CADTH Health Technology Review
Hip Protectors for Community-Dwelling Older Adults
Rapid Review
Authors: Keeley Farrell, Melissa Walter
Abbreviations
AMSTAR 2
A MeaSurement Tool to Assess systematic Reviews 2
AGREE
Appraisal of Guidelines for Research and Evaluation
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
RACGP
Royal Australian College of General Practitioners
RCT
randomized controlled trial
RNAO
Registered Nurses’ Association of Ontario
Key Messages
In community-dwelling older adults who wore hip protectors there was no difference in the risk of hip fractures or pelvic fractures, compared to those who did not wear hip protectors.
Three guidelines were identified that include recommendations around the use of hip protectors in older adults. One guideline suggests that hip protectors should be considered in adults at risk for falls and hip fracture. One guideline conditionally recommends hip protectors for frail older adults in the appropriate environment. One guideline suggests that hip protectors should not be considered in older adults in community settings.
Context and Policy Issues
Falls are common in older adults and are associated with both morbidity and mortality. Approximately 30% of community-dwelling adults over the age of 65 and 50% of community-dwelling adults over the age of 80 experience a fall at least once per year.1 Falls can result in fractures, traumatic brain injuries, depression, loss of autonomy, functional decline, and death.2 Approximately 30,000 hip fractures occur each year in Canada3 and more than 90% of hip fractures are attributable to falls.4 There are a number of risk factors associated with hip fractures such as female gender, older age, low cognitive function, and previous spine or hip fracture.4
There are several interventions that aim to reduce the number of hip fractures in older adults. These include regular exercise, pharmacological treatments (e.g., calcium, vitamin D), and the use of hip protectors.4 There are 2 main types of hip protectors that include either hard shells or soft pads that are usually held within specifically designed underwear.5 The purpose of hip protectors is to either shunt or absorb the force of impact to prevent fractures.5
There is uncertainty on the effectiveness of hip protectors which may be explained by limited user adherence in studies of hip protectors.6 A systematic review of barriers and facilitators to the use of hip protectors in long-term care settings found multiple barriers including discomfort, unwanted side effects, poor ergonomics, and distaste with the aesthetics of hip protectors.6
The aim of this report is to summarize the evidence regarding the clinical effectiveness of hip protectors for community-dwelling older adults. In addition, evidence-based guidelines with recommendations regarding hip protectors in preventing fall-related injuries among community-dwelling older adults will be reviewed.
Research Questions
1. What is the clinical effectiveness of hip protectors in preventing fall-related injuries among community-dwelling older adults?
2. What are the evidence-based guidelines regarding the use of hip protectors in preventing fall-related injuries among community-dwelling older adults?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the international HTA database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were hip protectors and community/home settings. No filters were applied to limit the retrieval by study type. The search was limited to English language documents published between January 1, 2014 and July 26, 2021.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
Population | Adults aged 55 years and older living independently in the community (i.e., home setting) |
Intervention | Hip protectors (any style/brand) |
Comparator | Q1: Alternate style/brand of hip protector; no hip protectors Q2: Not applicable |
Outcomes | Q1: Clinical effectiveness (e.g., incidence or number of fractured hips and other related injuries, user satisfaction, mortality) and harms (e.g., skin irritation, risk of pelvic fractures, impediment to activities of daily living) Q2: Recommendations regarding the use of hip protectors among community-dwelling older adults (e.g., optimal style of hip protectors, role of caregiver/home care staff in promoting adherence to, proper use of, and satisfaction with hip protectors) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, non-randomized studies, guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2014. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 for systematic reviews and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument8 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
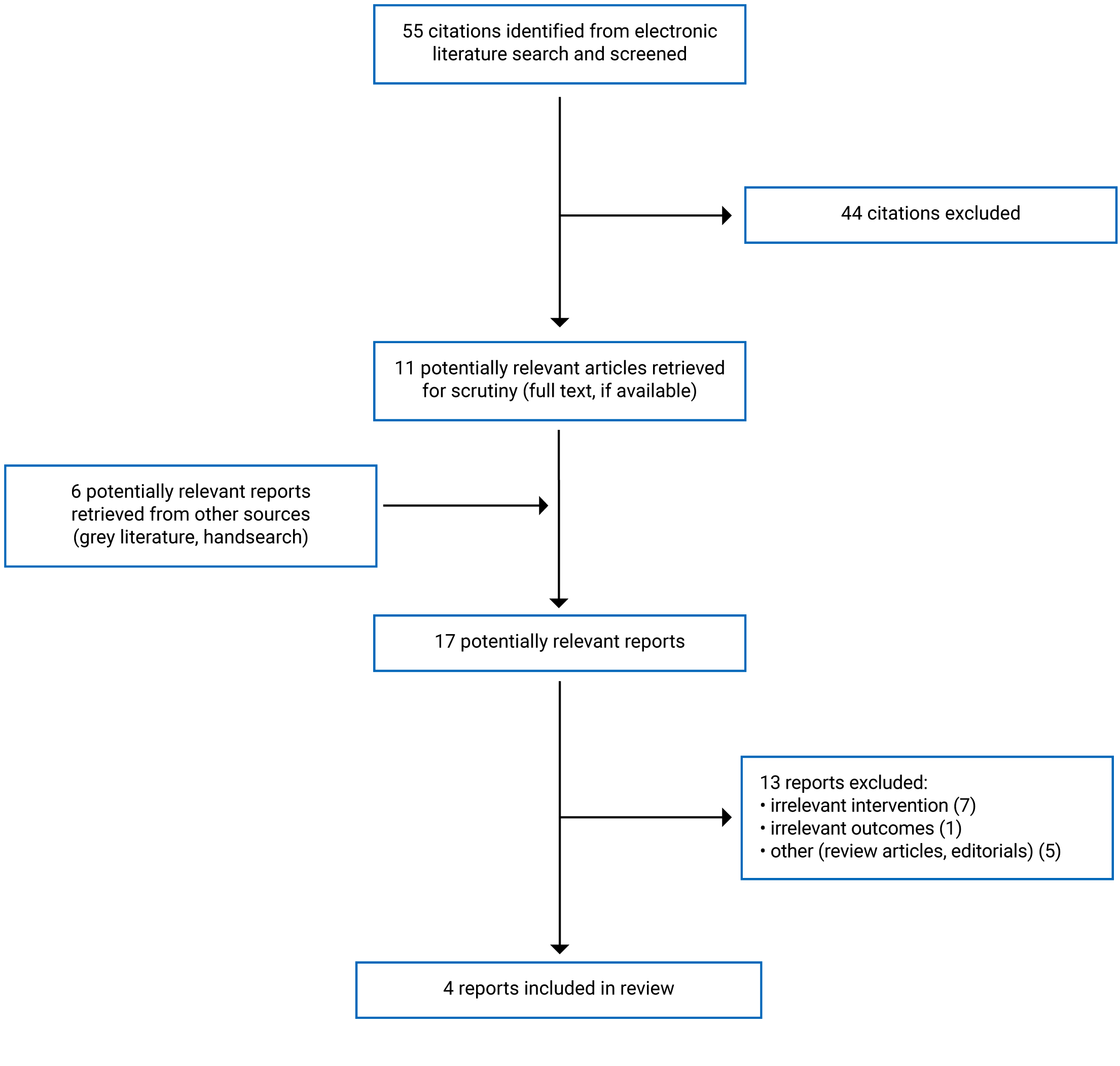
A total of 55 citations were identified in the literature search. Following screening of titles and abstracts, 44 citations were excluded and 11 potentially relevant reports from the electronic search were retrieved for full-text review. 6 potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 13 publications were excluded for various reasons, and 4 publications met the inclusion criteria and were included in this report. These comprised 1 systematic review and 3 evidence-based guidelines. Appendix 1 presents the PRISMA9 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The included systematic review by Santesso et al. (2014)5 had broader inclusion criteria than the present review. Specifically, the systematic review included studies in older adults living in institutionalized care settings in addition to those in community-dwelling older adults. Only the characteristics and results of the subset of relevant studies will be discussed in this report.
Three evidence-based guidelines10-12 were identified and included in this report. One guideline did not distinguish sex from gender and reported on their population as “postmenopausal women and men older than 50 years of age (p. i).”11 While we have retained the original language used when reporting on this guideline, we acknowledge that such language is not inclusive of trans and non-binary persons.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Santesso et al. (2014)5 was an update to a previous systematic review originally published in 1999. For the update the search time frame was limited to November 2009 until December 2012. Nineteen randomized controlled trials (RCTs) met the inclusion criteria and 5 were relevant to the present review. A meta-analysis was conducted, and data was pooled separately from trials in institutionalized and community settings. All 5 relevant RCTs were included in the meta-analysis.
Three evidence-based guidelines10-12 were included in the present review.
The Registered Nurses’ Association of Ontario (RNAO) guideline was published in 2017.10 A systematic literature search was conducted to identify relevant systematic reviews, and website searching was conducted to identify relevant guidelines. The authors appraised the systematic reviews using AMSTAR and RNAO’s scoring system that rates reviews as low, moderate, or strong. The guidelines were appraised by the authors using AGREE II and RNAO’s scoring system that rates guidelines as low, moderate, or strong. The authors excluded guidelines with a ‘low’ quality rating. A panel of experts was established to develop the recommendations and a modified Delphi technique was used to obtain panel consensus. Recommendations were assigned levels of evidence ranging from Ia (highest) to V (lowest).
The joint guideline by the Royal Australian College of General Practitioners (RACGP) and Osteoporosis Australia was published in 2017.11 The guideline was an update to a version published in 2010. A systematic literature search was conducted to identify relevant RCTs, prospective cohort studies, and systematic reviews of RCTs or prospective cohort studies. The body of evidence supporting each recommendation was rated according to the National Health and Medical Research Council body of evidence matrix. An expert working group developed the recommendations based on the evidence, or through consensus in the absence of sufficient evidence. Each recommendation was given a final grade based on the National Health and Medical Research Council grades of recommendation that ranged from A (highest) to D (lowest).
The Eastern Association for the Surgery of Trauma guideline was published in 2016.12 A systematic literature search was conducted to identify eligible RCTs, prospective and retrospective observational studies, case-control studies, and meta-analyses. The evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology and each study was assessed as being at low, moderate, or high risk of bias. The research questions were created using a modified Delphi technique and each reviewer independently assessed the evidence that was used to develop the recommendations. Based on the GRADE methodology, when formulating the recommendations, the phrases “we strongly recommend” or “we conditionally recommend” were used for strong evidence and weaker evidence, respectively.
Country of Origin
The systematic review by Santesso et al. (2014)5 was authored by a researcher in Canada. The relevant RCTs were conducted in Australia and the UK.
The RNAO guideline10 was conducted by authors from Canada. The RACGP and Osteoporosis Australia guideline11 was conducted by authors from Australia. The Eastern Association for the Surgery of Trauma guideline12 was conducted by authors from the US.
Patient Population
Santesso et al. (2014)5 included studies in older adults living in the community or institutionalized care. The population relevant to the present review included 5,614 community-dwelling older adults. The mean age of participants in the relevant trials ranged from 78 to 84 years.
The intended users of the RNAO guideline10 include nurses and other health-care providers, individuals and organizations responsible for the education of health-care providers, and managers, administrators, and policy-makers. The intended users for the recommendation on hip protectors are nurses and other health-care providers. The target population for the guideline is adults (greater than 18 years old) who are at risk for falls and fall injuries. The majority of evidence included in the guideline focused on older adults (greater than 65 years old) including evidence used to support the recommendation on hip protectors.
The intended users of the RACGP and Osteoporosis Australia guideline11 are general practitioners and other health professionals. The target population of the guideline is women who are postmenopausal and men older than 50 who may be at risk of minimal trauma fracture, have been diagnosed as having at least 1 minimal trauma fracture, or diagnosed with osteoporosis.
The intended users of the Eastern Association for the Surgery of Trauma guideline12 are not specified. The target population for the guideline is adults aged 65 years or older.
Interventions and Comparators
In Santesso et al. (2014)5 the intervention was hip protectors, and the comparator was no hip protectors. The follow-up period in the relevant studies ranged from 3 to 42 months.
In the RNAO guideline10 the relevant interventions considered were interventions for preventing falls and reducing the risk for falls or fall-related injury. In the RACGP and Osteoporosis Australia guideline11 the interventions considered were best practice in the identification, diagnosis, treatment, and management of osteoporosis. In the Eastern Association for the Surgery of Trauma guideline12 clinical interventions to reduce fall-related injuries were considered.
Outcomes
In Santesso et al. (2014)5 outcomes assessed in the relevant population included risk of sustaining a hip fracture, risk of sustaining a pelvic fracture, overall rate of pelvic and other fractures, rate of fall events, acceptance of and adherence to wearing protectors (compliance), and complications.
In the RNAO guideline10 hip fractures and falls were included in the discussion on the evidence around hip protectors. The potential benefits, harms, and barriers to adherence of hip protectors were also discussed. In the RACGP and Osteoporosis Australia guideline11 hip fracture risk was considered for the recommendation on hip protectors. In the Eastern Association for the Surgery of Trauma guideline12 injury due to falls, harms, and compliance were considered.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Review
The systematic review by Santesso et al. (2014)5 had a clear research objective. The authors state that the protocol was published before the review; however, they did not provide a reference for the protocol, and it is unclear which components of the research methods were established a priori and whether the protocol was registered. This has the potential to introduce bias if methods were adjusted after the review had begun. The review used a comprehensive literature search strategy. The study eligibility criteria were clearly defined, the literature search was conducted in multiple databases, the literature search dates were provided, restrictions and key terms used in the literature search were described, and a flow chart of study selection was provided. Providing details on these elements of the literature search increases its reproducibility. Both study selection and data extraction were performed independently by 2 authors. The risk of bias in the included studies was also assessed independently by 2 authors using appropriate methods. Performing these processes in duplicate decreases the likelihood of inconsistencies. A list of excluded studies and justifications was provided. Appropriate methods for meta-analysis were described and heterogeneity was assessed. Sensitivity analyses were conducted to explore impact on pooled results of removing studies assessed at high risk of bias in the domain of allocation concealment. The authors state that they did not detect publication bias; however, their investigation of publication bias was not described. The authors state their sources of funding for the systematic review, but the sources of funding for the individual studies included in the review were not reported. Therefore, it is impossible to discern whether the included studies were commercially or independently funded.
Guidelines
All of the included guidelines had clearly described objectives.10-12 Both the RNAO and Eastern Association for the Surgery of Trauma guidelines10,12 specifically described the health questions covered by the guidelines. The RACGP and Osteoporosis Australia guideline11 included a description of the scope and purpose of the guideline however, the health questions were not specifically described. All the guidelines clearly described their target populations. The guideline development groups for the RNAO and RACGP and Osteoporosis guidelines included individuals from all relevant professional groups.10,11 The Eastern Association of the Surgery of Trauma guidelines did not specify the roles or institutions of the members of the guideline development group.12 The RACGP and Osteoporosis Australia guideline had a limited consultation period that did not include the view or preferences of the target population.11 It is unclear if the views and preferences of the target populations were sought for the other 2 guidelines.10,12 The target users were clearly defined for the RNAO and RACGP and Osteoporosis Australia guidelines; however, the Eastern Association for the Surgery of Trauma guideline did not define the target users.10-12 All the guidelines used systematic methods to search for evidence however, the full search strategy was not provided for the RACGP and Osteoporosis Australia guideline.11 The RACGP and Osteoporosis Australia guideline11 did not provide details on the full inclusion and exclusion criteria or on who performed study screening and whether it was done in duplicate. The criteria for selecting the evidence were clearly described in the other 2 guidelines.10,12 In all the guidelines the quality of the evidence was assessed; however, discussion of the strengths and limitations of the body of evidence was limited. Further, in the RACGP and Osteoporosis Australia guideline11 the quality ratings for the included studies were not provided, thus limiting our interpretation of the evidence. The description of the methods for formulating the recommendations was limited in all the included guidelines. All the guidelines include a brief description of the methods used for formulating the recommendations; however, discussion of the outcomes of the recommendation development process (e.g., extent to which consensus was reached) and descriptions of how the development processes influenced the final recommendations (e.g., alignment with recommendations and final vote) were lacking. It is unclear what process was used to obtain consensus on the recommendations in the Eastern Association for the Surgery of Trauma guideline.12 The RNAO guideline10 included a discussion of the potential side effects and harms of hip protectors, and the other 2 guidelines did not. All the guidelines included a description of the evidence used to formulate the recommendations and there was an explicit link between the evidence and recommendations. Both the RNAO and RACGP and Osteoporosis Australia guidelines were reviewed externally by experts before publication.10,11 The Eastern Association for the Surgery of Trauma guideline12 did not describe an external review process. Out of the 3 included guidelines, only the RNAO guideline10 included a detailed procedure for updating the guideline. The RACGP and Osteoporosis Australia guideline included a recommendation around hip protectors that was specific and unambiguous. The other 2 included guidelines did not specify the appropriate setting for the use of hip protectors in their recommendations.10,12 The key recommendations were easily identifiable in all the included guidelines. The Eastern Association for the Surgery of Trauma guideline12 did not receive any funding and stated that the authors did not declare any conflicts of interest. The other 2 guidelines identified their funding sources and included explicit statements that the funding did not influence the content of the guidelines; however, the RACGP and Osteoporosis Australia guideline did not report if there were any competing interests within the guideline working group.10,11
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Hip Protectors
Falls and Fractures
In Santesso et al. (2014)5 results from the meta-analysis found that when compared to no hip protectors, that wearing hip protectors did not reduce the risk of hip fractures or pelvic fractures in community-dwelling older adults. Individuals wearing hip protectors also had a similar rate of other fractures compared to those who did not wear hip protectors.
The rate of falls in community-dwelling older adults was reported by individual RCT in Santesso et al. (2014).5 Mixed results were found for the effect of hip protectors on the rate of falls in community-dwelling older adults in the included studies that assessed this outcome. Results reported in these studies included an increase, decrease, or no difference in the rate of falls with the use of hip protectors compared to no hip protectors.
Acceptance and Adherence (Compliance)
Acceptance and adherence (also termed compliance) of hip protectors in community-dwelling older adults was reported by individual RCTs in the systematic review by Santesso et al. (2014).5 Compliance to hip protectors in community-dwelling older adults ranged from 31% to 51%.
Complications
In the systematic review by Santesso et al. (2014)5 there were 4 individual RCTs that reported on complications. In 2 of the RCTs no complications were reported. In 1 of the studies 1 hip fracture was reported as a result of falling while putting on a hip protector. In another study, 16 participants (5%) reported minor skin irritation caused by the hip protectors.
Guidelines
Three guidelines were identified that include recommendations regarding the use of hip protectors in older adults.10-12
The RNAO guideline10 suggests that hip protectors be considered as an intervention to reduce the risk of hip fracture among adults at risk for falls and hip fracture. This recommendation was based on moderate quality evidence from 1 systematic review. The RACGP and Osteoporosis Australia guideline11 suggests that hip protectors should not be considered to reduce the risk of hip fracture in community settings . This recommendation is based on 1 systematic review that the authors determined provided some support for the recommendation and that care should be taken in its application. The Eastern Association for Surgery of Trauma guideline12 conditionally recommends hip protectors for frail older adults in the appropriate environment; this recommendation is based on evidence from 2 reviews and 2 RCTs that the authors rated as weaker evidence.
Limitations
The findings in this report are limited by the quantity of the evidence. Only 1 systematic review was identified that included 5 relevant RCTs.5 Further, the recommendations around hip protectors in 2 of the included guidelines10,11 were based on this systematic review.
The guidelines included general recommendations on the use of hip protectors, but they did not include recommendations around the optimal style of hip protectors, or the role of caregivers/home care staff in promoting the adherence to, the proper use of, and strategies to improve satisfaction with hip protectors. The recommendations around hip protectors in 2 of the included guidelines10,12 were general recommendations that were not specific to community settings.
None of the relevant RCTs in the included systematic review were conducted in Canada.5 The RNAO guideline10 is specific to Canada; however, the other 2 included guidelines are not.11,12 Therefore it is unclear whether all of the results summarized in this report are generalizable to the Canadian context.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 systematic review5 and 3 evidence-based guidelines10-12 on the use of hip protectors in community-dwelling older adults.
The findings from the systematic review suggest that hip protectors do not reduce the risk of hip fractures or pelvic fractures, or the rate of other fractures in community-dwelling older adults, when compared to those who did not wear hip protectors.5 The effect of hip protectors on the rate of falls in community-dwelling older adults was unclear, as the findings were mixed.5 The rate of adherence to hip protectors in community-dwelling older adults in the relevant studies ranged from 31% to 51%,5 however, it is unknown whether the level of adherence to the hip protectors influenced the clinical outcomes. Of the 4 RCTs that reported on complications related to hip protectors in the systematic review, 2 of the RCTs reported no complications, 1 RCT reported the incidence of 1 hip fracture as a result of falling while putting on a hip protector, and in 1 RCT, 5% of patients reported minor skin irritation caused by hip protectors.5
The RNAO guideline10 suggests that hip protectors be considered as an intervention to reduce the risk of hip fracture among adults at risk for falls and hip fracture. The RACGP and Osteoporosis Australia guideline11 suggests that hip protectors should not be considered to reduce the risk of hip fractures in older adults in community settings. Both the RNAO and RACGP and Osteoporosis Australia guidelines10,11 based their recommendations on the systematic review by Santesso et al. (2014),5 which found that hip protectors did not reduce the risk of fractures in community settings. In the RNAO guideline10 the expert panel suggested that some individuals in the community may benefit from hip protectors such as those with osteoporosis engaging in high-risk activities despite the lack of evidence in this setting. The RNAO guideline10 suggests supporting individualized decisions around the use of hip protectors by reviewing the evidence as well as the potential benefits, harms, and barriers. For frail older adults, the Eastern Association for Surgery of Trauma guideline12 conditionally recommends hip protectors in the appropriate environment.
Limited evidence was identified on the effectiveness of hip protectors in community-dwelling older adults. Based on the results of 1 systematic review, hip protectors do not reduce the likelihood of hip fractures, pelvic fractures, or other fractures in community-dwelling older adults.5 Recommendations were mixed with 1 guideline10 that suggests hip protectors be considered among adults at risk for falls and hip fracture, 1 guideline12 that conditionally recommends hip protectors in for frail older adults in the appropriate environment, and 1 guideline11 that suggests that hip protectors should not be considered in older adults in community settings. Future research may be helpful to consider the potential influence of compliance with wearing hip protectors, as it is unclear whether the level of compliance with wearing hip protectors, which ranged from 31% to 51%, had an impact on the findings in the systematic review.5
References
1.National Institute for Health and Care Excellence. Assessment and prevention of falls in older people. (Clinical guideline CG161) 2013; https://www.nice.org.uk/guidance/cg161/evidence/falls-full-guidance-190033741. Accessed 2021 Aug 19.
2.Juckett LA, Bunger AC, Jarrott SE, et al. Determinants of fall prevention guideline implementation in the home- and community-based service setting. Gerontologist. 2020;15:15. PubMed
3.Leslie WD, O'Donnell S, Lagace C, et al. Population-based Canadian hip fracture rates with international comparisons. Osteoporos Int. 2010;21(8):1317-1322. PubMed
4.de Bot R, Veldman HD, Witlox AM, van Rhijn LW, Hiligsmann M. Hip protectors are cost-effective in the prevention of hip fractures in patients with high fracture risk. Osteoporos Int. 2020;31(7):1217-1229. PubMed
5.Santesso N, Carrasco-Labra A, Brignardello-Petersen R. Hip protectors for preventing hip fractures in older people. Cochrane Database Syst Rev. 2014(3):CD001255. PubMed
6.Korall AM, Feldman F, Scott VJ, et al. Facilitators of and barriers to hip protector acceptance and adherence in long-term care facilities: a systematic review. J Am Med Dir Assoc. 2015;16(3):185-193. PubMed
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
8.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2021 Jul 28.
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
10.Preventing falls and reducing injury from falls. 4th ed. Toronto (ON): Registered Nurses’ Association of Ontario; 2017: https://rnao.ca/bpg/guidelines/prevention-falls-and-fall-injuries. Accessed 2021 Jul 28.
11.Osteoporosis prevention, diagnosis and management in postmenopausal women and men over 50 years of age. 2nd ed. East Melbourne (AU): The Royal Australian College of General Practitioners and Osteoporosis Australia; 2017: https://www.racgp.org.au/getattachment/2261965f-112a-47e3-b7f9-cecb9dc4fe9f/Osteoporosis-prevention-diagnosis-and-management-in-postmenopausal-women-and-men-over-50-years-of-age.aspx. Accessed 2021 Jul 28.
12.Crandall M, Duncan T, Mallat A, et al. Prevention of fall-related injuries in the elderly: An Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2016;81(1):196-206. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review and Meta-Analysis
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
Santesso et al. (2014)5 Canada Peterborough and Stamford Hospitals NHS Foundation Trust, University of Otago, Hull York Medical School, Cochrane Bone, Joint and Muscle Trauma Group | 19 RCTs in total, 5 RCTs relevant to the present review 19 RCTs in total were included in the meta-analysis, 5 RCTs relevant to the present review | Inclusion criteria: older adults living in the community or institutionalized care Relevant population: Community-dwelling older adults, mean age of participants ranged from 78 to 84 years, proportion of male participants ranged from 0% to 30%, number of participants in the relevant trials ranged from 171 to 4169 | Intervention: hip protectors Comparator: no hip protectors | Outcomes: risk of sustaining a hip fracture, risk of sustaining a pelvic fracture, overall rate of pelvic and other fractures, rate of fall events, acceptance of and adherence to wearing protectors (compliance), complications Follow-up: 3 to 42 months |
NHS = National Health Service; RCT = randomized controlled trial.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
RNAO (2017)10 | ||||||
Intended users: Practice recommendations: nurses and other health-care providers Education recommendations: individuals and organizations responsible for the education of health care providers Organization and policy recommendations: managers, administrators, and policy-makers Target population: adults (> 18 years) who are at risk for falls and fall injuries | Interventions for preventing falls and reducing the risk for falls or falls-related injury, interventions or processes following a fall, education for nurses and other health-care providers, organizational policies and system-level supports | For hip protectors, hip fractures, falls and the potential benefits, harms, and barriers to adherence are discussed | A systematic literature search was conducted to identify relevant SRs. SRs were independently assessed for eligibility by 2 researchers. Data tables and research summaries were provided to expert panel members for review and discussion. Guidelines were identified through website searching and suggestions from the expert panel. Guidelines were appraised and those with a weak score were excluded. | SRs were appraised using AMSTAR and RNAO’s scoring system that rates reviews as low, moderate, or strong. Guidelines were appraised using AGREE II and RNAO’s scoring system that rates guidelines as low, moderate, or strong. Guidelines with a low quality rating were excluded. | RNAO established a panel of experts representing a range of sectors and practice areas. A modified Delphi technique was used to obtain panel consensus on recommendations. Recommendations were assigned levels of evidence based on the source of evidence used to support the recommendation. Levels of evidence:
| Prior to publication, feedback on the guideline was solicited from external stakeholders with subject matter expertise or who may be affected by the implementation of the guideline. |
RNAO (2017)10 Continued | ||||||
| ||||||
RACGP and Osteoporosis Australia (2017)11 | ||||||
Intended users: general practitioners and other health professionals. Target population: women who are postmenopausal and men older than 50 years of age who may be at risk of minimal trauma fracture, have been diagnosed as having at least 1 minimal trauma fracture, or diagnosed with osteoporosis. | Best practice in the identification, diagnosis, treatment, and management of osteoporosis. | Fracture, bone mineral density | Update to the 2010 version of the guideline. A systematic literature search was conducted. Evidence used to support recommendations was limited to RCTs, prospective cohort studies, and SRs of RCTs or prospective cohort studies. | The body of evidence supporting each recommendation was rated according to the NHMRC body of evidence matrix. | Recommendations were developed by an expert working group based on the systematic literature review. If evidence was insufficient or did not meet the minimum requirements, recommendations were developed through working group consensus. Each recommendation was given a final grade based on the NHMRC grades of recommendation. Grades of recommendations:
| The guideline was reviewed by general practitioner subject matter experts and the RACGP’s Expert Committee for Quality Care. |
RACGP and Osteoporosis Australia (2017)11 Continued | ||||||
Note: Grade D was also applied to recommendations where there was expert consensus in the absence of a strong body of evidence | ||||||
Eastern Association for the Surgery of Trauma (2016)12 | ||||||
Intended users: NR Target population: Adults aged 65 or older | Clinical interventions to reduce fall-related injuries | Injury due to falls | A systematic literature search was conducted by research librarians to identify eligible RCTs, prospective and retrospective observational studies, case-control studies, and meta-analyses. Three reviewers independently screened titles and abstracts for studies that met the inclusion criteria. Data were extracted from the studies and each reviewer was provided with a master copy. | Each designated reviewer independently assessed the evidence using the GRADE methodology. Studies were assessed as being at low, moderate, or high risk of bias. | The PICO questions were created using a modified Delphi method. Evidence was reviewed independently by each reviewer to answer the predetermined PICO questions and develop the recommendations. Based on the GRADE methodology, when formulating the recommendations, the phrases “we strongly recommend” or “we conditionally recommend” were used for strong evidence and weaker evidence, respectively. | NR |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; AMSTAR = A MeaSurement Tool to Assess systematic Reviews; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; NHMRC = National Health and Medical Research Council; NR = not reported; PICO = population, intervention, comparison, outcomes; RACGP = Royal Australian College of General Practitioners; RCT = randomized controlled trial; RNAO = Registered Nurses’ Association of Ontario; SR = systematic review.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Review and Meta-Analysis Using AMSTAR 27
Strengths | Limitations |
Santesso et al. (2014)5 | |
Clear objective Comprehensive literature search strategy and detailed methods described Study selection was performed in duplicate Data extraction was performed in duplicate List of excluded studies and justifications provided Characteristics of included studies were described in detail Two investigators independently assessed risk of bias using the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions Appropriate methods for meta-analysis were described and heterogeneity was assessed Sensitivity analysis was performed that excluded studies at high risk of bias Sources of funding for systematic review were reported | Unclear whether the protocol was registered, and which components of the research methods were established a priori Sources of funding for individual studies included in review were not reported Authors state that publication bias was not detected however, their investigation of publication bias was not described |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 5: Strengths and Limitations of Guidelines Using AGREE II8
Item | RNAO (2017)10 | RACGP and Osteoporosis Australia (2017)11 | Eastern Association for the Surgery of Trauma (2016)12 |
Domain 1: Scope and Purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Partially | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder Involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Unclear |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | No | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | No |
Domain 3: Rigour of Development | |||
7. Systematic methods were used to search for evidence. | Yes | Partially | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Partially | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Partially | No | Partially |
10. The methods for formulating the recommendations are clearly described. | Partially | No | Partially |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Unclear | Unclear |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Unclear |
14. A procedure for updating the guideline is provided. | Yes | No | No |
Domain 4: Clarity of Presentation | |||
15. The recommendations are specific and unambiguous. | Partially | Yes | Partially |
16. The different options for management of the condition or health issue are clearly presented. | NA | NA | NA |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | No | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Partially | No |
20. The potential resource implications of applying the recommendations have been considered. | No | No | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes | No | No |
Domain 6: Editorial Independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | No | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable; RACGP = Royal Australian College of General Practitioners; RNAO = Registered Nurses’ Association of Ontario.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings from the Included Systematic Review and Meta-Analysis
Study citation and study design | Results |
Hip fracture | |
Santesso et al. (2014)5 SR with MA (5 RCTs) | Risk ratio = 1.15 (95% CI, 0.84 to 1.58) |
Pelvic fracture | |
Santesso et al. (2014)5 SR with MA (3 RCTs) | Risk ratio = 1.04 (95% CI, 0.52 to 2.09) |
Other fractures (excluding pelvis) | |
Santesso et al. (2014)5 SR with MA (3 RCTs) | Rate ratio = 0.83 (95% CI, 0.65 to 1.04) |
Pelvic and other fractures | |
Santesso et al. (2014)5 SR with MA (5 RCTs) | Rate ratio = 0.86 (95% CI, 0.69 to 1.06) |
Falls | |
Santesso et al. (2014)5 SR (4 RCTs) | Cameron 2011a Rate ratio = 2.55 (95% CI, 1.06 to 6.14) |
Cameron 2011b Rate ratio = 2.12 (95% CI, 0.94 to 4.79) | |
Birks 2004 Rate ratio = 0.72 (95% CI, 0.63 to 0.83) | |
Cameron 2003 Rate ratio = 1.23 (95% CI, 1.11 to 1.37) | |
Acceptance and adherence (also termed compliance) | |
Santesso et al. (2014)5 SR (4 RCTs) | Cameron 2011a Adherence was 34% to 37% in patients who were initially hospitalized and later discharged to the community and 48% to 51% in participants in the community at 6 months |
Birks 2004 31% of participants were still wearing protectors daily by end of 28-month study | |
Birks 2003 Compliance = 34% | |
Cameron 2003 33% to 38% of participants were wearing protectors all the time by the end of 2-year study | |
Complications | |
Santesso et al. (2014)5 SR (4 RCTs) | Cameron 2011a and Cameron 2011b Participants were asked open-ended questions about complications and no complications were reported |
Birks 2004 1 hip fracture as a result of falling while putting on a hip protector | |
Cameron 2003 16 participants (5%) reported minor skin irritation caused by hip protectors | |
CI = confidence interval; MA = meta-analysis; SR = systematic review.
Note: A risk ratio or rate ratio less than 1 favours hip protectors
Table 7: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
RNAO (2017)10 | |
Recommendation: “Consider hip protectors as an intervention to reduce the risk of hip fracture among adults at risk for falls and hip fracture. Review the evidence, potential benefits, harms, and barriers to use with the person to support individualized decisions. (p. 13)”10 Supporting evidence: Evidence in long-term care settings came from systematic reviews and guidelines. Evidence in community settings came from 1 systematic review (Santesso et al. [2014]5) that reported that hip protectors had little or no effect in community-dwelling older adults. “Despite the lack of evidence, the expert panel suggests that some individuals may consider hip protectors—for example, those in hospital at risk for hip fracture, or those in the community with osteoporosis engaging in higher-risk activities (e.g., sports, walking on icy sidewalks, etc.). (p. 41)”10 | Quality of evidence: reviews = moderate, guidelines = strong Level of evidence: Ia (Evidence obtained from meta-analysis or systematic reviews of RCTs, and/or synthesis of multiple studies primarily of quantitative research) |
RACGP and Osteoporosis Australia (2017)11 | |
Recommendation: “Consider the use of hip protectors to reduce the risk of hip fracture in residential-care settings, but not in community settings.(p. 66)”11 Supporting evidence: Evidence came from 1 systematic review (Santesso et al. [2014]5) that found that hip protectors have little or no effect on hip fracture risk in community settings. | Recommendation grade = C (Body of evidence provides some support for recommendation[s] but care should be taken in its application.) |
Eastern Association for Surgery of Trauma (2016)12 | |
Recommendation: “We conditionally recommend hip protectors for frail elderly individuals in the appropriate environment. (p. 204)”12 Supporting evidence: Evidence came from 1 systematic review that concluded that hip protectors decrease hip fractures in older adults living in nursing homes and have a negligible effect in community-dwelling older adults. Evidence also came from several RCTs and a review that showed mixed results. | Strength of recommendation = conditional recommendation (based on weaker evidence) |
RACGP = Royal Australian College of General Practitioners; RCT = randomized controlled trial; RNAO = Registered Nurses’ Association of Ontario.
Appendix 5: References of Potential Interest
Previous CADTH Reports
13.Banerjee S, Gunn H, Spry C. Vitamin D supplementation for the prevention of falls and fractures in residents of long-term care facilities: a 2021 update. Can J Health Technol. 2021;1(7). https://www.cadth.ca/vitamin-d-supplementation-prevention-falls-and-fractures-residents-long-term-care-facilities-2021. Accessed 2021 Jul 28.
14.CADTH. Hip protectors. 2017; https://cadth.ca/index.php/hip-protectors. Accessed 2021 Jul 28.
15.Hip protectors: clinical and cost effectiveness. (CADTH Rapid response report: reference list). Ottawa (ON): CADTH; 2016: https://cadth.ca/hip-protectors-clinical-and-cost-effectiveness. Accessed 2021 Jul 28.
16.Fall prevention strategies for adult patients: comparative effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/fall-prevention-strategies-adult-patients-comparative-effectiveness-cost-effectiveness-and. Accessed 2021 Jul 28.
17.Fall risk assessment tools and prevention strategies: clinical effectiveness and guidelines. (CADTH Rapid response report: reference list). Ottawa (ON): CADTH; 2016: https://www.cadth.ca/fall-risk-assessment-tools-and-prevention-strategies-clinical-effectiveness-and-guidelines. Accessed 2021 Jul 28.
Review Articles
18.Fares A. Pharmacological and non-pharmacological means for prevention of fractures among elderly. Int J Prev Med. 2018;9:78.
19.Cianferotti L, Fossi C, Brandi ML. Hip protectors: are they worth it? Calcif Tissue Int. 2015;97(1):1-11.
Additional References
20.Keenan BE, Evans SL. Biomechanical testing of hip protectors following the Canadian Standards Association express document. Osteoporos Int. 2019;30(6):1205-1214.
21.Taylor SF, Coogle CL, Cotter JJ, Welleford EA, Copolillo A. Community-dwelling older adults' adherence to environmental fall prevention recommendations. J Appl Gerontol. 2019;38(6):755-774.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca