CADTH Health Technology Review
Pharmacological Thromboprophylaxis in Patients With Cancer
Rapid Review
Authors: Anusree Subramonian, Alison Adams
Abbreviations
ASCO
American Society of Clinical Oncology
ASH
American Society of Hematology
CHEST
American College of Chest Physicians
DIC
disseminated intravascular coagulation
DOAC
direct oral anticoagulant
DVT
deep vein thrombosis
ESVS
European Society for Vascular Surgery
GRADE
Grading of Recommendations, Assessment, Development and Evaluations
ITAC
International Initiative on Thrombosis and Cancer
LMWH
low-molecular-weight heparin
NICE
National Institute for Health and Care Excellence
PE
pulmonary embolism
RCT
randomized controlled trial
VKA
vitamin K antagonist
VTE
venous thromboembolism
Key Messages
Six evidence-based guidelines were identified regarding the long-term (6 months or longer) use of pharmacological thromboprophylaxis for the management of cancer-associated thrombosis. The guidelines used rigorous methodology, systematically searched for evidence, and were clearly reported.
Anticoagulation therapy for 6 months or longer is recommended by 5 guidelines for patients with active cancer and venous thromboembolism to prevent recurrences of venous thromboembolism. However, the recommendations are weak and made based on low-quality evidence or expert consensus.
Two guidelines recommend a low-molecular-weight heparin or direct oral anticoagulant for long-term use (6 months or longer) in patients with cancer. This recommendation is based on low- to high-certainty evidence.
Two guidelines strongly recommend direct oral anticoagulants in patients with cancers in locations other than gastrointestinal or genitourinary cancers. This recommendation is based on high-quality evidence.
No guidelines were identified regarding arterial thrombosis or chronic disseminated intravascular coagulation associated with cancer.
Context and Policy Issues
Thrombosis or coagulation of blood within a blood vessel is a common complication of cancer and has been recognized since the 19th century.1,2 Cancer-associated thrombosis is the second leading cause of death in patients with cancer.3,4 Cancer causes a hypercoagulable or prothrombotic state that, when combined with a stasis of blood flow or endothelial injury, can result in thrombosis. The 3 types of cancer-associated thrombosis are venous thromboembolism (VTE), arterial thrombosis, and chronic disseminated intravascular coagulation (DIC).1 It has been estimated that approximately 20% to 30% of all first VTEs are associated with cancer.4 A 4- to 7-fold increased risk of VTE is observed in patients with cancer.2 There are 2 types of VTE: pulmonary embolism (PE) and deep vein thrombosis (DVT). The risk factors for cancer-associated VTE include patient factors (e.g., older age, medical comorbidities, previous history of VTE), cancer-associated risk factors (e.g., primary site of cancer, advanced stage), and treatment-associated risk factors (e.g., chemotherapy, hospitalization, and surgery).1,2
Thromboprophylaxis or management strategies to prevent the occurrence of thrombotic events are warranted in patients with cancer due to the increased risk.5,6 Pharmacological thromboprophylaxis options include direct-acting oral anticoagulants (DOACs), such as apixaban, edoxaban, and rivaroxaban; low-molecular-weight heparins (LMWHs), such as dalteparin, enoxaparin, and tinzaparin; and vitamin K antagonists (VKAs), such as warfarin.5,6 The benefits and risks of extended or long-term anticoagulation (> 6 months) for the prevention of thrombotic events have been discussed in recent studies7 and reviews of trials.6 The purpose of this report is to summarize the evidence-based guidelines regarding the long-term use of pharmacological thromboprophylaxis for the management of cancer-associated thrombosis.
Research Question
What are the evidence-based guidelines regarding the long-term use of pharmacological thromboprophylaxis for the management of cancer-associated thrombosis?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Library, the University of York Centre for Reviews and Dissemination (CRD) databases, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were pharmacological thromboprophylaxis and cancer. Search filters were applied to limit retrieval to guidelines. Conference abstracts were excluded. When possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and September 27, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with cancer |
Intervention | Long-term (i.e., ≥ 6 months) pharmacological thromboprophylaxis (e.g., direct-acting oral anticoagulants [e.g., apixaban, edoxaban, rivaroxaban], low-molecular-weight heparins [e.g., dalteparin, enoxaparin, tinzaparin], unfractionated heparin, warfarin) |
Comparator | Not applicable |
Outcomes | Recommendations regarding best practices (e.g., appropriate patient populations, recommended treatment protocols or strategies, contraindications) |
Study designs | Evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2016. When multiple versions of a guideline from the same group were identified, inclusion was limited to the latest version. Guidelines with unclear methodology were excluded.
Summary of Evidence
Quantity of Research Available
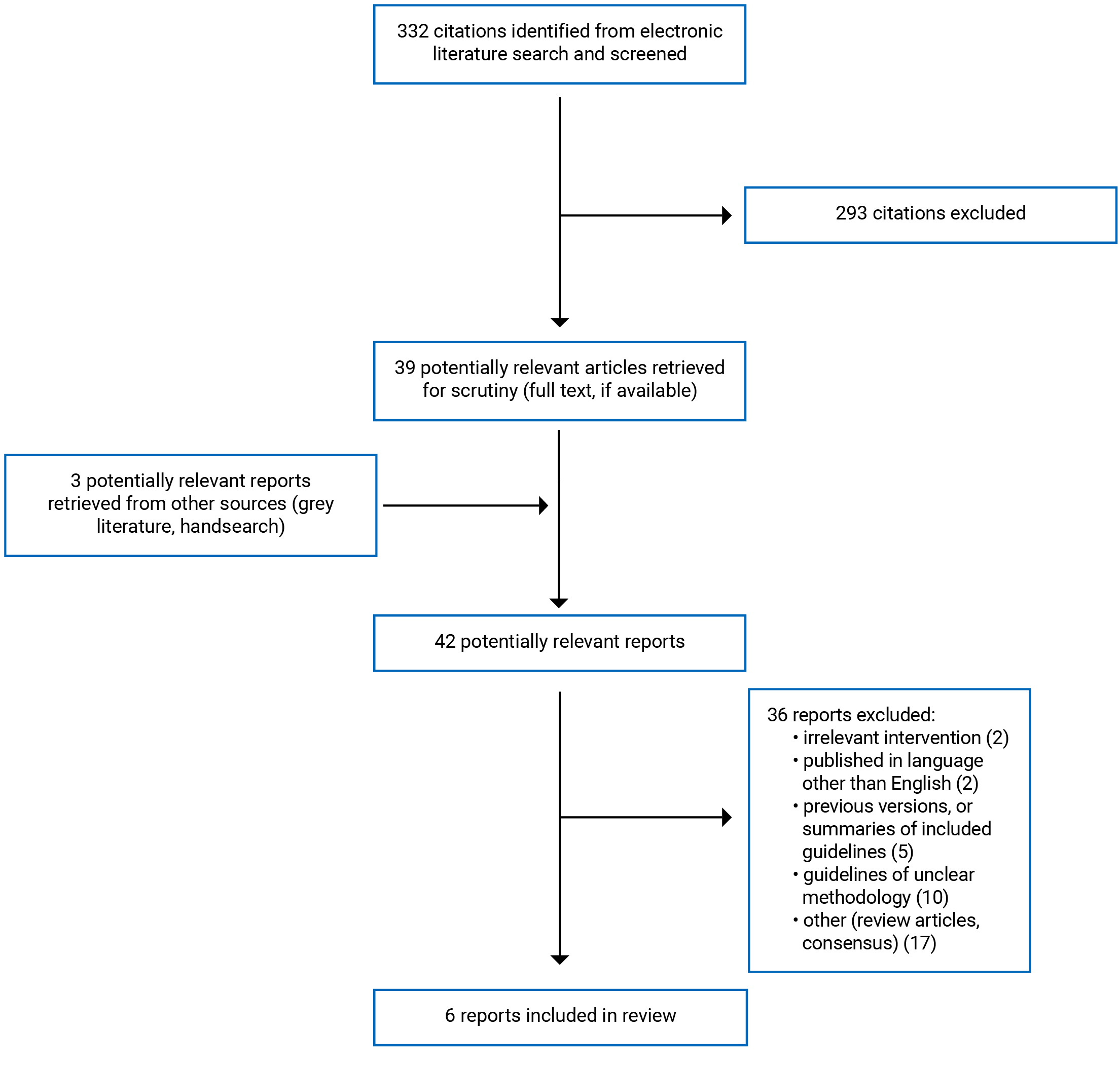
A total of 332 citations were identified in the literature search. Following screening of titles and abstracts, 293 citations were excluded and 39 potentially relevant reports from the electronic search were retrieved for full-text review. Another 3 potentially relevant publications were retrieved from the grey literature search or handsearch for full-text review. Of these potentially relevant articles, 36 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 6 evidence-based guidelines. Appendix 1 presents the PRISMA8 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Six evidence-based guidelines were included in the report.9-14 All included guidelines provided recommendations regarding several pharmacological and non-pharmacological interventions for the prevention and management of VTE.9-14 Three guidelines10,13,14 provided recommendations for all individuals with venous thromboses (with and without cancer). Only the recommendations relevant to the long-term (≥ 6 months) pharmacological thromboprophylaxis in patients with cancer will be described in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Six evidence-based guidelines were included in the report.9-14 They were the American Society of Hematology (ASH) guideline (2021),12 the American College of Chest Physicians (CHEST) guideline (2021),14 European Society for Vascular Surgery (ESVS) guideline (2021),10 American Society of Clinical Oncology (ASCO) guideline (2020),11 National Institute for Health and Care Excellence (NICE) guideline (2020),13 and the International Initiative on Thrombosis and Cancer (ITAC) guideline (2019).9
All included guidelines collected evidence using systematic literature review.9-14 Multiple electronic databases, as well as bibliographies and trial registries, were searched to identify evidence. Systematic reviews and randomized controlled trials (RCTs) were identified as evidence for developing recommendations. In the ESVS guideline, non-randomized studies were also included in the evidence base.10 In 3 guidelines, if limited or no evidence were identified for a particular question, expert judgment by the guideline panel was used to develop a recommendation.9,11,13
The quality assessment of the evidence was conducted using several methods. In 5 guidelines, the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach was used, and the certainty of evidence was graded from high quality to very low quality.9,11-14 In the ESVS guideline, certainty of evidence was graded from level A (evidence from multiple RCTs or meta-analyses) to level C (expert consensus or evidence from small retrospective studies).10
In terms of the development and evaluation of recommendations, the ASH guideline12 and the CHEST guideline14 used Evidence-to-Decision framework to formulate the recommendations. The recommendations were finalized after panel discussions (ASH guideline12) or panel consensus by modified Delphi technique (CHEST guideline14). In the ESVS guideline,10 ITAC guideline,9 ASCO guideline,11and the NICE guideline,13 the recommendations were formulated and finalized using panel discussions and consensus.
The strength of the recommendations was reported in the guidelines.9-14 The GRADE approach was employed in grading the recommendations in 4 guidelines.9,12-14 The recommendations were graded as strong or weak based on the degree of confidence in the benefit of the intervention over the risks.9,12-14 In the CHEST guideline14 and NICE guideline,13 the strength of the recommendation was noted in the wording of the recommendation. In the ITAC guideline,9 grades 1 and 2 were used to denote strong and weak recommendations, respectively. In the ASH guideline,12 recommendations were graded as strong (worded as “panel recommends”) or conditional (worded as “panel suggests”).
In the ESVS guideline,10 recommendations were graded from class I (intervention is beneficial and effective) to class III (intervention is not effective and may be harmful in some cases).10 In the ASCO guideline, recommendations were graded as strong, moderate, or weak based on the extent of confidence in the risk-benefit profile of the intervention.11
Country of Origin
The ASH guideline,12 CHEST guideline,14 and ASCO guideline11 were developed by North American groups. The ITAC guideline9 was developed by an international group. The ESVS10 guideline was developed by a European group, and the NICE guideline13 was developed in the UK.
Patient Population
The target population of the included guidelines, relevant to the current report, were patients with active cancer. The intended users of all guidelines included health care professionals such as clinicians (e.g., oncologists, internists, hematologists), nurses, and pharmacists. In 2 guidelines, patients, their families, and caregivers were also listed as intended users.11,13
Interventions and Comparators
The relevant interventions considered in the guidelines were anticoagulants such as LMWHs, VKAs, and DOACs prescribed for long-term (i.e., ≥ 6 months) pharmacological thromboprophylaxis.
Outcomes
Recurrence of VTE and risk of major bleeding were considered as outcomes of interest in all included guidelines.9-14 Mortality was considered in 3 guidelines.9,12,14 In addition, risk of minor bleeding and thrombocytopenia were also considered as outcomes in the 2019 ITAC guideline.
Summary of Critical Appraisal
All 6 guidelines9-14 provided a clear description of the scope and purpose of the guideline. Overall objectives, health questions covered in the guideline, and the target population were described. The guideline development groups included individuals from all relevant professional groups.9-14 Patient preferences were sought during the development phase in 3 guidelines.11-13 Patient stakeholders were given an opportunity to review the summary of draft recommendations in 2 guidelines.9,10 In the CHEST guideline,14 it was unclear whether the views and preferences of the patient population were obtained. The target users were not clearly described in the CHEST guideline, although it was likely clinicians.14
Among the included guidelines, 4 were updates to previously published versions and included an updated evidence base and recommendations.9,11,13,14 Two guidelines were newly developed.10,12 In all 6 guidelines, systematic methods were used to identify evidence, and selection criteria for the evidence were described.9-14 The strength and limitations of the evidence were reported in 4 guidelines9,12-14 but was unclear in the ESVS10 and ASCO11 guidelines. In all guidelines, methods for formulating and developing the guidelines were described. The ASH guideline12 and the CHEST guideline14 used Evidence-to-Decision framework, and the explicit link between evidence and recommendations were clearly described. Evidence contributing to each recommendation were also clear in 3 of the other guidelines.9-11 In the NICE guideline,13 The explicit link to evidence for each of the recommendations was unclear, although detailed discussions about the evidence base was included. The presentation was clear in all 6 guidelines.9-14 The recommendations were unambiguous and easy to identify. Different pharmacological and non-pharmacological treatment options for the condition of interest were considered. A procedure for updating the evidence base and recommendations was described in 3 guidelines.11-13 In the ESVS guideline, a plan for a future update was not included.10 In 2 other guidelines (by CHEST14 and by ITAC9), which were updates from previous versions, the process for update was unclear. Lastly, all guidelines were externally reviewed by stakeholders and experts before publication.9-14
In terms of the applicability of the recommendations, 5 guidelines9,11-14 described the facilitators and barriers to the implementation of the recommendations and addressed the potential resource implications. In the ESVS guideline,10 it was unclear whether these issues were considered. The ITAC guideline9 was accompanied by a web-based app for the implementations of the recommendations, which is likely beneficial to the users. In 3 guidelines, it was unclear whether any tools were provided to aid for that purpose.10,12,14 The NICE guideline13 included auditing criteria to monitor and evaluate whether the recommendations are being used and to obtain feedback from the users; similar monitoring or auditing criteria were not reported in 4 other guidelines9,10,12,14 and were unclear in the ASCO guideline.11
There was editorial independence in all included guidelines.9-14 Competing interests of all members of the guideline development panel were recorded. It was available as supplemental information in 4 guidelines.9,11-13 It was also unlikely that the funding sources would have influenced the recommendations.9-14
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the detailed recommendations and supporting evidence that are relevant to the current report.
Guidelines
Duration of Thromboprophylaxis
The ASH guideline12 suggests long-term anticoagulation (> 6 months) versus short-term anticoagulation (3 to 6 months) for patients with active cancer and VTE. This is a conditional recommendation based on low-certainty evidence. For patients with active cancer and VTE who receive long-term anticoagulation, the guideline suggests that indefinite duration is preferred over discontinuation of treatment after a definite period. This is a conditional recommendation based on very low–quality evidence.
The CHEST guideline14 strongly recommends extended-phase anticoagulation (> 6 months) with a DOAC in patients with VTE and a persistent risk factor. This recommendation is based on moderate-quality evidence. Active cancer is considered a persistent risk factor.
The ASCO guideline11 recommends long-term anticoagulation with an LMWH, a DOAC, or a VKA for longer than 6 months for select patients with active cancer. Recommended patient groups include those with metastatic disease and those receiving chemotherapy. Additionally, intermittent reassessments are recommended beyond 6 months to evaluate the risk-benefit profile. This is a weak to moderate recommendation based on low-quality evidence as well as informal consensus.
The NICE guideline13 similarly recommends (weak recommendation) to consider continuing anticoagulation beyond 6 months for patients with active cancer. Individual risk of VTE recurrence and bleeding should also be considered. They suggest that patient preferences also be taken into consideration. The evidence base for this recommendation is unclear.
The ITAC guideline9 recommends that patients with active cancer and established VTE should be treated for at least 6 months with an LMWH or a DOAC to prevent recurrences. This is a strong recommendation based on high-quality evidence. After 6 months, a decision regarding termination or continuation of anticoagulation should be made by considering the individual’s risk-benefit profile, resources, patient preference, and cancer activity. However, this recommendation was based on expert opinion and consensus due to lack of evidence.
Choice of Anticoagulants for Long-Term Thromboprophylaxis
The ASH guideline12 suggests using DOACs or LMWHs for long-term anticoagulation for patients with active cancer and VTE. This is a conditional recommendation based on very low–certainty evidence.
The CHEST guideline14 suggests anticoagulation with VKA, for patients with VTE and a persistent risk factor (e.g., active cancer) who cannot receive DOAC. This is a weak recommendation based on moderate-quality evidence. It was unclear whether any or all of the evidence was formed by studies among patients with cancer.
The ESVS guideline10 strongly recommends switching from an LMWH to a DOAC after 3 to 6 months of treatment in patients with cancer-associated DVT. This is a grade I recommendation based on high-quality (grade A) evidence. The guideline also recommends DOACs for extended anticoagulation (as well as initial and principal phases of treatment) in select patients with cancer-associated DVT, whose cancer is not located in the gastrointestinal or genitourinary systems. This is a moderate-to-strong (grade IIa) recommendation based on high-quality (grade A) evidence.
The ASCO guideline11 recommends LMWHs, such as edoxaban or rivaroxaban, for a minimum duration of 6 months in patients with cancer-associated thrombosis. VKAs, although inferior, may be used if LMWHs or DOACs are not accessible. DOACs are associated with a higher risk of major bleeding in patients with gastrointestinal or genitourinary cancers. This is a strong recommendation based on high-quality evidence.
The NICE guideline13 suggests that current anticoagulation treatment be continued if well tolerated in patients with active cancer. However, this is a weak recommendation and was based on the opinion of the committee members due to the lack of evidence.
Limitations
The main limitation of this report is the lack of high-quality evidence regarding long-term pharmacological thromboprophylaxis in patients with cancer. Several of the recommendations were based on evidence of very low to low quality, and some were based on the expert opinion of the guideline panel. The authors of the included guidelines also noted the knowledge gap and the need for future research. The long-term studies were mostly 6 to 12 months in duration; therefore, clinical evidence regarding the benefits and risks of treatment longer than 12 months is limited. The authors of the guidelines also noted that studies specifically in patients with cancer were also limited. Because the strength of recommendations depends on the quality of the evidence identified, several recommendations were weak or conditional.
No guidelines were identified regarding long-term thromboprophylaxis for the other types of cancer-associated thrombosis such as arterial thrombosis or chronic DIC.
Conclusions and Implications for Decision- or Policy-Making
Six evidence-based guidelines were identified regarding long-term use of pharmacological thromboprophylaxis for the management of cancer-associated thrombosis.9-14 They were generally well developed, used rigorous methods, were clearly presented, and were reviewed by stakeholders. Three9,11,12 of the guidelines were specific to patients with cancer-associated thrombosis, and 310,13,14 were more general and considered all patients with a VTE disease. Although the guidelines were developed by North American, European, and international groups, their use was not specifically restricted to those countries. No guidelines were identified regarding the long-term management of other types of cancer-associated thrombosis such as arterial thrombosis and chronic DIC.
In 5 guidelines,11-14 long-term (i.e., > 6 months) anticoagulation is recommended for patients with active cancer and VTE to prevent recurrence of VTE. These are conditional or weak recommendations based on low-quality evidence or by expert consensus. Three guidelines recommend regular reassessments of the risks and benefits of anticoagulation after 6 months of treatment.9,11,13 Patient preferences should also be taken into consideration.9,13 This recommendation is made based on expert consensus due to lack of evidence. One guideline makes a conditional recommendation to continue anticoagulation for an indefinite period, rather than discontinue after a definite period, in patients with active cancer.12
Regarding the type of anticoagulant to be used for long-term thromboprophylaxis, 2 guidelines11,12 recommend LMWHs or DOACs for patients with active cancer; 1 guideline12 based this recommendation on very low–certainty evidence and the other guideline11 based the recommendation on high-certainty evidence. The degree of certainty of evidence reflects the confidence of the guideline panel that the effect estimate is close to the true effect, ranging from high to very low. If the patients cannot receive DOACs or LMWHs, VKAs may be used, as recommended by 2 guidelines.11,14 The authors of 2 guidelines10,11 reported that in patients with gastrointestinal or genitourinary cancers there is high-quality evidence that DOACs are associated with a higher risk of major bleeding; therefore, DOACs are recommended for long-term treatment in patients with cancer not located in these sites (moderate-to-strong recommendation based on high-quality evidence).10 Lastly, 1 guideline13 suggests continuing current anticoagulation in patients with cancer, if it is well tolerated. However, the recommendation is weak and based on expert opinion.
Overall, the recommendations made by these different guidelines were consistent; however, several recommendations were weak or conditional due to a lack of high-quality evidence. The authors of the guidelines suggested that the weak evidence base was due to limited studies conducted specifically in patients with active cancer. As most of the long-term studies ranged from 6 months to 12 months in duration, the risks and benefits of anticoagulation beyond 12 months is less clear. Some recommendations about the duration of anticoagulation were therefore made based on expert judgment and consensus. Future research on the benefits and harms of pharmacological thromboprophylaxis beyond 12 months in patients with active cancer is warranted. Because some decisions were recommended to be made based on patient preferences and individual risk-benefit profiles, patient engagement may play an important role in clinical decision-making.
References
1.Abdol Razak NB, Jones G, Bhandari M, Berndt MC, Metharom P. Cancer-associated thrombosis: an overview of mechanisms, risk factors, and treatment. Cancers (Basel). 2018;10(10):380. PubMed
2.Noble S, Pasi J. Epidemiology and pathophysiology of cancer-associated thrombosis. Br J Cancer. 2010;102 Suppl 1(Suppl 1):S2-S9.
3.Fernandes CJ, Morinaga LTK, Alves JL, Jr., et al. Cancer-associated thrombosis: the when, how and why. Eur Respir Rev. 2019;28(151):180119. PubMed
4.Timp JF, Braekkan SK, Versteeg HH, Cannegieter SC. Epidemiology of cancer-associated venous thrombosis. Blood. 2013;122(10):1712-1723. PubMed
5.Lee AY, Peterson EA. Treatment of cancer-associated thrombosis. Blood. 2013;122(14):2310-2317. PubMed
6.Wang T-F, Li A, Garcia D. Managing thrombosis in cancer patients. Res Pract Thromb Haemost. 2018;2(3):429-438. PubMed
7.Napolitano M, Mansueto MF, Raso S, Siragusa S. Quality of life in patients with cancer under prolonged anticoagulation for high-risk deep vein thrombosis: a long-term follow-up. Clin Appl Thromb Hemost. 2020;26:1076029620918290. PubMed
8.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
9.Farge D, Frere C, Connors JM, et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019;20(10):e566-e581. PubMed
10.Kakkos SK, Gohel M, Baekgaard N, et al. Editor's Choice - European Society for Vascular Surgery (ESVS) 2021 clinical practice guidelines on the management of venous thrombosis. Eur J Vasc Endovasc Surg. 2021;61(1):9-82. PubMed
11.Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol. 2020;38(5):496-520. PubMed
12.Lyman GH, Carrier M, Ay C, et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. Blood Adv. 2021;5(4):927-974. PubMed
13.National Institute for Health and Care Excellence. Venous thromboembolic diseases: diagnosis, management and thrombophilia testing. (NICE guideline 158) 2020; https://www.nice.org.uk/guidance/ng158. Accessed 2021 Oct 6.
14.Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic therapy for VTE disease: second update of the CHEST Guideline and Expert Panel report. Chest. 2021:S0012-3692(0021)01506-01503.
15.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Oct 6.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
ASH Guideline, 202112 | ||||||
Intended users: patients, health care providers such as hematologists, oncologists, internists, general practitioners, and other clinicians. Target population: Patients with cancer | All modalities for the prevention and treatment of VTE for patients with cancer. Relevant intervention: long-term (≥ 6 months) pharmacological thromboprophylaxis | Mortality, PE, DVT, major bleeding, | Evidence collected using a systematic literature review | Quality assessment of the studies done using Cochrane Risk of bias tool. Certainty of evidence was assessed using the GRADE approach. (ranging from very low to high certainty)a | Recommendations were formulated using Evidence-to-Decision framework. Recommendations were developed by discussion and consensus by an expert interdisciplinary panel on balance of benefit and harms, assumptions and preferences related to the decision. Recommendations are labelled strong or conditional. | External review by stakeholders, reviews by Guideline Oversight Subcommittee and the ASH Committee on Quality, and peer review (before publication) |
CHEST Guideline, 202114 | ||||||
Intended Users: Not reported Target Population: Patients with venous thromboses. Relevant target population: Patients with active cancer and VTE | All modalities for the prevention and treatment of venous thromboses, Relevant intervention: Long-term (≥ 6 months) pharmacological thromboprophylaxis in patients with cancer | Recurrence of VTE, major bleeding, all-cause mortality | Evidence collected using a systematic literature review | Certainty of evidence was assessed using the GRADE approach. (ranging from very low to high certainty)a | Recommendations were formulated using Evidence-to-Decision framework. Consensus by expert panel (modified Delphi technique) was used to finalize the recommendations. Strength of recommendations grouped as 2 categories: Strong and weak, based on the extend of confidence in the risk-benefit profile. | External review and peer review before publication |
ESVS Guideline, 202110 | ||||||
Intended Users: clinical care team Target Population: Patients with venous thromboses. Relevant target population: Patients with active cancer and VTE | All modalities for the prevention and treatment of venous thromboses, Relevant intervention: Long-term (≥ 6 months) pharmacological thromboprophylaxis in patients with cancer | Recurrence of VTE, major bleeding | Evidence collected using a systematic literature review | Evidence levels A: evidence from multiple RCTs or meta-analyses B: evidence from single RCT or large non-randomized studies C: consensus of experts’ opinion or evidence from small retrospective studies | Recommendations were formulated using consensus among the guideline development group. Class of Recommendations: Class I: Evidence and/or general agreement that a given treatment or procedure is beneficial, useful, and effective Class II: Conflicting evidence Class IIa: Weight of evidence/opinion is in favour usefulness/ efficacy Class IIb: Usefulness/ efficacy is less well established by evidence/opinion Class III: Evidence or general agreement that the given treatment or procedure is not useful/ effective, and in some cases may be harmful | Lay summaries were evaluated by patients External review not reported |
ASCO Guideline, 202011 | ||||||
Intended Users: Oncologists, surgeons, oncology nurses and pharmacists, other health care professional, patients, and caregivers. Target Population: Adult individuals with cancer | All modalities for the prevention and treatment of VTE for patients with cancer Relevant intervention: long-term (≥ 6 months) pharmacological thromboprophylaxis | Recurrence of VTE, major bleeding | Evidence collected using a systematic literature review | Assessed using GRADE approacha | Guideline developed using GRADE methodology. Consensus by expert panel (modified Delphi technique) was used in situations with limited or lack of evidence. Strength of recommendations grouped as 3 categories: strong, moderate, and weak, based on the extent of confidence in the risk-benefit profile. | By an expert panel; and peer review before publication |
NICE Guideline, 202013 | ||||||
Intended Users: Health care professionals, commissioners, and providers of VTE services, patients, caregivers, and family of patients Target Population: Adult individuals with suspected or confirmed VTE Relevant target population: Patients with active cancer | All modalities for the diagnosis and management of VTE Relevant intervention: long-term (≥ 6 months) pharmacological thromboprophylaxis | Recurrence of VTE, major bleeding | Evidence collected using a systematic literature review | ROBIS tool for systematic reviews, PROBAST tool for individual studies Quality of evidence assessed using GRADE approacha | Recommendations were formulated by discussion and consensus among the guideline development group. Strength of recommendations were graded as strong or weak based on the risk-benefit profile. Strength of recommendations were indicated in the wording. | Stakeholder review of the draft guideline. |
ITAC Guideline, 20199 | ||||||
Intended Users: Clinicians Target Population: Individuals with cancer | All modalities for the diagnosis and management of cancer-associated thrombosis Relevant intervention: long-term (≥ 6 months) pharmacological thromboprophylaxis | Recurrence of VTE, major and minor bleeding, mortality, thrombocyte-penia | Evidence collected using a systematic literature review | Quality of evidence assessed using GRADE approacha And graded from A (high) to D (very low) | Recommendations were formulated using consensus among the guideline development group. Expert judgment based on professional experience and consensus of experts were used in situations with limited or no evidence. Strength of recommendations grouped as 2 categories: Strong (Grade 1) and weak (grade 2), based on the extend of confidence in the risk-benefit profile. | Reviewed by an advisory panel, which included clinicians, nurses, and patient advocates. Additional peer review was conducted before publication in the journal. |
ASCO = American Society of Clinical Oncology; ASH = American Society of Hematology; CHEST = The American College of Chest Physicians; DVT = deep vein thrombosis; ESVS = European Society for Vascular Surgery; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; ITAC = International Initiative on Thrombosis and Cancer; NICE = National Institute for Health and Care Excellence; PE = pulmonary embolism; PROBAST = Prediction model Risk Of Bias ASsessment Tool; RCT = randomized controlled trial; ROBIS = A Risk of Bias Assessment Tool for Systematic Reviews; VTE = venous thromboembolism
aCertainty of evidence was assessed using the GRADE approach, with the following ratings:
Very low: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
Low: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Moderate: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
High: We are very confident that the true effect lies close to that of the estimate of the effect.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Guidelines Using AGREE II15
Item | ASH Guideline, 202112 | CHEST Guideline, 202114 | ESVS Guideline, 202110 | ASCO Guideline, 202011 | NICE Guideline, 202013 | ITAC Guideline, 20199 |
|---|---|---|---|---|---|---|
Domain 1: Scope and Purpose | ||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | ||||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Unclear | Yes- in the form of review of lay summary of guideline | Yes | Yes | Yes- in the form of review of summary of guideline |
6. The target users of the guideline are clearly defined. | Yes | Unclear | Yes | Yes | Yes | Yes |
Domain 3: Rigour of Development | ||||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Unclear | Unclear | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes | Unclear but likely | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Unclear | No | Yes | Yes | Unclear |
Domain 4: Clarity of Presentation | ||||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Unclear | Yes | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear | Unclear | Unclear | Yes | Yes | Yes- using a web-based app |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Unclear | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | Unclear | Yes | No |
Domain 6: Editorial Independence | ||||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes-though not available with the publication | Yes-though not available with the publication | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASCO = American Society of Clinical Oncology; ASH = American Society of Hematology; CHEST = The American College of Chest Physicians; ESVS = European Society for Vascular Surgery; ITAC = International Initiative on Thrombosis and Cancer; NICE = National Institute for Health and Care Excellence.
Note that this table has not been copy-edited.
Appendix 4: Main Study Findings and Authors’ Conclusions
Table 4: Summary of Recommendations: Duration of Anticoagulation
Guideline | Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|---|
Long-term vs. short-term anticoagulation | ||
ASH Guideline, 202112 | Recommendation: “For patients with active cancer and VTEs, the ASH guideline panel suggests long-term anticoagulation for secondary prophylaxis (>6 months) rather than short-term treatment alone (3-6 months).” (p.957)12 Evidence: One study that directly compared short-term vs. long-term anticoagulation and 1 single-arm study provided evidence to inform this recommendation. Long-term anticoagulation had no impact on mortality (1 study), may lower recurrent thrombotic events (i.e., VTE, PE, DVT) (2 studies) in patients with cancer. Long-term anticoagulation may increase the risk of major bleeding (1 study) in patients with cancer. 10 RCTs conducted in patients without cancer provided additional indirect evidence to inform this recommendation. The guideline authors pointed out the knowledge gap and the need for additional data on this topic. | Quality of evidence: Low certainty Strength of recommendation: Conditional |
Recommendation: “For patients with active cancer and VTEs receiving long-term anticoagulation for secondary prophylaxis, the ASH guideline panel suggests continuing indefinite anticoagulation over stopping after completion of a definitive period of anticoagulation” (p.957)12 Evidence: 1 single-arm study provided evidence to inform this recommendation. Indefinite duration of anticoagulation had no impact or mortality (1 study) and may lower recurrent thrombotic events (i.e., VTE, PE, DVT) (1 study) in patients with cancer. Indefinite duration of anticoagulation increased the risk of major bleeding (1 study) in patients with cancer. (small effect). 8 RCTs conducted in patients without cancer provided additional indirect evidence to inform this recommendation. The guideline authors pointed out the knowledge gap and the need for additional data on this topic. | Quality of evidence: Very low certainty Strength of recommendation: Conditional | |
CHEST Guideline, 202114 | Recommendation: “In patients with VTE diagnosed in the absence of transient provocation (unprovoked VTE or provoked by persistent risk factor), we recommend offering extended-phase anticoagulation with a DOAC.” (p.e4)14 Note: Active cancer was considered as a ‘persistent risk factor’ in the guideline Evidence: A meta-analysis of 15 studies provided the evidence to form this recommendation. It was unclear whether any or all of these studies were among patients with active cancer. | Quality of evidence: Moderate Strength of recommendation: Strong |
ASCO Guideline 202011 | Recommendation: “Anticoagulation with LMWH, DOACs, or VKAs beyond the initial 6 months should be offered to select patients with active cancer, such as those with metastatic disease or those receiving chemotherapy. Anticoagulation beyond 6 months needs to be assessed on an intermittent basis to ensure a continued favorable risk-benefit profile.” (p.505)11 Evidence: Recommendation was formulated based on informal consensus. The authors noted the limited evidence about the risk-benefit profile of anticoagulation beyond 6 months. Expert panel suggested that, in selected patients, long-term anticoagulation (> 6 months) should be considered because of the risk of recurrence. | Quality of evidence: Low Strength of recommendation: Weak to moderate |
NICE Guideline, 202013 | Recommendation: “Consider continuing anticoagulation beyond 3 months (6 months for people with active cancer) after an unprovoked DVT or PE. Base the decision on the balance between the person's risk of venous thromboembolism (VTE) recurrence and their risk of bleeding. Discuss the risks and benefits of long-term anticoagulation with the person, and take their preferences into account.” (p.19)13 Evidence: Unclear. | Quality of evidence: Unclear. The committee members noted that the quality of the overall evidence base was very low. Strength of recommendation: Weak |
ITAC Guideline, 20199 | Recommendation: “LMWH or direct oral anticoagulants should be used for a minimum of 6 months to treat established VTE in patients with cancer.” (p.e569)9 Evidence: 1 meta-analyses (of 16 studies) provided evidence to formulate this recommendation. Compared to VKA, LMWH was associated with a statistically significant (42%) reduction in the risk of recurrence of VTE, and no difference were found in the rates of major or minor bleeding, 12-month mortality or thrombocytopenia (8 studies). The meta-analysis did not find any significant differences between VKA and DOACs for these outcomes (5 studies). | Quality of evidence: High (level A) Strength of recommendation: Strong (grade 1) |
Recommendation: “After 6 months, termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists) should be based on individual evaluation of the benefit–risk ratio, tolerability, drug availability, patient preference, and cancer activity (guidance in the absence of data).” (p.e569)9 Evidence: Recommendation was formulated based on expert judgment and consensus due to limited/lack of evidence. | Quality of evidence: NA Strength of recommendation: NA | |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASCO = American Society of Clinical Oncology; ASH = American Society of Hematology; CHEST = The American College of Chest Physicians; DOAC = direct oral anticoagulant; DVT = deep vein thrombosis; ESVS = European Society for Vascular Surgery; ITAC = International Initiative on Thrombosis and Cancer; LMWH = low-molecular-weight heparin; NA = not applicable; NICE = National Institute for Health and Care Excellence; PE = pulmonary embolism; VKA = vitamin K antagonist; VTE = venous thromboembolism.
Note that this table has not been copy-edited.
Table 5: Summary of Recommendations: Choice of Anticoagulants for Long-Term Thromboprophylaxis
Guideline | Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|---|
ASH Guideline, 202112 | Recommendation: “For patients with active cancer and VTEs requiring long-term anticoagulation (>6 months), the ASH guideline panel suggests using DOACs or LMWH.” (p.957)12 Evidence: One RCT provided evidence to inform this recommendation. Compared to LMWHs, DOACs may lower recurrent thrombotic events (i.e., VTE, PE, DVT) (1 study). DOACs may also increase the risk of mortality and major bleeding (1 study). | Quality of evidence: Very low certainty Strength of recommendation: Conditional |
CHEST Guideline, 202114 | Recommendation: “In patients with VTE diagnosed in the absence of transient risk factor (unprovoked VTE or provoked by a persistent risk factor) who cannot receive a DOAC, we suggest offering extended-phase anticoagulation with a VKA.” (p.e4)14 Note: Active cancer was considered as a ‘persistent risk factor’ in the guideline. Evidence: A meta-analysis of 15 studies provided the evidence to form this recommendation. It was unclear whether any or all of these studies were among patients with active cancer. Remarks: “The recommendation to offer extended-phase anticoagulation would not automatically imply that all patients with unprovoked VTE receive extended therapy. Patient preference and predicted risk of recurrent VTE or bleeding should also influence the decision to proceed with, or continue, extended-phase anticoagulation therapy.” (p.e4)14 “Patients who receive extended-phase anticoagulation should have this decision re-evaluated at least on an annual basis, and at times of significant change in health status.” (p.e4)14 “Extended-phase anticoagulation does not have a predefined stop date. However, studies of extended-phase anticoagulation followed patients for durations of about 2 to 4 years. Although most patients in these studies did not stop anticoagulation therapy at the end of follow-up, the risk-to-benefit balance of continuing extended anticoagulation therapy beyond this time is uncertain.” (p.e4)14 | Quality of evidence: Moderate Strength of recommendation: Weak |
ESVS Guideline, 202110 | Recommendation: “For patients with active cancer-associated deep vein thrombosis, switching from a low-molecular-weight heparin to an oral anticoagulant is recommended after three to six months of treatment for extended treatment.” (p.62)10 Evidence: From consensus. In a meta-analysis of 4 studies, it was found that DOACs are more effective that dalteparin in preventing recurrence of VTE. There were no significant differences in the rates of major bleeding between the 2 groups of drugs. | Quality of evidence: high (level A) Strength of recommendation: class I (given treatment or procedure is beneficial, useful, and effective) |
Recommendation: “In selected patients with cancer-associated deep vein thrombosis, with the malignancy not located in the gastrointestinal or genitourinary systems, an approved direct oral anticoagulant for initial, principal, and extended treatment should be considered.” (p.62)10 Evidence: 5 studies provided evidence to form this recommendation. | Quality of evidence: High (level A) Strength of recommendation: Class IIa (There is some conflicting evidence but, weight of evidence is favours a benefit of treatment) | |
ASCO Guideline, 202011 | Recommendation: “For long-term anticoagulation, LMWH, edoxaban, or rivaroxaban for at least 6 months are preferred because of improved efficacy over vitamin K antagonists (VKAs). VKAs are inferior but may be used if LMWH or DOACs are not accessible. There is an increase in major bleeding risk with DOACs, particularly observed in GI and potentially genitourinary malignancies. Caution with DOACs is also warranted in other settings with high risk for mucosal bleeding. Drug-drug interaction should be checked before using a DOAC.” (p.505)11 Evidence: Evidence from 4 meta-analyses found that LMWH is more effective than VKAs in reducing risk of recurrence of VTE. Evidence from 3 MAs showed that risk of recurrent VTE was similar in DOACs and LMWHs; however, DOACs were associated with a higher risk of major bleeding. Evidence from 8 MAs that found that the risk of recurrent VTE and major bleeding were not different between DOACs and VKAs (1 MA found a significant benefit with rivaroxaban) However, these studies were not specific to patients with active cancer, so findings should be interpreted with caution. | Quality of evidence: High Strength of recommendation: Strong |
NICE Guideline, 202013 | Recommendation: For people with renal impairment, active cancer, established triple positive antiphospholipid syndrome or extreme body weight (less than 50 kg or more than 120 kg), consider carrying on with the current treatment if it is well tolerated.”(p.19)13 Evidence: Unclear Guideline authors noted the lack of evidence on long-term treatment for patients with active cancer and other conditions. Committee members suggested continuing the current treatment for this group if the current treatment is well tolerated, after considering patient preferences and clinical situation. | Quality of evidence: Unclear. The committee members noted that the quality of the overall evidence base was very low. Strength of recommendation: Weak |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASCO = American Society of Clinical Oncology; ASH = American Society of Hematology; CHEST = The American College of Chest Physicians; DOAC = direct oral anticoagulant; DVT = deep vein thrombosis; ESVS = European Society for Vascular Surgery; ITAC = International Initiative on Thrombosis and Cancer; LMWH = low-molecular-weight heparin; MA = meta-analysis; NA = not applicable; NICE = National Institute for Health and Care Excellence; PE = pulmonary embolism; VKA = vitamin K antagonist; VTE = venous thromboembolism.
Note that this table has not been copy-edited.
Appendix 5: References of Potential Interest
Review Articles
Streiff MB, Abutalib SA, Farge D, Murphy M, Connors JM, Piazza G. Update on guidelines for the management of cancer-associated thrombosis. Oncologist. 2021;26(1):e24-e40. PubMed
Lee AY, Peterson EA, Wu C. Clinical practice guidelines on cancer-associated thrombosis: a review on scope and methodology. Thromb Res. 2016;140 Suppl 1:S119-27. PubMed
Lyman GH, Kuderer NM. Clinical practice guidelines for the treatment and prevention of cancer-associated thrombosis. Thromb Res. 2020;191 Suppl 1:S79-S84. PubMed
Consensus Statements
Jimenez-Fonseca P, Carmona-Bayonas A, Calderon C, et al. FOTROCAN Delphi consensus statement regarding the prevention and treatment of cancer-associated thrombosis in areas of uncertainty and low quality of evidence. Clin Transl Oncol. 2017;19(8):997-1009. PubMed
Guidance Documents, Methodology Not Reported
Kirschner M, N do O Hartmann, Parmentier S, et al. Primary thromboprophylaxis in patients with malignancies: daily practice recommendations by the Hemostasis Working Party of the German Society of Hematology and Medical Oncology (DGHO), the Society of Thrombosis and Hemostasis Research (GTH), and the Austrian Society of Hematology and Oncology (OGHO). Cancers (Basel). 2021;13(12):2905. PubMed
Wang TF, Zwicker JI, Ay C, et al. The use of direct oral anticoagulants for primary thromboprophylaxis in ambulatory cancer patients: Guidance from the SSC of the ISTH. J Thromb Haemost. 2019;17(10):1772-1778. PubMed
Streiff MB, Holmstrom B, Angelini D, et al. NCCN Guidelines Insights: cancer-associated venous thromboembolic disease, Version 2.2018. J Natl Compr Canc Netw. 2018;16(11):1289-1303. PubMed
Quintanar T, Font C, Gallardo E, Barba R, Obispo B, Diaz-Pedroche C. Consensus statement of the Spanish Society of Internal Medicine and the Spanish Society of Medical Oncology on secondary thromboprophylaxis in patients with cancer. Clin Transl Oncol. 2021;23(4):697-708. PubMed
Munoz Martin AJ, Gallardo Diaz E, Garcia Escobar I, et al. SEOM clinical guideline of venous thromboembolism (VTE) and cancer (2019). Clin Transl Oncol. 2020;22(2):171-186. PubMed
Tomkowski W, Kuca P, Urbanek T, et al. Venous thromboembolism-recommendations on the prevention, diagnostic approach and management. The 2017 Polish Consensus Statement. Acta Angiologica. 2017;23(2):35-71.
Wojtukiewicz MZ, Sierko E, Tomkowski W, et al. Guidelines for the prevention and treatment of venous thromboembolism in non-surgically treated cancer patients. Nowotwory. 2016;66(4):326-350.
Additional References
Carrier M, Blais N, Crowther M, et al. Treatment algorithm in cancer-associated thrombosis: Canadian expert consensus. Curr Oncol. 2018;25(5):329-337. PubMed
Napolitano M, Mansueto MF, Raso S, Siragusa S. Quality of life in patients with cancer under prolonged anticoagulation for high-risk deep vein thrombosis: a long-term follow-up. Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620918290. PubMed
Pulmonary embolism diagnosis & treatment guideline. Seattle (WA): Kaiser Permanente; 2020: https://wa.kaiserpermanente.org/static/pdf/public/guidelines/pulmonary-embolism.pdf. Accessed 2021 Oct 6.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca