CADTH Health Technology Review
Ketamine for Adults With Treatment-Resistant Depression or Post-Traumatic Stress Disorder
Rapid Review
Authors: Khai Tran, Quenby Mahood
Abbreviations
AE
adverse event
ALS-18
Affective Lability Scale short form
AGREE II
Appraisal of Guidelines for Research and Evaluation II
BDI-II
Beck Depression Inventory – II
CADSS
Clinician-Administered Dissociative State Scale
CAPS-5
Clinician-Administered PTSD Scale for DSM-5
CGI
Clinical Global Impression scale
COWAT
Controlled Oral Word Association Test
DSM-5
Diagnostic and Statistical Manual of Mental Disorders, 5th Edition
ECT
Electroconvulsive Therapy
GRADE
Grades of Recommendation Assessment, Development and Evaluation
HAM-A
Hamilton Anxiety Rating Scale
HAMD or HDRS
Hamilton Depression Rating Scale
IM
intramuscular
ITT
intention to treat
MADRS
Montgomery-Asberg Depression Rating Scale
MoCA
Montreal Cognitive Assessment
PANSS
Positive and Negative Syndrome Scale
PCL-5
PTSD Checklist for DSM-5
PHG-9
Patient Health Questionnaire-9
PTSD
post-traumatic disorder
TRD
treatment-resistant depression
RCT
randomized controlled trial
rTMS
Repetitive Transcranial Magnetic Stimulation
YMRS
Young Mania Rating Scale
Key Messages
Two randomized controlled trials reported mixed evidence on the efficacy of repeated IV ketamine infusions for improving post-traumatic stress disorder. One randomized controlled trial with small sample size found that repeated IV ketamine infusions significantly improved post-traumatic stress disorder symptoms compared with midazolam in civilian population, while the other randomized controlled trial with larger sample size could not demonstrate a significant efficacy on post-traumatic stress disorder symptoms compared with placebo in military population. The antidepressant effects of ketamine were rapid, but the effects were not sustained after few weeks of post-treatment follow-up.
One randomized controlled trial comparing IV ketamine with IV esketamine found both treatments had comparable acute antidepressant effects for treatment-resistant depression 24 hours following infusion.
Two randomized controlled trials provided mixed evidence on the efficacy of single infusion of IV ketamine that was used as anesthetic agent for electroconvulsive therapy for treatment-resistant depression. One randomized controlled trial involving military population showed that patients undergoing electroconvulsive therapy for treatment-resistant depression with ketamine anesthesia had similar improvement of depression when compared with patients undergoing electroconvulsive therapy with methohexital anesthesia. However, in other randomized controlled trial comparing with propofol-based anesthesia in a civilian population, ketamine-based anesthesia provided faster improvement in depressive symptoms and fewer electroconvulsive therapy treatments to achieve disease remission.
In a small randomized controlled trial, alternate infusions of subanesthetic dose of ketamine or midazolam with alternate electroconvulsive therapy showed no significant difference in antidepressant effects between groups.
The efficacy of oral ketamine was demonstrated in 1 randomized controlled trial that repeated administration of oral ketamine significantly reduced depressive symptoms compared with placebo.
A small retrospective chart review study showed that repeated administration of intramuscular ketamine had no significant differences in the improvement of depressive and anxiety symptoms compared with repeated transcranial magnetic stimulation.
Findings suggest overall safety and tolerability of ketamine for treatment of post-traumatic stress disorder or treatment-resistant depression. Most frequent side effects associated with ketamine were dissociative symptoms and cardiovascular changes such as increased blood pressure and heart rate, but these effects were transient.
The Danish guideline recommend against the use of IV ketamine in patients with treatment-resistant depression, due to low quality and insufficient evidence regarding the lack of long-term efficacy and the risk of abuse of ketamine. Likewise, the Canadian guideline recommends IV ketamine be considered as third-line treatment for adults with TRD, because of the short-lived efficacy of ketamine, its side effects, and the lack of strategies for relapse prevention after ketamine infusions.
Context and Policy Issues
Depression is a debilitating mental illness that affects approximately 5.4% of the Canadian population.1 Although there are many effective first-line pharmacotherapy treatments for depression, about 21.7% of Canadians remain non-responsive to at least 2 antidepressant medications from different classes. Patients with such limited responsiveness to medications are often considered to have treatment-resistant depression (TRD).2,3 They are known to experience longer depressive episodes, and are at increased risk of drug (including alcohol) abuse, suicide, and hospitalizations.4 A wide variety of antidepressant drug medications and 2 somatic treatments through brain stimulation, namely electroconvulsive therapy (ECT) and repetitive transcranial magnetic stimulation (rTMS), are available for TRD.4
Ketamine, an noncompetitive N-methyl-D-aspartate receptor antagonist, has been approved and primarily used as an IV anesthetic induction drug in doses ranging between 1.0 and 4.5 mg/kg.5 As it also interacts with other receptors, ketamine has been explored for other indications such as depressive disorders, suicidal ideation, substance use disorders, anxiety disorders, refractory status epilepticus, bronchial asthma exacerbations, and pain management.6 Over the past decades, numerous clinical and preclinical studies have demonstrated the rapid antidepressant effects of ketamine in subanesthetic dosages (e.g., 0.5 m/kg) in patients with major depressive disorders and TRD.7,8 Ketamine is a racemic mixture of 2 enantiomers, S(+)-ketamine (esketamine) and R(-)-ketamine (arketamine).9 Recently intranasal esketamine has received FDA approval for TRD in the US.10 There are limited research on the use of other formulations of ketamine for TRD including the oral, subcutaneous, and intramuscular forms.11
Post-traumatic stress disorder (PTSD) is a disabling mental condition that affects about 9.2% of Canadians in their lifetime.12 In Canadian war zone veterans, its prevalence has been estimated up to 10%.13 Although anyone can get PTSD, the risk factors for PTSD include being female, having experienced a prior trauma, having been abused as a child, having pre-existing mental health problems, and having a family of mental illness.12 People with PTSD commonly have associated problems including depression, panic attacks, alcohol and substance abuse, problems in relationship, and increased risk of other medical problems.12 There are few drugs with insufficient efficacy available for treatment of PTSD.14 A previous proof-of-concept RCT15 provided the first evidence of rapid reduction in PTSD and depressive symptoms 24 hours after a single dose of IV ketamine infusion compared to midazolam in primarily civilian population. However, a recent RCT16 involving patients with chronic pain with or without PTSD found no significant effects of a single infusion of ketamine in improving PTSD or pain symptoms compared with ketorolac.
This report aims to summarize the clinical effectiveness and cost-effectiveness of ketamine compared with all relevant comparators including placebo or no treatment for adults with TRD or PTSD. Additionally, this report also aims to summarize the recommendations from evidence-based guidelines regarding the use and administration of ketamine for those populations.
Research Questions
What is the clinical effectiveness of ketamine versus placebo or no treatment for adults with TRD or PTSD?
What is the clinical effectiveness of ketamine versus alternative interventions for adults with TRD or PTSD?
What is the clinical effectiveness of ketamine administered via different routes for adults with TRD or PTSD?
What is the cost-effectiveness of ketamine versus placebo or no treatment for adults with TRD or PTSD?
What is the cost-effectiveness of ketamine versus alternative interventions for adults with TRD or PTSD?
What is the cost-effectiveness of ketamine administered via different routes for adults with TRD or PTSD?
What are the evidence-based guidelines regarding the use and administration of ketamine for adults with TRD or PTSD?
Methods
Literature Search Methods
This report makes use of a literature search strategy developed for a previous CADTH report.17 For the current report, a limited literature search was conducted by an information specialist on key resources including MEDLINE, PsycInfo, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were ketamine and depression or PTSD. CADTH-developed search filters were applied to limit retrieval to guidelines, randomized controlled trials, controlled clinical trials, or any other type of clinical trial, health technology assessments, systematic reviews, meta-analyses, or network meta-analyses, and economic studies. The search was limited to documents published in English between January 1, 2017, and March 7, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. Titles and abstracts were reviewed in the first screening level, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with TRD or PTSD |
Intervention | Ketamine administered via any route (e.g., IV, intramuscular, subcutaneous, intranasal, oral, sublingual) |
Comparator | Q1 to Q4: Placebo, no treatment Q2 to Q5: Pharmacotherapy (e.g., antidepressants [e.g., SSRIs, SNRIs], antipsychotic drugs), psychotherapy (e.g., cognitive behavioural therapy), electroconvulsive therapy Q3 to Q6: Ketamine administered via alternative routes (e.g., IV, intramuscular, subcutaneous, intranasal, oral, sublingual) Q7: Not applicable |
Outcomes | Q1 to Q3: Clinical effectiveness (e.g., symptom severity [e.g., depressive symptoms, PTSD symptoms], suicidality, hospital admission rate, length of stay, quality of life, fatigue, and safety [e.g., adverse events]) Q4 to Q6: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q7: Recommendations regarding best practices (e.g., appropriate patient populations or clinical settings, treatment protocols, contraindications, and recommended patient monitoring strategies) |
Study designs | Health technology assessments, systematic reviews, randomized-controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
PTSD = post-traumatic stress disorder; SNRI = serotonin and norepinephrine reuptake inhibitor; SSRI = selective serotonin reuptake inhibitor; TRD = treatment-resistant depression.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017. Studies retrieved by the search were excluded if they were included in the previous CADTH reports.17,18
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: The Downs and Black checklist19 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument20 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
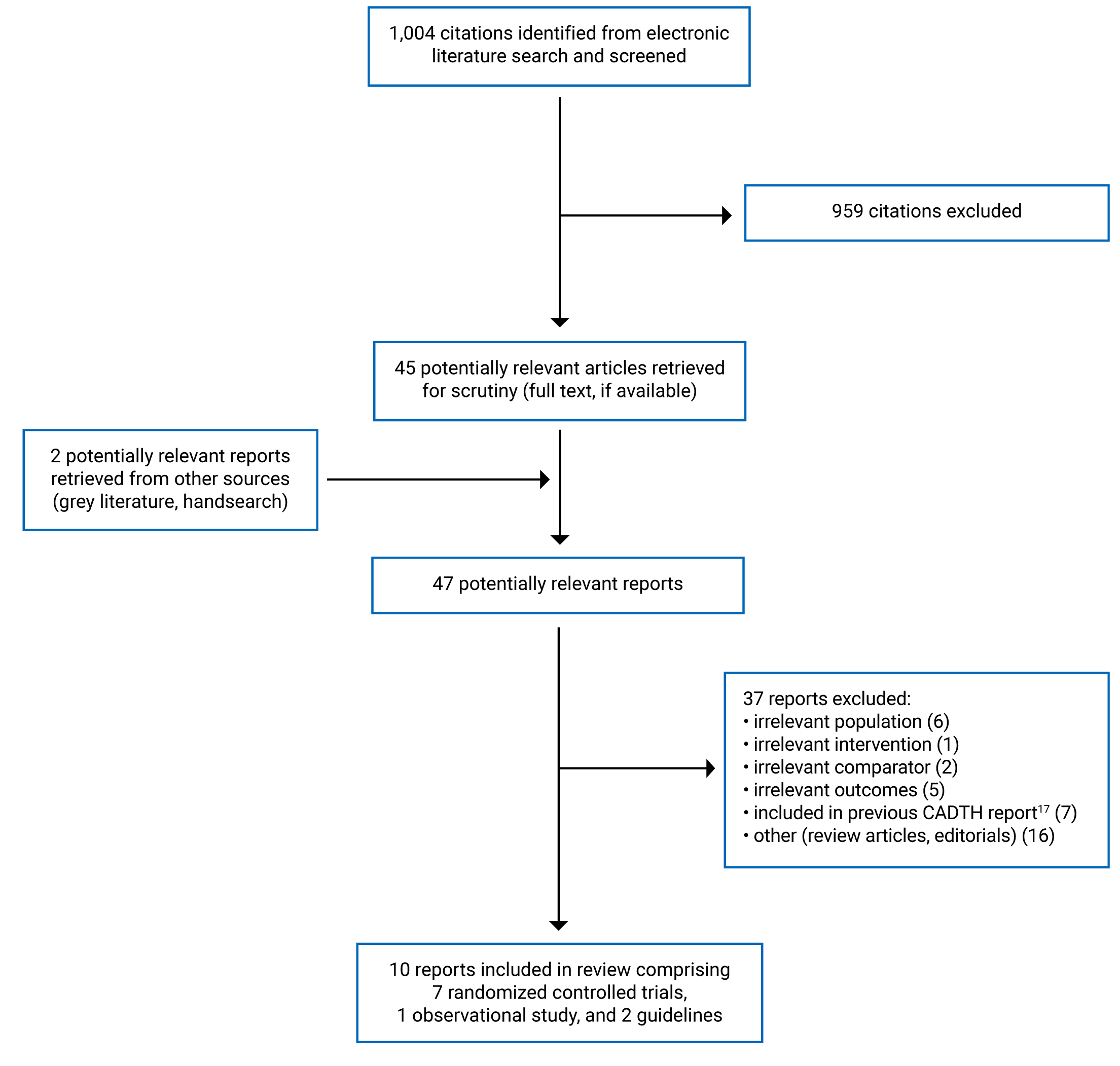
A total of 1,004 citations were identified in the literature search. Following screening of titles and abstracts, 959 citations were excluded and 45 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 37 publications were excluded for various reasons, and 10 publications met the inclusion criteria and were included in this report. These comprised 7 RCTs, 1 non-randomized study, and 2 evidence-based guidelines. Appendix 1 presents the PRISMA21 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Additional details regarding the characteristics of included primary clinical studies22-29 (Table 2) and guidelines30,31 (Table 3) are provided in Appendix 2.
Study Design
The 8 included primary clinical studies comprises 7 RCTs and 1 retrospective chart review study. The RCTs22-28 were published between 2018 and 2022, while the retrospective chart review study29 were published in 2021. All of the RCTs were parallel and double-blinded. Six RCTs22-24,26-28 reported that sample size calculation for primary outcomes was performed; however, 2 RCTs23,27 reported results from interim analysis based on smaller sample sizes than originally planned. The retrospective chart review study29 did not perform sample size calculation. Four RCTs23,24,26,27 analyzed the data using the intention-to-treat (ITT) approach, while 3 RCTs22,25,28 analyzed the data as per protocol.
Both included guidelines were evidence-based, providing recommendations on 6 interventions including ketamine in 1 guideline,30 and on the use of ketamine for treatment of TRD in the other.31 A systematic search of the literature was conducted, and the quality of evidence and the strength of recommendations were assessed and graded using the Grades of Recommendation Assessment, Development and Evaluation (GRADE) in 1 guideline,30 while the Cochrane risk of bias tool was used to assess the study quality in the other.31
Country of Origin
The primary clinical studies were conducted by authors from US,22,23,25,28 Brazil,24 Israel,26 Canada,27 and the Netherlands.29
The guidelines were conducted by authors from Denmark30 and Canada.31
Patient Population
One study22 involved veterans and service members with PTSD who failed previous antidepressant treatment, 1 study23 involved patients with chronic PTSD, who were stable with psychotropic medications for at least 3 months before randomization, and 4 studies involved patient with TRD, referring to patients who failed to respond to at least 1 antidepressant,24 or 2 antidepressants.25,26,28 Two studies did not provide definition for TRD.27,29 Mean age of patients among included studies ranged between 3925 and 4928 years. The percent of male ranged between 17%25 to 82%.26 The sample sizes of the studies ranged between 1225 to 158.22
In both guidelines30,31 the target population was patients with TRD, while the intended users were health care professionals who treat patients with TRD.
Interventions and Comparators
The interventions used in the included studies were IV ketamine, oral ketamine, or intramuscular (IM) ketamine. The comparators were placebo (i.e., saline), midazolam, IV esketamine, IV propofol, IV methohexital, and rTMS. Overall, 2 studies22,26 compared ketamine with placebo and 6 studies23-25,27-29 compared ketamine with other treatment modalities. One study22 compared IV ketamine with placebo, 1 study26 compared oral ketamine with placebo, 1 study24 compared IV ketamine with IV esketamine, 2 studies23,25 compared IV ketamine with midazolam, 2 studies compared anesthesia-based IV ketamine with IV propofol27 or IV methohexital28 for ECT, and 1 study29 compared IM ketamine with rTMS.
The Danish guideline30 formulated its recommendations concerning 6 selected interventions comprising unilateral high frequency rTMS, IV ketamine or esketamine, bright light therapy, cognitive behavioural analysis system of psychotherapy, psychotherapy targeting rumination, and cognitive remediation for treatment of TRD. The Canadian guideline31 provides recommendations for the use of ketamine in adults with TRD.
Outcomes
Seven RCTs22-28 reported both efficacy and safety outcomes, while the retrospective chart review study29 reported only efficacy outcomes. The efficacy outcomes comprised PTSD symptoms, depression, and anxiety. PTSD symptoms were measured using the PTSD Checklist for DSM-5 (PCL-5) or the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5). Depression was measured using the Montgomery-Asberg Depression Rating Scale (MADRS), the Hamilton Depression Rating Scale (HDRS or HAMD), the Beck Depression Inventory – II (BDI-II), the Patient Health Questionnaire-9 (PHQ-9), or the Clinical Global Impression scale (CGI). Anxiety was measured using the Hamilton Anxiety Rating Scale (HAM-A).
The safety outcomes assessed in the included studies included dissociation, presence and severity of positive and negative symptoms, anxiety, cognitive changes, verbal fluency, and sudden mood changes over the past week. Changes in those outcomes were measured, respectively, using the Clinician-Administered Dissociative State Scale (CADSS), the Positive and Negative Syndrome Scale (PANSS), the Young Mania Rating Scale (YMRS), the Montreal Cognitive Assessment (MoCA), the Controlled Oral Word Association Test (COWAT), and the short form of the Affective Lability Scale (ALS-18). Other adverse events (AEs) related to ketamine treatment were also reported.
Brief descriptions of the scorings of the tools used to measure the efficacy and safety outcomes are presented as footnotes of Table 2 in Appendix 2.
Three studies23,26,29 assessed the outcomes at the end of treatment, while 5 studies measured the outcomes after last treatment at 4 weeks,22 7 days,24 3 weeks,25 3 days28 and 30 days.27
Both guidelines30,31 considered all efficacy, tolerability, and safety outcomes that were clinically relevant for making recommendations.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included primary clinical studies (Table 4) and guidelines (Table 5) are provided in Appendix 3.
With respect to reporting, all primary studies including 7 RCTs22-28 and 1 retrospective chart review study29 clearly described the objective of the study, the interventions of interest, the main outcomes, and the main findings of the study. The baseline characteristics of the patients included in the study were clearly described in all studies, except in 1 study.25 Without a clear description of patient baseline characteristics, it was not possible to assess if there were potential confounders that could potentially affect the interpretation of the results. One RCT24 had no patients lost to follow-up. Two RCTs23,26 reported the reasons why patients were lost to follow-up, and 4 RCTs22,25,27,28 did not. None of the studies that lost patients to follow-up described the characteristics of those patients. In 1 RCT,22 missing data were treated as treatment failure (i.e., nonresponder). Three RCTs23,26,27 used the ITT approach in the data analyses to account for patients lost to follow-up. Not accounting for patients lost to follow-up in the analyses may increase potential risk of attrition bias. Actual P values (i.e., P values) and the random variability in the data for the main outcomes (e.g., confidence interval, standard deviation, or interquartile range) were reported in all included studies.22-29 In a non-inferiority study,24 the pre-specified margin was set at 20%, meaning a difference in remission rates between groups that was less than 20% would be considered non-inferiority. As the difference in remission rates between groups was only 5.3%, the margin was totally valid. Regarding external validity, all studies, except 1,22 had relatively small sample size (i.e., 15 to 52 patients in total), whose participants may not be representative of the entire population from which they were recruited.23-29 For internal validity, all RCTs were double-blinded to the investigators and patients; thus, the risk of biases for selection, performance, and detection were low. Two RCTs22,24 reported the methods of randomization and allocation concealment, while 4 RCTs23,25-27 did not report either, and 1 RCT28 only reported the method of randomization. Not performing allocation concealment may result in risk of selection bias. The retrospective chart review study29 may be prone to high risk of bias for selection, performance, and detection due to the nature of the observational study design. Additionally, confounding variables that may have significant impact to the findings were not identified and adjusted for in the analyses in this study.29
Appropriate statistical tests were used to assess the main outcomes, and reliable and validated outcome measures were used in all studies.22-29 Patients in different intervention groups appeared to be recruited from the same population and over the same period of time in all studies.22-29 Six studies22-24,26-28 reported sample size calculation, while 2 studies25,29 did not. Of those reported sample size calculation, 2 RCTs23,27 reported results from the interim analysis based on a much smaller sample sizes than that pre-determined by the calculation. It was unclear if using data from a smaller sample size than originally planned may have reduced the studies’ power to detect significant differences in certain outcomes. Patient compliance was not assessed in all studies.22-29 Overall, 5 included studies22-24,26,28 were of moderate methodological quality, and 3 studies25,27,29 were of low methodological quality.
Both guidelines30,31 were explicit in terms of scope and purpose (i.e., objectives, health questions, and populations), and had clear presentation (i.e., specific, and unambiguous recommendations, different options for management of the condition or health issue, and easy to find key recommendations). In terms of stakeholder involvement, both guidelines30,31 clearly defined target users and the development groups. However, it was unclear if the views and preferences of the patients were sought in the Canadian guideline.31 For rigour of development, both guidelines30,31 reported systematic methods used to search for evidence, criteria for selecting evidence, explicit link between recommendations and the supporting evidence, and methods of formulating the recommendations. Both guidelines30,31 considered health benefits, side effects, and risks in formulating the recommendations, and were externally peer-reviewed before publication. One guideline30 used GRADE methodology to assess and grade its recommendations, while the other31 used the Cochrane risk of bias tool to assess the study quality, based on which the line-of-treatment recommendations were determined by expert consensus after assessing the efficacy, tolerability, safety, and feasibility of the intervention. For clarity, the recommendations in both guidelines30,31 are specific and unambiguous, provide different options for management of the condition, and are easily identifiable. For applicability, both guidelines30,31 were not explicit in terms of facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, resource implications (e.g., considering costs in recommendations), and monitoring or auditing criteria. For editorial independence, both guidelines30,31 reported competing interests of guideline development group members, and that the views of the funding body did not have influence on the content of the guidelines. Overall, both included guidelines30,31 were of good methodological quality.
Summary of Findings
Appendix 4 presents the main study findings of the primary clinical studies22-29 (Table 6 to Table 9) and the summary of guideline recommendations30,31 (Table 10). The findings are presented by outcome, which are PTSD (Table 6), depression (Table 7), anxiety (Table 8), and safety (Table 9).
Clinical Effectiveness of Ketamine Versus Placebo or No Treatment for Adults With TRD or PTSD
Two RCTs compared IV ketamine22 or oral ketamine26 with placebo (i.e., saline) were identified.
PTSD
The RCT by Abdallah et al. (2022)22 tested whether IV ketamine at standard dose (0.5 mg/kg) and low dose (0.2 mg/kg) could reduce PTSD symptoms compared with placebo in veterans. Eight 40-minute IV infusions of ketamine or saline were administered twice weekly for 4 weeks, followed by 4 weeks follow-up. Analyses on the PCL-5 scores revealed that the scores improved over time in all treatment groups, and there was no significant difference in PCL-5 scores between standard dose and placebo after first infusion (i.e., 24 hour), at end of treatment (i.e., 4 weeks), and at 4 weeks of follow-up. Similarly, the PCL-5 scores between low dose and placebo were not significantly different after first infusion and at the end of treatment. There were no significant differences in PCL-5 scores between standard and low dose of ketamine. Similar results were obtained for the effect of ketamine on CAPS-5 scores. There were no significant differences in response rates among the 3 groups. Response was defined as a 25% or more improvement in PCL-5 scores from baseline.
Depression
The RCT by Abdallah et al. (2022)22 found that standard dose, but not the low dose, of ketamine significantly lowered MADRS scores compared with placebo at 24 hours post-infusion (P = 0.05), and at end of treatment (P = 0.01) However, the difference in MADRS scores between standard dose and placebo were not significant at 4 weeks of follow-up. There were no significant differences in MADRS scores between standard and low dose of ketamine.
The RCT by Domany et al. (2019)26 compared oral ketamine (1 mg/kg thrice weekly for 21 days) with placebo in patients with TRD and found that ketamine significantly reduced MADRS scores at end of treatment (P < 0.001). The response was defined as achieving a 50% or more reduction of MADRS scores from baseline. At 21 days, the response rate was significantly higher in the ketamine group (31.8%) than the placebo group (5.6%); P < 0.05. Similar results were obtained for the effect of ketamine on remission, defined as MADRS fewer than 10 points. After 21 days of treatment, 27.3% patients in the ketamine group achieved remission compared to none in the placebo group (P < 0.05).
Safety
The RCT by Abdallah et al. (2022)22 used CADSS to examine the dissociative effects of ketamine. Ketamine dose-dependently induced increase in the CADSS scores at 30 minutes from the start of infusion, and both the standard and low doses of ketamine had significantly higher CADSS scores than those of placebo (P < 0.05). However, the dissociative symptoms induced by ketamine returned to the placebo levels after the treatment was completed at 120 minutes. At post-treatment follow-up, there were no significant differences between treatment groups (P > 0.05). Additionally, the authors used the PANSS to examine the psychotomimetic effects of ketamine and found that there were no significant differences in PANSS scores between ketamine (both standard and low dose) and placebo during treatment. At post-treatment follow-up, both ketamine doses had significantly lower in PANSS scores compared to placebo (P < 0.05). The incidences of treatment-related AEs in the standard dose, low dose, and placebo were 39.5%, 39.5% and 21%, respectively. The AEs most likely associated with both ketamine doses and not present in the placebo were agitation (5.7%), anxiety (3.8%), irritability (7.6%), constipation (2.9%), and sweating (2.9%).
The RCT by Domany et al. (2019)26 found that 40% in the ketamine group compared to 18.2% in the placebo group had transient elevation of systolic blood pressure more than 20 mm Hg at first administration. Common AEs associated with ketamine included euphoria, dizziness, and drowsiness. The authors stated that those AEs and blood pressure increase were resolved within 1 hour and were milder at later administration of ketamine.
Clinical Effectiveness of Ketamine Versus Alternative Interventions for Adults With TRD or PTSD
Two RCTs23,25 compared IV ketamine with midazolam, 1 RCT24 compared IV ketamine with IV esketamine, 2 RCTs27,28 compared anesthesia-based IV ketamine with anesthesia-based IV propofol or IV methohexital, and 1 retrospective chart review29 compared IM ketamine with rTMS.
PTSD
The RCT by Feder et al. (2021)23 randomized patients with chronic PTSD, who were stable on psychotropic medications for at least 3 months before randomization to receive 6 infusions of ketamine (0.5 mg/kg per day) or midazolam (0.045 mg/kg per day) 3 days per weeks over 2 consecutive weeks. PTSD severity assessment using the CAPS-5 showed that improvement in the total scores over the course of treatment were significantly lower in the ketamine group compared with the midazolam group at week 1 (P = 0.030) and at week 2 (P = 0.004). Response rate, defined as a 30% or more reduction in CAPS-5 scores from baseline, was significantly higher in the ketamine group (67%) compared with the midazolam group (20%); P = 0.03. However, the effects of ketamine on CAPS-5 scores were gradually lost over time. The median time to loss of response (defined as < 30% improvement from baseline) among responders was 27.5 days (IQR: 23 days to 32 days).
Depression
The RCT by Feder et al. (2021)23 found that depressive symptoms in PTSD patients measured by MADRS scores was significantly improved in the ketamine group compared with the midazolam groups at week 1 and week 2 (P < 0.05).
The RCT by Altinay et al. (2019)25 compared ketamine (0.5 mg/kg) with midazolam (0.045 mg/kg) infused on alternate days with ECT days for 1 week in patients with TRD. Depressive symptoms measured using MADRS scores showed no significant difference between ketamine and midazolam groups. Similar results were also observed with the HAMD scores. The response rates and remission rates were also not statistically significantly different between the treatment groups.
The non-inferiority clinical trial by Correia-Melo et al. (2020)24 assessed the efficacy of esketamine compared to ketamine in patients with TRD. There were no significant differences in mean MADRS scores between the 2 treatments at 24 hours, 72 hours, and 7 days after a single infusion of ketamine 0.5 mg/kg or esketamine 0.25 mg/kg. There were also no significant differences between treatment groups in the response rates or the remission rates at all follow-up time points. Similar results were observed with the CGI scores, with both ketamine and esketamine groups showing improvement in depressive symptoms without significant differences between groups at any time point.
Two RCTs, 1 by Carspecken et al. (2018)28 and 1 by Gamble et al. (2018)27 evaluated the ketamine’s antidepressant effects in ECT as a primary anesthetic . In the RCT by Carspecken et al. (2018),28 veterans with TRD were infused with IV ketamine (1 mg/kg to 2 mg/kg) or IV methohexital (1 mg/kg to 2 mg/kg) for induction of general anesthesia for each ECT session, and ECT course was scheduled with consecutive sessions 3 times a week with length determined by clinical response per the treating psychiatrist. Patients in both groups had depressive symptom improvement (i.e., decreased of HAMD or PHQ-9 scores) after completing the ECT index course compared with baseline.28 However, there was no significant difference in HAMD scores or PHQ-9 scores between ketamine and methohexital groups at final ECT session or at 72 hours follow-up.28
The RCT by Gamble et al. (2018)27 also compared the antidepressive effects between IV ketamine-based anesthesia (0.75 mg/kg) and IV propofol-based anesthesia (1 mg/kg) in TRD patients referred to ECT. Compared to the propofol group, the ketamine group had higher response rates (100% versus 83%) and remission rates (100% versus 58%) assessed using MADRS scores. Multivariate survival analysis adjusted for age and sex showed that patients in the ketamine group were more than twice as likely to achieve response and remission compared with the propofol group. Patients allocated in the ketamine groups significantly required fewer number of ECT treatments to achieve a 50% reduction in MADRS scores compared with those in the propofol group (P = 0.01). There were no significant differences in the relapse rates (MADRS > 20) between groups at 30-day follow-up.
The retrospective chart review study by Mikellides et al. (2021)29 compared the antidepressant efficacy of both ketamine therapy and rTMS therapy in patients with TRD. Intramuscular ketamine was administered twice weekly for 8 sessions at an initial dose of 0.25 mg/kg, then the dosage was titrated upwards to a maximum of 1 mg/kg by session 4. There were significant decreases in HAMD and BDI-II scores in the post-treatment compared to pre-treatment in both groups. However, there was no significant differences in the response rates or remissions rates between groups.
Anxiety
In the retrospective chart review study by Mikellides et al. (2021),29 the HAM-A scores were significantly reduced in the post-treatment compared to pre-treatment in both IM ketamine and rTMS group, but there were no significant differences in the response rates or remissions rates between groups.
Safety
The RCT by Feder et al. (2021)23 found that the dissociative symptoms observed during ketamine infusions were transient, resolving by 2 hours after the start of infusion. No significant psychotic or manic symptoms were observed after ketamine infusions. There were no suicidal behaviours present during the assessment period. Most frequent AEs of ketamine compared with midazolam after the start of infusions included blurred visions (54% versus 0%), dizziness (33% versus 13%), headache (27% versus 13%), and nausea, or vomiting (20% versus 7%). Statistical comparisons were not reported.
The RCT by Altinay et al. (2019)25 found no significant difference between ketamine and midazolam groups in cognitive testing (by MoCA or COWAT scores), or in manic symptoms (by YMRS scores).
The RCT by Correia-Melo et al. (2020)24 found that no significant difference in dissociative symptoms between ketamine and esketamine groups. The authors reported that most common treatment emergent AEs associated with ketamine or esketamine were increased blood pressure, heart rate, nausea, and dissociation. However, proportions and statistical comparisons between groups were not described. Three patients (1 ketamine and 2 esketamine) had to pause the infusion due to increased blood pressure above 30% of the baseline values. The authors reported that no life-threatening or other serious adverse events were observed.
The RCT by Carspecken et al. (2018),28 found no significant difference in cognitive impairment between IV ketamine-based anesthesia and IV methohexital-based anesthesia administered before and after ECT. There were also no significant differences between groups in blood pressure, heart rate, mean number of seizures in index course per patient, mean seizure length, or mean length of post-anesthesia care unit stay. Two patients in the ketamine group experienced transient memorable dissociative symptoms during treatment, but no recurrences were reported during follow-up visits.
The RCT by Gamble et al. (2018)27 found no significant difference in dissociative symptoms between IV ketamine-based anesthesia and IV propofol-based anesthesia groups across ECT sessions. For both groups, there was a decrease in CADSS scores with an increased number of ECT treatments. The ALS-18 scores for measuring sudden mood change over the past week significantly decreased at 30-day follow-up, but the change did not significantly differ between groups. The rates of AEs such as blood pressure increase or decrease, nausea or vomiting, and headache were not significantly different between groups.
Clinical Effectiveness of Ketamine Administered Via Different Routes for Adults With TRD or PTSD
No studies comparing ketamine administered via different routes for adults with TRD or PTSD were identified; therefore, no summary can be provided.
Cost-effectiveness of Ketamine Versus Placebo or No Treatment for Adults With TRD or PTSD
No cost-effectiveness studies of ketamine versus placebo or no treatment for adults with TRD or PTSD were identified; therefore, no summary can be provided.
Cost-effectiveness of Ketamine Versus Alternative Interventions for Adults With TRD or PTSD
No cost-effectiveness studies of ketamine versus alternative interventions for adults with TRD or PTSD were identified; therefore, no summary can be provided.
Cost-effectiveness of Ketamine Administered Via Different Routes for Adults With TRD or PTSD
No cost-effectiveness studies of ketamine administered via different routes for adults with TRD or PTSD were identified; therefore, no summary can be provided.
Guidelines
The Danish guideline by Moeller et al. (2021)30 provides weak recommendation against the use of IV ketamine as add-on to usual antidepressant treatment in patients with TRD. The rationale for the recommendation was that the benefits was short-lived, while the evidence on long-term efficacy and side effects, including the risk of abuse, was unclear.
The Canadian guideline by Swainson et al. (2021)31 acknowledges the short-term efficacy of IV ketamine (relapse within 10 days for most patients), the lack of strategies for relapse prevention, and limited evidence on the efficacy of repeated ketamine treatment either by IV infusions of IV or different routes of administration, including oral, intranasal, and sublingual formulations. Therefore, the guideline recommends IV ketamine be considered as third line of treatment for adults with TRD.
Limitations
A general limitation of the included primary clinical studies was that 7 of 8 studies had small sample sizes that limit the generalizability of the findings. In double-blind RCTs, the high rate of transient dissociative symptoms in the ketamine group potentially affects the blinding that may lead to negative outcome expectations from the comparators, thus exaggerating differences between groups. Definition of TRD varied among studies, and 1 study23 examining the effect of ketamine in PTSD did not require history of nonresponse to antidepressant. As all studies used ketamine as add-on therapy that allow patients to continue using stable dosages of other psychotropic medications (e.g., antidepressants, antipsychotic drugs, or mood stabilizers) during treatment, the concomitant antidepressant treatments across studies were not standardized. The retrospective chart review study29 was limited by its retrospective design, without the advantages of randomization to minimize bias. The study29 was prone to selection and attrition biases as it selected only patients who completed the total number of rTMS or ketamine sessions required, and patients with complete clinical evaluations before and after treatment, without collecting information of patients who terminated the treatment prematurely or those with incomplete assessment.
The recommendations from both included guidelines30,31 were mostly based on low-quality evidence. No guidelines regarding the use of ketamine for treatment of PTSD were identified.
Conclusions and Implications for Decision- or Policy-Making
This report identified 7 RCTs,22-28 1 retrospective chart review study,29 and 2 guidelines.30,31 The identified primary clinical studies provided evidence for the efficacy and safety of ketamine compared with placebo or alternative interventions for treatment of TRD or PTSD in adults. Evidence comparing the clinical effectiveness of ketamine administered via different routes were not identified. Also, no evidence was identified regarding the cost-effectiveness of ketamine compared with placebo or alternative interventions; or of 1 ketamine formulation versus others for adults with TRD or PTSD.
The effects of ketamine on PTSD symptoms were reported in 2 RCTs22,23 with mixed findings. A small sample size RCT23 (15 patients per group) found that repeated IV ketamine infusions significantly improved PTSD symptoms compared with midazolam in civilian population of mostly females. A larger RCT22 (around 50 patients per groups) could not demonstrate a significant efficacy on PTSD symptoms compared with placebo in military population of mostly males. It is unclear if the population and sex differences may have played a role in differing outcomes. However, the standard dose of IV ketamine (0.5 mg/kg) in both studies was superior to placebo22 or midazolam23 to reduce depressive symptoms. The antidepressant effects of ketamine were rapid, but the effects were not sustained during 4 weeks of post-treatment follow-up.22 An RCT24 comparing IV ketamine with IV esketamine found both treatments had comparable acute antidepressant effects for TRD 24 hours following infusion. When a single infusion of IV ketamine was used as anesthetic agent for ECT, patients undergoing ECT for TRD with ketamine anesthesia had similar improvement of depression when compared with patients undergoing ECT with methohexital anesthesia.28 However, in another study27 comparing with propofol-based anesthesia, ketamine-based anesthesia provided faster improvement in depressive symptoms and required fewer ECT treatments to achieve disease remission. It is unclear if the differences in outcomes between studies27,28 may be due difference in comparators. In a small RCT,25 alternate infusions of ketamine or midazolam with alternate ECT showed no significant difference in antidepressant effects between groups. The efficacy of oral ketamine was demonstrated in 1 RCT26 in which repeated administration of oral ketamine significantly reduced depressive symptoms compared to placebo. A small retrospective chart review study29 showed that the reduction in depressive and anxiety symptoms with repeated administration of IM ketamine was not significantly different compared with rTMS. Findings from included RCTs suggest overall safety and tolerability of ketamine for treatment of PTSD or TRD.22-28 Most frequent AEs associated with ketamine were dissociative symptoms and cardiovascular changes such as increased blood pressure and heart rate, but these effects were transient. The Danish guideline30 recommend against the use of IV ketamine in patients with TRD, due to low-quality and insufficient evidence regarding the lack of long-term efficacy and the risk of abuse of ketamine. Likewise, the Canadian guideline31 recommends that IV ketamine be considered as third-line treatment for adults with TRD, because of the short-lived efficacy of ketamine, its side effects, and the lack of strategies for relapse prevention after ketamine infusions.
CADTH previously published 2 Rapid Response reports17,18 on this topic. The 2017 CADTH report18 identified 3 systematic reviews, 5 primary studies, and 2 evidence-based guidelines. The 2019 CADTH report17 identified 6 primary clinical studies and 1 evidence-based guideline. Overall, the included studies showed that the IV ketamine had rapid antidepressant effects for treatment of TRD and single-dose infusion of ketamine was effective at reducing PTSD severity. However, an RCT involving repeated infusions found no difference in depression severity or suicidal ideation between ketamine and placebo. All 3 guidelines included in the 2 previous CADTH reports17,18 recommended against the use of ketamine for patients with TRD or PTSD. The current report extends the scope of the 2 previous CADTH reports to include all ketamine formulations and all comparators of interest.
Given the aforementioned limitations of the included studies in this report, there is insufficient evidence to provide definitive conclusions about the clinical effectiveness of ketamine for treatment of TRD or PTSD. Future research is needed to address questions such as optimal dose regimens, patient selection, and treatment duration with longer follow-up period to determine whether ketamine should be used for treatment of TRD or PTSD.
References
1.Canadian Mental Health Association. Fast facts about mental health and mental illness. 2021; https://cmha.ca/brochure/fast-facts-about-mental-illness/. Accessed 2022 Mar 28.
2.Rizvi SJ, Grima E, Tan M, et al. Treatment-resistant depression in primary care across Canada. Can J Psychiatry. 2014;59(7):349-357. PubMed
3.Rybak YE, Lai KSP, Ramasubbu R, et al. Treatment-resistant major depressive disorder: Canadian expert consensus on definition and assessment. Depress Anxiety. 2021;38(4):456-467. PubMed
4.Mood Disorders Society of Canada. 2018 Treatment Resistant Depression Study. 2018; https://mdsc.ca/wp-content/uploads/2018/04/MDSC-Treatment-Resistant-Depression-Study-April-25.pdf. Accessed 2022 Mar 28.
5.Ketamine hydrochloride injection USP (ketamine hydrochloride): 10 mg/mL ketamine; 50 mg/mL ketamine [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2015: https://www.sandoz.ca/sites/www.sandoz.ca/files/Ketamine_HCl_PMe_20150506.pdf. Accessed 2022 Mar 28.
6.Gautam CS, Mahajan SS, Sharma J, Singh H, Singh J. Repurposing potential of ketamine: opportunities and challenges. Indian J Psychol Med. 2020;42(1):22-29. PubMed
7.Lent JK, Arredondo A, Pugh MA, Austin PN. Ketamine and treatment-resistant depression. AANA J. 2019;87(5):411-419. PubMed
8.Subramanian S, Haroutounian S, Palanca BJA, Lenze EJ. Ketamine as a therapeutic agent for depression and pain: mechanisms and evidence. J Neurol Sci. 2022;434:120152. PubMed
9.Andrade C. Ketamine for depression, 3: does chirality matter? J Clin Psychiatry. 2017;78(6):e674-e677. PubMed
10.Traynor K. Esketamine nasal spray approved for treatment-resistant depression. Am J Health Syst Pharm. 2019;76(9):573. PubMed
11.Iqbal SZ, Mathew SJ. Ketamine for depression clinical issues. Adv Pharmacol. 2020;89:131-162. PubMed
12.Veteran Affairs Canada. Learn about PTSD. 2019; https://www.veterans.gc.ca/eng/health-support/mental-health-and-wellness/understanding-mental-health/learn-ptsd#b3. Accessed 2022 Mar 28.
13.Veteran Affairs Canada. Post-traumatic stress disorder (PTSD) and war-related stress. 2019; https://www.veterans.gc.ca/eng/health-support/mental-health-and-wellness/understanding-mental-health/ptsd-warstress. Accessed 2022 Mar 28.
14.Hoskins M, Pearce J, Bethell A, et al. Pharmacotherapy for post-traumatic stress disorder: systematic review and meta-analysis. Br J Psychiatry. 2015;206(2):93-100. PubMed
15.Feder A, Parides MK, Murrough JW, et al. Efficacy of intravenous ketamine for treatment of chronic posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry. 2014;71(6):681-688. PubMed
16.Dadabayev AR, Joshi SA, Reda MH, et al. Low dose ketamine infusion for comorbid posttraumatic stress disorder and chronic pain: a randomized double-blind clinical trial. Chronic Stress (Thousand Oaks). 2020;4:2470547020981670. PubMed
17.Li K, Loshak H. Intravenous ketamine for adults with treatment resistant depression or post-traumatic stress disorder: a review of clinical effectiveness, cost-effectiveness and guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1203%20IV%20Ketamine%20for%20Depression%20and%20PTSD%20Final.pdf. Accessed 2022 Mar 7.
18.Kim J, Mierzwinski-Urban M. Ketamine for treatment resistant depression or post-traumatic stress disorder in various settings: a review of clinical effectiveness, safety, and guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/pdf/htis/2017/RC0855%20Ketamine%20for%20Resistant%20Depression%20Final.pdf. Accessed 2022 Mar 7.
19.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
20.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Mar 7.
21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
22.Abdallah CG, Roache JD, Gueorguieva R, et al. Dose-related effects of ketamine for antidepressant-resistant symptoms of posttraumatic stress disorder in veterans and active duty military: a double-blind, randomized, placebo-controlled multi-center clinical trial. Neuropsychopharmacology. 2022;19:19. PubMed
23.Feder A, Costi S, Rutter SB, et al. A randomized controlled trial of repeated ketamine administration for chronic posttraumatic stress disorder. Am J Psychiatry. 2021;178(2):193-202. PubMed
24.Correia-Melo FS, Leal GC, Vieira F, et al. Efficacy and safety of adjunctive therapy using esketamine or racemic ketamine for adult treatment-resistant depression: A randomized, double-blind, non-inferiority study. J Affect Disord. 2020;264:527-534. PubMed
25.Altinay M, Karne H, Anand A. Administration of sub-anesthetic dose of ketamine and electroconvulsive treatment on alternate week days in patients with treatment resistant depression: a double blind placebo controlled trial. Psychopharmacol Bull. 2019;49(1):8-16. PubMed
26.Domany Y, Bleich-Cohen M, Tarrasch R, et al. Repeated oral ketamine for out-patient treatment of resistant depression: randomised, double-blind, placebo-controlled, proof-of-concept study. Br J Psychiatry. 2019;214(1):20-26. PubMed
27.Gamble JJ, Bi H, Bowen R, et al. Ketamine-based anesthesia improves electroconvulsive therapy outcomes: a randomized-controlled study. Can J Anaesth. 2018;65(6):636-646. PubMed
28.Carspecken CW, Borisovskaya A, Lan ST, et al. Ketamine anesthesia does not improve depression scores in electroconvulsive therapy: a randomized clinical trial. J Neurosurg Anesthesiol. 2018;30(4):305-313. PubMed
29.Mikellides G, Michael P, Psalta L, Schuhmann T, Sack AT. A retrospective naturalistic study comparing the efficacy of ketamine and repetitive transcranial magnetic stimulation for treatment-resistant depression. Front Psychiatry. 2021;12:784830. PubMed
30.Moeller SB, Gbyl K, Hjorthoj C, et al. Treatment of difficult-to-treat depression - clinical guideline for selected interventions. Nord J Psychiatry. 2021:1-12. PubMed
31.Swainson J, McGirr A, Blier P, et al. The Canadian Network for Mood and Anxiety Treatments (CANMAT) Task Force recommendations for the use of racemic ketamine in adults with major depressive disorder: Recommandations du Groupe de Travail du Reseau Canadien pour les Traitements de L'humeur et de L'anxiete (CANMAT) concernant l'utilisation de la ketamine racemique chez les adultes souffrant de trouble depressif majeur. Can J Psychiatry. 2021;66(2):113-125. PubMed
32.U.S. Department of Veteran Affairs. PTSD checklist for DSM-5 (PCL-5). 2022; https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp. Accessed 2022 Mar 20.
33.U.S. Department of Veteran Affairs. Clinician-Administered PTSD Scale for DSM-5 (CAPS-5). 2021; https://www.ptsd.va.gov/professional/assessment/adult-int/caps.asp. Accessed 2022 Mar 20.
34.Blum L. Montgomery Asberg Depression Rating Scale (MADRS) In: Korner-Bitensky N, ed. Stroke Engine Assessments. Montreal (QC): Stroke Engine; 2009 Sept 21: https://strokengine.ca/en/assessments/montgomery-asberg-depression-rating-scale-madrs/.Accessed 2022 Mar 20.
35.Bremner JD, Krystal JH, Putnam FW, et al. Measurement of dissociative states with the Clinician-Administered Dissociative States Scale (CADSS). J Trauma Stress. 1998;11(1):125-136. PubMed
36.Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261-276. PubMed
37.Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56-62. PubMed
38.Lukasiewicz M, Gerard S, Besnard A, et al. Young Mania Rating Scale: how to interpret the numbers? Determination of a severity threshold and of the minimal clinically significant difference in the EMBLEM cohort. Int J Methods Psychiatr Res. 2013;22(1):46-58. PubMed
39.Rosenzweig A. Montreal Cognitive Assessment (MoCA) test for dementia. In: Opole IO, ed. Verywell Health. New York (NY): Verywell Health; 2022 Jan 29: https://www.verywellhealth.com/alzheimers-and-montreal-cognitive-assessment-moca-98617. Accessed 2022 Mar 20.
40.National Institute of Neurological Disorders and Stroke, Common Data Elements. Hopkins Verbal Learning Test - revised (HVLT-R). 2022; https://www.commondataelements.ninds.nih.gov/report-viewer/23964/Hopkins%20Verbal%20Learning%20Test%20-%20Revised%20(HVLT-R). Accessed 2022 Mar 20.
41.Controlled Oral Word Association Test (COWAT). In: Health ABC Study: operations manual. Vol XV. 2012; https://healthabc.nia.nih.gov/sites/default/files/COWATOMY16_0.pdf. Accessed 2022 Mar 20.
42.Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont). 2007;4(7):28-37. PubMed
43.Look AE, Flory JD, Harvey PD, Siever LJ. Psychometric properties of a short form of the Affective Lability Scale (ALS-18). Pers Individ Dif. 2010;49(3):187-191. PubMed
44.Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50-55. PubMed
45.Beck AT, Steer RA, Ball R, Ranieri W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J Pers Assess. 1996;67(3):588-597. PubMed
46.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-613. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
RCT | ||||
Abdallah et al. (2022)22 US Source of funding: US Department of Defense and US Department of Veteran Affairs | Multicenter, double-blind, parallel 1:1:1, placebo-controlled RCT Sample size calculation: Yes ITT analysis: No | Veterans and service members with PTSD (N = 158) who failed previous antidepressant treatment. % Male:
Mean age (SD), years:
Mean years of military services (SD):
Mean PCL-5a (SD):
Mean CAPS-5b (SD):
Mean MADRSc (SD):
| IV ketamine:
Placebo (n = 54): Saline Eight 40-minute IV infusions of ketamine or placebo (saline) were administered twice weekly | Outcomes: Primary:
Secondary:
AEs
Follow-up: 4 weeks post-treatment |
Feder et al. (2021)23 US Source of funding: Private funding | Single centre, double-blind, parallel 1:1, placebo-controlled RCT Sample size calculation: Yes; but enrolled only 30 patients instead of 40 as planned. ITT analysis: Yes | Patients with chronic PTSD, who were stable with psychotropic medications for at least 3 months before randomization (N = 30) % Male:
Mean age (SD), years:
Mean duration of PTSD (SD), years:
Mean CAPS-5b (SD):
Mean MADRSc (SD):
| IV ketamine (n = 15): 0.5 mg/kg Midazolam (n = 15): 0.045 mg/kg Three infusions per week for 2 weeks, with a total of 6 infusions Patients were assessed on each infusion day, 24 hours, and 2 weeks after the first infusion | Outcomes:
Follow-up: 2 weeks (end of treatment) after the first infusion; 100 days for loss of response |
Correia-Melo et al. (2020)24 Brazil Source of funding: Public funding | Bicentre, non-inferiority, double-blind, parallel-controlled, 1:1, RCT Sample size calculation: Yes ITT analysis: Yes Non-inferiority would be demonstrated if the difference in remission rates between ketamine and esketamine was less than the pre-specified margin of 20%. | Patients with TRD (N = 63) who failed to respond to at least 1 antidepressant. % Male:
Mean age (SD), years:
Mean MADRSc (SD):
| IV ketamine (n = 29): 0.5 mg/kg IV esketamine (n = 34): 0.25 mg/kg 40-minute single infusion | Outcomes:
Follow-up: 7 days CGI-S performed at baseline CGI-I performed at 24 hours, 72 hours and 7 days after infusion |
Altinay et al. (2019)25 US Source of funding: Cleveland Clinic Foundation Research Project Committee | Single centre, double-blind, parallel 1:1, placebo-controlled RCT Sample size calculation: No ITT analysis: Unclear | Patients with TRD (N = 12) who failed to respond to at least 2 antidepressants, and who were referred for ECT. % Male:
Mean age (SD), years:
HAMD (SD):
MoCA (SD):
| ECT + IV ketamine (n = 7) ECT + midazolam (n = 5) Ketamine: 0.5 mg/kg over 40-minute infusion Midazolam (as placebo): 0.045 mg/kg over 40-minute infusion ECT: Mondays, Wednesdays, and Fridays Infusions: Tuesdays and Thursdays | Outcomes:
Follow-up: 3 weeks |
Domany et al. (2019)26 Israel Source of funding: Private funding | Single centre, double-blind, parallel 1:1, placebo-controlled RCT Sample size calculation: Yes ITT analysis: Yes | Patients with TRD (N = 41) who had inadequate response to at least 2 antidepressants and were stable with current treatment. They were randomly assigned to ketamine or placebo on top of usual care. % Male:
Mean age (SD), years:
Mean MADRS (SD):
| Oral ketamine (n = 22): 1 mg/kg thrice weekly for 21 days Placebo (n = 19): Saline thrice weekly for 21 days | Outcomes:
Follow-up: 21 days (end of treatment) |
Carspecken et al. (2018)28 US Source of funding: US Department of Veterans Affairs | Single centre, double-blind (patients and outcome assessors, parallel 1:1, RCT Sample size calculation: Yes ITT analysis: No | Veterans and service members with TRD (N = 52) who failed to respond to at least 2 antidepressants and were referred for ECT. % Male:
Mean age (SD), years:
Mean number of psychiatric medication (SD):
Baseline PHQ-9: NR Baseline HAMD: NR | IV ketamine-based anesthesia (n = 27): 1 to 2 mg/kg IV methohexital-based anesthesia (n = 25): 1 to 2 mg/kg ECT course was scheduled with consecutive sessions 3 times a week with length determined by clinical response per the treating psychiatrist. | Outcomes:
Follow-up: 3 days after final ECT treatment for PHQ-9 and HAMD; 2 to 4 weeks after ECT completion for MoCA. |
Gamble et al. (2018)27 Canada Source of funding: Schulman Research Award (University of Saskatchewan) and the Royal University Hospital foundation (Saskatoon, Saskatchewan) | Single centre, double-blind, parallel 1:1, RCT Sample size calculation: Yes ITT analysis: Yes (modified) | Patients with TRD (N = 24) who were referred for ECT. Definition for TRD was not provided. % Male:
Mean age (SD), years:
Mean MADRSc (SD):
Mean ALS-18l (SD):
Previously had ECT:
| IV ketamine-based anesthesia (n = 12): 0.75 mg/kg IV propofol-based anesthesia (n = 12): 1 mg/kg Both arms received IV remifentanil 1 mcg/kg and succinylcholine 0.75 mg/kg All patients received 8 ECT sessions scheduled at 2 or 3 sessions/week. | Outcomes:
Follow-up: 30 days after the final ECT session |
NRSs | ||||
Mikellides et al. (2021)29 The Netherlands Source of funding: NR | Retrospective chart review from a single centre Sample size calculation: No Adjustment for confounders: No | Patients with TRD (N = 24). Definition for TRD was not provided. % Male:
Mean age (SD), years:
Mean number of failed antidepressants (SD):
Mean HDRS (SD):
Mean HAM-A (SD):
Mean BDI-II (SD):
| IM ketamine (n = 12): twice weekly for 8 sessions; 0.25 mg/kg first, then the dosage was titrated upwards to a maximum of 1 mg/kg by session 4. rTMS (n = 12): 5 iTBS sessions were administered per week for 6 weeks, over the left of dorsal lateral prefrontal cortex. | Outcomes:
Follow-up: Only pre- and post-treatment assessment (4 weeks for IM ketamine; 6 weeks for rTMS) |
AEs = adverse events; ALS-18 = the short form of the Affective Lability Scale (also known as ALS-SF); BDI-II = Beck Depression Inventory – II; CADSS = Clinician-Administered Dissociative State Scale; ALS-18 = the short form of the Affective Lability Scale; CAPS-5 = Clinician-Administered PTSD Scale for DSM-5; CGI = Clinical Global Impression; CGI-I = CGI-improvement; CGI-S = CGI-severity; COWAT = Controlled Oral Word Association Test; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition); ECT = electroconvulsive therapy; HAM-A = Hamilton Anxiety Rating Scale; HAMD = Hamilton Depression Scale; HDRS = Hamilton Depression Rating Scale; HVLT-R = Hopkins Verbal Learning Test – Revised; IM = intramuscular; iTBS = intermittent theta-burst stimulation; ITT = intention-to-treat; MADRS = Montgomery-Asberg Depression Rating Scale; MoCA = Montreal Cognitive Assessment; NR = not reported; NRS = non-randomized study; PANSS = Positive and Negative Syndrome Scale; PCL-5 = PTSD Checklist for DSM-5; PHQ-9 = Patient Health Questionnaire-9; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; rTMS = repetitive transcranial magnetic stimulation; SD = standard deviation; TRD = treatment-resistant depression; YMRS = Young Mania Rating Scale.
aThe PCL-5 is a 20-item self-report measure that assesses the 20 DSM-5 symptoms of PTSD. Each item was rated on a 5-point Likert (0 = “Not at all” to 4 = “Extremely”). A total symptom severity score (range - 0 to 80) can be obtained by summing the scores for each of the 20 items. A 5-to-10-point change represents reliable change (i.e., change not due to chance) and a 10-to-20-point change represents clinically significant change.32
bThe CAPS-5, a 30-item structured interview, is the gold standard in PTSD assessment. The frequency and intensity information were converted into a single 5-point (0 to 4) symptom severity scale. The anchor points for this severity scale are 0 = absent, 1 = mild/subthreshold, 2 = moderate/threshold, 3 = severe/markedly elevated, and 4 = extreme/incapacitating.33
cThe MADRS has 10 items and used by clinicians to assess the severity of depression in patients with a diagnosis of depression. Each item has a severity scale from 0 to 6, with higher scores reflecting more severe symptoms. Ratings can be added to form an overall score (from 0 to 60). The proposed cut-offs: scores of 0 to 6 indicate an absence of symptoms; 7 to 19 represent mild depression; 20 to 34 moderate; 35 to 60 indicate severe depression.34
dThe CADSS is a scale used to measure dissociative states, consisting of 23 clinician-administered items, each scored from 0 (not at all) to 4 (extreme).35
eThe PANSS is a standardized, clinical interview that rates the presence and severity of positive and negative symptoms, as well as general psychopathology for people with schizophrenia. It consists of 30 items, 7 are positive symptoms, 7 are negative symptoms, and 16 are general psychopathology symptoms. Symptom severity for each item is rated in the 7-point scale (1 = absent; 7 = extreme).36
fThe HAMD, also termed HDRS, is used to measure the severity of symptoms of depression based on 17-item scales rated on either a 3- or 5-point scale, with the sum of all items making up the total score. The scores of 0 to 7 are considered as being normal, 8 to 16 suggest mild depression, 17 to 23 moderate depression and scores over 24 are indicative of severe depression; the maximum score being 52.37
gThe YMRS is an 11-item rating scale used to assess manic symptoms. Four items are rated on a 0 to 8 scale, while the remaining 7 items are rated on a 0 to 4 scale. The optimal YMRS severity threshold of 25 (positive predictive value [PPV] = 83.0%; negative predictive value [NPV] = 66.0%) was determined to be classified as severely ill. The YMRS minimal clinically significant difference was 6.6 points.38
hThe MoCA is a 30-point screening test for detecting cognitive impairment. MoCA scores range between 0 and 30. A score of ≥ 26 is considered to be normal. People with mild cognitive impairment had an average score of 22.1. People with Alzheimer disease scored an average of 16.2.39
IThe HVLT-R provides a brief assessment of verbal learning and memory (delayed recall and recognition) for individuals aged 16 years and older. The test is a 12-item 3 learning trial verbal learning test with delayed recall and recognition memory test. Raw scores are derived from Total Recall, Delayed Recall, Retention (% retained), and a Recognition Discrimination Index.40
jThe COWAT is a verbal fluency test that measures spontaneous production of words with the given letter (C, F, or L). Individuals are also instructed to exclude proper nouns, numbers, and the same word with a different suffix.41
kThe CGI is a standardized assessment scale for determining the effect of mental health treatment among psychiatric patients. It has 2 separate global subscales: Severity Illness (CGI-S) and Global Improvement (CGI-I). The CGI-S rates the severity on a 1 to 7 scale, with 1 representing normal symptoms (patient is not ill), 4 representing moderately ill, and 7 representing most severely ill. The CGI-I taken after treatment and compared with baseline. It rates the improvement on a 1 to 7 scale, with 1 representing ‘very much improved,’ 7 for ‘very much worse’ due to treatment, and 4 for no change from treatment.42
lThe ALS-18 is an 18-item scale that retrospectively measures sudden mood change over the past week. Each item is rated on a 4-point (0 to 3) scale, ranging from 0 = “Very uncharacteristic of me” to 3 = “Very characteristic of me.” The ALS-18 also includes a total score and scores of three subscales: Anxiety/ Depression, depression/Elation, and Anger.43
mThe HAM-A that assesses anxiety severity, consists of 14 items measuring different symptoms. Each item is rated on a 5-point (0 to 4) scale, ranging from 0 = Not present to 4 = Very severe. Total score ranges from 0 to 56, where scores < 17 indicate mild severity, scores between 18 and 24 indicate mild to moderate severity, and scores between 25 to 30 indicate moderate to severe anxiety.44
nThe BDI-II that assesses depression severity, consists of 21 items. Each item is rated on a 4-point (0 to 3) scale, with a total score ranging from 0 to 63. Scores of 0 to 10 indicate absent or minimal depression, 14 to 19 for mild depression, 20 to 28 for moderate depression, and 29 to 63 for severe depression.45
oThe PHQ-9 is a 9-item depression scale. Each item is rated on 4-point (0 [not at all] to 3 [nearly every day]) scale, with a total score ranging from 0 to 27. Scores of 0 to 4 indicates none or minimal depression, 5 to 9 mild depression, 10 to 14 moderate depression, 15 to 19 moderately severe depression, and 19 to 27 severe depression.46
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations, development, and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
DHA, Moeller et al. (2021)30 | ||||||
Intended users: All health care professionals who treat patients with difficult-to-treat depression Target population: Patients with difficult-to-treat depression (defined as without remission despite at least 2 antidepressants; chronic depression [i.e., lasting for 2 or more years regardless of treatment], or treatment-resistant using an assessment scale) | Six selected interventions: unilateral high frequency, IV ketamine or esketamine, bright light therapy, cognitive behavioural analysis system of psychotherapy, psychotherapy targeting rumination, and cognitive remediation. | All efficacy, tolerability, and safety outcomes that were clinically relevant. | The evidence from literature was systematically identified. Data extraction was conducted independently by 2 reviewers. Data were synthesized using meta-analysis wherever appropriate. | Quality of evidence and strength of recommendations were graded using GRADE. The program MAGICapp was used to formulate the recommendations,a taking into considerations of 1) the quality of evidence, 2) the efficacy and tolerability of the intervention, 3) the patient preference concerning the intervention, and 4) practical issues (e.g., a demand for special training or equipment) | Recommendations were developed by a guideline working group comprising professionals in psychiatry, clinical psychology, nursing, general practice, academic experts in psychiatry and psychology, and a patient representative. The program Making GRADE the Irresistible Choice (MAGICapp) was used to formulate the recommendations. Options for recommendations: strong recommendation for/or against the intervention, weak recommendation for/or against the intervention or a good clinical practice (in the absence of relevant evidence). | The guideline was reviewed by various organizations before publishing in a peer-reviewed journal. |
CANMAT, Swainson et al. (2021)31 | ||||||
Intended Users: Clinicians who treat patients with TRD Target population: Patients with TRD | Racemic ketamine | All efficacy, tolerability, feasibility, and safety outcomes that were relevant to developer-specified research questions. | The evidence from literature was systematically identified. Recent consensus statement and guidelines were also reviewed. | The Cochrane risk of bias tool was used to assess the quality of evidence. Clinical recommendations were graded by line of treatmentb with level of evidencec supporting each recommendation. | A task force developed 14 clinical questions. The recommendations were given in a question-answer format. | Published in peer-reviewed journal. |
CANMAT = The Canadian Network for Mood and Anxiety Treatments; DHA = Danish Health Authority; GRAGE = Grades of Recommendation, Assessment, Development, and Evaluation; TRD = treatment-resistant depression.
aOptions for recommendations were as follows: strong recommendation for/or against the intervention, weak recommendation for/or against the intervention or good clinical practice (in the absence of sufficiently relevant evidence).
bLine of treatment31:
First: Level 1 or level 2 evidence for efficacy plus clinical support for safety/tolerability/feasibility.
Second: Level 3 or higher evidence for efficacy plus clinical support for safety/tolerability/feasibility.
Third: Level 4 evidence of higher for efficacy plus clinical support for safety/tolerability/feasibility.
Not recommended: Level 1 evidence for lack of efficacy or level 2 evidence for lack of efficacy plus expert consensus.
Level of evidence31:
Level 1: Meta-analysis with narrow confidence interval or replicated double-blind (DB), randomized controlled trial (RCT) that includes a placebo or active comparison condition (n ≥ 30 in each active treatment arm).
Level 2: Meta-analysis with wide confidence interval or 1 DB RCT with placebo or active comparison condition (n ≥ 30 in each active treatment arm).
Level 3: At least 1 DB RCT with placebo or active comparison condition (n = 10 to 29 in each active treatment arm).
Level 4: Pilot study (RCT with n < 10 participants in each active treatment arm), uncontrolled trial, anecdotal reports, or expert opinion.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Clinical Studies Using the Downs and Black checklist19
Strengths | Limitations |
|---|---|
Abdallah et al. (2022)22 | |
RCTs | |
Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
| Reporting:
Internal validity – bias:
|
Feder et al. (2021)23 | |
Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
| Reporting:
Internal validity — bias:
External validity:
Internal validity — confounding:
|
Correia-Melo et al. (2020)24 | |
Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
| External validity:
Internal validity — confounding:
|
Altinay et al. (2019)25 | |
Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
| Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
|
Domany et al. (2019)26 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity — confounding:
| External validity:
Internal validity —bias:
Internal validity — confounding:
|
Gamble et al. (2018)27 | |
Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
| Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
|
Carspecken et al. (2018)28 | |
Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
| Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
|
NRS | |
Mikellides et al. (2021)29 | |
Reporting:
External validity:
Internal validity — bias:
| Reporting:
External validity:
Internal validity — bias:
Internal validity — confounding:
|
CI = confidence interval; ITT = intention-to-treat; NRS = non-randomized study; RCT = randomized controlled trial.
Table 5: Strengths and Limitations of Guidelines Using AGREE II20
Item | DHA, Moeller et al. (2021)30 | CANMAT, Swainson et al. (2021)31 |
|---|---|---|
Domain 1: Scope and Purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder Involvement | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of Development | ||
7. Systematic methods were used to search for evidence. | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes |
14. A procedure for updating the guideline is provided. | Unclear | Unclear |
Domain 4: Clarity of Presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | Unclear | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Unclear | Unclear |
Domain 6: Editorial Independence | ||
22. The views of the funding body have not influenced the content of the guideline. | No | No |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; CANMAT = The Canadian Network for Mood and Anxiety Treatments; DHA = Danish Health Authority; NR = not reported; NA = not applicable.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome – PTSD symptoms
Study citation, study design, and patient model | Study findings |
|---|---|
PCL-5 scores | |
Standard dose IV Ketamine 0.5 mg/kg (n = 51) vs. Low dose IV ketamine 0.2 mg/kg (n = 53) vs. Placebo (n = 54) | |
Abdallah et al. (2022)22 RCT Veterans and service members with PTSD (N = 158) who failed previous antidepressant treatment | After 24 hour – MD ± SEM
End of treatment (i.e., 4 weeks) – MD ± SEM
At 4 weeks of follow-up – MD ± SEM
Response (≥ 25% improvement in PCL-5) after 24 hours:
|
CAPS-5 scores | |
Standard dose IV Ketamine 0.5 mg/kg (n = 51) vs. Low dose IV ketamine 0.2 mg/kg (n = 53) vs. Placebo (n = 54) | |
Abdallah et al. (2022)22 RCT Veterans and service members with PTSD (N = 158) who failed previous antidepressant treatment | After 24 hour – MD ± SEM
At 4 weeks of follow-up – MD ± SEM
|
IV Ketamine 0.5 mg/kg (n = 15) vs. IV Midazolam 0.045 mg/kg (n = 15) | |
Feder et al. (2021)23 RCT Patients with chronic PTSD, who were stable with psychotropic medications for at least 3 months before randomization (N = 30) | Total CAPS-5 scores were significantly lower in the ketamine group compared with the midazolam group:
Response (≥ 30% reduction from baseline):
Loss of response (< 30% improvement from baseline):
|
Adj. = adjusted; CAPS-5 = Clinician-Administered PTSD Scale for DSM-5; CI = confidence interval; IQR = interquartile range; MD = mean difference; OR = odds ratio; PCL-5 = PTSD checklist for DSM-5; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; SEM = standard error of the mean; vs. = versus.
Table 7: Summary of Findings by Outcome – Depression
Study citation, study design, and patient model | Study findings |
|---|---|
MADRS scores | |
Standard dose IV Ketamine 0.5 mg/kg (n = 51) vs. Low dose IV ketamine 0.2 mg/kg (n = 53) vs. Placebo (n = 54) | |
Abdallah et al. (2022)22 RCT Veterans and service members with PTSD (N = 158) who failed previous antidepressant treatment | After 24 hour – MD ± SEM
End of treatment (i.e., 4 weeks) – MD ± SEM
At 4 weeks of follow-up – MD ± SEM
|
IV Ketamine 0.5 mg/kg (n = 15) vs. IV Midazolam 0.045 mg/kg (n = 15) | |
Feder et al. (2021)23 RCT Patients with chronic PTSD, who were stable with psychotropic medications for at least 3 months before randomization (N = 30) | Depression was significantly improved in the ketamine group compared with the midazolam groups at week 1 and week 2 (P < 0.05). Data were presented graphically without numerical values. |
IV ketamine 0.5 mg/kg (n = 29) vs. IV esketamine 0.25 mg/kg (n = 34) | |
Correia-Melo et al. (2020)24 RCT Patients with TRD (N = 63) who failed to respond to at least 1 antidepressant | Mean MADRS scores at:
Remission rate (%) at:
Response rate (%; ≥ 50% reduction from baseline) at:
|
ECT + IV ketamine 0.5 mg/kg (n = 7) vs. ECT + midazolam 0.045 mg/kg (n = 5) | |
Altinay et al. (2019)25 RCT Patients with TRD (N = 12) who failed to respond to at least 2 antidepressants, and who were referred for ECT | There was no significant difference between ketamine and midazolam groups.
|
Oral ketamine 1 mg/kg thrice weekly for 21 days (n = 22) vs. Placebo (n = 19) | |
Domany et al. (2019)26 RCT Patients with TRD (N = 41) who had inadequate response to at least 2 antidepressants and were stable with current treatment. | Mean change of MADRS scores at day 21 from baseline:
Response (≥ 50% reduction from baseline) at day 21:
Remission (MADRS ≤ 10) at day 21:
|
IV ketamine-based anesthesia 0.75 mg/kg (n = 12) vs. IV propofol-based anesthesia 1 mg/kg (n = 12) | |
Gamble et al. (2018)27 RCT Patients with TRD (N = 24) who were referred for ECT. Definition for TRD was not provided. | Response (≥ 50% reduction from baseline):
Remission (MADRS ≤ 10):
Relapse (MADRS > 20) at 30-day follow-up:
Median (IQR) of ECT treatments to a 50% reduction in MADRS scores:
|
HAMD or HDRS scores | |
ECT + IV ketamine 0.5 mg/kg (n = 7) vs. ECT + midazolam 0.045 mg/kg (n = 5) | |
Altinay et al. (2019)25 RCT Patients with TRD (N = 12) who failed to respond to at least 2 antidepressants, and who were referred for ECT | There was no significant difference between ketamine and midazolam groups.
Response (≥ 50% decrease in scores):
Remission (HAMD < 8)
|
IV ketamine-based anesthesia 1 to 2 mg/kg (n = 27) vs. IV methohexital-based anesthesia 1 to 2 mg/kg (n = 25) | |
Carspecken et al. (2018)28 RCT Veterans and service members with TRD (N = 52) who failed to respond to at least 2 antidepressants, and who were referred for ECT. | Patients in both groups had depression score improvement (decreased) after completing the ECT index course.
|
IM ketamine 0.25 mg/kg first, then 1 mg/kg (n = 12) vs. rTMS (n = 12) | |
Mikellides et al. (2021)29 Retrospective chart review study Patients with TRD (N = 24). Definition for TRD was not provided. |
|
BDI-II | |
IM ketamine 0.25 mg/kg first, then 1 mg/kg (n = 12) vs. rTMS (n = 12) | |
Mikellides et al. (2021)29 Retrospective chart review study Patients with TRD (N = 24). Definition for TRD was not provided. |
|
PHQ-9 scores | |
IV ketamine-based anesthesia 1 to 2 mg/kg (n = 27) vs. IV methohexital-based anesthesia 1 to 2 mg/kg (n = 25) | |
Carspecken et al. (2018)28 RCT Veterans and service members with TRD (N = 52) who failed to respond to at least 2 antidepressants, and who were referred for ECT. | Patients in both groups had depression score improvement (decreased) after completing the ECT index course.
|
CGI scores | |
IV ketamine 0.5 mg/kg (n = 29) vs. IV esketamine 0.25 mg/kg (n = 34) | |
Correia-Melo et al. (2020)24 RCT Patients with TRD (N = 63) who failed to respond to at least 1 antidepressant | Median (IQR) of GCI-Improvement scores at:
|
adj. = adjusted; BDI-II = Beck Depression Inventory – II; CGI = Clinical Global Impression; CI = confidence interval; CGI = Clinical Global Impression; ECT = electroconvulsive therapy; HAMD = Hamilton depression scale; HDRS = Hamilton Depression Rating Scale; HR = hazard ratio; IQR = interquartile range; IV = IV; LB = lower bound; MADRS = Montgomery-Asberg Depression Rating Scale; LM = lower bound; MD = mean difference; PHQ-9 = Patient Health Questionnaire-9; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; rTMS = repetitive transcranial magnetic stimulation; SEM = standard error of the mean; SE = standard error; TRD = treatment-resistant depression; vs. = versus.
Table 8: Summary of Findings by Outcome — Anxiety
Study citation, study design, and patient model | Study findings |
|---|---|
HAM-A scores | |
IM ketamine 0.25 mg/kg first, then 1 mg/kg (n = 12) vs. rTMS (n = 12) | |
Mikellides et al. (2021)29 Retrospective chart review study Patients with TRD (N = 24). Definition for TRD was not provided. |
|
HAM-A = Hamilton Anxiety Rating Scale; TRD = treatment-resistant depression; rTMS = repetitive transcranial magnetic stimulation.
Table 9: Summary of Findings by Outcome — Safety
Study citation, study design, and patient model | Study findings |
|---|---|
CADSS scores | |
Standard dose IV Ketamine 0.5 mg/kg (n = 51) vs. Low dose IV ketamin 0.2 mg/kg (n = 53) vs. Placebo (n = 54) | |
Abdallah et al. (2022)22 RCT Veterans and service members with PTSD (N = 158) who failed previous antidepressant treatment |
|
IV Ketamine 0.5 mg/kg (n = 15) vs. IV Midazolam 0.045 mg/kg (n = 15) | |
Feder et al. (2021)23 RCT Patients with chronic PTSD, who were stable with psychotropic medications for at least 3 months before randomization (N = 30) | The authors reported that “Dissociative symptoms that emerged during ketamine infusions were transient, with highest levels reported at the infusion-end assessment (40 minutes), and had resolved by the next assessment,120 minutes after start of infusion.” |
IV ketamine 0.5 mg/kg (n = 29) vs. IV esketamine 0.25 mg/kg (n = 34) | |
Correia-Melo et al. (2020)24 RCT Patients with TRD (N = 63) who failed to respond to at least 1 antidepressant | No significant difference in mean CADSS scores between groups:
|
IV ketamine-based anesthesia 0.75 mg/kg (n = 12) vs. IV propofol-based anesthesia 1 mg/kg (n = 12) | |
Gamble et al. (2018)27 RCT Patients with TRD (N = 24) who were referred for ECT. Definition for TRD was not provided. |
|
PANSS scores | |
Standard dose IV Ketamine 0.5 mg/kg (n = 51) vs. Low dose IV ketamine 0.2 mg/kg (n = 53) vs. Placebo (n = 54) | |
Abdallah et al. (2022)22 RCT Veterans and service members with PTSD (N = 158) who failed previous antidepressant treatment |
|
YMRS scores | |
ECT + IV ketamine 0.5 mg/kg (n = 7) vs. ECT + midazolam 0.045 mg/kg (n = 5) | |
Altinay et al. (2019)25 RCT Patients with TRD (N = 12) who failed to respond to at least 2 antidepressants, and who were referred for ECT | There was no significant difference between ketamine and midazolam groups.
|
MoCA scores | |
ECT + IV ketamine 0.5 mg/kg (n = 7) vs. ECT + midazolam 0.045 mg/kg (n = 5) | |
Altinay et al. (2019)25 RCT Patients with TRD (N = 12) who failed to respond to at least 2 antidepressants, and who were referred for ECT | There was no significant difference between ketamine and midazolam groups.
|
IV ketamine-based anesthesia 1 to 2 mg/kg (n = 27) vs. IV methohexital-based anesthesia 1 to 2 mg/kg (n = 25) | |
Carspecken et al. (2018)28 RCT Veterans and service members with TRD (N = 52) who failed to respond to at least 2 antidepressants, and who were referred for ECT. | Patients in both groups had no cognitive impairment after completing the ECT index course.
|
COWAT scores | |
ECT + IV ketamine 0.5 mg/kg (n = 7) vs. ECT + midazolam 0.045 mg/kg (n = 5) | |
Altinay et al. (2019)25 RCT Patients with TRD (N = 12) who failed to respond to at least 2 antidepressants, and who were referred for ECT | There was no significant difference between ketamine and midazolam groups.
|
ALS-18 scores | |
IV ketamine-based anesthesia 0.75 mg/kg (n = 12) vs. IV propofol-based anesthesia 1 mg/kg (n = 12) | |
Gamble et al. (2018)27 RCT Patients with TRD (N = 24) who were referred for ECT. Definition for TRD was not provided. | At 30-day follow-up:
|
Other AEs | |
Standard dose IV Ketamine 0.5 mg/kg (n = 51) vs. Low dose IV ketamine 0.2 mg/kg (n = 53) vs. Placebo (n = 54) | |
Abdallah et al. (2022)22 RCT Veterans and service members with PTSD (N = 158) who failed previous antidepressant treatment |
|
IV Ketamine 0.5 mg/kg (n = 15) vs. IV Midazolam 0.045 mg/kg (n = 15) | |
Feder et al. (2021)23 RCT Patients with chronic PTSD, who were stable with psychotropic medications for at least 3 months before randomization (N = 30) |
|
IV ketamine 0.5 mg/kg (n = 29) vs. IV esketamine 0.25 mg/kg (n = 34) | |
Correia-Melo et al. (2020)24 RCT Patients with TRD (N = 63) who failed to respond to at least 1 antidepressant |
|
Oral ketamine 1 mg/kg thrice weekly for 21 days (n = 22) vs. Placebo (n = 19) | |
Domany et al. (2019)26 RCT Patients with TRD (N = 41) who had inadequate response to at least 2 antidepressants and were stable with current treatment. |
|
| |
Gamble et al. (2018)27 RCT Patients with TRD (N = 24) who were referred for ECT. Definition for TRD was not provided. | No significant differences in rates of other AEs:
|
IV ketamine-based anesthesia 1 to 2 mg/kg (n = 27) vs. IV methohexital-based anesthesia 1 to 2 mg/kg (n = 25) | |
Carspecken et al. (2018)28 RCT Veterans and service members with TRD (N = 52) who failed to respond to at least 2 antidepressants, and who were referred for ECT. | Effect of anesthesia on periprocedural clinical outcomes:
|
AE = adverse event; ALS-18 = the short form of the Affective Lability Scale; CADSS = Clinician-Administered Dissociative State Scale; COWAT = Controlled Oral Word Association Test; ECT = electroconvulsive therapy; MoCA = Montreal Cognitive Assessment; PACU = post-anesthesia care unit; PANSS = Positive and Negative Syndrome Scale; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; SD = standard deviation; SE = standard error; TEAE = treatment emergent adverse events; TRD = treatment-resistant depression; YMRS = Young Mania Rating Scale.
Table 10: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
DHA, Moeller et al. (2021)30 | |
“Do not use intravenous ketamine/esketamine in patients with DTD, as benefits are uncertain and short-lived. The adverse effects are considerable, and the long-term effects, including the risk of abuse, unknown.”30 (p. 6) Evidence supporting this recommendation came from 4 RCTs published from 2016 to 2019. | Weak recommendation against IV ketamine/esketamine |
CANMAT, Swainson et al. (2021)31 | |
“Efficacy
Evidence for recommendation on the efficacy of IV ketamine in acute treatment of DTD came from 7 meta-analyses, 6 RCTs, and 4 open-label studies. Evidence for recommendation on the efficacy of other formulations of ketamine came from 1 systematic review, 7 RCTs and 1 retrospective case series. | |
“Patient selection
Evidence for recommendation on who should receive ketamine came from previous CANMAT guidelines. | |
CANMAT = The Canadian Network for Mood and Anxiety Treatments; DHA = Danish Health Authority; DTD = difficult-to-treat depression.
Appendix 5: References of Potential Interest
Studies Included in the Previous CADTH Report17
Chen MH, Li CT, Lin WC, et al. Cognitive function of patients with treatment-resistant depression after a single low dose of ketamine infusion. J Affect Disord. 2018;241:1-7. PubMed
Chen MH, Lin WC, Wu HJ, et al. Antisuicidal effect, BDNF Val66Met polymorphism, and low-dose ketamine infusion: reanalysis of adjunctive ketamine study of Taiwanese patients with treatment-resistant depression (AKSTP-TRD). J Affect Disord. 2019;251:162-169. PubMed
Fava M, Freeman MP, Flynn M, et al. Double-blind, placebo-controlled, dose-ranging trial of intravenous ketamine as adjunctive therapy in treatment-resistant depression (TRD). Mol Psychiatry. 2018;03:03.
Ionescu DF, Bentley KH, Eikermann M, et al. Repeat-dose ketamine augmentation for treatment-resistant depression with chronic suicidal ideation: a randomized, double blind, placebo controlled trial. J Affect Disord. 2019;243:516-524. PubMed
Phillips JL, Norris S, Talbot J, et al. Single, repeated, and maintenance ketamine infusions for treatment-resistant depression: a randomized controlled trial. Am J Psychiatry. 2019;176(5):401-409. PubMed
Su TP, Chen MH, Li CT, et al. Dose-related effects of adjunctive ketamine in Taiwanese patients with treatment-resistant depression. Neuropsychopharmacology. 2017;42(13):2482-2492. PubMed
VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder. Washington (DC): Department of Veterans Affairs, Department of Defense; 2017: https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal012418.pdf. Accessed 2019 Oct 24.
Additional References
Bentley S, Artin H, Mehaffey E, et al. Response to intravenous racemic ketamine after switch from intranasal (S)-ketamine on symptoms of treatment-resistant depression and post-traumatic stress disorder in Veterans: A retrospective case series. Pharmacotherapy:The Journal of Human Pharmacology & Drug Therapy. 2022 Feb 05;05:05. PubMed
Melcer T, Walker GJ, Dye JL, et al. Is Prehospital Ketamine Associated With a Change in the Prognosis of PTSD? Mil Med. 2022 Feb 01;01:01. PubMed
Shiroma PR, Thuras P, Wels J, Erbes C, Kehle-Forbes S, Polusny M. A Proof-of-Concept Study of Subanesthetic Intravenous Ketamine Combined With Prolonged Exposure Therapy Among Veterans With Posttraumatic Stress Disorder. J Clin Psychiatr. 2020 11 10;81(6):10. PubMed
Ross C, Jain R, Bonnett CJ, Wolfson P. High-dose ketamine infusion for the treatment of posttraumatic stress disorder in combat veterans. Ann Clin Psychiatry. 2019 11;31(4):271-279. PubMed
Albott CS, Lim KO, Forbes MK, et al. Efficacy, Safety, and Durability of Repeated Ketamine Infusions for Comorbid Posttraumatic Stress Disorder and Treatment-Resistant Depression. J Clin Psychiatr. 2018 May/Jun;79(3). PubMed
Mion G, Le Masson J, Granier C, Hoffmann C. A retrospective study of ketamine administration and the development of acute or post-traumatic stress disorder in 274 war-wounded soldiers. Anaesthesia. 2017 Dec;72(12):1476-1483. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matter of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca