CADTH Health Technology Review
Floatation Therapy for Mental Health Conditions
Rapid Review
Authors: Khai Tran, Hannah Loshak
Abbreviations
ASI-3
Anxiety Sensitivity Index-3
DERS
Dysfunctional Emotional Regulation Scale
EDN
Experienced Deviation from Normal State Scale
GAD
generalized anxiety disorder
GAD-Q-IV
Generalized Anxiety Disorder Questionnaire 4th edition
ITT
intention-to-treat
MAAS
Mindful Attention and Awareness Scale
MADRS-S
Montgomery-Asberg Depression Rating Scale
OASIS
Overall Anxiety Severity and Impairment Scale
PANAS-X
Positive and Negative Affect Schedule Expanded Form
PHG-9
Patient Health Questionnaire 9-item depression scale
PSQI
Pittsburg Sleep Quality Index
PSWQ
Penn State Worry Questionnaire
PTSD
post-traumatic stress disorder
RCT
randomized controlled trial
REST
Restricted Environmental Stimulation Therapy
SD
standard deviation
SDS
Sheehan Disability Scale
SR
systematic review
STAI
State-Trait Anxiety Inventory
VAS
Visual Analogue Scale
Key Messages
Limited evidence from 2 randomized controlled trials suggested that floatation with restricted environmental stimulation therapy may provide some potential benefits in reducing anxiety and improving many of the symptoms associated with anxiety, including muscle tension, blood pressure, difficulties in emotion regulation, sleep difficulties, and depression, in individuals with anxiety disorders.
Both trials reported no serious adverse events or negative side effects associated with the floatation therapy.
No evidence was found on the cost-effectiveness of floatation therapy for the treatment of mental health conditions.
No evidence-based guidelines with recommendations regarding the use of floatation therapy for the treatment of mental health conditions were identified.
Context and Policy Issues
Mental health conditions including schizophrenia, depression, bipolar disorder, anxiety disorders, and personal disorders affect about 13% of people globally.1 In Canada, there are 10.4% of Canadians who have a mental health condition at any given time.1 Anxiety disorders are the most common mental health conditions in Canada, affecting 9% of men and 16% of women in any given year.1 They include generalized anxiety disorder (GAD), obsessive compulsive disorder, panic disorder, social anxiety disorder, phobias (including agoraphobia), post-traumatic stress disorder (PTSD), and eating disorders – anorexia (i.e., not eating) or bulimia (i.e., overeating followed by purging).1
Depending on the degree of a mental health condition, which can vary from mild to severe, there are different options for pharmacological and psychological therapy.1 Alternative therapies such as exercise, diet, acupuncture, meditation, or naturopathy may also provide benefits to individuals with mental health conditions.1
Floatation therapy with restricted environmental stimulation technique, namely floatation-REST, is a non-pharmacological intervention, during which an individual is lying horizontally in supine position in a shallow pool (usually a quiet and dark tank) of water saturated with Epsom salt (i.e., magnesium sulphate) and kept approximately at 35°C.2,3 The high buoyancy of the water allows a person to float comfortably and effortless.2,3 The environment is designed to reduce external stimulation such as sound, touch, and light.2,3 The technique is not recommended to individual with claustrophobia, epilepsy, low blood pressure, any contagious disease, open wounds, or skin ulcers.3 Research on mostly healthy populations has shown floatation-REST to reduce stress,4 anxiety,5 and pain.6
The aim of this report is to summarize the evidence regarding the clinical effectiveness and cost-effectiveness of floatation-REST for the treatment of mental health conditions. This report also aims to summarize the recommendations from evidence-based guidelines regarding the use of this technique for the treatment of mental health conditions.
Research Questions
What is the clinical effectiveness of floatation therapy for the treatment of mental health conditions?
What is the cost-effectiveness of floatation therapy for the treatment of mental health conditions?
What are the evidence-based guidelines regarding the use of floatation therapy for the treatment of mental health conditions?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE and PsycINFO via OVID, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were floatation tanks and mental health. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2016 and November 5, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2016. Primary studies were excluded if they were of single-arm before-and-after design (i.e., non-comparative).
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist7 for randomized controlled trials (RCTs). Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Criteria | Description |
|---|---|
Population | People with mental health conditions (e.g., depression, PTSD, anxiety disorders), with or without comorbid conditions |
Intervention | Floatation therapy (e.g., Floatation Restricted Environmental Stimulation Therapy), alone or in combination with other interventions (e.g., pharmacotherapy, psychotherapy) |
Comparator | Q1 and Q2: Pharmacological interventions; non-pharmacological interventions (e.g., psychotherapy, pool therapy); no treatment (e.g., waitlist); placebo (e.g., sham interventions) Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., severity of symptoms [e.g., depressive symptoms, PTSD symptoms, anxiety symptoms], functional status or disability, quality of life, safety [e.g., adverse events]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q3: Recommendations regarding best practices (e.g., appropriate patient populations of clinical settings, treatment protocols [e.g., frequency and length of treatment], contraindications, recommended safeguards) |
Study designs | HTAs, SRs, RCTs, non-randomized studies, economic evaluations, and guidelines |
HTA = health technology assessment; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; SR = systematic review.
Summary of Evidence
Quantity of Research Available
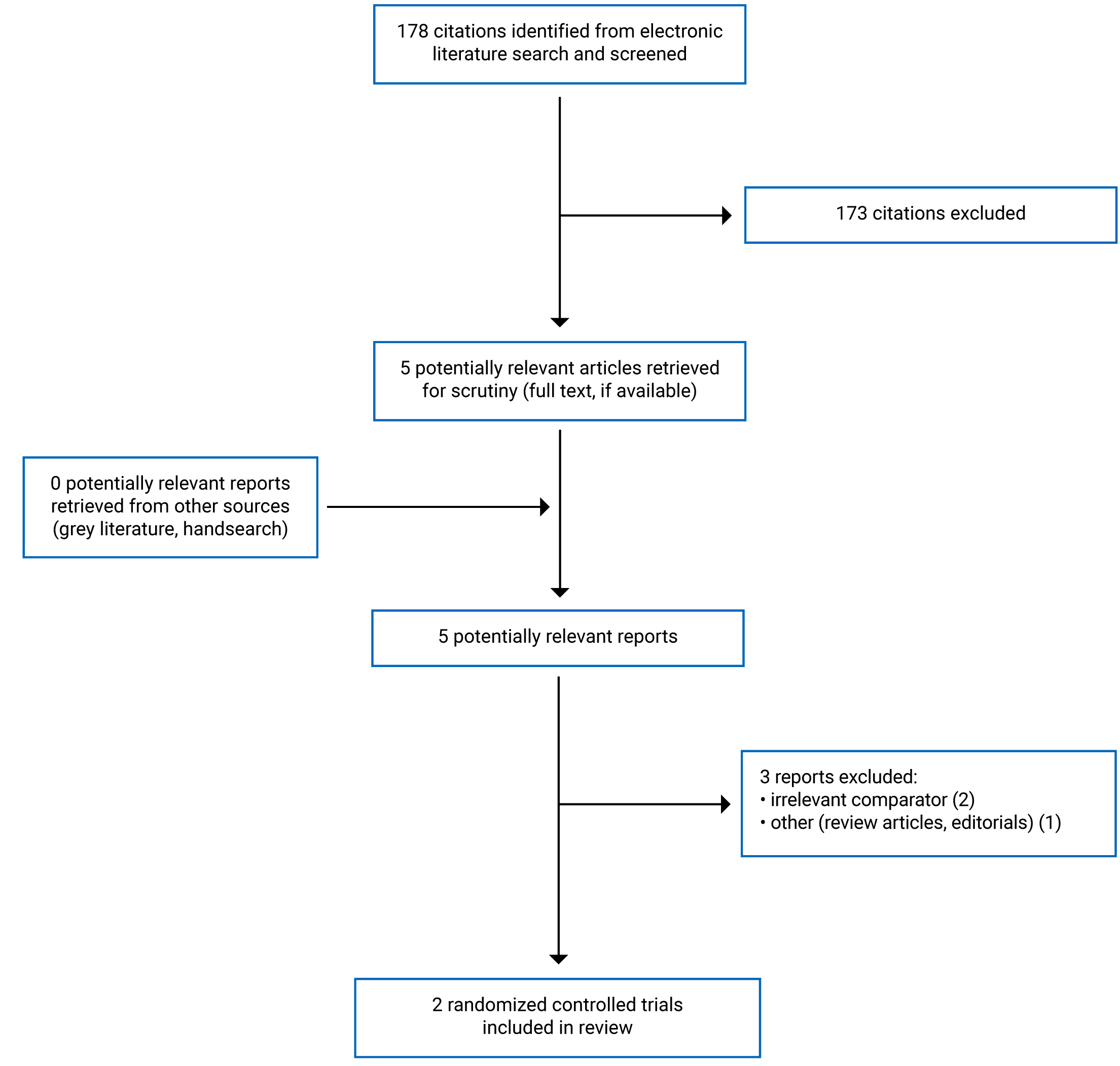
A total of 178 citations were identified in the literature search. Following screening of titles and abstracts, 173 citations were excluded and 5 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 3 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA8 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The detailed characteristics of the included publications, which were of primary clinical studies,9,10 are provided in Appendix 2.
Study Design
The 2 included primary clinical studies were RCTs; 19 was of open-label, within-subject crossover design, and the other10 was of open-label, parallel-group design. One RCT9 was published in 2018, and the other was published in 2016.10
Country of Origin
The primary clinical studies were conducted by authors from US9 and Sweden.10
Patient Population
Participants in 1 RCT9 comprised adults with high levels of anxiety sensitivity with a mix of comorbidities, including GAD, social anxiety disorder, panic disorder, agoraphobia, PTSD, and unipolar major depressive disorder. Participants in the other RCT10 were adults with GAD. The mean age of participants in the 2 RCTs was 39 years9 and 43 years,10 respectively. The percentage of male participants was 38.7%9 and 30%,10 respectively. The percentage of participants who were in stable condition on medication was 68% in 1 RCT9 and 40% in the other.10 One RCT10 reported that 34% of its participants had psychotherapy during the study.
Interventions and Comparators
One RCT9 compared floatation-REST, referred to as float condition, with an exteroceptive comparator, referred to as film condition, in which participants watched a nature documentary from the BBC Planet Earth series. Participants completed a 90-minute session of floatation-REST or the exteroceptive comparator. After the completion of 1 condition, participants crossed over the other condition approximately 1 week later. Both conditions were scheduled to occur at the same time of day for each participant.
The other RCT10 compared floatation-REST with waitlist. Floatation-REST consisted of 12 sessions (45 minutes each) extending over 7 weeks with 2 sessions per week. The 4th week was treatment-free. The waitlist control group was assessed at the corresponding time period. After the 7-week treatment period, the waitlist control group was offered a short floatation-REST treatment (4 sessions in total), but no data were collected.
Outcomes
The outcomes in 1 RCT9 were safety and tolerability, state anxiety, relaxation, muscle tension, serenity, blood pressure, and interoceptive measures. State anxiety was assessed using The Spielberger State Anxiety Inventory (STAI), which is a 20-item self-report questionnaire designed to assess an individual’s level of anxiety at the present moment with total scores ranging from 20 to 80; higher scores mean higher levels of anxiety. Relaxation was measured on a 100-point visual analogue scale (VAS), from 0 (Not at all relaxed or no relaxation) to 100 (Extremely relaxed or the most relaxed I have ever felt). Muscle tension was measured on a 100-point bipolar valence scale ranging from −50 (Extremely Unpleasant) to +50 (Extremely Pleasant), with the slider starting in the middle of the scale at 0 (Neutral). Serenity was assessed using the Positive and Negative Affect Schedule Expanded Form (PANAS-X), which is commonly used to measure mood. The scale has participants rate how calm, relaxed, and at ease they feel at the present moment using a 5-point Likert-type response scale, ranging from 1 (very slightly or not at all) to 5 (extremely). All measures were assessed before-and-after 90-minute treatment with either float condition or film condition. There were no other follow-up data in this study.
The outcome measures in the other RCT10 included the Penn State Worry Questionnaire (PSWQ), the Generalized Anxiety Disorder Questionnaire 4th edition (GAD-Q-IV), the Montgomery-Asberg Depression Rating Scale (MADRS-S), the Pittsburg Sleep Quality Index (PSQI), the Dysfunctional Emotional Regulation Scale (DERS), the Mindful Attention and Awareness Scale (MAAS), and the Experienced Deviation from Normal State Scale (EDN). The 16-item PSWQ is used to assess pathological worry. The instrument has a strong ability to differentiate patients with GAD from other anxiety disorders. Total scores range between 16 and 80. The cut-off score of 45 or higher indicates GAD. The 9-item GAD-Q-IV is a self-reported measure assessing the severity of GAD as defined by the 4th edition of the Diagnostic and Statistical Manual. The measure is used as a continuous variable, and the total score ranges between 0 and 12. A cut-off point of 5.7 or higher has been suggested to yield the optimal ratio between sensitivity and specificity for identifying severe GAD. The 9-item MADRS-S is a Swedish self-reported assessment of depressive symptoms. The total score ranges between 0 and 54. Cut-off values have been set at: 0 to 6 for no depression; 7 to 19 for mild depression; 20 to 34 for moderate depression; and 34 or higher for severe depression. The 19-item PSQI is used to assess subjective sleep quality. The instrument measures sleep disturbance during the previous month. The total score ranges between 0 and 21 and distinguishes between good and poor sleep, where a score of 5 or higher indicates poor-quality sleep. The 36-item DERS is a self-reported measure assessing emotion regulation difficulties. The total score ranges between 36 and 180. Higher scoring indicates greater difficulties in emotion regulation. The 15-item MAAS is a self-reported measure of trait mindfulness. It assesses the level of open and receptive attention to and awareness of ongoing experience. The score ranges from 1 to 6. Higher scoring indicates greater mindfulness. The EDN is a Swedish 29-item self-reported measure specifically designed to be used in floatation-REST experiments. It assesses the degree of relaxation and deviation from normal state experience during the flotation session. Each item is graded on VAS ranging from 0 to 100. A score of 30 on EDN at the first floatation session, and a score of 40 at the subsequent floatation sessions, are considered an indication of typical treatment response, in comparison with resting on a bed in a dark quiet room, which generally gives a score of 15. All measures were assessed at baseline, 4 weeks into treatment, and 7 weeks into treatment. Follow-up data were collected 6 months after the end of 7-week treatment from participants in the floatation-REST group only.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included RCTs9,10 are provided in Appendix 3.
With respect to reporting, both RCTs9,10 clearly described the objective of the study, the interventions of interest, the main outcomes, the baseline characteristics of the patients included in the study, and the main findings of the study. For both RCTs9,10 actual probability and standard deviation values for the main outcomes were reported. One RCT9 assessed the safety and tolerability of the intervention, while the other RCT10 did not. One RCT9 had 2 patients lost during study and used intention-to-treat (ITT) approach in the analyses of the main outcomes, while the other RCT10 had 4 patients lost during study but did not use ITT in the analyses. Not accounting for those patients in the analyses may have resulted in attrition bias. In both RCTs,9,10 all participants not lost to follow-up were assessed for the same period of time (i.e., 90 minutes in 1 RCT9; and 12 treatment sessions over 7 weeks and 6 months follow-up after treatment in the other RCT10). Actual P values and the random variability in the data for the main outcomes (e.g., confidence intervals or standard deviations) were reported in both RCTs.9,10 Regarding external validity, it was unclear if the participants were representative of the entire population from which they were recruited since the study populations in both RCTs were relatively small (i.e., 31 participants in 1 RCT9 and 50 participants in the other RCT10). For internal validity, both RCTs9,10 were open-label in design. The nature of the studies prevented the use of blinding in both participants and investigators. The lack of blinding may have resulted in performance and detection bias. Appropriate statistical tests were used to assess the main outcomes, and reliable and validated outcome measures were used in both RCTs.9,10 Patients in different intervention groups appeared to be recruited from the same population and over the same period of time in both RCTs.9,10 The authors of 1 RCT9 did not report whether a sample size calculation was performed, while a sample size calculation was performed in the other RCT.10 Without a sample size calculation, it is unclear whether the statistically non-significant findings for certain outcomes in the RCT9 were because the study was underpowered for those outcomes. Both RCTs9,10 were conducted at a university research setting, and thus it was unclear if staff, places, and facilities where the patients were treated were representative of the treatment the majority of patients receive. Overall, both RCTs9,10 were of moderate methodological quality.
Summary of Findings
Appendix 4 presents the main study findings of the included RCTs.9,10 The findings are presented by outcomes, which are safety and tolerability (Table 4), state anxiety (Table 5), muscle tension (Table 6), relaxation (Table 7), serenity (Table 8), blood pressure (Table 9), interoceptive measures (Table 10), pathological worry (Table 11), difficulties in emotion regulation (Table 12), mindfulness (Table 13), sleep difficulties (Table 14), depression (Table 15), experienced deviations from normal state (Table 16), and medication and psychotherapy (Table 17).
Clinical Effectiveness of Floatation Therapy for the Treatment of Mental Health Conditions
Safety and Tolerability
One RCT9 found no serious adverse events or major safety concerns that occurred during or after floatation-REST. No safety or tolerability results were reported for the film condition. Most participants finished the entire 90-minute float condition, with 5 participants exiting the pool after approximately 85 minutes. All participants completed the 90-minute film condition. The other RCT10 reported that no negative side effects were found, although adverse event was not pre-specified as an outcome in that study.
State Anxiety
One RCT9 found that, after 90-minute treatment, participants in both float and film condition groups reported reductions in state anxiety, assessed using STAI, but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001).
The other RCT10 found that GAD-symptomatology, assessed using GAD-Q-IV, was statistically significantly reduced for the floatation-REST group (P < 0.001), but not for the waitlist control group, when comparing post-treatment to baseline. Comparing between groups at post-treatment, the floatation-REST group had statistically significantly lower GAD-symptomatology than the waitlist control group (P < 0.05). The treatment effect on GAD-symptomatology was maintained in the floatation-REST group at 6-month follow-up, indicated by no statistically significant differences between post-treatment and follow-up scores.
Muscle Tension
One RCT9 found that, after 90-minute treatment, participants in both float and film condition groups reported reductions in muscle tension, assessed using VAS, but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001). The other RCT10 did not assess this outcome.
Relaxation
One RCT9 found that, after 90-minute treatment, participants in both float and film condition groups reported reductions in relaxation, assessed using VAS, but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001). The other RCT10 did not assess this outcome.
Serenity
One RCT9 found that, after 90-minute treatment, participants in both float and film condition groups reported improvement in serenity, assessed using PANAS-X, but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001). The other RCT10 did not assess this outcome.
Blood Pressure
One RCT9 found that, during treatment (up to 90 minutes), participants in the float condition had a statistically significant reduction in both systolic blood pressure (SBP) and diastolic blood pressure (DBP) (P < 0.001) compared with baseline. Between 15 and 75 minutes, the overall reduction in SBP and DBP in the float condition group was 5.5 mm Hg and 12.8 mm Hg, respectively. Participants in the film condition had no change in both SBP and DBP during treatment. The other RCT10 did not assess this outcome.
Interoceptive Measures
One RCT9 reported a statistically significant increase (P < 0.001) in the intensity of cardiorespiratory sensations (e.g., breath and heartbeat), a statistically significant increase (P < 0.001) in the attention and awareness of cardiorespiratory sensations (e.g., breath and heartbeat), and feeling more pleasant sensations (P < 0.05) in participants in the float condition compared with those in the film condition. The other RCT10 did not assess this outcome.
Pathological Worry
One RCT10 found that pathological worry, assessed using PSWQ, was statistically significantly reduced for both the float-REST group (P < 0.001) and the waitlist control group (P < 0.05), when comparing post-treatment to baseline. However, between the groups at post-treatment, there was no statistically significant difference in pathological worry. The treatment effect on pathological worry was maintained in the floatation-REST group at 6-month follow-up, indicated by no statistically significant differences between post-treatment and follow-up scores. The other RCT9 did not assess this outcome.
Difficulties in Emotion Regulation
One RCT10 found that difficulties in emotion regulation, assessed using DERS, was statistically significantly reduced for the floatation-REST group (P < 0.001), but not for the waitlist control group, when comparing post-treatment to baseline. Comparing between the groups at post-treatment, floatation-REST group had statistically significantly less difficulties in emotion regulation than the waitlist control group (P < 0.05). The treatment effect on difficulties in emotion regulation was maintained in the floatation-REST group at 6-month follow-up, indicated by no statistically significant differences between post-treatment and follow-up scores. The other RCT9 did not assess this outcome.
Mindfulness
One RCT10 found that mindfulness, assessed using MAAS, was statistically significantly increased for the floatation-REST group (P < 0.01), but statistically significantly decreased for the waitlist control group (P < 0.05), when comparing post-treatment to baseline. However, between the groups at post-treatment, there was no statistically significant difference in mindfulness. The treatment effect on mindfulness was maintained in the floatation-REST group at 6-month follow-up, indicated by no statistically significant differences between post-treatment and follow-up scores. The other RCT9 did not assess this outcome.
Sleep Difficulties
One RCT10 found that sleep difficulties, assessed using PSQI, was statistically significantly reduced for the floatation-REST group (P < 0.001), but not for the waitlist control group, when comparing post-treatment to baseline. Comparing between the groups at post-treatment, the floatation-REST group had statistically significantly less sleep difficulties than the waitlist group (P < 0.01). The treatment effect on sleep difficulties was maintained in the floatation-REST group at 6-month follow-up, indicated by no statistically significant differences between post-treatment and follow-up scores. The other RCT9 did not assess this outcome.
Depression
One RCT10 found that depression, assessed using MADRS-S, was statistically significantly reduced for the floatation-REST group (P < 0.001), but not for the waitlist control group, when comparing post-treatment to baseline. Comparing between the groups at post-treatment, the floatation-REST group had statistically significantly less depression than the waitlist group (P < 0.01). The treatment effect on depression was not maintained in the floatation-REST group at 6-month follow-up, indicated by a statistically significantly higher score at follow-up compared to post-treatment score (P < 0.05). The other RCT9 did not assess this outcome.
Experienced Deviations From Normal State
One RCT10 found that experienced deviations from normal state, assessed using EDN, were statistically significantly increased during the floatation-REST sessions from baseline to 4-week treatment (P < 0.05) and from baseline to post-treatment (P < 0.05). The outcome was not assessed for the waitlist control group; therefore, no comparison between the groups was made. This outcome was also not assessed at 6-month follow-up. The other RCT9 did not assess this outcome.
Medication and Psychotherapy
One RCT10 reported that there was no statistically significant difference in both the floatation-REST group and the waitlist control group with regard to received psychotherapy and the use of anxiolytics, antidepressants, as well as sleep medication, when comparing post-treatment with baseline. Follow-up data at 6 months were collected for the floatation-REST group, but no statistical comparison between follow-up and post-treatment data was made. The other RCT9 did not assess this outcome.
Cost-Effectiveness of Floatation Therapy for the Treatment of Mental Health Conditions
No studies evaluating the cost-effectiveness of floatation therapy for the treatment of mental health conditions were identified; therefore, no summary can be provided.
Guidelines
No evidence-based guidelines regarding the use of floatation therapy for the treatment of mental health conditions were identified; therefore, no summary can be provided.
Limitations
The included studies were not without limitations. Both RCTs9,10 had relatively small populations and no active comparator. As the RCT by Feinstein et al. (2018)9 only focused on acute effects following a single float session without assessments of cumulative effects of multiple float sessions and longitudinal follow-up, it was unclear if benefits of the interventions could be sustained long-term in populations with anxiety disorders. Given that all participants in the RCT by Feinstein et al. (2018)9 were recruited from a previous study where they completed an initial float session of 60 minutes (without any physiological measurement) to help acclimate them to a float environment, the current results may be biased by previous exposure to the first float condition. Participants in the film condition comparator sat upright in a chair while those in the float condition lied on their back.9 This difference in conditions likely affected the results particularly on the measurements of interoceptive awareness and muscle tension. In the RCT by Jonsson and Kjellgren (2016),10 there was a sizable proportion of participants receiving uncontrolled medication (40%) and/or psychotherapy (34%) during the study. The differences in the efficacy of these treatments among participants could impact the findings. Although randomization was applied in the RCT by Jonsson and Kjellgren (2016),10 some scores of the outcome measures at baseline, such as PSWQ for pathological worry and MAAS for mindfulness, were not balanced between the groups. These differences in scores were not adjusted for or considered in the analyses and might have significantly had an impact on the findings. In fact, it was unclear whether the lack of effect of the treatment by floatation-REST on pathological worry and mindfulness might have been affected by the imbalance in those baseline scores. As both studies9,10 investigated the effect of floatation-REST specifically in populations with anxiety disorders, the findings may not be generalizable to other mental health conditions.
Conclusions and Implications for Decision- or Policy-Making
This report identified 2 RCTs9,10 examining the effect of floatation-REST on individuals with high anxiety sensitivity9 or GAD.10 No relevant economic evaluation studies or guidelines on the use of floatation-REST were identified.
Findings from 1 RCT9 involving individuals with high anxiety sensitivity showed that floatation-REST provided a significant anxiolytic effect characterized by significant reductions in state anxiety and muscle tension, as well as significant increases in relaxation and serenity improvement, compared with a film condition. The floating condition significantly reduced blood pressure (both SBP and DBP) and significantly enhanced awareness and attention for cardiorespiratory sensations compared with the film condition. The study found no serious adverse events or major safety concerns during or after the 90-minute float session.
Findings from 1 RCT10 involving individuals with GAD showed that floatation-REST generated significant beneficial effects including reductions and improvements in GAD-symptomatology, difficulties in emotion regulation, sleep difficulties, and depression, compared with a waitlist control. However, pathological worry and mindfulness were not significantly different between the groups at post-treatment. Compared with post-treatment, treatment effects on most outcome measures, except depression, were maintained at 6-month follow-up.
The findings on floatation-REST interventions for populations with anxiety disorders obtained from the 2 RCTs9,10 should be considered as preliminary given the limitations of the evidence. Thus, interpretations and generalization of the findings should be made with caution. Future research with a larger sample size, with a longer follow-up, and with an active comparator should be conducted to replicate these findings. Also, the effect of floatation-REST should be tested in individuals with other mental health conditions, with and without a conventional treatment. Until then, the current findings only suggest that floatation-REST may have some potential therapeutic effects as complementary treatment to existing treatment protocols for individuals with anxiety disorders.
References
1.Quick facts: mental illness & addiction in Canada. Belleville (ON): Mood Disorders Society of Canada; 2019: https://mdsc.ca/docs/MDSC_Quick_Facts_4th_Edition_EN.pdf. Accessed 2021 Dec 6.
2.Evidence brief: risk of infection in the use of floatation tanks. Toronto (ON): Public Health Ontario; 2016: https://www.publichealthontario.ca/-/media/documents/e/2016/eb-floatation-tanks.pdf?sc_lang=en. Accessed 2021 Dec 6.
3.Government of Western Australia Department of Health. Floatation tanks. 2021; https://www.healthywa.wa.gov.au/Articles/F_I/Floatation-tanks. Accessed 2021 Dec 6.
4.van Dierendonck D, te Nijenhuis J. Flotation restricted environmental stimulation therapy (REST) as a stress-management tool: A meta-analysis. Psychology and Health. 2005;20.
5.Kjellgren A, Westman J. Beneficial effects of treatment with sensory isolation in flotation-tank as a preventive health-care intervention - a randomized controlled pilot trial. BMC Complement Altern Med. 2014;14:417. PubMed
6.Kjellgren A, Sundequist U, Norlander T, Archer T. Effects of flotation-REST on muscle tension pain. Pain Res Manag. 2001;6(4):181-189. PubMed
7.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
8.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. PubMed
9.Feinstein JS, Khalsa SS, Yeh H, et al. The Elicitation of Relaxation and Interoceptive Awareness Using Floatation Therapy in Individuals With High Anxiety Sensitivity. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018;3(6):555-562. PubMed
10.Jonsson K, Kjellgren A. Promising effects of treatment with flotation-REST (restricted environmental stimulation technique) as an intervention for generalized anxiety disorder (GAD): a randomized controlled pilot trial. BMC Altern Med. 2016;16:108. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Feinstein et al. (2018)9 US Funding: William K. Warren Foundation, Epsom Salt Council, and National Institute of Health Centres of Biomedical Research Excellence | Open-label RCT, within-subject crossover design Sample size calculation provided: No ITT: Yes | Adults with high levels of anxiety sensitivity (N = 31) Mean age, years (SD): 39.1 (11.1) % Male: 38.7 Comorbidities:
Condition on medication stable for 6 weeks or longer (n = 21) Mean anxiety sensitivity, measured with ASI-3a (SD): 28.1 (12.3) Mean anxiety severity, measured with OASISb (SD): 10.0 (3.8) Mean depression severity, measured with PHQ-9c (SD): 11.6 (5.5) Mean level of disability, measured with SDSd (SD): 14.7 (8.0) | Floatation-REST (float condition) (N = 15) Exteroceptive comparator (film condition)e (N = 16) Participants completed a 90-minute session of Floatation-REST or exteroceptive comparator. After completion of 1 condition, participants crossed over to the other condition approximately 1 week later. Both conditions were scheduled to occur at the same time of day for each participant. | Outcomes:
Follow-up: None other than immediately after 90 minutes of treatment |
Jonsson and Kjellgren (2016)10 Sweden Funding: Unrestricted grant from the County Council of Värmland, Sweden | Open-label RCT, parallel-group design Sample size calculation provided: Yes ITT: No | Adults with GAD (N = 50) Mean age, years (SD): 43.04 (13.37) % Male: 30 % Participants stable on medication: 40 % Participants having psychotherapy: 34 Mean pathological worry, measured with PSWQk (SD): 60.00 (10.84) Mean GAD-symptomatology, measured with GAD-Q-IVl (SD): 9.87 (2.19) Mean depression, measured with MADRS-Sj (SD): 22.48 (7.51) Mean sleep difficulties, measured with PSQIm (SD): 10.17 (3.70) Mean difficulties in emotion regulation, measured with DERSn (SD): 99.74 (20.13) Mean mindfulness, measured with MAASo (SD): 3.29 (0.78) | Floatation-REST (N = 25) Waitlist (N = 25) Floatation-REST consisted of 12 sessions (45 minutes each) extending over 7 weeks with 2 sessions per week. | Outcomes:
Follow-up: 6 months after the end of treatment |
ASI-3 = Anxiety Sensitivity Index-3; DERS = Dysfunctional Emotional Regulation Scale; EDN = Experienced Deviation from Normal State Scale; GAD = generalized anxiety disorder; GAD-Q-IV = Generalized Anxiety Disorder Questionnaire 4th edition; ITT = intention-to-treat; MAAS = Mindful Attention and Awareness Scale; MADRS-S = Montgomery-Asberg Depression Rating Scale; OASIS = Overall Anxiety Severity and Impairment Scale; PANAS-X = Positive and Negative Affect Schedule Expanded Form; PHG-9 = Patient Health Questionnaire 9-item depression scale; PSQI = Pittsburg Sleep Quality Index; PSWQ = Penn State Worry Questionnaire; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation; SDS = Sheehan Disability Scale; STAI = State-Trait Anxiety Inventory; VAS = visual analogue scale.
Note that this table has not been copy-edited.
aThe ASI-3 is an 18-item questionnaire with questions answered using a 4-point scale. The total ASI scores can range from 0 to 72. Healthy North Americans have a mean ASI-3 total score of 12.8 (SD = 10.6). Patients with anxiety and depression commonly have a total ASI score around 30.
bThe OASIS is a 5-item questionnaire, which is a continuous measure of anxiety severity and impairment over the past week. Each item is rated on a 5-point scale and the ratings are summed to obtain a total score ranging from 0 to 20. A cut-score of 8 has been shown to correctly classify 87% of individuals as having a current anxiety diagnosis.
cThe PHQ-9 is a 9-item measure for assessing the severity of depressive symptoms over the past 2 weeks. Scores of 1 to 4 are considered indicative of minimal depression, 5 to 9 mild depression, 10 to 14 moderate depression, 15 to 19 moderately severe depression, and 20 to 27 severe depression.
dThe SDS assesses how much the respondent’s mental health issues are perceived to have affected their daily activities in 3 functional domains: work/school, social/leisure activities, and family life/home responsibilities. Total disability scores range between 0 to 30, with scores ≥ 5 signifying impairment. Significant impairment in functioning in patients with anxiety disorders has been shown to be associated with mean total disability scores between 14 and 18.
eWatching a nature documentary from the BBC Planet.
fSTAI is a 20-item self-report questionnaire designed to assess an individual’s level of anxiety at the present moment with total scores ranging from 20 to 80; higher scores mean higher levels of anxiety.
gMeasured on a 100-point VAS scale, from 0 (Not at all relaxed or no relaxation) to 100 (Extremely relaxed or the most relaxed I have ever felt).
hMeasured on a 100-point bipolar valence scale ranging from −50 (Extremely Unpleasant) to + 50 (Extremely Pleasant), with the slider starting in the middle of the scale at 0 (Neutral).
iMeasured using the PANAS-X, which is commonly used to measure mood. The scale has participants rate how calm, relaxed, and at ease they feel at the present moment using a 5-point Likert-type response scale, ranging from 1 (Very slightly or not at all) to 5 (extremely).
jThe 9-item MADRS-S is a Swedish self-reported assessment of depressive symptoms. The total score ranges between 0 and 54. Cut-off values have been set at: 0 to 6 = no depression; 7 to 19 = mild depression; 20 to 34 = moderate depression; and 34 or higher = severe depression.
kThe 16-item PSWQ is used to assess pathological worry. The instrument has a strong ability to differentiate patients with GAD from other anxiety disorders. Total scores range between 16 and 80. The cut-off score of 45 or higher indicates GAD.
lThe 9-item GAD-Q-IV is a self-reported measure assessing the severity of GAD as defined by the 4th edition of the Diagnostic and Statistical Manual. The measure is used as a continuous variable and the total score ranges between 0 and 12. A cut-off point of 5.7 or higher has been suggested to yield the optimal ratio between sensitivity and specificity for identifying severe GAD.
mThe 19-item PSQI is used to assess subjective sleep quality. The instrument measures sleep disturbance during the previous month. The total score ranges between 0 and 21 and distinguishes between good and poor sleep, where a score of 5 or higher indicates poor-quality sleep.
nThe 36-item DERS is a self-reported measure assessing emotion regulation difficulties. The total score ranges between 36 and 180. Higher scoring indicates greater difficulties in emotion regulation.
oThe 15-item MAAS is a self-reported measure of trait mindfulness. It assesses the level of open and receptive attention to and awareness of ongoing experience. The score ranges from 1 to 6. Higher scoring indicates greater mindfulness.
pThe EDN is a Swedish 29-item self-reported measure specifically designed to be used in floatation-REST experiments. It assesses the degree of relaxation and deviation from normal state experience during the flotation session. Each item is graded on VAS ranging from 0 to 100. A score of 30 on EDN at the first floatation session, and a score of 40 at the subsequent floatation sessions, is considered an indication of typical treatment response, in comparison with resting on a bed in a dark quiet room, which generally gives a score of 15.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist7
Strengths | Limitations |
|---|---|
Feinstein et al. (2018)9 | |
|
|
Jonsson and Kjellgren (2016)10 | |
|
|
ITT = intention-to-treat; RCT = randomized controlled trial.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Safety and Tolerability
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Film condition | |
Feinstein et al. (2018)9 RCT, crossover Adults with high levels of anxiety sensitivity | No SAEs or major safety concerns during or after Floatation-REST. No safety or tolerability results were reported for the film condition. Most participants finished the entire 90-minute floatation, with 5 participants exiting the pool after approximately 85 minutes. All participants in the film condition group completed the 90-minute film. |
Floatation-REST vs. waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | No negative side effects were found. |
GAD = generalized anxiety disorder; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SAE = serious adverse event.
Table 5: Summary of Findings by Outcome — State Anxiety
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Film condition | |
Feinstein et al. (2018)9 RCT, crossover Adults with high levels of anxiety sensitivity | After 90-minute treatment, participants in both groups reported reduction in state anxiety (measured with STAI), but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001). The results were reported graphically only. |
Floatation-REST vs. Waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | GAD-symptomatology (measured with GAD-Q-IV) Floatation-REST, mean (SD)
Waitlist, mean (SD)
Comparing between the groups after treatment, the floatation-REST group had statistically significantly lower GAD-symptomatology than the waitlist group (P < 0.05). |
GAD = generalized anxiety disorder; GAD-Q-IV = Dimensional scoring from the Generalized Anxiety Disorder Questionnaire; PSWQ = Penn State Worry Questionnaire; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation; STAI = State-Trait Anxiety Inventory.
Table 6: Summary of Findings by Outcome — Muscle Tension
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Film condition | |
Feinstein et al. (2018)9 RCT, crossover Adults with high levels of anxiety sensitivity | After 90-minute treatment, participants in both groups reported reduction in muscle tension (measured with VAS), but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001). The results were reported graphically only. |
RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; VAS = visual analogue scale.
Table 7: Summary of Findings by Outcome — Relaxation
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Film condition | |
Feinstein et al. (2018)9 RCT, crossover Adults with high levels of anxiety sensitivity | After 90-minute treatment, participants in both groups reported improvement in relaxation (measured with VAS), but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001). The results were reported graphically only. |
RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; VAS = visual analogue scale.
Table 8: Summary of Findings by Outcome — Serenity
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Film condition | |
Feinstein et al. (2018)9 RCT, crossover Adults with high levels of anxiety sensitivity | After 90-minute treatment, participants in both groups reported improvement in serenity (measured with PANAS-X), but the magnitude of change was statistically significantly larger in the float condition compared to the film condition (P < 0.001). The results were reported graphically only. |
PANAS-X = Positive and Negative Affect Schedule Expanded Form; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy.
Table 9: Summary of Findings by Outcome — Blood Pressure
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Film condition | |
Feinstein et al. (2018)9 RCT, crossover Adults with high levels of anxiety sensitivity | During treatment (up to 90 minutes), participants in the float condition had a statistically significant reduction in both SBP and DBP (P < 0.001). Between 15 and 75 minutes, the overall reduction in SBP was 5.3 mm Hg, and the overall reduction in DBP was 12.8 mm Hg. Participants in the film condition had no change in both SBP and DBP during treatment. |
DBP = diastolic blood pressure; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SBP = systolic blood pressure.
Table 10: Summary of Findings by Outcome — Interoceptive Measures
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Film condition | |
Feinstein et al. (2018)9 RCT, crossover Adults with high levels of anxiety sensitivity | A statistically significant increase (P < 0.001) in the intensity of cardiorespiratory sensations (e.g., breath and heartbeat) was reported in participants in the float condition compared to those in the film condition. A statistically significant increase (P < 0.001) in the attention and awareness of cardiorespiratory sensations (e.g., breath and heartbeat) was reported in participants in the float condition compared to those in the film condition. Participants reported that these cardiorespiratory sensations felt statistically significantly more pleasant with the float condition than with the film condition (P < 0.05). |
RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy.
Table 11: Summary of Findings by Outcome — Pathological Worry
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | Pathological worry (measured with PSWQ) Floatation-REST, mean (SD)
Waitlist, mean (SD)
Comparing between the groups after treatment, there was no statistically significant difference in pathological worry (P > 0.05). |
GAD = generalized anxiety disorder; PSWQ = Penn State Worry Questionnaire; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation.
Table 12: Summary of Findings by Outcome — Difficulties in Emotion Regulation
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | Difficulties in emotion regulation (measured with DERS) Floatation-REST, mean (SD)
Waitlist, mean (SD)
Comparing between the groups after treatment, the floatation-REST group had statistically significantly less difficulties in emotional regulation than the waitlist group (P < 0.05). |
DERS = Dysfunctional Emotional Regulation Scale; GAD = generalized anxiety disorder; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation.
Table 13: Summary of Findings by Outcome — Mindfulness
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | Mindfulness (measured with MAAS) Floatation-REST, mean (SD)
Waitlist, mean (SD)
Comparing between the groups after treatment, there was no statistically significant difference in mindfulness (P > 0.05). |
GAD = generalized anxiety disorder; MAAS = Mindful Attention and Awareness Scale; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation.
Table 14: Summary of Findings by Outcome — Sleep Difficulties
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | Sleep difficulties (measured with PSQI) Floatation-REST, mean (SD)
Waitlist, mean (SD)
Comparing between the groups after treatment, the floatation-REST group had statistically significantly less sleep difficulties than the waitlist group (P < 0.01). |
GAD = generalized anxiety disorder; PSQI = Pittsburg Sleep Quality Index; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation.
Table 15: Summary of Findings by Outcome — Depression
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | Depression (measured with MADRS-S) Floatation-REST, mean (SD)
Waitlist, mean (SD)
Comparing between the groups after treatment, the floatation-REST group had statistically significantly less severe depression than the waitlist group (P < 0.01). |
GAD = generalized anxiety disorder; MADRS-S = Montgomery-Asberg Depression Rating Scale; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation.
Table 16: Summary of Findings by Outcome — Experienced Deviations from Normal State
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Waitlist | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | Experienced deviation from normal state (measured with EDN) Floatation-REST, mean (SD) • Baseline: 31.59 (15.43) • 4 weeks of treatment: 45.48 (15.43) • After treatment: 44.07 (16.25); P < 0.05 compared with baseline Waitlist, mean (SD) • No data collected No comparison between the groups was made. |
EDN = experienced deviation from normal state; GAD = generalized anxiety disorder; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy; SD = standard deviation.
Table 17: Summary of Findings by Outcome — Medication and Psychotherapy
Study citation, study design, and patient model | Study findings |
|---|---|
Floatation-REST vs. Waitlista | |
Jonsson and Kjellgren (2016)10 RCT, parallel group Adults with GAD | Psychotherapy
Anxiolytics
Antidepressants
Sleep medication
|
GAD = generalized anxiety disorder; RCT = randomized controlled trial; REST = Reduced Environmental Stimulation Therapy.
aNo between-group comparisons were performed.
Appendix 5: Additional References of Potential Interest
Khalsa SS, Moseman SE, Yeh HW, et al. Reduced environmental stimulation in anorexia nervosa: an early-phase clinical trial. Front Psychol. 2020;11:567499. PubMed
Feinstein JS, Khalsa SS, Yeh HW, et al. Examining the short-term anxiolytic and antidepressant effect of Floatation-REST. PLoS ONE. 2018;13(2):e0190292. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca