CADTH Health Technology Review
Obstetrical Ultrasound During Pregnancy
Rapid Review
Authors: Kylie Tingley, Jennifer Horton
Key Messages
No relevant evidence was identified comparing the safety of frequent obstetrical ultrasounds compared to the routine use of obstetrical ultrasound during pregnancy.
This review identified 10 evidence-based guidelines that provided recommendations regarding various indications for obstetrical ultrasound, as well as the frequency of obstetrical ultrasound; however, the methodological rigour of these guidelines is limited and recommendations should be interpreted with caution.
One guideline recommended against obstetrical ultrasound for non-medical purposes and recommended that ultrasound exposure be as low as reasonably possible during pregnancy. These recommendations were based on moderate-quality evidence and expert opinion, and should be interpreted with caution.
The guidelines made recommendations for specific patient populations for whom more frequent obstetrical ultrasound examinations may be required. These populations included pregnancies affected by certain congenital infections, people pregnant with twins, pregnant adolescents, and pregnant people at high risk for fetal anomalies or for whom mid-trimester transabdominal ultrasound would be challenging.
Context and Policy Issues
Obstetricians have been using ultrasound to diagnose intrauterine pregnancy since the 1960s and 1970s.1 Ultrasound is a non-invasive diagnostic modality that has typically been associated with little to no risk1; however, epidemiologic research on ultrasound is limited.2 A systematic review by Whitworth and colleagues (2014)3 demonstrated that there is debate in the literature about whether ultrasound examination, especially multiple exposures, is harmful in individuals who are pregnant. Currently, the Society of Obstetricians and Gynaecologists of Canada recommends that all pregnant individuals have 2 ultrasounds; 1 between 11 to 14 weeks’ gestation to date the pregnancy and 1 between 18 to 20 weeks’ gestation to assess anatomic features.4 Despite these recommendations, decision-makers have identified that that pregnant individuals may be receiving additional ultrasounds as part of their routine prenatal care at physicians’ offices and obstetrical clinics, and may also receive an ultrasound during an emergency room visit. This has led to a lack of consistency in the process and there is concern that this has contributed to the potential overuse of ultrasounds during pregnancy.
In response to these concerns regarding the frequent use of ultrasounds during pregnancy, there is a need to review the evidence and evidence-based guidance regarding obstetrical ultrasound to ensure that decision-makers have the best evidence to inform decisions about care pathways for individuals who are pregnant. The 2 objectives of this report are: 1) to identify and summarize the available evidence regarding the safety of routine versus more frequent use of obstetrical ultrasound among individuals who are pregnant; and 2) to identify and summarize the evidence-based guidance regarding the use of obstetrical ultrasound during pregnancy.
Research Questions
What is the clinical evidence for the safety related to the frequent use of obstetrical ultrasound during pregnancy?
What are the evidence-based guidelines for the use of obstetrical ultrasound during pregnancy?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were obstetrical ultrasound and adverse events. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or network meta-analyses; and randomized controlled trials, controlled clinical trials, or any other type of clinical trial. An additional search was done for obstetrical ultrasound, with CADTH-developed search filters applied to limit retrieval to guidelines. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2015 and November 1, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals who are pregnant |
Intervention | Q1: Frequent use of obstetrical ultrasound Q2: Obstetrical ultrasound |
Comparator | Q1: Routine use of obstetrical ultrasound (i.e., routine use as defined in the literature, 2 ultrasounds as recommended by the Society of Obstetricians and Gynaecologists of Canada) Q2: Not applicable |
Outcomes | Q1: Safety (e.g., adverse events associated with obstetrical ultrasound, clinical impacts of obstetrical ultrasound overuse, adverse maternal outcomes, adverse fetal outcomes related to obstetrical ultrasound overuse) Q2: Recommendations related to the best practice for the use of obstetrical ultrasound during pregnancy (e.g., appropriate patient populations or clinical settings, strategies to mitigate harms, adverse events, and misuse), recommendations related to the appropriate frequency of obstetrical ultrasounds received during pregnancy, recommendations related to clinical indication warranting further or more frequent obstetrical ultrasounds |
Study designs | Health technology assessment and systematics reviews, randomized controlled trials, non-randomized studies, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2015. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument5 for guidelines. The strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
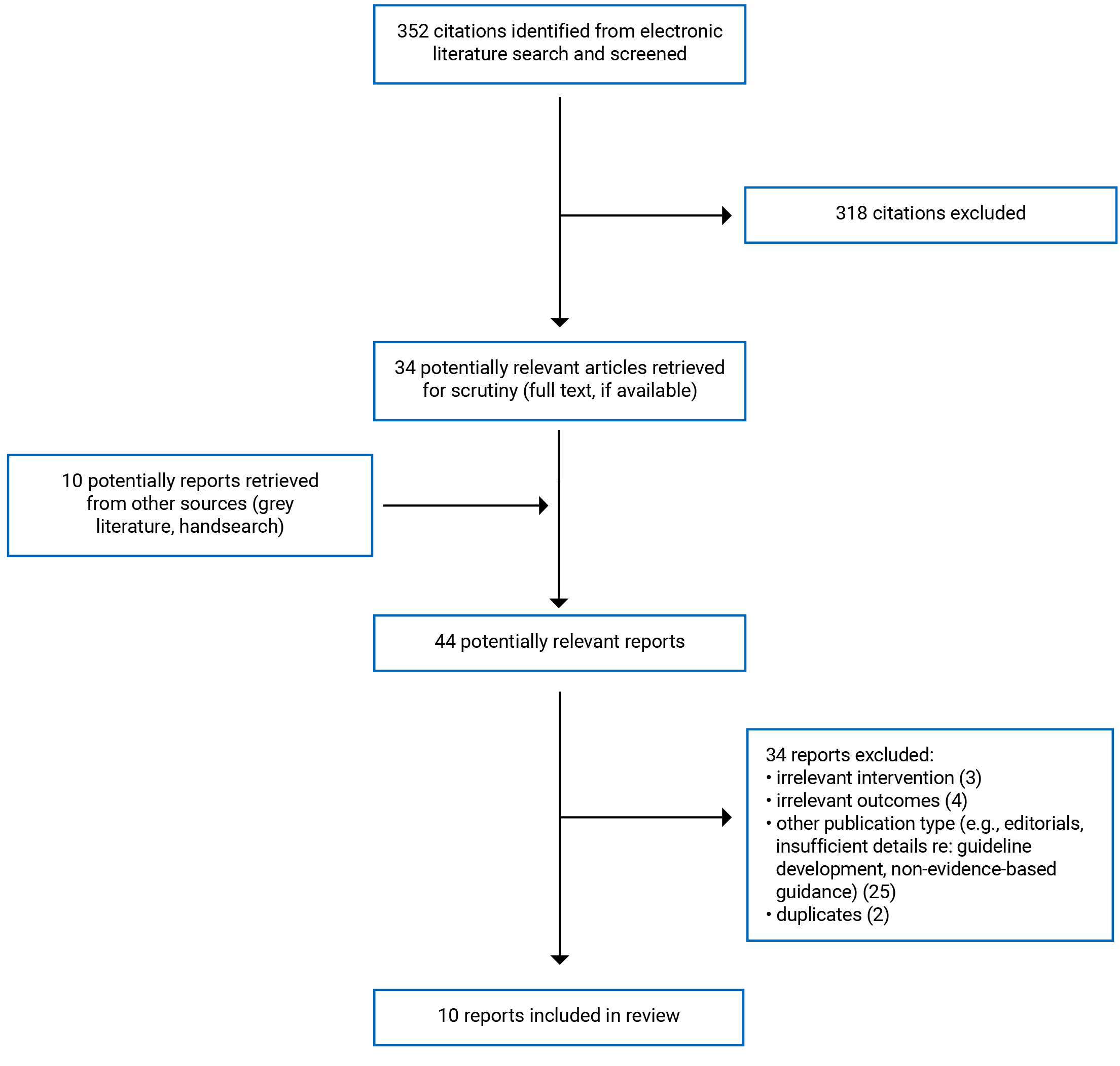
A total of 352 citations were identified in the literature search. Following the screening of titles and abstracts, 318 citations were excluded and 34 potentially relevant reports from the electronic search were retrieved for full-text review. Ten potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 34 publications were excluded for various reasons and 10 publications met the inclusion criteria and were included in this report. These 10 publications were evidence-based guidelines. Appendix 1 presents the PRISMA6 flow chart of the study selection.
Summary of Study Characteristics
No eligible health technology assessments, systematics reviews, randomized controlled trials, or non-randomized studies were identified. Ten evidence-based guidelines with recommendations regarding obstetrical ultrasound were identified.2,7-15
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Ten evidence-based guidelines with recommendations regarding obstetrical ultrasound were identified.2,7-15 Six of the guidelines were developed by the Society of Obstetricians and Gynaecologists of Canada,2,8,10-12,15 2 were developed by ISUOG ― the International Society of Ultrasound in Obstetrics and Gynecology,7,14 1 was developed by the U.S. Department of Veterans Affairs and the U.S. Department of Defense,9 and 1 was developed by the American College of Obstetricians and Gynecologists.13 Each of the 10 included guidelines collected evidence using a review of the literature and expert opinion, when needed.2,7-15 One of the guidelines also used patient focus groups to inform their recommendations.9 Five of the included guidelines2,8,10,11,15 used the criteria described by the Canadian Task Force on Preventive Health Care to determine the quality of evidence and classify the strength of recommendations. Evidence was graded from I (evidence obtained from at least 1 randomized controlled trial) to III (opinions of respected authorities and based on clinical experience, descriptive studies, or reports of expert committees). Two guidelines9,12 followed the Grading of Recommendations Assessment, Development and Evaluation system to assess the quality of evidence from high to very low and classify the strength of recommendations as strong or weak. Two guidelines7,14 used an 8-category rating for grading the quality of evidence coupled with a 5-category system for grading the strength of recommendations. Finally, 1 guideline9 followed a method outlined by the United States Preventive Services Task Force to review and evaluate the evidence and assigned 1 of 3 categories to the group’s recommendations.
Country of Origin
Six of the included guidelines were Canadian,2,8,10-12,15 2 were from the US,9,13 and 2 were international.7,14
Patient Population
The intended users for each of the 10 included guidelines were health care providers.2,7-15 In half of the included guidelines, the target population broadly covered pregnant individuals.2,7,8,10,13 Two of the guidelines focused on individuals who are pregnant with twins.11,14 One guideline focused specifically on service members or veterans belonging to the U.S. Department of Veterans Affairs or the U.S. Department of Defense and who are pregnant.9 One guideline focused on pregnant individuals with a higher risk of fetal anomalies or who may have complications with a mid-second trimester ultrasound.12 The last guideline focused on pregnant adolescents.15
Interventions and Comparators
All 10 guidelines discussed the role of obstetrical ultrasound during pregnancy.2,7-15 Comparators are not relevant to the guideline research question in this report.
Outcomes
The guidelines included in this review provided a series of recommendations related to various outcomes that are of relevance to the use of obstetrical ultrasound and, more broadly, to the management of pregnancy. The outcomes that were considered in the supporting literature for the guidelines included the clinical indications, the benefits and risks of obstetrical ultrasound,2,7,8,10-14 and the monitoring of healthy pregnancy.9,15
Summary of Critical Appraisal
The included evidence-based guidelines demonstrated both strengths and limitations. Strengths included the clarity of the scope and purpose for each of the included guidelines, as well as the clarity of presentation for each of the recommendations.2,7-15 Each of the included guidelines were also developed by groups of individuals from all relevant professional organizations.2,7-15 The guidelines also had limitations. Perspectives from members of the target audience (i.e., people who are pregnant) seemed to be present in only 1 of the included guidelines,9 which could limit the applicability of the recommendations.
There were also limitations regarding the rigour of development. While each of the included guidelines included a description of the sources that were searched, it was unclear whether that searching was done in a systematic fashion for 4 of the guidelines.2,7,8,10 One guideline9 adequately described the criteria for selecting the evidence and the methods for formulating the recommendations, whereas in the other 9 guidelines it was unclear from the authors’ reporting how the evidence was selected and how recommendations were developed. In addition, 6 guidelines2,7,8,10-12 did not include discussion of the strengths and weaknesses of the body of evidence used to formulate the recommendations. It was also unclear in 7 of the guidelines2,7,8,10,12-14 whether the recommendations had been externally reviewed by experts before publication. None of the included guidelines provided details of a procedure for updating the guideline. These limitations may limit the certainty of the recommendations provided.
None of the included guidelines2,7-15 discussed barriers or facilitators to the application of recommendations, provided advice or tools that could be put into practice, considered resource implications of applying the recommendations, or presented auditing or monitoring criteria. These limitations may further limit the applicability of the included recommendations. Finally, while each of the included guidelines2,7-15 indicated that competing interests of members of its guideline development group had been recorded, limited information was reported regarding the nature of any competing interests. In addition, the funder for each of the included guidelines2,7-15 was not clearly reported; thus, no comments can be made about potential conflicts of interest concerning the development of the guidelines.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Safety Related to Frequent Use of Obstetrical Ultrasound During Pregnancy
No relevant evidence was identified regarding the safety of frequent obstetrical ultrasounds during pregnancy compared to the routine use of obstetrical ultrasound during pregnancy; therefore, no summary can be provided.
Guidelines
This review identified 10 evidence-based guidelines2,7-15 that provided recommendations regarding various clinical indications for obstetrical ultrasound, as well as for the frequency of obstetrical ultrasound during pregnancy.
General Recommendations for Obstetrical Ultrasound
First Trimester Ultrasound
Van den Hof and colleagues (2019)8 made several recommendations regarding circumstances for when first trimester ultrasound would be warranted. The authors made 4 recommendations for first trimester ultrasound based on evidence that was assessed as good quality: 1) during diagnostic or therapeutic procedures requiring visual guidance (e.g., chorionic villus sampling) and before prophylactic cervical cerclage placement, 2) for suspected multiple gestation, 3) for suspected ectopic pregnancy, molar pregnancy, and suspected pelvic masses, and 4) as a component of the screening protocol for preeclampsia among pregnant people. The guideline development group made an additional 2 recommendations for first trimester ultrasound based on evidence assessed as fair quality: 1) for assessment of threatened abortion, and 2) before pregnancy termination.
The U.S. Department of Veterans Affairs and the U.S. Department of Defense management of pregnancy working group (2018)9 recommended first trimester ultrasound for 3 reasons: to establish gestational age and estimated birth date, to identify multiple pregnancies, and to confirm the presence of cardiac activity. Among those who present with pregnancy after the first trimester, this guideline development group recommends that a dating and anatomical ultrasound be performed at the earliest opportunity and preferably before 22 weeks.9 According to the group’s ranking system, this recommendation was strong and based on moderate-quality evidence.9
Morin and Lim (2017)11 reported specific recommendations for obstetrical ultrasound among people pregnant with twins, stating that a first trimester ultrasound is recommended if a twin pregnancy is suspected at the first physical examination or if the individual is at risk (e.g., those who have used assisted reproductive technologies). The authors made this recommendation based on evidence that was assessed as good quality.11These recommendations align with the previously mentioned guidelines by Van den Hof and colleagues (2019)8 and the U.S. Department of Veterans Affairs and U.S. Department of Defense management of pregnancy working group (2018).9
Second Trimester Ultrasound
Cargill and Morin (2017)10 recommended that people who are pregnant be offered a routine second trimester ultrasound between 18 and 22 weeks’ gestation. This recommendation was based on evidence that was assessed by the authors as fair quality.10 Similarly, Morin and Lim (2017)11 recommended that, for people who are pregnant with twins, a detailed ultrasound should be offered and preferably between 18 and 22 weeks’ gestation. Their recommendation was also based on evidence that was assesses to be of fair quality.11 The American College of Obstetricians and Gynecologists (2016)13 also recommended that without other specific indications, the best time for a single ultrasound examination is between 18 and 22 weeks’ gestation. This recommendation was based primarily on consensus and expert opinion.9
Recommendations for Increased Frequency of Obstetrical Ultrasound
Four of the guidelines7,12,14,15 reviewed in this report provided recommendations for specific patient populations for whom increased frequency of obstetrical ultrasound may be warranted.
People Who Have a Congenital Infection While Pregnant
Khalil and colleagues (2020)7 recommended that serial ultrasound monitoring should be done for the management of maternal and fetal parvovirus B19 infection based on moderate-quality evidence. The authors also recommend that serial ultrasound monitoring be performed for the management of maternal and fetal varicella-zoster virus infection based on low- to moderate-quality evidence, and for maternal and fetal Zika virus infection. However, this recommendation is based on the clinical experience of the guideline development group and is considered a “good practice point.” In addition, Khalil and colleagues (2020)7 recommended that, for those with a Zika virus infection, a third trimester ultrasound should be considered if the baseline scan is normal. However, this recommendation is based on the clinical experience of the guideline development group and is considered a “good practice point.”
People Who Are Pregnant With Twins
Khalil and colleagues (2016)14 recommended that people who have uncomplicated dichorionic twin pregnancies should have a first trimester scan, a detailed second trimester scan, and scans every 4 weeks thereafter. This recommendation was based on the clinical experience of the guideline development group and is considered a “good practice point.” In addition, the authors noted that individuals with complicated pregnancies of dichorionic twins should be scanned more frequently, depending on the condition of the individual and the severity of the complications.14 The authors also recommended that people who are pregnant with monochorionic twins in uncomplicated pregnancies should have a first trimester scan and be scanned every 2 weeks after 16 weeks’ gestation and that complicated cases should be scanned more frequently, depending on the condition and severity of the case.14 These 2 recommendations were based on evidence that the authors assessed as low- to moderate-quality.14
Adolescents Who Are Pregnant
Fleming and colleagues (2015)15 recommended that pregnant adolescents should have a first trimester ultrasound, an anatomical ultrasound at 16 to 20 weeks’ gestation, and an ultrasound to assess fetal well-being and fetal weight at 32 to 34 weeks’ gestation. These recommendations were based on evidence that the guideline development group assessed as good quality.15
People Who Are Pregnant and at High Risk for Fetal Anomalies or for Whom Mid-Trimester Transabdominal Ultrasound Would Be Challenging
Nevo and colleagues (2017)12 recommended that pregnant individuals who have a higher risk for fetal anomalies or for whom a mid-trimester transabdominal ultrasound may be challenging should be offered an early comprehensive fetal anatomic ultrasound at 13 to 16 weeks’ gestation. This ultrasound would not replace the routine 18- to 22-week anatomy scan.12 The recommendation was not graded, but the quality of evidence was rated high (i.e., very confident that the true effect lies close to that of the estimate of the effect).12 It was unclear from the reporting which evidence was used to develop the recommendation.
Recommendations for Mitigating Harms of Obstetrical Ultrasound
One guideline2 provided recommendations regarding mitigating the potential harms of obstetrical ultrasound. Van den Hof (2018)2 recommended that ultrasound only be used when the potential medical benefit outweighs any potential risk. According to the ranking system used, this recommendation was based on good-quality evidence.2 In addition, Van den Hof (2018)2 recommended against the use of obstetrical ultrasound for non-medical reasons (e.g., sex determination, non-medical photos, commercial purposes). This recommendation was based on evidence that was assessed by the guideline development group as fair quality.2 The author does make reference to supporting evidence for these recommendations, discussing potential adverse effects of repeat ultrasound exposure during pregnancy.2 Van den Hof (2018)2 also made 2 further recommendations for mitigating the potential harms of obstetrical ultrasound use: ultrasound exposure should be as low as reasonably achievable given the potential for tissue heating if the thermal index exceeds 1 (based on good-quality evidence); and spectral power and colour Doppler should be avoided for imaging in the first trimester, except if the pregnancy is at high risk for trisomy syndromes or anomalies (based on expert opinion of the guideline development group).
Limitations
No relevant evidence was identified regarding the safety of frequent obstetrical ultrasounds compared to the routine use of obstetrical ultrasound during pregnancy.
Two of the guidelines included in this report were broader in scope than the research question posed by this review (e.g., recommendations for management of pregnancy in specific populations);9,15 thus, the applicability of recommendations may be limited in their generalizability to other populations. Four of the identified guidelines were not developed for the Canadian context and therefore may limit the applicability of recommendations to the Canadian health care system.7,9,13,14
Important methodological limitations were identified in the critical appraisal conducted for the included guidelines, limiting the confidence with which the recommendations can be applied to various clinical settings. In addition, very few of the recommendations were based on high-quality evidence, as reported by the guideline authors. Consequently, the findings of this review should be interpreted with caution.
Conclusions and Implications for Decision- or Policy-Making
No relevant studies describing the safety of frequent obstetrical ultrasounds compared to routine versus more frequent use of obstetrical ultrasound were identified; therefore, no summary can be provided. However, this review did identify 10 evidence-based guidelines that included recommendations about various aspects of obstetrical ultrasound use, including clinical indication for obstetrical ultrasound, specific patient populations that may require more frequent obstetrical ultrasound examinations, and strategies to mitigate potential harms of obstetrical ultrasound overuse.
Regarding routine obstetrical ultrasound use, 3 guidelines made recommendations for the use of first trimester ultrasound8,9,11 and 3 guidelines made recommendations regarding the use of second trimester ultrasound, preferably between 18 and 22 weeks’ gestation.10,11,13 Specific patient populations for whom recommendations were made for more frequent obstetrical ultrasound examinations included those with pregnancies who are affected by certain congenital infections,7 people who are pregnant with twins,14 pregnant adolescents,15 and people who are pregnant and at high risk for fetal anomalies or for whom mid-trimester transabdominal ultrasound would be challenging.12 Finally, Van den Hof (2018)2 recommended against obstetrical ultrasound for non-medical purposes (e.g., sex determination, non-medical photos, and so forth) and recommended that ultrasound exposure be as low as possible. Decision-makers should take these recommendations into consideration when developing various care pathways and policies regarding the use and misuse of obstetrical ultrasound.
There is a moderate level of uncertainty regarding the recommendations discussed in this review. Given the important methodological limitations discussed for many of these recommendations, particularly those related to the rigour of guideline development and guideline applicability, and the lack of high-quality supporting evidence available for several of the recommendations, the findings of this review should be interpreted with caution. Better transparency in reporting the methodologies used for guideline development would improve the ability to conduct quality assessment and reduce uncertainties in guideline development.
No evidence regarding the safety of frequent obstetrical ultrasounds compared to the routine use of obstetrical ultrasound were identified. Future research to address this question may help to reduce uncertainty in the frequency of obstetrical ultrasound use during pregnancy and provide decision-makers with better evidence upon which to base their decisions.
References
1.Herbst MK TD, Shanahan MM. Obstetrical Ultrasound. Treasure Island (FL): StatPearls. 2021. In: https://www.ncbi.nlm.nih.gov/books/NBK470450/. Accessed 2021 Nov 22.
2.Van den Hof MC. No. 359-Obstetric Ultrasound Biological Effects and Safety. J Obstet Gynaecol Can. 2018;40(5):627-632. PubMed
3.Whitworth M, Bricker L, Mullan C. Ultrasound for fetal assessment in early pregnancy. Cochrane Database Syst Rev. 2015(7):CD007058. PubMed
4.The Society of Obstetricians and Gynaecologists of Canada. Your pregnancy: Routine tests. https://www.pregnancyinfo.ca/your-pregnancy/routine-tests/ultrasound/. Published 2021. Accessed 2021 Nov 22.
5.Consortium ANS. The AGREE II Instrument. In: [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Nov 22.
6.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
7.Khalil A, Sotiriadis A, Chaoui R, et al. ISUOG Practice Guidelines: role of ultrasound in congenital infection. Ultrasound Obstet Gynecol. 2020;56(1):128-151. PubMed
8.Van den Hof MC, Smithies M, Nevo O, Oullet A. No. 375-Clinical Practice Guideline on the Use of First Trimester Ultrasound. J Obstet Gynaecol Can. 2019;41(3):388-395. PubMed
9.Management of Pregnancy Work Group. VA/DoD clinical practice guideline for the management of pregnancy. Version 3.0. In: Washington (DC): Department of Veterans Affairs, Department of Defense; 2018: https://www.healthquality.va.gov/guidelines/WH/up/VADoDPregnancyCPG4102018.pdf. Accessed 2021 Nov 22.
10.Cargill Y, Morin L. No. 223-Content of a Complete Routine Second Trimester Obstetrical Ultrasound Examination and Report. J Obstet Gynaecol Can. 2017;39(8):e144-e149. PubMed
11.Morin L, Lim K. No. 260-Ultrasound in Twin Pregnancies. J Obstet Gynaecol Can. 2017;39(10):e398-e411. PubMed
12.Nevo O, Brown R, Glanc P, Lim K. No. 352-Technical Update: The Role of Early Comprehensive Fetal Anatomy Ultrasound Examination. J Obstet Gynaecol Can. 2017;39(12):1203-1211. PubMed
13.Committee on Practice B-O, the American Institute of Ultrasound in M. Practice Bulletin No. 175: Ultrasound in Pregnancy. Obstet Gynecol. 2016;128(6):e241-e256. PubMed
14.Khalil A, Rodgers M, Baschat A, et al. ISUOG Practice Guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol. 2016;47(2):247-263. PubMed
15.Fleming N, O'Driscoll T, Becker G, Spitzer RF, Canpago C. Adolescent Pregnancy Guidelines. J Obstet Gynaecol Can. 2015;37(8):740-756. PubMed
16.Woolf S, Battista R, Angerson G, Logan A, Eel W. Canadian Task Force on Preventive Health Care: New grades for recommendations from the Canadian Task Force on Preventive Health Care. CMAJ. 2003;169:207-208. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice, and major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
Khalil et al. (2020)7 | |||||
Intended users: Health care providers Target population: people who are pregnant | Intervention: Ultrasound examination for the diagnosis and management of congenital infection Outcomes: Ultrasound signs, timing of infection in relation to gestational age, diagnosis of maternal and fetal infection, and appropriate management | Searched the Cochrane Library, Cochrane Register of Controlled Trials, MEDLINE, the National Library for Health, the National Guidelines Clearing House, grey literature searches websites of health technology assessment agencies, clinical practice guideline collections, and clinical trial registers | Used an 8-category system for grading quality of evidence and a 5-category system for grading the strength of recommendationsa | NR | NR |
Van den Hof et al. (2019)8 | |||||
Intended Users: Health care providers Target Population: people who are pregnant | Intervention: First trimester ultrasound (includes all examinations at or before 14 weeks gestation) Outcomes: Indications for first trimester ultrasound; clinical benefit of first trimester ultrasound | “A MEDLINE search and bibliography reviews in relevant literature provided the evidence” (p. 388) | Level of evidence and classification of recommendations were determined using criteria described by the Canadian Task Force on Preventive Health Care (5-category system)b | NR | NR |
U.S. Department of Veterans Affairs and U.S. Department of Defense (2018)9 | |||||
Intended Users: Veteran’s Affairs and Department of Defense health care providers Target Population: Service Members or Veterans who are pregnant | Intervention: Treatment and management of pregnant women in the Department of Veteran’s Affairs or Department of Defense Outcomes: Care throughout pregnancy; 1-time interventions; referral; special considerations | Searched the Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Database of Abstracts of Reviews of Effects, Embase, Health Technology Assessment Database, MEDLINE/ PreMEDLINE, PsycINFO, and PubMed. Citations were reviewed systematically. | Followed the “Grading of Recommendations Assessment, Development and Evaluation system to assess the quality of the evidence base and assign a strength for each recommendation.” (p.11-12) | “The Work Group determined the relative strength of each recommendation (“Strong” or “Weak”). A “Strong” recommendation generally indicates a high confidence in the quality of the available scientific evidence, a clear difference in magnitude between the benefits and harms of an intervention, similar patient or provider values and preferences, and understood influence of other implications (e.g., resource use, feasibility). If the Work Group has less confidence after the assessment across these domains and believes that additional evidence may change the recommendation, it generally assigns a “Weak” recommendation.” (p. 12) | NR |
Van den Hof (2018)2 | |||||
Intended Users: health care providers Target Population: people who are pregnant | Intervention: Obstetrical ultrasound Outcomes: Biological effects and safety | “The 2005 version of this guideline was used as a | Level of evidence and classification of recommendations were determined using criteria described by the Canadian Task Force on Preventive Health Care (5-category system)b | NR | NR |
Cargill and Morin (2017)10 | |||||
Intended Users: health care providers Target Population: people who are pregnant | Intervention: Second trimester ultrasound Outcomes: Clinical benefit of second trimester ultrasound | Previous guidelines from the American Institute of Ultrasound in Medicine, the American College of Obstetricians and Gynecologists and the Royal College of Obstetricians and Gynaecologists were reviewed. PubMed and the Cochrane Database were also searched using the words “routine second trimester obstetrical ultrasound.” | Level of evidence and classification of recommendations were determined using criteria described by the Canadian Task Force on Preventive Health Care (5-category system)b | NR | NR |
Morin and Lim (2017)11 | |||||
Intended Users: health care providers Target Population: people who are pregnant with twins | Intervention: Diagnostic Ultrasound Outcomes: Perinatal mortality and morbidity; short-term and long-term neonatal morbidity; optimal use of ultrasound | Evidence collected using a systematic literature review, which searched multiple databases and the grey literature. Eligible study designs includes systematic reviews, randomized controlled trials, and observational studies. | Level of evidence and classification of recommendations were determined using criteria described by the Canadian Task Force on Preventive Health Care (5-category system)b | The guideline development group reviewed the evidence, with input from relevant experts and recommendations were made according to guidance from The Canadian Task Force on Preventive Health Careb | NR |
Nevo et al. (2017)12 | |||||
Intended Users: health care providers Target Population: people who are pregnant and for whom mid-second trimester ultrasound scanning may be technically challenging or who are at higher risk of fetal anomalies | Intervention: Early comprehensive fetal anatomic scanning Outcomes: Early identification of fetal anomalies | Comprehensively searched MEDLINE, Embase, Cochrane Register of Controlled Trials, Cochrane Database of Systematic Reviews, Scopus, and 4 clinical practice guideline repositories. Two-stage screening approach for search results. | “The quality of evidence was rated using the criteria described in the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology framework.” (p. 1206) Quality level of a body of evidence can be categorized from high to very low | Strength of recommendations defined as “strong” or “weak” | NR |
American College of Obstetricians and Gynecologists Committee on Practice Bulletins ― Obstetrics (2016)13 | |||||
Intended Users: obstetrician-gynecologists Target Population: people who are pregnant | Intervention: Obstetric ultrasonography Outcomes: Clinical indications, benefits, and risks associated with obstetric ultrasonography | Searched MEDLINE, the Cochrane Library, and the American College of Obstetricians and Gynecologists’ own internal resources. Various guidelines were also reviewed and additional studies were identified by reviewing bibliographies of included articles. | “Studies were reviewed and evaluated for quality according to the method outlined by the U.S. Preventive Services Task Force: I Evidence obtained from at least 1 properly designed randomized controlled trial. II-1 Evidence obtained from well-designed controlled trials without randomization. II-2 Evidence obtained from well-designed cohort or case-controlled analytic studies, preferably from more than 1 centre or research group. II-3 Evidence obtained from multiple time series with or without the intervention. Dramatic results in uncontrolled experiments also could be regarded as this type of evidence. III Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees.” (p. e256) | “Based on the highest level of evidence found in the data, recommendations are provided and graded according to the following categories: Level A—Recommendations are based on good and consistent scientific evidence. Level B—Recommendations are based on limited or inconsistent scientific evidence. Level C—Recommendations are based primarily on consensus and expert opinion.” (p. e256) | NR |
Khalil et al. (2016)14 | |||||
Intended Users: health care providers Target Population: people who are pregnant with twins | Intervention: Obstetrical ultrasound Outcomes: Monitoring of twin pregnancy | Searched MEDLINE, the Cochrane Library and Cochrane Register of Controlled Trials, National Library for Health and the National Guidelines Clearing House for published literature. Grey literature was identified through website searching of health technology assessment agencies, clinical practice guidelines collections, and clinical trial registries. | Used an 8-category system for grading quality of evidence and a 5-category system for grading the strength of recommendationsa | NR | NR |
Fleming et al. (2015)15 | |||||
Intended Users: health care providers Target Population: adolescents who are pregnant | Intervention: General management of pregnancy Outcomes: Healthy pregnancy | Evidence collected using database searches of PubMed and the Cochrane Library and the grey literature. Eligible study designs includes systematic reviews, randomized controlled trials, and observational studies. | The quality of evidence in this document was rated using the criteria described in the Report of the Canadian Task Force on Preventive Health Care (5 categories)b | NR | NR |
NR = not reported.
aEvidence assessment and recommendation grading system used by Khalil et al. (2020)7 and Khalil et al. (2016)20
Classification of evidence levels: 1++ = high-quality meta-analyses, systematic reviews of randomized controlled trials, or randomized controlled trials with very low risk of bias; 1+ = well-conducted meta-analyses, systematic reviews of randomized controlled trials, or randomized controlled trials with low risk of bias; 1– = meta-analyses, systematic reviews of randomized controlled trials, or randomized controlled trials with high risk of bias; 2++ = high-quality systematic reviews of case-controlled or cohort studies, or high-quality case-controlled or cohort studies with very low risk of confounding, bias, or chance and high probability that the relationship is causa; 2+ = well-conducted case-controlled or cohort studies with low risk of confounding, bias, or chance and moderate probability that the relationship is causal; 2– = case-controlled or cohort studies with high risk of confounding, bias, or chance and significant risk that the relationship is not causal; 3 = non-analytical studies (e.g., case reports, case series); 4 = expert opinion.
Grades of recommendation: A = at least 1 meta-analysis, systematic review, or randomized controlled trial rated as 1++ and directly applicable to the target population, or a systematic review of randomized controlled trials or body of evidence consisting principally of studies rated as 1+ applicable directly to the target population and demonstrating an overall consistency of results; B = body of evidence including studies rated as 2++ applicable directly to the target population and demonstrating an overall consistency of results, or evidence extrapolated from studies rated as 1++ or 1+; C = body of evidence including studies rated as 2+ applicable directly to the target population and demonstrating overall consistency of results, or evidence extrapolated from studies rated as 2++; D = evidence of level 3 or 4, or evidence extrapolated from studies rated as 2+. Good practice point: a recommended best practice based on clinical experience of the guideline development group.
bEvidence assessment and recommendation grading system from the Canadian Task Force on Preventive Health Care (Woolf et al., 2003)16
Quality of evidence assessment: I = evidence obtained from at least 1 properly randomized controlled trial; II-1 = evidence from well-designed controlled trials without randomization; II-2 = evidence from well-designed cohort (prospective or retrospective) or case-controlled studies, preferably from more than 1 centre or research group; II-3 =evidence obtained from comparisons between times or places with or without the intervention (dramatic results in uncontrolled experiments ― such as the results of treatment with penicillin in the 1940s ― could also be included in this category); III = opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees.
Classification of recommendations: A = there is good evidence to recommend the clinical preventive action; B = there is fair evidence to recommend the clinical preventive action; C = the existing evidence is conflicting and does not allow for making a recommendation for or against the use of the clinical preventive action; however, other factors may influence decision-making; D = there is fair evidence to recommend against the clinical preventive action; E = there is good evidence to recommend against the clinical preventive action; I = there is insufficient evidence (in quantity or quality) to make a recommendation; however, other factors may influence decision-making.
Note that this appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Guidelines Using AGREE II5
Item | Khalil et al. (2020)7 | Van den Hof et al. (2019)8 | U.S. Department of Veterans Affairs and U.S. Department of Defense (2018)9 | Van den Hof (2018)2 | Cargill and Morin (2017)10 | Morin and Lim (2017)11 | Nevo et al. (2017)12 | American College of Obstetricians and Gynecologists Committee on Practice Bulletins ― Obstetrics (2016)13 | Khalil et al. (2016)14 | Fleming et al. (2015)15 |
|---|---|---|---|---|---|---|---|---|---|---|
Domain 1: Scope and Purpose | ||||||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | ||||||||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Yes | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Unclear | Yes | Unclear | Unclear | Unclear | Unclear | Yes | Yes | Yes |
Domain 3: Rigour of Development | ||||||||||
7. Systematic methods were used to search for evidence. | Unclear | Unclear | Yes | Unclear | No | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | No | No | Yes | No | No | No | Yes | No | No | No |
9. The strengths and limitations of the body of evidence are clearly described. | No | No | Yes | No | No | No | No | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | No | No | Yes | No | No | No | No | No | No | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Unclear | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Unclear | Yes | Unclear | Unclear | No | No | No | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Unclear | Unclear | Yes | Unclear | Unclear | Yes | Unclear | Unclear | Unclear | Yes |
14. A procedure for updating the guideline is provided. | No | No | No | No | No | No | No | No | No | No |
Domain 4: Clarity of Presentation | ||||||||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Unclear | No | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||||||||
18. The guideline describes facilitators and barriers to its application. | No | No | No | No | No | No | No | No | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No | No | No | No | No | No | No | No | No |
20. The potential resource implications of applying the recommendations have been considered. | No | No | No | No | No | No | No | No | No | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | No | No | No | No | No | No | No |
Domain 6: Editorial Independence | ||||||||||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | No | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | No | Yes |
AGREE II = Appraisal of Guidelines for Research & Evaluation II.
Note that this appendix has not been copy-edited.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Khalil et al. (2020)7 | |
Outcome: management of maternal and fetal parvovirus B19 infection | |
“Serial ultrasound monitoring should start 4 weeks after infection or seroconversion and be performed every 1-2 weeks thereafter until 12 weeks after infection” (p. 140)7 Supporting evidence: None reported | Grade of recommendation: B (Body of evidence including studies rated as 2++ applicable directly to the target population and demonstrating overall consistency of results; or evidence extrapolated from studies rated as 1++ or 1+ ) |
“Serial ultrasound examinations, looking for evidence of ascites, cardiomegaly, hydrops fetalis and raised middle cerebral artery-peak systolic velocity, should be performed every 1-2 weeks for 8-12 weeks after exposure” (p. 140)7 Supporting evidence: None reported | Grade of recommendation: C (Body of evidence including studies rated as 2+ applicable directly to the target population and demonstrating overall consistency of results; or evidence extrapolated from studies rated as 2++ ) |
Outcome: management of maternal and fetal varicella-zoster virus | |
“Following maternal infection in the first 20 gestational weeks, serial ultrasound examinations should be performed from 5 weeks after the initial infection or from 16 gestational weeks, whichever is soonest” (p. 143)7 Supporting evidence: Since the ultrasound features of varicella syndrome (e.g., hydrocephalus, fetal growth restriction, limb defects) can be detected by ≥ 5 weeks after the initial maternal infection in majority of fetuses, the guideline authors suggests that serial ultrasound be started from 5 weeks of maternal infection. This recommendation was based on the clinical experience of the guideline development group. | Grade of recommendation: Good practice point (Recommended best practice based on clinical experience of the Guideline Development Group) |
Outcome: diagnosis of fetal Zika virus | |
“A baseline fetal ultrasound examination should be performed after potential maternal exposure to zika virus, with referral to an ultrasound or fetal-medicine specialist in case of concerning features” (p.144)7 Supporting evidence: None reported | Grade of recommendation: Good practice point (Recommended best practice based on clinical experience of the Guideline Development Group) |
“If the baseline scan is normal, a repeat scan in the third trimester can be considered” (p. 144)7 Supporting evidence: None reported | Grade of recommendation: Good practice point (Recommended best practice based on clinical experience of the Guideline Development Group) |
Outcome: management of pregnancies with congenital Zika syndrome | |
“Zika virus affected pregnancies should be managed in an ultrasound or fetal-medicine unit with serial ultrasound scans and the availability of further laboratory testing” (p. 145 to 146)7 Supporting evidence: None reported | Grade of recommendation: Good practice point (recommended best practice based on clinical experience of the Guideline Development Group) |
Van den Hof et al. (2019)8 | |
Outcome: clinical indications for first trimester ultrasound | |
“First trimester ultrasound if recommended for assessment of threatened abortion to document fetal viability or for incomplete abortion to identify retained products of conception” (p. 391)8 Supporting evidence: Unclear. The authors commented that ultrasound identification of fetal cardiac activity helps to guide management and to reassure the mother. If an incomplete abortion is suspected, ultrasound can be useful in identifying retained products of conception. If abortion is inevitable (indicated by dilated cervix), an ultrasound is not recommended. | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case-controlled studies, preferably from more than 1 centre or research group); Classification of recommendation: B (There is fair evidence to recommend the clinical preventive action.) |
“First trimester ultrasound is recommended prior to pregnancy termination” (p. 391)8 Supporting evidence: Unclear The authors commented that an ultrasound examination before induced abortion can help avoid an inaccurate estimation of gestational age or a missed diagnosis of ectopic pregnancy. | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case-controlled studies, preferably from more than 1 centre or research group); Classification of recommendation: B (There is fair evidence to recommend the clinical preventive action.) |
First trimester ultrasound is recommended during diagnostic or therapeutic procedures requiring visual guidance (e.g., chorionic villus sampling) and before prophylactic cervical cerclage placement” (p. 391)8 Supporting evidence: Evidence suggests that ultrasound guidance is relevant in the timing and placement of cervical cerclage, especially in patients with a known or potential cervical abnormality. Fetal cardiac activity should be confirmed and an early comprehensive pregnancy ultrasound should be conducted before this procedure. | Quality of evidence assessment: I (Evidence obtained from at least 1 properly randomized controlled trial); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
“First trimester ultrasound is recommended for suspected multiple gestation to allow for reliable determination of chorionicity and amnionicity and to establish early fetal genetic and anatomic screening” (p. 392)8 Supporting evidence: Unclear. The authors noted that an 11 to 14 week ultrasound assessment including nuchal translucencies is recommended for genetic screening in multiple gestation, if resources are available. In the first trimester, ultrasound can also define chorionicity or amnionicity. | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case-controlled studies, preferably from more than 1 centre or research group); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
“First trimester ultrasound is recommended in the workup for suspected ectopic pregnancy, molar pregnancy, and suspected pelvic masses” (p. 392)8 Supporting evidence: Evidence from 3 studies showed that ultrasound assessment along with Beta-human chorionic gonadotropin measurements “can detect as many as 96% of ectopic pregnancies with a specificity of 100%.” This approach also had a “positive predictive value of 100% and a negative predictive value of 92% in women with a clinical suspicion of ectopic pregnancy” (p. 392)8 Evidence from 3 studies suggested that ultrasound assessment is a “sensitive and reliable method for diagnosing a molar pregnancy”. Ultrasound can also be used to monitor ovarian cyst resolution and uterine involution after the treatment of molar pregnancy. | Quality of evidence assessment: II-1 (Evidence from well-designed controlled trials without randomization); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
“When appropriate expertise and resources are in place to screen women for the risk of preeclampsia, first trimester ultrasound is recommended as a valuable component of the screening protocol” (p. 393)8 Supporting evidence: “If a pelvic mass predates the pregnancy or is discovered incidentally, ultrasound can identify its location and characteristics. Pattern recognition and subjective evaluation of the ultrasound image can suggest whether the lesion is benign or malignant.41 Doppler assessment provides minimal contribution to the diagnosis.” (p. 392)8 | Quality of evidence assessment: I (Evidence obtained from at least 1 properly randomized controlled trial); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
U.S. Department of Veterans Affairs and U.S. Department of Defense (2018)9 | |
Outcome: clinical indications for imaging during pregnancy | |
“We recommend first-trimester ultrasound to establish or confirm the gestational age and estimated birth date, identify multiple pregnancies, and confirm the presence of cardiac activity. For pregnant women who present after the first trimester, we suggest performing a dating and anatomical ultrasound at the earliest opportunity, preferably prior to 22 weeks.” (p. 49)9 Supporting evidence: Evidence from a large prospective study showed that LMP estimate of gestational age and early ultrasound estimate of gestational age were similar. However, when they were discrepant LMP estimate was greater than ultrasound based gestational age. This meant a higher proportion of births grouped as ‘post-term’. In another large prospective study, it was found that first trimester ultrasound was “better” for the prediction of gestational age estimation compared to LMP based estimation. | Quality of evidence: “The Work Group determined confidence in the quality of the evidence was moderate in support of first-trimester ultrasound to establish or confirm the gestational age and estimated birth date. Other support for this recommendation stemmed from benefits of this recommendation outweighing the harms.” (p. 50); Classification of recommendation: Strong |
Van den Hof (2018)2 | |
Outcome: mitigating potential harm(s) of obstetrical ultrasound | |
“Obstetrical ultrasound should only be used when the potential medical benefit outweighs any theoretical or potential risk” (p. 627)2 Supporting evidence: None reported | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case-controlled studies, preferably from more than 1 centre or research group); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
“Obstetrical ultrasound should not be used for non medical reasons, such as sex determination, producing nonmedical photos or videos, or for commercial purposes” (p. 627)2 Supporting evidence: None reported. “No studies have shown a cumulative adverse effect with repeat exposures. Although obstetrical ultrasound has gained a reputation for safety, the possibility of subtle effects such as left- or non- righthandedness cannot be dismissed. The concern about bio-effects is particularly important, given that acoustic output from equipment intended for obstetric use has increased, and fetal imaging is being practiced at earlier gestations when the fetus is potentially more vulnerable. [9,10] For these reasons, obstetrical ultrasound should only be undertaken for medical reasons.” (p. 629)2 | Quality of evidence assessment: III (Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees); Classification of recommendation: B (There is fair evidence to recommend the clinical preventive action.) |
“Ultrasound exposure should be as low as reasonably achievable because of the potential for tissue heating when the thermal index exceeds 1. Exposure can be reduced through the use of output control and/or by reducing the amount of time the beam is focused on one place (dwell time) (p. 627-8)2 Supporting evidence: The guideline authors mentioned evidence from embryonic and fetal animal studies which suggested that, a temperature rise (by ultrasound heating) of < 1.5°C above physiologic level is not harmful. If more heat is generated, potential for harm to the embryonic and fetal tissues increases with both the duration of exposure and degree or rise in the in situ temperature. There is also an inverse relation between the rise in temperature and duration of exposure, which can be harmful. For example, rise in temperature of 4°C for 5 minutes or more could result in severe developmental sequelae in a fetus. | Quality of evidence assessment: II-1 (Evidence from well-designed controlled trials without randomization); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
“Spectral power and colour Doppler should be avoided while imaging the fetus in the first trimester, except in those circumstances where their use contributes to the investigation of pregnancies at high risk for trisomies or anomalies” (p.628)2 Supporting evidence: “Higher energy intensities are associated with pulsed, power, and colour flow Doppler studies. In this early gestational period, Doppler should not be used routinely. When Doppler is required for refining trisomy or anomaly risk, attention should be made to keep the thermal index ≤0.7 [29]. If greater output reflected by a higher thermal index (0.7–1.5) is needed, exposure time should be limited (usually <10 minutes). Output with a thermal index >1.5 is not recommended. These concerns do not apply to uterine artery Doppler studies since the fetus is outside of the area of focused insonation [29].” (p. 631)2 | Quality of evidence assessment: III (Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees); Classification of recommendation: B (There is fair evidence to recommend the clinical preventive action.) |
Cargill et al. (2017)10 | |
Outcome: indication for second trimester ultrasound | |
Pregnant women should be offered a routine second trimester ultrasound between 18 and 22 weeks’ gestation” (p. e148)10 Supporting evidence: Evidence suggests that more fetal anomalies can be detected if the ultrasound scan is done after 18 weeks of gestation. In a study, it was reported that a fetal anatomy survey for congenital anomalies were more likely to be incomplete before 18 weeks, in patients with normal or excess body weight. The authors noted that the Royal College of Obstetricians and Gynaecologists recommends second trimester fetal anatomical scan be performed between 20 and 23 weeks. | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case- controlled studies, preferably from more than 1 centre or research group); Classification of recommendation: B (There is fair evidence to recommend the clinical preventive action.) |
Morin et al. (2017)11 | |
Outcome: indication for first trimester ultrasound | |
“All patients who are suspected to have a twin pregnancy on first trimester physical examination or who are at risk (e.g., pregnancies resulting from assisted reproductive technologies) should have first trimester ultrasound performed.” (p. e401)11 Supporting evidence: “Ideally, determination of chorionicity should be done in the first trimester. The management of structural anomalies, screening for and identification of aneuploidy, determination of the etiology of fetal growth and/or fluid discordance, early diagnosis of twin-to-twin transfusion syndrome, and the management of a surviving twin following intrauterine demise are examples of clinical management depending on chorionicity. The high mortality and morbidity of monoamniotic twins is well-documented, and early and in- tensive monitoring and intervention may improve outcomes [4-6].” (p. e400)11 | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case- controlled l studies, preferably from more than 1 centre or research group); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
“Detailed ultrasound examination to screen for fetal anomalies should be offered, preferably between 18 and 22 weeks’ gestation, in all twin pregnancies.” (p. e404)11 Supporting evidence: In a study evaluating the accuracy of antenatal ultrasound for the detection of anomalies in twin pregnancies, 88% of anomalies were detected by ultrasound scan (in 245 twins). | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case- controlled studies, preferably from more than 1 centre or research group); Classification of recommendation: B (There is fair evidence to recommend the clinical preventive action.) |
Nevo et al. (2017)12 | |
Outcome: clinical indication for early comprehensive fetal anatomy ultrasound examination | |
“Early comprehensive fetal anatomic scanning at 13-16 weeks’ gestations should be considered for women who have higher risk for significant fetal anomalies or in whom it is anticipated that a midtrimester transabdominal scan will be technically challenging. This scan does not replace the routine 18- to 22-week anatomy scan.” (p. 1204)12 Supporting evidence: Unclear reporting | Quality of evidence: High (We are confident that the true effect lies close to that of the estimate of effect); Classification of recommendation: NR |
American College of Obstetricians and Gynecologists Committee on Practice Bulletins ― Obstetrics (2016)13 | |
Outcome: clinical indication for obstetrical ultrasound | |
“When a growth disturbance is suspected clinically or there is a medical or obstetric condition that increases the risk of a growth disturbance, ultrasonography is the modality of choice to identify abnormal fetal growth.” (p. e252)13 Supporting evidence: Unclear reporting | Quality of evidence: NR; Classification of recommendation: level B (based on limited or inconsistent evidence) |
“In the absence of other specific indications, the optimal time for a single ultrasound examination is at 18–22 weeks of gestation” (p. e251)13 Supporting evidence: Unclear reporting | Quality of evidence: NR; Classification of recommendation: level C (based primarily on consensus and expert opinion) |
Khalil et al. (2016)14 | |
Outcome: monitoring of twin pregnancy | |
“Women with an uncomplicated dichorionic twin pregnancy should have a first-trimester scan, a detailed second-trimester scan, and scans every 4 weeks thereafter. Complicated dichorionic twins should be scanned more frequently, depending on the condition and its severity.” (p. 249)14 Supporting evidence: None reported | Quality of evidence: 4 (expert opinion); Classification of recommendation: Good practice point (Recommended best practice based on the clinical experience of the guideline development group) |
“Uncomplicated monochorionic twins should have a first-trimester scan and be scanned every 2 weeks after 16 weeks in order to detect twin-to-twin transfusion syndrome and twin anemia–polycythemia sequence in a timely manner. Complicated monochorionic twins should be scanned more frequently, depending on the condition and its severity” (p. 249)14 Supporting evidence: “In uncomplicated monochorionic twins, an ultrasound scan should be performed in the first trimester There should then be scans every 2 weeks from 16 weeks onwards, as timely detection of twin-to-twin transfusion syndrome and twin anemia–polycythemia sequence has been shown to improve perinatal outcome [19,20].” (p. 250)14 | Quality of evidence: NR; Classification of recommendation: C (Body of evidence including studies rated as 2+ applicable directly to the target population and demonstrating overall consistency of results; or extrapolated evidence from studies rated as 2++ ) |
Fleming et al. (2015)15 | |
Outcome: management of adolescents who are pregnant “A first-trimester ultrasound is recommended not only for the usual reasons for properly dating the pregnancy, but also for assessing the increased risks of preterm birth.” (p. 744)15 Supporting evidence: unclear reporting | Quality of evidence assessment: III (Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
“An ultrasound anatomical assessment at 16 to 20 weeks is recommended because of increased rates of congenital anomalies in this population.” (p. 747)15 Supporting evidence: unclear reporting | Quality of evidence assessment: II-2 (Evidence from well-designed cohort (prospective of retrospective) or case- controlled studies, preferably from more than 1 centre or research group); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
As in other populations at risk of intrauterine growth restriction and low birth weight, an ultrasound to assess fetal well-being and estimated fetal weight at 32 to 34 weeks’ gestational age is suggested to screen for intrauterine growth restriction.” (p. 747)15 Supporting evidence: unclear reporting | Quality of evidence assessment: III (Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees); Classification of recommendation: A (There is good evidence to recommend the clinical preventive action.) |
LMP = last menstrual period; NR = not reported.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca