CADTH Health Technology Review
Melatonin for the Treatment of Insomnia: A 2022 Update
Rapid Review
Authors: Candyce Hamel, Jennifer Horton
Abbreviations
AGREE
Appraisal of Guidelines for Research and Evaluation
AMSTAR
A Measurement Tool to Assess Systematic Reviews
CBT-I
cognitive behavioural therapy for insomnia
DSM
Diagnostic and Statistical Manual of Mental Disorders
GRADE
Grading of Recommendations Assessment, Development and Evaluation
ICD
International Disease Classification
LSEQ
Leeds Sleep Evaluation Questionnaire
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PSQI
Pittsburgh Sleep Quality Index
RCT
randomized controlled trials
SR
systematic review
Key Messages
Two umbrella reviews, 7 systematic reviews, and 2 randomized controlled trials provided mixed results on the clinical effectiveness of melatonin for insomnia, when compared to placebo. Some studies reported improvement in sleep and quality of life outcomes with melatonin, and some studies reported no difference between patients who received melatonin and those who received placebo.
Efficacy of melatonin was measured both objectively (e.g., polysomnography, actigraphy) and subjectively (e.g., validated questionnaires, sleep diaries), and was measured across multiple outcomes.
Two guidelines recommend melatonin for insomnia, but the strength of the recommendations was not reported. One guideline recommends melatonin for insomnia, based on very low evidence (but the evidence was unclear). One guideline recommends against melatonin for chronic insomnia disorder (weak recommendation). The evidence for these recommendations was not well reported across the guidelines.
No studies were found that evaluated the clinical effectiveness of melatonin compared to prescription sedatives in people with insomnia that met the criteria for this review.
No studies were found for the cost-effectiveness of melatonin in people with insomnia that met the criteria for this review.
Context and Policy Issues
Insomnia is a sleep disorder which can be situational, recurrent, or chronic.1 The 4th cycle (2014 to 2015) of the Canadian Health Measures Survey classified 21.8% to 28.9% of adults 18 to 64 years old and 18.6% to 25.8% of adults 65 years and older of having nighttime insomnia (i.e., trouble going to sleep or staying asleep). Insomnia was more prevalent among females than males in both age groups.1
Several organizations have developed classifications for insomnia disorder, including the WHO International Disease Classification 11 (ICD-11),2 section 7A00 Chronic Insomnia, and the International Classification of Sleep Disorders.3 Chronic insomnia is described as: having sleep disturbances (e.g., difficulty falling asleep, difficulty staying asleep); having associated daytime symptoms (e.g., daytime sleepiness, mood disturbance/irritability); a situation that cannot be explained by inadequate opportunity or inadequate circumstances (e.g., safe, dark environment) to sleep; sleep disturbance and associated daytime symptoms occur at least 3 times a week for at least 3 months; sleep/wake difficulty cannot be better explained by another sleep disorder.2
Management and treatment options for insomnia include cognitive behavioural therapy for insomnia (CBT-I), light therapy, prescribed medications (e.g., benzodiazepine), over the counter sleep aids (e.g., doxylamine), and dietary supplements (e.g., melatonin).4,5 An UpToDate report states that the evidence base for CBT-I is stronger than for medications, therefore, CBT-I should be a part of the management approach for insomnia.4 The selection of medication for insomnia is highly individualized and should consider symptom pattern, past treatment response, medication availability and cost, side effects and contraindications, comorbidities, and patient preference.4
Melatonin is a dietary supplement which may help facilitate sleep onset. It is rapidly absorbed and although side effects from controlled studies are not well established, it is reported to have mild side effects (e.g., vivid dreams, headache, stomach cramps) from short-term and intermediate-term administration.4,6 However, the effectiveness of melatonin for the treatment of insomnia in adults is not clear, and may depend on type of insomnia (e.g., sleep onset insomnia, sleep maintenance insomnia) and comorbidities (e.g., dementia).4
This report is an update to a previous CADTH report published in 2019, which include 4 systematic reviews (SRs) and 2 randomized controlled trials (RCTs). All studies included in the previous report answered the clinical effectiveness question (i.e., no cost-effectiveness studies or guidelines were identified). The included SRs and RCTs suggested favourable effects of melatonin on global sleep outcomes, specific sleep outcomes, and outcomes related to functioning and mood. Effects around quality of life were unclear.7 The objective of this report is to summarize the evidence regarding the clinical effectiveness, cost-effectiveness, and guidelines pertaining to the use of melatonin for the treatment of insomnia in adults.
Research Questions
What is the clinical effectiveness of melatonin versus no treatment or placebo for the treatment of insomnia in adults?
What is the clinical effectiveness of melatonin versus prescription sedatives for the treatment of insomnia in adults?
What is the cost-effectiveness of melatonin versus no treatment or placebo for the treatment of insomnia in adults?
What is the cost-effectiveness of melatonin versus prescription sedatives for the treatment of insomnia in adults?
What are the evidence-based guidelines regarding the use of melatonin for the treatment of insomnia in adults?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were melatonin and insomnia. CADTH-developed search filters were applied to limit retrieval to health technology assessments, SR, meta-analyses, or network meta-analyses; RCTs, controlled clinical trials, or any other type of clinical trial; economic studies; and guidelines. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2019 and April 6, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with insomnia |
Intervention | Melatonin |
Comparator | Q1 and Q3: No treatment, placebo Q2 and Q4: Prescription sedatives (e.g., benzodiazepines [e.g., zopiclone, eszopiclone, zolpidem, temazepam, oxazepam], doxepin) Q5: Not applicable |
Outcomes | Q1 and Q2: Clinical effectiveness (e.g., objective sleep parameters [e.g., total sleep time, sleep latency, sleep efficiency, percentage of rapid eye movement sleep, etc.], quality of life), safety Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios) Q5: Recommendations regarding the use of melatonin for the treatment of insomnia |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, economic evaluations, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2019. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs or were captured in the 2019 CADTH report were excluded (unless additional outcomes were reported). Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)8 for SRs, the “Questionnaire to assess the relevance and credibility of a network meta-analysis”9 for network meta-analyses, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument10 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
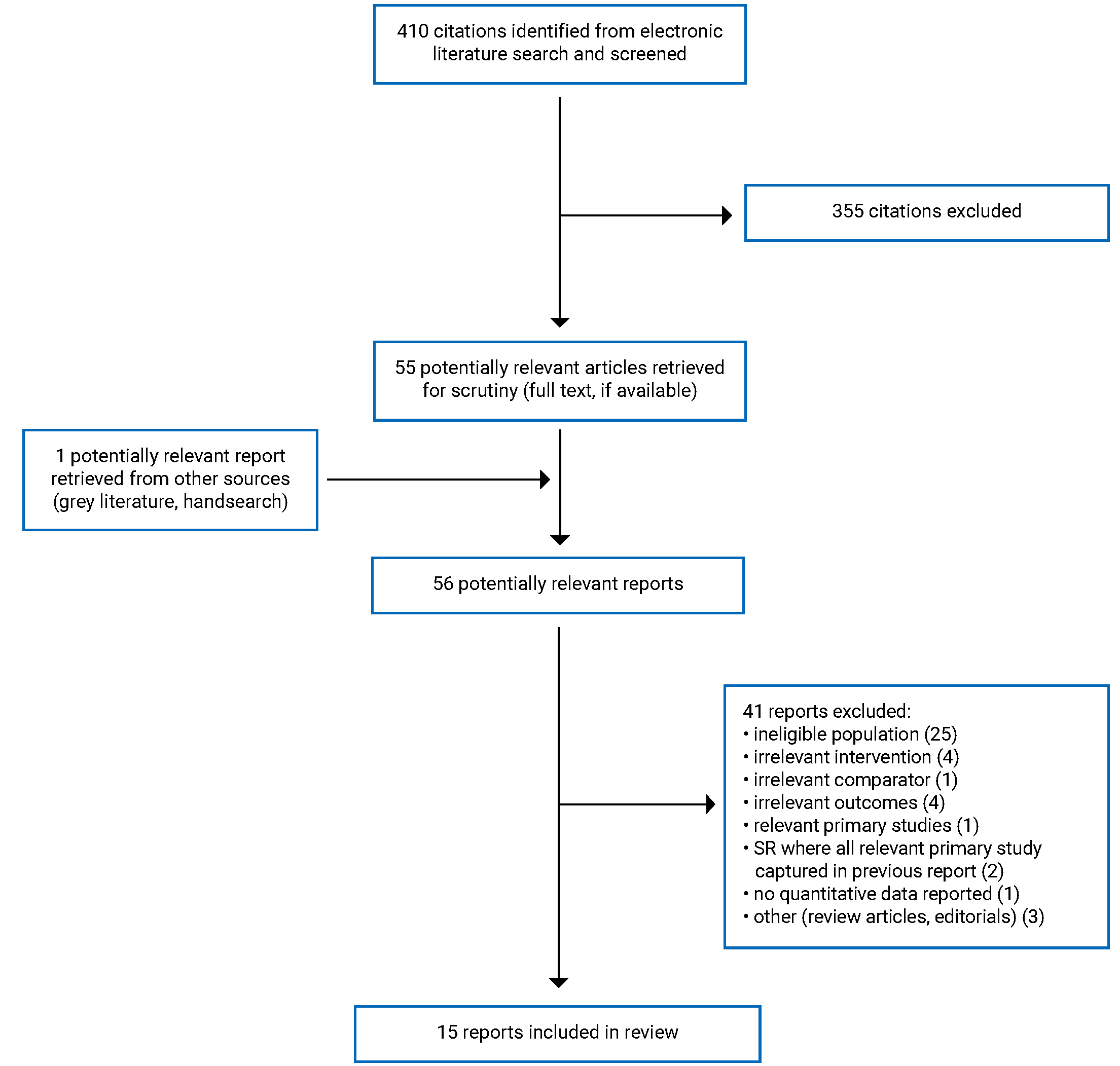
A total of 410 citations were identified in the literature search. Following screening of titles and abstracts, 355 citations were excluded and 55 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 41 publications were excluded for various reasons, and 15 publications met the inclusion criteria and were included in this report. These comprised 2 umbrella reviews, 7 SRs (including 1 network meta-analysis), 2 RCTs, and 4 evidence-based guidelines. Appendix 1 presents the PRISMA11 flow chart of the study selection.
One cohort study was also identified but was not eligible for inclusion based on the criteria for this review. Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Two umbrella reviews,12,13 7 SRs,14-20 (1 of which was a network meta-analysis17), 2 RCTs,21,22 and 4 guidelines23-26 were identified for inclusion in this review. No relevant economic evaluation studies were identified.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Two umbrella reviews published in 201913 and 202012 were identified for inclusion in this review. The 18 relevant SRs or meta-analyses in these umbrella reviews were published between 1997 and 2018, and 1 review was included in both umbrella reviews. Seven SRs14-20 were identified for inclusion in this review. Reviews were published between 2019 and 2022. The relevant primary studies included in these reviews were published between 1995 and 2018. The SRs included meta-analyses, RCTs, crossover RCTs, prospective and retrospective cohort studies, and placebo-drug-placebo studies. Searches ranges from database inception up to August 20, 2021. There were 14 primary studies included in the SRs, with some overlap of inclusion of primary studies between the SRs, particularly between Sys et al. (2020)19 and Pierce et al. (2019).20 Two SRs15,19 included Garfinkel et al. 1995, 2 SRs19,20 included Lemoine et al. 2007, 3 SRs17,19,20 included Wade et al. 2007, and 2 SRs included Wade et al. 2010.19,20 The overlap of included primary studies in included SRs is presented in Appendix 5. The outcome results of the overlapping primary studies were only reported once in this review. Some primary studies were captured in both this review and the 2019 CADTH report,7 as they provided additional outcomes not captured in the 2019 CADTH review. One umbrella review and SR included the same meta-analysis (Olde Rikkert et al. 2001). Both umbrella reviews and the 7 SRs had broader inclusion criteria than the present review. Specifically, eligible participants could include children and/or those with sleep problems, disorders, or difficulties, not specific to insomnia. Additionally, eligible interventions included non-pharmacological interventions (e.g., cognitive behavioural therapy, sleep restriction, yoga), other pharmacological interventions (e.g., benzodiazepines, over the counter sleep aids), other dietary supplements (e.g., Ayurveda, valerian), and melatonin receptor agonists. Only the characteristics and results of the subset of relevant studies will be described in this report.
Two RCTs published in 202121 and 202022 were identified in Appendix 2
Four guidelines, published between 2019 and 2021 were identified. One guideline was developed with several German medical societies,23 1 from Italian and French societies,24 1 from 5 Italian scientific societies,25 and 1 from the Department of Veterans Affairs and Department of Defense in the US.26 All 4 guidelines used a systematic review approach to form the evidence base for recommendations. SRs performed in the guidelines included guidelines,25 SRs and meta-analyses,24,25 RCTs,23,26 and cohort studies.26 One guidelines’ review also included “studies of lower evidence” if studies with high evidence were lacking.23 One guideline used an evidence classification according to standardized European Procedures, with a citation provided, but was not further described.23 Two guidelines used the RAND/UCLA Appropriateness Method,24,25 and 1 guideline used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system.26 Three guidelines used a Delphi method for recommendations development,23-25 and 1 used GRADE.26 Most guidelines did not adequately describe their rating system; however, the guideline that used GRADE to provide the strength of the recommendation described strong recommendations as those that “generally indicates high confidence in the quality of the available scientific evidence, a clear difference in magnitude between the benefits and harms of an intervention, similarity among patient or provider values and preferences, and the apparent influence of other implications (e.g., resource use, feasibility [p.12])”26 and weak recommendations if “the Work Group has less confidence after the assessment across these domains and believes that additional evidence may change the recommendation (p. 12).”26
Country of Origin
The 2 umbrella reviews had authorship teams in Canada13 and Singapore.12 One SR was published with the first author in Belgium,19 China,14 Germany,17 and the UK.18 Three SRs were published with the first author in the US.15,16,20
One RCT was conducted in Korea21 and the other in China.22
One guideline was meant to apply to the Italy as only available options in Italy were taken into consideration.25 The other 3 guidelines did not specifically state which country they were meant to apply; however, they were conducted by several German medical societies,23 Italian and French societies,24 and the US Department of Veterans Affairs and Department of Defense.26
Patient Population
The SRs included in the umbrella reviews included patients 18 years and older with primary or comorbid insomnia12 and adults 18 years and older with acute (< 3 months) or chronic (> 3 months) insomnia disorder according to Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnostic criteria, International Classification of Sleep Disorders, or Research Diagnostic Criteria for insomnia.13 Participants of the included studies were not always described but could have included adults (not otherwise described), elderly (not otherwise described), elderly patients with schizophrenia, dementia, Alzheimer disease, and patients who were medically ill.
Participants in the relevant studies of the included SRs include patients with Parkinson disease with insomnia,14 patients 65 years and older with long-term or chronic insomnia,15 patients with type 2 diabetes and insomnia,16 patients 55 years and older with insomnia disorder defined by DSM-IV and/or ICD-10,17 patients with dementia with insomnia (DSM-5 circadian cycle sleep disorder with insomnia),18 patients with long-term insomnia or DSM-IV insomnia,19 and patients 65 years and older with primary insomnia.20 Five reviews included patients with mean ages of 60 years or more,14-16,19,20 and 1 review included with patients 55 years and older.17
Participants in the RCTs included women 55 years of age and older with insomnia (i.e., PSQI score ≥ 5)21 and individuals aged 45 to 60 years old with primary insomnia (i.e., DSM-IV criteria).22 Both studies were in the hospital, either via recruitment or to measure objective outcomes. Participants were all female in 1 study21 and 47.5% male in the other.22
The target population for the guidelines included individuals with neurologic diseases and insomnia,23 adults with neuropsychiatric disorders (e.g., mood disorders, autism spectrum disorder, eating disorders) and insomnia,24 adults with insomnia,25 and adults treated in any Veterans Affairs or Department of Defense in the primary care setting with chronic insomnia disorder.26 Intended users include psychiatric clinical practice, clinical practice, and health care providers.
Interventions and Comparators
Two umbrella reviews, 7 SRs, and 2 RCTs examined immediate-release melatonin, prolonged-release melatonin, controlled-release melatonin, and melatonin (not otherwise described). The prescribed doses ranged from 0.5 to 6 mg. Duration of treatment ranged from 3 days to 6 months. Most studies were short-term (e.g., 8 weeks or less). Comparators consisted of placebo or inactive control (e.g., placebo/sham, wait list). One SR did not specify the comparator in the inclusion details, but stated in the discussion that all of the included studies reported adverse effects between melatonin and placebo.20 For this reason, we assumed the comparison was placebo in the relevant included studies.
The 4 guidelines evaluated immediate release, prolonged-release, and melatonin (not otherwise described). One guideline specified 2 mg of prolonged-release melatonin.25
Outcomes
Sleep Outcomes
Sleep outcomes were reported in the umbrella reviews using objective, subjective, or combined measures and were reported by sleep efficiency or quality,12,13 sleep onset latency,12,13 total sleep time,12,13 wake after sleep onset,12,13 and sleep satisfaction.13 Four SRs and 1 RCT measured sleep outcomes objectively through polysomnography or actigraphy using several sleep outcomes including sleep efficiency,15-17,22 total sleep time,14,15,17,22 wake time after sleep onset,15-17 sleep onset latency,15,17,22 number of awakenings,15-17 wake during sleep,22 and early wake.22 Four SRs and 2 RCTs measured sleep outcomes subjectively through sleep questionnaires (e.g., PSQI, Leeds Sleep Evaluation Questionnaire [LSEQ]), and sleep diaries, and reported several sleep outcomes including sleep quality,14,17-19,21,22 sleep onset latency,19 quality of night,19 and insomnia severity index.19 Last, 1 SR20 reported sleep outcomes using undefined measurement (i.e., no indication if objective or subjective), including sleep efficiency, sleep quality, sleep latency, night time awakenings, and nocturnal wake time. This SR also qualitatively reported combined sleep-related outcomes.
Functioning, Mood, and Quality of Life
Daytime parameters were measured with self-reported sleep questionnaires or scales (e.g., Epworth Sleepiness Scale), or were not described. These included morning alertness,12,19,20 behaviour following awakening,19 daytime sleepiness,14,17,22 quality of day,19 and overall functioning. Quality of life outcomes were measured with the Short Form Health Survey (SF-36) and reported on physical function and mental health,17 quality of life measured with the WHO-5 index,19 clinical global impression,19 and health-related quality of life12,13 or quality of life18 without clearly providing the measurement tool used. One SR that included patients with dementia evaluated cognition using the Mini Mental State Examination and activities of daily living measured with Lawton’s Instrumental Activities of Daily Living Scale.18
Adverse Events
Adverse events were reported in 1 umbrella review,12 3 SRs,15,18,19 and 1 RCT.22
Most guidelines did not report which outcomes were considered by the guideline panels. The guideline that used GRADE methodology included various outcomes depending on the key question being answered.26 Only outcomes that were rated as critical and important for decision-making were included, such as daytime functioning, insomnia severity, sleep efficiency, sleep onset latency, wake after sleep onset, sleep quality, total sleep time, quality of life, and harms.
Summary of Critical Appraisal
The critical appraisal of the included umbrella reviews, SRs, RCTs, and guidelines is presented here. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Umbrella Reviews
The umbrella reviews12,13 were assessed using AMSTAR 28 with additional questions specifically related to umbrella reviews (e.g., evaluating overlap of primary studies included in the SRs). Several strengths were identified. Both umbrella reviews were prospectively registered in the PROSPERO database, several electronic databases were searched with supplemental searching performed to identify reviews not found in electronic databases, and PRISMA flow diagrams were provided. One umbrella review13 described the method for study selection and critical appraisal and is considered sufficiently robust, performed a matrix of evidence to ascertain the degree of overlap, and used GRADE to ascertain the strength of the evidence. One umbrella review12 did not describe the method of study selection or critical appraisal, though they did sufficiently report the method for data extraction. Neither umbrella review provided a list of excluded studies or the source of funding of the included reviews.
Systematic Reviews
The SRs14-16,18-20 and the network meta-analysis17 were assessed using AMSTAR 28 and the network meta-analysis was further assessed using the ISPOR Questionnaire.9 There were strengths across the reviews. A PRISMA flow diagram was provided in all reviews. All but 1 review20 searched 2 or more electronic databases and provided details around the method for study selection. One Cochrane review18 provided the list of excluded studies and reported the funding of the included primary studies. This was not provided in any other review. There was also difference in limitations in quality of conduct and reporting across reviews. Four SRs did not mention a protocol.14,15,19,20 Three SRs did not perform any supplemental searching to identify studies not published in electronic databases.14,15,20 Not all elements of PICO were described for the inclusion criteria, primarily around comparators15,16,19,20 and outcomes.15,20 Three SRs did not report the method of data extraction.15,17,20 Two SRs did not report if critical appraisal or risk of bias of the included studies was performed,19,20 and 1 SR reported that critical appraisal was performed, but did not provide the results.15 At least some level of the characteristics of the included studies (e.g., population, control, dosage, setting) was not sufficiently reported in the reviews, in all but 3 reviews.15,18,19 The source of funding of the primary included studies was only reported in 1 SR,18 A formal assessment of publication bias was not performed in any of the reviews. Among the reviews that addressed reasons for not performing an assessment of publication bias was because there were too few studies16,18 or because there is still debate on how to perform publication bias for network meta-analyses.17 The network meta-analysis17 provided a rationale for using random-effects models, and graphical representation of the evidence networks for several outcomes were provided.
Randomized Controlled Trials
The RCTs21,22 were assessed using the Downs and Black checklist and several strengths were identified in both studies.27 The aim of the study, inclusion and exclusion criteria, intervention and comparison, main outcomes, and characteristics of the included patients of the studies were clearly described. In both studies, the placebo tablet was identical in appearance to the melatonin tablet, which would reduce the chance of patients knowing which group they were assigned to. Patients in both groups were recruited from the same population and follow-up was the same. Reporting of the outcomes was sufficient in both studies and included the number of patients contributing to the data in both groups, and results at baseline and at follow-up. However, the method of randomization was not well reported in 1 study22 and not reported at all in the other.21 Allocation concealment was not reported in 1 study.21 Neither study measured adherence to the medication.
Guidelines
The guidelines were assessed using the AGREE-II tool.10 All guidelines provided a description of the scope and purpose of the guideline, clearly presented the recommendations, and provided a statement around the competing interests of the members of the guideline development group. There was a lack of reporting around the methods of the conduct of the SRs (e.g., method of study selection, strengths and limitation of the body of evidence), if the guideline was externally reviewed, a procedure for updating the guideline, description of facilitators and barriers to guideline application, and resource implications in 3 guidelines.23-25 In the other guideline those items were well reported.26
Summary of Findings
There was some overlap in the primary studies that were included in the SRs; therefore, to avoid duplication of results, outcome data from an individual primary study are only reported once. A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Melatonin Versus No treatment or Placebo
Sleep Measures
The 2 umbrella reviews reported the outcomes as either subjective, objective, or combined. For this reason, the outcomes from the umbrella reviews are reported separately from the SRs and RCTs.
Results From Umbrella Reviews
Sleep efficiency or quality. Results from the included meta-analyses and SRs within the umbrella reviews were mixed with some reporting a statistically significant increase in sleep efficiency or quality with melatonin, while other reported no change or difference.12,13
Sleep latency, total sleep time, wake after sleep onset. Results from the included meta-analyses and SRs within the umbrella reviews were mixed with some reporting a statistically significant improvement in these sleep outcomes, while other reported no change or difference.12,13
Sleep satisfaction. Sleep satisfaction was reported in one included SR (with one included study) within the umbrella review and reported a significant increase in both percentage of nights scored “good” and percentage of “good mood.”13
Quality of life. One umbrella review reported a significant increase in health-related quality of life (undefined subjective measurement tool; evidence from 1 included primary study in 1 SR).13
Results From Primary Studies Within SRs and Primary Studies Identified in This Review
Objective sleep measures (i.e., polysomnography, actigraphy)
Sleep efficiency. Two SRs and 1 RCT reported on sleep efficiency using objective sleep measures. The 2 SRs reported on sleep efficiency comparing melatonin (2 mg or 3 mg) to placebo. In patients with primary insomnia, 2 RCTs in the SR by Almond et al.15 and in patients with type 2 diabetes with insomnia, 1 RCT in the SR by Kothari et al.,16 reported statistically significant improvements in sleep efficiency. In a RCT of patients with primary insomnia, there was no difference in sleep efficiency in patients who received melatonin (3 mg) compared to placebo.22
Total sleep time. Two SR, 1 network meta-analysis, and 1 RCT reported on total sleep time using objective sleep measures. The 2 SRs reported on total sleep time comparing melatonin (2 mg or 3 mg) to placebo. There were mixed results between the SRs and the studies within the reviews. One RCT in the SR by Ma et al.14 reported non-significant results in patients with Parkinson disease. In patients with primary insomnia in the SR by Almond et al.,15 1 RCT reported no difference in total sleep time and 1 placebo-drug-placebo study reported a significant increase in total sleep time. Additionally, the network meta-analysis by Baglioni et al. 202017 included outcome data on 1 RCT in patients with insomnia disorder (DSM-IV and/or ICD-10), but did not provide details around the impact of melatonin compared to placebo. In a RCT of patients with primary insomnia, there was no difference in total sleep time in patients who received melatonin (3 mg) compared to placebo.22
Wake time after sleep onset. Two SRs, 1 network meta-analysis, and 1 RCT reported on wake time after sleep onset using objective sleep measures. The 2 SRs reported on wake time after sleep onset comparing melatonin (2 mg or 3 mg) to placebo. In patients with primary insomnia, 2 RCTs in the SR by Almond et al.15 and in patients with type 2 diabetes with insomnia, 1 RCT in the SR by Kothari et al.,16 reported that melatonin significantly reduced wake time after sleep onset. Additionally, the network meta-analysis by Baglioni et al. 202017 included outcome data on 1 RCT in patients with insomnia disorder (DSM-IV and/or ICD-10), but did not provide details around the impact of melatonin compared to placebo. In a RCT of patients with primary insomnia, there was no difference in wake after sleep onset in patients who received melatonin (3 mg) compared to placebo.22
Sleep onset latency. One SR, 1 network meta-analysis, and 1 RCT reported on sleep latency using objective sleep measures. The 1 SR reported on sleep latency comparing melatonin (2 mg or 3 mg) to placebo. In patients with primary insomnia, 2 RCTs in the SR by Almond et al.15 reported no difference in sleep onset latency between melatonin and placebo. Additionally, the network meta-analysis by Baglioni et al. 202017 included outcome data on 1 RCT in patients with insomnia disorder (DSM-IV and/or ICD-10), but did not provide details around the impact of melatonin compared to placebo. In a RCT of patients with primary insomnia, there was no difference in sleep latency in patients who received melatonin (3 mg) compared to placebo.22
Number of awakenings. Two SRs and 1 network meta-analysis reported on number of awakening using objective sleep measures. The 2 SRs reported on number of awakenings in patients receiving melatonin (2 mg or 3 mg) or placebo. In patients with primary insomnia, 1 placebo-drug-placebo study in the SR by Almond et al.15 reported that the number of awakenings was not significantly affected. In patients with type 2 diabetes with insomnia, 1 RCT in the SR by Kothari et al.16 reported there was a significant effect of melatonin compared to placebo. Additionally, the network meta-analysis by Baglioni et al. 202017 included outcome data on 1 RCT in patients with insomnia disorder (DSM-IV and/or ICD-10), but did not provide details around the impact of melatonin compared to placebo.
Wake during sleep. In a RCT of patients with primary insomnia, there was no difference in wake during sleep (measured in minutes) in patients who received melatonin (3 mg) compared to placebo.22
Early wake. In a RCT of patients with primary insomnia, there was a significant decrease in early wake (measured in minutes) in patients who received melatonin (3 mg) compared to placebo.22
Subjective sleep measures (e.g., sleep questionnaires, sleep diary)
Sleep quality. Three SRs, 1 network meta-analysis, and 2 RCTs reported on sleep quality using sleep questionnaires and sleep diaries. In the 3 SRs, sleep quality was measured using subjective measures (e.g., PSQI, LSEQ, sleep diaries). In patients with Parkinson disease taking melatonin (3 mg), 1 SR found a statistically significant increase in sleep quality compared to placebo (measured with PSQI; evidence from 1 relevant RCT).14 In another SR in patients with dementia, there was no difference in carer-rated sleep quality between patients who received melatonin (5 mg) and placebo (measured with PSQI; evidence from 1 relevant RCT).18 In another SR, in patients with long-term insomnia, there was a statistically significant increase in sleep quality in those taking melatonin (2 mg) when measured with LSEQ and PSQI,19 but no difference was observed when reported in sleep diaries (evidence from 3 relevant RCTs).19 Additionally, the network meta-analysis by Baglioni et al. 202017 included outcome data on 2 RCTs in patients with insomnia disorder (DSM-IV and/or ICD-10). This was measured through LSEQ, PSQI, and sleep diaries, but did not provide details around the impact of melatonin compared to placebo. In 1 RCT, there was a significant difference in sleep quality in the patients who received melatonin (2 mg), but not in the patients who received placebo. However, there was no difference between groups (P = 0.158).21 In another RCT of patients with primary insomnia, there was no difference in the PSQI total score in patients who received melatonin (3 mg) compared to placebo.22
Sleep onset latency. In patients with long-term insomnia, 1 SR reported a statistically significant shortening of sleep latency with melatonin compared to placebo (measured with PSQI or undefined subjective measurement tool; evidence from 2 relevant RCTs), which continued up to 29 weeks in 1 included primary study.19
Quality of night. In patients with long-term insomnia, 1 SR reported no difference in sleep maintenance in patients who received melatonin (2 mg) compared to placebo (measured using sleep diaries; evidence from 1 relevant RCT).19
Insomnia severity index. In 1 RCT of patients with primary insomnia, there was no difference on the Insomnia Sleep Index in patients who received melatonin (3 mg) compared to placebo.22
Other Sleep Outcomes Using Undefined Measurement
Sleep efficiency. In patients with primary insomnia, 1 SR reported a trend for improved efficiency (undefined measure; evidence from 1 relevant RCT).20
Sleep quality. In patients with primary insomnia, 1 SR reported no positive effect or improvement on sleep quality (undefined measure; evidence from 2 relevant RCTs).20
Sleep latency. In patients with primary insomnia, 1 SR reported a significant decrease in sleep latency (undefined measure; evidence from 1 relevant RCT).20
Nighttime awakenings. In patients with primary insomnia, 1 SR reported a decreased number of nighttime awakenings (undefined measure; evidence from 1 relevant RCT).20
Nocturnal wake time. In patients with primary insomnia, 1 SR reported a significant increase in nocturnal wake time (undefined measure; evidence from 1 relevant RCT).20
Combined sleep-related outcomes. In patients with long-term insomnia, 1 SR reported no difference in total sleep time and sleep maintenance (measured with sleep diaries; evidence from 1 relevant RCT). In another SR in patients with primary insomnia, there was no statistically significant improvement or difference in total sleep time, sleep latency, sleep efficiency, or wake time (undefined measure; evidence from 3 relevant RCTs).20
Functioning, Mood, Quality of Life
Behaviour following wakening. In patients with long-term insomnia, 1 SR reported a statistically significant improvement with melatonin compared to placebo (measured with LSEQ; evidence from 1 relevant RCT).19
Alertness in morning. In patients with long-term insomnia and primary insomnia, 2 SR reported a significantly more alertness in the morning with melatonin compared to placebo or an increase in morning alertness (undefined measure; evidence from 2 relevant RCTs).19
Sleepiness. One SR, 1 umbrella review, and 1 RCT reported on sleepiness measured with the Epworth Sleepiness Scale (ESS). In patients with Parkinson disease, 1 SR reported that daytime sleepiness is not affected by melatonin (3 mg) compared to placebo (evidence from 1 relevant RCT).14 Additionally, the network meta-analysis by Baglioni et al. 202017 included outcome data on 1 RCT in patients with insomnia disorder (DSM-IV and/or ICD-10), but did not provide details around the impact of melatonin compared to placebo (evidence from 1 relevant RCT). In a RCT of patients with primary insomnia, there was no difference in on the ESS in patients who received melatonin (3 mg) compared to placebo.22
Quality of day. In patients with long-term insomnia, 1 SR reported no difference in quality of day (measured with sleep diaries; evidence from 1 relevant RCT).19
Quality of life. In patients with long-term insomnia, 1 SR reported mixed results for quality of life (measured with WHO-5 index; evidence from 2 relevant RCTs).19
Clinical Global Impression (CGI). In patients with long-term insomnia, 1 SR reported both no difference and a significant improvement in patients who received melatonin (2 mg) compared to placebo (measured using CGI scale; evidence from 2 relevant RCTs).19
Cognition and activities of daily living. In patients with dementia, 1 SR reported that there is no evidence that melatonin had either beneficial or harmful effects in these patients (cognition measured with Mini Mental State Examination, activities of daily living measured with Lawton’s Instrumental Activities of Daily Living Scale; evidence from 1 relevant RCT).18
Physical and mental function. The network meta-analysis by Baglioni et al. 202017 included outcome data on 1 RCT in patients with insomnia disorder (DSM-IV and/or ICD-10), but did not provide details around the impact of melatonin compared to placebo (measured with SF-36).
Adverse Events
Adverse events were reported in 3 SRs.15,18,19 Overall, these were reported as no or infrequent adverse events, mild or not serious (e.g., pruritus, headache), treatment was well-tolerated, or no difference between patients who received melatonin and placebo. In a RCT of patients with primary insomnia, there was no difference in the incidence of adverse events in patients who received melatonin (3 mg) compared to placebo, and melatonin was well-tolerated. Additionally, the RCT reported there were no clinically relevant changes in vital signs and laboratory blood and urine tests.22
Clinical Effectiveness of Melatonin Versus Prescription Sedatives
No relevant evidence regarding the clinical effectiveness of melatonin versus prescription sedatives for insomnia was identified; therefore, no summary can be provided.
Cost-Effectiveness of Melatonin Versus No Treatment or Placebo
No relevant evidence regarding the cost-effectiveness of melatonin versus no treatment or placebo for insomnia was identified; therefore, no summary can be provided.
Cost-Effectiveness of Melatonin Versus Prescription Sedatives
No relevant evidence regarding the cost-effectiveness of melatonin versus prescription sedatives for insomnia was identified; therefore, no summary can be provided.
Guidelines
Four evidence-based guidelines23-26 were identified providing recommendations for melatonin for treatment of insomnia.
Neurologic Disease and Neuropsychiatric Disorders
One guideline, by Mayer et al. (2021), recommends melatonin for patients with neurologic diseases (i.e., movement disorders, multiple sclerosis, epilepsy, dementia and prion-diseases),23 although the authors reported that these recommendations were based on very low evidence. However, it is unclear if this “low evidence” was specific to the recommendations for dementia and prion-diseases or for all recommendations in the guideline.
One guideline, by Pagalini et al. (2021), provides recommendations for patients with various neuropsychiatric disorders and recommends prolonged-release melatonin at 2 mg to 10 mg, 1 to 2 hours before bedtime for the treatment of insomnia symptoms or comorbid insomnia in mood disorders.24 Recommendations for anxiety disorders, attention-deficit/hyperactivity disorder, autism spectrum disorder, and eating disorders are given in the absence of well-conducted RCTs in adults and state that melatonin “might be useful” or “could be of interest.”24 Prolonged-release melatonin at 2 mg given 1 to 2 hours before bedtime and immediate-release melatonin at 2 mg to 6 mg given at bedtime might be useful in the treatment of insomnia in neurocognitive disorders.24 Prolonged-release melatonin at 2 mg given 1 to 2 hours before bedtime could be used in individuals 55 years of age and older with substance use disorder and in individuals with schizophrenia. Immediate-release melatonin for individuals with schizophrenia gave uncertain results and more studies are needed to be able to provide recommendations.24 The quality of evidence and strength of each recommendation was not reported in this guideline.
Insomnia
Two guidelines provided recommendations for insomnia, not specific to any other comorbidity. One guideline, by Palagini et al. (2020)25 recommends pharmacological treatments as the first-line option when CBT-Insomnia is not available. The drug selected should be based on factors such as type of insomnia, age, comorbidities, and potential side effects. If the choice is prolonged-release melatonin, in individuals 55 years of age and older, use it within 13 weeks. The quality of evidence and strength of the recommendations was not reported in this guideline. The guideline by the Department of Veterans Affairs and Department of Defense26 suggest against the use of melatonin for the treatment of chronic insomnia disorder (weak recommendation).
Limitations
Two umbrella reviews and 7 SRs were identified with primary studies that evaluated melatonin for insomnia. Overall, the quality of conduct and reporting for these reviews was mixed (e.g., no supplemental searching, lack of details around the methods of study selection, no list of excluded studies), making it difficult to determine if all relevant primary studies were captured by the SR and to determine which primary studies were relevant to this current review. For example, some reviews identified the primary studies as patients with insomnia. However, when evaluating those primary studies as part of this review, they did not qualify as having insomnia, but rather poor sleep quality.14 The definition of what was considered insomnia in general was mixed, with some reviews requiring a clinical diagnosis of insomnia (e.g., DSM-IV) and others accepting self-reported insomnia. This difference may impact the certainty of the results across the reviews. One umbrella review included a SR where the comparator was labelled as “control,” making it unclear if this group was given placebo, no treatment, or some other inactive comparison.13 The quality of reporting of the outcomes was insufficient in several reviews. It was not always stated how the outcome was measured, as some reviews combined subjective (e.g., polysomnography) and objective (e.g., validated questionnaires, sleep diaries) measures. Additionally, when the name of the questionnaire used to evaluate subjective sleep outcomes was provided, the scale of the questionnaire and the interpretation of the value (e.g., higher score is better sleep efficiency) was not provided. Some reviews provided results in which it is not possible to determine if the result was improved or worse for the melatonin group (e.g., mean difference with no descriptor if a negative or positive value was better). The network meta-analysis reported the mean and standard deviations for the comparisons, but did not provide an indication if the was a difference or no difference pre- and post-treatment or between those who received melatonin and those who received placebo. However, the authors did conclude that their findings do not support any of the selected therapies for insomnia disorder.17
Two RCTs were also identified for inclusion. One RCT stated that randomization was performed using a random number method,22 but did not further describe this process (e.g., computer-generated random number generation, selecting a number from a hat), so it is difficult to determine if there is any bias associated with the process that was used. The other RCT did not report on either the method of randomization or the process of allocation concealment, therefore it is unclear if there was any selection bias in this study.21 Neither RCT reported on if compliance (or nonadherence) to treatment was measured,21,22 which may lead to a failure to detect a true treatment effect.
The SRs were often conducted in specific populations (e.g., patients with cancer, patients with schizophrenia), resulting in few relevant included studies, often among a small group of patients. This heterogeneity makes it difficult to determine any trends across reviews. Primary studies were often short-term (e.g., < 8 weeks), therefore they did not provide any long-term evidence for the efficacy and safety of melatonin. Even among the short-term primary studies, harms data were rarely reported.
Both subjective and objective outcomes are reported using several different measures, including sleep efficiency, sleep quality, latency of sleep onset, total sleep time/duration of sleep, depth of sleep, wake time after sleep onset, number of awakenings, freshness on awakening, alertness in morning, morning headaches, morning mental dullness, daytime sleepiness, mood, overall functioning, physical function, mental status, quality of life. Therefore, depending on the individual and the measure that might be the most important to them, any or all of these measures could be considered when recommending melatonin.
Most guidelines did not provide a detailed description of the method of conduct of the systematic review that informed the recommendations. For example, the process of study selection was only reported in 1 guideline. Therefore, we cannot determine if all relevant studies were captured. Additionally, 3 of 4 guidelines did not provide formal ratings for the certainty of the evidence for each recommendation.23-25 One guideline provides 1 statement around the certainty of the evidence, but it is not clear if it is for all recommendations in the guideline or only in that particular section (i.e., dementia and prion-diseases).23 Veterans Affairs is the only guideline to recommend against melatonin for insomnia, but it also specifies that this recommendation if for chronic insomnia, which is defined as lasting longer than 3 months. This might be why it differs from Palagini et al. (2020), who state that it be used within 13 weeks (i.e., before it becomes chronic). Although none of the guidelines were produced specifically for the Canadian health care system, melatonin in the formulations included in the recommendations are available in Canada, making these recommendations generalizable to the Canadian health care system.
Last, we were not able to find any evidence for 3 of the research questions in this review. There was no evidence to evaluate the clinical effectiveness of melatonin versus prescription sedatives, the cost-effectiveness of melatonin versus no treatment or placebo, and the cost-effectiveness of melatonin versus prescription sedatives.
Conclusions and Implications for Decision- or Policy-Making
Two umbrella reviews, 7 SRs, and 2 RCTs were identified to address the effectiveness of melatonin versus no treatment or placebo for the treatment of insomnia. No evidence was identified to evaluate the clinical effectiveness of melatonin versus prescription sedatives for the treatment of insomnia. All included reviews were broader in scope than this review (e.g., broader population, broader interventions). Where possible, depending on the quality of the reporting, relevant primary studies were identified from these reviews. Generally, findings suggested that melatonin may be effective for some sleep-related outcomes, but may differ depending on how it is measured. For example, in patients with insomnia, the use of melatonin did not have any impact on sleep onset latency when measured objectively (evidence from 2 RCTs in 1 SR and 1 primary RCT),15,22 but significantly reduced sleep onset latency when measured subjectively (evidence from 2 RCTs in 1 SR).19 Efficacy may also be dependent on the population. For example, the systematic review by McCleery et al. (2020) found no beneficial or harmful effects in people with dementia due to Alzheimer disease.18 However, Ma et al. (2022) concluded that melatonin could be considered an effective treatment in patients with Parkinson disease.14 As the majority of the primary studies were 8 weeks or less, there is inadequate evidence to confirm the long-term efficacy of melatonin.13
Among the included reviews and primary studies, there is heterogeneity in terms of the included population and the methods of measuring the outcomes, which leads to uncertainty in the effectiveness of melatonin. For example, the reviews and primary studies included patients with clinically defined insomnia disorder (i.e., DSM-VI or ICD-10),13,17,22 either long-term (undefined) or DSM-IV defined insomnia combined,15,19 undefined primary insomnia,12,20 Parkinson disease,14 type 2 diabetes,16 dementia,18 or were all female.21 Authors of these studies often concluded that larger studies should be performed. The safety and harms of melatonin is poorly reported in primary studies, and 1 umbrella review,12 3 SRs,15,18,19 and 1 RCT22 reported that short-term use of melatonin was considered safe and well-tolerated. Interpretation of the results across these reviews was often hampered by the poor reporting in the details of the included primary studies (e.g., patients, setting, intervention, outcome measurement, outcome data). The 7 SRs and 2 RCTs included patients aged 55 years and older, which may impact the generalizability of the results to adults between the ages of 18 and 54.
Four guidelines were identified providing recommendations for melatonin for the treatment of insomnia in general,25,26 and for several neurologic diseases23 and neuropsychiatric disorders.24 Although the guidelines state that there is insufficient evidence23or an absence of well-conducted RCTs24 to help support the recommendations, they often state that melatonin may be used to treat insomnia. However, 1 guideline specific to chronic insomnia, recommends against the use of melatonin.26
This review is an update to a previously published CADTH from 2019.7 The results from this updated report are similar in terms of the clinical effectiveness of melatonin versus no treatment or placebo. The 2019 CADTH report did not identify any guidelines; however, this report has identified 4 guidelines published between 2019 and 2021. There was no evidence to evaluate the cost-effectiveness of melatonin in the 2019 report and no evidence was found in this update.
References
1.Chaput J-P, Yau J, Rao DP, Morin CM. Prevalance of insomnia for Canadians aged 6 to 79. Health Rep. 2018;29(12):16-20. PubMed
2.ICD-11 for Mortality and Morbidity Statistics. World Health Organization. https://icd.who.int/browse11/l-m/en. Published 2022. Accessed 2022 Apr 12.
3.International Classification of Sleep Disorders 3rd Ed. Darien (IL): Academy of Sleep Medicine; 2014.
4.DN N. Pharmacotherapy for insomnia in adults. In: TW P, ed. UpToDate. Waltham (MA)2022: http://www.uptodate.com/. Accessed 2022 Apr 12.
5.van Maanen A, Meijer AM, van der Heijden KB, Oort FJ. The effects of light therapy on sleep problems: A systematic review and meta-analysis. Sleep Med Rev. 2016;29:52-62. PubMed
6.Andersen LPH, Gogenur I, Rosenberg J, Reiter RJ. The Safety of Melatonin in Humans. Clin Drug Investig. 2016;36:169-175. PubMed
7.Melatonin for the Treatment of Insomnia: A Review of Clinical Effectiveness, Cost- Effectiveness, and Guidelines In: Ottawa (ON): CADTH; 2019: https://www.cadth.ca/melatonin-insomnia-review-clinical-effectiveness-cost-effectiveness-and-guidelines. Accessed 2022 Apr 12.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
10.Agree Next Steps Consortium. The AGREE II Instrument. In: Hamilton, ON: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Apr 12.
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Low TL, Choo FN, Tan SM. The efficacy of melatonin and melatonin agonists in insomnia - An umbrella review. J Psychiatr Res. 2020;121:10-23. PubMed
13.Rios P, Cardoso R, Morra D, et al. Comparative effectiveness and safety of pharmacological and non-pharmacological interventions for insomnia: an overview of reviews. Syst Rev. 2019;8(1):281. PubMed
14.Ma H, Yan J, Sun W, Jiang M, Zhang Y. Melatonin Treatment for Sleep Disorders in Parkinson's Disease: A Meta-Analysis and Systematic Review. Front Aging Neurosci. 2022;14:784314. PubMed
15.Almond SM, Warren MJ, Shealy KM, Threatt TB, Ward ED. A Systematic Review of the Efficacy and Safety of Over-the-Counter Medications Used in Older People for the Treatment of Primary insomnia. Sr Care Pharm. 2021;36(2):83-92. PubMed
16.Kothari V, Cardona Z, Chirakalwasan N, Anothaisintawee T, Reutrakul S. Sleep interventions and glucose metabolism: systematic review and meta-analysis. Sleep Med. 2021;78:24-35. PubMed
17.Baglioni C, Bostanova Z, Bacaro V, et al. A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials Evaluating the Evidence Base of Melatonin, Light Exposure, Exercise, and Complementary and Alternative Medicine for Patients with Insomnia Disorder. J Clin Med. 2020;9(6):22. PubMed
18.McCleery J, Sharpley AL. Pharmacotherapies for sleep disturbances in dementia. Cochrane Database Syst Rev. 2020;11:CD009178. PubMed
19.Sys J, Van Cleynenbreugel S, Deschodt M, Van der Linden L, Tournoy J. Efficacy and safety of non-benzodiazepine and non-Z-drug hypnotic medication for insomnia in older people: a systematic literature review. Eur J Clin Pharmacol. 2020;76(3):363-381. PubMed
20.Pierce M, Linnebur SA, Pearson SM, Fixen DR. Optimal Melatonin Dose in Older Adults: A Clinical Review of the Literature. Sr Care Pharm. 2019;34(7):419-431. PubMed
21.Kim Y, Kang HT, Lee DC. Melatonin Supplementation for Six Weeks Had No Effect on Arterial Stiffness and Mitochondrial DNA in Women Aged 55 Years and Older with Insomnia: A Double-Blind Randomized Controlled Study. International Journal of Environmental Research & Public Health [Electronic Resource]. 2021;18(5):04.
22.Xu H, Zhang C, Qian Y, et al. Efficacy of melatonin for sleep disturbance in middle-aged primary insomnia: a double-blind, randomised clinical trial. Sleep Med. 2020;76:113-119. PubMed
23.Mayer G, Happe S, Evers S, et al. Insomnia in neurological diseases. Neurol. 2021;3(1):15. PubMed
24.Palagini L, Manni R, Aguglia E, et al. International Expert Opinions and Recommendations on the Use of Melatonin in the Treatment of Insomnia and Circadian Sleep Disturbances in Adult Neuropsychiatric Disorders. Front Psychiatr. 2021;12:688890. PubMed
25.Palagini L, Manni R, Aguglia E, et al. Expert Opinions and Consensus Recommendations for the Evaluation and Management of Insomnia in Clinical Practice: Joint Statements of Five Italian Scientific Societies. Front Psychiatr. 2020;11:558. PubMed
26.The Management of Chronic Insomnia Disorder and Obstructive Sleep Apnea Work Group. VA/DoD clinical practice guideline for the management of chronic insomnia disorder and obstructive sleep apnea. In: Washington (DC): Department of Veterans Affairs; Department of Defense; 2019: https://www.healthquality.va.gov/guidelines/CD/insomnia/VADoDSleepCPGFinal508.pdf. Accessed 2022 Apr 26.
27.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Umbrella Reviews
Study citation, country, funding source | Study designs and numbers of studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Low et al. (2020)12 Singapore Funding: NR | Systematic reviews and meta-analyses Reviews published up to July 2018 were searched Number of reviews included: 18 Number of relevant reviews: 7 published between 2001 and 2018 (2 additional reviews on Ramelteon in adults) | Eligibility criteria: Treatment in primary or comorbid insomnia in any age group that included RCTs Included patients were 18 years and older (one study was > 16 years) who had primary or comorbid insomnia N studies included in reviews = 33 N patients included in reviews = 3654 | Eligible interventions: Melatonin/ melatonin receptor agonists Eligible comparators: Placebo or other medications Relevant intervention: Melatonin 0.3 to 75 mg Relevant comparators: Placebo Duration of interventions ranged from 3 days to 6 months (where reported) | Outcomes in included reviews: Sleep quality; Sleep efficiency; Sleep latency; Sleep onset; Total sleep time; REM latency; Ease of getting to sleep; Quality of night/day; Wake after sleep onset; Number of awakening; Morning alertness; Quality of Life; WHO-5 well-being index; Safety Outcomes reported in relevant reviews: Sleep efficiency; Total sleep time; Sleep latency |
Rios et al. (2019)13 Canada Funding: Canadian Institutes of Health Research | Systematic knowledge syntheses including primary studies of any design with or without a meta-analysis Reviews published up to June 14, 2017 Number of included reviews: 64 Number of relevant reviews: 12 (8 with meta-analyses) published between 1997 and 2017 | Eligibility criteria: Adults > 18 years of age diagnosed with acute (< 3 months) or chronic (> 3 months) insomnia disorder according to the DSM diagnostic criteria, International Classification of Sleep Disorders, or Research Diagnostic Criteria for insomnia N patients included in reviews = NR (reported in some reviews, but not all) | Eligible interventions: Prescription or non-prescription Pharmacological interventions, Non-pharmacological interventions (e.g., cognitive behavioural therapy, sleep restriction, Melatonin) Eligible comparators: Inactive controls (e.g., placebo/sham, wait list, symptom monitoring), Active controls (e.g., another available intervention) Relevant intervention: Melatonin Relevant comparator: Inactive controls (mostly placebo; one included systematic review states ‘control’) | Eligible outcomes: Effectiveness (e.g., sleep onset latency, total sleep time, wake after sleep onset); Harms (e.g., hangover/ morning sedation, accidental injuries) Outcomes reported in relevant reviews: Sleep onset latency; Total sleep time; Wake after sleep onset; Sleep quality; Sleep satisfaction; Sleep efficiency; Health-related quality of life |
Table 3: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Ma et al. (2022)14 China Funding: Project of Henan Province Science and Technology, the Key Projects of Medical Science and Technology in Henan Province and Medical Science and Technology Research in Henan Province | RCTs Studies published up to August 20, 2021 were searched Number of primary studies: 7 Number of relevant primary studies: 1 (2 other studies were categorized as insomnia but were evaluated at full-text as part of this review and were not for insomnia). Study published in 2007. | Inclusion criteria: Patients with Parkinson disease Relevant population: Patients who had Parkinson disease for an average of 6.4 years and insomnia. Average age was 62.9 years in the intervention group and 60.7 years in the control group; 77.8% male. N = 18 | Eligible interventions: Melatonin or prolonged-release melatonin Eligible comparator: Placebo or clonazepam Relevant interventions: 3 mg melatonin Relevant comparators: Placebo Duration of intervention: 4 weeks | Outcomes: At least one of the following: Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), RBD questionnaire (RBDQ) and polysomnography (PSG) sleep parameters Follow-up: End of treatment (4 weeks) |
Almond et al. (2021)15 US Funding: NR | Crossover RCTs, Placebo-drug-placebo Studies published up to May 8, 2020 were searched Number of primary studies: 5 Number of relevant primary studies: 2 (1 crossover RCT, 1 placebo-drug-placebo). Studies published in 1995 and 1999. | Inclusion criteria: Adult 65 years of age and older being evaluated on over the counter sleep aids for primary insomnia or sleep disorders in the outpatient setting Relevant population: Patients who had complained of long-term insomnia in one study and were diagnosed with chronic primary insomnia according to DSM-IV in the other. Patients were 68 to 93 and 66 to 86 years old; 40.9% male. N = 22 | Eligible interventions: Over the counter sleep aids Eligible comparators: NR Relevant interventions: 2 mg controlled-released melatonin in one study, 3 mg melatonin capsules in the other Relevant comparators: Placebo Duration of the included studies were 7 weeks (3 weeks melatonin/placebo, 1 week washout, 3 weeks melatonin/ placebo), and 19 days (placebo nights 1 to 3, melatonin nights 4 to 16, placebo nights 17 to 18) | Outcomes: Subjective and objective measures of changes in sleep, such as mean total sleep time, sleep latency, sleep efficiency, and number of awakenings; Safety end points, such as psychomotor ability, cognitive ability, and adverse effect profile Follow-up: Assessments were done at the end of the 3-week treatment period in one study, and on nights 1 to 5, 17 and 18 in the other |
Kothari et al. (2021)16 US Funding: No funding | RCTs, crossover RCTs, single-arm prospective studies Studies published up to August 1, 2019 were searched Number of primary studies: 22 Number of relevant studies: 1 crossover RCT (1 additional study evaluating Ramelteon). Study published in 2011. | Inclusion criteria: Adults aged ≥ 18 years with problems of sleep disturbances eg: insomnia, short sleep, poor sleep quality Relevant population: Patients with type 2 diabetes with insomnia. Average age of patients was 63 years old; 30.5% male. N = 36 | Eligible interventions: Sleep extension, sleep education or cognitive behavioural therapy for insomnia, and pharmacological interventions Eligible comparators: NR Relevant interventions: 2 mg of prolonged-release melatonin Relevant comparators: Placebo Duration of intervention: 3 weeks, followed by 5 months of open-label melatonin for all patients | Relevant outcomes: Sleep-related outcomes (e.g., objective sleep assessment, sleep parameters from questionnaires and sleep diaries) Other outcomes: At least one of the glycemic outcomes must be measured: glucose, insulin, Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) or hemoglobin A1C (A1C). Follow-up: 3 weeks |
Baglioni et al. (2020)17 Germany Funding: German Ministry for Education and Research | RCTs Studies published between January 1994 and September 2019 were searched Number of primary studies: 40 Number of relevant primary studies: 3 RCTs (4 additional studies evaluating Ramelteon). Studies published in 2007, 2009, and 2011. | Inclusion criteria: Individuals with insomnia disorder of any age Relevant population: Individuals aged 55 years and older with insomnia disorder (defined by DSM-IV and/or ICD-10); 37.5 to 60.5% male. N = 437 | Eligible interventions: Ayurveda, chelation, diet-based therapy, energy healing therapy, exercise, folk medicine, homeopathy, hypnosis, light exposure, massage, meditation, melatonin, music therapy, natural herbs, naturopathy, qi gong, reiki, tai chi, transcranial magnetic stimulation, valerian, vitamin, and yoga Eligible comparators: waiting list, no treatment, pharmacological and psychological (e.g., psychoeducation) placebo, standard therapy for insomnia: sleep pharmacotherapy (hypnotics: benzodiazepine and benzodiazepine receptor agonists and recommended psychological treatment, i.e., CBT-I [CBT-I, sleep restriction, stimulus control]). Relevant interventions: Melatonin Relevant comparators: Placebo | Outcomes: Objective and subjective standardized measures of sleep and/or insomnia Outcomes in relevant studies: Self-report questionnaires, polysomnography Follow-up: NR |
McCleery et al. (2020)18 UK Funding: National Institute for Health Research | RCTs Studies published up until February 19, 2020 were searched Number of primary studies: 9 Number of relevant primary studies: 2 RCTs. Studies published in 2014 and 2018. | Inclusion criteria: People with dementia with sleep problems identified on the basis of subjective and objectives measures Relevant population: Patients with mild or moderate dementia (CDR 1 and 2) with DSM-5 circadian cycle sleep disorder with insomnia in one study, and patients with dementia (diagnostic criteria not specified) with insomnia at baseline (defined as Pittsburgh Sleep Quality Index score ≥ 6). Mean age were 92.2 and 83.1 years in one study, and NR for the subgroup in the other; 22.6% male in one study, and NR for the subgroup in the other. N = 53 (one study included a subgroup with insomnia and reported on these patients) | Eligible interventions: Any drug primarily intended to improve patients' sleep Eligible comparators: Placebo Relevant interventions: 5 mg immediate-release melatonin in one study, 2 mg slow-release melatonin in the other Relevant comparators: Placebo Duration of intervention: 8 weeks in one study, 28 weeks (2-week run-in phase, 24-weeks treatment phase, 2-week run out phase) in the other | Relevant outcomes: Objective sleep outcomes measured with polysomnography or actigraphy; Quality of life; Adverse events Other outcomes: Carer ratings of patient's sleep using sleep diaries or validated observer scales; Cognition measured with any validated scale; Activities of daily living (ADLs) measured with any validated scale; Carer outcomes (well-being, quality of life, burden, sleep). Follow-up: End of treatment |
Sys et al. (2020)19 Belgium Funding: NR | RCTs, non-RCTs with parallel groups, prospective or retrospective cohort studies with control groups, and observational studies Studies published up until September 1, 2019 were searched Number of primary studies: 24 Number of relevant studies: 4 (3 RCTs and 1 crossover RCT) (4 additional studies evaluating Ramelteon). Studies published between 1995 and 2010. | Inclusion criteria: Patients ≥ 65 years with insomnia Relevant population: Patients with long-term insomnia or DSM-IV insomnia in outpatient clinics. Patients in all studies were ≥ 55 years’ old. N = 817 | Eligible interventions: Antidepressants, antipsychotic drugs, anticonvulsive medications, antihistamines, herbal therapies, melatonin receptor agonists, and orexin receptor antagonists Eligible comparators: NR Relevant interventions: 2 mg prolonged-release melatonin Relevant comparators: Placebo Duration of intervention: Studies ranged from 3 to 29 weeks, with some including run-in and run out periods or washout periods | Relevant outcomes: Sleep duration; Subjective sleep quality; Safety profile, number of adverse events Follow-up: End of treatment |
Pierce et al. (2019)20 US Funding: No funding | Meta-analyses, RCTs, and prospective and retrospective cohort studies Studies published up until October 10, 2018 were searched Number of studies: 3 meta-analyses, 21 RCTs, 1 cohort study Number of relevant studies: 1 meta-analysis, 7 RCTs (2 RCTs, 5 crossover RCTs). Studies published between 1998 to 2010. | Inclusion criteria: Adults 65 years of age and older Relevant population: Adults with primary insomnia. Mean age of the patients ranged from 65.67 to 71.7 years old; % male NR N = 874 | Eligible interventions: Exogenous melatonin Included comparators: Unclear Eligible interventions: 0.5 to 6 mg of controlled-release, immediate-release and prolonged-release melatonin Relevant comparators: Unclear (assumption has been made that comparator was placebo based on a statement made in the discussion section) Duration of intervention: Studies ranged from 8 nights to 26 weeks | Reported outcomes: Sleep efficiency; Sleep latency; Wake time following initiation; Follow-up: End of treatment |
NR = not reported; RCT = randomized controlled trials.
Table 4: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Kim et al. 202121 Korea Funding: Kuhnil Pharmacy (Seoul, Korea) | RCT | N = 38 Eligibility criteria: Women > 55 years old with insomnia (Pittsburgh Sleep Quality Index (PSQI) ≥ 5) who had not taken medication for depression, insomnia, or tranquilization in the past 3 months. Exclusion criteria: History of menopausal hormone replacement therapy; cerebrovascular diseases (including ischemic stroke and cerebral hemorrhage), cardiovascular diseases (including unstable angina, myocardial infarction, and coronary revascularization); chronic liver disease (including chronic hepatitis, liver cirrhosis, and hepatocellular carcinoma); chronic renal disease (including previous chronic kidney disease and kidney transplantation); malignant neoplasm; any treatment for depression, insomnia, or tranquilization at least 3 months before this study; aspartate aminotransferase (AST) > 100 IU/L, alanine aminotransferase (ALT) > 100 IU/L, or creatinine > 1.4 mg/dL. Setting: Patients recruited via Severance Hospital Age median (interquartile range): Melatonin: 61 (58, 71); Placebo: 61 (59, 65) % male: 0% | Intervention: 2 mg prolonged-release melatonin (Circadian) Comparator: Placebo Treatment was taken daily 2 hours before sleep | Relevant outcomes: Pittsburgh Sleep Quality Index Other outcomes: Arterial stiffness; Mitochondrial DNA Follow-up: 6 weeks |
Xu et al. 202022 China Funding: Shanghai Municipal Commission of Science and Technology | RCT | N = 61 Eligibility criteria: Chinese individuals aged 45 to 60 years who had primary insomnia according to the DSM-IV criteria Exclusion criteria: Use of hypnotics within the previous one month or any psychoactive treatment, had drugs such as neuroleptic, antidepressants and anticholinergic agents which could interfere on sleep structure within the previous 3 months; moderate-severe OSA or relevant periodic leg movements; sleep disorders associated with a psychiatric disorder; severe psychiatric disorders, especially psychosis, anxiety and depression; sleep disorders secondary to another medical condition; a lifestyle likely to interfere with sleep patterns; use of prohibited medication or alcoholism; patients with severe organic diseases or with other conditions not suitable for participating in the study at the investigator's discreet. Setting: Tertiary hospital Age mean (SD): Melatonin: 57.24 (5.59); Placebo: 56.53 (4.65) % male: 47.5% | Intervention: 3 mg fast-release melatonin tablet Comparator: Placebo Treatment was taken daily 1 hour before bedtime | Outcomes: Sleep quality (polysomnography); Subjective sleep performance and daytime somnolence (PSQI), Insomnia Severity Index; Epworth Sleepiness Scale; Serious adverse events and side effects Follow-up: 4 weeks |
DNA = DNA; PSQI = Pittsburgh Sleep Quality Index; SD = standard deviation.
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Mayer et al. (2021)23 | ||||||
Intended Users: NR Target Population: Insomnias in headaches, neurodegenerative movement disorders, multiple sclerosis, traumatic brain injury, epilepsies, stroke, neuromuscular disease and dementia | Cognitive behavioural therapy; Light therapy; Physical exercise; Pharmacological therapy (e.g., benzodiazepine); Non-pharmacological therapy (e.g., melatonin) Chronic insomnia (ICD 10) | Treatment of insomnia | Systematic review of randomized controlled trials, and “studies of lower evidence (p. 9)”23 if studies of high evidence were lacking | Literature was categorized independently by 2 experts according to Oxford Centre for Evidence-based Medicine Levels of Evidence (2001) | Nominal group process and Delphi technique Evidence classification (class 1-IV) was performed according to standardized European Procedures Levels of recommendation are A-D (not further described) | NR |
Palagini et al. (2021)24 | ||||||
Intended users: Psychiatric clinical practice Target population: Adults with neuropsychiatric disorders and insomnia and circadian sleep disturbances | Prolonged-release and immediate-release exogenous melatonin | Treatment of insomnia symptoms; Use of melatonin during sedative-hypnotics discontinuation | Systematic literature review including systematic reviews and meta-analyses | RAND/UCLA Appropriateness method which include critical appraisal of the evidence (not otherwise described) | RAND/UCLA Appropriateness Method for conceptualizing, designing, and carrying out the appropriateness procedures. Recommendation formulated using a modified Delphi method | NR |
Palagini et al. (2020)25 | ||||||
Intended users: Clinical practice Target population: Adult population with insomnia | Cognitive behavioural therapy; Pharmacological therapy (i.e., Melatonin 2 mg prolonged-release, sedating antidepressants, short/medium-acting benzodiazepines, Zdrugs) | Treatment of insomnia | Systematic literature review of guidelines, with additional systematic review of systematic reviews or meta-analyses | RAND/UCLA Appropriateness method which include critical appraisal of the evidence (not otherwise described) | RAND/UCLA Appropriateness Method for conceptualizing, designing, and carrying out the appropriateness procedures. Recommendation formulated using a modified Delphi method | NR |
Department of Veterans Affairs (2019)26 | ||||||
Intended Users: Health care providers Target Population: Adults 18 years or older treated in any VA/DoD primary care setting who have experienced sleep disorders | Key Question 1: Pharmacotherapy, including over the counter preparations (e.g., melatonin) | Patient health outcomes; Quality of life | Systematic review of clinical studies and systematic reviews, RCTs, and cohort studies | Not clearly reported, but included blinding of patients and professionals, allocation concealment | VA and DoD Evidence-Based Practice Work Group (www.healthquality.va.gov/policy/index.asp) Grading of Recommendations Assessment, Development and Evaluation (GRADE) system, considering:
Recommendations were strong (generally indicates high confidence in the quality of the available scientific evidence, a clear difference in magnitude between the benefits and harms of an intervention, similarity among patient or provider values and preferences, and the apparent influence of other implications) (e.g., resource use, feasibility) or weak (If the Work Group has less confidence after the assessment across these domains and believes that additional evidence may change the recommendation). | Posted on a wiki website for a period of 14 business days; American Academy of Sleep Medicine |
DoD = Department of Defense; ICD = International Classification of Diseases; NR = not reported; VA = Veterans Affairs.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Umbrella Reviews Using AMSTAR 28
Strengths | Limitations |
|---|---|
Low et al. 202012 | |
|
|
Rios et al. 201913 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 7: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 28 and the ISPOR Questionnaire9
Strengths | Limitations |
|---|---|
Ma et al. (2022)14 | |
|
|
Almond et al. (2021)15 | |
|
|
Kothari et al. (2021)16 | |
|
|
Baglioni et al. (2020)17 | |
|
|
McCleery et al. (2020)18 | |
|
|
Sys et al. (2020)19 | |
|
|
Pierce et al. (2020)20 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NR = not reported; PICO = participants, intervention, comparator, outcomes.
Table 8: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist27
Strengths | Limitations |
|---|---|
Kim et al. (2021)21 | |
|
|
Xu et al. (2020)22 | |
|
|
Table 9: Strengths and Limitations of Guidelines Using AGREE II10
AGREE scale item | Mayer et al. (2021)23 | Palagini et al. (2021)24 | Palagini et al. (2020)25 | Veterans Affairs (2019)26 |
|---|---|---|---|---|
Domain 1: Scope and Purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Unclear | Unclear | Yes |
6. The target users of the guideline are clearly defined. | No | Yes | Yes | Yes |
Domain 3: Rigour of Development | ||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | No | No | No | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | No | No | No | Yes |
10. The methods for formulating the recommendations are clearly described. | No | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Unclear | Unclear | Unclear | Yes |
14. A procedure for updating the guideline is provided. | No | No | No | Yes |
Domain 4: Clarity of Presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||
18. The guideline describes facilitators and barriers to its application. | No | No | No | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No | No | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | No | No | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | Yes |
Domain 6: Editorial Independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes (no funding) | Unclear | Unclear | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes (none) | Yes (none) | Yes (none) | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 10: Summary of Findings Included Umbrella Reviews
Main study findings | Authors’ conclusion |
|---|---|
Low et al. 202012 | |
Sleep outcomes 1. 3/5 studies showed improved sleep latency and sleep efficiency; Statistically significant improvement in sleep latency (Olde Rikkert et al. 2001) 2. “In 3 of 4 trials, sleep efficiency was significantly improved compared to placebo, while sleep latency was significantly improved in 2. In 2 others, total sleep time improved significantly. In 3 studies, melatonin significantly improved at least one actigraphic measure of sleep quality. (p. 19)”12; Statistically significant improvement in sleep latency (Harrington 2004) 3. 1/4 studies reported improvement in sleep quality; No statistically significant improvement in total sleep time or sleep latency (MacMahon et al. 2005) 4. Out of 4 studies, 2 favoured melatonin and 2 did not favour either melatonin or control (Costello et al. 2014) 5. Melatonin significantly lowers sleep latency [-2.48 (−4.56 to −0.40)] and significantly increases total sleep time [29.27 (6.68 to 51.86)], but had little effect on sleep efficiency (Li et al. 2018) 6. “Circadin 1–2 h before bedtime was associated with significant improvements in many sleep and daytime parameters, including sleep quality and latency, morning alertness and health-related quality of life. (p. 21)”12; Statistically significant improvement in sleep latency (Lyseng-Williamson et al. 2012) Adverse events
Other relevant review already captured in the 2019 CADTH report: Auld et al. 2017. | Findings were fairly consistently across reviews, however, there was considerable heterogeneity, which leads to uncertainty Most reviews did not specify timing of melatonin administration, and among those that did, timing was variable. “Hence, it is possible that conflicting conclusions are contributed by different and/or suboptimal timing of administration of melatonin. (p. 22)”12 “It appears that there is inadequate evidence to confirm the efficacy of melatonin in primary insomnia. (p. 22)”12 |
Rios et al. 201913 | |
Sleep onset latency (reported in 4 MAs and 3 SRs) measured with sleep diaries, polysomnography and/or actigraphy
Total sleep time (reported in 6 MAs and 4 SRs) measured with polysomnography, actigraphy, sleep diary, subjective report, and PSQI
Wake after sleep onset (reported in 3 MAs and 2 SRs) measured with sleep diary, polysomnography, actigraphy
Sleep quality (reported in 5 MAs and 5 SRs) measured with polysomnography, actigraphy, sleep scales questionnaires, carer-rated sleep quality, and various sleep questionnaires (e.g., LSEQ, PSQI)
Sleep satisfaction (reported in 1 SR) measured by % nights scored good; % good mood
Sleep efficiency (reported in 5 MAs and 3 SRs) measured by polysomnography, actigraphy, and sleep diary
Health-related quality of life (reported in 1 SR) measurement tool not reported
|
|
LSEQ = Leeds Sleep Evaluation Questionnaire; MA = meta-analysis; PSQI = Pittsburgh Sleep Quality Index; SR = systematic review.
Table 11: Summary of Findings Included Systematic Reviews and Network Meta-Analysis
Main study findings | Authors’ conclusion |
|---|---|
Ma et al. (2022)14 | |
Data from 1 relevant included study (Medeiros et al. 2007) Objective outcomes (measured with polysomnography) Total sleep time
Subjective outcomes Sleep quality (measured with PSQI)
Daytime sleepiness measured by mean change (measured with ESS)
|
|
Almond et al. (2021)15 | |
Data from 2 relevant included studies (Garfinkel et al. 1995, Monti et al. 1999) Objective outcomes (measured with wrist actigraphy or polysomnography) Sleep efficiency
Wake time after sleep onset
Total sleep time
Sleep latency
Number of awakenings (Monti et al. 1999)
Safety outcomes Adverse events
|
|
Kothari et al. (2021)16 | |
Data from 1 relevant included study (Garfinkel et al. 2011) Reported as melatonin vs placebo at 3 weeks Objective outcomes (measured using actigraphy) Sleep efficiency
Wake time after sleep onset
Number of awakenings
|
|
Baglioni et al. (2020)17 | |
Data from 2 relevant included studies (Lurthinger et al. 2019; Rondanelli et al. 2007) Other relevant primary studies already captured in 2019 CADTH review and not reported here: Wade et al. 2007 Reported as Melatonin pre-mean (SD) vs Placebo pre-mean (SD); Melatonin post mean (SD) vs Placebo post mean (SD) Objective outcomes (measured by polysomnography, actigraphy) Sleep onset latency (Luthringer et al. 2009)
Wake after sleep onset (Luthringer et al. 2009)
Total sleep time (Luthringer et al. 2009)
Number of awakenings (Luthringer et al. 2009)
Additional objective outcomes not reported here: Stage 1 sleep Stage 2 sleep, Stage 3 sleep, REM sleep Subjective outcomes Sleep (measured with PSQI) (Rondanelli et al. 2007)
Sleep quality (measured with LSEQ) (Luthringer et al. 2009, Rondanelli et al. 2007)
Sleep quality (measured with sleep diary) (Luthringer et al. 2009, Rondanelli et al. 2007)
Sleepiness (measured with ESS) (Rondanelli et al. 2007)
Physical function (measured with SF36) (Rondanelli et al. 2007)
Mental (measured with SF36) (Rondanelli et al. 2007)
|
|
McCleery et al. (2020)18 | |
Data from 1 relevant included study (Morales-Delgado et al. 2018) Other relevant primary study already captured in 2019 CADTH review and not reported here: Wade et al. 2014 Subjective outcomes Carer-rated sleep quality (measured with PSQI)
Cognition (measured with Mini Mental State Examination)
Activities of Daily Living (Lawton's Instrumental ADLs Scale)
Adverse events
|
|
Sys et al. (2020)19 | |
Data from 3 relevant included primary studies (Lemoine et al. 2017; Wade et al. 2007; Wade et al. 2010) Other relevant primary studies already captured and reported in a systematic review in this report: Garfinkel et al. 1995 Subjective outcomes Sleep quality
Sleep latency
Total sleep time and sleep maintenance
Quality of night (sleep diaries)
Quality of day (sleep diaries)
Quality of life
Next-day alertness, well-being, feelings and mood Behaviour following wakening (LSEQ)
Alertness in morning
Clinical Global Impression Scores
Adverse events
|
|
Pierce et al. (2019)20 | |
Meta-analysis including 6 RCTs (Olde Rikkert et al. 2001)
Also captured in the Low et al. 2021 umbrella review in this report, but this systematic review reported additional details Data from 4 relevant included primary studies (Baskett et al. 2003, Jean-Louis et al. 1998; Hughes et al. 1998, Dawson et al. 1998) Other relevant primary studies already captured and reported in a systematic review in this report: Wade et al. 2007; Lemoine et al. 2017 Method of measurement not reported Multiple outcomes reported qualitatively
Sleep quality
Sleep efficiency
Sleep latency
Night time awakenings
Nocturnal wake time
Morning alertness
|
|
AEs = adverse events; CI = confidence interval; ESS = Epworth Sleepiness Scale; LSEQ = Leeds Sleep Evaluation Questionnaire; MD = mean difference; PSQI = Pittsburgh Sleep Quality Index; RCT = randomized controlled trials; Std MD = standardized mean difference.
Table 12: Summary of Findings of Included Primary Clinical Studies
Main study findings | Authors’ conclusion |
|---|---|
Kim et al. (2021)21 | |
Median score (Interquartile range) at baseline and 6-weeks Subjective outcome Sleep quality index (PSQI)
|
|
Xu et al. (2020)22 | |
Outcomes reported as Reported as Difference in change (95% CI); p-value [calculated as (change in melatonin group) - (change in placebo group)] Objective outcomes (measured by polysomnography) Sleep efficiency (%) 3.19 (−3.23 to 9.60); 0.324 Total sleep time (in minutes)
Wake after sleep onset (in minutes)
Sleep latency (in minutes)
Wake during sleep (in minutes)
Early wake (in minutes)
Subjective outcomes PSQI total score
Insomnia Severity Index
Epworth Sleepiness Scale
Safety
Other outcomes reported but not extracted: Objective: REM latency, Micro-arousal index, N1%, N2%, N3%, REM%; Subjective: Component 1 to 7 scores of the PSQI |
|
CI = confidence interval; PSQI = Pittsburgh Sleep Quality Index; REM = rapid eye movement.
Table 13: Summary of Recommendations in Included Guidelines
Recommendations | Quality of evidence and strength of recommendations |
|---|---|
Mayer et al. (2021)23 | |
Movement disorders
Multiple sclerosis
Epilepsy
Dementia and prion-diseases
| Movement disorders NR Multiple sclerosis NR Epilepsy NR Dementia and prion-diseases “The recommendations are therefore of very low evidence and do not imply that certain treatments may not be helpful or efficacious. (p. 8)”23 |
Palagini et al. (2021)24 | |
Mood disorders 1. “The administration of prolonged-release melatonin at 2–10 mg, 1–2 h before bedtime, should be used in the treatment of insomnia symptoms or comorbid insomnia in mood disorders.” (p.8) 2. “The chronotype of patients should be taken into account to adapt the timing of the administration.” (p.8) 3. “The administration of immediate-release melatonin in the treatment of insomnia symptoms or comorbid insomnia in mood disorders gave uncertain results, more studies are needed for recommendation in the clinical practice.” (p.8) Anxiety disorders 1. “In the absence to date of well-conducted RCTs, the administration of melatonin might be useful in the treatment of insomnia symptoms or comorbid insomnia disorder in anxiety disorders according to international guidelines for insomnia disorder treatment (> 55 years 2 mg PR melatonin 1–2 h before bedtime).” (p.8) Attention-Deficit/Hyperactivity Disorder (ADHD) 1. “In the absence of well-conducted trials, the administration of immediate-release melatonin at sleep-promoting dose (2–6mg) before bedtime could be of interest to treat insomnia symptoms associated with ADHD.” (p.9) Autism Spectrum Disorder (ASD) 1. “In the absence to date of well-conducted trials in adults, the administration of prolonged-release melatonin at 2–5mg 1–2 h before bedtime could be useful in the treatment of insomnia in adults with ASD, as an extrapolation from solid available data in children.” (p.9) Eating Disorders 1. “In the absence to date of well-conducted trials, the administration of melatonin might be useful in the treatment of insomnia symptoms or comorbid insomnia in eating disorders according to international guidelines for insomnia treatment (prolonged-release melatonin at 2mg, 1–2 h before bedtime), but consensus was uncertain, more studies are needed for recommendation in the clinical practice.” (p.10) Neurocognitive Disorders 1. “The administration of prolonged-release melatonin at 2mg might be useful 1–2 h before bedtime in the treatment of insomnia in Neurocognitive Disorders.” (p.11) 2. “The administration of immediate-release melatonin 2–6mg at bedtime might be useful in the treatment of insomnia in Neurocognitive Disorders.” (p.11) 3. “The administration of prolonged-release melatonin at 2mg may be particularly useful in patients with Parkinson Disease and may contribute to improve sleep quality and other sleep disturbances including Rem Behavioral Disorder.” (p.11) Substance Use Disorder 1. “Melatonin might be useful in the treatment of insomnia symptoms or insomnia comorbid related to substances use disorders according to international guidelines for insomnia treatment, using prolonged-release melatonin at 2mg 1–2 h before bedtime if >55 years old.” (p.12) Schizophrenia 1. “Melatonin might be useful in the treatment of insomnia symptoms or comorbid insomnia in schizophrenia; the administration of prolonged-release melatonin at 2 mg, 1–2 h before bedtime, could be used in schizophrenia.” (p.12) 2. “The administration of immediate-release melatonin in the treatment of insomnia symptoms or comorbid insomnia in schizophrenia gave uncertain results, more studies are needed for recommendation in the clinical practice.” (p.12) | Not reported |
Palagini et al. (2020)25 | |
1. “Pharmacological treatment should be first-line option when CBT-Insomnia is not available. The choice of the drug should be based on different factors such as type of insomnia, age, comorbidities, and potential side effects among drugs available in Italy.” (p.2) 2. “If the choice is prolonged-release melatonin (>55 years old) use it in within 13 weeks.” (p.2) | Not reported |
Veteran Affairs (2019)26 | |
“32. We suggest against the use of melatonin for the treatment of chronic insomnia disorder. (p. 60)”26 | Weak against |
AD = Alzheimer dementia; ADHD = Attention-Deficit/Hyperactivity Disorder; ASD = Autism Spectrum Disorder; CBT = cognitive behavioural therapy; h = hours; PR = prolonged-release; RCT = randomized controlled trial.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 14: Overlap in Relevant Primary Studies between Included Systematic Reviews
Primary study citation | Ma (2022)14 | Almond (2021)15 | Kothari (2021)16 | Baglioni (2020)17 | McCleery (2020)18 | Sys (2020)19 | Pierce (2019)20 |
|---|---|---|---|---|---|---|---|
Baskett et al. Age Aging 2003; 32:164 to 70 | — | — | — | — | — | — | Yes |
Dawson et al. J Biol Rhythms 1998; 13:532 to 8. | — | — | — | — | — | — | Yes |
Garfinkel et al. Lancet Long Engl. 1995; 346(8974):541 to 544. | — | Yes | — | — | — | Yes | — |
Garfinkel et al. Diabetes, Metab Syndrome Obes Targets Ther 2011; 4:307e13. | — | — | Yes | — | — | — | — |
Hughes et al. Sleep 1998;21: 52 to 68. | — | — | — | — | — | — | Yes |
Jean-Louis et al. J Pineal Res 1998;25:177 to 83. | — | — | — | — | — | — | Yes |
Lemoine et al. J Sleep Res 2007; 16:372 to 80. | — | — | — | — | — | Yes | Yes |
Luthringer et al. Int. Clin. Psychopharmacol. 2009; 24: 239 to 249. | — | — | — | Yes | — | — | — |
Medeiros et al. J. Neurol. 2007; 254:459 to 464. | Yes | — | — | — | — | — | — |
Monti et al. Arch Gerontol Geriatr. 1999; 28(2):85 to 98. | — | Yes | — | — | — | — | — |
Morales-Delgado et al. Euro. Ger. Med. 2018;9(4):449 to 54. | — | — | — | — | Yes | — | — |
Rondanelli et al. J. Am. Geriatr. Soc. 2011; 59: 82 to 90. | — | — | — | Yes | — | — | — |
Wade et al. Curr. Med. Res. Opin. 2007, 23, 2597 to 2605. | — | — | — | Yes | — | Yes | Yes |
Wade et al. BMC Medicine 2010; 8:51. | — | — | — | — | — | Yes | Yes |
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Melatonin for the Treatment of Insomnia: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines Review. Ottawa (ON): CADTH; 2019. https://www.cadth.ca/melatonin-insomnia-review-clinical-effectiveness-cost-effectiveness-and-guidelines Accessed 2022 Apr 12.
Guidelines With Unclear Methods
Insomnia Guideline. Renton (WA): Kaiser Permanente. 2021. https://wa.kaiserpermanente.org/static/pdf/public/guidelines/insomnia.pdf Accessed 2022 Apr 24.
Review Articles
Integrative Review With Unclear Methods
Bueno APR, Savi FM, Alves IA, Bandeira VAC. Regulatory aspects and evidences of melatonin use for sleep disorders and insomnia: an integrative review. Review. Arquivos de Neuro-Psiquiatria. 2021;79(8):732-742. PubMed
Additional References
Relevant Primary Studies
Bologna C, Madonna P, Pone E. Efficacy of Prolonged-Release Melatonin 2 mg (PRM 2 mg) Prescribed for Insomnia in Hospitalized Patients for COVID-19: A Retrospective Observational Study. Journal of Clinical Medicine. 2021;10(24):14. PubMed
Additional reviews with primary studies evaluating Ramelteon
Moon E, Partonen T, Beaulieu S, Linnaranta O. Melatonergic agents influence the sleep-wake and circadian rhythms in healthy and psychiatric participants: a systematic review and meta-analysis of randomized controlled trials. Neuropsychopharmacology. 2022;04:04.
A systematic review which include a few studies on melatonin receptor agonists. There are several studies on melatonin, but none among those with insomnia.
Scharner V, Hasieber L, Sonnichsen A, Mann E. Efficacy and safety of Z-substances in the management of insomnia in older adults: a systematic review for the development of recommendations to reduce potentially inappropriate prescribing. Research Support, Non-U.S. Gov't Review. BMC Geriatrics. 2022;22(1):87. PubMed
Includes on study evaluating Benzodiazepine-like medication (BDLM) (Intervention) or selective melatonin receptor agonist {Ramelteon) (comparison).
Roehrs TA, Auciello J, Tseng J, Whiteside G. Current and potential pharmacological treatment options for insomnia in patients with alcohol use disorder in recovery. Research Support, Non-U.S. Gov't Review. Neuropsychopharmacology Reports. 2020;40(3):211-223. PubMed
Includes one study on Ramelteon for insomnia in patients with alcohol use disorder in recovery
Gottlieb JF, Benedetti F, Geoffroy PA, et al. The chronotherapeutic treatment of bipolar disorders: A systematic review and practice recommendations from the ISBD task force on chronotherapy and chronobiology. Bipolar Disorders. 2019;21(8):741-773. PubMed
A systematic review that includes one study evaluating Ramelteon in patients with bipolar disorders with manic symptoms and insomnia.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca