CADTH Health Technology Review
Monitoring Patients With Psychotic Disorders for Clozapine-Induced Myocarditis or Cardiomyopathy
Rapid Review
Authors: Chantelle C. Lachance, Monika Mierzwinski-Urban
Abbreviations
AWMF
Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (German)
English translation: Working Group of Scientific Medical Societies
DGPPN
Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (German)
English translation: German Association for Psychiatry, Psychotherapy and Psychosomatics
ECG
electrocardiogram
ECT
electroconvulsive therapy
NICE
National Institute for Health and Care Excellence
RANZCP
Royal Australian and New Zealand College of Psychiatrists
RCT
randomized controlled trial
Key Messages
Three evidence-based guidelines were identified about the use of clozapine for patients with psychotic disorders.
The included guidelines provide recommendations for testing and assessment of key health parameters for patients who are prescribed clozapine via various means such as laboratory tests and electrocardiogram.
The guidelines provide recommendations of co-prescription for patients who have not responded adequately to an optimized dose of clozapine alone.
Two guidelines offer specific recommendations on clozapine dosing.
The guidelines were generally well developed, clearly reported, and consistent in their recommendations. However, several of the recommendations were derived from sources of evidence that may not be considered of the highest quality, with the strength of recommendation not reported and unclear.
The diagnostic accuracy of high-sensitivity troponin I testing versus troponin T testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders is unknown as no relevant evidence was identified.
Given the limited availability and varying quality of evidence, the diagnostic accuracy of high-sensitivity troponin I testing and how best to monitor for clozapine-induced myocarditis and cardiomyopathy in patients with psychotic disorders remains uncertain.
Context and Policy Issues
Mental health conditions, including bipolar disorders, generalized anxiety disorders, major depressive disorders, and schizophrenia, affect about one-third of the Canadian population.1 In Canada, schizophrenia affects approximately 1% of the population over the age of 10 years old, and the all-cause mortality rate in those with the condition is 2.8 times higher than those without it.2 Different pharmacological and psychological therapy options are available for patients with mental health conditions; the most appropriate therapy option for patients depends on the type (e.g., generalized anxiety disorders versus schizophrenia) and degree (i.e., mild, moderate, or severe) of their mental health condition.3 For example, first-line therapy for those diagnosed with schizophrenia or bipolar disorder is often pharmacological therapy.4,5
Clozapine is a second-generation antipsychotic drug indicated for patients with psychotic disorders, including delusional disorder, schizophrenia, schizoaffective disorder, and bipolar disorder.6,7 Clozapine has shown clinical efficacy; for example, clozapine has shown benefits over other antipsychotic drugs for patients with treatment-resistant schizophrenia and in reducing the risk of suicide in patients with schizophrenia.4,8-10 Typically, clozapine is prescribed to patients who are resistant to first-line antipsychotic drugs due to the risk of unpredictable and serious adverse drug reactions, such as myocarditis and cardiomyopathy.6,11,12 Resistance to first-line antipsychotic drugs is common: for patients with schizophrenia, it is estimated that 50% do not respond adequately (i.e., partial or no response) after receiving their prescribed pharmacotherapy.13
Myocarditis is defined as inflammation of the heart muscle and typically develops within the first 4 weeks after initiating clozapine.10,14 Cardiomyopathy is a disease of the heart muscle that makes it harder for the heart to pump blood to the rest of the body and has a later onset.15,16 The incidence of clozapine-related myocarditis in Australia and Canada over the last few decades has been variably reported at between 0.01% and 3.88%, which is a higher incidence rate than that of clozapine-related cardiomyopathy.10,17-19 Recognizing how fatal these adverse events can be, health care providers require guidance around how to monitor for myocarditis and cardiomyopathy, as well as appropriate courses of action for when myocarditis or cardiomyopathy are detected (e.g., stop clozapine use and switch to a different antipsychotic).
There are different ways to screen and diagnose myocarditis and cardiomyopathy, including clinical examination, endomyocardial biopsy, electrocardiogram (ECG), echocardiogram, cardiac MRI, and biochemical markers of myocardial injury.20 A simply blood test can assess biochemical markers of myocardial injury, including cardiac troponin I and T, which can be less invasive for the patient and cost-saving for the health care system.21,22 However, concerns about the diagnostic test accuracy of high-sensitivity cardiac troponin assays still prevail.21,23
In 2021, CADTH produced a report providing a reference list of publications concerning the diagnostic accuracy of high-sensitivity troponin I testing versus troponin T testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders.24 In addition, the report provided a reference list of evidence-based guidelines on the use of clozapine for patients with psychotic disorders.24 The aim of this rapid review is to summarize and critically appraise the full text of relevant evidence regarding the diagnostic accuracy of high-sensitivity troponin I testing versus troponin T testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders. This report also aims to summarize and critically appraise the recommendations from evidence-based guidelines regarding the use of clozapine for patients with psychotic disorders.
Research Questions
What is the diagnostic accuracy of high-sensitivity troponin I testing versus troponin T testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders?
What are the evidence-based guidelines on the use of clozapine for patients with psychotic disorders?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were high-sensitivity troponin I testing and clozapine. No filters were applied to limit the retrieval by study type for question 1. CADTH-developed search filters were applied to limit retrieval to guidelines for question 2. Conference abstracts were excluded from the search results. The search was completed on April 20, 2022, and limited to English-language documents published since January 1, 2016.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with psychotic disorders (e.g., delusional disorder, schizophrenia [including treatment-resistant], schizoaffective disorder, and bipolar disorder) in any setting (e.g., acute, tertiary, or outpatient/community settings) |
Intervention | Q1: High-sensitivity troponin I test (index test) Q2: Clozapine (trade name: Clozaril) |
Comparator | Q1: Troponin T test (comparator test) Q2: Not applicable |
Reference standard | Q1: Biopsy or diagnosis by a cardiologist Q2: Not applicable |
Outcomes | Q1: Diagnostic accuracy for myocarditis or cardiomyopathy (e.g., sensitivity, specificity, negative predictive value, positive predictive value) Q2: Recommendations regarding:
|
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications, or if they were published before 2016. Guidelines with unclear methodologies were also excluded.
Critical Appraisal of Individual Studies
The included guidelines were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.25 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
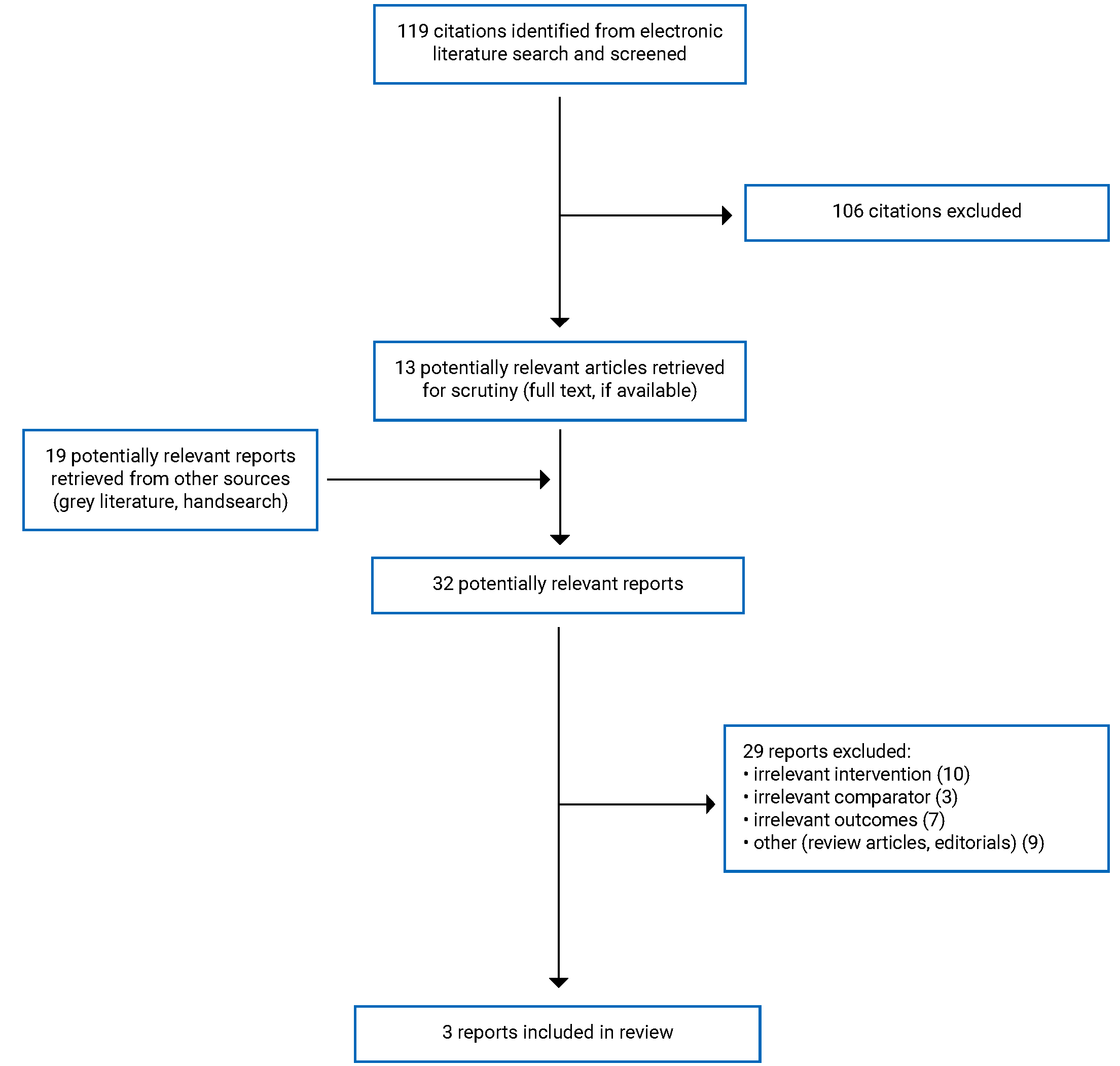
A total of 119 citations were identified in the literature search. Following screening of titles and abstracts, 106 citations were excluded and 13 potentially relevant reports from the electronic search were retrieved for full-text review. Nineteen potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 29 publications were excluded for various reasons, and 3 publications, all of which were evidence-based guidelines,26-28 met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA29 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
No health technology assessments, systematic reviews, randomized controlled trials (RCTs), or non-randomized studies were identified regarding the diagnostic accuracy of high-sensitivity troponin I testing versus troponin T testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders. Three guidelines, published between 2016 and 2020, were identified regarding the use of clozapine for patients with psychotic disorders.26-28 The Royal Australian and New Zealand College of Psychiatrists (RANZCP) guideline26 is an update for the previous 2005 clinical practice guidelines for the management of schizophrenia and related disorders.30 The German Association for Psychiatry, Psychotherapy and Psychosomatics (in German called Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde [DGPPN]) guideline28 is also an update to a previous guideline, but it is not clear when the last version was published.
Additional details regarding the characteristics of the included guidelines are provided in Appendix 2.
Study Design
The 3 guidelines were developed by the National Institute for Health and Care Excellence (NICE),27 DGPPN,28 and RANZCP.26
For the NICE27 and DGPPN28 guidelines, evidence informing the recommendations were collected through a well-defined literature search. The RANZCP group drafted its recommendations with reference to existing systematic reviews, informal literature reviews, and relevant international clinical practice guidelines.26
The guidelines used rating schemes to convey the quality of the evidence.26-28 Evidence informing the NICE guideline27 was rated based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology as being of high, moderate, low, or very low quality. Evidence informing the DGPPN guideline28 ranged from 1++ (highest; i.e., high-quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias) to 4 (lowest; i.e., expert opinion). For the RANZCP guideline,26 evidence for intervention studies was assigned grades ranging from I (highest; i.e., systematic review of RCTs) to IV (lowest; i.e., case series), according to Australian National Health and Medical Research Council levels of evidence. Grading recommendations for the DGPPN guideline28 were based on the methodology of the Scottish Intercollegiate Guidelines Network (Grade A [highest] to D [lowest]). Neither the NICE27 nor the RANZCP26 guidelines were clear on their rating schemes for strength of recommendations.
All 3 guidelines provide details on how their recommendations were developed and evaluated. For the NICE guideline,27 recommendations were drafted based on the committee’s interpretation of the available evidence, taking into account the trade-off between the benefits and harms, costs, or implications compared with the economic benefits, current practices, recommendations made in other relevant guidelines, people’s preferences, and equality issues. When evidence was of poor quality, or was conflicting or absent, the committee drafted recommendations based on expert opinion.27 The DGPPN guideline28 was developed in full accordance with the Working Group of Scientific Medical Societies (i.e., in German called Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften [AWMF]) Guidance Manual and Rules for Guideline Development.31 The DGPPN guideline28 is an evidence- and consensus-based guideline (i.e., with a representative committee, systematic review and synthesis of the evidence, and structured consensus development), classified as a level S3 guideline (i.e., the highest quality level for guidance development in Germany). Evidence-based recommendations for the RANZCP guideline26 were formulated when the guideline group judged that there was sufficient evidence on a topic. Where evidence was weak or lacking, consensus-based recommendations were formulated by a group of experts.26
Each guideline group took a slightly different approach to validate their guidelines. The NICE group conducted a stakeholder review of the draft guideline through a 6-week public consultation and feedback process; all comments received from registered key stakeholders were responded to in writing and posted on the NICE website.27 For the revision process, the DGPPN group involved experts within topic-specific, module working groups to update and expand the guideline texts.26 The RANZCP group invited review by its committees and members, an expert advisory committee, and key stakeholders (e.g., professional bodies, special interest groups).26
Country of Origin
The NICE guideline27 is intended for those living in the UK; the DGPPN guideline28 is intended for those living in Germany; and the RANZCP guideline26 is intended for those living in Australia and New Zealand.
Patient Population
The intended users of the NICE guideline27 are health care professionals, social care practitioners, and other practitioners providing public services for people with complex psychosis; commissioners and providers of mental health services; and people using mental health services, their families, and carers. The target population of this guideline is adults with complex psychosis (i.e., primary diagnosis of a psychotic illness with severe and treatment-resistant symptoms of psychosis and functional impairment).27
The intended users of the DGPPN guideline28 are practitioners who treat people with schizophrenia. The target population of this guideline is people with schizophrenia.28
The intended users of the RANZCP guideline26 are psychiatrists, psychiatry trainees, resident medical officers, and hospital interns in psychiatry. The authors mentioned that the guideline may also be useful to general practitioners, mental health nurses, other clinicians who work with people with schizophrenia and related psychoses, and policy-makers. The target population of this guideline is people with schizophrenia and related disorders.26
Interventions and Comparators
The included guidelines considered a range of evidence-based practices for the clinical management and rehabilitation of people with psychotic disorders. The relevant intervention for all included guidelines was clozapine for people with psychotic disorders (i.e., complex psychosis,27 schizophrenia,26,28 and related disorders26).
Outcomes
The relevant outcomes of the included guidelines were evidence about rates of physical and mental health conditions and substance misuse in this population;27 augmenting clozapine with a co-prescription,26,27 electroconvulsive therapy (ECT),26 or switching to another drug;26 drug treatment resistance comparing combination treatment with monotherapy;28 adverse events;26 metabolic and adverse event monitoring;26 prescriptions to reduce adverse events related to taking clozapine;26 lower value of therapeutic reference range for clozapine;28 efficacy and safety of different doses of clozapine;26 other guidelines and studies;27,28 the committee’s experience and knowledge;27 and clinical consensus.28
Summary of Critical Appraisal
All included guidelines26-28 were clear and specific with describing their overall objectives, health questions, population to whom the guideline is meant to apply, and target users of the guideline. The included guidelines all involved guideline development groups of relevant professions.26-28 The NICE27 and RANZCP26 guideline developers sought the views and preferences of the target population (e.g., patients, public), but this was unclear from the abbreviated English version of the DGPPN guideline.28 The NICE27 and DGPPN31 guidelines used systematic methods to search for evidence, which is a strategy that increases reproducibility and reduces potential bias. The RANZCP26 guideline used a different approach to search for evidence: the guideline development group used existing systematic reviews, informal literature reviews, and relevant international clinical practice guidelines to draft its recommendations. All guidelines26-28 described strengths and limitations of the body of evidence; described methods for formulating the recommendations; considered the health benefits, side effects, and risks in the formulation of the recommendations; provided an explicit link between the recommendations and the supporting evidence; were reviewed by external experts before its publication; and provided a procedure for updating the guideline. The 1 exception was that the RANZCP26 guideline did not indicate a procedure for updating the guideline. All guidelines26-28 provided specific and unambiguous recommendations, presented different options for management of the condition, and presented key recommendations in a way that is easily identifiable. The included guidelines26-28 provided advice or tools on how the recommendations can be put into practice and the potential resource implications of applying the recommendations have been considered. The NICE27 and RANZCP26 guidelines described facilitators and barriers to the application, but this was unclear for the DGPPN guideline.28 It was also unclear if any of the guidelines26-28 presented monitoring and/or auditing criteria. Regarding editorial independence, all guidelines26-28 were not clear nor did they provide an explicit statement that the funding body did not influence the content of the guideline. Moreover, while conflicts of interest for contributing authors were provided in the NICE27 and RANZCP26 guidelines, they were not clearly addressed in the DGPPN guideline.28 Given that guidelines were intended for use in the UK,27 Germany,28 Australia,26 and New Zealand,26 the recommendations may not be generalizable to Canadian settings.
Although the views and preferences of the target population, facilitators and barriers to the application, and competing interests were not mentioned in the abbreviated English version of the DGPPN guideline,28 it is possible these were addressed in the long version, published in German. For example, the DGPPN guideline was developed in full accordance with the AWMF Guidance Manual and Rules for Guideline Development,31 and this guidance advises that representatives of target users and patient target population should be included in the guideline development at an early stage. Thus, it is likely that the DGPPN followed this recommendation and included pertinent details about target user involvement in its long version of the guideline, published in German.31
Overall, the guidelines were clearly presented, were grounded in a generally comprehensive and transparently assessed evidence base, and appeared to provide unbiased recommendations on current clinical practice for clinical audiences. Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the detailed recommendations and supporting evidence that are relevant to the current report.
Diagnostic Accuracy of High-Sensitivity Troponin I Testing
No relevant evidence regarding high-sensitivity troponin I testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders was identified; therefore, no summary can be provided.
Guidelines
Clozapine Management Involving Testing and Assessment of Key Health Parameters
The NICE guideline27 provides a list of considerations for the rehabilitation service to examine during the initial physical comprehensive assessment (e.g., full blood count, drug levels where appropriate, ECG). An exhaustive list is provided in Table 4. This guideline also suggests that medicines should be reviewed regularly to manage complex psychosis and monitor effectiveness, adverse effects, and drug interactions, including monitoring for continence and constipation for those taking clozapine. Moreover, drug levels should be monitored to check adherence and guide dosing: at least annually and as needed for clozapine and mood-stabilizing anti-epileptic medicines. All of the NICE recommendations are derived from committee consensus based on evidence from the literature, expert opinions, and existing guidelines (the strength of this recommendation is not reported and unclear; the quality of the supporting evidence is not reported and unclear).27
The DGPPN guideline28 provides 3 recommendations regarding clozapine management with testing and assessment of health parameters. These recommendations are based on good clinical practice informed by clinical consensus (the strength of this recommendation is not reported and unclear; the quality of the supporting evidence is not reported and unclear). The DGPPN guideline28 recommends providing laboratory tests and recording an ECG before starting pharmacotherapy. This guideline also suggests the decision about the suitable antipsychotic drug and route of administration is made jointly by the service user and treating doctor and recommends considering and discussing a variety of health parameters. Moreover, the guideline recommends informing service users, family members, and close confidants, as well as carers, about the necessary monitoring tests, and recommends implementing the monitoring tests as part of the overall treatment plan. The full list of recommended tests is located in Table 9 of the DGPPN guideline.28
The RANZCP guideline26 suggests that clozapine monitoring protocols should be followed rigorously. This recommendation is based on level III-1 evidence from pseudo-RCT findings (the strength of this recommendation is not reported and unclear). This guideline also suggests that metabolic monitoring and interventions to manage the metabolic side effects of clozapine are essential. This recommendation is based on level II evidence from RCT findings (the strength of this recommendation is not reported and unclear).26
Clozapine Management in Patients with Co-Prescriptions and Adjunct Treatment
The NICE guideline27 provides 2 recommendations regarding clozapine management in patients with co-prescriptions. Both NICE recommendations are derived from committee consensus based on evidence from the literature, expert opinions, and existing guidelines (the strength of this recommendation is not reported and unclear; the quality of the supporting evidence is not reported and unclear).27 For people with complex psychosis whose symptoms have not responded adequately to an optimized dose of clozapine alone, NICE recommends augmenting clozapine with the following, depending on target symptoms: (1) an antipsychotic drug (e.g., aripiprazole for schizophrenia and related psychoses); (2) a mood stabilizer for psychosis with significant affective symptoms; and/or (3) an antidepressant if there are significant depressive symptoms in addition to the psychotic condition. NICE also recommends the following:
Only use multiple medicines, or doses above British National Formulary or summary of product characteristics limits, to treat complex psychosis: (i) if this is agreed and documented by the multidisciplinary team and the person (and their family, carer or advocate, as appropriate); (ii) as a limited therapeutic trial, returning to conventional dosages or monotherapy after 3 months, unless the clinical benefits of higher doses or combined therapy clearly outweigh the risks; (iii) if the medicines are being used to treat specific symptoms that are disabling or distressing; (iv) after taking into account drug interactions and side effects, for example be cautious when adding an antidepressant to clozapine for someone who has experienced symptoms of mania; (v) if systems and processes are in place for monitoring the person's response to treatment and side effects (monitoring may include physical examination, ECG and appropriate hematological tests) (p. 33).27
The DGPPN guideline28 provides various recommendations regarding clozapine management in patients with co-prescriptions. The guideline states treatment with olanzapine or risperidone may be suggested if clozapine is not tolerated. This recommendation is based on good clinical practice informed by clinical consensus (the strength of this recommendation is not reported and unclear; the quality of the supporting evidence is not reported and unclear). In case of drug treatment resistance, DGPPN suggests first offering treatment with an antipsychotic in monotherapy; this comes from level 1++ evidence (i.e., high-quality meta-analysis) and a grade A recommendation (i.e., highest grade). A combination of 2 antipsychotic drugs may be suggested, with monitoring of side effects and interactions, if adequate response is not achieved with monotherapy with 3 different antipsychotic drugs, including clozapine strategy (good clinical practice informed by clinical consensus; the strength of this recommendation is not reported and unclear; the quality of the supporting evidence is not reported and unclear). The DGPPN guideline recommends documenting this approach and, if there is still no treatment response, discontinuing this strategy (good clinical practice informed by clinical consensus; the strength of this recommendation is not reported and unclear; the quality of the supporting evidence is not reported and unclear). The DGPPN guideline recommends that the combination of IV or sublingual lorazepam and clozapine should be avoided.28 This recommendation is adapted from another guideline, based on 4 original studies, and classified as a grade B recommendation.28
The RANZCP guideline26 also provides 3 recommendations for this outcome. The RANZCP guideline26 advises the consideration of either of the following treatment options if positive symptoms persist despite an adequate trial of clozapine: continue clozapine and prescribe adjunctive medication; or reinstate the previous regimen that was most effective and well tolerated and prescribe adjunctive medication.26 This recommendation is based on level II evidence from RCT findings (the strength of this recommendation is not reported and unclear).26 The addition of ECT may be considered in people with treatment-resistant schizophrenia who have an inadequate response to clozapine. This is also based on level II evidence from RCT findings (the strength of this recommendation is not reported and unclear).26 Where clozapine monotherapy is ineffective, augmentation with other medicines or ECT can be considered (level III-1 evidence from pseudo-RCT findings; the strength of this recommendation is not reported and unclear).26
Management of Clozapine Dosing
The DGPPN guideline28 suggests reaching a serum level of clozapine of at least 350 ng/mL in case of treatment resistance as long as there are no tolerability issues (grade B recommendation based on level 2++ evidence [i.e., high-quality systematic reviews of case-control or cohort studies, and high-quality case-control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal]).28
The RANZCP guideline26 suggests 12.5 mg as the daily starting dose and 900 mg as the maximum recommended dose with the caveat that these doses may not be tolerated by some people. This recommendation is adapted from product information approved by “Australian Therapeutic Goods Administration, product information approved by Medsafe (the New Zealand Medicines and Medical Devices Safety Authority) and Therapeutic Guidelines – Psychotropic version 7 (Psychotropic Writing Group, 2013).” The strength of this recommendation is not reported and unclear.26
Limitations
The findings in this report are limited by the quantity of relevant evidence. No studies were identified that evaluated the diagnostic accuracy of high-sensitivity troponin I testing versus troponin T testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders; therefore, the diagnostic accuracy of high-sensitivity troponin I testing is unknown.
Three evidence-based guidelines26-28 were identified that included recommendations on the use of clozapine for patients with psychotic disorders; however, these guidelines did not provide specific recommendations for monitoring clozapine-induced cardiomyopathy or clozapine-induced myocarditis (e.g., physical symptoms to identify, type and magnitude of vital sign changes). This report identified 1 strong recommendation based on high-quality evidence, with several other recommendations that were based on sources of evidence that may not be considered highest quality, with the strength of recommendation not reported and unclear. The included guidelines were specific to the UK,27 Germany,28 Australia,26 and New Zealand;26 therefore, it is unclear whether the results summarized in this report are generalizable to Canada.
These limitations warrant the use of caution when interpreting the findings of this report.
Conclusions and Implications for Decision or Policy-Making
This rapid review is an upgrade of a 2021 CADTH report24 that provided a reference list of relevant studies on the topic identified from the literature. This report identified 3 evidence-based guidelines published since 2016 that captured current recommendations regarding the use of clozapine for patients with psychotic disorders.26-28 The included guidelines were generally well developed and clearly presented.26-28 No relevant studies were identified regarding diagnostic accuracy of high-sensitivity troponin I testing versus troponin T testing for detecting myocarditis or cardiomyopathy in patients receiving clozapine for psychotic disorders.
The 3 included guidelines provide recommendations for testing and assessment of key health parameters for patients who are prescribed clozapine.26-28 Two guidelines27,28 describe which assessments should be considered before initiating pharmacotherapy, including clozapine. These recommendations are based on evidence from the literature, expert opinions, and existing guidelines27 and good clinical practice informed by clinical consensus.28 Three guidelines highlight the importance of rigorously following clozapine monitoring protocols; monitoring medicines and drug levels; checking adherence; guiding dosing; monitoring effectiveness, adverse effects, and drug interactions (recommendations from level II [i.e., RCT] and III-1 [i.e., pseudo-RCT] evidence as well as committee consensus on evidence from the literature, expert opinions, and existing guidelines).26-28 Together, this guidance provides key information on which tests and assessments should be considered for monitoring the potential side effects of clozapine.
The 3 guidelines also provide recommendations of co-prescription and adjunct treatment for patients who have not responded adequately to an optimized dose of clozapine alone.26-28 Derived from varying levels of evidence, the guidelines recommend continuing clozapine and prescribing adjunctive medication, with the type dependent on target symptoms (e.g., antipsychotic, mood stabilizer, antidepressant);26-28 reinstating the previous regimen that was most effective and well tolerated and prescribing adjunctive medication26; and/or augmenting with ECT.26
Two guidelines provide recommendations about clozapine dosing. One guideline suggests 12.5 mg as the daily starting dose and 900 mg as the maximum recommended dose with an important caveat that these doses may not be tolerated by individuals.26 Based on level 2++ evidence (i.e., highest quality), 1 guideline suggests reaching a serum level of clozapine of at least 350 ng/mL in case of treatment resistance if there are no tolerability issues.28
Overall, the recommendations put forward by these different guideline groups were consistent; however, several of the recommendations were derived from sources of evidence that may not be considered highest quality, with the strength of recommendation not reported and unclear. Given that the guidelines were produced by guideline groups in other countries, it is unclear whether the recommendations summarized in this report are generalizable to Canada. New primary research on the diagnostic accuracy of high-sensitivity troponin I testing for detecting myocarditis or cardiomyopathy may further inform the research questions addressed in this report.
References
1.Mental illness in Canada. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/mental-illness-canada-infographic/mental-illness-canada-infographic.pdf. Accessed 2022 May 4.
2.Schizophrenia in Canada. Ottawa (ON): Public Health Agency of Canada; 2020: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/schizophrenia-canada/schizophrenia-canada-en.pdf. Accessed 2022 May 9.
3.National Health Services. Treatment - psychosis. 2019; https://www.nhs.uk/mental-health/conditions/psychosis/treatment/. Accessed 2022 May 9.
4.Chien WT, Yip AL. Current approaches to treatments for schizophrenia spectrum disorders, part I: an overview and medical treatments. Neuropsychiatr Dis Treat. 2013;9:1311-1332. PubMed
5.Shah N, Grover S, Rao GP. Clinical practice guidelines for management of bipolar disorder. Indian J Psychiatry. 2017;59(Suppl 1):S51-s66. PubMed
6.Sandoz clozapine (clozapine): 25 mg and 100 mg tablets [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2018 Aug 17: https://www.sandoz.ca/sites/www.sandoz.ca/files/Sandoz%20Clozapine%20Product%20Monograph.pdf. Accessed 2022 May 16.
7.National Alliance on Mental Ilness. Clozapine (Clozaril and FazaClo). 2020; https://www.nami.org/About-Mental-Illness/Treatments/Mental-Health-Medications/Types-of-Medication/Clozapine-(Clozaril-and-FazaClo)#:~:text=Clozapine%20is%20a%20medication%20that,thinking%2C%20mood%2C%20and%20behavior. Accessed 2022 May 9.
8.Tuunainen A, Wahlbeck K, Gilbody SM. Newer atypical antipsychotic medication versus clozapine for schizophrenia. Cochrane Database Syst Rev. 2000(2):Cd000966. PubMed
9.Siskind D, McCartney L, Goldschlager R, Kisely S. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 2016;209(5):385-392. PubMed
10.Haas SJ, Hill R, Krum H, et al. Clozapine-associated myocarditis: a review of 116 cases of suspected myocarditis associated with the use of clozapine in Australia during 1993-2003. Drug Saf. 2007;30(1):47-57. PubMed
11.Alawami M, Wasywich C, Cicovic A, Kenedi C. A systematic review of clozapine induced cardiomyopathy. Int J Cardiol. 2014;176(2):315-320. PubMed
12.Farooq S, Choudry A, Cohen D, Naeem F, Ayub M. Barriers to using clozapine in treatment-resistant schizophrenia: systematic review. BJPsych Bull. 2019;43(1):8-16. PubMed
13.Treatment-resistant schizophrenia in Canada: prevalence, impact, and treatment recommendations. Vaughan (ON): AA Pharma Inc.; 2017: https://www.aaspire.ca/resources/HealthCareProfessional/English/17-AA004_AAC0080E_Unbranded%20TRS%20brochure%2017163_EN_Print_Layout_V9_LR_Client-Friendly.pdf. Accessed 2022 May 16.
14.Knoph KN, Morgan RJ, Palmer BA, et al. Clozapine-induced cardiomyopathy and myocarditis monitoring: a systematic review. Schizophr Res. 2018;199:17-30. PubMed
15.Centers for Disease Control and Prevention. Cardiomyopathy. 2019; https://www.cdc.gov/heartdisease/cardiomyopathy.htm. Accessed 2022 May 9.
16.Mayo Clinic. Cardiomyopathy. 2022; https://www.mayoclinic.org/diseases-conditions/cardiomyopathy/symptoms-causes/syc-20370709. Accessed 2022 May 10.
17.Reinders J, Parsonage W, Lange D, Potter JM, Plever S. Clozapine-related myocarditis and cardiomyopathy in an Australian metropolitan psychiatric service. Aust N Z J Psychiatry. 2004;38(11-12):915-922. PubMed
18.Higgins JM, San C, Lagnado G, Chua D, Mihic T. Incidence and management of clozapine-induced myocarditis in a large tertiary hospital. Can J Psychiatry. 2019;64(8):561-567. PubMed
19.Youssef DL, Narayanan P, Gill N. Incidence and risk factors for clozapine-induced myocarditis and cardiomyopathy at a regional mental health service in Australia. Australas Psychiatry. 2016;24(2):176-180. PubMed
20.Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34(33):2636-2648, 2648a-2648d.
21.Sandoval Y, Smith SW, Apple FS. Present and future of cardiac troponin in clinical practice: a paradigm shift to high-sensitivity assays. Am J Med. 2016;129(4):354-365. PubMed
22.deFilippi CR, Tocchi M, Parmar RJ, et al. Cardiac troponin T in chest pain unit patients without ischemic electrocardiographic changes: angiographic correlates and long-term clinical outcomes. J Am Coll Cardiol. 2000;35(7):1827-1834. PubMed
23.Sandoval Y, Jaffe AS. Using high-sensitivity cardiac troponin T for acute cardiac care. Am J Med. 2017;130(12):1358-1365.e1351. PubMed
24.Monitoring patients with psychotic disorders for clozapine-induced myocarditis or cardiomyopathy. Ottawa (ON): CADTH; 2021: https://www.cadth.ca/monitoring-patients-psychotic-disorders-clozapine-induced-myocarditis-or-cardiomyopathy. Accessed 2022 May 9.
25.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 May 16.
26.Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders. Aust N Z J Psychiatry. 2016;50(5):1-117. https://www.ranzcp.org/files/resources/college_statements/clinician/cpg/schizophrenia-disorders-cpg.aspx. Accessed 2022 April 27. PubMed
27.National Institute for Heatlh and Care Excellence. Rehabilitation for adults with complex psychosis (NICE guideline NG181). 2020: https://www.nice.org.uk/guidance/ng181. Accessed 2022 May 13.
28.DGPPN e.V. (ed.) for the Guideline Group. S3 guideline for schizophrenia. Abbreviated version (English). Version 1.0 ed. Berlin (DE): German Association for Psychiatry, Psychotherapy and Psychosomatics, DGPPN; 2019: https://www.dgppn.de/_Resources/Persistent/b794e84f9cbdf0d761b26cb1bd323b65188cb9e6/038-009e_S3_Schizophrenie_2019-03.pdf. Accessed 2022 April 27.
29.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
30.Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of schizophrenia and related disorders. Aust N Z J Psychiatry. 2005;39(1-2):1-30. PubMed
31.Muche-Borowski C, Selbmann HK, Nothacker M, Müller W, Kopp I. AWMF guidance manual and rules for guideline development. 1st ed. Frankfurt (DE): German Association of the Scientific Medical Societies (AWMF) - Standing Guidelines Commission; 2012: https://www.awmf.org/fileadmin/user_upload/Leitlinien/AWMF-Regelwerk/AWMF-Guidance_2013.pdf. Accessed 2022 May 3.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and | Guideline validation |
|---|---|---|---|---|---|---|
NICE, 202027 | ||||||
Intended Users: Health care professionals, social care practitioners and other practitioners providing public services for people with complex psychosis; commissioners and providers of mental health services; people using mental health services, their families, and carers. Target Population: Adults with complex psychosis (i.e., primary diagnosis of a psychotic illness with severe and treatment-resistant symptoms of psychosis and functional impairment). | Guideline covers mental health rehabilitation for adults with complex psychosis. Relevant intervention: Clozapine for people with complex psychosis. | Evidence about rates of physical and mental health conditions and substance misuse in this population, evidence about augmenting clozapine with a co-prescription, another NICE guideline, and the committee’s experience and knowledge. | Evidence collected and selected from a systematic literature review. | GRADE | Recommendations were drafted based on the committee’s interpretation of the available evidence, taking into account the trade-off between the benefits and harms, costs or implications compared with the economic benefits, current practices, recommendations made in other relevant guidelines, people’s preferences and equality issues. When evidence was of poor quality, conflicting, or absent, the committee drafted recommendations based on expert opinion. | Stakeholder review of the draft guideline through a 6-week public consultation and feedback process. All comments received from registered key stakeholders were responded to in writing and posted on the NICE website. |
DGPPN, 201928 | ||||||
Intended Users: Practitioners who treat people with schizophrenia. Target Population: People with schizophrenia. | Guideline covers the diagnosis, treatment, rehabilitation, and care of people with schizophrenia. Relevant intervention: Clozapine for people with schizophrenia. | Evidence about drug treatment resistance comparing combination treatment with monotherapy, other guidelines (e.g., NICE, AWMF) and studies, lower value of therapeutic reference range for clozapine, and clinical consensus. | Evidence collected and selected from a systematic literature review with critical appraisal of the literature and assignment of the quality of evidence. | SIGN | Evidence- and consensus-based guideline (i.e., with a representative committee, systematic review and synthesis of the evidence, and structured consensus development), classified as a level S3 guideline (i.e., the highest quality level for guidance development in Germany). Developed in full accordance with the AWMF Guidance Manual and Rules for Guideline Development.31 | For the revision process, the DGPPN group involved experts within topic-specific, module working groups to update and expand the guideline texts. |
RANZCP, 201626 | ||||||
Intended Users: Psychiatrists, psychiatry trainees, resident medical officers, and hospital interns in psychiatry. It may also be useful to general practitioners, mental health nurses, other clinicians who work with people with schizophrenia and related psychoses, and policy-makers. Target Population: People with schizophrenia and related disorders. | Guideline covers clinical management of schizophrenia and related disorders. Relevant intervention: Clozapine for people with schizophrenia and related disorders. | Evidence about adverse events, metabolic and adverse event monitoring, prescriptions to reduce adverse events related to taking clozapine, augmenting clozapine with a co-prescription, ECT or switching to another agent, and efficacy and safety of different doses of clozapine. | RANZCP group drafted guidelines with reference to existing systematic reviews, informal literature reviews, and relevant international clinical practice guidelines. | For intervention studies, NHMRC levels of evidence. | Evidence-based recommendations were formulated when the guideline group judged that there was sufficient evidence on a topic. Where evidence was weak or lacking, consensus-based recommendations were formulated by a group of experts. | RANZCP invited review by its committees and members, an expert advisory committee, and key stakeholders (e.g., professional bodies, special interest groups). |
AWMF = Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (English translation: Working Group of Scientific Medical Societies); DGPPN = Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (English translation: German Association for Psychiatry, Psychotherapy and Psychosomatics); GRADE = Grading of Recommendations Assessment, Development and Evaluation; NHMRC = National Health and Medical Research Council ; NICE = National Institute for Health and Care Excellence; RANZCP = Royal Australian and New Zealand College of Psychiatrists; SIGN = Scottish Intercollegiate Guidelines Network; WG = working group.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II25
Item | NICE, 202027 | DGPPN, 201928 | RANZCP, 201626 |
|---|---|---|---|
Domain 1: Scope and Purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | Yes | Unclear | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes |
Domain 3: Rigour of Development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | No |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes | No |
Domain 4: Clarity of Presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | Yes | Unclear | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Unclear | Unclear | Unclear |
Domain 6: Editorial Independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Unclear | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; AWMF = Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (English translation: Working Group of Scientific Medical Societies); DGPPN = Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (English translation: German Association for Psychiatry, Psychotherapy and Psychosomatics); NICE = National Institute for Health and Care Excellence; RANZCP = Royal Australian and New Zealand College of Psychiatrists.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
NICE, 202027 | |
Management of clozapine involving testing and assessment of key health parameters Recommendation 1: “The initial physical health check in the comprehensive assessment by the rehabilitation service should include: body mass index; waist circumference; full blood count; pulse and blood pressure; glycosylated hemoglobin (HbA1c), blood lipid profile, liver function tests, renal function tests and thyroid function; prolactin levels (for people on medicines that raise prolactin levels); renal function tests and calcium levels (for people on lithium); drug levels where appropriate, for example mood stabilizing or anti-epileptic medicines, lithium and clozapine; …ECG; smoking, alcohol and illicit substance use; nutritional status, diet and level of physical activity; continence and constipation (particularly if the person is on clozapine); any movement disorders; sexual health; vision, hearing and podiatry; oral inspection of general dental health; any difficulties with swallowing (p. 24-5).”27 Evidence for Recommendation 1: “The committee used evidence about rates of physical and mental health conditions and substance misuse in this population to recommend what to consider as part of the initial assessment when people enter the rehabilitation service. The committee also drew on their experience to provide details about what a structured comprehensive biopsychosocial needs assessment should cover to assess people's complex needs and comorbidities. The committee agreed that baseline investigations before starting antipsychotic medicines recommended in the NICE guidelines on psychosis and schizophrenia in adults and bipolar disorder should form the core of the initial physical health check for people in rehabilitation services because most would be receiving antipsychotic medicines. The committee also drew on the evidence identifying the most common physical and mental health comorbidities to highlight conditions that staff need to be alert for because these may contribute to higher mortality or complexity in rehabilitation in this population. The committee also agreed that more understanding is needed about the likely impact of physical comorbidities on mortality among people with complex psychosis, so they made a research recommendation on coexisting physical health conditions (p.63 to 4).”27 Recommendation 2: “Regularly review medicines used to manage complex psychosis and monitor effectiveness, adverse effects and drug interactions, including monitoring for constipation for those taking clozapine. Follow recommendations in the NICE guidelines on medicines optimization and multimorbidity (p.33-4).”27 Evidence for Recommendation 2: “The committee made recommendations on dosing and interactions with other substances based on their experience and knowledge about the safety of various therapeutic options (p. 69).”27 Recommendation 3: “Monitor drug levels to check adherence and guide dosing: At least annually and as needed for clozapine and mood stabilizing anti-epileptic medicines (p. 34).”27 Evidence for Recommendation 3: “The committee agreed it was important to measure drug levels regularly to assess adherence and guide dosing. There was a lack of evidence on how frequently this should be done, so the committee used their own knowledge and experience, as well as drawing on NICE's guideline on bipolar disorder for monitoring of people taking lithium (p.69).”27 | Recommendations are derived from committee consensus based on evidence from the literature, expert opinions, and existing guidelines (strength of recommendation: NR and unclear; quality of supporting evidence: NR and unclear). |
Management of clozapine in patients with co-prescriptions and adjunct treatment Recommendation 4: “For people with complex psychosis whose symptoms have not responded adequately to an optimized dose of clozapine alone, consider augmenting clozapine with the following, depending on target symptoms:
Evidence for Recommendation 4: “There was some evidence from RCTs supporting augmentation with the agents in recommendation 1.9.9 [recommendation 2] for reducing psychosis symptoms in people with schizophrenia refractory to clozapine. The evidence was limited by small sample sizes and information on adverse events was very sparse. However, given the lack of treatment options, and considering that current prescribing for this population is inconsistent, the committee decided that augmentation should be considered an option (p.68).”27 Recommendation 5: “Only use multiple medicines, or doses above BNF or summary of product characteristics limits, to treat complex psychosis:
Evidence for Recommendation 5: “The committee made recommendations on dosing and interactions with other substances based on their experience and knowledge about the safety of various therapeutic options. They recommended therapeutic plasma levels because this may be useful in checking nonadherence or to confirm toxicity or pharmacokinetic drug interactions…The committee also agreed it was important to monitor the effects of specific medicines. However, again there was no evidence on how frequently to do this…The committee also wanted to highlight the importance of ECG monitoring. Antipsychotic medicines can cause cardiac abnormalities, for example lengthened QT interval on electrocardiography. Although the NICE guidelines on psychosis and schizophrenia in adults and bipolar disorder recommend ECGs only when starting antipsychotic medicines, the committee recommended considering ECGs annually (and more frequently for people with complex antipsychotic regimens or doses above BNF levels). They agreed this consideration was warranted for this population, many of whom have been on medicines long term, or combinations of medicines that may alter cardiac rhythm, or both. It is already common practice to perform ECGs if exceeding BNF limits for antipsychotics (p.69).”27 | Recommendations are derived from committee consensus based on evidence from the literature, expert opinions, and existing guidelines (strength of recommendation: NR and unclear; quality of supporting evidence: NR and unclear). |
DGPPN, 201928 | |
Management of clozapine involving testing and assessment of key health parameters Recommendations 1 to 3 below draw from Table 9 (p.40) in the DGPPN guideline. Refer to the original guideline for additional details pertaining to these recommendations. Recommendation 1: “Before starting pharmacotherapy, we recommend performing laboratory tests, as shown in Table 9, and recording an ECG. We recommend ruling out pregnancy in women of child-bearing age (p.24).”28 Evidence for Recommendation 1: Unclear Recommendation 2: “We recommend that the decision about the suitable antipsychotic and route of administration is made jointly by the service user and treating doctor. We recommend considering and discussing the following:
We recommend continually reviewing the risk-benefit assessment in the course of treatment and taking appropriate measures if there are any changes (p.24).”28 Evidence for Recommendation 2: Adapted and revised from the AWMF guideline ‘Schizophrenia’ 2006 (in German) and the NICE guideline ‘Psychosis and schizophrenia in adults 2014.’ Recommendation 3: “We recommend informing service users, family members and close confidants, as well as carers, about the necessary monitoring tests* (see Table 9), and we recommend implementing the monitoring tests as part of the overall treatment plan. *The legal regulations regarding confidentiality must hereby be observed (p.39).”28 Evidence for Recommendation 3: Unclear | Recommendations 1 to 3 are based on GCP informed by clinical consensus (strength of recommendation: NR and unclear; quality of supporting evidence: NR and unclear) |
Management of clozapine in patients with co-prescriptions and adjunct treatment Recommendation 4: “If clozapine is not tolerated, treatment with olanzapine or risperidone* may be suggested (p.35).”28 Evidence for Recommendation 4: “This recommendation is not based on a systematic search, but on a clinical consensus. *Important literature can be found in the background text (in German). The findings on risperidone were not as consistent as those for olanzapine (p.35).”28 Recommendation 5: “In case of drug treatment resistance, we recommend first offering treatment with an antipsychotic in monotherapy [5a]. A combination of two antipsychotics may be suggested, with monitoring of side effects and interactions, if adequate response is not achieved with monotherapy with three different antipsychotics, including clozapine [5b]). We recommend documenting this approach and, if there is still no treatment response, discontinuing this strategy[5c] (p.36).”28 Evidence for Recommendation 5: [5a] “evidence was derived from the “finding that the cited meta-analysis was unable to show additional value for the combination treatment compared with monotherapy if only methodologically high-quality studies were included. Most of the studies evaluated in this meta-analysis included people with drug treatment resistance, although the definition was not standardized across the studies ([5b-c], p.36).”28 Recommendation 6: “In case of comparable efficacy of lorazepam and antipsychotics in the acute treatment of aggression and psychomotor arousal, we suggest offering lorazepam* because of its more favourable side-effect profile. *The combination of intravenous or sublingual lorazepam and clozapine should be avoided (p.54).”28 Evidence for Recommendation 6 Adapted from another guideline, based on four original studies. | Recommendations 4 and 5b-c are based on GCP informed by clinical consensus (strength of recommendation: NR and unclear; quality of supporting evidence: NR and unclear). Recommendation 5a is based on level 1++ evidence (i.e., high-quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias), indicating a strong recommendation based on high-quality evidence. The level of evidence for recommendation 6 is not explicit (i.e., guideline developers mentioned evidence used was adapted from another guideline, based on four original studies). Recommendation 6 is a grade B recommendation. |
Management of clozapine dosing Recommendation 7: “In case of treatment resistance, we suggest reaching a serum level of clozapine of at least 350 ng/mL, as long as there are no tolerability issues (p. 25).”28 Evidence for Recommendation 7: Based on 5 studies and on the lower value of the therapeutic reference range for clozapine (source unknown). | Recommendation 7 is based on level 2++ evidence (i.e., high-quality systematic reviews of case-control or cohort studies; high-quality case-control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is causal) and is a grade B recommendation. |
RANZCP, 201626 | |
Management of clozapine involving testing and assessment of key health parameters Recommendation 1: “Clozapine monitoring protocols should be followed rigorously. (p.37)”26 Evidence for Recommendation 1: “Mandated blood monitoring (weekly for the first 18 weeks, every 4 weeks thereafter) means that blood dyscrasia is likely to be detected, but cardiomyopathy and myocarditis are also potentially dangerous side effects. There is little evidence that the cardiac adverse events can be predicted, but baseline ECG and troponin are advisable. Regular ECGs do not have a strong evidence base and it has been suggested that they be undertaken only if clinically indicated (Murch et al., 2013; Ronaldson et al., 2011, p.38).”26 Evidence for Recommendation 2: “Metabolic monitoring and interventions to manage the metabolic side effects of clozapine are essential (p.37).”26 Evidence for Recommendation 2: “Metabolic monitoring and advice about diet and exercise are essential. There is some evidence to support the use of metformin (500 mg bd) to minimize weight gain and insulin resistance for people taking clozapine (Chen et al., 2013). It is essential that the prescribing doctor is familiar with the unique profile of clozapine and can manage other less common side effects. If a person taking clozapine has a neutrophil count in the amber range, the addition of a low dose of lithium may be useful to protect against clozapine-induced neutropenia and maintain the person on clozapine (Paton and Esop, 2005, p.38).”26 | Recommendation 1 is based on level III-1 evidence from pseudo-RCT findings (strength of recommendation: NR and unclear). Recommendation 2 is based on level II evidence from RCT findings (strength of recommendation: NR and unclear). |
Management of clozapine in patients with co-prescriptions and adjunct treatment Recommendation 3 on the management of acute relapse: “If positive symptoms persist despite an adequate trial of clozapine, consider either of the following treatment options:
Evidence for Recommendation 3: Unclear Recommendation 4: “The addition of ECT may be considered in people with treatment-resistant schizophrenia who have an inadequate response to clozapine (p.49).”26 Evidence for Recommendation 4: “The combination of ECT with clozapine may be of particular benefit for people who have an inadequate response to clozapine alone (Havaki-Kontaxaki et al., 2006; Petrides et al.,2015, p.48).”26 Recommendation 5: “Where clozapine monotherapy is ineffective, augmentation with other medicines or electro-convulsive therapy can be considered (p.37).”26 Evidence for Recommendation 5: “It can take up to 12 months to see the full benefits of clozapine. If clozapine is ineffective, the choice is whether to augment clozapine with another drug or ECT, or switch to another agent. If there has been absolutely no response and/or side effects are severe, a switch is suggested. Care needs to be taken in down-titration. If clozapine has had some – even modest – benefit, augmentation is justifiable, although the evidence for this strategy is equivocal. On an individual level, the addition of a high affinity dopamine D2 blocking agent such as risperidone or amisulpride to clozapine can be effective for residual positive symptoms. The addition of aripiprazole to clozapine can effect significant weight reduction and improvement in metabolic parameters. Antidepressants and mood stabilizers cannot be recommended as adjuncts in the absence of mood or anxiety symptoms. N-acetyl cysteine (Berk et al., 2008) and ethyl-eicosapentaoic acid (EPA) (fish oil) (Porcelli et al., 2012) are undergoing evaluation as clozapine augmenters. ECT has a limited place in the management of people with treatment-resistant schizophrenia…, including those on clozapine (Petrides et al., 2015; Tharyan and Adams, 2005). Combination of antipsychotic agents. The concurrent use of two or more antipsychotics for people with treatment-resistant or refractory schizophrenia is common practice, despite limited evidence to support this practice. Compared with antipsychotic monotherapy, combined antipsychotic treatment has been associated with an increased side effect burden, high-dose prescribing, increased hospitalization rates and length of stay, higher treatment costs and increased mortality (Gallego et al., 2012). Switching from polypharmacy back to monotherapy is possible, and strategies to reduce polypharmacy by educating clinicians to change their prescribing behaviour have had some success (Tani et al., 2013, p.38).”26 | Recommendations 3 and 4 are based on level II evidence from RCT findings (strength of recommendation: NR and unclear). Recommendation 5 is based on level III-1 evidence from pseudo-RCT findings (strength of recommendation: NR and unclear). |
Management of clozapine dosing Recommendation 6:
Evidence for Recommendation 6: “Higher doses than those usually recommended may sometimes be required, but there is a lack of research about efficacy and safety. Higher doses should be used cautiously, and careful monitoring of safety and tolerability is essential. Clozapine should be considered when there is a poor response or significant side effects (p.33).”26 | Recommendation 6 is based on evidence adapted from product information approved by Australian Therapeutic Goods Administration, product information approved by Medsafe (the New Zealand Medicines and Medical Devices Safety Authority) and Therapeutic Guidelines – Psychotropic version 7 (Psychotropic Writing Group, 2013). The strength of this recommendation is NR and unclear. |
AWMF = ; BNF = British National Formulary; DGPPN = Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (English translation: German Association for Psychiatry, Psychotherapy and Psychosomatics); ECG = electrocardiogram; ECT = electroconvulsive therapy; GCP = Good Clinical Practice; NICE = National Institute for Health and Care Excellence; NR = not reported; RANZCP = Royal Australian and New Zealand College of Psychiatrists; RCT = randomized controlled trial.
Note that this table has not been copy-edited.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Clozapine initiation for schizophrenia: a review of clinical effectiveness and guidelines (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020. https://cadth.ca/clozapine-initiation-schizophrenia-review-clinical-effectiveness-and-guidelines. Accessed 2022 May 13.
Combination atypical antipsychotics in adolescents or adults with schizophrenia: a review of clinical and cost-effectiveness and guidelines (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2016. https://www.cadth.ca/sites/default/files/pdf/htis/2016/RC0805%20Combinations%20of%20Atypical%20Antipsychotics%20in%20Schizophrenia%20Final.pdf
Antipsychotics for pediatric patients: a review of the clinical effectiveness, safety, and guidelines (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2016. https://pubmed.ncbi.nlm.nih.gov/27077159/. Accessed 2022 May 13.
Guidance Documents With Unclear Methodology
MOH protocols for the management of patients with schizophrenia and bipolar affective disorder. Riyadh (SA): Saudi Arabia Ministry of Health; 2021. https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/SCHIZOPHRENIA-BIPOLAR-Affective-Disorder.pdf. Accessed 2022 May 13.
Clozapine treatment guidelines. London (GB): Camden and Islington NHS Foundation Trust; 2021. https://www.candi.nhs.uk/sites/default/files/Clozapine%20Treatment%20guidelines%20_PHA06_August%202021.pdf. Accessed 2022 May 13.
Clozapine management clinical guideline. Adelaide (AU): Government of South Australia; 2017. https://www.sahealth.sa.gov.au/wps/wcm/connect/059961804298b3078c77be80c298878e/1Clozapine+Management+Clinical+Guideline_13092017%5B1%5D.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-059961804298b3078c77be80c298878e-nPyR6Ln. Accessed 2022 May 13.
Queensland Psychotropic Medication Advisory Committee. Safe and quality use of clozapine in mental health alcohol and other drugs (MHAOD) services. Brisbane Queensland (AU): the State of Queensland (Queensland Health); 2021. https://www.health.qld.gov.au/__data/assets/pdf_file/0025/625354/qh-gdl-437.pdf. Accessed 2022 May 13.
Additional References
Griffin JM, Woznica E, Gilotra NA, Nucifora FC, Jr. Clozapine-associated myocarditis: a protocol for monitoring upon clozapine initiation and recommendations for how to conduct a clozapine rechallenge. J Clin Psychopharmacol. 2021;41(2):180-185. PubMed
Richardson N, Greenway SC, Bousman CA. Clozapine-induced myocarditis and patient outcomes after drug rechallenge following myocarditis: a systematic case review. Psychiatry Res. 2021 Nov 1;305:114247. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca