CADTH Health Technology Review
Computed Tomography-Derived Fractional Flow Reserve for the Diagnosis of Coronary Artery Disease
Rapid Review
Authors: Yi-Sheng Chao, Jennifer Horton
Abbreviations
CAD
coronary artery disease
CCTA
coronary computed tomography angiography
CTP
myocardial computed tomography perfusion
FFR
fractional flow reserve
CT-FFR
computed tomography-derived fractional flow reserve
ICA
invasive coronary angiography
ICER
incremental cost-effectiveness ratio
MACE
major adverse cardiovascular event
NICE
National Institute for Health and Care Excellence
PROMISE
Prospective Multicenter Imaging Study for Evaluation of Chest Pain
QALY
quality-adjusted life-year
SPECT
single-photon emission computed tomography
Key Messages
Computed tomography-derived fractional flow reserve (CT-FFR) may predict coronary artery disease or flow-limiting stenosis in adult patients with stable chest pain better than coronary CT angiography alone, based on the relevant studies in 2 systematic reviews.
CT-FFR is associated with a decreased need for invasive coronary angiography and revascularization in adult patients with stable chest pain, based on findings from 1 systematic review.
In the US settings, CT-FFR was dominant (i.e., less costly and more effective) compared to stress testing for the evaluation of low-risk stable chest pain, based on findings from 1 cost-effectiveness study.
Context and Policy Issues
Chest pain is a symptom that is frequently reported by patients and may originate from several organs, including the heart, lungs, and esophagus.1 Chest pain can relate to conditions of different severity, some of which can be life-threatening.1 One of the potentially life-threatening conditions that can cause chest pain is heart disease.2 Heart disease, including ischemic heart disease and angina, was the second-leading cause of death in 2012 in Canada and was the leading cause of hospitalization in 2013 and 2014.2
The typical chest pain associated with coronary artery disease (CAD) can feel like pressure or squeezing in the chest that might radiate into the arm or neck and is triggered by physical or emotional stress.3 This acute chest pain can be diagnosed using criteria in various tests, such as electrocardiography, and the pain can be alleviated using nitroglycerin.4 In contrast to typical chest pain, stable chest pain does not change in severity or frequency and it does not present with the signs of typical chest pain used in electrocardiography to form a diagnosis.4 Patients with stable chest pain are usually assessed noninvasively, such as through exercise electrocardiography, nuclear imaging, or pharmacological electrocardiography.5 More recently, there are several emerging technologies to help classify patients with chest pain based on their risks of CAD. Coronary CT angiography (CCTA), an imaging technique to assess coronary arteries, has been used to assess patients with an intermediate- to high-risk of CAD.5 Fractional flow reserve (FFR) measures the ratio between maximal blood flow in a diseased artery and the normal maximal blood flow.5 FFR can be measured invasively through invasive coronary angiography (ICA) or noninvasively through 3-dimensional models derived from CCTA images of sufficient quality.5
Differential diagnosis of chest pain, an important feature of acute coronary syndrome, has been a focus for primary care and in various settings in Canada.4 Among 197 legal actions or hospital complaints featuring acute coronary syndrome analyzed by the Canadian Medical Protective Association (or CMPA) between 2014 and 2018 in Canada, 116 are related to diagnostic error, particularly during the assessment and testing phases while diagnosing.6 There is a need for better strategies and tools for assessing a patient’s risk of CAD to improve health care quality.
With several options available to assess patients with chest pain, the use of invasive FFR has increased for more than 5-fold between 2010 and 2015 in Ontario, particularly in patients with stable CAD.7 It remains unclear whether FFR measured noninvasively using CCTA images (CT-FFR) can be as accurate and effective as other options in Canada. This review aims to systematically search for the literature on the diagnostic accuracy, clinical utility, and cost-effectiveness of CT-FFR for the diagnosis of CAD in patients with stable chest pain compared with other diagnostic tests.
Research Questions
What is the diagnostic accuracy of computed tomography-derived fractional flow reserve (CT-FFR) analysis for the diagnosis of coronary artery disease in patients with stable chest pain?
What is the clinical utility of CT-FFR analysis for the diagnosis of coronary artery disease in patients with stable chest pain?
What is the cost-effectiveness of CT-FFR analysis for the diagnosis of coronary artery disease in patients with stable chest pain?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were stable chest pain, CT scans, and fractional flow reserve. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or network meta-analyses; randomized controlled trials, controlled clinical trials, or any other type of clinical trial; and economic studies. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016 and September 27, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients with stable chest pain |
Intervention | CT-FFR |
Comparator | Q1 to Q3: Layering of tests (treadmill, myocardial perfusion scanning, invasive coronary angiography, stress echo), coronary CT angiography without CT-FFR, diagnostic invasive catheter angiography, PET, or single-photon emission CT |
Reference test | Q1: Invasive fractional flow reserve Q2 and Q3: Not applicable |
Outcomes | Q1: Diagnostic accuracy (e.g., sensitivity, specificity, positive predictive value, negative predictive value) Q2: Clinical utility (e.g., time to treatment, mortality, incidence of myocardial infarction, quality of life) Q3: Cost-effectiveness (e.g., cost per quality-adjusted life-years) |
Study designs | Health technology assessment, systematic reviews, non-randomized studies, randomized controlled trials, and economic evaluations |
CT-FFR = computed tomography-derived fractional flow reserve.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2016. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for systematic reviews and the Drummond checklist9 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
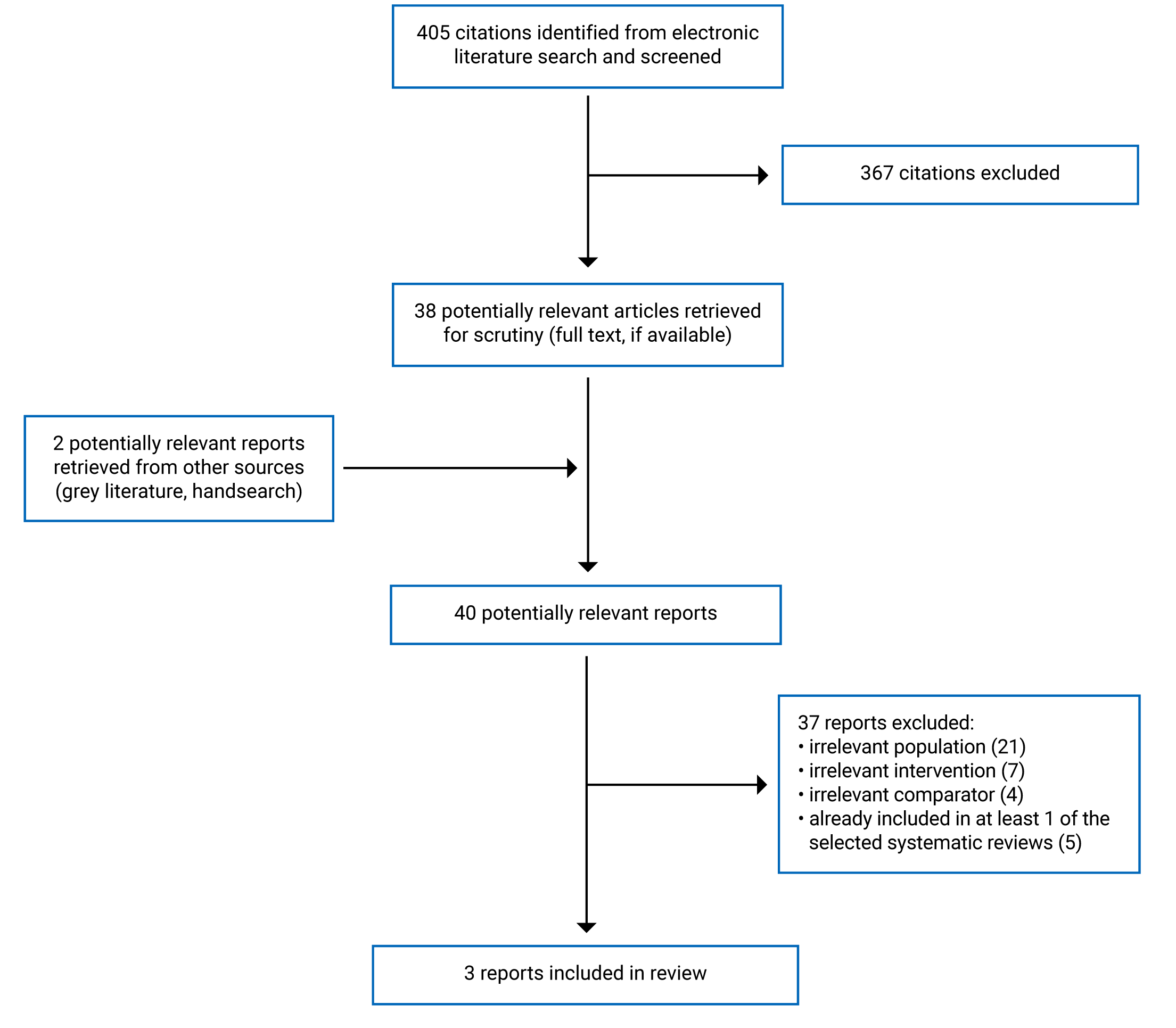
A total of 405 citations were identified in the literature search. Following screening of titles and abstracts, 367 citations were excluded and 38 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 37 publications were excluded for various reasons and 3 publications met the inclusion criteria and were included in this report. These comprised 2 systematic reviews and 1 economic evaluation. Appendix 1 presents the PRISMA10 flow chart of the study selection.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Two included systematic reviews had broader inclusion criteria than the current review.11,12 One systematic review was used for a medical technology guidance project by the National Institute for Health and Care Excellence (NICE) in the UK (the guidance11 and the systematic review13 published separately). This systematic review that NICE conducted was used to update a published guidance.11 The other systematic review by Hamon et al. searched for publications on the diagnostic accuracy of CT diagnostic techniques published in July 2018 or earlier.12 The NICE review searched for primary studies published between 2016 and 2021.13 Among the 23 studies included by NICE, 3 trials were relevant to this review.11 Hamon et al. identified 50 publications, 26 of which were relevant to this review, of which 8 publications examined CT-FFR for diagnostic accuracy at a per-patient level and 18 publications examined diagnostic accuracy at the per-vessel level.12
Karady et al. conducted an individual-based Markov microsimulation model funded by a manufacturer of CT-FFR, HeartFlow, using several sources of cost and utility data, mainly from the Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) trial.14 Karady et al. used a societal perspective to assess the cost-effectiveness in a lifetime.14 The cost data were from the PROMISE trial, the US Centers for Medicare & Medicaid Services website, and the Red Book.14 The effectiveness measures of anatomic approaches included ICA and revascularization, as well as major adverse cardiovascular events (MACEs) that included death and non-fatal myocardial infarction.14 The utility was measured with quality-adjusted life-years (QALYs).14
Country of Origin
The systematic reviews conducted by NICE and Hamon et al. were by authors from the UK and France, respectively.11,12
The first author of the cost-effectiveness analysis was based in the US.14
Patient Population
The NICE systematic review included patients with stable chest pain and other heart conditions; the 3 trials relevant to this report included patients with stable chest pain.11,13 Hamon et al. included studies enrolling patients with stable chest pain.12
Karady et al. used patient data from the PROMISE trial, which enrolled 10,003 patients with stable chest pain and 30% to 69% with stenosis.14 The median age was 60 years and 52.7% of them were female.14
Interventions and Comparators
CT-FFR was the intervention under investigation in the systematic reviews by the NICE11 and Hamon et al.12 The NICE systematic review specifically evaluated HeartFlow CT-FFR and compared it to several technologies.13 CT-FFR was compared to CCTA alone in the 3 relevant trials in the systematic review by NICE.11,13 In addition, 1 of the 3 trials also compared CT-FFR to CCTA with stress myocardial CT perfusion (CTP) and ICA with invasive FFR, and used invasive FFR as a reference standard.13 The relevant studies in Hamon et al. compared stress CTP, transluminal attenuation gradients, CT-FFR, and CCTA alone using invasive FFR as a reference standard.12
Karady et al. compared anatomic approaches and functional testing for low-risk chest pain in the cost-effectiveness analysis.14 The anatomic approaches included CCTA alone and CT-FFR, and the functional testing was stress testing including stress single-photon emission CT (SPECT), stress echocardiography, and exercise treadmill testing in this study.14 The PROMISE trial used invasive FFR as a reference standard.15
Outcomes
The 3 relevant trials in the systematic review by NICE evaluated several outcomes, including all-cause-death, any revascularization, diagnostic accuracy of vessel stenosis, and major adverse cardiac events.13 The lengths of follow-up were 4.7 years in 1 included trial and not described in the other trials.13 In the systematic review by Hamon et al., the outcomes extracted were diagnostic accuracy for the diagnosis of hemodynamic significant CAD and the length of follow-up was not described.12
Karady et al. assessed the costs, effectiveness, and utility of anatomical approaches to mainly derive incremental cost-effectiveness ratios (ICERs) of competing strategies.14 Other outcomes included cost and utility measured by QALYs (at 2 years, 5 years, and over a lifetime) and life-years gained over a lifetime.14
Summary of Critical Appraisal
Systematic Reviews
Both systematic reviews described population, intervention, comparator, and outcomes (or PICO) components and study design selection.11,12 However, neither reported that the review protocols had been published a priori12,13 and it was unclear whether there were any deviations to the review protocol.
Both conducted comprehensive literature searches and the study selection was done in duplicate12,13; thus, the chance of missing important studies might be small. However, the NICE systematic review did not explicitly report that data extraction was conducted in duplicate13 and it was unclear whether the accuracy of extracted data might be compromised.
Both systematic reviews described the included studies in detail and assessed the risks of bias in the included studies.12,13 Both described data synthesis.12,13 Hamon et al. meta-analyzed the diagnostic accuracy from the primary studies.12 Heterogeneity between included studies was recognized by both systematic reviews.12,13 However, neither reported the sources of funding for the included studies,12,13 and whether the sources of funding might lead to biased results in the included primary studies was not clear.
Hamon et al. did not provide a list of excluded studies12 and it was difficult to check the accuracy of their study selection results.
NICE reported that there were no potential biases identified in the primary studies but did not assess publication bias among the included studies.13 The impact of publication bias was not assessed in the NICE systematic review.13 In contrast, Hamon et al. assessed publication bias and concluded the publication bias was small.12
The authors of both systematic reviews declared no conflicts of interest.12,13
Economic Evaluations
Karady et al. described the research question, its economic importance, the viewpoint of the analysis, the rationale for the choice of interventions and comparators, the form of economic evaluation, the reason to choose the economic evaluation, the sources of cost and effectiveness estimates, the details of the effectiveness study (i.e., the PROMISE trial), the primary outcomes, the methods to value benefits, the characteristics of the patients, and the methods to estimate quantities and unit costs.14 The quantities of resource use were reported with unit cost.14 The currency and price data were reported.14 The details in currency adjustment for inflation and currency conversion were explained and justified.14 The discount rates were based on a published guideline.14 The simulation model was explained and the key parameters were justified.14 Multiple time horizons, up to a lifetime, were reported for the comparison of costs and effectiveness.14 The details in the sensitivity analysis, including the choice of variables and the ranges that the variables varied, were provided.14 Relevant comparators were compared in the study.14 The incremental analysis was reported.14 Major outcomes were listed by different time points and screening strategies.14 The answers to the research questions and the conclusions from the data were reported.14 The details in this cost-effectiveness analysis was well-described and the major parameters were justified.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
There was no overlap in the relevant studies in systematic reviews by NICE and Hamon et al.12,13 The 2 relevant trials in the systematic review by NICE were not included in the systematic reviews summarized by Hamon et al.12,13 There were primary studies reporting the clinical effectiveness and the diagnostic accuracy of CT-FFR in the systematic reviews.12,13 The cost-effectiveness of CT-FFR was reported by Karady et al.14
Appendix 4 presents the main study findings and authors’ conclusions.
Diagnostic Accuracy of CT-FFR
CT-FFR Versus CCTA alone
Both systematic reviews reported on the diagnostic accuracy of CT-FFR. Hamon et al. meta-analyzed the findings from 8, and 18, studies on CT-FFR for diagnostic accuracy at a per-patient and per-vessel level, respectively.12
Hamon et al. reported the ranges of pooled sensitivities and specificities at per-patient and per-vessel levels in the meta-analyses, using invasive FFR as a reference standard for the detection of hemodynamic significant CAD.12 Hamon et al. concluded that CT-FFR had incremental value, compared with CCTA, based on the positive likelihood ratios and specificity.12
One trial from 2019 was summarized in the NICE systematic review, which reported the diagnostic accuracy using the area-under-the-curve.13 Three approaches were compared: CCTA, CT-FFR, and CCTA with CTP in per-vessel‒ or per-patient‒based models.13 CT-FFR was statistically significantly better than CCTA with CTP or CCTA alone for the detection of flow-limiting stenosis.13
Clinical Utility of CT-FFR
Two of the 3 relevant trials in the systematic review by NICE reported the clinical utility of CT-FFR.13 Based on 1 trial with a median follow-up of 4.7 years, positive CT-FFR results predicted the primary end point (a composite of death from any cause, non-fatal myocardial infarction, and any revascularization) and MACE that was statistically significantly better than CCTA in patients with stable chest pain.13 Based on the other trial whose length of follow-up was not described by NICE, CT-FFR was significantly better in predicting revascularization or MACE than CCTA.13 When ICA was reserved for patients with CT-FFR of less than or equal to 0.8, there could be a 44% decrease in ICA among those with less than 50% stenosis and a 24% increase in revascularization due to ICA.13
Cost-Effectiveness of CT-FFR
Based on the model using the PROMISE trial data and other data sources, Karady et al. compared the cost-effectiveness of anatomic approaches (CCTA alone and CT-FFR) with functional testing (stress testing, including stress SPECT, stress echocardiography, and exercise treadmill testing).14 Although CT-FFR was associated with higher ICA and revascularization at 60 days, 2 years, and 5 years, compared with functional testing, the cost of CT-FFR could be outweighed by less ICA and revascularization after 5 years compared to CCTA alone.14 CT-FFR was more effective in selecting patients for ICA and led to an additional 6 months in perfect health in a lifetime compared with functional testing.14
By assessing the cost and effectiveness over a lifetime, CT-FFR was considered dominant (i.e., less costly and more effective) compared to functional testing.14 Based on the ICER, functional testing was dominated by CT-FFR.14 In subgroups, the ICER of CT-FFR was US$192 per QALY, and CT-FFR dominated functional testing in females or those below or above 60 years of age, compared to functional testing.14 In the quasi-probabilistic sensitivity analysis using the cost and QALY distributions derived from the data, the probability of CT-FFR being cost-effective was 65.4% compared to functional testing, assuming a willingness-to-pay threshold of US$100,000 per QALY.14
Limitations
There were relatively few studies that recruited patients with stable chest pain and tested CT-FFR. For example, most of the primary studies included in the systematic reviews recruited patients with suspected CAD.13 The conditions that studies aimed to diagnose were not the same.12,13 The interpretation of patient characteristics also varied across publications. For example, all of the populations analyzed in a meta-analysis by Celeng et al.16 were considered patients with stable chest pain by the authors of another systematic review.5 However, Celeng et al. did not specify that the patients in the primary studies had stable chest pain.16 In the systematic review by Hamon et al., the statistical significance for the comparison of diagnostic accuracy between CT-FFR and CCTA was not reported and it was unclear whether Hamon et al. made conclusions based on valid statistical inference.12 The conclusions in the systematic reviews were often made based on studies recruiting patients with stable chest pain and other heart conditions, except for the long-term follow-up of clinical effectiveness in a trial that only recruited patients with stable chest pain.12,13 Thus, the generalizability of the conclusions from these systematic reviews to patients with stable chest pain, particularly those without suspected CAD, requires further investigation. There are measures to ensure CCTA image quality and obtain precise measurements of FFR, such as using CT units of 64 slices or more.11 However, the variations in imaging quality might be a concern, but this was not well-reported.13 The evidence on the long-term clinical effectiveness of CT-FFR might be limited.13 There was only 1 cost-effectiveness analysis to assess lifetime costs and benefits, based on 1 trial comparing CT-FFR and CCTA in the US.14 There were few primary studies that had trial sites in Canada13 and whether this might impact the generalizability of the conclusions of the CT-FFR studies to the Canadian clinical practice is unclear.
Conclusions and Implications for Decision- or Policy-Making
Two systematic reviews reporting diagnostic accuracy or clinical utility were identified.12,13 The NICE systematic review was produced as an evidence synthesis to guide health care practice.13 One cost-effectiveness analysis was identified.14
The diagnostic accuracy of CT-FFR was reported in 2 systematic reviews, compared with CCTA.12,13 NICE identified a trial that used area-under-the-curve to compare diagnostic accuracy and concluded that CT-FFR was significantly better than CCTA for flow-limiting stenosis.13 Hamon et al. meta-analyzed primary studies and concluded that CT-FFR had incremental value based on the positive likelihood ratios and specificity, compared with CCTA alone, for the detection of hemodynamic, significant CAD.12
In a trial with a median follow-up of 4.7 years for the evaluation of clinical utility, CT-FFR was a statistically significantly better predictor of a composite outcome of all-cause-death, non-fatal myocardial infarction, and any revascularization compared to CCTA alone.13 In the other trial, in which the length of follow-up was not specified by NICE, CT-FFR predicted revascularization or MACE better than CCTA.13
In the NICE guidance updated in 2021, it is recommended to include HeartFlow CT-FFR for patients with stable and recent onset chest pain when offered CCTA for chest pain assessment, as HeartFlow CT-FFR is associated with a decreased need for ICA and revascularization.13
The cost-effectiveness analysis by Karady et al. used clinical data from the PROMISE trial and compared CT-FFR and functional approaches (i.e., stress testing, including stress SPECT, stress echocardiography, and exercise treadmill testing).14 CT-FFR was more effective in selecting patients for ICA and lead to an additional 6 months in perfect health in a lifetime compared with functional testing.14 By assessing the cost and effectiveness over a lifetime, CT-FFR dominated functional testing, based on the ICER.14
The limitations to the literature was related to a limited number of studies explicitly focusing on patients with stable chest pain, differences in the interpretation of population characteristics, the lack of statistical significance reporting in some studies, unclear generalizability of the conclusions based on studies recruiting patients with stable chest pain and other heart conditions, and the need for more long-term follow-up of patients with stable chest pain diagnosed using different imaging approaches.12,13 There were few trials that had sites in Canada.12,13
Two systematic reviews provide some evidence that CT-FFR derived from CCTA images had incremental value for the diagnosis of CAD or stenosis compared with CCTA.12,13 CT-FFR was more likely to be cost-effective than stress testing in the US settings.14 However, there remains a need for the assessment of long-term consequences of CT-FFR use, specifically for the diagnosis of CAD in patients with stable chest pain in Canadian contexts.
References
1.Thompson AD, Shea MJ. Chest Pain. Kenilworth, NJ: Merck & Co., Inc.; 2020: https://www.merckmanuals.com/en-ca/professional/cardiovascular-disorders/symptoms-of-cardiovascular-disorders/chest-pain. Accessed Oct 11, 2021.
2.Public Health Agency of Canada. Heart disease in Canada: Highlights from the Canadian Chronic Disease Surveillance System. Ottawa, ON: Government of Canada; 2017: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/heart-disease-fact-sheet/heart-disease-factsheet-eng.pdf. Accessed Oct 11, 2021.
3.American Heart Association. Angina Pectoris (Stable Angina). Dallas, TX: American Heart Association; 2015: https://www.heart.org/en/health-topics/heart-attack/angina-chest-pain/angina-pectoris-stable-angina. Accessed Oct 21, 2021.
4.Brenna CTA, Afgani FJ, Hanneman K, et al. Chest pain investigation in patients at low or intermediate risk. Can Fam Physician. 2020;66(1):24.
5.Helfand M, Anderson J, Peterson K, Bourne D. Evidence Assist: Coronary Computed Tomography Angiography Innovations in Noninvasive Diagnosis of Coronary Artery Disease. Portland, OR: Department of Veterans Affairs; 2019.
6.Canadian Medical Protective Association. The diagnostic challenges of chest pain: Recognizing acute coronary syndrome. Ottawa, ON: Canadian Medical Protective Association; 2019: https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2019/the-diagnostic-challenges-of-chest-pain-recognizing-acute-coronary-syndrome. Accessed Oct 11, 2021.
7.Elbaz-Greener G, Masih S, Fang J, Roifman I, Wijeysundera HC. Temporal trends in fractional flow reserve use in patients undergoing coronary angiography: a population-based study. CJC open. 2019;1(1):10-18.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed Oct 29, 2021.
10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
11.National Institute for Health and Clinical Excellence. HeartFlow FFRCT for estimating fractional flow reserve from coronary CT angiography. London, UK: National Institute for Health and Clinical Excellence; 2017: https://www.nice.org.uk/guidance/mtg32/resources/heartflow-ffrct-for-estimating-fractional-flow-reserve-from-coronary-ct-angiography-pdf-64371991952581. Accessed Oct 1, 2021.
12.Hamon M, Geindreau D, Guittet L, Bauters C, Hamon M. Additional diagnostic value of new CT imaging techniques for the functional assessment of coronary artery disease: a meta-analysis. Eur Radiol. 2019;29(6):3044-3061. PubMed
13.National Institute for Health and Care Excellence. Review of MTG32: HeartFlow FFRCT for estimating fractional flow reserve from coronary CT angiography. London, UK: National Institute for Health and Care Excellence; 2017: https://www.nice.org.uk/guidance/mtg32/evidence/review-decision-april-2021-pdf-9076795165. Accessed Oct 11, 2021.
14.Karady J, Mayrhofer T, Ivanov A, et al. Cost-effectiveness Analysis of Anatomic vs Functional Index Testing in Patients With Low-Risk Stable Chest Pain. JAMA Netw Open. 2020;3(12):e2028312. PubMed
15.Lu MT, Ferencik M, Roberts RS, et al. Noninvasive FFR Derived From Coronary CT Angiography: Management and Outcomes in the PROMISE Trial. JACC Cardiovasc Imaging. 2017;10(11):1350-1358. PubMed
16.Celeng C, Leiner T, Maurovich-Horvat P, et al. Anatomical and Functional Computed Tomography for Diagnosing Hemodynamically Significant Coronary Artery Disease: A Meta-Analysis. JACC Cardiovasc Imaging. 2019;12(7 Pt 2):1316-1325. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
National Institute for Health and Clinical Excellence (2021),11,13 UK Funded by the National Institute for Health and Clinical Excellence | Primary studies published between 2016 and 2021 23 studies included, 3 trials relevant to this report: NXT (Curzen et al. 2016), PROMISE (Lu et al. 2017), and PERFECTION (Pontone et al. 2019) | Inclusion criteria: Patients with stable chest pain, stable chest pain and without known CAD, suspected CAD, new onset chest pain, stable angina pectoris, or stable typical angina pectoris Patients with stable chest pain: 200 in the NXT trial, 271 in the PROMISE trial, and 147 in the PERFECTION trial | Inclusion criteria: HeartFlow CT-FFR compared with comparator technologies including PET, SPECT, and CCTA NXT trial CCTA alone vs. CT-FFR for clinical effectiveness CT-FFR compared with TAG320 and CCTA for diagnostic accuracy Reference standard: not reported PROMISE trial CT-FFR vs. CCTA Reference standard: invasive FFR PERFECTION trial “diagnostic accuracy of CCTA vs. CCTA+ CT-FFR vs. CCTA + Stress-CTP and ICA + invasive FFR as reference standard (p. 58)”13 Reference standard: ICA + invasive FFR | Outcomes: NXT trial Death from any cause, non-fatal myocardial infarction, and any revascularization PROMISE trial Diagnostic accuracy of revascularization or major adverse cardiac events PERFECTION trial Diagnostic accuracy of vessel stenosis by patients or per vessel Follow-up: A follow-up study of the NXT trial: 4.7 years (median); not described in the other studies |
Hamon et al. (2019),12 France No funding reported | Publications in English up to July 2018 50 articles published between 2008 and 2018 identified Diagnostic accuracy of CT-FFR at per-patient level (8 relevant publications) and per-vessel levels (18 relevant publications) | Inclusion criteria: patients with stable chest pain 3,024 subjects Mean ages summarized by primary studies Other population characteristics not reported | Inclusion criteria: CCTA, stress CTP, CT-FFR, and TAG as CT diagnostic techniques CT-FFR ≤ 0.80 as the threshold for hemodynamically significant CAD | Inclusion criteria: 1) the detection of hemodynamically relevant CAD; 2) numbers of true-positive, false-positive, true-negative, and false-negative; 3) invasive FFR as the reference standard Follow-up time not reported |
CAD = coronary artery disease; CCTA = coronary computed tomography angiography; CT-FFR = computed tomography-derived fractional flow reserve; CTP = myocardial computed tomography perfusion; FFR = fractional flow reserve; ICA = invasive coronary angiography; NXT = Next Steps; PERFECTION = PERfusion versus Fractional flow rEserve measured by computed tomography angiography In the evaluation of suspected cOroNary artery disease; PROMISE = Prospective Multicenter Imaging Study for Evaluation of Chest Pain; SPECT = single-photon emission computed tomography; TAG = transluminal attenuation gradient; vs. = versus.
Table 3: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Karady et al. (2020),14 US Funded by HeartFlow | Cost-effectiveness analysis Time horizons: 60 days, 2 years, and 5 years for health care utilization, lifetime for cost-effectiveness analysis Societal perspective | 10,003 participants with stable chest pain and 30% to 69% of stenosis in the Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) trial Median age = 60.0 years Female = 5,270; 52.7% White = 7,693; 77.4% | Anatomic approaches (CCTA, and CT-FFR) vs. functional testing (stress testing, including stress SPECT, stress echocardiography, and exercise treadmill testing) for the assessment of low-risk stable chest pain | Individual-based Markov microsimulation model Sensitivity analyses: (1) various adherence to medical therapy (2) expanding the indication of CT-FFR to those with luminal narrowing greater than 70% (3) do-nothing strategy (4) quasi-probabilistic sensitivity analysis by calculating cost-effectiveness acceptability curves for anatomic strategies compared with functional testing | Clinical and utility data from the PROMISE trial Health status data from the CONFIRM registry Cost data from the PROMISE trial and the US Centers for Medicare & Medicaid Services website; the 2017 edition of the Red Book for medication costs | Assumptions in clinical care and patient characteristics across lifetime Outcomes “Downstream ICA and coronary revascularization, MACE (death, non-fatal myocardial infarction), cost, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER) of competing strategies (p. 1)”14 |
CONFIRM = COroNary CT Angiography Evaluation For Clinical Outcomes: An InteRnational Multicenter; CCTA = coronary computed tomography angiography; CT-FFR = computed tomography-derived fractional flow reserve; ICA = invasive coronary angiography; ICER = incremental cost-effectiveness ratio; MACE = major adverse cardiovascular event; PROMISE = Prospective Multicenter Imaging Study for Evaluation of Chest Pain; QALY = quality-adjusted life-year; SPECT = single-photon emission computed tomography; vs. = versus.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 28
Strengths | Limitations |
|---|---|
National Institute for Health and Clinical Excellence (2021)11,13 | |
|
|
Hamon et al. (2019)12 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PICO = population, intervention, comparator, and outcomes.
Table 5: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist9
Strengths | Limitations |
|---|---|
Karady et al. (2020)14 | |
|
|
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcomes — Diagnostic Accuracy
Study citation, study design, and patient model | Study findings |
|---|---|
HeartFlow CT-FFR vs. CCTA alone | |
AUC for flow-limiting stenoses | |
National Institute for Health and Clinical Excellence (2021); the guidance11 and the systematic review13 published separately Systematic review of primary studies (randomized and non-randomized studies) Patients with stable chest pain in 1 trial | PERFECTION trial:
|
Unspecified CT-FFR vs. CCTA | |
Sensitivities and specificities for hemodynamic significant CAD | |
Hamon et al. (2019)12 Systematic review of publications Patients with stable chest pain in 50 publications | Patient level, 8 and 15 studies for CT-FFR and CCTA, respectively
Vessel level, 18 and 37 studies for CT-FFR and CCTA, respectively
|
CAD = coronary artery disease; CCTA = coronary computed tomography angiography; CT-FFR = computed tomography-derived fractional flow reserve; CTP = myocardial computed tomography perfusion; PERFECTION = PERfusion versus Fractional flow rEserve measured by computed tomography angiography In the evaluation of suspected cOroNary artery disease; vs. = versus.
Table 7: Summary of Findings by Outcomes — Clinical Utility
Study citation, study design, and patient model | Study findings |
|---|---|
CT-FFR vs. CCTA alone | |
Composite end point (composite of death from any cause, non-fatal myocardial infarction, and any revascularization) | |
National Institute for Health and Clinical Excellence (2021); the guidance11 and the systematic review13 published separately Systematic review of primary studies (randomized and non-randomized studies) Patients with stable chest pain in 1 trial | NXT trial (Curzenet al. 2016, Ihdayhid et al. 2019a, and 2019b)
Composite end point
|
Revascularization or major adverse cardiac events | |
National Institute for Health and Clinical Excellence (2021); the guidance11 and the systematic review13 published separately Systematic review of primary studies (randomized and non-randomized studies) Patients with stable chest pain in 1 trial | PROMISE trial
|
Frequency of MACE | |
National Institute for Health and Clinical Excellence (2021); the guidance11 and the systematic review13 published separately Systematic review of primary studies (randomized and non-randomized studies) Patients with stable chest pain in 1 trial | NXT trial
|
CCTA = coronary computed tomography angiography; CT-FFR = computed tomography-derived fractional flow reserve; FFR = fractional flow reserve; MACE = major adverse cardiovascular events; NXT = Next Steps; vs = versus.
Table 8: Summary of Findings of Included Economic Evaluation
Main study findings | Authors’ conclusion |
|---|---|
Karady et al. (2020)14 | |
Cost-effectiveness analysis, CT-FFR vs. functional testing Cost (95% CI), US dollars
QALY (95% CI)
Discounted ICER (US dollars/QALY)
Life-years gained (95% CI) in years
Sensitivity analyses, CT-FFR vs. functional testing Adherence to Medical Therapy
Expanding the Indication of CT-FFR to Patients With Greater Than 70%Luminal Narrowing
Do-Nothing Strategy
Quasi-probabilistic sensitivity analysis
| “anatomic strategies may present a more favorable initial diagnostic option in the evaluation of low-risk SCP compared with functional testing” (p. 2)14 |
CI = confidence interval; CT-FFR = CT-derived fractional flow reserve; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SCP = stable chest pain; vs. = versus.
Appendix 5: References of Potential Interest
Rapid Review
Helfand M, Anderson J, Peterson K, Bourne D. Evidence Assist: Coronary Computed Tomography Angiography Innovations in Noninvasive Diagnosis of Coronary Artery Disease. Porland, OR: Department of Veterans Affairs. https://www.hsrd.research.va.gov/publications/esp/non-invasive-cad.pdf Accessed Oct 29, 2021.
Additional References
Luo Y, Mao M, Xiang R, et al. Diagnostic performance of computed tomography-based fraction flow reserve in identifying myocardial ischemia caused by coronary artery stenosis: A meta-analysis. Hellenic J Cardiol. 2021;S1109-9666(21)00110-X.
Curzen N, Nicholas Z, Stuart B, et al. Fractional flow reserve derived from computed tomography coronary angiography in the assessment and management of stable chest pain: the FORECAST randofmized trial. Eur Heart J. 2021;42(37):3844-3852. PubMed
Qiao HY, Tang CX, Schoepf UJ, et al. Impact of machine learning-based coronary computed tomography angiography fractional flow reserve on treatment decisions and clinical outcomes in patients with suspected coronary artery disease. Eur Radiol. 2020;30(11):5841-5851. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca