CADTH Health Technology Review
Floatation Therapy for Physical Conditions
Rapid Review
Authors: Keeley Farrell, Hannah Loshak
Abbreviations
DoD
Department of Defense
GRADE
Grading of Recommendations Assessment, Development and Evaluation
NRS
numerical rating scale
RCT
randomized controlled trial
REST
restricted environmental stimulation therapy
VA
Department of Veterans Affairs
Key Messages
The clinical effectiveness of floatation therapy for the treatment of physical conditions remains uncertain. One randomized controlled trial was identified that evaluated floatation-restricted environmental stimulation therapy (REST) compared with placebo and waitlist control groups for the treatment of patients with chronic pain. The trial reported no significant differences between the 3 treatment groups on any of the outcomes measured including those related to pain, medication use, quality of life, sleep impairment, anxiety, or depression.
One guideline was identified that states that there is insufficient evidence to recommend for or against the use of sensory deprivation tanks in patients with symptoms attributed to mild traumatic brain injury.
The cost-effectiveness of floatation therapy for the treatment of physical condition is unknown as no relevant economic evaluations were identified.
Context and Policy Issues
Floatation therapy, also known as floatation-restricted environmental stimulation therapy (REST) is a therapy in which a person lies horizontally in a quiet, dark tank (sensory deprivation tank) filled with water saturated with magnesium sulphate (Epsom salt).1 The high concentration of magnesium sulphate in the water increases its buoyancy and allows individuals to float effortlessly on their back.1,2 The water in the tank is heated to outer skin temperature (approximately 35 °C).3 During a floatation therapy session, patients float on their back inside the tank for approximately 1 hour.4 It has been suggested that floatation therapy achieves beneficial effects through deep relaxation that is induced by sensory isolation.1 Floatation therapy has been used as a treatment for a variety of psychological and physical conditions, such as chronic pain, fibromyalgia, and multiple sclerosis.3 Floatation therapy may not be appropriate for patients with conditions including epilepsy, kidney disease, low blood pressure, any contagious disease, open wounds, or claustrophobia.4 Patients with physical conditions may be seeking alternative therapies due to dissatisfaction with current treatment options. For example, treatment for chronic pain is often only partially effective,5 which may lead some patients with chronic pain to seek alternative treatment options such as floatation therapy.
A summary of the available literature could help decision-makers determine the appropriate use of floatation therapy for patients with physical conditions.
This report is part of a series of 2 CADTH reports on the use of floatation therapy. The other report aimed to summarize the clinical effectiveness, cost-effectiveness, and guidelines of floatation therapy for the treatment of mental health conditions. The aim of the current report is to summarize the clinical effectiveness, cost-effectiveness, and evidence-based guidelines regarding the use of floatation therapy for the treatment of physical conditions.
Research Questions
What is the clinical effectiveness of floatation therapy for the treatment of physical conditions?
What is the cost-effectiveness of floatation therapy for the treatment of physical conditions?
What are the evidence-based guidelines regarding the use of floatation therapy for the treatment of physical conditions?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and PsycINFO via OVID, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was floatation tanks. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2016 and November 15, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People with physical conditions (e.g., chronic pain, fibromyalgia, multiple sclerosis, physical disabilities, neurodegenerative disease), with or without comorbid conditions |
Intervention | Floatation therapy (e.g., Floatation-Restricted Environmental Stimulation Therapy), alone or in combination with other interventions (e.g., pharmacotherapy, psychotherapy) |
Comparator | Q1 to Q2: Pharmacological interventions; non-pharmacological interventions (e.g., psychotherapy, pool therapy); no treatment (e.g., waitlist); placebo (e.g., sham interventions) Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., severity of symptoms [e.g., pain, anxiety symptoms, depressive symptoms], functional status or disability, quality of life, safety [e.g., adverse events]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q3: Recommendations regarding best practices (e.g., appropriate patient populations of clinical settings, treatment protocols [e.g., frequency and length of treatment], contraindications, recommended safeguards) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, guidelines, economic evaluations |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: the Downs and Black checklist6 for the randomized controlled trial (RCT) and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument7 for the guideline. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
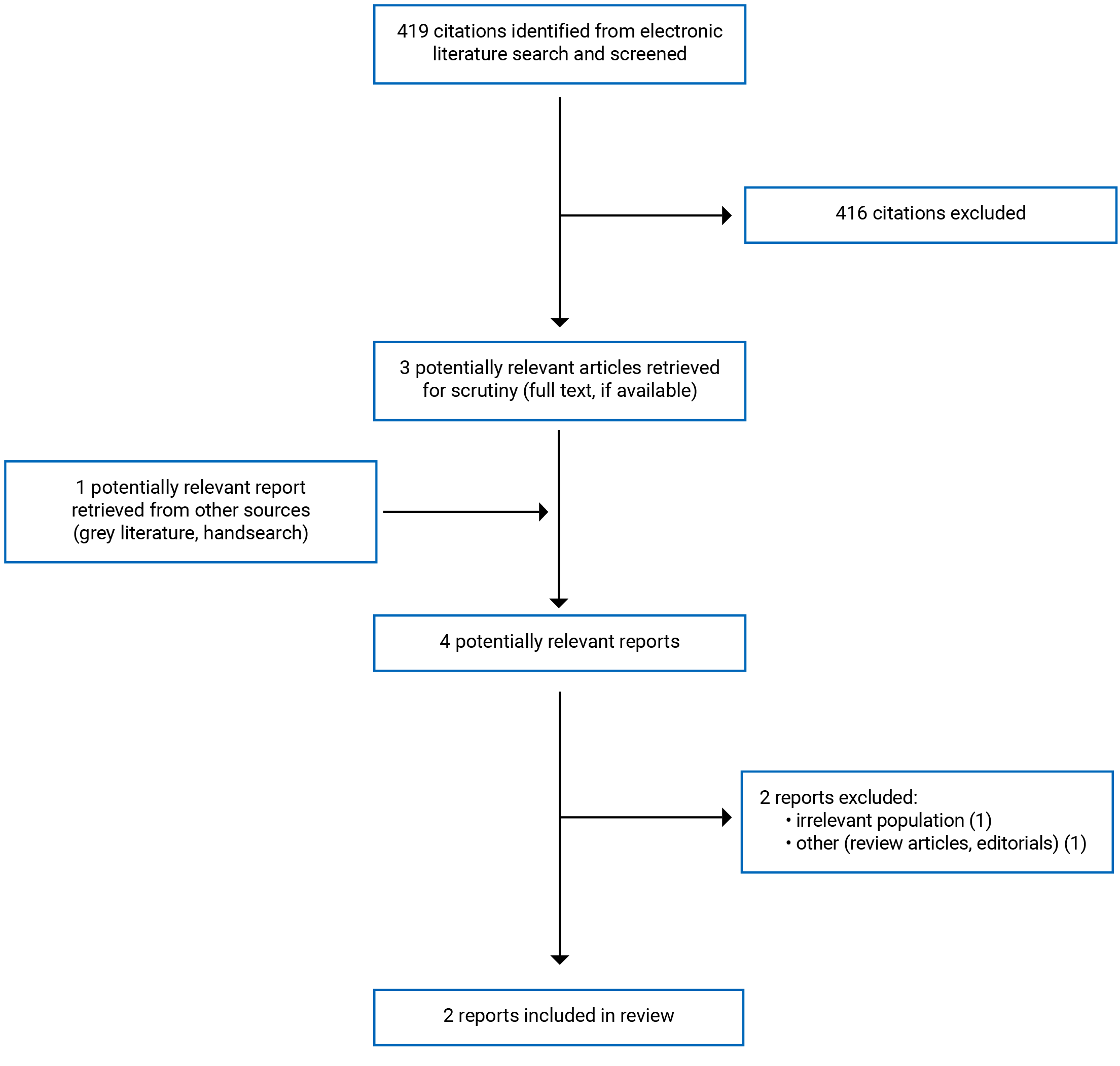
A total of 419 citations were identified in the literature search. Following screening of titles and abstracts, 416 citations were excluded and 3 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 2 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. These comprised 1 RCT and 1 evidence-based guideline. Appendix 1 presents the PRISMA8 flow chart of the study selection.
Summary of Study Characteristics
One RCT9 was identified that evaluated floatation-REST in patients with chronic pain. One evidence-based guideline10 was identified that included a recommendation around sensory deprivation tanks for the treatment of symptoms associated with mild traumatic brain injury. No relevant health technology assessments, non-randomized studies, or economic evaluations were identified.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
One single-centre, single-blind (patients were blinded), 3-arm RCT9 that evaluated the clinical effectiveness of floatation-REST was included in this report. The RCT reported both between-group comparisons and within-group comparisons (before and after treatment).9
One guideline10 developed by the Department of Veterans Affairs (VA) and Department of Defense (DoD) and published in 2021 was included in this report. The guideline was an update to a version published in 2016. As part of the guideline development process a systematic literature search was conducted to identify relevant clinical studies and systematic reviews. The evidence was rated based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology as being of high, moderate, low, or very low quality. A work group attended a recommendation development meeting in which they interpreted the systematic review’s findings and developed the recommendations. A detailed description of the methods used to formulate recommendations was not provided. Recommendations were either for or against an intervention and each recommendation was rated based on a modified GRADE and US Preventive Services Task Force method as being either strong or weak. In cases of interventions with insufficient evidence the recommendation was neither for nor against it.
Country of Origin
The RCT by Loose et al. (2021)9 was conducted in Germany.
The VA/DoD guideline10 is intended for use in the US.
Patient Population
Loose et al. (2021)9 included 99 patients (80 women, 19 men) diagnosed with chronic pain disorder with psychological and somatic factors. The mean age of patients was 51.7 (standard deviation = 12.3) years. The mean pain intensity numerical rating scale (NRS) scores for patients at baseline were 73.9 for maximum pain and 50.1 for mean pain. These scores correspond to moderate to severe pain. The mean Beck Depression Inventory II score at baseline was 22.3 and the mean State-Trait Anxiety Inventory score at baseline was 52.3. These scores correspond to moderate levels of depression and trait anxiety.
The intended users of the VA/DoD guideline10 are VA and DoD primary care providers involved with the care of patients with mild traumatic brain injury. The target population of the guideline is patients with symptoms attributed to mild traumatic brain injury who are eligible for care in VA/DoD health care systems.
Interventions and Comparators
In the RCT by Loose et al. (2021)9 the intervention was 5 sessions of floatation-REST that lasted 60 to 90 minutes and were each separated by 4 days. Sessions took place in a floatation pod in which the water was kept at skin temperature and high buoyancy was achieved by adding Epsom salt. The tank was located in a quiet, darkened room and patients wore sound-insulating wax earplugs. Patients were also encouraged to switch the lights off inside the tank. The placebo group received 5 sessions (60 to 90 minutes each) of an intervention that was designed to mimic floatation-REST but the degree of environmental stimulus restriction and effortless floating was reduced. Placebo sessions took place in the same tank but with reduced buoyancy and water depth, ensuring that patients rested on the bottom of the tank (with their head above water). The light inside the tank stayed on throughout the session and background music was played constantly. Patients in the placebo group wore soft earplugs instead of the more insulating earplugs worn by the intervention group. Additionally, a blood pressure cuff was attached to the lower leg of patients in the placebo group and inflated at random intervals and they were asked to rate their current pain and relaxation levels a mean of every 10.3 minutes. The goal was to prevent deep relaxation in the placebo group by changing stimuli and active cognitive processes. Treatment credibility and expectancy were assessed using the 4-item scale of Borkovek and Nau.9 There were no significant differences in credibility or expectancy between the floatation-REST and placebo groups.9 The trial also included a waitlist control group that did not receive any further intervention.
The VA/DoD guideline10 considered a range of evidence-based practices for the management and rehabilitation of patients with symptoms attributable to mild traumatic brain injury. Practices considered in the guideline included a variety of tests, assessment tools, and pharmacologic and non-pharmacologic interventions. The guideline included a recommendation around sensory deprivation tanks in general that was not specific to floatation therapy.
Outcomes
The primary outcome for the RCT by Loose et al. (2021)9 was change in pain intensity (maximum and mean) assessed retrospectively for 1 week using a validated 101-point NRS. The NRS scores range from 0 (no pain) to 100 (worst imaginable pain). Secondary outcomes included pain-related disability, pain area, pain widespreadness, trait anxiety, depression, quality of life, sleep quality, and use of medication. The primary and secondary outcomes were assessed at baseline as well as 3 follow-up visits (1, 12, and 24 weeks after the last intervention and 4, 15, and 27 weeks after baseline for the waitlist control group). Pain-related disability was assessed with the Pain Disability Index (scores range from 0 to 70 with higher scores indicating greater disability). Pain widespreadness (number of body regions affected by pain) was assessed by the Widespread Pain Index (scores range from 0 to 19 with higher scores indicating more body regions affected by pain). Both pain area and the Widespread Pain Index were derived from electronic pain drawings using the SymptomMapper application. Pain area ranges from 0 to 100% of the total body area.11 Trait anxiety was assessed using the State-Trait Anxiety Inventory (scores range from 20 to 80 with higher scores indicating greater anxiety). Depression was assessed using the Beck Depression Inventory II (scores range from 0 to 63 with higher scores indicating greater severity of depression). Quality of life was assessed by the 12-Item Short Form Health Survey (Mean [standard deviation] t score, 50 [10], with higher scores indicating better physical and mental health). Sleep quality was assessed retrospectively for 1 week using the NRS with scores ranging from 0 (not impaired by pain) to 100 (very much impaired). To assess medication use, the study defined medication steps based on the most potent medication taken by each patient (medication steps: 0 = no pain medication; 1 = nonopioid analgesics; 2 = analgesic adjuvants; 3 = cannabinoids; 4 = weak opioids; and 5 = strong opioids). In addition, current pain intensity, level of relaxation, pain area, pain widespreadness, and state anxiety were assessed before and after each treatment session in the intervention and placebo groups.
The major outcomes considered by the VA/DoD guideline10 were symptom improvement, functional independence and quality of life, as well as return to participating in activities, duties, work, and sports.
Summary of Critical Appraisal
Randomized Controlled Trial
In the RCT by Loose et al. (2021)9 the objective, outcomes, interventions, and patient characteristics were clearly described. However, adverse events were not reported. Additionally, actual P values and confidence intervals were not reported. Not reporting these measures limits the overall ability to interpret the results. The number of patients lost to follow-up in each group and dropout reasons were provided. The authors stated that they did not identify any systematic reasons for patient dropouts from the study.9 The proportion of patients recruited out of the total number of patients screened was reported. Additionally, patients in different intervention groups were selected over the same time period. Baseline characteristics appear to be balanced between the different treatment groups. Confounding factors were not discussed in the trial nor adjusted for in the analyses. Therefore, it is unclear whether there were any confounding factors that could have biased the outcomes of the trial. A placebo group was included in the trial to blind patients to the intervention they received; however, investigators were not blind to treatment assignment. Blinding investigators to the treatment assignment of patients reduces the risk of bias in the assessment and reporting of outcomes. There were differences between the interventions that the placebo and floatation-REST groups that may have resulted in some unblinding of patients. However, the credibility and expectancy of the intervention was measured, and no significant differences were found between the placebo and floatation-REST groups. Patients were assigned to 1 of the 3 treatment groups using a central telephone randomization procedure prepared by an investigator who was not involved in patient care. Ensuring that the assignment of patients to treatment groups is random reduces the risk of selection bias. Due to the nature of the intervention (patients were monitored during treatment sessions), compliance with the intervention was reliable. A power calculation was conducted a priori to determine sample size and an adequate number of patients was enrolled in each group. Because there were multiple outcomes assessed in the trial, multiplicity was adjusted for using a Bonferroni correction. Adjusting for multiplicity is important in trials that assess multiple outcomes due to the potential inflation of the type I error rate. Patients who were randomized to a treatment group but dopped out of the study before any measurement were not included in analyses. Analyzing all patients as per their initial randomization regardless of whether they actually received treatment (known as intention-to-treat analysis) preserves the balance between the groups achieved through randomization. Since the study was conducted in a single-centre in Germany, the results may not be generalizable to the Canadian population. The authors reported no conflicts of interest and stated that the sponsor did not influence the conduct or reporting of the study.
Guideline
The overall objective and health questions covered by the VA/DoD guideline10 were clearly described. The guideline development group included individuals from all relevant professional groups. As part of the guideline development process a patient focus group was held to obtain the views and preferences of the target population. Systematic methods were used to search for evidence. The search was conducted in multiple databases, the full search strategy and search terms were provided, and the inclusion and exclusion criteria for studies were clearly described. Providing details of these elements of the search strategy increases its reproducibility. However, it is unclear if the screening of articles was done in duplicate. Performing screening of articles in duplicate helps reduce the risk of bias. The methods for formulating the recommendations were clearly described and there was an explicit link between the recommendations and supporting evidence. The guideline was reviewed externally by experts before its publication. The procedure for updating the guideline includes a routine update every 3 to 5 years as well as an update if a recommendation is identified as harmful to patients. The recommendations are easily identifiable in the guideline, and they are specific and unambiguous. The guideline was funded by the VA Evidence-Based Practice, Office of Quality and Patient Safety, however, it does not include an explicit statement that the funding body did not influence the content of the guideline. The guideline reported that no conflicts of interest among the work group or guideline development team were identified. Since the VA/DoD guideline10 was intended for use in the US, the recommendations may not be generalizable to Canadian settings.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Floatation-REST
The results of 1 RCT9 that evaluated the clinical effectiveness of floatation-REST in patients with chronic pain are summarized below.
Pain Intensity
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for change in maximum pain or change in mean pain at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for the number of patients achieving a 30% reduction in maximum pain or mean pain at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).
Patients treated with floatation-REST experienced a significant improvement in mean pain intensity after the intervention compared with before the intervention (i.e., within-group comparison). Similarly, there was also a significant improvement in mean pain intensity after the intervention compared with before the intervention in the placebo group. When the 2 groups were compared, there was no significant between-group difference in mean pain intensity measured at pre-intervention and post-intervention in the floatation-REST group versus the placebo group.
Pain-Related Disability
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for change in mean Pain Disability Index score at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).
Pain Area
There was no significant difference in the change from baseline in mean pain area at 1 week between the floatation-REST and placebo groups. There was a significant improvement in mean pain area measured after the intervention compared with before the intervention in the floatation-REST group (i.e., within-group comparison). There was also a significant improvement in mean pain area measured after the intervention compared with before the intervention in the placebo group. When the 2 groups were compared, there was no significant between-group difference in mean pain area measured at pre-intervention and post-intervention in the floatation-REST group versus the placebo group.
Pain Widespreadness
There was no significant difference in the change from baseline in pain widespreadness (number of body regions affected by pain, measured by the Widespread Pain Index) at 1 week between the floatation-REST and placebo groups. Patients treated with floatation-REST experienced a significant improvement in the mean Widespread Pain Index score measured after the intervention compared with before the intervention in the intervention group (i.e., within-group comparison). Patients in the placebo group similarly experienced a significant improvement in mean Widespread Pain Index score measured after the intervention compared with before the intervention in the placebo group. When the 2 groups were compared, there was no significant between-group difference in mean Widespread Pain Index score measured at pre-intervention and post-intervention in the floatation-REST group versus the placebo group.
Trait Anxiety
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for change in mean State-Trait Anxiety Inventory score at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks). There was a significant improvement in mean State-Trait Anxiety Inventory score after the intervention compared with before the intervention in the floatation-REST group (i.e., within-group comparison). There was also a significant improvement in the mean State-Trait Anxiety Inventory score after the intervention compared with before the intervention in the placebo group. When the 2 groups were compared, there was no significant between-group difference in mean State-Trait Anxiety Inventory score measured at pre-intervention and post-intervention in the floatation-REST group versus the placebo group.
Depression
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for change in mean Beck Depression Inventory II scores at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).
Quality of Life
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for change in the physical component or mental component of the 12-Item Short Form Health Survey at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).
Sleep Impairment
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for change in mean sleep impairment at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).
Medication Use
There were no significant differences between the floatation-REST, placebo, and waitlist control groups for change in mean medication step at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).
Level of Relaxation
There was a significant improvement in mean relaxation after the intervention compared with before the intervention in the floatation-REST group (i.e., within-group comparison). There was also a significant improvement in mean relaxation after the intervention compared with before the intervention in the placebo group. When the 2 groups were compared, there was a significant between-group difference in mean relaxation measured at pre-intervention and post-intervention in the floatation-REST group versus the placebo group.
Cost-Effectiveness of Floatation-REST
No relevant evidence regarding the cost-effectiveness of floatation therapy for the treatment of physical conditions was identified; therefore, no summary can be provided.
Guidelines
One guideline10 was identified that included a recommendation regarding the use of sensory deprivation tanks in patients with symptoms attributable to mild traumatic brain injury.
The VA/DoD guideline10 states that there is insufficient evidence to recommend for or against the use of sensory deprivation tanks for the treatment of patients with symptoms attributed to mild traumatic brain injury. No relevant evidence on sensory deprivation tanks was identified.
Limitations
The findings in this report are limited by the quantity of relevant evidence. One randomized placebo-controlled trial was identified that evaluated the clinical effectiveness of floatation-REST in patients with chronic pain.9 This trial did not report on adverse events, therefore the safety of floatation-REST in patients with chronic pain is unknown. No studies were identified that evaluated the clinical effectiveness of floatation-REST in pediatric patients or for physical conditions other than chronic pain. Additionally, no studies were identified that compared treatment with floatation-REST versus other alternative therapies; therefore, the clinical effectiveness of floatation-REST versus alternative treatments is unknown. No relevant economic evaluations of floatation therapy for the treatment of physical conditions were identified, therefore, the cost-effectiveness of floatation therapy is unknown.
One evidence-based guideline was identified that included a recommendation on the use of sensory deprivation tanks for the treatment of patients with symptoms attributed to mild traumatic brain injury; however, this guideline did not identify any relevant evidence on the clinical effectiveness of sensory deprivation tanks.10
The VA/DoD guideline10 is specific to the US and the RCT by Loose et al. (2021)9 was conducted in Germany. Therefore, it is unclear whether the results summarized in this report are generalizable to Canada.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 RCT9 and 1 evidence-based guideline10 on the use of floatation therapy for the treatment of physical conditions. No literature assessing the cost-effectiveness of floatation therapy for the treatment of physical conditions was identified.
The RCT by Loose et al. (2021)9 evaluated floatation-REST in patients with chronic pain. The trial reported no significant differences between the floatation-REST, placebo, and waitlist control groups for pain intensity, pain-related disability, pain area, pain widespreadness, trait anxiety, depression, quality of life, sleep impairment, or medication use at any of the time points (baseline to 1 week, 12 weeks, or 24 weeks).9 While significant within-group improvements in pain intensity, pain area, pain widespreadness, trait anxiety, and level of relaxation were reported when measured before and after the intervention in the floatation-REST and placebo groups, there were no significant between-group differences for pain intensity, pain area, pain widespreadness, and trait anxiety when the floatation-REST and placebo groups were compared.9 However, there was a significant between-group difference in the level of relaxation measured before and after the intervention that favoured the placebo group versus the floatation-REST group.9 The trial did not report on adverse events.
The VA/DoD guideline10 states that there is insufficient evidence to recommend for or against the use of sensory deprivation tanks for the treatment of symptoms attributed to mild traumatic brain injury.10 No relevant evidence on sensory deprivation tanks was identified.10
Limited evidence was identified on the effectiveness of floatation therapy for the treatment of patients with physical conditions. Based on the results of 1 RCT,9 there are no significant differences between the effect of floatation-REST, placebo, or waitlist control on pain intensity, pain-related disability, pain area, pain widespreadness, trait anxiety, depression, quality of life, sleep impairment, or medication use in patients with chronic pain. One guideline10 states that there is insufficient evidence to recommend for or against the use of sensory deprivation tanks in patients with symptoms attributed to mild traumatic brain injury. Additional high-quality studies that compare floatation therapy to other alternative therapies for patients with physical conditions would help reduce the uncertainty around the clinical effectiveness and safety of floatation therapy.
References
1.Jonsson K, Kjellgren A. Promising effects of treatment with flotation-REST (restricted environmental stimulation technique) as an intervention for generalized anxiety disorder (GAD): a randomized controlled pilot trial. BMC Complement Altern Med. 2016;16:108. PubMed
2.Feinstein JS, Khalsa SS, Yeh HW, et al. Examining the short-term anxiolytic and antidepressant effect of Floatation-REST. PLoS ONE [Electronic Resource]. 2018;13(2):e0190292. PubMed
3.Hoffman JL. “Everything Old Is New Again”: A Review of Current Complementary and Alternative Medicine Trends. Holist Nurs Pract. 2021;35(6):300-305. PubMed
4.Government of Western Australia. Floatation tanks. https://www.healthywa.wa.gov.au/Articles/F_I/Floatation-tanks. Accessed 2021 Nov 30.
5.Canadian Pain Task Force Report. Chronic pain in Canada: laying a foundation for action. Ottawa (ON): Health Canada; 2019: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2019.html. Accessed 2021 Dec 9.
6.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
7.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Dec 10.
8.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
9.Loose LF, Manuel J, Karst M, Schmidt LK, Beissner F. Flotation Restricted Environmental Stimulation Therapy for Chronic Pain: A Randomized Clinical Trial. JAMA netw. 2021;4(5):e219627.
10.VA/DoD clinical practice guideline for the management and rehabilitation of post-acute mild traumatic brain injury. Washington (DC): Department of Veterans Affairs, Department of Defense; 2021: https://www.healthquality.va.gov/guidelines/Rehab/mtbi/VADoDmTBICPGFinal508.pdf. Accessed 2021 Nov 23.
11.Hanover Medical School. NCT03584750: Floating for chronic pain (Float4Pain). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://www.clinicaltrials.gov/ct2/show/NCT03584750. Accessed 2021 Dec 10.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Randomized Controlled Trial
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Loose et al. (2021)9 Germany Horst Görtz Foundation | Single-centre, single-blind, 3-arm RCT | Inclusion criteria: patients aged 18 to 75 years diagnosed with chronic pain disorder with psychological and somatic factors. Exclusion criteria: pregnancy, acute illness, contagious disease, acute major depression, epilepsy, claustrophobia, schizophrenia, incontinence, and suspected literacy and cognitive barriers to understanding the instructions. Baseline characteristics: 99 patients (80 women, 19 men) with a mean age of 51.7 (SD = 12.3) years, mean NRS scores of 73.9 (SD = 16.3) for maximum pain and 50.1 (SD = 17.3) for mean pain, mean Beck Depression Inventory II score of 22.3 (SD = 12.5) and mean State-Trait Anxiety Inventory part X2 score of 52.3 (SD = 11.9). | Intervention: 5 treatment sessions of floatation-REST that lasted 60 to 90 minutes Comparators: placebo (five 60-to-90-minute sessions designed to mimic floatation-REST with reduced levels of environmental stimulus restriction and effortless floating), waitlist control (did not receive any additional treatment) | Outcomes: pain intensity, pain-related disability, pain area, pain widespreadness, trait anxiety, depression, quality of life, sleep quality, use of pain medication, level of relaxation, heart rate variability, unusual body sensations during intervention Follow-up: 24 weeks |
NRS = numerical rating scale; RCT = randomized controlled trial; REST = restricted environmental stimulation therapy; SD = standard deviation.
Table 3: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
VA/DoD (2021)10 | ||||||
Intended users: VA and DoD primary care providers including physicians, nurse practitioners, physician assistants, nurses, pharmacists, psychologists, social workers, and others involved with the care of patients with mild traumatic brain injury. Target population: Patients with symptoms attributed to mild traumatic brain injury who are eligible for care in the VA or DoD health care systems, and those who receive care from community-based clinicians. | Evidence-based practices for the management and rehabilitation of patients with symptoms attributable to mild traumatic brain injury | Symptom improvement, functional independence/ quality of life, return to activity/ duty/ work/ sports | Update to the 2016 version of the guideline. A systematic literature search was conducted to identify relevant clinical studies and systematic reviews. Titles and abstracts were screened based on the inclusion criteria. Potentially relevant full-text articles were retrieved and underwent 2 rounds of screening. Included studies were discussed narratively. | The quality of the evidence supporting each recommendation was rated based on the GRADE methodology. The evidence was rated as being high, moderate, low, or very low quality. | The guideline work group attended a 4-day virtual recommendation development meeting in which they interpreted the systematic review’s findings and developed the recommendations. Where appropriate, modified recommendations from the 2016 guideline were carried forward. New recommendations based on the updated systematic review were also developed. Each recommendation was rated based on a modified GRADE and USPSTF methodology. Recommendations were rated based on an assessment of the overall quality of the evidence base, benefits and harms, patient values and preferences, and other implications. Strength and direction of recommendations and general corresponding text:
| A draft of the guidelines was sent to experts from the VA and DoD health care systems and outside organizations for review. |
DoD = Department of Defense; GRADE = Grading of Recommendations Assessment, Development and Evaluation; USPSTF = US Preventive Services Task Force; VA = Department of Veterans Affairs.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the Randomized Controlled Trial Using the Downs and Black Checklist6
Strengths | Limitations |
|---|---|
Loose et al. (2021)9 | |
Objective, outcomes, interventions, patient characteristics, and main findings clearly described Number of patients lost to follow-up in each group and dropout reasons were provided The proportion of patients recruited out of those screened was reported Patients in different intervention groups were selected over the same time period A placebo group was included in the study to blind individuals to the intervention they received Compliance with the intervention was reliable as patients were being monitored during the treatment sessions The main outcomes measures used were accurate Baseline characteristics appear to be balanced between the treatment groups Patients, care providers, and care setting were representative of the population and setting of interest Patients were randomly assigned to treatment groups using a central telephone randomization procedure prepared by an investigator who was not involved in patient care A power calculation was conducted a priori to determine sample size and an adequate number of patients was recruited to each group Multiplicity was adjusted for using a Bonferroni correction Length of follow-up was standardized across treatment groups Authors reported no conflicts of interest and stated that the sponsor did not influence the conduct or reporting of the study | Potential confounders were not discussed Adverse events were not reported Actual P values and confidence intervals were not reported Investigators were not blind to treatment assignment Patients who were randomized but dropped out of the study before any measurement were not included in analyses The results of the study may not be generalizable to Canadian patients |
Table 5: Strengths and Limitations of the Guideline Using AGREE II7
Item | VA/DoD (2021)10 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | NA |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | NA |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; DoD = Department of Defense; NA = not applicable; VA = Department of Veterans Affairs.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Pain
Outcome | Time point | Study citation | |||
|---|---|---|---|---|---|
Loose et al. (2021)9 | |||||
Intervention group | Placebo group | Waitlist group | P value | ||
Pain intensity | |||||
Maximum pain, NRS score Mean (SD) Note: scores range from 0 to 100 with higher scores indicating maximum pain. | Change from baseline at 1 week | −7.6 (19.7) | −5.8 (12.7) | 0.4 (14.0) | NS |
Change from baseline at 12 weeks | −3.6 (15.7) | −3.4 (14.7) | −2.5 (14.3) | NS | |
Change from baseline at 24 weeks | −2.4 (19.6) | −0.8 (15.3) | −2.1 (14.3) | NS | |
Mean pain, NRS score Mean (SD) Note: scores range from 0 to 100 with higher scores indicating maximum pain. | Change from baseline at 1 week | −2.1 (19.4) | −4.2 (16.2) | 2.0 (12.6) | NS |
Change from baseline at 12 weeks | −2.0 (19.6) | −1.8 (11.6) | −1.0 (13.8) | NS | |
Change from baseline at 24 weeks | −0.2 (13.7) | −2.4 (14.1) | −2.4 (13.4) | NS | |
Number of patients who experienced at least a 30% reduction in maximum pain from baseline, as measured using the NRS N (%) | 1 week | 5 (20) | 4 (16) | 2 (8) | NS |
12 weeks | 2 (8) | 2 (8) | 2 (8) | NS | |
24 weeks | 3 (12) | 3 (12) | 2 (8) | NS | |
Number of patients who experienced at least a 30% reduction in mean pain from baseline, as measured using the NRS N (%) | 1 week | 5 (20) | 5 (20) | 1 (4) | NS |
12 weeks | 8 (32) | 4 (16) | 3 (12) | NS | |
24 weeks | 4 (16) | 5 (20) | 5 (20) | NS | |
Pain intensity, NRS score Mean (SD) Note: scores range from 0 to 100 with higher scores indicating maximum pain. | Pre-intervention | 51.3 (20.6) | 46.0 (21.3) | NA | Intervention vs placebo: NS Intervention (pre-intervention vs post-intervention): P < 0.001 Placebo (pre-intervention vs post-intervention): P < 0.001 |
Post-intervention | 34.3 (20.4) | 22.7 (18.4) | NA | ||
Pain-related disability | |||||
Pain Disability Index score Mean (SD) Note: scores range from 0 to 70 with higher scores indicating greater disability. | Change from baseline at 1 week | −1.7 (10.7) | −4.2 (8.4) | 0.0 (5.1) | NS |
Change from baseline at 12 weeks | −4.8 (11.6) | −0.5 (8.9) | −0.2 (9.9) | NS | |
Change from baseline at 24 weeks | 0.2 (12.0) | −3.7 (11.2) | 0.9 (12.9) | NS | |
Pain area | |||||
Pain area, % Mean (SD) Note: pain area ranges from 0 to 100% of body area | Change from baseline at 1 week | −5.0 (14.7) | −3.1 (7.7) | NA | NS |
Pre-intervention | 10.6 (12.9) | 7.8 (9.2) | NA | Intervention vs placebo: NS Intervention (pre-intervention vs post-intervention): P < 0.001 Placebo (pre-intervention vs post-intervention): P < 0.001 | |
Post-intervention | 7.0 (11.2) | 4.4 (7.3) | NA | ||
Pain widespreadness (number of body regions affected by pain) | |||||
Widespread Pain Index score Mean (SD) Note: scores range from 0 to 19 with higher scores indicating more body regions affected by pain. | Change from baseline at 1 week | −3.1 (3.7) | −0.6 (3.5) | NA | NS |
Pre-intervention | 6.6 (4.5) | 5.4 (4.1) | NA | Intervention vs placebo: NS Intervention (pre-intervention vs post-intervention): P < 0.001 Placebo (pre-intervention vs post-intervention): P < 0.001 | |
Post-intervention | 4.6 (4.2) | 3.4 (3.7) | NA | ||
NA = not applicable; NRS = numerical rating scale; NS = not significant; SD = standard deviation.
Table 7: Summary of Findings by Outcome — Other Outcomes
Outcome | Time point | Study citation | |||
|---|---|---|---|---|---|
Loose et al. (2021)9 | |||||
Intervention group | Placebo group | Waitlist group | P value | ||
Trait anxiety | |||||
State-Trait Anxiety Inventory score Mean (SD) Note: scores range from 20 to 80 with higher scores indicating greater anxiety. | Change from baseline at 1 week | −1.7 (5.9) | −1.3 (5.6) | −1.8 (4.3) | NS |
Change from baseline at 12 weeks | −3.0 (6.4) | 0.0 (6.3) | −3.2 (3.5) | NS | |
Change from baseline at 24 weeks | −1.9 (5.9) | −0.8 (6.7) | −0.7 (4.8) | NS | |
Pre-intervention | 45.0 (12.0) | 44.6 (11.0) | NA | Intervention vs placebo: NS Intervention (pre-intervention vs post-intervention): P < 0.001 Placebo (pre-intervention vs post-intervention): P < 0.001 | |
Post-intervention | 34.8 (9.9) | 32.3 (8.4) | NA | ||
Depression | |||||
Beck Depression Inventory II score Mean (SD) Note: scores range from 0 to 63 with higher scores indicating greater severity of depression. | Change from baseline at 1 week | −3.3 (10.8) | −2.0 (4.7) | −2.2 (4.8) | NS |
Change from baseline at 12 weeks | −3.6 (9.0) | −0.5 (6.2) | −2.2 (4.4) | NS | |
Change from baseline at 24 weeks | −0.8 (7.2) | −0.9 (7.0) | −2.0 (6.5) | NS | |
Quality of life | |||||
SF-12 score – physical component Mean (SD) Note: Mean (SD) t score, 50 (10), with higher scores indicating better physical health. | Change from baseline at 1 week | 3.0 (5.9) | 2.3 (8.3) | 0.7 (4.5) | NS |
Change from baseline at 12 weeks | 3.0 (7.8) | 0.7 (6.0) | 0.9 (5.0) | NS | |
Change from baseline at 24 weeks | 2.7 (7.0) | 3.2 (8.2) | −0.1 (5.2) | NS | |
SF-12 score – mental component Mean (SD) Note: Mean (SD) t score, 50 (10), with higher scores indicating better mental health. | Change from baseline at 1 week | 2.9 (8.1) | 2.4 (6.1) | −0.7 (5.8) | NS |
Change from baseline at 12 weeks | −0.4 (8.9) | 1.4 (7.7) | −1.0 (5.5) | NS | |
Change from baseline at 24 weeks | 0.1 (5.9) | −1.0 (8.2) | −0.6 (6.2) | NS | |
Sleep impairment | |||||
Sleep impairment, NRS score Mean (SD) Note: scores range from 0 to 100 with higher scores indicating maximum impairment | Change from baseline at 1 week | −6.8 (27.2) | −17.4 (25.4) | −7.4 (15.6) | NS |
Change from baseline at 12 weeks | 1.6 (25.0) | −7.6 (22.6) | −8.4 (15.5) | NS | |
Change from baseline at 24 weeks | 2.6 (20.8) | −15.4 (28.3) | −8.0 (17.1) | NS | |
Medication use | |||||
Medication step Mean (SD) Note: steps range from 0 (no pain medication) to 5 (strong opioids) based on most potent medication used. | Change from baseline at 1 week | −0.3 (0.8) | 0.0 (0.7) | −0.4 (1.1) | NS |
Change from baseline at 12 weeks | 0.2 (1.0) | −0.2 (0.8) | −0.4 (1.1) | NS | |
Change from baseline at 24 weeks | 0.0 (1.2) | 0.0 (0.7) | −0.5 (1.4) | NS | |
Level of relaxation | |||||
Relaxation, NRS score Mean (SD) Note: scores range from 0 to 100 with higher scores indicating maximum relaxation. | Pre-intervention | 47.2 (24.2) | 46.9 (22.5) | NA | Intervention vs placebo: P < 0.01 Intervention (pre-intervention vs post-intervention): P < 0.001 Placebo (pre-intervention vs post-intervention): P < 0.001 |
Post-intervention | 71.1 (22.5) | 81.3 (17.9) | NA | ||
NA = not applicable; NRS = numerical rating scale; NS = not significant; SD = standard deviation; SF-12 = 12-Item Short Form Health Survey.
Table 8: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Strength of recommendations |
|---|---|
VA/DoD (2021)10 | |
Recommendation: There is insufficient evidence to recommend for or against the use of any of the following interventions for the treatment of patients with symptoms attributed to mild traumatic brain injury:
Supporting evidence: no evidence was identified on sensory deprivation tanks. | Neither for nor against |
DoD = Department of Defense; VA = Department of Veterans Affairs.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca