CADTH Health Technology Review
Temperature Management in Patients After Cardiac Arrest
Rapid Review
Authors: Diksha Kumar, Khai Tran, Zahra Premji
Abbreviations
AAN
American Academy of Neurology
CCCS
Canadian Critical Care Society
CCS
Canadian Cardiovascular Society
GRADE
Grading of Recommendations, Assessment, Development and Evaluations
ICU
intensive care unit
NMA
network meta-analysis
OCHA
out-of-hospital cardiac arrest
RCT
randomized controlled trial
ROSC
return of spontaneous circulation
SR
systematic review
TTM
targeted temperature management
Key Messages
Two systematic reviews (1 with a network meta-analysis and 1 with a meta-analysis), 1 randomized controlled trial, and 7 non-randomized studies were identified about the comparative clinical effectiveness of normothermia versus hypothermia in adult patients after cardiac arrest.
Normothermia was found to be similar to hypothermia for several clinical- and patient-related outcomes, such as survival, hospital mortality, and quality of life. There was limited evidence to suggest that either type of targeted temperature management was more efficacious, with findings suggesting that normothermia may be associated with greater protocol adherence and decreased prescription medication use coming from low-quality non-randomized studies.
Four evidence-based guidelines were identified regarding targeted temperature management (normothermia or hypothermia) in adult patients after cardiac arrest. All guidelines strongly recommend targeted temperature management for eligible patients, particularly for patients resuscitated following out-of-hospital cardiac arrest. Identified guidelines from the Canadian Cardiovascular Society and American Academy of Neurology present strong recommendations for hypothermic targeted temperature management.
Context and Policy Issues
An estimated 35,000 cardiac arrests occur annually in Canada, with the majority of them occurring outside of hospital settings.1 The abrupt loss of cardiac function is associated with poor clinical outcomes; the rate of survival to hospital discharge for out-of-hospital cardiac arrest (OCHA) ranges between 3.9% and 7.1%.2 Survival after cardiac arrest not only requires the coordination of emergency services to facilitate immediate resuscitation and return of circulation, but also critical care over the next 24 hours to ensure that the brain is adequately supplied with oxygenated blood.3 Fever is common among patients following cardiac arrest and resuscitation, and is thought to worsen brain damage.4 Brain injury is a major cause of both mortality and decreased function, therefore its prevention is an imperative aspect of post–cardiac arrest care.5
Hypothermic targeted temperature management (TTM) has been widely practised within this patient population to control body temperature.4 Also known as therapeutic hypothermia, the intervention involves the use of feedback-controlled intravascular cooling techniques in comatose patients to achieve a target body temperature typically in the range of 32°C to 34°C.3 Canadian guidelines have recommended therapeutic hypothermia for unresponsive patients following OCHA; however, the evidence base has been largely inconclusive.2 Results from a recently published randomized controlled trial (RCT)6 showed that hypothermic TTM may not provide significantly clinical improvements over targeted normothermia at 37°C, which raises the question of whether existing hypothermic TTM protocols in critical care settings are of clinical value to this patient population.
The objective of this report is to identify and review current evidence regarding the comparative clinical effectiveness of normothermia versus hypothermia in adult patients after cardiac arrest and summarize identified evidence-based guidelines and recommendations regarding TTM.
Research Questions
What is the comparative clinical effectiveness of normothermia versus hypothermia for targeted temperature management in adult patients after cardiac arrest?
What are the evidence-based guidelines regarding targeted temperature management (normothermia or hypothermia) in adult patients after cardiac arrest?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Library, the University of York Centre for Reviews and Dissemination (CRD) databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. For question 1, the main search concepts were cardiac arrest, hypothermia, and normothermia. No filters were applied to limit the retrieval by study type. For question 2, the main search concepts were cardiac arrest and temperature management. Search filters were applied to this search to limit retrieval to guidelines. When possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and December 16, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients treated in critical care (intensive or critical care units) after out-of-hospital or in-hospital cardiac arrest |
Intervention | Q1: Normothermia, also known as targeted normothermia (i.e., maintenance of a normal core body temperature) Q2: TTM (normothermia or hypothermia) |
Comparator | Q1: Hypothermia, also known as targeted hypothermia, therapeutic hypothermia, or protective hypothermia Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., health-related quality of life, degree of disability or dependence, functional status, mortality) and harms (e.g., pneumonia, sepsis, bleeding, arrhythmia, skin complications associated with the device used to achieve TTM) Q2: Recommendations regarding TTM (normothermia or hypothermia) in adult patients after cardiac arrest (e.g., use of normothermia versus hypothermia, temperature range, time to reach normothermic or hypothermic range, duration of normothermia or hypothermia, management of fever and/or shivering, starting point of timing of therapy for patient within goal temperature when hypothermia is used) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Q = question; TTM = targeted temperature management.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2016. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SR. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 for SR, the Professional Society for Health Economics and Outcomes Research (ISPOR) questionnaire8 for network meta-analyses, the Downs and Black checklist9 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument10 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
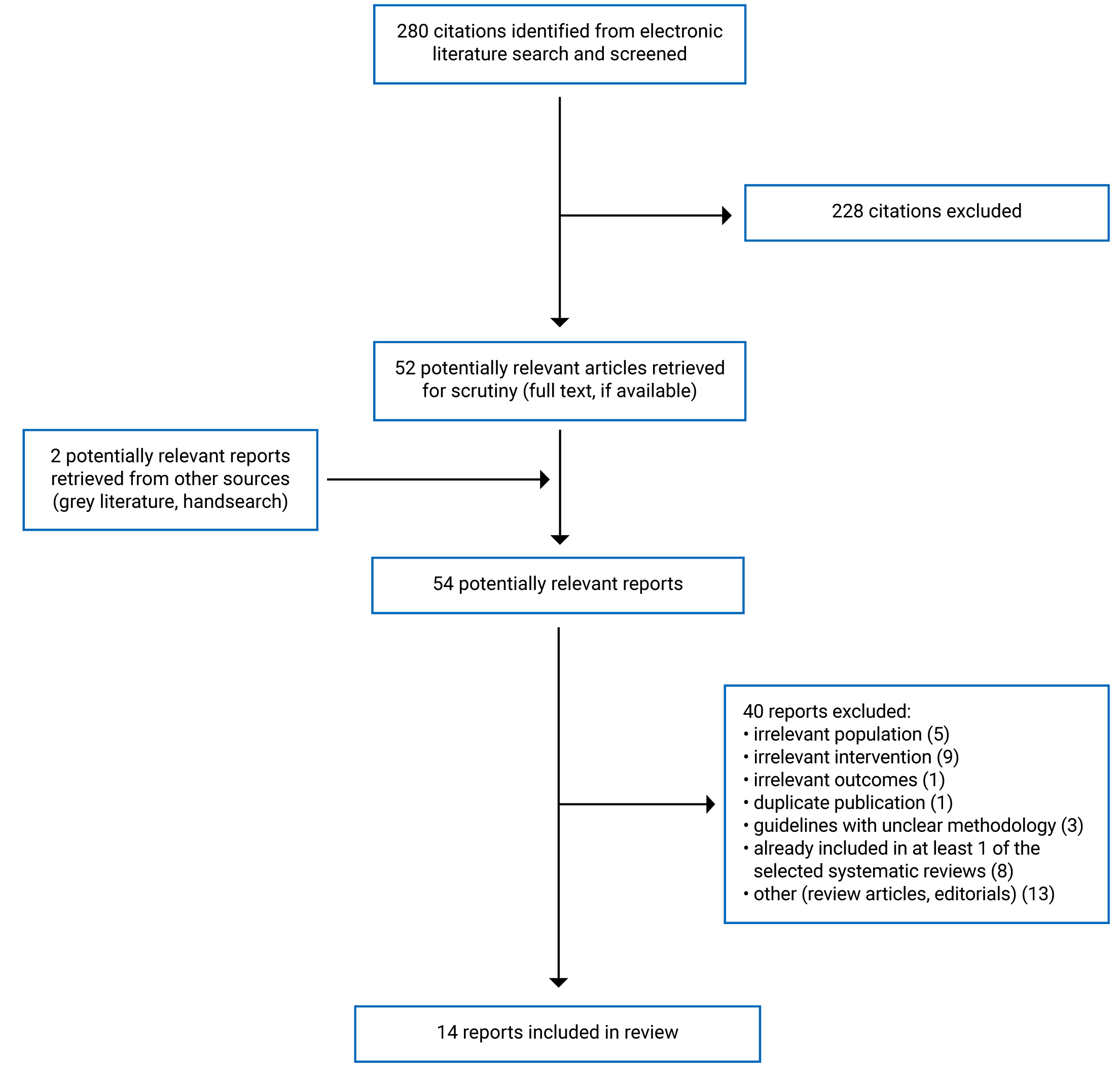
A total of 280 citations were identified in the literature search. Following screening of titles and abstracts, 228 citations were excluded and 52 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 40 publications were excluded for various reasons and 14 publications met the inclusion criteria and were included in this report. These comprised 2 SRs, 1 RCT, 7 non-randomized studies, and 4 evidence-based guidelines. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA)11 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Two SRs were identified, both published in 2021.5,12 The authors of 1 SR, which included RCTs published up to June 21, 2021, conducted a network meta-analysis (NMA) of 10 RCTs.5 Similarly, the other SR included RCTs that were published up to June 17, 2021, and included a meta-analysis of 9 RCTs.12 A table outlining the overlap between included primary studies within the 2 SRs included in this report is provided in Appendix 5.
The included RCT, published in 2016, was of non-blinded, parallel design.13 Seven non-randomized studies published between 2016 and 2021 were also identified, including 6 retrospective cohort studies14-19 and 1 observational post hoc analysis of an RCT.20
Additionally, 4 guidelines with recommendations regarding post–cardiac arrest TTM were included in this report.2,21-23 The most recent guideline, published in 2018, was developed by the French Intensive Care Society (FICS) and French Society of Anesthesia and Intensive Care Medicine.21 Two of the included guidelines were published in 2017, 1 by the American Academy of Neurology (AAN),22 and the other developed jointly by the Canadian Cardiovascular Society (CCS), Canadian Cardiovascular Critical Care Society, and Canadian Association of Interventional Cardiology.2 The final guideline from 2016 was developed by the Canadian Critical Care Society (CCCS), Canadian Neurocritical Care Society, and Canadian Critical Care Trials Group.23 Methods for the collection, selection, and synthesis of evidence informing the recommendations were reported in 3 guidelines, stating that a comprehensive literature search was performed2,22,23 and that the evidence was reviewed by committee members.2,22 Two guidelines classified the level of evidence for a recommendation from “very low” or “low” to “high.”21,23 The AAN guideline graded evidence as Class I, II, III, or IV.22 The authors of the CCS guideline used Grading of Recommendations, Assessment, Development and Evaluations (GRADE) methodology to assess the quality of evidence.2 Final recommendations were made using Delphi methodology,21,23 GRADE methodology,2,21 and nominal group technique.23 The strength of recommendations was classified in various ways; 2 of the included guidelines referred to them as either “strong” or “conditional,”2,23 1 graded them as A, B, C, or U (insufficient evidence),22 and the other organized them as positive or negative and as strong or weak.21
Country of Origin
One of the SRs listed first authors from Canada,5 and the other listed first authors from Denmark.12 The included primary clinical studies were conducted in Israel,17 Singapore,13,18 South Korea,16 Switzerland,14 the Netherlands,20 and Turkey.15 Two of the included guidelines were Canadian,2,23 1 was from the US,22 and 1 was from France.21
Patient Population
Both SRs5,12 included RCTs with adult patients after cardiac arrest, with the SR by Fernando et al. (2021)5 limiting inclusion to patients with OCHA who remained unresponsive following signs of return of spontaneous circulation (ROSC). The SR by Fernando et al. (2021)5 included 4,218 participants across 10 RCTs, and the SR by Granfeldt et al. (2021)12 included 2,968 participants from 9 RCTs.12 Patients’ mean age was similar between the 2 SRs (approximately 63 years5 and 6412 years). The majority of the included population in both SRs were male, ranging from 60% to 88.9% in 1 SR5 and from 56% to 100% in the other.12
There was some variation in the patient population among the 8 primary studies included in this report. All studies included adult patients hospitalized following cardiac arrest.13-20 The mean age of the patients ranged between 52.5 years and 65 years.13-20 Sex was reported in 7 of the 8 primary studies, and the majority of patients across the studies were male, ranging from 53.4% to 81.5%. One retrospective cohort study16 and 1 observational post hoc analysis20 limited inclusion to patients with OCHA, whereas the others did not specify between in-hospital and out-of-hospital cardiac arrest. The RCT13 and retrospective cohort study18 by Pang et al. included primarily patients who had an in-hospital cardiac arrest (90.5% to 92.4% of participants) and specifically comprised patients on extracorporeal life support. Three of the included retrospective cohort studies15,17,19 reviewed patient data from patients in the intensive care unit (ICU).
The relevant target population of the 4 included guidelines2,21-23 in this report was adult patients with cardiac arrest. One guideline21 contained recommendations for a broader population: both adult and pediatric patients with cardiac arrest, traumatic brain injury, stroke or other brain injuries, and shock. Authors of the CCS guideline2 specified that the recommendations pertained to patients with OCHA. The guideline developed by FICS21 was broadly intended for clinicians who provide neurologic care to critically ill patients. The intended users of the 3 other included guidelines2,22,23 were clinicians who provide care for patients with cardiac arrest; the AAN guideline22 is specifically for nontraumatic cardiac arrest and the CCS is guideline for OCHA.2
Interventions and Comparators
The SR with NMA by Fernando et al. (2021)5 compared normothermia (37°C to 37.8°C) with 3 temperature ranges of hypothermia: 31°C to 32°C (which they referred to as “deep hypothermia”), 33°C to 34°C (“moderate hypothermia”), and 35°C to 36°C (“mild hypothermia”). The SR with meta-analysis by Granfeldt et al. (2021)12 compared normothermia, whether it involved active cooling as part of TTM or not, with hypothermic TTM (32°C to 34°C).
Normothermia was defined in various ways in the included primary clinical studies. Therapeutic normothermia was described as a body temperature maintained at 36°C,14,19 37°C,13 36°C to 37°C,20 or higher than 35.5°C.16 Three retrospective studies15,17,18 considered normothermia as a comparison group but did not specify a temperature range; however, 115 of the studies considered normothermia as a non-TTM intervention. Targeted normothermia was specified to be maintained for 28 hours in the retrospective cohort study by Casamento et al. (2016).19
Hypothermia was also defined in various ways in the included primary studies. Targeted hypothermia was described as body temperature maintained at 33°C,14 34°C,13 32°C to 34°C,17,19,20 33°C to 35°C,15 or lower than 35.5°C.16 Hypothermia was specified as maintained for 24 hours in the studies by Pang et al.13,18 and Casamento et al. (2016).19
All included guidelines presented recommendations regarding TTM as part of in-hospital care following cardiac arrest.2,21-23 The AAN guideline defined therapeutic hypothermia, or hypothermic TTM, as cooling to a core body temperature of 32°C to 34°C.22 The CCS guideline broadly defined the intervention considered, TTM, as a strategy of intentional temperature management of a patient after cardiac arrest, which consists of active patient cooling, subsequent rewarming, and extended fever control.2
Outcomes
Several clinical outcomes of relevance were described in the studies included in this review. These outcomes included the following: survival with good neurologic outcome,5,12,13,18 overall survival,5,12,13,15-20 mortality,13-15,17,19 ICU or hospital length of stay,13-15,18,19 neurologic status,13-16,20 protocol adherence,14 quality of life,20 time spent in temperature target range,19 medication prescription,14,19 and adverse events.5,13,14,17-19
The modified Rankin Scale, Cerebral Performance Categories scale, and Pittsburgh Cardiac Arrest Category scale were the validated measures used to describe neurologic outcomes in 2 SRs,5,12 1 RCT,13 and 5 non-randomized studies.14-16,18,20 The modified Rankin Scale is commonly used to measure the degree of disability of people who have suffered a stroke or other causes or neurologic disability.24 The scale ranges from 0 to 6, with 0 for no symptoms, 3 for moderate disability (requires some help but able to walk without assistance), and 6 for dead.24 The Cerebral Performance Categories are the gold standard for describing the level of function and impairment after cardiac arrest.25 The categories, which rank from 1 to 5, are as follows: good cerebral performance, moderate cerebral disability, severe cerebral disability, coma or vegetative state, and brain death.25 Finally, the Pittsburgh Cardiac Arrest Category is a 4-level illness severity score with the following rankings: awake, coma with mild cardiopulmonary failure, coma with severe cardiopulmonary failure, and deep coma.26 Studies that investigated survival with good neurologic outcome defined a favourable neurologic outcome as any of the following: modified Rankin Scale score of 0 to 3,5,12 Cerebral Performance Categories scale score of 1 or 2,5,12,13,18 Pittsburgh Cardiac Arrest Category score of 1 or 2,5 or blinded assessment from a health professional indicating no, mild, or moderate disability.5
The authors of 1 retrospective cohort study14 reported protocol adherence as a primary outcome, and patients were considered to have adhered to the protocol if their body core temperature was within a range of 1°C around the target temperatures of 33°C and 36°C for the hypothermia and normothermia groups, respectively.
The authors of 2 retrospective cohort studies14,19 reported several outcomes related to the prescription and dose of catecholamines, sedatives, and relaxants administered to patients in the targeted normothermia and hypothermia groups.
The 4 guidelines included in this report regarded survival with good neurologic function as an outcome for consideration when developing recommendations.2,21-23
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 2.
Systematic Reviews and Network Meta-Analyses
Both SRs5,12 used comprehensive search and selection strategies, which is evident because most RCTs relevant to this report were excluded on the basis of inclusion within the SRs. Both SRs by Fernando et al. (2021)5 and Granfeldt et al. (2021)12 had registered published protocols with detailed search strategies. Fernando et al. (2021)5 searched 6 databases (MEDLINE, PubMed, Embase, Scopus, Web of Science, and the Cochrane Database of Systematic Reviews), conducted further surveillance searches, and performed a grey literature search, including the reference lists of all included studies and existing SR on TTM. Granfeldt et al. (2021) searched 3 databases (PubMed, Embase, and the Cochrane Central Register of Controlled Trials) as well as the International Clinical Trials Registry Platform and ClinicalTrials.gov for registered ongoing and unpublished trials. However, it is unclear whether content experts were consulted during the review process of either of the SRs5,12 and, in the case of Fernando et al. (2021),5 it is unclear whether trial registries were searched as part of the grey literature search outlined in the published protocol. Research questions and inclusion criteria were clearly reported and consisted of components of population, intervention, comparison, and outcomes.5,12 Although Fernando et al. (2021)5 explained their selection of RCTs for inclusion in the review, Granfeldt et al. (2021)5,12 did not justify their selection of randomized and non-randomized controlled studies for inclusion. The study selection and data extraction processes were performed in duplicate, and the included studies were described in adequate detail in supplementary materials.5,12 Reasons for exclusion cannot be easily verified because neither of the SRs published a list of excluded studies.
In terms of conducting meta-analyses, authors of both SRs5,12 justified combining the data in a meta-analysis or NMA and used assessment tools by Cochrane to assess the risk of bias of included studies. Statistical heterogeneity among trials were assessed using visual inspection of forest plots, the I2 statistic, and the Chi-square test.5,12 Heterogeneity was observed in the results of the reviews, but the authors investigated the potential sources of any heterogeneity in the results and discussed its impact in the findings.5,12
Fernando et al. (2021)5 initially performed pairwise MA using the random-effects model, and then evaluated the feasibility of conducting an NMA by checking the availability of evidence, transitivity assumption, connectivity, and agreement between direct and indirect evidence. With the assumption of a common heterogeneity parameter, the frequentist random-effects model was chosen to combine the included data.5 However, the authors did not provide a justification about why the analyses were performed with a frequentist instead of a Bayesian approach. Due to insufficient data, the authors were unable to conduct subgroup analyses or meta-regression to explain statistical heterogeneity.5 The authors presented a network graph of included studies, and given the geometry of the NMA, the comparisons between normothermia and deep and moderate hypothermia were direct, and the comparison between normothermia and mild hypothermia was indirect.5 In addition, Fernando et al. (2021)5 provided a clear summary of the main findings but did not perform any sensitivity analyses.
Randomized Controlled Trial
Several aspects of the included RCT13 were clearly described, such as the study objective, primary and secondary outcomes, patient characteristics, interventions, potential confounders, main findings, estimates of random variability, and adverse events. However, in reviewing the results section, it was unclear whether 1 of the 12 participants in the normothermia group was lost to follow-up given the discrepancy between the total number of participants and the number of patients discharged or deceased. The single-centre study was conducted in a tertiary referral centre, which may not be representative of where most patients seek immediate care after a cardiac arrest. In addition, due to the non-blinded design, investigators, outcomes assessors, and patients were aware of the treatment administered, which may have increased the risk of performance bias and detection bias. It is unclear whether the study was adequately powered because of its sample size of 21 participants. This RCT was also published as a letter to the editor, thus it is unclear whether the methodology and findings have been subject to peer review.
Non-Randomized Studies
Overall, the reporting was clear across the 7 non-randomized studies14-20 in terms of study objectives, patient characteristics, potential confounders, interventions, and estimates of random variability. In 3 studies,14,19,20 the characteristics of the patients lost to follow-up were not described. The authors of 2 studies17,18 did not specify a temperature range for the normothermia group. In Kocayigit et al. (2021),15 it was unclear when the survival and good neurologic results outcomes were measured. The external validity of the study findings to other similar settings was generally considered poor because 4 of the included non-randomized studies14,15,17,18 were single-centre, retrospective cohort studies. The other 3 studies consisted of patient data derived from either multiple centres19,20 or national registries,16 which may have increased generalizability. None of the included studies were conducted in Canada, which may limit relevance of the results in the Canadian context. Threats to the internal validity of the studies were primarily due to the non-randomized nature of the studies: 6 of the included studies14-19 were of retrospective cohort design, which means the investigators, outcome assessors, and patients may have been aware of the intervention. Additionally, there is uncertainty about whether there was a high level of compliance with the intervention and whether the recorded patient data are accurate. Participants across the intervention and comparator groups appeared to be recruited at the same sites or from the same population and over the same periods of time. Some studies16,17,19,20 considered potential confounders when adjusting main outcomes, whereas other studies15,18 did not take into account baseline differences between the groups. Only 1 included study19 provided power calculations, but sample size was noted to be a limitation in 3 studies.14,17,18
Guidelines
All included guidelines described a clear scope and purpose.2,21-23 Evidence of some stakeholder involvement was evident in the development of all guidelines; however, it was unclear whether the views and preferences of the target patient population were sought.2,21-23 In terms of rigour of development, all included guidelines conducted a comprehensive search to collect evidence to support recommendations and did not specify whether other systematic methods, such as screening and study selection in duplicate, were undertaken.2,21-23 The guidelines also did not provide a procedure for future updates.2,21-23 Nonetheless, the supporting evidence was clearly appraised and used to support recommendations, and there was an evident process and methodology for the development of recommendations.2,21-23 There was an explicit link between the recommendations and the supporting evidence, with varying strengths of recommendations associated with different levels of evidence.2,21-23 All relevant recommendations were easily identifiable and clearly presented.2,21-23 The authors of the guidelines adequately described potential facilitators and barriers to application of recommendations but did not provide intended users with additional guidance on how to implement the recommendations and monitor the implementation of relevant interventions.2,21-23 Finally, all the included guidelines appeared to have editorial independence, with clear disclosures of competing interests.2,21-23
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Normothermia Versus Hypothermia
Survival
Two SRs,5,12 1 RCT,13 and 1 retrospective cohort study18 evaluated the effect of TTM on survival rate with good neurologic or functional outcome. A favourable neurologic or functional outcome was defined as any of the following: modified Rankin Scale score of 0 to 3,5,12; Cerebral Performance Categories scale score of 1 or 2,5,12,13,18; Pittsburgh Cardiac Arrest Category score of 1 or 2,5 or blinded assessment from a health professional indicating no, mild, or moderate disability.5 No statistically significant differences were identified in the survival rate with good neurologic outcome between the normothermia and hypothermia groups.5,12,13,18 The SRs with NMA and meta-analysis reported odds ratios5 and risk ratios,12 respectively; however, the estimates were not statistically significant, suggesting no differences between interventions.
Two SRs, 1 RCT, 5 retrospective cohort studies, and 1 observational post hoc analysis of an RCT also evaluated overall survival, recorded at an unspecified time point,15,17 at hospital discharge,5,12,16,18,19 or within 30 days,12 90 days,5,12,20 6 months,5,12,13 or 1 year after discharge.20 The authors of 1 retrospective cohort study19 found a significantly greater proportion of survivors at discharge in the normothermia group compared with the hypothermia (TTM 32°C to 34°C) group, but no statistically significant differences were reported in the other studies.5,12,13,15-18,20
Mortality
Hospital and ICU mortality rates were evaluated in 1 RCT18 and 4 of the retrospective cohort studies14,15,17,19 included in this report. There were no statistically significant differences between the normothermia and hypothermia groups.
ICU or Hospital Length of Stay
One RCT13 and 4 retrospective cohort studies14,15,18,19 reported the average length of ICU14,19 or hospital13,15,18 stay as either a mean with standard deviation14 or median with interquartile range.13,15,18,19 The authors of 1 retrospective cohort study found that patients in the normothermia group who received standard supportive therapy experienced significantly longer hospital stays compared with patients in the hypothermia (TTM at 33°C to 35°C) group.15 There were no significant differences between the groups reported in the other studies.13,14,18,19
Neurologic Status
Neurologic status and function were measured in the studies included in this report using Cerebral Performance Categories scale scores13-16,20 and modified Rankin Scale scores.14 The authors of 1 retrospective cohort study15 found that a significantly greater proportion of patients in the hypothermia (TTM at 33°C to 35°C) group had good neurologic results, defined as a Cerebral Performance Categories scale score of either 1 or 2, compared with patients in normothermia (non-TTM) group. Although this finding was in favour of targeted hypothermia, no statistically significant differences were identified among the groups in other studies that also investigated this outcome.13,14,16,20
Protocol Adherence
One retrospective cohort study by Duggelin et al. (2021)14 investigated the proportion of patients adherent to the TTM protocol at 24 hours. Using a Cox proportional hazard model, it was demonstrated that a significantly higher proportion patients in the normothermia (36°C) group were adherent to the TTM protocol compared with patients in the hypothermia (33°C) group.14
Quality of Life
Quality of life at 1-year follow-up, measured using the 36-Item Short Form Survey, was reported in 1 included observational post hoc analysis.20 Patients in both groups reported similar physical and mental component scores.20 The risk ratio estimates were not statistically significant, suggesting no differences between interventions.
Time Spent in Temperature Target Range
The authors of 1 retrospective cohort study19 evaluated the median proportion of time spent in the prescribed temperature range among patients in the hypothermia (TTM 32 to 34°C) versus normothermia (TTM 36°C) groups and found no statistically significant differences.
Medication Prescription
The proportion of patients receiving sedatives and relaxants and the mean or median doses prescribed were reported in 2 retrospective cohort studies.14,19 There were no statistically significant differences in the proportion of patients receiving propofol, morphine, midazolam, fentanyl, and pethidine for sedation, but 1 of the studies found that a significantly lower proportion of patients in the normothermia (TTM 36°C) group received at least 1 dose of muscle relaxant compared with patients in the hypothermia (TTM 32 to 34°C) group. Patients in the normothermia (TTM 36°C) group were reported to have received significantly lower doses of midalozam14,19 and fentanyl19 compared with patients in the hypothermia (TTM 32 to 34°C) group.
Adverse Events
Several adverse events were reported in the studies included in this report: arrhythmia,5,13,14,19 bleeding,5,13,14,18,19 pneumonia,5,13,14 sepsis,5 seizures,5,17 limb ischemia,13,18 acute renal failure,13,18 continuous renal replacement therapy,13,18,19 thrombosis,14 bradycardia,14 hypoxic ischemia encephalopathy,18 stroke,18 ischemic hepatitis,18 cardiovascular instability,19 and mechanical ventilation.19 The authors of Duggelin et al. (2021)14 found that there was a significantly lower incidence of bradycardia among patients in the normothermia (TTM 36°C) group compared with patients in the hypothermia (TTM 33°C) group. However, no statistically significant differences were identified among the groups in other studies or for other adverse events.5,13,17-19
Guidelines
Among the 4 included guidelines, all strongly recommended the use of TTM to improve survival and neurologic outcome in patients resuscitated from OCHA with a shockable cardiac rhythm (ventricular tachycardia or ventricular fibrillation).2,21-23 The CCCS guideline23 extended the strong recommendation to patients presenting with pulseless ventricular tachycardia. In terms of patients with in-hospital cardiac arrest, the FICS guideline issued a positive recommendation for TTM at the level of expert opinion.21 However, the CCCS guideline contained a strong recommendation supported by low-level evidence in favour of TTM for patients with in-hospital cardiac arrest.23
The CCS guideline strongly recommended hypothermia (between 33°C and 36°C) for eligible patients who undergo TTM. The AAN guideline22 similarly specified in their recommendation that the TTM intervention should be hypothermia (32°C to 34°C for 24 hours); however, they also issued a lower-level recommendation supported by the same level of evidence for normothermia (36°C for 24 hours followed by 8 hours of rewarming to 37°C and temperature maintenance below 37.5°C until 72 hours) in patients who are comatose with either a shockable or non-shockable initial cardiac rhythm. The FICS guideline21 contains a weak recommendation for hypothermic (32°C to 36°C) TTM. Recommendations in the CCCS guideline23 do not state target temperature ranges for TTM.
With regard to specific technical recommendations, the CCS issued a lower-level recommendation supporting the use of surface cooling or intravascular cooling techniques.2
Limitations
Although there was a high quantity of eligible publications identified in this report for the clinical effectiveness question, the quality of the included primary studies5,12-20 was low. Some limitations were explicitly acknowledged by authors of the individual studies included in this review, such as the lack of generalizability of a single-centre retrospective cohort study and small sample sizes. Moreover, the critical appraisal performed as part of this review identified some important limitations of the included studies. For example, some of the included non-randomized studies represented outcomes with unclear time points and follow-up periods and lacked detail on important adverse events. With the exception of 1 RCT included in the SR by Fernando et al. (2021),5 none of the studies included in this report were conducted in a Canadian setting, which could be a limitation.
Furthermore, there was a significant amount of overlap identified across the 2 SRs included in this report; much of the available evidence identified in this review is based on the same trials. The 1 RCT included in this report that did not overlap with the SRs is a preliminary study with 21 participants. This limits the available evidence base to address research questions regarding the clinical effectiveness of targeted and non-targeted normothermia for patients in critical care after cardiac arrest.
The SRs included in this report had several strengths in methodology, but authors of both SRs5,12 reported heterogeneity in study characteristics, such as patient populations and interventions, among the included RCTs and did not perform subsequent meta-regression or subgroup analyses to investigate the heterogeneity due to insufficient data. The NMA by Fernando et al. (2021)5 also lacked direct comparative evidence evaluating the differences between normothermia and mild hypothermia (35°C to 36°C).
Although the guidelines included in this report were generally of high quality, some relevant recommendations regarding TTM were categorized as conditional and supported by low-quality evidence, as stated by guideline authors. The guidelines did not contain any recommendations pertaining to the management of fever and shivering or specifics on the timing of TTM therapy.
Conclusions and Implications for Decision- or Policy-Making
This report identified 2 SRs (1 with an NMA5 and 1 with a meta-analysis12), 1 RCT,13 and 7 non-randomized studies14-20 published since 2016 informing the comparative clinical effectiveness of normothermia versus hypothermia for adult patients after cardiac arrest. Overall, there were no statistically significant differences across all the studies for several clinical effectiveness and patient-related outcomes: survival with good neurologic outcome, overall survival, hospital mortality, quality of life, and time spent in the temperature target range. There was an indication that targeted normothermia at 36°C may offer slight benefits over hypothermic TTM. Outcomes in favour of normothermia, such as greater proportion of survivors at discharge, protocol adherence, and decreased dose and use of prescribed sedatives and relaxants, were identified in 2 retrospective cohort studies.14,19 However, the studies14,19 were characterized to be of low quality and with potentially limited generalizability to the Canadian context. Therefore, there is limited evidence to suggest that normothermic TTM may provide more clinical benefits over hypothermic TTM.
In addition, 4 evidence-based guidelines published since 2016 were identified regarding the use of TTM for adult patients after cardiac arrest. In general, TTM was strongly recommended by all included guidelines, particularly for adult patients resuscitated from OCHA. Patients presenting with shockable initial cardiac rhythm versus non-shockable cardiac rhythm were also more strongly recommended for TTM. Unlike the clinical evidence identified in this report, guidelines — particularly those developed by Canadian and American organizations — strongly recommended the use of hypothermia for eligible patients, either in the 33°C to 36°C or 32°C to 34°C ranges. The guidelines included in this report were found to be of moderate to high quality. It is important to acknowledge that these guidelines are older compared with some of the clinical studies included in this report, with the latest 1 published in 2018, which may be the cause of discrepancies between the evidence used to inform the recommendations and the current literature on the topic.
Baseline characteristics, such as age, location of cardiac arrest (in hospital vs. out of hospital), and initial cardiac rhythm, may play a role in determining which patients are mostly likely to benefit from either modality of TTM. Larger RCTs and additional SRs with less heterogeneity may allow for the necessary means to identify such subgroups.
References
1.Heart and Stroke Foundation of Canada. Saving lives. 2022; https://www.heartandstroke.ca/what-we-do/our-impact/saving-lives. Accessed 2022 Jan 19.
2.Wong GC, van Diepen S, Ainsworth C, et al. Canadian Cardiovascular Society/Canadian Cardiovascular Critical Care Society/Canadian Association of Interventional Cardiology Position Statement on the Optimal Care of the Postarrest Patient. Can J Cardiol. 2017;33(1):1-16. PubMed
3.Schafer A, Bauersachs J, Akin M. Therapeutic Hypothermia following Cardiac Arrest after the TTM2 trial - more Questions Raised than Answered. Curr Probl Cardiol. 2021:101046. PubMed
4.Kikutani K, Nishikimi M, Shimatani T, Kyo M, Ohshimo S, Shime N. Differential Effectiveness of Hypothermic Targeted Temperature Management According to the Severity of Post-Cardiac Arrest Syndrome. J Clin Med. 2021;10(23):5643. PubMed
5.Fernando SM, Di Santo P, Sadeghirad B, et al. Targeted temperature management following out-of-hospital cardiac arrest: a systematic review and network meta-analysis of temperature targets. Intensive Care Med. 2021;47(10):1078-1088. PubMed
6.Dankiewicz J, Friberg H, Belohlavek J, et al. Time to start of cardiopulmonary resuscitation and the effect of target temperature management at 33degreeC and 36degreeC. Resuscitation. 2016;99:44-49. PubMed
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
8.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
9.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
10.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2022 Jan 27.
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Granfeldt A, Holmberg MJ, Nolan JP, Soar J, Andersen LW, International Liaison Committee on Resuscitation Advanced Life Support Task F. Targeted temperature management in adult cardiac arrest: Systematic review and meta-analysis. Resuscitation. 2021;167:160-172. PubMed
13.Pang PY, Wee GH, Hoo AE, et al. Therapeutic hypothermia in adult patients receiving extracorporeal life support: early results of a randomized controlled study. J Cardiothorac Surg. 2016;11:43. PubMed
14.Duggelin R, Maggiorini M, Voigtsberger S, Schwarz U, Hilty MP. Increased protocol adherence and safety during controlled normothermia as compared to hypothermia after cardiac arrest. J Crit Care. 2021;63:146-153. PubMed
15.Kocayigit H, Suner KO, Kaya B, Tomak Y, Tuna AT, Erdem AF. Neurological Outcomes of Normothermia versus Targeted Temperature Management in Post-cardiac Arrest Syndrome. J Coll Physicians Surg Pak. 2021;30(5):497-501. PubMed
16.Kim JH, Park JH, Shin SD, et al. Effects of moderate hypothermia versus normothermia on survival outcomes according to the initial body temperature in out-of-hospital cardiac patients: A nationwide observational study. Resuscitation. 2020;151:157-165. PubMed
17.Eilam A, Samogalskyi V, Bregman G, Eliner-Avishai S, Gilad R. Occurrence of overt seizures in comatose survivor patients treated with targeted temperature. Brain Behav. 2017;7(11):e00842. PubMed
18.Pang PYK, Wee GHL, Huang MJ, et al. Therapeutic Hypothermia May Improve Neurological Outcomes in Extracorporeal Life Support for Adult Cardiac Arrest. Heart Lung Circ. 2017;26(8):817-824. PubMed
19.Casamento A, Minson A, Radford S, et al. A comparison of therapeutic hypothermia and strict therapeutic normothermia after cardiac arrest. Resuscitation. 2016;106:83-88. PubMed
20.Spoormans EM, Lemkes JS, Janssens GN, et al. Targeted Temperature Management in Out-of-Hospital Cardiac Arrest With Shockable Rhythm: A Post Hoc Analysis of the Coronary Angiography After Cardiac Arrest Trial. Crit Care Med. 2021;22:22. PubMed
21.Cariou A, Payen JF, Asehnoune K, et al. Targeted temperature management in the ICU: Guidelines from a French expert panel. Anaesth Crit Care Pain Med. 2018;37(5):481-491. PubMed
22.Geocadin RG, Wijdicks E, Armstrong MJ, et al. Practice guideline summary: Reducing brain injury following cardiopulmonary resuscitation: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2017;88(22):2141-2149. PubMed
23.Howes D, Gray SH, Brooks SC, et al. Canadian Guidelines for the use of targeted temperature management (therapeutic hypothermia) after cardiac arrest: A joint statement from The Canadian Critical Care Society (CCCS), Canadian Neurocritical Care Society (CNCCS), and the Canadian Critical Care Trials Group (CCCTG). Resuscitation. 2016;98:48-63. PubMed
24.Banks JL, Marotta CA. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38(3):1091-1096. PubMed
25.Balouris SA, Raina KD, Rittenberger JC, Callaway CW, Rogers JC, Holm MB. Development and validation of the Cerebral Performance Categories-Extended (CPC-E). Resuscitation. 2015;94:98-105. PubMed
26.Coppler PJ, Elmer J, Calderon L, et al. Validation of the Pittsburgh Cardiac Arrest Category illness severity score. Resuscitation. 2015;89:86-92. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Review and Network Meta-Analysis
Study, country, funding | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Fernando et al. (2021)5 Canada Funding: No funding received | SR with NMA Total: 10 RCTs (N = 4,218; range 30 to 1,861) included in NMA Year of publication: 2000 to 2021 | Adult patients with OHCA who remained unresponsive following ROSC Range of mean age: (56 to 75) years Range of % male: 60 to 88.9 Initial rhythm: any, VF, VF/VT, VF/VT/asystole, VF/asystole, asystole/PEA | Normothermia (37°C to 37.8°C) (n = 1,390) Deep hypothermia (31°C to 32°C) (n = 276) Moderate hypothermia (33°C to 34°C) (n = 2,086) Mild hypothermia (35°C to 36°C) (n = 466) | Primary outcome:
Secondary outcomes:
Follow-up: NR |
Granfeldt et al. (2021)12 Denmark Funding: NR | SR with MA Total 9 RCTs (N = 2,968; range: 16 to 1,861) Year of publication: 2001 to 2021 | Adult patients with cardiac arrest in any setting (in-hospital or out-of-hospital) underwent TTM Range of mean age:
Range of % male:
Initial rhythm: Shockable (VF/VT), non-shockable (asystole/PEA) | Normothermia (e.g., no TTM, no clear description of TTM, or TTM to maintain normothermia [generally 36.5°C to 38°C]) Hypothermia (TTM at 32°C to 34°C) | Survival with favourable neurological outcome at hospital discharge or 30 days Survival with favourable neurological outcome at 90 or 180 days Overall survival to hospital discharge or 30 days Overall survival at 90 or 180 days Follow-up: 90 or 180 days |
AE = adverse event; MA = meta-analysis; NMA = network met-analysis; NR = not reported; OHCA = out-of-hospital cardiac arrest; PEA = pulseless electrical activity; ROSC = return of spontaneous circulation; SR = systematic review; TTM = targeted temperature management; VF = ventricular fibrillation; VT = ventricular tachycardia.
Note: This table has not been copy-edited.
aGood functional outcome was defined on the basis of any of the following: (1) modified Rankin Scale score of 0 (no symptoms) to 3 (moderate disability); (2) Cerebral Performance Categories scale score of 1 (good cerebral performance) or 2 (moderate cerebral disability); (3) Pittsburgh cerebral performance category of 1 (good recovery) or 2 (moderate disability); or (4) blinded assessment from a health professional indication no, mild, or moderate disability.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized controlled trial | ||||
Pang et al. (2016)13 Singapore Funding: SingHealth Foundation | Non-blinded, parallel (1:1) RCT Sample size calculation provided: No ITT: NR | Adult patients receiving ECLS for cardiac arrest Mean age: 52.5 years % Male: 81.0 % In-hospital cardiac arrest: 90.5 % Acute coronary syndrome: 81.0 Mean duration of CPR: 25.7 minutes Mean duration of ECLS: 4.4 days Initial rhythm: Any | Normothermia (37°C) (n = 12) Targeted hypothermia (34°C maintained for 24 hours in the ICU) (n = 9) Cooling to 34°C was performed by modulating the heat exchanger component of the ECLS circuit. | Primary outcome: Survival to hospital discharge with good neurological function (defined as a CPCa of 1 or 2) Secondary outcomes:
Follow-up: 6 months |
Non-randomized studies | ||||
Duggelin et al. (2021)14 Switzerland Funding: No funding received | Retrospective cohort study Sample size calculation provided: No Adjustment for confounders conducted: No | Adult patients successfully resuscitated after out-of-hospital or in-hospital cardiac arrest Mean age: 61 years % Male: 81.5 Mean time to ROSC: 17.6 minutes % OHCA: 83.0 Initial rhythm: Any |
TTM was initiated by application of 30 mL/kg body weight of saline cooled to 4°C for TTM 33°C or no cooled saline for TTM 36°C. TTM was maintained for 24 hours. | Outcomes:
Follow-up: NA |
Kocayigit et al. (2021)15 Turkey Funding: NR | Retrospective cohort study Sample size calculation provided: No Adjustment for confounders conducted: No | Adult patients hospitalized in the ICU for cardiac arrest due to myocardial infarction receiving TTM Mean age: 58.1 years Median duration of CPR: 20 minutes % OHCA: 59.8 Initial rhythm: VF/asystole | Normothermia (non-TTM; temperature not specified) (n = 31) Hypothermia (TTM at 33°C to 35°C for 24 hours) | Outcomes:
Follow-up: NA |
Spoormans et al. (2021)20 The Netherlands Funding: The Netherlands Heart Institute, Biotronik, and AstraZeneca | Observational post hoc analysis of an RCT Sample size calculation provided: No Adjustment for confounders conducted: Yes | Adult patients successfully resuscitated after OHCA with an initial shockable rhythm Mean age: 65 years % Male: 78.6 Median time to ROSC: 15 minutes Median time arrest to basic life support: 2 minutes Initial rhythm: Shockable (VF/VT) | Normothermia (TTM at 36 to 37°C) (n = 190) Hypothermia (TTM at 32°C to 34°C) (n = 269) Cooling methods of TTM: Body surface cooling, intravascular cooling device | Primary outcome:
Secondary outcomes:
Follow-up: 90 days, 1 year |
Kim et al. (2020)16 South Korea Funding: National Fire Agency of Korea and the Korea Centers for Disease Control and Prevention | Retrospective cohort study Sample size calculation provided: No Adjustment for confounders conducted: Yes | OHCA patients who were hospitalized and underwent TTM Mean age: 59.8 years % Male: 76.7 Initial rhythm: Any | Normothermia (TTM at ≥35.5°C) (n = 116) Hypothermia (TTM at <35.5°C) (n = 628) Cooling methods of TTM: External conventional cooling, external device cooling, intra-cavity cooling, unknown) | Primary outcome: • Survival to hospital discharge Secondary outcome: • Good neurological status (defined as a CPCa of 1 or 2) Follow-up: NA |
Eilam et al. (2017)17 Israel Funding: NR | Retrospective cohort study Sample size calculation provided: No Adjustment for confounders conducted: Yes | Comatose adult patients post-CPR hospitalized in the ICU Mean age: 56.3 years % Male: 53.4 Initial rhythm: Any | Normothermia (temperature not specified) (n = 62) Targeted hypothermia (32°C to 34°C maintained for 24 hours in the ICU) (n = 26) | Outcomes:
Follow-up: NA |
Pang et al. (2017)18 Singapore Funding: Sing Health Foundation | Retrospective cohort study Sample size calculation provided: No Adjustment for confounders conducted: No | Adult patients received CPR for refractory cardiac arrest and being treated with ECLS Mean age: 49.9 years % Male: 78.5 % In-hospital cardiac arrest: 92.4 Mean duration of CPR: 32.0 minutes Mean duration of ECLS: 5.4 days Initial rhythm: VT/VF, PEA, asystole | Normothermia (temperature not specified) (n = 65) Targeted hypothermia (34°C maintained for 24 hours in the ICU) (n = 14) Cooling to 34°C was performed by modulating the heat exchanger component of the ECLS circuit. | Outcomes:
Follow-up: 60 days |
Casamento et al. (2016)19 Australia, New Zealand Funding: NR | Retrospective cohort study Sample size calculation provided: Yes Adjustment for confounders conducted: Yes | Adult patients with cardiac arrest admitted to ICU Mean age: 62.5 years % Male: 78.3 Mean time to ROSC: 21 minutes Initial cardiac rhythm: EMD, VT/VF, asystole | Strict therapeutic normothermia (36°C for 28 hours) (n = 69) Therapeutic hypothermia (32 to 34°C for 24 hours) Cooling methods were performed using external cooling devices. | Primary outcome:
Secondary outcomes:
|
AE = adverse events; CPC = cerebral performance category; CPR = cardiopulmonary resuscitation; ICU = intensive care unit; ECLS = extracorporeal life support; EMD = electromechanical dissociation; NA = not applicable; NR = not reported; OHCA = out-of-hospital cardiac arrest; PEA = pulseless electrical activity; QoL = quality of life; RCT = randomized controlled trial; ROSC = return of spontaneous circulation; VF = ventricular fibrillation; VT = ventricular tachycardia.
Note: This table has not been copy-edited.
aCPC is a 5-category scale for measuring neurological status after cardiac arrest ranging from 1 (conscious, alert, able to work and lead a normal life) to 5 (brain dead, circulation preserved).
bThe modified Rankin Scale is commonly used to measure the degree of disability of people who have suffered a stroke or other causes or neurological disability. It is a scale runs from 0 to 6, with 0 for no symptoms and 6 for dead.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
SRLF/SFAR, Cariou et al. (2018)21 | ||||||
Intended users: Clinicians who provide neurological care to critically ill patients. Target population: Adult and pediatric patients with cardiac arrest, traumatic brain injury, stroke, other brain injuries, and shock. | TTM in the ICU as a primary neuroprotective method. | Survival with good neurological outcome. | Methods for collection, selection and synthesis of evidence were not reported. | The quality of evidence was rated as high, moderate, low, and very low.a The strength of recommendation was either positive or negative, and strong or weak.b | Recommendations were developed by a group of experts for the SRLF and the SFAR. The committee defined a list of questions and assigned designated experts to address each questions. The recommendations were developed using the GRADE method. The strength of recommendation was determined and validated by the experts through a vote, using the Delphi and GRADE Grid method. | The guideline was reviewed by internal and external experts and published in peer-reviewed journal. |
AAN, Geocadin et al. (2017)22 | ||||||
Intended Users: Clinicians who provide care for patients with nontraumatic cardiac arrest. Target Population: Adult patients who are comatose after successful CPR after cardiac arrest. | TTM for neuroprotective interventions in adult patients who are comatose after successful CPR. Therapeutic hypothermia is defined as cooling to a core body temperature of 32°C to 34°C. | Survival with good neurological outcome | A comprehensive literature search was taken. Evidence was reviewed by the committee members. | The level of evidence was classified as Class I, II, III or IV.c The strength of the recommendations was classified as A, B, C, or Ud. | The committee members reviewed the articles and classified the level of evidence using the AAN classification scheme for therapeutic articles. Recommendations were formulated and linked to the strength of the evidence. | The guideline was reviewed by AAN committees and published in peer-reviewed journal. |
CCS/CCCCS/CAIC, Wong et al. (2017)2 | ||||||
Intended Users: Clinicians who provide in-hospital care for OHCA patients. Target Population: OHCA patients. | TTM for in-hospital care of OHCA patients. TTM was defined as a strategy of intentional temperature management of a postarrest patient comprising active patient cooling, subsequent rewarming, and extended fever control. | Survival with good neurological outcome. | A comprehensive literature search was taken. Evidence was reviewed by the committee. | GRADE methodology was used to assess the quality of evidencea The strength of recommendations was either “Strong” (desirable effects clearly outweigh undesirable effects or clearly do not) or “Conditional” (when trade-offs are less certain, either because of low-quality evidence or because the evidence suggests that desirable and undesirable effects are closely balanced). | The Writing Panel composed of cardiologists and critical care specialists developed a set of clinical questions. The members review the evidence and formulate the recommendations with the help of GRADE. Final recommendations were made by majority vote based on the quality of the available evidence. | The guideline was reviewed by internal and external experts and published in peer-reviewed journal. |
CCCS/CNCCS/CCCTG, Howes et al. (2016)23 | ||||||
Intended Users: Clinicians who provide care for patients with cardiac arrest. Target Population: Adult patients with cardiac arrest. | TTM use after cardiac arrest in adult patients. | Survival with good neurological outcome. | A comprehensive literature search was taken. | The level of evidence for a recommendation was graded as high, moderate, or low.a The “low” and “very low” designations were combined to a single “low” category. The strength of recommendation was defined as “Strong” or “Conditional,” based on consideration of the quality of evidence, balance between benefits and risks, feasibility, and cost.e | A committee composed of experts in neurocritical care created a set of clinical questions. Each section lead coordinated the work with its team to search, extract and grade the literature, and formulate the draft recommendations. The final recommendations were made using a combination of Delphi methodology and nominal group technique. | The guideline was reviewed by internal and external experts and published in peer-reviewed journal. |
AAN = American Academy of Neurology; CPR = cardiopulmonary resuscitation; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; ICU = intensive care unit; NCS = Neurological Care Society; OHCA = out-of-hospital cardiac arrest; SFAR = Société française d’anesthésie et de réanimation; SRLF = Société de réanimation de langue française; TTM = targeted temperature management.
Note: This table has not been copy-edited.
aLevel of evidence: High = Further research is very unlikely to change the confidence in the estimate of the effect; Moderate = Further research is likely to have an impact on the confidence in the estimate of the effect and may change the estimate of the effect itself; Low = Further research is likely to have an impact on the confidence in the estimate of the effect and is likely to change the estimate of the effect itself; Very low = Any estimate of the effect is very unlikely.
bStrength of recommendation: Strong = We recommend (GRADE 1+) or we do not recommend (GRADE 1-); Weak = We suggest (GRADE 2+) or we do not suggest (GRADE 2-).
cLevel of evidence: Class I = A randomized, controlled clinical trial of the intervention of interest with good methodology and masked or objective outcome assessment, in a representative population. Relevant baseline characteristics are presented and substantially equivalent among treatment groups or there is appropriate statistical adjustment for differences. Class II = A randomized, controlled clinical trial of the intervention of interest in a representative population with moderate quality and with masked or objective outcome assessment, relevant baseline characteristics are presented and substantially equivalent among treatment groups, or there is appropriate statistical adjustment for differences. Class III = All other controlled trials (including well-defined natural history controls or patients serving as own controls) in a representative population, where outcome is independently assessed, or independently derived by objective outcome measurement. Class IV = Studies not meeting Class I, II, or III criteria, including consensus or expert opinion.
dStrength of recommendation: A = Established as effective, ineffective, or harmful (or established as useful/predictive or not useful/predictive) for the given condition in the specified population. (Level A rating requires at least 2 consistent Class I studies.) B = Probably effective, ineffective, or harmful (or probably useful/predictive or not useful/predictive) for the given condition in the specified population. (Level B rating requires at least one Class I study or 2 consistent Class II studies.) C = Possibly effective, ineffective, or harmful (or possibly useful/predictive or not useful/predictive) for the given condition in the specified population. (Level C rating requires at least one Class II study or 2 consistent Class III studies.) U = Data inadequate or conflicting; given current knowledge, treatment (test, predictor) is unproven. *In exceptional cases, one convincing Class I study may suffice for an “A” recommendation if 1) all criteria are met, 2) the magnitude of effect is large (relative rate improved outcome > 5 and the lower limit of the confidence interval is > 2).
eStrength of recommendation: Strong = The panel is confident that the desirable effects of adherence to a recommendation outweigh the undesirable effects; Conditional = The panel concludes that the desirable effects of adherence to a recommendation probably outweigh the undesirable effects but is not confident.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews and Network Meta-Analysis Using AMSTAR 27 and the ISPOR Questionnaire8
Strengths | Limitations |
|---|---|
Fernando et al. (2021)5 | |
|
|
| |
Granfeldt et al. (2021)12 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CI = confidence interval; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; MA = meta-analysis; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist9
Strengths | Limitations |
|---|---|
Randomized controlled trial | |
Pang et al. (2016)13 | |
Reporting:
Internal validity (bias, confounding):
| Reporting:
External validity:
Internal validity (bias, confounding):
Power:
|
Non-randomized studies | |
Duggelin et al. (2021)14 | |
Reporting:
Internal validity (bias, confounding):
| Reporting: characteristics of patients lost to follow-up NR External validity:
Internal validity (bias, confounding):
Power:
|
Kocayigit et al. (2021)15 | |
Reporting:
Internal validity (bias, confounding):
| Reporting:
External validity:
Internal validity (bias, confounding):
Power: power calculations were not provided, but sample size was not noted as a limitation of the study. |
Spoormans et al. (2021)20 | |
Reporting:
External validity: observational post hoc analysis of COACT trial conducted in 19 hospitals in the Netherlands Internal validity (bias, confounding):
| Reporting:
External validity: non-Canadian sample Internal validity (bias, confounding):
Power: This was a substudy of a larger trial, and therefore sample size calculations were not performed. |
Kim et al. (2020)16 | |
Reporting:
External validity:
Internal validity (bias, confounding):
| Reporting: adverse events NR External validity: non-Canadian sample Internal validity (bias, confounding):
Power: power calculations were not provided, but sample size was not noted as a limitation of the study. |
Eilam et al. (2017)17 | |
Reporting:
Internal validity (bias, confounding):
| Reporting:
External validity:
Internal validity (bias, confounding):
Power:
|
Pang et al. (2017)18 | |
Reporting:
Internal validity (bias, confounding):
| Reporting:
External validity:
Internal validity (bias, confounding):
Power:
|
Casamento et al. (2016)19 | |
Reporting:
External validity: Multi-centre, international (Australia and New Zealand) retrospective review Internal validity (bias, confounding):
Power: power calculations provided | Reporting:
External validity:
Internal validity (bias, confounding):
|
APACHE = Acute Physiologic Assessment and Chronic Health Evaluation; COACT = Coronary Angiography after Cardiac Arrest; ECMO = extracorporeal membrane oxygenation; ICU = intensive care unit; IQR = interquartile range; NR = not reported; OCHA = out-of-hospital cardiac arrest; ROSC = return of spontaneous circulation; SD = standard deviation.
Table 7: Strengths and Limitations of Guidelines Using AGREE II10
Item | SRLF/SFAR, Cariou et al. (2018)21 | AAN, Geocadin et al. (2017)22 | CCS/CCCCS/CAIC, Wong et al. (2017)2 | CCCS/CNCCS/CCCTG, Howes et al. (2016)23 |
|---|---|---|---|---|
Domain 1: Scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | Unclear | Unclear | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes |
Domain 3: Rigour of development | ||||
7. Systematic methods were used to search for evidence. | Only a comprehensive search reported | Only a comprehensive search reported | Only a comprehensive search reported | Only a comprehensive search reported |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Unclear | Unclear | Unclear | Unclear |
Domain 4: Clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear | Unclear | Unclear | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear | Unclear | Yes | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Unclear | Unclear | Unclear | Unclear |
Domain 6: Editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcomes for Survival
Study citation, study design, and patient model | Study findings |
|---|---|
Survival with good neurological outcome | |
Fernando et al. (2021)5 SR (10 RCTs included in NMA) Adult patients with OHCA who remained unresponsive following ROSC | NMA estimate (OR [95% CI]) compared hypothermia with normothermia (i.e., 37°C to 37.8°C): Survival with good functional outcome at hospital discharge, or the latest time point reported up until 6 months post-discharge:
|
Granfeldt et al. (2021)12 SR (9 RCTs included in MA) Adult patients with cardiac arrest in any setting (in-hospital or out-of-hospital) underwent TTM | MA estimate (RR [95% CI]) compared hypothermia (i.e., 32°C to 34°C) with normothermia (e.g., no TTM, no clear description of TTM, or TTM to maintain normothermia [generally 36.5°C to 38°C]):
|
Pang et al. (2016)13 RCT Adult patients receiving ECLS for cardiac arrest | Survival rate to hospital discharge with good neurological function in hypothermia (TTM 34°C) versus in normothermia (37°C) groups:
|
Pang et al. (2017)18 Retrospective cohort study Adult patients received CPR for refractory cardiac arrest and being treated with ECLS | Survival rate with good neurological recovery (i.e., CPC of 1 or 2) in hypothermia (TTM 34°C) versus normothermia (temperature not specified) groups:
|
Overall survival | |
Fernando et al. (2021)5 SR (10 RCTs included in NMA) Adult patients with OHCA who remained unresponsive following ROSC | NMA estimate (OR [95% CI]) compared with normothermia (37°C to 37.8°C): Overall survival (i.e., survival at hospital discharge, or the latest time point reported up until 6 months post-discharge):
|
Granfeldt et al. (2021)12 SR (9 RCTs included in MA) Adult patients with cardiac arrest in any setting (in-hospital or out-of-hospital) underwent TTM | MA estimate (RR [95% CI]) compared hypothermia (i.e., 32 to 34°C) with normothermia (e.g., no TTM, no clear description of TTM, or TTM to maintain normothermia [generally 36.5°C to 38°C]):
|
Pang et al. (2016)13 RCT Adult patients receiving ECLS for cardiac arrest | Survival rate until 6 months in hypothermia (TTM 34°C) versus normothermia (37°C) groups:
|
Kocayigit et al. (2021)15 Retrospective cohort study Adult patients hospitalized in the ICU for cardiac arrest due to myocardial infarction receiving TTM | Survival rate in hypothermia (TTM at 33°C to 35°C) versus normothermia (non-TTM; temperature not specified) groups:
|
Spoormans et al. (2021)20 Observational post hoc analysis of an RCT Adult patients successfully resuscitated after OHCA with an initial shockable rhythm | Survival in hypothermia (TTM at 32°C to 34°C) versus normothermia (TTM at 36°C to 37°C) groups:
|
Kim et al. (2020)16 Retrospective cohort study OHCA patients who were hospitalized and underwent TTM | Survival to hospital discharge in hypothermia (TTM at <35.5°C) versus normothermia (TTM at ≥35.5°C) groups:
|
Eilam et al. (2017)17 Retrospective cohort study Comatose adult patients post-CPR hospitalized in the ICU | Survival rate in hypothermia (TTM 32°C to 34°C) versus Normothermia (temperature not specified):
|
Pang et al. (2017)18 Retrospective cohort study Adult patients received CPR for refractory cardiac arrest and being treated with ECLS | Survival rate to discharge in hypothermia (TTM 34°C) versus normothermia (temperature not specified) groups:
|
Casamento et al. (2016)19 Retrospective cohort study Adult patients with cardiac arrest admitted to ICU | Survival rate to discharge in hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C) groups:
|
CI = confidence interval; ECLS = extracorporeal life support; HR = hazard ratio; ICU = intensive care unit; MA = meta-analysis; NMA = network meta-analysis; OHCA = out-of-hospital cardiac arrest; OR = odds ratio; RCT = randomized controlled trial; ROSC = return of spontaneous circulation; RR = risk ratio; SR = systematic review; TTM = targeted temperature management.
Table 9: Summary of Findings by Outcomes for Mortality
Study citation, study design, and patient model | Study findings |
|---|---|
ICU/In-hospital death | |
Pang et al. (2016)13 RCT Adult patients receiving ECLS for cardiac arrest | Hospital mortality rate in hypothermia (TTM 34°C) versus normothermia (37°C) groups:
|
Duggelin et al. (2021)14 Retrospective cohort study Adult patients successfully resuscitated after out-of-hospital or in-hospital cardiac arrest | Hospital mortality rate in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
ICU mortality rate in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
|
Kocayigit et al. (2021)15 Retrospective cohort study Adult patients hospitalized in the ICU for cardiac arrest due to myocardial infarction receiving TTM | 30-day mortality rate in hypothermia (TTM at 33°C to 35°C) versus normothermia (non-TTM; temperature not specified) groups:
|
Eilam et al. (2017)17 Retrospective cohort study Comatose adult patients post-CPR hospitalized in the ICU | Hospital mortality rate in hypothermia (TTM 32°C to 34°C) versus Normothermia (temperature not specified):
|
Casamento et al. (2016)19 Retrospective cohort study Adult patients with cardiac arrest admitted to ICU | ICU mortality rate in hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C) groups:
Hospital mortality rate in hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C) groups:
|
CPR = cardiopulmonary resuscitation; ECLS = extracorporeal life support; ICU = intensive care unit; RCT = randomized controlled trial; TTM = targeted temperature management.
Table 10: Summary of Findings by Outcomes for ICU and Hospital Length of Stay
Study citation, study design, and patient model | Study findings |
|---|---|
Pang et al. (2016)13 RCT Adult patients receiving ECLS for cardiac arrest | Median (range) length of hospital stay in hypothermia (TTM 34°C) versus normothermia (37°C) groups:
|
Duggelin et al. (2021)14 Retrospective cohort study Adult patients successfully resuscitated after out-of-hospital or in-hospital cardiac arrest | Mean (SD) of ICU length of stay in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
Mean (SD) of hospital length of stay in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
|
Kocayigit et al. (2021)15 Retrospective cohort study Adult patients hospitalized in the ICU for cardiac arrest due to myocardial infarction receiving TTM | Median (range) length of hospital stay in hypothermia (TTM at 33°C to 35°C) versus normothermia (non-TTM; temperature not specified) groups:
Hospital stay before discharge (SD) in hypothermia (TTM at 33°C to 35°C) versus normothermia (non-TTM; temperature not specified) groups:
|
Pang et al. (2017)18 Retrospective cohort study Adult patients received CPR for refractory cardiac arrest and being treated with ECLS | Median (range) length of hospital stay in hypothermia (TTM 34°C) versus normothermia (temperature not specified) groups:
|
Casamento et al. (2016)19 Retrospective cohort study Adult patients with cardiac arrest admitted to ICU | Median (range) of ICU length of stay in hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C) groups:
Median (range) of hospital length of stay in hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C) groups:
|
ECLS = extracorporeal life support; ICU = intensive care unit; SD = standard deviation; RCT = randomized controlled trial; TTM = targeted temperature management.
Table 11: Summary of Findings by Outcomes for Neurological Status
Study citation, study design, and patient model | Study findings |
|---|---|
Pang et al. (2016)13 RCT Adult patients receiving ECLS for cardiac arrest | Severe neurological dysfunction (CPC 3 to 5) rate in hypothermia (TTM 34°C) versus normothermia (37°C) groups:
|
Duggelin et al. (2021)14 Retrospective cohort study Adult patients successfully resuscitated after out-of-hospital or in-hospital cardiac arrest | Proportion of patients with modified Rankin Score < 4 in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
Proportion of patients with CPC < 3 in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
|
Kocayigit et al. (2021)15 Retrospective cohort study Adult patients hospitalized in the ICU for cardiac arrest due to myocardial infarction receiving TTM | Proportion of patients with good neurologic results (i.e., CPC 1 or 2) in hypothermia (TTM at 33°C to 35°C) versus normothermia (non-TTM; temperature not specified) groups:
|
Spoormans et al. (2021)20 Observational post hoc analysis of an RCT Adult patients successfully resuscitated after OHCA with an initial shockable rhythm | Patients with good neurological function at 90-day follow-up in hypothermia (TTM at 32°C to 34°C) versus normothermia (TTM at 36°C to 37°C) groups:
CPC scores did not significantly differ between hypothermia (TTM at 32 to 34°C) versus normothermia (TTM at 36 to 37°C) groups:
|
Kim et al. (2020)16 Retrospective cohort study OHCA patients who were hospitalized and underwent TTM | Good neurological status (i.e., a CPC score of 1 or 2) in hypothermia (TTM at <35.5°C) versus normothermia (TTM at ≥35.5°C) groups:
|
CPC = cerebral performance category; ECLS = extracorporeal life support; ICU = intensive care unit; OR = odds ratio; RCT = randomized controlled trial; TTM = targeted temperature management.
Table 12: Summary of Findings by Outcomes for Protocol Adherence
Study citation, study design, and patient model | Study findings |
|---|---|
Duggelin et al. (2021)14 Retrospective cohort study Adult patients successfully resuscitated after out-of-hospital or in-hospital cardiac arrest | Proportion of patients adherent to the protocol at 24 hours in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
|
TTM = targeted temperature management.
Table 13: Summary of Findings by Outcomes for Quality of Life
Study citation, study design, and patient model | Study findings |
|---|---|
Spoormans et al. (2021)20 Observational post hoc analysis of an RCT Adult patients successfully resuscitated after OHCA with an initial shockable rhythm | Quality of life at 1-year follow-up (using SF-36-Item Health Survey) in hypothermia (TTM at 32°C to 34°C) versus normothermia (TTM at 36°C to 37°C) groups:
|
CI = confidence interval; OHCA = out-of-hospital cardiac arrest; RCT = randomized controlled trial; RR = risk ratio; TTM = targeted temperature management.
Table 14: Summary of Findings by Outcomes for Time Spent in Temperature Target Range
Study citation, study design, and patient model | Study findings |
|---|---|
Casamento et al. (2016)19 Retrospective cohort study Adult patients with cardiac arrest admitted to ICU | Median proportion (range) of time spent in the prescribed temperature range in hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C) groups:
|
ICU = intensive care unit; TTM = targeted temperature management.
Table 15: Summary of Findings by Outcomes for Medication Prescription
Study citation, study design, and patient model | Study findings |
|---|---|
Duggelin et al. (2021)14 Retrospective cohort study Adult patients successfully resuscitated after out-of-hospital or in-hospital cardiac arrest | Hypothermia (TTM 33°C) versus normothermia (TTM 36°C):
|
Casamento et al. (2016)19 Retrospective cohort study Adult patients with cardiac arrest admitted to ICU | Hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C):
|
ICU = intensive care unit; TTM = targeted temperature management.
Table 16: Summary of Findings by Outcomes for Adverse Events
Study citation, study design, and patient model | Study findings |
|---|---|
Fernando et al. (2021)5 SR (10 RCTs included in NMA) Adult patients with OHCA who remained unresponsive following ROSC | NMA estimate (OR [95% CI]) compared hypothermia with normothermia (i.e., 37°C to 37.8°C):
MA estimate (OR [95% CI]) compared hypothermia with normothermia (i.e., 37°C to 37.8°C):
|
Pang et al. (2016)13 RCT Adult patients receiving ECLS for cardiac arrest | AE incidence in hypothermia (TTM 34°C) versus normothermia (37°C) groups (i.e., ECLS-related complications within 7 days):
|
Duggelin et al. (2021)14 Retrospective cohort study Adult patients successfully resuscitated after out-of-hospital or in-hospital cardiac arrest | Proportion of patients with at least 1 AE in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
AE incidence in hypothermia (TTM 33°C) versus normothermia (TTM 36°C) groups:
|
Eilam et al. (2017)17 Retrospective cohort study Comatose adult patients post-CPR hospitalized in the ICU | Rate of seizure in hypothermia (TTM 32°C to 34°C) versus Normothermia (temperature not specified):
|
Pang et al. (2017)18 Retrospective cohort study Adult patients received CPR for refractory cardiac arrest and being treated with ECLS | AE incidence in hypothermia (TTM 34°C) versus normothermia (temperature not specified) groups:
|
Casamento et al. (2016)19 Retrospective cohort study Adult patients with cardiac arrest admitted to ICU | AE incidence in hypothermia (TTM 32°C to 34°C) versus normothermia (TTM 36°C):
|
AE = adverse event; CI = confidence interval; ECLS = extracorporeal life support; HR = hazard ratio; ICU = intensive care unit; MA = meta-analysis; NMA = network meta-analysis; OHCA = out-of-hospital cardiac arrest; OR = odds ratio; RCT = randomized controlled trial; ROSC = return of spontaneous circulation; RR = risk ratio; SR = systematic review; TTM = targeted temperature management.
Table 17: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
SRLF/SFAR, Cariou et al. (2018)21 | |
“We recommend using TTM in order to improve survival with good neurological outcome in patients resuscitated from out-of-hospital cardiac arrest (OHCA) with shockable cardiac rhythm (ventricular fibrillation and pulseless ventricular tachycardia) and who remain comatose after return of spontaneous circulation (ROSC).”21 (p.483) Evidence supporting this recommendation came from 7 MAs and 4 SRs assessed studies on TTM after CA. | Strength of recommendation: Grade 1+ |
“We suggest considering TTM in order to improve survival with good neurological outcome in patients resuscitated from OHCA with non-shockable cardiac rhythm (asystole or pulseless electrical activity) and who remain comatose after ROSC.”21 (p.483) This recommendation was developed based on evidence from 8 MAs and 4 reviews on TTM after CA. | Strength of recommendation: Grade 2+ |
“We suggest considering TTM in order to increase survival with good neurological outcome in patients resuscitated from in-hospital cardiac arrest (IHCA) who remain comatose after ROSC.”21 (p.483) There were no published RCTs with patients presenting in-hospital cardiac arrest (IHCA) patients. | Strength of recommendation: Expert opinion |
“We suggest considering TTM between 32 and 36 oC in order to improve survival with good neurological outcome after CA.”21 (p.483) One RCT and 1 SR of 6 RCTs provided evidence for this recommendation. However, it was not possible to define the optimal temperature within this range. | Strength of recommendation: Grade 2+ |
AAN, Geocadin et al. (2017)22 | |
“For patients who are comatose after an initial cardiac rhythm of VT/VF, TH (32–34°C for 24 hours) is highly likely to be effective in improving neurologic outcome and survival compared with non-TH and should be offered.”22 (p. 2142) The recommendation was developed based on 2 Class I studies. | Level of evidence: Class I Strength of recommendation: A |
“For patients who are comatose with an initial cardiac rhythm of either VT/VF or PEA/asystole, TTM (36°C for 24 hours followed by 8 hours of rewarming to 37°C and temperature maintenance below 37.58C until 72 hours) is likely as effective as TH in improving neurologic outcome and survival and is an acceptable alternative to TH. ”22 (p. 2142-2143) The recommendation was developed based on 1 Class I study. | Level of evidence: Class I Strength of recommendation: B |
“For patients who are comatose with an initial rhythm of VF, there is insufficient evidence to support or refute the use of 32°C vs 34°C TH because of lack of statistical precision.”22 (p. 2143) The recommendation was developed based on Class III studies. | Level of evidence: Class III Strength of recommendation: U |
“For patients who are comatose in whom the initial rhythm is PEA/asystole, treatment with TH vs non-TH possibly improves functional neurologic outcome and survival at hospital discharge and may be offered.”22 (p. 2143) The recommendation was developed based on 2 MAs of Class III studies. | Level of evidence: Class III Strength of recommendation: C |
“For patients who are comatose after cardiac arrest, prehospital cooling as an adjunct to in-hospital cooling is highly likely to be ineffective in further improving neurologic outcome and survival and should not be offered.”22 (p. 2144) The recommendation was developed based on multiple Class I studies. | Level of evidence: Class I Strength of recommendation: A |
CCS/CCCCS/CAIC, Wong et al. (2017)2 | |
“We recommend that TTM be used in unresponsive OHCA survivors with an initial shockable rhythm after ROSC.”2 (p.3) The recommendation was developed based on 3 RCTs of low quality. | Level of evidence: Low Strength of recommendation: Strong |
“We suggest TTM be used in unresponsive OHCA survivors with an initial nonshockable rhythm after ROSC.”2 (p.3) The recommendation was developed based on 7 observational studies. | Level of evidence: Very low Strength of recommendation: Conditional |
“We suggest that TTM be considered in unresponsive survivors of in-hospital cardiac arrest with any rhythm after ROSC.”2 (p.3) The recommendation was developed based on 3 observational studies. | Level of evidence: Very low Strength of recommendation: Conditional |
“We recommend that a temperature between 33°C and 36°C, inclusively, be selected and maintained for patients who undergo TTM.”2 (p.3) The recommendation was developed based on 2 RCTs. | Level of evidence: Moderate Strength of recommendation: Strong |
“We do not recommend the use of chilled intravenous fluids for prehospital cooling after ROSC.”2 (p.3) The recommendation was developed based on 2 RCTs. | Level of evidence: Moderate Strength of recommendation: Strong |
“We suggest that either surface cooling or intravascular cooling techniques may be used to induce and maintain TTM.”2 (p.4) The recommendation was developed based on 2 RCTs and 2 observational studies. | Level of evidence: Low Strength of recommendation: Conditional |
“We suggest that the cooling temperature selected for TTM be maintained for at least 24 hours.”2 (p.4) “We suggest TTM be continued beyond 24 hours from ROSC to prevent fever.”2 (p.4) The recommendations were developed based on 2 RCTs and 1 retrospective study. | Level of evidence: Very low Strength of recommendation: Conditional |
CCCS/CNCCS/CCCTG, Howes et al. (2016)23 | |
“We recommend that Targeted Temperature Management (TTM) be used for neuro-protection in eligible adult patients after resuscitation from cardiac arrest.”23 (p.52) The recommendation was developed based on 2 RCTs of high quality. | Level of evidence: High Strength of recommendation: Strong |
“We recommend that patients with a presenting rhythm of ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT)are eligible for TTM.”23 (p.52) The recommendation was developed based on 4 RCTs of high quality. | Level of evidence: High Strength of recommendation: Strong |
“We suggest that patients with a presenting rhythm of pulseless electrical activity (PEA) or asystole are eligible for TTM.”23 (p.52) The recommendation was developed based on 1 RCT and 1 retrospective study. | Level of evidence: Low Strength of recommendation: Conditional |
“We recommend that patients who suffer out-of-hospital cardiac arrest are eligible for TTM.”23 (p.53) The recommendation was developed based on 2 RCTs of high quality. | Level of evidence: High Strength of recommendation: Strong |
“We recommend that patients who suffer in-hospital cardiac arrest are eligible for TTM.”23 (p.53) The recommendation was developed based on 4 low-quality studies. | Level of evidence: Low Strength of recommendation: Strong |
“We recommend that patients who suffer a cardiac arrest of known cardiac cause or of an unknown cause are eligible for TTM.”23 (p.53) | Level of evidence: High Strength of recommendation: Strong |
CA = cardiac arrest; MA = meta-analysis; OHCA = out-of-hospital cardiac arrest; PEA = pulseless electrical activity; RCT = randomized controlled trial; ROSC = return of spontaneous circulation; SR = systematic reviews; TH = therapeutic hypothermia; TTM = targeted temperature management; VF = ventricular fibrillation; VT = ventricular tachycardia.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 18: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Fernando et al. (2021)5 | Granfeldt et al. (2021)12 |
|---|---|---|
Bernard SA et al. N Engl J Med 2002; 346:557–563 | Yes | Yes |
Dankiewicz J et al. Engl J Med 2021; 384:2283–2294 | Yes | Yes |
Hypothermia After Cardiac Arrest Study Group 2002; N Engl J Med 346:549–556 | Yes | Yes |
Hachimi-Idrissi S 2001; Resuscitation 51:275–281 | Yes | Yes |
Lascarrou JB et al. 2019; N Engl J Med 81:2327–2337 | Yes | Yes |
Laurent I et al. 2005; Am Coll Cardiol 46:432–437 | Yes | Yes |
Le May M et al. 2021; JAMA 326 : 1494-1503 | Yes | No |
Lopez-de-Sa E et al. 2012; Circulation 126:2826–2833 | Yes | No |
Lopez-de-Sa E et al. 2018; Intensive Care Med 44:1807–1815 | Yes | No |
Nielsen N et al. 2013; N Engl J Med 369:2197–2206 | Yes | No |
Callaway CW et al. 2002; Resuscitation 52(2):159–65 | No | Yes |
Zhang J 2005; Chin J Clin Rehabilitation 9:136–8 | No | Yes |
Hachimi-Idrissi S ewt al. 2005; Resuscitation 64:187–92 | No | Yes |
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Temperature settings for therapeutic hypothermia: guidelines. (CADTH rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/sites/default/files/pdf/htis/june-2016/RB0993%20Therapeutic%20Hypothermia%20Final.pdf. Accessed 2022 Jan 27.
Normothermia versus therapeutic hypothermia for adult patients after cardiac arrest: clinical evidence. (CADTH rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2014: https://www.cadth.ca/media/pdf/htis/dec-2014/RB0727%20Normothermia%20Final.pdf. Accessed 2022 Jan 27.
Additional References
National Institute for Health and Care Excellence. Arctic Sun 5000 for therapeutic hypothermia after cardiac arrest. (Medtech innovation briefing MIB112) 2017; https://www.nice.org.uk/advice/mib112. Accessed 2022 Jan 27.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca