CADTH Health Technology Review
Single-Use Negative Pressure Wound Therapy for Chronic Wounds
Rapid Review
Authors: Sara D. Khangura, Carolyn Spry
Abbreviations
NPWT
negative pressure wound therapy
sNPWT
single-use negative pressure wound therapy
tNPWT
traditional negative pressure wound therapy
Key Messages
Limited clinical effectiveness data suggest that single-use negative pressure wound therapy may reduce the frequency of dressing changes when compared with standard wound therapy (evidence from 1 single-arm study).
No clinical evidence was identified describing the impact of single-use negative pressure wound therapy on functionality, pain, mortality, length of hospital stay, quality of life, and safety.
It is unknown whether single-use or disposable negative pressure wound therapy is cost-effective for the management of chronic wounds (no eligible studies found).
One guideline provides recommendations relevant to single-use negative pressure wound therapy with chronic wounds; however, there is no clear link to a robust evidence review reported by the guideline developers.
Context and Policy Issues
Chronic wounds present a challenge for patients, clinicians, and health systems.1-5 Characterized by impaired and delayed healing, chronic wounds can include a variety of ulcerative wounds,1 as well as nonhealing surgical, traumatic, and other wounds.6
Both wound care treatment and innovation have advanced over the past several decades. A variety of available therapies are now available to treat chronic wounds — including negative pressure wound therapy (NPWT),6 which was developed and introduced in the 1990s.7 NPWT involves the application of a vacuum, or suction, to a wound to remove exudate and other matter from the wound bed.8,9 NPWT has been characterized as an adjunctive therapy,6 with the mechanisms of action thought to have a beneficial effect on both direct and indirect factors associated with local wound healing, including the stable environment provided by a semipermeable dressing, alterations in blood flow, and diminished inflammatory response.9 Possible adverse reactions that have been associated with the use of NPWT include bleeding, pain, and infection — as well as more serious outcomes, including death.9
Although NPWT is considered a useful tool in chronic wound care, the devices are generally large and heavy, limiting patient mobility, and limiting use of the devices to inpatient hospital settings.10 In response to broader health care trends toward the increased delivery of care in outpatient and community settings, single-use and disposable NPWT devices have been developed.11 Single-use NPWT (sNPWT) first became available in 2010, with devices that are smaller in size than those used in traditional NPWT (tNPWT).12 Consequently, sNPWT devices are typically portable due to their small size and lightweight, ranging between less than 1 pound (0.45 kg) to less than 2 pounds (0.91 kg) compared with tNPWT devices, which can weigh as many as 8 pounds (3.6 kg).12 Designed to be portable and disposable, sNPWT devices may use either electrical or mechanical power, and may support improved quality of life for patients who could still benefit from NPWT, but no longer require hospitalization.12,13 The sNPWT devices are intended for use with smaller wounds that produce less exudate as compared to larger wounds, and sNPWT may necessitate fewer dressing changes than tNPWT.12
Clinical evidence to date regarding the effectiveness and safety of NPWT has been characterized as inconclusive and of low quality.9 However, given the potential benefits that sNPWT devices may provide to ambulatory patients with chronic wounds in particular, it is imperative to identify and assess available evidence that can inform and support decision-making. The purpose of this report is to identify and summarize available evidence and evidence-based guidelines describing the clinical effectiveness, cost-effectiveness, and recommendations relevant to the use sNPWT in patients with chronic wounds.
Research Questions
What is the clinical effectiveness of single-use or disposable negative pressure wound therapy for the management of chronic wounds?
What is the cost-effectiveness of single-use or disposable negative pressure wound therapy for the management of chronic wounds?
What are the evidence-based guidelines regarding the use of single-use or disposable negative pressure wound therapy for the management of chronic wounds?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were negative pressure wound therapy and chronic wounds. No filters were applied to limit retrieval by study type. Comments, newspaper articles, editorials, and letters were excluded. When possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016, and September 8, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Individuals (of all ages) with chronic wounds of any etiology |
Intervention | Single-use or disposable negative pressure wound therapy |
Comparator | Q1 and Q2: Conventional wound dressings (e.g., silver dressings, moist wound healing dressings, alginate wound dressings, gauze) Q3: No comparator required |
Outcomes | Q1: Clinical effectiveness (e.g., wound healing, such as time to wound healing; functionality; pain; mortality; hospital stay; quality of life; safety, such as adverse events) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q3: Recommendations regarding best practices (e.g., appropriate patient populations; types of wounds; or clinical settings, contraindications; administration protocols, such as length of treatment; special considerations for use in remote settings) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, guidelines |
Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2016. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist14 for primary clinical studies and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument15 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
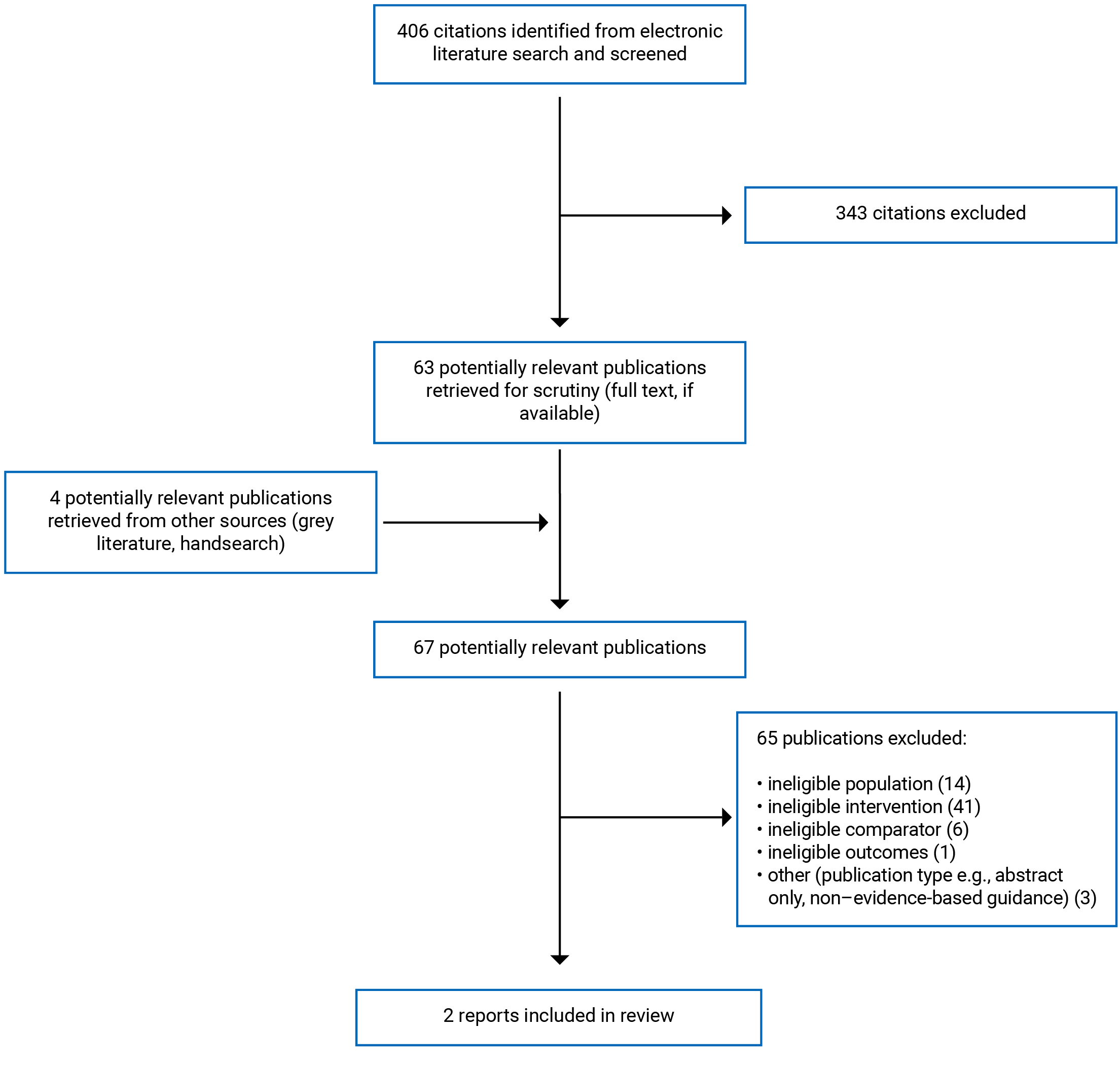
A total of 406 citations were identified in the literature search. Following screening of titles and abstracts, 343 citations were excluded and 63 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 65 publications were excluded for various reasons, and 2 publications met the inclusion criteria and were included in this report. These comprised 1 single-arm study reporting some comparative data describing clinical outcomes and 1 evidence-based guideline. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)16 flow chart for the study selection is presented in Appendix 1.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The single-arm clinical study included in this report was described by the authors as a “service evaluation”17 and included some limited comparative clinical effectiveness data eligible for this review. The study was published in 2020 and it assessed outcomes in 1 group of patients; there was not a separate control group of patients included in the study.
One evidence-based guideline was identified and included in this report.18 The scope of the guideline is broader than the criteria established for this review, including recommendations for the management of both chronic and acute wounds, as well as recommendations for both tNPWT and sNPWT. Recommendations of relevance to the present review are included and summarized here.
Additional details regarding the characteristics of included publications are provided in Table 2.
Study Design
The included single-arm clinical study assessed a novel wound care pathway involving both standard care and sNPWT (sNPWT) in a single group of patients in 7 centres for 12 weeks.17 Some comparative clinical outcome data were described between the sNPWT and standard care phases of the wound care pathway evaluation.
The International Consensus Panel Recommendations for the Optimization of Traditional and Single-use Negative Pressure Wound Therapy in the Treatment of Acute and Chronic Wounds guideline was published in 2021.18 The advice is intended to support and inform clinicians regarding the use of NPWT in general (i.e., whether and when) and, more specifically, to inform decisions concerning the use of tNPWT compared with sNPWT.18 The guideline provides a series of recommendations, characterized as consensus statements by the guideline authors. The guideline provides no description of either evidence assembly or a quality assessment undertaken by the authors; the development of the recommendations is described as relying on both a series of panel meetings and discussions, including a Delphi method.18 There is no external validation process described, while an internal validation exercise describes the final approval of the guideline document as being solicited from all panel experts who developed the recommendations. Likewise, no strength of recommendations is provided, nor is the quality of evidence supporting the recommendations described.18
Country of Origin
The single-arm clinical study was conducted in Ireland, with 5 of the 7 centres under study located in the Republic of Ireland and 2 of the 7 centres located in Northern Ireland.17
Although the first author of the guideline is indicated as being based in the US, the guideline group was international in its composition, including experts from Canada, Spain, the UK, and the US.18
Patient Population
The authors reported that the group of patients described in the single-arm clinical study were represented by 36 wounds.17 Wounds were included in the study if they were identified as “hard-to-heal”17, which was defined as those wounds with a duration of greater than 6 weeks and a less than 10% reduction in wound size (by area) with standard wound therapy for the previous 4 weeks. Wounds were ineligible if they had been treated previously with any form of NPWT. The median duration of wound was 3 months to 6 months, and the most common types of wounds were surgical (36.11%), leg ulcers (30.56%), and trauma (19.44%), with the remaining wounds being described as pressure ulcers (grades 3/4), skin tears, and “other” (≤ 6% for each category).17
The guideline describes recommendations of relevance to patients with either acute and/or chronic wounds18; however, the focus of this report is to summarize only the information within the guideline of relevance to patients with chronic wounds.
Interventions and Comparators
The clinical assessment described in the single-arm study evaluated a novel wound care pathway — dubbed by the authors as the “PICO™ sNPWT hard-to-heal pathway.”17. Researchers initiated sNPWT with eligible patients (as described previously) for a period of 2 weeks to 4 weeks (with the duration of sNPWT therapy subject to the judgment of the attending clinician), followed by a course of standard therapy for 8 weeks to 10 weeks, rendering a total 12 weeks of follow-up.17
The guideline describes recommendations of relevance to both tNPWT and sNPWT18; however, the focus of this report is to summarize only the information within the guideline of relevance to sNPWT.
Outcomes
The single-arm clinical study’s clinical assessment measured several outcomes, but only 2 reported comparative clinical data and were therefore eligible for inclusion in this report: dressing changes per week and wound healing, measured as the change in wound area per week.17
The single-arm clinical study also reported on the development of an economic model17; however, these data were not eligible for inclusion in this report because they only described a simple cost comparison as opposed to a robust description of cost-effectiveness.
The guideline included in this review provides a series of recommendations, characterized as consensus statements by the guideline authors, that are categorized by outcomes of relevance to clinical, patient-oriented, and systems-level priorities. For the purpose of this review, the focus is on guidance of particular relevance to chronic wounds treated with sNPWT, which included guideline recommendations addressing wound-related factors, patient satisfaction and quality of life, as well as care setting. The guideline also provides some guidance specific to cost-related factors; however, this was ineligible for inclusion in this review because the guidance only describes a simple cost comparison and therefore fell short of describing cost-effectiveness.18
Summary of Critical Appraisal
Single-Arm Clinical Study
The single-arm clinical study used a 1-arm design, with no control group of patients. Rather, there was 1 group of patients exposed to 2 interventions across a 12-week wound care pathway, with some limited comparisons drawn between the 2 interventions provided at the various time points within the wound care pathway (i.e., the patients served as their own controls).17 Single-arm studies are common but present several important limitations — among the most apparent, the fact that it is not possible to establish any effect caused by or associated with an intervention when there are no data describing what happens in the absence of the intervention.19 In this study, the authors had the benefit of observing the same group of patients with and without the sNPWT intervention; however, the patients were at different points in time in their healing so the study lacks the benefit of a concurrent control group comparison.17 This introduces important limitations to the study’s ability to generate a robust comparison that produces valid and reliable findings. There were several additional limitations and strengths identified with this study and its approach. Strengths observed included some clarity in reporting (i.e., the aim of the study and patient characteristics were described) and no loss to follow-up was reported. Because the assessment was completed with only 1 group of patients, confounding was not a threat to internal validity in this study, with all patients receiving the same 2 interventions and thereby serving as their own controls. Further, the statistical tests and the main outcome measures appear to be appropriate. Limitations of the clinical assessment of the single-arm clinical study were also noted; there was a lack of clarity and detail describing the outcomes, interventions, patient characteristics, main findings, and adverse events. In addition, no information on the representativeness of the patients assessed was provided, which prevents the reader from assessing how this may affect external validity. Further, blinding of the patients, health care workers, and assessors was not possible with the intervention under study. Compliance with the interventions (including time exposed to the sNPWT intervention) was also not described, which prevents the reader from considering whether bias may have impacted the internal validity of the study. Finally, no mention of sample size was reported, which prevents the reader from assessing whether the study was sufficiently powered to render valid and reliable results.
Funding was not reported by the study authors nor solicited by the checklist tools used in this critical appraisal; however, it was noted that potential conflicts of interest were reported for several of the authors in the form of paid consultation and/or employment with a for-profit corporation that manufactures medical equipment. Potential conflicts of interest are an important consideration when considering the extent to which there may be bias in the conduct and/or reporting of the research.20
Guideline
The included guideline also demonstrated both strengths and limitations. Strengths included the clarity of its scope and purpose, as well as the clarity with which its recommendations were presented. In addition, stakeholder involvement was described in part, with target users of the guideline being mentioned. The guideline also had limitations; it is missing information describing stakeholder involvement regarding the individual members on the expert panel (e.g., group membership, institution, location, and role in the guideline development group). Further, there is no description of consultation with patients or the general public to solicit their views on the guidance and recommendations developed. Rigour of development was a limitation of this guideline, with little information describing the use of evidence or the extent to which the literature was consulted to inform development of the recommendations. The guideline makes mention of “supplemental literature that further augmented current expertise and experience... (p. S2)”18 being provided for review before the initial guideline development meeting; however, there is no further description of how this literature was identified, assembled, assessed, or provided to the panel of experts, which prevents the reader from being able to assess whether a systematic approach to incorporating evidence was used in the development of the guideline. Further, each recommendation (or “consensus statement” as described by the authors) is followed by an explanatory section that references citations from published literature; however, no other explicit link to evidence is made clear by the authors. In addition, there is no strength of recommendation indicated for each of the consensus statements, nor is the quality of the evidence supporting each recommendation described. The applicability and editorial independence of the guideline is not described in sufficient detail to ensure the reader can assess whether and to what extent the guideline can appropriately be implemented in various health care settings. In addition, funding for the development of the guideline and an editorial contribution were provided by a for-profit corporation that manufactures medical equipment, constituting a potential conflict of interest concerning the development of the guideline.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings and authors’ conclusions.
Clinical Effectiveness of sNPWT
The single-arm clinical study found a statistically significant reduction in dressing changes per week during the sNPWT and post-sNPWT standard care phases of the wound care pathway compared with the pre-intervention standard care phase of the wound care pathway for 36 hard-to-heal wounds.17
Findings describing wound healing, indicated that the wounds reduced in area by 16.8% during the sNPWT phase and 18.9% during the post-sNPWT standard care phase of the research (no comparison statistic reported).17
Cost-Effectiveness of sNPWT
No eligible data describing single-use or disposable NPWT for chronic wounds was identified; therefore, no summary can be provided.
Guideline Recommendations
The included guideline makes a series of recommendations relevant to both clinical and economic outcomes.18 Recommendations addressing wound-related factors include guidance on the size of the wound and its impact on the selection of either tNPWT or sNPWT, as well as considerations specific to the particular sNPWT device being considered for use.18 Another recommendation addresses the importance of regular reassessment of the wound (i.e., every 2 weeks) to ascertain whether NPWT should continue at all and/or whether and when the patient can be transitioned from tNPWT to sNPWT, including the circumstances determining an appropriate transition (i.e., based on wound characteristics).18
Recommendations in the guideline also address patient satisfaction and quality of life, health care setting, and economic considerations, with several consensus statements provided in favour of earliest initiation of sNPWT to optimize patient-oriented outcomes, and to support the transition from inpatient to outpatient care settings.18 There was no description of the quality of the evidence supporting the recommendations, nor was any strength of the recommendations reported.
Limitations
Relative to the body of literature describing NPWT,21-26 the subset of available literature describing single-use or disposable NPWT devices for the treatment of chronic wounds remains limited.27 In this review, 2 eligible sources were identified that reported limited data on the clinical effectiveness of sNPWT and guideline recommendations.17,18
The single-arm clinical study and guideline identified by this review offer some early data and insights describing the use of sNPWT with chronic wounds; however, there were important limitations demonstrated by both sources. The eligible clinical effectiveness data did not rely on a comparison between 2 patient groups17 and the included guideline was broader in scope than the research questions posed in this review (e.g., recommendations apply to both acute and chronic wounds),18 which renders the findings of this review and their applicability of limited utility.
Comparative clinical effectiveness outcomes were limited to those describing the frequency of dressing changes and wound healing17; no eligible data were identified that described other key clinical outcomes, such as functionality, pain, mortality, length of hospital stay, patient quality of life, and adverse events. Similarly, clinical effectiveness data were limited to observations of 36 wounds from centres in Ireland, which may not be representative of the Canadian context — including those living in rural or remote settings.
Important methodological limitations were identified by the critical appraisal conducted for both included sources in this review, which limit the extent to which the summarized data can be applied effectively within various clinical contexts. In addition, the presence of potential conflicts of interest as well as funding from private, for-profit industry that was acknowledged in both sources included in this review warrant consideration regarding the utility of the data and the recommendations reported. Consequently, the findings of this review should be interpreted with caution.
Conclusions and Implications for Decision- or Policy-Making
This review identified 1 single-arm study reporting data on clinical effectiveness outcomes and 1 evidence-based guideline with recommendations relevant to the use of sNPWT with chronic wounds.17,18 No eligible data describing the cost-effectiveness of single-use or disposable NPWT for chronic wounds was identified; therefore, no summary can be provided.
Findings from the single-arm clinical study showed a statistically significant reduction in the number of dressing changes required and an improvement of wound healing (no statistical comparison reported) following initiation of the wound care pathway that used the sNPWT device.17 These findings corroborate hypotheses and limited case reports12,13 described elsewhere in the literature, suggesting that sNPWT devices may reduce the number of dressing changes required during wound care. However, the study reports findings for 36 wounds, which is a small sample size and limits generalizability of these findings to contexts outside of the study population described. This is a limitation characteristic of much of the current evidence (e.g., case series, or conference abstracts) available that describes sNPWT devices.13,28,29
Although the authors of the single-arm clinical study favoured sNPWT compared with standard wound therapy, there were also methodological limitations and potential conflicts of interest (i.e., paid contract work and/or employment within private industry) that were acknowledged by the study authors.17 In addition, the lack of available data on key clinical effectiveness outcomes, most notably safety, is an important limitation of this review, such as possible adverse events that have been associated with the use of NPWT in general, including bleeding, infection, pain, and mortality.9
The guideline included in this review also puts forward multiple recommendations that generally favour first-line use of sNPWT compared with tNPWT devices for the treatment of chronic wounds (as well as acute wounds). However, the lack of a clear link to a robust source of evidence — as well as the acknowledged funding source, which was provided by private industry — are important limitations of this guideline.18
In the broader context of wound care, single-use and disposable NPWT devices are being developed alongside other new hospital-based NPWT devices.26 Whereas hospital-based NPWT are undergoing development toward broader uses — including the addition of instillation systems that deliver saline and other substances to the wound bed — single-use and disposable devices are being developed to increase the availability and uptake of NPWT devices outside of inpatient settings.11 However, given the relative novelty of these devices, the evidence to support their clinical and cost-effectiveness remains scarce. Therefore, more high-quality research will be necessary to advance current understanding and best practices with regard to the use of single-use and disposable NPWT devices.
References
1.Frykberg RG, Banks J. Challenges in the Treatment of Chronic Wounds. Adv Wound Care (New Rochelle). 2015;4(9):560-582. PubMed
2.Bowers S, Franco E. Chronic Wounds: Evaluation and Management. Am Fam Physician. 2020;101(3):159-166. PubMed
3.Vogt TN, Koller FJ, Santos PND, Lenhani BE, Guimarães PRB, Kalinke LP. Quality of life assessment in chronic wound patients using the Wound-QoL and FLQA-Wk instruments. Invest Educ Enferm. 2020;38(3):e11. PubMed
4.Squitieri L, Tsangaris E, Klassen AF, et al. Patient-reported experience measures are essential to improving quality of care for chronic wounds: An international qualitative study. Int Wound J. 2020;17(4):1052-1061. PubMed
5.Chan BCF, Cadarette SM, Wodchis WP, Mittmann N, Krahn MD. Lifetime cost of chronic ulcers requiring hospitalization in Ontario, Canada: A population-based study. Wound Medicine. 2018;20:21-34.
6.Evans K, Kim PJ. Overview of treatment of chronic wounds. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Oct 08.
7.Téot L, Guillot-Masanovic M, Miquel P, et al. Clinical impact of negative-pressure wound therapy: a 1,126-patient observational prospective study. Wound Repair Regen. 2014;22(3):341-350. PubMed
8.Medical suction devices: using them safely and effectively. Plymouth Meeting (PA): ECRI Institute; 2020: www.ecri.org. Accessed 2021 Oct 08.
9.Gestring M. Negative pressure wound therapy. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2021: www.uptodate.com. Accessed 2021 Oct 08.
10.Hudson DA, Adams KG, Van Huyssteen A, Martin R, Huddleston EM. Simplified negative pressure wound therapy: clinical evaluation of an ultraportable, no-canister system. Int Wound J. 2015;12(2):195-201. PubMed
11.Apelqvist J, Willy C, Fagerdahl AM, et al. Negative Pressure Wound Therapy: Future Perspectives. EWMA J. 2017;18(2):33-36.
12.Crumley C. Single-Use Negative Pressure Wound Therapy Devices: A Technologic Analysis. J Wound Ostomy Continence Nurs. 2021;48(3):195-198. PubMed
13.Brandon T. Using a single-use, disposable negative pressure wound therapy system in the management of small wounds. Wounds UK. 2016;EWMA Special.
14.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
15.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Oct 08.
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
17.McCluskey P, Brennan K, Mullan J, et al. Impact of a single-use negative pressure wound therapy system on healing. J Community Nurs. 2020;34(1):36-43.
18.Hurd T, Kirsner RS, Sancho-Insenser JJ, et al. International Consensus Panel Recommendations for the Optimization of Traditional and Single-Use Negative Pressure Wound Therapy in the Treatment of Acute and Chronic Wounds. Wounds. 2021;33(suppl 2):S1-S11. PubMed
19.Cucherat M, Laporte S, Delaitre O, et al. From single-arm studies to externally controlled studies. Methodological considerations and guidelines. Therapie. 2020;75(1):21-27. PubMed
20.Romain PL. Conflicts of interest in research: looking out for number one means keeping the primary interest front and center. Curr Rev Musculoskelet Med. 2015;8(2):122-127. PubMed
21.Song YP, Wang L, Yuan BF, et al. Negative-pressure wound therapy for III/IV pressure injuries: A meta-analysis. Wound Repair Regen. 2021;29(1):20-33. PubMed
22.Janssen AH, Wegdam JA, de Vries Reilingh TS, Eskes AM, Vermeulen H. Negative pressure wound therapy for patients with hard-to-heal wounds: a systematic review. J Wound Care. 2020;29(4):206-212. PubMed
23.Liu S, He CZ, Cai YT, et al. Evaluation of negative-pressure wound therapy for patients with diabetic foot ulcers: systematic review and meta-analysis. Ther Clin Risk Manag. 2017;13:533-544. PubMed
24.Liu Z, Dumville JC, Hinchliffe RJ, et al. Negative pressure wound therapy for treating foot wounds in people with diabetes mellitus. Cochrane Database Syst Rev. 2018;10:CD010318. PubMed
25.Alfie V, Pichon-Riviere A, Augustovski F, et al. [Negative-pressure wound therapy]. Buenos Aires (AR): Institute for Clinical Effectiveness and Health Policy; 2018: https://database.inahta.org/article/20009. Accessed 2021 Sep 27.
26.Apelqvist J, Willy C, Fagerdahl AM, et al. EWMA Document: Negative Pressure Wound Therapy. J Wound Care. 2017;26(Sup3):S1-S154.
27.Klappenbach R CA, Pichon-Riviere A, Augustovski F, García Martí S, Alcaraz A, Bardach A, López A, Rey-Ares L. Single-use negative pressure wound therapy for chronic and acute wounds. Buenos Aires (AR): Institute for Clinical Effectiveness and Health Policy; 2016: https://www.crd.york.ac.uk/CRDWeb/ShowRecord.asp?ID=32016001129. Accessed 2021 Sep 20.
28.Single-use negative pressure therapy and the pediatric patient. Wound Management & Prevention. 2020: https://www.hmpgloballearningnetwork.com/site/wmp/article/single-use-negative-pressure-therapy-and-pediatric-patient. Accessed 2021 Oct 01.
29.Gombert A, Barbati ME, Wittens C, Grommes J, Jalaie H. Effect of a new incision management system (PREVENA R) on wound healing after endophlebectomy of the common femoral vein: a case series. J Med Case Rep. 2016;10:130. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
McCluskey (2020)17 Ireland Funding source NR | “Service evaluation”17 (p. 37) using an uncontrolled, single-arm design and assessing a wound care pathway with some comparative findings reported between interventions received across the duration of the pathway | Hard-to-heal wounds (N = 36) (i.e., > 6 weeks in duration; < 10% reduction in area over previous 4 weeks; no previous NPWT) Median wound duration: 3 to 6 months Wound types: Surgical wound (36.11%) Leg ulcer (30.56%) Trauma (19.44%) Pressure ulcer (grade 3/4); skin tear; other (< 6% for each category) | Intervention: PICO™ sNPWT Comparator: standard wound management | Outcome, measure: Dressing changes, n per week (summary statistic not described) Wound healing, mean change in wound area per week (%) Follow-up: 2-4 weeks (sNPWT); 8-10 weeks (standard care) |
NPWT = negative pressure wound therapy; NR = not reported; sNPWT = single-use negative pressure wound therapy
Table 3: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Hurd, 202118 | ||||||
Intended users: Clinicians Target population: Patients with acute and/or chronic wound(s) | tNPWT and sNPWT | Therapeutic goals, wound-related factors, patient satisfaction and quality of life, care setting-related factors, economic-related factors, NPWT system-related factors | Described only as the provision of “supplemental literature” (p. S2) | NR | During a meeting of international experts in wound care and NPWT use using a modified Delphi method and several rounds of group discussion, followed by final approval of all panel members | NR |
NPWT = negative pressure wound therapy; NR = not reported; sNPWT = single-use negative pressure wound therapy; tNPWT = traditional negative pressure wound therapy
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist14
Strengths | Limitations |
|---|---|
McCluskey, 202014 | |
Reporting
Internal Validity (bias)
Internal Validity (confounding)
| Reporting
External Validity
Internal Validity (bias)
Power
|
Table 5: Strengths and Limitations of Guideline Using AGREE II15
Item | Hurd et al., (2021)18 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Unclear |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | Unclear |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Unclear |
13. The guideline has been externally reviewed by experts prior to its publication. | Unclear |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Unclear |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NR = not reported
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings of Included Primary Clinical Study
Main study findings | Authors’ conclusion |
|---|---|
McCluskey, 202017 | |
Dressing changes, n per week (unit of measurement not otherwise reported)a Pre-PICO™ sNPWT phase of wound care pathway (standard care)
During PICO™ sNPWT phase of wound care pathway
Post-PICO™ sNPWT phase of wound care pathway (standard care)
Wound healing, mean change in wound area per week (%) relative to pre-PICO™ sNPWT phase of the hard-to-heal wound care pathway During PICO™ sNPWT phase of wound care pathway
Post-PICO™ sNPWT phase of wound care pathway (standard care)
| “Dressing-change frequency significantly reduced during PICO sNPWT treatment compared to the standard dressing regime before the evaluation (p<0.001).” (p. 36)17 “The mean percentage area of change per week [i.e., wound healing] clearly supports the mode of action of PICO sNPWT...” (p. 38)17 |
NR = not reported; sNPWT = single-use negative pressure wound therapy.
aSummary statistic is not indicated/described in the report
Table 7: Summary of Recommendations in Included Guidelines
Recommendations | Quality of evidence and strength of recommendations |
|---|---|
Hurd, 202118 | |
Outcome: Wound-related factors “Wounds appropriate for consideration of sNPWT are those that meet device IFU, based on wound size, depth, and exudate amount. The clinician must be familiar with the IFU of the sNPWT system utilized, as these factors can considerably vary between sNPWT devices.” (p. S3) “Wounds appropriate for consideration of tNPWT are those in which the size, depth, and volume of exudate are beyond the management capacity of a sNPWT system.” (p. S3) “The sNPWT system can be considered as a bolster dressing for wounds in which closure is being obtained via a split-thickness skin graft or application of a skin substitute.” (p. S4) “The wound should be reassessed at regular intervals (ideally every 2 weeks) to determine if NPWT treatment should be continued or discontinued and for the appropriateness of transition from tNPWT to sNPWT. Consideration should be made for reassessment of NPWT use if therapeutic goals have not been met or there is minimal or no change in wound size, amount of granulation tissue, or reduction in edema and exudate volume. Transition from tNPWT to sNPWT should be considered when the wound size, depth, and exudate amount are within the management capacity of the sNPWT system that is being considered for use.” (p. S5) Note: unclear whether the recommendations for this outcome are specific to chronic wounds or general to both acute and chronic wounds | Quality of evidence: NR for any of the recommendations Strength of recommendations: NR for any of the recommendations |
Outcome: Patient satisfaction and quality of life “When NPWT is deemed an appropriate treatment modality for acute and chronic wounds, sNPWT should be the first-line modality utilized to increase patient satisfaction and quality of life. Patient education on NPWT as a treatment modality, the benefits of its use, and the advantages of sNPWT over tNPWT can improve patient satisfaction and treatment compliance.” (p. S5) “sNPWT use may be an optimal choice for ambulatory patients with wounds eligible for sNPWT use who must return to work or face barriers to access follow-up medical appointments.” (p. S6) Note. unclear whether the latter recommendation for this outcome is specific to chronic wounds or general to both acute and chronic wounds | Quality of evidence: NR for any of the recommendations Strength of recommendations: NR for any of the recommendations |
Outcome: Health care setting “... Initial use of sNPWT or early conversion to sNPWT from tNPWT in eligible wounds should be considered to assist in transitioning patients from inpatient to outpatient care.” (p. S6) Note: unclear whether the recommendation for this outcome is specific to chronic wounds or general to both acute and chronic wounds | Quality of evidence: NR for any of the recommendations Strength of recommendations: NR for any of the recommendations |
Supporting evidence: described as supplemental literature reviewed by the expert panel i.e., methods for identifying and assessing the literature were not described, nor was a summary of the supporting evidence provided/available to the reader. | — |
IFU = instructions for use; NR = not reported; sNPWT = single-use negative pressure wound therapy; tNPWT = traditional negative pressure wound therapy.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Review Article
Literature Review and Case Series
Wee IJ, Mak M, O’Donnell G, et al. The smart negative pressure (SNaP) wound care system: a case series from Singapore. Int Wound J. 2019;16:891–896. PubMed
Additional References
Ineligible Population — Wounds Not Chronic
Kwon J, Staley C, McCullough M, et al. A randomized clinical trial evaluating negative pressure therapy to decrease vascular groin incision complications. J Vasc Surg. 2018;68(6):1744-1752. PubMed
Mixed Population — Data Describing Only Patients Who Received Single-Use NPWT Not Available
Danne J, Gwini S, McKenzie D, Danne P. A retrospective study of pilonidal sinus healing by secondary intention using negative pressure wound therapy versus alginate or gauze dressings. Ostomy Wound Manage. 2017;63(3):47-53. PubMed
Ineligible Comparator (i.e., NPWT Versus Alternative NPWT)
Kirsner RS, Delhougne G, Searle RJ. A cost-effectiveness analysis comparing single-use and traditional negative pressure wound therapy to treat chronic venous and diabetic foot ulcers. Wound Manag Prev. 2020;66(3):30-38. PubMed
Kirsner R, Dove C, Reyzelman A, Vayser D, Jaimes H. A prospective, randomized, controlled clinical trial on the efficacy of a single-use negative pressure wound therapy system, compared to traditional negative pressure wound therapy in the treatment of chronic ulcers of the lower extremities. Wound Repair Regen. 2019;27(5):519-529. PubMed
No Comparator
Cuomo R, Nisi G, Grimaldi L, Brandi C, D'Aniello C. Use of ultraportable vacuum therapy systems in the treatment of venous leg ulcer. Acta Biomed. 2017;88(3):297-301. PubMed
Guideline With Unclear Methodology; No Clear Guidance Specific to Single-Use NPWT and Chronic Wounds
British Columbia Provincial Nursing Skin & Wound Committee. Guideline: negative pressure wound therapy (reusable/disposable) for adults & children. Vancouver (BC): BC Patient Safety & Quality Council: 2019; https://www.clwk.ca/buddydrive/file/guideline-npwt-2019-april-final/. Accessed 2021 Oct 08.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca