CADTH Health Technology Review
Lenalidomide, Bortezomib, and Dexamethasone as Induction Therapy Before Autologous Stem Cell Transplant for Multiple Myeloma
Rapid Review
Authors: Sarah Goring, Lory Picheca
Abbreviations
ASCT
autologous stem cell transplantation
BSH
British Society for Haematology
CIBMTR
Center for International Blood and Marrow Transplant Research
CR
complete response
CyBorD
bortezomib-cyclophosphamide-dexamethasone
eGFR
estimated glomerular filtration rate
EHA
European Hematology Association
ESMO
European Society for Medical Oncology
IMiD
immunomodulatory imide drugs
ISS
international staging system
MSAG
Medical and Scientific Advisory Group
NCCN
National Comprehensive Cancer Network
ORR
overall response rate
PR
partial response
RCT
randomized controlled trial
R-ISS
revised international staging system
sCR
stringent complete response
VGPR
very good partial response
RVd
bortezomib-lenalidomide-dexamethasone
Key Messages
One relevant systematic review and network meta-analysis (which included 1 relevant randomized controlled trial), 4 non-randomized studies, and 6 evidence-based guideline reports, representing 5 evidence-based guidelines were identified in this report.
The clinical effectiveness regarding response, relapse, progression-free survival, and overall survival broadly favoured bortezomib-lenalidomide-dexamethasone (RVd) over bortezomib-cyclophosphamide-dexamethasone (CyBorD), although the magnitude and direction of association was not always consistent, and few estimates were statistically significant.
Limited evidence on the safety of RVd relative to CyBorD was found.
No evidence on the cost-effectiveness of RVd as induction therapy before autologous stem cell transplant for multiple myeloma was found.
Among the 5 included guidelines, 3 specifically recommend RVd as a first option for induction therapy among transplant-eligible newly diagnosed multiple myeloma patients, and 2 recommend more broadly defined 3-drug induction regimens that include RVd.
Context and Policy Issues
Multiple myeloma is a hematological cancer characterized by uncontrolled proliferation and improper function of plasma cells in the bone marrow. Build-up of these plasma cells can lead to clinical manifestations including bone pain, mineral imbalances (e.g., calcium), renal insufficiency, anemia, and infections. Although multiple myeloma is considered a rare disease, approximately 3,800 Canadians will be diagnosed in 2021 with the majority of new cases among men; age-standardized incidence rates in Canada are projected to be 10.9 per 100,000 males and 6.2 per 100,000 females in 2021.1
Recent estimates suggest that median overall survival for multiple myeloma is approximately 6 years, although the disease is heterogeneous, and survival can range from a few months to over 10 years.2,3 The International Staging System (ISS) risk stratification algorithm categorizes disease according to prognostic factors including tumour burden, renal function, and tumour microenvironment (measured via serum Beta2-microglobulin and serum albumin levels); higher stage is associated with worse prognosis.3 Molecular classification based on cytogentics is also prognostic, and patients are categorized as standard risk or high-risk according to chromosomal abnormalities. The more recently developed revised ISS (R-ISS) combines ISS stage with molecular cytogenics and serum lactate dehydrogenase levels (a marker for disease aggressiveness) into an updated prognostic staging system.4
Survival among individuals with multiple myeloma has improved over the past few decades, largely owing to improvements in disease management; in Canada, 5-year survival increased from 26% in the early 1990s to 50% between 2015 and 2017.1 Autologous stem cell transplantation (ASCT) represents a current standard of care for newly diagnosed patients who are transplant-eligible.5 Prior to ASCT, patients are given induction therapy to reduce the number of tumour cells in the bone marrow and peripheral blood. Novel drugs such as proteasome inhibitors (e.g., bortezomib) and/or immunomodulatory imide drugs (IMiDs) (e.g., thalidomide and lenalidomide) have demonstrated improved efficacy over older chemotherapy regimens and have been adopted into current clinical practice.6
The triplet therapy combination of botezomib, lenalidomide, and dexamethasone (RVd) is currently considered the standard of care in the US for induction therapy among newly diagnosed, transplant-eligible patients with multiple myeloma.2 A Health Canada Notice of Compliance does not exist for RVd induction therapy. While generic versions of lenalidomide, bortezomib and dexamethasone are available, CADTH’s Reimbursement Review process is not well suited for products associated with multiple manufacturers. Instead of RVd, current local standard of care for transplant-eligible multiple myeloma in Ontario and other provinces involves bortezomib, cyclophosphamide, and dexamethasone (CyBorD).7
The purpose of this report is to summarize the available evidence on the clinical effectiveness, safety, cost-effectiveness of RVd relative to CyBorD, along with evidence-based guidelines regarding the use of RVd for induction therapy among newly diagnosed transplant-eligible patients with multiple myeloma.
Research Questions
What is the clinical effectiveness of lenalidomide in combination with bortezomib and dexamethasone as induction therapy before autologous stem cell transplant for multiple myeloma?
What is the cost-effectiveness of lenalidomide in combination with bortezomib and dexamethasone as induction therapy before autologous stem cell transplant for multiple myeloma?
What are the evidence-based guidelines for treating patients requiring induction therapy before autologous stem cell transplant for multiple myeloma?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Library, the University of York Centre for Reviews and Dissemination (CRD) databases, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were multiple myeloma, autologous transplantation and induction chemotherapy. For question 2, search filters were applied to limit retrieval to economic studies and for question 3, search filters were applied to limit retrieval to guidelines. Comments, newspaper articles, editorials, and letters were excluded. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2016 and November 14, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with newly diagnosed myeloma (excluding smouldering myeloma) intended to receive autologous stem cell transplants who require induction therapy. |
Intervention | Induction therapy before transplant with lenalidomide in combination with bortezomib and dexamethasone (any dose; pulsed or non-pulsed). |
Comparator | Q1 to Q2: Induction therapy before transplant with cyclophosphamide, bortezomib, and dexamethasone. Q3: Not applicable. |
Outcomes | Q1: Clinical effectiveness (e.g., Response rate, complete response vs. partial response, time to progression post-transplant, progression-free survival, overall survival, duration of response, quality of life, safety [i.e., adverse events of ≥ grade 3 and grade 4, serious adverse events, deaths]). Q2: Cost-effectiveness outcomes (e.g., cost per quality-adjusted life-years gained, incremental cost-effectiveness ratios). Q3: Recommendations regarding best practices for patients requiring induction therapy for transplant-eligible myeloma. |
Study designs | Health technology assessments and systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, evidence-based guidelines. |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or they were duplicate publications. Health technology assessments, systematic reviews, randomized controlled trials (RCT), non-randomized studies, and economic evaluations were excluded if they were published before 2016. Guidelines published before 2019 were also excluded. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Single-arm and before-and-after studies involving RVd but not CyBorD were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for systematic reviews, the “Questionnaire to assess the relevance and credibility of a network meta-analysis”9 for network meta-analyses, the Downs and Black checklist10 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument11 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
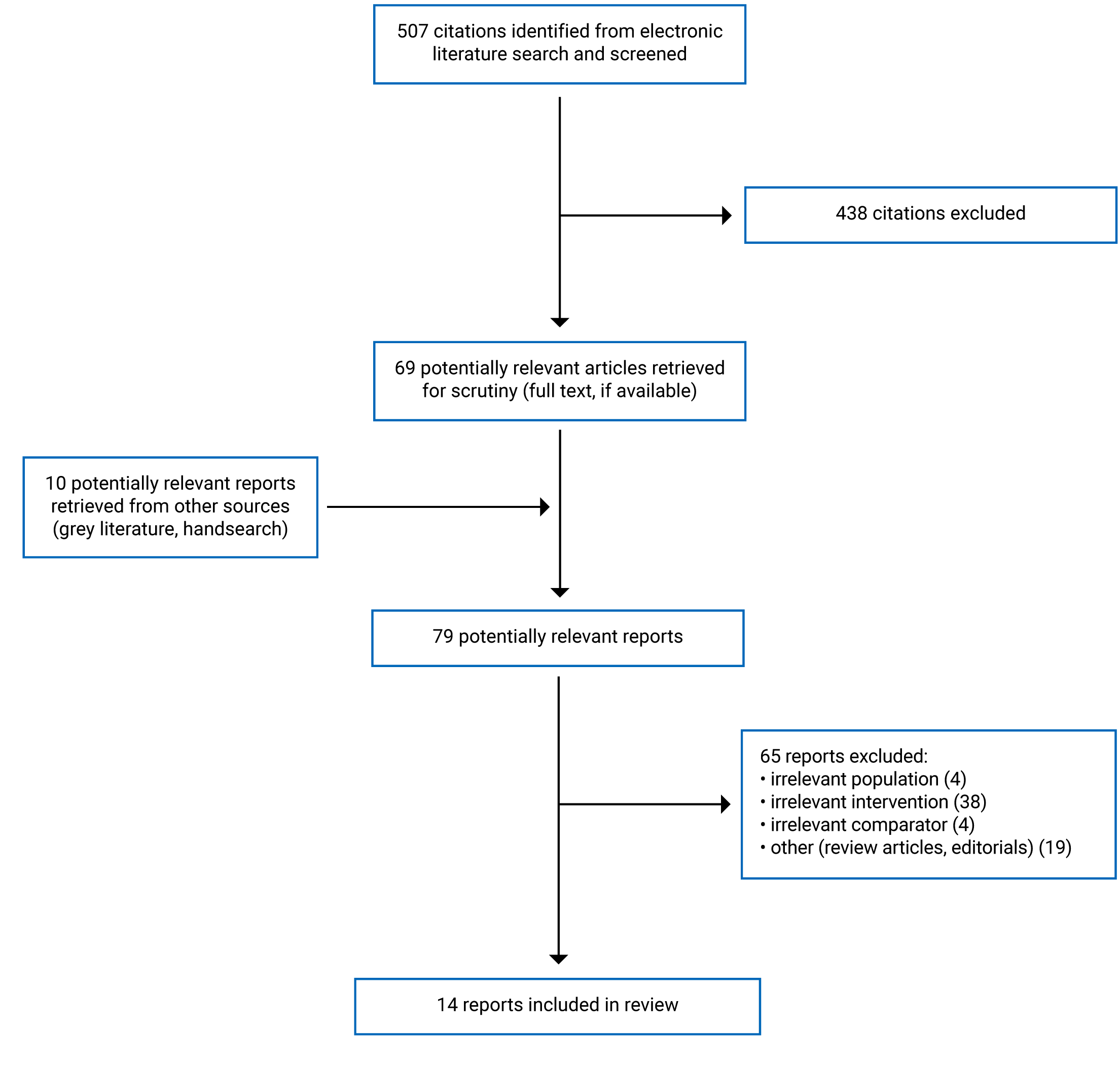
A total of 507 citations were identified in the literature search. Following screening of titles and abstracts, 438 citations were excluded and 69 potentially relevant reports from the electronic search were retrieved for full-text review. 10 potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 65 publications were excluded for various reasons, and 14 publications met the inclusion criteria and were included in this report. These comprised 4 systematic reviews, 4 non-randomized studies, and 6 evidence-based guideline reports, representing 5 evidence-based guidelines. Appendix 1 presents the PRISMA12 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Four systematic reviews were identified, published between 2016 and 2019.13-16 One14 systematic review included primary studies that were economic evaluations, published between 1990 and 2018. Two systematic reviews captured RCTs reporting on clinical efficacy and safety, published before November 2016 (Zeng et al. [2017]16) or May 2018 (Sekine et al. [2019]15). Both of these systematic reviews also involved network meta-analyses. A fourth systematic review captured RCTs and observational studies involving IMiD-based regimens and that reported adverse events relating to infection.13 This latter systematic review, current to May 2017, involved a meta-analysis across IMiD-based regimens to estimate the overall incidence rate associated with IMiD-based therapy, as well as pairwise meta-analysis between IMiD-based and non-IMiD-based regimens to estimate the relative risk of infection.
Across the 413-16 systematic reviews, 1 primary study relevant to the current report was identified (the phase II EVOLUTION RCT), in the systematic review by Zeng et al. (2017).16 No relevant studies were identified in the other 313-15 systematic reviews. The characteristics and results from the systematic review and network meta-analysis by Zeng et al. (2017),16 focusing on the results from the 1 relevant study (EVOLUTION), will be described in this report. The characteristics and results from the other 313-15 systematic reviews will not be described hereafter, aside from a brief summary of their critical appraisal.
Additionally, 417-20 non-randomized studies and 521-25 guidelines (captured in 6 reports21-26) were identified, and are described in the following subsections. Two relevant reports for were available for the National Comprehensive Cancer Network (NCCN) guidelines: the main guidelines22 and the NCCN Evidence BlocksTM.26 Hereafter, only the main guidelines will be cited in the text of the report, unless the NCCN Evidence BlocksTM are being specifically addressed; both reports will be cited in the tables.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The systematic review by Zeng et al. (2017)16 captured RCTs published before November 2016 that were conducted among transplant-eligible patients with newly diagnosed multiple myeloma, and that compared overall survival, progression-free survival or overall response rate (ORR) between different pre-ASCT induction therapies (not restricted to RVd and CyBorD). One relevant RCT was identified within this systematic review.
All 417-20 non-randomized studies were designed as retrospective cohort studies. Two of the studies involved data from the Center for International Blood and Marrow Transplant Research (CIBMTR), with 6-year study periods overlapping by 1 year: Cornell et al. (2017)18 captured data between 2008 and 2013, and Sidana et al. (2021)19 captured data between 2013 and 2018. The study by Uttervall et al. (2019)20 retrospectively captured data from 1 hospital in Sweden over a period of 10 years (2009 to 2018), and the study by Chakraborty et al. (2017)17 retrospectively captured data from the US-based Mayo Clinic over approximately 15 years (2000 to 2015).
The 5 guidelines were developed by: the National Comprehensive Cancer Network (NCCN)22; British Society for Haematology (BSH) and UK Myeloma Forum24; the European Hematology Association (EHA) and European Society for Medical Oncology (ESMO)21; Myeloma Australia’s Medical and Scientific Advisory Group (MSAG)23; and a group of co-authors from Belgium.25 Evidence informing the guidelines was collected through a literature search, which is well-defined in 124 guideline, yet not well reported in the other 4.21-23,25 All 5 guidelines use rating schemes to convey the quality of the evidence and strength of the recommendations, using numerical and alphabetical categories. Although the rating schemes differ from guideline to guideline (see Appendix 2 for details), 1 and A represent the highest levels in all 521-25 guidelines’ rating schemes. For the NCCN guidelines, the rating scheme differs in the main guidelines22 and the NCCN Evidence BlocksTM.26 In the main guidelines, category 1 recommendations represent the strongest rating based on quality of evidence and consensus within the NCCN Panel, and category 3 represents the lowest rating; whereas in the NCCN Evidence BlocksTM,26 the best ratings for quality of evidence, consistency of evidence, efficacy, safety and affordability, are rated as 5s (and worst ratings are 1s).
Country of Origin
The systematic review by Zeng et al. (2017)16 was conducted by a group of researchers from China. One20 of the 417-20 non-randomized studies was conducted in Sweden. The 317-19 other non-randomized studies had US-based lead authors, although the co-author group and CIBMTR data source were from international locations in 218,19 of those 317-19 studies.
The NCCN guidelines were developed by US group; the BSH/UK Myeloma Forum guidelines were developed by a British group; EHA-ESMO Clinical Practice Guidelines were developed by a European group; Myeloma Australia’s MSAG was an Australian group, and the guidelines by Vekemens et al. (2020)25 were developed by a Belgian group.
Patient Population
For the systematic review reported by Zeng et al. (2017),16 the patient characteristics from the relevant primary study (EVOLUTION) were summarized for the full population, rather than for the transplant-eligible subpopulation relevant to the current report. Patients’ median age was approximately 60 years, the majority of patients were male (57% to 58%), and the proportion of patients with ISS stage III differed slightly across arms, with 33% in the CyBorD arm and 19% in the RVd arm.
Three17,18,20 of the 417-20 non-randomized studies captured a broader patient population than considered in the current report: 217,18 studies captured patients receiving induction treatment regimens that are not relevant to the report, and 120 study captured patients who did not undergo ASCT. However, in all studies, baseline patient characteristics and outcomes were available for the subgroup of patients relevant to the current report: newly diagnosed patients with multiple myeloma receiving induction therapy with either RVd or CyBorD, before ASCT.
Across the relevant populations of the 417-20 non-randomized studies, median or mean ages ranged from 55 to 62 years across study groups, the proportion of male patients ranged from 54% to 65%, and the proportion of patients with ISS stage III ranged from 17% to 35%. Measures of renal function were captured, although using different metrics. In 317-19 of the 417-20 studies, renal function was measured at diagnosis or at-transplant as the proportion of patients with high serum creatinine levels (> 1.5 mg/dL or ≥ 2 mg/dL) or low estimated glomerular filtration rate (eGFR) (< 60 mL/min/1.73 m2) — both of which indicate poor renal function. In these 317-19 studies, renal function was worse among patients given CyBorD compared with those given RVd. In the fourth study, Uttervall et al. (2019)20 reported eGFR levels using an unclear metric (e.g., mean or median) and unclear timing of measurement (e.g., at diagnosis or at-transplant); the authors reported slightly better eGFR levels in the CyBorD group (67 mL/min/1.73m2) than in the RVd group (63 mL/min/1.73m2).
The proportion of high-risk patients, based on cytogenics, was reported in 317-19 of the 417-20 non-randomized studies, ranging from 11.5% to 37%. Definitions of high-risk disease consistently included patients with certain translocations (i.e., t[4;14], t[14;16], t[14;20]), and deletions (del17p), although inclusion of other cytogenic markers, such as chromosome 1 abnormalities, varied.
All 521-25 guidelines cover treatment recommendations for a broader patient population than the focus of the current report, including treatment recommendations for transplant-ineligible patients, or for smouldering myeloma. However, all 5 guidelines include specific guidance on initial treatment of newly diagnosed patients with symptomatic multiple myeloma who are transplant candidates. The intended users of all 5 guidelines are medical professionals, e.g., hematological oncologists, clinical practitioners.
Interventions and Comparators
In the systematic review, the induction therapy regimen in the 1 relevant study (EVOLUTION) involved 8 21-day cycles. In the RVd arm, this involved: a 25 mg dose of lenalidomide given on days 1 to 14; a 1.3 mg/m2 dose of bortezomib (on days 1, 4, 8, and 11); and 40 mg of dexamethasone given on days 1, 8, and 15. The CyBorD arm involved the same dosing of bortezomib and dexamethasone, and cyclophosphamide delivered at 500 mg/m2 on days 1 and 8.
Among the 417-20 non-randomized studies, 120 study provided details on dosing. The regimens delivered in that study involved 3-week cycles, similar to the EVOLUTION trial, yet with differences in dosing and delivery. Dexamethasone was dosed at 20 mg per day (rather than 40 mg as in EVOLUTION), yet delivered more frequently. Cyclophosphamide was delivered on the first day of every cycle, rather that twice per cycle in EVOLUTION, dosed at 1,000 mg/m2. The bortezomab dosing and timing was similar to EVOLUTION, although was delivered subcutaneously, and the lenalidomide schedule was also similar to EVOLUTION although was adjusted to kidney function and age of patients, ranging from 15 mg to 25 mg.
In 119 non-randomized study, the median number of induction therapy cycles before ASCT was 4 in both the RVd and CyBorD groups. In another non-randomized study,20 median number of induction cycles before high-dose treatment was 5 in the RVd group and 4 in the CyBorD group. The other 217,18 non-randomized studies included RVD, CyBorD, as well as other induction therapy regimens; the median number of cycles was calculated across all regimens (including those not relevant to the current report), and was reported as 4 cycles in both17,18 studies. Use of subsequent therapies varied across the 417-20 non-randomized studies. For example, 76% of patients captured in the study by Sidana et al. (2021)19 received maintenance therapy post-ASCT; whereas it was received by 8% of patients in the study by Uttervall et al. (2019).20
All 521-25 guidelines provide recommendations regarding primary therapy, and specifically the choice of induction therapy, for newly diagnosed patients with symptomatic multiple myeloma who are transplant candidates. Additionally, all 521-25 guidelines cover some aspects of RVd dosing and delivery. Regarding the delivery of bortezomib, Myeloma Australia’s MSAG recommend that delivery either subcutaneously or using the RVd-lite regimen of weekly rather than twice-weekly bortezomib.23 The BSH/UK Myeloma Forum and the NCCN both prefer weekly subcutaneous delivery of bortezomib.22,24 Regarding lenalidomide, the MSAG recommend using 1 of the following 2 regimens: 8 × 21 day cycles (14 days of lenalidomide); or 6 × 28 day cycles (21 days of lenalidomide),23 and the BSH/UK Myeloma Forum specify 4 to 6 cycles of induction regimen, typically, before ASCT.24 Several bodies provide specific considerations regarding use of lenalidomide before stem cell harvest. The NCCN broadly recommend harvesting stem cells before prolonged exposure to lenalidomide;22 whereas the BSH/UK Myeloma Forum and MSAG more specifically recommend a maximum of 4 cycles of RVd before stem cell harvest.23,24 The NCCN guidelines provide specific considerations for lenalidomide dosing among patients with renal impairment,22 and the Belgian and ESMO-EHA guidelines provide guidance on adjustment to dosing according to patient frailty.21,25
Outcomes
Response
Response rates were reported in the 116 relevant systematic review and network meta-analysis, and in all 417-20 non-randomized studies. In these 5 studies, response was defined according to the International Myeloma Working Group criteria.
In the systematic review by Zeng et al. (2017),16 response rates were reported as ORR, defined as partial response (PR) or better (i.e., PR, very good partial response [VGPR], complete response [CR], or stringent complete response [sCR]). In the 4 non-randomized studies, response rates were reported as: PR or better16,17; VGPR or better (i.e., VGPR, CR, or sCR)17,19; or else reported for each response category separately.18-20 The timing of assessment varied across studies. In 317-19 of the 417-20 non-randomized studies, response was measured pre-transplant (reported as a baseline patient characteristic),17,19 or at-transplant (reported as a study outcome),18 as well as post-transplant, specified as: at day 100 post-transplant,19 best response post-transplant (time frame not specified),17,19 or best response at day 100 post-transplant.18 In the 116 relevant systematic review, and in 120 non-randomized study, the exact timing of response with respect to ASCT was unclear: Zeng et al. (2017)16 reported post-induction response, and Uttervall et al. (2019)20 reported best post-high-dose treatment.
Relapse or Progression
The outcome of relapse or progression was captured in 1 non-randomized study, by Cornell et al. (2017),18 defined as the time from ASCT to first evidence of recurrence or progression of multiple myeloma post-ASCT.
Progression-Free Survival
Progression-free survival was captured in 417-20 non-randomized studies. In 218,19 studies, it was defined as time from ASCT to progression or death, in 1 study it was defined as time from diagnosis to progression or death,17 and in 1 study, it was not defined but assumed to be measured from diagnosis or treatment initiation.20 In the latter study,20 censoring occurred at the time of initiating maintenance therapy; whereas, in the other 317-19 studies, censoring occurred at the date of last follow-up (if event-free).
Overall Survival
Overall survival was captured in 417-20 non-randomized studies, measured as time to death. The start time for the analysis (i.e., diagnosis, treatment initiation, or ASCT), and criteria for censoring (i.e., start of maintenance therapy, or date of last known follow-up) was consistent with the analysis of progression-free survival.
Adverse Events
Secondary primary malignancy and death due to secondary primary malignancy were reported in 218,20 non-randomized studies. Other adverse events were not reported.
Outcomes Captured in Guidelines
In the 521-25 guidelines, outcomes that informed recommendations were based on efficacy outcomes such as response, depth of response, progression-free survival, and overall survival. Additionally, minimal residual disease negativity was considered in formulating guidance. Toxicity and adverse events focused on peripheral neuropathy. One guideline24 specifies patient preference, drug access, and funding as criteria for recommendations.
Summary of Critical Appraisal
Systematic Reviews and Network Meta-Analyses
The 313-15 systematic reviews and/or network meta-analyses that did not capture any studies relevant to the current report were assessed with a focus on the comprehensiveness and quality of search strategies to understand whether they may have missed key studies (Appendix 3). In 113 systematic review that involved broader eligibility criteria than the current review (i.e., not restricted to transplant-eligible patients), the EVOLUTION RCT was indeed captured; however, subgroup data for the population of interest to this report (i.e., transplant-eligible patients) were not provided. In another systematic review (with network meta-analysis),15 eligibility criteria were restricted to transplant-eligible patients, and the EVOLUTION RCT was not captured. This RCT may have been appropriately excluded (rather than accidentally missed) as it is unclear whether subgroup data for transplant-eligible patients are publicly available from that RCT. Furthermore, the search strategies of the latter systematic review15 were comprehensive (although clinical trial registries did not appear to be searched), study selection was performed in duplicate, and the eligibility were clearly specified according to a pre-defined study protocol. Hence it is likely that the EVOLUTION was actively and appropriately excluded, rather than missed due to inadequate search strategy, and it is not evident that other studies were missed. In another systematic review,13 the researchers collected data from RCTs and non-randomized studies that reported on serious infections, analyzed in a pairwise meta-analysis. In this systematic review, authors attempted to identify and include all relevant studies, and had broader eligibility criteria than in the current report. The authors did capture the EVOLUTION RCT, but not within the subgroup of transplant-eligible patients. Additionally, the RVd arm of the SWOG-S0777 trial was included, although this trial did not compare RVd with CyBorD hence is not relevant to the current report. It is unlikely that studies were missed due to the methodology of the systematic review. A third systematic review14 captured economic evaluations; however, did not capture any studies involving RVd. As the eligibility criteria was broader than for the current study, and multiple databases were searched with relevant records reviewed in duplicate, the lack of relevant studies identified in the review was not considered to be due to the search methodology, but rather due to absence of such studies. Based on this assessment, it is unlikely that any key studies comparing RVd and CyBorD were missed in these systematic reviews.
The systematic review by Zeng et al. (2017),16 which captured 1 relevant study, was based on a comprehensive search of multiple databases, conference proceedings, and clinical trial registries. Although the authors conducted data extraction in duplicate, it was unclear whether study selection was also performed in duplicate. The eligibility criteria for the systematic review were clearly presented, covering relevant aspects of population, intervention, comparator group, and outcomes, yet it was unclear whether the review methods were established before the conduct of the review. The assessment of the relevance and credibility of systematic review and network meta-analysis focused on the comparison between RVd and CyBorD within the larger network of evidence. Overall, the analysis was considered relevant to the current research questions; however, there was 1 major concern regarding credibility. In the network meta-analysis, the comparison between RVd and CyBorD was based on direct evidence from EVOLUTION RCT. This RCT enrolled both transplant-eligible and transplant-ineligible patients, whereas the target population of the network meta-analysis was transplant-eligible patients, as is the focus of the current report. Given that the EVOLUTION RCT was included in the response network but not in the overall survival or progression-free survival networks, it is unknown whether Zeng et al. (2017)16 may have contacted the EVOLUTION trial investigators and obtained subgroup-specific data for response but not overall survival or progression-free survival; however, individual study data were not provided by Zeng et al. (2017)16 to be able to confirm the source data. Hence, the main concern regarding the relevance and credibility of the findings rests on whether transplant-eligible subgroup data from EVOLUTION were used as inputs to the analysis. The impact of this is unclear without further research into relative effect sizes between RVd and CyBorD among transplant-eligible versus transplant-ineligible populations.
Non-Randomized Studies
Overall, the reporting was clear across the 417-20 non-randomized studies in terms of study objectives, outcomes, and patient characteristics. Additionally, the principal confounders and methods for adjustment of these potential confounders were well-described. However, in 120 study, the timing of baseline and outcome measurements were unclear, as were some aspects of the reported metrics. For example, the summary statistics describing baseline laboratory values were unclear, as were the timing of these measurements (i.e., whether at diagnosis or pre-transplant). Additionally in this same study, response was measured as best response post-high-dose treatment; however, it was unclear if this meant pre-transplant response, or response over a longer-term follow-up post-high-dose treatment and ASCT.
The external validity of the study findings to other similar settings was considered good, based on the use of registries or institutional databases which were assumed to have low sampling bias. The generalizability of the study setting to the Canadian setting was relatively low. The 2 CIBMTR-based studies18,19 may have captured Canadian centres (although it is unclear how many) yet the other 2 studies did not.17,20 However, the relative treatment effects estimated from the studies may be generalizable to the Canadian setting.
Threats to the internal validity of the studies were primarily due to the non-randomized nature of the studies, although in each study, efforts were made to adjust for ISS stage and high-risk multiple myeloma: both of which were associated with treatment choice (reflected by imbalances across treatment groups) and prognosis. In 317-19 studies, both of these factors were included during model development. In the fourth20 study, ISS was included as an adjustment factor but high-risk multiple myeloma was not, nor was R-ISS due to missing data for the majority of patients. Subgroup analysis from the study suggested that this would have been an important confounder to include in the multivariable model, and its omission may have biased the results although the baseline distribution by cytogenic risk was not reported, making it difficult to assess the direction of this potential bias. Other adjustment factors included hemoglobin levels, serum calcium, serum albumin, and serum Beta2-microglobulin levels in 120 study (the latter 2 were also captured in the ISS staging), estimated glomerular filtration rate in 120 study, subsequent therapies in 218,19 studies (planned use in 118 study and observed use in 119 study), age in 217,20 studies, sex in 117 study and transplant period in 117 study. All studies used Cox proportional hazards models for time-to-event analysis of overall survival and progression-free survival, which is considered appropriate; however, in 120 study, the reporting and interpretation of the multivariable model was unclear, and in 119 study, an adjustment factor (use of maintenance therapy) was based on observations post-baseline, yet was not analyzed using a time-varying framework.
No study provided power calculations; sample size was listed as a limitation in 120 study.
Guidelines
Among the 521-25 identified guidelines, 321,22,24 were from organizations that develop guidelines across multiple hematological or oncology indications, and external documents regarding the overall process of guideline development were available.27-29 The guidelines by the MSAG to Myeloma Australia identified in this report were an update to a previous 2019 guideline30 on the management of multiple myeloma, and specific to the use of RVd; details on the development of the update document were not reported.23 The Belgian guidelines were developed by a group of co-authors from Belgium, however, did not appear to represent a particular organization, and detailed documentation on the process of guideline development was not available.25
The scope and purpose of all 521-25 guidelines were clear. Within the guideline development documentation which was available for 321,22,24 guidelines, evidence of stakeholder involvement in guideline development was clear as a standard process across all guidelines developed by the groups, although the details for the specific guidelines identified in this report were not reported. Stakeholder involvement in the development of the guidelines was unclear in the other 223,25 guidelines.
In terms of the rigour of guideline development, all guidelines indicated some degree of systematic search; however, only 124 guideline provided details on the search strategy used. In the other guidelines, the broad approach to literature search was either obtained from supporting documentation,22 or was not described.21,23,25 Across all guidelines, the strengths and limitations of the supporting evidence were clear, primarily through the use of standardized schemes used to categorize the quality of the evidence.21-25
In all 521-25 guideline documents, the recommendations were specific, clearly presented, and provided different options for treatment; for example, alternatives for patients with renal insufficiency, or alternatives based on cost and health care coverage.
In terms of applicability, all 521-25 guidelines provided some mention of potential barriers, such as cost, renal function, and/or patient frailty, which may impact the choice of treatment, and provided alternative treatments and/or methods for dose adjustment of the RVd regimen to address these issues. Two21,22 guidelines were determined to have additional tools for putting the recommendations into practice.
Four21,22,24,25 of the 5 guidelines appeared to have editorial independence, and provided statements stating no sources of external funding. In the Australian guidelines, explicit statements regarding funding were not provided.23 Similarly, conflicts of interest for contributing authors were provided in 421,22,24,25 of the 521-25 guidelines, and not addressed in the fifth.23
Overall, the guidelines were clearly presented, based on a comprehensive and transparently assessed evidence base, and appeared to provide unbiased recommendations on current clinical practice for clinical audiences, taking into consideration individual patient characteristics, as well as the costs associated with treatment.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of RVd Versus CyBorD
Response
In the systematic review by Zeng et al. (2017),16 1 relevant study, the EVOLUTION RCT, was included in a network meta-analysis for the outcome of post-induction ORR; timing with respect to ASCT was unclear. EVOLUTION was the only RCT that informed the network connection between RVd and CyBorD, and no indirect evidence informed that connection. The odds ratio from the network meta-analysis comparing the ORR for RVd and CyBorD reflected a 40% increase in the odds of responding to treatment (i.e., a PR or better) associated with RVd, however, the estimate was not statistically significant. Study specific data inputs from the EVOLUTION RCT were not provided by Zeng et al. (2017).16
Of the 4 non-randomized studies,17-20 statistical comparisons between RVd and CyBorD were provided in 2,19,20 yet no statistically significant differences were identified. The other 217,18 studies included regimens that are not of interest to the current report. In these 217,18 studies, response rates were tested for differences across all 418 or all 617 regimens being compared in the study using chi-square tests, but comparisons of response rates specifically between RVd and CyBorD were not tested for statistical significance.
In the 317-19 studies reporting response pre-ASCT, the proportion of patients with VGPR or better was numerically higher among patients receiving RVd compared with CyBorD. In 119 study, the proportions of patients achieving VGPR or better were 65% for VRd and 59% for CyBorD, however the difference was not statistically significant. The other 217,18 studies did not test for statistical significance between RVd and CyBorD. The proportions of patients with VGPR or better in those 217,18 studies were: 41% and 40% for RVd and CyBorD, respectively, in 117 study; and 57% and 44% for RVd and CyBorD, respectively, in the other study.18 Proportions of patients achieving sCR were reported in 217,18 studies. Differences were not tested for statistical significance, yet were numerically higher among patients receiving RVd: 18% and 12% for RVd and CyBorD, respectively, in 117 study; and 5% and 4% for RVd and CyBorD, respectively, in the other study.18 The proportion of patients with CR or better was reported in 119 study, and was the same across treatment groups (17%; not statistically significant).
Post-ASCT, the proportion of patients with VGPR or better was numerically higher among those receiving RVd in 217,18 of the 317-19 studies, and numerically higher among patients receiving CyBorD in the third19 study. In the 217,18 studies with higher VGPR or better among patients receiving RVd, proportions were 83% for VRd versus 78% for CyBorD in 117 study, and 65% for VRd versus 58% for CyBorD in the other study18; differences were not tested for statistical significance. In the third19 study, which reported numerically higher proportions of VGPR or better among patients receiving CyBorD, the differences were not statistically significant (several estimates provided; see Appendix 4 for details). CR and sCR were also reported post-ASCT. In 217,19 of the 317-19 studies, numerically higher proportions of patients achieved CR or sCR among patients receiving VRd, and in the third18 study, the proportion of patients achieving sCR was the same (12%) in both groups. Among the 217,19 studies with numerically higher proportions of CR or sCR reported among patients receiving RVd, the CR proportions were not statistically significantly different (63% among patients receiving VRd versus 57% among patients receiving CyBorD) in 119 study, and in the other study,17 the sCR proportions were 46% among patients receiving VRd compared with 34% among patients receiving CyBorD (tests of statistical significance not reported, although the study authors concluded that RVd was associated with superior response rates compared with CyBorD).
In the 120 study reporting best response post-high-dose therapy, for which timing was unclear with respect to ASCT, no statistically significant differences were reported for the proportion of patients with PR or better (see Appendix 4 for details). The proportion of patients with CR or near-CR was numerically higher in the CyBorD group (50%) compared with the RVd group (42%), as was the proportion of patients with VGPR or better (78% in the CyBorD group, compared with 76% in the RVd group) (neither was tested for statistical significance).
Relapse and Progression
In the 118 study reporting the proportion of patients with relapse or progression, patients receiving RVd were statistically less likely to progress or relapse compared with patients receiving CyBorD. At 3 years, the proportion of patients who relapsed or progressed was 38% (95% confidence interval [CI]: 31% to 45%) in the RVd group, compared with 63% (95% CI, 49% to 77%) in the CyBorD group, although these estimates were not tested for statistical significance and not adjusted for potential confounding. However, a multivariable model, adjusted for high-risk disease and planned post-ASCT treatment, indicated a 32% reduction in the risk of relapse or progression associated with RVd, which was statistically significant.
Progression-Free Survival
Progression-free survival was reported in all 417-20 non-randomized studies as the proportion of patients with progression-free survival at set time points (e.g., 1 year), or as adjusted or unadjusted comparisons of time-to-event data, reported as P values and/or hazard ratios. The direction of association for all point estimates (except for 1 estimate of 1-year PFS18), consistently favoured RVd, and differences were statistically significant in 219,20 of the 417-20 studies. Multivariable models were presented in all 417-20 studies, and included adjustments for ISS stage, and/or high-risk disease (based on cytogenics). Hazard ratios for RVd versus CyBorD in the adjusted models were available in 317-19 of the 417-20 studies, and estimated a 17% to 30% reduction in risk of progression or death associated with RVd versus CyBorD, although the estimates were not statistically significant.
In 119 study, progression-free survival was analyzed according to subgroup based on renal function. Among patients with better renal function (eGFR ≥ 60 mL/min/1.73m2 at diagnosis), unadjusted differences in progression-free survival between RVd and CyBorD were statistically significant, favouring RVd. However, among patients with worse renal function (eGFR < 60 mL/min/1.73m2 at diagnosis), unadjusted differences in progression-free survival between RVd and CyBorD were non-significant.
Overall Survival
Overall survival was reported in all 417-20 non-randomized studies as the proportion of patients surviving at set time points (e.g., 1 year), or as adjusted or unadjusted comparisons of time-to-event data, reported as P values and/or hazard ratios. The direction of association for all point estimates consistently favoured RVd (except for 118 estimate of 1-year overall survival, and 117 estimate of 5-year overall survival, which were the same in both groups when rounded to the nearest percent), and differences were statistically significant in 217,19 studies. Multivariable models were presented in 317-19 of the 417-20 studies, and included adjustments for ISS stage, and/or high-risk disease (based on cytogenics). In the adjusted models, point estimates in 218,19 studies estimated a 25 to 30% reduction in risk of death associated with RVd versus CyBorD, although neither was statistically significant. In the third study,17 the hazard ratio was statistically significant and estimated more than a 3-fold increase in the risk of death associated with CyBorD compared with RVd, although with considerable uncertainty.
In 119 study, overall survival was analyzed according to subgroup based on renal function. Among patients with better renal function (eGFR ≥ 60 mL/min/1.73m2 at diagnosis), unadjusted differences in overall survival between RVd and CyBorD were not statistically significant. Whereas, among patients with worse renal function (eGFR < 60 mL/min/1.73m2 at diagnosis), unadjusted differences in overall survival between RVd and CyBorD were statistically significant, favouring RVd. In both subgroups, however, the P values were of similar magnitude (0.075, and 0.042, respectively), and the differences in statistical significance reflect minor fluctuations around the threshold of 0.05.
Adverse Events
Secondary primary malignancies were reported in 218,20 studies, although neither study tested for statistically significant differences between RVd and CyBorD. In 120 study, 2 patients among the 71 who received RVd (2.8%) were reported as having secondary primary malignancies. The authors did not address secondary primary malignancies among patients who received CyBorD. In the other study,18 deaths due to secondary primary malignancies were reported in 2 patients who received RVd (0.7%) and 1 patient who received CyBorD (1.2%).
Cost-Effectiveness of RVd
No relevant evidence regarding the cost-effectiveness of RVd for induction therapy before autologous stem cell transplant for multiple myeloma patients was identified; therefore, no summary can be provided.
Guidelines
Among the 5 included guidelines, the NCCN,22 the EHA-ESMO,21 and the MSAG23 specifically recommend RVd as a first option for induction therapy among transplant-eligible newly diagnosed multiple myeloma patients. The NCCN include the regimen as a category 1, indicating high-level evidence and that there is uniform consensus within the NCCN Panel that the intervention is appropriate. RVd is the only regimen listed in the NCCN guidelines as a preferred option (over other recommended options or regimens that are useful in certain circumstances) (p. 23).22 The EHA-ESMO guidelines list RVd as 1 of 2 regimens to consider as a “first option” (p. 313)21 (the other is daratumumab in combination with RVd). This recommendation is based on level II evidence (i.e., small RCTs, large RCTs with lower methodological quality, meta-analyses of such trials, and/or meta-analysis with demonstrated heterogeneity), and with a recommendation grade B (“strong or moderate evidence for efficacy but with a limited clinical benefit, generally recommended”) (Supplemental material, p. 20).21 The included MSAG guidelines specifically focus on RVd (as an update to earlier guidelines), and MSAG recommends RVd as “the current standard of care for induction therapy prior to ASCT” (p. 3).23 Their recommendation is based on level 1B evidence, and a grade A recommendation, indicating that it was based on least 1 good-quality RCT that addressed the specific recommendation.
Two other guidelines – issued by a group from Belgium,25 and the BSH-UK Myeloma Forum24 — recommend more broadly defined 3-drug induction regimens that include RVd. The Belgian guidelines25 recommend a 3-drug regimen including at least bortezomib and dexamethasone as the standard of care, with a guideline recommendation level IA, indicating that the recommendation was based on at least 1 good-quality RCT, and that there was consistency addressing the specific recommendation. In discussing this recommendation, the guideline authors state that adding thalidomide as a third drug is superior to adding cyclophosphamide (i.e., CyBorD), and that adding lenalidomide (i.e., RVd) results in “significantly higher response rates, response duration and PFS […] compared with previous studies using [bortezomib-thalidomide-dexamethasone]” (p. 5).25 However, the guideline authors do not specifically recommend use of RVd over bortezomib-thalidomide-dexamethasone or CyBorD. The guidelines issued by the BSH/UK Myeloma Forum24 similarly specify that patients should receive an induction regimen that includes a proteasome inhibitor (i.e., bortezomib or carfilzomib) and a corticosteroid (e.g., dexamethasone), graded as a level IA recommendation, indicating a strong recommendation based on high-quality evidence. A related recommendation is that triplet regimens are generally recommended, and that the addition of an IMiD (e.g., lenalidomide or thalidomide) is preferred over cyclophosphamide, also as a level IA recommendation. In their discussion regarding the choice between lenalidomide, thalidomide, or cyclophosphamide as the third drug, the BSH/UK Myeloma Forum guideline authors describe RVd as an “attractive, well-tolerated option,” and note that the reduced dose protocol (RVd-lite) is “well tolerated in older patients, making this a preferred, well-tolerated treatment option” (p. 251).24
Limitations
There are several limitations of the current review.
A main limitation is the lack of evidence on cost-effectiveness, and the limited evidence from RCTs identified in this review. Although there was 1 relevant RCT identified within a systematic review (the EVOLUTION RCT), a major limitation of that systematic review was the lack of clarity regarding whether transplant-eligible subgroup data were used in the analysis, rather than data from the full trial population which also included transplant-ineligible patients. The remaining evidence informing this report came from retrospective observational studies, which carry a higher risk of bias due to their non-randomized nature. Another phase III RCT was identified in abstract form, presented at a 2019 workshop (Appendix 5), although it was not included in the current review as there was no full-text publication. This RCT enrolled newly diagnosed patients with multiple myeloma, and randomized patients to RVd or CyBorD; however, it is unclear whether the population was restricted to transplant-eligible patients, or whether it captured both transplant-eligible and transplant-ineligible patients, similar to the EVOLUTION RCT. While the abstract reported statistically significant differences in CR after 4 cycles of RVd (35.4%) compared with 4 cycles CyBorD (18.3%) (P value < 0.02), it failed to meet its primary end point of VGPR or better, despite a numerically greater proportion of patients achieving VGPR or better in the RVd arm (61.5%) compared with the CyBorD arm (48.3%) (P value = 0.09). As the abstract was presented over 2 years ago and has not yet been published, it is unclear whether it will become available in a peer reviewed journal and hence other end points from this study may not become available in the public domain. As this study could not be critically appraised due to its abstract format, the findings should be interpreted with caution.
Another limitation is that, while all studies included adjustment factors for key confounders, the impact of potential effect modification was not clear. Although treatment-by-disease characteristic interaction terms were considered in 118 study, they were not included in any of the final models. Additionally, 120 study conducted a subgroup analysis by R-ISS stage and high-risk cytogenics; however, the analyses conducted within those subgroups were not designed to test for differences between treatment groups. Subgroups of interest may include those with worse prognosis; for example, those with high-risk cytogenics or stage III ISS. Additionally, poor renal function is associated with preferential choice of CyBorD over RVd,22,31 or else dose modifications of RVd,22 hence understanding the relative treatment effect among patients with renal insufficiency may be of interest.
Adverse event data were not well reported in the primary studies; available data were limited to secondary primary malignancy, for which there were few events, no statistical tests, and inconsistent direction of association. This lack of reporting may have been due to the retrospective nature of the non-randomized studies, from which adverse event data may not have been readily available. Peripheral neuropathy is a common adverse event associated with neurotoxic drugs such as bortezomib and lenalidomide, and is noted in several guidelines as a consideration for treatment choice. In the EVOLUTION RCT, grade 3 or higher peripheral neuropathy was reported in 17% of patients receiving RVd.32 Additional real-world evidence comparing these adverse events would be helpful for informing treatment choice and delivery.
Another limitation of the review were the limited details on regimen dosing and delivery in the non-randomized studies. While the median number of cycles was typically reported, no further details were available in 3 of the 4 non-randomized studies. For bortezomib, it was unclear whether the studies captured delivery on a once- or twice-weekly schedule, and whether delivered intravenously or subcutaneously. For lenalidomide, it was unclear whether dosing was adjusted for kidney function or frailty. For dexamethasone, it was unclear if delivered as 40 mg 3 days per cycle, similar to the EVOLUTION RCT, or at the lower dose of 20 mg, more frequently, as in the study by Utterval et al. (2019).20 Finally, for cyclophosphamide it was unclear if delivered on the first day of every cycle, as in the study by Utterval et al. (2019),20 or twice per cycle, as in EVOLUTION, dosed at 1,000 mg/m2. The impact of such changes to dosing and delivery on treatment efficacy and safety requires further review of the clinical literature.
The heterogeneity of subsequent therapy use across the studies was another limitation of note. Importantly, Sidana et al. (2021)19 identified the varied use of maintenance as a major factor determining long-term benefit following ASCT, and cited it as possible reason for differences in relative efficacy in the evidence base. While Sidana et al. (2021)19 adjusted for use of maintenance therapy in their analysis, and considered this to be a possible reason for the lack of significant treatment effect in their study, the approach of adjusting for factors observed post-baseline may have introduced bias in their analysis and should be interpreted with caution.
None of the studies were conducted in an entirely Canadian setting, which is a limitation. However, some of the study sites captured in the 2 CIBMTR-based studies (one limited to North America and 1 capturing international sites) were likely to have been Canadian. Furthermore, country was not identified as an important adjustment factor in either study and hence may not modify the relative effectiveness or safety estimates for RVd relative to CyBorD. Hence, while the lack of Canadian-specific studies may be seen as a limitation, the relative effect sizes measured in non-Canadian settings may generalize well to Canadian settings.
Conclusions and Implications for Decision- or Policy-Making
This report identified 417-20 non-randomized studies and 116 relevant systematic review with network meta-analysis published since 2017 informing the clinical effectiveness and safety of RVd relative to CyBorD, alongside 521-25 guidelines published since 2019 capturing current recommendations regarding RVd as induction treatment for newly diagnosed transplant-eligible patients with multiple myeloma. No relevant cost-effectiveness analyses were identified.
The clinical effectiveness regarding response, relapse, progression-free survival, and overall survival broadly favoured RVd over CyBorD, although there were inconsistencies in the magnitude and direction of association across the different outcomes and studies, and few estimates were statistically significant. Pre-transplant, response was the same or numerically better with RVd for all 317-19 studies and across all definitions of response; however, only 1 comparison was tested for statistical significance, which was reported as being non-statistically significant. Post-transplant, 117 study reported consistently better response with RVd across different categories of response, with a difference of 12% in sCR rates; the study authors concluded that RVd was associated with superior response rates compared with CyBorD, although did not present test statistics that supported the statistical significance of this particular comparison. In the other 218,19 studies reporting on post-transplant response, differences of this magnitude were not observed, and in the 119 study that tested for statistically significant differences in response rates between RVd and CyBorD, none were reported as being statistically significant. Notably, in the post-ASCT assessment of response, consolidation and maintenance therapies were not accounted for and may have influenced longer-term response.19 In the 216,20 studies for which ASCT-related timing was unclear, the numerical estimates for ORR (i.e., PR or better) were higher among patients receiving RVd, although were non-significant, and comparisons of other response definitions (VGPR or better; CR or better) showed numerical estimates that were higher among patients receiving CyBorD (statistical significance not reported).
For relapse or progression, the 1 study18 reporting this outcome found a statistically significant 32% reduction in the rate of relapse or progression associated with RVd compared with CyBorD, after adjusting for differences in baseline patient and disease characteristics. In the analyses of progression-free survival, none of the 3 multivariable adjusted models showed statistically significant differences between RVd and CyBorD; however, the direction of the estimated non-significant association was consistently in favour of RVd, with an effect size ranging from 17% to 30% reduction in risk. For overall survival, all 317-19 multivariable models similarly favoured RVd over CyBorD, with a statistically significant effect size in 117 model, and estimated effect sizes ranging from 25% to 68% reduction in risk.17-19
Taken together, the broad findings of clinical effectiveness that generally —but not always statistically — favoured RVd over CyBorD in the current report align with the evidence-based clinical practice guidelines in the US, Australia, and Europe, which recommend RVd as a first option for induction therapy over CyBorD, and from British and Belgian groups which position IMiD-based triplet therapy over CyBorD. The evidence informing these 5 guidelines were based on comparative evidence of RVd relative to other regimens, and/or single-arm data on RVd, but not necessarily from studies that directly compare RVd to CyBorD. The majority of the evidence informing these guidelines was outside the scope of the current review, and hence the findings from the current review represents complementary data with similar broad conclusions.
Despite the alignment between the clinical findings and guidelines regarding the value of RVd, and its coverage and wide use in countries such as Australia, Sweden, and the US, it is not reimbursed in several countries. For example, RVd is not covered by the National Health Service in the UK or in Belgium, despite being recommended in the Belgian and the BSH/UK Myeloma Forum guidelines.24,25,33 The New Zealand multiple myeloma guidelines did not recommend RVd as an option for induction therapy (and hence these guidelines were not included in the current review) specifically due to its lack of coverage despite an acknowledgement of its superior effectiveness.34
In Canadian provinces and territories, RVd is not currently reimbursed for transplant-eligible patients with multiple myeloma, although it is covered in Saskatchewan for transplant-ineligible patients and is being considered in several others.35 Although the findings of the current review suggested clinical benefits of RVd, the lack of cost-effectiveness studies in the newly diagnosed transplant-eligible population, the limited availability of high-quality published RCT evidence, and lack of statistically significant findings in the non-randomized studies may pose a challenge for clearly establishing the value of RVd over CyBorD, particularly in the Canadian setting. A more comprehensive systematic review incorporating a broader evidence base, and formal direct and indirect comparisons, along with new primary research on clinical and cost-effectiveness of RVd compared with CyBorD in the Canadian setting, may further inform the research questions addressed in this Rapid Review.
References
1.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society Statistics Canada and the Public Health Agency of Canada. Canadian cancer statistics 2021. Toronto (ON): Canadian Cancer Society; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2021 Nov 18.
2.Rajkumar SV. Multiple myeloma: 2020 update on diagnosis, risk-stratification and management. Am J Hematol. 2020;95(5):548-567. PubMed
3.Greipp PR, San Miguel J, Durie BG, et al. International staging system for multiple myeloma. J Clin Oncol. 2005;23(15):3412-3420. PubMed
4.Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised international staging system for multiple myeloma: a report from International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863-2869. PubMed
5.Rajkumar SV. Multiple myeloma: overview of management. In: Kyle RA, Connor RF, eds. UpToDate. Waltham (MA): UpToDate; 2021: http://www.uptodate.com. Accessed 2021 Nov 15.
6.Rajkumar SV, Kumar S. Multiple myeloma current treatment algorithms. Blood Cancer J. 2020;10(9):94. PubMed
7.Sunnybrook Health Sciences Centre. Plasma cell neoplasms. 2020; https://sunnybrook.ca/content/?page=hematology-treatments-plasma. Accessed 2021 Nov 18.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Agree Next Steps C. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Dec 16.
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Chen M, Zhao Y, Xu C, Wang X, Zhang X, Mao B. Immunomodulatory drugs and the risk of serious infection in multiple myeloma: systematic review and meta-analysis of randomized and observational studies. Ann Hematol. 2018;97(6):925-944. PubMed
14.Fu S, Wu C-F, Wang M, Lairson DR. Cost effectiveness of transplant, conventional chemotherapy, and novel agents in multiple myeloma: a systematic review. Pharmacoeconomics. 2019;37(12):1421-1449. PubMed
15.Sekine L, Ziegelmann PK, Manica D, et al. Frontline treatment for transplant-eligible multiple myeloma: a 6474 patients network meta-analysis. Hematol Oncol. 2019;37(1):62-74. PubMed
16.Zeng Z-H, Chen J-F, Li Y-X, Zhang R, Xiao L-F, Meng X-Y. Induction regimens for transplant-eligible patients with newly diagnosed multiple myeloma: a network meta-analysis of randomized controlled trials. Cancer Manag Res. 2017;9:287-298. PubMed
17.Chakraborty R, Muchtar E, Kumar S, et al. The impact of induction regimen on transplant outcome in newly diagnosed multiple myeloma in the era of novel agents. Bone Marrow Transplant. 2017;52(1):34-40. PubMed
18.Cornell RF, D'Souza A, Kassim AA, et al. Maintenance versus induction therapy choice on outcomes after autologous transplantation for multiple myeloma. Biol Blood Marrow Transplant. 2017;23(2):269-277. PubMed
19.Sidana S, Kumar S, Fraser R, et al. Impact of induction therapy with VRD vs. VCD on outcomes in patients with multiple myeloma in partial response or better undergoing upfront autologous stem cell transplantation. Transplant Cell Ther. 2021.
20.Uttervall K, Borg Bruchfeld J, Gran C, et al. Upfront bortezomib, lenalidomide, and dexamethasone compared to bortezomib, cyclophosphamide, and dexamethasone in multiple myeloma. Eur J Haematol. 2019;103(3):247-254. PubMed
21.Dimopoulos MA, Moreau P, Terpos E, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(3):309-322. PubMed
22.Multiple myeloma (version 3.2022). Plymouth Meeting (PA): National Comprehensive Cancer Network; 2021: www.nccn.org. Accessed 2021 Nov 18.
23.Quach H, Prince HM, Medical Scientific Advisory Group (MSAG). MSAG update: bortezomib, lenalidomide and dexamethasone (VRd) for initial treatment of multiple myeloma. Melbourne (AU): Myeloma Australia; 2020: https://myeloma.org.au/wp-content/uploads/2020/09/MSAG_clinical_practice_update_JUL20_final.pdf. Accessed 2021 Nov 18.
24.Sive J, Cuthill K, Hunter H, et al. Guidelines on the diagnosis, investigation and initial treatment of myeloma: a British Society for Haematology/UK Myeloma Forum Guideline. Br J Haematol. 2021;193(2):245-268. PubMed
25.Vekemans M-C, Doyen C, Caers J, et al. Recommendations on the management of multiple myeloma in 2020. Acta Clin Belg. 2020:1-17. PubMed
26.Multiple myeloma NCCN evidence blocks (version 3.2022). Plymouth Meeting (PA): National Comprehensive Cancer Network; 2021: www.nccn.org. Accessed 2021 Nov 18.
27.British Society for Haematology Guidelines Committee. BSH guidelines process 2018. London (GB): British Society for Haematology; 2018: https://b-s-h.org.uk/media/16732/bsh-guidance-development-process-dec-5-18.pdf. Accessed 2021 Nov 29.
28.National Comprehensive Cancer Network. Development and update of guidelines. 2021; https://www.nccn.org/guidelines/guidelines-process/development-and-update-of-guidelines. Accessed 2021 Nov 29.
29.ESMO Guidelines Committee (GLC). ESMO Standard Operating Procedures (SOPs) for Clinical Practice Guidelines (CPGs) and ESMO Magnitude of Clinical Benefit (ESMO-MCBS) scores. Lugano (CH): ESMO; 2021: https://www.esmo.org/content/download/77789/1426712/1/ESMO-Clinical-Practice-Guidelines-Standard-Operating-Procedures.pdf. Accessed 2021 Nov 26.
30.Quach H, Prince HM, Medical Scientific Advisory Group (MSAG). Clinical practice guideline: multiple myeloma. Melbourne (AU): Myeloma Australia; 2019: https://myeloma.org.au/wp-content/uploads/2019/10/myeloma_clinical_practice_guideline_oct19.pdf. Accessed 2021 Nov 29.
31.Mahindra A, Hari P, Fraser R, et al. Autologous hematopoietic cell transplantation for multiple myeloma patients with renal insufficiency: a center for international blood and marrow transplant research analysis. Bone Marrow Transplant. 2017;52(12):1616-1622. PubMed
32.Kumar S, Flinn I, Richardson PG, et al. Randomized, multicenter, phase 2 study (EVOLUTION) of combinations of bortezomib, dexamethasone, cyclophosphamide, and lenalidomide in previously untreated multiple myeloma. Blood. 2012;119(19):4375-4382. PubMed
33.Myeloma Group. Bortezomib, lenalidomide and dexamethasone (VRD). Redditch (GB): NHS Thames Valley Strategic Clinical Network; 2019: http://nssg.oxford-haematology.org.uk/myeloma/pdf-protocols/mm-6-bortezomib-len-dex.pdf. Accessed 2021 Nov 18.
34.Chien N, Romeril K, Baker B, Goodman H, Chan H. Consensus statement on the treatment of transplant-eligible patients with newly diagnosed multiple myeloma in New Zealand. N Z Med J. 2020;133(1527):104-110. PubMed
35.pCODR. Provincial funding summary for lenalidomide (Revlimid) (in combo) bortezomib + dexamethasone for newly diagnosed multiple myeloma Ottawa (ON): CADTH; 2020: https://www.cadth.ca/sites/default/files/pcodr/pcodr-provfund-10141-LenalidomideRevlimid_MM.pdf. Accessed 2021 Nov 18.
36.Smith A, Wisloff F, Samson D, UK Myeloma Forum, Nordic Myeloma Study Group, British Committee for Standards in Haematology. Guidelines on the diagnosis and management of multiple myeloma 2005. Br J Haematol. 2006;132(4):410-451. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews and Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Fu et al. 201914 US Funding source: None | Study designs included: This systematic review captured economic evaluations. Number primary studies included: 24 primary studies were included; 12 in first line, 11 in second line, and 1 in multi-line. None were relevant to the current report. | Eligible populations: Patients with multiple myeloma, irrespective of line of treatment, or transplant eligibility. Relevant population: Newly diagnosed patients with multiple myeloma, receiving an ASCT. | Eligible interventions and comparators: Treatments for patients with MM, including transplant, conventional chemotherapy, and novel agents. Relevant intervention and comparator: RVd vs. CyBorD (no studies captured). | Outcomes: Cost-effectiveness, or cost-utility. Follow-up: Time horizons ranged from 20 months to lifetime. |
Sekine et al. 201915 Brazil Funding source: None | Study designs included: This systematic review and network meta-analysis captured phase II or III RCTs comparing two or more frontline treatments for transplant-eligible patients. Number primary studies included: 10 primary studies (21 publications) were included. None evaluated RVd, hence none were relevant to the current review. | Eligible population: Patients with newly diagnosed transplant-eligible multiple myeloma, initiating frontline treatment. | Eligible interventions and comparators: Frontline treatments for patients with newly diagnosed MM. Relevant intervention and comparator: RVd vs. CyBorD (no studies captured). | Outcomes: Overall survival, progression-free survival, complete response, objective response rate, adverse events. Follow-up: 19 to 91 months. |
Chen et al. 201813 China Funding source: None reported | Study designs included: This systematic review and meta-analysis captured RCTs and observational studies involving patients with MM newly initiating a thalidomide-, lenalidomide, or pomalidomide-based regimen. | Eligible population: Patients with multiple myeloma, initiating a new regimen. | Eligible interventions: Newly initiated thalidomide-, lenalidomide, or pomalidomide-based regimen. | Outcomes: Adverse events relating to infection. Follow-up: 10 to 55 months. |
Chen et al. 201813 China Funding source: None reported (continued) | Number primary studies included: 92 primary studies were included. None directly compared RVd and CyBorD among transplant-eligible patients, hence none were relevant to the current review.a | Eligible comparators: Newly initiated non-thalidomide-, non-lenalidomide, and non-pomalidomide-based regimen. Relevant intervention and comparator: RVd vs. CyBorD (no studies captured). | ||
Zeng et al. (2017)16 China Funding source: None reported. | Study designs included: This systematic review and network meta-analysis captured RCTs comparing two or more pre-ASCT induction therapies. Number primary studies included: 14 primary RCTs were included. One RCT compared RVd and CyBorD, and was relevant to the current review.b | Eligible population: Patients with newly diagnosed transplant-eligible multiple myeloma, initiating pre-ASCT induction therapy. Relevant population: Characteristics of patients in the RVd vs. CyBorD arms of the relevant RCT:b
| Eligible interventions and comparators: Frontline treatments for patients with newly diagnosed MM. Relevant intervention and comparator: RVd vs. CyBorD (1 relevant RCT captured). In the relevant arms of the relevant RCT, 8 x 21-day cycles were given:
| Outcomes:
Follow-up: NR. |
ASCT = autologous stem cell transplant; CyBorD = bortezomib-cyclophosphamide-dexamethasone; ISS = international staging system; MM = multiple myeloma; NR = not reported; RCT = randomized controlled trial; RVd = bortezomib-lenalidomide-dexamethasone.
aThe phase II EVOLUTION trial by Kumar et al. was included in the synthesis. The EVOLUTION trial includes both transplant-eligible and transplant-ineligible patients, and based on the reporting by Chen et al. (2018)13 it does not appear that the data included in their systematic review and meta-analysis was exclusively from the transplant-eligible subgroup.
bThe phase II EVOLUTION trial by Kumar et al. was included in the synthesis. The EVOLUTION trial includes both transplant-eligible and transplant-ineligible patients, and based on the reporting by Zeng et al. (2017),16 it appears that outcomes data from the transplant-eligible subgroup of the EVOLUTION trial may have been included, although baseline characteristics appear to be based on the full trial population.
cA modified dosing CyBorD arm involving cyclophosphamide was also described (given on days 1,8,15) but did not appear to be included in the evidence synthesis.
Note that this appendix has not been copy-edited.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Sidana et al. (2021)19 US Funding source: CIBMTR© | Study design: Retrospective cohort Data source: CIBMTR Study period: January 2013 to December 2018 Relevant study objective: To compare outcomes of patients receiving RVd vs. CyBorD induction prior to ASCT. | Key eligibility criteria: Received RVd or CyBorD induction therapy, with at least a partial response prior to transplant; underwent upfront ASCT. Total sample size: 1,135 patients Key characteristics, RVd vs. CyBorD:
| RVd induction:
CyBorD induction:
| Key outcomes:
Follow-up: Range: 3 to 82 months (0.25 to 6.8 years). |
Uttervall et al. (2019)20 Sweden Funding source: Cancerfonden | Study design: Retrospective cohort Data source: Medical records from Karolinska University Hospital, Sweden, and the Swedish national death registry. Study period: January 2009 to December 2018 Relevant study objective: To compare outcomes among patients receiving RVd vs. CyBorD. | Key eligibility criteria: Patients with newly diagnosed MM receiving RVd or CyBorD in the first line, stratified by receipt of HDT plus ACST (only the stratum with HDT plus ACST is included in the report). Total sample size: 681 patients; 422 received HDT plus ASCT; 259 did not. Key characteristics, RVd vs. CyBorD:
| RVd induction:
CyBorD induction
Subsequent treatment (both groups): HDT given as C (2g/m2 IV); filgrastim SC for mobilization; melphalan 200 mg/m2 IV 2-4 weeks after harvest. No consolidation treatment given; maintenance given in 8% of patients. | Key outcomes:
Follow-up: Median: 18 months (RVd); 36 months (CyBorD). |
Chakraborty et al. (2017)17 US Funding source: Unclear | Study design: Retrospective cohort Data source: Mayo Clinic (Rochester, Minnesota, US) institutional database Study period: January 2000 to May 2015 Relevant study objective: To compare overall survival by treatment, among newly diagnosed MM patients receiving novel agent-based induction regimens and who underwent early ASCT. | Key eligibility criteria: Received early ASCT, received 1 induction therapy regimen, did not relapse before ASCT. Total sample size: 1,017 patients; 319 received RVd or CyBorD; 698 received an induction regimen not relevant to the current review. Key characteristics, RVd vs. CyBorD:
| RVd induction:
CyBorD induction
| Key outcomes:
Follow-up: Median (among all surviving patients): 32.1 months (RVd); 26.9 months (CyBorD). |
Cornell et al. (2017)18 US Funding source: CIBMTR | Study design: Retrospective cohort Data source: CIBMTR Study period: 2008 to 2013 Relevant study objective: To compare triplet therapy with doublet induction therapy among MM patients receiving upfront ASCT. | Key eligibility criteria: Received: 1 bortezomib- or lenalidomide-based induction therapy regimen (at least 2 cycles); melphalan conditioning regimen; ASCT ≤ 12 months post-diagnosis (first ASCT). Tandem transplant recipients excluded. Total sample size: 693 patients; 354 received RVd or CyBorD; 339 received an induction regimen not relevant to the current review. Key characteristics, RVd vs. CyBorD:
| RVd induction:
CyBorD induction:
| Key outcomes:
Follow-up:
|
ASCT = autologous stem cell transplant; CIBMTR = Center for International Blood and Marrow Transplant Research; C = cyclophosphamide; CyBorD = bortezomib-cyclophosphamide-dexamethasone; D = dexamethasone; eGFR = estimated glomerular filtration rate; HDT = high-dose treatment; ISS = international staging system; IV = intravenous; MM = multiple myeloma; NR = not reported; R = lenalidomide; SC = subcutaneous; V = bortezomib; RVd = bortezomib-lenalidomide-dexamethasone; vs. = versus.
aHigh-risk based on cytogenics: t(4;14), t(14;16), t(14;20), del17p, +1q, HR2.
bHigh-risk based on cytogenics: t(4;14), t(14;16), t(14;20), del17p.
cCalculated across the total sample of 1,017 patients (i.e., all induction regimens together), not for each specific induction regimen.
dHigh-risk based on cytogenics: t(4;14), t(14;16), t(14;20), del17p, hypodiploidy, and any abnormality in chromosome 1.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: Clinical practitioners Target population: The guideline covers all patients with multiple myeloma; the relevant population is patients with multiple myeloma (symptomatic), who are transplant candidates. | Guideline covers diagnosis and management of multiple myeloma. Relevant practice covered: Primary therapy for multiple myeloma transplant candidates | Response rates, depth of response, overall survival, progression-free survival, neuropathy, grade 3/4 adverse events. | PubMed search (prior to October 2020)a, selected for relevant, and discussed by the NCCN Guidelines Panel. | Based on NCCN categories of evidence and consensus:b
As well as NCCN blocks, in which quality of the evidence is categorized from 1 (lowest) to 5 (highest). | Guideline development follows a well-defined process, including: an annual institutional review, a literature review, third-party submissions, panel meetings, development of recommendations, and development of discussion. Complete details are provided online.28 | The guidelines are reviewed by the NCCN Panel chair / Vice-chair, and the full NCCN Guideline Panel. Complete details are provided online.28 |
British Society for Haematology/UK Myeloma Forum, 202124 | ||||||
Intended Users: Healthcare professionals Target population: The guideline covers all patients with multiple myeloma; the relevant population is patients with multiple myeloma (symptomatic), who are transplant candidates. | Guideline covers diagnosis and management of multiple myeloma. Relevant practice covered: Primary therapy for multiple myeloma transplant candidates | Response rates, depth of response, MRD negativity, overall survival, progression-free survival, side effects, patient preferences, drug access and funding. | Evidence was collected using MEDLINE, PubMed, Embase, Central, and Web of Science searches (January 2013 to July 2019). Guidance was developed according to pre-defined process.c | Based on the GRADE criteria, in which the quality of the evidence is graded as:
And strength of the recommendation is graded as:
Additional details available.27 | Guidance was developed according to pre-defined process,27 involving:
| The manuscript was reviewed by several parties, including: the BSH Guidelines Committee Haematology Oncology Task Force; the BSH Guidelines Committee; the Haematology Oncology sounding board of BSH; the UK Charity Myeloma UK. It was also posted to the BSH website for comment. |
EHA-ESMO Clinical Practice Guidelines, 202121 | ||||||
Intended Users: Clinical practice Target population: The guideline covers all patients with multiple myeloma; the relevant population is newly diagnosed patients with multiple myeloma, who are eligible for high-dose treatment and autologous transplantation. | Guideline covers diagnosis and management of multiple myeloma. Relevant practice covered: Induction regimen for newly diagnosed patients with multiple myeloma, who are eligible for high-dose treatment and autologous transplantation | Response rates, peripheral neuropathy, MRD negativity, progression-free survival. | Evidence was collected And synthesized according to ESMO standard operating procedures for clinical practice guideline development.29 Specific details on search strategies were not provided. | Adapted from the Infectious Diseases Society of America-US Public Health Service Grading System in which the quality of the evidence is graded from I (most high-quality) to IV (least high-quality), and grade of recommendation is rated from A (strongly recommended) to E (never recommended). Additional details available.c | Guidance was developed according to ESMO standard operating procedures for clinical practice guideline.29 | The manuscript was reviewed by reviewers nominated by ESMO and EHA. Guidelines were approved by the EHA Board and the ESMO guidelines committee. |
Myeloma Australia’s Medical and Scientific Advisory Group (MSAG), 202023 | ||||||
Intended users: Clinicians Target population: The guideline covers all patients with multiple myeloma; the relevant population is patients with multiple myeloma (symptomatic), who are transplant candidates. | Guideline covers treatment with RVd among transplant-eligible and -ineligible patients with multiple myeloma. Relevant practice covered: Primary therapy for multiple myeloma transplant candidates | Response rates, depth of response, MRD negativity, progression-free survival, peripheral neuropathy, hematologic toxicity, stem cell mobilization. | NR | Quality of the evidence is graded from 1A (most high-quality) to 4 (least high-quality), and grade of recommendation is rated from A (based on at least one level 1A or 1B evidence) to C (based on level 4 evidence). Additional details available.e | NR | NR |
Vekemens et al. (Belgium), 202025 | ||||||
Intended Users: Belgian hematologists Target population: The guideline covers all patients with multiple myeloma; the relevant population is patients with multiple myeloma (symptomatic), who are transplant candidates. | Guideline covers diagnosis and management of multiple myeloma. Relevant practice covered: Primary therapy for multiple myeloma transplant candidates | Response rates, depth of response, MRD negativity, progression-free survival. | Not stated. Described as an ‘extensive’ literature review. | Level of evidence is graded from 1A (most high-quality) to 4 (least high-quality), and grade of recommendation is rated from A (based on at least one level 1A or 1B evidence) to C (based on level 4 evidence). Additional details available.f | NR | NR |
BSH = British Society for Haematology; EHA = European Hematology Association; ESMO = European Society for Medical Oncology; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; MRD = minimal residual disease; NCCN = National Comprehensive Cancer Network; NR = not reported; RVd = bortezomib-lenalidomide-dexamethasone.
asearch date not provided, but was conducted prior to update, which was October 19, 2020.
bdefinitions are provided within the guidelines; interpretation for relevant categories provided in the summary of findings table.
cdetails available at: https://b-s-h.org.uk/media/16732/bsh-guidance-development-process-dec-5-18.pdf
cdetails in Supplemental Table 7 of the guidelines document.
eGrading is assumed to be the same as in the MSAG 2019 Clinical Practice Guidelines for Multiple Myeloma.30
eVekemens et al. (2020)25 cited a previous publication as to how recommendations are graded.36
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews and Network Meta-Analyses Using AMSTAR 28 and the ISPOR Questionnaire9
Strengths | Limitations |
|---|---|
Fu et al. (2019)14,a | |
| Unclear whether review methods were established prior to the conduct of the review. |
Sekine et al. (2019)15,a | |
| Clinical trial registries were not searched. |
Chen et al. (2018)13,a | |
|
|
Zeng et al. (2017)16 | |
• Eligibility criteria were clearly defined, covering the elements of PICO and study design choices • Extraction was performed in duplicate
Relevance:
Credibility:
|
Relevance:
Credibility:
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CyBorD = bortezomib-cyclophosphamide-dexamethasone; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; PICO = population, intervention, comparator group, outcome; RCT = randomized controlled trial; RVd = bortezomib-lenalidomide-dexamethasone.
aFor systematic reviews that did not capture any relevant studies, the assessment focused on the comprehensiveness of the literature search, to assess whether relevant studies were potentially missed.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist10
Strengths | Limitations |
|---|---|
Sidana et al. (2021)19 | |
Reporting:
External validity:
Internal validity (bias, confounding):
Power: Power calculations not provided. Sample size was not noted as a limitation of the study. | Reporting:
External validity:
Internal validity (bias, confounding):
|
Uttervall et al. (2019)20 | |
Reporting:
External validity:
Internal validity (bias, confounding):
| Reporting:
External validity: Single hospital; non-Canadian centre. Internal validity (bias, confounding):
Power: Power calculations not provided. Sample size in the RVd group was noted as a limitation of the study. |
Chakraborty et al. (2017)17 | |
Reporting:
External validity:
Internal validity (bias, confounding):
Power: Power calculations not provided. Large sample size and long duration of follow-up were used to “ensure statistical power.” (p. 35).17 | Reporting:
External validity: Non-profit academic setting (Mayo clinic) may not generalize to other US-based centres; non-Canadian centre.
|
Cornell et al. (2017)18 | |
Reporting:
External validity: North American sample; however, sampling methods were unclear. Internal validity (bias, confounding):
Power: Power calculations not provided. Sample size was not noted as a limitation of the study. | Reporting:
External validity:
Internal validity (bias, confounding):
|
CyBorD = bortezomib-cyclophosphamide-dexamethasone; ISS = international staging system; IV = intravenous; MM = multiple myeloma; RCT = randomized controlled trial; RVd = bortezomib-lenalidomide-dexamethasone.
Table 7: Strengths and Limitations of Guidelines Using AGREE II11
Item | British Society for Haematology/UK Myeloma Forum, 202124 | EHA-ESMO Clinical Practice Guidelines, 202121 | Myeloma Australia’s Medical and Scientific Advisory Group (MSAG), 202023 | Vekemens et al. (Belgium), 202025 | |
|---|---|---|---|---|---|
Domain 1: Scope and purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||||
4. The guideline development group includes individuals from all relevant professional groups. | Yesa | Yesa | Yesa | Unclear | Unclear |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yesa | Yesa | Unclear | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes | Yes |
Domain 3: Rigour of development | |||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Unclear | Unclear | Unclear |
8. The criteria for selecting the evidence are clearly described. | No | No | No | No | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes | Yes |
#10. #The methods for formulating the recommendations are clearly described. | Yesa | Yesa | Yesa | Unclear | Unclear |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts prior to its publication. | Yes | Yes | Yes | Unclear | Unclear |
14. A procedure for updating the guideline is provided. | Yesa | Yesa | Yesa | No | No |
Domain 4: Clarity of presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | |||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No | Yes | No | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | NA | NA | NA | NA | NA |
Domain 6: Editorial independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Yes – guideline development funded solely by membership dues; industry support is not accepted. | Yes – Funding is not accepted for guideline production, other than travel costs. | Yes – no external funding is accepted. Production costs covered by central funds. | Unclear | Yes – the authors declare no funding sources. |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | No | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable.
aAssumed to be yes, based on documentation within the general guideline development process.27-29
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 8: Summary of Findings by Outcome — Response
Study citation and study design | Outcome definition | Outcome time-point | % Response, RVd | % Response, CyBorD | RVd vs. CyBorD relative effect estimatea | RVd vs. CyBorD P value |
|---|---|---|---|---|---|---|
Pre- or at-ASCT | ||||||
Sidana et al. (2021)19 Retrospective cohort | CR | Pre-transplantb | 17% | 17% | NR | NR |
VGPR or better | Pre-transplantb | 65% | 59% | NR | 0.11 | |
Chakraborty et al. (2017)17 Retrospective cohort | sCR | Pre-transplantc | 17.5% | 12.4% | NR | NR |
VGPR or better | Pre-transplantc | 41.3% | 40.4% | NR | NR | |
Cornell et al. (2017)18 Retrospective cohort | sCR | At-ASCT | 5% | 4% | NR | NR |
VGPR or better | At-ASCT | 56.7% | 44.0% | NR | NR | |
Post-ASCT | ||||||
Sidana et al. (2021)19 Retrospective cohort | CR | Best response post-ASCT | 63% | 57% | NR | 0.07 |
VGPR or better | At day 100 post-ASCT | 74%, in text 76%, in table | 75%, in text 77%, in table | NR | 0.47, in text 0.68, in table | |
VGPR or better | Best response post-ASCT | 85%, in text 86%, in table | 89% | NR | 0.17, in text 0.31, in table | |
Chakraborty et al. (2017)17 Retrospective cohort | sCR | Post-ASCT | 46% | 34.2% | NR | NR |
VGPR or better | Post-ASCT | 82.5% | 77.7% | NR | NR | |
Cornell et al. (2017)18 Retrospective cohort | sCR | Best response 100 days post-ASCT | 12% | 12% | NR | NR |
VGPR or better | Best response 100 days post-ASCT | 64.8% | 58.3% | NR | NR | |
Unclear timing with respect to ASCT | ||||||
Zeng et al. (2017)16 Systematic review 1 RCT was eligible for the current review. | ORR | Post-induction | NR | NR | NMA odds ratio = 1.4 (95% CrI: 0.63 to 3.2)d | NMA P value NR |
ORR | Post-induction | NR | NR | Kumar et al. (2012) study specific results NR | Kumar et al. (2012) study specific results NR | |
Uttervall et al. (2019)20 Retrospective cohort | CR or nCR | Best response post-HDT | 42% | 50% | NR | NR |
VGPR or better | Best response post-HDT | 76% | 78% | NR | NR | |
PR or better | Best response post-HDT | 98% | 95% | NR | Not significant | |
ASCT = autologous stem cell transplant; CR = complete response; CrI = credible interval; CyBorD = bortezomib-cyclophosphamide-dexamethasone; HDT = high-dose treatment; NMA = network meta-analysis; nCR = near complete response; NR = not reported; ORR = overall response rate (defined as partial response or better); PR = partial response; RCT = randomized controlled trial; sCR = stringent complete response; VGPR = very good partial response; RVd = bortezomib-lenalidomide-dexamethasone.
aOdds ratios > 1 represent better response for RVd compared with CyBorD.
bAuthors reported this as a baseline characteristic rather than a study outcome, however, it has been included in the current table as it is an outcome of induction therapy. Note that in this study, eligibility was restricted to patients achieving pre-transplant partial response or better after induction therapy.
cAuthors reported this as a baseline characteristic rather than a study outcome, however, it has been included in the current table as it is an outcome of induction therapy.
dUnclear whether authors reported a credible interval or a confidence interval.
Note that this appendix has not been copy-edited.
Table 9: Summary of Findings by Outcome — Relapse and Progression
Study citation and study design | Outcome definition and time-point | R/P, RVd (95% CI) | R/P, CyBorD (95% CI) | RVd vs. CyBorD hazard ratio (95% CI) a | RVd vs. CyBorD P value |
|---|---|---|---|---|---|
Cornell et al. (2017)18 Retrospective cohort | 1-year relapse/progression, unadjusted | 17% (12% to 21%) | 16% (9% to 25%) | NR | NR |
2-year relapse/progression, unadjusted | 29% (23% to 35%) | 40% (29% to 53%) | NR | NR | |
3-year relapse/progression, unadjusted | 38% (31% to 45%) | 63% (49% to 77%) | NR | NR | |
Relapse/progression, adjustedb | NR | NR | 0.678 (0.465 to 0.990) | 0.0444 |
CI = confidence interval; CyBorD = bortezomib-cyclophosphamide-dexamethasone; NR = not reported; RVd = bortezomib-lenalidomide-dexamethasone.
aHazard ratios < 1 represent better (lower) relapse/progression rates for RVd compared with CyBorD.
bAdjusted for cytogenics (high-risk) and planned post-ASCT therapy.
Table 10: Summary of Findings by Outcome — Progression-Free Survival
Study citation and study design | Outcome definition and time-point | PFS, RVd (95% CI) | PFS, CyBorD (95% CI) | RVd vs. CyBorD hazard ratio (95% CI) a | RVd vs. CyBorD P value |
|---|---|---|---|---|---|
Sidana et al. (2021)19 Retrospective cohort | 2-year PFS, unadjusted | 72% (68% to 75%) | 60% (53% to 67%) | NR | 0.004 |
5-year PFS, unadjusted | 40% (34% to 46%) | 32% (24% to 41%) | NR | 0.152 | |
PFS, unadjusted | NR | NR | NR | 0.004 (via log-rank test) | |
PFS, adjustedb | NR | NR | 0.83 (0.65 to 1.05)c | 0.13 | |
PFS, unadjusted: eGFR < 60 mL/min/1.73m2 | 2-year: 71% 5-year: 39% | 2-year: 64% 5-year: 39% | NR | 0.555 (via log-rank test) | |
PFS, unadjusted: eGFR ≥ 60 mL/min/1.73m2 | 2-year: 73% 5-year: 41% | 2-year: 57% 5-year: 28% | NR | 0.003 (via log-rank test) | |
Uttervall et al. (2019)20 Retrospective cohort | 1-year PFS, unadjusted | 97% | 89% | NR | NR |
18-month PFS, unadjusted | 91% | 73% | NR | NR | |
PFS, unadjusted | NR | NR | NR | 0.022 (via log-rank test) | |
PFS, adjustedd | NR | NR | NR, favours RVd | < 0.001 | |
Chakraborty et al. (2017)17 Retrospective cohort | Median PFS, unadjusted | 32.6 months (30.3 to 42.5) | 32.6 months (30.2 to 38.2) | 0.94 (0.66 to 1.35)e | 0.76 |
PFS, adjustedf | 0.70 (0.44 to 1.10)g | 0.13 | |||
Cornell et al. (2017)18 Retrospective cohort | 1-year PFS, unadjusted | 82% (78% to 87%) | 83% (74% to 90%) | NR | NR |
2-year PFS, unadjusted | 70% (64% to 76%) | 59% (47% to 71%) | NR | NR | |
3-year PFS, unadjusted | 61% (53% to 68%) | 36% (23% to 50%) | NR | NR | |
PFS, adjustedh | NR | NR | 0.701 (0.483 to 1.018) | 0.0618 |
CI = confidence interval; CyBorD = bortezomib-cyclophosphamide-dexamethasone; eGFR = estimated glomerular filtration rate; NR = not reported; PFS = progression-free survival; RVd = bortezomib-lenalidomide-dexamethasone.
aHazard ratios < 1 represent better progression-free survival for RVd compared with CyBorD.
bAdjusted for international staging system (ISS) stage, cytogenics (high-risk), maintenance therapy, and pre-transplant response.
cFor CyBorD vs. RVd, author-reported HR = 1.20 (95% CI: 0.95 to 1.53); inverse estimates for RVd vs. CyBorD are presented in the table.
dAdjusted for age, serum lactate dehydrogenase, ISS, beta-2 microglobulin, serum albumin, serum calcium, hemoglobin, eGFR (MDRD formula).
eFor CyBorD vs. RVd, author-reported HR = 1.06 (95% CI: 0.74 to 1.51); inverse estimates for RVd vs. CyBorD are presented in the table.
fAdjusted for age, sex, transplant period (2000 to 2007 vs. 2008 to 2015), international staging system (ISS) stage, and cytogenics (high-risk).
gFor CyBorD vs. RVd, author-reported HR = 1.42 (95% CI: 0.91 to 2.26); inverse estimates for RVd vs. CyBorD are presented in the table.
hAdjusted for cytogenics (high-risk) and planned post-ASCT therapy.
Table 11: Summary of Findings by Outcome — Overall Survival
Study citation and study design | Outcome definition and time-point | OS, RVd (95% CI) | OS, CyBorD (95% CI) | RVd vs. CyBorD hazard ratio (95% CI) a | RVd vs. CyBorD P value |
|---|---|---|---|---|---|
Sidana et al. (2021)19 Retrospective cohort | 2-year OS, unadjusted | 92% (90% to 94%) | 87% (81% to 91%) | NR | 0.056 |
5-year OS, unadjusted | 79% (74% to 83%) | 60% (50% to 69%) | NR | <0.001 | |
OS, unadjusted | NR | NR | NR | 0.004 (via log-rank test) | |
OS, adjustedb | NR | NR | 0.75 (0.53 to 1.09)c | 0.13 | |
OS, unadjusted: eGFR < 60 mL/min/1.73m2 | 2-year: 93% 5-year: 84% | 2-year: 85% 5-year: 60% | NR | 0.042 (via log-rank test) | |
OS, unadjusted: eGFR ≥ 60 mL/min/1.73m2 | 2-year: 92% 5-year: 78% | 2-year: 90% 5-year: 61% | NR | 0.075 (via log-rank test) | |
Uttervall et al. (2019)20 Retrospective cohort | 1-year OS, unadjusted | 98% | 96% | NR | NR |
18-month OS, unadjusted | 98% | 95% | NR | NR | |
OS, unadjusted | NR | NR | NR | 0.093 (via log-rank test) | |
Chakraborty et al. (2017)17 Retrospective cohort | 5-year OS, unadjusted | 79% (65.7% to 88.1%) | 79.2% (63.5% to 88.5%) | NR | NR |
Median OS, unadjusted | Not reached | Not reached | NR | NR | |
OS, unadjusted | NR | NR | 0.88 (0.42 to 1.79)d | 0.72 | |
OS, adjustede | NR | NR | 0.32 (0.10 to 0.88)f | 0.03 | |
Cornell et al. (2017)18 Retrospective cohort | 1-year OS, unadjusted | 96% (94% to 98%) | 96% (91% to 99%) | NR | NR |
2-year OS, unadjusted | 92% (88% to 95%) | 86% (77% to 93%) | NR | NR | |
3-year OS, unadjusted | 85% (79% to 90%) | 67% (52% to 80%) | NR | NR | |
OS, adjustedg | NR | NR | 0.705 (0.398 to 1.251) | 0.2322 |
CI = confidence interval; CyBorD = bortezomib-cyclophosphamide-dexamethasone; eGFR = estimated glomerular filtration rate; NR = not reported; OS = overall survival; RVd = bortezomib-lenalidomide-dexamethasone.
aHazard ratios < 1 represent better overall survival for RVd compared with CyBorD.
bAdjusted for international staging system (ISS) stage, cytogenics (high-risk), maintenance therapy, and pre-transplant response.
cFor CyBorD vs. RVd, author-reported HR = 1.33 (95% CI: 0.92 to 1.90); inverse estimates for RVd vs. CyBorD are presented in the table.
dFor CyBorD vs. RVd, author-reported HR = 1.14 (95% CI: 0.56 to 2.36); inverse estimates for RVd vs. CyBorD are presented in the table.
eAdjusted for age, sex, transplant period (2000 to 2007 vs. 2008 to 2015), international staging system (ISS) stage, and cytogenics (high-risk).
fFor CyBorD vs. RVd, author-reported HR = 3.11 (95% CI: 1.14 to 9.96); inverse estimates for RVd vs. CyBorD are presented in the table.
gAdjusted for international staging system (ISS) stage, and cytogenics (high-risk).
Table 12: Summary of Findings by Outcome — Adverse Events
Study citation and study design | Outcome definition | n/N, RVd (%) | R/P, CyBorD (95% CI) | RVd vs. CyBorD hazard ratio (95% CI) a | RVd vs. CyBorD P value |
|---|---|---|---|---|---|
Uttervall et al. (2019)20 Retrospective cohort | Secondary primary malignancy | 2 / 71 (2.8%) | Unclear if NR or 0 | NR | NR |
Cornell et al. (2017)18 Retrospective cohort | Death due to secondary primary malignancy | 2 / 270 (0.7%) | 1 / 84 (1.2%) | NR | NR |
CI = confidence interval; CyBorD = bortezomib-cyclophosphamide-dexamethasone; NR = not reported; RVd = bortezomib-lenalidomide-dexamethasone.
Table 13: Summary of Authors’ Conclusions of Included Systematic Review, Network Meta-Analysis, and Primary Clinical Studies
Study citation | Authors’ conclusion |
|---|---|
Zeng et al. (2017)16 Systematic review and network meta-analysis | There were no relevant conclusions relating to RVd vs. CyBorD made by the study authors. |
Sidana et al. (2021)19 Retrospective cohort | “In conclusion, we did not observe any difference in VGPR or better response rates with RVd or [CyBorD] induction therapy amongst patients who achieved at least a partial response and proceeded to stem cell transplant. […] [T]he two regimens were found to have associated with comparable survival outcomes after adjusting for maintenance therapy and other known prognostic variables.” -p.1419 |
Uttervall et al. (2019)20 Retrospective cohort | “In conclusion, replacing [CyBorD] with RVd upfront improves response and PFS, both for patients eligible and not eligible for [high-dose treatment]. There also appears to be an overall better survival with upfront RVd. RVd is well tolerated and there was no evidence that it leads to a higher incidence of SPMs. We therefore recommend RVd to be given upfront to all [multiple myeloma] patients.” -p. 25320 |
Chakraborty et al. (2017)17 Retrospective cohort | “In this study, the RVd induction regimen was shown to have superior response rates and survival benefit over [CyBorD] […] in patients successfully completing induction therapy and undergoing early transplant, after controlling for important host and tumor characteristics.” -p. 3717 |
Cornell et al. (2017)18 Retrospective cohort | “It is notable that in comparing the 2 commonly used triplet therapies, RVd versus [CyBorD], we observed a trend for lower risk of progression among RVd induction recipients.” -p. 275.18 |
CyBorD = bortezomib-cyclophosphamide-dexamethasone; VGPR = very good partial response; RVd = bortezomib-lenalidomide-dexamethasone.
Table 14: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Primary therapy for transplant candidates:
The evidence supporting RVd includes data from 6 trials:
| The recommendation that RVd is the preferred option for primary treatment of transplant-eligible patients with MM is categorized as category 1, indicating high-level evidence and that there is uniform consensus within the NCCN Panel that the intervention is appropriate. The NCCN Evidence BlocksTM for RVd are (ranked 5 as highest/best, 1 as lowest/worst):
|
British Society for Haematology/UK Myeloma Forum, 202124 | |
The relevant recommendations regarding choice of initial treatment for transplant-eligible patients with MM are:
Broader evidence supporting the recommendation for a proteasome inhibitor backbone, such as bortezomib, is based on better response, progression-free survival, and overall survival, and evidence supporting the addition of an immunomodulary drug such as lenalidomide, is based on evidence of increased response. Evidence specific to the RVd regimen included:
| The first 3 recommendations are GRADE level 1A, indicating a strong recommendation based on high-quality evidence. The fourth recommendation is GRADE level 1C, indicating a strong recommendation based on low-quality evidence. |
EHA-ESMO Clinical Practice Guidelines, 202121 | |
The relevant recommendations regarding choice of initial treatment for transplant-eligible patients with MM are: RVd is considered to have the best risk-benefit profile among triplet regimens for induction therapy. RVd is listed as the first option to consider, along with the quadruplet regimen daratumumab plus bortezomib-thalidomide-dexamethasone. The key evidence specific to the recommendation for RVd was based on high VGPR rates, CR rates, MRD negativity rates, and prolonged PFS,in the following studies:
Additionally, improved VGPR and MRD negativity with RVd compared with bortezomib-thalidomide-dexamethasone was supported by evidence from: An integrated analysis of 3 RCTs, presented in abstract form by Rosinol et al. | The recommendation for RVd was categorized as level II (indicating that the evidence was based on small RCTs, large RCTs with lower methodological quality, or “meta-analyses of such trials or of trials with demonstrated heterogeneity”), and grade B (“strong or moderate evidence for efficacy but with a limited clinical benefit, generally recommended”). |
Vekemens et al., 202025 | |
The relevant recommendation regarding choice of induction therapy among transplant-eligible patients with MM is to use a 3-drug regimen, including at least bortezomib and dexamethasone. As supporting evidence, the guideline authors make the following comments regarding specific regimens, although these do not comprise a formal recommendation:
The latter statement relating to RVd was supported by evidence from:
| The recommendation was graded as category 1,A, indicating that the recommendation was based on at least one good-quality RCT, and that there was consistency addressing the specific recommendation. |
Myeloma Australia’s Medical and Scientific Advisory Group (MSAG)23 | |
The relevant recommendations regarding choice of induction therapy among transplant-eligible patients with MM are:
The relevant evidence supporting the recommendation for RVd as standard of care included:
| Recommendations 1, 5, and 6 were categorized as level 1B evidence (i.e., based on at least 1 RCT), and grade A recommendation (i.e., based on at least 1 good-quality RCT that addressed the specific recommendation). Recommendation 2 was level 2A evidence (i.e., based on at least one non-randomized trial [including phase II trials]), and grade B recommendation (i.e., the recommendation was based on well-conducted studies but that there were no RCTs addressing the specific recommendation). Recommendations 3 and 4 were not categorized according to level of evidence or strength of recommendation. |
ASCT = autologous stem cell transplant; CR = complete response; CyBorD = bortezomib-cyclophosphamide-dexamethasone; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; MM = multiple myeloma; MRD = minimal residual disease; NCCN = National Comprehensive Cancer Network; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; VGPR = very good partial response; RVd = bortezomib-lenalidomide-dexamethasone.
a“the purpose of classifying regimens as such is to convey the sense of the panel regarding the relative efficacy and toxicity of the regimens. Factors considered by the Panel include evidence, efficacy, toxicity, pre-existing comorbidities such as renal insufficiency, and in some cases access to certain agents.” -slide 47.22
bIn the discussion section, this is listed as a preferred primary therapy; this may reflect a recent change in the guidelines, as the discussion update is marked as being in progress.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Additional References
RCT With Comparisons Between RVd and CyBorD, Conference Abstract
37.Kumar L, Chellapuram Sk, Sahoo R, Gupta R. VRd versus VCd as induction therapy for newly diagnosed multiple myeloma: a phase III, randomized study. Clin Lymphoma Myeloma Leuk. 2019;19(10):e361.
A phase III trial, presented at 17th International Myeloma Workshop, which occurred September 12 to 15, 2019, in Boston, Massachusetts, US.
Non-Randomized Studies With Comparisons Between RVd and CyBorD, Yet Population Not Restricted to Newly Diagnosed Transplant-eligible Patients
38.Kumar L, Gundu N, Kancharia H, et al. Multiple myeloma-effect of induction therapy on transplant outcomes. Clin Lymphoma Myeloma Leuk. 2021;21(2):80-90.e5. PubMed
A retrospective single-centre study conducted in India, comparing triplet- versus doublet regimens. This study included patients undergoing ASCT after second or subsequent remission after salvage induction therapy, and the main results did not report outcomes by RVd vs. CyBorD; however, suboptimal stem cell mobilization was reported for the RVd (9.4%) and CyBorD (9.52%) groups separately, and it was noted in the discussion section that the VGPR or better was not statistically different in the RVd (69.8%) and CyBorD (63.4%) groups.
39.Nasr F, Ghoche AA, Diab S, et al. Lebanese real-world experience in treating multiple myeloma: a multicenter retrospective study. Leuk Res Rep. 2021;15:100252. PubMed
A retrospective study conducted using data from two hospitals in Lebanon, which provided Kaplan-Meier curves for progression-free survival and overall survival by treatment regimen, including RVd and CyBorD. However, this study included patients who did and who did not undergo ASCT.
Guidance Documents, Methodology Unreported
40.Iida S, Ishida T, Murakami H, et al. JSH practical guidelines for hematological malignancies, 2018: III. Myeloma-1. Multiple myeloma (MM). Int J Hematol. 2019;109(5):509-538. PubMed
Guidelines by the Japanese Society of Hematology, for which the methods of evidence grading and literature review could not be determined. Three-drug regimens, including but not limited to RVd, are recommended, but with a comment to for careful consideration due to increased toxicity over two-drug regimens.
Canadian and US-Based Guidance Documents, RVd Not Specifically Addressed
41.Mikhael J, Ismaila N, Cheung MC, et al. Treatment of Multiple Myeloma: ASCO and CCO Joint Clinical Practice Guideline. J Clin Oncol. 2019;37(14):1228-1263. PubMed
Guidelines by the American Society for Clinical Oncology and Cancer Care Ontario. Treatment guidelines are at the class-level, and do not specify RVd, however, the recommendation is for induction regimens that include a proteasome inhibitor, an immunomodulatory drug, and a steroid, which encompasses RVd.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca