CADTH Health Technology Review
Pembrolizumab for Microsatellite Instability-High or Mismatch Repair Deficient Small Bowel Adenocarcinoma or Appendiceal Adenocarcinoma
Rapid Review
Authors: Keeley Farrell, Jennifer Horton
Abbreviations
dMMR
mismatch repair deficient
MSI-H
microsatellite instability-high
NCCN
National Comprehensive Cancer Network
Key Messages
Some adult patients with microsatellite instability-high (MSI-H)/mismatch repair deficient (dMMR) small bowel adenocarcinoma might benefit from pembrolizumab in controlling the disease (i.e., some patients achieved a partial or complete response after treatment). These findings are based on 2 single-arm studies (i.e., no comparator) with fewer than 20 patients in each study, which limits the certainty of the findings. The longer-term benefit of pembrolizumab is unclear, as some outcomes (e.g., progression-free survival, overall survival) were not reached at the time of data analysis.
The safety of pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma is unknown (no evidence was found for this population).
No evidence was identified regarding the clinical effectiveness of pembrolizumab monotherapy for patients with MSI-H/dMMR appendiceal adenocarcinoma.
No evidence was identified regarding the cost-effectiveness of pembrolizumab monotherapy for patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma.
No evidence-based guidelines were identified regarding pembrolizumab monotherapy for patients with MSI-H/dMMR appendiceal adenocarcinoma.
One guideline was identified that recommends pembrolizumab as an option for initial or subsequent therapy in patients with advanced or metastatic MSI-H/dMMR small bowel adenocarcinoma.
Context and Policy Issues
Mismatch repair is an essential DNA repair mechanism that corrects errors that occur during DNA replication.1,2 Deficiency in mismatch repair can lead to increased mutations in the microsatellite regions of DNA, resulting in a phenotype termed microsatellite instability.3,4 The microsatellite instability-high (MSI-H)/mismatch repair deficient (dMMR) phenotype is seen in a variety of cancer types including small intestine and colorectal cancer.2 The MSI-H/dMMR phenotype can occur sporadically or result from Lynch syndrome, which is caused by a germline mutation (a mutation that occurs in the reproductive cells [eggs or sperm]) in 1 of the DNA mismatch repair genes.2 MSI-H/dMMR tumours are more likely to be susceptible to immunotherapy.5
In 2016, 850 people were diagnosed with small bowel cancer in Canada6 and approximately 40% of small bowel cancers are adenocarcinomas.7 The frequency of the MSI-H/dMMR phenotype in small bowel adenocarcinoma has been estimated to range from 5% to 35%.7 The 5-year overall survival for small bowel adenocarcinoma ranges from 14% to 33%.7 Appendiceal cancer has an estimated incidence of 1 to 2 per million, per year,8 and approximately 60% of appendiceal cancers are adenocarcinomas.9 The prevalence of the MSI-H/dMMR phenotype in appendiceal carcinomas is estimated to be 2.8%.10 The 5-year survival for appendiceal carcinoma ranges from 20% to 60%.10
Current standard of care for the treatment of small bowel adenocarcinoma is chemotherapy with fluorouracil-leucovorin-oxaliplatin (known as FOLFOX) or capecitabine-oxaliplatin (known as CAPOX).5 Anti-epidermal growth factor receptor therapy (e.g., cetuximab, panitumumab) and anti-vascular endothelial growth factor receptor therapy (e.g., bevacizumab) have been studied in small bowel adenocarcinoma. However, their place in therapy is uncertain.5 Current treatment options for appendiceal adenocarcinoma include surgery (e.g., appendectomy) and chemotherapy.11
Checkpoint inhibitors are immunotherapy drugs that reverse the immunosuppressive mechanisms elicited by tumour cells.2 Pembrolizumab, a humanized immunoglobulin G4 monoclonal antibody, is a checkpoint inhibitor that targets programmed cell death-1 receptor and has significant activity in MSI-H/dMMR tumours.2 Pembrolizumab has been studied in multiple types of cancer including MSI-H/dMMR colorectal cancer.4,12 Most of the adverse events associated with the use of pembrolizumab are thought to be immune-related and can occur in any organ.13 Severe adverse events (Grade 3 to 4) occur in up to 5% of patients treated with pembrolizumab.13 Pembrolizumab may have a role in treating a variety of MSI-H/dMMR cancers including small bowel adenocarcinoma and appendiceal adenocarcinoma.
The CADTH pan-Canadian Expert Review Committee (pERC) issued a final reimbursement recommendation for pembrolizumab as monotherapy for MSI-H/dMMR colorectal cancer if certain conditions are met.14 A Health Canada Notice of Compliance does not yet exist for pembrolizumab as monotherapy for MSI-H/dMMR small bowel adenocarcinoma and appendiceal adenocarcinoma. Furthermore, CADTH has not assessed any drugs through the reimbursement review process for small bowel adenocarcinoma and appendiceal adenocarcinoma.
The aim of this report is to summarize the evidence regarding the clinical effectiveness and cost-effectiveness, and evidence-based guidelines, of pembrolizumab monotherapy in patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma.
Research Questions
What is the clinical effectiveness of pembrolizumab monotherapy in patients with microsatellite instability-high or mismatch repair deficient (MSI-H/dMMR) small bowel adenocarcinoma or appendiceal adenocarcinoma?
What is the cost-effectiveness of pembrolizumab monotherapy in patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma?
What are the evidence-based guidelines regarding the use of pembrolizumab for the treatment of MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were pembrolizumab and small bowel or appendiceal cancer. No filters were applied to limit the retrieval by study type. Where possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2016 and August 23, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma |
Intervention | Q1 to Q3: Pembrolizumab monotherapy |
Comparator | Q1 and Q2: Chemotherapy, chemotherapy with or without bevacizumab, panitumumab OR cetuximab, no treatment, no comparator Q3: Not applicable |
Outcomes | Q1: Clinical effectiveness (progression-free survival, overall survival, response rate, duration of response, quality of life, safety [i.e., adverse events of ≥ Grade 3 and Grade 4, deaths]) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-years gained, incremental cost-effectiveness ratios) Q3: Recommendations regarding the use of pembrolizumab for MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, guidelines, economic evaluations |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high; Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2016. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess Systematic Reviews 2 (or AMSTAR 2)15 for systematic reviews, the Downs and Black checklist16 for non-randomized studies, and the Appraisal of Guidelines for Research and Evaluation (or AGREE) II instrument17 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
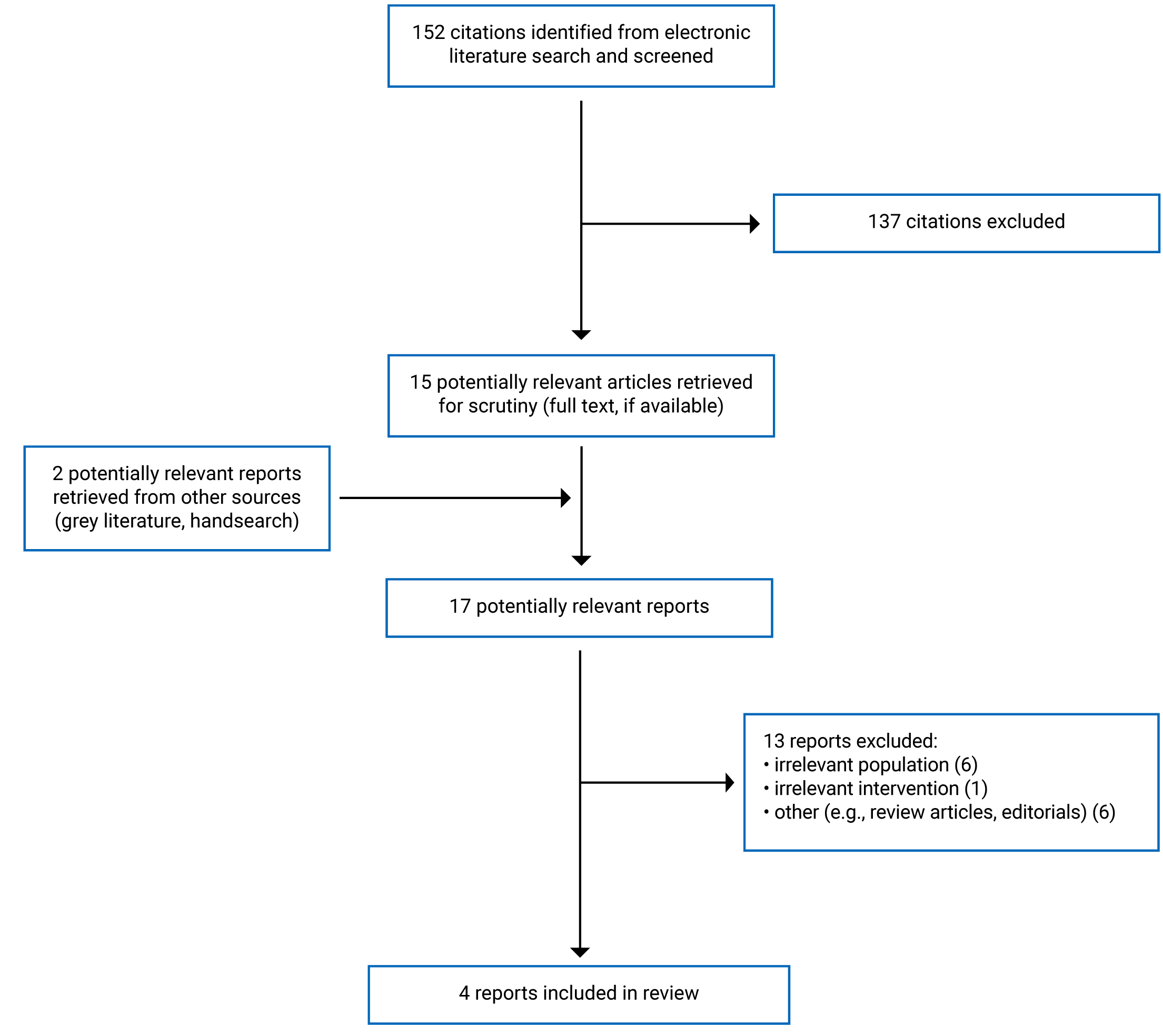
A total of 152 citations were identified in the literature search. Following the screening of titles and abstracts, 137 citations were excluded and 15 potentially relevant reports from the electronic search were retrieved for full-text review. Two potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 13 publications were excluded for various reasons and 4 publications met the inclusion criteria and were included in this report. These comprised 1 systematic review, 2 non-randomized studies, and 1 evidence-based guideline. Appendix 1 presents the PRISMA18 flow chart of the study selection.
All included publications were specific to MSI-H/dMMR small bowel adenocarcinoma. No publications related to patients with MSI-H/dMMR appendiceal adenocarcinoma were identified. No economic evaluations that assessed the cost-effectiveness of pembrolizumab monotherapy in patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma were identified.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The included systematic review19 had broader inclusion criteria than the present report. Specifically, studies of any checkpoint-based immunotherapy in patients with any Lynch syndrome–associated cancer were eligible. The systematic review did not include any primary studies relevant to the present report (i.e., studies in patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma).
The 2 included non-randomized studies also had broader inclusion criteria than the present report. The Pedersen et al. (2021)20 study included patients with small bowel adenocarcinoma and the Marabelle et al. (2020)21 study included patients with non-colorectal solid tumours. Only the characteristics and results specific to patients with MSI-H/dMMR small bowel adenocarcinoma will be discussed in this report.
One evidence-based guideline that included recommendations around the use of pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma was included in this report.22
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Therkildsen et al. (2021)19 conducted their search on November 3, 2020. Restrictions based on date of publication were not specified. In total, 31 studies were included in the systematic review; however, none of them were relevant to the current report.
Two phase II, open label, single-arm, prospective cohort studies that evaluated pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma were identified.20,21,23,24
One guideline was identified that was developed by the National Comprehensive Cancer Network (NCCN) and published in 2021.22 A search of the PubMed database was performed to identify relevant non-randomized studies, randomized controlled trials, systematic reviews, guidelines, and validation studies. A multidisciplinary panel reviewed and discussed the evidence and developed the recommendations by voting. The recommendations were assigned categories based on both the level of clinical evidence and the degree of consensus within the guidelines panel. The categories ranged from 1 (highest) to 3 (lowest).
Country of Origin
The systematic review was authored by a researcher in Denmark.19
The single-arm study by Pedersen et al. (2021)20 was authored by a researcher in the US and the study sites were in the US. The single-arm study by Marabelle et al. (2020)21 was authored by a researcher in France.
The NCCN guideline22 was conducted by authors in the US.
Patient Population
Therkildsen et al. (2021)19 included patients with any Lynch syndrome‒associated cancer. None of the included primary studies included patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma.
Pedersen et al. (2021)20 included 4 adults with MSI-H/dMMR small bowel adenocarcinoma with 1 or more prior line of systemic chemotherapy for unresectable or metastatic disease. The study by Marabelle et al. (2020)21 included 19 adults with advanced unresectable and/or metastatic-incurable MSI-H/dMMR small bowel adenocarcinoma with disease progression on or intolerance to prior standard therapy.
The intended users of the NCCN guideline22 include all individuals who impact decision-making in cancer care including physicians, nurses, pharmacists, payers, and patients and their families. The target population for the guideline is patients with small bowel adenocarcinoma.
Interventions and Comparators
The eligible interventions in Therkildsen et al. (2021)19 were checkpoint-based immunotherapies including pembrolizumab and others.
The intervention in both single-arm studies was IV pembrolizumab 200 mg administered once every 3 weeks for 35 cycles or until treatment intolerance or disease progression.20,21 Both single-arm studies were single-arm trials and did not include a control group.
The NCCN guideline22 considered interventions and practices that address diagnosis, pathologic staging, surgical management, perioperative treatment, patient surveillance, management of recurrent and metastatic disease, and survivorship.
Outcomes
The outcomes included in the systematic review by Therkildsen et al. (2021)19 were objective response rate, progression-free survival, and overall survival.
The primary and secondary outcomes in both single-arm studies applied to the whole study population,20,23 which was broader than the subset of the population relevant to this report. The primary outcome in Pedersen et al. (2021)20,23 was overall response rate. However, in the population relevant to this report, the overall response rate was not calculated; rather, the number of patients who achieved a complete response or a partial response to treatment was reported. The secondary outcomes were progression-free survival, overall survival, and adverse events.23 Adverse events were not reported separately for the population relevant to this report. Pedersen et al. (2021)20,23 also reported on duration of response; however, this outcome does not appear to have been pre-specified. The primary outcome in Marabelle et al. (2020)21,24 was objective response rate. The secondary outcomes were duration of response, progression-free survival, and overall survival.24
Both single-arm studies assessed objective (or overall) response rate as per the Response Evaluation Criteria in Solid Tumors (or RECIST) version 1.1 criteria.20,21 In Marabelle et al. (2020),21 the objective response rate was defined as the proportion of patients with a confirmed complete or partial response by an independent central radiographic review. In Pedersen et al. (2021),20,23 the overall response rate was defined as the percent of patients whose best response was complete response or partial response. In Pedersen et al. (2021),20 the scanning interval was every 12 weeks; and in Marabelle et al. (2020),21 the scanning interval was every 9 weeks in year 1 and every 12 weeks thereafter. In Pedersen et al. (2021),20 the overall response rate was confirmed by a second scan at least 4 weeks after the initial scan showing a response. Both studies assessed progression-free survival and overall survival. Progression-free survival was defined as the time from study registration20 or first dose of study medication21 to the first of either progressive disease or death. Overall survival was defined as the time from study registration20 or first dose of study medication21 to death from any cause. Both studies assessed duration of response. Marabelle et al. (2020)21 defined duration of response as the time from first documented evidence of complete or partial response until the first of either disease progression or death from any cause. Pedersen et al. (2021)20 did not provide a definition for duration of response. Both studies also assessed adverse events; however, they were not reported separately for the population of interest to this report (i.e., patients with MSI-H/dMMR small bowel adenocarcinoma).
The NCCN guideline22 considered objective response rate, progression-free survival, and adverse events.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Review
The systematic review by Therkildsen et al. (2021)19 had a clear research objective. The authors did not include a statement that the review methods were established a priori. This has the potential to introduce bias if methods were adjusted after the review had begun. The authors used a comprehensive literature search strategy. The study eligibility criteria were clearly defined, the search was conducted in multiple databases, and the search date and keywords used were provided. Providing details on these elements of the search strategy increases its reproducibility. Study selection was performed in duplicate and discrepancies were resolved by involving a third reviewer. A list of excluded studies and justifications was not provided. Unjustified exclusion of studies could bias the results of the review. The authors state that the funding sources for the included studies were reviewed to assess any conflicts of interest. Potential conflicts of interest of the authors were disclosed.
Non-Randomized Studies
In both studies,20,21 the objective, outcomes, patient characteristics, interventions, and main findings were clearly described. Both studies used a single-arm study design, where outcomes were examined in a single group of patients who received pembrolizumab, and neither study included a control group of patients who did not receive pembrolizumab. Therefore, these studies are both susceptible to multiple forms of bias that threaten both internal and external validity. Without a control group, it is unclear whether the results observed in these studies should be attributed to pembrolizumab alone, as there are many uncontrolled factors that could have impacted the results. Because both studies had single-arm designs, blinding of patients or study personnel was not possible. The main outcome measures used in the studies were objective measures (e.g., survival, objective response) that are unlikely to be influenced by blinding. Pedersen et al. (2021)20,23 reported on duration of response; however, this outcome does not appear to have been prespecified. Reporting results from outcomes that were not prespecified suggests that a study may be at risk of reporting bias (selective reporting). Neither of the studies discussed potential confounders; however, the authors of Pedersen et al. (2021)20 state that participants were excluded if they had confounding comorbidities. Only 1 patient was lost to follow-up in Marabelle et al. (2020).21 An overview of patient disposition was not provided in Pedersen et al. (2021);20 however, the authors state that all patients were evaluated for secondary survival end points. Details on the recruitment method for participants were not provided in either study. Therefore, it is unclear whether the study samples were representative of the source populations. Both studies were industry-funded and disclosed potential conflicts of interest.
Guideline
The NCCN guideline22,25 clearly described the overall objective, health questions covered by the guideline, the target population, and the target users. The guideline development group included individuals from all relevant professional groups. It is unclear whether the views and preferences of the target population were sought. External review of the guideline was not discussed. However, a patient advocate was included on the guidelines panel. There were some limitations to the methods used to search for evidence. Only 1 database (PubMed) was searched; it is unclear whether screening was done in duplicate and the full inclusion and exclusion criteria were not provided. The recommendations in the guideline were assigned categories based on the level of evidence supporting the recommendation. However, strengths and limitations of the body of evidence were not described. The methods for formulating the recommendations were clearly described. There is an explicit link between evidence and recommendations; however, the recommendation of pembrolizumab as a first-line option is not described in the discussion section. The guideline states that an update to the discussion section is currently in progress. External parties can make submissions requesting changes to NCCN guidelines and these submissions are reviewed by the guidelines panel. The recommendations are specific and unambiguous, and are outlined in treatment algorithms at the beginning of the guideline. The development of the guideline was solely funded by NCCN and conflict of interests of panel members were disclosed. The guideline procedures state that panel members are removed from deliberations and/or votes when there is a meaningful conflict.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Pembrolizumab
No relevant evidence regarding the clinical effectiveness of pembrolizumab monotherapy in patients with MSI-H/dMMR appendiceal adenocarcinoma was identified. However, a summary of the evidence in patients with MSI-H/dMMR small bowel adenocarcinoma is provided.
Response Rate: In the single-arm study by Pedersen et al. (2021),20 2 patients (50%) with MSI-H/dMMR small bowel adenocarcinoma achieved a confirmed partial response after treatment with pembrolizumab and no patients achieved a complete response. In the single-arm study by Marabelle et al. (2020),21 the objective response rate was 42.1% in patients treated with pembrolizumab, with 3 of 19 patients achieving a complete response and 5 of 19 achieving a partial response.
Duration of Response: The average duration of response in Pedersen et al. (2021)20 was 28.5 months. The median duration of response in Marabelle et al. (2020)21 was not reached. However, the range for having no progressive disease by the time of last disease assessment was 4.3 to 31.3 months.
Progression-Free Survival: In the single-arm study by Pedersen et al. (2021),20 the median progression-free survival was not reached in patients with MSI-H/dMMR small bowel adenocarcinoma treated with pembrolizumab but the lower boundary of the 95% confidence interval for the estimate was 2.5 months.
In the single-arm study by Marabelle et al. (2020),21 the median progression-free survival was 9.2 months and the upper boundary of the 95% confidence interval had not been reached at the time of analysis.
Overall Survival: The median overall survival was not reached in either study, but the lower boundary of the 95% confidence interval for the estimate of overall survival was 2.5 months in Pedersen et al. (2021)20 and 10.6 months in Marabelle et al. (2020).21
Cost-Effectiveness of Pembrolizumab
No relevant evidence regarding the cost-effectiveness of pembrolizumab monotherapy in patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma was identified. Therefore, no summary can be provided.
Guidelines
No evidence-based guidelines regarding the use of pembrolizumab for the treatment of MSI-H/dMMR appendiceal adenocarcinoma were identified. A summary of 1 evidence-based guideline regarding the use of pembrolizumab for the treatment of MSI-H/dMMR small bowel adenocarcinoma is provided.
The NCCN guideline22 recommends pembrolizumab as an option for initial or subsequent therapy in patients with advanced or metastatic MSI-H/dMMR small bowel adenocarcinoma who have not received previous treatment with a checkpoint inhibitor. The guideline also recommends pembrolizumab as an option for initial therapy in patients with advanced or metastatic MSI-H/dMMR small bowel adenocarcinoma with prior oxaliplatin exposure in the adjuvant setting or contraindication who have not received previous treatment with a checkpoint inhibitor. Both recommendations are based on lower-level evidence and there is uniform NCCN consensus that the intervention is appropriate.
Limitations
This report is limited by the small number of relevant publications. No relevant evidence regarding pembrolizumab in patients with MSI-H/dMMR appendiceal adenocarcinoma was identified. Additionally, no relevant evidence regarding the cost-effectiveness of pembrolizumab monotherapy in patients with MSI-H/dMMR small bowel adenocarcinoma was identified. The included systematic review19 did not include any relevant studies and no studies were identified that compared the clinical effectiveness of pembrolizumab to other standards of care in patients with MSI-H/dMMR small bowel adenocarcinoma.
The 2 non-randomized studies included in this report were single-arm studies that included 4 and 19 relevant patients and no control group.20,21 The results of these studies should be interpreted with caution. Neither of the included studies assessed quality of life.20,21 Additionally, adverse events were not reported separately for patients with MSI-H/dMMR small bowel adenocarcinoma in either study.20,21
The evidence that informed the relevant recommendations in the guideline22 was also limited to 2 single-arm studies (1 of which is included in this report and included 4 relevant patients).20
One of the single-arm studies was conducted in the US20 and the other study did not specify the locations of the study sites.21 The NCCN guideline is meant to apply in the US. Therefore, it is unclear whether the results summarized in this report are generalizable to Canada.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 systematic review19 that did not include any relevant studies, 2 single-arm studies,20,21 and 1 evidence-based guideline22 on the use of pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma. No relevant evidence in patients with MSI-H/dMMR appendiceal adenocarcinoma was identified. Additionally, no relevant evidence on the cost-effectiveness of pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma was identified.
The findings from the 2 single-arm studies suggest that pembrolizumab may provide some clinical benefit in patients with MSI-H/dMMR small bowel adenocarcinoma.20,21 Neither of the studies reported on adverse events separately for patients with MSI-H/dMMR adenocarcinoma, so the safety in this population is unknown.20,21 In Pedersen et al. (2021),20 2 patients (50%) with MSI-H/dMMR small bowel adenocarcinoma achieved a partial response after treatment with pembrolizumab and no patients achieved a complete response to treatment. The average duration of response was 28.5 months.20 The median progression-free survival and overall survival were not reached. However, the lower boundary of the 95% confidence interval was 2.5 months for both outcomes.20 In Marabelle et al. (2020),21 the objective response rate was 42.1% in the 19 patients with MSI-H/dMMR small bowel adenocarcinoma treated with pembrolizumab and 50% of the patients treated with pembrolizumab survived without disease progression for at least 9 months.21 The median overall survival was not reached; however, the lower boundary of the 95% confidence interval was 10.6 months.21 Both studies used a single-arm design and did not use a control group to compare the clinical effectiveness of pembrolizumab to other standard treatments or to patients who did not receive any treatment for MSI-H/dMMR small bowel adenocarcinoma, which limits the interpretation of the findings.
The NCCN guideline22 recommends pembrolizumab as an option for initial or subsequent therapy in patients with advanced or metastatic MSI-H/dMMR small bowel adenocarcinoma. The guideline also recommends pembrolizumab as an option for initial therapy in patients with advanced or metastatic MSI-H/dMMR small bowel adenocarcinoma with prior oxaliplatin exposure in the adjuvant setting or contraindication.22
Overall, the body of evidence was limited and gaps in the evidence, as well as methodological limitations of the included studies, make it difficult to draw conclusions on the clinical effectiveness of pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma. Specifically, the single-arm design precludes head-to-head comparisons and does not inform the clinical effectiveness of pembrolizumab compared to other interventions. Multiple outcomes in the included studies were not reached (i.e., progression-free survival, overall survival); therefore, longer-term follow-up is required to understand the benefit of pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma. Additional high-quality studies that compare the clinical effectiveness, as well as economic evaluations investigating the cost-effectiveness of pembrolizumab in patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma with other treatment options, would help stakeholders in decision-making on the use of pembrolizumab.
References
1.Arora S, Velichinskii R, Lesh RW, et al. Existing and Emerging Biomarkers for Immune Checkpoint Immunotherapy in Solid Tumors. Adv Ther. 2019;36(10):2638-2678. PubMed
2.Ciombor KK, Goldberg RM. Hypermutated Tumors and Immune Checkpoint Inhibition. Drugs. 2018;78(2):155-162. PubMed
3.Ruiz-Banobre J, Goel A. DNA Mismatch Repair Deficiency and Immune Checkpoint Inhibitors in Gastrointestinal Cancers. Gastroenterology. 2019;156(4):890-903. PubMed
4.Sahin IH. Immune checkpoint inhibitor response in mismatch repair-deficient colorectal cancer and other solid tumors: Is it truly disease-agnostic? Colorectal Cancer. 2020;9(4).
5.Mazlom H, Teuwen LA, Peeters M. Management of small bowel adenocarcinoma: making the most of the available evidence to inform routine practice. Curr Opin Oncol. 2021;33(4):368-371. PubMed
6.Society CC. Small intestine cancer statistics. 2021; https://cancer.ca/en/cancer-information/cancer-types/small-intestine/statistics. Accessed 2021 Sep 9.
7.Aparicio T, Zaanan A, Svrcek M, et al. Small bowel adenocarcinoma: epidemiology, risk factors, diagnosis and treatment. Dig Liver Dis. 2014;46(2):97-104. PubMed
8.Institute NC. Appendiceal cancer. 2021; https://www.cancer.gov/pediatric-adult-rare-tumor/rare-tumors/rare-digestive-system-tumors/appendiceal-cancer. Accessed 2021 Sep 9.
9.Kelly KJ. Management of Appendix Cancer. Clin Colon Rectal Surg. 2015;28(4):247-255. PubMed
10.Morales-Miranda A, Rosado ID, Núñez CC, Montero FC. Appendiceal carcinoma associated with microsatellite instability. Mol Clin Oncol. 2018;8(5):694-698. PubMed
11.Glasgow SC GW, Stewart D, et al. The American Society of Colon and Rectal Surgeons, Clinical Practice Guidelines for the Management of Appendiceal Neoplasms. Dis Colon Rectum. 2019;62(12):1425-1438. PubMed
12.André T, Shiu K-K, Kim TW, et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. N Engl J Med. 2020;383(23):2207-2218. PubMed
13.Kwok G, Yau TCC, Chiu JW, Tse E, Kwong Y-L. Pembrolizumab (Keytruda). Hum Vaccin Immunother. 2016;12(11):2777-2789. PubMed
14.CADTH Reimbursement Recommendation Pembrolizumab (Keytruda). Can J Health Technol. 2021;1(7).
15.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
16.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
17.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 1800 Jan 1.
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
19.Therkildsen C, Jensen LH, Rasmussen M, Bernstein I. An Update on Immune Checkpoint Therapy for the Treatment of Lynch Syndrome. Clin. 2021;14:181-197. PubMed
20.Pedersen KS, Foster NR, Overman MJ, et al. ZEBRA: A Multicenter Phase II Study of Pembrolizumab in Patients with Advanced Small-Bowel Adenocarcinoma. Clin Cancer Res. 2021;27(13):3641-3648. PubMed
21.Marabelle A, Le DT, Ascierto PA, et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/ mismatch repair-deficient cancer: Results from the phase II KEYNOTE-158 study. Journal of Clinical Oncology. 2020;38(1):1-10. PubMed
22.Benson AB, Venook AP, Al-Hawary MM, et al. Small Bowel Adenocarcinoma, Version 2.2020. Plymouth Meeting (PA): National Comprehensive Cancer Network. 2020. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1495 Accessed 2021 Sep 9. 2021.
23.Academic and Community Cancer Research United. NCT02949219: Pembrolizumab in Treating Patients With Small Bowel Adenocarcinoma That is Metastatic or Locally Advanced and Cannot Be Removed by Surgery. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021. https://clinicaltrials.gov/ct2/show/NCT02949219 Accessed 2021 Sep 17. 2021.
24.Merck Sharp & Dohme Corp. NCT02628067: Study of Pembrolizumab (MK-3475) in Participants With Advanced Solid Tumors (MK-3475-158/KEYNOTE-158). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2021. https://clinicaltrials.gov/ct2/show/NCT02628067 Accessed 2021 Sep 17. 2021.
25.Network NCC. Development and Update of Guidelines. Guidelines Process 2021; https://www.nccn.org/guidelines/guidelines-process/development-and-update-of-guidelines Accessed 2021 Sep 9.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Therkildsen et al. (2021)19 Denmark NR | 31 studies in total including 7 cohort studies and 24 case reports. None of the included studies were in patients relevant to the current report (i.e., patients with MSI-H/dMMR small bowel adenocarcinoma or appendiceal adenocarcinoma). | Inclusion criteria: Patients with Lynch syndrome‒associated cancer | Eligible interventions: FDA- and EMA- approved checkpoint-based immunotherapies targeting CTLA-4 (ipilimumab), PD-1 (pembrolizumab and nivolumab), or PD-L1 (atezolizumab, avelumab, and durvalumab) Eligible comparators: not specified | Outcomes: objective response rate, progression-free survival, overall survival Follow-up: NR |
CTLA-4 = cytotoxic T lymphocyte antigen 4; dMMR = mismatch repair deficient; EMA = European Medicines Agency; MSI-H = microsatellite instability-high; NR = not reported; PD-1 = programmed death-1; PD-L1 = programmed death-ligand 1.
Table 3: Characteristics of Included Non-Randomized Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Pedersen et al. (2021)20 US The Merck Investigator Studies Program, the Kavanagh Family Foundation, Kevin T. Doner Memorial Fund | Phase II, single-arm, open label, prospective cohort study | Inclusion criteria: Patients aged 18 years or older with small bowel adenocarcinoma with 1 or more prior line of systemic chemotherapy for unresectable or metastatic disease. Relevant population: Four patients with MSI-H/dMMR small bowel adenocarcinoma Population characteristics were not reported separately for the relevant population. | Intervention: IV pembrolizumab 200 mg once every 3 weeks until treatment intolerance, disease progression, or completion of 35 cycles Comparator: This study did not include a control group (i.e., no comparator). | Outcomes: complete response, partial response, duration of response, toxicity/safety, progression-free survival, overall survival Follow-up: 2 years |
Marabelle et al. (2020)21 France Merck Sharp and Dohme Corp., a subsidiary of Merck and Co., Inc. | Phase II, single-arm, open label, prospective cohort study | Inclusion criteria: Patients aged 18 years or older with advanced unresectable and/or metastatic incurable non-colorectal solid tumour with disease progression on or intolerance to prior standard therapy. Relevant population: Nineteen patients with MSI-H/dMMR small bowel adenocarcinoma Population characteristics were not reported separately for the relevant population. | Intervention: IV pembrolizumab 200 mg once every 3 weeks for 35 cycles (approximately 2 years) or until disease progression, unacceptable toxicity, or patient withdrawal Comparator: This study did not include a control group (i.e., no comparator). | Outcomes: objective response rate, duration of response, progression-free survival, overall survival, safety and tolerability Follow-up: median = 13.4 months (range, 0.4 to 34.2 months) |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: All individuals who impact decision-making in cancer care including physicians, nurses, pharmacists, payers, and patients and their families. Target population: Patients with small bowel adenocarcinoma | Interventions and practices that address diagnosis, pathologic staging, surgical management, perioperative treatment, patient surveillance, management of recurrent and metastatic disease, and survivorship. | Objective response rate, progression-free survival, adverse events | Electronic search of the PubMed database was performed to identify relevant literature. | Quality of data (e.g., trial design and how the results were derived) is considered during the guideline development panel’s deliberation process. | A multidisciplinary panel of cancer specialists, clinical experts and researchers reviewed and discussed the evidence to develop the recommendations. In the absence of high-level evidence, recommendations were based on expert consensus. The panel members deliberated on the interpretation of the clinical evidence and voted on how the evidence should be incorporated into the guidelines. The recommendations were assigned categories based on both the level of clinical evidence available and the degree of consensus within the guidelines panel. NCCN categories:
| External or internal review of guidelines was not discussed however, external parties can make submissions requesting changes to guidelines. These submissions are reviewed by the guidelines panel. |
NCCN = National Comprehensive Cancer Network.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Review Using AMSTAR 215
Strengths | Limitations |
|---|---|
Therkildsen et al. (2021)19 | |
Clear objective Comprehensive literature search strategy and detailed methods described Study selection was performed in duplicate and discrepancies were resolved by involving a third reviewer Authors disclosed potential conflicts of interest | Unclear if review methods were established a priori List of excluded studies and justifications not provided |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 6: Strengths and Limitations of Non-Randomized Studies Using the Downs and Black checklist16
Strengths | Limitations |
|---|---|
Pedersen et al. (2021)20 | |
Objective, outcomes, patient characteristics, interventions, and main findings were clearly described Main outcomes used were objective measures and unlikely to be influenced by blinding (e.g., survival, objective response) A power calculation was conducted a priori to determine sample size Authors disclosed funding source and potential conflicts of interest | This study did not include a control group; therefore, the results are susceptible to multiple forms of bias that threaten both internal and external validity Potential confounders were not discussed however, the authors state that participants were excluded if they had confounding comorbidities Overview of patient disposition was not provided however, authors state that all patients were evaluable for secondary survival end points Details on how the study sample was selected were not provided All study sites were located in the US; therefore, it is unclear whether the results are generalizable to patients in Canada |
Marabelle et al. (2020)21 | |
Objective, outcomes, patient characteristics, interventions, and main findings were clearly described Adverse events were reported Only 1 patient was lost to follow-up Main outcomes used were objective measures and unlikely to be influenced by blinding (e.g., survival, objective response) Responses were confirmed by independent central radiologic review Authors disclosed funding source and potential conflicts of interest | This study did not include a control group; therefore, the results are susceptible to multiple forms of bias that threaten both internal and external validity Potential confounders were not discussed Details on how the study sample was selected were not provided It is unclear if the authors conducted a power calculation a priori to determine sample size Multi-centre study however, authors do not specify locations of the study sites and therefore, it is unclear whether the results are generalizable to patients in Canada |
Table 7: Strengths and Limitations of Guideline Using AGREE II17
Item | |
|---|---|
Domain 1: Scope and Purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder Involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of Development | |
7. Systematic methods were used to search for evidence. | Partially |
8. The criteria for selecting the evidence are clearly described. | Partially |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Unclear |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of Presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | NA |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Partially |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial Independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable; NCCN = National Comprehensive Cancer Network.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Response and Duration
Study citation and study design | Results |
|---|---|
Objective response rate | |
Marabelle et al. (2020)21 Single-arm prospective cohort | 42.1% (95% CI, 20.3 to 66.5) |
Complete response | |
Pedersen et al. (2021)20 Single-arm prospective cohort | 0% |
Marabelle et al. (2020)21 Single-arm prospective cohort | 3 of 19 patients (16%) |
Partial response | |
Pedersen et al. (2021)20 Single-arm prospective cohort | 2 of 4 patients (50%) |
Marabelle et al. (2020)21 Single-arm prospective cohort | 5 of 19 patients (26%) |
Duration of response | |
Pedersen et al. (2021)20 Single-arm prospective cohort | Average = 28.5 months (range, 26.5 to 30.5) |
Marabelle et al. (2020)21 Single-arm prospective cohort | Median duration of response = not reached No progressive disease by the time of last disease assessment, range = 4.3 to 31.3 months |
CI = confidence interval.
Table 9: Summary of Findings by Outcome — Survival
Study citation and study design | Results |
|---|---|
Progression-free survival | |
Pedersen et al. (2021)20 Single-arm prospective cohort | Median = not reached (95% CI, 2.5 months to not reached) |
Marabelle et al. (2020)21 Single-arm prospective cohort | Median = 9.2 months (95% CI, 2.3 to not reached) |
Overall survival | |
Pedersen et al. (2021)20 Single-arm prospective cohort | Median = not reached (95% CI, 2.5 months to not reached) |
Marabelle et al. (2020)21 Single-arm prospective cohort | Median = not reached (95% CI, 10.6 months to not reached) |
CI = confidence interval.
Table 10: Summary of Recommendations in Included Guideline
Recommendations and supporting evidence | Category of evidence |
|---|---|
NCCN (2021)22 | |
Recommendations:
Supporting evidence: the recommendations are based on results from 2 single-arm prospective cohort studies. One single-arm study included a cohort of patients with MSI-H/dMMR small bowel adenocarcinoma as well as other types of non-colorectal cancer and found that treatment with pembrolizumab may control the disease in some patients. The other single-arm study was the study by Pedersen et al. (2021)20 included in this report. | Category 2A (based upon lower-level evidence, there is uniform NCCN consensus that the intervention is appropriate) |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high; NCCN = National Comprehensive Cancer Network.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
26.Keytruda for Squamous Non-Small Cell Lung Cancer. (CADTH Therapeutic Review). Ottawa (ON): CADTH; 2020. https://www.cadth.ca/keytruda-squamous-nsclc-details Accessed 2021 Sep 10.
27.Pembrolizumab (Keytruda) for HNSCC. (CADTH Therapeutic Review). Ottawa (ON): CADTH; 2020. https://cadth.ca/pembrolizumab-keytruda-hnscc-details Accessed 2021 Sep 10.
Review Articles
28.Pestana RC, Sen S, Hobbs BP, Hong DS. Histology-agnostic drug development - considering issues beyond the tissue. Nat Rev Clin Oncol. 2020;17(9):555-568. PubMed
29.Yamamoto H, Imai K. An updated review of microsatellite instability in the era of next-generation sequencing and precision medicine. Semin Oncol. 2019;46(3):261-270. PubMed
Additional References
30.Hirsch D, Gaiser T, Merx K, et al. Clinical responses to PD-1 inhibition and their molecular characterization in six patients with mismatch repair-deficient metastatic cancer of the digestive system. J Cancer Res Clin Oncol. 2021;147(1):263-273. PubMed
31.Le DT, Kim TW, Van Cutsem E, et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J Clin Oncol. 2020;38(1):11-19. PubMed
32.Al Attar L, Truong P. The Effect of Pembrolizumab in Absence of Programmed Death 1 Receptor. Cureus. 2018;10(6):e2896. PubMed
33.Le DT, Durham JN, Smith KN, et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science. 2017;357(6349):409-413. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca