CADTH Health Technology Review
Dexamethasone Intravitreal Implant for the Treatment of Macular Edema Following Retinal Detachment Surgery
Rapid Review
Authors: Gabrielle Brankston, Melissa Walter
Abbreviations
BCVA
best corrected visual acuity
CMT
central macular thickness
CRT
central retinal thickness
DEX
dexamethasone
logMAR
logarithm of the minimum angle of resolution
ME
macular edema
RD
retinal detachment
RRD
rhegmatogenous retinal detachment
SR
systematic review
Key Messages
Evidence from 1 systematic review and 2 observational studies suggests that dexamethasone intravitreal implant is associated with improvement in macular edema secondary to retinal detachment surgery.
The evidence primarily came from low- to moderate-quality studies.
It is challenging to draw definitive conclusions about the effectiveness of this intervention because of the paucity of data, the lack of controlled clinical studies, and the retrospective nature of the current literature.
No evidence was identified on the cost-effectiveness of dexamethasone intravitreal implant for the treatment of macular edema secondary to retinal detachment surgery.
Context and Policy Issues
Surgical procedures for retinal detachment (RD), including scleral buckling, pneumatic retinopexy, and pars plana vitrectomy, can be complicated by postoperative macular edema (ME), an important cause of postoperative visual impairment.1-3 Postoperative ME can occur in 6% to 47% of patients who have undergone a surgical procedure for RD.1-4 The etiology of this complication likely involves an inflammatory process triggered by the surgery.5 Conventional treatments for postoperative ME include topical nonsteroidal anti-inflammatory drugs, topical steroids, and intravitreal triamcinolone acetonide, which have shown variable results.5
A dexamethasone (DEX) intravitreal implant (Ozurdex; Allergan Inc, Irvine, CA) delivers sustained-release corticosteroid medication over several months.6 The DEX implant has been approved by Health Canada for the treatment of ME following central retinal vein occlusion, the treatment of non-infectious posterior uveitis, and for the treatment of adult patients with diabetic macular edema who are pseudophakic.7 Efficacy of the DEX implant has also been demonstrated in cases of ME after cataract surgery,8 epiretinal membrane peeling,9,10 radiation maculopathy,11 and retinitis pigmentosa.12 However, Ozurdex does not currently have a Health Canada–approved indication for ME following RD surgery.
Previous CADTH reimbursement reviews have summarized the evidence for the use of DEX implant for the treatment of ME following central retinal vein occlusion13 and the treatment of adult patients with diabetic ME who are pseudophakic.7 Also, 1 CADTH Rapid Response report examined clinical effectiveness of DEX implants for patients with uveitis.14 Each of the reviews reported limited direct evidence of clinical effectiveness, uncertainty about the duration of treatment effect, and uncertainty about the cost-effectiveness of DEX implant compared with sham or other medications.7,13,14
The clinical effectiveness and recommendation of DEX implant for ME after RD surgery are unclear. However, the effectiveness of the treatment for ME of other etiologies provides some optimism that a DEX implant might be effective for that indication. The objective of this report is to summarize the evidence regarding the clinical effectiveness and cost-effectiveness of DEX implant for the treatment of ME following RD surgery. If available, evidence-based clinical practice guidelines will also be summarized.
Research Questions
What is the clinical effectiveness of dexamethasone intravitreal implant versus no treatment or placebo for the treatment of macular edema following retinal detachment surgery?
What is the clinical effectiveness of dexamethasone intravitreal implant versus alternative interventions for the treatment of macular edema following retinal detachment surgery?
What is the cost-effectiveness of dexamethasone intravitreal implant versus no treatment or placebo for the treatment of macular edema following retinal detachment surgery?
What is the cost-effectiveness of dexamethasone intravitreal implant versus alternative interventions for the treatment of macular edema following retinal detachment surgery?
What are the evidence-based guidelines regarding dexamethasone intravitreal implant for the treatment of macular edema following retinal detachment surgery?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were dexamethasone intravitreal implant and retinal detachment surgery. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded. The search was completed on March 30, 2022, and was limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Single-arm, pretest-posttest studies were considered for inclusion.
Criteria | Description |
|---|---|
Population | Adults with macular edema following retinal detachment surgery |
Intervention | Dexamethasone intravitreal implant (e.g., Ozurdex) |
Comparator | Q1 and Q3: No treatment, placebo Q2 and Q4: Laser photocoagulation therapy, triamcinolone acetonide, anti-VEGF drugs (e.g., bevacizumab, ranibizumab, aflibercept) Q5: Not applicable |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., best corrected visual acuity, intraocular pressure, central foveal thickness, safety [e.g., adverse events, vision loss]) Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios) Q5: Recommendations regarding the use of dexamethasone intravitreal implant for the treatment of macular edema following retinal detachment surgery |
Study designs | Health technology assessments, systematic reviews, randomized-controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
VEGF = vascular endothelial growth factor.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017. Primary studies retrieved by the search were excluded if they were captured in the included systematic review.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)15 for the systematic review and the Downs and Black checklist16 for the non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
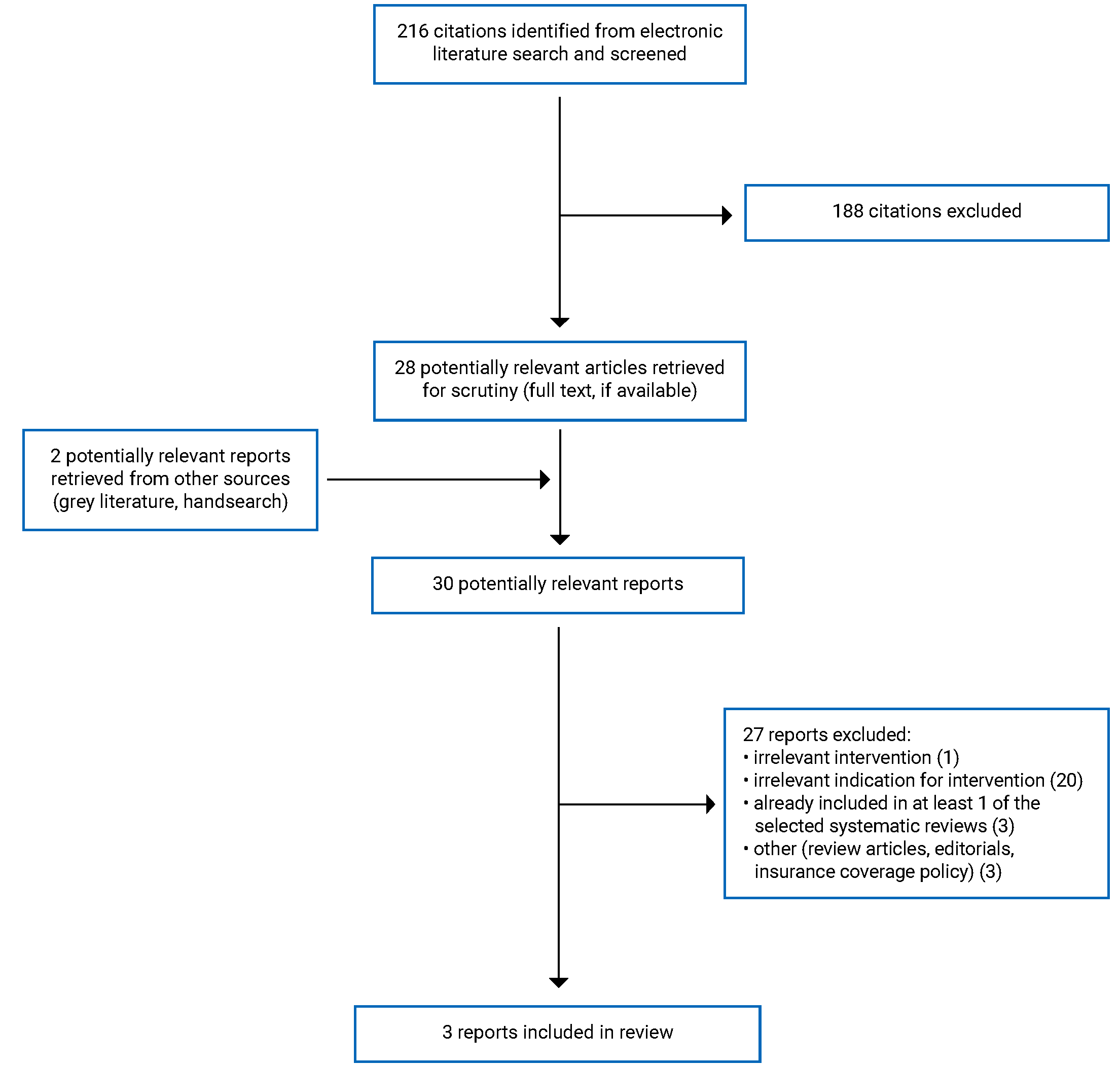
A total of 216 citations were identified in the literature search. Following screening of titles and abstracts, 188 citations were excluded and 28 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of the 30 potentially relevant articles, 27 publications were excluded for various reasons, and 3 publications met the inclusion criteria and were included in this report. These comprised 1 systematic review (SR) and 2 observational (uncontrolled retrospective before-and-after) studies. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)17 flow chart of the study selection is presented in Appendix 1.
Additional references of potential interest are provided in Appendix 5. These references are studies or SRs that do not appear to focus solely on the indication of interest but may provide information about the efficacy or safety of intravitreal DEX implant for the treatment of other indications in the population of interest.
Summary of Study Characteristics
Details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Three relevant reports were identified comprising 1 SR18 and 2 observational studies.19,20
The SR18 had broader inclusion criteria than this review. Specifically, the authors evaluated the clinical effectiveness of a DEX implant for ME secondary to surgery for RD or epiretinal membrane. However, only 3 of the included studies in the SR evaluated the treatment for the indication of interest for this report and data were analyzed by indication.18 Therefore, only the characteristics and results of this subset of relevant studies will be described in this report. The authors did not report the date range covered by the literature search.
The SR18 included 3 retrospective uncontrolled studies of patients with ME secondary to RD surgery who were assessed at baseline and at various follow-up periods using a single-arm, pretest-posttest design to assess clinical effectiveness of the treatment. Clinical effectiveness of the DEX implant was assessed using best corrected visual acuity (BCVA) and central macular thickness (CMT). The SR18 pooled data from the 3 individual studies. The publication years of the 3 relevant studies included in the SR ranged from 2018 to 2020. The total number of patients enrolled in the eligible studies ranged from 14 to 17.
Two observational studies included patients with ME secondary to RD surgery who were assessed at baseline and at various follow-up periods using a retrospective, uncontrolled, before-and-after design to assess clinical effectiveness of the DEX implant.19,20 Clinical effectiveness of the DEX implant was assessed using BCVA and CMT or central retinal thickness (CRT). Both observational studies were retrospective medical record reviews of 1419 and 1220 patients, respectively.
Country of Origin
The lead author of the SR was from Italy.18 One each of the observational studies was from Greece19 and Taiwan.20
Patient Population
Patients in all included studies were of similar age. The mean age of patients included in the SR18 ranged from 56.3 years to 67 years, while the mean age in the primary clinical studies was 54.6 (standard deviation [SD] = 10.2) years20 and 60.4 (SD = 9.2) years.19
Patients included in the SR18 and observational studies19,20 underwent pars plana vitrectomy for RD. Patients in 1 observational study underwent pars plana vitrectomy with silicone oil tamponade.20 One study reported the mean number of pars plana vitrectomy procedures before DEX implant (mean = 1.75; SD = 1.23).20
All included studies reported on lens status before implant. Of the patients included in the SR, 0% to 43% had eyes that were phakic and 57% to 100% of eyes were pseudophakic.18 In the primary clinical studies, pre-implant lens status was phakic in 17%20 to 43%19 of eyes, pseudophakic in 57%19 to 75% of eyes,20 and aphakic in 8% of eyes.20
Two studies reported ellipsoid zone integrity at baseline: 64%19 and 92%20 of included patients showed disrupted ellipsoid zone at baseline. Baseline BCVA ranged from 0.58 (SD = 0.17) logarithm of the minimum angle of resolution (logMAR) to 1.24 (SD = 0.34) logMAR18-20 and baseline CMT or CRT ranged from 505 μm (SD = 133) to 623 (SD = 142) μm.18-20 WHO defines low vision as a BCVA score greater than 0.5 logMAR and blindness as a BCVA score greater than 1.3 logMAR.21,22 Estimated average central macular thickness in healthy eyes is 182 (SD = 23) μm.23
DEX implant was used as monotherapy for ME in 1 observational study,19 whereas another observational study provided DEX implants for patients with ME that was unresponsive to conventional treatment after 1 month.20
Interventions and Comparators
All the included studies18-20 evaluated 0.7 mg DEX implant for treatment of ME secondary to vitrectomy for RD and used baseline (pretreatment) visual and anatomical measurements as comparators. One study examined the effect of a single DEX implant,20 whereas the other observational study19 and the SR18 allowed for multiple implants as needed.
Outcomes
Visual outcomes in all the studies18-20 were assessed using BCVA measurement by means of Snellen charts, slit-lamp biomicroscopy, and dilated fundoscopy. The BCVA was converted to the logMAR for statistical purposes.
Anatomical outcomes in all studies were assessed by CMT or CRT; optical coherence tomography was performed in all patients and evaluated for CRT or CMT measurement.
The main outcome measures for the SR were mean difference in BCVA and CMT from baseline to last available follow-up measure.18 The main outcome measures for 1 observational study were mean BCVA and CRT at month 1, month 6, and month 12 after DEX implant; the condition of the ellipsoid zone was also assessed.19 The main outcome measures for the other observational study were mean BCVA and CMT and intraocular pressure at 1 month, 3 months, and 6 months after the implant.20 For visual and anatomical outcomes, a lower value than baseline indicates clinical improvement.
The mean number of implants at the end of follow-up ranged from 1.0 to 1.4 for studies included in the SR.18 For the observational study that allowed for more than 1 implant per patient, the mean number of implants was 1.4 at the 12-month follow-up.19
Summary of Critical Appraisal
Systematic Review
All studies included in the SR18 were retrospective chart reviews of patients who had been treated with DEX implant for ME secondary to RD surgery. According to the authors, the methodology was based on the PRISMA guidelines and the Cochrane Handbook. Thus, they adhered to rigorous methodology and high reporting standards, including assessment of risk of bias among individual studies, exploration of heterogeneity between studies, robust statistical analyses, and evaluation of quality of the body of evidence.18 Further strengths of the SR were a search strategy that included a comprehensive list of search terms and more than 1 database; selection of studies and extraction of data in duplicate by 2 reviewers; use of random-effects models, if appropriate, to pool data in meta-analyses; and a thorough description of the characteristics and results of included studies.
However, there were several key limitations related to the quality of the individual studies. All included studies had small sample sizes and exclusively used a retrospective medical record review design in which a single-arm, pretest-posttest assessment of outcomes was used. Without comparison groups, the authors could not draw conclusions about whether the DEX implant was superior to another treatment, placebo, or no treatment at all. Using the Egger test, the authors also demonstrated a risk of publication bias for CMT change from baseline.
Other methodology-related limitations of the SR include not searching the grey literature or reference lists of included studies for potentially relevant citations, not providing a list of excluded studies and rational for exclusion, and not reporting the time frame included in the literature search.
Observational Studies
Both included studies were retrospective in nature and consisted of medical record reviews of patients who had been treated with DEX implant for ME secondary to RD surgery.19,20 Both studies used valid tests for outcome measures. It is unclear whether the patients included were representative of the population of interest. Patients included in each of the studies were selected from the patient population of only 1 or 2 select surgeons, which potentially limited inclusion to patients with a more complicated postoperative course with recalcitrant ME compared with the broader target population of interest.19,20 Therefore, the potential for selection bias limits the generalizability of study results. The retrospective nature of the observational studies may have resulted in relevant data that were missing or not recorded at all. For example, 1 included study reported that optical coherence tomography examinations were not performed at every outpatient visit, which means that the timeline of ME development and its resolution after DEX implant (described as injection) may not have been precisely observed.20 Finally, different individuals may have been involved in patient care and data entry at different times because the studies involved reviewing charts over a long time frame.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Clinical Effectiveness of Dexamethasone Intravitreal Implant Versus No Treatment or Placebo
Best Corrected Visual Acuity
Pooled data from the SR demonstrated statistically significant improvements in BCVA from baseline to 1 month and 6 months but not at 12 months following DEX implant for ME secondary to vitrectomy for rhegmatogenous RD surgery.18 Rhegmatogenous detachments occur when a hole or tear in the retina allows fluid to collect underneath the retina, pulling the retina away from underlying tissues.24 Significant heterogeneity was detected between studies for the 12-month measure.
One of the 2 observational studies demonstrated statistically significant improvements in BCVA from baseline to 1 month, 6 months, and 12 months follow-up.19 Patients included in this study were offered more than 1 implant as needed.19 In contrast, no statistically significant change from baseline BCVA was observed at 1 month, 3 months, and 6 months post-implant in patients who were offered a single implant.20
Central Macular Thickness and Central Retinal Thickness
Pooled data from the SR demonstrated statistically significant improvements in CMT from baseline to 1 month and 6 months but not at 12 months following DEX treatment for ME secondary to vitrectomy for rhegmatogenous RD.18 This indicates that, after 6 months, CMT measurements gradually started reverting toward baseline values. Significant heterogeneity was detected between studies for the 1-month and 12-month measures.
The included observational studies demonstrated statistically significant improvements in CMT at 1 month, 3 months, and 6 months following implant,20 and in CRT at 1 month, 6 months, and 12 months following implant, with the maximum effect observed 1 month after treatment.19 Although significant improvements in CMT or CRT persisted at 6 months and 12 months after a single DEX implant under silicone oil tamponade, these reductions showed signs of gradually reverting toward baseline values over time. Six (50%) eyes did not respond to treatment.20
Univariate and multivariate linear regression analyses showed a significant negative association between baseline CMT and efficacy of a single DEX implant at 6 months, indicating more severe ME at baseline was associated with lower treatment effectiveness.20 With a single DEX implant, half of eyes showed no response to the implant upon follow-up optical coherence tomography scans, 25% of eyes showed responsiveness to treatment, and 25% showed recurrent ME.20
Resolution of ME at 12-Month Follow-Up
One observational study observed a majority (71.4%) of cases showed a total resolution of ME and 1 (7.6%) case of persistent ME 12 months after DEX implant.19
Adverse Events
The SR reported no cases of post-implant infection (i.e., endophthalmitis) in the included studies.18 One observational study reported no endophthalmitis, RD, anterior chamber migration, intraocular pressure spikes beyond 30 mm Hg, or posterior entrapment in the retro–silicone oil space after DEX implant.20 The other observational study reported 1 case of vitreous hemorrhage 1 week post-implant, 2 cases of ocular hypertension 2 months post-implant, and 2 cases of cataract during the 12-month follow-up period; no serious adverse events were observed at the 12-month follow-up visit.19
Clinical Effectiveness of Dexamethasone Intravitreal Implant Versus Alternative Interventions
No relevant evidence regarding the clinical effectiveness for DEX intravitreal implant versus alternative interventions for ME following RD repair surgery was identified; therefore, no summary can be provided.
Cost-Effectiveness of Dexamethasone Intravitreal Implant Versus No Treatment or Placebo
No relevant evidence regarding the cost-effectiveness for DEX intravitreal implant versus no treatment or placebo for ME following RD repair surgery was identified; therefore, no summary can be provided.
Cost-Effectiveness of Dexamethasone Intravitreal Implant Versus Alternative Interventions
No relevant evidence regarding the cost-effectiveness for DEX intravitreal implant versus alternative interventions for ME following RD repair surgery was identified; therefore, no summary can be provided.
Evidence-Based Guidelines for Dexamethasone Intravitreal Implant
No relevant evidence-based guidelines were identified regarding DEX intravitreal implant for the treatment of ME following RD surgery.
The main study findings and authors’ conclusions are presented in Appendix 4.
Limitations
The included SR18 and observational studies19,20 on DEX implants in patients with ME secondary to RD surgery had several important limitations. The SR was reasonably well conducted and provided pooled estimates of effect; however, the included primary studies relevant to this report were uncontrolled before-and-after studies with no comparison to any active treatment or placebo.18 In addition, significant heterogeneity was found for the BCVA and CMT analyses which limited the authors’ ability to draw sound conclusions about clinical effectiveness.18 Thus, there is some uncertainty in terms of the validity of the results.
All included studies were characterized by retrospective data collection, small sample size, and the lack of a comparison or control group.18-20 The single-group design limited the ability of all included studies to determine a causal relationship between treatment and outcome. As such, there is no way to know whether ME would have improved with time in the absence of treatment. Therefore, it is impossible to draw conclusions about whether the DEX implant is superior to another treatment or no treatment. Furthermore, none of the included studies quantified what would qualify as a clinically important improvement; therefore, it was unclear to what extent the reported statistically significant improvement translates to clinically importance.
All included studies reviewed patients who had undergone only 1 type of RD surgery (i.e., vitrectomy). There were no studies identified that included patients who had undergone other surgical procedures for RD.
No evidence was identified for research question 3 to question 5. Therefore, knowledge gaps exist on the cost-effectiveness and clinical practice guidelines for DEX implant for the treatment of ME following RD surgery.
Conclusions and Implications for Decision- or Policy-Making
The management of postoperative ME remains challenging because conventional management with topical nonsteroidal anti-inflammatory drugs, topical steroids, and intravitreal triamcinolone acetonide demonstrate variable clinical effectiveness.5 Although the current review provides some evidence that DEX implants may be effective in the treatment of ME secondary to RD surgery, no data comparing DEX implants with no treatment, placebo, or standard treatment were identified, making it challenging to draw conclusions about the comparative effectiveness of DEX implant versus no treatment, placebo, or alternative interventions for the treatment of ME following RD surgery.
Evidence from the current report is somewhat inconsistent regarding the effectiveness of DEX implants for this indication. Evidence from 1 SR and 1 uncontrolled before-and-after study suggests that DEX implants result in improved visual acuity,18,19 whereas another uncontrolled before-and-after study found no statistically significant improvement in the outcome.20 In addition, results from the SR showed visual acuity improvement was short-lived and not statistically different from baseline by the 12-month follow-up assessment.18 All included studies reported significant improvements in anatomical outcomes (CMT or CRT)18-20; however, the SR reported that the improvement in CMT had waned and was no longer statistically different from baseline by the 12-month follow-up period.18
Differences in baseline pathology may explain the variability in results. Linear regression analyses from 1 observational study showed a significant negative association between baseline CMT and efficacy of a single DEX implant at 6 months.20 Differences in included baseline patient characteristics (e.g., phakic versus pseudophakic), differences between studies in terms of the number of DEX implants offered, and differences in adjunctive treatment with surgery (e.g., silicone oil) may have contributed to the inconsistency in results.
Because of the limited evidence, high-quality research studies are needed to provide more definitive evidence of the efficacy and safety of the DEX implant for ME following RD surgery. Future research should prospectively evaluate the use of DEX implants compared with control groups receiving standard treatment to investigate the comparative effectiveness of DEX. Further, outcomes stratified by severity of ME would allow for a more customized approach to treatment.
References
1.Gebler M, Pfeiffer S, Callizo J, Hoerauf H, Feltgen N, Bemme S. Incidence and risk factors for macular oedema after primary rhegmatogenous retinal detachment surgery: a prospective single-centre study. Acta Ophthalmol. 2022;100(3):295-301. PubMed
2.Lai TT, Huang JS, Yeh PT. Incidence and risk factors for cystoid macular edema following scleral buckling. Eye (Lond). 2017;31(4):566-571. PubMed
3.Tunc M, Lahey JM, Kearney JJ, Lewis JM, Francis R. Cystoid macular oedema following pneumatic retinopexy vs scleral buckling. Eye (Lond). 2007;21(6):831-834. PubMed
4.Kim SJ, Martin DF, Hubbard GB, et al. Incidence of postvitrectomy macular edema using optical coherence tomography. Ophthalmology. 2009;116(8):1531-1537. PubMed
5.Romano V, Angi M, Scotti F, et al. Inflammation and macular oedema after pars plana vitrectomy. Mediators Inflamm. 2013;2013:971758. PubMed
6.Kuppermann BD, Zacharias LC, Kenney MC. Steroid differentiation: the safety profile of various steroids on retinal cells in vitro and their implications for clinical use (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2014;112:116-141.
7.Drug Reimbursement Review: dexamethasone (Ozurdex) for diabetic macular edema. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/dexamethasone. Accessed 2022 Apr 14.
8.Bellocq D, Pierre-Kahn V, Matonti F, et al. Effectiveness and safety of dexamethasone implants for postsurgical macular oedema including Irvine-Gass syndrome: the EPISODIC-2 study. Br J Ophthalmol. 2017;101(3):333-341. PubMed
9.Taney LS, Baumal CR, Duker JS. Sustained-release dexamethasone intravitreal implant for persistent macular edema after vitrectomy for epiretinal membrane. Ophthalmic Surg Lasers Imaging Retina. 2015;46(2):224-228. PubMed
10.Hattenbach LO, Springer-Wanner C, Hoerauf H, et al. Intravitreal sustained-release steroid implants for the treatment of macular edema following surgical removal of epiretinal membranes. Ophthalmologica. 2017;237(4):232-237. PubMed
11.Bui KM, Chow CC, Mieler WF. Treatment of recalcitrant radiation maculopathy using intravitreal dexamethasone (Ozurdex) implant. Retin Cases Brief Rep. 2014;8(3):167-170. PubMed
12.Srour M, Querques G, Leveziel N, et al. Intravitreal dexamethasone implant (Ozurdex) for macular edema secondary to retinitis pigmentosa. Graefes Arch Clin Exp Ophthalmol. 2013;251(6):1501-1506. PubMed
13.Drug Reimbursement Review: dexamethasone (Ozurdex) for macular edema following central retinal vein occlusion. Ottawa (ON): CADTH; 2012: https://www.cadth.ca/dexamethasone-intravitreal-implant. Accessed 2022 Apr 20.
14.Intravitreal dexamethasone implants for non-infectious uveitis: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.cadth.ca/intravitreal-dexamethasone-implants-non-infectious-uveitis-review-clinical-effectiveness-cost. Accessed 2022 Apr 14.
15.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
16.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
17.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
18.Parisi G, Fallico M, Avitabile T, et al. Intravitreal dexamethasone implant for postoperative macular oedema secondary to vitrectomy for epiretinal membrane and retinal detachment: a systematic review and meta-analysis. J Ophthalmol. 2021;2021:6627677. PubMed
19.Chatziralli I, Theodossiadis G, Dimitriou E, Kazantzis D, Theodossiadis P. Macular edema after successful pars plana vitrectomy for rhegmatogenous retinal detachment: factors affecting edema development and considerations for treatment. Ocul Immunol Inflamm. 2021;29(1):187-192. PubMed
20.Hsu CR, Hsieh YT, Yang CM, Lin CP. Single-dose effect of intravitreal dexamethasone implant for post-vitrectomy macular edema under silicone oil. Ocul Immunol Inflamm. 2021:1-7. PubMed
21.Virgili G, Acosta R, Bentley SA, Giacomelli G, Allcock C, Evans JR. Reading aids for adults with low vision. Cochrane Database Syst Rev. 2018;4:CD003303. PubMed
22.9D90 Vision impairment including blindness. ICD-11 for Mortality and Morbidity Statistics (Version: 02/2022). Geneva (CH): World Health Organization; 2022: https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1103667651. Accessed 2022 May 1.
23.Chan A, Duker JS, Ko TH, Fujimoto JG, Schuman JS. Normal macular thickness measurements in healthy eyes using Stratus optical coherence tomography. Arch Ophthalmol. 2006;124(2):193-198. PubMed
24.Mayo Clinic. Retinal detachment 2020; https://www.mayoclinic.org/diseases-conditions/retinal-detachment/symptoms-causes/syc-20351344 Accessed 2022 May 2.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review and Meta-Analysis
Study citation, country, funding source | Study designs and numbers of primary studies included | Population | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Parisi et al. (2021)18 Italy Funding source: NR | Overall: 7 studies Relevant to the present review:
| Relevant to the present review:
| Relevant to the present review: Intervention: intravitreal 0.7 mg dexamethasone implant for the treatment of postoperative macular edema after vitrectomy for RRD Comparator: none; all included studies used a single-arm pretest-posttest design | Outcomes:
Follow-up: 1-month to 12-months follow-up |
BCVA = best corrected visual acuity; CMT = central macular thickness; ERM = epiretinal membrane; NR = not reported; RRD = rhegmatogenous retinal detachment.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Chatziralli et al. (2021)19 Greece Funding source: no specific funding received for this project | Retrospective uncontrolled before-and-after chart review |
| Intervention:
| Outcomes:
|
Hsu et al. (2021)20 Taiwan Funding source: No funding received | Retrospective uncontrolled before-and-after chart review |
| Intervention:
Comparator:
| Outcomes:
Follow-up:
|
BCVA = best corrected visual acuity; CMT = central macular thickness; CRT = central retinal thickness; IOP = intraocular pressure; PVR = proliferative vitreoretinopathy; SO = silicone oil; ME = macular edema; NR = not reported.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Review and Meta-Analysis Using AMSTAR 215
Strengths | Limitations |
|---|---|
Parisi et al. (2021)18 | |
The objectives and research question were well-defined. Provided a good description of the search strategy; included keywords searched; more than one database was included in the literature search. Two reviewers independently reviewed articles for inclusion and extracted data. PRISMA guidelines were followed. Authors assessed risk of bias of included studies. Authors used random-effects models to pool data in meta-analyses where applicable. Characteristics and results of individual studies were well-described. | None of the included studies had a comparison group. Individual study designs were exclusively pretest-posttest. Individual studies had small sample sizes. Authors did not report search of grey literature or hand search of references lists of included studies. Studies excluded upon full-text review were not listed, however, the rational for exclusion was aggregated and reported. Authors of 2 included studies had potential conflict of interest. Authors did not report the time frame included in the literature search. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist16
Strengths | Limitations |
|---|---|
Chatziralli et al. (2021)19 | |
Study objective and research question were well-defined. No loss to follow-up. Intervention and patient characteristics were well-defined. | Study was somewhat unclear but seems to be a retrospective chart review rather than a clinical trial. Study design was pretest-posttest and thus there is no way to know whether the eyes would have improved over time regardless of treatment. There was no control/comparison group. No sample size calculation. Small sample size. Characteristics of the target population were not described; therefore, it is unclear whether the sample population was representative of the target population. Neither patients nor outcome assessors were blinded to treatment. It is unclear whether the statistical analyses were appropriate. The outcome measure, best corrected visual acuity, was assessed using Snellen charts and converted to the logarithm of the minimum angle of resolution (logMAR) for analysis. Data from Snellen charts may not be normally distributed, and parametric tests were used but may not be appropriate. |
Hsu et al. (2021)20 | |
Study objective and research question were well-defined. No loss to follow-up. Intervention and patient characteristics were well-defined. | Study was a retrospective chart review rather than a clinical trial. Study design was pretest-posttest and thus there is no way to know whether the eyes would have improved over time regardless of treatment. The study timeline encompassed a 7-year period (surgeons may have become more skilled over time) There was no control/comparison group. No sample size calculation. Small sample size. Characteristics of the target population were not described; therefore, it is unclear whether the sample population was representative of the target population. Neither patients nor outcome assessors were blinded to treatment. Unplanned subgroup analyses were conducted however, no statistical analysis was performed. The methods of the regression analyses were not well-described. |
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings From the Included Systematic Review and Meta-Analysis
Main study findings | Authors’ conclusion |
|---|---|
Parisi et al. (2021)18 | |
Visual Outcome (BCVA change)
Macular Thickness Outcome (CMT change)
Adverse Events
| “The present meta-analysis showed favorable visual and anatomical outcomes following the use of dexamethasone implant for macular oedema secondary to ERM and RRD vitrectomy (p. 5).”18 “Our findings showed both visual and anatomical improvements following DEX treatment for macular oedema secondary to vitrectomy for ERM and RRD (p. 7).”18 “When considering the different follow-ups, significant visual and anatomical improvements were demonstrated in both groups at 1 and 6 months. At 12 months, significant visual and anatomical improvements were shown in the ERM group, while these were nonsignificant in the RRD group (p. 7).”18 “In conclusion, the use of intravitreal dexamethasone implant for macular oedema following vitrectomy for ERM and RRD allowed improving both visual and anatomical outcomes. The implant represents a valid therapeutic option for this sight-threatening condition (p. 10).”18 |
BCVA = best corrected visual acuity; CI = confidence interval; CMT = central macular thickness; DEX = dexamethasone intravitreal implant; ERM = epiretinal membrane; MD = mean difference; RRD = rhegmatogenous retinal detachment.
Table 7: Summary of Findings of Included Primary Clinical Studies
Main study findings | Authors’ conclusion |
|---|---|
Chatziralli et al. (2021)19 | |
BCVA
CRT
Resolution of ME at 12-month follow-up
Ellipsoid zone
Total number of implants
Adverse events
| “It is worthy to mention that patients with cystoid type of macular edema, pseudophakic lens status, long-standing macula off RRD and PVR had worse anatomical results with higher CRT at the end of the 12-month follow-up, which also affected the final visual outcome at month 12 post-treatment. The evolution of CRT in our study has shown that the maximum effect of intravitreal dexamethasone implant is prominent at month 1 after treatment (p. 5).”19 “Our results also suggested that intravitreal dexamethasone implant is a viable treatment option in patients with macular edema post PPV. This sort of treatment has been shown to provide resolution or significant reduction in CRT with improvement in VA and low recurrence rate associated with good safety profile, even with a limited number of dexamethasone implant with average 1.4 implants (p. 5).”19 |
Hsu et al. (2021)20 | |
Functional Outcomes BCVA
CMT
CMT subgroup analysis
Mean CMT decrement for patients with > 100 μm decrement:
Mean CMT decrement for patients with > 200 μm decrement:
Linear regression
Anatomic Outcomes
Complications and Adverse Events
| “The preliminary results show that CMT was significantly decreased at 6 months after the injection. A more prominent baseline ME before the injection was negatively correlated with DEX implant efficacy (p. 3).”20 “…this study explores the responsiveness of ME to a single steroid implant under SO endotamponade in a real-world scenario. We found that a sustained-release DEX implant may be an effective treatment for posterior segment inflammation in vitrectomized eyes and recalcitrant post-vitrectomy ME under SO tamponade. DEX implants could be safely administered to SO-filled eyes without any significant side effects (p. 6).”20 |
BCVA = best corrected visual acuity; CMT = central macular thickness; CRT = central retinal thickness; DEX = dexamethasone; ERM = epiretinal membrane; EZ = ellipsoid zone; IOP = intraocular pressure; OCT = optical coherence tomography; PPV = pars plana vitrectomy; PVR = proliferative vitreoretinopathy; RD = retinal detachment; SO = silicone oil.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Ozurdex for diabetic macular edema: clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: reference list). Ottawa (ON): CADTH; 2020. https://www.cadth.ca/ozurdex-diabetic-macular-edema-clinical-effectiveness-cost-effectiveness-and-guidelines. Accessed 2022 Apr 14.
Drug Reimbursement Review: dexamethasone (Ozurdex) for diabetic macular edema. Ottawa (ON): CADTH; 2018: https://www.cadth.ca/dexamethasone. Accessed 2022 Apr 14.
Drug Reimbursement Review: dexamethasone (Ozurdex) for macular edema following central retinal vein occlusion. Ottawa (ON): CADTH; 2012: https://www.cadth.ca/dexamethasone-intravitreal-implant. Accessed 2022 Apr 20.
Review Articles
Bonfiglio V, Reibaldi M, Fallico M, et al. Widening use of dexamethasone implant for the treatment of macular edema. Drug Des Devel Ther. 2017;11:2359-2372. . PubMed
Additional References
Aetna. Dexamethasone ophthalmic implants (Ozurdex and Dextenza). 2022; http://www.aetna.com/cpb/medical/data/700_799/0795.html. Accessed 2022 Apr 9.
Garli M, Aydin Kurna S, Acikalin B, Ceviker A. Evaluation of the effect of intravitreal dexamethasone (Ozurdex((R))) implant on intraocular pressure in vitrectomized and non-vitrectomized eyes with macular edema. Turk J Ophthalmol. 2021 Dec 28;51(6):365-372. . PubMed
Rajesh B, Zarranz-Ventura J, Fung AT, et al. Safety of 6000 intravitreal dexamethasone implants. Br J Ophthalmol. 2020 Jan;104(1):39-46. . PubMed
Chang YC, Liu PK, Kao TE, et al. Dexamethasone intravitreal implant (Ozurdex) for long-term macular edema after epiretinal membrane peeling surgery. J Ophthalmol. 2018;2018:5832186. . PubMed
Karaca Adiyeke S, Ture G, Talay E. Intravitreal dexamethasone implant for postvitrectomy macular edema: a retrospective cohort of patients with postvitrectomy macular edema treatment. J Ocul Pharmacol Ther. 2018 May;34(4):335-339. . PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matter of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca