CADTH Health Technology Review
Nabilone for the Treatment of Post-Traumatic Stress Disorder: A 2021 Update
Rapid Review
Authors: Keeley Farrell, Zahra Premji
Abbreviations
CBD
cannabidiol
PTSD
post-traumatic stress disorder
THC
delta-9-tetrahydrocannabinol
Key Messages
Two systematic reviews that met the inclusion criteria of this report were identified. Within these reviews, the clinical effectiveness of nabilone for the treatment of adult patients with post-traumatic stress disorder (PTSD) was evaluated in 1 relevant primary study. This single-arm, open-label study found that most patients with PTSD experienced total cessation or reduction of nightmares following treatment with nabilone. This study lacked a control group, limiting the certainty of these findings.
No evidence-based guidelines regarding the use of nabilone for the treatment of adult patients with PTSD were identified.
Context and Policy Issues
PTSD is a psychiatric disorder that can develop in individuals following exposure to trauma.1 Symptoms of PTSD include intrusive and distressing memories or dreams, dissociative reactions, and psychological or physiologic distress related to the traumatic event.2 According to the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) (known as DSM-5) definition of PTSD, the person must have been exposed to actual or threatened death, serious injury, or sexual violation.2 The person may have directly experienced or witnessed the traumatic event, learned that the event occurred to a close family member or friend, or experienced repeated exposure to details of the trauma.2 Sleep problems are common in PTSD, with approximately 50% to 70% of patients with PTSD having comorbid sleep disorders.3 Sleep problems can include nightmares, distressed awakenings, nocturnal panic attacks, sleep terrors, and insomnia.3 Other common comorbidities of PTSD include depression, substance use, and memory problems.1 Additionally, the risk of suicide attempts is 2- to 3-fold higher in those with PTSD.2
The lifetime prevalence of PTSD in Canada is estimated to be 9.2% and more than 76% of Canadians have reported exposure to a significant traumatic event.2 The prevalence of PTSD is approximately twice as high in women than men.2 Some of the most common forms of trauma associated with PTSD include the unexpected death of someone close, sexual assault, and having a child with serious illness.2
Current treatments for PTSD include both psychotherapy and pharmacotherapy.4 Cognitive behavioural therapy is a form of psychotherapy that is used to treat patients with PTSD.2,4,5 Pharmacological therapies such as selective serotonin reuptake inhibitors (e.g., fluoxetine, paroxetine, sertraline) and serotonin and noradrenaline reuptake inhibitors (e.g., venlafaxine, duloxetine) have also been recommended for the treatment of PTSD.2,4 Other pharmacological options for the treatment of PTSD include atypical antipsychotic drugs (e.g., risperidone, olanzapine, aripiprazole), antidepressants (e.g., mirtazapine, bupropion), and others (e.g., gabapentin, topiramate).2,5 Recently, cannabinoids have emerged as a potential treatment option for patients with PTSD.6 Cannabinoids is an umbrella term for the components of the cannabis plant and their synthetic analogues.7 Delta-9-tetrahydrocannabinol (THC) is the most abundant cannabinoid and is the primary psychoactive component of cannabis.7 Nabilone is a synthetic analogue of THC which has been studied as a potential therapeutic option for people with PTSD.6
This report is an update to a 2019 CADTH report8 on nabilone for the treatment of patients with PTSD. The previous report identified 2 primary clinical studies (1 randomized controlled trial and 1 retrospective chart review).8 The randomized controlled trial showed a statistically significant reduction in the frequency of nightmares in participants treated with nabilone versus placebo.8 The retrospective chart review showed a statistically significant reduction in PTSD symptoms (including insomnia and nightmares) after treatment with nabilone compared with before treatment.8
The aim of the current report is to summarize the clinical evidence and the evidence-based guidelines regarding the use of nabilone for the treatment of adult patients with PTSD that have been published since the 2019 CADTH report8 on this topic.
Research Questions
What is the clinical effectiveness of nabilone for the treatment of post-traumatic stress disorder in adults?
What are the evidence-based guidelines regarding the use of nabilone for the treatment of post-traumatic stress disorder in adults?
Methods
Literature Search Methods
This report is an update of a literature search strategy developed for the 2019 CADTH report.8 For the current report, a limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, APA PsycINFO, the Cochrane Database of Systematic Reviews, the University of York Centre for Reviews and Dissemination (CRD) databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. No filters were applied to limit the retrieval by study type. The initial search was limited to English-language documents published between January 1, 2013, and January 17, 2019. For the current report, database searches were rerun on October 20, 2021, to capture any articles published since the initial search date. The search of major health technology agencies was also updated to include documents published since January 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with a diagnosis of PTSD |
Intervention | Nabilone |
Comparator | Q1: Active treatments (e.g., pharmacotherapy, psychotherapy); placebo; no treatment Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., severity of PTSD symptoms, anxiety, depression, quality of life, safety [e.g., adverse events]) Q2: Recommendations regarding best practices (e.g., appropriate patient populations, recommended treatment protocols) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, guidelines |
PTSD = post-traumatic stress disorder; Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, were published before 2018, or were included in the 2019 CADTH report8 on this topic. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews or in the 2019 CADTH report8 were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included systematic reviews were critically appraised by 1 reviewer using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)9 as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
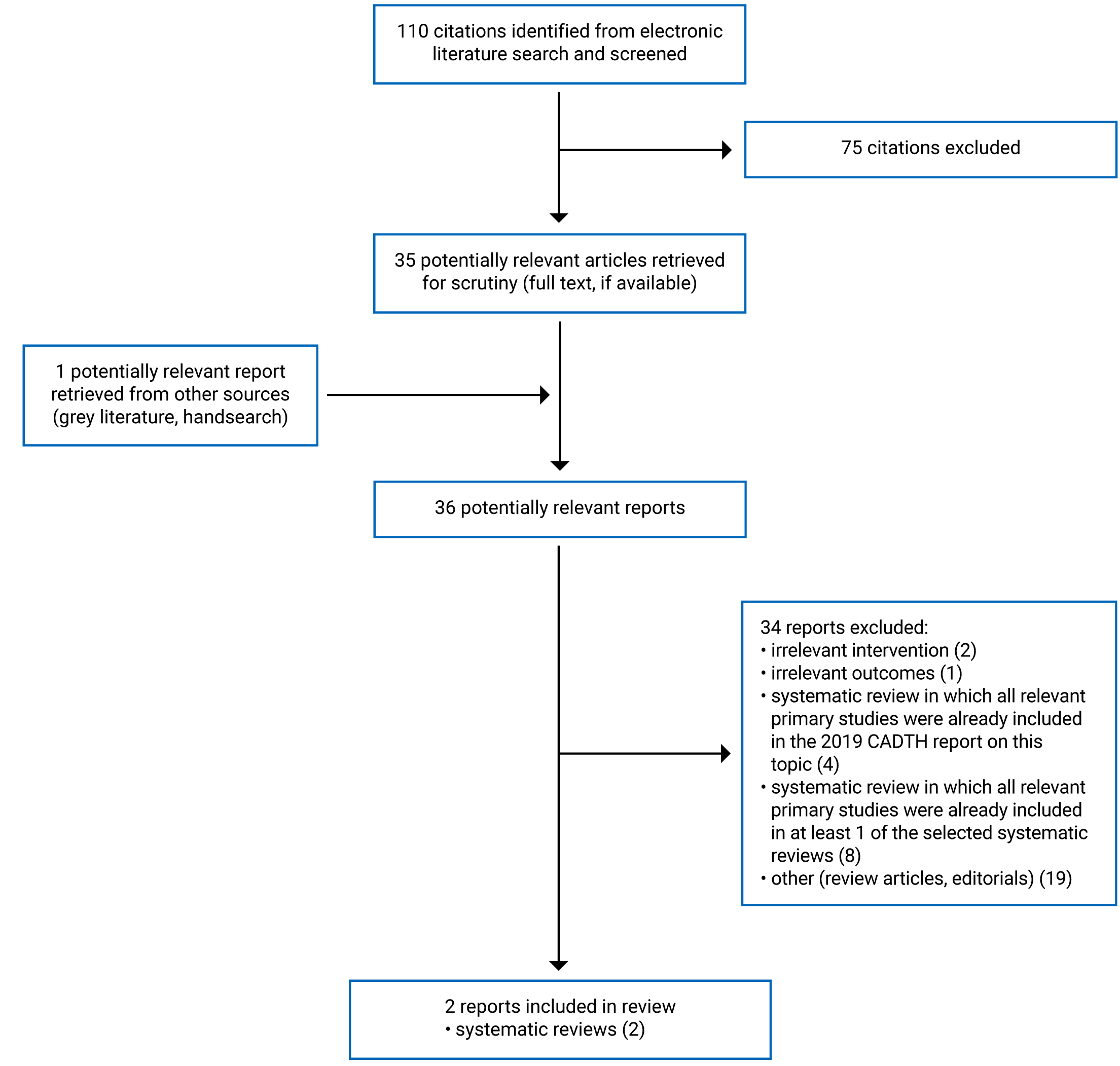
A total of 110 citations were identified in the literature search. Following screening of titles and abstracts, 75 citations were excluded and 35 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these 36 potentially relevant articles, 34 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. These comprised 2 systematic reviews.10,11 The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)12 flow chart of the study selection is presented in Appendix 1. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Two systematic reviews10,11 (that included a total of 1 relevant non-randomized study) were identified for inclusion in this review. No relevant health technology assessments, randomized controlled trials, or evidence-based guidelines were identified. Details regarding the characteristics of included publications are provided in Appendix 2
Both of the included systematic reviews10,11 had broader inclusion criteria than the present report. Specifically, the systematic review by Steardo et al. (2021)10 evaluated any medicinal cannabinoid for the treatment of PTSD in patients of any age. The systematic review by Raymundi et al. (2020)11 evaluated THC, dronabinol, or nabilone alone or in combination with cannabidiol (CBD) in healthy adults, patients of any age with anxiety, and patients of any age with PTSD. The search time frame in the systematic review by Raymund et al. (2020)11 was from 1974 to July 2020. In total, 22 studies met the inclusion criteria for the systematic review; however, none of the included studies were relevant to the current report (i.e., studies of nabilone in adults with PTSD). Only the characteristics and results of the subset of relevant studies will be discussed in this report.
Study Design
The authors of the systematic review by Steardo et al. (2021)10 included randomized controlled trials and non-randomized studies published up to November 23, 2020. Ten studies in total were summarized in the systematic review, including 1 single-arm, open-label study relevant to the present report. Additional details on the design of the relevant primary study were not reported in the systematic review. Additionally, the review by Steardo et al. (2021)10 included 2 studies of nabilone in adult patients with PTSD; however, because these studies were described in the 2019 CADTH report8 on this topic, they are not discussed in the current report.
Country of Origin
The systematic review by Steardo et al. (2021)10 was authored by researchers in Italy. The relevant trial included in this systematic review was conducted in Canada.
Patient Population
The relevant population in the relevant study in the systematic review by Steardo et al. (2021)10 comprised 47 patients with a Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision) (DSM-IV-TR) diagnosis of PTSD and treatment-resistant nightmares. The mean age of participants was 44 years. Twenty-seven patients were female and 20 were male.
Interventions and Comparators
The intervention in the relevant study in the systematic review by Steardo et al. (2021)10 was nabilone taken before bedtime at a starting dose of 0.5 mg and then titrated. Doses were kept below 6 mg/day. Patients received flexible duration of treatment with nabilone depending on clinical response.10 The relevant non-randomized study was a single-arm trial that did not include a control group.
Outcomes
The outcomes assessed in the relevant study in the systematic review by Steardo et al. (2021)11 were changes in the intensity of PTSD-related nightmares.
Summary of Critical Appraisal
Since the systematic review by Raymundi et al. (2020)11 did not include any relevant primary studies, only the sections relevant to this report (e.g., protocol, search strategy) were critically appraised. Neither of the included systematic reviews10,11 included a statement that the review methods were established a priori. This has the potential to introduce bias if the methods were adjusted after the review had begun. The authors of both reviews used a comprehensive literature search strategy. The searches were conducted in multiple databases, key search terms were provided, and the reference lists of included articles were handsearched for additional relevant literature. In the systematic review by Steardo et al. (2021),10 grey literature was also included if sufficient detail was provided. Providing details of these elements of the search strategy increases its reproducibility. The study eligibility criteria for the systematic review by Steardo et al. (2021)10 were clearly defined; however, eligible comparators were not specified. In the systematic review by Raymundi et al. (2020),11 the eligible interventions were not clearly defined. The authors stated that only studies that evaluated THC alone or in combination with CBD were eligible; however, studies that evaluated nabilone (a synthetic analogue of THC) were included in the review. Study selection was performed in duplicate in the systematic review by Steardo et al. (2021),10 and discrepancies were resolved through consensus or by involving a third reviewer when agreement could not be reached. In the systematic review by Raymundi et al. (2020),11 abstract screening was performed in duplicate; however, the authors did not state whether full-text screening was also performed in duplicate. Performing study selection in duplicate helps reduce the risk of bias in study selection. Neither of the reviews provided a list of excluded studies with justifications for exclusion. Unjustified exclusion of studies could bias the results of the review.
In the systematic review by Steardo et al. (2021),10 data extraction was performed independently by 2 blinded researchers; in cases of discrepancies, data were checked by all reviewers for accuracy. Limited details around study design and methods of included studies were provided in the systematic review by Steardo et al. (2021).10 The quality of evidence was assessed independently by 2 researchers in the systematic review by Steardo et al. (2021).10 The risk of bias in randomized controlled trials was assessed using the Revised Cochrane Risk of Bias Tool; however, it is unclear whether the risk of bias in non-randomized studies was assessed using an appropriate tool.10 The authors gave each of the included studies a quality rating based on the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach; however, GRADE is used to assess the overall quality of a body of evidence and is not an appropriate tool to assess the risk of bias in individual studies.13,14 The authors did not state whether an additional tool specifically designed to assess the risk of bias in individual non-randomized studies was used to determine the quality rating assigned to each study. This limits the trustworthiness of the quality ratings the authors assigned to the included studies. The risk of bias in the relevant study included in the systematic review by Steardo et al. (2021)10 was expected to be high due to its study design (i.e., uncontrolled single-arm study). The sources of funding for the individual studies included in the systematic review by Steardo et al. (2021)10 were not reported. Providing the sources of funding makes it possible to discern whether the funding agency could have influenced the results of the included studies. The authors of both systematic reviews10,11 disclosed their sources of funding for their reviews and stated that they did not have any potential conflicts of interest. The authors of the systematic review by Steardo et al. (2021)10 did not receive any external funding. The authors of the systematic review by Raymundi et al. (2020)11 stated that their funding sources had no role in the design, collection, analysis, and interpretation of data in the writing of the report or the decision to submit the paper for publication.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
The main study findings are presented in Appendix 4.
Clinical Effectiveness of Nabilone
PTSD-Related Nightmares
Of the 47 participants included in the relevant single-arm, open-label study included in the systematic review by Steardo et al. (2021),10 34 patients (72%) with PTSD experienced total cessation or reduction in nightmares after treatment with nabilone. Four patients (8%) with PTSD did not experience a recurrence of nightmares after discontinuation of nabilone.10 No further details on the results of this study were provided in the systematic review.
Guidelines
No evidence-based guidelines regarding the use of nabilone for the treatment of adults with PTSD were identified; therefore, no summary can be provided.
Limitations
This report is limited by the quantity and quality of relevant evidence. No evidence-based guidelines regarding the use of nabilone in patients with PTSD were identified. Two systematic reviews10,11 were included in this report; however, 1 of these reviews11 did not include any relevant studies. The systematic review by Steardo et al. (2021)10 included 1 relevant single-arm, open-label study. No studies were identified that compared treatment with nabilone versus alternative therapies; therefore, the clinical effectiveness of nabilone versus alternative treatments is unknown.
The results of the single-arm study included in the systematic review by Steardo et al. (2021)10 should be interpreted with caution. This single-arm, open-label study presented within-group comparisons in patients treated with nabilone. Because there was no control group of patients who did not receive treatment with nabilone, the results are susceptible to numerous forms of bias that threaten both internal and external validity. Any outcomes observed in the study’s participants should not be attributed to nabilone alone as there are many uncontrolled factors that may have contributed to the findings of this study. The outcomes reported for the relevant study included in the systematic review by Steardo et al. (2021)10 were changes in the intensity of PTSD-related nightmares.10 Other outcomes, such as overall measures of PTSD symptoms, depression, anxiety, and quality of life, were not assessed. Adverse events also were not reported for the relevant study.10
Conclusions and Implications for Decision- or Policy-Making
This report comprises 2 systematic reviews.10,11 The systematic review by Raymundi et al. (2020)11 did not include any studies relevant to the current report. The systematic review by Steardo et al. (2021)10 included 1 relevant single-arm, open-label study that assessed the clinical effectiveness of nabilone for the treatment of adults with PTSD. No evidence-based guidelines regarding the use of nabilone in patients with PTSD were identified.
The relevant single-arm, open-label study in the systematic review by Steardo et al. (2021)10 showed that 34 patients (72%) with PTSD experienced total cessation or reduction of nightmares after treatment with nabilone. The study also showed that 4 patients (8%) with PTSD did not experience a recurrence of nightmares after discontinuation of nabilone. Adverse events from the relevant study were not reported by Steardo et al. (2021).10 The relevant study used a single-arm design and did not include a control group to compare the clinical effectiveness of nabilone to other standard treatments or patients who did not receive any treatment, which limits the interpretation of the findings.
Two primary clinical studies (1 randomized controlled trial and 1 retrospective chart review) that evaluated nabilone in adult patients with PTSD were identified in the 2019 CADTH report8 on this topic. The randomized controlled trial showed a statistically significant reduction in the frequency of nightmares in participants treated with nabilone versus placebo.8 The retrospective chart review reported a statistically significant reduction in PTSD symptoms (including insomnia and nightmares) after treatment with nabilone compared to before treatment.8 The authors of the studies also reported on adverse events and that nabilone was well-tolerated.8 The most commonly reported adverse events in patients taking nabilone were dry mouth, sedation, and headache.8 The randomized controlled trial did not report the type of adverse events experienced by the placebo group, which limits the interpretation of the findings.8 Both included studies had important limitations as outlined in the previous CADTH report.8 These limitations included lack of generalizability to the overall PTSD population in Canada due to both studies including only male participants and lack of comparisons of nabilone versus alternative treatments.8 Further limitations are the crossover design of the randomized controlled trial (due to uncertainty about whether the washout period was adequate) and the lack of comparator group in the retrospective chart review.8
Overall, the limited quantity of evidence and the methodological limitations of the included studies make it difficult to draw conclusions about the clinical effectiveness of nabilone for adults with PTSD. Additional high-quality studies that directly compare patients treated with nabilone to patients treated with other treatment options or to a control group of patients who receive no treatment would help reduce uncertainty about the clinical effectiveness and safety of nabilone in patients with PTSD.
References
1.Sbarski B, Akirav I. Cannabinoids as therapeutics for PTSD. Pharmacol Ther. 2020;211:107551. PubMed
2.Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders. BMC Psychiatry. 2014;14(Suppl 1):S1. PubMed
3.El-Solh AA, Riaz U, Roberts J. Sleep disorders in patients with posttraumatic stress disorder. Chest. 2018;154(2):427-439. PubMed
4.Cohen J, Wei Z, Phang J, Laprairie RB, Zhang Y. Cannabinoids as an emerging therapy for posttraumatic stress disorder and substance use disorders. J Clin Neurophysiol. 2020;37(1):28-34. PubMed
5.Yabuki Y, Fukunaga K. Clinical therapeutic strategy and neuronal mechanism underlying post-traumatic stress disorder (PTSD). Int J Mol Sci. 2019;20(15):3614. PubMed
6.Hill MN, Campolongo P, Yehuda R, Patel S. Integrating endocannabinoid signaling and cannabinoids into the biology and treatment of posttraumatic stress disorder. Neuropsychopharmacology. 2018;43(1):80-102. PubMed
7.Fraguas-Sanchez AI, Torres-Suarez AI. Medical use of cannabinoids. Drugs. 2018;78(16):1665-1703. PubMed
8.Nabilone for the treatment of post-traumatic stress disorder: a review of clinical effectiveness and guidelines. Ottawa (ON): CADTH; 2019 Feb 20: https://www.cadth.ca/nabilone-treatment-post-traumatic-stress-disorder-review-clinical-effectiveness-and-guidelines. Accessed 2021 Nov 5.
9.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
10.Steardo L Jr, Carbone EA, Menculini G, Moretti P, Steardo L, Tortorella A. Endocannabinoid system as therapeutic target of PTSD: a systematic review. Life (Basel). 2021;11(3):214. PubMed
11.Raymundi AM, Da Silva TR, Sohn JMB, Bertoglio LJ, Stern CA. Effects of DELTA9-tetrahydrocannabinol on aversive memories and anxiety: a review from human studies. BMC Psychiatry. 2020;20(1):420. PubMed
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.What is GRADE? London (UK): BMJ Best Practice; 2021: https://bestpractice.bmj.com/info/toolkit/learn-ebm/what-is-grade/. Accessed 2021 Nov 4.
14.Schunemann HJ, Cuello C, Akl EA, et al. GRADE guidelines: 18. How ROBINS-I and other tools to assess risk of bias in nonrandomized studies should be used to rate the certainty of a body of evidence. J Clin Epidemiol. 2019;111:105-114. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Steardo et al. (2021)10 Italy No external funding received | Study design: Systematic review of RCTs and observational studies. Number of included studies: 10 studies in total including 2 RCTs and 8 observational studies; 1 single-arm, open-label study was relevant to the present report | Studies of patients of all ages with PTSD diagnosed according to DSM criteria were eligible for inclusion. Only studies of adults were considered relevant to the present report. Population of relevant primary study: 47 patients with a DSM-IV-TR diagnosis of PTSD and treatment-resistant nightmares, mean age of 44 ± 9 years, 27 patients were female and 20 were male. | Eligible interventions: medicinal cannabinoids Eligible comparators: not specified Relevant intervention: nabilone 0.5 mg (starting dose) before bedtime, then titrated; doses were kept below 6 mg/day Relevant comparator: This study did not include a control group. All comparisons were from before treatment to after treatment with nabilone | Outcomes: symptoms of PTSD Follow-up: varied by primary study |
Raymundi et al. (2020)11 Brazil Fundação Araucária; Conselho Nacional de Desenvolvimento Científico e Tecnológico; the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) | Study design: Systematic review of human studies and RCTs Number of included studies: 22 studies in total including 21 prospective controlled trials and 1 open-label study None of the included studies were relevant to the current report (i.e., none of the studies investigated nabilone in adults with PTSD) | Studies of healthy adults or patients with anxiety or PTSD were eligible for inclusion. Only studies of adults diagnosed with PTSD were considered relevant to the present report. | Eligible interventions: THC alone or in combination with CBD Eligible comparators: not specified | Outcomes: aversive memory extinction or reconsolidation, anxiety-related responses Follow-up: NR |
CBD = cannabidiol; DSM = Diagnostic and Statistical Manual of Mental Disorders; DSM-IV-TR = Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision); NR = not reported; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; SUD = substance use disorder; THC = delta-9-tetrahydrocannabinol.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews Using AMSTAR 29
Strengths | Limitations |
|---|---|
Steardo et al. (2021)10 | |
Comprehensive literature search strategy and detailed methods described The search was conducted in multiple databases, key search terms were provided, and the reference lists of included articles were handsearched for additional relevant literature Study selection was performed in duplicate, and disagreements were resolved through consensus or involving a third reviewer Data extraction was performed independently by 2 blinded researchers Authors accounted for risk of bias in included studies when discussing results of review Authors reported that no external funding was received and declared that they had no conflicts of interest | Unclear if review methods were established a priori Eligible comparators were not specified Authors did not provide justification for eligible study designs Authors did not provide a list of excluded studies with justifications for exclusion Details on study design and methods of included studies were lacking It is unclear how risk of bias of non-randomized studies was assessed The relevant included study was an uncontrolled single-arm study and therefore is susceptible to multiple forms of bias that threaten both internal and external validity Sources of funding for individual studies included in the review were not reported |
Raymundi et al. (2020)11 | |
Comprehensive literature search strategy and detailed methods described The search was conducted in multiple databases, key search terms were provided, and the reference lists of included articles were handsearched for additional relevant literature Authors reported their funding sources and declared that they had no competing interests Authors stated that funders had no role in the design, collection, analysis, and interpretation of data, in the writing of the report, or the decision to submit the paper for publication | Unclear if review methods were established a priori Eligible interventions were not clearly defined, and eligible comparators were not specified Abstracts were screened independently by 2 reviewers; however, it is unclear if full-text review was also performed in duplicate Authors did not provide a list of excluded studies with justifications for exclusion |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trial.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — PTSD-Related Nightmares
Study citation and study design | Findings |
|---|---|
PTSD-related nightmares | |
Steardo et al. (2021)10 SR (1 relevant prospective, single-arm, open-label study) | Fraser (2009) • 34 out of 47 patients (72%) experienced total cessation or reduction of nightmares after starting nabilone • 4 out of 47 patients (8%) did not experience a recurrence of nightmares after discontinuation of nabilone Note: the duration of treatment with nabilone in this study was flexible depending on clinical response |
PTSD = post-traumatic stress disorder; SR = systematic review.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
15.Medical marijuana for post-traumatic stress disorder: a review of clinical effectiveness and guidelines. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017: https://www.cadth.ca/index.php/medical-marijuana-post-traumatic-stress-disorder-review-clinical-effectiveness-and-guidelines. Accessed 2021 Nov 5.
Review Articles
16.Schlag AK, O'Sullivan SE, Zafar RR, Nutt DJ. Current controversies in medical cannabis: recent developments in human clinical applications and potential therapeutics. Neuropharmacology. 2021Jun 15;191:108586. PubMed
17.Tibbo PG, McKee KA, Meyer JH, et al. Are there therapeutic benefits of cannabinoid products in adult mental illness? Can J Psychiatry. 2021;66(2):185-194. PubMed
18.Mouhamed Y, Vishnyakov A, Qorri B, et al. Therapeutic potential of medicinal marijuana: an educational primer for health care professionals. Drug, Healthc Patient Saf. 2018;10:45-66. PubMed
Additional References
19.Morgenthaler TI, Auerbach S, Casey KR, et al. Position paper for the treatment of nightmare disorder in adults: an American Academy of Sleep Medicine position paper. J Clin Sleep Med. 2018;14(6):1041-1055. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca