CADTH Health Technology Review
Robotic-Assisted Surgical Systems for Knee Arthroplasty
Rapid Review
Authors: Rob Edge, Kelly Farrah
Abbreviations
AKSS
American Knee Society Score
COI
conflict of interest
HSS
Hospital for Special Surgery Knee Score
ICER
incremental cost-effectiveness ratio
ITT
intention to treat
KSFS
Knee Society Function Score
KSS
Knee Society Score
LOS
length of stay
MA
meta-analysis
MCID
minimal clinically important difference
NHS
national health service
OA
osteoarthritis
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-analyses
QALY
quality-adjusted life-year
QoL
Quality of Life
RCT
randomized controlled trial
ROM
range of motion
rTKA
robotic-assisted total knee arthroplasty
rUTK
robotic-assisted unicompartmental knee arthroplasty
SR
systematic review
TKA
total knee arthroplasty
UKA
unicompartmental knee arthroplasty
VAS
visual analogue scale
WOMAC
Western Ontario and McMaster Universities Osteoarthritis Index
WTP
willingness-to-pay
Key Messages
Overall, there was no consensus in the evidence to indicate that robotic-assisted knee arthroplasty provided any superior clinical effectiveness outcomes when compared to conventional techniques.
No evidence indicated that robot-assisted knee arthroplasty had worse clinical outcomes than conventional techniques. Evidence did support the association of robotic-assisted knee arthroplasty with decreased length of hospital stay and increased operative time.
Further adequately powered studies of short-term and long-term clinical effectiveness for robotic-assisted knee arthroplasty are required to definitively demonstrate any potential benefits for patients requiring knee arthroplasty.
Robotic-assisted knee arthroplasty was consistently modelled as cost-effective when clinical inputs included improved quality of life and reduced rates of surgical revisions when compared with conventional techniques. The clinical effectiveness evidence reviewed in this report was unable to adequately support these clinical inputs as accurate.
Context and Policy Issues
Osteoarthritis (OA) of the knee is a debilitating condition with an increasing incidence with age, currently estimated to affect 19% of people over 45 years old, and is associated with significant decreases in quality of life (QoL).1 As the Canadian population ages in the coming years, technological improvements have the potential to provide this increasing patient population with superior clinical and cost-effective treatments. Patients who receive knee replacement operations for OA or other indications, including osteonecrosis, typically see substantial improvements in pain, function, and overall QoL following conventional total knee arthroplasty (TKA) and unicompartmental knee arthroplasty (UKA).2,3 For patients who are refractory to nonsurgical treatment options, these knee replacement operations are considered cost-effective.3 However, significant room for improvement in clinical outcomes remains as the 2-year surgical revision rate has been reported to be as high as 9%,4 and lifetime revision rates as high as 35% have been observed in male patients who are in their early 50s.3 Surgical revision (i.e., revision from here on) of TKA and UKA is associated with a significant decrease in QoL, and decreased cost-effectiveness.3
Robotic-assisted knee arthroplasty interventions (rTKA and rUKA) have demonstrated increased surgical precision and greater accuracy in implant positioning.5,6 While US utilization rates for rTKA and rUKA remain modest (approximately 7% in 2019),3,5 it is hypothesized that the increased accuracy of rTKA and rUKA leads to decreased revision rates and improved functional outcomes.4 Robotic systems to facilitate rTKA and rUKA are associated with significant additional capital costs and resource utilization.7 Robotic-assisted knee arthroplasty must therefore be associated with improved clinical outcomes, and/or decreased revision rates to be cost-effective, and would be most cost-effective in centres that perform high procedure volumes to reduce per-patient costs.3,8-11
This report aims to retrieve and review the evidence for the clinical effectiveness and cost-effectiveness of robotic-assisted knee arthroplasty as compared to conventional knee arthroplasty techniques.
Research Questions
What is the clinical effectiveness of robotic-assisted surgical systems used for patients requiring knee arthroplasty?
What is the cost-effectiveness of robotic-assisted surgical systems used for patients requiring knee arthroplasty?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were robotic-assisted surgical systems and knee arthroplasty. No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and January 20, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients (of any age) requiring total or partial (i.e., unicompartmental) knee arthroplasty due to any cause (e.g., osteoarthritis, rheumatoid arthritis, psoriatic arthritis, trauma, dysplasia) |
Intervention | Arthroplasty performed using robotic-assisted surgical systems (e.g., Zimmer Biomet’s ROSA, Stryker’s MAKO) |
Comparator | Conventional and traditional surgery performed without robotic-assisted surgical systems |
Outcomes | Q1: Clinical effectiveness (e.g., postoperative functional status and mobility, range of motion, pain reduction, length of hospital stay, health-related quality of life, patient satisfaction, blood loss, operative time) and safety (e.g., rates of adverse events, hospital readmission, surgical revisions, complications [e.g., infections]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year, cost per health benefit gained) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, economic evaluations |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or were published before 2021 for clinical effectiveness outcomes or before 2017 for cost-effectiveness outcomes. Primary studies were excluded if they were captured in 1 or more included systematic reviews (SRs). Completely overlapping SRs, that is, SRs that included the same primary clinical effectiveness studies, were excluded if they also reported all outcomes from the identified studies.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)12 for systematic reviews, the Downs and Black checklist13 for randomized studies, and the Drummond checklist14 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
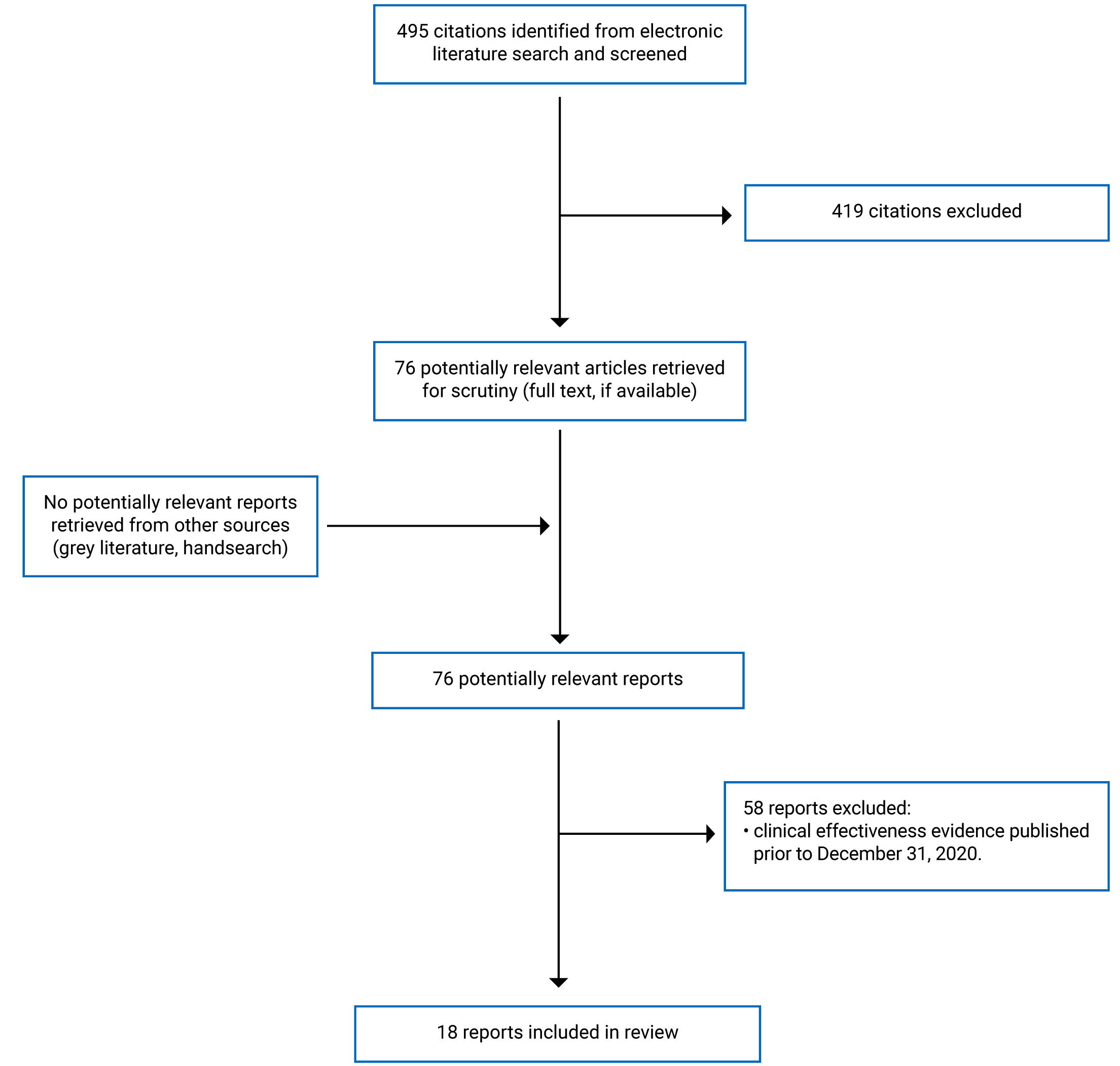
A total of 495 citations were identified in the literature search. Following screening of titles and abstracts, 419 citations were excluded and 76 potentially relevant reports from the electronic search remained. To reduce the number of studies to enable a rapid review, the time frame for inclusion for clinical effectiveness evidence was restricted to January 1, 2021, to January 20, 2022, while cost-effectiveness publication date inclusion criteria remained between January 1, 2017, and January 20, 2022. In addition, only SRs and randomized controlled trials (RCTs) were included in the clinical effectiveness evidence. This reduced study inclusion to a total of 18 reports that were retrieved for full-text review. No potentially relevant publications were identified from the grey literature. Of the 18 potentially relevant articles, all retrieved publications met the inclusion criteria and were included in this report. These comprised 10 SRs, 3 RCTs, and 5 economic evaluations. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)15 flow chart of the study selection.
Of note, the SRs contained significant overlap of 69 primary studies, which together with the 3 RCTs make a total of 72 primary studies contributing to the evidence summarized in this report. The overlap of primary study evidence contained within the SRs is outlined in Appendix 5.
A separate bibliography of studies that would have been included in this report based on the original search criteria time frame is provided in Appendix 6.
Summary of Study Characteristics
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
This report identified 10 SRs published since the beginning of 2021.4,6,7,16-22 In total, these 10 studies include 69 different primary studies published between 2002 and 2022. The date ranges covered by the systematic literature searches in the SRs ranged from not reported,6,17 2016 to 2020,16 all literature to 2019,4,7 1999 to 2019,18 and all literature to 2020.19-22 These searches yielded different quantities of studies relevant to this report. The quantity and study design determinations were reported as follows: Batailler et al. identified 14 comparative case-control studies;16 Bernard-de-Villeneuve et al. identified 2 RCTs and 4 non-randomized comparative studies;17 Chin et al. included 11 RCTs, 6 non-randomized comparative studies, and 3 case-control studies;7 Gaudiani et al. included 3 RCTs and 4 non-randomized comparative studies;18 Kort et al. examined 10 MAs;6 Kunze et al. identified 4 relevant RCTs;19 Negrin et al. identified 4 RCTs and 6 case-control studies;4 Sun et al. included 4 RCTs, 9 non-randomized comparative studies, and 3 case-control studies;20 Zhang J et al. included 16 comparative cohort studies;21 and Zhang P et al. included 3 RCTs and 7 comparative cohort studies.22
Three RCTs published in 2021 met the inclusion criteria for this report.2,23,24 All 3 studies were single-centre studies, and 2 were double-blinded studies.23,24
Five studies,3,8-11 all of which were based on a health care payer perspective, provided the cost-effectiveness evidence for this report. Cost-effectiveness was calculated for patient lifetime,3,8,10 20-year horizon,11 or 5-year horizon.9 The clinical input data used in the economic models was derived from prior cost-effectiveness studies in 1 study,8 while 1 study used a PRISMA-compliant SR to identify and include clinical evidence in an economic model.10 Two studies used clinical data from 2 independent sources for each intervention with the assumption that this noncomparative data were valid for direct comparison.9,11 Burn et al. derived clinical data from the UK’s National Health Service (NHS) data.3 Cost data were derived from Medicare reimbursement data,10 the NHS,3,8,9 prior cost-effectiveness studies,11 and costs from the device manufacturer.8 Utility data were sourced from prior cost-effectiveness studies8-11 and the NHS.3
The 5 economic analyses all used an economic Markov model approach, 4 of which were patient-level state-transition models.3,9-11 The model used by Clement et al. was a Markov decision analysis model.8
Country of Origin
The SRs were conducted in France,16,17 Singapore,7 the US,18,19 the EU,6 Chile,4 the UK,21 and China.20,22 The 3 RCTs included in this report were all conducted in the UK.2,23,24 The cost-effectiveness studies were conducted in the US,10 Belgium,11 the EU,3 and the UK.8,9 No identified evidence was conducted in Canada or intended to represent a Canadian health care setting.
Patient Population
The identified SRs did not sufficiently describe the patient population of interest, with 6 of the 10 SRs not defining the relevant patient population at all.4,7,16,20-22 Bernard-de-Villeneuve et al. simply defined the patient population as any human subjects,17 Gaudiani et al. included all studies that reported patients’ age and gender;18 Kort et al. used any indication that required UKA;6 and Kunze et al. included any indication in humans that required UKA.19 Despite not specifically defining the patient population of interest for systematic literature searches, the only indication mentioned in the included SRs was OA of the knee.4,6,7,17-22 The patient population of the included studies of the SRs was described briefly.4,6,7,16-22 The sex ratio of included patients was reported by 3 studies, but within these SRs not all included primary studies reported the sex of participants. Most primary studies enrolled a majority female population, and ranged from 47% to 100% female.7,16,22 The mean age of the study participants was reported by 7 SRs, and overall ranged from 57 to 71.4 years of age. Similarly, not all primary studies reported the age of participants.4,7,16-18,21,22 The total number of participants or knees included in the SRs ranged from 385 to 50,024.4,6,7,16-22
The identified RCTs all provided patient inclusion and exclusion criteria.2,23,24 Banger et al. enrolled consenting adults eligible for UKA surgery and excluded those patients with ligament insufficiency; inflammatory arthritis; deformity requiring augmentation; neurologic movement disorders; pathology of the feet, ankles, hips, or opposite knee; and patients requiring TKA.23 The RCT by Batailler et al. enrolled consenting adult patients who had isolated medial femorotibial OA or osteonecrosis of the femoral condyle, reducible deformity, and intact anterior cruciate ligament who were eligible for UKA. This study excluded patients with a lower limb coronal plane deformity greater than 15 degrees.2 The study by Blyth et al. enrolled consenting patients who had medial and lateral compartment OA suitable for TKA, with intact cruciate and collateral ligaments. Patients with rheumatoid or other inflammatory arthropathy, varus or valgus deformity of greater than 15 degrees, a fixed flexion contracture of greater than 10 degrees, single-compartment OA suitable for isolated UKA, patellofemoral OA greater than Kellgren and Lawrence grade 3, prior complicating surgery, or spine OA that may alter gait outcome were excluded from enrolment in this study.24
The identified cost-effectiveness studies all defined a patient age and a source supporting this as a representative age to model as this was a primary determinant of cost-effectiveness in the models.3,8-11 Patient ages used in the models were 60 years old,10 67 years old,11 71 years old,3 and 65 years old.8,9 Nherera et al. and Burn et al. included some different age categories in the model to evaluate the impact of age on cost-effectiveness and threshold prices, respectively.3,9
Interventions and Comparators
Clinical effectiveness of rTKA was compared to TKA in 5 SRs,6,7,16,21,22 and rUKA was compared to UKA in 7 SRs.4,6,7,17-20 Batailler et al. only included studies that examined a specific image-based robotic-assisted system (Stryker’s MAKO in the US).16
The 3 RCTs all described the specific robotic-assisted system used.2,23,24 Both Banger et al. and Blyth et al. used a system described similarly as Restoris MCK (made by Stryker in the US).23,24 Banger et al. used an Oxford phase 3 UKA as the description for the manual comparator,23 while Blyth et al. described the conventional technique as traditional TKA with a Nexgen LPS implant (made by Zimmer in the US).24 Batailler et al. compared a conventional UKA technique to the BlueBelt Navio image-free robotic surgical system (made by Smith and Nephew in the UK).2
The 5 cost-effectiveness studies modelled rTKA compared to TKA,3,11 non-CT rUKA compared to UKA,9 and rUKA compared to UKA and TKA.8 One cost-effectiveness study modelled a specific robotic-assisted system, the MAKO (made by Stryker in the US).11
Outcomes
In the SRs, clinical effectiveness outcomes included the following functional outcome scales: Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Knee Society Score (KSS), Knee Society Function Score (KSFS), Hospital for Special Surgery (HSS) knee score, American Knee Society Score (AKSS). WOMAC scores were reported by 5 SRs.4,6,7,16,21 WOMAC is a self-administered questionnaire that includes validated scores on pain, stiffness, and physical function with higher scores reflecting more severe symptoms. The minimal clinical important difference (MCID) for the WOMAC score has previously been estimated at 11 for pain, 9 for function, 8 for stiffness, and 10 for the total score.25 Other similar functional knee outcomes were included in evidence reported by the SRs: 4 included the KSS (0 to 100),6,7,16,21 2 included the KSFS (0 to 100),6,7 2 included the HSS knee score (0 to 100),6,7 and 2 included the AKSS (0 to 200).4,22 In these scales a higher score represents better knee function and/or clinical score. One SR included information on the MCID of KSS,21 though none of the other SRs or RCTs reported any results in relation to an MCID for any functional knee score. Range of motion (ROM) was another knee functional outcome reported in 4 SRs,4,6,16,22 though the clinical significance of ROM findings was not reported. Kort et al. reported ROM findings from the MA of Chin et al.; however, these results were not reported in the retrieved full-text of Chin et al.6,7 Results from the 12-Item Short Form Survey (SF-12), a patient-reported outcome measure that has both physical and mental components, was reported by Negrin et al. without any context for the clinical relevance of the reported numbers.4 Gaudiani et al. pooled some outcome measures in the meta-analysis (MA) to report a clinical outcome improvement that was the percentage improvement of a given clinical outcome measure between preoperative and postoperative measures such that difference scales could be combined in the analysis.18
Perioperative outcomes reported in the SRs included pain, length of stay (LOS), operative time, and time to attainment of physiotherapy. Pain was measured using a patient-reported visual analogue scale (VAS)6,16,18,22 from 0 to 10 with a higher number indicating greater relative pain. The pain component of the WOMAC was reported by 2 SRs.2,21 Gaudiani et al. reported on a study that measured pain using a numerical rating scale from 1 to 10 where higher numbers indicated greater patient-reported pain.18 LOS was reported by 3 SRs,4,16,17 operative time was reported by 2 SRs,7,19 and time to attainment of physiotherapy was reported by 2 SRs.4,17
Postoperative outcomes reported by the SRs included complications and revision rates. Complications were reported as an aggregate incidence in 8 of the 10 SRs.4,6,7,16,19-22 Similarly, revision rate was reported in 9 of the 10 SRs.4,6,7,16-20,22
Of note, Kort et al., did not report all outcomes from Chin et al., and Zhang P et al. Therefore, all 3 SRs are included in this report. To limit the overrepresentation of outcomes, each finding from these studies was reported once, to avoid multiple reporting of results published by more than 1 SR.
The 3 RCTs also reported revision rate, incidence of complications, and Forgotten Joint Score.2,23,24 The Forgotten Joint Score is a functional score that indicates the subjective feeling of the operated knee in everyday life.2 The RCTs also reported the Oxford Knee Score,23,24 the AKSS,23 VAS pain,23,24 VAS stiffness,23,24 satisfaction,23,24 ROM,23,24 the International Knee Society Score,2 and the New Knee Society Score.24 The University of California Los Angeles activity score is another validated score that instead reflects patient activity from 0 to 10 with greater activity associated with a greater score and was reported by 2 included RCTs.23,24 Batailler et al. also reported several objective outcome measures of gait, including walking speed, flexion/extension stance phase (maximum extension), flexion/extension swing phase (maximum flexion), adduction/abduction ROM, adduction/abduction maximum adduction, external/internal rotation, anterior/posterior translation swing phase, and anterior/posterior translation ROM.2
The 4 of the 5 identified cost-effectiveness studies reported outcomes of incremental cost-effectiveness ratio (ICER), which is the cost per quality-adjusted life-year (QALY) gained by using the intervention.8-11 Burn et al. instead report the clinical effectiveness required to meet the NHS willingness-to-pay (WTP) threshold.
Summary of Critical Appraisal
The SRs included in this report are generally at low risk of bias. While 2 SRs did not report a search time frame,6,17 all SRs described a comprehensive systematic literature search, provided inclusion and exclusion criteria, conducted study selection in duplicate, provided a PRISMA flow chart of literature selection that briefly described reasons for study exclusions, tabulated included study characteristics, and provided a discussion of the limitations of the SR.4,6,7,16-22 However, none of the included SRs provided a list of excluded studies or formulated a research question with PICO-defined terms. The patient population of interest was particularly vague in all SRs. Data extraction methodology was provided by 6 of the SRs.6,17,18,20-22 Batailler et al. did not clearly report the statistical significance of identified differences between rTKA and TKA.16 The risk of publication bias was assessed by 2 of the included SRs, both of which found no evidence of publication bias.7,20 Sun et al. reported that a limitation of their study was the small sample size of the included studies, which may have increased the risk of publication bias.20 Kort et al. reviewed MAs and failed to provide any analysis on the overlap of included studies.6 Zhang P et al. also reported that publication bias exists as a limitation of the study; however, this SR did not provide any analysis of publication bias or from what evidence that reported limitation was based on.22 Six SRs included an MA;7,18-22 however, 3 of these SRs did not discuss heterogeneity between the studies and the potential impact on the findings of the MA.7,18,21 One SR was an SR of MAs and it discussed concerns regarding heterogeneity between studies in the MAs.6 This report includes 4 of 10 SRs with a conflict of interest (COI),4,6,16,17 5 SRs that reported no COIs,7,18,20-22 and 1 SR that failed to provide a statement regarding COI.19
A critical appraisal of the identified evidence was included in 9 of the SRs.4,6,7,16,17,19-22 However, only 3 SRs provided some synthesis of critical appraisal results with findings.4,6,20 Kort et al. reported concerns regarding the heterogeneity of follow-up in the included MAs, that 6 of 9 MAs were evaluated as “critically low quality” (which included Chin et al.),7 the commercial bias within the primary study evidence, and the heterogeneity of the intervention as the technology has evolved.6 One MA not included in this report reported on the quantity of COIs in this field. This MA found that 91% of primary studies in this field involve financially conflicted authors, and that a statistically significant correlation between COIs with findings that favour robotic-assisted joint arthroplasty exists.5 Kort et al. was the only SR to make any comment regarding the potential for commercial bias within the primary literature, despite this high prevalence of industry funding.6 Negrin et al. highlighted a lack of type I evidence in the identified primary studies, and that more large prospective comparative studies are required to confirm or dismiss potential benefits of rUTK. The most common quality concerns regarding the identified evidence were related to blinding and selection bias.4 Sun et al. suggested that their conclusions lack reliability and that more studies are required.20
Three included primary RCTs2,23,24 contributed evidence to this report. These studies shared important methodological strengths, including information on patient recruitment and enrolment; an outline of statistical methodology, including an a priori sample size calculation; a clearly defined patient population, intervention, and outcomes; a description of randomization methodology; a discussion on limitations; and a quantification and discussion on complications. Common limitations were that all 3 studies were single-centre studies, with limited information on device training, and all 3 studies reported author COIs.2,23,24 Two of the studies were designed as double-blind studies;23,24 however, Banger et al. did not report clear assessment of the maintenance of blinding, nor was it clear if outcome assessment was blinded.23 Blyth et al. conducted a test of blinding at 1 year to assess the potential for bias that may have resulted from unintentional unblinding, and found no evidence that any unblinding had occurred.24 Both Batailler et al. and Blyth et al. identified statistically significant differences in relevant baseline patient characteristics,2,24 whereas Banger et al. failed to report important patient baseline characteristics.23 Banger et al. reported that an intention-to-treat (ITT) analysis was not feasible as loss to follow-up was associated with a loss of longitudinal information.23 Batailler et al. reported that results were analyzed as ITT but failed to report sufficient methodology,2 while Blyth et al. also reported an ITT analysis and included information on patients who were not treated per randomization.24 Blyth et al. compared robotic-assisted bi-UKA to manual TKA, and the authors cite relevant evidence to justify this direct comparison.24
Five economic studies3,8-11 contributed to the cost-effectiveness evidence in this report. Common strengths of the evidence included a well-formulated research question of economic significance, clearly stated objectives and outcomes, sources for clinical and cost model inputs, clearly stated model assumptions, a defined time horizon, and conclusions that follow from the model with appropriate caveats.3,8-11 Two of the 5 studies provided a definition of the patient population of interest.3,10 Three studies modelled cost-effectiveness for centres that have different volumes of cases, which was found to be an important determinant of cost-effectiveness.8,10,11 While all studies justified the methodological approach, none of the studies discussed or compared possible alternative approaches.3,8-11 Clement et al. was the only study that did not provide a sensitivity analysis or a discount rate in the model.8 Four of the studies included cost estimates from a single manufacturer.8-11 While Rajan et al. used several clinical studies as sources for clinical inputs,10 2 studies based a revision rate on a single noncomparative study,8,9 and Vermue et al. based revision rate on radiological alignment with minimal clinical data justification.11 Three studies reported author COIs,8-10 1 did not provide a COI statement,3 and 1 reported no COIs.11
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Robotic-Assisted Surgical Systems
Functional Outcomes
Systematic Review Findings
Many different functional outcome scales were used to compare knee function following robotic-assisted and conventional knee arthroplasty in the identified evidence. Knee function as assessed by the WOMAC was reported by 5 SRs.4,6,7,16,21 Batailler et al. found improved WOMAC scores for TKA over rTKA in both WOMAC total and WOMAC pain from 3 studies; however, the statistical significance of this difference was unclear.16 Kort et al. identified 1 of 3 studies that found a statistically significant difference in WOMAC scores favouring rTKA.6 Zhang J et al. pooled results from 2 studies and identified a statistically significant difference in WOMAC pain and WOMAC function favouring rTKA over TKA.21 The remaining evidence from Chin et al. and Negrin et al. did not find any differences in WOMAC outcomes.4,7
rUKA demonstrated better short-term knee function (up to 3 years) as measured by KSS in an MA by Chin et al., which was also reported in Kort.6,7 Zhang J et al. found superior KSS function scores following rTKA as compared to TKA but no statistically significant difference between rTKA and TKA in KSS satistfaction.21 One MA reported no statistically significant difference in KSS,6 while Batailler et al. reported no significant difference between rTKA and TKA without defining the meaning of significant difference.16
Two SRs identified the same reported statistically significant difference favouring rUKA in KSFS in pooled results from 3 primary studies.4,7 The MA of Chin et al. provides important context that this difference was observed during follow-up within 3 years.6,7 Kort et al. also identified 2 MAs that favoured rTKA in the HSS outcome, and 2 studies that did not.6 Negrin et al. identified 2 studies that found a statistically significant improvement in AKSS short-term functional outcomes within 1 year for rUKA over UKA; however, this difference did not remain after 1 year as reported by 1 of these 2 studies.4 The MA of Zhang P et al. pooled results from 4 studies and did not identify a statistically significant difference in AKSS functional outcomes between rUKA and UKA.22
Negrin also reported SF-12 physical and mental outcomes from 2 studies, and an International Knee Score from 2 studies, none of which were associated with a statistically significant difference between rUKA and UKA.4
Gaudiani et al. combined different functional outcome measures from 7 studies, and found no statistically significant difference in improvement between rUKA and UKA.18 ROM was reported by 4 identified studies,4,6,16,22 3 of which reported no statistically significant difference with robotic-assisted arthroplasty,4,6,22 and 1 that did not report on the statistical significance of the difference.16 Negrin et al. identified 2 studies that, in the short-term follow-up of 0 and 3 days, identified a statistically significant greater ROM for rUKA as compared to UKA.4
Overall, no consistent statistically significant differences emerged from the SRs and MAs in knee functional outcome scores. However, findings of Chin et al. and Negrin et al. suggest that there are potential functional outcome differences that are time dependent.4,7 Negrin et al. found a study that reported a better AKSS for rUKA over UKA that was not maintained at 1-year follow-up; however, overall, the significance of functional outcome score assessment timing in these results is not clear as there was a lack of longitudinal follow-up in this evidence. Zhang J et al. reported a statistically significant difference in KSS, although the difference did not reach the level of MCID.21 The clinical significance of the other identified statistically significant differences was not reported. Overall, regarding functional outcomes, the authors of the included SRs concluded similar clinical effectiveness outcomes at mid and long term,4,6,7,16,18,21,22 but better short-term functional outcomes for robotic-assisted interventions.7
Primary Study Findings
Batailler et al. found that walking speed was statistically faster for patients who had rUKA as compared to UKA. The authors of this study concluded that there was no significant difference between rUKA and UKA for clinical outcomes at 6 months.2 However, the other functional outcomes from the included RCTs did not indicate any statistically significant differences between robotic-assisted knee arthroplasty and conventional intervention. Despite all 3 RCTs conducting an a priori statistical power calculation, it is unclear if these studies were adequately powered to detect significant differences in functional outcome scores as 2 studies were designed to be powered for radiological outcomes not relevant to this report,2,23 and 1 was powered for sagittal knee moment.24 All the authors of these RCTs conclude that clinical outcomes were equivalent between the compared interventions.2,23,24
Perioperative Outcomes
Systematic Review Findings
The identified evidence also included perioperative outcomes of operative time, pain, LOS, and time to attainment of physiotherapy. Statistically significant shorter operative time was reported by 2 SRs for conventional arthroplasty techniques, UKA, and TKA.6,7 Differences in WOMAC and VAS pain of unknown statistical significance were reported by Batailler et al., while 1 of 2 studies in Gaudiani et al.,18 and 2 of 3 studies in Negrin et al.,4 and pooled results of 2 studies reporting WOMAC pain21 identified reduced postoperative pain with robotic-assisted arthroplasty. One SR identified no difference in postoperative pain between rUKA and UKA in an MA that pooled results from 4 studies.22 The identified evidence consistently reported decreased LOS following robotic-assisted arthroplasty as compared to conventional interventions from a total of 8 nonoverlapping primary studies.4,16,17 The time to attainment of physiotherapy was reported by 2 SRs on the same primary study that demonstrated that patients attained physiotherapy about 10 hours faster following UKA as compared to rUKA.4,17 Overall, this report finds some consistent evidence that while operative time was increased for robotic-assisted knee arthroplasty, it was associated with decreased pain, decreased LOS, and decreased time to attainment of physiotherapy.
Primary Study Findings
Blyth et al. reported that bi-rUTK required significantly more operative time, almost twice as much on average, as compared to UTK.24 No statistically significant differences were observed in the other perioperative outcomes in the included RCTs.
Postoperative Outcomes
Systematic Review Findings
Besides long-term functional outcomes, postoperative outcomes reported in the identified studies included complications and revisions. Eight included SRs reported on complications,4,6,7,16,19-22 and 9 SRs reported on revision rates.4,6,7,16-20,22 Sun et al. provided the most detail on reported complications and described that they mainly involved prosthetic loosening, subsidence, polyethylene bearing dislocation, periprosthetic fracture, knee ankylosis, wound complications, deep hematoma, infection, thrombosis, and persistent pain.20 Bernard-de-Villeneuve reported on a study that specified that the complications were minor wound complications,17 and Negrin reported medial-sided knee pain and wound complications as separate outcomes.4 Overall, limited information was provided about specific complications. One SR reported that complications were low for both interventions,16 and 3 MAs found no statistically significant difference in complication rates between the 2 interventions.7,21,22 Kort et al. reported that 1 of 3 MAs favoured rUKA over UKA with a significantly lower complication rate, while 2 MAs found no significant difference between rTKA and TKA complication rates.6 Both Kunze et al. and Sun et al. identified statistically significant differences favouring robotic-assisted arthroplasty interventions over the conventional counterpart for complication rates.19,20 Zhang P et al. reported pooled complication rates at less than 2 years, greater than 2 years, and overall from 8 primary studies. None of these time frames demonstrated a statistically significant difference in complication rates.22 The ability to draw conclusions from the mixed findings of complication rates in the identified SRs was limited by not having a definition for complication and the time frame in which they were recorded in the primary studies.
Rates of revision were reported in 9 SRs.4,6,7,16-20,22 Batailler et al. reported revision rates as low for both interventions.16 No statistically significant difference between robotic-assisted arthroplasty and its conventional comparator were found in pooled results from 9 primary studies in Chin et al.,7 7 studies in Gaudiani et al.,18 or 5 studies in Zhang P et al.22 Kort et al. did not identify any MAs that demonstrated a statistically significant difference in revision rates.6 However, significant differences in revision rates were observed in Negrin et al., where 1 of 2 identified studies found a higher revision rate in rUKA than UKA at 2-year follow-up.4 Additionally, Sun et al. pooled results from 10 studies to find that rUKA had a significantly lower revision rate than UKA.20 The authors stated that owing to important limitations, the findings on rates of revision and complications lacked reliability, and that more studies are required.20
Primary Study Findings
The included primary studies did not report any statistically significant differences in rates of complication or revision.2,23,24 Blyth et al. included a comprehensive table of all recorded complication categories, further classified as less than or greater than 3 months postoperative. The most frequently observed complications were falls, postoperative persistent pain, wound leakage, and upper gastrointestinal complaints.24 Banger et al. reported 6 instances of all-cause reintervention in patients who received TKA as compared to none in patients who received rTKA over 5 years. The authors narratively described the 6 observed reinterventions in the 49 patients who received TKA. Four of the 6 reinterventions were for pain, 1 was due to a fall, and 1 was for an infection following a biopsy. There were no malignment or component position errors in these patients.23
Cost-Effectiveness of Robotic-Assisted Surgical Systems
Of the 5 identified cost-effectiveness studies, 4 concluded that robotic-assisted knee arthroplasty would be cost-effective using their model, inputs, and assumptions.8-11 Burn et al.3 used a different approach and reported the clinical effectiveness required for robotic-assisted knee arthroplasty to be cost-effective for the NHS. This study concluded that robotic-assisted knee arthroplasty would have to lead to improvements in function and reductions in revision rates to be cost-effective.3 Rajan et al.10 used inputs of lower rates of revision and higher postoperative QoL. This study identified revision rate and case volume as important determinants of cost-effectiveness, with the ICER of US$92,823 for low volume centres (13 patients receiving rTKA per year), and an ICER of US$25,730 for high volume centres (200 patients receiving rTKA per year).10 A probabilistic sensitivity analysis using this model found that at US$50,000 and US$100,000 WTP thresholds, rTKA would be cost-effective 67.5% and 68.5% of the time, respectively.10 Vermue et al.11 also reported that reduced revision rates were a primary determinant of cost-effectiveness. This study used clinical data of alignment as a predictor of revision rate, with the authors cautioning against recommending robot-assisted surgery until there are data confirming that alignment predicts success.11 The study found that a minimum of 253 rTKA procedures per year were required to keep the ICER under US$50,000, and a probabilistic sensitivity analysis suggested that at US$50,000 WTP, rTKA would be cost-effective 2.18% of the time.11 Nherera et al.9 found that non-CT rUKA provided an ICER of ₤2, 831 when case volumes were 100 per year, and that at ₤20,000 per QALY WTP, non-CT robotic-assisted UKA was cost-effective 100% of the time. This study9 identified age and cost of robotics as important determinants of cost-effectiveness. The 2-year revision rates used in this study were 2.9% for UKA, from a large national database, and 0.78% for non-CT rUKA, from a noncomparative retrospective study.9 Clement et al.8 compared rUKA to both TKA and UKA and found that the ICER over TKA was ₤7,170, and the ICER over UKA was ₤8,604. Revision rates used in this model were 1.1% for UKA, 0.3% for TKA, and 0.5% for rUKA.8 Additional differences in clinical inputs included a lower postoperative QALY for TKA (0.671) versus UKA and rUKA (0.750), and increased mortality following TKA starting at 4-fold increased risk at 30 days with a decreasing difference in increased risk of mortality at 90 days, 1 year, 4 years, and 8 years.8 These cost-effectiveness studies provided consistent evidence that robotic-assisted knee arthroplasty could be cost-effective, and the clinical inputs for the economic models provided some insightful benchmarks for clinical effectiveness requirements for cost-effectiveness in the modelled settings.3,8-11
Limitations
This report is limited by the heterogeneity of the identified studies regarding important aspects that included interventions and follow-up intervals. This report is also limited by an unknown impact of overlapping evidence included within the SRs. Statistically significant findings were reported without reporting an MCID, making the clinical significance of statistically significant findings unclear. The included RCTs were not designed to be sufficiently powered for all outcomes; therefore, findings of no statistically significant difference for some outcomes may be limited by an insufficient sample size to detect a clinically significant difference. This limitation was acknowledged by the authors of the RCTs. The economic analyses were not designed to model a Canadian health care setting and the findings of these studies are limited by clinical input data that this report was unable to confirm as accurate.
Conclusions and Implications for Decision- or Policy-Making
This report identified 10 SRs and 3 RCTs representing a total of 72 primary studies that examined clinical effectiveness outcomes for robotic-assisted knee arthroplasty as compared to conventional techniques.2,4,6,7,16-24 To examine postoperative knee function, a total of 5 outcome scores were used in these studies and included WOMAC, KSS, KSFS, HSS, and AKSS. Across the identified evidence, none of these metrics consistently measured a statistically significant difference between the interventions, except for 1 MA7 that reported that pooled KSFS results from 3 studies indicated a higher function for rUKA than UKA in a short-term follow-up of 3 years or less. This MA also reported a long-term follow-up of greater than 10 years of pooled results from 2 studies and did not find a difference in KSFS between rTKA and TKA.7 None of the statistically significant differences identified reported an MCID, except 1 SR that identified a statistically significant improvement in KSS function for rTKA over TKA and stated that the difference was not greater than the MCID.21 Overall, while the findings from comparative studies reporting functional scores lacked consensus, and were not put in the context of the MCID, there was no evidence that robotic-assisted knee arthroplasty provided worse functional outcomes to patients, though it may be associated with some short-term functional benefits. Consistent evidence was identified from 5 MAs that operative time was shorter for conventional techniques,6,7 whereas robotic-assisted knee arthroplasty techniques were consistently associated with shorter LOS in 8 primary studies.2,4,16
Similar to functional outcomes, the evidence of revision and complication rates associated with robotic-assisted knee arthroplasty as compared to conventional techniques was mixed; however, no evidence supported conventional techniques as superior. Most of the identified evidence did not demonstrate statistically significant revision or complication rate differences between robotic-assisted knee arthroplasty when compared to conventional techniques.2,4,6,7,16-24
The evidence from the RCTs included in this report avoided potential bias of the MAs in which the clinical effectiveness of later device generations may have been inappropriately pooled with earlier technology.6 However, the 3 RCTs were also likely underpowered for most reported outcomes, as reported by the study authors, and were therefore unable to detect a potential clinical benefit of robotic-assisted knee arthroplasty. Otherwise, all 3 RCTs were also associated with concerns for bias regarding COI and baseline patient characteristics.2,23,24 There is a need for adequately powered RCTs to assess the comparative clinical effectiveness of robotic-assisted knee arthroplasty and conventional techniques at both short- and long-term follow-up.6,7,20,22
The cost-effectiveness of robotic-assisted knee arthroplasty was assessed in 5 included economic model studies.3,8-11 These studies were well-conducted studies and all modelled scenarios indicated that robotic-assisted knee arthroplasty was cost-effective. There is uncertainty associated with these conclusions because this report was unable to confirm the accuracy of the clinical effectiveness inputs, especially regarding decreased revision rates and increased QoL for patients treated with robotic-assisted knee arthroplasty. These models also identified additional factors that impacted the cost-effectiveness of robotic-assisted knee arthroplasty, including volume of cases and patient age.3,8-11
References
1.Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163-2196. PubMed
2.Batailler C, Lording T, Naaim A, Servien E, Cheze L, Lustig S. No difference of gait parameters in patients with image-free robotic-assisted medial unicompartmental knee arthroplasty compared to a conventional technique: early results of a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2021 Apr 11. PubMed
3.Burn E, Prieto-Alhambra D, Hamilton TW, Kennedy JA, Murray DW, Pinedo-Villanueva R. Threshold for computer- and robot-assisted knee and hip replacements in the English National Health Service. Value Health. 2020;23(6):719-726. PubMed
4.Negrin R, Ferrer G, Iniguez M, et al. Robotic-assisted surgery in medial unicompartmental knee arthroplasty: does it improve the precision of the surgery and its clinical outcomes? Systematic review. J Robot Surg. 2021;15(2):165-177. PubMed
5.DeFrance MJ, Yayac MF, Courtney PM, Squire MW. The impact of author financial conflicts on robotic-assisted joint arthroplasty research. J Arthroplasty. 2021;36(4):1462-1469. PubMed
6.Kort N, Stirling P, Pilot P, Muller JH. Robot-assisted knee arthroplasty improves component positioning and alignment, but results are inconclusive on whether it improves clinical scores or reduces complications and revisions: a systematic overview of meta-analyses. Knee Surg Sports Traumatol Arthrosc. 2021 Mar 5. PubMed
7.Chin BZ, Tan SSH, Chua KCX, Budiono GR, Syn NL, O'Neill GK. Robot-assisted versus conventional total and unicompartmental knee arthroplasty: A meta-analysis of radiological and functional outcomes. J Knee Surg. 2021;34(10):1064-1075. PubMed
8.Clement ND, Deehan DJ, Patton JT. Robot-assisted unicompartmental knee arthroplasty for patients with isolated medial compartment osteoarthritis is cost-effective: a markov decision analysis. Bone Joint J. 2019;101-B(9):1063-1070. PubMed
9.Nherera LM, Verma S, Trueman P, Jennings S. Early economic evaluation demonstrates that noncomputerized tomography robotic-assisted surgery is cost-effective in patients undergoing unicompartmental knee arthroplasty at high-volume orthopaedic centres. Adv Orthop. 2020 Apr 14;2020:3460675. PubMed
10.Rajan PV, Khlopas A, Klika A, Molloy R, Krebs V, Piuzzi NS. The cost-effectiveness of robotic-assisted versus manual total knee arthroplasty: A markov model-based evaluation. J Am Acad Orthop Surg. 2022 Feb 15;30(4):168-176. PubMed
11.Vermue H, Tack P, Gryson T, Victor J. Can robot-assisted total knee arthroplasty be a cost-effective procedure? A Markov decision analysis. Knee. 2021;29:345-352. PubMed
12.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2022 Feb 24.
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Batailler C, Fernandez A, Swan J, et al. MAKO CT-based robotic arm-assisted system is a reliable procedure for total knee arthroplasty: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2021;29(11):3585-3598. PubMed
17.Bernard-de-Villeneuve F, Kayikci K, Sappey-Marinier E, et al. Health economic value of CT scan based robotic assisted UKA: a systematic review of comparative studies. Arch Orthop Trauma Surg. 2021;141(12):2129-2138. PubMed
18.Gaudiani MA, Samuel LT, Kamath AF, Courtney PM, Lee GC. Robotic-assisted versus manual unicompartmental knee arthroplasty: Contemporary systematic review and meta-analysis of early functional outcomes. J Knee Surg. 2021;34(10):1048-1056. PubMed
19.Kunze KN, Farivar D, Premkumar A, Cross MB, Della Valle AG, Pearle AD. Comparing clinical and radiographic outcomes of robotic-assisted, computer-navigated and conventional unicompartmental knee arthroplasty: A network meta-analysis of randomized controlled trials. J Orthop. 2021;25:212-219. PubMed
20.Sun Y, Liu W, Hou J, Hu X, Zhang W. Does robotic-assisted unicompartmental knee arthroplasty have lower complication and revision rates than the conventional procedure? A systematic review and meta-analysis. BMJ Open. 2021;11(8):e044778. PubMed
21.Zhang J, Ndou WS, Ng N, et al. Robotic-arm assisted total knee arthroplasty is associated with improved accuracy and patient reported outcomes: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2021 Feb 6. PubMed
22.Zhang P, Xu K, Zhang J, Chen P, Fang Y, Wang J. Comparison of robotic-assisted versus conventional unicompartmental knee arthroplasty for the treatment of single compartment knee osteoarthritis: A meta-analysis. Int J Med Robot. 2021;17(1):1-11. PubMed
23.Banger M, Doonan J, Rowe P, Jones B, MacLean A, Blyth MJB. Robotic arm-assisted versus conventional medial unicompartmental knee arthroplasty: five-year clinical outcomes of a randomized controlled trial. Bone Joint J. 2021;103-B(6):1088-1095. PubMed
24.Blyth MJG, Banger MS, Doonan J, Jones BG, MacLean AD, Rowe PJ. Early outcomes after robotic arm-assisted bi-unicompartmental knee arthroplasty compared with total knee arthroplasty: a prospective, randomized controlled trial. Bone Joint J. 2021;103-B(10):1561-1570. PubMed
25.Clement ND, Bardgett M, Weir D, Holland J, Gerrand C, Deehan DJ. What is the minimum clinically important difference for the WOMAC index after TKA? Clin Orthop Relat Res. 2018;476(10):2005-2014. PubMed
26.Ferket BS, Feldman Z, Zhou J, Oei EH, Bierma-Zeinstra SM, Mazumdar M. Impact of total knee replacement practice: cost effectiveness analysis of data from the Osteoarthritis Initiative. BMJ. 2017;356:j1131. PubMed
27.Slover J, Espehaug B, Havelin LI, et al. Cost-effectiveness of unicompartmental and total knee arthroplasty in elderly low-demand patients. A Markov decision analysis. J Bone Joint Surg Am. 2006;88(11):2348-2355. PubMed
28.Moschetti WE, Konopka JF, Rubash HE, Genuario JW. Can robot-assisted unicompartmental knee arthroplasty be cost-effective? A markov decision analysis. J Arthroplasty. 2016;31(4):759-765. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Batailler et al. (2021), France16 Funding: No specific funding | SR - Comparative studies (n = 14) | Not defined in search. Included studies:
| MAKO (Stryker, USA) image-based robotic-assisted systems to perform TKA TKA | Outcomes:
Follow-up: Mean follow-up ranged from 7.3 weeks to 2 years |
Bernard-de-Villeneuve et al. (2021), France17 Funding: NR. Senior author is consultant for Stryker | SR - RCTs (n = 2), prospective cohort (n = 2), retrospective cohort (n = 5). | Search was any human subjects Included studies:
| Any image-based robotic-assisted systems to perform UKA Manual comparator | Outcomes:
Follow-up: Mean follow-up ranged from 3 months to 132 months. |
Chin et al. (2021), Singapore7 Funding: None | MA - RCTs (n = 11), prospective cohort (n = 3), retrospective cohort (n = 6), case-control (n = 3) | Not defined in search Included studies:
| Any robotic-assisted systems to perform TKA/UKA Manual comparator | Outcomes:
Follow-up: Mean follow-up ranged from 3 months to 45 months |
Gaudiani et al. (2021), USA18 Funding: NR | MA - RCTs (n = 3), retrospective cohort (n = 4) | Search was any studies that report patient’s gender and age Included studies:
| Any robotic-assisted systems to perform UKA Manual comparator | Outcomes:
Follow-up: Mean follow-up of included studies 25.5 months |
Kort et al. (2021), EU6 Funding: Stichting IMA. First author is consultant for Stryker | SR - Meta-analyses (n = 10) | Search was any indication Included studies:
| Any robotic-assisted systems to perform UKA/TKA Manual comparator | Outcomes:
Follow-up: Ranged from 12 to 132 months |
Kunze et al. (2021), USA19 Funding: NR | MA - RCTs (n=4 four relevant to robotic-assisted systems) | Search was for any indication in humans Included studies:
| Any computer or robotic-assisted systems to perform UKA Manual comparator | Outcomes:
Follow-up: |
Negrin et al. (2021), Chile4 Funding: NR. Some authors have some industry conflict of interest | SR - RCT (n = 4), retrospective cohort (n = 2), prospective case-control (n = 2), retrospective case-control (n = 5) | Not defined in search Included studies:
| Any robotic-assisted systems to perform UKA Conventional UKA | Outcomes:
Follow-up: Longer term outcomes follow-up ranged from 3 months to 2 years |
Sun et al. (2021), China20 Funding: Natural Science Foundation of China, Wu Jieping Medical Foundation, Shandong Provincial Key Research and Development Project. | MA - RCT (n = 4), prospective cohort (n = 4), retrospective cohort (n = 5), case control (n = 3) | Not defined in search Included studies:
| Any robotic-assisted systems to perform UKA Conventional UKA | Outcomes:
Follow-up: Mean follow-up ranged from 1 month to 5 years. |
Zhang J et al. (2021), UK21 Funding: No specific funding. Unclear conflict of interest. | MA - Prospective cohort (n = 11), retrospective cohort (n = 5) | Not defined in search Included studies:
| Any robotic-assisted systems to perform TKA Conventional TKA | Outcomes:
Follow-up: Ranged from 1 month to 15 months |
Zhang P et al. (2021), China22 Funding: National Natural Science Foundation of China, Jiangsu medical innovation team project. | MA - RCT (n = 3), prospective cohort (n = 3) retrospective cohort (n = 4), | Not defined in search Included studies:
| Any robotic-assisted systems to perform TKA Conventional TKA | Outcomes:
Follow-up: reported as > 2 years and < 2 years |
AKSS = American Knee Society Score; FJS = Forgotten Joint Score; HSS = Hospital for Special Surgery Knee Score; IKSS = International Knee Society Score; KSFS = Knee Society Function Score; KSS = Knee Society Score; LOS = length of stay; MA = meta-analyses; NR = not reported; OKS = Oxford Knee Score; RCT = randomized controlled trial; ROM = range of motion; SR = systematic review; TKA = total knee arthroplasty; UKA = unicompartmental knee arthroplasty; VAS = visual analogue scale; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index;
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
Banger et al. (2021), UK23 Funding: Stryker, USA | Double-blind single-center RCT | Consenting patients eligible for UKA surgery Exclusions: ligament insufficiency, inflammatory arthritis, deformity requiring augmentation, neurological movement disorders, pathology of the feet, ankles, hips, or opposite knee, patients requiring TKA | Restoris MCK (Stryker, USA) using the MAKO Robotic-arm Interactive Orthopaedic system (RIO) (Stryker, USA). MAKO technician collaborated on UKA surgical planning (n = 55) Oxford phase 3 UKA (Zimmer Biomet, USA) (n = 49) | Outcomes:
Follow-up: 1-, 2-, and 5-years post-operative |
Batailler et al. (2021)(2), France2 Funding: Smith & Nephew, UK | Single-center RCT | Consenting patients with isolated medial femorotibial OA or osteonecrosis of the femoral condyle, reducible deformity, and intact ACL eligible for UKA Exclusions: lower limb coronal plane deformity > 15° | BlueBelt Navio image-free robotic surgical system (Smith & Nephew, UK) (n = 33) Conventional technique (n = 33) | Outcomes:
Follow-up: 6 months |
Blyth et al. (2021), UK24 Funding: Efficacy and Mechanism Evaluation Programme and Stryker, USA | Double-blind single-center RCT | Consenting patients with medial and lateral compartment OA suitable for TKA, intact cruciate and collateral ligaments | bi-UKA with medial and lateral Restoris MCK (multicompartmental Knee) with aid of MAKO Robotic-Arm Assisted Technology (Stryker, USA) (n = 34) Traditional TKA with Nexgen LPS implant (Zimmer, USA) (n = 42) | Outcomes:
|
Blyth et al. (2021), UK24 Funding: Efficacy and Mechanism Evaluation Programme and Stryker, USA (continued) | Exclusions: rheumatoid or other inflammatory arthropathy, varus or valgus deformity of > 15°, a fixed flexion contracture of > 10°, single-compartment OA suitable for isolated UKA, patellofemoral OA > Kellgren and Lawrence grade III, prior complicating surgery, OA in spine that may alter gait outcome |
Follow-up: 6 weeks and 1 year |
ACL = anterior cruciate ligament; AKSS = American Knee Society Score; FJS = Forgotten Joint Score; HSS = Hospital for Special Surgery Knee Score; IKSS = International Knee Society Score; KSFS = Knee Society Function Score; KSS = Knee Society Score; LOS = length of stay; MA = meta-analyses; NKSS = New Knee Society Score; NR = not reported; OA = osteoarthritis; OKS = Oxford Knee Score; RCT = randomized controlled trial; ROM = range of motion; SR = systematic review; TKA = total knee arthroplasty; UCLA = University of California Los Angeles; UKA = unicompartmental knee arthroplasty; VAS = visual analogue scale; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index;
Table 4: Characteristics of Included Economic Evaluations
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Rajan et al. (2022), USA10 Funding: NR. Some authors have some industry conflict of interest | Lifetime cost-effectiveness for the healthcare payer | Patients aged 60 years with advanced knee degenerative joint disease treated with TKA | rTKA TKA | Markov model using patient-level state-transition | Clinical: 11 studies published between 2007 and 2020 Cost: Medicare reimbursement schedules Utility data: from similar cost-effectiveness studies | Fixed cost of robotic surgery QOL of suboptimal TKA the same for both interventions QOLs of all revisions the same Societal costs the same for both interventions One revision cycle |
Vermue et al. (2021), Belgium11 Funding: None | 20-year cost-effectiveness for the healthcare payer | Patients aged 67 years with primary asteoarthritis treated with TKA | MAKO (Stryker, USA) rTKA TKA | Markov model using patient-level state-transition | Clinical: Revision rate based on alignment and evidence for improved alignment with rTKA to determine implant survival Cost: Ferket et al., 201726 and Manufacturer (Stryker, USA) Utility data: 0.725 for primary TKA and 0.707 for revision TKA Slover et al., 200627 | Knee malalignment leads to equally to increased revision for rTKA and TKA One revision cycle Used publicly available cost for a specific rTKA device (Stryker, USA) |
Burn et al. (2020), EU3 Funding: NIHR | Lifetime threshold prices for the healthcare system | Average profile of patients undergoing knee and hip replacements (71 years old) | rTKA TKA | Markov model using patient-level state-transition | Clinical and Cost: the NHS - Clinical practice data link (CPRD), hospital episode statistics admitted patient care (HES APC) Utility: the NHS - CPRD HES patient-reported outcome measures (HES PROMS) | QOL increases over 6 months post-op QOL remains unchanged for patients not requiring revision Revised state is 75% QOL vs unrevised One revision cycle |
Nherera et al. (2020), UK9 Funding: NR. All authors have COIs | 5-year cost-effectiveness for the healthcare payer | Patients aged 65 years with primary asteoarthritis treated with TKA Also considered patients aged < 55 years, 65 - 74 years, and > 75 years | non-CT rUKA UKA | Markov model using patient-level state-transition | Clinical: rUKA from British National Joint Registry, cUKA from a two-year observational study Revision of non-CT rUKA = 2.99% Revision of UKA = 0.78% Cost: NHS reference cost in 2018/2019 Utility: Moschetti et al., 201628 | Clinical data from independent sources for each intervention are valid Impact of revisions limited to two years Equivalent mortality between interventions |
Clement et al. (2019), UK8 Funding: NR. All authors have COIs | Lifetime cost-effectiveness in the UK healthcare setting | Patients aged 65 undergoing UKA for unicompartmental end-stage OA | rUKA UKA and TKA | Markov model using decision analysis | Clinical: Moshetti et al., 201628 and Slover et al., 200627 Revision/y of rUKA = 0.5% Revision/y of UKA = 1.1% Revision/y of TKA = 0.3% Costs: Manufacturer (Stryker, USA) and NHS | Twelve-month lease of robot (Stryker, USA) Equivalent mortality between interventions One revision cycle Clinical data from independent sources for each intervention are valid |
COI = conflict of interest; NIHR = National Institute for Health Research; NHS = national health service; QoL = quality of life; rTKA = robotic-assisted total knee arthroplasty; rUKA = robotic-assisted unicompartmental knee arthroplasty; TKA = total knee arthroplasty; UKA = unicompartmental knee arthroplasty.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 212
Strengths | Limitations |
|---|---|
Batailler et al. (2021)16 | |
|
|
Bernard-de-Villeneuve et al. (2021)17 | |
|
|
Chin et al. (2021)7 | |
|
|
Gaudiani et al. (2021)18 | |
|
|
Kort et al. (2021)6 | |
|
|
Kunze et al. (2021)19 | |
|
|
Negrin et al. (2021)4 | |
|
|
Sun et al. (2021)20 | |
|
|
Zhang J. et al. (2021)21 | |
|
|
Zhang P. et al. (2021)22 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; COI = conflict of interest; PICO = population, intervention, comparator, outcome; PRISMA = Preferred Reporting Terms for Systematic Reviews and Meta-analyses
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black checklist13
Strengths | Limitations |
|---|---|
Banger et al. (2021)23 | |
|
|
Batailler et al. (2021)(2)2 | |
|
|
Blyth et al. (2021)24 | |
|
|
COI = conflict of interest; CONSORT = Consolidated Standards of Reporting Trials; ITT = intention to treat; MCID = minimal clinically important difference; TKA = total knee arthroplasty; UKA = unicompartmental knee arthroplasty;
Table 7: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist14
Strengths | Limitations |
|---|---|
Rajan et al. (2022)10 | |
|
|
Vermue et al. (2021)11 | |
|
|
Burn et al. (2020)3 | |
|
|
Nherera et al. (2020)9 | |
|
|
Clement et al. (2019)8 | |
|
|
COI = conflict of interest
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings Included Systematic Reviews
Main study findings | Authors’ conclusion |
|---|---|
Batailler, 202116 | |
Meaning of reported intervals unclear (95% CI, range, or STD). Statistical significance of reported findings unclear. Robotic vs. Manual WOMAC Total Marchand (2017): 7 ± 8 vs. 14 ± 8 Marchand (2019): 6 ± 6 vs. 9 ± 8 Robotic vs. Manual WOMAC Pain Marchand (2017): 3 ± 3 vs. 5 ± 3 Kayani (2018)(2): 2.6 vs. 4.5 Robotic vs. Manual VAS pain Bhimani (2020): 2.6 vs. 3.5 Robotic vs. Manual KSS Khlopas (2019): 67.2(16 - 100) vs. 65.5(18 - 99) Smith (2019): 80 vs. 73 Naziri (2019): 88.2 vs. 89.5 Robotic vs. Manual LOS Kayani (2018)(2): 77h vs. 105h Smith (2019): 2.1days vs. 2.6days Naziri (2019): 1.27days vs. 1.92days Mont (2019): 1.8days vs. 2.5days Bhimani (2020): 1.9days vs. 2.3days Cotter (2020): 1.2days vs. 1.6days Robotic vs. Manual ROM Smith (2019): 119° vs. 116° Naziri (2019): 121.3° (+3.8) vs. 109.8° (-8.7) Robotic vs. Manual Complication Rate Kayani (2019): 1.67% vs. 1.67% Smith (2019): 0 vs. 0 Naziri (2019): 0 vs. 0 Cotter (2020): 2.7% vs. 3.6% | “The CT-based robotic-assisted system for TKA reduced postoperative pain and improved implant positioning with equal or slightly superior improvement of the functional outcomes at one year, compared to conventional TKA.” (p3585) “The postoperative outcomes during hospitalization were equal or slightly superior for the robotic-assisted group compared to conventional TKA, without significant differences in clinical and functional results at short and mid-term. Current evidence shows advantages of image-based robotic-assisted TKA in mechanical knee alignment, implant positioning, ligamentous balance and soft tissue protection. However, powerful studies at longer term follow-up are critical to assess the long-term advantages of this robotic system, particularly for TKA survivorship or potential benefits of alternate alignment philosophies.”(p3596) “Currently, at mid-term, the use of the robotic-assisted system is at least equivalent to the conventional technique for functional outcomes, but not superior.” (p3594) “The complication and revision rates were low in both robotic-assisted and in conventional technique cohorts at short-term follow-up.” (p3594) |
Robotic vs. Manual Revision Rate Kayani (2019) 30d: 0 vs. 0 Smith (2019) 1yr: 0 vs. 0 Naziri (2019) 90d: 0 vs. 0 Cotter (2020) 90d: 2.7% vs. 3.6% | |
Bernard-de-Villeneuve, 202117 | |
Statistically significant results are indicated with reported P value. Robotic vs. Manual Revision Rate Blyth (2017): 0 vs. 0 Gilmour (2018): 0 vs. 3.7% Cool (2019): 0.81% vs. 5.28% (P = 0.002) St Mart (2020): 2.6% vs. 3.7% Wong (2019): 12% vs. 6.8% (P < 0.05) Vakharia (2019): 0.99% vs. 4.24% (P = 0.03) Robotic vs. Manual LOS Blyth (2017): 0.54days shorter for rTKA Kayani (2019)(2): 42.5h vs. 71.1h (P < 0.001) Cool (2019): 0.81% vs. 5.28% (P = 0.002) Hansen (2014): 8.8h less for rUKA Robotic vs. Manual Time to Attainment of Physiotherapy Hansen (2014): 42.17h vs. 52.47h (P = 0.024) | “Despite the relative short duration of follow-up of the selected studies (maximum 36 months), short-term revisions were rare and most of the studies did not report revisions after rUKA compared to conventional technique. Gilmour et al. found that patients in the robotic arm-assisted group have a 100% survivorship at 2 years, compared to 97% of those in the manual group.” (p2134) “Faster rehabilitation was found in the rUKA group compared with the mUKA group, but this was not significant [19]. Operating time appeared to be longer in robotic-assisted UKA procedures” (p2135) |
Chin, 20217 | |
*Statistically significant difference (P < 0.05) rUKA vs. UKA Operative Time Mean Difference (95%CI) 5 studies: 17.10 (13.24 to 20.97) favours UKA* rTKA vs. TKA Operative Time Mean Difference (95%CI) 6 studies: 24.36 (8.7 to 39.82) favours TKA* rUKA vs. UKA KSS (short-term) Mean Difference (95%CI) 3 studies: 19.67 (5.67 to 33.68) favours rUKA* rUKA vs. UKA KSFS (short-term) Mean Difference (95%CI) 3 studies: 4.31 (1.93 to 6.69) favours rUKA* rTKA vs. TKA WOMAC (mid-term) Mean Difference (95%CI) 3 studies: -1.63 (-3.45 to 0.19) rTKA vs. TKA HSS (mid-term) Mean Difference (95%CI) 3 studies: 1.14 (-0.42 to 2.70) | “Robot-assisted UKA was found to have significantly better short-term functional outcomes compared with conventional UKA (moderate-to-high quality evidence). Robot-assisted TKA, however, did not exhibit significantly better short- and midterm subjective knee outcome scores compared with its conventional counterpart (high-quality evidence). Robot-assisted TKA and UKA were associated with nonstatistically significant improved ROM and lesser rates of revision. Robot-assisted total and unicompartmental knee arthroplasty leads to better radiological outcomes, with no significant differences in mid- and long-term functional outcomes compared with conventional methods for the former. Larger prospective studies with mid- and long-term outcomes are required to further substantiate findings from the present study.” (p1064) |
rTKA vs. TKA KSFS (long-term) Mean Difference (95%CI) 2 studies: -1.79 (-5.04 to 1.46) rUKA vs. UKA Complications RR (95%CI) 5 studies: 1.07 (0.54 to 2.14) rTKA vs. TKA Complications RR (95%CI) 5 studies: 0.91 (0.30 to 2.75) rUKA vs. UKA Revisions RR (95%CI) 5 studies: 0.94 (0.47 to 1.89) rTKA vs. TKA Revisions RR (95%CI) 4 studies: 0.69 (0.37 to 1.28) | |
Gaudiani, 202118 | |
Robotic vs. Manual UKA Clinical Outcome Measure improvement ± STD 7 studies: 26 ± 12% vs. 24 ± 12% (P = 0.6) Robotic vs. Manual UKA Revision Rate 7 studies: 3% vs. 3% (P = 0.8) Robotic vs. Manual NRS Pain Kayani (2019)(2): 5.6 vs. 2.6 (P < 0.001) Robotic vs. Manual VAS Pain Blyth (2017): 8 vs. 9 (P = 0.161) | ”A systematic review of literature found similar positive clinical outcomes and revision rates between RA-UKA and manual UKA at short-term follow-up.” (p1054) “Longer term follow-up in direct comparison studies may inform the clinical advantages of robotic and manual UKA, along with any important differences with respect to long-term component durability and sustained functional improvement.” (p1055) “The principal argument for robotics may be then that it is an equalizer that allows lower volume surgeons to obtain results similar to high volume and experienced surgeons. While current comparative studies do not show superior outcomes with RA-UKA compared with manual instrumentation, there remains a role for robotics in partial knee replacement in low volume surgeons.” (p1054) |
Kort, 20216 | |
UKA Complications ES Zhang (2020): 0.62 favours rUKA (P =0.0041) Fu (2018): 1.56 (ns) Revision Rate ES Zhang (2020): 0.49 (ns) KSS ES Zhang (2020): 0.37 (ns) Operative Time ES Zhang (2020): 0.74 favours UKA (P =0.001) Fu (2018): 15.69 favours UKA (P < 0.00001) | ”Although robotic assistance affords improved component positioning, its benefits regarding clinical scores, patient satisfaction and implant survivorship remains to be confirmed. Finally, this overview revealed that six of the ten meta-analyses were of ‘critically low quality’, calling for caution when interpreting results.” (p14) “This overview of meta-analyses on robot-assisted knee arthroplasty highlighted discrepancies in pooling results across different generations of robotic systems and the level of assistance they provide. Long-term studies are needed to ascertain the impact of robotic assistance on clinical and functional scores, and rates of complications and revision. In addition, results should be stratified on the basis of generation and the level of robotic assistance, as this will provide more insights into the effect of matureness of these novel technologies.” (p9) |
TKA Complications ES Onggo (2020): 1.06 (ns) Ren (2019): 0.83 (ns) Revision Rate ES Onggo (2020): 0.57 (ns) WOMAC ES Agarwal (2020): -2.81 favours rTKA (P < 0.0001) Onggo (2020): -1.59 (ns) Ren (2019): -2.01 (ns) HSS ES Agarwal (2020): 1.71 favours rTKA (P < 0.00001) Onggo (2020): 1.62 favours rTKA (P < 0.00001) Ren (2019): 0.82 (ns) KSS ES Agarwal (2020): -0.50 (ns) Onggo (2020): -0.84 (ns) Ren (2019): 0.82 (ns) Pooled Functional Outcomes ES Karunaratne (2019): -0.51 favours NR ROM ES Agarwal (2020): 0.42 (ns) Onggo (2020): -0.91 (ns) Ren (2019): -0.84 (ns) Operative time ES Onggo (2020): 21.5 favours TKA (P =0.006) Ren (2019): 15.97 (ns) | “The overview also revealed that robot-assisted knee arthroplasty extended operation times by roughly 16–25 min. Only some of the meta-analyses found significant differences in clinical or functional scores between robot-assisted versus conventional knee arthroplasty. These findings, therefore, support the hypothesis that robot assistance improves the accuracy of component alignment and positioning, but are inconclusive regarding clinical scores, complications and revision rates.” (p4) |
Kunze, 202119 | |
*Statistically significant difference (P < 0.05) rUKA vs. UKA Operative Time Mean Difference (95%CI) 1 study: 16.0 (-7.28 to 39.28) rUKA vs. UKA Complications Odds Ratio (95%CI) 3 studies: 0.39 (0.18 to 0.85) favours rUKA (P = 0.018)* rUKA vs. UKA Revisions Odds Ratio (95%CI) 2 studies: 0.22 (0.02 to 2.33) | “Furthermore, the results of this study corroborate survivorship data from previous literature that has reported comparable revision and reoperation rates between robotic or computer navigation-assisted and conventional UKA” (p218) “Robotic-assisted UKA was found to result in a significantly lower likelihood of all-cause complications compared to conventional UKA; (2) no significant differences were found in operative time, all-cause reoperations, and postoperative tibiofemoral alignment among the three treatment groups, though the use of robotic or computer navigation-assisted trended towards increased operative times;” (p216) |
Negrin, 20214 | |
No statistically significant differences identified in WOMAC functional (2 studies), WOMAC pain (2 studies), WOMAC stiffness (2 studies), SF-12 physical (2 studies), SF-12 mental (2 studies), IKS score (2 studies), or wound complications (1 study). * Statistically significant findings only (P < 0.05) rUKA vs. UKA AKSS (± STD, 95%CI) Cobb (2006) 18w: 166.6 (± 18.36) vs. 137.4 (± 27.46)* Blyth (2017) 3m: 164 (131 to 178) vs. 143 (132 to 166)* Blyth (2017) -1y: 171 (153 to 179) vs. 164 (144 to 182) rUKA vs. UKA VAS Pain (± STD, 95%CI) Blyth (2017) 3m: 8/100 (2 to 21) vs. 9/100 (4 to 28) Kayani (2017)(2) 2d: 2.6/10 (± 0.7) vs. 5.6/10 (± 1.3)* rUKA vs. UKA ROM (± STD) Hansen (2014) 0d: 69.08° (± 15.9°) vs. 54.81° (± 20.26°)* Kayani (2017)(2) 3d: 98.5° (± 8.8°) vs. 93.3° (± 4.9°)* rUKA vs. UKA Time (h) to Physiotherapy (± STD) Hansen (2014): 42.17 (± 14.55) vs. 52.47 (± 19.77)* rUKA vs. UKA LOS (h) (± STD) Kayani (2017)(2): 42.5 (± 5.9) vs. 71.1 (± 14.6)* rUKA vs. UKA Post-Operative Medial Sided Knee Pain Hansen (2014) 6m: 20% vs. 3.3%* rUKA vs. UKA Revision Rate Batallier (2018) 2y: 7% vs. 9% Wong (2019) 2y: 12% vs. 6.8%* | “These excellent results in the orientation of the implant are in contrast with the fact that the current evidence still does not show benefits for RAS in its survivorship or in the functional results in the long term.” (p175) “Surgery with robotic-assistance is a useful tool in increasing the precision of the unicompartmental medial knee implant placement. While this may in theory improve clinical, functional and survival results, it is not possible to confirm so with the current evidence. There is still contradictory literature in relation to survivorship, initial clinical results and longterm functional results.” (p175) |
Sun, 202120 | |
rUKA vs. UKA Complications RR (95%CI) 16 studies: 0.52 (0.28 to 0.96) (favours rUKA, P = 0.0366) rUKA vs. UKA Revision Rate RR (95%CI) 10 studies: 0.42 (0.20 to 0.86) (favours rUKA, P = 0.017) | “To summarise, this meta-analysis study indicates that robotic-assisted UKA is associated with fewer complications and lower rates of revision surgery than conventional UKA. No evidence suggests that the use of robotic systems might increase the rate of non-implant- specific complications of UKA. Therefore, the study provides evidence that robotic-assisted UKA has fewer complications and lower revision rates than conventional UKA; however, owing to important limitations, the results lack reliability, and more studies are required.” (p8) |
Zhang J., 202121 | |
*Statistically significant difference (P < 0.05) rTKA vs. TKA WOMAC (function) Mean Difference (95%CI) 2 studies: -11.18 (-17.09 to -5.27) favours rTKA* rTKA vs. TKA WOMAC (pain) Mean Difference (95%CI) 2 studies: -2.76 (-4.88 to -0.64) favours rTKA* rTKA vs. TKA KSS (function) Mean Difference (95%CI) 2 studies: -3.09 (-4.55 to -1.62) favours rTKA* rTKA vs. TKA KSS (satisfaction) Mean Difference (95%CI) 2 studies: -0.65 (-1.46 to 0.16) rTKA vs. TKA Complications Odds Ratio (95%CI) 5 studies: 1.36 (0.63 to 2.94) | “rTKA demonstrated improved accuracy of component positioning and early patient-reported outcomes, though it may not be clinically significant. … Future well-powered studies should report on the knee alignment and balancing techniques utilised in rTKAs to enable greater comparisons to be made on which techniques maximally benefit patient outcomes and provide better insights into alternate alignment philosophies.” (p12) “Although there was a significant difference in the KSS of 1.23 points in favour of rTKA, this is not greater than the minimal clinical important difference (MCID) and, therefore, may not be clinically relevant. Similarly, for WOMAC scores, there was a statistically significant difference but may not be clinically relevant.” (p9) “Given that only 33% of the weighted studies (n = 2/6) in the current analysis had a minimum follow-up of 1 year, of which only one had a follow-up of 15 months for the RATKA group, there remains a need for improved evidence with longer follow-up to better assess longer term complication and revision rates. There are a few key limitations of the data” (p10) |
Zhang P., 202122 | |
rUKA vs. UKA AKSS Mean Difference (95%CI) 4 studies: -2.41 (-7.50 to 12.31) rUKA vs. UKA ROM Mean Difference (95%CI) 3 studies: -0.24 (-5.78 to 5.29) rUKA vs. UKA Pain Odds Ratio (95%CI) 4 studies: 0.59 (0.23 to 1.51) rUKA vs. UKA Revision Odds Ratio (95%CI) 5 studies: 0.88 (0.43 to 1.82) rUKA vs. UKA Complications Odds Ratio (95%CI) 4 studies <2y: 0.77 (0.32 to 1.85) 4 studies ≥2y: 1.41 (0.72 to 2.77) 8 studies all: 1.12 (0.66 to 1.91) | “Robotic-assisted UKA has better component position accuracy compared with conventional UKA. But there was no significant difference in clinical results. In order to further evaluate the utility of robotic-assisted UKA, long-term follow-up RCTs are needed, as well as studies to evaluate the correlation between post-operative alignment and long-term clinical results.” (p10) |
AKSS = American Knee Society Score; CI = confidence interval; d = days; ES = effect size; h = hours; HSS = Hospital for Special Surgery Knee Score; KSFS = Knee Society Function Score; KSS = Knee Society Score; LOS = length of stay; m = months; MCID = minimal clinically important difference; NR = not reported; ns = not statistically significant; NRS = numerical rating scale; ROM = range of motion; RR = relative risk; rTKA = robotic assisted total knee arthroplasty; rUKA = robotic assisted unicompartmental knee arthroplasty; SF-12 = Short Form Health Survey; STD = standard deviation; TKA = total knee arthroplasty; UKA = unicompartmental knee arthroplasty; VAS = visual analogue scale; vs. = versus; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index; y = year
Table 9: Summary of Findings of Included Randomized Controlled Trials
Main study findings | Authors’ conclusion |
|---|---|
Banger et al. (2021)23 | |
There were no statistically significant findings in any functional, satisfaction, complication, or revision outcomes in rTKA (n = 55) as compared to TKA (n = 49) at 5 years follow-up. Except: All Cause Reintervention over 5 years (includes all surgical procedures carried out on the knee). All Cause Reintervention rUKA: 0 UKA: 6 (P < 0.001) | “This study has shown a lower reintervention rate at five years for robotic arm-assisted UKA when compared with a manual approach. Excellent clinical outcomes were seen in both groups, with no statistical or clinical differences in outcomes was observed at five years.” (p1094) “There were no differences in postoperative complications between the two groups, nor in the number of attendances to the hospital outpatient clinic. None of the robotic arm-assisted group required further surgery, with six (9%) of the manual group requiring a reintervention. Of the six patients, two were complete revisions to TKA (one for early tibial loosening at 2.5 years in a patient following a fall, and one for pain). Four underwent arthroscopic procedures; three for pain plus a possible lateral meniscal tear and one for possible infection when a biopsy was carried out. There were no alignment or component position errors identified in any of these six patients.” (p 1091) |
Batailler et al. (2021)(2)2 | |
There were no statistically significant findings in any functional, satisfaction, gait, complication, or revision outcomes in rUKA (n = 33) as compared to UKA (n = 33) at 6 months follow-up. Except: Mean Walking Speed (km/h) (± STD [range]) rUKA: 2.4±0.7[1.2 to 4] UKA: 2.8±0.7[0.8 to 4] (P < 0.001) | “Gait parameters at 6 months after medial UKA were comparable between the techniques. There was no significant difference between these two techniques for clinical outcomes at 6 months after medial UKA.” (p9) |
Blyth et al. (2021)24 | |
There were no statistically significant findings in any functional, satisfaction, pain, activity, LOS, complication, or revision outcomes in TKA (n = 42) as compared to bi-rUKA (n = 34) at 1 year follow-up. Except: Mean Operative Time (minutes) (± STD) bi-rUKA: 159.4 (± 20.1) TKA: 96.8 (±15.8) (P < 0.001) | “Robotic arm-assisted, cruciate-sparing bi-UKA offered similar early clinical outcomes and rates of complications to a mechanically aligned TKA, both in the immediate postoperative period and up to one year following surgery.”(p1561) “However, on the basis of our results, we are unable to recommend bi-UKA as a routine alternative treatment for patients with OA of the knee at present. We are also unable to identify which patients might benefit from this approach with the limited data that this study generated. The accuracy of robotic arm-assisted technology,” (p1568) |
LOS = length of stay; OA = osteoarthritis; rTKA = robotic assisted total knee arthroplasty; rUKA = robotic assisted unicompartmental knee arthroplasty; STD = standard deviation; TKA = total knee arthroplasty; vs. = versus; UKA = unicompartmental knee arthroplasty;
Table 10: Summary of Findings of Included Economic Evaluations
Main study findings | Authors’ conclusion |
|---|---|
Rajan et al. (2022)10 | |
rTKA vs. TKA Cost-Effectiveness QALYs: 13.55 vs. 13.29 ICER ($/QALY) Low volume (13/y): $92,823 Mid volume (100/y): $29,261 High volume (200/y): $25,730 Sensitivity Analysis “All things being equal, if the annualized revision rate for conventional TKA is decreased to 0%, robotic-assisted TKA would still be the preferred method at the $100,000/QALY WTP. The robotic-assisted revision rate would have to increase from the base case of 0.6% to 1.6% or 2.2% for conventional TKA to become the preferred procedure at the $50,000 and $100,000/QALY WTPs, respectively.” (p6) Probabilistic Sensitivity Analysis “We found that at $50,000 and $100,000 WTPs, robotic-assisted TKA was cost-effective 67.5% and 68.5% of the time.” (p7) | “Robotic-assisted TKAs are associated with higher capital equipment and surgical costs. However, with lower annualized revision rates and higher postoperative QoL, robotic-assisted TKAs were found to be cost-effective.” (p8) |
Vermue et al. (2021)11 | |
rTKA vs. TKA Cost-Effectiveness QALYs: 9.22 vs. 9.19 ICER ($/QALY) Mid volume (70/y): $376,145 High volume (253/y): <$50,000 Probabilistic Sensitivity Analysis At $50,000 WTP, robotic-assisted TKA was cost-effective 2.18% of the time.” (p7) | “Robot-assisted TKA might be a cost-effective procedure compared to conventional TKA if a minimum of 253 cases are performed on a yearly basis. The cost-benefit of the robotic TKA surgery is mainly based on a decreased revision rate. This study is based on the assumption that alignment is a predictor of success in total knee arthroplasty. Until there is data confirming the assertion that alignment predicts success robot-assisted surgery cannot be recommended.” (p351) |
Burn et al. (2020)3 | |
To achieve cost-effectiveness threshold of ₤20,000/QALY, and NHS willing to pay up to an additional ₤10,000 for the robotic technology, post-primary unrevised QoL would need to be improved by 5% on average, or NHS willing to pay an additional ₤1,000 extra if robotic technology could halve the revision rate. | “At current prices, computer- and robot-assisted knee and hip replacement will likely need to lead to improvements in patient-reported outcomes in addition to any reduction in the risk revision.” (p719) |
Nherera et al. (2020)9 | |
Non-CT rUKA vs. UKA Cost-Effectiveness (100 patients) total QALYs: 440 vs. 431 ICER (₤QALY) Low volume (20/y): ₤43,581 High volume (100/y): ₤2,831 Sensitivity Analyses - (100 cases/year, 65yo) The cost per QALY ranges from conditions where non-CT rUKA dominates to conditions where cost per QALY is ₤33,704. Non-CT rUKA would dominate when patients are under 55 years old, and 7-year follow up. Highest costs/QALY for non-CT rUKA occur in patients over 75 (₤10,283), 2-year follow up (₤33,704), and upper estimates of the costs of robotics (₤5,676). Probabilistic Sensitivity Analysis At ₤20,000/QALY WTP, non-CT robotic-assisted UKA was cost-effective 100% of the time. | “According to our economic analysis, the use of non-CT robotics-assisted UKA may be more cost-effective when compared to traditional UKA for patients with knee osteoarthritis when performed at high-volume orthopaedic centres with experienced clinicians.” (p7) |
Clement et al. (2019)8 | |
rUKA vs. TKA vs. UKA Cost-Effectiveness (100 patients/y) total QALYs : 13.59 vs.11.80 vs. 12.20 ICER (₤QALY) (100/y) over TKA: ₤7,170 over UKA: ₤8,604 | “In conclusion, rUKA can be considered a cost-effective alternative to manual TKA and UKA for patients with isolated medial compartment OA of the knee. The cost per QALY is less than the lowest cost threshold defined by NICE and could be supported for use within the NHS. In the knowledge of improved functional outcomes and lower complication rates relative to TKA and improved implant survival relative to manual UKA, it would seem inevitable that cost-effective rUKA will be introduced to the NHS.” (p1069) |
CT = computed tomography; ICER = incremental cost-effectiveness ratio; NHS = national health service; OA = osteoarthritis; QALY = quality-adjusted life-year; rTKA = robotic assisted total knee arthroplasty; QoL = quality of life; rUKA = robotic assisted unicompartmental knee arthroplasty; STD = standard deviation; TKA = total knee arthroplasty; UKA = unicompartmental knee arthroplasty; vs. = versus; WTP = willingness-to-pay; y = year;
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
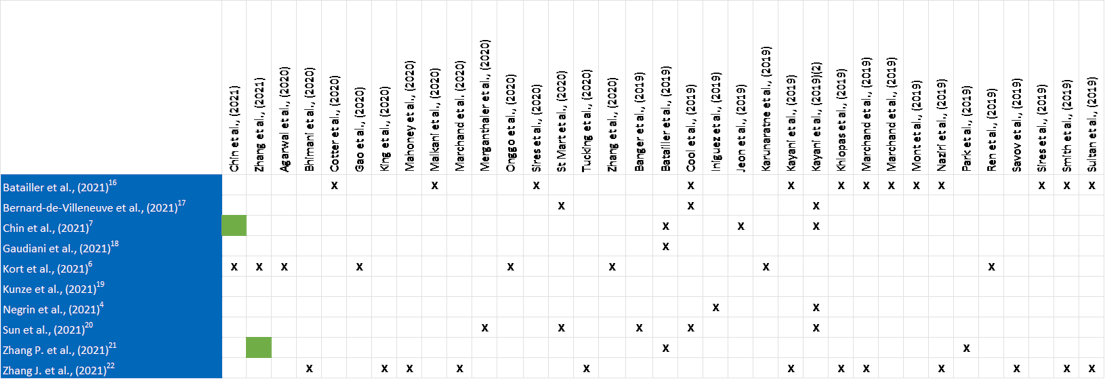
Green squares indicate that Kort et al. included Chin et al. and Zhang P et al. as indicated. Data from these two SRs was not reported more than once in this report.
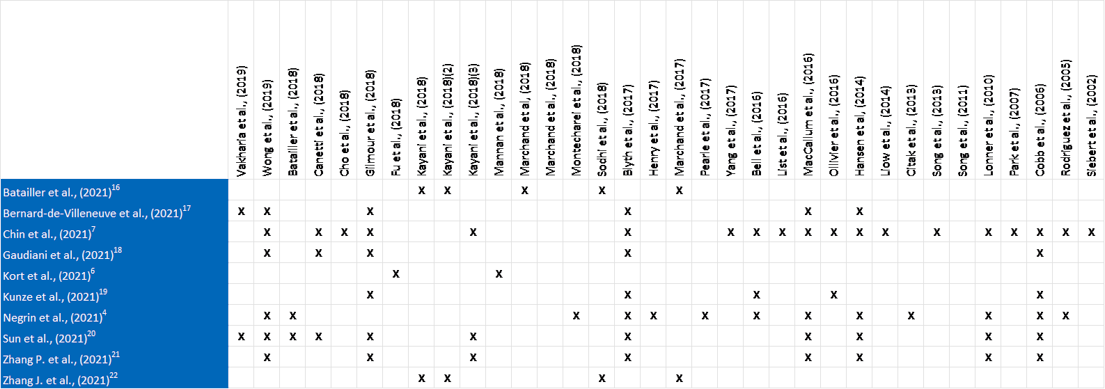
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Systematic Review of Conflict of Interest
DeFrance MJ, Yayac MF, Courtney PM, Squire MW. The impact of author financial conflicts on robotic-assisted joint arthroplasty research. J Arthroplasty. 2021;36(4):1462-1469. PubMed
Additional Clinical Efficacy References published between January 1, 2017 and December 31, 2020 and Non-randomized comparative studies
King CA, Jordan M, Bradley AT, Wlodarski C, Tauchen A, Puri L. Transitioning a practice to robotic total knee arthroplasty is correlated with favorable short-term clinical outcomes-a single surgeon experience. J Knee Surg. 2022;35(1):78-82. PubMed
Archer A, Salem HS, Coppolecchia A, Mont MA. Lengths of stay and discharge dispositions after total knee arthroplasty: a comparison of robotic-assisted and manual techniques. J Knee Surg. 2021 Oct 5. PubMed
Bendich I, Kapadia M, Alpaugh K, Diane A, Vigdorchik J, Westrich G. Trends of utilization and 90-day complication rates for computer-assisted navigation and robotic assistance for total knee arthroplasty in the United States from 2010 to 2018. Arthroplast Today. 2021;11:134-139. PubMed
Blyth MJG, Banger MS, Doonan J, Jones BG, MacLean AD, Rowe PJ. Early outcomes after robotic arm-assisted bi-unicompartmental knee arthroplasty compared with total knee arthroplasty: a prospective, randomized controlled trial. Bone Joint J. 2021;103-B(10):1561-1570. PubMed
Crizer MP, Haffar A, Battenberg A, McGrath M, Sutton R, Lonner JH. Robotic assistance in unicompartmental knee arthroplasty results in superior early functional recovery and is more likely to meet patient expectations. Adv Orthop. 2021 Jul 14;2021:4770960. PubMed
DeFrance MJ, Yayac MF, Courtney PM, Squire MW. The impact of author financial conflicts on robotic-assisted joint arthroplasty research. J Arthroplasty. 2021;36(4):1462-1469. PubMed
Emara AK, Zhou G, Klika AK, et al. Robotic-arm-assisted knee arthroplasty associated with favorable in-hospital metrics and exponentially rising adoption compared with manual knee arthroplasty. J Am Acad Orthop Surg. 2021;29(24):e1328-e1342. PubMed
Hamilton DA, Ononuju U, Nowak C, Chen C, Darwiche H. Differences in immediate postoperative outcomes between robotic-assisted TKA and conventional TKA. Arthroplast Today. 2021;8:57-62. PubMed
Held MB, Gazgalis A, Neuwirth AL, Shah RP, Cooper HJ, Geller JA. Imageless robotic-assisted total knee arthroplasty leads to similar 24-month WOMAC scores as compared to conventional total knee arthroplasty: a retrospective cohort study. Knee Surg Sports Traumatol Arthrosc. 2021 May 7. PubMed
Khan H, Dhillon K, Mahapatra P, et al. Blood loss and transfusion risk in robotic-assisted knee arthroplasty: A retrospective analysis. Int J Med Robot. 2021;17(6):e2308. PubMed
Marchand KB, Moody R, Scholl LY, et al. Results of robotic-assisted versus manual total knee arthroplasty at 2-year follow-up. J Knee Surg. 2021 Jun 29. PubMed
Mergenthaler G, Batailler C, Lording T, Servien E, Lustig S. Is robotic-assisted unicompartmental knee arthroplasty a safe procedure? A case control study. Knee Surg Sports Traumatol Arthrosc. 2021;29(3):931-938. PubMed
Mitchell J, Wang J, Bukowski B, et al. Relative clinical outcomes comparing manual and robotic-assisted total knee arthroplasty at minimum 1-year follow-up. HSS J. 2021;17(3):267-273. PubMed
Negrin R, Duboy J, Iniguez M, et al. Robotic-assisted vs conventional surgery in medial unicompartmental knee arthroplasty: a clinical and radiological study. Knee Surg Relat Res. 2021;33(1):5. PubMed
Shaw JH, Lindsay-Rivera KG, Buckley PJ, Weir RM, Banka TR, Davis JJ. Minimal clinically important difference in robotic-assisted total knee arthroplasty versus standard manual total knee arthroplasty. J Arthroplasty. 2021;36(7S):S233-S241. PubMed
Shearman AD, Sephton BM, Wilson J, Nathwani DK. Robotic-assisted unicompartmental knee arthroplasty is associated with earlier discharge from physiotherapy and reduced length-of-stay compared to conventional navigated techniques. Arch Orthop Trauma Surg. 2021;141(12):2147-2153. PubMed
Smith AF, Eccles CJ, Bhimani SJ, et al. Improved patient satisfaction following robotic-assisted total knee arthroplasty. J Knee Surg. 2021;34(7):730-738. PubMed
Stulberg BN, Zadzilka JD, Kreuzer S, et al. Safe and effective use of active robotics for TKA: early results of a multicenter study. J Orthop. 2021 Jul 23;26:119-125. PubMed
Wu C, Fukui N, Lin YK, et al. Comparison of robotic and conventional unicompartmental knee arthroplasty outcomes in patients with osteoarthritis: a retrospective cohort study. J Clin Med. 2021;11(1):31. PubMed
Zhang J, Ndou WS, Ng N, et al. Correction to: Robotic-arm assisted total knee arthroplasty is associated with improved accuracy and patient reported outcomes: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2021;18:18.
Agarwal N, To K, McDonnell S, Khan W. Clinical and radiological outcomes in robotic-assisted total knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty. 2020;35(11):3393-3409.e3392. PubMed
Bhimani SJ, Bhimani R, Smith A, Eccles C, Smith L, Malkani A. Robotic-assisted total knee arthroplasty demonstrates decreased postoperative pain and opioid usage compared to conventional total knee arthroplasty. Bone Jt Open. 2020;1(2):8-12. PubMed
Clement ND, Bell A, Simpson P, Macpherson G, Patton JT, Hamilton DF. Robotic-assisted unicompartmental knee arthroplasty has a greater early functional outcome when compared to manual total knee arthroplasty for isolated medial compartment arthritis. Bone Joint Res. 2020;9(1):15-22. PubMed
Gao J, Dong S, Li JJ, Ge L, Xing D, Lin J. New technology-based assistive techniques in total knee arthroplasty: a Bayesian network meta-analysis and systematic review. Int J Med Robot. 2020:e2189. PubMed
Greiner JJ, Wang JF, Mitchell J, Hetzel SJ, Lee EJ, Illgen RL. Opioid use in robotic-arm assisted total knee arthroplasty: a comparison to conventional manual total knee arthroplasty. Surg Technol Int. 2020;37:280-289. PubMed
Grosso MJ, Li WT, Hozack WJ, Sherman M, Parvizi J, Courtney PM. Short-term outcomes are comparable between robotic-arm assisted and traditional total knee arthroplasty. J Knee Surg. 2020 Oct 27. PubMed
Iturriaga C, Salem HS, Ehiorobo JO, Sodhi N, Mont MA. Robotic-assisted versus manual unicompartmental knee arthroplasty: a systematic review. Surg Technol Int. 2020;37:275-279. PubMed
Khlopas A, Sodhi N, Hozack WJ, et al. Patient-reported functional and satisfaction outcomes after robotic-arm-assisted total knee arthroplasty: early results of a prospective multicenter investigation. J Knee Surg. 2020;33(7):685-690. PubMed
Kim YH, Yoon SH, Park JW. Does robotic-assisted tka result in better outcome scores or long-term survivorship than conventional TKA? A randomized, controlled trial. Clin Orthop Relat Res. 2020;478(2):266-275. PubMed
Lin J, Yan S, Ye Z, Zhao X. A systematic review of MAKO-assisted unicompartmental knee arthroplasty. Int J Med Robot. 2020;16(5):1-7. PubMed
Mancino F, Cacciola G, Malahias MA, et al. What are the benefits of robotic-assisted total knee arthroplasty over conventional manual total knee arthroplasty? A systematic review of comparative studies. Orthop Rev (Pavia). 2020;12(Suppl 1):8657. PubMed
Ofa SA, Ross BJ, Flick TR, Patel AH, Sherman WF. Robotic total knee arthroplasty vs conventional total knee arthroplasty: a nationwide database study. Arthroplast Today. 2020;6(4):1001-1008.e1003. PubMed
Onggo JR, Onggo JD, De Steiger R, Hau R. Robotic-assisted total knee arthroplasty is comparable to conventional total knee arthroplasty: a meta-analysis and systematic review. Arch Orthop Trauma Surg. 2020;140(10):1533-1549. PubMed
Pelkowski JN, Wilke BK, Crowe MM, Sherman CE, Ortiguera CJ, Ledford CK. Robotic-assisted versus manual total knee arthroplasty in a crossover cohort: what did patients prefer? Surg Technol Int. 2020;37:336-340. PubMed
Shatrov J, Parker D. Computer and robotic - assisted total knee arthroplasty: a review of outcomes. J. 2020;7(1):70.
St Mart JP, de Steiger RN, Cuthbert A, Donnelly W. The three-year survivorship of robotically assisted versus non-robotically assisted unicompartmental knee arthroplasty. Bone Joint J. 2020;102-B(3):319-328. PubMed
Yun AG, Qutami M, Chen CM, Pasko KBD. Management of failed UKA to TKA: conventional versus robotic-assisted conversion technique. Knee Surg Relat Res. 2020;32(1):38. PubMed
Batailler C, White N, Ranaldi FM, Neyret P, Servien E, Lustig S. Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1232-1240. PubMed
Cho KJ, Seon JK, Jang WY, Park CG, Song EK. Robotic versus conventional primary total knee arthroplasty: clinical and radiological long-term results with a minimum follow-up of ten years. Int Orthop. 2019;43(6):1345-1354. PubMed
Cool CL, Needham KA, Khlopas A, Mont MA. Revision analysis of robotic arm-assisted and manual unicompartmental knee arthroplasty. J Arthroplasty. 2019;34(5):926-931. PubMed
Jeon SW, Kim KI, Song SJ. Robot-assisted total knee arthroplasty does not improve long-term clinical and radiologic outcomes. J Arthroplasty. 2019;34(8):1656-1661. PubMed
Karunaratne S, Duan M, Pappas E, et al. The effectiveness of robotic hip and knee arthroplasty on patient-reported outcomes: A systematic review and meta-analysis. Int Orthop. 2019;43(6):1283-1295. PubMed
Kayani B, Konan S, Ayuob A, Onochie E, Al-Jabri T, Haddad FS. Robotic technology in total knee arthroplasty: a systematic review. EFORT Open Rev. 2019;4(10):611-617. PubMed
Kayani B, Konan S, Tahmassebi J, Rowan FE, Haddad FS. An assessment of early functional rehabilitation and hospital discharge in conventional versus robotic-arm assisted unicompartmental knee arthroplasty: a prospective cohort study. Bone Joint J. 2019;101-B(1):24-33. PubMed
Marchand RC, Sodhi N, Anis HK, et al. One-year patient outcomes for robotic-arm-assisted versus manual total knee arthroplasty. J Knee Surg. 2019;32(11):1063-1068. PubMed
Naziri Q, Cusson BC, Chaudhri M, Shah NV, Sastry A. Making the transition from traditional to robotic-arm assisted TKA: What to expect? A single-surgeon comparative-analysis of the first-40 consecutive cases. J Orthop. 2019;16(4):364-368. PubMed
Park KK, Han CD, Yang IH, Lee WS, Han JH, Kwon HM. Robot-assisted unicompartmental knee arthroplasty can reduce radiologic outliers compared to conventional techniques. PLoS ONE. 2019;14(12):e0225941. PubMed
Ren Y, Cao S, Wu J, Weng X, Feng B. Efficacy and reliability of active robotic-assisted total knee arthroplasty compared with conventional total knee arthroplasty: a systematic review and meta-analysis. Postgrad Med J. 2019;95(1121):125-133. PubMed
Wong J, Murtaugh T, Lakra A, Cooper HJ, Shah RP, Geller JA. Robotic-assisted unicompartmental knee replacement offers no early advantage over conventional unicompartmental knee replacement. Knee Surg Sports Traumatol Arthrosc. 2019;27(7):2303-2308. PubMed
Zhang F, Li H, Ba Z, Bo C, Li K. Robotic arm-assisted vs conventional unicompartmental knee arthroplasty: a meta-analysis of the effects on clinical outcomes. Medicine (Baltimore). 2019;98(35):e16968. PubMed
Canetti R, Batailler C, Bankhead C, Neyret P, Servien E, Lustig S. Faster return to sport after robotic-assisted lateral unicompartmental knee arthroplasty: a comparative study. Arch Orthop Trauma Surg. 2018;138(12):1765-1771. PubMed
Fu J, Wang Y, Li X, et al. Robot-assisted vs. conventional unicompartmental knee arthroplasty: Systematic review and meta-analysis. Orthopade. 2018;47(12):1009-1017. PubMed
Gilmour A, MacLean AD, Rowe PJ, et al. Robotic-arm-assisted vs conventional unicompartmental knee arthroplasty. The 2-year clinical outcomes of a randomized controlled trial. J Arthroplasty. 2018;33(7S):S109-S115. PubMed
Kayani B, Konan S, Tahmassebi J, Pietrzak JRT, Haddad FS. Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty: a prospective cohort study. Bone Joint J. 2018;100-B(7):930-937. PubMed
Motesharei A, Rowe P, Blyth M, Jones B, Maclean A. A comparison of gait one year post operation in an RCT of robotic UKA versus traditional Oxford UKA. Gait Posture. 2018;62:41-45. PubMed
Naziri Q, Mixa PJ, Murray DP, et al. Robotic-assisted and computer-navigated unicompartmental knee arthroplasties: a systematic review. Surg Technol Int. 2018;32:271-278. PubMed
Blyth MJG, Anthony I, Rowe P, Banger MS, MacLean A, Jones B. Robotic arm-assisted versus conventional unicompartmental knee arthroplasty: Exploratory secondary analysis of a randomised controlled trial. Bone Joint Res. 2017;6(11):631-639. PubMed
Liow MHL, Goh GS, Wong MK, Chin PL, Tay DK, Yeo SJ. Robotic-assisted total knee arthroplasty may lead to improvement in quality-of-life measures: a 2-year follow-up of a prospective randomized trial. Knee Surg Sports Traumatol Arthrosc. 2017;25(9):2942-2951. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.