CADTH Health Technology Review
Clinical Effectiveness of Second-Generation Injectable Antipsychotic Drugs
Rapid Review
Authors: Nazia Darvesh, Danielle MacDougall, Quenby Mahood
Abbreviations
AIMS
Abnormal Involuntary Movement Scale
AE
adverse event
AMI
amisulpride
AQoL
Assessment of Quality of Life
ARI
aripiprazole
BARS
Barnes Akathisia Rating Scale
BPRS
Brief Psychiatric Rating Scale
CGI-I
Clinical Global Impression-Improvement
CGI-S
Clinical Global Impression-Severity
EPS
Extrapyramidal symptoms
ESRS
Extrapyramidal Symptom Rating Scale
FG
first-generation
GAF
Global Assessment of Function
HAM-A
Hamilton Anxiety Rating Scale
HDRS
Hamilton Depression Rating Scale
LAI
long-acting injectable
MADRS
Mongtomery-Asberg Depression Rating Scale
NRS
non-randomized study
OLA
olanzapine
PANSS
Positive and Negative Syndrome Scale
PP
paliperidone palmitate
PSP
Personal and Social Performance scale
QLS
Heinrichs-Carpenter QoL scale
QoL
quality of life
QUE
quetiapine
RIS
risperidone
SAS
Simpson-Angus Extrapyramidal Side Effects Scale
SES
Service Engagement Scale (SES)
SF-36 or SF-12
Short Form Health Survey, 36 questions, or Short Form Health Survey, 12 questions
SFS
Social Functioning Scale
SG
second generation
SOF
Scale of Functioning
SOFAS
Social and Occupational Functioning Assessment Scale
SQLS-R4
Schizophrenia Quality-of-Life Scale, Revision 4
SWN-S
Subjective Well-Being Under Neuroleptics Scale-Short Form
TSQM
Treatment Satisfaction Questionnaire for Medication
VAS
visual analogue scale
W-QOLI
Wisconsin Quality-of-Life Index
YMRS
Young Mania Rating Scale
ZIP
ziprasidone
Key Messages
The evidence in this report is limited because statistical information was not adequately reported in included studies.
When comparing second-generation paliperidone palmitate injections and first-generation haloperidol decanoate injections, there is little-to-no difference in treatment success or adverse events.
When comparing second-generation risperidone injections and first-generation haloperidol decanoate and fluphenazine decanoate injections given together, there is little-to-no difference in whether patients discontinue treatment.
Hospitalization appears higher for patients who receive haloperidol decanoate injections compared to those who receive second-generation risperidone or aripiprazole injections, but there is little-to-no difference when comparing injections of risperidone to those of haloperidol decanoate and fluphenazine decanoate given together.
There is little-to-no difference between patients who stop treatment when comparing risperidone injections to any oral second-generation antipsychotic drugs, second-generation olanzapine injections compared to oral olanzapine, or aripiprazole injections compared to oral aripiprazole. There is little-to-no difference in adverse events between patients given aripiprazole injections compared to those given oral aripiprazole.
Some studies showed a difference in relapse between second-generation injections compared to oral second-generation medication, while other studies showed little-to-no differences.
Patients may experience fewer hospital days when given olanzapine injections compared to those receiving oral olanzapine.
Context and Policy Issues
The population of patients affected by psychosis is large. In 2019, 23.6 million people had schizophrenia and 39.5 million people had bipolar disorder worldwide.1 Antipsychotic drug treatments are given to patients to manage psychosis symptoms, such as hallucinations and delusions.2 These medications work to clear confusion and increase calm in people with a variety of conditions.2 However, antipsychotic medications can have serious side effects such as involuntary movements, dizziness, and risk for diabetes.2
There are several antipsychotic medications on the market, and these are generally grouped into 2 categories; first-generation (FG) and second-generation (SG) antipsychotic drugs. FG drugs are older medications that block dopamine, and are referred to as typical antipsychotic drugs, whereas SG drugs block dopamine while also playing a role in controlling serotonin and are referred to as atypical antipsychotic drugs.2 Although SG antipsychotic drugs were first available in Canada in the 1990s, they have been prescribed more than FG antipsychotic drugs over time because they are thought to have fewer side effects.3 Both medication types are available as oral formulations and IV or intramuscular injections, with different doses and administration frequencies.2 Long-acting injectable (LAI) antipsychotic drugs are an option for patients who are unable to adhere to treatment involving frequent dosing and those who suffer from relapses.4 In some cases, oral administration therapies can cause immediate unwanted side effects.4 LAI antipsychotic drugs can therefore offer a solution to this, as they are administered every 2 or 4 weeks rather than being taken daily.4
Given the differences in prescription patterns, potential side effects, and treatment administration methods between antipsychotic drugs, there is a need to determine the effects of SG-LAIs when compared to other antipsychotic drugs based on generation type or route of administration. A previous CADTH report on antipsychotic medications published in 20215 focused on emergency settings and another 1 published in 20196 reviewed their effects in comparison to placebo. Therefore, this rapid review aims to summarize literature on the clinical safety and effectiveness of SG-LAIs compared to FG-LAIs, and SG-LAIs compared to oral SG antipsychotic drugs in non-emergency settings, in patients with schizophrenia and/or bipolar disorders.
Research Questions
What is the clinical effectiveness of second-generation injectable antipsychotic medications versus first-generation injectable antipsychotics?
What is the clinical effectiveness of second-generation injectable antipsychotic medications versus second-generation oral antipsychotics?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy was comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were injectable second-generation antipsychotic drugs, including aripiprazole, risperidone, olanzapine, paliperidone, and ziprasidone. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews (SRs), meta-analyses (MAs), or network meta-analyses, any types of clinical trials or observational studies, or economic studies. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2017 and March 1, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with a mental health condition |
Intervention | Second-generation injectable antipsychotic drugs (depots) |
Comparator | Q1: First-generation injectable (depots) antipsychotic drugs Q2: Second-generation oral antipsychotic drugs |
Outcomes | Clinical effectiveness, that is, efficacy (e.g., adherence to therapy; quality of life; reduction in the symptoms of the condition; hospital readmission and/or health care utilization) time to relapse; suicide/mortality; and safety (e.g., tolerability, adverse effects, relapse) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were duplicate publications. Studies were also excluded if the populations had dementia, the ages of patients were unclear, compared doses or frequencies of same medication, had unclear route of administration, or had no comparator group. Articles about antipsychotic use in chemotherapy, substance use, or withdrawal scenarios, and studies about rapid or short-acting antipsychotic drugs in emergency situations or combined use of antipsychotic drugs with another drug where the effect of the antipsychotic drugs could not be evaluated were also excluded. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. SRs with objectives that did not focus on SG antipsychotic drugs were also excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 for SRs and the Downs and Black checklist8 for randomized controlled trials (RCTs). Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
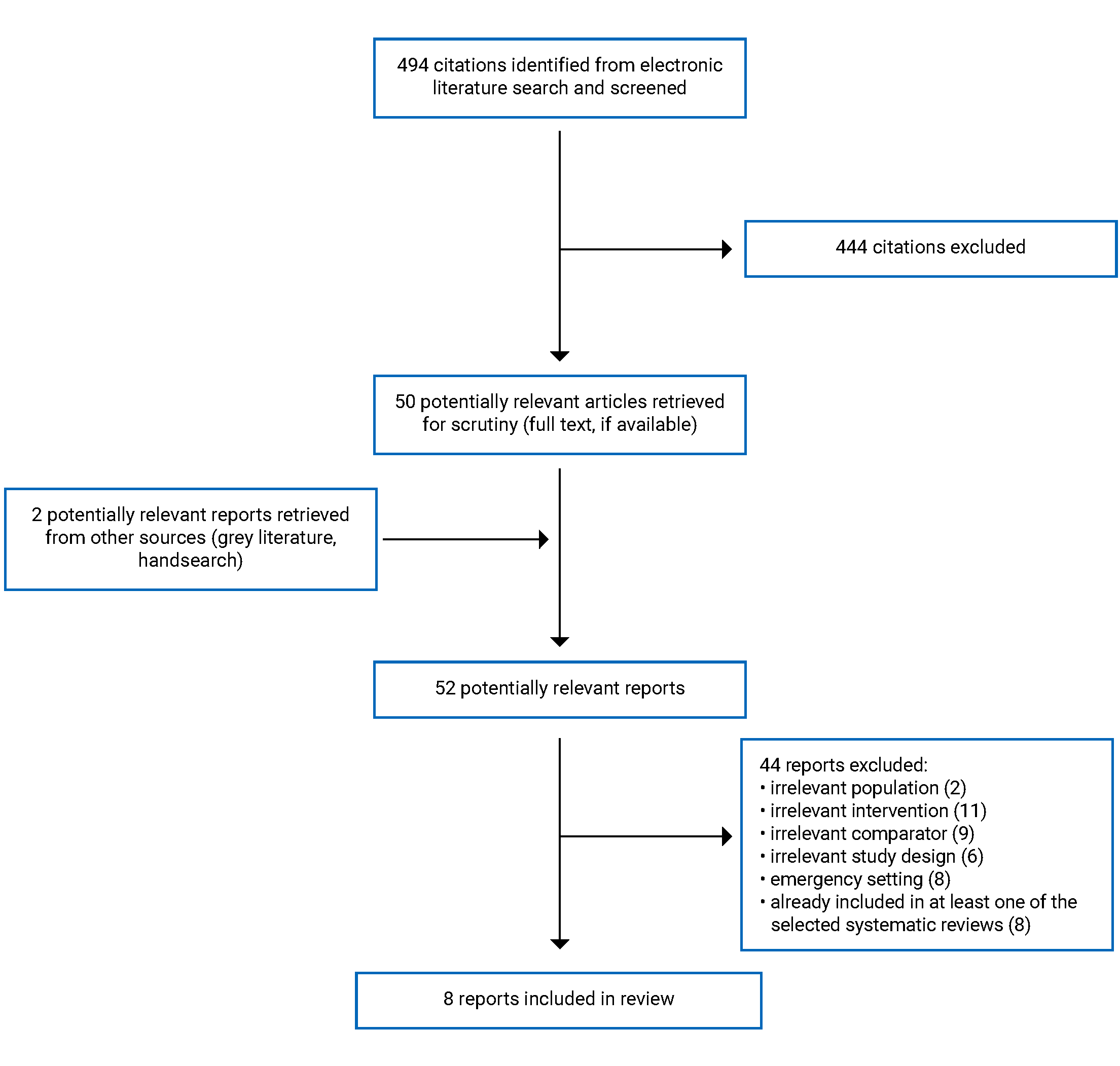
A total of 494 citations were identified in the literature search. Following screening of titles and abstracts, 444 citations were excluded and 50 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 44 publications were excluded for various reasons, and 8 publications met the inclusion criteria and were included in this report. These comprised 7 SRs and 1 RCT. Appendix 1 presents the PRISMA9 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
The scope of all 7 SRs10-16 was broader than the topic of the current review. Some primary studies included in these SRs were out of scope with no comparator group or comparator group of no interest to the current review. Therefore, only the characteristics and results of the subset of relevant studies are described in this report.
Study Design
The 7 SRs10-16 were published between 2017 and 2020 and they included literature published up to 2019. Three SRs13,14,16 MA results relevant to the current review so summary estimates were extracted for these SRs. Three SRs did not conduct MAs10,11,15 and 1 SR12 did not have MAs relevant to the current review; data for individual studies were extracted instead. The Saucedo Uribe et al. SR16 included 17 RCTs of which 2 were relevant to the current review. The Gentile SR10 included 51 studies of which 8 RCTs and 5 NRSs were relevant to the current review. The Keramatian et al. SR11 include 35 studies of which 2 RCTs and 3 non-randomized studies (NRSs) were relevant to the current review. The Olagunju et al. SR13 included 26 studies of which 8 RCTs were relevant to the current review. The Peters et al. SR15 identified 31 RCTs and 5 MAs from the literature; 4 of the RCTs were relevant to this review. The Park et al. SR14 included 17 RCTs and 13 NRSs of which all but 1 NRS was relevant to the current review. The SR14 had 4 MAs that were relevant to the current report. The McDonagh et al. SR12 from the Agency for Health care Research and Quality included 2 SRs and 29 RCTs of which 4 RCTs were relevant to the current review. These 4 RCTs were also captured in other SRs included in the current report; however, the McDonagh et al. SR12 reported some results that were not in the other SRs. The overlap across all SRs is presented in Appendix 5.
The 1 included RCT17 was published in 2022.
Country of Origin
For SRs, 1 had a first author from Italy,10 1 from Mexico,16 1 from Canada,11 1 from Australia,13 1 from Germany,15 1 from South Korea,14 and 1 from the US.12 For the included RCT,17 the first author was from China and the study was conducted across 15 centres in China.
Patient Population
Five SRs12-16 focused on populations with schizophrenia-related conditions only, and 2 SRs10,11 included populations with either schizophrenia- or bipolar-related disorders. Across SRs, the number of patients included in their primary studies ranged from 10 to 8,433. All SRs reported results for adult populations and for those that provided average age data, this ranged from 21.5 to 48.0 years. In the 1 included RCT,17 the population was 436 adults with schizophrenia with an average age of 34.2 years in the intervention group and 33.6 years in the comparator group.
Studies did not distinguish whether gender or sex were reported or whether nonbinary identification was recorded, so results are summarized as reported by the authors of the included studies. Based on 3 SRs,13,15,16 males ranged from 43.1% to 86.2% across studies. One SR12 reported on females which ranged from 22.0% to 39.2%. For the included RCT,17 both the intervention and comparator were comprised of 28.4% males and 71.6% females.
Interventions and Comparators
Five SRs10-12,15,16 included studies that compared SG-LAIs with FG-LAIs, 6 SRs10-15 included studies that compared SG-LAIs with oral SG antipsychotic drugs, and 1 RCT17 compared an SG-LAI plus oral placebo with oral SG antipsychotic plus placebo injection.
The SG-LAIs evaluated were aripiprazole (ARI) 50 mg to 400 mg,10-14 olanzapine (OLA) 150 mg to 600 mg,10,12-14 paliperidone palmitate (PP) 39 mg to 234 mg,10-12,15,16 risperidone (RIS) 12.5 mg to 50 mg,10-16 or ARI-LAI plus oral placebo,17 or any SG-LAI.14 Doses for any SG-LAI14 were not reported. FG-LAIs included haloperidol decanoate 25 to 200 mg,10-12,15,16 fluphenazine decanoate 37 mg and haloperidol decanoate 114 mg together,16 zuclopenthixol decanoate,10 or any FG-LAI.11 Studies did not provide the doses for zuclopenthixol decanoate LAI10 or any FG-LAI.11 Oral SG antipsychotic drugs included amisulpride (AMI),14 ARI 6 mg to 30 mg,10-14 OLA 5 mg to 20 mg,10,12-15 quetiapine (QUE) 300 mg to 500 mg,10,13,14 RIS 1 mg to 6 mg, ziprasidone (ZIP),14 paliperidone extended-release 6 mg to 12 mg,15 oral ARI plus placebo injection,17 or any SG antipsychotic.10,11,13-15 The doses for AMI,14 ZIP,14 or any oral SG antipsychotic were not provided.10,11,13-15 Specifically, 2 SRs10,11 reporting on FG-LAI, 2 SRs11,14 on SG-LAI, and 4 SRs10,11,13,14 on oral SG antipsychotic did not provide the doses that were evaluated.
LAIs were provided every 2 weeks or monthly. When reported, oral SG antipsychotic drugs were given to patients daily. Five SRs10,11,13,14,16 did not report how often treatments were provided.
Study duration ranged from 2.5 months to 2.5 years.
Outcomes
Effectiveness
Effectiveness was measured in as efficacy failure,12 discontinuation,10-12,14-16 non-compliance,14 remission,12,14 symptoms,11,12,14-17 functioning,11-15,17 quality of life,11-14 stabilization,15 and satisfaction.15
Specifically, symptoms were measured as individual symptoms or by using scales such as the Positive and Negative Syndrome Scale (PANSS), the Young Mania Rating Scale (YMRS), the Hamilton Depression Rating Scale (HDRS), the Hamilton Anxiety Rating Scale (HAM-A), the Brief Psychiatric Rating Scale (BPRS), the Mongtomery-Asberg Depression Rating Scale (MADRS), and the visual analogue scale (VAS).
The PANSS is a 30-item scale that measures positive symptoms (excess of function), negative symptoms (loss of function), and general psychopathology.18 Each item is rated from 1 to 7; higher numbers indicate increasing psychopathology.18 It is measured using a clinical interview with the patient, and includes input from care staff or family members.18
The YMRS is an 11-item scale that measures symptoms in those with mania, during a clinical interview.19-21 Each item has 5 severity score levels with higher scores indicating increased severity.19-21 Four items are scored out of 8 and 7 items are scored out of 4, with the total score ranging from 0 to 60.19-21
The HDRS can have 17, 21, or 29 items and is used by clinicians to measure depression symptoms in patients.22,23 Each item is scored from 0 to 2 or 0 to 4 with higher numbers indicating more severity.22,23
The HAM-A is a 14-item scale used by clinicians to measure anxiety symptoms.24,25 Each item is given a score from 0 to 4 with higher numbers indicating more severity.24,25
The BPRS is an 18-item scale that measures psychiatric symptoms during a clinical interview with a clinician.26,27 Each item is rated from 0 to 7 with higher numbers indicating more severity.26,27
The MADRS is a 10-item scale and is used by clinicians to measure depression symptoms in patients.28,29 Each item is scored from 0 to 6 with higher numbers indicating more severity.28,29 The total score ranges from 0 to 60.28,29
The VAS is a continuous scale that can be used by a patient to indicate the intensity of pain across a spectrum of no pain to worst pain.30
Functioning was measured using the Clinical Global Impression-Severity (CGI-S),11,12,14,15,17 the Clinical Global Impression-Improvement (CGI-I),11,12,17 the Global Assessment of Function (GAF),13 the Scale of Functioning (SOF),13 the Personal and Social Performance scale (PSP),13,17 the Social and Occupational Functioning Assessment Scale (SOFAS),13 the Subjective Well-Being Under Neuroleptics Scale-Short Form (SWN-S),15 and the Social Functioning Scale (SFS).13
The Clinical Global Impression scales measure symptoms, treatment response, and treatment efficacy.31,32 The CGI-S and the CGI-I sections are each on 7-point scales, where higher values indicate more illness or worsening of condition, respectively.31,32
The GAF measures social, occupational, and psychological functioning as a whole, and provides a score from 1 to 100, where higher numbers indicate more functioning in life’s activties.33,34
The PSP is based on the SOFAS, which was part of the DSM-IV.34-37 Both instruments assess social functioning in patients based on a 100-point scale; with higher numbers indicating higher functioning.34-37
The SWN is a scale that patients with psychotic disorders fill out to measure illness, treatment experiences, and life satisfaction.38,39 The long version contains 38 items, and the short version has 20 items.38,39 Each item is given a score from 1 to 6 representing “not at all” to “very much” as a response to each statement.38,39
The SFS is based on patient self-report and captures functioning in people with schizophrenia.40,41 There are 76 items and most are rated on 2 to 5 point scales; with higher numbers indicating more competent behaviour.40,41
Quality of life was measured using the Heinrichs-Carpenter QoL scale (QLS),13 the 12-item Short Form Health Survey (SF-12),13 the 36-item Short Form Health Survey (SF-36),12,13 the Schizophrenia Quality-of-Life Scale, Revision 4 (SQLS-R4),13 the Wisconsin Quality-of-Life Index (W-QOLI),13 and the Assessment of Quality of Life (AQoL).13
The QLS is a 21-item scale based on a semi-structured interview used by a clinician to document the quality of life in those with schizophrenic deficit syndrome.42 Each item is rated on a 5- or 7-point scale with higher numbers indicating better quality of life.42
The Short Form Health Surveys are self-reported by patients and measure health status in different domains including physical, mental, and emotional health.43,44 Each item has 2 to 5 response options ranging from values representing excellent health to poor health.43,44
The SQLS-R4 has 33 items and measures quality of life in patients with schizophrenia.45,46 Each item is scored on a 5-point scale, and each domain is given a score from 0 to 100, representing best to worst health status, respectively.45,46
The W-QOLI is a model that measures quality of life in 9 dimensions and can be filled out by a patient, clinician, or caregiver.47,48 Some questions have non-hierarchical responses, while others have an order of options (e.g., satisfaction from very dissatisfied to very satisfied).47,48
The AQoL are a group of instruments that measure different life dimensions such as independent living, mental health, and senses.49,50 There are 4 versions that include 12, 20, 26, or 35 items; each item has 4 to 6 response options.49,50
Satisfaction was measured using the Service Engagement Scale (SES),14 and the Treatment Satisfaction Questionnaire for Medication (TSQM).14
The SES is a 14-item questionnaire that was developed with people who had first episode psychosis, and measures engagement with community mental health services.51,52
The TSQM is a 14-tem instrument that measures effectiveness, convenience, side effects and global satisfaction in patients.53,54 One item uses a dichotomous response scale, while the other questions have a 7-point scale ranging from extremely satisfied to extremely dissatisfied.53,54
Safety
Safety was measured as EPS,11,12,14-17 hospitalizations,11,14-16 relapse,12,14,15 suicidal or homicidal ideation,12 death,12 and other adverse events (AEs).11,12,14,16,17 Drug-induced movements were captured by the Abnormal Involuntary Movement Scale (AIMS), the Simpson-Angus Extrapyramidal Side Effects Scale (SAS), the Extrapyramidal Symptom Rating Scale (ESRS), the Barnes Akathisia Rating Scale (BARS), and the global assessment of akathisia.
The AIMS is a 12-item scale used by clinicians to measure dyskinesias (i.e., involuntary movements) severity in patients.31,55 Each item is scored from 0 to 4 with higher numbers indicating greater severity.31,55
The SAS is a 10-item scale used by clinicians to measure involuntary movements in patients.56,57 Each item is scored from 0 to 4 with higher numbers indicating more severity.56,57
The ESRS is a scale used by clinicians to measure involuntary movements in patients.58 It has 8 subscales with questions about movements for each that can be scored from 0 up to 6, with higher numbers indicating greater severity.58
The BARS and the global assessment of akathisia are scales used by clinicians to measure akathisia (i.e., restlessness) in patients through observation.59,60 For the BARS, each item is scored from 0 to 3 or 0 to 5 with higher numbers indicating more severity and for the global assessment of akathisia, the score ranges from 0 to 5 with higher numbers indicating more severe akathisia.59,60
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Summary of Critical Appraisal
Systematic Reviews
All 7 SRs10-16 clearly stated the populations, interventions, and outcomes of interest. Six SRs10,12-16 also clearly stated the comparators to include in the reviews upfront. Three SRs12,14,16 established a protocol or study criteria beforehand. For 4 SRs,10,11,13,15 it is unclear whether a protocol was written; potential bias due to protocol deviation could not be determined.
Six SRs10-14,16 searched at least 2 databases and provided keywords or search strategies. For 1 SR,15 literature search was performed in 1 database, and it is unknown if it was enough to comprehensively capture relevant published literature. Five SRs10-13,15 conducted more comprehensive literature searches involving databases and other sources such as reference lists of included studies, reference lists of other reviews, clinical trial registries, expert recommendations, and grey literature.
Four SRs11,12,14,16 performed study selection in duplicate, 2 SRs11,12 conducted data extraction in duplicate with independent reviewers, and 4 SRs12-14,16 assessed the risk of bias for included studies. For SRs that did not conduct study selection or data extraction in duplicate, it is unclear if all relevant studies were included, and the completeness and accuracy of the extracted data are unknown. For the 3 SRs10,11,15 where it is unclear if risk of bias was assessed, it may be challenging to draw conclusions since potential weakness in study conduct are unclear.
Two SRs12,15 described study and population characteristics in sufficient detail. Five 5 SRs10,11,13,14,16 described some characteristics in detail, while other specifics such as treatment doses and frequencies were not provided. This limits the comparability of the studies to others, and it was difficult to determine the applicability of the findings.
Six SRs10-12,14-16 did not report quantitative data on comparative effects between study groups for all outcomes; it was unclear to determine whether there were meaningful differences between study groups.
In the 2 SRs13,16 that conducted relevant MAs, both combined study results appropriately and addressed heterogeneity. One SR13 assessed for publication bias but the other SR16 did not. Thus, in the latter,16 it is unclear whether included studies were published selectively.
For 2 SRs,10,16 authors indicated that there were no conflicts of interest. One SR14 did not provide a conflicts of interest statement. For 2 SRs,11,15 1 of the review authors of each study received funds from pharmaceutical companies and it is unclear how this may have affected conduct or interpretation of results. One SR13 indicated no conflicts of interest however the funding source of the review was unclear. In another SR,12 conflicts were collected; however, it is unclear whether any may have been related to review and interpretation of findings.
Randomized Controlled Trial
In the 1 included RCT,17 authors clearly stated objectives and study criteria. Patients were randomized and important factors that may have influenced outcomes were balanced between study groups. The study was conducted across 15 sites in China which may increase the generalizability of the findings; however, the exclusion of those who were of childbearing age, pregnant, or breastfeeding may mean that the results could not be generalizable to these populations.
Although the trial was described as double blind, the authors stated that investigators were blind to assignment but that drug managers who administered the treatments at each site were unblinded. It is unclear if the placebos administered adequately concealed treatment since the aripiprazole and placebo injections appear different. This is a limitation since knowledge of study assignment may have introduced performance bias (e.g., patients may have been treated differently if study personnel knew what treatment they received, patients may have self-reported outcomes differently with knowledge of their assignment) or detection bias if outcome assessors were also not blinded.
Around a quarter of each study group did not complete the study because of loss to follow-up, discontinuation of treatment, consent withdrawal, adverse event (AE), clinician advice, and other reasons; the missing data were handled using the last observation carried forward method. It is unclear if reasons for dropout were related to study assignment, or if they were similar between groups. This is a limitation as results may be skewed.
Some outcome data (e.g., symptoms, functioning) were collected subjectively through questionnaires completed by patients, clinicians, or family members. This is a limitation since there may have been bias due to knowledge of study assignment, and outcomes may be unreliable.
Three review authors received funding from pharmaceutical companies. It is unclear whether and how these potential conflicts may have affected results of the review.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings by outcome.
The summaries in this report may contain some data from the same trials as there was overlap in some of trials included within the SRs. This overlap across SRs is presented in Appendix 5. Where the same primary study results were reported in 2 or more SRs, they are presented once in this report from 1 of the included SRs.
Effectiveness of Second-Generation Versus First-Generation Injectable Antipsychotic Drugs
Effectiveness was measured as efficacy failure in 1 SR,12 discontinuation in 2 SRs,10,16 continuation in 1 SR,11 and as symptoms using the PANSS in 1 SR.16
Efficacy Failure
Results from 1 SR12 showed little-to-no difference in efficacy failure between PP-LAI and haloperidol decanoate LAI; these findings had low precision.
Discontinuation and Continuation
The results from 2 SRs10,16 showed that there were no differences between RIS-LAI and haloperidol decanoate LAI and fluphenazine decanoate LAI given together, and no difference between PP-LAI and haloperidol decanoate LAI. There is uncertainty regarding these findings because data on the comparative effects and measures of variability were not reported. For results from 1 SR,10 there appeared to be higher discontinuation in the haloperidol decanoate LAI group compared to the PP-LAI group, however no statistical comparison was reported. For results from 1 SR,10 there appeared to be higher discontinuation in the zuclopenthixol decanoate LAI group compared to the RIS-LAI group. Another SR11 showed what appeared to be higher treatment continuation in the RIS-LAI group compared to the FG-LAI group. However, no statistical comparison was reported in either study.
Symptoms
In 1 MA involving 2 RCTs reported in 1 SR,16 there was little-to-no difference in the PANSS score between SG-LAIs and FG-LAIs.
Safety of Second-Generation Versus First-Generation Injectable Antipsychotic Drugs
Extrapyramidal Symptoms
Two SRs12,16 reported results for extrapyramidal symptoms (EPS). In 1 SR,16 1 MA suggested little-to-no difference in tardive dyskinesia between SG-LAIs and FG-LAIs. In another SR,12 there appeared to be a higher AIMS score in the haloperidol decanoate LAI group compared to the PP-LAI group, and a higher global rating of akathisia in the PP-LAI group compared to the haloperidol decanoate LAI; interpretation of the statistical information provided in the SR is unclear.
Hospitalizations
Two SRs11,16 reported results for hospitalizations. In SR,16 authors stated that the number of hospitalizations was not statistically significantly different between the RIS-LAI group and the comparator group that received haloperidol decanoate LAI and fluphenazine decanoate LAI together; however, the magnitude and precision are uncertain because data on the comparative effects and measures of variability were not reported. In another SR,11 authors reported that the risk of all-cause hospitalization risk was significantly higher in the haloperidol decanoate LAI group compared to the ARI-LAI group; however, the precision is uncertain because data on the measures of variability were not reported. In this same SR,11 authors stated that after adjusting for confounders, those in the FG-LAI group had a higher risk of hospitalization for any mood episode and major depressive episode compared to the RIS-LAI group; however, results are imprecise.
Suicidal or Homicidal Ideation
One SR12 reported on suicidal or homicidal ideation, which appeared higher in the PP-LAI group compared to the haloperidol decanoate LAI group, however, there was no statistical comparison reported.
Treatment Emergent Adverse Events
Adverse events were reported in 1 SR.16 Authors stated that treatment emergent AEs were not statistically significantly different between the PP-LAI and haloperidol decanoate LAI groups, however, the magnitude and precision are uncertain because data on the comparative effects and measures of variability were not reported.
Effectiveness of Second-Generation Injectable Versus Second-Generation Oral Antipsychotic Drugs
Non-Compliance and Discontinuation
One SR14 reported non-compliance outcomes, with little-to-no difference between groups.
Four SRs10,12,14,15 reported discontinuation outcomes. In 2 SRs10,15 with results comparing RIS-LAI to any oral SG antipsychotic, there did not appear to be differences between groups, however, the authors did not report statistical comparisons. Based on 1 SR,10 the RIS-LAI group appeared to have a lower discontinuation rate compared to the QUE group, but a higher discontinuation rate compared to oral ARI and OLA groups. However, statistical data on comparative effects was not reported.
One SR10 showed what appeared to be a lower discontinuation rate in the PP-LAI group compared to the oral SG antipsychotic group; however, authors did not report comparative effects. One SR15 showed what appeared to be higher discontinuation rate in the PP-LAI group compared to the oral OLA group; however, data on the comparative effects was not reported.
In 1 SR15 authors stated that discontinuation rates during the treatment period was similar between PP-LAI and oral OLA groups.
Statistical analyses from 1 SR12 suggested little-to-no difference in all-cause discontinuation and time to all-cause discontinuation between OLA-LAI and oral OLA; precision is unknown because measures of variability were not reported.
Based on SR,12 there appeared to be more people discontinuing treatment in the oral ARI group compared to the ARI-LAI groups; statistical data on comparative effects was not reported. Other findings from this SR12 showed little-to-no difference in time to all-cause discontinuation between ARI-LAI and oral ARI groups.
Symptoms
Four SRs11,12,14,15 and 1 RCT17 reported on symptoms. One MA14 based on 2 RCTs showed a greater decrease in MADRS score with SG-LAI compared to the oral SG antipsychotic.
Two SRs11,15 compared RIS-LAI to oral SG antipsychotic drugs and stated that there were no differences in symptoms between groups; however, conclusions are uncertain because data on the comparative effects and measures of variability were not reported. One SR11 indicated that the RIS-LAI group had a higher number of positive clinical events and lower number of negative events; however, there were no statistical values reported.
One SR15 reported no significant differences between the PP-LAI and oral OLA groups for PANSS score; however comparative data were not reported.
One SR12 reported little-to-no difference in baseline-to-end point least squares mean change on PANSS total score; precision is unclear because measured of variability were not reported.
One SR12 and 1 RCT17 reported on ARI-LAI compared to oral ARI. The SR12 showed a higher positive change in PANSS score in the oral ARI group compared to the ARI-LAI groups but data on comparative values were not reported. The SR12 also showed little-to-no difference in non-exacerbation of psychotic symptoms; but measures of variability were not reported. The RCT17 showed little-to-no difference in PANSS outcomes between ARI-LAI and oral ARI groups.
Remission
One MA14 based on 5 RCTs showed little-to-no difference in remission between groups. Results from 1 SR12 showed what appeared to be lower remission in the ARI-LAI group compared to the oral ARI group; however, data on comparative effects were not reported.
Stabilization
One SR15 showed little-to-no difference in time to stabilization between the RIS-LAI group compared to oral SG antipsychotic drugs group; data on measures of variability were not reported.
Functioning
Five SRs11-15 and 1 RCT17 reported on functioning. One SR11 compared RIS-LAI to oral SG antipsychotic drugs; some results suggested significant decrease in CGI-S scores in patients who switched from oral SG antipsychotic to RIS-LAI, while other results showed RIS-LAI and oral SG antipsychotic groups were similar.
One SR15 suggested negative symptoms were more favourable for a PP-LAI group compared to oral paliperidone extended-release medication but that there was little-to-no difference in functioning measured using the PSP and SWN-S scales.
Based on 1 MA13 that included 7 RCTs, functional outcome was better in the SG-LAI group compared to the oral SG antipsychotic group.
One RCT17 comparing ARI-LAI plus oral placebo to oral ARI plus placebo injection showed little-to-no difference in functioning scores between groups. One SR12 did not report comparative data to form conclusions.
Quality of Life and Satisfaction
The authors of 1 SR15 stated that there were differences between patients for treatment satisfaction, convenience, and service engagement between the PP-LAI and oral paliperidone extended-release groups.
Safety of Second-Generation Injectable Versus Second-Generation Oral Antipsychotic Drugs
Extrapyramidal Symptoms
Four SRs11,12,14,15 and 1 RCT17 reported on EPS. One NRS in 1 SR11 stated that there was a decrease in EPS from baseline to 12 months in patients switched from oral SG antipsychotic drugs to RIS-LAI. Two SRs11,15 found little-to-no difference in EPS, AIMS scores, or SAS scores; measures of variability were not reported. In 1 SR,11 the RIS-LAI group appeared to have more akathisia compared to the oral SG antipsychotic group; data on comparative effects were not reported.
In 1 SR15 with results comparing PP-LAI to oral paliperidone extended-release medication, results were unclear.
In 1 SR,12 there appeared to be fewer EPS in the ORA-LAI group compared to the oral OLA group; data on comparative effects were not reported.
One SR12 comparing ARI-LAI to oral ARI did not report comparative data on EPS to form conclusions.
One RCT17 comparing ARI-LAI plus oral placebo to oral ARI plus placebo injection stated no difference between groups in EPS scales; however, no comparative effects were reported.
Relapse
One SR15 suggested little-to-no difference in relapse between RIS-LAI and oral SG antipsychotic groups.
In 1 MA14 based on 2 RCTs, the RIS-LAI group had a longer time to relapse compared to the oral ARI group.
In 1 SR12 comparing ARI-LAI with oral ARI, there was little-to-no difference in the estimated relapse rate. In the same SR,12 there appeared to be little-to-no difference in the ORA-LAI group compared to oral OLA in the rate of relapse and a difference between groups on time to relapse with data on comparative effects not reported; relapse findings are unclear since the results from these 2 outcomes are different.
Hospitalization
In 1 SR15 there appeared to be higher hospitalization in the RIS-LAI compared to the oral SG antipsychotic group; however data on comparative effects were not reported.
In 1 MA14 based on 2 RCTs, the OLA-LAI group had a shorter number of hospital days compared to the oral OLA group.
Other AEs
In 1 SR,11 some results showed little-to-no difference in AEs between RIS-LAI and oral SG antipsychotic group while other results showed a higher percentage of patients in the RIS-LAI group with somnolence, headache, tremors, and skin rash compared to oral SG antipsychotic group but data on these comparative effects were not reported.
One SR15 comparing PP-LAI to oral paliperidone extended-release medication, results were unclear.
In 1 SR,12 there appeared to be higher AEs and higher discontinuation due to AEs in the ORA-LAI group compared to the oral OLA group, and fewer overall AEs and fewer withdrawal due to AEs in the ARI-LAI group compared to the oral ARI group. Data on comparative effects were not reported for these findings.
One RCT17 comparing ARI-LAI plus oral placebo to oral ARI plus placebo injection stated little-to-no difference between groups in treatment emergent AEs and injection site reactions.
Suicidality and Death
In 1 RCT reported in 1 SR,12 there appeared to be little-to-no difference in suicidality in the ARI-LAI group compared to the oral ARI group; data on comparative effects were not reported.
In 1 RCT reported in 1 SR,12 there appeared to be more deaths in the oral ORA group compared to the OLA-LIS group; data on comparative effects were not reported.
Limitations
Limitations of the body of evidence were few results on SG-LAIs compared to FG-LAIs in recently published literature, a lack of statistical findings to form conclusions, unclear comparability across studies due to using different outcome measures to determine safety and effectiveness, unclear generalizability to the Canadian population, and unclear quality of the evidence. Five SRs10-12,15,16 published between 2017 and 2019 had data comparing SG-LAIs and FG-LAIs; however, there were few datum for each outcome, since for this comparison, efficacy failure, continuation, symptoms, suicidal or homicidal ideation and AEs were only reported in 1 primary study from these SRs.
The summaries from included SRs did not report quantitative findings sufficiently. In most cases, authors of SRs did not provide data on comparative effects or measures of variability between groups, and instead reported primary study-level frequency or percentage values for each study groups. In some cases, these data were supplemented with a narrative statement on statistical significance without providing statistical data. It is therefore challenging to derive conclusions from this evidence.
Another limitation was the variety of ways that effectiveness or safety were measured in included studies. The evidence included 7 scales to measure symptoms, 9 instruments to measure functioning, 8 scales to measure quality of life, 2 questionnaires to measure satisfaction, and 4 scales to measure EPS. Given the variability in measurement tools and their results, it is unclear how outcomes can be compared across studies.
Given that most of the evidence base was from SRs which included primary studies from different countries, it is unclear how generalizable the results are to the Canadian population.
In 3 of the 7 included SRs, it was unclear whether risk of bias assessment was conducted, which is another limitation since there is missing information about the quality and strength of the evidence.
Conclusions and Implications for Decision- or Policy-Making
A rapid review was conducted to determine the clinical effectiveness of SG-LAI compared to FG-LAI or oral SG antipsychotic drugs for patients with schizophrenia or bipolar disorders. Seven SRs10-16 and 1 RCT17 were found, which were published between 2017 and 2019. These studies reported effects on discontinuation, continuation, symptoms, remission, stabilization, functioning, quality of life, satisfaction, and AEs such as EPS, relapse, hospitalization, suicide or suicidal ideation, or death. Five SRs10-12,15,16 reported outcomes comparing SG-LAI to FG-LAI, and 6 SRs10-15 and 1 RCT17 reported outcomes comparing SG-LAI to oral SG antipsychotic drugs.
For the comparison of SG-LAI to FG-LAI, 2 SRs12,16 indicated little-to-no difference in efficacy failure between PP-LAI and haloperidol decanoate LAI groups, and little-to-no change in symptom severity between SG-LAI and FG-LAI groups. Three SRs11,12,16 showed little-to-no difference in tardive dyskinesia between SG-LAI and FG-LAI, EPS between PP-LAI and haloperidol decanoate LAI, treatment emergent AEs between PP-LAI and haloperidol decanoate LAI, or in hospitalizations between RIS-LAI and haloperidol decanoate LAI and fluphenazine decanoate LAI given together. However, a higher risk of hospitalization was reported in patients given FG-LAI compared to RIS-LAI, and between those given haloperidol decanoate LAI compared to those given ARI-LAI, although the precision of these latter findings is uncertain because data on the measures of variability were not reported.
For the comparison of SG-LAI to oral SG antipsychotic drugs, 2 SRs12,14 suggested little-to-no difference in non-compliance between RIS-LAI and oral SG antipsychotic, OLA-LAI and oral OLA, and ARI-LAI and oral ARI groups. Two other SRs11,15 showed little-to-no difference in symptom severity scores, depression, and mania between RIS-LAI and oral SG antipsychotic drugs; however, these SRs did not assess risk of bias or report quantitative data. Results from 2 SRs12,15 and 1 RCT17 suggested little-to-no difference in symptom severity between PP-LAI and oral OLA, between OLA-LIS and oral OLA, and between ARI-LAI and oral ARI. One MA14 based on 2 studies suggested a greater decrease in depression in patients given RIS-compared to patients given oral ARI or QUE.
One MA14 based on 5 studies suggested little-to-no difference in remission between SG-LAI and oral SG antipsychotic groups and another MA13 based on 7 RCTs suggested that patients given SG-LAI had more favourable psychosocial function compared to those given oral SG antipsychotic.
When comparing RIS-LAI to oral SG antipsychotic drugs, 1 SR15 suggested little-to-no difference in time to stabilization or relapse between patients who received RIS-LAI and those who received oral SG antipsychotic. Another SR11 found that illness severity decreased in patients who switched from oral SG antipsychotic to RIS-LAI. Both SRs11,15 also showed little-to-no difference in EPS between these groups.
One RCT17 reported little-to-no difference in illness severity, improvements from treatment, or social performance between ARI-LAI and oral ARI, and data from 2 SRs11,12 showed little-to-no difference in quality of life between ARI-LAI and oral ARI groups. One RCT17 showed little-to-no difference between ARI-LAI compared to oral ARI for AEs and injection site reactions.
Based on 1 SR,15 PP-LAI was more favourable than oral paliperidone extended-release for negative symptoms measured on some functioning scales, but there was no difference between groups on other functioning scales; PP-LAI was more favourable than oral paliperidone extended-release tablets for treatment satisfaction, convenience, and service engagement.
One SR12 showed that time to relapse differed between patients receiving OLA-LAI and those receiving oral OLA, however there was little-to-no difference in the rate of relapse. One MA14 suggested that mean hospital days were lower for the OLA-LAI group compared to the oral OLA group. Based on an SR12 that reported on ARI-LAI compared to oral ARI, findings suggested little-to-no difference in relapse rate between groups, but that the OLA-LAI group had a longer time to relapse compared to the oral OLA group. Based on MA data,14 patients given RIS-LAI showed longer time to relapse compared to those given oral ARI.
Based on the poor reporting of quantitative information and unclear quality of studies, the evidence in this report is insufficient to answer the research questions definitively. Future studies of strong methodological quality using standardized outcome measures and applying appropriate quantitative analyses are needed to determine conclusively the clinical effectiveness of SG injectable versus FG injectable antipsychotic drugs and versus SG oral antipsychotic medications.
References
1.GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137-150. PubMed
2.Centre for Addiction and Mental Health. Antipsychotic medications. 2022; https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/antipsychotic-medication. Accessed April 4, 2022.
3.Horn M, Procyshyn RM, Warburton WP, et al. Prescribing second-generation antipsychotic medications: practice guidelines for general practitioners. BCMJ.54:75-82.
4.Lauriello JC, A.R. Pharmacotherapy for schizophrenia: long-acting injectable antipsychotic drugs. In: Post TW, ed. UpToDate2022: https://www.uptodate.com/contents/pharmacotherapy-for-schizophrenia-long-acting-injectable-antipsychotic-drugs. Accessed 2022 Apr 4.
5.Brankston G, Picheca L. Antipsychotic drugs or benzodiazepines for rapid tranquilization in mental health facilities or emergency department settings. Cdn J Health Technol. 2021;1(8). https://canjhealthtechnol.ca/index.php/cjht/article/view/rc1373. Accessed 2022 Apr 4.
6.Narain T, Ford C. Atypical injectable antipsychotics for schizophrenia or bipolar disorder: a review of clinical effectiveness and cost-effectiveness. Ottawa (ON): CADTH; 2019: https://www.ncbi.nlm.nih.gov/books/NBK541213/. Accessed 2022 Apr 4.
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
8.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
10.Gentile S. Discontinuation rates during long-term, second-generation antipsychotic long-acting injection treatment: a systematic review. Psychiatry Clin Neurosci. 2019;73(5):216-230. PubMed
11.Keramatian K, Chakrabarty T, Yatham LN. Long-acting injectable second-generation/atypical antipsychotics for the management of bipolar disorder: a systematic review. CNS Drugs. 2019;33(5):431-456. PubMed
12.McDonagh MS, Dana T, Selph S, et al. Treatments for schizophrenia in adults: a systematic review. (Comparative Effectiveness Reviews, no. 198). Rockville (MD): Agency for Healthcare Research and Quality; 2017: https://www.ncbi.nlm.nih.gov/books/NBK487628/. Accessed 2022 Apr 4.
13.Olagunju AT, Clark SR, Baune BT. Long-acting atypical antipsychotics in schizophrenia: a systematic review and meta-analyses of effects on functional outcome. Aust N Z J Psychiatry. 2019;53(6):509-527. PubMed
14.Park SC, Choi MY, Choi J, et al. Comparative efficacy and safety of long-acting injectable and oral second-generation antipsychotics for the treatment of schizophrenia: a systematic review and meta-analysis. Clin Psychopharmacol Neurosci. 2018;16(4):361-375. PubMed
15.Peters L, Krogmann A, von Hardenberg L, Bodeker K, Nohles VB, Correll CU. Long-acting injections in schizophrenia: a 3-Year update on randomized controlled trials published January 2016-March 2019. Curr Psychiatry Rep. 2019;21(12):124. PubMed
16.Saucedo Uribe E, Carranza Navarro F, Guerrero Medrano AF, et al. Preliminary efficacy and tolerability profiles of first versus second-generation long-acting injectable antipsychotics in schizophrenia: a systematic review and meta-analysis. J Psychiatr Res. 2020;129:222-233. PubMed
17.Xiao L, Zhao Q, Li AN, et al. Efficacy and safety of aripiprazole once-monthly versus oral aripiprazole in Chinese patients with acute schizophrenia: a multicenter, randomized, double-blind, non-inferiority study. Psychopharmacology (Berl). 2022;239(1):243-251. PubMed
18.Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261-276. PubMed
19.Young Mania Rating Scale (YMRS). MEASURE: modeling effective antipsychotic therapeutic success by utizlizing real evidence: patient education tools. 2006; https://dcf.psychiatry.ufl.edu/files/2011/05/Young-Mania-Rating-Scale-Measure-with-background.pdf. Accessed 2022 Apr 4.
20.Lukasiewicz M, Gerard S, Besnard A, et al. Young Mania Rating Scale: how to interpret the numbers? Determination of a severity threshold and of the minimal clinically significant difference in the EMBLEM cohort. Int J Methods Psychiatr Res. 2013;22(1):46-58. PubMed
21.Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429-435. PubMed
22.Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56-62. PubMed
23.Hamilton Depression Rating Scale (HDRS). Gainesville (FL): University of Florida; 2011: https://dcf.psychiatry.ufl.edu/files/2011/05/HAMILTON-DEPRESSION.pdf. Accessed 2022 Apr 4.
24.Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50-55. PubMed
25.Hamilton Anxiety Rating Scale (HAM-A). Gainesville (FL): University of Florida; 2011: https://dcf.psychiatry.ufl.edu/files/2011/05/HAMILTON-ANXIETY.pdf. Accessed 2022 Apr 4.
26.Overall JE, Gorham DR. The Brief Psychiatric Rating Scale. Psychol Rep. 1962;10(3):799-812.
27.Brief Psychiatric Rating Scale (BPRS). [n.d.][n.d.]; . Accessed 2022 Apr 4.
28.Blum L. Montgomery Asberg Depression Rating Scale (MADRS). In: Korner-Bitensky N, ed. Stroke Engine Assessments. Montreal (QC): Stroke Engine; 2009: https://strokengine.ca/en/assessments/montgomery-asberg-depression-rating-scale-madrs/. Accessed 2022 Apr 4.
29.Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382-389. PubMed
30.Haefeli M, Elfering A. Pain assessment. Eur Spine J. 2006;15(Suppl 1):S17-24. PubMed
31.Guy W, National Institute of Mental Health, Psychopharmacology Research Branch, Early Clinical Drug Evaluation Program. ECDEU assessment manual for psychopharmacology. Rockville (MD): U.S. Dept. of Health, Education, and Welfare; 1976.
32.Clinical Global Impression (CGI). In: Guy W, ed. ECDEU assessment manual for psychopharmacology. Rockville (MD): U.S. Department of Health, Education, and Welfare; 1976: https://www.psywellness.com.sg/docs/CGI.pdf. Accessed 2022 Apr 4.
33.American Psychiatric Association. Global Assessment of Functioning (GAF) Scale. Diagnostic and statistical manual of mental disorders (DSM-IV-TR). 4th ed. Washington (DC): American Psychiatric Association; 2000:p.34.
34.American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV. Washington (DC): American Psychiatric Association; 1994.
35.American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington (DC): American Psychiatric Association; 2013.
36.Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101(4):323-329. PubMed
37.White S, Dominise C, Naik D, Killaspy H. The reliability of the Personal and Social Performance scale - informing its training and use. Psychiatry Res. 2016;243:312-317. PubMed
38.Naber D, Moritz S, Lambert M, et al. Improvement of schizophrenic patients' subjective well-being under atypical antipsychotic drugs. Schizophr Res. 2001;50(1-2):79-88. PubMed
39.Vothknecht S, Schoevers RA, de Haan L. Subjective well-being in schizophrenia as measured with the Subjective Well-Being under Neuroleptic Treatment scale: a review. Aust N Z J Psychiatry. 2011;45(3):182-192. PubMed
40.Burns T, Patrick D. Social functioning as an outcome measure in schizophrenia studies. Acta Psychiatr Scand. 2007;116(6):403-418. PubMed
41.Iffland JR, Lockhofen D, Gruppe H, Gallhofer B, Sammer G, Hanewald B. Validation of the German version of the Social Functioning Scale (SFS) for schizophrenia. PLoS One. 2015;10(4):e0121807. PubMed
42.Heinrichs DW, Hanlon TE, Carpenter WT, Jr. The Quality of Life Scale: an instrument for rating the schizophrenic deficit syndrome. Schizophr Bull. 1984;10(3):388-398. PubMed
43.Physiopedia. 36-item Short Form Survey (SF-36). [n.d.][n.d.]; ). Accessed 2022 Apr 4.
44.RAND Corporation. 36-Item Short Form Survey (SF-36). [n.d.][n.d.]; . Accessed 2022 Apr 4.
45.Isjanovski V, Naumovska A, Bonevski D, Novotni A. Validation of the Schizophrenia Quality of Life Scale Revision 4 (SQLS-R4) among patients with schizophrenia. Open Access Maced J Med Sci. 2016;4(1):65-69. PubMed
46.Martin CR, Allan R. Factor structure of the Schizophrenia Quality of Life Scale Revision 4 (SQLS-R4). Psychol Health Med. 2007;12(2):126-134. PubMed
47.Diamond R, Becker M. The Wisconsin Quality of Life Index: a multidimensional model for measuring quality of life. J Clin Psychiatry. 1999;60 Suppl 3:29-31. PubMed
48.University of South Florida. Wisconsin Quality of Life Index: W-QLI manual. [n.d.][n.d.]; . Accessed 2022 Apr 4.
49.Assessment of Quality of Life. Instruments. 2014; https://www.aqol.com.au/index.php/aqolinstruments. Accessed 2022 Apr 4.
50.Hawthorne G, Richardson J, Osborne R. The Assessment of Quality of Life (AQoL) instrument: a psychometric measure of health-related quality of life. Qual Life Res. 1999;8(3):209-224. PubMed
51.Tait L, Birchwood M, Trower P. A new scale (SES) to measure engagement with community mental health services. J Ment Health. 2002;11(2):191-198. PubMed
52.Tait L. Service Engagement Scale (SES), measuring engagement with community mental health services. [2002]; https://www.lyndatait.com/service-engagement-scale/. Accessed 2022 Apr 4.
53.Atkinson MJ, Sinha A, Hass SL, et al. Validation of a general measure of treatment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a national panel study of chronic disease. Health Qual Life Outcomes. 2004;2:12. PubMed
54.Bharmal M, Payne K, Atkinson MJ, Desrosiers MP, Morisky DE, Gemmen E. Validation of an abbreviated Treatment Satisfaction Questionnaire for Medication (TSQM-9) among patients on antihypertensive medications. Health Qual Life Outcomes. 2009;7(1):36. PubMed
55.Guy W. Abnormal Involuntary Movement Scale (AIMS). ECDEU assessment manual for psychopharmacology: revised (DHEW publicaiton number ADM 76-338). Rockville (MD): US Department of Health, Education and Welfare, Public Health Service, Alcohol, Drug Abuse and Mental Health Administration, NIMH Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976: https://www.waombudsman.org/files/2013/09/AIMS-Test-Abnormal-Involuntary-Movement-Test.pdf. Accessed 2022 Apr 4.
56.Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl. 1970;212(S212):11-19. PubMed
57.Modified Simpson-Angus Scale (MSAS): extrapyramidal side effects scale. Ontario (CAN): PsychDB; [n.d.][n.d.]: . Accessed 2022 Apr 4.
58.Chouinard G, Margolese HC. Manual for the Extrapyramidal Symptom Rating Scale (ESRS). Schizophr Res. 2005;76(2-3):247-265. PubMed
59.Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. 1989;154:672-676. PubMed
60.Barnes Akathisia Rating Scale (BARS) Syracuse (NY): Simple and Practical Mental Health; 2014: https://simpleandpractical.com/wp-content/uploads/2014/09/Barnes-Akathisia-Rating-Scale-BARS.pdf. Accessed 2022 Apr 4.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix was not copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Saucedo Uribe et al. (2020)16 Mexico Funding: No funding | Literature published between 1966 and May 2019 17 RCTs 2 RCTs and 1 MA relevant to current review | 62 to 290 patients with schizophrenia or schizoaffective disorder Average age across studies: 44 to 48 years Males across studies: 71% to 74% | Interventions: PP-LAI, RIS-LAI FG Comparators: haloperidol decanoate LAI alone, or fluphenazine decanoate LAI and haloperidol decanoate LAI together | Outcomes: discontinuation, symptoms, hospitalization, AEs Follow-up: 1 or 2 years |
Gentile (2019)10 Italy Funding: NR | Literature published between 2001 and October 2018 51 studies 8 RCTs, 5 NRSs relevant to current review | 102 to 2,053 adult patients with schizophrenia spectrum or bipolar disorders | Interventions: ARI-LAI, OLA-LAI, PP-LAI, RIS-LAI FG Comparators: haloperidol decanoate LAI, zuclopenthixol decanoate LAI Oral SG Comparators: ARI, OLA, QUE, or any SG antipsychotic | Outcome: discontinuation Follow-up: 9.5 to 30 months |
Keramatian et al. (2019)11 Canada Funding: No funding | Literature published up to November 2018 35 studies 2 RCTs, 3 NRSs relevant to current review | 10 to 3,916 adult patientsb with bipolar disorder or schizophrenia | Interventions: ARI-LAI, PP-LAI, RIS-LAI FG Comparators: FG-LAI, haloperidol decanoate LAI Oral SG Comparators: ARI, or any SG antipsychotic | Outcomes: discontinuation, symptoms, functioning, quality of life, AEs, hospitalization Follow-up: 1 year or more |
Olagunju et al. (2019)13 Australia Fundinga: Australian Government Research Training Programme Scholarship | Literature published up to March 2018 26 studies 8 RCTs and 1 MA relevant to current review | 41 to 1,182 adult patients with schizophrenia or schizoaffective disorders Males across studies: 48% to 72% | Interventions: ARI-LAI, OLA-LAI, RIS-LAI Oral SG Comparators: ARI, OLA, QUE, RIS, or any SG antipsychotic | Outcomes: psychosocial functioning, quality of life Follow-up: 12 to 130 weeks |
Peters et al. (2019)15 Germany Funding: NR | Literature published between January 2016 and March 2019 31 RCTs, 5 MAs 5 publications relevant to current review based on 4 RCTs | 57 to 290 adults with schizophrenia spectrum disorders Age range across studies: 22.7 to 46.4 years Males across studies: 43.1% to 86.2% | Interventions: PP-LAI, RIS-LAI FG Comparators: haloperidol decanoate LAI Oral SG Comparators: OLA, extended-release paliperidone, or any SG antipsychotic | Outcomes: stabilization, symptoms, discontinuation, satisfaction, functioning, hospitalization, relapse Follow-up: 13 to 96 weeks |
Park et al. (2018)14 South Korea Funding: National Evidence-based Health care Collaborating Agency | Literature published between 2000 and April 2015 17 RCTs, 13 NRSs 17 RCTs, 12 NRSs, 4 MAs relevant to current review | 21 to 8,433 adult patients with schizophrenia or schizoaffective disorders | Interventions: ARI-LAI, OLA-LAI, RIS-LAI, SG-LAI Oral SG Comparators: AMI, ARI, OLA, QUE, RIS, ZIP, or any SG antipsychotic | Outcomes: remission, non-compliance, quality of life, functioning, symptoms, discontinuation, relapse, hospitalization, AEs Follow-up: 3 months to 5 years |
McDonagh et al. (2017)12 US Funding: The Agency for Health care Research and Quality | Literature published between 2011 and February 2017 2 SRs, 29 RCTs 4 RCTs relevant to current review | 86 to 662 adults with schizophrenia Age range across studies: 21.5 to 45 years Females across studies: 22.0% to 39.2% | Interventions: ARI-LAI, OLA-LAI, PP-LAI, RIS-LAI FG Comparators: haloperidol decanoate LAI Oral SG Comparators: ARI, OLA, or RIS | Outcomes: efficacy failure, discontinuation, remission, symptoms, functioning, quality of life, relapse, AE, suicide, death Follow-up: 9.5 to 24 months |
AE = adverse event; AMI = amisulpride; ARI = aripiprazole; FG = first-generation; LAI = long-acting injectable; MA = meta-analysis; NR = not reported; NRS = non-randomized study; OLA = olanzapine; PP = paliperidone palmitate; QUE = quetiapine; RCT = randomized controlled trial; RIS = risperidone; SG = second-generation; SR = systematic review; ZIP = ziprasidone.
aThe publication indicates the authors received no funding for the article, the acknowledgement section mentions the research was support by an Australian Government Research Training Programme Scholarship.
bOne included primary study enrolled patients aged 15 years and older; it is included since the mean age of the population is an adult age.
Table 3: Characteristics of Included Randomized Controlled Trial
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Xiao et al. (2022)17 China Funding: individual authors funds from National Key Research and Development Program of China, Capital’s Funds for Health Improvement and Research, Demonstration research ward of Beijing Health Committee, Pfizer and Merck | RCT, multi-centre, double-blind | Inclusion criteria: 18 to 65 years old with schizophrenia Exclusion criteria: hospitalized ≥ 30 days in past 90 days; PANSS score improved by ≥ 30% between screening and baseline; resistant to antipsychotic drugs; people with childbearing potential, pregnant, or breastfeeding Intervention group: mean age 34.2 (SD 10.3), male sex 28.4%, female sex 71.6% Comparator group: mean age 33.6 (SD 10.9), male sex 28.4%, female sex 71.6% | Intervention (n = 218): 400 mg ARI-LAI once-monthly plus oral placebo SG Comparator (n = 218): 10 to 20 mg oral ARI daily plus monthly placebo injection | Outcomes: symptoms, functioning, AEs Follow-up: 10 or 12 weeks |
AE = adverse event; AP = antipsychotic; ARI = aripiprazole; LAI = long-acting injectable; mg = milligrams; PANSS = Positive and Negative Syndrome Scale; RCT = randomized controlled trial; SD = standard deviation.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix was not copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 27
Strengths | Limitations |
|---|---|
Saucedo Uribe et al. (2020)16 | |
Authors clearly stated the populations, interventions, comparators, and outcomes of interest. A protocol was established beforehand, and the review was registered on PROSPERO. Deviations to the original study plan were discussed. Authors searched at least 2 databases, provided keywords for their search, and did not limit by language. Authors performed study selection and risk of bias assessment in duplicate. Authors described treatment dose, study designs, and study duration in sufficient detail. Authors used a satisfactory technique for assessing risk of bias. Authors used a weighted technique to combine study results, considered heterogeneity, and conducted subgroup analyses when heterogeneity was present. Authors addressed risk of bias and heterogeneity when discussing the results of the review. Authors indicated that there were no conflicts of interest. | It is unclear whether additional sources (e.g., reference lists, experts, grey literature) were searched. It is unclear whether data extraction was conducted in duplicate. A list of excluded studies with justifications was not provided. Population diagnoses and morbidities, treatment frequency, quantitative data from results, and sources of funding from individual studies were not sufficiently described. Data on comparative effects were not reported for all outcomes. Publication bias could not be conducted because a small number of studies were found. Authors stated that due to the small number of studies, heterogeneity, incomplete reporting of data, risk of bias concerns, and different methods to measure outcomes, the inferences from the results and the applicability of the findings may be limited. |
Gentile (2019)10 | |
The author clearly stated the populations, interventions, comparators, and outcomes of interest. The author searched at least 2 databases, provided keywords for their search, and scanned reference lists of included studies. The author discussed limitations of the review based on the variety of study designs included. The author declared no conflict of interest. | It is unclear whether a protocol was established before conducting the review. Study selection was not conducted by reviewers independently. It is unclear how data extraction was conducted. A list of excluded studies with justifications was not provided. Population diagnoses and morbidities, treatment dose and frequency, average age of adults, statistical analysis results, and sources of funding from individual studies were not sufficiently described. Data on comparative effects were not reported for all outcomes. It is unclear whether individual studies were assessed for risk of bias. Authors noted that adherence to oral treatment is difficult to measure due to clinician ratings and self-reports; they can be overestimated in studies. |
Keramatian et al. (2019)11 | |
Authors clearly stated the populations, interventions, and outcomes of interest. Authors searched at least 2 databases, provided keywords for their search, and screened reference lists of reviews. Authors provided a list of excluded studies with justifications for exclusion. Authors performed study selection and data extraction in duplicate. Authors described outcomes, study designs, and study duration in sufficient detail. | It is unclear what study details the review protocol contained. Statistical analysis results, treatment dose and frequency, and sources of funding from individual studies were not sufficiently described. Data on comparative effects were not reported for all outcomes. It is unclear whether risk of bias of individual studies was assessed. The average age for individual studies was not extracted in detail. It is unclear whether the heterogeneity in the studies was investigated. Authors noted that the efficacy and tolerability of second-generation LAI antipsychotic drugs used for bipolar disorder in the studies they included may be overestimated, because the populations only contained patients who responded to the intervention of interest during an open-label stage. One review author received funds or was on boards for several organizations including pharmaceutical companies. |
Olagunju et al. (2019)13 | |
Authors clearly stated the populations, interventions, comparators, and outcomes of interest. Authors searched at least 2 databases, provided keywords for their search, searched clinical trial registries, and scanned reference lists of included studies and relevant reviews. Authors described outcomes, study designs, sources of funding, and study duration in sufficient detail. Authors used a satisfactory technique for assessing risk of bias. Authors justified statistical analyses for combining data from multiple studies and investigated heterogeneity. Authors discussed risk of bias and heterogeneity when interpreting results of the review. Authors assessed publication bias. Authors indicated that there were no conflicts of interest. | It is unclear whether a protocol was established before conducting the review. One author performed study selection and data extraction. A list of excluded studies with justifications was not provided. For the individual studies, data on the average age, treatment dose and frequency were not adequately reported. The funding source for the review was unclear. Authors indicated poor reporting in included studies and variation on how outcomes were measured. Authors indicated that most studies were industry-sponsored. |
Peters et al. (2019)15 | |
Authors clearly stated the populations, interventions, comparators, and outcomes of interest. Authors provided keywords for their search strategy and consulted expert recommendations. Authors described populations, interventions, comparators, outcomes, study designs, sources of funding, and study duration in sufficient detail. | It is unclear whether a protocol was established before conducting the review. Authors limited their search to one database and to literature published between 2016 and 2019. It is unclear whether study selection and data extraction were performed in duplicate. A list of excluded studies with justifications was not provided. It is unclear whether risk of bias of individual studies was assessed. Data on comparative effects were not reported for all outcomes. Heterogeneity in the included studies was not discussed. One review author received funds, provided advice or was a shareholder for one or more organizations including pharmaceutical companies. |
Park et al. (2018)14 | |
Authors clearly stated the populations, interventions, comparators, and outcomes of interest. The study criteria were established beforehand. Authors searched at least 2 databases and provided keywords for their search. Authors performed study selection and quality assessment in duplicate. Authors described populations, outcomes funding sources, study designs, and study duration in sufficient detail. Authors used a satisfactory technique for assessing risk of bias. Quality of the evidence was provided when presenting results of analyses. Authors judged the evidence to be moderate to high quality. Authors investigated heterogeneity and discussed it when interpreting results. | It is unclear whether data extraction was conducted independently. A list of excluded studies with justifications was not provided. The average age for individual studies, and treatment dose and frequency were not extracted in detail. Data on comparative effects were not reported for all outcomes. A statement about conflicts of interest was not provided. Authors indicated high heterogeneity due to follow-up time, disease severity, and small number of studies found. |
McDonagh et al. (2017)12 | |
Authors clearly stated the populations, interventions, comparators, and outcomes of interest. A protocol was established beforehand, and the review was registered on PROSPERO. Authors searched at least 2 databases, provided their search strategy, performed hand searching, and consulted grey literature. Authors performed study selection, data extraction, and quality assessment in duplicate. Authors provided a list of excluded studies with justifications. Authors described populations, interventions, comparators, outcomes, funding sources, study designs, and study duration in sufficient detail. Authors used a satisfactory technique for assessing the risk of bias in individual studies that were included in the review. Risk of bias and heterogeneity in included studies was considered when discussing results of the review. | Data on comparative effects were not reported for all outcomes. Conflicts were collected; however, it is unclear whether there were any potential conflicts of interest that could have affected the review. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; LAI = long-acting injectable; PROSPERO = The International Prospective Register of Systematic Reviews.
Table 5: Strengths and Limitations of an RCT Using the Downs and Black Checklist8
Strengths | Limitations |
|---|---|
Xiao et al. (2022)17 | |
Authors clearly stated the objectives, primary and secondary outcomes, patient characteristics, interventions, and main findings. Authors reported random variability in outcomes and exact P values. Patients were randomized to study groups. Authors reported on adverse events and patients lost to follow-up. The study was double-blind. The study was conducted across 15 sites in China which may increase the generalizability of the findings. | It is unclear whether the patients recruited, patients prepared to participate, or the staff, places, and facilities where patients were treated were representative of the source population. Drug managers who administered the treatments at each site were unblinded. It is unclear whether outcome assessors were blind. People who were of childbearing potential, pregnant, or breastfeeding were excluded from the study, limiting generalizability to these populations. Although placebo was used, authors indicated that the aripiprazole and placebo injections had different appearances and it’s unclear whether patients and investigators were aware of assignment. 27% of the intervention group and 24% of the comparator group did not complete the study because of loss to follow-up, discontinuation of treatment, consent withdrawal, adverse events, clinician advice, and other reasons. It is unclear if reasons for dropout were related to study assignment, or if they were similar between groups. Outcomes measured from the CGI-S, PANSS, SAS, AIMS, BARS, and PSP were assessed subjectively. It is unclear how adverse event data were collected. Authors indicated that the duration of the study was short and that the findings should be interpreted with caution due to confounding factors. Three review authors received funding from pharmaceutical companies. |
AIMS = Abnormal Involuntary Movement Scale; BARS = Barnes Akathisia Rating Scale; CGI-S = Clinical Global Impression-Severity; PANSS = Positive and Negative Syndrome Scale; PSP = Personal and Social Performance scale; SAS = Simpson-Angus Extrapyramidal Side Effects Scale.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix was not copy-edited.
Table 6: Second-Generation Injectable Antipsychotic Drugs Versus First-Generation Injectable Antipsychotic Drugs — Effectiveness
Study citation and study design | Detailed findings | |||
|---|---|---|---|---|
Primary studies | Intervention(s) and results | Comparator(s) and results | Group comparisons and overall results | |
Efficacy failure | ||||
McDonagh et al. (2017)12 SR | McEvoy et al. (2014) | PP-LAI (39 to 234 mg)a 49 patients (33.8%) | Haloperidol decanoate LAI (25 to 200 mg) 47 patients (32.4%) | PP-LAI compared to haloperidol decanoate LAI HR = 0.98 (95% CI, 0.64 to 1.47) |
Discontinuation | ||||
Saucedo Uribe et al. (2020)16 SR | Covell et al. (2012) | RIS-LAI (31 mg) | Haloperidol decanoate LAI (114 mg) and Fluphenazine decanoate LAI (37 mg) | Review authors stated that treatment discontinuation was not statistically significantly different between the 2 groups, however conclusions are uncertain because data on the comparative effects and measures of variability were not reported. |
Gentile (2019)10 SR | Decuypere et al. (2017) | PP-LAI (once/month) 69% to 80% | Haloperidol LAI 76% to 89% | Data on comparative effects were not reported. |
Cordiner et al. (2016) | RIS-LAI 28.0% to 33.0% | Zuclopenthixol decanoate LAI 38.0% | Data on comparative effects were not reported. | |
McEvoy et al. (2014) | PP-LAI (129 to 169 mg/month)a 66.2% | Haloperidol decanoate LAI 65.5% | Review authors stated that there were no differences between the groups. | |
Continuation | ||||
Keramatian et al. (2019)11 SR | Wu et al. (2016) | RIS-LAI (25 to 50 mg/2 wks) 21.7% | FG-LAI 8.7% | Data on comparative effects were not reported. |
Symptoms | ||||
Saucedo Uribe et al. (2020)16 SR | 1 MA of 2 studies Covell et al. (2012), McEvoy et al. (2014) | SG-LAIs | FG-LAIs | Change in PANSS score: MD = 0.54 (95% CI, −3.33 to 4.41), P = 0.78 |
CI = confidence interval; FG = first-generation; HR = hazard ratio; LAI = long-acting injectable; MA = meta-analysis; MD = mean difference; mg = milligrams; PANSS = Positive and Negative Syndrome Scale; PP = paliperidone palmitate; RIS = risperidone; SG-LAI = second-generation long-acting injectable; SR = systematic review.
aIt is unclear why the dose values for the McEvoy et al. (2014) study, which were reported in the McDonagh et al. (2017) and Gentile (2019) SRs, is different; the original McEvoy et al. (2014) was not consulted for this report.
Table 7: Second-Generation Injectable Versus First-Generation Injectable Antipsychotic Drugs — Safety
Study citation and study design | Detailed findings | |||
|---|---|---|---|---|
Primary studies | Intervention(s) and results | Comparator(s) and results | Group comparisons and overall results | |
Extrapyramidal symptoms | ||||
Saucedo Uribe et al. (2020)16 SR | 1 MA of 2 studies Covell et al. (2012) and McEvoy et al. | SG-LAIs | FG-LAIs | Tardive dyskinesia RR = 0.99 (95% CI, 0.47 to 2.07), P = 0.98 |
McDonagh et al. (2017)12 SR | McEvoy et al. (2014) | PP-LAI (39 to 234 mg) AIMSa: 29 people (21.4%) Global rating of akathisia: 0.73 (95% CI, 0.59 to 0.87) | Haloperidol decanoate LAI (25 to 200 mg) AIMSa: 30 people (23.85%) Global rating of akathisia: 0.45 (95% CI, 0.31 to 0.59) | AIMS, P = 0.57; Global rating scale of akathisia, P = 0.006 Authors stated that the mean change in AIMS global score, or tardive dyskinesia were not statistically significantly different between the two groups, however conclusions are uncertain because data on the comparative effects and measures of variability were not reported. |
Hospitalization | ||||
Saucedo Uribe et al. (2020)16 SR | Covell et al. (2012) | RIS-LAI (31 mg) | Haloperidol decanoate LAI (114 mg) and Fluphenazine decanoate LAI (37 mg) | Authors stated that number of hospitalizations was not statistically significantly different between the two groups, however conclusions are uncertain because data on the comparative effects and measures of variability were not reported. |
Keramatian et al. (2019)11 SR | Yan et al. (2018) | ARI-LAI | Haloperidol decanoate LAI | Authors stated that the risk of all-cause hospitalization risk was significantly higher in the haloperidol decanoate LAI group compared to the ARI-LAI group (OR = 1.49), however precision is uncertain because data on the measures of variability were not reported. |
Wu et al. (2016) | RIS-LAI (25 to 50 mg twice/month) Hospitalization for any mood episode decreased from 35.5% to 31.8% | FG-LAI Hospitalization for any mood episode increased from 34.0% to 36.5% | Hospitalization risk for any mood episode (FG-LAI vs. RIS-LAI) HR = 1.24, 95% CI, 1.08 to 1.44 Hospitalization risk for major depressive episodes (FG-LAI vs. RIS-LAI) HR = 1.68, 95% CI, 1.24 to 2.28 Authors stated that after adjusting for confounders, the FG-LAI group had a higher risk of hospitalization for any mood episode and major depressive episode compared to the risperidone LAI group. | |
Suicidal or homicidal ideation | ||||
McDonagh et al. (2017)12 SR | McEvoy et al. (2014) | PP-LAI (39 to 234 mg) 23 people (15.6%) | Haloperidol decanoate LAI (25 to 200 mg) 21 people (14.3%) | Data on comparative effects were not reported. |
Treatment emergent adverse events | ||||
Saucedo Uribe et al. (2020)16 SR | McEvoy et al. (2014) | PP-LAI (149 mg)d | Haloperidol decanoate LAI (75 mg)d | Authors stated that treatment emergent AEs were not statistically significantly different between the two groups, however conclusions are uncertain because data on the comparative effects and measures of variability were not reported. |
AE = adverse event; AIMS = Abnormal Involuntary Movement Scale; ARI = aripiprazole; EPS = extrapyramidal symptoms; FG = first-generation; LAI = long-acting injectable; mg = milligrams; OR = odds ratio; PP = paliperidone palmitate; RIS = risperidone; SAS = Simpson-Angus Extrapyramidal Side Effects Scale; SR = systematic review.
aAIMS Global Severity Score (incidence of AIMS > 2).
bSAS Mean Score (Incidence of SAS ≥ 1).
dIt is unclear why the dose values for the McEvoy et al. (2014) study, which were reported in the McDonagh et al. (2017) and Saucedo Uribe et al. (2020) SRs, is different; the original McEvoy et al. (2014) was not consulted for this report.
Table 8: Second-Generation Injectable Versus Second-Generation Oral Antipsychotic Drugs — Effectiveness
Study citation and study design | Detailed findings | |||
|---|---|---|---|---|
Primary studies | Intervention(s) and results | Oral comparator(s) and results | Group comparisons and overall results | |
Non-compliance | ||||
Park et al. (2018)14 SR | Weiden et al. (2012) | RIS-LAI | SG antipsychotic | Treated < 1 year RR = 0.58, 95% CI, 0.09 to 3.35 Treated for 1 year RR = 0.79, 95% CI, 0.47 to 1.31 Treated for > 1 year RR = 0.92, 95% CI, 0.51 to 1.66 |
Discontinuation | ||||
Park et al. (2018)14 SR | NR | SG-LAI | SG antipsychotic | Authors did not report which individual studies were included in MA for all-cause discontinuation and since 1 primary study in the SR was out of scope, the MA results could not be included. |
Gentile (2019)10 SR | Anderson et al. (2017) | PP-LAI (monthly) 27% | SG antipsychotic 51% | Data on comparative effects were not reported. |
Pilon et al. (2014) | PP-LAI (monthly) 61.3% | SG antipsychotic 72.4% | Data on comparative effects were not reported. | |
Vieta et al. (2012) | RIS-LAI 35.6% | OLA 25.1% | Data on comparative effects were not reported. | |
Gaebel et al. (2010) | RIS-LAI (25 mg to 50 mg/2 weeks) 54.1% | QUE 61.4% | Data on comparative effects were not reported. | |
Macfadden et al. (2010) | RIS-LAI (25 to 50 mg/2 weeks) 29.6% | ARI 28.4% | Data on comparative effects were not reported. | |
Buckley et al. (2015) | RIS-LAI (12.5 to 50 mg/2 weeks) 53% | SG antipsychotic 52.7% | Data on comparative effects were not reported. | |
Pilon et al. (2017) | RIS-LAI 71.7% | SG antipsychotic 71.7% | Data on comparative effects were not reported. | |
Peters et al. (2019)15 SR | Huang et al. (2018) | PP-LAI (monthly) 45.6% | OLA 43.9% | “The discontinuation rate during the treatment period was similar for PP1M (45.6%) and olanzapine (43.9%) (p. 22).”15 |
Bozzatello et al. (2019) | PP-LAI (50 to 150 mg/month) 8.3% | Paliperidone extended-release (6 to 12 mg/day) 11.1% | Data on comparative effects were not reported. | |
Malla et al. (2016) | RIS-LAI (25 to 50 mg) 22.1% | SG antipsychotic (300 to 500, 15 to 20, or 1 to 6 mg) 20.8% | “The discontinuation rate during the treatment period was comparable (p. 22).”15 | |
McDonagh et al. (2017)12 SR | Detke et al. (2014) | OLA-LAI (405 mg/month) All-cause discontinuation: 53.8% Time to all-cause discontinuation (median): 645 days | OLA (10 mg/day) All-cause discontinuation: 51.2% Time to all-cause discontinuation (median): 678 days | All-cause discontinuation rate, P = 0.600 Time to all-cause discontinuation, median days, P = 0.612 |
Fleischhacker et al. (2014) | ARI-LAI (400 mg/month) Discontinued: 69 people (26%) ARI (50 mg/month) Discontinued: 70 people (53.4%) | ARI (10 to 30 mg/day) Discontinued: 83 people (33.1%) | Data on comparative effects were not reported. | |
Ishigooka et al. (2015) | ARI-LAI (300 to 400 mg/month) All-cause discontinuation: 25.9% | ARI (6 to 24 mg/day) All-cause discontinuation: 33.5% | Time to all-cause discontinuation: HR = 0.74 (95% Cl, 0.52 to 1.03) | |
Symptoms | ||||
Park et al. (2018)14 SR | 1 MA based on de Arce Cordón et al. (2012), Smeraldi et al. (2013) | RIS-LAI | ARI, QUE | MADRS score SMD = −1.69, 95% CI, −2.95 to −0.43 Authors did not report which individual studies were included in MA for PANSS and since 1 primary study in the SR was out of scope, the MA results could not be included. |
Keramatian et al. (2019)11 SR | Han et al. (2007) | RIS-LAI (25 to 37.5 mg/2 weeks) | SG antipsychotic | Authors stated that there were no statistically significant changes in BPRS, HDRS, YMRS between the two groups, however conclusions are uncertain because data on the comparative effects and measures of variability were not reported. |
Yatham et al. (2007) | RIS-LAI (25 to 50 mg/2 weeks) | SG antipsychotic | “There were no significant between-group differences in changes from baseline to study end point in global, manic or depressive symptom severity (p. 449.)”11 | |
Chengappa et al. (2010) | RIS-LAI (25 to 50 mg/2 weeks) | SG antipsychotic | “Risperidone LAI group experienced higher number of positive clinical events and fewer negative events; both groups similar improvements in YMRS, MADRS (p. 441).”11 | |
Peters et al. (2019)15 SR | Huang et al. (2018) | PP-LAI (monthly) | OLA | “No significant difference between the 2 groups in any PANSS score (p. 6).”15 |
McDonagh et al. (2017)12 SR | Detke et al. (2014) | OLA-LAI (405 mg/month) Change in PANSS total score: −0.82 (SE 1.2) | OLA (10 mg/day) Change in PANSS total score: −1.14 (SE 1.2) | Baseline-to-end point least squares mean change on PANSS total score: P = 0.834 |
Xiao et al. (2022)17 RCT | NA | ARI-LAI (400 mg/month) plus oral placebo | ARI daily plus placebo injection/month | Difference of PANSS-positive score = −0.6 95% CI, −0.4 to 0.3, P = 0.198 Difference of PANSS negative score = 0.2 95% CI, −0.1 to 1.4, P = 0.706 Responder rate (≥ 30% reduction in PANSS total score) = 2.2, 95% CI, 1.0 to 4.7, P = 0.052 |
McDonagh et al. (2017)12 SR | Fleischhacker et al. (2014) | ARI-LAI (400 mg/month) Change in PANSS total score: −1.66 (SE 0.72) ARI-LAI (50 mg/month) Change in PANSS total score: 0.58 (SE 0.71) | ARI (10 to 30 mg/day) Change in PANSS total score: 3.08 (SE 1.01) | Data on comparative effects were not reported. |
Ishigooka et al. (2015) | ARI-LAI (300 to 400 mg/month) | ARI (6 to 24 mg/day) | Non-exacerbation of psychotic symptoms/non-relapse rate (Kaplan–Meier) Difference = 0.3 (95% Cl, −3.9 to 4.5) | |
Remission | ||||
Park et al. (2018)14 SR | 1 MA based on de Arce Cordón et al. (2012), Fleischhacker et al. (2014), Ishigooka et al. (2015), Keks et al. (2007), Smeraldi et al. (2013) | SG-LAI | SG antipsychotic | RR = 1.07, 95% CI, 0.99 to 1.15 |
McDonagh et al. (2017)12 SR | Ishigooka et al. (2015) | ARI-LAI (300 to 400 mg/month) 69.4% | ARI (6 to 24 mg/day) 71.1% | Data on comparative effects were not reported. |
Stabilization | ||||
Peters et al. (2019)15 SR | Malla et al. (2016) | RIS-LAI (25 to 50 mg) | SG antipsychotic (300 to 500, 15 to 20, or 1 to 6 mg) | No significant differences in time to stabilization, likelihood ratio = 0.07, 95% CI, 0.651 to 1.75 |
Functioning | ||||
Park et al. (2018)14 SR | NR | SG-LAI | SG antipsychotic | Authors did not report which individual studies were included in MA for CGI-S and since 1 primary study in the SR was out of scope, the MA results could not be included. |
Keramatian et al. (2019)11 SR | Han et al. (2007) | RIS-LAI (25 to 37.5 mg/2 weeks) | SG antipsychotic | Significant decrease in CGI-S in patients switched from oral SG antipsychotic to RIS-LAI |
Chengappa et al. (2010) | RIS-LAI (25 to 50 mg/2 weeks) | SG antipsychotic | Both groups were for similar improvements in CGI-S or CGI-I scores | |
Olagunju et al. (2019)13 SR | 1 MA based on 7 RCTs | SG-LAI | SG antipsychotic | Psychosocial function SMD = 0.16, 95% CI, 0.07 to 0.24, P = 0.0003 |
Peters et al. (2019)15 SR | Bozzatello et al. (2019) | PP-LAI (50 to 150 mg/month) | Paliperidone extended-release (6 to 12 mg/day) | “PP1M was superior for negative symptoms rated with the Clinical Global Impression-Schizophrenia scale (P = 0.012) (p. 11).”15 “no significant between-group emerged regarding PSP (p = 0.103) and SWN-S (p = 0.65) scores (p. 15).”15 |
Xiao et al. (2022)17 RCT | NA | ARI-LAI (400 mg/month) plus oral placebo | ARI daily plus placebo injection/month | Difference of least squares means of CGI-S score = −0.1 (95% CI, −0.3 to 0.1), P = 0.357 Difference of least squares means of CGI-I score = 0.0 (95% CI, −0.2 to 0.1), P = 0.779 Difference of least squares means of PSP score = −0.5 (95% CI, −2.7 to 1.7), P = 0.641 |
McDonagh et al. (2017)12 SR | Fleischhacker et al. (2014) | ARI-LAI (400 mg/month) CGI-S change from baseline, least square mean: −0.13 (SE 0.05) CGI-I change from baseline, least square mean: 3.27 (SE 1.16) ARI-LAI (50 mg/month) CGI-S change from baseline, least square mean: 0.23 (SE 0.07) CGI-I change from baseline, least square mean: 4.02 (SE 1.32) | ARI (10 to 30 mg/day) CGI-S change from baseline, least square mean: 0.05 (SE 0.05) CGI-I change from baseline, least square mean: 3.66 (SE 1.16) | Data on comparative effects were not reported. |
Quality of life | ||||
Park et al. (2018)14 SR | Ascher-Svanum et al. (2013), de Arce Cordón et al. (2012) | SG-LAI | SG antipsychotic | Data on comparative effects were not reported. |
Satisfaction | ||||
Peters et al. (2019)15 SR | Bozzatello et al. (2019) | PP-LAI (50 to 150 mg/month) | Paliperidone extended-release (6 to 12 mg/day) | “PP1M was superior to paliperidone extended-release in global treatment satisfaction (p = 0.001) and convenience (p = 0.037), measured by the Treatment Satisfaction Questionnaire for Medication (TSQM), as well as in service engagement (p = 0.001), measured by the Service Engagement Scale (SES) (p. 22)”15 |
ARI = aripiprazole; BPRS = Barnes Akathisia Rating Scale; CGI-I = Clinical Global Impression-Improvement; CGI-S = Clinical Global Impression-Severity; CI = confidence interval; HAM-A = Hamilton Anxiety Rating Scale; HDRS = Hamilton Depression Rating Scale; HR = hazard ratio; LAI = long-acting injectable; MA = meta-analysis; MADRS = Mongtomery-Asberg Depression Rating Scale; mg = milligrams; NA = not applicable; NR = not reported; OLA = olanzapine; PANSS = Positive and Negative Syndrome Scale; PP = paliperidone palmitate; PP1M = paliperidone palmitate one monthly; PSP = Personal and Social Performance scale; QUE = quetiapine; RCT = randomized controlled trial; RIS = risperidone; RR = relative risk; SE = standard error; SMD = standardized mean difference; SG = second-generation; SR = systematic review; TSQM = Treatment Satisfaction Questionnaire for Medication; VAS = visual analogue scale; YMRS = Young Mania Rating Scale.
Table 9: Second-Generation Injectable Versus Second-Generation Oral Antipsychotic Drugs — Safety
Study citation and design | Detailed findings | |||
|---|---|---|---|---|
Primary studies | Intervention(s) and results | Oral comparator(s) and results | Group comparisons and overall results | |
Extrapyramidal symptoms | ||||
Park et al. (2018)14 SR | NR | SG-LAI | SG antipsychotic | Authors did not report which individual studies were included in MA for AIMS, ESRS, and EPS and since 1 primary study in the SR was out of scope, the MA results could not be included. |
Keramatian et al. (2019)11 SR | Yatham et al. (2007) | RIS-LAI (25 to 50 mg/2 weeks) | SG antipsychotic | No significant differences between groups for EPS |
Chengappa et al. (2010) | RIS-LAI (25 to 50 mg/2 weeks) Akathisia: 13% vs 8% | SG antipsychotic Akathisia: 8% | Data on comparative effects were not reported. | |
Peters et al. (2019)15 SR | Malla et al. (2016) | RIS-LAI (25 to 50 mg) | SG antipsychotic (300 to 500, 15 to 20, or 1 to 6 mg) | “No significant change in AIMS or SAS scores in either group. BARS: small number of patients experienced akathisia during [(RLAI 5.6%); oral 10.3%] and following [(RLAI 7.7%); oral 9.2%] stabilization with no significant (p. 124).”15 |
McDonagh et al. (2017)12 SR | Detke et al. (2014) | OLA-LAI (405 mg/month) EPS/ akathisia: 7 people (2.7%) | OLA (10 mg daily) EPS/ akathisia: 10 people (3.8%) | Data on comparative effects were not reported. |
Fleischhacker et al. (2014) | ARI-LAI (400 mg/month) SAS total score, change from baseline at week 38, LSM: −0.16 (SE 0.09) AIMS movement rating score, change from baseline at week 38; LSM: −0.00 (SE 0.07) BARS global score, change from baseline at week 38, LSM: 0.06 (SE 0.03) ARI-LAI (50 mg/month) SAS total score, change from baseline at week 38, LSM: −0.21 (SE 0.16) AIMS movement rating score, change from baseline at week 38, LSM: −0.01 (SE 0.12) BARS global score, change from baseline at week 38, LSM: −0.06 (SE 0.06) | ARI (10 to 30 mg daily) SAS total score, change from baseline at week 38, least squares mean: −0.22 (SE 0.09) AIMS movement rating score, change from baseline at week 38, least squares mean: −0.11 (SE 0.07) BARS global score, change from baseline at week 38, least squares mean: −0.05 (SE 0.03) | Data on comparative effects were not reported. | |
Ishigooka et al. (2015) | ARI-LAI (300 to 400 mg/month) Extrapyramidal AE: 16.2% Tardive dyskinesia: 0% Akathisia: 6.6% | ARI (6 to 24 mg daily) Extrapyramidal AE: 14.1% Tardive dyskinesia: 0.4% Akathisia: 6.2% | Data on comparative effects were not reported. | |
Xiao et al. (2022)17 RCT | NA | ARI-LAI (400 mg/month) plus oral placebo | ARI daily plus placebo injection/month | “The changes in SAS total, AIMS movement rating, and BARS global scores from baseline to week 12 did not show any differences between the two groups (p. 247).”17 |
Relapse | ||||
Peters et al. (2019)15 SR | Malla et al. (2016) | RIS-LAI (25 to 50 mg) 26.2% | SG antipsychotic (300 to 500, 15 to 20, or 1 to 6 mg) 14.3% | HR = 2.57, 95% CI, 0.15 to 1.25 |
Park et al. (2018)14 SR | 1 MA based on De Arce Cordón et al. (2012) and Macfadden et al. (2010) | RIS-LAI | ARI | Time to relapse SMD = 0.42, 95% CI, 0.29 to 0.54 |
McDonagh et al. (2017)12 SR | Fleischhacker et al. (2014) | ARI-LAI (400 mg/ month) 7.12% ARI-LAI (50 mg/ month) 21.80% | ARI (10 to 30 mg/day) 7.76% | Estimated relapse rate, treatment difference: −0.6 (95% CI, −5.26 to 3.99) |
Ishigooka et al. (2015) | ARI-LAI (300 to 400 mg/month) Stabilization of psychotic symptoms/ relapse: 92.5% Exacerbation of psychotic symptoms/ relapse: 6.6% | ARI (6 to 24 mg/day) Stabilization of psychotic symptoms/ relapse: 92.5% Exacerbation of psychotic symptoms/ relapse: 6.6% | Time to exacerbation of psychotic symptoms/relapse (Kaplan–Meier): HR = 0.94, 95% Cl, 0.46 to 1.92 | |
Detke et al. (2014) | OLA-LAI (405 mg/month) Relapse: 20.1% Time to relapse (median): 539 days | OLA (10 mg/day) Relapse: 18.5% Time to relapse (median): 281 days | Rate of relapse, P = 0.659 Time to relapse/rescue, P < 0.001 | |
Hospitalization | ||||
Peters et al. (2019)15 SR | Malla et al. (2016) | RIS-LAI (25 to 50 mg) 19.1% | SG antipsychotic (300 to 500, 15 to 20, or 1 to 6 mg) 11.4% | Data on comparative effects were not reported. |
Park et al. (2018)14 SR | 1 MA based on Detke et al. (2014), Ascher-Svanum et al. (2013) | OLA-LAI | OLA | Mean hospital days SMD = −0.11, 95% CI, −0.22 to −0.01 |
Other adverse events | ||||
Park et al. (2018)14 SR | NR | SG-LAI | SG antipsychotic | Authors did not report which individual studies were included in the MA for drug-related side effects and since 1 primary study in the SR was out of scope, the MA results could not be included. |
Keramatian et al. (2019)11 SR | Yatham et al. (2007) | RIS-LAI (25 to 50 mg/2 weeks) | SG antipsychotic | “>10% receiving risperidone LAI reported insomnia, nausea, fatigue, headache. No significant differences between groups in AEs (p. 441).”11 |
Chengappa et al. (2010) | RIS-LAI (25 to 50 mg/2 weeks) Somnolence: 26% Headache: 17% Tremors: 17% Skin rash: 13% | SG antipsychotic Somnolence: 16% Headache: 12% Tremors: 8% Skin rash: 0% | Data on comparative effects were not reported. | |
McDonagh et al. (2017)12 SR | Detke et al. (2014) | OLA-LAI (405 mg/month) Any AE: 68.9% Discontinuations due to AEs: 9.8% | OLA (10 mg daily) Any AE: 67.7% Discontinuations due to AEs: 9.6% | Data on comparative effects were not reported. |
Fleischhacker et al. (2014) | ARI-LAI (400 mg/month) Discontinued due to AE: 3.0% ARI-LAI (50 mg/month) Discontinued due to AE: 5.3% | ARI (10 to 30 mg daily) Discontinued due to AE: 2.6% | Data on comparative effects were not reported. | |
Ishigooka et al. (2015) | ARI-LAI (300 to 400 mg/month) Overall, AE: 77.2% Withdrawal due to AE: 7.5% | ARI (6 to 24 mg daily) Overall, AE: 79.3% Withdrawal due to AE: 11.5% | Data on comparative effects were not reported. | |
Xiao et al. (2022)17 RCT | NA | ARI-LAI (400 mg/month) plus oral placebo | ARI daily plus placebo injection/month | “A total of 186 (85.7%) patients in the AOM group and 197 (90.8%) in the oral aripiprazole group experienced at least one TEAE (p = 0.135). The incidence rates of EPS-related TEAEs in the AOM and oral aripiprazole groups through week 12 were 39.6% and 47.9%, respectively, with no statistically significant difference in the two groups (p. 247).”17 “A small proportion of patients (< 3%) in the AOM and oral aripiprazole groups experienced mild injection site reactions, including pain, redness, swelling, and induration. There was no significant difference among the two groups (p. 247).”17 |
Suicidalitya | ||||
McDonagh et al. (2017)12 SR | Fleischhacker et al. (2014) | ARI-LAI (400 mg/month) Suicidality, LS mean (SE): −0.1 (1.0) ARI-LAI (50 mg/month) Suicidality LS mean (SE): 0.0 (0.0) | ARI (10 to 30 mg daily) Suicidality, LS mean: 0.1 (1.3) | Data on comparative effects were not reported. |
Death | ||||
McDonagh et al. (2017)12 SR | Detke et al. (2014) | OLA-LAI (405 mg/month) 0% | OLA (10 mg daily) 0.8% | Data on comparative effects were not reported. |
AE = adverse event; AIMS = Abnormal Involuntary Movement Scale; ARI = aripiprazole; BARS = Barnes Akathisia Rating Scale; CI = confidence interval; EPS = extrapyramidal symptoms; ESRS = Extrapyramidal Symptom Rating Scale; HR = hazard ratio; LAI = long-acting injectable; MA = meta-analysis; mg = milligrams; NA = not applicable; NR = not reported; OLA = olanzapine; PP = paliperidone palmitate; PP1M = paliperidone palmitate one monthly; RCT = randomized controlled trial; RIS = risperidone; SAS = Simpson-Angus Extrapyramidal Side Effects Scale; SE = standard error; SG = second-generation; SMD = standardized mean difference; SR = systematic review; TEAE = treatment emergent adverse event.
aMeasured using the Columbia Suicide Severity Rating Scale as the change from baseline to week 38.
Appendix 5: Overlap Between Included Systematic Reviews
Table 10: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Saucedo Uribe et al. (2020)16 | Gentile (2019)10 | Keramatian et al. (2019)11 | Olagunju et al. (2019)13 | Peters et al. (2019)15 | Park et al. (2018)14 | McDonagh et al. (2017)12 |
|---|---|---|---|---|---|---|---|
Bozzatello P, et al. Clin Drug Investig. 2019;39(2):169 to 178. | — | — | — | — | Yes | — | — |
Huang M, et al. Prog Neuropsychopharmacol Biol Psychiatry. 2018;81:122 to 130. | — | — | — | — | Yes | — | — |
Stroup TS, et al. J Clin Psychiatry. 2018; 80(1):18m12109. | — | — | — | — | Yes | — | — |
Yan T, et al. Curr Med Res Opin. 2018;34(1):41 to 47. | — | — | Yes | — | — | — | — |
Anderson JP, et al. BMC Psychiatry. 2017;17(1):346. | — | Yes | — | — | — | — | — |
Decuypere F, et al. PLoS One. 2017;12(6):e0179049. | — | Yes | — | — | — | — | — |
Pilon D, et al. BMC Psychiatry. 2017;17(1):207. | — | Yes | — | — | — | — | — |
Pilon D, et al. Clin Ther. 2017;39(10):1972 to 1985.e2. | — | Yes | — | — | — | — | — |
Cordiner M, et al. Ther Adv Psychopharmacol. 2016;6(1):22 to 32. | — | Yes | — | — | — | — | — |
Cordiner M, et al. Ther Adv Psychopharmacol. 2016;6(2):66 to 76. | — | Yes | — | — | — | — | — |
Malla A, et al. Clin Schizophr Relat Psychoses. 2016;9(4):198 to 208. | — | — | — | — | Yes | — | — |
Wu CS, et al. J Affect Disord. 2016;197:189 to 95. | — | — | Yes | — | — | — | — |
Buckley PF, et al. Schizophr Bull. 2015;41(2):449 to 59. | — | Yes | — | Yes | — | Yes | — |
Ishigooka J, et al. Schizophr Res. 2015;161(2 to 3):421 to 8. | — | Yes | — | — | — | Yes | Yes |
Ascher-Svanum H, et al. Neuropsychiatr Dis Treat. 2014;10:1125 to 31. | — | — | — | Yes | — | — | — |
Detke HC, et al. J Clin Psychopharmacol. 2014;34(4):426 to 34. | — | Yes | — | — | — | Yes | Yes |
Fleischhacker WW, et al. Br. J. Psychiatry 2014;205:135 to 144. | — | Yes | — | Yes | — | Yes | Yes |
McEvoy JP, et al. JAMA. 2014;311(19):1978 to 87. | Yes | Yes | — | — | Yes | — | Yes |
NCT00992407 2014a | — | — | — | Yes | — | — | — |
Ascher-Svanum H, et al. BMC Psychiatry. 2013;13:224. | — | — | — | — | — | Yes | — |
Huang SS, et al. Psychiatr Serv. 2013;64(12):1259 to 62. | — | — | — | — | — | Yes | — |
Rouillon F, et al. Acta Neuropsychiatr. 2013;25(5):297 to 306. | — | — | — | Yes | — | Yes | — |
Smeraldi E, et al. Ther Adv Psychopharmacol. 2013;3(4):191 to 9. | — | — | — | — | — | Yes | — |
Wykes T, et al. BMC Psychiatry. 2013;13:28. | — | — | — | Yes | — | Yes | — |
Covell NH, et al. J Clin Psychiatry. 2012;73(5):669 to 75. | Yes | — | — | — | — | — | — |
de Arce Cordón R, et al. Eur Arch Psychiatry Clin Neurosci. 2012;262(2):139 to 49. | — | — | — | — | — | Yes | — |
Suzuki H and Gen K. Ther Adv Psychopharmacol. 2012;2(1):23 to 9. | — | — | — | — | — | Yes | — |
Suzuki H, et al. Ther Adv Psychopharmacol. 2012;2(6):227 to 34. | — | — | — | — | — | Yes | — |
Vieta E, et al. Eur Neuropsychopharmacol. 2012;22(11):825 to 35. | — | Yes | — | — | — | — | — |
Weiden PJ, et al. J Clin Psychiatry. 2012;73(9):1224 to 33. | — | — | — | — | — | Yes | — |
Fe Bravo-Ortiz M, et al. Int J Psychiatry Clin Pract. 2011;15(4):286 to 95. | — | — | — | — | — | Yes | — |
McDonnell DP, et al. Hum Psychopharmacol. 2011;26(6):422 to 33. | — | — | — | — | — | Yes | — |
Chengappa KN, et al. Acta Neuropsychiatr. 2010;22(2):68 to 80. | — | — | Yes | — | — | — | — |
Gaebel W, et al. Neuropsychopharmacology. 2010;35(12):2367 to 77. | — | Yes | — | — | — | Yes | — |
Lang K, et al. Psychiatr Serv. 2010;61(12):1239 to 47. | — | — | — | — | — | Yes | — |
Macfadden W, et al. Psychiatry (Edgmont). 2010;7(11):23 to 31. | — | Yes | — | — | — | Yes | — |
Schmauss M, et al. Pharmacopsychiatry. 2010;43(2):73 to 80. | — | — | — | — | — | Yes | — |
Spill B, et al. Int J Psychiatry Clin Pract. 2010;14(1):53 to 62. | — | — | — | — | — | Yes | — |
Willis M, et al. Eur J Health Econ. 2010;11(6):585 to 94. | — | — | — | — | — | Yes | — |
Weiden PJ, et al. J Clin Psychiatry. 2009;70(10):1397 to 406. | — | — | — | — | — | Yes | — |
Kim B, et al. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(5):1231 to 5. | — | — | — | — | — | Yes | — |
Beauclair L, et al. J Med Econ 2007;10:427 to 442. | — | — | — | — | — | Yes | — |
Han C, et al. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(6):1219 to 23. | — | — | Yes | — | — | — | — |
Keks NA, et al. Br J Psychiatry. 2007;191:131 to 9. | — | — | — | Yes | — | Yes | — |
Schmauss M, et al. Int Clin Psychopharmacol. 2007;22(2):85 to 92. | — | — | — | — | — | Yes | — |
Yatham LN, et al. Acta Psychiatr Scand Suppl. 2007;(434):50 to 6. | — | — | Yes | — | — | — | — |
Bai YM, et al. Pharmacopsychiatry. 2006;39(4):135 to 41. | — | — | — | Yes | — | Yes | — |
Llorca PM, et al. Int J Psychiatry Clin Pract. 2006;10(4):276 to 84. | — | — | — | — | — | Yes | — |
Chue P, et al. Eur Neuropsychopharmacol. 2005;15(1):111 to 7. | — | — | — | — | — | Yes | — |
aNo associated citation, the study is from a ClinicalTrial.gov entry.
Appendix 6: References of Potential Interest
Previous CADTH Reports
Brankston G, Picheca L. Antipsychotic drugs or benzodiazepines for rapid tranquilization in mental health facilities or emergency department settings. C J Health Technol. 2021;1(8).
Narain T, Ford C. Atypical injectable antipsychotics for schizophrenia or bipolar disorder: a review of clinical effectiveness and cost-effectiveness (CADTH Rapid response reports). Ottawa (ON): CADTH; 2019.
Results Already in an Included Systematic Review
Pacchiarotti I, Tiihonen J, Kotzalidis GD, et al. Long-acting injectable antipsychotics (LAIs) for maintenance treatment of bipolar and schizoaffective disorders: a systematic review. Eur Neuropsychopharmacol. 2019;29(4):457-470. PubMed
Rapinesi C, Kotzalidis GD, Mazzarini L, et al. Long-Acting Injectable (LAI) aripiprazole formulations in the treatment of schizophrenia and bipolar disorder: a systematic review. Clin Drug Investig. 2019;39(8):713-735. PubMed
Alphs L, Bossie C, Mao L, Lee E, Starr HL. Treatment effect with paliperidone palmitate compared with oral antipsychotics in patients with recent-onset versus more chronic schizophrenia and a history of criminal justice system involvement. Early Interv Psychiatry. 2018;12(1):55-65. PubMed
Butler M, Urosevic S, Desai P, et al. Treatment for Bipolar Disorder in Adults: A Systematic Review (AHRQ Comparative Effectiveness Reviews). Rockville (MD): Agency for Healthcare Research and Quality (US); 2018.
Huang M, Yu L, Pan F, et al. A randomized, 13-week study assessing the efficacy and metabolic effects of paliperidone palmitate injection and olanzapine in first-episode schizophrenia patients. Prog Neuropsychopharmacol Biol Psychiatry. 2018;81:122-130. PubMed
Prajapati AR, Wilson J, Song F, Maidment I. Second-generation antipsychotic long-acting injections in bipolar disorder: systematic review and meta-analysis. Bipolar Disord. 2018;20(8):687-696. PubMed
Stroup TS, Bareis NA, Rosenheck RA, Swartz MS, McEvoy JP. Heterogeneity of treatment effects of long-acting injectable antipsychotic medications. J Clin Psychiatry. 2018;80(1):27. PubMed
Gentile S. Safety concerns associated with second-generation antipsychotic long-acting injection treatment. a systematic update. Horm Mol Biol Clin Investig. 2017;36(2):23. PubMed
Reviews Not Focused on Second-Generation Antipsychotic Drugs
Ostuzzi G, Bertolini F, Del Giovane C, et al. Maintenance treatment with long-acting injectable antipsychotics for people With nonaffective psychoses: a network meta-analysis. Am J Psychiatry. 2021;178(5):424-436. PubMed
Ostuzzi G, Bighelli I, So R, Furukawa TA, Barbui C. Does formulation matter? A systematic review and meta-analysis of oral versus long-acting antipsychotic studies. Schizophr Res. 2017;183:10-21. PubMed
Unclear Population Age and Drug Administration Routes
Sabe M, Zhao N, Crippa A, Kaiser S. Antipsychotics for negative and positive symptoms of schizophrenia: dose-response meta-analysis of randomized controlled acute phase trials. NPJ Schizophr. 2021;7(1):43. PubMed
Guinart D, Misawa F, Rubio JM, et al. Outcomes of neuroleptic malignant syndrome with depot versus oral antipsychotics: a systematic review and pooled, patient-level analysis of 662 case reports. J Clin Psychiatry. 2020;82(1):24. PubMed
Azorin JM, Simon N. Dopamine receptor partial agonists for the treatment of bipolar disorder. Drugs. 2019;79(15):1657-1677. PubMed
Salgueiro M, Segarra R. Long-acting injectable second-generation antipsychotics in first-episode psychosis: a narrative review. Int Clin Psychopharmacol. 2019;34(2):51-56. PubMed
Ineligible Due to Combination Treatments
Kishi T, Ikuta T, Matsuda Y, et al. Mood stabilizers and/or antipsychotics for bipolar disorder in the maintenance phase: a systematic review and network meta-analysis of randomized controlled trials. Mol Psychiatry. 2021;26(8):4146-4157. PubMed
Nuechterlein KH, Ventura J, Subotnik KL, et al. A randomized controlled trial of cognitive remediation and long-acting injectable risperidone after a first episode of schizophrenia: improving cognition and work/school functioning. Psychol Med. 2020:1-10. PubMed
Foster A, Buckley P, Lauriello J, Looney S, Schooler N. Combination antipsychotic therapies: an analysis from a longitudinal pragmatic trial. J Clin Psychopharmacol. 2017;37(5):595-599. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca