CADTH Health Technology Review
Robotic-Assisted Spinal Surgery
Rapid Review
Authors: Diksha Kumar, Charlotte Wells, Lory Picheca
Key Messages
The use of robotic systems to aid in surgical procedures, including spinal surgeries, has been on the rise over the past several years.
Systematic reviews and economic evaluations on the clinical and cost-effectiveness of robotic-assisted surgical systems used for patients requiring spinal surgeries that do not involve pedicle screw placement are lacking.
Context and Policy Issues
Spinal fusion procedures for conditions such as disc herniation, spondylolisthesis, and spinal stenosis have been traditionally performed by securing a bone graft that promotes fusion between vertebrae with metal pedicle screws, which are inserted using free-hand methods.1 Free-hand surgeries are associated with potential complications, as improper screw placement can lead to damage to the blood vessels and nerve roots close to the insertion sites, resulting in potential vascular, neurological, and visceral damage.2 Injuries and complications can include leakage of cerebrospinal fluid, blood loss, and deep wound infection.3 Approximately 30,000 adults living in Canada undergo spine surgery annually, thereby creating a demand for technological advances within the field to improve patient outcomes, reduce the risk of intraoperative and postoperative complications, and decrease the need for revision surgeries.4
Robotic assistance in spinal surgery was initially developed as a way to improve the accuracy of pedicle screw placement in fusion procedures and to reduce the risk of manual fixation, with the first robot approved by the FDA for this indication being the SpineAssist by Mazor Robotics in 2004.2 Mazor X, the latest robotic-guided system for spinal surgery approved for use in Canada, is marketed primarily for preoperative or intraoperative planning of procedures that involve screw placement.5 Compared to previous systems, the Mazor X has a more advanced camera system for intraoperative navigation as well as an improved robotic arm that allows for greater mobility.2,6 While there is considerable literature investigating the comparative clinical effectiveness of robotic-assisted spinal surgery systems versus conventional methods in the realm of pedicle screw placement,7,8 it is unclear whether robotic systems are beneficial for other types of complex spinal operations, such as tumour resections or laminectomy (i.e., partial or full removal of the vertebral bone).
The objective of this report is to summarize the evidence regarding the clinical and cost-effectiveness of robotic-assisted surgical systems used for patients requiring spinal surgery procedures that do not involve pedicle screw placement.
Research Questions
What is the clinical effectiveness of robotic-assisted surgical systems used for patients requiring spinal surgery?
What is the cost-effectiveness of robotic-assisted surgical systems used for patients requiring spinal surgery?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Library, the University of York Centre for Reviews and Dissemination databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were robotics and spinal surgery. No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and March 28, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Any patients requiring spinal surgery |
Intervention | Spinal surgery (any spinal surgery, not including pedicle screw placement) using robotic-assisted surgical systems (e.g., MAZOR Robotic Guidance System) |
Comparator | Conventional and traditional surgery performed without robotic-assisted surgical systems (including minimally invasive spinal surgery) |
Outcomes | Q1: Clinical effectiveness (e.g., postoperative functional status and mobility, range of motion, pain, length of hospital stay, health-related quality of life, patient satisfaction, blood loss, operative time, impact of anesthesia) and safety (e.g., rates of adverse events, hospital readmission, surgical revisions, complications [e.g., infections]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, cost per health benefit gained) |
Study designs | Health technology assessments, systematic reviews, and economic evaluations |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017.
Summary of Evidence
Quantity of Research Available
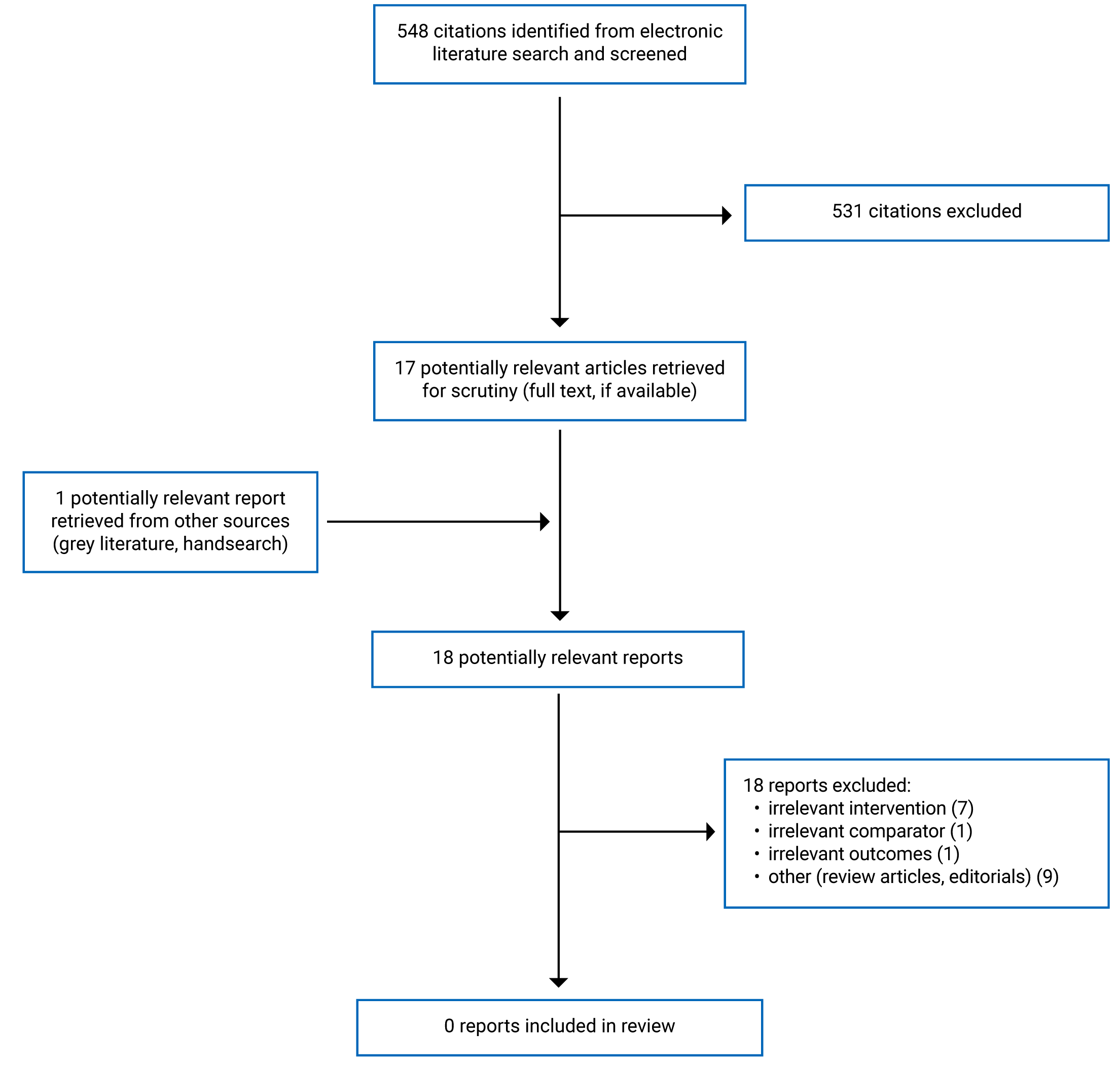
A total of 548 citations were identified in the literature search. Following screening of titles and abstracts, 531 citations were excluded and 17 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. None of these 18 potentially relevant articles met the inclusion criteria and were excluded for various reasons. Appendix 1 presents the PRISMA9 flow chart of the study selection. References of potential interest are provided in Appendix 2.
Summary of Findings
No relevant literature was identified regarding the clinical or cost-effectiveness of robotic-assisted surgical systems used for patients requiring spinal surgery that did not involve pedicle screw placement; therefore, no summary can be provided.
Limitations
Based on the findings of this report, published systematic reviews and economic evaluations regarding the clinical and cost-effectiveness of robotic-assisted surgical systems for performing spinal surgeries that do not involve pedicle screw placement seem to be lacking. This report is limited by the time frame used for literature searches (January 1, 2017, to March 28, 2022). It is possible that relevant literature published more than 5 years ago was excluded by the current date-limited search. A list of related publications that were not eligible for inclusion in this report due to their study design are provided in Appendix 2.
Conclusions and Implications for Decision- or Policy-Making
Conclusions could not be drawn regarding the clinical or cost-effectiveness of robotic-assisted surgical systems used for patients requiring spinal surgeries that do not involve pedicle screw placement because no literature that met the inclusion criteria for this report was identified.
It appears that the applications of robotic-guided systems in spinal procedures other than pedicle screw placement remain largely unexplored in clinical literature. Further research examining the clinical and cost-effectiveness of robotic-assisted surgical systems for these procedures is needed to investigate whether they are more effective than traditional methods and to inform decision-makers considering investment in these systems.
References
1.Huang J, Li Y, Huang L. Spine surgical robotics: review of the current application and disadvantages for future perspectives. J Robot Surg. 2020;14(1):11-16. PubMed
2.D'Souza M, Gendreau J, Feng A, Kim LH, Ho AL, Veeravagu A. Robotic-assisted spine surgery: history, efficacy, cost, and future trends. Robot Surg. 2019;6:9-23. PubMed
3.Campbell DH, McDonald D, Araghi K, Araghi T, Chutkan N, Araghi A. The clinical impact of image guidance and robotics in spinal surgery: a review of safety, accuracy, efficiency, and complication reduction. Int J Spine Surg. 2021;15(s2):S10-S20. PubMed
4.Cram P, Landon BE, Matelski J, et al. Utilization and outcomes for spine surgery in the United States and Canada. Spine (Phila Pa 1976). 2019;44(19):1371-1380. PubMed
5.Medtronic. Mazor X Stealth Edition. 2021; https://www.medtronic.com/us-en/healthcare-professionals/products/spinal-orthopaedic/spine-robotics/mazor-x-stealth-edition.html. Accessed 2022 May 04.
6.Molliqaj G, Paun L, Nouri A, Girod PP, Schaller K, Tessitore E. Role of robotics in improving surgical outcome in spinal pathologies. World Neurosurg. 2020;140:664-673. PubMed
7.Tovar MA, Dowlati E, Zhao DY, et al. Robot-assisted and augmented reality-assisted spinal instrumentation: a systematic review and meta-analysis of screw accuracy and outcomes over the last decade. J Neurosurg Spine. 2022:1-16. PubMed
8.Li J, Fang Y, Jin Z, Wang Y, Yu M. The impact of robot-assisted spine surgeries on clinical outcomes: A systemic review and meta-analysis. Int J Med Robot. 2020;16(6):1-14. PubMed
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Review Articles
Li Z, Yu G, Jiang S, Hu L, Li W. Robot-assisted laminectomy in spinal surgery: a systematic review. Ann Transl Med. 2021;9(8):715. PubMed
Non-Randomized Studies
Jin M, Ge M, Lei L, et al. Clinical and radiologic outcomes of robot-assisted kyphoplasty versus fluoroscopy-assisted kyphoplasty in the treatment of osteoporotic vertebral compression fractures: a retrospective comparative study. World Neurosurg. 2022;158:e1-e9. PubMed
Qian J, Fang C, Ge P, et al. Efficacy and safety of establishing an optimal path through unilateral pedicle under the assistance of surgical robot in percutaneous kyphoplasty. Pain Physician. 2022;25(1):E133-E140. PubMed
Wang TY, Mehta VA, Sankey EW, Lavoie S, Abd-El-Barr MM, Yarbrough CK. Operative time and learning curve between fluoroscopy-based instrument tracking and robot-assisted instrumentation for patients undergoing minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF). Clin Neurol Neurosurg. 2021;206:106698. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.