CADTH Health Technology Review
Melatonin for the Treatment or Prevention of Delirium
Rapid Review
Authors: Sara D. Khangura, Danielle McDougall
Abbreviations
AE
adverse event
CABG
coronary artery bypass
CAM
Confusion Assessment Method
CI
confidence interval
ICU
intensive care unit
LOS
length of stay
MDAS
Memorial Delirium Assessment Scale
RCT
randomized controlled trial
RR
relative risk
SAE
severe adverse event
SD
standard deviation
SE
standard error
SR
systematic review
Key Messages
Variable findings were reported for clinical effectiveness of melatonin for the prevention or treatment of delirium compared with placebo in the literature that met the criteria for this review.
No studies that met the criteria for this review were found on the clinical effectiveness of melatonin for the prevention and/or treatment of delirium versus antipsychotic drugs or cholinergic agents.
There was limited evidence available on the clinical effectiveness of melatonin for the prevention and/or treatment of delirium versus dexmedetomidine.
There were no statistically or clinically significant harms reported from the use of melatonin in the treatment of patients at risk from or experiencing delirium.
Limited guidance was found that provided recommendations for the use of melatonin in the prevention and//or treatment of delirium for hospitalized inpatients.
Context and Policy Issues
Delirium is an acute condition that is characterized by confusion and altered consciousness, which commonly develops during hospitalization.1 Delirium often affects older inpatients and those with comorbidities,2-5 including visual and or cognitive impairment (e.g., dementia),6,7 and has been characterized as the most common complication following surgery among older adults.4 In addition to patient characteristics, the risk for developing delirium has also been associated with health care factors, including poor nutrition, the need for use of restraints, and other iatrogenic events.6 Depending on the level of agitation and hyperactive behaviour, delirium may be more or less recognizable, making diagnosis a challenge in cases for which agitation is not apparent or is not severe enough to be noticed in a busy hospital or intensive care unit (ICU) setting.5,6
Much of the published literature focuses on delirium in hospitalized older adults,6 and/or those in the ICU; however, delirium can affect people of any age who are critically ill and in hospital,8 and often co-occurs with sleep disruption that is common when admitted to hospital and ICU environments.3,6 Delirium can contribute to significant morbidity, including falls, longer stays in the ICU and/or hospital, higher rates of long-term care placement following discharge from hospital, hospital readmission, functional decline, and mortality.3,4,6-8 The condition can have long-term effects for some patients, with a return to baseline cognition taking up to a year for some people; in others, the cognitive effects can be permanent.6 In addition to the deleterious effects that delirium can cause for patients, families, and health care providers, delirium has also been associated with higher costs of care. Its effective prevention and management is considered a health care quality indicator,6,8 making it an important priority for individuals, communities, and health care systems.4
There are several approaches to managing delirium in the hospital setting, including both preventive and therapeutic interventions that may be either pharmacological and non-pharmaceutical.6 Non-pharmaceutical interventions aimed at the prevention of delirium focus on identifying and mitigating risk factors for developing delirium before its onset.6 Some research has investigated the use of medical interventions for the prevention of delirium (e.g., preoperative administration of antipsychotic medications); however, the evidence is inconclusive about the effectiveness of these preventive measures.6 Treatment of delirium may initially involve the use of non-pharmacological interventions (e.g., assistance with reorientation from a health care provider, family member, or other caregiver), or escalate to more intensive interventions, such as the use of physical restraints.6 Often the prevention and/or management of delirium requires the use of pharmacological intervention, including the use of antipsychotic medications or cholinesterase inhibitors; however, these are not thought to treat the underlying cause of delirium,9 are not supported by conclusive evidence of any preventive or therapeutic benefit,5,8 and may cause harm.6
Melatonin has been suggested as a potentially useful intervention for the prevention and/or treatment of delirium in hospitalized patients3,5 because it is a hormone, produced by the pineal gland, that supports healthy circadian rhythms and sleep patterns.10 Melatonin is also believed to have a favourable safety profile, with few side effects described in the literature to date.3 Because of the association between delirium and poor sleep,10 melatonin could potentially be a clinically effective intervention for the prevention and management of delirium in hospitalized inpatients.4 Nonetheless, currently available research describing the use of melatonin for the prevention and/or treatment of delirium has produced variable findings and has not supported consensus about its clinical effectiveness or utility.3-5
Given the potential benefit that melatonin may offer to patients who are at risk for developing or experiencing delirium while hospitalized, this review aims to gather and summarize relevant evidence describing clinical effectiveness and evidence-based guidance.
Research Questions
What is the clinical effectiveness of melatonin versus no treatment or placebo for the treatment or prevention of delirium in adult patients in the hospital or intensive care unit?
What is the clinical effectiveness of melatonin versus antipsychotic drugs for the treatment or prevention of delirium in adult patients in the hospital or intensive care unit?
What is the clinical effectiveness of melatonin versus cholinergic agents for the treatment or prevention of delirium in adult patients in the hospital or intensive care unit?
What is the clinical effectiveness of melatonin versus dexmedetomidine for the treatment or prevention of delirium in adult patients in the hospital or intensive care unit?
What are the evidence-based guidelines regarding the use of melatonin for the treatment or prevention of delirium in adult patients in the hospital or intensive care unit?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, PsycINFO, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were melatonin and delirium. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded. If possible, retrieval was limited to the human population. The search was completed on March 23, 2022, and was limited to English-language documents published since January 1, 2017.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1 to Q5: Adults with delirium or at risk of delirium admitted to the hospital or intensive care unit |
Intervention | Q1 to Q5: Melatonin |
Comparator | Q1: No treatment, placebo Q2: Antipsychotic drugs (e.g., haloperidol, risperidone, olanzapine, quetiapine) Q3: Cholinergic agents (e.g., rivastigmine, donepezil, galantamine) Q4: Dexmedetomidine Q5: Not applicable |
Outcomes | Q1 to Q4: Clinical effectiveness (e.g., cognitive functioning, delirium severity, duration of delirium, short-term delirium symptoms, quality of life), safety Q5: Recommendations regarding the use of melatonin for the treatment or prevention of delirium |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, evidence-based guidelines |
Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2021. Systematic reviews (SRs) in which all relevant primary studies were captured in other more recent or more comprehensive SRs were excluded. SRs and primary studies retrieved by the search were excluded if they were captured in 1 or more included overviews of SRs or systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)11 for overviews of SRs and systematic reviews, the Downs and Black checklist12 for RCTs, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument13 for evidence-based guidelines. Summary scores were not calculated for the included studies and publications; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
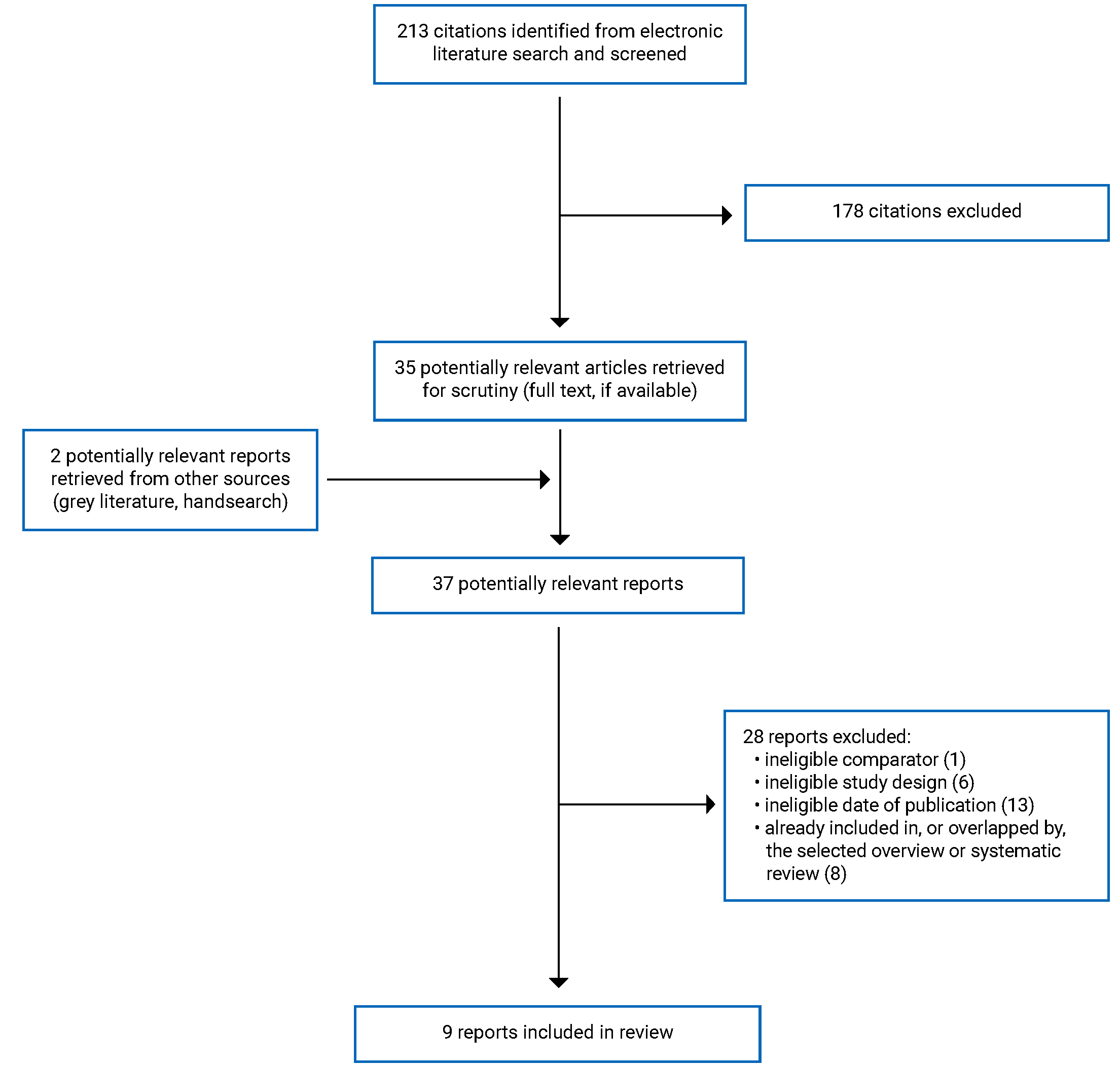
A total of 213 citations were identified in the electronic literature search. Following screening of titles and abstracts, 178 citations were excluded and 35 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 37 potentially relevant articles, 28 were excluded for various reasons, and 9 publications met the inclusion criteria and were included in this report. These comprised 1 overview of meta-analyses (with or without SRs), 1 SR, 6 randomized controlled trials (RCTs), and 1 evidence-based guideline. Appendix 1 presents the PRISMA14 flow chart outlining study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The overview and the SR in this report had broader inclusion criteria than this review.15,16 Specifically, the authors evaluated the clinical effectiveness of melatonergic drugs (i.e., both melatonin and Ramelteon) for the prevention of delirium in hospitalized patients.15,16 Similarly, the guideline included in this report was more broadly focused on sleep and circadian rhythm disorders (including those causing delirium);17 consequently, only the characteristics, results, and recommendations from the subset of studies and/or guidance that are relevant will be described in this report.
The overview was published in 2021 and sought meta-analyses (with or without SRs) published between January 2020 and August 2021.15 The overview included 3 meta-analyses of RCTs published between 2016 and 2020; however, none of the included studies were eligible for inclusion in this report. One study was a meta-analysis (conducted without an accompanying SR) that presented some data on melatonin separately; however, a meta-analysis without a SR was not an eligible study design for inclusion in this review. The other 2 were SRs with meta-analyses, with all data presented combining both melatonin and Ramelteon,15 which were not eligible for inclusion in this review because Ramelteon was not an eligible intervention. Thus, although the overview study itself met the eligibility criteria for this report, it was considered an empty overview because it contained no eligible studies (i.e., it was retained as an eligible study, but no data could be abstracted or summarized in this report).
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The SR was published in 2021.16 It included studies from the inception dates of the citation databases that were queried to May 2020 and included 9 RCTs, published between 2010 and 2020, that were eligible for inclusion in this report.16
Six RCTs were found to be eligible for this report, 2 of which were published in 202218,19 and 4 of which were published in 2021.20-23 Five of these RCTs used a double-blind, placebo-controlled design,18-21,23 and 1 did not specify whether participants, clinicians, and/or investigators were blinded to patient allocation to treatment.22 Four of the RCTs were conducted within a single centre,19-21,23 whereas 1 RCT was conducted across 12 centres;18 another did not report information describing whether the study was single- or multi-centre.22 Although 5 of the 6 RCTs were designed as superiority trials,18-20,22,23 1 was a feasibility study intended to assess the potential for conducting a large-scale RCT.21 Duration of follow-up ranged across 5 of the RCTs (and the outcomes measured) between 4 days and 90 days.18-23 One RCT did not clearly report follow-up time.20
The 1 guideline included in this report was published in 2021, and was developed by the Italian Society of Psychosomatic Medicine with several other organizations participating in and/or contributing to the development process: the Italian Association of Sleep Medicine, the Italian Association for the Fight Against Stigma, the Italian Society of Consultation-Liaison Psychiatry, the Italian Society of Neuropsychopharmacology, the Italian Society of Psychosomatic Medicine, the French Society for Sleep Research and Sleep Medicine, and the French Association of Biological Psychiatry and Neuropsychopharmacology.17 The guideline developers used a systematic literature review to identify and critically appraise relevant evidence. Following the synthesis of evidence, a modified Delphi technique was used to establish consensus on a set of recommendations between a panel of experts.17 The guideline developers did not report the use of a grading or rating system for the recommendations they published, and of the 9 recommendation statements included in the guideline, 1 recommendation addressed the use of melatonin for the treatment and prevention of delirium.17
Country of Origin
The SR was conducted by investigators based in Australia16 as were 2 of the RCTs included in this report.18,21 Two of the other RCTs were conducted in China,19,23 1 in Iran,20 and another in Egypt.22 The guideline does not specify a context to which its recommendations apply; rather, it characterizes itself as an international guideline led by Italian and French experts.17
Patient Population
The SR included in this report described RCTs of adults who were 18 years of age or older and were hospitalized in medical or surgical wards or the ICU. It included 1,712 patients in total, 1,303 of whom contributed to data that were eligible for this report.16 The conditions, or reasons for hospitalization, were not provided in the overview study, although a reference to a high degree of heterogeneity was identified and quantified.15 Patients included in the eligible primary studies from the SR represented a broad range of conditions and/or reasons for hospitalization, including hip surgery, liver resection, organophosphate poisoning, and elective cardiac and pulmonary thromboendarterectomy (as well as several studies for which no specific condition or reason for hospitalization provided other than medical, surgical, emergency, and elective patients).16 Similarly, the SR noted a high degree of heterogeneity in the 9 studies investigating melatonin and specified patient characteristics as being 1 of several sources of this heterogeneity.16
The multi-centre RCT enrolled and randomized 847 adult patients, aged 18 years or older (841 of whom were included in the analyses), and admitted to the ICU for various reasons (i.e., medical, surgical, elective, and emergency) and diagnoses (including cardiovascular, gastrointestinal, sepsis-related, metabolic, trauma-related, neurologic, and respiratory).18 Similarly, the Australian feasibility RCT enrolled patients (29 randomized; 28 analyzed) with various reasons for admission (although limited to medical reasons only), including sepsis, trauma, and cardiovascular and metabolic reasons; however, this RCT also limited its population to older adults who were aged 70 years and older.21 The remaining 4 RCTs focused on patients who had a particular condition (i.e., acute heart failure)19 and/or underwent a particular surgical procedure (i.e., coronary artery bypass graft surgery20,22 or percutaneous transluminal coronary intervention).23 Three of these 4 RCTs limited their populations of interest to older adults who were at least 60 years of age or older,19,22,23 whereas the fourth included patients as young as 30 years.20 The 2 Chinese studies had larger sample sizes than the Iranian and Egyptian studies, with 497 patients randomized (and 480 with complete follow-up)19 and 297 patients randomized (285 analyzed).23 Finally, the Iranian study randomized and analyzed 60 patients;20 the Egyptian study randomized and analyzed 110 patients.22
The guideline was developed to inform psychiatric clinicians about the preventive and therapeutic treatment of adult patients with neuropsychiatric disorders who suffer from sleep and circadian rhythm disturbances (including delirium).17 The recommendations specific to delirium are not particular to patients in a hospital and/or ICU setting; however, the evidence used to inform the recommendations was based on hospitalized patient data.17
Interventions and Comparators
The SR included studies that compared melatonin and/or Ramelteon (any dose) against placebo and/or usual care; studies eligible for this report described doses of melatonin between 0.5 mg/kg to 50 mg/kg.16 The SR described treatment durations ranging from 4 days to 14 days, and the daily doses for 8 of the 9 included RCTs eligible for this report, with a single preoperative dose administered in 1 of the RCTs.16
The 6 RCTs included in this report investigated melatonin at dosages ranging from 3 mg to 5 mg per day.18-23 Five of the 6 RCTs investigated melatonin administered orally,19-23 whereas 1 investigated the use of enterally administered melatonin.18 Five of the 6 RCTs included in this review compared melatonin against matching placebos,18-21,23 with the sixth comparing melatonin plus dexmedetomidine against dexmedetomidine only.22 Patients who experienced severely agitated dementia in both arms of this latter trial also received haloperidol as needed.22
The guideline provides recommendations for the use of melatonin at dosages ranging from 2 mg to 5 mg, depending on whether the dosage is immediate release versus prolonged release.17
Outcomes
The primary outcome for 7 of the 8 studies in this report that examined clinical effectiveness was the occurrence or presence of delirium,15,16,18-20,22,23 whereas 2 RCTs included severity of delirium in the primary outcome.20,21 All studies that measured the presence of delirium reported use of the Confusion Assessment Method (CAM) and/or the CAM-ICU instrument(s),16,18-20,22,23 with severity of delirium measured using the Memorial Delirium Assessment Scale (MDAS)20,21 and Confusion Assessment Method – Severity Scale (CAM-S).18 The CAM and CAM-ICU are diagnostic measures that detect the presence of delirium using an algorithm.24 The MDAS and CAM-S instruments are measures of the severity of delirium, with higher scores indicating more severe delirium.25,26 Additional measures of delirium were reported among some RCTs described in the SR, including the Abbreviated Mental Test and the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV).16
Secondary and other outcomes were measured without the use of standardized instruments, including those characterizing the prevention of delirium (i.e., time to onset of delirium)22 as well as those characterizing the management of delirium (i.e., duration of delirium)16,22 and adjunct interventions (i.e., not melatonin) to manage delirium.18,21,22 Additional outcomes measured included mortality,16,18,19,23 length of stay (LOS) in hospital16,18,19,22,23 and/or the ICU,16,18,20,22 as well as adverse events (AEs) and severe adverse events (SAEs).16,18-21
The evidence-based guideline described the effectiveness of melatonin for the prevention and treatment of sleep disorders, including those associated with delirium.17
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Overview of Meta-Analyses With or Without Systematic Reviews
The overview demonstrated both strengths and limitations, such as the research objectives and eligibility criteria (i.e., population, intervention, comparator, and outcomes) were made clear and a protocol was produced a priori.15 The search strategy reported in the overview paper met the criteria of a comprehensive search,15 which is a component of a well-conducted review because it assures the reader that efforts have been made to identify the maximum amount of eligible information. The overview report also described the use of duplicate screening at the title and abstract phase (with insufficient information reported concerning full-text review) as well as duplicate data abstraction.15 The overview did not provide a list of excluded studies and the authors did not report the source(s) of funding for the included studies.15 These features are important to ensure transparency of the methods and reproducibility of the findings.15,27
Systematic Review
The SR included in this review demonstrated both strengths and limitations, such as the research objectives and eligibility criteria were made clear,16 which is important for framing and establishing the aim and research question(s) of a review. The SR did not describe the production of a review protocol in advance of conducting the study, which is important to ensure transparency and reproducibility of the review and to mitigate the potential for introducing bias. Although the authors of the SR described a comprehensive search,16 neither duplicate screening nor duplicate data abstraction methods were reported.16 Screening by 2 independent reviewers is an important feature of a well-conducted SR because it helps ensure that all eligible studies are identified and included and reduces the potential for bias and error. Similarly, duplicate data abstraction is important for ensuring that data have been accurately and comprehensively identified. Risk of bias was assessed using the Cochrane risk of bias tool28 and authors were careful to assess and describe significant clinical heterogeneity and publication bias as limiting factors of their review — which may cause any potential effect of an intervention to be less clearly apparent29 — but also account for these limitations in their interpretation of findings.16,29 Similar to the overview, the SR was limited in its description of excluded studies as well as the source(s) of funding for the included studies.16,27 Other limitations included a lack of detail and interpretation describing the reported publication bias (e.g., the source or drivers), multiple typos and errors in the manuscript that interfered with the interpretation of findings for some outcomes, and failure to discuss the potential impact of risk of bias in the primary studies on the findings of the review.16
Randomized Controlled Trials
Similarly, the papers describing RCTs demonstrated strengths and limitations, with clear descriptions of several important features of the trial methods and findings.18-23 Nonetheless, multiple typos and errors in 2 of the manuscripts were sufficient to interfere with the readability, comprehensibility, and interpretation of findings for some outcomes.21,23 Furthermore, 3 of the papers were unclear about the outcomes and measures they described, which similarly rendered some of the findings unclear and challenging to interpret.20-22 One of these RCTs also failed to provide any narrative summary of the results, providing only tabulated data in the results section of the paper.22 This unusual presentation of the study results made it particularly challenging to contextualize and interpret some of the findings.
Four RCTs21,22 demonstrated sufficient external validity with apparently representative patient populations and hospital settings.18-20,23 The other 2 RCTs did not include sufficient information with which to assess the representativeness of the study populations, health care received and health care settings.21,22
Other strengths common to all RCTs included in this review and demonstrating internal validity were randomized assignment to treatment groups, adequate reporting of sufficient statistical testing methods, and no evidence of data dredging or post hoc analyses.18-23 However, 1 of the RCTs was not clear about the methods used to randomize patients to the treatment groups,22 which is an important limitation rendering uncertainty about whether the randomization process was robust and/or free from any biases. Another strength common to 4 of the trials included in this review was double-blind administration of study treatments,18,19,21,23 which is a methodological feature that helps to mitigate bias that could affect the measurement of treatment effects and contributes to confidence in the internal validity of these trials. Two of the RCTs did not report information about blinded allocation to treatment,20,22 which is a limitation that could negatively impact the internal validity of the findings.
Four of the RCTs in this report described the use of power calculations that demonstrated sufficient power to detect any statistically significant differences between treatment groups;18,19,22,23 however, 2 of the RCTs did not.20,21 One of these RCTs was designed as a feasibility trial, which was intentionally limited in scope and was primarily interested in demonstrating whether a larger trial is feasible and how best to design it (i.e., the authors explicitly stated that they were not pursuing a power calculation in favour of demonstrating the standard deviation for the primary outcome as part of the primary objective of demonstrating feasibility).21 The research objective and small sample size (28 patients analyzed) in this RCT21 are important considerations when weighing the utility of its findings in this review. In addition, the other study in which no power calculation was described also used a small sample size (60 patients analyzed) and demonstrated other limitations that require consideration (e.g., no baseline assessments for psychological comorbidities, limited assessment of complications) when interpreting the findings in the context of this review.20
Three of the RCTs had larger sample sizes (ranging from 285 to 841 patients analyzed) as well as robust methods for randomization and blinded allocation to treatment, which are strengths that warrant consideration about the value that their findings contribute to this review.18,19,23 Nonetheless, some limitations were present in these studies as well, such as the authors of 2 of these larger RCTs explicitly acknowledged uncertainty about the dosages of melatonin used in their studies, and point out that this may have been a limiting factor affecting the findings because they describe the clinical effectiveness of melatonin for the prevention and/or treatment of delirium.18,19 Finally, a limitation from the multicentre Australian study was clinical heterogeneity between patients included in the trial, including variability in the ages, diagnoses, and reasons for hospital admission.18 As in reviews of primary clinical studies, multiple differences in patient characteristics across a clinical study population can render variable findings that may lead to uncertainty in the potential effects of the intervention of interest.
Evidence-Based Guideline
The scope and purpose of the guideline included in this review was clear;17 however, because the scope is much broader than that of this report, there is limited information of relevance to the research question posed herein. Stakeholder involvement is a strength in terms of the multidisciplinary composition of the guideline developers, but there is no mention of patient or public involvement and the intended target users for the guideline are not made explicit.17 Rigour of development is strong regarding the use of an SR to identify evidence that is clearly linked to the relevant recommendations; however, there is no discussion of the quality of the evidence, how the evidence was used to develop the recommendations, nor the strength of the recommendations,17 which are key features of a robust evidence-based guideline.30 There is also no description of a policy or plans for updating the guideline.17 Furthermore, the guideline is very limited in its clarity of presentation regarding delirium; that is, the recommendations are ambiguous and fail to provide clear and specific guidance.17 Similarly, the applicability of the recommendations regarding delirium are not clear, with no information about suggestions for implementing the guideline into clinical practice.17 Finally, funding and potential conflicts of interest were not described within the published report of the guideline,17 leaving uncertainty concerning the extent to which the guideline developers were able to maintain editorial independence. Nonetheless, given the context and subject matter of the recommendations specific to this report (i.e., melatonin is a generic supplement), it may be that editorial independence (e.g., from corporate or financial conflicts of interest) is less of a limiting factor of relevance to this report. Further, the guideline developers in this case are nonprofit groups with no obvious ties to financial or other potential conflicts of interest. Instead, the fact that authors of the guideline have published unclear and nonspecific guidance particular to delirium, neither advising in favour or against the use of melatonin (i.e., due to the uncertainty present in the relevant evidence base) is a more important limiting factor because it applies to the research question being posed by this report.
Summary of Findings
Clinical Effectiveness of Melatonin Versus No Treatment or Placebo for the Treatment or Prevention of Delirium
Treatment of Delirium
One SR and 3 RCTs included in this review presented results on the clinical effectiveness of melatonin compared with placebo or usual care (i.e., not otherwise described) by describing 3 outcomes relevant to the treatment of delirium: duration, severity, and adjunct interventions.16,18,20,21
Duration of Delirium
The SR included 5 RCTs describing the duration of delirium. Note the findings of these were pooled in a meta-analysis of studies that included Ramelteon, which was not eligible for this report; therefore, the results for the quantitative synthesis were not eligible for inclusion in this report.16 These 5 RCTs had sample sizes ranging from 87 patients to 378 patients and mean ages ranging from 50 years to 84 years (as well as various diagnoses and reasons for admission) and dosages of melatonin ranging from 0.5 mg to 3 mg per day and follow-up durations between 5 days and 14 days. None reported a statistically significant difference between treatment groups in the duration of delirium.16
Severity of Delirium
Three RCTs included in this review reported on the severity of delirium, 2 of which used the MDAS measure20,21 and 1 of which used the CAM-S measure.18 The studies ranged in sample size from 28 patients to 841 patients, with mean ages of treatment groups ranging from 60.26 (standard deviation [SD] = 9.50) years and 86.1 (SD = 4.40) years (as well as various diagnoses and reasons for admission), dosages of melatonin ranging from 3 mg to 5 mg per day (with 1 RCT using enteral administration of the study drugs18), and follow-up durations between 5 days and 14 days (with 1 RCT not reporting on follow-up duration20).18,20,21 Two of the RCTs reported no difference between the treatment groups in severity of delirium,18,21 whereas the third reported a statistically significant difference between the treatment groups, but did not specify which intervention was favoured by the analysis, stating only that “The difference between the melatonin and control groups with regard to the severity of delirium and based on the MDAS was statistically significant (P=0.003) (p. 123).”20
Adjunct Interventions for Delirium
Two of the RCTs included in this review reported on adjunct interventions required to manage delirium in patients (sample sizes ranging from 28 patients to 841 patients with various diagnoses and reasons for admission, and mean ages among treatment groups ranging from 61.9 years to 86.1 years) who received either melatonin (dosages ranging from 4 mg to 5 mg per day) or matching placebo for a range of 7 days to 14 days of follow-up.18,21 One of the RCTs included enteral administration of the study drugs,18 and the other investigated orally administered study drugs.21 Both studies reported no statistically significant differences between treatment groups in the need for either rescue medications or restraints.18,21
Prevention of Delirium
All 6 of the studies reporting on the clinical effectiveness of melatonin compared with placebo or usual care described 1 outcome relevant to the prevention of delirium (i.e., occurrence of delirium).16,18-21,23
Occurrence of Delirium
Four of the 6 studies reporting on the occurrence of delirium showed no difference between the melatonin and placebo or usual care treatment groups,16,18,20,21 including pooled results reported in the included SR combining data from 9 RCTs representing 1,285 patients, which generated a risk ratio (RR) of 0.67 (95% confidence interval [CI], 0.41 to 1.09).16 Among the individual RCTs included in the SR, 5 of 9 RCTs pooled in the MA investigating the occurrence of delirium showed no statistically significant difference between melatonin and placebo, with 4 of 9 RCTs finding a statistically significant difference favoured melatonin.16 A subgroup analysis focusing on only medical patients also did not demonstrate any statistically significant difference between the treatment groups (RR = 0.88; 95% CI, 0.15 to 5.31).16
The 2 studies that produced a statistically significant difference between treatment groups both indicated a benefit of melatonin compared with placebo.19,23
Mortality
All-Cause Mortality
One SR and 3 RCTs presented data describing all-cause mortality in patients receiving melatonin versus placebo.16,18,19,23 None of the RCTs (either those included in the SR or those included in this review) found a statistically significant difference between treatment groups in the number of deaths among study participants.16,18,19,23
Health Care Utilization
One SR and 4 RCTs included in this review reported on the clinical effectiveness of melatonin compared with placebo or usual care by describing 2 outcomes relevant to the health care utilization (i.e., lengths of stay in hospital and/or ICU).16,18-20,23
Length of Stay in Hospital
One SR and 3 RCTs investigated the effect of melatonin compared with placebo on the LOS in hospital. The 3 RCTs were clear about measuring this outcome in days,18,19,23 the SR did not report the unit of measurement.16 Study sample sizes across the 5 eligible RCTs described in the SR and the 3 RCTs included in this review ranged from 87 patients to 841 patients with mean ages from 50 years to 84 years with various diagnoses and reasons for admission.16,18,19,23 Dosages of melatonin ranged from 0.5 mg to 5 mg per day,16,18,19,23 with 1 study investigating the use of study drugs administered enterally18 and the other 3 describing orally administered study medications.16,19,23 Of the 5 RCTs included in the SR that reported on this outcome, none reported a statistically significant difference in length of hospital stay between the melatonin and placebo treatment groups.16 Of the 3 RCTs included in this review that reported data on mean number of days in hospital, 2 reported a statistically significant benefit for patients receiving melatonin (P = 0.01 in both studies, although the data were subject to an apparent error in 1 of these reports23),19,23 whereas the third found no significant difference in the median days hospitalized between the treatment groups (P = 0.816).18
Length of Stay in ICU
The SR and 2 RCTs included in this review reported on duration of stay in the ICU.16,18,20 As with the outcome measuring LOS in hospital, the SR did not explicitly report the unit of measurement for this outcome,16 whereas the 2 RCTs were clear about reporting this outcome in mean number of days.18,20 The SR also published what appeared to be a typographical error in the forest plot for this outcome, indicating that the intervention arm was “tryptophan”; however, there is no other mention of tryptophan in the article. One of the primary studies from the forest plot was retrieved to verify that the intervention was, in fact, melatonin.16 Study sample sizes across the 3 eligible RCTs described in the SR and the 2 RCTs included in this review ranged from 36 patients to 841 patients with mean ages between 50 years and 84 years and various diagnoses and reasons for admission.16,18,20 Dosages of melatonin ranged from 0.5 mg to 5 mg per day,16,18,20 with 1 study investigating the use of study drugs administered enterally18 and the other 2 describing orally administered study medications.16,20 Of the 3 RCTs included in the SR that reported on this outcome, none reported a statistically significant difference in LOS in the ICU between the melatonin and placebo treatment groups.16 And of the 2 RCTs included in this review that reported data on number of days in hospital, 1 reported a statistically significant benefit for patients receiving melatonin (P = 0.04),20 whereas the other found no significant difference in the median days hospitalized between the treatment groups (P = 0.135).18
Safety
One SR and 4 RCTs included in this review reported on the safety of melatonin compared with placebo or usual care by describing 2 relevant outcomes: AEs and SAEs.16,18-20,23
Adverse Events
The SR and 3 RCTs reported on a variety of AEs, from measures of liver function,16,18 gastrointestinal symptoms,16,19 hallucinations and/or nightmares,16 falls, and new pressure areas.21 One RCT of 841 patients administered 4 mg per day for 14 days (or until ICU discharge) enterally to patients with a variety of diagnoses and reasons for admissions, and found no statistically significant differences in 3 measures of liver function: bilirubin, alanine transferase, and alkaline phosphatase.18 Another RCT including 497 patients measured mild liver dysfunction and found a statistically significant difference (P value not reported, i.e., reported narratively only) between the treatment groups that favoured placebo (melatonin group = 25 patients; as placebo group = 16 patients).19 The 2 studies reporting on diarrhea and gastrointestinal disorders were nonspecific in the description of their findings, with 1 RCT stating only that 2 patients in the melatonin group experienced diarrhea (and not reporting on the placebo group)19 and the SR describing gastrointestinal disorders as common in the melatonin group (with no information on the placebo group) from a narrative synthesis of 2 RCTs.16 Another RCT of 28 older adult patients with various diagnoses and reasons for hospital admission found no occurrences of new pressure areas, and reported 2 patients who experienced a fall in the melatonin group compared with no patients in the placebo group, but the difference was not statistically significant (P = 0.485).21
Severe Adverse Events
Two RCTs included in this review reported on the numbers of patients experiencing any SAE.18,20 Both studies included patients with median ages in the early sixties and representing a variety of diagnoses and reasons for hospital admission, with 1 RCT reporting findings on 841 patients18 and the other on 60 patients.20 Dosages of melatonin were 3 mg per day administered orally20 and 4 mg per day administered enterally.18 No SAEs were reported in either the melatonin or placebo groups in the larger study,18 and no SAEs were reported in the melatonin group in the smaller study (with no data reported on the placebo group).20
Clinical Effectiveness of Melatonin Versus Antipsychotic Drugs for the Treatment or Prevention of Delirium
No relevant evidence describing the clinical effectiveness of melatonin compared with antipsychotic drugs for the treatment or prevention of delirium was identified; therefore, no summary can be provided.
Clinical Effectiveness of Melatonin Versus Cholinergic Agents for the Treatment or Prevention of Delirium
No relevant evidence describing the clinical effectiveness of melatonin compared with cholinergic agents for the treatment or prevention of delirium was identified; therefore, no summary can be provided.
Clinical Effectiveness of Melatonin Versus Dexmedetomidine for the Treatment or Prevention of Delirium
Treatment of Delirium
The RCT describing the clinical effectiveness of melatonin (5 mg/day) plus dexmedetomidine as compared with dexmedetomidine only in older adults following coronary artery bypass graft surgery described outcomes relevant to the treatment of delirium (i.e., duration and adjunct interventions for the management of delirium).22
Duration of Delirium
Mean hours of delirium were measured across 4 days of follow-up, although the unit of analysis in the tabulated-only results was unclear (e.g., per patient versus per episode of delirium, and so on) with a statistically significant mean difference between treatment groups reported in favour of the melatonin plus dexmedetomidine group (mean difference = –23.5; standard error [SE] = 6.2; 95% CI, −36.5 to −10.5; P = 0.001).22 This finding was corroborated by a Kaplan-Meier survival analysis of time to recovery from delirium, showing a statistically significant benefit of melatonin added to dexmedetomidine compared with dexmedetomidine alone (P < 0.001).22
Adjunct Interventions for Delirium
The RCT also presented data on the need for haloperidol among the subset of patients in the study who experienced delirium (n = 21) and reported no statistically significant differences between melatonin plus dexmedetomidine versus dexmedetomidine alone (RR = 0.56; 95% CI, 0.17 to 1.85; P = 0.361).22
Prevention of Delirium
This RCT also described outcomes relevant to the prevention of delirium (i.e., occurrence and time to onset of delirium).22
Occurrence of Delirium
The study reported a statistically significant benefit of melatonin plus dexmedetomidine compared with dexmedetomidine alone in the proportion of patients who experienced delirium (RR = 0.40; 95% CI, 0.17 to 0.95; P = 0.029).22
Time to Onset of Delirium
This RCT also reported a statistically significant benefit in favour of melatonin plus dexmedetomidine compared with dexmedetomidine alone in both the mean hours to onset of delirium (mean difference = 23.1; SE = 7.7; 95% CI, 7.0 to 39.2; P = 0.007) and the probability of not experiencing delirium across 96 hours of follow-up (P = 0.020).22
Health Care Utilization
The RCT comparing melatonin plus dexmedetomidine to dexmedetomidine alone also described health care utilization outcomes, specifically, lengths of hospital and ICU stays.22
Length of Stay in Hospital
Although results from this RCT showed fewer mean days in hospital in the group that received melatonin plus dexmedetomidine versus the group that received dexmedetomidine alone (mean = 11.9 [SE = 5.3] days versus mean = 13.8 [SE = 6.2] days, respectively), the difference between the treatment groups was not statistically significant (P = 0.096).22
Length of Stay in ICU
The RCT also did not report a statistically significant difference in mean days admitted to the ICU between the group that received melatonin plus dexmedetomidine versus the group that received dexmedetomidine alone (mean difference = −0.5; SE = 0.3; 95% CI, −1.1 to 0.2; P = 0.160).22
Guidelines
The international guideline included in this review published 2 recommendations addressing melatonin for the prevention and treatment of sleep and circadian rhythm disorders associated with delirium.17 The first recommendation indicates that dosages of between 2 mg and 5 mg (depending on whether the medication is immediate release compared with prolonged release) may be useful for the treatment of delirium, but that the evidence remains inadequate to support consensus among the expert panel to establish a recommendation that can be used in clinical practice.17 Similarly, the recommendation addressing prevention of delirium suggests that dosages between 2 mg and 5 mg (depending on whether the medication is immediate release or prolonged release) taken before bedtime may be useful for at-risk populations, but that the evidence remains inadequate to support consensus among the expert panel to establish a recommendation that can be used in clinical practice.17
The recommendations were based on evidence identified from a SR of the literature and included 3 SRs and 1 scoping review.17 There was no information provided describing the quality of these reviews, neither was there information provided concerning the strength of the recommendations.17
The data from the included studies by outcome are presented in Appendix 4.
Limitations
This review identified 7 studies describing the clinical effectiveness of melatonin compared with placebo for the treatment and/or prevention of delirium,15,16,18-21,23 but is limited to 1 study of 60 patients describing the clinical effectiveness of melatonin compared with another intervention (i.e., melatonin plus dexmedetomidine versus dexmedetomidine alone).22 No evidence was found comparing melatonin with either antipsychotic medications or cholinesterase inhibitors. Further, there is limited available guidance to inform the use of melatonin for the treatment and/or prevention of delirium with 1 evidence-based guideline identified that had a broader scope than the current review and contained limited relevant information.17
Clinical heterogeneity between the study populations of several RCTs (i.e., within-study heterogeneity) was a common feature in this review,18,20,21 including various patient characteristics, such as age, diagnosis, and reason(s) for admission. This type of clinical heterogeneity can impact the treatment effect that is observed, either inflating or nullifying the effectiveness of an intervention.31 For this review, a variety of patients with a range of characteristics were examined within several of the included RCTs.18,20,21 Although it is beyond the scope of this narrative synthesis review to investigate the extent to which these broadly variable patient populations may or may not have affected the effects or effect sizes that were observed within the included studies, it is a potential limitation worth considering when interpreting the findings of this report.
In addition, clinical heterogeneity was identified between the included RCTs in this review (i.e., between-study heterogeneity),18-21,23 with significant statistical heterogeneity identified in the SR that included and/or reported on meta-analyses.16 Specifically, different patient groups across the studies (e.g., a variety of diagnoses, age groups, and types of reasons for admission to hospital), receiving different dosages of melatonin, using different modes of administration, across various durations of follow-up; and may be a contributing factor to the inconsistency in the findings observed across the trials included in this review.18-21,23 Clinical heterogeneity can also contribute to statistical heterogeneity, the latter of which was identified as significant in both the overview and SR included in this review.16 Notably, this problematic degree of heterogeneity has been identified in other similar reviews that were not eligible for inclusion in the current report,32,33 suggesting this may be a common current challenge within this body of evidence. Specific to this review, these fundamental differences between the studies examining the clinical effectiveness of melatonin for the treatment of delirium in hospitalized patients may be an important limiting factor when considering and interpreting the findings from the studies included in this review and the extent to which they can effectively answer the research questions posed herein.
In addition, authors of 2 of the RCTs included in this review made mention of the uncertainty about the optimal dosage of melatonin for the treatment or prevention of delirium.18,19 The question about dosing of melatonin in the prevention and/or treatment of inpatient delirium appears elsewhere in the literature as well.34 This suggests that there is uncertainty concerning this issue, which supports the need for additional research to help elucidate optimal dosing of melatonin for the treatment or prevention of delirium.
Clinical heterogeneity is also more broadly apparent as it concerns the evidence addressing the role of melatonin in the prevention and/or treatment of delirium, that is, the frequency with which melatonin receptor agonists are investigated in combination, particularly melatonin and Ramelteon,35-39 (including the reviews included in this study15,16). Currently, Ramelteon is not available in Canada,40 making these combined data less relevant to the Canadian context; evidence that did not present data specific to melatonin only limited the ability to answer research questions specific to the clinical effectiveness of melatonin in a Canadian context.
Finally, because it concerns the evidence describing clinical effectiveness, small sample sizes and important methodological limitations observed in several of the included trials in this review and their reports of findings20-22 limits the usefulness of these studies in answering the research questions and informing an understanding of the clinical effectiveness of melatonin for the prevention and/or treatment of delirium.
Conclusions and Implications for Decision- or Policy-Making
This review identified a large body of evidence addressing the use of melatonin for the prevention and/or treatment of delirium, but limited the eligible studies to those most recently published between 2021 and 2022. One overview of MAs, 1 SR, 6 RCTs and 1 evidence-based guideline were identified and summarized. As with other evidence syntheses and literature sources that have been published on this topic,32,33,35,37 this review found variability in the findings and conclusions of included studies, making it difficult to establish any conclusive interpretations about the available evidence. This level of uncertainty seems to be a hallmark of the evidence in this area3,4 and may be due to several factors, most notably clinical heterogeneity within and between studies, which also contributes to statistical heterogeneity in quantitative evidence syntheses.
The evidence is reasonably dichotomous (i.e., studies in this review generally report either no difference between melatonin and placebo18 or some benefit of melatonin).19,23 This, combined with limited evidence of harms caused by melatonin and the limited evidence on the clinical effectiveness of melatonin compared with other interventions, supports continued research into the clinical effectiveness of this intervention.
In addition to the variability in clinical factors within and between studies that have been suggested in the limitations portion of this report, other sources of heterogeneity may be present and have been posited in the literature, such as there may be clinically important variability in the quality and potency of melatonin products given their non-pharmacological production and classification.3 This is only 1 possibility among many that may affect the clarity of the evidence in this area of research.
There have been multiple calls for more research investigating the clinical effectiveness of melatonin for the prevention and/or treatment of delirium in hospitalized patients.4,35 The evidence identified in this review did share some important methodological components that may benefit future efforts to effectively synthesize quantitative data or the similar comparators across multiple studies (i.e., placebo or usual care) and frequently used outcome measures (e.g., the CAM, CAM-ICU, and MDAS). Future research investigating the role of melatonin in the prevention and/or treatment of delirium is likely to benefit from larger sample sizes and more homogeneous study patient populations.4,41
References
1.Francis J. Delirium and acute confusional states: Prevention, treatment, and prognosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 Apr 17.
2.Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825-e873. PubMed
3.Endriukaitis L. Is melatonin an effective treatment option for the prevention of hospital-induced delirium? Chicago (IL): Drug Information Group, Deparment of Pharmacy Practice, University of Illinois Chicago; 2020: https://dig.pharmacy.uic.edu/faqs/2020-2/february-2020-faqs/is-melatonin-an-effective-treatment-option-for-the-prevention-of-hospital-induced-delirium/. Accessed 2022 Apr 17.
4.Sigaut S, Couffignal C, Esposito-Farese M, et al. Melatonin for prevention of postoperative delirium after lower limb fracture surgery in elderly patients (DELIRLESS): study protocol for a multicentre randomised controlled trial. BMJ Open. 2021;11(12):e053908. PubMed
5.Marcantonio ER. Delirium in hospitalized older adults. N Engl J Med. 2017;377(15):1456-1466. PubMed
6.Wan M, Chase J. Delirium in older adults: Diagnosis, prevention, and treatment. BC Med J. 2017;59(3):165-170. https://bcmj.org/articles/delirium-older-adults-diagnosis-prevention-and-treatment. Accessed 2022 Apr 17.
7.Bush SH, Lawlor PG, Ryan K, et al. Delirium in adult cancer patients: ESMO Clinical Practice Guidelines. Ann Oncol. 2018;29(Suppl 4):iv143-iv165.
8.Siddiqi N, Harrison JK, Clegg A, et al. Interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2016;3:CD005563. PubMed
9.Daniels LM, Nelson SB, Frank RD, Park JG. Pharmacologic treatment of intensive care unit delirium and the impact on duration of delirium, length of intensive care unit stay, length of hospitalization, and 28-day mortality. Mayo Clin Proc. 2018;93(12):1739-1748. PubMed
10.Grover S, Dua D, Sahoo S, Chakrabarti S, Avasthi A. Effectiveness of melatonin in the management of delirium: A retrospective study. J Mental Health Hum Behav. 2019;24(2):78-84. https://www.jmhhb.org/article.asp?issn=0971-8990;year=2019;volume=24;issue=2;spage=78;epage=84;aulast=Grover;type=0. Accessed 2022 Apr 17.
11.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
12.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
13.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Mar 23.
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
15.Blodgett TJ, Blodgett NP. Melatonin and melatonin-receptor agonists to prevent delirium in hospitalized older adults: An umbrella review. Geriatr Nurs. 2021;42(6):1562-1568. PubMed
16.Khaing K, Nair BR. Melatonin for delirium prevention in hospitalized patients: A systematic review and meta-analysis. J Psychiatr Res. 2021;133:181-190. PubMed
17.Palagini L, Manni R, Aguglia E, et al. International expert opinions and recommendations on the use of melatonin in the treatment of insomnia and circadian sleep disturbances in adult neuropsychiatric disorders. Front Psychiatry. 2021;12:688890. PubMed
18.Wibrow B, Martinez FE, Myers E, et al. Prophylactic melatonin for delirium in intensive care (Pro-MEDIC): a randomized controlled trial. Intensive Care Med. 2022;27:27. PubMed
19.Yin B, Ye T, Liu X, Wan R, Gu L, Zong G. Effects of melatonin for delirium in elderly acute heart failure patients: a randomized, single-center, double-blind, and placebo-controlled trial. Heart Surg Forum. 2022;25(1):E037-E041. PubMed
20.Javaherforoosh Zadeh F, Janatmakan F, Shafaeebejestan E, Jorairahmadi S. Effect of melatonin on delirium after on-pump coronary artery bypass graft surgery: a randomized clinical trial. Iran J Med Sci. 2021;46(2):120-127. PubMed
21.Lange PW, Clayton-Chubb DI, Watson R, Maier AB. Results from a double blinded, randomised, placebo-controlled, feasibility trial of melatonin for the treatment of delirium in older medical inpatients. Intern Med J. 2021;51(1):33-41. PubMed
22.Mahrose R, ElSerwi H, Maurice A, Elsersi M. Postoperative delirium after coronary artery bypass graft surgery: Dexmedetomidine infusion alone or with the addition of oral melatonin. Egyptian J Anaesthesia. 2021;37(1):62-68.
23.Shi Y. Effects of melatonin on postoperative delirium after PCI in elderly patients: a randomized, single-center, double-blind, placebo-controlled trial. Heart Surg Forum. 2021;24(5):E893-E897. PubMed
24.Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941-948. PubMed
25.Inouye SK, Kosar CM, Tommet D, et al. The CAM-S: development and validation of a new scoring system for delirium severity in 2 cohorts. Ann Intern Med. 2014;160(8):526-533. PubMed
26.Breitbart W, Rosenfeld B, Roth A, Smith MJ, Cohen K, Passik S. The Memorial Delirium Assessment Scale. J Pain Symptom Manage. 1997;13(3):128-137. PubMed
27.Page MJ, Moher D, Fidler FM, et al. The REPRISE project: protocol for an evaluation of REProducibility and Replicability In Syntheses of Evidence. Syst Rev. 2021;10(1):112. PubMed
28.Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. PubMed
29.Gagnier JJ, Moher D, Boon H, Beyene J, Bombardier C. Investigating clinical heterogeneity in systematic reviews: a methodologic review of guidance in the literature. BMC Med Res Methodol. 2012;12(1):111. PubMed
30.Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. J Clin Epidemiol. 2010;63(12):1308-1311. PubMed
31.West SL, Gartlehner G, Mansfield AJ, et al. Comparative effectiveness review methods: clinical heterogeneity. Rockville (MD): Agency for Healthcare Research and Quality (AHRQ); 2010: https://www.ncbi.nlm.nih.gov/books/NBK53317/. Accessed 2022 Apr 17.
32.Ng KT, Teoh WY, Khor AJ. The effect of melatonin on delirium in hospitalised patients: A systematic review and meta-analyses with trial sequential analysis. J Clin Anesth. 2020;59:74-81. PubMed
33.Asleson DR, Chiu AW. Melatonin for delirium prevention in acute medically ill, and perioperative geriatric patients. Aging Med (Milton). 2020;3(2):132-137. PubMed
34.Campbell AM, Axon DR, Martin JR, Slack MK, Mollon L, Lee JK. Melatonin for the prevention of postoperative delirium in older adults: a systematic review and meta-analysis. BMC Geriatr. 2019;19(1):272. PubMed
35.Zhang Q, Gao F, Zhang S, Sun W, Li Z. Prophylactic use of exogenous melatonin and melatonin receptor agonists to improve sleep and delirium in the intensive care units: a systematic review and meta-analysis of randomized controlled trials. Sleep Breath. 2019;23(4):1059-1070. PubMed
36.Han Y, Wu J, Qin Z, et al. Melatonin and its analogues for the prevention of postoperative delirium: A systematic review and meta-analysis. J Pineal Res. 2020;68(4):e12644. PubMed
37.Lewandowska K, Malkiewicz MA, Sieminski M, Cubala WJ, Winklewski PJ, Medrzycka-Dabrowska WA. The role of melatonin and melatonin receptor agonist in the prevention of sleep disturbances and delirium in intensive care unit - a clinical review. Sleep Med. 2020;69:127-134. PubMed
38.Yang CP, Tseng PT, Pei-Chen Chang J, Su H, Satyanarayanan SK, Su KP. Melatonergic agents in the prevention of delirium: A network meta-analysis of randomized controlled trials. Sleep Med Rev. 2020;50:101235. PubMed
39.Walker CK, Gales MA. Melatonin receptor agonists for delirium prevention. Ann Pharmacother. 2017;51(1):72-78. PubMed
40.CAMH. Sleep disorders - pharmacotherapy. 2022; https://www.camh.ca/en/professionals/treating-conditions-and-disorders/sleep-disorders/sleep-disorders---treatment/sleep-disorders---pharmacotherapy. Accessed 2022 Apr 17.
41.Lawlor PG, McNamara-Kilian MT, MacDonald AR, et al. Melatonin to prevent delirium in patients with advanced cancer: a double blind, parallel, randomized, controlled, feasibility trial. BMC Palliat Care. 2020;19(1):163. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Overview of Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Blodgett et al. (2021)15 US Funding reported as follows: “This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.”(p. 1567) | Studies included:
Studies eligible for this report:
| Patients included (N = 2,859):
| Interventions included:
Comparators included:
| Outcomes:
Follow-up:
|
ICU = intensive care unit; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
Table 3: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Khaing et al. (2021)16 Australia Funding: Reported as none | Studies included:
Studies eligible for this report:
| Patients included (N = 1,712):
Patients eligible for this report (N = 1,303):
| Interventions included:
Interventions eligible for this report:
Comparators eligible for this report:
| Outcomes:
Follow-up:
|
ICU = intensive care unit; RCT = randomized controlled trial.
Table 4: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and | Clinical outcomes, |
|---|---|---|---|---|
Wibrow et al. (2022)18 Australia Funding: The Western Australia department of health; John Hunter Charitable Trust Fund | Multicentre (N = 12), double-blind, placebo-controlled RCT (Pro-MEDIC trial) | Adults ≥ 18y (N = 847 randomized; N = 841 analyzed) admitted to the ICU with an expected LOS of at least 72 hours Age, mean years (SD) Intervention: 61.9 (15.1) Control: 61.9 (15.2) Male sex, n pt (%) Intervention: 247 (59.1) Control: 280 (66.4) Regular alcohol use, n pt (%) Intervention: 141 (33.7) Control: 164 (38.9) Positive CAM at baseline, n pt (%) Intervention: 40 (9.6) Control: 35 (8.3) Elective admission, n pt (%) Intervention: 36 (8.6) Control: 41 (9.7) Emergency admission, n pt (%) Intervention: 343 (81.9) Control: 338 (80.1) Surgical admission, n pt (%) Intervention: 100 (23.9) Control: 113 (26.8) Medical admission, n pt (%) Intervention: 191 (45.6) Control: 197 (46.7) | Melatonin, 4 mg per day, administered enterally in the evening (n = 423 randomized; n = 419 analyzed) Placebo (matching) (n = 424 randomized; n = 422 analyzed) | Outcomes: Primary:
Secondary:
Follow-up:
Mortality: 28 days, 90 days |
Yin et al. (2022)19 China Funding: Top Talent Support Program for Young and Middle-Aged People of Wuxi Health Committee | Single-centre, double-blind, placebo-controlled RCT | Elderly adults ≥ 60 years with acute heart failure admitted to the ICU (N = 497 randomized; N = 480 with complete follow-up) Age, mean years (SD) Intervention: 69.1 (7.5) Control: 68.5 (7.1) Male sex, n pt (%) Intervention: 152 (61.3) Control: 143 (57.4) History of hypertension, n pt (%) Intervention: 184 (74.2) Control: 195 (78.3) Nicotine use, n pt (%) Intervention: 68 (27.4) Control: 72 (28.9) | Melatonin, 3 mg per day, administered orally (n = 248 randomized; n = 236 with complete follow-up) Placebo (n = 249 randomized; n = 244 with complete follow-up) | Outcomes: Primary:
Secondary:
Follow-up: Primary outcome: 7 days treatment regimen and follow-up Mortality: 30 days |
Javaherforoosh et al. (2021)20 Iran Funding: NR | Single-centre, double-blind, placebo-controlled RCT | Adults ≥ 30y following on-pump CABG (N = 60 randomized; N = 60 analyzed) Age, mean years (SD) Intervention: 60.26 (9.50) Control: 62.9 (8.08) Male sex, n pt (%) Intervention: 20 (66.6) Control: 22 (73.3) EuroSCORE, mean % (SD) Intervention: 2.63 (2.65) Control: 2.86 (2.83) History of hypertension, n pt (%) Intervention: 26 (86.6) Control: 29 (96.6) Smoking, n pt (%) Intervention: 10 (33.3) Control: 12 (40) Opium addiction, n pt (%) Intervention: 4 (13.3) Control: 6 (20) | Melatonin, 3 mg, administered orally on the evening and morning before surgery, and until the second postoperative day (n = 30 randomized and analyzed) Placebo (matching) (n = 30 randomized and analyzed) | Outcomes: Primary:
Secondary:
Follow-up: NR |
Lange et al. (2021)21 Australia Funding: Health-e-care pty ltd; Royal Melbourne Hospital | Single-centre, double-blind, placebo-controlled feasibility RCT | Elderly adult ≥ 70 years medical inpatients with delirium (N = 29 randomized; N = 28 analyzed) Age, mean years (SD) Intervention: 85.1 (6.5) Control: 86.1 (4.4) Female sex, n pt (%) Intervention: 8 (61.5) Control: 7 (46.7) Baseline MDAS, mean (SD) Intervention: 14.4 (6.7) Control: 16.7 (4.6) History of delirium, n pt (%) Intervention: 0 (0) Control: 2 (13.3) History of depression, n pt (%) Intervention: 4 (30.8) Control: 0 (0) History of dementia, n pt (%) Intervention: 6 (46.2) Control: 8 (53.3) Current smoker, n pt (%) Intervention: 0 (0) Control: 1 (6.7) Any alcohol use, n pt (%) Intervention: 4 (30.8) Control: 3 (20.0) | Melatonin, 5 mg/day, administered orally in the evening (n = 14 randomized and analyzed) Placebo (matching) (n = 15 randomized and n = 14 analyzed) | Outcomes: Primary:
Secondary:
Follow-up: Primary outcome: 5 days treatment regimen and follow-up Secondary outcomes: 7 days |
Mahrose et al. (2021)22 Egypt Funding: NR | RCT (information describing the setting[s] and the use of blinding were NR) | Adults ≥ 60y following CABG (N = 110 randomized and analyzed) Age, mean ears (SD) Intervention: 67.0 (6.7) Control: 66.1 (6.3) Male sex, n pt (%) Intervention: 42 (76.4) Control: 41 (74.5) Smoking, n pt (%) Intervention: 25 (45.5) Control: 29 (52.7) Hypertension, n pt (%) Intervention: 39 (70.9) Control: 26 (47.3) | Melatonin, 5 mg per day, administered orally on the evening before surgery, and every 24 hours until the third postoperative day, plus; dexmedetomidine, 20 minutes postoperative bolus of 0.4 mcg/kg upon arrival in the ICU, followed by 0.2 to 0.7 mcg/kg/h for a maximum 24 hours; patients with delirium who were severely agitated were also treated with IV haloperidol (increments of 1 to 5 mg every 30 to 60 minutes) as needed (n = 55 randomized and analyzed) Dexmedetomidine, 20 minutes postoperative bolus of 0.4 mcg/kg, upon arrival in the ICU, followed by 0.2 to 0.7 mcg/kg/hour for a maximum 24 hours; patients with delirium who were severely agitated were also treated with IV haloperidol (increments of 1 to 5mg every 30 to 60 minutes) as needed (n = 55 randomized and analyzed) | Outcomes: Primary:
Other outcomes:
Follow-up: Primary outcome: 5 days Onset and duration of delirium: 4 days 4 days |
Shi et al. (2021)23 China Funding: NR | Single-centre, double-blind, placebo-controlled RCT (with ITT analyses) | Adults > 60 years in the ICU following PCI (N = 297 randomized and N = 285 analyzed) Age, mean years (SD) Intervention: 71.5 (6.7) Control: 71.6 (6.6) Male sex, n pt (%) Intervention: 93 (62.8) Control: 89 (59.7) Nicotine use, n pt (%) Intervention: 45 (30.4) Control: 49 (32.9) History of hypertension, n pt (%) Intervention: 106 (71.6) Control: 112 (75.2) | Melatonin, 3 mg per day, administered orally for 7 days (n = 148 randomized and n = 143 completed follow-up) Placebo (matching) (n = 149 randomized and n = 142 completed follow-up) | Outcomes: Primary:
Secondary:
Follow-up: Primary outcome: 7 days Mortality: 30 days |
CABG = coronary artery bypass; CAM = Confusion Assessment Method; CAM-ICU = Confusion Assessment Method for the Intensive Care Unit; EuroSCORE = European System for Cardiac Operative Risk Evaluation; h = hour(s); ICU = intensive care unit; ITT = intention-to-treat; LOS = length of stay; MDAS = Memorial Delirium Assessment Scale; min = minute(s); NR = not reported; PCI = percutaneous transluminal coronary intervention; Pro-MEDIC = prophylactic melatonin for delirium in intensive care; pt = patient(s); RCT = randomized controlled trial; SD = standard deviation
Table 5: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality | Recommendations | Guideline validation |
|---|---|---|---|---|---|---|
Palagini et al. (2021)17 | ||||||
Intended users: Those in psychiatric clinical practice Target population: Adults with neuropsychiatry disorders having insomnia and/or circadian sleep disturbances | Melatonin | Effectiveness of melatonin for the treatment of insomnia and/or circadian sleep disturbances (including delirium) | SR using 3 databases; 2 researchers conducted the review | Evidence is described as having been critically appraised, but methods for doing so are not described | A modified Delphi approach using a panel of experts to review and iteratively develop recommendations | Consensus among the panel of experts was reached for each recommendation before publication |
SR = systematic review.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Overview of Systematic Reviews
Strengths | Limitations |
|---|---|
Blodgett (2021)15 | |
PICOS described within the research objectives and questions. Authors reported developing a protocol describing the methods a priori. A comprehensive literature search strategy was described. Study selection at the title and abstract stage was performed in duplicate. There was an implicit rationale provided to justify the inclusion of MAs as the eligible study design. The rationales for exclusion of sources were reported aggregately in the PRISMA diagram. Overlap between the primary studies of included SRs was mentioned. Risk of bias was assessed using the AMSTAR-211 checklist. Data abstraction was performed in duplicate. Heterogeneity and risk of bias were discussed in the interpretation of results. | Study selection at the full-text stage was not clearly described. Excluded studies were not listed. Overlap between the primary studies of included SRs was briefly mentioned but no citation matrix was presented or methods for avoiding over-representation of overlapped studies was discussed. Heterogeneity among included studies was identified as being significant. Sources of funding for included studies were not reported. The source of funding for the review was not clearly reported. |
AMSTAR-2 = A MeaSurement Tool to Assess systematic Reviews 2; MA = meta-analysis; PRISMA = Preferred Reporting Items of Systematic Reviews and Meta-Analyses; SR = systematic review.
Table 7: Strengths and Limitations of Systematic Review
Strengths | Limitations |
|---|---|
Khaing et al. (2021)16 | |
PICOS described within the research aim and methods section. A comprehensive literature search strategy was described. Included studies described in sufficient detail. Satisfactory methods were used to conduct risk of bias assessment. Appropriate methods were used for meta-analysis. Heterogeneity was measured and discussed in the interpretation of the findings. Publication bias was assessed. Funding for the review work was reported. | An explicit description of a review protocol or a priori method was not reported. RCTs only were included but a rationale for this limitation was not described. There was no mention of study selection or data abstraction being performed in duplicate. Excluded studies were not listed and the rationales for exclusion were not reported for individual studies. Multiple instances of errors and/or typos in reporting were identified, making interpretation of some findings challenging and unclear. Heterogeneity among included studies was identified as being significant. Sources of funding for included studies were not reported. The potential impact of risk of bias was not discussed in the interpretation of the results of the meta-analyses or the discussion/interpretation of the findings. |
Table 8: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist12
Strengths | Limitations |
|---|---|
Wibrow et al. (2022)18 | |
Reporting
External validity
Internal validity
Study power
| Reporting Adverse events not clearly reported. External validity
Other
|
Yin et al. (2022)19 | |
Reporting
External validity
Internal validity
Study power
| Other
|
Javaherforoosh et al. (2021)20 | |
Reporting
External validity
Internal validity
| Reporting
Internal validity
Study power
Other
|
Lange et al. (2021)21 | |
Reporting
External validity
Internal validity
| Reporting
External validity
Internal validity
Study power
Other
|
Mahrose et al. (2021)22 | |
Reporting
External validity
Internal validity
Study power
| Reporting
External validity
Internal validity
|
Shi et al. (2021)23 | |
Reporting
External validity
Internal validity
Study power
| Reporting
Other
|
RCT = randomized controlled trial.
Table 9: Strengths and Limitations of Guideline Using AGREE II13
Item | Palagini et al. (2021)17 |
|---|---|
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes (though, only implicitly) |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes (i.e., multidisciplinary) |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No (not reported) |
6. The target users of the guideline are clearly defined. | Unclear (not explicitly stated) |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | No (not reported) |
10. The methods for formulating the recommendations are clearly described. | Unclear (not explicitly described) |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Unclear (not explicitly described) |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Unclear (not explicitly described) |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | No |
16. The different options for management of the condition or health issue are clearly presented. | No |
17. Key recommendations are easily identifiable. | No |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 10: Summary of Findings for Clinical Effectiveness — Treatment of Delirium
Study citation and design | Outcomes |
|---|---|
Duration of delirium | |
Khaing et al. (2021)a16 SR (5 RCTs eligible for this report from an MA of 6 RCTs i.e., 1 of which investigated Ramelteon) | Ford 2020 (N = 202 of 210 patients), 7 days treatment regimen
|
Abbasi 2018 (N = 172 patients), 5 days treatment regimen
| |
Jaiswal 2018 (N = 87 patients), 14 days treatment regimen
| |
de Jonghe 2014 (N = 378 patients), 5 days treatment regimen
| |
Al-Aama 2011 (N = 122 patients), 14 days treatment regimen
| |
Mahrose et al. (2021)22 RCT | Hours of deliriumb across 4 days follow-up, mean (SD)
Kaplan-Meier survival analysis of time to recovery from delirium across 96 h follow-up, h
|
Adjunct interventions for delirium | |
Wibrow et al. (2022)18 RCT | Patients (N = 841 patients) who required antipsychotic drugs across 14 days follow-up, n (%)
Patients (N = 841 patients) who required sedatives across 14 days follow-up, n (%)
Patients (N = 841 patients) who required physical restraints across 14 days follow-up, n (%)
|
Lange et al. (2021)21 RCT | Restraints used (N = 28 patients; unit of measure NR), 5 days follow-up
Rescue medication used (N = 28 patients; unit of measure NR), 5 days follow-up
|
Mahrose et al. (2021)22 RCT | Patients with delirium (N = 21) requiring haloperidol, follow-up NR, n (%)
|
Severity of delirium | |
Wibrow et al. (2022)18 RCT | CAM-S scores (N = 841 patients), follow-up NR, mean (SD)
|
Javaherforoosh et al. (2021)20 RCT | Difference between treatment groups in MDAS scores (N = 60 patients)
|
Lange et al. (2021)21 RCT | Difference in MDAS (N = 28 patients), baseline (day 0) to treatment (days 1 to 5), mean (SD)
Difference in MDAS (N = 28 patients), treatment (days 1 to 5) to post-treatment (days 6 to 7), mean (SD)
|
CAM = Confusion Assessment Method; CAM-ICU = Confusion Assessment Method for the Intensive Care Unit; CI = confidence interval; ICU = intensive care unit; MDAS = Memorial Delirium Assessment Scale; NR = not reported; NS = not significant; RCT = randomized controlled trial; RR = relative risk; SD = standard deviation; SE = standard error; SR = systematic review.
aThese data were reported for both the duration of delirium and days in hospital outcomes in this article;16 it is unclear whether this is an error.
bThe study report was unclear as to whether the duration of delirium was per patient, per episode of delirium, or some other unit of analysis (i.e., NR)
Table 11: Summary of Findings for Clinical Effectiveness — Prevention of Delirium
Study citation and design | Outcomes |
|---|---|
Occurrence of delirium | |
Wibrow et al. (2022)18 RCT | Patients (N = 841 patients) who experienced delirium across 14 days follow-up, n/N (%)
Assessments identifying delirium across 14 days follow-up, n/N (%)
Proportion of delirium-free assessments per patient across 14 days follow-up, mean (SD)
Proportion of delirium-free days per patient across 14 days follow-up, mean (SD)
|
Yin et al. (2022)19 RCT | Patients (N = 497) who experienced delirium across 7 days follow-up, n/N (%)
|
Khaing et al. (2021)16 SR (9 RCTs eligible for this report from an MA of 14 RCTs i.e., 5 of which investigated Ramelteon) | Quantitative synthesis of 9 RCTs using MA with fixed effects (N = 1,285 patients)
|
Subgroup analysis of medical patients only from 2 eligible RCTs (14 days treatment regimens), quantitative synthesis using MA with fixed-effects model (N = 209 patients)
| |
Data from RCTs included in the MAs: | |
Abbasi 2018 (N = 172 patients), 5 days treatment regimen
| |
Jaiswal 2018 (N = 87 patients), 14 days treatment regimen
| |
Vijaykumar 2016 (N = 56 patients), 5 days treatment regimen
| |
de Jonghe 2014 (N = 378 patients), 5 days treatment regimen
| |
Al-Aama 2011 (N = 122 patients), 14 days treatment regimen
| |
Nickkholgh 2011 (N = 36 patients), follow-up NR
| |
Sultan 2010 (N = 102 patients), 4 days treatment regimen
| |
Javaherforoosh et al. (2021)20 RCT | Occurrence of delirium (N = 60 patients), day of surgery, n patients (%)
Occurrence of delirium (N = 60 patients), first day post-surgery, n patients (%)
Occurrence of delirium (N = 60 patients), second day post-surgery, n patients (%)
|
Lange et al. (2021)21 RCT | Days with CAM-positive findings (i.e., with delirium; N = 28 patients), median (IQR)
|
Mahrose et al. (2021)22 RCT | Patients who experienced delirium across 5 days follow-up, n (%)
|
Shi et al. (2021)23 RCT | Patients (N = 297) who experienced delirium across 7 days follow-up, n (%)
|
Time to onset of delirium | |
Mahrose et al. (2021)22 RCT | Hours to onset of delirium, mean (SD)
Kaplan-Meier survival analysis, probability of no delirium across 96h follow-up, mean (SD)
|
CAM = Confusion Assessment Method; CI = confidence interval; ICU = intensive care unit; IQR = interquartile range; MA = meta-analysis; NR = not reported; NS = not significant; RCT = randomized controlled trial; RR = relative risk; SD = standard deviation; SE = standard error; SR = systematic review.
Table 12: Summary of Findings for Clinical Effectiveness — Mortality
Study citation and design | Outcomes |
|---|---|
All-cause morality | |
Wibrow et al. (2022)18 RCT | Patients (N = 841 patients) who died in the ICU, n (%)
Survival analysis (N = 841 patients) of mortality in hospital at 90 days follow-up, HR (95% CI)
Mortality at 28 days, n (%)
Mortality at 90 days, n (%)
|
Yin et al. (2022)19 RCT | Mortality at 30 days follow-up, n/N (%)
|
Khaing et al. (2021)16 SR (3 RCTs eligible for this report from an MA of 5 RCTs i.e., 1 of which investigated Ramelteon) | Abbasi 2018 (N = 172 patients), 5 days treatment regimen
|
de Jonghe 2014 (N = 378 patients), 5 days treatment regimen
| |
Al-Aama 2011 (N = 122 patients), 14 days treatment regimen
| |
Shi et al. (2021)23 RCT | Patients who died from any cause across 30 days follow-up, n (%)
|
CI = confidence interval; HR = hazard ratio; ICU = intensive care unit; NS = not significant; RCT = randomized controlled trial; RR = relative risk; SR = systematic review.
Table 13: Summary of Findings for Clinical Effectiveness — Health Care Utilization
Study citation and design | Outcomes |
|---|---|
Length of stay (hospital) | |
Wibrow et al. (2022)18 RCT | Days in hospital (N = 841 patients), median (IQR)
|
Yin et al. (2022)19 RCT | Days in hospital (N = 497 patients), mean (SD)
|
Khaing et al. (2021)a16 SR (5 RCTs eligible for this report from an MA of 6 RCTs i.e., 1 of which investigated Ramelteon) | Ford 2020 (N = 202/210 patients), 7 days treatment regimen
|
Abbasi 2018 (N = 172 patients), 5 days treatment regimen
| |
Jaiswal 2018 (N = 87 patients), 14 days treatment regimen
| |
de Jonghe 2014 (N = 378 patients), 5 days treatment regimen
| |
Al-Aama 2011 (N = 122 patients), 14 days treatment regimen
| |
Mahrose et al. (2021)22 RCT | Days in hospital (N = 110 patients), mean (SE)
|
Shi et al. (2021)23 RCT | Data as tabulated in the report (p. E895): Days per patient (N = 297) in hospital, mean (SD)
Nonetheless, the narrative describing these data are presented as follows in the report of findings: “The mean length of stay in the Mel group was 13.4 days, and the mean length of stay in the placebo group was 15.9 days, which was a statistically significant difference between the two groups (P = 0.01).” (p. E895) Thus, it is unclear whether the data are as per the tabulated findings above, or as per the narrative summary above. |
Length of stay (ICU) | |
Wibrow et al. (2022)18 RCT | Days in ICU (N = 841 patients), median (IQR)
|
Javaherforoosh et al. (2021)20 RCT | Days in ICU (N = 60 patients), mean (SD)
|
Khaing et al. (2021)16 SR (3 RCTs eligible for this report from an MA of 5 RCTs i.e., 2 of which investigated Ramelteon) | Abbasi 2018 (N = 172 patients), 5 days treatment regimen
|
Vijaykumar 2016 (N = 56 patients), 5 days treatment regimen
| |
Nickkholgh 2011 (N = 36 patients), follow-up NR
| |
Mahrose et al. (2021)22 RCT | Days in ICU, mean (SD)
|
CI = confidence interval; ICU = intensive care unit; IQR = interquartile range; LOS = length of stay; MA = meta-analysis; NR = not reported; NS = not significant; RCT = randomized controlled trial; RR = relative risk; SD = standard deviation; SE = standard error; SR = systematic review.
aThese data were reported for both the duration of delirium and days in hospital outcomes in this article;16 it is unclear whether this is an error.
bWhereas the figure from which these data were abstracted indicates the intervention arm as ‘Tryptophan,’ the remainder of the paper refers only to melatonin for these studies and outcomes and has been assumed to be a typo or error in the paper.
Table 14: Summary of Findings for Clinical Effectiveness — Safety
Study citation and design | Outcomes |
|---|---|
Adverse events | |
Wibrow et al. (2022)18 RCT | Measures of liver function (N = 841 patients), median (IQR)
|
Yin et al. (2022)19 RCT | Patients (N = 497) who experienced diarrhea, n
Patients who experienced mild liver dysfunction, n
|
Khaing et al. (2021)16 SR (2 RCTs) | Narrative synthesis of 2 studies, (N = NR patients)
|
Lange et al. (2021)21 RCT | Falls (unit of measurement NR), 5 days follow-up, n
New pressure areas (unit of measurement NR), 5 days follow-up, n
|
Severe adverse events | |
Wibrow et al. (2022)18 RCT | Patients (N = 841) experiencing any severe adverse event, n
|
Javaherforoosh et al. (2021)20 RCT | Patients (N = 60) experiencing any severe adverse event, n
|
GI = gastrointestinal; IQR = interquartile range; NR = not reported; NS = not significant; RCT = randomized controlled trial; RR = relative risk; SR = systematic review.
Table 15: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Palgini et al. (2021)17 | |
Recommendations “The administration of PR melatonin at 2mg or IR melatonin at 2-5mg might be useful in the treatment of insomnia and circadian rhythm disturbances related to delirium, but consensus was uncertain, more studies are needed for recommendation in clinical practice.” (p. 10) “The administration of PR melatonin at 2mg or 3-5mg IR before bedtime might prevent the incidence of delirium in at-risk population, but consensus was uncertain, more studies are needed for recommendation in the clinical practice.” (p. 10) Supporting Evidence
| Quality of evidence
Strength of recommendation
|
IR = immediate release; NR = not reported; PR = prolonged release; SR = systematic review.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Melatonin for the treatment of insomnia: A review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Feb. https://www.cadth.ca/melatonin-insomnia-review-clinical-effectiveness-cost-effectiveness-and-guidelines
Current practice analysis: interventions for insomnia disorder. (CADTH technology review: no.7). Ottawa (ON): CADTH; 2017 Jun. https://www.cadth.ca/current-practice-analysis-interventions-insomnia-disorder-optimal-use-project-june-2017
Sleep medications for the treatment or prevention of delirium: clinical effectiveness and guidelines. (CADTH rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2016. https://www.cadth.ca/sleep-medications-treatment-or-prevention-delirium-clinical-effectiveness-and-guidelines
Articles Describing Ramelteon
Hamidi A, Roberts RJ, Weinhouse GL, et al. Characterization of nocturnal neuroactive medication use and related sleep documentation in critically ill adults. Crit Care Explor. 2021 Mar 15;3(3):e0367. PubMed
Oh ES, Leoutsakos JM, Rosenberg PB, et al. Effects of ramelteon on the prevention of postoperative delirium in older patients undergoing orthopedic surgery: the RECOVER randomized controlled trial. Am J Geriatr Psychiatry. 2021 Jan;29(1):90-100. PubMed
Hamblin SE, Burka AT. Ramelteon for ICU delirium prevention: is it time to melt away? Crit Care Med. 2019 Dec;47(12):1813-1815. PubMed
Hokuto D, Nomi T, Yoshikawa T, Matsuo Y, Kamitani N, Sho M. Preventative effects of ramelteon against postoperative delirium after elective liver resection. PLoS One. 2020 Nov 2;15(11):e0241673. PubMed
Jaiswal SJ, Vyas AD, Heisel AJ, et al. Ramelteon for prevention of postoperative delirium: a randomized controlled trial in patients undergoing elective pulmonary thromboendarterectomy. Crit Care Med. 2019 Dec;47(12):1751-1758. PubMed
Leon-Salas B, Trujillo-Martin MM, del Castillo LPM, et al. Pharmacologic interventions for prevention of delirium in hospitalized older people: A meta-analysis. Arch Gerontol Geriatr. Sep-Oct 2020;90:104171. PubMed
Lopez CN, Fuentes A, Dhala A, Balk J. Ramelteon for decreasing delirium in surgical intensive care unit patients. Clinical Medicine Insights: Psychiatry. January 2020.
Gupta PK, Verma R, Kohli M, Shukla N, Kannaujia S. The effect of ramelteon on postoperative delirium in elderly patients: A randomised double-blind study. J Clinical & Diagnostic Research. 2019 Dec;13(12):15-19.
Sanchez DL, Fusick AJ, Hudson WB, Schmitz JE, Catalano MC, Catalano G. Ramelteon in the treatment of delirium: New perspectives from reported findings and a case observation. Current Drug Therapy. 2019;14(3):184-191.
Thom R, Bui M, Rosner B, et al. Ramelteon is not associated with improved outcomes among critically ill delirious patients: a single-center retrospective cohort study. Psychosomatics. May-Jun 2019;60(3):289-297. PubMed
Wu YC, Tseng PT, Tu YK, et al. Association of delirium response and safety of pharmacological interventions for the management and prevention of delirium: a network meta-analysis. JAMA Psychiatry. 2019 May 1;76(5):526-535. PubMed
Nishikimi M, Numaguchi A, Takahashi K, et al. Effect of administration of ramelteon, a melatonin receptor agonist, on the duration of stay in the ICU: a single-center randomized placebo-controlled trial. Crit Care Med. 2018 Jul;46(7):1099-1105. PubMed
Luther R, McLeod A. The effect of chronotherapy on delirium in critical care - a systematic review. Nurs Crit Care. 2018 Nov;23(6):283-290. PubMed
Pinkhasov A, James SA, Fazzari M, Singh D, Lam S. Role of ramelteon in reduction of as-needed antipsychotics in elderly patients with delirium in a general hospital setting. Clin Drug Investig. 2017 Dec;37(12):1137-1141. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca