CADTH Health Technology Review
Melatonin for the Treatment of Insomnia in Children and Adolescents
Rapid Review
Authors: Khai Tran, Quenby Mahood
Abbreviations
AAN
American Academy of Neurology
ADHD
attention-deficit/hyperactivity disorder
AE
adverse event
ASD
autism spectrum disorder
CI
confidence interval
DLMO
dim light melatonin onset
MA
meta-analysis
MCID
minimal clinically important difference
MD
mean difference
RCT
randomized controlled trial
SOL
sleep onset latency
SOT
sleep onset time
SR
systematic review
TST
total sleep time
Key Messages
There is some evidence of benefit of melatonin compared with placebo for the short-term treatment of insomnia in children and adolescents with neurodisabilities.
The short-term safety profile of melatonin suggested that it was well-tolerated, although some severe adverse events may occur. There was a lack of long-term safety data.
The American Academy of Neurology guideline recommends high-grade melatonin should be prescribed for treatment of sleep disturbance in children and adolescents with autism spectrum disorder if first-line treatment with behavioural strategies is not helpful.
Evidence comparing the clinical effectiveness of melatonin with prescription sedatives for the treatment of insomnia in children and adolescents was not identified.
No evidence was found regarding the cost-effectiveness of melatonin compared with placebo or prescription sedatives for the treatment of insomnia in children and adolescents.
Context and Policy Issues
According to the Canadian Health Measures Survey of 2007 to 2015, the prevalence of nighttime insomnia symptoms among people living in Canada aged 6 years to 79 years increased over that time.1 In 2014 and 2015, approximately 8.8% and 15.3% of children (aged 6 years to 13 years) and adolescents (aged 14 years to 17 years), respectively, had nighttime insomnia symptoms.1 The symptoms were determined by how often the individuals had trouble going to sleep or staying asleep.1 Poor sleep in children and adolescents may result in daytime sleepiness and affect a child’s learning, school performance, and psychological and development growth.2
Insomnia is a general term for sleep disorders and disturbances caused by behavioural, biological or various neurologic conditions.3 The International Classification of Sleep Disorders, Third Edition, describes sleep disorders in children and adolescents in 7 major categories: insomnia disorders, sleep-related breathing disorders, central disorders of hypersomnolence, circadian rhythm sleep-wake disorders, sleep-related movement disorders, parasomnias, and other sleep disorders.4 Certain types of sleep disorders can be diagnosed and evaluated by actigraphy, polysomnography, or other sleep and neurologic tests.5
Melatonin is an endogenous hormone produced by the pineal gland that is responsible for the regulation of the sleep-wake cycle.6 It has been demonstrated that the time of sleep onset is associated with the initiation of melatonin synthesis.6 The misalignment of the endogenous melatonin rhythm and the sleep-wake cycle results in difficulty falling asleep and waking in the morning.6 Exogenous melatonin has been identified in foods of animal and plant origin.7 In foods of animal origin, melatonin is found at high concentrations in eggs, fish, meat, and milk.7 Melatonin is also identified in foods of plant origin, such as fruits, seeds, and cereals.7
Melatonin supplements have been produced by many manufacturers, and are available in different formulations (oral, topical, transdermal, and sublingual routes), and dosages (0.3 mg to 10 mg).8 In Canada, melatonin was licensed in 2005 as a natural health product for use to help re-set the body's sleep-wake cycle and to reduce the time of sleep onset in adults.9 Since 2011, melatonin-containing products have been licensed for use in Canada in children aged 12 years and older, but have not been authorized for use in children aged 11 years and younger.9 A safety review conducted by Health Canada has identified some common short-term side effects associated with the use of melatonin in the pediatric population, such as sleepiness, fatigue, aggression, abnormal dreams, and headache.9 There is limited evidence of benefit for the use of melatonin supplements for treating sleep disorders in some specific pediatric populations;8 however, concerns have been raised about its long-term safety regarding growth and psychological development in children.9
This report aims to summarize the clinical effectiveness and cost-effectiveness of melatonin compared with no treatment, placebo, or prescription sedatives for the treatment of insomnia in children and adolescents. This report also aims to summarize the recommendations from evidence-based guidelines regarding the use melatonin for the treatment of insomnia in the pediatric population.
Research Questions
What is the clinical effectiveness of melatonin versus no treatment or placebo for the treatment of insomnia in children and adolescents?
What is the clinical effectiveness of melatonin versus prescription sedatives for the treatment of insomnia in children and adolescents?
What is the cost-effectiveness of melatonin versus no treatment or placebo for the treatment of insomnia in children and adolescents?
What is the cost-effectiveness of melatonin versus prescription sedatives for the treatment of insomnia in children and adolescents?
What are the evidence-based guidelines regarding the use of melatonin for the treatment of insomnia in children and adolescents?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, PsycInfo, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were melatonin, insomnia, and pediatrics. No filters were applied to limit the retrieval by study type. Conference abstracts were omitted from the search results. The search was completed on April 19, 2022, and was limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Children and adolescents with insomnia |
Intervention | Melatonin |
Comparator | Q1 and Q3: No treatment, placebo Q2 and Q4: Prescription sedatives (e.g., benzodiazepines [e.g., zopiclone, eszopiclone, zolpidem, temazepam, oxazepam], doxepin) Q5: Not applicable |
Outcomes | Q1 and Q2: Clinical effectiveness (objective sleep parameters [e.g., total sleep time, sleep latency, sleep efficiency, percentage of rapid eye movement sleep], quality of life), safety Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios) Q5: Recommendations regarding the use of melatonin for the treatment of insomnia |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2017. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SR were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)10 for SR, the Downs and Black checklist11 for randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument12 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
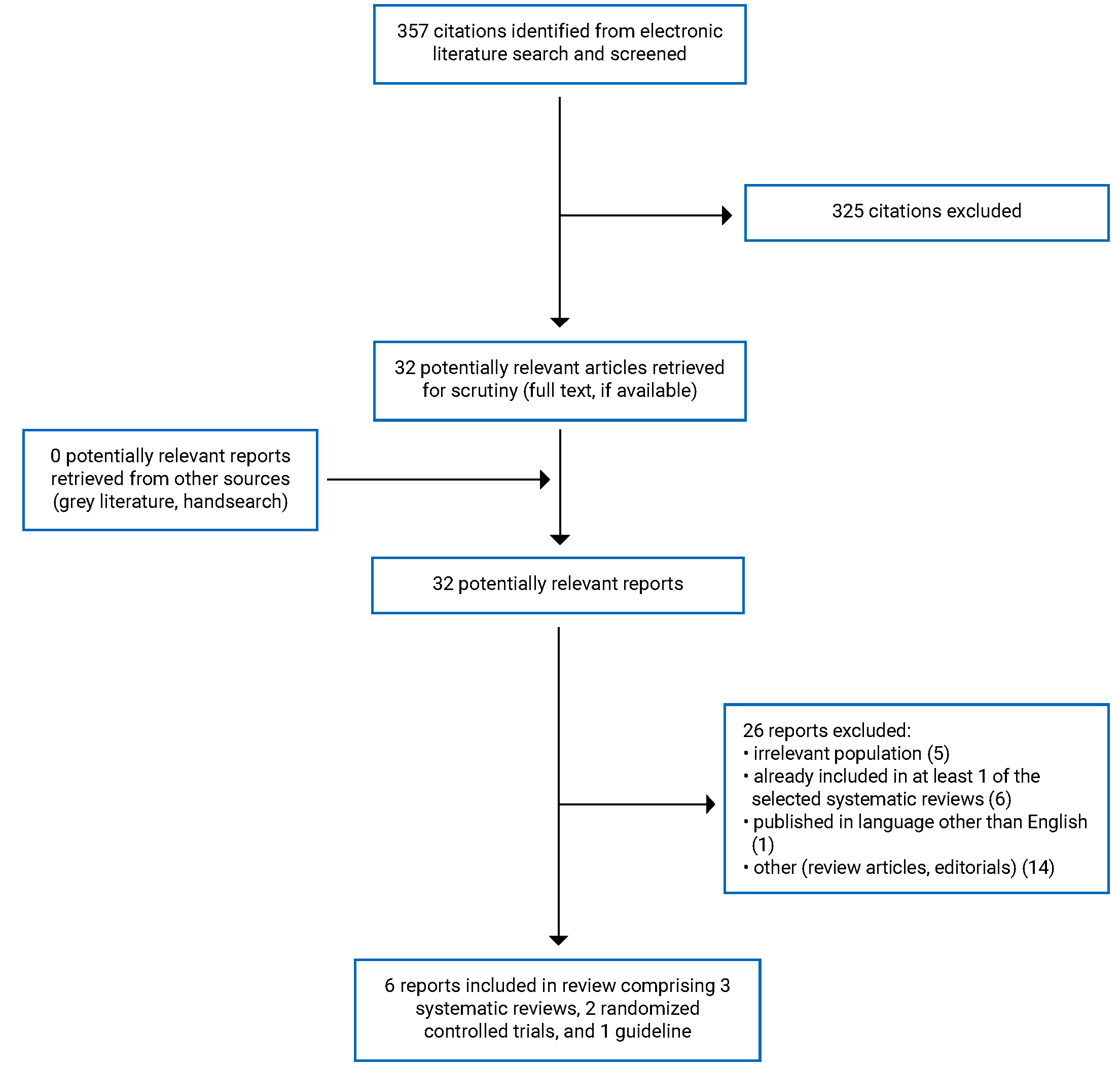
A total of 357 citations were identified in the literature search. Following screening of titles and abstracts, 325 citations were excluded, and 32 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of the 32 potentially relevant articles, 26 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 3 SRs, 2 randomized controlled trials (RCTs), and 1 evidence-based guideline. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)13 flow chart of the study selection is presented in Appendix 1.
Summary of Study Characteristics
Additional details regarding the characteristics of included SRs14-16 (Table 2), primary clinical studies17,18 (Table 3), and guideline19 (Table 4) are provided in Appendix 2.
Study Design
The SR by Wei et al. (2020)14 identified and included 7 RCTs (N = 387) in meta-analyses (MAs). The RCTs were published between 2001 and 2017. The SR by Parker et al. (2019)15 identified and included 11 RCTs (N = 695) in MAs. The RCTs were published between 1996 and 2015. The SR by Abdelgadir et al. (2018)16 identified and included 13 RCTs (N = 671) in MAs. The RCTs were published between 1998 and 2012. Both SRs by Parker et al. (2019)15 and Abdelgadir et al. (2018)16 had 8 overlapped primary studies with one another, and they had 1 overlapped study with the SR by Wei et al. (2020).14 The overlap in relevant primary studies between included SRs is presented in Appendix 5.
Both included primary clinical studies were RCTs,17,18 published in 202117 and 2017.18 Both RCTs17,18 were parallel and double-blinded. One RCT was multicentric,17 while the other was monocentric.18 One RCT17 reported a sample size calculation and analyzed the data using the intention-to-treat (ITT) approach, while the other18 did not.
The included evidence-based guideline was from the American Academy of Neurology (AAN),19 which provided recommendations on the use of behavioural strategies alone or combination with pharmacologic or nutraceutical approaches, including melatonin to improve sleep in children and adolescents with autism spectrum disorder (ASD) and sleep disturbance. A systematic search of the literature was conducted, and the quality of evidence and the strength of recommendations were assessed based on the methods described in the 2011 AAN guideline development process manual.20
Country of Origin
The SRs were conducted by authors from China14 and the UK.15,16 The primary clinical studies were conducted by authors from Japan17 and the Netherlands.18
The guideline was conducted by authors from the US.19
Patient Population
Patients in the RCTs included in the SR by Wei et al. (2020)14 were children with symptoms of sleep onset insomnia, including difficult in initiating sleep and daytime fatigue. Five of 7 trials reported that children had attention-deficit/hyperactivity disorder (ADHD), while 2 trials did not report comorbid conditions. The mean age of the children ranged from 8.9 years to 10.3 years, and 43% to 79% were male.
Patients in the RCTs included in the SR by Parker et al. (2019)15 were children with non-respiratory sleep disturbances, of any duration, related to initiation, maintenance, or scheduling of sleep. The comorbid conditions included developmental delay, ASD, ADHD, cerebral palsy, or epilepsy. The mean age of the children ranged from 5.5 years to 10.3 years. Gender or sex was not reported.
Patients in the RCTs included in the SR by Abdelgadir et al. (2018)16 were children with sleep disturbances and comorbid conditions including ASD, ADHD, girls with Rett syndrome, or fragile X syndrome. The mean of ages ranged from 1 year to 18 years. Gender or sex was not reported.
Patients in the RCT by Hayashi et al. (2021)17 were children with sleep disturbances and ASD. The mean age of patients was 11.2 years, and the percentage of males was 62%.
Patients in the RCT by van Maanen et al. (2017)18 were children with chronic sleep onset insomnia. The study did not report the children’s comorbid conditions, but it excluded psychiatric disorders other than ADHD or ASD. The mean age of patients was 10.0 years, and the proportion of males was 61%.
The target population of the included guideline is children and adolescents with sleep disturbance and ASD, while the intended users are clinicians who seek to improve sleep in this population.
Interventions and Comparators
All included SRs,14-16 and the primary clinical studies17,18 compared melatonin with placebo. Melatonin dosages (0.5 mg to 9 mg per day), duration of treatment (1 week to 13 weeks), regimens (fast release, sustained release) and administration times (at 4:30 p.m. to 9:00 p.m. or 20 minutes to 45 minutes before bedtime) varied across studies.
The included guideline provided recommendations about pharmacologic (i.e., melatonin) and nonpharmacologic strategies for treating sleep disturbances in children and adolescents with ASD.
Outcomes
All 3 SRs14-16 and 1 primary clinical study17 reported both efficacy and safety outcomes, while the other primary clinical study18 reported only efficacy outcomes. The efficacy outcomes comprised sleep onset latency (SOL; defined as the length of time in bed from when the lights are turned off until the onset of any sleep stage), sleep onset time (SOT; defined as the clock time at night when the patient goes into any sleep stage from wakefulness), total sleep time (TST; defined as the length of time between sleep onset and wake-up time), sleep efficiency (defined as the ratio of TST to total time in bed), number of wakenings after sleep onset, wake-up time after sleep onset (defined as total time staying awake between the time of falling asleep and wakening time), light-time off, dim light melatonin onset (DLMO; defined as the clock time between 7:00 p.m. and 11:00 p.m. when endogenous melatonin reaches 4 pg/mL in the saliva), and child’s behaviour. The sleep parameters were recorded by either electronic sleep diary or actigraphy (a wrist-worn device). Child’s behaviour was assessed by either parental perception or with the aberrant behaviour checklist.21
The included guideline19 considered all sleep outcomes and adverse events (AEs) in pharmacologic (i.e., melatonin) and nonpharmacologic strategies for making recommendations.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included SRs14-16 (Table 5), primary clinical studies17,18 (Table 6), and guideline19 (Table 7) are provided in Appendix 3.
All 3 SRs14-16 were explicit in their objectives and inclusion criteria for the review and selection of the study designs for inclusion as well as included a comprehensive literature search strategy. Providing details of the literature search strategy increases the reproducibility of the review. Study selection and data extraction were performed in duplicate in all SRs.14-16 Performing these activities in duplicate reduces the likelihood of missing relevant studies and making errors in data extraction. Two SRs14,15 provided details of the characteristics of the included studies, while 1 SR16 did not. Sufficient details of the included studies allow for assessment of the clinical heterogeneity among the studies and whether subgroup analyses are needed to explore the sources of the heterogeneity. None of the SRs14-16 provided a list of excluded studies, the reasons for exclusion, or the sources of funding for the included studies. Not having a list of, or the justifications for, the excluded studies makes it impossible to assess whether any relevant articles were excluded and, if so, for what reasons. Funding received from industry can introduce bias in favour of the intervention. The authors of all SRs14-16 assessed the methodological quality of the included studies using the Cochrane Risk of Bias tool and evaluated publication bias using the funnel plot method. One SR16 used the Grading of Recommendation, Assessment, Development and Evaluation (GRADE) system to assess the quality of the body of evidence associated with specific outcomes. The authors of all SRs14-16 used the software Review Manager (RevMan) in the MAs. The review authors of 2 of the SRs,14,15 (but not the third)16 assessed the potential impact of the risk of bias in individual studies on the results, and they accounted for risk of bias in the included studies when interpreting or discussing the results of the review. The review authors of 2 SRs14,16 declared that no funding was received for their work, while the authors of 1 SR15 received public funding. Conflicts of interest were also declared in all 3 SRs.14-16 Overall, all 3 SRs14-16 were of moderate methodological quality.
With respect to reporting in the RCTs, both 17,18 clearly described the objective of the study, the interventions of interest, the main outcomes, and the main findings of the study. The baseline characteristics of the patients included in the study were clearly described in 1 RCT,17 but not in the other.18 Without a clear description of patient baseline characteristics, it was not possible to assess if there were potential confounders that could affect the interpretation of the results. One RCT17 had 4% of patients who did not complete the study; however, all randomized patients were included in the full analysis set at the end of treatment. The other RCT18 did not report if there were any patients lost to follow-up. Not accounting for patients lost to follow-up in the analyses may increase potential risk of attrition bias. Actual P values and the random variability in the data for the main outcomes (e.g., confidence interval [CI], standard deviation, or standard error) were reported in 1 RCT,18 while the other17 only reported the actual P values. One RCT17 reported AEs, while the other18 did not. Regarding external validity, it was likely that patients were recruited from the same population, and over the same period of time. Both trials17,18 were conducted in both home and hospital settings, suggesting that the staff, places, and facilities where the patients were treated, were representative of the treatment the majority of the patients receive. For internal validity, both trials were double-blind RCTs in which the investigators and patients were blinded. Randomization would reduce selection bias, while blinding of investigators and patients would reduce the risk of performance and detection biases. Methods of randomization and allocation concealment were described in 1 RCT,17 but not in the other.18 No allocation concealment could risk selection bias. Appropriate statistical tests were used to assess the main outcomes, and reliable and validated outcome measures (both diary and actigraphy) were used in both RCTs.17,18 One RCT17 performed a sample size calculation, while the other18 did not. The non-significant differences in certain outcomes could result from a study that was underpowered for those outcomes. Overall, 1 RCT17 was of moderate methodological quality, and the other18 was of low methodological quality.
The included guideline19 was explicit in terms of scope and purpose (i.e., objectives, health questions, and populations), and had clear presentation (i.e., specific, and unambiguous recommendations, different options for management of the condition or health issue, and easy to find key recommendations). In terms of stakeholder involvement, the guidelines clearly defined target users and the development groups. The views and preferences of the target population (e.g., patients, public) were sought. For rigour of development, the guideline reported systematic methods used to search for evidence, criteria for selecting evidence, explicit links between recommendations and the supporting evidence, and methods of formulating the recommendations. The guideline considered health benefits, side effects, and risks in formulating the recommendations, and were externally peer reviewed before publication. The guideline assessed the quality of evidence and graded the level of recommendations based on the methods described in the 2011 AAN guideline development process manual.20 For clarity, the recommendations in the guideline are specific and unambiguous, provide different options for management of the condition, and are easily identifiable. For applicability, the guideline was not explicit in terms of facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, resource implications (e.g., considering costs in recommendations), and monitoring or auditing criteria. For editorial independence, the guideline reported competing interests of guideline development group members and that the views of the funding body did not have influence on the content of the guidelines. Overall, the guideline was of good methodological quality.
Summary of Findings
The main study findings of the SRs,14-16 primary clinical studies,17,18 and the summary of guideline recommendations are presented in Appendix 4.19 The findings are presented by outcomes, which are SOL, SOT, TST, sleep efficiency, number of wakenings after sleep onset, wake-up time after sleep onset, light-off time, DLMO, child’s behaviour, and safety.
Clinical Effectiveness of Melatonin Versus No Treatment or Placebo for the Treatment of Insomnia in Children and Adolescents
Sleep Onset Latency
Three SRs14-16 and 2 primary clinical studies17,18 reported the outcome SOL (Table 8).
The SR by Wei et al. (2020)14 combined both actigraphy and parent-reported sleep diary data of 6 RCTs MAs. The SOL of the melatonin group was significantly shorter than the placebo group by 0.36 hours (95% CI, −0.49 to −0.24; P < 0.00001). There was moderate statistical heterogeneity among studies because the I2 value was 34%.
The SR by Parker et al. (2019)15 included data from 12 RCTs in MAs, in which 6 trials had data for parent-reported sleep diary SOL, 5 trials had data for actigraphy-measured SOL, and 1 trial reported polysomnography-measured SOL. For sleep diary SOL, there was a significant decrease in SOL in the melatonin group compared with placebo. The pooled mean difference (MD) was −35.6 minutes (95% CI, −50.85 to −20.26; P < 0.001). Statistical heterogeneity was high because the I2 value was 89%. Subgroup analysis based on ASD reduced statistical heterogeneity among studies. There was a statistically significant difference in effect between studies of children with ASD and studies with mixed populations and studies with other neurodisability populations (P < 0.001; I2 = 92.5%). In the ASD subgroup, the MD in SOL between melatonin and placebo was −50.9 minutes (95% CI, −55.49 to −46.24; P < 0.00001; I2 = 0%) compared with −27.41 minutes (95% CI, −39.13 to −15.69; P < 0.00001; I2 = 56%) in other populations. For actigraphy-measured SOL, pooled analysis of data from 5 RCTs also revealed a significant decrease in actigraphy-measured SOL favouring melatonin compared with placebo. The pooled MD was −23.4 minutes (95% CI, −30.91 to −15.78; P < 0.00001; I2 = 48%). Subgroup analysis based on previous parent-directed sleep intervention (e.g., advice booklet, sleep hygiene, behavioural management) showed no statistically significant difference in effect between subgroups (P = 0.55; I2 = 0%). One RCT that used polysomnography reported a significant reduction in SOL for the melatonin group compared with the placebo group (MD = −11.4 minutes; 95% CI, −17.2 to −5.6; P = 0.02).
The SR by Abdelgadir et al. (2018) combined both actigraphy-measured and parent-reported sleep diary data of 11 RCTs in MAs and found a significant reduction in SOL in the melatonin group compared with the placebo group. The pooled MD was −28.97 minutes (95% CI, −39.78 to −18.17; P < 0.00001). Statistical heterogeneity was high because the I2 value was 82%. Subgroup analyses based on comorbidity (i.e., ASD, ADHD, and other neurodisability) reduced the I2 to 0% and showed no statistically significant difference in effect between subgroups (P = 0.05; I2 = 66.7%). Pooled analyses of parent-reported SOL using sleep diary or actigraphy-measured SOL showed a similar effect favouring melatonin compared with placebo. The pooled MD in SOL was −35.6 minutes and −22.6 minutes for sleep diary and actigraphy, respectively.
In the RCT by Hayashi et al. (2021),17 the median SOLs reported using sleep diary data between the last 7 days of the randomization phase and baseline were −5.0 minutes, −22.0 minutes, and −20.0 minutes for the placebo group, 1 mg melatonin group, and 4 mg melatonin group, respectively. The difference between each melatonin group and placebo group was statistically significant (P < 0.0001). Subgroup analyses were conducted with respect to sex, age, weight (< 40 kg, ≥ 40 kg), height (145 cm, ≥ 145 cm), SOL at baseline, history of ramelteon treatment, and ADHD. The results revealed that 1 mg melatonin significantly reduced SOL compared with placebo for all subgroups except female gender, previous history of ramelteon treatment, and height of 145 cm or greater. The 4 mg melatonin group had a significantly reduced SOL compared with the placebo group for all subgroups. For actigraphy-measured SOL, changes in median SOL recorded during the last 7 days of the randomization phase from baseline were 1.0 minutes, 21.0 minutes, and 20.0 minutes for the placebo group, 1 mg melatonin group, and 4 mg melatonin group, respectively. The difference between each melatonin group and the placebo group was statistically significant (P < 0.0001).
The RCT by Maanen et al. (2017)18 showed that melatonin treatment significantly reduced sleep diary–reported SOL (beta = −0.34; P < 0.001) and actigraphy-measured SOL (beta = −0.33; P < 0.001) compared with placebo.
Sleep Onset Time
One SR14 and 1 primary clinical study18 reported the outcome SOT (Table 9).
The SR by Wei et al. (2020)14 included 6 RCTs that reported SOT. Pooled analysis showed that children and adolescents in the melatonin group were falling asleep significantly earlier compared with those in the placebo group. The pooled MD for SOT was −0.62 hours (95% CI, −0.80 to −0.45; P < 0.00001). There was no statistical heterogeneity among studies because the I2 was 0%.
The RCT by Maanen et al. (2017)18 showed that melatonin treatment significantly reduced sleep diary–reported SOT (beta = −0.69; P < 0.001) and actigraphy-measured SOT (beta = −0.65; P < 0.001) compared with placebo.
Total Sleep Time
Three SRs14-16 and 2 primary clinical studies17,18 reported the outcome TST (Table 10).
The SR by Wei et al. (2020)14 included 6 RCTs that reported TST. Compared with the placebo group, TST was significantly increased for melatonin group (pooled MD = 0.38 hours; 95% CI, 0.09 to 0.66; P = 0.009). Statistical heterogeneity was moderate because the I2 value was 52%.
The SR by Parker et al. (2019)15 included data from 13 RCTs in MAs, in which 7 trials had data for sleep diary–reported TST, 5 trials had data for actigraphy-measured TST, and 1 trial reported polysomnography-measured TST. For sleep diary–reported TST, melatonin treatment significantly increased TST compared with placebo. The pooled MD was 29.6 minutes (95% CI, 6.91 to 52.35; P < 0.001). Statistical heterogeneity was high because the I2 value was 97%. Subgroup analyses based on ASD reduced statistical heterogeneity among studies. There was a statistically significant difference in effect between studies of children with ASD and those with mixed and other neurodisability populations (P < 0.001; I2 = 92.5%). In the ASD subgroup, the MD in TST between the melatonin and placebo groups was 64.7 minutes (95% CI, 58.81 to 70.65; P < 0.001; I2 = 0%) compared with 15.9 minutes (95% CI, 9.15 to 22.59; P < 0.001; I2 = 56%) in other populations. Subgroup analysis based on previous parent-directed sleep intervention showed no statistically significant difference in effect between subgroups (P = 0.09; I2 = 65.2%). For actigraphy-measured SOL, a pooled analysis of data from 5 RCTs also revealed a significant increase in actigraphy-measured TST favouring melatonin compared with placebo (pooled MD = 31.93 minutes (95% CI, 14.76 to 49.09; P < 0.001). Statistical heterogeneity was high because the I2 value was 76%. Subgroup analysis based on previous parent-directed sleep intervention showed no statistically significant difference in effect between subgroups (P = 0.48; I2 = 0%). One RCT that used polysomnography reported no significant difference in TST between the melatonin group and placebo group (MD = 39.3 minutes favouring placebo; 95% CI, −34.7 to 113.3; P = 0.26).
The SR by Abdelgadir et al. (2018)16 combined both actigraphy-recorded and parent-reported diary data of 9 RCTs in MAs and found a significant increase in TST in the melatonin group compared with the placebo group. The pooled MD was 48.26 minutes (95% CI, 36.78 to 59.73; P < 0.00001). Statistical heterogeneity was moderate because the I2 value was 31%. Subgroup analyses based on comorbidity (i.e., ASD and other neurodisability) reduced the I2 to 0% and showed a statistically significant difference in effect between subgroups (P = 0.01; I2 = 84.2%). In the ASD subgroup, the MD in TST between the melatonin and placebo groups was 61.30 minutes (95% CI, 50.48 to 72.13; P < 0.00001; I2 = 0%) compared with 27.91 minutes (95% CI, 4.23 to 51.60; P = 0.02; I2 = 0%) for other neurodisability populations. Pooled analyses of parent-reported TST using a sleep diary or actigraphy-measured TST showed a similar effect favouring melatonin compared with placebo. The pooled MD was 55.4 minutes and 43.4 minutes for sleep diary and actigraphy, respectively.
The RCT by Hayashi et al. (2021)17 found the changes in median TST reported using a sleep diary between the last 7 days of randomization phase and baseline were −1.0 minutes, 8.5 minutes, and −8.0 minutes for the placebo group, 1 mg melatonin group, and 4 mg melatonin group, respectively. The difference between each melatonin group (1 mg and 4 mg) and the placebo group was not statistically significant (P = 0.29 and P = 0.99, respectively).
The RCT by Maanen et al. (2017)18 showed that melatonin treatment significantly increased sleep diary–reported TST (beta = 0.49; P < 0.001) and actigraphy-measured SOT (beta = 0.23; P = 0.012) compared with placebo.
Sleep Efficiency
One SR15 and 2 primary clinical studies17,18 reported the outcome sleep efficiency (Table 11).
The SR by Parker et al. (2019)15 included 5 RCTs that reported sleep efficiency. One RCT had both actigraphy-recorded data and parent-reported data using a sleep diary, 3 RCTs had actigraphy-recorded data only, and 1 RCT measured sleep efficiency using polysomnography. For parent-reported sleep efficiency using a sleep diary, there was no statistically significant difference between the melatonin group and the placebo group (MD = 0.30%; 95% CI, −0.90 to 1.49; P = 0.62). For actigraphy-measured sleep efficiency, there was also no statistically significant difference between the melatonin group and the placebo group. The pooled MD was 4.76% (95% CI, −0.95 to 10.47; P = 0.10). Statistical heterogeneity was high because the I2 value was 94%. Subgroup analysis based on previous parent-directed sleep intervention did not reduce heterogeneity and showed no statistically significant difference in effect between subgroups (P = 0.34; I2 = 0%). One RCT that used polysomnography reported no significant difference in sleep efficiency between the melatonin group and the placebo group (MD = 3.8%; 95% CI, −2.5 to 10.1; P = 0.17).
The RCT by Hayashi et al. (2021)17 showed a small difference in sleep efficiency between 4 mg melatonin (2.4%) compared with placebo (−0.5%; P = 0.04). There was no significant difference in sleep efficiency between 1 mg melatonin (2.1%) compared with placebo (−0.5%; P = 0.14).
The RCT by Maanen et al. (2017)18 showed that melatonin treatment significantly increased actigraphy-measured sleep efficiency (beta = 1.51; P = 0.033) compared with placebo.
Number of Wakenings After Sleep Onset
Two SRs15,16 and 1 primary clinical study17 reported the number of wakenings after sleep onset as an outcome (Table 12).
The SR by Parker et al. (2019)15 included 4 RCTs that reported the number of wakenings after sleep onset using sleep diaries. There was no statistically significant difference in the number of night wakenings between the melatonin group and the placebo group. The pooled MD was −0.04 (95% CI, −0.22 to 0.13; P = 0.61). Statistical heterogeneity was high because the I2 value was 84%. Subgroup analyses showed no statistically significant difference in effect between studies of children with ASD and those of children in other neurodisability populations (P = 0.06; I2 = 71.7%).
The SR by Abdelgadir et al. (2018) combined both actigraphy-recorded and parent-reported diary data of 6 RCTs in an MA and found no statistically significant difference in the number of wakenings between melatonin group and placebo group. The pooled MD was −0.49 (95% CI, −1.71 to 0.73; P = 0.43). Statistical heterogeneity was high as the I2 value was 95%. Separate analyses by types of recording (i.e., diary or actigraphy) also showed no statistically significant differences in the number of wakenings between groups.
The RCT by Hayashi et al. (2021)17 showed that the changes in median number of wakenings recorded during the last 7 days of the randomization phase from baseline were 0.5, 1.5, and −0.5 for placebo, 1 mg melatonin, and 4 mg melatonin, respectively. There was no statistically significant difference between the 1 mg melatonin group and the placebo group (P = 0.09) or between the 4 mg melatonin group and the placebo group (P = 1.00).
Wake-Up Time After Sleep Onset
One SR14 and 2 primary clinical studies17,18 reported wake-up time after sleep onset as an outcome (Table 13).
The SR by Wei et al. (2020)14 included 4 RCTs reporting wake-up time. The MAs showed no statistically significant difference in wake-up time between the melatonin group and placebo group. The pooled MD was −0.16 hours (95% CI, −0.33 to 0.01; P = 0.07). There was no statistical heterogeneity because the I2 value was 0%.
In the RCT by Hayashi et al. (2021),17 the wake-up time in the 1 mg melatonin group extended significantly compared with the placebo group (12.5 minutes versus −6.0 minutes; P = 0.007), while there was no significant difference in wake-up time between the 4 mg melatonin group and placebo group (8.0 minutes versus −6.0 minutes; P = 0.30).
The RCT by Maanen et al. (2017)18 showed that melatonin treatment significantly increased actigraphy-measured wake-up time after sleep onset (beta = 0.17; P = 0.003) compared with placebo.
Light-Off Time
The SR by Wei et al. (2020)14 included 4 RCTs that reported light-off time (Table 14). The MAs showed no significant difference in light-off time between the melatonin group and placebo group. The pooled MD was −0.08 hours (95% CI, −0.35 to 0.18; P = 0.55). There was no statistical heterogeneity because the I2 value was 0%.
Dim Light Melatonin Onset
One SR14 and 1 primary clinical study18 reported the outcome DLMO (Table 15).
The SR by Wei et al. (2020)14 included 5 RCTs reporting DLMO. Compared with placebo, DLMO was significantly advanced (pooled MD = −0.82 hours; 95% CI, −1.23 to −0.41; P < 0.0001). Statistical heterogeneity was moderate because the I2 value was 49%.
The RCT by Maanen et al. (2017)18 showed that DLMO significantly advanced during melatonin treatment (beta = −0.99; P = 0.008) compared with placebo.
Child’s Behaviour
One SR16 and 1 primary clinical study17 included child’s behaviour as an outcome (Table 16).
The SR by Abdelgadir et al. (2018)16 included 7 RCTs reporting child’s behaviour according to parental perception. Four RCTs found that children’s behaviour changed favouring melatonin over placebo. However, 3 RCTs that assessed children with ADHD reported no differences in behaviour between melatonin and placebo groups.
In the RCT by Hayashi et al. (2021),17 child’s behaviour was assessed using the aberrant behaviour checklist.21 There were no significant differences between melatonin group and the placebo group with respect to all of 5 aberrant behaviours (i.e., excitability, inertia, stereotypic behaviour, hyperactivity, and inappropriate speech).
Safety
Three SRs14-16 and 1 primary clinical study17 reported safety outcomes (Table 17).
The SR by Wei et al. (2020)14 included 7 RCTs that reported dropout as a safety outcome and found no significant difference in the incidence of all-cause dropout or dropout due to AEs during melatonin treatment compared with placebo. The authors of the SR14 briefly described, without presenting any data, that most AEs in the included studies were reported as mild to moderate AEs after short-term use of melatonin, including tiredness, headache, gastrointestinal upset, and sometimes decreased mood; 1 reported 1 case of migraine as a severe AE.
The SR by Parker et al. (2019)15 included 11 RCTs reporting AEs. Three of those trials reported that no AEs were observed. AEs were reported in different ways across RCTs, and no MAs were possible. The AEs included abdominal pain; agitation; anxiety; behaviour change or problems; breathlessness; cold, flu, or infection; confusion; constipation; diarrhea; cough; daytime laziness; decreased mood; dizziness; drowsiness; gastrointestinal illness; impaired appetite; increased activity; increased excitability; mood swings; seizures; rash; hypothermia; fatigue; headache or migraine; “hung-over feeling”; tremor; nausea; vomiting; nightmares; rash; mood swings; hypothermia; irritation to skin hyperactivity; itching or painful lumps on the skin; sleep maintenance insomnia; somnolence; skin pigment changes; perspiration; regression of development; and visual disturbances.
The SR by Abdelgadir et al. (2018)16 included 11 RCTs that reported AEs, although these data were not enough to allow MAs. However, the authors of the SR16 reported no significant differences in AEs between the melatonin group and the placebo group.
The RCT by Hayashi et al. (2021),17 observed no serious AEs or death during the treatment period. The incidences of AEs were 18.2%, 13.8%, and 29.2% for the placebo group, the 1 mg melatonin group, and the 4 mg melatonin group, respectively. One incidence of somnolence provoked temporary interruption in the 1 mg melatonin group and 1 incidence of medication discontinuation in the 4 mg melatonin group. The most predominant AEs that occurred in all 3 groups (i.e., placebo, 1 mg, and 4 mg) during treatment were infections and infestations (7.6%, 4.6%, and 10.8%, respectively), nervous system disorders (3.0%, 3.1%, and 6.2%, respectively), and pharyngitis (6.1%, 3.1%, and 3.1%, respectively).
Clinical Effectiveness of Melatonin Versus Prescription Sedatives for the Treatment of Insomnia in Children and Adolescents
No studies comparing melatonin versus prescription sedatives for the treatment of insomnia in children and adolescents were identified; therefore, no summary can be provided.
Cost-Effectiveness of Melatonin Versus No Treatment or Placebo for the Treatment of Insomnia in Children and Adolescents
No studies comparing the cost-effectiveness of melatonin versus no treatment or placebo for the treatment of insomnia in children and adolescents were identified; therefore, no summary can be provided.
Cost-Effectiveness of Melatonin Versus Prescription Sedatives for the Treatment of Insomnia in Children and Adolescents
No studies comparing the cost-effectiveness of melatonin versus prescription sedatives for the treatment of insomnia in children and adolescents were identified; therefore, no summary can be provided.
Guidelines
The AAN guideline19 provides recommendations (level B) for the treatment of insomnia and disrupted sleep behaviour in children and adolescents with ASD. The guideline recommends that parental counselling regarding strategies for improvement of sleep habits and behavioural strategies should be the first-line treatment approach, used either alone or with concomitant medications. If the behavioural approaches have not been sufficient, the guideline recommends the use of high-grade melatonin, starting with a low dose (1 mg/day to 3 mg/day), 30 minutes to 60 minutes before bedtime, and titrating up to 10 mg/day. The guideline suggests that clinicians should inform parents and patients (as appropriate) about the potential AEs of melatonin use and the lack of long-term safety data.
Limitations
There are several limitations of the SRs,14-16 including the substantial heterogeneity in the demographics and characteristics of included studies. The heterogeneity and inconsistency among the included studies limited the overall quality of the evidence obtained. The included studies included mostly children between ages 6 years and 11 years, with various comorbidities; therefore, the findings may not be applicable to children outside this age range or to specific populations of children. There was no consensus regarding the dosage, treatment duration, and administration time of melatonin. The dosage of melatonin varied among the included studies ranging from 0.5 mg/day to 9 mg/day and the duration of treatment varied from 1 week to 13 weeks with no consistent pattern among studies. Melatonin was administered at 4:30 p.m. to 9:00 p.m. or 20 minutes to 45 minutes before bedtime. Administration time either before or after DLMO may affect the efficacy of melatonin. Recent evidence suggests that the chronobiological effect of melatonin could have been stronger if it was administered 3 hours to 5 hours before DLMO.22 Most included studies did not report detailed demographic and clinical characteristics, so any imbalances between groups could not be determined. This may have some risk of selection bias that could impact the reliability and the strength of the evidence. The included studies used a wide variety of different outcomes and measurement tools. The recording methods of sleep parameters using a sleep diary or actigraphy were not uniform among studies. The parent-reported method using a sleep diary was considered to be subjective and less accurate than the objective method using actigraphy. One included study used polysomnography to measure sleep outcomes. There was variability in the type of AEs reported, which limits the assessment of melatonin safety. Most of the included studies assessed the efficacy and safety immediately after the melatonin treatment was completed, without any follow-up evaluation for long-term effects. The washout periods between melatonin and placebo treatment varied among the crossover studies. Melatonin could have a carry-on effect on sleep parameters and circadian rhythm that likely affected the results. Most studies had small sample sizes (6 to 54 participants), so any non-significant differences in outcomes may be due to low statistical power.
As described previously, the included primary clinical studies17,18 had limited findings on melatonin long-term efficacy and safety.
The included guideline recognized the lack of well-designed studies of sleep-related treatments for children with ASD, optimal outcome measures, minimal clinically important differences (MCIDs) for most outcomes, and long-term AEs. Therefore, the strength of all recommendations was considered level B, corresponding to the helping verb “should.”
This review was limited with evidence only for the clinical efficacy and safety of melatonin compared with placebo; we did not identify any studies that compared melatonin with prescription sedatives or any cost-effectiveness studies of melatonin for the treatment of insomnia in children and adolescents. No evidence-based guidelines for the treatment of insomnia in other populations of children and adolescents were identified.
Conclusions and Implications for Decision- or Policy-Making
This report identified 3 SRs,14-16 2 primary clinical studies (both RCTs),17,18 and 1 guideline.19 The identified SRs and primary clinical studies provided evidence for the efficacy and safety of melatonin compared with placebo for treatment of sleep problems in children and adolescents with neurodisabilities, including ASD. No evidence that compared the clinical effectiveness of melatonin with prescription sedatives for the treatment of insomnia in children and adolescents was identified. Also, no evidence was identified regarding the cost-effectiveness of melatonin compared with placebo or prescription sedatives for the treatment of insomnia in children and adolescents.
Collective evidence from the included SRs14-16 and primary clinical studies17,18 suggested that melatonin was effective compared with placebo for SOL, SOT, TST, and DLMO. Subgroup analyses based on the etiology of the sleep disturbance suggested that the benefit of melatonin may be greatest for children with ASD. However, there was no evidence of benefit for melatonin compared with placebo regarding other sleep outcomes, such as sleep efficiency, number of wakenings after sleep onset, wake-up time after sleep onset, and light-off time. The effect of melatonin on child’s behaviour and its long-term safety were unclear. Short-term use of melatonin appears to be safe and tolerable despite variability in reporting AEs in the included studies. AEs were reported to be mild to moderate, including tiredness, headache, gastrointestinal upset, and sometimes decrease of mood. There was incidence of somnolence that provoked temporary interruption and medication discontinuation, prompting caution for the potential development of somnolence in melatonin treatment. The AAN guideline19 recommends that high-grade melatonin should be prescribed for treatment of sleep disturbance in children and adolescents with ASD if the first-line treatment with behavioural strategies is not helpful.
There is some evidence of the benefit and tolerability of melatonin compared with placebo in the short-term treatment of insomnia in children and adolescents with neurodisabilities. However, the clinical significance of the benefit remains uncertain. There were no MCIDs identified within the study findings; therefore, it was unclear if the differences in sleep parameters — although statistically significant — were clinically meaningful. With the previously mentioned limitations of the included studies, the findings are unlikely to be generalizable, and interpretation of the results should be done with caution. Well-designed trials are needed that have standardized measures, identify MCIDs in the outcome measures, have more relevant child and parent outcomes, and include longer-term follow-up. Future trials should also focus on populations with specific comorbidities and defined age ranges. It would be helpful if future trials compare the effectiveness of melatonin with alternative pharmacological interventions that have a different mechanism of action, such as prescribed sedatives, to provide evidence about which drugs may be of most benefit to particular populations.
References
1.Chaput J-P, Yau J, Rao DP, Morin CM. Prevalence of insomnia for Canadians aged 6 to 79. Health Rep. 2018;29(12):16-20. https://www150.statcan.gc.ca/n1/en/pub/82-003-x/2018012/article/00002-eng.pdf?st=EqZ1Kriy. Accessed 2022 May 6. PubMed
2.Gradisar M, Crowley SJ. Delayed sleep phase disorder in youth. Curr Opin Psychiatry. 2013;26(6):580-585. PubMed
3.Esposito S, Laino D, D'Alonzo R, et al. Pediatric sleep disturbances and treatment with melatonin. J Transl Med. 2019;17(1):77. PubMed
4.Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387-1394. PubMed
5.Ophoff D, Slaats MA, Boudewyns A, Glazemakers I, Van Hoorenbeeck K, Verhulst SL. Sleep disorders during childhood: a practical review. Eur J Pediatr. 2018;177(5):641-648. PubMed
6.Sletten TL, Vincenzi S, Redman JR, Lockley SW, Rajaratnam SM. Timing of sleep and its relationship with the endogenous melatonin rhythm. Front Neurol. 2010;1:137. PubMed
7.Pereira N, Naufel MF, Ribeiro EB, Tufik S, Hachul H. Influence of dietary sources of melatonin on sleep quality: a review. J Food Sci. 2020;85(1):5-13. PubMed
8.Abramova R, Campbell P, Baron J, Patel K, Parmar S. Review of melatonin supplementation for sleep disorders in pediatric special populations. J Pharm Pract. 2020;33(4):533-539. PubMed
9.Health Canada. Summary Safety Review: melatonin (n-acetyl-5-methoxytryptamine): review of the safety of melatonin in children and adolescents. 2015; https://www.canada.ca/en/health-canada/services/drugs-health-products/medeffect-canada/safety-reviews/summary-safety-review-melatonin-acetyl-methoxytryptamine-review-safety-melatonin-children-adolescents.html. Accessed 2022 May 09.
10.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
12.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 May 17.
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Wei S, Smits MG, Tang X, et al. Efficacy and safety of melatonin for sleep onset insomnia in children and adolescents: a meta-analysis of randomized controlled trials. Sleep Med. 2020;68:1-8. PubMed
15.Parker A, Beresford B, Dawson V, et al. Oral melatonin for non-respiratory sleep disturbance in children with neurodisabilities: systematic review and meta-analyses. Dev Med Child Neurol. 2019;61(8):880-890. PubMed
16.Abdelgadir IS, Gordon MA, Akobeng AK. Melatonin for the management of sleep problems in children with neurodevelopmental disorders: a systematic review and meta-analysis. Arch Dis Child. 2018;103(12):1155-1162. PubMed
17.Hayashi M, Mishima K, Fukumizu M, et al. Melatonin treatment and adequate sleep hygiene interventions in children with autism spectrum disorder: a randomized controlled trial. J Autism Dev Disord. 2021;28:28. PubMed
18.van Maanen A, Meijer AM, Smits MG, van der Heijden KB, Oort FJ. Effects of melatonin and bright light treatment in childhood chronic sleep onset insomnia with late melatonin onset: a randomized controlled study. Sleep. 2017;40(2):01.
19.Williams Buckley A, Hirtz D, Oskoui M, et al. Practice guideline: treatment for insomnia and disrupted sleep behavior in children and adolescents with autism spectrum disorder: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2020;94(9):392-404. PubMed
20.Gronseth GS, Woodroffe LM, Getchius TSD. Clinical practice guideline process manual. St Paul (MN): American Academy of Neurology; 2011: https://www.aan.com/siteassets/home-page/policy-and-guidelines/guidelines/about-guidelines/11guidelinedevmanual_v408_web.pdf. Accessed 2022 Apr 26.
21.Aman MG, Singh NN, Stewart AW, Field CJ. The aberrant behavior checklist: a behavior rating scale for the assessment of treatment effects. Am J Ment Defic. 1985;89(5):485-491. PubMed
22.Bruni O, Alonso-Alconada D, Besag F, et al. Current role of melatonin in pediatric neurology: clinical recommendations. Eur J Paediatr Neurol. 2015;19(2):122-133. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Wei et al. (2020)14 China No specific funding received | SR with MA Total: 7 placebo-RCTs; 5 parallel and 2 crossover (N = 387) included in MA Year of publication: 2001 to 2017 Sample size: 40 to 107 Assessment of risk of bias: Cochrane Collaboration’s risk-of-bias tool | Children with symptoms of sleep onset insomnia, including difficult in initiating sleep and daytime fatigue. Comorbidity: 5 of 7 trials reported that children had ADHD. 2 trials did not report comorbid. Mean age: 8.9 to 10.3 years % Male: 42.9 to 79 | Melatonin (n = 234) Placebo (n = 197) Melatonin dosage: 1 mg/day to 6 mg/day, fast-release) Administration time: 4:30 p.m. to 20 minutes before bedtime | Primary efficacy outcome:
Primary safety outcomes:
Secondary efficacy outcomes:
Sleep recording: Diary or actigraphy (a wrist-worn device) Treatment duration: ranging from 1 week to 4 weeks |
Parker et al. (2019)15 UK Health Technology Assessment Programme of the UK National Institute for Health Research | SR with MA Total: 11 placebo-RCTs; 3 parallel and 8 crossover (N = 685) Year of publication: 1996 to 2015 Sample size: 6 to 160 Assessment of risk of bias: Cochrane Collaboration’s risk-of-bias tool | Children with non-respiratory sleep disturbances, of any duration, related to initiation, maintenance, or scheduling of sleep. Comorbidity: DD alone or DD + other, ASD only or ASD + learning disability, ADHD, mixed, cerebral palsy, epilepsy Mean age: 5.5 to 10.3 years % Male: NR | Melatonin (n = 340) Placebo (n = 345) Melatonin dosage: 0.5 mg to 6 mg fast-release or 9 mg sustained-release Administration time: at 6 p.m. to 9 p.m. or 40 minutes to 45 minutes before bedtime | Outcomes:
Sleep recording: Diary or actigraphy Treatment duration: 10 days to 12 weeks |
Abdelgadir et al. (2018)16 UK No specific funding received | SR with MA Total: 13 placebo-RCTs (N = 671) Year of publication: 1998 to 2012 Sample size: 9 to 134 Assessment of risk of bias: Cochrane Collaboration’s risk-of-bias tool GRADE system was used to assess the quality of the body of evidence associated with specific outcomes. | Children with sleep disturbances Comorbidity: Neurodevelopment disorders, neurodevelopment disabilities, ASD, ADHD, girls with Rett syndrome, autism, fragile X syndrome, or autism and fragile X syndrome Age range: 1 to 18 years % Male: NR | Melatonin (n = 340) Placebo (n = 331) Melatonin dosage:
Administration time: NR | Outcomes:
Sleep recording: Diary, actigraphy, or polysomnography Treatment duration: 1 week to 13 weeks |
ADHD = attention-deficit/hyperactivity disorder; AE = adverse event; ASD = autism spectrum disorder; DD = developmental delay; DLMO = dim light melatonin onset; GRADE = Grading of Recommendation, Assessment, Development and Evaluation; NR = not reported; RCT = randomized controlled trial; SOL = sleep onset latency; SOT = sleep onset time; SR = systematic review; TST = total sleep time.
aSOT = the clock time when the patient went into sleep from wakefulness at night.
bDLMO = the clock time in the evening when endogenous melatonin reaches 4 pg/mL in saliva.
cSOL = time spent in bed from light turn off until the onset of any sleep stage.
dTST = time between sleep onset and wake-up time.
eSleep efficiency = ratio of TST to total time in bed.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Hayashi et al. (2021)17 Japan Nobelpharma Co., Ltd. | Multicentre, double-blind, 3 parallel-group 1:1:1, placebo-RCT Sample size calculation provided: Yes ITT: Yes | Children with sleep disturbances (N = 196) Comorbidity: ASD Mean age: 11.2 years % Male: 61.7 SOL:
History of ramelteon treatment:
| Melatonin 1 mg (n = 65) Melatonin 4 mg (n = 65) Placebo (n = 66) Administration time: 45 minutes before bedtime All children were under adequate sleep hygiene interventions. | Primary outcome (assessed with electronic sleep diary):
Secondary outcomes (assessed with actigraphy):
Safety outcomes (AEs) Sleep recording: Diary and actigraphy Treatment duration: 14 days |
Maanen et al. (2017)18 The Netherlands Pharma Nord; Physician Engineered Products | Single-centre, double-blind, 2 parallel-group 1:1, placebo-RCT Sample size calculation provided: No ITT: NR | Children with chronic sleep onset insomnia (N = 84) Comorbidity: NR, but the study excluded psychiatric disorders other than ADHD or ASD Mean age: 10.0 years % Male: 61.0 | Melatonin 3 mg, fast-release (n = 26) Bright light treatment (n = 30) Placebo (n = 28) Administration time: 7:00 p.m. Sleep hygiene instructions were handed out to all participants. | Outcomes:
Sleep recording: Diary and actigraphy Treatment duration: 3 to 4 weeks |
AE = adverse event; ASD = autism spectrum disorder; DLMO = dim light melatonin onset; ITT = intention-to-treat; NR = not reported; RCT = randomized controlled trial; SOL = sleep onset latency; SOT = sleep onset time; TST = total sleep time.
aSOL = time spent in bed from light turn off until the onset of any sleep stage.
bTST: time between sleep onset and wake-up time.
cSleep efficiency = ratio of TST to total time in bed.
dChild’s behaviours were assessed using the aberrant behaviour checklist by Aman MG et al. (1994).21
eSOT = the clock time when the patient went into sleep from wakefulness at night.
fDLMO = defined as the clock time between 7:00 p.m. to 11:00 p.m. when the endogenous melatonin reaches 4 pg/mL in saliva.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
AAN, Buckley et al. (2020)19 | ||||||
Intended users: Clinicians who treat children and adolescents with ASD and sleep disturbance Target population: Children and adolescents with ASD and sleep disturbance | Pharmacologic (i.e., melatonin) and nonpharmacologic strategies for treating sleep disturbances in children and adolescents with ASD. | Sleep outcomes (e.g., SOL, sleep efficiency, night awakenings, TST). | The evidence from literature was systematically identified. Studies were reviewed and rated using standard AAN methodology. | Level of evidencea and strength of recommendationb were classified according to the AAN methodology.20 | A multidisciplinary panel including child neurologists, psychiatrists, neuropsychologists, and developmental pediatricians was formed. Evidence-based medicine methodologists supported the project. Strength of recommendation was assigned through modified Delphi voting. | The guideline was internally reviewed and published in a peer-reviewed journal. |
AAN = American Academy of Neurology; ASD = autism spectrum disorder; RCT = randomized controlled trial; SOL = sleep onset latency; TST = total sleep time.
aLevel of evidence: I = Well-designed RCT that fulfills all criteria; II = Well-designed cohort study or RCT missing 1 or 3 criteria; III = Well-designed controlled studies; IV = Poor-designed or irrelevant studies.
bStrength of recommendation: A = Strongest recommendation level and is denoted by use of the helping verb “must.” These recommendations are rare. B = Corresponds to the helping verb “should.” These recommendations are more common, as the requirements are less stringent but are still associated with confidence in the rationale and a favourable benefit-risk profile. C = Corresponds to the helping verb “may.” These recommendations represent the lowest allowable recommendation level that the AAN considers useful within the scope of clinical practice and can accommodate the highest degree of practice variation.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 210
Strengths | Limitations |
|---|---|
Wei et al. (2020)14 | |
The research question or objective and the inclusion criteria for the review clearly include the components of PICO. A study protocol was published on the website. The review authors explained their selection of study designs, which were RCTs, including parallel and crossover designs. The literature search strategy was comprehensive and clearly described, increasing reproducibility. The review authors performed study selection and data extraction in duplicate, reducing the risk of missing relevant studies and making errors in data extraction. The characteristics of the included studies were described in adequate detail, including patient characteristics, dosages of melatonin, administration time, and the treatment duration were described. The methodological quality of the included studies was assessed using the Cochrane Risk of Bias tool. The software Review Manager (RevMan) was used in the meta-analysis. Investigation of the causes of heterogeneity was planned. The review authors provided a discussion of the heterogeneity observed in the results, which was the main limitation of the meta-analysis. The review authors assessed potential impact of risk of bias in individual studies on the results, and they accounted for risk of bias in the included studies when interpreting or discussing the results of the review. The review authors evaluated publication bias using funnel plot method. The review authors declared that no funding was received for this systematic review. Conflicts of interest were also declared. | A list of excluded studies and the reasons for exclusion were not provided. Therefore, it was not possible to assess whether any relevant articles were excluded and if so, for what reasons. The review authors did not report the sources of funding for the included studies. This is potentially a concern because funding received from industry can introduce bias in favour of the intervention. |
Parker et al. (2019)15 | |
The research question or objective and the inclusion criteria for the review clearly include the components of PICO. The study protocol had been registered on the website of the Centre for Reviews and Dissemination (PROSPERO). The review authors explained their selection of study designs, which were RCTs, including parallel and crossover designs. The literature search strategy was comprehensive and clearly described, increasing reproducibility. The review authors performed study selection and data extraction in duplicate, reducing the risk of missing relevant studies and making errors in data extraction. The characteristics of the included studies were described in adequate detail, including patient characteristics, dosages of melatonin, administration time, and the treatment duration were described. The methodological quality of the included studies was assessed using the Cochrane Risk of Bias tool. The software Review Manager (RevMan) was used in the meta-analysis. The causes of heterogeneity were investigated. The review authors provided a discussion of the heterogeneity observed in the results. The review authors assessed potential impact of risk of bias in individual studies on the results, and they accounted for risk of bias in the included studies when interpreting or discussing the results of the review. Investigation of publication bias was not applicable due to small number of included studies (i.e., less than 10). The review authors reported the source of funding and declared conflicts of interest. | A list of excluded studies and the reasons for exclusion were not provided. Therefore, it was not possible to assess whether any relevant articles were excluded and if so, for what reasons. The review authors did not report the sources of funding for the included studies. This is potentially a concern because funding received from industry can introduce bias in favour of the intervention. |
Abdelgadir et al. (2018)16 | |
The research question or objective and the inclusion criteria for the review clearly include the components of PICO. The study protocol had been registered on the website of the Centre for Reviews and Dissemination (PROSPERO). The review authors explained their selection of study designs, which were RCTs, including parallel and crossover designs. The literature search strategy was comprehensive and clearly described, increasing reproducibility. The review authors performed study selection and data extraction in duplicate, reducing the risk of missing relevant studies and making errors in data extraction. The methodological quality of the included studies was assessed using the Cochrane Risk of Bias tool. The software Review Manager (RevMan) was used in the meta-analysis. Investigation of the causes of heterogeneity was planned. The review authors provided a discussion of the heterogeneity observed in the results. The review authors evaluated publication bias using funnel plot method. The review authors declared that no funding was received for this systematic review. Conflicts of interest were also declared. | A list of excluded studies and the reasons for exclusion were not provided. Therefore, it was not possible to assess whether any relevant articles were excluded and if so, for what reasons. The review authors did not report the sources of funding for the included studies. This is potentially a concern because funding received from industry can introduce bias in favour of the intervention. The characteristics of the included studies were partially described. The review authors did not assess potential impact of risk of bias in individual studies on the results, and they did not account for risk of bias in the included studies when interpreting or discussing the results of the review. |
PICO = population, intervention, comparator, and outcome; RCT = randomized controlled trial.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist11
Strengths | Limitations |
|---|---|
Hayashi et al. (2021)17 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| Reporting:
|
Maanen et al. (2017)18 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| Reporting:
Internal validity – confounding:
|
RCT = randomized controlled trial.
Table 7: Strengths and Limitations of the AAN Guideline Using AGREE II12
Item | AAN, Buckley et al. (2020)19 |
|---|---|
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Unclear |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | No |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ANN = American Academy of Neurology; NR = not reported; NA = not applicable.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcomes for Melatonin Versus Placebo — Sleep Onset Latency
Study citation, study design, and patient model | Study findings |
|---|---|
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Six RCTs (N = 326) reported SOL (combining both actigraphy and parent-reported diary data).
|
Parker et al. (2019)15 SR with MA Children with non-respiratory sleep disturbances Comorbid: DD alone or DD + other, ASD only or ASD + learning disability, ADHD, mixed, cerebral palsy, epilepsy | Parent-reported SOL using sleep diaries Six RCTs (N = 223)
ASD subgroup analysis:
Actigraphy-measured SOL Five RCTs (N = 264)
Previous parent-directed sleep intervention subgroup analysis:
Polysomnography-measured SOL 1 RCT (N = 10)
|
Abdelgadir et al. (2018)16 SR with MA Children with sleep disturbances Comorbid: Neurodevelopment disorders, neurodevelopment disabilities, ASD, ADHD, girls with Rett syndrome, autism, fragile X syndrome, or autism and fragile X syndrome | Total trials reporting SOL (combining both actigraphy and parent-reported diary data) Thirteen RCTs reported SOL, but 11 RCTs (N = 581) provided sufficient data for MA.
Parent-reported SOL using sleep diaries Five RCTs (N = 219)
Actigraphy-measured SOL Six RCTs (N = 362)
Comorbid subgroup analysis
|
Hayashi et al. (2021)17 RCT Children with sleep disturbances (N = 196) Comorbid: ASD | Parent-reported SOL using sleep diaries Changes in median SOL recorded during the last 7 days of the randomization phase from baseline:
Sex subgroup analysis:
Age subgroup analysis:
Weight subgroup analysis:
SOL at baseline subgroup analysis:
Previous ramelteon treatment subgroup analysis:
|
Intellectual disabilities subgroup analysis:
ADHD subgroup analysis:
Height subgroup analysis:
Actigraphy-measured SOL Changes in median SOL recorded during the last 7 days of the randomization phase from baseline:
| |
Maanen et al. (2017)18 RCT Children with chronic sleep onset insomnia (N = 84) Comorbid: NR, but the study excluded psychiatric disorders other than ADHD or ASD | Parent-reported SOL using sleep diaries
Actigraphy-measured SOL
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; CI = confidence interval; MA = meta-analysis; MD = mean difference; SOL = sleep onset latency; RCT = randomized controlled trial; SE = standard error; SR = systematic review; vs. = versus.
Table 9: Summary of Findings by Outcomes for Melatonin Versus Placebo — Sleep Onset Time
Study citation, study design, and patient model | Study findings |
|---|---|
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Six RCTs (N = 364) reported SOT.
|
Maanen et al. (2017)18 RCT Children with chronic sleep onset insomnia (N = 84) Comorbid: NR, but the study excluded psychiatric disorders other than ADHD or ASD | Parent-reported SOT using sleep diaries
Actigraphy-measured SOT
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; CI = confidence interval; MA = meta-analysis; MD = mean difference; SOT = sleep onset time; RCT = randomized controlled trial; SE = standard error; SR = systematic review; vs. = versus.
Table 10: Summary of Findings by Outcomes for Melatonin Versus Placebo — Total Sleep Time
Study citation, study design, and patient model | Study findings |
|---|---|
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Five RCTs (N = 262) reported TST (combining both actigraphy and parent-reported diary data).
|
Parker et al. (2019)15 SR with MA Children with non-respiratory sleep disturbances Comorbid: DD alone or DD + other, ASD only or ASD + learning disability, ADHD, mixed, cerebral palsy, epilepsy | Parent-reported TST using sleep diaries Seven RCTs (N = 232)
ASD subgroup analysis:
Previous parent-directed sleep intervention subgroup analysis:
One RCT with low risk of bias (N = 110)
Actigraphy-measured TST Five RCTs (N = 265)
Previous parent-directed sleep intervention subgroup analysis:
Removal of a single RCT where the study population primarily had ASD (4 RCTs; N = 199)
Polysomnography-measured TST 1 RCT (N = 10) MD (95% CI) = 39.3 minutes favouring placebo (−34.7 to 113.3); P = 0.26 |
Abdelgadir et al. (2018)16 SR with MA Children with sleep disturbances Comorbid: Neurodevelopment disorders, neurodevelopment disabilities, ASD, ADHD, girls with Rett syndrome, autism, fragile X syndrome, or autism and fragile X syndrome | Total trials reporting TST (combining both actigraphy and parent-reported diary data) 9 RCTs (N = 541)
Parent-reported TST using sleep diaries Four RCTs (N = 187)
Actigraphy-measured TST Five RCTs (N = 354)
Comorbid subgroup analysis
|
Hayashi et al. (2021)17 RCT Children with sleep disturbances (N = 196) Comorbid: ASD | Actigraphy-measured TST Changes in median TST recorded during the last 7 days of the randomization phase from baseline:
|
Maanen et al. (2017)18 RCT Children with chronic sleep onset insomnia (N = 84) Comorbid: NR, but the study excluded psychiatric disorders other than ADHD or ASD | Parent-reported TST using sleep diaries
Actigraphy-measured TST
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; CI = confidence interval; DD = developmental delay; MA = meta-analysis; MCDI = minimum clinically important difference; MD = mean difference; RCT = randomized controlled trial; SR = systematic review; TST = total sleep time; vs. = versus.
Table 11: Summary of Findings by Outcomes for Melatonin Versus Placebo — Sleep Efficiency
Study citation, study design, and patient model | Study findings |
|---|---|
Parker et al. (2019)15 SR with MA Children with non-respiratory sleep disturbances Comorbid: DD alone or DD + other, ASD only or ASD + learning disability, ADHD, mixed, cerebral palsy, epilepsy | Parent-reported sleep efficiency using sleep diaries 1 RCT (N = 50)
Actigraphy-measured sleep efficiency Four RCTs (N = 254)
Previous parent-directed sleep intervention subgroup analysis:
Removal of a single RCT where the study population primarily had ASD (3 RCTs; N = 188)
Polysomnography-measured sleep efficiency 1 RCT (N = 10)
|
Hayashi et al. (2021)17 RCT Children with sleep disturbances (N = 196) Comorbid: ASD | Actigraphy-measured sleep efficiency Changes in median sleep efficiency recorded during the last 7 days of the randomization phase from baseline:
|
Maanen et al. (2017)18 RCT Children with chronic sleep onset insomnia (N = 84) Comorbid: NR, but the study excluded psychiatric disorders other than ADHD or ASD | Actigraphy-measured sleep efficiency
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; CI = confidence interval; DD = developmental delay; MA = meta-analysis; MD = mean difference; RCT = randomized controlled trial; SE = standard error; SR = systematic review; vs. = versus.
Table 12: Summary of Findings by Outcomes for Melatonin Versus Placebo — Number of Wakenings After Sleep Onset
Study citation, study design, and patient model | Study findings |
|---|---|
Parker et al. (2019)15 SR with MA Children with non-respiratory sleep disturbances Comorbid: DD alone or DD + other, ASD only or ASD + learning disability, ADHD, mixed, cerebral palsy, epilepsy | Parent-reported number of wakenings after sleep onset using sleep diaries 4 RCTs (N = 94)
ASD subgroup analysis:
|
Abdelgadir et al. (2018)16 SR with MA Children with sleep disturbances Comorbid: Neurodevelopment disorders, neurodevelopment disabilities, ASD, ADHD, girls with Rett syndrome, autism, fragile X syndrome, or autism and fragile X syndrome | Total trials reporting number of wakenings after sleep onset (combining both actigraphy and parent-reported diary data) Six RCTs (N = 277)
Parent-reported number of wakenings using sleep diaries Three RCTs (N = 87)
Actigraphy-measured number of wakenings Three RCTs (N = 190)
|
Hayashi et al. (2021)17 RCT Children with sleep disturbances (N = 196) Comorbid: ASD | Actigraphy-measured number of wakenings after sleep onset Changes in median number of wakening recorded during the last 7 days of the randomization phase from baseline:
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; CI = confidence interval; DD = developmental delay; MA = meta-analysis; MD = mean difference; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
Table 13: Summary of Findings by Outcomes for Melatonin Versus Placebo — Wake Time After Sleep Onset
Study citation, study design, and patient model | Study findings |
|---|---|
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Four RCTs (N = 209) reported wake-up time.
|
Hayashi et al. (2021)17 RCT Children with sleep disturbances (N = 196) Comorbid: ASD | Actigraphy-measured wake-up time after sleep onset Changes in median wakening time after sleep onset recorded during the last 7 days of the randomization phase from baseline:
|
Maanen et al. (2017)18 RCT Children with chronic sleep onset insomnia (N = 84) Comorbid: NR, but the study excluded psychiatric disorders other than ADHD or ASD | Actigraphy-measured wake-up time after sleep onset
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; CI = confidence interval; MA = meta-analysis; MD = mean difference; NR = not reported; RCT = randomized controlled trial; SE = standard error; SR = systematic review; vs. = versus.
Table 14: Summary of Findings by Outcomes for Melatonin Versus Placebo — Light-Off Time
Study citation, study design, and patient model | Study findings |
|---|---|
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Three RCTs (N = 179) reported light-off time.
|
ADHD = attention-deficit/hyperactivity disorder; CI = confidence interval; h = hour; MA = meta-analysis; MD = mean difference; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
Table 15: Summary of Findings by Outcomes for Melatonin Versus Placebo — Dim Light Melatonin Onset
Study citation, study design, and patient model | Study findings |
|---|---|
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Five RCTs (N = 271) reported DLMO.
|
Maanen et al. (2017)18 RCT Children with chronic sleep onset insomnia (N = 84) Comorbid: NR, but the study excluded psychiatric disorders other than ADHD or ASD | Actigraphy-measured DLMO
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; CI = confidence interval; DLMO = dim light melatonin onset; h = hour; MA = meta-analysis; MD = mean difference; RCT = randomized controlled trial; SE = standard error; SR = systematic review; vs. = versus.
Table 16: Summary of Findings by Outcomes for Melatonin Versus Placebo — Child’s Behaviour
Study citation, study design, and patient model | Study findings |
|---|---|
Abdelgadir et al. (2018)16 SR with MA Children with sleep disturbances Comorbid: Neurodevelopment disorders, neurodevelopment disabilities, ASD, ADHD, girls with Rett syndrome, autism, fragile X syndrome, or autism and fragile X syndrome |
|
Hayashi et al. (2021)17 RCT Children with sleep disturbances (N = 196) Comorbid: ASD | There were no significant differences between melatonin group and the placebo group with respect to all of 5 aberrant behaviours (i.e., excitability, inertia, stereotypic behaviour, hyperactivity, and inappropriate speech). |
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; MA = meta-analysis; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
Table 17: Summary of Findings by Outcomes for Melatonin Versus Placebo — Safety Outcomes
Study Citation, Study Design, and Patient Model | Study Findings |
|---|---|
All-cause dropout | |
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Seven RCTs (N = 431) reported all-cause dropout.
|
Dropout due to adverse events | |
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. | Seven RCTs (N = 431) reported dropout due to AEs.
|
Adverse events | |
Wei et al. (2020)14 SR with MA Children with symptoms of sleep onset insomnia Comorbid: Five of 7 trials reported that children had ADHD. Two trials did not report comorbid. |
|
Parker et al. (2019)15 SR with MA Children with non-respiratory sleep disturbances Comorbid: DD alone or DD + other, ASD only or ASD + learning disability, ADHD, mixed, cerebral palsy, epilepsy |
|
Abdelgadir et al. (2018)16 SR with MA Children with sleep disturbances Comorbid: Neurodevelopment disorders, neurodevelopment disabilities, ASD, ADHD, girls with Rett syndrome, autism, fragile X syndrome, or autism and fragile X syndrome |
|
Hayashi et al. (2021)17 RCT Children with sleep disturbances (N = 196) Comorbid: ASD | Overall AEs:
Drug-related AEs:
Serious AEs (none) Serious drug-related AEs (none) Severe AEs (none) AEs leading to death (none) AEs leading to temporary interruption:
AEs leading to discontinuation:
Infections and infestations:
Nervous system disorders:
Pharyngitis:
|
ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder; AE = adverse event; CI = confidence interval; DD = developmental delay; MA = meta-analysis; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
Table 18: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
AAN, Buckley et al. (2020)19 | |
“Clinicians seek improve sleep function in children and adolescents with ASD should counsel parents or guardians regarding strategies for improved sleep habits, with behavioral strategies as a first-line treatment approach either alone or in combination with pharmacologic or nutraceutical approaches, depending on individual circumstances.”19 (p. 399) The recommendation was supported by evidence from 8 studies. | Quality of evidence: III or higher Strength of recommendation: B |
“Clinicians should offer melatonin to children and adolescents with ASD if behavioral strategies have not been helpful and contributing coexisting conditions and use of concomitant medications have been addressed.”19 (p. 400) The recommendation was supported by evidence from 8 studies. | Quality of evidence: III or higher Strength of recommendation: B |
“Clinicians offering melatonin for sleep disturbance in children and adolescents with ASD should write a prescription for melatonin or recommend using a high-purity pharmaceutical grade of melatonin when available.”19 (p. 400) The recommendation was supported by evidence from 8 studies. | Quality of evidence: III or higher Strength of recommendation: B |
“Clinicians offering melatonin for sleep dysregulation in children and adolescents with ASD should start by initiating a low dose (1-3 mg/d), 30-60 minutes before bedtime, and titrate to effect, not exceeding 10 mg/d.”19 (p. 400) The recommendation was supported by evidence from 8 studies. | Quality of evidence: III or higher Strength of recommendation: B |
“Clinicians offering melatonin for sleep disturbance in children and adolescents with ASD should counsel children and adolescents with ASD and sleep disturbance (as appropriate) and their parents regarding adverse events of melatonin use and the lack of long-term safety data.”19 (p. 400) The recommendation was supported by evidence from 8 studies. | Quality of evidence: III or higher Strength of recommendation: B |
AAN = American Academy of Neurology; ASD = autism spectrum disorder.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 19: Overlap Between Relevant Primary Studies and Included Systematic Reviews
Primary study citation | Wei et al. (2020)14 | Parker et al. (2029)15 | Abdelgadir et al. (2018)16 |
|---|---|---|---|
Eckerberg B et al. Chronobiol Int 2012;29(9):1239e48. | Yes | No | No |
Smits MG et al. J Child Neurol 2001;16(2):86e92. | Yes | No | No |
Smits MG et al. J Am Acad Child Adolesc Psychiatry 2003;42(11):1286e93. | Yes | No | No |
van der Heijden KB et al. J Am Acad Child Adolesc Psychiatry 2007;46(2):233e41. | Yes | No | No |
van Geijlswijk IM et al. Psychopharmacology (Berl) 2010;212(3):379e91. | Yes | No | No |
van Maanen A et al. Sleep 2017;40(2). | Yes | No | No |
Weiss MD et al. J Am Acad Child Adolesc Psychiatry 2006;45(5):512e9. | Yes | Yes | Yes |
Appleton RE et al. Health Technol Assess 2012; 16: i-239. | No | Yes | Yes |
Camfield P et al. J Child Neurol 1996; 11: 341-3. | No | Yes | No |
Wasdell MB et al. J Pineal Res 2008; 44: 57-64. | No | Yes | Yes |
Cortesi F et al. J Sleep Res 2012; 21: 700-9. | No | Yes | Yes |
Van der Heijden KB et al. J Am Acad Child Adolesc Psychiatry 2007; 46: 233-41. | No | Yes | Yes |
Garstang J and Wallis M. Child Care Health Dev 2006; 32: 585-9. | No | Yes | Yes |
Wright B et al. J Autism Dev Disord 2011; 41: 175-84. | No | Yes | Yes |
Dodge NN and Wilson GA. J Child Neurol 2001; 16: 581-4. | No | Yes | Yes |
Jain SV, Horn PS et al. Sleep Med 2015; 16: 637-44. | No | Yes | No |
Wirojanan J et al. J Clin Sleep Med 2009; 5: 145-50. | No | Yes | No |
Gringras P et al. J Am Acad Child Adolesc Psychiatry 2017;56:948-57. | No | No | Yes |
McArthur AJ and Budden SS. Dev Med Child Neurol 1998;40:186-92. | No | No | Yes |
Mohammadi MR et al. Iran J Psychiatry 2012;7:87-92. | No | No | Yes |
Niederhofer H et al. J Autism Dev Disord 2003;33:469-72. | No | No | Yes |
Wirojanan J et al. J Clin Sleep Med 2009;5:145-50. | No | No | Yes |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca