CADTH Health Technology Review
Cognitive Remediation Therapy for People With Schizophrenia Spectrum Disorder: A Rapid Qualitative Review
Rapid Review
Authors: Umair Majid, Melissa Severn
Abbreviations
CRT
cognitive remediation therapy
SSD
schizophrenia spectrum disorders
Context and Policy Issues
Schizophrenia spectrum disorders (SSD) – which include schizophrenia affective disorder, delusional disorder, schizophreniform disorder, and schizophrenia – are serious mental illnesses that affect how a person thinks, feels, and behaves. According to WHO, schizophrenia affects 20 million people worldwide.1 A comprehensive systematic review of 188 studies estimated a median global point prevalence of 4.6 per 1,000.2 People with schizophrenia are more likely to die at an early age compared to the general population, primarily from preventable disease such as cardiovascular issues that go untreated or were missed.3 Schizophrenia is generally diagnosed between the late teens and early thirties.
Symptoms of SSD include psychotic symptoms, negative symptoms, and cognitive symptoms. Research suggests that up to 98% of people with schizophrenia experience some level of cognitive impairment including memory loss, reduced attention, and difficulty in reasoning and problem solving.4,5 Cognitive impairment may be the most salient predictor of daily functioning for people with SSD.6,7 Cognitive deficits may lead to unemployment, reduced independence, and lack of community and social engagement.8-14 While treatment for psychotic symptoms in SSD is common, research has shown antipsychotic therapy to have a low to modest impact on cognitive performance.15-19 This finding is especially important because early research showed that cognitive deficits may continue despite improvement in psychotic symptoms.20
Cognitive remediation therapy (CRT) is “a behavioural, training-based intervention that aims to improve cognitive processes (attention, memory, executive functions, social cognition or meta cognition) with the goals of durability and generalization.”21 There are 2 categories of CRT approaches. Compensatory approaches target functional outcomes by using environmental supports to bypass cognitive deficits.22 Restorative approaches, on the other hand, use the concept of brain neuroplasticity; whereby, the brain is amenable for cognitive repair given the appropriate stimuli.6,23 CRT can be facilitated by a clinician or be completed independently and can be facilitated in a group or individual format. CRT can also be computer-assisted or completed using pencil and paper exercises.
Research suggests that CRT leads to cognitive and functional improvement.21,24,25 For example, a meta-analysis of 40 studies on CRT published between 1973 and 2009 found a global cognition effect size of 0.45 from CRT on cognitive symptoms for SSD.21 Other research reported that CRT improves clinical, cognitive, and functional symptoms for patients with both early and chronic SSD.25 However, some research has found that participant’s motivation can influence whether CRT is effective in addressing cognitive deficits.6 CRT that leverages participant’s intrinsic motivation, allows meaningful participation in game-like tasks, and enables control over learning that may improve the effectiveness of CRT.26
While studies have shown that CRT is effective in addressing cognitive deficits, few studies that have explored how people with SSD perceive and experience CRT, including the challenges they face accessing CRT, the barriers they experience continuing CRT, and the benefits they perceive from CRT. This rapid review will analyze the findings from primary qualitative and mixed-methods studies to identify how people with SSD access, perceive, and engage with CRT.
Key Messages
This rapid qualitative review analyzed 8 studies describing the perspectives of people living with schizophrenia spectrum disorder (SSD) who use cognitive remediation therapy (CRT), and their caregivers and clinicians. The aim of this rapid review was to identify experiences with accessing CRT, expectations of CRT for treating and supporting recovery from SSD, and experiences engaging with CRT. From the participant’s perspective, this review found several perceived and realized benefits of CRT. People living with SSD reported notable improvements in their attention, memory, and problem solving. People living with SSD also reported improvement in their lives, when they applied the cognitive strategies acquired from CRT into daily life activities. People living with SSD also described improvement in communication skills, social engagement, motivation, independence, and a reduction in psychotic symptoms. This review found a common preference among people living with SSD and caregivers to provide personalized delivery and treatment of CRT. People living with SSD cited several ways to introduce personalized CRT: cognitive trainer or clinician’s support and guidance; the content, design, and implementation of CRT; using technology; and group environment and interacting with peers. The constant presence of a polite, friendly, empathetic, and encouraging clinician contributed to beneficial views of CRT. People living with SSD enjoyed the structure of sessions and cognitive tasks, specifically working on tasks at their own pace with gradual increases in difficult that gave them a sense of accomplishment and mastery. People living with SSD also enjoyed using technology and playing games to complete tasks; however, some found accessing a computer and a high-quality internet connection difficult. Finally, while people living with SSD reported several social benefits to group-based CRT, others found group-based CRT to be unconducive for their learning, especially when the group environment was not supportive or encouraging. One study described caregiver experiences and another described clinician experiences. Caregivers and clinicians in both studies recognized the importance of matching the type of cognitive exercises and structure of sessions to the cognitive needs of people living with SSD. Furthermore, caregivers preferred more examples of real-life strategies that they can use to help their loved one apply in their daily life.
Research Questions
What are the perspectives and experiences of people living (or caring for someone) with SSD, or their health care providers, regarding cognitive remediation therapy and:
the process of accessing cognitive remediation therapy as a treatment for SSD
their expectations for how cognitive remediation therapy will (or will not) treat and support recovery from SSD
the process of engaging with cognitive remediation therapy as a treatment for SSD.
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and PsycInfo. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were cognitive remediation and SSD. CADTH-developed search filters were applied to limit retrieval to qualitative studies. The search was also limited to English language documents published between January 1, 2011, and September 21, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Sample | Adults (≥ 18 years) who are living (or caring for someone) with SSD (e.g., schizophrenia, schizoaffective disorder, delusional disorder, schizophreniform disorder); health care providers for people living with SSD |
Phenomenon of interest | Perspectives and experiences of accessing and undergoing cognitive remediation therapy for SSD – with or without treatment as usual (pharmacotherapy) |
Design | Any qualitative design or the qualitative portions of mixed-method studies |
Evaluation | Perspectives on accessing cognitive remediation therapy for SSD; expectations of cognitive remediation therapy for treating and supporting recovery from SSD; experiences of engaging with cognitive remediation therapy |
Research type | Primary qualitative studies; qualitative components of primary mixed-methods studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2011. We also excluded articles that were specific to CRT for psychosis or prodromal symptoms, and any studies pertaining cognitive-behavioural therapy for SSD.
Critical Appraisal of Individual Studies
The included studies were critically appraised by 1 reviewer using the Quality of Reporting (QuaRT) tool.27 The tool evaluates the reporting quality of studies based on 4 characteristics: question and study design, selection of participants, methods of data collection, and methods of data analysis. Summary scores were not calculated to describe the quality of included studies; rather, the strengths and limitations of each included study were described narratively in Appendix 4. Results of the critical appraisal were not used to exclude studies from this review.
Data Analysis
Descriptive Analysis
One reviewer extracted the following study and methodological characteristics of included studies: research objectives, country of publication, study design and qualitative methodology or analytic approach, data collection method(s), inclusion criterion of participants, sample size, proportion of male respondents, age range, and the name of the treatment. One reviewer performed summary statistics of these characteristics that are summarized in the Summary of Included Literature section and Appendices 2 and 3.
Analytic Approach
Data analysis was performed using the qualitative meta-synthesis approach.28 This approach aims to aggregate the findings from multiple included studies to produce a holistic interpretation of the topic, while maintaining the original meaning of each study in the final interpretations. Using the constant comparative method and constructivist grounded theory,29 1 reviewer analyzed and synthesized the findings from all included studies to develop an integrative interpretation of the topic using Microsoft Word. The reviewer focused on developing an interpretation of the topic that answered the research questions and supported the relevant policy decisions.
One reviewer used a staged coding process to conduct analysis that comprised of the following: pilot coding, initial coding, and focused coding. In pilot coding, the reviewer analyzed the findings and discussion sections of 2 included studies and created a preliminary coding schema that outlined emerging themes and concepts. The reviewer analyzed the findings rapidly through a line-by-line analysis to acquire a broad sense of the data as well as salient issues in the experience and expectations of accessing and engaging with CRT for SSD. The reviewer discussed this preliminary coding schema with the CADTH reviewer/owner of this project to ensure that the preliminary findings were consistent with the research questions and policy decisions. In initial coding, the reviewer analyzed the remaining studies using the preliminary coding schema as a guide to identify relevant findings. The reviewer also pursued opportunities to compare findings between patients, caregivers, and clinicians. The reviewer refined the preliminary coding schema after the analysis of each article.
In the final stage of focused coding, the final coding schema was reviewed for comprehensiveness, representativeness, and relevance with the research questions and policy decisions. The reviewer reorganized all coding to achieve theoretical saturation between and within each theme by identifying consistency, redundancy, and divergence between themes. The reviewer used the final coding schema to develop a narrative summary of each theme, and all summaries were collated into 1 integrated and holistic interpretation of the topic.
Summary of Included Literature
Quantity of Research Available
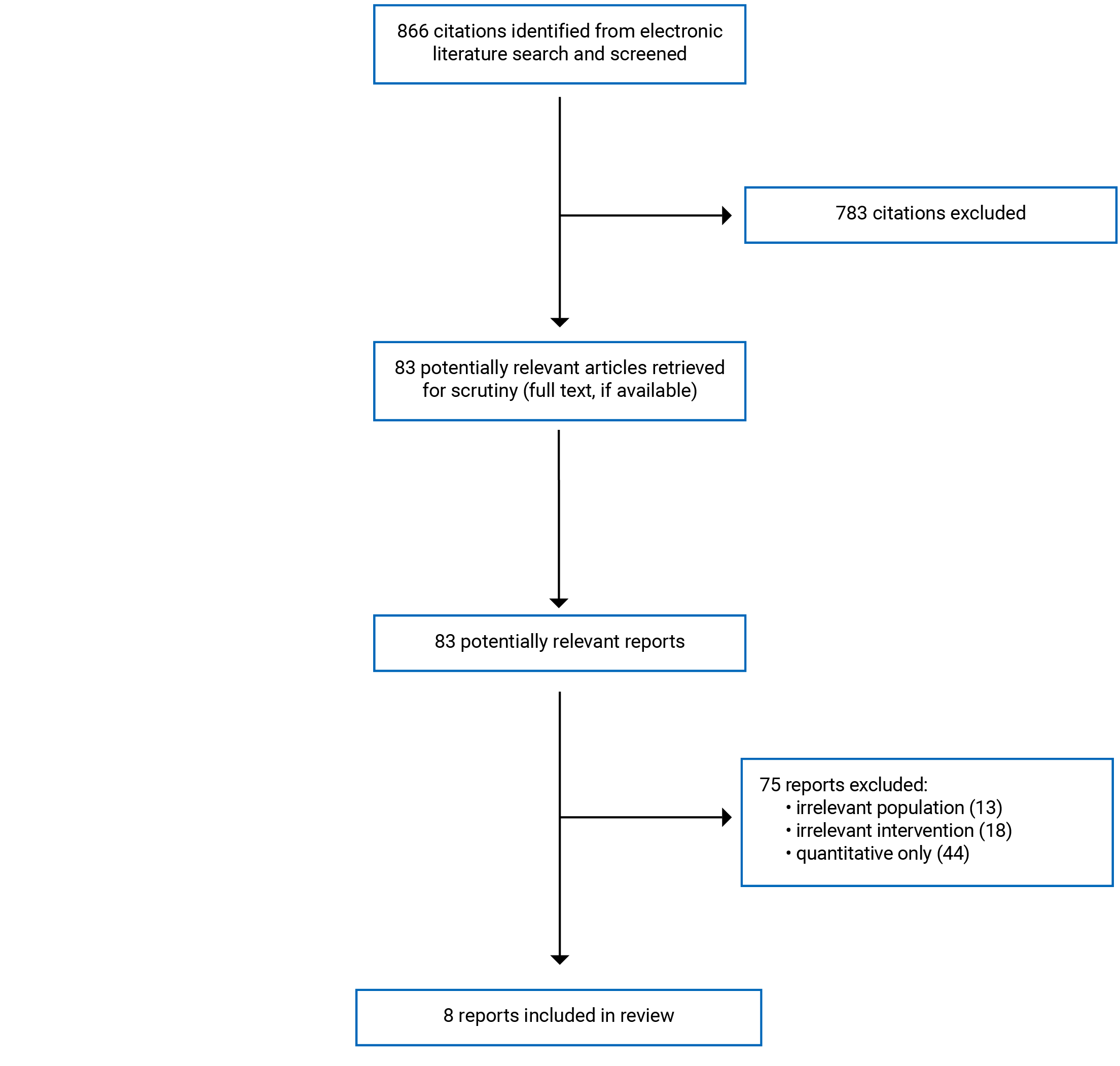
A total of 866 citations were identified in the literature search. Following the screening of titles and abstracts, 783 citations were excluded and 83 potentially relevant reports from the electronic search were retrieved for the full-text review. Of these potentially relevant articles, 75 publications were excluded for various reasons, and 8 publications met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA flow chart of the study selection process.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications and the people living with SSD are provided in Appendices 2 and 3.
Study Design, Qualitative Methodology or Analytic Approach, and Data Collection Methods
Four studies used a qualitative study design,30-33 and 4 studies employed a mixed-methods design.34-37 Of these studies, only 1 did not report its qualitative methodology or analytic approach.36 Of the remaining 7 studies that reported the methodology or approach, 4 used thematic analysis,30,31,34,37 and 1 of each of the others used content analysis,38 qualitative description,32 and ethnography.33 In terms of data collection, 5 studies used semi-structured interviews,32,34-37 2 used semi-structured surveys,30,31 and 1 used observation.33
Country of Origin
Two studies were published in Australia,30,31 2 in the US,35,36 1 in Canada,34 1 in France,33 1 in South Africa,32 and 1 in the UK.37
Patient Population
All except 1 study specified the type and number of participants included in the study.33 The perspectives of people with SSD, caregivers, and clinicians are included in this rapid review. One of each study reported caregiver34 and clinicial35 perspectives. Overall, this rapid review analyzed the perspectives of 127 people with schizophrenia, 20 caregivers, and 6 clinicians.
All studies included people with schizophrenia and/or schizoaffective disorder. One study included people who had both schizophrenia and HIV.32 The percentage of male research participants was reported in 4 studies,30-32,34 ranging from 45% and 55%. Furthermore, the age range was reported by 3 studies,30-32 ranging from 26 and 51 years.
Interventions (and Comparators)
All included studies focused on some type of cognitive training for schizophrenia, but they used slightly different terminology. Five studies used some variation of CRT.30,31,33,35,36 Other studies indicated a rehabilitation program for working memory,32 cognitive adaptation training,34 and cognitive enhancement therapy.36 One study compared CRT with computer games.30 Another study specified the delivery of cognitive adaptation training on the computer with the assistance of a caregiver.34
Five studies reported computer-assisted CRT,30-32,36,37 1 study reported a hybrid CRT approach,35 1 study did not use computer-assisted CRT,34 and 1 study did not indicate whether CRT was computer-assisted. Furthermore, 4 studies reported group-based CRT,30,31,35,36 and 3 studies reported individual-based CRT,32,34,37 One study reported on both group and individual-based CRT.33
Summary of Critical Appraisal
A summary of strengths and limitations of each included study can be found in Appendix 4.
Generally, included qualitative and mixed-method studies reported most of the 4 methodological characteristics in the QuaRT tool, giving an impression of good reporting quality. All except 1 study36 clearly identified their research question, study design, and qualitative analytic approach. Similarly, all except 1 study33 provided a detailed description of data collection methods, recruitment procedures, and sample size. However, approximately half of included studies did not provide sufficient description on data analysis procedures and strategies.33,34,36,37 Three of these studies were mixed-methods studies; the choice of study design may explain why there was little information regarding qualitative data analysis since authors must regularly balance methodological description of their study with the word count limitations of journals. Finally, none of the studies explicitly considered how they improved the quality or rigour of their study, while all studies employed some form of analysis in pairs and reflexive discussions on the analysis.
In conclusion, the reporting quality of included studies was generally high except for data analysis. Furthermore, no studies explicitly considered strategies that improved the rigour of their study. This has important implications for the findings of this rapid review. Since half of the included studies were mixed-methods, authors may be constrained in reporting the methodological information of 2 studies rather than 1. Having to balance rigid word count limitations may encourage the omission of essential methodological information from the final published manuscript.
Results
This section highlights the perspectives of people living with SSD using CRT, and their caregivers and clinicians. This section is divided into the following subsections: perceived and realized benefits from CRT, and personalized delivery and treatment (cognitive trainer or clinicians support and guidance; content, design, and implementation of CRT; using technology; and group environment and interacting with peers).
Perceived and Realized Benefits from CRT
People living with SSD in the included studies perceived several cognitive, functional, social, intrinsic, and symptomatic benefits from CRT. First, participants in 4 studies reported the following improvements in their cognitive skills: attention, concentration, reaction speed, problem solving, memory, retention, and planning.30,31,33,37
Second, people living with SSD described how they were able to apply the cognitive skills they learned from CRT — also referred to as functional benefits — in their daily lives: “I didn’t expect the computer programme...to help me with my general well-being and general planning...so I was impressed by it because I didn’t think it would work as much as it did actually.”37 People living with SSD in 3 studies transferred their CRT training skills into their daily lives, specifically in routines and social situations, and to improve strategies to resolve life problems.31,33,37 People living with SSD also found CRT training helpful for remembering things — since CRT taught them how to create and use memory aids — and maintaining high concentration when completing job applications and following cooking recipes.37 Similarly, caregivers mentioned how CRT guides that included detailed cognitive strategies and examples for daily life were the most useful to them. Caregivers also preferred to have more guidance that was available in an online format with convenient access, so they can help their loved ones improve their skills throughout the day.34
Third, people living with SSD reported several social benefits from group-based CRT. These benefits included pursuing shared goals with peers, improving communication and social skills, comparing symptoms and validating personal experiences, and offering support to others with mental illness.30,31,35 For example, this person living with SSD described how group-based CRT provided an opportunity to share experiences with others:
“[It was] nice to know others that had similar experiences and that it’s not just you. People that are at a similar stage of recovery, under control but experiencing similar milder symptoms. Not just crazy and doing it on your own.”30
And this other people living with SSD illustrated how group-based CRT helped to improve communication skills with the family:
“I used to have trouble with family. I would get too defensive but now I have realised how to step back and think more clearly about situations, before reacting. It showed me ways to attack problems.”31
Fourth, patients reported improved motivation, self-determination, confidence, and emotional and internal regulation.30,31,36,37 These benefits came from achieving a sense of accomplishment by completing CRT, having opportunities to reflect on personal strengths and weaknesses, being given the opportunity to confront and overcome challenges, and contest existing beliefs.30,37 Finally, people living with SSD in 1 study reported a reduction in their psychiatric, mood, and stress symptoms resulting from participating in CRT.30 However, this study did not elaborate on such improvements.
People living with SSD in the included studies mostly discussed perceived or realized benefits from CRT. However, some people living with SSD expressed limited benefits, either because they were unaware or unsure of whether CRT would provide them with cognitive benefits, or because they were unable to transfer cognitive strategies from CRT into their daily lives.30-32,37 Low awareness of CRT and its benefits was not mentioned in all included studies. People living with SSD in 1 study believed that CRT was intended for those with severe cognitive impairment, and they did not group themselves in that category.32 Other people living with SSD described being unable to transfer what they learned to their everyday lives, even if they reported some improvement in memory and attention,30,31,37 as this person living with SSD illustrated:
“I didn’t see correspondence between specific tasks and everyday life but I did see general improvements in attention, memory and problem solving.31
Personalized Delivery and Treatment
A common theme present across someone living with SSD, caregiver and clinician perspectives was delivering CRT in a personalized and tailored way. This theme was grounded in the idea that people living with SSD have different cognitive needs, requiring different types of activities, skills, and strategies. People living with SSD requested flexibility in the types of cognitive tasks, the structure of sessions, and the use of technology.30,31 The role of the cognitive trainer and clinician was important for delivering tailored CRT.31 2021,37 Caregivers preferred to have a menu of cognitive tasks that they can apply to match the cognitive needs of their loved one.34 Clinicians recognized the importance of tailoring CRT by recommending that participants with high cognitive impairment attend more frequent sessions, while other people living with SSD who were more independent complete at-home, asynchronous exercises.35 However, the lack of tailored CRT delivery can lead to inadvertent consequences. For example, applying cognitive exercises designed for severe cognitive impairment for people living with SSD with low cognitive impairment may lead to disinterest and demotivation, especially since people living with SSD in the included studies reported enjoyment in the gradual progression of difficulty in cognitive tasks.30,31 On the other hand, the implementation of tasks designed for lower cognitive impairment — and thereby more challenging to complete — to people living with SSD with high cognitive impairment may lead to frustration, which may also exacerbate pre-existing anxiety or other comorbidities.30,32,37
The number and length of sessions was mentioned by people living with SSD as another way to tailor CRT. Some people living with SSD suggested providing CRT in more frequent but shorter sessions; however, this was not the case for all people living with SSD as some preferred longer sessions.37 Preferences regarding the structure of sessions may depend on the participant’s lifestyle, and whether they have multiple competing priorities that they must manage alongside CRT. CRT can be implemented in-person at a medical facility or at-home, in a group or individual format, can use technology or pencil and paper exercises, or be a combination thereof. Delivering CRT in a tailored manner may also allow participants to choose their preferred delivery mode, depending on their current priorities and lifestyle. Similarly, participants preferred group-based CRT because of its social benefits,30,31,35,36 but preferred independent CRT when a supportive and encouraging environment was not present.30-32 Each of these aspects to personalized delivery and treatment will be discussed in detail in the following sections.
Cognitive Trainer or Clinician’s Support and Guidance
The constant presence of a cognitive trainer or clinician was mentioned as a key contributor to a beneficial CRT experience.31,35,37 Specifically, trainers and clinicians played an important role in guiding and encouraging people living with SSD through difficult tasks, as this person living with SSD illustrated: “there was a trust, a feeling of trust that I had and a feeling that I was sort of you know in a comfortable environment and in, in kind of like you know everything was being handled in a thoroughly professional manner.”37 People living with SSD identified several interpersonal qualities that they valued in trainers and clinicians: polite, friendly, patient, trustworthy, understanding, empathetic, and warm.31,35,37 People living with also appreciated when trainers and clinicians provided reminders to complete their homework, assisted in brainstorming strategies for assignments, explained tasks clearly, signposted activities that may interest people living with SSD, and tailored CRT tasks to their learning styles and emotional and psychological needs.31,37 On the other hand, people living with SSD reported a suboptimal CRT experience when there were limited interactions with trainers and clinicians.31,32,35 No studies reported unpleasant interactions with trainers and clinicians.
Clinicians acknowledged the need to support participants throughout CRT and deliver CRT in a tailored manner.35 To clinicians, tailored delivery referred to having people living with SSD who required more assistance to attend more sessions; whereas others who may be more independent and have access to technology complete CRT exercises at their convenience.
Content, Design, and Implementation of CRT
Some patients appreciated the design, layout, and structure of sessions and cognitive tasks.30,37 People living with SSD specifically valued CRT when tasks were easy to follow and complete, when there was the opportunity to ask for feedback, and when training was flexible to the needs of patients.30,31 People living with SSD also appreciated working through tasks at their own pace, with gradual increases in difficulty that allowed them to experience a sense of accomplishment, improvement, and mastery.30,31 Improvement in increasingly difficult tasks instilled enjoyment and genuine engagement in CRT.37 However, people living with SSD preferred exercises that were less repetitive and attending sessions in different settings.30,37
While some people living with SSD appreciated the content, design, and implementation of CRT, others did not. For example, half of the people living with SSD in 1 study found the content too challenging to complete.30 Discontent toward the structure of sessions and format of CRT tasks came from the following reasons: the amount of exposure to information required to complete tasks, anticipation of failure, experiencing failure when completing progressively difficult tasks, a fear of mental exhaustion from participating in CRT for many hours, and inability to incorporate learning from CRT to improve daily functioning.30,32,37 All of these issues made engagement in CRT exhausting and tiring: “it was quite draining. It was almost like it took a hell of a lot of energy from me...after I’d done it I felt tired; my mind was completely tired.”32 These issues were salient for patients who had pre-existing issues with anxiety, which were exacerbated by challenging cognitive tasks.32 Furthermore, some people living with SSD did not initiate CRT because of anxiety; they felt increased anxiety because they were exposed to the realities of their cognitive impairment, which was difficult to accept for some who believed they did not need therapy.32 People living with SSD who had low tolerance to frustration, high pre-existing anxiety, high vulnerability to mental fatigue, and low motivation were more likely to drop out.32 For these people living with SSD, CRT was viewed as a threat to their self-esteem, inadvertently causing emotional stress.32 To remedy this, some people living with SSD suggested providing CRT in more frequent but shorter sessions; however, this was not the case for all people living with SSD, as some preferred longer sessions.37
Caregivers preferred to have CRT guides and other supporting materials (e.g., signs, checklists, and worksheets) tailored to their loved one.34 Caregivers reported that engaging loved ones was a challenge.34 They found that 4 months was insufficient for engaging their loved ones in transferring cognitive strategies from CRT into daily life. Caregivers also found engagement difficult when their loved ones did not believe they had cognitive issues or rejected their schizophrenia diagnosis. Caregivers also found it difficult to follow CRT exercises in the recommended order when their loved ones wanted to pursue their own learning path. Alongside these conversations, 1 participant mentioned how CRT guides and supporting documents perpetuated dysfunctional narratives that did not reflect the severity of their loved one’s mental illness. In their view, CRT exercises assumed a specific level of severity that was not applicable to their loved one, thereby making exercises less effective. Caregivers found that motivating their loved one who had mild cognitive impairment to complete exercises designed for severe cognitive impairment was challenging because the tasks were completed quickly with minimal effort and stimulation. However, other people living with SSD used the dysfunctional language in CRT to discuss the realities of severe cognitive impairment with their loved ones, which helped motivate people living with SSD to engage in CRT.
Using Technology
People living in 5 studies reported an enjoyable experience using computers to complete cognitive exercises.30-32,36,37 People living with SSD found the use of computers relatively easy,30-32,36,37 especially for those who had previous experiences with computers.37 However, people living with SSD who did not have previous experience with technology found it hard to engage with CRT.32,35,37 People living with SSD expressed demotivation when they could not access a computer, when they needed to navigate the internet to complete tasks, when they had low-quality internet, and when they needed to set up a laptop.32,35,37 For example, as this person living with SSD described: “some days I struggled to connect to the internet and it made me feel so, so demotivated.”32 People living with SSD in 1 study also reported the high cost of internet as a barrier to completing CRT exercises in their home using their personal computer.32
Group Environment and Interacting with Peers
People living with SSD expressed some benefits to completing CRT in a group setting. People living with SSD found that group CRT provided an opportunity to exchange shared experiences about CRT and schizophrenia,30,31,35,36 as this 1 person living with SSD highlighted: “it was alright to have more persons. One on one might be too confronting. Groups are more comfortable. To have other people with similar problems it was a good experience because allow us to share perspectives.”31 People living with SSD found a constructive peer environment where everyone worked toward mutual goals, engaged in shared problem solving, and aided peers as an important feature that made group-based CRT a beneficial experience.30,31 However, people living with SSD also preferred working independently through CRT tasks.32,35 For these people living with SSD, group-based CRT was distracting and competitive, which made them feel insecure.30-32 People living with SSD reported how the lack of peer support in group-based CRT created an unpleasant environment that was not conducive for learning:32 “I just felt this place has, like, breaking me down. People aren’t encouraged...it feels like encouragement or more positivity or more group work or more teamwork.”32
On the other hand, people living with SSD who attended CRT in their homes reported frequent interruptions from outside noise, attending to family needs, and picking up phone calls.32,36 These people living with SSD also faced challenges in allocating a time block in their busy schedules for CRT sessions; for example, people living with SSD in 2 studies reported that their vacation schedule interfered with CRT sessions and completing homework.32,36
Clinicians believed that hybrid CRT (with group sessions and individual exercises) was better suited for clients who were more independently motivated and had some technological literacy. However, hybrid CRT overall placed a strain on a person’s time who is living with SSD since it required both in-person sessions and at-home exercises, as this clinician described:
“it became a little bit more challenging, because we had to find the time to not only just monitor the computer room...but also just to make sure that they understand how to manipulate the computer.”35
Limitations
This rapid review highlighted the experiences and perspectives of people living with SSD using CRT. However, there are some limitations of this work that reflect the limited quantity and depth of data available. First, there was a low number of studies included in this review, half of which used a mixed-methods study design that offered limited depth and breadth in the experiences and perspectives. This was especially the case for the perspectives of caregivers and clinicians. These perspectives offered more nuance on the topic, but they were limited to 2 studies. There is a clear need for research on the perspectives of clinicians and caregivers.
Second, almost all studies were unclear about how they designed and implemented CRT. Some studies implemented independent online-based CRT, others implemented in-person CRT, and others implemented a combination of the 2. Each CRT format may present unique challenges for people with SSD; however, the authors of included studies were unclear about how their CRT format presented unique challenges for people living with SSD. Wherever possible, this report highlighted the relationship between the CRT format and barriers to accessing and continuing treatment experienced by people with SSD, but this was not always possible. There is a need to compare how the experiences and perspectives of CRT differ across CRT formats. This information may help to understand, for example, how perceived benefits may differ between online and in-person CRT, or how technological literacy may be a more salient barrier for people with severe, chronic SSD.
Third, this report excluded studies on CRT for psychosis. Individuals who exhibit psychosis may be dissimilar to people with SSD in the severity of symptoms and level of impairment. As this rapid review discussed, the level of impairment may influence the types of challenges experienced by people with SSD. Including the psychosis literature may have broadened the nuance of this work, by providing more data on CRT for low impairment and cognitive deficits.
Conclusions and Implications for Decision- or Policy-Making
This rapid review found 8 studies that described the perspectives and experiences of people living with SSD using CRT, their caregivers, and clinicians who facilitated CRT.
People living with SSD listed several cognitive, functional, social, intrinsic, and symptomatic benefits from CRT. People living with SSD reported how they were able to apply the skills and strategies they acquired from CRT into their daily lives, ultimately improving daily function. People living with SSD also described how group-based CRT improved their confidence and ability to communicate with others. As for intrinsic benefits, some people living with SSD explained how they felt increased motivation, self-determination, confidence, and emotional regulation. Differences in experiences about whether CRT led to benefits came from not being able to transfer cognitive strategies from CRT into daily life, and confusion regarding the aim of CRT.
Those living with SSD, caregivers, and clinicians expressed the importance of delivering CRT in a personalized manner. People living with SSD described several characteristics that contributed to personalized CRT: cognitive trainer or clinician’s support and guidance; content, design, and implementation of CRT; using technology; and group environment and interacting with peers. First (cognitive trainer or clinician’s support and guidance), the constant presence of a clinician – who possessed qualities such as empathy and politeness – contributed to a beneficial CRT experience. People living with SSD also noted that the low availability of clinicians made CRT more challenging, contributing to an unpleasant experience. Similarly, cognitive trainers and clinicians acknowledged the importance of delivering CRT in a personalized manner. Second (content, design, and implementation of CRT), people living with SSD found the design, layout, and structure of sessions and cognitive tasks to be conducive for their learning. Specifically, participants enjoyed the opportunity to work through cognitive tasks at their own pace, with a gradual increase in the difficulty that allowed them to experience a sense of accomplishment or mastery. However, other people living with SSD found CRT to be time-consuming or challenging, especially for those who had severe cognitive impairment, anxiety, or other comorbidities. Caregivers expressed the desire for more guidance and examples of cognitive strategies that they can use to improve the daily functioning of their loved ones. Third (using technology), the use of technology to complete cognitive tasks was viewed as beneficial and unpleasant by different people living with SSD. Some people living with SSD enjoyed the opportunity to learn using a computer and play games when completing cognitive tasks. Others, however, found that not having access to a computer and high-quality internet connection was frustrating that interfered with the ability to engage in CRT meaningfully. On the other hand, clinicians also found that hybrid CRT was best suited for people living with SSD who were more independent, had lower cognitive impairment, and had multiple competing priorities. Finally (group environment and interacting with peers), while people living with SSD perceived several social benefits from participating in group CRT, others found group CRT to be distracting, especially when the group environment was not supportive or encouraging, or too competitive. People living with SSD who had low cognitive impairment preferred at-home, asynchronous sessions because of the inherent flexibility in completing cognitive tasks at their convenience while managing competing priorities.
Allowing delivery mode flexibility may reduce challenges in engaging with interventions for people with diverse needs, goals, and preferences.39 In the context of CRT, tailoring is essential to ensure that there is a balance between challenge and enjoyment, allowing people living with SSD to be fully immersed in cognitive exercises. However, decision-makers, program developers and clinicians may consider reflecting on how barriers to CRT, such as lack of computer access and multiple competing priorities mentioned in this rapid review, may exacerbate perceived cognitive challenge for people living with SSD, possibly leading to disinterest and demotivation overtime when the challenge is not accompanied by support and encouragement. Flexibility in CRT tasks may allow people living with SSD with different needs and goals to choose the level of challenge they desire. Flexible CRT may allow people living with SSD to modify their CRT learning pathway to cognitive needs. For example, CRT may permit people living with SSD to complete easier cognitive tasks on 1 day, and more difficult the next day, based on the preferences of people living with SSD. Furthermore, CRT should also allow people living with SSD who show faster improvement to be able to skip or modify the CRT curricula to pursue more challenging tasks. Future implementation of CRT may also consider allowing people living with SSD to choose group- or individual-based CRT and permit people living with SSD to change their choice throughout their participation in CRT to reflect changes in availability.
Transferring cognitive learning to real-life situations to improve daily function was also a common concern shared by both people living with SSD and their caregivers in included studies. While people living with SSD reported that they were able to apply some CRT skills in their daily lives, this was not the case for everyone.31,33,34,37 This is an important concern because an inability to transfer CRT skills to daily lives may be a gap in the design, content, and structure of CRT. Inability to transfer CRT to use in daily life may also lead to unpleasant CRT experiences and attrition, since people living with SSD may view CRT as an intense time commitment without the expected improvements in their daily lives. It may be beneficial to consider how to best support people living with SSD and their caregivers to implement CRT skills in daily lives, perhaps by implementing exercises that target the application of cognitive skills, providing more relevant and tangible examples, and teaching cognitive skills through active learning strategies. Cognitive trainers and clinicians can use the preferences and experiences of people living with SSD to guide the design of cognitive exercises that favour the application of skills into daily life. For example, if people living with SSD need to improve their memory or concentration, then trainers and clinicians can facilitate a cognitive exercise in a context of a daily life activity that interests the person living with SSD — such as cooking or completing a school assignment — while reminding them of the cognitive strategies they can implement throughout the process. In group-based CRT, trainers and clinicians can also facilitate a discussion on how people living with SSD have successfully applied cognitive skills from CRT to improve their daily lives. This discussion can create a space for exchanging strategies and ideas between those living with SSD, and if provided in a supportive environment, can make the CRT experience more genuine and meaningful to people living with SSD.
References
1.Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-1858. PubMed
2.Saha S, Chant D, Welham J, McGrath J. A systematic review of the prevalence of schizophrenia. PLoS Med. 2005;2(5):e141. PubMed
3.Laursen TM, Nordentoft M, Mortensen PB. Excess early mortality in schizophrenia. Annu Rev Clin Psychol. 2014;10:425-448. PubMed
4.Keefe RS, Eesley CE, Poe MP. Defining a cognitive function decrement in schizophrenia. Biol Psychiatry. 2005;57(6):688-691. PubMed
5.Nuechterlein KH, Barch DM, Gold JM, Goldberg TE, Green MF, Heaton RK. Identification of separable cognitive factors in schizophrenia. Schizophr Res. 2004;72(1):29-39. PubMed
6.Kaneko Y, Keshavan M. Cognitive remediation in schizophrenia. Clin Psychopharmacol Neurosci. 2012;10(3):125-135. PubMed
7.Bowie CR, Leung WW, Reichenberg A, et al. Predicting schizophrenia patients' real-world behavior with specific neuropsychological and functional capacity measures. Biol Psychiatry. 2008;63(5):505-511. PubMed
8.Eack SM, Hogarty GE, Greenwald DP, Hogarty SS, Keshavan MS. Cognitive enhancement therapy improves emotional intelligence in early course schizophrenia: preliminary effects. Schizophr Res. 2007;89(1-3):308-311. PubMed
9.Fett AK, Viechtbauer W, Dominguez MD, Penn DL, van Os J, Krabbendam L. The relationship between neurocognition and social cognition with functional outcomes in schizophrenia: a meta-analysis. Neurosci Biobehav Rev. 2011;35(3):573-588. PubMed
10.Green MF, Nuechterlein KH. Should schizophrenia be treated as a neurocognitive disorder? Schizophr Bull. 1999;25(2):309-319. PubMed
11.Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull. 2000;26(1):119-136. PubMed
12.Gold JM, Goldberg RW, McNary SW, Dixon LB, Lehman AF. Cognitive correlates of job tenure among patients with severe mental illness. Am J Psychiatry. 2002;159(8):1395-1402. PubMed
13.Bowie CR, Reichenberg A, Patterson TL, Heaton RK, Harvey PD. Determinants of real-world functional performance in schizophrenia subjects: correlations with cognition, functional capacity, and symptoms. Am J Psychiatry. 2006;163(3):418-425. PubMed
14.Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. 1996;153(3):321-330. PubMed
15.Hill SK, Bishop JR, Palumbo D, Sweeney JA. Effect of second-generation antipsychotics on cognition: current issues and future challenges. Expert Rev Neurother. 2010;10(1):43-57. PubMed
16.Mishara AL, Goldberg TE. A meta-analysis and critical review of the effects of conventional neuroleptic treatment on cognition in schizophrenia: opening a closed book. Biol Psychiatry. 2004;55(10):1013-1022. PubMed
17.Davidson M, Galderisi S, Weiser M, et al. Cognitive effects of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: a randomized, open-label clinical trial (EUFEST). Am J Psychiatry. 2009;166(6):675-682. PubMed
18.Keefe RS, Bilder RM, Davis SM, et al. Neurocognitive effects of antipsychotic medications in patients with chronic schizophrenia in the CATIE Trial. Arch Gen Psychiatry. 2007;64(6):633-647. PubMed
19.Woodward TS, Whitman JC, Arbuthnott K, Kragelj TL, Lyons J, Stip E. Visual search irregularities in schizophrenia depend on display size switching. Cogn Neuropsychiatry. 2005;10(2):137-152. PubMed
20.Harvey PD, Docherty NM, Serper MR, Rasmussen M. Cognitive deficits and thought disorder: II. An 8-month followup study. Schizophr Bull. 1990;16(1):147-156. PubMed
21.Birchwood M, Peters E, Tarrier N, et al. A multi-centre, randomised controlled trial of cognitive therapy to prevent harmful compliance with command hallucinations. BMC Psychiatry. 2011;11:155. PubMed
22.Draper ML, Stutes DS, Maples NJ, Velligan DI. Cognitive adaptation training for outpatients with schizophrenia. J Clin Psychol. 2009;65(8):842-853. PubMed
23.Medalia A, Choi J. Cognitive remediation in schizophrenia. Neuropsychol Rev. 2009;19(3):353-364. PubMed
24.McGurk SR, Twamley EW, Sitzer DI, McHugo GJ, Mueser KT. A meta-analysis of cognitive remediation in schizophrenia. Am J Psychiatry. 2007;164(12):1791-1802. PubMed
25.Deste G, Barlati S, Galluzzo A, et al. Effectiveness of Cognitive Remediation in Early Versus Chronic Schizophrenia: A Preliminary Report. Front Psychiatry. 2019;10:236. PubMed
26.Choi J, Fiszdon JM, Medalia A. Expectancy-value theory in persistence of learning effects in schizophrenia: role of task value and perceived competency. Schizophr Bull. 2010;36(5):957-965. PubMed
27.Carroll C, Booth A, Cooper K. A worked example of “best fit” framework synthesis: a systematic review of views concerning the taking of some potential chemopreventive agents. BMC Med Res Methodol. 2011;11:29. PubMed
28.Sandelowski M, Barroso J. Toward a metasynthesis of qualitative findings on motherhood in HIV-positive women. Res Nurs Health. 2003;26(2):153-170. PubMed
29.Charmaz K. Constructing Grounded Theory. Thousand Oaks (CA): Sage Publications Ltd; 2014.
30.Bryce S, Warren N, Ponsford J, Rossell S, Lee S. Understanding the lived experience of cognitive remediation in schizophrenia: A qualitative comparison with an active control. Psychiatr Rehabil J. 2018;41(4):302-311. PubMed
31.Contreras NA, Lee S, Tan EJ, Castle DJ, Rossell SL. “How is cognitive remediation training perceived by people with schizophrenia? A qualitative study examining personal experiences”. J Ment Health. 2016;25(3):260-266. PubMed
32.Ferreira-Correia A, Barberis T, Msimanga L. Barriers to the implementation of a computer-based rehabilitation programme in two public psychiatric settings. S Afr J Psychiatr. 2017;24(1):1-8. PubMed
33.Moutaud B. Cognitive Optimisation and Schizophrenia: Assembling Heterogeneity, Overcoming the Precariousness of Life, and Challenging Public Health Policies in Psychiatry in France. Cult Med Psychiatry. 2021;14:14. PubMed
34.Kidd SA, Ernest D, Arthur C, et al. A Pilot Study of a Family Cognitive Adaptation Training Guide for Individuals With Schizophrenia. Psychiatr Rehabil J. 2018;41(2):109-117. PubMed
35.Medalia A, Saperstein AM, Stefancic A, et al. Feasibility and acceptability of remotely accessed cognitive remediation for schizophrenia in public health settings. Psychiatry Res. 2021;301:113956. PubMed
36.Schutt RK, Seidman LJ, Eack SM, Deck B, Keshavan MS. Adapting cognitive remediation to a group home: A brief report. Asian J Psychiatr. 2017;25:184-187. PubMed
37.Reeder C, Pile V, Crawford P, et al. The Feasibility and Acceptability to Service Users of CIRCuiTS, a Computerized Cognitive Remediation Therapy Programme for Schizophrenia. Behav Cogn Psychother. 2016;44(3):288-305. PubMed
38.Keefe RS, Haig GM, Marder SR, et al. Report on ISCTM Consensus Meeting on Clinical Assessment of Response to Treatment of Cognitive Impairment in Schizophrenia. Schizophr Bull. 2016;42(1):19-33. PubMed
39.Cooper LA, Hill MN, Powe NR. Designing and evaluating interventions to eliminate racial and ethnic disparities in health care. J Gen Intern Med. 2002;17(6):477-486. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Publications
Study citation, country | Study design and analytic approach1 | Study objectives | Inclusion criteria | Data collection strategy |
|---|---|---|---|---|
Medalia 2021,35 US | Mixed-methods – content analysis | Consider the feasibility and acceptability of a hybrid approach to cognitive remediation | Adults referred for cognitive remediation therapy | Semi-structured interviews |
Moutaud 2021,33 France | Qualitative – ethnography | Describe CRT as an assemblage that lies at the intersection of multiple overlapping theories and spaces of mental disorders and psychiatric care | NR | Observation |
Bryce 2018,30 Australia | Qualitative – thematic analysis | Compare the experience of participating in cognitive remediation in a computer game setting | Outpatients with schizophrenia | Semi-structured survey |
Kidd 2018,34 Canada | Mixed-methods – thematic analysis | Examine changes in the self-assessed and caregiver-assessed outcomes of people with schizophrenia after exposure to a cognitive adaptation training guide that addressed pragmatic, in-home approaches to offset the cognitive impacts of the illness | Caregiver who has been actively involved in the support of the individual and having had regular in-home contact in the supported person's home environment, the supported individual was identified as having primary diagnosis of schizophrenia or schizoaffective disorder | Semi-structured interviews |
Ferreira-Correia 2017,32 South Africa | Qualitative – qualitative description | Explore the experiences of a group of volunteers with working memory deficits (associated with diagnoses of HIV and schizophrenia), in terms of perceived barriers they encountered during their participation in computer-based rehabilitation programs | Living with HIV and on antiretroviral treatment, and participants previously diagnosed with paranoid schizophrenia in full remission | Semi-structured interviews |
Schutt 2017,36 US | Mixed-methods – NR | Develop procedures for and test the feasibility of implementing cognitive enhancement therapy in a group home environment | Diagnosis of schizophrenia or schizoaffective disorder, stability of positive symptoms, maintenance antipsychotic medication regimen, presence of social and cognitive disability, an IQ of at least 80, and no medical contraindications | Semi-structured interviews |
Contreras 2016,31 Australia | Qualitative – thematic analysis | Explore the subjective experience of participants undertaking a cognitive remediation trial | Patients with a schizophrenia diagnosis, no history of traumatic brain injury or neurologic illness, receiving a stable dose of antipsychotic medication for at least 8 weeks before study, no electroconvulsive therapy in the previous 6 months, and no hearing or visual impairment | Semi-structured survey |
Reeder 2016,37 UK | Mixed-methods – thematic analysis | Assess the feasibility and acceptability of a new strategy-based computerized CRT program for people with psychosis | Patients who received the therapy as a part of a randomized controlled trial, diagnosis of schizophrenia, at least 1 year contact with mental health services, inefficient executive/memory performance, poor social functioning, no plan to change medication, no diagnosis of substance dependence, no evidence of organic cause to cognitive difficulties | Semi-structured interviews |
NR = not reported; CRT = cognitive remediation therapy.
Appendix 3: Characteristics of Study Participants
Note that this appendix has not been copy-edited.
Table 3: Study Participants’ Characteristics
Study citation, country | Sample size | Sex (% male) | Age range in years | Unemployment (%) | Treatment name |
|---|---|---|---|---|---|
Medalia 2021,35 US | 17 patients and 6 clinicians | NR | NR | NR | Cognitive remediation |
Moutaud 2021,33 France | NR | NR | NR | NR | Cognitive remediation therapy |
Bryce 2018,30 Australia | 42 patients | 52.4 | 31-51 | 66.7 | Cognitive remediation and computer games |
Kidd 2018,34 Canada | 20 patients and 20 caregivers | 50.0 | NR | 53.0 | Cognitive adaptation training |
Ferreira-Correia 2017,32 South Africa | 5 patients | 44.5 | 26-45 | 44.5 | Computer-based rehabilitation programs for working memory deficits - specifically CogMed Working Memory Training Program |
Schutt 2017,36 US | 6 patients | NR | NR | NR | Cognitive enhancement therapy |
Contreras 2016,31 Australia | 20 patients | 55.0 | 26-46 | 70.0 | Cognitive remediation training |
Reeder 2016,37 UK | 17 patients | NR | NR | NR | Computerized cognitive remediation therapy |
NR = not reported.
Appendix 4: Critical Appraisal of Included Studies
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Included Studies
Strengths | Limitations |
|---|---|
Medalia 202135 | |
Clearly identified study design and analytic approach Clearly described sample selection and recruitment Provided detailed data collection procedures Provided detailed data analysis methods | No explicit considerations on rigour or quality strategies for the qualitative analysis No justification for chosen analytic approach |
Moutaud 202133 | |
Clearly identified study design and analytic approach | No explicit considerations on rigour or quality strategies for the qualitative analysis No justification for chosen analytic approach No description of data collection instruments/measures and why they were used Very little description of qualitative data analysis Conceptual/reflection-based analysis of ethnographic data |
Bryce 201830 | |
Clearly identified study design and analytic approach Clearly described sample selection and recruitment Provided detailed data collection procedures Provided detailed data analysis methods | No explicit considerations on rigour or quality strategies for the qualitative analysis No justification for chosen analytic approach |
Kidd 201834 | |
Clearly identified study design and analytic approach Clearly described sample selection and recruitment Provided detailed data collection procedures | No explicit considerations on rigour or quality strategies for the qualitative analysis No justification for chosen analytic approach Very little description of qualitative data analysis |
Ferreira-Correia 201732 | |
Clearly identified study design and analytic approach Clearly described sample selection and recruitment Provided detailed data analysis methods | No explicit considerations on rigour or quality strategies for the qualitative analysis No justification for chosen analytic approach No description of data collection instruments/measures and why they were used |
Schutt 201736 | |
Clearly described sample selection and recruitment Provided detailed data collection procedures | Did not identify analytic approach No explicit considerations on rigour or quality strategies for the qualitative analysis No analysis approach or procedures No justification for chosen analytic approach |
Contreras 201631 | |
Clearly identified study design and analytic approach Clearly described sample selection and recruitment Provided detailed data collection procedures Provided detailed data analysis methods | No explicit considerations on rigour or quality strategies for the qualitative analysis No justification for chosen analytic approach |
Reeder 201637 | |
Clearly identified study design and analytic approach Clearly described sample selection and recruitment Provided detailed data collection procedures | No explicit considerations on rigour or quality strategies for the qualitative analysis No justification for chosen analytic approach Very little description of qualitative data analysis |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein do not necessarily reflect the views of Health Canada, Canada’s provincial or territorial governments, other CADTH funders, or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to requests@cadth.ca