CADTH Health Technology Review
Guidelines for Pediatric Immune Thrombocytopenia
Rapid Review
Authors: Daphne Hui, Angela Barbara, Sarah C. McGill
Abbreviations
ASH
American Society of Hematology
ITP
immune thrombocytopenia
IVIG
IV immune globulin
RCT
randomized controlled trial
SR
systematic review
TRA
thrombopoietin receptor agonist
Key Messages
Three guidelines included in this report recommend rituximab, thrombopoietic agents (drugs that promote platelet growth), and thrombopoietin receptor agonists (e.g., romiplostim, eltrombopag) over splenectomy as second-line treatment in children with immune thrombocytopenia who do not respond to first-line treatment.
Three guidelines included in this report recommend for children with persistent or chronic immune thrombocytopenia who have no response to 1 thrombopoietin receptor agonist or who lose an initial response that treatment can be switched to another thrombopoietin receptor agonist and/or combined with mycophenolate mofetil or another immunosuppressant. For individuals who do not respond to thrombopoietin receptor agonists, the recommendation is to consider rituximab and dexamethasone, especially for adolescent females.
No relevant evidence-based recommendation was identified regarding the use of dapsone for the treatment of children with immune thrombocytopenia.
Context and Policy Issues
Immune thrombocytopenia (ITP) is an acquired autoimmune disorder characterized by a low platelet count (< 100,000/μL) resulting from platelet destruction and impaired platelet production.1,2 The cause of ITP is not always known but it may be caused by a viral infection or an immune response.3 The Canadian Paediatric Society reported that ITP affects approximately 5 in 100,000 children in Canada per year.3 There is a greater incidence of ITP in individuals between the ages of 2 years to 5 years and a lower incidence during adolescence.3,4 ITP typically presents with bruising, bleeding, and/or a sudden petechial rash in an otherwise healthy child.4 Apart from bleeding of the skin and mucous membranes, systemic symptoms tend to be absent. Therefore, thrombocytopenia may be detected incidentally during evaluation of complete blood counts (including platelets), such as during routine or presurgical assessments.4 Approximately, 10% to 20% of children will develop chronic ITP, defined as platelet count of less than 100,000/μL persisting beyond 12 months from the time of initial presentation.2 Factors correlated with increased risk of chronic disease include older age, gradual and subtle onset of symptoms, higher platelet count at initial diagnosis, and lack of preceding infection or vaccination before development of ITP.2 Newly diagnosed and persistent ITP are defined as ITP within 3 months from diagnosis and ongoing ITP between 3 months and 12 months from initial diagnosis, respectively.5
Management of newly diagnosed ITP in children is based largely on the severity of bleeding, risk factors, degree of thrombocytopenia (condition of low blood platelet count), quality of life, and values and preferences of the patient, caregiver, and family. Initial management includes watchful waiting (i.e., no interventions used) or pharmacological interventions. Pharmacological interventions for newly diagnosed ITP include IV immune globulin (IVIG), anti-D immunoglobulin, and glucocorticoids such as methylprednisolone.5
Management of chronic ITP depends on the symptom type and duration.2 For instance, some patients will experience intermittent episodes of thrombocytopenia but remain relatively asymptomatic sometimes, whereas other patients may require continuous or intermittent therapy for ongoing or recurrent bleeding symptoms or risks. Selecting a particular pharmacologic treatment depends on risk factors for bleeding (e.g., active lifestyle, sports), continuous bleeding symptoms, concomitant medications and medical conditions (e.g., anxiety, fatigue), and access to care.2 Acute interventions for bleeding or risk of bleeding are similar to the first-line pharmacological interventions including IVIG, anti-D immunoglobulin, and glucocorticoids.2 However, clinicians prefer steroid-sparing agents such as rituximab and thrombopoietic agents, which include thrombopoietin receptor agonists (TRAs or TPO-RAs in some publications).2 TRAs (e.g., eltrombopag and romiplostim), which stimulate the production of platelets (thrombopoiesis) through the thrombopoietin receptor, may be used in children with chronic ITP. Based on evidence from randomized and non-randomized studies, eltrombopag and romiplostim appear to have comparable efficacy and produce a durable platelet response with less frequent bleeding-related adverse events.2 One randomized study on long-term use of romiplostim (n = 17) or placebo (n = 5) suggested that platelet levels can be maintained for over 4 years with good tolerability and without major toxicity.2
Dapsone is an immunosuppressive agent that may be used in children with late persistent or chronic ITP; however, it has not been demonstrated to exhibit a curative effect and is associated with some toxicity (e.g., hepatotoxicity).2 Splenectomy is an option that may be considered in a small percentage of patients who have severe thrombocytopenia with excessive bleeding requiring repeated or continuous pharmacologic interventions.2
The purpose of this Rapid Review is to evaluate recent evidence-based guidelines regarding the use of dapsone, rituximab, and TRAs for the treatment of ITP in children. There will be separate reports summarizing the clinical effectiveness and cost-effectiveness of these interventions for the treatment of ITP in children. CADTH is also conducting a systematic review (SR) on treatments for adults with ITP.
Research Questions
What are the evidence-based guidelines regarding dapsone for pediatric patients with immune thrombocytopenia?
What are the evidence-based guidelines regarding rituximab for pediatric patients with immune thrombocytopenia?
What are the evidence-based guidelines regarding thrombopoietin receptor agonists for pediatric patients with immune thrombocytopenia?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and Embase through the Ovid platform, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were immune thrombocytopenia and pediatrics. CADTH-developed search filters were applied to limit retrieval to guidelines. If possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and April 12, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Pediatric patients (< 18 years of age) with immune thrombocytopenia |
Intervention | Q1: Dapsone Q2: Rituximab Q3: Thrombopoietin receptor agonists (e.g., romiplostim, eltrombopag) |
Comparator | Not applicable |
Outcomes | Q1: Recommendations regarding the use of dapsone for pediatric patients with immune thrombocytopenia Q2: Recommendations regarding the use of rituximab for pediatric patients with immune thrombocytopenia Q3: Recommendations regarding the use of thrombopoietin receptor agonists for pediatric patients with immune thrombocytopenia |
Study designs | Evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017. Guidelines with unclear methodology were also excluded. Of note, guidelines on avatrombopag, (a TRA used to treat thrombocytopenia in people with ITP) are not discussed in this report because the drug is undergoing a CADTH Reimbursement Review.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument6 for guidelines as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
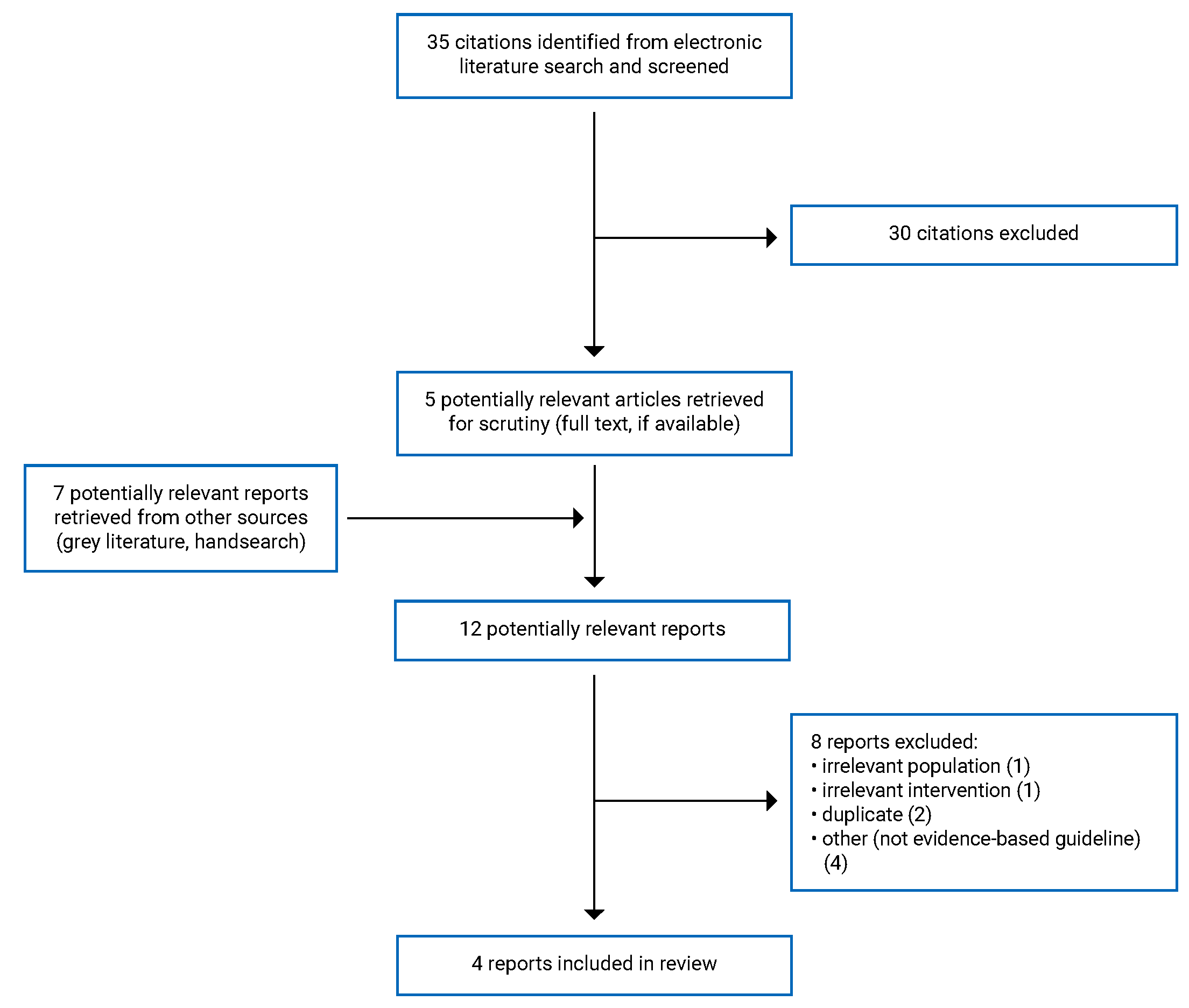
A total of 35 citations were identified in the literature search. Following screening of titles and abstracts, 30 citations were excluded and 5 potentially relevant reports from the electronic search were retrieved for full-text review. 7 potentially relevant publications were retrieved from the grey literature search for full-text review. Of the 12 potentially relevant articles, 8 were excluded for various reasons; 4 evidence-based guidelines1,7-9 met the inclusion criteria and were included in this report. Figure 1 presents the PRISMA10 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
A total of 4 evidence-based guidelines were included in this review.1,7-9 Additional details regarding the characteristics of the included publications are provided in Table 2.
Study Design
The 2021 guideline by the Working Group of Chinese Guideline for the Diagnosis and Treatment of Childhood Primary Immune Thrombocytopenia, referred to as the 2021 Chinese-adapted guidelines herein, is an adaptation of published guidelines in consideration of values, resources, and social and cultural factors specific to China.9 The adaptation was performed through a systematic search for guidelines (which would be adapted) and supplementary evidence (study design not reported) following ADAPTE methodology and the WHO Handbook for Guideline Development.9 Evidence levels based on the source of the evidence and grade of recommendations based on evidence requirements were adopted from the 2019 Updated International Consensus Report on the Investigation and Management of Primary Immune Thrombocytopenia.7,9 Evidence levels were designated as follows: Ia = evidence obtained from meta-analysis of RCTs; Ib = 1 or more RCTs; IIa = 1 or more well-designed controlled studies without randomization; IIb = 1 or more other type of well-designed quasi-experimental studies; III = well-designed nonexperimental descriptive studies (such as comparative studies, correlated studies, and case studies); and IV = expert committee reports or opinions and/or clinical experience of respected authorities). Grades of the recommendations were defined as follows: A = requires at least 1 RCT as part of a body of literature of overall good quality and consistency addressing specific recommendation; B = requires well-conducted clinical studies but not RCT on the topic of recommendation; and C = requires expert committee reports or opinions and/or clinical experiences of respective authorities.9 The Cochrane risk of bias tool and quality assessment tool for case series were used to evaluate methodological quality of RCTs and case series, respectively. The adapted guidelines and rationale were revised, improved, and finalized following 2 rounds of Delphi survey and an online consensus meeting.9
The 2019 guidelines for ITP by the American Society of Hematology (ASH) were developed based on SRs (performed following the general methods outlined in the Cochrane Handbook for Systematic Reviews of Interventions) of effects of interventions and evidence pertaining to baseline risks, costs, values, and preferences.1 Grading of Recommendations, Assessment, Development and Evaluations (GRADE) methodology was used to assess certainty in the evidence (i.e., quality of the evidence) for each effect estimate of the outcomes through 4 levels from very low to high.1 Various GRADE domains were considered, such as risk of bias, inconsistency, indirectness, imprecision, and publication bias. The strength of the recommendation was rated as strong (“recommends”) or conditional (“suggests”).1 Interpretations of the strength of the recommendations were reported separately for patients, clinicians, policy-makers, and researchers.1 Risk of bias was assessed at the outcome level using Cochrane tools for randomized and non-randomized studies. Guidelines were established based on consensus among the panel; however, in rare occasions, voting was implemented (e.g., 80% majority was required for a strong recommendation).1
The 2019 Updated International Consensus Report on the Investigation and Management of Primary Immune Thrombocytopenia (referred to as the 2019 updated international consensus report on primary ITP herein) is an update to a report published in 2010.7 This 2019 report was developed based on a search of PubMed for publications published between January 1, 2009, and July 23, 2018, to retrieve articles published since the last literature search of the original report. The updated recommendations followed the principles of the CheckUp guidelines.7 Two panel meetings were conducted to discuss the identified literature, draft consensus statements, and finalize updated recommendations. Consensus was required; however, 100% consensus was not reached on every recommendation — 85% of recommendations achieved 85% agreement. Recommendations were rated for the level of evidence: Ia = meta-analysis of RCTs, Ib = 1 or more RCTs, IIa = 1 or more well-designed controlled studies without randomization, IIb = 1 or more other well-designed quasi-experimental studies, III = well-designed nonexperimental descriptive studies (e.g., comparative studies, case studies), and IV = expert committee reports or opinions and/or experience of respected authorities. Grades of the recommendations were defined as follows: A = 1 or more RCTs of overall good quality and consistency addressing specific recommendations (Ia and Ib), B = well-conducted clinical studies when there are no randomized clinical trials available (IIa, IIb, and III); and C = evidence from expert committee reports or opinions and/or experiences of respected authorities which suggests absence of directly applicable clinical studies of good quality (IV).7 All authors provided input on each draft of the manuscript and approved the final version for submission.7
The 2018 guidelines from an interdisciplinary European working group did not report the methodology associated with development of the guidelines but were included because a grading system was used for supporting evidence and the recommendations, which indicates that the guidelines were evidence-based.8 The recommendations were developed by an interdisciplinary working group of experts from the German Society for Hematology and Medical Oncology, German Society for Transfusion Medicine and Immunohematology, Austrian Society for Hematology and Medical Oncology, Swiss Society for Hematology, and Society for Pediatric Oncology and Hematology.8 The recommendations were based on relevant publications published up to November 2017. Abstracts were also considered if they were presented at meetings in 2015 and thereafter. Rating of evidence levels followed the Oxford Centre of Evidence-Based Medicine: Levels of Evidence (March 2009) and grading of recommendations followed the National Program for Medical Service Guidelines Method Report of 2010.8 The grading designations for the recommendations were defined as follows: A = strong recommendation (“must”); B = recommendation (“should”); 0 = open recommendation (“can”); and expert consensus which was provided when there was insufficient supporting data.8 The authors noted this was when “there is insufficient scientific data.” Information such as the use of voting or a consensus system and validation methodology were not reported.8
Country of Origin
The 2021 Chinese-adapted guidelines were devised for clinical practice in China.9
The 2019 ASH guidelines did not specify a country where the guidelines were meant to apply. It was noted that the guidelines should be interpreted with consideration of local clinical practice, availability of resources, institutional policies, and limitations of time.1
The 2019 updated international consensus report on primary ITP was intended to provide a global perspective, with representation from Europe (13 individuals), North America (US: 4 individuals; Canada: 1 individual), China (2 individuals), Australia (1 individual), and Japan (1 individual) on the development panel.7
The 2018 interdisciplinary European working group guidelines did not specify a country where the guidelines were meant to apply. However, they were devised by experts representing Germany (2 societies). Austria (1 society), Switzerland (1 society), and another society that was not identified by country.8
Patient Population
The target population of the 2021 Chinese-adapted guidelines was children with primary ITP aged 1 month to 18 years living in China. Intended users were clinicians, health care decision-makers, and researchers.9
The 2019 ASH guidelines focused on adults and children with ITP (newly diagnosed, persistent, and chronic ITP refractory to first-line treatment) and non–life-threatening bleeding. Intended users were patients, clinicians, policy-makers, and other decision-makers.1
The 2019 updated international consensus report on primary ITP focused on adults, pregnant adults, and children with primary ITP. The intended users were not explicitly reported but appears to be individuals involved with the diagnosis and management of primary ITP.7
The 2018 interdisciplinary European working group guidelines focused on adults, children, and adolescents with ITP. Intended users were not reported but it was noted that the document was intended as an aid for medical decision-making.8
Interventions and Comparators
The interventions in the 2021 Chinese-adapted guidelines relevant to this report included rituximab and thrombopoietic agents.9 However, the recommendations did not specify the exact type of thrombopoietic agents.9
The 2019 ASH guidelines focused on first-line therapy (for newly diagnosed) and second-line management of ITP. The interventions relevant to this report included rituximab and TRAs.1
The 2019 updated international consensus report on primary ITP focused on emergency treatment and first-line therapy and beyond for children with persistent or chronic primary ITP (i.e., could include up to third-line treatment this is not specified).7
The 2018 interdisciplinary European working group guidelines focused on various pharmacological and surgical interventions for ITP. The interventions relevant to this report included treatment of chronic ITP. No specific treatments were mentioned in the recommendation although eltrombopag and romiplostim (TRAs) were discussed.8
Outcomes
The 2021 Chinese-adapted guidelines considered medical resources, the environment, cost-effectiveness, feasibility, values, and preferences of parents and/or guardians. These factors served as the basis for the rationale of the guidelines.9
The 2019 ASH guidelines were developed based on a population perspective considering a balance of harms and benefits with comparators, extent of resource use associated with alternative options, and assumptions of values and preferences. The guidelines were intended to provide recommendations based on patient-reported outcomes, adverse events, treatment impact, and platelet count response.1
The outcomes considered by the guideline panel in the 2019 updated international consensus report on primary ITP were not clearly reported. Eligible outcomes in the literature included from the PubMed search were also not reported. Nevertheless, implementation considerations (e.g., dosing), benefits, and risks were reported among the supporting evidence.7
The 2018 interdisciplinary European working group guidelines also did not report on the outcomes considered during development or if and which outcomes were eligible during selection of supporting evidence. However, common side effects were mentioned.8
Summary of Critical Appraisal
Overall, the 4 evidence-based guidelines were clear regarding clarity of presentation; namely, recommendations were specific, unambiguous, and easily identified and different management options were presented.1,7-9
The 2018 interdisciplinary European working group did not report the methodology associated with guideline development. However, its recommendations were rated using the National Program for Medical Service Guidelines Method Report of 2010 and supporting evidence levels were rated using the Oxford Centre of Evidence-Based Medicine: Levels of Evidence (March 2009).8 The guidelines went through an external review process, and the working group noted that the document was intended exclusively to aid medical decision-making and the guidelines were not suitable to define medical standards. Notable limitations in all the guidelines include limiting recommendations to the class of intervention without information about specific drugs. For example, the guidelines reporting on TRAs did not provide recommendations specific to romiplostim or eltrombopag.1,7,9 Further, the 2019 updated international consensus report recommendation was unclear about the place in therapy (e.g., first line or second line) of the treatment options for children with persistent or chronic ITP.7 Standards of practice and availability to certain treatments may differ across clinical practices across countries and within countries.
Regarding the scope and purpose, all guidelines clearly reported the objectives and the population to whom the guideline apply; however, the related health questions were not reported in the 2019 Updated International Consensus Report on Primary ITP and the 2018 Interdisciplinary European Working Group guidelines.7,8 The target users of the guideline were clearly defined for the 2021 Chinese-adapted guidelines and 2019 ASH guidelines and were not reported in the 2019 updated international consensus report and the 2018 interdisciplinary European working group guidelines.1,7-9 Regarding stakeholder involvement, 3 guidelines were developed with groups comprising clinical and methodological experts in addition to patient and guardian representation.1,7,9 The 2018 interdisciplinary European working group guidelines included clinical experts in the development group (a combination of hematology, oncology, and immunohematology experts), but there was no mention of patient and/or caregiver representation or consultation.8
Regarding rigour of development, systematic methods were used to search for evidence for the 2021 Chinese-adapted guidelines, 2019 ASH guidelines, and 2019 updated International consensus report.1,7,9 The 2021 Chinese-adapted guidelines reported the databases, main search terms, and inclusion criteria and performed quality assessments; however, the assessment tools were not reported.9 The 2019 ASH guidelines and 2019 updated international consensus report did not report details such as the inclusion and exclusion criteria; however, the ASH guidelines noted that they followed the methods of the Cochrane Handbook for SRs.1,7 The 3 guidelines had additional strengths, including consideration of the health benefits, side effects, and risks in the development of recommendations as well as reporting of guideline development methodology and supporting evidence.1,7,9 The 2019 ASH guidelines and 2019 updated international consensus report clearly reported methodology and explicit links between the recommendations and supporting evidence.1,7,9 However, the methodology and links between the recommendations and supporting evidence was not very clear in the 2021 Chinese-adapted guidelines.9 Moreover, the 2021 Chinese-adapted guidelines, 2019 ASH guidelines, and 2019 updated international consensus report did not clearly report the strengths and limitations of the evidence supporting the recommendations.1,7,9 The 2021 Chinese-adapted guidelines reported favourable and unfavourable implementation factors and the 2019 ASH guidelines reported the limitations of the guidelines.1,7,9 The 2019 ASH guidelines and 2019 updated international consensus report also reported procedures for updating the guidelines.1,7,9 The 2018 interdisciplinary European working group guidelines did not clearly describe the links between the recommendations and supporting evidence.8 All 4 guidelines underwent external review by experts before publication.1,7-9
The 2021 Chinese-adapted guidelines, 2019 ASH guidelines, and 2019 updated international consensus report reported information regarding applicability, facilitators and barriers to application, advice and/or tools on how put the recommendations into practice, and consideration of potential resource implications.1,7,9 The 2021 Chinese-adapted guidelines provided implementation instructions, the 2019 ASH guidelines reported good practice statements that were not based on a SR of available evidence, and the 2019 updated international consensus report provided dosages and considerations such as platelet count.1,7,9 The 2018 interdisciplinary European working group guidelines did not report facilitators and barriers to application, and it was unclear if potential resource implications of applying recommendations were considered; however, dosages for frequently used drugs for ITP were reported.8 Only the 2019 ASH guidelines reported monitoring and/or auditing criteria, which indicates ongoing review by experts and survey for new evidence will be conducted.1
Regarding editorial independence, all guideline documents reported competing interests. The 2021 Chinese-adapted guidelines reported the funding source as well.9 The 2019 updated international consensus report and 2018 interdisciplinary European working group guidelines did not report the funding of the guideline development although financial conflict of interest(s) were reported for authors.7,8 The ASH guidelines were likely influenced by ASH because funding of the work, panel formation, management of conflicts of interest, internal and external review, and organizational approval was guided by ASH policies and procedures. ASH also appointed the members of the guideline panel.1
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
A total of 4 evidence-based guidelines were included in this review.1,7-9 No guidelines informed the use of dapsone, 3 guidelines informed the use of rituximab,1,7,9 and 3 guidelines informed the use of TRAs (e.g., romiplostim, eltrombopag)1,7,9 as treatment for pediatric populations with ITP. The 2018 interdisciplinary European working group guidelines did not specify particular treatments in the recommendations.8 Appendix 4 presents the main study findings and authors’ conclusions.
Guidelines
Recommendations Regarding the Use of Dapsone for Pediatric Patients With ITP
No evidence-based guidelines were identified for the use of dapsone for pediatric patients with ITP.
Recommendations Regarding the Use of Rituximab for Pediatric Patients With ITP
For children with ITP who do not respond to first-line treatment, the Chinese-adaptation guideline development group suggest choosing conventional second-line treatment with rituximab rather than splenectomy (level III evidence, grade B recommendation).9
For children with ITP who do not respond to first-line treatment and have non-life-threatening mucosal bleeding and/or diminished health-related quality of life, the ASH guideline panel suggests the use of rituximab rather than splenectomy (conditional recommendation, very low certainty in the evidence) (recommendation 2).1
Recommendations Regarding the Use of TRAs for Pediatric Patients With ITP
For children with ITP who do not respond to first-line treatment, the Chinese-adaptation guideline development group suggest choosing conventional second-line treatment with thrombopoietic agents rather than splenectomy (level Ib evidence, grade A recommendation).9
For children with ITP who do not respond to first-line treatment and have non-life-threatening mucosal bleeding and/or diminished health-related quality of life, the ASH guideline panel suggests the use of TRAs rather than splenectomy (conditional recommendation, very low certainty in the evidence) (recommendation 20).1
For treatment of children with persistent or chronic ITP, the 2019 updated international consensus report on primary ITP recommends the use of TRAs for demonstrated good response, reduction in bleeding frequency, and absence of side effects in most patients (evidence level Ib, grade A recommendation). In patients with no response to 1 TRA or when an initial response is lost, an alternative TRA may be used alone or in combination with mycophenolate mofetil or another immunosuppressant (evidence level not reported, grade C recommendation). Rituximab and dexamethasone should be considered in those who fail TRAs, especially adolescent females (evidence level III, grade C recommendation).7
For children with ITP who have grade 4 bleeding, the Chinese-adaptation guideline suggest rescue therapy with combined platelet transfusion, pulse therapy of high-dose methylprednisolone, and pulse therapy of high-dose IVIG to ensure the most effective and rapid elevation of platelet counts for effective hemostasis. The addition of a thrombopoietic agent may be considered at the same time.9
The 2019 updated international consensus report on primary ITP recommended that TRAs be considered for emergency treatment of children with ITP of any stage to aid the acute response and prevent a decrease in platelet count if initial response to emergency therapy is lost (evidence level not reported, grade C recommendation).7
The 2018 interdisciplinary European working group noted that TRAs are effective for the treatment of chronic ITP in children and adolescents and provided supporting references. However, the group also stated that there is no standard treatment for chronic ITP in children and adolescents and patients should be referred to centres with expertise in pediatric hematology.8
Recommendations on Using Rituximab and TRAs for Pediatric Patients With ITP
For children with ITP who do not respond to first-line treatment, the Chinese-adaptation guideline development group suggests conventional second-line treatment with thrombopoietic agents rather than rituximab (level Ib evidence, grade A recommendation).9
For children with ITP who do not respond to first-line treatment and have non-life-threatening mucosal bleeding and/or diminished health-related quality of life, the ASH guideline panel suggests the use of TRAs rather than rituximab (conditional recommendation, very low certainty in the evidence) (recommendation 19).1
Limitations
Overall, the 4 evidence-based guidelines were associated with a few limitations as discussed in the Summary of Critical Appraisal section.1,7-9 The 2018 interdisciplinary European working group did not report the methodology associated with guideline development.8
None of the evidence-based guidelines included in this report provided recommendations for the use of dapsone in patients with ITP younger than 18 years of age. Moreover, none of the evidence-based guidelines were specific to the Canadian health care system, which limits generalizability because of differences in implementation considerations including access to treatments between countries and within Canadian jurisdictions (e.g., provincial public drug plans).
In the 3 guidelines that informed the use of TRAs (e.g., romiplostim, eltrombopag)1,7,9 as treatment for pediatric populations with ITP, the recommendations were not reported separately for the specific types of TRAs. The 2021 Chinese-adapted guidelines were provided for thrombopoietic agents and the 2019 ASH guidelines and the 2019 updated international consensus report on primary ITP were provided for TRAs. The broad reference to these interventions may not be informative because there are different drugs within these categories.2 Although there is evidence suggesting similar efficacy of romiplostim and eltrombopag in children with chronic ITP, data directly comparing the 2 drugs are not available.2
Conclusions and Implications for Decision- or Policy-Making
This report included information from 4 evidence-based guidelines,1,7-9 3 of which reported on the use rituximab and TRAs (e.g., romiplostim, eltrombopag)1,7,9 for the treatment of pediatric populations with ITP.
For children with ITP who do not respond to first-line treatment, rituximab, thrombopoietic agents, and TRAs were recommended over splenectomy as second-line treatment.1,9 For children with persistent or chronic ITP, it was recommended to switch to another TRA and/or consider combining with mycophenolate mofetil or another immunosuppressant if there is no response to 1 TRA or if the initial response is lost, and to consider using rituximab plus dexamethasone in those who fail TRAs, especially adolescent females.7 The 2018 interdisciplinary European working group stated there were no standard treatments for chronic ITP in children and adolescents, but noted that TRAs (e.g., eltrombopag and romiplostim) are effective for treatment of chronic ITP in children and adolescents.8
For rescue treatment of children with ITP who have grade 4 bleeding, the Chinese-adaptation guideline development group recommended considering thrombopoietic agent therapy combined with platelet transfusion, pulse therapy of high-dose methylprednisolone, and pulse therapy of high-dose IVIG.9 For emergency treatment of children with ITP of any stage, the 2019 updated international consensus report recommended TRAs be considered.7
Overall, there is a need for evidence-based guidelines specific to Canadian health care settings, with specific information on various TRAs, for the treatment of ITP in pediatric populations. Dapsone, rituximab, and romiplostim are used off-label in Canada to treat pediatric ITP. There are also data suggesting that newer generations of anti-CD20 monoclonal antibodies such as obinutuzumab may be more effective and better tolerated than rituximab, a first generation anti-CD20 monoclonal antibody.11 Therefore, there is a need for well-designed studies to support evidence-based guidelines that investigate the use of dapsone, rituximab, and newer anti-CD20 monoclonal antibody drugs in direct comparison with romiplostim and eltrombopag in the Canadian health care setting for the treatment of ITP children. No evidence-based guidelines were identified that recommended using dapsone to treat ITP in pediatric patients. Overall, the recommendations of the guidelines included in this report should be interpreted with caution due to methodological limitations and unknown generalizability in the Canadian context.
References
1.Neunert C, Terrell DR, Arnold DM, et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Advances. 2019;3(23):3829-3866. PubMed
2.Bussel JB. Immune thrombocytopenia (ITP) in children: management of chronic disease. In: Mahoney DHJ, Armsby C, eds. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Apr 11.
3.Friedman J, Beck C, Canadian Paediatric Society Acute Care Committee. Diagnosis and management of typical, newly diagnosed primary immune thrombocytopenia (ITP) of childhood. Paediatr Child Health 2019 24(1):54. Ottawa (ON): Canadian Pediatric Society; 2019: https://cps.ca/documents/position/immune-thrombocytopenia#ref1. Accessed 2022 May 12.
4.Bussel JB. Immune thrombocytopenia (ITP) in children: clinical features and diagnosis. In: O'Brien S, Armsby C, eds. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Apr 11.
5.Bussel JB. Immune thrombocytopenia (ITP) in children: initial management. In: O'Brien S, Armsby C, eds. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Apr 11.
6.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 May 12.
7.Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Advances. 2019;3(22):3780-3817. PubMed
8.Matzdorff A, Meyer O, Ostermann H, et al. Immune thrombocytopenia - current diagnostics and therapy: recommendations of a Joint Working Group of DGHO, ÖGHO, SGH, GPOH, and DGTI. Oncology Research and Treatment. 2018;41(suppl 5):1-30. PubMed
9.Working Group of Chinese Guideline for the Diagnosis and Treatment of Childhood Primary Immune Thrombocytopenia, Subspecialty Group of Hematologic Diseases Society of Pediatrics Chinese Medical Association, Editorial Board Chinese Journal of Pediatrics. Adapted guideline for the diagnosis and treatment of primary immune thrombocytopenia for Chinese children (2021). Pediatric Investigation. 2022:1-12.
10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
11.Du FH, Mills EA, Mao-Draayer Y. Next-generation anti-CD20 monoclonal antibodies in autoimmune disease treatment. Auto Immun Highlights. 2017;8(1):12-12. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality | Recommendations | Guideline validation |
|---|---|---|---|---|---|---|
Chinese-adapted guidelines (2021)9 | ||||||
Intended users:
Target population: children with primary ITP (1 month to 18 years of age) This guideline does not address neonatal ITP, secondary ITP, and non-immune mediated thrombocytopenia Guideline affiliated with the Working Group of Chinese Guideline for the Diagnosis and Treatment of Childhood Primary ITP | Intervention and comparators were not limited in inclusion criteria Interventions relevant to this report: rituximab and thrombopoietic agents | Outcomes of the clinical questions:
| 19 clinical questions (and associated outcomes) established through online consensus meetings with multiple discussions with core members of guideline adaptation working group. Multiple databases searched for published guidelines, which were adopted, adapted, or used to developed new recommendations; followed the ADAPTE approach Supplementary searches for additional evidence. Interviews with doctors, patients, and guardians | Methodological quality and risk of bias of supporting evidence assessed (e.g., Cochrane risk of bias tool for RCTs). Evidence levels (source of evidence):a,b
Grade of recommendation (level of evidence):a,c
| Guideline adaptation considered values, resources, and social and cultural factors specific to China; followed WHO Handbook for Guideline Development Development group (representing 11 provinces in China) included pediatric hematologists, a patient, a guardian, a guideline methodologist, an epidemiologist, and an editor of academic journals Medical resources, the environment, cost-effectiveness, feasibility, values, and preferences of parents and/or guardians were considered. 2 rounds of Delphi survey and online consensus meeting then revision, improvement, and finalization. | Survey to assess degree of agreement with recommendations, clarity, and clinical feasibility (completed by 57 clinicians and 3 guardians). External review by 5 hematologists and 1 methodologist. Revisions made based on the survey and external review. Consultation with Chinese Medical Association, Society of Pediatrics, and other guideline-issuing bodies and developers Final approval granted after review by steering committee. |
ASH guidelines (2019)1 | ||||||
Intended users:
Target population: adults and children with ITPb and non-life-threatening bleeding. Target population relevant to this report: children with ITPc and non–life-threatening bleeding. Guideline does not address treatments introduced after 2017 or emergency management of ITP. ASH previously published guidelines in 2011. | Management approaches discussed in guideline: observation, corticosteroids, IV immunoglobulin, anti-D immunoglobulin, rituximab, splenectomy, and TRAs. This guideline focused on first- and second-line management of ITP. Interventions relevant to this report: rituximab and TRAs (referred to as TPO-RA in this guideline). TRAs discussed include romiplostim and eltrombopag. | Outcomes of interest selected by panel for each a priori question based on relative importance for decision-making considering impact on patient outcomes:
Outcome definitions were consistent with published terminology. | Clinical questions selected by the panel through anonymous ranking and discussion until consensus was reached. Questions from the 2011 guidelines were reviewed and new questions were proposed. Clinical questions investigated with SRs (updated and original) following OUHSC guidance. SR methodology followed the Cochrane Handbook for SRs of Interventions. Evidence of baseline risks, costs, values, and preferences also searched. Evidence review followed GRADE EtD framework EtD tables summarized searched evidence (e.g., SR results) and addressed equity, acceptability, feasibility, intervention effects, resource utilization (cost-effectiveness), and values and preferences (relative importance of outcomes). | GRADE methodology to assess certainty in the evidence for each effect estimate of outcomes based on various domains Risk of bias assessed at outcome level using Cochrane tools for randomized trials and non-randomized studies. Strength of recommendation (interpretations of strength of recommendations were specified for patients,d clinicians,e policy-makers,f and researchersg):
| Development based on ASH policies GIN best practice. Panel (appointed by ASH) included adult and pediatric hematologists, methodologists, and patient representatives, Recommendations developed by panel based on review of EtD tables during 2 meetings that lasted 2 days each, online communication, and conference calls. Review conducted with a population perspective, considered balance of harms and benefits, resource use associated with alternative options, and assumptions of values and preferences. Consensus was required but in rare occasions voting was used (e.g., 80% majority required for a strong recommendation). | Draft recommendations reviewed and revised by all panel members. Reviewed by external stakeholders (i.e., medical professionals, allied organizations, patients, and public), and made accessible online on for comment. Reviewed by ASH Guideline Oversight Subcommittee. Approved by ASH Committee on Quality. |
Updated international consensus report on primary ITP (2019)7 | ||||||
Intended users: NR but likely to be individuals involved with the diagnosis and management of primary ITP. Target population: adults, pregnant adults, and children with primary ITP. Target population relevant to this report: children with primary ITP. Update to the International Consensus Report published in 2010. | Management approaches discussed in guideline: various pharmacological and surgical interventions for emergency treatment and first-line (newly diagnosed) therapy and beyond (lines NR but for children with persistent or chronic primary ITP). Interventions relevant to this report: rituximab and TRAs (referred to as TPO-RA in this guideline). TRAs discussed include romiplostim and eltrombopag. | Outcomes considered and eligible outcomes of the literature included from the PubMed search NR Implementation considerations (e.g., dosing), benefits, and risk were reported | PubMed search (January 1, 2009, to July 23, 2018, to retrieve articles published since the last literature search of the original report). | Evidence levels (source of evidence):b
Grade of recommendation (level of evidence):c
| Panelh members (from Europe, US, Canada, China, Australia, and Japan) included pediatric and adult hematologists, and a patient representative Update of the recommendations followed principles of CheckUp guidelines. 2 panel meetings held to discuss identified literature, draft consensus statements, and finalize updated recommendations. Consensus required; however, 100% consensus was not reached on every recommendation: 85% of recommendations achieved 85% agreement | All authors provided input on each draft of manuscript and approved the final version for submission. |
Interdisciplinary European working group (2018)8 | ||||||
Intended Users: Medical decision-making. Target Population: Adults, children, and adolescents with ITP. Target population relevant to this report: children and adolescents with ITP. | Management approaches discussed in guideline: various pharmacological and surgical interventions for ITP. Interventions relevant to this report: treatment of chronic ITP. No specific treatments were mentioned in recommendation but eltrombopag and romiplostim (TRAs) were discussed. | Methodology NR. Common side effects were mentioned. | Methodology NR. It was noted that recommendations were based on relevant publications published up until November 2017. Abstracts were also considered if they were presented at meetings in 2015 and thereafter. | Evidence level rating followed the Oxford Centre of Evidence-Based Medicine (March 2009). Recommendation rating (i.e., A, B, or 0) followed the National Program for Medical Service Guidelines, Method Report of 2010. Levels of recommendation:i
| Methodology NR. Recommendations developed by an interdisciplinary working group of experts from the German Society for Hematology and Medical Oncology, German Society for Transfusion Medicine and Immunohematology, Austrian Society for Hematology and Medical Oncology, Swiss Society for Hematology, Society for Pediatric Oncology and Hematology (country NR). | Methodology NR. |
ASH = American Society of Hematology; EC = expert consensus; EtD = evidence-to-decision; GIN = Guidelines International Network; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; HCP = health care professional; ITP = immune thrombocytopenia; IV = IV; MA = meta-analysis; NR = not reported; OUHSC = University of Oklahoma Health Sciences Center; RCT = randomized controlled trial; SR = systematic review; TPO-RA = thrombopoietin receptor agonist; TRA = thrombopoietin receptor agonist.
aAdopted processes from the 2019 updated international consensus report on primary ITP.7
bEvidence levels: Ia = MA of RCTs; Ib = ≥ 1 RCTs; IIa = ≥ 1 well-designed controlled studies without randomization; IIb = ≥ 1 other well-designed quasi-experimental studies; III = well-designed nonexperimental descriptive studies (e.g., comparative studies, case studies); IV = expert committee reports or opinions and/or experience of respected authorities.
cGrades of recommendation: A = ≥ 1 RCTs of overall good quality and consistency (Ia and Ib); B = well-conducted clinical studies when there are no randomized clinical trials available (IIa, IIb, and III); C = evidence from expert committee reports or opinions and/or experiences of respected authorities (IV).
cGuidelines focused on management of newly diagnosed, persistent, and chronic ITP refractory to first-line treatment.
dStrong recommendation for patients: Most individuals in this situation would want the recommended course of action, and only a small proportion would not. Conditional recommendation for patients: The majority of individuals in this situation would want the suggested course of action, but many would not. Decision aids may be useful in helping patients to make decisions consistent with their individual risks, values, and preferences.
eStrong recommendation for clinicians: Most individuals should follow the recommended course of action. Formal decision aids are not likely to be needed to help individual patients make decisions consistent with their values and preferences. Conditional recommendation for clinicians: Recognize that different choices will be appropriate for individual patients and that you must help each patient arrive at a management decision consistent with the patient’s values and preferences. Decision aids may be useful in helping individuals to make decisions consistent with their individual risks, values, and preferences.
fStrong recommendation for policy-makers: The recommendation can be adopted as policy in most situations. Adherence to this recommendation according to the guideline could be used as a quality criterion or performance indicator. Conditional recommendation for policy-makers: Policy-making will require substantial debate and involvement of various stakeholders. Performance measures about the suggested course of action should focus on whether an appropriate decision-making process is duly documented.
gStrong recommendation for researchers: The recommendation is supported by credible research or other convincing judgments that make additional research unlikely to alter the recommendation. On occasion, a strong recommendation is based on low or very low certainty in the evidence. In such instances, further research may provide important information that alters the recommendations. Conditional recommendation for researchers: This recommendation is likely to be strengthened (for future updates or adaptation) by additional research. An evaluation of the conditions and criteria (and the related judgments, research evidence, and additional considerations) that determined the conditional (rather than strong) recommendation will help identify possible research gaps.
hTwo members of the panel were experts in clinical trials methodology.
iLevels of recommendation: A = strong recommendation (“must”); B = recommendation (“should”); 0 = open recommendation (“can”); EC = the opinion of most experts on closest to good clinical practice when there is insufficient scientific data.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II6
Item | Chinese-adapted guidelines (2021)9 | ASH guidelines (2019)1 | Updated international consensus report on primary ITP (2019)7 | Interdisciplinary European working group guidelines (2018)8 |
|---|---|---|---|---|
Domain 1: Scope and Purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | No | No |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes — clinical and methodology personnel with patient and guardian representation. | Yes — clinical and methodology personnel with patient representation. | Yes — clinical and methodology personnel with patient representation. | No — only includes clinical experts |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes —13 parents and/or guardians provided preferences and values via survey. 1 patient and 1 guardian were on the GDP. | Yes — 2 patient representatives on guideline development panel. | Yes — 1 patient representative on guideline development panel. | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | No — NR but presumably individuals involved with diagnosis and management of primary ITP. | No — NR but presumably individuals involved with medical decision-making regarding ITP |
Domain 3: Rigour of Development | ||||
7. Systematic methods were used to search for evidence. | Yes — databases, main search terms, and inclusion criteria reported. | Yes — details NR but followed reputable methodology (e.g., Cochrane Handbook for SRs). | Yes — more details should be provided (e.g., inclusion and/or exclusion criteria). | No — NR |
8. The criteria for selecting the evidence are clearly described. | Yes | No | No | No — NR |
9. The strengths and limitations of the body of evidence are clearly described. | No but favourable and unfavourable factors of the instructions for implementation reported. | Not directly but limitations of the guidelines were reported. | No | No |
10. The methods for formulating the recommendations are clearly described. | Unclear — methodology could be more concise. | Yes | Yes | No — NR |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Unclear — although common side effects were discussed in the supporting evidence |
12. There is an explicit link between the recommendations and the supporting evidence. | Unclear — supplementary evidence was combined with source guideline evidence. Only supplementary evidence (i.e., searched by Chinese guideline development group) was reported. | Yes | Yes | Unclear |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes — guideline is published in Blood Advances journal but there was no mention of additional external review. | Unclear — NR but published in a peer-reviewed journal |
14. A procedure for updating the guideline is provided. | No | Yes | Yes — consensus report leadership will review need for updates yearly. | No |
Domain 4: Clarity of Presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes — instructions for implementation provided. | Yes — reported good practice statements that were not based on a SR of available evidence. | Yes — dosages and considerations such as platelet count reported. | Yes — dosages for frequently used drugs for ITP reported. |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Unclear | No — NR |
21. The guideline presents monitoring and/or auditing criteria. | No | Yes — ASH will conduct ongoing review by experts and survey for new evidence. | No | No |
Domain 6: Editorial Independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes — no reason to believe so, funding source reported. | Unlikely — funding entirely from ASH and guideline panel was appointed by ASH and most were ASH members. | Unclear — funding of the guideline development was NR but financial COIs were reported for authors. | Unclear — funding of the guideline development was NR but financial COIs were reported for authors |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes — no COIs to report. | Yes — COIs of guideline panel and/or SR team reported in main document and supplemental files. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASH = American Society of Hematology; COI = conflict of interest; GDP = guideline development group; ITP = immune thrombocytopenia; NR = not reported.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidencea | Quality of evidence and strength of recommendations |
|---|---|
Chinese-adapted guidelines (2021)9 | |
Second-line treatment (thrombopoietic agent, rituximab, or splenectomy as second-line treatment) in children with ITP who have no response to first-line treatment Recommendation(s):
Rationale for adaptation: Source guideline was adopted as supplementary evidence was consistent with source guideline evidence. Authors noted that in China, children and caregivers prefer to not undergo splenectomy upon failure of first-line treatment. Implementation consideration(s): 2 classes of thrombopoietic drugs are available in China — recombinant human thrombopoietin and TRAs.
Supplementary evidenceb:
| Recommendation 1: Level Ib evidence, Grade A Recommendation 2: Level Ib evidence, Grade A Recommendation 3: Level III evidence, Grade B |
Rescue treatment for children with ITP who have grade 4 bleeding Recommendation(s): “When grade 4 bleeding occurs in children with ITP, we suggest rescue therapy with combined platelet transfusion, pulse therapy of high-dose methylprednisolone, and pulse therapy of high-dose IVIG to ensure the most effective and rapid platelet counts elevation for effective hemostasis. At the same time, the addition of a thrombopoietic agent may be considered.” (p.9)9 Rationale for adaptation: Source guideline adopted with slight adaptations. The updated international consensus report on primary ITP (2019) recommended the use of TRAs for grade 4 bleeding to potentially elicit a quick response and prevent a drop in platelet count if initial emergency treatment fails. Guideline authors noted that while there was no direct evidence of recombinant human thrombopoietin use for grade 4 bleeding in children with ITP there was evidence from clinical experience in China. During administration for critical illness, it has been found that recombinant human thrombopoietin allows for the following advantages: faster onset of action compared to orally administered TRAs, facilitation of drug absorption via subcutaneous administration, and no hepatic metabolism. Implementation consideration(s): It was noted that grade 4 bleeding may occur at any stage of unremitting disease; thus, it is necessary to stabilize vital signs and rapidly elevate platelet counts to gain time for subsequent treatment. Authors highlighted that platelet transfusion is not recommended for children with ITP who do not have grade 4 bleeding. In such instances, emergency splenectomy may be performed or antifibrinolytics may be administered (especially in the event of gastrointestinal bleeding). Supplementary evidenceb: No supplementary evidence. |
|
ASH guidelines (2019)1 | |
Recommendation(s): “In children with ITP who have non–life-threatening mucosal bleeding and/or diminished HRQoL and do not respond to first-line treatment…”
Supporting evidencec:
Implementation consideration(s)d:
| Recommendation 19: Conditional recommendation with very low certainty in the evidence of effects Recommendation 20: Conditional recommendation with very low certainty in the evidence of effects Recommendation 21: Conditional recommendation with very low certainty in the evidence of effects |
Updated international consensus report on primary ITP (2019)7 | |
Emergency treatment of children with ITP of any stage Recommendation(s):
Supporting evidence: none specific to TPO-RAs. Implementation consideration(s): none specific to TPO-RAs. | Evidence level NR, Grade C |
Treatment of children with persistent or chronic ITP Recommendation(s):
Supporting evidence:
| Recommendation 4: evidence level Ib, Grade A Recommendation 5: evidence level NR, Grade C Recommendation 6: evidence level III, Grade C |
Interdisciplinary European working group guidelines (2018)8 | |
Treatment for chronic ITP in children and adolescents Recommendation(s): “As yet, there is no standard treatment for chronic ITP in children and adolescents. Patients should be referred to centers with expertise in pediatric hematology.” (p.19)8 Of note, authors noted that TRAs are effective for treatment of chronic ITP in children and adolescents with supporting references. Eltrombopag and romiplostim were discussed. | Evidence level: 5 (Range of evidence levels NR but followed the Oxford Centre of Evidence-Based Medicine [March 2009]) Degree of recommendation: expert consensus (EC) |
AE = adverse event; ASH = American Society of Hematology; HRQoL = health-related quality of life; IQR = interquartile range; ITP = immune thrombocytopenia; IVIG = IV immunoglobulin; NR = not reported; MMF = mycophenolate mofetil; QoL = quality of life; RCT = randomized controlled trial; TPO-RA = thrombopoietin receptor agonist; TRA = thrombopoietin receptor agonist; vs. = versus.
aImplementation considerations reported in this table do not include discussions related to cost in the source publications since none of the guidelines were specific to Canada. Please see source publications for this information.
bSupplementary evidence was combined with source guideline evidence. Only supplementary evidence (i.e., searched by Chinese guideline development group) was reported.
cGuideline authors were not able to estimate the relative effects regarding benefits, harms, and burdens due to lack of comparisons.
dIt was noted, during the guideline panel meetings, there was a lack of a liquid preparation for eltrombopag, which has since become available.
eSee p. 23 and p. 24 for supporting evidence and implementation considerations for TPO-RAs (as a whole).
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Guidelines With Unclear Methodology or Did Not Report a Systematic Approach to Guideline Development
Park YH, Kim DY, Kim S, et al. Management of immune thrombocytopenia: 2022 update of Korean experts recommendations. Blood Res. 2022;57(1):20-28. PubMed
Jang JH, Kim JY, Mun YC, et al. Management of immune thrombocytopenia: Korean experts recommendation in 2017. Blood Res. 2017 Dec;52(4):254-263. PubMed
Review Articles
Grainger JD, Kuhne T, Hippenmeyer J, Cooper N. Romiplostim in children with newly diagnosed or persistent primary immune thrombocytopenia. Ann Hematol. 2021 September;100(9):2143-2154. PubMed
Kuter DJ, Tarantino MD, Lawrence T. Clinical overview and practical considerations for optimizing romiplostim therapy in patients with immune thrombocytopenia. Blood Rev. 2021;49:100811. PubMed
Review of the 2019 ASH Guidelines
Sahi PK, Chandra J. Immune Thrombocytopenia: American Society of Hematology Guidelines, 2019. Indian Pediatr. 2020 09 15;57(9):854-856. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca