CADTH Health Technology Review
Chlorhexidine Oral Care in Critically Ill Adults
Rapid Review
Authors: Anusree Subramonian, Jennifer Horton
Abbreviations
BOAG
Barnason’s oral assessment guide
BOAS
Beck Oral Assessment Scale
CHX
chlorhexidine gluconate
ICU
intensive care unit
RCT
randomized controlled trial
RNAO
Registered Nurses’ Association of Ontario
SD
standard deviation
SR
systematic review
VAP
ventilator-associated pneumonia
VAT
ventilator-acquired tracheobronchitis
Key Messages
Three systematic reviews and 2 randomized clinical trials were identified regarding the clinical effectiveness of chlorhexidine oral care in adult patients who were in critical care and being mechanically ventilated. The evidence was of limited quality, with methodological limitations.
Compared to ozonated water and to Nanosil, chlorhexidine oral care was associated with a significantly higher risk of ventilator-associated pneumonia. Compared to bicarbonate, chlorhexidine oral care was associated with a significantly lower risk of ventilator-associated pneumonia. There was no significant difference in the risk of ventilator-associated pneumonia between chlorhexidine and other agents, such as potassium permanganate, hydrogen peroxide, or miswak.
There was no significant difference in the risk of mortality between oral care with chlorhexidine and that with other oral care drugs.
An evidence-based guideline targeting individuals who require assistance on oral care recommended a multi-component oral care protocol. No specific recommendation regarding the use of oral care agents for the prevention of ventilator-associated pneumonia was made because of lack of evidence.
There is a lack of evidence on the safety or cost-effectiveness of chlorhexidine oral care in adults who are in critical care and being mechanically ventilated.
Context and Policy Issues
Ventilator-associated pneumonia (VAP) is an important cause of mortality and morbidity in individuals who are critically ill and on ventilatory support.1 VAP is defined as a hospital-acquired pneumonia that develops after 48 hours or more on endotracheal intubation.1 Intubation can lower the immunity of the oral cavity, which, combined with the mechanical stress of the endotracheal tube, can introduce pathogens resulting in airway infections.2 It has been estimated that, in Canada, 10.6 cases of VAP are recorded per 1,000 ventilator days and approximately 230 deaths per year are due to VAP. The cost to the Canadian health care system from VAP is $46 million per year.1
Chlorhexidine gluconate (CHX) is an antiseptic drug widely used in the oral care protocol to prevent VAP.3 In spite of its broad use and inclusion in VAP-prevention bundles, some evidence suggests that CHX oral care may paradoxically increase the risk of mortality.4 Further, CHX harms the oral mucosa, resulting in oral lesions and bleeding.4 A previous CADTH report found that CHX was effective in preventing nosocomial pneumonia and bloodstream infections in hospitalized adults. The report highlighted the uncertainty of evidence regarding the benefit of CHX in preventing VAP.5
The purpose of this report is to summarize the evidence regarding the clinical effectiveness and cost-effectiveness of CHX for oral care in adult patients with artificial airways and/or who are in critical care being mechanically ventilated. Additionally, the report also aims to review evidence-based guidelines on oral care in adult patients with artificial airways and/or who are in critical care and being mechanically ventilated.
Research Questions
What is the clinical effectiveness regarding the routine use of chlorhexidine as a drug for oral care in adult patients with artificial airways and/or who are critically ill and on ventilators?
What is the cost-effectiveness of routine use of chlorhexidine as a drug for oral care in adult patients with artificial airways and/or who are critically ill and on ventilators?
What are the evidence-based guidelines regarding oral care drugs for routine use in adults with artificial airways or critically ill adults on ventilators to prevent ventilator-associated pneumonia?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were chlorhexidine, oral care, and critical care. No filters were applied to limit the retrieval by study type. Two additional searches were done. The first additional search was done for chlorhexidine and oral care, with CADTH-developed search filters applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or network meta-analyses; randomized controlled trials; and economic studies. The second additional search was done for oral care and critical care, with CADTH-developed search filters applied to limit retrieval to guidelines. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2018 and September 2, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with artificial airways and/or adults in critical care being ventilated |
Intervention | Q1 and Q2: Chlorhexidine oral solution (e.g., 0.12% solution) Q3: Oral care drugs |
Comparator | Q1 and Q2: Other types of oral care (e.g., sodium bicarbonate, hydrogen peroxide) Q3: Not applicable |
Outcomes | Q1: Clinical benefit (e.g., changes in rate of ventilator-associated pneumonia and improvement in oral hygiene) and harms (e.g., changes in rate of mortality, morbidity, oral sores and wounds) Q2: Cost per clinical benefit gained (e.g., incremental cost per health benefit, cost per quality-adjusted life-year gained) Q3: Recommendations regarding the use of chlorhexidine and alternative oral care drugs for routine use in critically ill adults to prevent ventilator-associated pneumonia |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, economic evaluations, and evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or if they were duplicate publications. Articles published before December 2018 were excluded to avoid overlapping with the previous CADTH report.5 Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more of the included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)6 for SRs, the Downs and Black checklist7 for randomized and non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument8 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
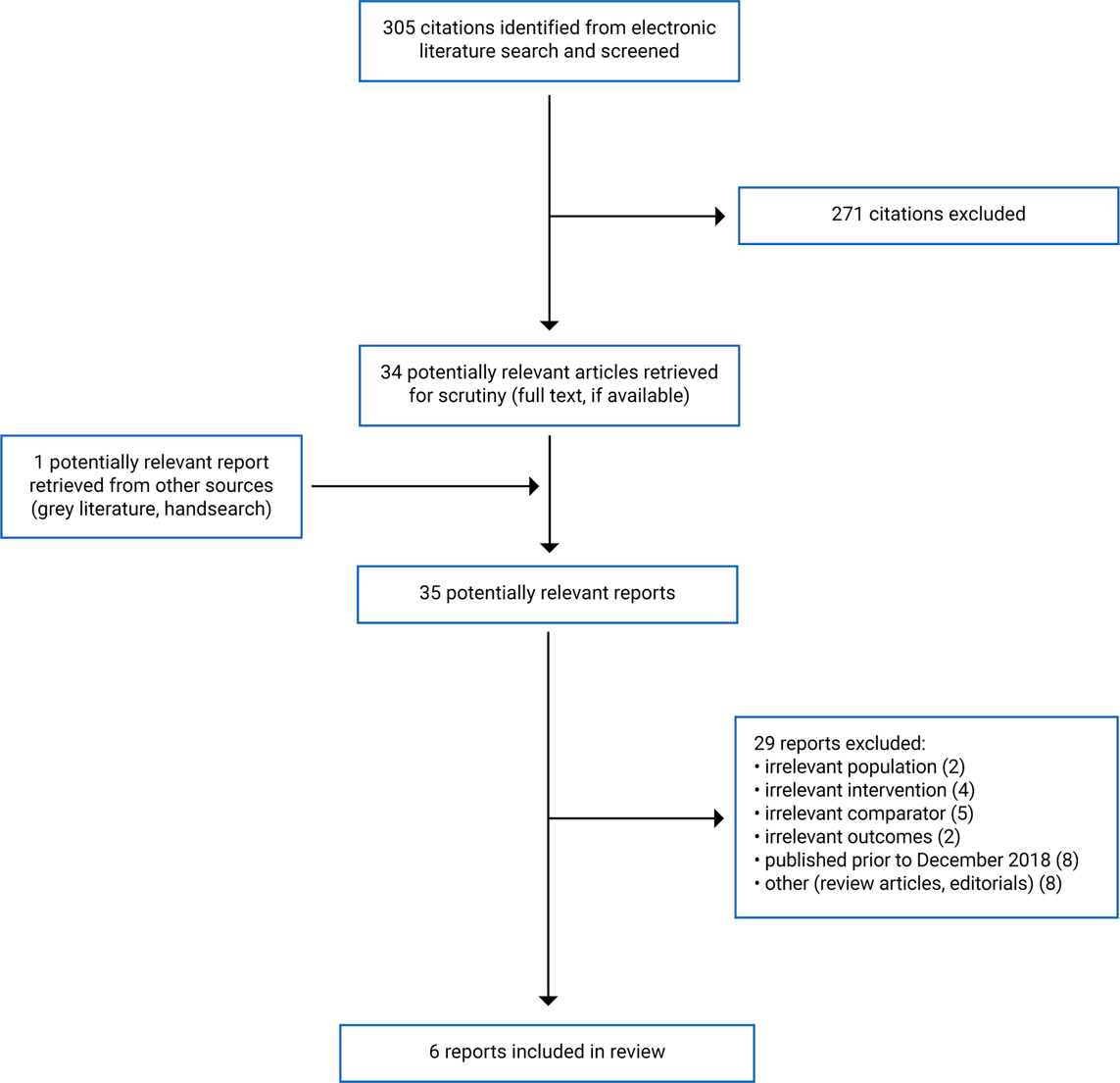
A total of 305 citations were identified in the literature search. Following screening of titles and abstracts, 271 citations were excluded and 34 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 29 publications were excluded for various reasons and 6 publications met the inclusion criteria and were included in this report. These comprised 3 SRs,9-11 2 randomized controlled trials (RCTs),12,13 and 1 evidence-based guideline.14 Appendix 1 presents the PRISMA15 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
Three SRs9-11 (2 with meta-analyses9,11), 2 RCTs,12,13 and an evidence-based guideline14 were included in the current report. All 3 SRs had broader inclusion criteria than the present review.9-11 In them, a number of interventions and comparators were of interest. Only the characteristics and results of the subset of the studies included in the SRs that are relevant to the present review are described in this report.
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
The 3 SRs included in this report were published in 2021,10 2020,11 and 2019.9 All individual studies contained within the 3 SRs were RCTs. There was some overlap of primary studies across the SRs, as shown in Appendix 5.
The SR by Mojtahedzadeh et al.10 searched for studies published until August 2020. It included 18 studies, among which 7 were relevant to the current report. The SR by Zhao et al.11 was an update to its 2016 version. In the 2020 version used in this report, studies identified until February 2020 were considered. The SR included 37 studies, among which 7 were relevant to the current report. Lastly, the SR by Lee et al.9 searched for studies published until September 2018. Eleven studies were included in the SR, among which 5 were relevant to this report.
The 2 included primary studies were RCTs, 1 double-blind12 and the other single-blind.13 Both studies were published in 2021.12,13 One RCT was published as a correspondence (i.e., a letter to the editor).12 Details regarding the study methodology and population were not available in the publication.
The included evidence-based guideline was developed by the Registered Nurses’ Association of Ontario (RNAO).14 Evidence for the formulation of the guideline was obtained through a systematic literature review, a review of previous guidelines, a guideline search and gap analysis, as well as expert consultation. The quality of evidence that was used to formulate recommendations was assessed using the Cochrane Risk of Bias tool (for RCTs), ROBINS-I (for observational studies), AMSTAR 2 (for SRs), and AGREE-II (for guidelines). Recommendations were developed through consensus and voting. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach and were rated as high, moderate, low, or very low. The strength of each recommendation was indicated as strong or conditional. A strong recommendation implies that a majority of persons will be best served by the recommended action. A conditional recommendation implies that some uncertainty exists and that not all persons will be best served by the recommended action, thus requiring a more careful consideration of personal circumstances, preferences, and values.
Country of Origin
The SRs were conducted by authors from Canada,9 China,11 and Iran.10
The RCTs were conducted in Iran12 and Turkey.13
The guideline was developed in Canada.14
Patient Population
The relevant patient population in the SR by Mojtahedzadeh et al.10 were adult patients undergoing tracheal intubation. Across the relevant studies, 534 patients were enrolled. Additional characteristics of the patients — such as age and the duration of intubation — were not reported. The SR by Zhao et al.11 included critically ill patients who were mechanically ventilated for 48 hours or more and did not have VAP or respiratory infections at baseline. Overall, there were 626 participants across the studies who were relevant to the current report. The mean age of the participants ranged from 34.4 years to 56.9 years. In the SR by Lee et al.,9 adult patients admitted to the intensive care unit (ICU) and on ventilators were included. The number of participants in the relevant subset of studies was not reported. The mean age of the participants ranged from 36.1 years to 58.7 years.
In the RCT by Izadi et al.,12 eligible participants were patients on mechanical ventilation. However, additional inclusion and exclusion criteria were not reported. The total number of participants was 78 (CHX group, n = 37; control group, n = 36). Although it was reported as if there were no differences between the 2 groups in baseline characteristics such as age, sex, comorbidities, and baseline oral health, specific demographic and clinical characteristics of the participants were not reported. In the RCT by Kes at al.,13 adult patients who were mechanically ventilated and admitted to the critical care unit were included. Patients who were ventilated for less than 48 hours, who had confirmed pneumonia prior to ICU admission, who were undergoing chemotherapy or radiation therapy, who had maxillofacial surgery or a tracheostomy, or who were pregnant were excluded. Accordingly, 76 patients were enrolled (CHX group, n = 38; control group, n = 38). The mean age of the patients was 72.79 years (standard deviation [SD] = 12 years) in the CHX group and 77.37 years (SD = 10.1 years) in the control group.
The target population for the guideline14 was adults who require assistance for their oral care. Relevant to this report, adult patients who were in critical care and being ventilated were part of the target population in the guideline. The intended users of the guideline were nurses, caregivers, educators, health service organizations, academic institutions, and families.
Interventions and Comparators
Several interventions and comparators were included in the SRs. Relevant to the current report, the included SRs considered various concentrations (0.12% to 2%) of CHX solution. In 1 SR,10 CHX was compared to any natural products or herbal products, including miswak, matrica, echinacea and aloe vera extract, zufa, and orthodentol mouthwash. In the SR by Zhao et al.,11 the relevant comparators were other oral care drugs, such as potassium permanganate, ozonated water, Nanosil, hydrogen peroxide, and miswak. Similarly, in the SR by Lee et al.,9 the comparators were other oral care drugs, such as bicarbonate, potassium permanganate, and saline.
In the RCT by Kes et al.,13 the intervention was oral care with 0.12% CHX gluconate every 8 hours. Patients in the control group received similar oral care with sodium bicarbonate. In the RCT by Izadi et al.,12 CHX mouthwash was used for oral care every 8 hours (strength not reported). Patients in the control group received ozonated water in the same frequency.
Oral care protocols and techniques for oral care were considered in the guideline.14
Outcomes
The relevant outcomes of interest in the SRs were VAP,9-11 mortality,9,11 and use of systemic antibiotics.11In the SRs by Zhao et al.11 and Lee et al.,9 VAP was defined as pneumonia in a patient who was on mechanical ventilation for at least 48 hours, and mortality was defined as either all-cause ICU mortality9,11 or 30 day all-cause mortality.11 Outcome definitions were not reported in the SR by Mojtahedzadeh et al.10
In the RCT by Izadi et al.,12 the outcome of interest was oral health measured using the Beck Oral Assessment Scale (BOAS). The scale comprises 5 subscales assessing the status of lips, mucous membranes and gums, teeth, tongue, and saliva. Each subscale measures oral health from 1 to 4, 4 indicating poorer health. Thus, the overall BOAS score ranges from 5 to 20, with a lower score indicating better oral health. The primary outcome in the RCT by Kes et al.13 was the incidence of VAP. Clinical diagnostic criteria for VAP were new or worsening infiltrates in a chest X-ray, together with 2 of the following: purulent tracheal aspirate, need for positive end-expiratory pressure of greater than 20% to maintain O2 saturation over 90%, white blood cell counts of less than 4,000/mm3 or greater than 11,000/mm3, body temperature of less than 35 0C or higher than 38.5 0C. Other outcomes assessed in the RCT were ventilator-associated tracheobronchitis (VAT) and oral health. VAT was defined using the same criteria as VAP, except for the presence of lung infiltrates. Oral health was assessed using Barnason’s oral assessment guide (BOAG), which evaluates 6 areas that assess teeth, lips, oral mucosa, saliva and gums, each on a 3-point scale. Overall scores range from 6 to 18, with a lower score indicating better oral health.13
Major outcomes considered in the included evidence-based guideline were oral health status, frequency of oral care, VAP, hospital-acquired pneumonia, and the knowledge and ability of health providers to provide oral care.14
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
The 3 included SRs9-11 described their objectives and inclusion criteria clearly, which included components of population, intervention, comparators, and outcomes. Multiple electronic databases were searched to identify eligible studies. Additional searches of bibliography and trial registries were also performed. The literature search was conducted within 24 months of completion and publication of the SRs. Study selection was conducted independently by 2 reviewers. Quality assessment of the included studies was done using validated tools.9-11 A list of excluded studies and the reasons for exclusion were reported in 2 SRs.9,11 Appropriate meta-analyses relevant to the current report were conducted in the SR by Zhao et al.11 using a fixed-effects model because of the low number of primary studies. In that SR,11 heterogeneity was assessed using the I2 statistic and reported as none (I2 = 0%) and low (I2 = 37%) for the VAP and mortality outcomes, respectively. Results of the meta-analyses in that SR11 were reported as effect sizes (i.e., risk ratios) with 95% confidence intervals and the quality of evidence was assessed using the GRADE approach. Detailed characteristics and results of the included studies were described in the SR by Zhao et al.11
The SRs had several limitations. In 2 SRs, it was unclear whether a protocol was published prior to the conducting of the review.9,10 In the SR by Mojtahedzadeh et al.,10 the characteristics of the included studies — such as the mean age and duration of ventilation — were not reported. As adult and pediatric patients were of interest to the SR,10 without the age of participants, it was not possible to confirm that the included studies relevant to the current report were conducted exclusively in adult populations. In that SR,10 results of the individual primary studies were not reported and the overall results of the SR were not reported clearly. Therefore, the comparative clinical effectiveness of CHX and the herbal oral care products were unclear from the SR.10 In the SR by Lee at al.,9 all comparators of interest (e.g., placebo, potassium permanganate, standard care) were grouped together as “control group” in the meta-analysis and separate analyses were not conducted with different comparators. Therefore, in that SR,9 the comparative effectiveness of CHX against other specific oral care products were unclear. Some details of the included studies such as the number of participants in the individual studies were not reported in the SR by Lee et al.9 In all 3 SRs, it was reported that the included relevant primary studies had several methodological limitations and high and unclear risk of bias.9-11 This could lower the validity and quality of the overall results of the SRs. Lastly, publication bias was not assessed in any of the SRs, either because of the low number of studies identified for each outcome11 or for unclear reasons.9,10
Randomized Controlled Trials
The objectives were clearly described in the 2 included RCTs.12,13 Both trials had randomized allocation and blinding (one12 was double-blinded and the other13 was single-blinded). In both RCTs, participants in both groups were enrolled from the same centres over the same period. Facilities at the study hospitals were likely representative of the treatment that the majority of patients receive. The outcome, oral health, was assessed using validated instruments in both RCTs.12,13
The RCT by Izadi et al.12 was published as a correspondence (i.e., a letter to the editor) and only limited details about the study methodology, participants, statistical analysis, and results were reported in the publication. Although the authors reported that the age, sex, underlying conditions, and baseline oral health were not different between the treatment and control groups, numerical or tabulated information of these baseline characteristics were not provided.12 Other potential confounding factors, such as the duration of ventilation, that could have affected the results were not reported in the RCT. Strength of CHX used in the treatment group, another factor which could affect the outcome, was also not reported. Therefore, a thorough critical appraisal of the study regarding internal and external validity was not possible. In the RCT by Kes et al.,13 a quarter of the enrolled participants (i.e., 19 out of 76 patients) dropped out of the study for various reasons (e.g., death, loss to follow-up) and these patients were excluded from the analysis. It is possible that this high study attrition could have affected the study results. Furthermore, according to the power calculation reported in the study, 38 patients were required in each group to ensure adequate power. However, 28 and 29 patients were included in the analysis of the treatment and control groups, respectively, suggesting that the study might not have been powered to detect statistically significant differences. The outcome for which the power calculation was performed was unclear. Patients were followed up for 3 days and it is unclear whether a longer duration of treatment could have affected the oral health outcome. The overall mean BOAG score, which was found to be significantly different between the groups, was calculated by including the baseline scores from day 1 (i.e., before treatment), together with scores on days 2 and 3 (i.e., after treatment), lowering the validity of the results. Change in oral health scores from baseline was not reported or compared in either of the included RCTs.12,13
Guidelines
The scope and purpose of the included RNAO guideline were described clearly.14 The target population and intended users of the guideline were clearly identified. The guideline was developed by an interdisciplinary group, whose members were listed. Systematic methods were used to search for evidence. The criteria for selecting the evidence and the quality assessment of the evidence were rigorous and appropriate. Recommendations were formulated by a consensus method involving the recommendation development group. The guideline was validated by a team of experts before publication. The process for guideline update was described. The recommendations were clear and easily identifiable. The evidence source for each recommendation was described and discussed. The certainty of evidence and the strength of each recommendation were assessed objectively and reported clearly. The criteria and instructions for the auditing and monitoring of the guideline were provided. There was adequate editorial independence.
The RNAO guideline14 was general to all persons requiring oral care assistance, which included patients on ventilators. Specific recommendations for oral care in critically ill and mechanically ventilated individuals were not provided. A research gap was identified in understanding the effect of oral care in the prevention of VAP. Because of the limitations of the identified evidence, the recommendations were of low certainty and conditional.
Summary of Findings
Results from the included studies are summarized here by outcome. Appendix 4 presents the main study findings.
Clinical Effectiveness of CHX
Ventilator-Associated Pneumonia
The SR by Zhao et al. reported that, compared to ozonated water, CHX oral care was associated with a statistically significantly higher rate of VAP occurrence.11 The evidence was from 1 RCT and no meta-analysis was conducted.
The same SR also reported that, compared to Nanosil, CHX oral care was associated with a statistically significantly higher rate of VAP occurrence.11 The evidence was from 1 RCT and no meta-analysis was conducted.
Evidence from an SR9 (reporting the results of 1 RCT) and a single-blind RCT13 suggested that CHX oral care was associated with statistically significantly lower rates of VAP occurrence compared to oral care with bicarbonate.
The SR by Lee et al. reported mixed results (from 2 RCTs) for the rates of VAP occurrence with CHX oral care compared to saline. While 1 RCT found that the rate of VAP occurrence was statistically significantly lower with CHX oral care, another RCT found no statistically significant difference between the groups.9
There were no statistically significant differences in the rates of VAP occurrence in patients who received CHX compared to those who received oral care with potassium permanganate (evidence from 2 SRs),9,11 hydrogen peroxide (evidence from 1 SR),11 or miswak (evidence from 1 SR).11
Mortality
There were no statistically significant differences in all-cause mortality or all-cause ICU mortality between CHX oral care and oral care with other agents, such as potassium permanganate (evidence from 2 SRs),9,11 Nanosil (evidence from 1 SR),11 saline (evidence from 1 SR),9 or bicarbonate (evidence from 1SR).9
Oral Health
Compared to ozonated water, oral care with CHX was associated with poorer oral health, as suggested by the evidence from an RCT.12 At day 3 and 5 of oral care, patients who received CHX had statistically significantly higher BOAS scores (indicating poorer oral health) compared to those who received ozonated water. Baseline and day 1 BOAS scores were not significantly different between the groups. Change in BOAS scores from baseline was not reported or compared.12
Evidence from 1 RCT showed that there were no statistically significant differences in oral health, measured with BOAG, between oral care with CHX and that with bicarbonate at days 2 and 3. The overall mean BOAG score of the CHX group was statistically significantly lower (indicating better oral health) than that of the bicarbonate group. It should be noted that the overall mean score was calculated by including the baseline scores (before study intervention) to the scores on days 2 and 3. Change in BOAG scores from baseline was not reported or compared.13
Ventilator-Associated Tracheobronchitis
Results from an RCT showed that there were no statistically significant differences in the rates of VAT occurrence in patients who received CHX oral care compared those who received bicarbonate.13
Use of Systemic Antibiotics
One SR (Zhao et al.11) reported results from an RCT that compared CHX with miswak. There were no statistically significant differences in the rates of systemic antibiotic usage between the CHX group and miswak group.11
Adverse Events
No relevant evidence regarding the safety of CHX for oral care in adult patients who are critically ill and on ventilators was identified; therefore, no summary can be provided.
Cost-Effectiveness of CHX
No relevant evidence regarding the cost-effectiveness of CHX for oral care in adult patients who are critically ill or on ventilators was identified; therefore, no summary can be provided.
Evidence-Based Guidelines Regarding Oral Care Drugs
No specific guidelines were identified regarding oral care for patients who were critically ill and mechanically ventilated. The RNAO guideline14 was general to all persons requiring oral care assistance, which included patients on ventilators. No recommendations were provided in the guideline regarding the use of CHX or other oral care drugs for routine use to prevent VAP in critically ill adults.14
The guideline suggested a multi-component oral care protocol for health providers. It should include components of standardized approach to assess oral health, individualized care plan, step-by-step guidance for oral care, and the identification of oral care tools and materials. The certainty of evidence was very low and the recommendation was conditional. A list of oral care tools and products was provided in the guideline, which included foam swabs, oral rinses, oral suctions, saliva substitutes, nystatin, tongue cleaners, toothbrushes, and toothpastes. The use of and evidence regarding rinses with oral care drugs such as CHX and povidone-iodine in lowering the risk of VAP was discussed; however, no recommendations were formulated.14
Limitations
The evidence summarized in this report was of low quality, with several methodological limitations, as described earlier. The SR by Zhao et al.11 was well-conducted; however, the primary studies included in the SR were at high risk of bias, lowering the validity of the results. No evidence regarding the safety and adverse effects of CHX was identified. No evidence regarding the cost-effectiveness of CHX for oral care in adult patients who are critically ill and on ventilators was identified. No specific guidelines were identified regarding oral care for patients who were critically ill and mechanically ventilated. Based on what was reported, none of the studies included in the 3 SRs9-11 and none of the included RCTs12,13 were conducted in Canada.
Conclusions and Implications for Decision- or Policy-Making
Three SRs9-11(2 with meta-analyses9,11) and 2 RCTs12,13 were identified regarding the clinical effectiveness of CHX oral care in adult patients with artificial airways and/or who were critically ill and mechanically ventilated. An evidence-based guideline14 for the oral care for adults who require assistance was included. No evidence regarding the cost-effectiveness of CHX for oral care was identified.
Overall, the evidence regarding clinical effectiveness was of low quality and the results should be interpreted with caution in light of the methodological limitations. Compared to ozonated water and to Nanosil, oral care with CHX was associated with significantly higher rates of VAP occurrence.11 Compared to bicarbonate, CHX oral care was associated with significantly lower rates of VAP occurrence.9,13 Evidence suggested that CHX was not significantly different from other oral care products, such potassium permanganate, hydrogen peroxide, and herbal agents (e.g., miskwak) in lowering the risk of VAP.9,11 There were no significant differences in all-cause mortality or all-cause ICU mortality between CHX and other oral care drugs.9,11 Low-quality evidence from RCTs suggested that CHX was associated with poorer oral health, compared to ozonated water,12 and no significantly different oral heath, compared to bicarbonate.13 One RCT of low quality also found that there were no significant differences in the rate of VAT occurrence between patients who received CHX and those who received bicarbonate for their oral care. Compared to the herbal product miswak, there were no significant differences in the use of systemic antibiotics associated with CHX oral care.11 There was no evidence regarding outcomes such as duration of ventilation or duration of ICU stay. Comparative evidence regarding the safety or adverse effects of CHX and other oral care drugs were not reported in any of the included publications.
The target population of the included guideline14 was all persons requiring oral care assistance. The guideline was developed with a comprehensive evidence search and rigorous methods. Because of the certainty of evidence being low or very low, conditional recommendations were made about a multi-component oral care protocol for health providers and educating persons and caregivers on the importance of oral care.14 No recommendations were provided in the guideline regarding the use of CHX or other oral care drugs for routine use to prevent VAP in critically ill adults.
A previous CADTH report published in 2019 examined the clinical effectiveness of CHX for oral care in adult patients who were hospitalized.5 The report highlighted the unclear evidence regarding the effectiveness of CHX in preventing VAP in medical and non-cardiac ICUs, where patients are more likely to be ventilated for longer durations. The included guideline also pointed to the research gaps in this topic.14 Well-designed, large, comparative trials are warranted to study the risks and benefits of oral care with CHX. Cost-effectiveness analyses could also play a role in informed decision-making and are therefore needed.
References
1.Pneumonia. Hospital Harm Improvement Resource. Ottawa (ON): Canadian Patient Safety Institute; 2016: http://www.patientsafetyinstitute.ca/en/toolsResources/Hospital-Harm-Measure/Documents/Resource-Library/HHIR%20Pneumonia.pdf. Accessed 2021 Oct 4.
2.Terezakis E, Needleman I, Kumar N, Moles D, Agudo E. The impact of hospitalization on oral health: a systematic review. J Clin Periodontol. 2011;38(7):628-636.PubMed
3.Klompas M, Li L, Kleinman K, Szumita PM, Massaro AF. Associations Between Ventilator Bundle Components and Outcomes. JAMA Intern Med. 2016;176(9):1277-1283.PubMed
4.Bouadma L, Klompas M. Oral care with chlorhexidine: beware! Intensive Care Med. 2018;44(7):1153-1155.PubMed
5.Chlorhexidine for Oral Care. A Review of Clinical Effectiveness and Guidelines. CADTH rapid response report: summary with critical appraisal. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1064%20Chlorhexidine%20for%20oral%20care%20Final.pdf. Accessed 2021 Oct 4.
6.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.PubMed
7.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384.PubMed
8.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Oct 4.
9.Lee S, Lighvan NL, McCredie V, et al. Chlorhexidine-Related Mortality Rate in Critically Ill Subjects in Intensive Care Units: A Systematic Review and Meta-Analysis. Respir Care. 2019;64(3):337-349.PubMed
10.Mojtahedzadeh M, Mashhadi Akbar Boojar M, Habtemariam S, et al. Systematic review: Effectiveness of herbal oral care products on ventilator-associated pneumonia. Phytother Res. 2021;35(7):3665-3672.PubMed
11.Zhao T, Wu X, Zhang Q, Li C, Worthington HV, Hua F. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst Rev. 2020;12:CD008367.PubMed
12.Izadi M, Bagheri M, Bahrami Far A, Sureda A, Soodmand M. Effect of ozonated water and chlorhexidine mouthwash on oral health in critically ill patients on mechanical ventilation: A double-blind randomised clinical trial. Intensive Crit Care Nurs. 2021;66:103083.PubMed
13.Kes D, Aydin Yildirim T, Kuru C, Pazarlıoglu F, Ciftci T, Ozdemir M. Effect of 0.12% Chlorhexidine Use for Oral Care on Ventilator-Associated Respiratory Infections: A Randomized Controlled Trial. J Trauma Nurs. 2021;28(4):228-234.PubMed
14.Oral health: Supporting adults who require assistance. Second edition. Toronto (ON): Registered Nurses’ Association of Ontario; 2020: https://rnao.ca/bpg/guidelines/oral-health-supporting-adults-who-require-assistance-second-edition. Accessed 2021 Oct 4.
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34.PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews and Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparators | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Mojtahedzadeh et al. (2021)10 Iran Funding source: NR | Systematic review of RCTs Number of included studies, n = 18 Number of relevant primary studies, n = 7 | Eligible population: Adult or pediatric participants undergoing tracheal intubation. Relevant population: Adult participants undergoing tracheal intubation Number of patients across the relevant primary studies, n = 534 Age: NR | Eligible interventions: Any natural products including raw materials, herbal extract, or products containing active ingredients Eligible comparators: placebo or standard care Relevant interventions:
Relevant comparator:
|
|
Zhao et al. (2020)11 China Funding source: Wuhan Young and Middle-aged Medical Talents Training Program, China; Cochrane Oral Health Global Alliance; NIHR, UK; CMB of New York, US | Systematic review and meta-analysis of RCTs Number of included studies, n = 37 Number of relevant primary studies, n = 9 | Critically ill hospitalized patients who were mechanically ventilated for ≥ 48 hours without VAP or respiratory infection at baseline. Overall number of patients, n = 5,675 Number of participants in the relevant studies, n = 894 Age of the relevant sample: Mean participant age ranged from 34.4 years to 58.4 years across the relevant studies. | Eligible interventions: Oral hygiene care procedures (e.g., oral and pharyngeal cavity rinse, professional assisted toothbrushing, antiseptics) Eligible comparators: no treatment, placebo, standard care or other oral hygiene care procedures. Relevant interventions:
Relevant comparators:
| Primary outcomes: incidence of VAP, mortality Relevant secondary outcomes: Duration of mechanical ventilation, duration of ICU stay, oral health (e.g., plaque index bleeding index), systemic antibiotic use, adverse events. Length of follow-up: Ranged from 3 to 9 days. |
Lee et al.,(2019)9 Canada Funding source: NR | Systematic review and meta-analysis of RCTs Number of included studies, n = 11 Number of relevant primary studies, n = 5 | Adult participants admitted to the ICU and were ventilated Overall number of patients, n = 1,769 Number of participants in the relevant studies, n = NR Age of the relevant sample: Mean participant age ranged from 36.1 years to 58.65 years across the relevant studies | Eligible interventions: Standard ICU care with CHX Eligible comparators: placebo, standard care Relevant interventions:
Relevant comparators:
| Outcomes: ICU mortality, incidence of VAP Length of follow-up: NR |
CHX = chlorhexidine; CMB = Chinese Medical Board; ICU = intensive care unit; n = number; NIHR = National Institute for Health Research; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; VAP = ventilator-associated pneumonia.
Note that this appendix has not been copy-edited.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Izadi et al.,(2021)12 Iran Funding source: NR Note: This RCT was published as a correspondence with limited details about the population and methods. | Double-blind RCT | Patients on mechanical ventilation Inclusion criteria: NR Exclusion criteria: NR Number of participants, n = 78 CHX group, n = 37 Control group, n = 36 Age of the participants: NR | Intervention: CHX mouthwash every 8 hours, strength NR Comparator: Ozonated water every 8 hours | Outcome: Oral health (measured with BOAS) Length of follow-up: 5 days |
Kes et al.,(2021)13 Turkey Funding source: Karabuk University Scientific Research Projects Coordination Unit | Single-blind RCT | Inclusion criteria: Patients ≥ 18 years of age, who were admitted to a critical care unit and were mechanically ventilated
Sex of the participants:
| Intervention: Oral care with 0.12% CHX gluconate thrice daily Comparator: Sodium bicarbonate thrice daily | Primary outcome: VAP, VAT Secondary outcomes: Oral health (measured with BOAG) Length of follow-up: 3 days |
BOAG = Barnason’s oral assessment guide; BOAS = Beck oral assessment scale; CHX = chlorhexidine; ICU = intensive care unit; n = number; RCT = randomized controlled trial; SD = standard deviation; VAP = ventilator-associated pneumonia; VAT = ventilator-associated tracheobronchitis.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Registered Nurses’ Association of Ontario (2020)14 | ||||||
Intended users: Nurses, caregivers, members of the interprofessional team, caregivers, educators, health service organizations, academic institutions, families Target population: Adults who require assistance to meet their oral care needs. | Oral care for adults who require assistance. Intervention relevant to the current report: Oral care agents for mechanically ventilated adults. | Persons oral health status, frequency of oral care, VAP, HAP, knowledge and ability of health providers to provide oral care | Evidence collected using a systematic literature review. Comprehensive search of the databases (e.g., CINAHL, MEDLINE, Cochrane database) was conducted for studies published from 2012 to 2019. A review of previous guidelines, guideline search and gap analysis, expert consultation and group discussions (with interprofessional teams and patients/caregivers) were also conducted. | Quality of the studies: assessed using Cochrane Risk of Bias tool, ROBINS-I, and AMSTAR 2. Certainty of evidence: assessed using the GRADE approach (ranging from very low to high certainty)a | Recommendations were formulated using evidence-to-decision framework. Decisions regarding recommendations were made by an expert panel, who considered certainty of evidence and evaluated the strength of recommendations. Strength of each recommendation indicated as strong or conditionalb based on context, certainty of evidence, balance of benefit and harms, health equity, and values and preferences. | Stakeholder review was done to obtain feedback on the drafted guideline. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CINAHL = Cumulative Index to Nursing and Allied Health Literature; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; HAP = hospital-acquired pneumonia; ROBINS-I = Risk of Bias in Non-randomized Studies - of Interventions; VAP = ventilator-associated pneumonia.
aCertainty of evidence was assessed using the GRADE approach, with the following ratings:
Very low: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
Low: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Moderate: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
High: We are very confident that the true effect lies close to that of the estimate of the effect.
bStrengths of recommendations included the following:
Strong recommendation: It implies that a majority of persons will be best served by the recommended action.
Conditional recommendation: Some uncertainty exists. Not all persons will be best served by the recommended action. A more careful consideration of personal circumstances, preferences, and values is needed.
Appendix 3: Critical Appraisal of Included Publications
Table 5: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 26
Strengths | Limitations |
|---|---|
Mojtahedzadeh et al. (2021)10 | |
The research question of the systematic review was described clearly. Clear inclusion and exclusion criteria were described. Inclusion criteria included the components of population, intervention, comparators, and outcome. Multiple databases were searched to identify eligible studies. Snowball searching of references was also conducted. The literature search was conducted within 24 months before the completion of the review. Two reviewers conducted study selection independently. There was good inter-rater agreement as assessed using the kappa statistic. Characteristics of the included studies such as interventions, comparators, study designs, and outcomes were described Risk of bias of the included studies was assessed using the CASP checklist. Risk of bias in the individual studies was reported. | It was unclear whether the review protocol was established before the conduct of the review. The rationale for the selection of study design for inclusion in the review was not described. It was unclear whether data extraction was conducted by 2 reviewers independently. A list of excluded studies was not provided. The population characteristics of the included studies such as mean age or sex of the participants were not provided. As adult and pediatric patients were of interest to the review, it was not possible to confirm that the included studies relevant to the current report were conducted exclusively in adult populations. Results of the individual studies were not reported. Overall results of the systematic review were not reported in detail. Sources of funding for the studies as well as potential sources of conflict of interest were not reported. Publication bias was not assessed. |
Zhao et al. (2020)11 | |
The research question of the systematic review was described clearly. Clear inclusion and exclusion criteria were described. Inclusion criteria included the components of population, intervention, comparators, and outcome. The systematic review was an update of a 2016 Cochrane review. Review methods were established before the conduct of the first version of the review. Deviations from the protocol were described and justified. Multiple databases were searched to identify eligible studies. Bibliographies and trial registries were searched. Expert and manufacturer consultation for additional studies was conducted. The literature search was conducted within 24 months before the completion of the review. Study selection and data extraction were conducted by 2 independent reviewers. Discrepancies were addressed and resolved through discussion. A list for excluded studies, along with the reasons for exclusion, was provided. Characteristics and details of the included studies were reported in detail. Sources of funding for the individual studies were also reported. Quality assessment of the included studies was performed using the Cochrane Risk of Bias tool. Detailed risk of bias of each of the included studies was provided. Appropriate methods were used for conducting meta-analyses. For the meta-analyses relevant to the current report, fixed effect models were used due to the low number of RCTs identified (2 RCTs). Results of the meta-analyses were reported as effect sizes (risk ratios) and 95% confidence intervals. Heterogeneity was assessed using the I2 statistic. Subgroup analyses were planned in case of considerable heterogeneity. Sensitivity analyses were planned to assess the effect of studies with high risk of bias or different diagnostic criteria for VAP. Quality of evidence was assessed using the GRADE approach. | The SR excluded quasi randomized and non-randomized studies. The rationale for the selection of study design for inclusion in the review was not described. All included relevant RCTs were reported to have high risk of bias. Methodological limitations and bias in the individual studies could lower the validity of the results of the SR and of the meta-analyses. It was planned that publication bias would be investigated using funnel plots if there were more than 10 studies for each outcome. Due to the low number of studies identified for each outcome, publication bias was not assessed. |
Lee et al. (2019)9 | |
The research question of the systematic review was described clearly. Clear inclusion and exclusion criteria were described. Inclusion criteria included the components of population, intervention, comparators, and outcome. Multiple databases were searched to identify eligible studies. Bibliographies were searched. The literature search was conducted within 24 months before the completion of the review. Study selection and data extraction were conducted by 2 independent reviewers. Discrepancies were addressed and resolved through discussion. A list for excluded studies, along with the reasons for exclusion, was provided. Characteristics and details of the included studies were reported in detail. Quality assessment of the included studies was performed using the Cochrane Risk of Bias tool. Risk of bias of each of the included studies was provided. A meta-analysis was conducted to statistically combine the results of the individual studies. However, this was not relevant to the current report. The authors had no conflicts of interests to declare. | It was unclear whether the review protocol was established before the conduct of the review. The rationale for the selection of study design for inclusion in the review was not described. Some details of the included studies such as the number of participants in the individual studies were not reported. Sources of funding for the studies as well as potential sources of conflict of interest were not reported. All comparators (e.g., placebo, potassium permanganate, standard care) were grouped together in the meta-analysis. Subgroup or sensitivity analyses were not conducted with different comparators. The comparative effectiveness of CHX against other specific oral care agents was not provided separately from other types of comparators. |
AMSTAR-2 = A MeaSurement Tool to Assess systematic Reviews 2; CASP = Critical Appraisal Skills Programme; CHX = chlorhexidine; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; RCT = randomized controlled trials; SR = systematic review; VAP = ventilator-associated pneumonia.
Note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist7
Strengths | Limitations |
|---|---|
Izadi et al. (2021)12 | |
The study was designed as a double-blind randomized controlled trial. Study objectives were reported. Participants of both groups were recruited over the same period of time from 2 hospitals. Facilities at the study centre were likely representative of the treatment that the majority of patients receive. The study outcome, oral health, was measured using a validated tool. Patients in treatment and control groups were followed up for the same period. | Note: The study was published as a correspondence (i.e., a letter to the editor). Only limited details about the study methodology, participants, statistical analysis and results were reported in the publication. Therefore, a thorough critical appraisal of the study regarding internal and external validity was not possible. Characteristics of patients included in the study, such as mean age, duration of ventilation, and comorbidities, were not reported. Strength of CHX used for oral care in the treatment group was not reported. A list of potential confounders was not provided. Since baseline and clinical characteristics of patients were not reported, any impact of confounding factors on the study results was unclear. Among the 78 patients included in the study, 5 were withdrawn. They were not included in the analysis. The reason for their exclusion was unclear. Adverse events in treatment and control groups were not reported. Patients were followed up for 5 days. It is unclear whether a longer duration of treatment would have affected the results of the study. The statistical tests used to compare the tests were unclear. Change in oral health score compared to baseline was not compared between the groups. It was unclear whether a sample size calculation was conducted to ensure adequate power. |
Kes et al. (2021)13 | |
The study was a single-blind randomized controlled trial. Critical care nurses who provided the treatment and most of the researchers were blinded to the allocation. The objectives of the study were clearly described, along with participant inclusion and exclusion criteria. Main study outcomes were described clearly in the methods section. Definitions of outcomes were provided and were assessed using validated tools. Study interventions and comparators were described. Main study findings were reported using simple outcome data (e.g., denominators and numerators). All patients who met the inclusion criteria from the source population were enrolled in the study. Patients in treatment and control groups were enrolled from the same centre. Facilities at the study centre were likely representative of the treatment that the majority of patients receive. | Although it was described as single-blind, it was unclear whether the patients were blinded to the treatment. In the main results, estimates of random variability (e.g., confidence intervals) were not reported. In some outcomes, actual P values were not reported, but rather indicted as “not significant.” Adverse events in treatment and control groups were not reported. Among 76 patients randomized in the trial, 19 (25%) dropped out due to various reasons (e.g., death, lost to follow-up). These participants were excluded from the analysis. According to the power calculation reported in the study, 38 patients were required in each group to ensure adequate power. The outcome for which this calculation was performed was not clear. Change in oral health score compared to baseline was not compared between the groups. Patients were followed up for 3 days. It is unclear whether a longer duration of treatment would have affected the results of the study. |
Table 7: Strengths and Limitations of Guideline Using AGREE II8
Item | Registered Nurses’ Association of Ontario (2020)14 |
|---|---|
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Probably yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Probably yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Yes |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings and Authors’ Conclusions
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome: Ventilator-Associated Pneumonia
Comparison | Study Citation and Study Design | Detailed Findings |
|---|---|---|
Incidence of VAP | ||
CHX vs. herbal oral care products | Mojtahedzadeh et al. (2021)10 SR (7 RCTs) | Among the relevant included studies, the herbal oral care products considered were Miswak (2 studies), Matrica (2 studies), Orthodentol mouthwash (1 study), Echinacea and aloe vera extract (1 study), and Zufa (1 study) Results: “Our assessment of the reviewed studies demonstrates that chlorhexidine and some other oral herbal medications have a critical role in the reduction of the oral microbial flora of the mouth and subsequently prevent hospital-acquired Infections including VAP.” (p.3667)10 Note: Results of the individual included studies were not reported in the publication. |
CHX vs. potassium permanganate | Zhao et al. (2020)11 SR and MA (2 RCTs) | Meidani et al. (2018) and Panchbhai et al. (2009): RR = 0.87 (95% CI, 0.50 to 1.52); P = 0.63; I2 = 0% |
Lee et al. (2019)9 SR (1 RCT) | Panchbhai et al. (2009): RR = 0.88 (95% CI, 0.42 to 1.71) | |
CHX vs. ozonated water | Zhao et al. (2020)11 SR and MA (1 RCT) | Hanifi et al. (2017): RR = 2.60 (95% CI, 1.12 to 6.03); P = 0.03 |
CHX vs. Nanosil | Zhao et al. (2020)11 SR and MA (1 RCT) | Khaky et al. (2018): RR = 8.76 (95% CI, 1.17 to 65.78); P = 0.03 |
CHX vs. hydrogen peroxide | Zhao et al. (2020)11 SR and MA (2 RCTs) | Dahiya et al. (2012): RR = 0.29 (95% CI, 0.06 to 1.28); P = 0.10 Bopp et al. (2006): CHX + toothbrushing (n = 2): 0 cases of VAP Control group (n = 3): 1 case of VAP |
CHX vs. miswak | Zhao et al. (2020)11 SR and MA (1 RCT) | Irani et al. (2019): RR = 13.00 (95% CI, 0.76 to 222.31); P = 0.08 |
CHX vs. bicarbonate | Lee et al. (2019)9 SR (1 RCT) | Fourrier et al. (2000): RR = 0.33 (95% CI, 0.14 to 0.81) |
Kes et al. (2021)13 Single-blind RCT | Number of participants: CHX group, n = 38; Control group, n = 38 Incidence of VAP:
| |
CHX vs. saline | Lee et al. (2019)9 SR (2 RCTs)a | Ozcaka et al. (2012): RR = 0.60 (95% CI, 0.37 to 0.98) Tantipong et al. (2008): RR = 0.43 (95% CI, 0.16 to 1.17) |
CHX = chlorhexidine; CI = confidence interval; MA = meta-analysis; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; VAP = ventilator-associated pneumonia.
aResults of the 2 RCTs were reported by more than 1 SR, but are presented once in the table, to avoid reporting results in duplicate.
Table 9: Summary of Findings by Outcome: Mortality
Comparison | Study citation and study design | Detailed findings |
|---|---|---|
CHX vs. potassium permanganate | Zhao et al. (2020)11 SR and MA (2 RCTs) | ICU or 30-day all-cause mortality: Meidani et al. (2018) and Panchbhai et al. (2009): RR = 1.11 (95% CI, 0.89 to 1.38); P = 0.34; I2 = 37% |
Lee et al. (2019)9 SR (1 RCT) | ICU mortality: Panchbhai et al. (2009): RR = 1.18 (95% CI, 0.96 to 1.46) | |
CHX vs. Nanosil | Zhao et al. (2020)11 SR and MA (1 RCT) | ICU or 30-day all-cause mortality: Khaky et al. (2018): RR = 4.87 (95% CI, 0.24 to 98.18); P = 0.30 |
CHX vs. bicarbonate | Lee et al. (2019)9 SR (1 RCT) | ICU mortality: Fourrier et al. (2000): RR = 0.43 (95% CI, 0.12 to 1.50) |
CHX vs. saline | Lee et al. (2019)9 SR (2 RCTs)a | ICU mortality: Ozcaka et al. (2012): RR = 0.99 (95% CI, 0.65 to 1.50) Tantipong et al. (2008): RR = 1.00 (95% CI, 0.69 to 1.45) |
CHX = chlorhexidine; CI = confidence interval; MA = meta-analysis; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; VAP = ventilator-associated pneumonia.
aResults of the 2 RCTs were reported by more than 1 SR, but are presented once in the table, to avoid reporting results in duplicate.
Table 10: Summary of Findings by Outcome: Oral Health
Comparison | Study citation and study design | Detailed findings |
|---|---|---|
CHX vs. ozonated water | Izadi et al.,(2021)12 Double-blind RCT | Number of participants: CHX group, n = 37; Control group, n = 36 Oral health measured using BOAS score:
|
CHX vs. bicarbonate | Kes et al. (2021)13 Single-blind RCT | Number of participants: CHX group, n = 38; Control group, n = 38 Oral health measured using BOAG score:
|
BOAG = Barnason’s oral assessment guide; BOAS = Beck oral assessment scale CHX = chlorhexidine; CI = confidence interval; RCT = randomized controlled trial; RR = risk ratio; SD = standard deviation.
Table 11: Summary of Findings by Outcome: Other Outcomes
Comparison | Study citation and study design | Detailed findings |
|---|---|---|
Use of systemic antibiotics | ||
CHX vs. miswak | Zhao et al. (2020)11 SR and MA (1 RCT) | Irani et al. (2019): RR = 1.04 (95% CI, 0.83 to 1.30) |
VAT | ||
CHX vs. bicarbonate | Kes et al. (2021)13 Single-blind RCT | Number of participants: CHX group, n = 38; Control group, n = 38 Incidence of VAT: CHX group, n (%) = 2 (6.9) Control group, n (%) = 4 (14.3) P = 0.318 |
CHX = chlorhexidine; CI = confidence interval; MA = meta-analysis; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; VAP = ventilator-associated tracheobronchitis.
Table 12: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Registered Nurses’ Association of Ontario (2020)14 | |
No specific recommendation regarding chlorhexidine and alternative oral care agents for routine use in critically ill adults to prevent VAP was made in the guideline. Recommendation: “The expert panel suggests that health providers follow a multi-component oral care protocol that includes:
Standardized approach:
Individualized oral care plan:
| Certainty of evidence:a Very low Strength of recommendation:b Conditional |
Step-by-step instructions:
Oral care tools and supplies:
A relevant summary is given below:
Povidone-iodine: “Povidone-iodine mouth rinse may be more effective than a saline mouth rinse in reducing the incidence of VAP, although the quality of the evidence is weak (150). ” (p.130)14 | |
VAP = ventilator-associated pneumonia.
aCertainty of evidence was assessed using the GRADE approach, with the following ratings:
Very low: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
Low: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Moderate: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
High: We are very confident that the true effect lies close to that of the estimate of the effect.
bStrengths of recommendations included the following:
Strong recommendation: It implies that a majority of persons will be best served by the recommended action.
Conditional recommendation: Some uncertainty exists. Not all persons will be best served by the recommended action. A more careful consideration of personal circumstances, preferences, and values is needed.
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 13: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Mojtahedzadeh et al. (2021)10 | Zhao et al., (2020)11 | Lee et al., (2019)9 |
|---|---|---|---|
Berry et al., Int J Nurs Stud 2011;48(6):681-688. | No | No | Yes |
Bopp et al., Journal of Dental Hygiene 2006;80(3):9. | No | Yes | No |
Dahiya et al., Nursing Journal of India 2012;103:89-91. | No | Yes | No |
Ebrahimian et al., Iranian Red Crescent Medical Journal, 21(5): e89639. | Yes | No | No |
Fourrier et al., Intensive Care Med 2000;26(9):1239-1247. | No | No | Yes |
Hafez et al., International Journal of Current Microbiology and Applied Sciences, 4:723–732. | Yes | No | No |
Hanifi et al., Iranian Red Crescent Medical Journal 2017;19(10):e60576. | No | Yes | No |
Irani et al., Medical Surgical Nursing Journal 2019;8(4):e100387. | Yes | Yes | No |
Khaky et al., Medicinski Arhiv 2018;72:206-9. | No | Yes | No |
Maarefvand et al., Modern Care Journal 2015;12(3):114–118. | Yes | No | No |
Meidani et al., International Journal of Preventive Medicine 2018;9(1):93. | No | Yes | No |
Mirzakhani et al., Journal of Client-Centered Nursing Care, 3(2): 161–166. | Yes | No | No |
Munro et al., Am J Crit Care 2009;18(5):428-437. | No | No | No |
O¨zcaka O¨, J Periodontal Res 2012;47(5):584-592. | No | Yes | Yes |
Panchbhai et al.,Chest 2009;135(5):1150-6. | No | Yes | Yes |
Rezaei et al., Journal of Indian Society of Periodontology, 20(4):404–408. | Yes | No | No |
Rezvani et al., 2018 Archives of Anesthesiology and Critical Care, 4(3):492–496. | Yes | No | No |
Tantipong et al., Infect Control Hosp Epidermiol 2008;29(2):131-136. | No | Yes | Yes |
Appendix 6: References of Potential Interest
Review Articles
1.Alecrim RX, Taminato M, Belasco A, Longo MCB, Kusahara DM, Fram D. Strategies for preventing ventilator-associated pneumonia: an integrative review. Rev Bras Enferm. 2019;72(2):521-530.PubMed
Guidelines of Unclear Methodology
2.Collins T, Plowright C, Gibson V, et al. British Association of Critical Care Nurses: Evidence-based consensus paper for oral care within adult critical care units. Nurs Crit Care. 2021;26(4):224-233.PubMed
Additional References
3.Burja S, Belec T, Bizjak N, Mori J, Markota A, Sinkovič A. Efficacy of a bundle approach in preventing the incidence of ventilator associated pneumonia (VAP). Bosn J Basic Med Sci. 2018;18(1):105-109.PubMed
4.Jackson L, Owens M. Does oral care with chlorhexidine reduce ventilator-associated pneumonia in mechanically ventilated adults? Br J Nurs. 2019;28(11):682-689.PubMed
5.Parreco J, Soe-Lin H, Byerly S, et al. Multi-Center Outcomes of Chlorhexidine Oral Decontamination in Intensive Care Units. Surg Infect (Larchmt). 2020;21(8):659-664.PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca