CADTH Health Technology Review
Metered-Dose Inhalers for Medical Cannabis Use
Rapid Review
Authors: Eugenia Palylyk-Colwell, Kelly Farrah
Abbreviations
AE
adverse event
CANTAB
Cambridge Neuropsychological Test Automated Battery
CBD
cannabidiol
MDI
metered-dose inhaler
RCT
randomized controlled trial
THC
tetrahydrocannabinol
VAS
visual analogue scale
Key Messages
Limited evidence of the clinical effectiveness of metered-dose inhalers for medical cannabis is available from patients who were prior users of medical cannabis (primarily by smoking) for treating chronic pain, chemotherapy-induced nausea, or spasticity.
No evidence was found for using metered-dose inhalers for medical cannabis in patients who were naive to medical cannabis.
Inhalation of medical cannabis using a metered-dose inhaler delivers low and precise doses of delta-9-tetrahydrocannabinol that provide a rapid onset of action and dose-dependent effects and is generally well tolerated.
No consistent or prolonged cognitive impairment occurred following inhalation of medical cannabis using a metered-dose inhaler in patients who had previously used medical cannabis for their medical condition.
No evidence was found that directly compared inhalation of medical cannabis using a metered-dose inhaler versus consumption of medical cannabis by an alternate route such as smoking, vapourizing, vaping, dabbing, mucosal administration, or oral ingestion.
No evidence-based guidelines were identified for using metered-dose inhalers for medical cannabis to inform best practices.
Context and Policy Issues
Cannabis is increasingly being used as a medical treatment for a wide range of health conditions such as chronic pain management, palliative care, dementia, emesis, epilepsy, cachexia, movement disorders, and post-traumatic stress disorder; however, there are many gaps in the evidence for using medical cannabis.1,2 As of March 2021, 292,399 individuals had registered in Canada to access cannabis for medical purposes.3 The average daily amount of medical cannabis authorized by health care practitioners for use by registered individuals who access their supply through Canadian federally licensed sellers is 2 g per day.3
There are many different ways to consume cannabis, such as smoking, vapourizing oil or ethanolic liquids, vaping, dabbing, administration of sublingual or mucosal tinctures, or oral ingestion.4,5 The onset, magnitude, and duration of the effects of cannabis are significantly affected by the route of administration.6 A strategy for the development of cannabis for medical use has been to alter the pharmacokinetics of cannabis delivery to maximize therapeutic effects while minimizing cognitive and behavioural psychoactive effects.6
Oral inhalation of cannabis by smoking, vaping, or using any form of inhalation device is a highly effective route of administration.5 Smoking cannabis produces a rapid onset of effect; however, plasma concentrations of active cannabinoids can be highly variable, and smoking is associated with numerous harms and health risks that generally preclude its use for therapeutic applications.6,7 Vapourization of cannabis oil and other products also presents health risks due to the presence of unsafe additives and the known health risks associated with vaping (e.g., dependence, formation of harmful chemicals such as formaldehyde when vaping liquid is heated).8,9 There is also a lack of evidence for using vapourization devices for medical cannabis.10
Currently, the precise dosing of medical cannabis by alternate routes of administration is hampered by a lack of standardization, which leads to batch-to-batch variability of the cannabis source due to differing potencies and ratios of the active cannabinoids (i.e., tetrahydrocannabinol [THC] and cannabidiol [CBD]). Moreover, the uncertainty associated with the dosing of medical cannabis due to lack of a standardized product can be a barrier to physician prescribing and the root of patient reluctance to use medical cannabis for their health condition. There is an increasing interest in the use of metered-dose inhalers (MDIs) to deliver medical cannabis in Canadian clinical practice as MDIs offer the delivery of medical cannabis by oral inhalation in a metered, precise, and consistent form. Additional benefits of oral inhalation of medical cannabis by MDI are reproducible dosing, a standardized product manufactured according to high pharmaceutical standards, the potential for the use of lower doses, fewer adverse events (AEs), avoidance of hazardous combustion products, portability, enhanced safety, and less potential for overconsumption, misuse, or diversion.5,11,12
There are currently 5 MDIs approved in Canada for the delivery of medical cannabis. These include the Syqe Inhaler (Syqe Medical Ltd., Tel Aviv, Israel),13 Volcano Medic (Storz & Bickel, GMBH),14 Volcano Medic 2 (Storz & Bickel, GMBH),15 Mighty Medic (Storz & Bickel, GMBH),16 and Mighty + Medic (Storz & Bickel, GMBH).17 Since the approval of MDIs for medical cannabis in Canada, there has been interest in understanding the clinical effectiveness of medical cannabis administered by these devices, particularly focusing on safety and potential strategies for best practices compared to the typical consumption methods.
The objective of this report is to summarize the evidence on the clinical effectiveness of MDIs for medical cannabis use and to identify evidence-based clinical practice guidelines to inform decisions about using MDIs for medical cannabis in Canadian clinical practice.
Research Questions
What is the clinical effectiveness of MDIs for medical cannabis use?
What are the evidence-based guidelines for MDIs for medical cannabis use?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International Health Technology Assessment (HTA) Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were metered-dose inhalers and cannabis. No filters were applied to limit the retrieval by study type. Conference abstracts, comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to documents in English published between January 1, 2017, and February 22, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first screening level, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 2, if they were duplicate publications, or if they were published before 2017.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist18 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively as detailed in Appendix 3.
Criteria | Description |
|---|---|
Population | Adults using cannabis for medical purposes |
Intervention | Metered-dose inhaler for medical cannabis use |
Comparator | Q1: Any other method of medical cannabis consumption Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., relief of signs and symptoms) and safety (e.g., any adverse events including but not limited to excessive impairment [panic attacks, paranoia, rapid heart rate or heart attack, uncontrollable shaking or seizures, unresponsiveness], side effects, morbidity, or mortality) Q2: Recommendations regarding best practices (e.g., appropriate patient populations or settings, recommended treatment strategies including dosage, strategies to mitigate harms, adverse events, and misuse) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Summary of Evidence
Quantity of Research Available
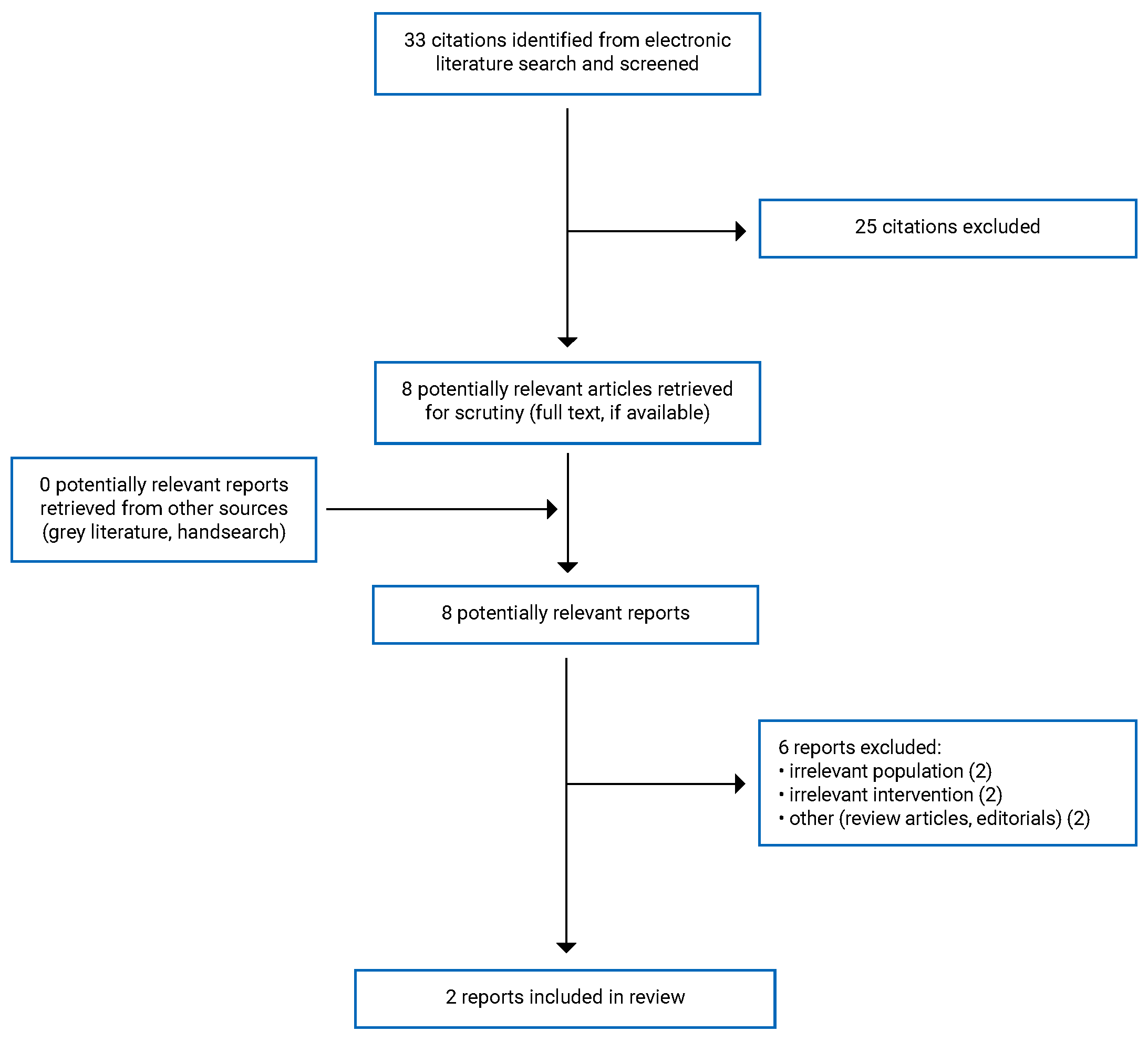
A total of 33 citations were identified in the literature search. Following the screening of titles and abstracts, 25 citations were excluded, and 8 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of the 8 potentially relevant articles, 6 publications were excluded for various reasons, and 2 publications met the selection criteria and were included in this report. These comprised 1 randomized controlled trial (RCT)11 and 1 non-randomized study.12 Appendix 1 presents the PRISMA19 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One RCT11 and 1 non-randomized study12 were included in this report. Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
The RCT11 was a randomized, double-blind (patients, investigators), placebo-controlled, single-centre, 3-period, 3-treatment crossover study conducted between March 2016 and July 2017.
The non-randomized study12 was a prospective, open-label, single-arm, single-centre, proof-of-concept cohort study that evaluated the change from baseline due to the intervention. The study was conducted between January 2016 and July 2017.
Country of Origin
The RCT11 and the non-randomized study12 were both conducted at the same single-centre site (i.e., the Pain Research Unit of the Rambam Health Care Campus in Haifa, Israel). The first authors of each study were also listed among the authors of the other study, which inferred that the same research group conducted both studies.
Patient Population
Both studies11,12 enrolled adult (18 years and older) patients who were ambulatory and recruited from the same pain research unit. Patients were required to have a valid licence from the Israeli Ministry of Health to consume medical cannabis as part of their ongoing medical treatment. Patients were also required to have baseline pain intensity of 6 or above on a 10 cm visual analogue scale (VAS). The RCT11 enrolled 27 patients. The mean age of patients was 48.3 years (range = 18 to 67), and most patients were male (70.4%).11 Pain diagnoses included painful radiculopathy, painful diabetic neuropathy, complex regional pain syndrome, other focal neuropathies, and phantom/stump pain.11 Baseline pain intensity was 7 or higher for 25 (92.6%) patients.11 Most patients (77.8%) had previously used smoking to administer cannabis, and monthly cannabis use ranged from 16 g to 30 g in the majority (74.1%) of patients.11
The non-randomized study12 included adult (18 years and older) patients who were hospitalized and held a valid licence to consume medical cannabis as part of their ongoing medical treatment from the Israeli Ministry of Health. A total of 22 patients were enrolled with diagnoses of oncologic pain and nausea, neuropathic pain, Crohn disease, and multiple sclerosis with spasticity. Median pain intensity before the intervention was 7 (range = 2 to 9) on a 10 cm VAS.12 The mean age of patients was 44.3 years (range = 25 to 78), and 54.5% of patients were female.12 Most (81.0%) patients had previously administered cannabis by smoking, and half (50.0%) of patients consumed cannabis 9 or more times per day before their hospitalization.12
Interventions and Comparators
In the RCT,11 each patient self-administered a single inhalation dose of 0.5 mg delta-9-THC or 1.0 mg delta-9-THC using the Syqe MDI (Syqe Medical Ltd., Tel Aviv, Israel) or a placebo dose using a matched MDI according to a 3-treatment crossover study design. The Syqe MDI is programmed to deliver doses of 0.5 mg to 1.5 mg aerosolized delta-9-THC. Patients received detailed instructions on using the Syqe MDI before dosing.11 There was at least a 2-day washout period between doses. Patients were required to abstain from cannabis-based medicines for 12 hours before the dose of study treatment; however, patients continued to receive their concurrent medications throughout the trial. Notably, 20 (74.1%) patients received simple analgesics, 18 (66.7%) patients received opioids, 12 (44.4%) patients received antidepressants, and 5 (18.5%) patients received sedatives.11
In the non-randomized study,12 patients self-administered individualized doses of delta-9-THC by inhalation using the Syqe MDI (Syqe Medical Ltd., Tel Aviv, Israel). Doses were based on the patient’s medical condition and the amount of cannabis used before hospitalization. A predefined number of self-administered inhalations was delivered during 4 dosing periods each day (i.e., at 8:00 a.m., 1:00 p.m., 6:00 p.m., and 9:00 p.m.), and a maximum number of daily rescue inhalations was also permitted for each patient.12 Patients received detailed instructions on the use of the Syqe MDI before dosing.12 The median number of inhalations prescribed during the study was 4 per day (range = 3 to 4), and the median number of rescue inhalations allowed was 3 per day (range = 2 to 4). The median number of actual inhalations administered was 3 per day (range = 1 to 6), and the median amount of cannabis used by patients per day was 51 mg (range = 20 mg to 96 mg).12 Patients also continued their routine medications, although no details pertaining to the type of medications or the distribution of use among the patients was provided.12
Outcomes
In the RCT,11 pain intensity was measured using a VAS where patients ranked their pain from 0, meaning no pain at all, to 10, meaning worst pain possible. Pain intensity was measured before inhalation and at 5, 15, 30, 60, 90, 120, and 150 minutes post-inhalation and results were reported and analyzed in the per-protocol population.11 Spontaneous AEs were recorded throughout the study. Patients were specifically asked to rate the severity of predetermined AEs known to be associated with the use of cannabis (i.e., drug high, dizziness, restlessness, headache, nausea, throat irritation, dry mouth, and general feeling) using a VAS at baseline and at the same times that pain intensity was measured.11 An increase of 2 or more points in the VAS score between 2 time points was recorded as an AE.11 Vital signs, including blood pressure and heart rate, were also recorded at baseline and 15, 30, 60, 90, 120, and 150 minutes post-inhalation.11 On each test day, cognitive function was assessed at baseline, 15, and 75 minutes post-inhalation using selected tests from the Cambridge Neuropsychological Test Automated Battery (CANTAB).11 Domains of interest in the CANTAB were processing speed (Reaction Time Test), episodic memory (Paired Associates Learning Task), working memory (Spatial Working Memory Test), and sustained attention (Rapid Visual Information Processing Test).11 A composite score for the CANTAB based on key outcome measures from these tests was also calculated.11
In the non-randomized study,12 outcome measures were obtained by self-administered questionnaires. Before each inhalation and 30 to 60 minutes post-inhalation, patients rated their pain, nausea, and/or spasticity (as appropriate) using a VAS where 0 meant no symptom and 10 meant symptom at maximum intensity.12 Upon completion of the study, each patient completed a treatment satisfaction questionnaire regarding ease of use and satisfaction with treatment on a scale of 1 to 7 where 1 meant absolutely do not agree, and 7 meant absolutely agree.12 At the end of the study, medical staff involved in training and monitoring patients completed a questionnaire on ease of use and satisfaction with the MDI using a scale of 1 to 5, where 1 meant do not agree and 5 meant agree.12
Summary of Critical Appraisal
An overview of the critical appraisal of the included publications is summarized in the following text. Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Randomized Controlled Trial
In the RCT,11 the objective, inclusion and exclusion criteria, patient characteristics, interventions, and outcome measures were clearly described. A sample size calculation was conducted; however, the authors did not report the results of the calculation, so it is unclear if an appropriate number of patients were included in the study to achieve sufficient power to detect a statistically significant difference between treatment groups for all comparisons. Patients and investigators were blinded to treatment, and the method of allocation concealment was reported, although it was not stated if other study personnel were also blinded to treatment. The study was conducted at a single centre, and all recruited patients were required to have a licence to use medical cannabis for the ongoing treatment of their medical condition. All included patients used medical cannabis before study entry (i.e., 74.1% of patients used 16 g to 30 g of cannabis per month); thus, the patient population represents a selected treatment-experienced population, which may complicate the generalizability of the study findings to patients with other medical conditions that would not fit the criteria for a licence for medical cannabis or to patients who are treatment naive. Regarding the latter, the study findings could underestimate the treatment effects and safety of medical cannabis in patients who have not previously used cannabis because patients who are treatment-experienced could have developed tolerance to medical cannabis.
Only 2 doses of delta-9-THC and 1 type of medical cannabis (i.e., dry flos; high THC and low CBD) were studied, so it is unknown if the study findings would be representative of other doses of medical cannabis or different ratios of cannabinoids. The study assessed outcomes after a single-dose administration, which is also not representative of the medical use of cannabis by the target patient population. There were 27 patients enrolled in the study; however, efficacy analyses were conducted in the per-protocol population (i.e., N = 22 for the 0.5 mg delta-9-THC dose; N = 24 for the 1.0 mg delta-9-THC dose; and N = 23 for placebo). While a per-protocol analysis ensured that each patient received all 3 study treatments, it may bias results in favour of the intervention because patients who had difficulties with the intervention or were not compliant could be excluded. In contrast, an intention-to-treat analysis evaluates patients based on the group to which they were originally randomized, regardless of whether or not they received the intervention. The main reasons for excluding patients from the per-protocol population were because they did not receive the intervention as randomized or were not eligible. Although the study was randomized, the distribution of known confounders, such as the concurrent use of pain medication (e.g., simple analgesics and opioids), which could have affected perception of pain intensity, was not described or adjusted for; however, given the crossover study design, it is expected that each patient would have acted as their own control, and this would have mitigated the impact of potential confounders.
Non-Randomized Trial
In the non-randomized study,12 the objective, inclusion criteria, patient characteristics, interventions, and outcome measures were clearly described. No exclusion criteria or sample size calculation was reported. The study enrolled 22 patients; however, 1 patient preferred not to use the MDI, so efficacy and safety analyses were performed on 21 patients. Due to the non-randomized design, it is not known if potential confounding factors were distributed evenly among the patient population (e.g., patients also continued their routine medications throughout the study, but the types of medications used were not described). The delta-9-THC doses were individualized based on a patient’s medical condition and prior cannabis use; however, the analysis did not adjust for the different delta-9-THC doses administered, and the publication did not mention if dose adjustments were done during the study. The study was not blinded, so patients, investigators, and assessors were aware of the active treatment, which could have biased the results, especially for subjective outcomes such as intensity of pain, nausea, spasticity, the severity of AEs, or treatment satisfaction. Patients’ and assessors’ awareness of who was receiving a dose of delta-9-THC could potentially bias the results in favour of a treatment effect due to the anticipation of a therapeutic response. No adjustment was made for the length of follow-up as patients were followed up until they were discharged from the hospital or withdrew from the study (i.e., median hospital stay was 4 days but ranged from 3 to 14 days). It is possible that chronologic factors could have confounded the study results if patients were followed for different lengths of time; however, the direction of bias in the results was unclear. An appropriate nonparametric statistical test (Wilcoxon signed-ranked test) was used due to the small sample size. All patients had previously used medical cannabis before hospitalization and possessed a licence to do so; therefore, the patient population represents a selected treatment-experienced hospitalized population, which could affect the generalizability of the study findings to patients who are non-hospitalized or treatment naive.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Clinical Effectiveness of MDIs for Medical Cannabis
The main findings from the included RCT11 and non-randomized study12 are summarized in the following sections and Appendix 4.
Pain Intensity
The RCT11 and non-randomized study12 both evaluated patient-reported pain intensity measured using a VAS before and after inhalation of a dose of medical cannabis via the MDI. In both studies, baseline pain intensity was approximately 7 points, which corresponds with pain of moderate to severe intensity.20
In the RCT,11 pain intensity at baseline was similar across all 3 treatment groups (Appendix 4). The maximum mean change from baseline in the reduction in pain intensity was dose-dependent. Therefore, using the MDI inhalation device resulted in pain intensity decreases of approximately 2 points (or 25%) with the 0.5 mg delta-9-THC dose and 3 points (or 39%) with the 1.0 mg delta-9-THC dose. The reduction in pain intensity from baseline was statistically significantly larger with the 1.0 mg delta-9-THC dose versus placebo and with the 1.0 mg delta-9-THC dose versus the 0.5 mg delta-9-THC dose. No statistical results for the 0.5 mg delta-9-THC dose versus placebo were reported for this outcome.
At 120 minutes post-inhalation of medical cannabis by MDI, the proportion of patients with a 30% or greater reduction in pain score by VAS was numerically highest following the 1.0 mg delta-9-THC dose (Appendix 4). The proportion of patients with a 30% or greater reduction in pain score by VAS appeared to follow a dose-dependent pattern, as numerically higher values were observed with the 1.0 mg delta-9-THC dose than the 0.5 mg delta-9-THC dose, which was higher than placebo. However, no within- or between-groups statistical comparisons results were reported for this outcome.
Similarly, a numerically higher a proportion of patients achieved a 2 point or greater reduction in pain score at 120 minutes with both the 1.0 mg and 0.5 mg delta-9-THC doses than placebo. However, no statistical comparisons within or between any of the treatment groups were reported for this outcome.
In the non-randomized study,12 when compared with pre-inhalation pain intensity, there was a statistically significant reduction in pain intensity by VAS at 30 to 60 minutes following inhalation of delta-9-THC by MDI (Appendix 4). In this study, doses of delta-9-THC were individualized based on a patient’s medical condition and prior medical cannabis use. The study results were not adjusted for the differences in the administered doses, so no inferences regarding a dose-response relationship can be made. No statistically significant within-patient differences in the reduction in pain intensity were found with repeated use. Of note, before hospitalization in this study, half (50.0%) of patients consumed medical cannabis 9 or more times a day. During hospitalization, patients used a median daily dose of 51 mg cannabis per day (range = 20 mg to 96 mg), which was administered over a median of 3 actual inhalations per day (range = 1 to 6). This implies a substantial reduction in the daily use of medical cannabis when administered using the MDI compared to the patients’ prehospitalization consumption of medical cannabis.
Nausea Intensity
In the non-randomized study, there was a statistically significant reduction in nausea intensity as measured by VAS 30 to 60 minutes post-inhalation of delta-9-THC by MDI compared to pre-inhalation nausea intensity (Appendix 4).
Spasticity Intensity
In the non-randomized study,12 there was a numerical reduction in spasticity intensity as measured by VAS 30 to 60 minutes post-inhalation of delta-9-THC by MDI (Appendix 4). No statistical testing was performed due to the small sample size.
Cognitive Impairment
In the RCT,11 there was no evidence of consistent or prolonged cognitive impairment following inhalation of either a 0.5 mg or 1.0 mg dose of delta-9-THC by MDI, as measured using the CANTAB instrument (Appendix 4). Significant impairment in cognition was detected at 1 time point, which was a statistically significant increase in the strategy score of the spatial working memory test at 15 minutes post-inhalation with the 1.0 mg delta-9-THC dose versus placebo. The difference between the 2 groups was no longer statistically significant at 75 minutes post-inhalation. There were no statistically significant differences between the 0.5 mg delta-9-THC dose and placebo at any time point. A statistically significant improvement in performance was observed with the 0.5 mg delta-9-THC dose compared with placebo at 15 minutes post-inhalation as measured by a faster movement time in the Real Time Test median 5-choice movement time, and a shorter response latency in the Rapid Visual Information Processing domains of the CANTAB. There were no statistically significant differences in the CANTAB composite cognitive score at 15 or 75 minutes for either the 0.5 mg dose or the 1.0 mg dose of delta-9-THC by MDI versus placebo.
Treatment Satisfaction
In the non-randomized study,12 patient and medical staff satisfaction with using MDIs to administer medical cannabis was high. Most patients strongly agreed that the MDI was easy to use, easy to inhale, and that the indication to end the inhalation was clear. Almost all patients either strongly agreed or agreed that they were overall satisfied with the use of the MDI. Medical staff also agreed that they were satisfied with the MDI and the ease of training and use by patients. No statistical comparisons of these data were performed.
Safety
The RCT11 captured data on spontaneously occurring AEs, as well as AEs that patients were specifically questioned about due to their association with cannabis use (Appendix 4). Of the 207 AEs reported, 4 were serious AEs deemed unrelated to the study intervention by the investigators (i.e., they were reported to be due to surgery complications in a single patient). Frequently occurring AEs (i.e., occurring in ≥ 5 patients in any treatment group) were drug high, cough, pain, weakness, restlessness, dry mouth, dizziness, and sleepiness.
There were statistically significant reductions in mean diastolic blood pressure with both the 0.5 mg and 1.0 mg delta-9-THC doses at 30 minutes and 60 minutes post-inhalation, respectively, compared with pre-inhalation values (Appendix 4). The mean heart rate was statistically significantly decreased with the 0.5 mg delta-9-THC dose at 90 minutes post-inhalation. With the 1.0 mg delta-9-THC dose, there was a statistically significant increase from pre-inhalation heart rate at 15 minutes post-inhalation. Blood pressure and heart rate resolved spontaneously and returned to normal with no intervention by 150 minutes post-inhalation.
There were limited safety data reported in the non-randomized study. No severe AEs were reported. Three patients experienced a mild cough following inhalation; however, the coughs resolved spontaneously within 1 minute.
Appendix 4 presents the main study findings and authors’ conclusions.
Guidelines
No relevant evidence-based guidelines for MDIs for medical cannabis use were identified; therefore, no summary can be provided.
Limitations
Various limitations prevent drawing definitive conclusions regarding the clinical effectiveness of MDIs for medical cannabis for this report. The number of relevant studies was small as only 1 RCT11 and 1 non-randomized study12 met the selection criteria. Both studies are limited by small sample sizes (i.e., 22 to 27 patients), which can lead to imprecise results due to the inclusion of relatively few patients and events, and potentially insufficient power to detect important treatment differences. Although a sample size calculation was done in the RCT,11 the calculated sample size was not reported, so it was impossible to determine if the study was adequately powered to measure treatment differences for all study outcomes. The non-randomized study12 is also limited by the lack of randomization and uncontrolled design, precluding knowing if potential confounding or prognostic factors were evenly distributed among the study patients.
No evidence was identified that directly compared MDI versus alternate methods of administrating medical cannabis, such as smoking, vapourizing, vaping, dabbing, mucosal administration, or oral ingestion. Consequently, there is no evidence available to assess the relative benefits or harms of administering medical cannabis by MDI versus other consumption methods. There was no evidence identified regarding the prevention of accidental exposure or overconsumption, misuse, or diversion of medical cannabis with using MDIs for medical cannabis.
Both included studies11,12 were single-centre studies conducted at the same pain research unit by the same research group over the same time period (i.e., 2016 to 2017). As a result, it is unknown if the study results are reproducible in other clinical settings or by other researchers. The generalizability of the findings of the studies to Canadian clinical practice is unknown due to likely differences in clinical practices and health care delivery between the different countries.
In both studies,11,12 patients had used medical cannabis before study entry to treat their medical condition. In fact, the requirement to have a licence to use medical cannabis was an inclusion criterion in both studies. According to the study authors, a medical licence for medical cannabis is granted only for specific indications; therefore, the study populations represent selected patients who were treatment-experienced and had a licence to use medical cannabis. This may affect the generalizability of the study findings in patients with medical conditions outside those for which the study participants had received licences for treatment with medical cannabis. Due to the previous ongoing use of medical cannabis, the study populations could have developed a relative tolerance to medical cannabis. So, it could be possible that patients who are treatment naive may be managed with lower doses of delta-9-THC than were evaluated in the studies. In addition, patients who are treatment naive may also experience more AEs than were observed in patients enrolled in the study who were treatment experienced. Additional sources of bias are the non-blinding of patients and study personnel in the non-randomized study,12 which may have led to performance and detection bias from the awareness of the active study intervention.
Both the RCT11 and non-randomized study12 evaluated the same MDI device (i.e., Syqe Inhaler), which utilizes a specific form of medical cannabis (i.e., pharmaceutical-grade cannabis flos containing 22% delta-9-THC, 0.1% cannabidiol, and 0.2% cannabinol). Consequently, the results of these studies may not be generalizable to other MDI devices or medical cannabis with different ratios of cannabinoids. The RCT11 evaluated only single-dose administration of medical cannabis, which is not reflective of use in the target patient population who use medical cannabis to treat chronic medical conditions. The non-randomized study12 evaluated individualized patient doses, with a collective median dose of 51 mg cannabis used per day (range = 20 mg to 96 mg) or 1.5 mg delta-9-THC per day (range = 1.0 mg to 3.0 mg). It is unknown if these doses reflect actual doses used in clinical practice in Canada. According to available data, for medical cannabis use from 2021, the average consumption of medical cannabis is 2 g per day for patients receiving their supply from federally regulated suppliers.3 It is important to note that the Canadian data did not specify the route of administration by which the 2 g per day of medical cannabis was consumed. It is also expected that the pharmaceutical-grade cannabis used in the included studies was of higher potency than would be routinely available to Canadian patients.
There is a lack of evidence of long-term efficacy and safety of MDIs used for medical cannabis as the included RCT11 investigated single-dose administration and the non-randomized study12 followed patients only during their hospitalization, which corresponds with a median length of stay of 4 days (range = 1 to 14 days). Patients were not followed up beyond the treatment period in the studies. As a result, no evidence was identified for the use of MDIs for medical cannabis beyond the treatment duration of the included studies.
No relevant evidence-based guidelines for MDIs used for medical cannabis were identified in the targeted literature searches, indicating an important evidence gap.
Conclusions and Implications for Decision- or Policy-Making
This report identified 1 RCT11 and 1 non-randomized study12 to inform the research question pertaining to the clinical effectiveness of MDIs for medical cannabis. Limited evidence from these studies is derived from a small number of patients licensed to use medical cannabis for the ongoing treatment of their medical conditions (e.g., chronic pain, chemotherapy-induced nausea, and spasticity). No evidence-based guidelines for MDIs for medical cannabis were identified to guide best practices.
The limited evidence supporting the clinical effectiveness of MDIs for medical cannabis is associated with a high level of uncertainty due to the small sample sizes, selected patient populations, short durations, and single-centre settings of the identified studies. No evidence was found of a direct comparison between medical cannabis administered by MDI versus another method of medical cannabis consumption (e.g., smoking, vapourizing, oral ingestion). Further, no evidence was identified to support that MDIs prevent accidental exposure, overconsumption, misuse, or diversion of medical cannabis to non-authorized users.
The included RCT11 demonstrated that in patients who are treatment experienced, inhalation of medical cannabis by MDI delivered precise and low inhalation doses of delta-9-THC, resulting in a dose-dependent treatment effect. Moreover, it was shown in both studies11,12 that patients used lower doses of medical cannabis following inhalation by MDI as compared to their pre-study consumption. Administration of medical cannabis by MDI was well tolerated based on the frequency of spontaneously reported AEs and AEs known to be associated with cannabis use. Although statistically significant reductions in mean diastolic blood pressure and a decrease or increase in heart rate were observed depending on dose and time post-inhalation, the changes were transient as values returned to baseline with no intervention by 150 minutes post-inhalation. The RCT11 also showed no consistent or prolonged cognitive impairment or enhancement associated with the doses of delta-9-THC administered in the study; however, it must be kept in mind that only single doses were used in this study and that patients were experienced users of medical cannabis. Patient and health care professional satisfaction with using MDIs for medical cannabis was high based on the results of treatment satisfaction questionnaires administered in the non-randomized study.12
No evidence was identified to support the long-term efficacy or safety of chronic use of MDIs for delivery of medical cannabis beyond the duration of the included studies. Lack of long-term efficacy and safety data for MDIs for medical cannabis is a major evidence gap, in addition to other evidence gaps associated with the use of cannabis for a variety of medical conditions.1
Two additional prospective, open-label, non-randomized, single-dose phase I studies21,22 were identified that evaluated the delivery of cannabis by different MDI devices (i.e., the CannaHaler by Kite-Systems in Tel Aviv, Israel,21 and a non-proprietary validated pressurized MDI22). The studies did not meet the selection criteria because they were both conducted in healthy volunteers, which is not an appropriate population for this report. Nonetheless, these studies provide additional information on the safety of MDIs used to deliver cannabis in individuals who were not previously using medical cannabis for ongoing treatment. Both studies reported that the MDIs were well tolerated with no reported AEs in 1 study21 and little or no coughing, moderate tachycardia, and only slight psychological AEs in the other study.22 A single-dose, open-label, non-randomized phase I study23 that evaluated the pharmacokinetics, efficacy, safety, and ease of use of the Syqe Inhaler in a cohort of 8 patients with chronic pain who were using medical cannabis was also identified but it was not included in this report because it was published in 2014. In this study, patients inhaled a single dose of 15.1 mg plus or minus 0.1 mg delta-9-THC using the Syqe Inhaler and reported a statistically significant 45% reduction in pain intensity compared to baseline at 20 minutes post-inhalation, returning to baseline within 90 minutes.23 The only reported AE was tolerable light-headedness lasting 15 to 30 minutes, requiring no intervention.23 These 3 studies are identified in Appendix 5.
Overall, there is limited evidence that the inhalation of medical cannabis using MDIs delivers low and precise doses of delta-9-THC associated with rapid onset of action and dose-dependent treatment effects, or that it is generally well tolerated in treatment-experienced users of medical cannabis. Larger prospective RCTs are needed to address the evidence gaps for direct comparisons of MDI with other methods of administering medical cannabis in patients who are treatment naive and to provide evidence of long-term efficacy and safety.
References
1.Medical cannabis - research gaps. Ottawa (ON): CADTH; 2020 Apr: https://www.cadth.ca/sites/default/files/pdf/research_gaps_medical_cannabis.pdf. Accessed 2022 Mar 12.
2.Health Canada. Information for health care professionals. Cannabis (marihuana, marijuana) and the cannabinoids. Ottawa (ON): Government of Canada; 2018: https://www.canada.ca/content/dam/hc-sc/documents/services/drugs-medication/cannabis/information-medical-practitioners/information-health-care-professionals-cannabis-cannabinoids-eng.pdf. Accessed 2022 Feb 24.
3.Health Canada. Data on cannabis for medical purposes. Ottawa (ON): Government of Canada; 2021: https://www.canada.ca/en/health-canada/services/drugs-medication/cannabis/research-data/medical-purpose.html. Accessed 2022 Mar 4.
4.Government of Canada. About cannabis. 2018 Oct 17; https://www.canada.ca/en/health-canada/services/drugs-medication/cannabis/about.html. Accessed 2022 Mar 12.
5.DocMJ. Everything you need to know about cannabis inhalers. 2019 Oct 25; https://docmj.com/everything-you-need-to-know-about-cannabis-inhalers/. Accessed 2022 Mar 15.
6.Huestis MA. Human cannabinoid pharmacokinetics. Chem Biodivers. 2007;4(8):1770-1804. PubMed
7.Government of Canada. Risks of smoking. 2016 May 17; https://www.canada.ca/en/health-canada/services/smoking-tobacco/effects-smoking/smoking-your-body/risks-smoking.html. Accessed 2022 Mar 15.
8.Government of Canada. Vaping-associated lung illness. 2020 Aug 20; https://www.canada.ca/en/public-health/services/diseases/vaping-pulmonary-illness.html. Accessed 2022 Mar 15.
9.Government of Canada. Risks of vaping. 2020 Jun 11; https://www.canada.ca/en/health-canada/services/smoking-tobacco/vaping/risks.html. Accessed 2022 Mar 15.
10.Freige C, Ryce A. Disposable handheld vaporization devices for inhalation of medical cannabis: clinical effectiveness and cost-effectiveness. (CADTH rapid response report: reference list). Ottawa (ON): CADTH; 2020 Mar: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RA1095%20Vape%20Devs%20for%20Cannabis%20Final.pdf. Accessed 2022 Mar 15.
11.Almog S, Aharon-Peretz J, Vulfsons S, et al. The pharmacokinetics, efficacy, and safety of a novel selective-dose cannabis inhaler in patients with chronic pain: A randomized, double-blinded, placebo-controlled trial. Eur J Pain. 2020;24(8):1505-1516. PubMed
12.Vulfsons S, Ognitz M, Bar-Sela G, Raz-Pasteur A, Eisenberg E. Cannabis treatment in hospitalized patients using the SYQE inhaler: Results of a pilot open-label study. Palliat Support Care. 2020;18(1):12-17. PubMed
13.Government of Canada. Syqe Inhaler. Syqe Medical Ltd; license no. 105910. Medical devices active licence listing (MDALL) 2021; https://health-products.canada.ca/mdall-limh/index-eng.jsp. Accessed 2022 Mar 4.
14.Government of Canada. Volcano Medic. Storz & Bickel GMBH; license no. 82405. Medical devices active licence listing (MDALL) 2010; https://health-products.canada.ca/mdall-limh/index-eng.jsp. Accessed 2022 Mar 4.
15.Government of Canada. Volcano Medic 2.Storz & Bickel GMBH; license no. 103842. Medical devices active licence listing (MDALL) 2019; https://health-products.canada.ca/mdall-limh/index-eng.jsp. Accessed 2022 Mar 4.
16.Government of Canada. Mighty Medic. Storz & Bickel GMBH; license no. 96431. Medical devices active licence listing (MDALL) 2016: https://health-products.canada.ca/mdall-limh/index-eng.jsp. Accessed 2022 Mar 4.
17.Government of Canada. Mighty + Medic. Storz & Bickel GMBH; licence no. 106942. Medical devices active licence listing (MDALL) 2021: https://health-products.canada.ca/mdall-limh/index-eng.jsp. Accessed March 4, 2022.
18.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
19.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
20.Jensen MP, Tomé-Pires C, de la Vega R, Galán S, Solé E, Miró J. What determines whether a pain is rated as mild, moderate, or severe? The importance of pain beliefs and pain interference. Clin J Pain. 2017;33(5):414-421. PubMed
21.Ben-Ishay O, Bar-On O, Kluger Y. Smokeless consumption of medical cannabis pharmacokinetics, safety and feasibility of the CannaHALER© a phase 1a study. J Cannabis Res. 2020;2(1):15. PubMed
22.Meyer P, Langos M, Brenneisen R. Human pharmacokinetics and adverse effects of pulmonary and intravenous THC-CBD formulations. Med Cannabis Cannabinoids. 2018;1(1):36-43. PubMed
23.Eisenberg E, Ogintz M, Almog S. The pharmacokinetics, efficacy, safety, and ease of use of a novel portable metered-dose cannabis inhaler in patients with chronic neuropathic pain: a phase 1a study. J Pain Palliat Care Pharmacother. 2014;28(3):216-225. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Almog et al., (2020)11 Israel Funding source: Syqe Medical Ltd. | Prospective, double-blind, 3-period, 3-treatment, crossover RCT Single centre: Rambam Health Care Campus, Haifa, Israel Sample size calculation: No | Adult ambulatory patients with chronic pain with BL pain intensity ≥ 6 on a 10 cm VAS licensed to receive medical cannabis (N = 27) Age, mean (SD): 48.3 (11.9) Female, n (%): 8 (29.6) BMI (kg/m2), mean (SD): 27.8 (5.0) BL pain intensity ≥ 7 on 10 cm VAS, n (%): 25 (92.6) 92.6% Pain diagnosis, n (%):
Prior cannabis use by smoking, n (%): 21 (77.8) Cannabis use per month 16 to 30 g, n (%): 20 (74.1) Use of concurrent pain medication, n (%): 22 (81.5) | Intervention: Single dose inhalation of 0.5 mg or 1 mg Δ9-THC using the Syqe MDI Comparator: Single dose inhalation of PBO via matched MDI | Outcomes:
Follow-up:
|
Vulfsons et al., (2020)12 Israel Funding source: Syqe Medical Ltd. | Prospective, open-label, single-arm, proof-of-concept before-after study Single centre: Rambam Health Care Campus, Haifa, Israel Sample size calculation: No | Adult hospitalized patients with a valid licence to consume medical cannabisa as part of ongoing medical treatment and who were prescribed a medical cannabis MDI for use during hospitalization (N = 22) Age, mean (SD): 44.3 (12.5) Female, n (%): 11 (52.4) Pain diagnosis, n (%):
Prior cannabis use by smoking, n (%): 17 (81.0) Cannabis consumed > 9 times per day pre-hospitalization n (%): 11 (52.4) | Intervention: Up to 4 prescribed daily doses of 0.5 mg Δ9-THC using the Syqe MDI based on patient’s medical condition and amount of cannabis used pre-hospitalization. Up to an additional 4 daily rescue inhalations were also permitted. Comparator: NA | Outcomes:
Follow-up: Until discharge from hospital or patient withdrew from study |
BL = baseline; BMI = basal metabolic rate; CANTAB = Cambridge Neuropsychological Test Automated Battery; CRPS = complex regional pain syndrome; MDI = metered-dose inhaler; NA = not applicable; PBO = placebo; RCT = randomized controlled trial; SD = standard deviation; Δ9-THC = deta-9 tetrahydrocannabinol; VAS = visual analogue scale.
aValid indications for a licence to consume medical cannabis as a last line of treatment from the Israeli Ministry of Health include pain of neuropathic origin, chemotherapy-induced nausea and vomiting, patients in palliative and end-of-life care, inflammatory bowel disease, spasticity, pain from multiple sclerosis, and cachexia from HIV and other infectious diseases.12
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist18
Strengths | Limitations |
|---|---|
Almog et al. (2020)11 | |
|
|
Vulfsons et al. (2020)12 | |
|
|
AE = adverse event; CANTAB = Cambridge Neuropsychological Test Automated Battery; CBD = cannabidiol; CI = confidence interval; ITT = intention-to-treat; MDI = metered dose inhaler; PP = per protocol; SD = standard deviation; SE = standard error; Δ9-THC = delta-9 tetrahydrocannabinol
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings of Included Primary Clinical Studies
Main study findings | Authors’ conclusion |
|---|---|
Almog et al. (2020)11 | |
Baseline pain score by VAS (Mean ± SD): Placebo: 7.4 ± 1.1 0.5 mg Δ9-THC: 7.8 ± 1.3 1.0 mg Δ9-THC: 7.6 ± 1.1 (P = 0.4266)a Reduction in pain intensity by VAS: 1.0 mg Δ9-THC vs. Placebo: (95% CI, 0.52; 2.23)b; P = 0.0015 1.0 mg Δ9-THC vs. 0.5 mg Δ9-THC: (95% CI, 0.35; 2.08)b; P = 0.0058b Mean maximum change from baseline in pain intensity by VAS, absolute difference (% reduction): Placebo: NR 0.5 mg Δ9-THC: −1.95 points (24.97) 1.0 mg Δ9-THC: −2.95 points (39.42) Proportion of patients with ≥ 30% reduction in pain score by VAS at 120 minutes, n (%): Placebo: 5 (21.74%) 0.5 mg Δ9-THC: 8 (36.36%) 1.0 mg Δ9-THC: 14 (60.87%) Proportion of patients with ≥ 2-point reduction in pain score by VAS at 120 minutes, n (%): Placebo: 6 (26.09%) 0.5 mg Δ9-THC: 14 (63.64%) 1.0 mg Δ9-THC: 16 (69.57%) AE in all patients: Total number of AEs: 207 Total number of SAEs: 4 Total number of patients with WDAE: 1 Most frequently occurring AEs (placebo vs. 0.5 mg Δ9-THC vs. 1.0 mg Δ9-THC), n (Number of reports)c: Drug high: 9 (9) vs. 12 (13) vs. 16 (16) Cough: 2 (2) vs. 4 (6) vs. 11 (13) Pain: 6 (6) vs. 7 (7) vs. 3 (3) Weakness: 5 (5) vs. 7 (7) vs. 6 (6) | “This feasibility trial demonstrated that a metered-dose inhaler delivered precise and low THC doses, produced a dose-dependent and safe analgesic effect in patients with neuropathic pain/complex-regional pain syndrome (CRPS). Thus, it enables individualization of medical cannabis regimens that can be evaluated pharmacokinetically and pharmaco-dynamically by accepted pharmaceutical models (p. 1505).”11 |
Restlessness: 7 (7) vs. 7 (7) vs. 3 (3) Dry mouth: 2 (2) vs. 8 (8) vs. 5 (5) Dizziness: 1 (1) vs. 2 (2) vs. 8 (8) Sleepiness: 2 (2) vs. 6 96) vs. 4 (4) Nausea: 2 (2) vs. 2 (2) vs. 4 (4) BP reduced: 2 (2) vs. 2 (2) vs. 2 (2) Hunger: 3 (3) vs. NR vs. 2 (2) Total 14 (41) vs. 22 (60) vs. 20 (66) Blood pressure and heart rate measurements: Mean (SD) diastolic blood pressure: Placebo: NR 0.5 mg Δ9-THC: Baseline: 78.8 (9.9) 30 minutes post-inhalation: 75.6 (10.4) Difference: P = 0.0452 1.0 mg Δ9-THC: Baseline: 77.7 (8.4) 60 minutes post-inhalation: 73.3 (9.8) Difference: P = 0.0052 Mean (SD) heart rate: Placebo: NR 0.5 mg Δ9-THC: Baseline: 76.2 (10.4) 90 minutes post-inhalation: 70.3 (10.8) Difference: P = 0.0042 1.0 mg Δ9-THC: Baseline: 74.7 (12.5) 15 minutes post-inhalation: 80.2 (13.9) Difference: P = 0.0229 Cognitive performance by CANTAB: Statistically significant differences vs. placebo, mean (SE) [95% CI]; P-value: 0.5 mg Δ9-THC vs placebo: RTI median 5-choice movement time at 15 minutes: −28.343 (12.765) [-53.649; −3.037]; P = 0.0285 Rapid visual information processing at 15 minutes: 0.014 (0.007) [0.000; 0.028]; P = 0.0493 | — |
1.0 mg Δ9-THC vs placebo: Spatial working memory strategy at 15 minutes: 0.515 (0.654) [-0.782; 1.812]; P = 0.0131 | — |
Vulfsons et al. (2020)12 | |
Cannabis consumption, median (range) (N = 21): Length of hospital stay (days): 4 (3 to 14) Number of prescribed inhalations per day: 4 (3 to 4) Number of rescue inhalations allowed per day: 3 (2 to 4) Number of actual inhalations per day: 3 (1 to 6) Cannabis dose per day (mg): 51 (20 to 96) Δ9-THC dose per day (mcg): 1500 (1000 to 3000) Number of inhalations during the study: 14 (15 to 25) Pain intensity by VAS, median (range) (N = NR) Pre-inhalation VAS: 7 (2 to 9) Post-inhalation VAS at 30 to 60 minutes: 4 (1 to 5) Wilcoxon signed rank test; Z = −3.059 (No within-subject differences were found with repeated use; Friedman test not significant) Nausea intensity by VAS, median (range) (N = 7) Pre-inhalation VAS: 3 (2 to 4) Post-inhalation VAS at 30 to 60 minutes: 2 (1 to 3) Wilcoxon signed rank-test; Z = −2.197 Spasticity intensity by VAS, median (range) (N = 4) Pre-inhalation VAS: 8 (7 to 9) Post-inhalation VAS at 30 to 60 minutes: 7 (6 to 8) No statistical test was performed due to the small sample Patient satisfaction using the inhaler based on scale of 1 = absolutely do not agree to 7 = absolutely agree), median (range): 6 (5 to 7) Patient satisfaction (% of patients who strongly agree/agree/ somewhat agree with following statements) (N = 10): Easy to use: 74/26/0 Easy to inhale: 78/11/11 The indication to end inhaling is clear: 89/11/0 Overall satisfaction with the inhaler: 47/47/5 Medical staff satisfaction (N = 6) It was stated that all agreed with above statements regarding their satisfaction with the device, ease of training, and use by patients | “Cannabis inhalation by combustion is not feasible for hospitalized patients. The use of the Syqe inhaler during hospitalization yielded high levels of patients and staff satisfaction with no complications (p. 12).”12 |
Safety No severe AEs were reported 3 patients experienced a mild cough immediately following inhalation that resolved spontaneously within a minute | — |
AE = adverse event; ANCOVA = analysis of covariance; BP = blood pressure; CANTAB = Cambridge Neuropsychological Test Automated Battery; CI = confidence interval; CRPS = complex regional pain syndrome; NR = not reported; RTI = reaction time test; SAE = serious adverse event; SD = standard deviation; SE = standard error; Δ9- THC = delta-9 tetrahydrocannabinol; VAS = visual analogue scale; WDAE = withdrawal due to adverse event
aP-value by repeated measures ANOVA
bNo point estimate was reported in the study
cEach patient could report more than one AE
Appendix 5: References of Potential Interest
Previous CADTH Reports
Freidge C, Ryce A. Disposable handheld vaporization devices for inhalation of medical cannabis: clinical effectiveness and cost-effectiveness (CADTH rapid response report: reference list). Ottawa (ON): CADTH; 2020 Mar: https://www.cadth.ca/sites/default/files/pdf/htis/2020/RA1095%20Vape%20Devs%20for%20Cannabis%20Final.pdf. Accessed 2022 Mar 15.
Medical cannabis - research gaps. Ottawa (ON): CADTH; 2020 Apr: https://www.cadth.ca/sites/default/files/pdf/research_gaps_medical_cannabis.pdf. Accessed 2022 Mar 12.
Non-Randomized Studies – MDI for Medical Cannabis in Healthy Volunteers
Ben-Ishay O, Bar-On O, Kluger Y. Smokeless consumption of medical cannabis pharmacokinetics, safety and feasibility of the CannaHALER© a phase 1a study. J Cannabis Res. 2020;2(1):15. PubMed
Meyer P, Langos M, Brenneisen R. Human pharmacokinetics and adverse effects of pulmonary and intravenous THC-CBD formulations. Med Cannabis Cannabinoids. 2018;1(1):36-43. PubMed
Non-Randomized Studies – Published Before 2017
Eisenberg E, Ogintz M, Almog S. The pharmacokinetics, efficacy, safety, and ease of use of a novel portable metered-dose cannabis inhaler in patients with chronic neuropathic pain: a phase 1a study. J Pain Palliat Care Pharmacother. 2014;28(3):216-225. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.