CADTH Health Technology Review
Vitamin B12 Testing in People With Suspected Vitamin B12 Deficiency
Rapid Review
Authors: Candyce Hamel, Carolyn Spry
Abbreviations
AUC
area under the curve
Hcy
homocysteine
HHcy
hyperhomocysteinemia
holoTC
holotranscobalamin
HTA
health technology assessment
MMA
methylmalonic acid
Key Messages
Findings from 3 diagnostic accuracy studies indicate that individual tests are insufficient to diagnose vitamin B12 deficiency, and a testing strategy that uses homocysteine and methylmalonic acid should be used in individuals suspected or at risk of vitamin B12 deficiency. This is supported by a health technology assessment that concluded that the current evidence does not provide enough information to determine the most appropriate test, or combination of tests to use in these patients.
The patient populations varied in the primary studies included in the systematic reviews and in the primary studies identified in this review, which may impact the generalizability of the results.
Reference standards and cut-off values (i.e., thresholds) used to diagnose vitamin B12 deficiency varied in the primary studies. Presentation of units (e.g., pg/mL, pmol/L) also varied, making it difficult to compare results across studies.
No studies were identified that evaluated the clinical utility of vitamin B12 testing in people with suspected vitamin B12 deficiency.
No studies were identified that evaluated the cost-effectiveness of vitamin B12 testing in people with suspected vitamin B12 deficiency.
No evidence-based guidelines were identified regarding the use of vitamin B12 testing in people with suspected vitamin B12 deficiency.
Context and Policy Issues
Vitamin B12, also called cobalamin, is a water-soluble B vitamin found in foods derived from animal products and from fortified cereals.1,2 The prevalence of vitamin B12 deficiency in the general population differs between older and younger people (e.g., in the UK 6% of those < 60 and 20% of those ≥ 60), and is also dependent on geographical location (e.g., 6% in the US, 40% in Latin American countries, 70% in East India).2 Most cases of vitamin B12 deficiency (in resource-rich settings) are due to malabsorption. This may be caused by pernicious anemia, an autoimmune condition in which antibodies to intrinsic factor are produced, which results in the inability for vitamin B12 to be absorbed. Other reasons for malabsorption may be from underlying diseases, such as Crohn disease and celiac disease, interaction with medication (e.g., proton pump inhibitor, metformin), and in those exposed to nitrous oxide (i.e., used for anesthesia or recreationally).1-3 Vitamin B12 deficiency may also be caused by diet (e.g., vegan diet, breastfed neonates born to individuals who are B12 deficient).1,4
As vitamin B12 is stored in body tissue (mainly the liver) subclinical deficiency develops over the course of several years (e.g., 5 to 10 years).1 Manifestations of vitamin B12 deficiency may be mild, such as fatigue and palpitations, but may progress to neurologic manifestations, such as peripheral neuropathy and dementia-like disease.3
There is currently no agreed-upon reference standard for measuring B12, and all are susceptible to confounding factors. A lack of agreement around cut-off levels (i.e., thresholds) to diagnose deficiency adds another layer of difficulty in diagnosing deficiency, as these thresholds may differ between guidelines, intuitions, and laboratories.
The 4 commonly used tests for vitamin B12 deficiency are briefly described in the following:
Serum vitamin B12 is typically the standard initial diagnostic test.1 It includes the total level of B12 in the blood, made up of active B12 (i.e., holotranscobalamin [holoTC]), which is available to be used by the body, and inactive B12 (i.e., holohaptocorrin), which cannot be used by the body.4 Deficiency typically presents in the serum once there is severe clinical deficiency.3 There is no agreed-upon total serum B12 level to diagnose deficiency, although lower than 148 pmol/L (200 ng/L) is often used.1,4
HoloTC measures the level of active (i.e., biologically available) B12 in the blood,1 and represents approximately 20% of the B12 measured in blood serum.5 The values for holoTC in healthy individuals are 35 pmol/L to 171 pmol/L, although lower and upper reference intervals vary greatly.4
Homocysteine (Hcy) levels may accumulate in the blood early in the course of vitamin B12 deficiency;4 however, elevated levels of Hcy might also be found in people with folate deficiency and those with some diseases (e.g., renal failure).1,4 There is no consensus on the reference range, although most laboratories use higher than 15 µmol/L as the level to define hyperhomocysteinemia (HHcy).4
Methylmalonic acid (MMA) can be measured in the blood or urine and raises with vitamin B12 deficiency.1 Although MMA may be falsely elevated in people with renal disease1 and small bowel bacterial overgrowth, high levels of MMA (e.g., > 0.75 µmol/L) are a strong marker of vitamin B12 deficiency.4 MMA is a high-cost test, which limits its widespread use.4
Current treatment for vitamin B12 deficiency includes supplements, which can be administered orally, sublingually, and parenterally (e.g., intramuscular injection). Route of administration may differ depending on the cause of deficiency. There are few safety concerns around vitamin B12 supplementation, as when stores of vitamin B12 are adequate, excess vitamin B12 is excreted.6
Routine evaluation for vitamin B12 deficiency in the general population was reviewed in a 2015 CADTH report.7 However, testing in populations suspected to be vitamin B12 deficient (e.g., people with the presence of unexplained neurologic abnormalities, people with vegan diets, neonates born to individuals who are vitamin B12 deficient, people taking metformin) may differ.
The objective of this report is to summarize the evidence regarding the diagnostic test accuracy, the clinical utility, the cost-effectiveness, and the recommendations from evidence-based guidelines of vitamin B12 testing in people with suspected vitamin B12 deficiency.
Research Questions
What is the diagnostic accuracy of vitamin B12 testing for the diagnosis of vitamin B12 deficiency in people with suspected vitamin B12 deficiency?
What is the clinical utility of vitamin B12 testing in people with suspected vitamin B12 deficiency?
What is the cost-effectiveness of vitamin B12 testing in people with suspected vitamin B12 deficiency?
What are the evidence-based guidelines regarding the use of vitamin B12 testing in people with suspected vitamin B12 deficiency?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international health technology assessment (HTA) database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Vitamin B12 deficiency and testing. A second search was conducted by applying the diagnostic test accuracy filter to the Vitamin B12 deficiency concept. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2012, and January 28, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People of all ages with suspected vitamin B12 deficiency (e.g., presence of unexplained hematologic or neurologic abnormalities [e.g., anemia, macrocytosis, peripheral neuropathy, dementia], or due to variables such as age, diet, family and medical history, or lifestyle) |
Intervention | Vitamin B12 testing using complete blood count, blood film, serum tests, or holotranscobalamin testing |
Comparator | Q1: No comparator Q2 to Q3: No testing for vitamin B12 deficiency Q4: Not applicable |
Reference standard | Q1: Any reference standard Q2 to Q4: Not applicable |
Outcomes | Q1: Diagnostic accuracy (e.g., sensitivity, specificity, positive predictive value, negative predictive value) Q2: Clinical utility (e.g., time to treatment, severity of symptoms [e.g., fatigue, mouth pain, numbness, weakness], quality of life, adverse events [e.g., irreversible neuropathy]) Q3: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q4: Recommendations regarding best practices (e.g., appropriate patient populations, recommended testing strategies) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications, or if they were published before 2012. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodologies were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)8 for systematic reviews and the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist9 for diagnostic test accuracy studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
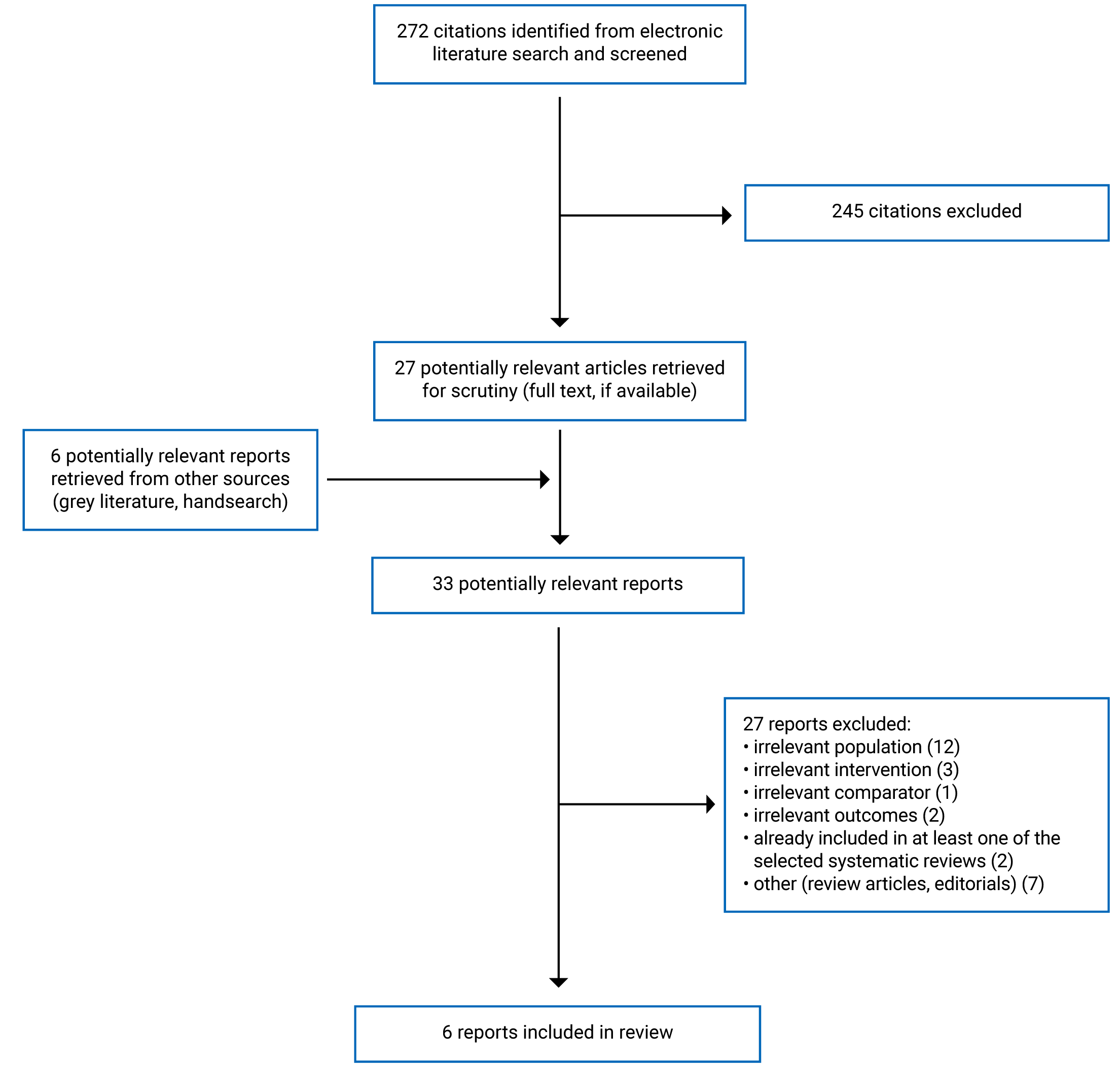
A total of 272 citations were identified in the literature search. Following screening of titles and abstracts, 245 citations were excluded and 27 potentially relevant reports from the electronic search were retrieved for full-text review. Six potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 27 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 1 HTA and 5 diagnostic test accuracy studies. Appendix 1 presents the PRISMA10 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
One HTA11 and 5 diagnostic test accuracy studies12-16 were identified for inclusion in this review. No relevant systematic reviews, randomized controlled trials, economic evaluation studies, or evidence-based guidelines were identified.
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
One health technology report11 included 4 systematic reviews to answer 4 research questions. Two of these research questions were relevant to the present review, and the systematic reviews to answer these research questions had broader inclusion criteria than the present review. Specifically, some of the included studies for the diagnostic test accuracy research question (research question 2), included primary studies that were not specific to people suspected of vitamin B12 deficiency. For example, 48% (26 out of 54) of the included studies in 1 systematic review had patients with no defined indications. Only the characteristics and results of the subset of relevant studies will be described in this report. Within the HTA report,11 1 systematic review did not identify any included studies and the other systematic reviews included 4 primary studies that were relevant to the current report and published between 2011 to 2015.
Five diagnostic test accuracy studies12-16 evaluated suspected vitamin B12 deficiency from participants diagnosed with existing conditions from various clinics, and included both outpatients and inpatients. One diagnostic test accuracy study, by Warendorf et al. (2021),12 used a respective cohort study design, a single-gate approach for patient selection, and a single set of eligibility criteria. Data were retrieved from first-referral outpatient records among those who had been diagnosed with polyneuropathy between January 1, 2013, and January 1, 2018, and whose records had laboratory test results for vitamin B12, MMA, and Hcy. Four diagnostic test accuracy studies used a cross-sectional design, a single-gate approach for patient selection, and a single set of eligibility criteria. Ao et al. (2017)13 included patients with Crohn disease attending the gastroenterology clinic at a university hospital. No date were provided for patient recruitment. Vashi et al. (2016)14 included a consecutive series of patients with cancer first seen at the Cancer Treatment Centers of America at the Midwestern Regional Medical Center between April 2014 and June 2014. Beletić et al. (2015) included patients with chronic obstructive pulmonary disease at the Clinic for Lung Disease and the Center for Medical Biochemistry of the Clinical Center of Serbia. Among the 50 patients included, 15 were attending the outpatient department of the clinic and 35 were hospitalized and enrolled upon remission. No date was provided for patient recruitment.15 Finally, Cinemre et al. (2015) included patients in the hematology department with a diagnosis of myeloproliferative disease. No date was provided for patient recruitment.16
Country of Origin
The HTA was conducted by the Swiss Federation and, as such, the applicability of the findings have been discussed within the Swiss context.11
The diagnostic test accuracy studies were conducted in, and enrolled patients from, Japan,13 the Netherlands,12 Serbia,15 Turkey,16 and the US.14
Patient Population
The HTA report11 included 2 systematic reviews relevant to this review that included patients with a clinical suspicion of vitamin B12 deficiency (e.g., those with macrocytosis, dementia, paresthesia, polyneuropathy, glossitis, malnutrition) and patients in high-risk populations (e.g., those who are post-bariatric surgery or gastric resection, vegans, vegetarians, age ≥ 65 years). In the other systematic review, among the 4 studies that are relevant to this review, the number of participants ranged from 77 to 1,279. The age of the participants was reported in 3 of these 4 studies, with mean ages of 55.09, 59, and 81. The setting in which the patients were identified from was not well reported, but included a natural medicine-oriented doctor’s office.
The diagnostic test accuracy study by Warendorf et al. (2021) included 311 first-referral outpatients diagnosed with polyneuropathy (mean age of 63.0 years).12 The study by Ao et al. (2017) included 48 outpatients of a gastroenterology clinic who had Crohn disease (mean age of 40.1 years).13 Vashi et al. (2016) included 316 patients with cancer from a Cancer Treatment Centres of America who were older than 18 (mean age of 52.5 years).14 Beletić et al. (2015) included 50 people from a clinic for lung diseases and a centre for medical biochemistry who had chronic obstructive pulmonary disease, diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (mean age of 49.0 years).15 Finally, Cinemre et al. (2015) included 58 patients followed in a hematology department who had myeloproliferative disorders (mean age of 61 years).16
Interventions and Comparators
The 2 systematic reviews in the HTA11 that are relevant to this review compared diagnostic serum testing (i.e., B12, holoTC, MMA) to no testing for the review on clinical effectiveness, and any diagnostic serum screening or test (i.e., total serum B12, holoTC, MMA) as the index test compared to any of these as the reference test. The 4 relevant primary studies extracted from this review evaluated the diagnostic accuracy of vitamin B12 with holoTC as the reference test, vitamin B12 with MMA as the reference test, and MMA with holoTC as the reference test.
The diagnostic test accuracy studies evaluated several index and reference tests. Warendorf et al. (2021) evaluated total vitamin B12 using 3 different reference tests (MMA, Hcy, and Hcy and/or MMA).12 Ao et al. (2017) evaluated serum concentrations of vitamin B12 with plasma concentration of Hcy as the reference test.13 Vashi et al. (2016) evaluated vitamin B12 with the Fedosov wellness quotient as the reference test. (The Fedosov wellness quotient uses a combined vitamin B12, MMA, and Hcy approach.)14 Beletić et al. (2015) used 3 different thresholds of Hcy as the index test and 2 different vitamin B12 thresholds as the reference tests.15 Cinemre et al. (2015) evaluated serum vitamin B12, holoTC, and total plasma as the index tests against serum MMA as the reference test.16 As the studies were a retrospective cohort and 4 cross-sectional designs, there were no follow-up periods.
In all of the diagnostic test accuracy studies, all participants received the same index and reference tests. For most studies, it was not clearly stated if there was an interval between tests; however, as they were cross-sectional, it is likely that testing occurred at the same time.13-16 As Warendorf et al. (2021) was a retrospective cohort study that used patient record, it was stated that the tests were done within 60 days of each other.12 In 4 of the diagnostic test accuracy studies,12,13,15,16 it was unclear if the results of the index tests were read without the knowledge of the results of the reference tests. Vashi et al. (2016) stated that the results of all tests were determined simultaneously in each patient.14
Outcomes
In the HTA report,11 the systematic review on clinical effectiveness aimed to report on safety (e.g., adverse events from testing), treatment (e.g., oral supplements), and effectiveness (e.g., improvement of symptoms) outcomes. The systematic review on the diagnostic accuracy of vitamin B12 testing reported on several statistical measures of diagnostic test accuracy, including sensitivity, specificity, and positive and negative predictive values.
The diagnostic test accuracy studies calculated various parameters of diagnostic performance. All 5 studies reported the area under the curve (AUC).12-16 Warendorf et al. (2021)12 also reported the threshold vitamin B12 levels to obtain 90% and 95% sensitivity. Vashi et al. (2016)14 reported the sensitivity and specificity. Cinemre et al. (2015)16 also reported the sensitivity, specificity, likelihood ratio positive, likelihood ratio negative, positive predictive value, and negative predictive value.
Summary of Critical Appraisal
Evidence Reviews
The systematic reviews in the HTA report11 were well-conducted and reported. The review methods were defined before the conduct of the reviews and a protocol was written and peer-reviewed by independent anonymous reviewers. The Participants, Intervention, Comparator, Outcomes (PICO) criteria were clearly defined for each of the systematic reviews that were undertaken. Several electronic databases were searched, reducing the risk of study selection bias, and the searches were provided, allowing for reproducibility. Identification of the included studies and risk of bias were performed by 2 independent reviews. The 1 minor limitation was around data extraction, which was performed by 1 reviewer and verified by a second reviewer.
Diagnostic Test Accuracy Studies
There were several common strengths in the 5 diagnostic test accuracy studies:12-16 the objectives, index tests, reference tests, and main outcomes were clearly described; all patients received the same index and reference tests; the thresholds used for the screening test were prespecified and supported by literature or by the manufacturers’ instructions; most studies included all participants in the analysis and among those that did not, the reasons for exclusion were provided and were clinically relevant; all studies avoided a case-control study design; and all studies disclosed the source of funding. One study described the method of patient selection.14 One study reported that the results of the screening tests were read without knowledge of the other tests.14 Four studies disclosed that their authors had no conflicts of interest.12-15 Although all studies included patients who were suspected of vitamin B12 deficiency, due to their underlying health conditions (e.g., cancer, myeloproliferative disease, Crohn disease, chronic obstructive pulmonary disease), the results from the individuals studies may not be generalizable to all patients who are suspected of vitamin B12 deficiency.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions. The data from the 4 relevant studies included in the systematic review of the HTA11 are reported in the Diagnostic Parameters section. Fourteen different index and reference tests were evaluated.
Diagnostic Accuracy of Vitamin B12 Testing
Area Under the Curve
Vitamin B12 Versus Homocysteine
Two diagnostic test accuracy studies reported the AUC for different thresholds of vitamin B12 with Hcy (> 14 µmol/L) as the reference test. Warendorf et al. (2021)12 reported an AUC of 0.61. Ao et al. (2017)13 reported an AUC of 0.73, which was statistically significant (95% confidence interval, 0.606 to 0.900), with the adequate cut-off value of 503 pg/mL for vitamin B12.
Vitamin B12 Versus Methylmalonic Acid
One diagnostic test accuracy study, by Warendorf et al. (2021),12 reported the AUC for vitamin B12 with MMA (> 0.29 µmol/L) as the reference test. This was the highest AUC (0.72) in the study, which also evaluated Hcy and MMA and/or Hcy as the reference tests.
Vitamin B12 Versus Methylmalonic Acid and/or Homocysteine
One diagnostic test accuracy study, by Warendorf et al. (2021),12 reported an AUC of 0.65 for vitamin B12 with MMA (> 0.29 µmol/L) and/or Hcy (> 14 µmol/L) as the reference test.
Vitamin B12, Homocysteine, Methylmalonic Acid Versus Fedosov Wellness Quotient (Combined Vitamin B12, Methylmalonic Acid, Homocysteine)
One diagnostic test accuracy study, by Vashi et al. (2016),14 reported the AUC for 3 index tests: vitamin B12 (< 300 pM/mL), Hcy (> 12 µmol/L), and MMA (> 260 nmol/L) with the combined vitamin B12, MMA, and Hcy as the reference test. MMA performed best with an AUC of 0.98. AUC for vitamin B12 and Hcy were similar, at 0.83 and 0.85, respectively.
Homocysteine Versus Vitamin B12
One diagnostic test accuracy study, by Beletić et al. (2015),15 reported the AUC for Hcy at 3 different thresholds (10 µmol/L, 12 µmol/L, and 15 µmol/L) with vitamin B12 at thresholds (203 ng/L and 473 ng/L) as the reference test. AUCs ranged from 0.504 to 0.842, with a Hcy of 15 µmol/L and a vitamin B12 of 203 ng/L having the highest AUC (0.842). However, none of the values were considered statistically significant of Hcy as a predictor of vitamin B12 deficiency.
Holotranscobalamin, Homocysteine Versus Methylmalonic Acid
One diagnostic test accuracy study, by Cinemre et al. (2015),16 reported the AUC for 2 index tests, holoTC (< 35 pmol/L) and Hcy (> 13 mol/L), with an age-adjusted MMA as the reference test. Both holoTC (AUC = 0.822; 95% confidence interval, 0.70 to 0.91; P ≤ 0.001) and Hcy (AUC = 0.662; 95% confidence interval, 0.53 to 0.78; P = 0.03) were found to be statistically significant.
Diagnostic Parameters
Vitamin B12 Versus Holotranscobalamin
Three diagnostic test accuracy studies reported the sensitivity and specificity for vitamin B12 with holoTC as the reference test. Schwarz et al. (2015), a primary study included in the HTA,11 evaluated the diagnostic accuracy of vitamin B12 using 2 different methods, chemiluminescent immunoassay (threshold of < 156 pmol/L) and microbiological tests with microtitre (threshold of < 212 pmol/L), with holoTC at 2 thresholds as the reference test. A holoTC threshold of less than 50 pmol/L was considered subclinical or possibly deficiency, and less than 35 pmol/L was considered probably deficient. Among these, the vitamin B12 microbiological tests with microtitre and holoTC (< 35 pmol/L) had the highest sensitivity at 71% (specificity = 95%). Sensitivity for other test comparisons ranged from 38% to 53% and specificity ranged from 90% to 96%.
Heil et al. (2012), included in the HTA,11 reported a sensitivity of 64% and a specificity of 88% for vitamin B12 (< 146 pmol/L) with holoTC (< 21 pmol/L). Schrempf et al. (2011) reported a lower sensitivity (56.3%), but at higher thresholds for both vitamin B12 (< 206 pmol/L) and holoTC (< 42 pmol/L).
Vitamin B12 Versus Homocysteine
Warendorf et al. (2021)12 reported that the best trade-off was at a vitamin B12 threshold of 257 pmol/L and a Hcy of greater than 14 µmol/L (sensitivity = 79%; specificity = 44%). At the higher vitamin B12 threshold of 374 pmol/L, sensitivity increased to 97%, but the specificity lowered to 10%.
Vitamin B12 Versus Methylmalonic Acid
Three diagnostic test accuracy studies evaluated different thresholds of vitamin B12 with MMA as the reference test. Heil et al. (2012), included in the HTA,11 reported a sensitivity of 53% and a specificity of 81% for vitamin B12 (< 146 pmol/L) with MMA (> 0.45 µmol/L) as the reference test. Both Schrempf et al. (2011) and Warendorf et al. (2021)12 reported higher sensitivity, but lower specificity than Heil et al. (Schrempf: sensitivity = 66.2%, specificity = 62.1%; Warendorf: sensitivity = 69%, specificity = 66%) using a higher vitamin B12 (Schrempf: < 206 pmol/L; Warendorf: < 213 pmol/L) and a lower MMA (Schrempf: > 0.298 µmol/L; Warendorf: > 0.29 µmol/L) threshold.
Vitamin B12 Versus Methylmalonic Acid and/or Homocysteine
Warendorf et al. (2021)12 evaluated vitamin B12 with the reference test of MMA (> 29 µmol/L) and/or Hcy (> 14 µmol/L). Results were similar between the reference test and using only Hcy (> 14 µmol/L).
Vitamin B12, Homocysteine, Methylmalonic Acid Versus Fedosov Wellness Quotient (Combined Vitamin B12, Methylmalonic Acid, Homocysteine)
One diagnostic test accuracy study, by Vashi et al. (2016),14 evaluated 3 index tests, vitamin B12, Hcy, and MMA, with a combined reference test that included vitamin B12, MMA, and Hcy. MMA (> 413.5 nmol/L) had the highest sensitivity and specificity, at 86% and 99%, respectively. Vitamin B12 (< 385 pg/mL) (86% and 80%, respectively) and Hcy (> 15.5 µmol/L) (71% and 95%, respectively) were less sensitive and specific.
Holotranscobalamin, Homocysteine Versus Methylmalonic Acid
One diagnostic test accuracy study, by Cinemre et al. (2015),16 reported that holoTC (≤ 40.6 pmol/L) had a greater sensitivity, specificity, positive likelihood ratio, positive predictive value, and negative predictive value than Hcy (> 14 mol/L), with age-adjusted MMA values as the reference test. HoloTC had a sensitivity of 75% and a specificity of 78%.
Methylmalonic Acid Versus Holotranscobalamin
Schwarz et al. (2015), a primary study in the HTA,11 evaluated the diagnostic accuracy of MMA (> 0.30 µmol/L) with holoTC at 2 thresholds as the reference test. A threshold of less than 50 pmol/L was considered subclinical or possibly deficiency, and less than 35 pmol/L was considered probably deficient. MMA was not sensitive at either holoTC threshold (41% and 40%).
Vitamin B12, Holotranscobalamin, Methylmalonic Acid Versus Red Cell Cobalamin
Valente et al. (2011), a primary study in the HTA report,11 evaluated the diagnostic accuracy of 3 different index tests, vitamin B12, holoTC, and MMA with red cell cobalamin (< 33 pmol/L) as the reference test. MMA (> 0.36 µmol/L) had the highest sensitivity, but the lowest specificity, at 81% and 63%, respectively.
Clinical Utility of Vitamin B12 Testing
No relevant evidence regarding the comparative clinical utility of vitamin B12 testing was identified; therefore, no summary can be provided.
Cost-effectiveness of Vitamin B12 Testing
No relevant evidence regarding the cost-effectiveness of vitamin B12 testing was identified; therefore, no summary can be provided.
Guidelines
No relevant evidence-based guidelines on vitamin B12 testing were identified; therefore, no summary can be provided.
Limitations
There were some limitations to the studies that would prevent a definitive conclusion on the diagnostic accuracy, clinical utility, and cost-effectiveness of vitamin B12 testing in those suspected of having vitamin B12 deficiency.
The systematic reviews conducted in the HTA included broader populations than were relevant for this review, particularly around the populations included in the primary studies. The HTA11 included studies that were conducted in WHO mortality stratum A countries, which may have omitted relevant studies. A common theme in the primary studies included in the systematic review was a lack of clear reporting around the clinical characteristics of the populations, which makes it difficult to determine if they are “suspected” of vitamin B12 deficiency. The primary studies that were identified as being relevant to this review had several different index and reference tests, and used different thresholds to define vitamin B12 deficiency.
Similar to the primary studies identified in the HTA, the diagnostic test accuracy studies12-16 used different index and reference tests, as well as different thresholds to define vitamin B12 deficiency. As this review included people with suspected vitamin B12 deficiency, the primary studies included people with underlying health conditions (e.g., cancer, myeloproliferative disorders, Crohn disease). These diseases may impact the health of these individuals differently; therefore, results in the studies may not be generalizable to all people suspected of vitamin B12 deficiency. Additionally, 3 of the 5 primary studies13,15,16 included fewer than 60 participants, which may not be considered a sufficient sample size.17 Several subpopulations were not identified in the included studies (for example, pregnant individuals suspected of vitamin B12 deficiency, babies born to individuals who are vitamin B12 deficient, and people with a vegan diet suspected of vitamin B12 deficiency).
No studies on the clinical utility or cost-effectiveness of vitamin B12 testing were identified. It is unclear which test(s) (e.g., serum vitamin B12, holoTC, Hcy, MMA) may result in improved clinical outcomes for patients who are suspected of having vitamin B12 deficiency and which, if any, would be cost-effective.
No evidence-based guidelines were included. One potential guideline was identified, but was excluded due to a lack of description of the methods to identify the included studies. This guideline has been listed in Appendix 5.
None of the included primary studies were conducted in Canada, and the HTA11 was not conducted or intended for professionals in Canada. Therefore, the generalizability of the findings from the included literature to the Canadian setting are unclear.
Conclusions and Implications for Decision- or Policy-Making
This review comprised 1 HTA,11 which included 4 relevant diagnostic test accuracy studies, and 5 diagnostic test accuracy studies.12-16 No relevant evidence was identified regarding the clinical utility or cost-effectiveness of vitamin B12 testing in people with suspected vitamin B12 deficiency, and no evidence-based guidelines regarding the use of vitamin B12 testing in people with suspected vitamin B12 deficiency were identified.
The results from this review are similar to the recently published HTA by the Swiss Federation.11 Although covering a similar publication period, the Swiss HTA only included studies from countries listed under the WHO mortality stratum A. This would have excluded 2 of the studies included in this review, which were conducted in Serbia15 and Turkey.16 Warendorf et al. (2021)12 would not have been captured by the search (November 4, 2020). As a list of excluded studies and the reason for exclusion was not provided, it is unclear why Ao et al. (2017)13 and Vashi et al. (2016)14 were not included in their review.
Evidence from 3 of the 5 diagnostic test accuracy studies12,14,15 identified by our search (i.e., not those in the HTA systematic review) reported that a single test is insufficient to diagnose vitamin B12 deficiency. Two of these studies12,14 concluded that Hcy and MMA should be used in this population in addition to serum B12. This was supported by the included HTA,11 published in 2021, which concluded that regardless of the results of the first-line test (i.e., total vitamin B12 or holoTC), these results needed to be supported with second-line testing to have sensitive and specific test results. The other 2 diagnostic test accuracy studies did not report on vitamin B12 as an index test, so could not contribute to this conclusion.13,16 Some studies did report statistically significant results. For example, 1 study, with 58 patients with myeloproliferative disorders, reported that holoTC was more sensitive and specific, had a greater positive likelihood ratio, and greater positive and negative predictive values than Hcy to diagnose vitamin B12 deficiency. However, caution must be taken when considering this result, as this was among a small group of patients with a rare disease, which may limit generalizability.16
Fourteen different index test and reference test comparisons were reported in the studies in this report. Vitamin B12, holoTC, Hcy, and MMA were all evaluated as both index and reference tests. Other reference tests included MMA and/or Hcy, the Fedosov wellness quotient (combined vitamin B12, Hcy, and MMA), and red cell cobalamin.
Vitamin B12 versus HoloTC: Three diagnostic test accuracy studies, all included in the systematic review in the HTA,11 reported sensitivities ranging from 38% to 71%, and specificities ranging from 50.5% to 96%, all using different thresholds for both vitamin B12 and holoTC.
Vitamin B12 versus Hcy: One study, in patients with Crohn disease, reported that serum vitamin B12 is a determinant for hyperhomocysteinemia, at a serum vitamin B12 threshold of 503 pg/mL.13 At a similar vitamin B12 threshold (374 pmol/L), 1 study in patients with polyneuropathy reported high sensitivity (97%), but low specificity (10%).12
Vitamin B12 versus MMA: Three diagnostic test accuracy studies, 2 of which were included in the systematic review in the HTA, varied in sensitivity and specificity, and the thresholds used.11,12 Two of these studies used similar thresholds for both tests and reported similar sensitivities (66.2% and 69%) and specificities (62.1% and 66%).
Vitamin B12 versus MMA and/or Hcy: One study used MMA and/or Hcy as the reference test and found similar results for AUC, sensitivity, and specificity as when Hcy was used as the reference test alone.12
Vitamin B12, Hcy, MMA versus Fedosov wellness quotient (combined vitamin B12, MMA, Hcy): One study, in patients with cancer, reported that MMA had the highest AUC (0.98) with the combined reference test compared to the index tests of vitamin B12 and Hcy.14
Hcy versus vitamin B12: Hcy evaluated at 3 thresholds, in patients with chronic obstructive pulmonary disease, was not found to be a good predictor of vitamin B12 deficiency with vitamin B12 as the reference test.15
HoloTC, Hcy versus MMA: One study, in patients with myeloproliferative disorders, reported that holoTC and Hcy were both statistically significant when compared to age-adjusted MMA, and that holoTC had greater sensitivity and specificity than Hcy.16
MMA versus HoloTC: One study, included in the systematic review in the HTA,11 reported that MMA was not sensitive at either of 2 different holoTC thresholds.
Vitamin B12, HoloTC, MMA versus red cell cobalamin: One study, included in the systematic review in the HTA,11 evaluated 3 different index tests with red cell cobalamin as the reference standard. MMA had the highest sensitivity among the 3 index tests, but the lowest specificity.
The limitations of the included literature should be considered when interpreting the findings of this report. The systematic review in the HTA11 was well-conducted and well reported, but the primary studies included were rated as having very low or low certainty of evidence, which impacts the confidence in the reported effect estimates. All included primary studies had clear objectives, well described tests and thresholds to define vitamin B12 deficiency, avoided a case-control design, and reported the source of funding, but they also had limitations that impact our confidence in the results. Four12,13,15,16 of 5 studies did not report on the method of patient selection, or whether the results of the index test were read without knowledge of the results of the reference standard. These limitations may result in bias in the selection of patients and in determining the results of the tests.
As levels of subclinical and clinical vitamin B12 deficiency varies in different countries, further research investigating the diagnostic accuracy of serum vitamin B12, holoTC, Hcy, and MMA in the Canadian setting would provide additional information on what tests should be used in this population. Additional studies in other people at risk should also be conducted (e.g., people with vegan diets). Clinical utility research is needed to evaluate the benefits and harms of testing in patients suspected of vitamin B12 deficiency. Cost-effectiveness studies in the Canadian health care context should also be undertaken, as the Canadian health care system and the disperse geographical landscape could contribute to the cost-effectiveness. The Hcy plasma sample must be kept cool and then centrifuged and removed from the red cells within 2 hours of collection, and MMA uses gas chromatography–mass spectrometry, which currently has a high cost;4 it is unknown if these factors would influence the cost-effectiveness of including Hcy and MMA in this population.
References
1.Means RT Jr, Fairfield KM. Clinical manifestations and diagnosis of vitamin B12 and folate deficiency. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: https://www.uptodate.com. Accessed 2022 Feb 8.
2.Langan RC, Goodbred AJ. Vitamin B12 deficiency: recognition and management. Am Fam Physician. 2017;96(6):384-389. PubMed
3.Vitamin B12 and health: vitamin B12 deficiency test. https://www.b12-vitamin.com/deficiency-test/. Accessed 2022 Feb 8.
4.Devalia V, Hamilton MS, Molloy AM, British Committee for Standards in Haematology. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol. 2014;166(4):496-513. PubMed
5.Thorpe S, Rigsby P, Roberts G, Lee A, Hamilton M, Craig D. An International Standard for holotranscobalamin (holoTC): international collaborative study to assign a holoTC value to the International Standard for vitamin B12 and serum folate. Clin Chem Lab Med. 2016;54(9):1467-1472. PubMed
6.Means RT Jr, Fairfield KM. Treatment of vitamin B12 and folate deficiencies. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: https://www.uptodate.com. Accessed 2022 Feb 8.
7.Vitamin B12 testing in the general population: clinical and cost-effectiveness and guidelines. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/htis/jan-2015/RB0781%20Vitamin%20B12%20Testing%20Final.pdf. Accessed 2022 Mar 4.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-536. PubMed
10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
11.Anastasi L, Jacobsen JH, Nicolopoulos K, Rochet E, Foerster V, Vreugdenburg T. Effectiveness and safety of vitamin B12 tests. Bern (CH): Federal Office of Public Health 2021: https://www.bag.admin.ch/bag/en/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/hta/hta-projekte/vitaminb12tests.html. Accessed 2022 Feb 8.
12.Warendorf JK, van Doormaal PTC, Vrancken A, et al. Clinical relevance of testing for metabolic vitamin B12 deficiency in patients with polyneuropathy. Nutr Neurosci. 2021:1-11. PubMed
13.Ao M, Tsuji H, Shide K, et al. High prevalence of vitamin B-12 insufficiency in patients with Crohn's disease. Asia Pac J Clin Nutr. 2017;26(6):1076-1081. PubMed
14.Vashi P, Edwin P, Popiel B, Lammersfeld C, Gupta D. Methylmalonic acid and homocysteine as indicators of vitamin B-12 deficiency in cancer. PLoS ONE. 2016;11(1):e0147843. PubMed
15.Beletic A, Mirkovic D, Dudvarski-Ilic A, et al. Questionable reliability of homocysteine as the metabolic marker for folate and vitamin B12 deficiency in patients with chronic obstructive pulmonary disease. J Med Biochem. 2015;34(4):467-472. PubMed
16.Cinemre H, Serinkan Cinemre BF, Cekdemir D, Aydemir B, Tamer A, Yazar H. Diagnosis of vitamin B12 deficiency in patients with myeloproliferative disorders. J Investig Med. 2015;63(4):636-640. PubMed
17.Bujang MA, Adnan TH. Requirements for minimum sample size for sensitivity and specificity analysis. J Clin Diagn Res. 2016;10(10):YE01-YE06. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Health Technology Assessment
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Anastasi et al. (2021)11 Switzerland Funding: NR | RQ1 study design: Systematic reviews, randomized, prospective non-randomized trials) Number of primary studies: 0 studies were identified RQ2 study design: SRs of diagnostic accuracy studies, if no SRs, primary diagnostic test accuracy studies will be considered Number of primary studies: One SR (54 primary) studies, plus 6 additional primary studies Number of relevant primary studies: 4 primary studies (based on information provided) | Patients with a clinical suspicion of, or at high-risk for, vitamin B12 deficiency Relevant population: patients with a clinical suspicion of vitamin B12 deficiency | Q1 Interventions: Diagnostic serum testing (total serum B12, holoTC, MMA) Q1 Comparator: No testing Q2 Index tests: Any diagnostic screening/test of vitamin B12 (total serum B12, holoTC, MMA) Q2 Reference tests: Any diagnostic screening/test of vitamin B12 (total serum B12, holoTC, MMA) | RQ1 outcomes: Safety [adverse events from testing (blood draw) or treatment (oral, nasal or intramuscular)]; Effectiveness [Improvement of symptoms, signs, or quality of life within a defined period (e.g. anaemia, neurological symptoms) and acceptable serum vitamin B12 levels established, or prevention of deficiency development within a defined period] RQ2 outcomes: Diagnostic test accuracy (sensitivity, specificity, positive/negative predictive values, false positives, false negatives, invalid/uninterpretable results, positive predictive value, negative predictive, value confirmed by a valid reference test) |
holoTC = holotranscobalamin; MMA = methylmalonic acid; NR = not reported; NA = not applicable; RQ = Research Question; SR = systematic review.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Warendorf et al. (2021)12 The Netherlands Funding: No funding | Retrospective cohort study | Inclusion criteria: First-referral outpatients diagnosed with polyneuropathy Exclusion criteria: folate deficiency (<6.8 μmol/L), vitamin B6 deficiency (<110 nmol/L), self-reported vitamin B supplement use up to 1 year prior to laboratory investigations, elevated (>3SD above the mean) blood levels of vitamin B12, folate or vitamin B6 suggestive of vitamin supplement use, or decreased renal function as indicated by age-adjusted estimated glomerular filtration rate Setting: NR Number of participants: 311 Age (years), mean (SD): 63.0 (11.4) Male sex, n (%): 235 (71.0) | Index test: Total vitamin B12 measured in plasma with Beckman Coulter DXI immunoenzymatic assay. Reference tests: (1) MMA; (2) Hcy; (3) Hcy and/or MMA. MMA was measured in plasma by chromatography-tandem mass spectroscopy. Hcy was measured with Atellica immunoassay. | Outcomes: Diagnostic test accuracy (threshold vitamin B12 levels to obtain 90% and 95% sensitivity, determined the optimum trade-off between sensitivity and specificity for the different reference metabolites, AUC) Follow-up: NA |
Ao et al. (2017)13 Japan Funding: JSPS KAKENHI | Cross-sectional | Inclusion criteria: Outpatients with Crohn’s disease Exclusion criteria: NR Setting: Gastroenterology Clinic at Kyoto University Hospital Number of participants: 48 Age (years), mean (SD): 40.1 (9.0) Age (years), median: 39.5 Male sex, n (%): 33 (68.8) | Index test: Serum concentrations of vitamin B12 was measured by chemiluminescent enzyme immunoassay (CLEIA) Reference test: Plasma concentration of Hcy was measured by High-performance liquid chromatography (HPLC) | Outcomes: Diagnostic test accuracy (AUC) Follow-up: NA |
Vashi et al. (2016)14 USA Funding: No funding | Cross-sectional (consecutive case series) | Inclusion criteria: Cancer patients greater than 18 years of age Exclusion criteria: No exclusion criteria Setting: Cancer Treatment Centers of America (CTCA) at Midwestern Regional Medical Center Number of participants: 316 Age (years), mean: 52.5 Age (years), median (range): 54 (22 to 82) Male sex, n (%): 134 (42.4) | Index test: Vitamin B12 measured using the ARCHITECT B-12 assay, MMA measured using Liquid chromatography/tandem mass spectrometry (LC/MS-MS), Hcy measured using the Dimension Vista ® System Reference test: Fedosov quotient (combined vitamin B12, MMA, and Hcy) | Outcomes: Diagnostic test accuracy (AUC, Sensitivity, Specificity) Follow-up: NA |
Beletić et al. (2015)15 Serbia Funding: Ministry of Education, Science and Technological Development of the Republic of Serbia | Cross-sectional | Inclusion criteria: People with chronic obstructive pulmonary disease (COPD) diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease Exclusion criteria: Smoking, alcohol consumption and supplementation with folic acid and/or vitamin B12, as well as the presence of coronary heart disease, cerebrovascular and gastrointestinal disorders, renal insufficiency, diabetes, malignant or autoimmune disease Setting: Clinic for Lung Diseases and the Center for Medical Biochemistry Number of participants: 50 Age (years), mean (SD): 49.0 (14.5) Male sex, n (%): 28 (56) | Index test: Hcy thresholds of 10, 12 and 15 µmol/L Reference test: Vitamin B12 thresholds of 203 ng/L and 473 ng/L The chemiluminescent micropartical immunoassays on the ARCHITECT® ci8200 Integrated System (Abbott Diagnostics, Wiesbaden, Germany) was applied for measurement of homocysteine and vitamin B12 concentrations. | Outcomes: Diagnostic test accuracy (AUC) Follow-up: NA |
Cinemre et al. (2015)16 Turkey Funding: Scientific Research Project Support Fund of Sakarya University | Cross-sectional | Inclusion criteria: Patients with myeloproliferative disorders Exclusion criteria: Those with gastrointestinal disorders such as Crohn disease, prior gastric or ileal resection, concurrent metformin use, a purely vegetarian diet, or serum creatinine levels greater than 1.1 mg/dL for women and greater than 1.3 mg/dL for men Setting: Hematology department Number of participants: 58 Age (years), mean (SD): 61 (15) Male sex, n (%): 29 (50) | Index test: (1) HoloTC measured using an automated commercial immunoassay (Architect i2000SR, Active B12; Abbott Laboratories, Abbott Park, IL) (2) Total plasma Hcy (Immulite 2000; Siemens Healthcare Di agnostics, Deerfield, IL) Reference test: Serum MMA measured using liquid chromatography-tandem mass spectrometry (HPLC 1200 binary pump and 1200 Autosampler; Agilent, Santa Clara, CA) and a detector (API 5500; ABSciex, Framingham, MA) | Outcomes: Diagnostic test accuracy (AUC) Follow-up: NA |
AUC = area under the curve; Hcy = Homocystein; MMA = methylmalonic acid; NA = not applicable; NR = not reported; SD = standard deviation
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 28
Strengths | Limitations |
|---|---|
Anastasi et al. (2021)11 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; GRADE = Grading of recommendations, assessment, development, and evaluations; PICO = Participants, intervention, comparator, outcomes; PRIMSA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Table 5: Strengths and Limitations of Diagnostic Test Accuracy Studies Using QUADAS-2
Strengths | Limitations |
|---|---|
Warendorf et al. (2021)12 | |
|
|
Ao et al. (2017)13 | |
|
|
Vashi et al. (2016)14 | |
|
|
Beletic et al. (2015)15 | |
|
|
Cinemre et al. (2015)16 | |
|
|
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings Included Systematic Reviews
Main study findings | Authors’ conclusion |
|---|---|
Anastasi et al. (2021)11 | |
|
|
CLIA = chemiluminescent immunoassay; Hcy = Homocysteine; holoTC = Holotranscobalamin; MMA = Methymalonic acid; MTP = microbiological tests with microtitre plates
Table 7: Summary of Findings of Included Diagnostic Test Accuracy Studies
Main study findings | Authors’ conclusion |
|---|---|
Warendorft 202112 | |
MMA > 0.29 µmol/L: AUC 0.72
Hcy > 14 µmol/L: AUC 0.61
MMA > 29 µmol/L and/or Hcy > 14 µmol/L: AUC 0.65
|
|
Ao 201713 | |
|
|
Vashi 201614 | |
|
|
Beletic 201515 | |
Results presented as AUC (SE) (95% CI); P value At a vitamin B12 cut-off level of 203 ng/L
At a vitamin B12 cut-off level of 473 ng/L
|
|
Cinemre 201516 | |
|
|
AUC = Area Under the Curve; CI = Confidence interval; Hcy = Homocysteine; HHcy = Hyperhomocysteinemia; HoloTC = Holotranscobalamin; MMA = Methylmalonic Acid; SE = Standard Error
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Vitamin B12 testing in the general population: clinical and cost-effectiveness. CADTH rapid response report: summary of abstracts Ottawa (ON): CADTH; 2015: https://www.cadth.ca/sites/default/files/pdf/htis/jan-2015/RB0781%20Vitamin%20B12%20Testing%20Final.pdf. Accessed 2022 Feb 25
Review Articles
Active B12 assay for diagnosing vitamin B12 deficiency. NICE MedTech Innovation Briefing [MIB40]. London (UK): National Institute for Health and Care Excellence; 2015: www.nice.org.uk/guidance/mib40. Accessed 2022 Feb 25
Guidance documents, methodology not reported
Devalia V, Hamilton MS, Molloy AM. Guidelines for the diagnosis and treatment of cobalamin and folate disorders. Br J Haematol. 2014 Aug; 166(4): 496-513. PubMed
Additional References
Vitamin B12 deficiency, including pernicious anaemia: diagnosis and management. NICE guidance in development [GID-NG10176]. London (UK): National Institute for Health and Care Excellence; Expected publication date: 01 Nov 2023: https://www.nice.org.uk/guidance/indevelopment/gid-ng10176. Accessed 2022 Feb 25
Vitamin B12 testing. Canberra (AU): Australian Department of Health; 2014: https://www1.health.gov.au/internet/main/publishing.nsf/Content/VitaminB12testing. Accessed 2022 Feb 25
Testing vitamin B12 levels in neuropathy, alopecia, dizziness, and fatigue: a rapid review. Toronto (ON): Health Quality Ontario; 2014: https://www.hqontario.ca/Portals/0/Documents/evidence/rapid-reviews/testing-vitamin-b12-levels-140203-en.pdf. Accessed 2022 Feb 25
Serum vitamin B12 testing: a rapid review. Toronto (ON): Health Quality Ontario; 2012: http://www.hqontario.ca/Portals/0/Documents/evidence/rapid-reviews/vitamin-b12-121212-en.pdf. Accessed 2022 Feb 25
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.