CADTH Health Technology Review
Orthopedic Footwear for People With Lower-Limb Conditions
Rapid Review
Authors: Angela M. Barbara, Aleksandra Grobelna
Abbreviations
DFU
diabetic foot ulcer
GRADE
Grading of Recommendations Assessment, Development and Evaluation
IWGDF
International Working Group on the Diabetic Foot
MTP
metatarsophalangeal joint
RA
rheumatoid arthritis
RCT
randomized controlled trial
SVS
Society for Vascular Surgery
Key Messages
In adults with rheumatoid arthritis, prefabricated orthopedic footwear may reduce foot pain and improve physical functioning, but not affect health-related quality of life. However, this is based on evidence of variable quality from within-group designs, comparing outcomes pre- and postintervention.
Due to conflicting results, evidence of variable quality from comparatives studies regarding the effectiveness of prefabricated orthopedic footwear for foot pain and foot function in people with inflammation of the soles of the feet (plantar fasciitis) or gout was inconclusive.
Evidence of variable quality from 2 systematic reviews suggested that prefabricated orthopedic footwear after a healed diabetic foot ulcer (DFU) may prevent the recurrence of the condition better than conventional shoes at 1 year but not at 2 years.
No economic evaluations were identified that evaluated the cost-effectiveness of prefabricated orthopedic footwear for treating people with lower-limb conditions.
Two evidence-based guidelines recommended against using orthopedic footwear for treatment in patients with DFUs and 2 recommended using orthopedic footwears for adults with healed DFUs to prevent a recurrence. One guideline recommended using orthopedic footwear by adults with rheumatoid arthritis.
Context and Policy Issues
In patients with systemic diseases such as diabetes mellites, rheumatoid arthritis (RA), plantar fasciitis, Charcot foot, and hallux valgus, the morbidity of the lower limb is compromised.1 Patients will experience pain, impairment, disability, and reduction in foot function and quality of life.2,3 The complications associated with these conditions place the lower limb at risk of infection, deformity, and amputation.1,3 Orthopedic footwear were designed to promote proper musculoskeletal movement and have biomechanical effects in people with these conditions.4
Orthopedic footwear (also known as therapeutic footwear) is a generic term for footwear with adaptations intended to treat conditions affecting the foot, ankle, and lower limbs.5 Because the type of footwear affects balance, gait velocity, cadence, stride time, and stride length, various types of shoe modifications have been used to decrease the forces applied on the foot and to change the location or distribution of applied forces.4,6 Examples included custom-made therapeutic shoes or sandals (i.e., uniquely manufactured for 1 individual), prefabricated orthopedic footwear, and ready-made or customized inserts. This report focuses on prefabricated orthopedic footwear, also referred to as off-the-shelf medical-grade footwear.5,7 These include prefabricated therapeutic shoes, sandals, or boots that are intended to offer therapeutic effect by providing extra depth, multiple width fittings, and other features not offered in conventional shoes.3,4,8,9 While the terms “orthopedic” and “therapeutic” are used interchangeably in the literature to refer to this type of footwear, “orthopedic” will be used throughout this report to encompass both terms.
Prefabricated orthopedic footwear falls under the broader category of nonsurgical offloading interventions. These are devices specifically designed to offload local stress, thus relieving mechanical pressure from a specific region of the foot.10 An example of offloading footwear is the rocker shoes, designed with a curvature in the sole intended to distribute pressure applied to the plantar surface of the foot to facilitate movement.1,6,7
Many health insurance plans cover orthopedic shoes to treat diagnosed medical conditions. To ensure that this policy is evidence-based, the objective of this report is to summarize the evidence on the clinical effectiveness and cost-effectiveness of prefabricated orthopedic footwear for the treatment of people with lower-limb conditions. Additionally, evidence-based guidelines regarding the use of prefabricated orthopedic footwear were sought.
Research Questions
What is the clinical effectiveness of orthopedic footwear for the treatment of people with lower-limb conditions?
What is the cost-effectiveness of orthopedic footwear for the treatment of people with lower-limb conditions?
What are the evidence-based guidelines regarding the use of orthopedic footwear for the treatment of people with lower-limb conditions?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including Medline, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was orthopedic footwear. No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and November 24, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People with lower-limb conditions (e.g., plantar fasciitis, diabetic foot ulcers, Charcot foot, hallux valgus, metatarsal amputation, clubfoot, rheumatoid arthritis) |
Intervention | Prefabricated orthopedic footwear (also known as therapeutic footwear) |
Comparator | Q1 to Q2: Alternative interventions (e.g., custom-made orthopedic footwear, foot orthotics, shoe inserts); no treatment with orthopedic shoes (i.e., use of regular footwear) Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., pain, functionality, quality of life, disability, amputations, safety [e.g., rates of adverse events]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q3: Recommendations regarding best practices (e.g., appropriate patient populations, recommended types or features of orthopedic footwear, guidance on the replacement of orthopedic footwear) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Systematic reviews in which all relevant studies were captured in other, more recent or more comprehensive systematic reviews were excluded.11,12 Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews.13-15
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess Systematic Reviews 216 for systematic reviews, the Downs and Black checklist17 for randomized and non-randomized studies, the Drummond checklist18 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation II instrument19 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
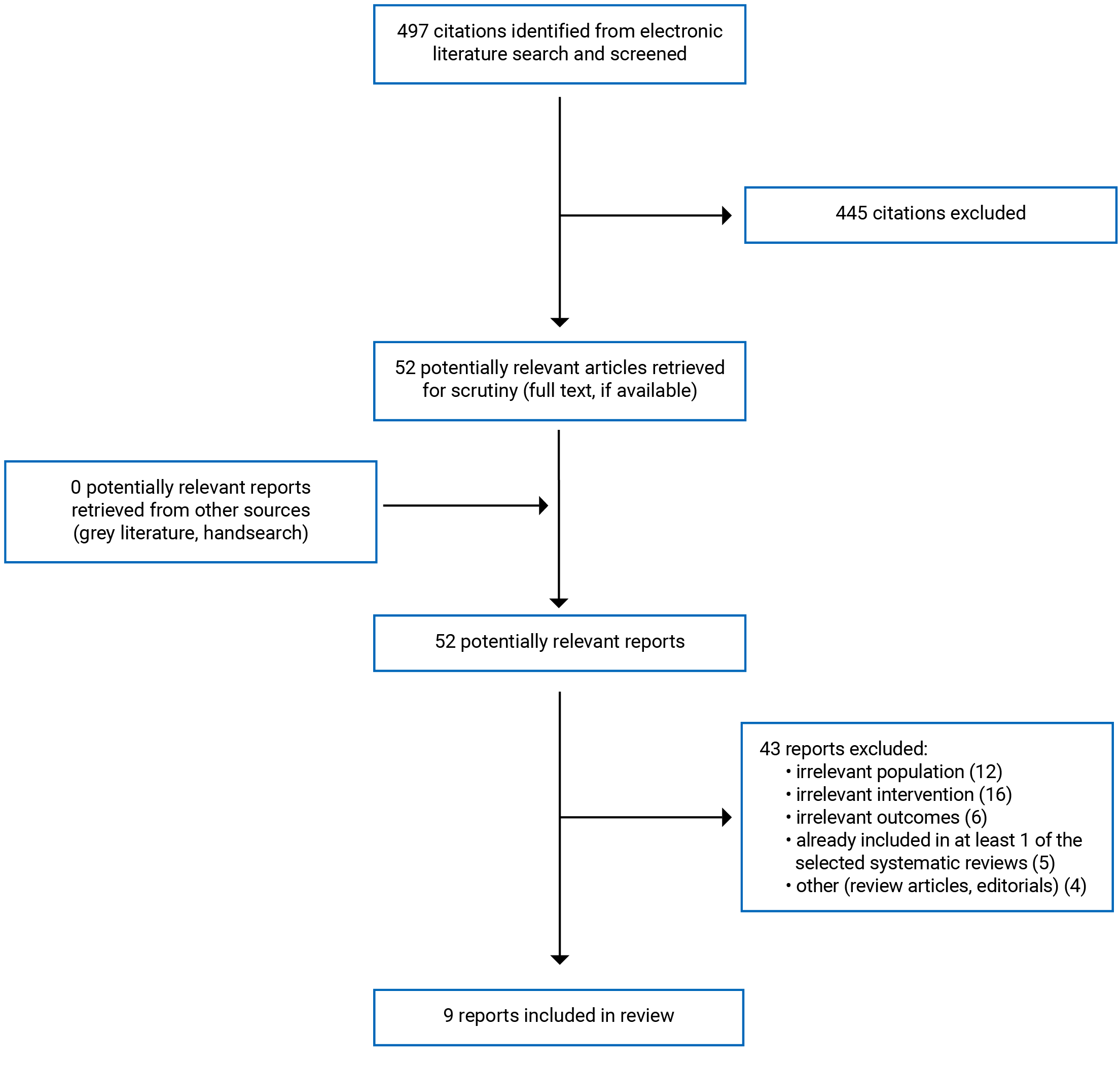
A total of 497 citations were identified in the literature search. Following the screening of titles and abstracts, 445 citations were excluded, and 52 potentially relevant reports from the electronic search were retrieved for full-text review. Of these potentially relevant articles, 43 publications were excluded for various reasons, and 9 publications met the inclusion criteria and were included in this report. These comprised 5 systematic reviews and 4 evidence-based guidelines. No relevant economic evaluations were identified. Appendix 1 presents the PRISMA20 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Five systematic reviews2-4,8,9 and 4 guidelines5,10,21,22 were included in this report.
Four systematic reviews2,4,8,9 had broader inclusion criteria for the interventions considered than the present review. Specifically, these systematic reviews investigated prefabricated orthopedic footwear and customized footwear,4,8,9 insoles,2,4,8 and/or other mechanical or offloading interventions (e.g., taping, ankle-foot orthoses, night splints).2 Only the subset of studies on prefabricated orthopedic footwear is presented here. There was some overlap in the studies included in the systematic reviews and the degree of overlap is summarized in Appendix 5.
The guideline by Bus et al.10 reported its methodology in a separate publication,23 which was used to supplement the information summarized in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Of the 5 systematic reviews,2-4,8,9 1 included meta-analyses.9 The number of relevant primary studies included in the systematic reviews ranged between 2 and 11. The included primary studies were 9 randomized controlled trials (RCTs), 2 randomized crossover trials, 4 prospective cohort studies, 1 retrospective cohort study, and 2 cross-sectional studies. The systematic reviews were published between 2016 and 2020, with latest literature search dates between January 2017 and March 2018.
All 4 evidence-based guidelines5,10,21,22 were informed by systematic reviews of the literature and included recommendations that were drafted using various consensus-generating methods. The guideline by Bus et al.10 was developed by the International Working Group on the Diabetic Foot (IWGDF), using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology for guideline development. The strength of the recommendations was scored as either strong or weak, based on the quality of evidence, balance between desirable and undesirable effects, values and preferences, resources, and costs, according to the GRADE framework. The quality of the evidence informing the recommendations was graded on study design (classified using the Scottish Intercollegiate Grouping Network criteria), risk of bias, inconsistency of results, publication bias, and presence of a large effect size and/or dose-response relationship.10
Two guidelines5,10 were updates to previously published versions and included updated evidence and recommendations, while 2 others21,22 were newly developed. The guideline by van Netten et al.,5 which was developed by Diabetic Foot Australia, used a systematic approach but did not follow a specific guideline development methodology or assess the quality of the evidence. The authors commented that many recommendations were predominantly based on expert opinion and standard of practice due to limited available evidence and might be seen as “good practice statements.”
The guideline by Tenten-Diepenmaat et al.21 was created by the RA Foot Expert Group. The quality of the evidence was assessed using the Evidence-Based Guideline Development of the Quality Institute for Public Healthcare in the Netherlands. The evidence was ranked on a 5-level scale, ranging from 1 (1 systematic review or at least 2 double-blind RCTs of good quality and of sufficient size) to 4b (opinion of the expert group). The strength of the recommendation was not specified.
The guideline by van Netten et al.5 was developed by the Society for Vascular Surgery (SVS) in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine, using the GRADE methodology. Recommendations were classified as strong (Grade 1) or weak (Grade 2). The level of evidence to support the recommendations was divided into 3 categories, defined as A (high-quality), B (moderate-quality), and C (low-quality).
Country of Origin
The first authors of the 5 systematic reviews were from Australia,8 New Zealand,3 Nigeria,4 and the Netherlands.2,9
The guidelines were intended for use in the Netherlands,21 Australia,5 the US,22 and worldwide.10 The members of the IWGDF guideline group were from 40 countries and 5 continents, and recruited representatives from more than 100 countries around the world to help implement the recommendations.10
Patient Population
Two systematic reviews reported on patients with active or healed diabetic foot ulcer (DFU),4,8 1 review included patients with plantar fasciitis,2 1 review included patients with RA, metatarsophalangeal joint (MTP) osteoarthritis, or gout, and another review reported only on patients with RA.9 The number of participants in the relevant primary studies included in these systematic reviews ranged from 15 to 150.
Four systematic reviews2,3,8,9 included only adults, and the mean ages in the included primary studies ranged from 38 years to 60 years. The other systematic review did not report the age of participants in the included studies.4 The proportion of females compared to males varied across studies, ranging from 5% to 100%. In the systematic review with the meta-analyses, there were 184 adults with relevant before-and-after-the-footwear intervention outcomes.9
The target population of the guidelines was patients with DFU5,10,22 and patients with RA.21 The intended users of the 4 guidelines were the clinicians and/or other health care providers who care for patients with diabetes or RA.
Interventions and Comparators
In all 5 systematic reviews, the relevant intervention was orthopedic footwear.2-4,8,9 In 1 systematic review,2 the intervention was specifically rocker-soled shoes with a stiff insole and proximal apex position (rocker shoes).2 Rocker soles are a commonly used shoe modification in which the soles of the shoe or sandal are curved.2 Rocker shoes are intended to transfer pressure applied to the plantar surface of the foot from some parts of the foot to others.6 The curvature of the rocker shoes leads to a better rolling of the body over the ground and reduces the need for foot movement.7 The systematic reviews2-4,8,9 assessed prefabricated orthopedic shoes on their own or paired with insoles or orthoses. The length of time that participants were assigned to the footwear intervention varied widely and ranged from a single laboratory visit to 2 years.2-4,8,9
Three systematic reviews3,4,8 listed the characteristics or technical requirements of orthopedic footwear. The footwear modifications included extra depth in the forefoot region to accommodate for foot orthoses or forefoot deformity, broad and squared toe box, low heel, padded health counter to improve fit, sufficient width, light weight, visible laces or Velcro, high value kid leather or fabric material, smooth lining to offer protection, and outside rocker profile. The systematic review by Tenten-Depenmaat9 et al. described the interventions in each included primary study (e.g., extra-depth shoes with long inside counter, pillow-back foam-padded collar, soft leather upper with removable cushion inlay, high-top shoes extended above the lateral malleoli, and wide toe box and Velcro closures adapted with a custom-made heel-to-toe rocker sole).9
The comparisons investigated were: prefabricated orthopedic footwear versus conventional shoes or own footwear,2-4 rocker shoes versus flat flip-flops,2 rocker shoes versus no footwear,2 prefabricated orthopedic footwear versus orthoses (i.e., own footwear plus insoles),2,3 and rocker shoes versus shoes with semi-rigid soles.8 The primary studies in the systematic reviews by Frecklington et al.3 and Tenten-Diepenmaat et al.9 also assessed effectiveness by comparing outcomes before and after wearing prefabricated orthopedic footwear.
In 2 guidelines,10,22 the interventions were offloading devices to manage DFUs, including orthopedic footwear. The interventions were medical-grade footwear in the Diabetic Foot Australia guideline5 and conservative treatment for people with RA, including ready-made orthopedic shoes, in the RA Foot Expert Group guideline.21
Outcomes
The outcomes reported in the selected systematic reviews included pain,2,3,9 functioning,2,3,9 health-related quality of life,9 recurrence of DFU,4,8 and adverse events.9
Pain, foot function, and physical functioning were measured by self-reported scores on various scales, such as the Visual Analogue Scale for foot pain during walking;2,3,9 the Numerical Rating Scale for pain and walking ability;2 the Foot Function Index for pain, disability and limitation;3,9 the Health Assessment Questionnaire for disability; the Foot Health Status Questionnaire for foot pain and physical activity;3,9 the Lower Extremity Function Scale;2 and the Toronto Activities of Daily Living Measure for walking and stairs.9 Foot function was also assessed by plantar pressure measurement and performance-based assessments such as the Robinson Bashall Functional Assessment.3,9
Health-related quality of life was assessed with the general well-being subscale of the Visual Analogue Scale and the Foot Health Status Questionnaire.9
For the guidelines, the outcomes considered by the guideline panels were pain,21 physical functioning,21 health-related quality of life,21 DFU healing,5,22,24 DFU recurrence,22 adverse events,21,24 and costs.24
Summary of Critical Appraisal
An overview of the critical appraisal of the included publications is summarized in the following text. Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Systematic Reviews
In the 5 selected systematic reviews,2-4,8,9 the objective and inclusion criteria were clearly stated; a literature search was conducted using multiple databases; the selection of articles was described and a flow chart presented; a list of the included primary studies was presented; and the characteristics of the included studies were described. Providing details of the literature search strategy increases the reproducibility of the review. One systematic review9 registered its study protocol in PROSPERO; and 4 systematic reviews did not report whether a protocol had been published before the conduct of the review; therefore, it is unknown whether any significant protocol deviations occurred that may impact the interpretation of the findings.
Study selection was done independently by 2 reviewers in 2 systematic reviews.2,9 and by 1 reviewer in 1 systematic review.8 However, the study selection approach was unclear in 2 systematic reviews.3,4 Data extraction was done by 1 reviewer in 1 systematic review.9 However, in 4 systematic reviews, it was unclear how data extractions were done.2,3,8,10 Therefore, the potential for errors cannot be ruled out. A list of excluded studies was not presented in any of the reviews.2-4,8,9 In the absence of justifications for excluding studies, it is unclear if the selection process captured all the relevant studies.
The quality of the included studies was assessed in 4 systematic reviews.2,3,8,9 In the systematic review by Ingiri et al.,8 the authors commented on the risk of bias for some of the primary studies but did not systematically assess the quality of the primary studies. The systematic review by Ahmed et al.8 critically appraised studies using an adapted version of the McMaster Critical Review Form for Quantitative Studies. In the systematic review by Schuitema et al.,2 the included studies had 1 or more domains assessed as high risk of bias on the Cochrane Risk of Bias tool. In the systematic review by Frecklington et al.,3 it was reported that Quality Index Tool scores ranged from 39% to 96% (higher scores indicated higher internal consistency, test–retest reliability, and inter-rater reliability). In the systematic review by Tenten-Diepenmaat et al.,9 scores on the 2 RCTs, evaluated using the PEDro checklist, were 50% (fair) and 80% (high). The PEDro checklist has been shown to be a valid, reliable, and a frequently used tool for assessing methodological quality.9 Scores for quality of within-group differences, evaluated using the Downs and Black checklist, ranged from 43% (low) to 86% (high). This checklist has been recommended by Cochrane for quality assessment of non-controlled trials.9
Meta-analyses were conducted in 1 systematic review and were appropriate.9 In the systematic review by Frecklington et al.,3 the authors decided that meta-analysis was not appropriate based on the variation in disease type and tools used to measure outcomes.
In 3 systematic reviews,3,4,8,25-29 the authors reported that there were no conflicts of interest. In 1 systematic review,2 conflicts of interest were not reported. In the remaining systematic review,9 the authors reported their conflicts of interest, and the first author had a cooperation with a company in producing orthopedic shoes. Therefore, the potential for bias cannot be ruled out.
Guidelines
All 4 guidelines5,10,21,22 provided a clear description of the scope and purpose of the guideline. Overall objectives, health questions covered in the guideline, target population, and target users were described. The guideline development groups included individuals from all relevant professional groups. Three guidelines10,21,22 considered patient input during the development phase, and 1 guideline5 did not report any patient involvement.
In all 4 guidelines,5,10,21,22 the systematic methods used to identify evidence and the selection criteria were described. The strengths and limitations of the evidence and the methods for formulating and developing the recommendations were reported in all guidelines. The explicit link between evidence and recommendations was clearly described. The recommendations were unambiguous and easy to identify. A procedure for updating the evidence base and recommendations was described in 3 guidelines.5,10,22 In the guideline by the Diabetic Foot Australia,21 a plan for future update was not included. All guidelines5,10,21,22 were externally reviewed by stakeholders and experts before publication.
Three guidelines5,10,22 described the facilitators and barriers to the implementation of the recommendations and addressed the potential resource implications. In the Diabetic Foot Australia guideline,21 it was not reported whether these issues were considered. There was editorial independence in all included guidelines. Competing interests of all members of the guideline development panel were recorded in all guidelines.5,10,21,22 Finally, while the funding sources did not influence the recommendations in 2 guidelines,10,21 it was unclear in the Diabetic Foot Australia guideline,5 and no funding was obtained for the SVS guideline.22
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Clinical Effectiveness of Orthopedic Footwear for the Treatment of People With Lower-Limb Conditions
The main findings from the included systematic reviews are summarized in the following sections and in Appendix 4. There was some overlap in the primary studies that were included in the systematic reviews. Therefore, to avoid duplication of reporting, outcomes data from an individual study is reported only once as part of 1 systematic review. If study outcomes were included in the meta-analyses by Tenten-Diepenmaat et al.,9 they are reported only in the pooled estimates (and not the individual study level results). A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Pain
The meta-analysis by Tenten-Diepenmaat et al.9 showed a statistically significant reduction in foot pain from baseline within a group of people with RA after wearing orthopedic shoes for between 30 days and 6 months. Statistical heterogeneity was moderate.
The included studies in the systematic review by Schuitema et al.2 reported that statistically significant lower pain scores were found in 1 RCT after the use of rocker shoes compared to conventional shoes at a single visit and in another RCT after the use of rocker shoes compared to flat flip-flops after 12 weeks. Another RCT included in the systematic review2 reported no statistically significant difference in pain after wearing rocker shoes compared to conventional running shoes for 6 months. Compared to bare feet, statistically significant less pain was reported with the rocker shoe plus insole after a single visit according to 1 RCT, but no statistically significant difference was reported after 12 weeks in another RCT included in the same systematic review.2
The systematic review by Frecklington et al.3 reported no statistically significant difference in foot pain between rocker shoes compared to conventional shoes plus orthoses after 12 weeks in people with MTP osteoarthritis in 1 RCT.
Functionality
The meta-analysis by Tenten-Diepenmaat et al.9 showed a statistically significant improvement in physical functioning in people from baseline within a group of people with RA after wearing orthopedic shoes for between 30 days and 2 months. Heterogeneity was moderate. Subgroup analyses showed a statistically significant improvement in self-reported physical functioning after wearing ready-made orthopedic shoes, but no effect on performance-based physical functioning was found. In the same systematic review,9 1 cross-sectional study reported an improvement in foot function (statistically significant reduced plantar pressure) in people with RA who wore orthopedic footwear compared to those who wore conventional footwear.
The systematic review by Schuitema et al.2 reported no significant difference in function after wearing rocker shoes compared to flip-flops and conventional shoes with insoles according to 1 RCT.
The systematic review by Frecklington et al.3 reported statistically significant plantar pressure reduction in people with MTP osteoarthritis after wearing rocker shoes compared to conventional shoes plus orthoses after a single visit in 1 RCT, but no significant difference after 12 weeks in another RCT.
Quality of Life
The results of the meta-analysis by Tenten-Diepenmaat et al.9 showed that health-related quality of life did not improve statistically significantly from baseline within a group of patients with RA after wearing orthopedic shoes for 8 weeks to 12 weeks. Despite using different measures to assess health-related quality of life, statistical heterogeneity was absent.
Recurrence of Diabetic Foot Ulcer
Two systematic reviews4,8 reported on the effect of prefabricated orthopedic footwear on the recurrence of DFUs. One systematic review reported no significant difference in ulcer relapse occurrence over 2 years between orthopedic footwear plus different types of inserts versus conventional footwear (1 RCT).4 However, the other systematic review found a reduction in DFU rates among participants who wore orthopedic footwear compared with conventional footwear (i.e., own usual footwear) at 1 year (1 prospective cohort study).8 The same systematic review found that rocker shoes with a rigid rocker sole reduced the risk of re-ulceration at the forefoot by 64% compared with semi-rigid rocker sole footwear (1 RCT).8
Safety
In the systematic review by Tenten-Diepenmaat et al.,9 adverse events were reported by 8% to 12% of participants in 3 studies. In 2 primary studies (1 RCT, 1 prospective cohort) assessed as fair quality by authors of the systematic review,9 the most common adverse events were that the heels slipped out of the shoes and that the shoes were hot to wear. One retrospective cohort study of low quality (as assessed by the systematic review’s authors) reported that poor fit was the most common adverse event.9
Cost-Effectiveness of Orthopedic Footwear for the Treatment of People With Lower-Limb Conditions
No economic evaluations were identified regarding the cost-effectiveness of prefabricated orthopedic footwear for people with lower-limb conditions; therefore, no summary can be provided.
Guidelines
Four evidence-based guidelines5,10,21,22 were identified that made recommendations regarding orthopedic footwear for the treatment of lower-limb conditions.
Treatment of Diabetic Foot Ulcers
Three evidence-based guidelines5,10 made recommendations regarding the use of orthopedic footwear for people with DFU. The IWGDF guideline10 made a strong recommendation, based on moderate-quality evidence, against the use orthopedic footwear to promote healing of neuropathic plantar DFU unless other offloading devices (e.g., knee- or ankle-high devices) were unavailable. The Diabetic Foot Australia guideline5 also recommended against medical-grade footwear for people with plantar DFUs, based on the Australian National Health and Medical Research Council and IWGDF guidelines, but the strength of the recommendation was not provided, and the quality of the evidence was not assessed. The Diabetic Foot Australia guideline5 did recommend medical-grade footwear plus orthoses or insoles for people with healed plantar DFUs, based on 2 RCTs; however, the strength of the recommendation and quality of evidence were not included. Similarly, the guideline by SVS with the American Podiatric Medical Association and the Society for Vascular Medicine 22 strongly recommended the use of orthopedic footwear plus insoles in patients considered high risk who have healed DFUs, based on low-quality evidence.
The Diabetic Foot Australia guideline5 included a recommendation that health care providers review prescribed footwear every 3 months for continued fit, protection, and support. This recommendation was based on 1 RCT and aligned with the Australian National Health and Medical Research Council guideline.
Treatment of Foot Problems in People With Rheumatoid Arthritis
The RA Foot Expert Group guideline21 recommended ready-made orthopedic footwear for people with RA to reduce forefoot plantar pressure and foot pain, and to improve gait characteristics, physical functioning, and health-related quality of life, based on low-quality controlled studies and uncontrolled studies. The recommendation further specified the patients who could be prescribed orthopedic footwear: patients with abnormal foot function, foot joint damage or deformity, or malalignment of the feet; and patients with feet that do not fit into over-the-counter shoes, but for whom custom-made shoes are not indicated. The guideline also contained a recommendation for the use of ready-made orthopedic shoes as 1 option for normalization of vertical plantar foot pressure and shearing forces in feet with hyperkeratotic lesions, based on expert opinion in the literature and by the expert group.
Limitations
There are a few limitations that prevent a definitive conclusion regarding the clinical effectiveness of prefabricated orthopedic footwear for all patients with lower-limb conditions. Although relevant systematic reviews were identified,2-4,8,9 most of their primary studies were limited by relatively small sample sizes: 61% (11 out of 18 studies) included fewer than 40 participants and a small percentage of studies (1%) had more than 100 participants. The meta-analyses in the systematic review by Tenten-Diepenmaat et al.9 were imprecise due to the small number of participants (ranging from 64 to 185). Also, the evidence from 3 systematic reviews that reported on patients with DFU2,4,8 was based on a relatively small number (2 or 3) of primary studies that fulfilled the inclusion criteria.
There was considerable heterogeneity among the primary studies identified in the systematic reviews, in terms of type of footwear, application of cointervention (i.e., insoles), duration of footwear intervention, and assessment of outcomes. Some primary studies assessed the impact of the footwear at a single visit, making it impossible to determine whether the effect was durable or fleeting. The authors of 1 systematic review9 pointed out that the ability to detect change over time is unknown for most of the assessment tools measuring foot pain, function, and disability in the included studies. Also, none of the instruments were validated for the measurement of foot pain, function, disability, and quality of life.2,3,9
The risk of bias ranged from fair to high for most of the primary studies in the included systematic reviews (as assessed by the systematic review authors). Common methodological limitations included nonblinding of participants and assessors to treatment allocation, nonblinding of assessors to outcomes, lack of external validity, and potential confounding. Any quality issues from the primary studies cause uncertainty in the findings presented in the systematic review.
In the included guidelines,5,10,21,22 the level of evidence of the recommendations also varied. The studies making up the evidence base for the recommendations were also small with varying risks of bias. Due to gaps in the literature, the relevant recommendations from the RA Foot Expert Group guideline21 were mostly based on expert opinion. Only 2 guidelines22,24 assessed the strength of their recommendations.
Evidence on clinical effectiveness was available for people with the following conditions: plantar fasciitis,2 DFUs,4,8 RA,3,9 gout,3 and MTP osteoarthritis.3 The included guidelines targeted people with DFUs5,10,22 and RA.21 No studies or guidelines were found that included people with Charcot foot (current, active condition), hallux valgus, metatarsal amputation, or clubfoot. Also, no studies were identified that reported the effect of orthopedic footwear on disability or amputation in people with lower-limb conditions. The information provided in the included systematic reviews2-4,8,9 was insufficient to determine the generalizability of the findings to Canadians in general and/or populations belonging to specific geographical, ethnic, or cultural groups in Canada.
One systematic review8 reported the countries in which the included studies were conducted (Italy and Germany), but 4 systematic reviews2-4,9 did not report this information. Similarly, the 4 included guidelines5,10,21,22 were not specifically intended for use in Canada, although the IWGDF guideline10 was intended for worldwide use. Taken together, the generalizability of the findings and recommendations to the Canadian context are unknown because of substantial variations in health care systems and available resources for delivering health services across countries.
No economic evaluations were identified regarding the cost-effectiveness of prefabricated orthopedic footwear for people with lower-limb conditions.
Conclusions and Implications for Decision- or Policy-Making
This review comprised 5 systematic reviews2-4,8,9 and 4 evidence-based guidelines.5,10,21,22
In within-group (before-and-after) designs, there was a medium-to-large effect in reducing foot pain, a small-to-medium effect on improved physical functioning, and a nonsignificant effect on health-related quality of life in adults with ready-made orthopedic shoes compared to before treatment.9 One systematic review3 found evidence that using orthopedic footwear resulted in statistically significant improvement in disability, but this was based on 1 primary study comparing before and after treatment findings in 38 patients. Adverse events were related to fit and comfort but were reported by a small proportion of patients in 3 small studies included in 1 systematic review.9 Evidence from within-group designs is limited because there are no comparison groups (i.e., outcomes are not compared between a group assigned to orthopedic footwear versus a group assigned to alternative footwear; rather 1 group’s outcomes are compared before and after the intervention).
In between-group designs, evidence from RCTs, ranked as high quality by authors of the systematic reviews, suggested statistically significant improvement in pain immediately following orthopedic footwear intervention,2,3 but there was conflicting evidence at medium-term (12 weeks) and longer-term (6 months to 8 months) concerning the same outcome. Similarly, there was improvement in foot function immediately after the intervention,2,3 but no effect at medium-term.2,3 The evidence regarding the improvement of foot function was also considered weak by the systematic review authors.2,3,9
Evidence from 2 systematic reviews4,8 indicated that the use of prefabricated orthopedic footwear prevented DFU recurrence at 1 year, but not at 2 years.4,8 There was also weak evidence that footwear with rocker soles are preferrable to semi-rigid soles to prevent DFU recurrence.8 No evidence was identified regarding the effectiveness of orthopedic footwear as an intervention to heal DFUs. Two guidelines5,24 specifically recommended against the use of prefabricated orthopedic footwear for treatment in patients with diabetes who have plantar foot. However, the guidelines recommended that adults with healed DFU,5,22 including people with a history of partial foot amputation or Charcot foot;22 people with diabetic foot deformity or pre-ulcerative lesion;5 and people with RA wear prefabricated orthopedic footwear.21
The limitations of the included literature should be considered when interpreting the findings of this report. Further research set in Canada and based on adequately powered high-quality RCTs with long-term follow-up is needed to better understand the clinical effectiveness of prefabricated orthopedic footwear in people with lower-limb conditions. Furthermore, to better assist with decision-making, economic evaluations regarding the cost-effectiveness of orthopedic footwear for treating people with lower-limb conditions need to be conducted.
References
1.Williams AE. An interpretive phenomenological study of user experiences of therapeutic footwear [thesis]. Manchester (UK): University of Salford; 2008.
2.Schuitema D, Greve C, Postema K, Dekker R, Hijmans JM. Effectiveness of mechanical treatment for plantar fasciitis: a systematic review. J Sport Rehabil. 2019;29(5):657-674. PubMed
3.Frecklington M, Dalbeth N, McNair P, et al. Footwear interventions for foot pain, function, impairment and disability for people with foot and ankle arthritis: a literature review. Semin Arthritis Rheum. 2018;47(6):814-824. PubMed
4.Igiri BE, Tagang JI, Okoduwa SIR, Adeyi AO, Okeh A. An integrative review of therapeutic footwear for neuropathic foot due to diabetes mellitus. Diabetes Metab Syndr. 2019;13(2):913-923. PubMed
5.van Netten JJ, Lazzarini PA, Armstrong DG, et al. Diabetic Foot Australia guideline on footwear for people with diabetes. J Foot Ankle Res. 2018;11(2):1-14. PubMed
6.Karimi MT. The evaluation of foot rockers on the kinematic parameters of individuals with diabetes. Foot Ankle Spec. 2018;11(4):322-329. PubMed
7.Hurst B, Branthwaite H, Greenhalgh A, Chockalingam N. Medical-grade footwear: the impact of fit and comfort. J Foot Ankle Res. 2017;10(2):1-7. PubMed
8.Ahmed S, Barwick A, Butterworth P, Nancarrow S. Footwear and insole design features that reduce neuropathic plantar forefoot ulcer risk in people with diabetes: a systematic literature review. J Foot Ankle Res. 2020;13(1):30. PubMed
9.Tenten-Diepenmaat M, van der Leeden M, Vliet Vlieland TPM, Roorda LD, Dekker J. The effectiveness of therapeutic shoes in patients with rheumatoid arthritis: a systematic review and meta-analysis. Rheumatol Int. 2018;38(5):749-762. PubMed
10.Bus SA, Armstrong DG, Gooday C, et al. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36(Suppl 1):e3274. PubMed
11.Dy SM, Bennett WL, Sharma R, et al. Preventing complications and treating symptoms of diabetic peripheral neuropathy. Rockville (MD): Agency for Healthcare Research and Quality; 2017. Accessed 2021 Nov 24.
12.Bus SA, van Deursen RW, Armstrong DG, et al. Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: a systematic review. Diabetes Metab Res Rev. 2015;32(Suppl 1):99-118. PubMed
13.Menz HB, Auhl M, Tan JM, Levinger P, Roddy E, Munteanu SE. Effectiveness of foot orthoses versus rocker-sole footwear for first metatarsophalangeal joint osteoarthritis: randomized trial. Arthritis Care Res (Hoboken). 2016;68(5):581-589. PubMed
14.Menz HB, Auhl M, Tan JM, Levinger P, Roddy E, Munteanu SE. Biomechanical effects of prefabricated foot orthoses and rocker-sole footwear in individuals with first metatarsophalangeal joint osteoarthritis. Arthritis Care Res (Hoboken). 2016;68(5):603-611. PubMed
15.López-Moral M, Lázaro-Martínez JL, García-Morales E, García-Álvarez Y, Álvaro-Afonso FJ, Molines-Barroso RJ. Clinical efficacy of therapeutic footwear with a rigid rocker sole in the prevention of recurrence in patients with diabetes mellitus and diabetic polineuropathy: a randomized clinical trial. PLoS One. 2019;14(7):e0219537. PubMed
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
18.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (UK): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2021 Nov 23.
19.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Nov 23.
20.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
21.Tenten-Diepenmaat M, van der Leeden M, Vliet Vlieland TPM, Dekker J, R. A. Foot Expert Group. Multidisciplinary recommendations for diagnosis and treatment of foot problems in people with rheumatoid arthritis. J Foot Ankle Res. 2018;11:37. PubMed
22.Hingorani A, LaMuraglia GM, Henke P, et al. The management of diabetic foot: a clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. J Vasc Surg. 2016;63(2 Suppl):3S-21S. PubMed
23.Bus SA, Van Netten JJ, Hinchliffe RJ, et al. Standards for the development and methodology of the 2019 International Working Group on the Diabetic Foot guidelines. Diabetes Metab Res Rev. 2020;36(Suppl 1):e3267. PubMed
24.Bus SA, Lavery LA, Monteiro-Soares M, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab Res Rev. 2020;36(Suppl 1):e3269. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Objective, study design, and number of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Ahmed et al. (2020)8 Australia Funding source: No funding | Objective: To summarize and evaluate the evidence for footwear and insole features that reduce pathological plantar pressures and the occurrence of diabetic neuropathy ulceration at the plantar forefoot in people with diabetic neuropathy Study designs: All study designs except for systematic reviews and case reports Search strategy: In July 2019, 6 electronic databases were searched (Medline, CINAHL, Amed, Proquest, Scopus, Academic Search Premier) using medical subject headings followed by a keyword subject heading. The search period was from 1987 to July 2019. Number of relevant primary studies: 2 studies (1 RCT, 1 prospective cohort study) | Participants were adult, had diabetes; all or some of the participants had neuropathy and foot deformity, history of plantar forefoot ulcers but no Charcot foot, history of heel ulcer or active foot ulcers Sample size: 51 and 92 % Female: NR Age: > 18 years | Intervention: Footwear as a long-term offloading intervention Comparators: Alternative footwear | Outcome: DFU recurrence Follow-up: 18 to 42 months |
Schuitema et al. (2020)2 The Netherlands Funding source: OIM Orthopedie, Assen, the Netherlands | Objective: To provide an overview of the effectiveness of all commonly used mechanical treatment options for plantar fasciitis Study designs: RCTs with a minimum number of 5 participants Search strategy: A systematic search was performed in 4 electronic databases (Medline, Embase, CINAHL, and Cochrane) using a combination of Medical Subject Headings terms and free-text words. Keywords used were plantar fasciitis, heel spur, calcaneal spur combined via a Boolean AND operator with orthotic devices, shoes, splints, rocker, soles, and tape. The search was performed up to March 26, 2017, and updated on March 8, 2018. Reference lists of all included articles were checked on additional relevant studies. Number of relevant primary studies: 2 RCTs, 1 randomized crossover trial | Adults aged (≥ 18 years) with plantar fasciitis, and only participants without a disease that could interfere with the symptoms of plantar fasciitis Sample size: Range 15 to 150 % Female: 68% to 80% Mean age: Range 38 to 52 years | Intervention: Rocker shoes Comparators: Alternative footwear | Outcomes:
Follow-up: Single visit, 12 weeks to 6 months |
Igiri et al. (2019)4 Nigeria Funding source: No funding | Objective: To review the technical requirements and efficacy of orthopedic footwear as an intervention for the amelioration and redistribution of mechanical pressure in the neuropathic foot particularly for people suffering with diabetes Study designs: RCTs, cohort studies Search strategy: Relevant scientific literature in PubMed, Medline and Google Scholar published between 2000 and 2017 were searched. The major keywords for the search included diabetic shoe, therapeutic footwear, foot ulcer, neuropathy, diabetic ulcer, diabetic foot, custom-made footwear intervention and diabetes. Number of relevant primary studies: 2 studies (1 RCT, 1 prospective cohort study) | People having neuropathic DFU due to diabetes mellitus and treated with an offloading technique Sample size: 92 and 400 % Female: NR Age: NR | Intervention: Therapeutic footwear interventions Comparators: Alternative footwear | Outcome: DFU recurrence Follow-up: 1 to 2 years |
Frecklington et al. (2018)3 New Zealand Funding source: NR | Objective: To conduct a literature review on the effectiveness of footwear on foot pain, function, impairment, and disability for people with foot and ankle arthritis Study designs: RCTs, prospective cohort studies, cross-sectional studies Search strategy: The following electronic databases (CINAHL, Medline, Scopus, SPORTDiscus and the Cochrane Library) were searched in September 2017, with no limitations were placed on the publication date. The search strategy comprised of the following keywords: arthritis, rheumatoid arthritis, gout, osteoarthritis, rheumatic disease, psoriatic arthritis, lupus erythematous, ankylosing spondylitis, systemic sclerosis, polymyalgia rheumatica with footwear, footwear intervention, foot orthoses, foot orthosis, foot orthotic, insole and shoe. Number of relevant primary studies: 11 studies (5 RCTs, 1 randomized crossover trial, 2 prospective cohort studies, 3 cross-sectional studies) | Adults with arthritis affecting the foot or ankle (rheumatoid arthritis, MTP osteoarthritis, or gout) Sample size: Range 18 to 98 % Female: 5% to 100% Mean age: Range 47 to 60 years | Intervention: Therapeutic footwear interventions Comparators: Alternative footwear | Outcomes:
Follow-up: Single visit, 30 days to 6 months |
Tenten-Diepenmaat et al. (2018)9 The Netherlands Funding sources: the Dutch Association of Podiatrists ‘NVvP’; the Dutch industry organization for orthopedic shoe technicians ‘NVOS Orthobanda’; the Dutch industry organization for pedicures ‘ProVoet’ | Objective: To systematically summarize the literature of the evidence on the effectiveness of orthopedic shoes in patients with rheumatoid arthritis Study designs: RCTs, randomized controlled crossover trials, quasi-experimental clinical trials, prospective- and retrospective cohort studies Search strategy: The following electronic databases were searched from inception to January 19, 2017: the Cochrane Central Registry for Controlled Trials, PubMed, EMBASE, and PEDro. A 2-way search strategy was employed using “rheumatoid arthritis” with “shoes” and related synonyms. The following database search strategy for PubMed was used: [“Arthritis, Rheumatoid” (Mesh) OR rheumatoid arthritis (tiab)] AND (“Shoes” (Mesh) OR shoe* (tiab) OR footwear* (tiab)]. Each database was searched independently by 2 researchers. In addition, reference lists of all selected publications were checked to retrieve relevant publications which have not been found with the computerized search. Number of relevant primary studies: 8 studies (4 RCTs, 2 randomized controlled crossover trials, 2 prospective cohort studies, 1 retrospective cohort study, 1 cross-sectional study) | Adult patients diagnosed with rheumatoid arthritis, or a defined subgroup of rheumatoid arthritis patients existing in the study population for whom data were presented separately Sample size: Range 18 to 80 % Female: NR Mean age: Range 47 to 60 years | Intervention: Orthopedic ready-made shoes for the treatment of rheumatoid arthritis -related foot problems Comparators: Alternative footwear | Outcomes:
Follow-up: Single visit, 30 days to 6 months |
DFU = diabetic foot ulcer; FFI = Foot Function Index; FHSQ = Foot Health Status Questionnaire; HAQ = Health Assessment Questionnaire; IWGDF = International Working Group on the Diabetic Foot; LEFS = Lower Extremity Function Scale; MTP = metatarsophalangeal joint; NR = not reported; NRS = numerical rating scale; RB = Robinson Bashall Functional Assessment; RCT = randomized controlled trial, TADL = Toronto Activities of Daily Living Measure; VAS = Visual Analogue Scale.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: Clinicians and other health care professionals Target population: Diabetic patients who have a foot ulcer and are at risk for infection, hospitalization, and amputation | Offloading interventions for the management of foot ulcers in people with diabetes | Benefits (DFU healing) and harms (adverse events), financial costs (resource utilization) | Using GRADE system, evidence came from systematic reviews, and expert opinion where evidence was not available | SIGN grading system was used as an initial guide for assigning level of evidence (excluding levels 3 and 4). Level 1 referred to RCTs and was considered “high”, and level 2 referred to case control, cohort, controlled before-and after designs, or interrupted time series and was considered “low”. The quality of evidence could then be lowered based on the presence of risk of bias, inconsistence of results and publication bias. The quality of evidence could also be raised based on the presence of a large effect size or evidence of a dose-response relationship (for observational studies only). | Guideline developed using GRADE methodology The initial guidelines, and each subsequent update, were developed by a consensus process and written by a panel of experts in the field. Using a multistep review process, the guidelines were revised by the IWGDF Editorial Board, followed by critical evaluation by global IWGDF representatives, culminating in an agreed upon text. All members of the working group participated in the discussion of the conclusions for each clinical question, reaching consensus on the content of the evidence statements and the strength of the recommendations. | The members of the IWGDF Editorial Board met in person on a number of occasions to thoroughly review each of the guideline chapters, which were then revised by the working groups based on this editorial review. The working groups then sent the guideline to the panel of independent international external experts for their critical review. The working group subsequently revised the document further based on these comments, after which, the IWGDF Editorial Board did a final review of the recommendations and the rationale provided. |
Diabetic Foot Australia (2018)5 | ||||||
Intended Users: Health care providers Target Population: People with diabetes | Medical-grade footwear for people with DFU | DFU healing | Information from the 2013 footwear guideline was updated by the primary author by reviewing and incorporating any new footwear-related recommendations from the most recent Australian NHMRC diabetic foot guideline and IWGDF guidance documents. The primary author then reviewed and incorporated common findings from all recent systematic reviews on footwear interventions for people with diabetes, recent RCTs included in these reviews, and any further studies obtained from hand searching reference lists of these articles and an additional non-systematic search of the literature. | NR | The first draft of this guideline was written by the first author and sent to 2 coauthors for critical review and expert opinion. A second draft incorporating consensus feedback from the 3 authors was written by the first author. | Drafts of the guideline incorporating feedback from all coauthors was sent to all coauthors for review, until consensus was reached from all authors, leading to the final version of the guideline, approved by all authors |
RA Foot Expert Group (2018)21 | ||||||
Intended Users: Rheumatologists, orthopedic surgeons, rehabilitation physicians, specialized nurses, podiatrists, orthopedic shoe technicians, and pedicurists Target Population: People with rheumatoid arthritis | Conservative treatment of foot problems in people with rheumatoid arthritis | Pain, physical functioning, health-related quality of life, adverse events | Literature was searched in PubMed. The available systematic reviews on the subject of interest were used to develop the draft recommendations. When no systematic review was available, core publications (according to the expert group) or available guidelines were used | The methodological quality was determined according to the “Evidence-Based Guideline Development” of the Quality Institute for Public Healthcare in the Netherlands. Five levels of evidence were distinguished, where: Level 1 = SR of at least 2 RCTs or 2 double-blind RCTs of good quality and of sufficient size; Level 2 = 1 study of double-blind RCTs of good quality and of sufficient size or 2 controlled trials of lesser quality; Level 3 = 1 study of controlled trial or lesser quality or 1 non-controlled study; Level 4a = expert opinion described in the literature; Level 4b = opinion of the expert group. | Draft recommendations were formulated (by the core members) based on relevant literature, to answer the research questions. The draft recommendations and semi-definitive frameworks were discussed with the experts during a second expert meeting and by email rounds and were refined into definitive recommendations and frameworks. | An anonymous voting procedure during an expert meeting was used to determine the level of agreement for each recommendation and framework. A recommendation was approved when ≥ 70% of the expert group voted a an agreement of ≥ 7, on a numeric rating scale from 0 (total disagreement) to 10 (total agreement). |
SVS With APMA and SVM (2016)22 | ||||||
Intended users: Clinicians Target population: Diabetic patients with diabetic foot disease | Offloading interventions for the management of DFU in people with diabetes | DFU healing, DFU recurrence | Full systematic review and meta-analysis for each key question. The evidence in several other areas was summarized. | Quality of evidence and strength of recommendations rated using GRADE approach. Recommendations are Grade 1 (strong) or Grade 2 (weak). Grade 1 recommendations are meant to identify practices for which benefit clearly outweighs risk. These recommendations can be made by clinicians and accepted by patients with a high degree of confidence. Grade 2 recommendations are made when the benefits and risks are more closely matched and are more dependent on specific clinical scenarios. Physician and patient preferences play a more important role in the decision-making process in these circumstances. | Guidelines developed using GRADE methodology | A consensus of the recommendations and level of evidence to support it was attained, and every recommendation in this guideline represented the unanimous opinion of the task force |
Intended users: Clinicians Target population: Diabetic patients with diabetic foot disease (continued) | The level of evidence to support the recommendation is divided into 3 categories: A (high quality), B (moderate quality), and C (low quality). | |||||
APMA = American Podiatric Medical Association; DFU = diabetic foot ulcer; GRADE = Grading of Recommendations Assessment, Development and Evaluation; IWGDF = International Working Group on the Diabetic Foot; NHMRC = National Health and Medical Research Council; NR = not reported; RA = rheumatoid arthritis; RCT = randomized controlled trial; SIGN = Scottish Intercollegiate Grouping Network; SVM = Society for Vascular Medicine; SVS = Society for Vascular Surgery.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 216
Item | Ahmed et al. (2020)8 | Schuitema et al. (2020)2 | Igiri et al. (2019)4 | Frecklington et al. (2018)3 | Tenten-Diepenmaat et al. (2018)9 |
|---|---|---|---|---|---|
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes | Yes | Yes | Yes | Yes |
2. Did the report of the review contain an explicit statement that the review methods were established before the conduct of the review and did the report justify any significant deviations from the protocol? | No | No | No | No | Yes |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes | Yes | Yes | Yes | Yes |
4. Did the review authors use a comprehensive literature search strategy? | Yes | Yes | Yes | Yes | Yes |
5. Did the review authors perform study selection in duplicate? | No | Yes | NR | NR | Yes |
6. Did the review authors perform data extraction in duplicate? | NR | NR | NR | NR | No |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | No | No | No | No | No |
8. Did the review authors describe the included studies in adequate detail? | Yes | Yes | Partially | Yes | Yes |
9. Did the review authors use a satisfactory technique for assessing the RoB in individual studies that were included in the review? | Yes – quality assessment form adapted from the McMaster Critical Review Form–Quantitative Studies | Yes – Cochrane Risk of Bias tool | NR | Yes – Quality Index Tool | Yes – PEDro Scale; Downs and Black checklist |
10. Did the review authors report on the sources of funding for the studies included in the review? | No | No | No | No | No |
11. If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | NA | NA | NA | NA | Yes |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | NA | NA | NA | NA | No |
13. Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? | No | Yes | Yes | No | Yes |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Yes | No | No | Yes | Yes |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | NA | NA | NA | NA | Partially (No investigation, but possible publication bias discussed) |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | No | NR | No | No | Yes |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NR = not reported; NA = not applicable; PEDro = Physiotherapy Evidence Database; PICO = population, intervention, comparator, outcomes; RoB = risk of bias.
Note: This table has not been copy-edited.
Table 5: Strengths and Limitations of Guidelines Using AGREE II19
Item | Diabetic Foot Australia (2018)5 | RA Foot Expert Group (2018)21 | SVS With APMA and SVM (2016)22 | |
|---|---|---|---|---|
Domain 1: Scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (e.g., patients, public) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (e.g., patients, public) have been sought. | Yes | No | Yes | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes |
Domain 3: Rigour of development | ||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes | No | Yes |
Domain 4: Clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | No | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | Yes | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | No | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | Yes | Yes | Yes |
Domain 6: Editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Unclear | Yes | NA |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; APMA = American Podiatric Medical Association; IWGDF = International Working Group on the Diabetic Foot; NA = not applicable; RA = rheumatoid arthritis; SVM = Society for Vascular Medicine; SVS = Society for Vascular Surgery.
Note: This table has not been copy-edited.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 6: Summary of Findings by Outcome – Pain
Comparison | Study citation and study design | Pain |
|---|---|---|
Rocker shoes vs. conventional shoes | Schuitema et al. (2020)2 SR (2 RCTs) | Fong et al. 2012a Pain (VAS score) at single visit in 15 people with plantar fasciitis
|
Ryan et al. 2006a Pain (VAS score) at 6 months in 12 people with plantar fasciitis
| ||
Rocker shoes vs. flat flip-flops | Schuitema et al. (2020)2 SR (1 RCT) | Vicenzino et al. 2015a Pain (NRS score) at 12 weeks in people with plantar fasciitis
|
Rocker shoes vs. barefoot | Schuitema et al. (2020)2 SR (2 RCT) | Vicenzino et al. 2015a Pain (NRS score) at 12 weeks in 150 people with plantar fasciitis
|
Fong et al. 2012a Pain (VAS score) at single visit in 15 in people with plantar fasciitis
| ||
Prefabricated orthopedic footwear vs. orthoses | Frecklington et al. (2018)3 SR (1 RCT) | Menz et al. 2016aa Pain (FHSQ score) at 12 weeks in people with 1 MTP osteoarthritis
|
Prefabricated orthopedic footwear – pre- and post | Frecklington et al. (2018)3 1 prospective cohort study | Rome et al. 2013 Pain (VAS score) at 8 months in 38 patients with gout
|
Tenten-Diepenmaat et al. (2018)9 SR and MA (4 RCTs, 1 prospective cohort study) | From the results of the MA, pooled scores showed a medium-to-large, statistically significant, effect for the reduction of foot pain (scores on various scales) in people with rheumatoid arthritis after wearing ready-made orthopedic shoes (SMD 0.60, 95% CI 0.28 to 0.92; P ≤ 0.001; I2 = 59%; n = 184). |
CI = confidence interval; FHSQ = Foot Health Status Questionnaire; MA = meta-analyses; MTP = metatarsophalangeal joint; NRS = Numerical Rating Scale; RCT = randomized controlled trial; SMD = standardized mean difference; SR = systematic review; VAS = Visual Analogue Scale.
aRaw data, effect sizes, and/or P values not reported in systematic review.
Note: This table has not been copy-edited.
Table 7: Summary of Findings by Outcome – Functioning
Comparison | Study citation and study design | Functioning |
|---|---|---|
Rocker shoes vs. flat flip-flops | Schuitema et al. (2020)2 SR (1 RCT) | Vicenzino et al. 2015a Function (LEFS score) at 12 weeks in people with plantar fasciitis
|
Rocker shoes vs. orthoses | Schuitema et al. (2020)2 SR (1 RCT) | Vicenzino et al. 2015a Function (LEFS score) at 12 weeks in people with plantar fasciitis
|
Rocker shoes vs. orthoses (continued) | Frecklington et al. (2018)3 SR (2 RCTs) | Menz et al. 2016aa Function (FFI-R SF score) at 12 weeks in people with MTP osteoarthritis
|
Menz et al. 2016bPlantar pressure (at same lab visit) in people with MTP osteoarthritis
| ||
Rocker shoes vs. orthoses (continued) | Tenten-Diepenmaat et al. (2018)9 SR (1 cross-sectional study) | Hennessy et al. 2007 In-shoe plantar peak pressure for total foot, mean (SD) in 20 people with rheumatoid arthritis
|
Prefabricated orthopedic footwear – pre- and post | Frecklington et al. (2018)3 SR (1 RCT) | Menz et al. 2016b Plantar pressure (at same lab visit) in people with MTP osteoarthritis
|
Prefabricated orthopedic footwear – pre- and post (continued) | Tenten-Diepenmaat et al. (2018)9 SR and MA (3 RCTs, 1 prospective cohort study) | From the results of the MA, pooled scores showed a small-to-medium, statistically significant, effect for the improvement of physical functioning in people with rheumatoid arthritis after wearing ready-made orthopedic shoes (SMD = 0.30; 95% CI, 0.04 to 0.56; P = 0.02; I2 = 28%; n = 150)
|
FFI = Foot Function Index; FFI-R SF = Foot Function Index—Revised (Short Form); LEFS = Lower Extremity Function Scale; MA = meta-analyses; MTP = metatarsophalangeal joint; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; SMD = standardized mean difference; SR = systematic review.
a.Raw data, effect sizes, and P values not reported in systematic review.
Note: This table has not been copy-edited.
Table 8: Summary of Findings by Outcome – Quality of Life
Comparison | Study citation and study design | QoL |
|---|---|---|
Prefabricated orthopedic footwear – pre- and post | Tenten-Diepenmaat et al. (2018)9 SR and MA (2 RCTs) | From the results of the MA, pooled scores showed a nonsignificant effect for the improvement of health-related quality of life (FHSQ or VAS scores) in people with rheumatoid arthritis after wearing ready-made orthopedic shoes (SMD 0.15, 95% CI −0.18 to 0.47; P = 0.38; I2 = 0% n = 64). |
CI = confidence interval; FHSQ = Foot Health Status Questionnaire; MA = meta-analyses; QoL = quality of life; SMD = standardized mean difference; SR = systematic review; VAS = visual analogue scale.
Note: This table has not been copy-edited.
Table 9: Summary of Findings by Outcome – DFU Recurrence
Comparison | Study Citation and Study Design | DFU Recurrence |
|---|---|---|
Prefabricated orthopedic footwear with rigid rocker sole vs. with semi-rigid sole | Ahmed et al. (2020)8 SR (1 RCT) | Lopez-Moral et al. (2019) Recurrent plantar DFU at 18 months in 51 patients with diabetes
|
Prefabricated orthopedic footwear vs. conventional shoes | Igiri et al. (2019)4 SR (1 RCT, 1 prospective cohort study) | Reiber et al. (2002) (RCT) Recurrent DFU at 2 years in 400 patients with diabetes (58% with neuropathy)
|
Prefabricated orthopedic footwear with rigid rocker sole vs. with semi-rigid sole | Ahmed et al. (2020)8 SR (1 RCT) | Busch and Chantelau (2003) Recurrent plantar DFU at 1 year in patients with diabetes, neuropathy and peripheral vascular disease
|
DFU = diabetic foot ulcer; RRR = relative risk reduction; RCT = randomized controlled trial; SR = systematic review.
Note: This table has not been copy-edited.
Table 10: Summary of Findings by Outcome – Adverse Events
Intervention | Study citation and study design | Adverse events |
|---|---|---|
Prefabricated orthopedic footwear | Tenten-Diepenmaat et al. (2018)9 SR (1 RCT, 1 prospective cohort study, 1 retrospective cohort study) | Williams et al. (2006) (RCT) Adverse events in in 40 people with rheumatoid arthritis
Moncur and Ward (1990) (prospective) Adverse events in in 25 people with rheumatoid arthritis
Pullar et al. (1983) (retrospective) Adverse events in in 39 people with rheumatoid arthritis
|
RCT = randomized controlled trial; SR = systematic review.
Note: This table has not been copy-edited.
Table 11: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
IWGDF (2019 Update)24 | |
Evidence-based guidelines regarding offloading interventions to promote healing of foot ulcers in persons with diabetes Recommendation 4(a): “In a person with diabetes and a neuropathic plantar forefoot or midfoot ulcer, do not use, and instruct the patient not to use, conventional or standard therapeutic footwear as offloading treatment to promote healing of the ulcer, unless none of the abovementioned offloading devices [nonremovable or removable, knee- or ankle-high devices] is available.” (p. 8) Supporting evidence: Data from 3 high-quality meta-analyses consistently favoured the use of offloading devices over conventional or standard orthopedic footwear to heal neuropathic plantar forefoot ulcers. Data from 4 low-quality RCTs and 1 high-quality meta-analysis reported worse outcomes for adverse events using orthopedic footwear. One low-quality RCT found similar preferences for therapeutic footwear compared to other offloading interventions. One low-quality RCT reported the material costs for modified footwear were lower than for total contact casts and nonremovable walkers in treating patients with a foot ulcer. However, a large health technology assessment showed that orthopedic footwear was far less cost-effective than other offloading devices. | Quality of evidence: Moderate Strength of recommendation: Strong |
Diabetic Foot Australia (2018)5 | |
Evidence-based guideline regarding footwear for people with diabetes Recommendation 7: “For people with a foot deformity or pre-ulcerative lesion, consider prescribing medical grade footwear.” (p. 7) Supporting evidence: Based on footwear requirements algorithms for prescription and footwear modifications in the literature Recommendation 8: “For people with a healed plantar foot ulcer, prescribe medical grade footwear with custom-made in-shoe orthoses or insoles with a demonstrated plantar pressure relieving effect at the high-risk areas.” (p. 7) Supporting evidence: 2 RCTs demonstrated > 30% reduction at the area of the highest plantar pressure with new medical-grade footwear with orthosis or insole compared to the patient’s current footwear. One of these RCTs reported that the risk of re-ulceration is smaller with medical-grade footwear. This aligns with the IWGDF recommendation. Recommendation 9: “Review prescribed footwear every three months to ensure it still fits, protects, and supports the foot.” (p. 9) Supporting evidence: One RCT that used a 3-month interval to ensure prescribed footwear remained appropriate, on expert opinion from seeing wear and tear in footwear in daily clinical practice, and aligns with the regular foot-screening interval for people at intermediate- or high-risk of foot ulceration as recommended in the Australian NHMRC diabetic foot guideline Recommendation 10: “For people with a plantar diabetic foot ulcer, footwear is not specifically recommended for treatment; prescribe appropriate offloading devices to heal these ulcers.” (p. 9) Supporting evidence: Australian NHMRC guideline and the IWGDF guidance documents | Quality of evidence: NR Strength of recommendation: NR |
RA Foot Expert Group (2018)21 | |
Evidence-based guideline regarding the treatment of foot problems in people with rheumatoid arthritis Recommendation: “Ready-made therapeutic shoes with extra depth, support, incorporated inlays, and optional technical adaptation can reduce forefoot plantar pressure and foot pain and improve gait characteristics, physical functioning, and health-related quality of life.* These ready-made shoes can be prescribed in patients with (i) abnormal foot function, foot joint damage/deformity, or malalignment of the feet, and (ii) feet that do not fit in over-the-counter shoes, but for whom custom-made shoes are not indicated.**” (p. 7) Supporting evidence: *Evidence from 3 low-quality controlled trials and 2 non-controlled studies; **opinion of the guideline group Recommendation: “Pressure and shearing forces should be normalized in feet with hyperkeratotic lesions. For normalization of pressure and shearing forces, i) an individual shoe- and sock advice can be given; or ii) foot orthoses, silicone toe orthosis, technical adaptations to over-the-counter shoes, ready- or custom-made therapeutic shoes, or a provisional therapy (e.g., felt padding or taping) can be prescribed.” (p. 7) Supporting evidence: Expert opinion described in 2 previously published guidelines; and opinion of the guideline group. | Quality of evidence: *Level 3 (based on controlled studies that may not be high quality or uncontrolled studies) ** Level 4b (opinion of the expert group) Strength of recommendation: NR Quality of evidence Level 4a/b (opinion described in the literature and opinion of the expert group) Strength of recommendation: NR |
SVS With APMA and SVM (2016)22 | |
Evidence-based guideline regarding the management of diabetic foot disease Recommendation: “In high-risk patients with healed DFU (including those with a prior history of DFU, partial foot amputation, or Charcot foot), we recommend wearing specific therapeutic footwear with pressure-relieving insoles to aid in prevention of new or recurrent foot ulcers” (p. 10S) Supporting evidence: Three prospective studies have demonstrated that patients wearing prescriptive pressure-relieving footwear have significantly fewer recurrences of ulceration compared with those persons not wearing orthopedic shoes. The same is true for all high-risk patients, including those with a prior history of DFU, partial foot amputations, or Charcot foot. Two systematic reviews demonstrated improved wound healing with total contact casting over RCW, orthopedic shoes, and conventional therapy. There was no advantage of irremovable cast walkers over total contact casting. There was improved healing with half-shoe compared with conventional wound care. orthopedic shoes and insoles reduced relapse rate in comparison with regular footwear. | Quality of evidence: Grade C (low) Strength of recommendation: Strong |
DFU = diabetic foot ulcer; IWGDF = International Working Group on the Diabetic Foot; NHMRC = National Health and Medical Research Council; NR = not reported; RA = rheumatoid arthritis; RCT = randomized controlled trial; RCW = removable cast walker.
Note: This table has not been copy-edited.
Appendix 5: Overlap Between Included Systematic Reviews
Table 12: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Ahmed et al. (2020)8 | Schuitema et al. (2020)2 | Igiri et al. (2019)4 | Frecklington et al. (2018)3 | Tenten-Diepenmaat et al. (2018)9 |
|---|---|---|---|---|---|
Lopez-Moral et al. PLoS One. 2019;14:e0219537. | Yes | NA | NA | NA | NA |
Menz et al. (RCT) Arthritis Care Res. 2016a; 68:581–9. | NA | NA | NA | Yes | NA |
Menz et al. Arthritis Care Res. 2016b; 68:603–11. | NA | NA | NA | Yes | NA |
Vicenzino et al. PLoS One. 2015;10(12):e0142789. | NA | Yes | NA | NA | NA |
Bagherzadeh Cham et al. Prosthet Orthot Int. 2014;38:310–5. | NA | NA | NA | Yes | Yes |
Stewart et al. Clin Biomech. 2014;29:1158–63. | NA | NA | NA | Yes | NA |
Fong et al. Clin Biomech. 2012;27(10):1072–1077. | NA | Yes | NA | NA | NA |
Cho et al. Clin Rehabil. 2009;23:512–21. | NA | NA | NA | Yes | Yes |
Ryan et al. Phys Sports Med. 2009;37(4):68–74. | NA | Yes | NA | NA | NA |
Hennessy et al. Clin Biomech. 2007;22:917–23. | NA | NA | NA | Yes | Yes |
Williams et al. Rheumatol. 2007;46:302–7. | NA | NA | NA | Yes | Yes |
Busch and Chantelau. Diabet Med. 2003;20(8):665. | Yes | NA | Yes | NA | NA |
Reiber et al. JAMA. 2002;287:2552e8. | NA | NA | Yes | NA | NA |
Chalmers et al. J Rheumatol. 2000;27:1643–7. | NA | NA | NA | Yes | Yes |
Fransen and Edmunds. Arthritis Care Res.1997;10:250–6. | NA | NA | NA | Yes | Yes |
Moncur and Ward. Arthritis Care Res. 1990;3:222–6. | NA | NA | NA | Yes | Yes |
Pullar et al. Health Bull. 1983;41(5):258–262. | NA | NA | NA | NA | Yes |
NA = not applicable; RCT = randomized controlled trial.
Note: This table has not been copy-edited.
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
25.Hill S, Ryce A. Orthotics material for patients requiring foot orthotics: clinical effectiveness and cost effectiveness. CADTH rapid response report: summary of abstracts. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RB1366%20Orthotics%20Material%20Final.pdf. Accessed 2021 Nov 30.
26.Tran K, Spry C. Custom-made foot orthoses versus pre-fabricated foot orthoses: a review of clinical effectiveness and cost-effectiveness. CADTH rapid response report: summary with critical appraisal. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1169%20Custom%20made%20orthotics%20versus%20prefabricated%20orthotics_Final.pdf. Accessed 2021 Nov 30.
Alternative Population
27.Bus SA, Lavery LA, Monteiro-Soares M, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes/Metabolism Res Rev. 2020;36(Suppl 1):e3269. PubMed
28.Crawford F, Nicolson DJ, Amanna AE, et al. Preventing foot ulceration in diabetes: systematic review and meta-analyses of RCT data. Diabetologia. 2020;63(1):49-64. PubMed
29.Preece SJ, Chapman JD, Braunstein B, Bruggemann GP, Nester CJ. Optimisation of rocker sole footwear for prevention of first plantar ulcer: comparison of group-optimised and individually-selected footwear designs. J Foot Ankle Res. 2017;10:27. PubMed
30.van Netten JJ, Raspovic A, Lavery LA, et al. Prevention of foot ulcers in the at-risk patient with diabetes: a systematic review. Diabetes/Metabolism Research and Reviews. 2020;36(Suppl 1):e3270. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.