CADTH Health Technology Review
Reconsolidation and Consolidation Therapies for the Treatment and Prevention of Post-Traumatic Stress Disorder
Rapid Review
Authors: Keeley Farrell, Quenby Mahood
Abbreviations
PTSD
post-traumatic stress disorder
RCT
randomized controlled trial
Key Messages
The evidence about the clinical effectiveness of reconsolidation and consolidation therapies for the treatment and prevention of post-traumatic stress disorder (PTSD) is uncertain because these therapies include a wide range of interventions and the study results varied widely.
The results from 1 systematic review suggest there were significantly greater improvements in PTSD severity in patients treated with reconsolidation therapy versus control. However, 3 other systematic reviews reported conflicting findings with some reconsolidation therapies indicating significant improvements in PTSD symptoms or severity versus control, whereas other reconsolidation therapies had no significantly different outcomes than the control groups.
There was limited evidence suggesting that multi-modular motion-assisted memory desensitization and reprocessing therapy reduced PTSD symptoms in veterans with treatment-resistant and combat-related PTSD; however, the significance of these results was not reported.
There was limited evidence suggesting a significant difference in PTSD incidence in favour of adults exposed to trauma treated with hydrocortisone versus control. There were no significant differences in PTSD incidence between adults exposed to trauma treated with any 1 of propranolol, omega-3 fatty acids, gabapentin, or paroxetine versus placebo.
Context and Policy Issues
Post-traumatic stress disorder (PTSD) is a psychiatric disorder that can develop in individuals following exposure to a traumatic event.1 Symptoms of PTSD include intrusive and distressing memories or dreams, dissociative reactions, and psychological or physiologic distress related to the traumatic event.2 The person with PTSD must have been exposed to actual or threatened death, serious injury, or sexual violation.2 The person may have directly experienced or witnessed the traumatic event, learned that the event occurred to a close family member or friend, or experienced repeated exposure to details of the trauma.2 Symptoms must be present for at least 1 month for a diagnosis of PTSD.3 PTSD is associated with a variety of comorbidities, including depression, substance use disorders, chronic pain, and sleep problems.1,2 Acute stress disorder has similar symptoms to PTSD; however, it is diagnosed between 3 days and 1 month after the traumatic event.3 Additionally, the risk of suicide attempts is 2- to 3-fold higher in those with PTSD.2 The lifetime prevalence of PTSD in Canada is estimated to be 9.2% and is approximately twice as high in women as in men.2
Treatment for PTSD includes both pharmacotherapy and psychotherapy. Some of the psychotherapies that have been used to treat PTSD include cognitive behavioural therapy, cognitive processing therapy, and prolonged exposure therapy.2 Some of the pharmacological therapies that have been used in the treatment of PTSD include selective serotonin reuptake inhibitors (e.g., fluoxetine, paroxetine, sertraline), serotonin and noradrenaline reuptake inhibitors (e.g., venlafaxine, duloxetine), and atypical antipsychotic drugs (e.g., risperidone, olanzapine).2 Reconsolidation and consolidation therapies are emerging as a potential treatment and preventive options, respectively, for PTSD.
Memories are thought to be initially modifiable when they are first acquired and then solidify through the synthesis of new proteins in a process known as consolidation.4 Thus, consolidation therapy aims to disrupt traumatic memories before the consolidation process takes place. Consolidation therapy uses pharmacological drugs such as propranolol or behavioural approaches administered shortly after a traumatic event to prevent the development of acute stress disorder or PTSD.5 An example of a behavioural approach that can be used in consolidation therapy is competing tasks, such as using a video game with high visuospatial demands aimed to interfere with the consolidation of traumatic memories.5
The traditional theory in the memory field was that memories could not be changed once the consolidation process had occurred.4,6 This theory was displaced after literature was published that showed that after memory retrieval, previously consolidated memories become destabilized and require protein synthesis for long-term storage in a process termed reconsolidation.4 A range of research into reconsolidation was conducted due to its potential as a therapeutic target for various disorders, including PTSD.6 Reconsolidation was first studied in animals; however, the interventions used to disrupt reconsolidation (e.g., hypothermia, pharmacological drugs with serious adverse effects or toxicity) were not translatable to humans.7 Later studies in animal models found that reconsolidation could be targeted through the use of propranolol.7 Propranolol was then studied in humans and has been found to help with diminishing emotions associated with fear memories.8
Reconsolidation therapy involves the combination of a memory reactivation therapy with a pharmacological drug or brain stimulation treatment.6,9 Pharmacological drugs used in reconsolidation therapy can include propranolol, D-cycloserine, oxytocin, and hydrocortisone. Brain stimulation treatments can include transcranial magnetic stimulation and transcranial electrical current stimulation.9 One example of a memory reactivation therapy that can be used in reconsolidation therapy is prolonged exposure therapy. During prolonged exposure therapy, participants work with a therapist and are exposed to stimuli that evoke fear and remind them of their past trauma with the goal of increasing their comfort and reducing their fear.10
Several brain regions, including the amygdala, prefrontal cortex, hypothalamus, and hippocampus, are involved in PTSD.11 The amygdala is regulated by the prefrontal cortex and has a critical role in fear and anxiety, and modulates memory consolidation.11 Hyperactivity of the amygdala in patients with PTSD leads to impairment of the fear extinction system.11 Additionally, the noradrenergic system (a system of neurons responsible for the neurotransmitter norepinephrine) plays a role in the regulation of some PTSD symptoms, including nightmares, sleep dysregulation, and hyperarousal.11 The consolidation of fear memories is associated with the beta-adrenergic receptors and norepinephrine system because the binding of norepinephrine to these receptors causes memory consolidation through promotion of the synthesis of certain proteins.8 Further, studies have suggested that glucocorticoids enhance fear extinction and reduce retrieval of aversive memories,3,11 and that fear extinction is linked to N-methyl-d-aspartate receptor–function in the amygdala.9
A wide range of pharmacological drugs may be used in consolidation and reconsolidation therapy. Due to the involvement of the noradrenergic system and beta-adrenergic receptors in PTSD, as well as the consolidation of fear memories, adrenoreceptor blockers (such as yohimbine) and beta-adrenergic blockers (such as propranolol) are potential therapeutic options.8,11 Additionally, glucocorticoids (e.g., dexamethasone and hydrocortisone) and N-methyl-d-aspartate—receptor agonists (e.g., D-cycloserine) may have a role in reconsolidation and consolidation therapy. Lastly, intranasal oxytocin has been shown to enhance fear extinction in healthy individuals and reduce amygdala hyperactivity in patients with PTSD.9
Nonpharmacological options used in reconsolidation therapy can include brain stimulation treatments, which target brain regions such as the prefrontal cortex, amygdala, or hippocampus and may reduce PTSD symptoms and be used in reconsolidation therapy.9 Fear extinction may be enhanced by transcranial magnetic stimulation and fear memory consolidation may be disrupted by transcranial direct current stimulation.9
The aim of the current report is to summarize the evidence regarding the clinical effectiveness of reconsolidation therapy for the treatment of adults with PTSD and consolidation therapy for the prevention of acute stress disorder or PTSD in adults who have experienced trauma.
Research Questions
What is clinical effectiveness of reconsolidation therapy versus placebo or no treatment for adults with PTSD?
What is clinical effectiveness of reconsolidation therapy versus alternative interventions for adults with PTSD?
What is clinical effectiveness of consolidation therapy versus placebo or no treatment placebo for the prevention of PTSD or acute stress disorder in adults who have experienced trauma?
What is clinical effectiveness of consolidation therapy versus alternative interventions for the prevention of PTSD or acute stress disorder in adults who have experienced trauma?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, PsycInfo, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were post-traumatic stress disorder and reconsolidation/consolidation therapy. A secondary search was conducted with the concepts post-traumatic stress disorder and pharmacotherapies. CADTH-developed search filters were applied to limit retrieval for this secondary search to health technology assessments, systematic reviews, meta-analyses, network meta-analyses, or any types of clinical trials or observational studies. The searches were completed on March 30, 2022, and limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1 and Q2: Adults (aged 18 years or older) with PTSD Q3 and Q4: Adults (aged 18 years or older) who have experienced trauma |
Intervention | Q1 and Q2: Reconsolidation therapy Q3 and Q4: Consolidation therapy |
Comparator | Q1 to Q3: Placebo or no treatment Q2 to Q4: Alternative interventions (e.g., psychotherapy, such as cognitive behavioural therapy; pharmacotherapy) |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., symptom severity [e.g., PTSD symptoms, depressive symptoms], quality of life, safety [e.g., rate of adverse events, side effects]) Q3 and Q4: Clinical effectiveness (e.g., incidence of PTSD, incidence of acute stress disorder, severity of PTSD, quality of life, safety [e.g., rate of adverse, side effects]) |
Study designs | Health technology assessments, systematic reviews |
PTSD = post-traumatic stress disorder.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017. Systematic reviews in which all relevant studies were captured in other, more recent or more comprehensive systematic reviews were excluded.3,12-19
Critical Appraisal of Individual Studies
The included systematic reviews were critically appraised by 1 reviewer using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2).20 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
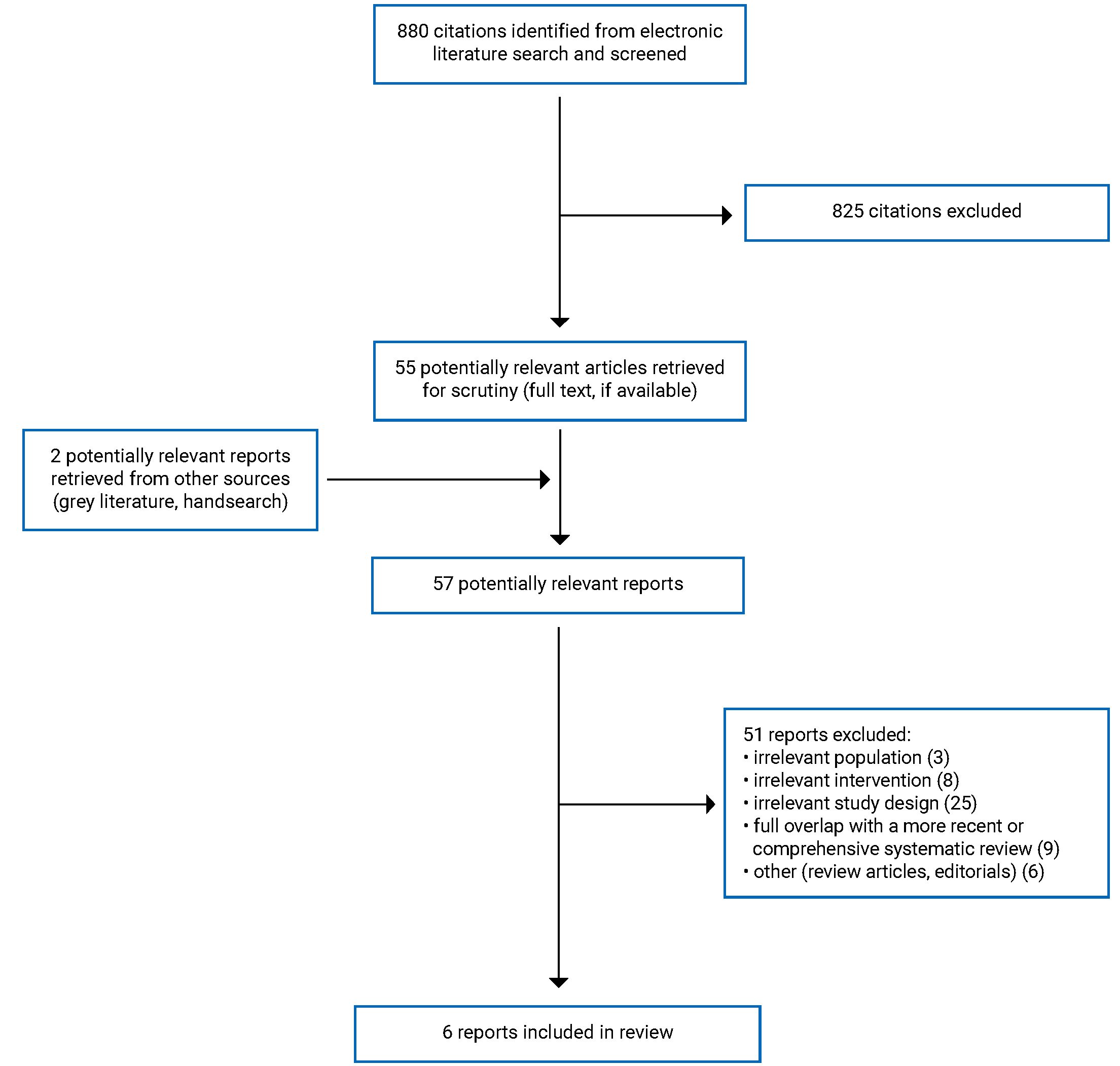
A total of 880 citations were identified in the literature search. Following screening of titles and abstracts, 825 citations were excluded and 55 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 51 publications were excluded for various reasons, and 6 systematic reviews met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA21 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
In total, 6 systematic reviews were included in this report comprising 2 with meta-analyses,22,23 1 with a network meta-analysis,24 and 3 others without pooled statistical analysis to estimate an overall combined treatment effect.25-27 There were 4 systematic reviews23,24,26,27 that included primary studies evaluating reconsolidation therapy, and 2 systematic reviews22,23 that included primary studies evaluating consolidation therapy.
All of the included systematic reviews had inclusion criteria that are broader than the present report. Specifically, 5 of the systematic reviews22,24-27 evaluated a range of interventions for PTSD other than consolidation or reconsolidation therapy. The systematic review by Baas et al. (2020)25 included studies evaluating any intervention for the treatment of PTSD in pregnant women with PTSD or exposure to trauma; however, none of the included studies evaluated reconsolidation or consolidation therapy for PTSD. Additionally, 1 of the systematic reviews23 included studies in pediatric participants in addition to studies in adult participants. Only the characteristics and results of the subset of relevant studies will be described in this report.
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
The systematic review and meta-analysis by Bertolini et al. (2022)22 included 13 randomized controlled trials (RCTs), 12 of which are relevant to the present report. Literature searches were conducted up to November 13, 2020, and no restrictions were imposed based on date of publication.22 The systematic review and meta-analysis by Astill Wright et al. (2021)23 included 25 RCTs, 24 of which are relevant to the present report. Literature searches were conducted up to March 20, 2020, and no restrictions were imposed based on date of publication.23 The systematic review by Baas et al. (2020)25 included 3 RCTs and 10 non-randomized studies, none of which are relevant to the present report. The search time frame was 1980 to June 2019.25 The systematic review by Knaust et al. (2020)26 included 18 studies in total, of which 6 RCTs, 1 single-arm before-after study, and 3 case studies are relevant to the present report. The search time frame was January 2013 to July 2020.26 The systematic review by Metcalf et al. (2020)27 included 34 RCTs, 12 of which are relevant to the present report. Literature searches were conducted up to December 21, 2018, and no restrictions were imposed based on date of publication.27 The systematic review and network meta-analysis by Merz et al. (2019)24 included 12 RCTs, 6 of which are relevant to the present report. The search time frame was January 1, 1980, to February 28, 2018.24 Results of the network meta-analysis are not presented in the present report due to overlap of relevant primary studies with other included systematic reviews and the inclusion of primary studies that are not relevant to this report in the network meta-analysis.
Four of the included systematic reviews22-24,27 had overlap in their included primary studies. Twelve primary studies were included in more than 1 systematic review. A citation matrix depicting the overlap between the included systematic reviews is provided in Appendix 5. Only primary studies that provide direct evidence that is relevant to this report were included in the overlap table.
Country of Origin
The included systematic reviews were conducted by authors in Italy,22 the UK,23 the Netherlands,25 Germany,26 Australia,27 and Switzerland.24
The relevant primary studies included in the systematic reviews by Bertolini et al. (2022),22 Astill Wright et al. (2021),23 and Knaust et al. (2020)26 were conducted in Canada, the US, Germany, Israel, the Netherlands, Japan, Romania, Brazil, Switzerland, and the UK. The countries where the relevant primary studies were conducted in the systematic reviews by Metcalf et al. (2020)27 and Merz et al. (2020)24 were not reported.
Patient Population
Two of the systematic reviews22,23 included studies of adults exposed to a traumatic event. In the systematic review by Bertolini et al. (2022),22 participants had to be exposed to the traumatic event within 3 months of receiving the intervention. The systematic review by Bertolini et al. (2022)22 excluded studies of participants who were symptomatic at baseline. In the systematic review by Astill Wright et al. (2021),23 participants were exposed to the traumatic event within 72 hours of receiving the intervention. The other 3 systematic reviews24,26,27 included studies of adults diagnosed with PTSD. The 5 included systematic reviews22-24,26,27 encompassed studies of participants that were exposed to a range of traumatic events, including assault, injury, motor vehicle accident, cardiac surgery, septic shock, Caesarean section, and combat-related events.
Interventions and Comparators
The systematic review by Bertolini et al. (2022)22 included studies of any pharmacological intervention administered with the intention to prevent the onset of PTSD or PTSD symptoms within 3 months of trauma. The consolidation interventions evaluated in the relevant studies include dexamethasone, hydrocortisone, propranolol, gabapentin, omega-3 fatty acids, paroxetine, and 5-hydroxytryptophan.22 The eligible comparators were placebo or any active pharmacological drug.
The systematic review by Astill Wright et al. (2021)23 included any consolidation- or reconsolidation-based prevention or treatment intervention. For reconsolidation, the interventions evaluated in the relevant studies include propranolol with memory reactivation, mifepristone with memory reactivation, mifepristone and D-cycloserine with memory reactivation, hydrocortisone with memory reactivation, sirolimus with memory reactivation, electroconvulsive therapy with memory reactivation, and reconsolidation of traumatic memories.23 The consolidation interventions evaluated in the relevant studies include hydrocortisone, dexamethasone, propranolol, oxytocin, a virtual reality pain task, a cognitive task memory interference procedure, and a cognitive task memory interference procedure with memory reactivation.23 The eligible comparators were placebo, pharmacological, or psychosocial interventions.
The systematic review by Knaust et al. (2020)26 included studies of any virtual trauma intervention that used immersive technology with the goal to reduce PTSD symptoms. Immersive technology was defined as technology that delivers an inclusive, extensive, surrounding, and vivid illusion of reality.26 The reconsolidation interventions evaluated in the relevant studies include multi-modular motion-assisted memory desensitization and reconsolidation, virtual reality exposure therapy with D-cycloserine, virtual reality exposure therapy with dexamethasone, virtual reality exposure therapy with alprazolam, and virtual reality exposure therapy with transcranial direct current stimulation.26 The eligible comparators were not specified.
The systematic review by Metcalf et al. (2020)27 included studies of any first-line PTSD treatment in combination with an augmentation intervention. Augmentation interventions were defined as any psychological, nonpsychological, or pharmacological intervention, delivered before, along with, or after a first-line PTSD treatment.27 The reconsolidation interventions evaluated in the relevant studies include prolonged exposure therapy in combination with 1 of the following: repetitive transcranial magnetic stimulation, D-cycloserine, oxytocin, yohimbine, hydrocortisone, methylene blue, paroxetine, or sertraline.27 The eligible comparators were first-line PTSD treatments alone.
The systematic review by Merz et al. (2019)24 included studies of any psychotherapeutic treatments, pharmacological treatments, or combinations of both. The reconsolidation interventions evaluated in the relevant studies include prolonged exposure therapy with sertraline or paroxetine, and exposure therapy with fluoxetine.24 The eligible comparators were any active psychotherapeutic or pharmacological PTSD treatment.
Outcomes
The systematic reviews22-24,26,27 used a range of scales to assess PTSD severity. These include the Clinician-Administered PTSD Scale, the PTSD Checklist, Post-Traumatic Stress Symptom 10-Question Inventory questionnaire, the Post-traumatic Stress Diagnostic Scale, the Post-traumatic Symptom Scale, Mini-International Neuropsychiatric Interview, and Davidson Trauma Scale.
The systematic reviews by Bertolini et al. (2022)22 and Astill Wright et al. (2021)23 assessed PTSD incidence using a range of tools, including the Clinician-Administered PTSD Scale, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (known as DSM-IV)—based interviews, Comprehensive International Diagnostic Interview PTSD, the Post-traumatic Symptom Scale, Post-Traumatic Stress Symptom 10-Question Inventory questionnaire, the Self-Rating Inventory for PTSD, the PTSD Checklist, and the revised Impact of Events Scale.
The systematic review by Astill Wright et al. (2021)23 assessed the severity of symptoms of re-experiencing traumatic memories using re-experiencing subscales and intrusive memories that were reported using a paper diary.
In the systematic review by Bertolini et al. (2022),22 quality of life was assessed using the 36-Item Short-Form Health Survey and depression was assessed using the Center for Epidemiologic Studies Depression scale, the Quick Inventory of Depressive Symptomatology, and the Montgomery-Asberg Depression Rating Scale. The systematic review by Metcalf et al. (2020)27 did not report the scales used to assess depression, anxiety, and quality of life.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Since the systematic review by Baas et al. (2020)25 did not include any relevant primary studies, only the sections relevant to this report (e.g., protocol, search strategy) were critically appraised. Additionally, the network meta-analysis conducted as part of the Merz et al. (2019)24 systematic review was not critically appraised given that it included results from studies that are not relevant to the present report.
The study eligibility criteria were clearly defined for all of the included systematic reviews. However, eligible comparators were not specified in the systematic reviews by Baas et al. (2020)25 and Knaust et al. (2020).26 The review methods were established before the conduct of the review for 4 of the systematic reviews.22-25The protocol of the Bertolini et al. (2022)22 systematic review was published and the other 3 systematic reviews registered their protocols.23-25 The authors of the Knaust et al. (2020)26 review stated that the inclusion criteria were established a priori; however, they do not state whether other methods (e.g., search strategy, research questions) were established before conducting the review. The authors of the Metcalf et al. (2020)27 systematic review do not state whether any of the review methods were established before conducting the review. This has the potential to introduce bias if the review methods were adjusted after the review had begun.
All of the searches were conducted in multiple databases and the key search terms used were provided.22-27 Five of the systematic reviews22-25,27 also searched trial registries. The authors of the Knaust et al. (2020)26 review do not state whether they searched trial registries. Additionally, the authors of the Knaust et al. (2020)26 and Metcalf et al. (2020)27 reviews do not state whether they handsearched the reference lists of the included articles to identify additional literature. Providing details of these elements of the search strategy increases its reproducibility. Study selection was performed by 2 independent reviewers in 3 of the systematic reviews.22,23,26 In 2 of the systematic reviews, full-text screening was performed in duplicate; however, abstract screening was done by a single reviewer in the review by Baas et al. (2020)25 and the authors of the Merz et al. (2019)24 review did not state whether abstract screening was performed in duplicate. The authors of the Metcalf et al. (2020)27 review did not state whether study selection was performed in duplicate. Performing study selection in duplicate helps reduce the risk of bias in study selection. A list of excluded studies with reasons for exclusion was provided in the systematic review by Bertolini et al. (2022).22 The other 5 systematic reviews23-27 did not provide lists of the excluded studies; however, they did provide reasons for exclusion in flow charts of study selection. Unjustified exclusion of studies could bias the results of the review.
Data extraction was performed in duplicate in 3 of the systematic reviews.22-24 In the systematic review by Metcalf et al. (2020),27 1 reviewer extracted data and another reviewer checked the data. The authors of the Knaust et al. (2020)26 systematic review do not state whether data extraction was performed in duplicate. Performing data extraction in duplicate increases the completeness and accuracy of data capture. The included primary studies were described in detail in the systematic review by Bertolini et al. (2022).22 In the other 4 systematic reviews,23,24,26,27 some details of the included primary studies were not reported. The time frame for follow-up and countries for the included primary studies were not specified in the systematic reviews by Metcalf et al. (2020)27 and Merz et al. (2019).24 The risk of bias in included primary studies was assessed using a satisfactory technique in 4 of the systematic reviews.22-24,27 In 3 of these systematic reviews,22,23,27 the risk of bias assessment was performed independently by 2 reviewers. Risk of bias in the included primary studies was not assessed in the systematic review by Knaust et al. (2020).26 Appropriate methods for the statistical combination of results were used in the meta-analysis by Bertolini et al. (2022).22 A random-effects model was used for the meta-analysis due to clinical heterogeneity among the included primary studies.22 Only results from studies assessing the same intervention were combined in meta-analysis.22 Subgroup analyses excluding studies at high risk of bias from the meta-analysis were pre-planned; however, they could not be carried out due to a lack of data.22 Additionally, publication bias could not be assessed through funnel plots due to the low number of studies per comparison.22 In the systematic review by Astill Wright et al. (2021)23 statistical heterogeneity was assessed and the choice of a fixed- or random-effects model for the meta-analysis followed from this assessment. However, due to the inclusion of heterogeneous interventions, a random-effects model may have been more appropriate for all analyses. Further, it may not have been appropriate to combine the results from studies that assessed a wide range of heterogenous interventions into a single pooled estimate. However, heterogeneity was assessed through several sensitivity analyses of subgroups of various interventions.23 Sensitivity analyses to assess the impact of risk of bias in individual studies on results of the meta-analysis were not performed and the authors do not state whether they assessed publication bias.23 The funding sources for the review were reported and potential conflicts of interest were disclosed in 3 of the systematic reviews.22,23,26 The funding source for the systematic review by Metcalf et al. (2020)27 was reported; however, the authors did not state whether they had any potential conflicts of interest. Potential conflicts of interest were disclosed by the authors of the Merz et al. (2019)24 systematic review; however, the funding source for the review was not reported.
Summary of Findings
The overall findings of the included studies are presented in the following text. Detailed summaries of the main findings are provided in Appendix 4. There was some overlap in the primary studies that were included in the systematic reviews; the pooled estimates from separate reviews thus contain some of the same data. A citation matrix illustrating the degree of overlap is presented in Appendix 5. When possible, data from relevant primary studies were presented only once.
Clinical Effectiveness of Reconsolidation Therapy
PTSD Severity
The meta-analysis conducted by Astill Wright et al. (2021)23 pooled results from studies that evaluated various reconsolidation interventions versus control groups. The meta-analysis suggested there were statistically significant differences in PTSD severity and re-experiencing severity at 1 to 4 weeks in favour of all pharmacological, electroconvulsive therapy, and psychological reconsolidation interventions (pooled result of a range of reconsolidation therapies) versus control.23 There were statistically significant differences in PTSD severity and re-experiencing severity at 2 weeks in favour of reconsolidation of traumatic memories versus control.23 There was no significant difference in PTSD severity at 1 to 4 weeks for all pharmacological and electroconvulsive therapy reconsolidation interventions versus control.23 There was no significant difference in PTSD severity at 1 week for propranolol with memory reactivation versus control.23
The systematic reviews by Knaust et al. (2020),26 Metcalf et al. (2020),27 and Merz et al. (2019)24 reported results from relevant primary studies individually. A wide range of reconsolidation therapies were evaluated. The results of some of the relevant primary studies suggested there were significant differences in PTSD symptoms or severity in favour of reconsolidation therapy versus control whereas results from other studies suggested there were no significant differences between treatment groups.
The systematic review by Knaust et al. (2020)26 reported that virtual reality exposure therapy with D-cycloserine was superior to virtual reality exposure therapy with placebo for PTSD severity (1 RCT). However, results from a different relevant RCT included in the systematic review suggested there were no significant difference in PTSD severity measured post-treatment between virtual reality exposure therapy with D-cycloserine and virtual reality exposure therapy with placebo.26 The systematic review reported a significant difference in PTSD severity measured at post treatment that favoured virtual reality exposure therapy with placebo versus virtual reality exposure therapy with alprazolam (1 RCT).26 Multi-modular motion-assisted memory desensitization and reconsolidation therapy reduced PTSD symptoms in veterans with treatment-resistant and combat-related PTSD (2 RCTs); however, the significance of these results versus control groups was not reported.26 The systematic review also reported modest therapy gains (1 single-arm before-after study) and positive treatment results (3 case studies) for patients with treatment-resistant and combat-related PTSD treated with multi-modular motion-assisted memory desensitization and reconsolidation therapy.26
The systematic review by Metcalf et al. (2020)27 reported no significant difference in PTSD symptoms for prolonged exposure with intranasal oxytocin (1 RCT), prolonged exposure with yohimbine (1 RCT), imaginal exposure with methylene blue (1 RCT), or prolonged exposure with sertraline (2 RCTs) versus control groups. The systematic review reported mixed results for prolonged exposure with D-cylcoserine.27 Results from 1 RCT included in the review suggested that patients treated with prolonged exposure with D-cycloserine were significantly more likely to show treatment response measured post-treatment.27 However, the systematic review also reported results from a different RCT that suggested that the prolonged exposure with D-cycloserine group performed significantly worse on measures of PTSD post treatment.27 Additionally, the review reported mixed results for prolonged exposure with paroxetine versus control groups.27 The systematic review reported results from 1 RCT that suggested there was a significant difference in improvement in PTSD symptoms in favour of the prolonged exposure with paroxetine group versus prolonged exposure alone.27 However, the systematic review also reported results from 2 other RCTs that suggested there were no significant differences for PTSD symptoms between prolonged exposure with paroxetine versus control groups.27
The systematic review by Merz et al. (2019)24 reported no significant difference in PTSD symptom severity measured at the end of treatment (12 weeks) for exposure therapy with fluoxetine versus fluoxetine alone; however, there was a significant difference in PTSD symptom severity in favour of the exposure therapy with fluoxetine group measured at the last available follow-up (length of follow-up not reported) (1 RCT).
Additional Efficacy Outcomes
Several relevant RCTs included in the Metcalf et al. (2020)27 systematic review reported on depression and quality of life. The systematic review reported results from 3 relevant RCTs that suggested there were no significant differences between treatment groups for depression.27 The systematic review also reported results from 1 RCT that suggested that reconsolidation therapy using prolonged exposure with D-cycloserine performed significantly worse on measures of depression than the control group at post treatment.27 Results from a different RCT included in the review suggested there were significant reductions in symptoms of depression within the prolonged exposure with repetitive transcranial magnetic stimulation group.27 There was a significant difference in favour of imaginal exposure with methylene blue versus control in quality of life for mental health (1 RCT).27 The systematic review reported results from another relevant RCT that suggested that the prolonged exposure with paroxetine group had significantly greater improvement in quality of life versus those in the control group.27
Safety
The systematic review by Metcalf et al. (2020)27 indicates that several of its included relevant RCTs reported adverse events. However, there were limited details on specific adverse events and distribution across study groups.27
Eleven relevant RCTs included in the Metcalf et al. (2020)27 and Merz et al. (2019)24 systematic reviews evaluated treatment dropout. There were statistically significant differences between treatment groups in dropout in some of the studies and in other studies there were no significant differences between groups. One relevant RCT included in the Metcalf et al. (2020)27 systematic review evaluated treatment adherence and the results suggested there were statistically significant differences between treatment groups.
Clinical Effectiveness of Consolidation Therapy
PTSD Incidence
The meta-analysis conducted by Bertolini et al. (2022)22 suggested that there were no significant differences between propranolol and placebo in PTSD rate at 3 months or at the studies’ end point (ranging from 6 weeks to 3 months). Four relevant RCTs included in the systematic review that were not included in the meta-analysis found no significant difference in PTSD rate between other consolidation therapies and control.22
The meta-analysis conducted by Astill Wright et al. (2021)23 pooled results from studies that evaluated various consolidation interventions versus control groups. The meta-analysis suggested there was a statistically significant difference in PTSD incidence at 1 month to 48 months in favour of all pharmacological, and psychological consolidation interventions (pooled result of a range of consolidation therapies) versus control.23 When studies evaluating hydrocortisone were removed from the analysis there was no significant difference in PTSD incidence at 1 month to 48 months for all pharmacological and psychological consolidation interventions (without hydrocortisone) versus control.23 There was a statistically significant difference in PTSD incidence at 3 months to 48 months in favour of all pharmaceutical consolidation interventions versus control.23 PTSD incidence at 3 months to 31 months was statistically significantly different in favour of hydrocortisone versus control.23 There was no significant difference in PTSD incidence at 1 month to 6 months for cognitive memory task interference procedure versus control.23
PTSD Severity
The meta-analysis conducted by Bertolini et al. (2022)22 suggested that there were no significant differences between propranolol and placebo in PTSD severity at 3 months or at the studies’ end point (ranging from 6 weeks to 3 months). The results for PTSD severity from 6 relevant RCTs evaluating other consolidation therapies were reported individually by study. The systematic review reported the results from 1 RCT that suggested that there is a statistically significant difference in PTSD severity in favour of 5-hydroxytryptophan versus placebo.22 There were no significant differences between treatment groups in PTSD severity in the other 5 RCTs included in the systematic review that reported on this outcome.22
The meta-analysis by Astill Wright et al. (2021)23 suggested there were no significant differences in PTSD severity at 2 weeks to 6 months or re-experiencing severity at 2 weeks to 48 months for all pharmacological and psychological consolidation interventions versus control. There was no significant difference in PTSD severity at 3 to 6 months for all pharmacological consolidation interventions versus control.23 Virtual reality pain task showed no significant differences in PTSD severity or re-experiencing severity at 6 months versus control.23 For cognitive memory task interference procedure versus control, there were no significant differences in PTSD severity at 2 weeks to 6 months or re-experiencing severity at 4 weeks.23
Intrusive Memory Frequency
The meta-analysis by Astill Wright et al. (2021)23 suggested that there was a significant difference in intrusive memory frequency at 1 week in favour of cognitive memory task interference procedure versus control.
Additional Efficacy Outcomes
Results for depression severity were reported individually for 4 relevant RCTs in the systematic review by Bertolini et al. (2022).22 There were no significant differences between treatment groups in depression severity in 3 of the RCTs.22 In 1 of the RCTs there were no significant differences in depression severity assessed at baseline and follow-up.22
Results for quality of life were reported individually for 3 relevant RCTs in the systematic review by Bertolini et al. (2022).22 There were no significant differences in quality of life between the treatment groups in any of the 3 RCTs.22
Safety
Dropouts due to adverse events were reported in 3 relevant RCTs in the systematic review by Bertolini et al. (2022).22 In 2 of the RCTs none of the participants dropped out due to adverse events.22 In 1 RCT there were no significant differences between treatment groups in dropouts rates due to adverse events.22
The meta-analysis conducted by Bertolini et al. (2022)22 suggested there were no significant differences between propranolol and placebo in dropout rates for any reason at 3 months or study end point (ranging from 6 weeks to 3 months). The meta-analysis suggested there were no significant differences between hydrocortisone versus placebo in dropout rates for any reason at study end point (ranging from 6 months to 49 months).22 The results for dropout for any reason from 4 relevant RCTs evaluating other consolidation therapies were reported individually by study. There were no significant differences between treatment groups in dropout rate for any reason at various time points in the 4 RCTs.22
Limitations
No evidence was identified that evaluated consolidation therapy for the prevention of acute stress disorder. Additionally, there was very limited evidence on the safety of reconsolidation and consolidation therapies reported in the included systematic reviews.
The relevant primary studies summarized in the included systematic reviews were of variable methodological quality. The systematic review authors’ ratings of the overall certainty of the evidence ranged from very low to low and many of the included primary studies were assessed as having moderate to high risk of bias.22-24,27 The authors of the Knaust et al. (2020)26 systematic review did not assess the risk of bias in the included primary studies; however, several relevant case studies and a single-arm before-after study were included, and are expected to be at high risk of bias due to the study design.
The relevant primary studies summarized in the included systematic reviews used a wide range of scales to assess PTSD severity. The minimal clinically important differences for these scales were not discussed in the systematic reviews; thus, it is unclear if the magnitude of benefits reported for of the reconsolidation and consolidation therapies are clinically meaningful.
Conclusions and Implications for Decision- or Policy-Making
This report summarizes evidence on the clinical effectiveness of reconsolidation therapy for the treatment of PTSD and consolidation therapy for the prevention of PTSD from 2 systematic reviews with meta-analyses,22,23 1 systematic review with a network meta-analysis,24 and 3 other systematic reviews25-27 that did not combine data from primary studies in a statistical analysis to estimate an overall treatment effect. Four of the systematic reviews23,24,26,27 reported on reconsolidation therapy and 2 systematic reviews22,23 reported on consolidation therapy.
The reconsolidation therapies varied widely across the included systematic reviews,23,24,26,27 and the evaluated interventions included a variety of memory reactivation procedures in combination with a range of pharmacological drugs and nondrug therapies, such as electroconvulsive therapy. The evidence was mixed with the results of some studies suggesting there were statistically significant differences in PTSD severity between patients treated with reconsolidation therapy versus control, and the results from other studies suggesting no significant differences between treatment groups. The meta-analysis conducted by Astill Wright et al. (2021)23 suggested there were statistically significant differences in PTSD severity and re-experiencing severity at 1 week to 4 weeks in favour of all pharmacological, electroconvulsive therapy, and psychological reconsolidation interventions versus control. The results of some of the relevant primary studies included in the systematic reviews by Knaust et al. (2020),26 Metcalf et al. (2020),27 and Merz et al. (2019)24 suggested there were significant differences in PTSD symptoms or severity in favour of reconsolidation therapy versus control, whereas results from other studies included in the systematic reviews suggested there were no significant differences between treatment groups. The systematic review by Knaust et al. (2020)26 reported that multi-modular motion-assisted memory desensitization and reprocessing therapy reduced PTSD symptoms in veterans with treatment-resistant and combat-related PTSD; however, the significance of these results was not reported. Although 1 systematic reviews27 reported primary study level adverse events, information on the specific adverse events was not provided. The other included systematic reviews did not report any safety outcomes.23,24,27
A wide range of consolidation therapies were evaluated in the included systematic reviews.22,23 The consolidation interventions evaluated included a range of pharmaceutical drugs, virtual reality pain tasks, and cognitive task memory interference procedures. The evidence was mixed with the results of some studies suggesting there were statistically significant differences in PTSD incidence or severity between patients treated with consolidation therapy versus those in the control group, and results from other studies suggesting there were no significant differences between treatment groups. The meta-analysis conducted by Bertolini et al. (2022)22 suggested that there were no significant differences between propranolol and placebo in PTSD incidence at 3 months or at the studies’ end point (ranging from 6 weeks to 3 months). Additionally, the systematic review reported results from relevant RCTs that suggested there were no significant differences in PTSD incidence between omega-3 fatty acids, gabapentin, or paroxetine versus placebo.22 The meta-analysis conducted by Astill Wright et al. (2021)23 suggested there was a statistically significant difference in PTSD incidence at 1 month to 48 months in favour of all pharmacological and psychological consolidation interventions versus control. However, when studies evaluating hydrocortisone were removed from the analysis, there was no significant difference in PTSD incidence at 1 month to 48 months for all pharmacological and psychological consolidation interventions (without hydrocortisone) versus control.23 The results of the meta-analysis suggested there was a statistically significant difference in PTSD incidence at 3 months to 31 months in favour of hydrocortisone versus control.23 One of the systematic reviews reported dropouts due to adverse events individually by study for the relevant studies.22 The other systematic review did not report any safety outcomes.23
Due to the wide range of heterogeneous reconsolidation and consolidation interventions evaluated in the included systematic reviews, it is difficult to draw conclusions around the clinical effectiveness of reconsolidation therapy for the treatment of PTSD or consolidation therapy for the prevention of PTSD. The limitations of the included literature (e.g., limited safety data, variable quality of primary studies in identified systematic reviews) should be considered when interpreting the findings of this report. Future research that focuses on specific reconsolidation or consolidation therapies or the comparative efficacy of different reconsolidation or consolidation approaches could help determine the clinical effectiveness of reconsolidation therapy for adults with PTSD or the clinical effectiveness of consolidation therapy for the prevention of PTSD or acute stress disorder in adults who have experienced trauma.
References
1.Castro-Vale I, Carvalho D. The pathways between cortisol-related regulation genes and PTSD psychotherapy. Healthcare (Basel). 2020;8(4):01.
2.Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders. BMC Psychiatry. 2014;14 Suppl 1:S1. PubMed
3.Astill Wright L, Sijbrandij M, Sinnerton R, Lewis C, Roberts NP, Bisson JI. Pharmacological prevention and early treatment of post-traumatic stress disorder and acute stress disorder: a systematic review and meta-analysis. Transl Psychiatry. 2019;9(1):334. PubMed
4.Monfils MH, Holmes EA. Memory boundaries: opening a window inspired by reconsolidation to treat anxiety, trauma-related, and addiction disorders. Lancet Psychiatry. 2018;5(12):1032-1042. PubMed
5.Brewin CR. Memory and forgetting. Curr Psychiatry Rep. 2018;20(10):87. PubMed
6.Dunbar AB, Taylor JR. Reconsolidation and psychopathology: moving towards reconsolidation-based treatments. Neurobiol Learn Mem. 2017;142(Pt A):162-171.
7.Beckers T, Kindt M. Memory reconsolidation interference as an emerging treatment for emotional disorders: strengths, limitations, challenges, and opportunities. Annu Rev Clin Psychol. 2017;13:99-121. PubMed
8.AlOkda AM, Nasr MM, Amin SN. Between an ugly truth and a perfect lie: wiping off fearful memories using beta-adrenergic receptors antagonists. J Cell Physiol. 2019;234(5):5722-5727. PubMed
9.Smith NB, Doran JM, Sippel LM, Harpaz-Rotem I. Fear extinction and memory reconsolidation as critical components in behavioral treatment for posttraumatic stress disorder and potential augmentation of these processes. Neurosci Lett. 2017;649:170-175. PubMed
10.American Psychological Association. Prolonged exposure (PE). Clinical practice guideline for the treatment of posttraumatic stress disorder. 2020; https://www.apa.org/ptsd-guideline/treatments/prolonged-exposure. Accessed 2022 May 4.
11.Akhtar A, Pilkhwal Sah S. Advances in the pharmacotherapeutic management of post-traumatic stress disorder. Expert Opin Pharmacother. 2021;22(14):1919-1930. PubMed
12.Hoskins MD, Sinnerton R, Nakamura A, et al. Pharmacological-assisted psychotherapy for post-traumatic stress disorder: a systematic review and meta-analysis. Eur J Psychotraumatol. 2021;12(1):1853379. PubMed
13.Eshuis LV, van Gelderen MJ, van Zuiden M, et al. Efficacy of immersive PTSD treatments: a systematic review of virtual and augmented reality exposure therapy and a meta-analysis of virtual reality exposure therapy. J Psychiatr Res. 2021;143:516-527. PubMed
14.Cassani R, Novak GS, Falk TH, Oliveira AA. Virtual reality and non-invasive brain stimulation for rehabilitation applications: a systematic review. J Neuroeng Rehabil. 2020;17(1):147. PubMed
15.Deng W, Hu D, Xu S, et al. The efficacy of virtual reality exposure therapy for PTSD symptoms: a systematic review and meta-analysis. J Affect Disord. 2019;257:698-709. PubMed
16.Walsh KH, Das RK, Saladin ME, Kamboj SK. Modulation of naturalistic maladaptive memories using behavioural and pharmacological reconsolidation-interfering strategies: a systematic review and meta-analysis of clinical and 'sub-clinical' studies. Psychopharmacology (Berl). 2018;235(9):2507-2527. PubMed
17.Kothgassner OD, Pellegrini M, Goreis A, et al. Hydrocortisone administration for reducing post-traumatic stress symptoms: a systematic review and meta-analysis. Psychoneuroendocrinology. 2021;126:105168. PubMed
18.Birk JL, Sumner JA, Haerizadeh M, et al. Early interventions to prevent posttraumatic stress disorder symptoms in survivors of life-threatening medical events: a systematic review. J Anxiety Disord. 2019;64:24-39. PubMed
19.Ma J, Hu D, Feng Z, et al. The effectiveness and safety of beta antagonist in burned patients: a systematic review and meta-analysis. Int Wound J. 2020;17(6):1881-1892. PubMed
20.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
22.Bertolini F, Robertson L, Bisson JI, et al. Early pharmacological interventions for universal prevention of post-traumatic stress disorder (PTSD). Cochrane Database Syst Rev. 2022;2:CD013443. PubMed
23.Astill Wright L, Horstmann L, Holmes EA, Bisson JI. Consolidation/reconsolidation therapies for the prevention and treatment of PTSD and re-experiencing: a systematic review and meta-analysis. Transl Psychiatry. 2021;11(1):453. PubMed
24.Merz J, Schwarzer G, Gerger H. Comparative efficacy and acceptability of pharmacological, psychotherapeutic, and combination treatments in adults with posttraumatic stress disorder: a network meta-analysis. JAMA Psychiatry. 2019;76(9):904-913. PubMed
25.Baas MAM, van Pampus MG, Braam L, Stramrood CAI, de Jongh A. The effects of PTSD treatment during pregnancy: systematic review and case study. Eur J Psychotraumatol. 2020;11(1):1762310. PubMed
26.Knaust T, Felnhofer A, Kothgassner OD, Hollmer H, Gorzka RJ, Schulz H. Virtual trauma interventions for the treatment of post-traumatic stress disorders: a scoping review. Front Psychol. 2020;11:562506. PubMed
27.Metcalf O, Stone C, Hinton M, et al. Treatment augmentation for posttraumatic stress disorder: a systematic review. Clin Psychol Sci Pract. 2020;27(1):e12310.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Bertolini et al. (2022)22 Italy University of York (UK), University of Verona (Italy), NIHR (UK) | Study design: SR and meta-analysis Included studies: 13 RCTs including 12 that are relevant to the present report. | Studies of adults aged 18 and older with history of a traumatic event. Studies that included participants who were symptomatic at baseline were excluded. | Eligible interventions: Any pharmacological intervention administered with the intention to prevent the onset of PTSD or PTSD symptoms within 3 months of the trauma. Eligible comparators: placebo or any active pharmacological agent. Note: 1 included RCT that compared 2 different enteral nutrition formulas is not relevant to the present report. | Outcomes: PTSD severity, PTSD rate, depression severity, quality of life, dropouts due to adverse events, dropout for any reason Follow-up: 2 weeks to 49 months |
Astill Wright et al. (2021)23 UK Wellcome Trust and Swedish Research Council | Study design: SR and meta-analysis Included studies: 25 RCTs including 24 that are relevant to the present report. | Studies of participants of any age exposed to a traumatic event. Only studies of adults were considered relevant to the present report. | Eligible interventions: consolidation or reconsolidation-based prevention or treatment interventions. Eligible comparators: placebo, pharmacological or psychosocial interventions. | Outcomes: PTSD incidence, PTSD severity, severity of re-experiencing symptoms, intrusive memory severity Follow-up: 1 week to 48 months |
Baas et al. (2020)25 The Netherlands NR | Study design: SR Included studies: 13 studies including 3 RCTs and 10 non-randomized studies. None of the included studies are relevant to the present report (i.e., none of the studies investigated consolidation or reconsolidation therapy). | Studies of pregnant women with PTSD or exposure to trauma. | Eligible interventions: interventions for the treatment of PTSD not limited to trauma-focused or evidence-based interventions. Eligible comparators: not specified | Outcomes: PTSD diagnosis, PTSD symptoms Follow-up: 6 weeks to 3 years |
Knaust et al. (2020)26 Germany University Hospital Hamburg-Eppendorf | Study design: SR Included studies: 18 studies including 6 RCTs, 1 single-arm before-after study, and 3 case studies that are relevant to the present report. | Studies of adults between the ages of 18 and 65 years diagnosed with PTSD. | Eligible interventions: any virtual trauma intervention with the goal to reduce PTSD symptoms that used immersive technology. Eligible comparators: not specified Relevant interventions: 3MDR; VRET with transcranial direct current stimulation; VRET with D-cycloserine; VRET with dexamethasone; VRET with alprazolam | Outcomes: PTSD severity, PTSD symptoms Follow-up: 1 month to 12 months |
Metcalf et al. (2020)27 Australia Centenary of Anzac Centre, a Department of Veterans’ Affairs funded initiative of Phoenix Australia | Study design: SR Included studies: 34 RCTs including 12 that are relevant to the current report | Studies of adults with diagnosed PTSD. | Eligible interventions: Any first-line PTSD treatment in combination with an augmentation intervention (any psychological, non-psychological, or pharmacological intervention, delivered before, concurrently, or after a first-line PTSD treatment) Eligible comparators: first-line PTSD treatment alone Relevant interventions: prolonged exposure therapy with rTMS, D-cycloserine, intranasal oxytocin, yohimbine, hydrocortisone, methylene blue, paroxetine, or sertraline | Outcomes: PTSD symptoms, PTSD severity, depression, anxiety, rate of remission, response rate, quality of life, treatment dropout, adverse events Follow-up: NR |
Merz et al. (2019)24 Switzerland NR | Study design: SR and network meta-analysis Included studies: 12 RCTs including 6 that are relevant to the present report. | Studies of adults with PTSD. | Eligible interventions: psychotherapeutic treatments, pharmacological treatments, or combinations of both. Eligible comparators: Any active psychotherapeutic or pharmacological PTSD treatment. Relevant interventions: prolonged exposure therapy with sertraline or paroxetine; exposure therapy with fluoxetine | Outcomes: PTSD symptom severity, patient dropouts Follow-up: NR |
3MDR = multi-modular motion-assisted memory desensitization and reconsolidation; NIHR = National Institute for Health Research; NR = not reported; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; rTMS = repetitive transcranial magnetic stimulation; SR = systematic review; VRET = virtual reality exposure therapy.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 220
Strengths | Limitations |
|---|---|
Bertolini et al. (2022)22 | |
|
|
Astill Wright et al. (2021)23 | |
|
|
Baas et al. (2020)25 | |
|
|
Knaust et al. (2020)26 | |
|
|
Metcalf et al. (2020)27 | |
|
|
Merz et al. (2019)24 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trial.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — PTSD, Depression, and Anxiety (Reconsolidation Therapy)
Study citation and study design | Intervention/ | Detailed findings |
|---|---|---|
Astill Wright et al. (2021)23 SR and meta-analysis | All pharmacological, electroconvulsive therapy, and psychological reconsolidation interventions vs control | PTSD severity at 1 to 4 weeks (9 RCTs; n = 372)
SMD < 0 favours pharmacological, electroconvulsive therapy, psychological reconsolidation interventions |
Re-experiencing severity at 1 to 4 weeks (7 RCTs; n = 235)
SMD < 0 favours pharmacological, electroconvulsive therapy, psychological reconsolidation interventions | ||
All pharmacological, and electroconvulsive therapy reconsolidation interventions vs control | PTSD severity at 1 to 4 weeks (5 RCTs; n = 215)
SMD < 0 favours pharmacological, electroconvulsive therapy reconsolidation interventions | |
Propranolol with MR vs control | PTSD severity at 1 week (2 RCTs; n = 78)
SMD < 0 favours propranolol with MR | |
Reconsolidation of traumatic memories vs waitlist control | PTSD severity at 2 weeks (4 RCTs; n = 157)
SMD < 0 favours reconsolidation of traumatic memories | |
Re-experiencing severity at 2 weeks (4 RCTs; n = 157)
SMD < 0 favours reconsolidation of traumatic memories | ||
Knaust et al. (2020)26 SR (6 RCTs, 1 single-arm before-after study, 3 case studies) | VRET with D-cycloserine vs VRET with placebo | Difede et al. 2013 (RCT)
“Significant decrease on the CAPS for both treatment groups. At 6 month-follow-up VRET with D-cycloserine were superior to active control group (p. 8).”26 |
VRET with dexamethasone vs VRET with placebo | Maples-Keller et al. 2018 (RCT) “Significant decrease on the CAPS for post-treatment but no significant differences between groups (p. 9).”26 | |
VRET with D-cycloserine vs VRET with alprazolam vs VRET with placebo | Rothbaum et al. 2014 (RCT) “All groups decreased significantly on the CAPS. The effect maintained over 12 months-follow-up. At post-treatment there was no significant difference between D-cycloserine and placebo group on the CAPS. However, there was a significant difference favoring placebo over alprazolam regarding the CAPS at post-treatment (p. 9).”26 | |
VRET with tDCS vs VRET with sham tDCS | Van’t Wout et al. 2018 (RCT)
“Both groups demonstrated significant reductions in PCL scores. There were no significant differences between groups at post time measurement, but VRET with tDCS were superior to VRET sham tDCS at 1 month-follow-up (p. 10).”26 | |
3MDR vs waitlist | Bisson et al. 2020 (RCT)
“Results indicated that 3MDR reduces PTSD symptoms in Veterans with treatment-resistant and combat-related PTSD (p. 10).”26 | |
3MDR vs non-trauma focused treatment (e.g., case management, stabilizing interventions, psychoeducation, etc.) | Van Gelderen et al. 2020 (RCT)
“Results showed that 3MDR reduces PTSD symptoms in Veterans with treatment-resistant and combat-related PTSD. However, no significant differences were found for secondary outcomes measures (e.g., PCL-5) and no long-term effects were assessed (p. 11).”26 | |
3MDR | Jetly et al. 2017 (single-arm before-after study) “Modest therapy gains for patients with treatment-resistant and combat-related PTSD (p. 10).”26 | |
Nijdam and Vermetten 2018 (case study) “Positive treatment results for a single patient with treatment-resistant and combat-related PTSD (p. 11).”26 | ||
Van Gelderen et al. 2018 (case study) “Positive treatment results for three patients with treatment-resistant and combat-related PTSD (p. 11).”26 | ||
Vermetten et al. 2013 (case study) “Preliminary results of two cases suggest that 3MDR is perhaps a treatment for treatment-resistant and combat-related PTSD (p. 12).”26 | ||
Metcalf et al. (2020)27 SR (12 RCTs) Note: Augmentation condition refers to the experimental group (i.e., either PE or IE in combination with a pharmacological agent). | PE with rTMS vs PE alone | Fryml et al. 2019 “PE + rTMS produced significant reductions in symptoms of depression in the fourth and fifth PE sessions (p ≤ .013) and a 15% greater reduction in CAPS scores at session five (p. 5).”27 |
PE with D-cycloserine vs PE alone | De Kleine et al. 2012 “No difference in PTSD symptoms between conditions; those in augmentation condition were more likely to show treatment response posttreatment (p = .040, OR = 2.83) (p. 8)”27 | |
Litz et al. 2012 “The augmentation condition performed significantly worse on measures of PTSD and depression at posttreatment (p < .05, g = 0.40–0.73). There were no significant effects at three- or six-month follow-up (p > .100) (p. 8).”27 | ||
PE with intranasal oxytocin vs PE alone | Flanagan et al. 2018 “No significant differences between conditions (p > .050) (p. 8).”27 | |
PE with yohimbine vs PE alone | Tuerk et al. 2018 “No differences between conditions in PTSD symptom reduction, remission rate, or depression (p. 9).”27 | |
PE with hydrocortisone vs PE alone | Yehuda et al. 2013 “PTSD symptoms change was greater for the augmentation condition (p < .050, d = 0.43); no differences between conditions posttreatment (p. 9).”27 | |
IE with methylene blue vs IE alone | Zoellner et al. 2017 There were no significant differences between groups on measures of PTSD severity or diagnosis, or depression. | |
PE with paroxetine vs PE alone vs paroxetine alone | Popiel et al. 2015
There were significant improvements in self-rated PTSD symptoms in all groups, and improvements were maintained at 12-month follow-up. However, there were no significant differences between groups in self-rated PTSD symptoms. | |
PE with sertraline vs PE alone vs sertraline alone | Rauch et al. 2019 “PTSD significantly improved for all conditions (p < .001); with no differences in PTSD symptom reduction (p ≥ .050), response rates (p = .360), or remission rates (p = .180) (p. 10)”27 | |
PE with sertraline vs sertraline alone | Rothbaum et al. 2006 “There was no difference between conditions in PTSD symptom reduction, depression, or anxiety at any time point (p > .050) (p. 10).”27 | |
PE with paroxetine vs PE alone | Schneier et al. 2012
There was a significant difference between treatment groups in improvement in PTSD symptoms favouring the PE with paroxetine group (P = 0.010). | |
Simon et al. 2008
There were no significant differences between treatment groups for PTSD symptoms or illness severity or improvement (P > 0.050; d = 0.20 to 0.35). | ||
Merz et al. (2019)24 SR (1 RCT) | ET with fluoxetine vs fluoxetine alone | Su et al. 2007
SMD < 0 favours ET with fluoxetine |
3MDR = multi-modular motion-assisted memory desensitization and reconsolidation; CAPS = clinician-administered PTSD scale; CAPS-5 = clinician-administered PTSD scale for Diagnostic and Statistical Manual of Mental Disorders 5th Edition; CI = confidence interval; ET = exposure therapy; IE = imaginal exposure; MR = memory reactivation; OR = odds ratio; PCL = PTSD checklist; PCL-5 = PTSD checklist for Diagnostic and Statistical Manual of Mental Disorders 5th Edition; PE = prolonged exposure; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; rTMS = repetitive transcranial magnetic stimulation; SMD = standardized mean difference; SR = systematic review; tDCS = transcranial direct current stimulation; VRET = virtual reality exposure therapy.
Table 5: Summary of Findings by Outcome — Treatment Dropout and Adherence (Reconsolidation Therapy)
Study citation and study design | Comparison | Detailed findings |
|---|---|---|
Treatment dropout | ||
Metcalf et al. (2020)27 SR (10 RCTs) | PE with D-cycloserine vs PE alone | De Kleine et al. 2012 No significant differences between groups in dropout. |
Litz et al. 2012
| ||
PE with intranasal oxytocin vs PE alone | Flanagan et al. 2018
| |
PE with yohimbine vs PE alone | Tuerk et al. 2018
| |
PE with hydrocortisone vs PE alone | Yehuda et al. 2013
| |
IE with methylene blue vs IE alone | Zoellner et al. 2017
| |
PE with paroxetine vs PE alone vs paroxetine alone | Popiel et al. 2015
| |
PE with sertraline vs sertraline alone | Rothbaum et al. 2006
| |
PE with paroxetine vs PE alone | Schneier et al. 2012
| |
Simon et al. 2008
| ||
Merz et al. (2019)24 SR (1 RCT) | ET with fluoxetine vs fluoxetine alone | Su et al. 2007 OR = 1.00 (95% CI, 0.02 to 55.8) OR < 1 favours ET with fluoxetine |
Treatment adherence | ||
Metcalf et al. (2020)27 SR (1 RCT) | PE with sertraline vs PE alone vs sertraline alone | Rauch et al. 2019
|
CI = confidence interval; ET = exposure therapy; IE = imaginal exposure; OR = odds ratio; PE = prolonged exposure; RCT = randomized controlled trial; SR = systematic review.
Table 6: Summary of Findings by Outcome — Additional Outcomes (Reconsolidation Therapy)
Study citation and study design | Comparison | Detailed findings |
|---|---|---|
Adverse events | ||
Metcalf et al. (2020)27 SR (6 RCTs) | PE with D-cycloserine vs PE alone | De Kleine et al. 2012 One participant from each treatment group was excluded due to adverse events. |
Litz et al. 2012 Three participants in the PE with D-cyclosporine group reported clinically significant symptom worsening. | ||
PE with intranasal oxytocin vs PE alone | Flanagan et al. 2018 One adverse event was reported in the PE alone group. | |
PE with yohimbine vs PE alone | Tuerk et al. 2018 One participant in the PE with yohimbine group administered rescue medication before the treatment session. | |
IE with methylene blue vs IE alone | Zoellner et al. 2017 One participant in the IE with methylene blue group discontinued due to adverse events. | |
PE with paroxetine vs PE alone | Simon et al. 2008 There were 2 adverse events that led to treatment discontinuation in the PE alone group and 1 adverse event that led to treatment discontinuation in the PE with paroxetine group. | |
Quality of life | ||
Metcalf et al. (2020)27 SR (2 RCTs) | IE with methylene blue vs IE alone | Zoellner et al. 2019 There were no significant differences between groups negative beliefs, disability, or quality of life (physical vitality) at 3-month follow-up. Quality of life (mental health) was greater in the IE and methylene blue group (P = 0.020, d = 0.58). |
PE with paroxetine vs PE alone | Schneier et al. 2012 Participants in the PE and paroxetine group had greater improvement in quality of life (P = 0.020). | |
IE = imaginal exposure; PE = prolonged exposure; RCT = randomized controlled trial; SR = systematic review.
Table 7: Summary of Findings by Outcome — PTSD (Consolidation Therapy)
Study citation and study design | Comparison | Detailed findings |
|---|---|---|
PTSD incidence | ||
Bertolini et al. (2022)22 SR and meta-analysis | Propranolol vs placebo | PTSD rate at 3 months (3 RCTs; n = 88)
RR < 1 favours propranolol |
PTSD rate at studies’ end point (4 RCTs; n = 127)
RR < 1 favours propranolol | ||
Omega-3 fatty acids vs placebo | Matsuoka et al. 2015 (RCT) PTSD rate at 3 months
RR < 1 favours omega-3 fatty acids | |
Propranolol vs gabapentin | Stein et al. 2007 (RCT) PTSD rate at 3 months
RR < 1 favours propranolol | |
Gabapentin vs placebo | Stein et al. 2007 (RCT) PTSD rate at 3 months
RR < 1 favours gabapentin | |
Paroxetine vs placebo | Borelli et al. 2019 (RCT) PTSD rate at 12 months
| |
Astill Wright et al. (2021)23 SR and meta-analysis | All pharmacological, and psychological consolidation interventions vs control | PTSD incidence at 1 to 48 months (12 RCTs; n = 2821)
RR < 1 favours pharmacological, psychological consolidation interventions |
All pharmacological, and psychological consolidation interventions (without hydrocortisone) vs control | PTSD incidence at 1 to 48 months (7 RCTs; n = 2695)
RR < 1 favours pharmacological, psychological consolidation interventions (without hydrocortisone) | |
All pharmacological consolidation interventions vs control | PTSD incidence at 3 to 48 months (10 RCTs; n = 2771)
RR < 1 favours pharmacological interventions | |
Hydrocortisone vs control | PTSD incidence at 3 to 31 months (5 RCTs; n = 126)
RR < 1 favours hydrocortisone | |
Cognitive memory task interference procedure with MR vs control | PTSD incidence at 1 to 6 months (3 RCTs; n = 157)
RR < 1 favours cognitive memory task interference procedure with MR | |
PTSD severity | ||
Bertolini et al. (2022)22 SR and meta-analysis | Propranolol vs placebo | PTSD severity at 3 months (2 RCTs; n = 86)
SMD < 0 favours propranolol |
PTSD severity at studies’ end point (4 RCTs; n = 125)
SMD < 0 favours propranolol | ||
Hydrocortisone vs placebo | Shaked et al. 2019 (RCT) PTSD severity at 1 month
MD < 0 favours hydrocortisone | |
Omega-3 fatty acids vs placebo | Matsuoka et al. 2015 (RCT) PTSD severity at 3 months
MD < 0 favours omega-3 fatty acids | |
Propranolol vs gabapentin | Stein et al. 2007 (RCT) PTSD severity at 3 months
| |
Gabapentin vs placebo | Stein et al. 2007 (RCT) PTSD severity at 3 months
| |
Paroxetine vs placebo | Borelli et al. 2019 (RCT) Mean change in PCL-C score from baseline to 3 months
Mean change in PCL-C score from baseline to 6 months
| |
5-hydroxytryptophan vs placebo | Tincu et al. 2016 (RCT) PTSD severity at 14 days
| |
Astill Wright et al. (2021)23 SR and meta-analysis | All pharmacological, and psychological consolidation interventions vs control | PTSD severity at 2 weeks to 6 months (8 RCTs; n = 411)
SMD < 0 favours pharmacological, psychological consolidation interventions |
Re-experiencing severity at 2 weeks to 48 months (6 RCTs; n = 1421)
SMD < 0 favours pharmacological, psychological consolidation interventions | ||
All pharmacological consolidation interventions vs control | PTSD severity at 3 to 6 months (4 RCTs; n = 202)
SMD < 0 favours pharmacological consolidation interventions | |
Virtual reality pain task vs control | PTSD severity at 6 months (1 RCT; n = 55)
SMD < 0 favours virtual reality pain task | |
Re-experiencing severity at 6 months (1 RCT; n = 55)
SMD < 0 favours virtual reality pain task | ||
Cognitive memory task interference procedure with MR vs control | PTSD severity at 2 weeks to 6 months (3 RCTs; n = 154)
SMD < 0 favours cognitive memory task interference procedure with MR | |
Re-experiencing severity at 4 weeks (2 RCTs; n = 127)
SMD < 0 favours cognitive memory task interference procedure with MR | ||
Intrusive memory frequency | ||
Astill Wright et al. (2021)23 SR and meta-analysis | Cognitive memory task interference procedure with MR vs control | Intrusive memory frequency at 1 week (3 RCTs; n = 166)
SMD < 0 favours cognitive memory task interference procedure with MR |
CAPS = clinician-administered post-traumatic stress disorder scale; CI = confidence interval; MD = mean difference; MR = memory reactivation; PCL-C = post-traumatic stress disorder checklist - civilian version; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; RR = relative risk; SMD = standardized mean difference; SR = systematic review.
Table 8: Summary of Findings by Outcome — Treatment Dropout (Consolidation Therapy)
Study citation and study design | Comparison | Detailed findings |
|---|---|---|
Dropouts due to adverse events | ||
Bertolini et al. (2022)22 SR and meta-analysis | Propranolol vs placebo | Orrey et al. 2015 (RCT) Dropouts due to adverse events at 6 weeks
RR < 1 favours propranolol |
Omega-3 fatty acids vs placebo | Matsuoka et al. 2015 (RCT) No participants dropped out due to adverse events in either treatment group. | |
Propranolol vs gabapentin | Stein et al. 2007 (RCT) No participants discontinued the assigned medication due to adverse events during the first treatment week. | |
Dropout for any reason | ||
Bertolini et al. (2022)22 SR and meta-analysis | Propranolol vs placebo | Dropout for any reason at 3 months (3 RCTs; n = 118)
|
Dropout for any reason at study end point (4 RCTs; n = 165)
| ||
Hydrocortisone vs placebo | Dropout for any reason at study end point (2 RCTs; n = 60)
| |
Dexamethasone vs placebo | Kok et al. 2016 (RCT) Dropout for any reason at 1.5 to 4 years
| |
Omega-3 fatty acids vs placebo | Matsuoka et al. 2015 (RCT) Dropout for any reason at 3 months
| |
Propranolol vs gabapentin | Stein et al. 2007 (RCT) Dropout for any reason at 3 months
| |
Gabapentin vs placebo | Stein et al. 2007 (RCT) Dropout for any reason at 3 months
| |
CI = confidence interval; RCT = randomized controlled trial; RR = relative risk; SMD = standardized mean difference; SR = systematic review.
Table 9: Summary of Findings by Outcome — Additional Outcomes (Consolidation Therapy)
Study citation and study design | Comparison | Detailed findings |
|---|---|---|
Depression severity | ||
Bertolini et al. (2022)22 SR and meta-analysis | Omega-3 fatty acids vs placebo | Matsuoka et al. 2015 (RCT) MADRS score at 3 months
MD < 0 favours omega-3 fatty acids |
Propranolol vs placebo | Stein et al. 2007 (RCT) Over the course of the study CES-D scores did not differ significantly between treatment groups. | |
Gabapentin vs placebo | Stein et al. 2007 (RCT) CES-D scores measured at 3 months did not differ significantly between treatment groups. | |
Paroxetine vs placebo | Borelli et al. 2019 (RCT) There were no significant differences between QIDS-SR scores assessed at baseline and follow-up at 8 weeks. | |
Quality of life | ||
Bertolini et al. (2022)22 SR and meta-analysis | Dexamethasone vs placebo | Kok et al. 2016 (RCT) There were no significant differences between treatment groups in SF-36 Mental Component Summary scores. |
Omega-3 fatty acids vs placebo | Matsuoka et al. 2015 (RCT) SF-36 Mental Component Summary score at 3 months
MD < 0 favours omega-3 fatty acids | |
Paroxetine vs placebo | Borelli et al. 2019 (RCT) Mean change in SF-36 scores from baseline to 12 months
| |
CES-D = Center for Epidemiologic Studies Depression Scale; CI = confidence interval; MADRS = Montgomery-Asberg Depression Rating Scale; MD = mean difference; PTSD = post-traumatic stress disorder; QIDS-SR = Quick Inventory of Depressive Symptomatology; RCT = randomized controlled trial; SF-36 = 36-Item Short-Form Health Survey; SR = systematic review.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 10: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Bertolini et al. (2022)22 | Astill Wright et al. (2021)23 | Metcalf et al. (2020)27 | Merz et al. (2019)24 |
|---|---|---|---|---|
Borrelli J Jr, et al. J Orthop Trauma. 2019;33(2): e58-63. | Yes | No | No | No |
Denke C, et al. Crit Care. 2008;12(2): P421. | Yes | Yes | No | No |
Hoge EA, et al. CNS Neurosci Ther. 2012;18(1): 21-7. | Yes | Yes | No | No |
Kok L, et al. Crit Care Med. 2016;44(3): 512 to 20. | Yes | Yes | No | No |
Matsuoka Y, et al. J Clin Psychiatry. 2015;76(8): e1015-22. | Yes | No | No | No |
Orrey DC, et al. Clin J Pain. 2015;31(1): 21-9. | Yes | No | No | No |
Pitman RK, et al. Biol Psychiatry. 2002;51(2): 189-92. | Yes | Yes | No | No |
Schelling G, et al. Biol Psychiatry. 2001;50(12): 978-85. | Yes | Yes | No | No |
Shaked G, et al. Eur J Trauma Emerg Surg. 2019;6: 1115-22. | Yes | No | No | No |
Stein MB, et al. J Trauma Stress. 2007;20(6): 923-32. | Yes | Yes | No | No |
Tincu R, et al. Crit Care. 2016;20 (Suppl 2):119. | Yes | No | No | No |
Weis F, et al. J Thorac Cardiovasc Surg. 2006;131(2): 277-82. | Yes | Yes | No | No |
Brunet A, et al. Am J Psychiatry. 2018;175: 427-33. | No | Yes | No | No |
Wood NE, et al. Psychiatry Res. 2015;225: 31-39. | No | Yes | No | No |
Suris A, et al. Ann Clin Psychiatry. 2010;22: 274-9. | No | Yes | No | No |
Suris A, et al. Ann Clin Psychiatry. 2013;25: 33-40. | No | Yes | No | No |
Corchs F, et al. Biol Psychiatry. 2018;83: S129eS455. | No | Yes | No | No |
Gray R and Bourke F. J Milit Vet Family Health. 2015;1: 13-20. | No | Yes | No | No |
Gray R, et al. Psychother Res. 2019;29: 621-39. | No | Yes | No | No |
Gray RM, et al. Psychol Trauma. 2021;13(6): 641-651. | No | Yes | No | No |
Tylee DG, et al. J Mil, Veteran Fam Health. 2017;3: 21-33. | No | Yes | No | No |
Delahanty DL, et al. CNS Spectr. 2013;18: 103-11. | No | Yes | No | No |
Schelling G, et al. Biol Psychiatry. 2004;55: 627-33. | No | Yes | No | No |
Zohar J, et al. Eur Neuropsychopharmacol. 2011;21: 796-809. | No | Yes | No | No |
van Zuiden M, et al. Biol Psychiatry. 2017;81: 1030-40 | No | Yes | No | No |
Freedman SA, et al. Eur J Psychotraumatol. 2020;11: 1750170 | No | Yes | No | No |
Horsch A, et al. Behav Res Ther. 2017;94: 36-47. | No | Yes | No | No |
Iyadurai L, et al. Mol Psychiatry. 2018;18: 674-82. | No | Yes | No | No |
Kanstrup MS, et al. Transl Psychiatry. 2021;11: 30 | No | Yes | No | No |
Popiel A, et al. J Behav Ther Exp Psychiatry. 2015;48: 17-26. | No | No | Yes | Yes |
Rothbaum BO, et al. J Trauma Stress. 2006;19(5): 625-638. | No | No | Yes | Yes |
Schneier FR, et al. Am J Psychiatry. 2012;169(1): 80-88. | No | No | Yes | Yes |
Simon NM, et al. J Clin Psychiatry. 2008;69(3): 400-405. | No | No | Yes | Yes |
Rauch SAM, et al. JAMA Psychiatry. 2018;76(2): 117-126. | No | No | Yes | Yes |
Su H, et al. Clin Rehab Tissue Engineering Res. 2007;11(39): 7783-7786. | No | No | No | Yes |
de Kleine RA, et al. Biol Psychiatry. 2012;71(11): 962-968. | No | No | Yes | No |
Litz BT, et al. J Psychiatr Res. 2012;46(9): 1184-1190. | No | No | Yes | No |
Tuerk PW, et al. Cogn Behav Ther. 2018;47(5): 351-371. | No | No | Yes | No |
Yehuda R, et al. Psychoneuroendocrinology. 2015;51: 589-597. | No | No | Yes | No |
Zoellner LA, et al. J Clin Psychiatry. 2017;78(7): e782-e789. | No | No | Yes | No |
Flanagan JC, et al. J Psychiatr Res. 2018;98: 64-69. | No | No | Yes | No |
Fryml LD, et al. J ECT. 2019; 35(1): 53-60. | No | No | Yes | No |
Note: Yes indicates the primary study was included within the systematic review; No indicates the primary study was not included within the systematic review.
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Propranolol for post traumatic stress disorder: a review of clinical effectiveness.(CADTH rapid response report: summary with critical appraisal). Ottawa(ON): CADTH; 2020 Mar: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RC1254%20Propranolol%20PTSD%20Final.pdf. Accessed 2022 May 4.
Review Articles
Kida S. Reconsolidation/destabilization, extinction and forgetting of fear memory as therapeutic targets for PTSD. Psychopharmacology (Berl). 2019;236(1):49-57. PubMed
Feduccia AA, Mithoefer MC. MDMA-assisted psychotherapy for PTSD: are memory reconsolidation and fear extinction underlying mechanisms? Prog Neuropsychopharmacol Biol Psychiatry. 2018;84(Pt A):221-228. PubMed
Randomized Controlled Trials
Brunet A, Sapkota RP, Guragain B, Tremblay J, Saumier D, Kirmayer LJ. Tackling the global problem of traumatic stress in low-income countries: a pilot clinical trial comparing reconsolidation therapy to paroxetine in Nepal. BMC Psychiatry. 2021;21(1):434. PubMed
Lehrner A, Hildebrandt T, Bierer LM, et al. A randomized, double-blind, placebo-controlled trial of hydrocortisone augmentation of prolonged exposure for PTSD in U.S. combat veterans. Behav Res Ther. 2021;144:103924. PubMed
Roullet P, Vaiva G, Very E, et al. Traumatic memory reactivation with or without propranolol for PTSD and comorbid MD symptoms: a randomised clinical trial. Neuropsychopharmacology. 2021;46(9):1643-1649. PubMed
Suris A, Holliday R, Adinoff B, Holder N, North CS. Facilitating fear-based memory extinction with dexamethasone: a randomized controlled trial in male veterans with combat-related PTSD. Psychiatry. 2017;80(4):399-410. PubMed
Tang VM, Trought K, Gicas KM, et al. Electroconvulsive therapy with a memory reactivation intervention for post-traumatic stress disorder: A randomized controlled trial. Brain Stimul. 2021;14(3):635-642. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.