CADTH Health Technology Review
Anakinra Therapy for Hemophagocytic Lymphohistiocytosis
Rapid Review
Authors: Sarah Ndegwa, Alison Adams
Abbreviations
HLH
hemophagocytic lymphohistiocytosis
IVIG
intravenous immunoglobulin
MAS
macrophage activation syndrome
pHLH
primary hemophagocytic lymphohistiocytosis
RCT
randomized controlled trial
sHLH
secondary hemophagocytic lymphohistiocytosis
sJIA
systemic juvenile idiopathic arthritis
Key Messages
Evidence from 1 retrospective cohort study (identified in 1 systematic review) suggested that anakinra may reduce 28-day mortality and the risk for death in adults diagnosed with hemophagocytic lymphohistiocytosis (HLH).
Due to the very low certainty of evidence from the single cohort study included in the systematic review, there is insufficient information to draw reliable conclusions regarding the clinical effectiveness of anakinra compared to standard treatments for patients diagnosed with HLH.
No evidence on the safety or cost-effectiveness of anakinra compared to current standard treatments or to placebo was identified.
Context and Policy Issues
Hemophagocytic lymphohistiocytosis (HLH) is a rare life-threatening syndrome characterized by uncontrolled activation of the immune system.1 HLH occurs most frequently in infants from birth to 18 months, but the syndrome has also been observed in children and adults of all ages.2 Symptoms of HLH are non-specific and are often difficult to differentiate from other hyperinflammatory disorders including sepsis and multiple organ dysfunction syndrome.1,3 Common findings include persistent fever, high serum ferritin, hepatosplenomegaly (swelling of the liver and spleen), rash, enlargement of the lymph nodes, neurologic symptoms, low blood cell counts, and liver function abnormalities.2 Unless diagnosed and treated early, patients with HLH typically progress to multi-organ failure associated with a high rate of mortality.
Nomenclature and diagnostic classification in this field are not clearly defined.4 Primary HLH (pHLH) is a term used to describe HLH that presents in infancy or early childhood as the result of inherited genetic mutations in inflammatory mediators.5 Secondary HLH (sHLH) refers to HLH triggered by viral infection, autoimmune disease, hematologic malignancy, or rheumatologic disease. Viral triggers (e.g., Epstein-Barr virus, cytomegalovirus, adenovirus, and herpes simplex virus) are the leading cause of sHLH.6,7 Recently, there have been reports of sHLH triggered by COVID-19.8-10 Macrophage activation syndrome (MAS) is typically used to describe sHLH when the underlying pathology is a rheumatologic disease (e.g., systemic juvenile idiopathic arthritis [sJIA], adult-onset Still’s disease).11 It is important to note that there is substantial overlap in the predisposing factors for pHLH and sHLH in that both can be triggered by infections or other immune activation events, and gene mutations can be found in individuals of any age.2
The diagnostic criteria for HLH have not been universally accepted or adopted, and current strategies (such as those based on HLH-2004 guidelines12 and HScore13) have substantial limitations.7,14 Prompt diagnosis is often hindered by the rarity of the syndrome, variable clinical presentation, and lack of specificity of clinical and laboratory findings.15 Treatment of HLH is centred on immunosuppressive therapy (including corticosteroids, IV immunoglobulin [IVIG], methotrexate, cyclosporin, and etoposide) combined with treatment of the triggering illness.3,16,17 However, this regimen has considerable treatment-related morbidity due to complications associated with immunosuppressive treatment, such as secondary infections, myelotoxicity, hepatic dysfunction, and secondary malignancies.1 Treatment with corticosteroids can hinder the diagnosis of certain malignancies (e.g., lymphoma), which is a concern in patients in whom the underlying HLH trigger is cancer.18 In addition, there are high costs associated with the use of IVIG.18 Hence, there is a need for alternative treatments that are cost-effective and have less treatment-associated toxicity.
Anakinra is a recombinant human interleukin-1 (IL-1) receptor antagonist.19 IL-1 is a proinflammatory mediator produced in response to infection and is central to the hyperinflammation process observed in HLH.7 In Canada, anakinra (Kineret) is approved for the treatment for adults with rheumatoid arthritis and adults, children, and infants over the age of 8 months diagnosed with Neonatal-Onset Multisystem Inflammatory Disease.19 Anakinra a promising treatment for HLH due to a short half-life and wide therapeutic range.20 Anakinra does not mask indicators of infection, but it is unclear whether anakinra is less myelosuppressive and less hepatotoxic than standard immunosuppressive therapy for HLH.7 It is unknown whether early treatment with anakinra has the potential to stabilize the hyperinflammatory process in HLH while acting as a bridging treatment to allow time for the diagnosis and treatment of the underlying triggering disease.18
The objective of the report is to summarize the evidence regarding the clinical and cost-effectiveness of anakinra for the treatment of HLH.
Research Questions
What is the clinical effectiveness of anakinra therapy for hemophagocytic lymphohistiocytosis?
What is the cost-effectiveness of anakinra therapy for hemophagocytic lymphohistiocytosis?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Library, the University of York Centre for Reviews and Dissemination databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were anakinra therapy and hemophagocytic lymphohistiocytosis. No filters were applied to limit the retrieval by study type. Conference abstracts were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2011 and December 14, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients of all ages with HLH including macrophage activation syndrome |
Intervention | Anakinra therapy |
Comparator |
|
Outcomes | Q1: Clinical effectiveness (e.g., mortality, end organ failure, hospital acquired infections, markers of MAS activity), safety (e.g., adverse events, serious adverse events, sepsis) Q2: Cost-effectiveness (e.g., cost per QALY) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations |
HLH = hemophagocytic lymphohistiocytosis; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2011. Articles describing patients with clinical features of excessive immune activation (e.g., hyperinflammatory syndromes, cytokine storm, or multi-organ failure) but without a specific diagnosis or HLH or MAS were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Narrative reviews, case series, case reports, and retrospective chart reviews were excluded from the main body of the report but are included in Appendix 5.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)21 for systematic reviews. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
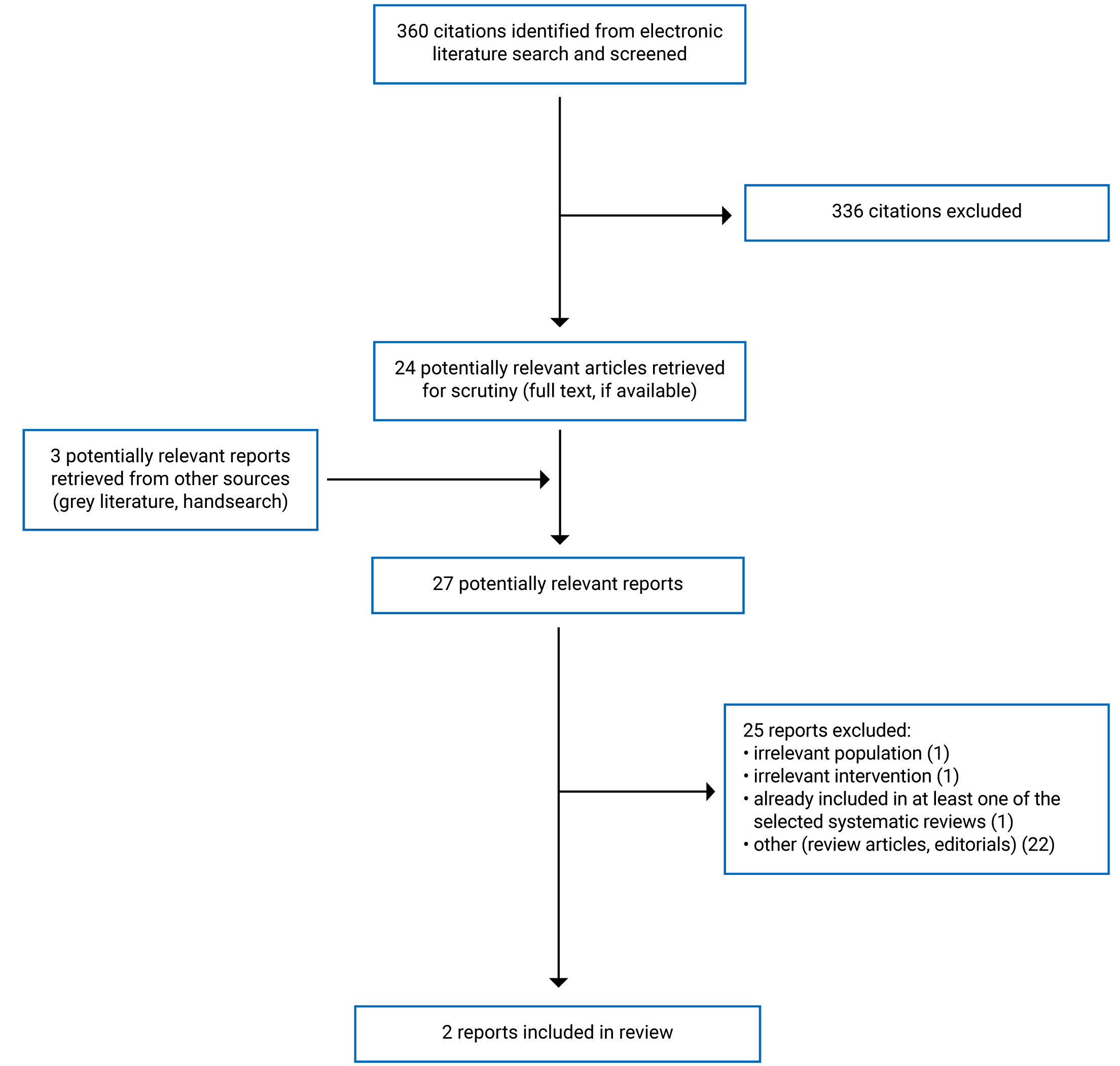
A total of 360 citations were identified in the literature search. Following screening of titles and abstracts, 336 citations were excluded and 24 potentially relevant reports from the electronic search were retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 25 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. Both the included publications were systematic reviews. No relevant randomized controlled trials, non-randomized studies, or economic evaluations were identified. Appendix 1 presents the PRISMA22 flowchart of the study selection.
Summary of Study Characteristics
Two systematic reviews23,24 (that included a total of 1 relevant primary study for this report) were identified for inclusion in this review. One systematic review23 published in 2020 had eligibility criteria that was more restrictive than the current review. The eligible patient population was restricted to patients of all ages with a diagnosis of sHLH triggered by COVID-19.23 Evidence related to other coronaviruses (e.g., severe acute respiratory syndrome or Middle East respiratory syndrome) was also considered. Eligible studies included systematic reviews, randomized controlled trials (RCTs), controlled clinical trials, and observational studies (including case series) published between 2000 and 2020. Case reports were also considered when no higher-level quality evidence was found. However, no relevant studies were identified. Two preliminary unpublished primary studies25,26 of interest were identified but neither met the selection criteria outlined in Table 1 for this report.
One systematic review24 published in 2020 had eligibility criteria that was closely aligned with the current review including (i.e., patients of all ages presenting with pHLH or sHLH, regardless of the trigger condition). Eligible studies included systematic reviews, clinical trials, and cohort studies published between 2010 and 2020. Case series were considered when no higher-level quality evidence was found. A total of 6 identified studies (1 comparative cohort study and 5 case series) published between 2016 and 2019 were included. The 5 case series each conducted a retrospective review of case notes in a single centre, spanning between 2 and 10 years from 2007 to 2017. However, since the case series did not include a comparator relevant to this report, the findings of these case series will not be discussed in this report. Only the characteristics and results of the relevant study will be discussed in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The relevant cohort study included in the systematic review24 was a non-randomized retrospective subgroup analysis of patients recruited to an earlier phase III RCT investigating patients with sepsis.
Country of Origin
Both systematic reviews were commissioned by NHS England in the UK.23,24 The relevant cohort study included within the systematic review,24 was conducted by researchers in the US. The original RCT was a multicenter study (91 centers from 11 countries in Europe and North America).24 However, the location of the patients included in the subgroup analysis of the cohort study was not reported.
Patient Population
The patient population in the 1 relevant cohort study included in the systematic review24 were adults with sepsis with multi-organ dysfunction and/or shock with features of MAS (defined as the presence of hepatobiliary dysfunction or disseminated intravascular coagulation). The systematic review authors stated that there were no between-group differences in baseline characteristics including age, gender, the severity of acute kidney injury or respiratory distress syndrome, or the risk of death.
Interventions and Comparators
Anakinra 2 mg/kg/hour given intravenously for 72 hours was assessed in the relevant cohort study included in the systematic review.24 The comparator was placebo 2 mg/kg/hour given intravenously for 72 hours. Concomitant treatments in each arm were not reported.
Outcomes
The relevant cohort study in the systematic review24 reported the 28-day mortality of patients receiving anakinra compared to placebo.
Summary of Critical Appraisal
Since 1 of the systematic reviews23 did not identify any relevant primary studies, only the sections regarding search methodology were critically appraised. Neither of the included systematic reviews23,24 indicated that a research protocol was established before conducting the review. The lack of a well-developed protocol has the potential to introduce bias if the methods used to conduct the review were adjusted during the review process. However, the authors of both systematic reviews did state that the methodology followed the NHS England guidance for developing evidence reviews. Both systematic reviews had a well-defined research question, clear eligibility criteria, and a comprehensive approach to the literature search. Multiple databases were searched to identify eligible studies and key search terms were provided. Providing details of these elements of the search strategy increases the reproducibility of the review. It was unclear if the authors of either systematic review performed study selection or data extraction in duplicate. This may have resulted in relevant studies being missed as well as errors in the data extraction. Only 1 of the systematic reviews24 provided a list of excluded studies with justifications for exclusion. Not having such information limits the reader’s ability to assess whether relevant articles were excluded and if so, for what reason. In addition, unjustified exclusion of studies could bias the results of the review.
In the 1 systematic review that identified a relevant primary study,24 the characteristics (when reported) of the included study including study design, baseline characteristics, interventions, comparators and study outcomes were provided in detailed evidence tables. Checklists from the Joanna Briggs Institute were used to critically appraise the methodological quality of the individual studies.27,28 The overall quality of the body of evidence available for each outcome was assessed using a modified version of the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.29 Based on risk of bias assessments, there was discussion around heterogeneity of findings and certainly of evidence within the narrative synthesis. The authors reported that the certainty of the evidence for the relevant outcomes was very low from the studies included in the systematic review. The authors of the systematic review reported several methodological weaknesses in the relevant cohort study, including a retrospective design with post-hoc analysis in which the original randomization process was no longer valid; lack of a defined comparator group (concomitant therapies were not defined); and a limited (N = 43) cohort of patients, meaning that the study was not powered to detect a difference in outcomes between the anakinra and placebo groups.24 Therefore, it is difficult to interpret the extent that findings can be attributable to treatment with anakinra alone.
The sources of funding for the individual studies included in the systematic review were reported. Providing the sources of funding makes it possible to discern whether the funding agency could have influenced the results of the included studies. Both systematic reviews23,24 were commissioned by NHS England. However, it was not reported if the authors of either systematic review had any potential conflicts of interest.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness and Safety of Anakinra
The authors of the systematic review24 evaluated the 28-day mortality and risk of death of patients receiving anakinra compared to standard treatments for HLH from the results of the single comparative cohort study. The authors stated that when assessed using modified GRADE, the certainty in the quality of the identified evidence from the single cohort study was very low.
Mortality, 28 Days
One comparative cohort analysis in the systematic review24 reported a statistically significantly lower 28-day mortality with a statistically significantly lower risk of death in adult patients with HLH treated with anakinra compared to those who received placebo.
Cost-Effectiveness of Anakinra
No relevant evidence regarding the cost-effectiveness of anakinra for HLH was identified; therefore, no summary can be provided.
Limitations
The findings in this report are limited by the quality and quantity of relevant evidence that was identified. The first systematic review23 which focused on anakinra treatment in patients with HLH triggered by COVID-19 was fairly well conducted; however, no relevant reports were identified leaving a gap in evidence to support the use of anakinra in this particular patient population.
The second systematic review24 evaluating anakinra for the treatment of HLH regardless of trigger condition was well conducted. However, 5 of 6 of the identified studies in this systematic review were non-comparative, retrospective, single-centre, case series and thus the findings were not included in this review. The single relevant cohort study described outcomes in middle-aged adults. Hence findings may not be generalizable to infants, children, or senior adults. Considering the inclusion period of the original RCT (which was published in 1997) on which this cohort study was based, a time during which sepsis management was different than what is practised today,30 and the location of patients included in the analysis in unknown, it is unclear how closely the findings are generalizable to the current clinical management of HLH in Canada.
No evidence was identified to evaluate the clinical effectiveness of anakinra compared to standard treatment for other clinically important outcomes including intensive care unit duration of stay, improvement of HLH symptoms, length of hospital stay, acquired infection with treatment, or other adverse events. Furthermore, no relevant studies regarding the cost-effectiveness of anakinra compared to standard treatments or placebo for HLH were identified, therefore no conclusions can be formed on this research question.
Conclusions and Implications for Decision- or Policy-Making
This review evaluated the existing evidence for the clinical effectiveness and cost-effectiveness of anakinra for the treatment of patients with HLH. The findings in this report are limited by the quantity and quality of the evidence that was identified. The key limitation to evaluating the effectiveness of anakinra compared to standard treatment for HLH is the lack of comparative studies. The rarity of the condition, inconsistent nomenclature, variable clinical diagnostic criteria, non-specific symptoms, and the heterogeneity of triggering factors have previously been identified in the literature as barriers to conducting prospective research on this topic.6
One systematic review23 focusing on the outcomes of anakinra in patients with HLH triggered by COVID-19 did not identify any relevant evidence; hence the efficacy of anakinra in this specific patient population is unclear. A second systematic review24 identified very low certainty evidence from 1 retrospective comparative cohort study, that compared to placebo, anakinra reduced 28-day mortality and the risk of death in adult patients with HLH.
An ongoing RCT is currently evaluating the safety of anakinra given as an adjunct to standard treatments compared to placebo in approximately 40 patients over the age of 1 year admitted to hospital with MAS.31 The specific primary objectives of the study are to determine whether giving anakinra results in no increased affects the rates of infection complications or mortality. Estimated study completion is September 2022.31
In conclusion, the very low certainty evidence from the relevant study included in this review is insufficient to draw reliable conclusions about the clinical effectiveness or safety of anakinra compared to standard treatments or placebo in patients with HLH. No evidence on the cost-effectiveness of anakinra compared to current standard treatments or placebo was identified, therefore no conclusions can be made on the cost-effectiveness of anakinra for HLH.
References
1.Hutchinson M, Tattersall RS, Manson JJ. Haemophagocytic lymphohisticytosis—an underrecognized hyperinflammatory syndrome. Rheumatology (Oxford). 2019;58(Supplement_6):vi23-vi30. PubMed
2.McClain KL. Clinical features and diagnosis of hemophagocytic lymphohistiocytosis. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA; 2021; https://www.uptodate.com/contents/clinical-features-and-diagnosis-of-hemophagocytic-lymphohistiocytosis#H2046407169. Accessed 2021 Dec 20.
3.Hines MR, von Bahr Greenwood T, Beutel G, et al. Consensus-Based Guidelines for the Recognition, Diagnosis, and Management of Hemophagocytic Lymphohistiocytosis in Critically Ill Children and Adults. Crit Care Med. 2021;05:05.
4.Nikiforow S, Berliner N. To “Lump” or to “Split” in Macrophage Activation Syndrome and Hemophagocytic Lymphohistiocytosis. Arthritis rheumatol. 2020;72(2):206-209. PubMed
5.Posas-Mendoza TF, McLeod C, Davis W, Zakem J, Quinet R. Etiologies and management of haemophagocytic lymphohistiocytosis: is it time for an updated protocol and targeted treatments? Rheumatology (Oxford). 2021;60(6):2927-2933. PubMed
6.Carter SJ, Tattersall RS, Ramanan AV. Macrophage activation syndrome in adults: recent advances in pathophysiology, diagnosis and treatment. Rheumatology (Oxford). 2018;58(1):5-17. PubMed
7.Mehta P, Cron RQ, Hartwell J, Manson JJ, Tattersall RS. Silencing the cytokine storm: the use of intravenous anakinra in haemophagocytic lymphohistiocytosis or macrophage activation syndrome. The Lancet Rheumatology. 2020;2(6):e358-e367. PubMed
8.Flower L, Laundy N, Khosravi M, et al. Haemophagocytic lymphohistiocytosis secondary to COVID-19: a case series. Lancet Rheumatol. 2021;3(11):e744-e747. PubMed
9.Dimopoulos G, de Mast Q, Markou N, et al. Favorable Anakinra Responses in Severe Covid-19 Patients with Secondary Hemophagocytic Lymphohistiocytosis. Cell host microbe. 2020;28(1):117-123.e111. PubMed
10.Schnaubelt S, Tihanyi D, Strassl R, et al. Hemophagocytic lymphohistiocytosis in COVID-19: Case reports of a stepwise approach. Medicine (Baltimore). 2021;100(12):e25170. PubMed
11.Crayne CB, Albeituni S, Nichols KE, Cron RQ. The Immunology of Macrophage Activation Syndrome. Frontiers in Immunology. 2019;10:119. PubMed
12.Henter JI, Horne A, Aricó M, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124-131. PubMed
13.Debaugnies F, Mahadeb B, Ferster A, et al. Performances of the H-Score for Diagnosis of Hemophagocytic Lymphohistiocytosis in Adult and Pediatric Patients. Am J Clin Pathol. 2016;145(6):862-870. PubMed
14.La Rosée P, Horne A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133(23):2465-2477. PubMed
15.Otrock ZK, Daver N, Kantarjian HM, Eby CS. Diagnostic Challenges of Hemophagocytic Lymphohistiocytosis. Clin Lymphoma Myeloma Leuk. 2017;17s:S105-s110. PubMed
16.Trottestam H, Horne A, Aricò M, et al. Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol. Blood. 2011;118(17):4577-4584. PubMed
17.Bergsten E, Horne A, Aricó M, et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study. Blood. 2017;130(25):2728-2738. PubMed
18.NHS. Clinical Commissioning Policy: Anakinra for Haemophagocytic Lymphohistiocytosis (HLH) for adults and children in all ages [210701P] (1924). 2021; https://www.england.nhs.uk/wp-content/uploads/2021/10/1924-Clinical-commissioning-policy-anakinra-for-haemophagocytic-lymphohistiocytosis-.pdf. Accessed 2021 Dec 20.
19.Swedish Orphan Biovitrum AB. Product Monograph. Kineret. 2018; https://pdf.hres.ca/dpd_pm/00044494.PDF. Accessed 2022 Jan 15.
20.Wampler Muskardin TL. Intravenous Anakinra for Macrophage Activation Syndrome May Hold Lessons for Treatment of Cytokine Storm in the Setting of Coronavirus Disease 2019. ACR Open Rheumatol. 2020;2(5):283-285. PubMed
21.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
22.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
23.NICE. Anakinra for COVID-19 associated secondary haemophagocytic lymphohistiocytosis. 2020; https://www.nice.org.uk/advice/es26/evidence/evidence-review-pdf-8768016685. Accessed 2021 Dec 20.
24.NHS England. Evidence review: Anakinra for Haemophagocytic Lymphohistiocytosis. 2020; https://www.england.nhs.uk/wp-content/uploads/2021/10/1924-Evidence-review-anakinra-for-haemophagocytic-lymphohistiocytosis.pdf. Accessed 2021 Dec 20.
25.Monteagudo LA, Boothby A, Gertner E. Continuous Intravenous Anakinra Infusion to Calm the Cytokine Storm in Macrophage Activation Syndrome. ACR Open Rheumatol. 2020;2(5):276-282. PubMed
26.Khan F, Stewart I, Fabbri L, et al. A systematic review and meta-analysis of Anakinra, Sarilumab, Siltuximab and Tocilizumab for Covid-19. medRxiv. 2021:2020.2004.2023.20076612.
27.The Joanna Briggs Institute. Checklist for Cohort Studies. 2017; https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Cohort_Studies2017_0.pdf. Accessed 2022 Jan 15.
28.The Joanna Briggs Institute. Checklist for Case Series. 2017;https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Case_Series2017_0.pdf. Accessed 2022 Jan 15.
29.What is GRADE? London (UK): BMJ Best Practice; 2021: https://bestpractice bmj com/info/toolkit/learn-ebm/what-is-grade/ Accessed 2022 Jan 15.
30.Grimaldi D, Goicoechea Turcott EW, Taccone FS. IL-1 receptor antagonist in sepsis: new findings with old data? J. 2016;8(9):2379-2382.
31.University of Alabama at Birmingham. NCT02780583: Treatment of Macrophage Activation Syndrome (MAS) With Anakinra (MAS). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022; https://clinicaltrials.gov/ct2/show/NCT02780583. Accessed 2022 Jan 5.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 1: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
NICE 202023 UK Funding: NHS England | Study designs: Systematic reviews, RCTs, controlled clinical trials, observational studies (including case series). Case reports considered if no higher-level evidence found. No relevant primary studies identified. | Adults and children with suspected or confirmed COVID-19 with features of sHLH triggered by COVID-19 or similar coronaviruses including SARS-CoV-1 or MERS-CoV. | Intervention: Anakinra 1 to 12 mg/kg/day, usually for 3 to 14 days by SC injection or IV infusion alone or in combination with corticosteroids, IVIG, etoposide or other therapies. Comparator: Best supportive care including treatment with corticosteroids, IVIG, etoposide, organ support (e.g., ventilation, renal replacement therapy transfusions) and antimicrobials | Outcomes:
Follow-up: NR |
NHS 202024 UK Funding: NHS England | Study designs: Systematic reviews, RCTs, controlled clinical trials, cohort studies. Case series considered if no higher-level evidence found. Included studies: 1 retrospective cohort study, which is relevant to this report (sample size: 43)a. | Adults and children presenting with pHLH or sHLH (regardless of trigger condition) requiring treatment for HLH as part of their clinical care. Relevant patient populations characteristics: Adults diagnosed with sepsis with multi-organ dysfunction and/or shock with features of MAS (defined as the presence of hepatobiliary dysfunction or disseminated intravascular coagulation). | Eligible interventions: Anakinra 1 to 10 mg/kg/day, usually for 3 to 14 days by SC injection or IV infusion as first- or- second-line treatment alone or in combination with corticosteroids, IVIG, cyclosporin, or etoposide. Eligible comparators: Current standard treatment with corticosteroids, IVIG, cyclosporin, methotrexate and/or etoposide without use of anakinra. | Eligible outcomes:
|
NHS 202024 UK Funding: NHS England (continued) | 1 single-centre retrospective case series (sample size: 8 to 44) (not eligible for the current report due to lack of a comparator). | Anakinra group baseline characteristics (n = 26)
Placebo group baseline characteristics (n = 17)
Risk of death: 0.53 ± 0.25 | Relevant intervention:
Relevant comparator: Placebo 2 mg/kg/hr IV for 72 hours (concomitant treatments NR) |
• Cost-effectiveness Relevant outcomes: 28-day mortality Follow-up: NR |
HLH = hemophagocytic lymphohistiocytosis; hr = hour; ICU = intensive care unit; IVIG = IV immunoglobulin; MAS = macrophage activation syndrome; mg = milligram; MERS-CoV = Middle East respiratory syndrome; NICE = national institute for health and care excellence ; NHS = national health service; NR = not reported; RCT = randomized controlled trial; SARS-CoV-1 = severe acute respiratory syndrome; SC = subcutaneous; SD = standard deviation; sHLH = secondary hemophagocytic lymphohistiocytosis; sJIA = systemic juvenile idiopathic arthritis; pHLH = primary hemophagocytic lymphohistiocytosis.
aOf the 763 patients (out of 906 originally recruited) who completed the original RCT for anakinra for severe sepsis. This study is an analysis of 43 adults who multi-organ dysfunction and/or shock with features of MAS (hepatobiliary dysfunction or disseminated intravascular coagulation).
Note that this appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Strengths and Limitations of Systematic Reviews Using AMSTAR 221
Strengths | Limitations |
|---|---|
NICE 202023 | |
|
|
NHS 202024 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; JBI = Joanna Briggs Institute NICE = national institute for health and care excellence; NHS = national health service.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 3: Summary of Findings of the Systematic Reviews
Findings | Authors’ Conclusions |
|---|---|
NHS 202024 | |
Mortality at 28 days: One comparative cohort study in adults with a diagnosis of sepsis with features of MAS (N = 43) reported a statistically significant lower mortality in patients treated with anakinra compared to placebo (34.6% vs. 64.7%; P = 0.0006) and a lower risk of death (HR 0.28; 95% CI 0.11 to 0.71; P = 0.0071). | “These studies provided very low certainty evidence that compared to standard treatment, anakinra reduces 30-day mortality in patients with HLH.” (p. 9) |
CI = confidence interval; HR = hazard ratio; MAS = macrophage activation syndrome; sHLH = secondary hemophagocytic lymphohistiocytosis; SD = standard deviation; SJIA = systemic juvenile idiopathic arthritis; SLE = systemic lupus erythematosus.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Review Articles
Mehta P, Cron RQ, Hartwell J, Manson JJ, Tattersall RS. Silencing the cytokine storm: the use of intravenous anakinra in haemophagocytic lymphohistiocytosis or macrophage activation syndrome. Lancet Rheumatol. 2020 Jun;2(6):e358-e367. PubMed
Wampler Muskardin TL. Intravenous Anakinra for Macrophage Activation Syndrome May Hold Lessons for Treatment of Cytokine Storm in the Setting of Coronavirus Disease 2019. ACR Open Rheumatol. 2020 May;2(5):283-285. PubMed
Additional References
Case Reports
Adults
Adamski J, Jaschke B, Nieminen T, Weigl W. Bowel Perforation During Haemophagocytic Lymphohistiocytosis Treatment with Corticosteroids and Anakinra. Eur J Case Rep Intern Med. 2021;8(10):002759. PubMed
Chizinga M, Kalra SS, Innabi A, Rackauskas M, Ataya A, Emtiazjoo A. Macrophage activating syndrome causing decompensated right heart failure. Respir Med Case Rep. 2021;33:101409. PubMed
Duminuco A, Palumbo G, Garibaldi B, et al. Hemophagocytic Syndrome in a Patient with ALL: Morphology Still Matters. Hemato. 2021;2(2):347-352.
Hardage J, Otto NB, Skaggs J, Travis S. Prompt Recognition of Hemophagocytic Lymphohistiocytosis in an Afebrile Patient with Lupus and Staphylococcus aureus Bacteremia. Am J Case Rep. 2021 Nov 09;22:e934092. PubMed
Hiraldo JDG, Dominguez-Mayoral A, Garcia-Gomez FJ, et al. Central nervous system involvement in adult-onset relapsing hemophagocytic lymphohistiocytosis responsive to maintenance treatment with anakinra. J Neuroimmunol. 2021 06 15;355:577552. PubMed
Lubnow M, Schmidt B, Fleck M, et al. Secondary hemophagocytic lymphohistiocytosis and severe liver injury induced by hepatic SARS-CoV-2 infection unmasking Wilson's disease: Balancing immunosuppression. Int J Infect Dis. 2021 Feb;103:624-627. PubMed
McCann N, Amarnani R, Shipa M, et al. Epstein-Barr virus associated haemophagocytic lymphohistiocytosis treated with anakinra and rituximab: A case report. Clin Infect Pract. 2021;9:100060.
Opalinska A, Kwiatkowska D, Burdacki A, et al. Multifocal Pyoderma Gangrenosum with an Underlying Hemophagocytic Lymphohistiocytosis: Case Report and the Review of the Literature. Dermatol Ther (Heidelb). 2021 Aug;11(4):1217-1237. PubMed
Thomson RJ, Singh A, Knight DS, Buckley J, Lamb LE, Captur G. Anakinra treats fulminant myocarditis from Neisseria meningitidis septicaemia and haemophagocytic lymphohistiocytosis: a case report. Eur Heart J Case Rep. 2021 Jun;5(6):ytab201. PubMed
Ajeganova S, De Becker A, Schots R. Efficacy of high-dose anakinra in refractory macrophage activation syndrome in adult-onset Still's disease: when dosage matters in overcoming secondary therapy resistance. Ther Adv Musculoskelet Dis. 2020;12:1759720X20974858. PubMed
Gabr JB, Liu E, Mian S, et al. Successful treatment of secondary macrophage activation syndrome with emapalumab in a patient with newly diagnosed adult-onset Still's disease: case report and review of the literature. Ann Transl Med. 2020 Jul;8(14):887. PubMed
Kanitkar T, Richardson C, Scobie A, et al. Fatal primary dengue-induced Haemophagocytic Lymphohistiocytosis (HLH) in a returning traveller from India treated with anakinra for the first time. Clin Infect Pract. 2020;7-8:100043.
Kubler L, Bittmann I, Kuipers JG. Macrophage activation syndrome triggered by active systemic lupus erythematosus: Successful treatment by interleukin-1 inhibition (anakinra). Z Rheumatol. 2020 Dec;79(10):1040-1045. PubMed
Lau A, Youn H, Caricchio R, Brent L. A Case of Cytomegalovirus-Induced Hemophagocytic Lymphohistiocytosis in a Patient with an Underlying Rheumatic Disease. Cureus. 2020 May 15;12(5):e8130. PubMed
Yip KP, Ali M, Avann F, Ganguly S. Pregnancy-induced haemophagocytic lymphohistiocytosis. J Intensive Care Soc. 2020 Feb;21(1):87-91. PubMed
Lange AV, Kazi S, Chen W, Barnes A. Fatal case of macrophage activation syndrome (MAS) in a patient with dermatomyositis and cytomegalovirus (CMV) viraemia. BMJ Case Rep. 2018 Jul 30; 2018:bcr2018225231. PubMed
Nusshag C, Morath C, Zeier M, Weigand MA, Merle U, Brenner T. Hemophagocytic lymphohistiocytosis in an adult kidney transplant recipient successfully treated by plasmapheresis: A case report and review of the literature. Medicine (Baltimore). 2017 Dec;96(50):e9283. PubMed
Ocon AJ, Bhatt BD, Miller C, Peredo RA. Safe usage of anakinra and dexamethasone to treat refractory hemophagocytic lymphohistiocytosis secondary to acute disseminated histoplasmosis in a patient with HIV/AIDS. BMJ Case Rep. 2017 Oct 04; 2017:bcr2017221264. PubMed
Parisi F, Paglionico A, Varriano V, Ferraccioli G, Gremese E. Refractory adult-onset Still disease complicated by macrophage activation syndrome and acute myocarditis: A case report treated with high doses (8 mg/kg/d) of anakinra. Medicine (Baltimore). 2017 Jun;96(24):e6656. PubMed
Young KJ, Savajiyani S, Sambhara VS, Rasche R. Anakinra for the treatment of systemic lupus erythematosus complicated by macrophage activation syndrome. Am J Respir Crit Care Med. 2017;195:A5918.
Agnihotri A, Ruff A, Gotterer L, Walker A, McKenney AH, Brateanu A. Adult Onset Still's Disease Associated with Mycoplasma pneumoniae Infection and Hemophagocytic Lymphohistiocytosis. Case Rep Med. 2016;2016:2071815. PubMed
Divithotawela C, Garrett P, Westall G, Bhaskar B, Tol M, Chambers DC. Successful treatment of cytomegalovirus associated hemophagocytic lymphohistiocytosis with the interleukin 1 inhibitor - anakinra. Respirol. 2016 Mar;4(1):4-6. PubMed
Kumar A, Kato H. Macrophage Activation Syndrome Associated with Adult-Onset Still's Disease Successfully Treated with Anakinra. Case Rep Rheumatol. 2016;2016:3717392. PubMed
Mehta MV, Manson DK, Horn EM, Haythe J. An atypical presentation of adult-onset Still's disease complicated by pulmonary hypertension and macrophage activation syndrome treated with immunosuppression: a case-based review of the literature. Pulm Circ. 2016 Mar;6(1):136-142. PubMed
Schafer EJ, Jung W, Korsten P. Combination Immunosuppressive Therapy Including Rituximab for Epstein-Barr Virus-Associated Hemophagocytic Lymphohistiocytosis in Adult-Onset Still's Disease. Case Rep Rheumatol. 2016;2016:8605274. PubMed
Merelli M, Quartuccio L, Bassetti M, et al. Efficacy of intravenous cyclosporine in a case of cytophagic histiocytic panniculitis complicated by haemophagocytic syndrome after visceral leishmania infection. Clin Exp Rheumatol. 2015 Nov-Dec;33(6):906-909. PubMed
Tayer-Shifman OE, Ben-Chetrit E. Refractory macrophage activation syndrome in a patient with SLE and APLA syndrome - Successful use of PET- CT and Anakinra in its diagnosis and treatment. Mod Rheumatol. 2015;25(6):954-957. PubMed
Kumar N, Goyal J, Goel A, Shakoory B, Chatham W. Macrophage activation syndrome secondary to human monocytic ehrlichiosis. Indian J Hematol Blood Transfus. 2014 Sep;30(Suppl 1):145-147. PubMed
Fischbach KE, Coe B, Radwan M, Rodriguez J, Carter J, Rumbak MJ. Macrophage activation syndrome in a patient with adult still's disease following rituximab: Presenting with “pseudo-septic shock”. ICU Dir. 2013 September;4(5):248-251.
Loh NK, Lucas M, Fernandez S, Prentice D. Successful treatment of macrophage activation syndrome complicating adult Still disease with anakinra. Intern Med J. 2012 Dec;42(12):1358-1362. PubMed
Infants and Children
McKeone DJ, DeMartini TKM, Kavanagh RP, Halstead ES. Case Report: Rapid Recognition and Immune Modulation of Secondary HLH Due to Disseminated HSV Infection. Front Pediatr. 2021;9:681055. PubMed
Vagrecha A, Patel HB, Mamdouhi T, et al. Effect of COVID-19 on anakinra-induced remission in homozygous STX11 hemophagocytosis lymphohistiocytosis. Pediatr Blood Cancer. 2021 Jun;68(6):e28897. PubMed
Derespina KR, Kaushik S, Mitchell W, Gorstein S, Ushay HM, Medar SS. E-cigarette or Vaping-Associated Acute Lung Injury and Hemophagocytic Lymphohistiocytosis. Pediatrics. 2020 Oct;146(4):10. PubMed
Kavirayani A, Charlesworth JEG, Segal S, et al. The Lazarus effect of very high-dose intravenous anakinra in severe non-familial CNS-HLH. Lancet Rheumatol. 2020 Dec;2(12):e736-e738. PubMed
Meneghel A, Martini G, Amigoni A, Pettenazzo A, Padalino M, Zulian F. Case Report: Life-Threatening Macrophage Activation Syndrome With Fulminant Myocarditis Successfully Rescued by High Dose Intravenous Anakinra. Front Pediatr. 2020;8:635080. PubMed
Hardman SJ, Tukur G, Waruiru C. Enterovirus-Associated HLH: Addition of Anakinra to IVIG and Corticosteroids. J Clin Immunol. 2019 May;39(4):373-375. PubMed
Kim SR, Kissoon-Larkin T, Horn B, Elder M. Anakinra as an agent to control hemophagocytic lymphohistiocytosis in Griscelli type 2. Pediatr Blood Cancer. 2019 Dec;66(12):e27997. PubMed
Lind-Holst M, Hartling UB, Christensen AE. High-dose anakinra as treatment for macrophage activation syndrome caused by refractory Kawasaki disease in an infant. BMJ Case Rep. 2019 Aug;12(8):04. PubMed
Barsalou J, Blincoe A, Fernandez I, et al. Rapamycin as an Adjunctive Therapy for NLRC4 Associated Macrophage Activation Syndrome. Front Immunol. 2018;9:2162. PubMed
Kerin V, Toplak N, Rajic V, Avcin T. Macrophage activation syndrome as a complication of systemic juvenile idiopathic arthritis - Case report. Zdravniski Vestnik. 2014;83(4):351-357.
Shafferman A, Birmingham JD, Cron RQ. High dose Anakinra for treatment of severe neonatal Kawasaki disease: a case report. Pediatr Rheumatol Online J. 2014;12:26. PubMed
Kahn PJ, Cron RQ. Higher-dose Anakinra is effective in a case of medically refractory macrophage activation syndrome. J Rheumatol. 2013 May;40(5):743-744. PubMed
Tammy P, Kwong JM, Cron RQ, et al. treatment of refractory macrophage activation syndrome in systemic juvenile idiopathic arthritis with high dose anakinra. J Rheum Dis Treat. 2015;1:014. https://clinmedjournals.org/articles/jrdt/jrdt-1-014.pdf
Case Series
Adults
Khalid M, Abdalla A, McCarthy G, Stack J. Haemophagocytic lymphohistiocytosis (HLH)-associated stress cardiomyopathy secondary to autoimmune conditions successfully treated with anakinra. BMJ Case Rep. 2021 Dec;14(12):09. PubMed
Schnaubelt S, Tihanyi D, Strassl R, et al. Hemophagocytic lymphohistiocytosis in COVID-19: Case reports of a stepwise approach. Medicine (Baltimore). 2021 Mar;100(12):e25170. PubMed
Dimopoulos G, de Mast Q, Markou N, et al. Favorable Anakinra Responses in Severe Covid-19 Patients with Secondary Hemophagocytic Lymphohistiocytosis. Cell host microbe. 2020 Jul;28(1):117-123.e111. PubMed
Rocco JM, Mallarino-Haeger C, McCurry D, Shah N. Severe anaplasmosis represents a treatable cause of secondary hemophagocytic lymphohistiocytosis: Two cases and review of literature. Ticks Tick Borne Dis. 2020 Sep;11(5):101468. PubMed
Wohlfarth P, Agis H, Gualdoni GA, et al. Interleukin 1 Receptor Antagonist Anakinra, Intravenous Immunoglobulin, and Corticosteroids in the Management of Critically Ill Adult Patients With Hemophagocytic Lymphohistiocytosis. J Intensive Care Med. 2019;34(9):723-731. PubMed
Kumar B, Aleem S, Saleh H, Petts J, Ballas ZK. A Personalized Diagnostic and Treatment Approach for Macrophage Activation Syndrome and Secondary Hemophagocytic Lymphohistiocytosis in Adults. J Clin Immunol. 2017;37(7):638-643. PubMed
Infants and Children
Charlesworth JEG, Wilson S, Qureshi A, et al. Continuous intravenous anakinra for treating severe secondary haemophagocytic lymphohistiocytosis/macrophage activation syndrome in critically ill children. Pediatr Blood Cancer. 2021 Sep;68(9):e29102. PubMed
Phadke O, Rouster-Stevens K, Giannopoulos H, Chandrakasan S, Prahalad S. Intravenous administration of anakinra in children with macrophage activation syndrome. Pediatr Rheumatol Online J. 2021 Jun;19(1):98. PubMed
Vicenzi P, Jiwani Z, Guirola R, Hamby T, Ray A. Comment on: The use of anakinra in the treatment of secondary hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2021 Apr;68(4):e28813. PubMed
Bami S, Vagrecha A, Soberman D, et al. The use of anakinra in the treatment of secondary hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2020 Nov;67(11):e28581. PubMed
Eloseily EM, Weiser P, Crayne CB, et al. Benefit of Anakinra in Treating Pediatric Secondary Hemophagocytic Lymphohistiocytosis. Arthritis rheumatol. 2020;72(2):326-334. PubMed
Gregory J, Greenberg J, Basu S. Outcomes Analysis of Children Diagnosed With Hemophagocytic Lymphohistiocytosis in the PICU. Pediatr Crit Care Med. 2019;20(4):e185-e190. PubMed
Sonmez HE, Demir S, Bilginer Y, Ozen S. Anakinra treatment in macrophage activation syndrome: a single center experience and systemic review of literature. Clinical Rheumatology. 2018;37(12):3329-3335. PubMed
Bruck N, Suttorp M, Kabus M, Heubner G, Gahr M, Pessler F. Rapid and sustained remission of systemic juvenile idiopathic arthritis-associated macrophage activation syndrome through treatment with anakinra and corticosteroids. J Clin Rheumatol. 2011 Jan;17(1):23-27. PubMed
Miettunen PM, Narendran A, Jayanthan A, Behrens EM, Cron RQ. Successful treatment of severe paediatric rheumatic disease-associated macrophage activation syndrome with interleukin-1 inhibition following conventional immunosuppressive therapy: case series with 12 patients. Rheumatology (Oxford). 2011 Feb;50(2):417-419. PubMed
Retrospective Chart Review
Adults
Sammut L, Murryam S, Vincent N, et al. EP18 Use of anakinra for haemophagocytic lymphohistiocytosis in adults. Rheumatology. 2020 Apr;59(Supp 2):keaa109.017. https://academic.oup.com/rheumatology/article/59/Supplement_2/keaa109.017/5822313
Monteagudo LA, Boothby A, Gertner E. Continuous Intravenous Anakinra Infusion to Calm the Cytokine Storm in Macrophage Activation Syndrome. ACR Open Rheumatol. 2020 May;2(5):276-282. PubMed
Lenert A, Yao Q. Macrophage activation syndrome complicating adult onset Still's disease: A single center case series and comparison with literature. Semin Arthritis Rheum. 2016 Jun;45(6):711-716. PubMed
Gerfaud-Valentin M, Maucort-Boulch D, Hot A, et al. Adult-onset still disease: manifestations, treatment, outcome, and prognostic factors in 57 patients. Medicine (Baltimore). 2014 Mar;93(2):91-99. PubMed
Infants and Children
Aytac S, Batu ED, Unal S, et al. Macrophage activation syndrome in children with systemic juvenile idiopathic arthritis and systemic lupus erythematosus. Rheumatol Int. 2016 Oct;36(10):1421-1429. PubMed
Barut K, Yucel G, Sinoplu AB, Sahin S, Adrovic A, Kasapcopur O. Evaluation of macrophage activation syndrome associated with systemic juvenile idiopathic arthritis: single center experience over a one-year period. Turk Pediatri Ars. 2015 Dec;50(4):206-210. PubMed
Rajasekaran S, Kruse K, Kovey K, et al. Therapeutic role of anakinra, an interleukin-1 receptor antagonist, in the management of secondary hemophagocytic lymphohistiocytosis/sepsis/multiple organ dysfunction/macrophage activating syndrome in critically ill children. Pediatr Crit Care Med. 2014 Jun;15(5):401-408. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca