CADTH Health Technology Review
Medication Administration With Inhalers or Nebulizers
Rapid Review
Authors: Khai Tran, Aleksandra Grobelna
Abbreviations
AE
adverse event
CO2
carbon dioxide
COPD
chronic obstructive pulmonary disease
DPI
dry powder inhaler
ED
emergency department
FEV1
forced expiratory volume in the first second
ICU
intensive care unit
MDI
metered-dose inhaler
O2
oxygen
RCT
randomized controlled trial
SR
systematic review
Key Messages
Delivery of medication via metered-dose inhalers to children or adults with asthma, or adults with chronic obstructive pulmonary disease at emergency departments or intensive care units, may be as effective as nebulizers in terms of clinical parameters and health care resource use.
Limited data on adverse events showed no significant differences between metered-dose inhalers and nebulizers.
No evidence was found on the clinical effectiveness of dry powder inhalers in comparison with nebulizers or metered-dose inhalers.
No evidence was found on the cost-effectiveness of medication administration via metered-dose inhalers, nebulizers, or dry powder inhalers in comparison with each other.
No evidence-based guidelines with recommendations regarding the comparative use of metered-dose inhalers, dry powder inhalers, or nebulizers for administration of medication were identified.
Context and Policy Issues
The Canadian Chronic Disease Surveillance System estimated that about 3.8 million Canadians aged 1 year or older were living with asthma, and about 2.0 million Canadians aged 35 years or older were living with chronic obstructive pulmonary disease (COPD), in 2011 to 2012.1 Medication administration through aerosol delivery is a crucial component for caring patients with respiratory distress such as asthma and COPD when they present at acute care settings such as emergency departments (EDs) or intensive care units (ICUs).2 There are 3 classes of medical aerosol devices: nebulizers, pressurized metered-dose inhalers (MDI), and dry power inhalers (DPI).3 Nebulizers are further divided by design into pneumatic jet nebulizers, ultrasonic nebulizers, and vibrating mesh nebulizers.3 In addition, there are different types, brands, and models of nebulizers with different performance characteristics.4
Nebulizers are popular aerosol-generating devices in acute care settings.4 The advantages of nebulizers are the ability to be used with a broad range of drug solutions and the convenience for patients who have difficulties coordinating themselves or following instructions such as infants, small children, and very old, debilitated, or distressed patients.4 The disadvantages of nebulizers are that the equipment may be large and cumbersome and requires a power source to operate, that there is potential for drug exposure to patients’ eyes (with face mask delivery) or to caregivers standing nearby, and that there is potential for contamination with improper handling or inadequate cleaning.4
The MDI was designed to deliver precise doses of specific drug formulations.4 The device consists of a canister, the medication, a propellant, a metering valve, a mouthpiece, and an actuator.4 Unlike nebulizers, an MDI does not require drug preparation, and its internal components are difficult to contaminate.4 Other advantages of MDIs are that the device is portable, convenient with multiple doses contained in a single device, and reproducible in terms of emitted doses.4 Several disadvantages of MDIs include the requirement of patients’ hand-breath coordination, activation, proper inhalation, and breath-hold, fixed-drug concentrations and doses, and negative reactions to propellants in some patients.4
The DPI was developed to overcome the hand-breath coordination required in the MDI and is propellant free, whereby drug delivery to the lungs is driven by inspiration.4 The device is portable, with a built-in dose counter.4 However, the patient’s inspiratory flow should be high enough to draw the drug from the device.4 Further, patients should know how the device works and how to use it for its proper application; for instance, they should not exhale into the mouthpiece, as humidity can impact the effect of the medication.4
Historically, it was believed that nebulizers were more effective than inhalers, and nebulizers have been the preferred choice of clinicians to treat patients in acute and critical care settings.2,4 However, with the advantages and disadvantages of each type of aerosol devices, it is unclear which 1 is more effective than the others, especially given that there are multiple factors to consider such as clinical settings, device and drug availability, devices with the ability to deliver multiple medications versus a single medication, patients’ ability to use a selected device correctly, drug administration time, costs, resource utilization, and patient and caregiver satisfaction.5
The aim of this report is to summarize the evidence regarding the clinical effectiveness and cost-effectiveness of nebulizers, MDIs, and DPIs in comparison with each other for administration of medication in hospital or ED settings. This report also aims to summarize the recommendations from evidence-based guidelines regarding the comparative use of these devices.
Research Questions
What is the clinical effectiveness of medication administration via metered-dose inhalers versus nebulizers?
What is the cost-effectiveness of medication administration via metered-dose inhalers versus nebulizers?
What is the clinical effectiveness of medication administration via dry powder inhalers versus nebulizers?
What is the cost-effectiveness of medication administration via dry powder inhalers versus nebulizers?
What is the clinical effectiveness of medication administration via dry powder inhalers versus metered-dose inhalers?
What is the cost-effectiveness of medication administration via dry powder inhalers versus metered-dose inhalers?
What are the evidence-based guidelines regarding dry powder inhalers, nebulizers, and metered-dose inhalers for medication administration?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were metered-dose inhalers, dry powder inhalers, and nebulizers. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English language documents published between January 1, 2016 and September 23, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients (any age) in hospital unit or ED settings |
Intervention | Q1 to Q2: Metered-dose (e.g., multi-dose) inhaler administration Q3 to Q6: Dry powder inhaler administration Q7: Metered-dose inhaler, dry powder inhaler, or nebulizer administration |
Comparator | Q1 to Q4: Nebulizer administration Q5 to Q6: Metered-dose inhalers Q7: Not applicable |
Outcomes | Q1, Q3, and Q5: Clinical effectiveness (e.g., length of hospital stay, symptom reduction, safety, and adverse events [e.g., tachycardia, dizziness, drowsiness, nasal itching, nosebleed, nose burning, stomachache]) Q2, Q4, and Q6: Cost-effectiveness (e.g., cost per quality-adjusted life-year, incremental cost-effectiveness ratios) Q7: Recommendations regarding the comparative use of metered-dose inhalers, dry powder inhalers, or nebulizers for administration of medication (i.e., if 1 should be used over the others) |
Study designs | HTAs, SRs, RCTs, non-randomized studies, economic evaluations, and guidelines |
ED = emergency department; HTA = health technology assessment; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications, or if they were published before 2016. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews (SRs). Guidelines with unclear methodology and those that did not provide recommendations regarding the comparative use of MDIs, DPIs, or nebulizers for administration of medication were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)6 for SRs, and the Downs and Black checklist7 for randomized and non-randomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
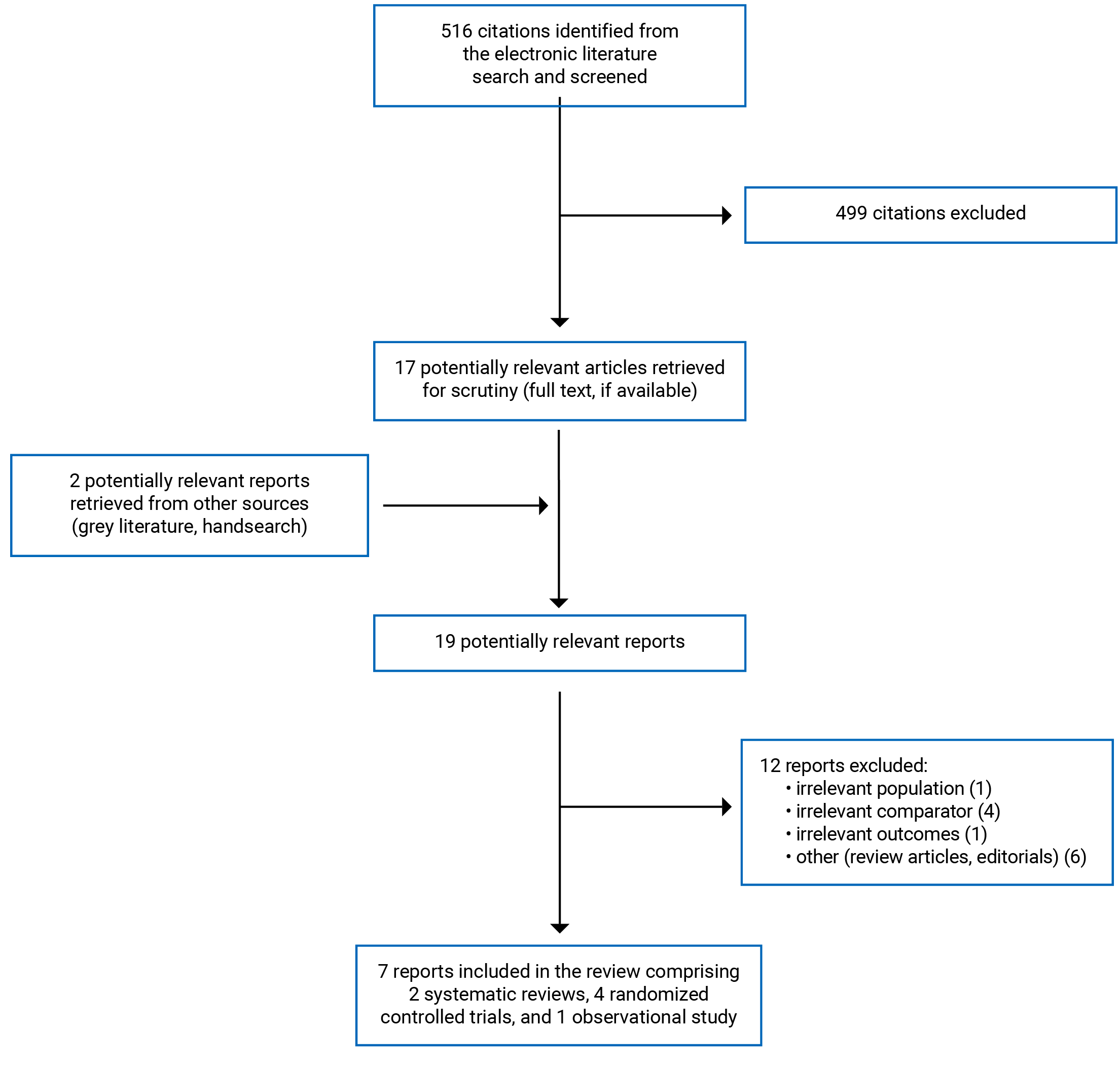
A total of 516 citations were identified in the literature search. Following screening of titles and abstracts, 499 citations were excluded, and 17 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 12 publications were excluded for various reasons, and 7 publications met the inclusion criteria and were included in this report. These comprised 2 SRs, 4 RCTs, and 1 non-randomized study. Appendix 1 presents the PRISMA8 flow chart of the study selection.
Summary of Study Characteristics
The detailed characteristics of the included SRs9,10 (Table 2) and primary clinical studies11-15 (Table 3) are provided in Appendix 2.
Study Design
The SR by Roncada et al. (2018)9 identified and included 9 RCTs (N = 1,307) in the meta-analyses. The RCTs were published between 1993 and 2006. The SR by van Geffen et al. (2016)10 identified and included 8 RCTs (N = 250) in the meta-analysis. The RCTs were published between 1985 and 2007.
The 5 included primary studies comprised 4 RCTs11-14 and 1 prospective cohort study.15 The RCTs11-14 were published between 2016 and 2019, while the prospective cohort study15 was published in 2021.
Country of Origin
The SRs were conducted by authors from Brazil9 and the Netherland.10 The primary studies were conducted by authors from Paraguay,11 US,12,15 Egypt,13 and Sweden.14
Patient Population
Patients in the RCTs included in the SR by Roncada et al. (2018)9 were children with mild-to-moderate asthma exacerbations treated at EDs. Patients in the included RCTs had mean age of 6.8 years, and 55% were male. Patient baseline characteristics were similar between treatment groups in term of age, heart rate, respiratory rate, O2 saturation, asthma clinical score, and forced expiratory volume in the first second (FEV1).
Patients in the RCTs included in the SR by van Geffen et al. (2016)10 were adult patients with COPD exacerbations treated at EDs. Three of the 8 included RCTs reported the mean age which were 55, 68, and 71 years; the other 5 RCTs did not provide age information. Other patient baseline characteristics were only reported as comparable between groups without any details provided.
Patients in the included primary studies were children with mild-to-moderate12,14,15 or moderate-to-severe11 asthma exacerbations treated at EDs11,12,14,15 or adult patients with asthma treated at ICU.13 The mean age of the children ranged from 23 months to 10 years, and the percentage of male ranged from 36 to 69. The adult population had a mean age of 61 years, and 50% of the population were male.
Interventions and Comparators
The SR by Roncada et al. (2018)9 included RCTs comparing the administration of a bronchodilator (i.e., salbutamol) by 2 inhalation techniques (i.e., MDI and nebulizer) for asthma treatment at pediatric ED units. The SR by van Geffen et al. (2016)10 included RCTs comparing pressurized MDIs with a spacer versus nebulizers as devices delivering different beta2-agonists and anticholinergics for the treatment of adult patients with COPD exacerbations in hospital ED settings.
Four included primary studies11,12,14,15 compared MDIs with nebulizers for the treatment of children with asthma exacerbations at EDs, and 1 primary study13 compared MDIs with nebulizers for the treatment of adult patients with asthma at ICU. Types of MDIs included MDIs with a valved-holding chamber,11 MDIs with AeroChamber Vent with or without humidification,13 and MDIs with a spacer.14 Two studies12,15 did not report the type of MDIs used. Types of nebulizers included breath-actuated nebulizers12 and vibrating mesh nebulizers with or without humidification.13 Three studies11,14,15 did not report the type of nebulizers used. The types of bronchodilators used for the treatment of asthma were salbutamol plus ipratropium bromide,11 albuterol,12,15 and salbutamol alone.14 One study13 did not report the type of medications used.
Outcomes
The clinical outcomes considered in the included SRs9,10 and primary studies11-15 can be broadly categorized as clinical parameters, health care resource use, and adverse events (AEs).
The clinical parameters included the heart rate,9,11,13,14 respiratory rate,9,13,14 O2 saturation,9-11,14 asthma severity score,9,11-13 change in FEV1,10 change in the dyspnea score in the first 24 hours after dosing,10 O2 partial pressure,13 CO2 partial pressure,13 pH,13 and skeletal muscle strength (i.e., grip).15 The asthma severity score evaluates the respiratory rate, presence of wheezing, cyanosis, chest retractions, and transcutaneous O2 saturation, with scores ranging from 0 to 15 points (i.e., mild exacerbation: < 7; moderate exacerbation: 8 to 11; severe exacerbation: ≥ 12).
Outcomes on health care resource use included ED or ICU length of stay,12-14 hospital admission rate,10-12,14 length of hospital stay,10 and mechanical ventilation days.13
One SR10 and 1 primary study12 reported on AEs.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of the included SRs9,10 (Table 4) and primary clinical studies11-15 (Table 5) are provided in Appendix 3.
Both SRs9,10 were explicit in their objectives and inclusion criteria for the review, selection of the study designs for inclusion, and included a comprehensive literature search strategy. Providing details of the literature search strategy increases the reproducibility of the review. Study selection and data extraction were performed in duplicate in 1 SR,10 but no such details were reported in the other SR.9 Performing these activities in duplicate reduces the likelihood of missing relevant studies and making errors in data extraction. One SR10 provided a list of excluded studies, the reasons for exclusion, and the sources of funding for the included studies, while the other SR did not.9 Not having a list of, or the justifications for, the excluded studies makes it impossible to assess whether any relevant articles were excluded and if so, for what reasons. Funding received from industry can introduce bias in favour of the intervention. One SR10 assessed the methodological quality of the included studies using the Cochrane risk of bias tool, while the other SR9 did not. Therefore, it was not possible to assess the trustworthiness of the meta-analysis findings from the latter SR.9 Both SR9,10 used the software Review Manager (RevMan) in the meta-analyses, and the authors of both SRs provided a discussion of the heterogeneity observed in the results, which was the main limitation of the meta-analyses. The review authors of both SRs9,10 declared that no funding was received for the reviews. Conflicts of interest were also declared in both SRs.9,10 Overall, 1 SR9 was of moderate methodological quality, and the other10 was of high methodological quality.
With respect to reporting, all primary studies including 4 RCTs11-14 and 1 prospective cohort study15 clearly described the objective of the study, the interventions of interest, the main outcomes, and the main findings of the study. The baseline characteristics of the patients included in the study were clearly described in all studies, except in 1 study.13 Without a clear description of patient baseline characteristics, it was not possible to assess if there were potential confounders that could potentially affect the interpretation of the results. Three studies11,13,14 had no patients lost to follow-up, 1 study15 did not report on patients lost to follow-up, and 1 study12 had about 9% of patients excluded due to various types of violation. The characteristics of these patients were not reported, and the analyses did not account for those patients. Not accounting for patients lost to follow-up in the analyses may have resulted in risk of attrition bias. Actual P values (i.e., P values) and the random variability in the data for the main outcomes (e.g., confidence interval, standard deviation, or interquartile range) were reported in all included studies.11-15 Regarding external validity, it was unclear if the patients were representative of the entire population from which they were recruited in 4 included studies,11,13-15 as their study populations were relatively small (i.e., 50 to 103 patients in total). For internal validity, 2 RCTs12,13 were non-blinded, 1 RCT14 had only the assessors blinded, and 1 RCT11 was double-blinded to the investigators and patients. The lack of blinding may result in risk of bias for selection, performance, and detection. Three RCTs12-14 did not report allocation concealment, the lack of which may result in risk of selection bias. The prospective cohort study15 may have been prone to high risk of bias for selection, performance, and detection due to the nature of the observational study design. However, confounding variables were identified and adjusted for in the analyses of this study.15 Appropriate statistical tests were used to assess the main outcomes, and reliable and validated outcome measures were used, in all studies.11-15 Patients in different intervention groups appeared to be recruited from the same population and over the same period of time in all studies, except in 1 study.15 Two13,15 of the 5 included studies did not report whether sample size calculations were performed, and it is unclear whether the non-significant differences in certain outcomes were because the studies were underpowered for those outcomes. Patient compliance was not reported in all included studies.11-15 Overall, 3 included studies11,12,14 were of moderate methodological quality, and 2 studies13,15 were of low methodological quality.
Summary of Findings
Appendix 4 presents the main study findings of the SRs9,10 and primary clinical studies.11-15 The findings are presented by outcome, which are clinical parameters (Table 6), health care resource use (Table 7), and AEs (Table 8).
Clinical Effectiveness of Medication Administration via Metered-Dose Inhalers Versus Nebulizers
Clinical Parameters in Pediatric Patients With Asthma Exacerbations Treated in EDs By MDIs Versus Nebulizers
Meta-analysis results of the SR by Roncada et al. (2018)9 found no statistically significant differences between MDIs with a spacer and nebulizers to administer a Beta2 agonist (i.e., salbutamol) in children with mild-to-moderate asthma exacerbations for the heart rate, respiratory rate, O2 saturation (P = 0.98), and asthma severity score.
The RCT by Iramain et al. (2018)11 showed that children with moderate-to-severe asthma exacerbations in the MDI group had a statistically significantly lower heart rate than those in the nebulizer group from 30 minutes of treatment (P < 0.003) up to until 4 hours of treatment (P < 0.00001). Both groups received ipratropium bromide between salbutamol treatments. Further, the MDI group had statistically significantly higher O2 saturation than those in the nebulizer group from 90 minutes of treatment (P < 0.00001) up to 4 hours of treatment (P < 0.00001). The asthma severity score was statistically significantly better (i.e., lower) from 60 minutes of treatment (P < 0.00001) up to 4 hours of treatment (P < 0.00001) in the MDI group than in the nebulizer group.
The RCT by Snider et al. (2018)12 found no statistically significant differences in post-treatment asthma severity scores between MDIs and breath-actuated nebulizers that delivered albuterol to children with mild-to-moderate asthma exacerbations treated at EDs.
The RCT by Mitselou et al. (2016),14 comparing MDI-spacers with nebulizers in delivering salbutamol to children with virus-induced wheezing or mild-to-moderate asthma exacerbations treated at EDs, found no statistically significant differences between groups in the heart rate, respiratory rate, and O2 saturation.
The prospective cohort study by Burger et al. (2020),15 comparing MDIs and nebulizers as the route of administration in delivering albuterol for treatment of children with mild-to-moderate asthma exacerbations at EDs, showed that children treated with nebulizer-delivered albuterol were associated with decreased skeletal muscle strength (measured by hand grip); whereas albuterol administration via MDIs was associated with no change in skeletal muscle strength. After adjustment for age and pre-treatment asthma severity scores, children treated with nebulizers had a 12.9% decrease in skeletal muscle strength compared with those treated with MDIs.
Clinical Parameters in Adult Patients With Asthma Exacerbations Treated in ICU By MDIs Versus Nebulizers
The RCT by Moustafa et al. (2017)13 found no statistically significant differences in various clinical parameters (i.e., heart rate, respiratory rate, asthma severity score, O2 partial pressure, CO2 partial pressure, and pH) between MDIs and nebulizers with or without humidification for the treatment of adult patients with asthma exacerbations at ICU.
Clinical Parameters in Adult Patients With COPD Exacerbations Treated in EDs By MDIs Versus Nebulizers
In the SR by van Geffen et al. (2016),10 comparing bronchodilators delivered by MDIs versus nebulizers for COPD exacerbations in adults treated in EDs, 1 included RCT showed no statistically significant difference in O2 saturation between the groups at different time points (i.e., 30 minutes, 6 hours, 24 hours, 48 hours, or 10 days). For the change in FEV1 1 hour after dosing, 2 RCTs found no statistically significant difference between the groups. For the change in FEV1 closest to 1 hour after dosing, a meta-analysis of 4 RCTs showed a statistically significant difference of 83 mL in favour of the nebulizer treatment (P = 0.03). For the change in the dyspnea score in the first 24 hours after dosing, 4 included RCTs reported no statistically significant difference between the groups.
Health Care Resource Use in Pediatric Patients With Asthma Exacerbations Treated in EDs By MDIs Versus Nebulizers
The RCT by Iramain et al. (2018)11 showed that statistically significantly fewer children with an asthma severity score of at least 7 in the MDI group needed to be hospitalized at the end of 4 hours of treatment compared with those in the nebulizer group (5.8% versus 27.5%; P = 0.003).
The RCT by Snider et al. (2018)12 found no statistically significant differences in ED length of stay and hospital admission rates between MDIs and breath-actuated nebulizers that delivered albuterol to children with mild-to-moderate asthma exacerbations treated at EDs, after adjustment for baseline asthma severity, ipratropium, and elevated versus standard dosing of albuterol.
The RCT by Mitselou et al. (2016)14 found no statistically significant difference in ED length of stay and hospital admission rates between MDI-spacers and nebulizers in delivering salbutamol to children with virus-induced wheezing or mild-to-moderate asthma exacerbations treated at EDs.
Health Care Resource Use in Adult Patients With Asthma Exacerbations Treated in ICU By MDIs Versus Nebulizers
The RCT by Moustafa et al. (2017)13 found that patients with asthma treated with vibrating mesh nebulizers had statistically significantly shorter ICU length of stay by about 1.42 days compared to those treated with MDIs (P = 0.039), with or without humidification. However, there was no statistically significant difference between the groups in mechanical ventilation days.
Health Care Resource Use in Adult Patients With COPD Exacerbations Treated in EDs By MDIs Versus Nebulizers
In the SR by van Geffen et al. (2016),10 1 RCT showed no statistically significant difference in hospital admission rates, and the other RCT showed no statistically significant difference in the length of hospital stay between the groups.
Adverse Events in Pediatric Patients With Asthma Exacerbations Treated in EDs By MDIs Versus Nebulizers
The RCT by Snider et al. (2018)12 found that there was a statistically significantly higher incidence of tachycardia in the nebulizer group compared with the MDI group (P = 0.002) for the treatment of children with mild-to-moderate asthma exacerbations in EDs. There were no statistically significant differences between the groups in nausea or vomiting.
Adverse Events in Adult Patients With COPD Exacerbations Treated in EDs By MDIs Versus Nebulizers
In the SR by van Geffen et al. (2016),10 3 RCTs reported AEs. One RCT reported 2 AEs in the nebulizer group, but the nature of the events was not reported. One RCT reported that there was 1 patient developing a marked fall in saturation from 88% to 73%, 15 minutes after taking the nebulizer treatment. One RCT reported 2 patients developing a pneumothorax and 1 patient requiring mechanical ventilation in the nebulizer group, and 3 patients developing a pneumothorax in the MDI group. The authors of the SR10 concluded that there were no significant differences between the groups concerning AEs in these studies.
Cost-Effectiveness of Medication Administration Via Metered-Dose Inhalers Versus Nebulizers
No studies comparing the cost-effectiveness of medication administration with MDIs versus nebulizers were identified; therefore, no summary can be provided.
Clinical Effectiveness of Medication Administration Via Dry Powder Inhalers Versus Nebulizers
No studies comparing the clinical effectiveness of medication administration with DPIs versus nebulizers were identified; therefore, no summary can be provided.
Cost-Effectiveness of Medication Administration Via Dry Powder Inhalers Versus Nebulizers
No studies comparing the cost-effectiveness of medication administration with DPIs versus nebulizers were identified; therefore, no summary can be provided.
Clinical Effectiveness of Medication Administration Via Dry Powder Inhalers Versus Metered-Dose Inhalers
No studies comparing the clinical effectiveness of medication administration with DPIs versus MDIs were identified; therefore, no summary can be provided.
Cost-Effectiveness of Medication Administration Via Dry Powder Inhalers Versus Metered-Dose Inhalers
No studies comparing the cost-effectiveness of medication administration with DPIs versus MDIs were identified; therefore, no summary can be provided.
Guidelines
No evidence-based guidelines with recommendations regarding the comparative use of MDIs, DPIs, or nebulizers for administration of medication were identified; therefore, no summary can be provided.
Limitations
The main limitation of both SRs9,10 was the substantial heterogeneity in patient baseline characteristics and significant variation in the type and dose of bronchodilators, as well as different frequencies of treatment among included studies. There was a lack of standardization of pulmonary function evaluations that were used to show improvements in lung function markers with the use of both inhalation techniques. The SR by van Geffen et al. (2016)10 included a low number of studies, each of which had relatively small numbers of patients. Some evidence in both SRs9,10 was relatively old. The oldest study was published in 1993 in 1 SR9 and in 1985 in the other SR.10 This may influence the results, since new devices may work in a different way than those used more than 28 years ago. Important clinical parameters such as hospital readmission in 30 days, change in peak FEV1, and change in quality of life were not available from the included studies. The type of nebulizers, compressors, and pressurized MDIs used in the studies might influence the results. Thus, these limitations might affect the generalizability of the findings.
A general limitation of the included primary clinical studies was that lung function was not evaluated. There was no follow-up on patients after being discharged from EDs. No data on the age of disease onset, previous severe exacerbations, and hospitalization were reported. The lack of these data prevents assessing whether they might have influenced the results.
This review did not identify any studies involving DPIs. Also, this review did not identify any economic evaluation studies or evidence-based guidelines with recommendations regarding the comparative use of MDIs, DPIs, or nebulizers for administration of medication. The findings in this review may have limited applicability and generalizability to the Canadian context.
Conclusions and Implications for Decision- or Policy-Making
This report identified 2 SRs9,10 and 5 primary clinical studies,11-15 including 4 RCTs11-14 and 1 prospective cohort study.15
Findings from 1 SR9 and 2 RCTs12,14 involving children with mild-to-moderate asthma exacerbations treated at EDs showed no significant differences between MDIs and nebulizers in post-treatment clinical parameters including the heart rate, respiratory rate, O2 saturation, and asthma severity score. In this population, evidence from 2 RCTs12,14 showed no significant differences between MDIs and nebulizers in health care resource use such as ED length of stay and hospital admission rates. One prospective cohort study15 reported that children treated with nebulizers had a 12.9% decrease in skeletal muscle strength compared with those treated with MDIs. With respect to AEs, 1 RCT12 reported a significantly higher incidence of tachycardia in the nebulizer group compared with the MDI group, but there were no significant differences between groups in nausea or vomiting.
Findings from 1 RCT11 involving children with moderate-to-severe asthma exacerbations treated at EDs showed that patients in the MDI group had a significantly lower heart rate, higher O2 saturation level, and better asthma severity score compared with the nebulizer group. Children in the MDI group had a significantly lower rate of hospital admission than those in the nebulizer group.
Findings from 1 RCT13 involving adult patients with asthma exacerbations treated in ICU showed no significant differences between MDIs and nebulizers in post-treatment clinical parameters including the heart rate, respiratory rate, asthma severity score, O2 partial pressure, CO2 partial pressure, and pH. Patients treated with nebulizers had significantly shorter in ICU length of stay compared to those treated with MDIs, without any significant difference in mechanical ventilation days.
Findings from 1 SR10 involving adult patients with COPD exacerbations treated at EDs showed no significant differences in O2 saturation, change in FEV1 1 hour after dosing, and change in the dyspnea score between the MDI and nebulizer groups. For health care resource use, there were no significant differences in hospital admission rates or length of hospital stay between the groups. With respect to AEs, the authors of the SR10 concluded that there were no significant differences between the groups in studies that reported AEs.
Taken together, evidence from the included SRs and primary clinical studies generally suggested that the delivery of medication via MDIs to patients with asthma or COPD at acute care settings may be as effective as nebulizers in terms of clinical parameters and health care resource use. Limited data on device-related AEs were available. No data were identified comparing DPIs with nebulizers or DPIs with MDIs. With the aforementioned limitations of the evidence, interpretation of the findings should be made with caution. More studies are needed to assess the optimal mode of delivery of bronchodilators in patients with respiratory distress, including studies on DPIs. Future studies should also assess patient important outcomes such as AEs and quality of life. Economic evaluation studies are also needed to compare the cost-effectiveness between devices in acute care settings.
References
1.Report from the Canadian Chronic Disease Surveillance System: asthma and chronic obstructive pulmonary disease (COPD) in Canada, 2018. Ottawa (ON): Public Health Agency of Canada; 2018: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/asthma-chronic-obstructive-pulmonary-disease-canada-2018.html. Accessed 2021 Oct 27.
2.Dailey PA, Shockley CM. Review of aerosol delivery in the emergency department. Ann Transl Med. 2021;9(7):591. PubMed
3.Lin HL, Fink JB, Ge H. Aerosol delivery via invasive ventilation: a narrative review. Ann. 2021;9(7):588. PubMed
4.Gardenhire DS, Burnett D, Strickland S, Myers TR. A guide to aerosol delivery devices for respiratory therapists, 4th edition. Irving (TX): American Association for Respiratory Care; 2017: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=12&ved=2ahUKEwjA3qHjqv_oAhUbCs0KHUxNATg4ChAWMAF6BAgCEAE&url=https%3A%2F%2Fwww.aarc.org%2Fwp-content%2Fuploads%2F2015%2F04%2Faerosol_guide_rt.pdf&usg=AOvVaw3G-vORTIyIJFLRscgi6K2A. Accessed 2021 Oct 27.
5.Dolovich MB, Ahrens RC, Hess DR, et al. Device selection and outcomes of aerosol therapy: evidence-based guidelines. American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127(1):335-371. PubMed
6.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
7.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
8.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
9.Roncada C, Andrade J, Bischoff LC, Pitrez PM. Comparison of two inhalational techniques for bronchodilator administration in children and adolescents with acute asthma crisis: a meta-analysis. Rev. 2018;36(3):364-371. PubMed
10.van Geffen WH, Douma WR, Slebos DJ, Kerstjens HA. Bronchodilators delivered by nebuliser versus pMDI with spacer or DPI for exacerbations of COPD. Cochrane Database Syst Rev. 2016(8):Cd011826. PubMed
11.Iramain R, Castro-Rodriguez JA, Jara A, et al. Salbutamol and ipratropium by inhaler is superior to nebulizer in children with severe acute asthma exacerbation: Randomized clinical trial. Pediatr Pulmonol. 2019;54(4):372-377. PubMed
12.Snider MA, Wan JY, Jacobs J, Kink R, Gilmore B, Arnold SR. A randomized trial comparing metered dose inhalers and breath actuated nebulizers. J Emerg Med. 2018;55(1):7-14. PubMed
13.Moustafa IOF, ElHansy MHE, Al Hallag M, et al. Clinical outcome associated with the use of different inhalation method with and without humidification in asthmatic mechanically ventilated patients. Pulm Pharmacol Ther. 2017;45:40-46. PubMed
14.Mitselou N, Hedlin G, Hederos CA. Spacers versus nebulizers in treatment of acute asthma - a prospective randomized study in preschool children. J Asthma. 2016;53(10):1059-1062. PubMed
15.Burger C, Vendiola DF, Arnold DH. Nebulized albuterol delivery is associated with decreased skeletal muscle strength in comparison with metered-dose inhaler delivery among children with acute asthma exacerbations. J Am Coll Emerg Physicians Open. 2021;2(2):e12422. PubMed
Appendix 1: Selection of Included Studies
Note that this appendix has not been copy-edited.
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Roncada et al. (2018)9 Brazil Funding: No funding received | SR with MA Total: 9 RCTs (N = 1,307) included in MA Year of publication: 1993 to 2006 Sample size: 33 to 580 Quality assessment tool: No tools were used. | Children with acute asthma crisis (mild-to-moderate exacerbations) treated at EDs Mean age: 6.8 years % Male: 55 Mean heart rate: 131 bpm Mean respiratory rate: 36 mpm Mean O2 saturation: 95% Mean asthma severity score (0 to 15):a 6.25 FEV1: 47% | MDI-spacer (N = 666) vs. nebulizer (N = 641) Medications:
| Outcomes:
Follow-up: NR |
van Geffen et al. (2016)10 The Netherlands Funding: No funding received | SR with MA Total: 8 RCTs (N = 250) included in MA Year of publication: 1985 to 2007 Quality assessment tool: Cochrane risk of bias instrument | Adult patients with COPD treated at EDs Mean age: 55, 68, and 71 years reported in 3 RCTs; NR in 5 RCTs. Other patient baseline characteristics were only reported as comparable between groups. | MDI-spacer vs. nebulizer Medications: Different beta2-agonists and anticholinergics | Outcomes: Primary:
Secondary:
Follow-up: NR |
AE = adverse event; bpm = beat per minute; COPD = chronic obstructive pulmonary disease; ED = emergency department; FEV1 = forced expiratory volume in 1 second; MA = meta-analysis; MDI = metered-dose inhaler; mpm = movements per minute; NR = not reported; O2 = oxygen; RCT = randomized controlled trial; SAE = serious adverse event; SR = systematic review.
aThe asthma severity score evaluates the respiratory rate, presence of wheezing, cyanosis, chest retractions, and transcutaneous O2 saturation, with scores ranging from 0 to 15 points (i.e., mild exacerbation: < 7; moderate exacerbation: 8 to 11; severe exacerbation: ≥ 12).
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, treatment duration, length of follow-up |
|---|---|---|---|---|
Randomized controlled trials | ||||
Iramain et al. (2019)11 Paraguay Funding: NR | RCT, investigators blinded, patients blinded, nurses and ED doctors non-blinded, single institution, parallel 1:1 ratio Sample size calculation provided: Yes ITT: Yes | Children (N = 103) with moderate-to-severe asthma treated at EDs Median age: 5 years (range 3 to 10 years) % Male: 55 Mean asthma severity score:a 7 Mean O2 saturation: ~85% No differences between groups in gender, age, atopy (dermatitis or rhinitis), exposure to tobacco, history of asthma, and treatment in the last 3 months. About 30% in both groups were diagnosed with asthma. | MDI with valved-holding chamber and mask along with O2 by a cannula separately (N = 52) vs. nebulizer (N = 51) Medications:
Both groups received ipratropium bromide between salbutamol administration. | Outcomes:
Treatment duration: 4 hours Follow-up: NR |
Snider et al. (2018)12 US Funding: NR | Non-blinded, non-inferiority RCT, single institution, parallel 1:1 ratio Sample size calculation provided: Yes ITT: No Non-inferiority margin: Admission rate difference ≤ 10% | Children (N = 890) with mild-to-moderate asthma exacerbations treated at EDs Mean age: 6 years % Male: 64.9 Pediatric asthma score:a
| MDI (N = 445) vs. breath-actuated nebulizer (N = 445) Medications: Albuterol dosing was based upon each participant’s randomized cohort, weight, and presenting asthma score. | Outcomes:
Treatment duration: 7 days Follow-up: NR |
Moustafa et al. (2017)13 Egypt Funding: NR | Non-blinded RCT, single institution, 6 arms, parallel 1:1:1:1:1:1 ratio Sample size calculation provided: No ITT: Unclear | Adult patients (N = 60) with asthma treated at ICU Mean age: 61 years % Male: 50 | Vibrating-mesh-nebulizer with humidification (N = 12) vs. vibrating-mesh-nebulizer without humidification (N = 12) vs. MDI-AV with humidification (N = 12) vs. MD-AV without humidification (N = 12) vs. jet nebulizer with humidification (N = 12) vs. jet nebulizer without humidification (N = 12) Medications: NR | Outcomes:
Treatment duration: NR Follow-up: NR |
Mitselou et al. (2016)14 Sweden Funding: NR | RCT, assessors blinded and non-blinded otherwise, single institution, parallel 1:1 ratio Sample size calculation provided: Yes ITT: Unclear | Preschool children (N = 98) with virus-induced wheezing or acute asthma exacerbations (mild-to-moderate) treated at EDs Mean age: 23 months % Male: 69 No difference between groups in parental smoking, fur-bearing animals at home, or asthma severity. | MDI-spacer (N = 53) vs. nebulizer (N = 45) Medications: Salbutamol | Outcomes:
Treatment duration: NR Follow-up: NR |
Non-randomized studies | ||||
Burger et al. (2021)15 US Funding: National Institutes of Health, National Center for Research Resources | Prospective cohort study Sample size calculation provided: No Adjustment for confounders conducted: Yes | Children (N = 50) with acute asthma exacerbations (mild-to-moderate) treated at EDs Median age: 9.8 years (range 7.4 to 12.3 years) % Male: 36 Median asthma severity score: 5.5 (range 2.5 to 8) | MDI (N = 40) vs. nebulizer (N = 10) Medications: Albuterol 10 mg for those treated with nebulizer and 0.72 mg to those treated with an MDI. | Outcomes:
Treatment duration: NR Follow-up: NR |
AE = adverse event; AV = AeroChamber Vent; COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; ED = emergency department; ICU = intensive care unit; min = minute; ITT = intention-to-treat; MDI = metered-dose inhaler; NR = not reported; O2 = oxygen; pCO2 = partial pressure of carbon dioxide; pO2 = partial pressure of oxygen; RCT = randomized controlled trial.
aThe asthma severity score evaluates the respiratory rate, presence of wheezing, cyanosis, chest retractions, and transcutaneous O2 saturation, with scores ranging from 0 to 15 points (i.e., mild exacerbation: < 7; moderate exacerbation: 8 to 11; severe exacerbation: ≥ 12).
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 26
Strengths | Limitations |
|---|---|
Roncada et al. (2018)9 | |
The research question or objective and the inclusion criteria for the review clearly include the components of PICO. The study protocol had been registered on the website of the Centre for Reviews and Dissemination (PROSPERO). This has low risk of bias in modifying the methods. The review authors explained their selection of study designs, which were RCTs with or without placebo. The literature search strategy was comprehensive and clearly described, increasing reproducibility. The characteristics of the included studies were described in adequate detail. A brief comparison of patient characteristics as to whether the treatment groups were balanced was provided. The dosages of medications in the intervention and comparator groups were described. The software Review Manager (RevMan) was used in the meta-analyses. The review authors provided a discussion of the heterogeneity observed in the results, which was the main limitation of the meta-analyses. The study did not receive any funding. The review authors declared that there were no conflicts of interest. | The review authors did not report whether study selection and data extraction were performed in duplicate. Therefore, it is unclear whether a fully systematic approach was taken in study selection and data extraction. A list of excluded studies and the reasons for exclusion were not provided. Therefore, it was not possible to assess whether any relevant articles were excluded and if so, for what reasons. The review authors did not report the sources of funding for the included studies. This is potentially a concern because funding received from industry can introduce bias in favour of the intervention. The review authors did not assess the quality, or risk of bias, of the included studies. Therefore, it was not possible to assess the trustworthiness of the meta-analysis findings. |
van Geffen et al. (2016)10 | |
The research question or objective and the inclusion criteria for the review clearly include the components of PICO. The study protocol had been registered on the website of the Centre for Reviews and Dissemination (PROSPERO). This has low risk of bias in modifying the methods. The review authors explained their selection of study designs, which were RCTs of both parallel and crossover designs. The literature search strategy was comprehensive and clearly described, increasing reproducibility. The review authors performed study selection and data extraction in duplicate, reducing the risk of missing relevant studies and making errors in data extraction. A list of excluded studies and the reason for exclusion were provided. The methodological quality of the included studies was assessed using the Cochrane risk of bias tool. The review authors reported on the sources of funding for the studies included in the review. The software Review Manager (RevMan) was used in the meta-analysis. The review authors accounted for risk of bias in the included studies when interpreting or discussing the results of the review. The review authors provided a discussion of the heterogeneity observed in the results, which was the main limitation of the meta-analysis. The review authors declared that no funding was received for this systematic review. Conflicts of interest were also declared. | The characteristics of the included studies were not described in adequate detail. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NR = not reported; PICO = population, intervention, comparator, and outcomes.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist7
Strengths | Limitations |
|---|---|
Iramain et al. (2019)11 | |
The objective of the study, the main outcomes to be measured, the characteristics of the patients included in the study, the interventions of interest, and the main findings were clearly described. This study had no patients lost to follow-up. Actual probability and standard deviation values were reported for the main outcomes. The study was conducted in a pediatric ED setting, where children with asthma exacerbations were treated. The investigators and patients were blinded. This may have been associated with low risk of performance bias. All patients were followed up for the same length of time (i.e., 4 hours). Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. Patients in different interventions groups appeared to be recruited from the same population and over the same period of time. Patients were randomly allocated using a computer random numbers table and a sealed enveloped technique for allocation concealment. This minimizes selection bias. A sample size calculation was performed. The sample size of 40 patients in each group provided a 90% power to detect a statistical difference in the hospitalization rate of 20%, with an Alpha of 0.05 and assuming a 2-tailed test. | As the study population was relatively small (N = 103), it was unclear if the study participants represented the entire population from which they were recruited. Patient compliance was not reported. |
Snider et al. (2018)12 | |
The objective of the study, the main outcomes to be measured, the characteristics of the patients included in the study, the interventions of interest, and the main findings were clearly described. Actual probability and standard deviation values were reported for the main outcomes. The study was conducted in a pediatric ED setting, where children with asthma exacerbations were treated. With a relatively large population, the study participants may represent the entire population from which they were recruited. All patients were followed up for the same length of time (i.e., 7 days). Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. Patients in different interventions groups appeared to be recruited from the same population and over the same period of time. The authors of the study performed a sample size calculation to detect a 10% difference in admission rate. With a power of 80%, the required sample size was 376 patients per treatment group. More than 376 patients were recruited for each treatment group. | About 9% of patients were excluded due to violation of different types. The characteristics of these patients were not reported, and the analyses did not account for those patients. This was a non-blinded RCT, in which investigators and patients were aware of the treatment. This may have resulted in high risk of performance bias. Patient compliance was not reported. |
Moustafa et al. (2017)13 | |
The objective of the study, the main outcomes to be measured, the interventions of interest, and the main findings were clearly described. Actual probability and standard deviation values were reported for the main outcomes. The study was conducted in an ICU, where adult patients with asthma were treated. Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. Patients in different interventions groups appeared to be recruited from the same population and over the same period of time. | The characteristics of the patients included in the study were not clearly described. As the study population was relatively small (N = 72), it was unclear if the study participants represented the entire population from which they were recruited. This was a non-blinded RCT, in which investigators and patients were aware of the treatment. This may have resulted in high risk of performance bias. Patient compliance was not reported. Length of follow-up was not reported; therefore, it was unclear if all patients were followed up for the same length of time. The authors of the study did not report whether a sample size calculation was performed. |
Mitselou et al. (2016)14 | |
The objective of the study, the main outcomes to be measured, the characteristics of the patients included in the study, the interventions of interest, and the main findings were clearly described. This study had no patients lost to follow-up. Actual probability, standard deviation, and 95% CI values were reported for the main outcomes. The study was conducted in a pediatric ED setting, where children with virus-induced wheezing or acute asthma exacerbations were treated. Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. Patients in different interventions groups appeared to be recruited from the same population and over the same period of time. A sample size calculation was performed. The authors of the study planned to have at least 100 patients, as the power estimation was 80% with 95% significance if there were 49 patients in each group for a 25% difference in the hospitalization rate, which was deemed to be clinically important. The study recruited 98 patients in total. | As the study population was relatively small (N = 98), it was unclear if the study participants represented the entire population from which they were recruited. This was a non-blinded RCT, in which investigators and patients were aware of the treatment. This may have resulted in high risk of performance bias. However, the assessors were blinded. Patient compliance was not reported. Length of follow-up was not reported; therefore, it was unclear if all patients were followed up with the same length of time. |
Burger et al. (2021)15 | |
The objective of the study, the main outcomes to be measured, the characteristics of the patients included in the study, the interventions of interest, and the main findings were clearly described. Actual probability and IQR values were reported for the main outcomes. Confounding variables were identified and adjusted for in the analyses. The study was conducted in a pediatric ED setting, where children with acute asthma exacerbations were treated. Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. | This was a non-randomized study, which is prone to high risk of bias for selection, performance, and detection. Patients lost to follow-up were not reported. As the study population was relatively small (N = 50), it was unclear if the study participants represented the entire population from which they were recruited. Patient compliance was not reported. Length of follow-up was not reported; therefore, it was unclear if all patients were followed up for the same length of time. It was unclear if patients in different interventions groups were recruited from the same population and over the same period of time. The authors of the study did not provide a sample size calculation. |
CI = confidence interval; ED = emergency department; ICU = intensive care unit; IQR = interquartile range; RCT = randomized controlled trial.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Clinical Parameters
Study citation, study design, and patient model | Study findings |
|---|---|
MDI vs. nebulizer | |
Heart rate | |
Roncada et al. (2018)9 SR Children with acute asthma crisis (mild-to-moderate exacerbations) treated at ED | Meta-analysis of 7 RCTs (N = 1,016)
|
Iramain et al. (2019)11 RCT Children (N = 103) with moderate-to-severe asthma treated at EDs | The MDI group had a statistically significantly lower heart rate (in bpm) than those in the nebulizer group from 30 minutes of treatment up to until 4 hours of treatment.
|
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | There was no statistically significant difference between MDIs and nebulizers with or without humidification (data not reported). |
Mitselou et al. (2016)14 RCT Preschool children (N = 98) with virus-induced wheezing or acute asthma exacerbations (mild-to-moderate) treated at EDs | No statistically significant difference between groups in the heart rate (in bpm).
|
Respiratory rate | |
Roncada et al. (2018)9 SR Children with acute asthma crisis (mild-to-moderate exacerbations) treated at EDs | Meta-analysis of 6 RCTs (N = 670)
|
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | There was no statistically significant difference between MDIs and nebulizers with or without humidification (data not reported). |
Mitselou et al. (2016)14 RCT Preschool children (N = 98) with virus-induced wheezing or acute asthma exacerbations (mild-to-moderate) treated at EDs | No statistically significant difference between groups in the respiratory rate (in mpm).
|
O2 saturation | |
Roncada et al. (2018)9 SR Children with acute asthma crisis (mild-to-moderate exacerbations) treated at EDs | Meta-analysis of 8 RCTs (N = 1,267)
|
Iramain et al. (2019)11 RCT Children (N = 103) with moderate-to-severe asthma treated at EDs | The MDI group had statistically significantly higher O2 saturation (in %) than those in the nebulizer group from 90 minutes of treatment up to until 4 hours of treatment.
|
van Geffen et al. (2016)10 SR Patients with COPD treated at EDs | One RCT (N = 42) showed no statistically significant difference between groups at different time points (i.e., 30 minutes, 6 hours, 24 hours, 48 hours, or 10 days).
|
Mitselou et al. (2016)14 RCT Preschool children (N = 98) with virus-induced wheezing or acute asthma exacerbations (mild-to-moderate) treated at EDs | No statistically significant difference between groups in O2 saturation (in %).
|
Asthma severity score | |
Roncada et al. (2018)9 SR Children with acute asthma crisis (mild-to-moderate exacerbations) treated at EDs | Meta-analysis of 7 RCTs (N = 667)
|
Iramain et al. (2019)11 RCT Children (N = 103) with moderate-to-severe asthma treated at EDs | The MDI group had statistically significantly better (i.e., lower) asthma severity score than those in the nebulizer group from 60 minutes of treatment up to until 4 hours of treatment.
A survival analysis showed that children in the MDI group had a statistically significantly higher chance to have a pulmonary score ≤ 6 compared with those in the nebulizer group (P < 0.0001). |
Snider et al. (2018)12 RCT Children (N = 890) with mild-to-moderate asthma exacerbations treated at EDs | There were no statistically significant differences in post-treatment asthma severity scores between groups. Score change after each treatment in EDs:
|
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | No statistically significant difference between MDIs and nebulizers with or without humidification (data not reported). |
Change in FEV1 | |
van Geffen et al. (2016)10 SR Patients with COPD treated at EDs | Change in FEV1 1 hour after dosing Two RCTs showed no statistically significant differences between the groups.
Change in FEV1 closest to 1 hour after dosing Meta-analysis of 4 RCTs (N = NR):
|
Change in the dyspnea score in the first 24 hours after dosing | |
van Geffen et al. (2016)10 SR Patients with COPD treated at EDs | 4 RCTs (N = NR) showed no statistically significant difference between the groups. Meta-analysis of 2 RCTs (N = 54):
|
O2 partial pressure | |
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | No statistically significant difference between MDIs and nebulizers with or without humidification (data not reported). |
CO2 partial pressure | |
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | No statistically significant difference between MDIs and nebulizers with or without humidification (data not reported). |
pH | |
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | No statistically significant difference between MDIs and nebulizers with or without humidification (data not reported). |
Skeletal muscle strength | |
Burger et al. (2021)15 Prospective cohort study Children (N = 50) with acute asthma exacerbations (mild-to-moderate) treated at EDs | Median (IQR) in change of grip:
*Adjusted for age and pre-treatment asthma severity score. |
bpm = beat per minute; CI = confidence interval; COPD = chronic obstructive pulmonary disease; ED = emergency department; FEV1 = forced expiratory volume in 1 second; hr = hour; ICU = intensive care unit; IQR = interquartile range; MD = mean difference; MDI = metered-dose inhaler; min = minute; mpm = movements per minute; NR = not reported; O2 = oxygen; RCT = randomized controlled trial; SR = systematic review; vs. = versus .
Table 7: Summary of Findings by Outcome — Health Care Resource Use
Study citation, study design, and patient model | Study findings |
|---|---|
MDI vs. nebulizer | |
ED or ICU length of stay | |
Snider et al. (2018)12 RCT Children (N = 890) with mild-to-moderate asthma exacerbations treated at EDs | No statistically significant difference between groups in ED length of stay:
*Adjusted for baseline severity, ipratropium, and elevated vs. standard dosing of albuterol. |
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | ICU length of stay:
ICU length of stay comparisons:
|
Mitselou et al. (2016)14 RCT Preschool children (N = 98) with virus-induced wheezing or acute asthma exacerbation (mild-to-moderate) treated at pediatric EDs | No statistically significant difference between groups in ED length of stay.
|
Hospital admission rate | |
van Geffen et al. (2016)10 SR Patients with COPD treated at EDs | One RCT (N = 22) showed no statistically significant difference between groups in hospital admission rates; OR (95% CI) = 0.8 (0.09 to 7.00); P = 0.84 |
Iramain et al. (2019)11 RCT Children (N = 103) with moderate-to-severe asthma treated at EDs | The need of hospitalization at the end of 4 hours of treatment in patients with pulmonary score ≥ 7 was statistically significantly lower in the MDI group compared to the nebulizer group.
|
Snider et al. (2018)12 RCT Children (N = 890) with mild-to-moderate asthma exacerbations treated at EDs | No statistically significant difference between groups in hospital admission rates:
*Adjusted for baseline severity, ipratropium, and elevated vs. standard dosing of albuterol. |
Mitselou et al. (2016)14 RCT Preschool children (N = 98) with virus-induced wheezing or acute asthma exacerbation (mild-to-moderate) treated at EDs | No statistically significant difference between groups in hospital admission rates:
|
Length of hospital stay | |
van Geffen et al. (2016)10 SR Patients with COPD treated at EDs | One RCT (N = 34) showed no statistically significant difference between groups in the length of hospital stay; MD (95% CI) = 0.80 days (−1.05 to 2.56); P = 0.40 |
Mechanical ventilation days | |
Moustafa et al. (2017)13 RCT Adult patients (N = 72) with asthma treated at ICU | Mechanical ventilation days:
Mechanical ventilation days comparisons:
|
CI = confidence interval; COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; ED = emergency department; ICU = intensive care unit; MDI = metered-dose inhaler; min = minute; OR = odds ratio; RCT = randomized controlled trial; RD = risk difference; RR = relative risk; SR = systematic review.
Table 8: Summary of Findings by Outcome — Adverse Events
Study citation, study design, and patient model | Study findings |
|---|---|
MDI vs. nebulizer | |
van Geffen et al. (2016)10 SR Patients with COPD treated at EDs |
|
Snider et al. (2018)12 RCT Children (N = 890) with mild-to-moderate asthma exacerbations treated at EDs |
|
AE = adverse event; CI = confidence interval; COPD = chronic obstructive pulmonary disease; ED = emergency department; MDI = metered-dose inhaler; O2 = oxygen; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca