CADTH Health Technology Review
Clinical Effectiveness of Opioid Substitution Treatment
Rapid Review
Authors: Sara D. Khangura, Melissa Walter
Abbreviations
AE
adverse event
DAM
diacetylmorphine
HAT
heroin-assisted therapy
HDM
hydromorphone
MA
meta-analysis
MAT
medication-assisted treatment
NRS
non-randomized studies
OAT
opioid agonist therapy
OST
opioid substitution treatment
OUD
opioid use disorder
RCT
randomized controlled trial
SAE
severe adverse event
SR
systematic review
SROM
slow or sustained-release oral morphine
Key Messages
A preponderance of evidence identified in this review indicates a relative benefit in the clinical effectiveness of heroin-assisted treatment, injectable hydromorphone, or diacetylmorphine compared to methadone in patients with opioid use disorder.
Most of the evidence in this review describing sustained-release oral morphine versus methadone shows no significant difference in measures of clinical effectiveness for patients with opioid use disorder.
There is a lack of evidence reported in systematic reviews and randomized controlled trials describing the clinical effectiveness of oral hydromorphone, fentanyl patches, and fentanyl buccal tablets.
Most of the evidence in this review, describing various forms of opioid substitution treatments, has been characterized as low quality and draws from the same several trials.
Context and Policy Issues
The opioid crisis is described as having reached epidemic proportions since the 1990s, with tens of thousands of related deaths in North America in the last several years alone.1-3 In addition to the impact that the opioid crisis is having on mortality, the effects on individuals, communities and all of society is significant (e.g., loss of employment and/or homelessness, multiple deleterious health effects for the individual, as well as crime-related activity and associated societal consequences).3
Opioid use disorder (OUD) can be treated with medication and/or psychotherapy, but these therapies are generally intended for long-term use, they are sometimes limited in their effectiveness, and the risk of relapse is considerable.4,5 Long-standing and conventional pharmacological therapy for OUD consists mostly of opioid agonist therapy (OAT) with methadone or buprenorphine, which have demonstrated effectiveness for treating OUD when compared to non-pharmacological therapy or no therapy.6 However, methadone and buprenorphine can cause considerable side effects, and many OUD patients remain refractory to them.5 In Canada, OAT with methadone has a long history of use, with federal oversight being transferred to the provinces in the 1990s, and various needs, approaches and available resources having developed across the country since then; 1 common feature, however, is an increasing need for access to effective treatments for OUD as the opioid crisis continues to worsen.7
Safe supply is the use of prescription opioid medications as safer alternatives to opioid drugs obtained illegally, and has been posited as an approach for addressing the opioid crisis.2,8 Safe supply programs using opioid substitution treatment (OST) have been established in several jurisdictions, including Canada, and have been shown to proffer health and social benefits to people living with OUD and their communities, including reduced criminal activity.3,6 In 2019, Health Canada announced its approval of injectable hydromorphone (HDM) and diacetylmorphine (DAM) for the treatment of OUD,9 with multiple safe supply programs becoming established across Canada since then. In addition to these medications, slow or sustained-release oral morphine (SROM), oral HDM and fentanyl patches or tablets are different types of OST that are undergoing investigation by various research groups for their clinical effectiveness in treating OUD.10-14
There is some debate and controversy concerning the safe supply concept; for example, the treatment of OUD with the same substance that has caused the condition has raised questions and concerns.15,16 In particular, the potential safety concerns (e.g., overdose, redistribution) with regard to the use of various forms of OST are not yet well understood, and this uncertainty alongside the societal stigma around the use of illicit opioids have presented some barriers to broader implementation of safe supply.6 Nonetheless, support in favour of the use of OST, based on early findings of its effectiveness for managing OUD, is gaining momentum.15,16 In recent years, OST has been 1 of several interventions being investigated in Canada as a means for addressing the current opioid crisis, as the importance of mitigating risk to people living with OUD who are being harmed and/or dying is critical.17
Whereas a great deal of data describing the effects of methadone used in OAT are available in the literature, it has been noted that data describing various forms of OST — including those that use SROM, HDM, DAM or fentanyl patches or tablets, among others — are less plentiful.18 The aim of this review is to identify and summarize evidence describing the clinical effectiveness of various types of OST for the treatment of OUD.
Research Questions
What is the clinical effectiveness of sustained-release oral morphine in opioid use disorder?
What is the clinical effectiveness of oral hydromorphone in opioid use disorder?
What is the clinical effectiveness of injectable hydromorphone or prescription diacetylmorphine in opioid use disorder?
What is the clinical effectiveness of fentanyl patches or fentanyl buccal tablets in opioid use disorder?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were sustained-release oral morphine, hydromorphone, heroin/diacetylmorphine, fentanyl patches, or fentanyl buccal tablets; and opioid substitution treatment/opioid use disorder. No filters were applied to limit the retrieval by study type. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2016 and November 11, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for eligibility. The final selection of full-text articles was based on the eligibility criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (18 years and older) requiring treatment for opioid use disorder. |
Intervention | Q1: Sustained-release oral morphine (also referred to as slow or extended-release oral morphine) Q2: Oral hydromorphone (also referred to as immediate release oral hydromorphone) Q3: Injectable hydromorphone or prescription diacetylmorphine (also referred to as heroin-assisted therapy or medical-grade heroin) Q4: Fentanyl patches (also referred to as transdermal fentanyl) or fentanyl buccal tablets (also referred to as sublingual fentanyl) Note: Used as part of safer supply programs (also known as safe supply), these interventions can be provided with or without concomitant non-pharmacological therapies. |
Comparator | Q1 to Q4: Placebo; standard of care (i.e., buprenorphine/naloxone, methadone); alternative interventions of interest (i.e., slow/sustained-release oral morphine, oral hydromorphone, injectable hydromorphone or prescription diacetylmorphine, fentanyl patches, or fentanyl buccal tablets). |
Outcomes | Q1 to Q4: Clinical effectiveness (e.g., retention in treatment, heroin use, use of other drugs of abuse [including opioids], transition to long-term recovery programs, health-related quality of life, change in rates of opioid-related substance use disorders, withdrawal symptoms, mental health scores, change in incidence of accessing primary care service, contracting HIV, or testing for hepatitis C) and safety (e.g., mortality, toxicity, adverse events). |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials. |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications, or if they were published before 2016. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more of the included SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)19 for overviews of SRs and SRs; and the Downs and Black checklist20 for randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
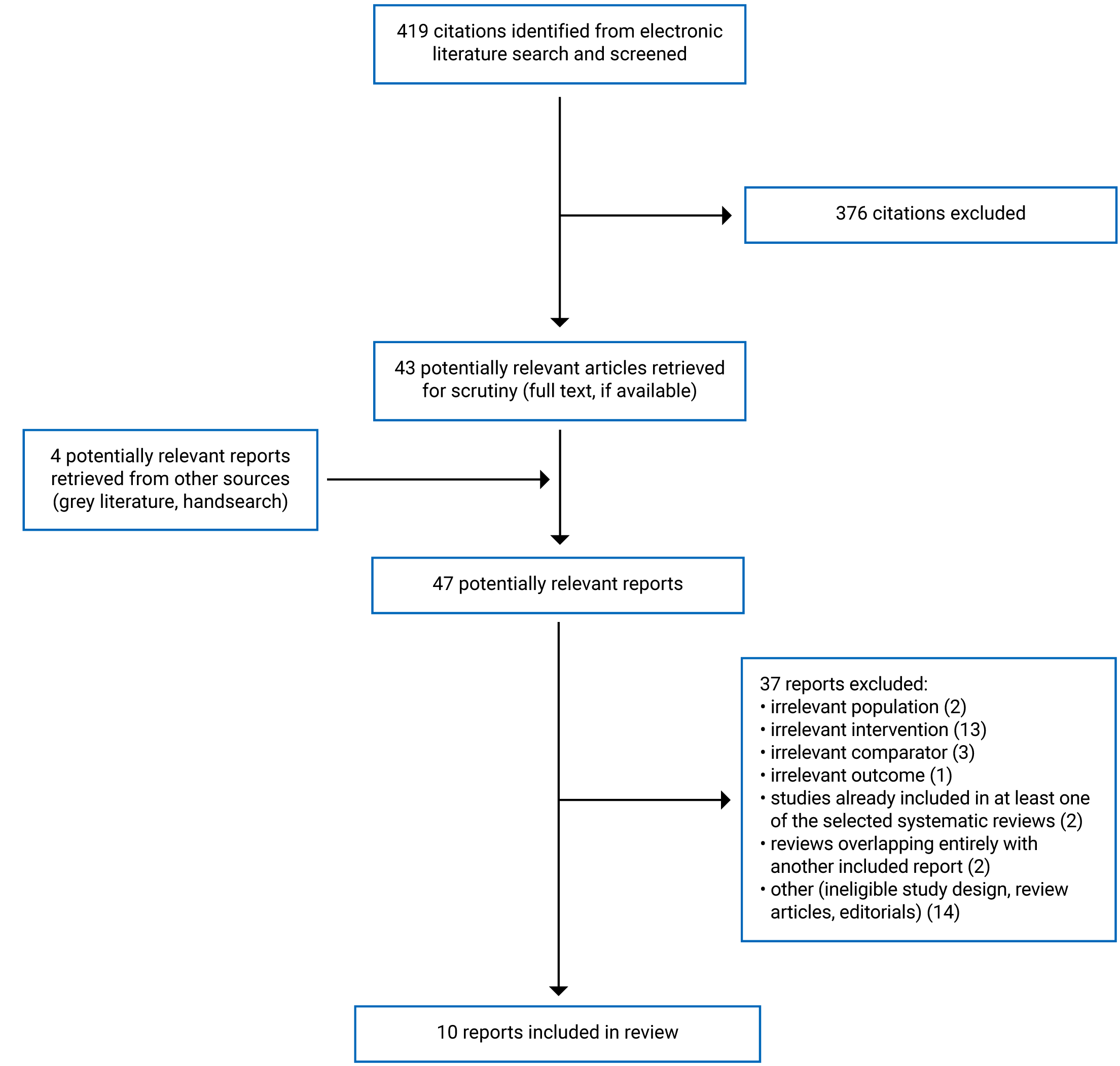
A total of 419 citations were identified in the literature search. Following screening of titles and abstracts, 376 citations were excluded and 43 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 37 publications were excluded for various reasons, and 10 publications met the eligibility criteria of this review and were included in this report.21-30 These comprised 4 reports that included overviews of SRs, SRs of primary studies, and/or primary studies in their reviews,23,25-27 3 SRs of primary studies21,22,24 and secondary analyses of data from other studies.28-30
Appendix 1 presents the PRISMA31 flow chart of the study selection.
Summary of Study Characteristics
All of the 7 reports that included overviews of SRs, SRs of primary studies, and/or primary studies had broader eligibility criteria than this review.21-27 Some of these reports focused on a broader set of interventions,21-23,27 whereas others were broader in their inclusion of eligible comparators.24-26 Because of the differences in scope and focus between this review and the eligible reports identified, some of the studies included in the 7 reports were not eligible for inclusion in the summary of this report. The other 3 reports described secondary analyses of data from other studies, including 3 RCTs that were relevant to this review.28-30
Details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The 4 reports that included overviews of SRs and/or SRs of primary studies were published between 2016 and 2020.23,25-27 The 2020 report was a rapid review that did not include any SRs of relevance to this review,23 and therefore none of the SRs were eligible for inclusion in this review. The 2018 report was a working paper that included 1 relevant overview of SRs and 9 relevant SRs published between 2005 and 2017.25 The 2017 report was an evidence brief that included 2 eligible SRs,26 which were also described in the 2018 working paper25; therefore, to avoid duplication, the 2 relevant SRs were summarized using information from the 2018 working paper25 and the portion of the 2017 evidence brief report that described those 2 SRs was not further summarized in this review. The 2016 report was a technical report that included 2 SRs relevant to this report, both of which were published in 2013.27
These 4 reports also included primary studies in their reviews.23,25-27 The 2020 rapid review did not limit their search by study design and included sources from any study design but did not include any primary studies of relevance to this review23; therefore there were no data eligible for inclusion in this review. The 2018 working paper sought RCTs to inform an assessment of patient-level outcomes (and other study designs to inform analyses of outcomes not relevant to this review [e.g., community-level outcomes]).25 This working paper narratively summarized 10 RCTs relevant to this review (across an unclear number of articles that were neither listed nor tabulated) but because these RCTs were also described by the SRs included the report25 these primary studies were not further summarized in this review to avoid redundancy. The 2017 evidence brief sought studies using any design reporting comparative data and included an unclear number of primary studies or reports that were neither listed nor tabulated, describing the findings from their review narratively only, with few quantitative data included.26 The 2016 technical report did not include any primary studies that were relevant to the current review.27 With regard to synthesis, these 4 reports provided narrative syntheses of the studies included in the reviews.
The 3 remaining SRs that described findings from primary studies only sought and included RCTs, conducted meta-analyses and were published between 2019 and 2021.21,22,24 The 2021 SR included 19 RCTs, 9 of which (reported across 16 reports) were relevant to this review, and were published between 2003 and 2016.21 The 2020 SR identified 4 RCTs,22 1 of which was published in 1999 and bore relevance to this review. The 2019 review included 4 RCTs, all of which were relevant to this review and were published between 2002 and 2014.24
The 3 reports describing secondary analyses of data from other studies were published between 2016 and 2019.28-30 One of the reports described secondary analyses of data from 3 studies — 2 RCTs and an observational study.28 Data from the observational cohort study were not eligible for inclusion in this review, but eligible data from the 2 RCTs — 1 of which was a multi-centre RCT, and the other, a phase III, double-blind noninferiority RCT — were included in this report.28 A 2018 report also described a subgroup analysis from the same phase III, double-blind noninferiority RCT described in the 2019 report.29 And the 2016 report described a 3-month extension of follow-up after the end of a 12-month open-label RCT, to investigate whether the relative benefits observed in the active intervention group would be sustained following the termination of treatment.30
A citation matrix outlining the overlap between relevant included studies within the reviews captured in this report, excluding reviews whose included SRs or primary studies were entirely captured by the other reviews, is presented in Appendix 5.
Country of Origin
Two of the reports that included overviews, SRs and/or primary studies listed first authors from the US.25,27 Two of the reports that included SRs and primary studies,23,26 as well as 2 of the SR reports,21,24 listed first authors from Canada, and 1 SR listed its first author from Italy.22
Two of the 3 RCTs described by the reports of RCT data included in this review were conducted in Canada,28,29 and the other RCT was conducted in Belgium.30
Patient Population
All 10 of the reports that were included in this review described study participants as those living with OUD.21-30 One report limited their population of interest to those treated in primary care settings,27 whereas another limited its population to those in outpatient settings.24 Two reports described sup-populations of interest: 1 SR focused on opioid-dependent pregnant women22 and another report presented secondary analyses of data from the SALOME trial32 describing study participants who self-identified as Indigenous.29 Few of the reports described details about the study participants (e.g., age, sex) and these are described in Appendix 2.
Interventions and Comparators
Several reports included in this review focused on a broad range of interventions and comparators, some of which were relevant to the current review. One report sought comparisons between any kind of harm reduction interventions for OUD used during the COVID-19 pandemic23; however, none of the included studies in this report was eligible for the current review. Another report was more broadly interested in medication-assisted treatment (MAT) models of care — some of which included pharmacological components that were relevant to this review (i.e., SROM).27 One SR sought studies describing any kind of OAT and OST, several of which described injectable HDM, DAM and SROM compared against methadone or DAM.21 Another SR was focused on any kind of pharmacological treatment for OUD, including 1 study on SROM versus methadone.22 Other reports sought to describe more specific interventions. One report was focused on heroin-assisted treatment (HAT) of any kind compared to any other treatment or no treatment.25 Another report sought information on injectable OAT and reported relevant findings comparing DAM to methadone.26 Another SR was focused on studies describing SROM against other medications, and presented data from studies comparing SROM with methadone.24
Two of the 3 reports of RCT data described findings from 2 RCTs comparing HDM to DAM28,29 and the third report described findings from an RCT comparing DAM with methadone.30 Of note, the 2019 paper was limited to describing a 3-day induction protocol of the interventions from the Canadian NAOMI and SALOME trials,28 and the report of the Belgian RCT was limited to an extended follow-up of the original treatment groups following the completion of the protocol-specified therapies (i.e., patients in the intervention arm were no longer receiving DAM during the extended 3-month follow-up period described in the paper, and were transferred to another therapy at the discretion of the clinicians overseeing their care; intervention[s] received by patients in the comparator arm following the end of the 12-month trial were not described clear).30
None of the evidence identified specified the use of oral HDM (i.e., all of the studies reporting data on HDM either specified injectable or inhalable HDM or did not specify the type of HDM used). Likewise, no evidence describing the use of fentanyl patches or buccal tablets was identified.
Outcomes
Several outcomes of relevance were described in the reports included in this review. These outcomes included the following: treatment retention22,24-27,29; use of illicit opioids and/or other drugs of abuse22,24-27,29,30; mental health21,22,25,26,29,30; physical and/or mental health26,29,30; quality of life24-26; adverse events (AEs) and severe adverse events (SAEs)22,24-26,28; and mortality.25,30
Summary of Critical Appraisal
Details regarding the strengths and limitations of included publications are provided in Appendix 3.
Reports Including Overviews, Systematic Reviews, and/or Primary Studies
Strengths and limitations were observed in the 7 reports including overviews of SRs, SRs of primary studies, and/or primary studies.21-27 For instance, whereas most of the included reviews did not specify the preparation of a protocol to inform their methods,23-27 2 of the reports did describe this important early step in the review process.21,22 On the other hand, with the exception of 1 included report,25 key review criteria i.e., population, intervention(s), comparator(s) and outcome(s), were clearly described.21-27 A clear description of these key criteria is important for framing and establishing the aim and research question(s) of a review. Similarly, a comprehensive search of the literature was also described in all21-27 but 126 of the reports. A comprehensive and detailed search strategy is a critical component of a well-conducted SR, as it assures the reader that calculated effort has been put into identifying a maximum amount of eligible information.
Duplicate study selection was reported in most of the reviews21,22,24,26,27; however 2 either did not describe their methods for study selection in sufficient detail or did not describe duplicate study selection.23,25 Independent review of potentially relevant citations by at least 2 reviewers is an important part of reducing the potential for bias and error in the SR process, and ensuring all eligible studies are identified and included in the review. Similarly, duplicate data abstraction is important for ensuring that data have been accurately and comprehensively identified; whereas 3 of the reports indicated that data were collected by 2 independent reviewers,21,22,26 the other reports did not clearly describe the methods used for data abstraction.23-25,27 In addition, some reviews included a clear and detailed description of the included studies,22,24 others did not include details describing this information.21,26 Similarly, while several reports listed and detailed the studies excluded from the review and the reasons for their ineligibility,22,25,27 others did not include this information,21,23,24,26 which is important for the reader of a review when considering how the eligibility criteria were applied and which evidence was not included in the findings and interpretation. A clear and comprehensive assessment of the risk of bias for included studies included is a key component of all SRs19; and while 5 of the included review reports described the risk of bias for included studies,21-24,26 others did not make mention of risk of bias at all,25,27 constituting a critical limitation. One of the reports provided an explicit assessment per comparison and outcome using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework,33 and reporting a low quality of evidence for all outcomes of relevance and included in this report.22 Another report clearly acknowledged the limitations of the evidence it reported on by describing it as limited and/or of low quality.27 The quality of a study is an important part of weighing the value and contribution of the evidence it provides in answer to a research question (i.e., a higher quality of evidence provides more confidence in the findings reported, while lower levels of evidence are cause for caution in the interpretation of findings). One report24 presented data that appeared inconsistent with its methods and procedures (i.e., an unusually high number of positive urine drug tests reported per patient [≥ 70 per group]), which did not seem logistically feasible within the methods and procedures of the study as described. All review reports included an acknowledgement of funding source(s),21-27 even if only an acknowledgement that no funding was used in support of the work.21 On the other hand, all21-27 but 122 of the included reviews did not describe the funding sources of their included studies, which constitutes important information for the reader toward understanding the extent to which any possible external conflicts of interest may have had an impact on the conduct and/or findings of the studies included in the review.19
Particular limitations were also noted with the reports that included various levels of synthesis, including overviews of SRs, SRs of primary studies, and primary studies; for instance, none of the 4 reports that were eligible for inclusion in this report were described by the authors as overviews of SRs. Two of them were very large reports with broad inclusion criteria with regard to study design (among others), hence the inclusion of SRs (among other study designs).25,27 The other 2 reports were presented as brief reports (i.e., an evidence brief26 and a rapid review)23; however, both included SRs and used methods that met the criteria necessary to be classified as overviews of SRs. But because the overarching aim of these 4 reports was not clearly stated as the conduct of a comprehensive and/or rigorous overview of SRs or SRs of primary studies, they demonstrated some important limitations. The presence of overlap between included SRs and/or included SRs with included primary studies was not always clear; reporting of included SRs was generally poor (i.e., no tabulated data); high-level results presented only briefly in the narrative and lacking in detail; as well as a limited assessment (if any) of risk of bias for included SRs. These limitations rendered a lack of relevant and available data and information that might otherwise have been available if robust overview and SR methods had been applied consistently to these reviews.
Reports of RCT Data
Because all 3 of the reports of RCT data were secondary,28 subgroup29 and follow-up30 analyses, some limitations in the basic reporting and description of details of the trials were observed. Specifically, these papers made reference to other/primary reports (that may not be available to all readers) of the RCTs they described, rather than describe the features of the RCT themselves. For instance, while the main outcomes of the studies were clearly described by all 3 papers,28-30 1 did not clearly describe the study aim or patient characteristics, referring instead to another report of the RCT.30 Other noted limitations in reporting included potential inconsistencies in the reporting of outcome and statistical data: 1 report described an unexpectedly and unusually high number of total injections across a 3-day induction protocol (i.e., > 40K per group of approximately 100 study participants each),28 which appears to be logistically improbable within the study procedures as described. In general, measures of internal validity suggested a relatively low risk of bias across the 3 trial reports;28-30 however, 1 RCT was open label, which constitutes an important potential risk of bias as the study participants, clinicians and investigators would have had knowledge of the intervention received by the study patients.30 There was insufficient information reported in any of the reports of RCT data to adequately assess the extent to which external validity was robust, or whether it constituted a risk of bias.28-30 Likewise, randomization procedures and other information critical to assessing the risk of bias due to confounding were not described in adequate detail to ascertain the strengths or limitations imposed by these risks in the 3 reports.28-30 Finally, sample sizes and the potential impact on study power were not discussed in any of the 3 reports of RCT data, despite the fact that the samples described were relatively small.28-30
Summary of Findings
Clinical Effectiveness of Opioid Substitution Treatment
Appendix 4 presents the main study findings and authors’ conclusions.
Treatment Retention
Five reports included in and contributing eligible information to this review reported relevant data describing the use of OST (i.e., HAT or SROM) compared with other therapies on patient retention in treatment programs or protocols.22,24,25,27,29
HAT Versus Methadone or Other Forms of HAT
Two of these 5 reports described various forms of HAT compared to either methadone and/or other forms of HAT.25,29 One report described an included overview of SRs that concluded, in general, there were no statistically significant differences identified in treatment retention between HAT and other traditional medications (described only as being primarily methadone).25 Nonetheless, based on the data from 1 SR (the number of trials or participants not reported) included in the overview that was summarized in the report, it was found that a benefit may be proffered in terms of treatment retention based on the type of HAT and comparator treatments being assessed. Specifically, the authors reported that methadone with injectable heroin was found to be more effective than HAT (RR, 1.17 [95% CI, 0.99 to 1.38]) and that methadone with inhalable heroin was also more effective than HAT (RR, 1.27 [95% CI, 1.11 to 1.46]).25 On the other hand, injectable HAT was found to be statistically significantly more effective for retaining patients in treatment compared to methadone alone (RR, 0.35 [95% CI, 0.21 to 0.59], calculated with injectable HAT as the control group).25 Other SRs (the number of trials or participants not reported) included in this report corroborated the latter finding, with 2 reporting a statistically significant benefit in favour of injectable HAT as compared to methadone alone (RR, 1.44 [95% CI, 1.16 to 1.79] from 1 SR and RR, 1.37 [95% CI, 1.03 to 1.83] from the other SR).25 Findings from an additional 2 SRs (the number of trials or participants not reported) summarized in the overview and addressing treatment retention were described narratively only, but also indicated an observed benefit of HAT when compared to methadone alone or traditional medication (which was not further specified).25 One of the reports of RCT data described treatment retention, measured by the proportion of patients in treatment for 28 days or more, among 61 Indigenous study participants with OUD treated with either HDM and DAM, and reported observing no statistically significant difference between the groups (mean risk difference, −3 [95% CI, −25 to 20], P > 0.05).29
SROM Versus Methadone or Other Medications
Three of the 5 reports describing treatment retention and including eligible data reported on comparisons of SROM with either methadone or other medications.22,24,27 The report focusing on MAT models of care delivered in primary care settings described the inclusion of an SR describing SROM, but explained that no data were summarized from the SR because it did not limit its analyses to the primary care setting.27 Nonetheless, some cursory data describing study characteristics were tabulated, including a narrative description of the findings and describing 2 relevant SRs of SROM: 1 SR (including 3 RCTs describing 195 patients) was reported as finding limited evidence that SROM was likely as effective or more effective for treatment retention than other medications (not specified); and the other SR (including 4 RCTs describing 271 patients) reported finding no significant difference between SROM and methadone.27 The direction of these findings were echoed in 2 other SRs included in this review.22,24 One SR reported no difference in treatment retention (as measured in 1 included RCT, using the number of patients having dropped out of treatment) between SROM as compared to methadone; that is, 0 study participants in both groups of 24 each (results reported narratively only).22 Notably, authors conducted a GRADE assessment of the evidence, characterizing the strength of evidence for this outcome as being of low quality.22 The other SR corroborating this finding combined results from 4 RCTs (describing 745 patients) and also reported no statistically significant difference between SROM and methadone in terms of treatment retention (i.e., RR 0.98 [95% CI, 0.94 to 1.02], P = 0.30).24 Similarly, these authors made note of the low quality of evidence identified and the impact this may have on their findings and interpretation.24
Use of Illicit Opioids and/or Other Drugs of Abuse
Two reports that included SRs,25,27 3 SRs22,24,26 and 2 reports of RCT data29,30 described the use of illicit opioids and/or other drugs of abuse in their findings comparing HAT or SROM with other medications.
HAT Versus Methadone or Other Forms of HAT
Four of the reports described findings from comparisons of HAT with either methadone or other forms of HAT (e.g., HDM, DAM).25,26,29,30 One report included 1 overview of SRs that concluded, in general, there was limited evidence to suggest any differences between HAT and other traditional medications for OUD (primarily methadone) with regard to illicit use of heroin.25 Nonetheless, results from 4 SRs (reported narratively only) included in the same report indicated otherwise, stating that all 4 SRs found a benefit favouring HAT when compared to methadone for reducing the use of illicit substances.25 However, in the 3-month extended follow-up study of the Belgian RCT evaluating 61 study participants, no significant difference in self-reported cocaine use or urinalysis for exposure to illicit heroin was found at 15 months post-baseline between participants who had received DAM during the 12 months of the trial as compared to those who had received methadone.30 Nonetheless, a sustained benefit was observed in self-reported use of street heroin in the group who had received DAM compared to those who had received methadone (i.e., a mean of 14 days during the 3-month follow-up versus a mean of 17 days, P = 0.00094).30
Another SR narratively described findings from 2 RCTs (number of study participants not reported) comparing HAT with other medications: 1 was a noninferiority trial concluding that HDM was noninferior to DAM when comparing urine markers of illicit opioid and/or heroin use; and the other reported the superiority of DAM as compared to other medications (which were not specified, nor was the outcome measure).26 On the other hand, the subgroup analysis of 61 Indigenous study participants randomized to either HDM or DAM found no statistically significant differences between the groups in 2 self-reported measures of illicit substance use (i.e., mean number of days using illicit heroin or street-acquired opioids) and 1 urinalysis measure (i.e., proportion of patients positive for exposure to street heroin).29 However, the authors reported a statistically significant difference in self-reported days of cocaine use between participants assigned to HDM and those assigned to DAM (mean difference −3.46 [95% CI, −7.87 to −0.10], P < 0.05, favouring DAM).29
SROM Versus Methadone
Three of the reports described findings of illicit substance use from comparisons of SROM with methadone.22,24,27 One report summarized findings from 1 SR (4 RCTs describing 271 patients, reported narratively only), indicating that no significant difference was found in the use of other illicit substances between patients receiving SROM as compared to those receiving methadone (measure not described).27 Likewise, an SR that pooled urinalysis results for heroin use across 3 trials (describing 677 participants) found no statistically significant difference between participants receiving SROM as compared to those receiving methadone (i.e., RR 0.96 [95% CI, 0.61 to 1.52], P = 0.86).24 Conversely, the SR reporting on findings from 1 small RCT of 48 pregnant participants comparing SROM with methadone observed statistically significantly less heroin use during the third trimester among those receiving SROM (measure not described) (RR, 2.40 [95% CI, 1.00 to 5.77], P = 0.05).22 Similarly, urinalysis from this RCT suggested a greater proportion of patients in the SROM arm had a negative test for exposure to benzodiazepines as compared to patients in the methadone arm (i.e., 89% versus 54%, no comparison statistic reported).22
Mental Health
Six reports described findings specific to mental health (i.e., 1 overview of SRs25; 3 SRs21,24,26; and 2 reports of RCTs29,30) in study participants receiving either various forms of HAT or SROM compared with other medications.
HAT Versus Methadone or Other Forms of HAT
One report presented mental health outcomes from 2 included SRs (number of participants not reported) comparing injectable HAT with methadone or other conventional treatments (not otherwise specified), with most results reported narratively only.25 The first SR reported on data from 1 RCT measuring depression and psychoticism using the Symptom Checklist-90-R (SCL-90-R) scale, and observing a statistically significant benefit in favour of supervised injectable heroin as compared to methadone (P = 0.002).25 The second SR narratively described the findings from multiple measures of mental health across 4 RCTs, 2 of which reported no difference in suicide attempts, severe depression, cognitive problems, difficult controlling aggression, and mental health (measures not reported) between groups receiving injectable HAT as compared to conventional medications (not specified) or methadone.25 Two RCTs from this second SR also described a significant improvement in scores on the SF-36 scale for study participants receiving injectable HAT as compared to conventional treatment (not specified) and significant improvements in mental health for participants receiving injectable HAT versus methadone (measures and comparative statistics not reported).25 One SR included in this review reported high-level findings narratively, indicating that improvements in SF-12 and the Addiction Severity Index Psychiatric Composite score were observed in extended follow-up (2 years) of 1 RCT (number of participants not reported) with DAM as compared to other treatments (not specified).26 Another SR in this review focused solely on measures of mental health, including meta-analyses for some outcomes and comparisons.21 One included RCT (describing 192 study participants) in this SR comparing HDM with DAM found no significant differences between the groups in composite scores of depressive symptoms, mental health symptomatology and addiction severity.21 Similarly, 1 of the RCT reports described a comparison of HDM and DAM in 61 Indigenous OUD patients by measuring psychological health using the Maudsley Addiction Profile (MAP), and reporting no statistically significant differences between scores among the study participant groups.29
On the other hand, the SR focused on mental health outcomes reported a series of meta-analyses of RCTs comparing DAM with methadone, finding a relative benefit of DAM: meta-analyses of 4 RCTs (1,474 study participants) found mental health symptomatology was statistically significantly improved in participants receiving DAM, using both fixed and random-effects models, (standardized mean difference: −0.233 [standard error 0.052], 95% CI, −0.336 to 0.131, P < 0.001).21 Similarly, a statistically significant benefit of DAM versus methadone in composite scores of addiction severity was observed in a meta-analysis of 4 RCTs (1,504 study participants), using a random-effects model (standardized mean difference: −0.189 [standard error 0.086], 95% CI −0.358 to −0.021, P = 0.028).21 Likewise, 1 of the reports of RCT data described extended, post-trial follow-up of a comparison of DAM with methadone by measuring mental health using the SCL-90-R Symptom Checklist, and reporting a benefit (though, not statistically significant) in favour of DAM (P = 0.056).30 Nonetheless, in a meta-analyses of 2 RCTs comparing DAM and methadone, no statistically significant differences were reported between groups in composite scores of both depressive symptoms (476 study participants) and mental health quality of life (144 study participants).21
SROM Versus Methadone
In 1 of the included SRs, 1 RCT comparing SROM with methadone found no statistically significant differences between study groups in composite scores of mental health symptomatology (241 study participants) and mental health quality of life (56 study participants).21 However, another SR found a statistically significant benefit favouring SROM over methadone in scores of depression (1 RCT with 55 study participants, measure not reported, P < 0.001); anxiety (1 RCT with 55 study participants, State Trait Anxiety scale, P < 0.01); and adverse mental symptoms (1 RCT with 157 study participants, outcome measure not reported, P < 0.01).24 However, when mental health and social functioning was measured using the BASIS-32 Behaviour and Symptom Identification Scale in a small RCT of 9 patients also reported in this SR, no difference was observed between the groups.21
Physical and/or Mental Health
Measures of physical and/or mental health were either mentioned or reported in 1 report describing an overview and an SR, and 2 reports of RCT data included in this review.26,29,30
HAT Versus Methadone or Other Forms of HAT
One SR briefly reported findings narratively, describing results from 1 RCT (number of study participants not reported) that reported no difference between DAM and methadone in physical/mental health, as measured by the SF-36 scale.26 On the other hand, the extended follow-up report of the Belgian RCT found a statistically significant benefit of DAM as compared to methadone that was sustained at the 3-month post-trial follow-up among the 61 study participants assessed using the Maudsley Addiction Profile (MAP) Health Symptoms Scale (HSS) score.30 Finally, the primary study report describing findings from a subgroup analysis of 61 Indigenous study participants in an RCT comparing HDM to DAM measured physical health using the MAP score and reported no statistically significant difference between the groups.29
Quality of Life
Measures of quality of life were either mentioned or reported in 1 overview of SRs and 2 SRs included in this review.24-26
HAT Versus Methadone or Other Forms of HAT
One report briefly mentioned in the narrative description of its findings that the overview of SRs included in its review concluded, in general, there were no significant differences identified in quality of life between HAT and other traditional medications (primarily methadone).25 One SR briefly reported findings narratively, describing results from 1 RCT (number of study participants not reported) that indicated health-related quality of life was improved in patients receiving DAM as compared to methadone.26
SROM Versus Methadone
One SR included in this review reported findings from 1 RCT (240 study participants) describing subscales of the Lancashire Quality of Life Profile, including family, finances and overall satisfaction, all of which indicated that methadone proffered a statistically significant benefit to study participants as compared to SROM.24
Adverse Events
One overview of SRs, 3 SRs and 1 report of RCT data described AEs and/or SAEs observed among study participants with OUD who received various forms of OST.22,24-26,28
HAT Versus Methadone or Other Forms of HAT
One report focused on HAT reported findings on SAEs from 3 SRs that described results from 7 RCTs (number of study participants not reported) comparing HAT to methadone, and indicating that there were statistically significantly fewer SAEs in all of the methadone groups relative to participants receiving HAT.25 One SR briefly mentioned in the narrative of its report findings from 1 RCT comparing HDM and DAM (number of study participants not reported), indicating that there were fewer SAEs observed in the HDM group as compared to study participants receiving DAM.26 On the other hand, the RCT describing 3-day induction protocols for HDM or DAM found no statistically significant difference between the groups in the rates per 100 injections for events of post-injection reaction and pruritis, somnolence, or overdose.28
SROM Versus Methadone
One SR reporting findings from 1 small RCT of 48 pregnant opioid-dependent study participants mentioned in the narrative of their results that no side effects were observed in the study, indicating no difference between groups.22 Notably, the authors of the SR assigned a low quality of evidence to this outcome using their GRADE assessment.22 Similarly, another SR describing findings from 1 RCT (157 study participants) found no statistically significant difference in AEs reported between the groups receiving SROM as compared to methadone (P = 0.62).24
Mortality
Two reports described mortality in study participants receiving various forms of HAT as compared to methadone.25,30 One report described an included overview of SRs that concluded, in general, there were no significant differences identified in mortality between HAT and other traditional medications (primarily methadone).25 Likewise, in its summary of 3 SRs with meta-analyses representing data from 9 RCTs of over 3,000 study participants, no statistically significant difference was found between study participants receiving various HAT protocols as compared methadone.25 The 1 RCT including data on mortality in a group of 61 study participants receiving either DAM or methadone reported 1 death in the experimental group and no deaths in the control group, with no statistical characterization of this difference between groups reported.30
Limitations
This review identified several relevant sources addressing 2 of the 4 research questions posed; however, none of the evidence identified in this review specified the use of oral HDM (i.e., all of the studies reporting data on HDM either specified injectable or inhalable HDM or did not specify the type of HDM used). Likewise, no evidence describing the use of fentanyl patches or buccal tablets was identified. These limitations constrain the extent to which this review can answer all of the 4 research questions posed.
While the quantity of eligible publications identified was plentiful, the quality of the eligible studies was generally low; and whereas this was clearly assessed and explicitly acknowledged by some of the authors of the studies included in this review, the critical appraisal performed as part of this review identified some important limitations of the included studies. For instance, several of the included reports on overviews of SRs and/or SRs of primary studies were poorly reported (e.g., included studies were neither listed nor tabulated; findings were often not presented quantitatively; no evidence of critical appraisal of included studies) and/or studies included in the reviews demonstrated a low quality of evidence. Similarly, the reports of RCT data lacked detail as they were supplementary publications from the RCT studies, describing only limited follow-up, limited interventions and outcomes or subgroup analyses.
Further, while the quantity of evidence addressing the use of OST for OUD appears to be plentiful, there was a great deal of overlap identified across the included reviews and there are multiple supplemental papers published describing the same trials i.e., much of the available evidence identified in this review (and other reviews included in this review) is based on the same several trials. This limits the available evidence base to address research questions querying the clinical effectiveness of OST and associated safe supply programs.
Conclusions and Implications for Decision- or Policy-Making
Ten reports were identified and found to be eligible for inclusion in this review: 4 reports that included overviews of SRs, SRs of primary studies, and/or primary studies23,25-27; 3 SRs21-24; and data from 3 RCTs.28-30 Studies reported on comparisons of various forms of injectable or inhalable HAT and SROM with methadone or other medications (some of which were not specified)21-30; whereas no studies explicitly described the use of oral HDM and no studies were found investigating the use of fentanyl patches or buccal tablets.
Evidence from multiple SRs indicated that HAT proffers higher treatment retention to individuals living with OUD as compared to methadone25; however, the quality of evidence for these findings was not reported and so, is unclear. On the other hand, there was no difference between SROM as compared to methadone for treatment retention22,24,27; notably, most of the evidence generating these findings was either poorly reported or was characterized by the authors as being of low quality. Evidence informing the effect of OST on the use of illicit opioids or other drugs of abuse was mixed and therefore unclear: whereas some studies favoured various forms of HAT over methadone, others found no difference between the interventions.25,30 Similarly, studies comparing HDM with DAM were mixed with regard to use of illicit opioids and/or other drugs of abuse26,29; importantly, these studies were either poorly reported, used small sample sizes and/or lacked a clear characterization of the quality of the evidence. As with the findings describing treatment retention, findings from SRs included in this review found no difference in the use of illicit opioids or other drugs of abuse among study participants receiving SROM as compared to methadone (though, the quality of the evidence was not reported).22,24,27 The 1 exception was a small trial of pregnant study participants described in 1 SR that identified a statistically significant benefit of SROM22; however, the generalizability of these findings should be interpreted with caution based on the small sample size and the particular subgroup of interest. Findings describing the effectiveness of OST for mental health, quality of life and physical health were mixed and based on evidence of unclear quality: while some evidence from systematic reviews indicated a benefit of injectable HAT or DAM as compared to methadone for some measures of mental health, other data from systematic reviews and RCTs found no difference between HAT and methadone, and no difference between HDM and DAM.21,24-26,29 Similarly, the data describing SROM compared to methadone for various measures of mental health produced mixed results, with some evidence indicating no difference between the groups,21 and other evidence reporting a benefit for study participants receiving SROM.24 Conversely, the 1 SR reporting on measures of quality of life in study participants receiving SROM or methadone found methadone to be more beneficial.24 Adverse events were generally found to be greater in frequency and severity with various forms of HAT as compared to methadone;25 whereas no difference was found when SROM was compared to methadone,22,24 and no consistent differences were found when HDM was compared with DAM. Similarly, limited available evidence describing mortality indicated no observed difference between HAT and methadone.26,28
These findings generally align, and somewhat overlap, with those produced by an earlier CADTH report in 2017, which summarized findings from 1 of the same reports as was included in this review, as well as several of the same trials and reviews (though, earlier publications of these studies).34 The earlier CADTH report similarly described mixed results concerning SROM versus methadone, as well as studies that generally reported improved clinical effectiveness in study participants receiving HDM, DAM or other forms of HAT as compared to methadone.34 The current review has identified mixed results across the eligible studies included, including lack of a clear relative benefit of various forms of HAT (e.g., injectable HDM, DAM) compared against other forms of OST, as well as the use of SROM compared to methadone — which has also been corroborated by other sources in the available literature.10
On the other hand, there does appear to be at least some preponderance of evidence assembled in this review that indicates a clinical benefit of injectable HDM and/or DAM over the use of methadone. In addition to the evidence presented here, there is a growing body of evidence using observational methods that describes a variety of associated interventions. For example, 1 Canadian study based in Ottawa investigated the use of injectable HDM combined with a housing program in a small sample of study participants with OUD and found that the combination of interventions was significantly effective for retaining individuals in treatment.35 This finding is supported by an environmental scan of injectable OAT programs conducted in Canada, suggesting that an important facilitator of benefit for individuals with OUD is the additional support of other health and social resources.36 Some of these facilitators were investigated in another Canadian study that used qualitative methods with OUD study participants to identify beneficial features of an HDM distribution program; these included: co-location with an overdose prevention centre, flexibility and the experience of having individual agency.37 Another Canadian study of pre-treatment factors associated with the effects of OAT in study participants with OUD corroborates this assertion, finding that the presence of additional supports during treatment increases the effectiveness of the OAT,38 suggesting that combined interventions may also be an important approach when investigating the effectiveness of OST interventions. Opportunities for future research investigating the clinical effectiveness of OST may therefore benefit from prioritizing the use of compound interventions that combine OST with other complementary supports and resources.
Given the mixed findings in this review, another opportunity for future research may be the investigation of specific subgroups that could benefit more significantly from a more tailored approach to the delivery of OST. For instance, an observational study conducted in Germany found some benefit of SROM for study participants refractory to OAT, suggesting that some individuals may benefit from switching to SROM more than others, including those patients having side effects of OAT with other treatments.39 And while much of the research describing more recent types of OST (e.g., HAT, HDM, DAM) to date focuses on its use in methadone refractory patients, there may also be opportunities to consider the role of these interventions as first-line therapy for individuals with OUD.
Other outcomes not identified by studies in this review may be critical to investigate as well e.g., the effect of various forms of OST on adherence to therapy for HIV and/or HCV — which has been indicated as a potential benefit of OAT using other forms of medication (i.e., buprenorphine, methadone, naltrexone).40-43 There may be a role for other types of OST (e.g., HAT, HDM, DAM) in addressing this outcome. Finally, given the lack of data identified describing fentanyl patches and/or buccal tablets, there is an opportunity to pursue research in this area as well; some case report data and other low-quality studies were found describing the use of fentanyl patches,12-14 indicating the need for RCTs and the generation of additional, high-quality evidence.
References
1.Link HM, Jones H, Miller L, Kaltenbach K, Seligman N. Buprenorphine-naloxone use in pregnancy: a systematic review and metaanalysis. Am J Obstet Gynecol MFM. 2020;2(3):100179. PubMed
2.Ivsins A, Boyd J, Beletsky L, McNeil R. Tackling the overdose crisis: The role of safe supply. Int J Drug Policy. 2020;80:102769. PubMed
3.Mielau J, Vogel M, Gutwinski S, Mick I. New approaches in drug dependence: opioids. Curr Addict Rep. 2021:1-8. PubMed
4.Saxon AJ, Strain E, Peavy KM. Approach to treating opioid use disorder. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: http://www.uptodate.com. Accessed 2021 Dec 12.
5.Noble F, Marie N. Management of opioid addiction with opioid substitution treatments: beyond methadone and buprenorphine. Front Psychiatry. 2018;9:742. PubMed
6.Strain E. Pharmacotherapy for opioid use disorder. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: http://www.uptodate.com. Accessed 2021 Dec 5.
7.Eibl JK, Morin K, Leinonen E, Marsh DC. The state of opioid agonist therapy in Canada 20 years after federal oversight. Can J Psychiatry. 2017;62(7):444-450. PubMed
8.Government of Canada. Safer supply. 2021; https://www.canada.ca/en/health-canada/services/opioids/responding-canada-opioid-crisis/safer-supply.html. Accessed 2021 Nov 12.
9.Government of Canada. Government of Canada approves new treatment options for opioid use disorder and supports research, treatment and harm reduction projects in Ontario. 2019; https://www.canada.ca/en/health-canada/news/2019/05/government-of-canada-approves-new-treatment-options-for-opioid-use-disorder-and-supports-research-treatment-and-harm-reduction-projects-in-ontario.html. Accessed 2021 Dec 3.
10.Socias ME, Wood E, Dong H, et al. Slow release oral morphine versus methadone for opioid use disorder in the fentanyl era (pRESTO): Protocol for a non-inferiority randomized clinical trial. Contemp Clin Trials. 2020;91:105993. PubMed
11.Braithwaite V, Fairgrieve C, Nolan S. Sustained-release oral hydromorphone for the treatment of opioid use disorder. J Addict Med. 2020;14(4):345-347. PubMed
12.Geile J, Maas A, Kraemer M, Doberentz E, Madea B. Fatal misuse of transdermal fentanyl patches. Forensic Sci Int. 2019;302:109858. PubMed
13.Taylor RG, Budhram A, Lee DH, Mirsattari SM. Opioid-associated amnestic syndrome observed with fentanyl patch use. CMAJ. 2019;191(12):E337-E339. PubMed
14.Tadrous M, Greaves S, Martins D, et al. Evaluation of the fentanyl patch-for-patch program in Ontario, Canada. Int J Drug Policy. 2019;66:82-86. PubMed
15.Steel D, Tekin S. Can treatment for substance use disorder prescribe the same substance as that used? The case of injectable opioid agonist treatment. Kennedy Inst Ethics J. 2021;31(3):271-301. PubMed
16.Pardo B, Reuter P. Facing fentanyl: should the USA consider trialling prescription heroin? Lancet Psychiatry. 2018;5(8):613-615. PubMed
17.Strike C, Watson TM. Losing the uphill battle? Emergent harm reduction interventions and barriers during the opioid overdose crisis in Canada. Int J Drug Policy. 2019;71:178-182. PubMed
18.Gastberger S, Baumgartner MR, Soyka M, et al. Concomitant heroin and cocaine use among opioid-dependent patients during methadone, buprenorphine or morphine opioid agonist therapy. Eur Addict Res. 2019;25(4):207-212. PubMed
19.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
20.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
21.Moazen-Zadeh E, Ziafat K, Yazdani K, et al. Impact of opioid agonist treatment on mental health in patients with opioid use disorder: a systematic review and network meta-analysis of randomized clinical trials. Am J Drug Alcohol Abuse. 2021;47(3):280-304. PubMed
22.Minozzi S, Amato L, Jahanfar S, Bellisario C, Ferri M, Davoli M. Maintenance agonist treatments for opiate-dependent pregnant women. Cochrane Database Syst Rev. 2020;11:CD006318. PubMed
23.What is the effect of the COVID-19 pandemic on opioid and substance use and related harms? Hamilton (ON): National Collaborating Centre for Methods and Tools; 2020: https://www.nccmt.ca/uploads/media/media/0001/02/3bb7203c61163ba3aceca1f88d49e81cc837f2c1.pdf. Accessed Nov 2021 Nov 15.
24.Klimas J, Gorfinkel L, Giacomuzzi SM, et al. Slow release oral morphine versus methadone for the treatment of opioid use disorder. BMJ Open. 2019;9(4):e025799. PubMed
25.Smart E. Evidence on the effectiveness of heroin-assisted treatment. Santa Monica (CA): RAND Corporation; 2018: https://www.rand.org/pubs/working_papers/WR1263.html. Accessed 2021 Nov 15.
26.Ontario Agency for Health Protection and Promotion (Public Health Ontario), Leece P, Tenenbaum M. Evidence Brief: Effectiveness of supervised injectable opioid agonist treatment (siOAT) for opioid use disorder. Toronto (ON): Public Health Ontario; 2017: https://www.publichealthontario.ca/-/media/documents/e/2017/eb-effectiveness-sioat.pdf?sc_lang=en. Accessed 2021 Nov 12.
27.Chou R, Korthuis PT, Weimer M, et al. Medication-assisted treatment models of care for opioid use disorder in primary care settings. (Technical Brief No. 28). Rockville (MD): Agency for Healthcare Research and Quality (AHRQ); 2016 https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/opioid-use-disorder_technical-brief.pdf. Accessed 2021 Nov 12.
28.Oviedo-Joekes E, Palis H, Guh D, et al. Adverse events during treatment induction with injectable diacetylmorphine and hydromorphone for opioid use disorder. J Addict Med. 2019;13(5):354-361. PubMed
29.Oviedo-Joekes E, Palis H, Guh D, et al. Characteristics and response to treatment among Indigenous people receiving injectable diacetylmorphine or hydromorphone in a randomised controlled trial for the treatment of long-term opioid dependence. Drug Alcohol Rev. 2018;37(1):137-146. PubMed
30.Demaret I, Quertemont E, Litran G, et al. Loss of treatment benefit when heroin-assisted treatment is stopped after 12 months. J Subst Abuse Treat. 2016;69:72-75. PubMed
31.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
32.Oviedo-Joekes E, Guh D, Brissette S, et al. Hydromorphone compared with diacetylmorphine for long-term opioid dependence: a randomized clinical trial. JAMA Psychiatry. 2016;73(5):447-455. PubMed
33.Siemieniuk R, Guyatt G. What is GRADE? BMJ Best Practice 2021; https://bestpractice.bmj.com/info/toolkit/learn-ebm/what-is-grade/.
34.Wells C, Jones S. Sustained-release oral morphine, injectable hydromorphone, and prescription diacetylmorphine for opioid use disorder: clinical and cost-effectiveness, and guidelines. (CADTH Rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sustained-release-oral-morphine-injectable-hydromorphone-and-prescription-diacetylmorphine-opioid. Accessed 2021 Dec 4.
35.Harris MT, Seliga RK, Fairbairn N, et al. Outcomes of Ottawa, Canada's Managed Opioid Program (MOP) where supervised injectable hydromorphone was paired with assisted housing. Int J Drug Policy. 2021;98:103400. PubMed
36.Eydt E, Glegg S, Sutherland C, et al. Service delivery models for injectable opioid agonist treatment in Canada: 2 sequential environmental scans. CMAJ Open. 2021;9(1):E115-E124. PubMed
37.Ivsins A, Boyd J, Mayer S, et al. Barriers and facilitators to a novel low-barrier hydromorphone distribution program in Vancouver, Canada: a qualitative study. Drug Alcohol Depend. 2020;216:108202. PubMed
38.Dong H, Hayashi K, Fairbairn N, et al. Long term pre-treatment opioid use trajectories in relation to opioid agonist therapy outcomes among people who use drugs in a Canadian setting. Addict Behav. 2021;112:106655. PubMed
39.Lehmann K, Kuhn S, Baschirotto C, et al. Substitution treatment for opioid dependence with slow-release oral morphine: Retention rate, health status, and substance use after switching to morphine. J Subst Abuse Treat. 2021;127:108350. PubMed
40.McNamara KF, Biondi BE, Hernandez-Ramirez RU, Taweh N, Grimshaw AA, Springer SA. A systematic review and meta-analysis of studies evaluating the effect of medication treatment for opioid use disorder on infectious disease outcomes. Open Forum Infect Dis. 2021;8(8):ofab289.
41.Johnson WD, Rivadeneira N, Adegbite AH, et al. Human immunodeficiency virus prevention for people who use drugs: overview of reviews and the ICOS of PICOS. J Infect Dis. 2020;222(Suppl 5):S278-S300. PubMed
42.Platt L, Minozzi S, Reed J, et al. Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs. Cochrane Database Syst Rev. 2017;9:CD012021. PubMed
43.Low AJ, Mburu G, Welton NJ, et al. Impact of opioid substitution therapy on antiretroviral therapy outcomes: a systematic review and meta-analysis. Clin Infect Dis. 2016;63(8):1094-1104. PubMed
44.Oviedo-Joekes E, Nosyk B, Brissette S, et al. The North American Opiate Medication Initiative (NAOMI): profile of participants in North America's first trial of heroin-assisted treatment. J Urban Health. 2008;85(6):812-825.Appendix 1: Selection of Included Studies
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Reports Describing an Overview, Systematic Reviews, and/or Primary Studies
Study citation, country, funding source | Number of reviews included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
NCCMT, 202023 Canada Funding: Public Health Agency of Canada | Study designs sought: Sources of any type (including commentary/expert opinion pieces) Studies included: 62 sources of various types Studies of relevance to this report: 0 (i.e., no relevant studies were included) | Population sought/included: People who use substances (no other description provided) N = NR | Interventions sought: Any harm reduction or treatment intervention used during the COVID-19 pandemic Interventions of relevance to the current review: None Comparators sought: Any harm reduction or treatment intervention used prior to the COVID-19 pandemic | Outcomes sought/of included studies relevant to this report:
Follow-up: NR |
Smart, 201825 USA Funding: RAND Corporation | Study designs sought: Studies of any design, including overviews, SRs and RCTs Studies included: 1 overview of SRs; 9 SRs; 10 RCTs across an unclear number of reports (i.e., not listed nor tabulated) Studies of relevance to this report: 1 overview of SRs; 9 SRs (which overlapped/included the 10 RCTs) Publication years of relevant studies, range: 2005 to 2017 N of included SRs/primary studies in relevant overview/SRs, range: 1 to 8 N of relevant SRs including MAs: 4 | Population sought/included/relevant to this report:
| Interventions/Comparators sought:
Comparators of included studies relevant to this report: Methadone and others (not specified) | Outcomes sought: Patient-level outcomes (no other restrictions/details reported) Outcomes of included studies relevant to this report:
Follow-up: NR |
Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726 Canada Funding: Ontario Government | Study designs sought: Primary or secondary research and data analyses Studies included: 36 (of various study designs including qualitative, economic analyses, etc.) Studies of relevance to this report: 2 SRs that were also described in another included report25 and therefore not further described from this report; an unclear number of RCTs that were neither tabulated nor listed (findings reported narratively only) | Population sought/included/relevant to this report:
| Interventions/comparators sought: Supervised injectable OAT using DAM or HDM/Other treatment or no treatment (not otherwise described) Interventions of included studies relevant to this report:
| Outcomes sought: Treatment retention, drug use patterns, and social, health or other outcomes Outcomes of included studies relevant to this report:
Follow-up: NR |
Chou, 201627 US Funding: AHRQ | Study designs sought: SRs, RCTs and NRS Studies included: 11 SRs and 17 RCTs Studies of relevance to this report: 2 SRs and 0 RCTs Publication years of relevant studies: 2013 N of included primary studies in relevant SRs: 3 and 4 N of relevant SRs including MAs: NR | Population sought/included/relevant to this report:
| Interventions/comparators sought: MAT models of care, including pharmacological/no treatment; other MAT; psychosocial interventions; medication and/or placebo (no other data/information reported) Interventions of included studies relevant to this review: SROM Comparators of included studies relevant to this review: Methadone; other MAT medications (not specified) | Outcomes sought:
Outcomes of included studies relevant to this review:
Follow-up: NR |
AHRQ = Agency for Healthcare Research and Quality; DAM = diacetylmorphine; HAT = heroin-assisted therapy; HDM = hydromorphone; MAT = medication-assisted treatment; NCCMT = National Collaborating Centre for Methods and Tools; NR = not reported; NRS = non-randomized study; OAT = opioid agonist therapy; OUD = opioid use disorder; QoL = quality of life; RCT = randomized controlled trial; SAE = severe adverse event; SR = systematic review; SROM = sustained-release oral morphine.
Table 3: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Moazen-Zadeh, 202121 Canada Funding: Reported as having received none | Study designs sought: RCTs Studies included: 19 RCTs Included studies of relevance to this report: 9 RCTs (described across 16 included reports), all of which were used in quantitative meta-analyses of outcomes relevant to this report | Population sought/included/relevant to this report:
| Interventions/comparators sought: OAT (any)/Placebo, waitlist or other forms of OAT Interventions of included studies relevant to this report: Injectable/inhalable HDM, DAM, SROM Comparators of included studies relevant to this report: Methadone, DAM | Outcomes sought: Mental health outcomes measured with a validated tool Outcomes of included studies relevant to this report:
Follow-up: >1mo post-baseline |
Minozzi, 202022 Italy Funding: National Institute on Drug Abuse; Mayor of Vienna; Schering Plough | Study designs sought: RCTs Studies included: 4 RCTs Included studies of relevance to this report: 1 RCT | Population sought/included/relevant to this report: Opiate-dependent pregnant women (relevant N=48) | Interventions/comparators sought: Any pharmacological maintenance treatment (alone or in combination with a psychosocial intervention)/No intervention, other pharmacological intervention or psychosocial interventions Interventions of included studies relevant to this report: SROM Comparators of included studies relevant to this report: Methadone | Outcomes sought: Child health status, neonatal mortality, retention in treatment, and reduced use of substances Outcomes* of included studies relevant to this report:
*GRADE level of evidence reported per outcome Follow-up: 15wks |
Klimas, 201924 Canada Funding: US National Institutes of Health (R25DA037756) | Study designs sought: RCTs Studies included: 4 RCTs Included studies of relevance to this report: 4 RCTs (3 of which were crossover RCTs), all of which were used in quantitative meta-analyses | Population sought/included/relevant to this report: Adults with OUD, according to DSM IV (N=471) treated in outpatient settings Mean age, yrs: 33.1 Female sex (3/4 studies reported), %: 24.4 | Interventions/comparators sought: SROM (with or without psychosocial intervention)/Other medications Interventions of included studies relevant to this report: SROM Mean dose, mg/day: 506.8 Comparators of included studies relevant to this report: Methadone Mean dose, mg/day: 67.2 | Outcomes sought/of included studies relevant to this review:
Follow-up, mean (range): 18wks (11 to 24) |
AE = adverse events; DAM = diacetylmorphine; DSM IV = Diagnostic and Statistical Manual of Mental Disorders, 4th edition; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HAT = heroin-assisted therapy; HDM = hydromorphone; MAT = medication-assisted treatment; mo = month(s); n/a = not applicable; N/n = number; NCCMT = National Collaborating Centre for Methods ; NR = not reported; NRS = non-randomized studies; OAT = opioid agonist therapy; OUD = opioid use disorder; QoL = quality of life; RCT = randomized controlled trial; SAE = severe adverse event; SF-12 = 12-item Short Form; SF-36 = 36-item Short Form; SR = systematic review; SROM = sustained-release oral morphine; wk = week(s); yr = year(s).
Table 4: Characteristics of Included Reports of RCT Data
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Oviedo-Joekes, 201928 Canada Funding: NAOMI trial: Canadian Institutes of Health Research, Canada Foundation for Innovation, Canada Research Chairs Program, University of British Columbia, Providence Health Care, the University of Montreal, Centre de Recherche et Aide aux Narcomanes, the Government of Quebec, Vancouver Coastal Health, and BC Centre for Disease Control SALOME trial: Canadian Institutes of Health Research, Providence Health Care, Inner Change Foundation, Providence Health Care Research Institute, St. Paul’s Hospital Foundation and Vancouver Coastal Health | Secondary analyses of data taken from 2 RCTs and an observational cohort study* *N.B. only some data from the 2 RCTs (SALOME trial32 and NAOMI trial44) were eligible for inclusion in this report i.e., relevant data from the NAOMI trial did not include information on the comparator arm (which used methadone as the comparison and was therefore not able to answer the research question posed in the analyses i.e., HDM vs. DAM); data from the observational cohort study was ineligible for inclusion in this report | Adults with OUD not sufficiently benefiting from conventional treatment (i.e., methadone, buprenorphine) Intervention group, n pt: 216 Comparator group, n pt: 124 | Intervention: 3-day induction protocol for injectable DAM with 1-3 injections administered per day Comparator: 3-day induction protocol for injectable HDM with 1-3 injections administered per day (SALOME trial only) | Outcomes:
Follow-up: Post-each injection, for 5 to 10 minutes and 15 to 30 minutes, respectively, per day of induction |
Oviedo-Joekes, 201829 Canada Funding: Canadian Institutes of Health Research (MCT-103817), Providence Health Care, Inner Change Foundation, Providence Health Care Research Institute, St. Paul’s Hospital Foundation and Vancouver Coastal Health | Secondary analyses of data taken from 1 double-blind, phase III non-inferiority RCT (SALOME trial)32 | Adults with OUD who self-identified as Indigenous and were not sufficiently benefiting from conventional treatment (i.e., methadone, buprenorphine) Intervention group, n pt: 32 Comparator group, n pt: 30* Mean age (SD): 40.89 (9.22) Proportion female (%): 46.77 | Intervention: Injectable HDM (no other details reported in this paper) Comparator: DAM (no other details reported in this paper) | Outcomes:
Follow-up: 6 mo |
*1pt died in the comparator group during the study and is therefore only included in the baseline assessments | ||||
Demaret, 201630 Belgium Funding: Federal Minister of Social Affairs and Public Health (80%); the City and the University of Liège (proportion NR) | Extended follow-up of 1 open-label RCT | Adults with OUD who have not benefited from drug treatment Intervention group, n pt: 31 Comparator group, n pt: 30 | Intervention: DAM (12 mo) followed by the most appropriate non-HAT Comparator: Oral methadone | Outcomes:
Follow-up: 3 mo (i.e., extended f/u, following 12 mo of f/u in the protocol-specified trial, rendering a total of 15 mo of follow-up data reported for relevant outcomes) |
AE = adverse event(s); BC = British Columbia; DAM = diacetylmorphine; f/u = follow-up; HDM = hydromorphone; mo = month(s); N/n = number; NAOMI = North American Opiate Medication Initiative; NR = not reported; OUD = opioid use disorder; pt = patient(s); RCT = randomized controlled trial; SAE = severe adverse event; SALOME = Study to Assess Long-term Opioid Maintenance Effectiveness.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Reports Including Overviews, Systematic Reviews, and/or Primary Studies Using AMSTAR 219
Strengths | Limitations |
|---|---|
Moazen-Zadeh, 202121 | |
|
|
Minozzi, 202022 | |
|
|
NCCMT, 202023 (No Relevant Studies Included) | |
|
|
Klimas, 201924 | |
|
|
Smart, 201825 | |
|
|
Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726 | |
|
|
Chou, 201627 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; mo = month(s); NCCMT = National Collaborating Centre for Methods and Tools; PICOS = population, intervention, comparator, outcome, study design; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review.
Table 6: Strengths and Limitations of Reports of RCT Data Using the Downs and Black Checklist20
Strengths | Limitations |
|---|---|
Oviedo-Joekes, 201928 | |
Reporting: The hypothesis, main outcomes and findings are clearly described Internal validity (bias):
Internal validity (confounding):
| Reporting:
External validity: Insufficient information provided to assess external validity Internal validity (confounding): Insufficient information provided describing randomization methods, adjustment for confounding and patient loss to follow-up Study Power: Not mentioned |
Oviedo-Joekes, 201829 | |
Reporting: The hypothesis, main outcomes, confounders, estimates of random variability and patient loss to follow-up are clearly described Internal validity (bias):
| Reporting:
External validity: • Insufficient information provided to assess external validity Internal validity (confounding): Insufficient information provided describing randomization methods, adjustment for confounding and pt loss to follow-up Study Power: Not mentioned |
Demaret, 201630 | |
Reporting: The main outcomes are clearly described Internal validity (bias):
Internal validity (confounding):
| Reporting:
External validity: Insufficient information provided to assess external validity Internal validity (bias):
Internal validity (confounding): Insufficient information provided describing randomization methods and adjustment for confounding Study Power: Not mentioned |
pt = patient(s); RCT = randomized controlled trial.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Summary of Findings Describing Treatment Retention
SROM
Main Study Findings
Chou, 201627
Treatment retention (reported narratively only):
SROM vs. other MAT medications (not specified): SROM reported as being at least similar to other MAT medications
SROM vs. Methadone: No significant differences reported between groups
Minozzi, 202022[
Treatment retention, n/N patients dropped out (reported narratively only; Grading of Recommendations, Assessment, Development and Evaluations [GRADE] level of evidence = LOW)
SROM: 0/24
Methadone: 0/24
Difference between groups: not reported (NR)
Klimas, 201924
Treatment retention at the end of the assessment period, n/N patients, meta-analyses
SROM vs. Methadone (4 trials representing 745 patients, inconsistency (a measure of heterogeneity across studies in meta-analyses) [I2] = 18%): SROM
331/376: Methadone
338/369: Difference between groups, risk ratio/relative risk (RR) (95% confidence interval [CI]), random-effects model
0.98 (0.94 to 1.02)
P = 0.30 (not significant [NS])
Relevant Authors’ Conclusion(s)
“There is not enough evidence to make conclusions for the comparison between methadone and slow-release morphine. Overall, the body of evidence is too small to make firm conclusions about the equivalence of the treatments compared. There is still a need for randomised controlled trials of adequate sample size comparing different maintenance treatments.”22 (p. 2)
“Meta-analysis of existing randomised trials suggests SROM may be generally equal to methadone in retaining patients in treatment and reducing heroin use... The methodological quality of the included RCTs was low-to-moderate.”24 (p. 1)
Oral HDM
Main Study Findings
No evidence identified.
Injectable HDM and/or DAM (HAT)
Main Study Findings
Smart, 201825
Treatment retention (reported in 1 included OV and 4 included SRs)
Findings from 1 OV of SRs (general conclusion)
HAT vs. other conventional treatments (primarily methadone)
No significant difference between groups (no other detail reported)
Findings from 1 OV of SRs (1 relevant SR included with meta-analysis), RR (95% CI)
HAT vs. Methadone + inhalable heroin
1.27 (1.11 to 1.46) (favours methadone + inhalable heroin)
HAT vs. Methadone + injectable heroin
1.17 (0.99 to 1.38) (favours methadone + inhalable heroin)
Injectable HAT vs. Methadone alone
0.35 (0.21 to 0.59) (favours injectable HAT)
Findings from 1 SR of RCTs (8 relevant RCTs included describing 2,032 participants), results reported narratively only
Injectable heroin treatment vs. traditional medication treatment (not specified)
Included RCTs generally favoured HAT but evidence was deemed to be of low quality
Findings from 1 SR of RCTs (6 relevant RCTs included with meta-analysis performed), RR (95% CI)
Injectable heroin vs. oral methadone
1.44 (1.16 to 1.79), favours injectable heroin
Findings from 1 SR of RCTs (N of relevant RCTs included NR with meta-analysis performed), RR (95% CI)
Injectable heroin vs. oral methadone
1.37 (1.03 to 1.83), favours injectable heroin
Findings from 1 SR of RCTs (N of relevant RCTs included NR), results reported narratively only
HAT vs. oral methadone
An association between HAT and treatment retention was reported
Oviedo-Joekes, 201829
Treatment retention (61 patients)
Receipt of study medication for ≥28 days, % patients (95% CI)
HDM: 75 (60 to 90)
DAM: 72 (56 to 89)
Difference between groups, mean difference (DAM less HDM) (95% CI)
-3 (-25 to 20)
P > 0.05 (NS)
Relevant Authors’ Conclusion(s)
"... supervised injectable HAT with optional oral methadone can offer benefits over oral methadone alone for treating opioid use disorder (OUD) among individuals who have tried traditional treatment modalities, including methadone, multiple times but are still injecting heroin. The strongest and most consistent effects across studies are shown for reducing illicit heroin use and improving treatment retention."25 (p. vi)
"While injectable DAM has shown to be effective [6,20], it is not currently licensed in many countries, including Canada and the United States. This study shows that hydromorphone could be an effective alternative. Expanding the supervised model of care with injectable hydromorphone (and DAM when available) offers an opportunity to integrate additional wholistic and culturally safe approaches to treatment to meet the needs of Indigenous patients."29 (p. 144)
Fentanyl Patches and/or Fentanyl Buccal Tablets
Main Study Findings
No evidence identified.
Summary of Findings Describing Use of Illicit Opioids and/or Other Drugs of Abuse
SROM
Main Study Findings
Chou, 201627
Use of substances (reported narratively only)
SROM vs. Methadone: No significant differences reported between groups
Minozzi, 202022
Use of heroin in the 3rd trimester (GRADE level of evidence = LOW)
SROM, n/N patients: 5/24
Methadone, n/N patients: 12/24
Difference between groups, RR (95% CI)
2.40 (1.00 to 5.77) (favours SROM)
P = 0.05
Use of other drugs of abuse, mean % of negative urine tests (GRADE level of evidence = NR)
Cocaine
SROM: 90
Methadone: 95
Difference between groups: NR
Benzodiazepines
SROM: 89
Methadone: 54
Difference between groups: NR
Klimas, 201924
Heroin use (n of positive drug urine tests per participant), meta-analyses
SROM vs. Methadone (3 trials representing 677 patients, I2 = 50%)
SROM: 70
Methadone: 75
Difference between groups, RR (95% CI), random-effects model
0.96 (0.61 to 1.52)
P = 0.86 (NS)
Relevant Authors’ Conclusion(s)
“Oral slow-release morphine may be superior to methadone for abstinence from heroin use during pregnancy (RR 2.40, 95% CI 1.00 to 5.77, one study, 48 participants, low-quality evidence). In the comparison between methadone and slow-release morphine, no side effects were reported for the mother...”22 (p. 2)
“Meta-analysis of existing randomised trials suggests SROM may be generally equal to methadone in retaining patients in treatment and reducing heroin use... The methodological quality of the included RCTs was low-to-moderate.”24 (p. 1)
Oral HDM
Main Study Findings
No evidence identified.
Injectable HDM and/or DAM (HAT)
Main Study Findings
Smart, 201825
Illicit substance use
Findings from 1 OV of SRs (general conclusion)
HAT vs. other conventional treatments (primarily methadone): Limited evidence to support any difference between groups (no other detail reported)
Findings from 4 SRs of RCTs (N of relevant RCTs included NR), results reported narratively only
HAT vs. methadone: All 4 SRs reported HAT to be more effective than methadone
Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726
Illicit substance use
HDM vs. DAM (1 RCT)
Street opioid/heroin use measured by urine markers, reported narratively only: HDM not inferior to DAM
DAM vs. other treatments (not specified) (1 RCT)
Street heroin use, measure NR, reported narratively only: Improved outcome in DAM group
Oviedo-Joekes, 201829
Use of illicit/street heroin/opioids (61 patients)
Days of illicit heroin use, mean (95% CI)
HDM: 4.56 (1.89 to 7.44)
DAM: 1.78 (0.46 to 3.90)
Difference between groups, mean difference (DAM less HDM) (95% CI)
-2.77 (-6.02 to 0.16)
P > 0.05 (NS)
Days using street-acquired opioids, mean (95% CI)
HDM: 5.10 (2.39 to 8.16)
DAM: 3.41 (1.14 to 6.53)
Difference between groups, mean difference (DAM less HDM) (95% CI)
-1.70 (-5.66 to 2.29)
P > 0.05 (NS)
Urine positive for street heroin, % patients (95% CI)
HDM: 32 (15 to 48)
DAM: 14 (1 to 26)
Difference between groups, mean difference (DAM less HDM) (95% CI)
-18 (-39 to 3)
P > 0.05 (NS)
Days of cocaine use, mean (95% CI)
HDM: 9.29 (5.98 to 13.13)
DAM: 5.83 (3.43 to 8.54)
Difference between groups, mean difference (DAM less HDM) (95% CI)
-3.46 (-7.87 to -0.10) (favours DAM)
P < 0.05
Demaret, 201630
Use of illicit substances (61 patients)
Self-reported use of street heroin at 3 mo post-trial (15 mo total f/u), mean* d
DAM: 14*
Methadone: 17*
Difference between groups, baseline to 15 mo follow-up:
Difference: NR (favours DAM)
P = 0.00094
Self-reported use of cocaine at 3 mo post-trial (15 mo total f/u), mean* d
DAM: 2*
Methadone: 3*
Difference between groups, baseline to 15 mo follow-up: P = 0.83 (NS)
Urinalysis for heroin use at 3 mo post-trial (15 mo total f/u), mean level of meconin per group (unit of measurement not specified)
DAM: NR
Methadone: NR
Difference between groups, baseline to 15 mo follow-up: P = 0.55 (NS)
*The type of summary statistic used was not reported; means were assumed from the reported use of ANOVA for the analyses
Relevant Authors’ Conclusion(s)
"... supervised injectable HAT with optional oral methadone can offer benefits over oral methadone alone for treating opioid use disorder (OUD) among individuals who have tried traditional treatment modalities, including methadone, multiple times but are still injecting heroin. The strongest and most consistent effects across studies are shown for reducing illicit heroin use and improving treatment retention." (p. vi)25
“As opioid-related harms increase in the population, many have called for additional treatment options for opioid use disorder. The current evidence supports siOAT as a second-line treatment. Recent policy changes in Canada allow physicians to apply for permission to prescribe DAM and permit jurisdictions to request the import of medical DAM for urgent public health reasons. These changes may facilitate the availability of this treatment option. Further evaluation of the emerging practice with siOAT in Canada can assist with understanding implementation issues and informing program decisions."26 (p. 8)
"While injectable DAM has shown to be effective [6,20], it is not currently licensed in many countries, including Canada and the United States. This study shows that hydromorphone could be an effective alternative. Expanding the supervised model of care with injectable hydromorphone (and DAM when available) offers an opportunity to integrate additional wholistic and culturally safe approaches to treatment to meet the needs of Indigenous patients."29 (p. 144)
“HAT is more effective than OMT for decreasing street heroin use for heroin-dependent individuals who pursue street heroin use in spite of a current or previous OMT. However, three months after a predetermined end of HAT (i.e., without a spontaneous demand by the patient), the use of street heroin increased again to reach levels very close to those observed in the control group. Therefore, HAT should be offered as an open-ended treatment as recommend [sic] by the WHO for other opioid treatment (World Health Organization, 2010) and the end of treatment should be a clinical decision based on the evolution of the patient.”30 (p. 74)
Note: siOAT means supervised injectable opioid agonist therapy.
Fentanyl Patches and/or Fentanyl Buccal Tablets
Main Study Findings
No evidence identified.
Summary of Findings Describing Mental Health
SROM
Main Study Findings
Moazen-Zadeh, 202121
Overall mental health symptomatology, meta-analyses of composite scores
SROM vs. Methadone (1 trial)
Sample size
SROM: 123
Methadone: 118
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.124 (0.129), -0.963 to 0.335
P = 0.335 (NS)
Random-effects model, standardized mean difference (standard error), 95% CI
-0.124 (0.129), -0.963 to 0.335
P = 0.335 (NS)
Mental health quality of life, meta-analyses of composite scores
SROM vs. Methadone (1 trial)
Sample size
SROM: 27
Methadone: 29
Difference between groups (NS)
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.350 (0.269), -0.878 to 0.178
P = 0.194 (NS)
Random-effects model, standardized mean difference (standard error), 95% CI
-0.350 (0.269), -0.878 to 0.178
P = 0.194 (NS)
Klimas, 201924
Mental Health
Mental health and social functioning (1 RCT representing 9 patients), BASIS-32 Behaviour and Symptom Identification Scale
SROM: NR
Methadone: NR
Difference between groups: No significant difference between groups was reported
Depression (1 RCT representing 55 patients), measure/scale NR
SROM: Drop from 17.84 at baseline to 10.51 at day 21
Methadone: NR
Difference between groups: P < 0.001 (favours SROM)
Anxiety (1 RCT representing 55 patients), State Trait Anxiety (described as being presented as charts only in the primary study paper)
SROM: NR
Methadone: NR
Difference between groups: P < 0.01 (favours SROM)
Adverse mental symptoms (1 RCT representing 157 patients), measure NR (standard deviation [SD])
SROM: 0.61 (0.56)
Methadone: 0.68 (0.60)
Difference between groups: P < 0.01 (favours SROM)
Relevant Authors’ Conclusions
"Opioid agonist treatments used for the treatment of opioid use disorder improve mental health independent of psychosocial services.”21 (p. 280)
“Overall, it appears that mental health symptomatology tends to improve in treatments with major opioid agonists, after accounting for the potential role of psychosocial interventions...”21 (p. 300)
No other conclusions particular to mental health reported.
Oral HDM
Main Study Findings
No evidence identified.
Injectable HDM and/or DAM (HAT)
Main Study Findings
Smart, 201825
Mental Health
Findings from 1 SR of RCTs (data from 1 relevant RCT included), results reported narratively only
Supervised injectable heroin vs. methadone
Depression and psychoticism, SCL-90-R: Significantly favours supervised injectable heroin, P = 0.002
Findings from 1 SR of RCTs (N of relevant RCTs included NR), results reported narratively only
Findings from 1 RCT of supervised injectable heroin vs. other conventional drug treatments
Mental health quality of life, “difference in SD units” (p. 27) on SF-36 scale (95% CI) (not otherwise explained/described): 0.58 (0.07 to 1.10), described as favouring supervised injectable heroin
Suicide attempts: No difference between groups
Severe depression (measure NR): No difference between groups
Cognitive problems (measure NR): No difference between groups
Problems controlling violent behaviour (measure NR): No difference between groups
Findings from 2 RCTs of supervised injectable heroin vs. methadone
Mental health: Significantly improved in the supervised injectable heroin group
Findings from 1 RCT of supervised injectable heroin vs. methadone:
Mental health: No difference between groups
Moazen-Zadeh, 202121
Depressive symptoms, meta-analyses of composite scores
DAM vs. HDM (1 trial)
Sample size
DAM: 97
HDM: 95
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.173 (0.145), -0.457 to 0.110
P = 0.230 (NS)
Random-effects model, standardized mean difference (standard error), 95% CI
-0.173 (0.145), -0.457 to 0.110
P = 0.230 (NS)
DAM vs. Methadone (2 trials, I2 = 32.448)
Sample size
DAM: 223
Methadone: 253
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.220 (0.092), -0.400 to -0.039 (favours DAM)
P = 0.017
Random-effects model, standardized mean difference (standard error), 95% CI
-0.255 (0.138), -0.525 to 0.015
P = 0.064 (NS)
Overall mental health symptomatology, meta-analyses of composite scores
DAM vs. HDM (1 trial)
Sample size:
DAM: 97
HDM: 95
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.154 (0.145), -0.437 to 0.129
P = 0.287 (NS)
Random-effects model, standardized mean difference (standard error), 95% CI
-0.154 (0.145), -0.437 to 0.129
P = 0.287 (NS)
DAM vs. Methadone (4 trials, I2 = 0.00)
Sample size
DAM: 736
Methadone: 738
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.233 (0.052), -0.336 to -0.131 (favours DAM)
P < 0.001
Random-effects model, standardized mean difference (standard error), 95% CI
-0.233 (0.052), -0.336 to 0.131 (favours DAM)
P < 0.001
Addiction severity, meta-analyses of composite scores
DAM vs. HDM (1 trial)
Sample size
DAM: 97
HDM: 92
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.070 (0.146), -0.355 to 0.216
P = 0.633 (NS)
Random-effects model, standardized mean difference (standard error), 95% CI
-0.070 (0.146), -0.355 to 0.216
P = 0.633 (NS)
DAM vs. Methadone (4 trials, I2 = 50.657)
Sample size
DAM: 748
Methadone: 756
Fixed-effects model, standardized mean difference (standard error), 95% CI
-0.148 (0.052), -0.249 to -0.046 (favours DAM)
P = 0.004
Random-effects model, standardized mean difference (standard error), 95% CI
-0.189 (0.086), -0.358 to -0.021 (favours DAM)
P = 0.028
Mental health quality of life, meta-analyses of composite scores
DAM vs. Methadone (2 trials, I2 = 0.00)
Sample size
DAM: 57
Methadone: 87
Fixed-effects model, standardized mean difference in scores (standard error), 95% CI
0.085 (0.175), -0.257 to 0.428
P = 0.624 (NS)
Random-effects model, standardized mean difference (standard error), 95% CI
0.085 (0.175), -0.257 to 0.428
P = 0.624 (NS)
Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726
Mental Health
DAM vs. other treatments (not specified) (1 RCT)
SF-12 score/Addiction Severity Index Psychiatric Composite score, reported narratively only: Improved outcomes observed in DAM group
Oviedo-Joekes, 201829
Mental Health (61 patients)
MAP psychological health score (higher score = poorer health), mean (95% CI)
HDM: 8.57 (5.41 to 11.73)
DAM: 8.73 (5.45 to 12.00)
Difference between groups, mean difference (DAM less HDM) (95% CI) (NS)
0.15 (-4.32 to 4.63)
P > 0.05
Demaret, 201630
Mental Health (61 patients)
Symptom Checklist (SCL-90-R) at 3 mo post-trial (15 mo total f/u), mean of total scores
DAM: 71
Methadone: 94
Difference between groups, baseline to 15 mo follow-up: P = 0.056 (NS)
Relevant Authors’ Conclusions
"Opioid agonist treatments used for the treatment of opioid use disorder improve mental health independent of psychosocial services.”21 (p. 280)
“Overall, it appears that mental health symptomatology tends to improve in treatments with major opioid agonists, after accounting for the potential role of psychosocial interventions, and this improvement favors DAM-assisted treatment in comparison to methadone.”21 (p. 300)
“As opioid-related harms increase in the population, many have called for additional treatment options for opioid use disorder. The current evidence supports siOAT as a second-line treatment. Recent policy changes in Canada allow physicians to apply for permission to prescribe DAM and permit jurisdictions to request the import of medical DAM for urgent public health reasons. These changes may facilitate the availability of this treatment option. Further evaluation of the emerging practice with siOAT in Canada can assist with understanding implementation issues and informing program decisions."26 (p. 8)
"While injectable DAM has shown to be effective [6,20], it is not currently licensed in many countries, including Canada and the United States. This study shows that hydromorphone could be an effective alternative. Expanding the supervised model of care with injectable hydromorphone (and DAM when available) offers an opportunity to integrate additional wholistic and culturally safe approaches to treatment to meet the needs of Indigenous patients."29 (p. 144)
Fentanyl Patches and/or Fentanyl Buccal Tablets
Main Study Findings
No evidence identified.
Summary of Findings Describing Physical and/or Mental Health
SROM
Main Study Findings
No evidence identified.
Oral HDM
Main Study Findings
No evidence identified.
Injectable HDM and/or DAM (HAT)
Main Study Findings
Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726
Physical/Mental Health
DAM vs. Methadone (1 RCT)
SF-36 scores, findings reported narratively only: No benefit observed in DAM group over methadone group
Oviedo-Joekes, 201829
Physical and Mental Health (61 patients)
MAP physical health score (higher score = poorer health), mean (95% CI)
HDM: 12.92 (10.02 to 15.82)
DAM: 11.61 (8.55 to 14.66)
Difference between groups, mean difference (DAM less HDM) (95% CI) (NS)
-1.31 (-5.45, 2.83)
P > 0.05
Demaret, 201630
Physical Health (61 patients)
Maudsley Addiction Profile, Health Symptoms Scale (MAP-HSS) at 3 mo post-trial (15 mo total f/u), mean of total scores
DAM: 13
Methadone: 18
Difference between groups, baseline to 15 mo follow-up: P = 0.0195 (favours DAM)
Relevant Authors’ Conclusion(s)
“As opioid-related harms increase in the population, many have called for additional treatment options for opioid use disorder. The current evidence supports siOAT as a second-line treatment. Recent policy changes in Canada allow physicians to apply for permission to prescribe DAM and permit jurisdictions to request the import of medical DAM for urgent public health reasons. These changes may facilitate the availability of this treatment option. Further evaluation of the emerging practice with siOAT in Canada can assist with understanding implementation issues and informing program decisions."26 (p. 8)
"While injectable DAM has shown to be effective [6,20], it is not currently licensed in many countries, including Canada and the United States. This study shows that hydromorphone could be an effective alternative. Expanding the supervised model of care with injectable hydromorphone (and DAM when available) offers an opportunity to integrate additional wholistic and culturally safe approaches to treatment to meet the needs of Indigenous patients."29 (p. 144)
Fentanyl Patches and/or Fentanyl Buccal Tablets
Main Study Findings
No evidence identified.
Summary of Findings Describing Quality of Life
SROM
Main Study Findings
Klimas, 201924
Quality of Life (Lancashire Quality of Life Profile)
Scores (type of summary statistic NR) on subscales of the Lancashire Quality of Life Profile (higher score is more favourable), 1 RCT representing 240 patients
Family
SROM: 3.4
Methadone: 5.8
Difference between groups (study includes a 3-way comparison with buprenorphine): P < 0.05 (favours methadone)
Finances
SROM: 2.6
Methadone: 4.4
Difference between groups (study includes a 3-way comparison with buprenorphine): P < 0.001 (favours methadone)
Overall satisfaction
SROM: 4.1
Methadone: 5.3
Difference between groups (study includes a 3-way comparison with buprenorphine) (favours methadone): P < 0.001 (favours ethadone)
Relevant Authors’ Conclusion(s)
"Unless future trials report contradictory findings, the public health crisis presented by illicitly manufactured opioids,2 and the known limitations of existing agonist therapies,14 34 these data should inform future investigations of SROM as a therapeutic tool among people undergoing treatment for OUD."24 (p. 7)
No other conclusions drawn specific to QoL.
Oral HDM
Main Study Findings
No evidence identified.
Injectable HDM and/or DAM (HAT)
Main Study Findings
Smart 201825
Quality of life
Findings from 1 OV of SRs (general conclusion)
HAT vs. other conventional treatments (primarily methadone): Limited evidence to support any difference between groups (no other detail reported)
Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726
Health-related quality of life
DAM vs. Methadone (1 RCT)
Measure not reported, findings reported narratively only: Higher (i.e., more favourable) in DAM group than methadone group
Relevant Authors’ Conclusion(s)
"... supervised injectable HAT with optional oral methadone can offer benefits over oral methadone alone for treating opioid use disorder (OUD) among individuals who have tried traditional treatment modalities, including methadone, multiple times but are still injecting heroin." (p. vi)25
“As opioid-related harms increase in the population, many have called for additional treatment options for opioid use disorder. The current evidence supports siOAT as a second-line treatment. Recent policy changes in Canada allow physicians to apply for permission to prescribe DAM and permit jurisdictions to request the import of medical DAM for urgent public health reasons. These changes may facilitate the availability of this treatment option. Further evaluation of the emerging practice with siOAT in Canada can assist with understanding implementation issues and informing program decisions."26 (p. 8)
Fentanyl Patches and/or Fentanyl Buccal Tablets
Main Study Findings
No evidence identified.
Summary of Findings Describing Adverse Events and Severe Adverse Events
SROM
Main Study Findings
Minozzi, 202022
Side effects, n patients (reported qualitatively only; GRADE level of evidence = LOW)
SROM: 0/24
Methadone: 0/24
Difference between groups: NR
Klimas, 201924
Side effects, n patients (reported qualitatively only; GRADE level of evidence = LOW)
AEs (1 RCT representing 157 patients), % patients
SROM: 81
Methadone: 79
Difference between groups: P = 0.62 (NS)
Relevant Authors’ Conclusion(s)
“Oral slow-release morphine may be superior to methadone for abstinence from heroin use during pregnancy (RR 2.40, 95% CI 1.00 to 5.77, one study, 48 participants, low-quality evidence). In the comparison between methadone and slow-release morphine, no side effects were reported for the mother... There is not enough evidence to make conclusions for the comparison between methadone and slow-release morphine. Overall, the body of evidence is too small to make firm conclusions about the equivalence of the treatments compared. There is still a need for randomised controlled trials of adequate sample size comparing different maintenance treatments.”22 (p. 2)
Oral HDM
Main Study Findings
No evidence identified.
Injectable HDM and/or DAM (HAT)
Main Study Findings
Smart, 201825
SAEs (reported in 3 SRs describing 7 relevant RCTs)
SAEs likely related to study medication, supervised injectable heroin vs. methadone
Findings from 1 SR w/MA of RCTs (N of RCTs included NR), RR (95% CI): 4.99 (1.66 to 14.99) (favours methadone)
Findings from 1 SR w/MA of RCTs (N of RCTs included NR), RR (95% CI): 13.50 (2.55 to 71.53) (favours methadone)
All SAEs, HAT vs. methadone
Findings from 1 SR w/MA of RCTs (N of RCTs included NR), RR (95% CI): 1.61 (1.11 to 2.33) (favours methadone)
Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726
SAEs
HDM vs. DAM (1 RCT)
N SAEs:
HDM: 5
DAM: 24
Difference between groups: NR
Oviedo-Joekes, 201928
AEs and SAEs during induction
Somnolence, n events (rate per 100 injections)
DAM: 34 (1.933)
HDM: 6 (0.563)
Difference between groups: NR
Overdose, n events (rate per 100 injections)
DAM: 4 (0.227)
HDM: 1 (0.094)
Difference between groups: NR
Post-injection reaction + injection site pruritis (reported for SALOME trial patients only)
N events (rate per 100 injections)
DAM (n patients = 102): 7 (0.784)
HDM (n patients = 100): 5 (0.588)
Difference between groups: NR
Relevant Authors’ Conclusion(s)
“As opioid-related harms increase in the population, many have called for additional treatment options for opioid use disorder. The current evidence supports siOAT as a second-line treatment. Recent policy changes in Canada allow physicians to apply for permission to prescribe DAM and permit jurisdictions to request the import of medical DAM for urgent public health reasons. These changes may facilitate the availability of this treatment option. Further evaluation of the emerging practice with siOAT in Canada can assist with understanding implementation issues and informing program decisions."26 (p. 8)
"This study suggests that a 3-day protocol allowed patients to safely reach high doses in a timely manner. Moreover, the few overdoses that occurred in the context of thousands of injections were safely treated onsite. Reaching and treating patients that have been injecting opioids for a long period of time requires approaches that ensure patient engagement by adjusting to their needs. As noted earlier, despite strong and compelling evidence, iOAT remains inaccessible outside of a few select settings in Canada and Europe. The findings of this study suggest that safety is not an evidence-based barrier to the implementation of treatment with injectable hydromorphone and diacetylmorphine."28 (p. 360)
Fentanyl Patches and/or Fentanyl Buccal Tablets
Main Study Findings
No evidence identified.
Summary of Findings Describing Mortality
SROM
Main Study Findings
No evidence identified.
Oral HDM
Main Study Findings
No evidence identified.
Injectable HDM and/or DAM (HAT)
Main Study Findings
Smart, 201825
Mortality (reported in 1 OV of SRs and 3 SRs)
Findings from 1 OV of SRs (general conclusion)
HAT vs. other conventional treatments (primarily methadone)
Limited evidence to support any difference between groups (no other detail reported)
HAT vs. methadone
Findings from 1 SR w/MA of RCTs (5 RCTs included describing 1,573 participants), RR (95% CI)
0.78 (0.32 to 1.89) (NS)
Supervised injectable heroin + optional oral methadone vs. oral methadone only
Findings from 2 SRs w/MA of RCTs (4 RCTs included describing 1,477 participants), RR (95% CI)
0.65 (0.25 to 1.69) (NS)
Demaret, 201630
Mortality
n patients
DAM: 1
Methadone: 0
Difference between groups, baseline to 15 mo follow-up: NR
Relevant Authors’ Conclusion(s)
"All three [SRs] showed an effect that pointed in the direction of a protective effect of HAT, but the differences between treatment and control groups were not statistically significantly [sic]."25 (p. 29-30)
Fentanyl Patches and/or Fentanyl Buccal Tablets
Main Study Findings
No evidence identified.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 7: Overlap in Relevant Systematic Reviews Between Included Reports of an Overview and/or Systematic Reviews
Systematic review citation | Smart, 201825 | Chou 201727 |
|---|---|---|
Ali, 2017 | Yes | No |
Timko, 2016 | Yes | No |
Fingleton, 2015 | Yes | No |
Perry, 2015 | Yes | No |
Strang, 2015 | Yes | No |
Koehler, 2014 | Yes | No |
Ferri, 2013 | No | Yes |
Minozzi, 2013 | No | Yes |
Ferri, 2011 | Yes | No |
Dalsbo, 2010 | Yes | No |
Egli, 2009 | Yes | No |
Amato, 2005 (overview of SRs) | Yes | No |
SR = systematic review.
Table 8: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Moazen-Zadeh, 202121 | Minozzi, 202022 | Klimas, 201924 | Ontario Agency for Health Protection and Promotion (Public Health Ontario), 201726 |
|---|---|---|---|---|
Oviedo-Joekes, 2017a | No | No | No | Yes |
Oviedo-Joekes, 2017b | No | No | No | Yes |
Palis, 2017 | No | No | No | Yes |
Oviedo-Joekes, 2016 | Yes | No | No | Yes |
Demaret, 2015 | Yes | No | No | Yes |
Falcato, 2015 | No | No | No | No |
Metrebian, 2015 | No | No | No | Yes |
Oviedo-Joekes, 2015 | Yes | No | No | No |
Verthein, 2015 | Yes | No | No | No |
Beck, 2014 | Yes | No | Yes | No |
Hammig, 2014 | No | No | No | No |
Blanken, 2012 | No | No | No | Yes |
Marchand, 2011 | No | No | No | Yes |
Reimer, 2011 | Yes | No | No | No |
Soyka, 2011 | No | No | No | Yes |
Verthein, 2011 | No | No | No | Yes |
Eiroa-Orosa, 2010a | No | No | No | Yes |
Eiroa-Orosa, 2010b | No | No | No | Yes |
Haasen, 2010 | No | No | No | Yes |
Karow, 2010 | Yes | No | No | No |
Nosyk, 2010 | No | No | No | Yes |
Oviedo-Joekes, 2010a | No | No | No | Yes |
Oviedo-Joekes, 2010b | No | No | No | Yes |
Schäfer, 2010 | No | No | No | Yes |
Strang, 2010 | Yes | No | No | No |
Haasen, 2009 | No | No | No | Yes |
Lobmann, 2009 | No | No | No | Yes |
Oviedo-Joekes, 2009 | Yes | No | No | Yes |
Perea-Milla, 2009 | No | No | Yes | |
Winklbaur, 2008 | Yes | No | No | No |
Haasen, 2007 | Yes | No | No | No |
Lintzeris, 2006 | Yes | No | No | No |
Giacomuzzi, 2006 | No | No | Yes | No |
March, 2006 | No | No | No | No |
Eder, 2005 | Yes | No | Yes | No |
Van den Brink, 2003 | Yes | No | No | No |
Clark, 2002 | No | No | Yes | No |
Fischer, 1999 | No | Yes | No | No |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca