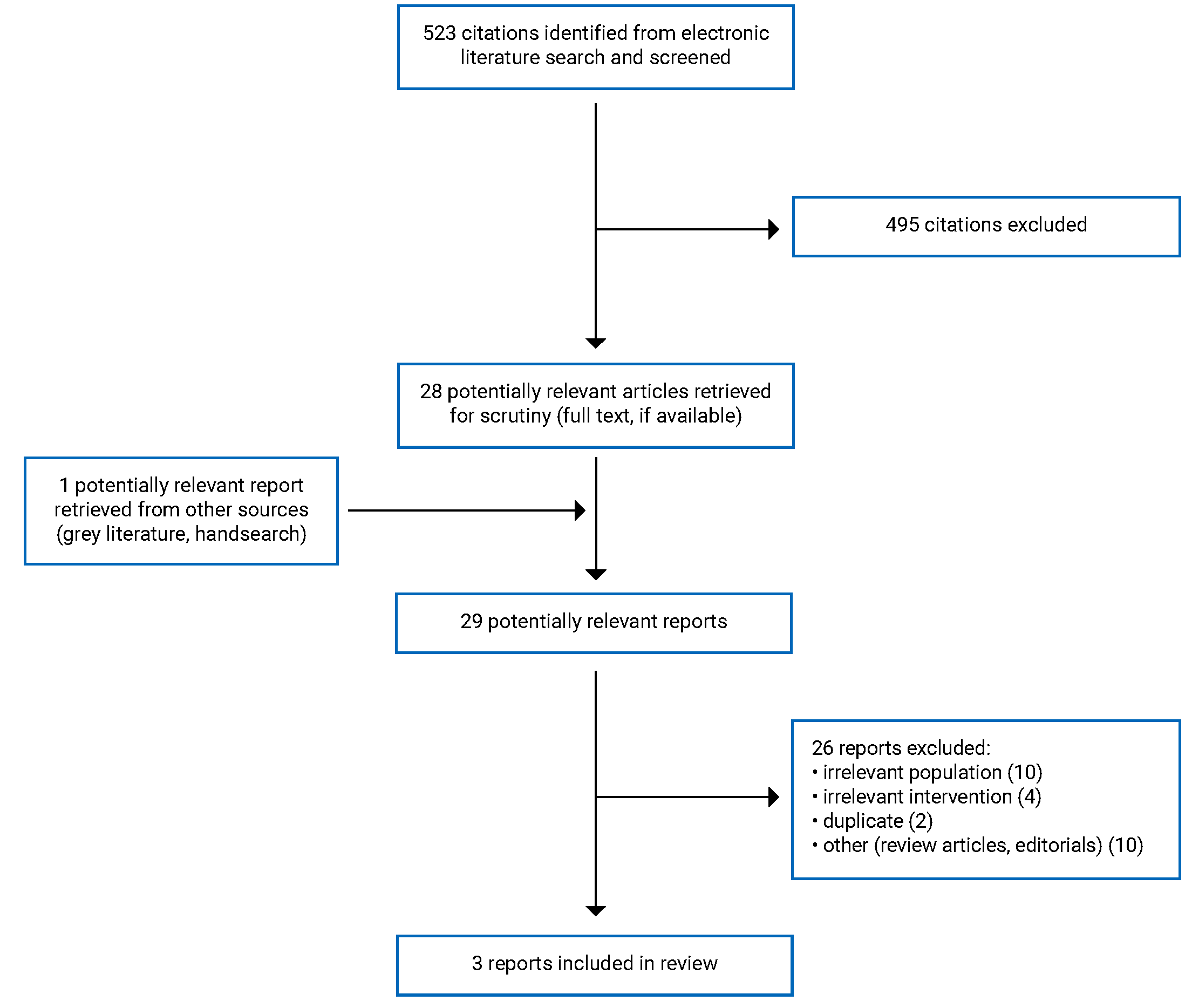
A total of 523 citations were identified in the literature search. Following screening of titles and abstracts, 495 citations were excluded and 28 potentially relevant reports from the electronic search were retrieved for full-text review. 1 potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 26 publications were excluded for various reasons, and 3 publications met the inclusion criteria and were included in this report. These comprised 1 SR,11 and 2 RCTs.12,13 No relevant evidence-based guidelines or economic evaluations were identified. Appendix 1 presents the PRISMA14 flow chart of the study selection.
Summary of Study Characteristics
One SR,11 and 2 RCTs,12,13 were identified and included in this report. Additional details regarding the characteristics of included publications are provided in Appendix 2.
The included SR11 had broader inclusions criteria than the present review. Specifically, Chen and Chang (2020) included adults of any gender undergoing supratentorial or infratentorial craniotomy, with the prophylactic use of at least 1 antiemetic drug compared to placebo or another antiemetic drug. However, only studies with aprepitant as an intervention are eligible for the current review. The characteristics and results of the subset of relevant studies will be described in this report.
Study Design
One SR with an NMA was included.11 It was published in 2020, and summarized RCTs published between the inception of the searched databases and June 2018. There were 17 RCTs identified in the SR and included in the NMA; 2 of these RCTs were directly relevant to this report (i.e., included direct comparisons between aprepitant and ondansetron). The NMA used a Bayesian approach using Markov chain Monte Carlo simulation and results were produced from random effects models for each outcome. In addition to the NMA, the authors also used pairwise meta-analysis and calculated pooled odds ratios for direct comparisons between all of the interventions and placebo and/or between interventions, if relevant RCTs were available.11 In terms of primary studies, 2 RCTs were identified and included in this report.12,13 There was no overlap between the primary studies included in this report and the RCTs included in the SR.
Country of Origin
The SR11 was conducted in China, and the 2 included studies that were relevant to this report were conducted in the US. One of the included RCTs was also conducted in the US12 and the other was conducted in Egypt.13
Patient Population
Patients in the 2 relevant studies in the included SR11 were adults of any gender undergoing supratentorial or infratentorial craniotomy, with the prophylactic use of at least 1 antiemetic drug. No details were provided about the study settings in the SR.
Patients in the study by Spaniolas et al.(2020)12 included adult patients undergoing laparoscopic sleeve gastrectomy at a single accredited bariatric centre. Patients in the study by Hasan and Abdelzaam (2019)13 included adult patients between 18 and 60 years old undergoing laparoscopic bariatric surgery with American Society of Anesthesiology I to II status who were also considered at high risk for PONV. This study was completed at an academic health centre (Aswan and Benha universities in Egypt).
Interventions and Comparators
The included SR11 had broader inclusion criteria than the current report with respect to interventions and comparators. Chen and Chang (2020)11 included RCTs that assessed the effects of any antiemetic drug (single or combination therapy) compared to either placebo or another antiemetic drug (single or combination therapy) on PONV. The 2 RCTs included in the SR that were relevant to the current review both included aprepitant (40 mg) as the intervention and ondansetron (4 mg) as the comparator. The NMA also included relevant indirect comparisons of aprepitant (40 mg) to other interventions, including: ramosetron, (0.3 mg), droperidol (0.625 mg or 1.15 mg), and fosaprepitant (150 mg).
In the study by Spaniolas et al. (2020)12 the intervention group received 2 antiemetic medications in the preoperative holding area (aprepitant 80 mg orally and scopolamine transdermal patch) and 2 antiemetic drugs intraoperatively (IV dexamethasone 8 mg and ondansetron 4 mg). The control group received the same intraoperative antiemetic drugs as the intervention group, but no preoperative antiemetic prophylaxis. In addition, the intervention group underwent total IV anesthesia (propofol based), while the control group underwent inhalation anesthesia. Patients in the study by Hasan and Abdelzaam (2019)13 were randomized to 1 of 3 intervention groups: oral placebo plus IV 4 mg of ondansetron; 80 mg of oral aprepitant plus 2 mL of IV normal saline; or 80 mg of oral aprepitant plus 4 mg of ondansetron by IV.
Outcomes
To assess the clinical effectiveness of aprepitant for the prevention of PONV in patients with the potential for life-threatening post-operative medical complications due to emesis, the main outcomes of interest were incidence of PONV up to 48 hours post operation,11,13 proportion of patients with a complete response,11,13 severity of PONV,12 proportion of patients requiring rescue antiemetic drugs,11,13 and PONV-related delay in hospital discharge.12 Complete response was defined as patients without PONV, those who did not require rescue antiemetic medications,11,13 and the severity of PONV was determined using a 10-point verbal rating scale and the Rhodes Index of nausea and emesis.12,13 One study also looked at PONV-related resource use, self-rated quality of recovery using the Quality of Recover (QoR-15), gastrointestinal quality of life using the Gastrointestinal Quality of Life Index, and broad-based quality of life using the EuroQoL 5-Dimensions 5-Levels (EQ-5D-5L).12 Adverse events including headache, dizziness, and excessive sedation were measured in the RCT by Hasan and Abdelzaam (2020) and reviewed in the SR by Chen and Chang (2020)11
Summary of Critical Appraisal
Systematic Review and Network Meta-analysis
Overall, the SR study design was of moderate quality as was the accompanying NMA.11 Strengths of the SR11 included a clearly stated the research question and inclusion criteria, methods that were established a priori, a search strategy across multiple electronic databases, and study selection conducted in duplicate. In addition, the authors did assess risk of bias of the individual studies included in the review using an appropriate tool. Together, these factors strengthen the methodological quality of the SR and help to reduce the risk of any bias in the results. Despite this, interpretation of the findings with respect to this current report was limited because only 2 of the included studies were relevant.
There were several limitations in the transparency of reporting with respect to study methods and interpretation of results for both the SR and the NMA; thus, limiting the ability to fully assess the validity and reliability of the study findings. First, it was unclear whether additional literature searches were conducted in trial registries, grey literature, or reference lists of included studies. Limiting the search strategy to electronic databases only could lead to some important and relevant literature being omitted from the SR. The authors also did not adequately discuss risk of bias of the individual studies when discussing their results. A discussion of risk of bias would be helpful to provide context and better understand the validity of results given a large proportion of studies were considered to have “unclear risk of bias” across several domains. The authors also did not adequately discuss the implications of any heterogeneity that was observed in their results, which also compromises the ability to fully assess the reliability of the overall study results. In terms of external validity, none of 17 RCTs included in the SR were conducted in Canada, which could limit the generalizability of results to a Canadian setting.
With respect to the NMA11 specifically, its strengths included a relevant study population, intervention, and effectiveness outcomes, including both direct and indirect comparisons, consistency between direct and indirect comparisons, and generally good reporting regarding all relevant and important results. However, there were some notable limitations with respect to reporting and transparency of the methods, the analysis, and the credibility of results. The authors did not adequately assess the baseline characteristics of patients in the included studies, so it is unclear if and how any differences among patients contribute to the interpretation of results. The authors also included a high proportion of studies that they reported as having an unclear risk of bias and 1 study described as having a high risk of bias, which could have an impact on the validity of the pooled results.
Based on the limitations described the results from the include SR and NMA11 should be interpreted with caution.
Randomized Controlled Trials
Two RCTs12,13 were included in the current review. In both studies the reporting of the research objective, inclusion and exclusion criteria, intervention, comparator, and main outcome were all well described, which is a strength when it comes to transparency and reproducibility of results. Patients in both studies were randomized using a computer-generated list of random numbers; thus, balancing potential unmeasured confounding factors and reducing the risk of selection bias. No patients were lost to follow-up in either study, which eliminates the risk of attrition bias. One of the RCTs13 reported that both patients and outcome assessors were blinded to the intervention, which minimizes any potential placebo effect or unconscious bias when evaluating outcomes in that study. Neither RCT reported whether randomized intervention assignment was concealed until recruitment was complete, which could have affected the internal validity of study results. Adverse events were not reported in either RCT. In the study by Hasan and Abdelzaam (2019), the authors report in the methods sections that adverse events would be assessed; however, adverse events were not reported in the results section of the paper, and the reason for this is unclear.13 In addition, the main findings from this study were not clearly described (i.e., unclear if estimate of variability for the mean was standard error or standard deviation).13 It also was not clear from the reporting of this study which 2 groups were being compared using the reported P values.13 Both RCTs had adequate statistical power to determine clinically important effects; however, in 1 RCT13 the authors used multiple t-tests to compare 3 treatment groups rather than analysis of variance (ANOVA) increasing the risk of type I error. In terms of external validity, both RCTs were limited in that the staff and setting were unlikely to be representative of the typical settings for bariatric surgery, particularly in Canada. In addition, it was difficult to determine whether the study populations in each RCT were representative of the entire population, which further limits the generalizability of study findings. Finally, in the study by Spaniolas et al. (2020),12 the type of anesthesia used differed between the 2 intervention groups (i.e., IV versus inhalation) and it is unknown whether that influenced the study findings.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Aprepitant for the Prevention of PONV in Patients With a History of PONV Refractory to Conventional Antiemetic Prophylaxis
No relevant evidence regarding aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis was identified; therefore, no summary can be provided.
Clinical Effectiveness of Aprepitant for the Prevention of PONV in Patients With the Potential for Life-Threatening Post-Operative Medical Complications Due to Emesis
One SR with meta-analysis and NMA in patients undergoing craniotomy, and 2 RCTs (1 with adults undergoing bariatric surgery, and the other with adults undergoing sleeve gastrectomy)12,13 were identified and included in this report.
The studies include in this review reported results pertaining to the incidence of PONV,11 proportion of patients with a complete response,11,13 severity of PONV,12,13 proportion of patients requiring rescue antiemetic drugs,11,13 and PONV-related delay in hospital discharge.12 None of the outcomes were common across all 3 studies.
Incidence of Post-Operative Vomiting
The overall incidence of post-operative vomiting, at different post-operative time points was reported in the included SR with NMA.11 Among the studies included in the SR, 2 considered aprepitant as an intervention with head-to-head comparisons with ondansetron. The pooled estimate of these 2 RCTs found that when aprepitant was compared to ondansetron, the odds of post-operative vomiting up to 48 hours post operation were lower for those treated with aprepitant.
Considering indirect comparisons from the NMA for post-operative vomiting, no therapy was favoured when aprepitant was compared to droperidol (at 0 to 2 hours post operation) or fosaprepitant (at 0 to 24 hours or 0 to 48 hours post operation).11
Incidence of Post-Operative Nausea
The overall incidence of post-operative nausea and the overall incidence of post-operative vomiting, at different post-operative time points was reported in the included SR with NMA.11 Among the studies included in the SR, 2 considered aprepitant as an intervention with head-to-head comparisons with ondansetron. The pooled estimate of these 2 RCTs found that when aprepitant was compared to ondansetron, there was little-to-no difference in the odds of post-operative nausea in the first 24 hours post operation.
Considering indirect treatment comparisons from the NMA for post-operative nausea, ramosetron was favoured compared to aprepitant in reducing post-operative nausea at 24 hours post operation; however, the results were imprecise.11
Severity of PONV
Both RCTs12,13 measured the severity of PONV. In the study by Spaniolas et al. (2020),12 the aprepitant intervention group reported statistically significantly less severe PONV measured by 2 different scales than the control group. In the study by Hasan and Abdelzaam (2019),13 the aprepitant plus ondansetron group rated the severity of nausea lower than the ondansetron alone or aprepitant alone groups, however, the statistical significance of the comparisons among the 3 treatment groups is unclear.
Rescue Antiemetic Drugs
Receipt of rescue antiemetic drugs was measured and reported in the SR11 and the RCT by Hasan and Abdelzaam (2019).13 Indirect comparison results from the SR with NMA11 suggest that ramosetron is favoured over aprepitant as the aprepitant group had higher odds of requiring rescue antiemetic drugs compared to the ramosetron group; however, the results are imprecise. The RCT13 reported a lower requirement for rescue antiemetic drugs in those treated with aprepitant and ondansetron (2%) compared to aprepitant alone (10%) or ondansetron alone (16%); however, the statistical significance of the comparisons among the 3 treatment groups is unclear.
Complete Response
Complete response was examined in 1 RCT13 and was defined as no post-operative nausea, retching, or vomiting and no need for rescue antiemetics. Hasan and Abdelzaam (2019)13 found that a higher percentage of patients in the ondansetron with aprepitant group showed a complete response compared to aprepitant or ondansetron alone; however, the statistical significance of these findings was not reported.
PONV-Related Delay in Hospital Discharge
One RCT12 evaluated the effectiveness of aprepitant and scopolamine plus dexamethasone and ondansetron compared to dexamethasone and ondansetron alone on how quickly patients were discharged from hospital following bariatric surgery. Findings from the trial demonstrated that there were no statistically significant differences in PONV-related delay in hospital discharge between treatment groups (0% aprepitant group versus 9.5% control group).
Quality of Life
A single RCT12 evaluated the effect of aprepitant and scopolamine plus dexamethasone and ondansetron compared to dexamethasone and ondansetron alone on patients’ quality of life. The aggregate index for the EQ-5D-5L was similar between groups at baseline, 24 hours, and 3 weeks; however, there were statistically significant improvement in the usual activity and mobility domains of the EQ-5D-5L and on the quality of recovery among the aprepitant group compared to the control group. The results from the Gastrointestinal Quality of Life Index showed little-to-no difference between the aprepitant group and the control group; however, the results are imprecise.
Cost-Effectiveness of Aprepitant for the Prevention of PONV in Patients With a History of PONV Refractory to Conventional Antiemetic Prophylaxis
No relevant cost-effectiveness evidence regarding aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis was identified; therefore, no summary can be provided.
Cost-Effectiveness of Aprepitant for the Prevention of PONV in Patients With the Potential for Life-Threatening Post-Operative Medical Complications Due to Emesis
No relevant evidence regarding aprepitant for the prevention of PONV in patients with the potential for life-threatening post-operative medical complications due to emesis was identified; therefore, no summary can be provided.
Guidelines
No relevant evidence-based guidelines were identified regarding aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis or in patients with potential for life-threatening medical complications due to emesis; therefore, no summary can be provided.
Limitations
This review is limited by the quantity of evidence identified regarding the clinical effectiveness, cost-effectiveness, and guidelines for the use of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis or in patients with potential for life-threatening medical complications due to emesis. Notably, no economic evaluations or guidelines were identified. Additionally, no clinical effectiveness literature was identified for use of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis. Furthermore, the current review only identified 2 subpopulations of patients with the potential for life-threatening medical complications due to emesis – patients undergoing craniotomy11 and patients undergoing laparoscopic bariatric surgery.12,13 Given the paucity of available evidence, further research is needed to draw robust conclusions on this topic.
Among the available evidence regarding the use of aprepitant for prevention of PONV in patients with the potential for life-threatening medical complications due to emesis, there was variability in the combination of therapies studied as well as variability in the outcomes that were assessed across studies. This variability limits the interpretation and synthesis of findings toward a more robust conclusion.
The 3 included studies11-13 also had limited external validity. The 2 relevant studies included in the SR11 and the 2 RCTs12,13 took place in settings outside of Canada; thus, the generalizability to the Canadian context is unclear. In addition, lack of detail about patient characteristics in the studies included in the SR11 and stringent eligibility criteria for both RCTs12,13 further limits the external validity of the findings.
Conclusions and Implications for Decision- or Policy-Making
This review identified 1 SR with NMA11 and 2 RCTs12,13 that addressed the clinical effectiveness of aprepitant for the prevention of PONV in patients who had a potential for life-threatening medical complications due to emesis. No relevant studies describing the cost-effectiveness or guidelines for the use of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis or in patients with potential for life-threatening medical complications due to emesis were found. In addition, no clinical effectiveness studies were found for the prevention of PONV in patients with a history of PONV refractory to conventional antiemetic prophylaxis.
Overall, among patients undergoing craniotomy or bariatric surgery the results supporting aprepitant were mixed depending on outcome and comparator. When compared to ondansetron, aprepitant reduced the odds of post-operative vomiting for up to 48 hours, but showed little-to-no difference in the odds of post-operative nausea within 24 hours.11 Indirect treatment comparisons favoured ramosetron compared to aprepitant for reducing post-operative nausea at 24 hours post operation, and for the need for rescue antiemetic drugs; however, both of these results were imprecise, thereby limiting the certainty in the findings.11 In addition, indirect comparisons found that no treatment was favoured for preventing post-operative vomiting when aprepitant was compared droperidol or fosaprepitant.11 The combination of aprepitant and ondansetron13 may lower the need for rescue antiemetic drugs compared to aprepitant alone or ondansetron alone. In addition, when compared to the control group, aprepitant may reduce the severity of PONV, but no difference was found in the length of stay in hospital, and there was little-to-no difference in aggregate quality of life scores.12
There were methodological limitations identified for each of the 3 included studies and considerable variability identified in reporting, including study populations and interventions, and assessed outcomes across the studies. Therefore, decision-makers should interpret these findings with caution when developing care pathways and policies regarding the expanded use of aprepitant to prevent PONV among patients with potential for life-threatening medical complications due to emesis. Better transparency in reporting the methodologies used for each study would improve the ability to critically appraise the studies, and further research to better understand the effects of aprepitant in other relevant subpopulations would reduce uncertainties with respect to clinical effectiveness.
No cost-effectiveness or evidence-based guidelines were identified for either subpopulation of interest and no clinical effectiveness evidence was found for the use of aprepitant for the prevention of PONV in patients with a history of PONV refractory to conventional anti-emetic prophylaxis. Future research to address the questions in this report may help reduce uncertainty and provide decision-makers with evidence to make their decisions.
References
1.Feinleib J, Kwan L, Yamani A. Postoperative nausea and vomiting. Waltham (MA): UpToDate; 2022 Mar 25: https://www.uptodate.com/contents/postoperative-nausea-and-vomiting. Accessed 2022 May 16.
2.Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. 1999 Sep;89(3):652-8. PubMed
3.Gan TJ, Belani KG, Bergese S, et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth Analg. 2020;131(2):411-448. PubMed
4.Jin Z, Gan TJ, Bergese SD. Prevention and Treatment of Postoperative Nausea and Vomiting (PONV): A Review of Current Recommendations and Emerging Therapies. Ther Clin Risk Manag. 2020;16:1305-1317. PubMed
5.Aprepitant: Drug information. Waltham (MA): UpToDate; 2022: www.uptodate.com. Accessed 2022 April 16.
6.Weibel S, Rucker G, Eberhart LH, et al. Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis. Cochrane Database Syst Rev. 2020;10:CD012859. PubMed
7.Merck Canada Inc. Emend aprepitant capsules 80 and 125 mg [product monograph]. Kirkland (QC): Merck Canada Inc.; 2014 Jan 22: https://www.merck.ca/static/pdf/EMEND-PM_E.pdf. Accessed 2022 May 16.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Chen Y, Chang J. Anti-emetic Drugs for Prophylaxis of Postoperative Nausea and Vomiting After Craniotomy: An Updated Systematic Review and Network Meta-Analysis. Front Med (Lausanne). 2020;7:40. PubMed
12.Spaniolas K, Nie L, Moller D, et al. A Comprehensive Approach for the Prevention of Nausea and Vomiting Following Sleeve Gastrectomy: a Randomized Controlled Trial. Obes Surg. 2020;30(11):4250-4257. PubMed
13.Hasan AME, Abdelzaam E-S. A Comparative Study between Aprepitant only versus Combined Ondansetron and Aprepitant as Antiemetic Therapy, Regarding Efficacy and Duration, in Patients Undergoing Laparoscopic bariatric Surgery Double-blinded, Randomized Control Clinical Trial https://www.longdom.org/open-access-pdfs/a-comparative-study-between-aprepitant-only-versus-combined-ondansetron-and-aprepitant-as-antiemetic-therapy-regarding-e.pdf. J Anesth Clin Res. 2019;10(5). Accessed 2022 May 16.
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review and Network Meta-Analysis
Study citation, country, funding source | Study designs and numbers of primary studies included | Population | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Chen and Chang, 202011 China Funding source not reported; however, authors report no conflicts of interest | Objective: To assess the effectiveness and safety of antiemetic drugs for PONV at different post-operative time intervals Study design: Systematic review and NMA of RCTs, also includes a pairwise meta-analysis Number of included studies: 17 RCTs were included in the NMA (relevant indirect treatment comparisons with aprepitant were included); 2 of the RCTs examined aprepitant and were relevant to current report (direct treatment comparisons) | Adults of any gender undergoing supratentorial or infratentorial craniotomy N = 1,433 patients across 17 RCTs included in the NMA (N = 95 and 104 in the 2 relevant RCTs with direct comparisons) | Eligible intervention: all antiemetic drugs Eligible comparators: placebo or other antiemetic drugs Relevant intervention: aprepitant Relevant comparators: ondansetron (direct comparison) Ramosetron, droperidol, fosaprepitant (indirect comparisons in NMA) | Outcomes:
Follow-up:
|
NMA = network meta-analysis; PONV = post-operative nausea and vomiting; RCT = randomized controlled trial.
Table 3: Characteristics of Included Randomized Controlled Trials
Study citation, country, funding source | Study design | Population | Intervention and | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Spaniolas et al., 202012 US Funded in part by a peer-reviewed grant by the Society for the Surgery of the Alimentary Tract Foundation | Study design: Prospective randomized controlled trial Setting: Single specialized bariatric surgery centre Objective: To evaluate the impact of a comprehensive approach on the prevention of PONV, minimization of severity, and related hospital resource utilization following sleeve gastrectomy. | Adult patients undergoing laparoscopic sleeve gastrectomy Number of patients:
Mean age, years (SD):
Mean BMI, kg/m2 (SD):
% Male:
| Intervention:
Comparator:
Both groups received routine scheduled antiemetics postoperatively (IV ondansetron 4 mg and metoclopramide 10 mg), as well as needed antiemetic drugs (compazine 10 mg as first line). | Outcomes:
Follow-up:
|
Hasan and Abdelzaam, 201913 Egypt Funding source not reported | Study design: Prospective, randomized double-blinded, controlled trial with 3 treatment arms Setting: Single academic care centre Objective: To examine PONV, the severity of nausea with a complete response up to 48 hours postoperatively, in 2 dual therapy groups and one triple therapy group. | All patients between 18 and 60 years of age with American Society of Anesthesiology I to II status who considered at high risk for PONV and who were undergoing a laparoscopic bariatric surgery under general anesthesia of at least 1- hour duration Number of patients:
Mean age, years (SD):
Mean weight, kg (SD)
% Male:
| Group A:
Group B:
Group C:
The oral aprepitant or placebo was given within 2 hours before their scheduled operation. 8 mg dexamethasone iv after the induction of anesthesia was given to all patients | Outcomes:
Follow-up:
|
PONV = postoperative nausea and vomiting; SD = standard deviation.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Review and Network Meta-Analysis Using AMSTAR 28 and the ISPOR Questionnaire9
Strengths | Limitations |
|---|---|
Chen and Chang, 202011 | |
AMSTAR 2:
ISPOR Questionnaire: Relevance
Credibility
Analysis
Reporting Quality and Transparency
Interpretation
| AMSTAR 2:
ISPOR Questionnaire: Credibility
Analysis
Reporting Quality and Transparency
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; PICO = population, intervention, comparator, outcome; PROSPERO = International Prospective Register of Systematic Reviews; RCT = randomized controlled trials; RoB = risk of bias; SR = systematic review.
Note that this table has not been copy-edited.
Table 5: Strengths and Limitations of Randomized Controlled Trials Using the Downs and Black Checklist10
Strengths | Limitations |
|---|---|
Spaniolas et al., 202012 | |
Reporting
Internal validity
Power
| Reporting
External validity
Internal validity
|
Hasan and Abdelzaam, 201913 | |
Reporting
Internal validity
Power
| Reporting
External validity
Internal validity
|
PONV = post-operative nausea and vomiting.
Note that this table has not been copy-edited.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 6: Summary of Findings Included Systematic Review and Network Meta-Analysis
Main study findings | Authors’ conclusion |
|---|---|
Chen and Chang, 202011 | |
SR with NMA of 17 RCTs examined the effectiveness and safety of antiemetic drugs for PONV at different post-operative time intervals after craniotomy. Two RCTs that directly compared aprepitant to conventional dual or triple antiemetic prophylaxis were relevant to this report, as were the indirect comparisons from the NMA that included aprepitant and a relevant comparator Findings of relevant head-to-head RCTs: Post-operative nausea at 0 to 24-hours post operation:
Post-operative vomiting at 0 to 2 hours post operation:
Post-operative vomiting at 0 to 24 hours post operation:
Post-operative vomiting at 0 to 48 hours post operation:
Overall findings from NMA:
Post-operative nausea during 0 to 24 hours post operation:
Post-operative vomiting during 0 to 2 hours post operation:
Post-operative vomiting during 0 to 24 hours post operation:
Post-operative vomiting during 0 to 48 hours post operation:
Requirement for rescue antiemetic drugs:
| “In this systematic review and NMA on patients who underwent craniotomy, direct, and indirect comparisons revealed ramosetron as the best antiemetic drug for post-operative nausea during the first 24h. Ramosetron was also associated with the lowest incidence of PONV and displayed the lowest requirement for rescue antiemetic drugs. Fosaprepitant was the best antiemetic drug for reducing POV on the first and second post-operative days, with droperidol representing the next best alternative. Furthermore, fosaprepitant was more effective than ondansetron for POV prophylaxis during the first and second postoperative days.” (p. 10) |
CI = confidence interval; CrI = credible interval; NMA = network meta-analysis; OR = odds ratio; PONV = post-operative nausea and vomiting; RCT = randomized controlled trial; SR = systematic review.
Note that this table has not been copy-edited.
Table 7: Summary of Findings of Included Randomized Controlled Trials
Main study findings | Authors’ conclusion |
|---|---|
Spaniolas et al., 202012 | |
A prospective RCT of 83 adult patients undergoing laparoscopic sleeve gastrectomy at a single academic bariatric centre to evaluate the impact of a comprehensive approach on the prevention of PONV, minimization of severity, and related hospital resource utilization. Summary of findings: PONV-related delay in hospital discharge, n (%):
Hospital stays in hours, median (IQR)
Severity of PONV
Quality of life using EQ-5D-5L aggregate index
Gastrointestinal Quality of Life Index, aggregate score
Quality of Recovery (QoR-15)
Hospital resource utilization:
| “The present study demonstrates improvement in patient- reported outcomes with a multilevel approach to PONV pre- vention following [sleeve gastrectomy]. Specifically, patients in the intervention group, with the combination of total intravenous anesthesia with propofol and multi-pharmacotherapy, reported improved self-rated experience with recovery early after surgery, as well as improved mobility and ability to perform daily activities 3 weeks after [sleeve gastrectomy].” (p. 4254) |
Hasan and Abdelzaam, 201913 | |
A prospective, randomized, double- blind controlled clinical trial of 150 patients undergoing laparoscopic bariatric surgery at a single centre to assess PONV, severity of nausea, and complete response among 3 groups: A) ondansetron alone, B) aprepitant alone, and C) ondansetron + aprepitant. Summary of findings: Nausea severity according to a verbal rating scale (0 = no nausea to 10 = “nausea as bad as it could be”), mean (estimate of variabilitya):
Requirement of rescue antiemetic drugs, n (%)
Complete response (no post-operative nausea, retching, or vomiting and no need for rescue antiemetics), %
| “In patients undergoing laparoscopic bariatric surgery, the addition of aprepitant to ondansetron significantly decreased postoperative vomiting rates and nausea severity and increased complete response for up to 48 hours postoperatively. Dexamethasone-aprepitant decreased postoperative vomiting rates and nausea severity in compared to dexamethasone-ondansetron but insignificantly. Finally, Oral aprepitant, when combined with intravenous ondansetron and dexamethasone, was effective in suppressing early PONV up to 48 h postoperatively.” (p. 6) |
aThe authors of this RCT did not report whether the estimate of variability of the mean was standard deviation or standard error.
bThe authors of this report used an inappropriate statistical test for comparing 3 treatment groups and it is unclear which groups the P value is comparing.
CI = confidence interval; IQR = interquartile range; PONV = post-operative nausea and vomiting; RCT = randomized controlled trial.
Note that this table has not been copy-edited.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca