CADTH Health Technology Review
Homelike Models of Long-Term Care: A 2021 Update
Rapid Review
Authors: Sarah Goring, Hannah Loshak
Key Messages
Among residents with dementia, positive effects of small-scale homelike models of care on social interaction were observed in 1 non-randomized study, whereas the evidence from relevant primary studies captured in 1 systematic review was mixed.
Residents with dementia living in small-scale homelike care facility compared with a traditional nursing home may spend more time in a positive mood or engagement, based on findings from 1 non-randomized study.
Evidence captured in 1 systematic review suggested lower use of restraints and psychotropic drugs in small-scale homelike settings compared with traditional nursing homes; however, a non-randomized study published in 2020 found no differences in psychotropic drug use.
Associations between homelike models of care and safety outcomes (e.g., COVID-19 infection, fall injuries) suggested a benefit of small-scale homelike long-term care settings over traditional large-scale settings.
Context and Policy Issues
In Canada, the number and proportion of older individuals is growing — a trend that is expected to continue in coming years. In 2020, there were 6.8 million adults aged 65 years and over, representing 18% of the total population.1 Prediction models suggest that this proportion will continue to increase, with the most rapid rate of increase occurring until 2030.2 The number of older seniors (aged 80 and over) is also expected to increase in coming years as the baby boomer cohort begins to enter this age group.
The aging population presents a challenge for the provision of long-term care in Canada. The demand for home and community care services is already unprecedented, with over 40,000 Canadians on wait lists for nursing homes.3 In response, the federal government has increased funding to improve the provision of home and community-based care. However, as systems of long-term care are implemented by provinces and territories, each region must address its current needs and challenges, and plan for future long-term care delivery.3
Over the past few decades, there has been a culture change in the delivery of long-term care.4 Traditional nursing homes in large-scale institutional settings have shifted toward person-centred care in small-scale homelike physical environments. Several innovative models of homelike care have been developed and adopted, encompassing aspects such as: a homelike physical environment (e.g., private bedrooms and bathrooms, natural sunlight, brightly coloured spaces, homelike furnishing and décor, plants, access to outdoor spaces, and absence of long hospital-like corridors, nursing stations, and staff uniforms); a person-centred approach to care (e.g., focus on warmth of interactions and relationships, empathy, and opportunities for meaningful activities); and flexibility (e.g., enabling resident autonomy and independence, having opportunities to participate in aspects of daily life that suit residents’ abilities [e.g., meal preparation and laundry], and having flexible daily schedules that allow for spontaneity and variety).4,5 Homelike care models are often designed with consistent assignment of staff, and high staff-to-resident ratios, and rely on leadership at the institutional level to empower and train staff and implement changes. Examples of homelike models of care include: Eden Alternative; Green House homes; The Butterfly Model of Care (for persons with dementia), and Dementia Villages (The Hogeweyk Care Concept).5
Several of these homelike models of care have recently been adopted in Canada. For example, the Butterfly Model of Care has now been adopted, either in part or in full, in several long-term care facilities in Alberta and in Eastern Ontario, and a Dementia village has been established in Langley, British Columbia.5 The provision of high-quality long-term care has been identified as a key priority in health regions across Canada; however, wider adoption of homelike models of care relies on evidence-based decision making. A previous CADTH review was conducted in 2019, and reported on limited-quality evidence from 9 non-randomized studies.6 The key findings from that review found no difference between homelike and traditional models of long-term care with respect to depression and affective state, and inconsistent findings for other psychosocial outcomes. No evidence on cost-effectiveness or evidence-based guidelines was identified.
The objective of the current report is to update the previously conducted review on homelike models of long-term care,6 and to summarize newly emerging evidence regarding the clinical effectiveness, cost-effectiveness, and guidelines regarding homelike models of care for residents of long-term care facilities.
Research Questions
What is the clinical effectiveness of homelike models of care (e.g., Eden Alternative and Greenhouse Concepts of Care) for residents of long-term care facilities?
What is the cost-effectiveness of homelike models of care for residents of long-term care facilities?
What are the evidence-based guidelines for homelike models of care for residents of long-term care facilities?
Methods
Literature Search Methods
The literature search strategy used in this report is an update of 1 developed for a previous CADTH report.6 For the current report, a limited literature search was conducted by an information specialist on key resources including MEDLINE via OVID, the Cochrane Database of Systematic Reviews, the international HTA database, Canadian and major international health technology agencies, as well as a focused internet search. No filters were applied to limit the retrieval by study type. The initial search was limited to English-language documents published between January 1, 2009 and May 7, 2019; due to the high volume of eligible studies, articles published before 2014 were excluded. For the current report, database searches were rerun on October 15, 2021 to capture any articles published since the initial search date. The search of major health technology agencies was also updated to include documents published since May 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Residents of long-term care facilities (with any condition, e.g., dementia, mental health, general aging) |
Intervention | Homelike models of care (e.g., Eden Alternative Care, Greenhouse Concepts, Butterfly Model [Dementia Care Matters], low density of residents) |
Comparator | Q1 and Q2: Traditional models of care (e.g., nursing homes, general population care, long-term care, residential care, long-term care with high density of residents) Q3: No comparator |
Outcomes | Q1: Clinical effectiveness (Physical [e.g., overall survival, mortality, activities of daily living] Psychosocial [e.g., cognitive status/functioning, mood, behaviour, social activities, quality of life], nutrition and food service clinical and safety outcomes [e.g., proper nutrition, choking risk, allergies] safety [e.g., adverse events, accidental falls, pressure ulcers] Q2: Cost-effectiveness outcomes (e.g., incremental cost per quality-adjusted life-year or health benefit) Q3: Evidence-based guideline recommendations for homelike models of care for residents of long-term care facilities |
Study designs | Q1: Health technology assessments and systematic reviews, randomized controlled trials, non-randomized studies Q2: Economic evaluations Q3: Guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2019. Studies captured in the 2019 CADTH review6 were also excluded. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 for systematic reviews, and the Downs and Black checklist8 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
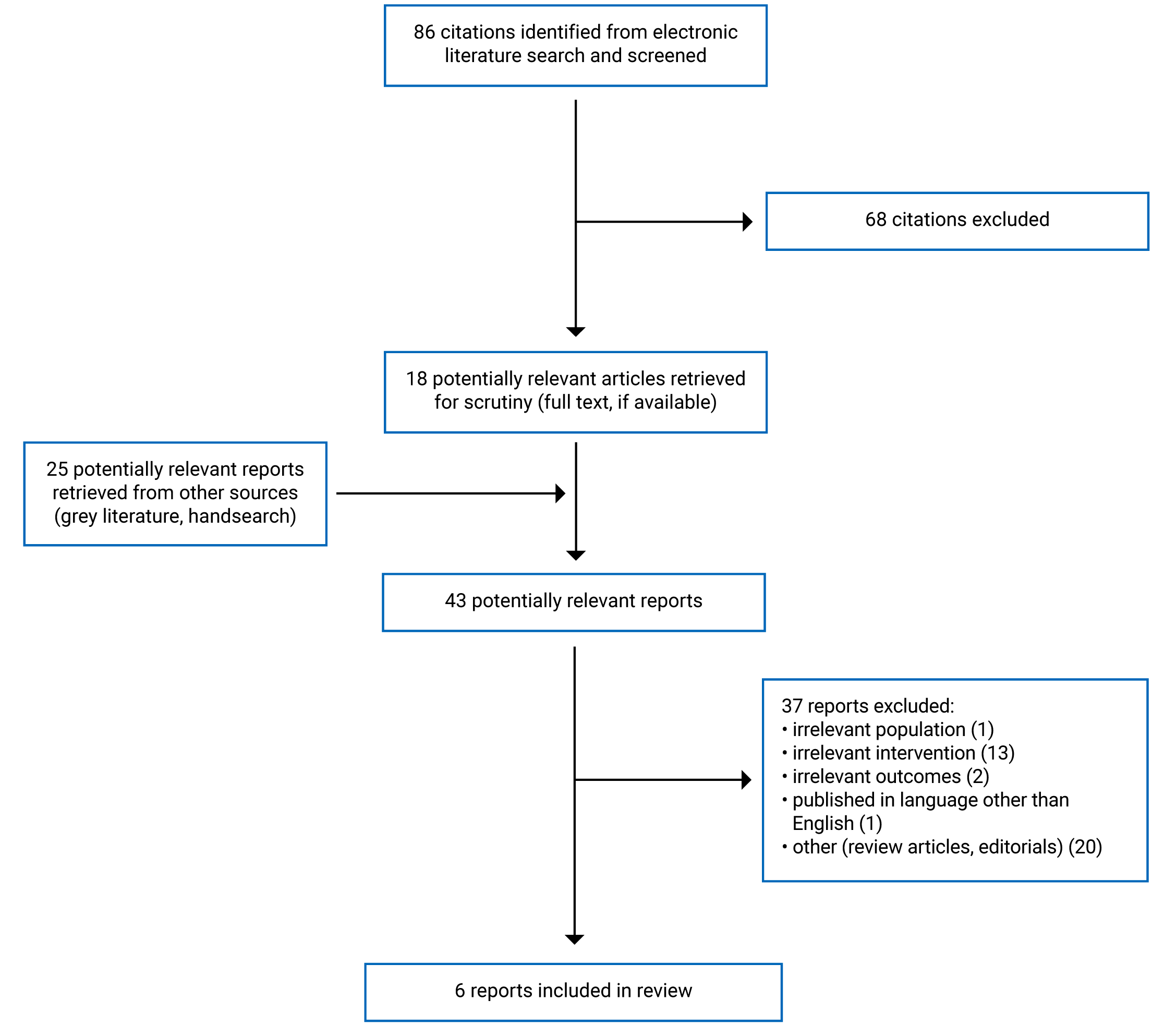
A total of 86 citations were identified in the literature search. Following screening of titles and abstracts, 68 citations were excluded and 18 potentially relevant reports from the electronic search were retrieved for full-text review. Twenty-five potentially relevant publications were retrieved from the grey literature search for full-text review. Of these 43 potentially relevant articles, 37 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 2 systematic reviews, and 4 non-randomized studies. No economic evaluations or evidence-based guidelines were identified. Appendix 1 presents the PRISMA9 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Two systematic reviews and 4 non-randomized studies, published between 2019 and 2021, were included. One systematic review captured studies published before July/August 2018,10 and the other systematic review captured studies published in the 5 years before May 2019.11
The systematic review by Adlbrecht et al. (2021)10 had eligibility criteria that was broader in some aspects, yet more restrictive in others, relative to the current review. In that systematic review, the population of interest was more restrictive, focusing exclusively on residents with dementia, yet included broader eligibility regarding interventions; not all were small-scale homelike models of care. The study designs eligible for the systematic review were also broader, capturing both comparative and non-comparative studies; however, the outcome of interest was more restrictive, limited only to social interactions. Overall, 6 of the 18 studies included in the systematic review were relevant to the current review, of which 3 were captured in the 2019 CADTH report.6 The 3 remaining studies are described in this report.
The second systematic review, by Dyer et al. (2019),11 had eligibility criteria that was closely aligned with the current review,11 and all 5 studies included in that systematic review were relevant to the current review. Of those 5 studies, 2 were captured in the 2019 CADTH report,6 leaving 3 eligible studies for this systematic review. One of the 3 studies was also captured in the more recent systematic review by Adlbrecht et al. (2021).10 (A citation matrix illustrating the degree of overlap is presented in Appendix 5). As such, summaries of the findings by Dyer et al. (2019)11 will be limited to the remaining 2 relevant studies.
Of the included non-randomized studies, 1 was a prospective cohort study,12 2 were retrospective studies,13,14 and 1 was a longitudinal study that incorporated a before-and-after design.15
Country of Origin
Of the 2 systematic reviews, 1 was conducted by a group in Austria (lead author) and Germany (co-authors),10 and the other was conducted in Australia.11 The 4 primary non-randomized studies were conducted in Canada and Sweden (with a lead author based in South Korea),12 the US,13 the Netherlands,15 and Germany.14
Population
Among the 2 systematic reviews, 1 was restricted to populations of long-term care residents with dementia.10 The other was not specifically restricted to residents with dementia; however, 1 of the 2 relevant primary studies in that systematic review was conducted among residents with dementia.11
Two of the 4 primary studies were restricted to long-term care residents with a form of dementia: 1 included residents defined as having with early-to-mid stage Alzheimer disease or related dementia,12 and the other was conducted among residents with dementia whose mean reported standardized mini mental state examination (sMMSE) score was 8.6 (out of a total of 30 points, indicating severely impaired cognitive functioning).15 A third study was not restricted to residents with dementia; however, the study was stratified by level of cognitive impairment. In that study, 46% of residents had no or slight cognitive impairment and 54% of residents had considerable or worse cognitive impairment.14 The fourth study was not restricted by residents’ cognitive function and residents’ characteristics were not described.13
Interventions and Comparators
In the 2 systematic reviews,10,11 1 included domestic small-scale living models considered to be innovative models of care — defined by the authors as models of care that are novel and not widely available in Australia.11 The other systematic review considered a broader set of special care or small-scale living facilities for persons with dementia, of which only small-scale homelike models of care were relevant to the current review.10
In the 4 non-randomized studies, all care homes were characterized as small-scale and having homelike features; however, the specific characteristics varied. Only the study by Zimmerman et al. (2021)13 described a specific model of care (the Green House model), whereas in the other 3 studies, the intervention was described as small-scale units (with 10 residents12; 7 to 8 residents,15 or not specified but defined as “small”14) with homelike features (based on a high homelike score12; presence of single-bedrooms and/or staff training12,15; or not specified but described as “homelike”14). One study included a before-and-after design component, in which residents were moved from a traditional large-scale facility to a small-scale or homelike model of care.
Outcomes
Psychosocial outcomes were reported in 2 systematic reviews10,11 and 2 non-randomized studies.12,15 This included: functional status (1 systematic review11), social interactions (1 systematic review,10 1 non-randomized study12); and behaviour and other neuropsychiatric outcomes (1 systematic review,11 2 non-randomized studies12,15).
Safety-related outcomes were reported in 2 non-randomized studies and 1 systematic review.11,13,14 Specifically, 1 non-randomized study13 reported on coronavirus disease 2019 (COVID-19) infection rates, admission/re-admission rates, and COVID-19-related mortality rates; 1 non-randomized study14 reported on fall-related injuries; and 1 systematic review11 reported a mixed grouping of outcomes considered to reflect quality of care, which included safety outcomes such as peptic ulcers.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
Two systematic reviews10,11 were assessed using the AMSTAR 27 critical appraisal tool.
One systematic review10 was assessed as being generally well-conducted in terms of having a well-defined research question and clear eligibility criteria, and included a comprehensive approach to the literature search. A limitation in the search implementation was that it was performed in 2018 while the systematic review was published in 2021, thus this systematic review would not have captured relevant studies for more than 2 years before publication. Regarding data extraction and summary of findings, tabular study-by-study summaries were provided and risk of bias assessments were conducted; however, there was limited discussion around heterogeneity of findings and threats to validity within the narrative synthesis. Furthermore, there was the potential for omissions and errors due to extractions having been done by a single researcher. For example, 1 relevant study identified in the systematic review was described as having been conducted in 2 countries (the Netherlands and Belgium), yet results from only 1 country (the Netherlands) were provided in the tabular summary. The extent to which the broad conclusions reached by Adlbrecht et al. (2021)10 were impacted cannot be assessed without independent data extraction from all relevant primary studies, which is beyond the scope of the current review.
The second systematic review was presented within a larger report covering a range of rapid scoping reviews and systematic reviews relating to innovative models of care.11 The report was not designed as a standalone systematic review on a single relevant topic (i.e., “comparing the impact of small-scale living designs with that of traditional residential aged care on resident-centred outcomes”) and hence reporting on the research question relevant to this report was limited. For example, although detailed search strategies and eligibility criteria were provided, it was unclear which ones applied to the systematic review of interest. Furthermore, detailed characteristics of the included studies were not provided, nor were quantitative outcome estimates, risk of bias assessments, or discussion of heterogeneity observed across the studies. The absence of these features in the systematic review impacts the ability to incorporate the findings in the present report, as the magnitude of effect size, and both the internal and external validity of the findings are all unknown. Finally, similar to the other systematic review, data extraction as performed by 1 researcher, leading to potential omissions and errors; however, the impact of this is unclear.
Non-Randomized Studies
Four non-randomized studies were assessed using the Downs and Black checklist.8
Across the 4 studies, reporting was clear in terms of the study objectives and outcomes of interest. However, descriptions of residents’ characteristics were limited, as were descriptions of the comparator. Regarding descriptions of the interventions, in 2 studies, select aspects of the interventions were clearly described: 1 study included long-term care units that followed a specific model of care (Green House homes),13 and another provided detailed descriptions for each of 4 long-term care facilities, including an assessment of the physical environment using the Therapeutic Environment Screening Survey for Nursing Homes (TESS-NH) tool.12 Conversely, in 1 study that analyzed secondary data, homelike care units were not described at all, aside from an operational definition “presence of small, homelike units.”14 With the exception of the study involving Green House homes,13 which follow a defined model of care, limited descriptions were provided in the studies regarding the overall philosophy of care or the staff’s approach to person-centred care.
With respect to generalizability to long-term care in Canada, the external validity of all studies was limited by having been conducted outside of Canada. Although 1 study included long-term care facilities in Vancouver, Canada, the comparison facility in that study was located in Sweden. Two studies had good external validity to the countries in which they were conducted (US, and Germany),13,14 given the broad geographic coverage and number of sampled units in those studies. While capturing a smaller sample size and fewer units, Kok et al. (2020)15 reported high participation rate, suggesting that the findings from that study may generalize to similar facilities.
Inherent to their non-randomized study design, imbalances in known and unknown resident characteristics that were related to the outcomes of interest was a concern across all studies; this may have affected the internal validity of some studies’ findings. Two of the study authors attempted to match or adjust for such differences.13,14 For example, in their comparison of COVID-19 incidence and mortality rates, Zimmerman et al. (2021)13 matched facilities based on geography (within 100 miles), given the geographic and temporal variability in COVID-19 prevalence across the US in 2020. However, they did not match on other potential factors (e.g., consistency of staff assignment to units) that may have been related to the risk of introducing COVID-19 to a given long-term care unit. Zimmermann et al. (2019)14 also attempted to adjust for potential confounding, using regression models to adjust for facility-level factors potentially associated with fall risk, and stratified the analysis by residents’ cognitive impairment level. Kok et al. (2020)15 did not use matching or adjustment strategies; however, they were able to leverage a management-level decision to move residents from 1 facility to small-scale units, while residents of another similar facility did not move. As there was no expectation of systematic differences in residents’ characteristics between the 2 facilities, and baseline characteristics were similar, there was low risk of bias due to confounding. The study with the greatest perceived risk of bias due to imbalances was the study by Lee et al. (2021).12 Observed imbalances in characteristics such as marital status (married versus widowed), age, activities of daily living, as well as other characteristics that were not reported, may have influenced the residents’ quality of life and confounded the study findings.
None of the 4 studies provided sample size calculations or reported on the study’s power to detect clinically meaningful differences in key outcomes; however, all study authors reported sample size as a study limitation. Lee et al. (2021)12 reported comparisons of homelike versus traditional long-term care facilities based on observations from 7 versus 5 residents, respectively, and acknowledged this as a limitation both to the ability to detect differences (which were statistically significant in 2 out of the 4 reported outcomes) as well as to the generalizability of the findings. Zimmerman et al. (2021)13 noted that having 0 cases of COVID-19 in over half of the Green House organizations and facilities with fewer than 50 beds was a limitation for comparing overall rates between these 2 settings, although the comparisons were statistically significant. Zimmermann et al. (2019)14 considered that the number of homelike units in their study sample (44 out of 220) to be a limitation, although it was unclear whether this referred to the study’s power (which detected significant differences within 1 of 2 study strata) or to the generalizability of the findings. Meanwhile, Kok et al. (2020)15 considered their study to have been sufficiently powered to detect differences in overall psychotropic use (despite non-statistically significant findings), although insufficient for detecting differences within more specific drug classes.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of Homelike Long-Term Care
Psychosocial outcomes: Functional Status
In the systematic review by Dyer et al. (2019),11 1 relevant study was cited to support the statement that the association between small-scale living homes and functional status was inconsistent; however, detailed results were not provided by Dyer et al. (2019).
Psychosocial outcomes: Social interactions
The association between small-scale homelike models of care and social interactions was evaluated in 1 included non-randomized study, and within 3 primary studies captured in the systematic review by Adlbrecht et al. (2021).10 In all studies, populations were restricted to residents with dementia.
Positive effects of small-scale homelike models of care were observed in the study by Lee et al. (2021)12: residents in the small-scale homelike facility in Sweden spent a statistically significantly lower proportion of time withdrawn compared with a large-scale traditional facility in Canada. However, among the relevant primary studies captured in the systematic review by by Adlbrecht et al. (2021),10 findings were inconsistent across studies. For example, the social relations subdomain of the quality of life in dementia (QUALIDEM) tool was used in 2 relevant studies captured by Adlbrecht et al. (2021).10 In 1 of these relevant studies, no differences were evident between settings, whereas statistically significant differences between small-scale and traditional nursing homes were reported in 1 country (the Netherlands) of a second study. In that latter study, statistically significant differences in the Revised Index of Social Engagement (RISE) metric were also observed. In the third relevant study identified by Adlbrecht et al. (2021),10 which was conducted in Ireland and used the Assessment Tool for Occupation and Social Engagement quality of life in dementia (ATOSE) to measure social engagement, significantly higher social engagement was observed among residents after renovating units to create household models of care, compared with the level of social engagement within the more traditional model of care that existed before renovations.
Psychosocial outcomes: Behaviour and other neuropsychiatric outcomes
The association between small-scale homelike settings and behaviour and other neuropsychiatric outcomes were inconsistent across specific outcomes within this domain.
Lee et al. (2021)12 reported a statistically significant difference in the overall well- or ill-being index (for which positive or negative values reflect overall time spent in positive or negative mood and engagement, respectively) among residents with dementia living in a homelike unit in Sweden compared with a traditional nursing care unit in Canada. However, the authors reported no significant differences in levels of agitation.
Two different interventions used for the treatment of behavioural and psychological symptoms of dementia were evaluated in the systematic review by Dyer et al. (2019): psychotropic drug use, and the use of physical restraints. Although the authors did not provide detailed study-by-study results or overall estimates of effect, Dyer et al. (2019) stated that small-scale care homes were associated with reduced use of psychotropic drugs and physical restraints, citing 2 studies relevant to the current review (Te Boekhorst et al. [2009] and Afendulis et al. [2016]). Conversely, in the included non-randomized study by Kok et al. (2020),15 no statistically significant differences in psychotropic drug use were identified among residents who moved to small-scale dementia special care units compared with those who remained in traditional large-scale dementia special care units.
Safety
Two included studies13,14 and a third relevant study captured in a systematic review11 reported on safety outcomes. The study populations were not restricted to residents with dementia, and in all 3 studies, improved safety was evident among small-scale homelike models of care compared with traditional models of long-term care.11,13,14
Zimmerman et al. (2021)13 found that during the first 7 months of 2020, the incidence and mortality rates of COVID-19, and the rates of admissions/re-admissions following a COVID-19 hospitalization, were statistically significantly lower among residents of small-scale Green House homes compared with geographically matched large-scale (≥ 50 beds), and small-to-mid-sized (< 50 beds) traditional nursing homes in the US. Addressing the fact that overall number of residents dictates the probability of observing at least 1 COVID-19 case, the researchers calculated case rates across entire Green House home organizations (capturing multiple units) rather than per unit, and thereby better aligning the number of residents at risk in these smaller-scale settings with other mid- and large-scale nursing home settings.
The risk of fall injuries was found to be lower in a subset of residents living in homelike models of care compared with traditional nursing homes. Based on observations collected from nursing homes across Germany, Zimmermann et al. (2019)14 reported a statistically significant reduced risk of fall injuries among cognitively impaired residents in homelike care units, compared with traditional (non-homelike care) units; however, no difference in the risk of fall injuries was detected among residents with low or slight cognitive impairment. Few details on the specific aspects of homelike care were available, thereby limiting the generalizability of the findings to other settings or further evaluating specifics aspects of the physical environment or resident care model leading to reductions in the risk of fall injuries.
A relevant study in the systematic review by Dyer et al. (2019),11 which evaluated Green House homes, was cited to support the statement that small-scale units were associated with improvements in quality-of-care indicators, including improvements in the proportion of bedfast residents, catheter use, low-risk pressure ulcers, hospital readmissions and avoidable hospital readmissions; however, no further details were provided.
Cost-Effectiveness of Homelike Long-Term Care
No relevant evidence regarding the cost-effectiveness of homelike models of long-term care was identified; therefore, no summary can be provided.
Guidelines
No relevant evidence-based guidelines on homelike models of long-term care were identified; therefore, no summary can be provided.
Limitations
The limitations of the current report echo those of the previous CADTH 2019 review.6
First, no evidence from randomized controlled trials was identified in this update, and there were threats to the internal validity and generalizability of the evidence from non-randomized studies. This leads to a relatively large risk of bias in the findings due to imbalances in the intervention and control groups that could not be adjusted for.
Second, 2 of 4 non-randomized studies, and 4 of the 5 relevant primary studies identified in the systematic reviews within this report were restricted residents with dementia and/or conducted in special dementia care units. While the majority of residents in long-term care live with dementia (in British Columbia, approximately 64% of residents have dementia),16 this does not apply to all residents in long-term care, and the impact of homelike models of care may differ across these populations. For example, in the non-randomized study that was stratified by cognitive function,14 the association between risk of fall and long-term care sitting differed among those with and without cognitive impairment.
Third, the interventions did not always follow a specific model of care, and the characteristics of the models of care were varied and often ill-defined —in particular, the homelike-ness of the setting was often unclear. One identified study13 and 1 relevant study identified from a systematic review11 followed a named model of care – specifically Green House homes — whereas the remaining models of care were not strictly defined. Furthermore, no comparative data were available from exclusively Canadian settings, thereby limiting generalizability of the findings to decision-making in Canada. As such, decisions around adopting specific models of care that were not captured in the review (e.g., the Butterfly model) that are relevant to a Canadian setting cannot be fully informed by studies identified in this review. Similarly, the comparator was varied, with traditional nursing homes varying in size and organizational structure and in located various countries around the world.
Finally, no relevant cost-effectiveness studies or evidence-based guidelines were identified. This may be related to the lack of supportive evidence available.
Conclusions and Implications for Decision- or Policy-Making
This report identified 4 non-randomized studies12-15 and 2 systematic reviews10,11 published since 2019, informing the clinical effectiveness and safety of homelike models of care for residents of long-term care facilities. No relevant evidence-based guidelines or cost-effectiveness analyses were identified.
This evidence provides insights into potential benefits associated with homelike models of long-term care that were identified since the publication of the 2019 CADTH review. Similar to the CADTH review published in 2019,6 associations between psychosocial outcomes and homelike models of care were inconsistent within the evidence included in this report. Specifically, there were inconsistent associations between long-term care settings and: functional status; social interactions; and behaviour and other neuropsychiatric outcomes. Some of these inconsistencies may have reflected heterogeneity in the delivery of care across the included studies’ homelike care models and traditional large-scale nursing homes. For example, Adlbrecht et al. (2021)10 noted that residents’ social interactions are strongly influenced by staffing features – not just physical environment. While all intervention groups captured in the current report were consistently small, other aspects of care, such as staff training, philosophy of care, and person-centred approach, may have varied, and may partly contribute to the observed inconsistencies in association. The conflicting evidence regarding psychotropic drug use may also reflect heterogeneity in philosophy of care, although study design issues may also have played a role. In their study, Kok et al. (2020)15 considered staffing considerations and study design in their explanation of why the non-significant findings in their study differed from previous work. First, they acknowledged that in their study, the transfer to a new care home may have caused stress to the residents which may have prevented reductions in psychotropic drug use; and second, they considered that staff training may have been insufficient, and/or that the similar ratio of staff to residents in the 2 settings may have had the result that nurses had to work alone in the small-scale setting with less flexibility to care for agitated residents.15
The findings of significantly reduced COVID-19 incidence and mortality rates in homelike care settings compared with traditional nursing homes13 may offer a tangible benefit on morbidity and mortality to residents of long-term care, who were disproportionately affected by the COVID-19 pandemic.17,18 While the retrospective cohort study captured in the current report was focused on COVID-19, these findings may also apply to infection control of other droplet-based and/or airborne communicable diseases. The study authors attributed lower COVID-19 case rates not only to the size of the facilities (i.e., number of beds), but also to other aspects of care homes such as the availability of private bedrooms and bathrooms (limiting spread), limited ancillary staff, and fewer admissions, which is consistent with research findings in the Canadian setting.17,19 Furthermore, the authors of this study considered that other features of the Green House model of care may have improved psychosocial well-being during the pandemic, such as having outdoor spaces to accommodate socially distanced visits from family, and having consistent universal staff to maintain social relationships, however, no data was reported to support this hypothesis.13
Additional associations between safety-related outcomes and small-scale homelike settings were observed in this review, such as an improvement in quality-of-care indicators (e.g., reduced risk of low-risk pressure ulcers) and reduced risk of fall-related injuries among cognitively impaired residents, demonstrating further potential benefits of homelike care settings over traditional long-term care homes.14
While further efforts to measure these outcomes in a comparative setting would be of benefit to decision-makers, the challenges of designing a study with sufficient power to detect clinically meaningful and statistically significant differences, and with high levels of internal and external validity remain.
As homelike models of care, such as dementia villages and the Butterfly model, have been adopted in several Canadian long-term care facilities,5 further research is needed to inform the cost-effectiveness, the benefits, and the potential risks associated with wider adoption, relative to maintaining traditional long-term care facilities.
References
1.Statistics Canada. Demographic estimates by age and sex, provinces and territories. 2020; https://www150.statcan.gc.ca/n1/pub/71-607-x/71-607-x2020018-eng.htm. Accessed 2021 Nov 1.
2.Statistics Canada. Population projections for Canada (2018 to 2068), provinces and territories (2018 to 2043). 2019; https://www150.statcan.gc.ca/n1/pub/91-520-x/2019001/hi-fs-eng.htm. Accessed 2021 Nov 1.
3.Enabling the future provision of long-term care in Canada. Toronto (ON): National Institute on Ageing; 2019: https://static1.squarespace.com/static/5c2fa7b03917eed9b5a436d8/t/5d9de15a38dca21e46009548/1570627931078/Enabling+the+Future+Provision+of+Long-Term+Care+in+Canada.pdf. Accessed 2021 Oct 18.
4.Armstrong P, Banerjee A, Armstrong H, et al. Models for long-term residential care: a summary of the consultants’ report to Long-Term Care Homes and Services, City of Toronto. Toronto (ON): City of Toronto; 2019: https://www.toronto.ca/legdocs/mmis/2019/ec/bgrd/backgroundfile-130891.pdf. Accessed 2021 Oct 18.
5.Dementia villages: innovative residential care for people with dementia. (CADTH issues in emerging health technologies issue 178). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/hs-eh/eh0071-dementia-villages.pdf. Accessed 2021 Nov 15.
6.Homelike models in long term care: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid Response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1125%20Homelike%20LTC%20models%20Final.pdf. Accessed 2021 Nov 15.
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
8.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
10.Adlbrecht L, Bartholomeyczik S, Hildebrandt C, Mayer H. Social interactions of persons with dementia living in special care units in long-term care: A mixed-methods systematic review. Dementia. 2021;20(3):967-984. PubMed
11.Dyer SM, van den Berg MEL, Barnett K, et al. Review of innovative models of aged care. Adelaide (AU): Royal Commission into Aged Care Quality and Safety; 2020: https://agedcare.royalcommission.gov.au/sites/default/files/2020-01/research-paper-3-review-innovative-models-of-aged-care.pdf. Accessed 2021 Nov 15.
12.Lee SY, Hung L, Chaudhury H, Morelli A. Effects of Physical Environment on Quality of Life among Residents with Dementia in Long-Term Care Facilities in Canada and Sweden: A longitudinal study in a large-scale institutional setting versus a small-scale homelike setting. Architectural Research. 2021;23(2):19-28.
13.Zimmerman S, Dumond-Stryker C, Tandan M, et al. Nontraditional Small House Nursing Homes Have Fewer COVID-19 Cases and Deaths. J Am Med Dir Assoc. 2021;22(3):489-493. PubMed
14.Zimmermann J, Swora M, Pfaff H, Zank S. Organizational factors of fall injuries among residents within German nursing homes: secondary analyses of cross-sectional data. Eur. 2019;16(4):503-512. PubMed
15.Kok JS, Oude Voshaar RC, Scherder EJA. Psychotropic drug use in residents with dementia living in small-scaled special care facilities; a longitudinal study. Aging Ment Health. 2020;24(4):689-696. PubMed
16.Seetharaman K, Chaudhury H, Kary M, Stewart J, Lindsay B, Hudson M. Best Practices in Dementia Care: A Review of the Grey Literature on Guidelines for Staffing and Physical Environment in Long-Term Care. Can J Aging. 2020:1-16. PubMed
17.Clarke J. Impacts of the COVID-19 pandemic in nursing and residential care facilities in Canada. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/n1/en/pub/45-28-0001/2021001/article/00025-eng.pdf?st=jsfA_jPs. Accessed 2021 Nov 9.
18.The impact of COVID-19 on long-term care in Canada: focus on the first 6 months. Ottawa (ON): Canadian Institute for Health Information; 2021: https://www.cihi.ca/sites/default/files/document/impact-covid-19-long-term-care-canada-first-6-months-report-en.pdf. Accessed 2021 Nov 9.
19.Factors associated with COVID-19 outbreaks, transmission and poor outcomes in Ontario’s LTC homes: presentation to the Ontario Long-Term Care Commission. Ottawa (ON): Canadian Institute for Health Information; 2021: http://www.ltccommission-commissionsld.ca/presentations/pdf/Canadian_Institute_for_Health_Information_March_3_2021.pdf. Accessed 2021 Nov 9.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Adlbrecht et al. (2021)10 Austria and Germany Funded by Senecura Kliniken- und HeimebetriebsgmbH | Study designs included: This mixed-methods systematic review captured qualitative and quantitative studies, not restricted by design. Number primary studies included: 18 primary studies; 6 quantitative non-randomized studies were relevant to the present report, of which 3 were captured in a the 2019 CADTH report. | Population characteristics: Residents of special care units or small-scale living facilities for persons with dementia in long-term care. | Intervention: The systematic review considered special care units or small-scale living facilities as an intervention; in the present review, we consider the subset of interventions with homelike care models. Comparators were not pre-defined and included: Traditional nursing care units; large-scale special care units; before/after environmental changes. | Outcomes: Social interactions. Metrics used in the relevant studies were: the RISE; the ATOSE; and the social relations subscale of the QUALIDEM tool. Follow-up: Variable |
Dyer et al. (2019)11 Australia Conducted “to assist the Royal Commission into Aged Care Quality and Safety” (funding unclear) | Study designs included: Comparative studies, not otherwise defined. Number primary studies included: 5, of which 3 were captured in a previous CADTH review. | Population characteristics: Residents of long-term care facilities that followed innovative models and complex interventions targeting the whole care environment. | Intervention: Small-scale domestic living models, as an innovative approach (defined as models of care that are novel and not widely available in Australia). Comparators: traditional residential aged care. | Outcomes: Broadly defined as resident-centred outcomes and included: social engagement; function; physical restraint; psychotropic drug use; quality-of-care; and caregiver relations. Follow-up: Variable |
ATOSE = Assessment Tool for Occupation and Social Engagement quality of life in dementia; QUALIDEM = quality of life in dementia; RISE = Revised Index of Social Engagement.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Lee et al. (2021)12 Canada, Sweden Ministry of Education, Science and Technology, Seoul, South Korea | Study design: Prospective cohort study Study objective: to compare QoL across different LTC settings in Canada and Sweden. Study sample: Two LTC dementia care facilities selected from 56 LTCs in Vancouver, Canada: 1) 1 with physical characteristics of a small-scale setting, and 2) 1 traditional large-scale setting. Two LTC dementia care facilities in Stockholm, Sweden selected from 10 dementia care facilities in a randomly selected municipality. The 2 selected LTC facilities had the greatest difference in physical environment features. | Number of residents in the comparative analysis = 12 across 2 LTC facilities.a Eligibility: Residents of a LTC (1 in Canada, 1 in Sweden) aged ≥ 60 years with early-to-mid stage Alzheimer disease or related dementia and able to ambulate. Key baseline characteristics (presented for each LTC facility): Mean age: 77.6 to 82.3 years % female: 60 to 71.4% Married: 20% to 57.1%. | Key comparisons were made between 2 LTCs.a Homelikeness was based on mean score (0 = unpleasant to 3 = favourable) from the relevant TESS-NH domain. Intervention: Edsberg Garden (Sweden) – 2 units with 10 residents per unit; single bedrooms; 1:4 ratio of staff to residents; mean homelike score = 2.50. Comparators: Maple Manor (Canada) – institutional care; 30 residents per unit; mixed single/semi-private bedrooms; double-loaded floor plan; 1:6 ratio of staff to residents; mean homelike score = 0.50. | Outcomes: Quality of life, measured using the Dementia Care Mapping tool, analyzed to capture 5 outcomes: 1. Potential positive engagement. 2. Diversity of occupation. 3. Agitation/distress. 4. Withdrawn behaviour. 5. Well- or ill-being Follow-up: Quality of life was measured 3 times over the course of 1 year. |
Zimmerman et al. (2021)13 US Funding source not reported | Study design: Retrospective cohort study Study objective: to compare rates of COVID-19 infection, admissions/readmissions, and mortality between: Green House/small nursing homes; traditional nursing homes with < 50 beds; and traditional nursing homes with ≥ 50 beds. Study sample: 43 Green House/small nursing home organizations (with 219 nursing homes) across 20 states. These were geographically matched (within 100 miles) to 177 nursing homes with < 50 beds, and 215 nursing homes with ≥ 50 beds. | Total number of residents not reported. Number of nursing homes presented by state, across 20 states. The state with the largest number of nursing homes was Ohio (23% of Green House homes; 33% of traditional nursing homes with < 50 beds; 28% of nursing homes with ≥ 50 beds. Other baseline characteristics not provided. | Intervention: Green House homesb (n = 219; across 43 organizations), described as housing 10 to 12 residents, universal staff assignment, private rooms and bathrooms, smaller overall space than traditional nursing homes, and a central entry. Comparators: Traditional nursing homes with < 50 beds (n = 177); and traditional nursing homes with ≥ 50 beds (n = 215). | Outcomes: COVID-19 infection rate per 1,000 resident days COVID-19 admission or readmission rate per 1,000 resident days COVID-19 mortality per 100 positive cases Follow-up: 193 days (January 20, 2020 to July 31, 2020) |
Kok et al. (2020)15 The Netherlands Funding source not reported | Study design: Non-randomized, controlled study Study objective: To explore changes in psychotropic drug use among residents with dementia when moving from large-scaled to small-scaled special care units, vs. residents remaining in large-scaled special care units. Study sample: Residents of 2 large nursing home facilities having large-scaled special care units. For organizational reasons, all residents of 1 facility were moved to a new facility with small-scaled units; residents in the second facility did not move. | Number of residents in intervention group = 72. Number of residents in comparator group = 56. Eligibility: Residents of large-scale special care units within 2 nursing homes, with a diagnosis of dementia, and whose legal representatives provided informed consent. Key baseline characteristics: No differences between groups. Across both groups:
| Intervention: Residents moved to a new facility with small-scaled units (7-8 residents), single bedrooms, staff trained on psychosocial interventions. Comparator: Residents in large-scaled units (did not move; 20-30 residents), shared bedrooms, and 1 living room per unit. | Outcomes: Psychotropic drug use, extracted from residents’ medical records and converted into average Defined Daily Doses given to each resident per psychotropic drug class. Length of follow-up: Drug use was measured at 2 months before planned move, and at 3 months and 6 months after transfer. |
Zimmermann et al. (2019)14 Germany The North Rhine-Westphalian Ministry of Culture and Science | Study design: Retrospective cohort study Relevant study objective: Whether organizational factors (especially staff mix, homelike units and dementia care units) influence the occurrence of fall injuries. Study sample: Secondary data from the EQisA Project; the study sample captured 220 nursing homes across Germany, with 18,985 residents. | Total number of residents included = 15,953 Eligibility: Residents of the 220 sampled nursing homes for whom consent was provided, excluding: residents who could not change their position in bed, residents receiving end-of-life care. Key baseline characteristics:
| Homelike units were included as a categorical variable in a multivariable model, with levels: Yes (intervention): homelike unit (20% of nursing homes), and No (comparator): not a homelike unit (80% of nursing homes). The operational definition was “presence of small, homelike units” and was not otherwise defined. | Outcome: The proportion of residents who were seriously injured by falling in the nursing home; fall-related injuries requiring medical treatment, including fractures wounds and persistent pain were considered serious fall injuries. Follow-up: 6 months; data were collected in 2016. |
EQisA = translated as quality outcomes in inpatient elderly care; LTC = long-term care; sMMSE = Standardized Mini-Mental State Examination; TESS-NH = Therapeutic Environment Screening Survey for Nursing Homes.
aTwo additional LTCs were included in the study; however, they were not included in the statistical comparison of quality of life between LTCs having the largest difference in physical environment.
bIncluding 1 additional small house facility in which the operations mirror Green House homes.
Appendix 3: Critical Appraisal of Included Publications
Note that that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 27
Strengths | Limitations |
|---|---|
Adlbrecht et al. (2021)10 | |
The research question and eligibility criteria were well-defined in terms of population, intervention, comparison, and outcomes. The literature search strategy was comprehensive, covering 5 bibliographic databases and the reference lists of relevant articles. Study selection was performed in duplicate. Detailed study-by-study summaries were provided, capturing population, interventions, comparators, outcomes, and study design, and follow-up. Risk of bias assessment was performed. | Search was conducted almost 3 years before the review’s publication date. Data extraction was performed by 1 researcher. Some relevant outcome estimates were omitted from the summary of study characteristics table. A list of excluded studies was not provided, although counts were summarized in a diagram. Results were synthesized narratively, with limited accounting for risk of bias or explanation of heterogeneity observed across the studies. |
Dyer et al. (2019) | |
The eligibility criteria regarding population, intervention and comparison was well-defined. Outcomes were not specified as an eligibility criterion, and assumed to be unrestricted. The literature search strategy was somewhat comprehensive. One bibliographic database appears to have been searched (though other databases were searched to address other research questions); however, the reference lists of relevant articles and grey literature sources were searched, and there was consultation with experts. | The systematic review was presented within a larger report covering a series of rapid scoping reviews, and systematic reviews only for specific topics. While it was stated that “a systematic review was conducted to compare the impact of small-scale living designs with that of traditional residential aged care on resident-centred outcomes”, the methodology for addressing that specific question was not clearly separated from the review methodology used to address other research questions within the report. Study selection was performed by 1 reviewer and reviewed by a second (not performed independently). Data extraction was performed by 1 researcher. Results were synthesized narratively without quantitative estimates, and study-by-study characteristics (population, intervention, comparison) and outcomes were not provided. Risk of bias was not assessed. There was limited interpretation/discussion of the findings; risk of bias and heterogeneity were not discussed. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist8
Strengths | Limitations |
|---|---|
Lee et al. (2021)12 | |
The main outcome measure was clearly described, and involved intensive, in-depth, real-time observations. The risk of bias due to reliability of the measurements across facilities was reduced by using the same mapper in both the Canadian and Swedish settings. Detailed description of the intervention and comparison LTC facility characteristics, including a detailed assessment of the physical environment using the Therapeutic Environment Screening Survey for Nursing Homes (TESS-NH) tool. | Subjects were not randomized. No adjustments or matching on potential confounders of the relationship between facility physical environment and QoL outcomes, leading to potential bias. The comparison between the main 2 LTCs may have been confounded by country (Sweden vs. Canada), year (2013 vs. 2016), and residents’ other characteristics (e.g., gender, activities of daily living, duration of residence). Loss to follow-up was not taken into account. The 17 residents who died or moved before study end were excluded; additional characteristics not provided. The intervention LTCs were not described as following a specific model of care, and thus may not generalize to other homelike models of care (e.g., Green House, Butterfly model). Similarly, the comparison LTC was not described as following a specific model of care and findings may not generalize to other traditional models of care. Actual P values not provided for the main outcomes; they were reported categorically as: not significant (> 0.05), < 0.05, or < 0.01. It is unclear if a statistical power calculation was done; however, the study may have had insufficient power to detect clinical important effects for all outcomes, given that the main statistical comparisons were made between 2 LTCs based on observations from 7 (intervention) and 5 (comparison) residents. The validity of selecting 2 LTCs post-hoc appeared to have been identified post-hoc for statistical comparison; other outcomes presented descriptively. |
Zimmerman et al. (2021)13 | |
Clearly stated objectives and outcome metrics. Study sample expected to be representative of source population, given the broad geographic coverage across the US, and high participation rates among Green House nursing homes 43 of 57 eligible Green House organizationsa participated). | Subjects were not randomized. No adjustments for potential differences between Green House and traditional nursing homes residents’ baseline risk of COVID-related mortality. Facilities were not randomized. Although facilities were matched geographically, no adjustment or matching was done for other characteristics related to funding model or staffing that may be related to the risk of introducing COVID-19 to a given nursing home. The main outcome measure may not have been accurate; COVID-19 case rates may have been systematically underestimated due to access to COVID-19 testing, particularly in the early portion of the study period. This is likely to apply to both intervention and comparison nursing homes. It is unclear if a statistical power calculation was done; however, all comparisons between Green House homes and traditional nursing homes were statistically significant. |
Kok et al. (2020)15 | |
Clearly stated objectives, hypothesis, and outcome metrics. High participation rate (legal representatives of 78% of eligible residents gave informed consent), likely to be representative of all eligible residents. Intervention and control group balanced at baseline Broad geographic coverage across the US, and high participation rates among Green House nursing homes 43 of 57 eligible Green House organizationsa participated). | Patients lost to follow-up were excluded and not described. The small-scale special care units were not described as following a specific model of care, and thus may not generalize to other homelike models of care (e.g., Green House, Butterfly model). The reliability of the outcome measured after residents were transferred to small-scale units is of concern, as the transfer itself may have caused stress and increased the use of psychotropic drugs. According to the authors, while the study had adequate power to detect differences in overall psychotropic drug use, the study did not have sufficient power to detect differences within more specific drug classes. |
Zimmermann et al. (2019)14 | |
Clearly stated objectives, hypothesis, and outcome metrics. Broad geographic coverage and sample size (n = 220 nursing homes; n = 15,953 residents) suggests reasonable external validity of the findings. As the analysis was based on secondary data, the staff collecting outcomes from the primary study were effectively blinded to the research question regarding homelike care interventions. Outcome measures are considered to be accurate; plausibility checks and local audits were performed as part of the primary study. Adjustment for confounding and effect modification was performed to reduce the risk of bias: analysis was stratified by baseline risk of falls (using cognitive ability as a proxy measure) and interaction terms for homelike care units x geography; other potential confounders were included in the multivariable model. | Few details provided with respect to residents’ characteristics and differences between residents of homelike care settings vs. non-homelike care settings. Consequently, imbalances could not be assessed. While the characteristics of typical German homelike care facilities were described, there was limited information regarding the implementation and admission criteria for the homelike care facilities within the study sample; variation across the sample may have biased the results and limits the external validity of the findings. Based on the number of homelike care units (44 out of 220), the study may have been underpowered to detect differences in fall injuries (sample size calculation not reported). |
LTC = long-term care; QoL = quality of life.
aIncluding 1 additional small house facility in which the operations mirror Green House homes.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that that this appendix has not been copy-edited.
Summary of Findings Included Systematic Reviews
Adlbrecht et al. (2021)10
Main study findings
The systematic review by Adlbrecht et al. (2021) identified 18 studies, of which 12 were not relevant to the current review.
The 6 remaining studies were relevant to the current review. Of these, 3 were included in the previous 2019 CADTH review and hence not reported here. The remaining 3 studies were De Rooij et al. (2012), Verbeek et al. (2010), and Morgan-Brown et al. (2013). These 3 studies were cited to support the following statement by Adlbrecht et al. (2021):
“Studies comparing special care units to traditional nursing homes and analysing social interactions in the subscales of quality of life report inconsistent results, indicating that residents of special care units still have little but probably slightly more social relations than traditional nursing home residents”. (p. 976)10
Study-specific findings, as reported by Adlbrecht et al. (2021),10 are as follows.
De Rooij et al. (2012)
The Netherlands; residents with dementia
In the social relations subscale of the QUALIDEM and for social engagement (RISE), there were significantly higher means aggregated over time (0, 6, 12 months) in small-scale units (n = 51 residents) compared with traditional nursing homes (n = 51 residents) in the Netherlands:
Social relations (QUALIDEM): mean value for small-scale units = 8.3; comparison vs. traditional homes P value < 0.001.a
Social engagement (RISE): mean value for small-scale units = 2.4; comparison vs. traditional homes P value < 0.01b
Verbeek et al. (2010)
The Netherlands; residents with dementia
In the social relations subscale of the QUALIDEM, as measured by nursing staff, there were no significant differences in group-by-time (small-scale vs. regular wards; at time 0, 6, and 12 months). Numerical estimates not provided by Adlbrecht et al. (2021).
Morgan-Brown et al. (2013)
Ireland; residents with dementia
Based on the ATOSE, there was significantly higher social engagement after implementation of household model units (daily mean = 57.9; standard deviation = 22.1) than in the same units before implementing household models (daily mean = 25.8; SD = 12.5) P value < 0.001.
Author’s conclusion
“The current review yielded fragmented evidence based on special care unit residents’ social interaction, highlighting the need for more profound research to make comprehensive recommendations for healthcare providers. Furthermore, persons with dementia living in special care units experience little, but more, social interaction than those not living in special care units… Nevertheless, the results are inconclusive regarding the influence of unit size and homelike characteristics on social interactions.” (p. 980)10
Dyer et al. (2019)11
Main study findings
Five studies were identified, of which 2 were included in the previous 2019 CADTH review, and 1 was included in the more recent SR by Adlbrecht et al. (2021).10 The remaining 2 studies were:
Afendulis et al. (2016)
In the systematic review by Dyer et al. (2019), this study was cited to support the statements that small-scale units were associated with “reduced physical restraint and psychotropic drug use” (p. 9)11 and “improvements in quality-of-care indicators” relative to traditional nursing homes. (p. 9)11
In a summary table, this study was also cited to support the following statement around quality-of-care indicators:
“Improvements in bedfast residents, catheter use, low-risk pressure ulcers, physical restraint use, hospital readmissions and avoidable hospital readmissions.” (p. 2 of Appendix 3)11
No quantitative metrics were provided.
Te Boekhorst et al. (2009)
In the systematic review by Dyer et al. (2019), this study was cited as showing “inconsistent effects on function” and “reduced physical restraint and psychotropic drug use.” No quantitative metrics were provided.
Authors’ conclusion
“Most of the approaches described in this report have limited evidence for their impact on recipient outcomes. Further evaluation would provide useful cost/benefit information to support wider implementation of promising approaches.” (p. 45)11
a Mean value for traditional homes not captured by Adlbrecht et al (2021).10
b Mean value for traditional homes not captured by Adlbrecht et al (2021).10
Summary of Findings of Included Primary Clinical Studies
Lee et al. (2021)12
Main study findings
Differences in QoL between a homelike small-scale LTC (Edsberg Arden) vs. a traditional LTC (Maple Manor), based on domains of the Dementia Care Mapping tool:
Data presented as: Edsberg Arden mean (SD) vs. Maple Manor mean (SD); P value (via t-test).
Positive Engagementa: 4.92 (6.89) vs. 2.83 (6.04); reported by authors as non-significant
Agitationa: 0.23 (0.26) vs. 0.31 (0.54); reported by authors as non-significant
Withdrawna: 5.93 (4.92) vs. 13.4 (5.23); P value < 0.05
Well- or ill-being indexb: 1.00 (0.05) vs. 0.61 (0.14); P value < 0.01
Authors’ conclusion
“Residents in a small-scale homelike setting with positive stimuli had a higher [QoL] compared to a large-scale institutional setting…” (p. 26)12
Zimmerman et al. (2021)13
Main study findings
Comparisons between Green House homes,c traditional nursing homes with < 50 beds and traditional nursing homes with ≥ 50 beds. P values based on log-rank tests.
COVID-19 case rate (per 1,000 resident days):
Percentiles: 50th, 75th, 90th:
Green House homesc: 0.00, 0.08, 0.30
Traditional (< 50 beds): 0.00, 0.15, 1.61
Traditional (≥ 50 beds): 0.06, 0.74, 2.10
P Values:
Green House homes vs. traditional (< 50 beds) = 0.014
Green House homes vs. traditional (≥ 50 beds) < 0.001
COVID-19 admission or readmissions (per 1,000 resident days):
Percentiles: 50th, 75th, 90th:
Green House homesc: 0.00, 0.00, < 0.01
Traditional (< 50 beds): 0.00, 0.13, 0.74
Traditional (≥ 50 beds): 0.00, 0.11, 0.49
P Values:
Green House homes vs. traditional (< 50 beds) < 0.001
Green House homes vs. traditional (≥ 50 beds) < 0.001
COVID-19 mortality (per 100 positive cases):
Percentiles: 50th, 75th, 90th:
Green House homesc: 0.00, < 0.01, 24.3
Traditional (< 50 beds): 10.0, 50.0, 80.5
Traditional (≥ 50 beds): 12.5, 30.0, 53.3
P Values:
Green House homes vs. traditional (< 50 beds) = 0.007
Green House homes vs. traditional (≥ 50 beds) = 0.007
Authors’ conclusion
“COVID-19 incidence and mortality rates are less in Green House/small [nursing homes] than rates in traditional [nursing homes] with < 50 and ≥ 50 beds, especially among the higher and extreme values.” (p. 492)13
Kok et al. (2020)15
Main study findings
No statistically significant differences in use of all central nervous system psychotropic medication categories between use among residents of in small-scaled and large-scaled special care units (small effect size based on η2 = 0.001d; P value = 0.790).
Defined daily dose of all central nervous system psychotropic medications (mean, standard deviation), by group and time, were:
Small-scaled dementia special care unit:
2 months before transfer: 1.47 (1.53)
3 months after transfer: 1.58 (1.78)
6 months after transfer: 1.65 (1.77)
Large-scaled dementia special care unit:
2 months before (non-)transfer: 1.30 (1.43)
3 months after (non-)transfer: 1.51 (1.72)
6 months after (non-)transfer: 1.40 (1.64)
For more specific drug classes, there was an increase in drug use over time for residents of small-scale units, vs. large-scaled units (presented as η2 [effect size]d), for:
Hypnotics and sedatives (0.596 [large effect size]; P value = 0.009)
Analgesics (0.071 [moderate effect size]; P value = 0.059)
Anti-Parkinsonian (0.062 [moderate effect size]; P value = 0.634)
Anxiolytics (0.068 [moderate effect size]; P value = 0.573)
Total psycholeptics (0.088 [moderate effect size]; P value = 0.053)
Anti-psychotics (0.036 [small effect size]; P value = 0.292)
For more specific drug classes, there was an increase in drug use over time for residents of large-scale units, vs. small-scaled units(presented as η2 [effect size]d), for:
Anti-epileptics (0.506 [large effect size]; P value = 0.048)
Anti-depressants (0.157 [large effect size]; P value = 0.084)
Total psychoanaleptics (0.088 [moderate effect size]; P value = 0.053).
Authors’ conclusion
“[o]ur hypothesis that replacement of residents from large- to small-scaled [special care units] would result in a reduction of psychotropic drugs had to be rejected. In contrast, we found a slight increase […] in overall psychotropic drug use over time in small versus large-scaled [special care units].” (p. 692)15
Zimmermann et al. (2019)14
Main study findings
Among residents with low-risk for fall injuries (i.e., low or slight cognitive impairment):
No statistically significant influence of homelike care units on the risk of fall injuries
Odds ratio of falls for homelike vs. non-homelike = 1.109; 95% CI, 0.891 to 1.379)
Among residents with high-risk for fall injuries (i.e., considerable or worse cognitive impairment):
Statistically significant reduction in risk of fall injuries among homelike care units
Odds ratio of falls for homelike vs. non-homelike = 0.833; 95% CI, 0.705 to 0.985)
No statistical interaction between geographic location and homelike care units.
Authors’ conclusion
“Cognitively impaired residents living in nursing homes with [homelike units] experienced fewer [fall injuries], regardless of the region of residence.” (p. 509)14
a Higher values represent a greater amount of time spent in a given state
b Positive or negative values reflect overall time spent in positive or negative mood and engagement, respectively
c Including 1 additional small house facility whose operations mirror Green House homes
d Effect size from multivariate analysis of variance (MANOVA) defined as: eta squared (η2) of > = 0.14 = large effect size; 0.06 to 0.13 moderate effect size; 0.01 to 0.05 = small effect size.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
There were 5 relevant primary studies captured in the 2 included systematic reviews; 1 primary study was common to both systematic reviews. Five additional relevant studies from these 2 systematic reviews were included in the previous CADTH review,6 and were excluded from this report and are not presented in Table 8.
Table 6: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Adlbrecht et al. (2021)10 | Dyer et al. (2019)11 |
|---|---|---|
Afendulis et al. Health Serv Res. 2016; 51 Suppl 1: 454-74 | No | Yes |
De Rooij et al. Int J Nurs Stud. 2012; 49(8):931-940 | Yes | Yes |
Morgan-Brown et al. Aging Ment Health. 2013; 17(10):57-65 | Yes | No |
Te Boekhorst et al. Int J Geriatr Psychiatry. 2009; 24(9):970-978 | No | Yes |
Verbeek et al. J Am Med Dir Assoc. 2010; 11(9):662-670 | Yes | No |
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
20.Dementia villages: innovative residential care for people with dementia. (CADTH issues in emerging health technologies issue 178). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/hs-eh/eh0071-dementia-villages.pdf. Accessed 2021 Nov 15.
21.Homelike models in long term care: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid Response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1125%20Homelike%20LTC%20models%20Final.pdf. Accessed 2021 Nov 15.
22.Eden Alternative and Green House concept of care: review of clinical effectiveness, cost-effectiveness, and guidelines. Ottawa (ON):CADTH; 2010: https://www.cadth.ca/sites/default/files/pdf/L0166_Eden_Alternative_Concept_final.pdf. Accessed 2021 Oct 18.
Review Articles
French language review (with English language summary)
23.État des connaissances: qualité du milieu de vie en centre d’hébergement pour les personnes âgées en perte d’autonomie. Québec (QC): Institut national d’excellence en santé et en services sociaux; 2018: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/ServicesSociaux/INESSS_Qualite_milieu_de_vie.pdf. Accessed 2021 October 18.
24.Living environment quality in long-term care facilities for dependent seniors. Québec (QC): Institut national d’excellence en santé et en services sociaux; 2018: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/ServicesSociaux/INESSS_Living_environment_long-term-care_facilitiese_EnglishSummary.pdf. Accessed 2021 October 18.
Policy papers and recommendations to government regarding adoption of homelike models of care
25.Improving quality of life for residents in facility-based continuing care. Edmonton (AB): Alberta Department of Health; 2021: https://open.alberta.ca/dataset/f680d1a6-bee5-4862-8ea4-e78d98b7965d/resource/22092c9c-99bb-4fee-9929-7ce06e71bbd1/download/health-improving-quality-life-residents-facility-based-continuing-care-2021-04-30.pdf. Accessed 2021 Oct 18.
26.Enabling the future provision of long-term care in Canada. Toronto (ON): National Institute on Ageing; 2019: https://static1.squarespace.com/static/5c2fa7b03917eed9b5a436d8/t/5d9de15a38dca21e46009548/1570627931078/Enabling+the+Future+Provision+of+Long-Term+Care+in+Canada.pdf. Accessed 2021 Oct 18.
Review of international guidelines on dementia care, encompassing unit size and homelike environment
27.Dementia-friendly care homes best practices in dementia care. Burnaby (BC): BC Care Providers, Alzheimers Society British Columbia, Simon Fraser University; 2020: https://bccare.ca/wp-content/uploads/2020/03/DFCH-Report_03_02web.pdf. Accessed 2021 Oct 18.
And associated publication
28.Seetharaman K, Chaudhury H, Kary M, Stewart J, Lindsay B, Hudson M. Best practices in dementia care: a review of the grey literature on guidelines for staffing and physical environment in long-term care. Can J Aging. 2020 Nov 16:1-16. PubMed
Additional References
Conference abstract
29.Verbeek H, De Boer B, Zwakhalen S, Hamers J. The impact of green care farms and other innovative nursing home models on BPSD symptoms in everyday life for people with dementia. Alzheimer's Dement. 2020:e039799.
Alternative publication date (i.e., published prior to 2019)
30.Dyer SM, Liu E, Gnanamanickam ES, et al. Clustered domestic residential aged care in Australia: fewer hospitalisations and better quality of life. Med J Aust. 208;208(10):433-438.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca