CADTH Health Technology Review
Radioiodine Resensitization for Radioiodine-Refractory Metastatic Differentiated Thyroid Cancer
Rapid Review
Authors: Sarah Goring, Quenby Mahood
Abbreviations
DTC
differentiated thyroid cancer
MAPK
mitogen-activated protein kinase
MEK
mitogen-activated kinase
NTRK
neurotrophic tyrosine receptor kinase
PET
positron emission tomography
PI3K
phosphoinositide 3-kinase
RAIRMDTC
radioiodine-refractory/resistant metastatic differentiated thyroid cancer
RECIST
Response Evaluation Criteria in Solid Tumours
RET
rearranged during transfection
Key Messages
Evidence of radioiodine resensitization was reported in 4 single-arm clinical trials and 3 uncontrolled retrospective cohort studies, which included between 3 and 20 patients. Over half of patients in these 7 studies demonstrated increased radioiodine avidity after resensitization treatment.
Where reported, at least half of radioiodine retreated patients remained progression free and/or had not initiated a new treatment by the end of study follow-up.
Adverse events associated with radioiodine resensitization therapies were typically mild, with skin-related adverse events being most common.
No studies comparing outcomes of radioiodine resensitization therapies against lenvatinib or to no treatment were identified.
No evidence on the cost-effectiveness of radioiodine resensitization therapy was found.
Context and Policy Issues
Thyroid cancer was among the 10 most commonly occurring cancers worldwide in 2020.1 In Canada, there were approximately 6,700 new cases in 2021, ranking eighth among all cancers for age-standardized incidence rate, and fifth among women.2
Over 90% of thyroid cancers involve the follicular cells,3 including papillary carcinoma, follicular carcinoma, and more rarely, Hürthle cell carcinoma; together these are classified as differentiated thyroid cancers (DTC). A specialized function of differentiated thyroid cells is to take up iodine from the blood. Consequently, an effective treatment for DTC is radioiodine (iodine-131, a radioactive iodine isotope), which is absorbed by the cells and causes cell death via beta radiation.4 Radioiodine is typically given post-surgery to destroy residual cancer cells, and is offered primarily to high-risk patients, such as those with distant metastases, which represents less than 10% of all DTCs.4,5
In approximately 50% of metastatic DTCs, cells lose the ability to perform specialized functions such as iodine uptake, causing them to be radioiodine-resistant or refractory.6 Prognosis is poor for patients with radioiodine-refractory/resistant metastatic DTC (RAIRMDTC), with approximately 90% of patients dying within 10 years of diagnosis.5 Treatment options for patients with RAIRMDTC are limited. Recent approvals of multikinase inhibitors have begun to address the unmet need for treatment of RAIRMDTC, demonstrating improvements in progression-free survival over placebo.7,8 In 2016, lenvatinib (a multikinase inhibitor) was approved by Health Canada and is currently reimbursed in several Canadian provinces9; however, treatment with lenvatinib is associated with substantial toxicity, and must be taken continuously until death or disease progression.8
An alternative approach to therapy has been explored in the past decade, using therapies that inhibit specific mediators of the mitogen-activated protein kinase (MAPK) and phosphoinositide 3-kinase (PI3K) pathways as a means to resensitize DTCs to radioiodine.10 Mutations within the MAPK pathway, (e.g., the BRAF V600E activating mutation) and PI3K pathway (e.g., RAS mutations), have been shown to reduce cells’ ability to import iodine (or radioiodine); approximately 70% of papillary thyroid cancers harbour such mutations.11 Targeting specific mutations within these pathways, using therapies such as BRAF inhibitors, mitogen-activated kinase (MEK) inhibitors, neurotrophic tyrosine receptor kinase (NTRK) inhibitors, and rearranged during transfection (RET) inhibitors can to restore cells’ ability to uptake iodine, and thereby resensitize previously radioiodine-refractory tumours to radioiodine therapy.
The purpose of the current report is to summarize evidence regarding the clinical effectiveness, safety, and cost-effectiveness of radioiodine resensitization therapies followed by treatment with radioiodine among patients with RAIRMDTC, relative to lenvatinib or no treatment, or as non-comparative estimates.
Research Questions
What is the clinical effectiveness of radioiodine resensitization followed by radioiodine in patients with radioiodine-refractory/resistant metastatic differentiated thyroid cancer?
What is the cost-effectiveness of radioiodine resensitization followed by radioiodine in patients with radioiodine-refractory/resistant metastatic differentiated thyroid cancer?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were thyroid cancer and resensitization, or thyroid cancer and radioiodine resensitizing drugs. Conference abstracts were omitted from the search results. The search was limited to English language documents published between January 1, 2013 and March 3, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with radioiodine-refractory/resistant metastatic thyroid cancera |
Intervention | Radioiodine resensitization (also known as redifferentiation) with: dabrafenib, vemurafenib (BRAF inhibitors); trametinib, selumetinib (MEK inhibitors); NTRK inhibitors (e.g., larotrectinib, entrectinib); or RET inhibitors (e.g., selpercatinib, pralsetinib), followed by radioiodine |
Comparator | Q1 and 2: Lenvatinib Q1: No treatment (e.g., waitlist, placebo); no comparator |
Outcomes | Q1: Clinical effectiveness (e.g., overall survival, progression-free survival [as defined by RECIST guidelines], radioiodine uptake, response rate [e.g., as determined by radiographic imaging], remission rate, health-related quality of life, need for subsequent treatments or change in therapy, emergency department visits, hospitalizations) and safety/harms (e.g., any grade treatment-related adverse events [e.g., hypertension, diarrhea, fatigue], withdrawal due to adverse events, mortality) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, cost per unit of health benefit) |
Study designs | Health technology assessments, systematic reviews, randomized-controlled trials, non-randomized studies, economic evaluations |
NTRK = neurotrophic tyrosine receptor kinase; MEK = mitogen-activated kinase; RET = rearranged during transfection.
aStudies with mixed populations regarding the stage of cancer (i.e., included metastatic, and locally advanced or early stages of differentiated thyroid cancer) were also eligible for inclusion.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2013. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)12 for systematic reviews, and the Downs and Black checklist13 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
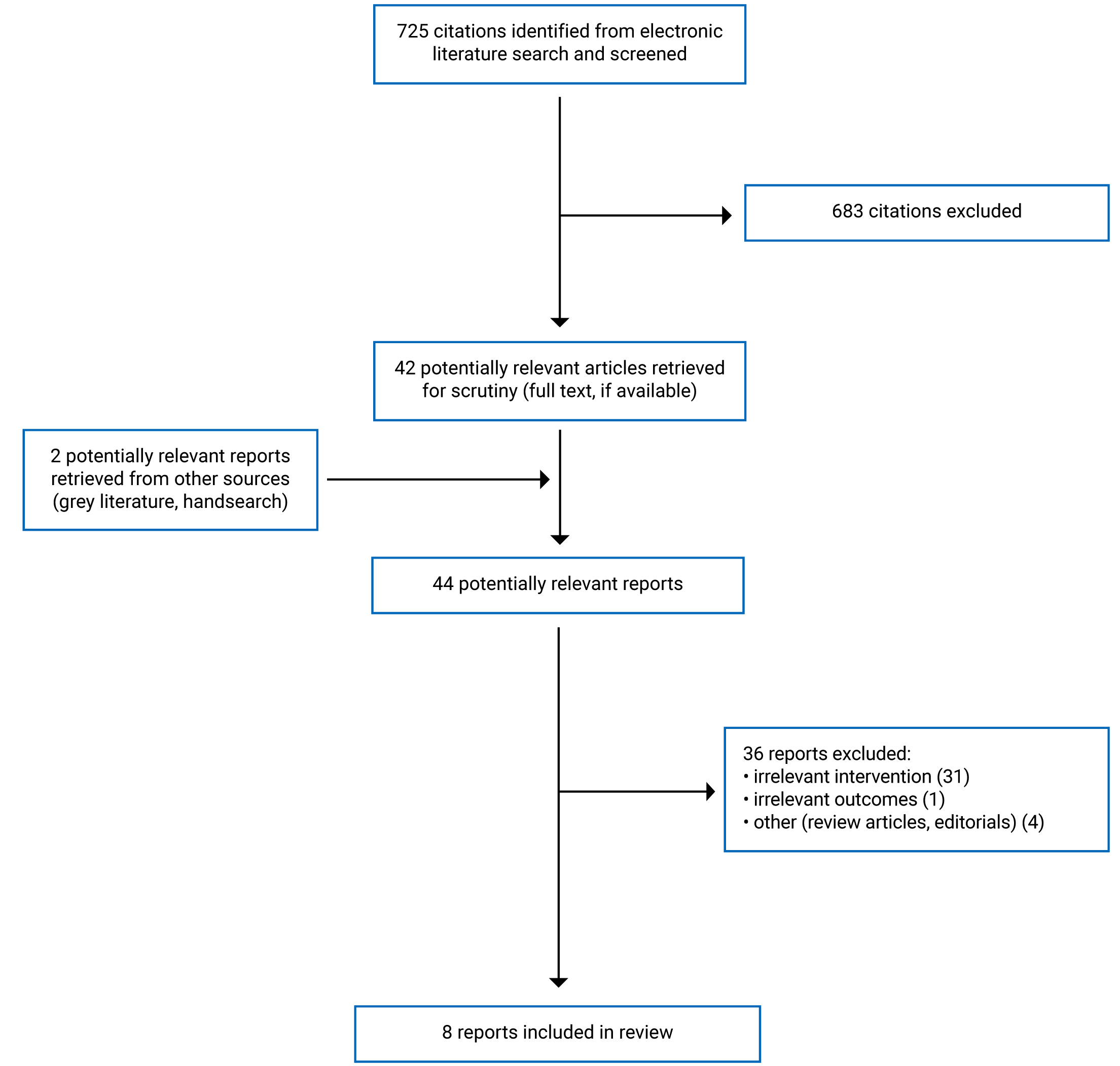
A total of 725 citations were identified in the literature search. Following screening of titles and abstracts, 683 citations were excluded and 42 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 36 publications were excluded for various reasons, and 8 publications met the inclusion criteria and were included in this report. These comprised 114 systematic review, and 715-21 non-randomized studies. Appendix 1 presents the PRISMA22 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One systematic review was identified, published in 2021, and including studies published up to December 2019.14 This systematic review was designed to identify studies involving treatment for advanced or refractory DTC, but captured a broader set of interventions than in the current report. Specifically, the systematic review eligibility criteria permitted inclusion of studies involving immunotherapies or tyrosine kinase inhibitor (any type), with or without re-treatment with radioiodine. Studies involving tyrosine kinase inhibitors were restricted to clinical trials of humans, whereas immunotherapy studies also included in vitro studies. Of the 23 studies identified in the systematic review, 315-17 were relevant to the current report. In the systematic review, brief summaries of each study were provided; there was no synthesis or additional interpretation provided. As these 315-17 studies were also identified as primary studies in the current review, the more comprehensive evidence from the primary studies was selected for inclusion, in lieu of the more limited evidence presented within this secondary source (i.e., the systematic review). As such, the characteristics and results from this systematic review will not be described hereafter, aside from a brief summary of its critical appraisal.
A total of 715-21 primary clinical studies were identified, including the 315-17 captured in the aforementioned systematic review, and 418-21 other studies. These 715-21 studies are described in the following subsections.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Of the 715-21 primary clinical studies identified in this report, none included a control group involving lenvatinib, placebo, or no treatment, nor were any designed to compare outcomes between radioiodine resensitization interventions. Four studies were single-arm clinical trials (i.e., had 1 intervention arm and no control arm) and 319-21 were uncontrolled retrospective cohort studies. In the 415-18 single-arm clinical trials and 121 of the retrospective cohort studies, all patients within each study received the same radioiodine resensitization regimen. In the other 219,20 uncontrolled retrospective cohort studies, several different radioiodine resensitization regimens were used; however, the studies were not designed to compare outcomes between these interventions.
Country of Origin
All 415-18 clinical trials were conducted in the US, of which 315,16,18 were conducted at the Memorial Sloan Kettering Cancer Centre in New York; the fourth17 was conducted at Massachusetts General Hospital. Among the 319-21 retrospective cohort studies, 120 was US-based, conducted at MD Anderson Cancer Centre in Texas, 121 was conducted in Croatia, and 119 in Australia.
Patient Population
All 715-21 studies included patients with RAIRMDTC. In 315,17,18 studies, patients with locally advanced or unresectable radioiodine-refractory DTC without distant metastasis were also eligible. In 115 of these 315,17,18 studies, 1 patient had locally advanced disease and all other patients had distant metastasis. In the other 217,18 studies, over 86% of patients (which represented all but 1 patient in each study) had distant metastasis to the lungs; it was unclear whether the remaining patient in each of these studies had distant or local metastasis. One21 retrospective study captured a broader patient population, but provided data on a relevant subset of patients with RAIRMDTC. The sample size was 3 patients in the relevant subset of the latter study21; in the remaining 615-20 studies, sample size ranged from 6 to 20 patients.
The median age across the 615-20 studies for which baseline patient characteristics were reported ranged from 56 to 68 years. In 515-18,20 of the 615-20 studies, there were more males than females (54% female to 86% male); in the remaining 119 study, which involved 6 patients, 2 patients (33%) were male.
Five15,17-19,21 of the studies were restricted to patients with RAIRMDTC harbouring BRAF V600E mutations, 119 of which also permitted NRAS mutations. In the other 216,20 studies, there were no mutation-related eligibility restrictions. In these studies, tumour genotype was reported among the baseline patient characteristics, and was most commonly BRAF V600E.
Where defined, the criteria for establishing radioiodine refractoriness differed slightly across studies. While all studies required 1 or more non-radioiodine-avid lesion(s) (including but not limited to metastatic sites), and/or progression despite previous radioiodine resensitization therapy, specific details within these criteria varied. Additionally, the 315,16,18 clinical trials conducted at the Memorial Sloan Kettering Cancer Center included a criterion that involved assessing 18F-fluorodeoxyglucose-avidity, whereas this criterion was not used in other studies.
The type of DTC varied within and across studies. The majority of patients had papillary cell thyroid cancer, including classical, tall, columnar, and clear cell papillary cell thyroid cancer. Five15,16,18-20 of the 715-21 studies also reported patients with poorly differentiated thyroid cancer, with proportions ranging from 15% to 43%; follicular cell and mixed types were also reported.
Interventions and Comparators
The 415-18 included single-arm clinical trials investigated the use of 4 different radioiodine resensitization regimens as interventions; none involved a comparator group. Three15,17,18 trials involved BRAF inhibitors: dabrafenib 150 mg twice daily,17 vemurafenib 960 mg twice daily,15 or vemurafenib 960 mg twice daily. in combination with the anti-ErbB3 monoclonal antibody CDX-3379 1,000 mg on alternating weeks (beginning on week 3).18 The fourth16 trial investigated the use of the MEK inhibitor selumetinib 75 mg twice daily. Across all 415-18 trials, treatment involved up to 8 weeks of treatment. Initially, patients received 415-17 to 618 weeks of radioiodine resensitization treatment, followed by a scan to re-assess radioiodine uptake (relative to baseline). In 315,16,18 studies, this assessment was done using an iodine-124 PET/CT (PET/CT) scan, and in 117 study, this was done using a whole body scan after low-dose (148 MBq) iodine-131. Patients whose tumours showed restored radioiodine avidity received approximately 2 additional weeks of radioiodine resensitization treatment (exact duration not reported in 215,16 studies), followed by a therapeutic dose of iodine-131. In the 315,16,18 studies using iodine-124 PET/CT, a dosimetry threshold had to be met, such that some patients showed radioiodine avidity that was insufficient to warrant a therapeutic dose of iodine-131. Radioiodine resensitization treatment was discontinued 215,16,18 to 517 days after receiving iodine-131.
Across the 319-21 uncontrolled retrospective cohort studies, clinical experience with several different radioiodine resensitization regimens were described. In 121 study, treatment was limited to vemurafenib 960 mg twice daily, with no comparison group. In the other 219,20 uncontrolled retrospective cohort studies, interventions included: dabrafenib, vemurafenib, trametinib, dabrafenib in combination with trametinib, dabrafenib in combination with vemurafenib, vemurafenib in combination with cobimetinib, and an investigational MEK inhibitor (doses provided in Appendix 2, reported by study authors); none of the studies compared outcomes between these interventions, nor did any include a comparison group involving lenvatinib or no treatment. In 220,21 studies, details were sparse regarding the planned duration of radioiodine resensitization regimens, assessment of radioiodine uptake, and subsequent therapeutic treatment with iodine-131, although in both20,21 studies it was stated that assessment of radioiodine uptake was evaluated using iodine-131 followed by a whole body scan. In the third19 study, treatment details were provided: patients received a 4-week course of radioiodine resensitization treatment, followed by an iodine-124 PET/CT scan to assess avidity, and patients with sufficient radioiodine avidity received a therapeutic dose of iodine-131. The duration of radioiodine resensitization treatment described in this study19 (four weeks) was broadly consistent with the duration reported in the clinical trials; whereas, the duration of radioiodine resensitization treatment described by Jaber et al. (2018),20 varied across patients, from less than 1 month to more than 6 years (median of 3.5 months; range of 0.9 to 76.4 months).
Outcomes
All 715-21 studies reported the proportion of patients with radioiodine resensitization as a key study outcome. Additionally, response, measured radiographically using Response Evaluation Criteria in Solid Tumours (RECIST) version 1.1, was reported in all 715-21 studies, with variability around the time point at which response was reported. Three15,18,19 studies reported progression-free survival. Mortality was reported in 121 study. All 715-21 studies reported on adverse events, either as radioiodine resensitization treatment-related,15,16,18 radioiodine-related,20 or all-cause adverse events.17,19,21
Summary of Critical Appraisal
Systematic Review
The 114 systematic review captured studies already included in the current report, and thus did not contribute additional evidence to the review. This systematic review was assessed with a focus on the comprehensiveness and quality of search strategies to understand whether it may have missed key studies; however, was not evaluated for the quality of reporting (Appendix 3).
In this 114 systematic review, the search covered multiple bibliographic databases, grey literature, and included a review of the reference lists from included studies; however, the lack of duplicate review during study selection may have led to the omission of relevant studies. Similarly, the search terms may have been overly broad: “TKI” and “tyrosine kinase inhibitor” were the only drug-related search terms (i.e., terms for specific drugs or more specific drug classes such as BRAF or MEK inhibitors were not used) and it is unclear whether these terms were applied to subject headings or to titles and abstracts alone. Hence there is a risk that some studies were missed due to the search sensitivity and study selection process.
Primary Clinical Studies
In 515-19 of the 715-21 studies, the objectives, outcomes, patient characteristics, interventions and main findings were clearly reported. In the other 220,21 studies, details regarding the intervention were lacking. The duration of treatment with vemurafenib was not described in the methods or results section of the study by Pešorda et al. (2020),21 and in the study by Jaber et al. (2018),20 the radioiodine resensitization treatment doses were not reported. Furthermore, in the latter study, the median duration of radioiodine resensitization treatment was reported as being 3.5 months (range 0.9 to 76.4 months), which, for some patients, vastly exceeded the duration of treatment in the other 5 studies (up to approximately 8 weeks), making it unclear the treatments were initially planned to be used for radioiodine resensitization, or whether this decision was made later in the treatment course. All 715-21 studies reported efficacy or effectiveness outcomes that were considered valid and reliable: radioiodine uptake was evaluated using either iodine-124 PET/CT or iodine-131 whole body scan, and tumour response was measured using RECIST v1.1 criteria. However, in 117 study, the timing of response assessment was unclear, with inconsistency between the methods (stating 3 months) and results (stating 6 months). Adverse events were well captured in 615-19,21 of the 7 studies, using the Common Terminology Criteria for Adverse Events version 4.0 classification system, or not stated. In the seventh study, Jaber et al. (2018)20 reported on radioiodine-related adverse events but did not report on adverse events related to the preceding radioiodine resensitization treatment, and hence was assessed as being not well captured.
A main limitation of all 715-21 studies was the non-comparative nature of the study designs. The 415-18 clinical trials were designed as single-arm trials; 121 of the retrospective cohort studies captured a single radioiodine resensitization treatment regimen; and the other 219,20 retrospective cohort studies were non-comparative despite capturing multiple treatments, due to the sample size relative to the number of treatments (6 patients and 3 regimens in the study by Iravani et al. [2019]19; 13 patients and 5 regimens in the study by Jaber et al. [2018]20). Given the non-comparative nature of the 715-21 studies, none involved blinding of patients, investigators, or outcome assessors. The implication of having non-comparative (i.e., uncontrolled) studies of investigational therapies is that direct comparisons of outcomes between groups of patients cannot be made, either between interventions, or against standard of care. As such, the findings from these studies do not enable robust evaluation of the relative benefits and harms of radioiodine resensitization treatment across interventions, or relative to the relevant comparators, lenvatinib or no treatment.
Another limitation related to the external validity of all studies, relative to the Canadian setting. This was assessed as being somewhat low, given that all 715-21 studies were single-centre studies conducted in non-Canadian settings, and therefore may not generalize to expected outcomes in all Canadian centres.
Sample size calculations were performed in 315,16,18 of the 415-18 clinical trials, and none of the 319-21 retrospective cohort studies. These 315,16,18 clinical trials were designed to reject a null hypothesis that up to 5% of patients would have radioiodine uptake. In 118 of these 315,16,18 studies, accrual was halted early and thus the study was underpowered; however, the primary end point was still met. In the other 215,16 trials, the target sample sizes were achieved and were sufficient for addressing the study objective of determining whether 5% or more of patients have radioiodine uptake.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings, by outcome.
Clinical Effectiveness of Radioiodine Resensitization Followed by Radioiodine
Resensitization
Across the 715-21 studies, between 50% and 71% of patients showed evidence of restored radioiodine avidity following resensitization therapy with vemurafenib-, dabrafenib-, trametinib- or selumetinib-based therapy, or other investigational MEK inhibitor. In 315,16,18 studies, some patients had evidence of restored radioiodine avidity but did not meet the dosimetry threshold to warrant therapeutic dose of radioiodine. With these patients removed, the proportion of patients who were retreated with radioiodine across the 715-21 studies ranged from 33% and 69%.
Resensitization according to tumour genotype was available in the 316,19,20 studies with mixed genotypes; the other 415,17,18,21 studies were restricted to patients whose tumours harboured BRAF V600E mutations. Across all 715-21 studies, the proportion of patients with BRAF V600E mutant tumours who were resensitized and retreated with radioiodine was 11% to 100%. Among patients with NRAS+ mutations, reported in 316,19,20 studies, the range was 33% to 100%. Two of the multi-genotype studies16,20 captured and reported on patients with wild-type tumours: in 120 study there was 1 patient who was resensitized and retreated with radioiodine (100%) and in the other study,16 1 out of 3 patients (33%) was resensitized and retreated with radioiodine. The latter study16 also reported on 3 patients whose tumours had RET/PTC translocations, of whom 1 was resensitized and retreated with radioiodine (33%).
Response
Tumour response following radioiodine treatment, based on RECIST v1.1 criteria, was reported in 615-20 of the 7 studies. This was measured as best response at 6 months in 415-18,20 studies, and as best response to the end of follow-up in 219,20 studies. All studies reported the response rates among patients treated with radioiodine, and 217,20 studies also reported response rates among all non-radioiodine-treated patients. The response rates among all included patients in the study was also calculated.
Across the 615-20 studies, none reported complete responses, either radioiodine-treated patients or those who were not resensitized. Among radioiodine-treated patients, at least 1 partial response was reported in each of the 6 studies, ranging from 33% to 75% of patients (in the 4 studies that reported best overall response at 6 months, this ranged from 33% to 63% of patients). The rest of the radioiodine-treated patients had stable disease at the pre-defined assessment time point (i.e., 6 months or the end of follow-up), with the exception of 118 study, in which 2 out of 4 radioiodine retreated patients (50%) had progressive disease by month 6. Details regarding tumour progression were provided by the study authors of that study,18 explaining that 1 of the 2 patients had initiated a new anti-cancer treatment despite having stable disease at 3 months (and so was categorized as having progressed), and that response had been mixed in second patient, with tumour regression in areas that had shown restored radioiodine avidity, but tumour growth in metastatic lesions that had not shown restored avidity.
Subsequent Therapy
Use of subsequent therapy was specified in 515,18-21 studies, among the subgroup of radioiodine-treated patients.
In 219,20 of these 5 studies, none of the radioiodine-treated patients had received subsequent treatment by the end of follow-up, with median follow-up times of 14.320 and 16.619 months.
In another 215,18 of these 5 studies, 50% of patients had received subsequent treatment by the end of the follow-up period. In 118 of these 215,18 studies, patients received unspecified systemic therapy (these patients were classified as having progressive disease). In the other study,15 patients received either radiation or vemurafenib re-treatment.
In the fifth21 of these 5 studies, it was reported that 1 out of 3 vemurafenib-treated patients received second-line sorafenib 2 years after successful redifferentiation with vemurafenib, but that the patient died shortly thereafter.
Progression-Free Survival or Time to Progression
In 115 clinical trial involving vemurafenib, individual patient-level data were provided regarding the timing of progression among 4 radioiodine-treated patients: progression events occurred at 9 months and 18 months post-progression, and censoring (i.e., event-free at last follow-up) occurred at 18 and 22 months.
Progression-free survival at 6 months was available from another clinical trial,18 among 4 radioiodine-treated patients, and findings were consistent with best overall response at 6 months from that trial: 50% patients had progressed by 6 months, and the other 50% of patients remained progression-free and alive at 6 months.
In 119 uncontrolled retrospective cohort study involving mixed treatments, all 6 patients (irrespective of treatment with radioiodine) were alive and progression-free at the end of follow-up (median = 16 months; range = 5 months to 40 months).
Mortality
Across the 715-21 studies, 1 death was reported in 121 uncontrolled retrospective cohort study, 2 years after successful resensitization to radioiodine. Mortality was not reported in any of the other 615-20 studies.
Adverse Events
Among the 615-19,21 studies reporting all-cause or targeted therapy-related adverse events, skin-related adverse events were the most common type of event. Maculopapular rash was common in vemurafenib-based studies, affecting approximately 3/4 of patients, and with grade 3 maculopapular rash affecting approximately 1/4 of patients in 215,18 studies. Rash was the most common selumetinib-related adverse event, affecting 90% of patients in 116 study, although all events were mild or moderate (grade 1 or 2). Skin-related lesions or changes were also the most common dabrafenib-related adverse event in the clinical trial by Rothenberg et al. (2015),17 affecting 80% of patients (all grade 1); these included skin darkening, actinic keratosis, verrucous keratosis, and other skin-related adverse events. Acneiform rash affected 2 out of the 3 trametinib-treated patients (67%) in the study by Iravani et al. (2019),19 both of which were grade 3 adverse events; grade 1 rash (unspecified) affected 2 out of the 2 (100%) vemurafenib plus cobimetinib-treated patients in that same study.
Other adverse events that affected more than 1 patient in any given study are provided in Table 11. Adverse events with frequencies of 50% or higher in at least 1 study included: nausea, diarrhea, fatigue, hand-foot syndrome (also known as palmar-plantar erythrodysesthesia syndrome), and pooled categories of events, such as increased levels of hepatic enzymes and gastrointestinal symptoms.
Cost-Effectiveness of Radioiodine Resensitization Followed by Radioiodine
No relevant evidence regarding the cost-effectiveness of radioiodine resensitization treatment for RAIMDTC was identified; therefore, no summary can be provided.
Limitations
While the present review captures a comprehensive synthesis of the available evidence on radioiodine resensitization among patients with RAIRMDTC, there are several noteworthy limitations.
First, no evidence on cost-effectiveness of radioiodine resensitization therapy was identified in this review and no studies identified that directly compared the efficacy and safety of radioiodine resensitization therapy against lenvatinib or no treatment. While it may be reasonable to assume that de-differentiated cancer cells are unlikely to spontaneously resensitize to radioiodine without treatment, and hence a resensitization rate of 0% might provide a reasonable benchmark against which to compare findings, the current evidence base does not enable robust comparisons of other relevant clinical outcomes (such as tumour response, progression-free survival, overall survival, health-related quality of life, and adverse event rates) against existing standards of care. Additionally, there was no evidence identified for NTRK or RET inhibitors; all identified evidence was related to BRAF and/or MEK inhibitor-based therapy.
Another key limitation of the identified evidence was the sample size (with all studies having fewer than 20 patients) and single-centred study design of the included studies. The clinical trials were designed to be adequately powered to reject a null hypothesis of a up to 5% resensitization rate. While the primary end points were met, and provided sufficient evidence for establishing proof-of-principle regarding resensitization, the sample sizes contributed to uncertainty around the true proportion of patients that resensitize to treatment. Precision was further reduced within genotype-specific subgroups, in which sample sizes were smaller (e.g., the sample sizes of patients harbouring a BRAF V600E mutation ranged from 3 to 12 patients), as well as for estimating radiographic response rates, as response was typically reported among the subset of patients treated with radioiodine. There are 2 newer single-arm phase II trials not captured in the current review that enrolled larger sample sizes: the SEL-I-METRY trial23 of selumetinib (n = 60 patients) is ongoing but results have not yet been reported, and the MERAIODE24 trial of trametinib plus dabrafenib (n = 24 patients) has been presented as a conference abstract, but the full-text manuscript is not yet available in the peer-reviewed literature. With their larger sample sizes, these trials should provide slightly more precise estimates of clinical effectiveness and safety. To help achieve these larger sample sizes, both trials were multi-centred, with 8 centres in each trial.23,24 In describing the SEL-I-METRY trial, Wadsley et al.25 reflected on the challenges of conducting multi-centred trials of radioiodine resensitization treatments, identifying several barriers such as: access to iodine-124 and to PET scanning facilities using iodine-124 as a tracer; and the calibration and validation of imaging measurements across sites to ensure consistent dosimetry and its associated costs. These barriers may explain the preponderance of single-centred trial designs identified in the current evidence base.
Another limitation of the current evidence base was the heterogeneity across the studies regarding tumour characteristics, including the baseline levels of radioiodine uptake across lesions. Tchekmedyian et al. (2022)18 pointed out that over half of patients in their study sample had at least 1 lesion with evidence of radioiodine uptake at baseline, despite meeting the criteria for being defined as radioiodine refractory. The authors posited that there may be differences in outcomes between patients with a lack of radioiodine avidity across all lesions at baseline, compared with those having mixed avidity, and recommended the need to revisit the definition of radioiodine refractoriness. Differences across trials in the definition of radioiodine refractoriness may have led to heterogeneity in the proportion of patients with resensitization as well as tumour response and progression-free survival rates among those who were resensitized to radioiodine. Other relationships between tumour characteristics, disease biomarkers, and clinical outcomes require further exploration.15
None of the studies were conducted in an entirely Canadian setting, which is a limitation, as the imaging techniques and medications used in the non-Canadian studies may not be available in all Canadian centres. Furthermore, it is unclear whether the patient and tumour characteristics in the US, Australian, and Croatian-based study samples would be similar to those of Canadian patients.
Conclusions and Implications for Decision- or Policy-Making
This report identified 415-18 single-arm clinical trials, 319-21 uncontrolled retrospective cohort studies, and 114 systematic review informing the clinical effectiveness and safety of radioiodine resensitization treatments for patients with RAIRMDTC. No relevant cost-effectiveness analyses were identified.
All 415-18 clinical trials met their primary objective of demonstrating radioiodine resensitization following treatment with a BRAF or MEK inhibitor (with or without the anti-ErbB3 monoclonal antibody CDX-3379), establishing the proof-of-concept that BRAF and MEK inhibitors can resensitize tumour to radioiodine. The clinical experience reported in the 319-21 uncontrolled retrospective cohort studies similarly showed increased radioiodine uptake following treatment, and study authors considered this to be feasible strategy. Across all 715-21 studies, all patients who were resensitized and retreated with radioiodine had partial responses or stable disease at the pre-defined response assessment time point (typically 6 months15-18,21), with the exception of 2 patients in 118 study, who had had stable disease or mixed response at 3 months, but subsequently initiated a new anti-cancer therapy and were categorized as having progressive disease. Adverse events in the included studies were primarily mild or moderate, although there was evidence of grade 3 acneiform rash associated with trametinib (in 2 out of 3 patients in 119 study), and grade 3 maculopapular rash associated with vemurafenib (in approximately 1-quarter of patients in 215,18 studies).
The demonstrated ability to resensitize tumours to radioiodine using BRAF and/or MEK inhibitors is consistent with emerging evidence from the MERAIODE24 trial, in which radioiodine resensitization rate was achieved in 95% of trametinib plus dabrafenib-treated patients with BRAF V600E mutated RAIRMDTC (95% confidence interval, 76% to 100%). The MERAIODE24 trial was not included in the current review as it was reported as a conference abstract and estimates may change when the full report is published reported in the peer-reviewed literature. However, this consistent evidence of resensitization, along with the evidence of tumour response among those resensitized, suggests there may be clinical benefit with radioiodine resensitization strategies using a shorter course of treatment (typically no more than 2 months) than the current standard of care with lenvatinib for which long-term maintenance treatment is required until death or progression. Furthermore, whereas the toxicity associated with lenvatinib has been cited as a concern (severe or life-threatening adverse events were experienced by approximately 3-quarters of patients in the lenvatinib arm of the SELECT trial),8 the resensitization therapies in the current review were primarily mild.
The limitations of the included literature, such as the small sample size of the included studies and the non-comparative evidence base does not lend itself to robust conclusions, and these limitations should be considered when interpreting the findings from this report. Given the potential challenges of setting up large, randomized trials of radioiodine resensitization treatment among patients with RAIRMDTC, even single-arm trials and observational studies involving multiple centres and larger sample sizes would improve the accuracy and precision of the proportion of patients whose tumours can be resensitized to radioiodine and other patient-relevant clinical outcomes, as well as enable exploration of predictive factors for successful resensitization. Findings from the SEL-I-METRY trial23 of selumetinib and the MERAIODE24 trial of trametinib plus dabrafenib, as well as additional data from new clinical trials and other evidence syntheses, may help better inform the role of radioiodine resensitization followed by radioiodine for the treatment of patients with RAIRMDTC.
References
1.Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. PubMed
2.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian cancer statistics 2021. Toronto (ON): Canadian Cancer Society; 2021: www.cancer.ca/Canadian-Cancer-Statistics-2021-EN. Accessed 2022 Mar 9.
3.Noone AM, Cronin KA, Altekruse SF, et al. Cancer incidence and survival trends by subtype using data from the surveillance epidemiology and end results program, 1992-2013. Cancer Epidemiol Biomarkers Prev. 2017;26(4):632-641. PubMed
4.Tuttle RM. Differentiated thyroid cancer: radioiodine treatment. In: Post TW, ed. UpToDate; 2022: https://www.uptodate.com/contents/differentiated-thyroid-cancer-overview-of-management. Accessed 2022 Feb 22.
5.Durante C, Haddy N, Baudin E, et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91(8):2892-2899. PubMed
6.Aashiq M, Silverman DA, Na'ara S, Takahashi H, Amit M. Radioiodine-refractory thyroid cancer: molecular basis of redifferentiation therapies, management, and novel therapies. Cancers (Basel). 2019;11(9):1382. PubMed
7.Brose MS, Nutting CM, Jarzab B, et al. Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 3 trial. Lancet. 2014;384(9940):319-328. PubMed
8.Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. 2015;372(7):621-630. PubMed
9.Provincial funding summary for Lenvatinib (Lenvima) for differentiated thyroid cancer (pCODR 10080). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pcodr/pcodr-provfund_lenvatinib-lenvima-dtc.pdf. Accessed Mar 25, 2022.
10.Fullmer T, Cabanillas ME, Zafereo M. Novel therapeutics in radioactive iodine-resistant thyroid cancer. Front Endocrinol (Lausanne). 2021;12:720723. PubMed
11.Nikiforova MN, Tseng GC, Steward D, Diorio D, Nikiforov YE. MicroRNA expression profiling of thyroid tumors: biological significance and diagnostic utility. J Clin Endocrinol Metab. 2008;93(5):1600-1608. PubMed
12.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Jones H, Green V, England J, Greenman J. Current understanding of nonsurgical interventions for refractory differentiated thyroid cancer: a systematic review. Future Sci OA. 2021;7(7):FSO738. PubMed
15.Dunn LA, Sherman EJ, Baxi SS, et al. Vemurafenib redifferentiation of BRAF mutant, RAI-refractory thyroid cancers. J Clin Endocrinol Metab. 2019;104(5):1417-1428. PubMed
16.Ho AL, Grewal RK, Leboeuf R, et al. Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer. N Engl J Med. 2013;368(7):623-632. PubMed
17.Rothenberg SM, McFadden DG, Palmer EL, Daniels GH, Wirth LJ. Redifferentiation of iodine-refractory BRAF V600E-mutant metastatic papillary thyroid cancer with dabrafenib. Clin Cancer Res. 2015;21(5):1028-1035. PubMed
18.Tchekmedyian V, Dunn L, Sherman EJ, et al. Enhancing radioiodine incorporation in BRAF-mutant, radioiodine-refractory thyroid cancers with Vemurafenib and the anti-ErbB3 monoclonal antibody CDX-3379: results of a pilot clinical trial. Thyroid. 2022;32(3):273-282. PubMed
19.Iravani A, Solomon B, Pattison DA, et al. Mitogen-activated protein kinase pathway inhibition for redifferentiation of radioiodine refractory differentiated thyroid cancer: an evolving protocol. Thyroid. 2019;29(11):1634-1645. PubMed
20.Jaber T, Waguespack SG, Cabanillas ME, et al. Targeted therapy in advanced thyroid cancer to resensitize tumors to radioactive iodine. J Clin Endocrinol Metab. 2018;103(10):3698-3705. PubMed
21.Pešorda M, Kusačić Kuna S, Huić D, et al. Kinase inhibitors in the treatment of thyroid cancer: institutional experience. Acta Clin Croat. 2020;59(Suppl 1):73-80. PubMed
22.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-34. PubMed
23.Brown SR, Hall A, Buckley HL, et al. Investigating the potential clinical benefit of Selumetinib in resensitising advanced iodine refractory differentiated thyroid cancer to radioiodine therapy (SEL-I-METRY): protocol for a multicentre UK single arm phase II trial. BMC Cancer. 2019;19(1):1-10. PubMed
24.Leboulleux S, Cao CD, Zerdoud S, et al. MERAIODE: a redifferentiation phase II trial with trametinib and dabrafenib followed by radioactive iodine administration for metastatic radioactive iodine refractory differentiated thyroid cancer patients with a BRAFV600E mutation (NCT 03244956). J Endocr Soc. 2021;5(Suppl 1):A876-A876.
25.Wadsley J, Gregory R, Flux G, et al. SELIMETRY-a multicentre I-131 dosimetry trial: a clinical perspective. Br J Radiol. 2017;90(1073):20160637. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Jones et al. (2021)14 UK Funding source: None | Study designs included: This systematic review captured clinical trials involving tyrosine kinase inhibitors, and any study design involving immunotherapies. Number primary studies included: 23 primary studies were included; 3 were relevant to the current report. | Eligible populations: For tyrosine kinase inhibitors: Patients with advanced/treatment refractory DTC. For immunotherapies: patients/tissues/cells of advanced/treatment refractory DTC Relevant population: patients with RAIRMDTC | Eligible interventions and comparators: Tyrosine kinase inhibitors or immunotherapies. Relevant interventions and comparators: Dabrafenib, vemurafenib, selumetinib. | Outcomes: Not restricted Follow-up: Not specified. |
DTC = differentiated thyroid cancer; RAIRMDTC = radioiodine-refractory/resistant metastatic differentiated thyroid cancer.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Tchekmedyian et al. (2022)18 US (Memorial Sloan Kettering Cancer Center) Funding: Kolltan Pharmaceuticals, NIH/NCI, and othersa | Study design: Single-arm single-centre pilot clinical trial Study period: 2015 to 2016 Relevant study objective: to evaluate the safety, tolerability, and redifferentiation potential of vemurafenib plus CDX-3379 in BRAF V600E+ RAIR patients. | Number patients: 7 Key eligibility criteria
Key baseline characteristics
| Intervention
| Outcomes
Follow-up: Up to 47 months |
Pešorda et al. (2020)21 Croatia Funding source not reported | Study design: Uncontrolled retrospective cohort study Study period: 2014 to 2020 Relevant study objective: to present experience with vemurafenib and its influence on tumour redifferentiation | Number patients: 3 (subgroup, among 17) Key eligibility criteria (for subgroup)
Key baseline characteristics: Not reported for subgroup | Intervention
| Outcomes
Follow-up: Unclearc |
Dunn et al. (2019)15 US (Memorial Sloan Kettering Cancer Center) Funding: Genentech, NIH/NCI, and othersa | Study design: Single-arm single-centre pilot clinical trial Study period: 2014 to 2015 Relevant study objective: to investigate enhancement of lesional iodide uptake with vemurafenib in patients with RAIR. | Number patients: 12 Key eligibility criteria
Key baseline characteristics
| Intervention
| Outcomes
Follow-up
|
Iravani et al. (2019)19 Australia No external funding | Study design: Uncontrolled retrospective cohort study Study period: 2015 to 2017 Relevant study objective: to assess the feasibility of MAPK-pathway blockade combined with thyroid hormone withdrawal for redifferentiation. | Number patients: 6 Key eligibility criteria:
Key baseline characteristics
| Intervention
| Outcomes
Follow-up: Median follow-up: 16 months; range: 5 to 40 months. |
Jaber et al. (2018)20 US (MD Anderson) Funding: NCI grant | Study design: Uncontrolled retrospective cohort study Study period: Not reported Relevant study objective: to describe patients receiving targeted therapy with demonstrated RAI update allowing for 131I administration. | Number patients: 13 Key eligibility criteria
Key baseline characteristics
| Intervention
| Outcomes
Follow-up: Median follow-up among post-RAI therapy: 14.3 months |
Rothenberg et al. (2015)17 US (Massachusetts General Hospital) Funding: GlaxoSmithKline; Ellison Foundation grant | Study design: Single-arm single-centre clinical trial Enrolment period: 2012 to 2013 Relevant study objective: to determine if dabrafenib can stimulate RAI among BRAF V600E+ RAIR patients. | Number patients: 10 Key eligibility criteria
Key baseline characteristics
| Intervention
| Outcomes
Follow-up: Unclearf |
Ho et al. (2013)16 US (Memorial Sloan Kettering Cancer Center) Funding: AstraZeneca, Genzyme, NIH, and othersa | Study design: Single-arm single-centre clinical trial Enrolment period: 2010 to 2011 Relevant study objective: to determine whether selumetinib Could reverse refractoriness to RAI among patients with metastatic TC. | Number patients: 20 Key eligibility criteria
Key baseline characteristics
| Intervention
| Outcomes
Follow-up: 6 months |
131I = iodine-131; b.i.d. = twice a day; FTC = follicular thyroid carcinoma; GBq = gigabecquerel; IV = intravenous; NIH/NCI = National Institutes of Health/National Cancer Institute; PDTC = poorly differentiated thyroid cancer; PFS = progression-free survival; PTC = papillary thyroid cancer; RAI = radioiodine; RAIR = radioiodine-refractory/resistant; WBS = whole body scan.
aAdditional funding source information: Dunn et al. (2019)15 and Tchekmedyian et al. (2022)18: Various NIH/NCI grants, the Geoffrey Beene Cancer Research Center and Cycle for Survival at Memorial Sloan Kettering Cancer Center; Ho et al. (2013)16: Grants from the American Thyroid Association, the Society of Memorial Sloan Kettering Cancer Centre, the NIH, the Lefkofsky Family, Margot Rosenberg Pulitzer, Byrne, and J Randolph Hearst foundations.
bRAIR definition: A) non-RAI-avid metastatic lesion on a diagnostic scan ≤ 2 years before enrolment; B) an RAI-avid lesion that is of stable size or that progressed despite RAI ≥ 6 months prior to study entry; or C) ≥1 18F-fluorodeoxyglucose-avid lesion(s). Note: for criterion C, Dunn et al. (2019)15 and Tchekmedyian et al. (2022)18 further specify a maximum standardized uptake value (SUVmax) >=5.
cOf the 3 patients, 1 was followed for 2 years post-radioiodine treatment; duration of follow-up for the other 2 patients was not reported.
dRAIR definition: A) minimal or no RAI avidity in some or all measurable sites of disease on appropriately performed RAI scans; B) imaging or biochemical progression despite RAI treatment within the past 12 months.
eRAIR definition: A) no RAI update at known sites of metastases; B) progressive disease despite previous RAI treatment with confirmed uptake; C) progressive disease within 1 year of RAI therapy.
fMethods state the end point of best response at 3 months; however, the results describe best response at 6 months.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the Systematic Review Using AMSTAR 212
Strengths | Limitations |
|---|---|
Jones et al. (2021)14, a | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PICO = population, intervention, comparator group, outcome; TKI = tyrosine kinase inhibitor.
aThe relevant studies captured within this systematic review are included as primary studies in the current report; therefore, the assessment focused on the comprehensiveness of the literature search, to assess whether any other relevant studies were potentially missed.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist13
Strengths | Limitations |
|---|---|
Tchekmedyian et al. (2022)18 | |
|
|
Pešorda et al. (2020)21 | |
|
|
Dunn et al. (2019)15 | |
|
|
Iravani et al. (2019)19 | |
|
|
Jaber et al. (2018)20 | |
|
|
Rothenberg et al. (2015)17 | |
|
|
Ho et al. (2013)16 | |
|
|
CTCAE = Common Terminology Criteria for Adverse Events.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Resensitization
Intervention | Study citation and study design | Resensitization definition (as described by study authors) | Estimate, n/N (%) |
|---|---|---|---|
Vemurafenib + CDX-3379 | Tchekmedyian et al. (2022)18 Single-arm trial BRAF V600E+ Sample size: n = 7 | Evaluable for 124I avidity | 6 / 7 (86) |
Increased 124I avidity after treatment | 5 / 7 (71) | ||
Sufficient change in avidity to warrant therapeutic dose of 131I | 4 / 7 (57)a | ||
Vemurafenib | Pešorda et al. (2020)21 Uncontrolled retrospective cohort BRAF V600E+ Sample size n = 3 | Showed restoration of RAI uptake evaluated with 131I imaging | 2 / 3 (67)b |
Vemurafenib | Dunn et al. (2019)15 Single-arm trial BRAF V600E+ Sample size n = 12 | New or increased RAI avidity in at least one tumour | 6 / 12 (50)c |
Met the lesional dosimetry threshold to warrant therapeutic dose of 131I (i.e., 124I responders) | 4 / 12 (33)c | ||
Mixedd | Iravani et al. (2019)19 Uncontrolled retrospective cohort BRAF V600E+ or NRAS+ Sample size n = 6 | Restoration of iodine avidity (based on 124I dosimetry) | 4 / 6 (67) |
Restoration of iodine avidity (based on 124I dosimetry) and received 131I RAI | 4 / 6 (67) | ||
Restoration of iodine avidity and received 131I RAI, among BRAF V600E+ patients receiving combination therapyd | 3 / 3 (100) | ||
Restoration of iodine avidity and received 131I RAI among NRAS+ patients receiving trametinibd | 1 / 3 (33) | ||
Mixede | Jaber et al. (2018)20 Uncontrolled retrospective cohort No genotype-based restrictions Sample size = 13 | Clinically meaningful uptake on pre-treatment WBS to warrant therapeutic dose of 131I | 8 / 13 (62) |
Received 131If | 9 / 13 (69) | ||
Received 131If, among BRAF V600E+ patients | 5 / 9 (56) | ||
Received 131If, among NRAS/KRAS+ patients | 3 / 3 (100) | ||
Received 131If, among wild-type patients | 1 / 1 (100) | ||
Dabrafenib | Rothenberg et al. (2015)17 Single-arm trial BRAF V600E + Sample size = 10 | Developed new RAI uptake after treatment | 6 / 10 (60) |
Developed new RAI uptake after treatment and received 131I RAI | 6 / 10 (60) | ||
Selumetinib | Ho et al. (2013)16 Single-arm trial No genotype-based restrictions Sample size n = 20 | 124I uptake that was new and/or increased after treatment | 12 / 20 (60) |
Received 131Ig | 8 / 20 (40) | ||
Received 131Ig, among NRAS+ patients | 5 / 5 (100) | ||
Received 131Ig, among BRAF V600E + patientsh | 1 / 9 (11) | ||
Received 131Ig, among RET/PTC+ patientsh | 1 / 3 (33) | ||
Received 131Ig, among wild-type patientsh | 1 / 3 (33) |
124I = iodine-124; 131I = iodine-131; RAI = radioiodine
a1 patient was not treated with 131I despite showing increased 124I avidity, including a new/increased iodine update in lung metastasis, because “a structural correlate for the former could not be identified on CT imaging.”
b1 patient did not want to perform a radioiodine scan. It is assumed that patients received a therapeutic dose of 131I however, this is unclear from the text.
creported by the authors as 6/10 (60%), as 2 patients did not receive a post-baseline 124I scan due to adverse events that precluded continuation of drug treatment. In the current report, the proportion has been re-calculated according to the intention-to-treat principle, for consistency across studies.
d3 patients with NRAS mutations received trametinib; 1 patient with BRAF V600E mutation received dabrafenib and trametinib; 2 patients with BRAF V600E mutation received vemurafenib and cobimetinib.
e3 patients with NRAS/KRAS mutations received trametinib (n=2) or investigational MEK inhibitor; 9 patients with BRAF V600E mutation received dabrafenib, vemurafenib, or dabrafenib and vemurafenib; 1 patient with wild-type tumour genotype received trametinib.
fDecision to administer 131I based on clinically meaningful uptake on pre-treatment scan to warrant therapeutic dose of 131I, or physician’s clinical judgment despite no evidence of uptake.
gDecision based on an “absorbed radiation dose in the lesion that would equal or exceed 2000 cGy with 300 mCi of RAI or less.” – Ho et al. (2013)16.
hAuthors also reported the proportion with 124I uptake by tumour genotype, irrespective of whether the uptake was sufficient to warrant a therapeutic dose of 131I: 4 / 9 (44%) patients with BRAF V600E+, 2 / 3 (67%) with RET/PTC+, and 1 / 3 (33%) with wild-type tumours.
Table 7: Summary of Findings by Outcome — Response
Response (RECIST v1.1) | Tchekmedyian et al. (2022)18 Single-arm trial | Dunn et al. (2019)15 Single-arm trial | Iravani et al. (2019)19 Uncontrolled retrospective cohort | Jaber et al. (2018)20 Uncontrolled retrospective cohort | Rothenberg et al. (2015)17 Single-arm trial | Ho et al. (2013)16 Single-arm trial |
|---|---|---|---|---|---|---|
Vemurafenib + CDX-3379 | Vemurafenib | Mixeda | Mixedb | Dabrafenib | Selumetinib | |
Assessment timing | 6 months | 6 months | End of follow-up | End of follow-up | 6 months | 6 months |
Among all patients | ||||||
Best overall response, n/N (%) | ||||||
CR | 0 / 7 (0) | 0 / 12 (0) | 0 / 6 (0) | 0 / 13 (0) | 0 / 10 (0) | 0 / 20 (0) |
PR | 2 / 7 (29) | 2 / 12 (17) | 3 / 6 (50) | 3 / 13 (23) | 2 / 10 (20) | 5 / 20 (25) |
SD | 0 / 7 (0) | 2 / 12 (17) | 1 / 6 (17) | 9 / 13 (46)c | 7 / 10 (70) | 3 / 20 (15) |
PD | 2 / 7 (29) | 3 / 12 (25) | 0 / 6 (0) | 0 / 13 (0) | 1 / 10 (10) | 0 / 20 (0) |
Mixed response | – | – | – | 1 / 13 (8)d | – | – |
Not assessed | 3 / 7 (43) | 5 / 12 (42) | 2 / 6 (33)e | – | – | 12 / 20 (60) |
Among 131I treated patients | ||||||
Best overall response, n/N (%) | ||||||
CR | 0 / 4 (0) | 0 / 4 (0) | 0 / 4 (0) | 0 / 9 (0) | 0 / 6 (0) | 0 / 8 (0) |
PR | 2 / 4 (50) | 2 / 4 (50) | 3 / 4 (75) | 3 / 9 (33) | 2 / 6 (33) | 5 / 8 (63) |
SD | 0 / 4 (0) | 2 / 4 (50) | 1 / 4 (25) | 6 / 9 (66)c | 4 / 6 (67) | 3 / 8 (38) |
PD | 2 / 4 (50) | 0 / 4 (0) | 0 / 4 (0) | 0 / 9 (0) | 0 / 6 (0) | 0 / 8 (0) |
Mixed response | – | – | – | 0 / 9 (0) | – | – |
Not assessed | – | – | – | – | – | – |
Among non-131I treated patients | ||||||
Best overall response, n/N (%) | ||||||
CR | – | – | – | 0 / 4 (0) | 0 / 4 (0) | – |
PR | – | – | – | 0 / 4 (0) | 0 / 4 (0) | – |
SD | – | – | – | 3 / 4 (75) | 3 / 4 (75) | – |
PD | – | 3 / 8 (38)e | – | 0 / 4 (0) | 1 / 4 (25) | – |
Mixed response | – | – | – | 1 / 4 (25)d | – | – |
Not assessed | 3 / 3 (100) | 5 / 8 (63) | 2 / 2 (100)f | – | – | 12 / 12 (100) |
131I = iodine-131; CR = complete response; PD = progressive disease; PR = partial response; RECIST = Response Evaluation Criteria in Solid Tumours; SD = stable disease.
a3 patients with NRAS mutations received trametinib; 1 patient with BRAF V600E mutation received dabrafenib and trametinib; 2 patients with BRAF V600E mutation received vemurafenib and cobimetinib.
b3 patients with NRAS/KRAS mutations received trametinib (n=2) or investigational MEK inhibitor; 9 patients with BRAF V600E mutation received dabrafenib, vemurafenib, or dabrafenib and vemurafenib; 1 patient with wild-type tumour genotype received trametinib.
cReported in the text as 5 131I-treated patients with stable disease; however, Figure 3b shows 6 131I-treated patients with stable disease. Extraction is based on the estimate from Figure 3b.
dSome lesions stable and others enlarged.
e3 patients were assessed off-protocol.
fPatients were reported as being “responsive” to subsequent treatment with lenvatinib at end of follow-up.
Table 8: Summary of Findings by Outcome — Subsequent Therapy
Intervention | Study citation and study design | Subsequent therapy definition | Estimate, n/N (%) |
|---|---|---|---|
Vemurafenib + CDX-3379 | Tchekmedyian et al. (2022)18 Single-arm trial Sample size: n=7 | Initiated systemic treatment after study, among 131I-treated | 2 / 4 (50) |
Did not initiate systemic treatment > 3 years post-study, among 131I-treated | 2 / 4 (50) | ||
Initiated systemic treatment after study, among non-131I-treated | 3 / 3 (100)a | ||
Vemurafenib | Pešorda et al. (2020)21 Uncontrolled retrospective cohort Sample size n = 3 | Received second-line sorafenib, among all patients | 1 / 3 (33)b |
Vemurafenib | Dunn et al. (2019)15 Single-arm trial Sample size n = 12 | Subsequent therapy, among 131I treated | — |
Radiation, ~9 months post-131I | 1 / 4 (25) | ||
Vemurafenib retreatment, ~18 months post31I | 1 / 4 (25) | ||
No subsequent treatment ≥ 22 months post131I | 2 / 4 (50) | ||
Mixedc | Iravani et al. (2019)19 Uncontrolled retrospective cohort BRAF V600E+ or NRAS+ Sample size n = 6 | Did not initiate new treatment by end of follow-up, among 131I-treated | 4 / 4 (100) |
Initiated lenvatinib, among non-131I-treatedd | 2 / 2 (100) | ||
Mixede | Jaber et al. (2018)20 Uncontrolled retrospective cohort No genotype-based restrictions Sample size = 13 | Median (range) time off systemic targeted therapy, post-131I, among 131I treatedf | 14.3 months (4.5 to 20.6) |
131I = iodine-13.1
aInitiated immediately for 1 patient, and initiated ~3 years after study treatment in 2 patients.
bDetails on subsequent treatment were provided for 1 patient. This patient (female) received second-line sorafenib 2 years after successful redifferentiation with vemurafenib. The patient died shortly after starting the second-line treatment.
c3 patients with NRAS mutations received trametinib; 1 patient with BRAF V600E mutation received dabrafenib and trametinib; 2 patients with BRAF V600E mutation received vemurafenib and cobimetinib.
dAll non-131I-treated patients received trametinib and had tumours harbouring NRAS mutations.
e3 patients with NRAS/KRAS mutations received trametinib (n=2) or investigational MEK inhibitor; 9 patients with BRAF V600E mutation received dabrafenib, vemurafenib, or dabrafenib and vemurafenib; 1 patient with wild-type tumour genotype received trametinib.
fUnclear if subsequent treatments were received of if patients remained off systemic targeted therapy at the end of the follow-up period.
Table 9: Summary of Findings by Outcome — Progression-Free Survival or Time to Progression
Intervention | Study citation and study design | Progression-free survival or time to progression |
|---|---|---|
Vemurafenib + CDX-3379 | Tchekmedyian et al. (2022)18 Single-arm trial Sample size: n=7 | Progression-free survival at 6 months, among 131I treated (n=4): • 2 / 4 (50%) patients progressed • 2 / 4 (50%) patients remained progression-free and alive |
Vemurafenib | Dunn et al. (2019)15 Single-arm trial Sample size n = 12 | Time to progression, among 131I treated (n=4):
|
Mixedb | Iravani et al. (2019)19 Uncontrolled retrospective cohort BRAF V600E+ or NRAS+ Sample size n = 6 | All patients (n=6) were alive and progression-free at the end of follow-up, irrespective of radioiodine treatment. |
131I = iodine-131.
aProgression assumed based on initiation of new anti-cancer therapy.
b3 patients with NRAS/KRAS mutations received trametinib (n=2) or investigational MEK inhibitor; 9 patients with BRAF V600E mutation received dabrafenib, vemurafenib, or dabrafenib and vemurafenib; 1 patient with wild-type tumour genotype received trametinib.
Table 10: Summary of Findings by Outcome — Mortality
Intervention | Study citation and study design | Deaths |
|---|---|---|
Vemurafenib | Pešorda et al. (2020)21 Uncontrolled retrospective cohort Sample size n = 3 | One patient died 2 years after successful redifferentiation, shortly after starting a second-line treatment. The other two patients were not reported to have died prior to the end of follow-up. |
Table 11: Summary of Findings by Outcome — Adverse Events
Intervention sample size | Adverse events experienced by > 1 patient | Grade 1 to 2 n (%) | Grade 3 to 5 n (%) | Any grade n (%) |
|---|---|---|---|---|
Tchekmedyian et al. (2022)18 | ||||
Vemurafenib + CDX-3379 Sample size: n=7 | Vemurafenib-related: | Total = 7 | Total = 7 | Total = 7 |
At least 1 adverse event | Not reported | Not reported | Not reported | |
Maculopapular rash | 3 (43) | 2 (29) | 5 (71) | |
Nausea | 4 (57) | 0 (0) | 4 (57) | |
Diarrhea | 2 (29) | 1 (14) | 3 (43) | |
Arthralgia | 2 (29) | 0 (0) | 2 (29) | |
Alanine aminotransferase elevation | 2 (29) | 0 (0) | 2 (29) | |
Alkaline phosphatase elevation | 2 (29) | 0 (0) | 2 (29) | |
Fatigue | 2 (29) | 0 (0) | 2 (29) | |
Hand-foot syndromea | 2 (29) | 0 (0) | 2 (29) | |
Pruritis | 2 (29) | 0 (0) | 2 (29) | |
Acneiform rash | 2 (29) | 0 (0) | 2 (29) | |
Vemurafenib + CDX-3379 Sample size: n=6b | CDX-3379-related: | Total = 6b | Total = 6b | Total = 6b |
At least 1 adverse event | Not reported | 0 (0) | Not reported | |
Diarrhea | 3 (50) | 0 (0) | 3 (50) | |
Nausea | 3 (50) | 0 (0) | 3 (50) | |
Arthralgia | 2 (33) | 0 (0) | 2 (33) | |
Hand-foot syndromea | 2 (33) | 0 (0) | 2 (33) | |
Alkaline phosphatase elevation | 2 (33) | 0 (0) | 2 (33) | |
Pešorda et al. (2020)21 | ||||
Vemurafenib Sample size n = 3 | Any adverse event: | Total = 3 | Total = 3 | Total = 3 |
At least 1 adverse event | Not reported | Not reported | Not reported | |
Squamous cell carcinoma of the skin | Not reported | Not reported | 2 (67) | |
Keratoacanthoma | Not reported | Not reported | 0 (67) | |
Dunn et al. (2019)15 | ||||
Vemurafenib Sample size n = 12 | Vemurafenib-related: | Total = 12 | Total = 12 | Total = 12 |
At least 1 adverse event | Not reported | Not reported | Not reported | |
Maculopapular rash | 7 (58) | 2 (17) | 9 (75) | |
Fatigue | 8 (67) | 0 (0) | 8 (66) | |
Hand-foot syndromea | 6 (50) | 1 (8) | 7 (58) | |
Nausea | 6 (50) | 0 (0) | 6 (50) | |
Alkaline phosphatase increased | 5 (42) | 0 (0) | 5 (42) | |
Arthralgia | 5 (42) | 0 (0) | 5 (42) | |
Bilirubin increased | 5 (42) | 0 (0) | 5 (42) | |
Alanine aminotransferase increased | 3 (25) | 0 (0) | 3 (25) | |
Diarrhea | 3 (25) | 0 (0) | 3 (25) | |
Neoplasm, benign (warts) | 3 (25) | 0 (0) | 3 (25) | |
Alopecia | 3 (25) | 0 (0) | 3 (25) | |
Skin/subcutaneous tissue disordersc | 2 (17) | 0 (0) | 2 (17) | |
Creatinine increased | 2 (17) | 0 (0) | 2 (17) | |
Aspartate aminotransferase increased | 2 (17) | 0 (0) | 2 (17) | |
Myalgia | 2 (17) | 0 (0) | 2 (17) | |
Dysgeusia | 2 (17) | 0 (0) | 2 (17) | |
Pruritus | 2 (17) | 0 (0) | 2 (17) | |
Iravani et al. (2019)19 | ||||
Trametinib Sample size = 3 | Any adverse event: | Total = 3 | Total = 3 | Total = 3 |
At least 1 adverse event | 1 (33) | 2 (67) | 3 (100) | |
Acneiform rash | 0 (0) | 2 (67) | 2 (67) | |
Vemurafenib + cobimetinib Sample size = 3 | Any adverse event: | Total = 2 | Total = 2 | Total = 2 |
At least 1 adverse event | 2 (100) | 0 (0) | 2 (100) | |
Rash | 2 (100) | 0 (0) | 2 (100) | |
Jaber et al. (2018)20 | ||||
Mixedd Sample size = 13 | RAI-related adverse events | Not reported by grade | Not reported by grade | Total = 9 |
At least 1 adverse event | 3 (33) | |||
Pneumonitis | 2 (22) | |||
Rothenberg et al. (2015)17 | ||||
Dabrafenib Sample size = 10 | Any adverse event: | Total = 10 | Total = 10 | Total = 10 |
At least 1 adverse event | 9 (90) | 1 (10)e | 10 (100) | |
Skin lesions or changes | 8 (80) | 0 (0) | 8 (80) | |
Fatigue | 5 (50) | 0 (0) | 5 (50) | |
Electrolyte abnormalities | 4 (40) | 1 (10)e | 5 (50) | |
Gastrointestinal symptoms | 5 (50) | 0 (0) | 5 (50) | |
Hand-foot syndromea | 4 (40) | 0 (0) | 4 (40) | |
Headache | 3 (30) | 0 (0) | 3 (30) | |
Epistaxis | 2 (20) | 0 (0) | 2 (20) | |
Eye disorders | 2 (20) | 0 (0) | 2 (20) | |
Creatinine increase | 2 (20) | 0 (0) | 2 (20) | |
Ho et al. (2013)16 | ||||
Selumetinib Sample size n = 20 | Selumetinb-related:f | Total = 20 | Total = 20 | Total = 20 |
At least 1 adverse event | Not reported | 0 (0) | Not reported | |
Rash | 18 (90) | 0 (0) | 18 (90) | |
Fatigue | 16 (80) | 0 (0) | 16 (80) | |
Hepatic enzymes increased | 14 (70) | 0 (0) | 14 (70) | |
Diarrhea | 9 (45) | 0 (0) | 9 (45) | |
Nausea | 8 (40) | 0 (0) | 8 (40) | |
Mucositis oral | 7 (35) | 0 (0) | 7 (35) | |
Edema limbs | 6 (30) | 0 (0) | 6 (30) | |
Constipation | 4 (20) | 0 (0) | 4 (20) | |
Hypoalbuminemia | 3 (15) | 0 (0) | 3 (15) | |
Pain | 3 (15) | 0 (0) | 3 (15) | |
White blood cell decreased | 3 (15) | 0 (0) | 3 (15) | |
Dry mouth | 2 (10) | 0 (0) | 2 (10) | |
Dry skin | 2 (10) | 0 (0) | 2 (10) | |
Edema face | 2 (10) | 0 (0) | 2 (10) | |
Hyperglycemia | 2 (10) | 0 (0) | 2 (10) | |
Hypoglycemia | 2 (10) | 0 (0) | 2 (10) | |
CTCAE = Common Terminology Criteria for Adverse Events.
aPlantar-palmar erythrodysesthesia syndrome.
b1 patient did not receive CDX-3379 due to vemurafenib-related toxicity (maculopapular rash) prior to initiating CDX-3379.
c1 case of seborrheic keratosis; 1 case of keratosis pilaris-like reaction.
d3 patients with NRAS/KRAS mutations received trametinib (n=2) or investigational MEK inhibitor; 9 patients with BRAF V600E mutation received dabrafenib, vemurafenib, or dabrafenib and vemurafenib; 1 patient with wild-type tumour genotype received trametinib.
eDeemed unrelated to study drug. In text this was listed as grade 2 but in table it was listed as severe according to CTCAE v4.0, which corresponds to grade 3.
fAdverse events deemed unrelated to selumetinib were reported by the study authors separately.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
CADTH. Lenvima for differentiated thyroid cancer - details. 2016; https://www.cadth.ca/lenvima-differentiated-thyroid-cancer-details. Accessed 2022 Mar 25.
Additional References
Groener JB, Gelen D, Mogler C, Herpel E, Toth C, Kender Z, Peichl M, Haufe S, Haberkorn U, Sulaj A, Zemva J. BRAF V600E and retinoic acid in radioiodine-refractory papillary thyroid cancer. Horm Metab Res. 2019;51(01):69-75. PubMed
Leboulleux S, Cao CD, Zerdoud S, et al. MERAIODE: a redifferentiation phase II trial with trametinib and dabrafenib followed by radioactive iodine administration for metastatic radioactive iodine refractory differentiated thyroid cancer patients with a BRAFV600E mutation (NCT 03244956). J Endocr Soc. 2021;5(Supplement_1):A876-A876.
Wadsley J, Gregory R, Flux G, et al. SELIMETRY - a multicentre I-131 dosimetry trial: a clinical perspective. Br J Radiol. 2017;90(1073):20160637. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca